Embed Size (px)
Citation preview

G
E
Dv
VMa
b
c
a
ARRA
KDMIR
1
wbcgettle
0d
ARTICLE IN PRESS Model
URR-5643; No. of Pages 8
European Journal of Radiology xxx (2011) xxx– xxx
Contents lists available at ScienceDirect
European Journal of Radiology
jo ur n al hom epage: www.elsev ier .com/ locate /e j rad
eeply infiltrating endometriosis: Evaluation of retro-cervical space on MRI afteraginal opacification
aleria Fiaschetti a, Sonia Cruscoa, Alessandro Meschinia,∗, Valentina Camaa, Livio Di Vitoa,assimiliano Marziali b, Emilio Piccioneb, Ferdinando Calabriac, Giovanni Simonetti a
Department of Diagnostic and Molecular Imaging, Interventional Radiology and Radiotherapy, Fondazione Policlinico “Tor Vergata”, Viale Oxford 81, Rome, ItalyDepartment of Gynecology and Obstetrics, Fondazione Policlinico “Tor Vergata”, Viale Oxford 81, Rome, ItalyDepartment of Nuclear Medicine and Diagnostic Imaging, IRCCS Neuromed, Pozzilli (IS), Italy
r t i c l e i n f o
rticle history:eceived 2 June 2011eceived in revised form 27 June 2011ccepted 29 June 2011
eywords:eep infiltrating endometriosisagnetic resonance
ntravaginal geletro-cervical space
a b s t r a c t
Objectives: To prospectively investigate diagnostic value and tolerability of MRI after intra-vaginal gelopacification for diagnosis and preoperative assessment of deeply infiltrating endometriosis.Methods: Sixty-three women with clinical suspicion of deeply infiltrating endometriosis were previouslyexamined with trans-vaginal ultrasonography and then with MRI pre and post administration of vaginalgel. We evaluated the tolerability of this procedure with a scoring scale from 0 to 3. We also assessedwith a score from 1 to 4 the visibility of four regions: Douglas-pouch, utero-sacral-ligaments, posterior-vaginal-fornix and recto-vaginal-septum. All patients underwent laparoscopic surgery after MRI.Results: Five patients considered procedure intolerable. Visibility of utero-sacral-ligaments and posterior-vaginal-fornix showed to be increased with gel (p < 0.001). In 57 out of 80 patients the MRI has allowedus to diagnose deeply infiltrating endometriosis.
Overall, the percentages of MRI-sensitivity, specificity, positive predictive value and negative predictivevalue were respectively 67.8%, 95.3%, 89.4 and 83.5% without gel, and 90.8%, 94.6%, 90.8% and 94.6%with gel; trans-vaginal ultrasonography sensitivity, specificity, positive predictive value and negativepredictive value were 57.5%, 96.6%, 90.9% and 79.5%.
In evaluation of utero-sacral-ligaments trans-vaginal ultrasonography, MRI without gel and with gel
sensitivity was respectively 61.9%, 47.6% and 81%; for recto-vaginal-septum these values were 12.5%,68.7% and 93.7%; for pouch of Douglas 82%, 87% and 97.4%; finally for posterior-vaginal-fornix 27.3%,36.4% and 81.8%.Conclusions: MRI with gel opacification of vagina should be recommended for suspicion of deep infiltrat-ing endometriosis, in particular for the added value in evaluation of recto-vaginal septum, utero-sacralagina
ligaments and posterior v. Introduction
Endometriosis is a common gynecological disorder that affectsomen in reproductive age; the exact prevalence is not defined
ut is estimated to be approximately 10% [1]. This pathology isharacterized by the presence of ectopic functional endometriallands and stroma outside the uterine cavity. Deeply infiltratingndometriosis (DIE) is a specific entity, histologically defined byhe presence of endometrial implants penetrating under the peri-
Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating enopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
oneal surface or under the wall of the pelvic organs to a depth of ateast 5 mm, inducing a fibro-muscular hyperplasia that surroundsndometriosis foci [2].
∗ Corresponding author. Tel.: +39 0620902401; fax: +39 0620902404.E-mail address: [email protected] (A. Meschini).
720-048X/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2011.06.058
l fornix.© 2011 Elsevier Ireland Ltd. All rights reserved.
Particularly, posterior DIE may involve anatomic structures thatsurround the pouch of Douglas, such as the utero-sacral ligaments(USL), the vaginal wall, the posterior vaginal fornix (PVF), the recto-vaginal septum (RVS) and the anterior wall of the rectum or recto-sigmoid junction [3].
Endometriosis is associated with a wide variety of symptoms,although in many patients it may be completely asymptomatic.Symptoms include dysmenorrhea, dyspareunia, noncyclical pelvicpain, dysuria, lower gastrointestinal symptoms and/or infertility[4].
Radical excision of all endometriotic implants is the treatmentof choice to control the symptomatology [5]; therefore, adequatepreoperative planning is essential for successful treatment.
dometriosis: Evaluation of retro-cervical space on MRI after vaginal
Diagnostic difficulties are posed by the multifaceted presenta-tion of pelvic endometriosis. In fact, pelvic exams may be reportedas normal in up to 40% of evaluations, despite disclosure of painfulnodularities in the posterior cul-de-sac, in case of DIE [6].
IN PRESSG Model
E
2 rnal of Radiology xxx (2011) xxx– xxx
Da[i[(s
atetuilmc
ew
fohsdmcmn
itabngnd
tmf
2
2
ec
mpiuw
ti
y6p
Table 1Patients characteristics.
Age (years ± SD) 34 ± 6Dysmenorrhea (%) 69/80 (86)Dyspareunia (%) 54/80 (67)Non-cyclic chronic pelvic pain (%) 48/80 (60)Dyschezia (%) 36/80 (45)
ARTICLEURR-5643; No. of Pages 8
V. Fiaschetti et al. / European Jou
Transvaginal ultrasounds (TVUS), used for the diagnosis ofIE, have shown variable diagnostic accuracy, depending on thenatomical affected sites and the experience of the investigators7]. Magnetic resonance imaging (MRI) remains the best non-nvasive method to evaluate the locations of pelvic endometriosis8]; standard MRI protocol include T2-weighted turbo spin-echoTSE) sequences in sagittal and transverse planes, T1-weighted TSEequences in axial planes with and without fat-suppression [9].
The challenge of MRI in posterior DIE is to capture a smallnatomic area encompassing several thin fibro-muscular struc-ures such as USL, vaginal and rectal wall, and to identifyndometriotic lesions, which as well are fibro-muscular configura-ions and have an MRI signal intensity similar to those surrounding;se of contrast media is still uncertain but for some Authors admin-
stration of gadolinium does not allow to discriminate between DIEesions from normal pelvic fibro-muscular structures and, further-
ore, contrast enhancement in small veins or normal parametriuman be misinterpreted with endometriotic foci [3].
Also, due to multiple closely related anatomical structures,ndometriosis implants may show variable imaging appearances,ith subtle signal alterations.
MRI features of endometriosis are heterogeneous: hemorrhagicoci can be detected as small implants with high signal intensity,ccasionally surrounded by solid fibrotic tissue; solid deep lesionsave low or moderate signal intensity, with point regions of highignal intensity on T1-weighted images. Likewise, signal intensityoes not help in distinguishing deep endometriosis of USL liga-ents, especially in case of lacking of hemorrhagic foci: in this
ase the diagnosis is based on the detection of bilateral or asym-etric thickening of the ligaments, or defined by the presence of
odularity inside the ligament.Intravaginal gel may be useful in identifying localizations of DIE,
n particular the posterior deep endometriosis because typicallyhe vaginal walls are directly opposed and the vaginal fornicesre collapsed around the cervix [10]. The use of gel allows a sta-le expansion of hollow organs such as the vagina and its viscousature prevents loss that would occur with a pure liquid; vaginalel opacification could delineate a better visualization of the for-ices and the cervix by relaxing vaginal walls, with a better view ofeep pelvis, as reported in literature [3].
The aim of our study is to demonstrate the diagnostic value andolerability of intra-vaginal contrast for preoperative MRI assess-
ent of DIE in retro-cervical space, compared with results obtainedrom TVUS, MRI without gel administration and histological exam.
. Materials and methods
.1. Patients’ selection
From January to December 2010, 83 women were prospectivelynrolled in the study; they were referred from Department of Gyne-ology and Obstetrics of our Institute for clinical suspicion of DIE.
All patients showed non-cyclic pelvic pain, dyspareunia, dys-enorrhea and/or infertility and were treated with estrogen and
rogestin medications and/or GnRH-agonist and non steroidal anti-nflammatory drugs (NSAIDs), for at least 1 year. All patientsnderwent physical examination and TVUS. Afterwards, patientsere examined with MRI of the pelvis.
Three patients were excluded by our study because they refusedhe procedure of gel opacification, therefore this approach was usedn 80 patients, with an acceptance rate of 96.4% (80/83).
Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating enopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
The 80 patients included in our study had a mean age of 34 ± 6ears (range 25–45 years), and were affected by dysmenorrhea in9/80 (86%), dyspareunia in 54/80 (67%), non-cyclic chronic pelvicain in 48/80 (60%), dyschezia in 36/80 (45%) and infertility in 22/80
Infertility (%) 22/80 (27)Previous surgery for endometriosis (%) 10/80 (12.5)
(27%); 10/80 patients (12.5%) had undergone a previous surgicalintervention for endometriosis Table 1.
The study was approved by our local ethical committee, andwritten informed consent was obtained from all enrolled patients.
2.2. Physical examination
In selected patients, it was considered suggestive of posteriorDIE when an area of thickening or a nodule was found in the USL,in the PVF and/or in the RVS.
2.3. TVUS protocol
TVUS scans were carried out by a single examiner with aniU22 (Philips medical systems, BEST, Netherlands) connected to aC5–9 MHz transducer. Each examination was interpreted in real-time with a standardized protocol by the same examiner with 10years of experience in gynecologic imaging at the outset of thestudy. The TVUS examination was used in the evaluation of pelvicpain to assess potential endometriotic lesions.
The examination protocol included, in addition to routine anal-ysis of the uterus and ovaries, the study of the pouch of Douglas,the USL, the PVF, and the RVS.
Abnormal hypoechoic linear thickening, nodules with or with-out regular contours and/or retractable masses on the retro-cervicalarea, including lesions on the USL, pouch of Douglas and/or vagina,were considered suspicious of deep retro-cervical endometriosis.
2.4. MRI acquisition
MRI was performed using a 1.5 T scanner (Achieva, Philips med-ical systems, BEST, Netherlands) using a pelvic phased-array coil.We intravenously administered peristaltic inhibitors (10 mg ofhyoscine-N-butylbromide, Buscopan) diluted in 10 ml saline solu-tion to reduce gastrointestinal tract artifacts, whereas the patienthad no contraindication.
Due to possibility of spontaneous T1 hyperintensity of bloodafter 8 days of bleeding, MRI should not be performed earlier thanday 8 of the menstrual cycle; therefore we examined the patientsbetween days 8 and 12 of the menstrual cycle.
The standard imaging protocol included a T1-weighted TSE(TR/TE, 613/10; matrix, 284 × 314; field of view, 228 × 320 mm;section thickness, 3 mm; intersection gap, 1 mm; voxel, 0.8 × 1.02;turbo factor, 5; nex 2); a T2-weighted TSE (TR/TE, 3204/90; matrix,420 × 225; field of view, 320 × 228 mm; section thickness, 3 mm;intersection gap, 1 mm; voxel, 0.76 × 1.02; turbo factor, 20; nex 4); aT1-weighted TSE fat-saturation (TR/TE, 553/10; matrix, 284 × 312;field of view, 228 × 320 mm; section thickness, 3 mm; intersectiongap, 1 mm; voxel, 0.8 × 1.02; turbo factor, 5; nex 2); a T2-weightedTSE fat saturation (TR/TE, 4103/50; matrix, 260 × 225; field of view,228 × 319 mm; section thickness, 3 mm; intersection gap, 1 mm;voxel, 0.88 × 1.4; turbo factor, 18; nex 3) performed in the trans-
dometriosis: Evaluation of retro-cervical space on MRI after vaginal
verse plane (perpendicular to the major axis of the uterus). AT2-weighted TSE sequences (TR/TE, 3000/90; matrix, 304 × 210;field of view, 230 mm × 230 mm; section thickness, 4 mm; inter-section gap, 1 mm; voxel, 0.76 × 1.08; turbo factor, 18; nex 3) and a
ARTICLE IN PRESSG Model
EURR-5643; No. of Pages 8
V. Fiaschetti et al. / European Journal of Radiology xxx (2011) xxx– xxx 3
F b). Thew
TfigfTst
otcw
ec1
N
sc
2
saaPo
io
D
i(
oloToct
of DIE and the symptomatology was referable a to pelvic varicocele(9 cases) and to uterine fibromyomas (8 cases); in 6 cases we werenot able to identify the cause of reported pelvic pain.
Table 2Localization of DIE as assessed by laparoscopic evaluation of the 57 patients.
Localization Number of lesions (%)
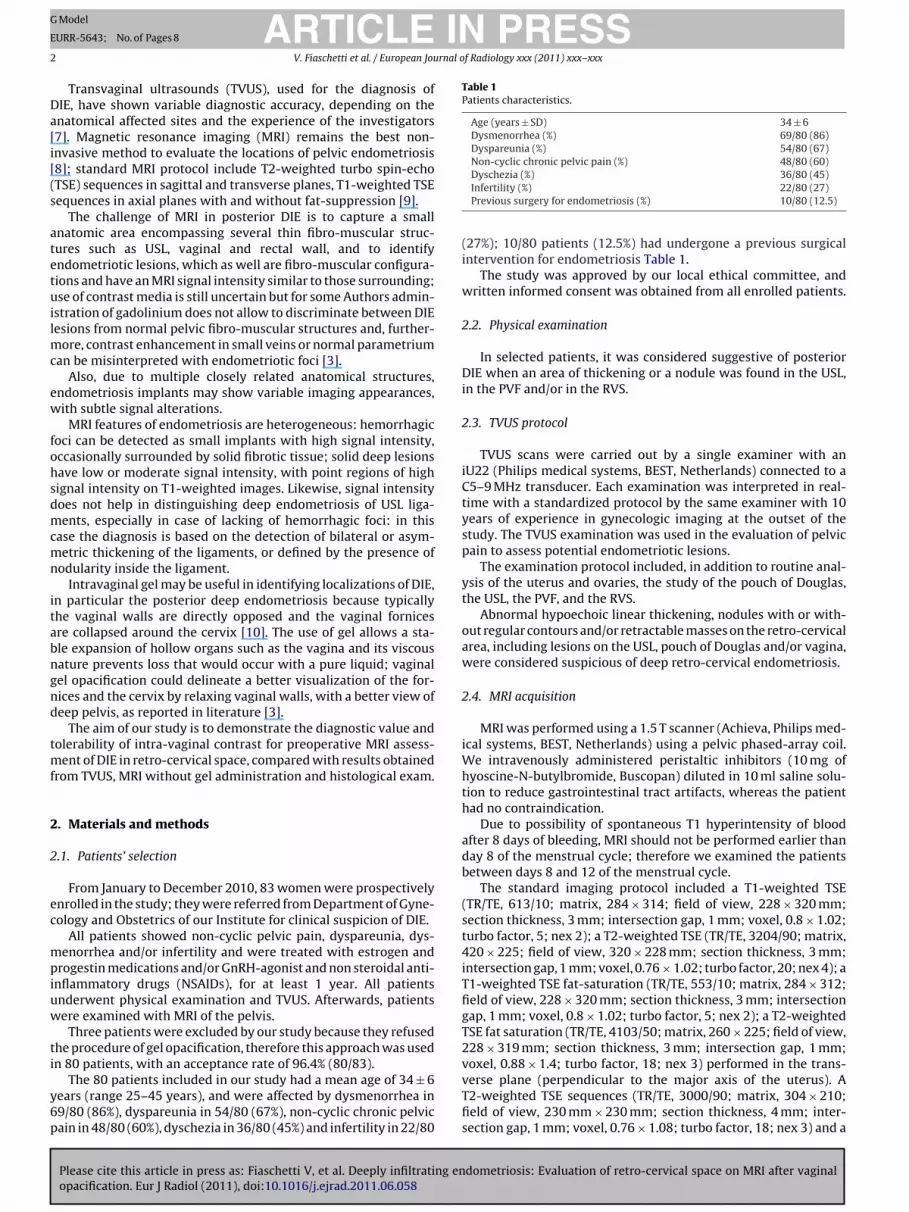
ig. 1. Sagittal T2-weighted MRI views pre (a) and post vaginal gel opacification (ith the hyposignal of the surrounding fibromuscolar anatomic structures.
1-weighted TSE fat-saturation (TR/TE, 632/10; matrix, 288 × 225;eld of view, 230 × 230 mm; section thickness, 4 mm; intersectionap, 1 mm; voxel, 0.8 × 1.02; turbo factor, 5; nex 2) were per-ormed on sagittal plane. The transverse and sagittal T1-weightedSE fat-saturation and the sagittal and transverse T2-weighted TSEequences were performed before and after vaginal gel opacifica-ion (Fig. 1).
The instillation of the gel was executed directly on the boardf the MR scanner, without changing the patient position. In par-icular, we used 100 ml of sterile US gel, introduced by a Foley’satheter into the vaginal canal to distend the fornices, a procedurehich takes about 3 min.
During the gel opacification a short questionnaire was made tovaluate the tolerability of the procedure; patients were asked toonsider this technique as: tolerable (score 0), fairly tolerable (score), hardly tolerable (score 2) and intolerable (score 3).
The duration of the whole MRI examination was about 25 min.o intravenous contrast medium was administered.
After MRI, all patients enrolled in our study underwent laparo-copic surgery to obtain definitive diagnose of histological sample,onsidered the gold standard for diagnosis of DIE.
.5. Data analysis
MRI data were evaluated in consensus by two radiologists, oneenior reviewer with almost 10 years of experience in pelvic MRInd one junior reviewer with more than two years of experience, on
designate workstation (Virtual Reading VR, Carestream Health).hysicians were blinded to clinical data of the patients and resultsf TVUS previously performed.
Pre- and post-vaginal opacification sequences were examinedn two separate sessions, leaving at least one week between thene and the other evaluation.
Four distinct anatomic regions were evaluated: the pouch ofouglas, the USL, the PVF, and the RVS.
Each region was classified with a grade based on their detectabil-ty, using a score from 1 to 4: excellent visibility (1), good visibility2), moderate visibility (3) and no visibility (4).
The diagnosis of posterior DIE was obtained by the presencef higher signal intensity and/or morphological abnormalities. Weooked for diagnostic characteristics such as a nodule or a massf fibrous nature, that showed very hypointense signal on T1- and
Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating enopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
2-weighted imaging; also, we searched for foci with hypersignaln T1-weighted imaging and T1-weighted fat-saturation, possiblyorresponding to hemorrhagic areas within the pouch of Douglas,he USL, the PVF and the RVS.
aqueous gel shows hypersignal intensity on T2-weighted image which contrasts
Involvement of the USL was defined as an irregularly shapednodule or as fibrous thickening compared with the controlateralUSL, with an iso- or hyposignal on T1- and T2-weighted sequences.Involvement of the pouch of Douglas and RVS was defined as thepresence of a nodule with irregular contours. Involvement of thePVF was assumed as mass and/or nodular thickening of the vaginalwall, located behind the posterior surface of the cervix.
2.6. Statistical analysis
We used dedicated software for the statistical analysis (Statis-tica release 7; Stat Soft, Tulsa, OK, USA).
The visibility of the four pelvic regions from MRI after gel opaci-fication was compared with the visibility without gel opacificationusing the Wilcoxon test.
Sensitivity, specificity, positive predictive value (PPV) and neg-ative predictive value (NPV) of TVUS and MRI scans, with andwithout gel opacification, in detecting the location of DIE in eacharea (pouch of Douglas, USL, PVF and RVS), were evaluated con-sidering the results from surgical laparoscopic sample as the goldstandard. The sensitivity of MRI with gel opacification was thencompared with the sensitivity without gel opacification, using theMcNemar test.
A p-value <0.05 was considered statistically significant.
3. Results
Laparoscopic surgery showed 87 endometriotic lesions in 57 outof 80 patients (71.2%), divided into 39/87 (45%) in the pouch ofDouglas, 21/87 (24%) in the USL, 11/87 (13%) in the PVF and 16/87(18%) in the RVS (Table 2).
In 23 out of 80 (28.8%) patients we did not observe localization
dometriosis: Evaluation of retro-cervical space on MRI after vaginal
Pouch of Douglas 39/87 (45%)Utero-sacral ligament 21/87 (24%)Posterior vaginal fornix 11/87 (13%)Recto-vaginal septum 16/87 (18%)
ARTICLE IN PRESSG Model
EURR-5643; No. of Pages 8
4 V. Fiaschetti et al. / European Journal of Radiology xxx (2011) xxx– xxx
Table 3Localizations of deep infiltrating endometriosis: correlation of TVUS and MRI findings and surgical laparoscopic findings.
Sensitivity (%) Specificity (%) PPV (%) NPV (%)
Total DIE locationsTVUS 57.5 (50/87) 96.6 (144/149) 90.9 (50/55) 79.5 (144/181)MRI without gel 67.8 (59/87) 95.3 (142/149) 89.4 (59/66) 83.5 (142/170)MRI with gel 90.8 (79/87) 94.6 (141/149) 90.8 (79/87) 94.6 (141/149)
DouglasTVUS 82 (32/39) 91.7 (22/24) 94.1 (32/34) 75.9 (22/29)MRI without gel 87 (34/39) 100 (24/24) 100 (34/34) 82.7 (24/29)MRI with gel 97.4 (38/39) 100 (24/24) 100 (38/38) 96 (24/25)
USLTVUS 61.9 (13/21) 94.6 (35/37) 86.7 (13/15) 81.4 (35/43)MRI without gel 47.6 (10/21) 91.9 (34/37) 76.9 (10/13) 75.5 (34/45)MRI with gel 81 (17/21) 91.9 (34/37) 85 (17/20) 89.5 (34/38)
PVFTVUS 27.3 (3/11) 97.8 (45/46) 75 (3/4) 84.9 (45/53)MRI without gel 36.4 (4/11) 97.8 (45/46) 80 (4/5) 86.5 (45/52)MRI with gel 81.8 (9/11) 97.8 (45/46) 90 (9/10) 95.7 (45/47)
RVSTVUS 12.5 (2/16) 100 (42/42) 100 (2/2) 75 (42/56)MRI without gel 68.7 (11/16) 92.8 (39/42) 78.6 (11/14) 88.6 (39/44)MRI with gel 93.7 (15/16) 90.5 (38/42) 78.9 (15/19) 97.4 (38/39)
D tic resr e.
3
(aParpuwo9pNp
3
s(cgw
wtfa
fi
TC
IE: deep infiltrating endometriosis; TVUS: transvaginal ultrasound; MRI: magneecto-vaginal septum; PPV: positive predictive value; NPV: negative predictive valu
.1. Transvaginal ultrasound results
TVUS allowed us to diagnose DIE properly in 50 out of 87 lesions45/80 patients) with a sensitivity of 57.5%; 5 false positive casesnd 37 false negative cases were observed, with specificity of 96.6%,PV 90.9% and NPV 79.5%. Particularly, we observed 2 false positivend 7 false negative cases, with sensitivity, specificity, PPV and NPVespectively of 82%, 91.7%, 94.1% and 75.9% in the evaluation of theouch of Douglas; sensitivity, specificity, PPV and NPV in the eval-ation of USL were respectively of 61.9%, 94.6%, 86.7% and 81.4%,ith 2 false positive and 8 false negative cases; in the evaluation
f PVF sensitivity, specificity, PPV and NPV results were of 27.3%,7.8%, 75% and 84.9%, with 8 false negative cases and only one falseositive; finally, in evaluation of RVS, sensitivity, specificity, PPV,PV were respectively of 12.5%, 100%, 100% and 75%, with no falseositive and 14 false negative cases observed (Table 3).
.2. Magnetic resonance imaging results
The gel instillation was accepted by 80 patients; among these,even patients (8.7%) considered the examination as intolerablescore 3), while the other 73 subjects (91.3%) expressed a final per-eption of well tolerability (score 0–2). The administration of USel (100 ml) was sufficient for adequate distension of the vaginalalls in the entire examined population.
We observed a significant difference between MRI with andithout intravaginal gel opacification, regarding the visibility of
he USL and the PVF (p < 0.0001 for both); while there was no dif-
Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating enopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
erence in terms of visibility at the level of the pouch of Douglasnd the RVS (p = 1.00 and p = 0.07, respectively) (Table 4).
In 57 patients (71.2%) the MRI was able to diagnose DIE. Somebrotic areas with or without a hemorrhagic core (hyperinten-
able 4omparison of visibility values with and without gel opacification.
Visibility grading without gel
1 2 3 4
Douglas 68 10 2 0
USL 44 27 9 0
PVF 33 27 19 1
RVS 65 11 4 0
a Wilcoxon test; USL: utero-sacral ligament; PVF: posterior vaginal fornix; RVS: recto-v
onance imaging; USL: utero-sacral ligament; PVF: posterior vaginal fornix; RVS:
sity on T1-weighted sequences with and without fat saturation) orhemorrhagic lesions, due to the cyclic bleeding of the endometri-otic tissue, were observed within the pouch of Douglas, the USL,the PVF and the RVS.
MRI with intravaginal gel allowed to diagnose a total of 79out of 87 true positive endometriotic lesions. Sixteen out of 79(20%) presented hemorrhagic foci inside, while the greatest partpresented fibrotic lesions. The hemorrhagic lesions were predom-inantly located in the RVS (7/16; 44%) (Fig. 2) and in the pouch ofDouglas (7/16, 44%) (Fig. 3); only 1 lesion had hemorrhagic charac-teristics in the PVF (1/16; 6%) and in the USL (1/16; 6%). Eight lesionson 87 total localizations of DIE (9.2%), diagnosed with laparoscopicsurgery, where not detected with MRI, therefore were consideredas false negatives.
The total values of sensitivity in the entire pelvis for DIE localiza-tions were of 90.8% with and 67.8% without gel opacification, withspecificity of 94.6% and 95.3% respectively. The PPV of the MRI withintravaginal gel was 90.8% with a NPV of 94.6%. The MRI withoutintravaginal gel showed a PPV of 89.4% and a NPV of 83.5%.
Also, we observed a total of 8 false positive lesions: 3 (37.5%) inthe USL, 1 (12.5%) in the PVF, 4 (50%) in the RVS but none in theDouglas pouch. All patients with false positive findings had under-gone previous surgical treatments for endometriosis and had signalintensity of the fibrotic tissue.
The MRI detection of lesions in the pouch of Douglas withoutgel opacification showed sensitivity of 87%, specificity of 100%, aPPV of 100% and a NPV of 82.7%; the MRI with gel opacification hadsensitivity of 97.4%, specificity of 100%, a PPV of 100% and a NPV of
dometriosis: Evaluation of retro-cervical space on MRI after vaginal
96%. There was no statistically significant difference in sensitivitybetween the two procedures (p = 0.15).
MRI without gel opacification showed sensitivity in detect-ing DIE in the USL of 47.6%, and it was increased up to
Visibility grading with gel p-Valuea
1 2 3 4
71 9 0 0 0.1161 18 1 0 <0.000160 20 0 0 <0.000168 12 0 0 0.07
aginal septum.

Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating endometriosis: Evaluation of retro-cervical space on MRI after vaginalopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
ARTICLE IN PRESSG Model
EURR-5643; No. of Pages 8
V. Fiaschetti et al. / European Journal of Radiology xxx (2011) xxx– xxx 5
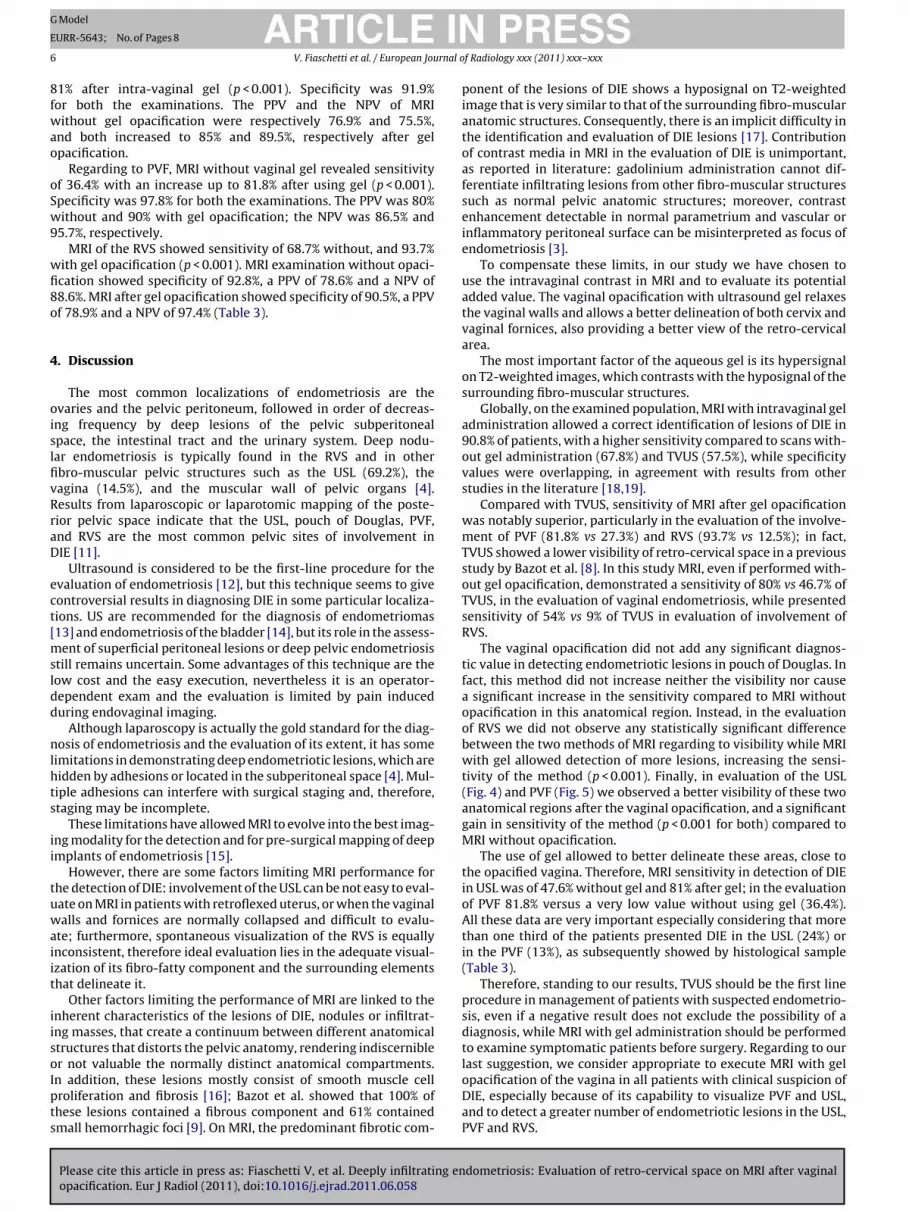
Fig. 2. Sagittal (a) and axial (b) T1-weighted TSE fat-saturation MRI view of patient with some DIE lesions in utero-vescical septum (dotted arrow), in the PVF (arrowhead)and hematic pouring in the pouch of Douglas. Corresponding sequences after vaginal gel opacification (c and d) show further localization on the RVS (arrow).
Fig. 3. Sagittal T1-weighted TSE fat-saturation MRI views before (a) and after gel opacification (b): hyperintense plaque of DIE in pouch of Douglas (arrow), poorly detectablewithout gel.
ING Model
E
6 rnal o
8fwao
oSw9
wfi8o
4
oislfivRraD
ect[msldd
nlhts
ii
tuwaiit
iisoIpts
ARTICLEURR-5643; No. of Pages 8
V. Fiaschetti et al. / European Jou
1% after intra-vaginal gel (p < 0.001). Specificity was 91.9%or both the examinations. The PPV and the NPV of MRIithout gel opacification were respectively 76.9% and 75.5%,
nd both increased to 85% and 89.5%, respectively after gelpacification.
Regarding to PVF, MRI without vaginal gel revealed sensitivityf 36.4% with an increase up to 81.8% after using gel (p < 0.001).pecificity was 97.8% for both the examinations. The PPV was 80%ithout and 90% with gel opacification; the NPV was 86.5% and
5.7%, respectively.MRI of the RVS showed sensitivity of 68.7% without, and 93.7%
ith gel opacification (p < 0.001). MRI examination without opaci-cation showed specificity of 92.8%, a PPV of 78.6% and a NPV of8.6%. MRI after gel opacification showed specificity of 90.5%, a PPVf 78.9% and a NPV of 97.4% (Table 3).
. Discussion
The most common localizations of endometriosis are thevaries and the pelvic peritoneum, followed in order of decreas-ng frequency by deep lesions of the pelvic subperitonealpace, the intestinal tract and the urinary system. Deep nodu-ar endometriosis is typically found in the RVS and in otherbro-muscular pelvic structures such as the USL (69.2%), theagina (14.5%), and the muscular wall of pelvic organs [4].esults from laparoscopic or laparotomic mapping of the poste-ior pelvic space indicate that the USL, pouch of Douglas, PVF,nd RVS are the most common pelvic sites of involvement inIE [11].
Ultrasound is considered to be the first-line procedure for thevaluation of endometriosis [12], but this technique seems to giveontroversial results in diagnosing DIE in some particular localiza-ions. US are recommended for the diagnosis of endometriomas13] and endometriosis of the bladder [14], but its role in the assess-
ent of superficial peritoneal lesions or deep pelvic endometriosistill remains uncertain. Some advantages of this technique are theow cost and the easy execution, nevertheless it is an operator-ependent exam and the evaluation is limited by pain induceduring endovaginal imaging.
Although laparoscopy is actually the gold standard for the diag-osis of endometriosis and the evaluation of its extent, it has some
imitations in demonstrating deep endometriotic lesions, which areidden by adhesions or located in the subperitoneal space [4]. Mul-iple adhesions can interfere with surgical staging and, therefore,taging may be incomplete.
These limitations have allowed MRI to evolve into the best imag-ng modality for the detection and for pre-surgical mapping of deepmplants of endometriosis [15].
However, there are some factors limiting MRI performance forhe detection of DIE: involvement of the USL can be not easy to eval-ate on MRI in patients with retroflexed uterus, or when the vaginalalls and fornices are normally collapsed and difficult to evalu-
te; furthermore, spontaneous visualization of the RVS is equallynconsistent, therefore ideal evaluation lies in the adequate visual-zation of its fibro-fatty component and the surrounding elementshat delineate it.
Other factors limiting the performance of MRI are linked to thenherent characteristics of the lesions of DIE, nodules or infiltrat-ng masses, that create a continuum between different anatomicaltructures that distorts the pelvic anatomy, rendering indiscernibler not valuable the normally distinct anatomical compartments.
Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating enopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
n addition, these lesions mostly consist of smooth muscle cellroliferation and fibrosis [16]; Bazot et al. showed that 100% ofhese lesions contained a fibrous component and 61% containedmall hemorrhagic foci [9]. On MRI, the predominant fibrotic com-
PRESSf Radiology xxx (2011) xxx– xxx
ponent of the lesions of DIE shows a hyposignal on T2-weightedimage that is very similar to that of the surrounding fibro-muscularanatomic structures. Consequently, there is an implicit difficulty inthe identification and evaluation of DIE lesions [17]. Contributionof contrast media in MRI in the evaluation of DIE is unimportant,as reported in literature: gadolinium administration cannot dif-ferentiate infiltrating lesions from other fibro-muscular structuressuch as normal pelvic anatomic structures; moreover, contrastenhancement detectable in normal parametrium and vascular orinflammatory peritoneal surface can be misinterpreted as focus ofendometriosis [3].
To compensate these limits, in our study we have chosen touse the intravaginal contrast in MRI and to evaluate its potentialadded value. The vaginal opacification with ultrasound gel relaxesthe vaginal walls and allows a better delineation of both cervix andvaginal fornices, also providing a better view of the retro-cervicalarea.
The most important factor of the aqueous gel is its hypersignalon T2-weighted images, which contrasts with the hyposignal of thesurrounding fibro-muscular structures.
Globally, on the examined population, MRI with intravaginal geladministration allowed a correct identification of lesions of DIE in90.8% of patients, with a higher sensitivity compared to scans with-out gel administration (67.8%) and TVUS (57.5%), while specificityvalues were overlapping, in agreement with results from otherstudies in the literature [18,19].
Compared with TVUS, sensitivity of MRI after gel opacificationwas notably superior, particularly in the evaluation of the involve-ment of PVF (81.8% vs 27.3%) and RVS (93.7% vs 12.5%); in fact,TVUS showed a lower visibility of retro-cervical space in a previousstudy by Bazot et al. [8]. In this study MRI, even if performed with-out gel opacification, demonstrated a sensitivity of 80% vs 46.7% ofTVUS, in the evaluation of vaginal endometriosis, while presentedsensitivity of 54% vs 9% of TVUS in evaluation of involvement ofRVS.
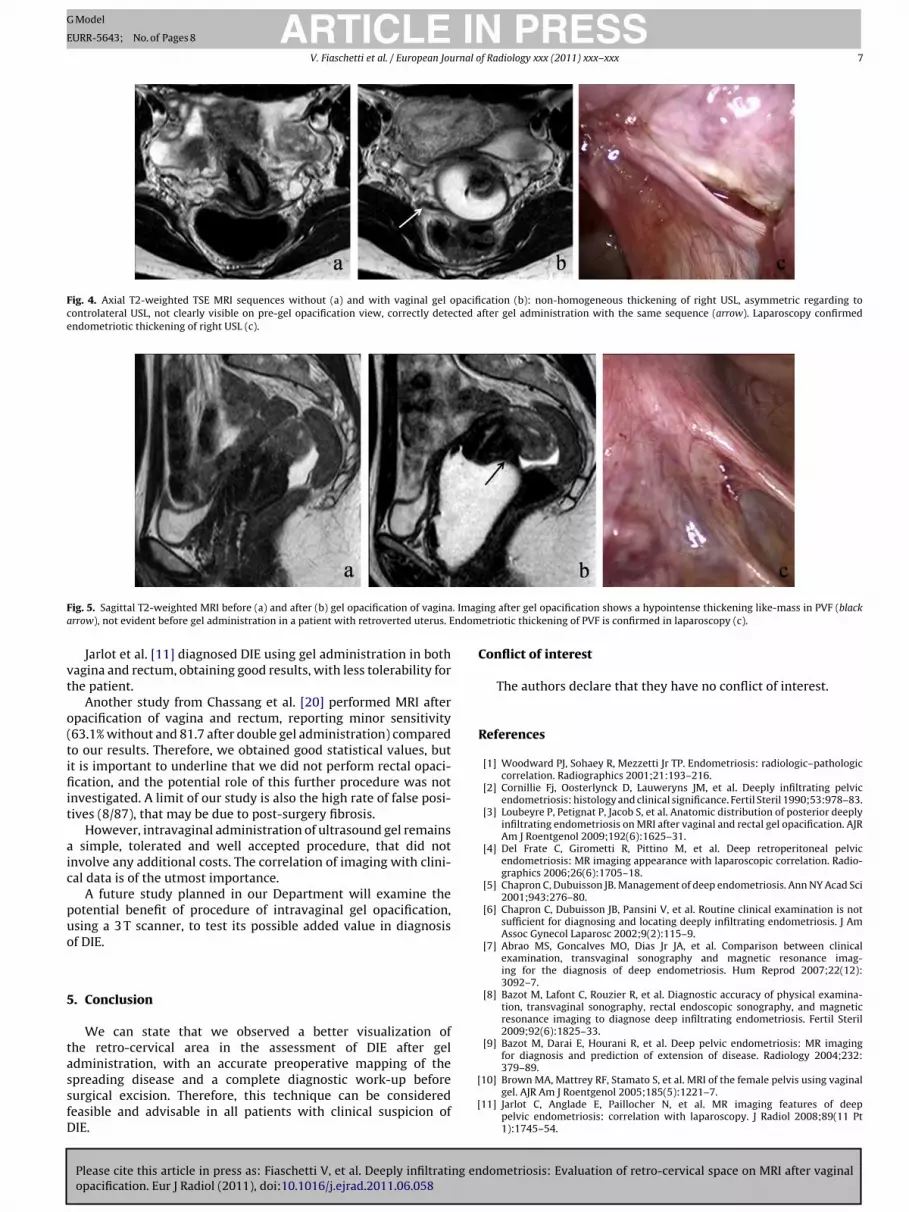
The vaginal opacification did not add any significant diagnos-tic value in detecting endometriotic lesions in pouch of Douglas. Infact, this method did not increase neither the visibility nor causea significant increase in the sensitivity compared to MRI withoutopacification in this anatomical region. Instead, in the evaluationof RVS we did not observe any statistically significant differencebetween the two methods of MRI regarding to visibility while MRIwith gel allowed detection of more lesions, increasing the sensi-tivity of the method (p < 0.001). Finally, in evaluation of the USL(Fig. 4) and PVF (Fig. 5) we observed a better visibility of these twoanatomical regions after the vaginal opacification, and a significantgain in sensitivity of the method (p < 0.001 for both) compared toMRI without opacification.
The use of gel allowed to better delineate these areas, close tothe opacified vagina. Therefore, MRI sensitivity in detection of DIEin USL was of 47.6% without gel and 81% after gel; in the evaluationof PVF 81.8% versus a very low value without using gel (36.4%).All these data are very important especially considering that morethan one third of the patients presented DIE in the USL (24%) orin the PVF (13%), as subsequently showed by histological sample(Table 3).
Therefore, standing to our results, TVUS should be the first lineprocedure in management of patients with suspected endometrio-sis, even if a negative result does not exclude the possibility of adiagnosis, while MRI with gel administration should be performedto examine symptomatic patients before surgery. Regarding to ourlast suggestion, we consider appropriate to execute MRI with gel
dometriosis: Evaluation of retro-cervical space on MRI after vaginal
opacification of the vagina in all patients with clinical suspicion ofDIE, especially because of its capability to visualize PVF and USL,and to detect a greater number of endometriotic lesions in the USL,PVF and RVS.
ARTICLE IN PRESSG Model
EURR-5643; No. of Pages 8
V. Fiaschetti et al. / European Journal of Radiology xxx (2011) xxx– xxx 7
Fig. 4. Axial T2-weighted TSE MRI sequences without (a) and with vaginal gel opacification (b): non-homogeneous thickening of right USL, asymmetric regarding tocontrolateral USL, not clearly visible on pre-gel opacification view, correctly detected after gel administration with the same sequence (arrow). Laparoscopy confirmedendometriotic thickening of right USL (c).
F . Imaga ndom
vt
o(tifiit
aic
puo
5
tassfD
ig. 5. Sagittal T2-weighted MRI before (a) and after (b) gel opacification of vaginarrow), not evident before gel administration in a patient with retroverted uterus. E
Jarlot et al. [11] diagnosed DIE using gel administration in bothagina and rectum, obtaining good results, with less tolerability forhe patient.
Another study from Chassang et al. [20] performed MRI afterpacification of vagina and rectum, reporting minor sensitivity63.1% without and 81.7 after double gel administration) comparedo our results. Therefore, we obtained good statistical values, butt is important to underline that we did not perform rectal opaci-cation, and the potential role of this further procedure was not
nvestigated. A limit of our study is also the high rate of false posi-ives (8/87), that may be due to post-surgery fibrosis.
However, intravaginal administration of ultrasound gel remains simple, tolerated and well accepted procedure, that did notnvolve any additional costs. The correlation of imaging with clini-al data is of the utmost importance.
A future study planned in our Department will examine theotential benefit of procedure of intravaginal gel opacification,sing a 3 T scanner, to test its possible added value in diagnosisf DIE.
. Conclusion
We can state that we observed a better visualization ofhe retro-cervical area in the assessment of DIE after geldministration, with an accurate preoperative mapping of the
Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating enopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
preading disease and a complete diagnostic work-up beforeurgical excision. Therefore, this technique can be consideredeasible and advisable in all patients with clinical suspicion ofIE.
[
[
ing after gel opacification shows a hypointense thickening like-mass in PVF (blacketriotic thickening of PVF is confirmed in laparoscopy (c).
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] Woodward PJ, Sohaey R, Mezzetti Jr TP. Endometriosis: radiologic–pathologiccorrelation. Radiographics 2001;21:193–216.
[2] Cornillie Fj, Oosterlynck D, Lauweryns JM, et al. Deeply infiltrating pelvicendometriosis: histology and clinical significance. Fertil Steril 1990;53:978–83.
[3] Loubeyre P, Petignat P, Jacob S, et al. Anatomic distribution of posterior deeplyinfiltrating endometriosis on MRI after vaginal and rectal gel opacification. AJRAm J Roentgenol 2009;192(6):1625–31.
[4] Del Frate C, Girometti R, Pittino M, et al. Deep retroperitoneal pelvicendometriosis: MR imaging appearance with laparoscopic correlation. Radio-graphics 2006;26(6):1705–18.
[5] Chapron C, Dubuisson JB. Management of deep endometriosis. Ann NY Acad Sci2001;943:276–80.
[6] Chapron C, Dubuisson JB, Pansini V, et al. Routine clinical examination is notsufficient for diagnosing and locating deeply infiltrating endometriosis. J AmAssoc Gynecol Laparosc 2002;9(2):115–9.
[7] Abrao MS, Goncalves MO, Dias Jr JA, et al. Comparison between clinicalexamination, transvaginal sonography and magnetic resonance imag-ing for the diagnosis of deep endometriosis. Hum Reprod 2007;22(12):3092–7.
[8] Bazot M, Lafont C, Rouzier R, et al. Diagnostic accuracy of physical examina-tion, transvaginal sonography, rectal endoscopic sonography, and magneticresonance imaging to diagnose deep infiltrating endometriosis. Fertil Steril2009;92(6):1825–33.
[9] Bazot M, Darai E, Hourani R, et al. Deep pelvic endometriosis: MR imagingfor diagnosis and prediction of extension of disease. Radiology 2004;232:379–89.
dometriosis: Evaluation of retro-cervical space on MRI after vaginal
10] Brown MA, Mattrey RF, Stamato S, et al. MRI of the female pelvis using vaginalgel. AJR Am J Roentgenol 2005;185(5):1221–7.
11] Jarlot C, Anglade E, Paillocher N, et al. MR imaging features of deeppelvic endometriosis: correlation with laparoscopy. J Radiol 2008;89(11 Pt1):1745–54.

ING Model
E
8 rnal o
[
[
[
[
[
[
[
[
ARTICLEURR-5643; No. of Pages 8
V. Fiaschetti et al. / European Jou
12] Piketty M, Chopin N, Dousset B, et al. Preoperative work-up for patients withdeeply infiltrating endometriosis: transvaginal ultrasonography must defi-nitely be the first-line imaging examination. Hum Reprod 2009;24(3):602–7.
13] Mais V, Guerriero S, Ajossa S, et al. The efficiency of transvaginal ultrasonogra-phy in the diagnosis of endometrioma. Fertil Steril 1993;60:776–80.
14] Fedele L, Bianchi S, Raffaelli R, et al. Preoperative assessment of bladderendometriosis. Hum Reprod 1997;12:2519–22.
Please cite this article in press as: Fiaschetti V, et al. Deeply infiltrating enopacification. Eur J Radiol (2011), doi:10.1016/j.ejrad.2011.06.058
15] Eskenazi B, Warner M, Bonsignor L, et al. Validation study of nonsurgical diag-nosis of endometriosis. Fertil Steril 2001;76(5):929–35.
16] Del Frate C, Girometti R, Pittino M, et al. Deep retroperitoneal pelvicendometriosis: MR imaging appearance with laparoscopic correlation. Radio-graphics 2006;26:1705–18.
[
PRESSf Radiology xxx (2011) xxx– xxx
17] Roy C, Balzan C, Thoma V, et al. Efficiency of MR imaging to orientatesurgical treatment of posterior deep pelvic endometriosis. Abdom Imaging2009;34:251–9.
18] Abrao MS, Gonc alves MO, Dias Jr JA, et al. Comparison between clinical exam-ination, transvaginal sonography and magnetic resonance imaging for thediagnosis of deep endometriosis. Hum Reprod 2007;22(12):3092–7.
19] Chamié LP, Blasbalg R, Gonc alves MO, et al. Accuracy of magnetic reso-
dometriosis: Evaluation of retro-cervical space on MRI after vaginal
nance imaging for diagnosis and preoperative assessment of deeply infiltratingendometriosis. Int J Gynaecol Obstet 2009;106(3):198–201.
20] Chassang M, Novellas S, Bloch-Marcotte C, et al. Utility of vaginal and rectalcontrast medium in MRI for the detection of deep pelvic endometriosis. EurRadiol 2010;20(4):1003–10.





























