Embed Size (px)
Citation preview

a r t i c l e s
Surgical prevention of posteriorcapsule opacificationPart 1: Progress in eliminating this complicationof cataract surgery
David J. Apple, MD, Qun Peng, MD, Nithi Visessook, MD,Liliana Werner, MD, PhD, Suresh K. Pandey, MD,Marcela Escobar-Gomez, MD, Jagat Ram, MD,Stephen B. Whiteside, MD, Robert Schoderbeck, BS,Edgar L. Ready, MS, Alfred Guindi, MD
ABSTRACT
Purpose: To evaluate over almost 2 decades the success of a component of cataractsurgery that represents a critical step in reducing the incidence of posterior capsuleopacification (PCO); namely, the efficacy of cortical cleanup.
Setting: Center for Research on Ocular Therapeutics and Biodevices, Storm Eye Institute,Department of Ophthalmology, Medical University of South Carolina, Charleston, SouthCarolina, USA.
Methods: Accessioned from the early 1980s to 1997, 3320 eyes obtained postmor-tem with posterior chamber intraocular lenses were analyzed with respect to for-mation of a postoperative Soemmering’s ring. This anatomic lesion, the precursor ofclinical PCO, represents an important and measurable indication of the quality ofcortical cleanup. Its formation was documented using Miyake–Apple posterior pho-tographic analysis.
Results: The quality and thoroughness of cortical cleanup and overall effectiveness ineliminating retained and/or regenerating cortical cells, as measured by scoring ofSoemmering’s rings, showed virtually no net change since the early 1980s. Theintensity of Soemmering’s ring was higher in the most recent specimens than inthose in the early 1980s.
Conclusion: The results indicate that renewed attention to cortical cleanup in cataractsurgery is warranted for significant reduction in incidence or the elimination ofPCO. More attention to the hydrodissection (cortical cleaving hydrodissection)step of the procedure is likely a practical, immediately implementable, and in-expensive remedy. J Cataract Refract Surg 2000; 26:180 –187 © 2000 ASCRS andESCRS
© 2000 ASCRS and ESCRS 0886-3350/00/$–see front matterPublished by Elsevier Science Inc. PII S0886-3350(99)00353-3

Posterior capsule opacification (PCO, secondary, orafter cataract) is a significant complication of extra-
capsular cataract extraction (ECCE) including phaco-emulsification. In 1992, we reviewed the literature onthis topic.1 The PCO rate has been documented to be ashigh as 50%.1–5 Progress has been made. However, arecent meta-analysis of published articles on PCO pro-vided pooled estimates of eyes that developed PCO 1, 3,and 5 years postoperatively; it found that the rate ofPCO remains unacceptably high, still greater than 25%in the first 5 years postoperatively.6
There are several increasingly urgent reasons toeradicate PCO. First, modern cataract surgery, withabout 2.5 million cases per year projected by 1999 in theUnited States, has become a procedure after which pa-tients expect perfect visual rehabilitation. Intraocularlens (IOL) implantation is now a refractive procedurethat is often performed in relatively young patients. Insuch cases, secondary complications such as PCO can-not be tolerated. Although pediatric IOL implantationhas become widespread,7–13 it is still characterized by arelatively high PCO incidence. Success in reducingPCO in children will help reduce the need for pri-mary posterior capsulotomy or posterior continuouscurvilinear capsulorhexis and will go far in preventingamblyopia.
Second, there are numerous medical reasons to limitthis complication and thus eliminate the need for sec-ondary neodymium:YAG (Nd:YAG) laser posteriorcapsulotomy. Among the significant complications of
Nd:YAG laser treatment are retinal–vitreal problems,secondary glaucoma, and IOL damage.14–18
Third, there are significant financial reasons to erad-icate this complication. The Nd:YAG laser posteriorcapsulotomy procedure is the second most expensivesurgical cost in the United States Medicare system,second only to the cost of the original cataract/IOLprocedure.
In our 1992 review of PCO,1 we discussed the op-tions to attack this problem including surgical tech-niques. It is now timely to analyze the efficacy of thevarious clinical approaches to prevent PCO.
In the current report, we analyzed autopsy globeswith posterior chamber IOLs (PC IOLs) accessioned inour laboratory since the early 1980s. We concentratedon a complication of cataract surgery that affects theincidence of PCO; namely, the formation of a Soem-mering’s ring.19,20 Cells within a Soemmering’s ring aredirect precursors of PCO. Our analysis provides the op-portunity to quantitatively measure the efficacy andthoroughness of cortical cleanup as the procedure hasevolved over the past 2 decades. Ram et al.21,22 analyzeda second important component of cataract surgery thatinfluences the occurrence of PCO—accuracy of capsular(in-the-bag) haptic fixation.
Materials and MethodsIn this study, 3320 eyes with PC IOLs obtained
postmortem were analyzed at the Center for OcularTherapeutics and Biodevices. These specimens were ac-cessioned between 1985 and 1988, when the center waslocated at the University of Utah, Salt Lake City, andfrom 1988 through 1997, after the center transferred toCharleston, South Carolina.
The globes were received randomly from eye banksnationwide. Because of the time span between IOL im-plantation and death, ranging in most cases from 1 to 5years, most specimens analyzed covered the period fromabout the beginning of serious PC IOL implantationworldwide in the late 1970s up to 1997. The markedincrease in numbers of accessioned globes that occurredin 1997 (Figure 1) is the result of a letter about this studydistributed to all United States eye banks.
All globes were photographed from behind usingthe Miyake–Apple posterior photographic tech-nique.23,24 Each globe was specifically analyzed for
Accepted for publication November 5, 1999.
From the Center for Research on Ocular Therapeutics and Biodevices,Storm Eye Institute, Department of Ophthalmology, Medical Universityof South Carolina, Charleston, South Carolina, USA.
Presented in part at the LXXXII annual meeting of the Oxford Ophthal-mological Congress, Oxford, United Kingdom, July 1997.
Supported in part by an unrestricted grant from Research to PreventBlindness Inc, New York, New York, USA.
None of the authors has a financial or proprietary interest in any productmentioned.
Teddy Redmon provided editorial assistance; Joyce Edmonds, HTL, pro-vided technical assistance.
Reprint requests to David J. Apple, MD, Storm Eye Institute, Depart-ment of Ophthalmology, Medical University of South Carolina, 167Ashley Avenue, PO Box 250676, Charleston, South Carolina 29425-2236, USA.
PREVENTION OF PCO: PROGRESS IN ELIMINATING
J CATARACT REFRACT SURG—VOL 26, FEBRUARY 2000 181

amount of Soemmering’s ring formation, which in es-sence is a measure of retained and regenerative corticalmaterial and cells after ECCE (including phacoemulsi-fication); these cells represent the basic source of mostcases of PCO. The scoring system was a modification ofone devised in the late 1980s.25,26 This analysis con-sisted of scoring 2 factors: the intensity of Soemmering’sring (SRI) and the area (number of involved quadrants)of capsular bag containing Soemmering’s ring (SRA).All eyes were graded from 0 (no retained material) to 4(marked ring) (Table 1).
Figures 2 to 4 are photographs of eyes that areexamples of how the scores of Soemmering’s ring forma-tion were tabulated. These demonstrate the morpho-logic types of profiles used to generate the scores,ranging from 0 to 4.
Figure 2 is an example of score 0–0 (no or veryminimal Soemmering’s ring formation), representing acase that had excellent cortical cleanup.
Figure 3 shows examples of the scoring according toSRI. Each ring covers a constant area (SRA grade 5 4):complete 360 degree coverage over all quadrants. Thevariable is, therefore, the intensity and density of re-tained material, which ranges from 1 to 4.
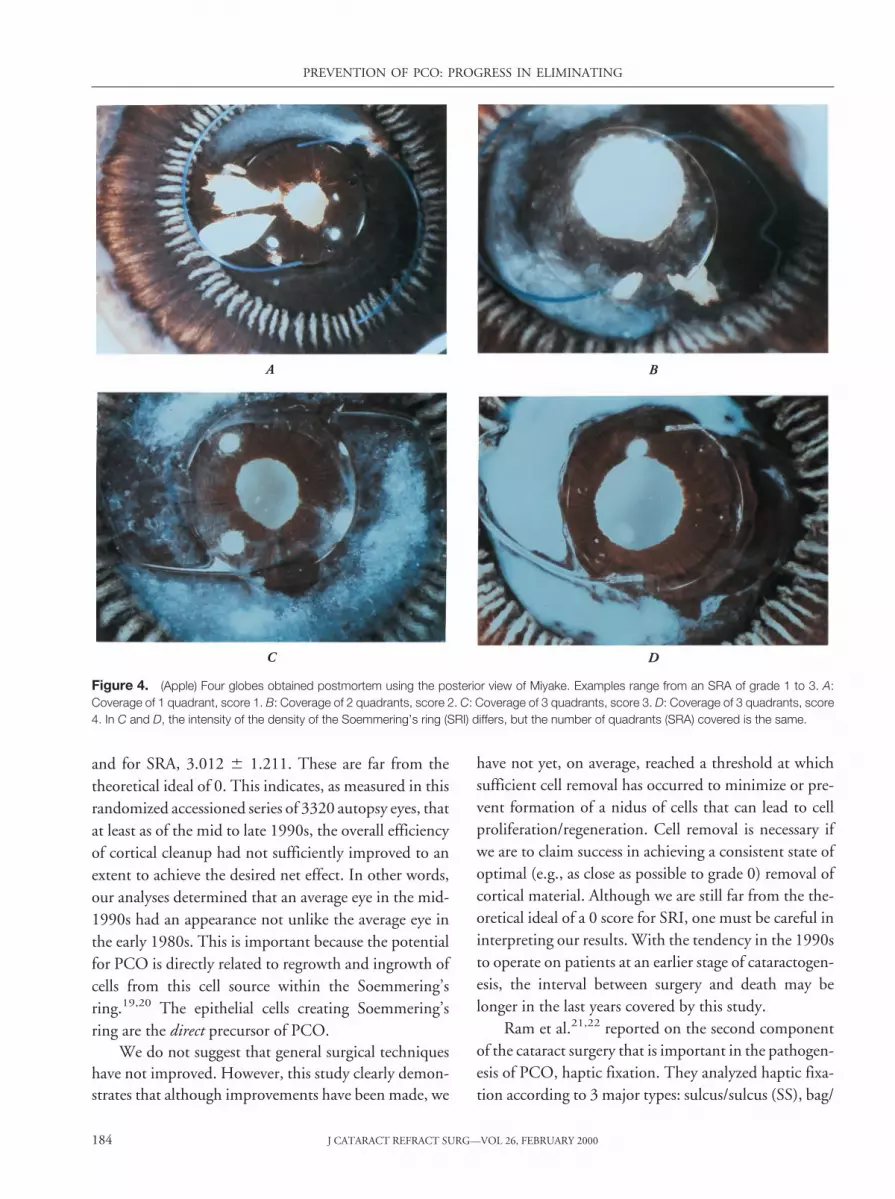
Figure 4 shows examples of Soemmering’s rings cat-egorized by SRA. These range from 1 quadrant (grade 1;Figure 4, A), to 2 quadrants (grade 2; Figure 4, B), to 3quadrants (grade 3, Figure 4, C, D).
The analyses were tabulated and charts prepared todemonstrate the annual and long-term variations in theSRI and SRA over the study. Computer-generated trendlines based on the raw data were also generated. Theanalysis of variance was used to compare the mean scoresof SRI and SRA over the years. A P value less than 0.05was considered statistically significant.
ResultsThe results of scoring for Soemmering’s ring are
shown in Figure 5. The SRI and SRA are results ofspecimens accessioned from 1985 to January 1998,which covers surgical procedures from the late 1970s tothe present. There was a slight decrease in mean SRAduring this period but a marked increase in mean SRI.The differences between the 1985 and 1997 mean SRIs
Figure 1. (Apple) Laboratory accessions of PC IOLs since 1985analyzed in this study (N 5 3320). Note the rapid increase in thenumber of accessions in 1997, in large part attributable to a world-wide notification regarding our interest in autopsy eyes with IOLs aswell as explanted IOLs.
Figure 2. (Apple) Gross photograph from behind (Miyake–Appleview) of 1 IOL in which cortical cleanup was excellent, leaving noresidual Soemmering’s ring. This represents 0 scores on both theSRA and SRI.
Table 1. Scoring system to analyze Soemmering’s ring formation.
Soemmering’s Ring Area(SRA)
Soemmering’s RingIntensity or Density
(SRI)
Grade Analysis Grade Analysis
0 No SR 0 No SR
1 1 quadrant 1 Minimal
2 2 quadrants 2 Mild
3 3 quadrants 3 Moderate
4 4 quadrants 4 Marked
SR 5 Soemmering’s ring
PREVENTION OF PCO: PROGRESS IN ELIMINATING
J CATARACT REFRACT SURG—VOL 26, FEBRUARY 2000182

and SRAs were statistically significant (P , .0001). Ta-ble 2 shows the mean and standard deviations of the SRIand SRA. This can best be appreciated by focusing onthe computer-generated trend lines seen in Figure 5 asbroken lines. Therefore, for practical purposes, the ap-parent effectiveness of surgical cortical cleanup in limit-ing the amount of retained and/or regenerated cortexand cells, as measured by this analysis of Soemmering’srings, has remained essentially unchanged over thisperiod.
DiscussionPosterior capsule opacification is a complication
with a very high rate—often greater than 50%, espe-cially in the 1980s. This corresponds to the early years
of modern ECCE and phacoemulsification.1 How-ever, although excellent clinical and experimental tech-niques are now available to measure and scorePCO,27–30 much of the data on PCO incidence remainanecdotal. Reports have shown that the incidence hasdecreased, but there are no studies to date that scientif-ically evaluate specific surgical techniques that mightexplain the decrease. We recently performed studies onsuch techniques, including cortical cleanup (in this re-port) and IOL fixation.21,22
The data on retained cortical material as measuredby Soemmering’s ring are surprising and disconcerting.Figure 5 shows virtually no decrease in residual Soem-mering’s ring throughout the study. For example, themean score for SRI in 1997 was 2.506 6 1.216 (SD)
Figure 3. (Apple) Four globes obtained postmortem viewed posteriorly (Miyake–Apple technique). In all cases, the area covered (SRA) is aconstant 4 (the ring covers all quadrants or 360 degrees); however, the density of retained material (SRI) ranges from 1 to 4. A: Intensity score is1. B: Intensity score is 2. C: Intensity score is 3. D: Intensity score is 4.
PREVENTION OF PCO: PROGRESS IN ELIMINATING
J CATARACT REFRACT SURG—VOL 26, FEBRUARY 2000 183
and for SRA, 3.012 6 1.211. These are far from thetheoretical ideal of 0. This indicates, as measured in thisrandomized accessioned series of 3320 autopsy eyes, thatat least as of the mid to late 1990s, the overall efficiencyof cortical cleanup had not sufficiently improved to anextent to achieve the desired net effect. In other words,our analyses determined that an average eye in the mid-1990s had an appearance not unlike the average eye inthe early 1980s. This is important because the potentialfor PCO is directly related to regrowth and ingrowth ofcells from this cell source within the Soemmering’sring.19,20 The epithelial cells creating Soemmering’sring are the direct precursor of PCO.
We do not suggest that general surgical techniqueshave not improved. However, this study clearly demon-strates that although improvements have been made, we
have not yet, on average, reached a threshold at whichsufficient cell removal has occurred to minimize or pre-vent formation of a nidus of cells that can lead to cellproliferation/regeneration. Cell removal is necessary ifwe are to claim success in achieving a consistent state ofoptimal (e.g., as close as possible to grade 0) removal ofcortical material. Although we are still far from the the-oretical ideal of a 0 score for SRI, one must be careful ininterpreting our results. With the tendency in the 1990sto operate on patients at an earlier stage of cataractogen-esis, the interval between surgery and death may belonger in the last years covered by this study.
Ram et al.21,22 reported on the second componentof the cataract surgery that is important in the pathogen-esis of PCO, haptic fixation. They analyzed haptic fixa-tion according to 3 major types: sulcus/sulcus (SS), bag/
Figure 4. (Apple) Four globes obtained postmortem using the posterior view of Miyake. Examples range from an SRA of grade 1 to 3. A:Coverage of 1 quadrant, score 1. B: Coverage of 2 quadrants, score 2. C: Coverage of 3 quadrants, score 3. D: Coverage of 3 quadrants, score4. In C and D, the intensity of the density of the Soemmering’s ring (SRI) differs, but the number of quadrants (SRA) covered is the same.
PREVENTION OF PCO: PROGRESS IN ELIMINATING
J CATARACT REFRACT SURG—VOL 26, FEBRUARY 2000184

bag (BB), and asymmetric fixation (bag/sulcus). Theyfound a not-unexpected decrease in ciliary SS fixation,from about 30% in the early 1980 seconds to about 10%as of 1998. Asymmetric fixation decreased from about60% to 30%. An increase in BB fixation was noted, fromless than 10% in the early years of the 1980s to almost60%. Of the 3320 IOLs included in this study, 258 werefoldable designs. Of these, 231 (89.5%) had BB fixa-tion. In summary, Ram et al. found that the quality of
haptic implantation and fixation has improved mark-edly over the period studied. The reason for the markedincrease in BB fixation is the availability of modern smallincision surgical techniques that allow more accuratehaptic placement. This is a positive finding in that it iswell established that this mode of fixation is clearly as-sociated with less PCO,1–3,31–35 largely because it en-hances the barrier effect of the IOL optic.
Cortical cleanup is an important prerequisite fortruly eradicating PCO; thus, this study prompted us torevisit a hypothesis we first entertained in 1989(D.J. Apple, MD, R. Casanova, MD, J. Davison, MD,et al, “Technique of PC IOL Implantation Using aSmall Smooth Circular Continuous Tear Capsuloto-my–Capsulorhexis. A Demonstration Using the Poste-rior Video Technique of Human Cadaver Eyes,” videopresented at the annual meeting of the American Acad-emy of Ophthalmology, New Orleans, Louisiana, USA,October 1989). We noted that enhanced and copioussubcapsular hydrodissection, in association with thethen relatively new procedure of continuous curvilinearcapsulorhexis, may be more useful for lens substanceremoval than previously assumed.
Hydrodissection was first documented by Faust in1984.36 A detailed clinical description was published byFine in 1992,37 who coined the term cortical cleavinghydrodissection. Although commonly done, sufficientcortical cleaving hydrodissection remains underem-phasized and underrated by most surgeons. It is oftenperformed as a rote maneuver that assists in the phaco-emulsification procedure and to enhance general safety,but not with the full intention of decreasing PCO. Wepostulate that this step, as performed in many cases, is aweak link in the cleanup procedure. Thus, we performedan experimental study regarding hydrodissection interms of efficacy and efficiency of removal of corticalmaterial and cells.38
Finally, the concept of the IOL’s barrier effect inreducing ingrowth of cells over the visual axis after sur-gery has been long hypothesized but poorly understood.We studied the nature of the barrier effect in detail in ahistopathological study of another series of postmortemeyes with PC IOLs.39
References1. Apple DJ, Solomon DK, Tetz MR, et al. Posterior cap-
sule opacification. Surv Ophthalmol 1992; 37:73–116
Figure 5. (Apple) Soemmering’s ring plotted for specimens acces-sioned between 1984 and January 1988 showing the intensity (SRI)and area (SRA). The curved lines represent the plot of the raw data.Each broken line represents the computer-generated trend line anal-ysis of each curve.
Table 2. Scoring of SRI and SRA in human globes obtained post-morten (N 5 3320 eyes).
YearNumber
of Globes
Mean 6 SD
SRI SRA
1985 47 1.489 6 1.013 3.085 6 1.546
1986 97 2.134 6 0.985 3.701 6 0.738
1987 208 2.212 6 1.160 3.534 6 1.002
1988 126 1.817 6 1.339 2.762 6 1.699
1989 122 1.721 6 1.232 2.861 6 1.606
1990 155 1.665 6 1.072 2.877 6 1.413
1991 101 1.960 6 1.170 3.149 6 1.493
1992 168 1.893 6 1.128 3.071 6 1.424
1993 182 1.929 6 1.145 2.912 6 1.584
1994 414 2.060 6 1.121 2.836 6 1.355
1995 239 1.992 6 1.336 2.594 6 1.681
1996 437 2.300 6 1.182 2.906 6 1.355
1997 1024 2.506 6 1.216 3.012 6 1.211
SRI 5 Soemmering’s ring intensity (0–4); SRA 5 Soemmering’s ringarea (0–4 quadrants)
PREVENTION OF PCO: PROGRESS IN ELIMINATING
J CATARACT REFRACT SURG—VOL 26, FEBRUARY 2000 185
2. Apple DJ, Kincaid MC, Mamalis N, Olson RJ. Intraoc-ular Lenses; Evolution, Designs, Complications, and Pa-thology. Baltimore, MD, Williams & Wilkins, 1989;317–361
3. Apple DJ, Rabb MF. Clinical Applications and Self-As-sessment, 5th ed. St Louis, MO, Mosby Year-Book,1998; 117–204
4. Dana MR, Chatzistefanou K, Schaumberg DA, FosterCS. Posterior capsule opacification after cataract sur-gery in patients with uveitis. Ophthalmology 1997;104:1387–1393; discussion by RE Smith, 1393–1394
5. Sourdille P. Overview of posterior capsule opacification(editorial). J Cataract Refract Surg 1997; 23:1431–1432
6. Schaumberg DA, Dana M, Christen WG, Glynn RJ. Asystematic overview of the incidence of posterior capsuleopacification. Ophthalmology 1998; 105:1213–1221
7. Wilson ME, Apple DJ, Bluestein EC, Wang X-H. In-traocular lenses for pediatric implantation: biomaterials,designs, and sizing. J Cataract Refract Surg 1994; 20:584–591
8. Brady KM, Atkinson CS, Kilty LA, Hiles DA. Cataractsurgery and intraocular lens implantation in children.Am J Ophthalmol 1995; 120:1–9
9. Wilson ME. Intraocular lens implantation: has it becomethe standard of care for children? (editorial) Ophthalmol-ogy 1996; 103:1719–1720
10. Gimbel HV, Basti S, Ferensowicz M, Debroff BM.Results of bilateral cataract extraction with posteriorchamber intraocular lens implantation in children.Ophthalmology 1997; 104:1737–1743
11. Gimbel HV. Posterior continuous curvilinear capsulo-rhexis and optic capture of the intraocular lens to preventsecondary opacification in pediatric cataract surgery.J Cataract Refract Surg 1997; 23:652–656
12. Vasavada A, Desai J. Primary posterior capsulorhexiswith and without anterior vitrectomy in congenital cata-racts. J Cataract Refract Surg 1997; 23:645–651
13. Zwaan J, Mullaney PB, Awad A, et al. Pediatric intraoc-ular lens implantation; surgical results and complicationsin more than 300 patients. Ophthalmology 1998; 105:112–118; discussion by RM Robb, 118–119
14. Javitt JC, Tielsch JM, Canner JK, et al. National out-comes of cataract extraction. Increased risk of retinalcomplications associated with Nd:YAG laser capsulot-omy. Ophthalmology 1992; 99:1487–1498
15. Newland TJ, Auffarth GU, Wesendahl TA, Apple DJ.Neodymium:YAG laser damage on silicone intraocularlenses; a comparison of lesions on explanted lenses andexperimentally produced lesions. J Cataract Refract Surg1994; 20:527–533
16. Holweger RR, Marefat B. Intraocular pressure changeafter neodymium:YAG capsulotomy. J Cataract RefractSurg 1997; 23:115–121
17. Ladas ID, Baltatzis S, Panagiotidis D, et al. Topical 2.0%
dorzolamide vs. oral acetazolamide for prevention of in-traocular pressure rise after neodymium:YAG laser pos-terior capsulotomy. Arch Ophthalmol 1997; 115:1241–1244
18. Kato K, Kurosaka D, Bissen-Miyajima H, et al. Elschnigpearl formation along the posterior capsulotomy marginafter neodymium:YAG capsulotomy. J Cataract RefractSurg 1997; 23:1556–1560
19. Soemmerring DW. Beobachtungen uber die organischenVeranderungen im Auge mit Staaroperationen. Frank-furt/Main, Wesche, 1828
20. Auffarth GU, Beischel CJ, Wesendahl TA, Apple DJ.Soemmering’s Ring Bildung nach Kataraktoperationund HKL Implantation: Eine Studie von 827 Autop-sieaugen (abstract). Klin Monatsbl Augenheilkd 1995;206(suppl):1–12
21. Ram J, Apple DJ, Peng Q, et al. Update on fixation ofrigid and foldable posterior chamber intraocular lenses.Part I. Elimination of fixation-induced decentration toachieve precise optical correction and visual rehabilita-tion. Ophthalmology 1999; 106:883–890
22. Ram J, Apple DJ, Peng Q, et al. Update on fixation ofrigid and foldable posterior chamber intraocular lenses.Part II. Choosing the correct haptic fixation and IOLdesigns to help eradicate posterior capsule opacification.Ophthalmology 1999; 106:891–900
23. Miyake K, Miyake C. Intraoperative posterior chamberlens haptic fixation in the human cadaver eye. Ophthal-mic Surg 1985; 16:230–236
24. Apple DJ, Lim ES, Morgan RC, et al. Preparation andstudy of human eyes obtained postmortem with theMiyake posterior photographic technique. Ophthal-mology 1990; 97:810 – 816
25. Hansen SO, Solomon KD, McKnight GT, et al. Poste-rior capsular opacification and intraocular lens decentra-tion. Part I: comparison of various posterior chamber lensdesigns implanted in the rabbit model. J Cataract RefractSurg 1988; 14:605–613
26. Tetz MR, O’Morchoe DJC, Gwin TD, et al. Posteriorcapsular opacification and intraocular lens decentration.Part II: experimental findings on a prototype circularintraocular lens design. J Cataract Refract Surg 1988;14:614–623
27. Lundgren B, Jonsson E, Rolfsen W. Secondary cataract.An in vivo model for studies on secondary cataract inrabbits. Acta Ophthalmol 1992; Suppl 205:25–28
28. Pande MV, Ursell PG, Spalton DJ, et al. High-resolutiondigital retroillumination imaging of the posterior lenscapsule after cataract surgery. J Cataract Refract Surg1997; 23:1521–1527
29. Tetz MR, Auffarth GU, Sperker M, et al. Photo-graphic image analysis system of posterior capsuleopacification. J Cataract Refract Surg 1997; 23:1515–1520
PREVENTION OF PCO: PROGRESS IN ELIMINATING
J CATARACT REFRACT SURG—VOL 26, FEBRUARY 2000186

30. Hayashi K, Hayashi H, Nakao F, Hayashi F. In vivoquantitative measurement of posterior capsule opacifica-tion after extracapsular cataract surgery. Am J Ophthal-mol 1998; 125:837–843
31. Apple DJ, Park SB, Merkley KH, et al. Posterior chamberintraocular lenses as in a series of 75 autopsy eyes. Part I.Loop location. J Cataract Refract Surg 1986; 12:358–362
32. Hansen SO, Tetz MR, Solomon KD, et al. Decentrationof flexible loop posterior chamber intraocular lenses in aseries of 222 postmortem eyes. Ophthalmology 1988;95:344–349
33. Apple DJ, Mamalis N, Loftfield K, et al. Complicationsof intraocular lenses. A historical and histopathologicalreview. Surv Ophthalmol 1984; 29:1–54
34. Apple DJ, Reidy JJ, Googe JM, et al. A comparison ofciliary sulcus and capsular bag fixation of posterior cham-ber intraocular lenses. Am Intra-Ocular Implant Soc J1985; 11:44–63
35. Vilhjalmsson GA, Lucas BC. Zur Nachstarinzidenz
sulkus-versus kapselsackfixierter Hinterkammerlinsen.Klin Monatsbl Augenheilkd 1992; 200:167–170
36. Faust KJ. Hydrodissection of soft nuclei. Am Intra-Ocu-lar Implant Soc J 1984; 10:75–77
37. Fine IH. Cortical cleaving hydrodissection. J CataractRefract Surg 1992; 18:508–512
38. Peng Q, Apple DJ, Visessook N, et al. Surgical preven-tion of posterior capsule opacification. Part 2: enhance-ment of cortical cleanup by focusing on hydrodissection.J Cataract Refract Surg 2000;26:189–197
39. Peng Q, Visessook N, Apple DJ, et al. Surgical preven-tion of posterior capsule opacification. Part 3: intraocularlens optic barrier effect as a second line of defense. J Cat-aract Refract Surg 2000; 26:198–213
Although the spelling of Soemmerring with two r’s is the correct Germanspelling,19 most authors in the English-speaking world have adopted thespelling with one r, and we have conformed to this usage.
PREVENTION OF PCO: PROGRESS IN ELIMINATING
J CATARACT REFRACT SURG—VOL 26, FEBRUARY 2000 187





























