Embed Size (px)
Citation preview
Techniques and Training with GreenLight HPS 120-W LaserTherapy of the Prostate: Position Paper
Gordon Muir a, Fernando Gomez Sancha b,*, Alexander Bachmann c, Benjamin Choi d,Edward Collins e, Jean de la Rosette f, Oliver Reich g, Shahin Tabatabaei h, Henry Woo i
aDepartment of Urology, King’s College Hospital, London, UKb Institute of Advanced Urological Surgery, Madrid, SpaincDepartment of Urology, University Hospital, Basel, SwitzerlanddDepartment of Urology, Weill Medical College of Cornell University, Ithaca, New York, USAeCalifornia Urological Services, San Francisco, California, USAfDepartment of Urology, Academic Medical Center, University of Amsterdam, The NetherlandsgDepartment of Urology, Ludwig-Maximilians-University, Munich, GermanyhDepartment of Urology, Massachusetts General Hospital, Boston, Massachusetts, USAiDepartment of Urology, Westmead Hospital, The University of Sydney, Australia
e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
Article info
Keywords:GreenLight HPS laserPhotoselective vaporizationof the prostateBenign prostatic hyperplasiaTechniqueTraining
Abstract
We report the technical recommendations of the International Green-Light User Group on photoselective vaporization of the prostate in menwith benign prostatic hyperplasia using the GreenLight HPS system(American Medical Systems, Minnetonka, Minnesota, USA). This high-power system employs a 120-W laser, which is a modification of theprevious 80-W potassium-titanyl-phosphate (KTP) laser. The objective ofthis report is to optimize the efficacy and safety of the procedure bydrawing on the experience of this multicentre international group. Inthis regard, recommendations for training are made, which relate toexisting users of the 80-W KTP laser as well as to new laser users.# 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Institute of Advanced Urological Surgery, Paseo de la Castellana 23,28046 Madrid, Spain. Tel. +34 91308 02 99; Fax: +34 9143 52877.E-mail address: [email protected] (F. Gomez Sancha).
1. Introduction
Photoselective vaporization of the prostate (PVP)using the 80-W potassium-titanyl-phosphate (KTP)532-nm laser is a recent technological developmentin the use of lasers as an alternative to transurethralresection of the prostate (TURP) for the treatment ofsymptomatic benign prostatic hyperplasia. Origi-
1569-9056/$ – see front matter # 2007 European Association of Urology. Publis
nally introduced by Malek et al. in 1998 utilizing a60-W KTP laser, a subsequent pilot study of PVP withthe 80-W KTP laser showed a good outcome andminimal side effects in men with prostate volumesof 24–76 ml [1]. PVP works on a different mechanismthan the existing holmium laser enucleation of theprostate, in that it involves prostate tissue ablationthrough vaporization as opposed to enucleation.
hed by Elsevier B.V. All rights reserved. doi:10.1016/j.eursup.2008.01.012

Fig. 2 – Photoselective vaporization of the prostate. The
fibre should be rotated in a sweeping fashion with rotation
amplitude reduced to an arc of 608 (c). This avoids an
e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7 371
Further progress with PVP has been the introductionof the high-performance system (HPS) 120-W laser,which aims to reduce lasing time and improveclinical outcomes while maintaining the samedegree of safety for patients. Technical recommen-dations on the GreenLight 80-W KTP laser (AmericanMedical Systems, Minnetonka, Minnesota, USA)have been published by the International GreenLightUser Group, in addition to training recommenda-tions [2]. In this paper, we discuss how the techniqueis used with the GreenLight HPS 120-W laser systemand what the new training requirements will be.
increase in the distance from the fibre to the tissue, which
would produce an oblique light footprint, reduce
vaporization efficiency, increase reflection of light, and
increase coagulation (a, b).
2. General principlesSeveral factors have to be considered when usingthe GreenLight HPS 120-W laser. The new HPSsystem operates with a fibre that emits a beam thatis more collimated and more powerful than the
Fig. 1 – Working distance of 120-W fibre from the
cystoscope: (a) at a distance where there is more
perspective and orientation is better; (b) close to the
cystoscope, where there is a higher risk of telescope
damage and orientation is worse.
80-W KTP laser. This translates in vitro as well asclinically into faster vaporization and a greater abilityto penetrate prostate tissue from longer fibre dis-tances. The increase in vaporization speed is asso-ciated with faster bubble generation and more tissuedebris, which has the potential to reduce the workingvisibility. For this reason, it is helpful to work withthe fibre slightly further from the cystoscope, whichalso reduces the risk of damage to the cystoscopefrom reflected energy. This also translates into betterorientation inside the prostatic fossa during surgery(Fig. 1). With this technique, it is important thatthe surgeon is sure that he/she is firing inside theprostatic fossa and not in the bladder. Caution isrecommended at the actual bladder neck, where thefibre should be kept closer to the cystoscope and thetissue to avoid damage to the ureteral orifices.
When handling the actual fibre during lasing,with the increased 120-W power it is important tomove the fibre slowly but constantly to avoid drillingholes in the prostate tissue, and spreading theenergy in this way will create a smooth surface. Inaddition, the rotation speed of the fibre must beadapted to the efficiency of vaporization: if effi-ciency is high, rotation can be speeded up, whereasif efficiency is low due to poor vascularization of aregion, rotation should be slowed down. Therotation angle of the fibre must be kept small(ie, from 5 to 7 o’clock, or 608) to keep the angle ofincidence of the beam as perpendicular to the tissueas possible (Fig. 2). The working distance of the laserfrom the tissue is a key issue. In vitro studies haveshown that it is possible to work slightly furtheraway with the 120-W laser compared with the80-W laser, at up to 4 mm, and still obtain goodvaporization (Fig. 3). However, a more efficient

Fig. 3 – Efficiency of vaporization at different working
distances for the 80-W KTP laser and the 120-W HPS lasers
based on in vitro studies with canine prostate tissue.
Based on data supplied by W. Kang (American Medical
Systems Research Group).
Fig. 4 – Relationship of the cystoscope and the laser fibre: (a)
moving the whole cystoscope to go from point A to B while
keeping the fibre and cystoscope in close proximity can
result in friction; (b) moving the fibre from point A to B
while keeping the cystoscope static can minimize trauma
to the gland. # IGLU Group.
e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7372
clinical vaporization effect is seen working atshorter distances in near contact mode. It is possiblethat at greater tissue distances the beam interferesmore with debris and bubbles arising from thetissue, thus compromising vaporization efficiency.As with the 80-W laser recommendations, it isimportant to avoid direct contact with the tissueas excessive heat reflection will char and damagethe fibre. Gentle fingertip movements of the laserfibre and cystoscope are recommended, and theapproach must be rather more static than themovements employed with TURP. This approachwill minimize bleeding and improve the chancesof completing the procedure with a small-calibrecystoscope, with reduced irrigation efficiency andwithout bleeding. One can also choose to move thefibre in association with the cystoscope when lasing,or the cystoscope can remain static while the fibre ismoved. The latter option can minimize friction tothe prostatic and urethral surfaces, again reducingthe likelihood of bleeding (Fig. 4).
Space restraints within the prostate may requirestarting the procedure at the lower power of 80 Wwith rapid fibre movement to avoid tissue contactuntil a working channel has been created and thenswitching to the 120-W power. This will also reducethe likelihood of damaging the fibre through excesscontact at 120 W. With experience, it may be possibleto use the 120-W power from start to finish even insmall prostates, but novice users and PVP userswithout experience with the 120-W laser shouldlower the power to 60 or 80 W initially. Expert users ofthe 120-W laser should aim to have only minimal,very short pauses during a lasing session. Anothernovel concept is fibre navigation, that is, the useof the fibre to navigate around the prostatic fossa
with a continuous beam operating at the correctworking distance. Spreading the energy inside thecavity in a symmetrical fashion—as opposed to thesequential approach (ie, middle lobe, then right lobe,and then left lobe) with a TURP—is analogous topeeling back layer after layer of prostate tissue.Another important distinction compared with someother lasing systems is the type of cavity being aimedfor with the HPS, which should be a ‘‘wine-glass’’ orTURP-like shape, as opposed to a small cylindricalchannel.
3. The modular approach to photoselectivevaporization of the prostate
The initial stages of patient evaluation, preparation,and anaesthesia as well as detailed approaches tovaporizing the prostate have been described pre-viously [2]. Given here are the basic principles for theHPS procedure, which can be divided into sixmodules.
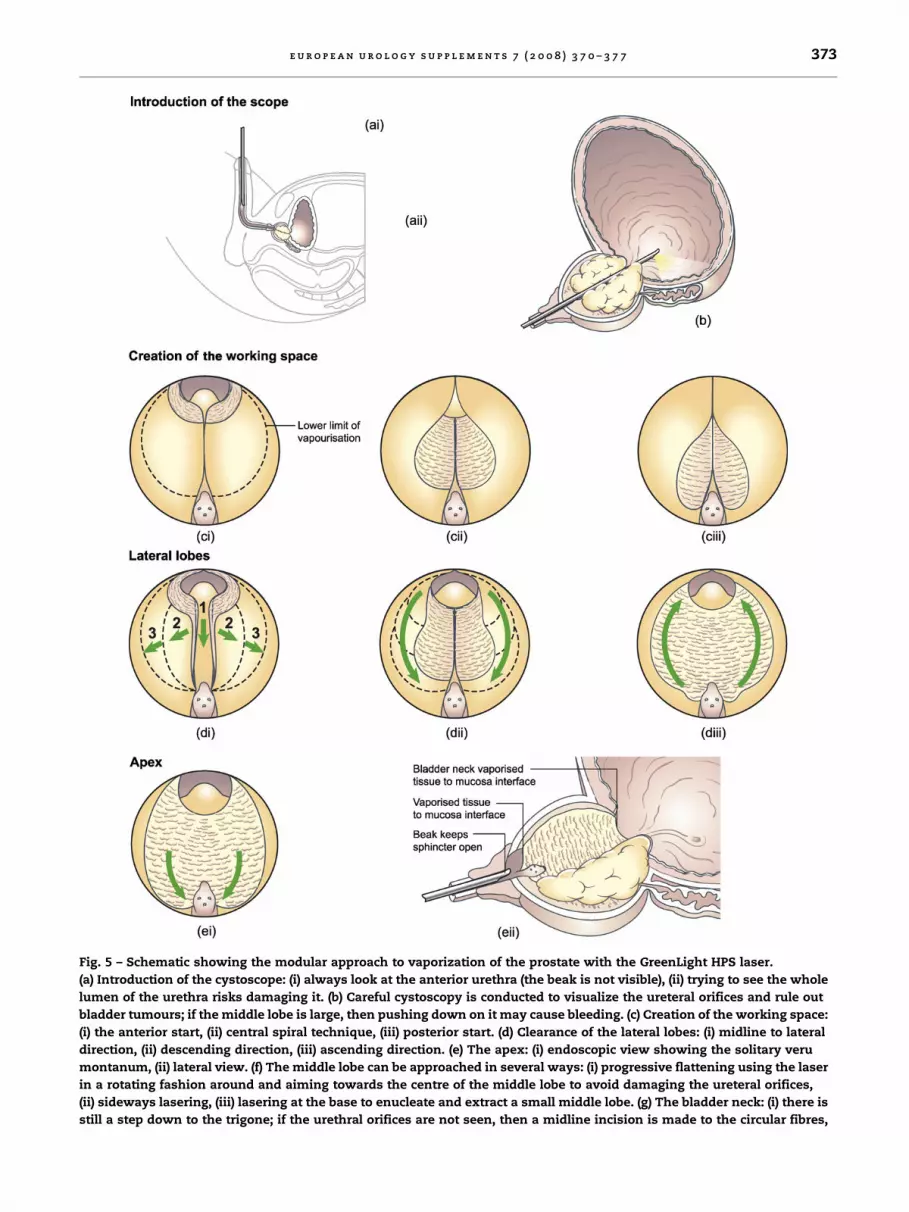
Fig. 5 – Schematic showing the modular approach to vaporization of the prostate with the GreenLight HPS laser.
(a) Introduction of the cystoscope: (i) always look at the anterior urethra (the beak is not visible), (ii) trying to see the whole
lumen of the urethra risks damaging it. (b) Careful cystoscopy is conducted to visualize the ureteral orifices and rule out
bladder tumours; if the middle lobe is large, then pushing down on it may cause bleeding. (c) Creation of the working space:
(i) the anterior start, (ii) central spiral technique, (iii) posterior start. (d) Clearance of the lateral lobes: (i) midline to lateral
direction, (ii) descending direction, (iii) ascending direction. (e) The apex: (i) endoscopic view showing the solitary veru
montanum, (ii) lateral view. (f) The middle lobe can be approached in several ways: (i) progressive flattening using the laser
in a rotating fashion around and aiming towards the centre of the middle lobe to avoid damaging the ureteral orifices,
(ii) sideways lasering, (iii) lasering at the base to enucleate and extract a small middle lobe. (g) The bladder neck: (i) there is
still a step down to the trigone; if the urethral orifices are not seen, then a midline incision is made to the circular fibres,
e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7 373

(ii) urethral orifices are now revealed, (iii) if the urethral orifices are visible, a bilateral incision opens the bladder neck,
(iv) bladder neck still elevated after removal of middle lobe. (h) Final steps: check that no major lumps protrude into the
lumen, no bleeders remain, and the cavity remains open when the bladder is empty. # IGLU Group.
e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7374
3.1. Preliminary cystoscopy
It is essential to introduce the cystoscope carefully,using either an optical obturator that smoothes thecystoscope’s beak or by tilting the cystoscopetowards the 6 o’clock position to avoid the beakcausing urethral or prostatic damage (Fig. 5a, b).Cystoscopy generates information on prostate size,length of the prostatic urethra, the presence of aurethral stricture and allows the ureteral orificesand the bladder neck to be localized. The cystoscopemust not be moved in and out unnecessarily, as thisis likely to cause bleeding; scratching of the prostaticsurface should also be avoided for the same reason.With large prostates or large middle lobes, it may bevery difficult to perform a cystoscopy without
causing bleeding, which might compromise visibil-ity during the subsequent operation. In such cases, itmay be more appropriate to rule out the presence ofany bladder tumours (if clinically relevant) usingflexible cystoscopy before surgery. Any congenitalabnormalities at the trigone (eg, ectopic ureters orduplex systems) should also be ruled out at thisstage.
3.2. Creation of the working space
Creating a working space at the start of theprocedure is imperative, because it allows the fibreto move more easily, thus avoiding contact withtissue and consequent fibre degradation (Fig. 5c).This space will provide good orientation during

e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7 375
surgery and also permit optimal irrigation duringlasing, which is important for visibility. The con-tinuous flow cystoscope through which the laserfibre is inserted can become obstructed with tissueparticles, so it is important to check that irrigationis working and that there is no pooling of irrigant orbladder distension. If particles do obstruct the flow,lasing should cease and the fibre carrier detachedfrom the outer sheath to allow the obstructingparticles to flow out. The use of a continuous flowpump can help regulate the flow and pressure ofirrigation, thus permitting high flow with limitedpressure. Pressure can be increased when needed,such as to improve visibility during bleeding. Theobjective is to maintain a filled but not overdistended bladder during surgery.
There are several approaches to generating theworking channel, including anterior, central spiral,and posterolateral. The anterior approach aims toreduce the chances of bleeding due to friction of thecystoscope on the prostatic urethral mucosa in largeprostates. The central approach is probably easierfor beginners working on small prostates. Theposterolateral approach can be performed respect-ing the bladder neck or middle lobe, or start byvaporizing them down to the circular fibres at thebladder neck. At the end of this module, thereshould be two perfectly defined landmarks: thebladder neck (ie, the transition between coagulatedtissue at the bladder neck and bladder mucosa) andthe lower limit of vaporization (ie, the transitionbetween coagulated tissue of the prostatic mucosaand the urethral sphincteric mucosa at the level ofthe veru montanum).
3.3. Lateral lobes
With two clearly defined landmarks, the bladderneck and the urethral sphincter, this phase of theoperation allows for safe and fast vaporization oftissue within those limits with minimal breaks inlasing (Fig. 5d). The lateral lobes are lasered in asymmetrical manner, layer by layer, with theobjective to obtain a smooth surface. This can beachieved if the laser is fired selectively againstpeaks of tissue on the surface (the mountains),flattening them out, instead of targeting areasalready vaporized (the valleys). One added benefitof the smooth surface is that it is much easier tocontrol any bleeds that may occur than if thesurface were irregular. The objective of this moduleshould be to achieve a concave surface on each side,with as complete a removal of lateral tissue aspossible, as this will facilitate further operativesteps.
3.4. Apex
Lasing at the apex should be very precise in orderto clear carefully the apical tissue and to avoiddamage to the sphincter (Fig. 5e). The objective isfor complete vaporization of paracollicular tissue.Care should be taken with anterior vaporizationat the level of the veru montanum; working withthe fibre far from the cystoscope allows for anteriorvaporization without rotating the cystoscope. Specialcare must be exerted here to avoid sphincterdamage, as the beak of the cystoscope can maintainan open sphincter when the cystoscope is withdrawnand compromise the sphincter localization. At theend of this stage, all apical tissue should havebeen removed and the ‘‘lonely veru’’ appearanceachieved.
3.5. Bladder neck/middle lobe
The bladder neck and middle lobe can be left to theend of the procedure, because it is much easier andsafer to vaporize the middle lobe once the laterallobes have been cleared (Fig. 5f, g). The first objectiveshould be to flatten the middle lobe. This can beaccomplished by firing left to right or right to left, orbetter, by progressively smoothening its contour,making sure that the beam is directed at the centreof the middle lobe, thus avoiding the ureteralorifices. With difficult middle lobes, experiencedusers might find it easier to detach a small middlelobe and push it into the bladder at this stage, but itmust be small enough to allow its extraction with alarge Zero-tip1 stone basket. Enucleation of largemiddle lobes is not recommended. Once the middlelobe has been flattened, the bladder neck might stillbe elevated. At this stage, a bilateral bladder neckincision (5 and 7 o’clock) down to the circular fibresdelineates the desired depth of vaporization. If theureteral orifices are not visualized, it might be saferto first perform a midline 6 o’clock incision untilthey are seen. The tissue between the incisions isvaporized until an unobstructed view of the trigoneis achieved.
3.6. Completion
It is important to empty the bladder to check ifbumps of obstructing tissue protrude into thecollapsed prostatic fossa (Fig. 5h). Any remainingbleeders should be identified and dealt with. Adigital rectal examination can also help to identifyremaining tissue in the posterolateral area. Atcompletion there should be visible a wide, open,concave cavity with a smooth surface (Fig. 6).

Fig. 6 – The final cystoscope image of the apex following
laser vaporization of the prostate.
e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7376
The energy usage perunit volume ofprostateglandcan be determined at the end of the procedure Fig. 7.illustrates the typical energy usage according toprostate volume for a new user of the 120-WGreenLight HPS laser. It should be noted that thetotal energy delivered does not seem to be associatedwith dysuria per se, but instead it is a symptom ofexcessive coagulation. With the 120-W laser and thecollimated beam, vaporization is more efficient andthere is no excess coagulation working at longerdistances of 1–3 mm, so there is less chance ofdysuria than with the 80-W laser and the divergentfibre. We believe that, in principle, it isbetter to obtaina wine-glass-shaped cavity using more energy thanto carve a small channel in the prostate due to theunfounded fear of producing dysuria.
Fig. 7 – Energy usage with the GreenLight HPS 120-W laser
according to preoperative prostate volume.
4. Training recommendations
The training recommendations with the 120-W HPSlaser are dependent on whether the user is anexperienced or inexperienced PVP user. For theexperienced PVP user, one who has completed30 cases, mentoring and proctoring should takeplace on at least one occasion. The inexperiencedPVP user who is a trained urologist should undertakea formal training course, watch several live proce-dures performed by an experienced surgeon, and besubsequently proctored for a minimum of two cases,although this number can vary at the proctor’sdiscretion. Any ongoing training should be con-ducted with the aid of the proctor. There is aperceived need for an international board of certifiedproctors, and this is critical for establishing a highstandard of excellence for this procedure. Werecommend that objective assessment milestonesbe established, as shown in Table 1. Twenty casesare required to be completed before an objectiveassessment can be carried out. These early casesshould involve prostates sized 25–60 ml (assessedusing TRUS), with a preference for smaller prostates.These patients should not be in retention or onanticoagulants or have prostates with large middlelobes.
Experience should be gained on the use of videoendoscopy, as this is the principle visual systemunder which the laser operates. The recommendedstepwise process for lasing is creating a workingchannel, then vaporizing the lateral lobes, apex, andmiddle lobe and bladder neck. We look forward tothe availability of computerized simulators underdevelopment that could greatly aid learning, butthe use of a wet lab, preferably one run by themanufacturer with certification, is an option untilsimulators are available. One possible future devel-opment is official certification for training inconjunction with one of the urological associations,
Table 1 – Objective assessment milestones in thetraining programme for the HPS laser
� Knowledge of
� anatomy
� laser physics
� laser-tissue interactions
� steps of the operation
� Handling of probe and cystoscope
� Management of bleeding
� Management of complications
� Management of damage to the ureteral orifices
� Catheter management
� Management of postoperative complications

e u r o p e a n u r o l o g y s u p p l e m e n t s 7 ( 2 0 0 8 ) 3 7 0 – 3 7 7 377
such as the European Association of Urology or theAmerican Urological Association.
Conflicts of interest
All authors have received honoraria from AMS formeeting attendance and the following authors actas paid consultants for AMS: J. de la Rosette, B. Choi,E. Collins and S. Tabatabaei. AMS have also providedlimited research funding for G. Muir.
References
[1] Hai MA, Malek RS. Photoselective vaporization of the pros-
tate: initial experience with a new 80 W KTP laser for the
treatment of benign prostatic hyperplasia. J Endourol
2003;17:93–6.
[2] Gomez Sancha F, Bachmann A, Choi BB, Tabatabaei S, Muir
GH. Photoselective vaporization of the prostate (Green-
Light PV): lessons learnt after 3500 procedures. Prostate
Cancer Prostatic Dis 2007;10:316–22.





























