Embed Size (px)
Citation preview

Archives of Medical Research 35 (2004) 348–358
0d
CASE REPORT
Severe Combined Immunodeficiency Syndrome Associatedwith Colonic Stenosis
Gabriela Lopez-Herrera,a Adriana Garibay-Escobar,a Bertha Judith Alvarez-Zavala,a AmaliaEsparza-Garcıa,b Marıa Eugenia Galindo-Rujana,b Leopoldo Flores-Romo,c Iris Estrada-Garcıa,d
Rogelio Hernandez-Pando,e Sergio Estrada-Parrad and Leopoldo Santos-Argumedoa
aDepartamentos de Biomedicina Molecular y cPatologıa Experimental, Centro de Investigacion y de Estudios Avanzados del IPN (CINVESTAV-IPN),Mexico City, Mexico
bHospital de Infectologıa Dr. Daniel Mendez Hernandez, Centro Medico La Raza, Instituto Mexicano del Seguro Social (IMSS), Mexico City, MexicodDepartamento de Inmunologıa, Escuela Nacional de Ciencias Biologicas del Instituto Politecnico Nacional (ENCB-IPN), Mexico City, Mexico
eDepartamento de Patologıa Experimental, Instituto Nacional de Ciencias Medicas y de la Nutricion Dr. Salvador Zubiran (INCMNSZ),Secretarıa de Salud (SSA), Mexico City, Mexico
Received for publication January 7, 2004; accepted April 21, 2004 (04/007).
Background. This is the first report in Mexico of a case of severe combined immu-nodeficiency syndrome (SCID) associated with colonic stenosis. The patient was an8-month-old Mexican female who died at this age. She suffered infections due to micro-organisms such as Mycobacterium tuberculosis, bacille Calmette-Guerin (BCG), Candidasp., and Pneumocystis carinii; and had frequent diarrhea. She was HIV-negative withoutfamilial history of immunodeficiency. The aim of the work was to analyze the immunologicstatus of this patient.
Methods. Peripheral blood from the patient and from a healthy matched control wereanalyzed by flow cytometry to determine peripheral leukocytes and production of cytokinesand their receptors in T-lymphocytes and monocytes. Immunohistochemical analysiswas performed in spleen and lymph node sections from the patient and control samples toassess alterations in architectural and cellular distribution within these lymphoid tissues.
Results. Peripheral blood analysis demonstrated reduced numbers of both T and B cellsand defective expression of cytokines by activated T cells. Postmortem analysis revealedvery small T and B cell zones in spleen and lymph nodes, absence of germinal centersand follicular dendritic cell networks, and two zones of stenosis at level of colon sigmoides.
Conclusions. As a whole, these data are consistent with severe combined immuno-deficiency (SCID) syndrome; thus, we conclude that this patient may have had a variantof SCID syndrome associated with intestinal stenosis. � 2004 IMSS. Published byElsevier Inc.
Key Words: Severe combined immunodeficiency syndrome, Intestinal stenosis.
Introduction
Severe combined immunodeficiency (SCID) is a life-threat-ening syndrome with recurrent infections, diarrhea, and fail-ure to thrive. Patients with SCID present persistent infections
Address reprint requests to: Leopoldo Santos-Argumedo, Ph.D., De-partamento de Biomedicina Molecular, CINVESTAV-IPN, Av. Instituto Po-litecnico Nacional #2508, Col. Zacatenco, 07360 Mexico, D.F., Mexico.Phone: (�52) (55) 5061-3800, exts. 3323 and 5020; FAX: (�52) (55) 5747-7134; E-mail: [email protected]
188-4409/04 $–see front matter. Copyright � 2004 IMSS. Published by Elsoi : 10.1016/ j .arcmed.2004.04.007
with opportunistic organisms such as Candida albicans,Pneumocystis carinii, adenovirus, respiratory syncytialvirus, bacille Calmette-Guerin (BCG), among others (1,2).This syndrome is characterized by disorders in T and B cellfunctions [reviewed in (3) and (4)] caused by mutations ingenes that encode intracellular proteins such as adenosinedeaminase (ADA) (5), JAK3 (6), ZAP-70 (7), p56lck (8),and RAG (9) and transmembrane proteins such as γc-chain(10), CD3γ (11), and CD45 (12). Most common causes ofSCID are X-linked forms, caused by mutations in JAK-3and IL2Rγc genes (2,13).
evier Inc.

A Case of SCID Associated with Colonic Stenosis 349
Clinically, patients have been classified in three groups ac-cording to presence or absence of T, B, and NK cells. Patientswithout T and B lymphocytes but with normal numbers ofNK cells (T-B-NK� SCID) caused by mutations in RAG1/RAG2 genes, patients lacking T lymphocytes and NK cellsbut with normal numbers of B cells (T-B�NK�SCID)caused by defects in γc-chain of cytokine receptors andJAK3 genes, and patients lacking all types of lymphocytes(T-B-NK� SCID), caused by deficiency of ADA activity.However, atypical forms of the disease have been reportedfor different mutations in a given gene or in the same muta-tion in different individuals; a clear example is the Omennsyndrome that is caused by defects in RAG1/RAG2 genesbut is in contrast with T-B-NK� SCID. These patients havea substantial number of oligoclonal-activated T cells butlack B cells (14,15) [reviewed in (16)].
There are other syndromes in which immunologic de-fects are unknown, for example, reticular dysgenesis (17)and hyper-IgE syndrome (18), among others. A new kind ofSCID associated with multiple intestinal atresia was reportedindependently by Walker (19), Rothenberg (20), and Moore(21), although genetic causes of this syndrome are unknown.These patients have variable numbers of total lymphocytesin peripheral blood, reduced numbers of T and B cells, andlow quantities of all immunoglobulin isotypes. They do nothave germinal centers in secondary lymphoid organs and,in some cases, familial history of multiple intestinal atresiahas been reported. In this work, we report a case of a patientwith SCID syndrome with two stenosis zones at level ofcolon sigmoides and whose immunologic findings suggesteda variant form of this syndrome.
Materials and Methods
Patient. The patient was an 8-month-old Mexican femaleseen at the Mexican Social Security Institute’s (IMSS) Dr.Daniel Mendez Hernandez Hospital de Infectologıa of theCentro Medico La Raza in Mexico City. She was bornweighing 2.8 kg, reaching 3.0 kg at 5 months. On the dayshe died, she weighed 2.0 kg. She received BCG vaccinationat birth; Sabin and pentavalent vaccines were given at 4months, according to the official Mexican ImmunizationProgram. At 4 months the patient presented abnormal growthof right axillary lymph node (LN) that under histologicexamination was suggestive of granulomatous reaction in-duced by BCG vaccination; however, PCR analysis formpt40 gene (present in Mycobacterium tuberculosis butabsent in BCG) (22) was positive; nonetheless, BCG infec-tion was not ruled out. She suffered frequent diarrhea epi-sodes and thrush. Pneumocystis carinii infection wasdiagnosed postmortem. No sample demonstrated HIV infec-tion, nor did her parents or other relatives have any apparentabnormality. No familial history of immunodeficiency wasrecorded. Peripheral blood (PB) was taken a few hours before
she died and tissue samples were obtained after autopsy; forcomparison, PB from a healthy female child of the sameage was analyzed simultaneously. Parents from both patientand healthy control gave informed consent for tests. Tissuesamples from another female child who died at a similarage due to kidney failure and without any evidence of immu-nodeficiency were used as control as well. These sampleswere taken with permission from the Pathology Service ofthe previously mentioned hospital.
Samples. PB was collected into sodium heparin Vacutainer�tubes (Becton-Dickinson, San Jose, CA, USA) from thepatient and from a healthy donor. Two milliliters of wholeblood was used for determination of different leukocyte pop-ulations and for detection of intracellular cytokines. Periph-eral blood mononuclear cells (PBMC) were isolated fromblood by Histopaque-1077 (Sigma Chemical Co., St.Louis, MO, USA) gradient centrifugation and cells wereresuspended (5 × 105 cells/mL) into RPMI 1640 (Gibco,Grand Island, NY, USA) supplemented with 10% fetalbovine serum (FBS) (Hyclone Laboratories, Logan, UT,USA), 2 mM glutamine, 100 U/mL penicillin, 100 U/mLstreptomycin, 25 µg/mL gentamicin, 1 mM pyruvate, andnonessential amino acids (Gibco). PBMC in RPMI wereused to study cytokine receptor expression. Tissue samplesfrom spleen and lymph nodes from patient and control wereconserved in formalin until processing.
Leukocyte immunophenotyping. Leukocyte subpopulationswere determined by extracellular staining. Briefly, aliquots ofwhole blood were incubated with the following combinationof monoclonal antibodies (mAb): Simultest Leuko-GATE anti-CD45 fluorescein isothiocyanate (FITC)/anti-CD14 phycoerythrin (PE) (Becton-Dickinson); Tritestanti-CD3 peridinin chlorophyll protein (PerCP)/anti-CD4FITC/anti-CD8 PE (Becton-Dickinson); Tritest anti-CD45PerCP/anti-CD3 FITC/anti-CD19 PE (Becton-Dickinson);Tritest anti-CD45 PerCP/anti-CD3 FITC/anti-CD16�CD56 PE (Becton-Dickinson); Tritest control anti-CD45PerCP/γ1FITC/γ1PE (Becton-Dickinson), and Tritestisotype control anti-CD3 PerCP/γ1FITC/γ1PE (Becton-Dickinson). Samples were incubated for 20 min at roomtemperature in the dark. After incubation, erythrocytes werelysed with FACS lysing solution (Becton-Dickinson) andsamples were further incubated for 10 min at room tempera-ture in the dark. Samples were washed with PBS containing1% BSA and fixed with PBS containing 1% formalin. Acqui-sition and analysis are described later.
Detection of intracellular cytokines
IL-2, IFN-g, IL-4, IL-1, IL-12, and TNF-a. Production ofcytokines was measured by intracellular staining [as de-scribed in (23)]. Briefly, capped polystyrene Falcon tubes(Becton-Dickinson) were used to incubate whole bloodsamples with 25 ng/mL phorbol myristate acetate (PMA)
Lopez-Herrera et al. /Archives of Medical Research 35 (2004) 348–358350
(Sigma), 1 µg/mL ionomycin (Sigma), and 10 µg/mL brefel-din A (BFA) (Sigma) or BFA only (control) for 5 h at37�C and 5% CO2. mAbs to cell surface markers anti-CD3peridinin chlorophyll protein (PerCP) (Becton-Dickinson)or anti-CD14PerCP (Becton-Dickinson) were added to ali-quots of stimulated and nonstimulated blood samples andsubsequently incubated for 15 min at room temperature inthe dark. After incubation, erythrocytes were lysed withFACS lysing solution (Becton-Dickinson), and samples wereincubated for an additional 10 min at room temperature inthe dark. Cells were then centrifuged for 5 min at 500 × gand supernatants were aspirated without disturbing pellets.FACS permeabilizing solution (Becton-Dickinson) wasadded to pellets and incubated for 10 min at room temperaturein the dark. Cell suspensions were then washed with phos-phate buffered saline (PBS) containing 0.1% bovine serumalbumin (BSA) (Research Organics, Cleveland, OH, USA)
and 0.01% sodium azide (PBA) and centrifuged for 5 min at500 × g; supernatants were removed. For intracellular stain-ing, anti-cytokine mAbs were added to pellets and cell sus-pensions were incubated at room temperature for 30 min inthe dark according to the following protocol: FastImmuneIFN-γ fluorescein isothiocyanate (FITC)/IL-4 phycoerythrin(PE) (Becton-Dickinson) or FastImmune� anti-Hu-IL-2FITC (Becton-Dickinson) and anti-CD69PE (Becton-Dickinson) were added to pellets previously stained withanti-CD3PerCP; anti-human IL-12(p40/p70)FITC (Phar-Mingen, San Diego, CA, USA), anti-CD69PE or anti-Hu-IL-1FITC (Becton-Dickinson), and anti-Hu-TNF-αPE(Becton-Dickinson) were added to pellets previously stainedwith anti-CD14PerCP. In these sets of experiments,Simultest γ2aFITC/γ1PE (Becton-Dickinson), with anti-CD3PerCP or anti-CD14PerCP were used as isotype con-trols. For all conditions, expression of CD69 was determined
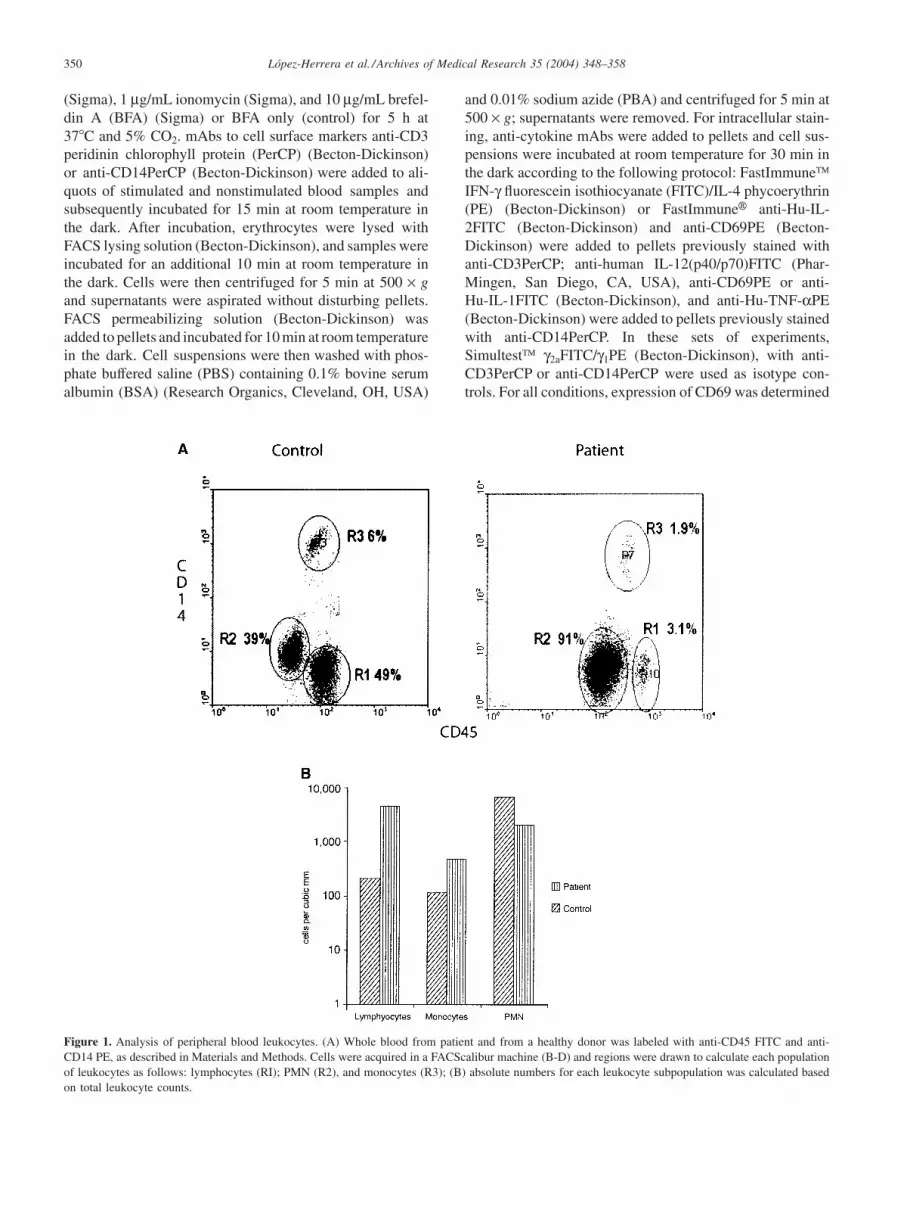
Figure 1. Analysis of peripheral blood leukocytes. (A) Whole blood from patient and from a healthy donor was labeled with anti-CD45 FITC and anti-CD14 PE, as described in Materials and Methods. Cells were acquired in a FACScalibur machine (B-D) and regions were drawn to calculate each populationof leukocytes as follows: lymphocytes (RI); PMN (R2), and monocytes (R3); (B) absolute numbers for each leukocyte subpopulation was calculated basedon total leukocyte counts.

A Case of SCID Associated with Colonic Stenosis 351
Figure 2. Lymphocyte subpopulations. Whole blood from patient and from a healthy donor was labeled with anti-CD45 PerCP, anti-CD3 FITC, and anti-CD19 PE or anti-CD16�56 PE as described in Materials and Methods. Events were analyzed in a FACScalibur machine (B-D) and regions were drawnto quantify each population. Lymphocytes were gated into a CD45� region (A) and each subpopulation was determined in this region by expression ofCD3 and CD19 (B), or CD3 and CD16�CD56 (C). Absolute numbers for each population were calculated taking data of absolute numbers of lymphocytesas 100%; results are shown in (D).
as activation control. Samples were washed with PBA andfixed with PBS containing 1% formalin. Finally, events wereacquired and analyzed as described later.
IL-2R, IFN-gR, IL-12R, and TNF-aR expression. Cytokinereceptors were determined as described by Garibay-Escobaret al. (23). Briefly, PBMC were stimulated for 48 h with 20µg/mL PHA (Sigma) or 200 ng/mL lipopolysaccharide (LPSEscherichia coli serotype O55:B5) (Sigma) in RPMI in 24-well, flat-bottom plates (Corning Glass Works, Corning, NY,USA) at 37�C and 5% CO2. After incubation, PBMC wereharvested by centrifugation at 500 × g for 5 min. Pelletswere resuspended and stained with the combination ofmAbs described later. PBMC stimulated with PHA werestained with a three-color combination using the follow-ing mAbs: anti-CD25(IL-2Rα)FITC (PharMingen); anti-IL12Rβ1PE (PharMingen), and anti-CD3PerCP. PBMCstimulated with LPS were stained with the following combi-nations using mAbs: anti-CD119(IFN-γR1)FITC (Serotec,Oxford, UK); anti-CD14PerCP or anti-CD120a(TNF-αRI)-FITC (Serotec), and anti-CD14PerCP. For isotype controls,cells were stained with Simultest γ2aFITC/γ1PE and anti-CD3PerCP or anti-CD14PerC. CD69 was measured as con-trol for activation (not shown). Samples were washed with
PBA and fixed with 1% formalin. Finally, events were ac-quired and analyzed as described later.
Acquisition and analysis. A fluorescence-activated cellsorter FACScalibur (Becton-Dickinson) equipped with 15mW argon ion laser and filter settings for FITC (530 nm),PE (585 nm), and PerCP emitting in deep red (�650 nm) wasused. For all samples, 10,000 cells were computed in listmode and analyzed gating in CD3 (T lymphocytes) or CD14(monocytes) using WinMdi 2.8 software.
Histology and immunohistochemistry analysis of lymphnodes and spleen. Spleen and LN samples were obtainedfrom patient and from a control subject. Stainings wereperformed on formalin-fixed, paraffin-embedded tissue sec-tions; the latter were exposed to high pressure and hightemperatures in sodium citrate solution (DAKO-Cytoma-tion, CA, USA). For immunohistochemical staining, basicDAB detection and V-Red detection kits (Ventana MedicalSystem, Inc., Tucson, AZ, USA) were used. Anti-CD3 andanti-CD20 antibodies (DAKO) were used to distinguish be-tween T- and B-cell zones, respectively: anti-CD68 (DAKO)was utilized as macrophage marker; anti-ki67 (DAKO) asproliferating cell-marker (germinal center reaction), and

Lopez-Herrera et al. /Archives of Medical Research 35 (2004) 348–358352
Figure 3. Helper and cytotoxic T lymphocytes. Whole blood from patient and from a healthy donor was stained with anti-CD3 PerCP, anti-CD4 FITC,and anti-CD8 PE. After staining as described in Materials and Methods, events were acquired in a FACScalibur machine (B-D) and regions were drawnto determine each population. Percentage for each subpopulation (A) was calculated in a CD3� region, absolute numbers were calculated taking the absolutenumber of T cells as 100%, and results are shown in (B).
anti-CD23 (Ventana Medical System) as marker for follicu-lar dendritic cell (FDC) networks within germinal centers(GC).
Results
Leukocyte immunophenotyping. Leukocyte populationswere identified by differential expression of CD45 and CD14(Figure 1A) and percentage of each population was calcu-lated in patient and control samples. Percentages of leuko-cytes from the patient were as follows: 3% lymphocytes; 1.9%monocytes, and 91% polymorphonuclear (PMN) cells. In
contrast, percentages of leukocytes from control were 49%lymphocytes, 6% monocytes, and 39%, PMN cells. Thestriking difference between lymphocytes from patient andcontrol was further evaluated analyzing absolute numbersof each cell population. As seen in Figure 1B, we found203 lymphocytes, 114 monocytes, and 6,879 PMN cells permm3 of whole blood in our patient, whereas in control subject4,518 lymphocytes, 464 monocytes, and 2,092 PMN permm3 whole blood were determined. These results clearlydemonstrated profound lymphopenia in the patient, compati-ble with SCID syndrome (3). Values calculated for controlsample were within normal ranges reported for healthychildren at this age (1,24).

A Case of SCID Associated with Colonic Stenosis 353
Figure 4. Cytokine production by activated T lymphocytes. For detection of cytokines produced by lymphocytes, whole blood from patient and from ahealthy donor was stimulated 5 h with PMA (25 ng/mL) plus ionomycin (1 µg/mL) in presence of BFA (10 µg/mL). After incubation, samples were stainedfor intracellular cytokines, as described in Materials and Methods. Activated T lymphocytes gated in CD3� cells (black lines) or nonstimulated cells (graydashed lines) were analyzed for expression of CD69 (A), IL2 (B), IFN-γ(C), and IL-4 (D). Percentages of positive cells and level of expression representedas mean fluorescence intensity (MFI) are indicated in each histogram.
To evaluate lymphocyte subpopulations, whole bloodwas stained with anti-CD45/anti-CD3/anti-CD19 or anti-CD45/anti-CD3/anti-CD16+CD56, as described in Materialsand Methods. Lymphocytes were gated in CD45� cells
(Figure 2A); subsequently, T, B, and NK cells were identifiedby expression of CD3 and CD19, or CD3 and CD16�CD56,respectively (Figures 2B and C). As shown in Figure 2D, wefound that all lymphocyte subpopulations examined were

Lopez-Herrera et al. /Archives of Medical Research 35 (2004) 348–358354
Figure 5. Cytokine production by activated monocytes. For detection of cytokines produced by activated monocytes, whole blood from patient and froma healthy donor was stimulated 5 h with PMA (25 ng/mL) plus ionomycin (1 µg/mL) in presence of BFA (10 µg/mL). After incubation, samples werestained for intracellular cytokines, as described in Materials and Methods. Activated monocytes gated in CD14� cells (black lines) or nonstimulated cells(gray dashed lines) were analyzed for expression of CD69 (A), IL-1 (B), IL-12 (C), and TNF-α (D). Percentages of positive cells and level of expressionrepresented as MFI are indicated in each histogram.
A Case of SCID Associated with Colonic Stenosis 355
reduced in the patient. We noted that both percentage andtotal amount of CD19� cells were deeply affected in thispatient, indicating a more severe B cell immunodeficiency.
T helper and cytotoxic cells were also quantified based onexpression ofCD4 andCD8, respectively.Cells gated withinaCD3� region showed normal proportions of these subpopu-lations: 75% of T cells were CD4� and 18% were CD8�in the patient, whereas 59 and 32% of T cells were CD4� andCD8� in control, respectively (Figure 3A). Nonetheless,absolute numbers of both CD4� and CD8� T cells werelower in patient compared with control (131 CD4� and30 CD8� cells/mm3 in patient, whereas control had 1,674CD4� and 898 CD8� cells/mm3) (Figure 3B).
Determination of intracellular cytokines IL-2, IFN-g, IL-12,and TNF-a. Patient CD3� lymphocytes activated with PMAand ionomycin expressed CD69 (87%), IL-2 (14%), IFN-γ(5%), and IL-4 (2%) (Figures 4A–D, respectively), whereasresults for control were CD69 (98%), IL-2 (21%), IFN-γ (21%),and IL-4 (14%), respectively (Figures 4A–D). Nonstimulatedcells did not show production of cytokines or expression ofactivation marker CD69. These results demonstrated that pa-tient T-cell function was defective for expression of CD69,IFNγ, and IL-4.
Cytokines produced by monocytes are shown in Figure 5. Inthe patient, 79% of monocytes expressed CD69 and IL-1 pro-duction was not detected; 12 and 48% of cells produced IL-12 and TNF-α, respectively. In contrast, in control subject 58%of monocytes expressed CD69 and 87, 34, and 46% producedIL-1, IL-12, and TNF-α, respectively (Figures 5A–D). Al-though expression of TNF-α was higher in patient than incontrol, cells from the patient were unable to produce IL-1(Figure 5). Nonstimulated cells neither produced cytokines norupregulated CD69 expression.
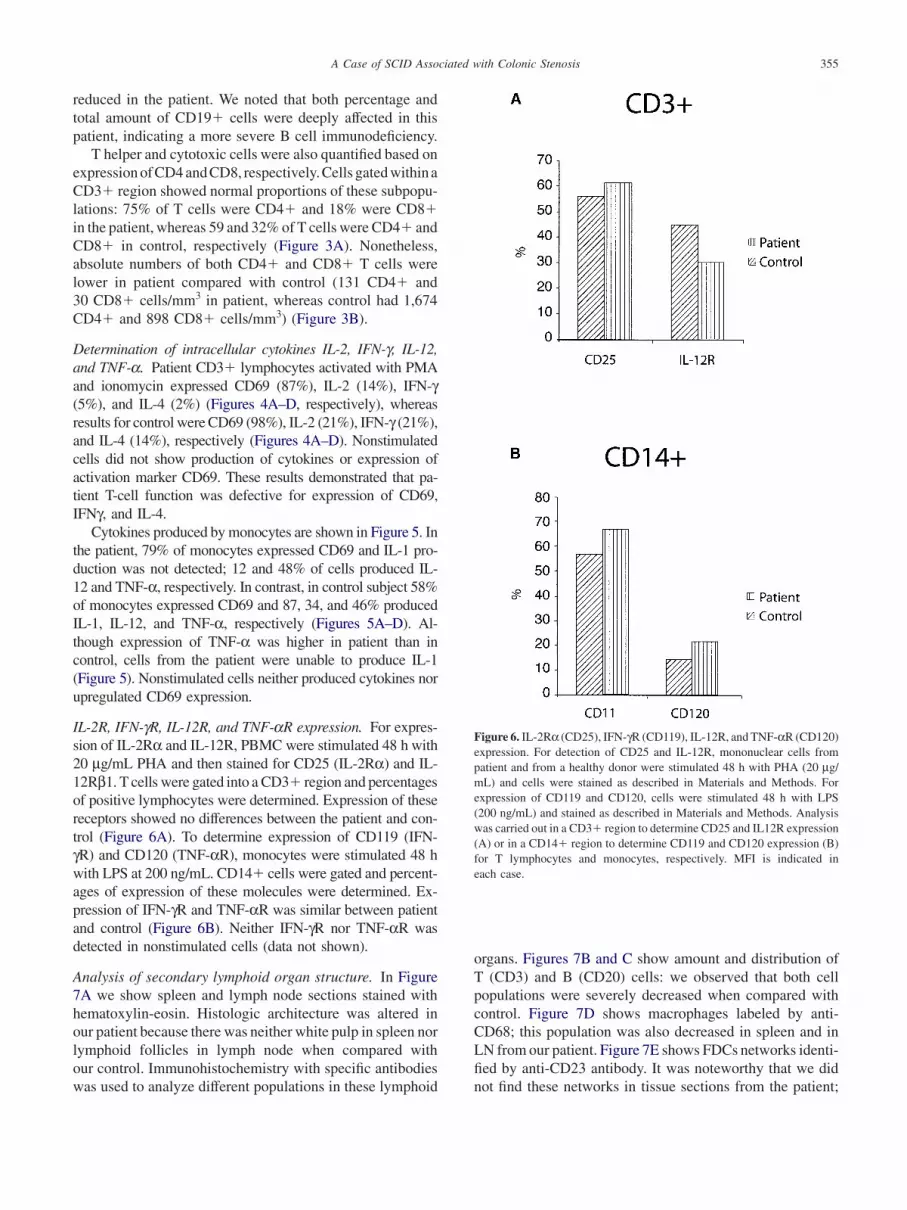
IL-2R, IFN-gR, IL-12R, and TNF-aR expression. For expres-sion of IL-2Rα and IL-12R, PBMC were stimulated 48 h with20 µg/mL PHA and then stained for CD25 (IL-2Rα) and IL-12Rβ1. T cells were gated into a CD3� region and percentagesof positive lymphocytes were determined. Expression of thesereceptors showed no differences between the patient and con-trol (Figure 6A). To determine expression of CD119 (IFN-γR) and CD120 (TNF-αR), monocytes were stimulated 48 hwith LPS at 200 ng/mL. CD14� cells were gated and percent-ages of expression of these molecules were determined. Ex-pression of IFN-γR and TNF-αR was similar between patientand control (Figure 6B). Neither IFN-γR nor TNF-αR wasdetected in nonstimulated cells (data not shown).
Analysis of secondary lymphoid organ structure. In Figure7A we show spleen and lymph node sections stained withhematoxylin-eosin. Histologic architecture was altered inour patient because there was neither white pulp in spleen norlymphoid follicles in lymph node when compared withour control. Immunohistochemistry with specific antibodieswas used to analyze different populations in these lymphoid
Figure 6. IL-2Rα (CD25), IFN-γR (CD119), IL-12R, and TNF-αR (CD120)expression. For detection of CD25 and IL-12R, mononuclear cells frompatient and from a healthy donor were stimulated 48 h with PHA (20 µg/mL) and cells were stained as described in Materials and Methods. Forexpression of CD119 and CD120, cells were stimulated 48 h with LPS(200 ng/mL) and stained as described in Materials and Methods. Analysiswas carried out in a CD3� region to determine CD25 and IL12R expression(A) or in a CD14� region to determine CD119 and CD120 expression (B)for T lymphocytes and monocytes, respectively. MFI is indicated ineach case.
organs. Figures 7B and C show amount and distribution ofT (CD3) and B (CD20) cells: we observed that both cellpopulations were severely decreased when compared withcontrol. Figure 7D shows macrophages labeled by anti-CD68; this population was also decreased in spleen and inLN from our patient. Figure 7E shows FDCs networks identi-fied by anti-CD23 antibody. It was noteworthy that we didnot find these networks in tissue sections from the patient;

Lopez-Herrera et al. /Archives of Medical Research 35 (2004) 348–358356
Figure 7. Immunohistochemical analysis of spleen and lymph node sections. Spleen (left) and lymph node (right) sections from a control (who died ofkidney failure) and the patient were stained with hematoxylin-eosin (A), anti-CD3 (brown) and anti-CD20 (red) [(B) and (C)], anti-CD68 (macrophages)(D), anti-CD23 (follicular dendritic cells) (E), and anti-ki67 (proliferating cells, germinal reaction) (F).
finally, we did not find clusters of proliferating cells in GCreaction, as observed in spleen and LN sections from thepatient stained with anti-ki67 antibody (Figure 7F). Thesefindings closely correlated with results obtained by flowcytometry in which strong reduction of peripheral lympho-cytes was detected with a more severe reduction in B-cellcompartment.
Finally, two zones of stenosis at level of colon sigmoideswere found in the patient (Figure 8A). Sections of one ofthese zones were obtained and stained with hematoxylin-eosin. Figure 8B shows a longitudinal section from this areain which there is wide hyperplasia of external muscular wallthat produced protrusion of mucosa associated with lumenreduction of colon; number and cellularity of nervous plexus

A Case of SCID Associated with Colonic Stenosis 357
Figure 8. Stenosis area in colon sigmoides. (A) Affected zone of colonsigmoides showing two stenotic zones (macroscopic view); (B) section fromnormal intestinal wall (arrows) transforming into stenotic zone was stainedwith hematoxylin-eosin and showed hyperplasia of external muscular layer(asterisk); there is neither inflammatory infiltrate nor fibrosis in this hy-perplastic area.
at this zone were normal (not shown), thus ruling out a case ofHirschsprung disease. There was no inflammatory infiltrateor fibrosis or granulomatous inflammation in hyperplasticmuscular wall, precluding existence of any chronic inflam-matory disease including tuberculosis.
Discussion
Results obtained by flow cytometry indicated that the patientsuffered severe lymphopenia, in agreement with decreaseof T-cell compartment in spleen and lymph nodes when
compared with control. However, B-cell compartment wasthe most severely affected both in percentage and absolutenumbers. These results clearly show a defect in number ofT and B lymphocytes as compared with either the controlthat we used or data from the literature (1,24). It was initiallyreported that the patient had very low levels of IgG, whereasIgM and IgA were reported as slightly high or normal,respectively. Data initially suggested a possible defectrestricted to the B-cell compartment; nevertheless, in thefinal analysis these data were discarded because the patientreceived several intravenous (i.v.) gamma globulin andplasma doses prior to immunoglobulin measurements. Tcells showed slightly defective expression of CD69, IL-2,IFN-γ, and IL-4 when activated with PMA plus ionomycin;however, function of T cells was present although in lowerrange of normality, as reported for children and healthyadults (23,25,26). Expression of CD69, IL-12, and TNF-αwas similar in control and patient, but expression of IL-1 wasnot observed in the patient, suggesting that activation ofmonocyte was partially affected, at least for this parameter.These results are also reinforced by data from the literaturefor children and healthy adults (23,27).
Analysis of spleen and lymph node tissue was even morestriking due to absolute lack of T- and B-cell compartments,FDCs networks, and germinal center areas, as well as re-duced number of macrophages. As a whole, these resultsindicated severe defect in immune response that could easilyexplain multiple infections that finally led to the death ofthis patient.
Additionally, two zones of stenosis at level of colon sig-moides were found in the patient. To date, the cause ofthese alterations is yet unknown, although they were notinflammatory infiltrate or fibrosis; thus, we consider thisabnormality a congenital malformation. It is interesting tomention that other cases of SCID associated with intestinalatresia have been reported, but genetic causes are unknown(19–21).
These observations together suggest that this case maybe a variant of severe combined immunodeficiency associ-ated with intestinal stenosis instead of atresia (19–21). Be-cause the patient died prematurely at the time of this study,we did not have the opportunity to make other determina-tions. To the best of our knowledge, this is the first reportof SCID associated with colonic stenosis in Mexico.
In conclusion, more work is needed to identify new casesof SCID associated with intestinal atresia or stenosis, as inthe present case. It is difficult to speculate with regard tothe genetic causes of this disease because to date theseare unknown. Thus, descriptions of new cases may help tounderstand possible causes and subsequently to look forgenetic defects.
AcknowledgmentsThis work was supported by grants from the Consejo Nacional deCiencia y Tecnologıa (CONACyT), Mexico (33497N 35047-M &

Lopez-Herrera et al. /Archives of Medical Research 35 (2004) 348–358358
40218Q). The authors thank QBP Blanca E. Reyes-Marquez andQFB Hector Romero-Ramırez for their technical assistance.
References1. Buckley RH, Schiff RI, Schiff SE, Markert ML, Williams LW, Har-
ville TO, Roberts JL, Puck JM. Human severe combined immunodefi-ciency: genetic, phenotypic, and functional diversity in one hundredeight infants. J Pediatr 1997;130:378–387.
2. Primary immunodeficiency diseases. Report of an IUIS Scientific Com-mittee. International Union of Immunological Societies. Clin ExpImmunol 1999;118(Suppl 1):1–28.
3. Buckley RH. Primary immunodeficiency diseases: dissectors of theimmune system. Immunol Rev 2002;185:206–219.
4. Candotti F, Notarangelo L, Visconti R, O’Shea J. Molecular aspects ofprimary immunodeficiencies: lessons from cytokine and other signalingpathways. J Clin Invest 2002;109:1261–1269.
5. Akeson AL, Wiginton DA, Hutton JJ. Normal and mutant humanadenosine deaminase genes. J Cell Biochem 1989;39:217–228.
6. Chen M, Cheng A, Candotti F, Zhou XJ, Hymel A, Fasth A, Notar-angelo LD, O’Shea JJ. Complex effects of naturally occurring mutationsin the JAK3 pseudokinase domain: evidence for interactions betweenthe kinase and pseudokinase domains. Mol Cell Biol 2000;20:947–956.
7. Chan AC, Kadlecek TA, Elder ME, Filipovich AH, Kuo WL, Iwa-shima M, Parslow TG, Weiss A. ZAP-70 deficiency in an autosomalrecessive form of severe combined immunodeficiency. Science 1994;264:1599–1601.
8. Goldman FD, Ballas ZK, Schutte BC, Kemp J, Hollenback C, NorazN, Taylor N. Defective expression of p56lck in an infant with severecombined immunodeficiency. J Clin Invest 1998;102:421–429.
9. Li W, Chang FC, Desiderio S. Rag-1 mutations associated with B-cell-negative SCID dissociate the nicking and transesterification stepsof V(D)J recombination. Mol Cell Biol 2001;21:3935–3946.
10. Noguchi M, Yi H, Rosenblatt HM, Filipovich AH, Adelstein S,Modi S. Interleukin-2 receptor gamma chain mutation results in X-linked severe combined immunodeficiency in humans. Cell 1993;73:147–157.
11. Arnaiz-Villena A, Timon M, Corell A, Perez-Aciego P, Martın-VillaJM, Regueiro JR. Brief report: Primary immunodeficiency caused bymutations in the gene encoding the CD3-gamma subunit of the T-lymphocyte receptor. N Engl J Med 1992;327:529–533.
12. Tchilian EZ, Wallace DL, Wells RS, Flower DR, Morgan GR, Bever-ley PC. A deletion in the gene encoding the CD45 antigen in a patientwith SCID. J Immunol 2001;166:1308–1313.
13. Leonard WJ. X-linked severe combined immunodeficiency: from mo-lecular cause to gene therapy within seven years. Mol Med Today2000;6:403–407.
14. Corneo B, Moshous D, Gungor T, Wulffraat N, Philippet P, LeDeist FL, Fischer A, de Villartay JP. Identical mutations in RAG1 or
RAG2 genes leading to defective V(D)J recombinase activity can causeeither T-B-severe combined immune deficiency or Omenn syndrome.Blood 2001;97:2772–2776.
15. Villa A, Sobacchi C, Notarangelo LD, Bozzi F, Abinun M, Abra-hamsen TG, Arkwright PD, Baniyash M, Brooks EG, Conley ME,Cortes P, Duse M, Fasth A, Filipovich AM, Infante AJ, Jones A, Mazzo-lari E, Muller SM, Pasic S, Rechavi G, Sacco MG, Santagata S,Schroeder ML, Seger R, Strina D, Ugazio A, Valiaho J, Vihinen M,Vogler LB, Ochs H, Vezzoni P, Friedrich W, Schwarz K. V(D)J recombi-nation defects in lymphocytes due to RAG mutations: severe immunode-ficiency with a spectrum of clinical presentations. Blood 2001;97:81–88.
16. Fontan CG. Primary immunodeficiencies. Clinical features and variantforms. Allergol Immunopathol 2001;29:101–107.
17. Emile JF, Geissmann F, Martin OC, Radford-Weiss I, Lepelletier Y,Heymer B, Espanol T, de Santes KB, Bertrand Y, Brousse N, Casa-nova JL, Fischer A. Langerhans cell deficiency in reticular dysgenesis.Blood 2000;96:58–62.
18. Pherwani AV, Madnani NA. Hyperimmunoglobulin E syndrome.Indian J Pediatr 2001;38:1029–1034.
19. Walker MW, Lovell MA, Kelly TE, Golden W, Saulsbury FT. Multipleareas of intestinal atresia associated with immunodeficiency and post-transfusion graft-versus-host disease. J Pediatr 1993;123:93–95.
20. Rothenberg ME, White FV, Chilmonczyk B, Chatila B. A syndromeinvolving immunodeficiency and multiple intestinal atresias. Immuno-deficiency 1995;5:171–178.
21. Moore SW, de Jongh G, Bouic P, Brown RA, Kirsten G. Immunedeficiency in familial duodenal atresia. J Pediatr Surg 1996;31:1733–1735.
22. Del Portillo P, Thomas MC, Martınez E, Maranon C, Valladares B,Patarroyo ME, Lopez MC. Multiprimer PCR system for differentialidentification of Mycobacteria in clinical samples. J Clin Microbiol1996;34:324–328.
23. Garibay-Escobar A, Estrada-Garcıa I, Estrada-Parra S, Santos-Argu-medo L. Integrated measurements by flow cytometry of cytokinesIL-2, IFN-γ, IL-12, TNF-α and their receptors in human blood fromhealthy donors. J Immunol Methods 2003;280:73–88.
24. de Vries E, Bruin-Versteeg S, Comans-Bitter WM, de Groot R, HopWC, Boerma GJ. Longitudinal survey of lymphocyte subpopulations inthe first year of life. Pediatr Res 2000;47:528–537.
25. Buck RH, Cordle CT, Thomas DJ, Winship TR, Schaller JP, DugleJE. Longitudinal study of intracellular T cell cytokine production ininfants compared to adults. Clin Exp Immunol 2002;128:490–497.
26. Cerbulo-Vazquez A, Valdes-Ramos R, Santos-Argumedo L. Activatedumbilical cord blood cells from pre-term and term neonates expressCD69 and synthesize IL-2 but are unable to produce IFN-gamma. ArchMed Res 2003;34:100–105.
27. Skrzeczynska J, Kobylarz K, Hartwich Z, Zembala M, Pryjma J.CD14�CD16� monocytes in the course of sepsis in neonates andsmall children: monitoring and functional studies. Scand J Immunol2002;55:629–638.





























