Embed Size (px)
Citation preview

851MR. R. H. RUSSELL: IRREDUCIBLE DISLOCATION AT THE ELBOW.
reaction, a specific gravity of 1015, a minute trace of
albumin, no sugar, a large deposit of amorphous and triplephosphates, and some epithelial cells. A subsequent acuteattack of renal colic was the prelude to a short illness in thecourse of which he had much trouble with his bladder, andwhich terminated fatally from sudden and unexpected coma.The details of this case are so interesting and the record
of symptoms is so graphic that I hope no apology is neces-sary for the length of the extracts which I have quoted.The entire disappearance of phosphaturia during the timehe was taking butter-milk suggests that the acids which itcontains so abundantly had probably something to do withneutralising the excess of phosphates, and if this be so itraises the question whether the large quantities of butter-milk which during his craze he was tempted to drink doesnot convey a hint that in the use of acids in ordinary formsof neutral or alkaline phosphatic urine we perhaps err indealing with inadequate doses.The presence of triple phosphates in the last analysis and
the co-existence of pain, heat, and straining on micturitiontoo clearly showed that the bladder had become the seat of acalculus, most probably a rapidly accumulating mass ofphosphates outside a uric acid nucleus. He died comatoseand this could hardly be ascribed to the condition of eitherhis bladder or kidney. It more closely resembled the comaso often met with in diabetes mellitus. The urine was per-sistently excessive in quantity but it never contained sugar.If the uric acid element in this case be left out the pictureof Tessier’s phosphatic diabetes is almost complete. Mostof the leading features of ordinary diabetes present them-selves but the urine contains as its abnormal constituent anexcess of phosphates instead of sugar.
Cases of this disorder are rare, but their diagnosis is easyif due attention is given to the urine, which is always neutralor alkaline in reaction, excessive in amount, usually of lowspecific gravity, and loaded with phosphates often of thestellar variety. The diseases with which it is most liable tobe confused are diabetes mellitus, diabetes insipidus, andchronic interstitial nephritis. The urine of diabetes mellituscontains sugar and that of interstitial nephritis albumin, sothat in straightforward cases either may be readily dis-tinguished from the urine of phosphaturia. The lattercondition, however, may occur in association with either orboth of the former, when the urine will be found to containphosphates, together with sugar or albumin, or with both.The effect upon the general health tends to be ultimately
serious and the prognosis should always be guarded. Theoccurrence of attacks of drowsiness, the onset of emaciation,the alternation of sugar with stellar phosphates, or a per-manent increase in the urea excretion are the more importantpoints which add to the gravity of the prognosis.Treatment is summed up, according to Ralfe, in rest anc
improvement of the general nutrition. Drugs seem to bEof little avail in checking the undue excretion of phosphateseven opium, which is of such value in true diabetes, has n(effect and is, on account of the tendency to drowsiness, riolaltogether free from risk. Butter-milk may be added to th4
daily dietary and will be found of considerable nutritiv4value. This case suggests that it may also possess soml
direct power over phosphates when these are present iimarked excess.Chesham-street, Belgrave-square, S.W.
CLERICAL, MEDICAL, ANDGENERAL LIFE ASSUR-ANCE SOCIETY.-The report of this society for the yearended June 30th, 1899, shows that the new assurances con-sisted of 810 policies, assuring .6641,353, and yielding inannual premiums f.2t.797. Re-assurances were effected tothe extent of f:46,OOO. with annual premiums of .61741.The net new business of the year was therefore .6595,353 insums assured, yielding annual premiums of f:20.056. Thetotal premium income was .6293,773, showing an increase ofE5148 over last year, and the whole income of the societywas raised from .6422.006 to f.431,776. The claims arisingfrom the death of 235 persons, assured under 299 policies,were for the aggregate amount of .6239,897. The excess ofrevenue over all expenditure amounted to no less than.6109,900 and raised the assurance fund at the close of theyear to .63,590,305. Three vacancies occurred in the boardof directors caused by the death of Sir John Mowbray (thechairman) and the resignation of Lord Curzon and LordLister. Sir Thomas Smith, F.R.C.S.Eng., was elected inLord Lister’s place.
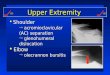
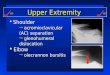
A CASE OF IRREDUCIBLE DISLOCATIONAT THE ELBOW.
BY R. HAMILTON RUSSELL, F.R.C.S. ENG ,SURGEON TO THE MELBOURNE HOSPITAL FOR SICK CHILDREN.
ON June 27th last a little boy, aged eight years, whileplaying at football fell with the left arm twisted under himand sustained a dislocation of both bones of the forearmbackwards at the elbow. He was attended by Dr. Loosli ofthis city, who was at once struck by certain peculiarities inthe casa; he also found that all efforts at reduction, evenunder chloroform, were of no avail, and asked me to see thepatient with him.On examination the fact of dislocation backwards of both
bones was very obvious, but there were unusual featureswhich, as the accident is one that, so far as I can ascertainqis now recorded for the first time, I will describe withsome minuteness. First, the arm was markedly straighterthan usual-so nearly straight, in fact, that it had beenfound possible to put the limb up somewhat loosely instraight cardboard splints ; secondly, there was an absenceof the usual marked fixity of the arm, so that the forearmcould be moved through a considerable angle but couldhardly be made to approach so near to a right angle withthe humerus as is usual in such a dislocation ; thirdly, onattempting reduction, the sensation imparted to me was
quite novel’: the forearm yielded to the pull quite easily, andthe deformity could be very nearly reduced but not quite,while directly the force was withdrawn the bones sprang backinto their false position with a kind of elastic rebound.There was also occasional slight crepitus. I was unable atthe time to make a correct diagnosis of the exact anatomicalnature of the injury which produced these phenomena, but Iadvised, with Dr. Loosli’s concurrence, an operation whichwas undertaken the next day.Through a longitudinal incbion over the extensor aspect
of the joint the triceps and aponeurotic investment of thejoints were divided and the interior of the articulation wasexposed to view. It was then found that the interior was
occupied by a mass of muscle which further investigationmade evident as the brachialis anticus. The internal epi-condyle was separated, which explained the slight crepit-usduring examination. ’lhe humerus at the time of the injuryhad pushed its way through the anterior ligament of the jointand passing to the outer side of the brachialis anticushad become lodged on the front of that muscle ; so that
when viewed through the operation wound the muscle lay: strapped over the back of the lower end of the humerus and, pinched tightly between that bone and the coronoid processI of the ulna. It was necessary to divide a portion of thedisplaced muscle, and when that wa<s done a strong curved, spatula was passed between the remainder of the muscle and, the bone and the humerus was easily pulled into place. The divided triceps was then sutured, the skin wound was com-apletely closed, and the arm was put up straight in a stifl
bandage. Six days later the bandage was taken off for theremoval of the stitches. The wound was quite healed, and thelittle boy was able to bend his arm without assistance twonear the right angle, in which position it was put up againin plaster-of-Paris for a further fortnight. Three weeksfrom the operation all apparatus was removed, but the childwas directed to wear a sling for one week more, withpermission, however, to take the arm out to use it when so,inclined, but to return it to the sling when not using it ;this was out of consideration for the partially dividedbrachialis anticus muscle. No passive motion was per-formed, although the elbow remained very stiff for someweeks. When last seen, five months after the accident, how-ever, the movement had all returned and the result was
perfect as to the utility of the arm, but on close inspectionduring flexion of the arm I had reason to think that thebrachialis anticus had never completely recovered and thatthe other muscles passing from the condyles to the forearmand wrist were called upon for a somewhat larger share thanusual in the production of flexion at the elbow. Thisseemed, however, to make no difference, as the child wasable to play cricket and other games, and there was no.
perceptible weakness or defect in the limb.Melbourne.

852 HOSPITAL MEDICINE AND SURGERY.
OF
HOSPITAL PRACTICE,BRITISH AND FOREIGN.
HOSPITAL FOR SICK CHILDREN, GREAT ORMOND-STREET.
A CASE OF CHRONIC INTESTINAL OBSTRUCTION ; NECROPSY.
(Under the care of Dr. D. B. LEES.)
Nulla autem est alia pro certo noscendi via, nisi quamplurimas etmorborum et dissectionum historias, tum aliorum tum propriascollectas habere, et inter se comparare.—MoBeeM De Sed. et G’a2tF.JMOf6., lib. iv. Procemiutn. -
INTESTINAL obstruction is a rare but very important com-plication of appendicitis. It is specially likely to occur incases in which localised abscesses have formed and
Hawkins 1 describes four deaths as due to this cause in tenfatal cases of local abscess ; these are generally acute cases.Obstruction of the intestine, when chronic in character, if dueto appendicitis, is more likely to result from matting togetherof the bowel as in the case recorded below. In thisinstance it is not improbable that tuberculous disease of theappendix was the cause of the adhesions. Fitz met witheight cases of perforation of the appendix resulting fromtuberculosis in 257 cases of appendicitis. For the notes of thecase we are indebted to Dr. Hugh Thursfield, medicalregistrar and pathologist.A boy, aged two and a half years, was admitted into the i
Hospital for Sick Children, Great Ormond-street, under the icare of Dr. D. B. Lees, at the end of June, 1899. He wasbrought to the hospital on account of constipation and wastreated in the out-patient department. The constipation wasfollowed by a bad attack of diarrhcea for which he was madean in-patient. The history given by his mother was that tillthe age of 18 months he was a healthy child, but he thenbegan to suffer from attacks of diarrhoea. Three monthslater his stomach was noticed to be getting larger and thediarrhcea was now accompanied by abdominal pain. He wastreated by a medical man and improved, but about Easter,1899, he began to have attacks of abdominal pain in which thestomach was, as his mother said, " drawn up in cord:" Hetwice passed blood by the rectum and vomited dark-brownfluid. He went to the country and improved for a time, but theabdominal troubles recurred and he was taken to the hos-
pital. As well as could be ascertained the family historyand the surroundings of the child were fairly good, thoughhis mother’s father was stated to have died from "con-sumption."
.
On admission the child was very thin and fretful but badno fever and at first no diarrhoea; his appetite was fairlygood and he did not appear to be very ill. The heart and
lungs were apparently sound, but the abdomen was enlarged ;there was visible peristalsis, and on the right side rather lowdown there was a mass which felt like a mass of enlargedglands. From time to time this mass could be felt in
slightly different positions, the most constant being just tothe right of, and below, the umbilicus. At first the child
improved greatly, but at the end of July diarrhoea with somefever set in and he began to lose ground. The motions werepale, slimy, and drab-coloured. There was never anyblood. In August and September he had several severeattacks of abdominal pain, which were accompanied byvisible peristalsis, the small intestines being especially con-cerned. The diagnosis lay between enlarged tuberculousglands with matting tcgether of coils of intestine anda chromic intussusception of the bowel. In the hope ofrelieving the obstruction laparotomy was performed by Mr.T. H. Kellock on Sept. 28th. He felt some large glands andsaw a few yellow tubercles on the peritoneum; some adherentcoils of intestine were separated and a small band of fibroustissue was divided. After the operation the child was com-pletely relieved of the attacks of abdominal pain but hiscondition otherwise remained unaltered. The diarrhcearecurred, he began to have an intermittent temperature, andgradually sank, and died on Oct. 12th.
1 Diseases of the Vermiform Appendix, p. 94.2 Mynter : Appendicitis, p. 89.
3 American Journal of the Medical Sciences, October, 1888.
Nee,ropsy.-The post-mortem examination was made 48hours atter death. In the head and thorax no abnormal con-dition was observed. On the parietal peritoneum in a fewplaces there were small scattered granular tubercles but nogeneral tuberculous peritonitis was present. On the rightside the liver was bound to the abdominal wall by denseadhesions. The lowest part of its right lobe was involved in amass which consisted of liver, intestine, peritoneum, andmesentery and they were so bound together that even carefuldissection could scarcely separate the various parts. Thismass lay to the right of, and rather below, the umbilicus,lying, in fact, over the lower half of the right kidney. Ondissecting the mass the appendix was found lying in a linepointing vertically upwards behind the colon. Its tip, how-ever, on the inner side of the colon was adherent to the lowestpart of the right lobe of the liver ; and matted roundthis point were loops of small intestine, the mesentery,the ascending colon, and several large glands, in one ofwhich there was a caseous focus. In two places at leastthere was a fistulous communication between the appendixand the small intestine which was much ulcerated. Theascending colon showed very little ulceration and no fistulawas found. On opening the loop of small intestine twosmall brownish bodies fell out which resembled the kernelof some fruit, such as an apricot. The small intestine abovethe portion involved in the tumour had its walls remark-
ably thickened and hypertrophied. The descending colonwas the site of very numerous small ulcerations, some ofwhich showed tubercles on the peritoneal surface, and allwere transverse to the gut and had edges slightly raised andmuch undermined. The lowest portion of the sigmoidflexure was caught up and fixed by strong adhesions to thetumour above. The spleen showed a few granular tuberclesand one small caseous patch. The mesenteric glands wererather larger than normal and in one of these there was afocus of caseation, but no mass of large glands was found.The glands elsewhere were normal.Remarks by Dr. Lu4 Es.-An accurate diagnosis of this case ’
may fairly be said to have been impossible. The mass felton admission was thought to be composed of caseous glandsand intestine matted together by a chronic tuberculous
process. The history given by the mother seemed to be inaccord with this view, the blood passed on two occasions perrectum and the diarrhoea being ascribed to tuberculousulcerations of the bowel. The attacks of abdominal pain andthe visible peristalsis were ascribed to the obstruction causedby the implication of the intestine in the mass which couldbe felt. But when the peristalsis became extreme, coils ofsmall intestine pushing forward the abdominal wall in
prominent ridges during the attacks of pain, it was deter-mined to try whether any relief could be given by operation.The laparotomy revealed adherent intestine, enlarged glands,and some tubercle. As much separation of the adhesions waseffected as seemed possible without incurring the risk of
rupture of the bowel. But the facts that a coil of smallintestine was adherent to a diseased appendix vermiformis,with two communications into it, that the tip of the
appendix was adherent to the liver, and that the adherentbowel contained two foreign bodies, were revealed only bythe necropsy. It may be added that the foreign bodies wereprecisely similar to one another, being oval in shape andquite unlike the feecal concretions " which often perforatethe appendix.
-Z?ev2,arks by Dr. THURSFIELD.-Pathologically the pointsof interest seem to me to be the unusual position of the
appendix and the question of the sequence of events-that is,whether the tuberculous infection preceded and determinedthe formation of the adhesions between the liver and
appendix or whether the tuberculous infection took placein a part of the intestine which was already the seat ofinflammation. I do not think that it is possible to advancebeyond speculation, but probability appears to me to point tothe first solution. The presence of the foreign bodies I
regard as accidental and quite recent.
BEDFORD COUNTY HOSPITAL.A CASE OF SUPPURATIVE APPENDICITIS WITH SECONDARY
LIVER ABSCESSES.
(Under the care of Mr. W. GIFFORD NASH.)ABSCESS of the liver occurring in the course of appen-
dicitis is nearly always the result of a septic thrombosis orof a pylephlebitis, but, as in the case here recorded, it may