Embed Size (px)
Citation preview

PROGRAM OVERVIEWThis program guide provides an overview of the 2018 Global Quality Pay for Performance (GQ P4P) Program for Independent Physician Associations (IPAs). In this third year of the program, IEHP has made program enhancements based on feedback from Providers in an effort to continually improve effectiveness. The IEHP GQ P4P program for IPAs is designed to reward IPAs for high performance and year-over-year improvement in key quality performance measures. This program overview is designed for IPAs and their staff as an easy guide to help maximize GQ P4P.
This year’s GQ P4P Program continues to provide financial rewards to IPAs for improving healthcare quality across multiple domains and measures. The 2018 GQ P4P program focuses on performance-based incentives to IPAs for services rendered in 2018.
If you would like to get more information about IEHP’s GQ P4P Program or best practices to help improve quality scores and outcomes, visit our Secure Provider Portal at www.iehp.org, email the Quality Team at [email protected] or call the IEHP Provider Relations Team at 909-890-2054.
What’s New?Two measures were retired • Annual Monitoring for Patients on Persistent Medications - Total • Childhood Immunizations - Combo 3
Three measures were added to the Clinical Quality Domain • Avoidance of Antibiotic Treatment in Adults with Acute Bronchitis • Weight Assessment and Counseling for Nutrition and Physical Activity for Children and Adolescents • Concurrent Use of Opioids and Benzodiazepines (monitoring only)
New Tier 1 and Tier 2 goal methodology includes a ‘practical significance’ standard
The budget was reduced from $30 million to $20 million, with removal of thecondition to pass through 33-50 percent of the funding to Primary Care Providers(PCPs), which was in place for previous program years.
1
To be eligible for incentive payments in the 2018 GQ P4P Program, IPAs must meet the following criteria:
• Have at least 5,000 IEHP Medi-Cal Members assigned as of January 2018 • Have at least 30 Members in the denominator as of December 2018 for each quality measure to qualify • Submit a GQ P4P Quality Work Plan to IEHP by March 1, 2018 in order to enroll in the program (see Work Plan details in Appendix 5) • Meet minimum Encounter Data Gates in order to qualify for incentive payments
Eligibility and Participation
Encounter Data Encounter data is foundational to performance scoring and is essential to success in the GQP4P Program. Complete, timely and accurate encounter data should be submitted throughnormal reporting channels for all services rendered to IEHP Members. Please use the codeslisted in Appendix 2 to help with proper coding to meet measure requirements. Lab Results Data from lab results is also foundational to Program performance scoring. Providers shouldensure they submit complete lab results data for services rendered to IEHP Members. IPAsshould work with their network Providers to ensure they are using the appropriate labvendors for IEHP Members, and submitting complete lab results data to IEHP.
Lab results that are performed in the office (e.g., point of care HbA1c testing, urinetests, etc.) should be coded and submitted through Providers’ encounter data. Immunizations To maximize performance in immunization-based measures, IEHP strongly encourages all Providers to report all immunizations via the California Immunization Registry (CAIR2). For more information on how to register for CAIR2, please visit http://cairweb.org/. IEHP is working closely with CAIR to establish a data sharing arrangement to be used in Global Quality P4P reporting.
Minimum Data Requirements
2

Supplemental Data What is Supplemental Data?When services are not captured in traditional encounter data systems, other Supplemental Data sources may be used to collect information about services rendered to Members to support Quality Reporting.
When Supplemental Data may be needed • For services that were provided prior to eligibility • When a Provider has “proof-of-service” for a noted gap in care (e.g. cervical cancer screening, immunizations rendered by another provider) • When Provider has “proof-of-service” for an eligible-population exclusion (e.g. total hysterectomy, bilateral mastectomy)
How to use Supplemental Data to support Global Quality P4PCreate an electronic log that includes minimum required data elements. See Appendix 6 for file layout requirements. Below is a listing of minimum data elements needed in a supplemental data log. • Member ID • Date of Service • Provider Identification • Provider Specialty • Diagnosis Code(s) – if applicable • Procedure Code(s) • Lab Results – if applicable
Requirements for using Supplemental Data in Global Quality P4P Reporting • The IPA must have clearly defined policies and procedures (in writing) that describe how Supplemental Data is collected, validated and used for P4P reporting • Policies/procedures must be shared with IEHP and must be in place to validate quality / accuracy of Supplemental Data • The IPA must collect “proof-of-service” documentation to confirm all services that are reported in the Supplemental Data log • The IPA must receive approval from IEHP’s Quality Team to use Supplemental Data in Global Quality Reporting (deadline for approval is October 31, 2018) • The IPA must complete a P4P Roadmap no later than December 1, 2018 • The IPA must complete IPA data validation activities prior to submitting Supplemental Data to IEHP • The IPA must submit a final Supplemental Data log to IEHP via SFTP no later than February 1, 2019
3

Data Validation Requirements for Supplemental Data in Global Quality P4P Reporting • To be counted in final IPA Global Quality P4P rates, Supplemental Data file must pass IEHP’s independent HEDIS® audit process • The IPA must present “proof-of-service” documents within required timeframes when requested by IEHP’s auditors • An auditor review will compare “proof-of-service” documents to submitted data • Supplemental Data records must pass 100 percent validation to be included in the final P4P reporting
Financial OverviewProviders are eligible to receive financial rewards for performance excellence and forperformance improvement. Financial rewards are based on a tiered system, providingincreasing financial rewards for reaching higher tiered level performance. The 2018 GQ P4PProgram incentive pool is $20 million for the IPA Program. Incentive dollars for the 2018 performance period will be distributed monthly via a new monthly per Member per month (PMPM) Quality Payment beginning in July 2019 and continuing through June 2020.
IPA Encounter Data GatesIPA encounter data submissions must meet minimum adequacy requirements in order to receiveGQ P4P Program incentive dollars. IPA encounter data performance is based on all professionalencounters submitted by the IPA for services rendered during the measurement year (e.g., 2018dates of service). IPA encounter data volume will be compared to established encounter databenchmarks for Seniors and Persons with Disabilities (SPD) and Non-SPD Members. IPAperformance will be calculated against each IPA’s proportion of SPD and Non-SPD Members.
Encounter data benchmarks have been established and correspond to an Encounter DataGate, reflecting higher encounter data volumes. As IPAs reach higher levels of encounter dataperformance, they become eligible for a larger percentage of the total possible GQ P4P incentive.Encounter rates are expressed as the number of encounters per Member per year (PMPY).An encounter is defined as a unique visit per Member per Provider per day. The table belowdescribes the Encounter Data Gates, performance levels, and their impact to IPA GQ P4PProgram incentive payments.
PERCENT OF POSSIBLE INCENTIVE PAYMENT
ENCOUNTER DATA GATE
NON-SPD PMPY
SPD PMPY
50% Gate 1 3.0 9.075% Gate 2 4.0 11.0
100% Gate 3 5.0 13.04

The Encounter Data Gating methodology only applies to the IPA methodology. Encounterdata must be submitted to IEHP in a timely way and must adhere to the reporting timeframesdelineated in IEHP’s Provider Policy and Procedure Manual - Policy 21A.
Appendix 1 provides a list of the 23 measures included in the 2018 GQ P4P Program andincludes the thresholds and benchmarks associated with respective tier goals. These measureshave been categorized into four domains: Clinical Quality; Behavioral Health Integration;Patient Experience; Encounter Data.
Most measures included in the Clinical Quality Domain primarily use standard Healthcare Effectiveness Data and Information Set (HEDIS®) process and outcomes measures that are based on the specifications published by the National Committee for Quality Assurance (NCQA). Non-HEDIS® measures that are included in the Clinical Quality Domain come from the California Department of Health Care Services (DHCS) Medi-Cal Managed Care Quality Program and the Pharmacy Quality Alliance (PQA). Clinical Quality Domain Measures: • Avoidance of Antibiotic Treatment in Adults with Acute Bronchitis (New) • Breast Cancer Screening • Cervical Cancer Screening • Childhood Immunizations – Combo 10 • Comprehensive Diabetes Care – Eye Exam • Comprehensive Diabetes Care – HbA1c Control < 8 • Concurrent Use of Opioids and Benzodiazepines (New) • Immunizations for Adolescents – Combo 2 • Initial Health Assessment • Medication Management for People with Asthma – 75% rate • Timely Postpartum Care • Timely Prenatal Care • Weight Assessment and Counseling for Nutrition and Physical Activity for Children and Adolescents (New) - Counseling for Physical Activity - Counseling for Nutrition - BMI Percentile • Well-Child 3-6 Years of Life
IEHP’s HEDIS® 2019 data set (measurement year 2018) will be used to evaluate Providers’ year-end performance. This measure set undergoes an independent audit review prior to rate finalization.
Performance Measures
5

The Initial Health Assessment (IHA) measure follows IEHP’s IHA internal compliance monitoring methodology and is not a HEDIS® measure.
The Concurrent Use of Opioids and Benzodiazepines measure specification is developed andmaintained by the PQA. This measure will not be used for incentive calculations but will becollected to establish a baseline rate for 2018. See Appendix 2 for measure details.
Behavioral Health Integration Domain Measures: The Behavioral Health Integration Domain includes two measures derived from the Centers forMedicare and Medicaid Services (CMS) Physician Quality Reporting System (PQRS) measure set.1 • Screening for Clinical Depression in Primary Care • Positive Depression Screening with Follow-Up Plan
Patient Experience Domain Measures: Patient Experience Domain measures include Member Satisfaction Survey questions from theConsumer Assessment of Healthcare Providers and Systems (CAHPS) survey that is published bythe Agency for Healthcare Research and Quality (AHRQ). IEHP conducts a Member SatisfactionSurvey that is a modified CAHPS survey and is the sole data source supporting the performancescoring methodology for this measure domain. The IEHP Member Satisfaction Survey is conductedbetween June and December of each year. Surveys received from the 2018 Member SatisfactionSurvey will be used to calculate the Patient Experience Domain measures. A copy of the currentMember Satisfaction Survey is included in Appendix 4. • Access to Care Needed Right Away • Access to Routine Care • Coordination of Care
Encounter Data Domain Measures: The fourth measure domain is Encounter Data. IPAs eligible for the GQ P4P Program becomeeligible to receive payment dollars once they have met the minimum encounter data gate.Higher encounter gate performance qualifies an IPA to receive a higher percentage of incentivedollars. See the ‘IPA Encounter Data Gates’ section of this program guide for additional detailson this methodology.
1 For information on the PQRS measure set: https://www.cms.gov/Medicare/Quality-Initiatives-Patient- Assessment-Instruments/PQRS/index.html.
6

2018 IPA Global Quality P4P Scoring and Payment Flowchart
PROGRAM ELIGIBILITY REQUIREMENTS
Membership will be determined as of 01/2018IPAs with 5,000 or more assigned Members
SCORING METHOD
Incentive eligible IPAs will receive a Quality Score for each Measure
IPAs must have 30 or more Members in each measure to be eligible for a Quality Score
The Quality Score is averaged to determine the Global Quality Performance Score
At least three measures are required to determine the Global Quality Performance Score
IPA PAYMENT CALCULATION[Global Quality Performance Score] x
[# Medi-Cal average Member months] = Member Points
[Member Points] x [payment amount per Member pint] = Max Payment Amount
[Max Payment Amount] x [Encounter Gate %] = Final Payment Amount
7

Scoring MethodologyPayment will be awarded to IPAs based on individual performance in reaching established Quality Goals (e.g., Tier Goals for each measure).
In the Clinical Quality Domain, HEDIS® measure results are based on each measure’s total eligible population assigned to the IPA. The eligible population is defined as the set of Members that meet the denominator criteria specified in the current year’s HEDIS® Technical Specifications (Volume 2) published by NCQA. Members in the eligible population are attributed to the assigned PCP on the anchor date of each measure, as defined within the HEDIS® measure. Members contribute to a IPA’s HEDIS® measure denominator if continuous enrollment criteria are met at the health plan level. For each measure, the HEDIS® score reflects the proportion of the eligible population that is in compliance with the numerator criteria, as defined in the current HEDIS® technical specifications (Volume 2).
In the Clinical Quality Domain, Non-HEDIS® measure results (i.e., Initial Health Assessment) are based on new health plan Members who are assigned to the IPA during the measurement year and who remain enrolled with IEHP and the IPA through the 120 day post enrollment period. See Appendix 2 for measure details.
In the Patient Experience Domain, monthly Member Satisfaction Survey measures are based onMembers who meet eligibility criteria to receive a mailed survey between June and December of themeasurement year. Members eligible to receive a Member Satisfaction Survey must have beencontinuously enrolled with IEHP for at least six months in the measurement year (2018) and musthave had an office visit in the prior six months, based on encounter data submitted to IEHP.Members who meet the survey eligibility criteria are randomly sampled to receive a survey. Surveymeasure results are attributed to the Member’s assigned IPA based on the most recent encounterthat qualified the Member for the survey. A Member is eligible to receive only one survey percalendar year.
For IPAs, the Encounter Data Domain measures assess the volume of IPA encounters received for all assigned IPA Members. The denominator is all assigned Medi-Cal Members each month of the measurement year (2018). All monthly assigned Members are summed to create the denominator (i.e., Member months). The numerator is the sum of all unique encounters (e.g., unique Member, Provider, date of service) in the measurement year for all assigned Members in the denominator. A Per Member Per Year (PMPY) rate is calculated following this formula:
(Total Unique Encounters / Total Member Months) x 12 = PMPY
8

Payment MethodologyIPA performance for each quality measure will be given a point value (i.e., a Quality Score). Pointsare assigned based on the Tier Goal achieved (e.g., Tier 1 = one point, Tier 2 = two points, Tier3 = three points) for each measure.
IPAs that have at least three quality measures which meet the minimum denominator size (n = 30)will be considered for payment calculations. An average of all eligible Quality Scores will determinethe overall GQ Performance Score. GQ P4P Program payments will be awarded according to thefollowing formula:
[Global Quality Performance Score] x [# Medi-Cal Average Member Months] = Member Points
[Member Points] x [Payment Amount per Member Point] = Incentive Payout Total
The payment amount per Member point is dependent on the total incentive money available for IPAs.
IPA PMPM Quality Payment Methodology From July 2019 – June 2020, IPAs will receive a monthly PMPM (per member per month) quality payment based on 2018 GQ P4P performance using the following formula:
2018 Global Quality P4P Payments
Total Medi-Cal Member Months
Quality PMPMPayment Amount
(A) Global P4P Payments: $2,656,800
Total Member Months: 1,440,000
Quality PMPM Payment Amount: $1.85
IPA payment example: IPA with monthly average of 120,000 Members (1,440,000 Member Months), 2.0 GQ Quality Score and Encounter Data Gate 2 met
*assuming stable membership volume
~ $221,400 monthly payment*~$2,656,800 annual payment*
9

Program Terms and Conditions • Participation in IEHP’s GQ P4P Program, as well as acceptance of incentive payments, does not in any way modify or supersede any terms or conditions of any agreement between IEHP and Providers or IPAs, whether that agreement is entered into, prior to or subsequent to, the date of this communication.• There is no guarantee of future funding for, or payment under, any IEHP Provider incentive program. The IEHP GQ P4P Program and/or its terms and conditions may be modified or terminated at any time, with or without notice, at IEHP’s sole discretion.• Criteria for calculating incentive payments are subject to change at any time, with or without notice, at IEHP’s sole discretion.• In consideration of IEHP’s offering of the IEHP GQ P4P Program, participants agree to fully and forever release and discharge IEHP from any and all claims, demands, causes of action, and suits, of any nature, pertaining to or arising from the offering by IEHP of the IEHP GQ P4P Program.• The determination of IEHP regarding performance scoring and payments under the IEHP GQ P4P Program is final.• As a condition of receiving payment under the IEHP GQ P4P Program, Providers and IPAs must be active and contracted with IEHP and have active assigned Members at the time of payment.
Quality Incentive Payout Timeline: Provider Communication Timeline
Dec2018
Nov2018
Oct2018
Sep2018
Aug2018
Jul2018
Jun2018
May2018
Apr2018
Mar2018
Feb2018
Jan2018
Interim 2017 GQ P4P payment (PCP & IPA) Final 2017 GQ P4P payment (PCP & IPA)
End of Traditional PCP P4P Program Monthly Quality PMPM payments based on 2017GQ P4P Performance year results (PCP only)
Dec2019
Nov2019
Oct2019
Sep2019
Aug2019
Jul2019
Jun2019
May2019
Apr2019
Mar2019
Feb2019
Jan2019
Monthly Quality PMPM payments based on 2018GQ P4P Performance year results (PCP & IPA)
Monthly Quality PMPM payments based on 2017GQ P4P Performance year results (PCP only)
Getting Help
Please direct questions and/or comments related to this program to IEHP’s Provider Call Center at 909-890-2054 or to IEHP’s Quality Department at [email protected].
10

1 New Measure for 2018 2Tier 3 goals set at the 90th percentile as published in the NCQA 2017 Mid-year Benchmarks and Thresholds and 2016 HEDIS® and Exclusion Audit Means, Percentiles source files ** Reporting Only Measure. Not eligible for incentive dollars*** Encounter Data measure benchmarks are “gates” not “tiers”
APPENDIX 1: 2018 IPA Global Quality P4P Program Measures2018 GQ P4P PROGRAM MEASURE LIST
Domain Measure Name Population Tier 1 Tier 2 Tier 32
Clinical Quality Avoidance of Antibiotic Treatment in Adults with Acute Bronchitis 1 Adult
Improvement demonstrated by meeting the
following 2 conditions:
10% reduction in non-
compliance
AND
Improvement of at least 2.0 percentage
points
Improvement demonstrated by meeting the
following 2 conditions:
20% reduction in non-
compliance
AND
Improvement of at least 3.0 percentage
points
39.0%
Clinical Quality Comprehensive Diabetes Care - HbA1c Control <8 Adult 58.0%
Clinical Quality Comprehensive Diabetes Care - Eye Exam Adult 68.0%
Clinical Quality Medication Management for People with Asthma - 75% Adult 48.0%
Behavioral Health Integration
Screening for Clinical Depression in Primary Care
Adult and Adolescent 50.0%
Behavioral Health Integration
Positive Depression Screening with Follow-Up Plan
Adult and Adolescent 90.0%
Clinical Quality Breast Cancer Screening Women 71.0%Clinical Quality Cervical Cancer Screening Women 70.0%Clinical Quality Timeliness of Prenatal Care Women 91.0%Clinical Quality Postpartum Care Women 74.0%Clinical Quality Childhood Immunizations - Combo 10 Child
Improvement demonstrated
by meeting the following 2 conditions:
10% reduction in non-
compliance
AND
Improvement of at least 2.0 percentage
points
Improvement demonstrated
by meeting the following 2 conditions:
20% reduction in non-
compliance
AND
Improvement of at least 3.0 percentage
points
46.0%
Clinical Quality Immunizations for Adolescents - Combo 2 Child 32.3%
Clinical Quality Well-Child Visits 3-6 Years of Life Child 83.0%
Clinical QualityWeight Assessment and Counseling
for Nutrition and Physical Activity for Children and Adolescents - Counseling
for Physical Activity 1Child 72.0%
Clinical QualityWeight Assessment and Counseling
for Nutrition and Physical Activity for Children and Adolescents - Counseling
for Nutrition 1Child 80.0%
Clinical QualityWeight Assessment and Counseling for Nutrition and Physical Activity
for Children and Adolescents - BMI Percentile 1
Child 86.0%
Clinical Quality Initial Health Assessment All 50.0%
Clinical Quality Concurrent Use of Opioids and Benzodiazepines 1 ** All Baseline Reporting Year
Patient Experience
Member Satisfaction Survey - Access to Care Needed Right Away All 84.00% 86.00% 88.0%
Patient Experience
Member Satisfaction Survey - Coordination of Care All 82.00% 84.00% 86.0%
Patient Experience
Member Satisfaction Survey – Access to Routine Care All 82.00% 85.00% 86.0%
Encounter Data Encounter Data for PCPs PMPY – SPD*** All 9.0 11.0 13.0
Encounter Data Encounter Data for PCPs PMPY - Non-SPD*** All 3.0 4.0 5.0
11
APPENDIX 2: Measures Overview
Population: Adult
Avoidance of Antibiotic Treatment in Adults With Acute Bronchitis (AAB)
Methodology: HEDIS® Measure Description: The percentage of adults 18-64 years of age with a diagnosis of acute bronchitis who were not dispensed an antibiotic prescription on or three days after the Index Episode Start Date (IESD). • Episode Date is the date of service for any outpatient or emergency department (ED) visit during the Intake Period (January 1, 2018-December 24, 2018) with a diagnosis of acute bronchitis • IESD: the earliest Episode Date during the Intake Period with a diagnosis of acute bronchitis that meets all of the following criteria: 1. Episode Date is the date of service for any outpatient or ED visit during the Intake Period with a diagnosis of acute bronchitis. 2. A 30-day Negative Medication History prior to the Episode Date. 3. A 12-month Negative Comorbid Condition History prior to and including the Episode Date. 4. A Negative Competing Diagnosis during the 38-day period from 30 days prior to the Episode Date through seven days after the Episode Date. 5. The member was continuously enrolled one year prior to the Episode Date through seven days after the Episode Date. • The measure is reported as an inverted rate [1 – (numerator/eligible population)]. A higher rate indicates appropriate treatment of adults with acute bronchitis (i.e., the proportion for whom antibiotics were not prescribed). • Members in hospice are excluded from the eligible population. • Exclude denied claims when assessing numerator criteria. • Do not include ED visits or observation visits that result in an inpatient stay. When an ED or observation visit and an inpatient stay are billed on separate claims, the visit results in an inpatient stay when the admission date for the inpatient stay occurs on the ED/ observation date of service or one calendar day after. An ED or observation visit billed on the same claim as an inpatient stay is considered a visit that resulted in an inpatient stay.
12

AAB ANTIBIOTIC MEDICATIONSDescription Prescription
Aminoglycosides • Amikacin • Tobramycin • Gentamicin • Streptomycin
Aminopenicillins • Amoxicillin • Ampicillin
Beta-lactamase inhibitors • Amoxicillin-clavulanate • Piperacillin-tazobactam • Ticarcillin-clavulanate • Ampicillin-sulbactam
First-generation cephalosporins • Cefadroxil • Cefazolin • Cephalexin
Fourth-generation cephalosporins • Cefepime
Ketolides • TelithromycinLincomycin derivatives • Clindamycin • Lincomycin
Macrolides • Azithromycin • Erythromycin • Erythromycin • Clarithromycin • Erythromycin lactobionate ethylsuccinate • Erythromycin stearate
Miscellaneous antibiotics • Aztreonam • Daptomycin • Metronidazole • Chloramphenicol • Erythromycin- • Vancomycin • Dalfopristin-quinupristin sulfisoxazole • Linezolid
Natural penicillins • Penicillin G benzathine- • Penicillin G procaine • Penicillin V potassium procaine • Penicillin G sodium • Penicillin G • Penicillin G potassium benzathine
Penicillinase resistant penicillins • Dicloxacillin • Nafcillin • Oxacillin
Quinolones • Ciprofloxacin • Levofloxacin • Norfloxacin • Gemifloxacin • Moxifloxacin • Ofloxacin
Rifamycin derivatives • RifampinSecond-generation
cephalosporin • Cefaclor • Cefoxitin • Cefuroxime • Cefotetan • Cefprozil
Sulfonamides • Sulfadiazine • Sulfamethoxazole-trimethoprimTetracyclines • Doxycycline • Minocycline • Tetracycline
Third-generation cephalosporins
• Cefdinir • Cefotaxime • Ceftibuten • Cefditoren • Cefpodoxime • Ceftriaxone • Cefixime • Ceftazidime
Urinary anti-infectives • Fosfomycin • Nitrofurantoin macrocrystals-monohydrate • Nitrofurantoin • Nitrofurantoin macrocrystals • Trimethoprim
Denominator: Members 18-64 years of age, who had an outpatient visit, an observation visit or an ED visit between January 1 – December 24 of the measurement year (2018) with a diagnosis of acute bronchitis. Numerator: Dispensed prescription for an antibiotic medication on or three days after IESD for the Members in denominator.
13

Comprehensive Diabetes Care (CDC) – HbA1c Control (<8.0)
Methodology: HEDIS®
Measure Description: The percentage of Members 18-75 years of age with diabetes (type 1 and type 2) who had the following: • HbA1c Control (<8.0%) – This includes diabetics whose most recent HbA1c test during the measurement year (2018) has a value <8.0%. - The Member is not numerator compliant if the result for the most recent HbA1c test is ≥8.0% or is missing a result, or if an HbA1c test was not done during the measurement year (2018). • The eligible population in this measure meets all of the following criteria: 1. Members who are 18-75 years old as of December 31 of the measurement year (2018). 2. Continuous enrollment in the measurement year (2018) with no more than one gap of up to 45 days during the measurement year. 3. Members who meet any of the following criteria during the measurement year (2018) or the year prior to the measurement year (2017). Count services that occur over both years: • At least two outpatient visits, observation visits, ED visits or nonacute inpatient encounters on different dates of service, with a diagnosis of diabetes. Visit type need not be the same for the two visits. • At least one acute inpatient encounter with a diagnosis of diabetes. • Members who were dispensed insulin or hypoglycemics/ antihyperglycemics on an ambulatory basis during the measurement year (2018) or the year prior to the measurement year (2017).
14

CODES TO IDENTIFY HbA1c TESTSService Code Type Code Code Description
HbA1c Test (<7.0%) CPT-CAT-II 3044F Hg A1c Level Lt 7.0%HbA1c Test CPT 83036 Hemoglobin Glycated
HbA1c Test CPT 83037 Hemoglobin; glycosylated (A1C) by device cleared by FDA for home use
HbA1c Test CPT-CAT-II 3044F Most recent hemoglobin A1c (HbA1c) level < 7.0%HbA1c Test CPT-CAT-II 3045F Most recent hemoglobin A1c (HbA1c) level 7.0-9.0%HbA1c Test CPT-CAT-II 3046F Most recent hemoglobin A1c (HbA1c) level > 9.0%HbA1c Test LOINC 17856-6 Hemoglobin A1c/hemoglobin.total In Blood By HplcHbA1c Test LOINC 4548-4 Hemoglobin A1c/hemoglobin.total In Blood
HbA1c Test LOINC 4549-2 Hemoglobin A1c/hemoglobin.total In Blood By Electrophoresis
• Members who meet any of the following criteria are excluded: 1. Members in hospice 2. Members who did not have a diagnosis of diabetes, in any setting, during the measurement year (2018) or the year prior to the measurement year (2017) and who had a diagnosis of gestational diabetes or steroid-induced diabetes, in any setting, during the measurement year (2018) or the year prior to the measurement year (2017)
Denominator: Members 18-75 years of age who meet all the criteria for eligible population.
Numerator: Members in the denominator who had the most recent HbA1c level <8 duringthe measurement year (2018).
15

Comprehensive Diabetes Care (CDC) – Eye Exam
Methodology: HEDIS®
Measure Description: The percentage of Members 18-75 years of age with diabetes (type 1 and type 2) who had the following: • Eye Exam (retinal) performed – This includes diabetics who had one of the following: - A retinal or dilated eye exam by an eye care professional (optometrist or ophthalmologist) in the measurement year (2018) - A negative retinal or dilated eye exam (negative for retinopathy) by an eye care professional in the year prior to the measurement year (2018) • The eligible population in this measure meets all of the following criteria: 1. Members who were 18-75 years old as of December 31 of the measurement year (2018). 2. Continuous enrollment in the measurement year (2018) with no more than one gap of up to 45 days during the measurement year. 3. Members who meet any of the following criteria during the measurement year (2018) or the year prior to the measurement year (2017). Count services that occur over both years: • At least two outpatient visits, observation visits, ED visits or nonacute inpatient encounters on different dates of service, with a diagnosis of diabetes. Visit type need not be the same for the two visits. • At least one acute inpatient encounter with a diagnosis of diabetes. • Members who were dispensed insulin or hypoglycemics/ antihyperglycemics on an ambulatory basis during the measurement year (2018) or the year prior to the measurement year (2017).
16

CODES TO IDENTIFY EYE EXAMS
Service Code Type Code Code Description
Diabetic Retinal Screening CPT 67028 Intravitreal Injection Of A Pharmacologic Agent (separate Procedure)
Diabetic Retinal Screening CPT 67030 Discission Of Vitreous Strands (without Removal) Pars Plana Approach
Diabetic Retinal Screening CPT 67031 Severing Of Vitreous Strands Vitreous Face Adhesions Sheets
Membranes Or Opacities Laser Surgery (one Or More Stages)Diabetic Retinal
Screening CPT 67036 Vitrectomy Mechanical Pars Plana Approach
Diabetic Retinal Screening CPT 67039 Vitrectomy Mechanical Pars Plana Approach With Focal Endolaser
PhotocoagulationDiabetic Retinal
Screening CPT 67040 Vitrectomy Mechanical Pars Plana Approach With Endolaser Panre Tinal Photocoagulation
Diabetic Retinal Screening CPT 67041 Vitrectomy Mechanical Pars Plana Approach With Removal Of
Preretinal Cellular Membrane (eg Macular Pucker)Diabetic Retinal
Screening CPT 67042 Vitrectomy Mechanical Pars Plana Approach With Removal Of Internal Limiting Membrane Of Retina (eg For Repair Of Macular Hole
Diabetic Retinal Screening CPT 67043
Vitrectomy mechanical pars plana approach, with removal of subretinal membrane (eg, Choroidal Neovascularization), includes, if performed, intraocular tamponade (ie, air, gas or silicone oil)
Diabetic Retinal Screening CPT 67101 Repair Retinal Detachment, Incld Drainage Of Subretinal Fluid When
Performed; CryotherapyDiabetic Retinal
Screening CPT 67105 Repair Retinal Detachment, Incld Drainage Of Subretinal Fluid When Performed; Photocoagulation
Diabetic Retinal Screening CPT 67107
Repair Of retinal detachment scleral buckling (such as lamellar scleral dissection, Imbrication or encircling procedure), including, when performed, implant, cryotherapy, photocoagulation, and drainage of subretinal fluid
Diabetic Retinal Screening CPT 67108 Repair Of Retinal Detachment With Vitrectomy Any Method With OR
Without Air Or Gas Tamponade Focal Endolaser PhotocoagulationDiabetic Retinal
Screening CPT 67110 Repair Of Retinal Detachment By Injection Of Air Or Other Gas (e G Pneumatic Retinopexy)
Diabetic Retinal Screening CPT 67112 Repair Of Retinal Detachment By Scleral Buckling Or Vitrectomy On
Patient Having Previous Ipsilateral Retinal Detachment Repair
Diabetic Retinal Screening CPT 67113
Repair Of Complex Retinal Detachment (eg, Proliferative Vitreoretinopathy Stage C-1 or greater, diabetic Traction Retinal Detachment, retinopathy of prematurity, retinal tear of greater than 90 degrees), with vitrectomy and membrane peeling, including, when performed, air, gas, or silicone oil tamponade, cryotherapy, endolaser photocoagulation, drainage of subretinal fluid, scleral buckling, and/or removal of lens
Diabetic Retinal Screening CPT 67121 Removal Of Implanted Material Posterior Segment Intraocular
17

CODES TO IDENTIFY EYE EXAMS
Service Code Type Code Code Description
Diabetic Retinal Screening CPT 67141 Prophylaxis Of Retinal Detachment (eg, retinal break lattice degeneration)
without drainage, 1 or more sessions; cryotherapy, diathermy
Diabetic Retinal Screening CPT 67145
Prophylaxis Of Retinal Detachment (eg, retinal break lattice degeneration) without drainage, 1 or more sessions; photocoagulation (laser or xenon arc)
Diabetic Retinal Screening CPT 67208 Destruction Of Localized Lesion Of Retina (eg Macular Edema
Tumors) One Or More Sessions Cryotherapy DiathermyDiabetic Retinal
Screening CPT 67210 Destruction Of Localized Lesion Of Retina (eg Macular Edema Tumors) One Or More Sessions Photocoagulation
Diabetic Retinal Screening CPT 67218 Destruction Of Localized Lesion Of Retina (eg Macular Edema
Tumors) One Or More Sessions Radiation By Implantation Of SourceDiabetic Retinal
Screening CPT 67220 Destruction Of Localized Lesion Of Choroid (eg Choroidal Neovasc Ularization) Photocoagulation (eg Laser) One Or More Sessions
Diabetic Retinal Screening CPT 67221 Destruction Of Localized Lesion Of Choroid (eg Choroidal Neovasc
Ularization) Photodynamic Therapy (includes Intravenous InfusionDiabetic Retinal
Screening CPT 67227 Destruction Of Extensive Or Progressive Retinopathy (eg Diabetic Retinopathy) One Or More Sessions Cryotherapy Diathermy
Diabetic Retinal Screening CPT 67228 Destruction of extensive or progressive retinopathy (eg, Diabetic
Retinopathy), 1 or more sessions; Photocoagulation
Diabetic Retinal Screening CPT 92002
Ophthalmological services: medical examination and evaluation with initiation of diagnostic and treatment program; Intermediate, new patient
Diabetic Retinal Screening CPT 92004
Ophthalmological services: medical examination and evaluation with initiation of diagnostic and treatment program; comprehensive, new patient, 1 or more visits
Diabetic Retinal Screening CPT 92012
Ophthalmological services: medical examination and evaluation with initiation or continuation of diagnostic and treatment program; intermediate, established patient
Diabetic Retinal Screening CPT 92014
Ophthalmological services: medical examination and evaluation with initiation or continuation of diagnostic and treatment program; comprehensive, established patient, 1 or more visits
Diabetic Retinal Screening CPT 92018
Ophthalmological examination and evaluation under general anesthesia with or without manipulation of globe for passive range of motion or other manipulation to facilitate diagnostic examination; complete
Diabetic Retinal Screening CPT 92019
Ophthalmological examination and evaluation under general anesthesia with or without manipulation of globe for passive range of motion or other manipulation to facilitate diagnostic examination; limited
Diabetic Retinal Screening CPT 92134
Scanning computerized ophthalmic diagnostic imaging posterior segment, with interpretation and report, unilateral or bilateral: optic nerve
Diabetic Retinal Screening CPT 92225 Ophthalmoscopy extended with retinal drawing (eg, for retinal
detachment melanoma), with Interpretation and report; initial
18

CODES TO IDENTIFY EYE EXAMS
Service Code Type Code Code Description
Diabetic Retinal Screening CPT 92226 Ophthalmoscopy Extended With Retinal Drawing (eg For Retinal
Detachment Melanoma) With Interpretation And Report Subsequent
Diabetic Retinal Screening CPT 92227
Remote imaging for detection of retinal disease (eg, Retinopathy in a patient with diabetes) with analysis and report under Physician supervision, unilateral or bilateral
Diabetic Retinal Screening CPT 92228
Remote imaging for monitoring and management of active retinal disease (eg, Diabetic Retinopathy) with Physician review, interpretation and report, unilateral or bilateral
Diabetic Retinal Screening CPT 92230 Fluorescein Angioscopy With Interpretation And Report
Diabetic Retinal Screening CPT 92235 Fluorescein Angiography (includes Multiframe Imaging) With
Interpretation And Report (unilateral Or Bilateral)Diabetic Retinal
Screening CPT 92240 Indocyanine-green Angiography (includes Multiframe Imaging) With Interpretation And Report (unilateral Or Bilateral)
Diabetic Retinal Screening CPT 92250 Fundus Photography With Interpretation And Report
Diabetic Retinal Screening CPT 92260 Ophthalmodynamometry
Diabetic Retinal Screening CPT 99203
Office or other patient visit for the evaluation and management of a new patient, which requires these 3 key components: A detailed history: A detailed exam: Medical decision making of low complexity.
Diabetic Retinal Screening CPT 99204
Office or other patient visit for the evaluation and management of a new patient, which requires these 3 key components: A comprehensive history: A comprehensive exam: Medical decision making of moderate complexity.
Diabetic Retinal Screening CPT 99205
Office or other patient visit for the evaluation and management of a new patient, which requires these 3 key components: A comprehensive history: A comprehensive exam: Medical decision making of high complexity.
Diabetic Retinal Screening CPT 99213
Office or other patient visit for the evaluation and management of an established patient, which requires at least 2 of these 3 components: An expanded problem focused history: An expanded problem focused examination: Medical decision making of low complexity.
Diabetic Retinal Screening CPT 99214
Office or other patient visit for the evaluation and management of an established patient, which requires at least 2 of these 3 components: A detailed history: A detailed exam: Medical decision making of moderate complexity.
Diabetic Retinal Screening CPT 99215
Office or other patient visit for the evaluation and management of an established patient, which requires at least 2 of these 3 components: A comprehensive history: A comprehensive exam: Medical decision making of high complexity.
19

CODES TO IDENTIFY EYE EXAMS
Service Code Type Code Code Description
Diabetic Retinal Screening CPT 99242
Office consultation for a new or established patient which requires these 3 key components: An expanded problem focused history: An expanded problem focused examination: and, Straightforward medical decision making.
Diabetic Retinal Screening CPT 99243
Office consultation for a new or established patient which requires these 3 key components: A detailed history: A detailed exam: and, Medical decision making of low complexity.
Diabetic Retinal Screening CPT 99244
Office consultation for a new or established patient which requires these 3 key components: A comprehensive history: A comprehensive examination: and, Medical decision making of moderate complexity.
Diabetic Retinal Screening CPT 99245
Office consultation for a new or established patient which requires these 3 key components: A comprehensive history: A comprehensive examination: and, Medical decision making of high complexity.
Diabetic Retinal Screening HCPCS S0620 Routine Ophthalmological Examination Including Refraction; New
Patient (s0620)Diabetic Retinal
Screening HCPCS S0621 Routine Ophthalmological Examination Including Refraction; Established Patient (s0621)
Diabetic Retinal Screening HCPCS S3000 Diabetic Indicator; Retinal Eye Exam, Dilated, Bilateral (s3000)
• Members who meet any of the following criteria are excluded: 1. Members in hospice 2. Members who did not have a diagnosis of diabetes, in any setting, during the measurement year (2018) or the year prior to the measurement year (2017) and who had a diagnosis of gestational diabetes or steroid-induced diabetes, in any setting, during the measurement year or the year prior to the measurement year Denominator: Members 18-75 years of age who meet all the criteria for eligible population.
Numerator: Members in the denominator who had an eye exam during the measurementyear (2018).
20

Medication Management for People with Asthma – 75% rate (MMA)
Methodology: HEDIS®
Measure Description: The percentage of Members 5–64 years of age during the measurement year (2018) who were identified as having persistent asthma and were dispensed appropriate medications which they remained on for at least 75 percent of their treatment period. (Treatment Period: The period of time beginning on the Index Prescription Start Date through December 31, 2018.) • Eligible population in this measure meets all of the following criteria: 1. Age 5- 64 as of December 31 of the measurement year (2018). 2. Continuous enrollment during the measurement year (2018) and the year prior to the measurement year (2017) with no more than one gap in enrollment of up to 45 days during each year of continuous enrollment. 3. Members had a) At least one ED visit with a principal diagnosis of asthma, OR b) At least one acute inpatient encounter with a principal diagnosis of asthma, OR c) At least four outpatient visits or observation visits on different dates of service, with any diagnosis of asthma and at least two asthma medication dispensing events for any controller medication or reliever medication. Visit type need not be the same for the four visits, OR d) At least four asthma medication dispensing events for any controller medication or reliever medication.
ASTHMA CONTROLLER MEDICATIONS:Description Prescription
Antiasthmatic combinations • Dyphylline-guaifenesin • Guaifenesin-theophylline
Antibody inhibitors • Omalizumab Anti-interleukin-5 • Mepolizumab • Reslizumab
Inhaled steroid combinations
• Budesonide-formoterol • Fluticasone-vilanterol • Fluticasone-salmeterol • Mometasone-formoterol
Inhaled corticosteroids • Beclomethasone • Flunisolide • Budesonide • Fluticasone CFC free • Ciclesonide • Mometasone
Leukotriene modifiers • Montelukast • Zafirlukast • ZileutonMast cell stabilizers • Cromolyn
Methylxanthines • Dyphylline • Theophylline
ASTHMA RELIEVER MEDICATIONSDescription Prescriptions
Short-acting, inhaled beta-2 agonists • Albuterol • Levalbuterol • Pirbuterol21

• Members who meet any of the following criteria are excluded: 1. Members who had no asthma controller medications dispensed during the measurement year (2018). 2. Members in hospice are excluded. 3. Members with the following diagnosis any time during the Member’s history through December 31 of the measurement year (2018) are excluded: COPD, Acute Respiratory Failure, Cystic Fibrosis, Chronic respiratory conditions and Emphysema.
Denominator: Members 5–64 years of age during the measurement year (2018) who were identified as having persistent asthma and were dispensed appropriate medications which they remained on during the treatment period.
Numerator: Members in denominator who remained on an asthma controller medication for at least 75 percent of their treatment period.
22

Population: Adult and Adolescent
Screening for Clinical Depression in Primary Care
Methodology: IEHP-defined Quality Metric – Modified from PQRS measure (NQF 0418)
Measure Description: The percentage of Members aged 12 years and older screened for clinical depression on the date of the encounter using an age appropriate standardized depression screening tool during the measurement year (2018).
Denominator: All Members aged 12 years and older with a PCP visit in the measurement year (2018). Member counted only once in the denominator.
PRIMARY CARE PROVIDER VISIT CODES:
Service Code Type Code Code Description
Screening for Clinical Depression in Primary Care CPT 99201
Office or other outpatient visit for the evaluation and management of a new patient which requires these three key components: A problem focused history; A problem focused examination; Straightforward medical decision making. Typically, 10 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care CPT 99202
Office or other outpatient visit for the evaluation and management of a new patient which requires these three key components: An expanded problem focused history; An expanded problem focused examination; Straightforward medical decision making. Typically, 20 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care CPT 99203
Office or other outpatient visit for the evaluation and management of a new patient which requires these three key components: A detailed history; A detailed examination; Medical decision making of low complexity. Typically, 30 minutes are spent face-to- face with the patient and/or family.
Screening for Clinical Depression in Primary Care CPT 99204
Office or other outpatient visit for the evaluation and management of a new patient which requires these three key components: A comprehensive history; A comprehensive examination; Medical decision making of moderate complexity. Typically, 45 minutes are spent face-to-face with the patient and/or family.
23

PRIMARY CARE PROVIDER VISIT CODES:
Service Code Type Code Code Description
Screening for Clinical Depression in Primary Care CPT 99205
Office or other outpatient visit for the evaluation and management of a new patient which requires these three key components: A comprehensive history; A comprehensive examination; Medical decision making of high complexity. Typically, 60 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care CPT 99212
Office or other outpatient visit for the evaluation and management of an established patient which requires at least two of these 3 key components: A problem focused history; A problem focused examination; Straightforward medical decision making. Typically, 10 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care CPT 99213
Office or other outpatient visit for the evaluation and management of an established patient which requires at least two of these 3 key components: An expanded problem focused history; An expanded problem focused examination; Medical decision making of low complexity. Typically, 15 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care CPT 99214
Office or other outpatient visit for the evaluation and management of an established patient which requires at least two of these 3 key components: A detailed history; A detailed examination; Medical decision making of moderate complexity. Typically, 25 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care CPT 99215
Office or other outpatient visit for the evaluation and management of an established patient which requires at least two of these 3 key components: A comprehensive history; A comprehensive examination; Medical decision making of high complexity. Typically, 40 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care HCPCS G0101
Office or other outpatient visit for the evaluation and management of an established patient which requires at least two of these 3 key components: A comprehensive history; A comprehensive examination; Medical decision making of high complexity. Typically, 40 minutes are spent face-to-face with the patient and/or family.
Screening for Clinical Depression in Primary Care HCPCS G0402 Initial preventive physical examination face-to-face visits
services limited to new beneficiary during the first 12 monthsScreening for Clinical
Depression in Primary Care HCPCS G0438 Annual wellness visit includes a personalized prevention plan of service (pps) initial visit
Screening for Clinical Depression in Primary Care HCPCS G0439 Annual wellness visit includes a personalized prevention
plan of service (pps) subsequent visit
24

Numerator: Members screened for clinical depression on the date of the encounter using an age appropriate standardized tool during the measurement year (2018).
PRIMARY CARE PROVIDER VISIT CODES:
Service Code Type Code Code Description
Screening for Clinical Depression in Primary Care HCPCS G0444 Annual depression screening 15 minutes
Screening for Clinical Depression in Primary Care CPT 97003 Occupational therapy evaluation
CODES TO IDENTIFY SCREENING FOR CLINICAL DEPRESSIONService Code Type Code Code Description
Screening for Clinical Depression in Primary Care CPT 1220F Patient screened for depression (sud)
Screening for Clinical Depression in Primary Care CPT 3351F
Negative screen for depressive symptoms as categorized by using a standardized depression screening/assessment tool (mdd)
Screening for Clinical Depression in Primary Care CPT 3352F No significant depressive symptoms as categorized by
using a stan dardized depression assessment tool (mdd)
Screening for Clinical Depression in Primary Care CPT 3353F
Mild to moderate depressive symptoms as categorized by using a standardized depression screening/assessment tool (mdd)
Screening for Clinical Depression in Primary Care CPT 3354F
Clinically significant depressive symptoms as categorized by usin g a standardized depression screening/assessment tool (mdd)
Screening for Clinical Depression in Primary Care CPT 3725F Screening for depression performed (dem)
Screening for Clinical Depression in Primary Care HCPCS G0444 Annual depression screening 15 minutes
Screening for Clinical Depression in Primary Care HCPCS G8431 Positive screen for clinical depression using a
standardized tool and a follow-up plan documentedScreening for Clinical
Depression in Primary Care HCPCS G8433 Screening for clinical depression using a standardized tool not documented patient not eligible/appropriate
Screening for Clinical Depression in Primary Care HCPCS G8510
Negative screen for clinical depression using a standardized tool patient not eligible/appropriate for follow-up plan documented
Screening for Clinical Depression in Primary Care HCPCS G8511
Screen for clinical depression using a standardize tool documented follow up plan not documented reason not specified
Screening for Clinical Depression in Primary Care HCPCS G8940
Screening for clinical depression documented follow-up plan not documented patient not eligible/appropriate
25
Definitions: Screening – Completion of a clinical or diagnostic tool used to identify people at risk of developing or having a certain disease or condition, even in the absence of symptoms.
Standardized Depression Screening Tool – A normalized and validated depression screening tool developed for the Member population in which it is being utilized. The name of the age appropriate standardized depression screening tool utilized must be documented in the medical record.
Examples of depression screening tools include but are not limited to: • Adolescent Screening Tools (12-17 years): Patient Health Questionnaire for Adolescents (PHQ-A), Beck Depression Inventory-Primary Care Version (BDI-PC), Mood Feeling Questionnaire (MFQ), Center for Epidemiologic Studies Depression Scale (CES-D), and PRIME MD-PHQ2 • Adult Screening Tools (18 years and older): Patient Health Questionnaire (PHQ-9 or PHQ-2), Beck Depression Inventory (BDI or BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Depression Scale (DEPS), Duke Anxiety-Depression Scale (DADS), Geriatric Depression Scale (GDS), Cornell Scale Screening, and PRIME MD-PHQ2
26

Positive Depression Screening with Follow Up Plan
Methodology: IEHP-defined Quality Metric – Modified from PQRS measure (NQF 0418)
Measure Description: The percentage of Members aged 12 years and older who screened positive for clinical depression using an age appropriate standardized depression screening tool who also have a follow-up plan documented during the measurement year (2018).
Denominator: All Members aged 12 years and older with a PCP visit with a positive depression screening in the measurement year (2018). Member counted only once in the denominator.
CODES TO IDENTIFY POSITIVE DEPRESSION SCREENING DURING A PRIMARY CARE PROVIDER VISIT:
Service Code Type Code Code Description
Positive Depression Screening with Follow Up Plan CPT 3353F
Mild to moderate depressive symptoms as categorized by using a standardized depression screening/assessment tool (mdd)
Positive Depression Screening with Follow Up Plan CPT 3354F
Clinically significant depressive symptoms as categorized by using a standardized depression screening/assessment tool (mdd)
Positive Depression Screening with Follow Up Plan HCPCS G8431 Positive screen for clinical depression using a
standardized tool and a follow-up plan documented
Positive Depression Screening with Follow Up Plan HCPCS G8511
Screen for clinical depression using a standardize tool documented follow up plan not documented reason not specified
Positive Depression Screening with Follow Up Plan HCPCS G8940
Screening for clinical depression documented follow-up plan not documented patient not eligible/appropriate
Numerator: Members screened positive for clinical depression with a follow-up plan documented during the measurement year (2018).
27

CODES TO IDENTIFY POSITIVE DEPRESSION SCREENING WITH FOLLOW-UP PLAN
Service Code Type Code Code DescriptionPositive Depression Screening
with Follow Up Plan CPT 0545F Plan for follow-up care for major depressive disorder documented (mdd adol)
Positive Depression Screening with Follow Up Plan HCPCS G8431 Positive screen for clinical depression using a
standardized tool and a follow-up plan documented
Positive Depression Screening with Follow Up Plan HCPCS G8940
Screening for clinical depression documented follow-up plan not documented patient not eligible/appropriate
Definitions:
Follow-Up Plan – Documented follow-up for a positive depression screening must include one or more of the following: • Additional evaluation for depression • Suicide Risk Assessment • Referral to a practitioner who is qualified to diagnose and treat depression • Pharmacological interventions • Other interventions or follow-up for the diagnosis or treatment of depression
28

Population: Women
Breast Cancer Screening (BCS)Methodology: HEDIS®
Measure Description: The percentage of women 50–74 years of age who had a mammogram to screen for breast cancer any time on or between October 1 two years prior to the measurement year (2016) and December 31 of the measurement year (2018). • The eligible population in the measure meets all of the following criteria: 1. Women 52-74 years as of December 31 of the measurement year (2018). 2. Continuous enrollment from October 1 two years prior to the measurement year (2016) through December 31 of the measurement year (2018) with no more than one gap in enrollment of up to 45 days for each calendar year of continuous enrolment. No gaps in enrollment are allowed from October 1 two years prior to the measurement year (2016) through December 31 two years prior to the measurement year (2016).
CODES USED TO IDENTIFY MAMMOGRAPHY:Service Code Type Code Code Description
Breast Cancer Screening CPT 77055 Mammography UnilateralBreast Cancer Screening CPT 77056 Mammography Bilateral
Breast Cancer Screening CPT 77057 Screening Mammography Bilateral (2-view Film Study Of Each Breast)
Breast Cancer Screening CPT 77061 Digital Breast Tomosynthesis UnilateralBreast Cancer Screening CPT 77062 Digital Breast Tomosynthesis Bilateral
Breast Cancer Screening CPT 77063 Screening Digital Breast Tomosynthesis Bilateral (list Separately In Addition To Code For Primary Procedure)
Breast Cancer Screening CPT 77065 Diagnostic Mammography W/computer-aided Detection; Unilateral
Breast Cancer Screening CPT 77066 Diagnostic Mammography W/computer-aided Detection; Bilateral
Breast Cancer Screening CPT 77067 Screening Mammography Bilateral (2-view Film Study Of Each Breast Including Computer-aided Detection (cad)
Breast Cancer Screening HCPCS G0202Screening Mammography, Bilateral (2-view Study Of Each Breast), Including Computer-aided Detection (cad) When Performed (g0202)
Breast Cancer Screening HCPCS G0204 Diagnostic Mammography, Including Computer-aided Detection (cad) When Performed; Bilateral (g0204)
Breast Cancer Screening HCPCS G0206 Diagnostic Mammography, Including Computer-aided Detection (cad) When Performed; Unilateral (g0206)
29
• Members who meet any of the following criteria are excluded: 1. Members who have had a bilateral mastectomy anytime during their history through December 31, 2018 may be excluded.
To exclude Members who meet the exclusion criteria, please complete Member Historical Data Form and fax to IEHP’s Quality Informatics Team at: 909-477-8568.
A copy of the Historical Data Form is available in Appendix 3.
2. Members in hospice are excluded.
Denominator: Women 52-74 years of age who met the criteria for eligible population.
Numerator: Members in denominator who had one or more mammograms any time on or between October 1 two years prior to the measurement year (2016) and December 31 of the measurement year (2018).
Cervical Cancer Screening (CCS)Methodology: HEDIS®
Measure Description: The percentage of Women 21–64 years of age who were screened for cervical cancer using either of the following criteria: • Women age 21–64 who had cervical cytology performed every 3 years. • Women age 30–64 who had cervical cytology/human papillomavirus (HPV) co-testing performed every 5 years. • The eligible population in the measure meets all of the following criteria: 1. Women 24-64 years as of December 31 of the measurement year (2018). 2. Continuous enrollment during the measurement year (2018) with no more than one gap in enrollment of up to 45 days.
CODES TO IDENTIFY CERVICAL CYTOLOGY:Service Code Type Code Code Description
Cervical Cancer Screening CPT 88141
Cytopathology Cervical Or Vaginal (any Reporting System) Requiring Interpretation By Physician (List separately In addition to code for technical service.)
Cervical Cancer Screening CPT 88142
Cytopathology Cervical Or Vaginal (any Reporting System) Collected In Preservative Fluid Automated Thin Layer Preparation Manual screening Under Physician Supervision
30

CODES TO IDENTIFY CERVICAL CYTOLOGY:Service Code Type Code Code Description
Cervical Cancer Screening CPT 88143
Cytopathology Cervical Or Vaginal (any Reporting System) Collec Ted In Preservative Fluid Automated Thin Layer Preparation; manual screening Under Physician Supervision: With manual screening and rescreening Under Physician Supervision
Cervical Cancer Screening CPT 88147 Cytopathology Smears Cervical Or Vaginal Screening By
Automated System Under Physician Supervision
Cervical Cancer Screening CPT 88148
Cytopathology Smears Cervical Or Vaginal Screening By Automated System With Manual Rescreening Under Physician Supervision
Cervical Cancer Screening CPT 88150 Cytopathology Slides Cervical Or Vaginal Manual Screening
Under Physician Supervision
Cervical Cancer Screening CPT 88152
Cytopathology Slides Cervical Or Vaginal With Manual Screening And Computer-assisted Rescreening Under Physician Supervision
Cervical Cancer Screening CPT 88153 Cytopathology Slides Cervical Or Vaginal With Manual
Screening And Rescreening Under Physician Supervision
Cervical Cancer Screening CPT 88154
Cytopathology Slides Cervical Or Vaginal With Manual Screening And Computer-assisted Rescreening Using Cell Selection And Review Under Physician Supervision
Cervical Cancer Screening CPT 88164 Cytopathology Slides Cervical Or Vaginal (the Bethesda System)
Manual Screening Under Physician Supervision
Cervical Cancer Screening CPT 88165
Cytopathology Slides Cervical Or Vaginal (the Bethesda System) With Manual Screening And Rescreening Under Physician Supervision
Cervical Cancer Screening CPT 88166
Cytopathology Slides Cervical Or Vaginal (the Bethesda System) With Manual Screening And Computer-assisted Rescreening Under Physician Supervision
Cervical Cancer Screening CPT 88167
Cytopathology Slides Cervical Or Vaginal (the Bethesda System) With Manual Screening And Computer-assisted Rescreening Using cell selection and review Under Physician Supervision
Cervical Cancer Screening CPT 88174
Cytopathology Cervical Or Vaginal (any Reporting System) Collected In Preservative Fluid Automated Thin Layer Preparation
Cervical Cancer Screening CPT 88175 Cytopathology Cervical Or Vaginal (any Reporting System)
Collected In Preservative Fluid Screening Automated By System
Cervical Cancer Screening HCPCS G0123
Screening Cytopathology, Cervical Or Vaginal (any Reporting System), Collected In Preservative Fluid, Automated Thin Layer Preparation, Screening By Cytotechnologist Under Physician Supervision (g0123)
Cervical Cancer Screening HCPCS G0124
Screening Cytopathology, Cervical Or Vaginal (any Reporting System), Collected In Preservative Fluid, Automated Thin Layer Preparation, Requiring Interpretation By Physician (g0124)
31

CODES TO IDENTIFY CERVICAL CYTOLOGY:Service Code Type Code Code Description
Cervical Cancer Screening HCPCS G0141
Screening Cytopathology Smears, Cervical Or Vaginal, Performed By Automated System, With Manual Rescreening, Requiring Interpretation By Physician (g0141)
Cervical Cancer Screening HCPCS G0143
Screening Cytopathology, Cervical Or Vaginal (any Reporting System), Collected In Preservative Fluid, Automated Thin Layer Preparation, With Manual Screening And Rescreening By Cytotechnologist Under Physician Supervision (g0143)
Cervical Cancer Screening HCPCS G0144
Screening Cytopathology, Cervical Or Vaginal (any Reporting System), Collected In Preservative Fluid, Automated Thin Layer Preparation, With Screening By Automated System, Under Physician Supervision (g0144)
Cervical Cancer Screening HCPCS G0145
Screening Cytopathology, Cervical Or Vaginal (any Reporting System), Collected In Preservative Fluid, Automated Thin Layer Preparation, With Screening By Automated System And Manual Rescreening Under Physician Supervision (g0145)
Cervical Cancer Screening HCPCS G0147
Screening Cytopathology Smears, Cervical Or Vaginal, Performed By Automated System Under Physician Supervision (g0147)
Cervical Cancer Screening HCPCS G0148
Screening Cytopathology Smears, Cervical Or Vaginal, Performed By Automated System With Manual Rescreening (g0148)
Cervical Cancer Screening HCPCS P3000 Screening Papanicolaou Smear, Cervical Or Vaginal, Up To Three
Smears, By Technician Under Physician Supervision (p3000)Cervical Cancer
Screening HCPCS P3001 Screening Papanicolaou Smear, Cervical Or Vaginal, Up To Three Smears, Requiring Interpretation By Physician (p3001)
Cervical Cancer Screening HCPCS Q0091
Screening Papanicolaou Smear; Obtaining, Preparing And Conveyance Of Cervical Or Vaginal Smear To Laboratory (q0091)
Cervical Cancer Screening LOINC 10524-7 Microscopic Observation [identifier] In Cervix By Cyto Stain
Cervical Cancer Screening LOINC 18500-9 Microscopic Observation [identifier] In Cervix By Cyto Stain
ThinprepCervical Cancer
Screening LOINC 19762-4 General Categories [interpretation] Of Cervical Or Vaginal Smear Or Scraping By Cyto Stain
Cervical Cancer Screening LOINC 19764-0 Statement Of Adequacy [interpretation] Of Cervical Or Vaginal
Smear Or Scraping By Cyto StainCervical Cancer
Screening LOINC 19765-7 Microscopic Observation [identifier] In Cervical Or Vaginal Smear Or Scraping By Cyto Stain
Cervical Cancer Screening LOINC 19766-5 Microscopic Observation [identifier] In Cervical Or Vaginal
Smear Or Scraping By Cyto Stain NarrativeCervical Cancer
Screening LOINC 19774-9 Cytology Study Comment Cervical Or Vaginal Smear Or Scraping Cyto Stain
32

CODES TO IDENTIFY CERVICAL CYTOLOGY:Service Code Type Code Code Description
Cervical Cancer Screening LOINC 33717-0 Cytology Cervical Or Vaginal Smear Or Scraping Study
Cervical Cancer Screening LOINC 47527-7 Cytology Report Of Cervical Or Vaginal Smear Or Scraping Cyto
Stain.thin PrepCervical Cancer
Screening LOINC 47528-5 Cytology Report Of Cervical Or Vaginal Smear Or Scraping Cyto Stain
CODES TO IDENTIFY HPV TESTS:Service Code Type Code Code Description
Cervical Cancer Screening CPT 87620 Infectious Agent Detection By Nucleic Acid (dna Or Rna)
Papillom Avirus Human Direct Probe TechniqueCervical Cancer
Screening CPT 87621 Infectious Agent Detection By Nucleic Acid (dna Or Rna) Papillom Avirus Human Amplified Probe Technique
Cervical Cancer Screening CPT 87622 Infectious Agent Detection By Nucleic Acid (dna Or Rna)
Papillom Avirus Human Quantification
Cervical Cancer Screening CPT 87624
Infectious Agent Detection By Nucleic Acid (dna Or Rna) Human Pap Illomavirus (hpv) High-risk Types (eg 16 18 31 33 35 39 45 51 52 56 58 59 68)
Cervical Cancer Screening CPT 87625
Infectious Agent Detection By Nucleic Acid (dna Or Rna) Human Pap Illomavirus (hpv) Types 16 And 18 Only Includes Type 45, If Performed
Cervical Cancer Screening HCPCS G0476
Infectious Agent Detection By Nucleic Acid (dna Or Rna); Human Papillomavirus (hpv), High-risk Types (e.g., 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68) For Cervical Cancer Screening, Must Be Performed In Addition To Pap Test (g0476)
Cervical Cancer Screening LOINC 21440-3 Human Papilloma Virus 16+18+31+33+35+45+51+52+56 Dna
[presence] In Cervix By Dna Probe
Cervical Cancer Screening LOINC 30167-1
Human Papilloma Virus 16+18+31+33+35+39+45+51+52+56+58+59+68 Dna [presence] In Cervix By Probe And Signal Amplification Method
Cervical Cancer Screening LOINC 38372-9
Human Papilloma Virus 6+11+16+18+31+33+35+39+42+43+44+45+51+52+56+58+59+68 Dna [presence] In Cervix By Probe And Signal Amplification Method
Cervical Cancer Screening LOINC 59263-4 Human Papilloma Virus 16 Dna [presence] In Cervix By Probe
And Signal Amplification MethodCervical Cancer
Screening LOINC 59264-2 Human Papilloma Virus 18 Dna [presence] In Cervix By Probe And Signal Amplification Method
Cervical Cancer Screening LOINC 59420-0
Human Papilloma Virus 16+18+31+33+35+39+45+51+52+56+58+59+66+68 Dna [presence] In Cervix By Probe And Signal Amplification Method
Cervical Cancer Screening LOINC 69002-4 Human Papilloma Virus E6+e7 Mrna [presence] In Cervix By
Probe And Target Amplification Method
33

CODES TO IDENTIFY HPV TESTS:Service Code Type Code Code Description
Cervical Cancer Screening LOINC 71431-1
Human Papilloma Virus 31+33+35+39+45+51+52+56+58+59+66+68 Dna [presence] In Cervix By Probe And Target Amplification Method
Cervical Cancer Screening LOINC 75694-0 Human Papilloma Virus 18+45 E6+e7 Mrna [presence] In Cervix
By Probe And Target Amplification MethodCervical Cancer
Screening LOINC 77379-6 Human Papiloma Virus 16 And 18 And 31+33+35+39+45+51+52+56+58+59+66+68 Dna [interpretation] In Cervix
Cervical Cancer Screening LOINC 77399-4 Human Papilloma Virus 16 Dna [presence] In Cervix By Probe
And Target Amplification MethodCervical Cancer
Screening LOINC 77400-0 Human Papilloma Virus 18 Dna [presence] In Cervix By Probe And Target Amplification Method
Cervical Cancer Screening LOINC 82354-2 Human Papilloma Virus 16 And 18+45 E6+e7 Mrna [identifier]
In Cervix By Probe And Target Amplification MethodCervical Cancer
Screening LOINC 82456-5 Human Papilloma Virus 16 E6+e7 Mrna [presence] In Cervix By Probe And Target Amplification Method
Cervical Cancer Screening LOINC 82675-0
Human Papilloma Virus 16+18+31+33+35+39+45+51+52+56+58+59+66+68 Dna [presence] In Cervix By Probe And Target Amplification Method
• Members who meet any of the following criteria are excluded: 1. Members who have had a hysterectomy with no residual cervix, cervical agenesis or acquired absence of cervix any time during their history through December 31, 2018 may be excluded.
To exclude Members who meet the exclusion criteria, please complete the Member Historical Data Form and fax to IEHP’s Quality Informatics Team at: 909-477-8568.
A copy of the Historical Data Form is available in Appendix 3.
2. Members in hospice are excluded.
Denominator: Women 24-64 years of age who met the criteria for eligible population.
Numerator: Women in the denominator who received a timely screen for cervical cancer.
34

Timeliness of Prenatal Care (PPC)
Methodology: HEDIS®
Measure Description: The percentage of deliveries of live births on or between November 6, 2017 and November 5, 2018 that received a prenatal care visit as a Member of the organization in the first trimester, on the enrollment start date or within 42 days of enrollment in the organization. • The eligible population in this measure meets all of the following criteria: 1. Continuous enrollment 43 days prior to delivery through 56 days after delivery with no allowable gap. 2. Members who delivered a live birth on or between November 6 of the year prior to the measurement year (2017) and November 5 of the measurement year (2018). This includes women who delivered in any setting. Women who had two separate deliveries (different dates of service) between November 6 of the year prior to the measurement year (2017) and November 5 of the measurement year (2018) count twice. Women who had multiple live births during one pregnancy count once.
CODES TO IDENTIFY STAND ALONE PRENATAL VISITS:Service Code Type Code Code Description
Prenatal Visit CPT 0500F Initial Prenatal Care VisitPrenatal Visit CPT 0501F Prenatal Flow SheetPrenatal Visit CPT 0502F Subsequent Prenatal Care VisitPrenatal Visit CPT 99500 Home Visit PrenatalPrenatal Visit HCPCS H1000 Prenatal Care, At-risk AssessmentPrenatal Visit HCPCS H1001 Prenatal Care, At-risk Enhanced Service; Antepartum ManagementPrenatal Visit HCPCS H1002 Prenatal Care, At Risk Enhanced Service; Care CoordinationPrenatal Visit HCPCS H1003 Prenatal Care, At-risk Enhanced Service; EducationPrenatal Visit HCPCS H1004 Prenatal Care, At-risk Enhanced Service; Follow-up Home VisitPrenatal Visit HCPCS Z1032 Initial Antepartum Office VisitPrenatal Visit HCPCS Z1034 Antepartum Follow-Up Visit
Prenatal care visit to an OB/GYN or other prenatal care practitioner or PCP. For visits to a PCP, a diagnosis of pregnancy must be present. Documentation in the medical record must include a note indicating the date when the prenatal care visit occurred, and evidence of one of the following. • A basic physical obstetrical examination that includes auscultation for fetal heart tone, or pelvic exam with obstetric observations, or measurement of fundus height (a standardized prenatal flow sheet may be used).
35

• Evidence that a prenatal care procedure was performed, such as: – Screening test in the form of an obstetric panel (must include all of the following: hematocrit, differential WBC count, platelet count, hepatitis B surface antigen, rubella antibody, syphilis test, RBC antibody screen, Rh and ABO blood typing), OR – TORCH antibody panel alone, OR – A rubella antibody test/titer with an Rh incompatibility (ABO/Rh) blood typing, OR – Echography of a pregnant uterus. • Documentation of LMP or EDD in conjunction with either of the following. – Prenatal risk assessment and counseling/education. – Complete obstetrical history. • Members in hospice are excluded.
Denominator: Members who delivered a live birth on or between November 6 of the year prior to the measurement year (2017) and November 5 of the measurement year (2018).
Numerator: Members in the denominator who had a prenatal care visit as a member of the organization in the first trimester, on the enrollment start date or within 42 days of enrollment in the organization.
Postpartum Care (PPC)
Methodology: HEDIS®
Measure Description: The percentage of deliveries of live births on or between November 6, 2017 and November 5, 2018 that had a postpartum visit on or between 21 and 56 days after delivery. • The eligible population in this measure meets all of the following criteria: 1. Continuous enrollment 43 days prior to delivery through 56 days after delivery with no allowable gap. 2. Members who delivered a live birth on or between November 6 of the year prior to the measurement year (2017) and November 5 of the measurement year (2018). This includes women who delivered in any setting. Women who had two separate deliveries (different dates of service) between November 6 of the year prior to the measurement year (2017) and November 5 of the measurement year (2018) count twice. Women who had multiple live births during one pregnancy count once.
36

CODES TO IDENTIFY POSTPARTUM CARE:Service Code Type Code Code Description
Postpartum Care CPT 57170 Diaphragm Or Cervical Cap Fitting With Instructions
Postpartum Care CPT 58300 Insertion Of Intrauterine Device (iud)
Postpartum Care CPT 59430 Postpartum Care Only (separate Procedure)
Postpartum Care CPT 99501 Home Visit Postnatal
Postpartum Care CPT-CAT-II 0503F Postpartum Care Visit
Postpartum Care HCPCS G0101 Cervical Or Vaginal Cancer Screening; Pelvic And Clinical Breast
Examination (g0101)Postpartum
Care ICD10CM Z01.411 [z01.411] Encounter For Gynecological Examination (general) (routine) With Abnormal Findings
Postpartum Care ICD10CM Z01.419 [z01.419] Encounter For Gynecological Examination (general)
(routine) Without Abnormal FindingsPostpartum
Care ICD10CM Z01.42 [z01.42] Encounter For Cervical Smear To Confirm Findings Of Recent Normal Smear Following Initial Abnormal Smear
Postpartum Care ICD10CM Z30.430 [z30.430] Encounter For Insertion Of Intrauterine Contraceptive
DevicePostpartum
Care ICD10CM Z39.1 [z39.1] Encounter For Care And Examination Of Lactating Mother
Postpartum Care ICD10CM Z39.2 [z39.2] Encounter For Routine Postpartum Follow-up
Postpartum Care HCPCS Z1038 Postpartum Follow-Up Office Visit
• Members in hospice are excluded.
Denominator: Members who delivered a live birth on or between November 6 of the year prior to the measurement year (2017) and November 5 of the measurement year (2018).
Numerator: Members in the denominator who had a postpartum visit on or between 21 and 56 days after delivery.
37

Population: Child
Childhood Immunizations (CIS) – Combo 10
Methodology: HEDIS®
Measure Description: The percentage of children 2 years of age who had four diphtheria, tetanus and acellular pertussis (DTaP); three polio (IPV); one measles, mumps and rubella (MMR); three haemophilus influenza type B (HiB); three hepatitis B (HepB), one chicken pox (VZV); four pneumococcal conjugate (PCV); one hepatitis A (HepA); two or three rotavirus (RV); and two influenza (flu) vaccines by their second birthday. The measure calculates a rate for each vaccine and one combination rate. • Combo 10 includes the timely completion of the following antigens: - DTaP; IPV; MMR; HiB; HepB; VZV; PCV; HepA; Rotavirus; Flu • The eligible population in this measure meets all of the following criteria: 1. Children who turn 2 years of age during the measurement year (2018). 2. Continuous enrollment 12 months prior to the child’s second birthday with no more than one gap in enrollment of up to 45 days during the 12 months prior to the child’s second birthday.
CHILDHOOD IMMUNIZATION CODE SET:Antigen Code Type Code Code Description
DTaP CPT 90698Diphtheria Tetanus Toxoids And Acellular Pertussis Vaccine And Hemophilus Influenza B Vaccine And Activated Poliovirus Vaccine, (DTaP-IPV/Hib), For Intramuscular Use
DTaP CPT 90700 Diphtheria Tetanus Toxoids And Acellular Pertussis Vaccine (dta P) For Intramuscular Use
DTaP CPT 90721 Diphtheria Tetanus Toxoids And Acellular Pertussis Vaccine And Hemophilus Influenza B Vaccine (dtap-hib) For Intramuscular Use
DTaP CPT 90723 Diphtheria Tetanus Toxoids Acellular Pertussis Vaccine Hepatitis B, and Inactivated poliovirus vaccine (dtap-hepb-ipv), For Intramuscular Use
IPV CPT 90698Diphtheria Tetanus Toxoids And Acellular Pertussis Vaccine And Hemophilus Influenza B Vaccine and activated poliovirus vaccine, (DTaP-IPV/Hib), For Intramuscular Use
IPV CPT 90713 Poliovirus Vaccine Inactivated (ipv) For Subcutaneous Use
IPV CPT 90723 Diphtheria Tetanus Toxoids Acellular Pertussis Vaccine Hepatitis B, and Inactivated poliovirus vaccine (dtap-hepb-ipv), For Intramuscular Use
MMR CPT 90707 Measles Mumps And Rubella Virus Vaccine (mmr) Live For Subcuta Neous Use
38

CHILDHOOD IMMUNIZATION CODE SET:Antigen Code Type Code Code Description
MMR CPT 90710 Measles Mumps Rubella And Varicella Vaccine (mmrv) Live For Subcutaneous Use
HiB CPT 90644Meningococcal Conjugate Vaccine, Serogroups C & Y And Hemophilus Influenzae Type B Vaccine (hib-mency), 4 dose schedule, When Administered to children 6 wks to 18 mos of age, For Intramuscular Use
HiB CPT 90645 Hemophilus Influenza B Vaccine (hib) Hboc Conjugate (4 Dose Schedule) For Intramuscular Use
HiB CPT 90646 Hemophilus Influenza B Vaccine (hib) Prp-d Conjugate For Booster Use Only Intramuscular Use
HiB CPT 90647 Hemophilus Influenza B Vaccine (hib) Prp-omp Conjugate (3 Dose S Chedule) For Intramuscular Use
HiB CPT 90648 Hemophilus Influenza B Vaccine (hib)prp-t Conjugate (4 Dose Sche Dule) For Intramuscular Use
HiB CPT 90698Diphtheria Tetanus Toxoids And Acellular Pertussis Vaccine And Hemophilus Influenza B Vaccine and activated poliovirus vaccine, (DTaP-IPV/Hib), For Intramuscular Use
HiB CPT 90721 Diphtheria Tetanus Toxoids And Acellular Pertussis Vaccine And Hemophilus Influenza B Vaccine (dtap-hib) For Intramuscular Use
HiB CPT 90748 Hepatitis B And Hemophilus Influenza B Vaccine (hepb-hib) For Intramuscular Use
HepB CPT 90723 Diphtheria Tetanus Toxoids Acellular Pertussis Vaccine Hepatitis B, and Inactivated poliovirus vaccine (dtap-hepb-ipv), For Intramuscular Use
HepB CPT 90740 Hepatitis B Vaccine Dialysis Or Immunosuppressed Patient Dosage (3 Dose Schedule) For Intramuscular Use
HepB CPT 90744 Hepatitis B Vaccine Pediatric/adolescent Dosage (3 Dose Schedule ) For Intramuscular Use
HepB CPT 90747 Hepatitis B Vaccine Dialysis Or Immunosuppressed Patient Dosage (4 Dose Schedule) For Intramuscular Use
HepB CPT 90748 Hepatitis B And Hemophilus Influenza B Vaccine (hepb-hib) For Intramuscular Use
HepB HCPCS G0010 Administration Of Hepatitis B Vaccine (g0010)
VZV CPT 90710 Measles Mumps Rubella And Varicella Vaccine (mmrv) Live For Subcutaneous Use
VZV CPT 90716 Varicella Virus Vaccine Live For Subcutaneous Use
PCV CPT 90669 Pneumococcal Conjugate Vaccine Polyvalent For Children Under Five Years For Intramuscular Use
PCV CPT 90670 Pneumococcal Conjucate Vaccine 13 Valent For Intramuscular UsePCV HCPCS G0009 Administration Of Pneumococcal Vaccine (g0009)
HepA CPT 90633 Hepatitis A Vaccine Pediatric/adolescent Dosage-2 Dose Schedule For Intramuscular Use
Rotavirus - 2 Dose CPT 90681 Rotavirus Vaccine Human Attenuated 2 Dose Schedule Live For Oral Use.
39

CHILDHOOD IMMUNIZATION CODE SET:Antigen Code Type Code Code Description
Rotavirus - 3 Dose CPT 90680 Rotavirus Vaccine Tetravalent Live For Oral Use
Flu CPT 90655 Flu Virus Vaccine, Trivalent (iiv3), Split Virus, Preservative Free, 0.25ml Dosage, For Intramuscular Use
Flu CPT 90657 Influenza Virus Vaccine Split Virus For Children 6-35 Months Of Age For Intramuscular Use
Flu CPT 90661 Influenza Virus Vaccine Derived From Cell Cultures Subunit Preservative And Antibiotic Free For Intramuscular Use
Flu CPT 90662 Influenza Virus Vaccine Split Virus Preservative Free Enhanced Immunogenicity Via Increased Antigen Content, For Intramuscular Use
Flu CPT 90673 Influenza Virus Vaccine Trivalent Derived From Recombinant Dna (r Iv3) Hemagglutinin (ha) Protein Only Preservative And Antibiotic
Flu CPT 90685 Influenza Virus Vaccine Quadrivalent (II4V) Split Virus preservative free, 0.25 ml dosage, For Intramuscular Use
Flu CPT 90686 Influenza Virus Vaccine Quadrivalent (II4V) Split Virus preservative free, 0.5 ml dosage, For Intramuscular Use
Flu CPT 90687 Influenza Virus Vaccine Quadrivalent (II4V) Split Virus, 0.25 ml dosage, For Intramuscular Use
Flu CPT 90688 Influenza Virus Vaccine Quadrivalent (II4V) Split Virus, 0.5 ml dosage, For Intramuscular Use
Flu HCPCS G0008 Administration Of Influenza Virus Vaccine (g0008)
• Members who meet any of the following criteria are excluded: 1. Members in hospice are excluded. 2. Children who had a contraindication for a specific vaccine are excluded from the denominator for all antigen rates and the combination rates.
Denominator: Children 2 years of age in the eligible population.
Numerator: Members in denominator who show timely completion of all antigens in combo10.
40

Immunizations for Adolescents (IMA) – Combo 2
Methodology: HEDIS®
Measure Description: The percentage of adolescents 13 years of age who had one dose of meningococcal conjugate; vaccine, one tetanus, diphtheria toxoids and acellular pertussis (Tdap); vaccine and two or three doses of the human papillomavirus (HPV) vaccine on or before their 13th birthday. The measure calculates a rate for each vaccine and a combination rate. • At least one dose of meningococcal conjugate vaccine on or between the Member’s 11th and 13th birthdays. • At least one tetanus, diphtheria toxoids and acellular pertussis (Tdap) vaccine on or between the Member’s 10th and 13th birthdays. • At least two HPV vaccines, with different dates of service on or between the Member’s 9th and 13th birthdays. – There must be at least 146 days between the first and second dose of the HPV vaccine. For example, if the service date for the first vaccine was March 1, then the service date for the second vaccine must be after July 25. OR At least three HPV vaccines, with different dates of service on or between the Member’s 9th and 13th birthdays. • The eligible population in this measure meets all of the following criteria: 1. Adolescents who turn 13 years of age during the measurement year (2018). 2. Continuous enrollment 12 months prior to the member’s 13th birthday with no more than one gap in enrollment of up to 45 days during the 12 months prior to the 13th birthday.
CODES TO IDENTIFY MENINGOCOCAL:Antigen Code Type Code Code Description
Meningococcal conjugate CPT 90734 Meningococcal Conjugate Vaccine Serogroups A, C, Y and W-135,
quadrivalent (MCV4 or MenACWY), For Intramuscular Use
CODES TO IDENTIFY TDAP:Antigen Code Type Code Code Description
Tdap CPT 90715Tetanus Diphtheria Toxoids And Acellular Pertussis Vaccine (Tdap) When Administered To Individuals 7 Years Or Older For Intramuscular Use
41

CODES TO IDENTIFY HPV:Antigen Code Type Code Code Description
HPV CPT 90649 Human Papilloma Virus (hpv) Vaccine Types 6 11 16 18 Quadrivalent (4vHPV), 2 or 3 Dose Schedule, For Intramuscular Use
HPV CPT 90650 Human Papilloma Virus (hpv) Vaccine Types 16, 18 bivalent (2vHPV) 2 or 3 Dose Schedule, For Intramuscular Use
HPV CPT 90651 Human Papilloma Virus Vaccine 6 11 16 18 31 33 45 52 58, nonavalent (9vHPV) 2 or 3 Dose Schedule, For Intramuscular Use
• Members who meet any of the following criteria are excluded: 1. Members in hospice are excluded. 2. Adolescents who had a contraindication for a specific vaccine are excluded from the denominator for all antigen rates and the combination rates.
Denominator: Adolescents 13 years of age who meet all the criteria for eligible population.
Numerator: Members in the denominator who had one dose of meningococcal conjugate vaccine, one tetanus, diphtheria toxoids and acellular pertussis (Tdap) vaccine, and have completed the human papillomavirus (HPV) vaccine series by their 13th birthday during the measurement year (2018).
42

CODES TO IDENTIFY WELL-CHILD: (NOTE: These codes must be provided by a Primary Care Provider in an office setting.)
Service Code Type Code Code Description
Well-Child 3-6 Years of Life CPT 99382
Initial comprehensive preventive medicine evaluation and management of an individual including an age and gender appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures, new patient: early childhood (age 1 through 4 years)
Well-Child 3-6 Years of Life CPT 99383
Initial comprehensive preventive medicine evaluation and management of an individual including an age and gender appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures, new patient: late childhood (age 5 through 11 years)
Well-Child 3-6 Years of Life CPT 99392
Periodic comprehensive preventive medicine reevaluation and management of an individual including an age and gender appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures, established patient; early childhood (age 1 through 4 years)
Well-Child 3-6 Years of Life CPT 99393
Periodic comprehensive preventive medicine reevaluation and management of an individual including an age and gender appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures, established patient; late childhood (age 5 through 11 years)
Well-Child 3-6 Years of Life HCPCS G0438 Annual Wellness Visit; Includes A Personalized Prevention Plan Of
Service (pps), Initial Visit (g0438)Well-Child 3-6
Years of Life HCPCS G0439 Annual Wellness Visit, Includes A Personalized Prevention Plan Of Service (pps), Subsequent Visit (g0439)
Well-Child 3-6 Years of Life ICD10CM Z00.121 Encounter For Routine Child Health Examination With
Abnormal FindingsWell-Child 3-6
Years of Life ICD10CM Z00.129 Encounter For Routine Child Health Examination Without Abnormal Findings
Well-Child 3-6 Years of Life ICD10CM Z00.5 Encounter For Examination Of Potential Donor Of Organ And Tissue
Well-Child 3-6 Years of life (W34)
Methodology: HEDIS®
Measure Description: The percentage of Members 3–6 years of age who had one or more well-child visits with a PCP during the measurement year (2018). • The eligible population in this measure meets all of the following criteria: 1. Age 3-6 years as of December 31 of the measurement year (2018). 2. Continuous enrollment in the measurement year (2018) with no more than one gap in enrollment of up to 45 days.
43

CODES TO IDENTIFY WELL-CHILD: (NOTE: These codes must be provided by a Primary Care Provider in an office setting.)
Service Code Type Code Code DescriptionWell-Child 3-6
Years of Life ICD10CM Z00.8 Encounter For Other General Examination
Well-Child 3-6 Years of Life ICD10CM Z02.0 Encounter For Examination For Admission To Educational Institution
Well-Child 3-6 Years of Life ICD10CM Z02.1 Encounter For Pre-employment Examination
Well-Child 3-6 Years of Life ICD10CM Z02.2 Encounter For Examination For Admission To Residential Institution
Well-Child 3-6 Years of Life ICD10CM Z02.5 Encounter For Examination For Participation In Sport
Well-Child 3-6 Years of Life ICD10CM Z02.6 Encounter For Examination For Insurance Purposes
Well-Child 3-6 Years of Life ICD10CM Z02.71 Encounter For Disability Determination
Well-Child 3-6 Years of Life ICD10CM Z02.79 Encounter For Issue Of Other Medical Certificate
Well-Child 3-6 Years of Life ICD10CM Z02.81 Encounter For Paternity Testing
Well-Child 3-6 Years of Life ICD10CM Z02.82 Encounter For Adoption Services
Well-Child 3-6 Years of Life ICD10CM Z02.83 Encounter For Blood-alcohol And Blood-drug Test
Well-Child 3-6 Years of Life ICD10CM Z02.89 Encounter For Other Administrative Examinations
Well-Child 3-6 Years of Life ICD10CM Z02.9 Encounter For Administrative Examinations, Unspecified
• Members in hospice are excluded.
Denominator: Members 3-6 years of age who meet all the criteria for eligible population.
Numerator: Members in the denominator who had at least one well-child visit with a PCP during the measurement year (2018).
The Well-Child visit must occur with a PCP, but the PCP does not have to be the practitioner assigned to the child.
44

Weight Assessment and Counseling for Nutrition and Physical Activity for Children and Adolescents (WCC)
Methodology: HEDIS®
Measure Description: The percentage of Members 3–17 years of age who had an outpatient visit with a PCP or OB/GYN and who had evidence of the following during the measurement year (2018). Report each of the three indicators below. • BMI percentile documentation* • Counseling for nutrition • Counseling for physical activity • The eligible population in this measure meets all of the following criteria: 1. Members who are 3-17 years of age as of December 31 of the measurement year (2018). 2. Continuous enrollment in the measurement year (2018) with no more than one gap up to 45 days. 3. An outpatient visit with a PCP or an OB/GYN during the measurement year (2018).
* Because BMI norms for youth vary with age and gender, this measure evaluates whether BMI percentile is assessed rather than an absolute BMI value.
CODES TO IDENTIFY BMI PERCENTILE:Code Code Type Description
Z68.51 ICD10 Body Mass Index (BMI) Pediatric, Less Than 5th Percentile For AgeZ68.52 ICD10 Body Mass Index (BMI) Pediatric, 5th Percentile To Less Than 85th Percentile For AgeZ68.53 ICD10 Body Mass Index (BMI) Pediatric, 85th Percentile To Less Than 95th Percentile For AgeZ68.54 ICD10 Body Mass Index (BMI) Pediatric, Greater Than Or Equal To 95th Percentile For Age
CODES TO IDENTIFY COUNSELING FOR PHYSICAL ACTIVITY:Code Code Type DescriptionG0447 HCPCS Face-to-face Behavioral Counseling For Obesity, 15 Minutes S9451 HCPCS Exercise Classes, Non-Physician Provider, Per Session Z02.5 ICD10 Encounter For Examination For Participation In Sport
Z71.82 ICD10 Exercise Counseling
45

CODES TO IDENTIFY COUNSELING FOR NUTRITION:Code Code Type Description
97802 CPT Medical Nutrition Therapy Initial Assessment And Intervention Individual Face-to-face With The Patient Each 15 Minutes
97803 CPT Medical Nutrition Therapy Re-assessment And Intervention Individual Face-to-face With The Patient Each 15 Minutes
97804 CPT Medical Nutrition Therapy Group (2 Or More Individual(s)) Each 30 Minutes
G0270 HCPCSMedical Nutrition Therapy; Reassessment And Subsequent Intervention(s) Following Second Referral In Same Year For Change In Diagnosis, Medical Condition Or Treatment Regimen (including Additional Hours Needed For Renal Disease), Individual, Face To Face
G0271 HCPCSMedical Nutrition Therapy, Reassessment And Subsequent Intervention(s) Following Second Referral In Same Year For Change In Diagnosis, Medical Condition, Or Treatment Regimen (including Additional Hours Needed For Renal Disease), Group (2 Or More Individuals)
G0447 HCPCS Face-to-face Behavioral Counseling For Obesity, 15 Minutes (G0447)S9449 HCPCS Weight Management Classes, Non-Physician Provider, Per Session (S9449)S9452 HCPCS Nutrition Classes, Non-Physician Provider, Per Session (S9452)S9470 HCPCS Nutritional Counseling, Dietitian Visit (S9470)Z71.3 ICD10 Dietary Counseling And Surveillance
Members who meet any of the following criteria are excluded: 1. Members in hospice are excluded. 2. Female Members who have a diagnosis of pregnancy during the measurement year (2018) are excluded. A diagnosis of pregnancy will be determined using claims and encounter data only.
Denominator: Members 3-17 years of age who meet all the criteria for eligible population.
Numerator: Members in the denominator who had evidence of BMI, counseling of nutrition or physical activity during the measurement year (2018).
46

Population: AllInitial Health Assessment (IHA)
Methodology: IEHP-Defined Compliance Metric
Measure Description: The IHA is a comprehensive assessment that is completed during theMember’s initial encounter with a PCP, appropriate medical specialist, or Non-Physician medical Provider and must be documented in the Member’s medical record. The IHA enables the Member’s PCP to assess and manage the acute, chronic and preventive health needs of the Member.
IEHP provides PCPs a monthly detailed Member roster on the IEHP Secure Provider Portal forall newly enrolled IEHP Members who are due for an IHA after 120 days of enrollment. • The eligible population is newly assigned Members with an IEHP effective enrollment date of January 1, 2018 through December 31, 2018. The IHA must be provided within 120 days of enrollment (e.g., Member enrolled in December 2018 must be seen by April 2019 and PCP must submit encounter by May 2019) • IHA visits completed during the 11 months prior to enrollment with IEHP count towards numerator compliance.
CODES TO IDENTIFY IHA VISITS:Code Code Type Description99201 CPT Office/Outpt E&M New Minor 1099202 CPT Office/Outpt E&M New Low-Mod99203 CPT Office/Outpt E&M New Mod Seve99204 CPT Office/Outpt E&M New Mod-Hi 499205 CPT Office/Outpt E&M New Mod-Hi 699211 CPT Office/Outpt E&M Estab 5 Min99212 CPT Office/Outpt E&M Estab Minor99213 CPT Office/Outpt E&M Estab Low-Mo99214 CPT Office/Outpt E&M Estab Mod-Hi99215 CPT Office/Outpt E&M Estab Mod-Hi99241 CPT Office Cons New/Estab Minor 199242 CPT Office Cons New/Est Lo Sever99243 CPT Office Cons New/Estab Mod 4099244 CPT Office Cons New/Estab Mod-Hi99245 CPT Office Cons New/Estab Mod-Hi99304 CPT Nursing Facility Care Init99305 CPT Nursing Facility Care Init99306 CPT Nursing Facility Care Init99307 CPT Nursing Fac Care Subseq
47

CODES TO IDENTIFY IHA VISITS:Code Code Type Description99308 CPT Nursing Fac Care Subseq99309 CPT Nursing Fac Care Subseq99310 CPT Nursing Fac Care Subseq99315 CPT Nurs Facil D/C Da Mgmt; 30 M99316 CPT Nurs Facil D/C Da Mgmt; > 3099318 CPT Annual Nursing Fac Assessmnt99324 CPT Domicil/R-Home Visit New Pat99325 CPT Domicil/R-Home Visit New Pat99326 CPT Domicil/R-Home Visit New Pat99327 CPT Domicil/R-Home Visit New Pat99328 CPT Domicil/R-Home Visit New Pat99334 CPT Domicil/R-Home Visit Est Pat99335 CPT Domicil/R-Home Visit Est Pat99336 CPT Domicil/R-Home Visit Est Pat99337 CPT Domicil/R-Home Visit Est Pat99341 CPT Home Visit E&M New Pt Lo Sev99342 CPT Home Visit E&M New Pt Mod Se99343 CPT Home Visit E&M New Pt Mod-Hi99344 CPT Home Visit E&M New Pt Hi Sev99345 CPT Home Visit E&M New Pt Unstbl99347 CPT Home Visit E&M Estab Minor-199348 CPT Home Visit E&M Estab Low-Mod99349 CPT Home Visit E&M Estab Mod-Hi99350 CPT Home Visit E&M Estab Mod-Hi99354 CPT Prolong Md Serv Outpt W/Pt;99355 CPT Prolong Md Serv Outpt W/Pt;99381 CPT Init Preven Meds E&M New Pt;99382 CPT Init Preven Meds E&M New Pt;99383 CPT Init Preven Meds E&M New Pt;99384 CPT Init Preven Meds E&M New Pt;99385 CPT Init Preven Meds E&M New Pt;99386 CPT Init Preven Meds E&M New Pt;99387 CPT Init Preven Meds E&M New Pt;99391 CPT Preven Meds E&M Estab Pt; In99392 CPT Preven Meds E&M Estab Pt; 1-99393 CPT Preven Meds E&M Estab Pt; 5-99394 CPT Preven Meds E&M Estab Pt; 1299395 CPT Preven Meds E&M Estab Pt; 1899396 CPT Preven Meds E&M Estab Pt; 4099397 CPT Preven Meds E&M Estab Pt; 65
48

CODES TO IDENTIFY IHA VISITS:Code Code Type Description99401 CPT Preven Med Counsl (Sep Pro);99402 CPT Preven Med Counsl (Sep Pro);99403 CPT Preven Med Counsl (Sep Pro);99404 CPT Preven Med Counsl (Sep Pro);99411 CPT Preven Med Counsl Grp (Sep P99412 CPT Preven Med Counsl Grp (Sep P99420 CPT Admin/Intrpt Health Risk Ass99429 CPT Unlisted Preven Meds Serv99444 CPT Online E/M By Phys99446 CPT Interprof Phone/Online 5-1099447 CPT Interprof Phone/Online 11-299448 CPT Interprof Phone/Online 21-399449 CPT Interprof Phone/Online 31/>99450 CPT Basic Life &/Or Disability E99455 CPT Work Relat/Disabl Exam-Treat99456 CPT Work Relat/Disabl Exam-Not TG0402 HCPCS Initial Preventive ExamG0438 HCPCS Ppps Initial VisitG0439 HCPCS Ppps Subseq VisitG0463 HCPCS Hospital Outpt Clinic VisitT1015 HCPCS Clinic ServiceZ00.00 ICD10CM Encounter for general adult medical examination without abnormal findingsZ00.01 ICD10CM Encounter for general adult medical examination with abnormal findings
Z00.121 ICD10CM Encounter for routine child health examination with abnormal findingsZ00.129 ICD10CM Encounter for routine child health examination without abnormal findings
Z00.5 ICD10CM Encounter for examination of potential donor of organ and tissueZ00.8 ICD10CM Encounter for other general examinationZ02.0 ICD10CM Encounter for examination for admission to educational institutionZ02.1 ICD10CM Encounter for pre-employment examinationZ02.2 ICD10CM Encounter for examination for admission to residential institutionZ02.3 ICD10CM Encounter for examination for recruitment to armed forcesZ02.4 ICD10CM Encounter for examination for driving licenseZ02.5 ICD10CM Encounter for examination for participation in sportZ02.6 ICD10CM Encounter for examination for insurance purposes
Z02.71 ICD10CM Encounter for disability determinationZ02.79 ICD10CM Encounter for issue of other medical certificateZ02.81 ICD10CM Encounter for paternity testingZ02.82 ICD10CM Encounter for adoption servicesZ02.83 ICD10CM Encounter for blood-alcohol and blood-drug testZ02.89 ICD10CM Encounter for other administrative examinationsZ02.9 ICD10CM Encounter for administrative examinations, unspecified 49

Concurrent Use of Opioids and Benzodiazepines
Methodology: IEHP-Defined Compliance Metric
Measure Description: The Concurrent Use of Opioids and Benzodiazepines measure specification is developed and maintained by the Pharmacy Quality Alliance (PQA). This measure examines the percentage of individuals 18 years and older with concurrent use of prescription opioids and benzodiazepines. The denominator includes individuals 18 years and older by the first day of the measurement year with two or more prescription claims for opioids filled on two or more separate days, for which the sum of the days supply is 15 or more days during the measurement period. The numerator includes individuals from the denominator with two or more prescription claims for benzodiazepines filled on two or more separate days, and concurrent use of opioids and benzodiazepines for 30 or more cumulative days.
Exclusion: Patients in hospice care and those with a cancer diagnosis are excluded.
Access to Care Needed Right Away
Methodology: Monthly Member Satisfaction Survey.
Measure Description: In the last six months, when you needed care right away, how often did you get care as soon as you needed it? • Valid response: never, sometimes, usually, always • Target response: usually, always
Measure Support: To help identify opportunities to improve customer service, IEHP conducts a monthly Member Satisfaction Survey between June-December annually. Member survey responses are analyzed and shared at the PCP level.
50

Coordination of Care
Methodology: Monthly Member Satisfaction Survey
Measure Description: In the last six months, how often did your Personal Doctor seem informed and up-to-date about the care you got from these doctors or other health providers? • Valid response: never, sometimes, usually, always • Target response: usually, always
Measure Support: To help identify opportunities to improve customer service, IEHP conducts a monthly Member Satisfaction Survey between June-December annually. Member Survey responses are analyzed and shared at the PCP level.
Rating of Access to Routine Care
Methodology: Monthly Member Satisfaction Survey
Measure Description: In the last six months, how often did you get an appointment for a check-up or routine care at a Doctor’s office or clinic as soon as you needed it? • Valid response: never, sometimes, usually, always • Target response: usually, always
Measure Support: To help identify opportunities to improve customer service, IEHP conducts a monthly Member Satisfaction Survey between June-December annually. Member Survey responses are analyzed and shared at the IPA level.
51

APPENDIX 3: Historical Data Form
52

APPENDIX 4: Member Satisfaction Survey
53

APPENDIX 4: Member Satisfaction Survey (continued...)
54

APPENDIX 5: 2018 IPA Global Quality P4P IPA Work Plan
Review Check List – DRAFT
ITEM NUMBER
IPA CHECK LIST - ELEMENTS OF A QUALITY PROGRAM
TOTAL POSSIBLE
POINTS
Clinical Quality Domain1 Key Leadership Support for Clinical Quality Improvement 52 Tools and Resources for Clinical Quality Improvement
a. Evidence-Based Clinical Practice Guidelines (CPGs) for Prevention, Wellness and Chronic Condition Management (CCM) 5
b. Toolkits for Team-Based Care including use of Targeted Member Lists from IEHP 5
3 Office and Practitioner Training Programs on Best Practices 54 Member Outreach and In-reach Activities to Address Care Gaps 55 Physician-level Reports and Monitoring of Clinical outcomes 56 Patient-centered Member Education Programs 57 Office Staff/ Practitioner Recognition Programs for High Performers 5
Behavioral Health Integration Domain8 Evidenced Based CPG for Depression Screening and Management 59 Office and Physician Training Programs on Best Practices 5
10 Development of resources for follow-up 511 Physician-level Reports and Monitoring of Performance Metrics 5
Encounter Data Domain12 Monthly Submission Volume Meeting IEHP Target Adequacy Rate 513 Monthly Submissions Accepted with <1% Error Rate 514 Tracking of Capitated Provider-Level Encounters 515 Use of Supplemental Data to improve data capture 516 Supplemental Data shared with IEHP timely and in agreed upon format 5
Patient Experience Domain17 Physician-level Reports and Monitoring of Performance Metrics 518 Office Staff and Physician Education Programs to Improve Patient Experience 519 Office Staff/ Practitioner Recognition Programs for High Performers 5
OVERALL PROGRAM SCORE 100
55

APPENDIX 6: Supplemental Claim File Data Dictionary
SUPPLEMENTAL CLAIM FILE DATA DICTIONARYField Name Data Type File Order NotesMemberKey Text (14) 1 IEHP Member ID.ProviderKey Text (25) 2 This should be the rendering provider’s NPI.
ClaimNumber Text (80) 3 Used to identify the claim source for Primary Source Verification.
DOS Date 4 The beginning Date of Service for the claim in MM/DD/YYYY format.
DOSThru Date 5 The ending Date of Service for the claim in MM/DD/YYYY format.
ICD9DxPri Text (5) 6ICD-9 diagnosis codes should contain all available digits (including all preceding zeros). Do not include the period that follows the third digit. If no fourth or fifth digit was coded, do not pad the missing spaces. For example, V42.0 should be loaded as V420. With the introduction of ICD-10 code set, IEHP will continue to support the ICD-9 code set as there are historical claims that rely on these codes (for HEDIS we recommend 3-4 years of historical claims data) in order to accurately calculate HEDIS rates.
ICD9DxSec1 Text (5) 7ICD9DxSec2 Text (5) 8ICD9DxSec3 Text (5) 9ICD9DxSec4 Text (5) 10ICD9DxSec5 Text (5) 11ICD9DxSec6 Text (5) 12ICD9DxSec7 Text (5) 13ICD9DxSec8 Text (5) 14ICD9DxSec9 Text (5) 15
ICD9DxSec10 Text (5) 16ICD10DxPri Text (7) 17
ICD-10 diagnosis codes should contain all available alphanumeric code. Do not include the decimal. For example, V39.00XS should be coded as V3900XS.
ICD10DxSec1 Text (7) 18ICD10DxSec2 Text (7) 19ICD10DxSec3 Text (7) 20ICD10DxSec4 Text (7) 21ICD10DxSec5 Text (7) 22ICD10DxSec6 Text (7) 23ICD10DxSec7 Text (7) 24ICD10DxSec8 Text (7) 25ICD10DxSec9 Text (7) 26
ICD10DxSec10 Text (7) 27
PCPFlag Bit 28Indicator for whether the claim provider serves as a PCP for the health plan. Refers to the provider’s contractual relationship to the plan, rather than medical specialty. Valid values are 0 (no), or 1 (yes)
HCFAPOS Text (2) 29
The Claim file contains claims for medical services. It may also contain lab services that do not have an associated result, pharmaceuticals administered in the practitioners office (usually documented by J codes in the CPT Field), and medical encounter data. The Claim file should contain one record per unique claim line.
56
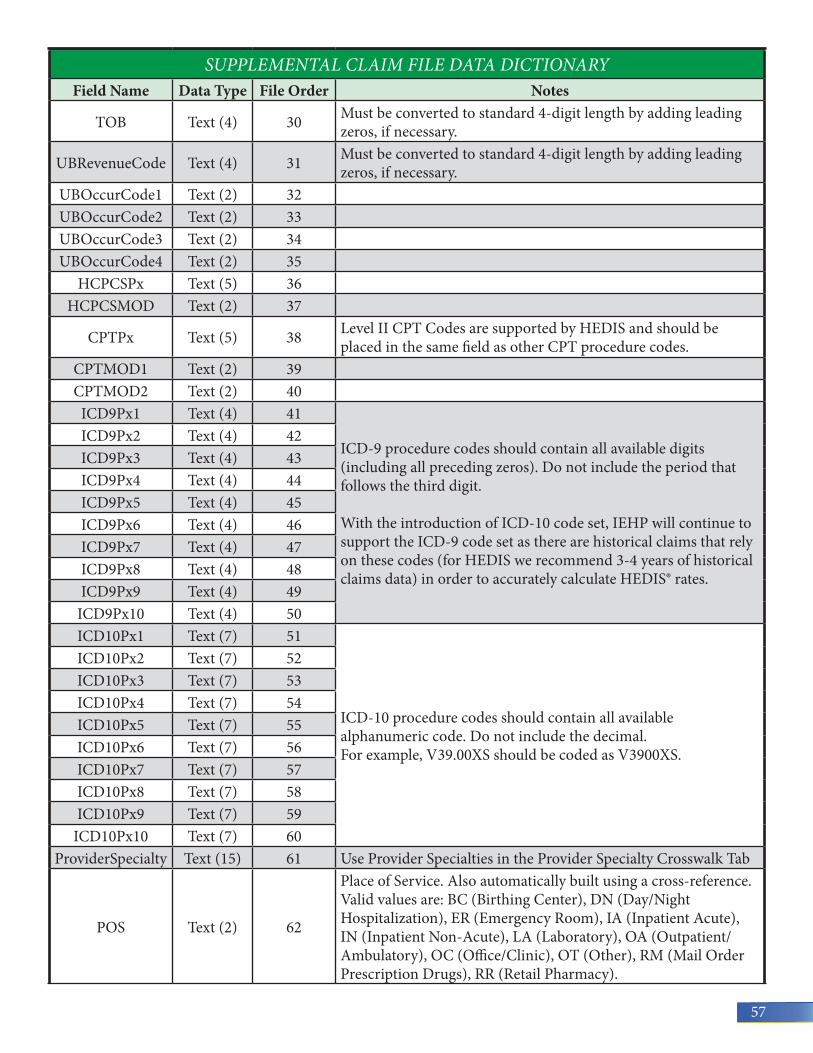
SUPPLEMENTAL CLAIM FILE DATA DICTIONARYField Name Data Type File Order Notes
TOB Text (4) 30 Must be converted to standard 4-digit length by adding leading zeros, if necessary.
UBRevenueCode Text (4) 31 Must be converted to standard 4-digit length by adding leading zeros, if necessary.
UBOccurCode1 Text (2) 32UBOccurCode2 Text (2) 33UBOccurCode3 Text (2) 34UBOccurCode4 Text (2) 35
HCPCSPx Text (5) 36HCPCSMOD Text (2) 37
CPTPx Text (5) 38 Level II CPT Codes are supported by HEDIS and should be placed in the same field as other CPT procedure codes.
CPTMOD1 Text (2) 39CPTMOD2 Text (2) 40
ICD9Px1 Text (4) 41
ICD-9 procedure codes should contain all available digits (including all preceding zeros). Do not include the period that follows the third digit. With the introduction of ICD-10 code set, IEHP will continue to support the ICD-9 code set as there are historical claims that rely on these codes (for HEDIS we recommend 3-4 years of historical claims data) in order to accurately calculate HEDIS® rates.
ICD9Px2 Text (4) 42ICD9Px3 Text (4) 43ICD9Px4 Text (4) 44ICD9Px5 Text (4) 45ICD9Px6 Text (4) 46ICD9Px7 Text (4) 47ICD9Px8 Text (4) 48ICD9Px9 Text (4) 49
ICD9Px10 Text (4) 50ICD10Px1 Text (7) 51
ICD-10 procedure codes should contain all available alphanumeric code. Do not include the decimal. For example, V39.00XS should be coded as V3900XS.
ICD10Px2 Text (7) 52ICD10Px3 Text (7) 53ICD10Px4 Text (7) 54ICD10Px5 Text (7) 55ICD10Px6 Text (7) 56ICD10Px7 Text (7) 57ICD10Px8 Text (7) 58ICD10Px9 Text (7) 59
ICD10Px10 Text (7) 60ProviderSpecialty Text (15) 61 Use Provider Specialties in the Provider Specialty Crosswalk Tab
POS Text (2) 62
Place of Service. Also automatically built using a cross-reference. Valid values are: BC (Birthing Center), DN (Day/Night Hospitalization), ER (Emergency Room), IA (Inpatient Acute), IN (Inpatient Non-Acute), LA (Laboratory), OA (Outpatient/Ambulatory), OC (Office/Clinic), OT (Other), RM (Mail Order Prescription Drugs), RR (Retail Pharmacy).
57

SUPPLEMENTAL LAB CLAIM FILE DATA DICTIONARYField Name Data Type File Order NotesMemberKey Text (30) 1ProviderKey Text (25) 2 This should be the rendering provider’s NPI.
ClaimNumber Text (80) 3 Used to identify the claim source for Primary Source Verification.
DOS Date 4 The Date of Service for the claim in MM/DD/YYYY format.
CPTPx Text (5) 5 Level II CPT Codes are supported by HEDIS and should be placed in the same field as other CPT procedure codes.
LOINC Text (7) 6 LOINC codes must contain the dash character that precedes the final digit.
HCPCSPx Text (5) 7 Used for medical services, that comes in through lab claims. Only one HCPCS code per claim line is allowed. If the claim contains multiple HCPCS codes, load them as separate claims.
HCPCSMod Text (2) 8
Result Decimal(28,10) 9 Used to document numeric lab results.
PosNegResult Bit 10 Used to document positive/negative lab results. Valid values are 0 (negative), or 1 (positive).
Supplemental Lab Claim File Data Dictionary The LabClaim file contains claims for laboratory services and allows lab results to be stored. The LabClaim file should contain one record per unique lab service claim.
58

APPENDIX 7: Constructing the IPA Payment Amount per Member Point
Using the formula below, the Payment Amount per Member Point is calculated as follows:
[Expected Global Quality Performance Score] x [Total Medi-Cal Membership as of 1/2018*] = Total Member Points
[Total Incentive Dollars Available] / [Total Member Points] = Payment Amount per Member Point
Final Payment Amount per Member Point Calculation:
EXPECTED GLOBAL QUALITY PERFORMANCE
SCORE
TOTAL MEDI-CAL MEMBERSHIP AS
OF 1/2018*MEMBER POINTS
1.88 720,776 1,355,058.88 x =
PROVIDER TOTAL INCENTIVE DOLLARS AVAILABLE
MEMBER POINTS
PAYMENT PER MEMBER POINT
IPA $20,000,000 1,355,058.88 $14.76** ÷ =*Excludes IEHP Direct, Kaiser, Allied Pacific IPA, Heritage Provider Network and Pomona Valley Medical Group Medi-Cal membership. ** Payment per Member Point is not finalized. Payment Per Member Point will be included in published status reports beginning in the Spring.
Rates will be shared with IPAs at least quarterly to track progress toward goals. Initial IPA reports will be available in March 2018.
59

NOTES
60
Provider Relations Team909-890-2054Monday-Friday, 8am - 5pm
©2018 Inland Empire Health Plan. All Rights Reserved. PS-18-776733
Follow us:






























