Embed Size (px)
Citation preview

Design and printing of this newsletter generously sponsored by
SPECIAL ISSUE: Tendon Rehabilitation, Surgery & Recovery
Chronic patellar tendinopathy
Achilles tendinopathy-Genetic Predisposition
Soft Tissue Tendon Management Protocols
New treatment methods: Sclerosing polidocanol injections and mini-surgical “scraping”
Accelerated Achilles Tendon repair
January 2011Volume 3 No 4
Sports Medicine Update

Sports Medicine Update Volume 3 No 4 January 2011Page 2
Dr Mark Ferguson Orthopaedic Surgeon
Johannesburg
Editorial
The content contained in this publication contains medical or health sciences information and is intended for professional use within the medical field. No suggested test or procedure should be carried out unless, in the reader’s judgment, its risk is justified. Because of rapid advances in the medical sciences, we recommend that the independent verification of diagnoses and drug dosages should be made. Discussions, views, and recommendations as to medical procedures, products, choice of drugs, and drug dosages are the responsibility of the authors. The views expressed by the editor or authors in this newsletter do not necessarily reflect those of the sponsors or publishers.
Production Editors: Ann Lake Publications Ann Lake/Helen GonçalvesDesign: Jane GouveiaSponsor: Pfizer SAEnquiries: Ann Lake Publications PO Box 265, Gallo Manor, 2052Fax to email: 086 671 9397Email: [email protected]: www.annlakepublications.co.za
Sports Medicine Update Page 2 Voume 1 No 1 June 2008Editorial Board
Dr Mark FergusonOrthopaedic SurgeonJohannesburg
Dr Jon PatriciosSports PhysicanJohannesburg
Dr Willem van der MerweOrthopaedic SurgeonCape Town
Dr Mike MarshallSports PhysicianDurban
Evan Speechly PhysiotherapistJohannesburg
While Achilles was in the temple of Apollo negotiating marriage to Polyxena, Paris discharged at him a poisoned arrow, which, guided by Apollo, fatally wounded him in the heel. This was his only vulnerable spot; for Thetis, having dipped him when an infant in the river Styx, had rendered every part of him invulnerable except that by which she held him. Although Homer talks of Achilles’ rage toward the Archaens many an athlete has cursed the pain of achilles tendon problems.
Tendon injuries account for a substantial proportion of overuse injuries in sport. Despite the morbidity associated with tendon injury in athletes, management is far from scientifically based. Only in 1990 did Clancy recognise the need for formalised nomenclature of the disorder. Tendinosis is the chief pathological label describing intratendinous degeneration. This is commonly due to aging, microtrauma and vascular compromise. Tendinopathy until recently was thought to be a purely inflammatory process caused by overuse but evidence now points to a multi-factorial aetiology for a condition that still remains defiant to all our forms of treatment. This issue was borne out of a recent conference held in South Africa on tendinopathy and featured many leading international speakers. We were fortunate to encourage
“Sing, Goddess, of the rage, of Peleus’ son Achillesthe accursed rage, which brought pain to thousands ”
Homer, Iliad
some of these presenters to share their knowledge in Sports Medicine Update.
Excellent research done at the Sports Science Institute by Mike Posthumus on genetic predisposition enables us to look into the future whereby susceptible individuals may be recognised and treated appropriately.
Although regrettably lost from our shores Helen Millson from the UK provides a thorough scientific approach to the conservative management of tendon problems. We are extremely fortunate to have received Prof Håkan Alfredson’s paper on his most recent research on invasive treatment modalities for achilles tendinopathy. Prof Alfredson has been one of the foremost researchers on tendinopathy over the last decade and we were honoured to have him here to present and perform live surgery at the Sports Centre in Rosebank. Barry Getz, who was instrumental in developing a functional rehabilitation programme for achilles tendon repairs, provides excellent guidelines for post-surgical therapy and recovery.
Our case report this issue from Glen Vardi reminds us that not only activity-related knee pains are sports injuries. Please, if you have any interesting cases please send them to the email below.
Chronic patellar tendinopathyChronic patellar tendinopathy (jumper’s knee) mainly affects athletes performing in sports that require an intensive use of the knee extensor mechanism such as jumping disciplines, e.g. track and field, volleyball, basketball, soccer and tennis. Clinically, it presents as an overuse syndrome with localised pain and some swelling over the inferior pole of the patella.
The diagnosis of patellar tendinopathy is clinical based on patients’ subjective reports of pain related to activity levels. The onset of symptoms is often insidious, but usually relates to an
increase in frequency or intensity of activity involving rapid repetitive ballistic movements of the knee joint. Initially, athletic patients will complain of a dull ache in the anterior knee after strenuous activity. Athletes who continue to play with these symptoms eventually experience pain that interferes with performance. On examination there is tenderness to palpation at the inferior pole of the patella.
There are numerous grading systems based the severity of the symptoms and the limitation of function. A recently developed 100 point system, The Victorian Institute of
Sport Assessment (VISA) is most commonly used. The primary benefit of the score is to monitor severity and response to therapy but it does not help with treatment plans or can be used as a prognostic tool.
Ultrasound and magnetic resonance imaging are the most commonly used modalities to confirm diagnosis and to quantify the severity of the condition. Ultrasound remains the investigation of choice at our Centre. Typical findings are hypoechogenic areas of the proximal tendon as well as irregularity of the tendinous envelope, intratendinous calcification, and erosion of the
Dr Mark Ferguson
Sports Medicine UpdateVolume 3 No 4 January 2011 Page 3
repair of macroscopic defects, scarification—that is, longitudinal tenotomy/tenoplasty of the tendon, percutaneous needling, percutaneous longitudinal tenotomy and arthroscopic assisted decompression of the tendon, possibly with excision of the inferior pole of the patella.
The aim of most surgical techniques has been to debulk the degenerative tissue, perform tenotomies and stimulate some healing response. Most technique interventions is aimed at the tendon or bone or both.
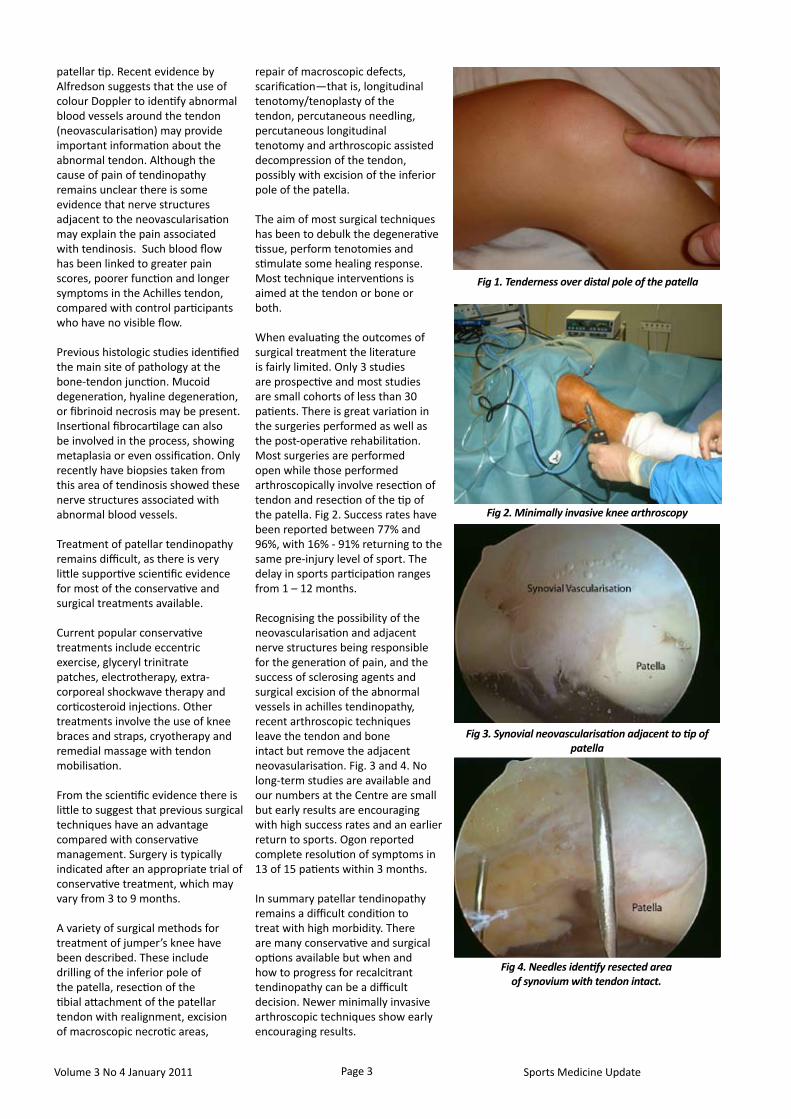
When evaluating the outcomes of surgical treatment the literature is fairly limited. Only 3 studies are prospective and most studies are small cohorts of less than 30 patients. There is great variation in the surgeries performed as well as the post-operative rehabilitation. Most surgeries are performed open while those performed arthroscopically involve resection of tendon and resection of the tip of the patella. Fig 2. Success rates have been reported between 77% and 96%, with 16% - 91% returning to the same pre-injury level of sport. The delay in sports participation ranges from 1 – 12 months. Recognising the possibility of the neovascularisation and adjacent nerve structures being responsible for the generation of pain, and the success of sclerosing agents and surgical excision of the abnormal vessels in achilles tendinopathy, recent arthroscopic techniques leave the tendon and bone intact but remove the adjacent neovasularisation. Fig. 3 and 4. No long-term studies are available and our numbers at the Centre are small but early results are encouraging with high success rates and an earlier return to sports. Ogon reported complete resolution of symptoms in 13 of 15 patients within 3 months.
In summary patellar tendinopathy remains a difficult condition to treat with high morbidity. There are many conservative and surgical options available but when and how to progress for recalcitrant tendinopathy can be a difficult decision. Newer minimally invasive arthroscopic techniques show early encouraging results.
Fig 1. Tenderness over distal pole of the patella
patellar tip. Recent evidence by Alfredson suggests that the use of colour Doppler to identify abnormal blood vessels around the tendon (neovascularisation) may provide important information about the abnormal tendon. Although the cause of pain of tendinopathy remains unclear there is some evidence that nerve structures adjacent to the neovascularisation may explain the pain associated with tendinosis. Such blood flow has been linked to greater pain scores, poorer function and longer symptoms in the Achilles tendon, compared with control participants who have no visible flow.
Previous histologic studies identified the main site of pathology at the bone-tendon junction. Mucoid degeneration, hyaline degeneration, or fibrinoid necrosis may be present. Insertional fibrocartilage can also be involved in the process, showing metaplasia or even ossification. Only recently have biopsies taken from this area of tendinosis showed these nerve structures associated with abnormal blood vessels.
Treatment of patellar tendinopathy remains difficult, as there is very little supportive scientific evidence for most of the conservative and surgical treatments available.
Current popular conservative treatments include eccentric exercise, glyceryl trinitrate patches, electrotherapy, extra-corporeal shockwave therapy and corticosteroid injections. Other treatments involve the use of knee braces and straps, cryotherapy and remedial massage with tendon mobilisation. From the scientific evidence there is little to suggest that previous surgical techniques have an advantage compared with conservative management. Surgery is typically indicated after an appropriate trial of conservative treatment, which may vary from 3 to 9 months. A variety of surgical methods for treatment of jumper’s knee have been described. These include drilling of the inferior pole of the patella, resection of the tibial attachment of the patellar tendon with realignment, excision of macroscopic necrotic areas,
Fig 2. Minimally invasive knee arthroscopy
Fig 3. Synovial neovascularisation adjacent to tip of patella
Fig 4. Needles identify resected area of synovium with tendon intact.

Sports Medicine Update Volume 3 No 4 January 2011Page 4
Genetic predisposition to Achilles tendinopathyAchilles tendinopathy is a complex multifactorial injury for which the exact aetiology is unknown. However, several intrinsic (from within the body) and extrinsic (environmental) risk factors have been identified.
It has been proposed that the intrinsic risk factors predispose the athletes for a specific injury. Once predisposed, susceptibility to injury is determined by exposure to extrinsic risk factors. It is important to note that these intrinsic and extrinsic risk factors do not cause or necessarily result in an injury. Genetic factors have recently been suggested as additional intrinsic risk factors for for chronic Achilles tendinopathy, as well as other musculoskeletal soft tissue injuries such as; Achilles tendon ruptures, rotator cuff tendon injuries, shoulder dislocations and ACL ruptures. Although the sequence of the 3.2 billion bases (A, C, G or T) of human DNA are over 99.9% identical, the sequence variations (polymorphisms) in human DNA contribute to the visible and measurable biological variation observed in individuals. In fact, many of the common intrinsic risk factors implicated in injuries, such as previous injury, somatotype, neuromuscular characteristics, biomechanical features, anatomical features and flexibility/laxity are, together with several other non-genetic factors, to a lesser or greater extent determined by genetic factors. Many of the intrinsic risk factors could therefore also in their own right be considered as complex multifactorial phenotypes.
We hypothesise that polymorphisms within specific genes that code for proteins involved in tendon biology are partially responsible for the observed inter-individual variation in:
susceptibility to tendon injuries 1. (intrinsic risk)adaptation to mechanical 2. loading (training)response to injury and repair 3. (healing), and response to treatment 4. modalities (surgical and non-surgical).
Based on this hypothesis, our research group at the UCT/MRC Research Unit for Exercise Science and Sports Medicine at the University of Cape Town have investigated several genetic sequence variants for their association with Achilles tendinopathy. To date, through the use of a candidate gene approach (selection of genes based on their biological function), various genetic sequence variants have been found to associate with risk of developing Achilles tendinopathy. Genes coding for structural proteins within tendons, as well as genes coding for proteins involved in various other biological functions within tendons have been investigated. The genes shown to associate with risk of chronic Achilles tendinopathy to date includes the α1 chain of type V colagen (COL5A1), tenacin-C (TNC), matrix metalloproteinase-3 (MMP3) and growth and differentiation factor 5 (GDF5) genes (Figure 1). The association of polymorphisms within the COL5A1 and GDF5
genes have already been repeated in a second independent population.
Although there are limitaioms to these initial association studies, the results suggest that chronic Achilles tendinopathy is caused by the poorly understood interaction of multiple genetic and environmental factors. Furthemore, these findings suggests that several biological processes such as:
synthesis of the collagne i. fibril within tendons (type V collagen),response to mechanical loading ii. (tenacin-C),
breakdown of collagen fibrils (MMP-3), and
signalling (growth and iii. differentiation factor 5),
play a role in the aetiology of chronic Achilles tendinopathy. The results support the hypothesis that sequence variants within specific genes contribute to inter-individual variation in susceptibility to chronic Achilles tendinopathy.
In addition to merely identifying ‘risk’, insights into the genetic contribution to injury susceptibility can help scientists better understand the precise molecular mechanism by which chronic Achilles tendinopathy occur. As previously mentioned, due to the design of these studies
(where candidate genes were identified and tested) all the genes identified to date encode for proteins directly involved in biological processes within tendons. Although there are biological reasons for the associated genes to be directly involved in the aetiology of these injuries, the exact reasons why
GeneProtein/
PolypeptidePopulations
COL5A1Type V collagen α1
chain2
TNC Tenascin C 1
MMP3Matrix
metalloproteinase 31
GDF5Growth and
Differentiation Factor 5
2
Figure 1. Genes associated with chronic Achilles tendinopathy are shown. The protein encoded for by the gene, as well as, the number of independent populations investigated to date are also summarised.
Prof M Collins2,1,3
1UCT/MRC Research Unit for Exercise Science and
Sports Medicine of the Department of Human
Biology, Faculty of Health Sciences, University of
Cape Town (UCT) Cape Town, South Africa
2The South African Medical Research Council (MRC) Cape Town, South
Africa 3International Olympic Centre (IOC)
Research Centre, University of Cape Town, Cape Town, South Africa.
Dr M Posthumus1,3,
Sports Medicine UpdateVolume 3 No 4 January 2011 Page 5
these variants are associated with these injuries still remains to be established. These genetic associations should therefore be tested for functional significance using appropriate molecular and cellular biology techniques.
For example, initial work from our laboratory has suggested that variants within the COL5A1 which are assocciated with chronic Achilles affect COL5A1 mRNA stability and by implication the production of type V collagen in tendons. Type V collagen, regulates fibril formation in tendons and it is possible that inherent differences in the levels of type V collagen could result in altered biochemical and biomechanical properties of tendons, which could predispose certain individuals to an increased injury risk.
Importantly for the sports clinician, the identification of genetic risk factors may identify individuals predisposed to musculoskeletal soft tissue injuries, such as Achille tendinopathy (Figure 1).
Individuals at increased risk of Achille tendinopathy could then benefit from customised training programmes and/or optimal exposure to extrinsic risk factors to reduce the incidence of injury. Furthermore, similar models could also be used to:
assist in determining which i. therapeutic interventions could be most effective in different individuals with musculoskeletal soft tissue injuries, and assist the clinician defining the ii. prognosis for these injuries. This approach is commonly referred to as “personalised medicine”.
The diagnosis and treatment of patients in the future may therefore be determined by traditional clinical examinations
and specialised investigations, as well as with the aid of the patient’s genetic profile (testing of multiple genetic variants). This concept of “personalised medicine”, as opposed to the more traditional approach of determining standards of care based on the average responses within large populations, is in its infancy.
The idea that genetic testing could one day be used in combination with other risk factors to determine risk (not diagnostic) for complex disorders, such as Achilles tendinopathy, either alone or in combination with other risk factors, is very attractive. However, more research is required before this becomes a reality. Although there could in the future be benefit in identifying athletes genetically predisposed to specific injuries, there are concerns that this information could be used to discriminate against athletes. Exercise scientists and sports clinicians need to take an active role in debating the ethical issues raised by the possible application of genetic testing in the discipline. Once consensus is reached, standard procedures need to be developed within this specific discipline.
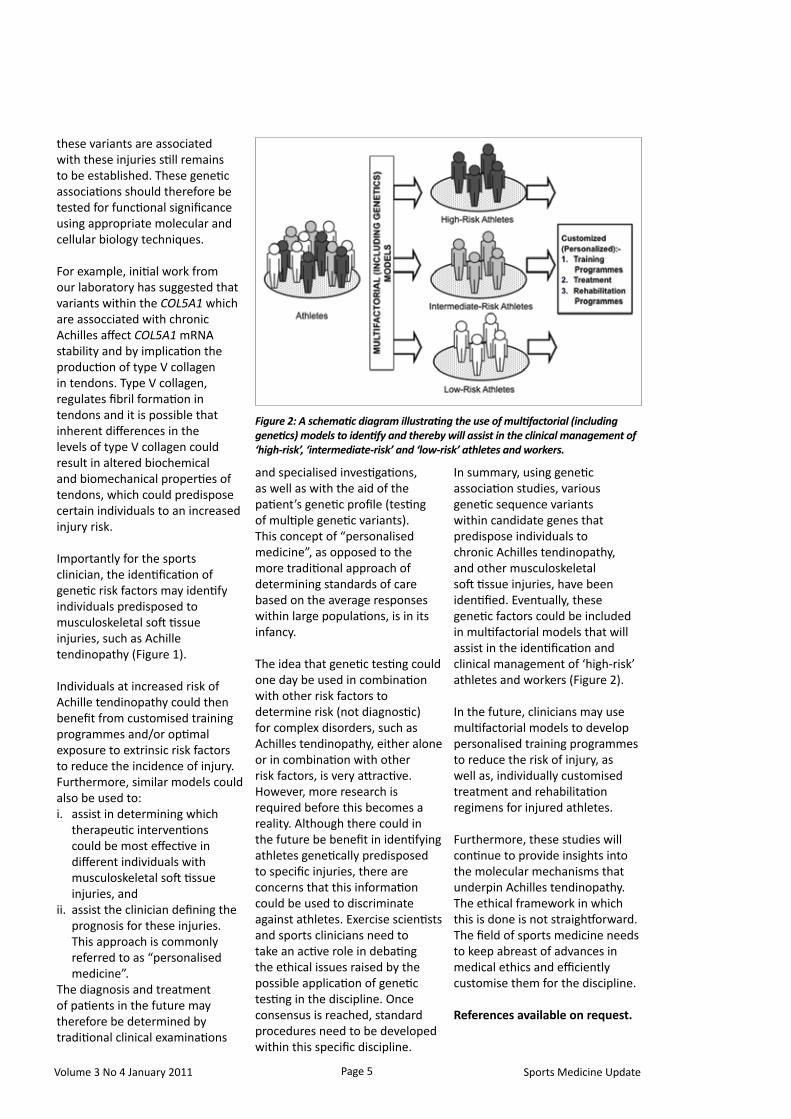
In summary, using genetic association studies, various genetic sequence variants within candidate genes that predispose individuals to chronic Achilles tendinopathy, and other musculoskeletal soft tissue injuries, have been identified. Eventually, these genetic factors could be included in multifactorial models that will assist in the identification and clinical management of ‘high-risk’ athletes and workers (Figure 2).
In the future, clinicians may use multifactorial models to develop personalised training programmes to reduce the risk of injury, as well as, individually customised treatment and rehabilitation regimens for injured athletes.
Furthermore, these studies will continue to provide insights into the molecular mechanisms that underpin Achilles tendinopathy. The ethical framework in which this is done is not straightforward. The field of sports medicine needs to keep abreast of advances in medical ethics and efficiently customise them for the discipline.
References available on request.
Figure 2: A schematic diagram illustrating the use of multifactorial (including genetics) models to identify and thereby will assist in the clinical management of ‘high-risk’, ‘intermediate-risk’ and ‘low-risk’ athletes and workers.
Sports Medicine Update Volume 3 No 4 January 2011Page 6
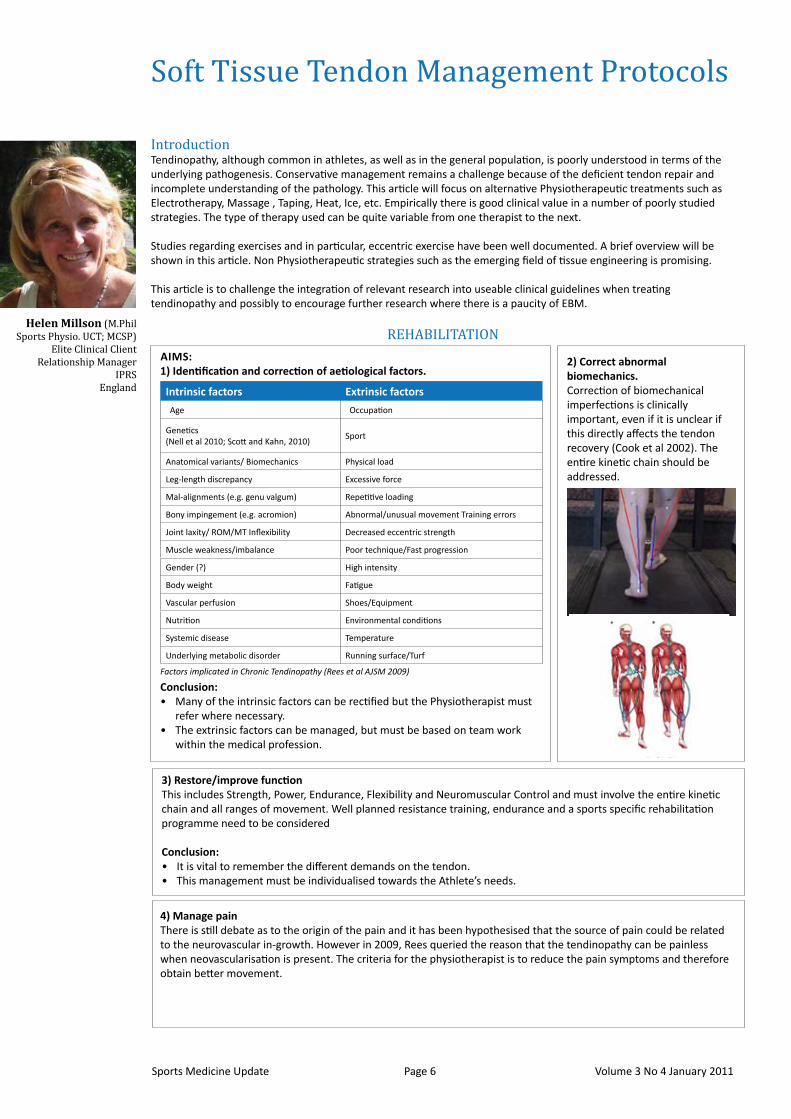
2) Correct abnormal biomechanics.Correction of biomechanical imperfections is clinically important, even if it is unclear if this directly affects the tendon recovery (Cook et al 2002). The entire kinetic chain should be addressed.
4) Manage pain There is still debate as to the origin of the pain and it has been hypothesised that the source of pain could be related to the neurovascular in-growth. However in 2009, Rees queried the reason that the tendinopathy can be painless when neovascularisation is present. The criteria for the physiotherapist is to reduce the pain symptoms and therefore obtain better movement.
IntroductionTendinopathy, although common in athletes, as well as in the general population, is poorly understood in terms of the underlying pathogenesis. Conservative management remains a challenge because of the deficient tendon repair and incomplete understanding of the pathology. This article will focus on alternative Physiotherapeutic treatments such as Electrotherapy, Massage , Taping, Heat, Ice, etc. Empirically there is good clinical value in a number of poorly studied strategies. The type of therapy used can be quite variable from one therapist to the next.
Studies regarding exercises and in particular, eccentric exercise have been well documented. A brief overview will be shown in this article. Non Physiotherapeutic strategies such as the emerging field of tissue engineering is promising.
This article is to challenge the integration of relevant research into useable clinical guidelines when treating tendinopathy and possibly to encourage further research where there is a paucity of EBM.
REHABILITATION
Soft Tissue Tendon Management Protocols
AiMS:1) Identification and correction of aetiological factors.
Conclusion:Many of the intrinsic factors can be rectified but the Physiotherapist must • refer where necessary.The extrinsic factors can be managed, but must be based on team work • within the medical profession.
intrinsic factors Extrinsic factors
Age Occupation
Genetics (Nell et al 2010; Scott and Kahn, 2010)
Sport
Anatomical variants/ Biomechanics Physical load
Leg-length discrepancy Excessive force
Mal-alignments (e.g. genu valgum) Repetitive loading
Bony impingement (e.g. acromion) Abnormal/unusual movement Training errors
Joint laxity/ ROM/MT Inflexibility Decreased eccentric strength
Muscle weakness/imbalance Poor technique/Fast progression
Gender (?) High intensity
Body weight Fatigue
Vascular perfusion Shoes/Equipment
Nutrition Environmental conditions
Systemic disease Temperature
Underlying metabolic disorder Running surface/Turf
Factors implicated in Chronic Tendinopathy (Rees et al AJSM 2009)
3) Restore/improve functionThis includes Strength, Power, Endurance, Flexibility and Neuromuscular Control and must involve the entire kinetic chain and all ranges of movement. Well planned resistance training, endurance and a sports specific rehabilitation programme need to be considered
Conclusion:It is vital to remember the different demands on the tendon.• This management must be individualised towards the Athlete’s needs.•
Helen Millson (M.Phil Sports Physio. UCT; MCSP)
Elite Clinical Client Relationship Manager
IPRSEngland

A) GeneralAs basic Science of Tendinopathy has evolved so have the treatment options for these conditions. Conservative treatment is the first Management strategy and may consist of the following non–Physiotherapy interventions: NSAID, Cortico steroids, Aprotonin, Glyceryl trinitrate patches, Sclerosing Polidocinal Injections and High Volume Injections (HVIGI) Some of these have shown to have some potential but there is little quality evidence.
There is an increasing interest in growth factors, stem cell therapy and cultured bone marrow and although the results have been encouraging (Obaid and Connell AJSM 2010), the debate remains as to their use. (de Vos et al., 2010; IOC Consensus -Engebretson et al 2010; Prof Roger Smith 2010)
B) Physiotherapy TreatmentElectrotherapyI. Cryotherapy/Compression II. Acupuncture, Dry Needling III. Manual techniquesIV. Stretching Exercises V. Proprioception/Neuromuscular Control VI. Taping/Bracing VII. Eccentric Exercises VIII. HydrotherapyIX.
ElectrotherapyProfessor Tim Watson (Cambridge Conference, 2010) has stated that the balance of evidence suggests that there is a role for electrotherapy in this area as long as one is selective.
Generally the use of ECSWT remains controversial except with calcific tendinopathy of Rotator Cuff Pathology. Although Professor Rompe at the Tendinopathy Conference in London September 2010 demonstrated his success with the use of ECSWT, the main conclusion generally is that the mechanism of action is not yet fully understood. The questions remain as to the intensity and dose required, as well as the best machine to be utilised and the physiotherapist’s preferences.Thus although there are many studies, more supportive than not, further research is needed.
Laser TherapyAlthough the American Physical Therapy Association (2010) stated that clinicians should consider the use of LLLT, Tumilty (Photomed Laser Surg. 2010) in his systematic review with meta-analysis stated that there were conflicting findings from multiple trials and essentially it is effective when recommended dosages are used.
Conclusion – Electrotherapy treatment: There is no substantive evidence and more quality research is required.
5) improve pathology The decision making regarding management revolves around the question – are the pathological changes a problem clinically and can we change the matrix turnover in tendinopathy? (Riley et al 2001) The question remains as to whether there is an inflammatory pathology? (Millar et al, 2010)
Conclusion: The knowledge is growing regarding the pathological changes in the tendon, but as yet there is no real consensus and it is imperative that there is good clinical reasoning when applying therapy.
REHABiLiTATiON: Stages of Healing
OTHER THERAPIES
Area Author Comment
Heat (via microwave)
Giombini et al., 2002; 2006
Patients who received hyperthermia experienced better pain relief compared with US or Excercise groups. Also better movement and function. Short term improvement maintained for 6 weeks
Hyperthermia with low frequency microwave compared with US.
Chapman Jones and Hill, 2002
Applied for 2 weeks = decrease pain at 12 months compared with conventional treatment.
Ultrasound Giombini, 2006US is ineffective as a thermal modality over large areas, as it can heat target areas up to only twice the size of the area of the transducer
UltrasoundHalfredson and Cook, 2008
Therapeutic US increases protein synthesis in tendons but there is an oversupply of poor quality protein in tendons suffering from overuse so may not improve clinical outcome to further increase protein production
UltrasoundProf Tim Watson, 2010
US good for tendon repair but not for chronic tendinopathy.
Low Intensity Pulsed US:
Warden et al., 2003; Walsh et al., 2007, Quin et al., 2006
Similar to shockwave, microcurrent and PMF in that established for wound healing and fracture. Also good demo for bone-tendon healing. ? Tendinopathy. More effective studies required.
UltrasoundPhiladelphia Panel, 2001
Effective for the tretament of Calcific tendonitis in the ShoulderLiterature shows possibly slightly effective in Lateral Epicondylitis
Ultrasound and LLLT
Rvan der Windt et al., 1999; Robertson and Bakker, 2001; Speed, 2001,Warden et al., 2008; Rees et al., 2009
US and LLLT possibly local heating of tissues. No other benefit.
Microcurrent Therapy
Some have methodological issues, human/ clinical studies less numerous. Generally encouraging. More effective studies required.
Pulsed Short Wave Therapy
Maryam et al., 2010 The thermal and non-thermal effects of high and low (PSWT) Significant physiological changes associated with the application of PSWT have been demonstrated
Ion/Phonophoresis
No real evidence. Limited evidence that US with phonophoresis may work with chronic tennis elbow
Hunter (2009) suggests that 50 – 60% of synthesis occurs during the regeneration phase. It is also important to be Objective when increasing the Rehabilitation. This may include the VISA -A Scale (Robinson et al, BJSM 2001) and the Visual Analogue Scale.
Tensile Strength
Lag Regeneration Remodelling
72Hrs
Time
4-6 days
5 days
10-12 wks
STAGE 1 STAGE 2 STAGE 3
3wks
6-12 mnths
Stages of Healing
MANAGEMENT
Sports Medicine UpdateVolume 3 No 4 January 2011 Page 7

Sports Medicine Update Volume 3 No 4 January 2011Page 8
C) Further physiotherapy interventions - Non Electrotherapy1) Cryotherapy and CompressionThere is evidence that combined cryotherapy and compression is superior to cryotherapy alone. (Speed 2004; Fink et al, 2002; Bleakley et al., 2005; Knobloch et al., 2008,.)
2) Acupuncture and Dry needling In their Cochrane Review, Green et al., 2008 showed that acupuncture might be able to provide short term relief of pain from tennis elbow. However, more research is needed.
Massage/FrictionIn reviewing the evidence it appears that transverse friction has no benefit over other treatments
4) Fascial ManipulationThere is a substantial decrease in pain in the short term with Patella tendinosis (Mayer et al., 2006; Pedrelli et al., 2009)
5) SSTMEmpirically, SSTM has clinical value in the treatment of soft tissue dysfunction. It may improve the biomechanical properties of healing tissue by increasing the collagen synthesis and improving collagen alignment. It may also increase the blood supply and help with pain relief (Glenn Hunter, 1998 to date). However, a neuro-physiological explanation may be the plausible explanation (Christenson, 2007). Conclusion: More research is needed.
6) Stretching - Tendinopathy Different sports require different strategies.A more stiff tendon is appropriate in low level sports such as cycling swimming, boxing sailing etc. By contrast, in sports with SSC movements (high loads), a more compliant MT unit requires high storage capacity for potential energy and must be sufficiently compliant to absorb energy e.g. basketball, high jump long jump etc. Therefore a more flexible tendon is appropriate.
The question is whether the Clinician can influence the compliance of tendons and whether ballistic or static type of stretching is relevant?
According to Rees et al (2009) there is no evidence to confirm either type of stretching and further research is needed. Witvrouw et al, (2007) hypothesised that perhaps eccentric exercises are similar to ballistic stretches.
Allison and Purdham, (2009) likened the eccentric heel drop exercises as an aggressive stretching programme suited to loading the passive structures. Further, the hypothesis is that a compliant tendon absorbs more energy, so little energy is transferred to the contractile apparatus and this reduces risk of injuring muscle. (Conf London Sep 2010)
Conclusion: FUNCTIONAL FLEXIBILITY is the key to this strategy.
7) Proprioception/NM Control This is a cornerstone of the management of Tendinopathy whereby there is modulation of afferent input to influence neuro-muscular regulation. Vincenzio (London Conference, Oct 2010), highlighted the involvement of the Central Neuronal mechanism.
8) TapingThere is general consensus regarding the proprioceptive effect of taping.However, there is little evidence to support this regarding Tendinopathy.Bracing, night splints, heel lifts and orthotics all have a role to play, but further research needs to be undertaken in this aspect.
9) Hydrotherapy may be undertaken in rehabilitation. Caution should be employed in pathology such as Achilles Tendinopathy where a brace should be worn in the water especially post surgery.
10) Eccentric ExercisesOver the years the use of Eccentric exercises has been used with positive effect and there are many studies to support this strategy (Hakan Alfredson 1998). However, what is most important is that there is much more convincing evidence that tendons respond to high load, regardless if concentric-eccentric, eccentric or isometric, rather than isolated eccentrics. (Alison and Purdham, 2009; Dr Peter Malliaris UK, 2010; Craig Purdham Australian Institute of Sport, 2010)
The exercise programme is performed for 6 – 12 weeks and if it is responding, one should continue for 6 – 12 months on a maintenance programme. Surgery is not considered until there has been at least 6 months of Conservative treatment.
Taping for Patella tendinopathy Taping for Wrist Extensors (Published in Rose McDonalds Taping) book, 2010)
Taping for Achilles Tendinopathy
Sports Medicine UpdateVolume 3 No 4 January 2011 Page 9
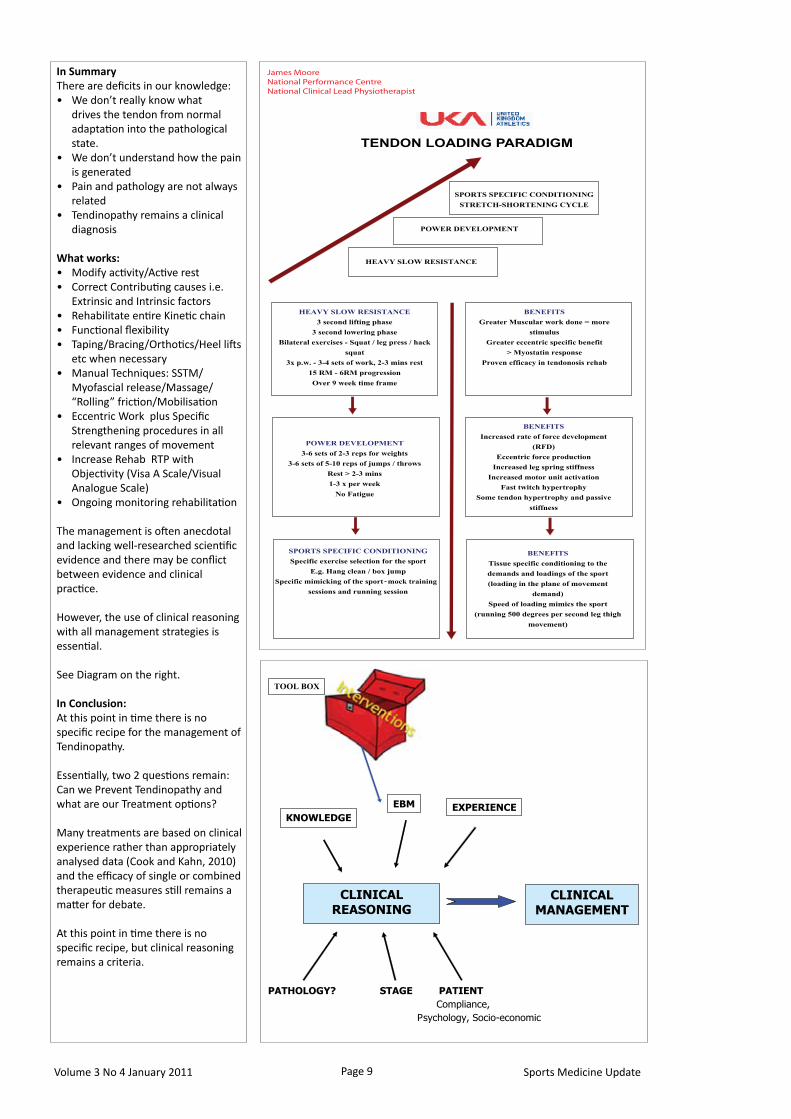
in SummaryThere are deficits in our knowledge:
We don’t really know what • drives the tendon from normal adaptation into the pathological state.We don’t understand how the pain • is generatedPain and pathology are not always • relatedTendinopathy remains a clinical • diagnosis
What works:Modify activity/Active rest• Correct Contributing causes i.e. • Extrinsic and Intrinsic factorsRehabilitate entire Kinetic chain• Functional flexibility• Taping/Bracing/Orthotics/Heel lifts • etc when necessaryManual Techniques: SSTM/• Myofascial release/Massage/ “Rolling” friction/MobilisationEccentric Work plus Specific • Strengthening procedures in all relevant ranges of movementIncrease Rehab RTP with • Objectivity (Visa A Scale/Visual Analogue Scale)Ongoing monitoring rehabilitation•
The management is often anecdotal and lacking well-researched scientific evidence and there may be conflict between evidence and clinical practice.
However, the use of clinical reasoning with all management strategies is essential.
See Diagram on the right.
in Conclusion:At this point in time there is no specific recipe for the management of Tendinopathy.
Essentially, two 2 questions remain:Can we Prevent Tendinopathy and what are our Treatment options?
Many treatments are based on clinical experience rather than appropriately analysed data (Cook and Kahn, 2010) and the efficacy of single or combined therapeutic measures still remains a matter for debate.
At this point in time there is no specific recipe, but clinical reasoning remains a criteria.
TENDON LOADING PARADIGM
SPORTS SPECIFIC CONDITIONING STRETCH-SHORTENING CYCLE
HEAVY SLOW RESISTANCE
POWER DEVELOPMENT
BENEFITS Tissue specific conditioning to the demands and loadings of the sport (loading in the plane of movement
demand) Speed of loading mimics the sport
(running 500 degrees per second leg thigh movement)
SPORTS SPECIFIC CONDITIONING Specific exercise selection for the sport
E.g. Hang clean / box jump Specific mimicking of the sport - mock training
sessions and running session
POWER DEVELOPMENT 3-6 sets of 2-3 reps for weights
3-6 sets of 5-10 reps of jumps / throws Rest > 2-3 mins 1-3 x per week
No Fatigue
BENEFITS
Increased rate of force development (RFD)
Eccentric force production Increased leg spring stiffness
Increased motor unit activation Fast twitch hypertrophy
Some tendon hypertrophy and passive stiffness
HEAVY SLOW RESISTANCE 3 second lifting phase
3 second lowering phase Bilateral exercises - Squat / leg press / hack
squat 3x p.w. - 3-4 sets of work, 2-3 mins rest
15 RM - 6RM progression Over 9 week time frame
BENEFITS Greater Muscular work done = more
stimulus Greater eccentric specific benefit
> Myostatin responseProven efficacy in tendonosis rehab
James MooreNational Performance CentreNational Clinical Lead Physiotherapist
CLINICAL REASONING
TOOL BOX
KNOWLEDGE
EBM EXPERIENCE
CLINICAL MANAGEMENT
PATHOLOGY? STAGE PATIENT Compliance, Psychology, Socio-economic

Sports Medicine Update Volume 3 No 4 January 2011Page 10
Figure 1. Neovascularisation adjacent to achilles
New treatment methods for the chronic painful Achilles tendon:
Sclerosing polidocanol injections and mini-surgical “scraping”IntroductionDuring the last fifteen years there has been at the Sports Medicine Unit in Umeåbeen intensive research on pain mechanisms related to the chronic painful tendon. Investigations using gray-scale ultrasound (US) together with colour Doppler (CD) have shown that chronic painful non-insertional Achilles tendinopathy had high blood flow, while pain-free normal tendons had no high blood flow.10 The structural tendon changes were located mainly in the ventral Achilles tendon, and the blood flow was seen mainly in regions with structural changes, and in the soft tissue just outside the ventral tendon.
These findings led to evaluation of pain in relation to the regions with high blood flow outside the ventral tendon. US+CD-guided injections of small volumes of a local anaesthetic, targeting only the regions with high blood flow on the ventral side of the tendon (just outside the tendon), led to a complete pain relief during tendon loading activity. The results from parallel immune-histochemical analyses of biopsies demonstrated nerves in close relation to blood vessels.1
MethodsSclerosing polidocanol injectionsThe findings using US+CD, immuno-histochemical analyses of biopsies, and injections of local anaesthesia, led to the hypothesis that blood vessels and nerves on the ventral side of the Achilles tendon were closely related to the tendon pain. Methods to interfere with blood vessels and nerves were discussed, and we started to use US+CD-guided injection treatment with the sclerosing substance polidocanol. Polidocanol is a well known substance, that has been in use for many years to treat varicose
veins and teleangiectasies, with very few side effects.6,7
We decided to start with a pilot study on patients with a long duration of pain symptoms from chronic midportion Achilles tendinosis, and to use the lowest concentration of polidocanol (5mg/ml).
Rehabilitation after treatmentOur traditional rehabilitation protocol after polidocanol injection treatment is as follows:
Follow-ups and additional treatments6-8 weeks after each injection treatment a new clinical and US+CD examination is performed. If there is remaining tendon pain during loading, together with remaining high blood flow on the deep side of the tendon, another injection treatment is performed-followed by the same rehabilitation protocol as after the first injection treatment.
We recommend a maximum of 5 injection treatments, with 6-8 weeks in between. Clinical studiesThe first study was a pilot study on 10 patients (7 males and 3 females, mean age 55 years) with chronic painful midportion Achilles tendinosis.11 (figure 1)After a mean of 2 polidocanol injection treatments, with 6-8 weeks in between, 8/10 patients were satisfied with the effect of the treatment and back to full Achilles tendon loading activity. At the 6 months follow-up, the same 8 patients were still satisfied but the two patients who were not satisfied (remaining tendon pain) had remaining high blood flow in the tendons.
Prof Håkan Alfredson MD, PhD
Sports Medicine Unit, University of Umeå
S-901 87 Umeå, Sweden
Rehabilitation after treatment
Day 1Rest-very light Achilles tendon loading.
Day 2-7Range of motion exercises and short walks in slow tempo.
Day 8-14Longer walks, light bicycling.
After 14 days
Gradual return to previous (before injury) tendon loading activity.

Sports Medicine UpdateVolume 3 No 4 January 2011 Page 11
An increased patient material allowed for follow-ups of larger groups. In a 2-year follow-up study (clinical and US+CD) of 42 patients (23 men and 19 women, mean age 53 years), 38 patients were still satisfied with the results of the treatment, and their VAS during Achilles tendon loading activity had decreased from 75 before treatment to 7 at follow-up.8
Ultrasound showed a significant reduction in the mean midportion tendon thickness (from 10 mm to 8 mm, p < 0.05) and a “more normal” tendon structure was seen. CD showed no, or a few, regions with remaining high blood flow (neovessels) in the majority of the successfully treated tendons, while there were multiple regions with high blood flow in the not satisfied patients. We concluded that initially good clinical results were associated with remaining good clinical results in the majority of the patients. Also, ultrasound showed a decreased tendon thickness and improved structure 2 years after treatment, indicating a remodelling, and possibly a regeneration, potential.8
Our good clinical results using US+CD-guided injections of polidocanol to treat midportion Achilles tendinosis have been reproduced by Clementsson et al. (2008),who showed good or excellent results in 20/26 midportion Achilles tendinosis tendons,4 and Torgalsen et al. in Oslo (non published material).
Complications using sclerosing polidocanol injection treatmentAt our clinic, patients undergoing this treatment are followed closely, and many are involved in research projects with long follow up periods. Therefore, we believe that we have reliable information about the complication rate in our material. After more than 1000 treated tendons, at the Sports Medicine Unit in Umeå and at the CapioArtro Clinic in
Stockholm, we have registered 6 total and 2 partial Achilles tendon ruptures. We believe this is a low complication rate. It should be remembered that we use a short rehabilitation period, with a relatively rapid return to full tendon loading activity.
PitfallsAlthough we have very few complications in our material, we have been informed about complications experienced by others. Complications such as thrombosis in the lower leg, excessive swelling around the Achilles and partial Achilles tendon rupture have been reported.
Mini-surgical “scraping”Again, the findings using US+CD, immuno-histochemical analyses of biopsies, and injections of local anaesthesia, together with the promising clinical results using sclerosing polidocanol injection treatment, raised the hypothesis that a surgical scraping procedure on the ventral side of the Achilles tendon would have a potential to cure the tendon pain. However, there were concerns about possible major formations of scar tissue, negatively affecting the tendon function. Therefore, we started slow, and didn´t involve athletes in the first trials. We used exactly the same pre-treatment evaluation as we use for sclerosing polidocanol injections, where the US and CD findings decide were the treatment is going to be targeted, and also the same rehabilitation protocol, with early walking and bicycling.
Clinical studiesAll tendons were examined with high resolution grey scale-ultrasound (US) and Colour Doppler (CD), AcusonSegoia (Siemens) at inclusion. A linear multifrequency (8 – 13 MHz) probe was used. CD was used to diagnose regions with high blood flow, and to locate where the blood flow entered the tendon. Both Achilles tendons were examined. Using US and CD the most proximal and most distal regions with high blood flow inside and outside the ventral Achilles were marked on the skin by a skin marker (Figure 1). After washing, local anaesthesia (5-10ml Xylocain+Adrenaline, 5mg/ml) was injected on the lateral and ventral side of the Achilles midportion. The skin was then draped with a sterile paper-cover exposing only the midportion of the Achilles tendon.
A longitudinal skin incision (1-2cm) was placed on the lateral side of the Achilles midportion, the sural nerve was kept aside, and the tendon was carefully identified (Figure 2). In the region with changes and high blood flow (marked by skin markers) the tendon was completely released from the ventral soft tissue, by sharp dissection with a knife, staying close to the ventral tendon. This was followed by haemostasis, using diathermy (figure 3). The skin was closed by single non-resorbable sutures.
The pilot study showed good clinical effects, with pain relief
Figure 2
Our good clinical results using US+CD-guided injections of polidocanol to treat midportion Achilles tendinosis have been reproduced by Clementsson et al. (2008)
New treatment methods for the chronic painful Achilles tendon:
Sclerosing polidocanol injections and mini-surgical “scraping”

Volume 3 No 4 January 2011Page 12Sports Medicine Update
and a rapid return to previous (before injury) activities without complications, in 8/10 patients.13 Because we had no serious side effects, the patient material was gradually increased to include also high level athletes. The clinical results in the now large patient material are still very promising, with a majority of the patients being satisfied and back in full Achilles tendon loading activity (non published material). Follow-
ups show a remodelling, with a gradually decreased tendon thickness and an improved tendon structure (non published material).
PitfallsThe few complications we have had have been related to poor wound care. Therefore, it is essential to keep the wound dry, and protect it from trauma such as rubbing from the shoe.
ConclusionsInterference on the ventral side of the Achilles midportion, where US+CD have shown high blood flow and biopsies have shown nerves in close relation to blood vessels, by targeted sclerosing polidocanol injections or targeted surgical “scraping”, have been shown to have a potential to cure the tendon pain and allow for a rapid return to full tendon
loading activity with low risks for complications. Pain relief and loading seems to be associated with a gradual improvement in terms of a decreased midportion tendon thickness and an improved structure. Mini-surgical “scraping” is a one-stage treatment, thereby saving time for the patients.
References - On request
Figure 3
Rehabilitation after mini-surgical “scraping
Day 1 Rest,elevated foot.
Day 2ROM, light stretching and short walks.
Day 3-7Gradually increased walking activity.
Day 8-14 Light bicycling
After 2 weeks
Sutures out, gradually increased load up to free activity after 4-6 weeks.
History 34 year old active female patient.with vague pain on the medial side of her right knee. Some catching and occasional locking. Intermittent swelling. She had been aware of these symptoms for about 2 years, and they were progressively getting worse.
Examination At her first visit, the knee was found to be effused. There was vague medial tibiofemoral joint line pain. She had an antalgic gait, but with no deformities. Menisical provocative tests were positive for pain, medially.
Investigations Xray showed metaphyseal changes in the proximal tibia and some bony irregularity of the medial femoral condyle.
Diagnosis Idiopathic bone infarcts
Progress: based on the above findings, an initial attempt at “revascularisation” was made, by bone grafting and drilling of the lesions, and debriding the damaged articular surface on both sides of the joint.
Case Study
Unfortunately, the latter did not work and eventually the articular surface and subchondral bone on the medial femoral condyle sloughed off and she could not cope with the ongoing symptoms of pain and swelling.
It was also noted that she developed varus pseudolaxity of the MCL, due to the relative destruction of the medial femoral condylae articular surface and about 5-10mm of subchondral bone.
She ended up having a total knee replacement.
Dr Glen VardiOrthopaedic Surgeon
Centre for Sports Medicine and Orthopaedics
Rosebank Johannesburg
Sports Medicine UpdateVolume 3 No 4 January 2011 Page 13
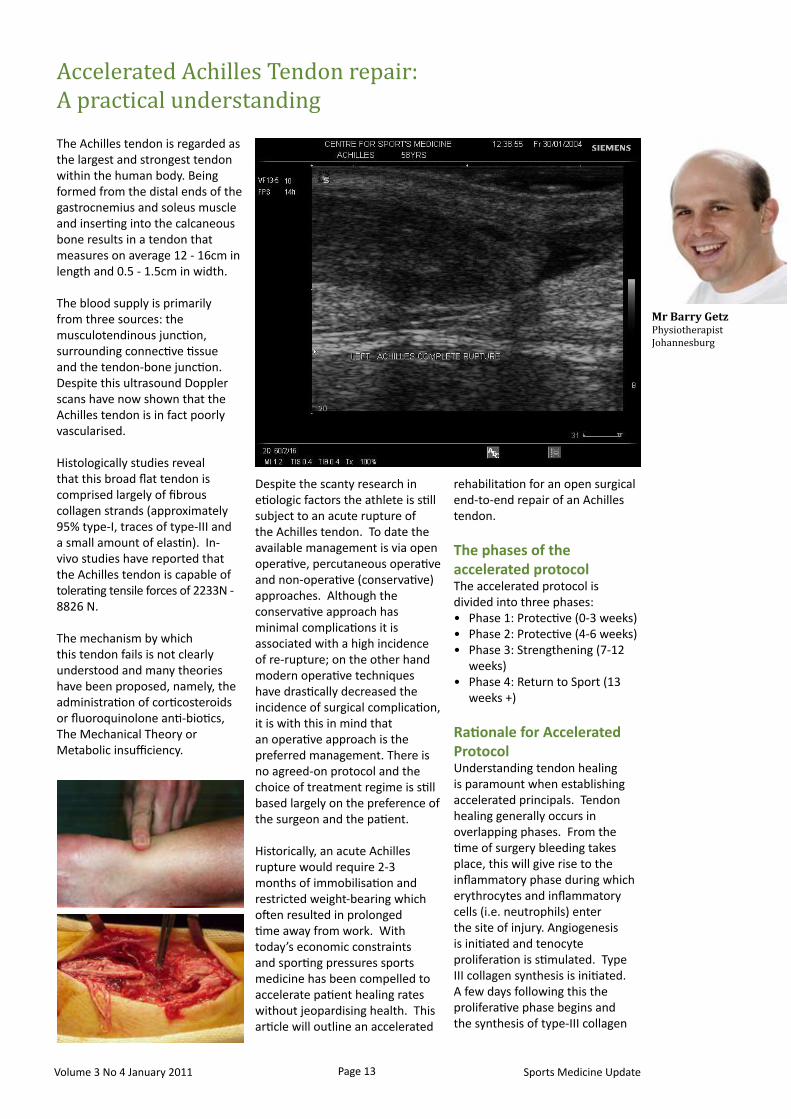
The Achilles tendon is regarded as the largest and strongest tendon within the human body. Being formed from the distal ends of the gastrocnemius and soleus muscle and inserting into the calcaneous bone results in a tendon that measures on average 12 - 16cm in length and 0.5 - 1.5cm in width.
The blood supply is primarily from three sources: the musculotendinous junction, surrounding connective tissue and the tendon-bone junction. Despite this ultrasound Doppler scans have now shown that the Achilles tendon is in fact poorly vascularised.
Histologically studies reveal that this broad flat tendon is comprised largely of fibrous collagen strands (approximately 95% type-I, traces of type-III and a small amount of elastin). In-vivo studies have reported that the Achilles tendon is capable of tolerating tensile forces of 2233N - 8826 N.
The mechanism by which this tendon fails is not clearly understood and many theories have been proposed, namely, the administration of corticosteroids or fluoroquinolone anti-biotics, The Mechanical Theory or Metabolic insufficiency.
Despite the scanty research in etiologic factors the athlete is still subject to an acute rupture of the Achilles tendon. To date the available management is via open operative, percutaneous operative and non-operative (conservative) approaches. Although the conservative approach has minimal complications it is associated with a high incidence of re-rupture; on the other hand modern operative techniques have drastically decreased the incidence of surgical complication, it is with this in mind that an operative approach is the preferred management. There is no agreed-on protocol and the choice of treatment regime is still based largely on the preference of the surgeon and the patient.
Historically, an acute Achilles rupture would require 2-3 months of immobilisation and restricted weight-bearing which often resulted in prolonged time away from work. With today’s economic constraints and sporting pressures sports medicine has been compelled to accelerate patient healing rates without jeopardising health. This article will outline an accelerated
rehabilitation for an open surgical end-to-end repair of an Achilles tendon.
The phases of the accelerated protocolThe accelerated protocol is divided into three phases:
Phase 1: Protective (0-3 weeks)• Phase 2: Protective (4-6 weeks)• Phase 3: Strengthening (7-12 • weeks)Phase 4: Return to Sport (13 • weeks +)
Rationale for Accelerated Protocol Understanding tendon healing is paramount when establishing accelerated principals. Tendon healing generally occurs in overlapping phases. From the time of surgery bleeding takes place, this will give rise to the inflammatory phase during which erythrocytes and inflammatory cells (i.e. neutrophils) enter the site of injury. Angiogenesis is initiated and tenocyte proliferation is stimulated. Type III collagen synthesis is initiated. A few days following this the proliferative phase begins and the synthesis of type-III collagen
Accelerated Achilles Tendon repair: A practical understanding
Mr Barry Getz PhysiotherapistJohannesburg

Sports Medicine Update Volume 3 No 4 January 2011Page 14
PHASE 1 (Protection)
Day of surgery
Patient placed into 30º equines back slab• Non weight-bearing crutch walking• Patient education on elevation and protection of • surgical repairDischarged•
Day 5
Placed into an orthopaedic boot with the ankle • adjusted to 30º equines e.g. VACOAchill©, Foam Walker (use heel wedges)Commence out of boot range of motion exercises•
inversion, eversion, restricted plantar and dorsi -flexion
Commence physiotherapy• Subtalar, mid and fore foot mobilisation -Soft tissue release and oedema massage -
Week 2
Initiate partial weight-bearing in orthopaedic boot (30º • equines)Commence resistant elastic activity (i.e. inversion, • eversion)Promote intrinsic foot muscle activity• Wound check by surgeon•
Week 3
Progress weight-bearing status• Commence gentle non weight-bearing stretching of • calfStationary cycling (heel is placed on pedal)• Hydrotherapy• Continue with physiotherapy (focus on ankle, subtalar • and foot mobilisation)Introduce core strength training•
PHASE 2 (Protection)
Week 4 - 6
Progressive weight-bearing• Full weight-bearing by week 5 -
Commence adjustment of heel wedge in boot• Aim to adjust 5mm per week. No heel wedge in boot -by end week 6
Continue physiotherapy (monitor lumbar spine/SIJ)• Increase resistance for all exercise (include plantar and • dorsi flexion)Continue physiotherapy (aggressive foot mobilisation)• Advance core strength training• Introduce proprioception exercises from week 5• Introduce cardiovascular exercises•
Phase 3 (Strengthening)
Week 7 - 12
Removal of all protective devices• 5mm heel wedge (bilaterally) in • all shoesGAIT retraining• Continue with strength, • proprioception training (NO BALLISTIC ACTIVITY!!)Full gym activity• Achieve full range of all • movementsCommence weight-bearing heel • raise

Sports Medicine UpdateVolume 3 No 4 January 2011 Page 15
patient satisfaction index was achieved when utilising early weight-bearing principles; this is compared to patients who are immobilised using casts and kept non-weight-bearing for up to six weeks.
ConclusionAn open end-to-end surgical repair combined with early mobilisation reduces range of motion loss, increases blood supply, and reduces the degree of
muscle atrophy but also decreases the time to resumption of normal activities.
The accelerated approach is not a modern gold standard for every patient, since a multitude of factors may influence the outcome. It is thus imperative that each surgeon carefully screen each patient intra-operatively prior to administering this type of protocol.
peaks. From about the sixth week the remodelling phase commences during which consolidation and maturation of the tendon occur. From the sixth week the repaired tissue changes from cellular to fibrous. Tenocyte metabolism still remains high and the tenocytes and collagen fibres begin to align based on the direction of stress. A high proportion of type-I collagen is now synthesised which is capable of tolerating higher tensile forces. From the tenth week maturation occurs and fibrous tissue changes into a scar-like tendon, this process continues for the subsequent months.
SummarySince the Achilles tendon is not capable of tolerating large tensile forces during the initial stages of rehabilitation the Achilles is placed into a shortened position, through the incorporation of orthopaedic boots and wedges, whilst permitting the gradual increase in intrinsic tendon force. This protective phase must compliment the production of collagen tissue without any delirious effects. In order to progress to the strengthening phase of the rehabilitation the Achilles tendon should have acquired sufficient tensile ability to tolerate everyday loads, excluding load spiking (e.g. ballistic activity).
The return to sport phase is only initiated once type-I collagen is present, since it is able to translate the greatest tensile force.
When reviewing early weight- bearing and mobilisation, clinical studies show that early weight- bearing and use of orthopaedic boots/splints following an open end-to-end repair allows for a faster recovery time and return to work with less use of rehabilitative resources. Moreover, a higher
Phase 4 (Return to Sport)
Week 13 +
Isokinetic strength test• Address relevant strength deficits• Walk–jog programme if concentric strength is within • 40% of non-involved leg
Month 4Isokinetic strength test• Functional sport rehabilitation if eccentric strength • is within 20% of non-involved leg
Month 5Isokinetic strength test• Return to sport if eccentric strength is within 10% of • non-involved leg