Embed Size (px)
Citation preview

A Comparison of Chlorhexidine-Alcohol Versus Povidone-Iodinefor Eliminating Skin Flora Before Genitourinary ProstheticSurgery: A Randomized Controlled Trial
Lawrence L. Yeung,* Shaun Grewal,*,† Arnold Bullock,‡ H. Henry Lai§and Steven B. Brandes�From the Division of Urology, Department of Surgery, Washington University in St. Louis, St. Louis, Missouri (SG, AB, HHL, SBB), and theDepartment of Urology, University of Florida, Gainesville, Florida (LLY)
Purpose: We defined the relevant skin flora during genitourinary prostheticsurgery, evaluated the safety of chlorhexidine-alcohol for use on the male geni-talia and compared chlorhexidine-alcohol to povidone-iodine in decreasing therate of positive bacterial skin cultures at the surgical skin site before prostheticdevice implantation.Materials and Methods: In this single institution, prospective, randomized, con-trolled study we evaluated 100 consecutive patients undergoing initial genitouri-nary prosthetic implantation. Patients were randomized to a standard skinpreparation with povidone-iodine or chlorhexidine-alcohol. Skin cultures wereobtained from the surgical site before and after skin preparation.Results: A total of 100 patients were randomized, with 50 in each arm. Pre-preparation cultures were positive in 79% of the patients. Post-preparationcultures were positive in 8% in the chlorhexidine-alcohol group compared to 32%in the povidone-iodine group (p � 0.0091). Coagulase-negative staphylococci werethe most commonly isolated organisms in post-preparation cultures in the povi-done-iodine group (13 of 16 patients) as opposed to propionibacterium in thechlorhexidine-alcohol group (3 of 4 patients). Clinical complications requiringadditional operations or device removal occurred in 6 patients (6%) with nosignificant difference between the 2 groups. No urethral or genital skin compli-cations occurred in either group.Conclusions: Chlorhexidine-alcohol was superior to povidone-iodine in eradicat-ing skin flora at the surgical skin site before genitourinary prosthetic implanta-tion. There does not appear to be any increased risk of urethral or genital skinirritation with the use of chlorhexidine compared to povidone-iodine. Chlorhexi-dine-alcohol appears to be the optimal agent for skin preparation before genito-urinary prosthetic procedures.
Key Words: chlorhexidine; penile implantation; urinary sphincter, artificial;
Abbreviations
and Acronyms
AUS � artificial urinary sphincter
CNS � coagulase-negativestaphylococci
GU � genitourinary
IPP � inflatable penile prosthesis
MUS � synthetic male urethralsling
PB � propionibacterium
Accepted for publication July 20, 2012.Study received institutional review board ap-
proval.Supported by a grant from the Sexual Medi-
cine Society of North America.* Nothing to disclose.† Correspondence: Department of Surgery,
Washington University in St. Louis, St. Louis,Missouri 63130 (telephone: 314-362-8227; FAX:314-367-5016; e-mail: [email protected]).
‡ Financial interest and/or other relationshipwith Pfizer, Astellas, American Medical SystemsInc. and Coloplast.
§ Financial interest and/or other relationshipwith Pfizer and Astellas.
� Financial interest and/or other relationshipwith Astellas, American Medical Systems Inc.and Allergan.
Editor’s Note: This article is the
third of 5 published in this issue
suburethral slings; povidone-iodine399.
136 www.jurology.com
WITH an aging population and in-creasing incidence of surgical treat-ment for prostate cancer, urologicalprosthetic procedures are being per-formed with increasing frequency. More
than 15,000 penile prostheses are im-0022-5347/13/1891-0136/0THE JOURNAL OF UROLOGY®
© 2013 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RES
planted per year in the United Statesand up to 10% of men seek treatmentfor stress urinary incontinence afterradical prostatectomy.1,2
Clinical infection remains the most
for which category 1 CME credits
can be earned. Instructions for
obtaining credits are given with
the questions on pages 398 and
dreaded complication of prosthetic sur-
http://dx.doi.org/10.1016/j.juro.2012.08.086Vol. 189, 136-140, January 2013
EARCH, INC. Printed in U.S.A.

GENITOURINARY PROSTHETIC SKIN PREPARATION 137
gery, resulting in additional operations in almost allcases. The primary route of implant infection isthought to be contamination before or during im-plantation in the majority of cases.3 The infectionrate of penile prostheses has traditionally been citedas 3% to 5%, increasing up to 8% in patients withdiabetes, although this rate has decreased in the eraof antibiotic coated prosthetics.4–6 Likewise, infec-tion rates of 5.5% have been reported for artificialurinary sphincters and 3% for male urethralslings.7,8
Elimination of skin flora at the time of surgicalsite antisepsis is a logical step in preventing contam-ination and infection during prosthetic surgery. Pov-idone-iodine has traditionally been the antisepticagent of choice for surgery involving the male geni-talia. However, studies from other specialties havedemonstrated that chlorhexidine-alcohol is superiorin eliminating skin flora at the surgical site.9,10 Wecompare the efficacy of chlorhexidine-alcohol (Chlora-Prep®, 2% chlorhexidine gluconate and 70% isopropylalcohol; Enturia, El Paso, Texas) to that of povidone-iodine (Betadine®, 7.5% iodine scrub and 10% iodinepaint; Purdue Products, Stamford, Connecticut) indecreasing the rate of positive bacterial skin cul-tures at the surgical skin site of GU prosthetic de-vice implantation. Furthermore, we evaluated thesafety of chlorhexidine-alcohol for use on the malegenitalia, and further defined the native flora of themale genitalia and perineum.
METHODS
A prospective, randomized study of patients undergoingurological prosthetic operations was performed. Institu-tional review board approval was obtained for the studyprotocol. The primary aim of the study was to demonstratethat chlorhexidine-alcohol is equivalent to povidone-io-dine at eradicating the skin flora before GU prostheticsurgery. Secondary aims of the study were to demonstratethe safety of chlorhexidine-alcohol for use on the male geni-talia and to define the native flora at the surgical siteduring prosthetic surgery. Patients undergoing virginplacement of an IPP, AUS, MUS or testicular implantwere included in the study. Patients were excluded fromstudy if they had a history of GU prosthetic implant pro-cedures, prior surgical site infection, or a documentedallergy to chlorhexidine, isopropyl alcohol or povidone-iodine.
Patients were randomized in a 1:1 ratio to surgical siteskin antisepsis with a standard povidone-iodine 10-min-ute scrub and paint process or a 2-minute chlorhexidine-alcohol scrub. The a priori size effect in our study wasdetermined to be 30% based on data from the orthopedicliterature. This resulted in a sample size of 49 patients ineach group to detect a 30% difference with a power of 0.8(� � 0.05). The randomization scheme was computer gen-erated. Allocation concealment was achieved by conceal-
ment of the randomization list from the surgeon at alltimes by the impartial circulating nurse. The randomiza-tion group was revealed by the nurse just before prepara-tion of the operating surgical suite.
Skin preparation was performed by the circulatingnurse or surgeon in all cases. Aerobic and anaerobic cul-tures were obtained by swabbing the incisional site with adry, sterile, cotton tipped swab before skin preparation. Asecond culture was obtained from the surgical site after alldrapes and instruments were on the field, just beforeincision. Specimens were sent immediately to the micro-biology laboratory for culture and sensitivity. Patientswere examined for local adverse reactions to the skinpreparation during the immediate postoperative periodand at the postoperative visit at 1 month.
All data analyses were performed using SPSS® version15.0. Descriptive statistics were created for all variablesusing means and standard deviations. Data analysiswas performed using the intent to treat principle. Per-centages were calculated for categorical data. Continuousvariables were compared using the 2-tailed t test andcategorical variables with the chi-square test. Multivari-ate logistic regression analysis was used to compare fordifferences in positive culture and clinical infection ratesbetween the treatment groups. Odds ratios with 95% con-fidence intervals are presented. Statistical significancewas defined as p �0.05. All data analyses were performedby an independent, unbiased statistician.
RESULTS
A total of 100 patients were included in the study,with 50 assigned to each group. The baseline char-acteristics of the patient population are shown in thetable. There were 65 patients who underwent place-ment of an IPP, 14 who underwent AUS placement,14 who underwent MUS placement, 5 who under-went combination IPP � MUS placement, and 2 whounderwent placement of a testicular implant (fig. 1).All penile prostheses were implanted through a pe-noscrotal approach. Mean followup was 9.75 months(range 4 to 15).
Mean operating room time was 86.2 minutes(�32.2, range 45 to 204). Of the cultures 79% werepositive before skin preparation and 20% were pos-
Baseline patient characteristics
Chlorhexidine Povidone-Iodine p Value
Mean pt age (SD) 62.2 (13.2) 65.1 (9.0) 0.2No. race:
White 41 34 0.1Black 9 16
No. smoking status:Yes 14 16 0.7No 36 34
No. diabetes:Yes 11 19 0.08No 39 31
Mean kg/m2 body 30.5 (6.3) 31.0 (5.4) 0.1
mass index (SD)
GENITOURINARY PROSTHETIC SKIN PREPARATION138
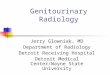
itive after skin preparation. Figure 2 displays theculture results before skin preparation. A total of 16(32%) cultures were positive in the povidone-iodinegroup after skin preparation compared to 4 (8%) inthe chlorhexidine-alcohol group (p � 0.0091, OR5.30; CI 1.51, 18.5).
Multivariate analyses were performed to evaluatethe effect of baseline risk factors on post-preparationculture and clinical complications. Main effects in-cluded in the multivariate regression model werediabetes, smoking status, age, body mass index andrace. The Hosmer-Lemeshow test was used to testthe goodness of fit. Diabetes was found to be a sig-nificant risk factor for positive skin culture afterskin preparation in our patient population (p � 0.04,OR 3.38, CI 1.04, 11.0). Furthermore, smoking sta-tus was found to be a significant risk factor forclinical complications (p � 0.046, OR 4.92, CI 1.03,23.26).
The most commonly isolated organisms after skinpreparation with povidone-iodine were CNS (13 pa-tients), followed by mixed gram-positive organisms(2 patients) and Staphylococcus aureus (1 patient).
0
5
10
15
20
25
30
35
40
IPP
AUS
MU
S
MU
S +
IPP
Tes�
cula
r Pr
osth
esis
chlorhexidine-alcohol
povidone-Iodine
Figure 1. Distribution of patients
05
101520253035404550
No
Gro
wth
Mix
ed O
rg.
Coag
Neg
Sta
ph
Gro
up B
Str
ep
Stap
h A
ureu
s
Pseu
dom
onas
Baci
llus S
p
Aspe
rgill
us N
iger
Prop
iono
bact
eriu
m
E. F
aeca
lis
Coag
Neg
Sta
ph +
Bac
illus
Num
ber o
f pa�
ents
Pre Prep Cultures
Figure 2. Culture results before skin preparation. Org., organ-isms. Coag Neg Staph, CNS. Strep, streptococci. E. Faecalis,
Enterococcus faecalis.PB was the only organism isolated after skin prep-aration in the chlorhexidine-alcohol group (fig. 3).
There was no significant difference in the inci-dence of clinical complications between the 2 groups.The overall incidence of clinical complications was7%. A superficial wound infection developed in 1patient and was successfully managed with oral an-tibiotics. Removal of the penile prosthesis was re-quired in 5 patients, and urethral erosion of a MUSoccurred in 1 patient and necessitated sling re-moval.
Subset analyses were performed for the group ofpatients undergoing a penoscrotal incision (IPP) vs aperineal incision (MUS or AUS). A significant differ-ence was noted in the post-preparation positive cul-ture rate for povidone-iodine vs chlorhexidine-alco-hol in the IPP subgroup (22.2% vs 8.8%, p � 0.02).No significant difference was noted in the positiveculture rate in the AUS/MUS subgroup (30.7% vs6.7%, p � 0.13). No urethral (dysuria) or genitalcomplications (skin irritation) were noted in eithergroup during the perioperative and postoperativeperiod or at 1 and 6-month followup.
DISCUSSION
Device infection remains the most dreaded compli-cation of GU prosthetic surgery. A device infectioncan lead to additional operations, which can resultin significant patient morbidity.3 Presumably themajority of infections are caused by contaminationof the prosthetic by microorganisms at the time ofimplantation, resulting in biofilm formation. Bio-film, a layer that is formed around the implant sur-face, is composed of extracellular polymers and ma-trix produced by microorganisms that becomeattached to the surface of the implant.11 This biofilmlayer suppresses the host immune response and al-
0
2
4
6
8
10
12
14
CNS SA PB FMS
chlorhexidine-alcohol
povidone-iodine
Figure 3. Post-preparation culture results. SA, S. aureus. FMS,few mixed organisms.
lows the organisms to remain viable with reduced

GENITOURINARY PROSTHETIC SKIN PREPARATION 139
growth rates, which can promote resistance to anti-biotics.12,13 Therefore, surgical site antisepsis is oneof the most important steps in preventing prostheticcolonization, which can result in biofilm formationand lead to clinical infections.
Chlorhexidine-alcohol has a rapid onset of actiondue to the alcohol component of the solution causingdenaturation of protein and disruption of cell mem-branes. It also has antimicrobial persistence out to48 hours because of the binding of chlorhexidine tothe skin.14,15 The appropriate application method isa 2-minute scrubbing followed by a 3-minute dryingperiod to allow the alcohol to evaporate to preventinadvertent ignition by electrocautery.
In comparison, povidone-iodine functions by dam-aging proteins and DNA via free iodine that is re-leased from solution after approximately 2 minutesof surface contact.16 The recommended scrub timefor povidone-iodine is 5 minutes, followed by a paint-ing process, and then allowing the preparation todry. This 2-step process typically takes approxi-mately 10 minutes and is the length of time advo-cated by many experts in GU prosthetic implanta-tion.17
Traditionally, chlorhexidine-alcohol has been con-sidered contraindicated for use on the genitalia dueto concerns of urethral irritation from the desiccat-ing effects of the alcohol component of the prepara-tion. Additionally, concerns over the flammability ofalcohol on the genitalia have led to resistance to theuse of alcohol based preparations on this region ofthe body.18 As a result, many operating room nursesand surgeons advocate the use of aqueous basedsolutions instead, such as povidone-iodine.
However, operating room fires due to the flamma-bility of alcohol are exceedingly rare. As a result, theNational Fire Protection Association, which sets na-tional fire safety standards, lifted its ban on the useof alcohol based surgical preparation solutions in theoperating room in 2005.19 Ignition of the alcohol canbe prevented by allowing for proper drying and pre-venting the pooling of the alcohol based agent.
Literature from other specialties has documentedthe superiority of chlorhexidine compared to povi-done-iodine for surgical site antisepsis. Saltzman etal published a series showing a decreased skin con-tamination rate (7% vs 31%, respectively) on post-preparation culture swabs before orthopedic shoul-der surgery.9 In addition, Darouiche et al revealed astatistically significant decrease in wound infectionrates (9.5% vs 16.1%, respectively) during clean con-taminated surgery in a randomized trial comparingchlorhexidine to povidone-iodine for surgical site an-tisepsis.10
Our data show a lower positive culture rate withchlorhexidine-alcohol compared to povidone-iodine
with a skin colonization rate of 8% vs 32%, respec-tively, after antisepsis. On the basis of our findings,5 patients would need to undergo skin preparationwith chlorhexidine-alcohol instead of povidone-io-dine to prevent 1 positive skin culture.
In a subset analysis chlorhexidine appeared to besuperior for penoscrotal and perineal incisions, withthe lack of statistical significance in the AUS/MUSsubgroup presumably explained by the small num-ber of positive cultures in this group (5). Addition-ally, chlorhexidine-alcohol appears to be superior topovidone-iodine at eliminating CNS, the most com-monly isolated organisms from prosthetic biofilm.20
PB was the predominant organism cultured fromthe surgical site after skin preparation with chlor-hexidine. It has infectious potential, and has beendescribed in infections of joint prostheses, shuntsand prosthetic heart valves.21 However, no reportsto date have described the involvement of Propi-onibacterium in infections of urological implants.Further research is needed to define the role of thisorganism in GU prosthetic infections as well as theoptimal method of eliminating this potentiallypathogenic skin flora at the time of skin antisepsis.
Diabetes status appeared to be a risk factor forpositive skin culture after surgical site antisepsis inour patient cohort and the reason for this finding isunclear. However, it may be related to higher base-line bacterial colony counts or differences in thenative skin flora in this population. This findingcould, in part, explain the higher rates of clinicalinfection in patients with diabetes demonstrated inlarger cohorts.4,5 In addition, smoking status was arisk factor for clinical complications in our study. Apopulation based analysis of National SurgicalQuality Improvement Program data has shownsmoking to be a risk factor for wound infections inbreast cancer surgery.22 To our knowledge, this isthe first study to demonstrate smoking as a riskfactor for clinical complications in prosthetic sur-gery. We hypothesize that this finding is related tothe associated peripheral vascular disease and im-paired wound healing in this patient population.Patients who smoke should be counseled regardingthe potential increased risk of complications beforeprosthetic implantation.
In addition to superior effectiveness in the elimi-nation of skin flora, surgical site antisepsis withchlorhexidine-alcohol is more cost-effective in termsof operating room costs because of the decreasedskin preparation time required for adequate anti-sepsis. At our institution the hospital cost for chlor-hexidine-alcohol is almost 40% more than for povi-done-iodine ($3.64 for povidone-iodine, $5.94 forchlorhexidine-alcohol). However, assuming operat-ing room fees of $62 per minute and anesthesia feesof $4 per minute, the total cost of a standard 10-
minute povidone-iodine paint and scrub would be
GENITOURINARY PROSTHETIC SKIN PREPARATION140
$525.70 more expensive than a 2-minute chlorhexi-dine preparation.23 Even if the recommended 3-min-ute drying time recommended for chlorhexidine-al-cohol is accounted for (which typically occurs duringthe draping process and adds no additional waitingperiod), skin preparation with chlorhexidine-alcoholis still $327.70 more cost-effective than povidone-iodine.
Our study has several limitations. While we wereable to demonstrate a significant difference in de-creasing the rate of positive bacterial skin culturesat the surgical skin site with chlorhexidine-alcohol,we could not detect a significant difference in clinicalinfection rates because the study was not powered todo so. A study would require the enrollment of 1,141patients to show a reduction in clinical infectionrates from 4% to 2%. In addition, as a single centerstudy, our results may not have external validity toother institutions where there may be differences innative skin flora, surgical techniques and operatingroom practices. We also analyzed qualitative ratherthan quantitative culture results. It is possible thatquantitative analyses of culture specimens afterskin preparation may show a correlation with clini-cal infection rates in a larger study, which we werenot able to perform. Lastly, our sample represents a
heterogeneous patient cohort, with possible differ-REFERENCES
177: 1021. is best? Rev Urol 2009; 11
ences in flora between the penoscrotal and perinealincisions.
Nonetheless, effective elimination of skin florabefore incision is a logical step in minimizing therisk of infection during prosthetic implantation.Given the lack of urethral or genital skin irritationand the cost benefit with the use of chlorhexidine-alcohol, this agent appears to be the superior choicefor surgical site antisepsis before GU prosthetic pro-cedures.
CONCLUSIONS
Chlorhexidine-alcohol appears to be superior to pov-idone-iodine in eliminating skin flora at the surgicalsite before GU prosthetic procedures. Chlorhexi-dine-alcohol has persistent antimicrobial effects forup to 48 hours after application, is safe for use on themale genitalia and is more cost-effective than povi-done-iodine. Although larger studies are needed todetermine a difference in clinical outcome, chlor-hexidine-alcohol appears to be the optimal agent forskin preparation before urological prosthetic proce-dures.
ACKNOWLEDGMENTS
Liu Yang assisted with statistical analysis.
1. Kojic EM and Darouiche RO: Candida infectionsof medical devices. Clin Microbiol Rev 2004; 17:255.
2. Stanford JL, Feng Z, Hamilton AS et al: Urinaryand sexual function after radical prostatectomyfor clincally localized prostate cancer: the Pros-tate Cancer Outcomes Study. JAMA 2000; 283:354.
3. Wilson SK and Costerton JW: Biofilm and penileprosthesis infections in the era of coated im-plants: a review. J Sex Med 2012; 9: 44.
4. Jarow JP: Risk factors for penile prosthetic in-fection. J Urol 1996; 156: 402.
5. Wilson SK, Carson CC, Cleves MA et al: Quanti-fying risk of penile prosthesis infection with el-evated glycosylated hemoglobin. J Urol 1998;159: 1537.
6. Wilson SK, Henry GD, Delk JR et al: Prevention ofinfection in revision of penile prosthesis usingantibiotic coated prosthesis and Mulcahy salvageprotocol. J Urol, suppl., 2003; 169: 325, abstract1264.
7. Lai HH, Hsu EI, Teh BS et al: 13 Years of expe-rience with artificial urinary sphincter implanta-tion at Baylor College of Medicine. J Urol 2007;
8. Guimarães M, Oliveira R, Pinto R et al: Interme-diate-term results, up to 4 years, of a bone-anchored male perineal sling for treating malestress urinary incontinence after prostate sur-gery. BJU Int 2009; 103: 500.
9. Saltzman MD, Nuber GW, Gryzlo SM et al: Effi-cacy of surgical preparation solutions in shouldersurgery. J Bone Joint Surg Am 2009; 91: 1949.
10. Darouiche RO, Wall MJ, Itani KM et al: Chlor-hexidine-alcohol versus povidone-iodine for sur-gical site antisepsis. N Engl J Med 2010; 362: 18.
11. Jefferson KK: What drives bacteria to produce abiofilm? FEMS Microbiol Lett 2004; 236: 163.
12. Von Eiff C, Neilman C and Peters G: New aspectsin the molecular basis of polymer-associated in-fections due to Staphylococcus. Eur J Clin Micro-biol Infect Dis 1999; 18: 843.
13. Costerton W, Veeh R, Shirtliff M et al: Theapplication of biofilm science to the study andcontrol of chronic bacterial infections. J Clin In-vest 2003; 112: 1466.
14. Data on file. CareFusion, Inc., San Diego, Califor-nia.
15. Hemani ML and Lepor H: Skin preparation for theprevention of surgical siteinfection: which agent
: 190.
16. Trostle SS and Hartmann FA: Surgical infection.In: Equine Surgery, 2nd ed. Edited by JA Auer.Philadelphia: WB Saunders 1992; p 47.
17. Henry GD, Kansal NS, Callaway M et al: Centersof excellence concept and penile prostheses: anoutcome analysis. J Urol 2009; 181: 1264.
18. Armstrong EP, Patrick KL and Erstad BL: Compar-ison of preoperative skin preparation products.Pharmacotherapy 2001; 21: 345.
19. Segal CG: Infection control: start with skin. NursManage 2006; 37: 46.
20. Henry GD, Wilson SK, Delk JR 2nd et al: Revisionwashout decreases penile prosthesis infection inrevision surgery: a multicenter study. J Urol 2005;173: 89.
21. Perry A and Lambert P: Propionibacterium acnes:infection beyond the skin. Expert Rev Anti InfectTher 2011; 9: 1149.
22. de Blacum C, Ogunleye A and Momoh A: Highbody mass index and smoking predict morbidity inbreast cancer surgery: a multivariate analysis of26,998 patients from national surgical qualityimprovement database. Ann Surg 2012; 255: 551.
23. Macario A: What does one minute of operating
room time cost? J Clin Anesth 2010; 22: 233.