Embed Size (px)
Citation preview

Thyroid Disease in Pregnancy
2011 Update
Endocrinology RoundsFebruary 16, 2011
Selina LiuPGY5 Endocrinology

Objectives
To briefly review thyroid anatomy and physiology in pregnancy and fetal thyroid physiology
To review causes of thyroid disease in pregnancy
To review the maternal and fetal outcomes of thyroid disease in pregnancy
To discuss the controversy surrounding screening for thyroid disease in pregnancy

Objectives
To review special considerations in management of thyroid disease in pregnancy
To highlight recent 2009-2011 articles published on thyroid disease in pregnancy

Thyroid in Pregnancy
non-pregnant: 10-30 g (North America)
in pregnancy, increased vascularity
thyroid gland hyperplasia
if enlargement noted incidentally on exam, may lead to lab evaluation of thyroid function
normal pregnancy - significant but reversible changes in maternal thyroid physiology

Casey BM & Leveno KJ. Obstet Gynecol 2006;1081283-9
Total T4: 150 % above normal non-pregnant reference
interval

Clinical Importance of Physiological Changes
Increased TBG
Placental de-iodination of T4
Increased iodine clearance (renal clearance and fetal transfer)
Need for T4 production total T4, T3 interference with fT4 assay
Need for T4 production T4 and T3 metabolism
need for iodine supplementation risk of maternal & fetal hypothyroidism and goitre
Keely E & Casey BM (2010). Thyroid disease in pregnancy. In RO Powrie, MF Greene, W Camann (Eds) deSwiet’s Medical Disorders in Obstetric Practice (5th Edition pp322-34). West Sussex, Wiley-Blackwell

Clinical Importance of Physiological Changes
hCG (1st trimester)
TSH-R Abs (TSI/TBII)
thyroid antibodies (post-partum)
fT4 and TSH
may have mild transient thyrotoxicosis
Graves’ disease may improve during pregnancy exacerbation of Graves’ disease precipitation of postpartum thyroiditis
Keely E & Casey BM (2010). Thyroid disease in pregnancy. In RO Powrie, MF Greene, W Camann (Eds) deSwiet’s Medical Disorders in Obstetric Practice (5th Edition pp322-34). West Sussex, Wiley-Blackwell

Fetal Thyroid Physiology
12 weeks gestational age: embryogenesis of fetal thyroid gland is complete
synthesis of thyroid hormone
fetal TSH also detectable
Mid-gestation: negative feedback control of thyroid hormone synthesis develops
Throughout gestation: pituitary-thyroid axis continues to develop

Fetal Thyroid Physiology
What crosses the placenta?
iodine
T3, T4 (poorly) – but large maternal–fetal gradient
maternal TRH – but negligible amount in maternal circulation
TSH-R antibodies (TSI/TBII) anti-thyroid medication – methimazole, PTU
Maternal TSH does NOT cross the placenta

Fetal Thyroid Physiology
Prior to 12 weeks gestation, fetus dependent on maternal thyroid hormone production critical time for fetal neural development (as well as later in gestation)
Throughout pregnancy, T4 and iodine supplied by mother to fetus
maternal iodine supply very important throughout unclear role of maternal T4 after fetal T4 production begins

Thyroid Disease in Pregnancy
Hyperthyroidism
Hypothyroidism
Post-partum Thyroiditis
Thyroid Nodules

Hyperthyroidism in Pregnancy
~ 0.2% of pregnancies complicated by hyperthyroidism
Causes: gestational transient thyrotoxicosis hyperemesis gravidarum gestational trophoblastic disease familial gestational thyrotoxicosis
hCG-mediated
Graves’ Disease toxic nodule/MNG thyroiditis exogenous iodine TSHoma struma ovarii
non hCG-mediated

Hypothyroidism in Pregnancy
overt hypothyroidism ~ 0.1-0.3% of pregnancies
subclinical hypothyroidism ~ 3-5% of pregnancies
Causes: Hashimoto’s Thyroiditis iodine deficiency prior RAI ablation/thyroidectomy medications (lithium, amiodarone) central hypothyroidism (rare)
(developed world)(worldwide)
? genetic susceptibility

Subclinical Hypothyroidism
TSH variable ~ 40-60% of TSH variability under genetic control?
Genome Wide Association Scanning:
SNP in PDE 8B gene associated with circulating TSH levels
PDE 8 B – catalyzes hydrolysis of cAMP
responsible for 2.3% of variance in TSH each copy of allele present – associated with an increase in TSH concentration of 0.13 mIU/L
Arnaud-Lopez L et al. 2008 Am J Hum Genet 82:1270-80

Subclinical Hypothyroidism – PDE8B
Arnaud-Lopez L et al. 2008 Am J Hum Genet 82:1270-80

1014 healthy pregnant women at 28 wks TFTs, anti-TPO, PDE8B genotype (AA, AG, GG)
developed reference range (based on anti-TPO – subjects)
TSH 0.49-4.21 mIU/L AA group had highest, GG group had lowest TSH AA group - greater proportion with TSH >4.21 mIU/L (ULN)

SNP in PDE8B associated with TSH - AA highest, GG lowest
no difference in fT3, fT4 or prevalence of anti-TPO + Abs

Post-partum Thyroiditis (PPT)
due to rebound autoimmunity post-partum
lymphocytic infiltration, transient changes in thyroid function
+ anti-TPO in >90% women with PPT those with high titres in early pregnancy more likely to be affected (50-60%)
high incidence in T1DM (18-25%) (high prevalence anti-TPO)

Post-partum Thyroiditis (PPT)
Pearce EN et al. 2003 N Engl J Med 348:2646-55

Thyroid Nodules in Pregnancy
nodule > 1cm – FNAB
if 1st or early 2nd trimester and malignant OR rapid growth, offer surgery in 2nd trimester
if follicular or papillary, no advanced disease – can defer surgery until post-partum
can suppress TSH if: previously treated thyroid cancer, FNAB suspicious or positive for malignancy, or if delaying surgery until post-partum
to detectable levels (keep fT4 in normal range)
J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47

Thyroid Nodules in Pregnancy
RAI with I131 should NOT be given to pregnant women or those breastfeeding
women with thyroid cancer treated with therapeutic doses of RAI should avoid pregnancy for 6-12 months post-ablation
J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47

Maternal Outcomes - Hyperthyroidism
increased risk of: spontaneous pregnancy loss CHF thyroid storm preterm birth preeclampsia perinatal morbidity & mortality

Fetal Outcomes – Maternal Hyperthyroidism
depends on degree of thyrotoxicosis, cause, and treatment of mother
in most cases, fetus is euthyroid but, transplacental transfer of TSH-R Abs (TSI/TBII) can cause fetal Graves’ disease
1-10% of neonates of affected women
risk directly related to maternal Ab titre in 3rd trimester
manifestations: fetal tachycardia high output heart failure hydrops fetalis
craniosynostosis IUGR fetal goitre

Endocrine Society Clinical Practice Guidelines 2007
measure TSH-R Abs prior to pregnancy or before end of 2nd trimester in women with:
current Graves’ Disease
prior history of Graves’ Disease and I131 treatment or thyroidectomy
previous neonate with Graves’ Disease
if – TSH-R Abs and don’t require anti-thyroid Rx
low risk of fetal/neonatal thyroid dysfunction
J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47
Fetal Outcomes – Maternal Hyperthyroidism

if + TSH-R Abs, need close fetal monitoring: fetal heart rate at each OB visit - ?tachycardia
fetal ultrasound – assess growth, ?goitre – especially if mother on anti-thyroid medication
consider serial U/S q2-4 wks in 3rd trimester – if very high TSH-R Abs titres
? fetal blood sampling for thyroid indices – not routine
if high maternal TSH-R Abs, evidence of IUGR, fetal CHF, or fetal goitre J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47
ACOG Practice Bulletin Obstet Gynecol 2002, 100(2):387-396
Fetal Outcomes – Maternal Hyperthyroidism

Maternal Outcomes - Hypothyroidism
increased risk of: early pregnancy failure preeclampsia placental abruption
treatment of women with overt hypothyroidism associated with improved pregnancy outcomes

Fetal Outcomes – Maternal Hypothyroidism
increased risk of: low birthweight stillbirth intellectual impairment
especially if overt maternal hypothyroidism in 1st trimester

Outcomes – Subclinical Thyroid Disease
less clear effect of: subclinical hypo/hyperthyroidism
euthyroid thyroid autoimmunity (+ autoantibodies)
maternal hypothroxinemia
normal TSH but low fT4
on both maternal and fetal outcomes

population-based cohort - Netherlands 3659 children and their mothers (Apr/02-Jan/06) examined association between early pregnancy thyroid function and cognitive function in early childhood
maternal TFTs (mean 13.3 wk GA) verbal/nonverbal cognitive development – as per mailed parent-report measures (18 and 30 months)
specifically looked at maternal hypothyroxinemia(normal TSH, but fT4)

TSH range 0.35-2.5fT4 11-25 (non-preg)
Hypothyroid TSH>2.5, fT4 <11
HyperthyroidTSH <0.03, fT4>25
Mild hypothyroxinemiaNormal TSH
fT4 <11.76 (10th %ile)
Severe hypothyroxinemiaNormal TSH
fT4 < 10.96 (5th %ile)

mild hypothyroxinemia significantly related to expressive language delay across ages severe hypothyroxinemia predicted likelihood of expressive language delay at 18m, 30m, and across ages

severe hypothyroxinemia predicted likelihood of nonverbal cognitive delay at 30m

Conclusions:
maternal hypothyroxinemia predicted a higher risk of verbal and nonverbal cognitive delay in early childhood
maternal TSH did not predict cognitive outcomes
need more studies assessing potential benefit of iodine or T4 supplementation in early pregnancy before can justify implementation of fT4 screening in early pregnancy

Screening in Pregnancy ?
What is a normal TSH in pregnancy?
Gestational age-specific TSH reference range?
several studies, in variety of populations
reference ranges in non-pregnant populations are not applicable to pregnancy

Gestational Age-Specific TSH Range
Dashe JS et al. 2005 Obstet Gynecol 106:753-7
13 731 pregnancies 13 599 singleton and 132 twin pregnancies
measured TSH
assay reference 0.4 – 4
created nomogram basedon gestational age

Dashe JS et al. 2005 Obstet Gynecol 106:753-7
342 women (singleton) with TSH above 97.5%ile
95 (28%) would not have been identified with TSH elevation as per assay reference value
340 women (singleton) with TSH below 2.5%ile
1448 (11%) euthyroid women would have been incorrectly characterized as abnormal as per assay reference value

Gestational Age-Specific TSH Range
Gestational-age specific normal TSH range
converted TSH values to MoM “multiples of median” to facilitate use in other populations
Dashe JS et al. 2005 Obstet Gynecol 106:753-7

goal – to calculate gestational age-specific TSH, fT4 and fT3 reference intervals in an iodine sufficient, thyroid antibody-negative population
also – to establish association between BMI and fT4, fT3
prospective population-based cohort Northern Finland Birth Cohort 1986 (9632 singleton births)
Thyroid 2011 Jan 22 epub ahead of print

Thyroid 2011 Jan 22 epub ahead of print
0.35
Assay reference range TSH 0.35-4.94

Thyroid 2011 Jan 22 epub ahead of print
Assay reference rangefT4 9-19
Assay reference rangefT3 2.62-5.7
5.7
19

Thyroid 2011 Jan 22 epub ahead of print
95%ile selected as upper limit therefore, upper limit of 2.7-3.1 mU/L in 1st trimester and 2.8-3.5 mU/L in early 2nd trimester

Thyroid 2011 Jan 22 epub ahead of print
TSH increases and fT4 decreases with increasing BMI
fT3 increases with increasing BMI

Screening in Pregnancy?
YES - ? potential harm to fetus if undiagnosed thyroid disease
NO – ? unclear benefits of screening in preventing adverse events
screening of only high-risk women failed to detect 30% of hypothyroid and 69% of hyperthyroid women
Vaidya B et al. 2007 J Clin Endocrinol Metab 92:203-7

J Clin Endocrinol Metab 2010 95(4):1699-707
4562 women, 2 centres in Italy randomized to universal screening or case-finding stratified as high risk or low risk all women in universal screening group, and high risk women in case-finding group, had TSH, fT4, antiTPO
low risk women in case-finding group: serum frozen, tested post-partum
Rx LT4 if TSH >2.5 if +anti-TPO, or Rx antithyroid medication if hyperthyroid

J Clin Endocrinol Metab 2010 95(4):1699-707

J Clin Endocrinol Metab 2010 95(4):1699-707
No difference in total number of adverse outcomes in case finding vs screening Majority of adverse outcomes in euthyroid groups

J Clin Endocrinol Metab 2010 95(4):1699-707
36/39 had at least 1
adverse outcom
e
19/51 had at least 1
adverse outcom
e
Interaction between thyroid status and trial arm: low risk women: adverse outcomes less likely in screening vs case finding inferred NNT = 1.8

J Clin Endocrinol Metab 2010 95(4):1699-707

J Clin Endocrinol Metab 2010 95(4):1699-707
universal screening vs case-finding did not result in less adverse outcomes
BUT - low risk women in universal screening group with abnormal thyroid function (who were treated) avoided adverse outcomes more often than low risk women in case finding group with abnormal thyroid function (not detected, so not treated)
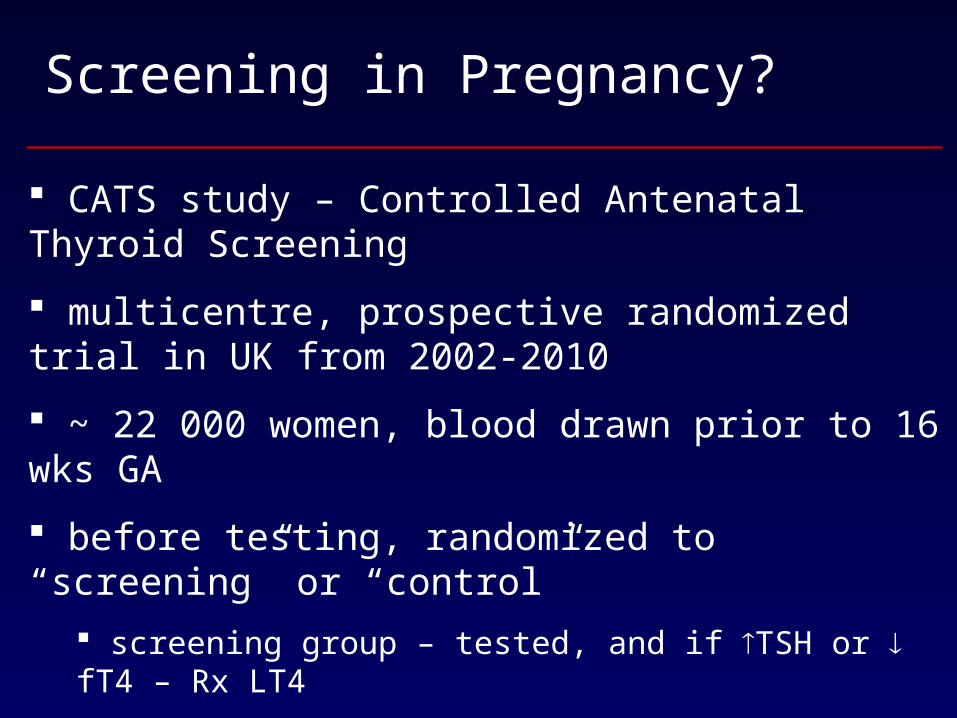
Screening in Pregnancy?
CATS study – Controlled Antenatal Thyroid Screening
multicentre, prospective randomized trial in UK from 2002-2010
~ 22 000 women, blood drawn prior to 16 wks GA
before testing, randomized to “screening” or “control”
screening group – tested, and if TSH or fT4 – Rx LT4
control group – tested post-partum, and if TSH or fT4 – Rx LT4 post-partum
1o outcome: children’s IQ at 38-40 months - no difference

J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47

Management – Special Considerations
Hyperthyroidism
goal – fT4 in upper limit normal range using lowest possible dose, monitor q4 weeks
PTU vs. methimazole ? – both equally effective
benefits of PTU: crosses placenta less readily, less excreted in breastmilk
decreased conversion fT4 to fT3
methimazole – risk of aplasia cutis, esophageal/choanal atresia (or is it due to hyperthyroidism itself?)

Management – Special Considerations
Endocrine Society Clinical Practice Guidelines – 2007
PTU is first line, especially during 1st trimester (organogenesis)
J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47
However – concern re: PTU and hepatotoxicity
2009 – meeting between American Thyroid Association and U.S. FDA reviewing role of PTU vs. methimazole in pregnancy
consider changing to methimazole in 2nd trimester?
Cooper DS & Rivkees SA. 2009 J Clin Endocrinol Metab, 94(6):1881-2

systematic review to assess the effects of interventions for preventing or treating hyperthyroidism in pregnant women
criteria – RCTs (or “quasi-randomized” trials), including abstracts, comparing antithyroid treatments in pregnant women
Cochrane Database Syst Rev 2010 (9):CD008633
unable to identify any eligible studies….

Conclusions:
unable to comment on implications for practice
early identification of hyperthyroidism before pregnancy may allow a woman to choose RAI or surgery before planning to have a child
Cochrane Database Syst Rev 2010 (9):CD008633

PTU in Pregnancy
Br J Clin Pharmacol 2009, 68(4):609-17
prospective observational controlled cohort study – 1994-2004 115 PTU-exposed pregnancies and 1141 controls 1o outcome – rate of major structural anomalies
PTU exposure between weeks 4-13 GA 2o outcomes – rate of fetal/neonatal thyroid dysfunction +/- goitre
PTU exposure beyond 13 weeks GA other – pregnancy outcomes, pre-term delivery, birth weight

PTU in Pregnancy
Rosenfeld et al. 2009 Br J Clin Pharmacol, 68(4):609-17
median daily dose of PTU 150 mg

PTU in Pregnancy
Rosenfeld et al. 2009 Br J Clin Pharmacol, 68(4):609-17
data on neonatal thyroid function in 87 cases and fetal thyroid ultrasound in 89 cases
16/87 had thyroid dysfunction: hypothyroidism - 7/74 (9.5%) pregnancies with PTU exposure after 13wks resulting in live birth
dose range 150-300 mg/day – dose constant until goitre found 3 without goitre, 4 with goitre
hyperthyroidism – 9/87 (10.3%) dose range 25-200 mg/day – 50% dose constant, 50% dose had been decreased 7 without goitre, 2 with goitre

PTU in Pregnancy
Rosenfeld et al. 2009 Br J Clin Pharmacol, 68(4):609-17
Conclusions:
no increased risk of major anomalies with PTU exposure from 4-13 weeks GA PTU exposure after 13th week GA:
9.5% neonatal hypothyroidism 10.3% neonatal hyperthyroidism
<50% goitre in neonates with thyroid dysfunction
role of directed fetal thyroid ultrasound in prenatal diagnosis of thyroid dysfunction, and for modification of PTU dosing ?

PTU in Pregnancy
Obstet Gynecol 2010, 116 Suppl 2:485-7
started PTU 1st trimester for Graves’ Disease at 30 wks GA, fever, sore throat, malaise, cough, dyspnea WBC 0.7 x109/L (3-10 x109/L), neutrophils 0.1x109/L (1.5-8 x109/L), lymphocytes 0.5 x109/L (1-3.5 x109/L) PTU stopped, Rx antibiotics & B, expectant management required thyroidectomy at 35 wks GA

Management – Special Considerations
Hypothyroidism – LT4
if diagnosed pre-pregnancy, target TSH <2.5 prior to pregnancy
if diagnosed during pregnancy, normalize TFTs as rapidly as possible
goal – TSH < 2.5 mIU/L in 1st trimester < 3.0 mIU/L in 2nd and 3rd
trimesters or to trimester-specific normal TSH range
J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47

Management – Special Considerations
Hypothyroidism – LT4
thyroid hormone requirements by 20-40% in pregnancy
? best way to meet these increased requirements in women with pre-existing hypothyroidism already on replacement

Management – Special Considerations Endocrine Society guidelines do not specify how
J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47

prospective randomized trial enrolled 60 pregnant women with 1o hypothyroidism on LT4, either seeking pregnancy or newly pregnant (<11wks GA)
on stable dose of LT4 for at least 6 wks prior, with normal baseline TSH within 6 months of conception
after pregnancy confirmed, randomized to either: group A – increase by 2 tablets/week (extra tablet Sat, W)
29% dose increase group B – increase by 3 tablets/week (extra tablet M, W, Fri)
43% dose increase
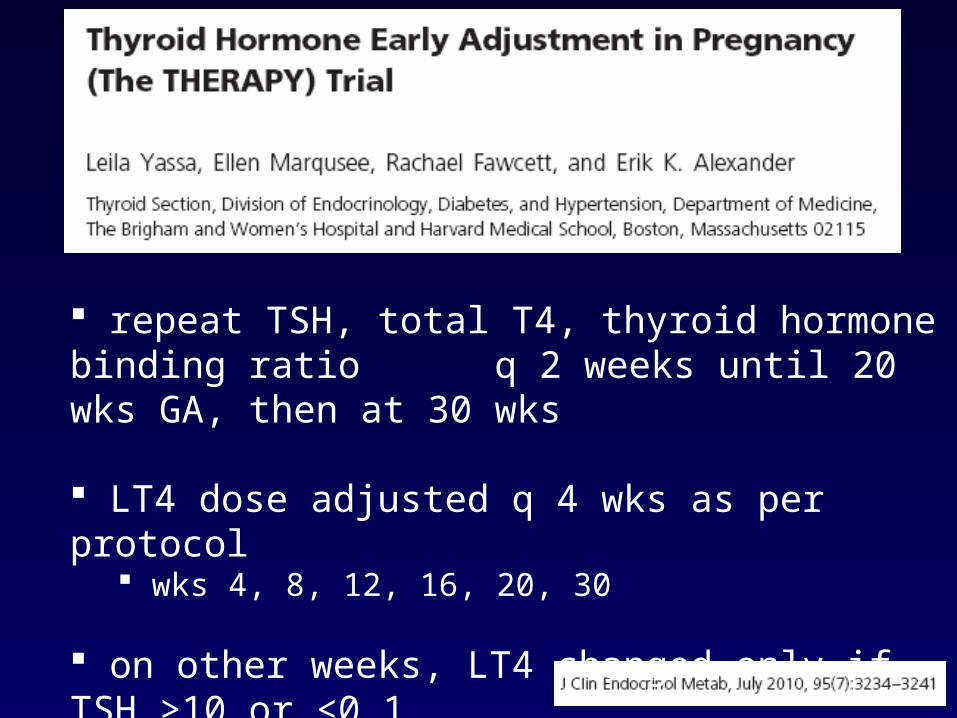
repeat TSH, total T4, thyroid hormone binding ratio q 2 weeks until 20 wks GA, then at 30 wks
LT4 dose adjusted q 4 wks as per protocol wks 4, 8, 12, 16, 20, 30
on other weeks, LT4 changed only if TSH >10 or <0.1
wks 6, 10, 14, 18

10 miscarriages (16.6%)1 stillbirth (20 wks – incompetent cervix)1 molar pregnancy




initial LT4 dose increase normalized TSH <5 in all patients for the remainder of the 1st trimester
initial LT4 increase caused TSH suppression <0.5 (or <0.1 in thyroid cancer patients) in:
8/25 = 32% in Group A 15/23 = 65% in Group B
P <0.01

P=0.02
18/29
13/20
20/32

also investigated optimal frequency of TSH evaluation
in 25 patients in Group A:
if tested every 4 wks, 24/26 (92%) of abnormal TSH values would have been detected
if tested every 6 wks, 19/26 (73%) of abnormal TSH values would have been detected

Conclusions:
a 29% LT4 dose increase (2 tablets extra/week) significantly decreased risk of maternal hypothyroidism throughout 1st trimester q4 week TSH required to detect further changes in dose requirements predictors of suppression: pre-pregnancy LT4 dose, pre-pregnancy TSH and etiology of hypothyroidism

2010 Thyroid 20(10):1175-8
retrospective study 53 pregnant women on LT4, with pre-conception (within 6 months) TSH <2.5, but within normal range stable LT4 dose pre-conception as at first visit divided into:
Group 1 – women who required LT4 dose increase Group 2 – women who did not require dose increase

2010 Thyroid 20(10):1175-8
pre-conception TSH higher in Group 1 vs. Group 2
1.55 + 0.62 mU/L vs. 0.98 + 0.67 mU/L (p<0.005)
when pre-conception TSH 1.2-2.4 – 50% needed when pre-conception TSH 0.1-1.2 – 17.2% needed
(p<0.02)

Management – Special Considerations
Subclinical Hypothyroidism
recall: ~3-5% of pregnancies
does this require treatment? is there any evidence showing benefit in treating?
what about euthyroid women with + antibodies?

to identify interventions used in management of clinical and subclinical hypothyroidism in pregnancy
to ascertain the impact of these interventions on important maternal, fetal, neonatal and childhood outcomes
Cochrane Database Syst Rev 2010 (7):CD007752

1o outcomes:
Maternal – pre-eclampsia (variously defined)Infant – pre-term delivery (<37 weeks GA)Infant as child – neurodevelopmental delay (variously defined)
Cochrane Database Syst Rev 2010 (7):CD007752

2o outcomes:
Cochrane Database Syst Rev 2010 (7):CD007752
Maternalmiscarriageanemiagestational HTNexcessive weight gainplacental abruptionpreterm laboursymptomatic hypothyroidism
PP hemorrhagePP depressionmaternal deathQOLinfertility
FetalIUFD
InfantSGAcretinismgoitreadmission to special care nurseryjaundice requiring Rxpoor feedinghoarse cryconstipation
lethargymacroglossiahypotonia

3 trials involving 314 women, all in Italy moderate iodine-deficient area
compared: levothyroxine vs. no treatment selenomethionine (selenium) vs. placebo levothyroxine adjusted dose vs. no adjusted dose
all at moderate risk of biasCochrane Database Syst Rev 2010 (7):CD007752

Results - LT4 vs. none: euthyroid women with +anti-TPO
risk of pre-term birth
non-significant trend towards fewer miscarriages (1st trimester)
Cochrane Database Syst Rev 2010 (7):CD007752
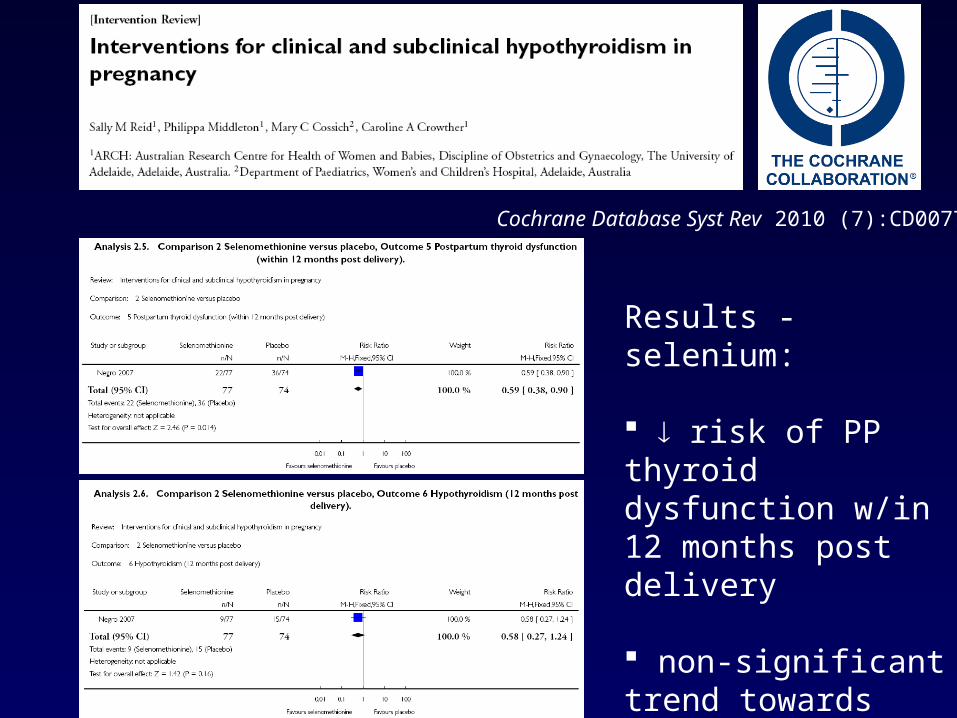
Results - selenium:
risk of PP thyroid dysfunction w/in 12 months post delivery
non-significant trend towards less overt hypothyroidism 12 months post delivery
Cochrane Database Syst Rev 2010 (7):CD007752

Conclusions:
LT4 in overt hypothyroidism – standard practice
“Whether levothyroxine should be utilised in autoimmune and subclinical hypothyroidism remains to be seen, but it may prove worthwhile, given a possible reduction in preterm birth and miscarriage.”
selenium – promising, but needs further studyCochrane Database Syst Rev 2010 (7):CD007752

Management – Special Considerations
Endocrine Society Clinical Practice Guidelines – 2007
LT4 treatment recommended in all pregnant women with subclinical hypothyroidism
not proven to modify long-term neurological development in offspring, but improvement in obstetrical outcomes
potential benefits outweigh potential risks
J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47

Objectives
To briefly review thyroid anatomy and physiology in pregnancy and fetal thyroid physiology
To review causes of thyroid disease in pregnancy
To review the maternal and fetal outcomes of thyroid disease in pregnancy
To discuss the controversy surrounding screening for thyroid disease in pregnancy
Objectives
To review special considerations in management of thyroid disease in pregnancy
To highlight recent 2009-2011 articles published on thyroid disease in pregnancy

References
Casey BM & Leveno KJ. Obstet Gynecol 2006;1081283-9 Keely E & Casey BM (2010). Thyroid disease in pregnancy. In RO Powrie, MF Greene, W Camann (Eds) de Swiet’s Medical Disorders in Obstetric Practice (5th Edition pp322-34). West Sussex, Wiley-Blackwell Arnaud-Lopez L et al. 2008 Am J Hum Genet 82:1270-80 Shields BM et al. 2009 J Clin Endocrinol Metab 94(11):4608-12 Pearce EN et al. 2003 N Engl J Med 348:2646-55 J Clin Endocrinol Metab 2007, 92(8):Suppl:S1-47 Cooper DS & Rivkees SA. 2009 J Clin Endocrinol Metab, 94(6):1881-2 Earl R et al. 2010 Cochrane Database Syst Rev, (9):CD008633 Rosenfeld H et al. 2009 Br J Clin Pharmacol, 68(4):609-17 Murji A et al. 2010 Obstet Gynecol, 116 Suppl 2:485-7 ACOG Practice Bulletin Obstet Gynecol 2002, 100(2):387-396 Yassa L et al. 2010 J Clin Endocrinol Metab, 95:3234-41 Abalovich M et al. 2010 Thyroid 20(10):1175-8 Reid SM et al. 2010 Cochrane Database Syst Rev, (7):CD007752

References
Negro R et al. 2006 J Clin Endocrinol Metab 91(7):2587-91 Negro R et al. 2007 J Clin Endocrinol Metab 92(4):1263-8 Rotondi M et al. 2004 Eur J Endocrinol 151:695-700 Dashe JS et al. 2005 Obstet Gynecol 106:753-7 Männistö T et al. 2011 Thyroid Jan 22 epub ahead of print Vaidya B et al. 2007 J Clin Endocrinol Metab 92:203-7 Negro R et al. 2010 J Clin Endocrinol Metab 95(4):1699-707 Henrichs J et al. 2010 J Clin Endocrinol Metab 95(9):4227-34


Negro R. et al. 2006 J Clin Endocrinol Metab 91(7):2587-91
115 euthyroid anti-TPO+ women randomized to LT4 vs. no treatment
0.5 ug/kg/d if TSH <1 mIU/L, 1.0 ug/kg/d if TSH 1-2 mIU/L, 1.5 ug/kg/d if TSH >2 mIU/L or anti-TPO > 1500 kIU/L
euthyroid anti-TPO- women were controls
gestational HTN, severe pre-eclampsia, pre-term birth, TSH, fT4, miscarriage, abruption, neonatal characteristics
Cochrane Database Syst Rev 2010 (7):CD007752

Negro R. et al. 2007 J Clin Endocrinol Metab 92(4):1263-8
169 euthyroid anti-TPO+ women randomized to selenium 200 ug/d) at or after 12 wks GA vs. placebo anti-TPO- women were controls
permanent hypothyroidism, PP thyroid dysfunction, TSH, fT4, anti-TPO Ab levelsCochrane Database Syst Rev 2010 (7):CD007752

Rotondi M. et al. 2004 Eur J Endocrinol 151:695-700
25 women with 1o hypothyroidism (Hashimotos or thyroidectomy) on LT4 who were anticipating pregnancy within next 1 yr, randomized to “modified” (target low-normal TSH) vs. “non-modified” (same dose), then seen at <12 wks GA
TFTs pre-conception and post-conceptionCochrane Database Syst Rev 2010 (7):CD007752











![For Selina Wallis LC 05.09[1]](https://img.dokumen.tips/doc/110x75/577dac301a28ab223f8d8b51/for-selina-wallis-lc-05091.jpg)