Embed Size (px)
Citation preview

8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 1/8
ORIGINAL CONTRIBUTION
Fluorouracil vs Gemcitabine Chemotherapy
Before and After Fluorouracil-BasedChemoradiation Following Resectionof Pancreatic AdenocarcinomaA Randomized Controlled TrialWilliam F. Regine, MD
Kathryn A. Winter, MS
Ross A. Abrams, MD
Howard Safran, MDJohn P. Hoffman, MD
Andre Konski, MD
Al B. Benson, MD
John S. Macdonald, MD
Mahesh R. Kudrimoti, MD
Mitchel L. Fromm, MD
Michael G. Haddock, MD
Paul Schaefer, MD
Christopher G. Willett, MD
Tyvin A. Rich, MD
DESPITE POTENTIALLY CURA-tive resection for pancre-atic adenocarcinoma, pat-terns of failure analyses
demonstrate a 50% to 85% compo-nent of local relapse associated withliver and intra-abdominal failure and a5-year survival of less than 20%.1-5 Thefrequency and pattern of failure makethe combination of adjuvant postop-erative chemotherapy and radiation animportant consideration. Phase 3 trials
have demonstrated long-term survivalof up to 20% of patients with resectedadenocarcinoma of the pancreastreatedwith adjuvant fluorouracil-based che-moradiation (chemotherapy plus ra-diation).6-8 Although these trials have
been small, their findings, combinedwith large institutional results,9,10 havesupported the use of postoperative ad- juvant chemoradiation with fluoroura-cil as a standard of care in the UnitedStates for more than 20 years.
TheUSFoodandDrugAdministrationapprovedgemcitabinein1996as thefirst
chemotherapeuticagent forpatientswithpancreaticcancersinceitsapprovaloffluo-rouracilnearly35yearsago.Approvalwasbasedon theresultsofstudiesonadvanced
For editorial comment see p 1066.
Author Affiliations are listed at the end of this article.Corresponding Author: William F. Regine, MD, Uni-versity of Maryland, 22 S Greene St, Baltimore, MD21030 ([email protected]).
Context Among patients with locally advanced metastatic pancreatic adenocarci-noma, gemcitabine has been shown to improve outcomes compared with fluorouracil.
Objective To determine if the addition of gemcitabine to adjuvant fluorouracil che-
moradiation (chemotherapy plus radiation) improves survival for patients with re-sected pancreatic adenocarcinoma.
Design, Setting, and Participants Randomized controlled phase 3 trial of pa-tients with complete gross total resection of pancreatic adenocarcinoma and no prior radiation or chemotherapy enrolled between July 1998 and July 2002 with follow-upthrough August 18, 2006, at 164 US and Canadian institutions.
Intervention Chemotherapy with either fluorouracil (continuous infusion of 250 mg/m2
per day; n=230) or gemcitabine (30-minute infusion of 1000 mg/m2 once per week;n= 221) for 3 weeks prior to chemoradiation therapy and for 12 weeks after chemo-radiation therapy. Chemoradiation with a continuous infusion of fluorouracil (250 mg/m2
per day) was the same for all patients (50.4 Gy).
Main Outcome Measures Survival for all patients and survival for patients with pan-creatic head tumors were the primary end points. Secondary end points included toxicity.
Results A total of 451 patients were randomized, eligible, and analyzable. Patientswith pancreatic head tumors (n=388) had a median survival of 20.5 months and a3-year survival of 31% in the gemcitabine group vs a median survival of 16.9 monthsand a 3-year survival of 22% in the fluorouracil group (hazard ratio, 0.82 [95% con-fidence interval, 0.65-1.03]; P =.09). The treatment effect was strengthened on mul-tivariate analysis (hazard ratio, 0.80 [95% confidence interval, 0.63-1.00]; P =.05).Grade 4 hematologic toxicity was 1% in the fluorouracil group and 14% in the gem-citabine group (P .001) without a difference in febrile neutropenia or infection. Therewere no differencesin the ability to complete chemotherapyor radiation therapy (85%).
Conclusions The addition of gemcitabine to adjuvant fluorouracil-based chemora-diation was associated with a survival benefit for patients with resected pancreatic can-cer, although this improvement was not statistically significant.
Trial Registration clinicaltrials.gov Identifier: NCT00003216
JAMA. 2008;299(9):1019-1026 www.jama.com
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 5, 2008—Vol 299, No. 9 1019

8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 2/8
disease.11,12 Inarandomizedtrialofgem-citabine vs fluorouracil as a first-linetherapyin 126patientswith advanced or
metastatic adenocarcinoma of the pan-creas, the median survival for patientstreatedwithgemcitabinewas5.7monthsand 1-year survival was 18% comparedwithamediansurvivalof4.4monthsand1-year survivalof2%for patientstreatedwithfluorouracil (P=.003).11 The activ-ityofgemcitabineinadvancedpancreaticcancer ledto theevaluationofgemcitab-ineincombinationwith chemoradiationwithfluorouracilinanattempttoimprovesurvivalforpatientswithresectedpancre-atic adenocarcinoma. This study repre-sents the first US cooperative group ad- juvantpancreaticphase3trialin3decades.
METHODS
Eligibility
An intergroup trial was conductedby thefollowing US National Cancer Institute–sponsored cooperative groups: the Ra-diation Therapy Oncology Group
(RTOG), the Eastern Cooperative On-cology Group, and the Southwest On-cology Group, inclusive of Canadianaf-filiates. The RTOG served as the leadgroup with the trial designation RTOG97-04.
The eligibility criteria included his-tologically confirmed adenocarci-noma of thepancreas andgross total tu-mor resection, confirmed by centralreview of operative and pathology re-ports. In addition, postoperative com-puted tomographic (CT) imaging wasrequired within 3 weeks of randomiza-tion to exclude patients who had evi-dence of persistent or recurrent localdisease or developed metastatic dis-ease prior to therapy. Surgical resec-tion margins were categorized as nega-tive, microscopically positive, or
unknown (defined as those having nocomment regarding margins in the pa-thology report).
Eligibility requirements also in-cluded stages T1 to T4, N0 to N1, andM0 according to the 1997 staging cri-teria of the American Joint Commis-sion on Cancer (BOX).13 If there wereno identifiable lymph nodes within theresection specimen, the patient was in-eligible. Patients were required to havea Karnofsky performance status of 60or higher; adequate hematologic, re-
nal, and hepatic function as defined bythe following: a white blood cell countof 3103 /µL or higher, a platelet countof 100103 /µL or higher, serum bili-rubin andcreatinine less than 1.5theupper limit of institutional normal, a se-rum aspartate aminotransferase con-centration 5 the upper limit of insti-tutional normal, and a documentedcaloric intakeof more than 1500 kcal/d.Patients with any prior radiotherapy toany site or chemotherapy were ineli-gible for this study, as were patients
with any prior malignancy other thannonmelanoma of the skin or in situ of thecervix. Theserum tumor marker CA19-9 was submitted for central testingand review. Protocol therapy was re-quired to begin 3 to 8 weeks after re-section and within 5 days of random-ization. All patients required writtenand informed consent according to in-
stitutional andfederal guidelines. All in-stitutions were required to have cur-rent institutional review board approvalon file with their respective group priorto registration of anypatients. The trialwas routinely monitored for excessive
toxicity by the RTOG Data Monitor-ing Committee, which functions inde-pendently of the RTOG.
Treatment Plan
After undergoing tumor resection, pa-tients were randomly assigned to eitherfluorouracil (group 1) or gemcitabine(group 2). Randomization was per-formed 3 to 8 weeks after surgery by adynamic balancing procedure, whichincluded stratification according to tu-mor diameter (3cmvs3 cm), nodalstatus (negative vs positive), and sur-
gical margins (negative vs positive vsunknown). Chemotherapyprior to che-moradiation therapy in group 1 con-sisted of a continuous infusion of 250mg/m2 of fluorouracil per day for 3weeks. Chemotherapy prior to chemo-radiation therapy in group 2 consistedof a 30-minute infusion of 1000 mg/m2
of gemcitabine onceweeklyfor 3 weeks.Between 1 and 2 weeks after comple-tion of chemotherapy, chemoradia-tion was initiated and was the same forboth groups (50.4 Gy with a continu-
ous infusion of 250 mg/m2
of fluoro-uracil daily throughout radiationtherapy).
Another phase of chemotherapy wasinitiated 3 to 5 weeks after completionof chemoradiation therapy. Group 1 re-ceived 3 months of a continuous infu-sion of fluorouracil daily [(4 weeks onplus 2 weeks off)2]. Group 2 re-ceived 3 months of gemcitabine [(3weeks onplus 1 weekoff)3]. Radia-tion therapy was delivered in 28 frac-tions (5 days per week) to the tumor
bed andregional nodes. Thetumor bedwas defined by preoperative CTimaging. Local pancreatic, celiac, mes-enteric, periaortic, pancreatic, duode-nal, and hepatic portal lymph nodeswere included in the radiation therapyfields.14 After an initial dose of 45 Gy,the final dose of 5.4 Gy was limited tothe tumor bed as defined by the pre-
Box. 1997 Staging Criteria
of the American
Joint Commission on Cancer
Primary tumor
T1: Tumor limited to the pancreas
and 2 cmor less ingreatest dimen-sion.
T2: Tumor limited to the pan-creas and more than 2 cm ingreatest dimension.
T3: Tumor extends directly intoany of the following: duodenum,bile duct, peripancreatic tissues.
T4: Tumor extends directly intoany one of the following: stom-ach, spleen, colon, adjacent largevessels.
Regional lymph nodes
N0: No regional lymph nodemetastasis.
N 1 : R e g i o n a l l y m p h n o d emetastasis.
Distant metastasis
M0: No distant metastasis.
M1: Distant metastasis.
CHEMOTHERAPY WITH FLUOROURACIL VS GEMCITABINE PLUS CHEMORADIATION
1020 JAMA, March 5, 2008—Vol 299, No. 9 (Reprinted) ©2008 American Medical Association. All rights reserved.

8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 3/8
operative tumor volume. At least 4-MVphotons and a minimum 3 to 4 field ap-proach was used. Doses were limited toless than 60% of hepatic volume re-ceiving more than 30 Gy. At least two-thirds of one functioning kidney was
spared fromradiation therapy fields andthe spinal cord was limited to less than45 Gy. Prospective quality assurance of radiation therapy was required for all.This was inclusive of submission of apreoperative abdominal CT scan and ra-diation therapy fieldsto be used for cen-tral review and approval prior to thestart of chemoradiation.
Follow-up of Patients
A follow-up visit was required at 2 to 4weeks after completion of chemoradia-tion and prior to the start of the second
phase of chemotherapy after chemora-diationtherapy.Thereafter, follow-upoc-curred at 3-month intervals for 1 year,then at6-month intervalsfor 3 years,andyearly thereafter. The last date of pa-tient follow-upwasAugust 18,2006.Fol-low-up consisted of physical examina-tion, complete blood cell count, liverfunction testing, chest x-ray, and CTscanning as clinically indicated. Eleva-tion in CA 19-9 level in and of itself wasnot to be considered a criterion for dis-ease recurrence.
Statistical Considerations
Survival for all patients and for pa-tients withpancreatic headtumors werethe primary end points. Secondary endpoints were disease-free survival andtoxicity, which was scored per the USNational Cancer Institute’s CommonToxicity Criteria version 2.0. All endpoints were prespecified in the origi-nal design of the trial and all analyseswere conducted on an intention-to-treat basis. Failure for overall survival
was defined as death due to any causeand was measured from date of ran-domization to date of death or last fol-low-up for censored patients. Failurefor disease-free survival was defined aslocal, regional, or distant relapse, ap-pearance of a second primary, or deathdue to any cause and measured fromdate of randomization to date of first
failureor lastfollow-upfor censoredpa-tients. Patients who did not have a fail-ure for overall survival or disease-freesurvival were censored as of their lastfollow-up visit.
Patients were stratified by nodal sta-
tus (uninvolved vs involved), tumor di-ameter (3cmvs3 cm), andsurgicalmargin status(negative vspositivevsun-known). The permuted block random-ization methodwasusedwith patientfac-tors balanced according to thepermutedblock randomization method.15 At anoriginal expected accrualof5 patients permonth,330patients were targeted to de-tect a 33% reduction in the hazard rateof overall survival for the chemoradia-tion plus gemcitabine group comparedwiththe chemoradiation plusfluoroura-cil group (increase in median survival
from 18to 27months; hazardratio[HR],0.67) with 80% power and a 2-sided level of .05,assuming an exponential dis-tribution. In early 2001, based on unex-pectedly rapid accrual (13 patients permonth) andafter approval by the US in-tergroup, the RTOG data monitoringcommittee,andtheNationalCancer In-stitute, the samplesize was increased tofind a smaller treatment effectwith morepower. Four hundred seventy analyz-able patients wouldprovide 85% powerto detect a 28% decrease in the HR of
overallsurvival (increase in mediansur-vival from 18 to 25 months; HR, 0.71)for all patients and 80% power in pa-tients with pancreatic head lesions.
All analyses were performed usingSAS version 9.1 statistical software(SASInstitute Inc, Cary, North Carolina).The 2 tests were used to compare dif-ferences among pretreatment charac-teristics between treatment groups. ForCA 19-9, the variable was categorizedas less than 180 U/mL vs 180 U/mL orhigher to be consistent with a protocol-
specified CA 19-9 analysis to be per-formed subsequentlyand based on pub-lished literature.16 Thez tests were usedto test for differences in binomial pro-portions of grade 3 toxic effects orhigher (worst overall, worst nonhema-tologic, and worsthematologic). Overalland disease-free survival were esti-mated univariately using the Kaplan-
Meier method17 and treatment groupswere compared using thelog-rank test.18
Multivariate analyses were performedwith Cox proportional hazard mod-els19 to test for treatment differences(between groups) while adjusting for
the stratification variables of nodal in-volvement (no vs yes), tumor diam-eter (3cmvs3 cm), andmargin sta-tus (negative vs positive and negativevs unknown), as well as any other vari-ablesthat were imbalanced between thetreatment groups. A tumor diameter of 3 cm was used for stratification basedon a prior large institutional study.9 Alltests were performed at a significancelevel of .05. All variables arecoded suchthat an HRof more than 1 indicates anincreasedrisk for thesecondlevel of thevariable and an HR of less than 1 indi-
cates a benefit for the second level of the variable.
RESULTS
Demographic Characteristics
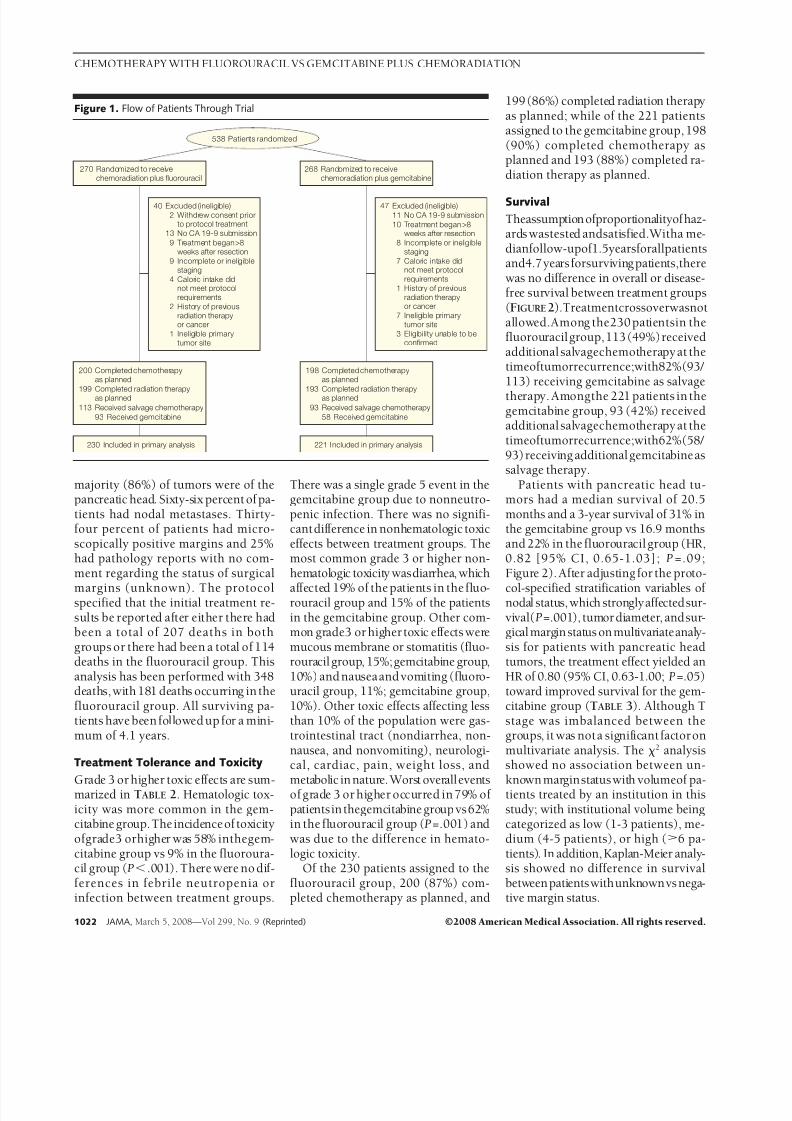
Between July 1998 and July 2002, 538patients at 164 institutions were ran-domized. Based on additional informa-tion obtained perprotocol after random-ization,87 patients (16%) wereineligibledue to lack of submission of serum tu-mor marker CA 19-9 (n=24), therapystarted more than 8 weeks after resec-
tion (n= 19), staging was incomplete orineligible (n= 17), caloric intakedid notmeet protocol requirements (n= 11), in-eligible primary tumor site (n=8), eli-gibility unable to be confirmed (n=3),history of previous radiation therapy orcancer (n=3), and/or patients with-drew consent(n=2). Thesepatients andreasons for ineligibility were evenly dis-tributed between treatment groups. Of the remaining 451 patients, 230 wererandomly assigned to chemoradiationplus fluorouracil and 221 to chemora-
diation plus gemcitabine (FIGURE 1
).Demographic factors were similar be-tween groups with the exception of Tstage (TABLE 1). The chemoradiationplus gemcitabine group had a higherpercentage of patients with T3 or T4disease (81%) compared with those ran-domized to the chemoradiation plusfluorouracil group (70%; P= .01). The
CHEMOTHERAPY WITH FLUOROURACIL VS GEMCITABINE PLUS CHEMORADIATION
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 5, 2008—Vol 299, No. 9 1021
8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 4/8
majority (86%) of tumors were of thepancreatic head. Sixty-six percent of pa-tients had nodal metastases. Thirty-four percent of patients had micro-scopically positive margins and 25%had pathology reports with no com-ment regarding the status of surgical
margins (unknown). The protocolspecified that the initial treatment re-sults be reported after either there hadbeen a total of 207 deaths in bothgroups or there had been a total of 114deaths in the fluorouracil group. Thisanalysis has been performed with 348deaths, with 181 deaths occurring in thefluorouracil group. All surviving pa-tients have been followed up for a mini-mum of 4.1 years.
Treatment Tolerance and Toxicity
Grade 3 or higher toxic effects are sum-marized in TABLE 2. Hematologic tox-icity was more common in the gem-citabine group.Theincidenceof toxicityofgrade3 orhigher was 58% inthegem-citabine group vs 9% in the fluoroura-cil group (P .001). There were no dif-ferences in febrile neutropenia orinfection between treatment groups.
There was a single grade 5 event in thegemcitabine group due to nonneutro-penic infection. There was no signifi-cantdifference in nonhematologic toxiceffects between treatment groups. Themost common grade 3 or higher non-hematologic toxicity wasdiarrhea, which
affected 19% of the patients in the fluo-rouracil group and 15% of the patientsin the gemcitabine group. Other com-mon grade3 or higher toxic effects weremucous membrane or stomatitis (fluo-rouracil group, 15%;gemcitabine group,10%) and nauseaand vomiting (fluoro-uracil group, 11%; gemcitabine group,10%). Other toxic effects affecting lessthan 10% of the population were gas-trointestinal tract (nondiarrhea, non-nausea, and nonvomiting), neurologi-cal, cardiac, pain, weight loss, and
metabolic in nature. Worst overalleventsof grade 3 or higher occurred in 79% of patientsinthegemcitabine group vs62%in the fluorouracil group (P=.001) andwas due to the difference in hemato-logic toxicity.
Of the 230 patients assigned to thefluorouracil group, 200 (87%) com-pleted chemotherapy as planned, and
199 (86%) completed radiation therapyas planned; while of the 221 patientsassigned to the gemcitabine group, 198(90%) completed chemotherapy asplanned and 193 (88%) completed ra-diation therapy as planned.
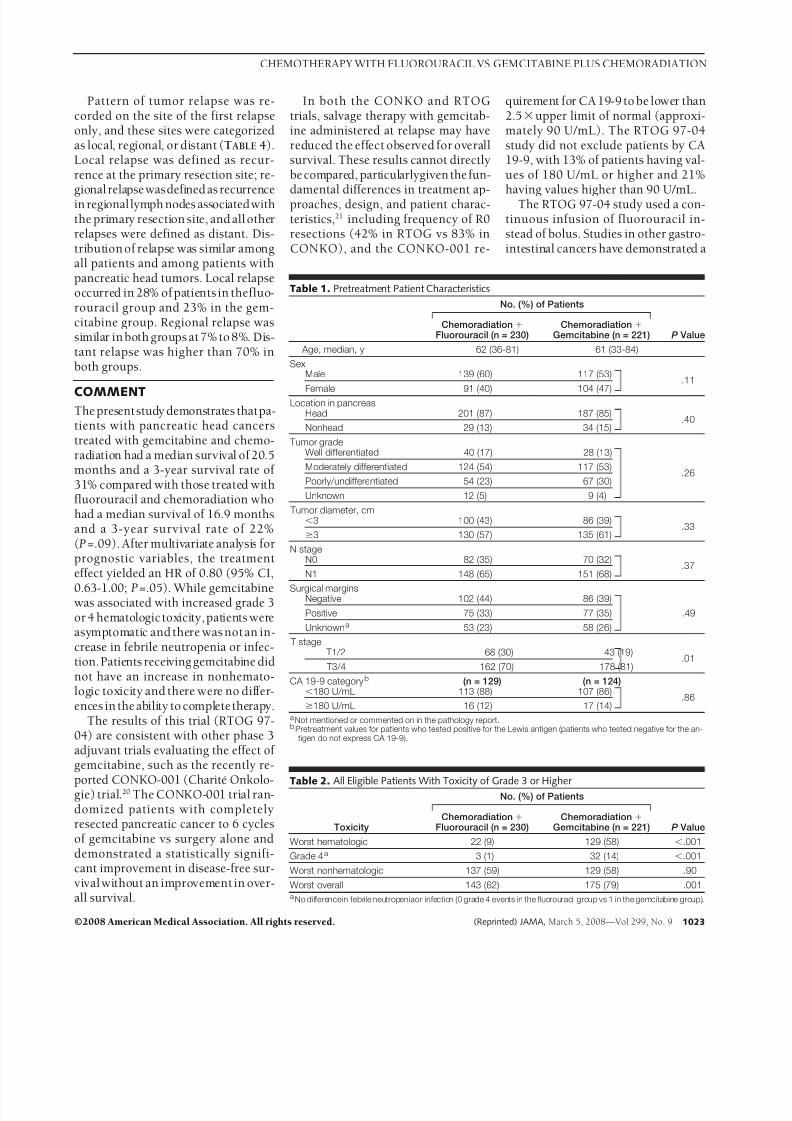
Survival
Theassumptionofproportionalityofhaz-ards wastested andsatisfied.Witha me-dianfollow-upof1.5yearsforallpatientsand4.7yearsforsurviving patients,therewas no difference in overall or disease-free survival between treatment groups(FIGURE2).Treatmentcrossoverwasnotallowed.Among the230 patientsin thefluorouracil group,113 (49%)receivedadditional salvagechemotherapy at thetimeoftumorrecurrence;with82%(93/ 113) receiving gemcitabine as salvage
therapy. Amongthe 221 patients in thegemcitabine group, 93 (42%) receivedadditional salvagechemotherapy at thetimeoftumorrecurrence;with62%(58/ 93)receiving additional gemcitabineassalvage therapy.
Patients with pancreatic head tu-mors had a median survival of 20.5months and a 3-year survival of 31% inthe gemcitabine group vs 16.9 monthsand 22% in the fluorouracil group (HR,0.82 [95% CI, 0.65-1.03]; P=.09;Figure 2). After adjusting for the proto-
col-specified stratification variables of nodal status, which stronglyaffectedsur-vival(P=.001), tumor diameter, andsur-gical margin status onmultivariateanaly-sis for patients with pancreatic headtumors, the treatment effect yielded anHR of 0.80 (95% CI, 0.63-1.00; P=.05)toward improved survival for the gem-citabine group (TABLE 3). Although Tstage was imbalanced between thegroups, it was nota significant factor onmultivariate analysis. The 2 analysisshowed no association between un-
known marginstatuswith volumeof pa-tients treated by an institution in thisstudy; with institutional volume beingcategorized as low (1-3 patients), me-dium (4-5 patients), or high (6 pa-tients). In addition, Kaplan-Meier analy-sis showed no difference in survivalbetweenpatientswithunknownvs nega-tive margin status.
Figure 1. Flow of Patients Through Trial
270 Randomized to receivechemoradiation plus fluorouracil
268 Randomized to receivechemoradiation plus gemcitabine
200 Completed chemotherapyas planned
199 Completed radiation therapyas planned
113 Received salvage chemotherapy
93 Received gemcitabine
198 Completed chemotherapyas planned
193 Completed radiation therapyas planned
93 Received salvage chemotherapy
58 Received gemcitabine
230 Included in primary analysis 221 Included in primary analysis
40 Excluded (ineligible)
2 Withdrew consent priorto protocol treatment
13 No CA 19-9 submission
9 Incomplete or ineligiblestaging
1 Ineligible primarytumor site
2 History of previousradiation therapyor cancer
4 Caloric intake didnot meet protocolrequirements
9 Treatment began>8weeks after resection
47 Excluded (ineligible)
11 No CA 19-9 submission
8 Incomplete or ineligiblestaging
1 History of previousradiation therapyor cancer
3 Eligibility unable to beconfirmed
7 Ineligible primarytumor site
7 Caloric intake didnot meet protocolrequirements
10 Treatment began >8weeks after resection
538 Patients randomized
CHEMOTHERAPY WITH FLUOROURACIL VS GEMCITABINE PLUS CHEMORADIATION
1022 JAMA, March 5, 2008—Vol 299, No. 9 (Reprinted) ©2008 American Medical Association. All rights reserved.
8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 5/8
Pattern of tumor relapse was re-corded on the site of the first relapseonly, and these sites were categorizedas local, regional, or distant (TABLE 4).Local relapse was defined as recur-rence at the primary resection site; re-
gional relapsewasdefined as recurrencein regionallymph nodes associatedwiththe primary resection site, and all otherrelapses were defined as distant. Dis-tribution of relapse was similar amongall patients and among patients withpancreatic head tumors. Local relapseoccurred in 28% of patients in thefluo-rouracil group and 23% in the gem-citabine group. Regional relapse wassimilar in both groups at 7% to 8%. Dis-tant relapse was higher than 70% inboth groups.
COMMENTThe presentstudy demonstrates thatpa-tients with pancreatic head cancerstreated with gemcitabine and chemo-radiation had a median survival of 20.5months and a 3-year survival rate of 31% compared with those treated withfluorouracil and chemoradiation whohad a median survival of 16.9 monthsand a 3-year survival rate of 22%(P=.09). After multivariate analysis forprognostic variables, the treatmenteffect yielded an HR of 0.80 (95% CI,
0.63-1.00; P=.05). While gemcitabinewas associated with increased grade 3or 4 hematologictoxicity, patients wereasymptomatic and there was not an in-crease in febrile neutropenia or infec-tion.Patients receiving gemcitabine didnot have an increase in nonhemato-logic toxicity and there were no differ-ences in the ability to completetherapy.
The results of this trial (RTOG 97-04) are consistent with other phase 3adjuvant trials evaluating the effect of gemcitabine, such as the recently re-
ported CONKO-001 (Charite Onkolo-gie) trial.20 The CONKO-001 trial ran-domized patients with completelyresected pancreatic cancer to 6 cyclesof gemcitabine vs surgery alone anddemonstrated a statistically signifi-cant improvement in disease-free sur-vival without an improvement in over-all survival.
In both the CONKO and RTOGtrials, salvage therapy with gemcitab-ine administered at relapse may havereduced the effect observed for overallsurvival. These results cannot directlybe compared, particularlygiven the fun-
damental differences in treatment ap-proaches, design, and patient charac-teristics,21 including frequency of R0resections (42% in RTOG vs 83% inCONKO), and the CONKO-001 re-
quirement for CA 19-9 to be lower than2.5upper limit of normal (approxi-mately 90 U/mL). The RTOG 97-04study did not exclude patients by CA19-9, with 13% of patients having val-ues of 180 U/mL or higher and 21%
having values higher than 90 U/mL.The RTOG 97-04 study used a con-tinuous infusion of fluorouracil in-stead of bolus. Studies in other gastro-intestinal cancers have demonstrated a
Table 1. Pretreatment Patient Characteristics
No. (%) of Patients
P ValueChemoradiation
Fluorouracil (n = 230)Chemoradiation
Gemcitabine (n = 221)
Age, median, y 62 (36-81) 61 (33-84)
SexMale 139 (60) 117 (53)
.11
Female 91 (40) 104 (47)Location in pancreas
Head 201 (87) 187 (85).40
Nonhead 29 (13) 34 (15)
Tumor gradeWell differentiated 40 (17) 28 (13)
Moderately differentiated 124 (54) 117 (53).26
Poorly/undifferentiated 54 (23) 67 (30)
Unknown 12 (5) 9 (4)
Tumor diameter, cm3 100 (43) 86 (39)
.333 130 (57) 135 (61)
N stageN0 82 (35) 70 (32)
.37N1 148 (65) 151 (68)
Surgical marginsNegative 102 (44) 86 (39)
Positive 75 (33) 77 (35) .49
Unknowna 53 (23) 58 (26)
T stage T1/2 68 (30) 43 (19)
.01 T3/4 162 (70) 178 (81)
CA 19-9 categoryb (n = 129) (n = 124)180 U/mL 113 (88) 107 (86)
.86180 U/mL 16 (12) 17 (14)
a Not mentioned or commented on in the pathology report.b Pretreatment values for patients who tested positive for the Lewis antigen (patients who tested negative for the an-
tigen do not express CA 19-9).
Table 2. All Eligible Patients With Toxicity of Grade 3 or Higher
Toxicity
No. (%) of Patients
P ValueChemoradiation
Fluorouracil (n = 230)Chemoradiation
Gemcitabine (n = 221)
Worst hematologic 22 (9) 129 (58) .001
Grade 4a 3 (1) 32 (14) .001
Worst nonhematologic 137 (59) 129 (58) .90
Worst overall 143 (62) 175 (79) .001a No differencein febrile neutropeniaor infection (0 grade 4 events in the fluorouracil group vs 1 in the gemcitabine group).
CHEMOTHERAPY WITH FLUOROURACIL VS GEMCITABINE PLUS CHEMORADIATION
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 5, 2008—Vol 299, No. 9 1023
8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 6/8
benefit of the continuous infusion of fluorouracil compared with bolus incombination withradiation therapy and
safety in pancreatic cancer has beendemonstrated.22-24 In comparing RTOG97-04 with previous adjuvant trials
using chemoradiation, this study is thefirst phase 3 trial requiring prospec-tive quality assurance of radiationtherapy. This was influenced by a priorUS intergroup phase 3 trial experi-ence with upper abdominal radiationtherapy reporting a 35% risk of majoror minor deviation from protocol-prescribed radiation therapy, most of which required correction prior to thestart of radiation therapy due to theriskof toxic effects on critical organs or fail-
ure to treat the appropriate target vol-umes.25 The RTOG 97-04 study com-pares favorably with the outcome insimilar phase 3 trials using chemora-diation in patients with pancreatic headadenocarcinoma (TABLE5).6,7 In RTOG97-04, 75% ofpatients had T3or T4dis-ease, 66%had lymph node–positive dis-ease, 34% had microscopically posi-tive margins, and the associatedoveralllocalrecurrence rate was 26%. TheGas-trointestinal Study Group (GITSG)trial6 included only patients with nega-
tive surgical margins andonly 30% hadlymph node–positive disease; the lo-cal recurrence rate in the chemoradia-tion group was 47%. The European Or-ganization for the Research andTreatment of Cancer (EORTC) trial7 in-cluded only patients with T1 or T2 dis-ease, 47%had lymph node–positive dis-ease, and 19% had microscopically
Table 3. Overall Survival for Patients With Pancreatic Head Tumors Only (n = 388)
Variable
No. ofPatients
Who Died
TotalNo. of
Patients % Adjusted HR
(95% CI)aP
Valueb
TreatmentChemoradiation fluorouracil 138 201 74
0.80 (0.63-1.00) .05Chemoradiation gemcitabine 138 187 80
Nodal statusN0 87 127 69
1.53 (1.18-1.97) .001N1 212 261 81
Tumor diameter, cm3 126 171 73
1.21 (0.95-1.53) .123 173 217 80
Surgical margin status
Negative 118 153 771.05 (0.80-1.37) .74
Positive 110 136 81
Negative 118 153 770.97 (0.72-1.31) .84
Unknown 71 99 72
Abbreviations: CI, confidence interval; HR, hazard ratio.a An HR of 1 indicates no differencebetween the2 subgroups. An HR higherthan 1 indicates an increased riskof death for
thesecondlevelof thevariableslisted. An HR of lessthan 1 indicatesa benefitfor thesecondlevelof thevariableslisted.b2 Test using the Cox proportional hazards model.
Table 4. Site of First Relapse
Site
No. (%) of Patients With Relapses a
Chemoradiation Fluorouracil Chemoradiation Gemcitabine
All Patients(n = 197)
Pancreatic Head(n = 173)
All Patients(n = 184)
Pancreatic Head(n = 155)
Local 55 (28) 49 (28) 43 (23) 35 (23)Regional 15 (8) 14 (8) 13 (7) 13 (8)
Distant 140 (71) 123 (71) 138 (75) 119 (77)a Because patients could have multiple simultaneous sites of relapses, the total number of relapses are greater than
the numbers of patients in each group.
Figure 2. Overall Survival Among All Eligible Patients
100
30
60
50
40
70
80
90
20
Log-rank P = .34
10
0
No. at Risk
Chemoradiation + gemcitabine
Chemoradiation + fluorouracil
0 1 2 3 4 5
221 152 87 55 35 21
230 160 80 49 36 16
Years From Randomization
% A
l i v e
All Patients
100
30
60
50
40
70
80
90
20
Log-rank P = .09
10
00 1 2 3 4 5
187 134 77 49 30 18
201 139 68 40 28 12
Years From Randomization
% A
l i v e
Patients With Pancreatic Head Tumors
Chemoradiation + gemcitabine
Chemoradiation + fluorouracil
Patients with pancreatic head tumors had a median survival of 20.5 months and a 3-year survival of 31% in the gemcitabine group vs 16.9 months and 22% in thefluorouracilgroup (hazard ratio,0.82 [95% confidenceinterval, 0.65-1.03]; P=.09).Amongall patients,of 221patientsin thechemoradiation plus gemcitabine group,167 died; of 230 patients in the chemoradiation plus fluorouracil group, 181 died. Among patients with pancreatic head tumors, of 187 patients in the chemoradiationplus gemcitabine group, 138 died; of 201 patients in the chemoradiation plus fluorouracil group, 161 died.
CHEMOTHERAPY WITH FLUOROURACIL VS GEMCITABINE PLUS CHEMORADIATION
1024 JAMA, March 5, 2008—Vol 299, No. 9 (Reprinted) ©2008 American Medical Association. All rights reserved.

8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 7/8
positive margins; the local recurrencerate in the chemoradiation group was51%. Thesurvivaland localrelapse out-comes in RTOG 97-04 comparewellde-spite having a much greater propor-tion of patients with T3 or T4 disease,
lymph node–positive disease, and mi-croscopically positive margins com-pared with these trials. To more easilycompare future adjuvant pancreatictrials, uniform eligibility criteriaare needed. The RTOG 97-04 study isthe first prospective,phase 3 trial evalu-a t i n g t h e c o r r e l a t i o n o f p o s t -operative CA 19-9 values to outcome.The results of this planned secondaryanalysis will help determine whetherpostoperative CA 19-9 values higherthan 180 U/mL should be a stratifica-tion variable.
The RTOG 9704 study was pow-eredto analyzesurvival for patients withpancreatic head tumors. Patients withpancreatic head tumors may presentwith different clinical features at diag-nosis such as obstructive jaundice com-pared with pancreatic body or tail tu-mors. A different operation is typicallyused for pancreatic head vs pancreatictail tumors (pancreaticoduodenec-tomy vs distal pancreatectomy). Pa-tients with resected pancreatic body ortail tumors have been generally found
to have a worse outcome than thosewith pancreatic head tumors.26,27
The finding of 25% of patients hav-ing unknown surgical margin status
warrants further comment. Althoughthis rate of unknown margin status ishigher than that reported in previoustrials,6,7,28,29 in these trials a lack of at-tainment and review of a patient’s pa-thology report was categorized as un-
known. In contrast, in RTOG 97-04 inwhich the review of pathology reportswas100%, unknown margin status wasspecifically defined as having no com-ment regarding margins in the pathol-ogy report. Interestingly, there was nodifference in survival observed amongpatients with unknown or negative sur-gical margin status.
TheRTOG 97-04 study included che-moradiation therapy with fluorouracilin both treatment groups. Therefore, theeffect of chemoradiation therapy can-not be assessed. The European Study
Group for Pancreatic Cancer 1 (ES-PAC-1) phase 3 adjuvant trial ques-tionedthe role of adjuvant chemoradia-tion.28,29 However, the ESPAC-1 trial hasbeen specifically critiqued,30-34 includ-ing with regard to its lack of specifica-tion of radiation therapyguidelines, lackof radiation therapy quality assurance,and wide range of radiation therapydoses—as high as 60 Gy.35 The resultsof the fluorouracil plus chemoradia-tion therapy after surgery group of ESPAC-1 appear inferior to those seen
in the EORTC and GITSG trials (13.9months vs 17.1 and 21 months, respec-tively) which used similar fluorouracilplusradiation therapy. Furthermore, in
ESPAC-1, 63% of patients developed alocal recurrence. The European StudyGroup for Pancreatic Cancer 3 (ES-PAC-3) is currently comparing adju-vant fluorouracil and gemcitabine in pa-tients with resected pancreatic cancer;
while an EORTC phase 2/3 trial evalu-ating the feasibility and potential ben-efit of combining concurrent gemcitab-ineplusradiation therapy intheadjuvantsetting is ongoing.
The RTOG 97-04 study was not de-signed to determine the role of adju-vant radiation because chemoradia-tion was given in both groups. Basedon CONKO-001and ESPAC-1, a single-agent modality with gemcitabine orfluorouracil could be considered an op-tion for patients with resected pancre-atic cancer and negative margins. How-
ever, patients with resected pancreaticcancer develop both systemic and lo-cal recurrence. Unfortunately, sys-temic therapies with fluorouracil andgemcitabine have only modest activ-ity. Therefore, it may not be possibleto demonstrate a survival benefit froma local modality such as fluorouracil andchemoradiation therapy when fluoro-uracil and gemcitabine have only amodest impact on delaying systemic re-currence. The ESPAC-1 study demon-strated a local recurrence of 63%. Even
though one-third of the patients in theRTOG 97-04 study had positive mar-gins, the local recurrence rate in thegemcitabine and chemoradiation group
Table 5. Previously Reported Phase 3 Postoperative Adjuvant Therapy Trials for Pancreatic Adenocarcinoma: Summary Results of AdjuvantTherapy Groups
GITSG6 EORTC7 ESPAC-128,29a CONKO-00120
RTOG
ChemoradiationFluorouracil
ChemoradiationGemcitabine
No./total (%) of patientsMi croscopicall y posit ive margins 0 20/ 104 (19)b 19/147 (28) 34/179 (19) 75/230 (33) 77/221 (35)
T3 or T4 disease NA 0 NA 154/179 (86) 162/230 (70) 178/221 (81)
Lymph node–posit ive disease 6/20 (30) 23/49 (47) 73/147 ( 50) 127/ 179 (71) 148/230 (65) 151/221 (68)Local recurrence rate, % (No./total) 47 (7/15) 51 (34/67)b 63 (99/158)c 37 (NA) 28 (49/173) 23 (35/155)
Median survival, mo 21 17.1 20.1 22.1 16.9 20.6
3-Year survival, % 24 30 30 34 22 31
5-Year survival, % 19 20 21 22.5 NA NA
Abbreviations: CONKO, Charite Onkologie; EORTC, European Organization for the Research and Treatment of Cancer; ESPAC, European Study Group for Pancreatic Cancer;GITSG, Gastrointestinal Study Group; NA, data not provided in the original study; RTOG, Radiation Therapy Oncology Group.
a Chemotherapy only group.b Includes patients with periampullary cancers.c Among all patients.
CHEMOTHERAPY WITH FLUOROURACIL VS GEMCITABINE PLUS CHEMORADIATION
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, March 5, 2008—Vol 299, No. 9 1025

8/3/2019 5fu vs gem -JAMA
http://slidepdf.com/reader/full/5fu-vs-gem-jama 8/8
was only 23%. Laboratory correlativestudies from RTOG 97-04 are ongo-ing and are evaluating molecular ge-netic alterations that promote local andsystemic relapse. Future trials shouldemphasize novel systemic treatments to
reduce systemic metastases and mod-ern image-guided radiation to preventlocal recurrence while reducing radia-tion-related toxic effects.
Author Affiliations: Department of Radiation Oncol-ogy, University of Maryland Medical Center, Balti-more (Dr Regine); Radiation Therapy Oncology Group,Philadelphia,Pennsylvania(Ms Winter); RushUniver-sity Medical Center, Chicago, Illinois (Dr Abrams); Di-vision of Hematology-Oncology, Brown University,Providence, Rhode Island (Dr Safran);Fox Chase Can-cer Center, Philadelphia, Pennsylvania (Drs HoffmanandKonski); Division of Hematology-Oncology,North-western University, Chicago, Illinois (Dr Benson); StVincent’s Cancer Care Center, New York, New York
(Dr Macdonald); Department of Radiation Medicine,University of Kentucky, Lexington (Dr Kudrimoti); Ak-ronGeneral MedicalCenter, Akron, Ohio(Dr Fromm);Mayo Clinic, Rochester, Minnesota (Dr Haddock); Na-talie Warren Cancer Center, Tulsa, Oklahoma (Dr Schaefer); Department of Radiation Oncology, DukeUniversity, Durham, North Carolina (Dr Willett); andDepartment of RadiationOncology, Universityof Vir-ginia, Charlottesville (Dr Rich).
Author Contributions: Dr Reginehad full accessto allof the data in the study and takes responsibility for the integrity of the data and the accuracy of the dataanalysis. Study conceptand design: Regine, Abrams, Hoffman,Benson, Macdonald, Willett, Rich.Acquisitionof data:Regine, Winter,Abrams, Hoffman,Safran.Analysis and interpretation of data: Regine, Winter,Abrams, Safran, Hoffman, Benson, Macdonald,Kudrimoti, Haddock, Willett.Drafting of the manuscript: Regine, Winter, Abrams,Safran, Hoffman, Benson.Critical revision of the manuscript for important in-tellectual content: Regine, Winter, Abrams, Safran,Hoffman, Benson, Konski, Macdonald, Kudrimoti,Fromm, Haddock, Schaefer, Willett, Rich.
Statistical analysis: Winter.Administrative, technical, or material support:Hoffman, Konski, Benson, Kudrimoti, Fromm,Haddock, Schaefer, Willett, Rich. Study supervision:Regine, Abrams, Safran, Hoffman,Benson, Macdonald, Willett, Rich.Financial Disclosures: Dr Benson reported receivingfunding fromEli Lillyfor an advisoryand researchrole.All funding goes directly to Northwestern University.
None of the other authors reported financial disclo-sures.Funding/Support: The National Cancer Institute sup-portedthe cooperativeclinical trials groups,whichpar-ticipatedin thisstudy,including theRadiation TherapyOncologyGroup (RTOG), the Eastern CooperativeOn-cology Group, andthe Southwest Oncologygroupviagrants U10 CA21661, U10 CA37422, and U10CA32115. Eli Lilly, the makers of gemcitabine, pro-vided financial support to RTOGHeadquartersand thestatistical center.Role of the Sponsor: The sponsors of this trial wereinvolved in the design of the study but were not in-volved in the conduct of the study, collection, man-agement, analysis, and interpretation of the data; or in the preparation, review, or approval of the manu-script.
REFERENCES
1. Nitecki SS, Sarr MG, Colby TV, et al. Long-termsurvival after resection for ductal adenocarcinoma ofthe pancreas: is it really improving? Ann Surg . 1995;221(1):59-66.2. Piorkowski RJ, Believernicht SW, Lawrence W Jr,et al. Pancreatic and periampullary carcinoma: expe-rience with 200 patients over a 12-year period. Am J Surg . 1982;143(2):189-193.3. Gudjonsson B. Cancer of the pancreas: 50 yearsof surgery. Cancer . 1987;60(9):2284-2303.4. Tepper J, Nardi G, Suit H. Carcinoma of the pan-creas:review of MGH experience from 1963-1973—analysis of surgical failure and its implications for ra-diation therapy. Cancer . 1976;37(3):1519-1524.5. Griffin JF, Smalley SR, Jewell W, et al. Patterns offailure after curativeresection of pancreatic carcinoma.Cancer . 1990;66(1):56-61.6. Kalser MH, Ellenberg SS. Pancreatic cancer: adju-vant combined radiation and chemotherapy following
curative resection. Arch Surg . 1985;120(8):899-903.7. Klinkenbijl JH, Jeekel J, Sahmoud T, et al. Adju-vantradiotherapyand 5-fluorouracilafter curative re-section of cancer of the pancreas and periampullaryregion: phase III trial of the EORTC GastrointestinalTract Cancer Cooperative Group. Ann Surg . 1999;230(6):776-782.8. Garofalo MC, Tan MT, Regine WF. On statisticalreanalysis, the eortc trial is a positive trial for adju-vant chemoradiation in pancreatic cancer. Ann Surg .2006;244(2):332-333.9. Yeo CJ, Abrams RA, Grochow LB, et al. Pancreat-icduodenectomy for pancreatic adenocarcinoma: post-operative adjuvant chemoradiation improves sur-vival: a prospective,single-institution experience.Ann Surg . 1997;225(5):621-636.10. Abrams RA, Yeo CJ. Combined modality adju-vant therapy for resectedperiampullarypancreaticandnonpancreatic adenocarcinoma: a review of studies
and experience at the Johns Hopkins Hospital,1991-2003. Surg Oncol Clin N Am. 2004;13(4):621-638.11. Burris HA,Moore MJ,AndersonJ, et al.Improve-ments in survival and clinical benefit with gemcitab-ineas first-line therapy forpatients withadvanced pan-
creas cancer: a randomized trial. J Clin Oncol. 1997;15(6):2403-2413.12. Rothenberg ML, Moore MJ, Cripps MC, et al. Aphase II trial of gemcitabine in patients with 5-FU-refractory pancreas cancer. Ann Oncol. 1996;7(4):347-353.13. Fleming ID,CooperJS, HensonDE,et al,eds.Exo-crinepancreas. In: AJCC Cancer Staging Manual. 5thed.Philadelphia,PA: Lippincott RavenPublishers; 1997:121-126.14. Regine WF. Postoperative adjuvanttherapy: past,present, and future trial development. In: Evans DB,Pisters PW, AbbruzzeseJL, eds.PancreaticCancer.NewYork, NY: Springer; 2006:235-242.15. Zelen M. Therandomization andstratification ofpatients to clinical trials. J Chronic Dis. 1974;27(7-8):365-375.16. Montgomery RC, Hoffman JP, Riley LB, Ro-gatko A, Ridge JA, Eisenberg BL. Prediction of recur-
rence and survival by post-resection CA 19-9 valuesin patients withadenocarcinoma of the pancreas. Ann Surg Oncol. 1997;4(7):551-556.17. Kaplan EL, Meier P. Non-parametric estimationfrom incomplete observation. J Am Stat . 1958;53:457-481.18. MantelN. Evaluationof survivaldataand twonewrank order statistics arising in its consideration. Can-cer Chemother Rep. 1966;5:163-170.19. CoxDR. Regressionmodelsand lifetables. J Royal Stat Soc B. 1972;34:187-229.20. OettleH, Post S, Neuhaus P, et al.Adjuvantche-motherapy with gemcitabine vs observation in pa-tients undergoing curative-intent resection of pan-creatic cancer. JAMA. 2007;297(3):267-277.21. Benson AB. Adjuvanttherapyfor pancreatic cancer. JAMA. 2007;297(3):311-313.22. O’ConnellMJ, MartensonJA, Wienand HS,et al.Improving adjuvant therapy for rectal cancer by com-
bining protracted-infusion fluorouracil with radiationtherapy after curative surgery. N Engl J Med . 1994;333(8):52-57.23. Cohen SJ, Dobelbower R, Lipsitz S, et al. A ran-domizedphasae III study of radiotherapy alone or with5-fluorouraceal and mitomycin C in patients with lo-
cally advanced adenocarcinom of the pancreas: East-ern Cooperative Oncolog Group study E8282. Int JRadiat Oncol Biol Phys. 2005;62(5):1345-1350.24. Whittington R, Neuberg D, TesterWJ, et al.Pro-tracted intravenous fluorouracil infusion with radia-tion therapy management of localized pancreatico-biliarycarcinoma: a phase I EasternCooperative Grouptrial. J Clin Oncol. 1995;13(1):227-232.25. MacdonaldJS, Smalley SR,BenedettiJ, etal. Che-moradiotherapy after surgery compared with sur-geryalonefor adenocarcinoma of thestomachor gas-troesophageal junction. N Engl J Med . 2001;345(10):725-730.26. Dalton RR, Sarr MG, van Heerden JA, et al. Car-cinoma of the body and tail of the pancreas: is cura-tive resection justified? Surgery. 1992;111(5):489-494.27. Nordback IH, HrubanRH, Boitnott JK, et al.Car-cinomaof thebodyand tailof thepancreas. AmJ Surg .
1992;164(1):26-31.28. NeoptolemosJP, Dunn JA,StockenDD, et al.Ad- juvant chemoradiotherapy in resectablepancreatic can-cer: a randomised controlled trial. Lancet . 2001;358(9293):1576-1585.29. Neoptolemos JP, Stocken DD, Friess H, et al. Arandomized trial of chemoradiotherapy and chemo-therapy after resection of pancreatic cancer. N Engl J Med . 2004;350(12):1200-1210.30. Abrams RA, Lillemoe KD, Piantadosi S. Continu-ing controversy over adjuvant therapy of pancreaticcancer. Lancet . 2001;358(9293):1565-1566.31. Choti MA. Adjuvant therapy for pancreatic can-cer: the debate continues. N Engl J Med . 2004;350(12):1249-1251.32. Morris SL, Beasley M, Leslie M. Chemotherapyfor pancreatic cancer. N Engl J Med . 2004;350(26):2713.33. Crane CH, Small W. Chemotherapy for pancra-
etic cancer. N Engl J Med . 2004;350(26):2713-2714.34. Bydder S, Spry N. Chemotherapy for pancreaticcancer. N Engl J Med . 2004;350(26):2714.35. Koshy MC,Landry JC,Cavanaugh SX,et al.A chal-lenge to the therapeutic nihilism of ESPAC-1. Int J Ra-diat Oncol Biol Phys. 2005;61(4):965-966.
CHEMOTHERAPY WITH FLUOROURACIL VS GEMCITABINE PLUS CHEMORADIATION
1026 JAMA, March 5, 2008—Vol 299, No. 9 (Reprinted) ©2008 American Medical Association. All rights reserved.

![Jama Baredine - Cjenik '19 R [HR]...JAMA BAREDINE JAMA BAREDINE • TRAKTOR STORY • SPELEOLIT - Cjenik ponuda za 2019. stranica | 2 Jama je geomorfološki spomenik prirode od 1986](https://img.dokumen.tips/doc/110x75/5e267633fcdea00a470bfa32/jama-baredine-cjenik-19-r-hr-jama-baredine-jama-baredine-a-traktor-story.jpg)