Embed Size (px)
Citation preview

NATURE MEDICINE • VOLUME 6 • NUMBER 9 • SEPTEMBER 2000 971
NEWS & VIEWS
in a Cbfa1+/– background maintained theirosteosclerotic phenotype1.
A second model suggests that an excessof Fra1 or ∆FosB molecules could het-erodimerize with, and titer out, a tran-scriptional inhibitor of osteoblastdifferentiation (Fig. 1b). Because Fra1 and∆FosB are not required for osteoblast dif-ferentiation in vivo1,6, this type of domi-nant-negative interaction could occuronly if Fra1 and ∆FosB heterodimerize inthe transgenic animals with a proteinwith which they do not heterodimerizeunder physiological circumstances. Asthe authors of both reports acknowledge,there is currently not enough evidence tosupport either of these models.
Through the use of the gene deletiontechnology, a wide array of molecules hasbeen identified that regulates bone re-modeling. Many of these molecules areunexpected, ranging from hormonessuch as leptin7 to tyrosine kinases such c-src and c-abl (refs. 8,9) to transcriptionfactors such as Pu-1, c-fos, NF-κB, Msx2,Cbfa1 (ref. 8). Moreover, overexpression
studies such as those by Jochum, et al.1
and Sabatakos, et al.2 show that even mol-ecules that normally do not control os-teoblast differentiation can, under certainconditions, tilt the precarious equilib-rium of bone remodeling toward a diseasestate.
Analysis of various animal models hasmade it clear that uncontrolled bone for-mation eventually leads to ex-tramedullary hematopoiesis, anemia andearly death. Likewise, a failure to resorbbone properly also causes diseases such asosteopetrosis. Bone remodeling, like mostother homeostatic functions, is a highlycomplex process, and improper regula-tion can lead to many different types ofdiseases, explaining why the list of regu-lators is so long. Given the new questionsraised by these two important mousemodels, and by others, it is safe to assumethat the list is not complete yet.
1. Jochum, W., et al. Increased bone formation andosteosclerosis in mice overexpressing the tran-scription factor Fra-1. Nature Med. 6, 980–984(2000).
2. Sabatakos, G., et al. Overexpression of ∆FosB tran-scription factor(s) increases bone formation andinhibits adipogenesis. Nature Med. 6, 985–990(2000).
3. Grigoriadis, A.E., Wang, Z.Q. & Wagner, E.F. Fosand bone cell development: lessons from a nu-clear oncogene. Trends Genet. 112, 436–441(1995).
4. Matsuo, K. et al. Fos/1 is a transcriptional target ofc-Fos during osteoclast differentiation. NatureGenet. 24, 184–187 (2000).
5. Metz, R., Kouzaride, T. & Bravo, R. A C-terminaldomain in fosB, absent in FosB/SF and Fra-1,which is able to interact with the TATA bindingprotein is required for altered c ell growth. EMBO13, 3832–3842 (1994).
6. Brown, J.R., Ye, H., Bronson, R.T., Dikkes, P. &Greenberg, M.E. A defect in nurturing in micelacking the immediate early gene fosB. Cell 86,297–309 (1996).
7. Ducy, P., et al. Leptin inhibits bone formationthrough a hypothalamic relay: a central control ofbone mass. Cell 100, 197–207 (2000).
8. Karsenty, G. The genetic transformation of bonebiology. Genes Dev.13, 3037–3051 (1999).
9. Li, B., et al. Mice deficient in Abl are osteoporoticand have defects in osteoblast maturation. NatureGenet. 24, 304–308 (2000).
Department of Molecular and Human GeneticsBaylor College of MedicineOne Baylor Plaza, Houston, Texas 77030Email: [email protected]
Pain, plasticity, and premature birth: a prescription forpermanent suffering?
A collection of clinical and animal studies suggest that exposure to pain during the neonatal period leads to long-term changes in neural circuitry and behavior, contradicting the theory that infants don’t ‘remember’ painful experiences.
K.J.S. ANANDABOUT 11,000 NEWBORN infants are receiv-ing intensive care in the U.S. today,
and many of these will be exposed to mul-tiple painful invasive procedures1–3. In con-trast to similar invasive proceduresperformed in the adult intensive care unit(ICU), few of these neonates will receiveanalgesic therapy in preparation for tissuedamaging procedures1–3. An inflammatoryresponse lasting from hours to days willfollow, leading to increased pain sensitiv-ity (hyperalgesia) around the area of dam-aged tissue. This inflammatory responseusually goes untreated. It is commonly be-lieved that “babies can’t remember thesepainful experiences”. However, recentstudies suggest that although early painfulmemories are not accessible to consciousrecall, they may be encoded in “proceduralmemory” and lead to abnormal behavioralpatterns or altered sensory processing inlater life4,5. In a recent issue of Science, Rudaet al. 6 made the startling discovery that lo-calized inflammation during the neonatalperiod permanently alters neuronal circuits
that process pain in the spinal cord.In an elegant series of experiments,
these researchers injected completeFreund’s adjuvant into the left hindpaw of0, 1, or 3 day-old rat pups to produce local-ized inflammation that lasted for 5 to 7days. When these animals reached adult-hood, they had increased numbers of pri-mary sensory (afferent) fibers exiting thesciatic nerve, and these fibers connectedwith superficial layers of the spinal corddorsal horn that are involved in pain pro-cessing (laminae I / II, called the substantiagelatinosa). These thinly myelinated orunmyelinated nerve fibers also extendedinto caudal segments of the spinal cord(L6, S1) that don’t normally receive sen-sory input from the sciatic nerve. Dorsalhorn neurons receiving input from theseterminals were hyperexcitable, demon-strating increased activity at rest and in re-
sponse to tactile or noxious stimuli. Thisled to an increase in pain response behav-iors in adult rats6.
Thus, neonatal painful experiences mayleave a legacy of altered sensitivity to sub-sequent pain, a concept proposed 13 yearsago7. For example, neonatal rats exposedto four daily needle sticks during the firstweek of life were more sensitive to pain at16 and 22 days of age8. Other studies re-ported that excessive sprouting of cuta-neous nerve fibers occurs followingneonatal skin wounds, associated withlowered thresholds for the withdrawal re-flex for several weeks following the injury9.The excessive nerve sprouting was inhib-ited by antibodies against nerve growthfactor (NGF) in adult but not neonatal rats,suggesting that more than one growth fac-tor induces nerve growth during this de-velopmental time period10. The cutaneousnerve sprouting in neonates was not in-hibited by sciatic nerve blockade, suggest-ing that nerve fiber function is notrequired for this sprouting to occur11.
© 2000 Nature America Inc. • http://medicine.nature.com©
200
0 N
atu
re A
mer
ica
Inc.
• h
ttp
://m
edic
ine.
nat
ure
.co
m

972 NATURE MEDICINE • VOLUME 6 • NUMBER 9 • SEPTEMBER 2000
NEWS & VIEWS
Another study reported that in-jection of carrageenan into thehindpaws of 1 day-old rats12 led tosignificant (33%) reductions inthe receptive field size (area of skinfrom which a dorsal horn neuronreceives sensory stimuli) of spinalcord sensory neurons in adult rats.Collectively, the long-term effectsof neonatal pain include hyperin-nervation in areas of woundedskin9, with increased sprouting ofprimary afferent fibers and hyper-excitability of sensory neurons6.The enhanced sensory input from“hypersensitive” skin may lead to adaptivechanges within the spinal cord dorsalhorn that decrease the receptive field sizeof afferent neurons12. The reduction in re-ceptive field size may be caused by reduceddendritic arborization of afferent neurons,increased connections with inhibitory in-terneurons, up-regulation of inhibitory re-ceptors or ion channels, or enhancedactivity of the descending inhibitory con-trols from supraspinal centers13.
Similar results have also been seen in in-fants. Clinical data suggest that the physi-ological or behavioral responses to painare altered by exposure to repetitive or pro-longed pain during early development4,5,14.For example, healthy infants undergoingroutine vaccination at 4-6 months of agewere noted to have accentuated behav-ioral responses (measured by facial expres-sions, duration of crying, and visualanalogue scales by blinded observers) ifthey were exposed to unanesthetized cir-cumcision at birth, as compared with un-circumcised infants or those receivingtopical anesthesia before circumcision15.
However, in evaluating the clinical rele-vance of these findings, Ruda et al. mustconsider the large differences in complex-ity and adaptability between human androdent brains, and also developmental dif-ferences between neonatal rats and hu-mans. The authors’ experimental systeminvolved induction of localized inflamma-tion for 5-7 days in neonatal rats. In hu-mans, this would correspond to inducingseveral weeks of continued pain duringlate gestation, which rarely occurs in theclinical setting. Also, such an inflamma-tory response would be expected to causelocalized fibrosis, limb deformities, andother trophic changes, which may con-tribute to the spinal cord changes reportedby Ruda et al. Injection of completeFreund’s adjuvant also induces a systemicinflammatory response leading to general-ized arthritis and spinal cord changes 16,
which may have contributed to these find-ings.
Studies on preterm neonates that spent4 weeks in the neonatal ICU have also re-ported dampened behavioral responses topainful procedures, such as to the heellance required for blood sampling.Dampened behavioral responses were cor-related with the number of painful proce-dures that the neonates received17.Measurements of facial behavioral and car-diac autonomic reactivity during a finger-lance blood collection showed similarresults in groups of 4 month-old infantswho were born either preterm or full-term18. Similarly, 18 month-old ex-preterm infants were less sensitive toeveryday pain when compared withmatched controls who were born full-term19. The greater the number of painfulprocedures infants had experienced asneonates, the less responsive they were topain as toddlers. Altered behavior was alsoseen in older children that had spent timein the neonatal ICU as infants20,21. Thesestudies suggest that painful experiences inlate human gestation seem to enhance,whereas painful experiences in earlyhuman gestation seem to dampen the be-havioral responses to subsequent pain.
Given the plasticity of supraspinal fociinvolved in sensory processing, repetitivepain during infancy may cause wide-spread changes in the immature brainleading to abnormal behaviors in adult-hood. Exposure of neonatal rat pups todaily needle-stick pain led to decreasedpain thresholds in late infancy, alongwith increased alcohol preference andanxiety-mediated behaviors during adult-hood. These behavioral changes resemblesome of the behaviors seen in older chil-dren that were born prematurely and ex-posed to painful procedures in theneonatal ICU8.
Across the different laboratory models,it is becoming increasingly clear that ex-
periences of pain will be “remem-bered” by the developing nervoussystem, perhaps for the entire lifeof the individual. These findingsshould focus the attention of clin-icians on the long-term impact ofearly painful experiences, andhighlight the urgent need for de-veloping therapeutic strategies forthe management of neonatalpain. Otherwise, future genera-tions will pay the price for med-ical procedures performedtoday22.
1. Barker, D.P. & Rutter, N. Exposure to invasiveprocedures in neonatal intensive care unit admis-sions. Arch. of Dis. in Childhood Fetal & Neonat.72, F47–48 (1995).
2. Johnston, C.C., Collinge, J.M., Henderson, S.J. &Anand, K.J.S. A cross-sectional survey of pain andpharmacological analgesia in Canadian neonatalintensive care units. Clinical Journal of Pain 13,308–312 (1997).
3. Porter, F.L. & Anand, K.J.S. Epidemiology of painin neonates. Research & Clinical Forums 20, 9–16.(1998).
4. Porter, F.L., Grunau, R.V.E. & Anand, K.J.S. Long-term effects of neonatal pain. J. Behav. Develop.Pediatr. 20, 253–261 (1999).
5. Anand, K.J. Clinical importance of pain and stressin preterm neonates. Biology of the Neonate 73,1–9 (1998).
6. Ruda, M.A., Ling, Q.-D., Hohmann, A.G., Peng,Y.B. & Tachibana, T. Altered nociceptive neuronalcircuits after neonatal peripheral inflammation.Science 289, 628–631 (2000).
7. Anand, K.J.S. & Hickey, P.R. Special Article: Painand its effects in the human neonate and fetus.New Engl. J. Med. 317, 1321–1329 (1987).
8. Anand, K.J.S., Coskun, V., Thrivikraman, K.V.,Nemeroff, C.B. & Plotsky, P.M. Long-term behav-ioral effects of repetitive pain in neonatal ratpups. Physiology & Behavior 66, 627–637 (1999).
9. Reynolds, M.L. & Fitzgerald, M. Long-term sen-sory hyper-innervation following neonatal skinwounds. Journal of Comparative Neurology 358,487–498 (1995).
10. Reynolds, M., Alvares, D., Middleton, J. &Fitzgerald, M. Neonatally wounded skin inducesNGF-independent sensory neurite outgrowth invitro. Brain Res. Dev. Brain Res. 102, 275–283(1997).
11. De Lima, J., Alvares, D., Hatch, D.J. & Fitzgerald,M. Sensory hyperinnervation after neonatal skinwounding: effect of bupivacaine sciatic nerveblock. Br. J. Anaesth. 83, 662–664 (1999).
12. Rahman, W., Fitzgerald, M., Aynsley-Green, A. &Dickenson, A.H. The effects of neonatal exposureto inflammation and/or morphine on neuronal re-sponses and morphine analgesia in adult rats. inProceedings of the 8th World Congress on Pain, Vol.8 (eds. Jensen, T.S., Turner, J.A. & Wiesenfeld-Hallin, Z.) 783–794 (IASP Press, Seattle, 1997).
13. Ren, K., Blass, E.M., Zhou, Q. & Dubner, R.Suckling and sucrose ingestion suppress persis-tent hyperalgesia and spinal Fos expression afterforepaw inflammation in infant rats. Proc. Natl.Acad. Sci. U.S.A. 94, 1471–1475 (1997).
14. Anand, K.J.S. Effects of perinatal pain. Prog. BrainRes. 122, 117–129 (1999).
15. Taddio, A., Katz, J., Ilersich, A.L. & Koren, G.Effect of neonatal circumcision on pain responseduring subsequent routine vaccination. Lancet349, 599–603 (1997).
16. Calza, L. et al. Peptide plasticity in primary sen-sory neurons and spinal cord during adjuvant-in-duced arthritis in the rat: animmunocytochemical a nd in situ hybridization
© 2000 Nature America Inc. • http://medicine.nature.com©
200
0 N
atu
re A
mer
ica
Inc.
• h
ttp
://m
edic
ine.
nat
ure
.co
m
NATURE MEDICINE • VOLUME 6 • NUMBER 9 • SEPTEMBER 2000 973
NEWS & VIEWS
NON-STEROIDAL ANTI-INFLAMMATORY drugs(NSAIDs) such as aspirin or ibuprofen
are widely used to alleviate fever, pain andinflammation. Because they also inhibitplatelet aggregation, NSAIDs are also usedto prevent myocardial infarction andstroke. Epidemiological studies suggestthat the use of NSAIDs may reduce the riskof developing Alzheimer disease (AD), andclinical trials are underway to test their ef-ficacy in the treatment of AD (ref. 1). Astudy, recently published by Lim et al.2 inThe Journal of Neuroscience, lends new ex-perimental support to the idea thatNSAIDs may be useful for the treatment ofAD. The investigators tested the effects oforally administered ibuprofen, a com-monly used NSAID, in a transgenic mousemodel of AD. After 6 months of treatment,the mice showed less AD-type pathologythan untreated controls.
AD is the most common form of demen-tia. The relentless cognitive decline in ADpatients is associated with the abnormal ac-cumulation of amyloid deposits (plaques)in the brain. Amyloid proteins are a groupof diverse proteins that have a tendency toform aggregates3. Different types of amy-loid aggregates share histologic stainingcharacteristics, and depending on theorgan in which they accumulate, cause avariety of diseases. Organs can be affectedby primary amyloidoses as well as by sec-ondary amyloidoses that result fromchronic inflammation induced by otherdiseases3. The findings of Lim et al. suggestthat molecular targets of NSAIDs play a keyrole in the development of brain amyloido-sis2, an important element, if not the maincause, of AD (refs. 4–6).
The amyloid protein that is deposited inAD brains is the Aβ peptide, which is de-rived from the larger amyloid protein pre-
cursor (APP) (refs. 4–6). APP mutationsthat increase the production of fibrillo-genic Aβ peptides cause rare forms of auto-somal dominant familial AD. Neuronalexpression of mutant APP elicits various
AD-like pathological alterations in trans-genic mice, including amyloid plaquesand distortions of neuronal processes(neuritic dystrophy). The plaques in thebrains of AD patients and APP mice triggerreactions of local astrocytes and microglia(gliosis). These injury-responsive cells pro-duce a large number of inflammatory me-diators including cytokines such asinterleukin (IL)-1. The gliosis observed inAD patients and the reduced incidence ofAD in people taking NSAIDs raise the ques-tion of whether inflammatory processesplay a prominent role in the pathogenesisof AD (ref. 1). If so, anti-inflammatorydrugs such as NSAIDs might prevent or re-duce AD-like pathology.
Lim et al. tested this hypothesis by treat-ing APP transgenic mice with ibuprofen2.Treatment was initiated when the micewere 10 months old, the age at whichplaque deposition typically begins in thismodel. The brains of treated and untreatedmice were compared 6 months later. Thetreated mice showed significant reduc-tions in cerebral plaque load, soluble andinsoluble Aβ, neuritic dystrophy, plaque-associated gliosis and IL-1 concentrations.
Although the study by Lim et al. was notdesigned to determine the mechanism ofibuprofen action or the relationship be-tween inflammatory changes and cogni-tive deficits, the findings, along with theongoing clinical trials of NSAIDs for AD,make it interesting to speculate aboutthese issues. Three molecular targets ofNSAIDs have been identified as potentialmediators of their anti-inflammatory ac-tions. NSAIDs inhibit the constitutivelyexpressed cyclooxygenase (COX-1) andthe inducible form of this enzyme (COX-2), both of which produce prostaglandins7.NSAIDs also activate the nuclear peroxi-
Ibuprofen, inflammation and Alzheimer diseaseMounting evidence suggests that non-steroidal anti-inflammatory drugs may be useful in reducing the risk of
Alzheimer disease. After much study, the mechanism by which these drugs reduce the amyloid deposition associated with the disease is still open to speculation.
TONY WYSS-CORAY & LENNART MUCKE
study. Neuroscience 82, 575–589 (1998).17. Johnston, C.C. & Stevens, B.J. Experience in a
neonatal intensive care unit affects pain response.Pediatrics 98, 925–930 (1996).
18. Oberlander, T.F. et al. Biobehavioral pain re-sponses in former extremely low birth weight in-fants at four months corrected age. Pediatrics105, e6 (2000).
19. Grunau, R.V., Whitfield, M.F. & Petrie, J.H. Painsensitivity and temperament in extremely low-birth-weight premature toddlers and pretermand full-term controls. Pain 58, 341–346 (1994).
20. Grunau, R.V., Whitfield, M.F., Petrie, J.H. & Fryer,E.L. Early pain experience, child and family fac-tors, as precursors of somatization: a prospectivestudy of extremely premature and fullterm chil-dren. Pain 56, 353–359 (1994).
21. Grunau, R.V.E., Whitfield, M.F. & Petrie, J.Children’s judgments about pain at age 8-10years: do extremely low birthweight (<1000 g)children differ from full birthweight peers. J.Child. Psychol. Psychiatr. 39, 587–594 (1998).
22. Anand, K.J.S. & Scalzo, F.M. Can adverse neona-tal experiences alter brain development and sub-
sequent behavior? Biol. Neonate 77, 69–82(2000).
Pain Neurobiology LaboratoryUniversity of Arkansas for Medical Sciences,Arkansas Children’s HospitalS-431800 Marshall StreetLittle Rock, Arkansas 72202Email: [email protected]
00.0583A1.Journal.eps
Neuro-protective?NSAIDs
AβActivation
ClearanceImmunization
Other Mediators
Anti-inflammatory
NeurotoxicNeurotoxic
COX-2
InjuredNeuron
ActivatedMicroglia
PPARγCOX-1, COX-2
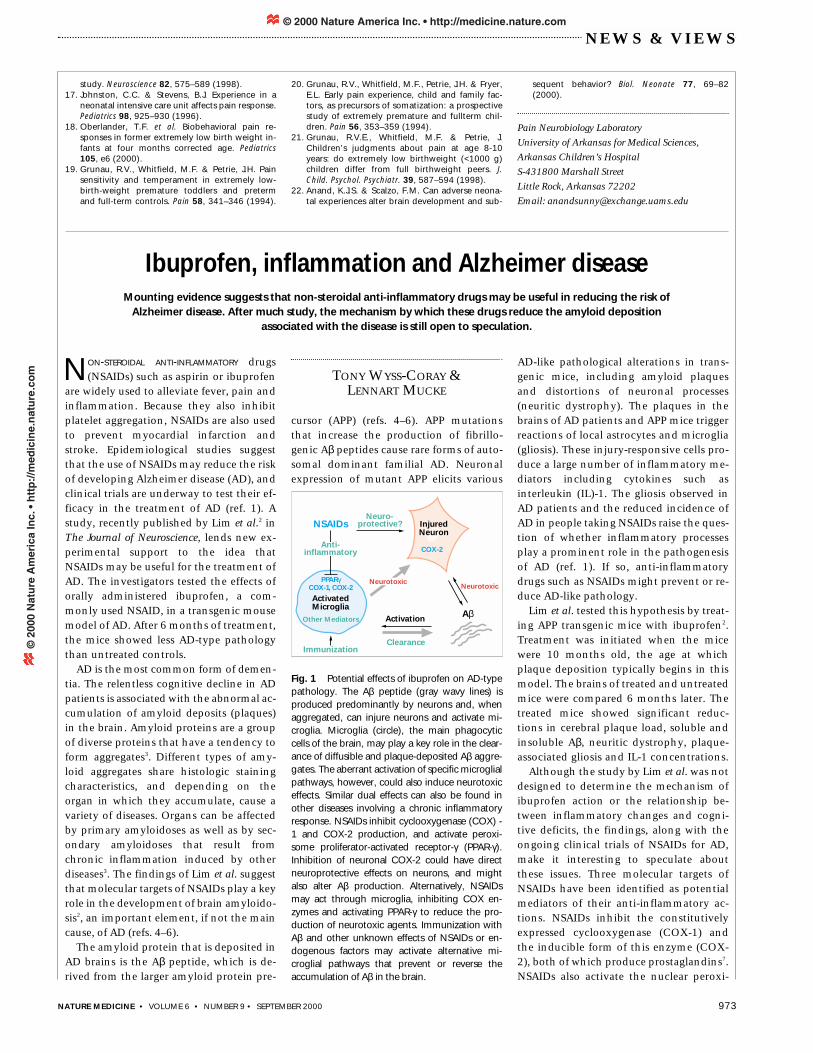
Fig. 1 Potential effects of ibuprofen on AD-typepathology. The Aβ peptide (gray wavy lines) isproduced predominantly by neurons and, whenaggregated, can injure neurons and activate mi-croglia. Microglia (circle), the main phagocyticcells of the brain, may play a key role in the clear-ance of diffusible and plaque-deposited Aβ aggre-gates. The aberrant activation of specific microglialpathways, however, could also induce neurotoxiceffects. Similar dual effects can also be found inother diseases involving a chronic inflammatoryresponse. NSAIDs inhibit cyclooxygenase (COX) -1 and COX-2 production, and activate peroxi-some proliferator-activated receptor-γ (PPAR-γ).Inhibition of neuronal COX-2 could have directneuroprotective effects on neurons, and mightalso alter Aβ production. Alternatively, NSAIDsmay act through microglia, inhibiting COX en-zymes and activating PPAR-γ to reduce the pro-duction of neurotoxic agents. Immunization withAβ and other unknown effects of NSAIDs or en-dogenous factors may activate alternative mi-croglial pathways that prevent or reverse theaccumulation of Aβ in the brain.
© 2000 Nature America Inc. • http://medicine.nature.com©
200
0 N
atu
re A
mer
ica
Inc.
• h
ttp
://m
edic
ine.
nat
ure
.co
m





























