Embed Size (px)
Citation preview

TRACHEOSTOMY CARE
BILL WOJCIECHOWSKI, MS, RRTDEPARTMENT OF CARDIORESPIRATORY CAREUNIVERSITY OF SOUTH ALABAMAMOBILE, ALABAMA

TRACHEOSTOMY CARE
Upper airway functionsbypassed whenpatient hastracheotomyperformed.

UPPER AIRWAY FUNCTIONS
Heat/moisture exchange
Thermoregulation Gustation (taste) Olfaction (smell) Filtration

CLINICAL COMPLICATIONS
Altered or loss of voice Speech & language delays (young
children) Loss of smell & taste Compromised nutritional status Impaired swallowing/increased risk
of aspiration Secretion control issues/infection Psychological distress Loss of physiologic PEEP

CLINICAL COMPLICATIONS
Absence of airflow often creates Frustration Anxiety Psychological distress
For children: delayed speech & language development

CLINICAL COMPLICATIONS
Absence of airflow decreases sensations Smell Taste Poor appetite Skin health Supplemental
feeding Difficulty swallowing Risk of aspiration

CLINICAL COMPLICATIONS
Cuffed trach tubes anchor larynx & sometimes interfere with: Laryngeal elevation Epiglottic inversion Airway protection
Cuffed trach tubes secure larynx,Deflated cuff: more freedom.

Three phases of normal swallowing:1) Oral phase2) Pharyngeal phase3) Esophageal phase




UPPER AIRWAY FUNCTIONS
Normal swallowing (pharyngeal phase): Oral & nasal cavities sealed Vocal cords close Positive pressure generated below
cords Air prevented from entering larynx Larynx elevates & moves forward Acts as a lever (mechanical event) Epiglottis seals larynx Food/liquid directed into esophagus

UPPER AIRWAY FUNCTIONS
Swallowing with Trach Tube Inserted: Vocal cords close Air flows through trach tube No subglottic
positive pressure Reduced sensations in
larynx & pharynx Pooling of airway secretions Increase risk of aspirationMost patients OK!!

CLINICAL COMPLICATIONS
Absence of upper airway airflow (inability to nose-breathe) compromises: Heat/moisture exchange Increased secretion viscosity Increased secretion volume Frequent suctioning Increase risk of airway
trauma/infection Presence of trach tube stimulates
secretions


http://www.brucemedical.com/filandcov.html

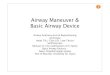
CLINICAL COMPLICATIONS
With cuff inflated: No physiologic PEEP Possible
micro-atelectasis Decreased
alveolar ventilation Compromised
oxygenation

Cuff deflated
Cuff inflated
Physiologic PEEPPresent
Physiologic PEEPAbsent

TRACHEOSTOMY CARE
Inspect stoma daily: irritation/inflammation.
Tracheostomy care is done every 8 to 12 hours and PRN.
Avoid dressings trapping moisture. Check secretions: white & clear;
greenish-yellow Odor often indicates infection. Assess need for suctioning q2h.

TRACHEOSTOMY CARE Signs of Infection:
Yellow or green secretions (pink or blood-tinged)
Thicker mucus Greater volume of mucus Stoma site bleeding Foul odor from stoma Febrile patient Pulmonary congestion Increased RR Listlessness Discomfort with trach/tender stoma site

CLEANING INNER CANNULA
PROCEDURE

CLEAN INNER CANNULA
1. Loosen inner cannula.
2. Hold outer cannula with one hand. Turninner cannula to right with other hand tounlock.

CLEAN INNER CANNULA
3. Remove the inner cannula bysteadily pulling it down and towardyour chest until it is out.

CLEAN INNER CANNULA
4. Place inner cannula in the solution of hydrogenperoxide & normal saline, and don sterile gloves.

CLEAN INNER CANNULA
5. Use trach brush, or pipe cleaner, to clean inner cannula of mucus and dried secretions.

CLEAN INNER CANNULA
6. Place it in bowl of normal saline (NS).
7. Shake off excess NS. Moisture will act as lubricant during inner cannula reinsertion.

CLEAN INNER CANNULA
8. Reinsert inner cannula, keeping curved portion facing downward.

CLEAN INNER CANNULA
9. Lock inner cannula into position.
10. Wash bowls thoroughly and allow to air dry. Soak trach brush soak in hydrogen peroxide-NS solution &, rinse with NS. Air to dry. Discard pipe cleaners.


CUFF PRESSURE
Goal: maintain cuff pressure below tracheal mucosal capillary perfusion pressure which is: 25 to 30 mm Hg.
Cuff pressure maintained: 20 to 25 mm Hg, or 25 to 35 cm H2O
Higher cuff pressures Cut off tracheal mucosal blood flow Tracheal wall damage
(necrosis/tracheomalcia)

CPR - TRACHEOSTOMY
Caregivers must receive CPR training. Suction if indicated. Change trach tube if clogged.
Spare tubes (cuffless &/or cuffed): same size & 1 size smaller
Pinch nose & mouth (cuffless trach). 2 breaths with manual
resuscitator/mouth-to-trach/mouth-to-stoma: STOMA LEAK
Mouth-to-mouth/bag-mask with finger over stoma: STOMA LEAK

TRACHEOSTOMY & SPEECH
Fenestrated: Weaning Speech
Granuloma formation
Increased risk of aspiration

TRACHEOSTOMY & SPEECH
Some space around tube
Snug fit: tube too large non-fenestrated:
poor or no speech


TRACHEOSTOMY TUBE PRECAUTIONS
Use extreme caution with baths and water
No swimming Avoid powder, talc, chlorine
bleach, ammonia, aerosol sprays, or colognes and perfumes
Prevent foreign objects from entering trach tube

TRACHEOSTOMY TUBE PRECAUTIONS
Avoid dust Avoid sand and beach Watch play with other children to
assure toys, fingers or other foreign bodies are not put into trach and trach is not pulled
No contact sports Frequent hand washing

EDUCATION
Teach airway anatomy Teach about equipment Teach CPR Teach infection control Teach humidification Teach suctioning Teach about speaking
valves/fenestrated trach tubes Teach communication through speech
therapy