Embed Size (px)
Citation preview

5/12/2015
1
Chienying Liu MD
Common Thyroid ProblemsCase‐Based Discussion
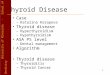
Schematic diagram of a follicular cell, illustrating the steps involved in thyroid hormone synthesis.
Park S M , and Chatterjee V K K J Med Genet 2005;42:379-389
©2005 by BMJ Publishing Group Ltd
cAMP

5/12/2015
2
Case 1 ‐ Hyperthyroidism
63 yo man not feeling himself, with unintentional weight loss and eyes feeling irritated
• Exam
– Thyroid, not enlarged, somewhat firm, no nodules, no bruits
– Subtle exophthalmos in the right eye with mild conjunctival erythema
• Came to us with the following labs
– TSH < 0.01
– Free T4 1.09 (<1.8)
– Free T3 4.40 (< 4.2)
– TPO antibody 101 (<34)
– Tg antibody positive
T3 toxicosis
(Common) Causes of Hyperthyroidism
• Graves disease– The most common cause of hyperthyroidism
– Caused by stimulating autoantibodies to the TSH receptor ( measured by TSI or TBII)
– TPO and or Tg AB frequently present 70‐90 %
• Toxic nodule/Toxic MNG
– 1.5‐44.5% of hyperthyroidism, depending on the iodine intake
– 2% in the United States
www.thyroidmanager.org

5/12/2015
3
Causes of Hyperthyroidism• Thyroiditis
– Autoimmune (painless) = subacute lymphocytic thyroiditis (1‐ 5%)• Postpartum thyroiditis also an example• TPO present in 50% of these patients at the time of diagnosis • Clinically, may not be differentiated from Graves disease on PE
– Infectious (very painful gland)• Post‐viral: Subacute granulomatous thyroiditis = de Quervain's thyroiditis ( < 1%)
– Strongly associated with HLA‐B35– ESR very elevated
• Acute Bacterial infection: fevers/chills, unilateral neck pain. May have hyperthyroidism
– Drug induced• Interferon‐alfa→ induced autoimmunity: painless thyroidi s or Graves disease• Interleukin 2 (for leukemia) • Lithium → mostly hypothyroidism but can induce autoimmune: Graves or painless thyroidi s• TKIs → usually hypothyroid but may also have destruc ve thyroidi s• Amiodarone induced type II hyperthyroidism → destruc ve thyroidi s
– Others• Radiation , palpation
Iodine ScanUptake 0 or very low
Causes of Hyperthyroidism
• Exogenous thyroid hormone
• Rare– TSH mediated (TSH secreting pituitary adenoma)
– Struma Ovarii• Autonomous functioning thyroid tissue in the teratoma
– Trophoblastic disease• Hydatidiform mole or choriocarcinoma (↑
– Metastatic thyroid cancer
– Familial non‐autoimmune hyperthyroidism• Due to a gain of function in the TSHR• Autoantibodies negative• Neonatal hyperthyroidism
– Thyroid hormone resistance

5/12/2015
4
Case 1 ‐ Hyperthyroidism
Diagnostic Test of Choice
• TSH receptor antibody testing
– TSI 433 (< 140 %)
• Iodine Uptake scan
– Diffuse uptake
– 4h 10% and 24 h 21%
– TSH < 0.01
– Free T4 1.09 (<1.8)
– Free T3 4.40 (< 4.2)
– TPO antibody 101 (<34)
– Thyroglobulin antibody positive
CourseStarted on Methimazole
Euthyroid on 5mg 5 months later
T3 toxicosis
Case 2 ‐ Hyperthyroidism• 60 yo presented with apparent exophthalmos and chemosisand atrial fibrillation
– TSH < 0.01
– Free T4 20 (9‐24)
– Free T3 436 (145‐348)
– TPO and TgAB negative
– TSI negative
• Thyroid gland mildly enlarged 2‐3 x, firm
Additional Test(s)?
• TBII Positive
• Iodine scan Not done (not needed)
T3 toxicosis

5/12/2015
5
TSH Receptor Autoantibodies
• TSH receptor is the major auto‐antigen in Graves’ disease (GD)
Antibodies include:
– Stimulating, most common
– Inhibitory/blocking
• Thyroid atrophy and hypothyroidism
– Neutral
– In GD hyperthyroidism, the stimulating type predominates
Best Practice & Research Clinical Endocrinology & Metabolism Vol. 19, No. 1, pp. 33–52, 2005
TSH Receptor Autoantibodies‐ Clinical Use• Differentiate GD from other causes of hyperthyroidism
• Predict risk of fetal or neonate hyperthyroidism
• ?? Predict remission or relapse in GD after antithyroid medications– In a meta‐analysis from 1994**:
• AB+ pts 3 times more likely to relapse• But 25% of AB‐ pts relapsed
25% of AB+ pts stayed in remission
– Recent studies: utility in prediction is yet to be proven*• heterogeneous populations, different assays, timing, duration of follow up, different cut offs to define positivity
* Kamath et al J of Thyroid Research 2012 **Feldt‐Rasmussen et al JCEM 1994

5/12/2015
6
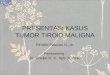
Kamath et al J of Thyroid Research 2012
Graves’ DiseaseAssessment of TSH Receptor Autoantibodies (TRAb)
TSI = Thyroid Stimulating Immunoglobulin
Bioassay
TBII = Thyroid Binding Inhibitory Immunoglobulin
Immunoassay

5/12/2015
7
Graves’ Disease Assessment ‐TSI
• Bioassay detecting cAMP production
(Measures the final balance of all TRAb) – 2nd generation (2 steps), cumbersome
• Detect cAMP using RIA
• Sensitivity 85‐90%, Specificity 99%
– 3rd generation• Employing luciferase reporter gene
• Higher sensitive
• Quest/Labcorp: 92% sensitive and 99.3% specific
– Advocates of this test: reflect clinical phenotype better
J Clin Endocrinol Metab 98 (2013): 2247–2255Lytton et al. Autoimmunity Review 2010
Graves’ Disease Assessment‐ TBII
• Competitive Immunoassay
(Measures TRAb of all types)– 1st generation – poor sensitivity
– 2nd generation • Used labeled TSH to TSH receptor from CHO or a recombinant TSH receptor protein preparation
• Sensitivity 97.1%, Specificity 97.4% (meta‐analysis)*
– 3rd generation• Replaced labeled TSH with specific TSH human monoclonal stimulating antibody M22
• Sensitivity 98.3%, Specificity 99.2% (meta‐analysis)*
Quest: Sensitivity 92%, specificity 100% (kronus)
Mayo Clinic: Sensitivity 95%, specificity 97% (Roche)
• There can be between method variability and suboptimal inter‐assay precision
*Autoimmunity Reviews 12 (2012): 107–113

5/12/2015
8
Case 2 ‐ Hyperthyroidism
• 60 yo women presented with apparent exophthalmos and chemosis and atrial fibrillation– TSH < 0.01
– Free T4 20 (9‐24)
– Free T3 436 (145‐348)
– TPO and TgAB negative
– TSI negative
• Thyroid exam – mildly enlarged, firm
Additional Test(s)?
• TBII positive 81% (<16%) inhibition
Clinical Course
• On methimazole
• Eye disease improved
• On MMI 10‐15mg 2‐3 years later– No side effects
– Wants to continue MMI
Case 3 ‐ Hyperthyroidism
• 47 yo woman presented with palpitations and some weight loss
• Maybe some URI symptoms 1‐2 months prior to presentation
– TSH 0.03
– Free T4 18 (10‐18)
– Free T3 6.5 (<5.7)
• Came to us for a consultation, 2.5 weeks later
• Exam
– Non‐tender gland, palpable but not grossly enlarged, no nodules
– No ophthalmopathy, not grossly hyperthyroid
Another case of T3 toxicosis

5/12/2015
9
Case 3 ‐ Hyperthyroidism
• Repeat labs + TSHR Ab at the time of the visit
– TSI negative
– TSH 0.38
– Free T4 9
– Free T3 3.6
3/4/2015 3/30/2015
TSH 18.90 (H) 4.58 (H)
Free T4 10 ‐ 18 pmol/L 7 (L) 8 (L)
Free T3 2.6 ‐ 5.7 pmol/L 3.7 2.8
TPO >850
Subacute Lymphocytic Thyroiditis = Silent Thyroiditis If uptake scan were performed early on when
hyperthyroid, uptake = very low
Monitor TFT – at risk for hypothyroidism
Course• Not symptomatic of hypothyroidism• Feeling better with time• Wants to be monitored
Case 4 ‐ Thyroid Nodule
• 32 yo woman presented with right neck pain that turned out to be musculoskeletal
• Found to have a 2.5 cm hypoechoic nodule
• Exam not remarkable other than the palpable nodule
• Work up:
– TSH 0.11, then 0.39
– TSH 0.46 (0.4‐4.0)
– Free T4 11 (9‐24)
– Free T3 284 (145‐384)
– TPO 119 (<60)
– TSI negative

5/12/2015
10
Case 4 – Thyroid Nodule
• Biopsy = follicular neoplasm
• Iodine uptake scan showed a hot nodule in the right with suppression of the rest of the gland
Treatment Options• Monitor given normal TFT• RAI• Surgery• ATD
• New strategies– Ethanol injection– Percutaneous laser thermal ablation
Hyper‐functioning Thyroid Nodule• Usually a follicular adenoma
– 57% of 75 toxic adenomas found to have TSHR mutations, 3%‐ Gsαmutations in a study– When biopsied – FNA shows either a benign nodule or follicular lesion/neoplasm
• Definitive diagnosis of follicular adenoma cannot be made on biopsy• Surgical resection needed to exam the capsule
• Risk of malignancy is said to be very low, biopsy not needed in most patients– Not completely free of cancer .– Case reports of malignancy, especially in children
• Progression from a hyperfunctioning nodule to a toxic nodule ‐ 4% year– Risk higher in older pts, nodules > 3 cm, in areas of low iodine intake
• Heterogeneity in clinical behavior of hyperfunctioning nodules– Thyrotoxicosis is usually not common < 2.5 cm – there are exceptions– Only about 30‐40% of hyperfunctioning nodules > 3‐4.5 cm are toxic
Krohn et al. Endocrine Reviews 26(4):504–524 2005; Corvilain Ann. Endocrinol 2003 (217 pts in Belgium)

5/12/2015
11
Treatment Modalities & Risk of Hypothyroidism
• Radioactive Iodine Treatment– Risk of hypothyroidism, variably reported– Incidence of hypothyroidism may increase with time
• 11% at 1 year, 33% at 5 years, and 49% at 10 years in a study of 105 patient
– Euthyroidism ( 9.7% vs 1.5% with hyperthyroid hot nodule) is a risk factor– Presence of thyroid antibody status is a risk factor– Pretreatment with ATD (raise TSH) is a risk factor– No correlation demonstrated with nodule size and radioiodine dose, or iodine uptake,
or degree of adjacent suppression on scans
• Surgery– Risk of hypothyroidism, 4.4% in one study, 14% in another– May also depend on antibody status
• ATD– Not curative, but may be considered in selected cases
Thyrotoxicosis of Other Etiology. ThyroidManager.org
Case 4 – Thyroid Nodule
• Biopsy = follicular neoplasm
• Uptake scan showed a hot nodule in the right with suppression of the rest of the gland
Treatment Options• Monitor given normal TFTs• RAI• Surgery• ATD?
• Newer strategies– Ethanol injection– Percutaneous laser thermal ablation
• Course• Elected surgery – Lobectomy• Path‐ Benign adenoma• On T4 25 mcg

5/12/2015
12
Case 5 – Hyperthyroidism + Nodule
• 30 yo woman presented with nausea, headaches, and malaise
• Exam – right thyroid fullness
• TFT– TSH 0.01
– Free T4 17
• US showed a 2.9 cm ill defined right nodule
• Uptake scan showed a hyperfunctioning nodule
Papillary Thyroid Cancer
Mirfakhraee et al. Thyroid Research 2013Review of cases 1950‐2012

5/12/2015
13
Hyperthyroidism Work UP‐ Take Home Messages
• Given that Graves disease is the most common in the iodine replete areas, obtaining a TSH receptor antibody testing ie either TSI or TBII is most cost effective
• TPO and Tg antibodies usually not every helpful in the work up of hyperthyroidism in most cases
• Uptake scan should be considered as the next step– If TSH receptor antibody testing is negative and thyroid function results are not
improving– If a nodule is present (> 1 cm)
• Especially if negative TSH receptor antibodies
– T4 and T3 profile can be helpful but is an overall relatively insensitive assessment of etiologies for hyperthyroidism
• Risk of malignancy is low in hyperfunctioning nodules but not zero– Biopsy is not needed in most cases
• Look at ultrasound characteristics and biopsy suspicious appearing nodules
32 yo woman not responding to LT4
• Graves disease, status post RAI ablation in 2013
• Started on LT4 one month later
• Never had normal TSH levels by report
• 02/13/2015: TSH 38.8 when on 75 mcg
• 02/25/2015: TSH 72 (0.5‐4.8) on 150mcg– FT4 0.92 (0.8‐1.7)
– T3 48 (55‐170)
• 03/12/2015: on 225mcg
• Exam – Weight 51 kg
– Mildly tachycardic
– Mild tremors and warmth on the outstretched hands
Differential Diagnoses
1. Noncompliance
2. Interfering drugs or supplements
3. Malabsorption
4. Lab error/issuesHeterophile antibodies
MacroTSH (anti TSH IgG‐TSH complex)
5. Conversion?
6. Others?
Preissner JCEM 2003

5/12/2015
14
Levothyroxine (l‐thyroxine)• Synthetic form of thyroid hormone, structurally identical to human thyroxine secreted
by the thyroid gland– Various brands have slightly different preparations and fillers, but with the same active
ingredient– ½ life is 7 days
• Absorption takes place in the small intestine– 45% upper jejunum, 34% lower jejunum and ileum, 21% duodenum (End Rev 2014)
• Gastric acid (acidic PH) important for its subsequent absorption– Best absorbed when fasting
• 70‐80% of the given dose is absorbed → IV conversion
• Metabolized in liver, eliminated by kidneys
Endocrine Reviews 2014
Food and beverages Interfering L‐thyroxine Absorption
• Best absorption to poorest absorption
60 min prior to breakfast
Bedtime (3 hours after last meal)
30 min prior to breakfast
With breakfast
– Most consistent TSH levels achieved at fasting states
• Coffee, especially espresso coffee – Probably by sequestering LT4 in the small intestine
• Fiber
• Soy products – Problematic for infants with CH, fed with soy formula
• Others– Cotton seed meal
– Walnuts
ATA guidelines on Treatment of Hypothyroidism Thyroid 2014Endocrine Reviews 2014

5/12/2015
15
Supplements/Drugs Interfering Absorption
• Calcium supplements• Ferrous iron• MVI that has calcium and/or iron• Phosphate binders (sevelamer)• Aluminum antacids• PPI and H2 blocker
– Short term co‐administration PPI ‐> no change in absorption
• Sucralfate (mixed results)• Orlistat• Rolaxifene (decreased absorption)• Cholestyramine• Colesevelam
• Chromium picolinate• Charcoal• Ciprofloxacin• Kayexelate
• Synthroid package insert:– Iron, calcium supplements and antacids should not be
administered within 4 hours – Has a caution statement on soy regarding its effects on
absorption– Other food cautions: cotton seed meal, walnuts, fibers
• Soy ? 4 hours
ATA 2014 Hypothyroid Guidelines
ATA guidelines on Treatment of Hypothyroidism Thyroid 2014
Gastro‐Intestinal Disease Affecting Absorption
• Diseases affect gastric acid production– H‐Pylori – Autoimmune atrophic gastritis
• Anti‐parietal cell antibody or IF antibody
• Disease affecting the small intestine– Celiac disease
• IgA antiendomysial antibody or tissue transgluaminase IgA antibody
– GI surgeries affecting the small bowel• (there are also data showing L‐thyroxine absorption preserved in Roux‐en‐Y patients)
– Lactose intolerance• Case reports of 900mcg requirement to 150ug after lactose free diet
– Intestinal giardiasis

5/12/2015
16
32 yo woman not responding to LT4
• Her husband vouched for her compliance
• We lowered her T4 dose empirically to 150mcg and repeat blood tests and obtained additional work up:
• 4/6/2015 on 150mcg
Take Home Message
• Consider various causes of high T4 requirement
– ? Lab issue or error in this case
– Autoimmune gastritis in this case
3/12/2015
TSH (0.45 ‐ 4.12 mIU/L) 0.26 (L)
Free T4 (10 ‐ 18 pmol/L) 25 (H)
T3, Total (0.9 ‐ 2.4 nmol/L) 1.7
3/12/2015
Tissue Transglutaminase Antibody, IgA
<20.0 CU
<10.0
Vitamin B12 211 ‐ 911 ng/L 245
Intrinsic Factor Blocking Antibody POSITIVE
4/6/2015
TSH 3.83
Free T4 10 ‐ 18 pmol/L 15
T3, Total 0.9 ‐ 2.4 nmol/L 1.3
20 yo woman TSH high normal, feeling tired
• Healthy otherwise
• FH positive for hypothyroidism
• Exam ‐ small goiter (right>left), firm by palpitation
• Ultrasound
– Prominent thyroid with diffuse heterogeneous echo‐texture with minimal increase in vascularity
• 1/10/2014: TSH 3.01
• 8/22/2014: TSH 5.43, FT4 1.08 (0.89‐1.76)
• TPO negative, Tg AB positive
• 1/05/2015: TSH 3.96, FT4 0.81
Do you treat?

5/12/2015
17
TSH TargetsNo known thyroid disease/goiter and Antibodies Negative
NHANES III NHANES III Distribution by Age
Hollowel J Clin Endocrinol Metab 2002 Surks J Clin Endocrinol Metab 2007
TSH 0.45 – 4.12 mIU/L = 2.5 to 97.5 percentile
Age Specific Distribution of TSH
Surks J Clin Endocrinol Metab 2007

5/12/2015
18
Age Specific TSH Reference Range
Boucai et al THYROID 2011
TSH ‐ 97.5 centile by Age Group

5/12/2015
19
Subclinical Hypothyroidism
• TSH ≥10 → Treat
– Meta‐analyses
• Increased HF (Gencer et al Circulation 2012)– Also some increase with TSH >7 ‐9.9 but more significant when TSH ≥ 10
– 80 yo or older, risk not increased
• Increased CV events and CV mortality (Rondondi JAMA 2010)
– One meta‐analysis suggested significance in younger patients only (<65 yo) (Razvi JCEM 2008)
– No randomized studies to evaluate benefits of treatment
Subclinical Hypothyroidism
• TSH 4.5‐10 →Mixed data/treatment is controversial (studies were in older individuals)
– Not as clearly associated with adverse CV events from observational studies
– No clear CV benefits, inconsistent LDL benefits with tx *
• Possible benefits of tx in CV events in patients 40‐70 yo but not older than 70 yo(Razi Arch Intern Med 2012, retrospective study )
– No demonstrated improvement in quality of life or cognitive function in older patients with tx (50s‐70s yo)*
– ATA 2012 guidelines: Consider antibody status, symptoms before treatment
– DO NOT OVERTREAT older individuals
• Older individuals (>70 yo) may have TSH in this range, because of normal aging
*Rugge Ann Intern Med 2015

5/12/2015
20
Subclinical Hypothyroidism
• TSH 2.5‐4.5
– Small studies showed benefits of tx in lipids, endothelial function, intima media thickness
– But no clinical outcome data
– Exception: women considering pregnancy
• Increased pregnancy loss for TSH 2.5‐5.0 during 1st trimester (Negro R JCEM 2010)
• Keep TSH < 2.5 prior to conception (Endocrine Society guidelines 2012)
• During pregnancy: TSH goal: 1st Trimester 0.1‐2.5; 2nd trimester 0.2‐3; 3rd trimester 0.3‐3.
Treatment of Subclinical Hypothyroidism
• Full replacement dose 1.6mcg/kg body weight (more lean body weight dependent)– Older patients require less, lower lean body weight
• Patients with subclinical hypothyroidism do not need full replacement– 25‐50mcg if TSH ≤10 *
– Consider age and risk for CAD when dosing, use lower dose
• Monitor TSH, 4‐6 weeks after initiation or a dose change*– Target range depending on ‘age and comorbidities’ , typically 0.5‐3.5 to 4 mIU/L *
– Target range 4‐6 mIU/L for persons >70‐80 yo* *ATA guidelines Thyroid 2014

5/12/2015
21
20 yo woman TSH high normal, feeling tired
• High normal TSH
• FH of hypothyroidism, evidence of thyroiditis (exam)
• What could be the ‘proven’ benefit of treatment?– A reduction in goiter size
(Romaldini Thyroid 1996)
• What could be the potential harm of treatment?– Likely minimal in this young pt
• May consider a trial of LT4
• TSH goal ‐ the lower half of the normal range for this young patient
• Also work up other causes of fatigue
• If she were to consider pregnancy → keep TSH < 2.5 mIU/L
THANK YOU