Embed Size (px)
Citation preview

5/1/15
1
Chienying Liu MD
Common Thyroid Problems Case-‐Based Discussion
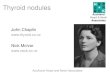
Schematic diagram of a follicular cell, illustrating the steps involved in thyroid hormone synthesis.
Park S M , and Chatterjee V K K J Med Genet 2005;42:379-389
©2005 by BMJ Publishing Group Ltd
cAMP

5/1/15
2
Case 1 -‐ Hyperthyroidism
63 yo man not feeling himself, with unintenFonal weight loss and eyes feeling irritated • Exam
– Thyroid, not enlarged, somewhat firm, no nodules, no bruits
– Subtle exophthalmos in the right eye with mild conjuncFval erythema
• Came to us with the following labs – TSH < 0.01 – Free T4 1.09 (<1.8) – Free T3 4.40 (< 4.2)
– TPO anFbody 101 (<34) – Tg anFbody posiFve
T3 toxicosis
(Common) Causes of Hyperthyroidism
• Graves disease – The most common cause of hyperthyroidism – Caused by sFmulaFng autoanFbodies to the TSH receptor ( measured by TSI or TBII)
– TPO and or Tg AB frequently present 70-‐90 %
• Toxic nodule/Toxic MNG – 1.5-‐44.5% of hyperthyroidism, depending on the iodine intake – 2% in the United States
www.thyroidmanager.org

5/1/15
3
Causes of Hyperthyroidism
• Thyroidi8s – Autoimmune (painless) = subacute lymphocy8c thyroidi8s (1-‐ 5%)
• Postpartum thyroidiFs also an example • TPO present in 50% of these paFents at the Fme of diagnosis • Clinically, may not be differenFated from Graves disease on PE
– InfecFous (very painful gland) • Post-‐viral: Subacute granulomatous thyroidiFs = de Quervain's thyroidiFs ( < 1%)
– Strongly associated with HLA-‐B35 – ESR very elevated
• Acute Bacterial infecFon: fevers/chills, unilateral neck pain. May have hyperthyroidism
– Drug induced • Interferon-‐alfa → induced autoimmunity: painless thyroidiFs or Graves disease • Interleukin 2 (for leukemia) • Lithium → mostly hypothyroidism but can induce autoimmune: Graves or painless thyroidiFs • TKIs → usually hypothyroid but may also have destrucFve thyroidiFs • Amiodarone induced type II hyperthyroidism → destrucFve thyroidiFs
– Others • RadiaFon , palpaFon
Iodine Scan Uptake 0 or very low
Causes of Hyperthyroidism • Exogenous thyroid hormone
• Rare – TSH mediated (TSH secre8ng pituitary adenoma)
– Struma Ovarii • Autonomous funcFoning thyroid Fssue in the teratoma
– Trophoblas8c disease • HydaFdiform mole or choriocarcinoma (↑𝐻𝐶𝐺)
– Metasta8c thyroid cancer
– Familial non-‐autoimmune hyperthyroidism • Due to a gain of funcFon in the TSHR • AutoanFbodies negaFve • Neonatal hyperthyroidism
– Thyroid hormone resistance

5/1/15
4
Case 1 -‐ Hyperthyroidism
DiagnosFc Test of Choice • TSH receptor anFbody tesFng
– TSI 433 (< 140 %)
• Iodine Uptake scan – Diffuse uptake – 4h 10% and 24 h 21%
– TSH < 0.01 – Free T4 1.09 (<1.8) – Free T3 4.40 (< 4.2)
– TPO anFbody 101 (<34) – Thyroglobulin anFbody posiFve
Course
Started on Methimazole Euthyroid on 5mg 5 months later
T3 toxicosis
Case 2 -‐ Hyperthyroidism • 60 yo presented with apparent exophthalmos and chemosis and atrial fibrillaFon – TSH < 0.01 – Free T4 20 (9-‐24) – Free T3 436 (145-‐348) – TPO and TgAB negaFve – TSI negaFve
• Thyroid gland mildly enlarged 2-‐3 x, firm
AddiFonal Test(s)? • TBII PosiFve
• Iodine scan Not done (not needed)
T3 toxicosis

5/1/15
5
TSH Receptor AutoanFbodies
• TSH receptor is the major auto-‐anFgen in Graves’ disease (GD) AnFbodies include:
– SFmulaFng, most common – Inhibitory/blocking
• Thyroid atrophy and hypothyroidism
– Neutral – In GD hyperthyroidism, the sFmulaFng type predominates
Best PracFce & Research Clinical Endocrinology & Metabolism Vol. 19, No. 1, pp. 33–52, 2005
TSH Receptor AutoanFbodies-‐ Clinical Use • DifferenFate GD from other causes of hyperthyroidism
• Predict risk of fetal or neonate hyperthyroidism
• ?? Predict remission or relapse in GD aner anFthyroid medicaFons – In a meta-‐analysis from 1994**:
• AB+ pts 3 Fmes more likely to relapse • But 25% of AB-‐ pts relapsed 25% of AB+ pts stayed in remission
– Recent studies: uFlity in predicFon is yet to be proven* • heterogeneous populaFons, different assays, Fming, duraFon of follow up, different cut offs to define posiFvity
* Kamath et al J of Thyroid Research 2012 **Feldt-‐Rasmussen et al JCEM 1994

5/1/15
6
Kamath et al J of Thyroid Research 2012
Graves’ Disease Assessment of TSH Receptor AutoanFbodies (TRAb)
TSI = Thyroid SFmulaFng Immunoglobulin Bioassay
TBII = Thyroid Binding Inhibitory Immunoglobulin
Immunoassay

5/1/15
7
Graves’ Disease Assessment -‐TSI
• Bioassay detecFng cAMP producFon (Measures the final balance of all TRAb)
– 2nd generaFon (2 steps), cumbersome • Detect cAMP using RIA • SensiFvity 85-‐90%, Specificity 99%
– 3rd generaFon • Employing luciferase reporter gene • Higher sensiFve • Quest/Labcorp: 92% sensiFve and 99.3% specific
– Advocates of this test: reflect clinical phenotype beser
J Clin Endocrinol Metab 98 (2013): 2247–2255 Lyson et al. Autoimmunity Review 2010
Graves’ Disease Assessment-‐ TBII
• CompeFFve Immunoassay (Measures TRAb of all types)
– 1st generaFon – poor sensiFvity – 2nd generaFon
• Used labeled TSH to TSH receptor from CHO or a recombinant TSH receptor protein preparaFon
• SensiFvity 97.1%, Specificity 97.4% (meta-‐analysis)* – 3rd generaFon
• Replaced labeled TSH with specific TSH human monoclonal sFmulaFng anFbody M22 • SensiFvity 98.3%, Specificity 99.2% (meta-‐analysis)* Quest: SensiFvity 92%, specificity 100% (kronus) Mayo Clinic: SensiFvity 95%, specificity 97% (Roche) • There can be between method variability and subopFmal inter-‐assay precision
*Autoimmunity Reviews 12 (2012): 107–113

5/1/15
8
Case 2 -‐ Hyperthyroidism • 60 yo women presented with
apparent exophthalmos and chemosis and atrial fibrillaFon – TSH < 0.01 – Free T4 20 (9-‐24) – Free T3 436 (145-‐348) – TPO and TgAB negaFve – TSI negaFve
• Thyroid exam – mildly enlarged, firm
AddiFonal Test(s)? • TBII posiFve 81% (<16%) inhibiFon
Clinical Course • On methimazole • Eye disease improved • On MMI 10-‐15mg 2-‐3 years later
– No side effects – Wants to conFnue MMI
Case 3 -‐ Hyperthyroidism
• 47 yo woman presented with palpitaFons and some weight loss • Maybe some URI symptoms 1-‐2 months prior to presentaFon
– TSH 0.03 – Free T4 18 (10-‐18) – Free T3 6.5 (<5.7)
• Came to us for a consultaFon, 2.5 weeks later • Exam
– Non-‐tender gland, palpable but not grossly enlarged, no nodules – No ophthalmopathy, not grossly hyperthyroid
Another case of T3 toxicosis

5/1/15
9
Case 3 -‐ Hyperthyroidism • Repeat labs + TSHR Ab at the Fme of the visit
– TSI negaFve – TSH 0.38 – Free T4 9 – Free T3 3.6
3/4/2015 3/30/2015 TSH 18.90 (H) 4.58 (H)
Free T4 10 -‐ 18 pmol/L 7 (L) 8 (L) Free T3 2.6 -‐ 5.7 pmol/L 3.7 2.8
TPO >850
Ø Acute Lymphocy8c Thyroidi8s = Silent Thyroidi8s § If uptake scan were to performed early on
when hyperthyroid, uptake = very low
Ø Monitor TFT – at risk for hypothyroidism
Course • Not symptoma8c of hypothyroidism • Feeling be]er with 8me • Wants to be monitored
Case 4 -‐ Thyroid Nodule • 32 yo woman presented with right neck pain that turned out to be musculoskeletal
• Found to have a 2.5 cm hypoechoic nodule
• Exam not remarkable other than the palpable nodule
• Work up: – TSH 0.11, then 0.39 – TSH 0.46 (0.4-‐4.0) – Free T4 11 (9-‐24) – Free T3 284 (145-‐384)
– TPO 119 (<60) – TSI negaFve

5/1/15
10
Case 4 – Thyroid Nodule
• Biopsy = follicular neoplasm
• Iodine uptake scan showed a hot nodule in the right with suppression of the rest of the gland
Treatment OpFons • Monitor given normal TFT • RAI • Surgery • ATD • New strategies
– Ethanol injecFon – Percutaneous laser thermal ablaFon
Hyper-‐funcFoning Thyroid Nodule • Usually a follicular adenoma
– 57% of 75 toxic adenomas found to have TSHR mutaFons, 3%-‐ Gsα mutaFons in a study – When biopsied – FNA shows either a benign nodule or follicular lesion/neoplasm
• DefiniFve diagnosis of follicular adenoma cannot be made on biopsy • Surgical resecFon needed to exam the capsule
• Risk of malignancy is said to be very low, biopsy not needed in most paFents – Not completely free of cancer . – Case reports of malignancy, especially in children
• Progression from a hyperfuncFoning nodule to a toxic nodule -‐ 4% year – Risk higher in older pts, nodules > 3 cm, in areas of low iodine intake
• Heterogeneity in clinical behavior of hyperfuncFoning nodules – Thyrotoxicosis is usually not common < 2.5 cm – there are excepFons – Only about 30-‐40% of hyperfuncFoning nodules > 3-‐4.5 cm are toxic
Krohn et al. Endocrine Reviews 26(4):504–524 2005; Corvilain Ann. Endocrinol 2003 (217 pts in Belgium)

5/1/15
11
Treatment ModaliFes & Risk of Hypothyroidism • RadioacFve Iodine Treatment
– Risk of hypothyroidism, variably reported – Incidence of hypothyroidism may increase with Fme
• 11% at 1 year, 33% at 5 years, and 49% at 10 years in a study of 105 paFent – Euthyroidism ( 9.7% vs 1.5% with hyperthyroid hot nodule) is a risk factor – Presence of thyroid anFbody status is a risk factor – Pretreatment with ATD (raise TSH) is a risk factor – No correlaFon demonstrated with nodule size and radioiodine dose, or iodine uptake, or degree of adjacent suppression on scans
• Surgery – Risk of hypothyroidism, 4.4% in one study, 14% in another – May also depend on anFbody status
• ATD – Not curaFve, but may be considered in selected cases
Thyrotoxicosis of Other EFology. ThyroidManager.org
Case 4 – Thyroid Nodule • Biopsy = follicular neoplasm
• Uptake scan showed a hot nodule in the right with suppression of the rest of the gland
Treatment OpFons • Monitor given normal TFTs • RAI • Surgery • ATD?
• Newer strategies
– Ethanol injecFon – Percutaneous laser thermal ablaFon
• Course
• Elected surgery – Lobectomy • Path-‐ Benign adenoma • On T4 25 mcg

5/1/15
12
Case 5 – Hyperthyroidism + Nodule
• 30 yo woman presented with nausea, headaches, and malaise
• Exam – right thyroid fullness • TFT
– TSH 0.01 – Free T4 17
• US showed a 2.9 cm ill defined right nodule
• Uptake scan showed a hyperfuncFoning nodule
Papillary Thyroid Cancer
Mirfakhraee et al. Thyroid Research 2013 Review of cases 1950-‐2012

5/1/15
13
Hyperthyroidism Work UP-‐ Take Home Messages • Given that Graves disease is the most common in the iodine replete areas,
obtaining a TSH receptor anFbody tesFng ie either TSI or TBII is most cost effecFve
• TPO and Tg anFbodies usually not every helpful in the work up of hyperthyroidism in most cases
• Uptake scan should be considered as the next step – If TSH receptor anFbody tesFng is negaFve and thyroid funcFon results are not improving
– If a nodule is present (> 1 cm) • Especially if negaFve TSH receptor anFbodies
– T4 and T3 profile can be helpful but is an overall relaFvely insensiFve assessment of eFologies for hyperthyroidism
• Risk of malignancy is low in hyperfuncFoning nodules but not zero – Biopsy is not needed in most cases
• Look at ultrasound characterisFcs and biopsy suspicious appearing nodules
32 yo woman not responding to LT4
• Graves disease, status post RAI ablaFon in 2013
• Started on LT4 one month later • Never had normal TSH levels by report • 02/13/2015: TSH 38.8 when on 75 mcg • 02/25/2015: TSH 72 (0.5-‐4.8) on 150mcg
– FT4 0.92 (0.8-‐1.7) – T3 48 (55-‐170)
• 03/12/2015: on 225mcg • Exam
– Weight 51 kg – Mildly tachycardic – Mild tremors and warmth on the outstretched
hands
DifferenFal Diagnoses 1. Noncompliance 2. Interfering drugs or supplements 3. MalabsorpFon 4. Lab error/issues
Heterophile anFbodies MacroTSH (anF TSH IgG-‐TSH complex)
5. Conversion? 6. Others?

5/1/15
14
Levothyroxine (l-‐thyroxine) • SyntheFc form of thyroid hormone, structurally idenFcal to human thyroxine secreted
by the thyroid gland – Various brands have slightly different preparaFons and fillers, but with the same acFve
ingredient – ½ life is 7 days
• AbsorpFon takes place in the small intesFne – 45% upper jejunum, 34% lower jejunum and ileum, 21% duodenum (End Rev 2014)
• Gastric acid (acidic PH) important for its subsequent absorpFon – Best absorbed when fasFng
• 70-‐80% of the given dose is absorbed → IV conversion
• Metabolized in liver, eliminated by kidneys
Endocrine Reviews 2014
Food and beverages Interfering L-‐thyroxine AbsorpFon
• Best absorpFon to poorest absorpFon 60 min prior to breakfast BedFme (3 hours aner last meal)
30 min prior to breakfast With breakfast – Most consistent TSH levels achieved at fasFng states
• Coffee, especially espresso coffee – Probably by sequestering LT4 in the small intesFne
• Fiber • Soy products
– ProblemaFc for infants with CH, fed with soy formula
• Others – Coson seed meal – Walnuts
ATA guidelines on Treatment of Hypothyroidism Thyroid 2014 Endocrine Reviews 2014

5/1/15
15
Supplements/Drugs Interfering AbsorpFon • Calcium supplements • Ferrous iron • MVI that has calcium and/or iron • Phosphate binders (sevelamer) • Aluminum antacids • PPI and H2 blocker
– Short term co-‐administraFon PPI -‐> no change in absorpFon
• Sucralfate (mixed results) • Orlistat • Rolaxifene (decreased absorpFon) • Cholestyramine • Colesevelam
• Chromium picolinate • Charcoal • Ciprofloxacin • Kayexelate
• Synthroid package insert: – Iron, calcium supplements and antacids should not be
administered within 4 hours – Has a cauFon statement on soy regarding its effects on
absorpFon – Other food cauFons: coson seed meal, walnuts, fibers
• Soy ? 4 hours
ATA 2014 Hypothyroid Guidelines
ATA guidelines on Treatment of Hypothyroidism Thyroid 2014
Gastro-‐IntesFnal Disease AffecFng AbsorpFon • Diseases affect gastric acid producFon
– H-‐Pylori – Autoimmune atrophic gastriFs
• AnF-‐parietal cell anFbody or IF anFbody • Disease affecFng the small intesFne
– Celiac disease • IgA anFendomysial anFbody or Fssue transgluaminase IgA anFbody
– GI surgeries affecFng the small bowel • (there are also data showing L-‐thyroxine absorp6on preserved in Roux-‐en-‐Y pa6ents)
– Lactose intolerance • Case reports of 900mcg requirement to 150ug aner lactose free diet
– IntesFnal giardiasis

5/1/15
16
32 yo woman not responding to LT4 • Her husband vouched for her compliance
• We lowered her T4 dose empirically to 150mcg and repeat blood tests and obtained addiFonal work up:
• 4/6/2015 on 150mcg
Take Home Message
• Consider various causes of high T4 requirement – ? Lab issue or error in this case – Autoimmune gastriFs in this case
3/12/2015 TSH (0.45 -‐ 4.12 mIU/L) 0.26 (L) Free T4 (10 -‐ 18 pmol/L) 25 (H) T3, Total (0.9 -‐ 2.4 nmol/L) 1.7
3/12/2015 Tissue Transglutaminase An8body, IgA <20.0 CU
<10.0
Vitamin B12 211 -‐ 911 ng/L 245 Intrinsic Factor Blocking An8body
POSITIVE
4/6/2015 TSH 3.83 Free T4 10 -‐ 18 pmol/L 15 T3, Total 0.9 -‐ 2.4 nmol/L 1.3
20 yo woman TSH high normal, feeling Fred
• Healthy otherwise • FH posiFve for hypothyroidism • Exam -‐ small goiter (right>len), firm by palpitaFon
• Ultrasound – Prominent thyroid with diffuse heterogeneous echo-‐texture with minimal increase in vascularity
• 1/10/2014: TSH 3.01 • 8/22/2014: TSH 5.43, FT4 1.08 (0.89-‐1.76) • TPO negaFve, Tg AB posiFve • 1/05/2015: TSH 3.96, FT4 0.81
Do you treat?

5/1/15
17
TSH Targets No known thyroid disease/goiter and AnFbodies NegaFve
NHANES III
NHANES III Distribu8on by Age
Hollowel J Clin Endocrinol Metab 2002 Surks J Clin Endocrinol Metab 2007
TSH 0.45 – 4.12 mIU/L = 2.5 to 97.5 percenFle
Age Specific DistribuFon of TSH
Surks J Clin Endocrinol Metab 2007

5/1/15
18
Age Specific TSH Reference Range
Boucai et al THYROID 2011
TSH -‐ 97.5 cenFle by Age Group

5/1/15
19
Subclinical Hypothyroidism
• TSH ≥10 → Treat – Meta-‐analyses
• Increased HF (Gencer et al CirculaFon 2012) – Also some increase with TSH >7 -‐9.9 but more significant when TSH ≥ 10 – 80 yo or older, risk not increased
• Increased CV events and CV mortality (Rondondi JAMA 2010)
– One meta-‐analysis suggested significance in younger paFents only (<65 yo) (Razvi JCEM 2008)
– No randomized studies to evaluate benefits of treatment
Subclinical Hypothyroidism
• TSH 4.5-‐10 →Mixed data/treatment is controversial (studies were in older individuals) – Not as clearly associated with adverse CV events from observaFonal studies – No clear CV benefits, inconsistent LDL benefits with tx *
• Possible benefits of tx in CV events in paFents 40-‐70 yo but not older than 70 yo (Razi Arch Intern Med 2012, retrospecFve study )
– No demonstrated improvement in quality of life or cogniFve funcFon in older paFents with tx (50s-‐70s yo)*
– ATA 2012 guidelines: Consider anFbody status, symptoms before treatment – DO NOT OVERTREAT older individuals
• Older individuals (>70 yo) may have TSH in this range, because of normal aging
*Rugge Ann Intern Med 2015

5/1/15
20
Subclinical Hypothyroidism
• TSH 2.5-‐4.5 – Small studies showed benefits of tx in lipids, endothelial funcFon, inFma media thickness
– But no clinical outcome data – ExcepFon: women considering pregnancy
• Increased pregnancy loss for TSH 2.5-‐5.0 during 1st trimester (Negro R JCEM 2010) • Keep TSH < 2.5 prior to concepFon (Endocrine Society guidelines 2012) • During pregnancy: TSH goal: 1st Trimester 0.1-‐2.5; 2nd trimester 0.2-‐3; 3rd trimester 0.3-‐3.
Treatment of Subclinical Hypothyroidism • Full replacement dose 1.6mcg/kg body weight (more lean body weight dependent) – Older paFents require less, lower lean body weight
• PaFents with subclinical hypothyroidism do not need full replacement – 25-‐50mcg if TSH ≤10 * – Consider age and risk for CAD when dosing, use lower dose
• Monitor TSH, 4-‐6 weeks aner iniFaFon or a dose change* – Target range depending on ‘age and comorbidiFes’ , typically 0.5-‐3.5 to 4 mIU/L *
– Target range 4-‐6 mIU/L for persons >70-‐80 yo* *ATA guidelines Thyroid 2014

5/1/15
21
20 yo woman TSH high normal, feeling Fred • High normal TSH • FH of hypothyroidism, evidence
of thyroidiFs (exam)
• What could be the ‘proven’ benefit of treatment? – A reducFon in goiter size (Romaldini Thyroid 1996)
• What could be the potenFal harm of treatment? – Likely minimal in this young pt
• May consider a trial of LT4
• TSH goal -‐ the lower half of the normal range for this young paFent
• Also work up other causes of faFgue
• If she were to consider pregnancy → keep TSH < 2.5 mIU/L
THANK YOU