Embed Size (px)
Citation preview

“ A STUDY OF PERINATAL OUTCOME IN PRETERM PREMATURE RUPTURE OF
The Tamil Nadu Dr. M.G.R Medical University
In partial fulfilment of the requirement for the award of the Degree of
M.S. OBSTETRICS AND GYNAECOLOGY
THE TAMIL NADU Dr. M.G.R MEDICAL UNIVERSITY
INSTITUTE OF OBSTETRICS AND GYNAECOLOGY,
GOVERNMENT HOSPITAL FOR WOMEN & CHILDREN,
MADRAS MEDICAL COLLEGE.
A STUDY OF PERINATAL OUTCOME IN PRETERM PREMATURE RUPTURE OF
MEMBRANES” Dissertation submitted to
The Tamil Nadu Dr. M.G.R Medical University
In partial fulfilment of the requirement for the award of the Degree of
M.S. OBSTETRICS AND GYNAECOLOGY
BRANCH II
THE TAMIL NADU Dr. M.G.R MEDICAL UNIVERSITY
INSTITUTE OF OBSTETRICS AND GYNAECOLOGY,
GOVERNMENT HOSPITAL FOR WOMEN & CHILDREN,
MADRAS MEDICAL COLLEGE.
APRIL-2018
A STUDY OF PERINATAL OUTCOME IN PRETERM PREMATURE RUPTURE OF
The Tamil Nadu Dr. M.G.R Medical University
In partial fulfilment of the requirement for the award of the Degree of
M.S. OBSTETRICS AND GYNAECOLOGY
THE TAMIL NADU Dr. M.G.R MEDICAL UNIVERSITY
INSTITUTE OF OBSTETRICS AND GYNAECOLOGY,
GOVERNMENT HOSPITAL FOR WOMEN & CHILDREN,
MADRAS MEDICAL COLLEGE.

BONAFIDE CERTIFICATE
This is to certify that this dissertation entitled “A STUDY OF
PERINATAL OUTCOME IN PRETERM PREMATURE
RUPTURE OF MEMBRANES” is the bonafide original work done by
Dr.S.YOGALAKSHMI , post graduate in the Department of Obstetrics
and Gynaecology, under the guidance of Dr.ARASI SRIVATHSAN,
MD, OG., Professor, Institute of Social Obstetrics and Gynaecology,
Kasturba Gandhi Hospital, Madras Medical College, Chennai, towards
partial fulfilment of the requirement of the Tamil Nadu Dr. M.G.R
Medical University for the award of M.S Degree in Obstetrics and
Gynaecology, March 2018. The period of post graduate study is from
June 2015 to June 2018.
Prof.Dr.ArasiSrivathsan MD, OG Prof Dr.T.K.ShanthyG unasinghMD, DGO
Professor, Director and Superindent,
ISO-KGH IOG
Prof R. NARAYANABABU MD, DCH
Dean.
Madras Medical College.
DECLARATION
I solemnly declare that this dissertation “A STUDY OF
PERINATAL OUTCOME IN PRETERM PREMATURE
RUPTURE OF MEMBRANES” was prepared by me under the
guidance and supervision of Dr.Arasi Srivathsan, MD, OG., Professor,
Institute of Social Obstetrics and Gynaecology, Kasturba Gandhi
Hospital, Madras Medical College, Triplicane, Chennai.
This dissertation is submitted to The Tamil Nadu Dr. M.G.R.
Medical University, Chennai in partial fulfilment of the University
regulations for the award of the degree of M.S. (Obstetrics and
Gynaecology).
Place: Chennai Date: Dr.S.YOGALAKSHMI

ACKNOWLEDGEMENTS
I gratefully acknowledge and sincerely thank Dr.R.Narayana Babu,
MD, DCH., Dean, Madras Medical College, for allowing me to use
thefacilities and clinical materials available in the hospital.
I extend my sincere thanks and gratitude to Dr.T.K.Shanthy
Gunasingh, MD, DGO., Director and Superintendent, IOG, for granting me
permission to utilize the facilities of the institute for my study.
I am extremely grateful to our beloved Professor, Dr.Arasi Srivathsan,
MD, OG., Professor of Obstetrics &Gynaecology, ISO-KGH, for her valuable
guidance, motivation and encouragement given during the study.
I humbly thank all the Professors and Assistant Professors of IOG,
Egmore and Government Kasturba Gandhi Hospital, Triplicane for all their
help during the course of the study.
My sincere thanks to my statistician Mr.Padmanabhan who patiently
helped me in analysing the results of this study.
My special thanks to my family and friends for their physical help and
moral support without which nothing would have been possible.
I am immensely grateful to all the patients who took part in the study.

CONTENTS
SL.NO TITLE PAGE NO.
1 INTRODUCTION 1
2 AIM AND OBJECTIVES 3
3 MATERIALS AND METHODS 4
4 REVIEW OF LITERATURE 7
5 OBSERVATION AND RESULTS 24
6 DISCUSSION 81
7 CONCLUSION 83
8 BIBLIOGRAPHY 84
9 INFORMED CONSENT FORM 88
10 PROFORMA 90
MASTER CHART

ABBREVIATION
ROM - Rupture of membranes
PPROM - Preterm premature Rupture of membranes
MMPs - matrix metallo proteinase
fFN - Fetal fibronectin
HMD - Hyaline membrane disease
RDS - Respiratory Distress syndrome
ACOG - American college of obstetrics and gynaecology
NICE - National institute of clinical Excellence
H/O - History of
MOD - Mode of delivery
LSCS - Lower segment cesarean section
B - booked
UB - unbooked
AFI - amniotic fluid index
NICU - neonatal intensive care unit
BMI - body mass index
NEC - necrotizing Enterocolitis
INTRODUCTION
1
INTRODUCTION
Preterm premature rupture rupture of membranes is defined as
rupture of fetal membrane before onset of labour at less than
37 completed weeks of gestation and after 28 weeks of gestation.
Incidence ranges from 3-10% of all deliveries. Preterm premature rupture
of membrane is one of the important causes of preterm birth can result in
high perinatal morbidity and mortality.
Preterm premature rupture of membranes complicates 3% of
pregnancies and leads to one third of preterm birth. Preterm delivery
affects one in 10 birth in USA and even greater birth in developing
continues and causes 40-75% neonatal death.
There are numerous risk factors for preterm premature rupture of
membrane such as maternal, socioeconomic class, infection at early
gestational age and associated co-morbid condition. Both mother and
fetus are at greater risk of infection after preterm premature rupture of
membrane.
The fetal and neonatal morbidity and mortality risks are
significantly affected by severity of oligohydrominos, duration of latency
and gestation at preterm premature rupture of membrane .
Complication of preterm premature rupture of membrane for the
fetus and newborn consist of prematurity, fetal distress, altered
2
pulmonary development leading to pulmonary hypoplasia, pulmonary
hypertension, necrotizing enterocolitis and neurological disorder.
The treatment relies on accurate diagnosis and gestational age is
dependent. The diagnosis of preterm premature rupture of membrane is
made by a combination of clinical suspicious, patient history and some
simple test.
Any evidence of infection , fetal distress and cord accidents is an
indication for delivery. A gestational age approach to therapy is important
and should be adjusted to each hospitals neonatal care unit. Antenatal
antibiotics and steroids have clear benefits and should be offered to all
women without complication.
The management of patients with preterm premature rupture of
membrane has changed markedly in the past several years. The basis for
this is a combination of better understanding of newborn physiology,
improved neonatal care and the widespread use of fetal monitoring.
An important recent advance is the recognition that an active
observation of program is associated with less morbidity and mortality.
Moreover advances in perinatal and antenatal care will continue to
improve the outcomes of these of these women and their children.

AIMS AND OBJECTIVES

3
AIM & OBJECTIVES
AIM:
To study perinatal outcome in preterm premature rupture of
membrane.
OBJECTIVE:
1. To study risk factors associated with preterm premature
rupture of membrane.
2. To study perinatal morbidity and mortality associated with
preterm premature rupture of membrane.
3. To study the outcome of labour in preterm premature rupture
of membrane.

MATERIALS ANDMETHODS

4
MATERIALS AND METHODS
This study was conducted in ISO-KGH from may 2016-may 2017
under Madras Medical College. Institutional Ethical committee clearance
was obtained from Madras Medical College.
SAMPLE SIZE:
200 patients
STUDY DESIGN:
Prospective observational study
DURATION OF STUDY:
One year
STUDY CENTRE:
Department of obstetrics and gynaecology in ISO KGH, Chennai.
INCLUSION CRITERIA:
All pregnant women with a singleton pregnancy between 28-37
weeks of gestation admitted in labour room were shifted after considering
inclusion and exclusion criteria.
5
EXCLUSION CRITERIA:
1. Multiple pregnancy
2. Fetal growth restriction
3. Uterine anomalies
4. Foetal anomalies
5. Hypertensive disorder complicating pregnancy
6. Gestational diabetes
7. Antepartum haemarrhage ( Placenta praevia, Abruption )
8. Class 2-4 cardiac disease
9. Tumour complicating pregnancy ( Fibroid, Ovarian tumour )
10. Medical disorder complicating pregnancy ( Chronic hypertension,
Chronic renal disease and SLE
STUDY METHOD:
This was prospective observational study which was carried out
those pregnant women admitted with preterm premature rupture of
membranes between 28-36 weeks of gestation. The gestational age was
calculated from LMP, if there is discrepancy of more than seven days

6
between LMP and early weeks USG and consecutive two coincide then
USG EDD should be taken.
For above mentioned patients we will do baseline investigation like
Hb, pcv, Blood grouping and Typing and High vaginal swab. Per
speculum examination should be done to confirm the diagnosis of
preterm premature rupture of membranes. Digital examination only be
done only when the patient is in the active labour.
The above mentioned patients are closely monitored throughout
labour. Immediately after delivery paediatrician was called over and look
sign of infection and Respiratory distress syndrome.
All the information was attached in pretested questionare. In study
all patients are observed until discharge from hospital. The study was
conducted after getting consent from patient. Close monitoring of all
patients of preterm premature rupture of membrane during labour and
baby immediately after delivery and upto discharge.

REVIEW OF LITERATURE

7
REVIEW OF LITERATURE
ROM:
Rupture of membrane or amniorrhexis is a term said during
pregnancy to describe a rupture of the amniotic sac. Normally it occurs
spontaneously at full term either during or at the beginning of lobour.
PPROM:
Preterm premature rupture of membrane defined as rupture of
membrane before 37 completed weeks of gestation.
TYPES OF PPROM
Early preterm: 28-32 weeks
Moderate preterm: 32-34 weeks
Late preterm: 34-36 weeks
INCIDENCE:
Incidence of PPROM ranges from 3.0-10.0% of all deliveries.
PPROM complicates approximately 3% of pregnancies and leads to one
third of preterm birth.

8
STRUCTURE OF FETAL MEMBRANES:
These are the membrane that develop outside the embryo but in
close association with it and they carry out certain specific functions.
Fetal membrane consist of amnion, chorion, allantois and yolk sac. The
amnion was innermost membrane of fetus and forms amniotic cavity that
contains amniotic fluid. The chorion was between amnion and decidua.
AMNION:
The amnion is the membrane that closely covers the embryo.
Pregnancy is the period of time during which a child matures with in the
womb of the mother. The period is important for the development of the
fetus. During this time the fetus must be protected from internal
environment of the mothers body and this is achieved in many ways. One
of the primary form of protection is the amniotic sac which is the
protective sac and fluid that surrounds the fetus and prevents damage.
The membrane that forms this sac is known as amnion. The amniotic
fluid provides a shock absorbing effect to the embryo against womb
infections etc. The watery fluid around the embryo helps in maintaining
constant temperature and pressure and protects the embryo in case the
mother has a fall. The amniotic fluid is derived from the mothers blood
and contains foetal cells. This is made use of in the prenatal sex test for
the fetus- known as amniocentesis. In amniocentesis the amniotic fluid is

9
drawn out with a syringe and the cells are tested for the presence of sex
chromosomes.
CHORION:
Chorion is a membrane that develops at the beginning of a
pregnancy between the developing fetus and the mother and continuous
to grow through out the pregnancy. It is formed by two layers the
embryonic mesoderm and double layers of trophoblasts. Chorion protects
the embryo and forms placenta for metabolic exchange between mother
and fetus.
YOLK SAC:
This is the formed below the embryo. In human beings this contains
a fluid but no yolk. It is vestigial organ. Its wall is made of trophoblast
and endoderm. The yolk sac functions as the region of the formation of
blood cells upto about 6th week of development when liver of fetus takes
up this function.
ALLANTOIS:
This is a small bag like structure that develops from the gut of the
embryo and near the yolk sac. This membrane develops around the third
week of development. Gradually the allantois shrinks in size and get

10
enclosed in umbilical cord. Allantois helps in the formation of umbilical
arteries and veins. The allantois also forms blood cells.
ETIOPATHOGENESIS:
WEAKENED FETAL MEMBRANE:
Fetal membrane likely break because they become fragile and
weak. This weakening is a normal process that typically happens at term
as the body prepares for labor and delivery. But, this can be a problem
when it occurs preterm (preterm). The natural weakening of fetal
membrane is thought to be due to one or combination of the following. In
preterm premature rupture rupture of membranes, these process are
activated too early;
CELL DEATH;
When cells undergoes programmed cell death, they release
chemical markers that are detected in high concentration in cases of
preterm premature rupture of membrane
Poor assembly of collagen:
Collagen is a molecule that gives fetal membrane their strength. In
cases of preterm premature rupture of membranes proteins that bind and
cross link collagen to increase its tensile strength are altered.

11
BREAKDOWN OF COLLAGEN:
Collagen is broken down by enzymes called matrix
metalloproteinases (MMPs), which are found at higher level in PPROM
amniotic fluid, this MMPs will break down the strength- bearing
collagen, so prostaglandin production will be synthesized in high amount
to prompt the uterine contraction and cervical ripening. MMPs are
inhibited by tissue inhibitors of MMPs which are found lower levels in
PPROM amniotic fluid.
INFECTION:
Infection and inflammation likely explains why membrane break
earlier than they are supposed to. In studies bacteria have been found in
the amniotic fluid one third of cases of PPROM. Often, testing of
amniotic fluid is normal, but a subclinical infection (too small to detect)
or infection of maternal tissues next to the amniotic fluid, may still be
contributing. In response to infection, the body creates inflammation by
making chemicals (ex: cytokines) that weaken the fetal membrane and
put them at risk for rupture. PPROM is also risk factor in the
development of neonatal infection.

12
GENETICS:
Many genes play role in inflammation and collagen production,
therefore inherited genes may play a role in predisposing a person to
PPROM.
RISK FACTORS:
The cause of PPROM is not clearly understood, but the following
are risk factors that have been shown to increase the chance of it
happening. In many cases however no risk factors is identified.
1.Infectins: urinary tract infection, sexually transmitted diseases, lower
genital infections ( ex: Bacterial vaginosis)
2. Cigarette smoking during pregnancy
3. Illicit drug use during pregnancy
4. Having had PPROM in previous pregnancies
5. Hydrominos: too much amniotic fluid
6. Multiple gestation: being pregnant with two or more fetuses at one
time
7. Having had episodes of bleeding anytime during pregnancy
8. Invasive procedure like amniocentesis and chorionic villous sampling

13
9. Nutritional deficits
10. Cervical insufficiency: having short or prematurely dilated cervix
during pregnancy
11. Low socio economic status
12. Being overweight
DIAGNOSIS OF PPROM:
To know for sure if a women has experienced PPROM a health
care clinician must prove that the fluid leaking from the vagina is
amniotic fluid, and the lobor has not yet started. To do this, a health care
clinician will take a medical history, do a gynecological exam using a
sterile speculum and ultrasound.
HISTORY:
A person with PPROM typically recalls a sudden gush of fluid loss
from the vagina, or steady loss of small amount of fluid.
SPECLUM EXAMINATION:
A health care clinician will insert a sterile speculum into the vagina
in order to see inside and perform the following evaluation. Digital
cervical exams, in which gloved fingers are inserted into the vagina to
14
measure the cervix, are avoided until the women is in active labor to
reduce the risk of infection.
POOLING TEST;
Pooling is when a collection of amniotic fluid can be seen in the
back of vagina (vaginal fornix). Sometimes leakage of fluid from the
cervical opening can be seen when the person coughs or does a valsalva
maneuver.
NITRAZINE TEST:
A sterile cotton swab is used to collect fluid from the vagina and
place it on nitrazine paper (phenaphthazne). Amniotic fluid is mildly
basic (ph 7.1-7.3) compared to normal vaginal secretion which are acidic
( ph 4.5-6 ). Basic flid, like amniotic fluid, will turn the nitrazine paper
from orange to dark blue.
FERN TEST:
A sterile cotton swab is used to collect fluid from vagina and place it
on a microscope slide. After drying, amniotic fluid will form a
crystallization pattern called arborization which resembles leaves of a
fern plant when viewed under a microscope.

15
FETAL FIBRONECTIN :( fFN )
It is the protein produced in pregnancy that determine the risk of
preterm delivery. The fFN test measures the amount of fetal fibronectin in
vaginal secretion and is performed like a pap smear test. A negative test is
a predictor that delivery will not occur in the next two weeks, but a
positive test does not necessarily indicate that preterm delivery is
imminent,
IMMUNOLOGICAL TEST:
Immune- chromatological tests ( Amnisure, Actim PPROM test,
Biosynex Amnioquick ). These are commercially available test kits that
detect chemicals present in amniotic fluid; placental alpha microglobulin-
1 (AmniSure ) and insulin like growth factor binding protein-1 ( Actim
PPROM test ). These are helpful if negative to rule out PPROM, but are
not that helpful if positive because the false positive rate is 19-30%.
DYE TEST
In this test a needle is used to inject indigo carmine dye (blue) into
the amniotic fluid that remains in the uterus through the abdominal wall.
In the case of PPROM, blue dye can be seen on a stained tampon or pad
after about 15-30 minutes. This method can be used to definitively make
a diagnosis, but is rarely done because it is invasive and increase risk of

16
infection. But, can be helpful if the diagnosis is still unclear after the
above evaluations have been done.
ULTRASOUND:
Ultrasound can measure the amount of amniotic fluid still in the
uterus surrounding the fetus. If the fluid levels are low, PPROM is more
likely. This is helpfl in cases when diagnosis is not certain, but is not, by
itself, definitive.
OTHER TESTS:
1. Detection of fetal cells in amniotic fluid
2. Detection of vernix and lanugo hair in amniotic fluid
FALSE POSITIVES:
Like amniotic fluid, blood, semen, vaginal secretion, antiseptics,
basic urine and cervical mucus also have a basic ph and also turn
nitrazine paper blue, Cervical mucus can also make a pattern similar to
ferning on a microscope slide, but it is usually patchy and less branching.
DIFFERENTIALDIAGNOSIS:
Other things to keep in mind that may present similarly to PPROM
are the following:

17
• Urinary incontinence: Leakage of small amounts of urine is
common in the last part of pregnancy
• Normal vaginal secretion of pregnancy
• Increased cervical discharge: this can happen when there is a
genital tract infection
• Semen
• Douching
• Vesicovaginal fistula: an abnormal connection between the bladder
and the vagina
• Loss of the mucus plug
COMPLICATION OF PPROM
COMPLICATIONS INCIDENCE (%)
1. Cord compression 32 to 76
2. Chorioamnionitis 13 to 60
3. Abruptio placentae 4 to 12
4. Antepartum fetal death 1 to 2
5. Respiratory distress syndrome 35

18
MATERNAL
1. Choriomnionitis (acute and subclinical)
This was most common complication occurring in PPROM .Clinical
chorioamnionitis is Diagnosed solely based on clinical signs since access
to uncontaminated amniotic fluid or placenta for culture is invasive and
usually avoided. Typically, the presence of fever with in addition two
other signs like uterine tenderness, maternal or fetal tachycardia and foul
or purulent amniotic fluid. Chorioamnionitis is an indication for
termination of pregnancy not cesarean section the latter was indicated in
obstetric indication only.
2. Postpartum endometritis
This was another maternal complication of PPROM. Endometritis
was usually associated with chrioamnionitis. The duration of antibiotic
therapy after preterm premature rupture of membrane does not affect the
neonatal morbidity and maternal morbidity.
FETAL
1. Prematurity
2. Hyaline membrane disease
3. Infection
4. Neurological damage
5. Pulmonary hypoplasia

19
6. Cerebral palsy
7. Musculoskeletal deformity
THE ROLE OF CORTICOSTEROIDS:
Corticosteroids decrease perinatal morbidity and mortality after
PPROM. A recent meta-analysis found that corticosteroids after PPROM,
versus no administration, reduced the risk of respiratory distress
syndrome (20 versus 35.4%) intraventricular hemorrhage (7.5 versus
15.9%) and necrotizing enterocolitis (0.8 versus 4.6%) without an
increase in the risk of maternal and fetal infection. The most widely used
and recommended regimens include intramuscular betamethasone 12mg
every 24 hours for two days, or intramuscular dexamethasone 6mg every
12 hours for two days. The National institutes of Health recommends
administration of corticosteroids nefore 30-32 weeks gestation, assuming
fetal viability and no evidence of intra-amniotic infection. Use of
corticosteroids between 32-34 weeks is controversial. Adminstration of
corticosteroids after 34 weeks gestation is not recommended unless there
is evidence of fetal lung immaturity by amniocentesis. Multiple courses
are not recommended because studies have shown that two or more
courses can result in cerebral palsy.
20
ROLE OF ANTIBIOTICS IN PPROM:
Giving antibiotics to patients with PPROM can reduce neonatal
infection and the latent period. A meta- analysis showed that a patient
receiving antibiotics after PPROM, compared those not receiving
antibiotics experienced reduced postpartum endometritis,
chorioamnionitis, neonatal sepsis, neonatal pneumonia and
intraventricular hemorrhage. Another meta-analysis found a decrease in
neonatal intraventricular hemorrhage and sepsis. The regimen studied by
the National institute of Child Health and Human Development trial uses
an intravenous combination of 2 gms of ampicilin and 250 mg of
erythromycin every 6 hours for 48 hours, followed by 250 mg of
amoxicillin and 333 mg of erythromycin every 8 hours for 5 days.
TOCOLYTIC THERAPY:
Limited data are available to help determine whether tocolytic
therapy is indicated after PPROM. As described above, corticosteroids
and antibiotics are beneficial when administered to patients with PPROM,
but no studies of these therapies combined with tocolysis are available.
Tocolytic therapy is not improve neonatal outcome. Long term tocolytic
therapy in patients with PPROM is not recommended; consideration of
this should await further research. ACOG guideline, there is no clear
evidence that tocolytic drug improve outcome and therefore it is
21
reasonable not to use them. However tocolysis should be considered if the
few days gained would be put to good use, such as completing a course of
corticosteroids or in utero transfer.
ACOG GUIDELINE:
There is no clear evidence that tocolytic drugs improve outcome
and therefore it is reasonable not to use them. However, tocolysis should
be considered if the few days gained would be put to good use, such as
completing course of corticosteroids or in utero transfer.
MANAGEMENT OF PPROM
1. 28-31 WEEKS
Delivery before 32 weeks gestation may lead to severe neonatal
morbidity and mortality. In the absence of intra-amniotic infection
pregnancy may be prolonged under antibiotics and corticosteroids until
34 weeks of gestation. Contraindication for conservative management is
chorioamnionitis, abruption and non reassuring fetal heart patterns.
Despite these measures many patients will deliver with in two weeks of
PPROM. During conservative treatment should watch for maternal
temperature, uterine contractions, uterine tenderness and laboratory
evidence of infection like leucocytosis or elevated ESR. Evidence

22
suggests that prolonged latency lead to increased incidence of intra-
amniotic infection.
2. 32-33 WEEKS
PPROM between 32-33 weeks of gestation should be induction of
labor after transport of patients to intensive neonatal care should be
considered. Prolonging pregnancy after documentation of pulmonary
maturity unnecessarily increases the likelihood of maternal infection,
umbilical cord compression and neonatal infection. There are few data to
guide the care of patients without documented pulmonary maturity.
Physicians must balance the risk of respiratory distress syndrome and
other sequelae of premature delivery with the risk of pregnancy
prolongation, such as neonatal sepsis and core accidents. Physician
should administer a course of corticosteroids and antibiotics to patients
without documented lung maturity consider delivery 48 hrs later or
perform careful assessment of fetal well being, observe for intra amniotic
infection, and deliver at 34 weeks.
3. 34-36 WEEKS
When PPROM occurs between 34-36 weeks gestation, physician
should avoid to urge to prolong the pregnancy. Studies shown that labor
induction clearly is beneficial at or after 34 weeks of gestation. One study
showed that Conservative management between 34-36 weeks of
gestational age resulted in an increased risk of chorio amnionitis and a

23
lower average umbilical cord ph. PPROM is not a contraindication to
vaginal delivery.
PREVENTION:
Both intravaginal progesterone and cervical cerclage are used
prophylactically to prevent PPROM in different circumstances, although
evidence is lacking on which is more effective and the relative costs and
benefits of each. In the UK, NICE has the following recommendations for
women who, on a transvaginal ultrasound scan between 16 and 34 weeks,
have a cervical length of <25mm. Women who have previously had a
preterm birth or pregnancy loss between 16 and 34 weeks, should be
offered either intravaginal progesterone or cervical cerclage. Women with
no history of a preterm birth or pregnancy loss between 16 and 34 weeks,
should be offered intravaginal progesterone. Women who have had
PPROM in a previous pregnancy or have a history of cervical trauma,
should be offered cervical cerclage. ACOG does not recommend
intravaginal progesterone or cervical cerclage and either of which not
improve maternal and perinatal outcome.
OBSERVATION AND RESULTS

24
OBSERVATION AND RESULTS
AGE GROUP Vs PPROMGROUP
TABLE 1
PPROMGROUP (GA in weeks) Total
28-32 33-34 <37
AG
E G
RO
UP
UPTO 25
Count 20 16 72 108
% within AGE GROUP
18.5% 14.8% 66.7% 100.0%
% within PPROMGROUP
45.5% 30.8% 69.2% 54.0%
% of Total 10.0% 8.0% 36.0% 54.0%
26-30
Count 20 28 24 72
% within AGE GROUP
27.8% 38.9% 33.3% 100.0%
% within PPROMGROUP
45.5% 53.8% 23.1% 36.0%
% of Total 10.0% 14.0% 12.0% 36.0%
>30
Count 4 8 8 20
% within AGE GROUP
20.0% 40.0% 40.0% 100.0%
% within PPROMGROUP
9.1% 15.4% 7.7% 10.0%
% of Total 2.0% 4.0% 4.0% 10.0%
Total
Count 44 52 104 200
% within AGE GROUP
22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

25
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 22.875a 4 .000
Likelihood Ratio 23.350 4 .000
Linear-by-Linear
Association 8.000 1 .005
N of Valid Cases 200
Patients with Preterm premature rupture of membrane occur in all
age group. 54% belong to age group 22<20 years.36% belongs to age
group 20-25 years. 10% belong to age group >30 years. But it was more
common in age group of < 25 years.
a. 1 cells (11.1%) have expected count less than 5. The minimum
expected count is 4.40.
The distribution of age classification among PPROM group is
statistically significant. Chi =22.8 P=0.005

26

27
TABLE 2
SOCIOECONOMIC CLASS VS PPROMGROUP
PPROMGROUP (GA in weeks ) Total
28-32 33-34 <37
SO
CIO
EC
ON
OM
IC C
LAS
S
3
Count 8 4 16 28
% within SE CLASS 28.6% 14.3% 57.1% 100.0%
% within PPROMGROUP 18.2% 7.7% 15.4% 14.0%
% of Total 4.0% 2.0% 8.0% 14.0%
4
Count 32 48 84 164
% within SE CLASS 19.5% 29.3% 51.2% 100.0%
% within PPROMGROUP 72.7% 92.3% 80.8% 82.0%
% of Total 16.0% 24.0% 42.0% 82.0%
5
Count 4 0 4 8
% within SE CLASS 50.0% 0.0% 50.0% 100.0%
% within PPROMGROUP 9.1% 0.0% 3.8% 4.0%
% of Total 2.0% 0.0% 2.0% 4.0%
Total
Count 44 52 104 200
% within SE CLASS 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP 100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

28
Chi-Square Tests
Value Df
Asymp. Sig.
(2-sided)
Pearson Chi-Square 8.261a 4 .082
Likelihood Ratio 9.809 4 .044
Linear-by-Linear
Association .180 1 .671
N of Valid Cases 200
a. 3 cells (33.3%) have expected count less than 5. The minimum
expected count is 1.76.
Socio economic class distribution among PPROM is statistically
significant Chi=8.26 P=0.81
82% of patient of preterm premature rupture of membrane belongs
to class 4 socioeconomic class as per modified Kuppusamy classification.

29
SOCIO ECONOMIC CLASS

30
BMI GROUP vs PPROMGROUP
TABLE 3
PPROMGROUP
(GA in weeks)
28-32 33-34 <37
BM
I GR
OU
P
NORMAL
Count 8 8 16
% within BMI GROUP
25.0% 25.0% 50.0%
% within PPROMGROUP
18.2% 15.4% 15.4%
% of Total 4.0% 4.0% 8.0%
OVERWEIGHT
Count 28 36 56
% within BMI GROUP
23.3% 30.0% 46.7%
% within PPROM
GROUP 63.6% 69.2% 53.8%
% of Total 14.0% 18.0% 28.0%
OBESE
Count 8 8 32
% within BMI GROUP
16.7% 16.7% 66.7%
% within PPROMGROUP
18.2% 15.4% 30.8%
% of Total 4.0% 4.0% 16.0%
Total
Count 44 52 104
% within BMI GROUP
22.0% 26.0% 52.0%
% within PPROMGROUP
100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0%
31
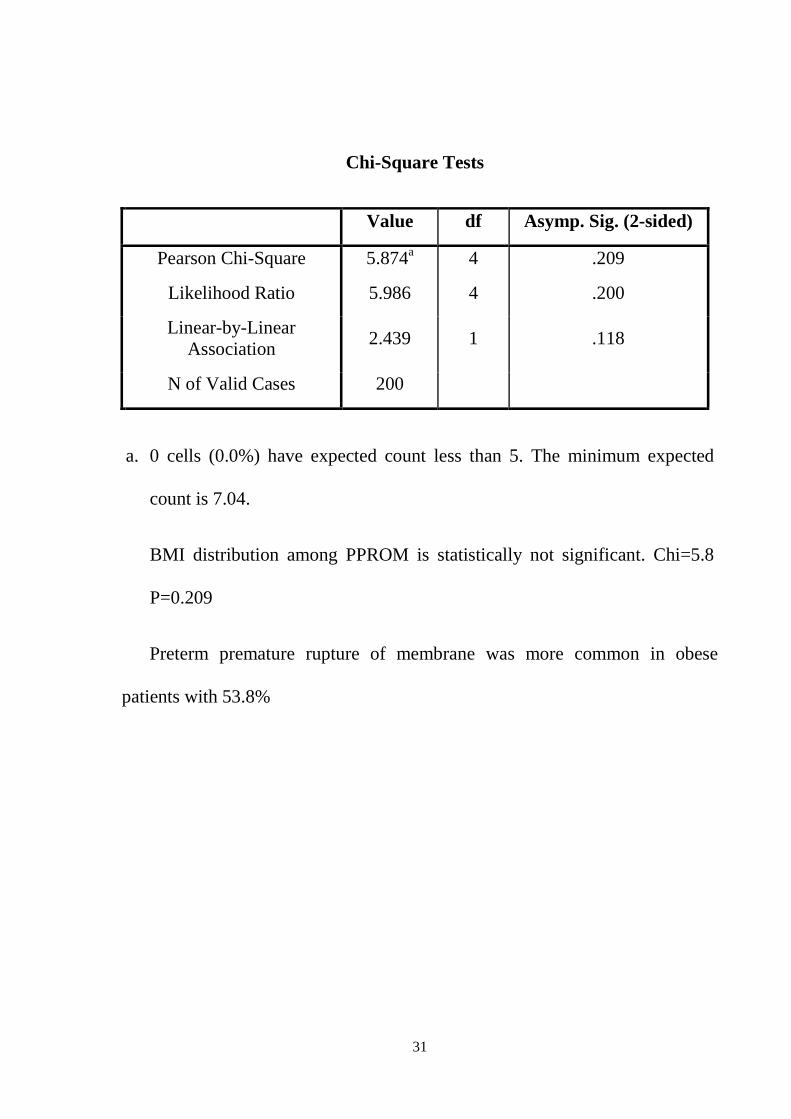
Chi-Square Tests
Value df Asymp. Sig. (2-sided)
Pearson Chi-Square 5.874a 4 .209
Likelihood Ratio 5.986 4 .200
Linear-by-Linear Association
2.439 1 .118
N of Valid Cases 200
a. 0 cells (0.0%) have expected count less than 5. The minimum expected
count is 7.04.
BMI distribution among PPROM is statistically not significant. Chi=5.8
P=0.209
Preterm premature rupture of membrane was more common in obese
patients with 53.8%

32

33
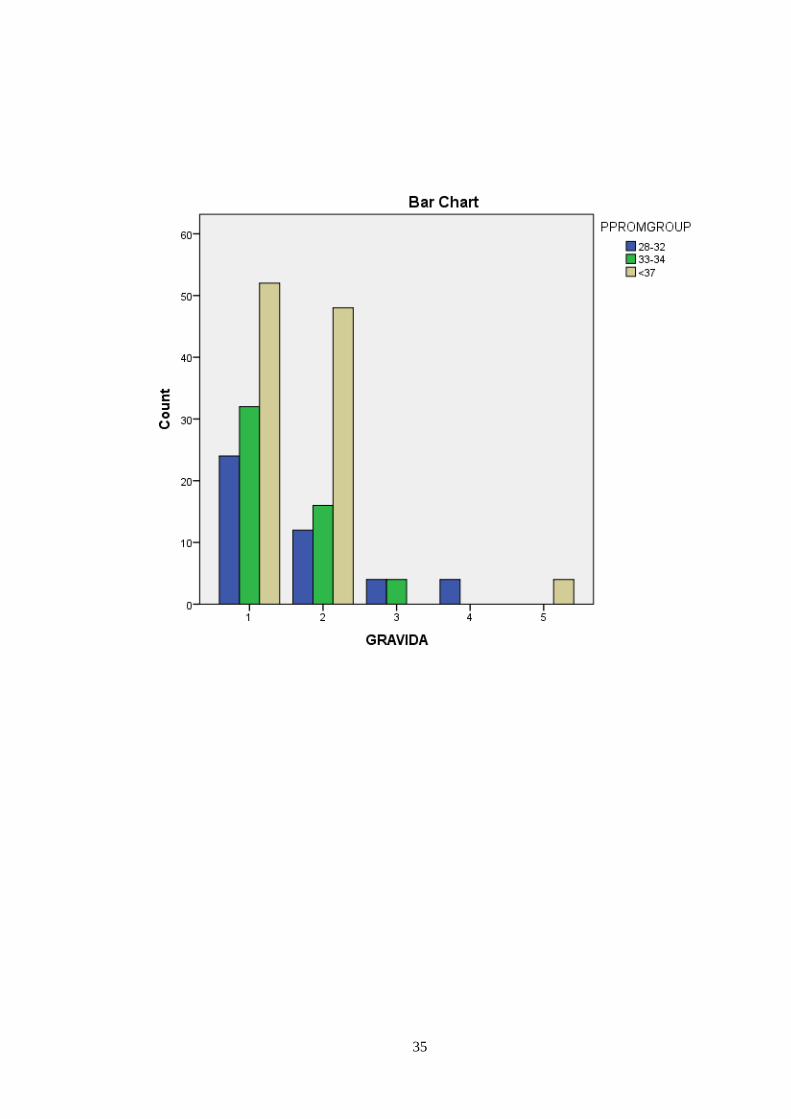
GRAVIDA vs PPROMGROUP
TABLE 4
PPROMGROUP (GA in weeks) Total
28-32 33-34 <37
GR
AV
IDA
1
Count 24 32 52 108 % within GRAVIDA 22.2% 29.6% 48.1% 100.0%
% within PPROMGROUP
54.5% 61.5% 50.0% 54.0%
% of Total 12.0% 16.0% 26.0% 54.0%
2
Count 12 16 48 76 % within GRAVIDA 15.8% 21.1% 63.2% 100.0%
% within PPROMGROUP
27.3% 30.8% 46.2% 38.0%
% of Total 6.0% 8.0% 24.0% 38.0%
3
Count 4 4 0 8 % within GRAVIDA 50.0% 50.0% 0.0% 100.0%
% within PPROMGROUP
9.1% 7.7% 0.0% 4.0%
% of Total 2.0% 2.0% 0.0% 4.0%
4
Count 4 0 0 4 % within GRAVIDA 100.0% 0.0% 0.0% 100.0%
% within PPROMGROUP
9.1% 0.0% 0.0% 2.0%
% of Total 2.0% 0.0% 0.0% 2.0%
5
Count 0 0 4 4 % within GRAVIDA 0.0% 0.0% 100.0% 100.0%
% within PPROMGROUP
0.0% 0.0% 3.8% 2.0%
% of Total 0.0% 0.0% 2.0% 2.0%
Total
Count 44 52 104 200 % within GRAVIDA 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
34
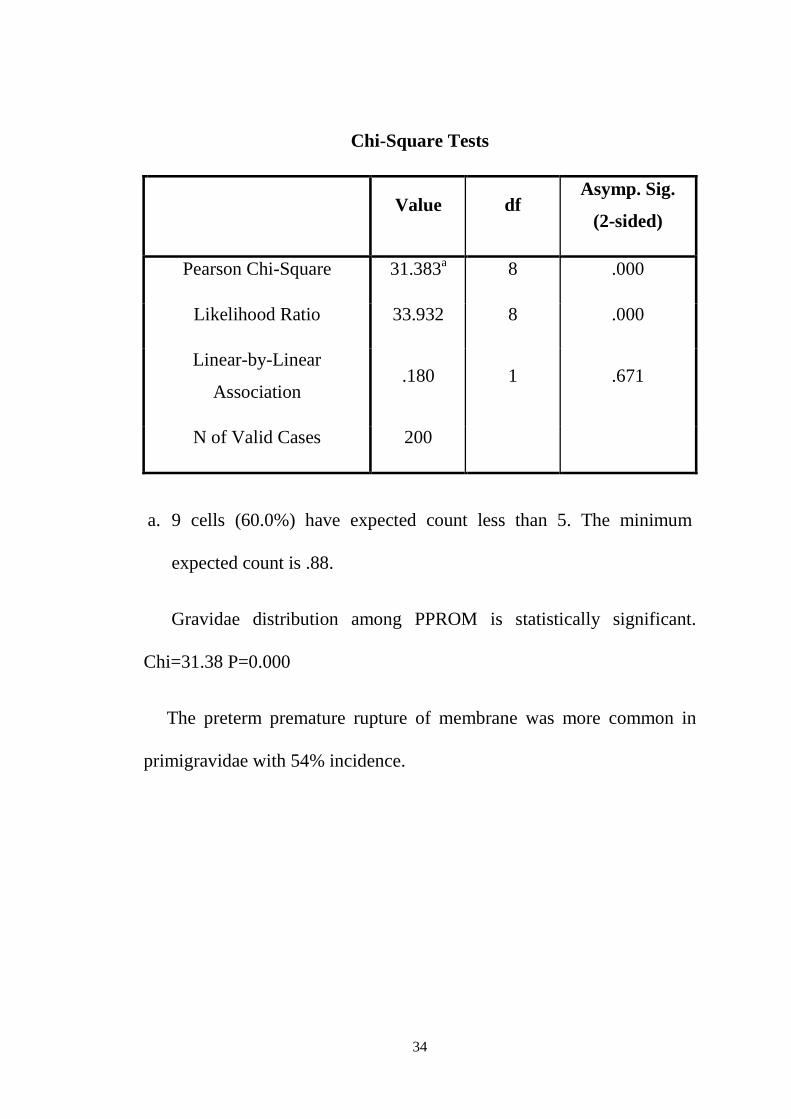
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 31.383a 8 .000
Likelihood Ratio 33.932 8 .000
Linear-by-Linear
Association .180 1 .671
N of Valid Cases 200
a. 9 cells (60.0%) have expected count less than 5. The minimum
expected count is .88.
Gravidae distribution among PPROM is statistically significant.
Chi=31.38 P=0.000
The preterm premature rupture of membrane was more common in
primigravidae with 54% incidence.
35

36
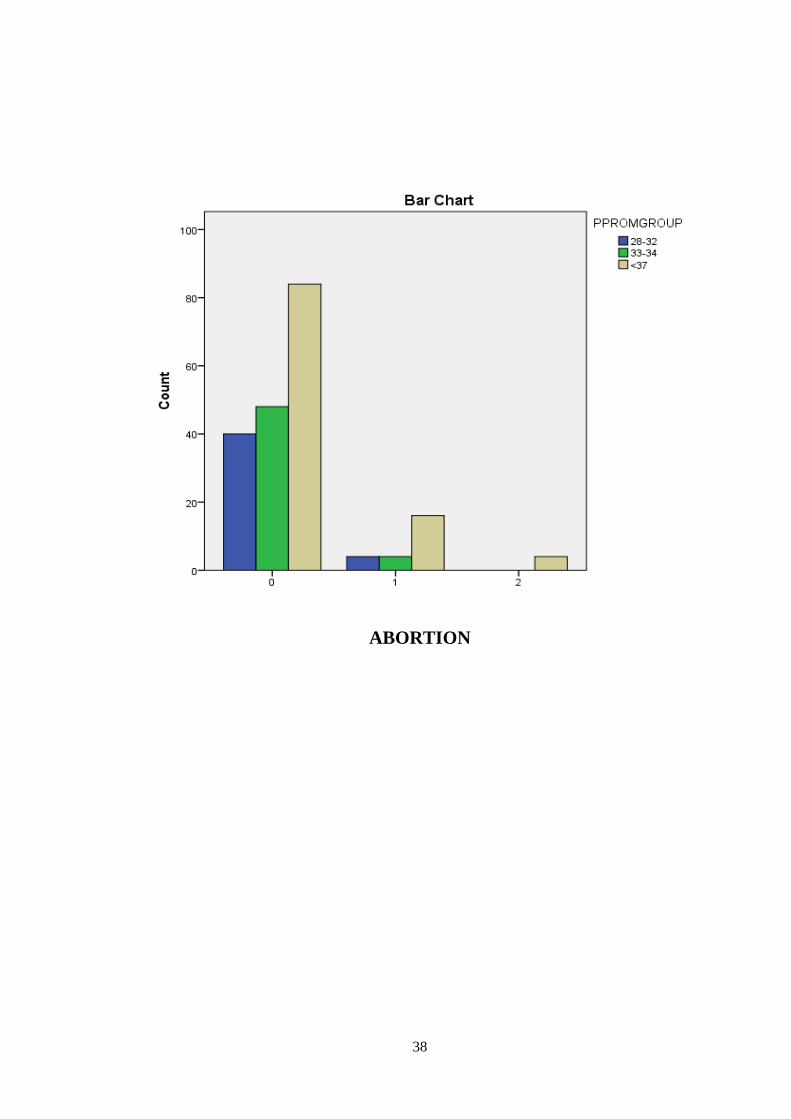
ABORTION VS PPROMGROUP
TABLE 5
PPROMGROUP
(GA in weeks) Total 28-32 33-34 <37
AB
OR
TIO
N
0
Count 40 48 84 172
% within ABORTIO 23.3% 27.9% 48.8% 100.0%
% within
PPROMGROUP 90.9% 92.3% 80.8% 86.0%
% of Total 20.0% 24.0% 42.0% 86.0%
1
Count 4 4 16 24
% within ABORTIO 16.7% 16.7% 66.7% 100.0%
% within
PPROMGROUP 9.1% 7.7% 15.4% 12.0%
% of Total 2.0% 2.0% 8.0% 12.0%
2
Count 0 0 4 4
% within ABORTIO 0.0% 0.0% 100.0% 100.0%
% within
PPROMGROUP 0.0% 0.0% 3.8% 2.0%
% of Total 0.0% 0.0% 2.0% 2.0%
Total
Count 44 52 104 200
% within ABORTIO 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

37
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 6.494a 4 .165
Likelihood Ratio 8.097 4 .088
Linear-by-Linear Association 4.747 1 .029
N of Valid Cases 200
a. 3 cells (33.3%) have expected count less than 5. The minimum
expected count is .88.
Previous abortion distribution among PPROM group is statistically
not significant. Chi=6.4 P=0.16
82% of patients with preterm premature rupture of membrane with
previous history of abortion.
38
ABORTION
39
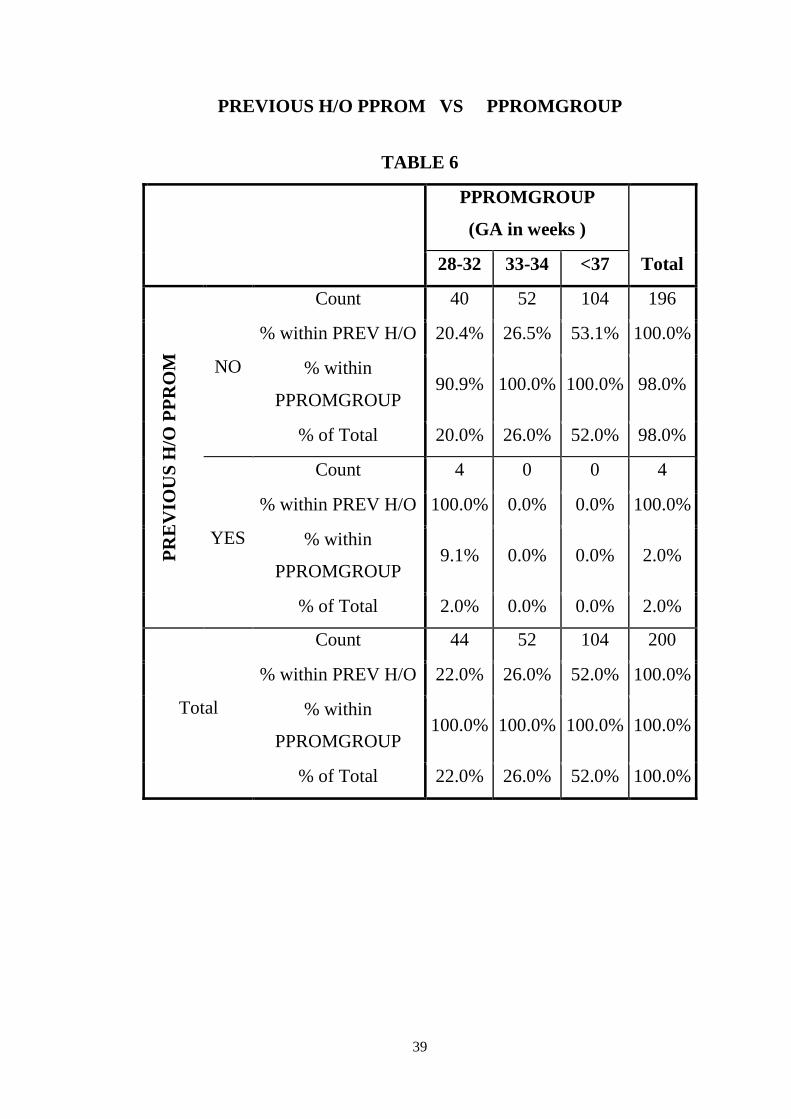
PREVIOUS H/O PPROM VS PPROMGROUP
TABLE 6
PPROMGROUP
(GA in weeks )
Total 28-32 33-34 <37
PR
EV
IOU
S H
/O P
PR
OM
NO
Count 40 52 104 196
% within PREV H/O 20.4% 26.5% 53.1% 100.0%
% within
PPROMGROUP 90.9% 100.0% 100.0% 98.0%
% of Total 20.0% 26.0% 52.0% 98.0%
YES
Count 4 0 0 4
% within PREV H/O 100.0% 0.0% 0.0% 100.0%
% within
PPROMGROUP 9.1% 0.0% 0.0% 2.0%
% of Total 2.0% 0.0% 0.0% 2.0%
Total
Count 44 52 104 200
% within PREV H/O 22.0% 26.0% 52.0% 100.0%
% within
PPROMGROUP 100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
40
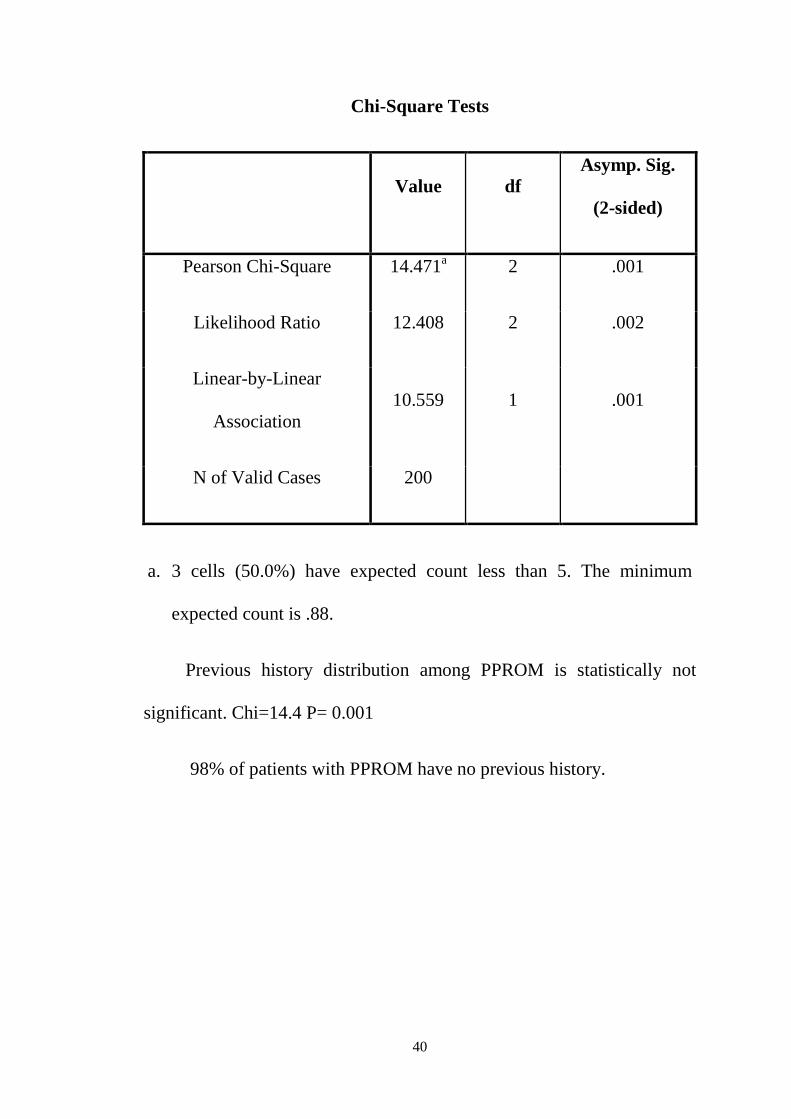
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 14.471a 2 .001
Likelihood Ratio 12.408 2 .002
Linear-by-Linear
Association 10.559 1 .001
N of Valid Cases 200
a. 3 cells (50.0%) have expected count less than 5. The minimum
expected count is .88.
Previous history distribution among PPROM is statistically not
significant. Chi=14.4 P= 0.001
98% of patients with PPROM have no previous history.

41
PREVIOUS H/O PPROM

42
MODE OF DELIVERY VS PPROMGROUP
TABLE 7
PPROMGROUP
(GA in weeks )
Total 28-32 33-34 <37
MO
DE
OF
DE
LIV
ER
Y
NORM
AL
Count 40 40 48 128
% within MOD 31.3% 31.3% 37.5% 100.0%
% within PPROM
GROUP 90.9% 76.9% 46.2% 64.0%
% of Total 20.0% 20.0% 24.0% 64.0%
LSCS
Count 4 12 56 72
% within MOD 5.6% 16.7% 77.8% 100.0%
% within PPROM
GROUP 9.1% 23.1% 53.8% 36.0%
% of Total 2.0% 6.0% 28.0% 36.0%
Total
Count 44 52 104 200
% within MOD 22.0% 26.0% 52.0% 100.0%
% within PPROM
GROUP
100.0
% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

43
Chi-Square Tests
Value df
Asymp. Sig.
(2-sided)
Pearson Chi-Square 31.974a 2 .000
Likelihood Ratio 34.819 2 .000
Linear-by-Linear
Association 30.700 1 .000
N of Valid Cases 200
a. 0 cells (0.0%) have expected count less than 5. The minimum
expected count is 15.84.
Mode of delivery among PPROM distribution is statistically
significant, Chi=31.9 P=0.00
64% of patients among present study PPROM delivered vaginally.

44
MODE OF DELIVERY

45
BOOKED CASE VS PPROMGROUP
TABLE 8
PPROMGROUP
(GA in weeks ) Total
28-32 33-34 <37
BO
OK
ED
CA
SE
Count 44 52 104 200
% within B /UB 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP 100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
Total
Count 44 52 104 200
% within B /UB 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP 100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

46
BOOKED CASES
a. No statistics are computed because B /UB is a constant.
Booked and Unbooked among PPROM distribution is statistically not
significant.
All patients with PPROM in present study is booked case.

47
ANEMIA VS PPROMGROUP
TABLE 9
PPROMGROUP
(GA in weeks )
Total 28-32 33-34 <37
AN
EM
IA
NO
Count 32 40 92 164
% within ANEMIA 19.5% 24.4% 56.1% 100.0%
% within
PPROMGROUP 72.7% 76.9% 88.5% 82.0%
% of Total 16.0% 20.0% 46.0% 82.0%
YES
Count 12 12 12 36
% within ANEMIA 33.3% 33.3% 33.3% 100.0%
% within
PPROMGROUP 27.3% 23.1% 11.5% 18.0%
% of Total 6.0% 6.0% 6.0% 18.0%
Total
Count 44 52 104 200
% within ANEMIA 22.0% 26.0% 52.0% 100.0%
% within
PPROMGROUP 100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

48
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 6.413a 2 .040
Likelihood Ratio 6.426 2 .040
Linear-by-Linear Association 6.048 1 .014
N of Valid Cases 200
a. 0 cells (0.0%) have expected count less than 5. The minimum
expected count is 7.92.
Anaemia distribution among PPROM group is statistically not
signicant. Chi=6.4 P=0.04
The above table illustrates that PPROM has no correlation with
preexisting anemia in mother (n=164 ) with a incidence of 64% without
anemia.

49

50
INFECTION vs PPROMGROUP
TABLE 10
PPROMGROUP
(GA in weeks ) Total
28-32 33-34 <37
INF
EC
TIO
N
NO
Count 36 52 100 188
% within INFECTION 19.1% 27.7% 53.2% 100.0%
% within
PPROMGROUP 81.8% 100.0% 96.2% 94.0%
% of Total 18.0% 26.0% 50.0% 94.0%
YES
Count 8 0 4 12
% within INFECTION 66.7% 0.0% 33.3% 100.0%
% within
PPROMGROUP 18.2% 0.0% 3.8% 6.0%
% of Total 4.0% 0.0% 2.0% 6.0%
Total
Count 44 52 104 200
% within INFECTIO 22.0% 26.0% 52.0% 100.0%
% within
PPROMGROUP 100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

51
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 15.752a 2 .000
Likelihood Ratio 15.154 2 .001
Linear-by-Linear Association 7.838 1 .005
N of Valid Cases 200
a. 2 cells (33.3%) have expected count less than 5. The minimum
expected count is 2.64.
Infection distribution among PPROM group is statistically not
significant.
The above table illustrates that PPROM has no correlation with
history of maternal infection ( n= 188) with a incidence of 84% without
maternal infection and 6% of patients with anemia have PPROM.

52
INFECTION

53
LIQUOR VS PPROMGROUP
TABLE 11
PPROMGROUP
(GA in weeks ) Total
28-32 33-34 <37
LIQ
UO
R (
AF
I)
>8
Count 40 28 68 136
% within LIQUOR 29.4% 20.6% 50.0% 100.0%
% within
PPROMGROUP 90.9% 53.8% 65.4% 68.0%
% of Total 20.0% 14.0% 34.0% 68.0%
5-8
Count 0 12 4 16
% within LIQUOR 0.0% 75.0% 25.0% 100.0%
% within
PPROMGROUP 0.0% 23.1% 3.8% 8.0%
% of Total 0.0% 6.0% 2.0% 8.0%
<5
Count 4 12 32 48
% within LIQUOR 8.3% 25.0% 66.7% 100.0%
% within
PPROMGROUP 9.1% 23.1% 30.8% 24.0%
% of Total 2.0% 6.0% 16.0% 24.0%
Total
Count 44 52 104 200
% within LIQUOR 22.0% 26.0% 52.0% 100.0%
% within
PPROMGROUP 100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%

54
Chi-Square Tests
Value df
Asymp. Sig.
(2-sided)
Pearson Chi-Square 31.650a 4 .000
Likelihood Ratio 31.586 4 .000
Linear-by-Linear
Association 7.344 1 .007
N of Valid Cases 200
a. 2 cells (22.2%) have expected count less than 5. The minimum
expected count is 3.52.
The amount of liquor distribution among PPROM group is
statistically not significant.
The above table illustrates that that PPROM patients have adequate
liquor (n=136) with a incidence of 68% and ( n=48) 48 patients have
severe oligohydrominos with a incidence of 24%.

55

56
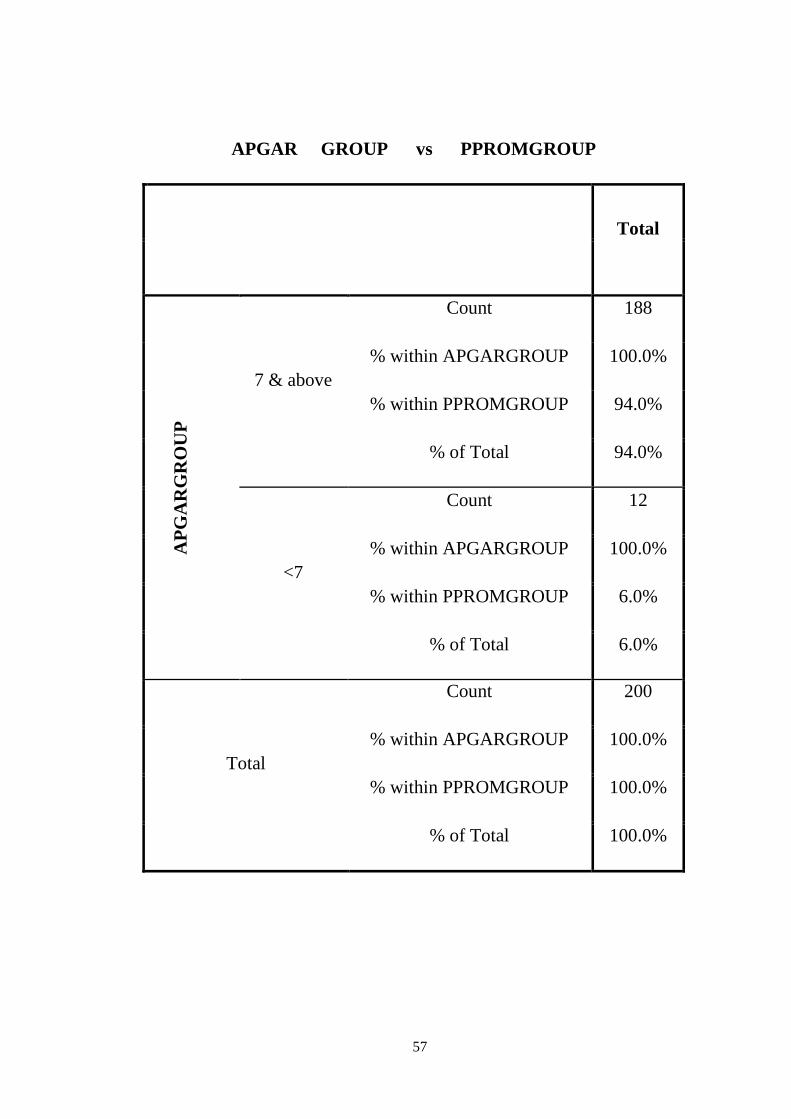
APGAR GROUP vs PPROMGROUP
TABLE 12
PPROMGROUP
(GA in weeks)
28-32 33-34 <37
AP
GA
RG
RO
UP
7 & above
Count 40 48 100
% within
APGARGROUP 21.3% 25.5% 53.2%
% within
PPROMGROUP 90.9% 92.3% 96.2%
% of Total 20.0% 24.0% 50.0%
<7
Count 4 4 4
% within
APGARGROUP 33.3% 33.3% 33.3%
% within
PPROMGROUP 9.1% 7.7% 3.8%
% of Total 2.0% 2.0% 2.0%
Total
Count 44 52 104
% within
APGARGROUP 22.0% 26.0% 52.0%
% within
PPROMGROUP 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0%
57
APGAR GROUP vs PPROMGROUP
Total
AP
GA
RG
RO
UP
7 & above
Count 188
% within APGARGROUP 100.0%
% within PPROMGROUP 94.0%
% of Total 94.0%
<7
Count 12
% within APGARGROUP 100.0%
% within PPROMGROUP 6.0%
% of Total 6.0%
Total
Count 200
% within APGARGROUP 100.0%
% within PPROMGROUP 100.0%
% of Total 100.0%
58
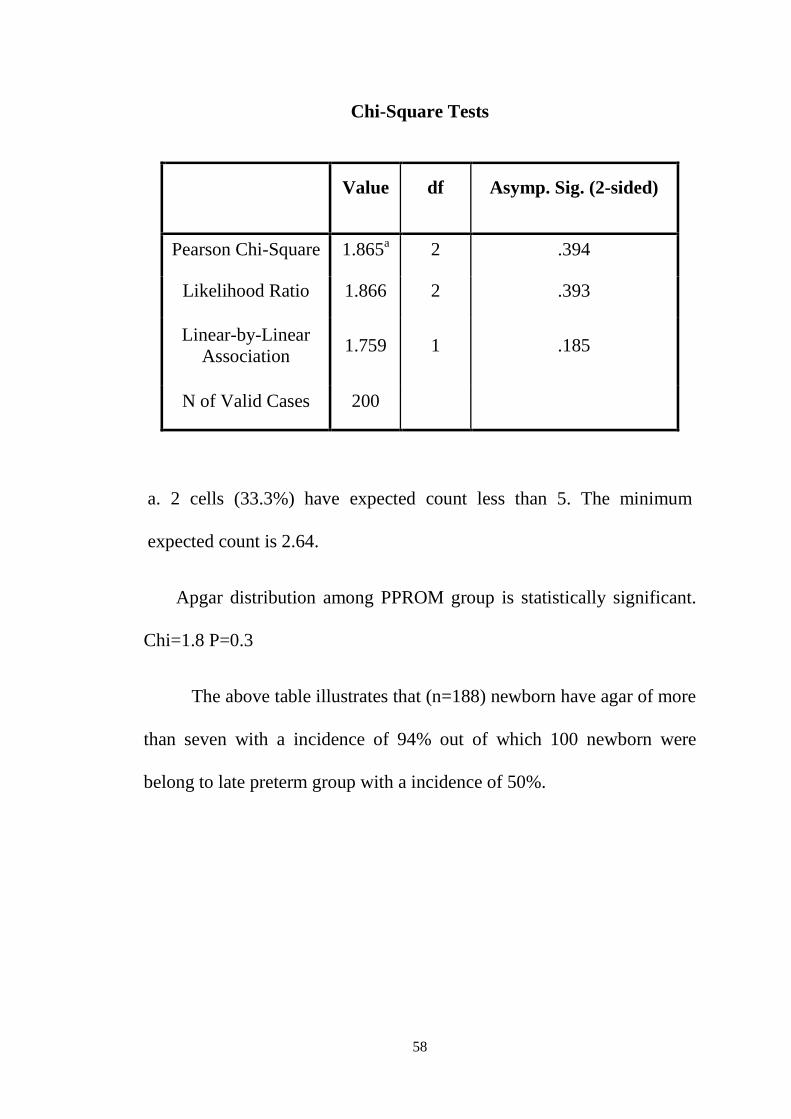
Chi-Square Tests
Value df Asymp. Sig. (2-sided)
Pearson Chi-Square 1.865a 2 .394
Likelihood Ratio 1.866 2 .393
Linear-by-Linear Association
1.759 1 .185
N of Valid Cases 200
a. 2 cells (33.3%) have expected count less than 5. The minimum
expected count is 2.64.
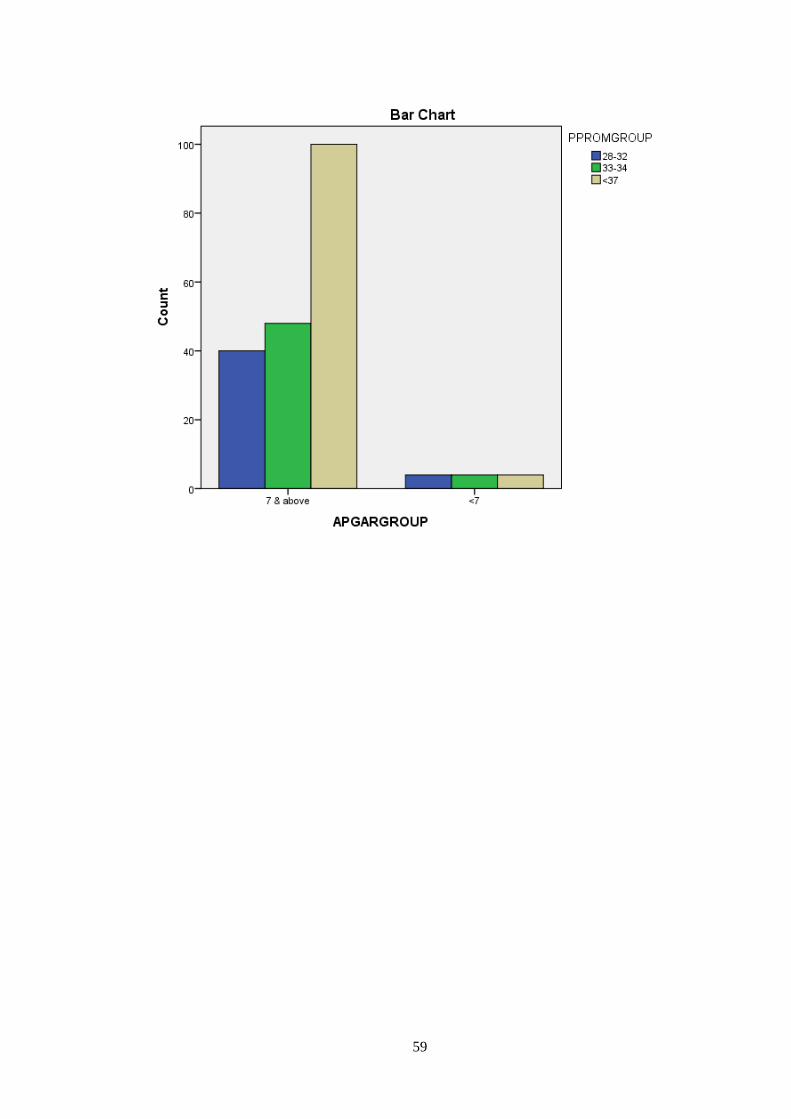
Apgar distribution among PPROM group is statistically significant.
Chi=1.8 P=0.3
The above table illustrates that (n=188) newborn have agar of more
than seven with a incidence of 94% out of which 100 newborn were
belong to late preterm group with a incidence of 50%.
59

60
NICU vs PPROMGROUP
TABLE 13
PPROMGROUP( GA in
weeks ) Total 28-32 33-34 <37
NIC
U
NO
Count 0 4 32 36
% within NICU 0.0% 11.1% 88.9% 100.0%
% within PPROMGROUP
0.0% 7.7% 30.8% 18.0%
% of Total 0.0% 2.0% 16.0% 18.0%
YES
Count 44 48 72 164
% within NICU 26.8% 29.3% 43.9% 100.0%
% within PPROMGROUP
100.0% 92.3% 69.2% 82.0%
% of Total 22.0% 24.0% 36.0% 82.0%
Total
Count 44 52 104 200
% within NICU 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 24.891a 2 .000
Likelihood Ratio 31.967 2 .000
Linear-by-Linear Association
23.306 1 .000
N of Valid Cases 200

61
a. 0 cells (0.0%) have expected count less than 5. The minimum
expected count is 7.92.
The NICU admission among PPROM group is statistically
significant. Chi =24.8 P =0.0
The above table illustrates that (n=164) 82% of newborn was
admitted in NICU out of which all early PPROM newborn got admitted
in NICU.

62
RESPIRATORY DISTRESS VS PPROMGROUP
TABLE 14
PPROMGROUP( GA in
weeks ) Total 28-32 33-34 <37
RE
SP
IRA
TO
RY
IST
RE
SS
NO
Count 0 8 34 42 % within RD 0.0% 19.0% 81.0% 100.0%
% within PPROMGROUP
0.0% 15.4% 32.7% 21.0%
% of Total 0.0% 4.0% 17.0% 21.0%
YES
Count 44 44 70 158 % within RD 27.8% 27.8% 44.3% 100.0%
% within PPROMGROUP
100.0% 84.6% 67.3% 79.0%
% of Total 22.0% 22.0% 35.0% 79.0%
Total
Count 44 52 104 200 % within RD 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 21.255a 2 .000
Likelihood Ratio 29.482 2 .000
Linear-by-Linear
Association 21.128 1 .000
N of Valid Cases 200

63
RESPIRATORY DISTRESS
a. 0 cells (0.0%) have expected count less than 5. The minimum
expected count is 9.24.
The above table illustrates that (n=158) 79% of newborn have got RD out
of which all early PPROM newborn have got RD.

64
PHOTOTHERAPY vs PPROMGROUP
TABLE 15
PPROMGROUP (GA in weeks ) Total
28-32 33-34 <37
PH
OT
OT
HE
RA
PY
NO
Count 8 36 76 120
% within PHOTO 6.7% 30.0% 63.3% 100.0%
% within PPROMGROUP
18.2% 69.2% 73.1% 60.0%
% of Total 4.0% 18.0% 38.0% 60.0%
YES
Count 36 16 28 80
% within PHOTO 45.0% 20.0% 35.0% 100.0%
% within PPROMGROUP
81.8% 30.8% 26.9% 40.0%
% of Total 18.0% 8.0% 14.0% 40.0%
Total
Count 44 52 104 200
% within PHOTO 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
Chi-Square Tests
Value df
Asymp. Sig.
(2-sided)
Pearson Chi-Square 41.317a 2 .000
Likelihood Ratio 42.129 2 .000
Linear-by-Linear
Association 32.656 1 .000
N of Valid Cases 200
65
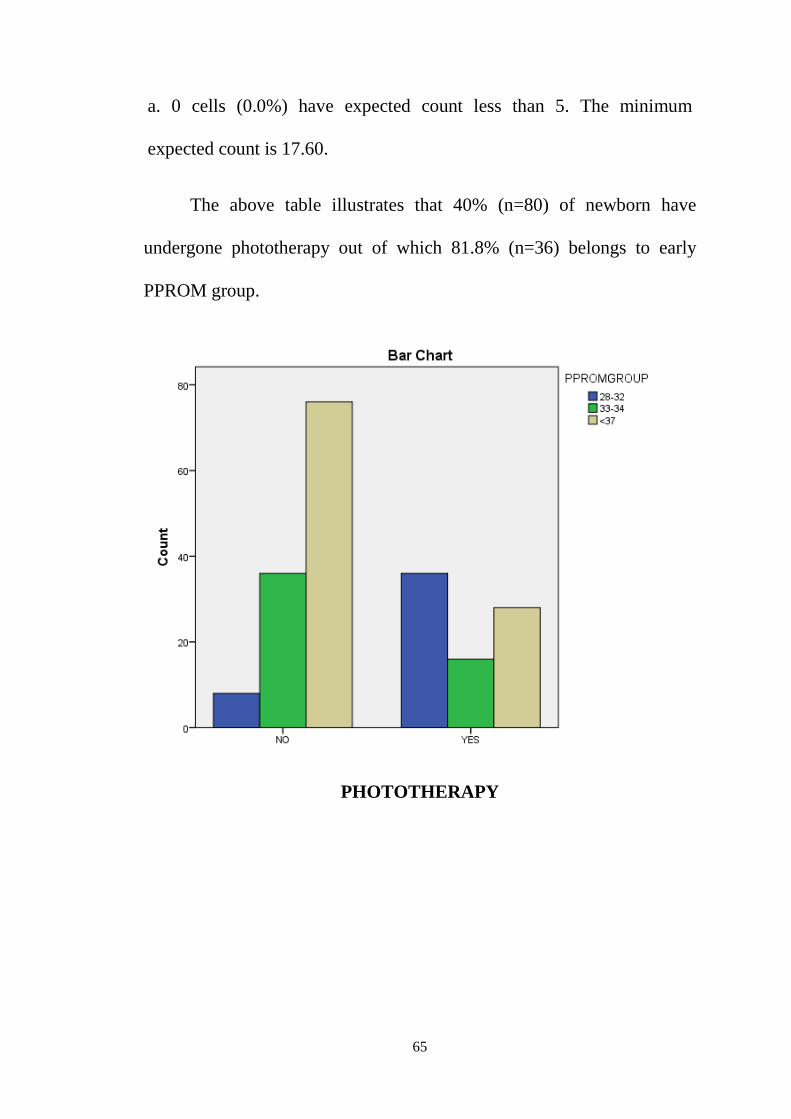
a. 0 cells (0.0%) have expected count less than 5. The minimum
expected count is 17.60.
The above table illustrates that 40% (n=80) of newborn have
undergone phototherapy out of which 81.8% (n=36) belongs to early
PPROM group.
PHOTOTHERAPY

66
FETAL INFECTION vs PPROMGROUP
TABLE 16
PPROM GROUP (GA in weeks ) Total
28-32 33-34 <37
FE
TA
L IN
FE
CT
ION
NO
Count 32 52 100 184
% within FET INFEC 17.4% 28.3% 54.3% 100.0%
% within PPROMGROUP
72.7% 100.0% 96.2% 92.0%
% of Total 16.0% 26.0% 50.0% 92.0%
YES
Count 12 0 4 16
% within FET INFEC 75.0% 0.0% 25.0% 100.0%
% within PPROMGROUP
27.3% 0.0% 3.8% 8.0%
% of Total 6.0% 0.0% 2.0% 8.0%
Total
Count 44 52 104 200
% within FET INFEC 22.0% 26.0% 52.0% 100.0%
% within PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Pearson Chi-Square 29.165a 2 .000
Likelihood Ratio 26.035 2 .000
Linear-by-Linear Association
17.038 1 .000
N of Valid Cases 200
67
FETAL INFECTION
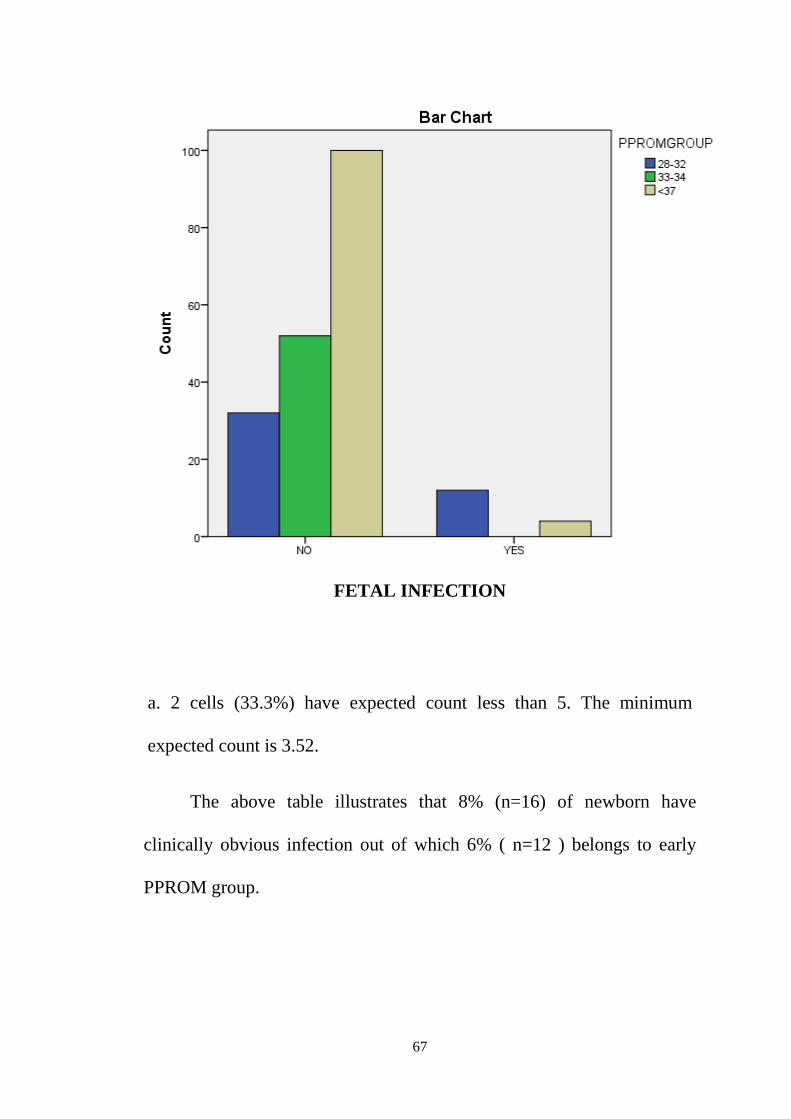
a. 2 cells (33.3%) have expected count less than 5. The minimum
expected count is 3.52.
The above table illustrates that 8% (n=16) of newborn have
clinically obvious infection out of which 6% ( n=12 ) belongs to early
PPROM group.

68
DEATH vs PPROMGROUP
TABLE 17
PPROMGROUP (GA in weeks ) Total
28-32 33-34 <37
DE
AT
H
NO
Count 32 48 100 180
% within DEATH 17.8% 26.7% 55.6% 100.0%
% within PPROMGROUP
72.7% 92.3% 96.2% 90.0%
% of Total 16.0% 24.0% 50.0% 90.0%
YES
Count 12 4 4 20
% within DEATH 60.0% 20.0% 20.0% 100.0%
% within PPROMGROUP
27.3% 7.7% 3.8% 10.0%
% of Total 6.0% 2.0% 2.0% 10.0%
Total
Count 44 52 104 200
% within DEATH 22.0% 26.0% 52.0% 100.0%
% wiSthin PPROMGROUP
100.0% 100.0% 100.0% 100.0%
% of Total 22.0% 26.0% 52.0% 100.0%
69
Chi-Square Tests
Value df Asymp. Sig. (2-
sided)
Pearson Chi-Square 19.270a 2 .000
Likelihood Ratio 16.357 2 .000
Linear-by-Linear
Association 16.668 1 .000
N of Valid Cases 200
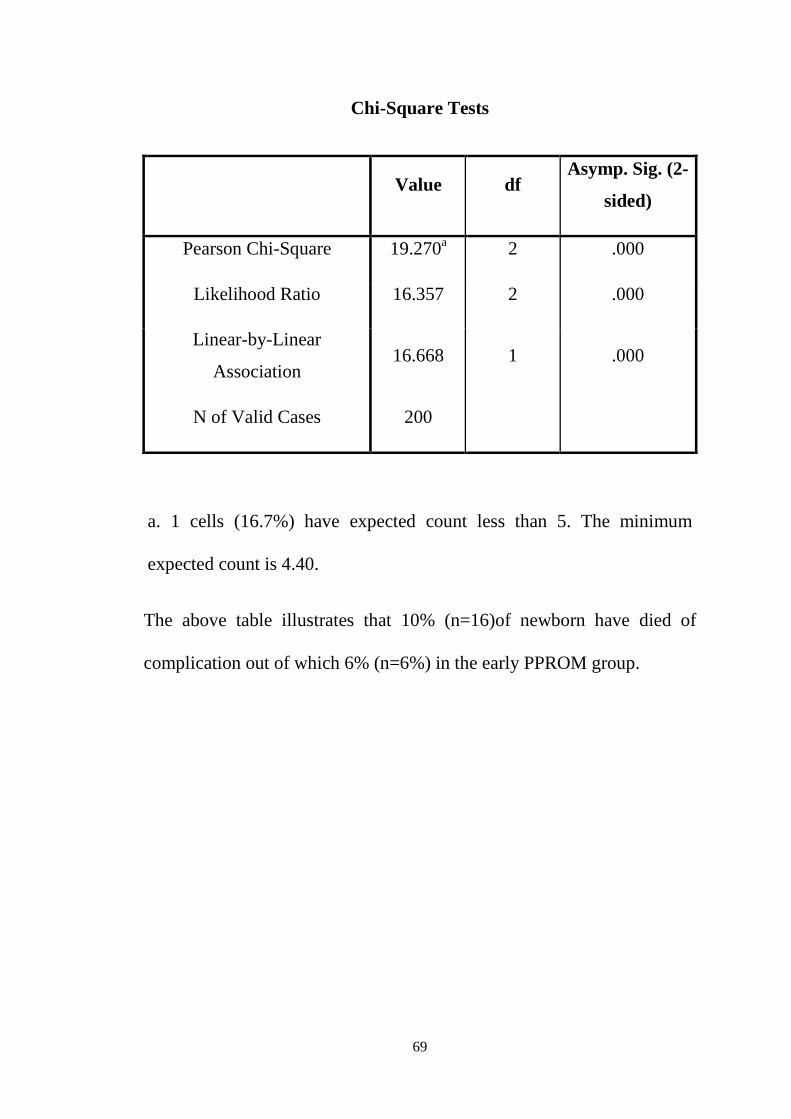
a. 1 cells (16.7%) have expected count less than 5. The minimum
expected count is 4.40.
The above table illustrates that 10% (n=16)of newborn have died of
complication out of which 6% (n=6%) in the early PPROM group.

70

71
GA
0 20 40 60 80 1000
20
40
60
80
100
100-Specificity
Sen
sitiv
ity
Sensitivity: 45.0 Specificity: 93.3 Criterion : ≤32
ROC curve
Variable GA
Classification variable PHOTO
Sample size 200
Positive group : PHOTO = 1 80
Negative group : PHOTO = 0 120
Disease prevalence (%) unknown
72
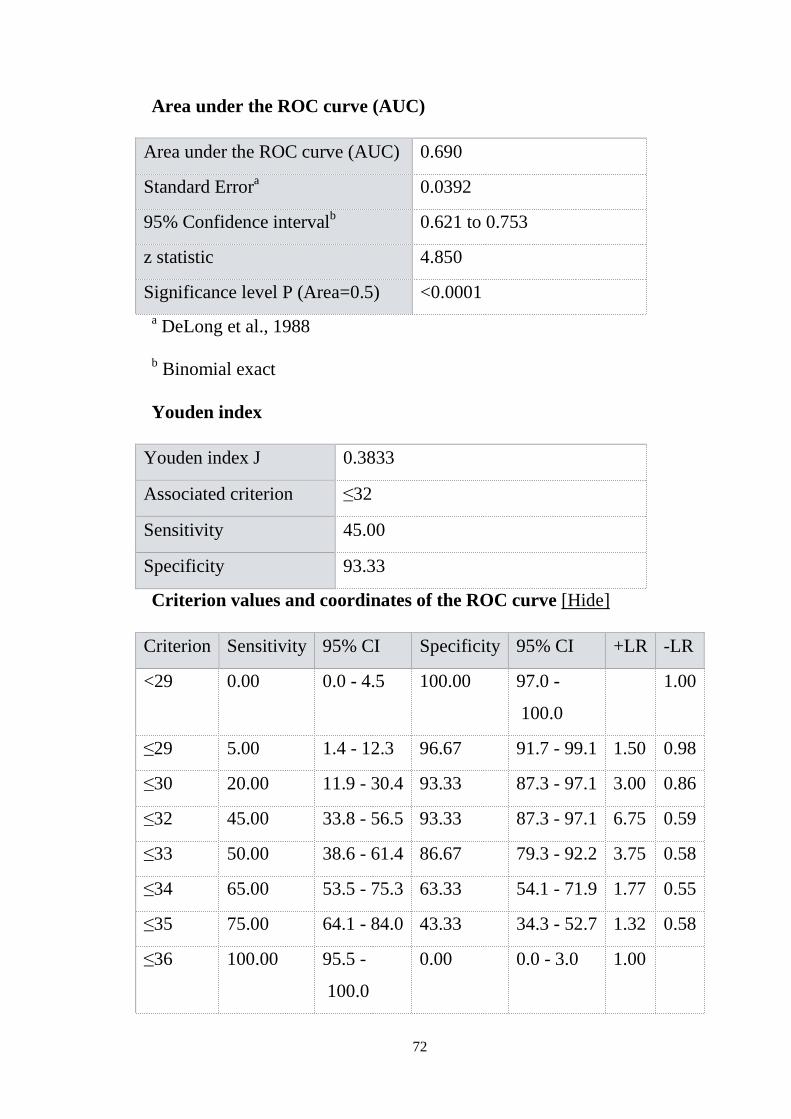
Area under the ROC curve (AUC)
Area under the ROC curve (AUC) 0.690
Standard Errora 0.0392
95% Confidence intervalb 0.621 to 0.753
z statistic 4.850
Significance level P (Area=0.5) <0.0001 a DeLong et al., 1988
b Binomial exact
Youden index
Youden index J 0.3833
Associated criterion ≤32
Sensitivity 45.00
Specificity 93.33
Criterion values and coordinates of the ROC curve [Hide]
Criterion Sensitivity 95% CI Specificity 95% CI +LR -LR
<29 0.00 0.0 - 4.5 100.00 97.0 -
100.0
1.00
≤29 5.00 1.4 - 12.3 96.67 91.7 - 99.1 1.50 0.98
≤30 20.00 11.9 - 30.4 93.33 87.3 - 97.1 3.00 0.86
≤32 45.00 33.8 - 56.5 93.33 87.3 - 97.1 6.75 0.59
≤33 50.00 38.6 - 61.4 86.67 79.3 - 92.2 3.75 0.58
≤34 65.00 53.5 - 75.3 63.33 54.1 - 71.9 1.77 0.55
≤35 75.00 64.1 - 84.0 43.33 34.3 - 52.7 1.32 0.58
≤36 100.00 95.5 -
100.0
0.00 0.0 - 3.0 1.00

73
The above ROC curve implies that less than 32 weeks of gestation
newborn had phototherapy has sensitivity of 45% and specificity of
93.3%.
GA
0 20 40 60 80 1000
20
40
60
80
100
100-Specificity
Sen
sitiv
ity
Sensitivity: 73.2 Specificity: 77.8 Criterion : ≤35
ROC curve
Variable GA
Classification variable NICU
Sample size 200
Positive group : NICU = 1 164
Negative group : NICU = 0 36
Disease prevalence (%) unknown

74
Area under the ROC curve (AUC)
Area under the ROC curve (AUC) 0.778
Standard Errora 0.0365
95% Confidence intervalb 0.714 to 0.833
z statistic 7.604
Significance level P (Area=0.5) <0.0001 a DeLong et al., 1988 b Binomial exact
Youden index
Youden index J 0.5095
Associated criterion ≤35
Sensitivity 73.17
Specificity 77.78
Criterion values and coordinates of the ROC curve [Hide]
Criterion Sensitivity 95% CI Specificity 95% CI +LR -LR
<29 0.00 0.0 - 2.2 100.00 90.3 -
100.0
1.00
≤32 26.83 20.2 - 34.3 100.00 90.3 -
100.0
0.73
≤33 31.71 24.7 - 39.4 88.89 73.9 - 96.9 2.85 0.77
≤34 56.10 48.1 - 63.8 88.89 73.9 - 96.9 5.05 0.49
≤35 73.17 65.7 - 79.8 77.78 60.8 - 89.9 3.29 0.34
≤36 100.00 97.8 -
100.0
0.00 0.0 - 9.7 1.00

75
The above ROC curve implies that less than 35 weeks of gestation
new born had NICU admission which had 73.2% sensitivity and 77.8%
specificity.
GA
0 20 40 60 80 1000
20
40
60
80
100
100-Specificity
Sen
sitiv
ity
Sensitivity: 72.8 Specificity: 69.0 Criterion : ≤35
ROC curve
Variable GA
Classification variable RD
Sample size 200
Positive group : RD = 1 158
Negative group : RD = 0 42
Disease prevalence (%) unknown

76
Area under the ROC curve (AUC)
Area under the ROC curve (AUC) 0.740
Standard Errora 0.0377
95% Confidence intervalb 0.674 to 0.800
z statistic 6.370
Significance level P (Area=0.5) <0.0001 a DeLong et al., 1988 b Binomial exact
Youden index
Youden index J 0.4183
Associated criterion ≤35
Sensitivity 72.78
Specificity 69.05
Criterion values and coordinates of the ROC curve [Hide]
Criterion Sensitivity 95% CI Specificity 95% CI +LR -LR
<29 0.00 0.0 - 2.3 100.00 91.6 -
100.0
1.00
≤32 27.85 21.0 - 35.5 100.00 91.6 -
100.0
0.72
≤33 32.28 25.1 - 40.2 88.10 74.4 - 96.0 2.71 0.77
≤34 55.70 47.6 - 63.6 80.95 65.9 - 91.4 2.92 0.55
≤35 72.78 65.1 - 79.6 69.05 52.9 - 82.4 2.35 0.39
≤36 100.00 97.7 -
100.0
0.00 0.0 - 8.4 1.00

77
The above ROC curve implies that less than 35 weeks of gestation
of newborn had RD and has sensitivity of 72.8% and specificity of 69%.
GA
0 20 40 60 80 1000
20
40
60
80
100
100-Specificity
Sen
sitiv
ity Sensitivity: 66.7 Specificity: 89.4 Criterion : ≤31
ROC curve
Variable GA
Classification variable INFECTIO
Sample size 200
Positive group : INFECTIO = 1 12
Negative group : INFECTIO = 0 188
Disease prevalence (%) unknown

78
Area under the ROC curve (AUC)
Area under the ROC curve (AUC) 0.759
Standard Errora 0.0673
95% Confidence intervalb 0.693 to 0.816
z statistic 3.844
Significance level P (Area=0.5) 0.0001 a DeLong et al., 1988 b Binomial exact
Youden index
Youden index J 0.5603
Associated criterion ≤31
Sensitivity 66.67
Specificity 89.36
Criterion values and coordinates of the ROC curve [Hide]
Criterion Sensitivity 95% CI Specificity 95% CI +LR -LR
<29 0.00 0.0 - 26.5 100.00 98.1 -
100.0
1.00
≤29 0.00 0.0 - 26.5 95.74 91.8 - 98.1 0.00 1.04
≤30 33.33 9.9 - 65.1 89.36 84.0 - 93.4 3.13 0.75
≤31 66.67 34.9 - 90.1 89.36 84.0 - 93.4 6.27 0.37
≤34 66.67 34.9 - 90.1 53.19 45.8 - 60.5 1.42 0.63
≤35 100.00 73.5 -
100.0
38.30 31.3 - 45.7 1.62 0.00
≤36 100.00 73.5 -
100.0
0.00 0.0 - 1.9 1.00

79
The above ROC curve implies that less than 35 weeks of gestation
of newborn had infection with 66.7% sensitivity and 89.4% specificity.
GA
0 20 40 60 80 1000
20
40
60
80
100
100-Specificity
Sen
sitiv
ity
Sensitivity: 60.0 Specificity: 93.3 Criterion : ≤30
ROC curve
Variable GA
Classification variable DEATH
Sample size 200
Positive group : DEATH = 1 20
Negative group : DEATH = 0 180
Disease prevalence (%) unknown

80
Area under the ROC curve (AUC)
Area under the ROC curve (AUC) 0.807
Standard Errora 0.0494
95% Confidence intervalb 0.745 to 0.859
z statistic 6.203
Significance level P (Area=0.5) <0.0001 a DeLong et al., 1988 b Binomial exact
Youden index
Youden index J 0.5333
Associated criterion ≤30
Sensitivity 60.00
Specificity 93.33
Criterion values and coordinates of the ROC curve [Hide]
Criterion Sensitivity 95% CI Specificity 95% CI +LR -LR
<29 0.00 0.0 - 16.8 100.00 98.0 - 100.0 1.00
≤29 20.00 5.7 - 43.7 97.78 94.4 - 99.4 9.00 0.82
≤30 60.00 36.1 - 80.9 93.33 88.6 - 96.5 9.00 0.43
≤33 60.00 36.1 - 80.9 75.56 68.6 - 81.6 2.45 0.53
≤34 80.00 56.3 - 94.3 55.56 48.0 - 62.9 1.80 0.36
≤35 100.00 83.2 - 100.0 40.00 32.8 - 47.6 1.67 0.00
≤36 100.00 83.2 - 100.0 0.00 0.0 - 2.0 1.00
The above ROC curve implies that less than 30 weeks of gestation
had died with 60% sensitivity and 93.3% specificity.

DISCUSSION

81
DISCUSSION
PPROM was more common in age group of less than 25 years with
a incidence of 54% out of which 36% late PPROM and 10% early
PPROM. Ina study by Noor et al in Ayub medical college in 2006
demonstrated that ( 58.8% ) higher incidence among younger age group.
PPROM was more common in low socio economic class with a
incidence of 82%. In a study done by Sheela et al demonstrated that
62.8% were belongs to low socio economic class.PPROM was more
common in primigravidae with a incidence of 54%. In a study conducted
by Ghandhi M et al majority were primigravidae 42.3% and another study
by Dkeke et al majority were primigravidae 29.1%.
PPROM was not associated with previous history of PPROM and
abortion with a incidence of 2% and 12% respectively. In a syudy by
Revathy et al 17% had previous abortion and 10% had previous history of
PPROM.
In our study 64% of patients had delivered vaginally and 36% had
delivered by LSCS. In a study by Sheela at al 65% had vaginal delivery
compared to 16% by LSCS.
Majority of neonatal morbidity noted in our study was Respiratory
distress contributing to 79% followed by hyperbilirubinaemia by 40%
and followed by sepsis by 8%. Respiratory distress was common in early
PPROM and hyper bilirubinaemia common in late preterm.

82
A study by Emeche et al showed 61% RDS Singel S et al obtained
92% in early PPROM. A study by Emeche et al showed 22% RDS,
17.8% hyper bilirubinaemia and 16% sepsis. Similar study by Signel S et
al in late PPROM showed 6.6% RDS and 16% sepsis. In present study
79% had RDS, 40% had hyper bilirubinaemia and 8% had sepsis.
CONCLUSION
83
CONCLUSION
PPROM was more common in younger age group, low socio
economic class and pimigravidae in present study.
PPROM was not associated with previous history ,booked or un
booked and previous abortion.
In present study most of newborn had better 5min apgar especially
late preterm group.
Majority of neonatal morbidity was due to RDS followed by hyper
bilirubinaemia then followed by sepsis.
In present study RDS was common in early preterm group and
hyper bilirubinaemia common in late preterm group.
In current study most of patients delivered vaginally compared to
36% of LSCS.
BIBL IOGRAPHY

84
BIBLIOGRAPHY
1. Bartfield MC , Carlan SJ, The home management ofpreterm
premature ruptured membranes. Clini Obstet Gynecol.
1998;41(3); 503-14.
2. Goldenberg RL, Rouse DJ, Prevention of premature birth. N
Eng J Med, 1998;339(5);313-20.
3. Jayaram VK, Sudha S. A study of PPROM management and
outcome . J Obstet Gynecol India. 2001;51;58-60.
4. Khuppel Ka, Curtis C, Robert LK Premature rupture of
membranes. Am J Obstet Gynecol.1979;134(6);655-61.
5. Noor S, Nazar AF, Bashir R, Sulthana R. Prevalenceof
PPROM AND ITS OUTCOME. J Ayub Med Coll
Abbottabad.2007;19(4);14-7.
6. Gandhi M, Shah F, Panchal C, Obstetric outcome in premature
rupture of membrane. Internet JGynecol Obstet. 2012;
16(2);1-5.
7. Okeke TC, Enwereji JO, Okoro OS, Airi CO, Ezugwu EC, Agu
PU. The incidence and management outcome of preterm
premature rupture of membrane in a tertiary hospitalin Nigeria.
Am J Clini Med RES, 2014;2910;14-7.

85
8. Revathi V, Sowjanya R, Lavanya S Maternal and perinatal
outcome in preterm premature rupture of membranre at term.
IOSR-JDMS.2015;14;12-5.
9. Singhal S Puri M, Gami N. An analysis of factors affecting the
duration of latency period and its impacton neonatal outcome
in patients with PPROM. Arch Gynecol Obstet,
2011;284(6);1339-43.
10. Allens. Epidemiology of preterm premature of membranes.
Clinic Obst Gynecol 1991; 19; 339-51.
11. French JI Mc Gregor JA.The patho-biology of preterm
premature rupture of membranes.Semin perinatal 1966;20;
344-68.
12. Wingfield M, Turner J,Stronge M. Significance of absent
amniotic fluid in labor follow rupture of membrane.J Obs
Gynecol 1993;13; 12-15.
13. Novak-antolic Z, Panzntar M, Verdenik I.Preterm premature
ruptre of membranes and postpartum infection.Eur J Obs Gyn
14. DepartmentofObetetrics and Gyneacology, Women’s Health
Research Centre, Imam Reza Hospital, Mashhad, University of
Medical Sciences, Mashhad, Iran.
86
15. Saira Dars, MS Obstetrics and Gynaecology, Department of
Obstetrics and Gynaecology, Liaquat UniversityHospital,
Hyderabad, Singh,Pakistan.
16. Maxwell GL. Preterm premature rupture of membranes. Obstet
Gynecol Surv 1993;48:576-83.
17. Merenstein GB, Weisman LE. Premature rupture of the
membranes: neonatal cnnsequences. Semin Perinatol
1996;20:375-80.
18. Douvas SG, Brewer JM, McKayML, Rhodes PG, Kahlstorf JH,
Morrison JC. Treatment of premature rupture of the
membranes. J Reprod Med 1984;29:741-4.
19. Cotton DB, Hill, Strassner HT, Platt LD, Ledger WJ. Use of
amniocentesis in preterm gestation wiyh ruptured membranes.
Obstet Gynecol 1984;63:38-43.
20. CarrollSG, Sebire NJ, Nicolaides KH. Preterm prelabour
amniorrhexis. New York/ London:Parthenon;1996.
21. Broekhuizen FF, Gliman M, Hamilton PR. Amniocentesisfor
gram stain and culture in preterm premature rupture of
membranes. Obstet Gynecol 1985;66:316-21.
22. Galask RP,Varner MW, Petzold CR, Wilbur SL. Bacterial
attachment to the chorionic membranes. Am J Obstet Gynecol
1984;148:915-28.

87
23. Gyr TN, Malek A, MathezLoic F, Altermatt HJ, Bodmer T,
Nicolaides K, et al. Permeation of human chorionic membranes
by Escherichia coli in vitro. Am j Obstet Gynecol
1994;170:223-7.
24. Royal college of Obstetricians and Gynaecologist. Clinical
Governance Advice 1c; Developing a clinical practice
guideline; producing a clinical practice guideline. London;
RCOG: 2006.
25. Baptisti A, Chemical test for the determination of ruptured
membranes. Am J Obstet Gynecol 1938;35:688-90.
26. Abe T, The detecyion of rupture of the fetal membranes with
nitrazine indicator. Am J Obstet Gynecol 1940;39;400-4.
27. Paavola A, Methods based on the study of crystals and fat
staining; use in diagnosing rupture of membranes. Ann Chir
Gynecol Fenn 1958;47:22-8.
28. Volet B, MorierGenoud J, The crystallization test in amniotic
fluid. Gynaecologia 1960;149;151-61.
29. Brosens I, Gordon H. The cytological diagnosis of ruptured
membranes using Nile Blue Sulfate staining. J Obstet Gynecol
Br Commonwealth 1965;72:342-6

INFORMED CONSENT
FORM

88
INFORMATION SHEET
• We are conducting a study on “PERINATAL OUTCOME IN
PRETERM PREMATURE RUPTURE OF MEMBRANES” in
KGH, Chennai. Your participation in the study is very valuable to us.
• The purpose of this study to evaluate the perinatal morbidity and
mortality and outcome of labour in preterm premature rupture of
membranes.
• We will follow those patients admitted to hospital labour ward with
history of draining P/V after 28 weeks and before 37 weeks of
gestation. We will monitor the outcome of labour and neonatal
outcome. Those babies followed upto period of hospitalization and
followed for morbidity and mortality.
• The privacy of the patients in the research will be maintained
throughout the study. In the event of any publication or presentation
resulting from the research, no personally identifiable information will
be shared.
• Taking part in the study is voluntary. You are free to decide whether
to participate in this study or to withdraw at any time, your decision
will not result in any loss of benefits to which you are itherwise
entitled.
• I have been given an information sheet giving details of the study.
• The results of the special study may be intimated to you at end of the
study period or during the study if anything is found abnormal which
may aid in the management or treatment.
Signature of the participant Signature of the investigator
Institution:
Date:

89
Muha;r;rp gw;wpa jfty; gbtk;
ehq;fs; Fiwgpurt mfhy rt;T KwpT gw;wp xU Ma;T
elj;jp tUfpNwhk;. ,e;j Ma;tpy; cq;fs; gq;Nfw;G ngUkjpg;G
tha;e;jJ.
,e;j Ma;tpy; Fiwgpurt mfhy rt;T Kwptpy; tUfpd;w
gpurt KiwAk; NkYk; mjdhy; cq;fs; Foe;ijf;F tUfpd;w
gpd; tpisTfSk; fz;fhzpf;fg;gLk;.
cq;fs; Foe;ij> Foe;ijfs; gphptpy; mDkjpf;fg;gl;lhy;
cq;fs; Foe;ijia tPl;bw;F mDg;Gk; tiu fz;fhzpf;fg;gLk;.
Nehahspfs; gw;wpa Fwpg;Gfs; Muha;r;rp KbAk; tiu
ufrpakhf ghJfhf;fg;gLk;. ,e;j Muha;r;rpia ntspapLk;NghJ
Nehahspfspd; jdpg;gl;l tptuq;fs; vJTk; ghjpf;fg;glkhl;lhJ.
,e;j Muha;r;rpapy; gq;FngWtJ Nehahspfspd; jdpg;gl;l
tpUg;gk;. NkYk; Nehahspfs; ,e;j Muha;r;rpapypUe;J vg;NghJ
Ntz;LkhdhYk; tpyfpf;nfhs;syhk;. Nehahspapd; ,e;j
Kbtpdhy; mtUf;Nfh my;yJ Muha;r;rpahsUf;Nfh ve;jtpj
ghjpg;Gk; fpilahJ.
,e;j Muha;r;rpapd; KbTfs; NehahspfSf;F Muha;r;rpapd;
,ilapNyh my;yJ KbtpNyh njhptpf;fg;gLk;. ,jpy; VNjDk;>
gpd; tpisTfs; Vw;gl;lhy; mij rhpnra;a rpfpr;iraspf;f jFe;j
cjtpfs; nra;ag;gLk;.
Ma;thshpd; ifnahg;gk; gq;Nfw;ghsh; ifnahg;gk;.
Njjp:
,lk;:

PROFORMA

90
PROFORMA
� NAME
� AGE
� IP NO
� PARITY
� SOCIO ECONOMIC STATUS
� PREVIOUS OBSTETRIC HISTORY
� PREVIOUS H/O ABORTION
� LMP/EDD
� WEIGHT GAIN DURING PREGNANCY (kg)
� BMI
� MANAGEMENT BASED ON GESTATIONAL AGE
� HIGH RISKS DURING PREGNANCY AND DELIVERY
� BABY DETAILS
• Mode of delivery
• Preterm neonatal complication
• Birth weight
• Apgar
• Mother side/ admitted
� POST PARTUM NEONATAL FOLLOW UP

MASTER CHART

S.no
NAME
AGE
SE CLASS
BMI
GRAVIDA
ABORTIO
GA
PREV H/O
MOD
B /UB
ANEMIA
INFECTIO
LIQUOR
5min APG
NICU
RD
PHOTO
FET INFEC
DEATH
1N
ith
ya
27
42
32
03
20
1B
00
07
11
10
0
2S
ug
an
ya
22
32
11
03
60
1B
00
08
00
00
0
3A
nit
ha
22
42
51
03
60
1B
00
08
00
00
0
4Is
hw
ary
a2
84
25
10
30
01
B0
00
81
11
00
5O
ma
tha
l2
33
27
10
32
01
B0
00
91
11
00
6K
art
hik
a1
95
28
10
35
01
B1
10
90
01
00
7T
am
ilse
lvi
27
43
35
23
50
1B
00
08
11
00
0
8Je
nn
ath
ma
ry
23
32
52
03
40
1B
00
08
11
10
0
9Je
ya
sri
23
32
62
03
60
1B
00
08
00
00
0
10
Na
nd
hin
i2
64
28
10
34
01
B0
00
81
00
00
11
Pra
bh
a3
24
29
10
33
01
B0
00
91
01
00
12
Lath
ara
ja2
64
30
10
36
01
B0
00
51
01
00
13
Re
va
thy
29
43
21
03
50
2B
10
09
10
00
0
14
De
vi
30
42
73
13
40
1B
00
19
10
00
0
15
Ila
kiy
a2
64
22
20
34
01
B0
01
91
00
00
16
Ve
nu
ma
dh
av
i2
74
25
20
34
01
B0
01
91
11
00
17
Sh
ali
ni
22
43
22
13
60
2B
00
28
11
10
0
18
De
vi
20
43
02
13
60
2B
10
21
01
10
00
19
Sri
na
nd
hin
i2
04
29
20
36
02
B0
02
91
10
00
20
Joth
i2
44
28
10
35
02
B0
02
91
10
00
21
Ma
lath
i2
34
36
10
36
02
B0
02
80
01
00
22
Ay
sha
20
43
32
03
60
2B
00
29
11
00
0
23
Inb
av
all
i3
04
25
41
32
01
B0
00
91
11
10
24
Am
ud
ha
20
42
61
03
40
2B
00
28
11
00
0
25
Lax
mi
21
42
81
03
50
1B
00
09
11
10
1
26
Me
racu
lin
23
42
32
03
60
1B
00
09
00
00
0

27
Sa
ran
ya
25
42
51
03
40
1B
00
09
11
00
0
28
Sa
ran
ya
26
43
71
03
30
1B
00
09
11
00
0
29
Pri
ya
24
52
83
03
21
1B
10
08
11
10
0
30
Lali
tha
27
42
62
03
50
1B
00
08
11
00
0
31
Ra
va
na
mm
al
18
43
22
13
60
1B
00
09
11
00
0
32
Ela
kiy
a3
24
30
20
31
01
B1
10
81
11
00
33
Ary
a1
84
22
10
29
01
B0
00
71
11
00
34
Go
ma
thy
24
32
21
03
60
1B
00
09
00
00
0
35
Re
shm
a2
54
28
10
33
01
B1
00
70
00
00
36
Pa
thch
iya
mm
al
37
42
72
03
50
2B
00
08
11
00
0
37
No
orj
ah
an
22
42
71
03
60
2B
00
08
11
10
0
38
Sh
ali
ni
25
42
51
03
60
2B
00
09
11
00
0
39
Su
mit
hra
28
42
82
03
60
2B
00
08
00
00
0
40
Ch
itra
31
42
72
03
60
2B
00
17
11
10
0
41
Pa
tta
mm
al
29
42
32
13
50
2B
00
27
11
00
0
42
Jen
ife
r2
13
29
10
36
02
B0
02
91
10
00
43
Jey
ara
ni
25
42
81
03
60
1B
00
08
11
01
0
44
Ma
ha
lax
mi
21
42
81
03
00
1B
00
08
11
11
0
45
Ga
jap
riy
a3
04
27
10
34
01
B0
00
91
11
00
46
Um
a2
64
24
10
34
02
B1
02
91
10
00
47
Re
va
thy
23
42
92
03
00
2B
00
08
11
00
1
48
An
ge
l3
04
26
10
29
01
B0
02
81
10
01
49
Pri
ya
29
33
01
03
00
1B
11
05
11
11
1
50
Lax
mi
32
43
02
03
40
2B
10
22
11
00
1
51
Ind
ira
ni
27
42
32
03
20
1B
00
07
11
10
0
52
Ma
ri2
23
21
10
36
01
B0
00
80
00
00
53
Ka
ma
tch
i2
44
25
10
36
01
B0
00
80
00
00
54
Re
nu
ka
28
42
51
03
00
1B
00
08
11
10
0
55
Aji
tha
23
32
71
03
20
1B
00
09
11
10
0
56
Sa
rojo
19
52
81
03
50
1B
11
09
00
10
0
57
Ka
dh
arb
ee
27
43
35
23
50
1B
00
08
11
00
0

58
Jey
ala
xm
i2
53
25
20
34
01
B0
00
81
11
00
59
Pa
lan
iya
mm
al
23
32
62
03
60
1B
00
08
00
00
0
60
Pa
ttu
26
42
81
03
40
1B
00
08
11
00
0
61
Kri
shn
av
en
i3
24
29
10
33
01
B0
00
91
11
00
62
Me
ga
bu
26
43
01
03
60
1B
00
05
11
10
0
63
Su
nd
ari
29
43
21
03
50
2B
10
09
11
00
0
64
Ra
dh
ab
ai
30
42
73
13
40
1B
00
19
11
00
0
65
Ma
ry2
64
22
20
34
01
B0
01
91
10
00
66
Ush
a2
74
25
20
34
01
B0
01
91
11
00
67
Mu
rug
am
ma
l2
24
32
21
36
02
B0
02
81
11
00
68
Gn
an
ap
ush
pa
m2
04
30
21
36
02
B1
02
10
11
00
0
69
Sa
ray
a2
04
29
20
36
02
B0
02
91
10
00
70
An
ura
dh
a2
44
28
10
35
02
B0
02
91
10
00
71
Pa
ttu
23
43
61
03
60
2B
00
28
00
10
0
72
Mu
niy
am
ma
l2
04
33
20
36
02
B0
02
91
10
00
73
Ma
rgre
t3
04
25
41
32
01
B0
00
91
11
10
74
Va
div
am
mig
ai
20
42
61
03
40
2B
00
28
11
00
0
75
Ch
inn
ap
on
nu
21
42
81
03
50
1B
00
09
11
10
1
76
Ra
jala
xm
i2
34
23
20
36
01
B0
00
90
00
00
77
Re
nu
ka
25
42
51
03
40
1B
00
09
11
00
0
78
Am
ud
ha
26
43
71
03
30
1B
00
09
11
00
0
79
Pit
cha
iya
mm
al
24
52
83
03
21
1B
10
08
11
10
0
80
Ga
ng
a2
74
26
20
35
01
B0
00
81
10
00
81
Se
lvi
18
43
22
13
60
1B
00
09
11
00
0
82
Pre
ma
32
43
02
03
10
1B
11
08
11
10
0
83
Ra
ni
18
42
21
02
90
1B
00
07
11
10
0
84
Ba
ckia
m2
43
22
10
36
01
B0
00
90
00
00
85
Ch
inn
ath
ai
25
42
81
03
30
1B
10
07
00
00
0
86
Pa
ram
esh
wa
ri3
74
27
20
35
02
B0
00
81
10
00
87
Ko
kil
a2
24
27
10
36
02
B0
00
81
11
00
88
Bh
av
an
i2
54
25
10
36
02
B0
00
91
10
00

89
Pa
vit
hra
28
42
82
03
60
2B
00
08
00
00
0
90
Pa
dm
ap
riy
a3
14
27
20
36
02
B0
01
71
11
00
91
Dh
ara
ni
29
42
32
13
50
2B
00
27
11
00
0
92
Ma
nu
sya
21
32
91
03
60
2B
00
29
11
00
0
93
Ka
laiv
an
i2
54
28
10
36
01
B0
00
81
10
10
94
He
ma
lath
a2
14
28
10
30
01
B0
00
81
11
10
95
Va
lli
30
42
71
03
40
1B
00
09
11
10
0
96
Sa
rith
a2
64
24
10
34
02
B1
02
91
10
00
97
Ka
na
ga
va
lli
23
42
92
03
00
2B
00
08
11
00
1
98
Ka
na
ga
lax
mi
30
42
61
02
90
1B
00
28
11
00
1
99
So
un
da
ri2
93
30
10
30
01
B1
10
51
11
11
10
0V
ara
lax
mi
32
43
02
03
40
2B
10
22
11
00
1
10
1G
racy
27
42
32
03
20
1B
00
07
11
10
0
10
2G
om
ath
i2
23
21
10
36
01
B0
00
80
00
00
10
3S
an
ka
ri2
44
25
10
36
01
B0
00
80
00
00
10
4T
am
ilse
lvi
28
42
51
03
00
1B
00
08
11
10
0
10
5M
an
jula
23
32
71
03
20
1B
00
09
11
10
0
10
6E
ruth
ay
am
ary
19
52
81
03
50
1B
11
09
00
10
0
10
7S
ha
rmil
a2
74
33
52
35
01
B0
00
81
10
00
10
8S
iva
ga
mi
25
32
52
03
40
1B
00
08
11
10
0
10
9Jo
thi
23
32
62
03
60
1B
00
08
00
00
0
11
0S
ara
ny
a2
64
28
10
34
01
B0
00
81
10
00
11
1M
ee
na
32
42
91
03
30
1B
00
09
11
10
0
11
2Je
ya
nth
i2
64
30
10
36
01
B0
00
51
11
00
11
3S
ou
nd
ari
29
43
21
03
50
2B
10
09
11
00
0
11
4D
ha
na
lax
mi
30
42
73
13
40
1B
00
19
11
00
0
11
5T
hu
lasi
26
42
22
03
40
1B
00
19
11
00
0
11
6La
xm
i2
74
25
20
34
01
B0
01
91
11
00
11
7M
ala
rko
di
22
43
22
13
60
2B
00
28
11
10
0
11
8M
ala
thy
20
43
02
13
60
2B
10
21
01
10
00
11
9S
ug
an
thi
20
42
92
03
60
2B
00
29
11
00
0
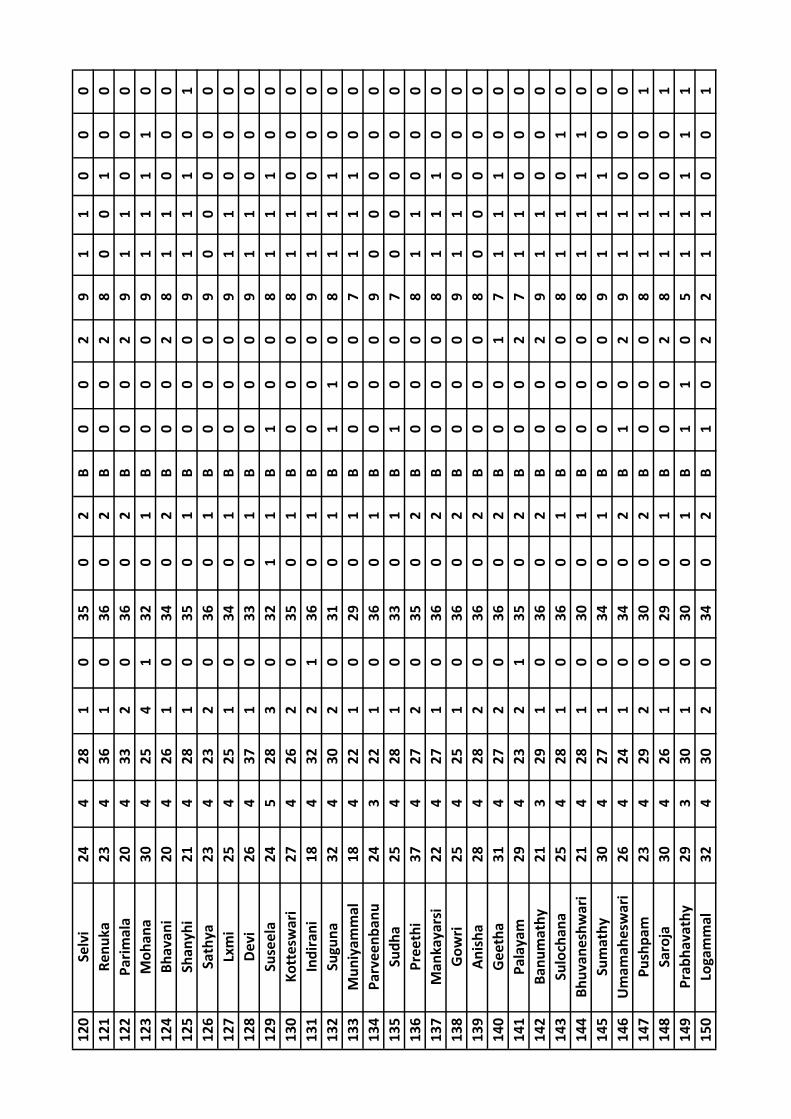
12
0S
elv
i2
44
28
10
35
02
B0
02
91
10
00
12
1R
en
uk
a2
34
36
10
36
02
B0
02
80
01
00
12
2P
ari
ma
la2
04
33
20
36
02
B0
02
91
10
00
12
3M
oh
an
a3
04
25
41
32
01
B0
00
91
11
10
12
4B
ha
va
ni
20
42
61
03
40
2B
00
28
11
00
0
12
5S
ha
ny
hi
21
42
81
03
50
1B
00
09
11
10
1
12
6S
ath
ya
23
42
32
03
60
1B
00
09
00
00
0
12
7Lx
mi
25
42
51
03
40
1B
00
09
11
00
0
12
8D
ev
i2
64
37
10
33
01
B0
00
91
10
00
12
9S
use
ela
24
52
83
03
21
1B
10
08
11
10
0
13
0K
ott
esw
ari
27
42
62
03
50
1B
00
08
11
00
0
13
1In
dir
an
i1
84
32
21
36
01
B0
00
91
10
00
13
2S
ug
un
a3
24
30
20
31
01
B1
10
81
11
00
13
3M
un
iya
mm
al
18
42
21
02
90
1B
00
07
11
10
0
13
4P
arv
ee
nb
an
u2
43
22
10
36
01
B0
00
90
00
00
13
5S
ud
ha
25
42
81
03
30
1B
10
07
00
00
0
13
6P
ree
thi
37
42
72
03
50
2B
00
08
11
00
0
13
7M
an
ka
ya
rsi
22
42
71
03
60
2B
00
08
11
10
0
13
8G
ow
ri2
54
25
10
36
02
B0
00
91
10
00
13
9A
nis
ha
28
42
82
03
60
2B
00
08
00
00
0
14
0G
ee
tha
31
42
72
03
60
2B
00
17
11
10
0
14
1P
ala
ya
m2
94
23
21
35
02
B0
02
71
10
00
14
2B
an
um
ath
y2
13
29
10
36
02
B0
02
91
10
00
14
3S
ulo
cha
na
25
42
81
03
60
1B
00
08
11
01
0
14
4B
hu
va
ne
shw
ari
21
42
81
03
00
1B
00
08
11
11
0
14
5S
um
ath
y3
04
27
10
34
01
B0
00
91
11
00
14
6U
ma
ma
he
swa
ri2
64
24
10
34
02
B1
02
91
10
00
14
7P
ush
pa
m2
34
29
20
30
02
B0
00
81
10
01
14
8S
aro
ja3
04
26
10
29
01
B0
02
81
10
01
14
9P
rab
ha
va
thy
29
33
01
03
00
1B
11
05
11
11
1
15
0Lo
ga
mm
al
32
43
02
03
40
2B
10
22
11
00
1

15
1V
asa
nth
a2
74
23
20
32
01
B0
00
71
11
00
15
2P
riy
a2
23
21
10
36
01
B0
00
80
00
00
15
3G
ow
ri2
44
25
10
36
01
B0
00
80
00
00
15
4S
ara
ny
a2
84
25
10
30
01
B0
00
81
11
00
15
5S
rala
23
32
71
03
20
1B
00
09
11
10
0
15
6S
he
eja
19
52
81
03
50
1B
11
09
00
10
0
15
7V
ija
ya
27
43
35
23
50
1B
00
08
11
00
0
15
8K
um
ari
25
32
52
03
40
1B
00
08
11
10
0
15
9C
hin
na
po
nn
u2
33
26
20
36
01
B0
00
80
00
00
16
0A
lam
elu
26
42
81
03
40
1B
00
08
11
00
0
16
1U
sain
ab
an
u3
24
29
10
33
01
B0
00
91
11
00
16
2V
ara
lax
mi
26
43
01
03
60
1B
00
05
11
10
0
16
3S
um
ath
y2
94
32
10
35
02
B1
00
91
10
00
16
4P
ush
ph
ala
tha
30
42
73
13
40
1B
00
19
11
00
0
16
5La
tha
raja
26
42
22
03
40
1B
00
19
11
00
0
16
6K
am
atc
hi
27
42
52
03
40
1B
00
19
11
10
0
16
7M
all
iga
22
43
22
13
60
2B
00
28
11
10
0
16
8M
ah
ala
xm
i2
04
30
21
36
02
B1
02
10
11
00
0
16
9R
aji
na
ma
la2
04
29
20
36
02
B0
02
91
10
00
17
0M
ala
rko
di
24
42
81
03
50
2B
00
29
11
00
0
17
1M
all
iga
23
43
61
03
60
2B
00
28
00
10
0
17
2V
asa
nth
i2
04
33
20
36
02
B0
02
91
10
00
17
3A
nja
lam
30
42
54
13
20
1B
00
09
11
11
0
17
4S
um
ith
ra2
04
26
10
34
02
B0
02
81
10
00
17
5S
ha
nth
i2
14
28
10
35
01
B0
00
91
11
01
17
6S
un
da
ri2
34
23
20
36
01
B0
00
90
00
00
17
7K
av
ith
a2
54
25
10
34
01
B0
00
91
10
00
17
8M
ala
26
43
71
03
30
1B
00
09
11
00
0
17
9B
rin
dh
a2
45
28
30
32
11
B1
00
81
11
00
18
0M
all
iga
27
42
62
03
50
1B
00
08
11
00
0
18
1S
ara
la1
84
32
21
36
01
B0
00
91
10
00

18
2S
ha
lin
i3
24
30
20
31
01
B1
10
81
11
00
18
3B
ha
va
ni
18
42
21
02
90
1B
00
07
11
10
0
18
4A
lam
elu
24
32
21
03
60
1B
00
09
00
00
0
18
5P
usp
ha
25
42
81
03
30
1B
10
07
00
00
0
18
6V
ara
lax
mi
37
42
72
03
50
2B
00
08
11
00
0
18
7A
na
nd
hi
22
42
71
03
60
2B
00
08
11
10
0
18
8S
ub
bu
lax
mi
25
42
51
03
60
2B
00
09
11
00
0
18
9C
hit
ra2
84
28
20
36
02
B0
00
80
00
00
19
0D
ee
pa
31
42
72
03
60
2B
00
17
11
10
0
19
1P
an
jav
arn
am
29
42
32
13
50
2B
00
27
11
00
0
19
2S
iva
ran
jin
i2
13
29
10
36
02
B0
02
91
10
00
19
3N
ad
hiy
a2
54
28
10
36
01
B0
00
81
10
10
19
4K
an
ag
a2
14
28
10
30
01
B0
00
81
11
10
19
5M
an
ime
ga
lai
30
42
71
03
40
1B
00
09
11
10
0
19
6N
ag
am
ax
mi
26
42
41
03
40
2B
10
29
11
00
0
19
7S
ow
miy
a2
34
29
20
30
02
B0
00
81
10
01
19
8R
an
i3
04
26
10
29
01
B0
02
81
10
01
19
9P
ad
ma
pri
ya
29
33
01
03
00
1B
11
05
11
11
1
20
0B
ab
y3
24
30
20
34
02
B1
02
21
10
01




![Preterm labor. Preterm termination of pregnancy Abortion: …22 week of gestation Abortion: …22 week of gestation Premature labor [PTL]: Premature labor](https://img.dokumen.tips/doc/110x75/56649edb5503460f94bebbb7/preterm-labor-preterm-termination-of-pregnancy-abortion-22-week-of-gestation.jpg)