Embed Size (px)
Citation preview

Using Quantitative and Qualitative Data to Evaluate and Refine a Self-help Kit for Lowering Fat Intake
KIM M. G A N S , ~ ~ ~ H. JOAN LOVELL, ' THOMAS M . L A S A T E R , ' . ~ J A N I C E B. M C P H I L L I P S , ~ MARJORIE R A D E N , ' A N D RICHARD A . CAR LET ON^.^
'Division of Health Education, Memorial Hospital of Rhode Island, Pawtucket, Rhode Island 02860;
2Department of Community Health, Brown University School of Medicine, Providence, Rhode
Island 02912; "currently Beth Israel Hospital, Boston, Massachussetts 02215; 4Division of Cardiology
and Department of Medicine, Memorial Hospital of Rhode Island, Pawtucket, Rhode Island 02860
and Brown University School of Medicine, Providence, Rhode Island 02912
ABSTRACT This paper describes the use of quantitative and qualitative research techniques to evaluate and refine "Let's Eat," a self-help kit for lowering fat intake. A quantitative telephone survey of kit recipients indicated that the original "Let's Eat" kit often was used incorrectly and that the most useful information, the goal-setting checklists and food choice lists, often was ignored. To elicit specific recommendations for "Let's Eat's" improvement, we conducted focus groups that provided quali- tative information that was used to significantly revise the kit. The new kit was then tested with pilot participants in a research project. Results indicated that recipients of the revised kit were significantly more likely to use the goal-setting checklists and to report positive dietary change than were recipients of the original kit.
INTRODUCTION
Despite declining blood cholesterol levels in recent years, high blood cholesterol remains an important public health problem in the U.S.',2Thus, there is a need to develop effec- tive cholesterol-lowering information that is practical and inexpensive for individuals who have their cholesterol mea- sured in a variety of settings. Minimal Contact Education for Cholesterol Change (MC) is a research project funded by the National Heart, Lung and Blood Institute to test the cost effectiveness of a variety of minimal-contact educational approaches to lowering blood cholesterol.This study is being conducted at various sites throughout southern New Eng- land and will recruit up to 13,000 participants.The purpose of this paper is to describe how we used both qualitative and quantitative formative research methods to evaluate and
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Address for corrcspondcncr: Dr. Kim Gans, I'h.13.. M.P.H., L.I>.N., Dlvlslon ofHcalth Education, Mrmorial Hosp~tal of Khode Icland, 1 1 1 Brewcter St., Pawtucket, RI 02860;Tel: (401) 729.2866; Fax: (401) 729-2494. 01996 SOCIETY FOR NUTRITION EI3UCATION
develop the "Let's Eat" kit, a self-help kit for lowering fat intake, for use in this study.
The "Let's Eat" kit was used both as a self-help tool for individuals and as part of the Pawtucket Heart Health Pro- gram (PHHP) cholesterol Screening, Counseling, Referral Events (SCORES) from 1989-1992. These events were a minimal-contact approach to cholesterol screening, educa- tion, and referral.3 Participants had their weight and total blood cholesterol measured, completed a brief eating pattern assessment entitled RateYour Plate,4 and underwent a 10- to 12-minute counseling session with a trained lay educator.The educator discussed the participant's heart disease risk factors, blood cholesterol level, and current eating pattern; helped participants set goals for behavior change; made referral rec- ommendat ion~,~ and described how to use take-home edu- cational materials including "Let's Eat," a self-help kit that focused on lowering total and saturated fat intake.
The original "Let's Eat" kit included two parts: an 8 y x 11" booklet and a 5" x 8" envelope containing additional materials.The booklet contained two pages of instructions, an eating pattern self-assessment entitled "Rat eYour Plate" (RYP), which was used to evaluate fat intake,4 and six pages of information on reading labels, dining out, cooking with less fat, and general information about cholesterol.
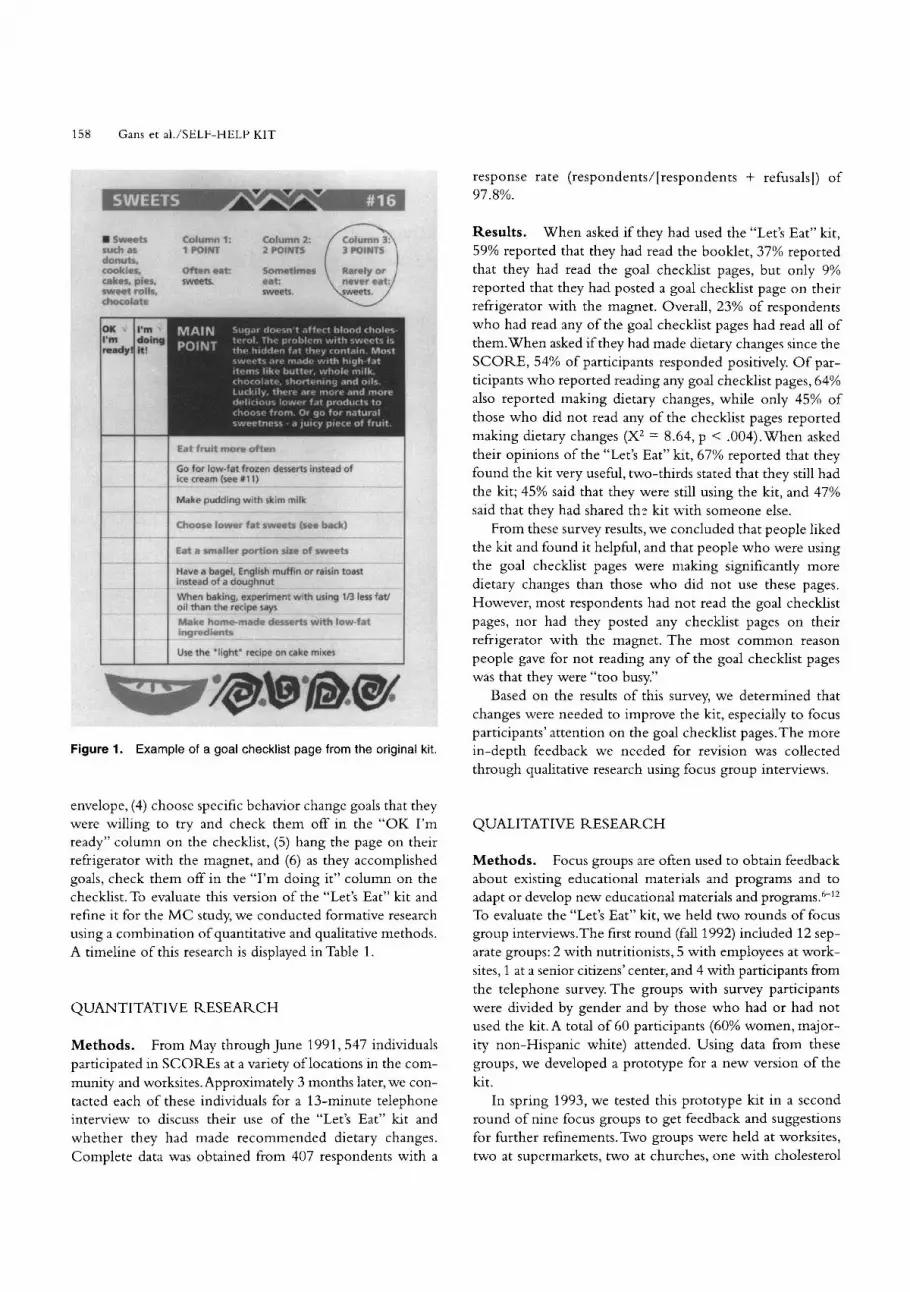
The envelope contained a PHHP magnet, a page of instructions, and 19 separate goal checklist pages. Each checklist page corresponded to a specific food category on the RYP (Fig. l) .The front of each page displayed a check- list of recommended goals for improving eating habits in rela- tion to that specific food category. These checklists were designed to facilitate goal setting and monitoring.The back of each page provided a list ofC'Better Choices" and foods to "Eat Less" as well as recipes, nutrient comparison charts, other tips, and/or graphics.
Participants were instructed to (1) complete the RYP, (2) choose one food category in which to make a change, (3) find the appropriate goal checklist for that category in the
158 Gans et al./SELF-HELP K I T
response rate (respondents/[respondents + refusals]) of 97.8%.
Results. When asked if they had used the "Let's Eat" kit, 59% reported that they had read the booklet, 37% reported that they had read the goal checklist pages, but only 9% reported that they had posted a goal checklist page on their refrigerator with the magnet. Overall, 23% of respondents who had read any of the goal checklist pages had read all of them.When asked if they had made dietary changes since the SCORE, 54% of participants responded positively. O f par- ticipants who reported reading any goal checklist pages, 64% also reported making dietary changes, while only 45% of those who did not read any of the checklist pages reported making dietary changes (X2 = 8.64, p < .004).When asked their opinions of the "Let's Eat" kit, 67% reported that they found the kit very useful, two-thirds stated that they still had the kit; 45% said that they were still using the kit, and 47% said that they had shared thz kit with someone else.
From these survey results, we concluded that people liked the kit and found it helpful, and that people who were using the goal checklist pages were making significantly more dietary changes than those who did not use these pages. However, most respondents had not read the goal checklist pages, nor had they posted any checklist pages on their refrigerator with the magnet. The most common reason
weetc h as -uts, 11, as, 05 , pies. qnt rnllr
Column 1: 7 pn!nlT
Colum 2 P'JlV
Often e a t sweets.
Some? eat: sweets.
a d
w ~ t h using I/:
~ r t s with IOU
Go for low-fa, ~ ~ u c c , 8 uc..cs ,i instead 04 ice cream (set
Choose lower fat sweets (see back1
r portion siz Eat a smatle e of sweets
Have a bagel, . - . - . . A .L .
English muff louohnut
in or raisin to lnxeao or a c
When baking oil than the r
Make home i r m r ~ d 1 ~ n t 6
I, experiment e t - I ~ P says
-made desse
3 less fat/
Use the 'ligh ake mixer people gave for not reading any of the goal checklist pages was that they were "too busy."
Based on the results of this survey, we determined that changes were needed to improve the kit, especially to focus participants' attention on the goal checklist pages.The more in-depth feedback we needed for revision was collected through qualitative research using focus group interviews.
Figure 1. Example of a goal checklist page from the original kit.
envelope, (4) choose specific behavior change goals that they were willing to try and check them off in the "OK I'm ready" column on the checklist, (5) hang the page on their refrigerator with the magnet, and (6) as they accomplished goals, check them off in the "I'm doing it" column on the checklist. To evaluate this version of the "Let's Eat" kit and refine it for the M C study, we conducted formative research using a combination of quantitative and qualitative methods. A timeline of this research is displayed in Table 1.
QUALITATIVE RESEARCH
Methods. Focus groups are often used to obtain feedback about existing educational materials and programs and to adapt or develop new educational materials and program^.^-'^ To evaluate the "Let's Eat" kit, we held two rounds of focus group interviews.The first round (fall 1992) included 12 sep- arate groups: 2 with nutritionists, 5 with employees at work- sites, 1 at a senior citizens' center, and 4 with participants from the telephone survey. The groups with survey participants were divided by gender and by those who had or had not used the kit. A total of 60 participants (60% women, major- ity non-Hispanic white) attended. Using data from these groups, we developed a prototype for a new version of the kit.
In spring 1993, we tested this prototype kit in a second round of nine focus groups to get feedback and suggestions for further refinements. Two groups were held at worksites, two at supermarkets, two at churches, one with cholesterol
QUANTITATIVE RESEARCH
Methods. From May through June 1991,547 individuals participated in SCORES at a variety of locations in the com- munity and worksites.Approximately 3 months later, we con- tacted each of these individuals for a 13-minute telephone interview to discuss their use of the "Let's Eat" kit and whether they had made recommended dietary changes. Complete data was obtained from 407 respondents with a

Journal of Nutrition Education Volume 28 Number 3 May June 1996 159
Table 1. Timeline of quantitative and qualitative research. -- -
Summer Fall Fall Winter Spring Spring-Summer Winter
1991 1991 1992 1992-93 1993 1993 1994
547 participants Telephone survey
receive original (n = 407) about
LE Kit at original kit.
cholesterol
SCORES.
Major Findings:
Recipients are not
using food-specific
behavior change
information
contained on the
goal checklist
pages in the
envelope.
Round 1 Prototype LE Kit Round 2 New LE Kit
12 focus groups developed 9 focus groups developed.
(n = 60) (n = 106)
Major Findings:
Checklist pages in
envelope not read
because instructions
not read and
unclear, pages in
envelope too easily
disorganized.
3-ring binder
suggested.
Support for checklist
format and
breakdown of goals
into steps, "Eat
Less" lists, graphs,
logo, and title.
Includes 3-ring
binder,
reformatted RYP,
kit components
labeled with
large numerals,
illustrated
instructions.
Major Findings:
Organize kit so
additional
information appears
in separate section
for more motivated
readers. Include
information on
reading labels,
dining out, weight
loss, etc.; include a
shopping list and a
separate recipe
section; include
name on spine of
kit; add icons to tie
kit to RYP.
Binder includes
RYP, magnet, and 3
tabbed sections:
goal checklists, A
Closer Look section,
and recipes.
Illustrations redone.
Icons and laminated
shopping list added.
Items on goal
checklists ordered
according to buying,
eating, and cooking
goals. Food-specific
information updated.
Telephone survey
with pilot study
participants
receiving
new kit.
Major Findings:
Users of new kit
more likely to
use goal-setting
checklists and to
report positive
dietary change
than recipients
of original kit.
screening participants from a hospital screening, one with patients from a low-income medical clinic, and one with nurses from this clinic. A total of 106 participants (75% women, majority non-Hispanic white) participated in these focus groups.
The groups were led by PHHP's social marketing coor- dinator and a co-moderator who assisted with recruitment, paperwork, and analysis of results. The majority of groups were interviewed at the site from which they were recruited. Participants were mailed the kit prior to the interview with instructions to read it beforehand. Each focus group inter- view lasted 2 hours and refreshments were served. In the first round, participants were paid $10; however, we found that this amount was an inadequate incentive to motivate partici- pants to read the entire kit prior to attending the interview. Therefore, in the second round, we increased the payment to $25.This increase in incentive appeared to increase the per- centage of participants who had read the kit before attend- ing the interview.
The moderator developed a script/discussion guide that she used to guide the sequence of questioning for the focus groups.This technique allowed for flexibility since the group discussion could flow naturally while the guide ensured that all important topics were covered. Using a discussion guide rather than a rigid script also allowed us to better obtain
unanticipated information. Discussion guides were modified depending on the audience (i.e., nutritionists vs. consumers reviewing the original kit vs. consumers reviewing the pro- totype kit); however, major topics were consistent across all three guides.
All focus groups were audiotaped. Following each inter- view, the moderator and co-moderator taped a brief synop- sis of their impressions of the discussion. The focus group tapes were transcribed by a professional transcription service. The moderator read the transcripts and listened to each tape several times, making notes and listening for threads of com- mentary reflecting a pattern or theme. All comments made in the focus group were considered in terms of the context of the comment, its relevance to the research questions, and the inferred motivation of the speaker. A report was then generated summarizing the primary conclusions from the groups with supporting quotations.
Results. In general, the focus groups provided much posi- tive feedback, specifically indicating support for the overall concept of the kit and the information it contained. Results showed that participants especially appreciated the food-spe- cific information and the breakdown of broad behavior change concepts into small steps on the goal checklists. Spe- cific recommendations for improvement included presenting

160 Gans et al./SELF-HELP KIT
the information in a more conventional format, clarifying and simplifying instructions, and adding information on cer- tain t0pics.A summary of the results follows along with sup- porting quotations drawn from the transcripts.
The title,"Let's Eat," was the subject of discussion in sev- eral groups.While some felt that the title should convey the concept ofC'eating for good health," the majority liked "Let's Eat" because it made the topic of healthful eating sound appetizing and enjoyable (as opposed to a "special diet"). Sev- eral participants also mentioned that, because the kit did not have a title on the spine, it was difficult to find on a shelf with their cookbooks.
The groups identified several problems with the original format of the kit. Many never even opened the envelope of goal checklist pages and those who did felt confused about what to do with them: "I wouldn't have the envelope to be honest with you. I opened the envelope first, but once I had all these pages all over the place, it's like, 'What the heck is this?' I think if you were to incorporate it all into one pack- age I could at least understand it."The concept of using a three-ring binder format instead of the booklet and envelope was suggested at several of the early focus groups: "There's a zillion little pieces of paper here. If I ever dropped this on the floor ... It would be more interesting if this were stapled together into a little booklet.Then you would have a ten- dency to look at both sides."
Focus groups also observed that the instructions in the original kit were complex and that very few people read them:"I went to the next page (How to Use the Let's Eat Kit) and I didn't want to read this. So I ignored that." Some sug- gested illustrating the instructions to make them c1earer:"Pic- tures, as they say, mean a thousand words.There are very few people who read ... I mean, they read for pleasure, but they don't read for ... structural things."
Focus group participants liked the goal checklist format and the fact that the broader recommendations were broken down into smaller, more manageable steps: " ... this [the 'Let's Eat' kit] presents little things that you could do, one thing at a time, instead of having this big thing to look through." One surprising result of the focus groups was that a large number of people interpreted the goal checklists to be self-assessment forms as well as tools for setting new goals. Instead of just choosing new goals from the lists, they checked all of the healthful behaviors that they had already incorporated into their lives. This unintended use of the checklists provided positive reinforcement for these partici- pants: "It's reassuring to know that you're accomplishing things when you see the check marks.This is what I want to do and this is what I've done ..."
There was broad approval of the food-specific "Better Choices" and "Eat Less" lists on the back of each goal check- list page, and participants wanted more of this information. Many were surprised to see that they were eating so many foods on the "Eat Less" lists. Some participants mentioned that most nutrition materials list only the healthful choices and thought listing foods to "Eat Less" was a strength of the
kit: "I liked it because I could figure which one is the best one at the market ..." In addition, participants liked the vari- ety of information in the graphic comparisons of fat content and miscellaneous tips, such as a chart comparing fat and calories in frozen desserts:"I usually eat any kind of ice cream ... and then I'm looking here and I say 'Wow! There's a lot of things you can eat that are better for you."'
The recipes were very popular and some participants reported having tried several of them. Most participants wanted more recipes, but in a separate section of the kit instead of on the back of the goal checklist pages. Several sug- gested including nutrient information for recipes:"If you had a section in the back that was recipes so you could have this [goal checklist] page on the refrigerator and yet take the recipe page to make something ... it would help you reach the goal that you were trying to achieve."
Participants liked the colors and logo of the kit. For the prototype kit, we produced "Let's Eat" magnets featuring the kit's logo. Participants felt that, even if they did not use the magnet to post pages of the kit, they would still put it on their refrigerator where it would serve as a reminder of healthful eating. Reviews of the illustrations, however, were mixed.The original illustrations were stylized and somewhat abstract. Many people liked them; however, older people, in particu- lar, had difficulty relating to the illustrations: "Like the illus- trations - they're almost surreal. Like what is this? A chicken? I don't know.They should look more realistic.""I found myself looking at some of them wondering what they were supposed to be. I kind of like them, but I think they might be sort of a distraction from the information on the page."
The RYP eating pattern assessment was also criticized in the focus groups. In particular, we received negative feedback regarding the original RYP instructions and on the mix of colors on the form: "I said, 'Oh my [gosh], what am I going to do here? ... This is complicated. What am I supposed to do?"' O n the original RYP, there were numbers directing the reader to the appropriate food page in the envelope. During the focus groups, we found that these numbers were either "not noticed" or noticed but not understood.
Scoring of the RYF', which required addition and multi- plication, was also difficult for some participants. Most par- ticipants indicated that they liked having a score to rate their eating pattern, but thought that the scoring could be made simpler: "Yeah, I think most people do like to see a score, because we all understand measurements ... so I think that's good."" ... I got confused on the subtotals. Like one page is a subtotal and now I have to add those two numbers together. Maybe we could just forget the subtotal and just have 'total everything together."'
In our attempt to focus attention on the goal checklist pages, some of the more general information from the origi- nal kit was omitted in development of the prototype. In the second round of focus groups, however, participants recom- mended adding some of these topics such as "label reading" and "dining out." In addition, all groups suggested adding fea- tures such as a shopping card:"The only thing I wanted ... was
May June 1996 161 Journal of Nutrition EducationVolume 28 Number 3
I wish I could take this with me to the market, because you see it has information about what meats to buy and what not - well, you get to the market and you forget. So I was think- ing 'well too bad they don't have little cards where you could bring the information with you,' because that's really where you start .... is buying.""It's very hard when you go out there. You have to take almost every package. Like I spend an hour when I can be spending only a half hour in the store. Hav- ing a list with you would be so much easier."
The focus groups also discussed issues relating to literacy 1evels.They suggested that readers with limited reading skills may want less information that is more basic, while more knowledgeable readers may want more extensive and com- plex information: "[How about] ... a 3-ring binder? The first section would be the explanation.The middle section would be all your food tips that could come out and be posted, and then the back section would be your extra that only some people would read."
wanted the kit to stand out visually from other health care materials.
We revised RYP to include 21 instead of 18 food cate- gories and added check boxes for responses, in contrast to the old version in which readers circled the entire question for their response. In addition, we reduced the amount of col- ored type to enhance readability and simplified the scoring instructions and scoring formula.To better cue participants to the relationship between RYP food categories and their corresponding goal checklist pages, we added icons to each RYP category that match illustrations on the corresponding food pages.
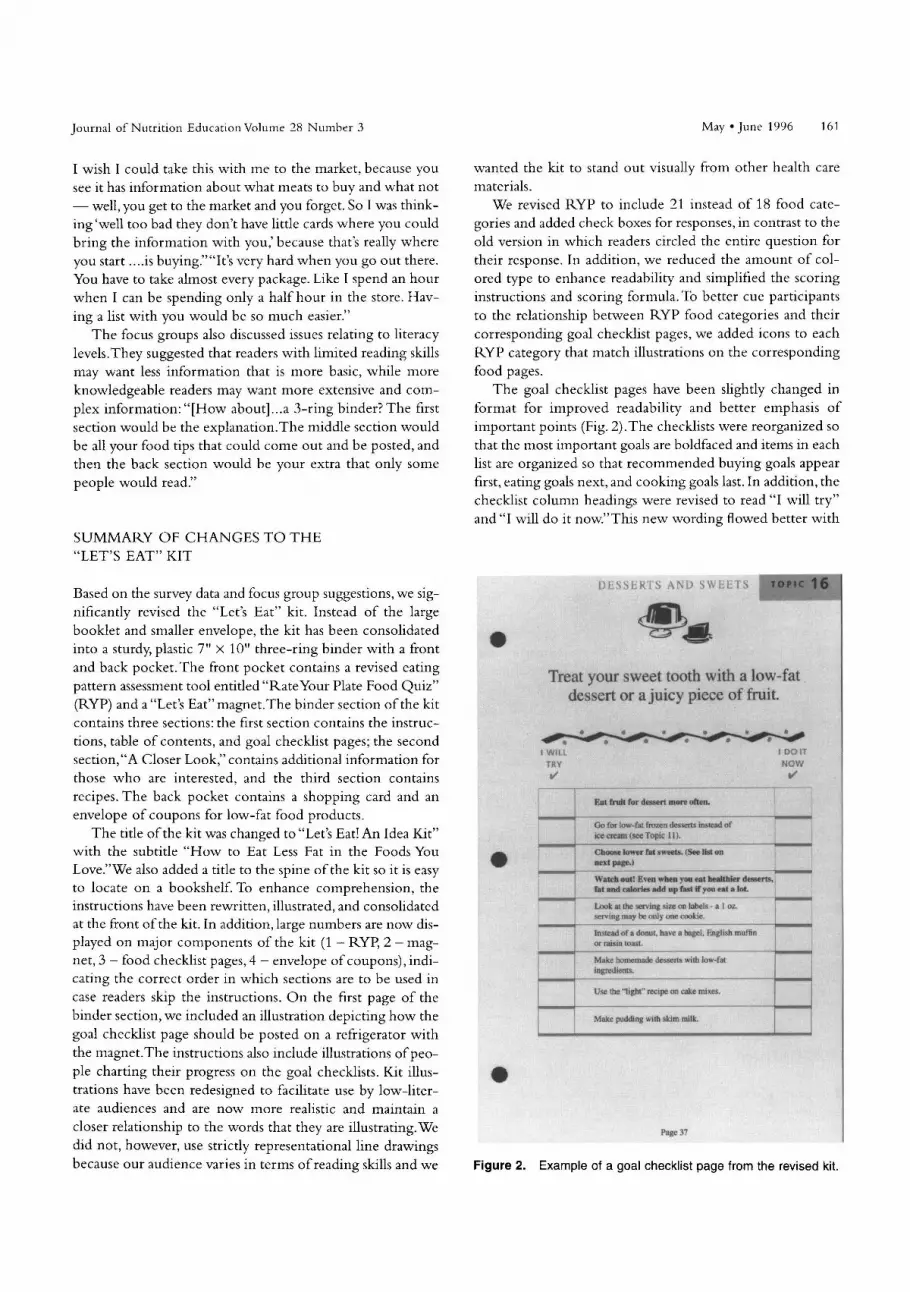
The goal checklist pages have been slightly changed in format for improved readability and better emphasis of important points (Fig. 2).The checklists were reorganized so that the most important goals are boldfaced and items in each list are organized so that recommended buying goals appear first, eating goals next, and cooking goals last. In addition, the checklist column headings were revised to read "I will try" and "I will do it now."This new wording flowed better with
SUMMARY O F CHANGES TO THE "LET'S EAT" KIT
Based on the survey data and focus group suggestions, we sig- nificantly revised the "Let's Eat" kit. Instead of the large booklet and smaller envelope, the kit has been consolidated into a sturdy, plastic 7" x 10" three-ring binder with a front
Treat your sweet tooth with a low-fat dessert or a juicy piece of fruit.
and back pocket.The front pocket contains a revised eating pattern assessment tool entitled "Rateyour Plate Food Quiz" (RYP) and a "Let's Eat" magnet.The binder section of the kit contains three sections: the first section contains the instruc-
& I V ILL
TRY w' 1 - - - '
?st huh for d-rt Inom ottm.
fmzen & w e n s s
tions, table of contents, and goal checklist pages; the second section,"A Closer Look," contains additional information for those who are interested, and the third section contains
NOW d
- - recipes. The back pocket contains a shopping card and an envelope of coupons for low-fat food products.
The title of the kit was changed to "Let's Eat! An Idea Kit" with the subtitle "How to Eat Less Fat in the Foods You Love."We also added a title to the spine of the kit so it is easy to locate on a bookshelf. To enhance comprehension, the instructions have been rewritten, illustrated, and consolidated at the front of the kit. In addition, large numbers are now dis- played on major components of the kit (1 - RYP, 2 - mag- net, 3 - food checklist pages, 4 - envelope of coupons), indi- cating the correct order in which sections are to be used in case readers skip the instructions. O n the first page of the binder section, we included an illustration depicting how the goal checklist page should be posted on a refrigerator with the magnet.The instructions also include illustrations of peo- ple charting their progress on the goal checklists. Kit illus- trations have been redesigned to facilitate use by low-liter- ate audiences and are now more realistic and maintain a closer relationship to the words that they are illustrating.We did not, however, use strictly representational line drawings because our audience varies in terms of reading skills and we
Go for imu-far ice cream (cpe
C h o w lower next pa=.) - -- - ,U-L .̂.., w.
TOPIC 1 l i . - fsr svr rs . (See I
bl m m t calnrits add up fml i f : - Lmk a1 the ur wwng rnry k
~ ~ a r c a n!gct. r.spirs r t l ~ i c l r ,
or raicin feast. -- Make honxma inpiedienrs. --
& desserts with I
wilh %k!m milk.
Figure 2. Example of a goal checklist page from the revised kit.

162 Gans et al./SELF-HELP KIT
the recommendations and appeared to be clearer to the focus group participants.We also updated the food lists on the back of the goal checklist pages to reflect new foods in the market. All recipes were moved from these pages to a sepa- rate section in the binder, and graphs and other food-specific information were added to replace the recipes on the back of the goal checklist pages.
After the goal checklist pages, we added a new section entitled "A Closer Look," which includes information on reading labels, vegetarian diets, low-fat recipe substitutions, the food guide pyramid, dining out, weight reduction and exercise, a form for recording blood cholesterol measure- ments, and a brief bibliography of recommended reading.The recipe section presents 30 low-fat recipes including nutrient information and numbered instructions.The back pocket of the kit includes an envelope of coupons for healthful food products and a laminated shopping card listing brand-specific food choices and nutrient criteria for choosing low-fat foods at the market.
EVALUATION O F THE REFINED KIT
To evaluate whether the new version of the kit was more user friendly than the older version, we reviewed data from 3- month follow-up telephone surveys of 375 pilot participants from the M C study (response rate 98.7%). Comparing this data with the 1992 telephone survey data showed that a higher percentage of those receiving the new kit reported reading the goal checklist pages (90% vs. 37%, X2 = 208.79, p < .0001) and posting a goal checklist page on their refrig- erator with the magnet (27% vs. 9%, X2 = 13.43, p < ,001). In addition, a higher percentage (64%) of participants who received the new "Let's Eat" kit self-reported making dietary changes compared to those receiving the old kit (54%) (X2 = 5.73, p < .02).
O f those who read at least one or more goal checklist page, 37% read all of them and the mean number read was 7.5 pages.Almost one-third reported using recipes from the kit, and 40% reported using coupons from the kit. Forty- three percent of respondents reported sharing the kit with others, 84% reported that they still had the kit, and 50% reported that they were still using the kit. We are currently using the new version of the "Let's Eat" kit in the ongoing M C study, and will continue to collect process data on its use and effectiveness.
IMPLICATIONS
This paper illustrates how both quantitative and qualitative formative research methods can be used to evaluate and improve an existing educational material. We recommend using both quantitative and qualitative methods in the devel- opment or adaptation of educational materials. Quantitative survey data can provide general information about the use
and effectiveness of materials, but often fail to provide spe- cific feedback needed for revisions. O n the other hand, quali- tative data from focus groups can yield specific, in-depth information about how to improve or develop educational materials, but cannot be generalized because of the small number and narrow range of participants involved. Each method has different strengths and weaknesses, so using a combination of methods provides the most comprehensive and useful feedback.
As a result of our findings, we recommend that other self- help nutrition education kits and materials include brief, illustrated instructions or be self-explanatory with sequen- tially numbered pieces; include food- and brand-specific information on foods to "eat less" as well as "better choices"; break recommendations into small, manageable steps and provide a tool for selecting and monitoring goals; provide colorful, realistic illustrations; include pieces that can be removed for ease of use such as recipes, checklists, and shop- ping cards; and include an eating pattern self-assessment form with simple scoring. Furthermore, we recommend that ongoing formative evaluation of educational materials using both qualitative and quantitative methods continue indefi- nitely as resources allow.
ACKNOWLEDGMENTS
The authors wish to acknowledge everyone involved in the ongoing development and evolution of the "Let's Eat" kit over the years including Nancy Beauchene, Susan Connery, Raul For tune t , Mary Lynne Hixson , Nancy Johnson, Catherine McMahon, and Elli Panichas. We would also like to thank Leonard and Cecelia Doaks at Patient LearningAsso- ciates in Potomoc, MD and BarbaraVan Horn at the Institute for the Study ofAdult Literacy at Penn State University.This work was supported by Grant HL23629 Pawtucket Heart Health Program, Grant HL48250 Worksites, Occupational Nurses and Cholesterol Change, and Grant HL47624 Mini- mal Contact Education for Cholesterol Reduction.
REFERENCES
1. Sempos CT, Cleeman JI, Carroll MD, et al. Prevalence of high blood
cholesterol among U.S. adults: an update based on guidelines from the
second report of the National Cholesterol Education Program Adult
Treatment Panel. JAMA 1993;269:3009-14.
2. Johnson CL, Rikind BM, Sempos CT, et al. Declining serum total cho-
lesterol levels in US adults. JAMA 1993; 269:3002-8.
3. Gans KM, LasaterTM, Linnan L, Lapane K, Carleton RA.A cholesterol
screening and education program: differences between older and
younger adults. J Nutr Educ 1990; 22:275-83.
4. Gans KM, Sundaram S, Hixson ML, McPhillips J, Linnan L, Carleton
RA. Rate Your Plate: an eating pattern assessment tool used at choles-
terol screening and education programs. J Nutr Educ 1993; 25:29-36.

Journal of Nutrition Education Volume 28 Number 3 May June 1996 163
5. National Cholesterol Education Program. Second report of the Expert
Panel on Detection, Evaluation and Treatment O f High Blood
Cholesterol in Adults. Circulation 1994;89:1333-445.
6. Hartman TJ, McCarthy PR, Park RJ, Schuster E, Kushi LH. Focus
group responses of potential participants in a nutrition education
program for individuals with limited literacy skills. J Am Diet Assoc
1994;94:744-8.
7. Murphy B, Ruth D, Hodge MM.The use of qualitative research in the
development of the Heartwise program for general practitioners. Med
J Aust 1993;158:626-8.
8. An evaluation of dietary guidance graphic alternatives: the evolution
of the eating right pyramid. Nutr Rev 1992; 50:275-82.
9. White SL, Maloney SK. Promoting healthy diets and active lives to
hard-to-reach groups: market research study. Public Health Rep
1990;105:224-31.
10. Crockett SJ, Heller KE, Merkel JM, Peterson JM. Assessing beliefs of
older rural Americans about nutrition education: use of the focus group
approach. J Am Diet Assoc 1990;90:563-7.
11. Mullis RM, Lansing D. Using focus groups to plan worksite nutrition
programs. J Nutr Educ 1986;18:S32.
12. Quatrornoni PA, Milbauer M, Posner BM, Carballeira NP, et al. Use of
focus groups to explore nutrition practices and health beliefs of urban
Caribbean Latinos with diabetes. Diabetes Care 1994;17:869-73.
INTERNATIONAL DIARY/MEETINGS
The International 14th Puijo Symposium "Physical Activity, Diet and Cardiovascular Diseases - A Fresh Look Beyond Old Facts" will be held on June 24-28, 1996, in Kuopio, Finland. For more information and registration forms please contact Paivi Smeds-Oravainen, Secretary, Puijo Symposium Secretariat,Tel: +358-71-2613 448, Fax: +358-71-2631 515, E-mail: [email protected].
The Office of Minority Health Resource Center, a nationwide service of the Office of Minority Health, U.S. Depart- ment of Health and Human Services, is distributing the Directory ojAfvican American Nutrition Programr.The directory was produced by the National Council of Negro Women and the Proctor and Gamble Company.To obtain free copies, call OMH-RC at 1-800-444-6472 and ask to speak with an information specialist.
The International Stress Management Association, in cooperation with several other organizations, will conduct ISMA-6, an international conference on stress and health, on October 5-8, 1996 in Sydney,Australia. For information, contact: F. J. McGuigan, Ph.D., Institute for Stress Management, 10455 Pomerado Road, San Diego, CA 92131 .Tel: (619) 635-4698; Fax: (619) 635-4669; e-mail: [email protected].
New Developments in the Pathogenesis and Treatment of NIDDM (Non-insulin Dependent Diabetes Mellitus)
Sponsored by the American Diabetes Association ofArizona and the National Institute of Diabetes and Digestive and Kid- ney Diseases, thls conference will feature presentations by internationally recognized experts who will review recent advances in the epidemiology, pathogenes, is and treatment of NIDDM. Highlights will include sessions on the genetics of NIDDM, the roles of insulin resistance and insulin secretory defects in the pathogenesis of NIDDM, prospects for prevention of NIDDM, and lessons learned from the UK Prospective Diabetes Study.The conference will be held November 1-3,1996 at the Radisson Resort, Scottsdale, AZ, USA. For more information, contact the American Diabetes Association, Arizona Afiliate, Inc., 2328 W. Royal Palm Rd., Suite D, Phoenix,AZ 85021;Tel: (602) 995-1515; Fax: (602) 995-0004.





























