Embed Size (px)
Citation preview

M. Saiful Huq, PhD, FAAPM, FInstP
Professor and Director of Medical Physics
University of Pittsburgh Cancer Institute and UPMC CancerCenter
Pittsburgh, Pennsylvania, USA
AAPM TG-100 : A new paradigm for quality
management in radiation therapy
1

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Disclosures
2
• I have nothing to disclose

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Acknowledgement
3
• Special thanks to Frank Rath from the University of
Wisconsin because I have taken many slides shown in this
presentation from his summer school presentations.

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Authors of TG100
4
M. Saiful Huq
(Chair)
Benedick Fraass
Peter Dunscombe John Gibbons
Geoffrey Ibbott
Sasa Mutic
Jeffrey Williamson
Bruce Thomadsen
Frank Rath
Jatinder Palta
Arno Mundt
Ellen Yorke
(Vice Chair)

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
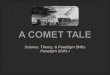
TG100 analysis of causes of failure for IMRT
5
Human
failure
35%
Lack of
standardized
procedures
15% Inadequate training
15%
Inadequate
communication
10%
Hardware/Software
failure
9%
Lack of resources
6%
Design failure
5%
Inadequate
commissioning
3%
Defective
materials/tools
2%

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Recent reports
6
2000
2009
2008
2008 2012
As technology and processes change
Retrospective approaches to QM are not
sufficient
All-inclusive QC checks may not be
feasible
Develop proactive approaches to failure
modes
Evaluate risks from each failure mode
Develop risk based approaches to QM

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
• Hazard identification and control approach is the basis for
safety planning procedures for manufacturing
• The design phase of the ISO safety strategy includes
identifications of hazards
assessment of the associated risk
removal of the hazards as much as practicable
Safety approach in industry

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Quality management in industry
• Systematic application of specific tools that improve process
controls producing more consistent and closer to optimal
outcomes and reduce the risk of mistakes, errors or
hazardous outcomes

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
• Process controls for grilling a steak
– Experience/training – how much charcoal to pile in the
middle of the grill, etc.
– Measurement tools – watch (steak goes on the grill 20
minutes after igniting the coals)
– Because there are some variables that are difficult to
control – meat thermometer (135 deg. F)
Process controls
9

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
• Can the concept of risk identification and process control be
applied to healthcare to improve the quality of care for patients?
• Yes, of course. Healthcare situations readily lend themselves to
a similar risk identification and control approach
Healthcare environment

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
What is risk?
• Risk: frequently defined as the answers to three questions
What can go wrong?
How likely is it to go wrong?
What are the consequences if it goes wrong?

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Risk assessment
• Risk assessment is the process of analyzing the hazards
involved in a process
• Many risk assessment and analysis tools/techniques
exist in industry
• These tools can be easily adapted to RT to enhance
safety and quality of treatment process
• TG100 used some of these tools to develop new
guidelines for RT QM

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
• Process tree (mapping)
• Failure mode and effects analysis (FMEA)
• Fault tree analysis (FTA)
• Establishment of a risk based QM program
Used IMRT as a case
study
Risk assessment tools

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
What is a process tree?
• Visual representation of the various steps in a process
• Demonstrates the flow of steps from process start to end
• Delineate and then understand the steps in the process

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Simple example of a process map
15
patient enters
linac vault
TP shift
instruction shift
treat
setup
patient to
CT marks
Courtesy: Darek Brown

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Complicated example: TG100 IMRT process tree
Patient database
information entered
Immobilization
and positioning
CT simulation
Other pre-
treatment imaging
Transfer images and
other DICOM data
Initial treatment
planning directive
RTP anatomy
contouring
Treatment planning
Plan approval
Plan preparation
Initial tx
(Day 1)
Subsequent tx
(Day N)
End of tx
Start of tx

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
TG100 IMRT process tree
17
Successful treatment
Imaging and
diagnosis
12 Subsequent
treatments
Chart filing
Immobilization
equipment
fabricated
Immobilization equipment
documented,
labeled, and stored
Immobilization for
Imaging study
Set up data
documented
Time out
Positioning
Imaging (port films, CBCT, etc) 27
Documentation
Treatment 3
Treatment 3
Documentation
Immobilization
equipment
documented,
labeled, and stored
Scheduling
Approve
plan 7, 20
7 RTP anatomy
contouring
1 Patient database
information entered
Data into electronic
Database 22
Data into written
chart 22
Review of patient
medical history
Immobilization
equipment fabricated
Import and fuse images 16
MD: delineate
GTV/CTV 2,5
PTV construction
Edit density map
for artifacts
Delineate ROIs and
planning structures
Indicate motion/uncertainty
Management 13, 14
Specify registration goals 23, 38
Specify protocol for delineating
target and structures 17
Specify images for
target/structure delineation 11
Specify dose limits and goals 26
Suggest initial guidelines for
treatment parameters
Enter prescription
And planning constraints 18, 21, 45
Setup fields
Setup dose
calc parameters
Optimization/
Dose calculation 12, 31
Evaluate plan 10, 28
6 Initial treatment
planning directive
8 Treatment planning
2 Immobilization
and positioning
3 CT simulation
9 Plan
approval
11 Initial treatment
Patient Identified
Special Instructions
(pacemakers, allergies,
preps, etc.) 9
Account for previous treatments
or chemotherapy 4
Motion management 8
Tx Unit operation
and calibration 3Information on
Previous or
concomitant treatment 22
Protocol for delineation
of targets 17
Patient ID
Treatment Site
Treatment settings
Imaging
Motion
Management 8
Protocol for PTV
Margin 6
Specify PTV Margin
Select Images 25
4D imaging correct 13
Optimization
ROI 33, 44
Optimization
settings 45
Treatment accessories 24
Boolean operations 29, 46
Changes noted 32, 34
Patient information 35
Monitor Pt/Tx 37, 43
Monitor Pt/Tx 37, 43
Specify ROI for optimization 19
Treatment settings
Positioning
Pt prep 35
Changes correct 40, 42Run leaf sequencer
Pt changes noted 42
Imaging Studies
Patient prepped
(contrast, tattoos,
BBs etc.)
Treatment accessories 24
4 Other imaging
Patient informed
Of imaging requirements
Images
Interpreted 1
Position
patient
Make images
5 Transfer
images
Transfer
Other datasets
Transfer CT
Dataset 41
Create case
4D representation
Save patient
Calculate dose
to optimization points
and dose distribution 12, 31
Heterogeneity correction 30
Evaluate leaf sequencer
Evaluate delivery
system limitations
Complete formal
prescription 36
Manual data entry and plan modification 39
Specify treatment course
Delivery protocols
Scheduling
Automatic data entry and plan modification
Prepare DRR and other images
Check version of
plan and patient ID
Annotate localization anatomy
Order fields
Prepare paper chart
Prepare electronic chart 15
Transfer patient data to treatment delivery 15
Define localization imaging
10 Plan
preparation
Enter demographics
Patient Position
Recorded in database
Patient information
Tx Unit operation
and calibration 3

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
FMEA
• A risk assessment tool used to identify weaknesses or
deficiencies (inadequate controls) in processes that could
lead to mistakes, errors, and potential hazardous outcomes

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Strategy for improving patient safety: FMEA & FTA
• Begins with a complete and thorough understanding of the
process – flow charts, process maps
• Perform a Process FMEA (P-FMEA) to identify weaknesses
or inadequate controls in the process
• Develop process controls that either reduce the risk or
improve the process
• Use FTA to identify root causes of potential process failures
and develop recommendations to improve quality control of
the process

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Completing an process FMEA
• Create a team
Ideally cross functional representing every function involved in the
process
Oncologists, medical physicists, dosimetrists, therapists, IT
personnel, administrators
Effort should be led by a facilitator trained in or familiar with the tools
used in the analysis
Consider providing training

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Completing an process FMEA
• Select a process – key step
Scale is important
Opportunity – Quality issues, past problems, not happy with the level
of success, …
Realistic opportunity to make improvements
Complexity or size

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Process FMEA – for each step in a process
Failure Modes
Cause
Detect
Effects
FM: Inability of a process
step to produce the
desired optimal outcome

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Completing an FMEA
23
Step Potential
failure
modes
Potential
causes of
failure
Potential
effects of
failure
O S D RPN Comment
For a given process:
RPN = O x S x D [ 1 ≤ RPN ≤ 1000 ]

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Completing an FMEA
1. For each process step – identify all potential failure modes
– always best to define failure modes as “not” meeting
process requirements
2. For each potential failure mode – identify all of the causes
that could produce that failure
a. Focus on process related causes of failure modes

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Completing an FMEA
3. For each potential failure mode – identify the effects of that
failure mode

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Completing an FMEA
4. Current controls – judge the current capabilities of
the process controls to:
a. Prevent the cause of a failure from occurring
b. Detect a failure when it occurs
c. Moderate the severity of a failure when it
occurs

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Completing an FMEA
• Most effective and lowest cost controls are those that
prevent causes of failure modes

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
FMEA ranking scales for Occurrence, Detection, Severity*
Occurrence of the cause of failure mode : O
Detection of failure mode: D
Severity of the effect when failure mode occurs: S
*Not used by TG100

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
• Risk Priority Number (RPN)
Occurrence ranking X Severity ranking X Detection ranking
Range of RPNs (1 -1000)
RPN of 125 or higher is problematic either in terms of safety or
process capability
Typical scenario –RPNs over 400!
Highest RPNs must be addressed first
Then work down to lower risk process steps
Completing an FMEA
29

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
• Risk Priority Number (RPN)
– Beware of patterns potentially hidden by low overall RPNs
Occurrence = 10, Severity =10, Detection=1 - RPN of 100 but
……
Occurrence=1, Severity=10, Detection=10 – RPN of 100 but ….
Severity of 10 – even if Occurrence and Detection are both a 1
can you or do you want to risk it?
Completing an FMEA
30

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Top/Down FMEA approach
• Start with the major “branches” of the selected process
• Perform a PFMEA to identify which ‘branches” are the
weakest (most likely to produce sub-optimal results or
errors/mistakes
• Drill down deeper into those “branches” – more detailed
process map and PFMEA

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Evaluates propagation of failures
Visual representation of propagation of failures
Begins on the left with a failure mode
Works backwards in time
(to the right to identify causes of failure)
Fault Tree
32

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Evaluates propagation of failures
Visual representation of propagation of failures
Begins on the left with a failure mode
Works backwards in time
(to the right to identify causes of failure)
Fault Tree
33
Error in calculated value
for patient
Error in data
Error in data input
Error in calculation algorithm
Error in prescription
OR

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Fault Tree
34
Errorin data
Errorin QC
Error in data input
Errorin QC
Error in Calculation algorithm
Errorin QC
Error in prescription
Errorin QC
Error in calculation
Errorin QA
Error in Calculated value for patient

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013 TG100

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
• Current QA guidance documents are based on prescriptive
approaches evaluating technical performances of
radiotherapy equipment
• There has been a growing recognition that quality and
safety impairment arises from weakness in radiotherapy
processes
• Hence the change in approach in QM in TG100
Summary
36

Saiful Huq – AAPM TG100: ORVC and Penn-Ohio Chapter Meeting, 2013
Our job is not to prevent
errors, but to keep the
errors from injuring the
patients.
Lucian Leape
It is useful to report
all accidents before
consequences appear
It is impossible to make anything
foolproof because fools are so
ingenious.
Arthur Bloch, Murphy’s law
Thank you
![ELECTRONIC MEDICAL RECORDS (EMR) STREAMLINE …chapter.aapm.org/pennohio/2013FallSympPresentations/SI7... · 2013. 11. 12. · Microsoft PowerPoint - Ppt0000033.ppt [Read-Only] Author:](https://img.dokumen.tips/doc/110x75/5fe0a80f4c1efe2f7a2f5c72/electronic-medical-records-emr-streamline-2013-11-12-microsoft-powerpoint.jpg)