Embed Size (px)
Citation preview
Lens
An In Vitro Evaluation of the Anew Zephyr Open-Bag IOLin the Prevention of Posterior Capsule Opacification Usinga Human Capsular Bag Model
Julie A. Eldred,1 David J. Spalton,1,2 and I. Michael Wormstone1
1School of Biological Sciences, University of East Anglia, Norwich, United Kingdom2King Edward VII Hospital, London, United Kingdom
Correspondence: I. Michael Worm-stone, School of Biological Sciences,University of East Anglia, Norwich,UK NR4 7TJ;[email protected].
Submitted: July 23, 2014Accepted: September 8, 2014
Citation: Eldred JA, Spalton DJ,Wormstone IM. An in vitro evaluationof the Anew Zephyr open-bag IOL inthe prevention of posterior capsuleopacification using a human capsularbag model. Invest Ophthalmol Vis Sci.2014;55:7057–7064. DOI:10.1167/iovs.14-15302
PURPOSE. During cataract surgery an IOL is placed within the capsular bag. Clinical studiesshow that IOLs with a square edge profile and complete contact between the IOL and theanterior capsule (AC) are currently the best way to prevent posterior capsule opacification(PCO). This has been challenged by recent clinical and experimental observations, whichsuggest that if the capsular bag is kept open with separation of contact between the AC andposterior capsule (PC) by an ‘‘open-bag device’’ PCO is dramatically reduced. Therefore, thecurrent study set out to evaluate the putative merits of an open-bag IOL (Anew Zephyr) in ahuman capsular bag model.
METHODS. An in vitro organ culture model using the bag–zonular–ciliary body complexisolated from fellow human donor eyes was prepared. A capsulorhexis and lens extractionwere performed, and an Alcon Acrysof IOL or Anew Zephyr IOL implanted. Preparationswere secured by pinning the ciliary body to a silicone ring and maintained in 6 mL Eagle’sminimum essential medium (EMEM) or EMEM supplemented with 2% vol/vol human serum(HS) and 10 ng/mL TGF-b2 for 28 days. Cell growth and capsular modifications weremonitored with phase-contrast and modified dark-field microscopy.
RESULTS. In serum-free EMEM culture conditions, cells were observed growing onto the PC ofpreparations implanted with an Anew Zephyr IOL, but this was retarded relative toobservations in match-paired capsular bags implanted with an Alcon Acrysof IOL. In the caseof cultures maintained in 2% HS-EMEM plus TGF-b2, the movement on to the PC was againdelayed with the presence of an Anew Zephyr IOL. Differences in the degree of growth on thePC and matrix modifications were apparent with the different donors, but in each case thematch-paired Alcon Acrysof implanted bag exhibited significantly greater coverage andmodification of the capsule.
CONCLUSIONS. The Anew Zephyr open-bag IOL performs consistently better than the AlconAcrysof IOL in the human capsular bag model. We propose that the benefits observed withthe Anew Zephyr result from a reduction in growth factor levels available within the capsularbag and a barrier function imposed by the ring haptic.
Keywords: intraocular lens, posterior capsule opacification, cataract, human, in vitro, model
Cataract is a consequence of the ageing of the lens and is themajor priority in the global initiative to eliminate avoidable
blindness by the year 2020.1 At present, the only means oftreating cataract is by surgery, which initially restores high-quality vision and this is currently the most performedoperation in developed countries. Unfortunately, posteriorcapsule opacification (PCO), the most common complicationof cataract surgery develops in a significant proportion ofpatients to such an extent that secondary visual loss occurs.2
A modern cataract operation generates a capsular bag (thebasement membrane of the lens), which comprises a propor-tion of the anterior and the entire PC.2 The bag remains in situand partitions the aqueous and vitreous humors, and usuallyhouses the IOL. Following surgery, light can pass freely alongthe visual axis through the transparent IOL and thin acellularPC. However, lens epithelial cells (LECs) remain at the time ofsurgery and recolonize denuded regions of the anterior capsule
(AC), and most importantly colonize the previously cell-freePC.2 Subsequent changes to the matrix and cell organizationresult in light scatter. If these changes are sufficiently severe,vision can become seriously impaired and corrective neodym-ium-doped yttrium aluminium garnet (Nd:YAG) laser surgery isrequired to remove the opacified PC,2 which is both expensive,logistically difficult with elderly patients, and not withoutmedical risk.3
There are a number of factors that can increase theincidence of PCO, for example, young age, intraocularinflammation, and surgical factors.2 However, studies haveshown that PCO rates can be diminished by improved IOLdesign,4,5 especially a square edge profile, which produces abarrier to LEC migration. However, in spite of these improve-ments approximately 10% of patients still require a Nd:YAGlaser capsulotomy within 2 years of surgery, which places astrain on healthcare resources, medical time, and the quality of
Copyright 2014 The Association for Research in Vision and Ophthalmology, Inc.
www.iovs.org j ISSN: 1552-5783 7057

a patient’s life.6 These problems are exacerbated in pediatricpatients, when cataract surgery is performed on patients withocular inflammation or following insertion of multifocal IOLsthat have a reduced barrier function. Therefore, PCO impact isa socioeconomic, geographic, and ageing problem, and novelapproaches in PCO prevention need to be developed.
At present, it is widely considered that an IOL with a squareedge profile and a capsulorhexis completely in contact withthe anterior surface offers the best PCO prevention, but thishas been challenged by clinical and experimental observationsin rabbit and monkey eyes, which demonstrate that if the ACand PC components are kept apart there is a profoundreduction in PCO.7–9 Similar results in rabbit eyes have beenshown with a novel disc design of IOL, which keeps the bagopen.10 This animal work has been corroborated by clinicalobservations with the Synchrony dual optic IOL (Abott MedicalOptics, Santa Ana, CA, USA), which was developed as anaccommodating IOL and consists of two linked IOLs implantedin the capsular bag which, by coincidence, keep the capsuleopen; an impressive observation has been that these eyes haveextremely low PCO rates. Further support in human eyescomes from a recent Japanese study using a ring device toseparate the capsules showing a consistent reduction in PCOwith up to 7 years post surgery.11 In summary, there is now asubstantial body of evidence, which shows that various devicesthat keep the capsular bag open, limit PCO. Anew Optics(Bristol, TN, USA) has developed a novel disc design of IOL,
which keeps the bag open and using rabbits as a test system,this has proven to be successful in reducing PCO forma-tion.10,12 it is now important to understand the relationshipbetween the IOL and human lens capsule and its associatedcells. Therefore, in the current study, we used an in vitrohuman capsular bag system to evaluate the ability of the AnewOptics Zephyr IOL in the prevention of PCO.
METHODS
All reagents were from Sigma (Poole, Dorset, UK) unlessotherwise stated.
Capsular Bag Preparation
Cataract surgery generates a clear capsular bag, and it is thisprocedure that has been transferred from the operating theaterto the laboratory. The model previously described by Liu etal.13 and developed by Cleary et al.14 was employed. Pairs ofdonor eyes (corneas previously removed for eye banking;Table) were obtained within 48-hours post mortem withnational research ethics committee approval and used inaccordance with the tenets of the Declaration of Helsinki. Theprocedure involves washing the lens briefly with Eagle’sminimum essential medium (EMEM) before creating a smallrhexis and removing the central lens mass from donor globesto leave a capsular bag for implantation of the IOL. Thecapsular bag containing the IOL was removed from the eyefollowing careful separation from the ciliary body andtransferred to a tissue-culture dish. The ciliary body wassecured to a silicone ring using entomologic pins. Using thismethod, the lens capsule remains intact and the capsular bagphysiologically suspended from zonules. As a control IOL wetested an Alcon Acrysof single piece IOL, which is recognizedto have excellent performance in suppressing PCO and is oftenregarded as a gold standard2 (Fig. 1A). The test IOL used wasthe Anew Zephyr open-bag design. This is an IOL with acircular fenestrated 3608 ring haptic connected by spokes tothe optic. The design of the ring haptic separates and preventsadhesion of the ACs and PCs and allows aqueous to percolateinto the equatorial bag10,12 (Fig. 1B). Capsular bag preparationswere maintained in nonsupplemented (serum-free; SF) EMEMor EMEM supplemented with 2% human serum (HS), 10 ng/mLTGF-b2 and 50 lg/mL gentamicin for a 28-day period. Ongoing
TABLE. Relevant Information Associated With Donors Used in ThisStudy
Donor
Age Sex Cause of Death Culture Conditions
79 Male Cerebrovascular
accident
SF EMEM
56 Female Pneumonia SF EMEM
61 Male Prostate cancer SF EMEM
84 Male Unknown 2% HS þ 10 ng/mL TGF-b53 Male Unknown 2% HS þ 10 ng/mL TGF-b63 Male Bowel cancer 2% HS þ 10 ng/mL TGF-b
SF, serum-free.
FIGURE 1. A schematic diagram illustrating the position of (A) a conventional square edge IOL and (B) the open-bag Anew Zephyr IOL within thecapsular bag and how their physical properties could provide a barrier to cell movement.
Open-Bag IOLs Reduce PCO IOVS j November 2014 j Vol. 55 j No. 11 j 7058
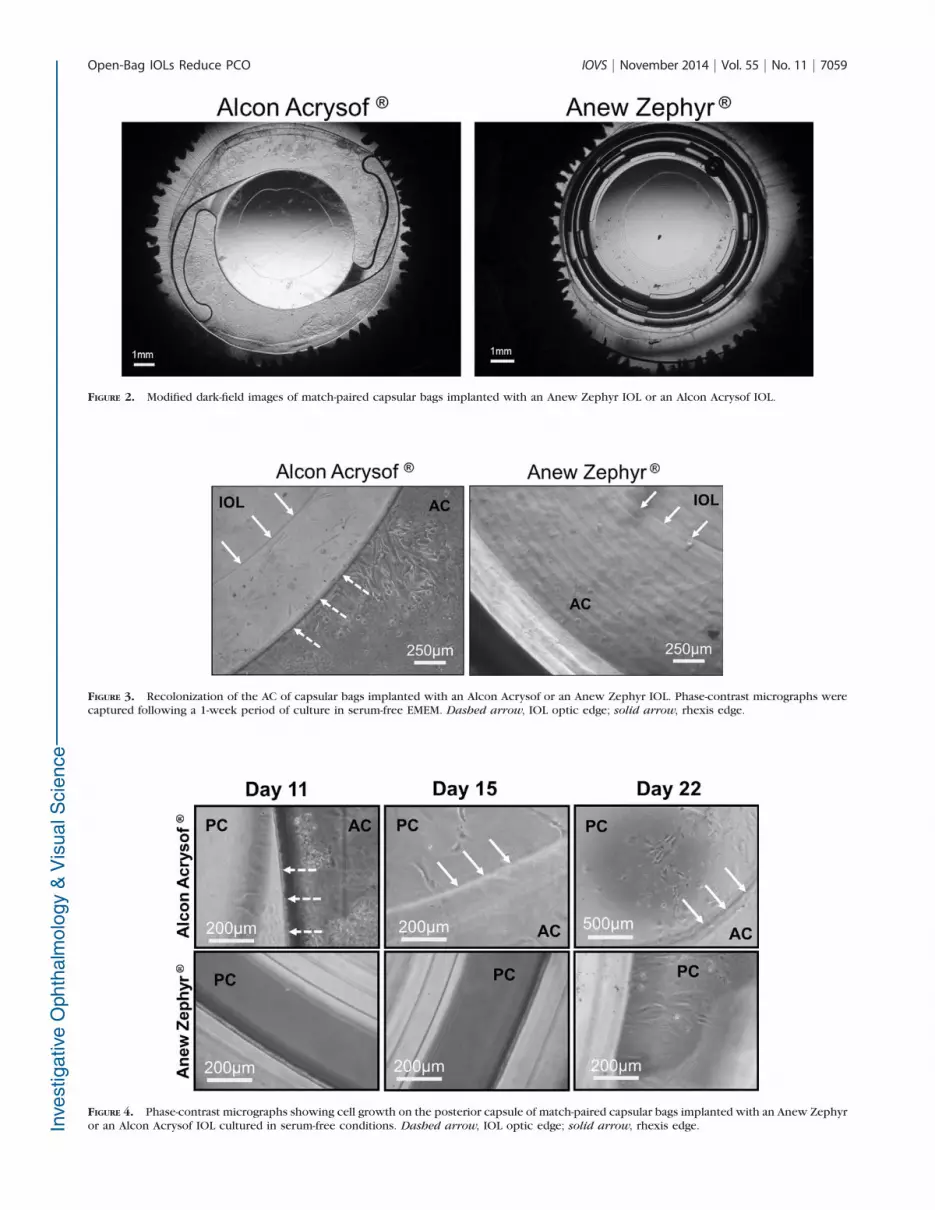
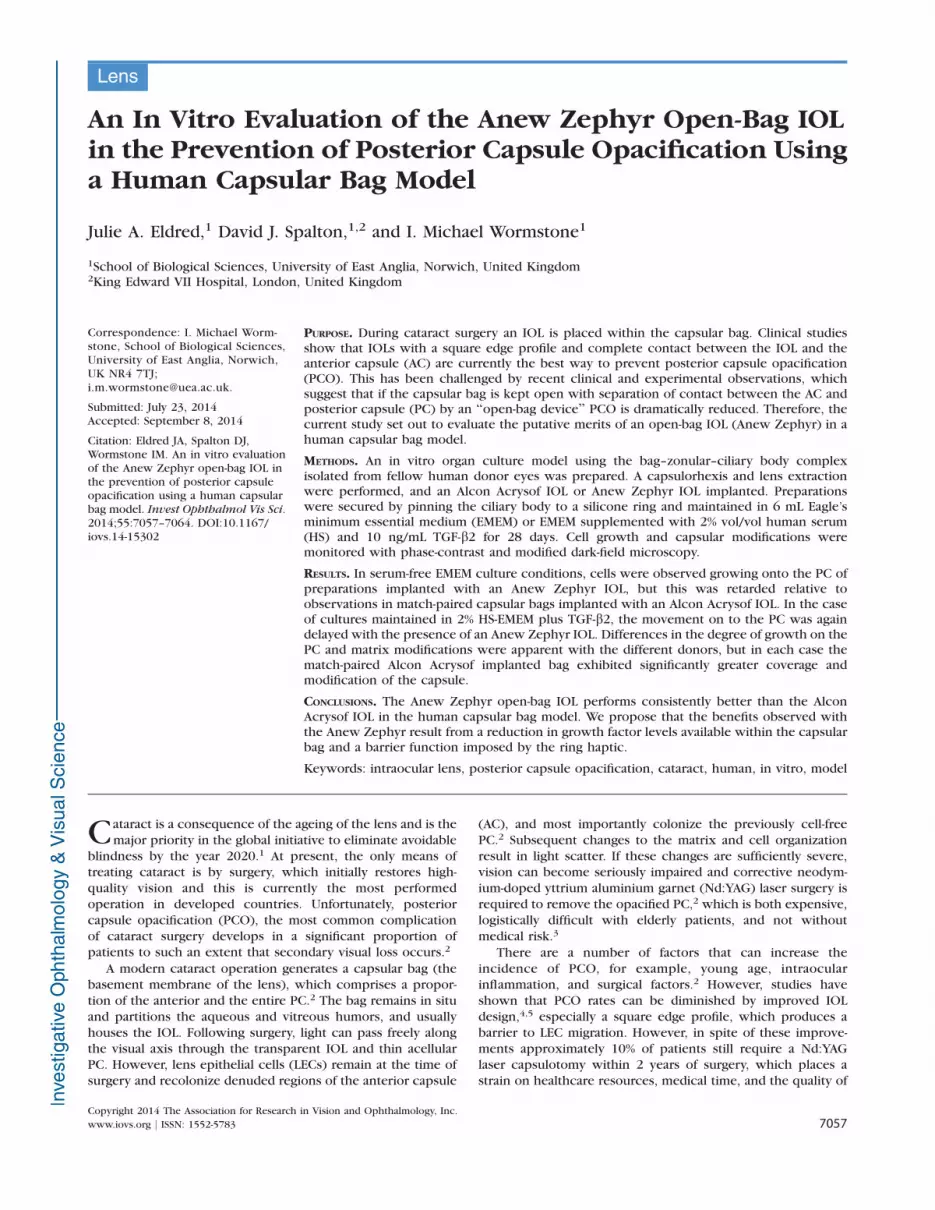
FIGURE 2. Modified dark-field images of match-paired capsular bags implanted with an Anew Zephyr IOL or an Alcon Acrysof IOL.
FIGURE 3. Recolonization of the AC of capsular bags implanted with an Alcon Acrysof or an Anew Zephyr IOL. Phase-contrast micrographs werecaptured following a 1-week period of culture in serum-free EMEM. Dashed arrow, IOL optic edge; solid arrow, rhexis edge.
FIGURE 4. Phase-contrast micrographs showing cell growth on the posterior capsule of match-paired capsular bags implanted with an Anew Zephyror an Alcon Acrysof IOL cultured in serum-free conditions. Dashed arrow, IOL optic edge; solid arrow, rhexis edge.
Open-Bag IOLs Reduce PCO IOVS j November 2014 j Vol. 55 j No. 11 j 7059

observations were captured using phase-contrast microscopy.Cell coverage of the central PC was determined usingImageJ1.45s analysis software (http://imagej.nih.gov/ij/; pro-vided in the public domain by the National Institutes of Health,Bethesda, MD, USA). To establish a measure of light scatter inthe central PC, Image Pro Premier software (Media Cybernet-ics, Warrendale, PA, USA) was employed using a methodadapted from Wormstone et al.15 In this present study, imageswere placed through a single pass of a Laplacian filter, whichidentifies light scattering regions. These regions appear bright,and thus have a high intensity per pixel. The mean intensity ofall pixels within the rhexis region was determined. Capsularbags without cells present on the PC were used to establishbackground levels, which was subtracted from test values.
RESULTS
Both Anew Zephyr and Alcon Acrysof IOLs were successfullyhoused within the capsular bag of each donor pair (Fig. 2). Inthe case of the Alcon Acrysof IOL, the capsulorhexis edge layon the anterior optic in each preparation; with the AnewZephyr IOL, the ACs and PCs were separated. It should bepointed out that the relative number of cells remaining aftersurgery is similar in both match-paired bags from a singledonor; however, variation in cell number following surgerybetween donors does occur. This is reflective of the variationalso seen in cataract patients. Recolonization of the AC withinboth bags of a donor matched-pair also occurs in a similarfashion, therefore the differences between the matched-pairedbags are largely associated with events on the PC.
The first series of capsular bags employed to compare theIOLs was maintained in serum-free EMEM, to test the influenceof IOL design on LEC behavior under baseline conditions.Following 1 week of culture, cells could be clearly seenrecolonizing denuded regions of the AC of capsular bags
implanted with an Alcon Acrysof IOL (Fig. 3) or an AnewZephyr IOL (Fig. 3). Observation of cell growth on theperipheral PC can be difficult in capsular bags implanted withthe Alcon Acrysof IOL because of the close proximity of theAC; however, cells could be observed growing beyond theedge of the optic body within the first 2 weeks of culture. Atcomparable times, match-paired cultures implanted with anAnew Zephyr IOL exhibited a marked reduction in growthacross the PC, which is illustrated in Figure 4. Cells continuedto grow throughout culture in all preparations; however, theextent of coverage at a given time-point was always greater inthe presence of an Alcon Acrysof IOL. At end point (day 28),cells could be observed on the PC beyond the capsulorhexismargin in all preparations. Mean percent coverage of thecentral PC with an Alcon Acrysof IOL implanted was 39.53 618.93% and with an Anew Zephyr IOL 9.36 6 7.87% (Fig. 5B).Due to general differences in the scale of wound-healingresponse between donors this was not a significant difference,but a common pattern was observed with each donor, suchthat capsular bags implanted with the Anew Zephyr IOLconsistently had less coverage on the central PC at day 28 thanwith an Alcon Acrysof implanted. Match-paired comparison ofcoverage at day 28 showed a significant reduction (84.44%) incoverage with an Anew Zephyr IOL relative to that seen withthe Alcon Acrysof implanted (Fig. 5C). It should also be notedthat coverage was often asymmetric regardless of which IOLwas implanted, suggesting a point of weakness in the barrierfunction of both IOLs.
A second series of match-paired capsular bag experimentswas maintained in 2% HS-EMEM and 10 ng/mL TGF-b2 toprovide comparison of IOLs in conditions known to drivegrowth and contraction.16 In these conditions, dramaticchanges were seen, such that in preparations implanted withan Acrysof or Anew Zephyr IOL cells covered the entire AC andtheir morphology was fibroblastic in appearance (Fig. 6). Inaddition matrix contraction (wrinkling) was evident in the
FIGURE 5. The Anew Zephyr IOL reduces cell coverage of the PC in serum-free conditions over a 1-month culture period. (A) Modified dark-fieldmicrographs of capsular bags captured at end point following removal of the respective IOL and fixation. The modified dark-field images present theAC, capsulorhexis (arrowed), and PC. In the case of the Anew Zephyr IOL implanted capsular bag, a section of the AC has been folded back toexpose the underlying cells on the PC; for the purpose of clarity, the solid white line indicates the natural location of the rhexis edge. (B) Pooleddata showing coverage of the central PC in the presence of an Alcon Acrysof or Anew Zephyr IOL. (C) Pooled data showing coverage in AnewZephyr implanted capsular bags relative to their match-paired Alcon Acrysof implanted counterpart. Data are presented as mean 6 SEM (n ¼ 3).*Indicates a significant difference between groups (Student’s t-test; P � 0.05).
Open-Bag IOLs Reduce PCO IOVS j November 2014 j Vol. 55 j No. 11 j 7060

peripheral regions of capsular bags. The coverage observed on
the PC at specific time-points varied between donors; however,it was consistently observed that coverage of the PC was
retarded in the presence of the Anew Zephyr IOL (Fig. 7). Forexample, at Day 13, cells were observed below the Alcon
Acrysof optic in all cases, but no cells were observed in the
fenestrations (i.e., the peripheral PC at this time-point). At end-point this order was still apparent, but not significantly
different. However, the degree of light scatter observed in
the central PC, resulting from cell and matrix modificationsignificantly differed between the two implants, such that
capsular bags implanted with an Acrysof IOL presented more
than double the level of light-scatter observed than their AnewZephyr IOL implanted counterparts (Fig. 8). Further assess-
ment of the capsular bags was made following IOL removal.
This was achieved by creating radial incisions in the AC andfolding it back, such that the central and peripheral PC is
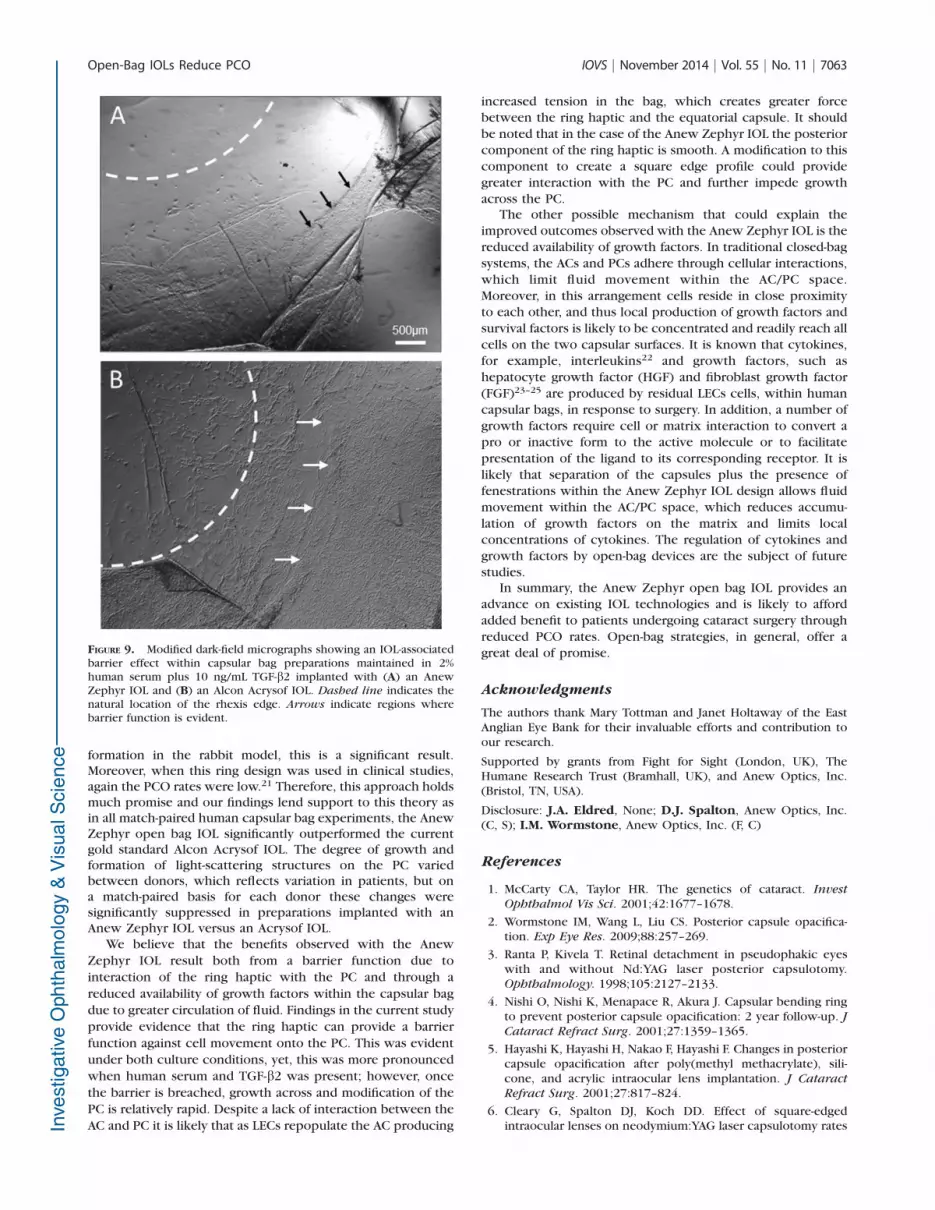
exposed; this allowed greater evaluation of cell distribution inthis region and assessment of IOL barrier function. There was
evidence of a barrier effect in association with both IOLs (Fig.
9). At day 28, there is evidence that this has been breached inplaces, however, a better retention of a barrier was observed
with the Anew Zephyr IOL (Fig. 9).
DISCUSSION
Posterior capsule opacification is associated with a progressivedeterioration in vision and its management adds substantialcosts to healthcare providers, therefore, improved manage-ment of PCO is an important healthcare need.2 A number ofapproaches to resolve PCO are being developed that target thebiological mechanisms of the condition, such as preventingLEC migration/proliferation, transdifferentiation to myofibro-blasts, matrix contraction, and in some cases annihilation ofthe LEC population.2 In all cases the objective is to retain aclear and uninterrupted passage of light along the visual axis.Biological processes face clinical and regulatory issues and atpresent these approaches have yet to reach the clinic, and thusIOL design remains the leading approach in the management ofPCO. Perhaps, the most significant advance in the last 20 yearshas been the incorporation of a square edge on the IOL optic,17
which through interaction with the lens capsule forms a‘‘barrier’’ to the cells and consequently impedes migrationonto the central PC. This effect is not limited to material18 andthe sharpness of the IOL posterior edge appears to be the mostimportant factor.19 The barrier effect is believed to be optimalwhen the capsulorhexis is fully seated on the anterior opticsurface.20 As the anterior and PCs come in contact the cellular
FIGURE 6. Recolonization of the AC of capsular bags implanted with an Alcon Acrysof or an Anew Zephyr IOL, following a 1-week period of culturein EMEM supplemented with 2% human serum plus 10 ng/mL TGFb2; solid arrow, rhexis edge.
FIGURE 7. Phase-contrast micrographs showing cell growth on the PC of match-paired capsular bags implanted with an Anew Zephyr or an AlconAcrysof IOL cultured in 2% human serum plus 10 ng/mL TGF-b2. Dashed arrow, IOL optic edge; solid arrow, rhexis edge.
Open-Bag IOLs Reduce PCO IOVS j November 2014 j Vol. 55 j No. 11 j 7061

interactions effectively ‘‘shrink-wrap’’ the capsular bag around
the IOL, which pushes the IOL against the PC creating a
pressure point at the square edge against the capsule, and thus
a mechanical barrier to LEC migration. However, while a
significant improvement on previous designs, these square
edge IOLs retard the progression of PCO rather than prevent it.
Changes in IOL engineering carry a less onerous burden of
regulation than biological techniques to inhibit LEC function
and, therefore, prevention or further retardation in the rate of
PCO formation through improved IOL designs is of obvious
benefit.
A series of developments have suggested an alternative
strategy to the traditional closed-bag, square edge IOL. Studies
in rabbit eyes to evaluate a capsular ring, which maintains
separation of the AC and PC, demonstrated significantly
reduced PCO rates.7,8 Considering the severity of PCO
FIGURE 8. The Anew Zephyr IOL appears to reduce cell coverage and formation of light scattering structures on the PC of capsular bags maintainedin 2% human serum plus 10 ng/mL TGF-b2 for 1 month. (A) Modified dark-field micrographs from three match-paired capsular bag experimentscaptured following removal of the respective IOL and fixation. The modified dark-field images present the AC, capsulorhexis (arrowed), and PC. (B)Pooled data showing coverage of the central PC in the presence of an Alcon Acrysof or Anew Zephyr IOL. (C) Pooled data showing coverage inAnew Zephyr implanted capsular bags relative to their match-paired Alcon Acrysof implanted counterpart. (D) Pooled data showing the level oflight scatter in the central PC in the presence of an Alcon Acrysof or an Anew Zephyr IOL. (E) Pooled data showing the level of light scatter in AnewZephyr implanted capsular bags relative to their match-paired Alcon Acrysof implanted counterpart. Data are presented as mean 6 SEM (n ¼ 3).*Indicates a significant difference between groups (Student’s t-test; P � 0.05).
Open-Bag IOLs Reduce PCO IOVS j November 2014 j Vol. 55 j No. 11 j 7062
formation in the rabbit model, this is a significant result.Moreover, when this ring design was used in clinical studies,again the PCO rates were low.21 Therefore, this approach holdsmuch promise and our findings lend support to this theory asin all match-paired human capsular bag experiments, the AnewZephyr open bag IOL significantly outperformed the currentgold standard Alcon Acrysof IOL. The degree of growth andformation of light-scattering structures on the PC variedbetween donors, which reflects variation in patients, but ona match-paired basis for each donor these changes weresignificantly suppressed in preparations implanted with anAnew Zephyr IOL versus an Acrysof IOL.
We believe that the benefits observed with the Anew
Zephyr IOL result both from a barrier function due to
interaction of the ring haptic with the PC and through a
reduced availability of growth factors within the capsular bag
due to greater circulation of fluid. Findings in the current study
provide evidence that the ring haptic can provide a barrier
function against cell movement onto the PC. This was evident
under both culture conditions, yet, this was more pronounced
when human serum and TGF-b2 was present; however, once
the barrier is breached, growth across and modification of the
PC is relatively rapid. Despite a lack of interaction between the
AC and PC it is likely that as LECs repopulate the AC producing
increased tension in the bag, which creates greater forcebetween the ring haptic and the equatorial capsule. It shouldbe noted that in the case of the Anew Zephyr IOL the posteriorcomponent of the ring haptic is smooth. A modification to thiscomponent to create a square edge profile could providegreater interaction with the PC and further impede growthacross the PC.
The other possible mechanism that could explain theimproved outcomes observed with the Anew Zephyr IOL is thereduced availability of growth factors. In traditional closed-bagsystems, the ACs and PCs adhere through cellular interactions,which limit fluid movement within the AC/PC space.Moreover, in this arrangement cells reside in close proximityto each other, and thus local production of growth factors andsurvival factors is likely to be concentrated and readily reach allcells on the two capsular surfaces. It is known that cytokines,for example, interleukins22 and growth factors, such ashepatocyte growth factor (HGF) and fibroblast growth factor(FGF)23–25 are produced by residual LECs cells, within humancapsular bags, in response to surgery. In addition, a number ofgrowth factors require cell or matrix interaction to convert apro or inactive form to the active molecule or to facilitatepresentation of the ligand to its corresponding receptor. It islikely that separation of the capsules plus the presence offenestrations within the Anew Zephyr IOL design allows fluidmovement within the AC/PC space, which reduces accumu-lation of growth factors on the matrix and limits localconcentrations of cytokines. The regulation of cytokines andgrowth factors by open-bag devices are the subject of futurestudies.
In summary, the Anew Zephyr open bag IOL provides anadvance on existing IOL technologies and is likely to affordadded benefit to patients undergoing cataract surgery throughreduced PCO rates. Open-bag strategies, in general, offer agreat deal of promise.
Acknowledgments
The authors thank Mary Tottman and Janet Holtaway of the EastAnglian Eye Bank for their invaluable efforts and contribution toour research.
Supported by grants from Fight for Sight (London, UK), TheHumane Research Trust (Bramhall, UK), and Anew Optics, Inc.(Bristol, TN, USA).
Disclosure: J.A. Eldred, None; D.J. Spalton, Anew Optics, Inc.(C, S); I.M. Wormstone, Anew Optics, Inc. (F, C)
References
1. McCarty CA, Taylor HR. The genetics of cataract. Invest
Ophthalmol Vis Sci. 2001;42:1677–1678.
2. Wormstone IM, Wang L, Liu CS. Posterior capsule opacifica-tion. Exp Eye Res. 2009;88:257–269.
3. Ranta P, Kivela T. Retinal detachment in pseudophakic eyeswith and without Nd:YAG laser posterior capsulotomy.Ophthalmology. 1998;105:2127–2133.
4. Nishi O, Nishi K, Menapace R, Akura J. Capsular bending ringto prevent posterior capsule opacification: 2 year follow-up. J
Cataract Refract Surg. 2001;27:1359–1365.
5. Hayashi K, Hayashi H, Nakao F, Hayashi F. Changes in posteriorcapsule opacification after poly(methyl methacrylate), sili-cone, and acrylic intraocular lens implantation. J Cataract
Refract Surg. 2001;27:817–824.
6. Cleary G, Spalton DJ, Koch DD. Effect of square-edgedintraocular lenses on neodymium:YAG laser capsulotomy rates
FIGURE 9. Modified dark-field micrographs showing an IOL-associatedbarrier effect within capsular bag preparations maintained in 2%human serum plus 10 ng/mL TGF-b2 implanted with (A) an AnewZephyr IOL and (B) an Alcon Acrysof IOL. Dashed line indicates thenatural location of the rhexis edge. Arrows indicate regions wherebarrier function is evident.
Open-Bag IOLs Reduce PCO IOVS j November 2014 j Vol. 55 j No. 11 j 7063

in the United States. J Cataract Refract Surg. 2007;33:1899–1906.
7. Hara T, Hara T, Sakanishi K, Yamada Y. Efficacy of equator ringsin an experimental rabbit study. Arch Ophthalmol. 1995;113:1060–1065.
8. Hashizoe M, Hara T, Ogura Y, Sakanishi K, Honda T, Hara T.Equator ring efficacy in maintaining capsular bag integrity andtransparency after cataract removal in monkey eyes. Graefes
Arch Clin Exp Ophthalmol. 1998;236:375–379.
9. Alon R, Assia EI, Kleinmann G. Prevention of posterior capsuleopacification by an intracapsular open capsule device. Invest
Ophthalmol Vis Sci. 2014;55:4005–4013.
10. Kavoussi SC, Werner L, Fuller SR, et al. Prevention of capsularbag opacification with a new hydrophilic acrylic disk-shapedintraocular lens. J Cataract Refract Surg. 2011;37:2194–2200.
11. Hara T, Narita M, Hashimoto T, Motoyama Y. Long-term studyof posterior capsular opacification prevention with endocap-sular equator rings in humans. Arch Ophthalmol. 2011;129:855–863.
12. Leishman L, Werner L, Bodnar Z, et al. Prevention of capsularbag opacification with a modified hydrophilic acrylic disk-shaped intraocular lens. J Cataract Refract Surg. 2012;38:1664–1670.
13. Liu CS, Wormstone IM, Duncan G, Marcantonio JM, Webb SF,Davies PD. A study of human lens cell growth in vitro. A modelfor posterior capsule opacification. Invest Ophthalmol Vis Sci.1996;37:906–914.
14. Cleary G, Spalton DJ, Zhang JJ, Marshall J. In vitro lens capsulemodel for investigation of posterior capsule opacification. J
Cataract Refract Surg. 2010;36:1249–1252.
15. Wormstone IM, Anderson IK, Eldred JA, Dawes LJ, Duncan G.Short-term exposure to transforming growth factor betainduces long-term fibrotic responses. Exp Eye Res. 2006;83:1238–1245.
16. Dawes LJ, Illingworth CD, Wormstone IM. A fully human invitro capsular bag model to permit intraocular lens evaluation.Invest Ophthalmol Vis Sci. 2012;53:23–29.
17. Hollick EJ, Spalton DJ, Ursell PG, et al. The effect ofpolymethylmethacrylate, silicone, and polyacrylic intraocularlenses on posterior capsular opacification 3 years after cataractsurgery. Ophthalmology. 1999;106:49–54.
18. Nishi O. Posterior capsule opacification. Part 1: experimentalinvestigations. J Cataract Refract Surg. 1999;25:106–117.
19. Nanavaty MA, Spalton DJ, Boyce J, Brain A, Marshall J. Edgeprofile of commercially available square-edged intraocularlenses. J Cataract Refract Surg. 2008;34:677–686.
20. Hollick EJ, Spalton DJ, Meacock WR. The effect of capsulo-rhexis size on posterior capsular opacification: one-year resultsof a randomized prospective trial. Am J Ophthalmol. 1999;128:271–279.
21. Hara T, Hara T, Narita M, Hashimoto T, Motoyama Y, Hara T.Long-term study of posterior capsular opacification preventionwith endocapsular equator rings in humans. Arch Ophthal-
mol. 2011;129:855–863.
22. Dawes LJ, Duncan G, Wormstone IM. Age-related differencesin signaling efficiency of human lens cells underpin differentialwound healing response rates following cataract surgery.Invest Ophthalmol Vis Sci. 2013;54:333–342.
23. Dawes LJ, Angell H, Sleeman M, Reddan JR, Wormstone IM.TGFbeta isoform dependent Smad2/3 kinetics in human lensepithelial cells: a Cellomics analysis. Exp Eye Res. 2007;84:1009–1012.
24. Wormstone IM, Del Rio-Tsonis K, McMahon G, et al. FGF: anautocrine regulator of human lens cell growth independent ofadded stimuli. Invest Ophthalmol Vis Sci. 2001;42:1305–1311.
25. Wormstone IM, Tamiya S, Marcantonio JM, Reddan JR.Hepatocyte growth factor function and c-Met expression inhuman lens epithelial cells. Invest Ophthalmol Vis Sci. 2000;41:4216–4222.
Open-Bag IOLs Reduce PCO IOVS j November 2014 j Vol. 55 j No. 11 j 7064





























