Embed Size (px)
Citation preview

Journal of the European Academy of Dermatology & Venereology, 2 (1993) 31-34© 1993 Elsevier Science Publishers B.V. All rights reserved 0926-9959/93/$06.00
31
DERVEN 00057
Acne fulminans (acute febrile ulcerative conglobate acne) treatedwith isotretinoin: a case report
Thomas Maher and Sarah RogersThe City of Dublin Skin and Cancer Hospitat, Dublin, Ireland
Abstract
A 16-year-old boy was treated for acne fulminans (AF) with isotretinoin when the acuteinflammatory stage had been suppressed with oral corticosteroids. From our experience of thiscase and from our review of the hterature, we recommend that isotretinoin should be withheldduring the acute, inflammatory phase of AF in order to prevent exacerbation of the condition.
Key words: Acute fulminans; Isotretinoin; Case report
Introduction
A case of acne fulminans (AF) or acutefebrile ulcerative conglobate acne with jointpains, is reported. The condition respondedto oral erythromyein, corticosteroids andisotretinoin but resulted in severely disfigur-ing facial scarring.
Case report
A 14-year-old schoolboy presented with asudden deterioration of his acne vulgaris.For the previous 3 years he had sufferedfrom mild papulo-pustular aene which hetreated with over-the-eounter preparations.
Correspondence to: Dr Sarah Rogers, The City ofDublin Skin and Cancer Hospital, Hume Street, Dublin2. Ireland. Phone: 353-766935; Fax: 353-762967.
Over a one-month period he developed eystson the face, neck, upper trunk and upperarms. He was given minocycline, 50 mg BD,by his family doctor but was referred quicklyto the skin chnic when the condition contin-ued to deteriorate. Until this time the boyhad enjoyed good health and was on nomedication. His brother had mild aene.
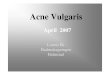
Examination revealed a pale, thin, miser-able-looking young man. There was weepingand crusting over the cheeks and around thehairline and large cysts, pustules and nod-ules, some ulcerated, were present on theface (Fig. 1), trunk, neck and upper arms.The cervical lymph nodes were enlarged andtender but the patient was apyrexial. Labora-tory investigations showed a haemoglobin(Hb) of 12.4 g% (13.0-18.0) and a white cellcount (WCC) of 13.2 x lO*" (4-11) with 87%polymorphonuciear leucocytes (PMNL). Theerythrocyte sedimentation rate (ESR) was

32
raised at 75 mm/h. Biochemical and lipidprofiles were normal. Swabs from skin grewStaphylococcus aureus and, from the nose,commensals only. Skin biopsies showed aperifollicular, neutrophiiic infiltrate.
The patient was admitted to hospital wheretreatment was initiated for secondary infec-tion with flucloxacillin, 500 mg TID, orally,chlorhexidine nasal cream BD, potassiumpermanganate baths daily and fusidic acidtulle dressings. Dihydrocodeine tartrate, 30mg was given eight hourly, for pain. Fivedays later he developed a pyrexia of 39°C.This was accompanied by arthralgia of thehips, shoulders and knees and severe malaise.The diagnosis of AF was made. Flucloxacillinwas discontinued and erythromycin was in-troduced at a dose of 500 mg, 6 hourly,intravenously, with the rationale that this
Fig. 1. Weeping and crusting of acne lesions on face.
would be both antistaphyloeoccal as well asbeing a therapeutic agent for acne. In addi-tion, he was given prednisolone, 20 mg daily,and naproxen, 500 mg BD orally. This regi-men produced a rapid response with symp-tomatic relief and the temperature returningto normal. Two weeks later isotretinoin wasintroduced at 1 mg/kg/day.
Over the eourse of the next 2 months thepatient continued to have arthralgia of de-creasing severity. The prednisolone wasgradually tailed off and naproxen discontin-ued. The dose of erythromycin was reducedto 500 mg twice daily and eventually discon-tinued as isotretinoin began to take effect.The ESR remained elevated at 70-80 mm/h.A large cyst on the left cheek was injectedwith triamcinolone. On completion of 4months of isotretinoin therapy the acne wascompletely inactive. However, though the pa-tient was clinically well, his ESR was 48mm/h.
Six months after onset of AF, the patienthas returned to school and resumed normalactivities including playing sport. The ESRwas 17 mm/h. There is now disfiguring scar-ring of his face with rope-like tracks of keloidextending from the ear to the mandible (Fig.2). The scarring on his back, while extensive,is not so severe.
Discussion
Acne fulminans was first described byBurns and Colville [1] in 1958. it was subse-quently named acute febrile ulcerative con-globate acne in 1971 by Kelly and Burns [2].The main features include the sudden onsetof severe and often ulcerating acne, fever,polyarthralgia, failure to respond to antibac-terial therapy and a response to debridementand steroid therapy. An elevated WCC witha predominance of PMNL is characteristicand a leukaemoid reaction has been de-scribed [3]. An elevated ESR usually accom-panies. Our patient had all these features.

33
Fig. 2. Rope-like keloid scarring on cheeks after treatment.
He also had a mild anaemia which has beendescribed previously but is not a consistentfeature [4]. The ESR is a useful marker tofollow disease activity but it is of note thatour patient was clinically improved somemonths before the ESR returned to normal.Osteolytic cysts, which may present as bonetenderness, can be detected by technetiumscintillography [5]. Our patient had no radio-logical investigations but, as he had no bonytenderness or arthritis and has recoveredcompletely from his arthralgia, he is unlikelyto have had osteolytic cysts.
Acne fulminans is rare with only 40 easesreported by Nault et al. in 1985 [5]. We havefound 13 eases reported since then [7,8,13-19]. The cause of AF is unknown. It has beenreported twice in twins which suggests a ge-netic predisposition [6,7]. Reports of accom-
panying erythema nodosum, circulating im-mune complexes [8] and a severe necrotiereaction to subcutaneous injection of Propi-onibacterium acnes antigen at 36 h [9] suggestan immune-complex disorder. This is furthersupported by the response to systemicsteroids. Cultures of blood, joint fluid andbone lesions are negative [2,4,10].
Most reported cases pre-date the intro-duction of isotretinoin and so it is hard tofind definite guidelines for its use in AF. Asit is the most effective treatment for acneone is tempted to introduce it as soon aspossible. Isotretinoin has been shown to ex-acerbate acne vulgaris initially in about onethird of patients [11], and has been reportedas a precipitating factor in AF by Kellett etal. [8]. A successful outcome was reportedwith isotretinoin therapy alone by Darley et

34
al. [7], but in that case the drug was intro-duced 6 months after the onset of AF whenthe condition had already improved consid-erably. The aim of treatment in the acutephase of AF is the suppression of inflamma-tory effects. We, therefore, followed Cun-liffe's adviee to give oral steroids combinedwith antibiotics initially and to introduceisotretinoin only after the acute phase [12].
References
1 Burns RE, Colville JM. Acne conglobata and septi-caemia? Arch Dermatol 1959;79:361-363.
2 Kelly P, Burns RE, Acute febrile ulcerative conglo-bate acne with polyarthralgia. Arch Dermatol197l;104:l82-]87.
3 Strom S, Thyresson N, Bostrom H. Acute febrileulceralive conglobate acne with leukaemoid reac-tion. Acta Dermatol Venereol (Stockholm) 1973;53:306-312.
4 Goldschmitt H, Lcyden JJ, Stein KH. Acne fulmi-nans. Arch Dermatol 1977;113:444-449.
5 Naull P, Lassonde M, St. Antoine P. Acne fulmi-nans with osteoiytic lesions. Arch Dermatol1985;121:662-664.
6 Palatsi R, Oikarincn A. Hormonal analysis anddelayed hypersensitivity in identical twins with se-vere acne. Acta Dermatol Vcncreol (Stockholm)1979;59:I57-16O.
7 Darley CR, Currey HLF, Baker H. Acne fulminanswith arthritis in identical twins treated withisotretinoin. J R Soc Med 1984;77:328-330.
8 Kellett JK, Beck MH, Chalmers RJG. Erythemanodosum and circulating immune complexes in aenefulminans after treatment with isotretinoin. Br MedJ 1985;290:820.
9 Williamson DM, Cunliffe WJ. Gatccliff M, et al.Acute ulcerative acne conglobata (acne fulminans)with erythema nodosum. Clin Exp Dermatol1977;2:35t.
10 Lane JM, Leyden JJ, Spcigcl RJ. Acne arthralgia. JBone Joint Surg l976;58A:673-675.
11 Buckley D, Rogers S, Daly P. Isotretinoin therapyfor acne vulgaris:results in an Irish population. Ir JMed Sci, 1990; 159:2-5.
12 Cunliffe WJ. Acne. London, Martin Dunitz Ltd.1989;36,
13 Statham BN, Holt PJA, Pritchard MH. Acne fulmi-nans: report of a case with polyarthritis. Clin ExpDermato! 1983;8:4ni-404.
14 Martin RW, Klingler WG. Acne fulminans. Am JFam Prac 1989;40:135-139.
15 Traupe H, von Muhlendahl KE, Bramswig J. et al.Acne of the fulminans type following testosteronetherapy in three excessively tall boys. Arch Derma-tol 1988;I24:414-417.
16 Heydcnrcich G. Testosterone and anabolic steroidsand acne fulminans. Arch Dermatol 1989;125:571-572.
17 van Schaardenburg D, Lavrijsen S, Vermcer BJ.Acne fulminans associated with painful splenomeg-aly. Arch Dermatol 1989;125:I32-133.
18 Siegel D, Strosbcrg JM, Wiese F. et al. Acne fulmi-nans with a lytic bone lesion responsive to dapsone.J Rheumatol 1982;9:344-346.
19 Vcrbov J. Acne fulminans in a 14 year old. Practi-tioner 1985;229:691.