Embed Size (px)
DESCRIPTION
Ben Spurr, PAS & Health Information Manager, Royal Hobart Hospital presented this at the 5th Annual Clinical Documentation, Coding and Analysis Conference. This event is the only case study led conference in Australia looking solely at clinical documentation, coding and analysis. For more information, please visit http://www.healthcareconferences.com.au/clinicaldocs
Citation preview
Royal Hobart Hospital: Preparing Clinical Coding for ABF
Ben Spurr – PAS & Health Information Manager

Royal Hobart Hospital - Background
Major Acute Hospital for THO - South
Royal Hobart Hospital - Background
RHH is the Tertiary Referral Hospital for Tasmania
Served Hobart for over 200 years
First Opened in 1804
Is Australia’s second oldest Hospital
It has been on the current site since 1820.
Oldest current buildings on site date to 1939.

Royal Hobart Hospital - Background
Services a population of 240 000 people
550 Beds (460 overnight, 90 day stay)
Provides State-wide services such as cardiac surgery, neurosurgery, extensive burns treatment, hyperbaric medicine, neonatal and paediatric intensive care and high risk obstetrics.
Averages 65 000 separations per year

Royal Hobart Hospital
Undergoing $586 million redevelopment

RHH Redevelopment
Major Redevelopments include:
New Inpatient Precinct
New Outpatients Department
New DCCM (ICU)
New Integrated Cancer Centre
New Medical Imaging Facility
New Assessment & Planning Unit (APU)
New Production Kitchen
RHH prior to National Health Reforms and ABF
Historical Block Funding
Changing to ABF
Whole new focus on clinical coding & casemix funding
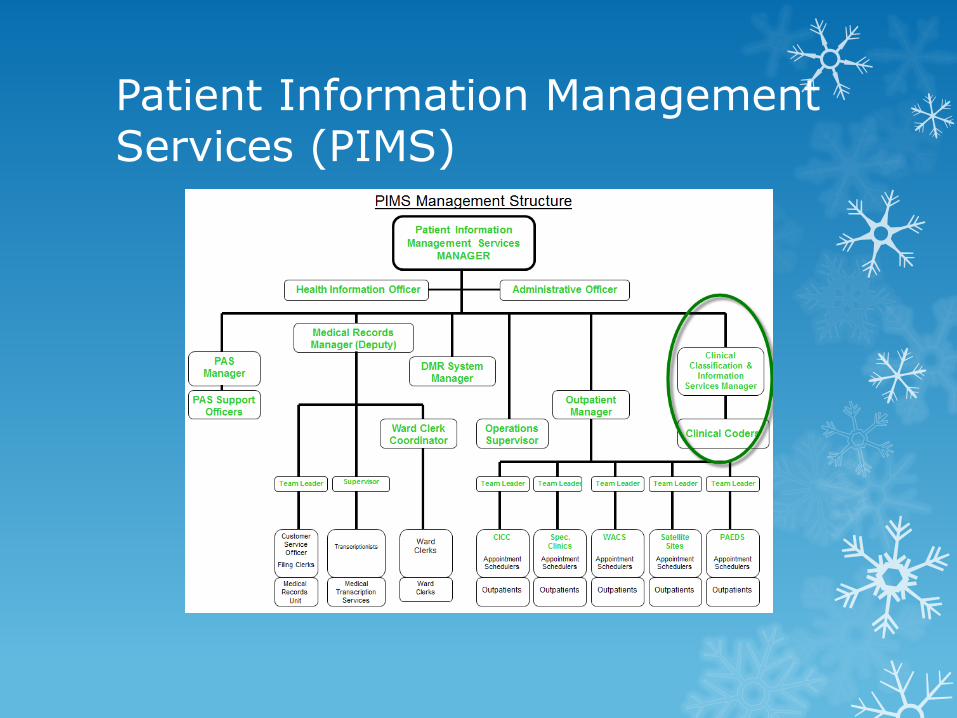
Patient Information Management Services (PIMS)

Clinical Coding Office
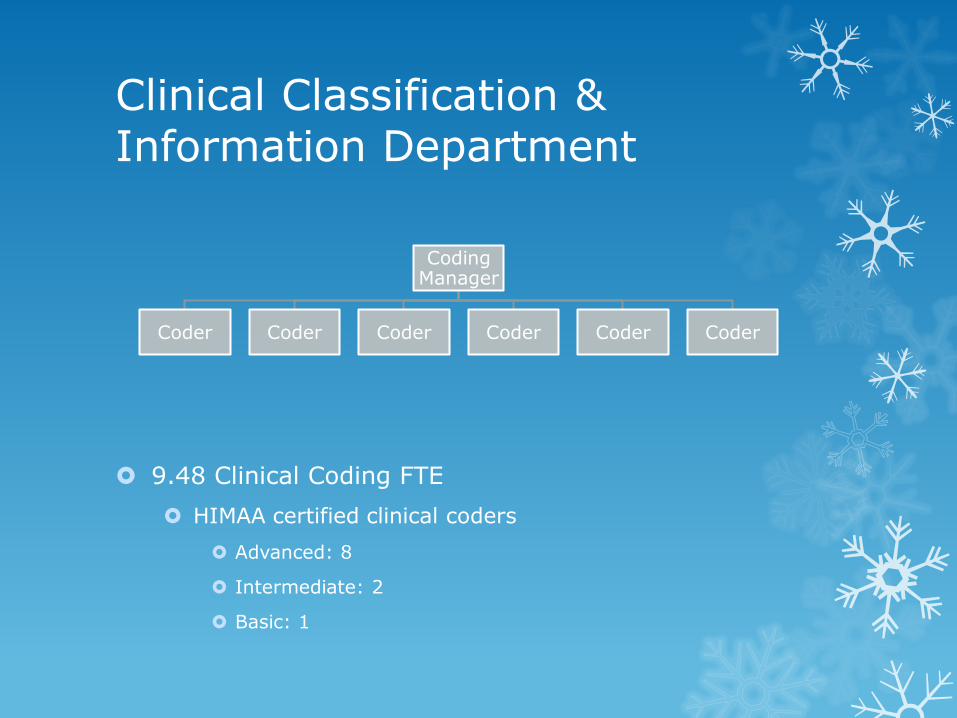
Clinical Classification & Information Department
9.48 Clinical Coding FTE
HIMAA certified clinical coders
Advanced: 8
Intermediate: 2
Basic: 1
Coding Manager
Coder Coder Coder Coder Coder Coder
Clinical Classification & Information Department
Health Roundtable peer Hospitals:
Average 13 FTE
Recruitment is extremely challenging
Although currently fully staffed
Clinical Coders sourced internally from previous administrative roles:
Clinical transcription
Ward Clerks
Medical Records
Offer staff Clinical Coding Experience:
Asses suitability to the role
Clinical Coding Training
Internal training (1:1 manager)
Aligned with experienced coding mentor (colleague)
HIMAA coding courses
At commencement often only completed terminology course
Undertake Basic HIMMA certificate on the job
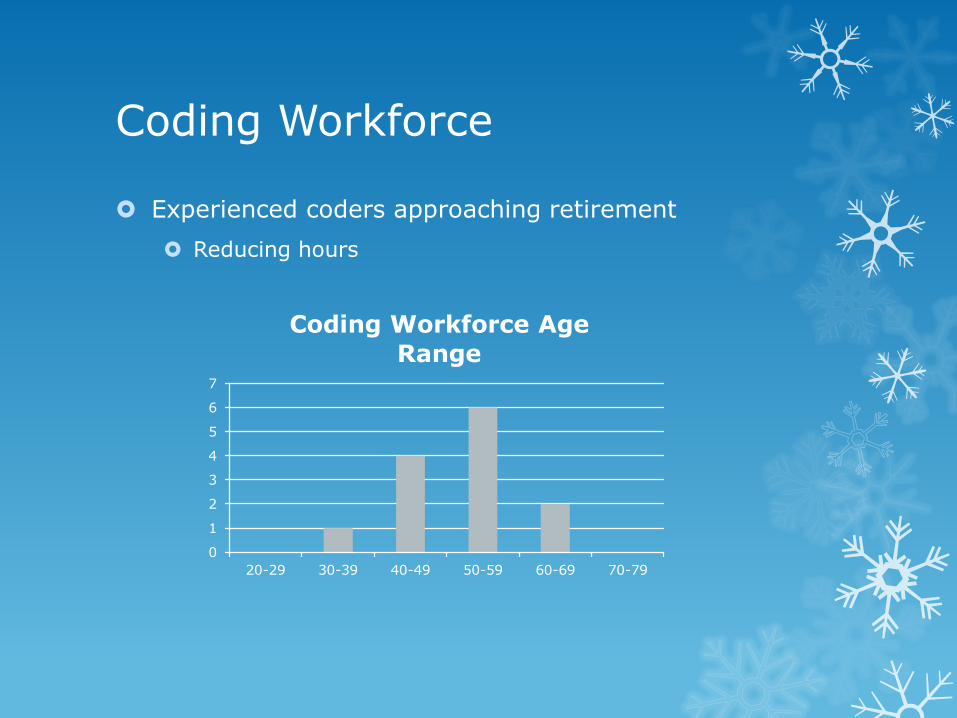
Coding Workforce
Experienced coders approaching retirement
Reducing hours
0
1
2
3
4
5
6
7
20-29 30-39 40-49 50-59 60-69 70-79
Coding Workforce Age
Range
Coding Workforce challenges
Nil Career Progression Pathway
Due to organisational structure of Department
General Administrative Award
All one award
Basic vs Advanced = (same award)
Stagnation
Motivation for personal development
Interstate recruitment
Hampered by Tasmanian award.
Coding Workforce challenges
No Leave Coverage
No Overtime
No Contractors
No Casuals
High Long Service Leave accrual
Clinical Coding Audits
Prior to 2012/13 no internal audit program
Annual external coding Audit:
Random Sample of 100 records
8% DRG Change
2010 DHHS State-wide Clinical Coding Baseline Audit:
19% Recommended DRG change
19% Potential DRG Change
Recommended that THOs undertake a review of their clinical coding workforce and their capacity to meet the increasing demand.
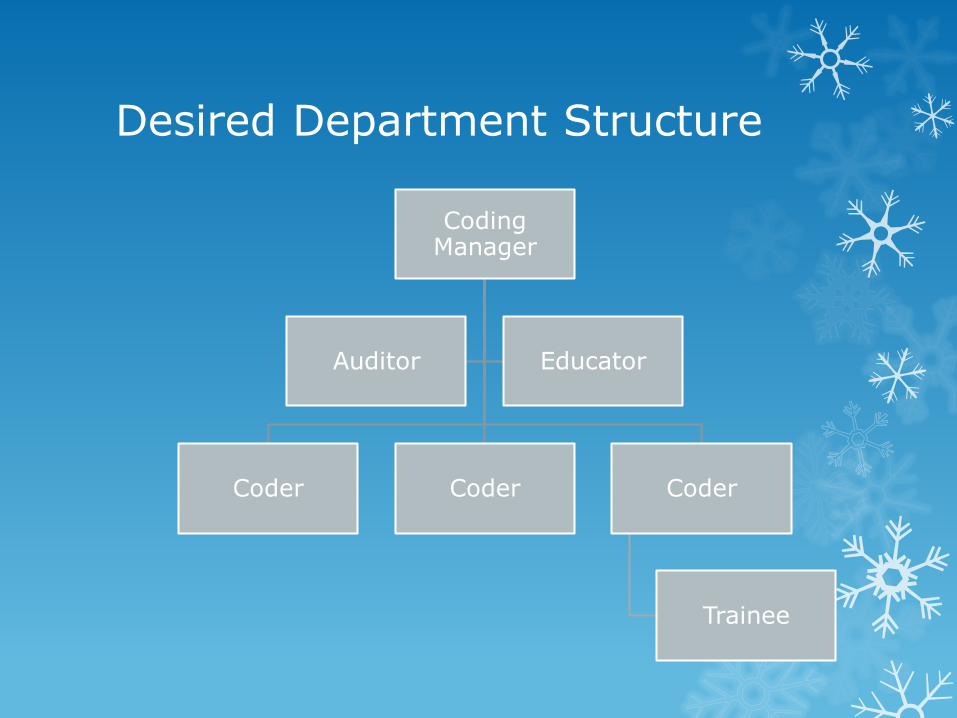
Desired Department Structure
Coding Manager
Coder Coder Coder
Trainee
Auditor Educator
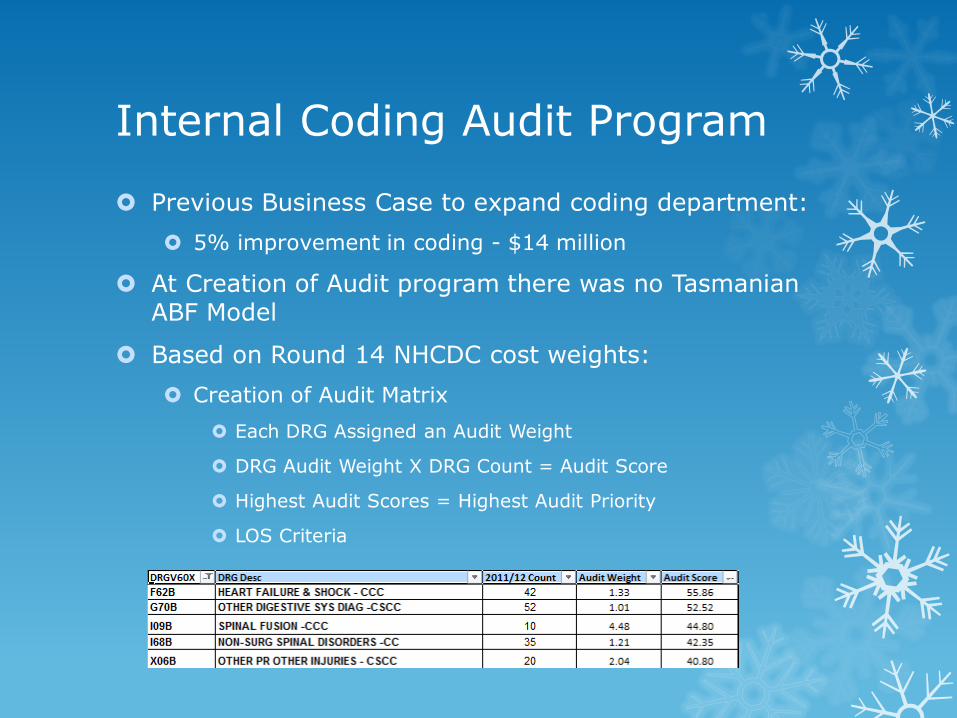
Internal Coding Audit Program
Previous Business Case to expand coding department:
5% improvement in coding - $14 million
At Creation of Audit program there was no Tasmanian ABF Model
Based on Round 14 NHCDC cost weights:
Creation of Audit Matrix
Each DRG Assigned an Audit Weight
DRG Audit Weight X DRG Count = Audit Score
Highest Audit Scores = Highest Audit Priority
LOS Criteria
Internal Coding Audit Program
Created an extract template to identify audit cases
Audit conducted at completion of monthly coding
Peer Audit Program
All Coders to be assigned cases for audit
Distributed by Coding Manager
Creating Audit Culture
Initial resistance / hesitance to peer audit
Peer audit Necessary due to resources:
Lack of auditor / educator position
Coding Manager time restrictions
Lack of familiarity with internal audits
Accustomed to yearly external audit process
Overcome initially with de-identification of original coder details
All appear to be coded by Coding Manager.
Monthly open forum to discuss results
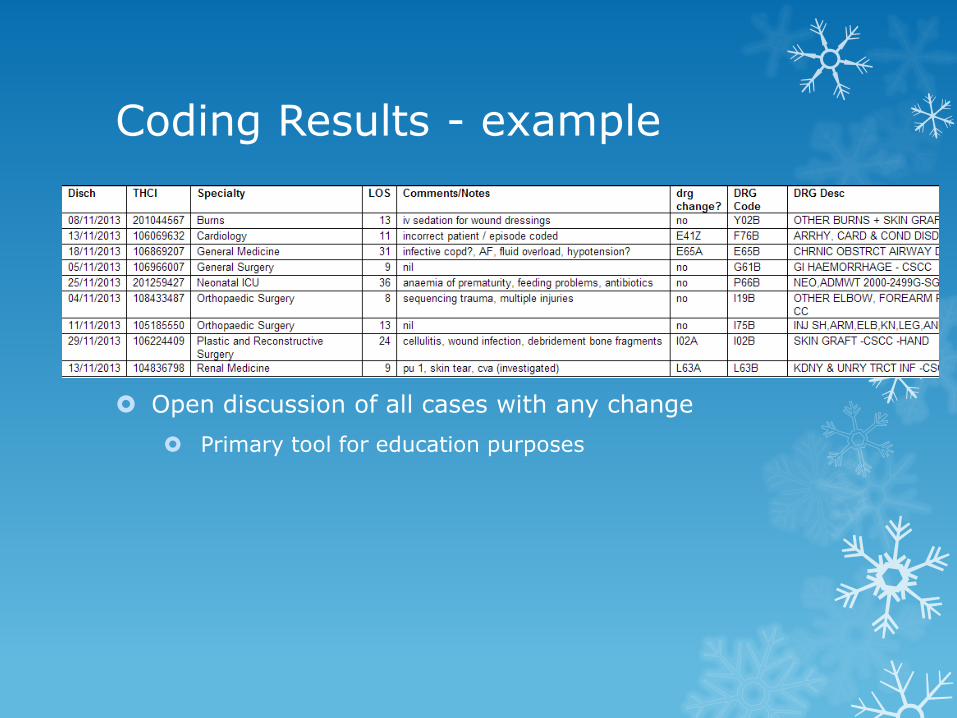
Coding Results - example
Open discussion of all cases with any change
Primary tool for education purposes
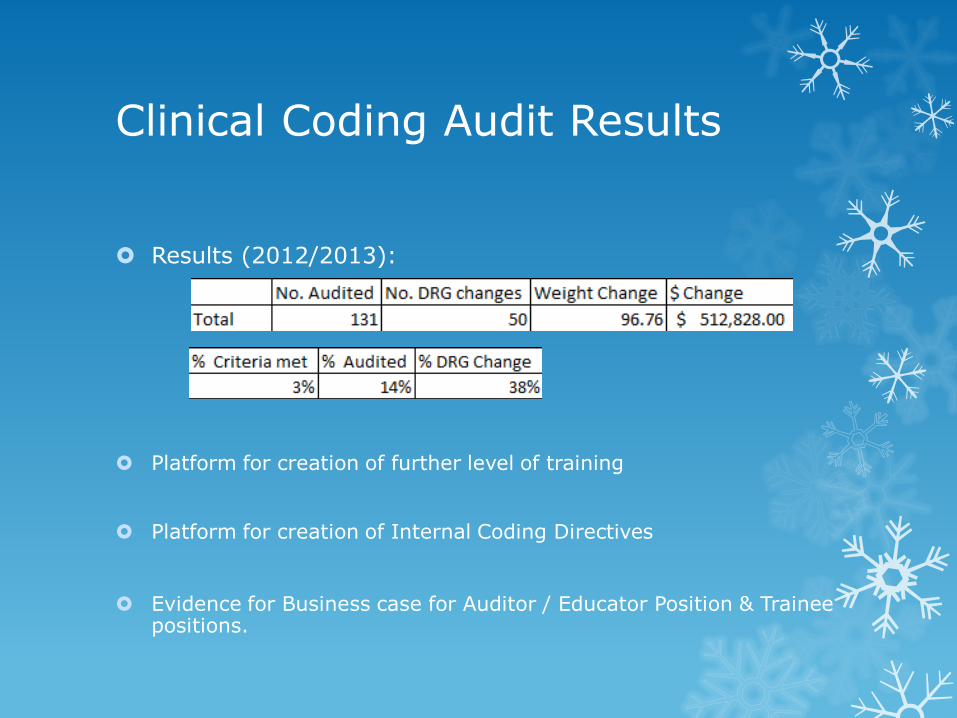
Clinical Coding Audit Results
Results (2012/2013):
Platform for creation of further level of training
Platform for creation of Internal Coding Directives
Evidence for Business case for Auditor / Educator Position & Trainee positions.
Clinical Coding Audit Results
Over time the continual feedback and response from audit results has been seen as positive in continuing education
Differing opinions / interpretations of standards highlighted
3M Codefinder pathway discussions
Navigation of DMR & Source Systems
Monthly internal audits are business as usual
Coders have embraced audit culture – thirst for knowledge
Positive attitude to audit & wider discussion and dissemination of findings
Coder Education
Education for coders to create queries for clinicians
Weekly coder education sessions
Clinical coder queries
Clinical & Coding
Challenge scenarios for further discussion
Clinical in-services with clinical specialties
Admissions Policy
Admission criteria
Care types
Clinical Engagement prior to ABF
Clinical Engagement
Clinicians keen to learn about ABF
Think they get the money!
Accountable for their own activity
Clinical Champions
Oncology
Obstetrics
Respiratory
General Medicine
Cardiology
Anaesthetics
Paediatrics
Surgery – work in progress
Clinical Engagement (cont)
Clinical Documentation Guidelines for RHH
Specific to each RHH specialty
Distributed to unit heads
Based on the “Good Clinical Documentation Guidelines”
Regular Presentations to interns / RMO’s / UTas Medical Students
Documentation Requirements
Px Dx & Additional Diagnosis.
Care Type Changes
Clinical Coding & DRG’s
Clinical Engagement (cont)
Clinical in services
Coding to Clinical – Clinical to Coding
Requested due to topical issues
Clinician reports
Coder questions
Engagement with GP Liaison officers
Primary focus is to the GP’s
Strong focus on Documentation and Communication.
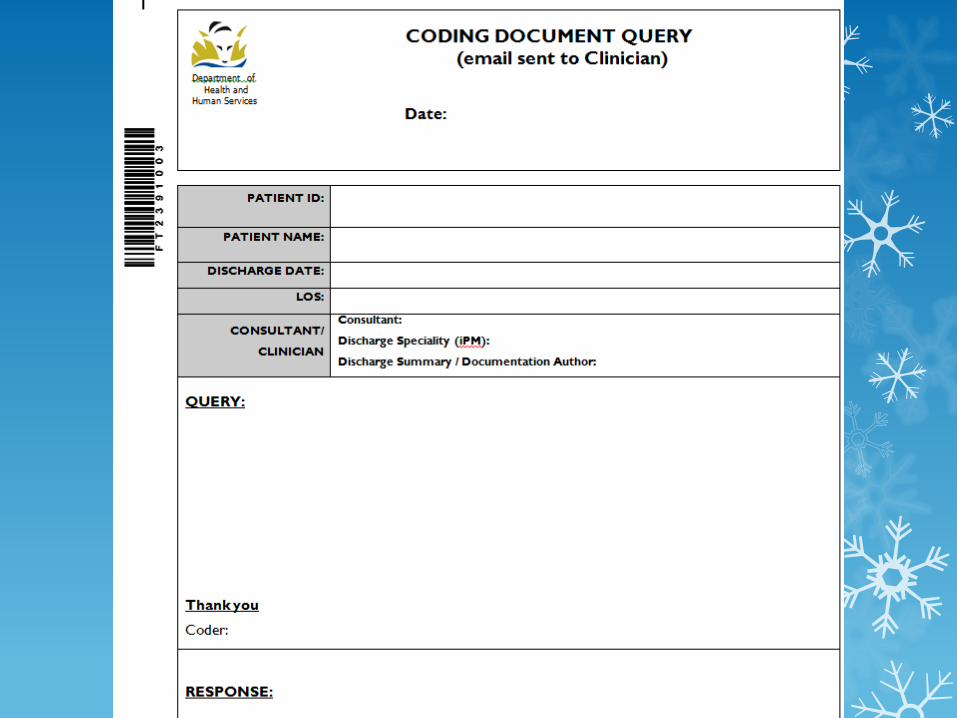
Clinical Engagement – Documentation Queries
Clinicians have improved their understanding of documentation requirements for clinical coding
Documentation Queries
DMR facilitates easier review and correspondence
Email queries & replies
Either screen shots or page reference
Evidence of replies scanned to DMR
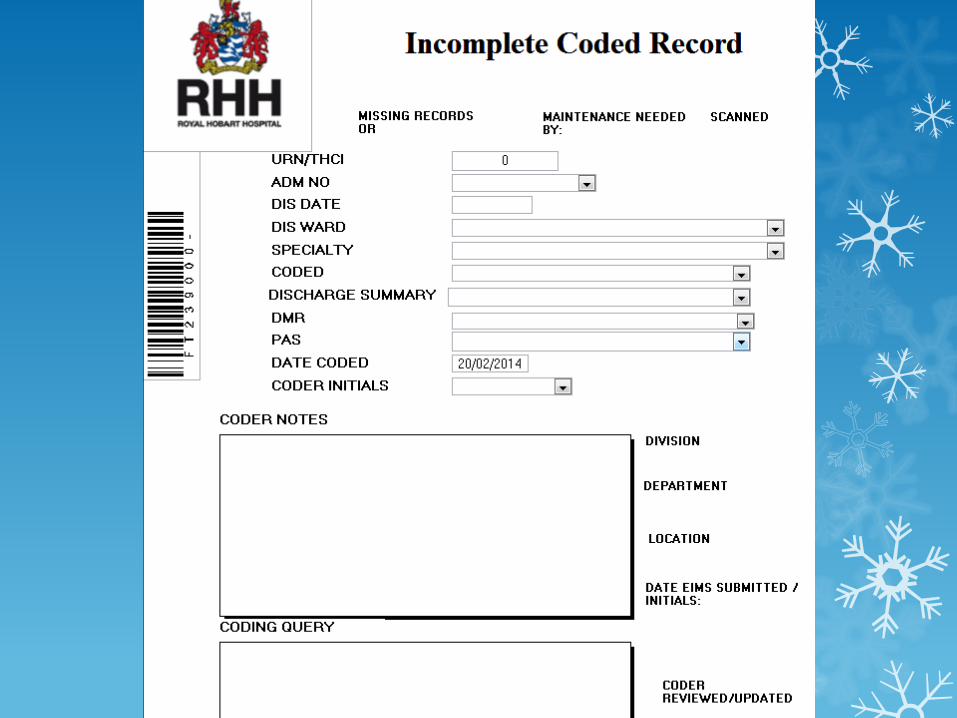
Incomplete Coding Database
Episodes where coding is adversely impacted are captured in incomplete Coding Database:
Nil Discharge Summary available
Missing Notes
Missing Operation Notes
Admission criteria not met
Incorrect care typing
Monthly Coding Reports
Results from Incomplete Coding Database
Missing notes by ward / specialty
Incomplete discharge summaries by ward / specialty
Incorrect care type changes by ward / specialty
Clinical Query Response Rate
Reported to Group Managers Monthly
Trended by month
Ward / specialty (all above)
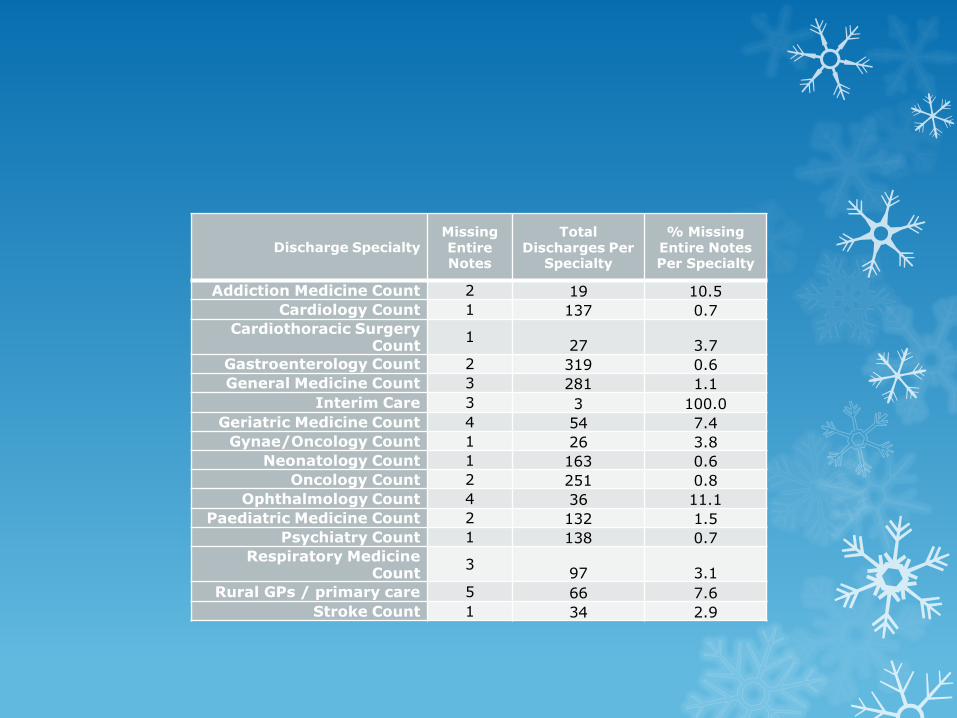
Discharge Specialty
Missing Entire Notes
Total Discharges Per
Specialty
% Missing Entire Notes Per Specialty
Addiction Medicine Count 2 19 10.5
Cardiology Count 1 137 0.7
Cardiothoracic Surgery Count
1 27 3.7
Gastroenterology Count 2 319 0.6
General Medicine Count 3 281 1.1
Interim Care 3 3 100.0
Geriatric Medicine Count 4 54 7.4
Gynae/Oncology Count 1 26 3.8
Neonatology Count 1 163 0.6
Oncology Count 2 251 0.8
Ophthalmology Count 4 36 11.1
Paediatric Medicine Count 2 132 1.5
Psychiatry Count 1 138 0.7
Respiratory Medicine Count
3 97 3.1
Rural GPs / primary care 5 66 7.6
Stroke Count 1 34 2.9
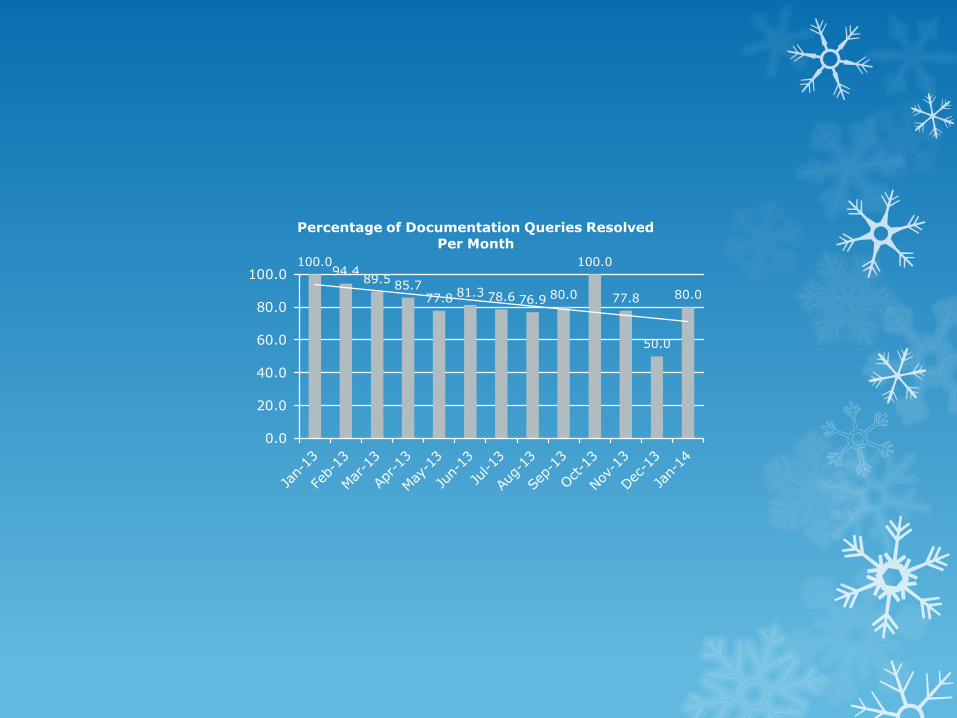
100.0 94.4
89.5 85.7
77.8 81.3 78.6 76.9 80.0
100.0
77.8
50.0
80.0
0.0
20.0
40.0
60.0
80.0
100.0
Percentage of Documentation Queries Resolved Per Month
Information Technology Projects Assisting Coding
Electronic Discharge Summaries
Training Delivery to clinicians - content
Legibility
Clinical Worklists
“incomplete summaries”
Statistical reports available
Completed Summaries messaged directly to DMR
DMR
Electronic Operation reports
Progress notes (limited at this stage)
ARIA
Real time clinical & admin data for Medical Oncology
Short coding turnaround times (real time clinical entry)
Information Technology (cont)
Future Developments
E-forms
Care type forms
Electronic operation reports (specialist)
Neurosurgery
DCCM / NICU
Clinical Systems
Auto CMV hours / progress notes / charts
Data / Coding edits
Business Intelligence Unit
DHHS
Challenges
Ageing workforce
Most experienced staff reducing hours
Approaching Retirement
Recruiting
Regional Area
Award Rate
Career pathway
Clinical Coding Auditor / Educator Position / Trainee position
Obtaining funding
Challenges
DHHS - Tasmanian Admissions Policy
Funding model = Financial Year
Admissions Policy = Calendar year
Clinical Coding Auditing from the DHHS
Awaiting release of State-wide Coding Action Plan
THO’s Requesting Coding Audits for quality improvement processes
Tasmanian Activity Based Funding Model
RHH exceeding Weighted Sep targets
No alternative public hospitals
N emphasis to audit to improve weighted separations at this time.
Questions?
Contact Details
Ben Spurr
PAS & Health Information Manager
Ph: 03 6222 6838





























