Embed Size (px)
Citation preview

Pharmacology

Local Anesthetics

Local Anesthetics• Amides vs. Esters• Pharmacodynamics and Pharmacokinetics• Calculating LAs• Injections

Amides
• Metabolized in the liver
Esters
• Metabolized by pseudocholinesterase in plasma
Amides
• Lidocaine• Bupivicaine• Mepivicaine• Articaine• Prilocaine
Esters
• Procaine• Cocaine• Tetracaine• Benzocaine• More toxic, more
allergic (methylparaben)

Amides• Lidocaine (Xylocaine) safest in children• Bupivicaine (Marcaine) not safe in children• Mepivicaine (Carbocaine, Polocaine) causes least vasodilation• Articaine (Septocaine) has one ester chain• Prilocaine (Citanest) methemglobinemia

Esters• Procaine• Cocaine vasoconstrictor• Tetracaine• Benzocaine

Pharmacodynamics
• Sodium channel blocker• Only non-ionized (free base) form can
penetrate neuron membrane• Critical length

Pharmacokinetics• ↑ blood flow shorter duration of action• ↑ lipid solubility/hydrophobicity more potent
longer duration of action• ↑ protein binding longer duration of action• ↓ pKa faster onset of action
– Mepivicaine: 7.6– Lidocaine, prilocaine, articaine: 7.8– Bupivicaine: 8.1

Calculating Local Anesthetic
• 1mL of liquid at sea level weighs 1g• Carpule/cartridge of anesthetic contains
1.8mL• So entirety of liquid in carpule weighs how
much?• 1.8g or 1800mg• But this isn’t very relevant clinically…

Calculating Local Anesthetic
• For 100% solution, 1.8g or 1800mg• For 1% LA,
• For 2% lidocaine, 36mg per carpule• For 4% articaine, 72mg per carpule
18mg
Practice Question
• A carpule of 2% lidocaine solution with 1:100,000 epinephrine would contain how much epinephrine in mg?
• For .001% epinephrine, 0.018mg

Vasoconstrictor
1. Prolong numbness2. Reduce toxicity3. Promote hemostasis

Toxicity
• Max epinephrine for ASA I patient= 0.2mg• Max epinephrine for cardiac patient= 0.04mg• Max lidocaine without vasoconstrictor= 4.4mg/kg• Max lidocaine with vasoconstrictor= 7mg/kg

Local Anesthetics

Delivering Local Anesthetic
• “Slow” injection is 1 carpule per minute

Needle Dimensions
• Length– Short= 20mm– Long= 32mm
• Diameter– 30-gauge= 0.3mm– 27-gauge= 0.4mm– 25-gauge= 0.5mm

Inferior Alveolar Nerve Block
• Highest failure rate• Halstead= classic• Gow-Gates= open mouth• Akinosi= closed mouth
3/4 carpule

Buccal Nerve Block
• Done in tandem with IAN block
1/4 carpule

Mental Nerve Block
• Locate rubbery bundle with finger
• Mental foramen by apices of premolars
1/3 carpule

Incisive Nerve Block
• Same as mental nerve block except hold pressure for 2 minutes after injection to force anesthetic into mental foramen
1/3 carpule

Posterior Superior Alveolar Block
• Maxillary molars• 16mm depth (half the
length of long needle)• High hematoma risk
1/2 carpule

Infraorbital Block
• Maxillary anteriors + premolars
• Also called true ASA block• Infraorbital foramen
1/2 carpule

Greater Palatine Nerve Block
• Posterior hard palate• Greater palatine foramen
1/4 carpule

Nasopalatine Block
• Hard palate from canine to canine
• Most painful
1/4 carpule

Local Infiltration
• Enter in vestibule• Aim for root apex• Works well in anterior
because facial cortical plate is thin
1/2 carpule


Antibiotics

Sulfonamides
• Bacteriostatic• Folate synthesis inhibitor (competes with
PABA)• Sulfadiazine, Sulfamethoxazole

Fluoroquinolones
• Bactericidal• DNA synthesis inhibitor• Ciprofloxacin, Levofloxacin

Penicillins• Bactericidal• Cell wall synthesis inhibitor, β-lactam• Cross-allergenic with cephalosporins because they are chemically related
• Penicillin G IV, more sensitive to acid degradation• Penicillin V oral• Amoxicillin broad spectrum• Augmentin amoxicillin + clavulanic acid (β-lactamase-resistant)• Methicillin β-lactamase-resistant• Dicloxacillin “• Ampicillin best/broadest gram-negative spectrum• Carbenicillin used specifically against pseudomonas
Cephalosporins
• Bactericidal• Cell wall synthesis inhibitor, β-lactam• 1st Gen= Cephalexin (Keflex)• 2nd Gen= Cefuroxime• 3rd Gen= Ceftriaxone• 4th Gen= Cefepime• 5th Gen= Ceftaroline

Monobactams
• Bactericidal• Cell wall synthesis inhibitor, β-lactam• Aztreonam

Carbapenems
• Bactericidal• Cell wall synthesis inhibitor, β-lactam• Imipenem

Tetracyclines
• Bacteriostatic• Protein synthesis inhibitor (30S ribosomal
subunit)• Tetracycline, Doxycycline, Minocycline• Broadest antimicrobial spectrum

Macrolides
• Bacteriostatic• Protein synthesis inhibitor (50S ribosomal
subunit)• Erythromycin, Clarithromycin, Azithromycin
Mac likes to throw mice

Lincosamides
• Bacteriostatic• Protein synthesis inhibitor (50S ribosomal
subunit)• Clindamycin, Lincomycin
Link also hides mice

When is Antibiotic Prophylaxis Required?
• Cardiovascular conditions– Prosthetic heart valve– History of endocarditis– Heart transplant with valvulopathy/valve dysfunction– Congenital heart problems
• Compromised immunity– Organ transplant– Neutropenia– Cancer therapy

Rx for Infective Endocarditis Prophylaxis
• First choice Amoxicillin 2g 1 hr before tx• Children, first choice Amoxicillin 50mg/kg 1 hr before tx• PCN allergy Clindamycin 600mg 1 hr before tx• Children, PCN allergy Clindamycin 20mg/kg 1 hr before tx• Non-oral (IV or IM) Ampicillin 2g 30 min before tx• Children, non-oral Ampicillin 50mg/kg 30 min before tx

Rx for Prosthetic Joint Prophylaxis
• First choice Keflex 2g 1 hr before tx

When is Antibiotic Prophylaxis NOT Required?
• Cardiovascular conditions– Cardiac pacemaker– Rheumatic fever without valvular dysfunction– Mitral valve prolapse without valvular
regurgitation

Side Effects• What causes GI upset and pseudomonas colitis? Clindamycin
• What is most likely to cause superinfection? Broad spectrum antibiotics
• What is associated with aplastic anemia? Chloramphenicol
• What is associated with liver damage? Tetracycline
• What is associated with allergic cholestatic hepatitis? Erythromycin estolate

Drug Interactions
• Cidal and static drugs cancel each other out• Penicillin & probenecid• Tetracycline & antacids/dairy• Broad spectrum antibiotics & anticoagulants• Antibiotics & oral contraceptives• Macrolides & seldane/digoxin

Drug Concentration
• Clindamycin à bone• Tetracycline à gingival crevicular fluid

Antivirals & Antifungals
• Acyclovir, Valcyclovir à herpes• Fluconazole, Ketoconazole à candidiasis– Clotrimazole (Mycelex) is in troche form

Analgesics

NSAIDs• Aspirin (ASA) COX 1 and 2 blocker (irreversible) GI• Ibuprofen (Motrin, Advil) COX 1 and 2 blocker (reversible) kidney• Naproxen (Aleve) COX 1 and 2 blocker (reversible)• Ketorolac (Acular) COX 1 and 2 blocker (reversible) IV, IM, or oral• Indomethacin COX 1 and 2 blocker (reversible) blood dyscrasias• Phenylbutazone (“Bute”) COX 1 and 2 blocker (reversible) for animals• Diflunisal (Dolobid) COX 1 and 2 blocker (reversible) longer half-life• Celecoxib (Celebrex) COX 2 blocker• Meloxicam (Mobic) COX 2 blocker arthritis
Acetaminophen• Acetaminophen inhibits pain in CNS liver• Drug of choice in feverish child, whereas aspirin can cause Reye’s Syndrome

Maximum Dose
• Ibuprofen 3.2g/day• Acetaminophen 4g/day

Therapeutic Effects of Aspirin
• Analgesic à inhibit COX 1 and 2 (PG synthesis)• Anti-inflammatory à same• Antipyretic à inhibit PG synthesis in
temperature regulation center of hypothalamus
• Bleeding time à inhibit TXA2 synthesisthereby inhibiting platelet aggregation

Toxic Effects of Aspirin
• Occult bleeding from GI tract• Tinnitus• Nausea and vomiting• Metabolic acidosis• Decreased tubular resorption of uric acid• Salicylism• Delirium• Hyperventilation

Corticosteroids
• Prednisone• Hydrocortisone• Triamcinolone• Dexamethasone

Therapeutic Effects of Steroids
• Analgesic à inhibit phospholipase A2 (AA synthesis)
• Anti-inflammatory à same

Side Effects of Steroids
• Gastric ulcers• Immunosuppression• Acute adrenal insufficiency• Osteoporosis• Hyperglycemia• Redistribution of body fat
Narcotics/Opioids• mu-opioid receptor agonists (in CNS)• Morphine• Hydrocodone• Oxycodone• Oxycontin controlled release• Codeine suppresses cough reflex, cough syrup• Tramadol (Ultram) similar to codeine• Heroin• Fentanyl• Sufentanil• Carfentanil• Meperidine (Demerol) lethal if combined with an MAOI
Combination Narcotics
• Vicodin Hydrocodone + APAP• Percocet Oxycodone + APAP• Tylenol 1 300mg APAP + 8mg Codeine• Tylenol 2 300mg APAP + 15mg Codeine• Tylenol 3 300mg APAP + 30mg Codeine• Tylenol 4 300mg APAP + 60mg Codeine
Therapeutic & Side Effects of Morphine
• Miosis• Out of it• Respiratory depression• Pneumonia• Hypotension• Infrequency• Nausea and vomiting• Euphoria and dysphoria

Overdose and Addiction
• Naloxone inverse agonist, emergency• Naltrexone antagonist, treat addiction• Methadone treat addiction• Pentazocine mixed agonist-antagonist• Nalbuphine mixed agonist-antagonist• Buprenorphine mixed agonist-antagonist

Nitrous Oxide
• Horace Wells was first to use for own extraction by his assistant
• Sensation before onset à tingling• Side effect à nausea• Long term exposure à peripheral neuropathy• MAC 105%• Diffusion hypoxia

General Principles
• Pharmacokinetics– pH– First Pass Effect– Volume of Distribution– Phase I vs. Phase II Metabolism– First-order vs. Zero-order Kinetics– Drug-drug interactions
• Pharmacodynamics – Type I vs. Type II Dose Response Curves
Pharmacokinetics
0. Administration1. Absorption2. Distribution3. Metabolism4. Clearance/Elimination
What the body does to the drug
(0) Administration
• Oral= ingestion through mouth• Sublingual= dissolved under the tongue• Subcutaneous= injected under the skin• IM= intramuscular, injected into muscle• IV= intravenous, injected into vein• Inhalation= breathed in• Topical= applied to skin or mucous membrane
How is a drug delivered?
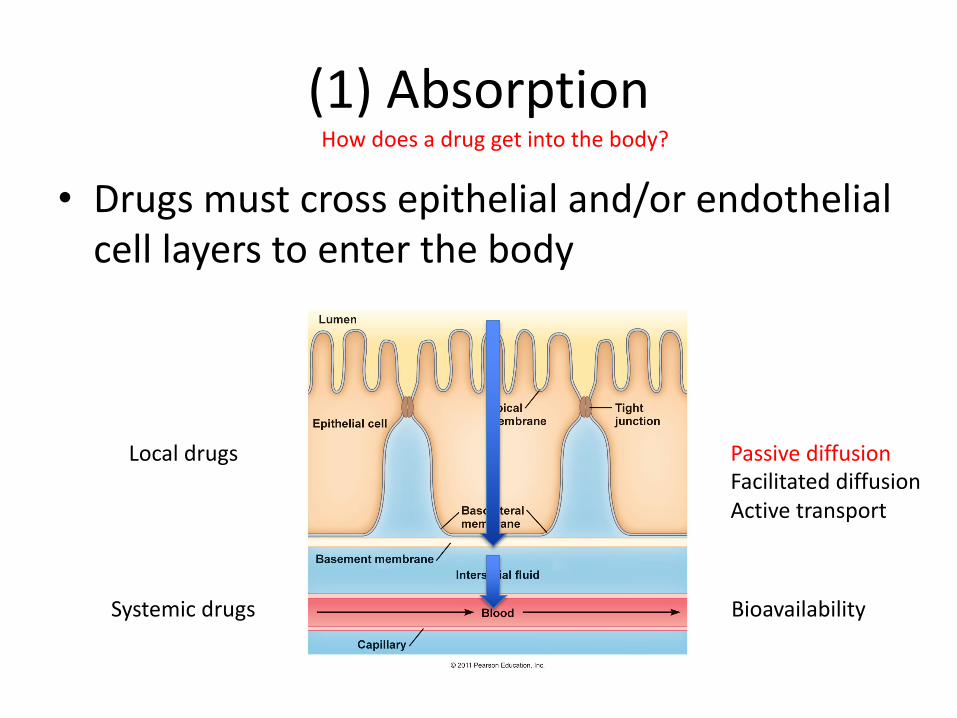
(1) Absorption
• Drugs must cross epithelial and/or endothelial cell layers to enter the body
How does a drug get into the body?
Local drugs
Systemic drugs
Passive diffusionFacilitated diffusionActive transport
Bioavailability

pH Considerations
• Acid/base properties of drug and pH of the environment can affect the charge state of a drug and hence alter its absorption– For weak acids, we want pH < pKa– For weak bases, we want pH > pKa
Acid Drug Base Drug
Acidic Environment
Non-ionized Ionized
Basic Environment
Ionized Non-ionized

(2) Distribution
• Most drugs must reach the blood in order to be distributed effectively
How does a drug get to the target site?

• Oral drugs undergo the first pass effect
First Pass Effect
Hepatic portal system

Volume of Distribution (Vd)
• Describes distribution of drug across the three body water compartments– Plasma (4%)– Interstitial (16%)– Intracellular (40%)
• Women, obese, and older people generally have less body water than the “average man”– Adipose has lowest water content– Brain and muscle have highest water content
• Binding to serum proteins lowers Vd and “traps” drugs in the blood as hydrophilic molecules
75 kg

(3) Metabolism
• Phase I– Functionalization (oxidation, reduction, hydrolysis)– Cytochrome P450
• Phase II– Conjugation (glucouronide, glutathione, glycine)– UDP-glucouronosyltransferase
How is a drug molecule chemically altered by the body?
Drug Metabolite Inactive(possibly inactive)
Phase I Phase II

Acetaminophen
Reduction GlutathionationPhase I Phase II

(4) Clearance/EliminationHow is a drug molecule eliminated from the body?
Urine
Drug
Feces
Phase I Phase II

Elimination Kinetics
• First-order kinetics– Constant fraction of drug is eliminated per unit
time (%/hour)– More common
• Zero-order kinetics– Constant amount of drug is eliminated per unit
time (mg/hour)– Less common– Higher risk of drug accumulation

Drug-Drug Interactions
• One drug affects the pharmacokinetics of another drug, most commonly metabolism– Induction à drug #1 induces liver cytochrome
enzymes resulting in increased metabolism and reduced effect of drug #2
– Inhibition à drug #1 competes for metabolism or directly inhibits liver cytochrome enzymes resulting in decreased metabolism and increased toxicity of drug #2

Drug-Drug InteractionsDental Drug Interacting Drug Effect
Diazepam Clarithromycin Increased sedation because of reduced metabolism of benzodiazepine
Tetracyclines Oral antacids (TUMS)
Reduced absorption of tetracyclines
Aspirin Anticoagulants Increased bleeding tendency
Aspirin Probenecid Decreased effect of probenecid
Aspirin Methotrexate Increased methotrexate toxicity
Acetaminophen Alcohol Increased risk of liver toxicity in chronic alcoholics
Local anesthetics Acetylcholinesterase inhibitors
Reduced effectiveness of acetylcholinesterase inhibitor

PrescribedDose
AdministeredDose
Active Dose
Intensity of effect
Medical errorsPatient compliance
AbsorptionDistributionMetabolismClearance
Pharmacokinetics
Drug-receptor interaction Pharmacodynamics


General Principles
• Pharmacokinetics– pH– First Pass Effect– Volume of Distribution– Phase I vs. Phase II Metabolism– First-order vs. Zero-order Kinetics– Drug-drug interactions
• Pharmacodynamics – Type I vs. Type II Dose Response Curves

Pharmacodynamics
• Almost all drug targets are proteins– Receptors– Ion channels– Enzymes– Carriers
• How a drug interacts with its target to produce therapeutic (and toxic) effects– Agonist– Antagonist– Inverse agonist
What the drug does to the body
Agonist
• Mimics the effects of an endogenous agonist molecule– Full agonist= can produce 100% of its desired effect– Partial agonist= cannot produce 100% of its desired
effect
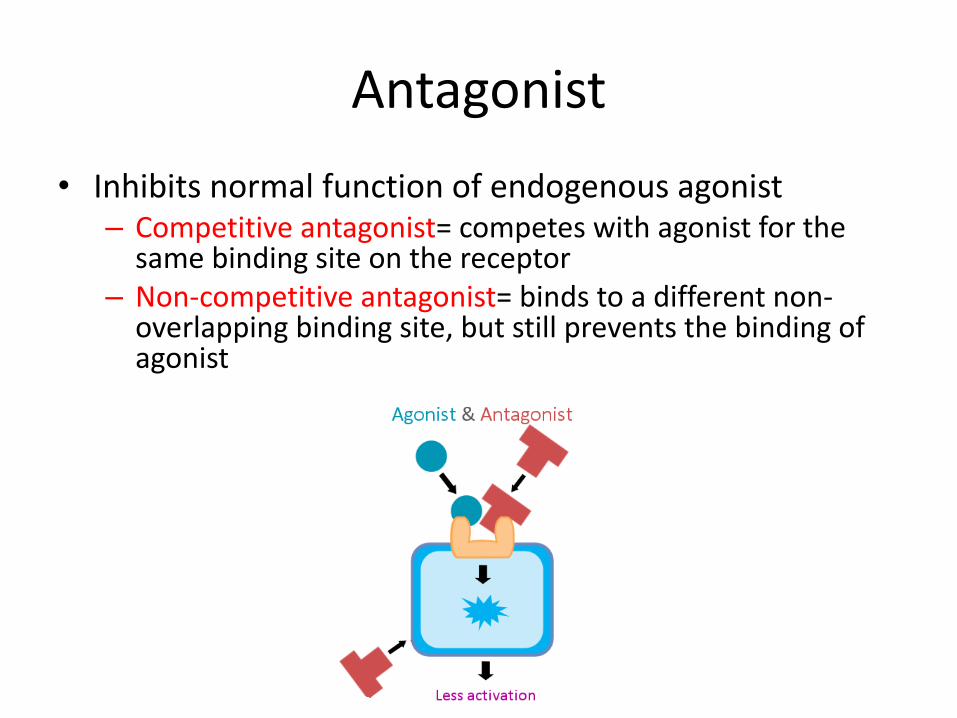
Antagonist• Inhibits normal function of endogenous agonist– Competitive antagonist= competes with agonist for the
same binding site on the receptor– Non-competitive antagonist= binds to a different non-
overlapping binding site, but still prevents the binding of agonist

Inverse Agonist
• Inhibits the basal activity of a receptor in the absence of the normal agonist
• Binds to a special kind of receptor that is active at rest in order to inhibit its basal activity

Type I Dose Response Curve
• X-axis indicates dose of drug• Y-axis indicates response/efficacy of drug• Can be either hyperbolic or sigmoid/log form

Type I Dose Response Curve
• Intrinsic activity= maximal effect (Emax) of a drug– Full agonist has intrinsic
activity of 1– Partial agonist is between
0 and 1– Antagonist has intrinsic
activity of 0
Type I Dose Response Curve
• Efficacy= effect of a drug as a function of binding• Affinity= attractiveness of a drug to its receptor– The lower the dissociation constant (Kd) the higher
the affinity
• Potency= power of a drug at a specific concentration– Usually measured by the effective concentration of
drug (EC50) leading to half its maximal effect (50% response)

Type I Dose Response Curve
• Competitive antagonist shifts agonist curve RIGHT• Noncompetitive antagonist shifts agonist curve DOWN

Type II Dose Response Curve• X-axis still indicates dose of drug• Y-axis indicates number of subjects responding to
a drug, rather than the efficacy of a drug

Type II Dose Response Curve• ED50= effective dose where 50% of population responded effectively
(treated)• TD50= toxic dose where 50% of population experienced toxic side effects• LD50= lethal dose where 50% of population responded lethally (died)
TI= LD50/ED50In animal studies
TI= TD50/ED50In human studies
Therapeutic window

Dose Response Curves
• Type I: dose vs. efficacy of drug• Type II: dose vs. response of patient

Additive
• Combining drugs combines their individual degrees of effect

Antagonistic• Combining drugs causes a lesser effect than either one alone
– Chemical antagonism= drug binds directly to another drug to put it out of commission
– Receptor antagonism= competition between two drugs for a single receptor– Pharmacokinetic antagonism= one drug affects the PK of another via pH, etc.– Physiologic antagonism= two drugs producing opposing effects on the same
tissue via distinct receptors

Synergistic
• Combining drugs leads to more than the sum of the two independently


ANS Pharmacology
• Autonomic Nervous System– Sympathetic Nervous System– Parasympathetic Nervous System
• Receptors in the ANS• Cholinergic Drugs (PSNS)• Adrenergic Drugs (SNS)

ANS Physiology• In general, PSNS and SNS
nerves control the same organs, but have opposing effects on them!– SNS is fight or flight– PSNS is rest and digest, feed
and breed• All nerve pathways originate
from the CNS (brain + spinal cord)– 12 cranial– 0 cervical– 12 thoracic– 5 lumbar– 5 sacral
PSNS SNS

Fight or Flight• Pupil dilation
• Dry mouth
• Increased heart rate
• Airway relaxation
• Slowed digestion
• Bladder relaxation
Rest and Digest, Feed and Breed • Pupil constriction
• Stimulated salivation
• Decreased heart rate
• Airway constriction
• Stimulated digestion
• Bladder constriction

Receptors in the ANS
• Ionotropic= ion channel• Metabotropic= G-protein coupled receptor

Receptors in the ANS• Cholinergic= binds acetylcholine– Nicotinic (nAChR)= also binds nicotine; ionotropic– Muscarinic (mAChR)= also binds muscarine; metabotropic
• Adrenergic= binds Epi/NE; metabotropic
SNS
PSNS

M
A
A
N
N
N
Receptors in the ANS
SNS
PSNS
• Cholinergic= binds acetylcholine– Nicotinic (nAChR)= also binds nicotine; ionotropic– Muscarinic (mAChR)= also binds muscarine; metabotropic
• Adrenergic= binds Epi/NE; metabotropic

SNS vs. PSNS• By the distinct effects they have on the same organs
– PSNS à promote “rest and digest” and “feed and breed”– SNS à promote “fight or flight”
• By the region of the spinal cord from which they arise– PSNS à craniosacral– SNS à thoracolumbar
• By the lengths of their pre- and postganglionic neurons– PSNS à long pre-ganglionic, short post-ganglionic near target organ– SNS à short pre-ganglionic to sympathetic trunk, long post-ganglionic
• By the neurotransmitters they use– PSNS à ACh everywhere– SNS à ACh to the ganglion, NE from nerves and Epi/NE from adrenal gland
• By the neurotransmitter receptors that they use– PSNS à muscarinic metabotropic receptors on target organs– SNS à adrenergic metabotropic receptors on target organs
Synthesis of Acetylcholine
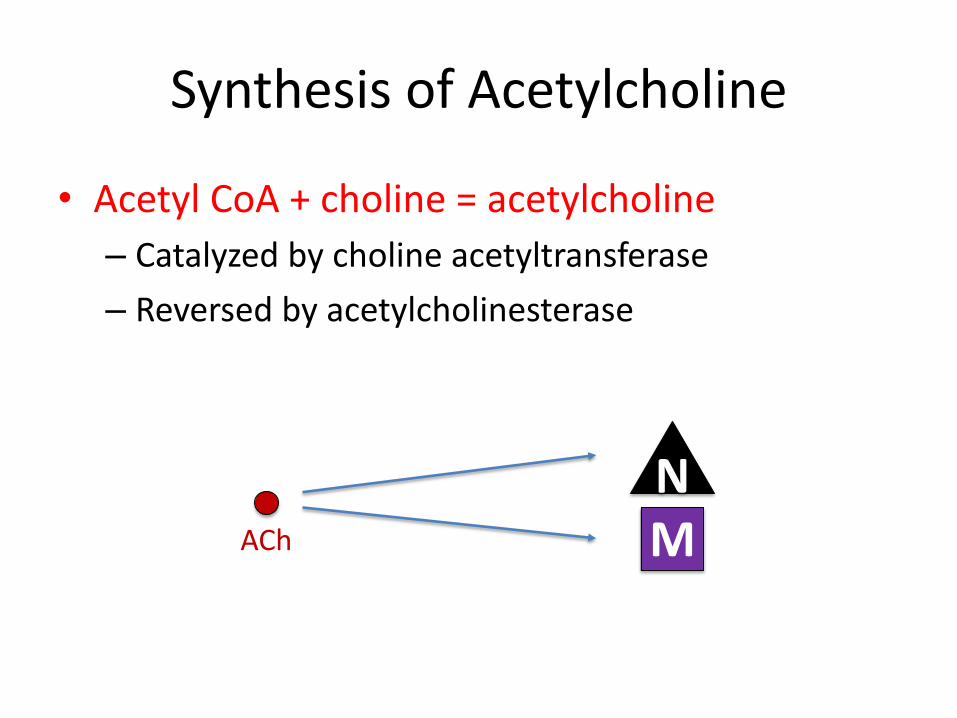
• Acetyl CoA + choline = acetylcholine– Catalyzed by choline acetyltransferase– Reversed by acetylcholinesterase
NMACh

Muscarinic Receptors
M2M1 M3 M4 M5
CNS Heart CNS CNSSmoothmuscle

Muscarinic Receptors
• Bradycardia= ↓ heart rate (chronotropy) and ↓ electrical conduction (dromotropy)
• SLUDS= salivation, lachrymation, urination, defecation, sweating
• BAM= bronchoconstriction, abdominal cramps, miosis
M2
M3
M Agonists
• Non-selective for muscarinic receptors so will affect all of them (M1-5) if systemic
• Therefore should not be used systemically with:– Peptic ulcers—gastric acid– Asthma/COPD—bronchoconstriction– CHF—decreased cardiac output
M

M AgonistsDirect-acting activates M receptor, congener (mimic) of ACh
Pilocarpine stimulates saliva or eye drops to constrict pupils
Methacholine methacholine acetylcholine
Indirect-acting non-competitively inhibits acetylcholinesterase (anticholinesterase)
Neostigmine reversibly inhibits cholinesterase, but can also directly affect NMJ
Physostigmine “
Edrophonium “
Organophosphate insecticides
irreversibly inhibits cholinesterase, poisoning can be treated with Pralidoxime
Nerve gases “
M

M Antagonists/AntimuscarinicsCompetitive inhibitors block M receptor, compete with ACh
Atropine reduces saliva or emergency drug to treat bradycardia (can also cause tachycardia)
Scopolamine “
Propantheline “
M

N Antagonists/Ganglionic BlockersNon-depolarizing blocks N receptor at allosteric site
Mecamylamine used to be used as an antihypertensive
Hexamethonium “
Depolarizing binds to N receptor but cannot be removed
Nicotine addictive substance found in tobacco products
N

N Antagonists/Neuromuscular Blockers
Non-depolarizing blocks N receptor at active site
Tubocurarine arrow poison
Depolarizing binds to N receptor but cannot be removed
Succinylcholine prevent laryngospasm and as a skeletal muscle relaxant during surgery
N
N

Synthesis of Epinephrine and Norepinephrine
• Tyrosine à L-DOPA à dopamine à NE à Epi– Catecholamines= dopamine, NE, Epi– Monoamines= dopamine, NE, Epi, serotonin (5-
HT), histamine
AEpi
NE

Adrenergic Receptors
α1 α2 β1 β2
Heart Smoothmuscle
Smoothmuscle
Smoothmuscle

α-receptors
• Vasoconstriction, urinary retention, pupil dilation (mydriasis)
• Vasoconstriction*
α1
α2

β-receptors
• Tachycardia= ↑ heart rate and ↑ electrical conduction and ↑ strength of contraction (inotropy)
• Renin release from kidneys
• Bronchodilation, vasodilation*, stop peristalsis
β1
β2

Adrenergic Agonists
Isoproterenol activates all β receptors
Norepinephrine activates all α receptors and β1
Epinephrine activates all α and β receptors
Phenylphrine (Sudafed) activates α1 receptor, reduce swelling via peripheral vasoconstriction
Oxymetazoline (Afrin nasal spray) “
Dobutamine activates β1 receptor, kickstarts the heart
Albuterol activates β2 receptor, bronchodilator used as an emergency inhaler
A

Adrenergic AntagonistsCompetitive antagonists block adrenergic receptors, compete with NE
Prazosin blocks α1 receptor
Chlorpromazine (CPZ) blocks α1 receptor and D2 receptor
Metoprolol blocks β1 receptor (cardioselective)
Atenolol “
Propranolol blocks all β receptors, prolongs lidocaine duration
Carvedilol blocks all β receptors and α1
Phentolamine blocks all α receptors
Phenoxybenzamine “
A

Sympathomimetics
Amphetamine stimulates release of stored NE
Tyramine (wine, cheese, chocolate) “
Ephedrine “
Cocaine inhibits reuptake of NE and dopamine
Methylphenidate “ psychostimulant for ADHD
Tricyclic antidepressants inhibits reuptake of serotonin and NE
Monoamine oxidase inhibitors blocks enzymatic degradation of monoamines
ANE

Sympatholytics
Guanethidine inhibits release of NE
Reserpine depletes NE stores thus inhibiting release
Clonidine α2 agonist (CNS) which actually blocks SNS signal
Methyldopa α2 agonist (CNS) which actually blocks SNS signal
ANE

Epinephrine Reversal
• Vasoconstrictor effect of epinephrine is converted into a vasodilator effect in the presence of an α-blocker whereby the β2 vasodilator effect becomes the major vascular response
• Basically α-blocker cancels out epinephrine’s α activation effects and it only activates β receptors

Vasovagal Reflex
• NE can activate baroreceptors which stimulate vagal reflex to reduce heart rate, leading to an opposite response to what NE usually does
• Atropine blocks this reflex


Circulatory System
• Human circulatory system is a closed system
• Pump= cardiac output (CO)• Tubing= peripheral
resistance (PR)• Fluid= blood volume (SV)

Circulatory System• BP= CO x PR• CO= SV x HR• Systole= pressure in arteries
when heart contracts• Diastole= pressure in arteries
when heart relaxes• Preload= pressure in
ventricles before heart contracts
• Afterload= pressure in arteries against which the ventricles must pump
BP= SV x HR x PR
120/80
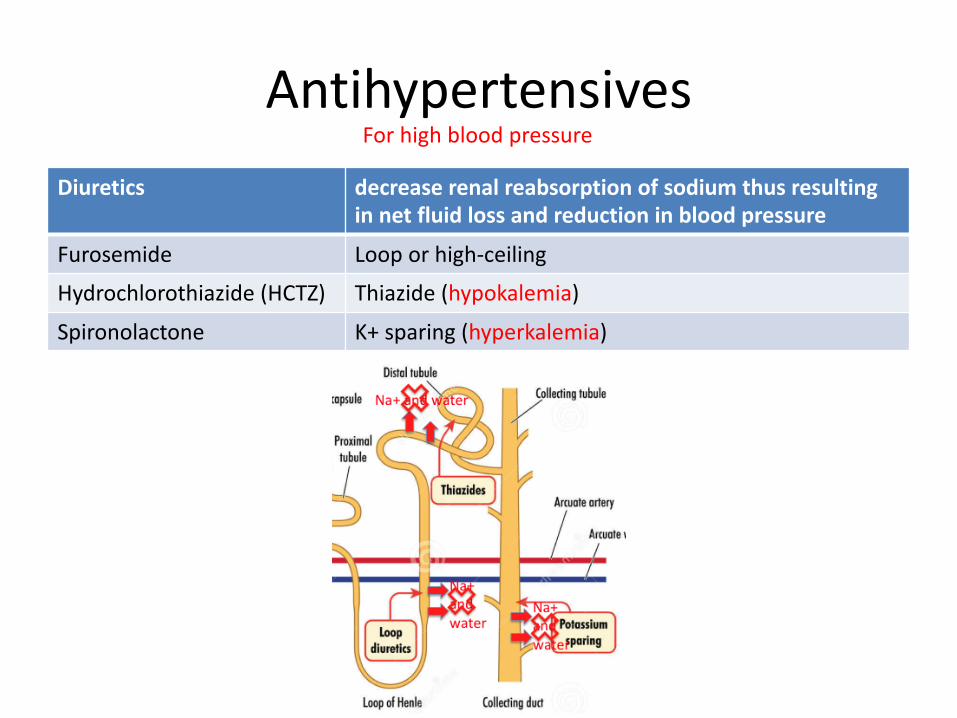
AntihypertensivesFor high blood pressure
Diuretics decrease renal reabsorption of sodium thus resulting in net fluid loss and reduction in blood pressure
Furosemide Loop or high-ceiling
Hydrochlorothiazide (HCTZ) Thiazide (hypokalemia)
Spironolactone K+ sparing (hyperkalemia)

AntihypertensivesFor high blood pressure
Vasodilators open K+ channels to cause vasodilation
Hydralazine
CCBs block calcium influx in order to cause vasodilation
Verapamil may induce gingival hyperplasia
Diltiazem “
Amlodipine “
Nifedipine “

AntihypertensivesACE Inhibitors blocks the enzyme that converts angiotensin I into angiotensin
II the latter of which is a potent vasoconstrictor
-prils
ARBs competitive antagonist at angiotensin II receptor again blocking a potent vasoconstrictor
-sartans
For high blood pressure
Renin
ACE

AntianginalsFor insufficient oxygen to cardiac muscle
Antianginals
Nitroglycerin vasodilation of smooth muscle in coronary arteries to ↑ O2 supply
Propranolol reduces oxygen demand by relaxing the heart
CCBs reduces oxygen demand by reducing peripheral resistance via vasodilation

Anti-CHF DrugsFor failure of heart to pump enough blood
Cardiac Glycosides block Na/K ATPase to increase calcium influx and promote positive inotropy in cardiac muscle cells only
Digoxin
Digitalis
ACE Inhibitors blocks the enzyme that converts angiotensin I into angiotensin II the latter of which is a potent vasoconstrictor
-prils

Anti-ArrhythmicsFor an irregular heartbeat
• Type 1 drugs= Na+ channel blockers for cardiac muscle only– 1A= lengthens refractory period to slow heartbeat– 1B= shortens refractory period to hasten
heartbeat
• Type 2 drugs= beta blockers• Type 3 drugs= K+ channel blockers• Type 4 drugs= Ca2+ channel blockers (CCBs)

Anti-ArrhythmicsFor an irregular heartbeat
Drug Name Type Arrhythmia
Quinidine Type 1A a-fib, supraventricular tachyarrhythmia
Procainamide “ “
Lidocaine Type 1B ventricular arrhythmia
Propranolol Type 2 paroxysmal tachycardia
Verapamil Type 4 a-fib, paroxysmal tachycardia, supraventricular tachyarrhythmia
Digitalis Cardiac glycoside
a-fib, paroxysmal tachycardia; digitalis-induced arrhythmia can be reversed with Phenytoin


Continuum of CNS Excitability
D S GABA
N M A

Antipsychotics
1st Generation D2 blocker
Haloperidol tardive dyskinesia
Phenothiazines tardive dyskinesia; specific examples are Chlorpromazine, Thioridazine, and Fluphenazine
2nd Generation D and 5HT blocker
Clozapine not as many side effects
For schizophrenia
D
S

AntidepressantsSSRI selective serotonin reuptake inhibitor
Fluoxetine anticholinergic side effects
Citalopram “
Trazodone “
SNRI/TCA serotonin and NE reuptake inhibitor, tricyclic antidepressants
Amitriptyline “
Imipramine “
MAOI monoamine oxidase inhibitors
Phenelzine “
Tranylcypromine “
Lithium is drug of choice for manic depression (bipolar disorder).
For depression

Anxiolytics/Sedatives
• Benzodiazepines• Barbiturates
For anxiety or sedation

Benzodiazepines• Increase GABA binding and chloride
ion influx to slow down the CNS• Ideal drug for oral sedation in the
dental setting• Propylene glycol can induce
thrombophlebitis in large veins
GABA
Benzodiazepine (BZD)
Diazepam 2-10mg Valium 1 hour before dental appointment
Triazolam Halcion
Chlordiazepoxide

Barbiturates
• Same mechanism as BZD• Barbs are contraindicated in patients with
intermittent porphyria because they will aggravate the disease
• Barb overdose causes respiratory depression
GABA
Barbiturate
Thiopental quick onset, short duration of action

• The more soluble the agent in blood, the more you need to reach critical tension in the brain
• Stage I: analgesia/feeling better• Stage II: delirium• Stage III: surgical anesthesia• Stage IV: medullary paralysis
General Anesthetics
General Anesthetic
Halothane hepatotoxicity

Parkinson’s Disease
• Substantia nigra to striatum is main pathway• Due to dopamine deficiency in brain• Dopamine cannot cross the BBB, but its precursor
levodopa (L-DOPA) can• Carbidopa blocks DOPA decarboxylase, allowing
L-DOPA to cross the BBB where it can be converted to dopamine once in the brain






![PHARMACOLOGY FOR OPTOMETRY - School of Medical · PDF file[PHAR3306 Pharmacology for Optometry 2013] 3 PHAR3306 COURSE INFORMATION UNITS OF CREDIT (UOC) Pharmacology for Optometry](https://img.dokumen.tips/doc/110x75/5aac711e7f8b9a8d678cebdd/pharmacology-for-optometry-school-of-medical-phar3306-pharmacology-for-optometry.jpg)







