Embed Size (px)
Citation preview
TTOOWWNN OOFF BBUURRLLIINNGGTTOONN Meeting Posting
Email Posting to [email protected] or Bring to the Clerks Office. Thank you Notice of Public Meeting – (As required by G.L. c. 30 A, c. §18-25)
29 CENTER STREET BURLINGTON, MASSACHUSETTS 01803 TEL (781) 270-1660 FAX (781) 238-4692 www.burlington.org [email protected]
DEPT./BOARD: Board of Health Regular Meeting DATE: February 25, 2020 TIME: 7:00 pm PLACE: Town Hall Main Meeting Room, 2nd Floor
AGENDA
This meeting is recorded and aired on BCAT Open Meeting/Pledge of Allegiance Approval of Minutes: January 28, 2020, February 11, 2020 Citizen’s Time Chairman’s Report Subcommittee Reports: • Protocol for Providing Vaccinations to Children in Cooperation with Burlington Public Schools Discussion
• 2020-2021 Flu Vaccine Purchase Recommendation • Protocol for Providing Vaccinations to Children in Cooperation with Burlington Public Schools • Revision to BOH Meeting Schedule
Staff Reports
• Environmental Engineer • Supervisory Nurse • Director of Public Health
Adjourn
Approved: DRAFT Town Clerk:
TOWN OF BURLINGTON, MA BOARD OF HEALTH
MINUTES Main Meeting Room, Town Hall
TUESDAY, JANUARY 28, 2020
______________________________________________
1 29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 l TEL (781) 270-1660 l FAX (781) 238-4692
www.burlington.org l [email protected]
Board Members Present: Ed Weiner, PhD, Chairman; David McSweeney, Vice Chairman; and Maribeth Welch
Not Present: Dr. Wayne Saltsman, MD, PhD and Libby Walendziewicz, RN, MSN
Staff Members Present: Susan Lumenello, REHS/RS, CHMM, Director of Public Health; Christine Mathis, Environmental Engineer; Chris Paulik, Supervising Nurse and Samantha Hardy, Associate Health Inspector
Dr. Weiner called the Board of Health meeting to order at 7:00 PM followed by the Pledge of Allegiance.
Approval of Minutes: January 14, 2020
MOTION: Mr. McSweeney moved to approve the Board of Health Meeting Minutes of January 14, 2020 as amended. The motion was seconded by Ms. Welch and unanimously approved. (3-0-0)
Citizen's Time: No one spoke.
Chairman's Report:
Dr. Weiner stated that Town Meeting met last night and zoning articles passed unanimously. There was discussion on the biosafety regulations that we adopted.
Subcommittee Reports: Ray Avenue Sewer Lines & FY2021 BOH Budget
Dr. Weiner stated that the minutes of the subcommittees will be discussed during the item that they address.
Variances:
● Café Escadrille, 26 Cambridge Street – Variance Modification, BOH Grease Interceptor Requirements For Food Service Establishments
Michael Murray appeared for the variance for Café Escadrille. Also in attendance was the DPW Director John Sanchez. Dr. Weiner stated that there are still problems with the system. Mr. Sanchez stated that a few years ago the DPW would do monthly checks for grease back up on the Ray Street sewer line. They are still finding grease. The last inspection was done on January 15, 2020 and there was still grease in the line and system. Mr. Murray stated that they don’t want to contribute to the problem. He asked that the Board revoke the variance and they will do more cleaning of the system.
Mr. McSweeney stated that the subcommittee met last week. It’s been over 2 years since the variance was approved and there is still FOG coming into the sewer line. We can either revoke the variance or require more doses and require that the exterior grease tank be cleaned more than twice a year. We need a plan. If
TOWN OF BURLINGTON BOARD OF HEALTH MINUTES
JANUARY 28, 2020
2
29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 ⧫ TEL (781) 270-1660 ⧫ FAX (781) 238-4692 www.burlington.org [email protected]
they choose not to use the protein matrix then they will have to go back to regular cleaning. Mr. Murray stated that the internal grease traps look great but the external grease tank still has build up. Mr. Sanchez stated that we have had issues prior to the protein matrix but we did not do as many clean ups of the sewer system. Mr. Murray stated that they would like the variance revoked. They will clean the system and start with a baseline and then try to figure out the problem.
Ms. Lumenello asked if all of the protein matrix will be stopped even internally. Mr. Murray replied he is not sure. If a variance is not obtained for the internal grease interceptors, then they must be cleaned and maintained when they reach 25% capacity or at 3 months, whichever comes first. Mr. Lumenello stated that the external grease interceptor needs to be cleaned in February and this should include maintenance of the entire system and lines. The applicant must notify the Board of Health and DPW when this is being done. The applicant was asked to email the office on their decision regarding the protein matrix. Mr. Sanchez stated that once the grease trap and service line is cleaned we can get a baseline. We will still monitor the line on a monthly basis until we see no evidence of grease.
MOTION: Mr. McSweeney moved to rescind the grease trap variance for 26 Cambridge Street. The motion was seconded by Ms. Welch and unanimously approved. (3-0-0)
Discussions:
● 10 Sunset Drive, Plumbing Variance Recommendation
Daniel Miniello appeared for a plumbing variance for 10 Sunset Drive. He would like to install 2 unapproved sink basins in his house. These 2 sinks are not on the approved state list.
MOTION: Mr. McSweeney moved to send a letter of no objection to the State Plumbing Board on behalf of Mr. Miniello in regards to the 2 sink basins. The motion was seconded by Ms. Welch and unanimously approved. (3-0-0)
● FY2021 BOH Budget
Ms. Lumenello presented the FY2021 Board of Health budget. The overview is there will be a 3.86% overall increase. There will be a .90% increase in salaries, 0% net increase in expenses and a 26.19% in special accounts. They are expecting a 30-40% increase in Household Hazardous Waste. This increase is based on the fact that Stericycle is no longer an approved vendor and the State now requires PCB testing. In looking at the numbers, they believe that FY15 was the most accurate count for Household Hazardous Waste day. They will be adding $50,000 as the line item. Ms. Lumenello stated that they are adding a line item for the Burlington Volunteer Reserve Corp (BVRC) with an amount of $1,000. Most of the activities through the MRC are funded by grants but they can’t use the money for refreshment, apparel or recruiting. This line item will cover these items. The BVRC assists in so many activities including Health Fairs, Bladder Cancer Screening, Household Hazardous Waste Day, Stop the Bleed training, Flu Clinics, Blood Drives, First Aid stations, etc.
Dr. Weiner stated that the elected officials are not getting a raise, only the appointed officials. Dr. Weiner asked if we could set up a revolving fund for donations for the BVRC. Ms. Lumenello replied that she could
TOWN OF BURLINGTON BOARD OF HEALTH MINUTES
JANUARY 28, 2020
3
29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 ⧫ TEL (781) 270-1660 ⧫ FAX (781) 238-4692 www.burlington.org [email protected]
look into this but we need to be careful because we shouldn’t take any donations from companies that we regulate.
MOTION: Mr. McSweeney moved to approve the FY2021 Board of Health budget. The motion was seconded by Ms. Welch and unanimously approved. (3-0-0)
Mr. McSweeney asked what the next steps are. Ms. Lumenello stated that the BOH will meet with the Ways and Means subcommittee and then on March 4, 2020, go before the Ways and Means Committee and then the budget will be voted on at the May Town Meeting.
Staff Reports
Environmental Engineer
Ms. Mathis presented her report:
● All mailings regarding Hazardous Material registrations have been completed. There are now 125 companies in Burlington that we inspect.
Mr. McSweeney asked what the issue with 4 Lowell Street was. Ms. Mathis stated that they received a pumping record from a realtor. They tied into the town sewer but the abandonment of the septic was never witnessed as required. We sent a letter to the contractor. Dr. Weiner asked if there is a penalty. Ms. Mathis stated that this is their first offense, so a letter was sent. Ms. Lumenello added that if there is another offense, then they will be issued a fine. Mr. McSweeney asked what the status of 207 Cambridge Street is. Ms. Mathis stated that they have received tentative approval from MassDOT. They are just waiting on the traffic plan because they have to close 3A when they tie in the system. Ms. Mathis stated that she will keep in contact with the applicant.
MOTION: Ms. Welch moved to approve the Environmental Engineer’s report. The motion was seconded by Mr. McSweeney and unanimously approved. (3-0-0)
Supervisory Nurse
Ms. Paulik presented her report:
● They will have nursing students from Northeastern for this semester.
● They still have flu shots if anyone needs them.
MOTION: Mr. McSweeney moved to approve the Supervisory Nurses’ report. The motion was seconded by Ms. Welch and unanimously approved. (3-0-0)
Associate Health Inspector
Ms. Hardy presented her report:
● All tobacco inspections have been completed.
● They are working on a training schedule for the BRVC for the next fiscal year.
TOWN OF BURLINGTON BOARD OF HEALTH MINUTES
JANUARY 28, 2020
4
29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 ⧫ TEL (781) 270-1660 ⧫ FAX (781) 238-4692 www.burlington.org [email protected]
● She has become a certified pool operator.
MOTION: Ms. Welch moved to approve the Associate Health Inspector’s report. The motion was seconded by Mr. McSweeney and unanimously approved. (3-0-0)
Director of Public Health
Ms. Lumenello presented her report:
● There is a tabletop exercise on February 4th from 12:30 to 4:30 PM dealing with critical staff dispensing. This will include the Burlington Police and Fire and 5-6 towns.
● There will be a training session at the Harvard School of Public Health on Workers Safety on February 19th from 6:00 to 8:00 PM.
● There will be a Food Code Training Review for all the food establishments on February 19th from 2:00 to 5:00 PM at the Burlington High School. There will be discussion on cleaning chemicals in the food establishments.
Mr. McSweeney asked if the staff has received any calls on the Coronavirus. Ms. Lumenello stated that we did receive one phone call from a school. She has been listening in on the CDC weekly phone calls.
Dr. Weiner stated that some of the restaurants in the Burlington Mall had to be shut down due to no water. Ms. Lumenello replied that yesterday, they had to visit the mall due to a water issue. Most of the restaurants closed on their own but 1 ticket was issued. They reminded the owners that if there is no water or electricity they need to close.
MOTION: Mr. McSweeney moved to approve the Director of Public Health’s report. The motion was seconded by Ms. Welch and unanimously approved. (3-0-0)
Dr. Weiner reminded residents to wash their hands and stay warm.
Adjourn
MOTION: Mr. McSweeney moved to adjourn the Board of Health meeting at 7:55 PM. The motion was seconded by Ms. Welch and unanimously approved. (3-0-0)
Respectfully Submitted by Dawn Cathcart, Recording Clerk
TOWN OF BURLINGTON BOARD OF HEALTH MINUTES
JANUARY 28, 2020
5
29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 ⧫ TEL (781) 270-1660 ⧫ FAX (781) 238-4692 www.burlington.org [email protected]
DOCUMENTS REVIEWED AT MEETING – TUESDAY, JANUARY 28, 2020
Agenda
Minutes: January 14, 2020
Chairman’s Report: None
Subcommittee Reports: Subcommittee Minutes dated 1/17/20 regarding Ray Avenue Sewer Line & FY2021 BOH Budget
Variances:
● Café Escadrille, 26 Cambridge Street – Variance Modification, BOH Grease Interceptor Requirements for Food Service Establishments
Memo from S. Lumenello dated 1/28/20, Approved variance request dated 12/3/18 with 2 attachments
Discussion:
● 10 Sunset Drive, Plumbing Variance Recommendation
Memo from S. Lumenello dated 1/21/20, Memo request, State Plumbing Board Variance application with attachments
● FY2021 BOH Budget: Presentation, Cover sheet, Budget Guidelines from P. Sagarino
Staff Reports: Environmental Engineer’s Report; Supervisory Nurse’s Report, Associate Health Inspector’s Report; Director of Public Health’s Report
Approved: DRAFT Town Clerk:
TOWN OF BURLINGTON, MA BOARD OF HEALTH
MINUTES Main Meeting Room, Town Hall
TUESDAY, FEBRUARY 11, 2020
______________________________________________
1 29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 l TEL (781) 270-1660 l FAX (781) 238-4692
www.burlington.org l [email protected]
Board Members Present: Ed Weiner, PhD, Chairman; David McSweeney, Vice Chairman; and Dr. Wayne Saltsman, MD, PhD
Not Present: Maribeth Welch, Libby Walendziewicz, RN, MSN
Staff Members Present: Susan Lumenello, REHS/RS, CHMM, Director of Public Health; Marlene Johnson, Health Agent
Dr. Weiner called the Board of Health meeting to order at 7:00 PM followed by the Pledge of Allegiance.
Approval of Minutes: January 28, 2020
Dr. Weiner stated that minutes will be tabled until the members that were present at that meeting are here.
Citizen's Time: No one spoke.
Chairman's Report:
Dr. Weiner thanked Ms. Lumenello and Dr. Saltsman for all their work getting information out on the Coronavirus. Dr. Weiner also thanked Mr. McSweeney for all the work he does on the various subcommittees.
Subcommittee Reports: There were no Subcommittee Reports.
Hearing:
● King Bibis, 45 Winn Street – Food Code Violation
Mrs. de Paula and Mr. Silva representing King Bibis appeared for the violation discussion. Ms. Johnson stated that the owner and sole proprietor, Julio Cesar de Paula is sick and could not come tonight. Mrs. De Paula is his wife and Mr. Silva is his brother and the interpreter but neither work in the store. Dr. Saltsman is concerned with hearing these issues without the owner being present. Dr. Weiner replied that we should hear the report, have discussion and vote on a direction to give them. If the owner does not agree we can suspend or close the establishment.
Ms. Johnson read her report of February 11, 2020 into the record. The memo includes the history, violations and recommendations. She has spoken to Mr. de Paula and he has been cooperative and is eager to learn.
Mr. McSweeney asked if they are open 7 days a week and is the Person in Charge (PIC) full time. Ms. Johnson replied they are open 7 days a week and there were 3 PICs when they first opened including the owner.
TOWN OF BURLINGTON BOARD OF HEALTH MINUTES
FEBRUARY 11, 2020
2
29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 ⧫ TEL (781) 270-1660 ⧫ FAX (781) 238-4692 www.burlington.org [email protected]
Dr. Weiner stated that the Board wants the establishment to be successful but they need to protect the community. There needs to be education on proper food safety to protect the public. Ms. Johnson stated that there was an obvious breakdown and she is not sure if it is language or knowledge. She has recommended that they hire a food consultant.
Dr. Saltsman asked if the establishment is still open for business. Ms. Johnson replied yes. Dr. Saltsman stated that is a concern due to the seriousness of the violations. He would like the food consultant hired by the end of this week and recommended that the community not be served until the consultant has signed off. Ms. Johnson stated that would be a suspension of their food permit with notice. Mr. McSweeney would agree that the need for a food consultant is more urgent than waiting until February 25th.
Dr. Weiner asked how we have assurances that the violations have been corrected. Ms. Johnson stated that most of the violations were corrected while she was still onsite during the inspection. The only one outstanding was the labeling of packaged bakery items but they have purchased a label machine to correct that issue. Ms. Johnson added that she has already re-inspected the facility and there were no violations. Dr. Weiner stated that staff should inspect the facility at least one more time and the food consultant should be hired by February 15th, the name should be given to the Board of Health by February 17th and they should appear back before the Board on March 24th. Ms. Johnson stated that she will inspect them this Friday. Dr. Weiner stated that if there is no progress, then Ms. Johnson should close them down.
MOTION: Dr. Saltsman moved to approve the recommendations of the Health Agent regarding King Bibis with the following changes: 1) The owner shall hire a professional food consultant by February 15, 2020; 2) The owner shall provide the name of the professional food consultant by February 17, 2020 to the Health Agent; 3) The owner shall come before the Board of Health on March 24, 2020 for an update; 4) the Health Agent shall inspect the establishment on February 14, 2020. The motion was seconded by Mr. McSweeney and unanimously approved. (3-0-0)
Staff Reports
Environmental Engineer
Ms. Mathis was not present so her report was not reviewed.
Health Agent
Ms. Johnson presented her report:
● Almost all of the indoor pools have been inspected with no issues. 1 pool is remaining.
● They have received calls on mice in the Burlington Mall. There is an increase of mice activity due to construction but all of the food establishments are clean.
● The larger number of emergency response calls were to the Burlington Mall when they had no running water.
Dr. Weiner asked if Spencer Gifts were going to be selling tobacco. Ms. Johnson replied no.
TOWN OF BURLINGTON BOARD OF HEALTH MINUTES
FEBRUARY 11, 2020
3
29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 ⧫ TEL (781) 270-1660 ⧫ FAX (781) 238-4692 www.burlington.org [email protected]
MOTION: Dr. Saltsman moved to approve the Health Agent’s report. The motion was seconded by Mr. McSweeney and unanimously approved. (3-0-0)
Director of Public Health
Ms. Lumenello presented her report:
● All applications have been received for the Health Fair. It will be March 28th. They are full with 59 exhibitors.
● There will be an emerging infectious disease workshop on February 19th from 6:00 to 7:30 PM.
● They received the technical assessment from the MRC ASPER office and Burlington received a score of 93%. This will now be done annually. The last time this assessment was done was in 2012 and Burlington received in the 70s.
MOTION: Mr. McSweeney moved to approve the Director of Public Health’s report. The motion was seconded by Dr. Saltsman and unanimously approved. (3-0-0)
Dr. Saltsman stated that the Coronavirus is significant but Massachusetts has a low threat with only 1 confirmed case. He is much more concerned with influenza. There were 300 new flu cases last week. Dr. Saltsman added that it is not too late to get your flu shot especially in elderly and kids. Make sure to wash your hands, stay home if you are sick and see your provider. Ms. Lumenello stated that the link to information of the Coronavirus is on the website.
Dr. Weiner stated that the biosafety regulations are also on the website.
Adjourn
MOTION: Dr. Saltsman moved to adjourn the Board of Health meeting at 7:36 PM. The motion was seconded by Mr. McSweeney and unanimously approved. (3-0-0)
Respectfully Submitted by Dawn Cathcart, Recording Clerk
DOCUMENTS REVIEWED AT MEETING – TUESDAY, FEBRUARY 11, 2020
Agenda
Minutes: January 28, 2020 (Tabled)
Chairman’s Report: None
Subcommittee Reports: None

TOWN OF BURLINGTON BOARD OF HEALTH MINUTES
FEBRUARY 11, 2020
4
29 CENTER STREET lBURLINGTON, MASSACHUSETTS 01803 ⧫ TEL (781) 270-1660 ⧫ FAX (781) 238-4692 www.burlington.org [email protected]
Hearing:
● King Bibis, 45 Winn Street – Food Code Violation
Memo from M. Johnson dated February 11, 2020
Staff Reports: Health Agent’s Report; Director of Public Health’s Report
Subcommittee Meeting Minutes: 02/12/2020
Present at this meeting were Susan Lumenello, Director of Public Health, Dr. Ed Weiner, BOH Chairman, Dr. Wayne Saltsman, BOH Medical Director & BOH Member, Patrick Larkin, Assistant Superintendent of Schools, Barbara Conley, BPS Lead Nurse
The BOH Draft Policy was reviewed and the following items discussed:
• Attachment 3 and 4 of the draft policy would need to be signed by the parent/guardian prior to the visit. • Attachment 4 designates a member of the school staff as a temporary agent for the child. The temporary agent
takes responsibility for the child and must be present during vaccination. The temporary agent would also be responsible for signing the Vaccine Screening Form on the day of vaccination.
• The BOH asked about the use of an Uber and raised concerns about the child arriving before the school representative. Patrick Larkin stated they will look into this – perhaps a permission slip for the child to ride in the representative’s vehicle.
• If second or third vaccinations are needed, the school will be responsible for ensuring the child gets a physical examination before vaccine administration.
• It was agreed that the routine flu vaccine should be included as part of the vaccinations.
Flu Vaccine Purchase Memo
Prepared by Christine Paulik MSN RN
DATE: February 25, 2020
2019-2020 Flu Season
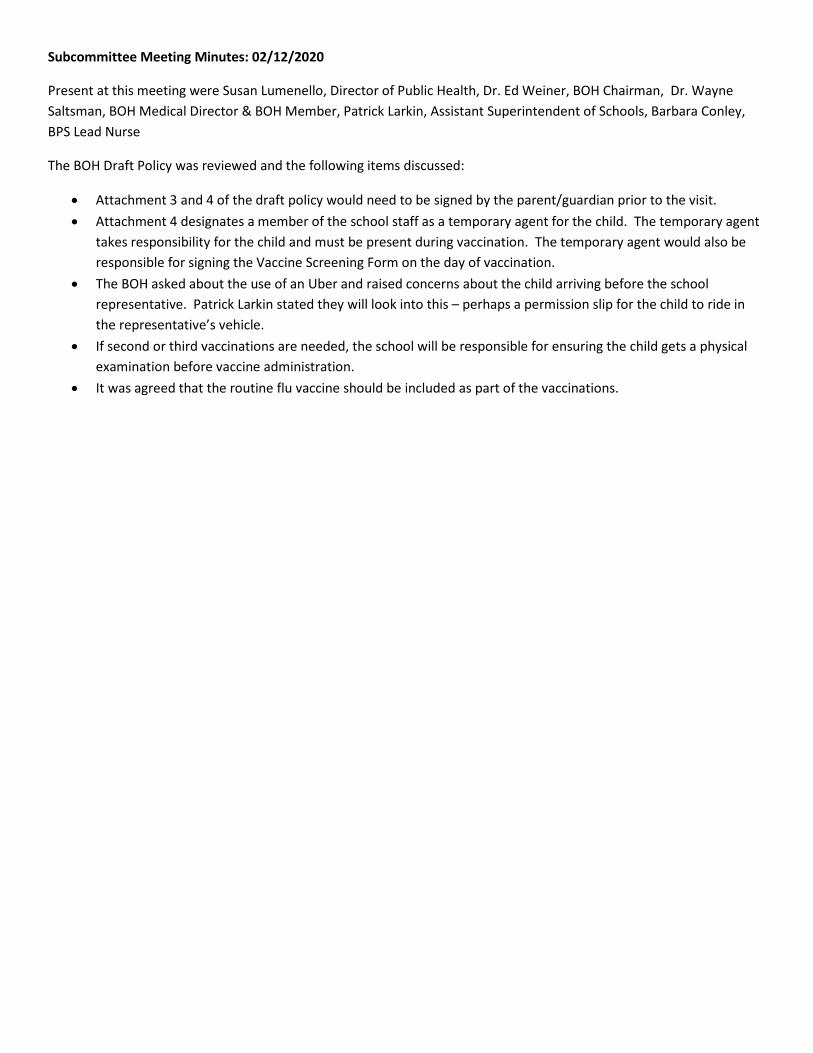
The BOH purchased Fluzone MDV 600 doses, Afluria MDV 200 doses, and Fluzone High Dose 70 doses. Fluzone MDV 150 doses will be returned for reimbursement. This flu season we gave 180 doses of state supplied flu vaccine through pediatric flu clinics at the BOH in October 2019 and during the annual flu clinic on October 26, 2019.
2019 Flu Shipment Delay Memo
Because of the Flu vaccine manufacturing and shipment delays (approximately 4 weeks), only 70 doses of High Dose vaccine were received prior to October 26th, 2019. The remaining doses were not guaranteed to arrive prior to the end of November. There was a delay in the last shipment of the Fluzone MDV, 210 doses, which did not arrive till mid November 2019. To ensure enough flu vaccine was available to the public for the town flu clinic, 200 doses of Afluria MDV vaccine was purchased.
6 mos. - 18 years
19 -29 years 30-49 years 50 - 64 years
65 years + Total
2019-2020 (492)
177 21 114 128 52 492
2017-2018 (527)
173 26 137 127 64 527
2016-2017 (467)
134 9 122 98 105 468
020406080
100120140160180200
2019-2020 (492) 2017-2018 (527) 2016-2017 (467)
# of
Vac
cine
s Di
spen
sed
Year
Total Flu Vaccine Dispensed at Clinic/EDS by Year
6 mos - 18 years
19 -29 years
30-49 years
50 - 64 years
65 years +
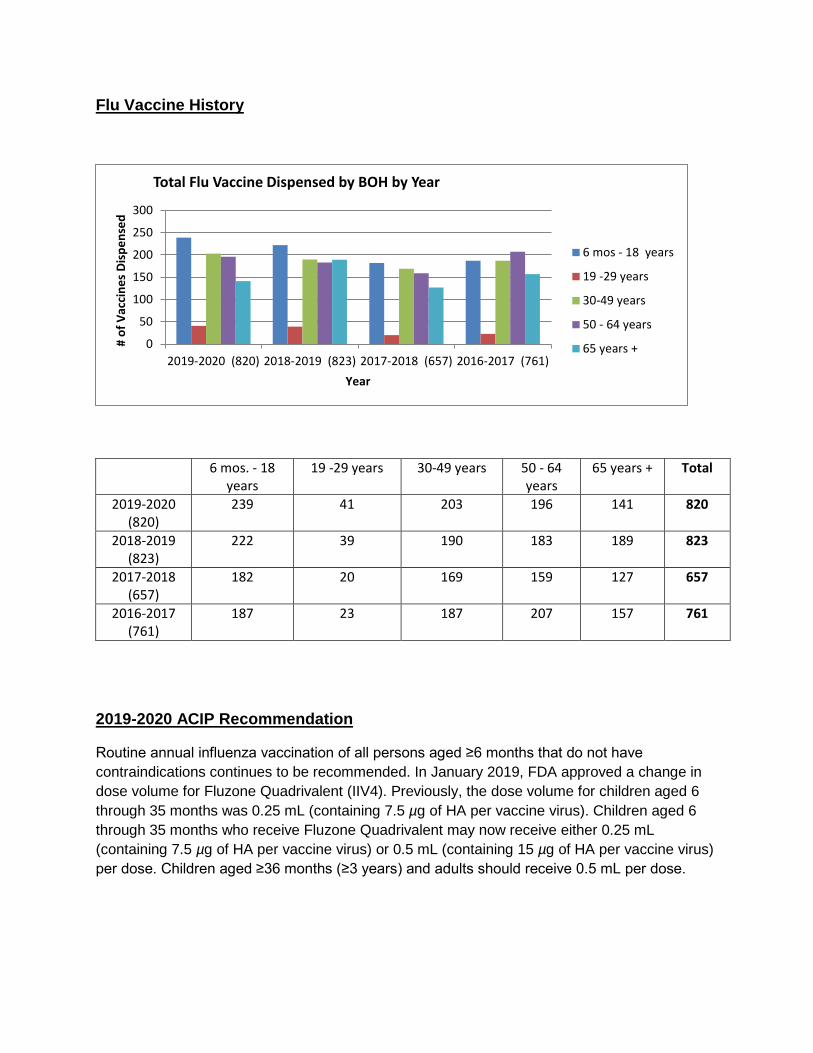
Flu Vaccine History
6 mos. - 18 years
19 -29 years 30-49 years 50 - 64 years
65 years + Total
2019-2020 (820)
239 41 203 196 141 820
2018-2019 (823)
222 39 190 183 189 823
2017-2018 (657)
182 20 169 159 127 657
2016-2017 (761)
187 23 187 207 157 761
2019-2020 ACIP Recommendation
Routine annual influenza vaccination of all persons aged ≥6 months that do not have contraindications continues to be recommended. In January 2019, FDA approved a change in dose volume for Fluzone Quadrivalent (IIV4). Previously, the dose volume for children aged 6 through 35 months was 0.25 mL (containing 7.5 µg of HA per vaccine virus). Children aged 6 through 35 months who receive Fluzone Quadrivalent may now receive either 0.25 mL (containing 7.5 µg of HA per vaccine virus) or 0.5 mL (containing 15 µg of HA per vaccine virus) per dose. Children aged ≥36 months (≥3 years) and adults should receive 0.5 mL per dose.
0
50
100
150
200
250
300
2019-2020 (820) 2018-2019 (823) 2017-2018 (657) 2016-2017 (761)
# of
Vac
cine
s Di
spen
sed
Year
Total Flu Vaccine Dispensed by BOH by Year
6 mos - 18 years
19 -29 years
30-49 years
50 - 64 years
65 years +
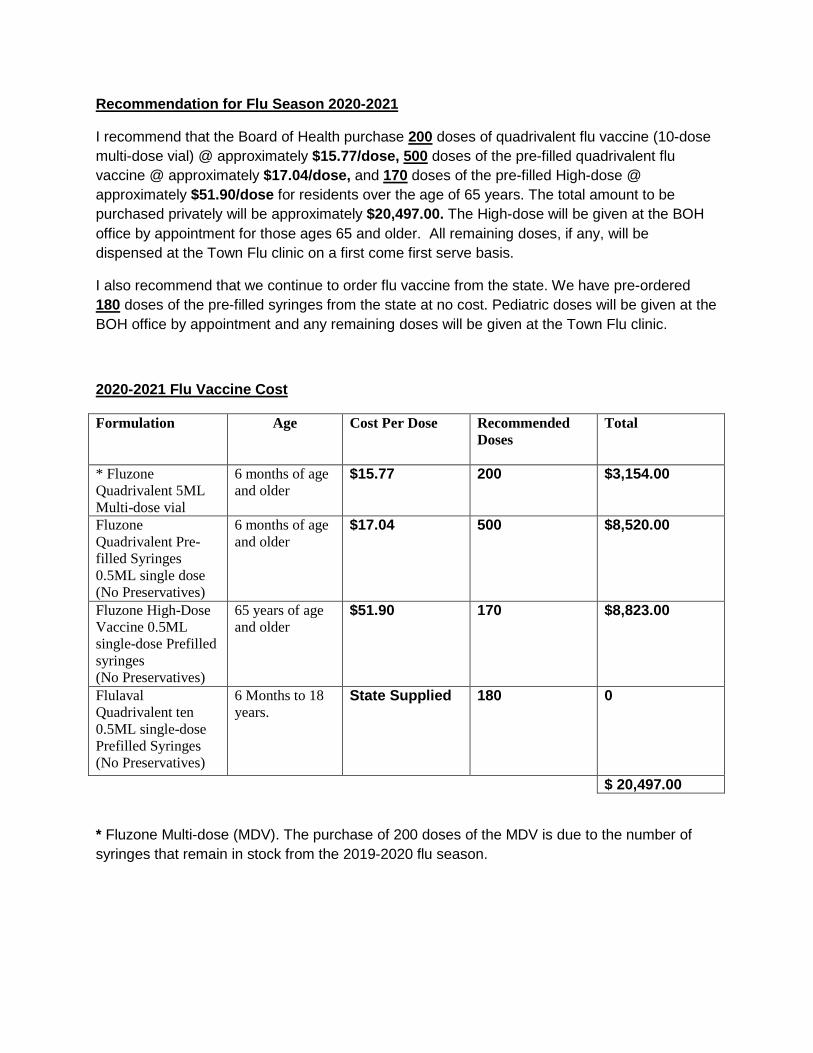
Recommendation for Flu Season 2020-2021
I recommend that the Board of Health purchase 200 doses of quadrivalent flu vaccine (10-dose multi-dose vial) @ approximately $15.77/dose, 500 doses of the pre-filled quadrivalent flu vaccine @ approximately $17.04/dose, and 170 doses of the pre-filled High-dose @ approximately $51.90/dose for residents over the age of 65 years. The total amount to be purchased privately will be approximately $20,497.00. The High-dose will be given at the BOH office by appointment for those ages 65 and older. All remaining doses, if any, will be dispensed at the Town Flu clinic on a first come first serve basis.
I also recommend that we continue to order flu vaccine from the state. We have pre-ordered 180 doses of the pre-filled syringes from the state at no cost. Pediatric doses will be given at the BOH office by appointment and any remaining doses will be given at the Town Flu clinic.
2020-2021 Flu Vaccine Cost
Formulation Age Cost Per Dose Recommended Doses
Total
* Fluzone Quadrivalent 5ML Multi-dose vial
6 months of age and older
$15.77 200 $3,154.00
Fluzone Quadrivalent Pre-filled Syringes 0.5ML single dose (No Preservatives)
6 months of age and older
$17.04 500 $8,520.00
Fluzone High-Dose Vaccine 0.5ML single-dose Prefilled syringes (No Preservatives)
65 years of age and older
$51.90 170 $8,823.00
Flulaval Quadrivalent ten 0.5ML single-dose Prefilled Syringes (No Preservatives)
6 Months to 18 years.
State Supplied 180 0
$ 20,497.00
* Fluzone Multi-dose (MDV). The purchase of 200 doses of the MDV is due to the number of syringes that remain in stock from the 2019-2020 flu season.
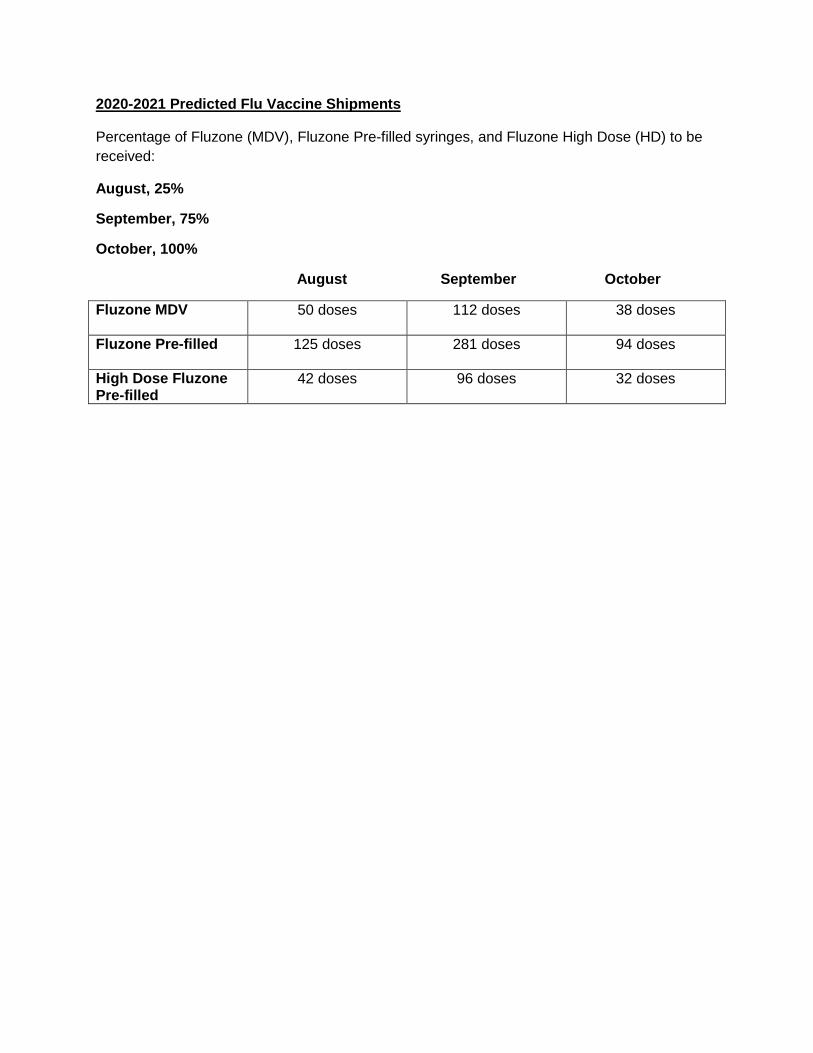
2020-2021 Predicted Flu Vaccine Shipments
Percentage of Fluzone (MDV), Fluzone Pre-filled syringes, and Fluzone High Dose (HD) to be received:
August, 25%
September, 75%
October, 100%
August September October
Fluzone MDV
50 doses 112 doses 38 doses
Fluzone Pre-filled
125 doses 281 doses 94 doses
High Dose Fluzone Pre-filled
42 doses 96 doses 32 doses
l3lJR I CiT() BOAR!) ()F HEALTJI 6 I Center ~trcct
Burlington. MA 01803
lei: 781-270-1955 h1.: 781-2T'-7687 Public Health Preven t . Promote . Pr o t ec t.
Protocol for Providing Vaccinations to Children in Cooperation with Burlington Public Schools
Approved by Board of Health: DRAFT
1. Standard Operating Procedures for the MA Department of Public Health (DPH) Vaccine for Children (VFC) Program must be followed. Note: A child is eligible for the VFC Program if he or she is younger than 19 years of age and is one of the following: (1) Medicaid-eligible (2) Uninsured (3) Underinsured (4) American Indian or Alaska Native.
2. The School Nurse will call the BOH Supervisory Nurse at 781-505-1139 to report that a child needs vaccination(s) to enter school. The School Nurse will fax the contact information of the child's parent or guardian and a completed "Vaccine Administration · Record" to 781-270-1605. The School Nurse will inform the parent or guardian to call the BOH office to schedule an appointment (walk-ins will not be accepted). Note: Only written documentation will be accepted as evidence of previous vaccination. If adequate documentation is not provided, the child will be considered susceptible and the BOH will start the child on the age-appropriate vaccination schedule.
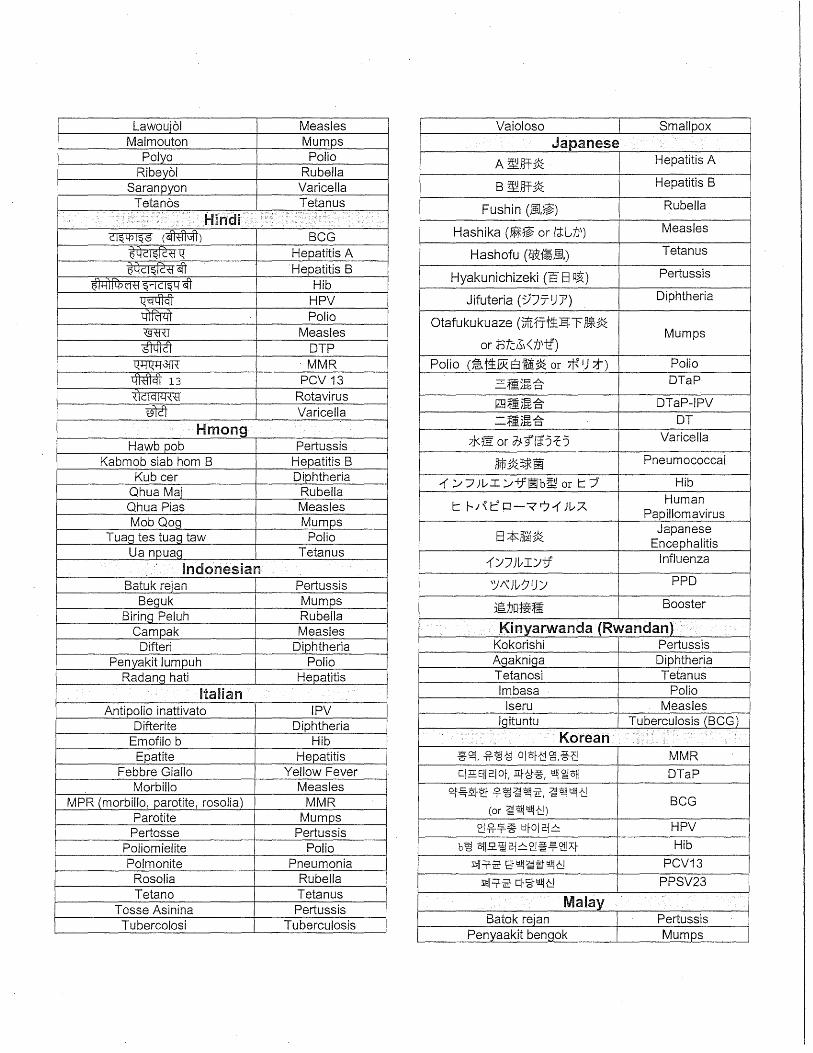
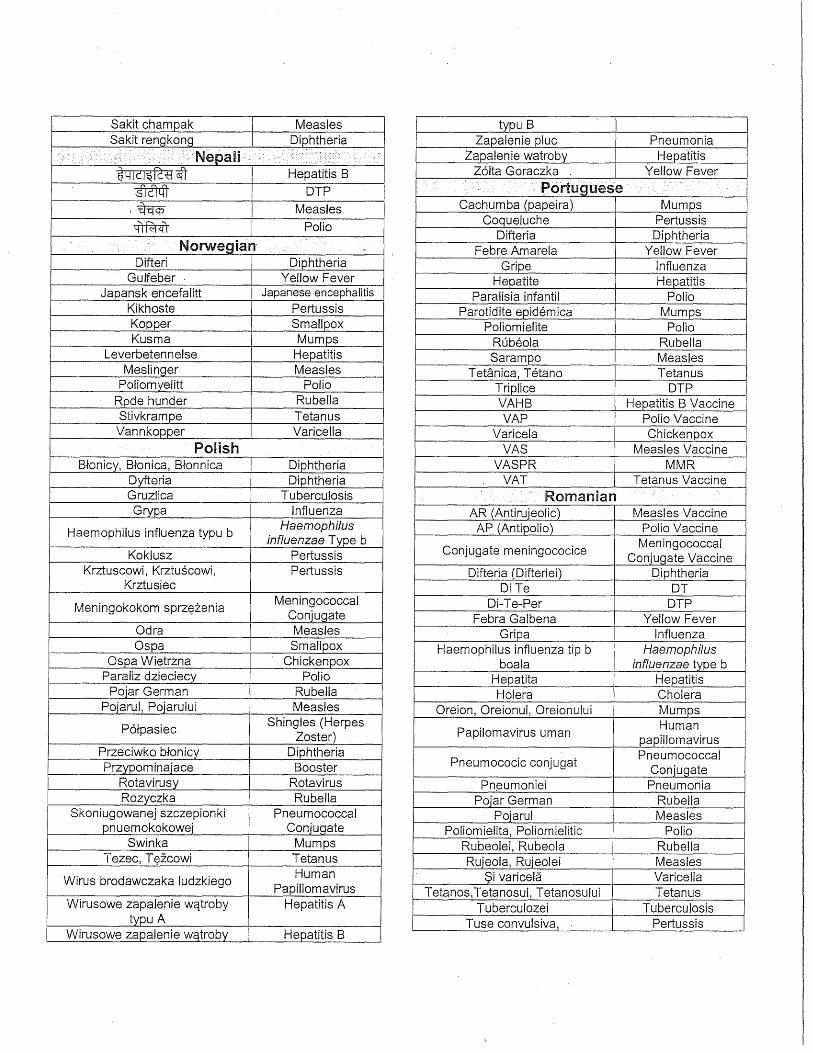
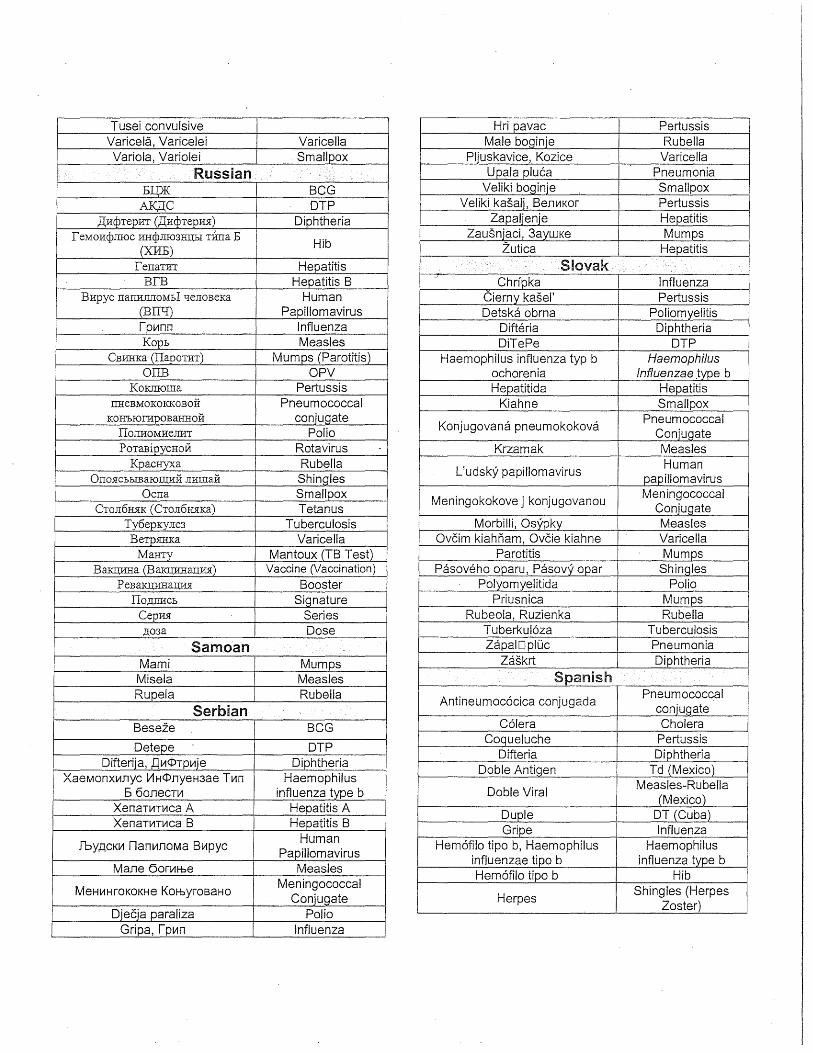
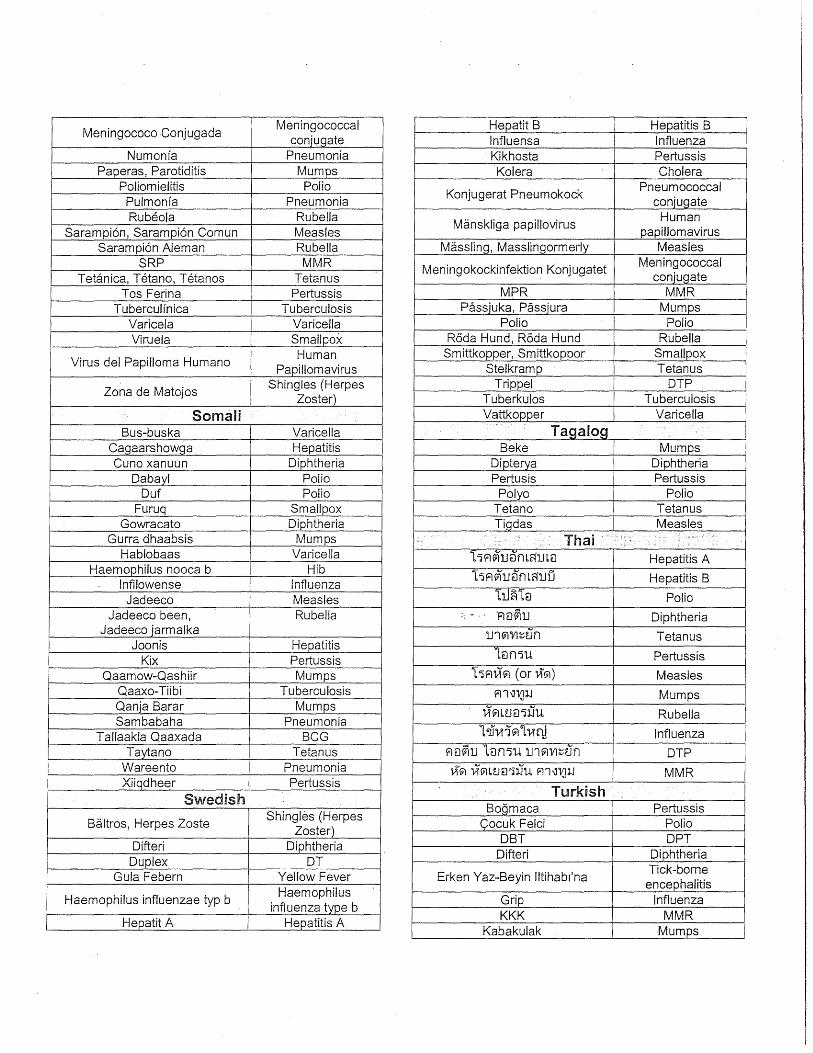
3. In the event that a Vaccine Administration Record is provided in a language other than English, the BOH Supervising Nurse will utilize the most current version of the CDC's Epidemiology and Prevention of Vaccine-Preventable Diseases (a.k.a. the "Pink Book") (Attachment 1) to interpret the vaccination record. If records cannot be translated, the child will be considered susceptible and will be started on the age-appropriate vaccination schedule in accordance with ACIP General Best Guidance for Immunization: Special Situations (Attachment 2).
4. The Supervisory Nurse will provide the parent or guardian with a Vaccine Information Sheet (VIS) for all vaccines that his/her child receives. In the event that a parent or guardian does not speak English, VIS will be provided in the appropriate language (Note: VIS can be found in several languages at immunize.org).
5. The child's parent or guardian must be present during vaccination unless alternate arrangements have been made with Burlington Public Schools. If the parent or guardian will not be present, a school representative will (1) obtain parent signature on the BOH Consent and Release Form (Attachment 3) md tilL I c n_porar) .\gent I orm (. tl<tchmcnt !2 (Burlington Public Schools will provide translation of~ ttachmcnt 1 and 4 paperworJ, to the appropriate language, if necessary); and, (2) \ ccompany the child to receive the vaccination(s) <tnd act ,1s till. child s I unporal) \gent dS dcstgnatulm Atta(.hmcnt 4.
G:\Protocols\Nursing\Vaccination & BPS\2019-08-VFC Program.doc
BURLINGTON BOARD OF HEALTH 61 Center Street
Burlington, MA 01803
Tel: 781-270-1955 Fax: 781-273-7687
Attachment 1 CDC's ''Pink Book''
G:\Protocols\Nursing\ Vaccination & BPS\20 19-08-VFC Program.docG:\Protoeols\Nursing\20 19 08 VFC Program.doe
Public Health Prevent. Promote. Pr otect.
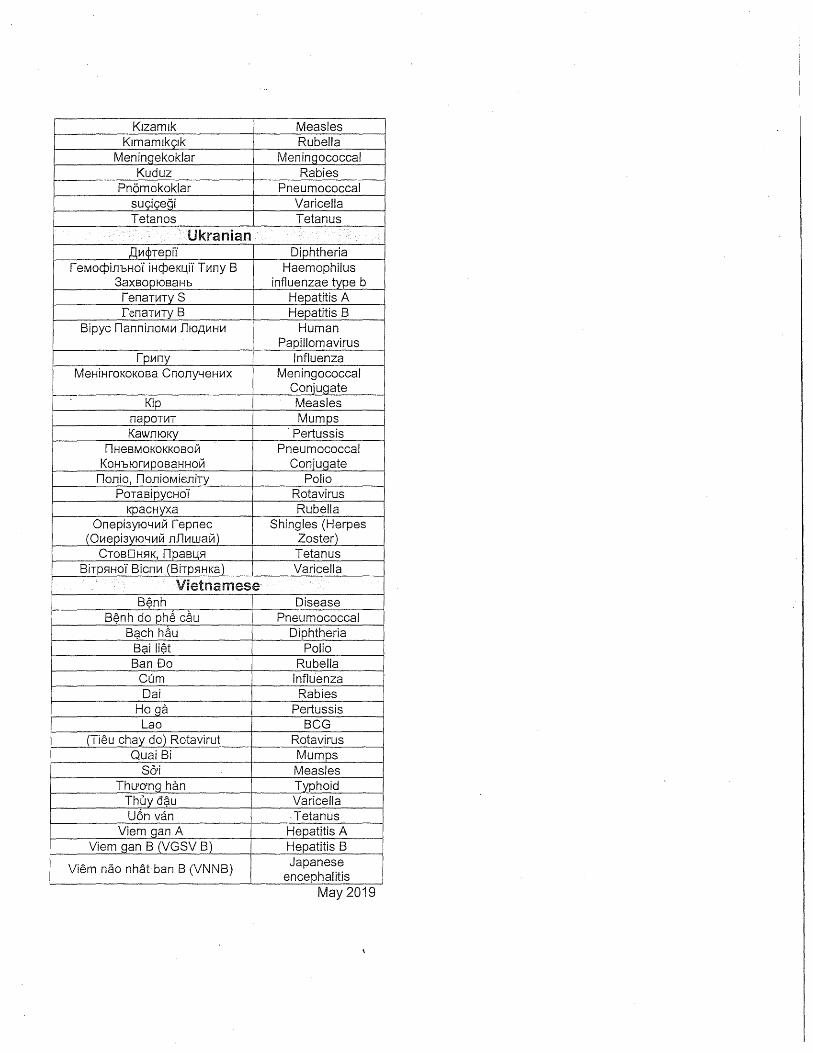
Foreign language Terms ' Aids to Translating Foreign Immunization Records ~
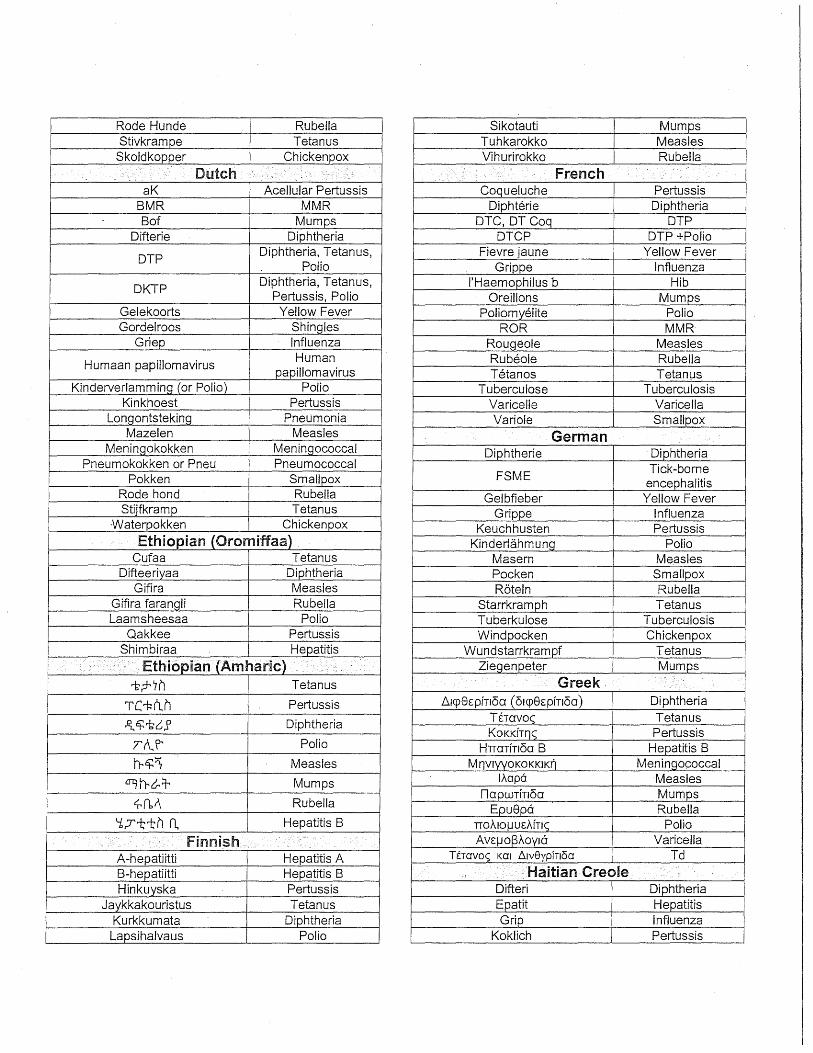
Table 1 Diseases, Vaccine, and Related Terms
This table lists terms, by language, for vaccine-preventable diseases and vaccines, and other terms that can be found on immunization records.
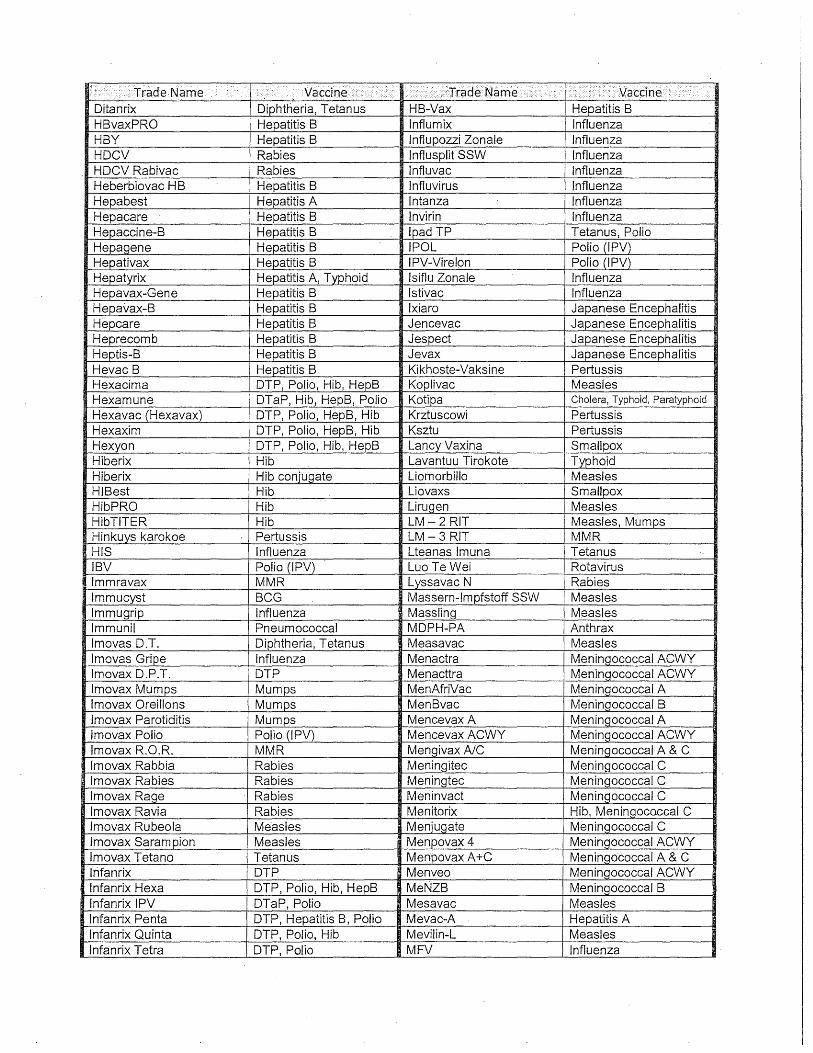
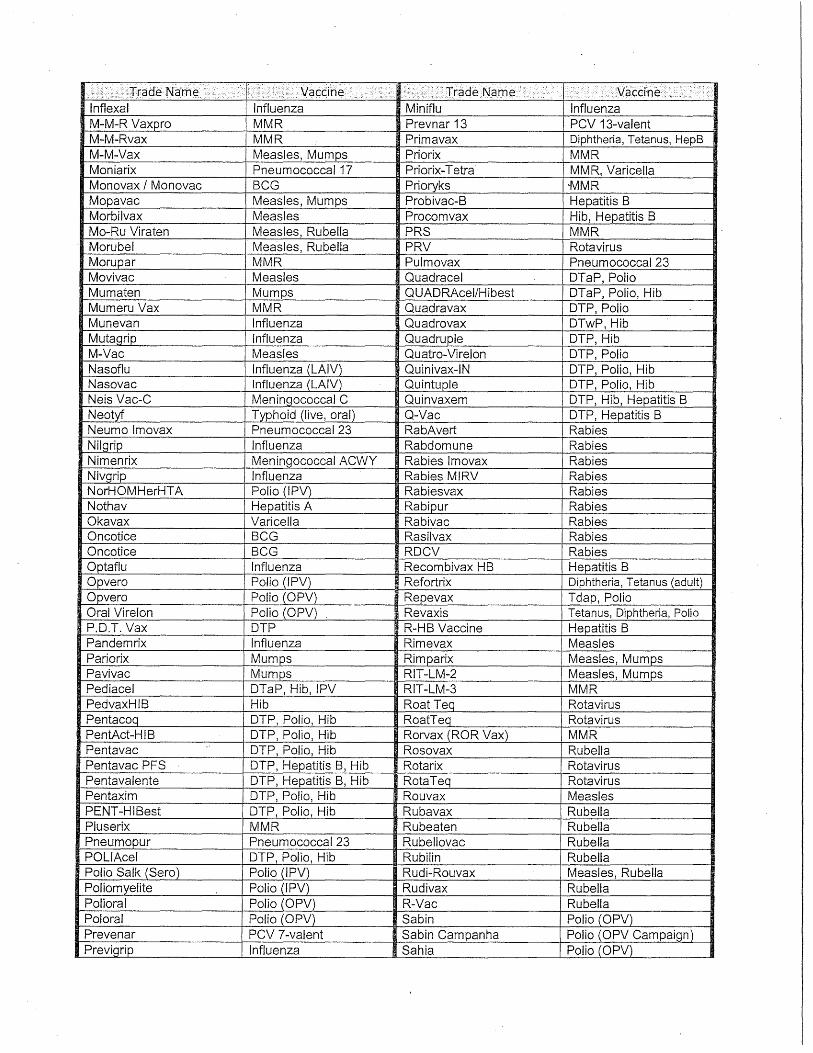
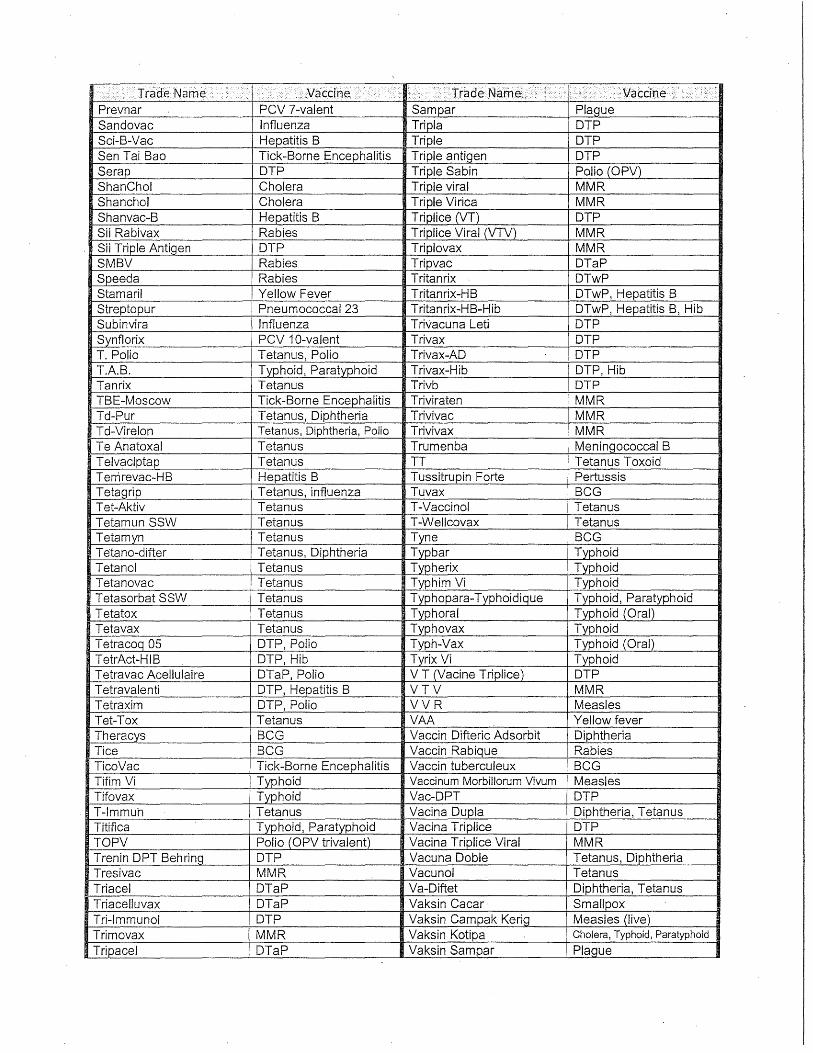
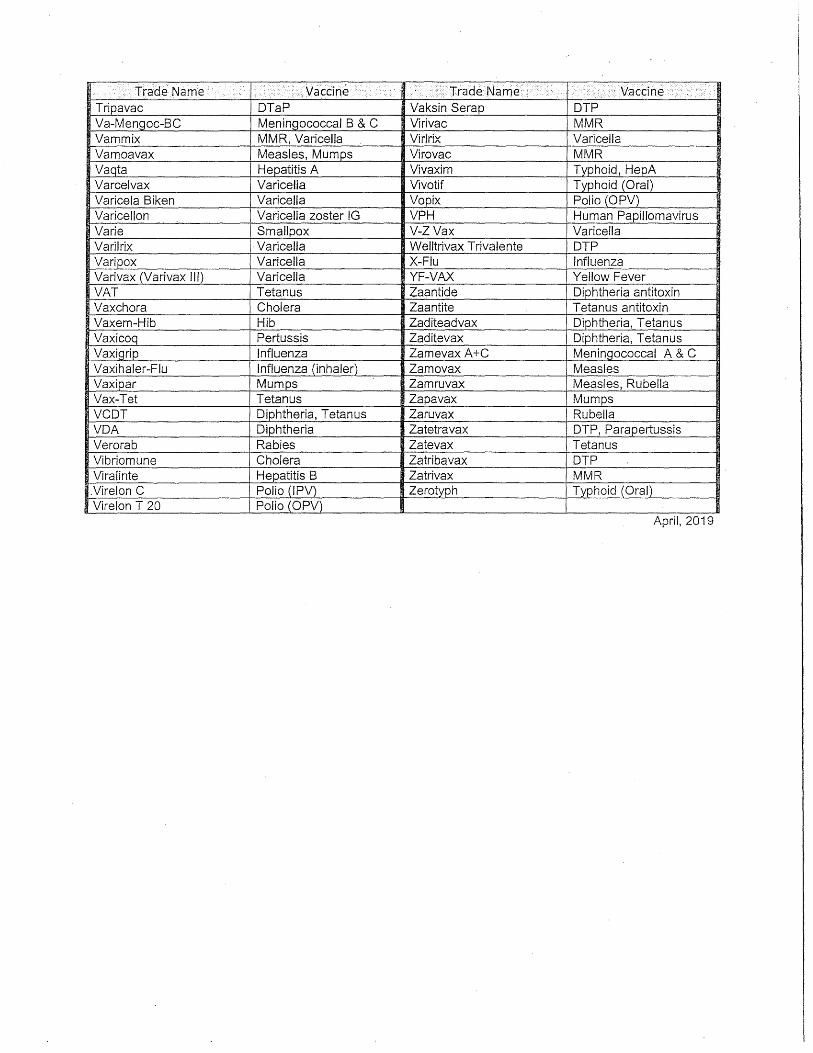
Table 2 Vaccines by Trade Name
This table identifies internationally used vaccines by trade name.
These tables have been created using a variety ofsources including lists developed by
the Minnesota Department of Health Immunization Program and
Washington State Department of Health.
See also: http://www.immunize.org/izpractices/p5121.pdf
These lists are not comprehensive. We have checked sources, but cannot claim complete accuracy.
May 2019
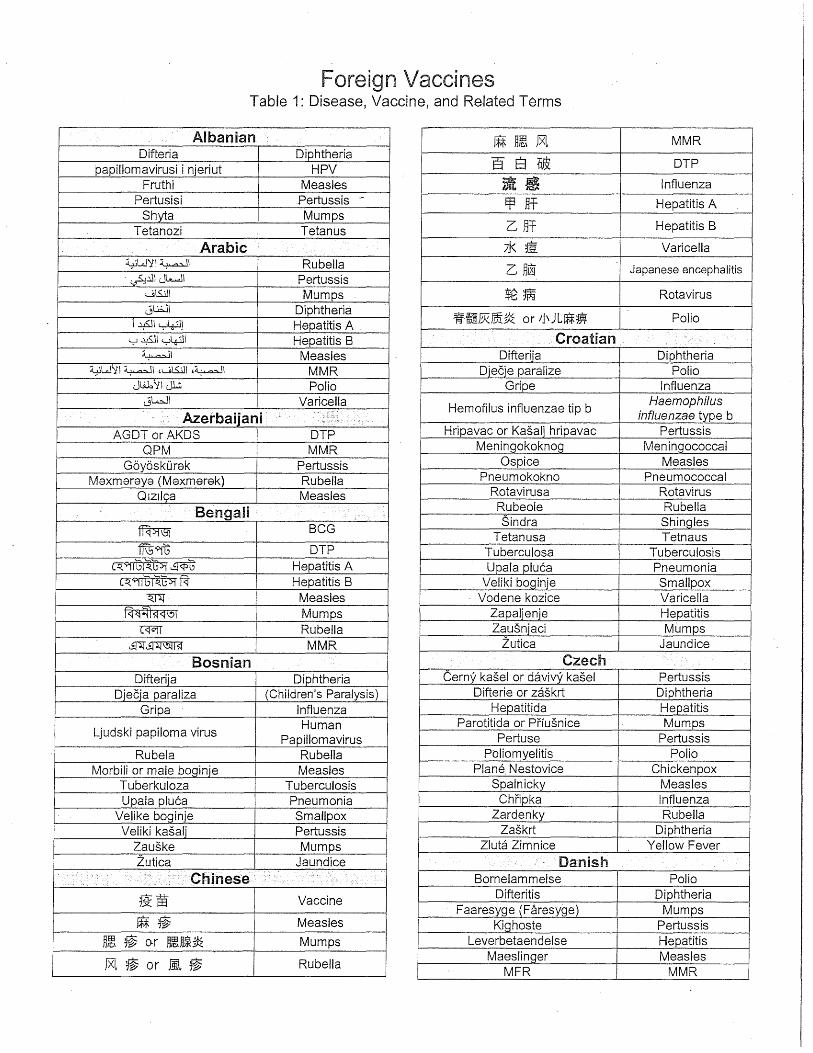
Foreign Vacc4nes Table 1: Disease, Vaccine, and Re~ated Terms
·.· Albanian ~ nm JXl MMR
8 E1 E~ DTP
»im Influenza
Difteria Diphtheria papillomavirusi i njeriut HPV
Fruthi Measles
Ef3Jff Hepatitis A
G ~f Hepatitis B
Pertusisi Pertussis .-
Shyta Mumps Tetanozi Tetanus
Arabic ;J< ~ Varicella
G ~~ Japanese encephalitis ~W':!I~I Rubella · "="~.lll Jk...JI Pertussis
t.,.j\S.jJI Mumps $~~ Rota virus
WREkmf~ or Jj\JL~m Polio 0\.l;JI Diphtheria
l~ly~) Hepatitis A . y~ly~l Hepatitis B Croatian ~I Measles Difterija Diphtheria
~W~I~I ,u\..S..i.ll ,~1 MMR Diecje paralize Polio Jt.i.b y I JL;, Polio Gripe Influenza
Hemofilus influenzae tip b Haemophilus
influenzae type b HripavacorKa§aljhripavac Pertussis
jlc...ll Varicella
Azerbaijani .... '\: .-::,.: .. ·····>
AGDT or AKDS DTP QPM MMR Meningokoknog Meningococcal
Ospice Measles Pneumokokno Pneumococcal
Rotavirusa Rota virus Rubeole Rubella Sindra Shingles
Tetanusa Tetnaus
Goyoskurak Pertussis Maxmaraya (Maxmarek) Rubella
OlzJiga Measles Bengali '
~ BCG
ffi59ffi DTP Tuberculosa Tuberculosis ~~~ Hepatitis A Upala pluca Pneumonia ~~~ Hepatitis B Veliki boginje Smallpox ~ Measles Vodene kozice Varicella
1<:1(;!--!1~<:1\!>1 Mumps Zapaljenje Hepatitis ~ Rubella Zausnjaci Mumps
~~ ~1.J\5mf MMR Zutica Jaundice
Bosnian Czech Difterija Diphtheria Cerny ka§el or davivy kasel Pertussis
Djecja paraliza (Children's Paralysis) Difterie or zaskrt Diphtheria Gripa Influenza Hepatitida Hepatitis
Parotitida or Prfusnice Mumps Pertuse Pertussis Ljudski papiloma virus
Human Papilloma virus
Rube Ia Rubella Poliomyelitis Polio Morbili or male boginje Measles Plane. Nestovice Chickenpox
Tuberkuloza Tuberculosis Spain icky Measles Upala pluca Pneumonia Chripka Influenza
Velike boginje Smallpox Zardenky Rubella Veliki kasalj Pertussis Zaskrt Diphtheria
Zauske Mumps Zluta Zimnice Yellow Fever Zutica Jaundice Danish
Bornelammelse Polio . ·, . . .... ··.· Chinese . ··'··.·.·.··.: :. :··· . .· :-.· . :''
Difteritis Diphtheria Faaresyge (Faresyge) Mumps
Kighoste Pertussis
19:ffi Vaccine
JU~ Measles
Hm ~ o.r ~~~~ Mumps Leverbetaendelse Hepatitis Maeslinger Measles
MFR MMR Jxl ~ or i.L ~ Rubella
Rode Hunde Rubella Sikotauti Mumps Stivkrampe Tetanus Tuhkarokko Measles
Skoldkopper Chickenpox Vihurirokko Rubella
Dutch .,,
.. .· ... --c
French .
aK Acellular Pertussis Coqueluche Pertussis BMR MMR Diphterie Diphtheria Bof Mumps DTC, DT Coq DTP
Difterie Diphtheria DTCP DTP +Polio
DTP Diphtheria, Tetanus,
Polio Fievre jaune Yellow Fever
Grippe Influenza
DKTP Diphtheria, Tetanus,
Pertussis, Polio I'Haemophilus b Hib
Oreillons Mumps Gelekoorts Yellow Fever Poliomyelite Polio Gordelroos Shingles ROR MMR
Griep Influenza Rouqeole Measles
Humaan papillomavirus Human
papillomavirus Rubeole Rubella Tetanos Tetanws
Kinderverlamming (or Polio) Polio Tuberculose Tubercu.losis Kinkhoest Pertussis Varicelle Varicella
Longontsteking Pneumonia Variole Smallpox Mazelen Measles German
Meninqokokken Meningococcal Pneumokokken or Pneu Pneumococcal
Pokken Smallpox Rode hand Rubella
Diphtherie · Diphtheria
FSME Tick-borne
encephalitis Gelbfieber Yellow Fever
Stijfkramp Tetanus ·Waterpokken Chickenpox
Grippe Influenza Keuchhusten Pertussis
Ethiopian (Oromiffaa) Kinderlahmung Polio Cufaa Tetanus Mas ern Measles
Difteeriyaa Diphtheria Pock en Smallpox Gifira Measles Roteln Rubella
Gifira faranqli Rubella Starrkramph Tetanus Laamsheesaa Polio Tuberkulose Tuberculosis
Qakkee Pertussis Windpocken Chickenpox Shimbiraa Hepatitis Wundstarrkrampf Tetanus .. ·.
• ··.: Ethiopian (Amharic) .• · .. :'. .. : . Zieqenpeter Mumps
.-s;r1n Tetanus Greek .
TC'i:dUI Pertussis fll<p8£pfTIOa (61cp8£pfn6a) Diphtheria
.fL tt: 1-~ .P Diphtheria
Tr\..P' Polio
Tbavoc Tetanus KoKKfrr,c Pertussis
Hnarfr16a B Hepatitis 8 !rtt:~ Measles M r)VIYYOKO KKIK~ Meningococcal
crtttr~::r Mumps
4-(bt\ Rubella
lf..apa Measles naowrfr1oa Mumps
EpuSpa Rubella 'i7ttn n.. Hepatitis 8 TTOAIO!JU£AfTI( Polio
.. Finnish .... . . AV£!JOr3AOVIC Varicella
A-hepatiitti Hepatitis A T£ravo<; KG! fl.JV8ypfTJ6a Td
B-hepatiitti Hepatitis B Haitian Creole .:.
Hinkuyska Pertussis Difteri Diphtheria Jaykkakouristus Tetanus Epa tit Hepatitis
Kurkkumata Diphtheria Grip Influenza Lapsihalvaus Polio Koklich Pertussis
Lawoujol Measles Vaioloso Smallpox Mal mouton Mumps Japanese
Pol yo Polio Ribeyol Rubella
Saranpyon Varicella
A~Bf~ Hepatitis A
8~Bf~ Hepatitis 8
Tetanos Tetanus ., ... · ·'· ''·:' ... ,., H·d····· < ,·.·.'· .,'< ','::,· · .. ·.
.. , ... •·•·'•·, .. ::'·' ·,: 1n · 1.'.·· · •.•. '· ...•
ci~Cf51~6 c<S!Nft:Jif) BCG
Fushin (&~) Rubella
Hashika (at~ or ld:G1.n Measles
~qc:1~~~-o: Hepatitis A ~ck1~~~ "it ·Hepatitis B
~~R$~~ ~"it Hib
~ HPV
Hashofu (~~{~&) Tetanus
Hyakunichizeki (s 8 Q_$:) Pertussis
Jifuteria (::J'Jj~J') Diphtheria
~ Polio ~ Measles mtt DTP
Otafukukuaze ()mff•I1:~TJl,~~ Mumps
or tit:.~-s, (i.J'if')
~JfR ·MMR Polio (~, 11:13< 8 a~ or iG 1) ;;t) Polio
-cftmclT 13 PCV13 .=w).EEil OTaP {IC:IC!!q~~ Rota virus
rna Varicella
Hmong Hawb pob Pertussis .
Q:9~i5i~ DTaP-IPV
=~.m;i~ DT
7.km or JJ. 9'1£:S.:C:S Varicella
Kabmob siab hom 8 Hepatitis 8 ~$~l3.K"i" Pneumococcal Kub cer Diphtheria
Qhua Maj Rubella Qhua Pias Measles Mob Qoq Mumps
Tua~ tes tuaq taw Polio Ua npuaq Tetanus
Indonesian
1' ~ 7 )I..- .I ~-!fmb~ or t: 7 Hib
t: r- J ~ t:o P-x rJ-{ 11..- .A Human
Papillomavirus
B=*~~~ Japanese
Encephalitis
1:YJ Jlti:Y"if' Influenza
Batuk rejan Pertussis 'YI\Jl--? 1)/
PPD
8eguk Mumps Siring Peluh Rubella
Campak Measles
~not~w Booster
: · .. Kinyarwanda (Rwandan) · Difteri Diphtheria Kokorishi Pertussis
Penyakit lumpuh Polio Agakniga Diphtheria Radanq hati Hepatitis Tetanosi Tetanus
Italian lmbasa Polio
Antipolio inattivato IPV Difterite Diphtheria
Emofilo b Hib
lseru Measles lgituntu Tuberculosis (8CG)
' '
Korean .' '· ,,
.. · ' ''·' :': ·'·
Epatite Hepatitis. .§~,-?f.~~ o!or~~,%~ MMR Febbre Giallo Yellow Fever Cj.E!=.E1j2jOt, IIr-2{%, ~ ~oH DTaP
Morbillo Measles MPR (morbillo, parotite, rosalia) MMR
Parotite Mumps Pertosse Pertussis
Qf&£r~ .5f~~~-rr, ~~~-tl 8CG
(or ~~~tl)
8 -*Ef-~ CltO! c1 ~ HPV
Poliomielite Polio b~ 'O:ll£~c1~'2.1~.Ef.'C!!;J::r Hib
Polmonite Pneumonia :rr~l.:::ri! 8~~gr~~ PCV13 Rosalia Rubella nf=jl it Ct t@" ~ ~ PPSV23 Tetano Tetanus
Tosse Asinina Pertussis Tubercolosi Tuberculosis
Malay Batok rejan Pertussis
Penyaakit bengok Mumps
Sakit champak Measles typu 8 Sakit rengkong Diphtheria Zapalenie pluc Pneumonia
I .' ::_ ·.· . < ···.•··Nepali .· .: >< } ..•. ., ........... _'_ .·· Zapalenie watroby Hepatitis
~q1c1~~~m Hepatitis 8
mm DTP
Z61ta Goraczka Yellow Fever .
Portuguese ' .
. ·.
\~ Measles
~ Polio
. Norwegian -
Cachumba (papeira) Mumps Coqueluche Pertussis
Difteria Diphtheria Febre Amarela Yellow Fever
Difteri Diphtheria Gulfeber Yellow Fever
Japansk encefalitt Japanese encephalitis
Gripe Influenza Hepatite Hepatitis
Paralisia infantil Polio Kikhoste Pertussis Kopper Smallpox
Parotidite epidemica Mumps Poliom ielite Polio
Kusma Mumps Rubeola Rubella Leverbetennelse Hepatitis Sarampo Measles
Meslinger Measles Tetanica, Tetano Tetanus Poliom:i_elitt Polio Triplice DTP
Rpde hunder Rubella VAHB Hepatitis 8 Vaccine Stivkrampe Tetanus VAP Polio Vaccine Vannkopper Varicella Varicela Chickenpox
Polish VAS Measles Vaccine Btonicy, 81-onica, Btonnica Diphtheria VASPR MMR
Dyfteria Diphtheria VAT Tetanus Vaccine Gruzlica Tuberculosis Romanian Grypa Influenza AR (Antirujeolic) Measles Vaccine
Haemophilus influenza typu b Haemophilus influenzae Type b
Koklusz Pertussis
AP (Antipolio) Polio Vaccine
Conjugate meningococice Meningococcal
Conjugate Vaccine Krztuscowi, Krztuscowi, Pertussis Difteria (Difteriei) Diphtheria
Krztusiec DiTe DT
Meningokokom sprz~zenia Meningococcal
Conjugate Di-Te-Per DTP
Febra Galbena Yellow Fever Odra Measles Ospa Smallpox
Os_Q_a Wietrzna Chickenpox Paraliz dzieciecy Polio
Gripa Influenza Haemophilus influenza tip b Haemophilus
boa Ia inf/uenzae type b Hepatita Hepatitis
Polar German Rubella Holera Cholera Pojarul, Pojarului Measles
P6tpasiec Shingles (Herpes
Zoster) Przeciwko btonicy Diphtheria Przypominajace Booster
Oreion, Oreionul, Oreionului Mumps
Papilomavirus uman Human
_Qapillom avirus
Pneumococic conjugat Pneumococcal
Conjugate Rotavirusy Rotavirus Pn~umoniei Pneumonia Rozyczka Rubella Pojar German Rubella
Skoniugowanej szczepionki Pneumococcal Pojarul Measles pnuemokokowej ConjuQate Poliomielita, Poliomielitic Polio
Swink a Mumps Rubeolei, Rubeola Rubella 1 ezec, T~zcowi Tetanus Rujeola, Rujeolei Measles
Wirus brodawczaka ludzkiego Human
Papillomavirus $i varicela Varicella
Tetanos,Tetanosul, Tetanosului Tetanus Wirusowe zapalenie wqtroby Hepatitis A Tuberculozei Tuberculosis
!t:Q_uA Wirusowe za_Qalenie Wqtroby He_Qatitis 8
Tuse convulsiva, Pertussis
Tusei convulsive Hri pavac Pertussis Varicela, Varicelei Varicella Male boginje Rubella Variola, Variolei SmaiiQ_ox Pljuskavice, Kozice Varicella
Russian "__ U_2_ala pluca Pneumonia
EI()K BCG Veliki boginje Smallpox
AK,I(C DTP Veliki kasalj, Bemt1Kor Pertussis
,lJ)-rqnep:aT ():(mlnepiDI) Diphtheria Zapaljenje Hepatitis
reMOH4_:>moc HH4_)1ll03HIU>I Tima J3 Hib (XI1.B)
Zausnjaci, 3aywKe Mumps Zutica Hepatitis
renaTHT Hepatitis Slovak BrB Hepatitis B Chrfpka Influenza
B:apyc namm.rroM:si qeJioBeKa Human Cierny kasel' Pertussis (BITY:) Papillomavirus Detska obrna Poliomyelitis lpvmn Influenza Difteria Diphtheria Kop:s Measles DiTePe DTP
CBnnKa (IIapoTHT) Mumps (Parotitis) Haemophilus influenza typ b Haemophilus OIIB OPV ochorenia lnfluenzae _type b
KoKJIIOma Pertussis Hepatitida Hepatitis ITHeBMOKOICKOBOH Pneumococcal Kiahne Smallpox
KOH'.h!OnipOBaHHOH conjugate IIoJrn:OMHeJIHT Polio Konjugovana pneumokokova
Pneumococcal Conjugate
PoTaBipycHo~ Rotavirus Krzamak Measles Kpacrryxa Rubella
Ono5Ic:s:srBa:FOm;:a:H JI:ama:H Shingles L'udsky papillomavirus
Human papillomavirus
Ocna Smallpox CToJI6H5IK ( CTOJI6H5!Ra) Tetanus
Meningokokove j konjugovanou Meningococcal Conjugate
Ty6epRyJie3 Tu bercu los is Morbilli, Osypky Measles Berp5IHKa Varicella Ovcim kiahnam, Ovcie kiahne Varicella
MaRTY Mantoux (TB Test)_ Parotitis Mumps Bai<Wilia (B~auiDI) Vaccine (Vaccination) Pasoveho oparu, Pasovyopar Shingles
p eBai<JJ;HHai.J;IDI Booster Polyomyelitida Polio IIo,n:Jrn:c:s Signature Priusnica Mumps
CepiDI Series Rubeola, Ruzienka Rubella ,n:o3a Dose Tuberkul6za Tuberculosis
Samoan Zap a I o piUc Pneumonia
Mami Mumps zaskrt Diphtheria
Misela Measles Spanish Rupela Rubella
Serbian Antineumoc6cica conjugada
Pneumococcal conjugate
Beseze BCG C61era Cholera
Detepe DTP Difterija, Avt<Drpvtje Diphtheria
XaeMonxvmyc V1H<DnyeH3ae Tvtn Haemophilus 5 6onecrvt influenza type b
Xenarvtrvtca A Hepatitis A XenaTII!TIIICa B Hepatitis B
fby.D,CKIII nanvtnoMa Blllpyc Human
Papillomavirus Mane 6orvt1-be Measles
MeHIIIHroKOKHe Kol-byrosaHo Meningococcal
Conjugate Djecja paraliza Polio
Coqueluche Pertussis Difteria Diphtheria
Doble Antigen Td (Mexico)
Doble Viral Measles-Rubella
(Mexico) Duple DT (Cuba} Gripe Influenza
Hem6filo tipo b, Haemophilus Haemophilus influenzae tipo b influenza type b Hem6filo tipo b Hib
Herpes Shingles (Herpes
Zoster)
Gripa, lpvtn Influenza
Meningococo .conjugada Meningococcal
conjugate Hepatit B Hepatitis B lnfluensa Influenza
Numonfa Pneumonia Kikhosta Pertussis Paperas, Parotiditis Mumps Kolera Cholera
Poliomielitis Polio Pulmonfa Pneumonia
Konjugerat Pneumokock Pneumococcal
conjugate Rubeola Rubella
Sarampi6n, Sarampi6n Comun Measles Manskliga papillovirus
Human papillomavirus
Sarampi6n Aleman Rubella Massling, Masslingormerly Measles SRP MMR
Tetanica, Tetano, Tetanos Tetanus Meningokockinfektion Konjugatet
Meningococcal conjugate
Tos Ferina Pertussis MPR MMR Tuberculfnica Tuberculosis Passjuka, Passjura Mumps
Varicela Varicella Polio Polio Viruela Smallpox Roda Hund, Roda Hund Rubella
Virus del Papilloma Humano Human
Papillomavirus Smittkopper, Smittkoppor Smallpox
Stelkramp Tetanus
Zona de Matojos Shingles (Herpes
Zoster) Trippel DTP
Tuberkulos Tuberculosis
Somali Vattkopper Varicella
Bus-buska Varicella Tagalog Cagaarshowga Hepatitis Beke Mumps Cuno xanuun Diphtheria Dipterya Diphtheria
Dabayl Polio Pertusis Pertussis Duf Polio Pol yo Polio
Furuq Smallpox Tetano Tetanus Gowracato Diphtheria Tigdas Measles
Gurra dhaabsis Mumps Thai . · ..•. ····: ....
·,· ·. < .... Hablobaas Varicella
Haemophilus nooca b Hib lnfilowense Influenza
Jadeeco Measles
1 '1A\1lll e)n LGilJ LfJ Hepatitis A 1 '1At1lue)n L~llU Hepatitis B
11J~18 Polio Jadeeco been, Rubella ; ·- -AeJ&'ilJ Diphtheria
Jadeeco jarmalka Joonis Hepatitis
Kix Pertussis
1J1~VJ::;cJ'n Tetanus
1eJtl'1U Pertussis
Qaamow-Qashiir Mumps 1'1A~~ (or "'G1) Measles Qaaxo-Tiibi Tuberculosis Qanja Barar Mumps Sambabaha Pneumonia
Tallaakla Qaaxada BCG
A1-Jl(]:W Mumps
~~ltl8'1iJU Rubella
1onvt1~"lvtf1! Influenza
Taytano Tetanus AfJ~lJ 1eJtl'1U 1J1~VJ::;cJtl DTP Wareento Pneumonia Xiiqdheer Pertussis
Swedish
Baltros, Herpes Zoste Shingles (Herpes
Zoster) Difteri Diphtheria Duplex DT
Gula Febern Yellow Fever
Haemophi!us influenzae typ b Haemophilus
influenza type b Hepatit A Hepatitis A
"'G1 ~~LtJeJ'1iJU A1\ll(]:W MMR
Turkish Bog maca Pertussis
Cocuk Felci Polio DBT OPT
Difteri Diphtheria
Erken Yaz-Beyin lltihab1'na Tick-borne
encephalitis Grip Influenza KKK MMR
Kabakulak Mumps
Krzamrk Measles K1mamrkgrk Rubella
Meningekoklar Meningococcal Kuduz Rabies
Pnomokoklar Pneumococcal sugigegi Varicella Tetanos Tetanus
Ukranian <
.QI!I<j>Teprl Diphtheria reMocjJinbHo"i iHcjJeKL(i"i Tl!lny B Haemophilus
3axsopf{)saHb influenzae type b renaTI!ITY S Hepatitis A fenaTI!ITY B Hepatitis B
Bipyc nanninOMI!I nf{)AI!IHI!I Human Papillomavirus
rp111ny Influenza MeHiHroKoKosa CnonyYeHI!IX Meningococcal
Conjugate Kip Measles
napOTI!IT Mumps Kawnf{)KY , Pertussis
n HeBMOKOKKOBOL7! Pneumococcal KoHbf{)rl!lposaHHOL71 Conjugate
nonio, noniOMieniTy Polio PoTasipycHo"i Rota virus
KpacHyxa Rubella Onepi3yf{)Lli!IL1 repnec Shingles (Herpes
(01!1epi3yf{)Lli!IL4 nn111waL:1) Zoster) CTOB0Hs:JK, npaBL(s:! Tetanus
BiTps:!HO'i Bicn111 (BiTps:!HKa) Varicella Vietnamese·
B$nh Disease B$nh do phe cau Pneumococcal
Bc;1ch hau Diphtheria Bc;1i li$t Polio Ban Do Rubella
Cum lnflu'enza Dai Rabies
Ho ga Pertussis Lao BCG
(Tieu chay do) Rotavirut Rota virus Quai Bi Mumps
sa.; Measles ThU'O'ng_ han Typhoid
Thuy a~u Varicella Uon van -Tetanus
Viem gan A Hepatitis A Viem gan B (VGSV B) Hepatitis B
Viem nao nhat ban B (VNNB) Japanese enceph alit is
May 2019
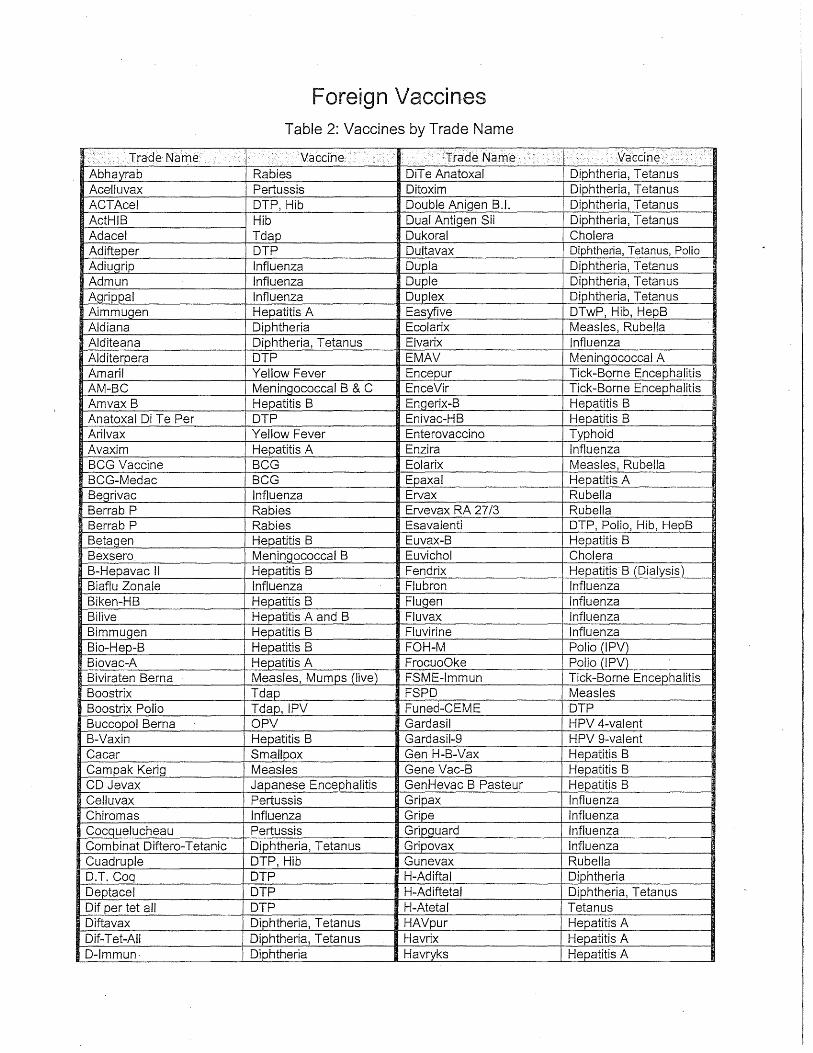
Foreign Vaccines Table 2: Vaccines by Trade Name
1: > :• ... ··Trade Name Vaccine .•.. ·····.·· .. · ..... · .. ·· .··
·trade Name ·•· < ·. .··vaccine.... > . .-· ........ . ... · . · ...... Abhayrab Rabies DiT e Anatoxal Diphtheria, Tetanus Ace-lluvax Pertussis Ditoxim Diphtheria, Tetanus ACTAcel DTP, Hib Double Anigen B.l. Diphtheria, Tetanus ActHIB Hib Dual Anti'gen Sii Diphtheria, Tetanus Adacel Tdap Dukoral Cholera Adifteper DTP Dultavax Diphtheria, Tetanus, Polio Adiugrip Influenza Dupla Diphtheria, Tetanus Admun Influenza Duple Diphtheria, Tetanus Agrippal Influenza Duplex Diphtheria, Tetanus Aimmugen Hepatitis A Easyfive DTwP, Hib, HepB Aldiana Diphtheria Ecolarix Measles, Rubella Alditeana Diphtheria, Tetanus Elvarix Influenza Alditerpera DTP EMAV Meningococcal A Amari! Yellow Fever Encepur Tick-Borne Encephalitis AM-BC Meningococcal B & C EnceVir Tick-Borne Encephalitis Amvax B Hepatitis B Engerix-B Hepatitis B Anatoxal Di T e Per DTP Enivac-HB Hepatitis B Arilvax Yellow Fever Enterovaccino Typhoid Avaxim Hepatitis A Enzira Influenza BCG Vaccine BCG Eolarix Measles, Rubella BCG-Medac BCG Epaxal Hepatitis A Begrivac Influenza Ervax Rubella Berrab P Rabies Ervevax RA 27/3 Rubella Berrab P Rabies Esavalenti DTP, Polio, Hib, HepB Betag_en Hepatitis B Euvax-B Hepatitis B Bexsero Meningococcal B Euvichol Cholera B-Hepavac II Hepatitis B Fendrix Hepatitis B (Dialysis) Biaflu Zonale Influenza Flubron Influenza Biken-HB Hepatitis B Flugen Influenza Bilive Hepatitis A and B Fluvax Influenza Bimmugen Hepatitis B Fluvirine Influenza Bio-Hep-8 Hepatitis B FOH-M Polio (IPV) Biovac-A Hepatitis A FrocuoOke Polio (IPV) Biviraten Berna Measles, Mumps (live) FSME-Immun Tick-Borne Encephalitis Boostrix Tdap FSPD Measles Boostrix Polio Tdap, IPV Funed-CEME DTP Buccopol Berna OPV Gardasil HPV 4-valent B-Vaxin Hepatitis B Gardasil-9 HPV 9-valent Cacar Smallpox Gen H-B-Vax Hepatitis B Campak Kerig Measles Gene Vac-B Hepatitis B CD Jevax Japanese Encephalitis GenHevac B Pasteur Hepatitis B Celluvax Pertussis Gripax Influenza Chiromas Influenza Gripe Influenza Cocquelucheau Pertussis Gripguard Influenza Combinat Diftero-Tetanic Diphtheria, Tetanus Gripovax Influenza Cuadruple DTP, Hib Gunevax Rubella D.T. Coq DTP H-Adiftal Diphtheria Deptacel DTP H-Adiftetal Diphtheria, Tetanus Dif per tet all DTP H-Atetal Tetanus Diftavax Diphtheria, Tetanus HAVpur Hepatitis A Dif-Tet-AII Diphtheria, Tetanus Havrix Hepatitis A D-lmmun- Diphtheria Havryks Hepatitis A
.•• TradeNa111e . . .......... Vaccine · •· •. i:·rrade Ni:une .······ 1··········:········: ......... ,
:.::o:. .... . .. • .... . .. ......
Ditanrix Diphtheria, Tetanus HB-Vax Hepatitis B HBvaxPRO Hepatitis B lnflumix Influenza HBY Hepatitis B lnflupozzi Zonale Influenza HDCV Rabies lnflusplit SSW Influenza HDCV Rabivac Rabies lnfluvac Influenza Heberbiovac HB Hepatitis B lnfluvirus Influenza Hepabest Hepatitis A lntanza Influenza Hepacare Hepatitis B lnvirin Influenza Hepaccine-B Hepatitis B lpad TP Tetanus, Polio Hepagene Hepatitis B I POL Polio (IPV) Hepativax Hepatitis B IPV-Virelon Polio (IPV) Hepatyrix Hepatitis A, Typhoid lsiflu Zonale Influenza Hepavax-Gene Hepatitis B lstivac Influenza Hepavax-B Hepatitis B lxiaro Japanese Encephalitis Hepcare Hepatitis B Jencevac Japanese Encephalitis Heprecomb Hepatitis B Jespect Japanese Encephalitis Heptis-B Hepatitis B Jevax Japanese Encephalitis Hevac B Hepatitis B Kikhoste-Vaksine Pertussis Hexacima DTP, Polio, Hib, HepB Koplivac Measles Hexamune DTaP, Hib, HepB, Polio Kotipa Cholera, Typhoid, Paratyphoid
Hexavac (Hexavax) DTP, Polio, HepB, Hib Krztuscowi Pertussis Hexaxim DTP, Polio, HepB, Hib Ksztu Pertussis Hexyon DTP, Polio, Hib, HepB Laney Vaxina Smallpox Hiberix Hib Lavantuu Tirokote Typhoid Hiberix Hib conjugate Liomorbillo Measles HI Best Hib Liovaxs Smallpox HibPRO Hib Lirugen Measles HibTITER Hib LM-2 RIT Measles, Mumps Hinkuys karokoe Pertussis LM-3 RIT MMR HIS Influenza Lteanas lmuna Tetanus IBV Polio (IPV) Luo Te Wei Rota virus lmmravax MMR Lyssavac N Rabies lmmucyst BCG Massern-lmpfstoff SSW Measles lmmugrip Influenza Massling Measles lmmunil Pneumococcal MDPH-PA Anthrax lmovas D.T. Diphtheria, Tetanus Measavac Measles lmovas Gripe Influenza Menactra Meningococcal ACWY lmovax D.P.T. DTP Menacttra Meningococcal ACWY lmovax Mumps Mumps MenAfriVac Meningococcal A lmovax Oreillons Mumps MenBvac Meningococcal B lmovax Parotiditis Mumps Mencevax A Mening_ococcal A lmovax Polio Polio (IPV)_ Mencevax ACWY Mening_ococcal ACWY lmovax R.O.R. MMR Mengivax AJC Mening_ococcal A & C lmovax Rabbia Rabies Meningitec Meningococcal C lmovax Rabies Rabies Meningtec Meningococcal C lmovax Rag_e Rabies Meninvact Meningococcal C lmovax Ravia Rabies Menitorix Hib, Meningococcal C lmovax Rubeola Measles Menjugate Meningococcal C lmovax Sa ram pion Measles Menpovax 4 Meningococcal ACWY lmovax Tetano Tetanus Menpovax A+C Meningococcal A & C lrifanrix DTP Menveo Meningococcal ACWY lnfanrix Hexa DTP, Polio, Hib, HepB MeNZB Meningococcal B lnfanrix IPV DTaP, Polio Mesavac Measles lnfanrix Penta DTP, Hepatitis B, Polio Mevac-A Hepatitis A lnfanrix Quinta DTP, Polio, Hib Mevilin-L Measles lnfanrix Tetra DTP, Polio MFV Influenza
, .. : : :. <J}ade·Nam~ .. ·.· ............ ·· •> I< i n , :: ~:;;:; ....... .... :: · · Jrade.Name •;. > ................. · ((;:.. ::; '. < > .<.:·· .••.••. ·.va~.;<""'ltlc;;., ·: .. :-: :·.:.:, • >· . .- ... .. :.::·· .... ·. lnflexal Influenza Miniflu Influenza M-M-R Vaxpro MMR Prevnar 13 PCV 13-valent M-M-Rvax MMR Primavax Diphtheria, Tetanus, HepB M-M-Vax Measles, Mumps Priorix MMR Moniarix Pneumococcal 17 Priorix-Tetra MMR, Varicella Monovax I Monovac BCG Prioryks ·MMR Mopavac Measles, Mumps Probivac-8 Hepatitis B Morbilvax Measles Procomvax Hib, Hepatitis 8 Mo-Ru Viraten Measles, Rubella PRS MMR Morubel Measles, Rubella PRV Rota virus Moru~ar MMR Pulmovax Pneumococcal 23 Movivac Measles Quadracel DTaP, Polio Mumaten Mumps QUADRAcei/Hibest DTaP, Polio, Hib Mumeru Vax MMR Quadravax DTP, Polio Munevan Influenza Quadrovax DTwP, Hib Mutagrip Influenza Quadruple DTP, Hib M-Vac Measles Quatro-Virelon DTP, Polio Nasoflu Influenza (LAIV) Quinivax-IN DTP, Polio, Hib Nasovac Influenza (LAIV) Quintuple DTP, Polio, Hib Neis Vac-C Meningococcal C Quinvaxem DTP, Hib, Hepatitis B Neotyf Typhoid (live, oral) Q-Vac DTP, Hepatitis B Neumo lmovax Pneumococcal 23 RabAvert Rabies Nilgrip Influenza Rabdomune Rabies Nimenrix Meningococcal ACWY Rabies lmovax Rabies Nivgrip Influenza Rabies MIRV Rabies NorHOMHerHTA Polio (IPV) Rabiesvax Rabies Nothav Hepatitis A Rabipur Rabies Okavax Varicella Rabivac Rabies Oncotice BCG Rasilvax Rabies Oncotice BCG RDCV Rabies Optaflu Influenza Recombivax HB Hepatitis B Opvero Polio (!PV) Refortrix Diphtheria, Tetanus (adult) Opvero Polio (OPV) Repevax Tdap, Polio Oral Virelon Polio (OPV) Revaxis Tetanus, Diphtheria, Polio P.D.T. Vax DTP R-H8 Vaccine Hepatitis B Pandemrix Influenza Rimevax Measles Pariorix Mumps Rimparix Measles, Mumps Pavivac Mumps RIT-LM-2 Measles, Mumps Pediacel DTaP, Hib, IPV RIT-LM-3 MMR PedvaxHIB Hib RoatTeg Rotavirus Pentacoq DTP, Polio, Hib RoatTeq Rotavirus PentAct-HIB DTP, Polio, Hib Rorvax (ROR Vax) MMR Pentavac
.. DTP, Polio, Hib Rosovax Rubella
Pentavac PFS DTP, Hepatitis B, Hib Rotarix Rota virus Pentavalente DTP, Hepatitis B, Hib RotaTeq Rota virus Pentaxim DTP, Polio, Hib Rouvax Measles PENT-HI Best DTP, Polio, Hib Rubavax Rubella Pluserix MMR Rubeaten Rubella Pneumopur Pneumococcal 23 Rubellovac Rubella POLl Ace! DTP, Polio, Hib Rubilin Rubella Polio Salk (Sera) Polio (IPV) Rudi-Rouvax Measles, Rubella Poliomyelite Polio (IPV) Rudivax Rubella Polioral Polio (OPV) R-Vac Rubella Poloral Polio (OPV) Sabin Polio (OPV) Prevenar PCV 7 -valent Sabin Campanha Polio (OPV Campaign) Previgrip Influenza Sahia Polio (OPV)
:·: .··':<:Trade Name ·.' .··'••,. · ·>• •• vaccine > .·.'·•· .. <: >·. Trade Name; · · '\/accine }'.,•:,.,, •• ·:.· .. ' << : ·:·· ::: . .-·< ..
Prevnar PCV 7 -valent Sam par PlaQue Sandovac Influenza Tripi a DTP Sci-B-Vac Hepatitis B Triple DTP Sen Tai Bao Tick-Borne Encephalitis Triple antigen DTP Serap DTP Triple Sabin Polio (OPV) ShanChol Cholera Triple viral MMR Shanchol Cholera Triple Virica MMR Shanvac-8 Hepatitis B Triplice (VT) DTP Sii Rabivax Rabies Triplice Viral (VTV) MMR Sii Triple Antigen DTP Triplovax MMR SMBV Rabies Tripvac DTaP Speed a Rabies Tritanrix DTwP Stamaril Yellow Fever Tritanrix-HB DTwP, Hepatitis B Streptopur Pneumococcal 23 Tritanrix-HB-Hib DTwP, Hepatitis 8, Hib Subinvira Influenza Trivacuna Leti DTP Synflorix PCV 1 O-va lent Trivax DTP T. Polio Tetanus, Polio Trivax-AD DTP T.A.B. Typhoid, Paratyphoid Trivax-Hib DTP, Hib Tanrix Tetanus Trivb DTP TBE-Moscow Tick-Borne Encephalitis Triviraten MMR Td-Pur Tetanus, Diphtheria Trivivac MMR Td-Virelon Tetanus, Diphtheria, Polio Trivivax MMR Te Anatoxal Tetanus Trumenba Meningococcal B T elvaclptap Tetanus TT Tetanus Toxoid T em revac-H B Hepatitis B Tussitrupin Forte Pertussis Tetagrip Tetanus, influenza Tuvax BCG Tet-Aktiv Tetanus T-Vaccinol Tetanus Tetamun SSW Tetanus T-Wellcovax Tetanus Tetamyn Tetanus Tyne BCG T etano-difter Tetanus, Di~htheria Typbar Typhoid Tetanal Tetanus Typherix Typhoid Tetanovac Tetanus Typhim Vi Typhoid T etasorbat SSW Tetanus Typhopara-Typhoidique Typhoid, Paratyphoid Tetatox Tetanus Typhoral Typhoid (Oral) Tetavax Tetanus Typhovax Typhoid Tetracoq 05 DTP, Polio Typh-Vax Typhoid (Oral) TetrAct-HIB DTP, Hib Tyrix Vi Typhoid Tetravac Acellulaire DTaP, Polio V T (Vacine Tripi ice) DTP T etravalenti DTP, Hepatitis B VTV MMR Tetraxim DTP, Polio VVR Measles Tet-Tox Tetanus VAA Yellow fever Theracys BCG Vaccin Difteric Adsorbit Diphtheria Tice BCG Vaccin Rabique Rabies TicoVac Tick-Borne Encephalitis Vaccin tuberculeux BCG Tifim Vi Typhoid Vaccinum Morbillorum Vivum Measles Tifovax Typhoid Vac-DPT DTP T-lmmu·n Tetanus Vacina Dupla Diphtheria, Tetanus Titifica Typhoid, Paratyphoid Vacina Triplice DTP TOPV Polio _(OPV trivalent) Vacina Triplice Viral MMR Trenin OPT Behring DTP Vacuna Doble Tetanus, Diphtheria Tresivac MMR Vacunol Tetanus Triacel DTaP Va-Diftet Diphtheria, Tetanus Triacelluvax DTaP · Vaksin Cacar Smallpox Tri-lmmunol DTP Vaksin Campak Kerig Measles (live) Trimovax MMR Vaksin Kotipa Cholera, Typhoid, Paratyphoid Tripacel DTaP Vaksin Sampar Plague
· ..
} •.. TradeNanie··· · I> · VacCine _ .. .·.: TradeNarne ... v. ·• • .... ••> · •.
I····· ... >. , ::_> .· accme .. · / Tripavac DTaP Vaksin Serap DTP Va-Mengoc-8C Meningococcal 8 & C Virivac MMR Vammix MMR, Varicella Virlrix Varicella Vamoavax Measles, Mumps Virovac MMR Vaqta Hepatitis A Vivaxim Typhoid, HepA Varcelvax Varicella Vivotif Typhoid (Oral) Varicela 8iken Varicella Vopix Polio (OPV) Varicellon Varicella zoster IG VPH Human Papillomavirus Varie Smallpox V-Z Vax Varicella Varilrix -Varicella Welltrivax Trivalente DTP Varipox Varicella X-Flu Influenza Varivax (Varivax Ill) Varicella YF-V/\X Yellow Fever VAT Tetanus Zaantide Diphtheria antitoxin Vaxchora Cholera Zaantite Tetanus antitoxin Vaxem-Hib Hib Zaditeadvax Diphtheria, Tetanus Vaxicoq Pertussis Zaditevax Diphtheria, Tetanus Vaxigrip Influenza Zamevax A+C Meningococcal A & C Vaxihaler-Fiu Influenza (inhaler) Zamovax Measles Vaxipar Mumps Zamruvax Measles, Rubella Vax-Tet Tetanus Zapavax Mumps VCDT Diphtheria, Tetanus Zaruvax Rubella VDA Diphtheria Zatetravax DTP, Parapertussis Verorab Rabies Zatevax Tetanus Vibriomune Cholera Zatribavax DTP Viralinte Hepatitis 8 Zatrivax MMR .Virelon C Polio (IPV) Zerotyph Typhoid (Orall Virelon T 20 Polio (OPV)
Apnl, 2019
BURLINGTON BOARD OF HEALTH 61 Center Street
Burlington, MA 01803
Tel: 781-270-1955 Fax: 781-273-7687
Attachment 2
Public Health Prevent. Promote. Pro t ect.
ACIP General Best Guidance for Immunizations
G:\Protocols\Nursing\ Vaccination & BPS\2019-08-VFC Program.docG:\Protoeols\l'lursing\20 19 08 VFC Program.doe
however, MMR or varicella vaccination during pregnancy should not'be considered a
reason to terminate pregnancy (3,10,50).
Persons who receive MMR vaccine do not transmit the vaccine viruses to contacts (10).
Transmission of varicella vaccine virus to contacts is exceedingly rare (3). MMR and
varicella vaccines should be administered when indicated to children and other
household contacts of pregnant women (1 o). Infants living in households with pregnant
women should be vaccinated with rotavirus vaccine according to the same schedule as
infants in households -without pregnant women.
Pregnant women should be evaluated for evidence of immunity to rubella and varicella
and be tested for the presence of HBsAg during every pregnancy (10,20,52). Women.
without evidence of immunity to rubella and varicella should be vaccinated immediately
after delivery. A second dose of varicella vaccine should be administered 4-8 weeks
later. ·A woman found to be HBsAg positive should be followed-up carefully to ensure
that the infant receives HBIG and begins the hepatitis B vaccine series no later than 12
hours after birth and that the infant completes the recommended hepatitis B vaccine
series on schedule (20). No known risk exists for the fetus from passive immunization of
pregnant women with immune globulin preparations.
Persons Vaccinated Outside the United States
Clinicians have a limited ability to determine whether persons are protected on the basis
of their country of origin and their vaccination records alone. Vaccines administered
outside the United States generally can be accepted as valid if the schedule (i.e.,
minimum ages and intervals) is similar to that recommended in the United States. With
the exception of influenza vaccine, only written documentation should be accepted as
evidence of previous vaccination. Written records are more likely to predict protection if
the vaccines, dates of administration, intervals between doses, and age at the time of
vaccination are comparable to U.S. recommendations. Although vaccines with
inadequate potency have been produced in other ~ountries (53,54), the majority of
General Best Practice Guidelines for Immunization: Special Situations 154
vaccines used worldvvide are produced vvith adequate quality control standards and are
potent.
Persons vaccinated outside of the United States can enter the country through a number
of different mechanisms. Those seeking to immigrate to the United States may be
vaccinated under the authority of a civil surgeon or a panel physician. Some enter the
United States as refugees and are vaccinated under the authority of the Office of Refugee
Resettlement, part of the Administration for Children and Families, in the Department
of Health and Human Services.
Adopted children's birth countries often have vaccination schedules that differ from the
recommended childhood vaccination schedule in the United States. Differences in the
U.S. schedule and those used in other countries include the vaccines administered, the
recommended ages of administration, and the number and timing of doses.
Data are inconclusive regarding the extent to which an internationally adopted child's
vaccination record reflects the child's protection. A child's record might indicate
administration of MMR vaccine when only single-antigen measles vaccine was
administered. A study of children adopted from orphanages in the People's Republic of
China, Russia, and countries in Eastern Europe determined that 67% of children vvith
documentation of > 3 doses of DTP before adoption had nonprotective titers to these
antigens (54). In contrast, children adopted from these countries who received
vaccination in the community (not only from orphanages) and had documentation of ;::::1
doses of DTP exhibited protective titers 67% of the time (54). However, antibody testing
was performed by using a hemagglutination assay, which tends to underestimate
protection and cannot directly be compared with antibody concentration (55). Data are
likely to remain limited for areas other than the People's Republic of China, Russia, and
Eastern Europe. Health care providers should ensure that household contacts of
international adoptees are vaccinated adequately, particularly for measles, hepatitis A,
and hepatitis B (56).
General Best Practice Guidelines for Immunization: Special Situations 155
Health care providers may use one of multiple approaches if the immunogenicity of
vaccines or the completeness of series administered to persons outside the United States
is in question. Repeating the vaccinations is an acceptable option that usually is safe and
prevents the need to obtain and interpret serologic tests. If avoiding unnecessary
injections is desired, judicious use of serologic testing might help determine which
vaccinations are needed. For some vaccines, the most readily available serologic tests
cannot document protection against infection. This best practices document provides
guidance on possible approaches to evaluation and revaccination for each vaccine
recommended in the United States (Table g-1).
DTaP Vaccine
Vaccination providers can revaccinate children younger than 7 years of age with DTaP
vaccine without regard to recorded doses; however, data indicate increased rates of local
adverse reactions after the fourth and fifth doses of DTaP (57). If a revaccination
approach is adopted and a severe local reaction occurs, serologic testing for specific IgG
antibody to tetanus and diphtheria toxins can be measured before administering
additional doses. Protective concentrationCa) indicates that additional doses are
unnecessary and subsequent vaccination should occur as age appropriate. No
established serologic correlates exist for protection against pertussis.
For a child whose record indicates receipt of 2::3 doses of DTP or DTaP, serologic testing
for specific IgG antibody to both diphtheria and tetanus toxin before additional doses is
a reasonable approach. If a protective concentration is present, recorded doses are
considered valid, and the vaccination series should be completed as age appropriate. An
indeterminate antibody concentration might indicate immunologic memory but waning
antibody; serologic testing can be repeated after a booster dose if vaccination providers
or parents want to avoid revaccination with a complete series.
Alternately, for a child whose records indicate receipt of ?::3 doses, a single booster dose
can be administered followed by serologic testing after 1 month for specific IgG antibody
to both diphtheria and tetanus toxins. Ifthe child has a protective concentration, the
General Best Practice Guidelines for Immunization: Special Situations 156
recorded doses are considered valid, and the vaccination series should be completed as
age appropriate. Children with an indeterminate concentration after a booster dose
should be revaccinated with a complete series.
Hepatitis A Vaccine
Children aged 12-23 months without documentation of hepatitis A vaccination or
serologic evidence of immunity should be vaccinated on arrival in the United States
(45). Persons who have received 1 dose should receive the second dose if 6-18 months
. have passed since the first dose was administered.
Hepatitis B Vaccine
Persons not knovvn to be vaccinated for hepatitis B should receive an age-appropriate
series of hepatitis B vaccine. A person whose records indicate receipt of ::::::3 doses of
vaccine is considered protected, and additional doses are not needed if ::::::1 dose was
administered at age ::::::24 weeks. Persons who received their last hepatitis B vaccine dose
at an age <24 .weeks should receive an additional dose at age ::::::24 weeks. People who
have received <3 doses of vaccine should complete the series at the recommended
intervals and ages.
All foreign-born persons and immigrants, refugees, and internationally adopted
children born in Asia, the Pacific Islands, Africa, and other regions of high or
intermediate hepatitis B endemicity should be tested for HBsAg, regardless of
vaccination status (58). Those determined to be HBsAg positive should be monitored for
development of liver disease. Household members of HBsAg-positive children or adults
should be vaccinated if they are not already immune.
Hib Vaccine
Interpretation of a serologic test to verify whether children who were vaccinated > 2
months previously are protected against Hib bacteria can be difficult. Because the
number of vaccinations needed for protection decreases with age and because adverse
General Best Practice Guidelines for Immunization: Special Situations 157
events are rare (59), age-appropriate vaccination should be provided. Hib vaccination is
not recommended routinely for persons aged ~5 years (59).
Meningococcal Vaccine
Quadrivalent meningococcal conjugate vaccines are not routinely used in other
countries in adolescents (the United Kingdom is the exception). Unless patients have
documented receipt they should be considered unvaccinated and receive the age
appropriate doses.
MMR Vaccine
The simplest approach to resolving concerns about MMR vaccination is to revaccinate
vvith 1 or 2 doses of MMR vaccine, depending on age. Serious adverse events after MMR
vaccinations are rare (10). No evidence indicates that administering MMR vaccine
increases the risk for adverse reactions among persons who are already immune to
measles, mumps, or rubella as a result of previous vaccination or natural disease. Doses
of measles.-containing vaccine administered before the first birthday should not be
counted as part of the series (10 ). Alternatively, serologic testing for IgG antibody to
vaccine viruses indicated on the vaccination record can be considered. Serologic testing
is widely available for measles and rubella IgG antibody. A person whose record
indicates receipt of monovalent measles or measles-rubella vaccine on or after the first
birthday and who has protective antibody against measles and rubella should receive 1
or 2 doses of MMR or MMRV as age appropriate to ensure protection against mumps
and varicella (and rubella if measles vaccine alone had been administered). If a person
whose record indicates receipt of MMR at age ~12 months has a protective
concentration of antibody to measles, no additional vaccination is needed unless a
second dose is required for school entry.
General Best Practice Guidelines for Immunization: Special Situations 158
Pneumococcal Vaccines
Many indus,trialized countries now routinely use pneumococcal vaccines. Although
recommendations for pneumococcal polysaccharide vaccine also exist in many
countries, the pneumococcal conjugate vaccine might not be routinely administered.
PCV13 and PPSV23 should be administered according to age-appropriate vaccination
schedules or as indicated by the presence of underlying medical conditions (43,60).
Poliovirus Vaccine
The simplest approach to vaccinating with poliovirus vaccine is to revaccinate persons
aged <18 years with IPV according to the U.S. schedule. Adverse events after IPV are
rare (42). Children appropriately vaccinated with 3 doses of OPV in economically
developing countries might have suboptimal seroconversion, including to type 3
poliovirus (42).
Rotavirus Vaccine
.Rotavirus vaccination should not be initiated for infants aged ;;:::15 weeks, o days. Infants
who began the rota virus vaccine series outside the United States but who did not
complete the series and who are still aged s8 months, o days, should follow the routine
schedule and receive doses to complete the series. If the brand of a previously
administered dose is live, reassortment pentavalent rota virus vaccine or is unknown, a
total of 3 doses of rota virus vaccine should be documented for series completion. All
doses should be administered by age 8 months, o days.
Td and Tdap Vaccines
Children aged ;;:::7 years who are not considered fully vaccinated for pertussis should
receive Tdap vaccine. "Fully vaccinated" means at least 5 doses of DTaP before the
seventh birthday or at least 4 doses of DTaP before the seventh birthday if the fourth
dose is given after the fourth birthday. One dose of Tdap is recommended after the
General Best Practice Guidelines for Immunization: Special Situations 159
seventh birthday. If additional doses of vaccine are needed, Td should be administered
as age appropriate.
Varicella Vaccine
Varicella vaccine is not available in most countries. A person who lacks evidence of
varicella immunity should be vaccinated as age appropriate (3,59).
Zoster Vaccine
In the United States, zoster vaccination is recommended for all persons aged ;;::6o years
who have no contraindications, including persons who report a previous episode of
zoster or who have chronic medical conditions. For persons who do not have
documentation of receipt of zoster vaccine, the vaccine should be offered at the patient's
first clinical encounter with the health care provider. The vaccine is administered as a
single o.6s-mL subcutaneous dose. Zoster vaccination is not indicated to treat acute
zoster, to prevent persons "With acute zoster from developing postherpetic neuralgia, or
to treat ongoing postherpetic neuralgia. Patients do not need to be asked about their
history of varicella or to have serologic testing conducted to determine zoster immunity
prior to administration of zoster vaccine.
Vaccinating Persons with Increased Bleeding Risk
Providers often avoid giving intramuscular injections or choose alternative routes for
persons with bleeding disorders because of the risk for hematoma formation after
injections. In one study, hepatitis B vaccine was administered intramuscularly to 153
persons with hemophilia. The vaccination was administered with a 23-gauge or smaller
caliber needle, followed by application of steady pressure to the site for 1-2 minutes. The
vaccinations resulted in a low (4%) bruising rate, and no patients required factor
supplementation (61). Whether antigens that produce more local reactions (e.g.,
pertussis) would produce an equally low rate of bruising is unknown.
General Best Practice Guidelines for Immunization: Special Situations 160
When hepatitis B or any other intramuscularly administered vaccine is indicated for a
patient with a bleeding disorder, the vaccine should be admip.istered intramuscularly if a
physician familiar with the patient's bleeding risk determines that the vaccine can be
administered by this route with reasonable safety. If the patient receives antihemophilia
or similar therapy, intramuscularly administered vaccinations can be scheduled shortly
after such therapy is administered. A fine-gauge needle (23-gauge or smaller caliber)
should be used for the vaccination, followed by firm pressure on the site, without
rubbing, for at least 2 minutes. The patient or family should be given information on the
risk for hematoma from the injection. Patients receiving anticoagulation therapy
presumably have the same bleeding risk as patients with clotting factor disorders and
should follow the same guidelines for intramuscular administration. If possible,
vaccination could be scheduled prior to the use of these medications, so that the
patients' risk of bleeding is not increased by their therapeutic action.
(a} Enzyme immunoassay tests are available. Physicians should contact the laboratory performing the test for interpretive standards
and limitations. Protective concentrations for antibody to diphtheria and tetanus toxins are defined as >O.l IU jmL.
General Best Practice Guidelines for Immunization: Special Situations 161
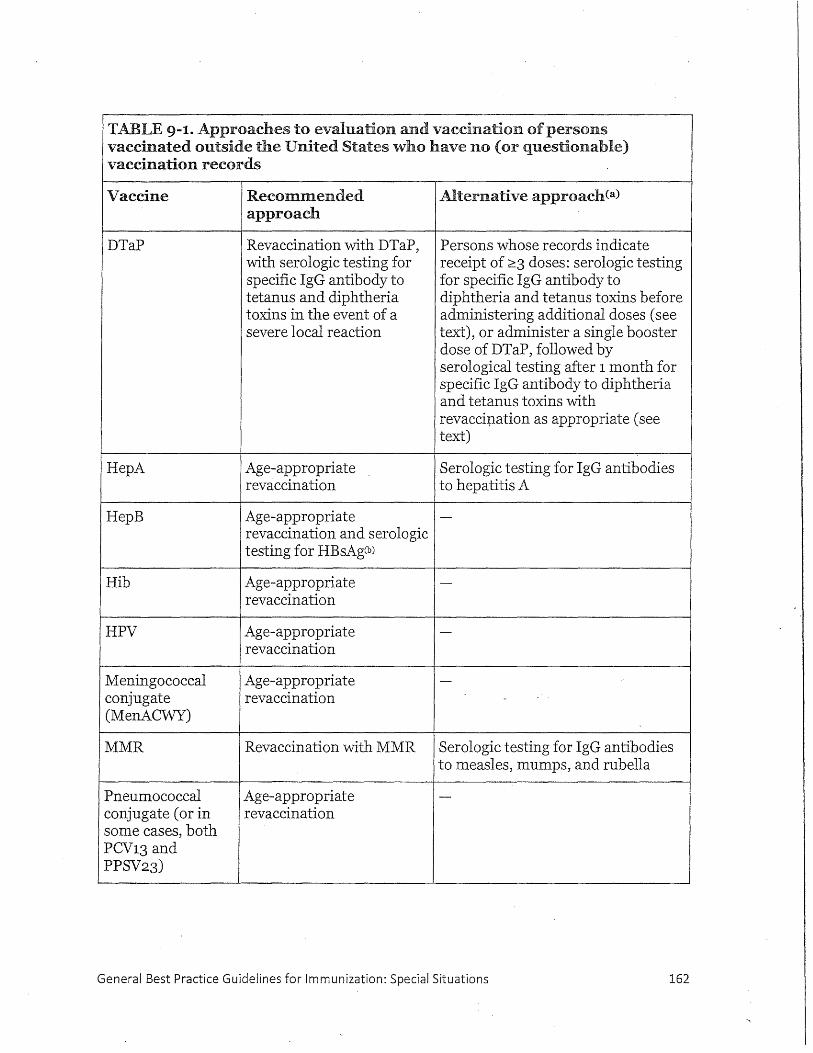
TABLE 9-1. Approaches to evaluation and vaccination of persons vaccinated outside the United States who have no (or questionable) vaccination records
Vaccine Recommended Alternative approach Ca)
approach
DTaP Revaccination with DTaP, Persons whose records indicate with serologic testing for receipt of :2::3 doses: serologic testing specific IgG antibody to for specific IgG antibody to tetanus and diphtheria diphtheria and tetanus toxins before toxins in the event of a administering additional doses (see severe local reaction text), or administer a single booster
dose of DTaP, followed by serological testing after 1 month for specific IgG antibody to diphtheria and tetanus toxins with revaccipation as appropriate (see text)
HepA Age-appropriate Serologic testing for IgG antibodies revaccination to hepatitis A
HepB Age-appropriate -revaccination and serologic testing for HBsAgCb)
Hib P. ... ge-appropriate -revaccination
HPV Age-appropriate -revaccination
Meningococcal Age-appropriate -conjugate revaccination (MenACWY)
MMR Revaccination with MMR Serologic testing for IgG antibodies to measles, mumps, and rubella
Pneumococcal Age-appropriate -conjugate (or in revaccination some cases, both PCV13 and PPSV23)
General Best Practice Guidelines for Immunization: Special Situations 162
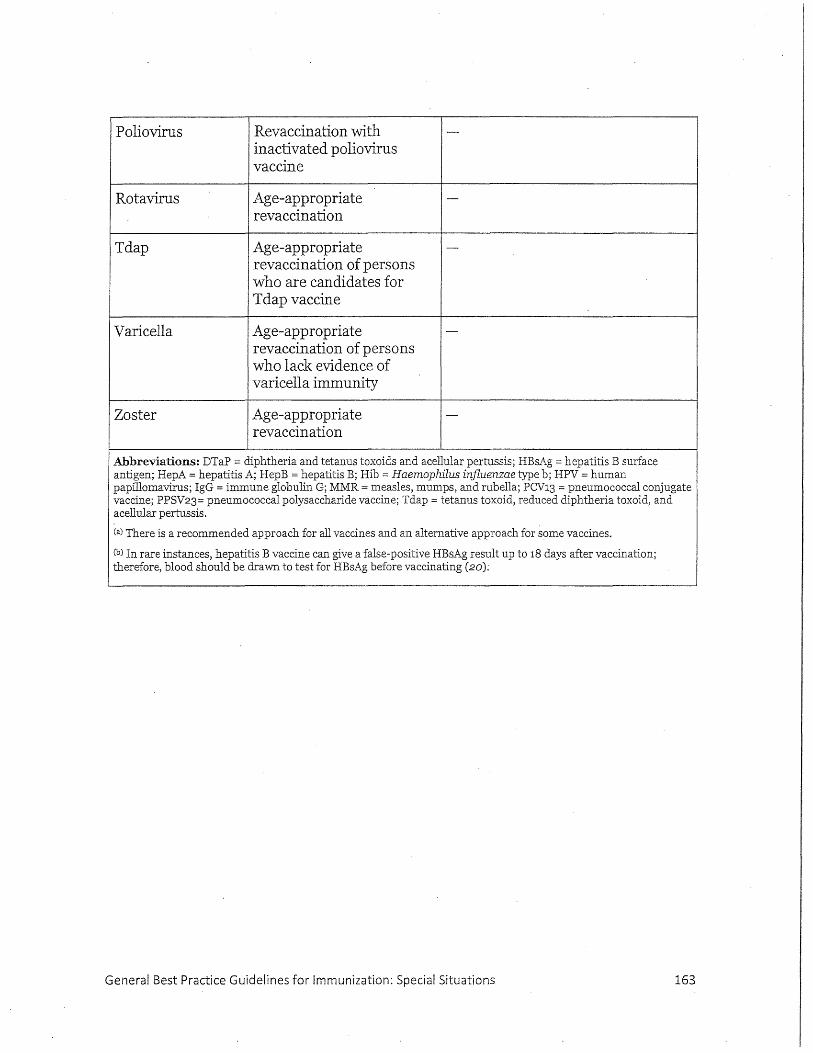
Poliovirus
Rota virus
Tdap
Varicella
Zoster
Revaccination with inactivated poliovirus vaccine
Age-appropriate revaccination
Age-appropriate revaccination of persons who are candidates for Tdap vaccine
Age-appropriate revaccination of persons who lack evidence of varicella immunity
Age-appropriate revaccination
Abbreviations: DTaP = diphtheria and tetanus toxoids and acellular pertussis; HBsAg = hepatitis B surface antigen; HepA =hepatitis A; HepB =hepatitis B; Hib = Haemophilus injluenzae type b; HPV =human papillomavirus; IgG = immune globulin G; MMR =measles, mumps, and rubella; PCV13 = pneumococcal conjugate vaccine; PPSV23= pneumococcal polysaccharide vaccine; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis.
Ca) There is a recommended approach for all vaccines and an alternative approach for some vaccines.
Cb) In rare instances, hepatitis B vaccine can give a false-positive HBsAg result up to 18 days after vaccination; therefore, blood should be dra"WTI. to test for HBsAg before vaccinating (20):
General Best Practice Guidelines for Immunization: Special Situations 163
BURLINGTON BOARD OF HEALTH 61 Center Street
Burlington, MA 01803
Tel: 781-270-1955 Fax: 781-273-7687
Attachment 3 Consent & Release Form
G:\Protocols\Nursing\Vaccination & BPS\2019-08-VFC Program.docG:\Protocols\i'iursing\20 19 08 VFC Program.doc
Public Health Prevent. Promote . Protect.
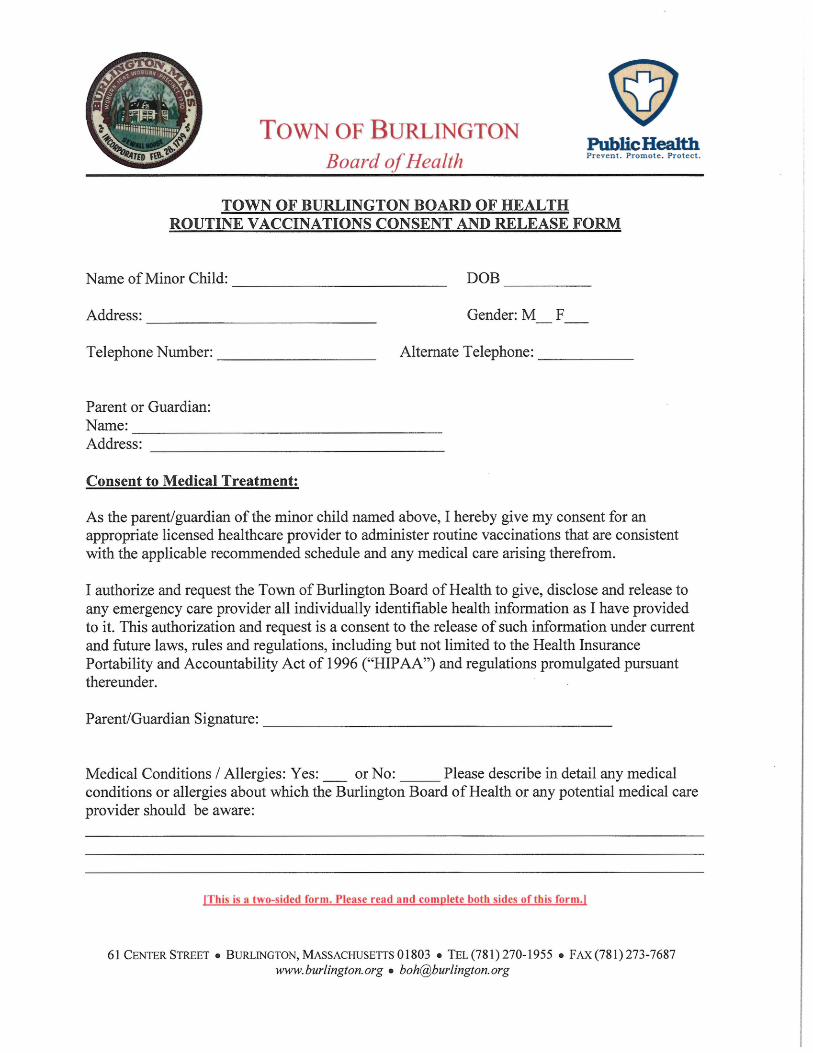
TOWN OF BURLINGTON Board of Health
Public Health Prevent . Promot e . Pro tect.
TOWN OF BURLINGTON BOARD OF HEALTH ROUTINE VACCINATIONS CONSENT AND RELEASE FORM
Name of Minor Child: DOB ------------------------ -----
Address: Gender: M F --------------------------
Telephone Number: _______________ _ Alternate Telephone: ____ __
Parent or Guardian: Name: -----------------------------------Address:
Consent to Medical Treatment:
As the parent/guardian of the minor child named above, I hereby give my consent for an appropriate licensed healthcare provider to administer routine vaccinations that are consistent with the applicable recommended schedule and any medical care arising therefrom.
I authorize and request the Town of Burlington Board of Health to give, disclose and release to any emergency care provider all individually identifiable health information as I have provided to it. This authorization and request is a consent to the release of such information under current and future laws, rules and regulations, including but not limited to the Health Insurance Portability and Accountability Act of 1996 ("HIP AA") and regulations promulgated pursuant thereunder.
Parent/Guardian Signature: ---------------------------------------
Medical Conditions I Allergies: Yes:_ or No: ____ Please describe in detail any medical conditions or allergies about which the Burlington Board of Health or any potential medical care provider should be aware:
!This is a two-sided form. Please read and complete both sides of this form.!
61 CENTER STREET • BURLINGTON, MASSACHUSETTS 01803 • TEL (781) 270-1955 • FAX (781) 273-7687 www. burlington. org • boh@burlington. org
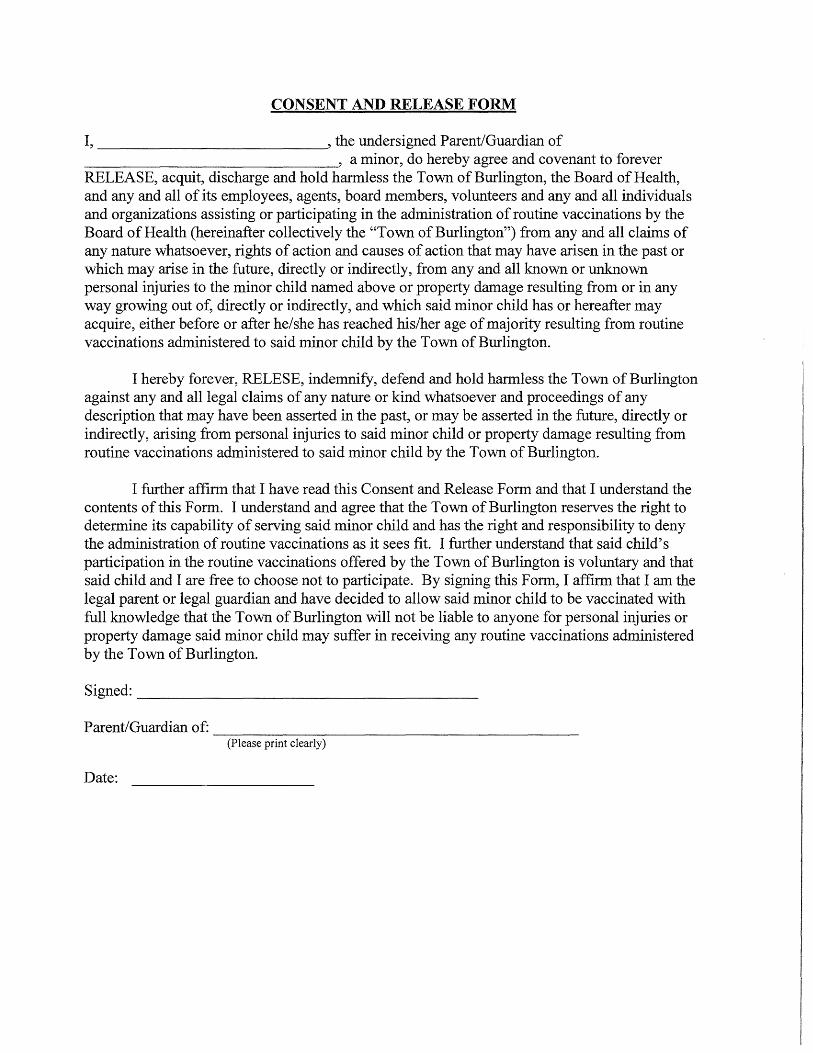
CONSENT AND RELEASE FORM
I, , the undersigned Parent/Guardian of ______________ , a minor, do hereby agree and covenant to forever RELEASE, acquit, discharge and hold harmless the Town of Burlington, the Board of Health, and any and all of its employees, agents, board members, volunteers and any and all individuals and organizations assisting or participating in the administration of routine vaccinations by the Board of Health (hereinafter collectively the "Town of Burlington") from any and all claims of any nature whatsoever, rights of action and causes of action that may have arisen in the past or which may arise in the future, directly or indirectly, from any and all known or unknown personal injuries to the minor child named above or property damage resulting from or in any way growing out of, directly or indirectly, and which said minor child has or hereafter may acquire, either before or after he/she has reached his/her age of majority resulting from routine vaccinations administered to said minor child by the Town of Burlington.
I hereby forever, RELESE, indemnify, defend and hold harmless the Town of Burlington against any and all legal claims of any nature or kind whatsoever and proceedings of any description that may have been asserted in the past, or may be asserted in the future, directly or indirectly, arising from personal injuries to said minor child or property damage resulting from routine vaccinations administered to said minor child by the Town of Burlington.
I further affirm that I have read this Consent and Release Form and that I understand the contents of this Form. I understand and agree that the Town of Burlington reserves the right to determine its capability of serving said minor child and has the right and responsibility to deny the administration of routine vaccinations as it sees fit. I further understand that said child's participation in the routine vaccinations offered by the Town of Burlington is voluntary and that said child and I are free to choose not to participate. By signing this Form, I affirm that I am the legal parent or legal guardian and have decided to allow said minor child to be vaccinated with full knowledge that the Town of Burlington will not be liable to anyone for personal injuries or property damage said minor child may suffer in receiving any routine vaccinations administered by the Town of Burlington.
Signed: ______________________ ___
Parent/Guardian of: --------------------------------(Please print clearly)
Date:
BURLINGTON BOARD OF HEALTH 61 Center Street
Burlington, MA 01803
Tel : 781-270-1955 Fax: 781-273-7687
Attachment 4 Temporary Agent Form
G:\Protocols\Nursing\ Vaccination & BPS\20 19-08-VFC Program.docG:\Protocols~J"ursing\2019 08 VFC Program.doc
Public Health Pr event. Promote . Protec t.
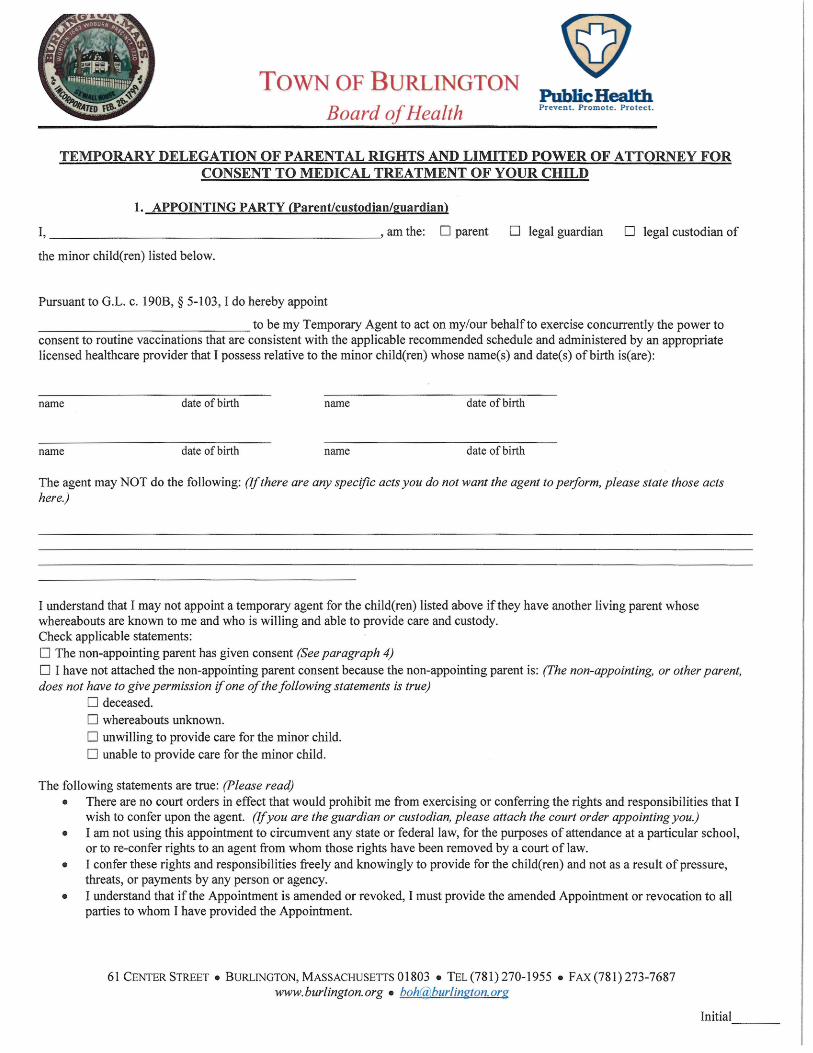
TOWN OF BURLINGTON Board of Health
Public Health Prevent. Promote. Protect.
TEMPORARY DELEGATION OF PARENTAL RIGHTS AND LIMITED POWER OF ATTORNEY FOR CONSENT TO MEDICAL TREATMENT OF YOUR CHILD
1. APPOINTING PARTY (Parent/custodian/guardian)
I,----------------------' am the: 0 parent 0 legal guardian D legal custodian of
the minor child(ren) listed below.
Pursuant to G.L. c. 190B, § 5-103, I do hereby appoint
______________ to be my Temporary Agent to act on my/our behalfto exercise concurrently the power to consent to routine vaccinations that are consistent with the applicable recommended schedule and administered by an appropriate licensed healthcare provider that I possess relative to the minor child(ren) whose name(s) and date(s) of birth is( are):
name date ofbirth name date of birth
name date of birth name date of birth
The agent may NOT do the following: (If there are any specific acts you do not want the agent to perform, please state those acts here)
I understand that I may not appoint a temporary agent for the child(ren) listed above if they have another living parent whose whereabouts are known to me and who is willing and able to provide care and custody. Check applicable statements: 0 The non-appointing parent has given consent (See paragraph 4)
0 I have not attached the non-appointing parent consent because the non-appointing parent is: (The non-appointing, or other parent, does not have to give permission if one of the following statements is true)
0 deceased. 0 whereabouts unknown. 0 unwilling to provide care for the minor child. 0 unable to provide care for the minor child.
The following statements are true: (Please read) • There are no court orders in effect that would prohibit me from exercising or conferring the rights and responsibilities that I
wish to confer upon the agent. (If you are the guardian or custodian, please attach the court order appointing you.) • I am not using this appointment to circumvent any state or federal law, for the purposes of attendance at a particular school,
or to re-confer rights to an agent from whom those rights have been removed by a court of law. • I confer these rights and responsibilities freely and knowingly to provide for the child(ren) and not as a result of pressure,
threats, or payments by any person or agency. • I understand that if the Appointment is amended or revoked, I must provide the amended Appointment or revocation to all
parties to whom I have provided the Appointment.
61 CENTERSTREET • BURLINGTON,MASSACHUSETTS01803 • TEL(781)270-1955 • FAX(781)273-7687 www.burlington.org • [email protected]
Initial ---
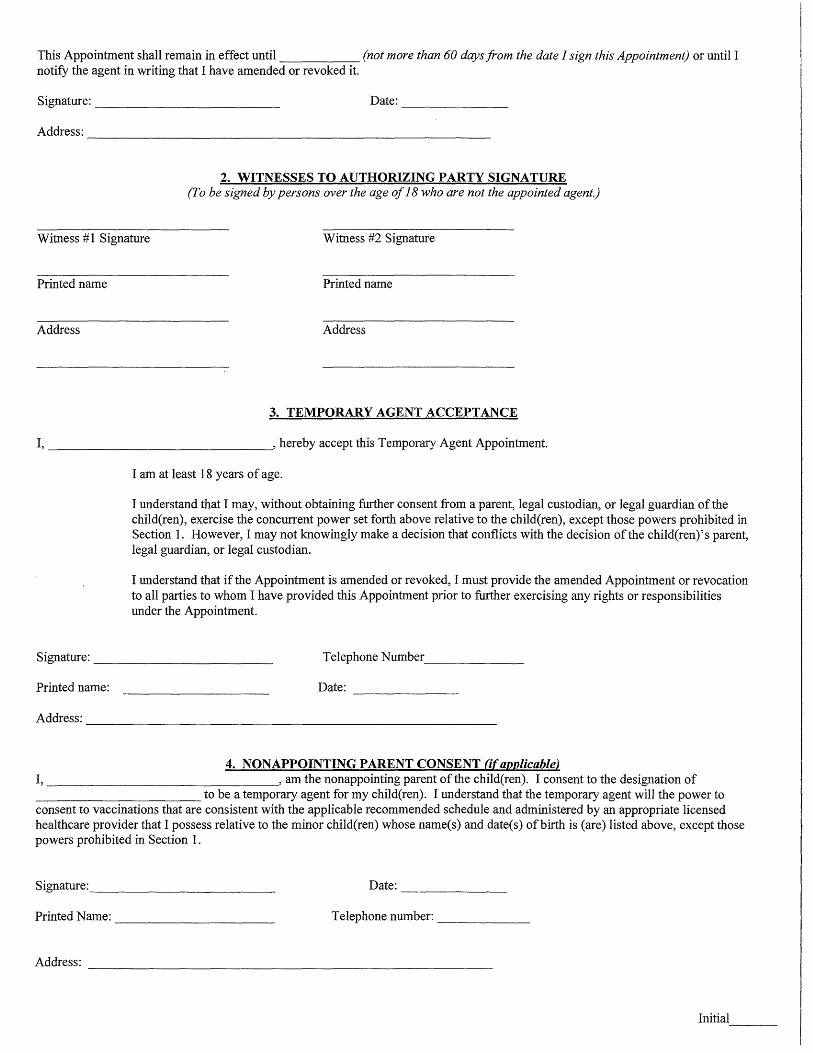
This Appointment shall remain in effect until (not more than 60 days from the date I sign this Appointment) or until I notify the agent in writing that I have amended or revoked it.
Signature: ______________ _ Date: _________ _
Ad&ess: __________________________________________ _
2. WITNESSES TO AUTHORIZING PARTY SIGNATURE (To be signed by persons over the age of 18 who are not the appointed agent.)
Witness #1 Signature Witness #2 Signature
Printed name Printed name
Ad&ess Ad&ess
3. TEMPORARY AGENT ACCEPTANCE
I, ------------------------' hereby accept this Temporary Agent Appointment.
I am at least 18 years of age.
I understand that I may, without obtaining further consent from a parent, legal custodian, or legal guardian of the child(ren), exercise the concurrent power set forth above relative to the child(ren), except those powers prohibited in Section 1. However, I may not knowingly make a decision that conflicts with the decision of the child(ren)'s parent, legal guardian, or legal custodian.
I understand that if the Appointment is amended or revoked, I must provide the amended Appointment or revocation to all parties to whom I have provided this Appointment prior to further exercising any rights or responsibilities under the Appointment.
Signature: ___________ _ Telephone Number ______ _
Printed name: Date: ______ _
Address: _____________________________________________ __
4. NONAPPOINTING PARENT CONSENT (ifapplicable) I, , am the nonappointing parent of the child(ren). I consent to the designation of -----------------to be a temporary agent for my child(ren). I understand that the temporary agent will the power to consent to vaccinations that are consistent with the applicable recommended schedule and administered by an appropriate licensed healthcare provider that I possess relative to the minor child(ren) whose name(s) and date(s) of birth is (are) listed above, except those powers prohibited in Section 1.
Signature: ___________ _ Date: ______ _
Printed Name: _______________ _ Telephone number: _____ _
Address: --------------------------
Initial ----
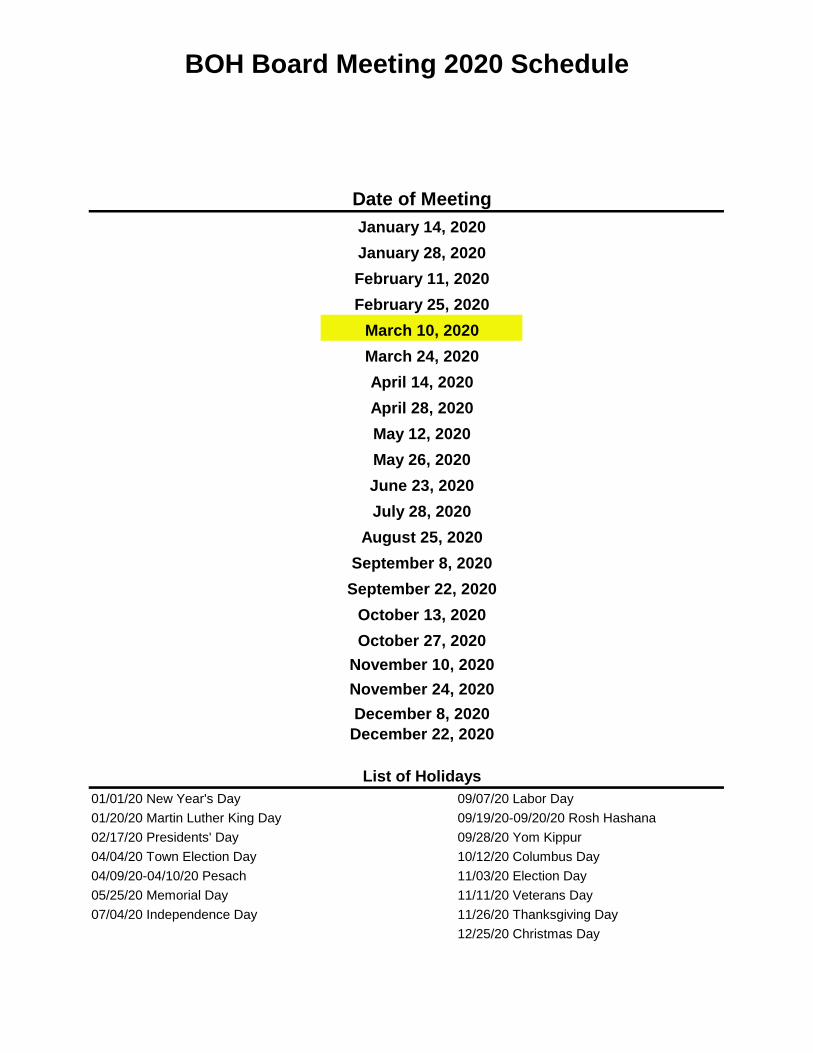
BOH Board Meeting 2020 Schedule
Date of Meeting
09/19/20-09/20/20 Rosh Hashana
List of Holidays
April 14, 2020April 28, 2020May 12, 2020May 26, 2020June 23, 2020
11/11/20 Veterans Day11/26/20 Thanksgiving Day12/25/20 Christmas Day
07/04/20 Independence Day
04/04/20 Town Election Day02/17/20 Presidents' Day
05/25/20 Memorial Day
July 28, 2020August 25, 2020
September 8, 2020
January 14, 2020January 28, 2020February 11, 2020February 25, 2020
March 10, 2020March 24, 2020
September 22, 2020October 13, 2020October 27, 2020
November 10, 2020November 24, 2020
10/12/20 Columbus Day11/03/20 Election Day04/09/20-04/10/20 Pesach
09/07/20 Labor Day01/01/20 New Year's Day
09/28/20 Yom Kippur01/20/20 Martin Luther King Day
December 8, 2020December 22, 2020
TOWN OF BURLINGTON
Board of Health Board of Health Staff:
Susan Lumenello, REHS/RS, CHMM, Director
Christine Mathis, Environmental Engineer
Marlene Johnson, R.S., Health Agent
Christine Paulik, R.N., Supervising Nurse
Samantha Hardy, Associate Health Inspector
Board of Health Members:
Ed Weiner, Ph.D., Chairman
David McSweeney, Vice Chairman
Wayne Saltsman, MD, Ph.D., BOH Member
Elizabeth Walendziewicz, BOH Member
Maribeth Welch, BOH Member
61 CENTER STREET BURLINGTON, MASSACHUSETTS 01803 TEL (781) 270-1955 FAX (781) 273-7687
www.burlington.org [email protected]
MEMORANDUM
To: Board of Health
From: Christine Mathis, Environmental Engineer
Date: February 11, 2020
RE: Environmental Engineer’s Report: January 17 – February 13, 2020
Hazardous Materials Inspections
Sarepta Pharmaceutical – 55 Network Drive
Boston Marriott Burlington – 1 Burlington Mall Road
Pre-Renovations/Demolition Permits
Renovation
6 Wayside Road, Suite G2
41 Burlington Mall Road, EP Lab 2, 5th
floor
41 Burlington Mall Road, Nuclear Medicine Deptartment
5 Wall Street, 5th
floor
12 A Street
259 A Cambridge Street
95 Network Drive, 4th
floor
35 Network Drive, 2nd
floor
55 Network Drive, 1st floor – A wing
55 Network Drive, 1st floor – B wing
11 Center Street
171 Cambridge Street, Suite 101
40 Burlington Mall Road
99 South Bedford Street, Suite 7
200 Summit Drive, 4th
floor
Demolition
14 Burlington Street
58 Beaverbrook Road
25 Sunset Drive
Investigations
Sumner Street – hydraulic oil release
52 Second Avenue – diesel fuel release
Meetings/Correspondence/Calls/Emails, Administrative Meetings
Weekly meeting with Director (1/22 and 1/29)
Nick Foote, ACV Enviro – Spring HHW event (1/24)
Sarepta IBC meeting (1/24)
EMMCP Executive Committee meeting (1/28)
BOH meeting (1/28)
Removal of elevator pit at former Sears, Burlington Mall (2/5)
Staff meeting (2/6)
Correspondence/Calls/Emails
Phil Lorocco, Stericycle – no longer providing services for HHW events
Glen Wilkinson, Tradebe – providing HHW services for April 2020
Elizabeth Bonaventre, Senior Planner – BOH Biological Safety Regulations
Alexa Balbo, Sarepta - BOH Biological Safety Regulations
Glenn Paparo, Plumbing Inspector – piping proposal at AMRI
Scott Tereshak, AMRI – waste collection process and aboveground storage tank
Joel Prellwitz, TRC – removal of freight elevators at Burlington Mall
Robert Beaudoin, Lexington DPW – Hartwell Avenue Regional HHW facility
Krista Gloden, Clean Harbors – HHW availability and pricing
Nancy Santilli, Burlington Recreation – schedule for 2020 HHW
Whitney Haskell, Chief Procurement Officer – soliciting bids under the statewide
Operational Service Division contract
Resident – disposal of mercury containing light bulbs
Bobby Young, EHS Manager Millipore – Biosafety regulations and new permit
James Curran, EMS Manager Abbott - Biosafety regulations
Brian Farless, EMMCP – 2020 mosquito budget
Anupam Gildyal, VulcanForms – Special Permit needed for 3D printing
April Antonelli, MassDOT – review of traffic plan for modifications at 207 Cambridge Street
Tom Murphy, Esq. – 108 Muller Road decision appeal
Ken Sanderson, MassDEP – follow-up to mercury release at residential home
Margret Hanley, LSP Isosceles Group – follow-up to hazardous materials inspection at
Network Drive Central Utility Plant
Kristine Hung, Esq., Riemer & Braunstein – VulcanForms Special Permit application and
subcommittee meeting
Eileen Coleman, Conservation – Stormwater brochure mailing recipients
Tom Hayes, DPW Engineering – MEC at 99 South Bedford Street
Eileen Ferren, BFD – 2020 Fire Department flammables permits
Administrative
Research on “Chemicals in the Workplace” portion of the Food Code Review Presentation
Article on Biological Safety Regulations for MRC newsletter
Draft Biological Safety Permit application
Household hazardous waste day preparations including: quotes and contract for collection of
chemicals, facilities use request, notification to town departments, advertising and vendor
confirmation for bulbs, batteries and propane tanks
Planning Department Reviews BOH Staff Review with No Comments:
1 Van De Graaff Drive – Insignificant Change
20 Second Avenue – Insignificant Change
154 Cambridge Street – Insignificant Change
TOWN OF BURLINGTON
Board of Health Board of Health Staff:
Susan Lumenello, REHS/RS, CHMM, Director
Christine Mathis, Environmental Engineer
Marlene Johnson, R.S., Health Agent James Dion, BOH Member
Christine Paulik, MSN, R.N., Supervising Nurse
Samantha Hardy, Associate Health Inspector
Board of Health Members:
Ed Weiner, Ph.D., Chairman
David McSweeney, Vice Chairman
Wayne Saltsman, MD, Ph.D., BOH Member
Elizabeth Walendziewicz, BOH Member
Maribeth Welch, BOH Member
61 CENTER STREET BURLINGTON, MASSACHUSETTS 01803 TEL (781) 270-1955 FAX (781) 273-7687
www.burlington.org [email protected]
January 29, 2020
Via Certified Mail
Ms. Alexa Balbo
EHS Manager
Sarepta Therapeutics
100 Federal Street
Andover, MA 01810
RE: 55 Network Drive, Burlington, MA
Dear Ms. Balbo:
On January 24, 2020, I inspected the above referenced Sarepta facility as required by the Town
of Burlington Control of Toxic and Hazardous Material Bylaw (Article XIV, Section 2.14).
During my inspection, I noted the following conditions requiring modification for your operation
to comply with the local bylaw.
1. Some of the satellite accumulation hazardous waste containers were not closed. The
storage requirements of the bylaw require that wastes containing toxic or hazardous
materials be stored in product-tight containers (Article XIV, Section 2.14.7.2)). The
Massachusetts Hazardous Waste Regulations require hazardous waste containers to be
closed except when waste is being added or removed. (Section 310 CMR 30.351(4)(e)).
2. In the water treatment room, incompatible materials (acids and bases) were stored in
close proximity to each other. Section 2.14.7.1 of the Town of Burlington Control of
Toxic and Hazardous Material bylaw states that “storage areas with containers of toxic or
hazardous materials that are incompatible with other materials stored nearby in other
containers shall be separated from these materials or wastes by means of a dike, berm,
wall or other suitable containment method”.
Corrective action of these items should be completed within 30 days of receipt of this letter and
documented in a letter or email to the Board of Health. Failure to resolve the issues regulated by
Article XIV, Section 2.14 may result in the issuance of a $200 fine per violation per day of non-
compliance. The Town of Burlington Control of Toxic and Hazardous Material Bylaw can be
reviewed at the Board of Health website at http://www.burlington.org.
Thank you for your attention to these matters. Please do not hesitate to contact me with any
questions.
Sincerely,
Christine Mathis
Environmental Engineer
cc: file, Board of Health
TOWN OF BURLINGTON
Board of Health Board of Health Staff:
Susan Lumenello, REHS/RS, CHMM, Director
Christine Mathis, Environmental Engineer
Marlene Johnson, R.S., Health Agent James Dion, BOH Member
Christine Paulik, MSN, R.N., Supervising Nurse
Samantha Hardy, Associate Health Inspector
Board of Health Members:
Ed Weiner, Ph.D., Chairman
David McSweeney, Vice Chairman
Wayne Saltsman, MD, Ph.D., BOH Member
Elizabeth Walendziewicz, BOH Member
Maribeth Welch, BOH Member
61 CENTER STREET BURLINGTON, MASSACHUSETTS 01803 TEL (781) 270-1955 FAX (781) 273-7687
www.burlington.org [email protected]
February 5, 2020
Via Certified Mail
Mr. Stephen Kenney
Director of Engineering
Boston Marriott Burlington
1 Burlington Mall Road
Burlington, MA 01803
Dear Mr. Kenney:
On January 31, 2020, I inspected your facility as required by the Town of Burlington Control of Toxic
and Hazardous Material Bylaw (Article XIV, Section 2.14). During my inspection, I noted the following
condition requiring modification for your operation to comply with the local bylaw.
In the basement Mechanical Pump Room, incompatible materials (a corrosive biocide and an
organic refrigerant) were stored in close proximity to each other. Section 2.14.7.1 of the bylaw
states that “storage areas with containers of toxic or hazardous materials that are incompatible
with other materials stored nearby in other containers shall be separated from these materials or
wastes by means of a dike, berm, wall or other suitable containment method”.
Corrective action of this item should be completed within 30 days of receipt of this letter and documented
in a letter or email to the Board of Health. Failure to resolve the issues regulated by Article XIV, Section
2.14 may result in the issuance of a $200 fine per violation per day of non-compliance. The Town of
Burlington Control of Toxic and Hazardous Material Bylaw can be reviewed at the Board of Health
website at http://www.burlington.org.
Thank you for your attention to these matters. Please do not hesitate to contact me with any questions.
Sincerely,
Christine Mathis
Environmental Engineer
cc: file, Board of Health
TOWN OF BURLINGTON Board of Health
Board of Health Staff: Susan Lumenello, REHS/RS, CHMM, Director Christine Mathis, Environmental Engineer Marlene Johnson, R.S., Health Agent Christine Paulik MSN, R.N., Supervising Nurse Samantha Hardy, Associate Health Inspector
Board of Health Members: Wayne Saltsman, MD, Ph.D., Chairman
Ed Weiner, Ph.D., Vice Chairman David McSweeney, BOH Member
Elizabeth Walendziewicz, BOH Member Maribeth Welch, BOH Member
61 CENTER STREET BURLINGTON, MASSACHUSETTS 01803 TEL (781) 270-1955 FAX (781) 273-7687 www.burlington.org [email protected]
Memorandum
To: Board of Health From: Christine Paulik MSN RN, Supervising Nurse Date: February 25th, 2020 RE: Supervising Nurse's Report: 1/17/20 - 2/13/20 _________________________________________________________________________________ Meetings:
• Weekly meeting with Susan Lumenello, 1/21, 1/28, 2/4, 2/11 • Shelby Aston (Sanofi) and Susan Lumenello, 1/21 • Kathy Tracy NEU Instructor, and Cassidy Sorenson NEU intern, 1/28 • Wellness Committee meeting 1/29 • Critical Staff Dispensing Table Top Exercise 2/4 • Staff Meeting 2/6 • Kathy Whittaker RN., Winchester BOH 2/10 • Health fair meeting with Sara Courtemanche, and Susan Lumenello, 2/12 • Sub Committee Meeting, 2/12
Calls/ Emails: • Susan Hoag, RN Boxboro PH nurse RE: DOT • Roberta, RN Lahey TB Clinic and Myrna Leiper RN, MDPH RE: DOT discharge and
follow-up appt. • Amy Warfield, Town Clerk’s Office, and Mike Wick, Library Director RE: PH table info • Christine Taylor, Director, Sunrise Assisted Living RE: illness reporting • Lisa Kinsley- Rocker RN, Lahey Hospital ER Director, Shannon Mc Grath, Infection
Control, RE: ER Protocol for Coronavirus, 2/3 Administrative:
• Monitor State weekly Flu report • Monthly AED checks • Public Health information table for February topic: Heart Health • Flu Vaccine Purchase Memo for 2020-2021 • Revised Rabies PSA and PSA for Council on Aging (COA) Newsletter • Community Health Fair planning • Bladder cancer screening planning
Mailed result letters to Firefighters, 2/6 • MRC Conference planning
Communicable Disease and Surveillance: • TB -case management and Direct Observational Therapy • (2) Coronavirus self-monitoring with Public Health Supervision • No follow-up needed per MDPH; (1) Lyme Disease, (15) Influenza, (1) Hep C, (1)
Varicella,(2) Hep B • Completed cases; TB DOT 1/23, (2) Pertussis
Immunizations and other injections: • (1) B12 Injection • Flu vaccine by appointments
Conferences/Seminars/Webinars and Trainings: • Webinar: Commissioner Bharel's Webinar with Local Public Health 1/22 • Webinar: LBOH and MDPH Discussion on Novel Coronavirus (2019-nCoV), 2/3, 2/13 • Webinar: CDC 2019 n-CoV response: Strategies for Ensuring Healthcare Systems • Webinar: Preparedness and Optimizing the N95 supplies, 2/11
Events: • Stop the Bleed Training for town employees and BVRC, 1/23 • Bladder Cancer Screenings for Firefighters, 1/27, 1/28, 1/29, 1/30, and 1/31 (Total= 33) • Stop the Bleed instructor training for nurse interns , 2/3 • Flu clinic at BOH, 2/3 • Critical Staff Dispensing Table Top Exercise 2/4
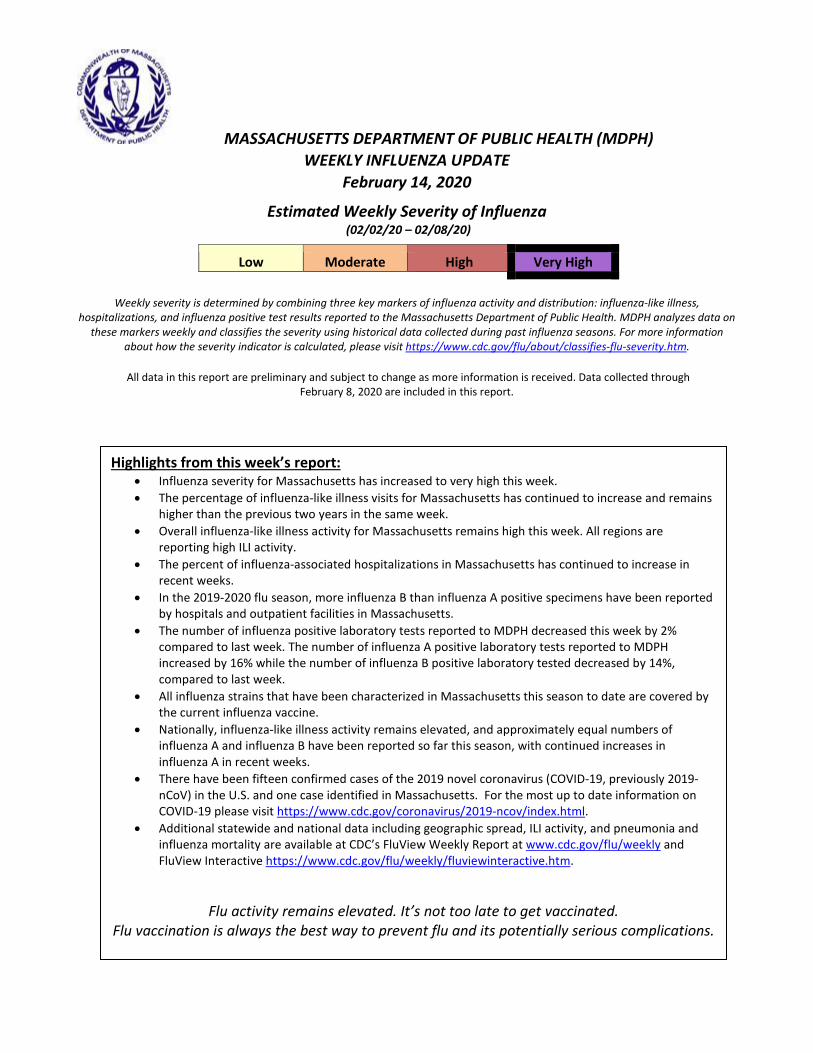
MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH (MDPH) WEEKLY INFLUENZA UPDATE
February 14, 2020
Estimated Weekly Severity of Influenza (02/02/20 – 02/08/20)
Low Moderate High Very High
Weekly severity is determined by combining three key markers of influenza activity and distribution: influenza-like illness,
hospitalizations, and influenza positive test results reported to the Massachusetts Department of Public Health. MDPH analyzes data on these markers weekly and classifies the severity using historical data collected during past influenza seasons. For more information
about how the severity indicator is calculated, please visit https://www.cdc.gov/flu/about/classifies-flu-severity.htm.
All data in this report are preliminary and subject to change as more information is received. Data collected through February 8, 2020 are included in this report.
Highlights from this week’s report: • Influenza severity for Massachusetts has increased to very high this week. • The percentage of influenza-like illness visits for Massachusetts has continued to increase and remains
higher than the previous two years in the same week. • Overall influenza-like illness activity for Massachusetts remains high this week. All regions are
reporting high ILI activity. • The percent of influenza-associated hospitalizations in Massachusetts has continued to increase in
recent weeks. • In the 2019-2020 flu season, more influenza B than influenza A positive specimens have been reported
by hospitals and outpatient facilities in Massachusetts. • The number of influenza positive laboratory tests reported to MDPH decreased this week by 2%
compared to last week. The number of influenza A positive laboratory tests reported to MDPH increased by 16% while the number of influenza B positive laboratory tested decreased by 14%, compared to last week.
• All influenza strains that have been characterized in Massachusetts this season to date are covered by the current influenza vaccine.
• Nationally, influenza-like illness activity remains elevated, and approximately equal numbers of influenza A and influenza B have been reported so far this season, with continued increases in influenza A in recent weeks.
• There have been fifteen confirmed cases of the 2019 novel coronavirus (COVID-19, previously 2019-nCoV) in the U.S. and one case identified in Massachusetts. For the most up to date information on COVID-19 please visit https://www.cdc.gov/coronavirus/2019-ncov/index.html.
• Additional statewide and national data including geographic spread, ILI activity, and pneumonia and influenza mortality are available at CDC’s FluView Weekly Report at www.cdc.gov/flu/weekly and FluView Interactive https://www.cdc.gov/flu/weekly/fluviewinteractive.htm.
Flu activity remains elevated. It’s not too late to get vaccinated. Flu vaccination is always the best way to prevent flu and its potentially serious complications.
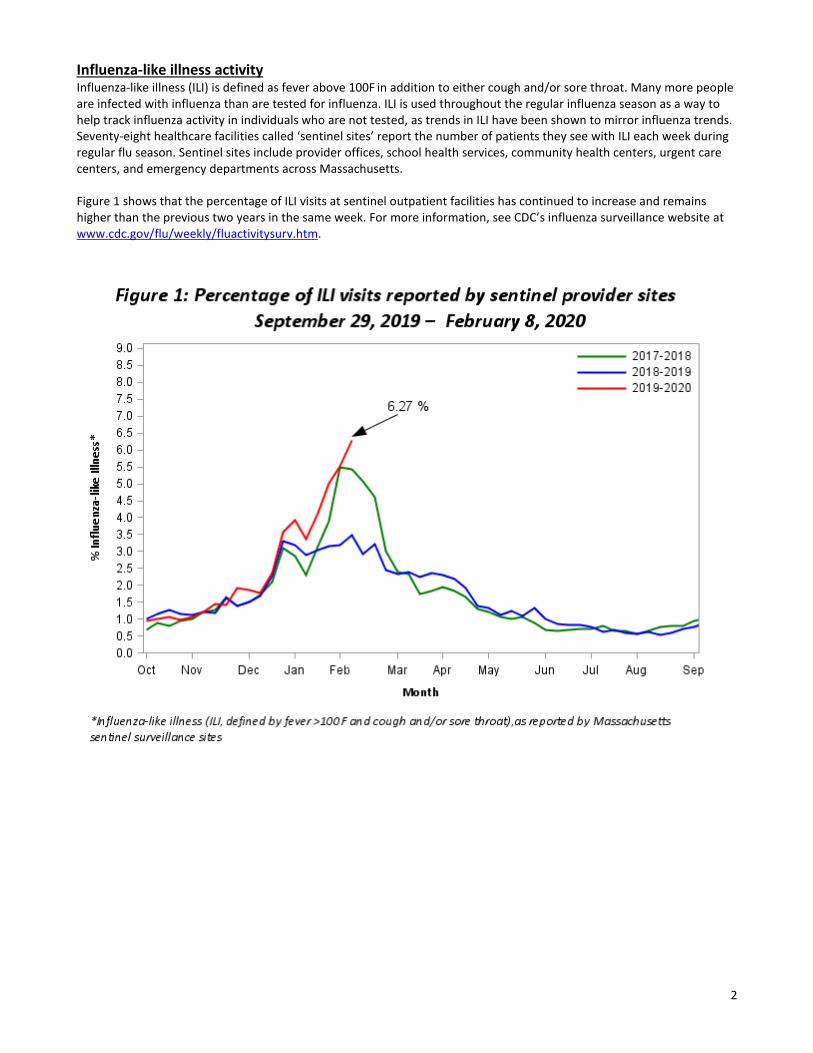
2
Influenza-like illness activity Influenza-like illness (ILI) is defined as fever above 100F in addition to either cough and/or sore throat. Many more people are infected with influenza than are tested for influenza. ILI is used throughout the regular influenza season as a way to help track influenza activity in individuals who are not tested, as trends in ILI have been shown to mirror influenza trends. Seventy-eight healthcare facilities called ‘sentinel sites’ report the number of patients they see with ILI each week during regular flu season. Sentinel sites include provider offices, school health services, community health centers, urgent care centers, and emergency departments across Massachusetts. Figure 1 shows that the percentage of ILI visits at sentinel outpatient facilities has continued to increase and remains higher than the previous two years in the same week. For more information, see CDC’s influenza surveillance website at www.cdc.gov/flu/weekly/fluactivitysurv.htm.
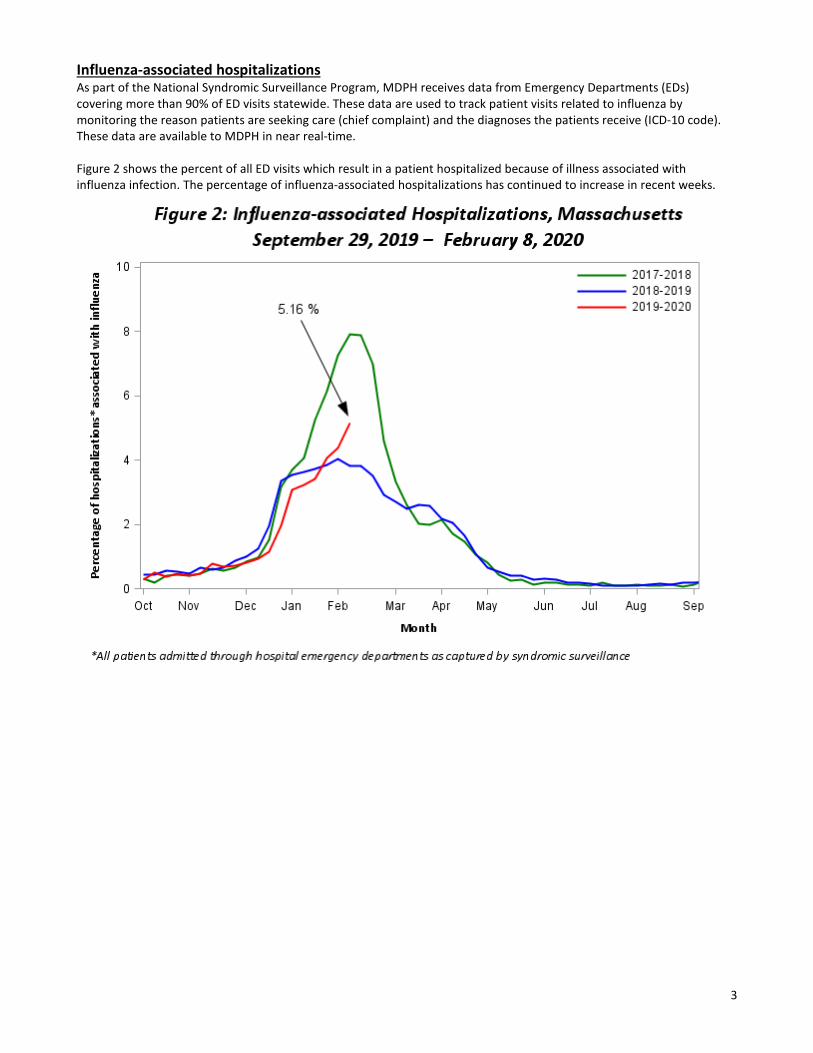
3
Influenza-associated hospitalizations As part of the National Syndromic Surveillance Program, MDPH receives data from Emergency Departments (EDs) covering more than 90% of ED visits statewide. These data are used to track patient visits related to influenza by monitoring the reason patients are seeking care (chief complaint) and the diagnoses the patients receive (ICD-10 code). These data are available to MDPH in near real-time. Figure 2 shows the percent of all ED visits which result in a patient hospitalized because of illness associated with influenza infection. The percentage of influenza-associated hospitalizations has continued to increase in recent weeks.
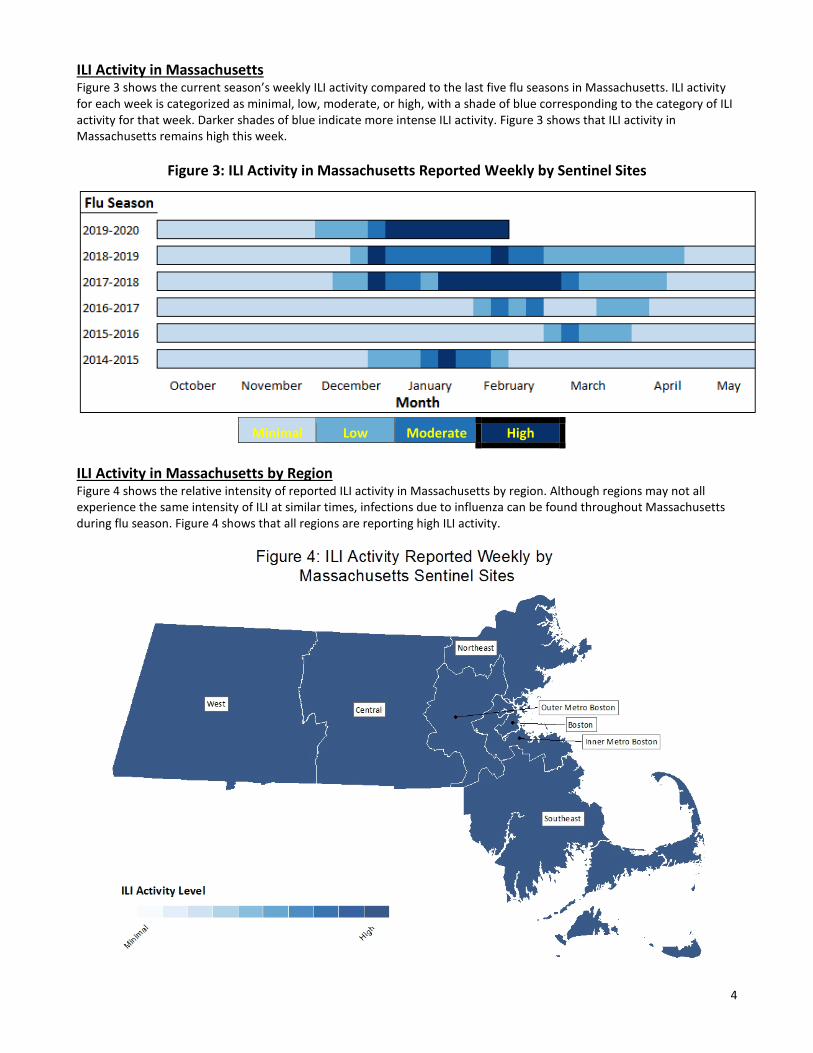
4
ILI Activity in Massachusetts Figure 3 shows the current season’s weekly ILI activity compared to the last five flu seasons in Massachusetts. ILI activity for each week is categorized as minimal, low, moderate, or high, with a shade of blue corresponding to the category of ILI activity for that week. Darker shades of blue indicate more intense ILI activity. Figure 3 shows that ILI activity in Massachusetts remains high this week.
Figure 3: ILI Activity in Massachusetts Reported Weekly by Sentinel Sites
Minimal Low Moderate High
ILI Activity in Massachusetts by Region Figure 4 shows the relative intensity of reported ILI activity in Massachusetts by region. Although regions may not all experience the same intensity of ILI at similar times, infections due to influenza can be found throughout Massachusetts during flu season. Figure 4 shows that all regions are reporting high ILI activity.
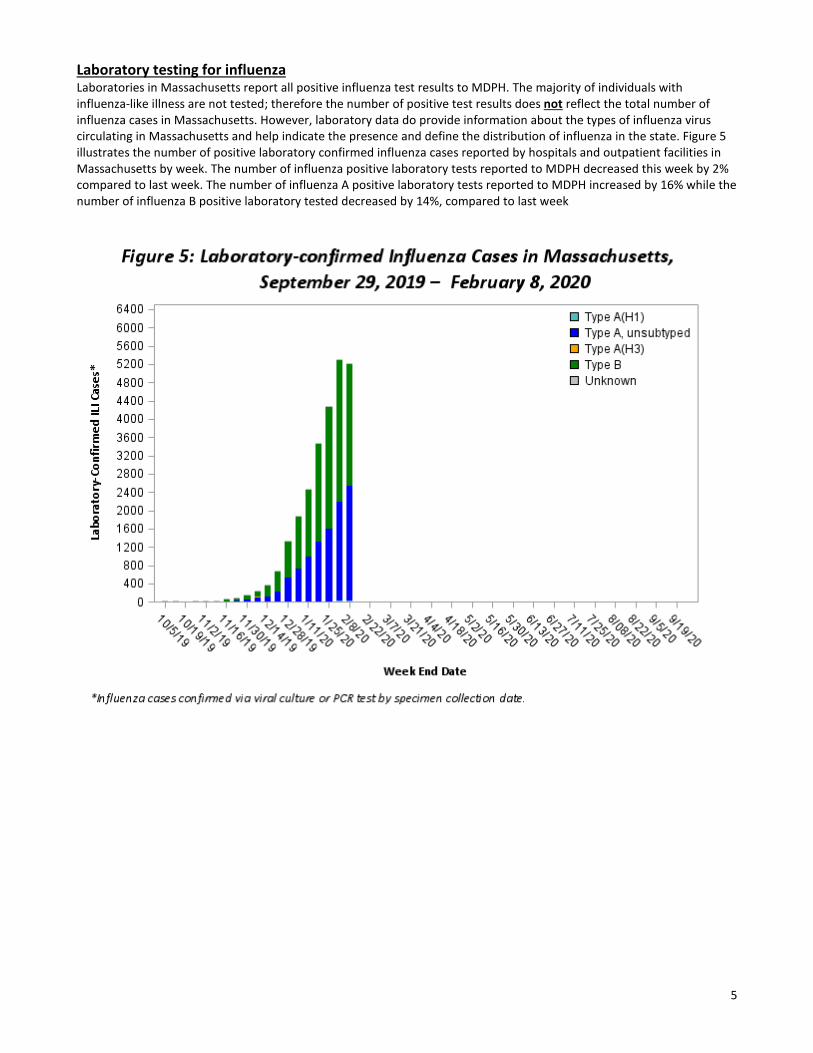
5
Laboratory testing for influenza Laboratories in Massachusetts report all positive influenza test results to MDPH. The majority of individuals with influenza-like illness are not tested; therefore the number of positive test results does not reflect the total number of influenza cases in Massachusetts. However, laboratory data do provide information about the types of influenza virus circulating in Massachusetts and help indicate the presence and define the distribution of influenza in the state. Figure 5 illustrates the number of positive laboratory confirmed influenza cases reported by hospitals and outpatient facilities in Massachusetts by week. The number of influenza positive laboratory tests reported to MDPH decreased this week by 2% compared to last week. The number of influenza A positive laboratory tests reported to MDPH increased by 16% while the number of influenza B positive laboratory tested decreased by 14%, compared to last week
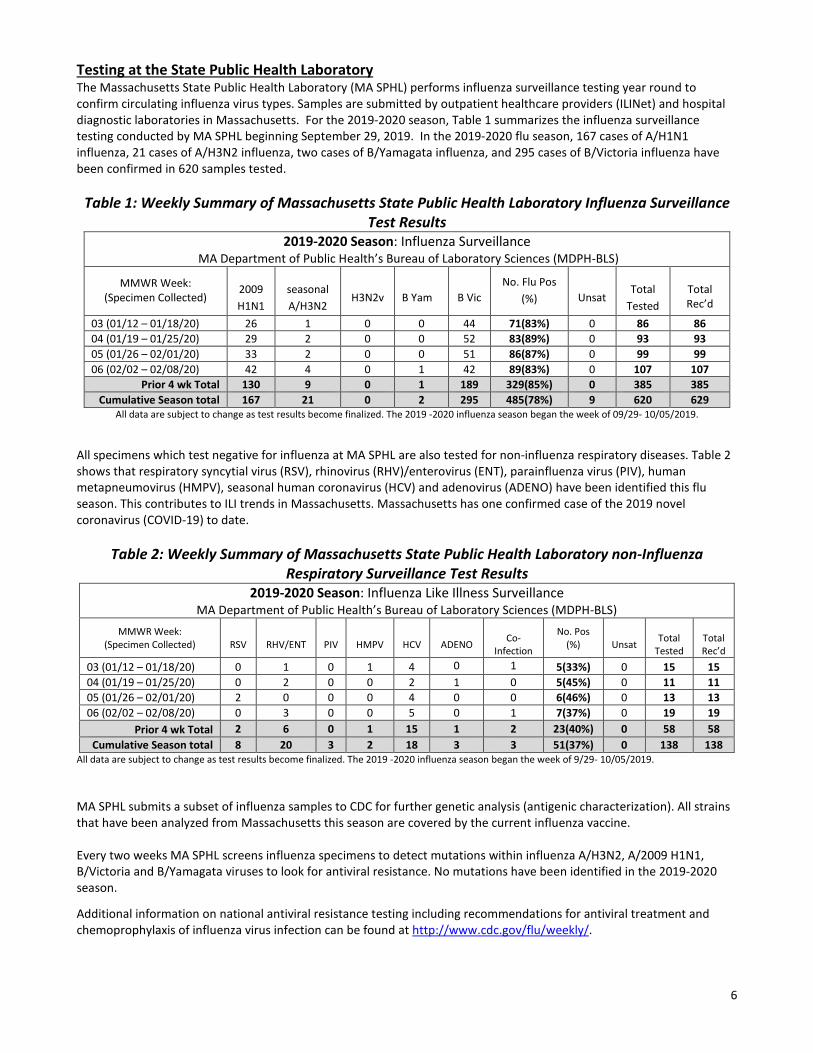
6
Testing at the State Public Health Laboratory The Massachusetts State Public Health Laboratory (MA SPHL) performs influenza surveillance testing year round to confirm circulating influenza virus types. Samples are submitted by outpatient healthcare providers (ILINet) and hospital diagnostic laboratories in Massachusetts. For the 2019-2020 season, Table 1 summarizes the influenza surveillance testing conducted by MA SPHL beginning September 29, 2019. In the 2019-2020 flu season, 167 cases of A/H1N1 influenza, 21 cases of A/H3N2 influenza, two cases of B/Yamagata influenza, and 295 cases of B/Victoria influenza have been confirmed in 620 samples tested.
Table 1: Weekly Summary of Massachusetts State Public Health Laboratory Influenza Surveillance Test Results
2019-2020 Season: Influenza Surveillance MA Department of Public Health’s Bureau of Laboratory Sciences (MDPH-BLS)
MMWR Week: (Specimen Collected)
2009 H1N1
seasonal A/H3N2
H3N2v
B Yam
B Vic
No. Flu Pos (%)
Unsat
Total
Tested
Total Rec’d
03 (01/12 – 01/18/20) 26 1 0 0 44 71(83%) 0 86 86 04 (01/19 – 01/25/20) 29 2 0 0 52 83(89%) 0 93 93 05 (01/26 – 02/01/20) 33 2 0 0 51 86(87%) 0 99 99 06 (02/02 – 02/08/20) 42 4 0 1 42 89(83%) 0 107 107
Prior 4 wk Total 130 9 0 1 189 329(85%) 0 385 385 Cumulative Season total 167 21 0 2 295 485(78%) 9 620 629
All data are subject to change as test results become finalized. The 2019 -2020 influenza season began the week of 09/29- 10/05/2019.
All specimens which test negative for influenza at MA SPHL are also tested for non-influenza respiratory diseases. Table 2 shows that respiratory syncytial virus (RSV), rhinovirus (RHV)/enterovirus (ENT), parainfluenza virus (PIV), human metapneumovirus (HMPV), seasonal human coronavirus (HCV) and adenovirus (ADENO) have been identified this flu season. This contributes to ILI trends in Massachusetts. Massachusetts has one confirmed case of the 2019 novel coronavirus (COVID-19) to date.
Table 2: Weekly Summary of Massachusetts State Public Health Laboratory non-Influenza Respiratory Surveillance Test Results
2019-2020 Season: Influenza Like Illness Surveillance MA Department of Public Health’s Bureau of Laboratory Sciences (MDPH-BLS)
MMWR Week: (Specimen Collected)
RSV
RHV/ENT
PIV
HMPV
HCV
ADENO
Co-
Infection
No. Pos (%)
Unsat
Total
Tested
Total Rec’d
03 (01/12 – 01/18/20) 0 1 0 1 4 0 1 5(33%) 0 15 15 04 (01/19 – 01/25/20) 0 2 0 0 2 1 0 5(45%) 0 11 11 05 (01/26 – 02/01/20) 2 0 0 0 4 0 0 6(46%) 0 13 13 06 (02/02 – 02/08/20) 0 3 0 0 5 0 1 7(37%) 0 19 19
Prior 4 wk Total 2 6 0 1 15 1 2 23(40%) 0 58 58 Cumulative Season total 8 20 3 2 18 3 3 51(37%) 0 138 138
All data are subject to change as test results become finalized. The 2019 -2020 influenza season began the week of 9/29- 10/05/2019. MA SPHL submits a subset of influenza samples to CDC for further genetic analysis (antigenic characterization). All strains that have been analyzed from Massachusetts this season are covered by the current influenza vaccine. Every two weeks MA SPHL screens influenza specimens to detect mutations within influenza A/H3N2, A/2009 H1N1, B/Victoria and B/Yamagata viruses to look for antiviral resistance. No mutations have been identified in the 2019-2020 season.
Additional information on national antiviral resistance testing including recommendations for antiviral treatment and chemoprophylaxis of influenza virus infection can be found at http://www.cdc.gov/flu/weekly/.

TOWN OF BURLINGTON Board of Health
Public Health Prevent . Promote. Protect .
Board o) HeaLth Sta}}: Board of Health Members: Susan Lumenello, REHS/RS, CHMM, Director Christine Mathis, Environmental Engineer Marlene Johnson, R.S., Health Agent Christine Paulik, R.N., Supervising Nurse Samantha Hardy, Associate Health Inspector
Ed Weiner, Ph.D., Chairman Wayne Saltsman, MD, Ph.D, Vice Chairman
David McSweeney, BOH Member Elizabeth Walendziewicz, BOH Member
Maribeth Welch, BOH Member
MEMORANDUM To: Board of Health From: Susan Lumenello, Director of Public Health
February 25, 2020 Date: RE: Director of Public Health's Report -January 31, 2020 through February 13, 2020
Meetings/Events ~ Individual Staff Meetings: Marlene Johnson (2/5/20. 2/12/20); Chris Paulik (2/11120); Samantha
Hardy (2/12/20); Sarah Courtemanche (2/7 /20); ~ Subcommittee Meeting on Protocol for Providing Vaccinations to Children in Cooperation with
Burlington Public Schools w/ Dr. Ed Weiner, Dr. Wayne Saltsman, Chris Paulik & Patrick Larkin, Assistant Superintendent of Schools & Barbara Conley, Lead Nurse for BPS, 2/13/20
Administrative, Phone Calls, E-mails ~ MA DPH Conference Call on Coronavirus, 2/3/20 ~ CDC Conference Call on Coronavirus, 2/3/20 ~ Barbara Conley, Burlington School Lead Nurse RE: Coronavirus ~ Board of Health Letter on Corona virus for Dissemination by Burlington Public Schools ~ Dr. Wayne Saltsman, BOH Medical Director RE: Coronavirus Letter ~ Dr. Ed Weiner, BOH Chairman RE: Coronavirus Letter; Subcommittee on School Vaccination
Program ~ David McSweeney, BOH Vice Chairman RE: Coronavirus Update ~ Maribeth Welch, BOH Member RE: Coronavirus Update ~ Dr. Ed Weiner, BOH Chairman RE: Pertussis Case ~ Dr. Wayne Saltsman, BOH Medical Director RE: Pertussis Case ~ Barbara Conley, Burlington School Lead Nurse RE: Pertussis Case ~ Review/edit 1128/20 BOH meeting minutes ~ Mike Hanafin, Burlington Fire Prevention RE: FD Inspections of Mobile Food Trucks with
Propane ~ Judy Wasserman, Burlington Union RE: Article on Biotechnology Regulations ~ Burlington Fire Department RE: Diesel Fuel Oil Spills at 2 Sumner Street and 52 Second
A venue on 2/13/20 ~ Paul Giddings, MA Department of Environmental Protection RE: Diesel Fuel Oil Spills at 2
Sumner Street and 52 Second A venue on 2/13/20 ~ Meeting Notes for 2/13/20 Subcommittee Meeting ~ Jen Murphy, Director Winchester Board of Health RE: MRC Background for Region 4A and 4B
61 C ENTER STREET • BURLINGTON, MASSACHUSETTS 01803 • TEL (781) 270-1955 • FAX (781) 273-7687 www. burlington. org • boh@burlington. org
~ 2019 BOH Annual Report ~ Meeting on Health Fair with Chris Paulik & Sarah Courtemanche ~ Assign Exhibitors Tables at Health Fair/Review Applications ~ CDC Information Call on Coronovirus, 2111120
Burlington Volunteer Reserve Corps (MRC) ~ Samantha Hardy & Katie Capobianco RE: FY21 BVRC Training Plan, 2/3/20 ~ Region 4B Medical Reserve Corps Advisory Board Meeting, 2/13/20 ~ Meeting on new BVRC Website (burlingtonmrc.org) w/Cathy Piccolo, Sarah Courtemanche, &
Katie Capobiance
Emergency Preparedness ~ Region 4AB Executive Committee Meeting, 2/5/20 ~ Tabletop Exercise on Critical Staff Dispensing, 2/4/20 ~ Region 4AB General Coalition Meeting, 2113/20
BOARD OF HEALTH
BOARD OF HEALTH MEMBERS Back row (l tor) Wayne Saltsman, MD, Ph.D; Maribeth Welch; Elizabeth Walendziewicz, RN
Front row (l tor) David McSweeney, Vice Chairman; Edward Weiner, Ph.D, Chairman
DEPARTMENT STAFF Susan Lumenello, REHS/RS, CHMM, Director Christine Mathis, Environmental Engineer Marlene Johnson, RS, Health Agent Samantha Hardy, Associate Health Inspector Christine Paulik, RN, Supervising Nurse Sarah Courtemanche, Administrative Assistant Cathy Piccolo, Administrative Assistant Kathleen Capobianco, Medical Reserve Corps (MRC) Administrative Assistant
WEBSITE http://www. burlington.org/departments/board of health/index.php
PURPOSE The mission of the Burlington Board of Health is to protect, promote, and prepare for all public health issues or potential crises that occur within the community. The Board of Health enforces state-mandated and local public health regulations, conducts inspections as mandated, issues town permits, investigates community-based complaints or concerns, and supports the goals of public health by providing education and community programs. In addition, the Board of Health is responsible for the review of many aspects of proposed land use and development issues--including drainage, safety and quality of life--and thus is a protector of town natural resources as well (i.e., its aquifers). The Board of Health specifically oversees and regulates (but is not limited to) town food service establishments, mobile food trucks, swimming pools, recombinant DNA-use industries, and any necessary actions that may occur as a consequence of communicable disease surveillance.
The Board of Health has and continues to play a critical role in both the investigation and coordination of care required for short and long-term remediation of the multiple "historical" contaminated sites within the community. Through local programming, routine investigations, establishment of by-laws and policies, as well as overseeing a bi-annual, household hazardous waste (HHW) program, the Board of Health is the organization for the protection of the Burlington environment.
The Burlington Board of Health is the sponsoring agency of the Burlington Volunteer Reserve Corps (BVRC), a federally recognized Medical Reserve Corps (MRC) unit under the Office of the Assistant Secretary for Preparedness and Response (ASPR), established to meet the public health needs of the community. BVRC volunteers support the Board of Health in providing public health services and programs, such as the annual flu clinic, the Community Health Fair, the semi-annual household hazardous waste collections, and blood pressure screenings throughout the community. BVRC volunteers participate in a variety of training opportunities to be able to assist the Town of Burlington, if needed, in emergency response efforts, such as disease outbreaks or sheltering.
The Board continues ongoing work as the leader in preparation for and response to any and all public health emergencies that may arise in the town. The Board focuses on the needs of the community with specific programming and education for emergency preparedness, including "drills," a community "health fair," and a "sharps" disposal program. The Board also works with the boards of surrounding towns, when needed, to promote public health safety and wellness.
GOALS Goals for the Board of Health include an emphasis in public health-focused training, exercises and drills, and programming for both Board staff and the Burlington Volunteer Reserve Corps (BVRC), a unique, independent volunteer group that is sponsored by the Board itself. The Board of Health will strive to improve the town's capabilities in emergency preparedness, provide health-related information and services to residents, and maintain the current level of regulatory oversight required to protect the Burlington community.
CHANGES Development and re-development in the past several years has increased the demands on the Board of Health. The number of food service establishments requiring inspections has steadily increased. In addition, the BOH is conducting more complex plan reviews and inspections for food service establishments with more specialized processes that require the review and approval of variances and specialized plans. During fiscal year 2018, the Board ofHiring hired a full time Associate Health Inspector to alleviate demands on the department and increase the quality of service. The Associate Health Inspector conducts inspections of food service establishments as well as recreational camps, tanning, tobacco, animals, kennels, housing, trash, and nuisance complaints. In 2019, the Associate Health Inspector completed classroom work to become a Certified Pool Operator (CPO) and received in field training from Burlington's Health Agent. The Board of Health now has two inspectors proficient in conducting pool inspections and no longer needs to rely on part time contracted inspectors to conduct those inspections.
2019 IDGHLIGHTS
• Biological Safety Regulations: In 2019, the Burlington Planning Board began taking proactive steps to attract biotechnology and life science companies to Burlington. One of the first steps was to host a Life Science Forum that featured a panel of industry and academic biotechnology
Page2
experts including Dr. Edward Weiner, Chairman of the Board of Health. The forum was well attended by town meeting members, town board and department representatives, town businesses and the public. The panelists offered their perspectives on the biotechnology industry and answered questions from the audience. Also in 2019 and following the forum, Burlington's biotechnology rating from the Massachusetts Biotechnology Council was upgraded to platinum level, the highest rating in terms of attractiveness to potential life science companies. By the end of 2019, discussions on new zoning regulations surrounding biotechnology companies began and zoning changes were expected to be brought before Town Meeting in January, 2020. The Board of Health raised concerns regarding the proposed zoning regulation changes, specifically that the changes allowed biotechnology companies to come to certain areas of Burlington "by right" and thereby not undergoing a formal review by the Board of Health. In response, the Board of Health enacted Biological Safety Regulations for the permitting and oversight of companies utilizing regulated biological agents which include recombinant or synthetic DNA molecules, Risk Group 3 Agents, or Select Agents as defined by the US Department of Health and Human Services. The regulations also prohibit the use ofBiosafety Level4 containment and/or Risk Group 4 Agents.
Dr. Ed Weiner, Board of Health Chairman (shown in the middle) was a panelist on a special Life Science Forum (from BCAT Special "Life Science Forum: January 16, 2019'')
• "Matter of Balance" Program for Residents: In 2019, the Board of Health and the Burlington Volunteer Reserve Corps (BVRC) collaborated with Lahey Health to conduct Matter of Balance classes for Burlington residents. Matter of Balance is an evidence based fall prevention program where participants achieve practical and personal solutions to reduce the fear of falling by replacing this fear with more constructive, confidence building concepts. The Board of Health Nurse and several BVRC volunteers have been trained by Lahey Health to be Matter of Balance coaches and are now certified to teach this course consisting of a two hour session each week for eight weeks. Each session contains a different topic for active discussion among participants on their fall related concerns, fears, risk factors and behaviors. The program provides guest speakers, discussions on videos watched in class, as well as handouts and other resources on how to remove potential hazards within the home and work place. In addition, low impact balance and strengthening exercises based on one's own abilities are practiced at each session. It is expected that future "Matter of Balance" courses will be held twice per year.
Page 3
Graduates of the 2019 Matter of Balance Course (holding certificates) with BVRC Coaches Carolyn Abruzzo, RN (far left) and Urvi Argawalla, RN (far right) and BOH Nurse Interns
Juliana Bernard & Matt Davis (kneeling, center) (photo by C. Paulik)
• Minimum Standards for the Keeping of Animals: During 2019, the Board of Health reviewed their current regulations on the keeping of animals, which apply to all animals kept as domesticated animals except household pets (animals kept indoors for non-agricultural purposes). A public hearing was held on March 12 and new Minimum Standards for the Keeping of Animals became effective on March 18. The new regulations incorporate the MA Department of Agriculture Best Management Practices, requiring that permit holders adhere to best management practices. The previous regulations had allowed residents to own up to three chickens or other fowl without obtaining a permit. The new regulations require anyone who is housing chickens in their backyard, no matter the number, to obtain a permit. In addition, the previous regulations capped the number of animals allowed under the permit. This cap has been removed; however, the Board may limit the number of animals allowed under the permit at their discretion.
A Burlington resident's chicken coop inspected by the Board of Health (photo by S. Hardy)
Page4
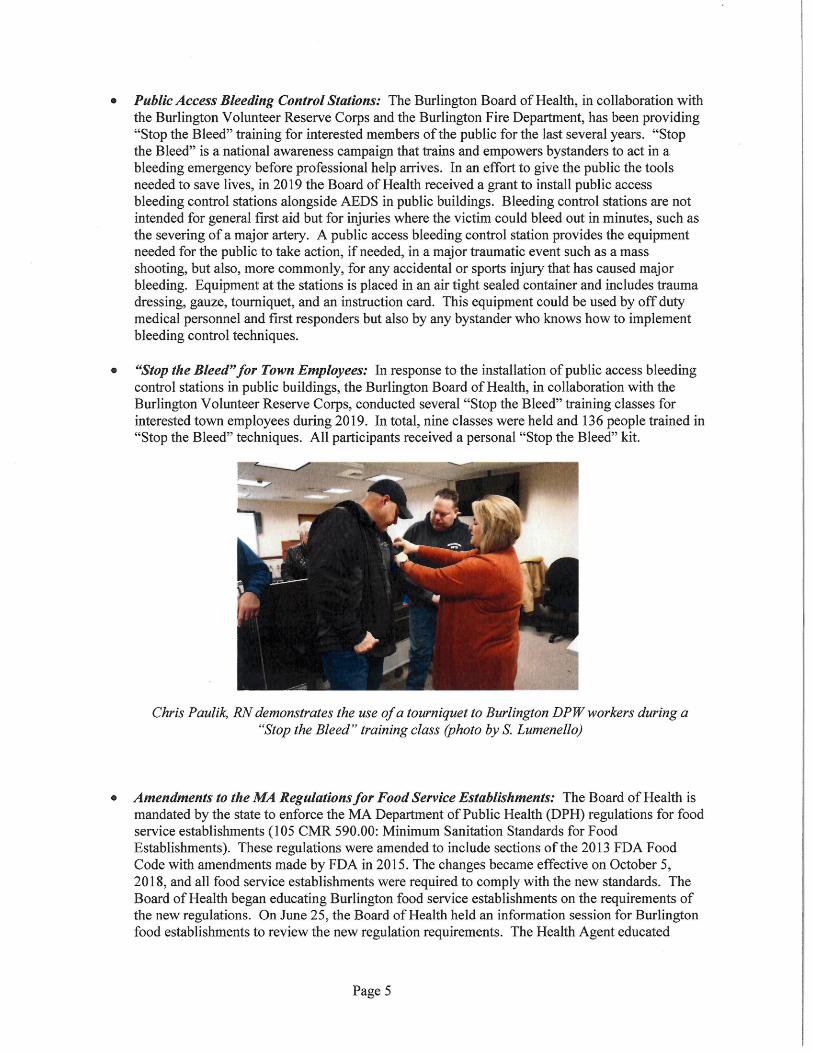
• Public Access Bleeding Control Stations: The Burlington Board of Health, in collaboration with the Burlington Volunteer Reserve Corps and the Burlington Fire Department, has been providing "Stop the Bleed" training for interested members of the public for the last several years. "Stop the Bleed" is a national awareness campaign that trains and empowers bystanders to act in a bleeding emergency before professional help arrives. In an effort to give the public the tools needed to save lives, in 2019 the Board of Health received a grant to install public access bleeding control stations alongside AEDS in public buildings. Bleeding control stations are not intended for general first aid but for injuries where the victim could bleed out in minutes, such as the severing of a major artery. A public access bleeding control station provides the equipment needed for the public to take action, if needed, in a major traumatic event such as a mass shooting, but also, more commonly, for any accidental or sports injury that has caused major bleeding. Equipment at the stations is placed in an air tight sealed container and includes trauma dressing, gauze, tourniquet, and an instruction card. This equipment could be used by off duty medical personnel and first responders but also by any bystander who knows how to implement bleeding control techniques.
• "Stop the Bleed" for Town Employees: In response to the installation of public access bleeding control stations in public buildings, the Burlington Board of Health, in collaboration with the Burlington Volunteer Reserve Corps, conducted several "Stop the Bleed" training classes for interested town employees during 2019. In total, nine classes were held and 136 people trained in "Stop the Bleed" techniques. All participants received a personal "Stop the Bleed" kit.
Chris Paulik, RN demonstrates the use of a tourniquet to Burlington DPW workers during a "Stop the Bleed" training class (photo by S. Lumenello)
• Amendments to the MA Regulations for Food Service Establishments: The Board of Health is mandated by the state to enforce the MA Department of Public Health (DPH) regulations for food service establishments (1 05 CMR 590.00: Minimum Sanitation Standards for Food Establishments). These regulations were amended to include sections of the 2013 FDA Food Code with amendments made by FDA in 2015. The changes became effective on October 5, 2018, and all food service establishments were required to comply with the new standards. The Board of Health began educating Burlington food service establishments on the requirements of the new regulations. On June 25, the Board of Health held an information session for Burlington food establishments to review the new regulation requirements. The Health Agent educated
Page 5
establishments on the changes such as terminology, inspection forms, employee illness reporting, and clean up procedures.
Marlene Johnson, Health Agent, presented a review of the new regulations governing food service establishments to over one hundred managers of Burlington food establishments (photo
byBCAT)
• Temporary Food Events: Temporary food events are defined by the MA Department of Public Health regulations for food service establishments as one that operates for no more than 14 consecutive days in conjunction with a single event that is open to the public. Pot luck events that are not conducted for commercial purposes are not considered to be a temporary food event, however, participants must be informed that neither the food nor the facilities have been inspected by the state or a local public health department. In 2019, temporary food service permits increased by 3 7%. Events permitted included events that have been occurring for many years such as Celebrate Burlington and the Taste, as well as new events such as the Gluten Free New England Expo.
Page 6
Marlene Johnson, Health Agent, inspects a booth at the 2019 Gluten Free New England Expo held at the Marriott Hotel (photo by Susan Lumenello)
STATISTICS
(Excel Table)
Page 7
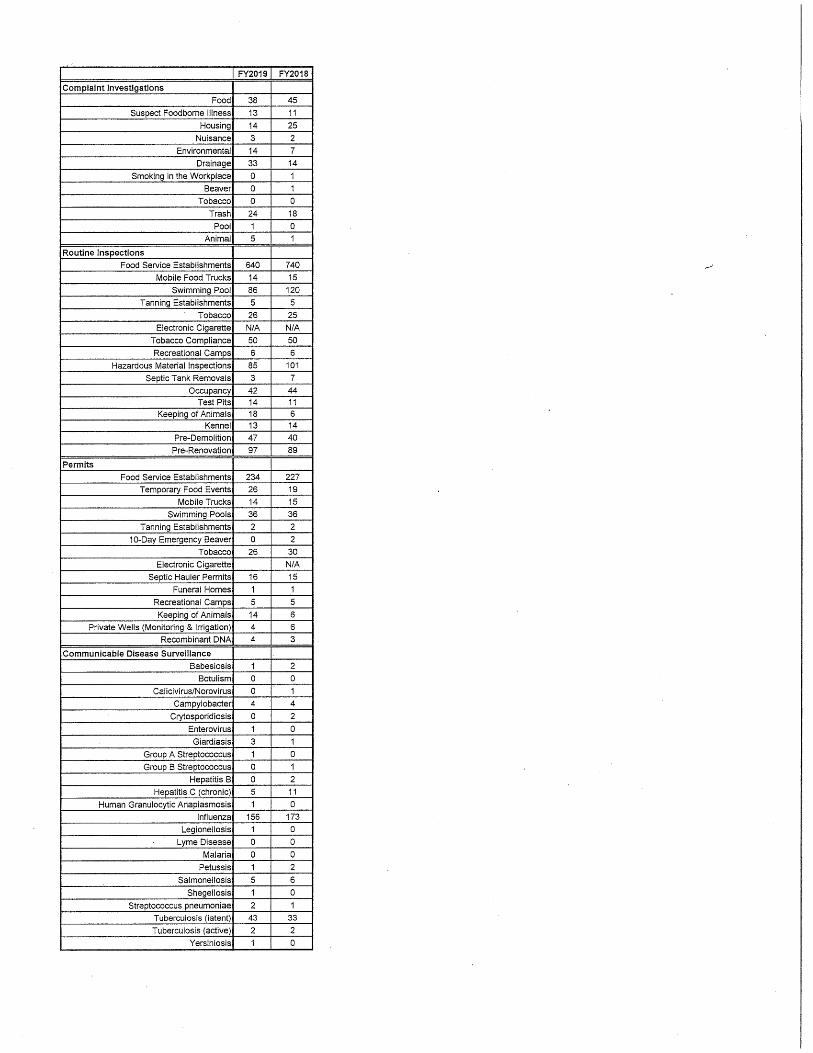
..
FY2019 FY2018
Complaint Investigations
Food 38 45
Suspect Foodborne Illness 13 11
Housing 14 25
Nuisance 3 2
Environmental 14 7
Drainage 33 14
Smoking in the Workplace 0 1
Beaver 0 1
Tobacco 0 0
Trash 24 18
Pool 1 0
Animal 5 1
Routine Inspections
Food Service Establishments 640 740
Mobile Food Trucks 14 15
Swimming Pool 86 120
Tanning Establishments 5 5
Tobacco 26 25
Electronic Cigarette N/A N/A
Tobacco Compliance 50 50
Recreational Camps 6 6
Hazardous Material Inspections 85 101
Septic Tank Removals 3 7
Occupancy 42 44
Test Pits 14 11 Keeping of Animals 18 6
Kennel 13 14
Pre-Demolition 47 40
Pre-Renovation 97 89
Permits
Food Service Establishments 234 227
Temporary Food Events 26 19
Mobile Trucks 14 15
Swimming Pools 36 36
Tanning Establishments 2 2
1 0-Day Emergency Beaver 0 2
Tobacco 26 30
Electronic Cigarette N/A
Septic Hauler Permits 16 15
Funeral Homes 1 1
Recreational Camps 5 5
Keeping of Animals 14 6
Private Wells (Monitoring & Irrigation) 4 6
Recombinant DNA 4 3
Communicable Disease Surveillance
Babesiosis 1 2
Botulism 0 0
Calicivirus/Norovirus 0 1
Campylobacter 4 4
Crytosporidiosis 0 2
Enterovirus 1 0
Giardiasis 3 1
Group A Streptococcus 1 0
Group B Streptococcus 0 1
Hepatitis B 0 2
Hepatitis C (chronic) 5 11
Human Granulocytic Anaplasmosis 1 0
Influenza 156 173
Legionellosis 1 0
Lyme Disease 0 0
Malaria 0 0
Petussis 1 2
Salmonellosis 5 6
Shegellosis 1 0
Streptococcus pneumoniae 2 1
Tuberculosis (latent) 43 33
Tuberculosis (active) 2 2
Yersiniosis 1 0

1edical ·eserve corps
TOWN OF BURLING1-,0N Board (~/'Health
· Public Health Prevent. Promote. Protect.
Board o) Health Staff: Susan Lumenello, REHSIRS, CHMM, Director Christine Mathis, Environmental Engineer Marlene Johnson, R.S, Health Agent Christine Paulik, MSN, R.N., Supervising Nurse Samantha Hardy, Associate Health Inspector
February 6, 2020
Dear Parent/Guardian,
Board a} Health Members: Ed Weiner, Ph.D., Chairman
David McSweeney, Vice Chairman Wayne Saltsman, MD, Ph.D., BOH Member
Elizabeth Walendziewicz, BOH Member Maribeth Welch, BOH Member
On February 5, 2020, the MA Department of Public Health informed the Burlington Board of Health that a student at Burlington High School has been diagnosed with a confirmed case of pertussis (whooping cough). It is possible that your child may have been exposed to pertussis. Please note that the incubation period for this case has passed, therefore, if your child is currently not exhibiting symptoms of pertussis then they were likely not infected.
Additional information, including the symptoms of pertussis, is outlined in the attached fact sheet. Parents/guardians should be aware ofthe signs and symptoms of pertussis. If your child has symptoms then medical evaluation and testing is recon11nended and five days of antibiotic treatment will likely be prescribed. Children with pertussis, if their medical condition allows, may return to school five (5) days after starting appropriate antibiotics and must continue taking the antibiotics until completed.
If you have any further questions or concerns, please do not hesitate to call Chris Paulik, RN, Board of Health Nurse at 781-505-1139.
Sincerely,
Dr. Wayne Saltsman, MD, Ph.D. Board of Health Medical Director
Susan Lumenello, REHS/RS, CHMM Director of Public Health
61 CENTERSTREET • BURLINGTON,MASSACHUSETTS01803 • TEL(781)270-1955 • FAX(781)273-7687 www. burlington. org • boh@burlington. org
October 20181 Page 1 of 3
Pertussis, also called "whooping cough," is a disease caused by bacteria (germs) that is easily spread from person to person. Pertussis is usually mild in older children and adults, but it often causes serious probletns in very young children.
s Pertussis sytnpt01ns have three stages. The first stage begins like a cold with a runny nose, sneezing and cough. The cough lasts for a week or two then slowly gets worse. The second stage is marked by uncontrolled coughing spells, vomiting after coughing, and sometimes a whooping noise that you can hear when the person breathes in. During severe coughing spells or spasms, a person may stop breathing or becotne blue in the face from lack of air. Between spells, the person often appears to be well. This stage lasts for about 2 to 6 weeks. The final stage is when the symptoms begin to gradually lessen. The person still may have coughing spells, but is beginning to get better. The duration of classic pertussis is about 6 to 10 weeks. Adults, teens and vaccinated children often have milder sytnptoms that can be like bronchitis or some other cough illness.
The germs that cause pertussis live in the nose, mouth and throat, and are sprayed into the air when an infected person sneezes, coughs or talks. Other people nearby can then breathe in the germs. Touching a tissue or sharing a cup used by someone with pertussis can also spread the disease. The first symptoms appear about 7 to 10 days after a person is exposed. People with pertussis can spread the disease starting up to 2 weeks before until 3 weeks after the cough starts, or until they have finished 5 days of an appropriate antibiotic treatment.
In Massachusetts, pertussis is most common among people over 10 years old who have lost the protection they got from childhood vaccines. Infants are also very likely to get the disease since they are often too young to have full protection from the vaccine. However, anyone can catch pertussis and it can be hard to diagnose because symptoms may resemble a cold, followed by a nagging cough that lasts for weeks or months.
It can be, especially for infants. Pertussis can cause breathing problems, pneumonia, and swelling of the brain (encephalitis), which can lead to seizures and brain damage. Pertussis can also cause death, especially in very young infants, but this is rare. In older children, teens and adults, the disease is milder but may last for weeks or months.
Massachusetts Department of Public Health I Bureau of Infectious Disease and Laboratory Sciences
f®'l ··~~~--#·
October 20181 Page 2 of 3
Pertussis can be very hard to diagnose. A doctor may think a patient has pertussis because of the symptoms, but a laboratory test is the only way to be sure. Pertussis is often diagnosed using a swab taken from the back of the nose. A blood test can also be done in some adolescents and adults.
The main treatment is plenty of rest and fluids, and antibiotics. Oxygen, medicine to help the patient breathe and mild sedatives are s01netitnes needed to help control severe coughing spells. Antibiotics can make the disease milder and the person less able to spread the disease if they are started early enough. Anyone who has been exposed to pertussis should see a doctor for antibiotics to prevent the disease, even if they were vaccinated.
in can I it Although pertussis disease is likely to provide immunity against pertussis, the duration of such immunity decreases over time. For this reason, people exposed to pertussis should see their doctor for antibiotics, even if they had the disease in the past. Children younger than 7 years old should have their immunization record reviewed by their doctor, in case they need more DTaP (diphtheria, tetanus and acellular pertussis) shots. Older children and adults who have never received a single dose ofTdap (tetanus, diphtheria and acellular pertussis) vaccine should talk to their doctor about getting a Tdap shot.
Vaccination is the best way to protect against pertussis. Pertussis vaccine is given with diphtheria and tetanus vaccines in the same shot. The shot that is currently used for children less than 7 years old is called DTaP (diphtheria, tetanus, acellular pertussis). Tdap (tetanus, diphtheria, acellular pertussis) is a vaccine for children 7 years of age and older, adolescents and adults. Currently only 1 dose ofTdap is recommended. Before the Tdap vaccine was available, adolescents and adults did not have a good way to prevent pertussis because immunity to pertussis frotn childhood vaccines decreases over time.
All vaccines, like other medicines, can cause side effects in some people. The DTaP · vaccine can cause redness, swelling where the shot was given, fever, drowsiness, or fretfulness. More serious reactions, including seizures and persistent crying lasting for more than 3 hours, are very rare. Getting the DTaP vaccine is much safer than getting pertussis, and most people do not have any problems with the vaccine. Many more young children will get pertussis if parents stop getting them vaccinated.
The Tdap vaccine can cause pain, redness, swelling where the shot was given, fever, headache, nausea, vomiting, diarrhea and other mild probletns. More serious reactions are
Massachusetts Department of Public Health I Bureau of Infectious Disease and Laboratory Sciences
October 20181 Page 3 of 3
very rare. Getting the Tdap vaccine is much safer than getting pertussis, and most people do not have any problems with the vaccine.
ld p All children younger than 7 years old should get this vaccine unless they have a history of seizures or other brain problem or had a serious health probletn after getting DTaP before. If not, your child should get DTaP when he or she is: 2 months old, 4 months old, 6 months old, 12-15 months old, and 4-6 years old.
p Older children and adults should get one shot ofTdap instead of a regular tetanus shot (Td). Adolescents usually get the Tdap shot at their 11-12 year old visit. It is especially important for adults in contact with young infants, such as parents, grandparents, health care workers and child care providers, to get a single Tdap shot. Children 7 to 10 years of age can get a dose ofTdap if they have not received all of their doses ofDTaP and are not fully protected against pertussis.
more i ,., ..... ,.~,,. ... """" • Your doctor, nurse or clinic, or your local board of health (listed in the phone book
under local government). • The Massachusetts Department of Public Health, Divisions of Epidemiology
and Immunization (617) 983-6800, or on the MDPH website at www. m ass.gov I dph/.
• Boston providers and residents may also call the Boston Public Health Commission at (617) 534-5611.
• CDC National Imtnunization Information Hotline: o English: 1-800-232-2522 (Mon- Fri, 8am- 11 pm) or Spanish: 1-800-232-
0233 (Mon- Fri, 8am- 11 pm) o TTY: 1-800-243-7889 (Mon- Fri, 1 Oam- 1 Opm)
Massachusetts Department of Public Health I Bureau of Infectious Disease and Laboratory Sciences
4~··~\ ·~~l
TOWN OF BUP~INGTON Board of Health
Public Health Prevent. Promote. Protect.
Board o) HeaLth Staj}: Susan Lumenello, REHSIRS, CHMM, Director Christine Mathis, Environmental Engineer Marlene Johnson, R.S., Health Agent Christine Paulik, MSN, R.N., Supervising Nurse Samantha Hardy, Associate Health Inspector
February.3, 2020
Woburn District Court 30 Pleasant Street Woburn, MA 01801 Attention: Clerk Magistrate
RE: An Act Modernizing Tobacco Control
Dear Sir/Madame:
Board o} Health Members: Ed Weiner, Ph.D., Chairman
David McSweeney, Vice Chairman Wayne Saltsman, MD, Ph.D., BOH Member
Elizabeth Walendziewicz, BOH Member Maribeth Welch, BOH Member
On November 27, 2019, Governor Charlie Baker signed into law An Act Modernizing Tobacco Control. This law amends several existing state laws addressing both tobacco products (cigarettes, cigars, chew/spit tobacco, pipe tobacco) and electronic vaping products. This letter focuses on the new fining and enforcement sections of the law only.
Historically, MGL Ch. 270, §6 has prohibited the sale of tobacco products to persons under the minimum legal sales age. The new law has been expanded to prohibit the sale of ALL flavored tobacco products, including menthol products, except for on-site consumption onl¥ in "Smoking Bars" (cigar bars, hookah bars, vape bars). Included in this law is a rewrite regarding fines. For decades, the fining scheme in the state law has been "not less than $1 00" for a first offense, "not less than $200" for a second offense and "not less than $300" for a third or subsequent offense. Our local health regulations have also included permit suspensions for second, third and subsequent offenses. The new mandated fining scheme is $1,000 for a first offense, $2,000 for a second offense and $5,000 for a third or subsequent offense within a 36-month period. These new fines apply to violations regarding sales to persons under the minimum legal sales age and sales of flavored tobacco product sales only.
It is routine for the Massachusetts Department of Public Health to enact regulations to facilitate enforcement of new laws. The state's Public Health Council has enacted an emergency regulation. This regulation does not, and will not, alter the state law's fining scheme. We will notify our retailers of this mandated increase in fines. Our compliance check protocol will not change in light of this state law update. We will take care to only issue the higher fines for violations of retailers failing a compliance check regarding sales to persons under 21 and sales of flavored tobacco products.
If you have any questions or concerns, please feel free to contact me.
Sincerely, · A 17 /; -~~u~~ Susan Lumenello, REHS/RS, CHMM Director of Public Health
61 CENTER STREET 0 BURLINGTON,MASSACHUSETTS01803 a TEL(781)270-1955 e FAX(781)273-7687 www. burlington. org (9 boh@burlington. org