Embed Size (px)
Citation preview

Genitourinary
System
&
Gastrointestinal
System

Anatomy of the Urinary System
How does the urinary system work?
The body takes nutrients from food and converts them to energy. After the body has taken the food that it
needs, waste products are left behind in the bowel and in the blood.
The urinary system keeps the chemicals, such as potassium and sodium, and water in balance by removing
a type of waste called urea from the blood. Urea is produced when protein, found in meat products, is broken
down in the body. Urea is carried in the bloodstream to the kidneys.
Other important functions of the kidneys include blood pressure regulation, and the production of
erythropoietin, which controls red blood cell production in the bone marrow.
Urinary system parts and their functions:
two kidneys - a pair of purplish-brown organs located below the ribs toward the middle of the back. Their function is to:
o remove liquid waste from the blood in the form of urine.
o keep a stable balance of salts and other substances in the blood.
o produce erythropoietin, a hormone that aids the formation of red blood cells.
The kidneys remove urea from the blood through tiny filtering units called nephrons. Each nephron
consists of a ball formed of small blood capillaries, called a glomerulus, and a small tube called a
renal tubule. Urea, together with water and other waste substances, forms the urine as it passes
through the nephrons and down the renal tubules of the kidney.

two ureters - narrow tubes that carry urine from the kidneys to the bladder. Muscles in the ureter walls continually tighten and relax forcing urine downward, away from the kidneys. If urine backs up, or is allowed to stand still, a kidney infection can develop. About every 10 to 15 seconds, small amounts of urine are emptied into the bladder from the ureters.
bladder - a triangle-shaped, hollow organ located in the lower abdomen. It is held in place by ligaments that are attached to other organs and the pelvic bones.The bladder's walls relax and expand to store urine, and contract and flatten to empty urine through the urethra.
two sphincter muscles - circular muscles that help keep urine from leaking by closing tightly like a rubber band around the opening of the bladder.
nerves in the bladder - alert a person when it is time to urinate, or empty the bladder.
urethra - the tube that allows urine to pass outside the body. The brain signals the bladder muscles to tighten, which squeezes urine out of the bladder. At the same time, the brain signals the sphincter muscles to relax to let urine exit the bladder through the urethra. When all the signals occur in the correct order, normal urination occurs.
Female anatomy

Male anatomy
Facts about urine:
Adults pass about a quart and a half of urine each day, depending on the fluids and foods consumed.
The volume of urine formed at night is about half that formed in the daytime.
Normal urine is sterile. It contains fluids, salts and waste products, but it is free of bacteria, viruses and fungi.
The tissues of the bladder are isolated from urine and toxic substances by a coating that discourages bacteria from attaching and growing on the bladder wall.
Overview of Genitourinary Disorders
What does genitourinary mean?
Genitourinary is a word that refers to the urinary and genital organs.
Urology is the branch of medicine concerned with the urinary tract in both genders and the genital tract of the
reproductive system in males.
Nephrology is the branch of medicine concerned with the kidney.
What is the urinary tract?

The urinary tract includes the organ system primarily responsible for cleaning and filtering excess fluid and
waste material from the blood. The urinary system is comprised of the following:
kidneys ureters bladder urethra
The kidneys also function as glands that produce hormones necessary for building red blood cells and
regulating blood pressure.
What causes problems in the urinary system?
Problems of the urinary system include acute and chronic kidney failure, urinary tract infections, obstructions
along the urinary tract, and abnormalities present at birth.
Diseases of the kidneys often produce temporary or permanent changes to the small functional structures
and vessels inside the kidney. Frequent urinary tract infections can cause scarring to these structures
leading to renal (kidney) failure. Some diseases that cause kidney damage include:
glomerulonephritis hemolytic uremic syndrome polycystic kidney disease hydronephrosis urinary tract infections
Disorders of the urinary tract are often related to a blockage that prevents complete emptying of the bladder
and often leads to reverse flow of urine. A urinary tract obstruction can cause damage to the urinary tract and
kidneys because urine backs-up and pools in various areas along the tract. Pooling of urine in the bladder,
ureters, or kidneys can lead to infection, scarring, and long-term kidney failure. Some disorders that cause
obstruction of the urinary tract include:
megaureter posterior urethral valves ureterocele or ureteral duplication vesicoureteral reflux neurogenic bladder
Several disorders of the urinary tract only affect males, which are largely related to the male anatomy as well
as fetal development. Disorders that affect males may involve the penis, urethra, or testes. Some of the male
urogenital disorders include:
undescended testes or cryptorchidism hydrocele hypospadias inguinal hernia micropenis testicular torsion
Disorders of the genitourinary system in children are often detected by fetal ultrasound prior to birth. If not
detected on fetal ultrasound, often children will develop a urinary tract infection that will prompt your child's
physician to perform special diagnostic tests that may detect an abnormality. Some diseases of the kidney do
not reveal themselves until later in life or after a child has a bacterial infection or an immune disorder.


Overview of Kidney Disorders
How do the kidneys work?
The body takes nutrients from food and converts them to energy. After the body has taken the food that it needs, waste products are left behind in the bowel and in the blood.
The kidneys and urinary system keep chemicals, such as potassium and sodium, and water in balance by
removing a type of waste, called urea, from the blood. Urea is produced when foods containing protein, such
as meat, poultry, and certain vegetables, are broken down in the body. Urea is carried in the bloodstream to
the kidneys.
Two kidneys, a pair of purplish-brown organs, are located below the ribs toward the middle of the back. Their
function is to:
remove liquid waste from the blood in the form of urine
keep a stable balance of salts and other substances in the blood
produce erythropoietin, a hormone that aids the formation of red blood cells.
The kidneys remove urea from the blood through tiny filtering units called nephrons. There are about one
million nephrons in each kidney, located in the medulla and the cortex. Each nephron consists of a ball
formed of small blood capillaries, called a glomerulus, and a small tube called a renal tubule.
Urea, together with water and other waste substances, forms the urine as it passes through the nephrons
and down the renal tubules of the kidney. Urine collects in the calyces and renal pelvis and moves into the
ureter, where it flows down into the bladder.
In addition to filtering waste from the blood and assisting in the balance of fluids and other substances in the
body, the kidneys perform other vital functions. These functions include:
production of hormones that help to regulate blood pressure and heart function

production of corticosteroids that help to regulate kidney function and the body’s inflammatory response system
assisting in converting vitamin D into a form that can be used by the body’s tissues
What causes problems with the kidneys?
In children, problems of the urinary system include acute and chronic kidney failure, urinary tract infections,
obstructions along the urinary tract, and abnormalities present at birth.
Diseases of the kidneys often produce temporary or permanent changes to the small functional structures
and vessels inside the kidney. Frequent urinary tract infections can cause scarring to these structures
leading to renal (kidney) failure. Some diseases that cause kidney damage include:
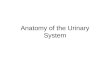
Glomerulonephritis, also known as glomerular nephritis, abbreviated GN, is a renal disease characterized by inflammation of the glomeruli, or small blood vessels in the kidneys. It may present with isolated hematuria and/or proteinuria (blood resp. protein in the urine); or as a nephrotic syndrome, a nephritic syndrome, acute renal failure, or chronic renal failure. They are categorized into several different pathological patterns, which are broadly grouped into non-proliferative or proliferative types. Diagnosing the pattern of GN is important because the outcome and treatment differs in different types. Primary causes are ones which are intrinsic to the kidney, whilst secondary causes are associated with certain infections (bacterial, viral or parasitic pathogens), drugs, systemic disorders (SLE, vasculitis) or diabetes.
Photomicrograph of a kidney biopsy from a patient with crescentic glomerulonephritis showing prominent fibrocellular crescent formation and moderate mesangial proliferation in a glomerulus. Hematoxylin and
eosin stain.
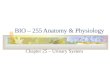
Polycystic kidney disease (PKD or PCKD, also known as polycystic kidney syndrome) is a cystic genetic disorder of the kidneys.It occurs in humans and other animals. PKD is characterized by the presence of multiple cysts (hence, "polycystic") in both kidneys. The cysts are numerous and fluid-filled cysts resulting in massive enlargement of the kidneys. The disease can also damage the liver, pancreas, and rarely, the heart and brain. The two major forms of polycystic kidney disease are distinguished by their patterns of inheritance.
Polycystic kidneys
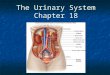
Hydronephrosis is distention and dilation of the renal pelvis and calyces, usually caused by obstruction of the free flow of urine from the kidney, leading to progressive atrophy of the kidney.

Specimen of a kidney that has undergone extensive dilation due to hydronephrosis. Note the extensive
atrophy and thinning of the renal cortex.
The signs and symptoms of hydronephrosis depend upon whether the obstruction is acute or chronic, partial or complete, unilateral or bilateral. Unilateral hydronephrosis may occur without any symptoms, while acute obstruction can cause intense pain.
Blood tests can show raised creatinine and electrolyte imbalance. Urinalysis may show an elevated pH due to the secondary destruction of nephrons within the affected kidney.
Symptoms that occur regardless of where the obstruction lies include loin or flank pain. An enlarged kidney may be palpable on examination.
Where the obstruction occurs in the lower urinary tract, suprapubic tenderness (with or without a history of bladder outflow obstruction) along with a palpable bladder are strongly suggestive of acute urinary retention, which left untreated is highly likely to cause hydronephrosis.
Upper urinary tract obstruction is characterised by pain in the flank, often radiating to either the abdomen or the groin. Where the obstruction is chronic, renal failure may also be present. If the obstruction is complete, an enlarged kidney is often palpable on examination.
Urinary tract infection (UTI) is a bacterial infection that affects any part of the urinary tract. Although urine contains a variety of fluids, salts, and waste products, it usually does not have bacteria in it.[1] When bacteria get into the bladder or kidney and multiply in the urine, they cause a UTI. The most common type of UTI is a bladder infection which is also often called cystitis. Another kind of UTI is a kidney infection, known as pyelonephritis, and is much more serious. Although they cause discomfort, urinary tract infections can usually be quickly and easily treated with a short course of antibiotics.
Disorders of the genitourinary system in children are often detected by fetal ultrasound prior to birth. If not detected on fetal ultrasound, often children will develop a urinary tract infection that will prompt your child's physician to perform special diagnostic tests that may detect an abnormality. Some diseases of the kidney do not reveal themselves until later in life or after a child has a bacterial infection or an immune disorder.
Renal Cortex

Important Terms
A
analgesic - any drug intended to alleviate pain.
B
biopsy - a procedure in which tissue samples are removed (with a needle or during surgery) from the body for examination under a microscope; to determine if cancer or other abnormal cells are present.
bladder - a triangle-shaped, hollow organ located in the lower abdomen that holds urine.
C
circumcision - surgical procedure to remove the skin covering the end of the penis, called the foreskin.
computed tomography scan (Also called a CT or CAT scan.) - a diagnostic imaging procedure that uses a combination of x-rays and computer technology to produce cross-sectional images (often called slices), both horizontally and vertically, of the body. A CT scan shows detailed images of any part of the body, including the bones, muscles, fat, and organs. CT scans are more detailed than general x-rays.
cryptorchidism (Also called undescended testes.) - a condition seen in newborns whereby one or both of the male testes has not passed down into the scrotal sac.
cystoscopy (Also called cystourethroscopy.) - an examination in which a scope, a flexible tube and viewing device, is inserted through the urethra to examine the bladder and urinary tract for structural abnormalities or obstructions, such as tumors or stones.
cystourethrogram (Also called a voiding cystogram.) - a specific x-ray that examines the urinary tract. A catheter (hollow tube) is placed in the urethra (tube that drains urine from the bladder to the outside of the body) and the bladder is filled with a liquid dye. X-ray images will be taken as the bladder fills and empties. The images will show if there is any reverse flow of urine into the ureters and kidneys.
D
dialysis - a medical procedure to remove wastes and additional fluid from the blood after the kidneys have stopped functioning.
E
electroencephalogram (EEG) - a procedure that records the brain's continuous electrical activity by means of electrodes attached to the scalp.
enuresis - involuntary discharge of urine usually during sleep at night; bedwetting beyond the age when bladder control should have been established.
epispadias - occurs when the urethral opening is in an abnormal location. In males, the opening is usually on the topside of the penis and not the tip.
exstrophy of the bladder - the bladder is essentially inside out and exposed on the outside of the abdomen. Because the bladder and other structures are exposed to the outside of the body, urine constantly trickles onto the skin causing local irritation.
glomerulonephritis - a type of glomerular kidney disease in which the kidneys' filters become inflamed and scarred, and slowly lose their ability to remove wastes and excess fluid from the blood to make urine.
glomerulosclerosis - the term used to describe scarring that occurs within the kidneys in the small balls of tiny blood vessels called the glomeruli. The glomeruli assist the kidneys in filtering urine from the blood.
H
hematuria - the presence of red blood cells in the urine.

hemolytic uremic syndrome - a rare kidney disorder that mostly affects children under the age of 10. It is often characterized by damage to the lining of blood vessel walls, destruction of red blood cells, and/or kidney failure.
horseshoe kidney - as the kidneys of the fetus arise from the pelvic area they abnormally fuse together at the lower end or base. By fusing, they form a "U" shape, which gives it the name "horseshoe."
hydronephrosis - a condition that occurs as a result of urine accumulation in the upper urinary tract. This usually occurs from a blockage somewhere along the urinary tract.
I
inguinal hernia - when a section of intestine protrudes through a weakness in the abdominal muscles in the groin area.
intravenous pyelogram (IVP ) - a series of x-rays of the kidney, ureters, and bladder with the injection of a contrast dye into the vein - to detect tumors, abnormalities, kidney stones, or any obstructions, and to assess renal blood flow.
K
kidney stone - a solid piece of material that forms from crystallization of excreted substances in the urine.
kidney transplantation - a procedure that places a healthy kidney from one person into a recipient's body.
kidneys - a pair of bean-shaped organs located below the ribs toward the middle of the back.
M
magnetic resonance imaging (MRI) - a diagnostic procedure that uses a combination of large magnets, radiofrequencies, and a computer to produce detailed images of organs and structures within the body.
megaureter - an expanded or widened ureter that does not function normally. The size of a megaureter is usually greater than 7 millimeters in diameter.
micropenis - a normally structured penis that is below the normal size range for an infant.
N
nephrectomy - surgery to remove the kidney; the most common treatment for kidney cancer.
nephrology - the medical specialty concerned with diseases of the kidneys.
nephrotic syndrome - a condition characterized by high levels of protein in the urine, low levels of protein in the blood, tissue swelling, and high cholesterol.
neurogenic bladder (Also called neuropathic bladder.) - a bladder disorder that can be caused by a tumor or other condition of the nervous system.
O
orchiopexy - a surgical repair that involves moving an unlowered testicle into the sac that holds the testicles (scrotum).
overflow incontinence - leakage that occurs when the quantity of urine produced exceeds the bladder's capacity to hold it.
P
paraphimosis - occurs when the foreskin is retracted behind the corona (or crown) of the penis and cannot be returned to the unretracted position.
phimosis - a constriction of the opening of the foreskin so that it cannot be drawn back over the tip of the penis.
polycystic kidney disease (PKD) - a genetic disorder characterized by the growth of numerous cysts filled with fluid in the kidneys.

posterior urethral valves - an abnormality of the urethra where the urethral valves, (small leaflets of tissue) have a narrow, slit-like opening that partially impedes urine outflow. Reverse flow occurs and can affect all of the urinary tract organs including the urethra, bladder, ureters, and kidneys.
priapism - inflammation of the penis.
proteinuria - large amounts of protein in the urine.
prune belly syndrome - a triad of symptoms that include multiple urinary tract abnormalities. The common abnormalities include absence of abdominal muscles, undescended testes, and abnormalities of the upper urinary tract.
R
renal angiography (Also called renal arteriography.) - a series of x-rays of the renal blood vessels with the injection of a contrast dye into a catheter, which is placed into the blood vessels of the kidney, to detect any signs of blockage or abnormalities affecting the blood supply to the kidneys.
renal ultrasound - a non-invasive test in which a transducer is passed over the kidney producing sound waves which bounce off of the kidney, transmitting a picture of the organ on a video screen. The test is used to determine the size and shape of the kidney, and to detect a mass, kidney stone, cyst, or other obstruction or abnormalities.
S
sphincter muscles - circular muscles that help keep urine from leaking by closing tightly like a rubber band around the opening of the bladder.
T
testicular torsion - a twisting of the testicles and the spermatic cord (the structure extending from the groin to the testes that contains nerves, ducts and blood vessels).
U
urea - the nitrogen part of urine produced from the breakdown of protein.
ureterocele - the portion of the ureter closest to the bladder becomes enlarged because the ureter opening is very tiny and obstructs urine outflow; urine backs up in the ureter tube.
ureteroscope - an optical device which is inserted into the urethra and passed up through the bladder to the ureter; to inspect the opening of the ureters.
ureters - two narrow tubes that carry urine from the kidneys to the bladder.
urethra - narrow channel through which urine passes from the bladder out of the body.
urethritis - infection limited to the urethra.
urinalysis - laboratory examination of urine for various cells and chemicals, such as red blood cells, white blood cells, infection, or excessive protein.
urinary incontinence - loss of bladder control.
urinary tract infection - an infection that occurs in the urinary tract; often caused by bacteria such as Escherichia coli. A urinary tract infection often causes frequent urination, pain, burning when urinating, and blood in the urine.
urology - the branch of medicine concerned with the urinary tract in both genders, and with the genital tract or reproductive system in the male.
urogenital - refers to the urinary and reproductive systems.
V
vesicoureteral reflux (VUR) - the abnormal flow of urine from the bladder back into the ureters; often as a result of a urinary tract infection or birth defect.

Gastrointestinal SystemANATOMY AND PHYSIOLOGY
Functions of the Gastrointestinal System To prepare food for absorption into the body and utilization by the cells To excrete any food material of no use to the body
Gastrointestinal System composed of: Gastrointestinal tract Accessory organs and structures
Gastrointestinal Tract Approx 4.5 meters in length Almost doubled when no muscle tone A fibromuscular tube
Gastrointestinal tract is made up of: Mouth Pharynx Esophagus Stomach Small intestine Large Intestine
Accessory organs & structures are: Salivary glands Teeth Tongue Liver Gall bladder Pancreas
Digestive Processes - 5 stages:1. Ingestion 2. Movement of food
Peristalsis3. Digestion
Mechanical Chemical
4. Absorption 5. Defecation
Mucosal layers (3) protection secretion absorption
Mouth Provides an entrance to the gastrointestinal system Initiates digestion by the mechanical breakdown of food material Normal swallowing mechanisms move the food bolus to the esophagus Mediated by Cranial nerves IX, X, and XII
Functions of the Mouth Chewing, grinding and mixing of food Formation of a bolus Initiation of digestive processes Swallowing

Taste These functions assisted by teeth, tongue, salivary glands and sensory nerve endings
Pharynx Food passes through the oropharynx and laryngopharynx to reach the esophagus Once a bolus of food reaches the pharynx swallowing is no longer voluntary
Swallowing swallowing initiates peristalsis
Peristalsis An involuntary activity of the longitudinal and circular layers of smooth muscle within the wall of the
tract Rhythmic, pulsatile contractions of these muscle layers move the contents of the tract forward
Esophagus Hollow tube connecting mouth to stomach Runs through mediastinum Attaches to the stomach just below the diaphragm Mucus membrane lining secreting protective mucoid substance
Functions of the esophagus Transport of food Movement of food by peristalsis Mechanical dispersion of food as the first part of digestion
Cardiac Sphincter A one-way valve preventing reflux of stomach contents into the esophagus Relaxes as peristaltic wave approaches so that food can enter the stomach Also known as the lower esophageal sphincter
Stomach A dilation of the intestinal tract between the esophagus and the beginning of small intestine Separated form the small intestine by the pyloric sphincter Has three regions:
1. fundus 2. body 3. pylorus
Food bolus enters the stomach moving slowly towards the pylorus (2 - 6 hours) Fluid mass in stomach called chyme Chyme pumped through pyloric sphincter into the small intestine Rate of movement of stomach contents depends on:
1. food type and consistency 2. rate of pancreatic and biliary secretions
Functions of the Stomach 1. Temporary storage 2. Mixing 3. Exocrine secretions
hydrochloric acid intrinsic factor pepsinogen mucus
4. Outflow regulation of processed food particles to the small intestine 5. Extraction of iron from food 6. Limited absorption
Control of Gastric Activity Gastric secretion is regulated by nervous and hormonal activity Gastric emptying is stimulated in response to stretch, stomach gastrin, and certain food types Gastric emptying is inhibited by reflex and hormonal activity
Small Intestine

2.5cms wide and 6m long Fills most of the abdomen Begins at the pyloric sphincter and ends with its connection to the large intestine at the ileocecal
valve 3 parts:
1. Duodenum First 25cms of small intestine Receives chyme from the stomach through the pyloric sphincter Fluids from the pancreas and gall bladder via the common bile duct Manufactures intestinal juice Susceptible to inflammatory processes
Function: Neutralizes the acidic chyme from the stomach Mixes chyme with pancreatic, biliary and intestinal secretions
2. Jejunum Jejunum – the largest section of small intestine 8 feet Absorption of Magnesium, Calcium, Iron
3. Ileum last 40cms of small intestine Chyme moves slowly towards the ileocecal valve (3 - 10 hours)
Functions of Small Intestine 1. Forward propulsion of contents 2. Major site of digestion 3. 90% absorption 4. Protection against infection 5. Hormone secretion 6. Intestinal juice secretion
Large intestine 2.5cms wide 1.5m long Stretches from ileocaecal valve to rectum Often described in 7 parts
o cecum o ascending colon o transverse colon o descending colon o sigmoid colon o rectum o anal canal
Exit tract controlled by anal sphincters Functions of the Large Intestine
o Reabsorption water and electrolytes o Microbial activity o Mass movement o Defecation – reflex action, abdo/diaphragmatic contraction o Feces
Water Inorganic salts Eplithelial cells Bacteria Undigested food
Peptic Ulcer Disease
- a hole in the mucosal wall of the esophagus, stomach or duodenum
Cause:

o increased HCl than alkaline mucus secreted by the goblet cells
Typeso esophageal ulcero gastrico duodenalo stresso drug-induced
Risk factorso Type O bloodo Type A personalityo Irregular meals/eating lateo Highly emotional
3 phases of secretiono Cephalic à smells, tastes, sees food à increased gastric secretiono Gastric à when food enters the stomacho Intestinal à when food enters the small intestines à decreased gastric secretion
Signs and symptomsGastric Duodenal
Location: Antrum (least blood supply) Small intestinesPain: Left mid-epigastric Mid-epigastricOnset: 1-3o pc 2-4o pcPain with food: (+) (-)Pain at night (-) (+)Weight Weight loss Weight gain
Diagnostic tests1. Gastroscopy2. X-Ray (UGIS – Barium swallow)
- mouth to duodenum3. Occult blood (Guaiac test)
Management:1. Antacids – alkaline substances to ↑ pH of the stomach2. H2 Blockers3. Anticholinergic4. Cytoprotectors5. Proton-pump inhibitors6. Prostaglandin agonists7. Antibiotics
Complications of PUD1. Hemorrhage/bleeding
s/s melena mgt: NPOrestlessness monitor v/sdizziness iced-saline lavage↑HR & shocks symptoms aluminum antacids
2. Perforations/s severe, sharp, abd pain mgt: NPO
tense, board-like abdomen sx↑temp rest
3. Intractability- symptoms persist despite mgt is done

Surgical management:
1. Partial gastrectomy
a. Billroth I (gastroduodenostomy) - Billroth I, more formally Billroth's operation I, is an operation in which the pylorus is removed and the distal stomach is anastomosed directly to the duodenum.
Comp: pernicious anemiadumping syndromealkaline gastritis
b. Billroth II (gastrojejunostomy) - Billroth II, more formally Billroth's operation II, is an operation in which the lower part of the stomach (antrum) is removed and a loop of small bowel (jejunum) is brought up and joined to it in a (side-to-side manner) for drainage (gastrojejunostomy).
Comp: pernicious anemiadumping syndromeless likely alkaline gastritis
c. Roux-en-Y procedure - . A surgical procedure performed to “bypass” the stomach. A smaller “pouch” is formed and becomes the functional stomach for the individual.
Comp: pernicious anemiadumping syndromerarely to manifest alkaline gastritis
Roux-en-Y image
Details of the gastric bypass procedureGastric bypass is just what the name. In a Roux-En-Y surgery, a pouch of one ounce or less is formed at the end of the esophagus. A length of intestine is then anastamosed (surgically connected) to this pouch and is called the “Roux limb”. This limb completely bypasses the stomach. The portion of intestine that is still connected to the stomach includes the pyloris, and duodenum and is now considered the “bypassed limb” This limb still contributes digestive juices from the stomach but these juices are not mixed within the Roux limb. The Roux limb and the bypassed limb join together below the stomach to form the “common channel”. Exactly where this common channel is formed depends on individual anatomical structure. It is important to know that, since digestive juices from the bypassed limb do not mix with the food passing through the Roux limb, the greater chance for malabsorption problems to occur. Hence, “The longer the Roux limb, the longer the portion of intestine trying to absorb nutrients without the benefit of these digestive juices. Both of these changes result in less absorption of nutrients and contribute to weight loss, and are called the Malabsorptive components of the procedure” (Obesity Surgery Center, 2008).

The Roux-En-Y gastric bypass surgery can be performed either by open incision or by laparoscopic means. Most surgeons today will attempt the latter unless it becomes evident that an open procedure must be performed. This can be either due to large amounts of fat obscuring the scope lens or any number of problems.
2. Vagotomy - A vagotomy is a surgical procedure in humans and animals that involves resection (removal of, or at least severing) of part of the vagus nerve. It is not to be confused with vasectomy.
Complications of gastrectomy1. Pernicious anemia
- Vit B12 deficiency (needed for maturation of RBC and brain functioning)s/s - ↓RBC
- pallor, fatigue- CNS changes à paresthesia, altered balance and gait- red smooth beefy tongue/strawberry tongue
Diagnostic test: Schilling’s test
Step 1 – 24hr urine specimen after intake of oral vit B– absence of vit B12 in urine means not absorbed
Step 2 – give IM vit B12 and check urine (vit b12 present) to confirm step 1 Bone marrow aspiration
à (+) large RBC’s (Pernicious anemia is a type of macrocytic anemia) Romberg’s test à balance
2. Dumping syndrome - Gastric dumping syndrome, or rapid gastric emptying, happens when the lower end of the small intestine, the jejunum, expands too quickly due to the presence of hyperosmolar food from the stomach. "Early" dumping begins concurrently or immediately succeeding a meal. Symptoms of early dumping include nausea, vomiting, bloating, cramping, diarrhea, dizziness and fatigue. "Late" dumping happens 1 to 3 hours after eating. Symptoms of late dumping include weakness, sweating, and dizziness. Many people have both types. The syndrome is most often associated with gastric surgery.
10-30 mins pc Self-limiting (will disappear in 6-9 mos) s/s hypovolemia due to osmosis
hypoglycemia due to oversecretion of insulindiarrheasteatorrhea
mgt:small frequent feedingschew foods slowlylie down pc 1-2 hrsavoid liquid with mealslow CHOmoderate CHON↑ fatlow Na
HIATAL HERNIA
- protrusion of a portion of the stomach upward through the diaphragm-

Types:- Sliding (Type I)- Paraesophageal “rolling” (Type II)
Risk factors:- congenital abnormality- penetrating wound- age- women > men- obesity- ascites- pregnancy- history of constipation
Assessment:- substernal pressure- epigastric pain- burning sensation- heartburn- reflux esophagitis- dysphagia- cough and dyspnea- bleeding à hematemesis
à melena- symptoms aggravated when lying flat
Diagnostic tests:- chest X-ray- gastric analysis- CBC- barium swallow
Health teachings:- provide small, frequent meals; avoid highly seasoned foods- maintain upright position during and after meal- give the following medications:
à antacidsà histamine antagonistà anticholinergics agentsà antiemetic drugs
- Avoid the following:à smoking, peppermintà fatty foodsà calcium channel blockersà diazepamà β-adrenergic agentsà constrictive clothing

à activities that increase intraaabdominal pressure- Elevate hed of bed while sleeping- Weight reduction- Upright position after eating at least 1 hour
Surgical management:- Nissen-Fundoplication
Post-op care:- Deep breathing and coughing exercise- Check patency of NGT- Position patient on semifowler’s position- Turning every 2 hours- Maintain closed-chest drainage if needed- Check for return of bowel sounds- Promote comfort and good nutrition
o IV solutions and electorlytes
PANCREATITIS
- Inflammatory condition of the pancreas
Risk factors:- obesity- alcohol consumption- biliary tract disease- abdominal trauma- surgery- drugs, infection- carcinoma, adenoma
Assessment- pain location- nausea and vomiting- dyspnea, ↓ breath sounds, crackles, cyanosis- signs of shock- F&E imbalance- ↓ bowel sounds, abdominal tenderness with guarding- steatorrhea- pale, cold, moist and jaundiced skin- supine position increases pain- presence of:
o Grey-Turner’s signo Cullen’s sign
Laboratories:- ↑ serum amylase and lipase- ↑ AST/SGOT- ↑ alkaline phosphatase- ↑ bilirubin- ↑ glucose (serum and urine)- ↑ WBC- ↑ BUN, creatinine- ↓ serum electrolytes
Diagnostic tests:- chest x-ray- ultrasound- endoscopic retrograde cholangiopancreatography
CHOLELITHIASIS / CHOLECYSTITIS

- Presence of gallstones in the gallbladder- Inflammation of the gallbladder
2 types:cholesterol stonespigmented stones
Risk factors:- 5 Fs- cirrhosis of the liver- pancreatic disease- hyperlipidemia
Assessment:- Pain: RUQ that radiates to back, scapular, heart
Murphy’s sign: pain after putting pressure at the RUQ after taking a deep breath- GIT signs and symptoms- Vital signs- Chills, jaundice- dark, amber urine
Laboratory workups:- ↑ WBC and alkaline phosphatase- ↑ serum amylase and lipase- ↑ AST (SGOT), bilirubin, PT
Diagnostic tests:- Ultrasound- ERCP
Management:- medical intervention:
o gallstone dissolution therapy à Ursodeoxycholic (Ursofalk)- ESWL- surgical interventions:
o cholecystectomy abdominal laparoscopic
o choledochostomyo choledocholelithotomyo cholecystotomy
HEPATITIS
- inflammation of the liver
Types:- toxic- viral
Stages:- pre-icteric- icteric- post-icteric
Assessment:- ↓ metabolism
o CHOo CHONo ↓ albumin synthesiso ↓ clotting factor synthesiso FATS

- ↓ production of bile salts- ↓ bilirubin metabolism- Impaired detoxification- ↓ absorption of vitamins ADEK and minerals
Diagnostic tests:- Liver function test
o ↑ serum bilirubin, enzymes, prothrombin time, ammoniao ↓ BUN
- Liver biopsy- Ultrasound
LIVER CIRRHOSIS
- a chronic degenerative disease of the liver in which the lobes are covered with fibrous tissue, the parenchyma degenerates, and the lobules are infiltrated with fat
Types:- Laennec’s cirrhosis- Post-necrotic cirrhosis- Biliary cirrhosis- Cardiac cirrhosis
Risk factors:- Alcohol- Nutritional deficiency- Hepatotoxins
Diagnostic tests:- Liver scan- Liver biopsy- Laboratory workups
o ↓ albumin, potassium, magnesium, BUNo ↑ prothrombin time, ammonia, AST(SGOT), ALT(SGPT), LDH, alkaline phosphatase, uric
acid, blood sugar
Complications of liver cirrhosis- Hepatic encephalopathy
o ↓ level of consciousnesso confused, irritable and with memory impairmento asterexiso fetor hepatitis
- Esophageal varices
APPENDICITIS
- Inflammation of the appendix
Risk factors- Men > Women- 10-30 years old- History of constipation- Low fiber diet
Assessment- Pain location
o Rebound tendernesso Rovsing’s sign - pain after pressure @ LLQ is pushed to RLQ

o Psoa’s sign - knee-chest position à right leg- Anorexia, N/V, fetid odor breath- ↑ temperature, shallow RR- Constipation- ↓ or absent bowel sound
Diagnostic tests:- ↑ WBC count, ↑ neutrophils- Enema containing a radiographic contrast agent
Surgeryà appendectomyPost-op care:
- Similar to other general surgery- Avoid lifting heavy objects/increasing abdominal pressure
ULCERATIVE COLITIS/CROHN’S DISEASEUC: a chronic, episodic, inflammatory disease of the large intestine and rectum, characterized by profuse watery diarrhea containing varying amounts of blood, mucus, and pusCD: a chronic inflammatory bowel disease of unknown origin, usually affecting the ileum, the colon, or both structures. Diseased segments may be separated by normal bowel segments. Also called regional enteritisSurgery
- Proctocolectomy- Continent ileostomy (Kock pouch)- Colectomy with ileoanal anastomosis- Ileoanal reservoir
Stoma care- color à pinkish, reddish with slight edema for 5-7 days- empty pouch when 1/3 to 1/2 full- wash skin with mild soap and warm water- administer skin barrier - prevent skin infection
Manage odor- Avoid gas forming and foul odor foods- Rinse pouch with tepid water, weak vinegar solution- Place deodorant tablet, small amount of mouthwash, a piece of charcoal into the pouch- Avoid foods that could obstruct the pouch
HEMORRHOIDS - a varicosity in the lower rectum or anus caused by congestion in the veins of the hemorrhoidal plexusTypes:
- External- Internal
Risk factors:- Chronic constipation- Obesity, pregnancy- Wearing constrictive clothing- Prolonged standing/sitting- ↓ fiber diet- Familial tendency- ↑ intraabdominal pressure
Assessment:- Discomfort, anal pruritus, pain- Bleeding especially during defecation- Narrowing of stool- Grapelike clusters around the anus (pink, red, blue)
Diagnostic tests:- External visualization- Internal-digital exam à proctoscopy, proctosigmoidoscopy
Surgical management- Sclerotherapy (internal)- Cryosurgery- Photocoagulation- Ligation (internal)

- HemorrhoidectomyPost-op
o analgesics as orderedo position: SL, proneo apply ice pack then warm compresso ↑ fluid intakeo use foam pillow or pads under the buttockso monitor bleeding, infection, emboli, phlebitiso Facilitate evacuation of stools
stool softeners laxative suppositories oil enemas
o Perform perineal care especially after defecationo Encourage ambulationo Encourage ↑ fiber diet