Embed Size (px)
Citation preview

terms/def
All of the following sites are generally accepted for IM injections EXCEPT one. Which one is the EXCEPTION?
• the buttocks
• the biceps muscle
• the deltoid muscle
• the anterior thigh
1 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
terms/def
Which term refers to a drug that binds to physiological receptors to result in specific cellular effects producing a predictable pharmacologic response?
• pharmacologic agonist
• pharmacologic antagonist
PHARMACOLOGY
2 copyright©2013-2014-Dental Decks

the biceps muscle
*** For young children, the anterior thigh is usually the place to give IM injections.
Absorption from an intramuscular injection is often faster and there is a higher bioavailability than with oral administration.
Proper depth of needle in muscle: In big muscle (adult) go in one inch; in children go in one-quarter of an inch. Never go beyond two-thirds of the needle length.
• pharmacologic agonist
Drugs that bind to physiologic receptors and mimic the regulatory effects of endogenous signaling compounds will produce a pharmacologic effect as a result of binding to the receptor. A drug that elicits a full response through this process is referred to as a pharmacologic agonist.
A partial agonist is a drug which acts on the physiologic receptor but elicits an effect which is only partly as effective as an agonist drug.
An antagonist is a drug which binds to the physiologic receptor but does not trigger an effect. When antagonist is present, the agonist drug cannot reach the receptor site to produce an effect.
1. Competitive antagonism occurs when a response can be achieved by increasing the dose of agonist in the presence of antagonist. 2. Noncompetitive antagonism occurs when a response cannot be achieved with increasing doses of agonist in the presence of antagonist.

terms/def
Which of the following routes of drug administration is generally used for local drug effects?
• topical administration
• oral ingestion
• subcutaneous injection
• intravenous injection
PHARMACOLOGY copyright © 2013-2014 - Dental Decks
The most important enzyme systems molecules are found in:
• lungs
• liver
• brain
• kidneys
• gastrointestinal tract
terms/def
for the biotransformation of drug
4 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

' topical administration
Common routes of administration of drugs: 1 Parenteral administration (not by way of intestine or GI tract)
• Intravenous (IV) - directly into the bloodstream. Acts very rapidly. • Intramuscular (fM) - injected into a muscle area, where it is promptly absorbed • Subcutaneous - injection beneath the skin. Absorption may be less rapid.
2. Enteral administration (by way of the intestine or GI tract) • Buccal or sublingual - a tablet is placed under the tongue or in the cheek • Oral - (most common route), the drug is swallowed. It is the most convenient for safe drug administration. It is safe, painless and economical. • Rectal - the drug in solution (enema) or suppository form is inserted into the rectum
3. Inhalation - the drug is given as an aerosol into the respiratory tract.
4. Topical administration - the drug is placed on the skin for a local effect.
5. Transdermal - the drug is placed within a "patch" and placed on the skin to be absorbed into the systemic circulation.
• liver
Hepatic metabolism of drugs occurs in Phase I reactions catalyzed by a microsomal mixed-function oxidase system (also known as the P-450 system) and in Phase II reactions known as conjugation reactions.
Phase I reactions: • Occur in the liver microsomal enzyme system (mixed-function oxidase system or P-450 system). In this system, drug metabolism occurs in three basic patterns. First, the active parent drug can be converted to the inactive metabolite. Second, an active parent drug may be converted to a second active compound which is subsequently converted to an inactive compound; and thirdly, an inactive parent drug may be transformed to an active compound. • The most common reaction in drug metabolism is an oxidation reaction in which oxygen in the form of hydroxy 1 group is attached to the drug molecule. • There are at least eight distinct groups of microsomal drug metabolizing enzymes: These enzyme "families" are identified as a cytochrome (CYP prefix) followed by their numerical digestion (e.g., 1A2). Thus the enzyme CYP 1A2 is a distinct drug metabolizing enzyme that converts a variety of drugs to the oxidized product.
Phase II reactions: • Conjugation reactions involve coupling the drug with an acid present in cells (usually glucuronic acid). When coupled to glucuronic acid, the process is known as glu-curonide conjugation with the resulting metabolite referred to as the "glucuronide." • Conjugations occur in the liver, kidney and to a lesser extent in other tissues. • Conjugation of drugs results in polar, water-soluble compounds that are rapidly excreted in urine. Thus, the parent drug is effectively rendered inactive and transported out of the body by this process.

terms/def Implicit in the interaction of a drug with its physiological receptor is that the drug create effects, but rather, modulates physiological cell functions.
• does; extrinsic
• does not; extrinsic
• does; intrinsic
• does not; intrinsic
5 copyright © 2013-2014 - Dental Decks
ADOIODVIATOVHd s p a a lejuarj -1,LOZ-E iOZ @
9
jep/suud)
1ll6!jAdoD
:s]
uo!ie|Bqu|.
|BP3J •
Ah
|BJO •
i uojiejismjiupe 6mp JOJ ainoj jsaisea pue isajes a q i

• does not; intrinsic
There are four major families of physiological receptors that drugs can bind to produce effects:
• Receptors as enzymes (i.e., cell surface protein kinases): These kinases exert their regulatory effects by phosphorylating proteins within the cell which alters the cellular biochemical activities. By binding to these kinases, drugs can also cause the alteration in biochemical activities resulting in a drug effect.
• Ion channels: Drugs can bind to ion channels in cell membranes to cause opening or closing. This alters the cell's membrane potential to result in a drug effect.
• G protein-coupled receptors: When drug binds to these receptors, second messengers are produced such as cyclic AMP to produce an effect within the cell. This results in a drug effect.
• Receptors in cell nucleus: Receptors for steroid hormones are soluble DNA-transcription factors within the nucleus that regulate the transcription of specific genes. Modification of the transcriptions of these genes results in a drug effect.
• oral —*** abbreviated P.O.
However, it is also the most unpredictable and least effective route available. Drugs taken by mouth have to be absorbed (usually from the small intestine) before they can be transported to their site of action. Absorption may be slow, unpredictable and irregular due to the presence of variable amounts of food in different stages of digestion and to the varying degrees of acidity and alkalinity of the digestive juices. Moreover, blood from the intestinal tract passes first to the liver: some drugs are metabolized in the liver and others may be stored there to be released only slowly. These considerations make it clear that oral administration is usually unsuitable in emergencies or on other occasions when a rapid effect is needed.
Note: After oral administration, drugs will generally be absorbed best from the duodenum. The duodenum has a large surface area due to the presence of villi and microvilli.
Note: A major advantage of IV administration of a drug is it allows for titration of the drug.
Other advantages of IV administration include: • Rapid onset • Drugs that cause irritation when administered subcutaneously can be given IV with no irritation • In case of emergency, there is an open line through which emergency drugs can be injected
One major disadvantage of IV injection is that since it has such a rapid onset of action, overdosage may have effects so immediate that it is impossible to reverse them.

The majority of drugs penetrate biomembranes by membrane phospholipids.
terms/def
through
• active transport
• facilitated diffusion
•filtration
• simple diffusion
PHARMACOLOGY
A teaspoon can hold what volume of liquid?
• 5 milliliters
• 10 milliliters
• 15 milliliters
• 20 milliliters
copyright S 2013-2014 - Dental Decks
terms/def
PHARMACOLOGY
8 copyright 6 2013-2014 - Dental Decks

• simple diffusion
The mechanism of drug transfer across biological membranes is by:
1. Passive transfer — is essential to various processes of metabolism • Simple diffusion: lipid-soluble substances move across the lipoprotein membrane by this process. The majority of drugs penetrate biomembranes by this process through membrane phospholipids. The amount of drug dissolving in the membrane at any time is directly proportional to the concentration gradient and its degree of lipid solubility (Note: Only nonionized drugs are soluble in lipid). • Filtration: water-soluble molecules small enough to pass through membrane channels may be carried through the pores by the bulk flow of water. Drugs of molecular weights of 60,000 or less can "filter" through capillary membranes.
2. Specialized transport • Active transport: lipid-insoluble substances (for example glucose) are shuttled across plasma membranes by forming complexes with specific membrane constituents called carriers. These carrier molecules within a cell furnish energy for transportation of the drug to regions of higher concentration. Facilitated diffusion is the term given to carrier-based transfer when the driving force is simply the concentration difference of the drug across the membrane.
Note: Osmosis is the movement of a pure solvent, as water, through a semipermeable membrane from a solution that has a lower solute concentration to one that has a higher concentration. The membrane is impermeable to the solute but is permeable to the solvent.
Remember: The physiochemical properties of drugs that influence their passage across biologic membranes are: lipid solubility, degree of ionization, and molecular size and shape.
5 milliliters
Approximate Household Measures and Weights
Teaspoons
1
3
48
Tablespoons
1
16
Cups or Glasses
1
Fluid Ounces
0.166
0.50
8
Milliliters
5
15
240
Grams
5
15
240

Which of the following drugs are known to as an adverse reaction. Select all that apply.
• levodopa (Larodopa, Dopar)
• prazosin (Minipress)
• indomethacin (Indocin)
• morphine
PHARMACOLOGY
produce
terms/def
orthostatic hypotension
g copyright©2013-2014-Dental Decks
terms/def
Pain that has no organic basis and is fixed upon some portion of the anatomy is referred to as:
• intractable pain
• referred pain
• psychogenic pain
• phantom pain
10 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY

• levodopa (Larodopa, Dopar) • prazosin (Minipress) • morphine
Orthostatic hypotension (also called postural hypotension) is abnormally low blood pressure occurring when an individual assumes the standing posture.
Drags that may produce orthostatic hypotension: • Antihypertensives: for example prazosin (Minipress) • Phenothiazines: for example chlorpromazine and thioridazine (Mellaril) • Tricyclic antidepressants: for example doxepin (Sinequan), amitriptyline (Elavil) and imipramine (Tofranil) • Narcotics: for example meperidine (Demerol) and morphine • Antiparkinson drugs: for example levodopa (Larodopa, Dopar) and carbidopa + levodopa (Sinemet)
Note: Indomethacin (fndocin) is an NSAID which may cause GI bleeding, ulcers and possible stomach perforation.
Important: Following vasovagal syncope, orthostatic hypotension is the most likely cause of transient unconsciousness in the dental office. Many factors have been identified that may be responsible for the development of orthostatic hypotension, including several which are important to the practice of dentistry. They include the administration and ingestion of drugs, prolonged recumbency and convalescence, an inadequate postural reflex, pregnancy, various defects in the legs, Addison's disease, physical exhaustion and starvation and chronic orthostatic hypotension (Shy-Drager syndrome). The incidence increases with age.
• phantom pain
**•* For example, the sensation of pain felt in a limb, although that limb has been amputated.
Other terms to know: • Intractable pain: is pain that is resistant or refractory to ordinary analgesic agents • Referred pain: is pain felt in an area other than the site of origin, such as pain near the shoulder associated with biliary disease • Psychogenic pain: is pain produced or caused by psychic or mental factors rather than organic factors
Remember: Pain threshold refers to the lowest level of pain a patient will detect.

terms/def
Which schedule of drugs would include a drug that is considered to have a strong potential for abuse or addiction, but which has legitimate medical use?
• schedule 1
• schedule II
• schedule III
• schedule IV
• scheduleV
PHARMACOLOGY
11 copyright © 2013-2014 - Dental Decks
terms/def
A drug with a high LD50 and a low ED50 has a:
high therapeutic index and is, therefore, very dangerous
• high therapeutic index and is, therefore, relatively safe
• low therapeutic index and is, therefore, very dangerous
i low therapeutic index and is, therefore, relatively safe
12 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• schedule II
Schedule I - a category of drugs not considered legitimate for medicinal use. Among the substances so classified by the DEA are mescaline, LSD, heroin, and marijuana. Special licensing procedures must be followed to use these or other Schedule I substances.
Schedule II - a category of drugs considered to have a strong potential for abuse or addiction, but which have legitimate medical use. Among the substances so classified by the DEA are Morphine, Cocaine, Pentobarbital, Oxycodone, Methadone, and straight Codeine.
Schedule III - a category of drugs considered to have less potential for abuse or addiction than Schedule I or II drugs. Among the substances so classified by the DEA are various analgesic combination compounds containing codeine (i.e., acetaminophen and codeine - Tylenol #3) and various analgesic combination compounds containing hy-drocodone (i.e., hydrocodone and acetaminophen— Vicodin; Lorcet).
Schedule IV - a category of drugs that have less potential for abuse or addiction than those of Schedules I to III. Among the substances so classified by the DEA are diazepam (Valium), lorazepam (Ativan), triazolam (Halcion), alprazolam (Xanax), and chloral hydrate.
Schedule V - a category of drugs that have a small potential for abuse or addiction. Among the substances so classified by the DEA are many commonly prescribed medications that contain a small amount of Codeine.
Note: Schedule II and III must have a written prescription signed by the health professional (laws vary from state to state). The FDA determines which drags are to be sold by prescription only. The prescription must have the address of the patient and dentist as well as the DEA number of the dentist.
• high therapeutic index and is, therefore, relatively safe
Explanation: The purpose of an acute toxicity test is to determine the nature and extent of the untoward reactions which might follow the administration of a single dose (or an overdose) of a drag. A quantitative aspect of acute toxicity testing is the determination of the drag's lethal dose using mice. This is usually expressed as the LD50. Standing alone, it conveys less information than does the ratio of the lethal to the effective doses (LD50/ED50), a quantity which is often known as the therapeutic index (a measure of drug safety). The greater a drug's therapeutic index, the less likely that fatalities will follow an accidental overdose.
1. EDS0 is the effective dose at which 50% of people will respond. Notes 2. LD50 is the lethal dose at which, in theory, 50% of people will die.
*** Lethal doses are always determined in mice, not people 3. The concept of therapeutic window is not the same as therapeutic index. The therapeutic window describes the range between the lowest therapeutic concentration and the beginning of toxicity. Some drags have a very narrow therapeutic window, making patient monitoring especially important. 4. Toxicity results when the dose of the drug is excessive for the particular patient. 5. Side effect: an adverse effect that occurs within the therapeutic dose range of the drug. 6. Idiosyncratic reaction: a reaction to a medication that is unusual and unpredictable, specific to a particular person. Unlike an allergic reaction, it can occur on first exposure to the medication, unlike a side effect, it affects only very few individuals.

terms/def
Which route of administration of a drug listed below is most known for its significant hepatic "first pass" metabolism?
• intramuscular
• inhalation
• sublingual
• oral
13 copyright©2013-2014-Dental Decks
PHARMACOLOGY
terms/def
The term bioavailability of a drug refers to:
• the movement of a drug into the body tissues over time
• the dissolution of a drug in the GI tract
• the measurement of the rate and amount of therapeutically active drug that reaches
the systemic circulation
• the relationship between the physical and chemical properties of a drug and the sy
stemic absorption of the drug
• the amount of drug destroyed by the liver prior to systemic absorption from the GI
tract
14 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

oral
The oral administration of a drug is the one most acceptable to the patient. It is convenient because drags can be given in the form of tablets or capsules which contain an exact dose. It is easy and the patient can take the drug without help from anyone else.
One of the disadvantages of drags taken by mouth is that they have to be absorbed (usually from the small intestine) before they can be transported to their site of action. Blood from the intestinal tract passes first to the liver: some drags are metabolized in the liver ("first-pass effect") and others maybe stored there to be released slowly. This consideration makes it clear that oral administration in usually unsuitable in emergencies or on other occasions when a rapid effect is needed.
Intramuscular injection is an injection made into a large muscle. The advantages of IM injection are that it results in uniform absorption and that it can be used for solutions too irritant for subcutaneous injection. The speed of absorption of drugs given by IM injection depends on the vehicle in which they are dissolved: absorption is rapid from aqueous solutions and slow from oily solutions.
• the measurement of the rate and amount of therapeutically active drug that reaches the systemic circulation
The bioavailability of a drug is affected by: • The dissolution of a drug in the GI tract • The destruction of a drug by the liver
Pharmacokinetics focuses on the processes concerned with absorption, distribution, biotransformation (metabolism), and excretion (elimination) of drugs.
• Absorption: there are four primary factors that must be considered in evaluating drug absorption:
1. Drug characteristics: • Formulation of the drug • Concentration of the drug: the higher the concentration, the more quickly the drug is absorbed • Lipophilic drug formulations are more readily absorbable: nonionized drugs are more lipid soluble and may readily diffuse across cell membranes • Acidic drugs become nonionized in the acidity of the stomach and then diffuse across membranes: basic drugs tend to ionize and are not well absorbed in the stomach
2. Routes of administration: the most common routes for giving medications include oral, topical, subcutaneous, intramuscular, intravenously, and rectal. 3. Blood flow: circulation at the site of administration is important in the drug absorption process. Decreased circulation (as seen in congestive heart failure) will result in decreased drug absorption.
4. Cell membrane characteristics: drugs cross membranes via passive diffusion or active transport.
• Distribution: is the transport of a drug in body fluids from the bloodstream (at the site of absorption) to various tissues in the body
• Biotransformation (metabolism): is the chemical inactivation of a drug through conversion to a more water-soluble compound that can be excreted from the body. It occurs primarily in the liver. Involves two major steps: Phase I makes the drug more hydrophilic through oxidation, reduction, or hydrolysis. Phase II is called glu-curonidation, it involves conjugation.
• Elimination: is the process by which drugs and their metabolites are removed from the body. The liver and the kidney are two major organs responsible for elimination. Most elimination occurs through excretion by the kidneys. The processes involved in renal elimination consist of glomerular fdtration, tubular secretion, and partial reabsorption.

terms/def
Factors influencing hepatic drug metabolism include which of the following?
microsomal enzyme inhibition
microsomal enzyme induction
• plasma protein binding
• genetic factors
> liver disease
• all of the above
15 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
terms/def
The urinary elimination of drugs is controlled by which of the following? Select all that apply.
• glomerular filtration
• microsomal enzyme induction
• renal tubular reabsorption
• active transport through renal tubular cells
16 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• all of the above
Factors Influencing Hepatic Drug Metabolism: • Microsomal enyzme inhibition: many drags and environmental agents can inhibit many of the CYP isoforms of the P-450 microsomal drug metabolizing system. Thus many drugs which ordinarily are metabolized by the particular CYP inhibited will not be effectively metabolized and will achieve higher than expected blood levels. • Microsomal enzyme induction: agents which induce higher levels of the microsomal drug metabolizing enzymes may cause a more rapid metabolism of other drags thus resulting in lower than expected blood levels of a drag. • Plasma protein binding: drugs highly bound to plasma proteins will not enter the liver to be metabolized, thus resulting in a longer plasma half-life of the drag. • Genetic factors: there is individual variance through genetic factors which contribute to differing rates of drag metabolism in the hepatic microsomal enzyme system. • Liver disease: hepatic impairment and liver disease most often will result in impairment of the microsomal drag metabolizing system. This most often results in elevated levels of unmetabolized drag. Note: Most drags are given at lower doses in hepati-cally impaired individuals.
• glomerular filtration • renal tubular reabsorption • active transport through renal tubular cells
• Glomerular filtration: all drags are filtered through the glomerulus to enter the renal tubules. The amount of drag varies according to the degree of plasma protein binding, and bound drags are not subjected to filtration.
• Tubular reabsorption: once they enter the renal tubules, drugs may be reabsorbed back into the blood stream through the renal tubular cells. Reabsorption favors the highly lipid soluble agents; the converse is that highly polar compounds are not effectively reabsorbed and are effectively excreted from the renal tubules.
• Active transport through renal tubular cells: the rate of renal elimination also depends on whether active transport into or out of the tubular fluid occurs.
Other excretory pathways for drugs: • The gastrointestinal tract excretes some drugs through the feces. This is not as preva
lent as urinary excretion. • Most drags can be detected in saliva after administration, but the salivary glands are not considered a route of drug excretion since the drug is re-swallowed along with the saliva. • Lungs excrete volatile compounds that were originally inhaled into the system. Nitrous oxide and the volatile general anesthetics are excreted by this route. • Some drugs are excreted in the sweat, but this route accounts for only a small per
centage of drag excretion.

The average time for the onset of drug effect after: tion is:
• immediate
• 5 minutes
• 15 minutes
• 30 minutes
terms/def
subcutaneous administra-
17 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY
terms/def
Which term is a compulsive, uncontrollable dependence on a substance, habit or practice to such a degree that cessation causes severe emotional, mental or physiological reactions?
• habituation
• tolerance
• addiction
• none of the above
18 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY

• 15 minutes
Routes of Drag Administration: • Oral route: It takes approximately 30 minutes for onset of drag effect after drag is swallowed. Oral route allows for use of many different dosage forms including tablets, capsules and liquids,
• Intramuscular injection: Onset of action of drags injected into muscle occurs rapidly (approximately 5 minutes) because of high blood flow through the muscles.
• Subcutaneous injection: Onset of action of drags injected under the skin takes about 15 minutes.
• Inhalation: Gases such as nitrous oxide are absorbed rapidly through the lungs and gain access to the general circulation within 5 minutes.
• Topical: This route includes ointments and creams applied to the skin and mucous membranes. It is not intended for systemic drag administration.
• Patch delivery: Onset of action of drags in skin patches is about 15 minutes and similar to subcutaneous injection. Skin patches release drag into the blood stream over a 12 to 24 hour period.
addiction
Habituation is an acquired tolerance from repeated exposure to a particular stimulus. Psychological and emotional dependence on a drug, tobacco or alcohol result from the repeated use of the substance but without the addictive, physiological need to increase dosage.
Tolerance is the phenomenon of decreased responsiveness to a drug following chronic administration.
Note: Physiological dependence is common to all forms of drag dependence and abuse. These drags of abuse all have the ability to change one's mood and sensory perception.

terms/def
Which route of drug administration will give the most rapid onset of pharmacological effect?
• oral administration
• subcutaneous injection
• intravenous injection
• intramuscular injection
19 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
terms/def
When a drug is administered repeatedly, a higher concentration of the drug than is desired may be achieved. The effect of this excessive accumulation is known as:
• additive effect
• synergistic response
• cumulative action
• idiosyncrasy
PHARMACOLOGY
20 copyright © 2013-2014 - Dental Decks

• intravenous injection
When a drag is given intravenously, it is placed directly into the systemic circulation. The drug is delivered rapidly to all tissues, including the drug receptor sites. For all other routes of drug administration (with the exception ofintra-arterial injection), the drag must be systemically absorbed prior to distribution to the drug receptor sites, and therefore the onset of pharmacological effects is slower.
Also, when a drag is given by IV injection there is a complete (100%) bioavailability. The entire dose is placed into the systemic circulation. With other routes of administration, the drug may be lost prior to reaching the systemic circulation. For example, with first-pass effects, a portion of an orally administered drag is eliminated, usually through degradation by liver enzymes, before the drag reaches its receptor sites.
Remember: The initial distribution of a drag into the tissues is determined chiefly by the rate of blood flow to the tissue, whereas drug affinity for the tissue will determine whether the drag will concentrate at that site.
Note: Gastric emptying time and degree of plasma protein binding also have an effect on drug distribution but are less important than the rate of blood flow to the tissues.
• cumulative action
An additive effect occurs when additive drugs are administered. The response is no greater than that which would be expected had the drags been given one at a time. There is no enhancement of potential of the individual drags as a result of being used in combination.
A synergistic response occurs when the combined action of two drags is greater than the sum of their individual actions. Examples of synergism: Alcohol is synergistic with diazepam (Valium), narcotics, barbiturates and phenothiazines and therefore should be avoided if an individual is taking these drags.
Idiosyncrasy is a response to a drug that is unusual or abnormal or one that grossly deviates from the routine reaction.

terms/def
The Controlled Substance Act of 1970 uses which criteria for inclusion of a drug into one of the five schedules?
• potential for abuse
• medical usefulness
• degree to which it produces physiological dependence
• degree to which it produces physical dependence
• all of the above
21 copyright B 2013-2014- Dental Decks
PHARMACOLOGY
terms/def
Which of the following refers to the efficacy of a drug?
• the relative concentrations of two or more drugs that produce the same drug effect
• the ability of a drug to produce a desired therapeutic effect regardless of dosage
• the dose of a drug that will kill a patient
22 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• all of the above
The Controlled Substance Act of 1970 uses the following criteria for inclusion of a drug into one of the five schedules:
1. Potential for abuse (most important) 2. Medical usefulness 3. Degree to which it produces physiological dependence 4. Degree to which it produces physical dependence
Remember: Schedule I drugs (LSD, heroin, etc.) cannot be prescribed and are made available only for specific approved research projects. Schedule II drugs (amphetamines, morphine, codeine, oxycodone etc.) can be prescribed but can not be refilled. A new prescription must be written for refills. Prescriptions for Schedule II drugs can not be called into the pharmacy over the telephone. Schedule III drugs (hydrocodone with acetaminophen, codeine with acetaminophen, etc.) may be called in to the pharmacy over the telephone. The prescriber can authorize refills without need of a new written prescription.
*** The prescriber must have a Drug Enforcement Agency authorization number (DEA #) in order to prescribe scheduled drags.
Clinical testing of drugs: Before a drug can be approved for sale to the public there is a set of clinical tests that must be performed. There is the Pre-Clinical Research Stage. Here the drug is synthesized and purified. Animal tests are performed, and institutional review boards assess the studies and make recommendations on how to proceed. If the recommendations are positive, then an application to the FDA occurs and clinical tests begin.
• Phase 1: clinical studies in this phase represent the first time that an investigational new drug is tested on humans either healthy volunteers or sometimes patients. The purpose of these studies is to study in a clinical setting, the metabolism, structure-reactivity relationships, mechanism of action, and side effects of the drug in humans. If possible, phase 1 studies are used to determine how effective the drug is. Phase 1 studies are usually conducted on 20 to 80 subjects. • The purpose of phase 2 clinical trials is to determine the efficacy of a drug to treat patients with a specific disease or condition, as well as learn about common short-term side effects or risks. These studies are conducted on a larger scale than phase 1 studies and typically involve several hundred patients. • Phase 3 clinical trials provide more information about the effects and safety of the drug and they allow scientists to extrapolate the results of clinical studies to the general population. Phase 3 studies generally involve several hundred to several thousand people. *** After a successful phase III, the drug company submits to the Food and Drug Administration (FDA) a New Drug Application (NDA) to market the drug.
• the ability of a drug to produce a desired therapeutic effect regardless of dosage
*** Efficacy refers to the number of receptors that must be activated to yield a maximal response. A drug with high efficacy needs to stimulate only a small percentage of receptors, whereas a drug with lesser efficacy (but still considered to be a full agonist) has to activate a larger proportion of receptors.
Factors Governing Drug Action: Two factors that determine the effect of a drug on physiologic processes are affinity and intrinsic activity. Affinity is a measure of the tightness that a drug binds to the receptor. Intrinsic activity is a measure of the ability of a drug once bound to the receptor to generate an effect activating stimulus and producing a change in cellular activity.
Potency is the relative concentrations of two or more drugs that produce the same drug effect. The effect usually chosen is 50% of the maximal effect and the dose causing this effect is called the EC50. Potency is determined mainly by the affinity of the receptor for the drug. Note: The smaller the EC50, the greater the potency of the drug. Potency is a comparative term (one drug is more potent than another drug).
Example: Drag #1 in a dose of 10 mg produces the same magnitude of response as Drag #2 in a dose of 50 mg. The following is true: Drag #1 is five times as potent as Drug #2.
Also: If Drag #1 has a greater efficacy than Drug #2, then Drug #1 is capable of producing a greater maximum effect than Drag #2.
When comparing drugs with respect to intensity of response, the drug that produces the greatest maximum effect is the one with the highest efficacy.

terms/def
When two drugs having similar effects are administered in combination, and the resulting response is the sum of the individual actions of each drug when given alone, then this result is referred to as:
• an additive effect
1 a synergistic response
• an antagonistic effect
1 cumulative action
PHARMACOLOGY
23 copyright e 2013-2014 - Dental Decks
adrenergics
Amphetamines are sympathomimetic amines that cause rapid release of?
Select all that apply.
• dopamine in the brain
• serotonin in the brain
• norepinephrine in the brain
• acetylcholine in the brain
24 copyrights 2013-2014- Dental Decks
PHARMACOLOGY

an additive effect
An additive effect occurs when additive drugs are administered. The response is no greater than the sum of the individual actions of each drag when given alone. There is no enhancement of potential of the individual drugs as a result of being used in combination.
A synergistic response occurs when the combined action of two drugs having similar pharmacological effects is greater than the sum of the individual actions. Alcohol is synergistic with the Valium family of drugs (i.e., Valium, Xanax, Halcion, etc), narcotics and barbiturates. Alcohol should be avoided when taking these medications.
• dopamine in the brain • serotonin in the brain • norepinephrine in the brain
Amphetamines pass readily into the CNS and cause a rapid release of norepinephrine in the brain. Amphetamines increase systolic and diastolic blood pressures and act as weak bronchodilators and respiratory stimulants. They have a high potential for abuse, resulting in tolerance, psychological dependence, and severe social disability. Abuse causes extreme violence and paranoid psychotic behavior. Note: Amphetamines and ephedrine are indirectly acting sympathomimetic (sympathetic-type) drugs. These drugs demonstrate tolerance and are orally active, unlike epinephrine and norepinephrine.
The physical effects of amphetamines (e.g., increased blood pressure, bronchodilation) are largely due to the adrenergic effects of norepinepherine. The psychological effects of amphetamines (e.g., dependence, addiction, euphoria) are largely due to increases in dopamine and serotonin.
Therapeutic uses of amphetamines: • Attention Deficit Hyperactivity Disorder (ADHD; hyperkinesis) - dextroamphetamine (Dexedrine) and a mix of dextroamphetamine with amphetamine (Adderall); (Adderall XR) sometimes used instead of methylphenidate (Ritalin). • Narcolepsy - dextroamphetamine (Dexedrine) is used to prevent daytime sleepiness in these patients. • Weight loss - phentermine (Ionamin) - structurally similar to dextroamphetamine.
1. Tyrosine hydroxylase catalyzes the rate limiting step in the synthesis of norepi-N'otes nephrine (NE) and epinephrine. The enzyme is inhibited by metyrosine.
2. Termination of transmission by NE takes place primarily by the reuptake of NE into prejunctional nerves and secondarily into other cells. Monoamine oxidase (MAO) and catechol-O-methyl transferase (COMT) then play a role in metabolizing the NE.

adrenergics
The following effects result from what type of pharmacological agent: lower blood pressure vasodilation orthostatic hypotension
an alpha-adrenergic receptor blocker (alpha-blocker)
a beta-adrenergic receptor blocker (beta-blocker)
25 copyright © 2013-2014- Dental Decks
PHARMACOLOGY
adrenergics
A drug that reduces the actions of the sympathetic nervous system is called a:
• sympathomimetic
• sympatholytic
• sympathetic amine
• adrenergic agent
26 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• an alpha-adrenergic receptor blocker (alpha-blocker)
Examples of selective alphaj-blockers used in medicine: • Doxazosin (Cardura) - used to treat hypertension • Prazosin (Minipress) - used to treat hypertension • Terazosin (Hytrin) - manage mild/moderate hypertension; treatment of benign prostatic hyperplasia (BPH)
• Tamsulosin (Flomax) - used to treat benign prostatic hyperplasia (BPH)
*** These drags selectively block a 1-type receptors but not a2-type.
Important: Alphaj-blockers cause orthostatic hypotension, also known as postural hypotension. This is a fainting spell which occurs because of a rapid fall in blood pressure when moving from the supine to the upright position, as in getting rapidly out of the dental chair. The symptoms are similar to simple fainting, however the condition is related to positioning. Note: Other adverse effects include tachycardia, nasal congestion and dry mouth.
*** Orthostatic hypotension can also result from centrally acting drags (i.e., clonidine and methyldopa) and direct vasodilators (i.e., hydralazine and diazoxide)
-...,. 1. Alpha-blockers inhibit the vasoconstrictor response to epinephrine and lev-Notes onordefrin.
2. Beta-blockers increase the vasoconstrictor response to epinephrine, but reduce the tachycardia resulting from epinephrine. 3. MAO inhibitors (i.e., phenelzine and tranylcypromine) should not be used with indirectly acting sympathetic drugs (i.e., Tyramine and amphetamines) and with several other drags such as opioids, especially meperidine. 4. Epinephrine and levonordefrin have exaggerated effects when given with neuron depleting agents like reserpine and guanethidine.
• sympatholytic *** Also called adrenergic blocking agent or adrenergic receptor blockers
Four kinds of adrenergic receptor blockers: (Note: They are all used to treat hypertension)
1. Beta-adrenergic blockers: • Nonselective: blocks both be ta r and beta2-receptors
• Propranolol • Carteolol • Sotalol • Nadolol • Penbutolol • Timolol
• Betaj-selective:
• Atenolol • Esmolol • Betaxolol • Metoprolol • Bisoprolol • Acebutolol
2. Alpha-adrenergic blockers
• Nonselective: blocks both alpha,- and alpha2- receptors
• Phentolamine • Phenoxybenzamine
• Alphaj-selective: • Prazosin • Doxazosin • Terazosin • Tamsulosin
3. Centrally acting alpha2-agonists: Act through stimulation of central inhibitory alpha2-adrenergic re-ceptors.They inhibit sympathetic cardioaccelerator and vasoconstrictor centers. Stimulation of alpha-adrenergic receptors in the brainstem results in reduced sympathetic outflow from the CNS.
• Clonidine • Methyldopa
4. Neuronal depleting agents: encompasses a wide variety of drugs having different mechanisms of action. Whatever their specific mechanism, the result is usually the same — a depletion of mediator in the neuron terminal or an inability of the mediator to be released from the terminal.
• Reserpine - depletes granules containing NE in nerve endings, releases NE • Guanethidine - blocks adrenergic nerve endings by a series of actions • Metyrosine - inhibits tyrosine hydroxylase; used to treat pheochromocytoma
Note: Carvedilol and labetalol are nonselective beta-blockers that also block alpharreceptors. They are
used for heart failure.

adrenergics
The following drugs belong to which pharmacologic category? epinephrine (Adrenalin) phenylephrine (Neo-Synephrine) albuterol (Proventil; Ventolin) isoproterenol
adrenergic agonists
• adrenergic antagonists
27 copyright©2013-2014-Dental Decks
PHARMACOLOGY
Adrenaline (epinephrine) stimulates:
• alpha-|-receptors only
• beta}-receptors only
• both alpha! 2 and bet^ 2-receptors
• both alpha1 and beta-,-receptors only
adrenergics
28 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

' adrenergic agonists
Note: The adrenergic receptors are divided into the subtypes of: • alphaj (etj) and alpha2 (cc2) • beta, (p,) andbeta2 (|32).
Some common adrenergic agonists, their main uses and receptor preference:
• Epinephrine: reverse anaphylaxis, vasoconstriction, bronchodilation - alphab alpha2, beta,, and beta2
• Norepinephrine: vasoconstriction -alphaj, alpha2, and beta,
• Isoproterenol: bronchodilation - betaj, and beta2
• Phenylephrine: nasal vasoconstriction - alpha;, and alpha2
• Albuterol: bronchodilation - beta2
• Terbutaline: bronchodilation - beta2
• Clonidine: antihypertensive - alpha2
• Methyldopa: antihypertensive - alpha2
• Dobutamine: cardiac stimulation - alphaj, and betaj
• both alpha., 2 and beta1 2-receptors
Adrenergic Receptor Type
Alpha,
Alpha
Beta
Beta.
Characteristics
Most common alpha receptor
Less common alpha receptor
Less common beta receptor (found on cells in heart)
Most common beta receptor
Neurotransmitters that Combine With Receptors
Norepinephrine or Epinephrine
Norepinephrine or Epinephrine
Norepinephrine or Epinephrine
Epinephrine (Norepinephrine generally combines either weakly or not at all)
Remember: Alpha receptor responses are predominantly excitatory in nature, while beta receptor responses are excitatory in nature in the heart and inhibitory elsewhere.
Comparison of Adrenergic Receptors
Receptor
Alpha,
Alpha2
Beta,
Beta,
Site
Smooth muscle in blood vessels Stomach, intestine Kidney Liver
Smooth muscle in blood vessels
Cardiac Kidney
Bronchial, vascular, coronary arteriole, uterine smooth muscle, skeletal muscle
Pancreas Liver
Effect of Stimulation
Vasoconstriction Decreased motility and tone Increased renin secretion Gluconeogenesis
Vasodilation
Increased rate and force of contraction Increased renin secretion
Vasodilation
Decreased secretion Gluconeogenesis

adrenergics
All of the following drugs are alpha-adrenergic receptor blockers EXCEPT one. Which one is the EXCEPTION?
• doxazosin (Cardura)
• phenoxybenzamine hydrochloride (Dibenzyline)
• phentolamine hydrochloride (Regitine)
• prazosin (Minipress)
• propranolol (Inderal)
• terazosin (Hytrin)
30 copyright S 2013-2014 - Dental Decks
PHARMACOLOGY
adrenergics
All of the following drugs are indirect-acting adrenergic agonists, EXCEPTone. Which one is the EXCEPTION?
• tyramine
• amphetamine
• epinephrine
• methamphetamine
• hydroxyamphetamine
29 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• propranolol (Inderal)
*** Propranolol is a beta-blocker (specifically a non-selective beta-blocker)
Alpha-blockers are medications that act by competitively inhibiting the action of catecholamines at the alpha receptor site. They act on blood vessels, causing them to relax. Alpha-blockers are commonly used to reduce high blood pressure and to treat an enlarged prostate. There are two types of alpha-blockers, which are classified according to the alpha receptor that they block (alpha! or alphaj.
• Selective alpha antagonists: only block alphaj-receptors and are more commonly used to treat cardiac conditions (hypertension) and benign prostatic hyperplasia. • Non-selective alpha antagonists: block both types of receptors and are generally not used for cardiac conditions because blocking both receptors can cause tachycardia (rapid heart beat) and palpitations (pounding heart beat). They are used in the presurgical management of pheochromocytoma and sometimes in treating Raynaud's phenomenon.
Some examples of alpha-blockers: • Doxazosin - selective alpharblocker. Among the alpha]-blockers it is the preferred agent for hypertension due to a longer duration of action. • Terazosin - selective alpharblocker. Used to treat benign prostatic hypertrophy. • Prazosin - selective alpha]-blocker. It is a second-line choice for the treatment of high blood pressure. • Phenoxybenzamine and phentolamine - both are nonselective alphaj and alpha2-blockers. They are used in the presurgical management of pheochromocytoma.
*** Aside from hypotension, which is a major effect of alpha-blockade, alpha-blockers cause relatively few adverse reactions.
• epinephrine
Two types of adrenergic agonists: 1. Indirect-acting: are those that cause the release of stored norepinephrine at the postganglionic nerve endings to produce their effects. Tyramine and amphetamines cause release of norepinephrine. 2. Direct-acting: are those that interact directly with the alpha or beta receptors.
Direct-acting adrenergic agonists may be receptor selective or receptor non-selective: • Phenylephrine = alphaj selective agonist • Clonidine = alpha2 selective agonist • Dobutamine = alphaj and betaj selective agonist • Terbutaline = beta2 selective agonist • Albuterol = beta2 selective agonist • Epinephrine = alphaj 2 and beta1>2 agonist • Norepinephrine = alphaj 2 and betaj agonist • Isoproterenol = betaj 2 agonist
Remember: Some literature refers to direct and indirect-acting adrenergic agonists as direct and indirect-acting sympathomimetic agents. These terms are almost always synonymous. They are agents that bring about tissue responses resembling those produced by stimulation of the sympathetic nervous system.

adrenergics
The heart is generally considered to have predominantly which type of adrenergic receptors?
• alpha] (a-,) receptors
• betaj (Bj) receptors
• alpha2 (a2) receptors
• beta2 (B2) receptors
PHARMACOLOGY
31 copyright e 2013-2014 - Dental Decks
Alpha adrenergic receptors are located on:
• vascular smooth muscle
• presynaptic nerve terminals
• blood platelets
• fat cells
• neurons in theCNS
• all of the above
adrenergics
32 copyright©2013-2014-Dental Decks
PHARMACOLOGY

• beta, (Bj) receptors
Receptor Types in the Sympathetic (Adrenergic) System
Receptor Type
Alpha,
Alpha2
Beta,
Beta2
Prominent Effector Organs
• Arterioles in skin, mucosa, viscera, and kidney (resistance vessels)
• Veins
• Presynaptic nerve endings • Postsynaptic in CNS
• Heart
• Arterioles (and arteries in skeletal muscle) • Bronchial and uterine smooth muscle
Response to Receptor Activation
• Constriction
• Constriction
• Inhibit norepinephrine release • Decreased sympathetic tone
• Increased heart rate • Increased force of contraction
• Dilation • Relaxation
all of the above
There are two main types of adrenergic receptors: 1. Alpha (a) receptors - responsible for most of the excitatory effects such as vasoconstriction and contraction of the uterus and spleen. 2. Beta (13) receptors - responsible for most of the inhibitory effects such as vasodilation and relaxation of respiratory smooth muscle.
Note: Two important EXCEPTIONS to the above: some alpha receptors mediate relaxation of gastrointestinal smooth muscle, and some beta receptors mediate increases in the force and rate of contractions of the heart.
Alpha receptors fall into two groups: 1. Postjunctional alphaj adrenergic receptors are found in radial smooth muscle of the iris, arteries, arterioles, and veins; in the GI tract. 2. Prejunctional alpha2 adrenergic receptors mediate the inhibition of the release of norepinephrine.
Beta receptors fall into two groups: 1. Postjunctional betaj adrenergic receptors are found in the myocardium (heart), the intestinal tract smooth muscle, and adipose tissue. 2. Postjunctional beta2 adrenergic receptors are found in bronchiolar and vascular smooth muscle.

All of the following neurons are cholinergic EXCEPTION?
• preganglionic sympathetic neurons
• preganglionic parasympathetic neurons
• postganglionic sympathetic neurons
• postganglionic parasympathetic neurons
EXCEPT one
copyri
adrenergics
. Which one is the
33 ght © 2013-2014 - Dental Decks
PHARMACOLOGY
adrenergics
What substance produces all of the following physiologic actions? constricts arteriolar blood vessels (vasoconstriction) relaxes bronchial smooth muscle (bronchodilation) decrease blood volume in nasal tissues causes a hypertensive response produces physiological actions opposite to that of histamine
• serotonin
• epinephrine
• dopamine
• acetylcholine
34 copyright <8 2013-2014 - Dental Decks

• postganglionic sympathetic neurons The autonomic nervous system (ANS) controls involuntary (smooth) muscle and gland activity. Blood pressure, pulse, sweating, bladder, and rectal sphincter tone are regulated by the ANS. Function of the heart, eyes, uterus, urinary bladder, and gastrointestinal tract, from the salivary glands to the anal sphincter, is governed and maintained by the ANS.
The ANS is a complex set of neurons that originate from the CNS (specifically the hypothalamus); it is composed of two antagonistic systems. The sympathetic nervous system (from thoraco-lumbar outflow) and the parasympathetic nervous system (from cranial-sacral outflow). The autonomic nervous system has cholinergic neurons that secrete acetylcholine and adrenergic neurons that secrete norepinephrine. Preganglionic neurons of both divisions (sympathetic and parasympathetic) are cholinergic, as are the postganglionic neurons of the parasympathetic branch. Postganglionic neurons of the sympathetic branch are usually adrenergic. One EXCEPTION is the sympathetic postganglionic neurons that innervate the sweat glands (they are cholinergic = secrete acetylcholine). Note: Adrenergic blocking agents block the effect of impulses transmitted by the adrenergic postganglionic neurons of the sympathetic branch.
CNS Somatic Nervous System <ACh- Striated
muscle
•3
G
Autonomic Nervous System
Sympathetic division < ACh' Q :NE
; ACh' Q-
Heart Smooth muscle
" Glands
Sweat glands Some blood vessels
Reproduced with permission, from Neidle EA, and Yagiela JA. Pharmacology and Therapeutics for Dentistry. Mosby, 1989.
<ACh* ' Adrenal ' medulla *NE JJ
Parasympathetic division
~<ACti 'Q-
* Nicotinic site | Muscarinic
Heart CAChJ" Smooth muscle
Glands
Fibers of the somatic and autonomic nervous systems, with the structures innervated by the different fibers and the chemical mediators responsible for transmission at the various loci. Dashed lines indicate postganglionic autonomic fibers.
• epinephrine
Therapeutic indications for epinephrine:
• To alleviate symptoms of an acute asthma attack • To treat bronchospasm associated with hypotension, as in anaphylaxis • To treat hypersensitivity reactions • Agent of choice for anaphylactic reactions (given sublingually or subcutaneously) • It is added to local anesthetics as a vasoconstrictor to prolong the activity of the local anesthetic solutions, by decreasing the rate of diffusion and absorption from the injection site • To restore cardiac activity in cardiac arrest • To relieve congestion of the nose, sinuses, and throat
Common side effects: headaches, agitation (anxiety), and tachycardia.
Important: Epinephrine should be used with caution in patients with high blood pressure and hyperthyroidism. These patients may have an increased sensitivity to epinephrine.

adrenergics
Epinephrine is the agent of choice for treating an anaphylactic reaction because of its stimulatory effects on both alpha and beta adrenergic receptors.
All of the following are desirable effects of epinephrine that make it the agent of choice for treating an anaphylactic reaction.
it has vasopressor activity it has bronchodilator properties it causes increased cardiac output it has a rapid onset of action
• both statements are true
• both statements are false
• the first statement is true, the second is false
• the first statement is false, the second is true
35 copyright © 2013-2014- Dental Decks
PHARMACOLOGY
adrenergics
"Epinephrine reversal" is a predictable result of the use of epinephrine in a patient who has received a/an:
• beta-blocker
• alpha-blocker
• adrenergic agonist
• all of the above
36 copyright © 2013-2014 - Dental Decks

• both statements are true
Epinephrine is the agent of choice for treating an anaphylactic reaction because of its stimulatory effects on both alpha and beta adrenergic receptors. Alpha receptor stimulation results in a vasopressor response (elevation of blood pressure). Beta receptor stimulation results in air way dilation and increased cardiac output. In this way, epinephrine counteracts the vascular effects of histamine-related anaphylaxis.
Note: Epinephrine is administered either intravenously, sublingually, subcutaneously or intramuscularly. There is a very rapid onset of action when given by these routes.
Other therapeutic indications for the use of epinephrine:
• To control superficial hemorrhage • As a component of local anesthetic solutions to prolong duration of anesthesia • Asthma — bronchodilator properties
• alpha-blocker
Explanation of answer: One of the best known effects of the alpha-receptor blocking agents (antiadrenergic) is their ability to reverse the pressor action of adrenaline (epinephrine). In the absence of blocking agents, epinephrine and norepinephrine both cause the blood pressure to rise. After the alpha-receptors have been blocked by an alpha-blocker, the pressor effect of norepinephrine is reduced or abolished while epinephrine brings about a fall in blood pressure.
This is because epinephrine stimulates both alpha and beta-receptors in the cardiovascular system but norepinephrine only stimulates alpha-receptors (norepinephrine lacks beta2 effects). After blockage of the alpha-receptors, only the beta-receptors can be stimulated.
Note: A pressor response (produces an increase in blood pressure) is mediated by alpha-receptors and a depressor response (produces a decrease in blood pressure) is mediated by beta2 receptors.
Important: In the absence of a-receptor blockers, the pressor response of a receptors in vascular smooth muscle predominates over the dilator response of |3 receptors.

adrenergics
Of the following, which is a clinically significant adverse reaction due to Meto-prolol?
• drowsiness
• hallucinations
• arthralgia
• dry mouth
37 copyright©2013-20l4-Dental Decks
PHARMACOLOGY
adrenergics
If norepinephrine or epinephrine were to stimulate or combine with the alpha receptors in the eye, which response would you expect?
• miosis (contraction of the pupil)
• mydriasis (dilation of the pupil)
• neither of the above; norepinephrine and epinephrine do not stimulate or combine with alpha receptors in the eye
38 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• drowsiness
Metoprolol (Lopressor, Toprol-XL) is a competitive, beta,-selective adrenergic receptor blocker (cardioselective), which is most similar to Atenolol. It is used in the treatment of hypertension, acute angina pectoris and may be helpful after a heart attack.
Atenolol (Tenormin) is a competitive, betarselective adrenergic receptor blocker (cardioselective), with a long plasma half life (long duration of action). It is used in the treatment of hypertension and chronic angina pectoris. Due to its low lipid solubility, Atenolol is renally eliminated, minimally metabolized, and has a low potential for causing CNS side effects compared to lipid soluble beta-blockers (e.g., Propranolol).
*** Metoprolol and Atenolol are both longer-acting and more predictable than Propranolol in producing therapeutic plasma levels. Because they are betaj selective adrenergic receptor-blockers, they are also safer to use in patients with a history of asthma or bronchitis.
Acebutolol (Sectral) is a betai-selective adrenergic receptor blocker (cardioselective). It is used to treat hypertension and to control ventricular arrhythmias. It has a low lipid solubility, which reduces its likelihood of producing adverse CNS effects. It also has mild intrinsic sympathomimetic activity (partial agonist activity at beta2 receptors) similar to Pindolol.
Important points: 1. With all "selective" beta-blockers, selectivity for the betaj receptor is lost at high doses. As the dose is increased they also block the beta2 receptors, thereby having effects on bronchial smooth muscle. 2. The most common side effects of beta-blockers are weakness and drowsiness.
> mydriasis (dilation of the pupil)
Organ/Tissue
Heart
Arterioles
Eye
Lung
Intestine
Urinary bladder
Uterus
Receptor Type
P> P> Pi Pi
a,.
P2
a.
P2
ai,2Pi,2 Oti
Cti
Pi
Cti
P2
Response to Adrenergic Agonists
Increases conduction velocity Increases contraction force Increases contraction rate Increases cardiac output
Constricts cerebral arterioles Dilates skeletal muscle arterioles
Contracts dilator muscle, producing mydriasis
Relaxes tracheal and bronchial muscles
Decreases peristalsis Contracts sphincter
Contracts trigone and sphincter muscles Relaxes detrusor muscle
Excites uterine contractions Inhibits uterine contractions

adrenergics
All of the following drugs are bronchodilators EXCETTone. Which one is the EXCEPTION?
• epinephrine
• levalbuterol (Xopenex)
< albuterol (Proventil)
• salmeterol (Serevent)
< metaproterenol (Alupent)
> histamine
• aminophylline
39 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY
adrenergics
Pharmaceutical agents that bring about tissue responses resembling those produced by stimulation of the sympathetic nervous system are called?
• cholinomimetic
• antiadrenergic
• parasympathomimetic
• sympathomimetic
40 copyright © 2013-2014- Dental Decks
PHARMACOLOGY

• histamine
Asthma is a respiratory disorder characterized by recurring episodes of paroxysmal dyspnea, wheezing on expiration, coughing, and viscous mucoid bronchial secretions. The episodes may be precipitated by inhalation of allergens or pollutants, infection, vigorous exercise, or emotional stress.
Management and prevention of an acute asthma attack: • Epinephrine, levalbuterol, albuterol, salmeterol and metaproterenol are beta2 adrenergic receptor agonists. Thus they stimulate the beta receptors in the airway to cause bronchodilation. They are taken via aerosol inhalers and nebulizers. Important: Albuterol is the drug of choice as a "rescue" agent during an acute asthmatic attack.
Note: Aminophylline is an example of a theophylline compound. Theophylline compounds are administered orally as bronchodilators in reversible airway obstruction due to asthma or COPD (chronic obstructive pulmonary disease). These drugs relax bronchial smooth muscle to improve airway function.
• sympathomimetic
The terms sympathomimetics, sympathomimetic amines, adrenergic agonists and adrenergic agents are almost always synonymous.
Epinephrine is the sympathomimetic agent used in dentistry. It is the vasoconstrictor for anesthetic solutions and the vasoconstrictor component in gingival retraction cords. As a component of local anesthetic preparations, it is used to prolong the duration of local anesthesia.
In medicine, sympathomimetics are used as pressor agents to maintain blood pressure in vascular shock. They are used as bronchodilators for asthma attacks and for allergic states including anaphylactic shock. Sympathomimetics used in medicine include dopamine, epinephrine, norepinephrine, isoproterenol, and phenylephrine.
Important: Epinephrine is indicated in medicine to treat bronchospasm and hypersensitivity reactions. It is the agent of choice for reversing anaphylactic reactions. It is used to restore cardiac activity in cardiac arrest.

The medical uses of a drug having adrenergic which of the following?
• reverse an anaphylactic reaction
• treat hypertension
• prevent angina pectoris
• reduce anxiety
• all of the above
adrenergics
: agonist actions would include
41 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
adrenergics
A fear reaction activates the sympathetic division of the autonomic nervous system to result in:
• miosis
• bradycardia
• hypertension
• increased salivation
42 copyright © 2013-2014 - Dental Decks

• reverse an anaphylactic reaction
The prototypical adrenergic agonist agent is epinephrine. Epinephrine stimulates both beta adrenergic receptors and alpha adrenergic receptors within the sympathetic division of the autonomic nervous system. Anaphylaxis is characterized by rapid, extreme reduction in blood pressure and bronchospasms. Epinephrine, upon injectable administration, will rapidly reverse the hypotension by causing vasoconstriction via the alphaj receptor stimulation; it will dilate the bronchial tubes via beta2 receptor stimulation; it will increase cardiac output via betaj receptor stimulation on the cardiac muscle.
Epinephrine is: • Ineffective in treating hypertension because of its alpha receptor stimulatory actions on the vasculature which could cause an even further elevation of blood pressure • Contraindicated in angina conditions because its cardiostimulatory effects would aggravate this condition • Will not reduce anxiety but will likely increase anxiety since it has central nervous system stimulatory effects
• hypertension
Activation of the sympathetic portion of the autonomic nervous system will cause alphaj-adrenergic receptor activation to result in arteriolar vasoconstriction with an associated elevation of blood pressure leading to hypertension.
1. Sympathetic activation of the eye would result in mydriasis (dilation) not Notes miosis.
2. Sympathetic activation of the heart would result in tachycardia, not bradycardia. 3. Sympathetic activation of the salivary glands would result in a thick ropey-type salivary flow, not increased salivation.
Miosis (pupillary constriction), bradycardia, and increased salivation are physiological effects all resulting from activation of the parasympathetic division of the autonomic nervous system.

The amide local anesthetics are metabolized
• lungs
• plasma
• liver
• kidney
PHARMACOLOGY
primarily
anesthetics
in the:
43 copyright © 2013-2014 - Dental Decks
anesthetics
What are some adverse side effects of local anesthetics?
44 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• liver
The amide-type local anesthetics that are used in dentistry and metabolized by the liver include: • Lidocaine (Xylocaine) • Prilocaine (Citanest) • Articaine (Ultracaine) • Mepivacaine (Carbocaine) ' Bupivacaine (Marcaine) • Etidocaine (Duranest)
These anesthetics are metabolized by the hepatic microsomal enzyme system, with the exception of articaine, which is metabolized by serum esterases. The products formed do not have anesthetic actions and are excreted primarily in the urine as metabolites. These agents should be used with caution or not at all in patients with compromised liver function. Note: The most abundant urinary metabolite of lidocaine is 4-hydroxyxy-
Amides are metabolized by three types of reactions: 1. Dealkylation of the amino terminus 2. Hydrolysis of the amide bond 3. Hydroxylation of the aromatic ring
The amides vary in protein binding. Lidocaine and mepivacaine are bound moderately. Etidocaine and bupivacaine are highly bound. Note: Bupivacaine is more selective for sensory nerves than etidocaine.
Product
Carbocaine 3% (Mepivacaine)
Citanest Plain 4% (Prilocaine)
Citanest Forte w/epinephrine (Prilocaine 4% w/epinephrine 1:200,000)
Lidocaine 2% w/epinephrine( 1:100,000)
Marcaine 0.5% w/epinephrine (Bupivacaine w/epinephrine 1:200,000)
Articaine 4% w/epinephrine (1:100,000)
Infiltration
20 minutes
20 minutes
2.25 hours
60 minutes
> 60 minutes
60 minutes
Inferior Alveolar Block
40 minutes
2.5 hours
3 hours
90 minutes
5-7 hours
60 minutes
Note: Bupivacaine has the longest duration of action of any dental local anesthetic presently available.
Adverse effects caused by local anesthetics are categorized into two major groups:
1. Effects resulting from toxicity 2. Effects resulting from allergy
Toxicities: • Too much anesthetic in the bloodstream can cause toxicities to the central nervous system
(CNS) and cardiovascular system • Opioids can increase the systemic toxicity of local anesthetics • Esters will show greater toxicity in patients with a hereditary deficiency of plasma esterases. Remember: Esters are metabolized by the plasma enzyme plasma pseudo-cholinesterase, which is a plasma esterase. • The CNS effects include: restlessness, stimulation, tremors, convulsive seizures followed by CNS depression, slowed respiration and even coma • The cardiovascular effects include: bradycardia and reduction of cardiac output
Allergy: • Hypersensitivities or allergic reactions to local anesthetics, particularly from the amides, are rare. These reactions are manifested as dermatological reactions and edema at the injection site. • Asthmatic wheezing syndromes have occurred in response to local anesthetic injections • Allergic reactions are more prevalent with the ester-type rather than the amide-type anesthetics. They also display cross-allergenicity. • Ester local anesthetic allergic manifestations include: nasolabial swelling, itching, and oral mucosal swelling • Methylparaben, which was used as a perservative, can also cause allergies

anesthetics
Which statement best describes the mechanism of action of local anesthetics on the nerve axon?
• decreases sodium uptake through sodium channels of the axon
' increases potassium outflow from inside to outside the nerve
• increases the membrane's permeability to sodium
• increases the excitability of the nerve axon
45 copyright © 2013-2014 - Dental Decks
Which form of a local anesthetic can
• ionized form
• nonionized free-base form
anesthetics
readily penetrate tissue membranes?
• both ionized and nonionized free-base forms
46 copyright©2013-2014-Dental Decks
PHARMACOLOGY

• decreases sodium uptake through sodium channels of the axon
When a local anesthetic solution is injected near the nerve, the solution interferes with the uptake of sodium from outside to inside the nerve. The local anesthetic blocks the specific sodium channels thereby blocking the sodium uptake. This decreases the nerve excitability below a critical level and nerve impulses fail to propagate along the axon. Since axons carry pain sensations, these sensations will not be carried and a blockage of pain results.
1. Local anesthetics reversibly block nerve impulse conduction and produce reversible loss of sensa-h tion at their administered site.
2. Local anesthetics have no effects on potassium at the nerve axon. 3. Small, nonmyelinated nerve fibers, which conduct pain and temperature sensations, are affected first, followed by touch, proprioception (pressure), and skeletal muscle tone (motor).
Pharmacokinetics of Local Anesthetics
Drug
Shor t Acting
Procaine
Chloroprocaine
Intermediate Acting
Lidocaine
Mepivacaine
Prilocaine
Long Acting
Bupivacaine
Etidocaine
Tetracaine
Amide or ester
Ester
Ester
Amide
Amide
Amide
Amide
Amide
Ester
Onset of Action
2-5 min
6-12 min
<2 min
3-5 min
<2 min
5 min
3-5 min
15 min %.
Duration of Action
15-60 min
30 min
30-60 min
45-90 min
60-120 min
2-4 hr
5-10 hr
2-3 hr
Protein Bound
5.8%
64.3%
77.5%
55%
95.6%
94%
75.6%
Pregnancy Category
C
C
B
C
B
C
B
C
How Supplied
I % , 2 % , 10%
1%,2%,3%
0.5%, 1%, 2%, 4%, with and without epinephrine
1%, 1.5%, 2%, 3 %
4% with and without epinephrine
0.25%, 0.5%, 0.75% with and without epinephrine
1%, 1.5% with and without epinephrine
1%, 2%, 3%
• nonionized free-base form
Local anesthetic free bases are fat-soluble (lipophilic) drugs. They are converted to their water-soluble (hydrophilic) hydrochloride salts to allow preparation of an injectable solution. In solution an equilibrium is established between the ionized and the nonionized forms of the local anesthetic. The proportion of the drug in the ionized form depends on the pKa of the drug and the pH of the solution. At the usual solution pH of 6.0 or lower, most local anesthetics are almost completely in the ionized form.
This is important because only the nonionized free-base form of the drug can readily penetrate tissue membranes. Local anesthesia can only be obtained if sufficient free-base is available. The lower the pKa of the drug and the higher the pH of the solution or injected tissues, the more free-base will be available.
Once the local anesthetic is injected the buffering capacity and pH of the tissues (normally 7.4) shifts the equilibrium in favor of free-base formation. At physiologic pH of 7.4 approximately 5-20% of the local anesthetic is in free-base form which is enough to penetrate and cause anesthesia. If infection or inflammation is present, the pH of the tissues may be acidic and there is a significant reduction in the concentration of the free-base form. In this situation, the local anesthetic may not be effective.
Key point of all this: The potential action of all local anesthetics depends on the ability of the anesthetic salt to liberate the free-base.
Note: If you inject lidocaine (pKa = 7.8) into tissue that has a pH of 7.8, the lidocaine will exist in an equal mixture of ionized and nonionized forms which will be more than enough to produce anesthesia.

anesthetics Which of the following are sedatives often used in the management of anxious pediatric dental patients? Select all that apply.
midazolam
• diazepam
• hydroxyzine
• pentobarbital
• secobarbital
• chloral hydrate
• meperidine
47 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
Ester-type local anesthetics are metabolized where?
• liver
• lungs
• plasma
• kidneys
copy;
anesthetics
48 right © 2013-2014 - Dental Decks
PHARMACOLOGY

• midazolam • diazepam • hydroxyzine • chloral hydrate • meperidine
Traditionally chloral hydrate has been used orally in the preoperative management of the anxious pediatric dental patient. It has an unpleasant odor and a bitter, caustic taste, which can be partially masked in a flavored syrup. Chloral hydrate is rapidly absorbed after oral administration with an onset of 15 to 30 minutes. Its duration of action is about 4 hours.
For use in children, chloral hydrate is available as a 500 mg/5 ml solution. The usual dose for a child is 50 mg/kg up to a maximum of 1 g. Important: Children will often enter a period of excitement and irritability before becoming sedated. It affects brain centers that control wakefulness and alertness. Chloral hydrate does not relieve pain.
1. Chloral hydrate is a prodrug and is metabolized to the active metabolite, trichloro-oethanol. Notes ^' Chloral hydrate's metabolite (trichloroethanol) may displace warfarin from its protein binding
sites resulting in an increase in the hypoprothrombinemic response to warfarin. 3. Sedative effects and/or respiratory depression with chloral hydrate may be additive with other CNS depressants — monitor for increased effect. These other CNS depressants include ethanol, antidepressants, narcotic analgesics, and benzodiazepines. 4. Be careful when using Chloral hydrate, serious toxicity can result if the dose is not controlled. 5. Meperidine (Demerol): a narcotic that produces sedation and relieves pain. 6. Midazolam (Versed): this is a very useful drug which is primarily an anti-anxiety agent, produces retrograde amnesia, and is a muscle relaxant and reduces the chance of seizures. Short acting (great for short procedures). 7. Hydroxyzine (Vistaril or Atarax): is a milder medication. Primarily an anti-histamine. Is often used in combination with other medications. 8. Diazepam (Valium): is an anti-anxiety agent.
• plasma
Ester-type local anesthetics all have an ester grouping within their chemical structure. An ester grouping is essentially a bridge or link containing the - COOCH2-configuration. Amide-type local anesthetics all have an amide grouping within their chemical structure. An amide grouping is essentially a bridge or link containing the - CONHCH2-configuration.
Ester-type local anesthetics are mainly available as topical anesthetics and include benzocaine (which does not have an amino terminus and therefore does not become charged, thus it is poorly soluble in water), tetracaine, and dibucaine. They are also available as medical anesthetic preparations such as propoxycaine (Ravocaine). Ester-type local anesthetics are no longer available as dental anesthetic injectable preparations because of their relatively high incidence of allergy. Only the amides are presently available as dental injectable local anesthetic agents. These include lidocaine, mepivacaine, prilocaine, bupivacaine, and articaine.
Ester-type local anesthetics are metabolized by the plasma enzyme plasma cholinesterase. Another name for this enzyme is pseudocholinesterase. This enzyme splits the ester linkage within the chemical structure rendering the anesthetic ineffective. Procaine (Novocaine) was one of the original ester-type anesthetics. When procaine is metabolized by plasma cholinesterase, a highly allergic compound called para aminobenzoic acid (PABAfor short) is formed. Many patients developed an allergy to PABA. Note: PABA can decrease the effectiveness of sulfonamides (antibiotics).
Note: Other chemicals that act like local anesthetics: • Diphenhydramine: Hj antihistamine • Tetrodotoxin: found in a number of tissues of the puffer or blowfish • Saxitoxin: is produced by certain strains of algae
Remember: Dyclonine hydrochloride is unusual in that it has a ketone linkage between the aromatic moiety and the rest of the anesthetic molecule. It is used as a topical.

Which of the following is a contraindication caine?
• biliary tract disease
• type II diabetes
• rheumatoid arthritis
• hepatic disease
anesthetics
or precaution to the use of Prilo-
49 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
Which local anesthetic has no place in
• articaine
• cocaine
• lidocaine
• bupivacaine
• prilocaine
anesthetics
i the routine practice of dentistry?
50 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• hepatic disease
*•** Remember: All amides are metabolized primarily in the liver, and the metabolites are then renally excreted.
Prilocaine (Citanest) is a local anesthetic of the amide class, used for nerve block, epidural and regional anesthesia. It has an intermediate duration of action and is longer acting than Lidocaine. Prilocaine produces less vasodilation than does an equal amount of Lidocaine (it is somewhat less potent than Lidocaine). It is available as a 4% solution with or without epinephrine, which prolongs the anesthetic effect.
Prilocaine is metabolized to orthotoluidine, a product that can produce methemoglobinemia, a condition that is characterized by increased levels of methemoglobin in the blood. Note: This methemoglobin is less effective than hemoglobin in carrying oxygen in the blood.
Prilocaine is about one-half as toxic as Lidocaine, but since methemoglobinemia is a possible reaction, Prilocaine is not used for patients with hypoxic conditions of any kind.
Note: EMLA Cream is a eutectic mixture of lidocaine 2.5% and prilocaine 2.5% formulated as an oil in water emulsion. In this eutectic mixture, both anesthetics are liquid at room temperature and the penetration and subsequent systemic absorption of both prilocaine and lidocaine are enhanced over that which would be seen if each component in crystalline form was applied separately as a 2.5% topical cream.
• cocaine
Cocaine is a naturally occurring ester of benzoic acid and was the first local anesthetic used in dentistry and medicine. It is potent and extremely toxic, and it is the only local anesthetic that causes definite vasoconstriction (all other local anesthetics are vasodilators). Cocaine is commercially available in a variety of forms and is applied to mucous membranes of the oral, laryngeal, and nasal cavities for use as a topical anesthetic. Cocaine causes significant euphoria (most likely due to its blockade of reuptake of dopamine in the brain), and abuse can lead to a physical dependence. Despite being an excellent local anesthetic, the risk of abuse and the intense local vasoconstriction it produces prevent cocaine from being more widely used clinically. Important: Cocaine has no place in the routine practice of dentistry.
The pharmacology of cocaine is unique among local anesthetics in that the drug inhibits the uptake of catecholamines by adrenergic nerve terminals. It therefore potentiates the action of endogenously released and exogenously administered sympathomimetic amines such as dobutamine, dopamine, or epinephrine. It increases the risk of developing cardiac arrhythmias and hypertension (i.e., cocaine increases the pressor activity of these sympathomimetic amines).

anesthetics
Local anesthetics theoretically should be less effective in acutely inflamed tissue than in normal tissue because in inflamed tissue what happens?
• the pH rises, thus inactivating the anesthetic
• the pH rises, thus decreasing available free base
• the pH decreases, thus decreasing available free base
• the pH remains the same, the extracellular fluid dilutes the anesthetic
51 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
AOOIODVlATOVHd sipaQ |eji»a - f 10Z-E10E O m6ijAdoa
zs
auuiidamda 6ui 8 LO'O pue ameDopij 6iu 9£ •
auuqdauida 6ai 8 L'O pue aiueDopn Bui 9£ •
auuqdauida 6iu 8 LO'O pue ame:)op!| 6ai g/£ •
auuqdamda but 8 L'O Pue auiBDopi| 6w g-£ •
£Uje)uos a|ndjBD aq) saop auuqdainda pue auiesopji qaniu MOH 'auuqdauida 000'QOLU qJIM aumDopji to uoijn|os o/0z e jo |ui 8' L sujejuoa a|ndje:> 3|iaqjsaue (eiuap y
S3i;aL|isaue

• the pH decreases, thus decreasing available free base
At body pH (7.4), a local anesthetic when infiltrated, will chemically exist as a portion which is ionized (has a proton attached) and as a portion which is non-ionized (has no proton attached). Note: A proton is nothing more than a hydrogen (H+) atom. That portion which is ionized has difficulty penetrating the nerve and will not be effective. That portion which is non-ionized will penetrate the nerve to cause anesthesia. That portion which is non-ionized is also known as the free base. The more proportion of the anesthetic which is in the free base form, the more effective it will be.
When tissue conditions are normal (pH 7.4), approximately 10-20% portion of an infiltrated local anesthetic is in the form of the free base (non-ionized form). This is enough to penetrate the nerve to cause anesthesia. When tissues are acidic, as in the case of tissue infection, less free base portion exists and more ionized portion is present. There is not enough free base form to penetrate the nerve to cause anesthesia. Therefore, the local anesthetic when infiltrated to the tissue site is not effective at the normal anesthetic doses.
• 36 mg lidocaine and 0.018 mg epinephrine
Key to question: 1 ml of a 2% solution of lidocaine with 1:100,000 epinephrine contains 20 mg of lidocaine and 0.010 mg of epinephrine.
A dental carpule contains 1.8 ml solution. Therefore, 1.8 ml of 2% solution of lidocaine with 1:100,000 epinephrine contains 36 mg of lidocaine and 0.018 mg epinephrine.
Epinephrine (vasoconstrictor) is included in local anesthetics for the following reasons: • It prolongs the duration of action • It reduces toxicity • It reduces the rate of vascular absorption • It provides a hemostatic effect to reduce bleeding at injection site

anesthetics
The maximal recommended adult dose of Lidocaine is 300 mg. How many milliliters of 2% Lidocaine need to be given
• 7.5 milliliters
• 10 milliliters
• 15 milliliters
• 20 milliliters
to reach this level?
53 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anesthetics
The maximum recommended dose of a local anesthetic that can be administered to a child < 10 years of age is determined by:
age
• weight
-height
• gender
54 copyright © 2013-2014- Dental Decks
PHARMACOLOGY

r
15 milliliters
Important information to solve questions of this type: • There are 20 mg of Lidocaine in every milliliter of 2% Lidocaine • 300 mg (maximal recommended dose) + 20 mg (in every mL) = 15 mLs • 20 mg x 1.8 mL (in every carpule) = 36 mg / 1 carpule • 300 mg * 36 mg = 8.3 carpules (8 carpules of 2% Lidocaine can be used)
Maximum Recommended Doses of Local Anesthetic
Drug
Lidocaine (Xylocaine)
Mepivacaine (Carbocaine)
Prilocaine (Citanest)
Bupivacaine (Marcaine)
Maximal Recommended
Dose mg ml
300 15
300 10
400 10
90 18
Concentration Used (%)
2
3
4
0.5
Approximate Number of Carpules
8.3
5.6
5.6
10
Guidelines Based on Weight
7mg/kg adult; 4.4 mg/kg child
7mg/kg adult; 4.4 mg/kg child
6mg/kg adult; 6mg/kg child
2mg/kg adult; 1.3 mg/kg child
Remember: Lidocaine has serious drug interactions with beta-blockers and cimetidine that decrease lidocaine clearance 30% or more. Propranolol, metoprolol, and nadolol are reported to reduce lidocaine clearance due to the decrease in cardiac output caused by the beta-blockers. Decreased cardiac output results in reduced liver blood flow which explains the decline in lidocaine clearance caused by these drugs. Cimetidine also decreases lidocaine clearance, but the mechanism of the interaction is different. Because cimetidine does not change liver blood flow, it is believed that cimetidine decreases lidocaine clearance by inhibiting hepatic microsomal enzymes. Lidocaine clearance may be accelerated by concomitant use of phenobarbital or pheny-toin. Both of these agents are known to be hepatic drug metabolizing drug inducers, and this is the probable mechanism of their drag interaction with lidocaine.
• weight — (mg/kg)
Example: For Lidocaine (2%) with epinephrine, a dosage of 4.4 mg/kg should not be exceeded (maximum is 300 mg).
Maximum Recommended Doses of Lidocaine for Children < 10 Years Old
Patient Weight (kg/lb)
10/23
15/34.5
20/46
25/57.5
Mg
44
66
88
100
Number of Carpules
1.2
1.8
2.4
2.6
Note: 1 kg = 2.3 lbs
2% = 20 mg / mL x 1.8 mL /l carpule = 36 mg/1 carpule

anesthetics
Local anesthetics depress which of the following nerve fibers first?
• large myelinated fibers
small unmyelinated fibers
small myelinated fibers
large unmyelinated fibers
55 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY
anesthetics
The maximum dose of articaine (Septocaine) that is recommended in one appointment is expressed as mg per kilogram body weight rather than total milligrams. Which dose is the maximum recommended dose for articaine in children and adults?
• 7 mg/kg
• 100 mg/kg
• 1 mg/kg
- 300 mg/kg
56 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

small unmyelinated fibers
*** These conduct pain and temperature
Important: They depress the large myelinated fibers last. The small nerves have the greater surface-volume ratio (this accounts for the rapid onset of action).
Clinically the general order of loss of function is as follows:
l.Pain 2. Temperature 3. Touch 4. Proprioception 5. Skeletal muscle tone
Note: Pain threshold refers to the lowest level of pain a patient will detect.
Remember: Local anesthetics reversibly block nerve impulse conduction and produce the reversible loss of sensation at their administration site. They do not produce a loss of consciousness. They appear to become incorporated within the nerve membrane or to bind to specific membrane sodium ion channels, restricting sodium permeability in response to partial depolarization.
• 7 mg/kg
In a typical 70 kg adult male, the dose of 7 mg/kg would equate to a total of 490 mgs. Thus, the maximum recommended amount of articaine that could be given to a 70 kg adult in one appointment is 490 mgs.
The table below shows the following number of dental cartridges containing 1.7 ml volume of solution to provide the indicated amounts of articaine hydrochloride 4% and epinephrine 1:100,000.
Number of Cartridges (1.7 ml)
1
2
3
4
5
6
7
8
Articaine HCL (4%) (mg)
68
136
204
272
340
408
476
544
Epinephrine 1:100,000 (mg)
0.017
0.034
0.051
0.068
0.085
0.102
0.119
0.136

anesthetics Which is the most frequently utilized route of administration for sedation in pediatric patients?
• oral
• inhalation
IV
PHARMACOLOGY 57
copyright © 2013-2014- Dental Decks
anesthetics
Which of the following are true regarding the use of nitrous oxide analgesia? Select all that apply.
rapid onset of action
lowers pain threshold
• produces euphoria
• respiratory irritant
• titratable
• slow recovery time
• virtually no adverse effects in absence of hypoxia
• therapeutic sedative for many medically compromised patients
58
• qenerally suitable for all ages . In , 13 ' 3 copyright ©2013-2014-Dental Decks
PHARMACOLOGY

• inhalation
*** The agent used most frequently is nitrous oxide.
Nitrous oxide is a slight sweet smelling, colorless, inert gas. It must always be coupled with no less than 30% oxygen. Nitrous oxide is quickly absorbed from the lungs and is physically dissolved in the blood. There is no biotransformation, and the gas is rapidly excreted by the lungs when the concentration gradient is reversed. It is recommended that the patient be maintained on oxygen for 5 to 10 minutes after the sedation period.
Dose response for nitrous oxide (always given in mixture with oxygen): • 10% - 20%: tingling of hands, feet, body warmth • 20% - 40%: mild sleepiness, relaxation, some analgesia, mind dissociation, heightened auditory perception •Above 50%: this is too much nitrous — nausea, sweating
*** Rapid onset: 5 minutes *** Rapid recovery: 5 minutes
Note: Nitrous oxide does not provide enough analgesic effect to preclude the use of local anesthesia in dental surgery or restorative procedures. Local anesthetics must be used along with nitrous oxide.
Remember: Nitrous oxide has minimal depressant effects on the cardiovascular system and no skeletal muscle relaxant properties.
• rapid onset of action • produces euphoria • titratable • virtually no adverse effects in absence of hypoxia • therapeutic sedative for many medically compromised patients • generally suitable for all ages
Important points about nitrous oxide: • The main therapeutic effect of nitrous oxide is relaxation/sedation (it is used in conscious sedation). Mild analgesia is a secondary effect. It is not a respiratory depressant. • The first symptom of nitrous oxide onset is tingling of the hands. • Nitrous oxide has no local anesthetic properties. Therefore, the addition of local anesthesia is necessary in procedures in which pain is anticipated. • Nitrous oxide elevates pain threshold. • Long term exposure to low doses of nitrous oxide has been shown to increase the incidence of spontaneous abortions. Environmental contamination by nitrous oxide can be kept to a minimum by employing a scavenger system. • Nitrous oxide is stored under pressure (750 psi) in steel cylinders (in a liquid state) painted blue. Oxygen is stored in green tanks. • Nitrous oxide delivery machines come pre-equipped with a fail-safe mechanism that will not allow less than 20% oxygen to be delivered to the patient. • It is a nonirritating, colorless gas with a slightly sweet odor and tasteless. It is very stable and inert chemically at room temperatures. • It has a rapid onset (blood:gas solubility coefficient = 0.47) and termination. • It is 1.5 times heavier than air. • Nitrous oxide will diffuse into air-containing cavities within the body faster than nitrogen diffuses out. This results in a temporary increase in either the pressure and/or volume of the cavity depending upon the dis-tensibility of its walls. This is most noticeable in the bowel. • Nitrous oxide interacts with vitamin B 1 2 synthesis in the human body by interfering with the enzyme methionine synthase, depleting the body of vitamin B | 2 . When nitrous oxide is used heavily and over an extended period of time, vitamin B 1 2 depletion will probably become a major problem, as it can cause brain and nerve damage.

anesthetics
All the following are considered to be what type of anesthetic?
• halothane
• enflurane
isoflurane
•sevoflurane
desflurane
59 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anesthetics
Which of the following are reasons why epinephrine is included in dental local
anesthetics? Select all that apply.
• it prolongs the duration of local anesthesia
• to increase the local pH and therefore increase the available free base form of the
local anesthetic
• to provide local hemostasis
• to delay the absorption of anesthetic into the systemic circulation thus reducing the
chance of systemic toxicities

• inhalation anesthetics
Inhalation anesthetics are drugs which are vaporized from the liquid form and inhaled to produce general anesthesia. These drugs are relatively simple lipophilic molecules ranging from halogenated hydrocarbons (halothane) to halo-genated ethers (isoflurane, enflurane, sevoflurane, desflurane). Note: Vaporization of these liquids occurs in a vaporizer and delivery to the patient occurs through an anesthesia machine via a nasal mask.
Essential Components of General Anesthesia: • Analgesia - perception of pain eliminated • Hypnosis - unconsciousness • Depression of spinal motor reflexes • Muscle relaxation
Hypotheses of General Anesthesia: • Lipid Theory: based on the fact that anesthetic action is correlated with the oil/gas coefficients. The higher the solubility of anesthetics is in oil, the greater is the anesthetic potency. No longer accepted as the primary mechanism. • Protein (Receptor) Theory: based on the fact that anesthetic potency is correlated with the ability of anesthetics to inhibit enzymatic activity of a pure, soluble protein. Also, attempts to explain that GABAA receptor is a potential target of anesthetics action. • Binding theory: anesthetics bind to hydrophobic portion of the ion channel.
Pharmacokinetics of Inhaled Anesthetics: • Amount that reaches the brain - Indicated by oihgas ratio (lipid solubility)
• Partial Pressure of anesthetics - 5% anesthetics = 38 mmHg
• Solubility of gas into blood (blood:gas solubility coefficient) - The lower the blood: gas ratio, the more anesthetics will arrive at the brain
• Cardiac Output - Increased CO = greater induction time
MAC (mean alveolar concentration): • A measure of potency • 1 MAC is the concentration necessary to prevent responding in 50% of population • Values of MAC are additive: - Avoid cardiovascular depressive concentration of potent agents
• it prolongs the duration of local anesthesia • to provide local hemostasis • to delay the absorption of anesthetic into the systemic circulation thus reducing the chance of systemic toxicities
Epinephrine, a vasoconstrictor, is included in dental local anesthetic preparations for the following three reasons:
1. It prolongs the duration of local anesthesia.
2. To provide a hemostasis such that local bleeding is controlled or reduced.
3. To delay the absorption of anesthetic into the systemic circulation thus reducing the chance of systemic toxicities.
Note: Epinephrine has no effect on pH or the amount of free base form of a local anesthetic.

Which stage of general anesthesia
• stage 1
• stage II
• stage III
• stage IV
begi ns with
anesthetics
unconsciousness?
61 copyright © 2013-2014 - Denta! Decks
PHARMACOLOGY
anesthetics
Nitrous oxide is used as a single agent to produce general anesthesia.
Nitrous oxide is used to produce sedation and mild analgesia.
• both statements are true
• both statements are false
• the first statement is true, the second is false
• The first statement is false, the second is true
62 copyright e 2013-2014- Dental Decks
PHARMACOLOGY

• stage II Four stages of general anesthesia:
• Stage 1: Amnesia/analgesia • Stage II: Delerium: begins with unconsciousness and ends with loss of eyelid reflex, purposeless movements and hyper reaction, dilated pupils, reflex vomiting, tachycardia, and hypertension • Stage III: Surgical anesthesia: four planes with progressive loss of reflexes and muscle control • Stage IV: Medullary paralysis: cessation of respiration, ending with death without proper treatment
Note: These four stages of anesthesia apply to the inhalants and not to the intravenous general anesthetics.
Agents used for general anesthesia: • Inhalation agents: volatile halogen-containing liquids
- Halothane: poses a risk with epinephrine; associated with hepatitis; poor skeletal muscle relaxant. However, it is one of the more widely used anesthetics for general surgical anesthesia. - Desflurane, sevoflurane, isoflurane and enflurane: pose less risk with epinephrine; not associated
with hepatitis; good skeletal muscle relaxants.
Note: Nitrous oxide (N20) is not considered a general anesthetic since hypoxic levels are required to produce anesthesia. It is considered a sedative. It is used alone to produce sedation or in combination with the above agents to supplement the anesthetic response. It is a gas at room temperature and pressure.
• Intravenous agents: • Ultrashort-acting barbiturates: thiopental (Pentothal) and methohexital (Brevital) • Benzodiazepines: diazepam (Valium), midazolam (Versed), and lorazepam (Ativan) • Neuroleptic-opioid combinations which are called neuroleptanalgesics combine fentanyl (opioid) and droperidol (a phenothiazine). When administered with nitrous oxide, neuroleptanalgesia can be converted to neuroleptanesthesia. • Other agents:
• Propofol (Diprivan): a short-acting hypnotic agent; vasodilator • Ketamine (Ketalar): is considered a dissociative anesthetic. It blocks yV-methyl-D-asparate (NMDA) (glutamate) receptors. Note: In some circumstances, ketamine has been known to produce illusions or hallucinations that are enhanced by environmental stimuli upon emergence from anesthesia. Diazepam is given with ketamine to avoid this. • Etomidate (Amidate): is a carboxylated imidazole derivative which acts similar to the ultrashort-acting barbiturates.
• the first statement is false, the second is true
Nitrous oxide is unable to produce general anesthesia except if it is given at concentrations greater than 80%. At these concentrations, the lack of oxygen would cause hypoxia in the patient. Inhalant anesthetics such as halothane and isoflurane can produce general anesthesia at concentrations approximating 3-5%. As such they are very useful in anesthesia.
Nitrous is used to produce sedation and mild analgesia. It is usually used in concentrations of 30-50%> along with pure oxygen. It is a colorless, nonirritating gas at room temperature and pressure, and is not flammable nor explosive. The onset of sedation is within 5 minutes and the recovery is just as rapid. It is excreted unchanged by the lungs. The most common complaint from patients taking nitrous oxide is mild nausea.
Note: Always give patient 100% oxygen at the end of the procedure to prevent diffusion hypoxia.
Adverse effects of nitrous oxide: • Decreased mental performance, audiovisual ability, and manual dexterity • At high doses and/or high exposure: reduced fertility, spontaneous abortions, neurological and kidney disease as well as bone marrow suppression
Nitrous oxide is contraindicated in patients: • Head injury • With bowel obstruction • Pneumothorax • Middle ear and sinus disease • With upper respiratory infections • COPD (emphysema or bronchitis) • In the first trimester of pregnancy • With whom communication is difficult (i.e., autistic patients) • Having a contagious disease since it is difficult to sterilize entire tabes
Important: Prolonged exposure (e.g., more than 24 hours) causes bone marrow depression.

anesthetics
Which component of a lidocaine local anesthetic solution causes an allergy?
• water
• bisulfites
• lidocaine
• epinephrine (vasoconstrictor)
63 copyright©2013-2014-Dental Decks
PHARMACOLOGY
Of the amide-type local anesthetics, which stream rather than the liver? Select all that apply.
• articaine (Septocaine, Zorcaine)
• mepivacaine (Carbocaine)
• lidocaine (Xylocaine)
• prilocaine (Citanest)
• bupivacaine (Marcaine)
anesthetics
is/are metabolized in the blood-
64 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• bisulfites
Patients may exhibit hypersensitivity to sulfites contained in some anesthetic solutions. Sodium metabisulfite prevents the oxidation (deterioration) of the epinephrine vasoconstrictor in those commercial preparations containing epinephrine. Most of the patients reacting to bisulfites have a history of asthma and the airway is hyperactive to the sulfites. Allergic reaction usually results in an asthmatic syndrome of wheezing and bronchial constriction. Bisulfites are present in only those commercial preparations containing vasoconstrictor. Preparations without vasoconstrictor such as mepivacaine 3%o (Carbocaine 3%) do not contain bisulfites.
Important: All local anesthetics except cocaine are vasodilators, however, mepivacaine has less of a vasodilator effect compared to the others and, therefore, is the drug chosen when a vasoconstrictor is not used with the local anesthetic.
1. Hypersensitivity or allergic reactions to local anesthetics, particularly the Notes amides, are much more rare than allergic reactions to the bisulfites.
2. Methylparaben is another local anesthetic preservative that may cause an allergic reaction.
• articaine (Septocaine, Zorcaine)
Articaine (Septocaine, Zorcaine) is an amide-type local anesthetic. However, it is chemically unique in that it has an ester group attached to its molecule which can be acted upon by plasma cholinesterase to render it ineffective. Therefore, it is the only amide which is metabolized in the bloodstream and not the liver. Rapid metabolism of this ester bond gives it a short half life.
Articaine is supplied as articaine HCL 4%o solution with epinephrine 1; 100,000 and as articaine HCL 4%> solution with epinephrine 1:200,000. It is indicated for local, infiltrative, or conductive anesthesia in both simple and complex dental and periodontal procedures. The onset of anesthesia following administration of articaine has been shown to be 1 to 6 minutes after injection. Complete anesthesia lasts approximately 1 hour.
Articaine is contraindicated in patients with a known history of hypersensitivity to local anesthetics of the amide type, or in patients with known hypersensitivity to sodium metabisulfite.

anesthetics
When phentolamine mesylate (OraVerse) is given after a dental procedure to reverse the local anesthetics effects, approximately how fast is the return to normal nerve sensation compared to the normal time for the anesthetic to wear off?
• 10% decrease in the time for normal sensation to return
• 25% decrease in the time for normal sensation to return
• 50% decrease in the time for normal sensation to return
• 80% decrease in the time for normal sensation to return
65 copyright © 2013-2014- Dental Decks
PHARMACOLOGY
anesthetics
Phentolamine mesylate (OraVerse) is a drug used to reverse soft tissue anesthesia and the associated functional deficits resulting from a local dental anesthetic containing a vasoconstrictor. Which statement best describes its mechanism of action?
• prevents the influx of sodium into the neuron by blocking neuronal channels
• causes vasodilation and increased blood flow in injection area
• prevents the efflux of sodium out of the neuron
• causes vasoconstriction and decreased blood flow in injection area
66 copyright © 2013-2014 - Dental Decks

• 50% decrease in the time for normal sensation to return
Thus if a local anesthetic such as lidocaine with epinephrine normally takes about 180 minutes to wear off, after phentolamine injection, the anesthetic will wear off in approximately 90 minutes. This represents a 50% decrease in time for normal sensation to be re-tored.
Note: OraVerse dose is based upon the number of cartridges of local anesthetic with vasoconstrictor administered.
• 1/2 a cartridge (0.2 mg) of OraVerse if 1/2 cartridge of anaesthetic was administered • 1 cartridge (0.4 mg) of OraVerse if 1 cartridge of anesthetic was administered • 2 cartridges (0.8 mg) of OraVerse if 2 cartridges of anesthetic were administered
Note: OraVerse (solution for injection/dental cartridge) is administered as a submucosal injection.
• causes vasodilation and increased blood flow in injection area
Phentolamine mesylate (OraVerse) is an alphat-adrenergic receptor blocker. Phentolamine mesylate competitively blocks alpha-adrenergic receptors to produce brief antagonism of circulating epinephrine and norepinephrine and antagonism of the vasoconstrictor in the anesthetic preparation. This results in vasodilation of the blood vessels. The local anesthetic is thus carried away at a more rapid rate from the injection site resulting in a more rapid return to normal nerve sensation.

anti-anxiety agents
All of the following drugs are benzodiazepines EXCEPT one. Which one is the EXCEPTION?
• chlordiazepoxide (Librium)
• diazepam (Valium)
• fiurazepam (Dalmane)
• midazolam (Versed)
• alprazolam (Xanax)
< Zolpidem (Ambien)
• triazolam (Halcion)
• oxazepam (Serax)
• temazepam (Restoril)
< clorazepate (Tranxene) 67
copyright©2013-2014-Dental Decks
PHARMACOLOGY
anti-anxiety agents
The most common adverse effects associated with the benzodiazepines include all of the following EXCEPT one. Which one is the EXCEPTION?
> CNS depression (drowsiness and sedation)
• GI disturbances (nausea, vomiting and diarrhea)
< confusion
• respiratory depression
• disorientation
• ataxia
68 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• Zolpidem (Ambien)
The benzodiazepines are used as oral preparations to alleviate anxiety and to induce sleep, and intravenously to cause conscious-sedation for outpatient surgery. Benzodiazepines act by potentiating the action of GAB A, an amino acid and an inhibitory neurotransmitter, which results in increased neuronal inhibition and CNS depression. Tolerance and physical dependence can occur with prolonged high dosage. They seem to be much safer than barbiturates. Other useful properties include being an anticonvulsant and a skeletal muscle relaxant.
Pharmacological effects of benzodiazepines: antianxiety, sedation, anticonvulsant, amnesia, and skeletal muscle relaxation.
Adverse effects: • CNS effects - fatigue, slurred speech, drowsiness/sleepiness and confusion (do not drive a car) • GI effects - dry mouth, nausea • Other effects - hypotension, muscle relaxation
Benzodiazepines used orally as tranquilizers: chlordiazepoxide (Librium), diazepam (Valium), alprazolam (Xanax) and lorazepam (Ativan). Those used as hypnotics to overcome insomnia: flurazepam (Dalmane) and triazolam (Halcion). Diazepam (Valium) and Clonazepam (Klonopin) can be used as anticonvulsants. Midazolam (Versed) comes as a liquid for preoperative sedation in children and as injectable for IV conscious sedation.
Note: Benzodiazepines should never be taken with any form of alcohol. Serious potentiation of the sedative effects of each will occur leading to unexpected inebriation and respiratory depression.
Important: Zolpidem (Ambien), eszopiclone (Lunesta), and zaleplon (Sonata) are anti-insomnia agents (called GABA-BZ Agonists). These agents appear to act through the potentiation of GAB A on benzodiazepine receptors, especially the omega-1 subunit. Note: They have shown no potential for causing addiction.
• respiratory depression
The benzodiazepines have clinically useful antianxiety, sedative-hypnotic, anticonvulsant and skeletal muscle relaxant properties. They exert their main effect on central GABA-nergic neurons. With normal dosing, the benzodiazepines have little effect on respiratory systems in healthy individuals.
The benzodiazepines (especially diazepam, lorazepam and midazolam) are important adjuncts in the practice of anesthesiology. They may be used as preoperative sedatives and induction agents, as well as supplemental agents for the maintenance of anesthesia. Important: The benzodiazepines, barbiturates and narcotic analgesics all produce sedation and have the ability to produce dependence.
The pharmacokinetics of individual benzodiazepines differ, and therefore there is a wide range in speed of onset and duration of action among these compounds. Following oral administration, most of the benzodiazepines are rapidly absorbed and highly bound to plasma protein. In general, most of the metabolites are conjugated with glucuronic acid and excreted in the urine and feces. Note: a-Hydroxylation is a rapid route of metabolism that is unique to triazolam, midazolam, and alprazolam, however, under normal circustances in healthy patients, the hydroxylation of these medications is of little clinical significance. This accounts for the very rapid metabolism and short sedative actions of these drugs.
1. The term tranquilizer refers to a drug that promotes tranquility by calming, soothing, qui-IS'otes eting or pacifying without sedating or depressant effects. Antipsychotic agents are consid
ered to be major tranquilizers and antianxiety agents (benzodiazepines) are considered to be minor tranquilizers. 2. For the treatment of insomnia due to anxiety the benzodiazepines flurazepam, temazepam and triazolam are usually prescribed. 3. Important: Flumazenil (Mazicon), a benzodiazepine antagonist, may be used to reverse the residual effects of benzodiazepines in the event of an overdose. 4. If the benzodiazepines are ineffective in helping with insomnia, Zolpidem (Ambien), eszopiclone (Lunesta), or zaleplon (Sonata) are often useful. These are anti-insomnia agents (called GABA-BZ Agonists).

Buspirone (BuSpar) is a partial agonist at a
• GABA (gamma-aminobutyric acid) receptor
• norepinephrine receptor
• dopamine receptor
• serotonin receptor
anti
specific:
-anxiety agents
copyrights 2013-2014
69 - Dental Decks
PHARMACOLOGY
anti-anxiety agents
Which of the following side effects are most common with the use of Diazepam (Valium)?
• rash, itch
• mouth, throat ulcers
• drowsiness, fatigue
• difficulty with urination

• serotonin receptor
Buspirone (BuSpar) is an orally administered antianxiety agent with a short half-life (2-4 hours). It is not chemically related to the benzodiazepines, or any other anxiolytic agent. Buspirone also differs from other antianxiety agents in that it does not possess anticonvulsant or muscle relaxant properties, does not impair psychomotor function and does not cause sedation (lacks CNS depressant activity) or physical dependence.
The exact mechanism of action of buspirone is unknown. However, it has a higher affinity for serotonin receptors in the CNS and a lesser affinity for the benzodiazepine -GABA receptors.
Important: The antianxiety effect is achieved via a partial agonist effect on CNS serotonin 5 -HT l a receptors that occurs without affecting the benzodiazepine receptors or causing CNS depression.
Remember: GABA-BZ agonists have a chemical structure that is dissimilar from those of the benzodiazepines and on the sedative hypnotics. These agents appear to act through the potentiation of GAB A on benzodiazepine receptors, especially the omega-1 subunit. They are used primarily for insomnia. They have exhibited some anxiolytic action but they have little effect on skeletal muscle or seizure thresholds. They appear to have minimal disruptive action on the normal sleep cycle, thus preserving deep sleep. Note: They have shown no potential for causing addiction. Examples include Zolpidem (Ambien), es-zopiclone (Lunesta), and zaleplon (Sonata). These drugs have short half-lives (1 to 2 hours).
• drowsiness, fatigue
Diazepam is prescribed in the treatment of anxiety, nervous tension, muscle spasm, and as an anticonvulsant. Contraindication to use: Acute narrow angle glaucoma.
It is used intravenously as the agent of choice to reverse status epilepticus induced by a local anesthetic overdose. Diazepam affects the limbic system of the brain (controls emotion). It has a high therapeutic index, produces some degree of amnesia, and can be locally irritating to tissue and may produce local thrombophlebitis when given intravenously.
Note: Propylene glycol, which is in the IV mixture, is the main cause of thrombophlebitis.

anti-anxiety agents
The barbiturates Phenobarbital (Luminal), Mephobarbital (Mebaral), and Primidone (Mysoline) are classified as what type of barbiturate?
• ultrashort-acting
• short-acting
• intermediate-acting
• long-acting
71 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
The brief duration of general anesthetic biturate is due to what factor?
• rapid rate of metabolism in the liver
anti-anxiety agents
action of an ultra-short-acting bar-
• low lipid solubility, resulting in a minimal concentration in the brain
• high degree of binding to plasma proteins
• rapid rate of redistribution from the brain to
• slow rate of excretion by the kidneys
PHARMACOLOGY
peripheral tissues
72 copyright©2013-2014-Dental Decks

• long-acting
The length of action can be related to the lipid solubility with the ultrashort being the most lipid soluble and the long acting having the least lipid solubility. They are metabolized in the liver. These drugs possess serious drug dependence potential. They do not possess significant analgesic properties. The length of hypnotic action of the four different classes after a single dose are as follows:
• Ultrashort-acting: 5 to 20 minutes • Short-acting: 1 to 3 hours • Intermediate-acting: 3 to 6 hours • Long-acting: 6 to 10 hours
Agents: • Ultrashort-acting: for induction of general anesthesia. Examples include thiopental (Pentothal) and methohexital (Brevital). • Short-acting: for treating insomnia. Examples include secobarbital (Seconal) and pentobarbital (Nembutal). • Intermediate-acting: for treating insomnia. Examples include amobarbital (Amytal) and butabar-bital (Butisol). • Long-acting: for treating certain types of seizures. Examples include phenobarbital (Luminal), me-phobarbital (Mebaral) and primidone (Mysoline).
Remember: Barbiturates do not possess analgesic properties.
Important concept for anticonvulsant effect of long-acting barbiturates (i.e. phenobarbital): Barbiturates work by inhibiting the depolarization of neurons by binding to the GAB A receptors, which enhances the transmission of chloride ions. They also increase the threshold for electrical stimulation of the motor cortex. Remember: Benzodiazepines work similarly to barbiturates, but they also increase the number of chloride channels while facilitating the transmission of chloride ions. This suppresses the spread of seizure activity but does not abolish abnormal discharge from a focus.
Note: The cause of death from acute barbiturate poisoning or overdosage is respiratory failure. Other adverse reactions include CNS depression, euphoria, and habituation. The most important therapeutic measure to be taken in a case of barbiturate poisoning is to assure adequate respiration.
• rapid rate of redistribution from the brain to peripheral tissues
Remember: These agents will maintain anesthesia only while in the brain. Because of their high lipid solubility, these agents will rapidly leave the brain for other tissues; thus the patient wakes up within a few minutes of administration.
Examples of ultra-short-acting barbiturates include thiopental (Pentothal) and methohexital (Brevital). These agents are administered by intravenous injection.
Contraindications to the use of ultra-short-acting barbiturates for general anesthesia: • Porphyria • Liver dysfunction (they are metabolized in the liver)
• Emphysema • Previous addiction to sedative hypnotic drugs
Remember: These drugs have the ability to produce dependence.

anti-anxiety agents
Which of the following statements concerning barbiturates are true? Select all that apply.
» barbi turates may increase the half-lives of drugs metabol ized by the liver
• barbiturates depress neuronal activity by increasing membrane ion conductance (primarily chloride), reducing glutamate-induced depolarizations and potentiating the inhibitory effects of GABA
• compared with benzodiazepines, the barbiturates exhibit a steeper dose-response relationship
• barbiturates may precipitate acute porphyria in susceptible patients
73 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-epileptics
All the following are classified as antiepileptics EXCEPT one. Which one is the EXCEPTION?
• gabapentin (Neurontin)
• carbamazepine (Tegretol)
• phenytoin (Dilantin)
• propafenone (Rythmol)
• phenobarbital (Luminal)
• diazepam (Valium)
• valproic acid (Depakene)
• ethosuximide (Zarontin)
• primidone (Mysoline) 74 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• barbiturates depress neuronal activity by increasing membrane ion conductance (primarily chloride), reducing glutamate-induced depolarizations and potentiating the inhibitory effects of GABA
• compared with benzodiazepines, the barbiturates exhibit a steeper dose-response relationship
• barbiturates may precipitate acute porphyria in susceptible patients
*** The first statement is false; barbiturates may decrease the half-lives of drugs metabolized by the liver. Barbiturates induce the formation of the liver microsomal enzymes that metabolize drugs. This leads to an increased clearance of the affected drugs and possibly leads to a decrease in the drugs effectiveness.
The uses of the barbiturates are determined by their duration of action:
1. The ultrashort-acting agents are used intravenously for the induction of general anesthesia. For extensive procedures, they are used to induce stage III surgical anesthesia. For very brief procedures, they may be used alone. 2. The short-acting agents can be used orally for their hypnotic, calming effect. These agents can be given preoperatively, before a dental appointment, to allay anxiety. 3. The intermediate-acting agents can also be prescribed to relieve anxiety before a dental appointment, although their effects will last longer than those of the short-acting agents. These agents are used for daytime sedation and for the treatment of insomnia (they suppress REM sleep). 4. The long-acting barbiturates are used primarily for daytime sedation and the treatment of epilepsy.
Generally the primary pharmacological effects of the barbiturates involve the brain and spinal cord (CNS — depression of. At sedative doses barbiturates do not effect or have little effect on the cardiovascular and respiratory systems. Barbiturates are metabolized in the liver. The chronic use of the barbiturates causes an increase in liver microsomal enzyme activity that appears to be the result of increased synthesis of enzyme. These drugs possess serious drug dependence potential. They do not possess sig-
• propafenone (Rythmol)
*** Propafenone (Rythmol) is an antiarrhythmic agent used to treat both ventricular arrhythmias and supraventricular tachycardias.
A seizure is an alteration in behavior, function, and/or consciousness that results from an abnormal electrical discharge of neurons in the brain. Epilepsy, or the term seizure disorder, is used to describe chronic unprovoked recurrent seizures. Seizures as classified as either partial or generalized, based on how the abnormal brain activity begins.
• Partial seizures: when seizures appear to result from abnormal activity in just one part of the brain. • Generalized seizures: seizures that seem to involve all of the brain. Four types of generalized seizures exist: absence (also called petit mal), myoclonic, atonic and tonic-clonic seizures (also called grand mal).
For most antiepileptic (anticonvulsant) drugs, the exact mechanism for reducing seizure activity is not clearly understood. All increase the threshold of the CNS to convulsive stimuli or inhibit the spread of seizure activity. The antiepileptic drugs (AEDs) can be grouped into the following classes:
1. Hydantoins: Phenytoin (Dilantin) is used in the treatment of tonic-clonic (grand mal) seizures. It prolongs the effective refractory period by blocking neuronal sodium channels. Phenytoin-induced gingival hyperplasia is common and may partially or totally obscure the crowns of teeth. The rate of development of this condition can be diminished by proper oral hygiene. 2. GABA analogs: The exact mechanism of action of valproic acid (Depakene) and the newer GABA analogs is not clearly understood. All of them increase the actions of GABA, an inhibitory neurotransmitter. They may inhibit the voltage-dependent sodium channel, thereby stabilizing the neuronal membranes. Examples of the newer GABA analogs include: gabapentin (Neurontin), divalproex sodium (Depakote), felbamate (Felbatol), lamotrig-ine (Lamictal), pregabalin (Lyrica), tiagabine (Gabitril), and topiramate (Topamax). 3. Succinimides: Ethosuximide (Zarontin): used in the treatment of absence seizures. 4. Barbiturates: Phenobarbital (Luminal) works by inhibiting depolarization of neurons by binding to the GABA receptors, which enhances the transmission of chloride ions. Primidone (Mysoline) is metabolized to phenobarbital and phenylethylmalonamide (PEMA), which have anticonvulsant activity. 5. Benzodiazepines: work similarly to barbiturates, but they also increase the number of chloride channels while facilitating the transmission of chloride ions. Examples include diazepam (Valium), clonazepam (Klonopin), and lorazepam (Ativan). Note: Diazepam (Valium) is used for status epilepticus and in emergency treatment of seizures. May cause drowsiness, dizziness, and ataxia. 6. Miscellaneous: oxcarbazepine (Trileptal), levetiracetam (Keppra), and carbamazepine (TregretoI).Carba-mazepine is used as prophylaxis for partial seizures with complex symptomatology including psychomotor and temporal lobe seizures. It is also used to treat tonic clonic seizures (grand mal) and trigeminal neuralgia. It rarely causes aplastic anemia.

anti-depressants
The most widely used tricyclic antidepressant (TCA) drug is:
• imipramine (Tofranil)
• amitriptyline (Elavil)
• desipramine (Norpramin)
• nortriptyline (Pamelor)
• doxepin (Sinequan)
75 copyright <3 2013-2014 - Dental Decks
PHARMACOLOGY
anti-depressants
Which drug is the current drug of choice for the treatment of the manic phase of bipolar disorder (or manic-depressive syndrome)?
• phenobarbital
> imipramine
• lithium
• haloperidol
76 copyright O 2013-2014 - Dental Decks

• amitriptyline (Elavil)
The tricyclic antidepressants are generally considered to be the drugs of first choice for the treatment of unipolar disorder (depression). These drugs inhibit the neuronal re-uptake of norepinephrine and serotonin (5-HT) in the brain. This results in the potentiation of their neurotransmitter actions at postsynaptic receptors.
Important: Amitriptyline displays the greatest anticholinergics effects (especially xe
rostomia), desipramine the least.
Drowsiness is the most frequent CNS adverse reaction. Anticholinergic adverse side effects include: dry mouth, constipation, blurred vision and tachycardia.
The selective serotonin reuptake inhibitors (SSRIs) have revolutionized the treatment of depression. The most important clinical distinction of the SSRIs from all other antidepressants is their very high specificity for blocking the reuptake of serotonin. Fluoxetine (Prozac) is the prototype and has the longest half-life. Paroxetine (Paxil), Sertraline (Zoloft) and Fluvoxamine (Luvox) have shorter half-lives and can be given once daily. Citalopram (Celexa) and escitalopram (Lexapro) are used for generalized anxiety disorders. These drugs are also effective for treating panic attacks. Side effects include nausea, headaches, anxiety, agitation, insomnia, and sexual dysfunction.
• lithium
Bipolar disorder (or manic-depressive syndrome) is characterized by cyclical changes in affective state between the manic and depressive phases of behavior. Bipolar patients cycle between the two affected states.
Lithium salts are by far the most important drugs for suppressing mania in patients with affective disorders. It is not useful for the acute manic episodes. Lithium can prevent the occurrence of both the depressive as well as the manic episodes in some but not all the patients. Antidepressants are often administered with lithium to manage the depressive phase of the illness if lithium alone is not sufficient. Note: Lithium works inside the cell to prevent the degradation of inositol triphosphate by IMPase, thus increasing its cytoplasmic concentration.These substances serve as second messengers within the CNS and may have widespread influence on neuronal function.
Approximately 25% of patients who suffer from mania do not respond to lithium. Carbamazepine (an anticonvulsant) and valproic acid (also an anticonvulsant) may be effective in some refractory cases. Note: Carbamazepine blocks sodium channels and valproic acid blocks both sodium and calcium channels.
Neuroleptic agents (also referred to as anti-psychotic agents or major tranquilizers) are used in the acute manic episodes. Chlorpromazine, which is a phenothiazine, and Haloperidol, which is not a phenothiazine but acts in a similar fashion, are effective in quelling the extreme mania and psychotic behavior.
1. The most common side effects of lithium, including GI irritation, fine hand tremor, Notes muscular weakness, polyuria, thirst, sleepiness, and a sluggish feeling, are often asso
ciated with initial therapy and usually fade within 1 to 2 weeks. 2. Severe intoxication results in vomiting, diarrhea, unconsciousness, and convulsions. 3. Sodium restriction leads to greater retention of lithium in the kidney. 4. Diuretics and some NSAIDs reduce lithium excretion and may cause lithium toxicity.

anti-depressants
Monoamine Oxidase (MAO) inhibitors are often used as third-line agents in cases of refractory and atypical depression. Which of the following drugs are MAO inhibitors?
• citalopram (Celexa)
• fluoxetine (Prozac)
• tranylcypromine (Parnate)
• phenelzine (Nardil)
• doxepin (Sinequan)
• imipramine (Tofranil)
77 copyright©2013-2014-Dental Decks
PHARMACOLOGY
anti-depressants
The vasoconstrictor epinephrine in local anesthetic injections must be used cautiously in patients taking all of the following antidepressant drugs EXCEPT one in order to avoid transient and significant increases in blood pressure. Which one is the EXCEPTION?
• tricyclic antidepressants (i.e., Elavil)
• selective serotonin reuptake inhibitors (i.e., Prozac and Paxil)
• serotonin and norepinephrine reuptake inhibitors (i.e., Effexor and Cymbalta)
78 copyright©2013-2014-Dental Decks
PHARMACOLOGY

• tranylcypromine (Parnate) • phenelzine (Nardil)
MAO inhibitors are used are often used as third-line agents in cases of refractory and atypical depression. MAO inhibitors antagonize the action of monoamine oxidase (MAO) responsible for the degradation of the naturally occurring monoamines — epinephrine, norepinephrine, dopamine, and serotonin. It is theorized that the increased level of monoamines in the brain is responsible for the antidepressant effect of the MAO inhibitors.
Note: Local anesthetics containing epinephrine are generally contraindicated inpatients who are taking MAO inhibitors.
The major limitation for the widespread use of the MAO inhibitors for the treatment of depression has been the potential for serious adverse side effects, including hypertensive crisis, which can be fatal. A hypertensive crisis can occur within several hours after ingestion of a substance that contains tyramine. Tyramine releases norepinephrine and other sympathomimetic amines, thereby raising blood pressure. Early symptoms include occipital headache, palpitations, stiff neck, nausea, vomiting, and sweating. Among the drugs that interact with MAO inhibitors are meperidine (Demerol), epinephrine and ephedrine.
1. Miscellaneous antidepressants include: Notes . Mirtazapine (Remeron): alpha2 -noradrenergic antagonnist
• Bupropion (Wellbutrin SL): norepinephrine/dopamine reuptake inhibitor • Trazodone (Desyrel): mechanism not clear; possible serotonin reuptake inhibitor
• selective serotonin reuptake inhibitors (i.e., Prozac and Paxil)
These two categories (tricyclic antidepressants and serotonin and norepinephrine reuptake inhibitors) of antidepressant drugs significantly increase norepinephrine levels in tissues. In the presence of a vasoconstrictor administered via a local anesthetic injection, the patient could experience significant elevation of blood pressure due to the vasopressor actions of the combination.
Note: The selective serotonin reuptake inhibitors (i.e., Prozac and Paxil) have no such effect on norepinephrine in tissues and interaction with a vasoconstrictor like epinephrine is not an issue.

anti-depressants
Which TWO groups of antidepressant drugs has the highest incidence of dry mouth (xerostomia)?
• tricyclic antidepressants (i.e., Elavil)
• selective serotonin reuptake inhibitors (i.e., Prozac and Paxil)
• serotonin and norepinephrine reuptake inhibitors (i.e., Effexor and Cymbalta)
• monoamine oxidase inhibitors (i.e., Nardil)
79 copyright © 2013-2014 - Dental Decks
anti-depressants
All of the following anti-depressant drugs are serotonin and norepinephrine reuptake inhibitors EXCEPT one. Which one is the EXCEPTION?
> venlafaxine (Effexor)
< nortriptyline (Pamelor)
- desipramine (Norpramin)
• desvenlafaxine (Pristiq)
• sertraline (Zoloft)
• duloxetine (Cymbalta)

r
• tricyclic antidepressants (i.e., Elavil) • serotonin and norepinephrine reuptake inhibitors (i.e., Effexor and Cymbalta)
These two categories of antidepressant drugs induce significant dry mouth in up to 75% of patients taking these medications. These effects are due to the secondary anticholinergic nature of these agents. Note: Drug-induced dry mouth must be treated palliatively with artificial salivary substitutes.
The selective serotonin reuptake inhibitors (i.e., Prozac, Paxil) and monoamine oxidase inhibitors have no secondary anticholinergic effects and therefore do not cause any significant dry mouth.
> sertraline (Zoloft)
Five major categories of antidepressant drugs: • Tricyclic antidepressants:
• Amitriptyline (Elavil) • Doxepin (Sinequan) • Imipramine (Tofranil)
• Serotonin and norepinephrine reuptake inhibitors: • Venlafaxine (Effexor) • Desvenlafaxine (Pristiq) • Nortriptyline (Pamelor) • Duloxetine (Cymbalta) • Desipramine (Norpramin)
• Selective serotonin reuptake inhibitors: • Citalopram (Celexa) • Paroxetine (Paxil) • Escitalopram (Lexapro) • Sertraline (Zoloft) • Fluoxetine (Prozac)
• Second generation miscellaneous: • Bupropion (Wellbutrin) • Trazodone (Desyrel) • Nefazodone (Serzone) • Mirtazipine (Remeron)
• Monoamine oxidase inhibitors: • Phenelzine (Nardil) • Tranylcypromine (Parnate) • Isocarboxazide (Marplan)

anti-histamines
All of the following are H rreceptor blockers EXCEPT one. Which one is the EXCEPTION?
• diphenhydramine HCL (Benadryl)
< chlorpheniramine maleate (Chlor-Trimeton)
cimetidine (Tagamet)
• loratadine (Claritin)
• desloratadine (Clarinex)
81 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-histamines
For which of the following conditions can Ranitidine be used?
prostatitis
• GERD (heartburn)
• toxic-shock syndrome
• renal failure
82 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• cimetidine (Tagamet)
*** Cimetidine is an antihistamine H2-receptor blocker.
Antihistamines are antagonizing agents that compete for receptor sites with natural histamine, which is stored preformed in cytoplasmic granules of tissue mast cells and blood basophils. It is released in response to IgE-mediated (immediate) allergic reactions and plays an important role in hay fever, urticaria and angioneurotic edema. Note: Histamine also plays an important role in the control of acid secretion (HCL) in the stomach.
There are two types of histamine receptors, Hrreceptors, which play an extremely important role in allergic reactions and H2-receptors, which are important in gastric acid secretion. The antihistamines are divided into H,and H2-receptor blockers depending on the histamine receptor they compete for.
Hj receptor blockers include: 1. First-generation (classical) agents:
• Diphenhydramine HCL (Benadryl) and chlorpheniramine maleate (Chlor-Trimetron) *** These agents have a broad spectrum of action which includes antihistaminic, anticholinergic, antiserotonergic, antibradykinin and sedative properties.
2. Second-generation agents: • Cetirizine HCL (Zyrtec), fexofenadine HCL (Allegra), loratadine (Claritin) and deslo-ratadine (Clarinex) *** Most of these agents, because of their poor CNS penetration (do not cross the blood-brain barrier), cause less sedation and drowsiness than the first-generation agents.
Important points: All of the Hrreceptor blockers do not prevent the release of histamine but rather compete with free histamine for binding at Hrreceptor sites. In general, the binding is competitive, however, some second-generation agents bind non-competitively at higher doses. Common side effects include drowsiness, dizziness, anticholinergic effects (dry mouth, nose and throat), and nausea. They can both stimulate and depress the CNS.
• GERD (heartburn)
H2-receptor antagonists compete with histamine at the H2-receptor. Histamine produces a wide variety of physiologic actions in many tissues. While H2-receptors are located in the GI tract and in vascular and bronchial smooth muscle, H2-receptor antagonists compete with histamine only in the GI tract. Inhibition of histamine at the parietal cell interferes with one of several mediators for signaling the parietal cell to secrete acid.
H2-blockers include: cimetidine (Tagamet), ranitidine (Zantac), famotidine (Pepcid) and nizatidine (Axid). These agents are all reversible competitive antagonists of the actions of histamine on H2-receptors. These agents are used to treat acid-peptic disease, especially duodenal ulcers and occasionally gastric peptic ulcers. These drugs are also used to treat Zollinger-Ellison syndrome (a hypersecretory disease) and gastroesophageal reflux disease (GERD).
Note: Cimetidine has an antiandrogen effect (can lead to impotence, loss of libido, and gynomastia). It also inhibits liver metabolism which can lead to an increase in activity of other drugs such as warfarin and carbamazepine.

anti-histamines
Diphenhydramine HCL (Benadryl), chlorpheniramine maleate (Cblor-Trime-ton), loratadine (Claritin), and desloratadine (Clarinex) are antihistamines at which histamine receptor site listed below?
Hj-receptor site
H2-receptor site
83 copyright©2013-2014-Dental Decks
PHARMACOLOGY
anti-infectives
Antibiotic regimens for patients with prosthetic implants include all of the following drugs as standard therapy of first choice in patients not allergic to penicillin EXCEPT one. Which one is the EXCEPTION?
• cephalexin
• cephradine
• amoxicillin
• tetracycline
84 copyright© 2013-2014- Dental Decks
PHARMACOLOGY

• H.,-receptor site
Antihistamines are antagonizing agents that compete for receptor sites with natural histamine. The two types of histamine antagonists are:
1. Hrreceptor antagonists: competitively block Hj-receptors blocking the effects of histamine at these receptors. They block the vasodilation, they block the constriction of the bronchi and they block capillary permeability which histamine ordinarily causes. The blockade of these effects of histamine overcomes the symptoms of seasonal allergies.
•Actions of Hj antihistamines: - Blocks pain and itch, vasodilation and bronchoconstriction due to histamine - Reduces motion sickness: first-generation only (i.e., Diphenhydramine HCL
and chlorpheniramine maleate) - Promotes sleep: first-generation only
Remember: The second generation Hj-receptor antagonists have the following characteristics: Longer half-lives than first generation (12-24 hours as opposed to 3-6 hours for first generation), they do not cross the blood-brain barrier, they produce little or no sedation, and have a higher risk of cardiac arrhythmias (long QT effect). Examples include Cetirizine HCL (Zyrtec), fexofenadine HCL (Allegra), loratadine (Claritin) and deslo-ratadine (Clarinex).
2. H2-receptor antagonists: competitively block H2-receptors, blocking the effects of histamine at these receptors. Examples of these drugs include: cimetidine (Tagamet), ranitidine (Zantac), famotidine (Pepcid) and nizatidine (Axid). They block secretion of stomach acid and are used in the treatment of duodenal ulcers.
Note: Histamine is found in all tissues, particularly in mast cells and blood basophils. It is released in allergic and inflammatory reactions.
• tetracycline
From the "Advisory Statement, Antibiotic Prophylaxis for Dental Patients with Total Joint Replacement" published by the American Dental Association and the American Academy of Orthopedic Surgeons, in the J Amer Dent Assoc 1997; 128(7):1004-8 and J Amer Dent Assoc 2003;134:895-898 — either cephalexin, or cephradine or amoxicillin can be used as the drugs of choice for standard prophylaxis medication in the patient with a total joint replacement.
• Cephalexin (Keflex) is a 1st generation cephalosporin; prophylaxis dose is 2 grams orally 1 hour prior to the dental procedure.
• Cephradine (Velosef) is a 1 st generation cephalosporin; prophylaxis dose is 2 grams orally 1 hour prior to the dental procedure.
• Amoxicillin is a member of the penicillin family; prophylaxis dose is 2 grams orally 1 hour prior to the dental procedure.
Note: For patients not allergic to penicillin and unable to take oral medications the suggested medications are cefazolin (a 1st generation cephalosporin) or ampicillin (member of the penicillin family). The regimen is as follows:
• Cefazolin (Ancef) 1 g or ampicillin 2 g intramuscularly or intravenously 1 hour prior to the dental procedure

anti-infectives
Which of the following antibiotics exerts its mode of action on the bacterial cell wall? Select all that apply.
• penicillin
• cephalexin
• clindamycin
• tetracycline
• erythromycin
• vancomycin
• chloramphenicol
• sulfonamides 85
• S t r e p t o m y c i n copyright©2013-20l4-DentalDecks
PHARMACOLOGY
Mefloquine (Lariam) belongs to a class which of the following conditions?
• malaria
• AIDS
• hepatitis
• cancer
• chlamydia
PHARMACOLOGY
of drugs
anti-infectives
which is useful in treating
86 copyright S 2013-2014 - Dental Decks

• clindamycin • tetracycline • erythromycin •chloramphenicol • streptomycin
Mechanisms of action of antibiotics on the bacteria cell: • Agents affecting cell wall:
- Penicillins - Vancomycin - Imipenem - Cephalosporins - Cycloserine - Bacitracin - Aztreonam
• Agents interfering with protein synthesis: - Tetracycline - Erythromycin - Azithromycin - Aminoglycosides - Lincomycin - Clarithromycin - Chloramphenicol - Clindamycin
• Agents interfering with normal biosynthetic pathways: - Sulfonamides - Trimethoprim - Fluoroquinolones (i.e., ciprofloxacin, norfloxacin, levofloxacin, moxifloxacin, and gemifloxacin)
Note: The most common clinical cause of bacterial resistance is the use of antibiotics when they are not indicated.
malaria
Malaria is a devastating parasitic disease transmitted through the bite of infected Anopheles mosquitoes. Endemic to tropical and subtropical areas of Asia, North and South America, the Middle East, North Africa, and the South Pacific. Plasmodium vivax is the most common of four human malaria species (P. falciparum, malariae, ovale, and vivax). P. vivax causes up to 65% of malaria in India and is becoming increasingly resistant to malaria drugs. By contrast, P. falciparum is the most deadly species and the subject of most malaria-related research and literature.
Mefloquine (Lariam) has been shown to be effective in treating malaria caused by all four malaria species.
Other antimalarial drugs are: • Chloroquin (Aralen) • Combination of atovaquone and proguanil (Malarone) • Halofantrine • Quinine • Combination of sulfadoxine and pyrimethamine (Fansidar)

anti-infectives
Which of the following antibiotics are considered broad-spectrum antibiotics? Select all that apply.
• penicillin VK
• cefaclor (Ceclor)
• ticarcillin
• penicillin G
• piperacillin
• cephalexin (Keflex)
87 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
Tetracyclines are the drugs of first choice in the lowing EXCEPT one. Which one is the EXCEPTION?
• mycoplasma pneumonia
• chlamydia infections
• rickettsial infections
• staphylococcal infections
PHARMACOLOGY
anti-infectives
treatment of all of the fol-
88 copyright © 2013-2014 - Dental Decks

• cefaclor (Ceclor) • ticarcillin • piperacillin
Cefaclor is a member of the cephalosporin family of antibiotics. The cephalosporins are penicillin-like in action against bacteria. They are bactericidal antibiotics and act like the penicillins and interfere with cell wall synthesis through inhibition of the synthesis of the peptidoglycan in the cell wall. The antibiotic binds to the enzymes (i.e., transpeptidase) that build/maintain the cell wall. This makes the cell wall osmotically unstable. Bacteria eventually lyse, resulting in death of the cell. Cephalosporins act against a wide range of gram-positive and gram-negative bacteria.
Currently there are four generations of cephalosporins. Each newer generation has significantly greater gram-negative antimicrobial properties than the preceding one, and a decreased maximum activity against gram-positive organisms.
Important cephalosporins within each generation:
• First: cephalexin (Keflex), cephradine (Velosef), cefadroxil (Duricefl, cefazolin (Ancefi. Most active against S. aureus, Group A Beta-hemolytic streptococci, and Pneumococcus. • Second: cefaclor (Ceclor), ceiuroxime (Ceftin), cefoxitin (Mefoxin), cefprozil (Cefzil), cefpodoxime (Vantin). Still have efficacy against gram-positive organisms but also possess good activity against E. coli and H. influenzae. • Third: cefixime (Suprax), cefoperazone (Cefobid), ceftriaxone (Rocephin). Have the broadest spectrum of activity of all cephalosporins and are extremely effective against gram-negative organisms. They are more active against E. coli, Klebsiella pneumoniae, Enterobacter, Salmonella, and Shigella. • Fourth: cefepime (Maxipime). Effective against Pseudomonas aeruginosa.
Note: Approximately 10% of individuals expressing allergy to the penicillin family of antibiotics will have cross allergenicity to the cephalosporins.
Remember: Antibiotics containing this beta-lactam ring are referred to collectively as beta-lactam antibiotics and include the penicillins, cephalosporins, and the two newer groups of agents, the carbapen-ems and the monobactams.
. staphylococcal infections
Popular Tetracyclines include: n a t i e n t s allergic to pent-
infections, and Rickettsia infections.
. Minocycline m^ciny. osed to « . acne, - r a x and menrngococca, prophylaxrs.
,„)• nsed to treat infections cansed by Rickettsia, Chlamydia
syphilis.

Azithromycin (Z-Pak, Zithromax) is an e
• macrolide class of antibiotics
• cephalosporin class of antibiotics
• quinolone class of antibiotics
• glycopeptide class of antibiotics
intibioticof the
anti-infectives
:
89 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
Erythromycin is well known to cause adverse:
• CNS effects
• GI effects
• hematologic effects
• renal effects
anti-infectives
90 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• macrolide class of antibiotics
Azithromycin (Z-Pak, Zithromax) and clarithromycin (Biaxin) are members of the macrolide class of antibiotics in which erythromycin is the prototype agent.
The bacterial spectrums of activity of azithromycin and clarithromycin are similar to that of erythromycin but possess greater intrinsic activity against H. influenzae and Helicobacter pylori. These two macrolides concentrate within macrophages, making them useful against organisms that are taken up by macrophages such as Mycobacterium avium intracellulare.
The significant tissue penetration of both agents and the prolonged elimination half-life of azithromycin (11-14 hours) allows for once-daily dosing for azithromycin and twice-daily dosing for clarithromycin.
Note: Macrolide antibiotics are generally used to treat infections caused by streptococcal bacteria and respiratory infections generally. They are also active against syphilis, Lyme disease and leprosy and tuberculosis. The macrolides can have a toxic effect on the liver, causing liver toxicity and jaundice and so should not be given to people who have an underlying liver problem such as an infection with hepatitis C.
Macrolides are bacteriostatic. The mechanism of action involves inhibition of protein synthesis that results from binding specifically to the 50s ribosomal subunit. This causes the RNA to dissociate from the ribosome and prevents protein synthesis.
Remember: Intrinsic activity is a measure of the ability of a drug once bound to the receptor to generate an effect activating stimulus and producing a change in cellular activity.
• GI effects
Adverse GI effects are reported for approximately 21% of patients receiving erythromycin, about 10% of patients receiving clarithromycin, and less than 5% for azithromycin.
In general, oral bioavailability of erythromycin is poor. It is readily inactivated by stomach acid, and several salts have been developed to overcome this drawback.
• Erythromycin stearate (Erythrocin) • Erythromycin ethylsuccinate (E.E.S.)
*** Since they are destroyed by stomach acid, erythromycins are usually enteric coated. This is a term designating a special coating applied to tablets or capsules which prevents their release and absorption of their contents until they reach the intestines.
Note: Erythromycin is metabolized in the liver, excretion is mainly via the bile.

The most commonly used aminoglycoside is:
• neomycin
• streptomycin
• tobramycin
• gentamicin
PHARMACOLOGY
anti-infectives
91 copyright 0 2013-2014 - Dental Decks
anti •infectives
Sulfonamides (also known as sulfa drugs) are structurally similar to:
• penicillins
• erythromycins
• acetylsalicyclic acid (Aspirin)
• para-aminobenzoic acid (PABA)
PHARMACOLOGY copyright©
92 2013-2014-Dental Decks

• gentamicin
Aminoglycosides are potent bactericidal antibiotics that act by creating fissures in the outer membrane of the bacterial cell. They are particularly active against aerobic, gram-negative bacteria and act synergistically against certain gram-positive organisms. Gentamicin is the most commonly used aminoglycoside, but amikacin may be particularly effective against resistant organisms. Aminoglycosides are used in the treatment of severe infections of the abdomen and urinary tract, as well as bacteremia and endocarditis. They are also used for prophylaxis, especially against endocarditis. Resistance is rare but increasing in frequency. Avoiding prolonged use, volume depletion and concomitant administration of other potentially nephrotoxic agents decreases the risk of toxicity. Single daily dosing of aminoglycosides is possible because of their rapid concentration-dependent killing and post-antibiotic effect and has the potential for decreased toxicity.
Aminoglycosides: • Gentamicin (Garamycin), Amikacin (Amiken), and Tobramycin (Nebcin). These are effective against serious infections caused by aerobic gram-negative bacteria, including E. Coli, En-terobacter, Klebsiella, Proteus, Pseuodomonas aeruginosa, and Serratia. • Streptomycin: The first aminoglycoside and was shown to be effective in the treatment of tuberculosis. Is seldom used today. • Neomycin (Mycifradin) and Kanamycin (Kantrex): Due to its toxic potential neomycin is used only topically or locally (e.g., in the GI tract). Kanamycin is rarely used because of its marked tendency to cause ototoxicity.
1. Aminoglycosides may cause severe neuromuscular weakness lasting hours to days Notes because of their potential curare-like effect. Aminoglycosides may aggravate muscle
weakness in patients with muscular disorders such as myasthenia gravis, infant botulism, or parkinsonism. 2. Aminoglycosides bind irreversibly to the 30s ribosomal subunit of bacteria, subsequently inhibiting protein synthesis. 3. Two well-known adverse effects are ototoxicity and nephrotoxicity.
• para-aminobenzoic acid (PABA)
Sulfonamides are often referred to as "sulfa drugs" because their molecules contain sulfur atoms. They have a different antibacterial mechanism from that of the antibiotics. The sulfonamides are structurally similar to PABA and this similarity is the basis for their antibacterial actions. PABA is needed by bacteria for the synthesis of folic acid. In turn, folic acid is needed for the synthesis of cellular components within the bacteria to allow for cell growth. Because of structural similarities between sulfonamides and PABA, the sulfonamides compete with PABA and are able to inhibit the actions of PABA. With PABA inhibited, folic acid is not synthesized within the bacteria, and bacterial cellular growth is inhibited. Sulfonamides are predominantly bacteriostatic agents.
Examples of sulfonamides: Sulfacetamide, Sulfadiazine, Sulfadoxine, Sulfamethizole, Sulfamethoxazole, Sulfanilamide, Sulfasalazine, and Sulfisoxazole.
1. Sulfonamides are not used for treatment of dental infections because of a Notes> low degree of effectiveness against oral pathogens.
2. Sulfonamides are used in medicine primarily for the treatment of urinary tract infections. 3. Bactrim is the brand name for the combination of trimethoprim and sulfamethoxazole. It is considered the drug of choice for many urinary tract infections. Bacteria susceptible to Bactrim include E. coli, Pneumocystis carinii, Klebsiella pneumoniae, Haemophilus influenzae and Salmonella species. 4. The trimethoprim component is an antimicrobial and the sulfamethoxazole is one of the sulfonamides. 5. Hypersensitivity reactions are common. Although blood dyscrasias are relatively rare, they can be fatal.

anti-infectives
Which antibiotic is not only effective against most staphylococci, aerobic and anaerobic streptococci, but is most effective in treating infections due to bac-teroides species?
• penicillin VK
• erythromycin
• tetracycline
• cephalexin (Keflex)
• clindamycin (Cleocin)
• vancomycin
93 copyright S 2013-2014 - Dental Decks
PHARMACOLOGY
Which antibiotic may cause bone marrow has limited use due to the side effects?
• penicillin
• tetracycline
• chloramphenicol
• doxycycline
disturbai
anti-infectives
ices [aplastic anemia) and
94 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• clindamycin (Cleocin)
Clindamycin binds to the 50s ribosomal subunit, blocking bacterial protein synthesis. Its use is restricted by its side effects such as severe diarrhea and pseudomembranous colitis. These side effects are caused by the overgrowth of the bacterium known as Clostridium difficile.
Clindamycin is bacteriostatic and is active against most gram-positive (i.e., Streptococcus pneumoniae, viridans, and pyogenes as well as Staphylococcus aureus) and many anaerobic organisms, including the anaerobic gram-negative bacteria Bacteroides frag-ilis.
In dentistry, clindamycin is an alternate antibiotic in the following situations: • When amoxicillin cannot be used for the standard regimen for prevention of bacterial endocarditis in patients undergoing dental procedures • For treatment of common oral-facial infections caused by aerobic gram-positive cocci and susceptible anaerobes • For prophylaxis for dental patients with total joint replacement
Important: Clindamycin can be given to patients allergic to penicillins since there is no cross allergenicity between penicillins and clindamycin.
Note: Vancomycin is given IV and is used most often in serious or life-threatening staphylococcal or streptococcal infections. It remains the drug of choice for severe cases of Clostridium difficile. Adverse effects include ototoxicity which may be permanent and the "red man" syndrome which is characterized by a sudden and profound fall in blood pressure with or without a maculopapular rash over the face, neck, upper chest, and extremities.
• chloramphenicol
Chloramphenicol is a broad-spectrum antibiotic effective against gram-positive and gram-negative bacteria and against anaerobes. It is used as a second or third line drug in medicine to treat serious infections due to organisms resistant to other less toxic antibiotics. For example it can be used to treat the following: Typhoid Fever, Bacterial Meningitis, Anaerobic Infections, Rickettsial Diseases, and Brucellosis.
Chloramphenicol inhibits protein synthesis in bacteria and, to a lesser extent, in eukary-otic cells. The drug readily penetrates bacterial cells, probably by facilitated diffusion. Chloramphenicol acts primarily by binding reversibly to the 50s ribosomal subunit.
The most important adverse effect of chloramphenicol is on the bone marrow. Chloramphenicol affects the hematopoietic system in two ways:
• by an non-dose-related idiosyncratic response manifested by aplastic anemia, leading in many cases to fatal pancytopenia
• by a dose-related toxic effect that presents as anemia, leukopenia, or thrombocytope
nia
Important: The risk of aplastic anemia does not contraindicate the use of chloramphenicol in situations in which it is necessary; however, it emphasizes that the drug should never be employed in undefined situations or in diseases readily, safely, and effectively treatable with other antimicrobial agents.
Note: Fatal chloramphenicol toxicity may develop in neonates, especially premature babies, when they are exposed to excessive doses of the drug. The illness, the gray baby syndrome, usually begins 2 to 9 days after treatment is started.

anti-infectives
Nitazoxanide (Alinia) is an oral antiprotozoal agent used to treat which of the following conditions?
leprosy
• malaria
• AIDS
• diarrhea caused by Clostridium difficile
• diarrhea caused by Giardia lamblia
95 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-infectives
All of the following drugs are useful for treating which disease? isoniazid streptomycin rifampin ethambutol pyrazinamide
• malaria
• AIDS
• rheumatoid arthritis
• tuberculosis
96 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• diarrhea caused by Giardia lamblia
*** This type of diarrhea is an intestinal infection also known as Giardiasis, and is the most common protozoan infection in the United States.
Antiprotozoal Agents: • Nitazoxanide (Alinia): is an antiprotozoal agent which is used in the treatment of Giardia, and those protozoal infections caused by Cryptosporidium parvum. Its mechanism is to interfere with the electron transfer reaction within the protozoa essential to anaerobic metabolism. • Atovaquone (Mepron): is an antiprotozoal agent used to treat Pneumocystitis carinii pneumonia (PCP) in patients who are intolerant to Cotrimoxazole. • Eflornithine (Vaniqa): has orphan drug status for the treatment of meningoen-cephalitic stage of Trypanosoma brucei gambiense infection (sleeping sickness). This drug is also indicated to be used as a cream to reduce unwanted hair from face and adjacent areas under the chin. • Furazolidone (Furoxone): is a antiprotozoal agent used to treat diarrhea caused by susceptible Giardias lamblia and Vibrio cholerae. • Metronidazole (Flagyl): is a synthetic antibacterial and antiprotozoal agent that is effective against Trichomonas vaginalis, which causes trichomoniasis. In addition, it is one of the most effective drugs available against anaerobic bacterial infections. These include infections caused by Helicobacter pylori, Clostridium difficile, Bacteroides species and Fusobacterium species. Note: Alcohol should be avoided because metronidazole and alcohol together can cause severe nausea, vomiting, cramps, flushing, and headache. It should is not used in pregnancy because of potential adverse effects on the fetus.
• tuberculosis
Tuberculosis is a bacterial infection caused by Mycobacterium tuberculosis. The anti-tubercular drugs either inhibit the growth of the bacteria or kill the bacteria. Because the Mycobacterium organism tends to develop resistance to any single antitubercular drug, combination drug therapy is standard in the treatment of tuberculosis.
Antitubercular drugs: • Isoniazid: often given in a four drug regimen along with rifampin, pyrazinamide and ethambutol • Streptomycin: often given in combination with isoniazid • Rifampin: usually given in combination with other agents • Ethambutol: usually given in combination with other agents • Pyrazinamide: popular in combination with rifampin
Mechanism of action: • Isoniazid: is bacteriostatic for resting organisms and bactericidal for dividing organisms. It interferes with lipid and nucleic acid biosynthesis in growing organisms. • Streptomycin: is a bactericidal antibiotic. It acts by interfering with normal protein synthesis. • Rifampin: inhibits DNA-dependent RNA-polymerase activity, thereby suppressing RNA synthesis. It can be bacteriostatic or bactericidal and is most active against bacteria undergoing cell division. • Ethambutol: inhibits cell wall synthesis by preventing the incorporation of mycolic acids. It is bacteriostatic and is active only against mycobacterium. • Pyrazinamide: the mechanism of action is unknown. It may be bacteriostatic or bactericidal against M. tuberculosis, depending on whether the mycobacteria are actively dividing.

The antiviral agent penciclovir (Denavir)
• herpes zoster
• genital herpes
• herpes simplex type 1 (HSV-i)
• papilloma virus
is active
anti-infectives
against which virus?
97 copyright 0 2013-2014 - Dental Decks
PHARMACOLOGY
anti-infectives
The following drugs are used to treat which viral disease? didanosine zidovudine ritonavir indinavir delavirdine
• herpes
• mumps
• AIDS
• chicken pox
98 copyright S> 2013-2014- Dental Decks

• herpes simplex type 1 (HSV-1)
Penciclovir (Denavir) is a cream formulation indicated for the treatment of recurrent herpes labialis (coldsores) in adults. This condition is caused by the herpes simplex type 1 virus. Penciclovir is not available for systemic dosing.
Penciclovir (Denavir) inhibits viral action by selectively inhibiting herpes viral DNA synthesis and therefore resulting in the inhibition of viral replication.
Other agents indicated for use in treating the condition of herpes labialis are: • Acyclovir tablets • Acyclovir cream • Docosanol cream (Abreva) • Lysine tablets • Valacyclovir caplets (Valtrex)
AIDS
AIDS (acquired immunodeficiency syndrome) has been recognized since 1981 as a unique clinical syndrome brought on by infection with the human immunodeficiency virus 1 (HIV-1) or virus 2 (HIV-2). The major cellular defect caused by infection with HIV is a depletion of T cells, primarily the sub-type T-helper cells known as CD4 cells. This results in a compromised immune system, which becomes susceptible to opportunistic infections.
HIV is a type of retrovirus that is responsible for the fatal illness from AIDS. A retrovirus has RNA as its nucleic acid and uses the enzyme reverse transcriptase to copy its genome into the DNA of the host's cells chromosomes. This DNA segment is then permanently incorporated into the host cell's DNA within the nucleus. The integrated DNA segment can produce new RNA in the cytoplasm of the host cell. The new RNA in turn synthesizes viral proteins, which are eventually passed on to other host cells such as the immune system macrophages. Ultimately enough of the human immune cells are compromised such that immune function is lost.
The HIV drugs such as didanosine (brand name Videx), zidovudine (brand name Retrovir), ritonavir (brand name Norvir), and indinavir (brand name Crixivan) work by inhibiting certain steps in the HIV infection process within the target cells to halt the destruction of the immune system by the HIV retrovirus.

anti-infectives Which of the following is classified as an antifungal agent?
1 bacitracin
amphotericin-B
• polymyxin-B
neomycin
99 copyright © 2013-2014- Dental Decks
PHARMACOLOGY
The drug of choice for treating Candidiasis is:
penicillin
erythromycin
• nystatin
• chloramphenicol
anti-infectives
PHARMACOLOGY
100 copyright © 2013-2014 - Dental Decks

• amphotericin-B
This is an antifungal agent given intravenously or orally for the treatment of severe systemic fungal infections caused by fungi such as Candida species. Bacitracin, polymyxin-B and neomycin are not antifungal agents. These are antibiotics effective against susceptible bacteria. Antibiotics in general do not have antifungal properties.
Summary of Some Antifungal Agents
Topical Agents (dissolve and swallow)
Clotrimazole (Mycelex Troche) Nystatin (Mycostatin)
Topical Agents (cream/ointment)
Amphotericin-B (Fungizone) Ketoconazole (Nizoral) Nystatin (Mycostatin)
Systemic Agents
Amphotericin-B (Fungizone) Ketoconazole (Nizoral) Fluconazole (Diflucan)
Use
Oropharyngeal Candidiasis Oral Cavity Candidiasis
Use
\ Cutaneous and Mucocu -J taneous candidiasis
Use
Systemic Candida Oral Esophageal Candidiasis Oralpharyngeal Candidiasis
Mechanism on Fungal Cell
Alters cell membrane Alters cell membrane
Mechanism on Fungal Cell
Alters cell membrane Alters cell membrane Alters cell membrane
Mechanism on Fungal Cell
Alters cell membrane Alters cell membrane Alters cell membrane
Form
Troche Oral Suspension
Form
Cream Cream Ointment
Form
IV injection Tablets Tablets
Note: Systemic amphotericin-B is associated with high incidence of kidney toxicity.
• nystatin
Candidiasis is an infection, usually of the oral cavity or vagina, with a Candida species, usually C. albicans, which causes an inflammatory, pruritic infection characterized by a thick, white discharge. It is common, especially in patients who have a deficiency in T-lymphocytes, or who are receiving chemotherapy, and in immunosuppressed individuals (AIDS patients). This yeast-like fungi is a normal inhabitant of the oral cavity and vaginal tract, however it is normally held in check by the indigenous bacteria of these areas. Note: Angular cheilitis (bilateral ulcers at the corner of the mouth) has been linked to C. albicans.
Remember: Nystatin and clotrimazole are the two antifungals that are used as "swish and swallow" to treat oral Candida infections. Nystatin (Mycostatin) is taken as an oral suspension to be swished around the mouth and swallowed. Clotrimazole (Mycelex) is taken as a troche (lozenge) which is slowly dissolved in the mouth and swallowed. They work by binding to sterols in the fungal cell membrane, increasing permeability and permitting the leakage of intracellular components. This leads to the death of the affected fungal cell.
Note: The suffixes of the following generic drug names are indicative of the corresponding drug classes:
• "azole" = azole-type antifungal drugs (e.g., clotrimazole) • "coxib" = COX-2 inhibitors (e.g., celecoxib) • "dipine" = dihydropyridine calcium channel blockers (e.g., nicardipine) • "olol" = beta-adrenergic receptor blockers (e.g., nadolol) • "ilol" or "alol" = beta-adrenergic receptor blocker that also blocks alpharadrenergic receptors (e.g., carvedilol or labetalol) • "onium" or "urium" = quaternary ammonium compounds, usually competitive peripheral acting skeletal muscle relaxerc (e.g., pancuronium) • "osin" = alpharadrenergic receptor blockers (e.g., terazosin) • "pril" = ACE inhibitors (e.g., enalapril) • "sartan" = angiotensin II receptor blockers (e.g., olmesartan) • "statin" = HMG-CoA reductase inhibitor (e.g., atorvastatin)

Which of the following is known as the original
• penicillin V
• penicillin G
• ampicillin
• amoxicillin
anti-infectives
! penicillin?
101 copyright 0 2013-2014 - Dental Decks
PHARMACOLOGY
Which penicillin is degraded in stomach acid and ally (by injection)?
• penicillin VK
• amoxicillin
• penicillin G
• ampicillin
PHARMACOLOGY
anti-infectives
is usually given parenter-
102 copyright © 2013-2014 - Dental Decks

• penicillin G
All penicillins are derivatives of 6-aminopenicillanic acid and contain a beta-lactam ring structure joined to a thiazolidine ring. The beta-lactam ring is essential for its antibacterial activity. This basic structure is synthesized by the penicillium mold from two amino acids, L-cysteine and L-valine. Antibiotics containing this beta-lactam ring are referred to collectively as beta-lactam antibiotics and include the penicillins, cephalosporins, and the two newer groups of agents, the carbapenems and the monobac-tams.
Penicillin G (benzylpenicillin) is the prototype for comparison. By side chain substitutions (specifically, this means substituting other groups at the R position of the penicillin molecule) of the basic 6-aminopenicillanic acid molecule, the semi-synthetic penicillins are produced which are more acid stable, have a broader spectrum, or are penicillinase resistant.
Other naturally occurring penicillins include: • Penicillin VK (Pen Vee K, V-cillin K) - preferred for treating oral infections because it is more acid stable (more reliable oral absorption) • Penicillin G parenteral (Pfizerpen) - always given parenterally (IM,IV or subcuta-neously) • Penicillin G benzathine (Bicillin C-R) - always given by IM route. It is used for the treatment of syphilis and prevention of rheumatic fever
Remember: 1. Penicillins are bactericidal; they inhibit cell wall synthesis. 2. Probenecid increases blood levels of natural penicillins and may be given concurrently for this purpose.
' penicillin G
Acid stable penicillins (may be used orally) include: • Penicillin VK • Amoxicillin • Ampicillin • Nafcillin • Oxacillin • Cloxacillin • Dicloxacillin
Extended spectrum penicillins include: • The aminopenicillins — Ampicillin and Amoxicillin
Broad spectrum penicillins include: • Piperacillin • Ticarcillin *** These two penicillins have the widest spectrum of all the penicillins
Penicillinase-resistant penicillins include: • Nafcillin • Oxacillin • Cloxacillin • Dicloxacillin

The antibiotic of choice for standard prophylactic reg erage for the prevention of bacterial endocarditis is:
• penicillin VK
• tetracycline
• erythromycin
• amoxicillin
anti-infectives
imen of antibiotic cov-
103 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti- infectives
Of the drugs listed which is the most preferable antibiotic for the treatment of non-penicillinase-producing gram-positive staphylococcal infections?
• tetracycline
• clindamycin
• ampicillin
• cefaclor (Celcor)
• penicillin VK
PHARMACOLOGY
104 copyright © 2013-2014 - Dental Decks

• amoxicillin
Premedication requirements for patients with valvular heart disease or congenital cardiac defects. If in doubt, have patient consult their physician as to need.
Current American Heart Association Guidelines: Published June 2007, JADA Volume 138, page 142.
Standard Regimen • Amoxicillin
- Adults: 2.0 g orally 30-60 minutes prior to appointment - Children: 50 mg/kg (not to exceed adult dose) orally 30-60 minutes prior to appointment
Allergy to Amoxicillin:
Note: Only if allergy is not of anaphylactic type. Any one of the following can be used. • Clindamycin
-Adults: 600 mg orally 30-60 minutes prior to appointment -Children: 20 mg/kg orally 30-60 minutes prior to appointment
• Cephalexin -Adults: 2.0 g orally 30-60 minutes prior to appointment -Children: 50 mg/kg orally 30-60 minutes prior to appointment
• Azithromycin -Adults: 500 mg orally 30-60 minutes prior to appointment -Children: 15 mg/kg orally 30-60 minutes prior to appointment
• Clarithromycin -Adults: 500 mg orally 30-60 minutes prior to appointment -Children: 15 mg/kg 30-60 minutes prior to appointment
penicillin VK
It is prudent to use an antibiotic with narrow spectrum of action and one that is bactericidal in order to minimize the development of bacterial resistance. Penicillin VK has these properties. Ampicillin has a broader spectrum of action than penicillin VK and cefaclor is a broad spectrum cephalosporin. Tetracycline and clindamycin are bacteriostatic antibiotics and not bacteriocidal.
Note: The major disadvantage of the penicillins is their rather high incidence of allergic reactions. Approximately 10% of the general population is allergic to penicillins. This incidence probably holds for any of the specific penicillins since there is cross allergy from one to the other. Skin rash (a delayed reaction) is the most prevalent allergic manifestation. Life threatening anaphylaxis can occur, but is very rare, particularly with oral dosing. In non-allergic individuals, penicillins at normal therapeutic doses have virtually no side effects what so ever. Penicillins are bactericidal, that is, they actually cause death of the invading bacteria.

Which of the following penicillin antibiotics have the tibacterial activity? Select all that apply.
• penicillin VK
• dicloxacillin
• ticarcillin
• amoxicillin
• piperacillin
• nafcillin
anti-infectives
widest spectrum of an-
105 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-infectives
Which of the following has a clinically significant drug interaction with Amoxicillin?
• triazolam (Halcion)
• methotrexate
• calcitrol
• candesartan
106 copyr ight©20l3-2014-Dental Decks
PHARMACOLOGY

• ticarcillin • piperacillin
Members of the penicillin family having the broadest spectrums of action are piperacillin and ticarcillin. In addition to being active against gram-positive cocci (streptococci, staphylococci, pneumococci), and gram-positive rods (bacillus and others), these agents are active against Pseudomonas, Proteus, Klebsiella, and Bacteroides.
These antibiotics are recommended for the treatment of urinary tract infections and other infections caused by susceptible gram-negative Pseudomonas species and Proteus species.
Penicillin VK has a relative limited spectrum of action against aerobic gram-positive cocci and anaerobes.
Dicloxacillin has a similar spectrum as penicillin VK but is active against penicillinase-producing staphylococcus.
Amoxicillin is an aminopenicillin which has an extended spectrum of action which includes not only aerobic gram-positive cocci and anaerobes, but some gram-negative bacilli such as Hemophilus, Proteus and Salmonella. Ampicillin also falls into the category of an aminopenicillin.
Important: None of the penicillins are active against viruses, fungi, rickettsiae or other nonbacterial organisms.
• methotrexate
*** Amoxicillin in large doses inhibits the renal tubular secretion of methotrexate, thereby causing higher, prolonged serum levels of methotrexate.
Aminopenicillins (ampicillin and amoxicillin) are characterized by the amino substitution of penicillin G. They are able to penetrate gram-negative bacteria more readily than are the natural penicillins or the penicillinase-resistant penicillins. However, the aminopenicillins are not stable to beta-lactamases (penicillinase) of either gram-positive or gram-negative bacteria.
Note: Gram-negative bacteria that are susceptible to aminopenicillins include: H.in-fluenzae, some E.Coli and Proteus mirabilis.
Ampicillin (Polycillin, Onipen) and Amoxicillin (Amoxil, Parotid) are used primarily to treat infections such as otitis media, bronchitis, sinusitis, and acute bacterial cystitis caused by susceptible organisms. Compared with ampicillin, amoxicillin has a higher oral absorption, higher serum levels, a longer half-life, and is less likely to cause adverse GI effects (diarrhea). Amoxicillin is given orally; ampicillin can be given orally or IV
Note: Ampicillin and amoxicillin are preferred agents in the treatment of urinary tract infections caused by susceptible enterococci (which are facultatively anaerobic, gram-positive cocci that grow in short chains under extreme conditions mainly in the intestine).

anti-infectives
What do all of the following penicillin antibiotics have in common? amoxicillin and clavulanate potassium (Augmentin) ampicillin and sulbactam (Unasyn) cloxacillin dicloxacillin
broad spectrum
penicillinase resistant
active against viruses
they are all aminopenicillins
107 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-
Beta-lactamases (enzymes) include which of the following? Select all that apply.
• cephalosporinase
• penicillinase
• ATPase
• protein kinase
PHARMACOLOGY
•infectives
108 copyright © 2013-2014 - Dental Decks

• penicillinase resistant
A functional part of the chemical molecule of all the penicillins is the so-called betalac-tam ring, which is a four-membered imbedded ring structure consisting of three carbons and one nitrogen atom which is responsible for the antibacterial activity of penicillins. Any alteration to the beta-lactam ring will also alter the antibacterial activity. Penicillinase is an enzyme secreted by bacteria which splits open the beta-lactam ring. This renders the penicillin molecule ineffective against those penicillinase secretors.
Cloxacillin and dicloxacillin resist the actions of penicillinase because they have a protected beta-lactam ring which prevents the actions of the enzyme.
Augmentin and Unasyn contain the agents clavulanate potassium and sulbactam respectively which block the actions of penicillinase from reaching the beta-lactam ring.
The majority of penicillins are directly excreted into the urine through renal tubular cell secretion. Probenecid (Benemid), an inhibitor of renal tubular cell secretion raises the blood levels of the penicillins by diminishing their tubular secretion. Probenecid is sometimes given simultaneously with penicillin to raise the blood levels for increased activity. Note: Probenecid is a drug used to treat gout.
• cephalosporinase • penicillinase
Beta-lactamases are enzymes produced and secreted by a wide range of gram-positive and gram-negative bacteria as a defense weapon against cephalosporin and penicillin antibiotics. These enzymes destroy the beta-lactam nucleus within these antibiotics by splitting open the beta-lactam ring structure. This action renders the antibiotic ineffective. Those beta-lactamases that work against cephalosporins are called cephalospori-nases, and those that work against penicillins are called penicillinases.
By combining clavulanic acid with a penicillin, the beta-lactamase enzyme is permanently inhibited by the acid, and the antibacterial activity of the penicillin is maintained. One popular commercial preparation is Augmentin, which contains amoxicillin and clavulanate potassium. Augmentin is used orally as pill or liquid form. Sulbactam is another beta-lactamase inhibitor. It is available for intravenous and intramuscular use combined with ampicillin under the brand name Unasyn.

Which of the following is often co-i renal clearance of the antibiotic?
• imipenem
• probenecid
• hydrochlorothiazide
• aztreonam
anti -infectives
administered with antibiotics to delay the
copyright©
109 2013-2014-Dental Decks
PHARMACOLOGY
Which antibiotic is used cautiously due to its colitis, severe GI upset)?
• azithromycin (Zithromax;Z-Pak)
• clindamycin
• penicillin VK
• cephalexin (Keflex)
PHARMACOLOGY
anti-infectives
side effects (pseudomembranous
110 copyright©2013-2014-Dental Decks

' probenecid
*** This elevates and prolongs the serum concentrations of the antibiotic when high tissue concentrations are necessary.
The majority of penicillins are handled by the kidneys as organic acids and excreted by tubular excretion. Probenecid interferes with tubular handling of organic acids within the nephron. Drugs affected by probenecid include most cephalosporins and natural penicillins, and other beta-lactam-related antibiotics such as aztreonam and imipenem.
Note: In some cases, probenecid administration can more than double the serum concentration of the affected drug. The half-life is prolonged as well.
Important: Nafcillin, oxacillin, cloxacillin and dicloxacillin are lipophilic and are excreted by biliary means. No combination with probenecid or dosage adjustment for renal dysfunction is necessary for these penicillins.
Notes 1. Imipenem is a beta-lactam antibiotic derived from thienamycin and is the first drag to be classified as a carbapenem antibiotic. It is currently the drug of choice for infections due to Enterobacter and Pseudomonas aeruginosa. It is usually combined with cilastatin and is used to treat severe or resistant infections, especially those that are nosocomial in origin. 2. Aztreonam is a parenteral synthetic beta-lactam antibiotic (classified as a monobactum). The spectrum is limited to aerobic gram-negative rods (i.e., Klebsiella, Pseudomonas, and Serratia). It has no gram-positive or anaerobic activity. It is synergistic with aminoglycosides.
clindamycin
Summary of Important Antibiotics
Drug
Penicillins: Penicillin VK Amoxicillin Amoxicillin/Clav. Acid (Augmentin) Ampicillin
Cephalosporins: Cephalexin (Keflex) Cefaclor {Ceclor)
Other: Clindamycin
Macrolides: Azithromycin (Z-Pak) Clarithromycin (Biaxin) Erythromycin
Tetracyclines: Tetracycline Doxyxycline (Vibramycin) Minocycline (Minocin; Arestin)
Aminoglycosides: Streptomycin Gentamycin
Miscellaneous: Ciprofloxacin (Cipro) Bacitracin Chloramphenicol
Antibacterial Action
Inhibits cell wall synthesis Same Same Same
Inhibits cell wall synthesis Same
Inhibits 50S ribosomes
Inhibits 50S ribosomes Same Same
Inhibits 30S ribosomes Same Same
Inhibits 30S ribosomes Same
Inhibits DNA Inhibits cell wall synthesis Inhibits 50S ribosomes
Antibacterial Mechanism
Bactericidal Same Same Same
Bactericidal Same
Bacteriostatic
Bacteriostatic Same Same
Bacteriostatic Same Same
Bactericidal Same
Bactericidal Same Bacteriostatic
Important Adverse Effects
Hypersensitivity Same Same Same
Hypersensitivity Same
Pseudomembranous colitis
None significant GI hyperactivity Same
Superinfection None significant Same
Ototoxicity, Nephrotoxicity Same
Nausea, Headache Nephrotoxicity Blood disorders

Which antibiotic/antimicrobial is drug allergy?
• ciprofloxacin (Cipro)
• penicillin VK
• clindamycin
• metronidazole (Flagyl)
anti-infectives
associated with the highest incidence of
111 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-infectives
Stavudine (also known as d4T, orZerit) is an antiretroviral drug used in the treatment of adults with HIV infection in combination with other antiretroviral agents. Which of the following categories does this agent belong to?
• nucleoside reverse transcriptase inhibitor
• protease inhibitor
• non-nucleoside reverse transcriptase inhibitor
112 copyright©2013-2014-Dental Decks
PHARMACOLOGY

• penicillin VK
Three groups of allergic reactions to the penicillins: 1. Acute (anaphylactic shock): occurs within 30 minutes. Characterized by urticaria, angioedema, bronchoconstriction, GI disturbances, and shock. Death can result in a short time if treatment is not instituted immediately (parenteral administration of epinephrine). 2. Accelerated: occurs 30 to 48 hours after. Manifestations include urticaria, praritis, wheezing, mild laryngeal edema, and local inflammatory reactions. Not life threatening. 3. Delayed: occurs after 2 to 3 days. Approximately 80-90% of all allergic reactions occurring with penicillin are of this type. Manifested by skin rashes.
Hypersensitivity reactions occur in up to 10% of patients receiving penicillin. Manifestations range from a mild rash to anaphylaxis. The rash may be urticarial, vesicular, bullous, or maculopapular. Rarely, thrombopenic purpura develops.
Note: A rash is the most common sign of an allergy to penicillin.
Remember: The mechanism of action of the fluoroquinolones is inhibition of DNA gy-rase, an enzyme that is essential in the transcription, replication, and repair of bacterial DNA. Drags in this class include ciprofloxacin (Cipro), norfloxacin (Noroxin), lev-ofloxacin (Levaquin), moxifloxacin (Avelox), and gemifloxacin (Factive). Fluoroquinolones are active against many gram-positive organisms and gram-negative aerobes, including Moraxella catarrhalis, Haemophilus influenzae, E. coli, chlamydia, and Mycoplasma pneumoniae. They are not active against Clostridium difficile. These drags are well tolerated, however, the most common adverse effects are GI (e.g., nausea, vomiting, diarrhea, abdominal pain), CNS (e.g., headache, dizziness, confusion) and dermatologic (e.g., rash, pruritis).
• nucleoside reverse transcriptase inhibitor
These agents chemically are nucleosides and work by inhibiting the viral enzyme known as reverse transcriptase. This results in an inhibition of the HIV viral RNA from being made into a DNA segment; thus the genome of the HIV virus is not copied from RNA. Other agents in this class include didanosine (Videx), zalcitabine (Hivid; ddC) and zidovudine (Retrovir; AZT).
Protease inhibitors suppress viral replication by inhibiting protease, the enzyme responsible for cleaving viral precursor peptides into infective virions. Some agents in this class include indinavir (Crixivan), nelfinavir (Viracept), ritonavir (Norvir), and saquinivir (Invirase).
Non-nucleoside reverse transcriptase inhibitors inhibit the catalytic reaction of reverse transcriptase that is independent of nucleotide binding. Some agents in this class include delavirdine (Rescriptor) and nevirapine (Viramune).
Note: Adefovir (Hepsera) is a nucleotide analog and although it is technically non-nucleoside, it is rarely included in the NNRTI classification because of its differing structure.

anti-infectives
All of the following are common adverse effects caused by the use of tetracyclines EXCEPT one. Which one is the EXCEPTION?
• photosensitivity
• nausea
• bone marrow disturbances
• diarrhea
• discoloration of teeth and enamel hypoplasia in young children
113 copyright © 2013-2014- Dental Decks
PHARMACOLOGY
Which of the following are referred to Select all that apply.
• penicillin VK
• ampicillin (Polycillin)
• cloxacillin (Cloxapen)
• dicloxacillin
• nafcillin
• amoxicillin (Amoxil)
• oxacillin
PHARMACOLOGY
as am inopenici!
anti-
llins?
-infectives
114 copyright© 2013-2014- Dental Decks

• bone marrow disturbances
Another common adverse effect is the occurrence of opportunistic (superinfection) infections caused by Candida albicans. This is due to the wide spectrum of antibacterial action which alters normal flora. Examples include both vaginal and oral candidiasis. These conditions are also known as vaginal and oral yeast infections.
Members of the tetracycline family of antibiotics include:
Short acting: • Tetracycline (Generic) Intermediate acting: • Demeclocycline (Declomycin) Long acting: • Minocycline (Minocin)
• Doxycycline (Vibramycin)
Remember: The usefulness of the tetracyclines in the treatment of odontogenic infections is limited since they can cause "yeast" infections very easily. They have been used as alternatives to penicillin in patients with ANUG (acute necrotizing ulcerative gingivitis) who require antibiotics.
Note: In adults, Fanconi syndrome can be caused by various things that damage the kidneys, including certain medications (azathioprine, cidofovir, gentamicin, and tetracycline). Fanconi syndrome is a disorder of the kidney tubules in which certain substances normally absorbed into the bloodstream by the kidneys are released into the urine instead.
• ampicillin (Polycillin) • amoxicillin (Amoxil)
These two antibiotics are characterized by the amino substitution of penicillin G. They work against many gram-positive organisms and some gram-negative bacteria such as Haemophilus influenzae, some Escherichia coli, and Proteus mirabilis. They are not penicillinase resistant. They are used for upper respiratory infections. .
The major difference in the drags is the higher oral absorption, higher serum levels, and longer half-life for amoxicillin compared with ampicillin. Amoxicillin is given orally; ampicillin can be given orally and IV.
Remember: Oral amoxicillin is recommended as the drug of choice for standard general prophylaxis for bacterial endocarditis in patients undergoing invasive dental procedures.
Note: Parenteral ampicillin is recommended as the drug of choice in patients unable to take oral medications and who are not allergic to penicillin for prophylaxis for bacterial endocarditis.

Cephalosporins have which of the following
• affect bacterial cell wall
• affect bacterial DNA
• affect bacterial protein synthesis
• interfere with bacterial metabolic pathways
anti-
modes of action?
infectives
115 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-infectives
Which of the following is the mode of action of the Tetracyclines?
• bacterial cell wall destruction
• prevent protein synthesis in the bacterial cell
• interfere with nucleic acid synthesis
• cause mutations within bacterial DNA
116 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• affect bacterial cell wall
Basic mechanisms of actions of antibiotics:
• Affect bacterial cell wall: - Penicillin family - Cephalosporin family
• Agents affecting bacterial DNA: - Fluoroquinolone family (i.e., ciprofloxacin) - Metronidazole (Flagyl)
• Agents affecting bacterial protein synthesis: - Tetracycline family - Erythromycin family - Clindamycin - Chloramphenicol
• Agents interfering with bacterial metabolic pathways: - Sulfonamides (sulfa drugs)
• prevent protein synthesis in the bacterial cell
The tetracyclines inhibit protein synthesis by binding to the 30 S subunit of the bacterial ribosome. The inhibition of this ribosomal function interferes with the attachment of the growing amino acid chain thus preventing complete formation of peptides from the ribosome. Since no peptides are formed, no proteins are formed. Since proteins are necessary for the bacterial cell to metabolically function, the lack thereof will cause a static state in which the bacterium becomes vulnerable to phagocytosis by the body's immune system.
Absorption of the tetracyclines from the GI tract is inhibited by divalent and trivalent cations such as CA++, Mg^, Fe^, and Al+++. These ions form chelation products with the tetracyclines and thus prevent their absorption. This is why tetracyclines should not be given with milk and dairy products (contain Ca++), iron-containing vitamins (contain Fe"), mineral supplements containing these irons, or antacids (contain Mg**).

anti-infectives
Which antibiotics exert their antibacterial activity through inhibition of protein synthesis in the bacterial cell? Select all that apply.
• cephalosporins
• tetracycline
• penicillin VK
• macrolides
• clindamycin
• sulfonamides
117 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
Erythromycin is a antibiotic wl of susceptible bacteria. The result is
• bactericidal; 30s
• bactericidal; 50s
• bacteriostatic; 30s
• bacteriostatic; 50s
PHARMACOLOGY
anti-infectives
lich binds to the ribosomal subunit the inhibition of protein synthesis.
t
•
118 copyright © 2013-2014 - Dental Decks

• tetracycline • macrolides • clindamycin
The tetracyclines are a group of broad-spectrum, bacteriostatic antibiotics that inhibit protein synthesis in the susceptible organism by binding to the 30S ribosome subunit, thereby impeding the binding of aminoacyl tRNA to the receptor site on the messenger RNA ribosome complex. The inhibition of this ribosomal function interferes with the attachment of the growing amino acid chain thus preventing complete formation of peptides from the ribosome. Since no peptides are formed, no proteins are formed. Since proteins are necessary for the bacterial cell to metabolically function, the lack thereof will cause a static state in which the bacterium becomes vulnerable to phagocytosis by the body's immune system.
Tetracyclines are useful in treating the following infections: • Medical infections caused by susceptible gram-positive and gram-negative bacteria • Infections caused by Mycoplasma, Chlamydia , Protozoa or Rickettsia • Exacerbations of chronic bronchitis • Lyme disease (caused by Borrelia burgdorferi) • Treatment of acne • Treatment of gonorrhea and syphilis in patients allergic to penicillin • Dental: treatment of periodontitis associated with the presence of Actinobacillius actino-mycetemcomitans (AA) (i.e., localized aggressive periodontitis)
Important: Tetracyclines are not the drug of choice for Streptococcus or Staphylococcus.
Clindamycin is bacteriostatic and is active against most gram-positive (i.e., Streptococcus pneumoniae, viridans, and pyogenes as well as Staphylococcus aureus) and many anaerobic organisms, including the anaerobic gram-negative bacteria Bacteroides fragilis.
The macrolides include: erythromycin, clarithromycin, and azithromycin.
• bacteriostatic; 50s
Erythromycin-type antibiotics are members of the Macrolide family of antibiotics.
Members of the Macrolide family (generic and brand names) are: • Azithromycin (Zithromax; Z-Pak) • Clarithromycin (Biaxin) • Erythromycin base (E-mycin; Eryc) • Erythromycin ethylsuccinate (E.E.S.) • Erythromycin stearate (Erythrocin)
All of the erythromycins are very effective against gram-positive bacteria but not so effective against gram-negative bacteria.
All of the erythromycins act through the same mechanism to bind to the 50s ribosomal subunit of susceptible bacteria. This causes the RNA to dissociate from the ribosome and prevents protein synthesis.
Note: GI Tract upset is the most common side effect of the erythromycins (take with food).

Which antimicrobial below is assoc
• tetracycline
• penicillin VK
• metronidazole (Flagyl)
• clindamycin
iated with
anti-infectives
photosensitivity?
119 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
Which of the following antivirals are Select all that apply.
• acyclovir (Zovirax)
• oseltamivir (Tamiflu)
• amantadine (Symmetrel)
• rimantadine (Flumadine)
• zanamivir (Relenza)
PHARMACOLOGY
classified
anti-infectives
as neuraminidase inhibitors?
120 copyright © 2013-2014 - Dental Decks

• tetracycline
The photosensitivity reaction caused by the tetracycline family of antibiotics results in the appearance of red rashes or blotches over the skin in the presence of sunlight.
Common adverse effects caused by the other agents: • Penicillin VK: hypersensitivity resulting in skin rash and rare anaphylaxis • Metronidazole (Flagyl): dizziness, headache, and nausea
Note: Metronidazole is not a true antibiotic since it is not found in natural organisms; it is a synthetic substance produced in the chemical laboratory.
• Clindamycin: diarrhea, abdominal pain; known to cause pseudomembranous colitis
• Oseltamivir (Tamiflu) • Zanamivir (Relenza)
Oseltamivir (Tamiflu) and zanamivir (Relenza) inhibit influenza virus neuraminidase enzymes, potentially altering virus particle aggregation and release. Tamiflu and Relenza are both used to treat acute illness due to influenza (A or B) infection.
Acyclovir (Zovirax) is an antiviral that inhibits DNA synthesis rather than neuraminidase enzymes.
Amantadine is a synthetic anti-viral drug that can inhibit the replication of viruses in cells. It was initially used to prevent influenza A during flu season, and, if given within 24 to 48 hours of the onset of flu symptoms, to decrease the severity of the flu. Later amantadine was found to cause improvement in the symptoms of Parkinson's disease.
Note: The mechanism of amantadine's antiviral activity involves interference with a viral protein, M2, which is required for the viral particle to become "uncoated" once taken inside a cell by endocytosis.
Rimantadine is a synthetic anti-viral drag that can prevent viruses in cells from multiplying. Like amantadine, rimantadine initially was used to prevent influenza A during flu season, and, if given within 24 to 48 hours after the onset of flu symptoms, to decrease the severity of the flu. Rimantadine is chemically related to amantadine, but rimantadine has fewer side effects on the nervous system than amantadine. Note: Rimantadine appears to exert its inhibitory effect early in the viral replicative cycle, possibly inhibiting the un-coating of the virus (similar to amantadine's mechanism of action).

anti-infectives Which drug can be used in the pregnant patient?
• tetracycline
• doxycycline (Vibramycin)
• minocycline (Minocin)
• penicillin VK
121 copyright © 2013-2014 - Dental Decks
A patient was given penicillin 15 minutes signs and symptoms. What kind of reaction
• laryngeal edema
• urticaria (welts that itch)
• severe hypotension
• GI disturbances
• bronchoconstriction (airway constriction)
• shock
ago isth
anti-infectives
and develops the following is patient having?
122 copyright ©2013-2014-Dental Decks
PHARMACOLOGY

• penicillin VK
Penicillin VK is not harmful to the fetus when taken by pregnant mothers. It is not incorporated into bony tissue or in the teeth of children like the tetracyclines.
Note: Tetracycline and all members of the tetracycline family are contraindicated in children up to 8 years old and in pregnant women. Tetracyclines have the ability to chelate calcium ions and become incorporated in the bony tissues. The teeth of children who have been given the drag may develop a greenish-brown discoloration. This effect is sometimes seen in the newly erupted teeth of infants whose mothers have received tetracycline during pregnancy.
Remember: Penicillins, which are bactericidal against susceptible organisms, disrupt synthesis of the bacterial cell wall and compete for and bind to specific enzyme proteins that catalyze transpeptidation and cross-linking. The enzymes to which they bind are called penicillin-binding proteins (PBPs). They consist of transpeptidases, transglyco-sylases, and D-alanine caboxykinases and are implicated in the final phases of building and reshaping of the bacterial cell wall while it is growing and dividing.
• anaphylactic reaction (anaphylacticshock)
*** This reaction most commonly occurs with parenteral administration of penicillin.
This reaction can be fatal if countermeasures such as the injection of epinephrine are not taken promptly. Epinephrine prevents the release of substances from mast cells and antagonizes the actions of histamine and leukotrienes of smooth muscle.
The most common adverse effect of penicillin therapy is an allergic reaction. These reactions occur in up to 10% of patients receiving penicillin. The most common manifestation is a mild rash.
Allergic reactions to penicillin are classified into three groups: 1. Immediate - onset reactions (anaphylaxis) occur within 30 minutes; Ig-E mediated. 2. Accelerated - allergic reactions arise 30 minutes to 48 hours after administration. Urticaria, pruritis, wheezing, and local inflammatory reactions. In general, not life-threatening. 3. Delayed - allergic reactions take longer than two days to develop. 80-90% of penicillin reactions are of this type. Basic skin rashes, which are generally mild.

Antipsychotic drugs include all of the EXCEPTION?
• the phenothiazines
• the thioxanthenes
• the butyrophenones
• the benzodiazepines
anti-
following EXCfP7"one.
copyright
•psychot ics
Which one is the
123 ©2013-2014-Dental Decks
PHARMACOLOGY
anti-psychotics
All of the following are phenothiazines EXCEPT one. Which one is the EXCEPTION?
• chlorpromazine (Thorazine)
• haloperidol (Haldol)
• prochlorperazine (Compazine)
• thioridazine
• perphenazine
• trifluoperazine (Stelazine)
124 copyright © 2013-2014 - Dental Decks

• the benzodiazepines
Antipsychotics, also known as major tranquilizers or neuroleptics, are used commonly in the treatment of a variety of psychotic disorders. By far the most widely used group of antipsychotic agents used in medicine are the phenothiazines, followed by the butyrophenones and the thioxanthenes.
The first antipsychotic on the market, chlorpromazine, is the key drug among the phenothiazine antipsychotic agents. Currently, antipsychotics are divided into two generations. The first generation includes the older, "typical" drugs that treat the positive but not the negative symptoms associated with a psychotic state. Second-generation drugs have far fewer extrapyramidal symptoms (EPS) and tardive dyskinesia (TD), and they are used to treat both positive and negative symptoms of schizophrenia. Note: With the exception of risperidone, they are prolactin sparing.
The exact mechanism of antipsychotic drug action is unknown. These drugs are thought to work by blocking postsynaptic dopamine receptors in the hypothalamus, basal ganglia, limbic system, brainstem, and medulla, and to some extent serotonin receptors.
Typical antipsychotic drugs (first generation) are more potent antagonists of D2 dopamine receptors than of D[ receptors. First generation drugs include the phenothiazines (chlorpromazine, fluphenazine, perphenazine, prochlorperazine, trifluoperazine, mesoridazine, and thioridazine), the thioxanthines (thiothixene) and the butyrophenones (haloperidol).
Newer (second generation) or atypical antipsychotic agents affect different receptor sites compared with first generation antipsychotics. They bind dopamine, including D l s D2, D4, and D5 receptors, with selectively for limbic dopamine receptors. They have increased affinity for serotonin (5-HT£ receptors compared with D2 receptors. They exhibit reduced ability or an inability to induce EPS. Second generation agents include clozapine, risperidone, olanzapine, quetiapine, ziprasidone, and aripiprazole.
Important: 1. Aripiprazole (Abilify) is the first of a new class of atypical antipsychotic agents called dopamine system stabilizers or dopamine partial agonists. It combines the actions of D2 and serotonin 5-HT2a
receptor antagonism. 2. Clozapine is specific for limbic receptors and not for striated (muscle) receptors, which explains the low incidence of EPS and TD.
• haloperidol (Haldol)
Antipsychotic agents include: • First generation (typical) agents:
1. Phenothiazines: • Chlorpromazine (Thorazine) • Mesoridazine • Perphenazine • Fluphenazine • Thioridazine • Prochlorperazine (Compazine) • Trifluoperazine (Stelazine)
2. Butyrophenones:
• Haloperidol is a highly effective antipsychotic drag used to treat schizophrenia. In addition, it has been found to be effective in the treatment of Tourette's syndrome.
3. Thioxanthenes: • Thiothixene is a less potent antipsychotic. It is used for the treatment of schizophrenia.
• Second generation (atypical) agents: this group includes clozapine, risperidone, olanzapine, quetiapine, ziprasidone, and aripiprazole. These drags are effective in treating schizophrenia and exhibit reduced ability or an inability to induce EPS.
Adverse effects of antipsychotic drugs: • Dystonia and akathisia (an unpleasant sensation of motor restlessness) • Long QT-interval syndrome and ultimately increase the risk of fatal arrhythmias • Neuroleptic malignant syndrome • Parkinsonism • Antimuscarinic effects • Orthostatic hypotension • Convulsions

anti-psychotics
Which of the following drugs are used to treat psychosis? Select all that apply.
• chlorpromazine
• doxepin
• risperidone (Risperdal)
• azelastine (Astelin)
• diazepam (Valium)
• clozapine (Clozaril)
• omeprazole (Prilosec)
• haloperidol (Haldol) 125
copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
anti-psychotics
Which statement describes the extrapyramidal syndrome (EPS) caused by the
phenothiazine-type antipsychotics?
• orthostatic hypotension
• sedation
• headache
• dry mouth
• muscle spasms of the oral-facial region
126 copyright©2013-2014-Dental Decks

• chlorpromazine • risperidone (Risperdal) • clozapine (Clozaril) • haloperidol (Haldol)
Antipsychotics are primarily indicated for treatment of psychosis associated with schizophrenia, paranoia, and manic symptoms of manic-depressive illness.
Typical antipsychotic drags (first generation) are more potent antagonists of D2
dopamine receptors than of Dj receptors. First generation drugs include the phenothiazines (chlorpromazine, fluphenazine, perphenazine, prochlorperazine, trifluoperazine, mesoridazine, and thioridazine), the thioxanthines (thiothixene) and the butyrophenones (haloperidol). Note: Haloperidol is a potent dopamine antagonist.
Newer (second generation) or atypical antipsychotic agents affect different receptor sites compared with first generation antipsychotics. They bind dopamine, including DT, D2, D4, and D5 receptors, with selectively for limbic dopamine receptors. They have increased affinity for serotonin (5-HTf) receptors compared with D2 receptors. They exhibit reduced ability or an inability to induce EPS. Second generation agents include clozapine, risperidone, olanzapine, quetiapine, ziprasidone, and aripiprazole.
1 .Azelastine (Astelin) is an antihistamine nasal spray. Notes 2. Doxepin is a tricyclic antidepressant used for treating depression and anxi
ety. 3. Diazepam (Valium) is a benzodiazepine used for anxiolysis. 4. Omeprazole (Prilosec) is a proton pump inhibitor used for the treatment of GERD.
• muscle spasms of the oral-facial region
Extrapyramidal syndrome (EPS) refers to a variety of signs and symptoms that are a result of the blockade of dopamine receptors in specific brain regions. These symptoms include: Parkinson-like movements (shuffled gait, pill-rolling effect of fingers), muscle rigidity, spasms of neck and facial muscles, tremors, and loss of muscle movement.
Tardive Dyskinesia (TD) is a serious, potentially irreversible neurological disorder that can appear at any age. Tardive Dyskinesia is a side effect of taking antipsychotic/neuroleptics drags. Symptoms involve uncontrollable movement of various body parts, including the body trunk, legs, arms, fingers, mouth, lips, or tongue. About 20 percent of people taking antipsychotic/neuroleptic drugs for more then one year will be affected.
Remember: Newer (second generation) or atypical antipsychotic agents affect different receptor sites compared with first generation antipsychotics. They bind dopamine, including Dr, D2, D4, and D5 receptors, with selectively for limbic dopamine receptors. They have increased affinity for serotonin (5-HTT) receptors compared with D2 receptors. They exhibit reduced ability or an inability to induce EPS. Second generation agents include clozapine, risperidone, olanzapine, quetiapine, ziprasidone, and aripiprazole.
Important: Clozapine is specific for limbic receptors and not for striated (muscle) receptors, which explains the low incidence of EPS and TD.

asp/acet/NSAIDs Which of the following are symptoms of acute aspirin toxicity? Select all that apply.
• tinnitus
• respiratory alkalosis
• vertigo
• muscle twitching
• nausea and vomiting
• myocardial infarction
127 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
The main ingredient in Advil is also lowing prescription products?
• percodan
• vicodin ES
• motrin
• naprosyn
PHARMACOLOGY
the mai
asp/acet/NSAIDs
in ingredient in which of the fol-
128 copyright © 2013-2014 - Dental Decks

• tinnitus • respiratory alkalosis • vertigo • nausea and vomiting
An overdosage of salicylates (acute aspirin toxicity) is life threatening and requires intensive supportive treatment in a hospital. Initial symptoms include respiratory alkalosis with hyperpnea and tachypnea, nausea, vomiting, hypokalemia, tinnitus, headache, dizziness, confusion, dehydration, hyperthermia, hyperactivity, and hematologic abnormalities, progressing to coma and respiratory collapse.
Chronic aspirin toxicity presents with the following signs and symptoms: salicylism, CNS effects, bleeding and GI
disturbances.
Aspirin inactivates the enzyme known as cyclooxygenase. Since cyclooxygenase synthesizes the prostaglandins, the inhibition of this enzyme results in the inhibition of prostaglandin synthesis. As a result, aspirin is analgesic, antipyretic (fever reducing), and anti-inflammatory. Aspirin is an irreversible platelet inhibitor and can reduce blood clotting to prolong bleeding. Note: Aspirin inhibits both COX-1 and COX-2.
Low doses of aspirin taken regularly can have a cardioprotective effect. These doses reduce thromboxane production in platelets to result in the inhibition of platelet aggregation. In this way, aspirin has the ability to inhibit the formation of life-threatening thrombi (blood clots).
The liver appears to be the principal site for salicylate metabolism, although other tissues may also be involved. The three chief metabolic products of salicylic acid are salicyluric acid, the ether or phenolic glucuronide and the ester or acyl glucuronide. Excretion of salicylates occurs principally via the kidney, through a combination of glomerular filtration and tubular excretion, in the form of free salicylic acid, salicyluric acid, as well as phenolic and acyl glu-curonides.
Contraindications to the use of aspirin: • Bleeding disorders (aspirin will increase bleeding time) • Do not use in children with viral infections (i.e., influenza or chickenpox) with or without fever due to a potential association with Reye's syndrome (this syndrome is a serious neurological defect) • Pregnancy (especially during the third trimester) • Peptic ulcers (aspirin may cause bleeding of the GI tract) • Asthma; rhinitis; nasal polyps • Concomitant use of anticoagulants
• motrin
Both Advil and Motrin are available over-the-counter and contain 200 mg of ibuprofen. Prescription-strength Motrin is also available and contains 400 mg or more ibuprofen.
Nonsteroidal anti-inflammatory drags (NSAIDs) have anti-inflammatory effects resulting from their ability to inactivate the enzyme prostaglandin endoperoxide synthase (cyclooxygenase). By doing this they inhibit the cyclooxygenase step of the arachidonic acid cascade and thus reduce local prostaglandin synthesis. NSAIDs also have analgesic, and antipyretic actions.
Remember: The traditional NSAIDs such as ibuprofen, naproxen and aspirin inhibit COX-2 along with COX-1. Thus they are effective in reducing pain and inflammation, but are capable of inducing gastrointestinal ulcers. The COX-2 selective inhibitors will reduce pain and inflammation without any significant risk of causing gastrointestinal ulcers.
For the traditional NSAIDs such as ibuprofen, naproxen, and aspirin, because they inhibit both COX-1 and COX-2 enzymes, they belong to the category of non-selective COX inhibitors. For celecoxib (Celebrex), because it inhibits COX-2 enzyme only, it belongs to the category of COX-2 selective inhibitors.
Note: Rofecoxib (Vioxx) and Valdecoxib (Bextra) are also COX-2 selective inhibitors that were removed from the market because they were found to have added cardiovascular risks in some patients.

Which non-narcotic analgesics would anti-coagulant medication?
• ibuprofen (Motrin, Advil)
• acetaminophen (Tylenol)
• aspirin
• naproxen sodium (Aleve)
you most 1
asp/acet/NSAIDs
ikely use in a patient taking
129 copyrightO2013-2014-Dental Decks
PHARMACOLOGY
Which agent has anti-
• codeine
• acetaminophen
• hydrocodone
• ibuprofen
inflammatory properties?
PHARMACOLOGY
asp/acet/NSAIDs
130 copyright©2013-2014-Dental Decks

• acetaminophen (Tylenol)
Acetaminophen has no effect on platelets nor the coagulation pathways and does not affect bleeding times or prothrombin times even with high doses.
Acetaminophen has two major pharmacological actions: an analgesic effect and an antipyretic (fever reducer) effect. Acetaminophen is not effective enough to reduce severe pain, but it is effective in reducing mild to moderate pain. Acetaminophen is a weak inhibitor of prostaglandin formation.
Large doses of acetaminophen can cause liver toxicity. Alcohol can seriously increase the hepatotoxic potential of acetaminophen. There are approximately 100 deaths annually due to liver toxicity produced by ingesting large continuous doses of acetaminophen. Acetaminophen very rarely causes drag sensitivities and can be given to patients having an allergy to aspirin.
Differences Between Acetaminophen and Aspirin
Affect blood clotting
Gastrointestinal ulcers
Associated with Reye's syndrome
Anti-inflammatory effects
Analgesic effects
Acetaminophen
No
No
No
No
Yes
Aspirin
Yes
Yes
Yes
Yes
Yes
ibuprofen
Ibuprofen inhibits the production of prostaglandins in peripheral tissues at sites where pain and inflammation are present. Inhibition of prostaglandin production reduces the inflammatory response at sites of surgery, injury or infection. Reduction of inflammation results in reduction of perceived pain.
Acetaminophen is a weak inhibitor of prostaglandin production in peripheral tissues. Thus, the inflammatory response is not affected to any great degree. Acetaminophen reduces pain through mechanisms other than inflammatory reduction. It is unclear exactly how acetaminophen works to reduce pain.
Codeine and hydrocodone are narcotic analgesics that effectively reduce pain but do not reduce inflammation. Narcotics work within the brain to block ascending pain impulses traveling from the periphery into the brain.

asp/acet/NSAIDs
Your patient has a history of drug abuse. Which agent could be given (if needed in the treatment plan) with no liability to cause an addiction?
• phenobarbital
ibuprofen
• hydrocodone
• meperidine
• codeine
131 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
NSAIDs reduce the production of. inflammation.
asp/acet/NSAIDs
. associated with pain and
• ieukotrienes
• cytokines
• prostaglandins
• interferons
132 copyright ©> 2013-2014 - Dental Decks
PHARMACOLOGY 109

• ibuprofen
Ibuprofen is an NSAID and is classified as a non-narcotic analgesic. Non-narcotic analgesics have no liability for abuse or addiction. They are not a controlled substances.
Phenobarbital is a barbiturate used as a sedative and to treat epilepsy. Barbiturates all have the potential to cause abuse and addiction, and are controlled substances requiring a DEA number from the prescriber.
Hydrocodone (Vicodin), meperidine (Demerol) and codeine are narcotic analgesics with the potential to cause abuse and addiction. They are all controlled substances requiring a DEA number from the prescriber.
Important: NSAIDs can inhibit the antihypertensive effect of ACE inhibitors, beta-blockers, and diuretics.
• prostaglandins
Nonsteroidal anti-inflammatory drugs (NSAIDs) inhibit the cyclooxygenase step of the arachidonic acid cascade and thus inhibit the activity of prostaglandin synthetase. Prostaglandins are a group of hormone-like substances that mediate a range of physiological functions, such as metabolism and nerve transmission. NSAIDs have analgesic, antipyretic, and anti-inflammatory properties (similar to aspirin). They are used for pain control, arthritis, and painful menstruation. Adverse reactions include GI upset (possible ulcers), and prolongation of bleeding time (reduction in platelet aggregation). Contraindications to the use of NSAIDs are impaired renal function, pregnancy, and GI disease (ulcers).
Examples of NSAIDs: • Proprionic acid derivatives: • Flurbiprofen (Ansaid) • Oxaprozin (Daypro) • Naproxen sodium (Anaprox, Aleve) • Ibuprofen (Motrin, Advil) • Ketoprofen (Orudis) • Naproxen (Naprosyn) • Fenoprofen (Nalfon)
• Acetic acid derivatives: • Indomethicin (Indocin) • Diclofenac sodium (Votaren) • Etodolac (Lodine) • Ketorolac (Toradol) • Sulindac (Clinoril)
• Alkanoic acid derivatives: • Nabumetone (Relafen)
• Fenamic acid derivatives: • Meclofenamate (Meclomen) • Mefenamic acid (Ponstel)
• Oxicams • Piroxicam (Feldene) • Meloxicam (Mobic)
• Cox-2 inhibitors • Celecoxib (Celebrex)

Which of the following agents has little
• ibuprofen
• acetaminophen
• aspirin
• naproxen
• nabumetone
ivalue
asp/acet/NSAIDs
in treating acute inflammation?
s
133 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY
asp/acet/NSAIDs
Your patient is taking the following medications. Which are used to reduce the signs and symptoms of rheumatoid arthritis? Select all that apply?
• amlodipine (Norvasc)
• enalapril (Vasotec)
• piroxicam (Feldene)
• prednisone
• fosamax (Alendronate sodium)
134 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• acetaminophen — (Tylenol)
Acetaminophen inhibits central prostaglandin synthesis — it is analgesic for low intensity pain and antipyretic. Because it is less effective than salicylates (aspirin) in blocking peripheral prostaglandin synthesis, it has no anti-inflammatory activity and does not affect platelet function and therefore will not affect clotting time. Note: In large doses (>7.5 g within 8 hours), acetaminophen can cause hepatic necrosis. Concurrent use with the following drugs may increase the risk of hepatotoxicity: barbiturates, hydantoins, carbamazepine, rifampin, sulfinpyrazone, and ethanol. Acute overdosage of acetaminophen can result in hepatotoxicity and is life threatening. Acetaminophen is metabolized to a highly toxic intermediate product, which normally is detoxified by glutathione. When glutathione is depleted, the toxic intermediate attacks other cells, causing necrosis. Symptoms that appear in the first 24 hours are nausea, vomiting, drowsiness, lethargy, malaise, and confusion. Note: N-acetylcysteine (NAC) is the specific antidote for acetaminophen poisoning.
Acetaminophen is preferred over aspirin when an analgesic or antipyretic drag is indicated and also the patient:
• Is asthmatic • Is allergic to aspirin • Is at added risk for an ulcer • Is taking drugs such as probenecid or methotrexate • Is experiencing bleeding • Is taking anticoagulants
Remember: Aspirin and Nonsteroidal Anti-inflammatory Agents (Ibuprofen, Naproxen, Nabumetone, and others) inactivate the enzyme known as cyclooxygenase. Since cyclooxygenase synthesizes the prostaglandins, the inhibition of this enzyme results in the inhibition of prostaglandin synthesis. Cyclooxygenase has an acronym of COX. Thus the Nonsteroidal Anti-inflammatory Agents (NSAIDs) are also known as COX inhibitors. As a result, they have analgesic, antipyretic, and anti-inflammatory actions. NSAIDs must be used cautiously in patients with peptic ulcer disease.
• Piroxicam (Feldene) • Prednisone
Piroxicam (Feldene) is a nonsteroidal anti-inflammatory drug (NSAID) that inhibits prostaglandin synthesis. It is used to manage inflammatory disorders and used for the symptomatic treatment of acute and chronic rheumatoid arthritis and osteoarthritis.
Prednisone is a corticosteroid and has anti-inflammatory actions. It is used for the treatment of a wide variety of inflammatory diseases including rheumatoid arthritis and osteoarthritis.
Remember: • Common side effects of NSAIDs such as piroxicam (Feldene) include:
- Gastric irritation - Heart burn - Nausea
• Short-term side effects of corticosteroids such as prednisone include: - Insomnia - Indigestion - Arthralgia
• Long-term side effects of corticosteroids include: - Edema (abdominal distension) - Psychological disturbances - Peptic ulcer - Osteoporosis - Muscle weakness

asp/acet/NSAIDs
Celecoxib (Celebrex) is a member of which category of drugs?
• salicyclates
• opiates
• COX-2 selective inhibitors
• non-selective COX inhibitors
• steroidal anti-inflammatories
135 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
cholinergic
The autonomic nervous system has cholinergic neurons that secrete:
• epinephrine
• norepinephrine
• acetylcholine
• dopamine
136 copyright © 2013-2014 - Dental Decks

• COX-2 selective inhibitors
Cyclooxygenase, or COX, is the enzyme which produces prostaglandins. Two forms of COX exist: COX-1, and COX-2. The COX-1 enzyme produces prostaglandins in the GI Tract. The prostaglandins formed act as a protective substance against the formation of gastrointestinal ulcers. The traditional NSAIDs such as ibuprofen, naproxen, aspirin, and others inhibit the COX-1 enzyme thus diminishing the formation of the protective prostaglandins. Gastrointestinal ulcers are therefore a potential adverse effect with these drugs. The COX-2 enzyme produces prostaglandins at the sites of surgery, infection and inflammation. When this enzyme is inhibited, less prostaglandins are produced and there is less pain and inflammation. The traditional NSAIDs such as ibuprofen, naproxen and aspirin inhibit COX-2 along with COX-1. Thus they are effective in reducing pain and inflammation, but are capable of inducing gastrointestinal ulcers. The COX-2 selective inhibitors will reduce pain and inflammation without any significant risk of causing gastrointestinal ulcers.
For the traditional NSAIDs such as ibuprofen, naproxen, and aspirin, because they inhibit both COX-1 and COX-2 enzymes, they belong to the category of non-selective COX inhibitors. For celecoxib (Celebrex), because it inhibits COX-2 enzyme only, it belongs to the category of COX-2 selective inhibitors.
The COX-2 selective inhibitors: - Are not salicylates because they are not aspirin drags - Are not opiates because they do not work like morphine - Are not steroidal anti-inflammatories because they are not corticosteroids such as hydrocortisone
• acetylcholine
Cholinergic is a term for a nerve ending that releases acetylcholine (ACh) as the primary neurotransmitter; also, a synapse in which acetylcholine is the primary neurotransmitter.
Acetylcholine receptors are called cholinergic receptors. They are subdivided as follows: • Muscarinic receptors (sites):
- At neuroeffector sites for all postganglionic cholinergic neurons (this is characteristic of all parasympathetic postganglionic nerves) - At neuroeffector sites of postganglionic sympathetic nerves to the sweat glands and a few blood vessels (these postganglionic nerves are also cholinergic)
• Nicotinic receptors (sites): - At the skeletal neuromuscular junction (involving somatic nerves) - At ganglionic sites (*** The same type of nicotinic receptor is present in sympathetic ganglia, parasympathetic ganglia, and the adrenal medulla)
*** Drugs that resemble ACh in chemical structure and bind to these receptors imitate the effects of parasympathetic postganglionic activity. Important:
1. Preganglionic neurons of both divisions (parasympathetic and sympathetic) are cholinergic, as are postganglionic neurons of the parasympathetic division. 2. Postganglionic neurons of the sympathetic division are usually adrenergic.
1. The action of acetylcholine at postganglionic parasympathetic sites is often Notes referred to as a muscarinic response.
2. The term nicotinic response is used to describe the stimulating action of ACh on the ganglia, as well as its action at the neuromuscular junction of skeletal muscle. 3. Muscarinic receptors are usually linked to Gq, phospholipase C (PLC), and Ca2+.

cholinergic
Which of the following are cholinergic actions? Select all that apply.
• slowing of the heart
• dilation of the pupils
• the stimulation of the smooth muscles of the bronchi, GI tract, gallbladder, bile duct, bladder and ureters
> The stimulation of sweat, salivary, tear and bronchial glands
137 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
All of the following are antimuscarini EXCEPTION?
• atropine
• scopolamine
• glycopyrrolate (Robinul)
• mecamylamine (Inversine)
• propantheline (Pro-Banthine)
PHARMACOLOGY
cholinergic
c agents EXCEPT one. Which one is the
138 copyright © 2013-2014 - Dental Decks

• slowing of the heart • the stimulation of the smooth muscles of the bronchi, GI tract, gallbladder, bile duct, bladder and ureters
• the stimulation of sweat, salivary, tear and bronchial glands
Cholinergic actions: • The stimulation of sweat, salivary, tear and bronchial glands • The stimulation of the smooth muscles of the bronchi, GI tract, gallbladder, bile duct, bladder and ureters (i.e., urination) • Slowing of the heart (bradycardia) • Constriction of the pupils (miosis)
Important: Acetylcholine is the chemical mediator at all autonomic ganglia and parasympathetic postganglionic synapses. It is also the transmitter substance of the neuromuscular junction in skeletal muscle (local anesthetics prevent or reduce the liberation of ACh at the NMJ) and sweat glands. Acetylcholine causes an alteration in cell membrane permeability to produce the above actions.
Anticholinergic actions: •The secretions of all glands in the nose, mouth, pharynx and respiratory tract is inhibited (unpleasant "dry mouth ") • An inhibitory effect on motility throughout the GI tract (may cause constipation and urinary retention) • The heart rate increases (tachycardia) • A rise in body temperature • Dilation of the pupils (mydriasis)
Note: Termination of transmission by ACh takes place primarily by metabolism by acetylcholinesterase located on postsynaptic or postjunctional membranes.
• mecamylamine (Inversine)
*** Mecamylamine is a nicotinic ganglion-blocking drag.
The typical effects of anticholinergic drags include mydriasis, antispasmodic actions and reduction in gastric and salivary secretions (dry mouth). Important: These drags are con-t ra indicated in patients with glaucoma.
These drags have no intrinsic activity of their own; they simply occupy the receptor site and prevent acetylcholine from occupying the same receptor. Accepted therapeutic indications include treating Parkinson's disease, motion sickness, postoperative bladder syndrome and traveler's diarrhea.
Synthetic Anticholinergic Drugs
Drug Name
Glycopyrrolate (Robinul)
Propantheline bromide (Pro-Banthine)
Benztropine mesylate (Cogentin)
Trihexyphenidyl HCL (Artane)
Atropine
Scopolamine
Major Use
Inhibit salivation and excessive secretions preoperatively; control of upper airway secretions
Traveler's diarrhea and antisecretory
Antiparkinsonism
Antiparkinsonism
To produce mydriasis and cycloplegia
To prevent or reduce motion sickness

The currently available ganglionic
• mecamylamine
• hexamethonium
• tetraethylammonium
• trimethaphan
blocker for clinical
cholinergic
1 use is:
139 copyright©2013-2014-Dental Decks
PHARMACOLOGY
cholinergic
The prototype depolarizing neuromuscular blocking agent is:
• tubocurarine (Curare)
• mivacurium (Mivacron)
• succinylcholine (Anectine)
• vecuronium (Norcuron)
• doxacurium (Nuromax)
• pancuronium (Pavulon)
• atracurium (Tracrium)
• cisatracurium (Nimbex)
• rocuronium (Zemuron) 140 copyright © 2013-2014 - Dental Decks

• mecamylamine
*** Hexamethonium, trimethaphan, and tetraethylammonium are no longer available in the U.S. for clinical use.
Nicotinic receptor antagonists (nicotinic blocking agents) are divided into ganglion-blocking drags and neuromuscular blocking drags.
Remember: two major types of nicotinic receptors: 1. Those at the skeletal neuromuscular junction of the somatic system
*** Neuromuscular blockers act here 2. Those at the autonomic ganglionic sites (both sympathetic and parasympathetic)
*** Ganglionic blockers act here
Although they are among the most potent agents available, ganglionic-blocking drugs are seldom used because of the annoying and sometimes disabling parasympathetic blockade. The side effects (caused by parasympathetic blockade) include a very pronounced xerostomia, constipation, blurred vision, and postural hypotension. These drags have only very limited clinical uses.
Mecamylamine (Inversine) is used clinically for: • The treatment of severe or malignant hypertension • An emergency hypertensive crisis *** It causes a rapid and reversible fall in blood pressure that enables it to immediately reverse an emergency hypertensive crisis. • A "bloodless field" surgery
• succinykholine (Anectine)
Neuromuscular blocking drugs are important for producing complete skeletal muscle relaxation and facilitate endotracheal intubation, as an adjunct to surgical anesthesia. These agents interact with nicotinic receptors at the skeletal neuromuscular junction. There are two classes of neuromuscular blockers:
1. Nondepolarizing: These agents competitively compete with acetylcholine at the nicotinic receptor. These agents bind to nicotinic cholinergic receptors and prevent acetylcholine from stimulating motor nerves, resulting in muscle paralysis. The prototype nondepolarizing agent is tubocurare (Curare). Other agents include mivacurium, vecuronium, doxacurium, pancuronium, atracurium, cisatracurium and rocuronium. Note: Neostigmine or pyridostigmine (which are cholinesterase inhibitors) can reverse the blockade of these agents. 2. Depolarizing (non-competitive): Succinylcholine (Anectine) is the only member of this group used in the United States. It acts like a nicotinic agonist and depolarizes (desensitizes) the neuromuscular end plate. It binds to the ACh receptor and stimulates depolarization causing initial excitation followed by block of neurotransmission and muscle paralysis. Important: Succinylcholine should be used with caution in patients with low levels of pseudo-cholinesterase, which breaks down succinylcholine. Respiratory failure may result.
*** Succinylcholine may cause muscarinic responses such as bradycardia and increased glandular secretions.
Very important: The major danger of all of these neuromuscular blocking drugs is too much paralysis (thepatient cannot breathe).
1. Dantrolene is an skeletal muscle relaxing agent that acts within the skeletal muscle fiber Notes rather than on the neuromuscular junction (does not block the nicotinic receptors). It inhibits
the depolarization-induced release of Ca2+ from the sarcoplasmic reticulum. The principal therapeutic applications of dantrolene are for the relief of spasticities associated with upper motor neuron disorders (i.e., stroke, cerebral palsy, and multiple sclerosis) and for the prophylaxis and treatment of malignant hyperthermia. 2. Botulinum toxin A (Botox) acts on the motor nerve terminal to prevent the release of ACh. It is used in ophthalmology to relax the extraocular muscles, and for muscle dystonias as well as to remove wrinkles.

cholinergic
All of the following are cholinesterase inhibitors EXGEPTone. Which one is the EXCEPTION?
• physostigmine
• edrophonium
• pyridostigmine
• phentolamine
• neostigmine
141 copyright©2013-2014-Dental Decks
PHARMACOLOGY
All of the following are cholinergic EXCEPTION?
• acetylcholine
• methacholine
• bethanechol (Urecholine)
• dobutamine
• carbachol (Isopto-Carbachol)
• pilocarpine hydrochloride
cholinergic
drugs EXCEPT one. Which one is the
142 copyright©2013-2014-Dental Decks
PHARMACOLOGY

•kick
• phentolamine
Phentolamine (and phenoxybenzamine) axe prototypes of non-selective alpha-adrenergic
receptor blockers.
Cholinesterase inhibitors act by blocking the enzyme (acetylcholinesterase) that degrades acetylcholine in the brain. This results in more acetylcholine in the synaptic cleft and enhances cholinergic transmission. These drugs act as indirect agonists at both muscarinic and nicotinic sites. Examples of cholinesterase inhibitors include:
• Edrophonium: reversible; very short duration of action; used to reverse curare-type drugs • Neostigmine: reversible; extended duration of action; used to reverse curare-type drugs and to treat myasthenia gravis • Physostigmine: reversible; short duration of action; used for glaucoma, and for an anti
dote for atropine • Pyridostigmine: reversible; extended duration of action; used to treat myasthenia gravis • Tacrine: reversible; extended duration of action; used to treat Alzheimer's disease • Donepezil: reversible; extended duration of action; used to treat Alzheimer's disease • Malathion: irreversible; long duration of action; used as an insecticide • Sarin: irreversible; long duration of action; used as a nerve gas
Three cholinesterase inhibitors are commonly prescribed for Alzheimer's disease: • Donepezil (Aricept), approved to treat all stages of Alzheimer's disease • Rivastigmine (Exelon), approved to treat mild to moderate Alzheimer's • Galantamine (Razadyne), approved to treat mild to moderate Alzheimer's
Note: The stimulation of the skeletal muscle by excess acetylcholine eventually results
in muscle paralysis.
• dobutamine
*** Dobutamine is an adrenergic agonist.
Cholinergic drugs are compounds that mimic the actions of the endogenous neurotransmitter acetylcholine (ACh). Direct-acting, or cholinomimetic, agents combine with cholinergic receptors (muscarimic or nicotinic or both), to cause a response in an effector. These drugs include ACh, various choline-ester congeners of ACh, and some alkaloids. With few exceptions (i.e., nicotine and other ganglionic stimulants), these agents exert prominent muscarinic or parasympathomimetic effects. These drugs are longer-lasting than ACh because they are not subject to rapid metabolism like ACh. ACh is metabolized by acetylcholinesterase, located near receptors for ACh. In the plasma and other sites, ACh (and many other esters) are metabolized by pseudocholinesterase. The other cholinergic agonists used as drugs are metabolized slowly or not at all by these enzymes.
Direct-acting agents: • Choline esters: The most noticeable effects of these drugs are a fall in blood pressure attributable to generalized vasodilation, flushing of the skin, a slowing of the heart rate, and an increased tone and activity of both the GI and urinary tracts. Topical application of these drugs to the eye causes miosis and a decrease in intraocular pressure. These drugs include:
• Acetylcholine chloride: used in ophthalmology to produce miosis • Bethanechol: used for postoperative abdominal distension and urinary retention • Carbachol: used in ophthalmology to produce miosis
• Cholinergic alkaloids: These drugs include muscarine, pilocarpine, nicotine and lobeline. Pilocarpine is the most useful alkaloid being employed as a miotic and to treat open angle glaucoma. Pilocarpine is also used to stimulate salivary flow in patients suffering from xerostomia due to radiation therapy in the treatment of head and neck cancer.
Indirect-acting agents: • Cholinesterase inhibitors: These drugs include physostigmine, edrophonium, pyridostigmine, neostigmine, malathion and sarin. They inhibit acetylcholinesterase at both muscarinic and nicotinic sites. They are indirect agonists at both muscarinic and nicotinic sites.
Note: If any of the cholinergic agents are administered before acetylcholine, the action of acetycholine will be enhanced and prolonged.

cholinergic
In dentistry, a cholinergic drug is used to:
• produce a dry field for taking impressions
• calm an anxious patient
• treat dry mouth by inducing salivation
• reduce nausea
143 copyright©2013-2014-Dental Decks
PHARMACOLOGY
cholinergic
All of the following statements concerning edrophonium are true EXCEPT one. Which one is the EXCEPTION?
• It is a direct-acting cholinergic agonist (cholinomimetic)
> It is a rapid-acting, short-duration, injectable cholinesterase inhibitor
• It is the drug of choice for diagnosing myasthenia gravis because of its rapid onset of action and reversibility
• It is also useful in differentiating a myasthenic crisis from a cholinergic crisis
144 copyright©2013-2014-Dental Decks
PHARMACOLOGY

• treat dry mouth by inducing salivation
Cholinergic drugs used in dentistry are: Pilocarpine (Salagen), and Cevimeline (Evoxac).
• Pilocarpine (Salagen) - is indicated for treatment of xerostomia caused by salivary gland hypofunction resulting from radiotherapy for cancer of the head and neck. It's pharmacologic category is cholinergic agonist. Prevalent side effects are excess sweating and nausea/heartburn/diarrhea due to the cholinergic nature of the drug.
• Cevimeline (Evoxac) - is indicated for the treatment of symptoms of xerostomia in patients with Sjogren's syndrome. It's pharmacologic category is cholinergic agonist. Prevalent side effects are increased sweating and nausea/heartburn/diarrhea due to the cholinergic nature of the drag.
• it is a direct-acting cholinergic agonist (cholinomimetic)
*** This is false; edrophonium is an indirect-acting cholinergic agonist (cholinomimetic) as are pyridostigmine, physostigmine, and neostigmine (they are all cholinesterase inhibitors). Note: These drugs are indirect agonists at both muscarinic and nicotinic sites.
Pyridostigmine is prescribed in the treatment of myasthenia gravis, however edrophonium is used to diagnose myasthenia gravis and not in the treatment of it due to its very short duration of action.
Symptoms of a cholinergic crisis include: bradycardia (decreased heart rate), lacrimation, extreme salivation, vasodilation and muscle weakness. Because a cholinergic crisis can result in muscle weakness like that of a myasthenic crisis, distinguishing the two conditions may be difficult. Administration of a short-acting cholinomimetic such as edrophonium will improve a myasthenic crisis but worsen a cholinergic crisis.
Remember: Typical cholinergic effects caused by stimulation of acetylcholine receptors (cholinergic receptors) include salivation, miosis, excessive sweating, flushing, increased GI motility and bradycardia.

cholinergic
Poisoning with an organophosphate cholinesterase inhibitor can be treated with:
• edrophonium
• carbachol
• pralidoxime
• nicotine
145 copyright © 2013-2014 - Dental Decks
cholinergic
The muscarinic effects of cholinergic agonists include all of the following EXCEPT one. Which one is the EXCEPTION?
• miosis
• flushing
• bronchoconstriction
• increased GI motility
• increased urination
• tachycardia
• salivation
• sweating
146 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• pralidoxime
Pralidoxime (Protopam) is a cholinesterase reactivator which is used as an antidote to reverse muscle paralysis resulting from organophoshate anticholinesterase pesticide poisoning. It is also used to reverse the effects of an overdosage of anticholinesterase agents used in the treatment of myasthenia gravis (i.e., pyridostigmine and ambenomium).
Symptoms of organophosphate poisoning include: excessive salivation, bronchocon-striction, diarrhea and skeletal muscle fasciculations (twitching).
Organophosphates are esters of phosphoric acid and an organic alcohol that inhibit the enzyme cholinesterase.
Examples include: • Isoflurophate: used in the treatment of glaucoma • Malathion: a widely used insecticide • Parathion: an insecticide
• Echothiophate: used in the treatment of glaucoma • Tabun: one of the most potent and toxic nerve gases • Soman: nerve gas • Sarin: nerve gas
• tachycardia
*** Bradycardia is a muscarinic effect of cholinergic agonists.
Direct-acting cholinergic drugs include: methacholine, carbachol, bethanecol and pilocarpine.
Indirect-acting cholinergic drugs (cholinesterase inhibitors) include: physostigmine, edrophonium,
neostigmine, pyridostigmine, malathion, echothiophate, sarin and soman.
Effects of anticholinesterases: Muscarinic: Nicotinic: • Miosis • Bronchoconstriction • Muscle twitching • Salivation • Increased GI motility • Weakness • Sweating • Urination • Tachycardia • Bradycardia • Increase in BP
Antimuscarinic drugs block the effect of acetylcholine and all drugs that stimulate muscarinic receptors. Atropine and scopolamine are prototypes. Other antimuscarinic drugs include: glycopyrrolate, propantheline, benztropine, cyclopentolate, tropicamide, trihexyphenidyl, homatropine, oxybutynin, and ipratropium. Antimuscarinic drugs produce the following effects:
• Salivary glands: reduced secretion (atropine) • GI tract: reduced peristalsis, reduced secretion (propantheline, glycopyrrolate) • Sweat glands: reduced secretion (atropine) • Eyes: mydriasis (homatropine, cyclopentolate, tropicamide) • Bronchi: bronchodilation, reduced secretion (ipratropium) • Bladder: urinary retention (oxybutynin) • CNS: antimotion sickness (scopolamine)
antitremor activity — to treat parkinsonism (benztropine, trihexyphenidyl)
1. Contraindications for using antimuscarinic drugs include: narrow-angle glaucoma, pro-Notes static hyperplasia, and tachycardia.
2. Pilocarpine and cevimeline (both cholinergic agonists) are used to stimulate salivary flow. 3. SAL-TROFJNE(atropine sulfate, USP tablets) is indicated to reduce salivation and is endorsed with the ADA Seal of Acceptance.

cholinergic
All of the following drugs may be useful in controlling salivary secretions to help in obtaining a dry field EXCEPT one. Which one is the EXCEPTION?
• atropine sulfate
•carbachol
• glycopyrrolate (Robinul)
• belladonna derivatives
• propantheline bromide (Pro-banthine)
147 copyright S 2013-2014 - Dental Decks
PHARMACOLOGY
The major natural glucocorticoid is:
• triamcinolone
• Cortisol
• dexamethasone
• prednisone
• prednisolone
corticosteroids
148 copyright © 2013-2014 - Dental Decks

•carbachol
*** Carbachol is a direct-acting cholinergic drag.
The other drags are all classified as anticholinergics. They block postganglionic cholin
ergic fibers.
Contraindications to their use include: • Glaucoma • Cardiovascular problems • Obstruction of the GI or GU tract
• Asthma
These drags also reduce spasms of smooth muscle in the bladder, bronchi, and intestine; relax the iris sphincter; decrease gastric, bronchial, and salivary secretions; decrease perspiration; and accelerate impulse conduction through the myocardium by blocking vagal impulses.
• Cortisol
The corticosteroids are steroid hormones produced by the adrenal cortex. They consist of two major groups:
1. Glucocorticoids: have important effects on metabolism, catabolism, immune responses and inflammation. The majority of the anti-inflammatory and immunosuppressive actions of the glucocorticoids are probably the result of their action on arachidonic acid metabolism. They induce the synthesis of a protein that inhibits phospholipase A2, thus decreasing the production of both prostaglandins and leukotrienes.
The major natural glucocorticoid is Cortisol. The synthetic glucocorticoids include hydrocortisone (Cortefi, cortisone, prednisone (Delatasone), prednisolone (Delta-Cortef, dexamethasone (Decadron), triamcinolone (Aristocort), methylyprednisolone (Medral), and betamethasone (Ce-stone). Glucocorticoids are most often used as anti-inflammatory and immunosuppressive agents.
Adverse effects of the short-term administration of systemic glucocorticoids include secondary infections, hyperglycemia, and a range of mood and behavioral changes. Long-term therapy may cause osteoporosis, cataracts, hypertension, myopathy, and adrenal insufficiency.
2. Mineralocorticoids: regulate sodium and potassium reabsorption in the collecting tubules of the kidney. The major natural mineralocorticoid in humans is aldosterone. Other mineralocorticoids include deoxycorticosterone and fludrocortisone. Mineralocorticoids are used in replacement therapy in hypoadrenocorticism or Addison's disease.
Note: Corticosteroids do not cure any disease. Inpatients with Addison's disease, corticosteroids serve as a replacement for the lack of steroid hormones being produced by the patient.
Contraindications to corticosteroid use include: latent TB or fungal infection, AIDS, herpes infections and patients with peptic ulcer disease (specifically, gastric ulcers) — these drugs themselves may cause
Toxic effects of the corticosteroids include growth inhibition, hyperglycemia, osteoporosis, psychosis and salt retention.

corticosteroids
All of the following are pharmacologic effects of glucocorticoids EXCEPT one. Which one is the EXCEPTION?
• stimulate protein breakdown, which results in increased plasma amino acid levels
• stimulate gluconeogenesis in the liver and inhibit peripheral glucose use
• impaired wound healing
• reduce the immune response
• decreased lipolysis
• inhibit local edema, capillary dilation, migration and activation of white blood cells, and phagocytosis by macrophages
• increase hemoglobin concentration and increase the numbers of circulating red blood cells and platelets
r 149 copyright S 2013-2014- Dental Decks
PHARMACOLOGY
The major natural mineralocorticoid in humans is:
• dexamethasone
• aldosterone
• Cortisol
• prednisone
• triamcinolone
PHARMACOLOGY
corticosteroids
150 copyright © 2013-2014 - Dental Decks

• decreased lipolysis
*** This is false; glucocorticoids affect the mobilization of fats from areas of deposition. Increased lipolysis occurs in areas of adipose accumulation, and serum fatty acid concentration increases.
Other effects of glucocorticoids include an anti-inflammatory action, immunosuppression, and an anti-allergenic action. Note: These effects occur in target cells following the interaction of the steroid with a specific glucocorticoid receptor.
Common Disorders Treated with Glucocorticoids
Disorder
Allergic conditions
Dermatologic
Respiratory
Endocrine
Collagen, vascular
Rheumatic
Neurologic
Ophthalmic
Examples
Seasonal allergic rhinitis, Serum sickness, Drug hypersensitivity reaction
Contact dermatitis, Erythema multiforme, Psoriasis, Pemphigus, Stevens-Johnson syndrome, Seborrheic dermatitis
Bronchial asthma, Sarcoidosis, COPD
Adrenocortical insufficiency
Systemic lupus erythematosus, Polymyositis, Temporal arteritis
Rheumatoid arthritis, Psoriatic arthritis, Acute gouty arthritis
Multiple sclerosis, Cerebral edema, Acute stroke and spinal cord injury
Allergic conjunctivitis, Uveitis, Herpes zoster ophthalmicus
Note: Beclomethasone, budesonide and flunisolide are special glucocorticoids (used as inhalers) that have been developed for use in chronic asthma and bronchial disease. These agents readily penetrate the airway mucosa but have very short half-lives after they enter the blood, so that systemic effects and toxicity are greatly reduced.
Remember: The pharmacologic effects of mineralocorticoids include an increase in sodium retention and an increase in potassium depletion which can lead to edema and hypertension if excessive and may lead to dehydration and hypotension if insufficient.
• aldosterone
*** Cortisol, prednisone, dexamethasone, and triamcinolone are all glucocorticoids.
Aldosterone is secreted by cells located in the zona glomerulosa of the adrenal cortex. The secretion of aldosterone is regulated by ACTH and by the renin-angiotensin system and is very important in the regulation of blood volume and pressure. Aldosterone promotes reabsorption of sodium into the blood from the glomerular filtrate. Potassium is lost in the urine because of the electronegativity that is created by the reabsorption of sodium in the kidney tubules.
Note: Increased blood aldosterone levels will result in high sodium and low potassium levels in the plasma.
Remember: Decreased sodium concentration causes the juxtaglomerular cells of the kidneys to secrete renin, which converts angiotensinogen to angiotensin I. Angiotensin I is converted to angiotensin II, which, in turn, stimulates the adrenal cortex to release aldosterone.
1. Addison's disease is caused by the hyposecretion of aldosterone and corti-Notcs sol.
2. ADH (Vasopressin) decreases the production of urine by increasing the reabsorption of water by the renal tubules (it increases the permeability of the collecting ducts and distal tubules). Without ADH, there would be extreme loss of water into the urine.
3. At high concentrations, ADH causes arterioles to constrict (increases blood pressure).

corticosteroids
Which corticosteroid is administered by inhalation to treat asthma?
• hydrocortisone
• prednisone
• cortisone
• fluticasone (Flonase)
• methylprednisolone (Medrol)
151 copyright © 2013-2014 - Dental Decks
corticosteroids
Which of the following drugs are classified as corticosteroids (steroids).
Select all that apply.
• hydrocortisone
• methylprednisolone
• prednisone
• compazine
• fluoxetine
• triamcinolone
• dexamethasone
152 opyright © 2013-2014 - Dental Decks

• fluticasone (Flonase)
Corticosteroids in the inhaled form, decrease the inflammation in the airway in asthma. Reduction of inflammation enhances the bronchodilating effects of the beta2-adrenergic agonists.
The following are some of the other popular inhaled corticosteroids used in the treatment
of asthma: • Triamcinolone (Azmacort) • Beclomethasone (Beconase) • Budesonide (Pulmicort) • Flunisolide (AeroBid)
Note: Inhaled steroids very often cause a fungal infection of the mouth and throat.
Combination products used in the treatment of COPD and asthma include:
• albuterol/ipratropium (Combivent)
• fluticasone/salmeterol (Advair Diskus)
• budesonide/formoterol (Symbicort)
Important: Leukotriene modifiers act on inflammatory mediators of asthma, the LTs (also known as slow-reacting substance of anaphylaxis [SRS-AJ), which contributes to airway obstruction. There are two subclasses: (1) Leukotriene receptor antagonists which include montelukast (Singulair) and zafirlukast (Accolate) (2) 5-lipoxygenase inhibitor (leukotriene synthesis inhibitor) which includes zileuton (Zyflo).
• hydrocortisone • methylprednisolone • prednisone • triamcinolone • dexamethasone
*** Prochlorperazine (Compazine) is an anti-psychotic medication in a group of drugs called phenothiazines. Fluoxetine (Prozac) is a drug used in the treatment of depression.
Two types of corticosteroids: 1. Glucocorticoids affect carbohydrate, lipid, and protein metabolism. They are used to treat numerous disorders, primarily through their anti-inflammatory and immunosuppressive actions. 2. Mineralocorticoids regulate sodium and potassium metabolism.
1. These drugs are used to treat a variety of conditions which include asthma, arthritis, al-Notes lergies, aphthous stomatitis, lupus erythematosus, and TMJ pain.
2. Contraindications to their use include latent infections (fungal, viral, or bacterial), AIDS, herpes infections, gastric ulcers, and congestive heart failure. 3. Adverse reactions include Cushing's syndrome (obesity and weakening of muscles), hyperglycemia, osteoporosis, peptic ulcers, and an increased risk of infection. 4. Corticosteroids do not cure any disease.
Inhaled corticosteroids used for asthma do not achieve significant blood levels to cause the adverse effects listed above for systemic agents. Popular aerosol corticosteroids are triamcinolone (Azmacort), beclomethasone (Beconase), fluticasone (Flovent) and budesonide (Pulmicort). Localized infections with Candida albicans occur frequently in the mouth and pharynx with repetitive use of inhalant corticosteroids.
Nasal spray corticosteroids used for seasonal allergies also do not achieve significant blood levels, and are used for their localized effects. Popular nasal spray corticosteroid products are triamcinolone (Nasocort), fluticasone (Flonase) and budesonide (Rhinocort).

cardiovascular
All of the following drugs are direct vasodilators EXCEPT one. Which one is the EXCEPTION?
• hydralazine (Apresoline)
• diazoxide (Proglycem)
• captopril (Capoten)
• sodium nitroprusside (Nipride)
• nitroglycerin (Nitrostat)
PHARMACOLOGY
153 copyright©2013-2014-Dental Decks
All of the following drugs are used to prevent or to pectoris EXCEPT one. Which one is the EXCEPTION?
• nitroglycerin (Nitrostat)
• isoflurophate
• nifedipine (Procardia)
• diltiazem (Cardizem)
• propranolol (Inderal)
• isosorbide (Isordil)
cardiovascular
provide relief of angina
154 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• captopril (Capoten)
*** Captopril is an angiotensin-converting enzyme inhibitor.
Direct vasodilators exert their antihypertensive effect by a direct vasodilator action on the smooth muscle of arterioles, resulting in a decrease in peripheral resistance and blood pressure. Compensatory responses may be marked and include salt retention and tachycardia. Adverse side effects include GI upset, headache, dizziness and tachycardia.
Note: nitroprusside, diazoxide, hydralazine and nitroglycerin are parenteral vasodilators which are used in hypertensive emergencies.
Calcium channel blockers are also effective vasodilators (indirect) and have been applied to the management of hypertension. Verapamil (Calan SR), Nifedipine (Procardia), and Diltiazem (Cardizem) have been given orally for the treatment of mild to moderate hypertension.
Remember: Hydralazine and minoxidil are peripheral vasodilators.
• isoflurophate
*** Isoflurophate is an organophosphate cholinesterase inhibitor used in the treatment of glaucoma
Angina pectoris is pain in the heart and chest which occurs during the occlusion of coronary arteries. Triggers that can cause occlusion are physical exertion, increased blood pressure, and vasoconstriction. Antianginal drags work by reducing cardiac rate and force, reducing peripheral vascular resistance, or dilating coronary blood vessels.
Nitroglycerin is a coronary artery vasodilator. It relaxes blood vessels to provide increased blood flow and oxygenation to the heart muscle. It is sublingually effective within 2-4 minutes. The nitroglycerin skin patch releases the drag over a 12 hour period to provide sustained blood levels for prevention of angina. The two most common adverse effects caused by nitroglycerin are orthostatic hypotension and headache.
Nifedipine (Procardia) and diltiazem (Cardizem) are calcium channel blockers used to prevent angina attacks. These drags are used to dilate coronary blood vessels for improved blood flow to heart muscle. Note: Calcium channel blockers as a class have been associated with causing gingival hyperplasia.
Propranolol (Inderal) is representative of the beta-blockers used to prevent angina attacks. Atenolol (Tenormin) is another popular beta-blocker used for this purpose. Beta-blockers are used to decrease the work load of the heart such that less oxygen is required.

Amyl nitrite is used in the emergency treatment • it:
• oxidizes hemoglobin
• irreversibly binds cyanide
• competes with cyanide for binding of cytochromes
• inhibits tubular reabsorption of cyanide
cardiovascular
Df cyanide poisoning because
155 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
cardiovascular
The positive inotropic effect of Digoxin (Lanoxin):
is dependent upon a normal cardiac rhythm
directly increases the force of myocardial contractions
• is antagonized by beta-blockers
• all of the above
156 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• oxidizes hemoglobin
*** Amyl nitrite oxidizes hemoglobin to methemoglobin which binds cyanide tightly,
keeping it in the peripheral circulation and preventing its access to tissues.
Amyl nitrite is a vasodilator and a highly volatile substance administered by inhalation
only. It is the most rapidly acting of the antianginal drags, producing effects within 10
seconds. Its duration of action is only 3 to 5 minutes. Because of its extreme potency there are uncomfortable side effects that invariably occur with its use (fainting and a
pounding headache). Important: This drag is rarely prescribed and is not the first drag
of choice in treating angina. It is abused to produce euphoria and as a sexual stimulant.
Other antianginal drugs include:
1. Nitrate: Nitroglycerin
*** This drag is the single most effective agent available for the management of acute angina episodes. Note: It dilates mostly veins.
2. Non-nitrate vasodilator: Dipyridamole (Persantine)
3. Beta adrenergic blocking drugs: reduce cardiac rate and force • Propranolol (Inderal)
• Nadolol (Corgard)
• Atenolol (Tenormin)
4. Calcium channel blocking drugs: dilate peripheral and coronary blood vessels • Verapamil (Isoptin, Calan) • Diltiazem (Cardizem) • Nifedipine (Procardia)
• directly increases the force of myocardial contractions
*** This positive inotropic effect is independent of a normal sinus rhythm and adrenergic stimulation. The cardiac glycosides are often called "digitalis" because several come from the digitalis (foxglove) plant. Digoxin (Lanoxin) is the most versatile and widely used.
Note: They are used to treat most supraventricular arrhythmias, cardiogenic shock and chronic heart failure. These drugs help the heart beat more strongly (positive inotropic effect), more slowly (bradycardia) and more efficiently. Cardiac glycosides inhibit the Na+-K+-ATPase membrane pump by inhibiting the adenosine triphosphate enzymes (transport ATPase or Na-K-ATPase). Na+-K+-ATPase splits adenosine triphosphate in the nerve and muscle cell and thus provides the energy necessary for transporting sodium across the cell membrane. Key point: This inhibition of the Na+-K+-ATPase enzyme leads to an increased calcium ion influx which augments the positive inotropic effect of cardiac glycosides. Adverse side effects include nausea and vomiting, appetite loss, diarrhea, ventricular arrhythmias, heart block, and visual and mental disturbances. Contraindications to their use include ventricular fibrillation and ventricular tachycardia.
Drug interactions: Many drugs affect digoxin levels. However, digoxin does not affect the levels of other drugs. In addition, when beta-blockers are added to digoxin in patients with AV conduction abnormalities, complete heart block can result. Erythromycin, clarithromycin and tetracycline may increase digitalis absorption and toxicity. Thyroid replacement therapy increases dose requirements of digoxin. Drugs that lower plasma potassium levels (e.g., thiazide and loop diuretics) increase digitalis toxicity. Drug treatment of mild to moderate heart failure proceeds in the following order:(l) Diuretics in patients with fluid retention (2) ACEIs or ARBs in all patients unless contraindicated (3) Beta-blockers in all stable (minimal fluid retention) patients unless contraindicated and (4) Digoxin. Note: If these medications are not sufficient to control heart failure, the following additional drugs may be given: (1) Spironolactone (an aldosterone antagonist) (2) Nitrates and hydralazine and (3) Calcium channel blockers (i.e., amlodipine andfelodipine only)
Remember: Most drugs useful in treating cardiac arrhythmias act primarily by increasing the refractory period of cardiac muscle.

All of the following are EXCEPT one. Which one is
• captopril (Capoten)
• hydralazine (Apresoline)
• enalapril (Vasotec)
• lisinopril (Zestril)
• fosinopril (Monopril)
cardiovascular
angiotensin-converting enzyme (ACE) the EXCEPTION?
copyright©2013-2014
inhibitors
157 - Dental Decks
PHARMACOLOGY
All of the following drugs are Class II Which one is the EXCEPTION?
• propranolol (Inderal)
• acetbutolol (Sectral)
• metoprolol (Lopressor)
• verapamil (Calan)
PHARMACOLOGY
cardiovascular
antiarrhythmic agents EXCEPT one.
158 copyright © 2013-2014 - Dental Decks

• hydralazine (Apresoline)
*** Hydralazine is a direct peripheral vasodilator.
ACE inhibitors interfere with the conversion of angiotensin I (a weak vasoconstrictor) to angiotensin II (a highly effective constrictor). They do this by being inhibitors of angiotensin-converting enzyme (ACE). These drugs are used to treat hypertension and congestive heart failure. Adverse effects include cough, hypotension, neutropenia, anorexia and polyuria. Note: They can alter the sense of taste and in a few rare cases, cause angioneurotic edema.
Angiotensin II is a potent vasoconstrictor and is a stimulus for aldosterone release from the adrenal glands. Reduction in aldosterone secretion results in less water absorption and sodium/potassium exchange in the distal renal tubule, causing a slight increase in serum potassium. ACE inhibitors inhibit the breakdown of bradykinin, a potent and naturally occurring vasodilator, by blocking the enzyme kin-inase II. This though, is thought to be the cause of the cough commonly experienced by patients who take this class of drugs.
Other ACE inhibitors (ACEIs) include:
• Benazepril (Lotensin) • Moexipril (Univasc) • Quinapril (Accupril) • Captopril (Capoten) • Ramipril (Altace) • Trandolapril (Mavik) • Lisinopril (Zestril) • Elanapril (Vasotec)
Angiotensin II receptor blockers (ARBs) include:
• Losartan (Cozaar) • Eprosartan (Teveten) • Irbesartan (Avapro) • Valsartan (Diovan) • Olmesartan (Benicar) • Candesartan (Atacand) • Telmisartan (Micardis)
*** ARBs block the effects of angiotensin II by blocking the binding of angiotensin II to its receptors. They do not affect bradykinin. Adverse effects include dizziness, diarrhea and myalgia.
The antihypertensive effects of ARBs have been proven comparable with those of the ACEIs. ACEIs and ARBs are of particular values for the treatment of hypertensive patients who have concomitant illnesses such as diabetes, renal insufficiency, left ventricular dysfunction, and CHE
Note: ACE inhibitors and Angiotensin II receptor blockers indirectly inhibit fluid volume increases when interfering with angiotensin II because angiotensin II stimulates the release of aldosterone, which promotes sodium and water retention.
• verapamil (Calan)
The Vaughan-Williams classification system traditionally has been used to classify antiarrhythmic drugs. This scheme places the available agents into one of four classes, usually denoted by Roman numerals I - IV. This system is loosely based on the channel or receptor involved.
Class I: Sodium channel blockers • Class I drugs are further classified on the basis of their effects on action potential duration:
• IA agents include: Quinidine (Quinidex), procainamide (Procan SR) and disopyramide (Nor-pace). These agents prolong the action potential. • IB agents include: Lidoca.ine(Xylocaine), mexiletine (Mexitil) and tocainide (Tonocard. These agents shorten the action potential. • IC agents include: Flecainide (Tambocor) and propafenone (Rythmol). These agents have no effect on action potential duration.
Class II: Beta-adrenergic blockers - Propranolol (Inderal) is the prototype antiarrhythmic beta-blocker. Other drugs in this class include: esmolol (Brevibloc) acetbutolol (Sectral) and metoprolol (Lopressor). These agents increase refractory period, decrease conduction velocity and reduce automaticity.
Class III: Potassium channel blockers - Amiodarone (Cordarone) is the prototype drug in this class. Sotalol (Betapace), ibutilide (Corvert) and dofetilide (Tikosyn) are also in this class. These drags increase refractory period and reduce automaticity.
Class IV: Calcium channel blockers - Verapamil (Calan) is the prototype. Diltiazem is also included in this group. These drugs increase refractory period, decrease conduction velocity and reduce automaticity.
Note: Miscellaneous antiarrhythmic drags include: adenosine (Adenocard) which increases refractory period and reduces automaticity and digoxin (Lanoxin) which increases the force of contraction of the heart muscle and decreases conduction velocity.

cardiovascular
Amiodarone (Cordarone) is the most potent and "broad-spectrum"antiar-rhythmic compound currently available.
Procainamide is an antihypertensive drug used to treat high blood pressure.
• both statements are true
• both statements are false
• The first statement is true, the second is false
• The first statement is false, the second is true
159 copyright©2013-2014-Dental Decks
PHARMACOLOGY
cardiovascular
Verapamil is useful for the treatment of:
• angina
• hypertension
• supraventricular tachyarrhythmias
• all of the above
160 copyright©2013-2014-Dental Decks
PHARMACOLOGY

• the first statement is true, the second is false
Procainamide is a Class IA antiarrhythmic agent that is used in the treatment of several cardiac arrhythmias including atrial fibrillation, atrial flutter, paroxysmal atrial tachycardia, and ventricular tachycardia. It is not used as an antihypertensive. It is a derivative of the ester local anesthetic procaine. Procainamide has properties similar to those of other Class IA agents, quinidine and disopy-ratnide. These drugs decrease myocardial conduction velocity, excitability, and contractility by inhibiting the influx of sodium through "fast" channels of the myocardial cell membrane, thereby increasing the recovery period after repolarization. Note: Quinidine is primarily used to treat supraventricular tachyarrhythmias.
Remember: Generally speaking, the use of beta-blockers (Class II agents) as antiarrhythmics is reserved for patients who require only control of ventricular rate during atrial tachyarrhythmias or who have mildly symptomatic ventricular arrhythmias. Side effects include bradycardia and hypotension.
Important: Amiodarone (Cordarone) is generally considered a Class III agent even though it also blocks sodium channels, a Class I action. It is unique in that it is the most potent and "broad-spectrum" antiarrhythmic compound currently available. It blocks sodium, calcium, and potassium channels as well as beta receptors. It has impressive efficacy in suppressing both supraventricular and ventricular arrhythmias. Note: Adverse effects include pulmonary fibrosis, thyroid abnormalities, skin discoloration, and peripheral neuropathy.
, 1. Common adverse effects of some antiarrhythmics: 'Notes • Procainamide: mental changes, torsade de pointes (TDP - is an uncommon vari
ant of ventricular tachycardia) • Quinidine: hypotension, cinchonism (headache, ringing in the ears, deafness), and torsade de pointes • Lidocaine: convulsions • Propranolol: bronchoconstriction, heart block • Calcium channel blockers: flushing, headache, hypotension, gingival hyperplasia and reduced contractility of the heart
• all of the above
Verapamil is the prototypical Class IV (calcium channel blockers) antiarrhythmic agent. It inhibits the intracellular entry of calcium through the slow channels of the calcium dependent tissues of the myocardium, which are concentrated in the SA and AV nodes. It is the drug of choice for the suppression of paroxysmal supraventricular tachycardias stemming from the AV node (which is characterized by a rapid cardiac rate, usually 160-190 per minute). Of the calcium channel antagonists available, only verapamil and diltiazem possess significant antiarrhythmic activity.
Note: Calcium channel blockers (e.g., verapamil, diltazem and nifedipine) are useful as antianginal agents and antihypertensive agents as well. They block calcium entry through the membranous calcium ion channels of cardiac and vascular smooth muscle. This has three effects:
1. Peripheral arterioles dilate (vasodilators) and total peripheral resistance decreases, reducing after-load and reducing myocardial oxygen requirements. 2. Increases oxygen delivery to the myocardium. 3. Reduces blood pressure if hypertension is present.
Important: Nitrites (amyl nitrite) and nitrates (nitroglycerin) are fast-acting antianginal agents that are used to relieve acute anginal attacks.
Note: For angina, nitroglycerin and nifedipine are usually used before verapamil.
Drugs used in acute hypertension
Hypertensive emergencies (parenteral)
Sodium nitroprusside
Nitroglycerin
Trimethaphan
Diazoxide
Hydralazine
Hypertensive urgencies (oralpreferred)
Clonidine
Nifedipine
Captopril
Labetalol

cardiovascular
All of the following drugs are classified as low molecular weight heparin type anticoagulants EXCEPT one. Which one is the EXCEPTION?
< enoxaparin (Lovenox)
• dalteparin (Fragmin)
• tinzaparin (Innohep)
• clopidogrel (Plavix)
161 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
cardiovascular
All of the following drugs are classified as glycoprotein llb/llla inhibitor type of anti-platelet agents EXCEPT one. Which one is the EXCEPTION?
• abciximab (Reopro)
• anagrelide (Agrylin)
• eptifibatide (Integrilin)
• tirofiban (Aggrastat)
162 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

Notes
• clopidogrel (Plavix)
Clopidogrel (Plavix) inhibits blood clotting by inhibiting platelet aggregation in an irreversible manner.
1. These type of anticoagulants agents (low molecular weight heparins) are used to treat acute symptomatic deep vein thrombosis. They are used to prevent deep vein thrombosis following knee or hip surgery. 2. They are administered subcutaneously since they are unable to be absorbed from the GI tract. 3. Standard heparin consists of components with molecular weights ranging from 4,000 to 30,000 dal-tons with a mean of 16,000 daltons. Low molecular-weight heparins range in molecular weights from 2,000 to 8,000 daltons. 4. Heparin acts at multiple sites in the coagulation system and binds with antithrombin III at two specific sites, resulting in its anticoagulant effect. At the first site factor Xa is neutralized and at the second site factor Ha (thrombin) is neutralized. 5. Low molecular weight heparins have a small effect on partial thromboplastin time but strongly inhibit factor Xa (not Ha). 6. The antidote for heparin is protamine; the antidote for warfarin is vitamin K.
Some Anticoagulants
Class
Heparin group
Oral anticoagulants
Subclass
Heparin
Low molecular weight heparin
Heparinoids
Direct thrombin inhibitors
Generic/trade Name
heparin sodium.
enoxaparin/Lovenox
dalteparin/Fragmin
tinzaparin/Innohep
danap ar oid/Orgaran
fotidap arimix/ AriXtra
bivalirudin/Angiomax
argatroban/Argatrobari •
lepirudin/Refludan
warfarin/Cournadin
anisindione/Miradon
• anagrelide (Agrylin)
Glycoprotein Ilb/IIIa inhibitors are reversible anti-platelet agents used to prevent acute cardiac ischemic complications and used in patients with acute coronary syndrome. They are administered intravenously. These agents block the platelet glycoprotein Ilb/IIIa receptor, the binding site for fibrinogen, von Willebrand factor, and other ligands. Inhibition of binding at this final common receptor reversibly blocks platelet aggregation and prevents thrombosis. Platelet aggregation inhibition is reversible following cessation of the IV administration of the drug minutes after an intravenous infusion. Note: The glycoprotein Ilb/IIIa inhibitors have a rapid onset of action. Their maximal antiplatelet effect occurs within minutes after an intravenous infusion. Important: The most serious adverse effects of GPIIb/IIIa antagonists include major bleeding, intracerebral hemorrhage and thrombocytopenia.
Some Anticoagulants
Class
Platelet aggregation inhibitors
Platelet-reducing agent
Thrombolytic agents
Subclass
Traditional
Adensosine diphosphate-induced platelet-fibrinogen binding inhibitors
Platelet glycogen Ilb/IIIa inhibitors
Phosphodiesterase III inhibitors
Generic/trade Name
acetyl salicylic acid/aspirin
dipyri damo le/Persantine
c 1 opidogre l/Plavix
ticlopidine/Ticlid
abciximab/ReoPro
eptifibatide/Inte grelin
tiroiiban/Aggrastat
anagreli de/Agrylin
cilostazol/Pletal
alteplas e/Activase
reteplase/Retavase
streptokinase/Streptase
tenecteplase/TNKase
urokinase/Abbokinase

cardiovascular
All of the following drugs are classified as what type?
lepirudin (Reflidan) argatroban danaparoid (Orgaran) bivalirudin (Angiomax)
' adrenergic antagonists
• thrombin-inhibitor type anticoagulants
• thioxanthenes
• ACE inhibitors
PHARMACOLOGY
163 copyright © 2013-2014 - Dental Decks
cardiovascular
For a patient who is taking anticoagulants, what is the most valuable test used in evaluating the patient as a surgical risk?
PTT (Partial Thromboplastin Time)
PT (Prothrombin Time)
platelet count
164 copyright C 2013-2014 - Dental Decks
PHARMACOLOGY

• thrombin-inhibitor type anticoagulants
These agents are administered intravenously for prevention of post-operative deep vein thrombosis following elective hip replacement surgery; for prophylaxis or treatment of thrombosis m adults with heparin-induced thrombocytopenia.
Their mechanism of action is through the direct inhibition of thrombin within the coagulation pathway, thus inhibiting fibrin formation.
• PT (Prothrombin Time)
This test is a one-stage test for detecting certain plasma coagulation defects owing to a deficiency of factors V, VII, or X. Thromboplastin and calcium are added to a sample of the patient's plasma and simultaneously, to a sample from a normal control. The length of time required for clot formation in both samples is observed. Thrombin is formed from prothrombin in the presence of adequate calcium, thromboplastin, and the essential tissue coagulation factors. A prolonged PT therefore indicates deficiency in one of the factors, as in liver disease, vitamin K deficiency, or anticoagulation therapy with the drug Coumadin.
International Normalized Ratio (MR). Once prothrombin times are determined, they are expressed as an INR value. INR stands for International Normalized Ratio and essentially is the ratio of the prothrombin time measured in the patient divided by a standard prothrombin time value, and multiplied by a constant. An INR value of 1 means normal prothrombin times of approximately 12 seconds; normal blood clotting would be present. INR values greater than 1 indicate that there is an anticoagulant effect. The higher the INR value, the greater the anticoagulant effect. Many patients taking anticoagulants have INR values of 2,3 and even up through 6.

All of the following conditions are managed by anti-platelet agents EXCEPT one. Which
• coronary artery disease (CAD)
• angina pectoris (UnstableAngina)
• myocardial infarction (Heart Attack)
• stroke
• hypertension
cardiovascular
using anticoagulants and one is the EXCEPTION?
-
165 copyright© 2013-2014-Dental Decks
PHARMACOLOGY
cardiovascular
Which of the following class of drugs lower blood cholesterol levels by inhibiting a key enzyme in the cholesterol synthesis pathway in the liver?
• HPG-CoB Reductase Inhibitors
• HCG-CoG Reductase Inhibitors
• HMG-CoA Reductase Inhibitors
• HCG-CoB Reductase Inhibitors
16 copyright©2013-2014-Dental Decks
PHARMACOLOGY

r
• hypertension
Anticoagulants such as warfarin (Coumadin) and anti-platelet agents such as aspirin and clopidogrel (Plavix) are used in the conditions listed for the following reasons:
• Coronary artery disease (CAD): will help prevent threat of myocardial infarction in CAD patients. • Angina pectoris (unstable angina): will help prevent thrombus from forming within the coronary arteries. • Myocardial infarction (MI): drugs that prevent blood clotting have been shown to prevent the threat of future infarcts. • Stroke: will help prevent thrombus from forming thus preventing threat of a cerebral embolism.
Note: Unless there are other accompanying cardiovascular problems such as those listed above, anticoagulant drags are not necessary in the treatment and management of hypertension. These drugs do nothing to lower blood pressure.
• HMG-CoA Reductase Inhibitors
Coronary artery disease (CAD) is a condition of narrowing of the blood vessels of the heart restricting oxygen flow to heart muscle. It has been correlated with the levels of blood cholesterol and triglycerides. If not treated, CAD can lead to myocardial infarction (heart attack). Drugs such as the statins, which lower blood cholesterol are effective in minimizing the threat of CAD.
Currently, six classes of antihyperlipidemic drugs are available, and each class has its own mechanism for lowering lipid levels. Note: The two major lipoproteins that are targeted are VLDLs and LDLs. The primary lipids of VLDLs are the triglycerides, whereas the primary lipids of LDLs are cholesteryl esters. Higher levels of LDL increase the risk of cardiovascular disease, whereas higher levels of VLDL increase the risk of pancreatitis.
• HMG-CoA Reductase inhibitors: the enzyme 3-hydroxy-3-methylglutaryl coenzyme A (IIMG-CoA) reductase is necessary in the key step to synthesize cholesterol. When the "statin" drugs inhibit this enzyme, cholesterol is not produced in the liver and blood levels decrease. The family of "statin drugs" include atorvastatin (Lipitor), simvastatin (Zocor), fluvastatin (Lescol), lovastatin (Mevacor) pravastatin (Pravachol) and rosu-vastatin (Crestor).
' Fibric acid derivatives: their primary lipoprotein effect is to decrease triglyceride and raise HDL concentrations. They do this by increasing lipoprotein lipase activity, which results in increased catabolism of VLDL. Examples include gemfibrozil (Lopid) and fenofibrate (TriCor).
• Bile acid sequestrants: these drugs bind to bile acids; bile acid sequestrants increase the diversion of cholesterol to bile acid synthesis, lower intracellular stores of cholesterol, and result in increased catabolism of LDL by the liver. Examples include cholestyramine (Questran), and colesevelam (WelChol).
• Other agents: nicotinic acid (niacin) is believed to act on a hormone-sensitive lipase; this leads to inhibition of release of free fatty acids from adipose tissue (lipolysis). The inhibition of lipolysis leads to reduced free fatty acid transport to the liver and therefore decreased synthesis of VLDL.
• Combination products: examples include lovastatin/niacin (Advicor) and ezetimibe/simvastatin (Vytorin).
• Selective cholesterol absorption inhibitors: ezetimibe (Zetia) is the first agent in a new class of drugs that appear to act on the brush border of intestinal epithelial cells, where it selectively inhibits the absorption of cholesterol from dietary and biliary sources.
Important: The "statin" drugs have the capability to increase the breakdown of skeletal muscle thereby releasing muscle protein. If the protein overloads the kidneys, renal failure could result. The erythromycin drugs enhance the capabilities of the "statins" to cause this effect. It is advisable for patients medicated with a "statin" drug not to be given erythromycin products.

cardiovascular
Antihypertensive agents lower blood pressure by reducing total peripheral resistance and by reducing cardiac output through a variety of mechanisms.
ACE inhibitors inhibit the conversion of inactive angiotensin I to the angiotensin II, a vasoconstrictor.
• both statements are true
• both statements are false
• the first statement is true, the second is false
• the first statement is false, the second is true
PHARMACOLOGY
167 copyright O 2013-2014 - Dental Decks
Which of the drugs below can prolong conduction and thus can increase the ri
• erythromycin
• ibuprofen
• hydrocodone
• penicillin VK
• azithromycin (Z-Pak)
PHARMACOLOGY
cardiovascular
the QT interval of cardiac electrical sk of cardiac arrhythmias?
168 copyright©2013-2014-Dental Decks

• both statements are true
Antihypertensive agents are classified by mechanisms of action: • Diuretics: include thiazide and thiazide-like ([NaCl] inhibitors) such as hydrochlorothiazide (HCTZ) and loop diuretics such as furosemide (lasix) and bumetanide (Bumex). These drugs inhibit sodium reabsorption in renal tubular cells within the kidney to cause excess sodium and urinary excretion resulting in reduced blood volume.
• Beta-adrenergic receptor blockers (beta-blockers): reduce the volume of cardiac output into the circulation resulting in reduce peripheral pressure. Two types:
1. Cardioselective beta-blockers (betaj-receptor block in heart muscle): examples include atenolol (Tenormin), metoprolol (Lopressor; ToprolXL), acebutolol (Secral), esmolol (Brevibloc) 2. Non-cardioselective (betaj and beta^ beta-blockers: examples include nadolol (Corgard), propranolol (Inderal), timolol (Betimol), penbutolol (Levatol), and sotalol (Betapace) *** Note: labetalol (Trandate) and carvedilol (Coreg) are non-selective beta-blockers that also block alphaj receptors.
• Alpha-adrenergic receptor blockers: cause dilation of arterioles and veins and reduce peripheral vascular resistance.Two types:
1. Cardioselective alpha-blockers (alpharreceptor blockers): examples include doxazosin (car-dura), prazosin (Minipress) and terazosin (Hytrin). 2. Non-cardioselective (alphaj and alphaj alpha-blockers: examples include phentolamine (Regit-ine) and phenoxybenzamine (Dibenzyline).
• Angiotensin-converting enzyme inhibitors (ACEInhibitors): examples include lisinopril (Prinivil; Zestril), ramipril (Altace) and enalapril (Vasotec): inhibit the conversion of inactive angiotensin I to the angiotensin II, a vasoconstrictor. This results in peripheral vasodilation and secondarily, an increase in urinary volume excretion. Both actions result in reduced blood pressure.
• Angiotensin II receptor blockers (ARBs): examples include losartan (Cozaar), valsartan (Dio-van), and candesartan (Atacand). ARBs block the effects of angiotensin II by blocking the binding of angiotensin II to its receptors. They do not effect bradykinin.
• Calcium channel blockers examples include Verapamil (Calan), amlodipine (Norvasc), diltiazem (Cardizem), and nifedipine (Procardia): inhibit calcium entry into vascular smooth muscle causing vasodilation of coronary and peripheral blood vessels thus lowering blood pressure.
• erythromycin
Erythromycin is one of the drugs confirmed to prolong the QT interval and is accepted as having a risk of causing arrhythmias. The QT interval is measured as the time and distance between the Q point of the QRS complex and the end of the T wave in the ECG tracing. A long QT syndrome was first described in the 1950's as a congenital syndrome involving QT interval prolongation and syncope and sudden death. These congenital long QT syndromes were characterized by a peculiar electrocardiographic appearance of the QRS complex involving a premature atria beat followed by a pause, then a subsequent sinus beat showing marked QT prolongation and deformity. This type of cardiac arrhythmia was originally termed "torsade de pointes" (from thefrench "twisting of the points ").
Erythromycin, an antibiotic used to treat bacterial infections, is considered as having a risk of causing torsade de pointes, an unusual adverse reaction for an antibiotic.
Clarithromycin, an antibiotic within the erythromycin family also causes prolongation of the QT interval.
Azithromycin, another member of the erythromycin family of antibiotics is not associated with prolonging the QT interval.

cancer/chemo Exemestane (Aromasin) and letrozole (Femara) are anticancer drugs classified under what category listed below?
• antibiotics
• aromatase inhibitors
• antimetabolites
• alkylating agents
• antimicrotubular
169 copyright e 2013-2014 - Dental Decks
PHARMACOLOGY
cancer/chemo
Alkylating agents are most effective in treating all of the following EXCEPT one. Which one is the EXCEPTION?
• chronic leukemias
• lymphomas
• AIDS
• myelomas
• carcinomas of the breast and ovary
170 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• aromatase inhibitors
Exemestane is an irreversible, steroidal aromatase inactivator. It prevents conversion of androgens to estrogens by tying up the enzyme aromatase. In breast cancers where growth is estrogen dependent, this drug will lower circulating estrogens.
Exemestane is used in the treatment of advanced cancer in post menopausal women whose disease has progressed following tamoxifen therapy.
Letrozole (Femora) works by a similar mechanism as above. It is used as first line treatment of hormone receptor positive or metastatic breast cancer in postmenopausal women. It is also indicated as an extended adjuvant treatment of early breast cancer in postmenopausal women who have received 5 years of adjuvant tamoxifen therapy.
AIDS
The alkylating agents contain a diverse group of compounds which all form alkyl bonds to nucleic acids. All of these agents share a similar mechanism of action and mechanism of resistance. The alkylating agents form covalent bonds with nucleic acids, and proteins. The N-7 position of guanine is a common binding site.
Major Alkylating Agents
Drug
Nitrogen Mustards: Mechlorethamine (Mustargen) Cyclophosphamide (Cytoxan)
Chlorambucil (Leukeran) Melphalan (Alkeran)
Nitrosoureas: Carmustine (BCNU.BiCNU) Lomustine (CCNU, CeeNU) Semustine (Methyl-CCNU)
Busulfan (Myleran)
Use
Hodgkin's disease and other lymphomas Lymphomas, leukemias, multiple myeloma, neuroblastoma, retinoblastoma, and cancers of the breast and ovary Chronic lymphocytic leukemia Hodgkin's disease and other lymphomas
Several types of cancer, including brain cancer Several types of cancer, including brain cancer and Hodgkin's disease Several types of cancer, including brain cancer
Chronic myelogenous leukemia

cancer/chemo The following drugs belong to what pharmaceutical class of agents:
Darbepoetin alpha Pegfilgrastim Sargramostin
• immune modulators
• monoclonal antibodies
• colony stimulating factors
• interferons
• immunosuppressants
PHARMACOLOGY
171 copyright © 2013-2014 - Dental Decks
cancer/chemo
Name the eight classes of drugs used in cancer chemotherapy.
172 copyright © 2013-2014 - Dental Decks

• colony stimulating factors
These drugs stimulate the production of neutrophils and erythroid progenitor cells in the hematopoietic process.
Colony stimulating factors: • Darbepoetin alpha: induces erythropoiesis by stimulating the division and differentiation of erythroid progenitor cells. It is used to treat anemia associated with chronic renal failure.
• Pegfilgrastim (Neulasta): stimulates the production, maturation and activation of neutrophils. It is used to decrease the incidence of infection by stimulation of granulocyte production in patients with nonmyeloid malignancies.
• Sargramostin (Leukine): is used for myeloid reconstitution after autologous bone marrow transplantation.
Listed below are the eight classes of drugs used in chemotherapy: 1. Alkylating agents - these agents alkylate DNA such that it cannot replicate. Popular agents include Cisplatin and Cyclophosphamide. 2. Anthracyclines - these agents destroy DNA such that the cell cannot replicate. Popular agents include Daunorubicin and Doxorubicin. 3. Antibiotics - these antibiotics are not used for antibacterial therapy but were specifically designed for cancer chemotherapy. The agent in this class is Dactinomycin. 4. Antimetabolites - these agents interfere which selected biochemical reactions necessary for cell growth. Popular agents are 5-Fluorouracil (5-FU), 6-Mercaptopurine and Methotrexate. 5. Antimicrotubular - affects the microtubular assembly with cells to inhibit cell mitosis. The popular agent is Paclitaxel (Taxol). 6. Antiestrogen - these agents block the tumors on which estrogen has a stimulatory effect. The popular agent is Tamoxifen (Nolvadex). 7. Vinca Alkaloids - these are mitotic spindle poisons. Examples include Vinblastine and Vincristine. 8. Gonadotropin hormone-releasing antigen - these inhibit gonadotropin secretion, an action which is effective in reducing certain carcinomas. The popular agent is Leuprolide.
Note: The anticancer drugs Asparaginase and Interferons do not fall within any category but are used in the treatment of certain cancers. Asparaginase deprives tumor cells of certain amino acids such that protein production is blocked. Interferons boost the immune system.
Agents used in treating breast cancer: • Antiestrogens: tamoxifen (Nolvadex), fulvestrant (Faslodex), and toremifene (Fareston). • Aromatase inhibitors: letrozole (Femara) and exemestane (Aromasin)

cancer/chemo
Your patient with a history of breast cancer is undergoing chemotherapy with a drug called cisplatin (Platinol). All of the following are expected adverse effects of cisplatin EXCEPT one. Which one is the EXCEPTION?
• nausea and vomiting
• hair loss (alopecia)
• blood test abnormalities (low magnesium, low calcium, low potassium)
• peptic ulcers
• changes within the tissues of the oral cavity such as mucositis
• low white blood cells
• low red blood cells (anemia)
• xerostomia 173
copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
cancer/chemo
Antimetabolites are cell cycle-specific drugs acting primarily in the:
• G0 phase or resting phase of the cell cycle
• S phase of the cell cycle
• G-, phase of the cell cycle
• G2 phase of the cell cycle
174 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• peptic ulcers
Cisplatin is an anti-cancer ("antineoplastic") chemotherapy drug. It is classified as an "alkylating agent."
Remember: Alkylating agents - these agents alkylate DNA such that it cannot replicate. Popular agents include Cisplatin and Cyclophosphamide.
Notes about cisplatin side effects (and most chemotherapy drugs): • Most people do not experience all of the side effects • The side effects are often predictable in terms of their onset and duration • The side effects are almost always reversible and will go away after treatment is complete. • The side effects and their severity depend on how much of the drug is given. In other words, high
doses may produce more severe side effects.
The most common side effects of chemotherapy are: • Anemia • Fatigue • Hair loss • Increased chance of bruising, bleeding, and infection • Nausea and vomiting
• Low WBCs • Xerostomia • Mucositis
Other less common side effects include: • Appetite and weight changes • Nerve and muscle problems • Dry and/or discolored skin
• Kidney and bladder irritation • Sexual and fertility issues because of effects on reproductive organs
Note: Mucositis is a common reaction to cancer chemotherapy. It is an inflammation of the mucous membranes. During chemotherapy and radiation therapy, mucosal tissues begin to desquamate and develop into ulcerations. The mucosal integrity is broken and is secondarily infected by oral flora. Palliative treatment is indicated for mucositis. The antineoplastics such as 5-fluorouracil (5FU), methotrexate and doxorubicin are commonly associated with the development of oral mucositis.
• S phase of the cell cycle
The S phase of the cell cycle = DNA synthesis
Antimetabolites are one of the oldest and most important classes of antineoplastic agents. They attack the cells in the S phase of the reproduction cycle by interfering with the biosynthesis of the purine and pyrimidine bases.
Antimetabolites used as Antineoplastic Agents niiuu.™™,, "•» »" "• " "-"l" » v " 5 V
Drug
Folic acid analog: Methotrexate (Amethopterin)
Pyrimidine analogs: Fluorouracil (5-FU) Floxuridine (FUDR) Cytosine arabinoside (Cytosar-U)
Purine analogs: Mercaptopurine (Purinethol) Thioguanine (6-TG, Tabloid)
Use
Choriocarcinoma, leukemia in the spinal fluid, osteogenic sarcoma, breast cancer, and head and neck cancer
Several types of cancers including colon and head and neck cancers Some cancers involving the liver Treating acute leukemias
Treating several types of leukemias Treating acute nonlymphocytic leukemia
Important: Alopecia (hair loss) occurs with the administration of most chemotherapeu-tic agents one to two weeks after treatment. Other common side effects include GI upset, increased incidence of infection (especially Candidiasis), and degeneration of lymphatic tissue.
Remember: Most chemotherapy drugs have been shown to be teratogenic in humans and should be avoided by pregnant women.

The prototype loop diuretic is:
• hydrochlorothiazide (HCTZ)
• furosemide (Lasix)
• spironolactone (Aldactone)
• triamterene (Dyrenium)
diuretics
175 copyright 0 2013-2014 - Dental Decks
PHARMACOLOGY
Which of the following is a pharmacologic collecting tubule?
• mannitol (Osmitrol)
• glycerin (Glyrol)
• spironolactone (Aldactone)
• urea (Ureaphil)
PHARMACOLOGY
diuretics
: antagonist of aldosterone in the
176 copyright<S2013-2014-Dental Decks

• furosemide (Lasix)
Diuretics are used to treat congestive heart failure by relieving edema and symptoms of dyspnea arising from pulmonary congestion. They are also used to treat hypertension, and in the management of edema associated with hepatic or renal disease.
Categories of widely used diuretics: • Thiazides: inhibit sodium reabsorption in the distal portion of the renal tubule within the kidney causing increased excretion of sodium and water. Prototype agent is hydrochlorothiazide (HCTZ). Other examples include chlorothiazide (Diuril), indapamide (Lozol), and metolazon (Zaroxolyn). Note: These drugs can cause hypokalemia (abnormally low level of potassium in the blood) , hyponatremia (abnormally low level of sodium in the blood) and may increase plasma uric acid. • Loop diuretics: inhibit reabsorption of sodium and chloride in the ascending Loop of Henle thus causing increased secretion of water, sodium and chloride. Prototype agent is furosemide (Lasix). Other examples include bumetanide (Bumex), ethacrynic acid (Edecrin), and torsemide (Demadex). Note: These drugs can cause hyperuricemia, tinnitus, hearing loss, hyponatremia and excessive fluid loss. • Potassium-sparing diuretics:
• Sodium channel blockers: these agents inhibit sodium reabsorption through sodium channels in renal epithelial cells. This inhibition creates a negative potential in the luminal membranes of principal cells, located in the distal convoluted tubule and collecting duct. Negative potential reduces secretion of potassium and hydrogen ions. Conserve potassium while causing diuresis. Thus, no potassium is lost from the body as is the case with other diuretics such as the thiazides and loops. Triamterene (Dyrenium) and amiloride (Midamor) are examples of this drug group. • Aldosterone antagonists: these drugs competitively inhibit the aldosterone receptor. This causes increased amounts of sodium and water to be excreted, while potassium is retained. Spironolactone (Aldactone) and eplerenone (Inspra) are examples.
*** Fixed-dose combination therapy: Dyazide is the brand name for the combination of triamterene and hydrochlorothiazide (HCTZ). This product combines the potassium-sparing diuretic with HCTZ for greater efficacy than either one individually.
Note: Positive inotropic drugs (drugs that make muscle contract more forcefully) can be used in the acute treatment of heart failure, these include dobutamine, dopamine, inamrinone, and milrinone. These drugs may be given intravenously to stimulate heart contractions and help keep blood circulating. They are only used temporarily because long-term use shortens life.
• spironolactone (Aldactone)
Potassium-sparing diuretics result in increased sodium and decreased potassium concentrations at the end of the distal convoluted tubules. There are two categories of potassium-sparing diuretics:
1. Antagonist of aldosterone in the collecting tubules: • Spironolactone (Aldactone)
Note: Spironolactone has been found to be effective in the treatment of primary aldosteronism. It may be useful in the treatment of heart failure because hyperal-dosteronism is commonly seen in this condition.
2. Block the sodium channels in the collecting tubules:
• Triamterene (Dyrenium) • Amiloride (Midamor)
*** The most important toxic effect of potassium-sparing diuretics is hyperkalemia.
Osmotic diuretics are highly filtered by the glomerulus and exert a solute-induced diuresis in the proximal tubule. They are used to reduce excess edema associated with neurosurgery or trauma to the CNS. Examples include: mannitol, glycerin, and urea.
Remember: Carbonic anhydrase inhibitors (i.e., Acetazolamide) are relatively weak diuretics because of the ability of more distal sites in the loop of Henle to increase their reabsorption of sodium. Note: Acetazolamide is used to prevent and reduce the symptoms of altitude sickness.

All the following drugs are second Which one is the EXCEPTION?
• glyburide (DiaBeta)
• metformin (Glucophage)
• glipizide (Glucotrol)
• glimepiride (Amaryl)
-generation
hypoglycemics
sulfonylureas EXCEPT one.
177 copyright © 2013-2014- Dental Decks
PHARMACOLOGY
hypoglycemics
Insulin regular, also known as Humulin R, is considered a/an:
• short-acting insulin with a duration of 6-8 hours
• long-acting insulin with a duration of 20-24 hours
• intermediate-acting insulin with a duration of 10-16 hours
• rapid-acting insulin with a duration of 3-4 hours
178 copyright©2013-2014-Dental Decks

• metformin (Glucophage)
*** Metformin is classified as a biguanide
Antidiabetic agents or oral hypoglycemic agents are drugs used as adjuncts to diet to treat non-insulin dependent diabetes mellitus (type 2 diabetes) that cannot be controlled by diet alone.
• Sulfonylureas, the first drug group introduced into the U.S. in 1955, close potassium channels in cell membranes, stimulate the beta cells to produce more insulin., and increase the sensitivity of target organs to insulin.
• The original "first generation" sulfonylureas include tolbutamide (Orinase), tolazamide (Tali-nose), and chlorpropamide (Diabinese). These drugs work well in lowering the blood sugar, but they have a major drawback. Because they bind to proteins in the blood, they can be dislodged by other medications that bind to these same proteins. Once dislodged, their activity can increase rapidly and lead to low blood sugars.
• Second generation sulfonylureas include glipizide (Glucotrol), glyburide (Micronase) and glimepiride (Amaryl). These drugs have an advantage for those who use other medications since they do not bind to carrier proteins in the blood. Because of this, drug interactions that may cause low blood sugars are less likely.
• Biguanides: metformin (Glucophage) primarily decreases hepatic glucose production. It also has minor effects on insulin sensitivity in both the liver and peripheral tissues. It has no direct effect on the pancreas and therefore does not enhance insulin secretion.
• Thiazolidinediones: rosiglitazone (Avandia) and pioglitazone (Actos) increase sensitivity in the muscle and liver by improving control of glycemic utilization. This in turn reduces circulating insulin levels. Note: Functioning beta-cells are required for these medications to work.
• Meglitinides: repaglinide (Prandin) and nateglinide (Starlix) lower blood sugar by stimulating the release of insulin from the pancreas in short bursts. Note: Functioning beta-cells are required for these medications to work.
• a-Glucosidase inhibitors: acarbose (Precose) and miglitol (Glyset) act through inhibition of pancreatic a-amylase and membrane-bound intestinal a-glucoside hydrolase enzymes. This enzyme inhibition delays glucose absorption. These enzymes do not enhance insulin secretion.
• short-acting insulin with a duration of 6-8 hours
Insulin preparations mimic the activity of endogenous insulin, which is required for the proper
utilization of glucose in normal metabolism. They are used in type 1 diabetes and in type 2 di
abetes which cannot be controlled completely by the oral antidiabetic drugs or by diet alone.
Impor apy. S3 Admin
Rapid-acting
Insulin aspart (NovoLog)
Insulin glulisine (Apidra)
Insulin lispro (Humalog)
Short-acting
Insulin regular (Humulin R)
Intermediate-acting
NPH (Humulin N)
Long-acting
Insulin detemir (Levemir)
Insulin glargine (Lantus)
Onset
5-15 min
5-15 min
5-15
30-60 min
2-4 hours
1 hour
2 hours
Peak
1-3 hours
30-90 min
30-90 min
2-4 hours
6-10 hours
No peak
No peak
Duration
3-5 hours
3-4 hours
3-4 hours
6-8 hours
10-16 hours
6-24 hours
20-24 hours
tant: Hypoglycemia (low blood sugar) is the most serious complication of insi /mptoms include: sweating, weakness, confusion, slurred speech and blurrec istration of a concentrated glucose source will relieve mild hypoglycemia.
tlin ther-I vision.

All of the following are effects of EXCEPTION?
• decreased gluconeogenesis
• increased triglyceride storage
• decreased protein synthesis
• increased glycogen synthesis
PHARMACOLOGY
insulin EXCEPT
hypoglycemics
one. Which one is the
179 copyright <B 2013-2014 - Dental Decks
hypoglycemics
Humulin 70/30 is the brand name for a mixture of insulins containing: 70% insulin NPH and 30% regular insulin injection. The advantage of this insulin mixture is which of the following?
• fast onset, short duration
• slow onset, short duration
• fast onset, long duration
• slow onset, long duration
180 copyrighte>2013-20l4-Dental Decks
PHARMACOLOGY

decreased protein synthesis
*** This is false; insulin increases protein synthesis.
Insulin is a pancreatic hormone secreted by the pancreatic beta-cells of the islets of Langerhans and is essential for the metabolism of glucose and for the homeostasis of blood glucose (it reduces blood glucose by increasing the conversion to glycogen and fat). Insulin injection is by subcutaneous administration.
Remember: Insulin is required in treating type 1 diabetes mellitus because the beta cells of the pancreas are devoid of insulin. In treating type 2 diabetes mellitus, oral hypoglycemics can often be used because the beta cells are able to secrete insulin, although in a more sluggish manner.
• fast onset, long duration
Humulin 70/30 mixture is a popular form of insulin that many diabetic patients take. Its advantage is that after a single injection, the regular insulin component (30%) provides a fast onset of blood sugar control beginning one-half hour after injection and the insulin NPH component (70%) starts acting within a couple of hours to provide a long duration of blood sugar control.
Note: Using either agent alone would not provide both the fast onset of insulin action along with the long duration.
Premixe rapid-ac the bran
Mixtures
Humulin 70/30
Novolin 70/30
Novolog 70/30
Humulin 50/50
Humalog 75/25
Onset
30 min
30 min
10-20 min
30 min
15 min
Peak
2-4 hours
2-12 hours
1-4 hours
2-5 hours
30 min-2hours
Duration
14-24 hours
Up to 24 hours
Up to 24 hours
18-24 hours
16-20 hours
d insulins are a combination of specific proportions of intermediate-act ting or short-acting insulin in one bottle or insulin pen (the numbers fo d name indicate the percentage of each type of insulin).
ng and 'lowing

misc. Which of the following is a high molecular weight heteropolysaccharide that inactivates thrombin and other coagulation factors and thus prevents blood clotting?
• prothrombin
• fibrin
1 heparin
• plasmin
181 copyright O 2013-2014- Dental Decks
PHARMACOLOGY
misc.
The following drugs are classified as what type of drugs? Etanercept (Enbrel) Infliximab (Remicade) Adalimumab (Humira)
• anti-anxiety agents
• anti-malarial agents
• immunosuppressants
• anti-rheumatic agents
182 copyright © 2013-2014 - Dental Decks

• heparin
Heparin is contained within mast cells and basophils. These cells occur in connective tissue and in extracellular spaces near blood vessels.
Remember: Heparin not only neutralizes tissue thromboplastin, but also blocks thromboplastin generation.
1. The administration of heparin will result in an increase in bleeding time due Notes to a potentiation of antithrombin III thereby inactivating thrombin. This pre
vents the conversion of fibrinogen to fibrin. 2. It is used for prophylaxis and treatment of thromboembolic disorders.
• anti-rheumatic agents
There are currently three tumor necrosis factor alpha (TNF) inhibitors FDA approved for the treatment of RA (listed in order of their approval for RA):
• Etanercept (Enbrel) is used to reduce the signs and symptoms of active rheumatoid arthritis in patients who have had inadequate response to one or more disease-modifying anti-rheumatic drugs (DMARDs). It is a recombinant DNA-derived protein which binds to tumor necrosis factor alpha (TNF).
• Infliximab (Remicade) is used to treat Crohn's disease and rheumatoid arthritis. Infliximab is a chimeric monoclonal antibody that binds to tumor necrosis factor alpha (TNF) thereby reducing the inflammatory actions of this endogenous compound.
• Adalimumab (Humira) is a fully human anti-TNP monoclonal antibody with high specificity for TNF. Adalimumab binds specifically to TNF and blocks its interaction with the p55 and p75 cell surface TNF receptors, thereby interfering with endogenous TNF activity. Adalimumab binds to both soluble as well as cell bound TNF. It is administered by subcutaneous injection every two weeks but can be increased to weekly, if needed. Adalimumab is effective in RA, Psoriatic arthritis, and ankylosing spondylitis, and Crohn's disease.
Note: Tumor necrosis factor alpha (TNF) is a pro-inflammatory cytokine produced by macrophages and lymphocytes. It is found in large quantities in the rheumatoid joint and is produced locally in the joint by synovial macrophages and lymphocytes infiltrating the joint synovium. TNF is one of the critical cytokines that mediate joint damage and destruction due to its activities on many cells in the joint as well as effects on other organs and body systems.

misc. Triazolam (Halcion), a pre-operative sedative in dentistry, is metabolized in the liver by the P-450 isoform CYP 3A4 enzyme. Drugs which inhibit the actions of CYP 3A4 would affect triazolam in which way?
• cause an increase in serum levels of triazolam
• cause a decrease in serum levels of triazolam
• cause no change in serum levels of triazolam
183 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc. When writing a prescription, b.i.d. is the abbreviation for:
• twice a day
• every 4 hours
• three times a day
• four times a day
184 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• cause an increase in serum levels of triazolam
Triazolam is known to interact with drugs that inhibit its metabolism via the CYP 3 A4 enzyme. Drugs that inhibit the metabolic pathway may have a profound effect on the clearance of triazolam. The resultant effects would be an increase in serum concentrations with an associated unexpected increase in the actions of triazolam. Consequently, triazolam should be avoided in patients receiving very potent inhibitors of CYP 3A4.
For example, antifungal agents (itraconazole, ketoconazole, fluconazole, miconazole, voriconazole) can significantly elevate the serum levels of triazolam resulting in toxicity with therapeutic doses. These antifungal agents inhibit the CYP 3 A4 isoform responsible for hepatic metabolism of triazolam. Thus the normal metabolism of triazolam is inhibited.
Do not administer triazolam to patients taking any of these antifungal agents.
• twice a day
Other popular and common abbreviations used when writing prescriptions:
• b.i.d. = twice a day • t.i.d. = three times a day • q.l2.h. = every 12 hours • q.4.h. = every 4 hours • stat. = immediately • h.s. = at bedtime • p.r.n. = as needed • a.c. = before meals • p.c. = after meals • p.o. = by mouth • Sig. = Label
Note: Always document prescriptions that are given to a patient in the patient's chart, along with the date they were written and any specific instructions for patient use.
Remember: • 1 grain = 65 mg • 1 ounce = 30 g or 30 mL

misc. All of the following drugs are useful in treating what medical condition?
pilocarpine (Isopto-Carpine) latanoprost (Xalatan) betaxolol (Betoptic) bimatoprost (Lumigan)
• pinkeye
• blepharitis
glaucoma
• uveitis
185 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
The following drugs are noted for causing what prominent oral side effect?
amitriptyline (Elavil) diphenhydramine (Benadryl) atropine diazepam (Valium)
geographic tongue
• xerostomia
• mucositis
• desquamative gingivitis
186 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• glaucoma
Glaucoma is characterized by an increase in intraocular pressure. It is caused by poor drainage of the aqueous humor (fluid in the eye) and can cause blindness.
• Pilocarpine (Isopto-Carpine): eye drops in the eyes causes papillary constriction thus allowing for drainage of the aqueous humor to reduce pressure • Latanoprost (Xalatan): a prostaglandin analog; eye drops in the eye reduces intraocular pressure by increasing the outflow of the aqueous humor • Betaxolol (Betoptic): a beta-blocker; eye drops in the eye reduces intraocular pressure by reducing the production of aqueous humor • Bimatoprost (Lumigan): same action as latanoprost (Xalatan)
• xerostomia
Xerostomia can be caused by certain drag classes that inhibit the production and secretion of saliva.
•Amitriptyline (Elavil) is representative of the tricyclic antidepressants, a class of drugs that causes significant xerostomia. They probably work through an anticholinergic action. • Diphenhydramine (Benadryl) is representative of the sedating-type antihistamines, a class of drugs that causes significant xerostomia. They probably work through an anticholinergic action. • Atropine is a powerful anticholinergic which blocks the production of saliva in the salivary glands. Other anticholinergics will have a similar action.
• Diazepam (Valium) is representative of the benzodiazepine tranquilizers. These drugs have moderate anticholinergic actions to reduce the outflow of saliva.
Note: The xerostomia actions produced by these classes of drugs are reversible with normal salivary flow regained after discontinuation of the drag.
Management of Salivary Dysfunction
Moisture /Lubrication
General - Drink: sip water, other liquids (that lack fermentable carbohydrate and carbonic acid) - Avoid ethanol, tobacco, coffee, tea, and hot spicy foods - Use sugarless candy/gum
Over-the-counter (OTC) products - Oral balance: apply 1/2 tsp. 5 to 6 times daily
Prescription (Rx) products - Pilocarpine HCL 2% (Salagen) 5mg 3 or 4 times daily - Anethole trithione (Sialor) 25mg 3 times daily - Bethanechol chloride (Urecholine)25mg 3 times daily - Cevimeline (Evoxac) 30mg caps 3 times daily - Artificial salivas: Glandosane Spray, Moi-Stir, Mouthkole, Optimoist, Roxane Saliva Substitute,
Salivart Spray, Salix Lozenges, or generic (sodium carboxymethylcellulose 0.5% aqueous solution)

misc. Levodopa is used in the treatment of Parkinson's disease to replenish the brain's supply of serotonin, the neurotransmitter that is deficient in this disorder.
Administering carbidopa in combination with levodopa reduces the required dose of levodopa by about 75%.
• both statements are true
• both statements are false
• the first statement is true, the second is false
• the first statement is false, the second is true
187 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
Which antiarrhythmic agent is effective only on the ventricle and is often administered IV to treat life-threatening ventricular arrhythmias?
• quinidine (Quinidex)
• lidocaine (Xylocaine)
• flecainide (Tambocor)
• propafenone (Rythmol)
• none of the above
copyright ©2013-2014-
188 Dental Decks
PHARMACOLOGY

• the first statement is false, the second is true
*** Levodopa is used in the treatment of Parkinson's disease to replenish the brain's supply of dopamine, the neurotransmitter that is deficient in this disorder.
Parkinson's disease (PH) results from a relative excess of cholinergic activity and a deficiency of dopaminergic activity in the basal ganglia. It is a chronic, debilitating disease with no known cure. Drug treatment for PD has centered on increasing the availability of dopamine in the CNS, inhibiting the effects of acetylcholine, and attempting to prevent further cell membrane damage through neuroprotective trials. Note: The D2~recep-tor subtype is the primary modulator of both clinical improvement and adverse reactions such as dystonia and hallucinations.
Levodopa has been the single most important drug in the treatment of PD. Administering carbidopa in combination with levodopa (Sinemet) reduces the required dose of levodopa by about 75%. When levodopa is given alone, much of the dose is metabolized before the drug reaches the brain. Therefore, large doses are required, and these are apt to cause unwanted side-effects. Carbidopa inhibits the peripheral decarboxylation of levodopa. This action simultaneously reduces the likelihood of peripheral side effects and allows more levodopa to reach the brain. Since carbidopa does not cross the blood-brain barrier, the levodopa in the brain is converted there to dopamine. Thus, co-administration of carbidopa plus levodopa in the form of Sinemet allows a significant reduction of levodopa dosage without reducing the desired effects.
Other antiparkinson agents: • Monoamine oxidase B (MAO-B) inhibitors: selegiline (Eldepyrl) and rasagiline (Azilect). These drugs irreversibly inhibit the enzyme MAO-B, which is responsible for the oxidative deamination of dopamine in the brain. This causes dopamine to accumulate in surviving nerve cells and reduces the symptoms of PD. • Glutamate antagonist (antiviral): amantadine (Symmetrel) appears to potentiate dopaminergic responses. • Dopamine agonists: bromocriptine, pergolide, apomorphine (Apokyn), pramipexole (Mirapex), and ropini-role (Requip). These drugs are direct dopamine receptor agonists. • Anticholinergic agents (antimuscarinic drugs): benztropine (Cogentin) and trihexyphenidyl (Tasmar). These drugs suppress central cholinergic activity and may inhibit reuptake and storage of dopamine in the CNS, thus prolonging the action of dopamine. • Catechol-O-methyl transferase (COMT) inhibitors: tolcapone (Tasmar) and entacapone (Comtan). These drugs are inhibitors of COMT, another enzyme that metabolizes dopamine. • Certain antidepressants and antihistamines such as diphenhydramine that have antimuscarinic actions may be given in the early stages of disease.
• lidocaine
When lidocaine is used IV to treat ventricular arrhythmias, it acts on the fibrillating ventricles to decrease the cardiac excitability and spares the atria. It can effectively reverse a life-threatening situation.
Quinidine is considered as the prototype antiarrhythmic agent and is used primarily to treat atrial fibrillation. It is not effective in treating life-threatening ventricular fibrillation.
Flecainide (Tambocor) is a potent antiarrhythmic agent, effective in a wide range of ventricular and atrial arrhythmias and tachycardias.
Propafenone (Rythmol) is used to treat both ventricular arrhythmias and supraventricular tachycardias.

misc. Write up a sample prescription, illustrating all of the pertinent information that needs to be included when writing a prescription for a patient.
189 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
All of the following drugs are useful for treating which common medical condition?
prednisone gold injections methotrexate nabumetone (Relafen) piroxicam (Feldene)
• osteoarthritis
• systemic lupus erythematosus
• lyme disease
• rheumatoid arthritis
190 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

Dr. John Doe, DDS License # 11 Any Street Federal Drug Registry # Any City, Any State 00000 (000)555-1212
Patient's Name: Age: Patient's Address: Date:
Rx: Amoxicillin 500 mg. tablets Disp. Four (4) tabs Sig: Take 4 tabs (2000 mg) 30-60 minutes prior to dental appointment
Signature:
Substitution permissible Substitution not permissible Number of refills
Notes: • Superscription - Patient's name, address, age, date • Inscription -Name of drug and the strength of the drug (i.e., 500 mg tablets) • Subscription - Directions to the pharmacist (dosage form and amount to be given Disp.) • Transcription or signa - Directions to the patient (Sig.) • Signature - Signature of person prescribing medication must appear
• rheumatoid arthritis
Rheumatoid arthritis (RA) is a chronic inflammatory disease of joints that results in joint pain, swelling, and destruction. RA is characterized by chronic inflammation of the synovium, which lines the joint. With disease progression, there is the accumulation of prostaglandins, leukotrienes and other mediators in the inflammatory changes and tissue destruction in the synovial lining.
How these drugs work in treating rheumatoid arthritis: • Prednisone: decreases the inflammatory response • Gold injections: may decrease prostaglandin production • Methotrexate: unknown, but may affect immune function • Nabumetone (Relafen): an NSAID that inhibits prostaglandin synthesis • Piroxicam (Feldene): an NSAID that inhibits prostaglandin synthesis
Note: All of the above drugs except gold injections are also useful in the treatment of osteoarthritis (OA). OA is characterized by progressive loss of articular cartilage. This may be the result of excessive loads on the joint or other factors. Agents useful in treating OA provide an analgesic and anti-inflammatory action to reduce pain within the joint.

misc. Which of the following gastrointestinal drugs reduce the formation of stomach acid by inhibiting the proton pump of the stomach parietal cells? Select all that apply.
• ranitidine (Zantac)
> omeprazole (Prilosec)
• cimetidine (Tagamet)
• famotidine (Pepcid)
< lansoprazole (Prevacid)
191 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
Which of the following drugs inhibit blood clotting by affecting the tion pathway to prevent fibrin formation? Select all that apply.
• heparin
• vitamin K
• aspirin
• clopidogrel (Plavix)
• warfarin (Coumadin)
copyright ©2013-2014-
misc.
i coagula-
192 • Dental Decks
PHARMACOLOGY

• lansoprazole (Prevacid) • omeprazole (Prilosec)
Hydrochloric acid (HO) is produced by the parietal cells of the stomach through a pump within each cell which pumps protons (H+) into the stomach contents. The pump is called the H+/K+ ATPase pump. HC1 is used for food digestion but an abundancy can cause heart burn and acid indigestion. Omeprazole and lansoprazole inhibit the pump such that no protons are pumped into the stomach contents and thus no HC1 is produced. These two drugs are classified as proton-pump inhibitors.
Stomach acid can also be reduced by inhibiting the effects of histamine in the stomach at the histamine type-2 receptors (H2 receptors). Ordinarily, histamine stimulates the gastric parietal cells to produce hydrochloric acid. Ranitidine, cimetidine and famotidine block the effects of histamine by blocking at the H2-receptors. These three drugs are classified as H2-receptor blockers.
Both the proton-pump inhibitors and H2-blockers are used to treat heartburn, indigestion, sour stomach, active duodenal ulcer disease and gastroesophageal reflux disease (GERD).
Remember: Antacids neutralize excess stomach acid by a chemical reaction. Antacids include aluminum hydroxide (Amphogel), bismuth subsalicylate (Pepto-Bismol), calcium carbonate (Turns) magnesium hydroxide (Maalox) and sodium bicarbonate.
' heparin • warfarin (Coumadin)
Heparin inactivates thrombin and prevents the conversion of fibrinogen to fibrin (blood clot); warfarin (Coumadin) interferes with the hepatic synthesis of vitamin-K dependent coagulation factors II, VII, IX and X resulting in the inability of the coagulation pathway to form fibrin (blood clot).
Vitamin K is a group of fat soluble vitamins that are essential for the synthesis of coagulation factors II, VII, IX and X, and prothrombin in the liver. Vitamin K will enhance blood clotting rather than inhibit blood clotting.
Aspirin inhibits blood clotting by inhibiting platelet aggregation in an irreversible manner. Inhibition of platelet aggregation prevents activation of the coagulation pathway; thus no fibrin (clot) is formed. Aspirin does not affect the coagulation pathway. Discontinuation of aspirin for 5 to 7 days allows for normal clotting time to reappear due to the synthesis of new platelets.
Clopidogrel (Plavix) inhibits blood clotting by inhibiting platelet aggregation in an irreversible manner. Thus the effects on blood clotting are the same as aspirin. Clopidogrel (Plavix) does not cause gastric ulcers like aspirin does and is the antiplatelet agent of choice in patients with history of ulcers.
Note: Clopidogrel, aspirin, abciximab (ReoPro), and anticoagulants (i.e., heparin) are used to lessen the chance of heart attack in people who need percutaneous coronary intervention (PCI), a procedure to open blocked arteries of the heart.

misc. What serious dental effect is associated with the following drugs:
zolendronic acid (Zometa) pamidronate (Aredia) risedronate (Actonel) ibandronate (Boniva) alendronate (Fosamax)
• mucositis
• osteonecrosis of the jaw bone
• angular cheilitis
• oral yeast infection
• xerostomia
193 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
Which substance is an enzyme formed in the kidney and released into the bloodstream where it has an important role in the formation of angiotensin?
plasmin
lysozyme
' renin
• heparin
194 copyright© 2013-2014- Dental Decks
PHARMACOLOGY

r
• osteonecrosis of the jaw bone
Zoledronic acid (Zometa), pamidronate (Aredia), risedronate (Actonel), ibandronate (Boniva), and alendronate (Fosamax) are members of the bisphosphonate class of drugs used to treat and manage Paget's disease, osteoporosis and to prevent hypercalcemia of malignancy. Bisphoshonate therapy has been associated with osteonecrosis, primarily of the jaw; this has been observed mostly in cancer patients, but also in patients with postmenopausal osteoporosis and other diagnoses. Risk factors include a diagnosis of cancer, with concomitant chemotherapy, radiotherapy or corticosteroids; anemia, coagulopathy, infection or pre-existing dental disease. Symptoms include a nonhealing extraction socket or an exposed jawbone. There is no data addressing whether discontinuation of therapy reduces the risk of developing osteonecrosis. However, as a precautionary measure, dental exams and preventative dentistry should be performed prior to placing patients with risk factors on chronic bisphosphonate therapy.
Important: Bisphosphonates have an affinity for hydroxyapatite crystals in bone and act as antiresorptive agents. Their primary mechanism of action involves inhibition of osteoclastic bone resorption. Adverse effects (besides osteonecrosis of the jaw bone) include GI symptoms and esophageal erosions.
Other agents that have an effect on bone:
• SERMs (Selective estrogen receptor modulators): Raloxifene (Evista) reduces resorption of bone and decreases overall bone turnover. It is used for treating osteoporosis. • Hormones:
• Calcitonin: is a naturally occurring hormone that is produced by parafollicular C-cells in the thyroid gland. It is known to block bone resorption through its potent inhibitory effects on osteoclasts. • Parathyroid hormone: PTH is the primary regulator of calcium and phosphate metabolism in bone and kidney. Physiologic actions include regulation of bone metabolism, renal tabular reabsorption of calcium and phosphate, and intestinal calcium absorption. Once-daily administration of PTH (teriparatide [For-teof) stimulates new bone formation via preferential stimulation of osteoblastic activity over osteoclastic activity. Note: PTH also acts on the kidneys by reducing renal clearance of calcium which increases plasma calcium. It also stimulates the production of the active form of vitamin D in the kidney.
• Vitamin D: helps to ensure that the body absorbs and retains calcium and phosphorus, which are critical for building bone. Note: 1,25-dihydroxycholecalciferol is the biologically active form of vitamin D (Chole-calciferol)
renin
Renin is proteolytic enzyme produced by and stored m the juxtaglomerular apparatus that surrounds each arteriole as it enters a glomerulus. Renin acts on the precursor substance anglotensmogen, which is manufactured by the liver and is present in the blood. Renin converts angfotensmogen to angiotensin I. In turn, angiotensin I is converted o angiotensin II by a converting enzyme associated with the walls of capillaries, particularly in the lungs.
Important: "The converting enzyme that converts ^angiotensin I to angiotensin II is
known as angiotensin converting enzyme or ACE."
Angiotensin II is a potent vasopressor. It not only increases total peripheral resistance but by stimulating aldosterone release, leads to an increase in plasma volume, venous return, stroke volume, and ultimately an increase m cardiac output.
Note: Aliskiren (Tekturna) is a renin inhibitor used to treat hypertension. This is the first of a new class of drugs and little information is available. It is used alone or m combination with other agents for the treatment of hypertension.

misc.
Disulfiram (Antabuse) is used in the management of:
• nicotine abuse
• ethanol abuse
• opioid abuse
• NSAID abuse
195 copyright © 2013-2014- Dental Decks
PHARMACOLOGY
misc.
Antacids do not prevent the overproduction of acid.
Antacids do neutralize the acid once it is in the stomach.
• both statements are true
• both statements are false
• the first statement is true, the second is false
• the first statement is false, the second is true
196 copyright © 2013-2014 - Dental Decks

• ethanolabuse
Disulfiram is not a cure for alcoholism but is a deterrent to ethanol consumption. Disulfiram is an antioxidant that interferes with the hepatic oxidation of the acetaldehyde metabolized from alcohol. Specifically it inhibits aldehyde dehydrogenase, a mitochondrial enzyme found in the liver. Even the ingestion of small amounts of ethanol results in high concentrations of acetaldehyde in the body. The unpleasant reaction that occurs (called the Disulfiram-Ethanol Reaction or DER) consists of a throbbing headache, dyspnea, throbbing in the neck, nausea, copious vomiting, thirst, tachycardia and hypotension. Note: Metronidazole, also inhibits aldehyde dehydrogenase.
Ethanol is a sedative-hypnotic drug and is the most important alcohol of pharmacologic interest. Its abuse is responsible for many socioeconomic problems. Drugs that are synergistic with ethanol include diazepam, meperidine, pentobarbital and chlorpromazine. When combined with alcohol these drugs could cause fatal oversedation.
Remember: Synergism refers to the combined action of two or more drugs that is greater than that achieved with a single drug.
• both statements are true
Gastric antacids are drugs that directly neutralize the gastric acid (HCL) secreted in the stomach. Antacid therapy is directed at decreasing the concentration and total load of gastric acid.
Some common over-the-counter antacid products: • Sodium bicarbonate products:
- Alka-Seltzer • Calcium carbonate products:
- Amitone - Turns
• Aluminum hydroxide products: - Alterna GEL - Amphojel
• Magnesium hydroxide products: - Milk of magnesia
• Bismuth salt products: - Pepto-Bismol
• Magnesium and aluminum products: - Maalox - Mylanta
*** Aluminum hydroxide is the most potent of these but has less neutralizing capacity than calcium carbonate or sodium bicarbonate.
Note: Dyspepsia means an impairment of the power or function of digestion.

misc.
Inhaled ammonia is the drug of choice for acting against:
• anaphylaxis
• heart attack
• syncope
• urticaria
197 yrlght © 2013-2014 - DentalDecks
PHARMACOLOGY
misc.
E t h y | alcohol (ethanol) causes a production of which hormone?
well marked diuresis by inhibiting the
. growth hormone
. insulin
.antidiuretic hormone (ADH)
. epinephrine
PHARMACOLOGY
198
copyright©2013-2014 Dental Decks

• syncope
Inhaled ammonia irritates trigeminal nerve sensory endings, with a resulting reflex stimulation of medullary respiratory and vasomotor centers. An aromatic ammonia vaporole is crushed between the fingers and held near the patient's nose. Note: The administration of oxygen will aid in combating tissue anoxia.
The symptoms of syncope include beads of sweat on the upper lip, a weak thready pulse, cold clammy skin, pallor and a dizzy feeling. The loss of normal vasomotor tonus produces pooling of blood peripherally so that the normal blood volume becomes insufficient. Placing the patient in a supine position and elevating the feet gives the patient a transfusion of whole blood by utilizing the forces of gravity. Note: The head should not be more than about 10 degrees lower than the rest of the body.
Types of syncope: • Vasovagal x • Neurogenic V Treat with high-flowing 100% oxygen • Orthostatic ) • Hyperventilation syndrome - Oxygen is not indicated
Note: 100% oxygen is contraindicated for a person who suffers from chronic obstructive pulmonary disease (COPD).
• antidiuretic hormone (ADH)
ADH (also called vasopressin) is a hormone that decreases the production of urine by increasing the reabsorption of water by the renal tubules. Without ADH, there would be extreme loss of water into the urine. Ethanol (ethyl alcohol) inhibits the production of ADH.
Remember: Ethyl alcohol dilates blood vessels of the skin, depresses the CNS, and in blood levels in excess of 400 mg % usually results in coma and death. Alcohol acts primarily on the nerve cells within the brain. Alcohol interferes with communication between nerve cells and all other cells, suppressing the activities of excitatory nerve pathways and increasing the activities of inhibitory nerve pathways.
Note: Recent evidence has shown that frequent ingestion of moderate amounts of alcohol in any form (beer, wine, distilled spirits) will reduce the risk of heart disease, particularly in men.
The order in which alcohol affects the various brain centers is as follows: • Cerebral cortex • Limbic system • Cerebellum • Hypothalamus and pituitary gland • Medulla (brain stem)

misc. Growth hormone is also called:
• dopamine
• aldosterone
• vasopressin
• somatotropin
199 copyright©2013-2014-Dental Decks
PHARMACOLOGY
misc.
All of the following drugs are useful in the treatment of which medical condition?
colchicine indomethacin sulfinpyrazone probenecid allopurinol
• colitis
• gout
• jaundice
- rheumatoid arthritis
200 copyright 0 2013-2014- Dental Decks
PHARMACOLOGY

' somatotropin
Growth hormone (GH) is produced by, and secreted from the anterior pituitary gland.
Basic Metabolic effects of growth hormone: • Increased rate of protein synthesis in all cells of the body • Decreased rate of carbohydrate utilization throughout the body • Increased mobilization of fats and use of fat for energy
Human growth hormone is prepared commercially and used as replacement therapy in patients with growth hormone deficiency. The commercial preparation is prepared as the purified polypeptide hormone of recombinant DNA origin with the same amino acid sequence as that produced by the pituitary gland.
Human growth hormone is indicated in children for the treatment of growth failure due to lack of adequate endogenous growth hormone secretion. It has been used in adults who have a growth hormone deficiency as a result of pituitary disease.
Note: Human growth hormone is administered as subcutaneous injection or intramuscular injection, usually three times per week.
• gout
The therapeutic management of gout involves three different aspects of the disease: 1. Reducing the inflammation during acute attacks: The drug of choice is colchicine. Colchicine impairs leukocytic migration to inflamed areas and disrupts urate deposition and the subsequent inflammatory response. It is most effective when initiated 12 to 36 hours after symptoms begin.
Notes: 1. Colchicine should never be given IM or subcutaneously (it causes tissue irritation). 2. Colchicine can severely damage the liver and kidney; long-term therapy may cause bone marrow depression.
Remember: NSAIDs are also important for the treatment of acute gouty arthritis. Indomethacin (may cause renal damage or bone marrow depression) is most commonly used.
2. Decreasing uric acid production: Allopurinol (Zyloprim) is the drug of choice in the management of chronic gout. It inhibits xanthine oxidase, an enzyme that converts hypoxanthine to xanthine, and xanthine to uric acid. May cause GI disturbances.
3. Enhancing uric acid clearance: Uricosuric agents include probenecid (Benemid) and sulfinpyrazone (Anturane). These agents act primarily in the kidney (specifically, the proximal convoluted tubules) and inhibit the secretion of other weak acids (i.e., penicillin), in addition to inhibiting the reabsorption of uric acid.
Remember: Normally penicillins and cephalosporins have to be given in high and frequent doses due to their high rate of elimination by the kidneys. Their excretion is slowed by giving probenecid.

misc. All of the following are catecholamines EXCEPT one. Which one is the EXCEPTION?
• epinephrine
• norepinephrine
chlorpromazine
• isoproterenol
• dopamine
'dobutamine
201 copyright e 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
Of the following drugs, which ones are skeletal muscle relaxants? Select all that apply.
• methocarbamol (Robaxin)
• cyclobenzaprine (Flexeril)
• baclofen (Lioresal)
• succinylcholine (Anectine)
• carisoprodol (Soma)
• omeprazole (Prilosec)
202 copyrighte2013-2014-Dental Decks
PHARMACOLOGY

r
• chlorpromazine
*** Chlorpromazine is a dopamine antagonist and antipsychotic agent.
Catecholamines are any one of a group of sympathomimetic compounds composed of a catechol molecule and the aliphatic portion of an amine. Some catecholamines are produced naturally by the body (called endogenous) and function as key neurological chemicals (i.e., epinephrine, norepinephrine and dopamine). Note: Epinephrine, Norepinephrine and Isoproterenol are considered to be direct-acting catecholamines.
-Sympathomimetics
Drug (Catecholamine)
Epinephrine
Norepinephrine
Isoproterenol
Dopamine
Dobutamine
Drug (Not Catecholamine)
Amphetamine, phenmetrazine
Ephedrfne
Phenylephrine
Albuterol, metaproterenol, terbutalihe
Oxymetazoline, xylometazoline
Clinical Applications
Anaphylaxis, glaucoma, asthma, to cause vasoconstriction
To cause vasoconstriction in hypotension
Asthma
Shock, heart failure
Shock, heart failure
Narcolepsy, obesity, attention deficit disorder
Urinary incontinence, to cause vasoconstriction, decongestion
To cause mydriasis, vasoconstriction, decongestion
Asthma, premature labor
To cause nasal decongestion (long acting)
Comments
Stimulates the myocardium
Stimulates the myocardium
Imrriediate precursor of NE
. methocarbamol (Robaxin) • cyclobenzaprine (Flexeril) • baclofen (Lioresal) • carisoprodol (Soma)
*** Succinylcholine is the prototype depolarizing neuromuscular blocking drug. Omeprazole is a
proton pump inhibitor. Skeletal muscle relaxants (spasmolytic drugs) are agents that relieve muscle spasms without paralysis They act in the CNS or in the skeletal muscle cell rather than at the neuromuscular end plate. 1 hese drugs are used in certain chronic diseases of the CNS (i.e., multiple sclerosis, cerebral palsy cerebrovascular accidents) that are associated with painful muscle spasms. By reducing the spasms there is a reduction in pain and improved mobility for the patient.
Drugs used for chronic muscle spasm: . • Baclofen (Lioresal): is a derivative of GABA; its site of action in reducing muscle spasms is the spinal cord. It stimulates GABAB receptors that are linked to the G protein, G b resulting in an increase in K+ conductance and a decrease in Ca2+ conductance. Used in the treatment of multiple sclerosis and other spinal cord diseases. All of the other skeletal muscle relaxants do not bind to the GABAB receptors: Diazepam (Valium) and tizanidine (Zanaflex) also act in the spinal cord and are effective muscle relaxants. . • Carisoprodol (Soma): is used in the treatment of muscle spasms and pam associated with acute temporomandibular joint pam. Its precise mechanism of action is not clear but many effects have been ascribed to its central depressive action.
Drags used for acute muscle spasm: • Cyclobenzaprine (Flexeril): relieves muscle spasm through a central action, possibly at the brain stem level. It is used to relieve acute, painful musculoskeletal conditions. It is not effective for muscle spasm secondary to cerebral or spinal cord disease. • Methocarbamol (Robaxin): is a centrally acting muscle relaxant that is used to relieve acute, painml musculoskeletal conditions and in the management of tetanus.
Note: Quinine is widely used for the effective relief of nocturnal leg cramps.

misc. All of the following drugs are used in the treatment of Parkinson's disease EXCEPT one. Which one is the EXCEPTION?
• levodopa (Dopar)
• bromocriptine (Parlodel)
• pergolide (Permax)
• haloperidol (Haldol)
• selegiline (Eldepryl)
• amantadine (Symmetrel)
203 copyright B 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
All of the following are CNS stimulants EXCEPT one. Which one is the EXCEPTION?
• caffeine
• doxapram (Dopram)
• phenobarbital
• methylphenidate
• phendimetrazine
• strychnine
204 copyright© 2013-2014- Dental Decks

• haloperidol (Haldol)
*** Haloperidol is used to treat psychotic syndromes.
Parkinson's disease is a slowly progressing, degenerative disorder of the nervous system. It has several distinguishing characteristics: tremor (shaking) when at rest, sluggish initiation of movements and muscle rigidity. In Parkinson's disease, nerve cells in the basal ganglia degenerate, resulting in lower production of dopamine. It may be treated (but not cured) with a wide variety of drugs:
• Levodopa (in combination with carbidopa) is the precursor of dopamine. It is the main treatment for Parkinson's disease. It is given with carbidopa to increase effectiveness and reduce side effects. • Bromocriptine or pergolide are dopamine agonists which are often given in addition to levodopa early in the treatment to enhance levodopa's action, or may be given later when levodopa's side effects become more of a problem. • Selegiline is a selective inhibitor of MAO Type B, the enzyme that is responsible for the oxidative deamination of dopamine in the brain. It is used as an adjunct to levodopa. • Amantadine appears to potentiate dopaminergic responses. Antiparkinsonian actions are unrelated to the antiviral effects. It is used in the early stages for mild disease. • Anticholinergic drugs (benztropine and trihexyphenidyl, certain antidepressants and antihistamines such as diphenhydramine) may be given without levodopa in the early stages of disease, with levodopa in later stages.
1. Dental implications of Anti-Parkinson's agents: Notes * Anti-Parkinson's agents (mainly levodopa, the direct dopamine agonists and the
COMT inhibitors) have been associated with orthostatic hypotension. • Xerostomia (caused by anticholinergics and MAO-B inhibitors). • Schedule appointment times based on when the patient is feeling the best. • Dyskinesia (abnormal muscle movements) caused by some of the drugs (mainly levodopa, the direct dopamine agonists, and the COMT inhibitors) can present a challenge when trying to perform dental treatment.
• phenobarbital
«** phenobarbital is a barbiturate (sedative-hypnotic).
CNS stimulants are a heterogenous group of compounds that produce various degrees of stimulation. Analeptic is a term that refers to a CNS stimulant which has the ability to overcome drug-induced respiratory depression and hypnosis. In the past the CNS stimulants were widely used therapeutically, but today they have only limited clinical application. Note: Their use for respiratory depression caused by an overdose of CNS depressants is generally not safe or recommended.
Analeptics and respiratory stimulants: doxapram and strychnine. These agents have limited use, but are occasionally indicated to stimulate respiration when a patient has pulmonary disease or to hasten recovery from a general anesthetic.
Xanthines include caffeine, theophylline and theobromine. These stimulants improve mental alertness, reduce the urge to sleep and elevate the mood. Caffeine is the only approved OTC stimulant. Theophylline and theobromine are weaker CNS stimulants than caffeine. Theophylline is the only xanthine important in the treatment of asthma. It stimulates the respiratory centers of the medulla and is able to cause bronchial dilation in patients with asthma. Note: It has a low therapeutic index and its metabolism is affected by several other drugs.
Sympathomimetic amines include the amphetamines and other related agents (i.e., methylphenidate, phendimetrazine, etc.). They are potent CNS stimulants. They are used to treat narcolepsy, obesity and attention deficit disorder.

misc. The symptoms of chronic caffeine consumption can include all of the following EXCEPT one. Which one is the EXCEPTION?
• feelings of anxiety and nervousness
• sleep disruption
• coughing
• irritability
• diuresis
• stomach complaints
• palpitations and arrhythmias
205 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
All of the following drugs are used to treat what condition? dexmethylphenidate (Focalin) extended-release methylphenidate (Concerto) mixed amphetamine salts (Adderal) atemoxetine (Strattera)
controlled-delivery methylphenidate (Metadate CR) lisdexamfetamine (Vyvanse)
• insomnia in adults
• tourette's syndrome in children
• attention deficit hyperactivity disorder (ADHD)
• insomnia in children
206 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• coughing
Caffeinism is a term used for people who are dependent upon caffeine (i.e., suffer side effects from having too much caffeine, take larger amounts and need to keep drinking caffeine to function properly). It is thought to occur if you have an intake above 600 to 750 mg of caffeine per day (more than 10 cups of coffee). Drinking more than 1000 mg per day is well into the toxic range.
Important: Caffeine stimulates the CNS unequally, with the cortex being the most affected and the spinal cord being the least affected.
Caffeine Content of Commonly Ingested Products
Product Beverages (1 cup or glass)
Brewed coffee
Instant coffee
Decaffeinated coffee
Tea
Cola drinks
OTC Drugs
Anacin
Excedrin
NoDoz
Vivarin
Caffeine Content (mg)
100-150
50-100
2-35
40-110
35-60
32
65
100
200
> attention deficit hyperactivity disorder (ADHD)
Drugs used to treat ADHD: • Methylphenidate (Ritalin): a mild central nervous system stimulant. In children with ADHD, this drug results in an increase in attention span, reduction in hyperactivity, and an improvement in behavior. • Dexmethylphenidate (Focalin): a form of methylphenidate called dexmethylphen-idate. • Adderal (dextroamphetamine): the trade name for mixed amphetamine salts which
act the same as methylphenidate in treating ADHD. • Atemoxetine (Strattera): the first non-stimulant approved for treating ADHD. It is approved for use in children and adults. • Metadate CR: the brand name for a controlled-delivery methylphenidate, another long acting form of the drug. • Lisdexamfetamine (Vyvanse): Lisdexamfetamine is a prodrug; after administration it is converted to dextroamphetamine (Adderall) in the intestines and/or liver. The dextroamphetamine, an amphetamine and stimulant for the brain, is responsible for the effect of lisdexamfetamine in ADHD. • Extended-release methylphenidate (Concerto): a long-acting form of methylphenidate.

misc. Which drug belongs to the opioid family and reduces GI motility ?
• loperamide (Imodium)
• lorazepam (Ativan)
• prochlorperazine (Compazine)
• propranolol (Inderal)
207 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
All of the following are prominent toxic effects of one is the EXCEPTION?
• irritability
• xerostomia
• loosened teeth
• gum disorders
• slurred speech
• tremors
PHARMACOLOGY
misc.
mercury EXCEPTone. Which
copyright© 2013-2014
-
208 - Dental Decks

• loperamide (Imodium)
Antidiarrheals: • Opiate and opioid derivatives
- Loperamide (Immodium): 1. Is an antidiarrheal which acts on intestinal muscles to inhibit peristalsis. 2. Is a member of the opioid family. It does not penetrate the central nervous system like the opioids such as codeine; thus it can be sold over the counter. 3. Has no evidence of drug abuse or dependence (unlike other opioids such as codeine, morphine and meperidine).
- Diphenoxylate is an antidiarrheal and inhibits excessive GI tract motility and GI propulsion. Commercial preparations contain a sub-therapeutic amount of atropine to discourage abuse. Diphenoxylate and atropine (Lomotil), unlike loperamide (Imodium), requires a prescription.
• Antisecretory:bismuth subsalicylate (Pepto-Bismol) •Adsorbents: attapulgite (Kaopectate)
Remember: Laxatives act in the reverse manner of the antidiarrheals and increase the motility of the GI tract. They are used to treat constipation. Examples include: magnesium hydroxide (Milk of Magnesia), castor oil, Metamucil and methylcellulose.
Antiemetics: act on the "vomiting center" in the medulla. This center has four different sources of stimuli. The chemoreceptor trigger zone (CTZ) is located outside the blood-brain barrier near the vomiting center in the medulla. It communicates with the vomiting center after input is received from drugs and hormones. The classes of antiemetics are:
• Antidopaminergic: • Phenothiazines: prochlorperazine (Compazine) and promethazine (Phenergan) • Benzamides: metoclopramide (Reglan) and trimethobenzamide HCL (Tigan)
• Anticholinergics: • Antihistamines: meclizine (Antivert), dimenhydrinate (Dramamine), and scopolamine (Transderm-Scop)
• Serotonin 5-HT3 receptor antagonists: ondansetron HCL (Zofran), dolasetron (Anzemet), granisetron HCL (Kytril) and palonosetron (Aloxi)
• xerostomia
*** Excessive saliva is a prominent toxic effect of mercury not xerostomia
These symptoms are all of the chronic form, which results from the inhalation of the vapors of dust of mercurial compounds or from repeated ingestion of very small amounts. The presence of mercury in the body is determined by a urine test. Treatment may include gastric lavage with milk and egg white or sodium bicarbonate, chelation with British anti-lewisite (BAL), and fluid therapy.
Note: British Anti-Lewisite (BAL) or Dimercaprol and penicillamine are two drugs currently marketed for promoting the excretion of mercury, lead, and several other agents. A few additional agents are available for the treatment of poisoning by metals other than mercury (e.g., edetate calcium disodium for lead and deferoxamine for iron).
Mercury that is absorbed into the circulatory system may be deposited in any tissue. Higher-than-average accumulations occur in the brain, liver, and kidney. Mercury does not collect irreversibly in human tissues. There is an average half-life of 55 days for transport through the body to the point of excretion. Thus, mercury that came into the body years ago is no longer present in the body.
1. Children and adults who are to be treated for lead poisoning should only be given the Notes Edetate Calcium Disodium (Calcium Disodium Versenate) form of "EDTA."
2. Penicillamine is also a highly effective chelator of copper and is of primary importance in the management of Wilson's disease (hepatolenticular degeneration). 3. Deferoxamine is a drug that chelates to absorbed iron very well and is eliminated in urine. 4. For carbon monoxide poisoning the treatment is 100% oxygen therapy (involves breathing oxygen through a tight-fitting mask). 5. Cyanide poisoning can be treated with rapid oxygen administration and the antidotes sodium nitrite and sodium thiosulfate.

misc.
Of the amino acid neurotransmitters listed below which one is an excitatory neurotransmitter?
• glycine
• glutamate
• GABA (g -aminobutyricacid)
• none of the above
PHARMACOLOGY
209 copyright© 2013-2014- Dental Decks
misc.
Oral contraceptives block ovulation by mones below? Select all that apply.
inhibiting which anterior pituitary hor-
. follicle stimulating hormone (FSH)
. growth hormone (GH)
.thyroid stimulating hormone (TSH)
. luteinizing hormone (LH)
.adrenocorticotropichormone (ACTH)
PHARMACOLOGY
210
• n o 2013-2014 -Dental Decks copyright © 2U13 t-v

r
• glutamate
Chemicals that transmit the signal from one neuron to the next are called neurotransmitters. They are synthesized in the cell body or nerve terminal of the presynaptic neuron. Neurotransmitters are released from the synapse and cross the synaptic cleft. The dendrite on the nerve cell body receives the signal. Various receptors on the postsynaptic membrane of the dendrite accept only certain neurotransmitters.
In the brain, 30 different neurotransmitters have been classified as amino acids, amines, and neuropeptides.
• Amino acid neurotransmitters: - Glutamate, GABA, and glycine. Glutamate is an excitatory neurotransmitter. GABA and glycine are inhibitory neurotransmitters. GABA is the major inhibitory neurotransmitter within the CNS.
•Amines: - Include the catecholamines — dopamine, norepinephrine, and epinephrine — as well as serotonin, histamine, and acetylcholine.
• Neuropeptides — most are also hormones; these include vasopressin, oxytocin, insulin, somatostatin, gastrin, substance P, endorphin, and enkephalin.
Remember: • Acetylcholine: effects in CNS generated by interaction with a mixture of nicotinic and muscarinic receptors • Dopamine: a catecholamine which acts through at least two subtypes Dl (activates adenyl cyclase), D2 (inhibits adenyl cyclase) • Serotonin: is 5-hydroxytryptamine which works through at least 14 subreceptor "tryptominergic" type neurons
1. Biosynthetic pathway of ACH: Step (1) Choline (taken up into nerve via action of permease) Notes Step (2) Choline acetylcholinesterase catalyzes the synthesis of
Ach from acetyl CoA and choline
2.Biosynthesis of NE and E: Step (1) Tyrosine to DOPA (enzyme is tyrosine hydroxylase Step (2) DOPA to Dopamine (enzyme is aromatic L-amino acid decarboxylase) Step (3) Dopamine to NE (enzyme is dopamine beta hydroxylase) Step (4) (mostly in the adrenal medulla): NE to E (enzyme is phenylethanolamine N-methyltransferase)
• follicle stimulating hormone (FSH) • luteinizing hormone (LH)
In addition to the above effects, oral contraceptives produce alterations in the genital tract, including changes in cervical mucus, rendering it unfavorable for sperm penetration even if ovulation occurs. Changes in the endometrium may also occur rendering it unfavorable for nidation (implantation of the fertilized ovum). Estrogens and progesterone-like compounds (progestins) are used for oral contraception.
• Estrogens: are a group of chemically similar steroid hormones. In humans, estrogens are made primarily in the female ovaries and in small amounts in the male testes and the adrenal glands, brain, and fat of both sexes. Estradiol is the most abundant and potent natural estrogen in humans. Other estrogens include ethinyl estradiol and mestranol.
• Progestins: are a group of chemically similar steroid hormones as well. In humans, progestins are made primarily in the female ovaries and male testes. Progesterone is the most abundant and potent progestin in humans. Other progestins include levonorgestrel, norethindrone, medroxyprogesterone, norgestimate and norgestrel.
Types of oral contraceptives:
• Combination: oral contraceptive agents usually contain both an estrogen agent and a progestin agent. Combination drugs include:
• ethinyl estradiol and norethindrone (Ovcon50, Brevicon 21, and Modicon 28) • ethinyl estradiol and levonorgestrel (Portia 0.15/30, Alesse 28 andAviane 21) • ethinyl estradiol and norgestrel (Cryselle, Ovral, and Orgestrel)
• Progestin-only: norethindrone (Micronor) • Emergency contraception: levonorgestrel (Plan B)
Warnings/Precautions with Oral Contraceptives:
• The risk of cardiovascular side effects increases in women who smoke cigarettes, especially those who are >35 years of age. • May increase the risk of thromboembolism. Women with hypertension should be encouraged to use a non-hormonal form of contraception.
Note: Antibiotics have the potential to diminish the effectiveness of oral contraceptives. Advise patients to use additional method of birth control when taking antibiotics and oral contraceptives concurrently.

misc. Drugs travel through the blood stream by binding to albumin plasma protein.
However, only a small number of drugs travel through the blood stream by this mechanism.
• both statements are true
• both statements are false
• the first statement is true, the second is false
• the first statement is fals, the second is true
211 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
What are four criteria to consider when selecting an analgesic agent for a patient?
• type of pain
• location of pain
• age of patient
• sex of patient
• patient's weight
• concurrent medication
• pregnancy
212 copyright © 2013-2014 - Dental Decks

• the first statement is true, the second is false
*** Most drugs travel through the blood stream by binding to albumin protein, which is abundant in plasma. In this way, drugs can be carried to all the tissues and organs.
A drug which is bound to plasma albumin always has some fraction which is not bound. The unbound portion is free to leave the blood compartment to be taken up by tissues where the drug will elicit its pharmacological effect. The remaining bound fraction of drug then continuously releases more free drag to be taken up by tissues. Eventually all drug in the blood compartment will be taken up by this process.
Important: Interactions between two or more drags can occur if they compete for binding on the plasma albumin. If drag A is bound to albumin prior to the patient taking drug B, and drug B has a greater binding affinity to albumin than drag A, then when drag B is taken, it will displace drag A from albumin to result in large amounts of unbound drug A which could lead to adverse reactions due to the sudden large amounts gaining access to the tissues.
One of the most fundamental aspects of drug action is the relationship between dose administered and the effect obtained (drugs are dose dependent). Dose and response are related and can be represented by a dose-response curve. There are two basic types of dose-response curves:
• The graded dose-response (DR) curve plots the degree of a given response against the concentration of the drag. These curves are useful for determining characteristics of agonists and antagonists. • The quantal dose-effect curve: In this case, a given quantal effect is chosen (e.g., a certain degree of cough suppression), and the concentration of the drag is plotted against the percentage of a specific population in which the drug produces the effect. The median effective dose (ED50 or the dose at which 50% of the individuals exhibit the specified quantal effect) and the median lethal dose (LD50 or the dose at which death is produced in 50%> of the experimental animals in preclinical studies) can be estimated from quantal dose-effect curves. With this type of curve, the relative effectiveness of various drugs for producing a desired or undesired effect, as well as the relative safety between various drugs, can be determined.
• type of pain • age of patient • concurrent medications • pregnancy
Criteria considered when selecting an analgesic agent:
1. Type of pain: • Severe •Mild • Moderate
2. Age of the patient: • Infant -» When calculating dosage, the height, weight, body surface area and renal hepatic
• Child J function must be taken into account
• Adult • Elderly: drug response is affected by age-related changes in physiology and pharmo-kinetics
3. Concurrent medications: Consider unwanted interactions, especially with the elderly. 4. Pregnancy: Because virtually any drag a pregnant woman takes can cross the placenta and enter the fetal circulation, drug use in pregnant patients is a source of special concern (check with patient's OB/GYN).
FDA Rating System for the Teratogenic Effects of Drugs: The FDA, the government agency that oversees the safety of drugs, provides the most widely used system to grade the teratogenic effects of medications. The FDA assigns a safety category for medications by using a 5-letter system: A, B, C, D, and X, with A being considered the most safe. X category medications: Studies in'animals or humans have demonstrated fetal abnormalities or there is positive evidence of fetal risk based on adverse reaction reports from investigational or marketing experience, or both, and the risk of the use of the drug in a pregnant woman clearly outweighs any potential benefit.

misc. Which of the following competitively blocks vitamin K-binding sites and inhibits the synthesis of vitamin K-dependent coagulation factors VII, IX, X, and II (prothrombin) and anticoagulant proteins C and S?
• heparin
• warfarin (Coumadin)
• aspirin
• anagrelide
213 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
Which drugs below act to induce gene transcription, inhibit cellular growth and alter the state of cell differentiation.
• immune globulins
• immunosuppressants
• keratinocyte growth factor
> interferons
214 copyright© 2013-2014- Dental Decks
PHARMACOLOGY

warfarin (Coumadin)
At therapeutic levels, warfarin decreases liver synthesis of vitamin K-dependent clotting factors by 30% to 50%. These clotting factors have different half-lives. Factor VII has the shortest half-life (6-9 hr) vs. factor II and X (up to 72 hr). Oral anticoagulants do not reverse ischemic damage or lyse an established thrombus but rather prevent extension of the existing thrombus and the formation of new thrombi by blocking synthesis of clotting factors.
Oral anticoagulants are used after a myocardial infarction to prevent coronary occlusion, in the treatment of pulmonary embolism, and in the treatment of venous thrombosis.
Note: Enhanced anticoagulant effects are seen when these drugs are combined with aspirin. For this reason, use acetaminophen (Tylenol) for pain control.
Patients on anticoagulant therapy may have excess bleeding after dental treatment. Always check medical history. If patient is on anticoagulants, his/her physician should have documentation of INR values to assess anticoagulant effects. INR stands for International Normalized Ratio and essentially is the ratio of the prothrombin time measured in the patient divided by a standard prothrombin time value, and multiplied by a constant. An INR value of 1 means normal prothrombin times of approximately 12 seconds; normal blood clotting would be present. INR values greater than 1 indicate that there is an anticoagulant effect. The higher the INR value, the greater the anticoagulant effect. Many patients taking anticoagulants have INR values of 2, 3 and even up through 6.
• interferons
Interferons are used for a variety of conditions including: hairy cell leukemia (interferon alpha-2a) chronic hepatitis B (interferon alpha-2b), recurring genital warts (interferon alpha-n3) and treatment of multiple sclerosis (interferon beta-la).
Immune globulins provide passive immunity by increasing antibody titers.
Immunosuppressants are drugs such as cyclosporin which prevent organ transplant rejection.
Growth factors such as keratinocyte growth factor promote cell proliferation and angio-genesis.

misc.
Granisetron (Kytril) and ondansetron (Zofran) are selective 5-HT3 receptor antagonists used to treat what condition?
• breast cancer
• osteoporosis
• emesis caused by cancer chemotherapy
• mucositis caused by radiation therapy
215 copyright © 2013-2014 - Dental Decks
misc.
The following drugs belong to what pharmaceutical class of agents:
pimecrolimus sirolimus tacrolimus
• immune modulators
• monoclonal antibodies
• immunosuppressants
• interferons
• colony stimulating factors
PHARMACOLOGY
216
copyright © 2013-2014 - Dental Decks

• emesis caused by cancer chemotherapy
The 5-HT3 receptor is a serotonin receptor which when activated during chemotherapy for cancer, causes emesis (nausea and vomiting). Both granisetron and ondansetron are indicated for prophylaxis of chemotherapy-related emesis, prophylaxis of nausea and vomiting associated with radiation therapy, and prophylaxis and treatment of postoperative nausea and vomiting (PONV).
Other serotonin 5-HT3 receptor antagonists include: dolasetron (Anzemet) and palonosetron (Aloxi)
Note: 5-HT3 stands for 5-hydroxytryptamine type 3 receptor.
• immunosuppressants
Pimecrolimus (Elidel) is an immunosuppressant agent used for treatment of mild to moderate atopic dermatitis.
Sirolimus (Rapamune) is an immunosuppressant agent used for prophylaxis of organ rejection in patients receiving renal transplants.
Tacrolimus (Protopic) is an immunosuppressant agent used to treat moderate to severe atopic dermatitis in patients not responsive to conventional therapy.

misc. The following drugs belong to what pharmaceutical class of agents:
adalimumab alefacept infliximab trastuzumab
• immune modulators
• monoclonal antibodies
• immunosuppressants
• interferons
• colony stimulating factors
217 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
Your patient's medication history includes modafinil (Provigil). Your patient is probably using this drug in order to:
. improve wakefulness during daytime sleepiness
• improve salivary flow in dry mouth disorders
• manage psychotic disorder
«treat mental depression
218 copyright © 2013-2014 - Dental Decks

monoclonal antibodies
Adalimumab (Humira) is a recombinant monoclonal antibody that binds to human tumor necrosis factor alpha (TNF-alpha) receptor sites. It is used to treat active rheumatoid arthritis.
Alefacept (Amevive) is a monoclonal antibody used to treat moderate to severe plaque psoriasis.
Infliximab (Remicade) is a monoclonal antibody used to treat ankylosing spondylitis, Crohn's disease, and rheumatoid arthritis. Like adalimumab, infliximab works by binding to TNF-alpha receptor sites.
Trastuzumab (Herceptin) is a monoclonal antibody which binds to the extracellular domain of the human epidermal growth factor receptor 2 protein (HER-2). It is used for the treatment of patients with metastatic breast cancer whose tumors overexpress the HER-2 protein and who have not received chemotherapy for their metastatic disease.
improve wakefulness during daytime sleepiness
Modafinil (Provigil) represents a class of central nervous system stimulants used to improve wakefulness in patients with excessive daytime sleepiness associated with narcolepsy and shift work sleep disorder. It also has an unlabeled use to treat attention deficit/hyperactivity disorder (ADHD).
The exact mechanism of modafinil is unclear; however part of its action may be due to decreased GABA-mediated neurotransmission.

1
misc. Which herbal supplement below is known to be somewhat effective in treating mild forms of mental depression?
• ginkgo biloba
• St Johns Wort
• garlic
• echinacea
• ginseng
219 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
St Johns Wort is a herbal supplement which can interact with some conventional medications to:
• increase the effectiveness of medications
• decrease the effectiveness of medications
• increase the toxicity of medications
220 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

St Johns Wort
Some studies have shown that St Johns Wort can inhibit the re-uptake of serotonin at neuronal synapses resulting in the elevation of serotonin within the CNS. This effect is similar to those antidepressants within the fluoxetine (Prozac) family. Of all the herbal supplements available to the consumer, St Johns Wort is associated with use as a mild antidepressant.
Ginkgo biloba is a herbal supplement used as a peripheral artery vasodilator.
Garlic is a herbal supplement used to lower cholesterol and to inhibit platelet aggregation resulting in a decrease in blood clotting.
Echinacea is a herbal supplement and immune stimulator used to minimize the severity of the common cold and seasonal flu.
Ginseng is a herbal supplement used to stimulate the immune system.
Chamomile has a long history of use in Europe for digestive ailments. The active constituents of chamomile have anti-inflammatory properties, and ease spasm and discomfort in the digestive tract. Note: Chamomile contains coumarin, a naturally-occurring compound with anticoagulant or blood-thinning effects. It should not be combined with warfarin or other anticoagulants.
Saw palmetto has long been used in Europe to treat an enlarged prostate or benign prostatic
hyperplasia (BPH).
• decrease the effectiveness of medications
St Johns Wort may induce the cytochrome P450 enzyme system to result in a more rapid metabolism of many drugs in this pathway. More rapid metabolism of a drug equates to less active drug available and less (decreased) effectiveness. Specifically, data indicates probable interactions between St Johns Wort and its effect in decreasing the actions of the following drugs:
• The HIV-1 protease inhibitor indinavir • The antirejection medication cyclosporin • The sedative midazolam • The antihypertensive nifedipine
Drug-drug interactions can involve prescription or nonprescription (over-the-counter) drugs. Drugs interact by acting at the same receptor or signal transduction pathway, or more commonly, a drug may affect the pharmacokinetics of another drag. The most common form of drug-drug interaction is one drug affecting the metabolism of another drag, involving either induction or inhibition of metabolizing enzymes.
• Induction of metabolism: is a reaction to certain drugs in which the number of liver enzymes increases, resulting in a reduction in the effect of the other drug. • Inhibition of metabolism: is a process by which one drug either competes for metabolism of another or directly inhibits drug-metabolizing enzymes.
1. Herbal medicines such as garlic, ginseng, and ginkgo (ginkgo biloba) are thought to interact with an-Notes ticoagulant or antiplatelet therapy. Remember: Chamomile contains coumarin and should not be
used in patients taking warfarin for fear of an additive affect. 2. St. John's wort is the herbal product most often reported to be involved in drag-herb interactions. 3. Echinacea has potential interactions with immunosuppressants. 4. Many herbal weight loss and "herbal speed" products rely on the pharmacodynamic interaction between ephedra and caffeine. Two primary alkaloids contained in ephedra—ephedrine and pseudoephedrine — have additive cardiovascular effects when taken with caffeine. At higher doses, the ephedra-caffeine interaction has been cited as a cause of death.
Important:The rate of drug metabolism can vary greatly, depending on the cytochrome p450 isozyme profile of a patient. Over the next few years, genetic screening of the cytochrome p450 system will be able to identify which patients are likely to develop toxicity or drug-drug interactions, and with which drugs. Ultimately, metabolic screening based on studies using highly-specific probes could help decide whether or not a drug is prescribed.

misc. All of the following drugs are serotonin 5-HT1D receptor agonists used to treat migraines EXCEPT one. Which one is the EXCEPTION?
• sumatriptan (Imitrex)
• frovatriptan (Frova)
> naratriptan (Amerge)
• donepezil (Aricept)
> rizatriptan (Maxalt)
• almotriptan (Axert)
> zolmitriptan (Zomig)
221 copyright o 2013-2014 - Dental Decks
PHARMACOLOGY
misc.
All of the following are drugs used to treat hypothyroidism EXCEPT one. Which one is the EXCEPTION?
> levothyroxine sodium (Synthroid)
• liothyronine (Cytomel)
> liotrix (Thyrolar)
• methimazole (Tapazole)
222 copyright e 2013-2014 - Dental Decks
PHARMACOLOGY

r • donepezil (Aricept)
*** Donepezil (Aricept) is a cholinesterase inhibitor used in the treatment of Alzheimer's disease.
Migraine medications: • The most commonly used migraine medications are the serotonin 1 (5-HTj) receptor agonists, commonly known as the "triptans." All 5-HTj receptor agonists (triptans) have a similar chemical structure and a comparable mechanism of action. 5-HT1B and 5-HT1D receptors located on the extracerebral, intracranial blood vessels that become dilated during a migraine attack and on nerve terminals in the trigeminal system. Therapeutic activity is caused by activation of these receptors, which results in cranial vessel constriction, inhibition of neuropeptide release, and reduced transmission in trigeminal pain pathways.
• Ergotamine derivatives demonstrate partial agonist and/or antagonist activity against dopamine, tryptaminergic, and alpha-adrenergic receptors, depending on their site. Ergotamine derivatives have three primary actions. They (1) depress central vasomotor center, (2) constrict peripheral and cranial blood vessels, and (3) reduce extracranial blood flow and decrease hyperfusion of the basilar artery area. Examples include: erotamine tartrate (Cafergot) and dihydroergotamine (DHE-45)
• Combination drugs: Midrin is a combination capsule that contains 65 mg of isomethep-tene mucate (an ergotamine derivative), 325 mg of acetaminophen, which exerts an analgesic effect, and 100 mg of dichloralphenazone, a mild sedative that acts centrally to allay anxiety. Note: Caffeine, which is added to many migraine combinations, helps to promote constrictive properties, and enhances absorption.
Note: Methylsergide (Sansert) blocks 5-HT2 receptors (serotonin antagonist) and is used for prophylaxis against migraines.
• methimazole (Tapazole)
Thyroid medications:
• Thyroid supplements: used to treat hypothyroidism • Levothyroxine sodium (synthetic Tj) • Liothyronine (synthetic T$) • Liotrix (T4:T3 = 4:1) Note: These drugs are usually taken orally in a single daily dose, preferably before breakfast. The treatment of choice for hypothyroidism is T4. It has a relatively slow onset of action, and its effects are cumulative over several weeks. T3 has a more rapid onset of action and dissipation of action. Adverse side effects include nervousness, nausea, diarrhea, tachycardia, tremor, weight loss and heat intolerance.
• Thyroid suppressants: used to treat hyperthyroidism • Methimazole (Tapazole) • Propylthiouracil (PTU)
Note: These drags inhibit thyroid peroxidase, which is an enzyme expressed mainly in the thyroid that liberates iodine for addition onto tyrosine residues on thyroglob-ulin for the production of the thyroid hormones — thyroxine (T4) or triiodothyronine (T3). Through reduced absorption of iodine, thyroid hormone synthesis is diminished. Adverse effects include rash, nausea, and agranulocytosis.
Note: Thyrogen is a recombinant DNA source of human TSH useful in the management and treatment of thyroid cancer patients.

misc. Nicotine is rapidly absorbed across the pulmonary capillary membrane and is delivered to the brain in high concentration within seconds of inhalation.
The nasal spray has the fastest delivery of the NRTs and more closely resembles the onset of the nicotine effects of smoking.
• both statements are true
• both statements are false
• the first statement is true, the second is false
• the first statement is false, the second is true
223 copyright B 2013-2014 - Dental Decks
PHARMACOLOGY
narcotic analgesics
Opioid drugs (narcotics) can be used as: Select all that apply.
• analgesics
• anti-inflammatories
• antitussives
• antidiarrheals
• preanesthetic medications
224 copyright© 2013-2014- Dental Decks
PHARMACOLOGY

r • both statements are true
Many pharmacologic approaches have been used to help people stop smoking. In current use are the nicotine replacement therapy (NRT) products, bupropion (Zyban, Wellbutrin) and varenicline (Chantix).
Nicotine replacement products are meant to help patients stop smoking. They are not meant to help get a patient through a long flight or an all-day meeting in a nonsmoking building.
Class
Nicotine replacement therapy
Antidepressant
Nicotine receptor agonist
Generic Name
Nicotine polacrilex
Nicotine
Bupropion
Varenicline
Trade Name
Nicorette
Nicoderm CQ Habitrol Nicotrol ProStep Nicotrol NS Nicotrol inhaler Commit
Zyban, Wellbutrin
Chantix
Formulation
Gum
Transdermal Transdermal Transdermal Transdermal Nasal spray Oral inhaler Lozenge
Tablet
Tablet
1. The patch (transdermal) is the most commonly used type of NRT. Patches are available in 15 and Notes "^ m § s t rengths for treatment initiation.
2. The gum delivers nicotine faster than the patch and can be used for incidence of craving. The gum is available in two strengths: 2 mg and 4 mg. 3. The lozenge also comes in 2 mg and 4 mg doses and delivers about 25% more nicotine than gum. 4. The nasal spray has the fastest delivery of nicotine of the NRTs. 5. Inhaled nicotine (using the nicotine inhaler) is absorbed in the mouth — not in the lungs. Each cartridge contains 10 mg nicotine and delivers 4 mg. It also contains 1 mg menthol. 6. Bupropion as a systemic medication seems to reduce the craving for cigarettes or the urge to smoke. Its mechanism of action is unclear. 7. Varenicline is the newest drug in the smoking cessation arsenal. Note: The FDA has issued an alert to providers to monitor patients taking this medication for depression, severe mood swings, abnormal dream states, and thoughts of suicide.
• analgesics • antitussives • antidiarrheals • preanesthetic medications
Opiates are very effective analgesics. They suppress the cough reflex (antitussive). They cause constipation and thus are effective antidiarrheal agents. When used as preanesthetic medications, opiates permit a reduction in the amount of general anesthetic required for surgical anesthesia.
Some common side effects of opiates (narcotics) include: sedation/drowsiness, dizziness and nausea. Other less common adverse effects are vomiting, hypotension, irregular/labored breathing (dyspnea), lightheadedness, nightmares and insomnia.
Notes 1. Respiratory depression is dose related and is the cause of death in narcotic drug overdose. It can happen with any of the narcotics. 2. Abuse can and does occur with all the narcotics. They are all controlled drugs falling under DEA Schedule II or DEA Schedule III of the schedules of controlled substances. 3. A DEA number is required in order to prescribe narcotics.

narcotic analgesics
Which drug is the standard to which all opiates (narcotics) are compared?
• codeine
• oxycodone
• hydrocodone
• meperidine
• morphine
• fentanyl
225 copyright© 2013-2014- Dental Decks
PHARMACOLOGY
narcotic analgesics
Which adverse effect is associated with opioid analgesics and not non-nar
cotic pain relievers?
allergic response
* nausea
• vomiting
• respiratory depression
226 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

• morphine
Opioid analgesics are thought to inhibit painful stimuli in the substantia gelatinosa of the spinal cord, brainstem, reticular activating system, thalamus, and limbic system. Opiate receptors in each of these areas interact with neurotransmitters of the autonomic nervous system, producing alterations in reaction to painful stimuli. The opioid action of the drug manifests as:
• Analgesia • Drowsiness 1 Euphoria • Mental clouding • Miosis (pupillary constriction)
• Decreased peristaltic motility 1 Nausea and vomiting • Respiratory depression ' Depression of the cough reflex 1 Orthostatic hypotension
Morphine is a naturally occurring opiate that is metabolized chiefly through glucuronidation by uridine diphosphate glucuronosyl transferase (UGT) enzymes in the liver. These enzymes produce an active analgesic metabolite (morphine-6-glucuronide).
Signs and symptoms of acute opioid intoxication:fhe intoxicated person is stuporous or asleep and has constricted pupils (pin-pointpupils) and depressed respiration. As the severity of intoxication increases, coma ensues. Note: Death from acute intoxication by an opioid analgesic is the result of profound, direct respiratory depression.
Remember: 1. Codeine is weaker (less potent) than morphine and less addictive. It is converted to morphine by cytochrome p450 2D6. Note: It differs from morphine in that a methoxy (— OCH3) substitution replaces the hydroxyl (— OH) group on the aromatic ring of the molecule. This relatively minor structural change provides codeine with significant oral effectiveness. 2. Oxycodone has a similar potency as morphine. In combination with acetaminophen it is known as Per-cocet or Tylox. 3. Hydrocodone has a similar potency as morphine. In combination with acetaminophen it is known as Vi-codin and Lorcet. 4. Meperidine (Demerol) is more potent than codeine but less potent than morphine but just as addictive. It has a shorter duration of action. It is the only narcotic agent that does not cause miosis (pupillary constriction).
5. Methadone (Dolophine) is an opioid agonist used in maintenance for treating opioid addiction. 6. Buprenorphine (Subutex) is an opioid partial agonist used to treat opioid dependence.
• respiratory depression
The most significant and well-known adverse reaction to opioids is respiratory depression. Death secondary to opioid overdose is nearly always due to respiratory depression. When opioids are appropriately used, the risk of severe respiratory depression is generally small as tolerance rapidly develops to this effect.
Opioid Analgesics
Drug
Morphine
Codeine
Meperidine
Methadone
Propoxyphene
Levorphanol
Hydrocodone
Oxycodone
Pentazocine
Length of Effectiveness
IV or IM: 2-3 hours By mouth: 3-4 hours Sustained release: 8-12 hours
By mouth: 3-4 hours Taken with aspirin or acetaminophen
IV or IM: about 3 hours By mouth: not very effective
By mouth: 4-6 hours, sometimes longer
By mouth: 3-4 hours
IV or IM: 4 hours By mouth: 4 hours
By mouth: 4-6 hours
By mouth: 3-4 hours
By mouth: up to 4 hours
Other Information
Starts to work quickly. Oral form can be very effective for cancer pain.
Less potent than morphine
Can cause seizures, tremors, and muscle spasms
Also used for treating heroin withdrawal
Generally taken with aspirin or acetaminophen to treat mild pain
Oral form is strong. Can be used instead of morphine
Usually combined with acetaminophen
Usually combined with aspirin or acetaminophen
Can block painkilling action of other opioids. About as strong as codeine. Can cause confusion and anxiety, especially in the elderly.

All of the following are opium < EXCEPTION?
• meperidine
• morphine
• codeine
ilkaloids.
narcotic analgesics
EXCEPT one. Which one is the
227 copyright©2013-20l4-Dental Decks
PHARMACOLOGY
Which drug is the prototype opioid
• morphine
• naloxone
• propranolol
• ibuprofen
antagonist?
narcotic analgesics
228 copyright © 2013-2014 - Dental Decks
PHARMACOLOGY

' meperidine
Chemical classification of opioid analgesics: Opium alkaloids:
• Morphine • Codeine
Synthetic derivatives: • Morphine group:
• Hydromorphone (Dilaudid) • Oxymorphone (Numorphan) • Nalbuphine (Nubain)
• Codeine group: • Hydrocodone (in Vicodin) • Oxycodone (in Percodan, Percocet and Tylox)
Synthetic narcotics: • Meperidine group:
• Meperidine (Demerol) • Alphaprodine (Nisentil) • Alfentanil (Alfenta) • Fentanyl (Sublimaze) • Sufentanil (Sufenta) • Diphenoxylate (in Lomotil) • Loperamide (in Imodium)
• Methadone group: • Methadone (Dolophine) • Propoxyphene (Darvon)
naloxone
Naloxone (Narcan) is a narcotic antagonist and is used in medical emergencies to reverse narcotic overdose. Overdose of narcotics results in respiratory depression and death due to respiratory shut down. Naloxone will reverse the respiratory depressant effects of the narcotics thus counteracting the lethal effects of these agents. Naloxone is given intravenously, intramuscularly or subcutaneously. Note: Naloxone does not have agonist activity at any opioid receptors.
Nalmefene (Revex) and naltrexone (ReVia) are the other two narcotic reversal agents used to reverse the respiratory depressive effects of the narcotic analgesics.
Typical narcotic analgesic drugs which are reversed by naloxone (Narcan), nalmefene (Revex), and naltrexone (ReVia) include:
• Codeine • Morphine • Hydrocodone • Oxycodone • Meperidine (Demerol) • Fentanyl
Note: Naltrexone (ReVia) is also used to treat alcohol dependence.

narcotic analgesics
The central nervous system contains three types of endogenous opioids. Which one of the following is NOT one of them?
beta-endorphins
• morphine
enkephalins
dynorphins
229 copyright e 2013-2014 - Dental Decks
PHARMACOLOGY
Which narcotic is not used in dentistry?
• morphine
• hydrocodone (component of Vicodin)
• oxycodone (component of Percocet)
• meperidine (Demerol)
• codeine
• fentanyl
narcotic analgesics
PHARMACOLOGY
230 copyright S 2013-2014 - Dental Decks

• morphine
Opiate receptors in the CNS mediate analgesic activity. Opioid agonists occupy the same receptors as endogenous opioid peptides, and both alter the central release of neurotransmitters from afferent nerves sensitive to noxious stimuli. They decrease presynaptic release of neurotransmitters and increase postsynaptic potential. The opioid receptors all have a common general structure. They are characteristically G protein-linked receptors embedded in the plasma membrane of neurons. Once the receptors are bound, a portion of the G protein (Gp is activated, allowing it to diffuse within the plasma membrane. The G protein moves within the membrane until it reaches its target — either an enzyme or an ion channel.
Opioid receptors in the central nervous system are thought to be activated by endogenous chemicals under physiologic conditions. The body contains three types of these chemicals that produce morphine-like effects (reduce pain):
• Beta-endorphins bind to opioid receptors in the brain and have potent analgesic activity. • Enkephalins bind to opioid receptors in the brain and are more widely distributed in the brain than the beta-endorphins. Seem to play a role in pain perception, movement, mood, and behavior. • Dynorphins are the most powerful of these chemicals and are found throughout the central and peripheral nervous systems. Some research supports the theory that they regulate pain at the spinal cord level, influence feeding behavior at the hypothalamic level and function with other endogenous opioids to regulate the cardiovascular system.
Opioid receptors: 1. urn (u) - mediate morphine-like supraspinal analgesia, miosis, respiratory depression, euphoria, physical dependence, and suppression of opiate withdrawal. Note: The prototypical opioid agonist for this receptor is morphine, and its analgesic activity is considered to depend on its binding to this receptor. 2. delta (5) - mediate antagonist activity. Note: The enkephalins are considered to be the typical agonist for this receptor. 3. kappa (K) - mediate spinal analgesia, respiratory depression, and sedation. Note: The dynorphins are thought to be the typical agonist for this receptor.
Sites of analgesic action of opioids: The opioid drugs produce analgesia by actions at several levels of the nervous system, in particular, inhibition of neurotransmitter release from the primary afferent terminals in the spinal cord and activation of descending inhibitory controls in the midbrain.
*** Opioid analgesics (i.e., morphine, codeine, meperidine, propoxyphene, etc.) mimic endogenous opioids at CNS opiate receptors, raising the pain threshold and increasing pain tolerance.
• morphine
Therapeutic indication for opioids (narcotic analgesics) are the relief of moderate-to-severe pain, as preanesthetic medications, as analgesic adjuncts during anesthesia, as antitussives, and as antidiarrheals. Note: They are administered with caution to patients with head injury or those with a history of drug abuse and dependency.
1. Morphine is not used in dentistry because of its high addictive liability. Notes 2. Hydrocodone in combination with acetaminophen is known as Vicodin,
Lorcet, Lortab, Maxidone, and Zydone. 3. Hydrocodone in combination with ibuprofen is known as Vicoprofen. 4. Oxycodone in combination with acetaminophen is known as Roxicet, Per-cocet, and Tylox. 5. Oxycodone in combination with ibuprofen is known as Combunox. 6. Oxycodone alone is known as OxyContin. It is more potent than codeine. 7. Meperidine (Demerol) in combination with promethazine is known as Mepergan Fortis. 8. Codeine in combination with acetaminophen is known as Tylenol #3. 9. Fentanyl is available as a transmucosal preparation known as Actiq, a transdermal patch formulation known as Duragesic and as an intravenous preparation known as Sublimaze.
Among the opiates available for use in dentistry, hydrocodone products are commonly
the drugs of choice.

narcotic analgesics
Which of the following analgesics may interact with warfarin (Coumadin) to cause increased bleeding? Select all that apply.
acetaminophen
ibuprofen
hydrocodone with acetaminophen
aspirin
oxycodone with acetaminophen
231 copyright O 2013-2014 - Dental Decks
PHARMACOLOGY
narcotic analgesics
Your patient has a history of neuropathic pain. They are currently taking oxycodone (OxyContin), which is an opiate analgesic. Which of the following are adverse effects of oxycodone? Select all that apply.
• nausea
• peptic ulcers
• insomnia
• constipation
• xerostomia
• excessive perspiration
232 copyright 0 2013-2014- Dental Decks

• ibuprofen • aspirin
Ibuprofen and other non-selective NSAIDs (inhibitors of both cyclooxygenase 1 and cyclooxygenase 2 enzymes) such as naproxen (Anaprox) and flurbiprofen (Ansaid) inhibit platelet aggregation. This action would enhance the anti-coagulant effect of warfarin (Coumadin) to increase the risk of bleeding. Aspirin inhibits platelet aggregation to potentiate the anticoagulant effects of warfarin (Coumadin) and increase the risk of bleeding.
Acetaminophen is a non-narcotic analgesic that does not affect platelet aggregation nor does it affect the coagulation pathway. Thus, it will not affect the anticoagulant nature of warfarin (Coumadin). Acetaminophen can be given safely to patients taking warfarin (Coumadin).
Hyrocodone with acetaminophen is a combination of a narcotic analgesic with acetaminophen. Common brand names for this combination are Vicodin, Lorcet and Lortab. Hydrocodone and the entire drug class of narcotic analgesics do not affect blood clotting and will not enhance the anticoagulant effects of warfarin (Coumadin). Narcotics with acetaminophen can be given safely to patients taking warfarin (Coumadin).
• nausea • constipation
The most common side effect of the narcotic (opiate) analgesics is nausea. The most serious side effect of the narcotic analgesics is respiratory depression. The cause of death from overdose of narcotics is almost always due to respiratory depression and shut down of the respiratory system.
Narcotic analgesics do not cause peptic ulcers, xerostomia, or excessive perspiration. Nor do they cause insomnia, but rather would cause drowsiness and sedation since narcotics depress the conscious centers of the brain.

narcotic analgesics
Which drug is a synthetic opioid analgesic used as an intravenous sedative and is more potent than morphine?
• meperidine (Demerol)
> pentazocine (Talwin)
• propoxyphene (Darvon)
• fentanyl
All of the following analgesics can produce EXCEPT one. Which one is the EXCEPTION?
• codeine
• morphine
• hydrocodone
• meperidine (Demerol)
• oxycodone
• voltaren
PHARMACOLOGY
narcotic analgesics
drug dependence and addiction
234 copyright © 2013-2014 - Dental Decks

•fentanyl
Fentanyl (Sublimaze)is a potent narcotic analgesic used primarily as an intravenous supplement during conscious sedation procedures or procedures requiring general anesthesia. Fentanyl is 80-100 times more potent than morphine.
Fentanyl is also available as a lollipop-type lozenge (brand name Actiq) for transmucosal absorption and as a transdermal patch (brand name Duragesic) for delivery through a patch applied to the skin. Note: Fentanyl congeners include Alfentanil, Sufentanil, and Remifentanil.
Meperidine (Demerol) is used as an intravenous supplement during conscious sedation procedures. However, it is less potent than morphine and much less potent than fentanyl. Meperidine (Demerol) is also used as an oral medication for pain control after dental surgery. Note: A metabolite, normeperidine, is a CNS stimulant. Important: Contraindicated with MAO inhibitors (e.g., phenylzine and tranylcypromine)
Pentazocine (Talwin) is chemically related to morphine and has weak analgesic properties. It is a mixed agonist-antagonist drug, having agonist activity at some receptors and antagonist activity at other receptors. It is not used intravenously to produce conscious sedation. Pentazocine has abuse liability. Note: Talwin NX tablets contain naloxone which is added to deter misuse.
Propoxyphene (Darvon) in the form of propoxyphene napsylate with acetaminophen is known as Darvocet-N 100 and is useful for pain control after dental surgery. It is taken orally and not used intravenously. Darvocet-N 100 has low abuse liability. Note: It is less potent than codeine and a metabolite, norpropoxyphene, is a CNS stimulant.
Tramadol (Ultram) is an opioid partial agonist. It is not a scheduled drug. Use great caution in combination with MAOIs (e.g., phenylzine and tranylcypromine).
• vu i ia ieu
*'** Voltaren is a NSAID which do not produce drug dependence and addiction.
The other analgesics belong to the opiate class of drugs. They are also known as narcotic analgesics since the actions of this family is to cause drowsiness and sleep as a side effect.
The opiates produce drug dependence leading to addiction. Psychic dependence, physical dependence, and tolerance can develop upon repeated administration. Psychic dependence is unlikely if an opiate is taken for a short period for pain relief. Physical dependence is a condition in which continued administration of the drug is required to prevent unpleasant withdrawal symptoms. Tolerance occurs when increasingly large doses of opiate are required in order to produce the same degree of analgesia.
Opiate drugs used in dentistry to provide pain relief after dental surgery include: • Codeine • Hydrocodone (Vicodin)
• Oxycodone (Percocet; Tylox) • Meperidine (Demerol)














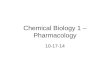
![Basic Pharmacology[1]](https://img.dokumen.tips/doc/110x75/577ce6e41a28abf10393dca7/basic-pharmacology1.jpg)










![Applies Fish Pharmacology[1]](https://img.dokumen.tips/doc/110x75/552ce87c4a795978658b4578/applies-fish-pharmacology1.jpg)

