Embed Size (px)
Citation preview

Voluntary Sector Partnership Joint
Commissioning and Procurement
Presentation
20th October 2016
Ian Mello, Borough SRO Locality Plan
Susan Crutchley, Programme Manager

Agenda1) What is joint commissioning?
2) Why RMBC & CCG are doing it?
3) How it is being done (i.e. staff working as teams around theme such as dementia, older people, children, joint commissioning boards etc.)?
4) Will there be the opportunity for co-design of services with the sector and the communities they serve as part of joint commissioning?
5) Will there be a commissioning strategy developed, if so, will this be shared with the sector?
6) How will this affect current funding/contracting arrangements between the sector and CCG or between the sector and RMBC?
7) STAR Procurement – short presentation about the process –Development of Tender Specifications, Advertising the opportunity, Pre-Qualification Questionnaire, Invitation to Tender, Timeframes for submission of documents, decision making
8) Locality Plan update

1) What is joint commissioning?
Joint Commissioning is a strategic approach to planning and delivering services in a holistic, integrated joined-up way. It is a means for the different partners commissioning public health and health services and social care provision, to deliver positive outcomes for local populations. We also jointly commission with other north east sector localities such as Bury and Oldham.
2) Why RMBC & CCG are doing it?
The NHS Five Year Forward View set policy clearly that CCG’s and Councils must deliver integrated services and work towards new models of health and social care in one single joint commissioning context. The Greater Manchester Health and Social Care Partnership is also taking this policy forward more locally.
3) How it is being done (i.e. staff working as teams around theme such as dementia, older people, children, joint commissioning boards etc.)?
To date we have created an Integrated Commissioning Board and throughout this financial year we are in a shadow or learning year for adult services commissioning. We have also worked together on major projects such as the Oasis Unit at Rochdale Infirmary.

4) Will there be the opportunity for co-design of services with the sector and
the communities they serve as part of joint commissioning?
Both the CCG and Council are fully committed to this principle and want to
take this forward locally. Last year we held over 40 engagement events for
the Locality Plan and we will be establishing another programme of them
very soon.
5) Will there be a commissioning strategy developed, if so, will this be shared
with the sector?
The Locality Plan will soon have an Operational Plan and this effectively will
be our five year commissioning strategy. This has to be completed by third
week of February 2017 for submission to GMHSCP: we want to engage and
consult with you and the public and our stakeholders about this.

6) How will this affect current funding/contracting arrangements between the
sector and CCG or between the sector and RMBC?
We are currently working with CVS and partners on the Health and Well-Being
Alliance model and see this as a formal part of our Locality Plan. We are also
working towards one single procurement and contracting approach across the
CCG and Council: we are happy to develop this with the sector going forward.
7) STAR Procurement
See following slides

STAR Procurement – The Process.
• All clients must complete a Procurement Initiation Document before
starting their process. This includes budget available, current arrangement
and service outcomes. This is then signed off by Finance and Operational
Leads. Any contracts above £250,000 total value are sent for Cabinet
approval at Rochdale.
• Needs Assessments, Market Engagement Sessions, Service User Feedback
are all collected as part of developing the Tender Specifications.
• All Procurements over £50,000 are advertised via the Procurement Portal
The Chest. This is a clear audit trail of the process from start to finish.
https://www.the-chest.org.uk/ Procurements over EU Thresholds are
advertised for Minimum 30 days

STAR Procurement – The Documentation .
• Suitability Assessment Questionnaire - Pass/Fail Document which checks
Organisations Policies E.g Health and Safety, Safeguarding, Financial
Standing and Economic Capability.
• Invitation to Tender – Document which instructs all bidders on timescales
and evaluation criteria for each project. Organisational proposals are also
detailed in this document. These are evaluated using a strict Quality
Guidance document briefed with Evaluation Panel.
• Decision Making – All bids are evaluated in conjuntion with the Council’s
Contract Procedure Rules and Best Practice. Moderation meetings to
determine an agreed score and bidder feedback is undertaken. Common
place to try and get Service User representation on the panel providing no
conflict of interests occur

Locality Plan Update
• LCO development
• Transformation Fund Bid
• Locality Plan Service Model: (over 50
engagement and co-production sessions held
to develop service model, biggest process in
any GM Locality Plan: will be repeated
throughout Winter 2016 until February 2017)

As you are no doubt aware the locality has to
establish an LCO under the Greater Manchester
Strategic Plan and guidance on this is clear:
“ Fully integrated Locality Care Organisations (LCOs) will be established in
each part of Greater Manchester. These Organisations, including all health
and social care providers in a locality will be working together collaboratively
to provide care to a defined population within a defined budget with primary
care at the centre, predicated on the GP registered list. Each area will develop
and design their delivery models. However, there will be core features of these
new organisations to be defined and agreed locally.”

What are LCOs?
• Multiple organisations working together to deliver health and care services within a defined budget;
• Have the ability to manage and co-ordinate the care of individuals along full length of clinical and social care pathways;
• Demonstrate a standardised approach to quality improvement activity, including patient safety;
• They treat and support patients in different more appropriate settings as a result of improved co-ordination;
• Importantly they demonstrate increased involvement and engagement of patients and service users in design, delivery and improvement of services;
• They are proactive in the management of population groups to inform early intervention and prevention;
• They have integrated IT solutions to support the collaboration.

Developing Accountable Care Local Care Organisation
1 Impact aspiration What difference will we make?
What are needs of population by population, activity, spend, needs2
3
4
5
6
7
8
Population needs
Changes in Care
Delivery
requirements
Changes in
information
Changes in
payment
Governance
Development
What are the highest priorities to address?
What are the key changes in how care is delivered to key segments of population?
What changes are required in who does what from where?
(core processes, workforce, delivery in person vs electronic, setting)?
How will flow of information will change to enable these changes?
(Information governance, patient level data set, core functions of delivery, engaging
patients, performance and payment)
What changes in payment need to be made to: a) directly reimburse costs, b)
incentivise behaviour, c) transfer accountability/risk will be made?
How will this operate and how will it be phased in?
What are key functions the need changes (e.g, function of teams, operational control,
managing financial risk, accessing capabilities)?
Identify changes in governance and delivery model (e.g., accountable care, group, etc)
Support the transformational changes needed in behaviour and interactions in the
system31

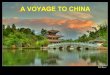
Example of LCO operating model
13
Review of performance andprocesswithin thecareteam
5
ü
ü
12
Multi-disciplinarycare team Case conference toworking discusscomplex
cases/issues
7
Navigation to
Specialist1 Patient access supportresources
1 2
Identification Patient
ofhigh risk enrollmentpatients In CC programme
3
Identificationofpatienthealth goals
4
Developmentofcare planwith patient
GPP2 Alliedhealth
professional
Care
coordinator Social
worker
Pharmacist
Behavioral
health
8
Discharge planningand coordination 11
Regular reviewandupdate ofcare plan
9 with patient/family
Accessto specialistopinion
10
Integrated healthand social careteam in home
1 Specialists in both inpatient or outpatient settings 2 Includes primary care physicians, advanced practice nurses, physicians assistants37
SOURCE: North West London Integrated Care Pilot; Dorling, & Richardson - Evidenced interventions for integrated care (2014)

GM Devolution Plan: Transformation
Fund• The Plan enabled GM to secure a £450 million Transformation Fund.
• The Fund was designed to enable places to develop new models of care
which began to change the nature of demand and to keep existing services
safe and sustainable while the radical change was happening.
• The agreed £450m is to be used to drive the transformation required by
the 5 Year Forward View and as such the funding from NHSE is to be
phased through a 5 year period, as outlined below.16/17 17/18 18/19 19/20 20/21 Total
TF (£m) 60 120 150 70 50 450

In order to align the spending of the TF with the wider work of GM
Devolution, outlined in the Strategic Plan, the following outlines the approximate resource assigned to each GM Theme
GM Theme Size of Fund
Radical upgrade in prevention £75m-£100m
Transforming care in the localities £250m-£275m
Standardising Acute Care £25m-£40m
Standardisation of support and back office £15m-£30m
Enabling better care £40m-£60m

Five assessment criteria for the Fund have been approved by the Strategic
Partnership Board
The assessment criteria for funding proposals will be based around five main areas outlined below.
Alignment to GM
strategy
• The proposal will need
to demonstrate
alignmentto the GM
transformation
initiatives in both its
strategy and vision as
well as its plan design.
• This will includecreating a link between
the programme and
GM/STP outcomes as
well as articulating
how the proposed
solution will close the
financial gap.
Readiness to deliver
• The proposal will need
to demonstrate that it
is ready to be
delivered.
• This will include
demonstrating:
Ø Project management
infrastructure is in
place
Ø The local system is
capable of delivery
Ø The intervention
specifics, such as
target patient groups
have been developed
Stakeholder engagement
• In order to be
successful, applicants
need to provide
evidence of wider
stakeholder support.
• This will need to be in
the form of:
Ø Formal sign-offs and
agreements
Ø Evidence of co-design
Ø Patient engagement
Robust financials
• Proposals will need to
clearly demonstrate
that the locality 5 year
financial and activity
plan contributes to
closing the gap and
underlying opportunity
for GM (or specific
localities).
• The programme
specific finance
template (see slide 10)
should demonstrate
the investment ask,
impacton activity and
finance and therefore
the return on
investment (ROI).
Foundation for Further
Transformation
• Final proposals will
need to demonstrate
the replicability and
forward planning
involved in their
programmes.
• This will include:
Ø Identifying the
evaluation framework
in place
Ø Identifying the
approach to sharing
best practice and
lessons learnt
The five criteria will be the same for GM initiatives, however the requirements will be adjusted to ensure they are appropriate.51

• Six main programmes within locality plan:
Prevention Thriving and Coping, Getting Help in the Community
and Getting More Help, Mental Health and Specialist Help and
System Transformation(enablers such as estate, IT and workforce
• Hubs x 4 located in Heywood, Middleton, Pennines and
central Rochdale: indicative locations identified
• Integrated Neighbourhood Teams and Integrated
Intermediate Care Service (health, social care and voluntary
sectors working under prime provider model)
• Prevention and Wellbeing Service Directory
• Behaviour Change Programme
• Health and Wellbeing Alliance model
Service Model

But this is a lot to do so…..
• GM has offered ‘Seed Corn’ Funding
– Any allocation of development funding will be based on detailed
costing and kept to the minimum amount commensurate with
producing a full business case.
– Localities will need to show evidence of demonstrable commitment
to the delivery of their development funding proposal
– This is to get team/governance/partnership/risk etc arrangements
and costed plans together to:
• Put a bid in for Transformation funding by 3rd Week February
2017
– But this will form part of the TF and needs to show 3:1 ROI as well
– And seed corn funding bid needs to be in very soon so allow time to
develop full TF bid