Embed Size (px)
Citation preview

Acute kidney injury in Sepsis
SubBag Nefrologi / Hipertensi
Bag. Penyakit Dalam FK UNDIP / RS. Dr. Kariadi
S E M AR A N G
Lestariningsih

Critical ill patient potentially AKI


AKI in ICU 5 –25% Mortality AKI 40-80%


Definition and diagnostic criteria for AKI
An abrupt (within 48 hr) reduction in kidney functioncurrently defined as an absolute increase in serum creatinine of either >0,3 mg/dl (25 umol/L) or presentage increase of >50% or reduction in OUP (documented oliguria of < 0,5 ml / kg per h for > 6hr )
Mehta RL. Nephrology Self Ass-vol 6, No 5, Sept 2007
More than different definitions of acute renal failure have been used in the literature

RIFLE criteria for Acute Renal Dysfunction
Risk
Injury
Failure
Loss
ESRD
Abrupt (1-7 days) decrease (> 25%) in GFR orScr x 1.5Sustained (> 24 hrs)
ARF ~ earliest time point for provision of RRT
Irreversible ARF or persistent ARF > 4 wks
ESRD > 3 months
Non-Oliguria Oliguria
UO < .5/ml/kg/hx 24 hrAnuria x 12 hrs
UO < 0.5/ml/kg/hx 12 hr ??
Decreased UO relative to the fluid inputUO < 0.5/ml/kg/h x 6hr
Adjusted creat or GFR decrease> 50% orScr x 2
Adjusted creat or GFR decrease > 75%Scr x 3 or Scr > 4mg%When acute > 0.5mg%
Spec
ific
ity

Klasifikasi/staging AKI modifikasi RIFLE
Stadium kriteria kreatinin kriteria urin output
1.
Risk
serum kreatinin meningkat > 0,3 mg/dl atau meningkat lebih dari 150-200 % dari awal
< 0,5ml/kg per jam untuk >6jam
2.
Injury
serum kreatinin meningkat sampai > 200% sampai 300% dari data awal
< 0,5 ml/kg per jam untuk 12 jam
3.
Failure
serum kreatinin meningkat > 300%, (serum kreatinin > 4mg/dl dengan peningkatan akut 0,5mg/dl, indikasi untuk renal replacement therapy
<0,3 ml/kg per jam x 24 jam atau anuria x 12 jam
Mehta RL. Nephrology Self Assesment Program , Vol 6, No 5, Sept 2007
Loss Persistent renal failure for >4 weeks
ESRD Persistent renal failure for >3 months
Murray PT, Palevsky PM. Nephrology Self Assesment Program , Vol 6, No 5, Sept 2007


SepsisIschemic insult
Nephrotoxic insult
Complement activationEndotoxin releaseIschemia-reperfusion
Cellular activation(PMN, endothelial cells…)
Arachidonic acid metabolities
Proteases
Chemokines
Platelet activating factor
Serum creatinine
Oxygen free radicals
Nitric oxide
Heat shock proteins
Endothelins
Acute kidney injury Urinary KIM-1, NAG
Urine output GFR
Anti-inflamatorymediators
Pro-inflamatorymediators -
+
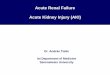
Pathogenic mechanism of sepsis related acute kidney injury

(1)Vasoconstriction
Renin-angiotensinendothelin
PGI2NO
(2)Obstruction
by casts
(3)Tubularbackleak
IschemiaNephrotoxins
Tubular damage(proximal tubules andascending thick limb)
(5)? Direct glomerular
effectGFR Oliguria
Tubularfluid flow
Intratubularpressure
Possible pathogenetic mechanisms in ATN.
(4)Interstitial
inflammation

Effects of ischemia on renal tubules in the pathogenesis of ischemic AKI
Schrier et al, J Clin Invest 2004, 114:5-14

Hemodynamic mechanism of ATN

We can identify different milestones along the timeline of AKI. Injury begins inducing molecular modifications subsequently evolving into cellular damage. Cells start to produce biomarkers of injury and only later does the clinical picture of the syndrome develop with typical sign and symptoms
Analyze biology by time zone with adequate and precission clock



The potential interventions in sepsis related AKI
1. Effective prevention/protection strategies for the kidney
in patient at risk2. Early recognition and attenuation of renal
damaged3. Pathophysiology driven pharmacology support4. Efficient extracorporeal blood purification therapy5. Strategies that promote recovery of renal function
Ronco . ASN 2008

Renal protection, there is damage before any symptom
MAP> 65 mmHg
CVP 8-12 mmHg (no ventilator)
12-15 mmHg (ventilator)
Urine > 0,5ml/BW/hour
SaO2 >70%
Koloid ,albumin ?
Renal Protection
•
•
•
•
•
•

Vasopressor therapy should be started early and not as a last resort in moribund patients. In a retrospective analysis of patient requiring NE, both the degree of organ dysfunction (SOFA score) and time to administer NE are associated with worse outcome
In conclusion, NE can be used to restore blood pressure without jeopardizing the renal function in fluid-resuscitated patients with distributive shock. Whether other vasopressors offer advantages over NE should be further investigated
M.Schetz, Blood Purification 20:243-251,2002
Vasopressors and the kidney

Loop diuretics in ARF: a double-blind randomized controlled trial
• Over 3 years, 278 oliguric patients were assessed as potential ARF. Twenty five percent recovered with simple rehydration.
• Ninety six patients were enrolled in the study. Study patients received i.v. dopamine 2 microgram/kg per min for 3 days ; mannitol i.v., 100 ml 6-hourly for 3 days, and randomized medication - i.v. torasemide 3 mg/kg, furosemide 3 mg/kg, or placebo- 6- hourly for 21 days or until renal recovery,dialysis, or death.
• Apache II scores were similar in the three groups.
Shilliday IR et al. Nephrol Dial Transplant 11: 1684, 1996.

Intensive insulin therapy sepsis by 45%
Blood glucose 80-110 mg/dl morbidity and mortality
Mechanism : bacterial phagocytosis and antiapoptotic effect of insulin
Tight control of blood glucose

Effect of control of mean blood glucose in ICU patients
Van den Berghe et al Crit Care Med2003, 31:359-366

Other therapy
- Ventilator ; low tidal volume
- Dietary nutrition
- N-acetil cystein
- Eritropoietin
- Stem cell



Treatment parameters in IHD dose study
Characteristic Alternate day hemodialysis
Daily hemodialysis
Duration of session (hr)
Blood flow rate ml/mnt
Dose (Kt/V)
Prescribed
Delivered
Weekly delivered
Time averaged BUN (mg/dl)
UF volume (L/session)
3.4+0.5
243+25
1.21+0.09
0.94+0.11
3.0+0.6
104+18
3.5+0.3
3.3+0.4
248+45
1.19+0.11
0.92+ 0.16
5.8+0,4
60+20
1.2+0.5
P<0.001 vs alternate day group

• AKI is a new terminology, which is identically to ARF type ATN ?
• AKI sepsis, RIFLE modified
• Early detection of AKI by biomarker
• Management
– Early detection
– Blood glucose control 80-110mg/dl
– Renal perfusion (MAP>70mmHg, CVP 8-12/12-15 mmHg, diuresis >0.5cc/BW/hour,SaO2 >70%
– Ventilator low TV, nutrition, Erithropoeitin, stem cell
– Extracorporeal therapy, CRRT, SLED
Conclusion

terima kasihterima kasih

Management of AKI

CRRTSLED
IHD
Treatment modalities for AKI in ICU