Embed Size (px)
Citation preview
ARTERIAL BLOOD GASES
PART 1 BACK TO BASICS
SSR OLIVIA ELSWORTH
SEPT 2017

• pH = measure of hydrogen ion concentration (acidity or alkalinity)
• PaCO2 = partial pressure of carbon dioxide dissolved in arterial blood
• HCO3- = bicarbonate (a base)
• B.E. = base excess (measurement of excess or insufficient bicarbonate in the blood)
• PaO2 = partial pressure of oxygen dissolved in arterial blood
• SaO2 = arterial oxygen saturation of haemoglobin
WHAT INFORMATION DOES AN ABG GIVE US?

WHAT’S NORMAL?
•pH – 7.35 – 7.45
•PaCO2 – 4.5- 6.0 kPa
•HCO3 – 22 – 26 mmol/l
•B.E. - -2 - +2 mmol/l
•PaO2 – 10 – 14 kPa
•SaO2 – 94% - 99%

Step 1 Look at pH
Acid-base disorder?
ABGS TAKE IT STEP BY STEP - 1

• In order for normal metabolism to take place, the pH of the blood must be maintained between 7.35 and 7.45
• The measurement of pH is directly affected by the number of hydrogen ions (H+) in the blood. The more H+ ions in the blood, the lower the pH and the more acidic it is. The less H+ ions in the blood, the higher the pH and the more alkalotic it is.
• If pH falls much below 6.8 or rises much above 7.8, cellular breakdown starts to occur leading to eventual death if left uncorrected.
STEP 1 - DOES PH MATTER?
Step 2 Look at PaCO2
Respiratory problem?
ABGS TAKE IT STEP BY STEP - 2
STEP 2 IS THERE A RESPIRATORY PROBLEM? • The waste product carbon dioxide (CO2) is produced during
normal cellular metabolism, and is carried in the blood to the lungs for excretion.
• If high levels of CO2 are allowed to build up in the lungs, the CO2 combined with water (H2O) will form carbonic acid (H2CO3) leading to a lowering of blood pH = acidosis
• If there are low levels of CO2 in the lungs, pH will rise = alkalosis

STEP 2 - LOOK AT PACO2 IS THERE A RESPIRATORY PROBLEM?
High pH
Low PaCO2
Respiratory Alkalosis
Low pH
High PaCO2
Respiratory Acidosis

Any condition that results in hypoventilation can cause respiratory acidosis.
RESPIRATORY ACIDOSIS - CAUSES

CAUSES OF HYPOVENTILATION
Respiratory Acidosis
CNS Depression
Impaired respiratory
muscle function
Pulmonary Disorders
Impaired respiratory ventilation
Any condition that results in hyperventilation can cause respiratory alkalosis.
RESPIRATORY ALKALOSIS - CAUSES

CAUSES OF HYPERVENTILATION
Respiratory Alkalosis
CNS Lesions
Psychological Response
Stimulation
Increased Metabolism
Step 3 Look at HCO3
Metabolic problem?
ABGS TAKE IT STEP BY STEP - 3
STEP 3 IS THERE A METABOLIC PROBLEM?
• Metabolic acidosis is caused by either a deficit of base in the bloodstream or an excess of acids, other than CO2.
• Metabolic alkalosis is caused by either an excess of base in the bloodstream or a loss of acids, other than CO2.

STEP 3 - LOOK AT HCO3 IS THERE A METABOLIC PROBLEM?
High pH
High HCO3
Metabolic Alkalosis
Low pH
Low HCO3
Metabolic Acidosis
CAUSES OF METABOLIC ACIDOSIS
Metabolic Acidosis
Ketones
Lactic Acid
Kidney disease
Poisoning
Hyperchloremia
Rhabdomyolysis

METABOLIC ALKALOSIS • The two systems most commonly involved in generating a
metabolic alkalosis are the kidneys and the GI tract. • Metabolic alkalosis is the most common acid-base
disturbance observed in hospitalized patients, accounting for approximately 50% of all acid-base disorders.
• Mortality rates have been reported as 45% in patients with an arterial blood pH of 7.55 and 80% when the pH was greater than 7.65

CAUSES OF METABOLIC ALKALOSIS
Metabolic Alkalosis
Loss of H+ ions
Alkali admin
Kidney disease
Shift of H+ ions
Diuretics
Step 4 Look at PaO2
& SaO2
Hypoxaemia?
ABGS TAKE IT STEP BY STEP - 4

• SpO2 and PaO2 too low? - hypoxaemia exists
• The amount of oxygen dissolved in arterial blood (PaO2) will directly affect the amount of oxygen bound to haemoglobin (SaO2). However, several factors will affect the strength with which oxygen binds to the hemoglobin molecule and the subsequent O2 delivery of the oxygen to the tissues e.g. age, fever, CO2 levels, temperature.
• Hypoxaemia can still exist with SpO2 of 99% if Hb is low.
• An interpretation of hypoxaemia should be made with consideration of the percentage of oxygen delivered at the time the arterial blood was drawn.
STEP 4 IS THERE HYPOXAEMIA?

If pH and PaCO2 are moving in opposite directions then the problem is primarily respiratory.
If pH and HCO3 are moving in the same direction then the problem is primarily metabolic.
TOP TIP!

ABG ANALYSIS – WHAT ABOUT COMPENSATION?
Is pH normal?
NO
Is this a respiratory problem?
Is this a metabolic problem?
YES
Is there compensation?

• When a patient develops an acid-base imbalance, the body attempts to compensate in order to return pH into the normal range.
• A patient can be uncompensated, partially compensated, or fully compensated.
• When an acid-base disorder is either uncompensated or partially compensated, the pH remains outside the normal range. In fully compensated states, the pH has returned to within the normal range, although the other values may still be abnormal.
IS THERE COMPENSATION?

BUFFER SYSTEMS
pH 7.35-7.45
Renal Buffer System
Respiratory Buffer System

• An abnormal pH triggers the lungs to either increase or decrease the rate and depth of ventilation.
•As pH falls, respiratory rate will increase to ‘blow off’ CO2. As pH rises, the respiratory rate will fall in order to retain more CO2.
•This compensatory action can be activated within 1-3 minutes of an acid-base imbalance occurring.
RESPIRATORY BUFFER SYSTEM

• The kidneys also have the ability to respond to changes in blood pH by retaining or excreting bicarbonate (HCO3-), a base or alkaline, through the urine.
• As pH falls, HCO3- is retained, as pH rises, HCO3- is excreted.
• The renal buffer response takes longer to compensate for an aid-base imbalance than the respiratory response, taking hours or days to correct pH.
RENAL BUFFER SYSTEM

pH PaCO2 HCO3
Respiratory Acidosis ↓ ↑ normal
Respiratory Alkalosis ↑ ↓ normal
Metabolic Acidosis ↓ normal ↓
Metabolic Alkalosis ↑ normal ↑
UNCOMPENSATED STATE

pH PaCO2 HCO3
Respiratory Acidosis ↓ ↑ ↑
Respiratory Alkalosis ↑ ↓ ↓
Metabolic Acidosis ↓ ↓
↓
Metabolic Alkalosis ↑ ↑
↑
PARTIALLY COMPENSATED STATE

pH PaCO2 HCO3
Respiratory Acidosis normal, but <7.40
↑ ↑
Respiratory Alkalosis normal, but >7.40
↓ ↓
Metabolic Acidosis normal, but <7.40
↓
↓
Metabolic Alkalosis normal, but >7.40
↑
↑
FULLY COMPENSATED STATE
ARTERIAL BLOOD GASES PART 2
FROM THEORY TO PRACTICE
SSR OLIVIA ELSWORTH
SEPT 2017

1. A BLOOD GAS SAMPLE IS TAKEN FROM A PATIENT PRESENTING WITH A HISTORY OF SEVERE ABDOMINAL PAIN AND VOMITING FOR 12 HOURS. A BLOOD GAS IS TAKEN ON AIR AND SHOWS ……
pH: 7.58
PaCO2: 5.0
PaO2: 11.0
HCO3: 30
SpO2: 95%

Step 1 – high pH = alkalosis Step 2 - normal PaCO2 Step 3 – high HCO3 + high pH = metabolic alkalosis Step 4 – normal oxygenation
This blood gas represents a metabolic alkalosis with no compensation
Hydrogen ions in the form of hydrochloric acid found in gastric secretions will be lost through severe vomiting. Whenever a hydrogen ion is excreted, a bicarbonate ion is gained in the extracellular space, leading to a state of alkalosis

2. A 22-YEAR-OLD ASTHMATIC PATIENT PRESENTS WITH AN ACUTE ONSET OF BREATHLESSNESS AND DIFFICULTY IN TALKING. A BLOOD GAS IS TAKEN ON AIR AND SHOWS ……
pH: 7.21
PaCO2: 7.0
PaO2: 8.0
HCO3: 24
SpO2: 86%

Step 1 – low pH = acidosis Step 2 - high PaCO2 + low pH = respiratory acidosis Step 3 – normal HCO3 Step 4 - hypoxaemia
This blood gas represents a respiratory acidosis with no compensation
This patient is having an acute asthma attack and is in Type 1 respiratory failure as a result of ineffective or hypoventilation
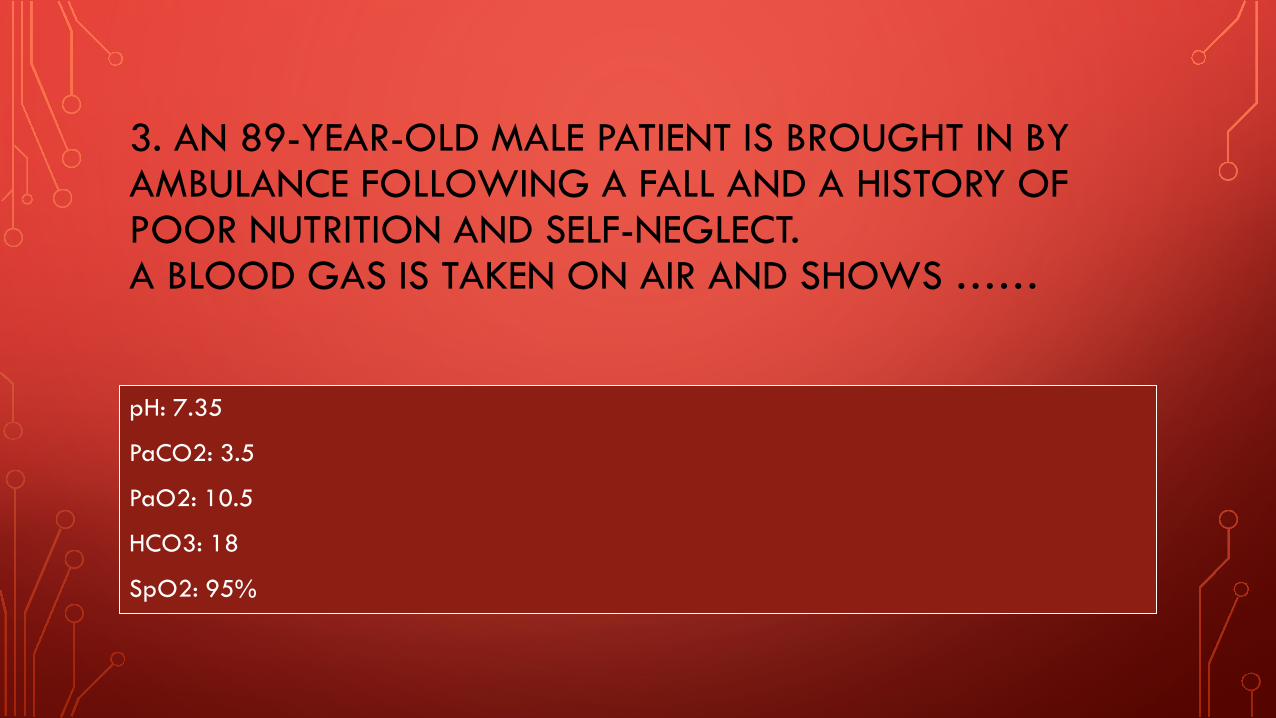
3. AN 89-YEAR-OLD MALE PATIENT IS BROUGHT IN BY AMBULANCE FOLLOWING A FALL AND A HISTORY OF POOR NUTRITION AND SELF-NEGLECT. A BLOOD GAS IS TAKEN ON AIR AND SHOWS ……
pH: 7.35
PaCO2: 3.5
PaO2: 10.5
HCO3: 18
SpO2: 95%

Step 1 – normal, but <7.40 Step 2 - low PaCO2 + normal pH = full respiratory compensation Step 3 – low HCO3 = metabolic acidosis Step 4 – normal oxygenation
This blood gas represents a metabolic acidosis with full compensation
This patient has been able to build up a level of compensation via the respiratory buffer system to a chronically worsening ketoacidosis as a result of chronic malnutrition
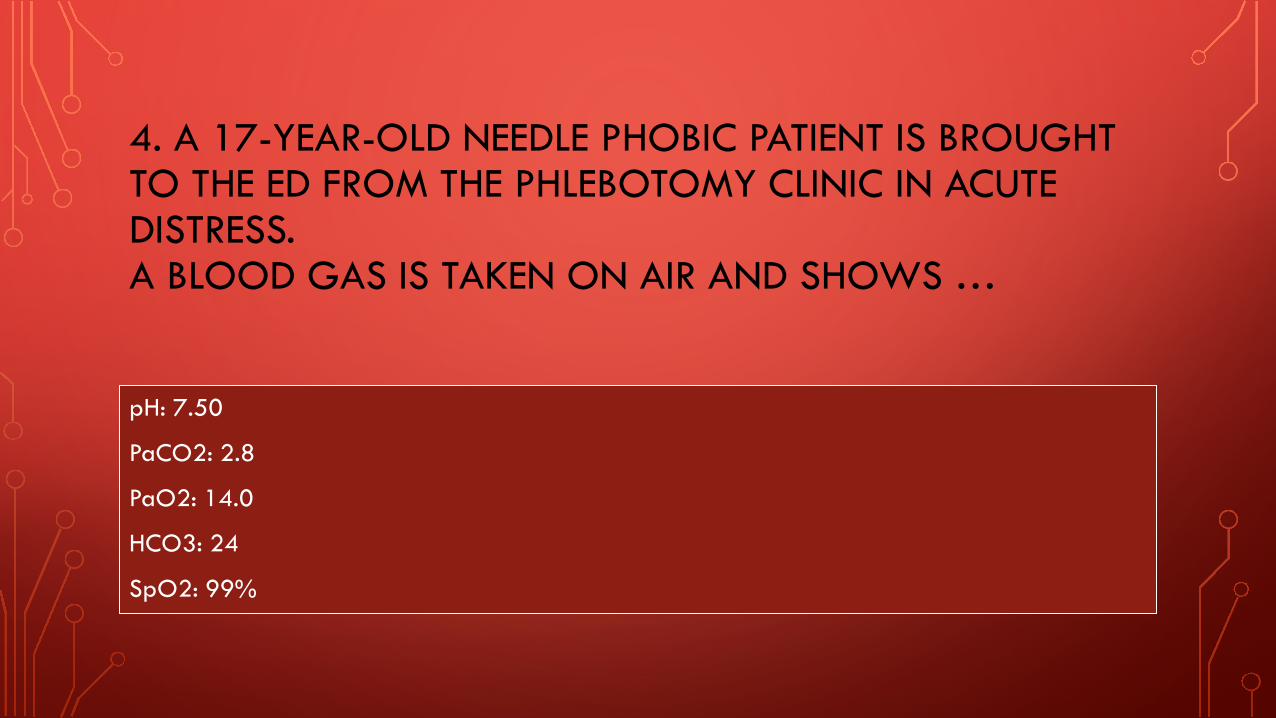
4. A 17-YEAR-OLD NEEDLE PHOBIC PATIENT IS BROUGHT TO THE ED FROM THE PHLEBOTOMY CLINIC IN ACUTE DISTRESS. A BLOOD GAS IS TAKEN ON AIR AND SHOWS …
pH: 7.50
PaCO2: 2.8
PaO2: 14.0
HCO3: 24
SpO2: 99%
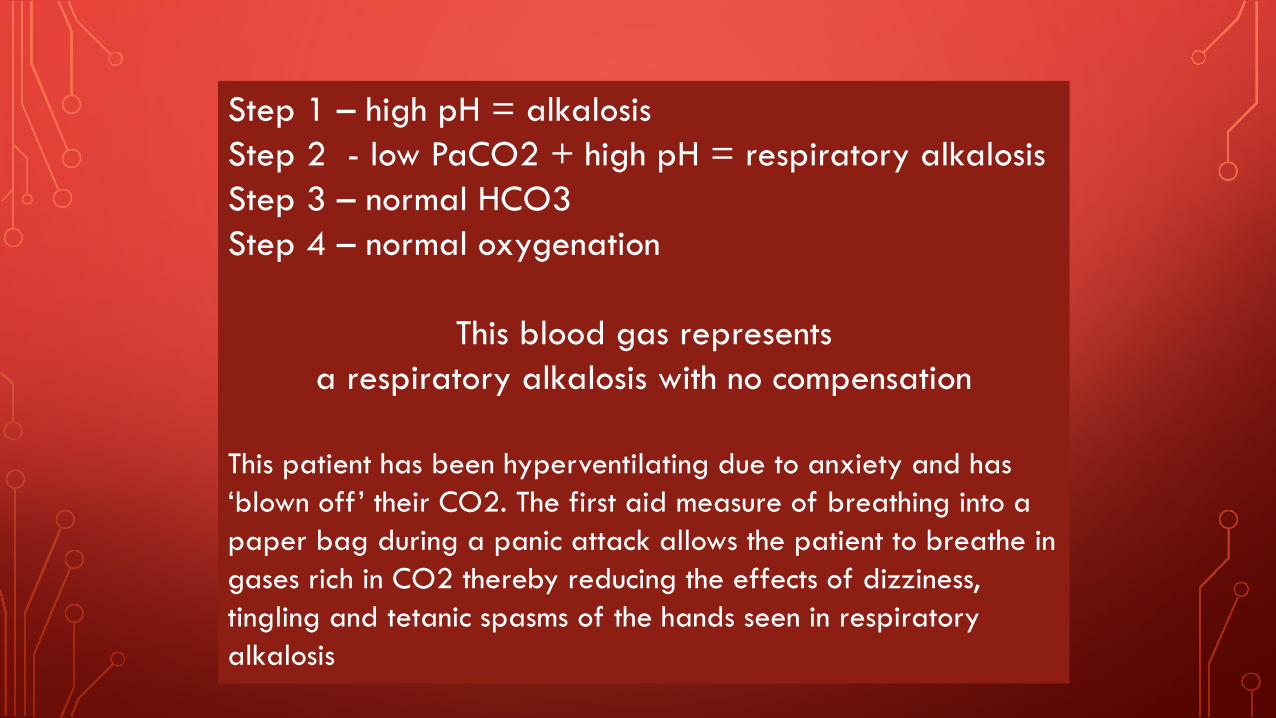
Step 1 – high pH = alkalosis Step 2 - low PaCO2 + high pH = respiratory alkalosis Step 3 – normal HCO3 Step 4 – normal oxygenation
This blood gas represents a respiratory alkalosis with no compensation
This patient has been hyperventilating due to anxiety and has ‘blown off’ their CO2. The first aid measure of breathing into a paper bag during a panic attack allows the patient to breathe in gases rich in CO2 thereby reducing the effects of dizziness, tingling and tetanic spasms of the hands seen in respiratory alkalosis

5. A 75-YEAR-OLD FEMALE PATIENT WITH KNOWN COPD IS BROUGHT IN BY AMBULANCE FOLLOWING A MECHANICAL FALL AND NEW LEFT HIP PAIN. A BLOOD GAS IS TAKEN ON AIR AND SHOWS ……
pH: 7.35
PaCO2: 7.2
PaO2: 10.5
HCO3: 26
SpO2: 93%

Step 1 – normal, but <7.40 Step 2 - high PaCO2 + normal pH = respiratory acidosis with full compensation Step 3 – normal HCO3 Step 4 – normal oxygenation
This blood gas represents a respiratory acidosis with full compensation
This patient has a chronic obstructive respiratory pattern and at baseline function the renal buffer system is able compensate for a respiratory acidosis, and pH remains at a normal level
6. A 25-YEAR-OLD INSULIN-DEPENDENT MALE PATIENT PRESENTS TO THE ED WITH A HISTORY OF VOMITING, LETHARGY AND CONFUSION AND SMELLS STRONGLY OF ALCOHOL. A BLOOD GAS IS TAKEN ON AIR AND SHOWS ……
pH: 7.21
PaCO2: 4.8
PaO2: 11.0
HCO3: 18
SpO2: 95%
Step 1 – low pH = acidosis Step 2 - normal PaCO2 Step 3 – low HCO3 + low pH = metabolic acidosis Step 4 – normal oxygenation
This blood gas represents a metabolic acidosis with no compensation
This patient is in DKA – diabetic ketoacidosis. In the absence of sufficient insulin, free fatty acids are released from adipose tissue which are then converted to ketone bodies by the liver. Ketone bodies serve as an energy source in the absence of insulin-mediated glucose delivery. The respiratory buffer system will try and compensate for the acidosis by increasing respiratory rate and efficiency often seen as the deep sighing breathing of Kaussmal respiration of DKA





























