Embed Size (px)
Citation preview

Acute and Chronic Treatment of Severeand Malignant Hypertension with the Oral
Angiotensin-converting Enzyme Inhibitor CaptoprilDAVID B. CASE, M.D., STEVEN A. ATLAS, M.D., PATRICIA A. SULLIVAN, R.N.,
AND JOHN H. LARAGH, M.D.
SUMMARY Ten patients with severe and 10 with accelerated or malignant hypertension were treated withthe angiotensin-converting enzyme inhibitor captopril. Captopril acutely reduced blood pressure in all patientsexcept two who had suppressed plasma renin activity. Four patients with encephalopathy showed immediateimprovement after the first dose. Two patients could be withdrawn from nitroprusside infusion upon adminis-tration of captopril. Nineteen of 20 patients have remained on captopril for 12-32 months. Blood pressure iscontrolled in 18 and improved in two. Eleven required addition of diuretic and one addition of clonidine. Themaximal antihypertensive effect of captopril with or without diuretics was evident after 3 months of continuoustherapy and was associated with elevated plasma renin levels, normal aldosterone excretion and preservation ofrenal function. Captopril was well-tolerated, but produced occasional rash, loss of taste and proteinuria. Weconclude that captopril, alone or in combination with other drugs, is effective in both the acute and long-termmanagement of severe and malignant hypertension.
EFFECTIVE TREATMENT of patients with severeand accelerated forms of hypertension is a complextherapeutic challenge. Patients are often treated ini-tially with potent parenteral vasodilators such asdiazoxide or sodium nitroprusside and are thenswitched to oral therapy, usually with several drugs.Malignant and severe hypertension are frequentlyassociated with hyperactivity of the renin-angioten-sin-aldosterone axis.'-4 As a result, drugs that block orinhibit the renin system, such as propranolol, the non-apeptide angiotensin-converting enzyme inhibitorteprotide (SQ 20881), and the angiotensin antagonistsaralasin, have been shown to lower blood pressure inthese forms of hypertension. 9̀ Captopril (Capoten,SQ14225) is an orally active inhibitor of angiotensin-converting enzyme, the peptidase that converts the in-active decapeptide angiotensin I to the vasopressoraldosterone-stimulating octapeptide angiotensin II.The present study was designed to determine theclinical effectiveness of captopril in severe and malig-nant hypertension. In addition to its renin-blockingaction, the drug has a rapid onset of action, with anantihypertensive effect that begins 15 minutes after thefirst dose.'0 It is available as an oral preparation suit-able for long-term therapy.
Materials and MethodsPatient Selection
Ten patients with severe hypertension (diastolicpressure greater than 120 mm Hg) and 10 with
From the Hypertension and Cardiovascular Center, Departmentof Medicine, The New York Hospital-Cornell University MedicalCollege, New York, New York.
Supported by grants HL 18323 (SCOR) and RR47, ClinicalResearch Center, and from the Squibb Institute of MedicalResearch.
Presented in part at the 52nd Scientific Session of the AmericanHeart Association, November 1979, Anaheim, California.
Address for correspondence: Dr. David B. Case, HypertensionCenter, 525 East 68th Street, New York, New York 10021.
Received July 29, 1980; revision accepted January 22, 1981.Circulation 64, No. 4, 1981.
accelerating or malignant hypertension (grade III orIV neuroretinopathy) were selected for study. Eachpatient gave written consent to the use of captoprilafter a protocol approved by the Human Rights inResearch Committee of The New York Hospi-tal-Cornell Medical Center. Clinical characteristics ofthese patients are listed in table 1. The patients were10-67 years old. Eleven of the patients had under-lying renovascular hypertension, seven with bilateralrenal artery stenosis and four with unilateral lesions.One patient had systemic lupus erythematosis andseven patients had essential hypertension; in onepatient (no. 4), no diagnosis was established. At thetime captopril was started, six of the patients werereceiving other medications: All six were onpropranolol; two were also on clonidine and twoothers were being given i.v. sodium nitroprusside. The14 other patients were not taking any drugs.Four patients with malignant hypertension had a
course complicated by mild-to-moderate enceph-alopathy, and one patient had a type III dissectingaortic aneurysm. None of the subjects had acute con-gestive cardiac failure, stroke or advanced renal in-sufficiency.
Study DesignEach patient underwent a complete history,
physical examination and routine blood chemistryanalysis. Blood pressure was taken at 2-minute inter-vals by Arteriosonde in 18 patients; in the remainingtwo, direct intraarterial pressure was monitored. Aftera stable baseline during which blood pressure wasrecorded in the head-up position, a single dose of cap-topril, 10-50 mg orally, was given. Blood pressurerecordings were continued for 90 minutes after thefirst dose.The dose of captopril was gradually increased over
the next 3-5 days to 300-600 mg/day except in twopatients who initially received 800 mg/day and onepatient who was given 225 mg/day. During thisperiod, all other drugs were withdrawn except for
765
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 64, No 4, OCTOBER 1981
propranolol in one patient with a dissecting aneurysmand in another with angina. Patients who had am-bulatory diastolic pressure greater than 105 mm Hgafter 1 week of captopril therapy received a diuretic:chlorthalidone, 25-50 mg/day, in six patients andfurosemide, 40-80 mg/day, in two. Drug dosages werereduced during outpatient follow-up to determine thelowest dose required for blood pressure control.At each follow-up visit, plasma renin activity,"
urinary aldosterone,'2 24-hour urine protein, bloodurea nitrogen, serum creatinine and other routinechemistries were measured.
Statistical Methods
Mean values have been expressed, with the standarderror of the mean as the index of dispersion. Statisticalsignificance was determined using the t test for paireddata; confirmation was obtained using Wilcoxon'srank-sum test for small samples. Correlations weremade using Spearman's correlation coefficient.
ResultsResponse to the First Dose
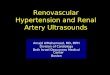
The blood pressure responses to the first oral dosesof captopril in 18 of the 20 patients who were notreceiving i.v. sodium nitroprusside are shown in figure1. Diastolic pressure fell in all but two patients, whohad suppressed levels of plasma renin activity (0.16and 0.38 ng AI/ml/hour). After 90 minutes, meandiastolic blood pressure in 18 patients had declinedfrom 132 ± 4 mm Hg to 107 ± 4 mm Hg (p <0.001).Heart rate did not change significantly (from 74 ± 6to 79 ± 9 beats/min). In the two patients alreadyreceiving sodium nitroprusside to maintain diastolicblood pressure at about 100 mm Hg, nitroprussidewas gradually withdrawn during the 30-minute periodafter the first oral dose of captopril.
For the group as a whole, the logarithm of thepretreatment plasma renin activity and the percentreduction in diastolic pressure correlated well(r = 0.82, p < 0.001).
Within one-half hour of the initial dose, all fourpatients with encephalopathy had relief from head-ache and a clearing of nausea, mental confusion anddecreased visual acuity. These benefits were main-tained even though blood pressure sometimes rosetransiently during the first week of therapy.'3
Responses after 1 Week
In 19 of the patients, diastolic blood pressure levelsafter one week of captopril therapy (fig. 1) were com-parable to those after the first dose (mean 107 ± 4mm Hg vs 108 ± 14 mm Hg). In one patient, diastolicpressure returned to control levels after 1 week on cap-topril alone; but he had been receiving furosemide upuntil the administration of the first dose, so his initialresponse was greatly exaggerated (fig. 1).
Long-term Effects
In 13 patients whose diastolic pressure remained
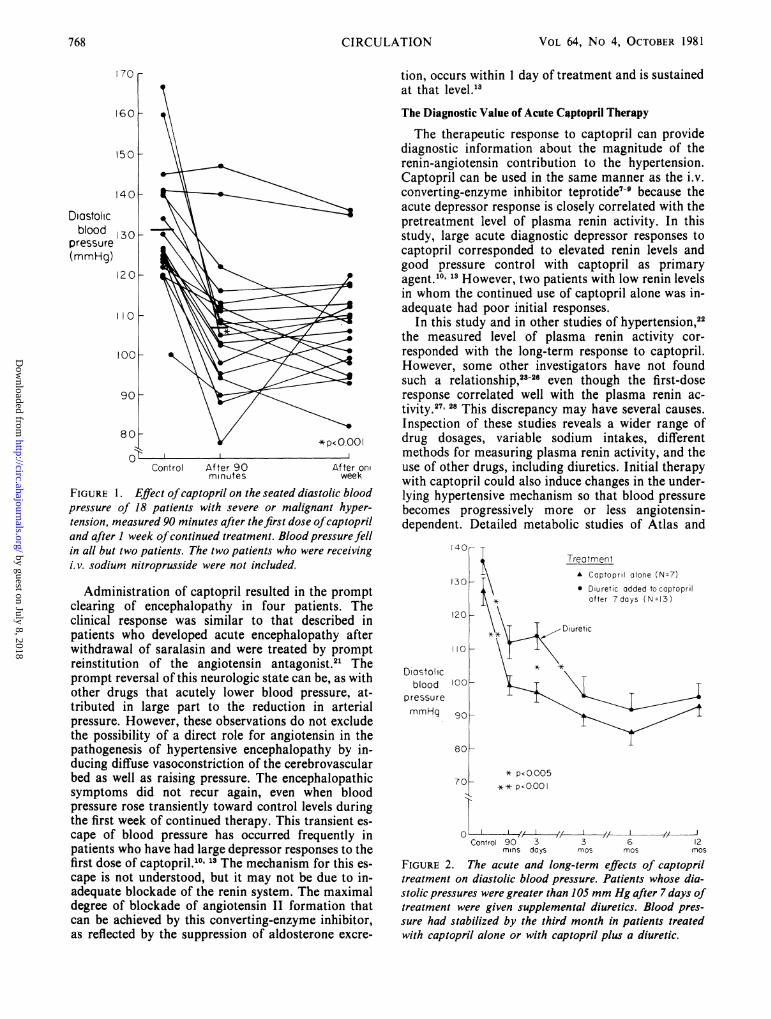
of captopril therapy, resulting in a further fall indiastolic pressure (from 114.0 ± 4.0 mm Hg to 96 ± 6mm Hg). The long-term pressure responses of thesepatients were comparable to those of the sevenpatients who were adequately controlled with capto-pril alone (fig. 2). The antihypertensive effect wasmaximal by the third month of therapy and stablethereafter. After 1 year, the mean diastolic pressurewas 93 ± 3 mm Hg for patients treated with captoprilalone and 96 i 4 mm Hg for those treated with cap-topril plus a diuretic.
Neuroretinopathy cleared in all patients during theinitial months of therapy. After 12 months treatment,there was no funduscopic evidence of acceleratedhypertension in any of the 10 patients who hadpresented initially with retinal hemorrhages or ex-udates.The effects of treatment on renal function are shown
in figure 3. Pretreatment serum creatinine was1.4 ± 0.02 mg/dl and blood urea nitrogen was 15 ± 2mg/dl in the group of patients who responded to cap-topril alone and were 1.6 ± 1.9 mg/dl and 22 i 5mg/dl, respectively, for the group of patients who re-quired addition of a diuretic after 7 days of captopril.These values remained unchanged during the firstweek of captopril treatment. The addition of diureticto captopril led to a modest rise in blood urea nitrogen(range of 30-35 mg/dl) after 3 and 6 months oftherapy, which returned to baseline after 12 months.Patients treated with captopril alone had a slight butsignificant rise in blood urea nitrogen (15 ± 2 to20 ± 2 mg/dl, p < 0.02), but not in serum creatinine,during the 12-month treatment period.Among all patients, plasma renin activity rose from
a mean of 15 ± 3 AI/ml/hour to 40 ± 6 ngAI/ml/hour (p < 0.001) after 3 months of therapyand remained in that range throughout the study (fig.4). Urinary aldosterone excretion remained in the nor-mal range (less than 25 gg/day) despite' adjunctivediuretic therapy in 13 of these patients. Control ratesof urinary aldosterone excretion were not determinedin most patients because treatment was initiatedbefore such a specimen could be obtained.
Sixteen of the 20 patients in this study have beenmaintained on captopril therapy for 20-35 months(table 2). One patient was withdrawn from captopril atthe time of corrective renal artery surgery. Patient 20was withdrawn from captopril after 2 years of con-trolled blood pressure and has remained normo-tensive for at least 3 months without treatment. Threepatients developed proteinuria; in two (patients 1 and5), proteinuria receded spontaneously on the samedose of captopril. Only patient 2 required discontinua-tion of therapy because of the development ofnephrotic syndrome associated with a decline in renalfunction. Since stopping captopril, renal function andurinary protein excretion in this patient have returnedto pretreatment levels.
In addition to diuretics, fl-adrenergic blockingagents were used in four patients for management ofangina, dissecting aneurysm or arrhythmias. In onepatient, addition of clonidine produced further im-
above 105 mm Hg, a diuretic was added after 1 week
CIRCULATION766
provement in blood pressure control.
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

ANTIHYPERTENSIVE TREATMENT WITH CAPTOPRIL/Case et al.
Side Effects of Captopril
Two patients had transient rashes lasting less than 1week during the initiation of therapy and one had lossof taste lasting for 1 month. These side effects clearedspontaneously without alteration of captopril dosage.Three patients developed proteinuria, but this was
transient in two patients, regressing spontaneouslydespite continued therapy. One patient required with-drawal of the drug.
DiscussionThis study demonstrates the success of the orally
active angiotensin-converting enzyme inhibitor capto-pril in both the initial treatment and the long-termmaintenance therapy of patients with severe, ac-celerated or malignant hypertension. A drug thatblocks the renin system is ideal for patients with severeand malignant hypertension, because such patientsfrequently have elevated plasma renin activity.'-" Theuse of captopril, other converting-enzyme inhibitors,and new, potent vasodilators such as minoxidil shouldvirtually eliminate the need to recommend bilateralnephrectomy for severe, drug-resistant hypertension.4
Acute Therapeutic Response to Captopril
The onset of action of captopril was within 15minutes of the first oral dose, reaching a maximaleffect within 30-90 minutes. Because of this rapidonset of action, captopril is suitable for initial treat-ment of severe hypertension. While blood pressurefalls promptly after the first dose of captopril, thedecline is not as precipitous as that which occurs fre-quently with diazoxide. There is recent evidence of therisks of abrupt hypotension, including irreversibleblindness.',, 1' In addition, captopril does not inducesignificant reflex tachycardia, in contrast to the direct-acting vasodilators diazoxide, hydralazine and minox-idil,'7 thereby averting potential tachyarrhythmias andangina. Captopril, however, like other angiotensionantagonists, can produce hypotension in sodium-depleted patients.'0' 18
Because of the rapid onset of captopril, we couldwean two patients from i.v. sodium nitroprusside ascaptopril was administered. The rationale for thisprocedure is that direct vasodilators such as hydrala-zine"' and nitroprusside20 stimulate renin release and,thus, the possible additive effect of these agents withcaptopril could lead to hypotension.
TABLE 1. Pretreatment Clinical Characteristics of Patients
Sex DiagnosisF RV-1M RV-1
3 29 M EHM
FM
RV-2RV-2RV-2
7 25 M EH
8 55 M EH
M
FEHRV-1
Bloodpressure(mm Hg)
180/120230/130196/130180/132230/134206/122*180/134178/125180/120198/140
196 ± 6/129 ± 2
PretreatmentPRA
(ng AI/ml/hr)
1311
6.78.77.33.02.5
7.01.57.3
6.8 ± 1.2
Acceleratedor malignant
11 15 F SLE
121314
474610
FM
M
EHEH
UNK15 39 M RV-2, AA16171819
20
Mean ± SEM
2256595620
M
FM
M
F
RV-1EHRV-1RV-2RV-2
244/160*270/152180/122140/110*t140/95*t170/100*220/140190/124220/135158/124
260 ± 14/132 ± 7
Grade ofhypertension
Severe
Pt
1
2
Age(years)
3067
4
56
565250
910
55
30
Mean ± SEM
Blood ureanitrogen(mg/dl)
10
16
10
28161910
19
14
13
15 ± 2
Serumcreatinine(mg/dl)
1.23.11.62.21.31.51.51.51.21.5
1.5 ± 0.1
9.1
300.1635252.50.38
21
3528
18.6 ± 4.5t
7831
19
16142214
132011
24 ± 6
3.02.91.30.9
0.81.61.41.31.51.2
1.6 ± 0.2
Abbreviations: EH = essential hypertension; RV-1 = unilateral renovascular hypertension; RV-2 = bilateral renovascularhypertension; SLE = systemic lupus erythematosis; AA = dissecting aortic aneurysm; UNK = unknown.*On propranolol.tDuring nitroprusside infusion.tp < 0.05 compared with patients with severe hypertension.
767
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 64, No 4, OCTOBER 1981
tion, occurs within 1 day of treatment and is sustainedat that level."3The Diagnostic Value of Acute Captopril Therapy
Control After 90minutes
FIGURE 1. Effect of captopril on the seated diaspressure of 18 patients with severe or maligntension, measured 90 minutes after thefirst dosecand after 1 week ofcontinued treatment. Blood pressure fellin all but two patients. The two patients who were receivingi. v. sodium nitroprusside were not included.
Administration of captopril resulted in the promptclearing of encephalopathy in four patients. Theclinical response was similar to that described inpatients who developed acute encephalopathy afterwithdrawal of saralasin and were treated by promptreinstitution of the angiotensin antagonist.21 Theprompt reversal of this neurologic state can be, as withother drugs that acutely lower blood pressure, at-tributed in large part to the reduction in arterialpressure. However, these observations do not excludethe possibility of a direct role for angiotensin in thepathogenesis of hypertensive encephalopathy by in-ducing diffuse vasoconstriction of the cerebrovascularbed as well as raising pressure. The encephalopathicsymptoms did not recur again, even when bloodpressure rose transiently toward control levels duringthe first week of continued therapy. This transient es-cape of blood pressure has occurred frequently inpatients who have had large depressor responses to thefirst dose of captopril.10' 13 The mechanism for this es-cape is not understood, but it may not be due to in-adequate blockade of the renin system. The maximaldegree of blockade of angiotensin TI formation thatcan be achieved by this converting-enzyme inhibitor,as reflected by the suppression of aldosterone excre-
The therapeutic response to captopril can providediagnostic information about the magnitude of therenin-angiotensin contribution to the hypertension.Captopril can be used in the same manner as the i.v.converting-enzyme inhibitor teprotide7-9 because theacute depressor response is closely correlated with thepretreatment level of plasma renin activity. In thisstudy, large acute diagnostic depressor responses tocaptopril corresponded to elevated renin levels andgood pressure control with captopril as primaryagent.". 13 However, two patients with low renin levelsin whom the continued use of captopril alone was in-
adequate had poor initial responses.In this study and in other studies of hypertension,22
the measured level of plasma renin activity cor-responded with the long-term response to captopril.However, some other investigators have not foundsuch a relationship,23 28 even though the first-doseresponse correlated well with the plasma renin ac-tivity.27' 28 This discrepancy may have several causes.Inspection of these studies reveals a wider range of
P<0001 drug dosages, variable sodium intakes, differentmethods for measuring plasma renin activity, and the
After on use of other drugs, including diuretics. Initial therapyweek with captopril could also induce changes in the under-
tolic blood lying hypertensive mechanism so that blood pressure
!ant hyper- becomes progressively more or less angiotensin-)fcaptopril dependent. Detailed metabolic studies of Atlas and
i40_
130
120
110 _
Diostolicblood 100o
pressure
mmHg 90 _
TreotmentA Captopril alone (N=7)0 Diuretic added tocaptopril
after 7days (N=13)
80_
70
0
* p<0005I-
** p<O.I
Control 90 3 3 6 12mins days mos mos mos
FIGURE 2. The acute and long-term effects of captopriltreatment on diastolic blood pressure. Patients whose dia-stolic pressures were greater than 105 mm Hg after 7 days oftreatment were given supplemental diuretics. Blood pres-sure had stabilized by the third month in patients treatedwith captopril alone or with captopril plus a diuretic.
170
160
150
140
Diastolicblood 130
pressure(mmHg)
120 _
I 10o
1O0 _
90 _
80
0 _
768 CIRCULATION
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

ANTIHYPERTENSIVE TREATMENT WITH CAPTOPRIL/Case et al.
42r
Blood ureanitrogenmg/d
TreatmentA Captopril alone (N=7)* Diuretic added to coptopril
after 7 days (N= 13)
34k
26F
1 8$
n.
4----t
t p< 025tt p< ,0
2
Serumcreatinine 5 -A
mg/dl
Control 90 3 6 12mins doys mos mos mos
FIGURE 3. Effect of captopril treatment on blood urea
nitrogen and serum creatinine. A slight rise in blood urea
nitrogen, but not serum creatinine, occurred in the patientstreated with captopril plus diuretics. The standard errorforserum creatinine in patients treated with captopril was so
small that it is obscured in the symbol for the mean value.
colleagues29 revealed significant reductions in aldo-sterone excretion and loss of sodium and water.Removal of extracellular volume, even in low-reninpatients,30 results in increased renin release, and wouldthus produce increased responsiveness to converting-enzyme blockade. This issue requires further study.The close relationship between the activity of the
renin system and the initial antihypertensive responseto captopril does not exclude the participation of otherantihypertensive mechanisms in the action of capto-pril, such as kinin accumulation. Although these othermechanisms have not been clarified, they appear towork in parallel with the effect of angiotensinblockade.
60 r
50o
* Plosma renin activity
Urine aidosierone
Plasm 4 0renin
activityng AI/mi /hr 30
20f
10
0
Control 3 months 6months 12months
20
Urineao oldosterone
ug/24hr
O
*P 0o, I
FIGURE 4. Effects of captopril on plasma renin activityand urine aldosterone excretion. Plasma renin activity rose
on captopril, although urine aldosterone excretion was nor-
mal during treatment despite concomitant diuretic therapyin 13 of these 20 patients.
A single dose of a converting-enzyme inhibitor hasalso been used in screening for renovascular hyper-tension, because both teprotide and captopril inducediagnostically large increases in plasma renin activityin renovascular hypertension.31 32 This test, however,produces false-positive results in patients withaccelerated hypertension.32
Long-term Response to Captopril
The patients treated in this study with captopril foras long as 3 years have remained controlled. How-ever, they were treated at a relatively early and un-complicated stage: Renal function was relatively in-tact and none had pulmonary edema, intracerebralhemorrhage, or myocardial infarction. Captoprilalone controlled pressure in seven of these 20 patients,while 13 required a diuretic. The addition of diureticsto captopril resulted in improved blood pressure con-trol, as noted previously.'0' 33,8 Clonidine and capto-pril were used in one patient. The possible supplemen-tary antihypertensive effect of fl-blocker therapy infour patients could not be evaluated since their usewas dictated by other indications (arrhythmia, anginaand dissecting aneurysm). Empirical multidrugtherapies have been used to control severe hyper-tension.33-40 Therefore, a converting-enzyme inhibitoralone or with diuretic or one other drug may be asimpler and less costly regimen than those usedpresently.Although specific mild drug toxicity occurred in
several patients in the form of rash, altered taste andproteinuria, there were no complaints of diminishedmental acuity, dry mouth, postural hypotension,altered sexual function, abnormal hair growth or gas-trointestinal distress. Three of 20 patients developedproteinuria while on captopril, and in one of them thedrug was discontinued because of nephrotic syndromewith deterioration of renal function. The nephrotox-icity of captopril has been described.41' 42 Proteinuriahas occurred in less than 3% of all patients treated4'and has been associated with biopsy evidence of mem-braneous glomerulopathy.40' 41 However, the pro-teinuria regressed even when the drug was continuedin the same or lower dosage.4'Serum creatinine remained unchanged both acutely
and after 12 months of captopril treatment, whetheror not diuretic therapy was added. Blood ureanitrogen rose, however, in those patients treated withdiuretics, reaching a peak after 6 months and thengradually decreasing toward baseline. Preservation ofrenal function despite large reductions in arterialpressure suggests that captopril may produce renalvasodilation. This is in keeping with the finding thatangiotensin antagonists reverse the renal vaso-constricting action of angiotensin.43Plasma renin activity rose during captopril therapy,
as demonstrated previously.'0' 23 24 This is probablyrelated to stimulation of baroreflex mechanisms by thereduction of pressure, and to interruption of the nega-tive feedback of angiotensin II on renin release. In
769
u
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 64, No 4, OCTOBER 1981
TABLE 2. Long-term Captopril Therapy
Duration Blood pressure Dose of
Gradeoof therapy (mm g) captopril Other drugshypertension (months) Sitting Supine (mg/day) (mg/day) Comment
Severe1 20 106/78 126/88 300 C-50 Proteinuria from third month, re-
ceded to 0.2 g/day2 12t 196/108 198/108 600 F-200 Persistent proteinuria, decreased
renal function
3 16 120/85 105/85 400 C-254 18 160/110 164/106 300 C-50, P-605 30 134/88 142/90 400 E-200 Proteinuria from 3rd month, re-
ceded to 1 g/day6 22 140/98 160/86 400 C-50, M-50 Angina has cleared7 17 112/80 116/80 400 -8 30 128/94 122/84 400 -9 22 120/100 132/90 400 C-10010 20 128/88 130/92 300 -
Mean SEM 134 ± 8/93 3 140 ± 9/91 3 390 ± 28
Malignant11 17 135/85 132/80 200 M-100, F-80 No new problems, SLE inactive12 32 128/94 140/100 400 C-50 Angina has cleared13 25 142/95 145/98 150 H-25, S-5014 20 120/80 126/86 200 -15 16 138/66 136/72 300 P-32016 it 140/88 134/84 400 CL-0.317 30 148/106 120/100 75 H-100, F-8018 22 134/86 145/86 450 -19 24 150/84 136/90 400 -20 24t 106/70 102/74 100 -
Mean SEM 134 ± 4/85 4 132 ± 4/87 3 268 ± 44
Abbreviations: C = chlorthalidone; F = furosemide; P = propranolol; E = ethacrynic acid; M = metoprolol; S = spirono-lactone; CL = clonidine; SLE = systemic lupus erythematosis.
tCaptopril withdrawn, in patient 2 because of persistent proteinuria and nephrotic syndrome; patient 16 underwentcorrective renal artery surgery; patient 20 remained normotensive after captopril was withdrawn and renal arteries weredilated by balloon catheter angioplasty.
some patients, renin levels have been reported todecline over time,23 but they did not decline signifi-cantly in our patients.
Suppression of aldosterone excretion during capto-pril therapy is associated with potassium retentionand, in most patients, a mild natriuresis during thefirst week of therapy.29 In these patients, aldosteroneexcretion remained normal despite marked increasesin renin activity and, in over half of the patients, theaddition of diuretics. Because of the acute nature oftheir illness, most of the patients did not have the rateof aldosterone excretion measured before captopriltherapy, which is markedly raised in malignant hyper-tension.' These findings indicate that the converting-enzyme inhibitor prevented hyperaldosteronismsecondary to hyperreninemia. Reactive rises in plasmarenin activity and aldosterone excretion have beenassociated with reduced antihypertensive effective-ness of thiazide diuretics.4'"
In summary, the oral converting-enzyme inhibitorcaptopril was an effective antihypertensive treatment
for patients with severe, accelerated, and malignanthypertension. Captopril has a rapid onset of action, soit is suitable for initial therapy in patients who requireurgent blood pressure reduction. The magnitude of theinitial antihypertensive response was closely related tothe pretreatment plasma renin activity. Immediatereversal of encephalopathic signs was observed in theacute treatment period. Continued captopril therapyalone or with other agents resulted in satisfactorylong-term blood pressure control. Renal function waswell-preserved on captopril, and hyperaldosteronismsecondary to concomitant diuretic therapy wasblocked. Because of its relative potency and safety,oral converting-enzyme inhibitors should be con-sidered for patients with severe and malignant hyper-tension for oral long-term and acute therapy.
AcknowledgmentThe authors thank the medical housestaff of The New York
Hospital and the staff of the Cardiovascular Center for theirassistance in managing these patients. We also thank Kathy Fallon
770 CIRCULATION
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

ANTIHYPERTENSIVE TREATMENT WITH CAPTOPRIL/Case et al.
and Lupe Corrier for their help in the preparation of thismanuscript.
References1. Laragh JH, Ulick S, Januszewicz V, Deming QB, Kelly WG,
Lieberman S: Aldosterone excretion and primary and malig-nant hypertension. J Clin Invest 39: 1091, 1960
2. Helmer OM: Renin activity in blood from patients with hyper-tension. Can Med Assoc J 90: 221, 1964
3. Genest J, Boucher R, deChamplain J, Veyrat M, Chr6tien P,Biron P, Tremblay G, Roy P, Cartier P: Studies on the reninangiotensin system in hypertensive patients. Can Med Assoc J90: 263, 1964
4. Brown JJ, Davies DL, Lever AD, Robertson JIS: Plasma reninconcentrations in human hypertension. I. Relationship betweenrenin, sodium, and potassium. Br Med J 2: 144, 1965
5. Biuhler FR, Laragh JH, Vaughan ED Jr, Brunner HR, GavrasH, Baer L: Antihypertensive action of propranolol: specificanti-renin responses in high and normal renin forms of essen-tial, renal, renovascular, and malignant hypertension. Am JCardiol 32: 511, 1973
6. Brunner HR, Gavras H, Laragh JH, Keenan R: Hypertensionin man. Exposure of the renin and sodium components usingangiotensin II blockade. Circ Res 34 (suppl I): 1-35, 1974
7. Gavras H, Brunner HR, Laragh JH, Sealey J, Gavras 1,Vukovich R: An angiotensin converting enzyme inhibitor toidentify and treat vasoconstrictive and volume factors in hyper-tensive patients. N Engl J Med 291: 817, 1974
8. Case D, Wallace J, Keim H, Weber M, Sealey J, Laragh JH:Possible role of renin in hypertension as suggested by renin-so-dium profiling and inhibition of converting enzyme. N Engl JMed 296: 641, 1977
9. Tifft CP, Gavras H, Kershaw GR, Gavras I, Brunner HR,Liang CS, Chobanian AV: Converting enzyme inhibition inhypertensive emergencies. Ann Intern Med 90: 43, 1979
10. Case DB, Atlas SA, Laragh JH, Sealey JE, Sullivan PA,McKinstry DN. Clinical experience with blockade of the renin-angiotensin-aldosterone system by an oral converting enzymeinhibitor (SQ 14225, captopril) in hypertensive patients. ProgCardiovasc Dis 21: 195, 1978
11. Sealey JE, Laragh JH: How to do a plasma renin assay. Car-diovasc Med 2: 1079, 1977
12. Sealey JE, Laragh JH: Measurement of urinary aldosterone ex-cretion in man. In Hypertension Manual, edited by Laragh JH.New York, Dun-Donnelley, 1974, pp 641-654
13. Case DB, Atlas SA, Laragh JH, Sullivan PA, Sealey JE: Use ofthe first-dose response on plasma renin activity to predict thelong-term effect of captopril: identification of a triphasic pat-tern of blood pressure response. J Cardiovasc Pharm 2: 339,1980
14. Kaplan NM: Clinical Hypertension, 2nd ed. Baltimore,Williams & Wilkins, 1978
15. Cove DH, Seddon M, Fletcher RF. Blindness after treatmentfor malignant hypertension. Br Med J 2: 245, 1979
16. Ledingham JGG, Rajagopalan B: Cerebral complications in thetreatment of accelerated hypertension. Q J Med 189: 25, 1979
17. Koch-Weser J: Hypertensive emergencies. N Engl J Med 290:211, 1974
18. Atkinson AB, Brown JJ, Morton JJ, Leckie B, Fraser R, LeverAF, Robertson JI: Captopril in a hyponatraemic hyperten-sive: need for caution in initiating therapy. Lancet 1: 557, 1979
19. Ueda H, Yagi S, Keneko Y: Hydralazine and plasma renin ac-tivity. Arch Intern Med 122: 387, 1968
20. Kaneko Y, Ikeda T, Takeda T, Ueda H: Renin release duringacute reduction of arterial pressure in normotensive subjectsand patients with renovascular hypertension. J Clin Invest 46:705, 1967
21. Keim HJ, Drayer JI, Case DB, Lopez-Ovejero J, Wallace JM,Weber MA, Laragh JH: A role for renin in rebound hyper-tension and encephalopathy after infusion of saralasin acetate(sarl-ala8-angiotensin II). N Engl J Med 296: 1175, 1976
22. MacGregor GA, Markandu ND, Roulston JE, Jones JC:Essential hypertension: effect of an oral inhibitor of angio-tensin converting enzyme. Br Med J 2: 1106, 1979
23. Gavras H, Brunner HR, Turini GA, Kershaw GR, Tifft CP,Cuttelod S, Gavras I, Vuokvich RA, McKinstry DN: Anti-hypertensive effect of the oral angiotensin converting enzymeinhibitor SQ 14225 in man. N Engl J Med 298: 991, 1978
24. Bravo EL, Tarazi RC: Converting enzyme inhibition with anorally active compound in hypertensive man. Hypertension 1:39, 1979
25. Sullivan JM, Ginsburg BA, Ratts TE, Johnson JG, Barton BR,Kraus DH, McKinstry DN, Muirhead EE. Hemodynamic andantihypertensive effects of captopril, an orally active angio-tensin converting enzyme inhibitor. Hypertension 1: 397, 1979
26. Johns DW, Baker KM, Ayers CR, Vaughan ED Jr, Carey RM,Peach MJ, Yancey MR, Ortt EM, Williams SC: Acute andchronic effects of captopril in hypertensive patients. Hyper-tension 2: 567, 1980
27. Brunner HR, Gavras H, Waeber B, Textor SC, Turini GA,Wauters JP: Clinical use of an orally acting converting enzymeinhibitor: captopril. Hypertension 2: 558, 1980
28. Spark RF, O'Hare CM, Regan RM: Low-renin hypertension:restoration of normotension and renin responsiveness. ArchIntern Med 133: 205, 1974
29. Atlas SA, Case DB, Sealey JE, Laragh JH, McKinstry DN.Interruption of the renin-angiotensin system in hypertensive pa-tients by captopril induces sustained reduction in aldosteronesecretion, potassium retention and natriuresis. Hypertension 1:274, 1979
30. Spark RF, O'Hare CM, Regan RM: Low-renin hypertension:restoration of normotension and renin responsiveness. ArchIntern Med 133: 205, 1974
31. Case DB, Laragh JH: Reactive hyperreninemia followingangiotensin blockade with either saralasin or converting en-zyme inhibitor: a new approach to screen for renovascularhypertension. Ann Intern Med 91: 153, 1979
32. Case DB, Atlas SA, Laragh JH: Reactive hyperreninemia toangiotensin blockade identified renovascular hypertension. ClinSci 57: 313S, 1979
33. Johnston CI, McGrath BP, Millar JA, Matthews PG: Long-term effects of captopril (SQ 14225) on blood pressure and hor-mone levels in essential hypertension. Lancet 2: 493, 1979
34. Waeber B, Brunner HR, Turini GA, Curlet N, Keller I, GavrasH: Potentiation of the antihypertensive effect of captopril bydiuretics. Ann Cardiol Angeiol (Paris) 28: 9, 1979
35. Hansson L, Olander R, Aberg H, Malmcrona R, WesterlundA: Treatment of hypertension with propranolol and hydrala-zine. Acta Med Scand 190: 531, 1971
36. Kincaid-Smith P: The management of severe hypertension. AmJ Cardiol 32: 575, 1973
37. Curry CL, Hosten AO: Current treatment of malignant hyper-tension. JAMA 232: 1367, 1975
38. Gifford RW Jr: Management and treatment of malignanthypertension and hypertensive emergencies. In Hypertension:Physiopathology and Treatment, edited by Genest J, Koiw E,Kuchel 0. New York, McGraw-Hill, 1977, pp 1024-2038
39. Wilburn RL, Blaufuss A, Bennett CM: Long-term treatment ofsevere hypertension with minoxidil, propranolol andfurosemide. Circulation 52: 706, 1975
40. Keusch GW, Weidmann P, Campese V, Lee DB, Upham AT,Massry SG: Minoxidil therapy in refractory hypertensionanalysis of 155 patients. Nephron 21: 1, 1978
41. Case DB, Atlas SA, Mouradian JA, Fishman RA, ShermanRL, Laragh JH: Proteinuria during long-term captopriltherapy. JAMA 244: 346, 1980
42. Hoorntje SJ, Weening JJ, The TH, Kallenberg CGM, DonkerAJM, Hoedemaeker PJ: Immune complex glomerulopathy inpatients treated with captopril. Lancet 1: 1212, 1980
43. Hollenberg NK, Williams GH, Burger B, Ishikawa I, AdamsDF: Blockade and stimulation of renal, adrenal, and vascularangiotensin II receptors with 1-Sar, 8-ala angiotensin lI in nor-mal man. J Clin Invest 57: 39, 1976
44. Weber MA, Drayer JIM, Rev A, Laragh JH: Disparate pat-terns of aldosterone response during diuretic treatment ofhypertension. Ann Intern Med 87: 55.2, 1977
45. Vaughan ED Jr, Carey RM, Peach MJ, Ackerley JA, AyersCR: The renin response to diuretic therapy. A limitation ofantihypertensive potential. Circ Res 42: 376, 1978
771
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from

D B Case, S A Atlas, P A Sullivan and J H Laraghangiotensin-converting enzyme inhibitor captopril.
Acute and chronic treatment of severe and malignant hypertension with the oral
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1981 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.64.4.765
1981;64:765-771Circulation.
http://circ.ahajournals.org/content/64/4/765the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 8, 2018http://circ.ahajournals.org/
Dow
nloaded from