-
7/28/2019 A Middle Aged Woman With Nausea Weight Loss and
Orthostatic Hypotension
1/7
A middle-aged woman with nausea, weightloss, and orthostatic
hypotension
W. Singer, MD
I.O. Yung, MD
R. Wollmann, MD,
PhD
T. Kelly, MD
B.M. Keegan, MD,
FRCP(C)
CASE PRESENTATION A 54-year-old, right-
handed, Caucasian woman presented with intermit-
tent nausea, vomiting, and orthostatic hypotension
of 1 year duration. Following every meal, she would
belch and vomit nonbloody undigested food. She re-
ported constipation and fatigue and felt lightheaded
and occasionally lost consciousness on standing. She
denied visual changes, dysphagia, dysarthria, weak-
ness, involuntary movement, or loss of urinary or fe-
cal continence. She denied fever, chill, dysuria,
diarrhea, or coughing. At one point, she was hospi-
talized for rehydration every 2 weeks. She had lostnearly 80
pounds over the prior year.
She had a history of osteoarthritis with bilateral
knee replacements. Her current medications were
lansoprazole, midodrine hydrochloride, fludrocorti-
sone acetate, and metoclopramide without signifi-
cant relief. Her family history was remarkable for
cancer and a brother had Down syndrome. She pre-
viously worked as a draftsman. She did not use to-
bacco or recreational drugs and rarely drank alcohol.
NEUROLOGIC EXAMINATION General examina-
tion was significant for orthostasis. Supine blood pres-sure was
143/89 mm Hg with heart rate of 88 beats per
minute. Upon standing, her blood pressure dropped to
63/44 mm Hg with heart rate increasing to 102 beats
per minute. Mental status, language, and cranial nerve
examination were normal. Sensation to vibration and
pinprick was decreased distally in the lower extremities
bilaterally. Light touch and temperature sensation were
normal. Romberg sign was negative. Muscle strength
and tone was normal in all extremities. Deep tendon
reflexes were intact in biceps, triceps, brachioradialis,
and patellar but absent at the Achilles. Plantar responses
were flexor. Limb coordination was normal. She could
stand without assistance for only under 1 minute before
becoming lightheaded, requiring sitting.
INVESTIGATIONS Extensive gastrointestinal
workup at different hospitals including mesenteric
lymph node biopsy led to the diagnosis of sclerosing
mesenteritis. Treatment with prednisone provided
only transient relief. Her endocrine evaluation did not
reveal a cause for the orthostasis. Transthoracic echocar-
diogram showed mild left ventricular hypertrophy with
diastolic dysfunction. EKG recorded a prolonged cor-
rected QT interval of 0.495 seconds (reference range:
0.44 seconds or less). CT chest, abdomen, and pelvis
with contrast showed increased density in the left lower
quadrant mesentery compatible with sclerosing mesen-
teritis with soft tissue thickening encasing the celiac axis
raising the question of lymphoma, pancreatic cancer, or
vasculitis. FDG-PET demonstrated mildly increasedFDG activity in
the left lower quadrant mesentery likely
related to sclerosing mesenteritis.
She was anemic with a hemoglobin of 10.3 g/dL
(reference range 11.515.5 g/dL) and MCV 90.3 fL.
Comprehensive metabolic panel was normal. Hemo-
globin A1c was normal. Serum vitamin B12 was 276
pg/mL (reference range 240900 pg/mL), total ho-
mocysteine was elevated at 22.8 mol/L (reference
range 4.513 mol/L), but methylmalonic acid level
and parietal cell antibody titer were normal and in-
trinsic factor blocking antibody was positive. Para-neoplastic
autoantibody panel was negative. Serum
protein electrophoresis (SPEP) with immunofixation
showed a monoclonal immunoglobulin A spike.
Angiotensin converting enzyme (ACE) and thyroid
stimulating hormone (TSH) were normal. Syphilis
screen was nonreactive. SSA and SSB antibodies were
negative. HIV-RNA level was undetectable.
Brain MRI with and without contrast displayed
normal sella and parasellar regions, craniocervical
junction, seventh and eighth nerve complexes. CSF
was clear with normal cell count (3 white blood cells;0 red
blood cells), normal glucose (49 mg/dL; 0.64
CSF-to-serum glucose ratio), and elevated protein at
52 mg/dL (reference range 1545 mg/dL), without
unique CSF oligoclonal bands, or malignant cells.
CSF herpes simplex virus, acid fast bacilli, and fungal
cultures were negative.
CME
Scan this code with yoursmartphone to access thisfeature
Address correspondence and
reprint requests to Dr. B. Mark
Keegan, Department of
Neurology, Mayo Clinic Collegeof Medicine, 200 First St. SW,
Rochester, MN 55905
[email protected]
From the Department of Neurology (W.S., B.M.K.), Mayo Clinic,
Rochester, MN; and Departments of Neurology (I.O.Y., T.K.) and
Pathology
(R.W.), University of Chicago, Chicago, IL.
Disclosure: Author disclosures are provided at the end of the
article.
NEUROLOGY
CLINICAL
PATHOLOGICAL
CONFERENCE
Section Editors
Joseph E. Parisi, MD
B. Mark Keegan, MD
Copyright 2011 by AAN Enterprises, Inc. 489
-
7/28/2019 A Middle Aged Woman With Nausea Weight Loss and
Orthostatic Hypotension
2/7
Nerve conduction study and EMG (NCS/EMG)
evaluations were as follows: sural sensory responses
were unobtainable bilaterally, the right radial sensory
response was normal. Left peroneal motor amplitude
was reduced with mild slowing of conduction veloc-
ity. The right tibial motor amplitude was mildly re-
duced; the distal latency and conduction velocity
were normal. The left peroneal F wave was unobtain-
able. The right tibial F wave latency was minimallyprolonged.
The right ulnar motor response and F
wave latency were normal. Needle examination of
the right lower extremity musculature showed mild
spontaneous activity in the medial gastrocnemius.
These findings were consistent with a length-
dependent, axonal, sensorimotor polyneuropathy.
A single 5-day trial of IV immunoglobulin (IVIg)
did not result in substantial improvement.
E XP ER T D IS CU SS IO N: D R. W OL FG AN G
SINGER A middle-aged woman presented with a1-year history of
upper and lower gastrointestinal
symptoms, orthostatic hypotension (OH), fatigue,
and considerable weight loss. Physical examination
confirmed the presence of OH, detected hypesthesia
in a stocking distribution affecting small and large
fiber modalities, and absent Achilles tendon reflexes.
Comprehensive workup is remarkable for several
findings: 1) EMG evidence of a length-dependent
axonal-predominant sensorimotor peripheral neu-
ropathy, 2) mild left ventricular hypertrophy with
diastolic dysfunction and QT prolongation, 3) in-creased CT
density and FDG-PET activity in the left
lower quadrant mesentery, compatible with a diag-
nosis of sclerosing mesenteritis as also suggested by
mesenteric lymph node biopsy, but also soft tissue
thickening encasing the celiac axis, 4) monoclonal
gammopathy (IgA ), and 5) normocytic anemia
with positive intrinsic factor blocking antibody but
without evidence of overt vitamin B12 deficiency.
Notably negative were CSF studies apart from a
mildly elevated protein, MRI of the brain, paraneo-
plastic panel, and ACE. A transient positive response
to prednisone and no response to 5 days of IVIg areof
interest.
A major aspect of this patients presentation is
that of severe OH. Neurogenic and non-neurogenic
etiologies of OH exist, but a severe orthostatic blood
pressure drop as documented along with only mild,
inadequate cardioacceleration and negative endocri-
nologic workup would argue for a neurogenic cause.
Formal autonomic testing would have been helpful
to further document this with abnormal blood pres-
sure responses to autonomic reflex maneuvers, such
as the Valsalva maneuver. Formal autonomic testing
would have also been helpful to document severity
and distribution of autonomic failure which can re-
veal important diagnostic clues. Neurogenic OH has
a broad differential diagnosis that includes peripheral
and central etiologies, including autonomic neuropa-
thies, pure autonomic failure, myelopathy, multiple
system atrophy, Parkinson disease, and several other
parkinsonian syndromes. Clinical presentation and ex-
amination findings argue against multiple system atro-
phy, a parkinsonian syndrome, or myelopathy. While
constipation is common in pure autonomic failure, up-
per gastrointestinal symptoms, particularly of the degree
reported in this patient, would be highly unusual for
that condition.1,2 The presentation would be most con-
sistent with an autonomic neuropathy.
Apart from neurogenic OH, this patient presents
with persistent postprandial belching, nausea, vomit-
ing, and weight loss. The patient carries a diagnosis
of sclerosing mesenteritis based on mesenteric lymph
node biopsy. This condition is characterized by such
upper gastrointestinal symptoms, and has been asso-ciated with
mechanical small bowel obstruction and
chronic intestinal pseudo-obstruction.3,4 Conversely,
gastroparesis as seen in autonomic neuropathies pres-
ents with similar symptoms and may be more likely
to be the underlying etiology here considering the
consistent postprandial occurrence of symptoms,
vomiting of undigested food, apparent lack of signif-
icant pain, and association with constipation and
neurogenic OH. Yet another consideration could be
a gastrointestinal infiltrative process such as gastroin-
testinal amyloidosis.5,6
Apart from the patients symptoms and examina-
tion findings, we are provided with additional clues
to the diagnosis. The patient was documented to
have clinical and EMG findings suggestive of a
length-dependent peripheral neuropathy with elec-
trophysiologic characteristics suggestive of a predom-
inantly axonal process. Considering that the patient
was apparently asymptomatic in regards to a somatic
peripheral neuropathy, there is a possibility that this
is an incidental, unrelated finding, but nonetheless,
this finding is intriguing and would lend further sup-
port to our suspicion of a peripheral neuropathicprocess
underlying this patients presentation.
The differential diagnosis for peripheral neuropa-
thies with autonomic involvement is broad. Dispro-
portionate involvement of autonomic fibers in a
peripheral neuropathic process is helpful in that the
differential diagnosis can be significantly narrowed.
Further narrowing of the differential can usually be
achieved by considering the onset of symptoms
(acute/subacute vs insidious/chronic) and differential
involvement of sympathetic and parasympathetic
function through a comprehensive autonomic review
490 Neurology 77 August 2, 2011
-
7/28/2019 A Middle Aged Woman With Nausea Weight Loss and
Orthostatic Hypotension
3/7
of systems and standardized autonomic testing. A
broad differential in this case would include amyloid
neuropathy, autoimmune/paraneoplastic etiologies
such as autoimmune autonomic ganglionopathy or
connective tissue disorders, genetic etiologies includ-
ing Fabry disease and hereditary sensory and auto-
nomic neuropathies (HSAN), metabolic etiologies
such as diabetes mellitus, toxic etiologies, and several
infectious etiologies.
The patient does not have a history of diabetes
mellitus with a normal comprehensive metabolic
panel. Vitamin B12 deficiency, even though autoim-
mune gastric disease appears to be present, should
not account for the majority of symptoms and find-
ings described. The patient does not have clinical or
electrophysiologic characteristics of Guillain-Barre
syndrome, botulism, or porphyria. There is no his-
tory of exposure to chemotherapy or other med-
ications and toxins associated with autonomic
neuropathies. Connective tissue disorders associated
with peripheral neuropathies can have various auto-nomic
involvement but the laboratory testing pro-
vided would argue at least against more common
entities in that category such as Sjogren syndrome.
Although the possibility of a vasculitic process was
raised based on imaging, the clinical picture does not
seem consistent with a vasculitic neuropathy. Lack of
family history, clinical presentation, and age at onset
argue against inherited autonomic neuropathies in
the different categories of HSAN. OH and gastroin-
testinal symptoms have been reported in female car-
riers of Fabry disease, but the patients age, lack of
family history, EMG findings, lack of neuropathic
pain, lack of reported cutaneous or ocular findings,
inability to account for the monoclonal gammopa-
thy, and described CT/PET findings make that diag-
nosis highly unlikely.7,8 Leprosy, AIDS, diphtheria,
Lyme disease, and celiac disease can all affect auto-
nomic fibers but the clinical presentation is inconsis-
tent with these diagnoses.
Autoimmune autonomic ganglionopathy cer-
tainly would be a consideration. Many cases of idio-
pathic autonomic neuropathy (AAG) have long been
assumed to be of autoimmune etiology, but it wasnot until the
recent discovery of specific antibodies
targeted against ganglionic nicotinic acetylcholine re-
ceptors (nAChR) that this concept could be proven.
Patients with this disorder are typically previously
healthy young or middle-aged individuals who de-
velop severe panautonomic failure over the course of
a few days to weeks with subsequent slow spontane-
ous recovery, which is often incomplete.911An ante-
cedent respiratory or gastrointestinal viral syndrome
is reported in many cases while an association with
preceding immunization or minor surgical proce-
dures has been made in other cases. Subacute auto-
nomic failure indistinguishable from AAG with a
paraneoplastic etiology has also been described.12,13
The typical patient with AAG has diffuse autonomic
dysfunction. Sympathetic failure results in OH and
widespread anhidrosis; parasympathetic failure pres-
ents as dry mouth, dry eyes, sexual dysfunction, uri-
nary retention, impaired pupillary responses, and
abnormal heart rate variation. Problems with the en-
teric autonomic nervous system present as gastroin-
testinal dysmotility with anorexia, early satiety,
postprandial abdominal pain, vomiting, diarrhea,
constipation, and intestinal pseudo-obstruction. Pa-
tients present with different combinations of these
signs and symptoms, with the most common pre-
senting symptoms being OH and gastrointestinal
dysmotility, each occurring in 70% to 80% of pa-
tients.9,14 Patients typically have normal strength and
reflexes. About 25% of patients describe minor sen-
sory symptoms, but objective sensory loss is usually
not present. EMG and nerve conduction studies aretypically
normal. Laboratory autonomic testing re-
veals evidence of diffuse autonomic failure, with
characteristically severe adrenergic failure resulting in
OH, but also cardiovagal and baroreflex failure, as
well as widespread anhidrosis.9 The most frequent
pattern of sweat loss seen on thermoregulatory sweat
testing is a ganglionopathy pattern rather than a
length-dependent pattern.15 AAG is associated with
antibodies specifically binding to the ganglionic nico-
tinic acetylcholine receptor (AChR) in approximately
50% of cases.13,14 Although subacute symptom onset,
sicca complex, pupillary abnormalities, and lower gas-
trointestinal tract symptoms are more common in the
antibody-positive group, the clinical presentation is
overall similar in seropositive and seronegative cases.16
The concept of an antibody-mediated disorder has been
thoroughly studied and confirmed using animal models
of experimental AAG, passive transfer studies, and stud-
ies on in vitro effects of antibodies on ganglionic
AChRs.14,1719 In addition to the classic presentation of
subacute pandysautonomia, several other clinical phe-
notypes of AAG have been described, including chronic
diffuse autonomic failure similar to pure autonomicfailure, and
limited forms of autonomic dysfunction
such as isolated gastrointestinal dysmotility, isolated
cholinergic autonomic failure, and cases of postural
tachycardia syndrome.9,13,14 There are a number of
reports on immunomodulatory and immunosup-
pressive therapy of AAG with promising results, al-
though no controlled trials have been conducted to
date.2022 Lack of response to an IVIg treatment trial
does not rule out the diagnosis, as not all patients
may respond to immunomodulatory therapy and
some patients have been reported to respond to
Neurology 77 August 2, 2011 491
-
7/28/2019 A Middle Aged Woman With Nausea Weight Loss and
Orthostatic Hypotension
4/7
plasma exchange or immunosuppressant agents afternot responding
to IVIg.21,22
The fact that a paraneoplastic panel in this case
was negative does not rule out the possibility of an
autoimmune or paraneoplastic autonomic neuropathy,
particularly not an autonomic neuropathy associated
with lymphoma. In fact, the presence of a monoclonal
gammopathy could argue for that. Also arguing for that
diagnosis would be the lymph node biopsy findings felt
to be consistent with sclerosing mesenteritis, along with
CT/PET mesentery findings and soft tissue thickening
encasing the celiac axis. Lymphoma has been reported
to be associated with sclerosing mesenteritis or has
beenmistaken for that condition.2325 Lymphoma has also
been described in association with autoimmune auto-
nomic ganglionopathy.12
Not explained by a paraneoplastic autonomic
neuropathy associated with lymphoma, however,
would be the cardiac findings of mild left ventricular
hypertrophy, diastolic dysfunction, and QT prolon-
gation. That last piece of the puzzle could however
be explained by a condition associated with mono-
clonal gammopathy, lymphoma, and peripheral neu-
ropathy with prominent autonomic features, namely
AL amyloidosis. The described cardiac findings are
somewhat nonspecific but have all been reported as
features of amyloid cardiomyopathy.26,27 While the
elevated homocysteine level may relate to vitamin de-
ficiencies (including B6, folate, and less likely B12
based on available data) in the setting of significant
weight loss, an alternative but purely speculative ex-
planation could be the presence of subclinical amy-
loid nephropathy, considering the known influence
of renal function on homocysteine levels.28
Among the different types of amyloidosis, only
some have been associated with amyloid neuropathy.
Among those, the most common type represents pri-mary (AL)
amyloidosis. The fibrils in AL amyloid
consist of monoclonal or light chains. Rarely,
monoclonal heavy chains are found. Familial (AF)
amyloidosis represents another, less common cause
of amyloid neuropathy with precursor proteins most
commonly variants of the transthyretin (TTR) mole-
cule. While the clinical presentation of TTR amyloid
neuropathy can be similar to that of primary amy-
loidosis, it would not account for the monoclonal
gammopathy and CT/PET findings.
Amyloid neuropathy is typically associated with
fatigue and weight loss. The neuropathy is frequently
a sensorimotor peripheral neuropathy or polyradicu-
loneuropathy with loss of pain and temperature sen-
sation, paresthesias, neuropathic pain, weakness, and
characteristically prominent autonomic dysfunc-
tion.29 EMG findings are characteristically those of
an axonal neuropathy.30 On nerve biopsy, axonal de-
generation, sometimes with predominant involve-
ment of small myelinated and unmyelinated fibers, is
seen.29 Deposits of a homogenous, amorphous sub-
stance are found infiltrating epineurial and endo-
neurial connective tissue and blood vessel walls,which stain
pink with hematoxylin & eosin (H&E),
metachromatically with methyl violet, and produce
apple-green birefringence when stained with Congo
red and viewed under polarized light.29,31 Immunos-
tains are available to help distinguish the different
types of amyloid in pathologic specimens, and most
recently, laser microdissection along with mass
spectrometry based proteomic analysis of amyloid de-
position has been introduced with promising results.32
A recent manuscript describes patterns of neurop-
athy and autonomic failure in patients with amyloid-
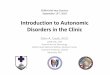
Figure1 Hematoxylin & eosinstained section of sural nerve
biopsy
demonstrating hyaline deposits in wallsof endoneurial
blood vessels
Figure2 Toluidine bluestained epoxy section of nerve showing
amorphous
material (amyloid)surrounding endoneurial vessels (arrows)
492 Neurology 77 August 2, 2011
-
7/28/2019 A Middle Aged Woman With Nausea Weight Loss and
Orthostatic Hypotension
5/7
osis.33A total of 62% of patients were found to have
generalized autonomic failure and polyneuropathywith pain, 17%
had generalized autonomic failure
and polyneuropathy without pain, and 11% had iso-
lated autonomic failure. Only 6% of patients had
peripheral neuropathy without autonomic failure,
and 5% had autonomic failure and somatic small-
fiber neuropathy. The most common autonomic
symptoms associated with amyloid neuropathy were
orthostatic intolerance (74%) and gastrointestinal
(71%) symptoms. Autonomic function testing
showed moderately severe to severe autonomic fail-
ure in all domains (sudomotor, cardiovagal, cardio-
vascular adrenergic), with cardiovagal function most
severely affected.
While no somatic neuropathic symptoms, including
neuropathic pain, were reported for the patient dis-
cussed here, there were unequivocal physical and elec-
trophysiologic findings of a somatic neuropathic
process. The electrophysiologic findings showed pre-
dominant axonal features as typically seen in amyloid
neuropathy. Autonomic failure as evidenced by neuro-
genic OH would also be characteristic for that condi-
tion. The gastrointestinal symptoms could be explained
by a combination of autonomic neuropathy, gastroin-
testinal amyloidosis, and the described sclerosing mes-
enteritis. The cardiac findings could indicate early
amyloid cardiomyopathy. This diagnosis would fur-
thermore account for the reported monoclonal gam-
mopathy. In the vast majority of cases, AL amyloidosis
relates to a monoclonal gammopathy with or without
multiple myeloma. Although rare, both focal and sys-
temic forms of amyloidosis have been reported in lym-
phoma.34,35 Alternatively, the imaging findings could
relate to amyloid deposition rather than lymphoma, al-
though a correlation between amyloid and sclerosing
mesenteritis has not been reported.
Therefore, the diagnosis that would seem to bestfit the whole
clinical picture would be primary (AL)
amyloidosis with amyloid neuropathy, possibly in
the setting of underlying lymphoma. Still to be consid-
ered, however, would have to be the possibility of a
paraneoplastic autonomic neuropathy in the setting of
lymphoma. I have to again emphasize that formal auto-
nomic testing, including tests to assess cardiovascular
adrenergic, cardiovagal, and sudomotor function,
would likely have provided a higher degree of diagnostic
certainty, as the pattern of autonomic dysfunction can
give important diagnostic clues. Specifically, a length-
dependent pattern of sweat loss and severe cardiovagalfailure
would have further supported the diagnosis of
amyloid neuropathy, while a ganglionopathy pattern of
sweat loss and moderate cardiovagal impairment would
have made a stronger case for an autoimmune/paraneo-
plastic autonomic ganglionopathy.
Regardless, at this point, a comprehensive search
for amyloid deposition is clearly indicated, perhaps
starting with a search in tissue obtained previously
(mesenteric lymph node biopsy) and fat aspirate, and
consideration for a peripheral nerve (sural) biopsy,
bone marrow biopsy, rectal biopsy, or rebiopsy of thedescribed
CT/PET abnormality if negative. If de-
tected, hematologic treatment approaches, including
peripheral stem cell transplantation, will have to be
considered, which have shown benefit in the treat-
ment of AL amyloidosis.36,37
Clinical diagnosis. Primary (AL) amyloidosis with
amyloid neuropathy.
NEUROPATHOLOGIC FINDINGS Based on her
NCS/EMG abnormalities, the patient underwent bi-
opsy of the left sural nerve. The H&E stain demon-
Figure3 Congo redstained section demonstrating amyloid deposits
within
nervefascicle
Figure4 Congored stain, higher
magnification,demonstratingamyloid deposits
in a perivascular distribution around endoneurial vessels
Neurology 77 August 2, 2011 493
-
7/28/2019 A Middle Aged Woman With Nausea Weight Loss and
Orthostatic Hypotension
6/7
strated pale hyaline deposits within nerve fascicles,
most of which were centered on blood vessels (figure
1). There were no inflammatory cell infiltrates. The
trichrome stain showed a mild diffuse loss of myelin-
ated axons from all fascicles at all levels. The trans-
verse semithin Epon sections also demonstrated
hyaline thickening of endoneurial vessels with a
mild diffuse loss of large myelinated axons (fig-
ure 2). A rare acutely degenerating axon was seen
in a few fascicles.
A diagnostic stain was employed. The Congo red
stain highlighted amyloid deposits in the walls of
most endoneurial vessels and also in a rare epineurial
vessel (figures 3 and 4). The amyloid was not immu-
noreactive with the amyloid A antibody. Despite a
monoclonal IgA spike in SPEP, immunohisto-
chemical staining did not specifically demonstrate
or immunoglobulin (Ig) light chain likely related
to the background Ig in paraffin embedded periph-
eral nerve, a common technical problem in nerve bi-
opsies. Mass spectrometrybased proteomic analysisof
microdissected amyloid deposits can provide a de-
finitive diagnosis of the amyloid subtype. Further
analysis was not pursued as the result was unlikely to
affect the overall treatment plan.
Final pathologic diagnosis. Amyloid neuropathy.
COMMENTS Based on her predominantly auto-
nomic and neurologic symptoms and nerve biopsy
result, we referred the patient to hematology to eval-
uate for amyloidosis. Our hematologist suspected
primary amyloidosis. Given the severity of her symp-toms and the
involvement of multiple organs, fur-
ther d iagnostic s tudy was not p ur sued to
distinguish among primary, secondary, or familial
amyloidosis as the distinction was unlikely to
change the overall poor prognosis or treatment de-
cision. After a cycle of melphalan and dexametha-
sone, the patient and her family requested
palliative care in a local hospice.
Amyloidosis is a multisystem disorder resulting
from excessive monoclonal plasma cell expansion or
mutation in the transthyretin gene. The tissue depo-sition of
insoluble amyloid fibrils leads to organ dys-
function. The clinical presentation depends on the
organs affected. Typical clinical findings include pro-
teinuria, restrictive cardiomyopathy, hepatospleno-
megaly, and polyneuropathy. Tissue biopsy is needed
to confirm the diagnosis. While amyloidosis has a
poor prognosis, chemotherapy and hematopoietic
cell transplantation may prolong survival. To avoid
delayed diagnosis and treatment, amyloidosis should
be considered in patients with unexplained auto-
nomic and neurologic dysfunction.
AUTHOR CONTRIBUTIONS
Dr. Singer contributed the expert discussion format. Dr. Yung
drafted and
revised the manuscript. Dr. Wollmann revised the manuscript. Dr.
Kelly
revised the manuscript. Dr. Keegan accepted the final revised
manuscript.
DISCLOSURE
Dr. Singer is a consultant for Pfizer Inc. Dr. Yung reports no
disclosures.
Dr. Wollmann examines neuromuscular biopsies at the Department
of
Pathology at the University of Chicago (about 50% effort). Dr.
Kelly
reports no disclosures. Dr. Keegan serves as Clinical
Pathological Confer-
ence Section Co-Editor for Neurologyand NeurologyPodcast panel
and
Chief Editor for eMedicine; and has served as a consultant for
Novartis.
REFERENCES
1. Low PA, Bannister R. Multiple system atrophy and pure
auto-
nomic failure. In: Low PA, ed. Clinical Autonomic Disorders,
2nd ed. Philadelphia: Lippincott-Raven; 1997:555575.
2. Polinsky RJ, Kopin IJ, Ebert MH, Weise V. Pharmaco-
logic distinction of different orthostatic hypotension syn-
dromes. Neurology 1981;31:17.
3. Akram S, Pardi DS, Schaffner JA,Smyrk TC. Sclerosing
mesen-
teritis: clinical features, treatment, and outcome in
ninety-two
patients. Clin Gastroenterol Hepatol 2007;5:589596.4. Schuffler
MD, Rohrmann CA, Chaffee RG, Brand DL,
Delaney JH, Young JH. Chronic intestinal pseudo-ob-
struction: a report of 27 cases and review of the
literature.
Medicine 1981;60:173196.
5. Battle WM, Rubin MR, Cohen S, Snape WJ Jr.
Gastrointestinal-motility dysfunction in amyloidosis.
N Engl J Med 1979;301:2425.
6. Tada S, Iida M, Yao T, Kitamoto T, Yao T, Fujishima M.
Intestinal pseudo-obstruction in patients with amyloidosis:
clinicopathologic differences between chemical types of
amyloid protein. Gut 1993;34:14121417.
7. Germain DP. Fabry disease. Orphanet J Rare Dis 2010;5:30.
8. Mutoh T, Senda Y, Sugimura K, et al. Severe
orthostatichypotension in a female carrier of Fabrys disease.
Arch
Neurol 1988;45:468472.
9. Klein CM, Vernino S, Lennon VA, et al. The spectrum of
autoimmune autonomic neuropathies. Ann Neurol 2003;
53:752758.
10. Suarez GA, Fealey RD, Camilleri M, Low PA. Idiopathic
autonomic neuropathy: clinical, neurophysiologic, and
follow-up studies on 27 patients. Neurology 1994;44:
16751682.
11. Young RR, Asbury AK, Corbett JL, Adams RD. Pure pan-
dysautonomia with recovery: description and discussion of
diagnostic criteria. Brain 1975;98:613636.
12. McKeon A, Lennon VA, Lachance DH, Fealey RD, Pit-
tock SJ. Ganglionic acetylcholine receptor autoantibody:
oncological, neurological, and serological accompani-
ments. Arch Neurol 2009;66:735741.
13. Vernino S, Low PA, Fealey RD, Stewart JD, Farrugia G,
Lennon VA. Autoantibodies to ganglionic acetylcholine
receptors in autoimmune autonomic neuropathies. N Engl
J Med 2000;343:847 855.
14. Vernino S, Sandroni P, Singer W, Low PA. Invited
Article:
Autonomic ganglia: target and novel therapeutic tool.
Neurology 2008;70:19261932.
15. Kimpinski K, Iodice V, Sandroni P, Fealey RD, Vernino
S, Low PA. Sudomotor dysfunction in autoimmune auto-
nomic ganglionopathy. Neurology 2009;73:15011506.
494 Neurology 77 August 2, 2011
-
7/28/2019 A Middle Aged Woman With Nausea Weight Loss and
Orthostatic Hypotension
7/7
16. Sandroni P, Vernino S, Klein CM, et al. Idiopathic auto-
nomic neuropathy: comparison of cases seropositive and
seronegative for ganglionic acetylcholine receptor anti-
body. Arch Neurol 2004;61:44 48.
17. Vernino S, Ermilov LG, Sha L, Szurszewski JH, Low PA,
Lennon VA. Passive transfer of autoimmune autonomic
neuropathy to mice. J Neurosci 2004;24:70377042.
18. Vernino S, Low PA, Lennon VA. Experimental autoim-
mune autonomic neuropathy. J Neurophysiol 2003;90:
20532059.
19. Wang Z, Low PA, Jordan J, et al. Autoimmune
autonomicganglionopathy: IgG effects on ganglionic acetylcholine
re-
ceptor current. Neurology 2007;68:19171921.
20. Hollenbeck R, Black BK, Peltier AC, et al. Long-term
treatment with rituximab of autoimmune autonomic gan-
glionopathy in a patient with lymphoma. Arch Neurol
2011;68:372375.
21. Iodice V, Kimpinski K, Vernino S, Sandroni P, Fealey
RD, Low PA. Efficacy of immunotherapy in seropositive
and seronegative putative autoimmune autonomic gangli-
onopathy. Neurology 2009;72:20022008.
22. Iodice V, Kimpinski K, Vernino S, Sandroni P, Low PA.
Immunotherapy for autoimmune autonomic ganglionopa-
thy. Auton Neurosci 2009;146:2225.
23. Ehrenpreis ED, Rao AS, Aki R, Brown H, Pae T, Boiskin
I. Normal positron emission tomography-computerized
tomogram in a patient with apparent mesenteric pannicu-
litis: biopsy is still the answer. Case Rep Gastroenterol
2009;3:131137.
24. Hiridis S, Hadgigeorgiou R, Karakitsos D, Karabinis A.
Sclerosing mesenteritis affecting the small and the large
intestine in a male patient with non-Hodgkin lymphoma:
a case presentation and review of the literature. J Med Case
Reports 2008;2:388.
25. Hoffmann JC, Lamberts R, Huppert P, Kaiserling E,
Gregor M. Intestinal obstruction, progressive weight loss,
and recurrent fever in two patients with mesenteric lesions.
Digestion 1998;59:86 90.
26. Desai HV, Aronow WS, Peterson SJ, Frishman WH. Car-
diac amyloidosis: approaches to diagnosis and manage-
ment. Cardiol Rev 2010;18:111.
27. Falk RH, Dubrey SW. Amyloid heart disease. Prog Car-
diovasc Dis 52:347361.
28. Arnadottir M, Hultberg B, Nilsson-Ehle P, Thysell H.
The effect of reduced glomerular filtration rate on plasma
total homocysteine concentration. Scand J Clin Lab Invest
1996;56:4146.29. Kyle RA, Kelly JJ, Dyck PJ, eds. Amyloidosis
and Neurop-
athy, 4th ed. Philadelphia: Elsevier Saunders; 2005.
30. Kelly JJ Jr. The electrodiagnostic findings in
peripheral
neuropathy associated with monoclonal gammopathy.
Muscle Nerve 1983;6:504509.
31. Elghetany MT, Saleem A. Methods for staining amyloid in
tissues: a review. Stain Technol 1988;63:201212.
32. Klein CJ, Vrana JA, Theis JD, et al. Mass Spectrometric-
based proteomic analysis of amyloid neuropathy type in
nerve tissue. Arch Neurol 2011;68:195199.
33. Wang AK, Fealey RD, Gehrking TL, Low PA. Patterns of
neuropathy and autonomic failure in patients with amyloido-
sis. Mayo Clin Proc 2008;83:12261230.
34. Ikee R, Kobayashi S, Hemmi N, Suzuki S, Miura S. Amy-
loidosis associated with chronic lymphocytic leukemia.
Amyloid 2005;12:131134.
35. Telio D, Bailey D, Chen C, Crump M, Reece D, Kukreti
V. Two distinct syndromes of lymphoma-associated AL
amyloidosis: a case series and review of the literature. Am
J
Hematol 2010;85:805808.
36. Gertz MA, Zeldenrust SR. Treatment of immunoglobulin
light
chain amyloidosis. Curr Hematol Malig Rep 2009;4:9198.
37. Palladini G, Merlini G. Transplantation vs.
conventional-
dose therapy for amyloidosis. Curr Opin Oncol 2011;23:
214220.
Neurology 77 August 2, 2011 495