Embed Size (px)
Citation preview

Nutrit ion Therapyfor ALI and ARDS
Anna Krzak, RDa, Melissa Pleva, PharmDb,Lena M. Napolitano, MDc,*
KEYWORDS
� Nutrition therapy � Enteral nutrition� Acute respiratory distress syndrome � Acute lung injury
The importance of nutrition support in critically ill patients with acute lung injury (ALI)and acute respiratory distress syndrome (ARDS) cannot be overstated. ALI and ARDSare characterized by a proinflammatory response associated with hypercatabolismthat could lead to significant nutrition deficits. Nutrition support is necessary toprevent cumulative caloric deficits, malnutrition, loss of lean body mass, and deterio-ration of respiratory muscle strength.1–3 Furthermore, early delivery of enteral nutrition(EN) has been associated with modulation of stress and the systemic immuneresponse as well as attenuation of disease severity.1 Such factors make the deliveryof EN in critically ill patients, particularly in high-risk patients, such as those with ALIand ARDS, a vital component of quality care and management.
NUTRITION REQUIREMENTS AND SUBSTRATE USE
Although the importanceof nutrition in this patient population iswidely accepted, deter-mining nutrition requirements and designing a nutrition support regimen is challenging.Secondary diagnoses in patients with ALI and ARDS, such as sepsis, trauma, majorsurgery, and multisystem organ failure, significantly alter metabolism.4,5 Variouscomorbidities, sedation, and neuromuscular blockade use further complicate compre-hensive assessment of energy expenditure and implementation of a safe and appro-priate nutrition support regimen.5
Determining Energy Requirements
The many metabolic and nutrition-related manifestations associated with ALI, ARDS,and common secondary diagnoses make standard equations for determining energyexpenditure highly inaccurate.4 Indirect calorimetry (IC) is considered the gold standard
Conflicts of interests: none.a Nutrition Services, University of Michigan Health System, Ann Arbor, MI, USAb Department of Pharmacy Services, University of Michigan Health System, Ann Arbor, MI, USAc Division of Acute Care Surgery, Department of Surgery, University of Michigan Health System,1500 East Medical Center Drive, 1C340A-UH, SPC 5033, Ann Arbor, MI 48109–5033, USA* Corresponding author.E-mail address: [email protected]
Crit Care Clin 27 (2011) 647–659doi:10.1016/j.ccc.2011.05.004 criticalcare.theclinics.com0749-0704/11/$ – see front matter � 2011 Published by Elsevier Inc.

Krzak et al648
for assessing energy requirements.1 Unfortunately, because of cost and lack of trainedpersonnel, IC is frequently unavailable. Even when available, technical factors, such asFiO2 greater than or equal to 60%, positive end expiratory pressure greater than 12 cmH2O, and hyperventilation/hypoventilation (acute changes altering body CO2 stores),prohibit accurate study measurement.4,5 When available, IC captures shifts in metab-olism during critical illness, allowing clinicians to design safe and appropriate nutritionsupport regimens while minimizing complications of underfeeding or overfeeding.4,5
Although traditionally respiratory quotient was thought to represent substrate use, itis nowmore often used to confirm the validity of the study.4 Ideally, the aim is to obtainIC at baseline and repeat when the patient clinical status changes in an effort to providethe safest and most appropriate nutrition therapy.4,5
Hypercapnia and Substrate Use
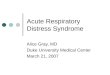
Previously, high carbohydrate provision was considered most detrimental in terms ofhypercapnia associated with overfeeding. However, Talpers and colleagues6 demon-strated that increasing caloric provision rather than excessive carbohydrate substratecorrelated more closely with CO2 production (Fig. 1). When the carbohydrate-to-fat-calorie ratio was constant, increasing total calorie intake resulted in a statisticallysignificant increase in VCO2 production.
6
Before the Talpers and colleagues study in 1992, a study (n5 20) reported a reductionin duration of mechanical ventilation with the use of a high-fat, low-carbohydrate formulacomparedwith a standard formula.1,7,8 Additional reviewof other pertinent literature on thissubject demonstrates no improvement in CO2 production or improved outcomes corre-latedwith use of high-fat, low-carbohydrate formulas.1,7,8 Moreover, the American Societyfor Parenteral and Enteral Nutrition (ASPEN)/Society of Critical Care Medicine (SCCM)consensus guidelines for nutrition support therapy in adult, critically ill patients publishedin 2009, state that, “Specialty high-lipid low-carbohydrate formulations designed to ma-nipulate the respiratory quotient and reduce CO2 production are not recommended forroutine use in [intensive care unit] ICU patients with acute respiratory failure.”1
Because of a high risk of CO2 retention, patients with ALI and ARDS on nutritionsupport should be frequently monitored for signs of underfeeding or overfeeding. Atten-tion should be paid to unanticipated acid/base changes or difficulty weaningfrom mechanical ventilation.5 Nutrition requirements for these patients should be
Fig. 1. Effect of carbohydrate versus total calories on CO2 production. Increasing caloricprovision rather than excessive carbohydrate substrate correlated more closely with CO2
production. When carbohydrate-to-fat-calorie ratio was constant, increasing total calorieintake resulted in a statistically significant increase in VCO2 production. Abbreviations: CHO,carbohydrate; REE, resting energy expenditure. (Adapted from Talpers SS, Romberger DJ,Bunce SB, et al. Nutritionally associated increased carbon dioxide production. Excess totalcalories vs high proportion of carbohydrate calories. Chest 1992;102:551–5; with permission.)

Nutrition Therapy for ALI and ARDS 649
reevaluated and the nutrition support regimen adjusted frequently as indicated by thepatients’ clinical status.
Complications of Underfeeding and Overfeeding
The fundamental goal of providing adequate nutrition support therapy to critically illpatients is to avoid gross underfeeding or overfeeding. The metabolic implicationscharacteristic of ALI and ARDS place these patients at higher risk for complicationsrelated to underfeeding or overfeeding (Table 1). Deleterious effects of underfeedingin patients with ALI and ARDS, such as a reduction in respiratory muscle strength andventilatory drive, could lead to failure to wean from mechanical ventilation.9 Under-feeding is also associated with immunosuppression, poor wound healing, andincreased risk of nosocomial infections.9 The effects of inadequate nutrition in criticallyill patients are more frequently highlighted, but it should be recognized that over-feeding may also lead to undesirable outcomes. Similar to the consequences ofunderfeeding, hypercapnia resulting from overfeeding may delay ventilator weaning.9
Stress hyperglycemia, which is common in critically ill patients, is exacerbated byoverfeeding and may also prolong wound healing and increase risk of infection.9
TIMING OF THERAPY: EARLY ENTERAL NUTRITION
Early initiation of enteral nutrition in critical illness is important to achieve clinicalbenefit. See Box 1 for a summary of the clinical benefits of early enteral nutrition.Once patients are fluid resuscitated and hemodynamically stable, enteral nutritionshould be initiated within 24 to 48 hours and advanced to goal over the next 48 to72 hours.1,10,11 Feeding initiated within 24 to 72 hours of ICU admission, comparedwith feeding started later, is associated with reduced gastrointestinal permeability;reduced activation and release of inflammatory cytokines; and decreased infectiousmorbidity, mortality, and hospital length of stay.1,10,11
ROUTE OF DELIVERY (GASTRIC VS SMALL-BOWEL FEEDS)
The most appropriate route of delivery of enteral nutrition is an area of intense debate.Although small-bowel feeding may decrease the incidence of gastroesophagealreflux, meta-analyses evaluating gastric and small-bowel feeding reported no
Table 1Complications of underfeeding and overfeeding
Underfeeding Overfeeding
Decreased ventilatory drive Hypercapnia
Depressed respiratory musclestrength
Azotemia
Failure to wean frommechanicalventilation
Failure towean frommechanicalventilation
Immunosuppression Electrolyte imbalances
Poor wound healing Hyperglycemia
Infections Infections
Poor wound healing
Immunosuppression
Hepatic steatosis
Data from Refs.3,6,9

Box 1
Benefits of early enteral nutrition
Attenuation of hypercatabolism
Decreased gastrointestinal permeability
Improved hepatic and visceral blood flow
Reduced activation and release of inflammatory cytokines
Decreased infectious morbidity
Decreased mortality
Shorter hospital length of stay
Data from Refs.1,10,11
Krzak et al650
significant difference in pneumonia, ICU length of stay, or mortality.12–15 Some of thebenefits of gastric feeding include ease of tube placement and earlier feedinginitiation.13 In fact, ASPEN/SCCM guidelines recognize that gastric feeding is appro-priate for many critically ill patients.1 However, at the height of critical illness, patientsare prone to gastrointestinal dysfunction, gastroparesis, and potential feedingintolerance.1 Therefore, small-bowel feeding tube placement should be consideredfor high-risk patients, particularly those with a history of aspiration or intolerance togastric feeding.1,5 Frequent withholding of EN because of elevated gastric residualvolumes also warrants evaluation for small-bowel feeding.1
SPECIAL CONSIDERATIONS FOR NUTRITION SUPPORT IN ALI AND ARDS
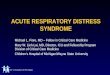
ALI and ARDS are characterized by a persistent production of oxygen free radicalsand arachidonic acid (AA)-derived inflammatory mediators.16–20 These mediatorsresult in lung inflammation, edema, and diffuse alveolar damage. A key aim in treatingpatients with ALI and ARDS is to modulate pulmonary inflammation and permeabilitycharacteristic of the disease, thereby improving oxygenation.16 A diet enriched witheicosapentaenoic acid (EPA) and g-linolenic acid (GLA) has been shown to modifythe availability of AA in tissue and cell phospholipids as well as stimulate proinflam-matory eicosanoid production from AA.16–20 Additionally, EPA shifts production ofcytokines from the highly proinflammatory 4-series leukotrienes and dienoic prosta-glandins to the less-inflammatory 5-series leukotrienes and trienoic prostaglandins.Through a series of pathways, GLA is metabolized to prostaglandin E1, a potent vaso-dilator of pulmonary and systemic circulation. Consequently, a combination of EPAand GLA may favorably reduce the pulmonary inflammatory response and supportvasodilation and oxygenation (Fig. 2).16–20
CLINICAL TRIALS WITH IMMUNE-MODULATING NUTRITION IN ALI/ARDS
Several studies in patients with ALI or ARDS have shown that the use of omega-3 fattyacids, specifically EPA and GLA, and antioxidants may prevent oxidative cellularinjury, modify the metabolic response caused by stress, and modulate immunityand inflammation.16–20 This specialized nutrition support therapy was associatedwith improved outcomes, including improved ventilation and oxygenation, shorterICU length of stay, and decreased morbidity and mortality.21–23

Fig. 2. Pathophysiology: metabolism of omega-6 fatty acids and omega-3 fatty acids. Themajor product of omega-6 fatty acid metabolism is arachidonic acid. Cyclooxygenase and lip-oxygenase enzymes use arachidonic acid to form prostaglandins of the 2 series and leukotri-enes of the 4 series. These compounds are known to be proinflammatory. The metabolites ofomega-3 fatty acids (primarily EPA and docosahexaenoic acid) compete with arachidonicacid for use of the same enzymes. As a result, more omega-3 fatty acids lead to both anincrease in antiinflammatory mediators and a decrease in proinflammatory mediators.(Created by Todd W. Rice, MD, MSc and Arthur P. Wheeler, MD and Presented at A.S.P.E.N.Clinical Nutrition Week 2011; with permission.)
Nutrition Therapy for ALI and ARDS 651
Three prospective, randomized clinical trials highlighted the use of omega-3 fattyacids and antioxidants in patients with ALI and ARDS. Two of these studies weresingle-center studies and one study was completed at 5 sites in the United States.The sample size in each study ranged from 100 to 165 patients. All three trials fol-lowed a similar study design comparing a diet enriched with EPA, GLA, and antioxi-dants (Oxepa; Abbott Nutrition, Abbott Laboratories, Columbus, OH, USA) with anisocaloric and isonitrogenous control diet (Pulmocare; Abbott Nutrition, AbbottLaboratories).4,5,9,16
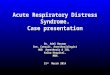
In a meta-analysis of these 3 trials, the diet enriched with EPA, GLA, and antioxi-dants was associated with the following outcomes: (1) a 60% reduction in 28-day,in-hospital, all-cause mortality (odds ratio [OR] 0.404; 95% confidence interval [CI]0.241–0.678; P 5 .001); (2) a mean increase of 4.9 ventilator-free days; (3) a meanincrease of 4.3 ICU-free days; (4) an 83% reduction in the risk of developing new organfailures, (The study reported by Singer and colleagues was excluded because it didnot assess the development of new organ failures); and (5) improvement in oxygena-tion status (Figs. 3 and 4).16,21–23
However, a recent study reported different findings. The ARDSNet EDEN-Omegastudy was entitled “Early Versus Delayed Enteral Feeding and Omega-3 Fatty Acid/Antioxidant Supplementation for Treating People With Acute Lung Injury or AcuteRespiratory Distress Syndrome.”24 This phase III clinical trial was a prospective,randomized trial of initial trophic enteral feeding followed by advancement to full-calorie enteral feeding versus early advancement to full-calorie enteral feeding. Thistrial was run simultaneously with a trial of omega-3 fatty acid, GLA, and antioxidant

Fig. 3. Effect of inflammation-modulating diet on mortality in ALI/ARDS. Effect of the EPA and GLA diet when compared with the control diet on28-day, in-hospital, all-cause mortality. Data are presented as OR for each study (boxes), 95% CI (horizontal lines), and summary as OR with 95% CI(diamond). (Adapted from Pontes-Arruda A, Demichele S, Seth A, et al. The use of an inflammation-modulating diet in patients with acute lung injuryor acute respiratory distress syndrome: a meta-analysis of outcome data. JPEN J Parenter Enteral Nutr 2008;32:596; with permission.)
Krza
ketal
652

Fig. 4. Effect of inflammation-modulating diet on ventilator-free (A) and ICU-free days (B) in patients with ALI and ARDS. Std diff, standard difference.(Adapted from Pontes-Arruda A, Demichele S, Seth A, et al. The use of an inflammation-modulating diet in patients with acute lung injury or acuterespiratory distress syndrome: a meta-analysis of outcome data. JPEN J Parenter Enteral Nutr 2008;32:596; with permission.)
Nutritio
nTherapyforALI
andARDS
653

Krzak et al654
supplementation versus comparator enteral solution. The primary outcome measureswere number of ventilator-free days and mortality before hospital discharge with un-assisted breathing. This trial added an omega-3 fatty acid and antioxidant supplementto usual feeding (did not use a commercially available product). This difference isimportant in this trial design from prior studies in that it separated the immune-modulating nutrients from the continuous delivery of EN.Participants assigned to initial minimal enteral feedings received feedings at 10
mL/h and continued at this rate for 144 hours, provided that the participant remainedon mechanical ventilation. After 144 hours, the feeding rate was advanced to thefull-calorie target rate. Participants assigned to initial full-calorie enteral feedingsreceived feedings at 25 mL/h, and the feeding rate was increased by 25 mL in-crements every 6 hours until the goal rate was reached. Omega-3 fatty acid, antiox-idant, and placebo supplements were administered with a syringe into theparticipant’s feeding tube every 12 hours until day 21 or discontinuation of theventilator.The Data Safety and Monitoring Board performed an interim analysis and examined
the data of the EDEN-Omega study. The study was terminated early for futility. Ina brief report in Surgery News,25 the preliminary data was reviewed. The mortalityrate at 60 days was significantly lower at 16.3% in the control group versus 26.6%in the experimental cohort (P 5 .05). In addition, patients randomized to the omega-3 fatty acid–supplement group had significantly fewer ventilator-free days within 28days (14.6 days, compared with 17.4 days for the control group, P 5 .03) and signif-icantly fewer ICU-free days within 28 days (13.9 days, compared with 16.8 days for thecontrol group, P 5 .02; Tables 2 and 3). Further review of the data from this prospec-tive clinical trial awaits peer-reviewed publication.
CONTROVERSIES WITH IMMUNE-MODULATING NUTRITION IN ALI/ARDS
Despite several reports regarding the positive effects of omega-3 fatty acids on the inflam-matory response in patients with ALI and ARDS, there are still areas of uncertainty andcontroversy.First, in the original 3 trials on omega-3 fatty acids, the medical management of the
patients is not consistently controlled or reported. The recent ARDSNet EDEN-Omegastudy was the first to report important components of medical management, such asfluid therapy and tidal volume.5,16,24
Second,many studies on the use of enteral omega-3 fatty acids used a comparatorformula (Pulmocare) that was high in fat and low in carbohydrate. The fat source in thiscomparator formula is primarily omega-6 fatty acids.16 Omega-6 fatty acids have beenassociated with proinflammatory characteristics in critically ill patients.1,26–28 It couldbe presumed that the results reported in studies using this high-fat, low-carbohydrateformula as the control were distorted because of the potential proinflammatory char-acteristics of omega-6 fatty acids.Third, timing of initiation of therapy, optimal dose, and duration of therapy remain
uncertain. As previously mentioned, early delivery of EN is pivotal to obtain clinicalbenefit.1,10,11 The same is true when using immune-modulating, specialized nutritionsupport. Studies suggest that delivery of more than 50% to 65% of goal calories ismore closely associated with positive outcomes of EN, when compared with lowercalorie provision.1 The period of time needed from delivery to clinical effect mayvary based on the dose and the route of delivery. See Table 3 for more informationregarding the dosing ranges of EPA, docosahexaenoic acid, and GLA in importanttrials. Additional studies are needed to come to a definitive conclusion.

Table 2Antiinflammatory immune-modulating enteral nutrition versus standard enteral nutrition in ALI, ARDS, and sepsis
Study Population Study Groups Mortality LOS Days, Mean ± SD Ventilator Days, Mean ± SD New Organ Dysfunction
Gadek et al,21 1999 ARDS (n 5 146) EPA/GLA/AOControl ENEPA/GLA/AOControl EN
11/70 (16%)19/76 (25%)ICU mortality
11.0 � 0.9 ICUa
14.8 � 1.3 ICU27.9 � 2.1 Hospital31.1 � 2.4 Hospital
9.6 � 0.9a
13.2 � 1.47/70 (10%)a
19/76 (25%)
Singer et al,22 2006 ARDS and ALI(n 5 100)
EPA/GLA/AOControl EN
14/46 (30%)a
26/49 (53%)28d mortality
13.5 � 11.8 ICU15.6 � 11.8 ICU
12.1 � 11.314.7 � 12.0
NR
Pontes-Arrudaet al,23 2006
Severe sepsis(n 5 165)
EPA/GLA/AOControl EN
26/83 (31%)a
38/82 (46%) 28dmortality
17.2 � 4.9 ICUa
23.4 � 3.5 ICU14.6 � 4.3a
22.2 � 5.132/83 (39%)a
66/82 (80%)
Abbreviations: AO, antioxidants; EN, enteral nutrition; EPA, eicosapentaenoic acid; GLA, g-linolenic acid; LOS, length of stay; NR, not reported; SD, standarddeviation.
a P �.05.Data from McClave SA, Martindale RG, Vanek VW, et al; A.S.P.E.N. Board of Directors; American College of Critical Care Medicine; Society of Critical Care
Medicine. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM)and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2009;33(3):277–316.
Nutritio
nTherapyforALI
andARDS
655

Table 3Summary of clinical studies
Gadek et al21 Singer et al22Pontes-Arruda et al23
ARDSNetEDEN-Omega24
Design P, R, C, DBFull feeds
P, R, CFull feeds
P, R, C, DBFull feeds
P, R, CFull feeds/trophic feeds
Setting Multicenter Single center Single center Multicenter
Patients 146 ARDS 100 ALI 165 severe sepsis/septic shock
272 ALI/ARDS
Interventions Omega-3FA 1 AO
Omega-3FA 1 AO
Omega-3FA 1 AO
Omega-3FA 1 AO
Mean fatty-acid intake
EPA (g/d) 6.9 5.4 4.9 6.8
DHA (g/d) 2.9 2.5 2.2 3.4
GLA (g/d) 5.8 5.1 4.6 5.9
Omega-3delivery
Continuous Continuous Continuous Bolus BID
Controlformula
High fat(omega-6, 9)
High fat(omega-6, 9)
High fat(omega-6, 9)
High carbohydrate
Tidal volume Uncontrolled Uncontrolled Uncontrolled 6 mL/kg PBW
Fluid therapy Uncontrolled Uncontrolled Uncontrolled Conservative
Outcomesa
Improvedoxygenation
X X X —
Reducedvent days
X X X X
Reduced ICUlength of stay
X X X X
Reduced neworgan failure
X Not assessed X —
Reduced 28-daymortality
— X X —
Abbreviations: AO, antioxidants; C, controlled; CD, control diet; DB, double blind; DHA, docosa-hexaenoic acid; EPA, eicosapentaenoic acid; FA, fatty acid; GLA, g-linolenic acid; P, prospective;PBW, predicted body weight; R, randomized.
a X: statistically significant (P<.05) for EPA 1 GLA versus control diet.Data from Pontes-Arruda A, Demichele S, Seth A, et al. The Use of an inflammation-modulating
diet in patients with acute lung injury or acute respiratory distress syndrome: a meta-analysis ofoutcome data. JPEN J Parenter Enteral Nutr 2008;32:596.
Krzak et al656
RECOMMENDATIONS FOR NUTRITION SUPPORT IN CRITICALLY ILL PATIENTS WITHALI AND ARDSGeneral
� EN is preferred when the gastrointestinal tract is functional.� Initiate early EN after patients are resuscitated.� Initiate within 24 to 48 hours and advance to the goal over the next 48 to 72hours.
� Withhold EN if patients are hypotensive or on increasing doses of vasopressors.� Polymeric formula is preferred.

Nutrition Therapy for ALI and ARDS 657
� Either gastric or small-bowel feeds are acceptable.� Consider small-bowel feeding tube placement in high-risk patients with historyof aspiration or intolerance to gastric feeding.
� Consider prokinetics in patients with feeding intolerance.� Provide antioxidants and trace minerals.� Fluid-restricted formulas should be considered in patients with respiratory failure.� Aggressively replace phosphorus in patients with normal renal function.
Evidence-based consensus guidelines on nutrition support in adult, critically illpatients endorse the following:
ASPEN/SCCM Guidelines
The ASPEN/SCCM Guidelines for the Provision and Assessment of Nutrition SupportTherapy in the Adult Critically Ill Patient published in 20091,2 recommend the following:
Patients with ARDS and severe ALI should be placed on an enteral formulationcharacterized by an anti-inflammatory lipid profile (ie, omega-3 fish oils, borageoil) and antioxidants.
Canadian Clinical Practice Guidelines
The “Canadian Clinical Practice Guidelines for Nutrition Support in MechanicallyVentilated, Critically Ill Adult Patients,” published in the January 2009 update, recom-mends the following:10
“Based on one level 1 study and four level 2 studies, we recommend the use of anenteral formula with fish oils, borage oils and antioxidants in patients with ALI andARDS.”
SUMMARY
Nutrition support is a critical component of care in patients with ALI/ARDS. Early ENsupport is recommended, using either gastric or small-bowel feeding dependent onpatient tolerance. Indirect calorimetry is the ideal method for determination of caloricrequirements in patients with ALI/ARDS. Specialized nutrition support, with an enteraldiet enriched with omega-3 fatty acid, GLA, and antioxidant supplementation, shouldbe considered in patients with ALI and ARDS based on the available clinical trial data.However, results from the recent ARDSNet EDEN-Omega study are not yet published.The optimal dosage, composition of fatty acids, and the ratio of individual immune-modulating nutrients in specialized enteral formulations remain controversial.
REFERENCES
1. McClave SA, Martindale RG, Vanek VW, et al, A.S.P.E.N. Board of Directors,American College of Critical Care Medicine, Society of Critical Care Medicine.Guidelines for the provision and assessment of nutrition support therapy in theadult critically ill patient: Society of Critical Care Medicine (SCCM) and AmericanSociety for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter EnteralNutr 2009;33(3):277–316.
2. Martindale RG, McClave SA, Vanek VW, et al, American College of Critical CareMedicine, A.S.P.E.N. Board of Directors. Guidelines for the provision and assess-ment of nutrition support therapy in the adult critically ill patient: Society of Critical

Krzak et al658
Care Medicine and American Society for Parenteral and Enteral Nutrition: execu-tive summary. Crit Care Med 2009;37(5):1757–61.
3. Fraser IM. Effects of refeeding on respiration and skeletal muscle function. ClinChest Med 1986;7:131–9.
4. Wooley JA, Sax HC. Indirect calorimetry: applications to practice. Nutr Clin Pract2003;18(5):434–9.
5. Turner KL, Moore FA, Martindale RG. Nutrition support for the acute lung injury/adult respiratory distress syndrome patient: a review. Nutr Clin Pract 2011;26:14.
6. Talpers SS, Romberger DJ, Bunce SB, et al. Nutritionally associated increasedcarbon dioxide production. Excess total calories vs high proportion of carbohy-drate calories. Chest 1992;102:551–5.
7. al-Saady NM, Blackmore CM, Bennett ED. High fat, low carbohydrate, enteralfeeding lowers PaCO2 and reduces the period of ventilation in artificially venti-lated patients. Intensive Care Med 1989;15:290–5.
8. Barale F, Verdy S, Boillot A, et al. Calorimetric study of enteral low-carbohydratediet in patients with respiratory insufficiency and decompensation. Agressologie1990;31:77–9.
9. McClave SA. The consequences of overfeeding and underfeeding. J Respir CarePract 1997;10:57–64.
10. Heyland DK, Dhaliwal R, Drover JW, et al, Canadian Critical Care Clinical Prac-tice Guidelines Committee. Canadian clinical practice guidelines for nutritionsupport in mechanically ventilated, critically ill adult patients. JPEN J ParenterEnteral Nutr 2003;27(5):355–73. Update January 2009. Available at: http://www.criticalcarenutrition.com/docs/cpg/srrev.pdf. Accessed April 24, 2011.
11. Marik PE, Zaloga GP. Early enteral nutrition in acutely ill patients: a systematicreview. Crit Care Med 2001;29:2264–70.
12. Heyland DK, Drover JW, MacDonald S, et al. Effect of postpyloric feeding ongastroesophageal regurgitation and pulmonary microaspiration: results ofa randomized controlled trial. Crit Care Med 2001;29:1495–501.
13. Ho KM, Dobb GJ, Webb SA. A comparison of early gastric and post-pyloric feedingin critically ill patients: a meta-analysis. Intensive Care Med 2006;32:639–49.
14. Marik PE, Zaloga GP. Gastric versus post-pyloric feeding: a systematic review.Crit Care 2003;7:R46–51.
15. Heyland DK, Drover JW, Dhaliwal R, et al. Optimizing the benefits and minimizingthe risks of enteral nutrition in the critically ill: role of small bowel feeding. JPEN JParenter Enteral Nutr 2002;26(Suppl 6):S51–5.
16. Pontes-Arruda A, Demichele S, Seth A, et al. The use of an inflammation-modulating diet in patients with acute lung injury or acute respiratory distresssyndrome: a meta-analysis of outcome data. JPEN J Parenter Enteral Nutr2008;32:596.
17. DeMichele SJ, Wood SM, Wennberg AK. A nutritional strategy to improveoxygenation and decrease morbidity in patients who have acute respiratorydistress syndrome. Respir Care Clin N Am 2006;12:547–66.
18. Mizock BA. Nutritional support in acute lung injury and acute respiratory distresssyndrome. Nutr Clin Pract 2001;16:319–28.
19. Mizock BA, DeMichele SJ. The acute respiratory distress syndrome: role of nutri-tional modulation through dietary lipids. Nutr Clin Pract 2004;19:563–74.
20. Nelson JL, DeMichele SJ, Pacht E, et al, Enteral Nutrition in ARDS Study Group.Effect of enteral feeding with eicosapentaenoic acid, gamma-linolenic acid, andantioxidants on antioxidant status in patients with acute respiratory distresssyndrome. JPEN J Parenter Enteral Nutr 2003;27:98–104.

Nutrition Therapy for ALI and ARDS 659
21. Gadek JE, DeMichele SJ, Karlstad MD, et al. Effect of enteral feeding with eico-sapentaenoic acid, gamma-linolenic acid, and antioxidants in patients with acuterespiratory distress syndrome. Crit Care Med 1999;27:1409–20.
22. Singer P, Theilla M, Fisher H, et al. Benefit of an enteral diet enriched with eico-sapentaenoic acid and gamma-linolenic acid in ventilated patients with acutelung injury. Crit Care Med 2006;34:1033–8.
23. Pontes-Arruda A, Aragao AM, Albuquerque JD. Effects of enteral feeding witheicosapentaenoic acid, gamma-linolenic acid, and antioxidants in mechanicallyventilated patients with severe sepsis and septic shock. Crit Care Med 2006;34:2325–33.
24. Early versus delayed enteral feeding and omega-3 fatty acid/antioxidant supple-mentation for treating people with acute lung injury or acute respiratory distresssyndrome (The EDEN-Omega Study). Available at: http://clinicaltrials.gov/ct2/show/NCT00609180. Accessed April 24, 2011.
25. Available at: http://www.facs.org/surgerynews/1209.pdf. Accessed April 24,2011.
26. Battistella FD, Widergren JT, Anderson JT, et al. A prospective, randomized trialof intravenous fat emulsion administration in trauma victims requiring total paren-teral nutrition. J Trauma 1997;43:52–8.
27. Mayer K, Kiessling A, Ott J, et al. Acute lung injury is reduced in fat-1 miceendogenously synthesizing n-3 fatty acids. Am J Respir Crit Care Med 2009;179:474–83.
28. Pluess T, Hayoz D, Berger MM, et al. Intravenous fish oil blunts the physiologicalresponse to endotoxin in healthy subjects. Intensive Care Med 2007;33:789–97.