-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
1/18
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
2/18
vessels into the portal system and simultaneous remodeling of
the paired right and leftcardinal veins into the
renal/adrenal/gonadal veins (subcardinal) and the azygous/
hemiazygos veins (supracardinal) lead ultimately to the mature
venous system. Thedevelopment of these systems is important when
approaching gastric varices (GV)
Henry et al372
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
3/18
and ectopic varices (ECV) because the connections that arise are
often related to theiranatomic origins. For example, in patients
with splenic vein thrombosis (SVT) and sub-sequent GV, the
hypertensive short gastric veins in the fundus of the stomach,
whichoriginate from the vitelline veins, often communicate with the
azygous vein, which orig-inates from the s upracardinal veins,
through small portosystemic collaterals in thedistal esophagus. 1
Understanding these anastomoses and the direction of theseveins
afferent and efferent flow based on their anatomy can help gu ide
therapeuticinterventions, which the authors note in future sections
of this review. 2
GV IN CIRRHOSIS
In patients with cirrhosis and no underlying splanchnic vein
thrombosis, studies havefound the prevalence of GV to be 17% to 25%
compared with a prevalence of esoph-ageal varices (EV) of 50% to
60%. 3,4 GV bleed less frequently than EV but tend to bemore
severe. 4 Fundal varices tend to bleed more often than varices in
the cardia orantrum. 4 The natural history of GV has rarely been
reported; but in one study of 132patients, the bleeding risk was
estimated at 16%, 36%, and 44% at 1 year, 3 years,and 5 years,
respectively. The presence of a red spot, a varix greater than 5 mm
insize, and advanced Child-Pugh class were all found to be
predictors of bleeding. 3
The absence of forward flow in the splenic vein has also
recently been establishedas a predictor of GV bleeding, with a
5-year risk of 59% versus 39% when comparedwith those with forward
flow. 5 This finding is consistent with a much earlier study
thatnoted, in comparison with EV, GV are much more likely to have
reversed or to-and-froflow in the splenic vein. 6
The management of GV in patients with cirrhosis depends greatly
on how they areclassified because this can provide a guide for the
prognosis and treatment approach.The most common system used is the
Sarin classification ( Fig. 2 ).4 Using this classi-fication system
helped identify gastric fundal varices as higher-risk lesions for
bleedingand has guided other studies in evaluating responses to
different therapies. Forinstance, sclerotherapy for GV has not had
the same success that it had in the treat-ment of EV, except in
subsets of patients with gastroesophageal varices (GOV)
1.Physiologically, this makes sense because, as the Sarin
classification has shown,GOV1 GV are located near the
gastroesophageal junction and are often fed fromthe same venous
source as EV. However, with fundal varices, GOV2 and IGV 1, the
Sarin classification does not truly describe the underlying
vascular heterogeneity,
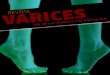
Fig. 1. The embryologic development of the portal venous and
systemic venous circulationof the abdomen. In gold are the
vitelline veins that merge over time to form the intrahe-patic
portal and hepatic veins as well as the superior portion of the
intrahepatic inferiorvena cava (IVC). These veins also form the
main portal vein and go on to form the splenicand mesenteric veins.
In red are the umbilical veins. Over time, the right umbilical vein
at-rophies and the left umbilical vein maintains a connection to
the left portal venous systemand forms the ductus venosus with the
vitelline veins; the ductus venosus becomes the lig-amentum venosum
and the umbilical vein atrophies after birth. This vestigial link
explainsthe presence of a recanalized umbilical vein in portal
hypertension. Colored teal blue arethe paired subcardinal veins,
which merge over time to form the abdominal IVC and bilat-eral
renal, adrenal, and gonadal veins. In green are the azygous and
hemiazygos veins,which are derived from the supracardinal veins and
run inferiorly into the abdomen wherethe hemiazygos connects into
the left adrenal vein. These vestigial connections should atro-phy
over time but are likely the source of small portosystemic
collaterals in portal hyperten-sion 1 and likely play a role in
gastrorenal shunt formation. 2 SVC, superior vena cava.
=
Gastric and Ectopic Varices 373
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
4/18
which has made it difficult to use this system alone to
standardize an approach totreatment and highlights the need for a
better understanding of the vascular anatomy.
Clinical investigators in the 1980s and 1990s, especially in
Japan, can be creditedwith bringing a new appreciation of the
architecture of the venous collateral bed un-derlying cardiofundal
varices; these typically involve collaterals arising from the
shortgastric veins and the posterior gastric veins leading to an
outflow trunk that ends in theleft renal vein. 6 This study also
highlights the difference between a right-sided portalcirculation
and a left-sided portal circulation in relation to GV. Proposed
vascular clas-sifications are based on the afferent veins feeding
the varices combined with thevenous outflow tract, whether it is
through a direct shunt or multiple small collaterals( Figs. 3 and 4
).7,8 The vascular classifications can be used in conjunction with
theendoscopic classification to determine the best therapy.
The management strategies for bleeding GV have varied over the
years but aregenerally categorized into either endoscopic or
radiologic approaches. Appropriate
Fig. 2. The Sarin endoscopic classification for GV. 4 GOV,
gastroesophageal varices; IGV,
isolated GV.
Henry et al374
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
5/18
medical management of acute GV bleeding is unclear because there
are no trials spe-cifically evaluating the use of octreotide or
vasopressin analogues; however, the diver-sion of splanchnic blood
flow should decrease bleeding similar to the effect seen inacute
esophageal variceal bleeding and should be considered in this
population.Balloon tamponade is likely a more effective method to
stop bleeding in the acutesetting; however, this usually must be
followed up by more definitive endoscopic orvascular therapy.
Fig. 3. The Kiyosue vascular classification of GV.7
Type 1 refers to a single afferent vein foreither the right or
left portal circulation; type 2 refers to multiple afferent vessels
contrib-uting to the varix; type 3 is consistent with type 2 with
the addition of small afferent vesselsin direct continuity with the
outflow track. Type A consists of a gastrorenal shunt (GRS) asthe
sole outflow; type B describes the presence of a GRS in conjunction
with small peri-diaphragmatic portosystemic collaterals; type C
describes the presence of both a GRS anddirect gastro-caval shunt;
type D consists of small portosystemic collaterals as the
soleoutflow track. Types 1, 2, and 3 can be combined with types A,
B, C, and D to describethe inflow and outflow of a GV.
Gastric and Ectopic Varices 375
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
6/18
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
7/18
Endoscopic Treatment of GV
Endoscopic therapies have focused mainly on injection therapy
with cyanoacrylateglues, but variceal band ligation has also been
evaluated . Cyanoacrylate injectionhas excellent rates of acute
hemostasis, greater than 90%, 914 but has variable rates
of rebleeding, with an average rate of around 20% within 1
year.9,10,13,15
Whencompared directly with band ligation, cyanoacrylate
injection is superior at both initialhemostasis as well as
long-term rebleeding. In one study, initial hemostasis was 87%with
cyanoacrylate versus 45% with band ligation, with rebleeding rates
of 31%versus 54%, respectively. 11 A more recent study comparing
the two did not show adifference in acute hemostasis (both achieved
93%); however, rebleeding with cyano-acrylate was 23.0% at 1 year
compared with 33.5% with the band ligation group. 9 Thisstudy also
showed a much higher rate of recurrence of GV with band ligation
versuscyanoacrylate, 60% versus 23%, respectively. One of the
concerns with cyanoacry-late injection is the risk of embolization
of the glue thrombus. The risk of severe and
potentially fatal embolization with the most commonly used
4-carbon N-butyl-2-cyanoacrylate is estimated to be 0% to 2%.
9,10,13,15 In one of the largest series, therisk of thrombotic
complication was only 0.7%; these all occurred in a technique
usinglarge volumes of lipiodol, which delays polymerization. 16 The
authors own datacomparing the ex vivo polymerization times of
various cyanoacrylate mixtures haveshown a roughly 2-fold increase
in the polymerization time by adding the iodinatedplant oil
ethiodized oil (Ethiodol) (identical to lipiodol) to
N-butyl-2-cyanoacrylate.These results suggest that the use of
iodinated contrast oils, although probablydecreasing the risk of
needle impaction, increases the risk of embolization. 17
TIPS Treatment of GV
Transjugular intrahepatic portosystemic shunt (TIPS) has been
evaluated in the treat-ment of GV. In comparison with EV, large GV
often have lower portal pressures andlower portosystemic gradients
before TIPS placement. 6,18 In a study from 1997, re-sults of TIPS
procedures in patients with EV and/or GV were compared
revealingthat EV had a notable reduction in size after TIPS, as
would be expected; but 50%of GV did not change in size despite
achieving a portosystemic gradient less than12 mm Hg. 19 These
findings were again noted in a study from 2007 comparing
cyano-acrylate injection with TIPS for the treatment of GV. Despite
a slightly lower rebleeding
rate in the TIPS group when follow-up endoscopy was performed,
those that under-went glue injection had a much lower r at e of
persistent GV compared with the TIPSgroup, 20% versus 57%,
respectively. 14 This phenomenon is likely caused by thepresence of
spontaneous shunts, such as gastrorenal and splenorenal shunts.
6
In a study from 2003, TIPS had a lower 30-day rate of rebleeding
when comparedwith cyanoacrylate injection, 15% versus 30%,
respectively. But there was no mortal-ity difference between the
groups, and the c ost analysis at 6 months revealed a sig-nificant
benefit of glue injection over TIPS. 20 In the authors own data,
they found alower 1-year rebleeding rate in the cyanoacrylate group
compared with the TIPSgroup, 10% and 25% respectively, and also
showed no mortality difference. 21 The au-thors did, however, show
an increased morbidity with TIPS caused by hepatic en-cephalopathy.
In an earlier study with this same population, the authors also
founda cost benefit to cyanoacrylate treatment when compared with
noncyanoacrylatetherapy. 22 Although TIPS remains a common and
widely accepted means of manag-ing GV bleeding, its application
remains problematic in many patients; it is sometimesineffective.
18,23 This ineffectiveness is especially so in patients with
far-left shunts, inwhom transhepatic occlusion of the shunt,
usually performed by delivering a coil
Gastric and Ectopic Varices 377
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
8/18
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
9/18
endoscopic injection of cyanoacrylate along with one other
patient with a red spot on aduodenal varix. All 3 acutely ble eding
patients achieved initial hemostasis, and therewere no rebleeds
among all 4. 46 Two other case reports reveal success with
cyanoac-rylate injection with no rebleeding out to 1 yea r, an d
another investigator reports suc-cess in a single case with
thrombin injection. 4749 Most DV have an afferent venoussupply from
either the portal vein or the superior mesenteric vein with an o
utflow trackdirectly into the inferior vena cava, making TIPS and
BRTO possible. 44,50 In one caseof failed endoscopic management,
rescue BRTO was performed for DV bleeding withcomplete obliteration
of the varix after 3 months of follow-up and no rebleeding. 51
Another series of 5 patients who underwent BRTO for DV reported
100% technicalsuccess and no rebleeding out to 1 year. 50 TIPS has
also been successful in onecase report of DV in the setting of
cirrhosis as a bridge to transplant. 52 Other reportson the general
use of TIPS for all kinds of ECV bleeding have shown modest results
inthe patients with DV. 53 Because of the lack of randomized
trials, an exact recommen-dation for the treatment of DV cannot be
made; but the evidence noted here suggeststhat, similar to GV,
there are many viable modalities with similar rates of success.
COLORECTAL VARICES
Rectal varices (RV) are the most prevalent of the ECV, with
rates reported as high as77% of all ECV. Their prevalence in
patients with cirrhosis is between 28% and 56%,whereas their
prevalence in extrahepatic portal vein obstruction is 63% to 94%.
5456
Bleeding from RV is rare but can be massive and fatal. 57,58
Most of the data on man-agement are related to TIPS placement in
these patients; however, there are a fewcase reports and case
series on endoscopic therapies, BRTO, and even surgical
man-agement. Endoscopically there are case reports of cyanoacrylate
use as well as bandligation. In contrast to GV, band ligation shows
superior results with excellent initial he-mostasis and low
rebleeding rates compared with glue injection. 5860 There have
beencase reports of standard BRTO therapy as well as a
transumbilical approach to aBRTO procedure; in both cases, the RV
were completely obliterated and there wasno rebleeding. 61,62 There
have been many retrospective studies evaluating TIPS re-sults in
these patients; although initial hemostasis results are quite good,
there arereble eding rates from 10% to 20% despite adequately
reduced portal pres-sure. 53,6365 This finding is similar to the
findings in some patients with GV afterTIPS and suggests that,
because of the complex vascular outflow pathways seen inthese
varices, TIPS alone may not be effective. In some cases, BRTO or
TIPS withdirect embolization of the varix may be necessary.
GV AND ECV IN PORTAL VEIN THROMBOSIS
A discussion of GV and ECV would be incomplete without also
addressing thesometimes-important role of portal vein thrombosis
(PVT) whether in cirrhotic or non-cirrhotic patients.
Cirrhotic PVT and GV/ECV Bleeding
Cirrhotic patients with PVT and variceal bleeding have a much
worse prognosis. 6669In addition, PVT is much more prevalent in
cirrhotic patients when compared with thegeneral population, with
an average prevalence around 10% and a range between2.1% and 23.0%.
70 There are only a few studies that remark on the incidence of
PVT, one with a cumulative incidence of 7.4% and another with an
annual incidenceof 16%. 71,72 The rates of variceal bleeding in
cirrhotic patients with PVT range fromabout 39% to 50% at
presentation; however, most of these bleeds are secondary
Gastric and Ectopic Varices 379
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
10/18
to EV. 73 There are very little data regarding gastric variceal
bleeding or ectopic varicealbleeding in cirrhotic patients with
PVT; of the data available, there are only case re-ports or very
small case series.
A case report of DV and GV in a patient with cirrhosis and PVT
note d h emostasiswithout rebleeding out to 1 year after endoscopic
injection of Histoacryl. 47 TIPS (usu-ally along with postprocedure
anticoagulation) is also a viable option in these patient s,even
with occlusive PVT provided intrahepatic portal branches can be
visualized. 74
This approach has the advantage of offering variceal
decompression but carries tech-nical challenges and an increased
risk of hepatic decompensation with higher MELDscores. 19 There are
a few prospective trials that have evaluated the use of
anticoagu-lation in PVT related to cirrhosis and have noted very
few bleeding events. 71,74,75 Inone of these studies, there was a
significantly higher rate of recanalization in patientson
anticoagulation; variceal bleeding was worse in patients that did
not receive anti-coagulation compared with those that did. 74
Certainly, long-term anticoagulationneeds to be considered in this
population, especially in patients with an
underlyingthrombophilia.
Noncirrhotic PVT and GV/ECV Bleeding
Although cirrhosis-related portal hypertension may be the most
common cause of GVand ECV, PVT and SVT are also known to cause both
GV and ECV. Noncirrhotic PVT isthe second leading cause of portal
hypertension in the Western world, with a preva-lence of 5% to 10%
in patients with portal hypertension. 76 Within this group of
pa-tients, EV are most prevalent at about 78% to 90% in all cases
of noncirrhotic PVT,with GV having a reported prevalence from 14%
to 50%. 68,7779 ECV have been re-
ported in 27% to 40% of cases of splanchnic vein thrombosis (PVT
alone or withSVT or mesenteric vein thrombosis) and have been noted
to be much more commonthan in cirrhosis. 55,77
In a study examining 60 patients with splanchnic vein
thrombosis, 54 of which hadchronic noncirrhotic portal-mesenteric
vein thrombosis, Orr and colleagues 78 notedthat 91% had EV on
initial endoscopy and 50% had GV. Of those 60 patients,
50%presented with gastrointestinal bleeding. Of all bleeding
events, the sentinel bleedingepisodes were from EV alone; but the
secondary bleeding episodes were morecommonly GV and ECV, with
bleeding rates of 26% and 33%, respectively. Fatal hem-orrhage was
more often from GV and ECV, suggesting that, although less
prevalent,
GV and ECV bleeding is more severe. A second study, by Spaander
and colleagues, 80revealed similar results. They found that gastric
fundal varices were associated with anincreased risk of rebleeding
by a factor of 5 (hazard ratio 5.07). Despite rebleedingrisks, the
overall mortal ity f or these patients is still more closely
related to the under-lying cause of the PVT. 69,81
Anticoagulation in the setting of PVT remains a challenging
aspect of treatment. Hy-percoagulable risks and myeloproliferative
disorders (MPD) should be assessed. Theprevalence of an inherent
clotting disorder, such as factor V Leiden, prothrombin mu-tation,
protein C or S deficiency, or MPD, in these patients is 50% to 60%
and can alterlong-term management in regard to anticoagulation.
68,8285 Currently, the Baveno Vcriteria, and other studies,
recommend treating acute PVT for at least 3 to 6 months;however, if
there is an underlying coagulopathy or MPD, then lifelong therapy
needs tobe considered. 86,87 In contrast, the data for
anticoagulation in chronic PVT, with cav-ernoma formation, are less
persuasive but still suggest that, in the setting of a
hyper-coagulable state, lifelong anticoagulation should be
considered. The risk of bleedingwhile on anticoagulation is low,
and some series showed that bleeding is less commonwith
anticoagulation than without, likely because of decreased portal
pressures
Henry et al380
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
11/18
secondary to recanalization. 78,88 Amitrano and colleagues 68
evaluated 121 patientswith PVT or mesenteric vein thrombosis noting
all follow-up bleeding events occurredin the patients that were not
on anticoagulation. Despite this low risk of bleeding fromvarices
in this population, experts recommend screening for varices early
after diag-nosis, performing follow-up endoscopy 6 months later, a
nd t hen annually from thereon, treating the varices as you would
in cirrhotic patients. 86,89 Although recanalizationdecreases the
risk of bleedi ng, not all patients achieve recanalization. In
separatestudies by Hall and Condat, 88,90 there were recanalization
rates of 82% and 90%,respectively. 88,90 However, in most studies,
the rates of recanalization on anticoagu-lation are in the range of
30% to 50%. 87,91 The rates of spontaneous recanalizationwithout
anticoagulation range from 0% to 32% in these studies. 8690
Overall, the mor-tality risk in these patients is related to the
thrombosis itself and/or the underlying dis-order causing the
thrombosis and not from bleeding risk, suggesting
thatanticoagulation is beneficial and should be considered in all
patients, especially thosewith an underlying thrombophilic
disorder. 69,92
Noncirrhotic SVT and GV/ECV Bleeding
SVT must also be considered separate from PVT and cirrhosis
because the underlyingcause is much different. The most common
causes of isolated SVT are chronicpancreatitis, acute pancreatitis,
pancreatic pseudocyst, and neoplasm, with pancre-atitis the most
frequent cause. 1,9397 The overall incidence of SVT ranges from
13%to 45%, with most of these studies evaluating populations of
patients wi th panc rea-titis. It is estimated that 60% of cases of
SVT are caused by pancreatitis. 94,9799 Theincidence of GV in SVT
ranges from 15% to almost 57%, with higher rates in studies
that looked specifically at acute and chronic
pancreatitis.1,93,94,98,99
The presentin gsymptom in patients w ith SVT is gastrointestinal
bleeding in 45% to 72% of cases. 97
Heider and colleagues 93 looked at a large group of patients
with pancreatitis over a10-year period and noted 53 that had SVT.
Of these 53 patients, they initially reportedthat 41 of them were
noted to have GV, a prevalence of almost 80%; however, most of
these were noted on computed tomography findings. On further
analysis, only 36 of these 53 patients underwent
esophagogastroduodenoscopy (EGD); of those patients,only 11 had
endoscopically notable GV, or about 30%. Another study by Agarwal
andcolleagues 98 evaluated the incidence and management of SVT in
patients with chronicpancreatitis. There was an incidence of SVT of
22% and, within that group, an inci-
dence of all varices of 41%. Of those with GV, 43% experienced a
bleeding event.The definitive treatment of GV bleeding in the
setting of SVT is splenectomy; however,
performing splenectomy in all patients with SVT is a contentious
subject. 93,96,98 Heiderand colleagues 93 found that, in their
patients with SVT, the overall bleeding risk was only4%; however,
the patients that bled were all patients with GV on EGD.
Additionally, Agarwal and colleagues 98 noted a bleeding rate from
varices (EV vs GV not specified)of approximately 10% and also noted
that, in patients who underwent splenectomy,there was no GV
bleeding out to 2 years compared with a 14% GV bleeding rate in
thosewho did not. This finding suggests that splenectomy may
prevent GV bleeding.
SUMMARY
In conclusion, GV and ECV have several underlying causes and,
therefore, cannot betreated with any one particular intervention.
Acute management of both GV and ECVshould focus on the
stabilization of patients while concurrently attempting to
definethe underlying cause so that therapy can be tailored to the
individual. More random-ized controlled trials are needed in the
future to better define the subsets of
Gastric and Ectopic Varices 381
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
12/18
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
13/18
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
14/18
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
15/18
29. Kim ES, Kweon YO, Cho CM, et al. The clinical efficacy of
the balloon occludedretrograde transvenous obliteration (BRTO) in
gastric variceal bleeding. J Hep-atol 2003;38:62 .
30. Ninoi T, Nakamura K, Kaminou T, et al. TIPS versus
transcatheter sclerotherapyfor gastric varices. AJR Am J Roentgenol
2004;183(2):36976 .
31. Ferral H, Patel NH. Selection criteria for patients
undergoing transjugular intra-hepatic portosystemic shunt
procedures: current status. J Vasc Interv Radiol2005;16(4):44955
.
32. Saad WE, Darwish WM, Davies MG, et al. Transjugular
intrahepatic portosyste-mic shunts in liver transplant recipients
for management of refractory ascites:clinical outcome. J Vasc
Interv Radiol 2010;21(2):21823 .
33. Uehara H, Akahoshi T, Tomikawa M, et al. Prediction of
improved liver functionafter balloon-occluded retrograde
transvenous obliteration: relation to hepaticvein pressure
gradient. J Gastroenterol Hepatol 2012;27(1):13741 .
34. Kumamoto M, Toyonaga A, Inoue H, et al. Long-term results of
balloon-occludedretrograde transvenous obliteration for gastric
fundal varices: hepatic deteriora-tion links to portosystemic shunt
syndrome. J Gastroenterol Hepatol 2010;25(6):112935 .
35. Saad WE, Wagner CC, Al-Osaimi A, et al. The effect of
balloon-occluded trans-venous obliteration of gastric varices and
gastrorenal shunts on the hepatic syn-thetic function: a comparison
between Child-Pugh and model for end-stage liverdisease scores.
Vasc Endovascular Surg 2013;47(4):2817 .
36. Cho SK, Shin SW, Yoo EY, et al. The short-term effects of
balloon-occludedretrograde transvenous obliteration, for treating
gastric variceal bleeding, on
portal hypertensive changes: a CT evaluation. Korean J Radiol
2007;8(6):52030 .37. Tanihata H, Minamiguchi H, Sato M, et al.
Changes in portal systemic pres-
sure gradient after balloon-occluded retrograde transvenous
obliteration ofgastric varices and aggravation of esophageal
varices. Cardiovasc InterventRadiol 2009;32(6):120916 .
38. Saad WE, Wagner CC, Lippert A, et al. Protective value of
TIPS against thedevelopment of hydrothorax/ascites and upper
gastrointestinal bleeding afterballoon-occluded retrograde
transvenous obliteration (BRTO). Am J Gastroen-terol
2013;108(10):16129 .
39. Cho SK, Shin SW, Do YS, et al. Development of thrombus in
the major systemicand portal veins after balloon-occluded
retrograde transvenous obliteration fortreating gastric variceal
bleeding: its frequency and outcome evaluation withCT. J Vasc
Interv Radiol 2008;19(4):52938 .
40. Mishra SR, Chander Sharma B, Kumar A, et al. Endoscopic
cyanoacrylate injec-tion versus beta-blocker for secondary
prophylaxis of gastric variceal bleed: arandomised controlled
trial. Gut 2010;59(6):72935 .
41. Mishra SR, Sharma BC, Kumar A, et al. Primary prophylaxis of
gastric varicealbleeding comparing cyanoacrylate injection and
beta-blockers: a randomizedcontrolled trial. J Hepatol
2011;54(6):11617 .
42. Norton ID, Andrews JC, Kamath PS. Management of ectopic
varices. Hepatol-ogy 1998;28(4):11548 .
43. Lebrec D, Benhamou JP. Ectopic varices in portal
hypertension. Clin Gastroen-terol 1985;14(1):10521 .
44. Hashizume M, Tanoue K, Ohta M, et al. Vascular anatomy of
duodenal varices:angiographic and histopathological assessments. Am
J Gastroenterol 1993;88(11):19425 .
Gastric and Ectopic Varices 385
http://refhub.elsevier.com/S1089-3261(14)00003-8/sref29http://refhub.elsevier.com/S1089-3261(14)00003-8/sref29http://refhub.elsevier.com/S1089-3261(14)00003-8/sref29http://refhub.elsevier.com/S1089-3261(14)00003-8/sref30http://refhub.elsevier.com/S1089-3261(14)00003-8/sref30http://refhub.elsevier.com/S1089-3261(14)00003-8/sref31http://refhub.elsevier.com/S1089-3261(14)00003-8/sref31http://refhub.elsevier.com/S1089-3261(14)00003-8/sref31http://refhub.elsevier.com/S1089-3261(14)00003-8/sref32http://refhub.elsevier.com/S1089-3261(14)00003-8/sref32http://refhub.elsevier.com/S1089-3261(14)00003-8/sref32http://refhub.elsevier.com/S1089-3261(14)00003-8/sref33http://refhub.elsevier.com/S1089-3261(14)00003-8/sref33http://refhub.elsevier.com/S1089-3261(14)00003-8/sref33http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref40http://refhub.elsevier.com/S1089-3261(14)00003-8/sref40http://refhub.elsevier.com/S1089-3261(14)00003-8/sref40http://refhub.elsevier.com/S1089-3261(14)00003-8/sref41http://refhub.elsevier.com/S1089-3261(14)00003-8/sref41http://refhub.elsevier.com/S1089-3261(14)00003-8/sref41http://refhub.elsevier.com/S1089-3261(14)00003-8/sref42http://refhub.elsevier.com/S1089-3261(14)00003-8/sref42http://refhub.elsevier.com/S1089-3261(14)00003-8/sref43http://refhub.elsevier.com/S1089-3261(14)00003-8/sref43http://refhub.elsevier.com/S1089-3261(14)00003-8/sref44http://refhub.elsevier.com/S1089-3261(14)00003-8/sref44http://refhub.elsevier.com/S1089-3261(14)00003-8/sref44http://refhub.elsevier.com/S1089-3261(14)00003-8/sref44http://refhub.elsevier.com/S1089-3261(14)00003-8/sref44http://refhub.elsevier.com/S1089-3261(14)00003-8/sref44http://refhub.elsevier.com/S1089-3261(14)00003-8/sref43http://refhub.elsevier.com/S1089-3261(14)00003-8/sref43http://refhub.elsevier.com/S1089-3261(14)00003-8/sref42http://refhub.elsevier.com/S1089-3261(14)00003-8/sref42http://refhub.elsevier.com/S1089-3261(14)00003-8/sref41http://refhub.elsevier.com/S1089-3261(14)00003-8/sref41http://refhub.elsevier.com/S1089-3261(14)00003-8/sref41http://refhub.elsevier.com/S1089-3261(14)00003-8/sref40http://refhub.elsevier.com/S1089-3261(14)00003-8/sref40http://refhub.elsevier.com/S1089-3261(14)00003-8/sref40http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref39http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref38http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref37http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref36http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref35http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref34http://refhub.elsevier.com/S1089-3261(14)00003-8/sref33http://refhub.elsevier.com/S1089-3261(14)00003-8/sref33http://refhub.elsevier.com/S1089-3261(14)00003-8/sref33http://refhub.elsevier.com/S1089-3261(14)00003-8/sref32http://refhub.elsevier.com/S1089-3261(14)00003-8/sref32http://refhub.elsevier.com/S1089-3261(14)00003-8/sref32http://refhub.elsevier.com/S1089-3261(14)00003-8/sref31http://refhub.elsevier.com/S1089-3261(14)00003-8/sref31http://refhub.elsevier.com/S1089-3261(14)00003-8/sref31http://refhub.elsevier.com/S1089-3261(14)00003-8/sref30http://refhub.elsevier.com/S1089-3261(14)00003-8/sref30http://refhub.elsevier.com/S1089-3261(14)00003-8/sref29http://refhub.elsevier.com/S1089-3261(14)00003-8/sref29http://refhub.elsevier.com/S1089-3261(14)00003-8/sref29
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
16/18
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
17/18
64. Shibata D, Brophy DP, Gordon FD, et al. Transjugular
intrahepatic portosystemicshunt for treatment of bleeding ectopic
varices with portal hypertension. Dis Co-lon Rectum
1999;42(12):15815 .
65. Nayar M, Saravanan R, Rowlands PC, et al. TIPSS in the
treatment of ectopicvariceal bleeding. Hepatogastroenterology
2006;53(70):5847 .
66. Merkel C, Bolognesi M, Bellon S, et al. Long-term follow-up
study of adult pa-tients with non-cirrhotic obstruction of the
portal system: comparison withcirrhotic patients. J Hepatol
1992;15(3):299303 .
67. Condat B, Pessione F, Hillaire S, et al. Current outcome of
portal vein thrombosisin adults: risk and benefit of anticoagulant
therapy. Gastroenterology 2001;120(2):4907 .
68. Amitrano L, Guardascione MA, Scaglione M, et al. Prognostic
factors in noncir-rhotic patients with splanchnic vein thromboses.
Am J Gastroenterol 2007;102(11):246470 .
69. Janssen HL, Wijnhoud A, Haagsma EB, et al. Extrahepatic
portal vein throm-bosis: aetiology and determinants of survival.
Gut 2001;49(5):7204 .
70. Rodriguez-Castro KI, Porte RJ, Nadal E, et al. Management of
nonneoplasticportal vein thrombosis in the setting of liver
transplantation: a systematic review.Transplantation
2012;94(11):114553 .
71. Francoz C, Belghiti J, Vilgrain V, et al. Splanchnic vein
thrombosis in candi-dates for liver transplantation: usefulness of
screening and anticoagulation.Gut 2005;54(5):6917 .
72. Zocco MA, Di Stasio E, De Cristofaro R, et al. Thrombotic
risk factors in patientswith liver cirrhosis: correlation with MELD
scoring system and portal vein throm-
bosis development. J Hepatol 2009;51(4):6829 .73. Amitrano L,
Guardascione MA, Brancaccio V, et al. Risk factors and clinical
pre-sentation of portal vein thrombosis in patients with liver
cirrhosis. J Hepatol2004;40(5):73641 .
74. Senzolo M, Sartori T, Rossetto V, et al. Prospective
evaluation of anticoagulationand transjugular intrahepatic
portosystemic shunt for the management of portalvein thrombosis in
cirrhosis. Liver Int 2012;32(6):91927 .
75. Amitrano L, Guardascione MA, Menchise A, et al. Safety and
efficacy of antico-agulation therapy with low molecular weight
heparin for portal vein thrombosis inpatients with liver cirrhosis.
J Clin Gastroenterol 2010;44(6):44851 .
76. Valla DC, Condat B, Lebrec D. Spectrum of portal vein
thrombosis in the West.J Gastroenterol Hepatol 2002;17(Suppl
3):S2247 .
77. Sarin SK, Sollano JD, Chawla YK, et al. Consensus on
extra-hepatic portal veinobstruction. Liver Int 2006;26(5):5129
.
78. Orr DW, Harrison PM, Devlin J, et al. Chronic mesenteric
venous thrombosis:evaluation and determinants of survival during
long-term follow-up. Clin Gastro-enterol Hepatol 2007;5(1):806
.
79. Spaander VM, van Buuren HR, Janssen HL. Review article: the
management ofnon-cirrhotic non-malignant portal vein thrombosis and
concurrent portal hyper-tension in adults. Aliment Pharmacol Ther
2007;26(Suppl 2):2039 .
80. Spaander MC, Darwish Murad S, van Buuren HR, et al.
Endoscopic treatment ofesophagogastric variceal bleeding in
patients with noncirrhotic extrahepaticportal vein thrombosis: a
long-term follow-up study. Gastrointest Endosc2008;67(6):8217 .
81. Primignani M. Portal vein thrombosis, revisited. Dig Liver
Dis 2010;42(3):16370 .82. Primignani M, Martinelli I, Bucciarelli
P, et al. Risk factors for thrombophilia in
extrahepatic portal vein obstruction. Hepatology 2005;41(3):6038
.
Gastric and Ectopic Varices 387
http://refhub.elsevier.com/S1089-3261(14)00003-8/sref64http://refhub.elsevier.com/S1089-3261(14)00003-8/sref64http://refhub.elsevier.com/S1089-3261(14)00003-8/sref64http://refhub.elsevier.com/S1089-3261(14)00003-8/sref65http://refhub.elsevier.com/S1089-3261(14)00003-8/sref65http://refhub.elsevier.com/S1089-3261(14)00003-8/sref66http://refhub.elsevier.com/S1089-3261(14)00003-8/sref66http://refhub.elsevier.com/S1089-3261(14)00003-8/sref66http://refhub.elsevier.com/S1089-3261(14)00003-8/sref67http://refhub.elsevier.com/S1089-3261(14)00003-8/sref67http://refhub.elsevier.com/S1089-3261(14)00003-8/sref67http://refhub.elsevier.com/S1089-3261(14)00003-8/sref68http://refhub.elsevier.com/S1089-3261(14)00003-8/sref68http://refhub.elsevier.com/S1089-3261(14)00003-8/sref68http://refhub.elsevier.com/S1089-3261(14)00003-8/sref69http://refhub.elsevier.com/S1089-3261(14)00003-8/sref69http://refhub.elsevier.com/S1089-3261(14)00003-8/sref70http://refhub.elsevier.com/S1089-3261(14)00003-8/sref70http://refhub.elsevier.com/S1089-3261(14)00003-8/sref70http://refhub.elsevier.com/S1089-3261(14)00003-8/sref71http://refhub.elsevier.com/S1089-3261(14)00003-8/sref71http://refhub.elsevier.com/S1089-3261(14)00003-8/sref71http://refhub.elsevier.com/S1089-3261(14)00003-8/sref72http://refhub.elsevier.com/S1089-3261(14)00003-8/sref72http://refhub.elsevier.com/S1089-3261(14)00003-8/sref72http://refhub.elsevier.com/S1089-3261(14)00003-8/sref73http://refhub.elsevier.com/S1089-3261(14)00003-8/sref73http://refhub.elsevier.com/S1089-3261(14)00003-8/sref73http://refhub.elsevier.com/S1089-3261(14)00003-8/sref74http://refhub.elsevier.com/S1089-3261(14)00003-8/sref74http://refhub.elsevier.com/S1089-3261(14)00003-8/sref74http://refhub.elsevier.com/S1089-3261(14)00003-8/sref75http://refhub.elsevier.com/S1089-3261(14)00003-8/sref75http://refhub.elsevier.com/S1089-3261(14)00003-8/sref75http://refhub.elsevier.com/S1089-3261(14)00003-8/sref76http://refhub.elsevier.com/S1089-3261(14)00003-8/sref76http://refhub.elsevier.com/S1089-3261(14)00003-8/sref77http://refhub.elsevier.com/S1089-3261(14)00003-8/sref77http://refhub.elsevier.com/S1089-3261(14)00003-8/sref78http://refhub.elsevier.com/S1089-3261(14)00003-8/sref78http://refhub.elsevier.com/S1089-3261(14)00003-8/sref78http://refhub.elsevier.com/S1089-3261(14)00003-8/sref79http://refhub.elsevier.com/S1089-3261(14)00003-8/sref79http://refhub.elsevier.com/S1089-3261(14)00003-8/sref79http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref81http://refhub.elsevier.com/S1089-3261(14)00003-8/sref82http://refhub.elsevier.com/S1089-3261(14)00003-8/sref82http://refhub.elsevier.com/S1089-3261(14)00003-8/sref82http://refhub.elsevier.com/S1089-3261(14)00003-8/sref82http://refhub.elsevier.com/S1089-3261(14)00003-8/sref81http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref80http://refhub.elsevier.com/S1089-3261(14)00003-8/sref79http://refhub.elsevier.com/S1089-3261(14)00003-8/sref79http://refhub.elsevier.com/S1089-3261(14)00003-8/sref79http://refhub.elsevier.com/S1089-3261(14)00003-8/sref78http://refhub.elsevier.com/S1089-3261(14)00003-8/sref78http://refhub.elsevier.com/S1089-3261(14)00003-8/sref78http://refhub.elsevier.com/S1089-3261(14)00003-8/sref77http://refhub.elsevier.com/S1089-3261(14)00003-8/sref77http://refhub.elsevier.com/S1089-3261(14)00003-8/sref76http://refhub.elsevier.com/S1089-3261(14)00003-8/sref76http://refhub.elsevier.com/S1089-3261(14)00003-8/sref75http://refhub.elsevier.com/S1089-3261(14)00003-8/sref75http://refhub.elsevier.com/S1089-3261(14)00003-8/sref75http://refhub.elsevier.com/S1089-3261(14)00003-8/sref74http://refhub.elsevier.com/S1089-3261(14)00003-8/sref74http://refhub.elsevier.com/S1089-3261(14)00003-8/sref74http://refhub.elsevier.com/S1089-3261(14)00003-8/sref73http://refhub.elsevier.com/S1089-3261(14)00003-8/sref73http://refhub.elsevier.com/S1089-3261(14)00003-8/sref73http://refhub.elsevier.com/S1089-3261(14)00003-8/sref72http://refhub.elsevier.com/S1089-3261(14)00003-8/sref72http://refhub.elsevier.com/S1089-3261(14)00003-8/sref72http://refhub.elsevier.com/S1089-3261(14)00003-8/sref71http://refhub.elsevier.com/S1089-3261(14)00003-8/sref71http://refhub.elsevier.com/S1089-3261(14)00003-8/sref71http://refhub.elsevier.com/S1089-3261(14)00003-8/sref70http://refhub.elsevier.com/S1089-3261(14)00003-8/sref70http://refhub.elsevier.com/S1089-3261(14)00003-8/sref70http://refhub.elsevier.com/S1089-3261(14)00003-8/sref69http://refhub.elsevier.com/S1089-3261(14)00003-8/sref69http://refhub.elsevier.com/S1089-3261(14)00003-8/sref68http://refhub.elsevier.com/S1089-3261(14)00003-8/sref68http://refhub.elsevier.com/S1089-3261(14)00003-8/sref68http://refhub.elsevier.com/S1089-3261(14)00003-8/sref67http://refhub.elsevier.com/S1089-3261(14)00003-8/sref67http://refhub.elsevier.com/S1089-3261(14)00003-8/sref67http://refhub.elsevier.com/S1089-3261(14)00003-8/sref66http://refhub.elsevier.com/S1089-3261(14)00003-8/sref66http://refhub.elsevier.com/S1089-3261(14)00003-8/sref66http://refhub.elsevier.com/S1089-3261(14)00003-8/sref65http://refhub.elsevier.com/S1089-3261(14)00003-8/sref65http://refhub.elsevier.com/S1089-3261(14)00003-8/sref64http://refhub.elsevier.com/S1089-3261(14)00003-8/sref64http://refhub.elsevier.com/S1089-3261(14)00003-8/sref64
-
8/10/2019 2014 04 Varices Gastricas y Ectopicas (1)
18/18
83. Primignani M, Mannucci PM. The role of thrombophilia in
splanchnic vein throm-bosis. Semin Liver Dis 2008;28(3):293301
.
84. De Stefano V, Teofili L, Leone G, et al. Spontaneous
erythroid colony formationas the clue to an underlying
myeloproliferative disorder in patients with Budd-Chiari syndrome
or portal vein thrombosis. Semin Thromb Hemost 1997;23(5):4118
.
85. Colaizzo D, Amitrano L, Tiscia GL, et al. The JAK2 V617F
mutation frequentlyoccurs in patients with portal and mesenteric
venous thrombosis. J ThrombHaemost 2007;5(1):5561 .
86. de Franchis R, Baveno VF. Revising consensus in portal
hypertension: report ofthe Baveno V consensus workshop on
methodology of diagnosis and therapy inportal hypertension. J
Hepatol 2010;53(4):7628 .
87. Plessier A, Darwish-Murad S, Hernandez-Guerra M, et al.
Acute portal veinthrombosis unrelated to cirrhosis: a prospective
multicenter follow-up study.Hepatology 2010;51(1):2108 .
88. Hall TC, Garcea G, Metcalfe M, et al. Impact of
anticoagulation on outcomes inacute non-cirrhotic and non-malignant
portal vein thrombosis: a retrospectiveobservational study.
Hepatogastroenterology 2013;60(122):3117 .
89. Garcia-Pagan JC, Hernandez-Guerra M, Bosch J. Extrahepatic
portal veinthrombosis. Semin Liver Dis 2008;28(3):28292 .
90. Condat B, Pessione F, Helene Denninger M, et al. Recent
portal or mesentericvenous thrombosis: increased recognition and
frequent recanalization on anti-coagulant therapy. Hepatology
2000;32(3):46670 .
91. Turnes J, Garcia-Pagan JC, Gonzalez M, et al. Portal
hypertension-related com-
plications after acute portal vein thrombosis: impact of early
anticoagulation.Clin Gastroenterol Hepatol 2008;6(12):14127 .92.
Donadini MP, Dentali F, Ageno W. Splanchnic vein thrombosis: new
risk factors
and management. Thromb Res 2012;129(Suppl 1):S936 .93. Heider
TR, Azeem S, Galanko JA, et al. The natural history of
pancreatitis-
induced splenic vein thrombosis. Ann Surg 2004;239(6):87680
[discussion:8802] .
94. Bernades P, Baetz A, Levy P, et al. Splenic and portal
venous obstruction inchronic pancreatitis. A prospective
longitudinal study of a medical-surgical se-ries of 266 patients.
Dig Dis Sci 1992;37(3):3406 .
95. Bradley EL 3rd. The natural history of splenic vein
thrombosis due to chronicpancreatitis: indications for surgery. Int
J Pancreatol 1987;2(2):8792 .
96. Butler JR, Eckert GJ, Zyromski NJ, et al. Natural history of
pancreatitis-inducedsplenic vein thrombosis: a systematic review
and meta-analysis of its incidenceand rate of gastrointestinal
bleeding. HPB (Oxford) 2011;13(12):83945 .
97. Weber SM, Rikkers LF. Splenic vein thrombosis and
gastrointestinal bleeding inchronic pancreatitis. World J Surg
2003;27(11):12714 .
98. Agarwal AK, Raj Kumar K, Agarwal S, et al. Significance of
splenic vein throm-bosis in chronic pancreatitis. Am J Surg
2008;196(2):14954 .
99. Sakorafas GH, Sarr MG, Farley DR, et al. The significance of
sinistral portal hy-
pertension complicating chronic pancreatitis. Am J Surg
2000;179(2):12933 .
Henry et al388
http://refhub.elsevier.com/S1089-3261(14)00003-8/sref83http://refhub.elsevier.com/S1089-3261(14)00003-8/sref83http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref85http://refhub.elsevier.com/S1089-3261(14)00003-8/sref85http://refhub.elsevier.com/S1089-3261(14)00003-8/sref85http://refhub.elsevier.com/S1089-3261(14)00003-8/sref86http://refhub.elsevier.com/S1089-3261(14)00003-8/sref86http://refhub.elsevier.com/S1089-3261(14)00003-8/sref86http://refhub.elsevier.com/S1089-3261(14)00003-8/sref87http://refhub.elsevier.com/S1089-3261(14)00003-8/sref87http://refhub.elsevier.com/S1089-3261(14)00003-8/sref87http://refhub.elsevier.com/S1089-3261(14)00003-8/sref88http://refhub.elsevier.com/S1089-3261(14)00003-8/sref88http://refhub.elsevier.com/S1089-3261(14)00003-8/sref88http://refhub.elsevier.com/S1089-3261(14)00003-8/sref89http://refhub.elsevier.com/S1089-3261(14)00003-8/sref89http://refhub.elsevier.com/S1089-3261(14)00003-8/sref90http://refhub.elsevier.com/S1089-3261(14)00003-8/sref90http://refhub.elsevier.com/S1089-3261(14)00003-8/sref90http://refhub.elsevier.com/S1089-3261(14)00003-8/sref91http://refhub.elsevier.com/S1089-3261(14)00003-8/sref91http://refhub.elsevier.com/S1089-3261(14)00003-8/sref91http://refhub.elsevier.com/S1089-3261(14)00003-8/sref92http://refhub.elsevier.com/S1089-3261(14)00003-8/sref92http://refhub.elsevier.com/S1089-3261(14)00003-8/sref93http://refhub.elsevier.com/S1089-3261(14)00003-8/sref93http://refhub.elsevier.com/S1089-3261(14)00003-8/sref93http://refhub.elsevier.com/S1089-3261(14)00003-8/sref94http://refhub.elsevier.com/S1089-3261(14)00003-8/sref94http://refhub.elsevier.com/S1089-3261(14)00003-8/sref94http://refhub.elsevier.com/S1089-3261(14)00003-8/sref95http://refhub.elsevier.com/S1089-3261(14)00003-8/sref95http://refhub.elsevier.com/S1089-3261(14)00003-8/sref96http://refhub.elsevier.com/S1089-3261(14)00003-8/sref96http://refhub.elsevier.com/S1089-3261(14)00003-8/sref96http://refhub.elsevier.com/S1089-3261(14)00003-8/sref97http://refhub.elsevier.com/S1089-3261(14)00003-8/sref97http://refhub.elsevier.com/S1089-3261(14)00003-8/sref98http://refhub.elsevier.com/S1089-3261(14)00003-8/sref98http://refhub.elsevier.com/S1089-3261(14)00003-8/sref99http://refhub.elsevier.com/S1089-3261(14)00003-8/sref99http://refhub.elsevier.com/S1089-3261(14)00003-8/sref99http://refhub.elsevier.com/S1089-3261(14)00003-8/sref99http://refhub.elsevier.com/S1089-3261(14)00003-8/sref98http://refhub.elsevier.com/S1089-3261(14)00003-8/sref98http://refhub.elsevier.com/S1089-3261(14)00003-8/sref97http://refhub.elsevier.com/S1089-3261(14)00003-8/sref97http://refhub.elsevier.com/S1089-3261(14)00003-8/sref96http://refhub.elsevier.com/S1089-3261(14)00003-8/sref96http://refhub.elsevier.com/S1089-3261(14)00003-8/sref96http://refhub.elsevier.com/S1089-3261(14)00003-8/sref95http://refhub.elsevier.com/S1089-3261(14)00003-8/sref95http://refhub.elsevier.com/S1089-3261(14)00003-8/sref94http://refhub.elsevier.com/S1089-3261(14)00003-8/sref94http://refhub.elsevier.com/S1089-3261(14)00003-8/sref94http://refhub.elsevier.com/S1089-3261(14)00003-8/sref93http://refhub.elsevier.com/S1089-3261(14)00003-8/sref93http://refhub.elsevier.com/S1089-3261(14)00003-8/sref93http://refhub.elsevier.com/S1089-3261(14)00003-8/sref92http://refhub.elsevier.com/S1089-3261(14)00003-8/sref92http://refhub.elsevier.com/S1089-3261(14)00003-8/sref91http://refhub.elsevier.com/S1089-3261(14)00003-8/sref91http://refhub.elsevier.com/S1089-3261(14)00003-8/sref91http://refhub.elsevier.com/S1089-3261(14)00003-8/sref90http://refhub.elsevier.com/S1089-3261(14)00003-8/sref90http://refhub.elsevier.com/S1089-3261(14)00003-8/sref90http://refhub.elsevier.com/S1089-3261(14)00003-8/sref89http://refhub.elsevier.com/S1089-3261(14)00003-8/sref89http://refhub.elsevier.com/S1089-3261(14)00003-8/sref88http://refhub.elsevier.com/S1089-3261(14)00003-8/sref88http://refhub.elsevier.com/S1089-3261(14)00003-8/sref88http://refhub.elsevier.com/S1089-3261(14)00003-8/sref87http://refhub.elsevier.com/S1089-3261(14)00003-8/sref87http://refhub.elsevier.com/S1089-3261(14)00003-8/sref87http://refhub.elsevier.com/S1089-3261(14)00003-8/sref86http://refhub.elsevier.com/S1089-3261(14)00003-8/sref86http://refhub.elsevier.com/S1089-3261(14)00003-8/sref86http://refhub.elsevier.com/S1089-3261(14)00003-8/sref85http://refhub.elsevier.com/S1089-3261(14)00003-8/sref85http://refhub.elsevier.com/S1089-3261(14)00003-8/sref85http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref84http://refhub.elsevier.com/S1089-3261(14)00003-8/sref83http://refhub.elsevier.com/S1089-3261(14)00003-8/sref83