Embed Size (px)
Citation preview

Originally Published in: Susan Young , Gisli H. Gudjonsson & Rachel Terry (2006)
The development of a forensic clinical psychology service in a community mental
health team, The Journal of Forensic Psychiatry & Psychology, 17:4, 626-635, DOI:
10.1080/14789940600911635
The Journal of Forensic
Psychiatry & Psychology http://www.tandfonline.com/loi/rjfp20
The development of a forensic
clinical psychology service in a
community mental health team
Susan Young a , Gisli H. Gudjonsson
a & Rachel Terry
b
a Institute of Psychiatry , London, UK
b David Salomons Estate , Kent, UK Published online: 17 Feb 2007.
To link to this article: http://dx.doi.org/10.1080/14789940600911635

The Journal of Forensic Psychiatry & Psychology, December 2006; 17(4): 626 – 635
The development of a forensic clinical psychology service in a
community mental health team
SUSAN YOUNG1, GISLI H. GUDJONSSON
1, & RACHEL TERRY
2
1Institute of Psychiatry, London, UK and
2David Salomons Estate, Kent, UK
Abstract This study provides detailed psychometric data on the patients in the care of a community forensic team in south-east London. Out of 59 patients referred to the psychology service, 39 (66%) attended at least one appointment. Overall, about 42% of all psychology appointments offered were not attended. The great majority (93%) of the patients were male, typically with a history of major mental illness and an index offence of either violence or sexual assault. The results from the psychometric testing confirmed that most of the patients have serious mental illness problems, which are often combined with marked antisocial personality traits, criminality proneness, and low self-esteem. Taken together, these findings suggest that many of the patients have a variety of complex psychiatric and psychological problems, which require intense intervention by a specialist team.
Introduction Recent developments in mental health care have resulted in increased forensic outpatient services and the development of community forensic mental health teams (CFMH)
throughout the United Kingdom (Mohan, Judge, & Fahy, 2004). According to Mohan et al.
(2004), two different kinds of CFMH models have evolved: (1) an integrated model, where
the forensic specialists work as part of the community mental health teams; and (2) a parallel model where they work as a separate service alongside community mental health teams. The two CFMH models differ in several service-related characteristics, including physical location, management, Correspondence: Susan Young, Department of Forensic Mental Health Science, Institute of Psychiatry, P.O. Box 23, De Crespigny Park, London SE5 8AF, UK. E-mail: [email protected] ISSN 1478-9949 print/ISSN 1478-9957 online ª 2006 Taylor & Francis DOI: 10.1080/14789940600911635
caseload, referral procedures, and liaison with criminal justice agencies (Mohan et al., 2004).
The advantage of the parallel model is that it has the potential to deliver a more specialized
treatment programme to a complex group of patients, while the disadvantage is that this
service model may discourage clinicians without forensic training from developing the skills
needed for the satisfactory risk assessment and management of violent patients (Snowden,
McKenna, & Jasper, 1999). About 80% of CFMH teams in England and Wales consider
themselves to follow the parallel model with emphasis on risk assessment rather than offence-
related therapy (Judge, Harty, & Fahy, 2004). Anger management was the most common
treatment offered by the various teams, with less treatment provision for sex offenders and
patients with personality disorders.
The purpose of this paper is to provide an audit of the psychological service of one parallel
CFMH team. The Forensic Psychology Service of the Croydon Community Forensic Team
(CCFT) was set up in December 2000 following an internal identification of service need.
This paper details the findings of an audit which examines the clinical service provided by the
CCFT Forensic Psychology Service between December 2000 and the end of July 2003. A
similar audit of the service was published on the contribution of the CCFT to multi-agency
public protection panels (MAPPP) for dangerous offenders (Young, Gudjonsson, &
Needham-Bennett, 2005). The current audit evaluates the type of referrals received, the basic
characteristics of the patients referred, the attendance rate of patients, the types of assessment
and treatment offered, and the psychological characteristics of the patients seen. In order to
obtain a better understanding of the patients’ personalities and clinical problems a number of
psychometric tests were administered. It was expected that the patients would display a range
of personality and clinical problems relevant to evaluating their risk, managing that risk, and
providing appropriate treatment.
Method Measures During the first one or two appointment sessions patients were asked to complete the following psychometric tests.
Eysenck Personality Questionnaire – Revised (EPQ-R; Eysenck & Eysenck, 1991). This 106-item questionnaire is a self-report measure of the following personality characteristics: psychoticism (P), extraversion (E), neuroticism (N), lie (L), addiction (A), and criminality (C).
Eysenck Impulsiveness Questionnaire (IVE; Eysenck & Eysenck, 1991). This 54-item questionnaire is a self-report measure of impulsiveness (I), venturesomeness (V), and empathy (E).
Culture-Free Self-Esteem Inventory (SEI; Battle, 1986). This 40-item questionnaire measures self-esteem on three scales: general (G), social (S), and personal (P).
Gough Socialization Scale (Megargee, 1972). This 54-item scale measures prosocial behaviour.
State-Trait Anger Expression Inventory – 2 (STAXI-2; Spielberger 1999). This 57-item
questionnaire measures an individual’s anger. According to the STAXI-2 manual, scores
between the 25th and 75th percentiles fall in the normal range. Individuals with anger scores
above the 75th percentile experience and/or express angry feelings to a degree that may
interfere with optimal functioning.
Symptom Checklist – 90 – R (SCL-90-R; Derogatis, 1994). This 90-item self-report
questionnaire is designed to reflect the psychological symptom patterns of community,
medical, and psychiatric respondents. Individuals are required to rate how much a problem
has distressed or bothered them during the previous seven days. Each item is rated on a five-
point scale of distress ranging from ‘not at all’ to ‘extremely’. It is scored in terms of nine
primary symptom dimensions: somatization, obsessive – compulsive, inter-personal
sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism.
Additionally, there are three global indices of distress associated with the SCL-90-R: (1) the global severity index, which provides the most sensitive single numeric indicator of a respondent’s psychological status, combining the number of symptoms reported with the intensity of perceived distress; (2) the positive symptom distress index, which reflects the average level of distress reported for the symptoms that were endorsed (i.e., a measure of symptom intensity); and (3) the
positive symptom total, which reflects the number of symptoms endorsed by the respondent, regardless of the level of distress reported (i.e., a measure of symptom breadth).
Procedure All patients referred to the service were sent a psychology appointment. Those who attended
completed a psychometric assessment of personality, anger, self-esteem, and mental state, and
where appropriate were offered treatment. More specifically, the data collection and analysis
consisted of the following:
gathering and recording of information about the number of referrals (this was
achieved by keeping a detailed log of all referrals to the forensic team)
examination of attendance rates (i.e., how many appointments were offered and attended, and reason for failure to attend)
breakdown of reasons for referral (e.g., assessment versus treatment, type of assessment conducted, and treatment provided)
analysis and presentation of psychometric test results (e.g., mean scores, standard deviations, comparison with appropriate normative samples, effect sizes, and scores falling outside normal limits).
Results Patient characteristics During the period December 2000 – July 2004, 59 patients (55 males and four females: 93%
males and 7% females) were referred to the psychology team. Their mean age was 34.2 years
(SD 9.7; range 18 – 63). The ethnic background of the patients was as follows: 34 (57.6%) were white; 12 (20.3%) were black Caribbean; six were black ‘other’ (10.2%); and there were
seven ethnic minorities classified as ‘other’ (11.9%).
The individuals referred had the following primary diagnoses: 36 (61%) were suffering from schizophrenia or affective disorder; 15 (25.4%) were suffering from personality
disorder; four (6.8%) from substance misuse; two (3.4%) from attention deficit hyperactivity disorder; one (1.7%) from Aspergers syndrome; and one (1.7%) from post-traumatic stress
disorder. Their index offences were as follows: 24 (41%) were offences of violence (e.g., actual
bodily harm, grievous bodily harm, manslaughter, and threats to kill); 10 (16.8%) were sexual offences; 10 were acquisitive offences (16.9%); five were arson (8.5%); and there were 10 others (16.8%).
Expansion of the service During the period of study the clinical caseload of the service as a whole expanded greatly. It increased by one-third (from 72 to 95 referrals between October 2001 and September 2002) with an average of two referrals per week. By the end of July 2003, the number of patients managed by the CCFT was 108 (representing a 50% increase in the team’s caseload).
Attendance Out of the 59 patients referred to the psychology team, 39 (66.1%) attended at least once. A
total of 366 appointments were offered to the 59 patients and, of those, 212 (58%) were taken
up. Very few appointments were missed because patients were unable to attend for a specific
reason (e.g., unwell due to sickness or deterioration in mental state, or conflict with social
welfare appointments).
Reason for referral The direct clinical psychology service was defined as the psychological assessment and treatment of outpatients, although periodically assessments at inpatient settings were conducted.
Out of the 366 appointments offered, 205 (56%) were for assessment and 161 (44%) were
for treatment. Of the treatment sessions offered, 91 (25%) were for individual cognitive
behaviour therapy (CBT) sessions, 48 (13%) for CBT group sessions, and 22 (6%) for
individual psychodynamic interventions.
In 2001, the first year of the forensic psychology service, there was a greater emphasis on
psychological assessment (75% of appointments offered), which is to be expected from a new
service. This gradually decreased and by 2003 around 40% of appointments offered were for assessment and 60% were for psychological treatment.
Assessment appointments were offered for a broad range of complex clinical work and risk
assessments, including the assessment and treatment of psychosexual problems, personality
problems, insight and attitude towards offending, anger and violent behaviour, anxiety and
depression, cognitive problems (e.g., IQ and memory), delusions and voices, and arson.
Treatments provided included: psychodynamic and/or cognitive therapy for offence-related
work with violent and/or sexual offenders; CBT treatment for anger, anxiety, depression,
psychosis, and personality disorder; and motivational interviewing for substance misuse.
Sometimes, in addition to these direct treatments, work was carried out with hostel staff. For
example, one patient with intellectual limitations who presented with sexually disinhibited
behaviour needed indirect psychological treatment and this was provided by a functional
analysis of his behaviour, and the development, implementation, and analysis of a treatment
programme within the hostel. In addition to the individual treatments offered, group
workshops were run on topics relating to anger, anxiety, victim empathy, and interpersonal
problems. These groups were run as one-off intensive workshops lasting one afternoon, as
opposed to traditional hourly group sessions run over a series of weeks. This approach was
taken to avoid a large number of drop-outs during treatment.
Psychometric test results Table I gives the mean scores, standard deviations, range of scores, effect size using Cohen’s
d (Cohen, 1988), and the number and percentage of patients who had scores that fell outside
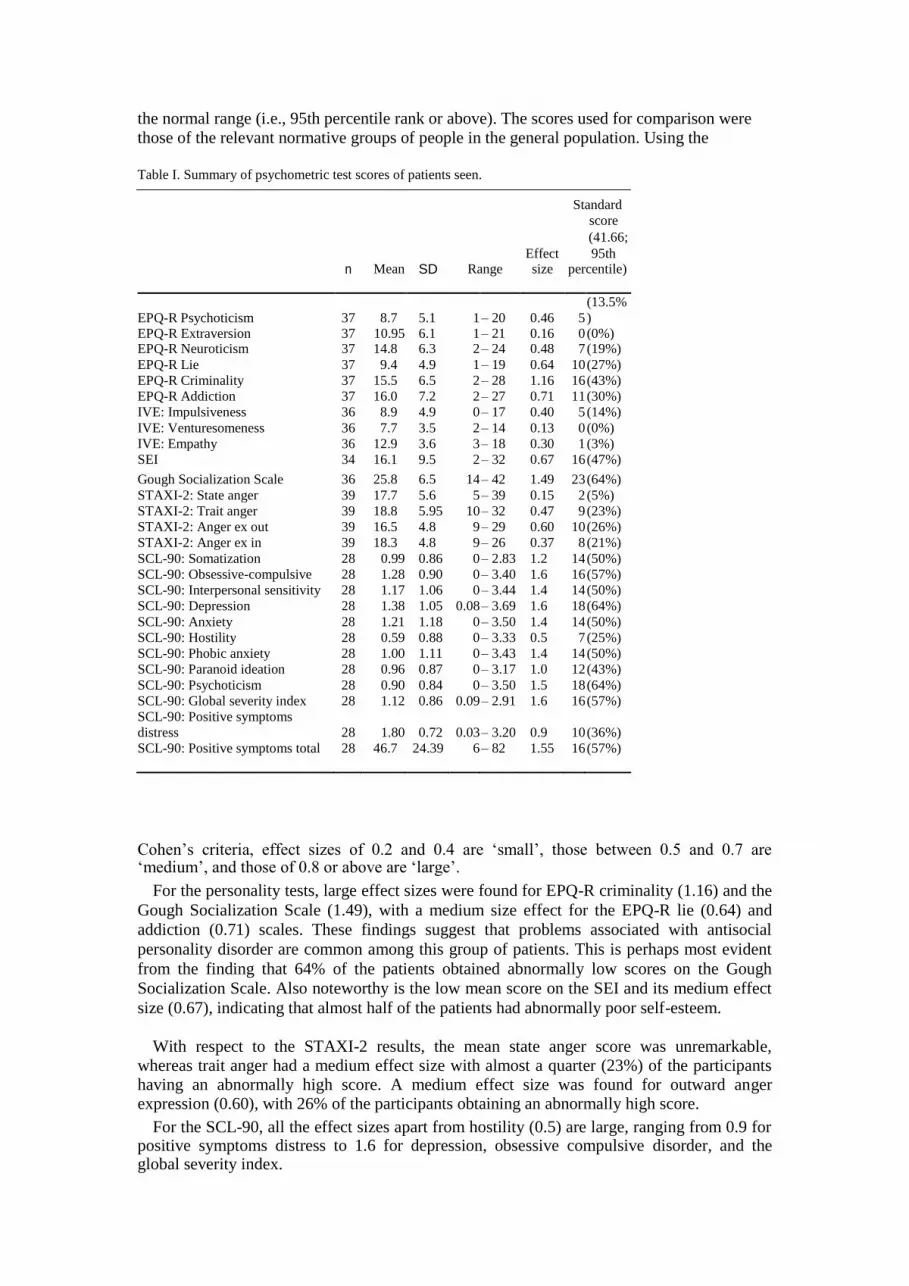
the normal range (i.e., 95th percentile rank or above). The scores used for comparison were
those of the relevant normative groups of people in the general population. Using the
Table I. Summary of psychometric test scores of patients seen. Standard
score
(41.66;
Effect 95th n Mean SD Range size percentile)
EPQ-R Psychoticism 37 8.7 5.1 1 – 20 0.46 5
(13.5%
) EPQ-R Extraversion 37 10.95 6.1 1 – 21 0.16 0 (0%) EPQ-R Neuroticism 37 14.8 6.3 2 – 24 0.48 7 (19%)
EPQ-R Lie 37 9.4 4.9 1 – 19 0.64 10 (27%)
EPQ-R Criminality 37 15.5 6.5 2 – 28 1.16 16 (43%)
EPQ-R Addiction 37 16.0 7.2 2 – 27 0.71 11 (30%)
IVE: Impulsiveness 36 8.9 4.9 0 – 17 0.40 5 (14%)
IVE: Venturesomeness 36 7.7 3.5 2 – 14 0.13 0 (0%)
IVE: Empathy 36 12.9 3.6 3 – 18 0.30 1 (3%)
SEI 34 16.1 9.5 2 – 32 0.67 16 (47%)
Gough Socialization Scale 36 25.8 6.5 14 – 42 1.49 23 (64%)
STAXI-2: State anger 39 17.7 5.6 5 – 39 0.15 2 (5%)
STAXI-2: Trait anger 39 18.8 5.95 10 – 32 0.47 9 (23%)
STAXI-2: Anger ex out 39 16.5 4.8 9 – 29 0.60 10 (26%)
STAXI-2: Anger ex in 39 18.3 4.8 9 – 26 0.37 8 (21%)
SCL-90: Somatization 28 0.99 0.86 0 – 2.83 1.2 14 (50%)
SCL-90: Obsessive-compulsive 28 1.28 0.90 0 – 3.40 1.6 16 (57%)
SCL-90: Interpersonal sensitivity 28 1.17 1.06 0 – 3.44 1.4 14 (50%)
SCL-90: Depression 28 1.38 1.05 0.08 – 3.69 1.6 18 (64%)
SCL-90: Anxiety 28 1.21 1.18 0 – 3.50 1.4 14 (50%)
SCL-90: Hostility 28 0.59 0.88 0 – 3.33 0.5 7 (25%)
SCL-90: Phobic anxiety 28 1.00 1.11 0 – 3.43 1.4 14 (50%)
SCL-90: Paranoid ideation 28 0.96 0.87 0 – 3.17 1.0 12 (43%)
SCL-90: Psychoticism 28 0.90 0.84 0 – 3.50 1.5 18 (64%)
SCL-90: Global severity index 28 1.12 0.86 0.09 – 2.91 1.6 16 (57%)
SCL-90: Positive symptoms
distress 28 1.80 0.72 0.03 – 3.20 0.9 10 (36%)
SCL-90: Positive symptoms total 28 46.7 24.39 6 – 82 1.55 16 (57%)
Cohen’s criteria, effect sizes of 0.2 and 0.4 are ‘small’, those between 0.5 and 0.7 are ‘medium’, and those of 0.8 or above are ‘large’.
For the personality tests, large effect sizes were found for EPQ-R criminality (1.16) and the
Gough Socialization Scale (1.49), with a medium size effect for the EPQ-R lie (0.64) and
addiction (0.71) scales. These findings suggest that problems associated with antisocial
personality disorder are common among this group of patients. This is perhaps most evident
from the finding that 64% of the patients obtained abnormally low scores on the Gough
Socialization Scale. Also noteworthy is the low mean score on the SEI and its medium effect
size (0.67), indicating that almost half of the patients had abnormally poor self-esteem.
With respect to the STAXI-2 results, the mean state anger score was unremarkable,
whereas trait anger had a medium effect size with almost a quarter (23%) of the participants having an abnormally high score. A medium effect size was found for outward anger expression (0.60), with 26% of the participants obtaining an abnormally high score.
For the SCL-90, all the effect sizes apart from hostility (0.5) are large, ranging from 0.9 for positive symptoms distress to 1.6 for depression, obsessive compulsive disorder, and the global severity index.
Discussion This audit of the CCFT Forensic Psychology Service examines the clinical service provided
from December 2000 to the end of July 2003. The results of the audit show that many patients
offered clinical psychology appointments failed to keep them. Indeed, about 42% of all
psychology appointments offered were not attended. Out of the 59 patients referred to the
psychology team, 39 (66.1%) attended at least once. This may not be markedly different to
other clinical psychology services. For example, the non-attendance rates for generic clinical
psychology services have been reported to range between 23% and 33% (Aubrey, Self, &
Halstead, 2003; Markham & Beeney, 1990). Rates reported for attrition range between 35%
and 40% (Aubrey et al., 2003; Trepka, 1986). It is likely that those who fail to turn up for
their psychological appointments are more disordered in their personality than the other
patients (Gudjonsson et al., 2004), which means that they are particularly in need of
psychological intervention focusing on criminogenic factors (Andrews, 1995).
Their failure to attend psychology appointments means that no direct psychological
evaluation can be conducted on these patients. The consequence is that formal assessment of
risk and detailed risk management may not take place, personality and clinical problems may
not be adequately assessed, and appropriate treatment is not provided. It is important to
identify methods to improve the attendance rate for psychological assessment and treatment.
User-involvement research has shown that attendance rates improve when patients are
provided with written information relating to their proposed treatment (Markham & Beeney,
1990) and this is used as a basis for discussion with a keyworker or care coordinator prior to
treatment. In addition, other members of the CMHT or forensic team, such as doctors and
nurses, could emphasize to the patient the importance of attending the psychological
assessment and treatment.
The findings from this small study involve one outreach team in south-east London. The great majority (93%) of the referrals were males. Over half of the patients had an index offence involving either violence (41%) or a sexual crime (16.8%). The great majority had a primary diagnosis of major mental illness, namely schizophrenia (61%) or affective disorder (25.4%).
Only four (6.8%) had a primary diagnosis of personality disorder. The results from the SCL-
90 confirm that many of the patients have serious mental illness problems which require
treatment. In addition, psychometric results from the personality tests indicate that the
majority of the patients who attended their initial assessment had marked antisocial
personality traits, criminality proneness, and low self-esteem. Taken together, these findings
suggest that many of the patients have a variety of complex psychiatric and psychological
problems, which require intense intervention by a specialist team.
In view of the low Gough Socialization and SEI scores among many of the patients,
suggesting antisocial personality disorder problems and poor self-esteem, effective treatment
will need to involve important lifestyle changes (Gottfredson & Hirschi, 1990; McGuire,
2002; Walters, 2002). The present findings also highlight important psychiatric problems,
which will need to be treated alongside the criminogenic problems (Prins, 2005). Among
some of the patients, the acting out of angry impulses needs to be treated, although anger
management programmes with offenders may need to be long, intensive, and well focused in
order to achieve an improvement beyond an ‘educational’ level (Howells et al., 2005).
The present findings regarding psychopathology need to be considered in the light of the
moderately high effect size of the EPQ lie score of many of the patients. Indeed, over one
quarter (27%) of the patients had an abnormally high lie score during psychological
evaluation. The lie score indicates a strong tendency among many of the patients to present
themselves in a socially desirable light. Gudjonsson and Moore (2001) found that high ‘other
deception’ (also known as ‘impression management’; Paulhus, 1998) is particularly
problematic among forensic patients who, as a result, are reluctant to be open about their
psychological problems and risk to others. This means that the reporting of psychopathology
in the current study may represent an underestimate of patients’ real problems both in terms
of type and severity. In spite of this, many patients were reporting a great deal of
psychopathology.
There is also a tendency among some forensic patients to present themselves as more
distressed than is actually the case. A limitation of this study was that the EPQ-R only
identifies the tendency to minimize symptoms, whereas both these response styles (i.e.,
minimization and exaggeration) can be captured by alternative measures such as the Millon
Clinical Multiaxial Inventory-III (MCMI-III; Millon, 1997).
Where there is a parallel forensic service, there is generally a need for clear exit criteria to
general mental health services. This would avoid some patients being held in a service that
implies they remain ‘dangerous’ and reduce stigma and marginalization (Burns, 2001).
Assertive outreach teams in London, whose remit is to support people with enduring mental
health difficulties and for whom other services have been unable to sustain engagement, are
including individuals with a history of violent and/or antisocial behaviours on their caseload,
which keeps patients within generic services (Priebe et al., 2003). The advantage of a parallel
model is that it may be better resourced to address and treat the complex issues surrounding
the patients’ risks, needs, and responsivity. However, where there is a parallel service, there
needs to be collaboration between the two services to maximize patients’ attendance,
involvement, and treatment effectiveness, while addressing and minimizing risks to the
public. References Andrews, D. (1995). The psychology of criminal conduct and effective treatment. In J. McGuire (Ed.),
What works: Reducing reoffending. (pp. 35–62). Chichester: John Wiley & Sons.
Aubrey, R., Self, R., & Halstead, J. E. (2003). Early non-attendance as a predictor of continued non-
attendance and subsequent attrition from psychological help. Clinical Psychology, 32, 6–10.
Battle, J. (1986). Culture-free SEI: Self esteem inventories for children and adults. Seattle:
Special Child Publications. Burns, T. (2001). To outreach or not to outreach. Journal of Forensic Psychiatry, 12, 13–17. Cohen,
J. (1988). Statistical power analysis for the behavioural sciences. Hillsdale, NJ: Erlbaum.
Derogatis, L. R. (1994). Symptom Checklist – 90 – R: Administration, scoring, and procedures manual (3rd ed.). Minneapolis: National Computer Systems, Inc.
Eysenck, H. J., & Eysenck, S. B. G. (1991). Manual of the Eysenck Personality Questionnaire. London: Hodder and Stoughton.
Gottfredson, M. R., & Hirschi, T. (1990). A general theory of crime. Stanford, CA: Stanford University Press.
Gudjonsson, G. H., Hannesdottir, K., Agustsson, T. P., Sigurdsson, J. F., Gudmundsdottir, A., Pordardottir, P., et al. (2004). Personality predictors of the failure of alcoholics to come for follow-
up treatment. Personality and Individual Differences, 37, 805–813. Gudjonsson, G. H., & Moore, E. (2001). Self-deception and other-deception among admissions to a
maximum security hospital and medium secure hospital. Psychology, Crime and Law, 7, 25–31. Howells, K., Day, A., Williamson, P., Bubner, S., Jauncey, S., Parker, A., & Heseltine, K. (2005). Brief
anger management programs with offenders: Outcomes and predictors of change. The Journal of Forensic Psychiatry and Psychology, 16, 296–311.
Judge, J., Harty, M.-A., & Fahy, T. (2004). Survey of community psychiatry services in England and
Wales. Journal of Forensic Psychiatry and Psychology, 15, 244–253. Markham, P., & Beeney, E. (1990). DNA rates and the effect of ‘‘opting in’’ to a clinical psychology
service. Clinical Psychology Forum, 29, 9–10. McGuire, J. (2002). Motivation for what? Effective programmes for motivated offenders. In M.
McMurran (Ed.), Motivating offenders to change (pp. 157–172). Chichester: John Wiley & Sons
Ltd. Megargee, E. I. (1972). The California Psychological Inventory handbook. London: Jossey-Bass,
Inc. Millon, T. (1997). Millon Clinical Multiaxial Inventory-III: Manual (2nd ed.). Minneapolis: NCS
Pearson Inc. Mohan, R., Judge, J., & Fahy, T. (2004). Community Forensic Psychiatry, Forensic Psychiatry, 3,
11–14. Mohan, R., Slade, M., & Fahy, T. (2004). Clinical characteristics of community forensic mental health
services. Psychiatric Services, 55, 1294–1298. Paulhus, D. L. (1998). Paulhus Deception Scales (PDS): The balanced inventory of desirable
responding 7. New York: MHS. Priebe, S., Fakhoury, W., Watts, J., Bebbington, P., Burns, T., Johnson, S., et al. (2003). Assertive
outreach teams in London: Patients’ characteristics and outcomes: Pan-London Assertive Outreach
Study, part 3. British Journal of Psychiatry, 183, 148–154. Prins, H. (2005). Offenders, deviants or patients? Hove: Routledge. Snowden, P., McKenna, J., & Jasper, A. (1999). Management of conditionally discharged patients and
others who present similar risks in the community: Integrated or parallel? Journal of Forensic Psychiatry, 10, 583–596.
Spielberger, C. D. (1999). STAXI-2. State-Trait Anger Expression Inventory-2. Odessa, FL: Psychological Assessment Resources.
Trepka, C. (1986). Attrition from an out-patient psychology clinic. British Journal of Medical Psychology, 59, 181–186.
Walters, G. D. (2002). Maintaining motivation for change using resources available in an offender’s natural environment. In M. McMurran (Ed.), Motivating offenders to change (pp. 121–135).
Chichester: John Wiley & Sons Ltd. Young, S., Gudjonsson, G. H., & Needham-Bennett, H. (2005). Multi-agency public protection panels
for dangerous offenders: One London forensic team’s experience. Journal of Forensic Psychiatry and Psychology, 16, 312–327.





























