Embed Size (px)
Citation preview
1
University of UtahDepartment of
Pediatrics
Resident Clinical Resource Handbook
This book is intended for the sole use of pediatric, family medicine residents and
medical students while rotating at Primary Children's Hospital.
If found, please call (801) 662-5704
or send to
graphics by Pamela Carpenter
Department of Pediatrics
Updated June 2015
Pediatric Residency Office PCH Eccles Outpt Bld, 1st Floor
81 N. Mario Capecchi DriveSalt Lake City, UT 84113
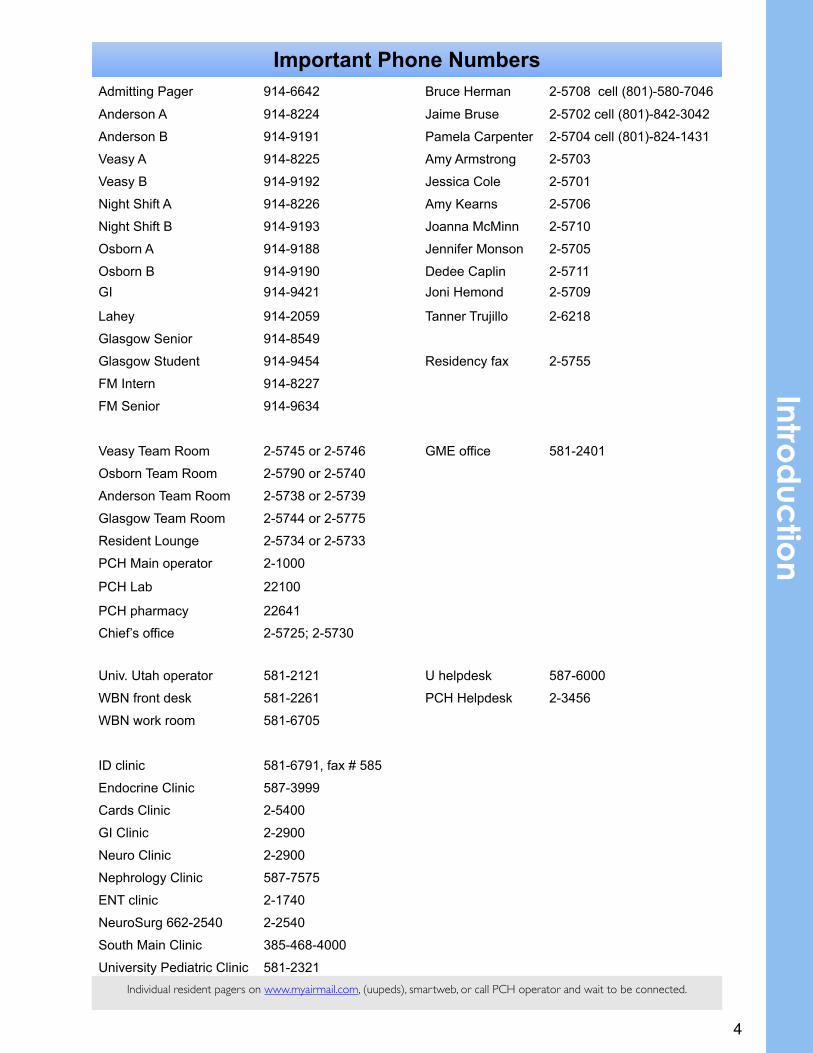
Important Phone NumbersImportant Phone NumbersImportant Phone NumbersImportant Phone NumbersAdmitting Pager 914-6642 Bruce Herman 2-5708 cell (801)-580-7046
Anderson A 914-8224 Jaime Bruse 2-5702 cell (801)-842-3042
Anderson B 914-9191 Pamela Carpenter 2-5704 cell (801)-824-1431
Veasy A 914-8225 Amy Armstrong 2-5703
Veasy B 914-9192 Jessica Cole 2-5701
Night Shift A 914-8226 Amy Kearns 2-5706
Night Shift B 914-9193 Joanna McMinn 2-5710
Osborn A 914-9188 Jennifer Monson 2-5705
Osborn B 914-9190 Dedee Caplin 2-5711GI 914-9421 Joni Hemond 2-5709
Lahey 914-2059 Tanner Trujillo 2-6218
Glasgow Senior 914-8549
Glasgow Student 914-9454 Residency fax 2-5755
FM Intern 914-8227
FM Senior 914-9634
Veasy Team Room 2-5745 or 2-5746 GME office 581-2401
Osborn Team Room 2-5790 or 2-5740
Anderson Team Room 2-5738 or 2-5739
Glasgow Team Room 2-5744 or 2-5775
Resident Lounge PCMC main operator
2-5734 or 2-5733
PCH Main operator 2-1000
PCH Lab 22100
PCH pharmacy 22641
Chief’s office 2-5725; 2-5730
Univ. Utah operator 581-2121 U helpdesk 587-6000
WBN front desk 581-2261 PCH Helpdesk 2-3456
WBN work room 581-6705
ID clinic 581-6791, fax # 585 3789Endocrine Clinic 587-3999
Cards Clinic 2-5400
GI Clinic 2-2900
Neuro Clinic 2-2900
Nephrology Clinic 587-7575
ENT clinic 2-1740
NeuroSurg 662-2540 2-2540
South Main Clinic 385-468-4000
University Pediatric Clinic 581-2321Individual resident pagers on www.myairmail.com, (uupeds), smartweb, or call PCH operator and wait to be connected.Individual resident pagers on www.myairmail.com, (uupeds), smartweb, or call PCH operator and wait to be connected.Individual resident pagers on www.myairmail.com, (uupeds), smartweb, or call PCH operator and wait to be connected.Individual resident pagers on www.myairmail.com, (uupeds), smartweb, or call PCH operator and wait to be connected.
4
Introd
uctio
n
5
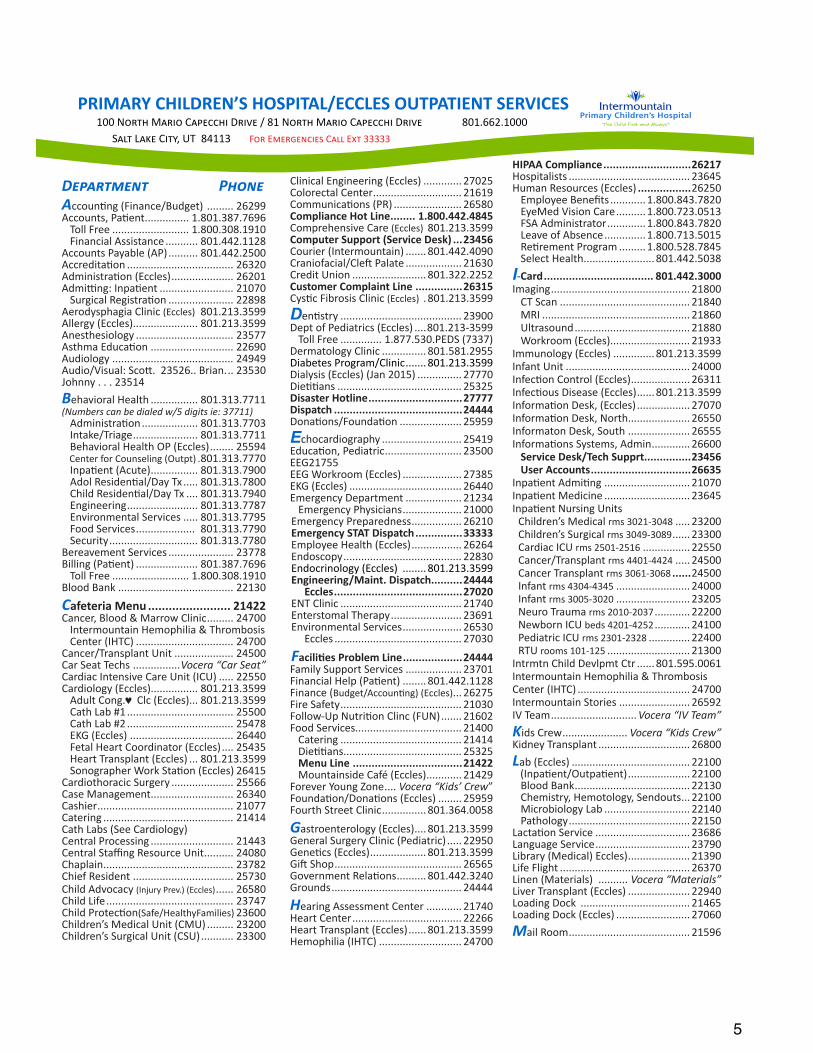
HIPAA Compliance ............................26217 Hospitalists ......................................... 23645 Human Resources (Eccles) .................26250ŵƉůŽLJĞĞĞŶĞĮƚƐ ............1.800.843.7820EyeMed Vision Care ..........1.800.723.0513FSA Administrator ............. 1.800.843.7820Leave of Absence .............. 1.800.713.5015ZĞƟƌĞŵĞŶƚWƌŽŐƌĂŵ .........1.800.528.7845Select Health ........................ 801.442.5038I-Card ................................... 801.442.3000/ŵĂŐŝŶŐ ............................................... 21800
CT Scan ............................................ 21840MRI .................................................. 21860Ultrasound ....................................... 21880Workroom (Eccles)........................... 21933
/ŵŵƵŶŽůŽŐLJ;ĐĐůĞƐͿ .............. 801.213.3599Infant Unit .......................................... 24000/ŶĨĞĐƟŽŶŽŶƚƌŽů;ĐĐůĞƐͿ .................... 26311/ŶĨĞĐƟŽƵƐŝƐĞĂƐĞ;ĐĐůĞƐͿ ......801.213.3599/ŶĨŽƌŵĂƟŽŶĞƐŬ;ĐĐůĞƐͿ .................. 27070/ŶĨŽƌŵĂƟŽŶĞƐŬEŽƌƚŚ..................... 26550/ŶĨŽƌŵĂƚŽŶĞƐŬ^ŽƵƚŚ ..................... 26555/ŶĨŽƌŵĂƟŽŶƐ^LJƐƚĞŵƐĚŵŝŶ ............. 26600
Service Desk/Tech Supprt...............23456User Accounts ................................26635
/ŶƉĂƟĞŶƚĚŵŝƟŶŐ ............................. 21070/ŶƉĂƟĞŶƚDĞĚŝĐŝŶĞ ............................. 23645/ŶƉĂƟĞŶƚEƵƌƐŝŶŐhŶŝƚƐ
Children’s Medical rms 3021-3048 ..... 23200ŚŝůĚƌĞŶ Ɛ^ƵƌŐŝĐĂůrms 3049-3089 ...... 23300Cardiac ICU rms 2501-2516 ................ 22550Cancer/Transplant rms 4401-4424 ..... 24500Cancer Transplant rms 3061-3068 ......24500Infant rms 4304-4345 ......................... 24000Infant rms 3005-3020 ......................... 23205EĞƵƌŽdƌĂƵŵĂrms 2010-2037 ............ 22200EĞǁďŽƌŶ/hbeds 4201-4252 ............ 24100WĞĚŝĂƚƌŝĐ/hrms 2301-2328 .............. 22400RTU rooms 101-125 ............................ 21300
/ŶƚƌŵƚŶŚŝůĚĞǀůƉŵƚƚƌ ......801.595.0061Intermountain Hemophilia & Thrombosis Center (IHTC) ...................................... 24700Intermountain Stories ........................ 26592IV Team ............................. Vocera “IV Team”KŝĚƐƌĞǁ ...................... Vocera “Kids Crew”Kidney Transplant ............................... 26800Lab (Eccles) ........................................ 22100;/ŶƉĂƟĞŶƚKƵƚƉĂƟĞŶƚͿ ..................... 22100
Blood Bank ....................................... 22130ŚĞŵŝƐƚƌLJ ,ĞŵŽƚŽůŽŐLJ ^ĞŶĚŽƵƚƐ ... 22100DŝĐƌŽďŝŽůŽŐLJ>Ăď ............................. 22140WĂƚŚŽůŽŐLJ ......................................... 22150
>ĂĐƚĂƟŽŶ^ĞƌǀŝĐĞ ................................ 23686>ĂŶŐƵĂŐĞ^ĞƌǀŝĐĞ ................................ 23790Library (Medical) Eccles) ..................... 21390>ŝĨĞ&ůŝŐŚƚ ............................................ 26370Linen (Materials) .......... Vocera “Materials”Liver Transplant (Eccles) ..................... 22940>ŽĂĚŝŶŐŽĐŬ ..................................... 21465>ŽĂĚŝŶŐŽĐŬ;ĐĐůĞƐͿ ......................... 27060Mail Room ......................................... 21596
PRIMARY CHILDREN’S HOSPITAL/ECCLES OUTPATIENT SERVICES ϭϬϬEÊÙã«DÙ®ÊÖ«®Ù®òϴϭEÊÙã«DÙ®ÊÖ«®Ù®òϴϬϭϲϲϮϭϬϬϬ^½ã>»®ãù hdϴϰϭϭϯ&ÊÙÃ٦Įݽ½øãϯϯϯϯϯ
ÖÙãÃÄãW«ÊÄAĐĐŽƵŶƟŶŐ;&ŝŶĂŶĐĞƵĚŐĞƚͿ ......... 26299ĐĐŽƵŶƚƐWĂƟĞŶƚ ............... 1.801.387.7696
Toll Free .......................... 1.800.308.1910Financial Assistance ........... 801.442.1128
ĐĐŽƵŶƚƐWĂLJĂďůĞ;WͿ .......... 801.442.2500ĐĐƌĞĚŝƚĂƟŽŶ .................................... 26320ĚŵŝŶŝƐƚƌĂƟŽŶ;ĐĐůĞƐͿ ..................... 26201ĚŵŝƫŶŐ/ŶƉĂƟĞŶƚ ......................... 21070^ƵƌŐŝĐĂůZĞŐŝƐƚƌĂƟŽŶ ...................... 22898
ĞƌŽĚLJƐƉŚĂŐŝĂůŝŶŝĐ(Eccles) 801.213.3599ůůĞƌŐLJ;ĐĐůĞƐͿ...................... 801.213.3599ŶĞƐƚŚĞƐŝŽůŽŐLJ ................................. 23577ƐƚŚŵĂĚƵĐĂƟŽŶ ............................ 22690ƵĚŝŽůŽŐLJ ......................................... 24949ƵĚŝŽsŝƐƵĂů^ĐŽƩϮϯϱϮϲƌŝĂŶ .. 23530Johnny . . . 23514Behavioral Health ................ 801.313.7711(Numbers can be dialed w/5 digits ie: 37711)ĚŵŝŶŝƐƚƌĂƟŽŶ ................... 801.313.7703/ŶƚĂŬĞdƌŝĂŐĞ ...................... 801.313.7711ĞŚĂǀŝŽƌĂů,ĞĂůƚŚKW;ĐĐůĞƐͿ ........ 25594
ĞŶƚĞƌĨŽƌŽƵŶƐĞůŝŶŐ;KƵƚƉƚͿ .801.313.7770/ŶƉĂƟĞŶƚ;ĐƵƚĞͿ ................ 801.313.7900ĚŽůZĞƐŝĚĞŶƟĂůĂLJddž ..... 801.313.7800ŚŝůĚZĞƐŝĚĞŶƟĂůĂLJddž .... 801.313.7940ŶŐŝŶĞĞƌŝŶŐ ........................ 801.313.7787Environmental Services ..... 801.313.7795Food Services .................... 801.313.7790Security .............................. 801.313.7780
Bereavement Services ...................... 23778ŝůůŝŶŐ;WĂƟĞŶƚͿ ..................... 801.387.7696
Toll Free .......................... 1.800.308.1910Blood Bank ....................................... 22130
Cafeteria Menu ........................ 21422ĂŶĐĞƌ ůŽŽĚΘDĂƌƌŽǁůŝŶŝĐ ......... 24700
Intermountain Hemophilia & Thrombosis Center (IHTC) ................................. 24700
Cancer/Transplant Unit .................... 24500Car Seat Techs ................Vocera “Car Seat”Cardiac Intensive Care Unit (ICU) ..... 22550ĂƌĚŝŽůŽŐLJ;ĐĐůĞƐͿ................ 801.213.3599ĚƵůƚŽŶŐj Clc (Eccles)... 801.213.3599Cath Lab #1 .................................... 25500Cath Lab #2 .................................... 25478EKG (Eccles) ................................... 26440Fetal Heart Coordinator (Eccles) .... 25435Heart Transplant (Eccles) ... 801.213.3599^ŽŶŽŐƌĂƉŚĞƌtŽƌŬ^ƚĂƟŽŶ;ĐĐůĞƐͿ 26415
ĂƌĚŝŽƚŚŽƌĂĐŝĐ^ƵƌŐĞƌLJ ..................... 25566ĂƐĞDĂŶĂŐĞŵĞŶƚ ............................ 26340Cashier .............................................. 21077ĂƚĞƌŝŶŐ ............................................ 21414ĂƚŚ>ĂďƐ;^ĞĞĂƌĚŝŽůŽŐLJͿĞŶƚƌĂůWƌŽĐĞƐƐŝŶŐ ............................ 21443ĞŶƚƌĂů^ƚĂĸŶŐZĞƐŽƵƌĐĞhŶŝƚ .......... 24080Chaplain ............................................ 23782Chief Resident .................................. 25730Child Advocacy ;/ŶũƵƌLJWƌĞǀ Ϳ;ĐĐůĞƐͿ ...... 26580Child Life ........................................... 23747ŚŝůĚWƌŽƚĞĐƟŽŶ(Safe/HealthyFamilies) 23600Children’s Medical Unit (CMU) ......... 23200ŚŝůĚƌĞŶ Ɛ^ƵƌŐŝĐĂůhŶŝƚ;^hͿ ........... 23300
ůŝŶŝĐĂůŶŐŝŶĞĞƌŝŶŐ;ĐĐůĞƐͿ ............. 27025 Colorectal Center .............................. 21619ŽŵŵƵŶŝĐĂƟŽŶƐ;WZͿ ....................... 26580Compliance Hot Line ........ 1.800.442.4845Comprehensive Care (Eccles) 801.213.3599Computer Support (Service Desk) ...23456Courier (Intermountain) ....... 801.442.4090 ƌĂŶŝŽĨĂĐŝĂůůĞŌWĂůĂƚĞ ................... 21630Credit Union ......................... 801.322.2252Customer Complaint Line ...............26315LJƐƟĐ&ŝďƌŽƐŝƐůŝŶŝĐ(Eccles) . 801.213.3599DĞŶƟƐƚƌLJ ......................................... 23900 ĞƉƚŽĨWĞĚŝĂƚƌŝĐƐ;ĐĐůĞƐͿ ....801.213-3599
Toll Free .............. ϭϴϳϳϱϯϬW^;ϳϯϯϳͿĞƌŵĂƚŽůŽŐLJůŝŶŝĐ ............... 801.581.2955ŝĂďĞƚĞƐWƌŽŐƌĂŵůŝŶŝĐ ....... 801.213.3599ŝĂůLJƐŝƐ;ĐĐůĞƐͿ;:ĂŶϮϬϭϱͿ ............... 27770ŝĞƟƟĂŶƐ .......................................... 25325Disaster Hotline ..............................27777Dispatch .........................................24444ŽŶĂƟŽŶƐ&ŽƵŶĚĂƟŽŶ ..................... 25959EĐŚŽĐĂƌĚŝŽŐƌĂƉŚLJ ........................... 25419ĚƵĐĂƟŽŶWĞĚŝĂƚƌŝĐ .......................... 23500EEG 21755EEG Workroom (Eccles) .................... 27385EKG (Eccles) ...................................... 26440ŵĞƌŐĞŶĐLJĞƉĂƌƚŵĞŶƚ ................... 21234ŵĞƌŐĞŶĐLJWŚLJƐŝĐŝĂŶƐ .................... 21000
ŵĞƌŐĞŶĐLJWƌĞƉĂƌĞĚŶĞƐƐ ................. 26210Emergency STAT Dispatch ...............33333 Employee Health (Eccles) ................. 26264Endoscopy ........................................ 22830ŶĚŽĐƌŝŶŽůŽŐLJ;ĐĐůĞƐͿ ........ 801.213.3599Engineering/Maint. Dispatch..........24444 Eccles .........................................27020EdůŝŶŝĐ ......................................... 21740Enterstomal Therapy ........................ 23691Environmental Services .................... 26530 Eccles ........................................... 27030
FĂĐŝůŝƟĞƐWƌŽďůĞŵ>ŝŶĞ ...................24444Family Support Services ................... 23701&ŝŶĂŶĐŝĂů,ĞůƉ;WĂƟĞŶƚͿ ........ 801.442.1128Finance (ƵĚŐĞƚĐĐŽƵŶƟŶŐͿ;ĐĐůĞƐͿ ... 26275Fire Safety ......................................... 21030&ŽůůŽǁͲhƉEƵƚƌŝƟŽŶůŝŶĐ;&hEͿ ....... 21602Food Services.................................... 21400ĂƚĞƌŝŶŐ ......................................... 21414ŝĞƟƟĂŶƐ........................................ 25325Menu Line ...................................21422Mountainside Café (Eccles) ............ 21429
&ŽƌĞǀĞƌzŽƵŶŐŽŶĞ .... Vocera “Kids’ Crew”&ŽƵŶĚĂƟŽŶŽŶĂƟŽŶƐ;ĐĐůĞƐͿ ........ 25959Fourth Street Clinic ............... 801.364.0058
GĂƐƚƌŽĞŶƚĞƌŽůŽŐLJ;ĐĐůĞƐͿ .... 801.213.3599'ĞŶĞƌĂů^ƵƌŐĞƌLJůŝŶŝĐ;WĞĚŝĂƚƌŝĐͿ ..... 22950'ĞŶĞƟĐƐ;ĐĐůĞƐͿ ................... 801.213.3599'ŝŌ^ŚŽƉ ........................................... 26565'ŽǀĞƌŶŵĞŶƚZĞůĂƟŽŶƐ .......... 801.442.3240Grounds ............................................ 24444
HĞĂƌŝŶŐƐƐĞƐƐŵĞŶƚĞŶƚĞƌ ............ 21740Heart Center ..................................... 22266 Heart Transplant (Eccles) ...... 801.213.3599Hemophilia (IHTC) ............................ 24700
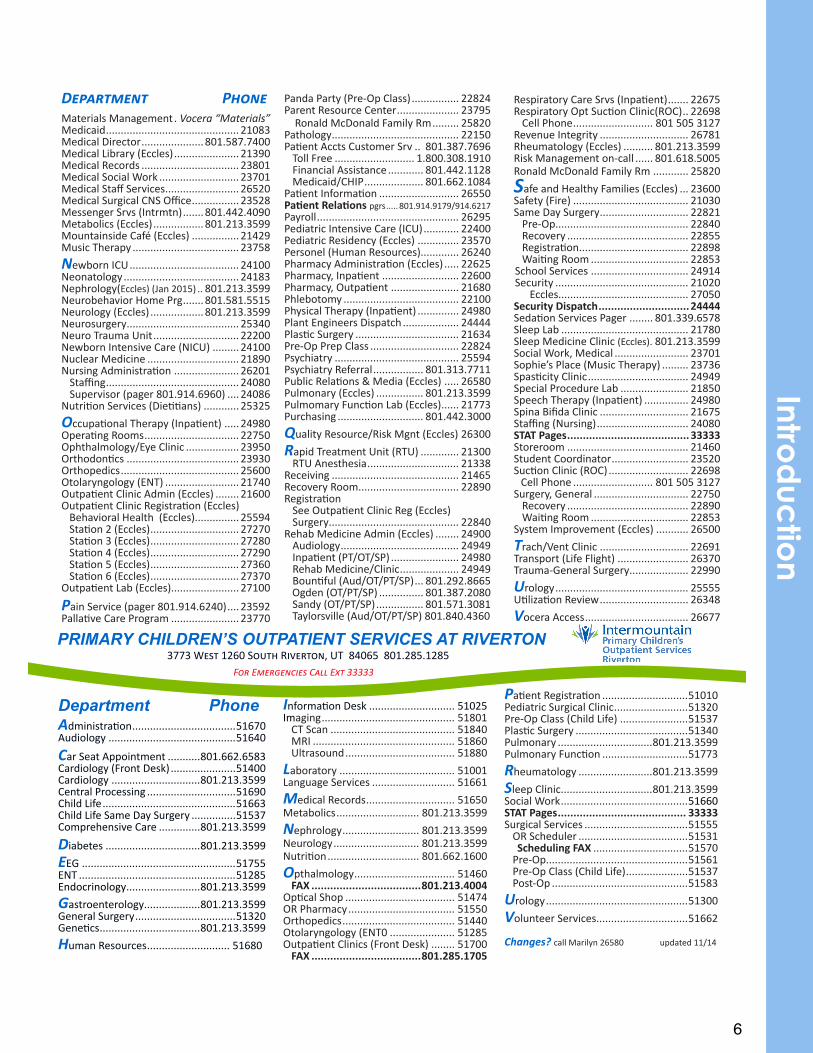
6
ÖÙãÃÄãW«ÊÄDĂƚĞƌŝĂůƐDĂŶĂŐĞŵĞŶƚ . Vocera “Materials”Medicaid ............................................. 21083DĞĚŝĐĂůŝƌĞĐƚŽƌ ..................... 801.587.7400Medical Library (Eccles) ...................... 21390Medical Records ................................. 23801Medical Social Work ........................... 23701DĞĚŝĐĂů^ƚĂī^ĞƌǀŝĐĞƐ ......................... 26520DĞĚŝĐĂů^ƵƌŐŝĐĂůE^KĸĐĞ ................ 23528DĞƐƐĞŶŐĞƌ^ƌǀƐ;/ŶƚƌŵƚŶͿ .......801.442.4090 Metabolics (Eccles) ................. 801.213.3599Mountainside Café (Eccles) ................ 21429Music Therapy .................................... 23758
NĞǁďŽƌŶ/h ..................................... 24100EĞŽŶĂƚŽůŽŐLJ ....................................... 24183EĞƉŚƌŽůŽŐLJ;Eccles) (Jan 2015) .. 801.213.3599EĞƵƌŽďĞŚĂǀŝŽƌ,ŽŵĞWƌŐ .......801.581.5515EĞƵƌŽůŽŐLJ;ĐĐůĞƐͿ .................. 801.213.3599EĞƵƌŽƐƵƌŐĞƌLJ ...................................... 25340EĞƵƌŽdƌĂƵŵĂhŶŝƚ ............................. 22200EĞǁďŽƌŶ/ŶƚĞŶƐŝǀĞĂƌĞ;E/hͿ ......... 24100EƵĐůĞĂƌDĞĚŝĐŝŶĞ ............................... 21890EƵƌƐŝŶŐĚŵŝŶŝƐƚƌĂƟŽŶ ...................... 26201^ƚĂĸŶŐ ............................................. 24080^ƵƉĞƌǀŝƐŽƌ;ƉĂŐĞƌϴϬϭϵϭϰϲϵϲϬͿ .... 24086
EƵƚƌŝƟŽŶ^ĞƌǀŝĐĞƐ;ŝĞƟƟĂŶƐͿ ............ 25325
OĐĐƵƉĂƟŽŶĂůdŚĞƌĂƉLJ;/ŶƉĂƟĞŶƚͿ ..... 24980KƉĞƌĂƟŶŐZŽŽŵƐ ................................ 22750KƉŚƚŚĂůŵŽůŽŐLJLJĞůŝŶŝĐ .................. 23950KƌƚŚŽĚŽŶƟĐƐ ...................................... 23930KƌƚŚŽƉĞĚŝĐƐ ........................................ 25600KƚŽůĂƌLJŶŐŽůŽŐLJ;EdͿ ......................... 21740KƵƚƉĂƟĞŶƚůŝŶŝĐĚŵŝŶ;ĐĐůĞƐͿ ........ 21600KƵƚƉĂƟĞŶƚůŝŶŝĐZĞŐŝƐƚƌĂƟŽŶ;ĐĐůĞƐͿ Behavioral Health (Eccles)............... 25594^ƚĂƟŽŶϮ;ĐĐůĞƐͿ .............................. 27270^ƚĂƟŽŶϯ;ĐĐůĞƐͿ .............................. 27280^ƚĂƟŽŶϰ;ĐĐůĞƐͿ .............................. 27290^ƚĂƟŽŶϱ;ĐĐůĞƐͿ .............................. 27360 ^ƚĂƟŽŶϲ;ĐĐůĞƐͿ .............................. 27370KƵƚƉĂƟĞŶƚ>Ăď;ĐĐůĞƐͿ....................... 27100
WĂŝŶ^ĞƌǀŝĐĞ;ƉĂŐĞƌϴϬϭϵϭϰϲϮϰϬͿ .... 23592WĂůůĂƟǀĞĂƌĞWƌŽŐƌĂŵ ....................... 23770
ZĞƐƉŝƌĂƚŽƌLJĂƌĞ^ƌǀƐ;/ŶƉĂƟĞŶƚͿ ....... 22675ZĞƐƉŝƌĂƚŽƌLJKƉƚ^ƵĐƟŽŶůŝŶŝĐ;ZKͿ .. 22698ĞůůWŚŽŶĞ ........................... 801 505 3127
ZĞǀĞŶƵĞ/ŶƚĞŐƌŝƚLJ .............................. 26781ZŚĞƵŵĂƚŽůŽŐLJ;ĐĐůĞƐͿ .......... 801.213.3599ZŝƐŬDĂŶĂŐĞŵĞŶƚŽŶͲĐĂůů ...... 801.618.5005ZŽŶĂůĚDĐŽŶĂůĚ&ĂŵŝůLJZŵ ............ 25820
Safe and Healthy Families (Eccles) ... 23600Safety (Fire) ....................................... 21030^ĂŵĞĂLJ^ƵƌŐĞƌLJ .............................. 22821WƌĞͲKƉ............................................. 22840Recovery ......................................... 22855ZĞŐŝƐƚƌĂƟŽŶ ..................................... 22898tĂŝƟŶŐZŽŽŵ ................................. 22853
School Services ................................. 24914Security ............................................. 21020 Eccles............................................ 27050Security Dispatch .............................24444 ^ĞĚĂƟŽŶ^ĞƌǀŝĐĞƐWĂŐĞƌ ........ 801.339.6578Sleep Lab ........................................... 21780Sleep Medicine Clinic (Eccles) . 801.213.3599^ŽĐŝĂůtŽƌŬDĞĚŝĐĂů ......................... 23701^ŽƉŚŝĞ ƐWůĂĐĞ;DƵƐŝĐdŚĞƌĂƉLJͿ ......... 23736^ƉĂƐƟĐŝƚLJůŝŶŝĐ .................................. 24949^ƉĞĐŝĂůWƌŽĐĞĚƵƌĞ>Ăď ....................... 21850^ƉĞĞĐŚdŚĞƌĂƉLJ;/ŶƉĂƟĞŶƚͿ ............... 24980^ƉŝŶĂŝĮĚĂůŝŶŝĐ .............................. 21675^ƚĂĸŶŐ;EƵƌƐŝŶŐͿ ............................... 24080STAT Pages .......................................33333Storeroom ......................................... 21460Student Coordinator .......................... 23520^ƵĐƟŽŶůŝŶŝĐ;ZKͿ ........................... 22698ĞůůWŚŽŶĞ ........................... 801 505 3127
^ƵƌŐĞƌLJ 'ĞŶĞƌĂů ................................ 22750Recovery ......................................... 22890tĂŝƟŶŐZŽŽŵ ................................. 22853
System Improvement (Eccles) ........... 26500
Trach/Vent Clinic .............................. 22691dƌĂŶƐƉŽƌƚ;>ŝĨĞ&ůŝŐŚƚͿ ........................ 26370dƌĂƵŵĂͲ'ĞŶĞƌĂů^ƵƌŐĞƌLJ .................... 22990
UƌŽůŽŐLJ ............................................. 25555hƟůŝnjĂƟŽŶZĞǀŝĞǁ .............................. 26348
Vocera Access ................................... 26677
WĂŶĚĂWĂƌƚLJ;WƌĞͲKƉůĂƐƐͿ ................ 22824WĂƌĞŶƚZĞƐŽƵƌĐĞĞŶƚĞƌ ..................... 23795ZŽŶĂůĚDĐŽŶĂůĚ&ĂŵŝůLJZŵ ......... 25820WĂƚŚŽůŽŐLJ ........................................... 22150 WĂƟĞŶƚĐĐƚƐƵƐƚŽŵĞƌ^ƌǀ .. 801.387.7696
Toll Free ........................... 1.800.308.1910Financial Assistance ............ 801.442.1128DĞĚŝĐĂŝĚ,/W .................... 801.662.1084
WĂƟĞŶƚ/ŶĨŽƌŵĂƟŽŶ ........................... 26550WĂƟĞŶƚZĞůĂƟŽŶƐ ƉŐƌƐ ..... 801.914.9179/914.6217WĂLJƌŽůů ................................................ 26295WĞĚŝĂƚƌŝĐ/ŶƚĞŶƐŝǀĞĂƌĞ;/hͿ ............ 22400WĞĚŝĂƚƌŝĐZĞƐŝĚĞŶĐLJ;ĐĐůĞƐͿ .............. 23570WĞƌƐŽŶĞů;,ƵŵĂŶZĞƐŽƵƌĐĞƐͿ............. 26240WŚĂƌŵĂĐLJĚŵŝŶŝƐƚƌĂƟŽŶ;ĐĐůĞƐͿ ..... 22625WŚĂƌŵĂĐLJ /ŶƉĂƟĞŶƚ .......................... 22600WŚĂƌŵĂĐLJ KƵƚƉĂƟĞŶƚ ....................... 21680WŚůĞďŽƚŽŵLJ ....................................... 22100WŚLJƐŝĐĂůdŚĞƌĂƉLJ;/ŶƉĂƟĞŶƚͿ .............. 24980WůĂŶƚŶŐŝŶĞĞƌƐŝƐƉĂƚĐŚ ................... 24444WůĂƐƟĐ^ƵƌŐĞƌLJ ................................... 21634WƌĞͲKƉWƌĞƉůĂƐƐ .............................. 22824WƐLJĐŚŝĂƚƌLJ .......................................... 25594WƐLJĐŚŝĂƚƌLJZĞĨĞƌƌĂů ................. 801.313.7711WƵďůŝĐZĞůĂƟŽŶƐΘDĞĚŝĂ;ĐĐůĞƐͿ ..... 26580WƵůŵŽŶĂƌLJ;ĐĐůĞƐͿ ................ 801.213.3599WƵůŵŽŵĂƌLJ&ƵŶĐƟŽŶ>Ăď;ĐĐůĞƐͿ ...... 21773WƵƌĐŚĂƐŝŶŐ ............................. 801.442.3000
QƵĂůŝƚLJZĞƐŽƵƌĐĞZŝƐŬDŐŶƚ;ĐĐůĞƐͿ 26300
Rapid Treatment Unit (RTU) ............. 21300RTU Anesthesia ............................... 21338
ZĞĐĞŝǀŝŶŐ ........................................... 21465Recovery Room .................................. 22890ZĞŐŝƐƚƌĂƟŽŶ^ĞĞKƵƚƉĂƟĞŶƚůŝŶŝĐZĞŐ;ĐĐůĞƐͿ^ƵƌŐĞƌLJ ............................................ 22840
Rehab Medicine Admin (Eccles) ........ 24900ƵĚŝŽůŽŐLJ ........................................ 24949/ŶƉĂƟĞŶƚ;WdKd^WͿ ....................... 24980Rehab Medicine/Clinic .................... 24949ŽƵŶƟĨƵů;ƵĚKdWd^WͿ ... 801.292.8665
KŐĚĞŶ;KdWd^WͿ ............... 801.387.2080^ĂŶĚLJ;KdWd^WͿ ................ 801.571.3081dĂLJůŽƌƐǀŝůůĞ;ƵĚKdWd^WͿϴϬϭϴϰϬϰϯϲϬ
PRIMARY CHILDREN’S OUTPATIENT SERVICES AT RIVERTON
ϯϳϳϯtÝãϭϮϲϬ^Êçã«Z®òÙãÊÄhdϴϰϬϲϱϴϬϭϮϴϱϭϮϴϱ &ÊÙÃ٦Įݽ½øãϯϯϯϯϯ
Department PhoneAĚŵŝŶŝƐƚƌĂƟŽŶ ...................................51670ƵĚŝŽůŽŐLJ ...........................................51640
Car Seat Appointment ...........801.662.6583ĂƌĚŝŽůŽŐLJ;&ƌŽŶƚĞƐŬͿ ......................51400ĂƌĚŝŽůŽŐLJ ..............................801.213.3599ĞŶƚƌĂůWƌŽĐĞƐƐŝŶŐ ..............................51690Child Life .............................................51663ŚŝůĚ>ŝĨĞ^ĂŵĞĂLJ^ƵƌŐĞƌLJ ...............51537Comprehensive Care ..............801.213.3599
Diabetes ................................801.213.3599
EEG ....................................................51755Ed .....................................................51285ŶĚŽĐƌŝŶŽůŽŐLJ .........................801.213.3599
GĂƐƚƌŽĞŶƚĞƌŽůŽŐLJ...................801.213.3599'ĞŶĞƌĂů^ƵƌŐĞƌLJ ..................................51320'ĞŶĞƟĐƐ ..................................801.213.3599
Human Resources ............................ 51680
IŶĨŽƌŵĂƟŽŶĞƐŬ ............................. 51025ImĂŐŝŶŐ ............................................. 51801
CT Scan .......................................... 51840MRI ................................................ 51860Ultrasound ..................................... 51880
Laboratory ....................................... 51001>ĂŶŐƵĂŐĞ^ĞƌǀŝĐĞƐ ............................ 51661
Medical Records .............................. 51650 Metabolics ............................ 801.213.3599
NĞƉŚƌŽůŽŐLJ .......................... 801.213.3599EĞƵƌŽůŽŐLJ ............................. 801.213.3599EƵƚƌŝƟŽŶ ............................... 801.662.1600
OƉƚŚĂůŵŽůŽŐLJ .................................. 51460FAX ...................................801.213.4004
KƉƟĐĂů^ŚŽƉ ..................................... 51474KZWŚĂƌŵĂĐLJ .................................... 51550KƌƚŚŽƉĞĚŝĐƐ ...................................... 51440KƚŽůĂƌLJŶŐŽůŽŐLJ;EdϬ ...................... 51285KƵƚƉĂƟĞŶƚůŝŶŝĐƐ;&ƌŽŶƚĞƐŬͿ ........ 51700
FAX ...................................801.285.1705
WĂƟĞŶƚZĞŐŝƐƚƌĂƟŽŶ .............................51010WĞĚŝĂƚƌŝĐ^ƵƌŐŝĐĂůůŝŶŝĐ .........................51320WƌĞͲKƉůĂƐƐ;ŚŝůĚ>ŝĨĞͿ .......................51537WůĂƐƟĐ^ƵƌŐĞƌLJ ......................................51340WƵůŵŽŶĂƌLJ ................................801.213.3599WƵůŵŽŶĂƌLJ&ƵŶĐƟŽŶ .............................51773
RŚĞƵŵĂƚŽůŽŐLJ .........................801.213.3599
Sleep Clinic...............................801.213.3599Social Work ...........................................51660STAT Pages ......................................... 33333^ƵƌŐŝĐĂů^ĞƌǀŝĐĞƐ ...................................51555KZ^ĐŚĞĚƵůĞƌ .....................................51531Scheduling FAX ................................51570WƌĞͲKƉ................................................51561WƌĞͲKƉůĂƐƐ;ŚŝůĚ>ŝĨĞͿ .....................51537WŽƐƚͲKƉ ..............................................51583
UƌŽůŽŐLJ ................................................51300
Volunteer Services...............................51662
Changes? call Marilyn 26580 updated 11/14
Introd
uctio
n
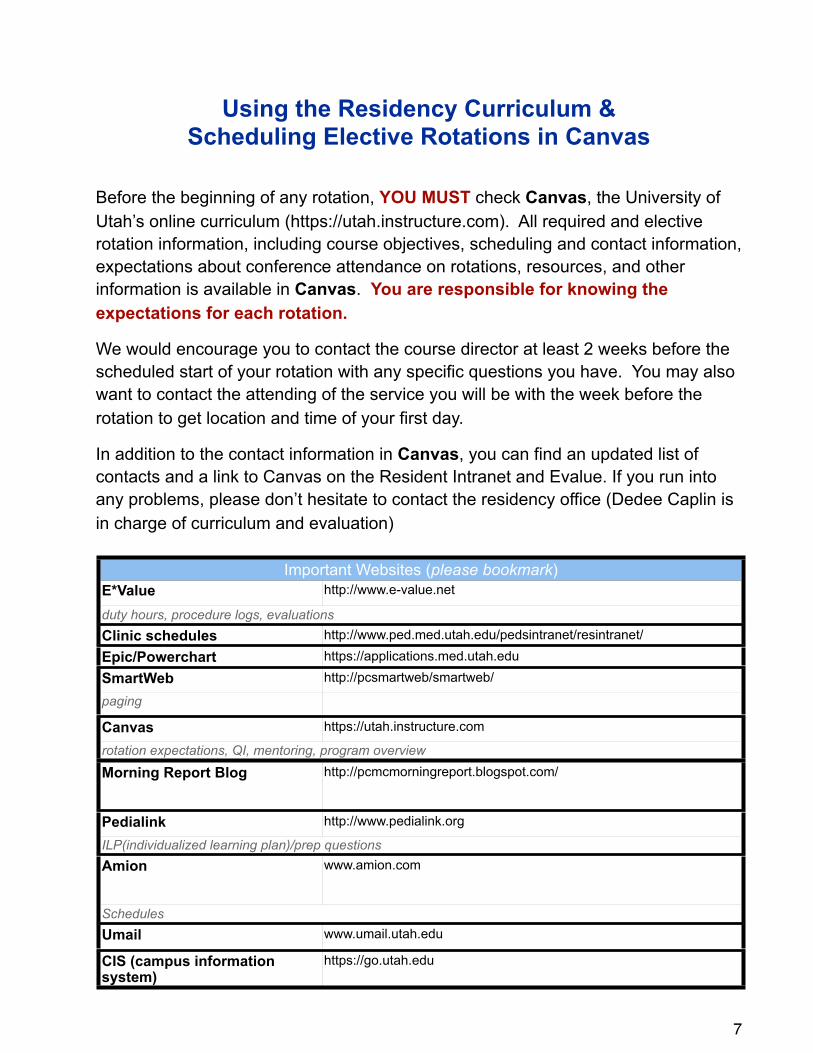
Using the Residency Curriculum & Scheduling Elective Rotations in Canvas
Before the beginning of any rotation, YOU MUST check Canvas, the University of Utah’s online curriculum (https://utah.instructure.com). All required and elective rotation information, including course objectives, scheduling and contact information, expectations about conference attendance on rotations, resources, and other information is available in Canvas. You are responsible for knowing the expectations for each rotation.
We would encourage you to contact the course director at least 2 weeks before the scheduled start of your rotation with any specific questions you have. You may also want to contact the attending of the service you will be with the week before the rotation to get location and time of your first day.
In addition to the contact information in Canvas, you can find an updated list of contacts and a link to Canvas on the Resident Intranet and Evalue. If you run into any problems, please don’t hesitate to contact the residency office (Dedee Caplin is in charge of curriculum and evaluation)
7
Important Websites (please bookmark) Important Websites (please bookmark) E*Value http://www.e-value.net
duty hours, procedure logs, evaluationsduty hours, procedure logs, evaluationsClinic schedules http://www.ped.med.utah.edu/pedsintranet/resintranet/
Epic/Powerchart https://applications.med.utah.edu
SmartWeb http://pcsmartweb/smartweb/
paging
Canvas https://utah.instructure.com
rotation expectations, QI, mentoring, program overviewrotation expectations, QI, mentoring, program overview
Morning Report Blog http://pcmcmorningreport.blogspot.com/
Pedialink http://www.pedialink.org
ILP(individualized learning plan)/prep questionsILP(individualized learning plan)/prep questionsAmion www.amion.com
SchedulesSchedulesUmail www.umail.utah.edu
CIS (campus information system)
https://go.utah.edu
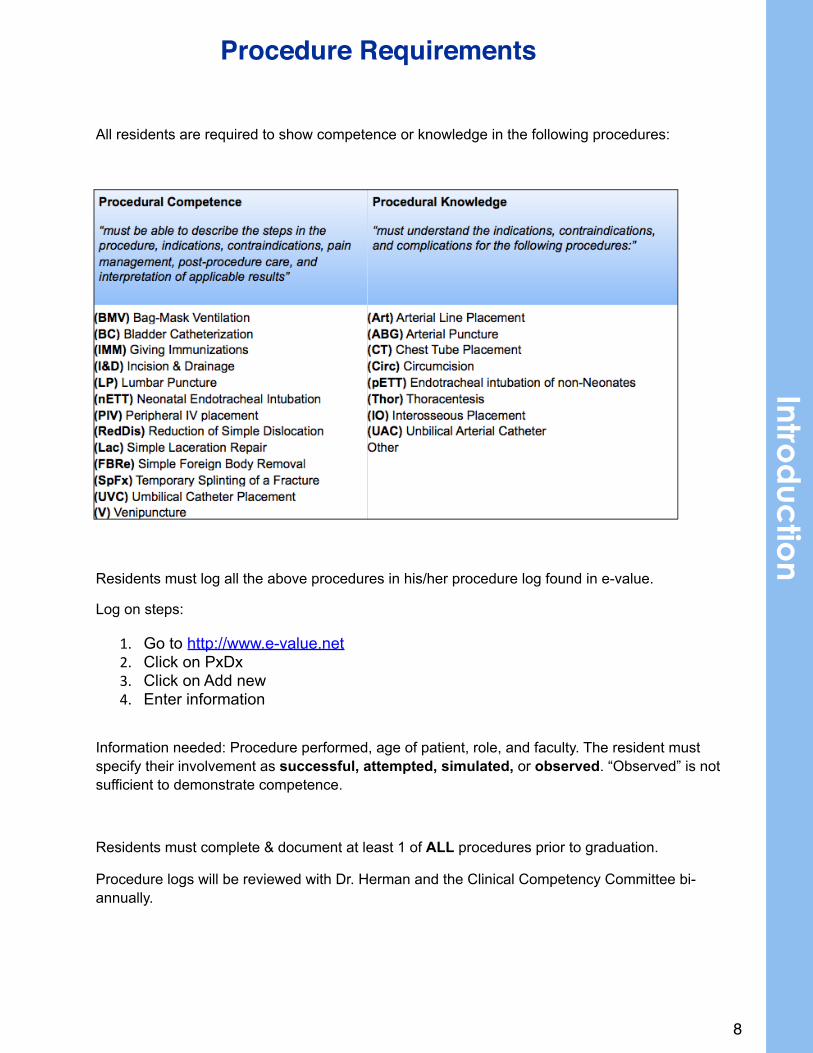
All residents are required to show competence or knowledge in the following procedures:
Residents must log all the above procedures in his/her procedure log found in e-value.
Log on steps:
1. Go to http://www.e-value.net2. Click on PxDx3. Click on Add new4. Enter information
Information needed: Procedure performed, age of patient, role, and faculty. The resident must specify their involvement as successful, attempted, simulated, or observed. “Observed” is not sufficient to demonstrate competence.
Residents must complete & document at least 1 of ALL procedures prior to graduation.
Procedure logs will be reviewed with Dr. Herman and the Clinical Competency Committee bi-annually.
8
Procedure RequirementsIntro
duc
tion
AFTER SCHOOL• Alphabet Blocks Child Care: child or after-school care, ages 6 weeks to 13 years, sliding
scale, for children with or without disabilities. Phone: 801-287-9502. Address: 3550 S 700 W.
• Neighborhood House: Offers before and after school programs for low-income children ages 5–12, including transportation to and from neighborhood schools. Neighborhood House also offers summer programs.Phone: 801-363-4589. Address: 1050 W. 500 S. Website: www.nhutah.org
• Sorenson Multicultural Center: free or low-cost after-school, summer, recreation, and arts programs in the Glendale area Phone: 801-974-2420. Address: 855 California Ave (1330 S)
• Boys and Girls Clubs: free or low-cost recreation, after school programs, and summer camp for kids 5–18 years old
o Capitol West Club: 567 West 300 North 801-531-7652o Lied Club: 464 South Concord (1235 West) 801-364-9118o Sugar House Club: 968 East Sugarmont Dr. (2225 So.) 801-484-0841o Tooele Club: 438 W 400 N, Tooele 435-843-5719o Website: www.bgcgsl.org
• West Valley Community Center: open gym, mentoring, youth groups, sports camps, youth group events, free or low cost. Phone: 801-654-0446. Address: 3818 W 4700 S. Website: westvalleycommunitycenter.org
• Youth City: serves Salt Lake City's young people ages 9-18 with innovative and enriching activities created with input from participants. YouthCity currently provides teen, after-school and summer, arts, employment, sports, government and service learning programming. Website: www.slcgov.com/publicservices/youthcity/
o Central City Teen Program: 801-535-7917, 615 S. 300 E. o Northwest Teen Program: 801-535-7917, 1300 W. 300 N.
• Salt Lake County Parks and Recreation: offers sports leagues, recreation centers, child care, after-school programs, adaptive sports. Scholarships available for sports league participation. Phone: 801-468-2299 or 801-270-7260
• SPLORE: specializes in affordable outdoor recreation activities for disabled, special needs, and at-risk youth through affordable, customized, inclusive recreation and education programs for people of all abilities. Scholarships are available. Phone: 801-484-4128. Website: www.splore.org
• National Youth Sports Program at the University of Utah: five-week sport and education program targeted toward low-income, at-risk youth ages 10 to 16 who reside in the Salt Lake School District. Phone: 801-585-5764
MENTORING• Big Brothers, Big Sisters of Utah: for children ages 6–12 from single-parent families that
pairs a child with a role model, building a one-on-one relationship built on trust and friendship. It includes community-based and school-based programs. There is also a high school mentoring program. Phone: 801-313-0303. Website: www.bbbsu.org
• Youth & Families with Promise: prevention program designed to enhance the school performance, social skills, and family bonds of at-risk youth aged 10–14. Phone: (435) 797-1543. Website: extension.usu.edu/yfp
CHILD ABUSE• Child Abuse and Neglect Hotline: 24-hour statewide hotline1-800-678-9399• The Center for Safe & Healthy Families at Primary Children’s Medical Center• Primary Children’s Medical Center- Primary Children’s Center for Safe and Healthy
Families: provides evaluations, treatment and medical examinations for children who have been physically and sexually abused. The center offers group treatment to parents and
9
Community Resources
children as well as individual treatment. 100 North Medical Drive., Salt Lake City, Utah 84113, (801)588-3650
CHILD CARE/RESPITE• Child Care Resource & Referral: provides free referrals to child care services and guides to
choosing quality child care.Salt Lake & Tooele Counties (Children’s Service Society): provides pregnancy counseling, parenting advocacy, infant and special needs adoption, child care resource, referral, and provider training. Fee based on ability to pay.
Salt Lake County: 801-355-4847. Toll Free: 1-866-GET HUGS (438-4847). Website: http://www.cssutah.org/
Utah, Wasatch & Summit: Orem: 801-863-8220. Toll Free: 1-800-952-8220. Website: http://www.uvu.edu/ccrr/
Box Elder, Cache & Rich Counties: Logan: 435-797-1552. Toll Free: 1-800-670-1552. http://www.usuchild.usu.edu/
Daggett, Duchesne, Uintah, Carbon, Emery, Grand & San Juan Counties:Price: 435-613-5619. Toll Free: 1-888-637-4786. Website: http://www.ceu.edu/childcare/ Juab, Piute, Wayne, Millard, Sanpete, Sevier, Iron, Washington, Kane, Garfield & Beaver Counties:St George: 435-628-4843. Cedar City: 435-586-8722. Toll Free: 1-888-344-4896. Website: http://childcarehelp.org/
• Department of Workforce Services Office of Child Care: offers information about child care cost assistance, referrals, and out-of-school time. Address: 1385 S. State St., Salt Lake City. Phone: (801) 468-0049 or toll free: (800) 622-7390
• Head Start and Early Head Start of Salt Lake: early childhood development programs serving low-income children from ages birth to 5 years. Children participate in a school-readiness curriculum and receive medical and dental services. Website: www.saltlakeheadstart.org. Phone: 801-977-1122
• Alphabet Blocks Child Care: child or after-school care, ages 6 weeks to 13 years, sliding scale, for children with or without disabilities. Phone: 801-287-9502. Address: 3550 S 700 W.
• Neighborhood House: offers a nursery/toddler preschool for low-income children ages 2–5, provided in a multilingual environment. Phone: 801-363-4589. Address: 1050 W. 500 S. Website: www.nhutah.org
• Family Support Center Crisis Nursery (3 locations): offers free 24/7 crisis nursery care for any child aged 0–11 for parents who are stressed, need a break, have an emergency arise, or have no one else to help take care of their children. Website: www.familysupportcenter.org
Sugar House: 2020 Lake Street (740 East), 801-487-7778Midvale: 777 W. Center Street (7720 South), 801-255-6881West Valley: 3663 South 3600 West, 801-967-4259 (Open 24/7)
DOMESTIC/COMMUNITY VIOLENCE• Domestic Violence LINK Line: information on and referrals to counseling, shelters, safe
houses, support groups, police, mental, health services, human service agencies, legal services, victims assistance groups and more. Phone: 1-800-897-LINK (5465)
• National Domestic Violence Hotline: 1-800-799-SAFE (7233)• Rape & Sexual Assault Crisis Line: 1-888-421-1100• YWCA Women in Jeopardy: 24-hour crisis line and shelter that provides safety, shelter, and
basic needs for women and children fleeing violent homes. Also includes advocacy and case management, therapeutic discussion groups, academic support, afterschool and
10
Introd
uctio
n
summer camp, teen program, child care, and parenting support. Childcare available. Address: 322 East 300 South. Phone: 801-537-8600
• Shelters: Link to shelters in Utah. Includes info about # of beds, children’s services, transient housing, pet boarding, availability of outreach coordinators, and contact numbers. Website: http://www.udvc.org/linkline_shelters.pdf
• Legal Aid Society: assists adults and children who are victims of domestic violence to obtain protective orders and civil stalking injunctions from the court regardless of their income. Address: 205 North 400 West. Phone: (801) 328-8849. Website: legalaidsocietyofsaltlake.org
• Cornerstone Counseling Center: outpatient substance abuse and domestic violence treatment programs including a mother/child program. Address: 47 W Bearcat Dr. Phone: 801-355-2846
• South Valley Sanctuary: provides safe shelter and supportive services to men, women and children who have been forced to leave their homes due to violence from a family member. Includes case management, crisis counseling, support groups, resource referral, etc. Phone: 801-255-1095. Website: www.southvalleysanctuary.com
EARLY INTERVENTION/DEVELOPMENT• Baby Watch/Early Intervention Services: Utah’s network of services for children (birth to age
3) with developmental delay or disabilities. Hotline: 1-800-961-4226 DDI Vantage (Ages 0–3) 801-266-3939 (Salt Lake, Granite, Murray School Districts, and Tooele County) Child Development Center (Ages 0–3) 801-412-2510 (Jordan district) Over age 3: Contact your school district School Districts: Granite: 801-646-5000, Salt Lake: 801-578-8599, Murray: 801-264-740, Jordan: 801-567-8100
• Utah Children with Special Health Care Needs: provides and promotes family-centered, coordinated care and facilitates the development of community-based systems for children with special needs and their families. Activities focus on reduction of preventable death, disability and illness in children due to chronic and disabling conditions. Also provides evaluation, diagnosis, prescriptions, and case management. Phone: 801-584-8284 or 1-800-829-8200. Address: 44 N. Mario Capecchi Dr. Website: www.health.utah.gov/cshcn
EDUCATION RESOURCES• Neighborhood House: offers before and after school programs for low-income children ages
5–12, including transportation to and from neighborhood schools. Neighborhood House also offers summer programs. Phone: 801-363-4589. Address: 1050 W. 500 S. Website: www.nhutah.org
• Guadalupe Educational Programs: educational services to disadvantaged children birth- 9yr. Includes preschool, an in-home program for ages 0–3, and school for grades K–3. Phone: 801-531-6100. Address: 340 S. Goshen St. (1040 W.)
EMPLOYMENT/JOB TRAINING• Salt Lake Community Action Program: Multiple neighborhood centers offering employment
assistance, weatherization, food assistance, housing assistance, head start programs, utility assistance job placement, and crisis intervention. Phone: 801-359-2444. Address: 764 S. 200 W. Website: www.slcap.org
FOOD/NUTRITION/BREASTFEEDING• WIC (Women, Infants, and Children): supplemental food program for pregnant women and
children under 5 years old. Phone: 1-877-WIC-KIDS (942-5437). Website: www.health.utah.gov/wic
11
• SNAP (Formerly Food Stamps): supplemental financial assistance for food for low-income families. Phone: (801) 526-0950 or 1-866-453-7410. Website: http://jobs.utah.gov/opencms/customereducation/services/foodstamps/index.html
• Catholic Community Services: St. Vincent de Paul provides hot, nutritious meals or sack lunches daily to low-income and homeless individuals.. Address: 437 West 200 South. Phone: (801) 363-7710. Website: http://www.ccsutah.org
• Free School Meals: Contact School District• Child Nutrition Program: administers several nutrition programs including the Summer Food
Service Program, which provides meals to low-income children during summer vacations, interim, and off-track periods. Phone: 801-538-7680. Website: www.schools.utah.gov/cnp
• Commodity Supplemental Food Program (CSFP): provides nutritious foods to low-income children, women, and older adults and is only available for those not participating in WIC. Interested individuals must apply in person at a participating food pantry. Phone: (801) 887-1275. Website: www.utahfoodbank.org/csfp
• Utahns Against Hunger: advocacy group provides referrals and information about food assistance programs and food pantries. Phone: 801-328-2561 or 1-800-453-3666. Website: www.uah.org
• Salt Lake Community Action Program: several neighborhood food pantries providing emergency 3-day food supply. Phone: 801-359-2444. Website: www.slcap.org/fdpntry
• Nutrition Clinic at Primary Children’s Medical Center: clinic w/ registered dietitians who specialize in children; provide consultation and dietary recommendations for children with special nutritional needs. Phone: 801-662-5313
• La Leche League: La Leche League is an international nonprofit, nonsectarian organization dedicated to providing education, information, support, and encouragement to women who want to breastfeed. National Toll-free: 1-800-525-3243. International Website: www.llli.org. Utah chapter: 801-264-LOVE (5683). www.lllusa.org/UT/Utah
LOW COST HEALTH CARE/INSURANCE• Baby Your Baby: Temporary financial assistance to low-income pregnant women. Phone:
1-800-826-9662. Website: www.babyyourbaby.org• Children’s Health Insurance Program (CHIP): affordable health insurance for low-income
working families that earn too much for Medicaid and have children. Phone: 1-877-KIDS-NOW (543-7669)/. Website: www.health.utah.gov/chip
• Medicaid: various health coverage options for low-income and disabled individuals. Website: ww.health.utah.gov/bep. Toll-free hotline: 1-800-662-9651. Utah: 801-538-6155
• Immunizations Hotline: vaccine information, including no-cost or low-cost vaccines for eligible children through the Utah Vaccines for Children Program (VCF). Phone: 1-800-275-0659
• Primary Care Network: health plan that covers services provided by a primary health care provider for low-income, uninsured Utahns that don’t qualify for Medicaid. Phone: 1-888-222-2542. Website: http://www.health.utah.gov/pcn/
• Together Rx Access: helps low-income individuals and families without prescription drug insurance receive discounts on medications. Phone: 1-800-250-2839. Website: www.TogetherRxAccess.com
FREE HEALTH CLINICS• Maliheh Free Clinic: provides free medical services for uninsured individuals and low
income families. Call for an appointment; no walk-ins. Address: 415 East 3900 South. Phone: 801-266-3700. Website: www.malihehfreeclinic.org
• Utah Hope Clinic: free medical facility providing treatment and referrals for those who are without insurance and at or below 150% Federal Poverty Guidelines. Open Tuesdays and
12
Introd
uctio
n
Wednesdays. Address: 65 East 6850 South. Phone: 801-568-6700. Website: www.utahhopeclinic.org
HOUSING• Salt Lake Community Action Program: multiple neighborhood centers offering employment
assistance, weatherization, food assistance, housing assistance, head start programs, utility assistance job placement, and crisis intervention.Phone: 801-359-2444. Address: 764 S. 200 W. Website: www.slcap.org
• Housing Authority: promotes affordable housing and rent subsidies for low-income individuals and families.
Salt Lake City: 801-487-2161. http://www.haslcutah.org/ Salt Lake County: 801-284-4400. http://www.hacsl.org/ West Valley: 801-963-3320
• Community Development Corporation of Utah: provides home ownership opportunities, home improvements, foreclosure assistance, down payment assistance, and housing education for low-income families. Phone: 801-994-7222. 1-866-994-7222. Website: http://www.cdcutah.org/
• Assist, Inc.: provides housing, accessibility design assistance, and home repairs to low income households or persons with disabilities. Website: www.assistutah.org. Phone: 801-355-7085
• Salt Lake Habitat for Humanity: Habitat builds and rehabilitates simple, decent, affordable houses for low-income families with the help of the homeowner (partner) families. Phone: 801-263-0136. Web: www.habitatsaltlake.com
IMMIGRATION/REFUGEE SERVICES• Utah Refugee Employment and Community Center/Asian Association of Utah: provides
services such as tutoring, language classes, translation, cultural activities and family counseling to all immigrants and refugees. Address: 1588 S. Major St (50 E). Phone: 801-467-6060. Website: www.aau-slc.org
• Catholic Community Services: offers refugee resettlement, job placement, education, help with immigration legal issues, and foster care for refugee children. Phone: (801) 977-9119. Website: www.ccsutah.org
• International Rescue Committee of Salt Lake: helps refugees find urnished home, rent help, health care, food, English language classes, job skills, education, social and community services, and legal services toward residency & citizenship. Address: 231 East 400 South, Suite 50. Phone: (801) 328-1091. www.rescue.org/us-program/us-salt-lake-city-ut
• Lutheran Social Services of Utah: works with recent arrivals of people fleeing Afghanistan, Bhutan, Bosnia, Burma, Congo, Croatia, Eritrea, Iran, Iraq, Lebanon, Liberia, Sudan, Somalia, Thailand, and Sierra Leone. http://www.lssu.org/
• Centro de la Familia de Utah: provides self-sufficiency programs, parenting resource center, Head Start, and breast care program for Hispanic families. Phone: 801-521-4473. Website: http://www.cdlfu.org/
LEGAL SERVICES• Disability Law Center: legal aid for persons with disabilities. Address: 205 North 400 West.
Phone: 1-800-662-9080 (toll free) or 1-801-363-1347. Website: www.disabilitylawcenter.org• Legal Aid Society: assists adults and children who are victims of domestic violence to obtain
protective orders and civil stalking injunctions from the court regardless of their income.Legal Aid Society of Salt Lake also provides low cost legal representation to low-
13
income individuals with family law cases in Salt Lake County. Address: 205 North 400 West. Phone: (801) 328-8849. Website: legalaidsocietyofsaltlake.org
• Utah Legal Services: provides legal representation, advocacy, education, and referral for low-income individuals. Phone: (801) 328-8891. Toll Free (800) 662-4245 (outside S.L. County). Website: www.utahlegalservices.org
• Tuesday Night Bar: free, brief one-on-one consultations to help determine their legal rights. First four Tuesdays of each month from 5:30–7:00 p.m. at the Utah Law & Justice Center. No walk-ins; call for an appointment at least 8 days in advance. Address: 645 South 200 East. Phone: 801-297-7037. www.utahbar.org/public/tuesday_night_bar.html
LITERACY
• English as a Second Language: low cost or free. West Valley Community Center. Phone: 801-654-0446
• Horizonte Instruction Center: 1234 S. Main Street. 801-578-8574. Web: horizonte.slcschools.org/programs/?index=ell
• Guadalupe Schools: ESL evening classes, limited child care. Address: 340 South Goshen St (1040 West). Phone: 801-531-6100 ext. 1105 or 1107. Website: www.guadalupe-schools.org/programs/CLC/clc.htm\
• English Skills Center: variety of English classes, including group classes and one-on-one tutoring. Phone: 801-328-5608. Website: www.eslcenter.org/
• Inglés Para Latinos: English classes with a flexible schedule for working adults, includes child care services. Phone: 801-556-1763. Website: www.inglesparalatinos.org
• Granite Peaks: English classes through continuing education, locations in Salt Lake City, West Valley, and Kearns. Phone: 385-646-5435. Website: www.granitepeaks.org
• Murray District: English classes for adults at Murray High School; year-round program. Address: 5440 South State Street. Phone :801-264-7460. Website: www.murrayschools.org/wworks/parents_adulteducation.shtml
• Asian Association : day and evening ESL classes. Phone: 801-461-6060. http://www.aau-slc.org/services-a-departments/esl-and-life-skills
• Holy Cross Ministries: ESL classes in Wendover. Phone: 801-261-3440. Web: www.holycrossministries.org
• Southpointe Adult High School: English classes for low-cost or free. Address: 9301 South Wight Fort Road (3400 West). Phone: 801-256-5952. Website: southpointe.jordandistrict.org/esol.htm
• Salt Lake Community Education : extensive English-as-a-Second-Language courses taught at Salt Lake Community College campuses. Phone: 801-957-3212. Website: www.slcc.edu/esl
BEHAVIOR• Utah Youth Village: counseling for troubled children and families. Offers residential care in
treatment foster homes or group homes as well as in-home help. Address: 5800 South Highland Drive. Phone: (801) 272-9980. Website: www.youthvillage.org
• Youth Support Systems: offers programs to help youth with delinquent and substance abuse behaviors. Address: 3500 South 3392 West. Phone: 801-969-3307. Website: www.yss.utah.org
• Youth & Families with Promise: prevention program designed to enhance the school performance, social skills, and family bonds of at-risk youth aged 10–14. Phone: (435) 797-1543. Website: extension.usu.edu/yfp
14
Introd
uctio
n
COUNSELING• Valley Mental Health:counseling services w/ fees based on ability to pay. Phone: (888)
949-4864. www.vmh.com• The Children’s Center: provides mental health services and early intervention for preschool
aged children with emotional and behavioral problems. Website: www.tccslc.orgSalt Lake City: 350 South 400 East, 801-582-5534Kearns: 5242 South 4820 West, 801- 966-4251
• Family Counseling Center: individual and family counseling, sliding pay scale. Address: 5250 S. Commerce Dr. (320 W), Suite 250. Phone: 801-261-3500 (24-hr number). Web: www.familycounselingcenterutah.com
• LDS Family Services: counseling and adoption services, various locations throughout Utah. 724 East 2100 South, Suite B. Phone: 801-487-0499. Web: providentliving.org
• New Life Foundation: support groups and referrals for those with eating disorders. Phone: 801-983-6441
• The Sharing Place: provides a safe and caring environment where children, teens, and their families who are grieving the death of a loved one may share their feelings while healing themselves. Address: 1695 East 3300 South. Phone: 801-466-6730. Website: thesharingplace.org
• Caring Connections: grief counseling and support groups, sponsored by the University of Utah College of Nursing. Phone: 801-585-9522. Website: nursing.utah.edu/practice/caringconnections
• Primary Children’s Bereavement Services: free support services available to families (individuals >6 years) who have experienced the death of a child in the family. Groups meet at PCH. Phone: 801-662-3774. Website: http://intermountainhealthcare.org/hospitals/primarychildrens/services/pages/service.aspx?service=bereavement%20services
• Sharing Parents of Utah: support group for families experiences a pregnancy loss, stillbirth, or newborn death. Phone: 801-272-5355. Website: www.shareparentsofutah.org
ADDICTION• Utah Tobacco Quit Line: provides private phone-based coaching and information about
programs your area to help you or a loved one quit smoking. Phone: 1-800-QUIT-NOW (784-8669). Website:
• Utah QuitNet: online support group and forum with resources for quitting smoking. Website: utahquitnet.com
• Youth Support Systems: offers programs to help youth with delinquent and substance abuse behaviors. Address: 3500 South 3392 West. Phone: 801-969-3307. Website: www.yss.utah.org
• Alcoholics Anonymous: free 12-step program for individuals with alcohol-abuse problems. Address: 80 West Louise (2860 S). Phone: 801-484-7871. Website: www.saltlakeaa.org
• Narcotics Anonymous: free 12-step fellowship for recovering from the disease of addiction. English: 801-25-CLEAN (801-252-5326)Spanish: 801-33-AYUDA (801-332-9832)www.uwana.org (Salt Lake area)www.nautah.org (statewide)
• Salt Lake County Behavioral Health Services: administers substance abuse prevention and treatment services. Fee based on ability to pay. Phone: 801-468-2009. Website: behavioralhealthservices.slco.org
• Cornerstone Counseling Center: outpatient substance abuse and domestic violence treatment programs including a mother/child program. Address: 47 W Bearcat Dr. Phone: 801-355-2846
• St. Mary’s Home for Men: residential substance abuse treatment facility designed to help clients overcome addictions and transition to independence, security, and good health.
15
Address: 745 E. 300 South. Phone: 801-977-9119. Website: www.ccsutah.org/programs/treatment-services
• Odyssey House: provides substance abuse treatment, education, and prevention services including individual, group and family therapy, milieu therapy, medication management, some medical services, life skills training, vocational rehabilitation, educational services, transitional housing, psychiatric services, and recreation. Phone: (801) 322-3222. Website: www.odysseyhouse.org
• House of Hope: provides comprehensive alcoholism and chemical dependency treatment services for men, women, pregnant women, women with children and mothers working to reunify with their child(ren). Community educational services and DUI PRIME for Life classes are also available. Address: 857 East 200 South. Phone: 801-487-3276 ext. 1201. Website: www.houseofhopeut.org
• Rescue Mission of Salt Lake: free year-long New Life Addiction Recovery Program is for men addicted to alcohol, drugs, pornography or gambling and includes free Bible-based recovery services. Address: 463 S. 400 West. Phone: 801.355.1302. Website: rescuesaltlake.org
PARENTING• Centro de la Familia de Utah: provides various parenting classes catered specifically to
people of Latino descent. Address: 3780 S West Temple. Phone: (801) 521-4473. Website: www.cdlfu.org
• The Family Support Center: free, confidential, and personalized in-home mentored parenting program for overwhelmed parents, as well as parenting classes at three locations. Website: www.familysupportcenter.org. Phone: 801-955-9110
• Jordan Family Education Center: parenting classes, support groups, short-term counseling on topics like parenting skills, dealing with adolescence, attention deficit, anger, grief, single parenting, blended families and many more. Phone: 801-565-7442. Website: www.jordandistrict.org/departments/jfec
• DDI Vantage: free parenting classes geared toward parents with children under age 3 on various topics from discipline to potty training. Phone: 801-266-3939. Website: www.ddivantage.com/parent_training.htm
• Grandfamilies (Children’s Service Society): support groups, family building, and counseling for those caring for grandchildren or relatives’ children. Phone: 801-355-7444. www.cssutah.org/grandfamilies-relatives-as-parents
• Children’s Service Society: parenting classes and resources, kindergarten readiness, parent group meetings, and in-home visits. Phone: 801-355-7444 or 1-800-839-7444. Website: http://www.cssutah.org/utah-parents-as-teachers
ADOPTION• Catholic Community Services:provides adoption and pregnancy counseling, immigration,
and refugee resettlement and other family services. Phone: (801) 977-9119. Website: www.ccsutah.org
• LDS Family Services: free pregnancy counseling and adoption services for teen or unwed mothers of all religions. Phone: 1-800-537-2229. Website: itsaboutlove.org
PREGNANCY AND INFANT RESOURCES• Baby Your Baby: resource to answer your questions and locate the services you and your
family may need before, during, and after pregnancy. Phone: 1-800-826-9662. Website: www.babyyourbaby.org
• Pregnancy Risk Line: provides accurate and current information about the effects of environmental exposures, including medications and herbs, on pregnancy and breastfeeding. Phone: 1-800-822-2229
16
Introd
uctio
n
• Catholic Community Services: provides adoption and pregnancy counseling, immigration, and refugee resettlement and other family services. Phone: (801) 977-9119. Website: www.ccsutah.org
• Children’s Service Society: provides pregnancy counseling, parenting advocacy, infant and special needs adoption, child care resource, referral, and provider training. Phone: (801) 355-7444 or 1-800-389-7444. www.cssutah.org
• Planned Parenthood: Salt Lake: 801-322-5571. West Valley: 801-973-9675. Web: www.plannedparenthood.org/utah
• Pregnancy Resource Center: pregnancy testing, peer counseling, support groups, temporary shelter, adoption assistance, medical and legal referrals. Address: 644S 900E. Phone: 801-363-543. Web: www.pregnancyresource.net
• University of Utah Teen Mother and Child Program: comprehensive medical care and social work services for teen mothers (under 18) and their children. Address: 3690 S. Main St. Phone: 385-468-3690
• Nurse-Family Partnership: free program that partners first-time moms with nurse home visitors. Specially trained nurses visit participants throughout pregnancy and until the baby turns 2yr. Address: 3690 South Main Street. Phone: 385-468-3690. www.nursefamilypartnership.org/Locations/Utah
SAFETY RESOURCES• Safe Kids Utah: car seat installation help and inspection sites. Phone: 801-538-6852. Web:
www.safekidsutah.org• Primary Children’s Care Seat Inspections: free car seat inspections by appointment only.
Phone: 801-662-CARS• Child Car Seat Inspection Station Locator: find the nearest car seat inspection station,
where certified technicians will inspect car seats and installation, usually for free. Website: stnw.nhtsa.gov/cps/cpsfitting/
SHELTERS• YWCA Women in Jeopardy: 24-hour crisis line and shelter that provides safety, shelter, and
basic needs for women and children fleeing violent homes. Also includes advocacy and case management, therapeutic discussion groups, academic support, afterschool and summer camp, teen program, child care, and parenting support. Childcare available. Address: 322 East 300 South. Phone: 801-537-8600
• South Valley Sanctuary: provides safe shelter and supportive services to men, women and children who have been forced to leave their homes due to the violence perpetrated by a family member. Includes case management, crisis counseling, support groups, resource referral, and more. Phone: 801-255-1095. www.southvalleysanctuary.com
• Salt Lake Community Action Program: multiple neighborhood centers offering employment assistance, weatherization, food assistance, housing assistance, head start programs, utility assistance job placement, and crisis intervention. Phone: 801-359-2444. Address: 764 S. 200 W. Website: www.slcap.org
• Rescue Haven: safe place where women and women with children can find safety from abusive relationships, counseling for addiction and the love of Jesus. As a ministry of the Rescue Mission of Salt Lake, Rescue Haven also gives homeless and low-income women access to emergency shelter, food, clothing, job placement and much more. Address: 1165 South State Street. Phone: 801-521-5925
• Rescue Mission of Salt Lake: shelter, chapel services, meals, lunches, day room, mail reception, showers, clothing for men and women. Address: 463 S. 400 West. Phone: 801.355.1302. Website: rescuesaltlake.org
• The Road Home: provides shelter, support, and programs for homeless individuals and families. Address: 210 South Rio Grande Street. Phone: 801-359-4142. Website: www.theroadhome.org.
17
• Homeless Youth Resource Center: delivers services to homeless street youth through street outreach, a drop-in center, and a transitional home. Services include meals, laundry, classes, referrals, and case management. Address: 655 South State Street. Phone: 801-364-0744. Website: http://www.voaut.org/Services/Homeless-Outreach--Housing-Programs/Homeless-Youth-Resource-Center
SPECIAL NEEDS/AUTISM• Access Utah: info, referrals, and services for people with disabilities. Phone:
1-800-333-8824. Web: accessut.org• The Family Support Center: autism respite care for children ages 0–11, fee based on ability
to pay. Address: 2020 South Lake Street (740 East). Phone: 801-487-7778. Web: www.familysupportcenter.org/autismrespite.php
• Utah Children with Special Health Care Needs: family-centered, coordinated care and facilitates the development of community-based systems for children with special needs and their families. Activities focus on reduction of preventable death, disability and illness in children due to chronic and disabling conditions. Also provides evaluation, diagnosis, prescriptions, and case management. Phone: 801-584-8284 or 1-800-829-8200. Address: 44 N. Mario Capecchi Dr. Website: www.health.utah.gov/cshcn
• Utah parent Center and Autism Information Resource: information, training, advocacy, support groups, parent workshops, and referrals for parents of disabled or autistic children. Phone: 801-272-1051 or 801-272-1067 (Spanish). Toll free: 1-800-468-1160. Website: www.utahparentcenter.org
• Foundations for Independence (Cerebral Palsy of Utah): family support, parent networking, respite services for families with children of all types of disabilities. Phone: 801-266-1805. Website: www.ffiutah.org
• Special Olympics Utah: sports training and competitions for children and adults with intellectual disabilities. Phone: 801-363-1111. Website: www.sout.org
• Disability Support Center for Families: helps community members with disabilities and/or their families learn more about available resources and community groups, including information, referral assistance, help with paperwork, training, support groups, and more. Phone: 801-973-0129. Web: www.disabilitysupportcenter.org
TEEN PREGNANCY• University of Utah Teen Mother and Child Program: comprehensive medical care and social
work services for teen mothers (under 18) and their children. Phone: 385-468-1000• UPAT Teen Parent Program: provides home visits, support, referrals, parenting and
developmental information, and group meetings with other teen parents. Phone: 801-326-4407. Web: www.cssutah.org/teen-parent-program
• LDS Family Services: free pregnancy counseling, adoption services, and foster care for teen or unwed mothers of all religions. Phone: 1-800-537-2229. Website: itsaboutlove.org
• Planned Parenthood: Salt Lake: 801-322-5571; West Valley: 801-973-9675; Web: www.plannedparenthood.org/utah
• Pregnancy Resource Center: pregnancy testing, peer counseling, support groups, temporary shelter, adoption assistance, medical & legal referrals. Address: 644 South 900 East. Phone: 801-363-5433. www.pregnancyresource.net
TEEN RESOURCES• Youth & Families with Promise: prevention program designed to enhance the school
performance, social skills, and family bonds of at-risk youth aged 10–14. Phone: (435) 797-1543. Website: extension.usu.edu/yfp
18
Introd
uctio
n
• Youth City: innovative and enriching activities for children 9-18. Provides teen, after-school and summer, arts, employment, sports, government and service learning programming. Web: www.slcgov.com/publicservices/youthcity/
Central City Teen Program: 801-535-7917, 615 S. 300 E. Northwest Teen Program: 801-535-7917, 1300 W. 300 N.
• University of Utah Adolescent Clinic: clinic focusing on adolescent issues including behavior issues, substance abuse, eating disorders, and gynecology. Phone: 801-587-7574
• National Runaway Switchboard: national hotline for runaways and their families to work through problems and find local help. Phone: 1-800-RUN-AWAY (24-hr hotline). Website: www.1800runaway.org
• Job Corps: provides vocational training, job placement, and GED attainment for economically disadvantaged youth. Phone: 1-800-733-JOBS. Website: www.jobscorp.gov
• Youth Employ Ability Services: helps low-income youth ages 14–21 to obtain their diploma or GED, and find job training and employment. Phone: 801-468-0115. Website: www.justforyouth.utah.gov/employment.htm
• Odyssey House: provides substance abuse services, including individual, group, and family therapy, milieu therapy, medication management, some medical services, life skills training, vocational rehabilitation, educational services, transitional housing, psychiatric services, and recreation. Phone: (801) 322-3222
• GED Testing: Info on testing locations, dates, and preparations. Phone: 801-538-7821. Web: www.utahged.org
• Teen Emotions Anonymous: 12-step program to help teens deal with emotional problems including depression, anxiety, and substance abuse. Hotline: 801-281-4778
• Tooele Youth Center (Teen Center): free or low-cost recreation, after school programs, and summer camp. Address: 102 North 7th Street. Phone: 435-843-5719. Website: www.bgcgsl.org
19

20
Zero Harm
22
Zero
Ha
rm
23
24
Zero
Ha
rm
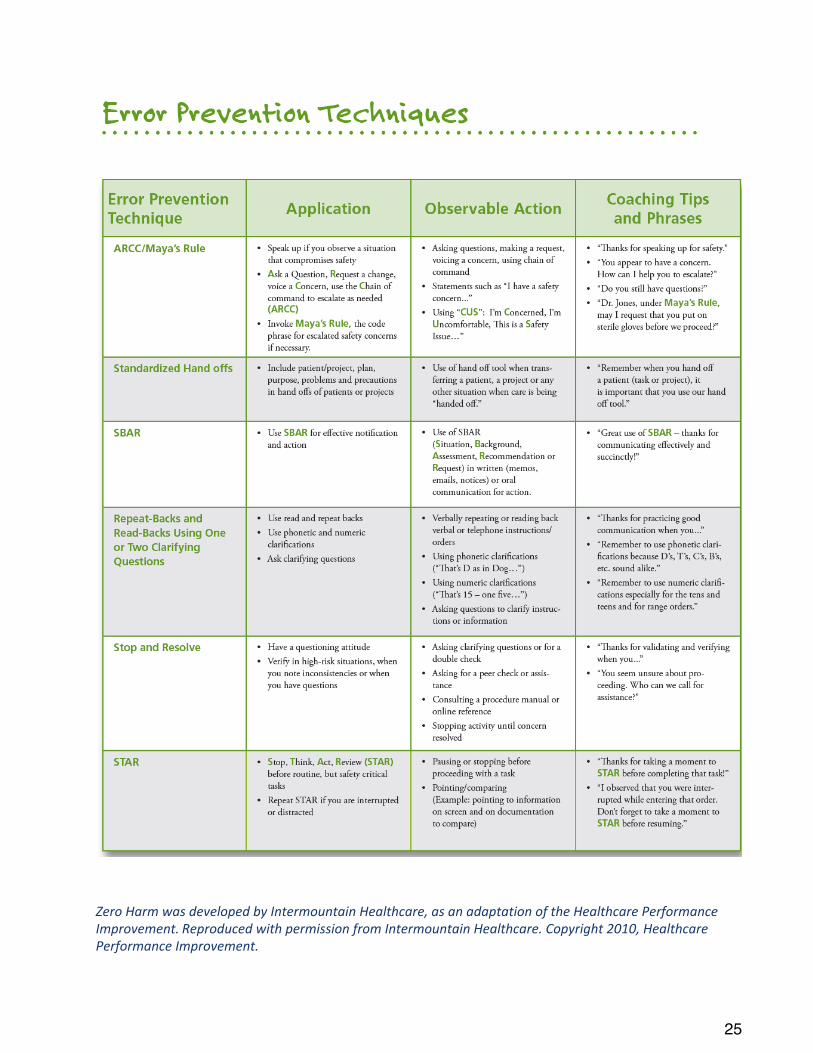
Zero%Harm%was%developed%by%Intermountain%Healthcare,%as%an%adaptation%of%the%Healthcare%Performance%Improvement. Reproduced%with%permission%from%Intermountain%Healthcare.%Copyright%2010,%Healthcare%Performance%Improvement.
25

26
Adolescent Medicine
28
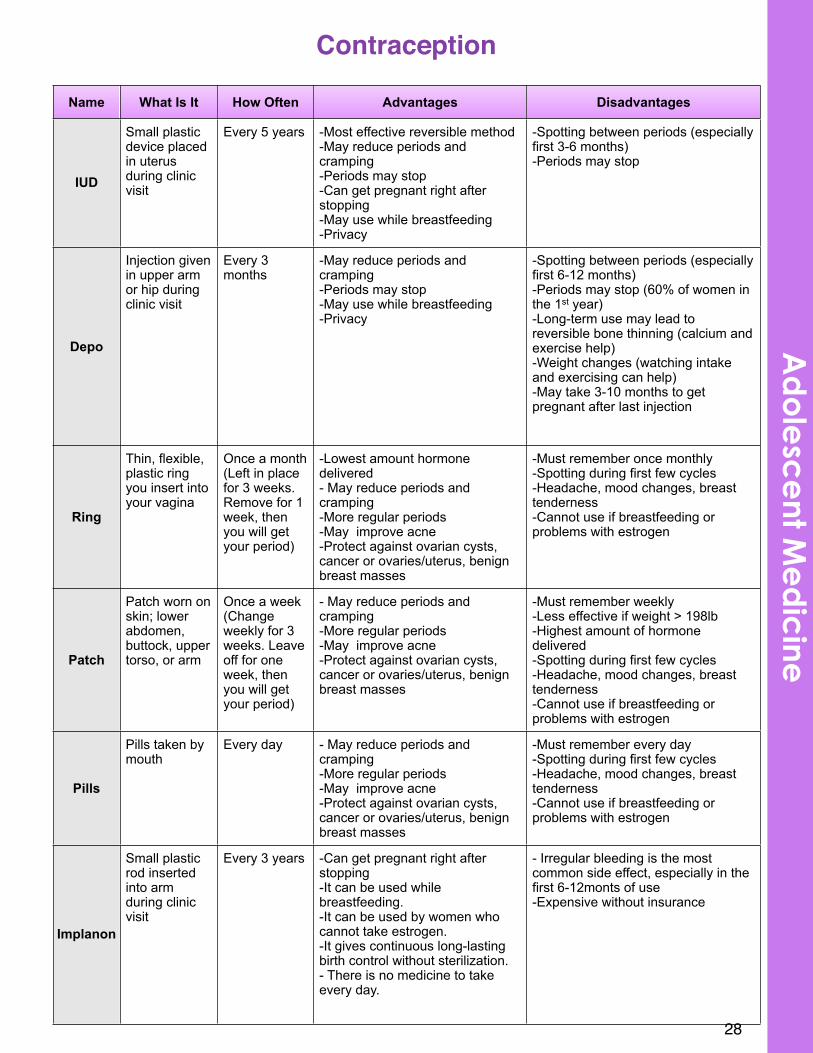
Contraception
Name What Is It How Often Advantages Disadvantages
IUD
Small plastic device placed in uterus during clinic visit
Every 5 years -Most effective reversible method-May reduce periods and cramping-Periods may stop-Can get pregnant right after stopping-May use while breastfeeding-Privacy
-Spotting between periods (especially first 3-6 months)-Periods may stop
Depo
Injection given in upper arm or hip during clinic visit
Every 3 months
-May reduce periods and cramping-Periods may stop-May use while breastfeeding-Privacy
-Spotting between periods (especially first 6-12 months)-Periods may stop (60% of women in the 1st year)-Long-term use may lead to reversible bone thinning (calcium and exercise help)-Weight changes (watching intake and exercising can help)-May take 3-10 months to get pregnant after last injection
Ring
Thin, flexible, plastic ring you insert into your vagina
Once a month(Left in place for 3 weeks. Remove for 1 week, then you will get your period)
-Lowest amount hormone delivered- May reduce periods and cramping-More regular periods-May improve acne-Protect against ovarian cysts, cancer or ovaries/uterus, benign breast masses
-Must remember once monthly-Spotting during first few cycles-Headache, mood changes, breast tenderness-Cannot use if breastfeeding or problems with estrogen
Patch
Patch worn on skin; lower abdomen, buttock, upper torso, or arm
Once a week(Change weekly for 3 weeks. Leave off for one week, then you will get your period)
- May reduce periods and cramping-More regular periods-May improve acne-Protect against ovarian cysts, cancer or ovaries/uterus, benign breast masses
-Must remember weekly-Less effective if weight > 198lb-Highest amount of hormone delivered-Spotting during first few cycles-Headache, mood changes, breast tenderness-Cannot use if breastfeeding or problems with estrogen
Pills
Pills taken by mouth
Every day - May reduce periods and cramping-More regular periods-May improve acne-Protect against ovarian cysts, cancer or ovaries/uterus, benign breast masses
-Must remember every day-Spotting during first few cycles-Headache, mood changes, breast tenderness-Cannot use if breastfeeding or problems with estrogen
Implanon
Small plastic rod inserted into arm during clinic visit
Every 3 years -Can get pregnant right after stopping-It can be used while breastfeeding.-It can be used by women who cannot take estrogen.-It gives continuous long-lasting birth control without sterilization.- There is no medicine to take every day.
- Irregular bleeding is the most common side effect, especially in the first 6-12monts of use-Expensive without insurance
Ad
ole
sce
nt Me
dic
ine
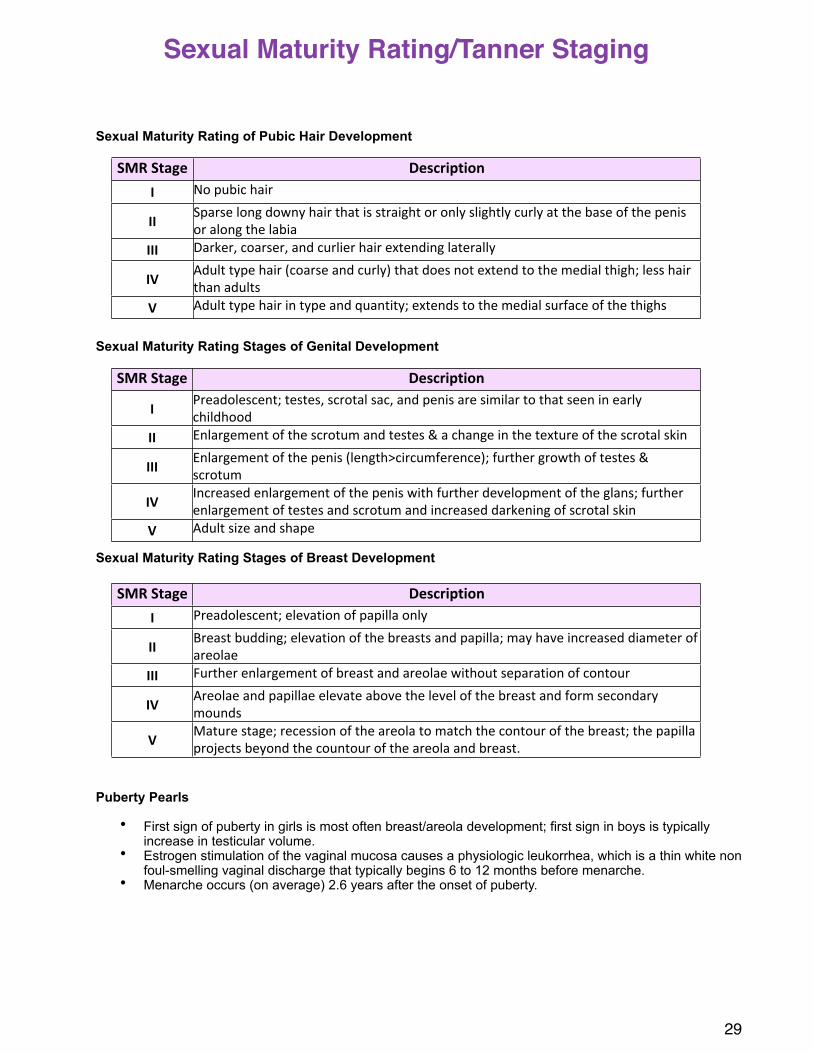
Sexual Maturity Rating of Pubic Hair Development
Sexual Maturity Rating Stages of Genital Development
Sexual Maturity Rating Stages of Breast Development
Puberty Pearls
• First sign of puberty in girls is most often breast/areola development; first sign in boys is typically increase in testicular volume.
• Estrogen stimulation of the vaginal mucosa causes a physiologic leukorrhea, which is a thin white non foul-smelling vaginal discharge that typically begins 6 to 12 months before menarche.
• Menarche occurs (on average) 2.6 years after the onset of puberty.
29
Sexual Maturity Rating/Tanner Staging
SMR$Stage DescriptionI No#pubic#hair
II Sparse#long#downy#hair#that#is#straight#or#only#slightly#curly#at#the#base#of#the#penis#or#along#the#labia
III Darker,#coarser,#and#curlier#hair#extending#laterally
IV Adult#type#hair#(coarse#and#curly)#that#does#not#extend#to#the#medial#thigh;#less#hair#than#adults
V Adult#type#hair#in#type#and#quantity;#extends#to#the#medial#surface#of#the#thighs
SMR$Stage Description
I Preadolescent;#testes,#scrotal#sac,#and#penis#are#similar#to#that#seen#in#early#childhood
II Enlargement#of#the#scrotum#and#testes#&#a#change#in#the#texture#of#the#scrotal#skin
III Enlargement#of#the#penis#(length>circumference);#further#growth#of#testes#&#scrotum
IV Increased#enlargement#of#the#penis#with#further#development#of#the#glans;#further#enlargement#of#testes#and#scrotum#and#increased#darkening#of#scrotal#skin
V Adult#size#and#shape
SMR$Stage DescriptionI Preadolescent;#elevation#of#papilla#only
II Breast#budding;#elevation#of#the#breasts#and#papilla;#may#have#increased#diameter#of#areolae
III Further#enlargement#of#breast#and#areolae#without#separation#of#contour
IV Areolae#and#papillae#elevate#above#the#level#of#the#breast#and#form#secondary#mounds#
V Mature#stage;#recession#of#the#areola#to#match#the#contour#of#the#breast;#the#papilla#projects#beyond#the#countour#of#the#areola#and#breast.
30
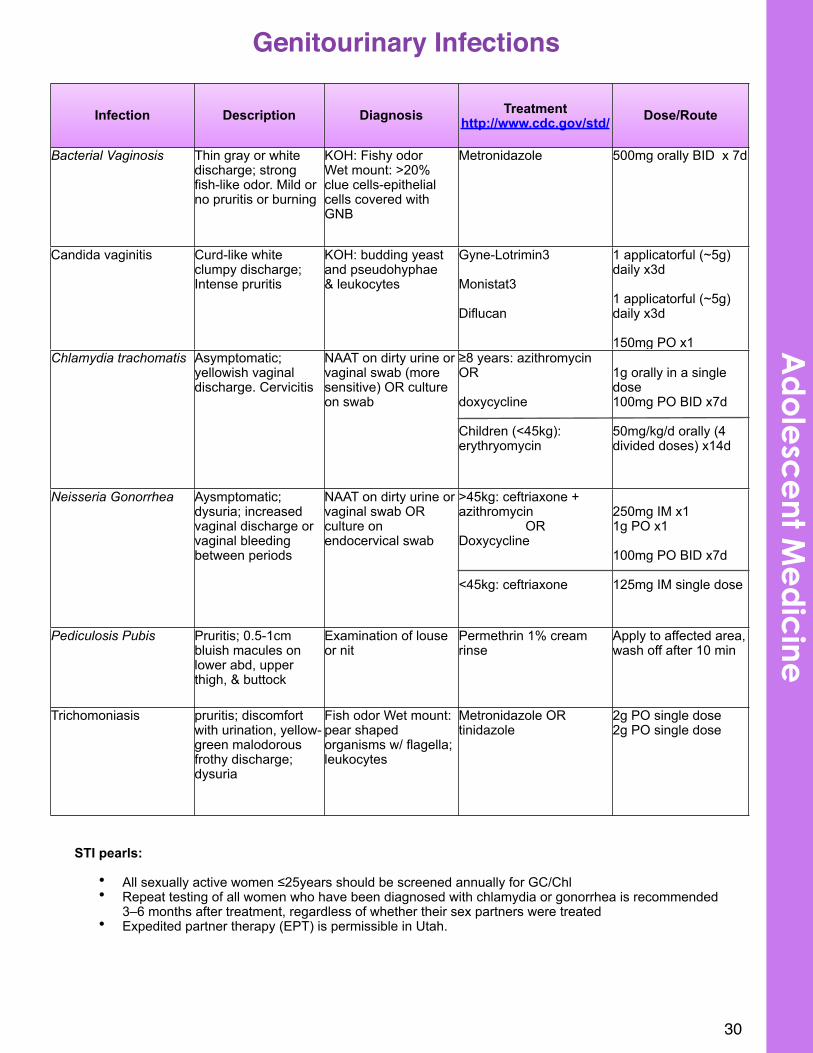
Genitourinary Infections
Infection Description Diagnosis Treatmenthttp://www.cdc.gov/std/ Dose/Route
Bacterial Vaginosis Thin gray or white discharge; strong fish-like odor. Mild or no pruritis or burning
KOH: Fishy odorWet mount: >20% clue cells-epithelial cells covered with GNB
Metronidazole 500mg orally BID x 7d
Candida vaginitis Curd-like white clumpy discharge; Intense pruritis
KOH: budding yeast and pseudohyphae& leukocytes
Gyne-Lotrimin3
Monistat3
Diflucan
1 applicatorful (~5g) daily x3d
1 applicatorful (~5g) daily x3d
150mg PO x1Chlamydia trachomatis Asymptomatic;
yellowish vaginal discharge. Cervicitis
NAAT on dirty urine or vaginal swab (more sensitive) OR culture on swab
≥8 years: azithromycin OR
doxycycline
Children (<45kg): erythryomycin
1g orally in a single dose100mg PO BID x7d
50mg/kg/d orally (4 divided doses) x14d
Neisseria Gonorrhea Aysmptomatic; dysuria; increased vaginal discharge or vaginal bleeding between periods
NAAT on dirty urine or vaginal swab OR culture on endocervical swab
>45kg: ceftriaxone +azithromycin
ORDoxycycline
<45kg: ceftriaxone
250mg IM x11g PO x1
100mg PO BID x7d
125mg IM single dose
Pediculosis Pubis Pruritis; 0.5-1cm bluish macules on lower abd, upper thigh, & buttock
Examination of louse or nit
Permethrin 1% cream rinse
Apply to affected area, wash off after 10 min
Trichomoniasis pruritis; discomfort with urination, yellow-green malodorous frothy discharge; dysuria
Fish odor Wet mount: pear shaped organisms w/ flagella; leukocytes
Metronidazole OR tinidazole
2g PO single dose2g PO single dose
STI pearls:
• All sexually active women ≤25years should be screened annually for GC/Chl• Repeat testing of all women who have been diagnosed with chlamydia or gonorrhea is recommended
3–6 months after treatment, regardless of whether their sex partners were treated• Expedited partner therapy (EPT) is permissible in Utah.
Ad
ole
sce
nt Me
dic
ine
What is PID? Infection of the upper female genital tract.Incidence: >750,000 cases annually in the US; 10-15% may become infertileCause: N. gonorrhoeae and C. trachomatis; vaginal flora (e.g., anaerobes, G. vaginalis, Haemophilusinfluenzae, enteric Gram-negative rods, and Streptococcus agalactiae) have also been associated.Symptoms: Asymptomatic commonly; may have lower abdominal pain, fever, abnormal bleeding, dyspareunia, and vaginal discharge.Diagnosis: Sexually active woman with lower abdominal pain AND one of the following: cervical motion tenderness, uterine tenderness, or adnexal tenderness.Specificity of diagnosis will be increased if any of the following is present:
• oral temperature >101° F (>38.3° C);• abnormal cervical or vaginal mucopurulent discharge;• presence of abundant numbers of WBC on saline microscopy of vaginal fluid;• elevated erythrocyte sedimentation rate;• elevated C-reactive protein; and• laboratory documentation of cervical infection with N. gonorrhoeae or C. trachomatis
Outpatient treatment: • Option #1: Ceftriaxone 250mg IM x1 + doxycycline 100mg PO BID x14d +/-
metronidazole 500mg PO x14d• Option #2: Cefoxitin 2g IM x1 and Probenecid 1g PO administered concurrently in a
single dose + doxycycline 100mg PO BID x14d +/- metronidazole 500mg PO x14d• Option #3: 3rd generation cephalosporin + doxycycline 100mg PO BID x14d +/-
metronidazole 500mg PO BID x14dMonitoring of therapy: If no improvement in 72 hours, patient should be re-evaluatedIndications for hospitalization: severe illness, outpatient treatment failure, inability to follow an outpatient treatment regimen, pregnancy, tubo-ovarian abscess, surgical emergencies cannot be excludedInpatient treatment:
• Option #1: Cefotetan 2g IV q12H (or cefoxitin 2g IV q6H) + doxycycline 100mg PO or IV q12H
• Option #2: Clindamycin 900mg IV q8H + Gentamicin loading dose IV or IM (2mg/kg) followed by maintenance dose (1.5mg/kg) q8H; single daily dosing (3-5mg/kg) can be substituted
Information obtained from http://cdc.gov/std/
31
Pelvic Inflammatory Disease
32
Cardiology
# # # #
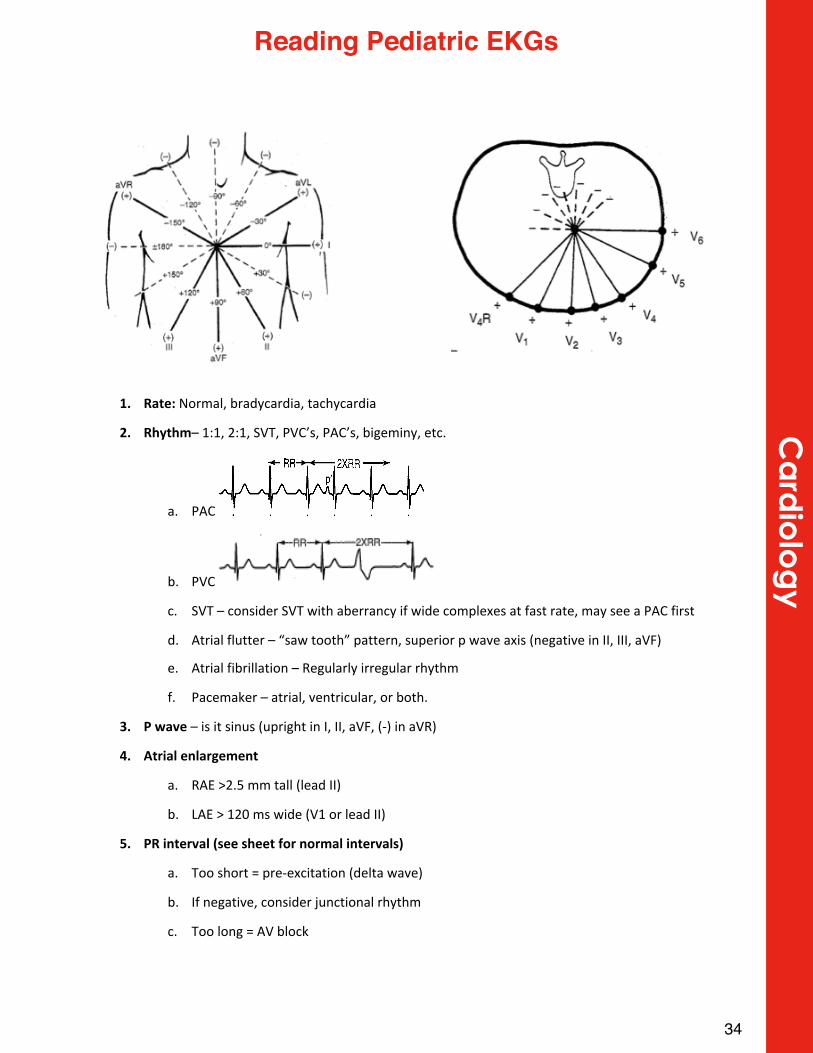
1. Rate:$Normal,#bradycardia,#tachycardia
2. Rhythm–#1:1,#2:1,#SVT,#PVC’s,#PAC’s,#bigeminy,#etc.
a. PAC
b. PVC
c. SVT#–#consider#SVT#with#aberrancy#if#wide#complexes#at#fast#rate,#may#see#a#PAC#first
d. Atrial#flutter#–#“saw#tooth”#pattern,#superior#p#wave#axis#(negative#in#II,#III,#aVF)
e. Atrial#fibrillation#–#Regularly#irregular#rhythm
f. Pacemaker#–#atrial,#ventricular,#or#both.#
3. P$wave#–#is#it#sinus#(upright#in#I,#II,#aVF,#(X)#in#aVR)
4. Atrial$enlargement
a. RAE#>2.5#mm#tall#(lead#II)
b. LAE#>#120#ms#wide#(V1#or#lead#II)
5. PR$interval$(see$sheet$for$normal$intervals)
a. Too#short#=#preXexcitation#(delta#wave)
b. If#negative,#consider#junctional#rhythm
c. Too#long#=#AV#block
34
Ca
rdio
log
yReading Pediatric EKGs
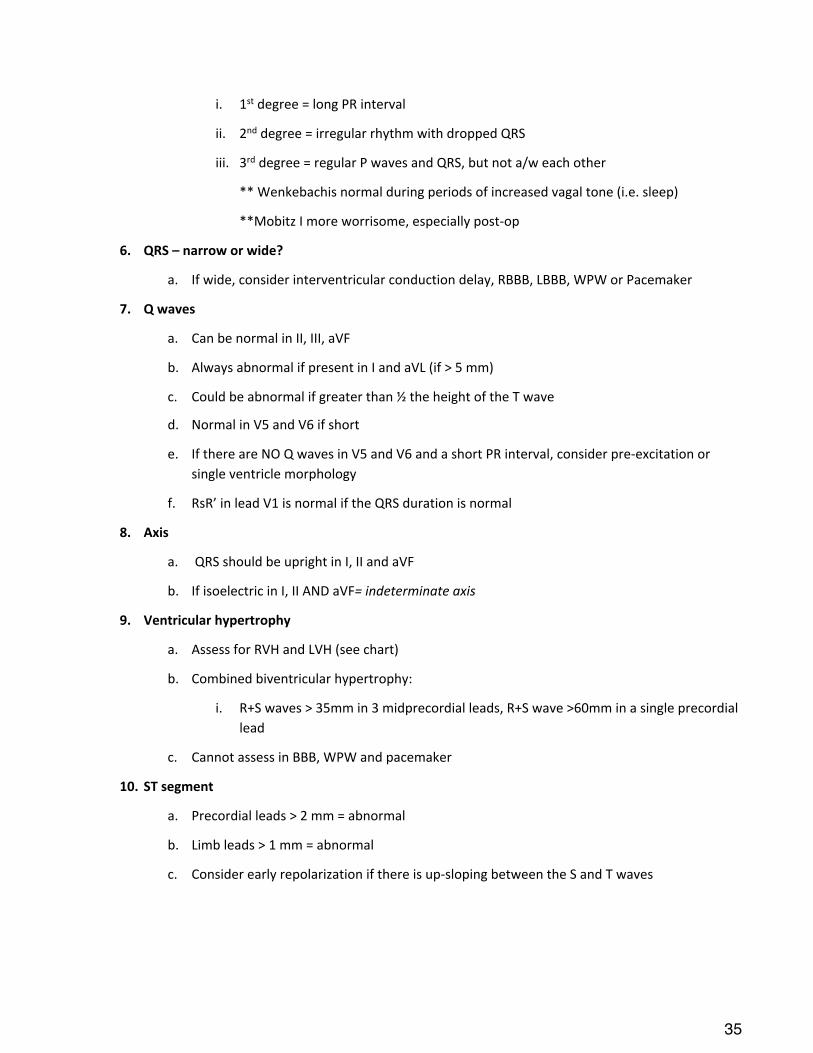
i. 1st#degree#=#long#PR#interval
ii. 2nd#degree#=#irregular#rhythm#with#dropped#QRS
iii. 3rd#degree#=#regular#P#waves#and#QRS,#but#not#a/w#each#other
**#Wenkebachis#normal#during#periods#of#increased#vagal#tone#(i.e.#sleep)
**Mobitz#I#more#worrisome,#especially#postXop
6. QRS$–$narrow$or$wide?
a. If#wide,#consider#interventricular#conduction#delay,#RBBB,#LBBB,#WPW#or#Pacemaker
7. Q$waves
a. Can#be#normal#in#II,#III,#aVF
b. Always#abnormal#if#present#in#I#and#aVL#(if#>#5#mm)
c. Could#be#abnormal#if#greater#than#½#the#height#of#the#T#wave
d. Normal#in#V5#and#V6#if#short
e. If#there#are#NO#Q#waves#in#V5#and#V6#and#a#short#PR#interval,#consider#preXexcitation#or#
single#ventricle#morphology
f. RsR’#in#lead#V1#is#normal#if#the#QRS#duration#is#normal
8. Axis$
a. #QRS#should#be#upright#in#I,#II#and#aVF
b. If#isoelectric#in#I,#II#AND#aVF=%indeterminate%axis
9. Ventricular$hypertrophy
a. Assess#for#RVH#and#LVH#(see#chart)
b. Combined#biventricular#hypertrophy:#
i. R+S#waves#>#35mm#in#3#midprecordial#leads,#R+S#wave#>60mm#in#a#single#precordial#
lead
c. Cannot#assess#in#BBB,#WPW#and#pacemaker
10. ST$segment$
a. Precordial#leads#>#2#mm#=#abnormal
b. Limb#leads#>#1#mm#=#abnormal
c. Consider#early#repolarization#if#there#is#upXsloping#between#the#S#and#T#waves
35
11. T$wave$
a. Should#become#more#positive#in#lateral#precordial#leads#and#within#60°#of#the#QRS
b. Can#be#upright#in#V1#x#48#hours,#then#should#be#downward#from#48#hrs#to#puberty
i. If#remains#upright#after#1#week,#consider#RVH
c. All#T#waves#should#be#upright#in#adults
d. If#tall#T#waves,#consider#hyperkalemia;#If#u#wave,#consider#hypokalemia
e. Strain#–#wide#QRSXT#angle,#abnormal#T#wave#axis
12. QTc
a. Manually#check#in#leads#II#and#V5#(use#the#QT#interval#after#the#longest#RXR)
b. If#a#u#wave#is#present,#include#with#T#wave#if#>#½#the#height#of#the#T#wave#in#>#3#leads
c. Cannot%be%analyzed%if%there%is%a%BBB
d. QTc#>#460#ms,#possibly#450#in#males
e. Short#QTc#is#300X320ms,#usually#a/w#a#tall#T#wave
36
Ca
rdio
log
y
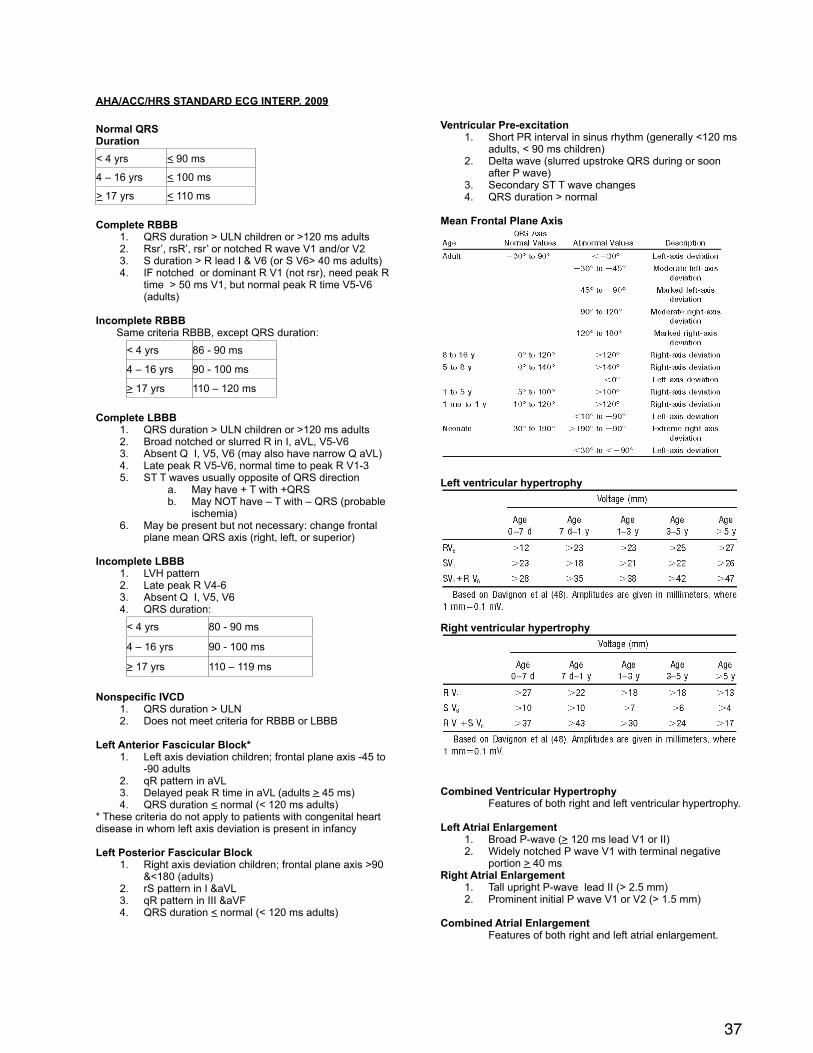
AHA/ACC/HRS STANDARD ECG INTERP. 2009
Normal QRS Duration < 4 yrs < 90 ms
4 – 16 yrs < 100 ms
> 17 yrs < 110 ms
Complete RBBB 1. QRS duration > ULN children or >120 ms adults2. Rsr’, rsR’, rsr’ or notched R wave V1 and/or V23. S duration > R lead I & V6 (or S V6> 40 ms adults)4. IF notched or dominant R V1 (not rsr), need peak R
time > 50 ms V1, but normal peak R time V5-V6 (adults)
Incomplete RBBB Same criteria RBBB, except QRS duration:
< 4 yrs 86 - 90 ms
4 – 16 yrs 90 - 100 ms
> 17 yrs 110 – 120 ms
Complete LBBB1. QRS duration > ULN children or >120 ms adults2. Broad notched or slurred R in I, aVL, V5-V63. Absent Q I, V5, V6 (may also have narrow Q aVL)4. Late peak R V5-V6, normal time to peak R V1-35. ST T waves usually opposite of QRS direction
a. May have + T with +QRSb. May NOT have – T with – QRS (probable
ischemia)6. May be present but not necessary: change frontal
plane mean QRS axis (right, left, or superior)
Incomplete LBBB1. LVH pattern2. Late peak R V4-63. Absent Q I, V5, V64. QRS duration:
< 4 yrs 80 - 90 ms
4 – 16 yrs 90 - 100 ms
> 17 yrs 110 – 119 ms
Nonspecific IVCD1. QRS duration > ULN 2. Does not meet criteria for RBBB or LBBB
Left Anterior Fascicular Block*1. Left axis deviation children; frontal plane axis -45 to
-90 adults2. qR pattern in aVL3. Delayed peak R time in aVL (adults > 45 ms) 4. QRS duration < normal (< 120 ms adults)
* These criteria do not apply to patients with congenital heart disease in whom left axis deviation is present in infancy
Left Posterior Fascicular Block1. Right axis deviation children; frontal plane axis >90
&<180 (adults)2. rS pattern in I &aVL3. qR pattern in III &aVF4. QRS duration < normal (< 120 ms adults)
Ventricular Pre-excitation1. Short PR interval in sinus rhythm (generally <120 ms
adults, < 90 ms children)2. Delta wave (slurred upstroke QRS during or soon
after P wave)3. Secondary ST T wave changes4. QRS duration > normal
Mean Frontal Plane Axis
Left ventricular hypertrophy
Right ventricular hypertrophy
Combined Ventricular HypertrophyFeatures of both right and left ventricular hypertrophy.
Left Atrial Enlargement1. Broad P-wave (> 120 ms lead V1 or II)2. Widely notched P wave V1 with terminal negative
portion > 40 msRight Atrial Enlargement
1. Tall upright P-wave lead II (> 2.5 mm)2. Prominent initial P wave V1 or V2 (> 1.5 mm)
Combined Atrial EnlargementFeatures of both right and left atrial enlargement.
37
38
Ca
rdio
log
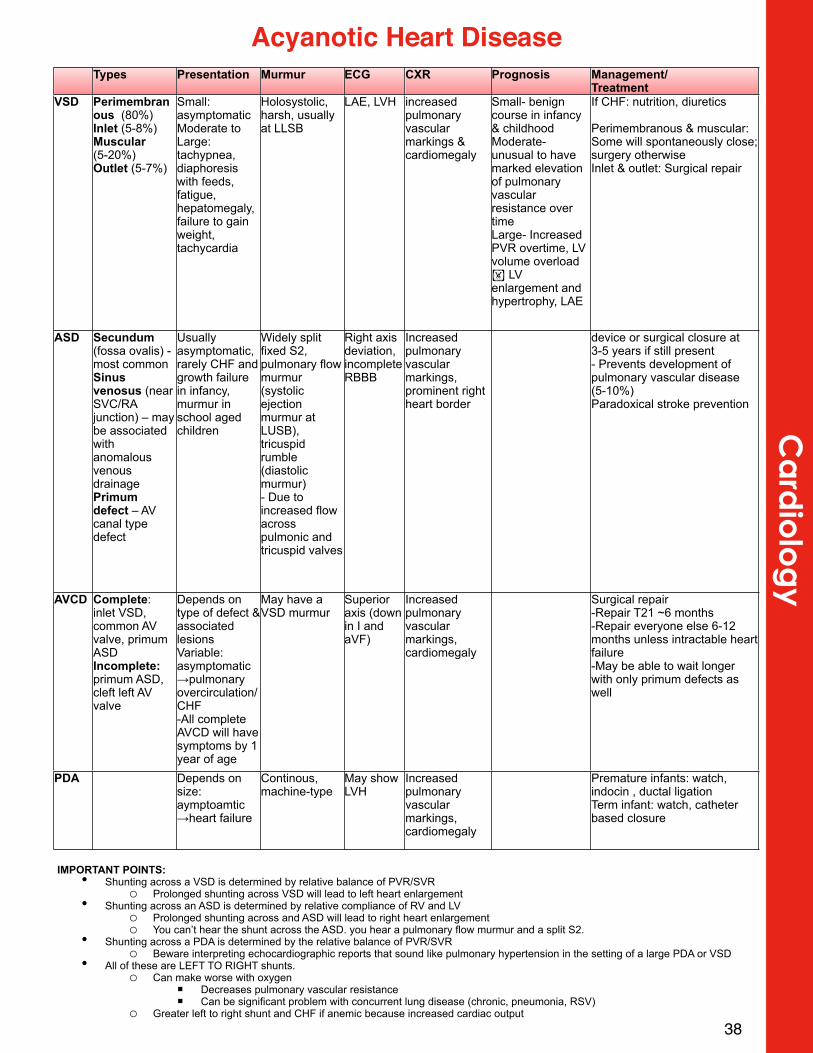
yTypes Presentation Murmur ECG CXR Prognosis Management/
TreatmentVSD Perimembran
ous (80%)Inlet (5-8%)Muscular (5-20%)Outlet (5-7%)
Small: asymptomaticModerate to Large: tachypnea, diaphoresis with feeds, fatigue, hepatomegaly, failure to gain weight, tachycardia
Holosystolic, harsh, usually at LLSB
LAE, LVH increased pulmonary vascular markings & cardiomegaly
Small- benign course in infancy & childhoodModerate- unusual to have marked elevation of pulmonary vascular resistance over timeLarge- Increased PVR overtime, LV volume overload ! LV enlargement and hypertrophy, LAE
If CHF: nutrition, diuretics
Perimembranous & muscular: Some will spontaneously close; surgery otherwiseInlet & outlet: Surgical repair
ASD Secundum (fossa ovalis) - most commonSinus venosus (near SVC/RA junction) – may be associated with anomalous venous drainagePrimum defect – AV canal type defect
Usually asymptomatic, rarely CHF and growth failure in infancy, murmur in school aged children
Widely split fixed S2, pulmonary flow murmur (systolic ejection murmur at LUSB), tricuspid rumble (diastolic murmur)- Due to increased flow across pulmonic and tricuspid valves
Right axis deviation, incomplete RBBB
Increased pulmonary vascular markings, prominent right heart border
device or surgical closure at 3-5 years if still present- Prevents development of pulmonary vascular disease (5-10%)Paradoxical stroke prevention
AVCD Complete: inlet VSD, common AV valve, primum ASDIncomplete: primum ASD, cleft left AV valve
Depends on type of defect & associated lesionsVariable: asymptomatic→pulmonary overcirculation/CHF-All complete AVCD will have symptoms by 1 year of age
May have a VSD murmur
Superior axis (down in I and aVF)
Increased pulmonary vascular markings, cardiomegaly
Surgical repair-Repair T21 ~6 months-Repair everyone else 6-12 months unless intractable heart failure-May be able to wait longer with only primum defects as well
PDA Depends on size: aymptoamtic →heart failure
Continous, machine-type
May show LVH
Increased pulmonary vascular markings, cardiomegaly
Premature infants: watch, indocin , ductal ligationTerm infant: watch, catheter based closure
Acyanotic Heart Disease
IMPORTANT POINTS: • Shunting across a VSD is determined by relative balance of PVR/SVR
o Prolonged shunting across VSD will lead to left heart enlargement• Shunting across an ASD is determined by relative compliance of RV and LV
o Prolonged shunting across and ASD will lead to right heart enlargemento You can’t hear the shunt across the ASD. you hear a pulmonary flow murmur and a split S2.
• Shunting across a PDA is determined by the relative balance of PVR/SVRo Beware interpreting echocardiographic reports that sound like pulmonary hypertension in the setting of a large PDA or VSD
• All of these are LEFT TO RIGHT shunts.o Can make worse with oxygen
! Decreases pulmonary vascular resistance! Can be significant problem with concurrent lung disease (chronic, pneumonia, RSV)
o Greater left to right shunt and CHF if anemic because increased cardiac output
What is it?generalized systemic vasculitis involving blood vessels throughout the bodyTrigger: Unknown (possibly virus or immune response)Complications: coronary artery aneurysms or ectasia in ≈15% to 25% of untreated children
May lead to myocardial infarction (MI), sudden death, or ischemic heart disease
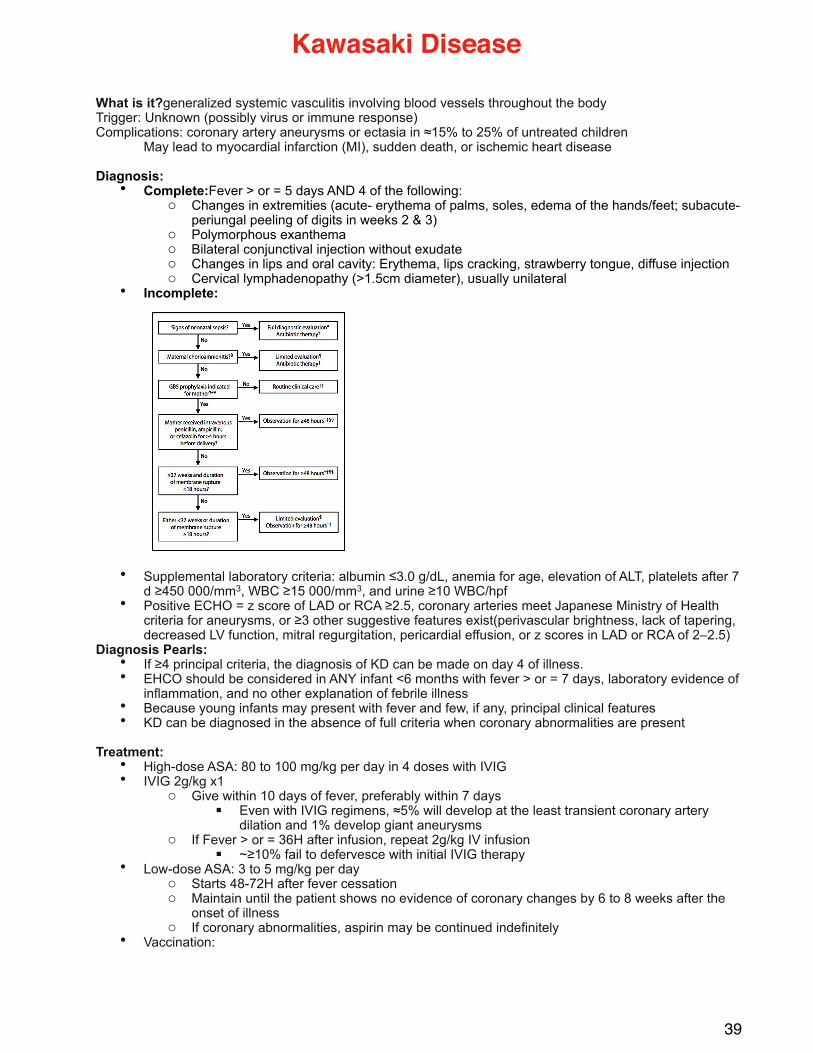
Diagnosis: • Complete:Fever > or = 5 days AND 4 of the following:
o Changes in extremities (acute- erythema of palms, soles, edema of the hands/feet; subacute- periungal peeling of digits in weeks 2 & 3)
o Polymorphous exanthemao Bilateral conjunctival injection without exudateo Changes in lips and oral cavity: Erythema, lips cracking, strawberry tongue, diffuse injectiono Cervical lymphadenopathy (>1.5cm diameter), usually unilateral
• Incomplete:
• Supplemental laboratory criteria: albumin ≤3.0 g/dL, anemia for age, elevation of ALT, platelets after 7 d ≥450 000/mm3, WBC ≥15 000/mm3, and urine ≥10 WBC/hpf
• Positive ECHO = z score of LAD or RCA ≥2.5, coronary arteries meet Japanese Ministry of Health criteria for aneurysms, or ≥3 other suggestive features exist(perivascular brightness, lack of tapering, decreased LV function, mitral regurgitation, pericardial effusion, or z scores in LAD or RCA of 2–2.5)
Diagnosis Pearls:• If ≥4 principal criteria, the diagnosis of KD can be made on day 4 of illness.• EHCO should be considered in ANY infant <6 months with fever > or = 7 days, laboratory evidence of
inflammation, and no other explanation of febrile illness• Because young infants may present with fever and few, if any, principal clinical features• KD can be diagnosed in the absence of full criteria when coronary abnormalities are present
Treatment:• High-dose ASA: 80 to 100 mg/kg per day in 4 doses with IVIG• IVIG 2g/kg x1
o Give within 10 days of fever, preferably within 7 days! Even with IVIG regimens, ≈5% will develop at the least transient coronary artery
dilation and 1% develop giant aneurysmso If Fever > or = 36H after infusion, repeat 2g/kg IV infusion
! ~≥10% fail to defervesce with initial IVIG therapy• Low-dose ASA: 3 to 5 mg/kg per day
o Starts 48-72H after fever cessationo Maintain until the patient shows no evidence of coronary changes by 6 to 8 weeks after the
onset of illness o If coronary abnormalities, aspirin may be continued indefinitely
• Vaccination:
39
Kawasaki Disease

o Yearly influenza vaccination recommended o Measles and varicella immunizations should be deferred for 11 months after a child receives
high-dose IVIG
Follow-up:• If no coronary artery involvement, f/u with cardiology in 4-6 weeks with ECHO• If coronary artery involvement, f/u per cardiology team
40
Ca
rdio
log
y
42
Dermatology
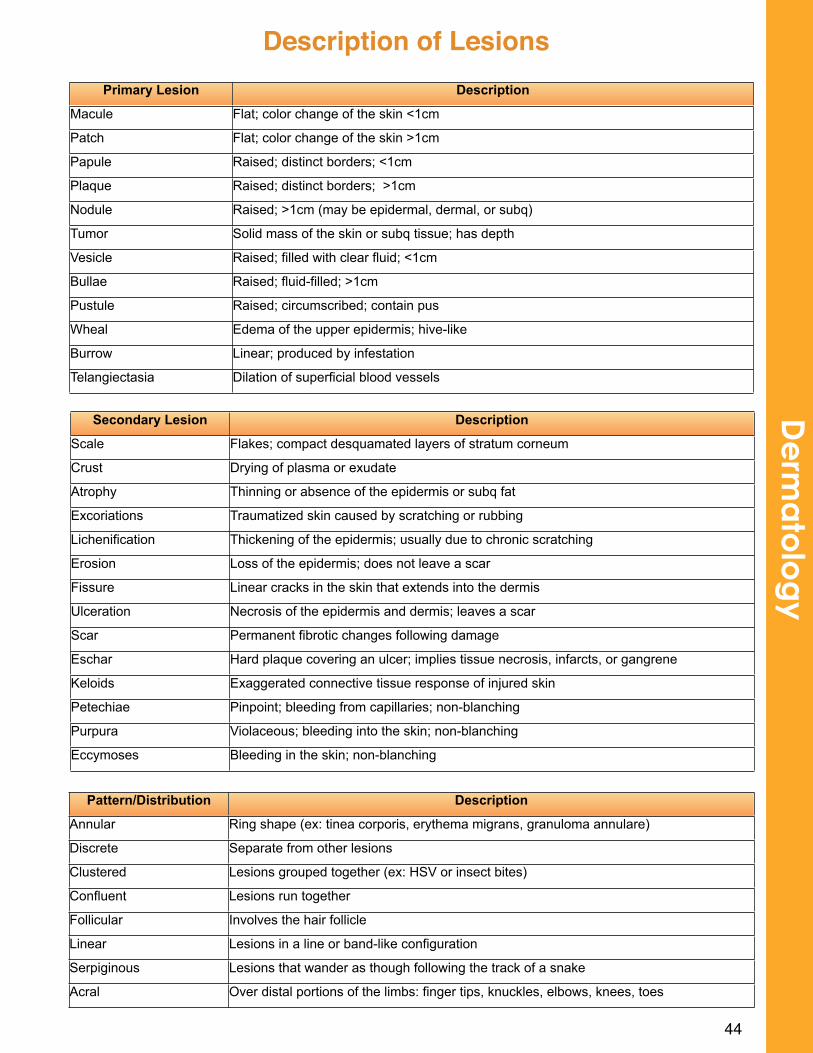
44
De
rma
tolo
gy
Description of LesionsPrimary Lesion Description
Macule Flat; color change of the skin <1cm
Patch Flat; color change of the skin >1cm
Papule Raised; distinct borders; <1cm
Plaque Raised; distinct borders; >1cm
Nodule Raised; >1cm (may be epidermal, dermal, or subq)
Tumor Solid mass of the skin or subq tissue; has depth
Vesicle Raised; filled with clear fluid; <1cm
Bullae Raised; fluid-filled; >1cm
Pustule Raised; circumscribed; contain pus
Wheal Edema of the upper epidermis; hive-like
Burrow Linear; produced by infestation
Telangiectasia Dilation of superficial blood vessels
Secondary Lesion Description
Scale Flakes; compact desquamated layers of stratum corneum
Crust Drying of plasma or exudate
Atrophy Thinning or absence of the epidermis or subq fat
Excoriations Traumatized skin caused by scratching or rubbing
Lichenification Thickening of the epidermis; usually due to chronic scratching
Erosion Loss of the epidermis; does not leave a scar
Fissure Linear cracks in the skin that extends into the dermis
Ulceration Necrosis of the epidermis and dermis; leaves a scar
Scar Permanent fibrotic changes following damage
Eschar Hard plaque covering an ulcer; implies tissue necrosis, infarcts, or gangrene
Keloids Exaggerated connective tissue response of injured skin
Petechiae Pinpoint; bleeding from capillaries; non-blanching
Purpura Violaceous; bleeding into the skin; non-blanching
Eccymoses Bleeding in the skin; non-blanching
Pattern/Distribution Description
Annular Ring shape (ex: tinea corporis, erythema migrans, granuloma annulare)
Discrete Separate from other lesions
Clustered Lesions grouped together (ex: HSV or insect bites)
Confluent Lesions run together
Follicular Involves the hair follicle
Linear Lesions in a line or band-like configuration
Serpiginous Lesions that wander as though following the track of a snake
Acral Over distal portions of the limbs: finger tips, knuckles, elbows, knees, toes
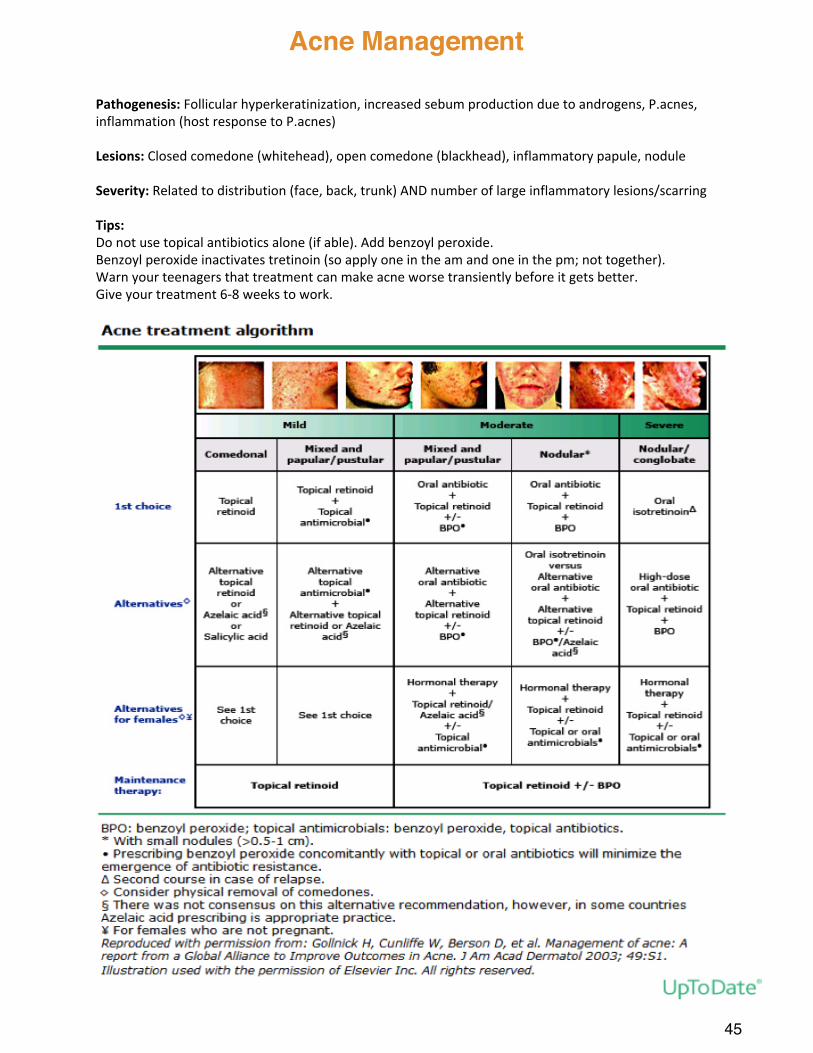
Pathogenesis:#Follicular#hyperkeratinization,#increased#sebum#production#due#to#androgens,#P.acnes,#inflammation#(host#response#to#P.acnes)
Lesions:#Closed#comedone#(whitehead),#open#comedone#(blackhead),#inflammatory#papule,#nodule
Severity:#Related#to#distribution#(face,#back,#trunk)#AND#number#of#large#inflammatory#lesions/scarring
Tips:Do#not#use#topical#antibiotics#alone#(if#able).#Add#benzoyl#peroxide.Benzoyl#peroxide#inactivates#tretinoin#(so#apply#one#in#the#am#and#one#in#the#pm;#not#together).Warn#your#teenagers#that#treatment#can#make#acne#worse#transiently#before#it#gets#better.Give#your#treatment#6X8#weeks#to#work.#
45
Acne Management
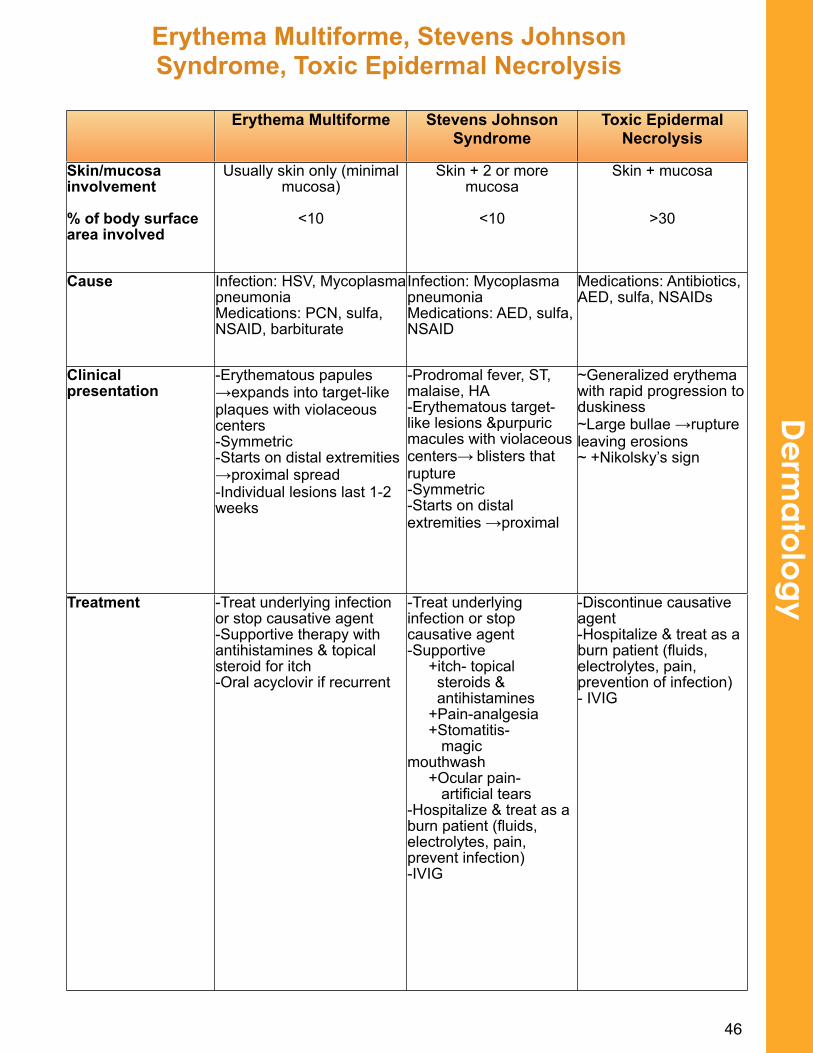
46
De
rma
tolo
gy
Erythema Multiforme, Stevens Johnson Syndrome, Toxic Epidermal Necrolysis
Erythema Multiforme Stevens Johnson Syndrome
Toxic Epidermal Necrolysis
Skin/mucosa involvement
% of body surface area involved
Usually skin only (minimal mucosa)
<10
Skin + 2 or more mucosa
<10
Skin + mucosa
>30
Cause Infection: HSV, Mycoplasma pneumoniaMedications: PCN, sulfa, NSAID, barbiturate
Infection: Mycoplasma pneumoniaMedications: AED, sulfa, NSAID
Medications: Antibiotics, AED, sulfa, NSAIDs
Clinical presentation
-Erythematous papules →expands into target-like plaques with violaceous centers-Symmetric -Starts on distal extremities →proximal spread-Individual lesions last 1-2 weeks
-Prodromal fever, ST, malaise, HA-Erythematous target-like lesions &purpuric macules with violaceous centers→ blisters that rupture-Symmetric-Starts on distal extremities →proximal
~Generalized erythema with rapid progression to duskiness~Large bullae →rupture leaving erosions~ +Nikolsky’s sign
Treatment -Treat underlying infection or stop causative agent-Supportive therapy with antihistamines & topical steroid for itch-Oral acyclovir if recurrent
-Treat underlying infection or stop causative agent-Supportive +itch- topical steroids & antihistamines +Pain-analgesia +Stomatitis- magicmouthwash +Ocular pain- artificial tears-Hospitalize & treat as a burn patient (fluids, electrolytes, pain, prevent infection)-IVIG
-Discontinue causative agent-Hospitalize & treat as a burn patient (fluids, electrolytes, pain, prevention of infection)- IVIG
48
Emergency Medicine
1. Communication with the ED nurses and staff is key. Tell the nurse when you are going to see the patient, what orders you write, and keep them informed of any changes. They are very experienced and helpful.
2. Ask for feedback at the start and at the end of each ED shift. This is how we help your education. ED attending physicians have different styles, and your initiative to seek feedback opens the conversation.
3. Efficiency. Some patients need treatment immediately. ABCs come first. One can always go back and gather more detailed information that is needed (i.e., SH, FH), but not required to begin interventions.
4. Brief presentations where you formulate your own assessment and plan. See next page for more details.
5. Patient ownership. You are the primary provider for your patients. Follow up on your patients during the ED stay. Keep families informed about any delays, changes in plans, lab and x-ray results. Make sure families always understand the plan of care.
6. Completely document patient encounters on the paper chart. The ED attending relies on you to completely fill in all this information. Document information in all areas: HPI, PMH, ROS, FH, SH, ALLERGIES, MEDS, and IMMUNIZATIONS.
7. Detailed discharge instructions are extremely important. Always include written information about when to follow up with primary care provider. Always include specific information about when to return to the ED. Do not simply say return to the ED “as needed.”
50
Eme
rge
ncy
Tips for Success in the ED
ED Patient Presentation
The ED patient presentation is different, and is your chance to shine. Ask for feedback. Always offer up your assessment and plan, as this is what sets residents apart. Key components:
• Brief < 3 minutes• Pertinent history and exam• Think of “worst first” in differential
o CC fever: meningitis, pneumonia, UTIo CC abdominal pain: appendicitis, ovarian/testicular torsion, bowel obstructiono CC headache: brain tumor, meningitis
• Present your assessment, and why you do or do not think the child has a “worst first” condition
• Offer your plan• Ask for feedback
Basic structure
1. Chief complaint (CC)2. HPI
a. Start with a one-liner (name, age, gender, PMH pertinent to the CC)b. The description of the CC: duration, severity, character, location, what makes it
better or worse, progression (worsening, stable, improving)c. Why did the patient come to the ED today?
3. ROS pertinent to CC4. Exam
a. Always mention Vital Signs firstb. Always describe the general appearance of the childc. Pertinent Exam Findings that help your assessment
5. Labs/X-Rays: mention if labs had been done prior to the PCH ED visit 6. Summary statement
a. One-linerb. Pertinent important symptoms c. Pertinent important exam findings
7. Problem Assessment: a. This is what I think and whyb. This is why I do or do not think the problem is a “worst-first” etiology
8. Plan:a. Any interventions: medications, fluidsb. Any tests: labs, x-rays, ECGsc. Consultsd. Disposition: home, admit, re-assess after intervention
References1. Davenport C. The 3-minute emergency medicine medical student presentation: a
variation on a theme. Acad Emerg Med 2008;15:683–687.
51
Differential of RLQ pain: mesenteric adenitis, enterocolitis, testicular/ovarian, intussusception, RLL pneumonia, IBD, septic hip, ovarian cyst, PID
Presentation:o Pain- classically begins in periumbilical region & then moves to RLQo Other symptoms/signs- anorexia, nausea, vomiting, fevero If perforated – can present with peritoneal signs
Physical Exam:o Pain on palpation in periumbilical region that migrates to RLQo Rovsing’s sign: palpation of LLQ causes pain in RLQo Psoas sign: increased abdominal pain when patient flexes right hip against resistanceo Obturator sign: increased abdominal pain when patient’s right leg is raised with knee flexed
and then internally rotated at the hipo Pain with jumpingo If perforated: guarding and/or rebound
Diagnostic studies: o Laboratory: CBC, CRP, U/A (may show sterile pyuria), urine HCG (girls)o Imaging: Ultrasound imaging of the appendix
! A non-visualized appendix is NOT always considered a negative test • For a nonvisulized appendix (depending on lab test results & clinical concern/
follow-up ability)- o Repeat US in 8-12 hourso Proceed to CT abdomen with rectal and IV contrast.
Diagnosis: The Pediatric Appendicitis ScoreItem# Score#(point)#Anorexia 1
Nausea#or#vomiting 1
Migration#of#pain 1
Fever#>38°C#(100.5°F) 1
Pain#with#cough,#percussion#or#hopping 2
Right#lower#quadrant#tenderness 2
White#blood#cell#count#>10,000#cells/microL 1Neutrophils#plus#band#forms#>7500#cells/microL 1Total 10$points
• A PAS ≤2 suggests a low risk for appendicitis. Children with a PAS score in this range may be discharged home as long as their caretakers understand that persistent pain or additional symptoms warrant repeat evaluation.
• A PAS ≥7 indicates a high risk for appendicitis. Children with a PAS score in this range warrant surgical consultation. It is unclear if the PAS alone can be used to determine the need for appendectomy, since 4-22 percent of such patients won’t have appendicitis.
• A PAS of 3 to 6 is indeterminate for appendicitis and the best approach is not clear. Options include surgical consultation, diagnostic imaging, serial abdominal examinations while being observed at home or in the hospital, or a combination of these approaches depending upon local resources
Data from: Samuel, M. Pediatric appendicitis score. J Pediatr Surg 2002; 37:877.
Management: o NPOo Surgical consulto IV abx: ceftriaxone 75mg/kg IV (max 2g) & metronidazole 10mg/kg IV (max 500mg)
52
Eme
rge
ncy
Appendicitis
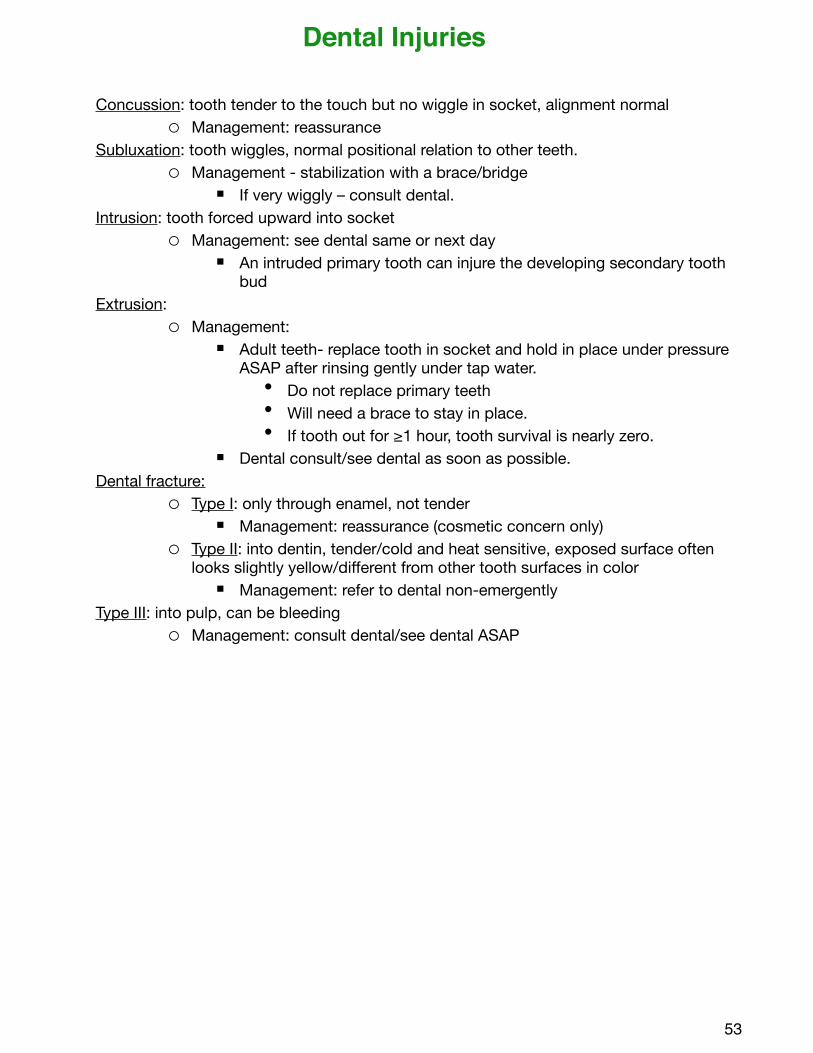
Concussion: tooth tender to the touch but no wiggle in socket, alignment normal o Management: reassurance
Subluxation: tooth wiggles, normal positional relation to other teeth. o Management - stabilization with a brace/bridge
! If very wiggly – consult dental.Intrusion: tooth forced upward into socket
o Management: see dental same or next day! An intruded primary tooth can injure the developing secondary tooth
budExtrusion:
o Management:! Adult teeth- replace tooth in socket and hold in place under pressure
ASAP after rinsing gently under tap water. • Do not replace primary teeth• Will need a brace to stay in place. • If tooth out for ≥1 hour, tooth survival is nearly zero.
! Dental consult/see dental as soon as possible. Dental fracture:
o Type I: only through enamel, not tender! Management: reassurance (cosmetic concern only)
o Type II: into dentin, tender/cold and heat sensitive, exposed surface often looks slightly yellow/different from other tooth surfaces in color
! Management: refer to dental non-emergentlyType III: into pulp, can be bleeding
o Management: consult dental/see dental ASAP
53
Dental Injuries
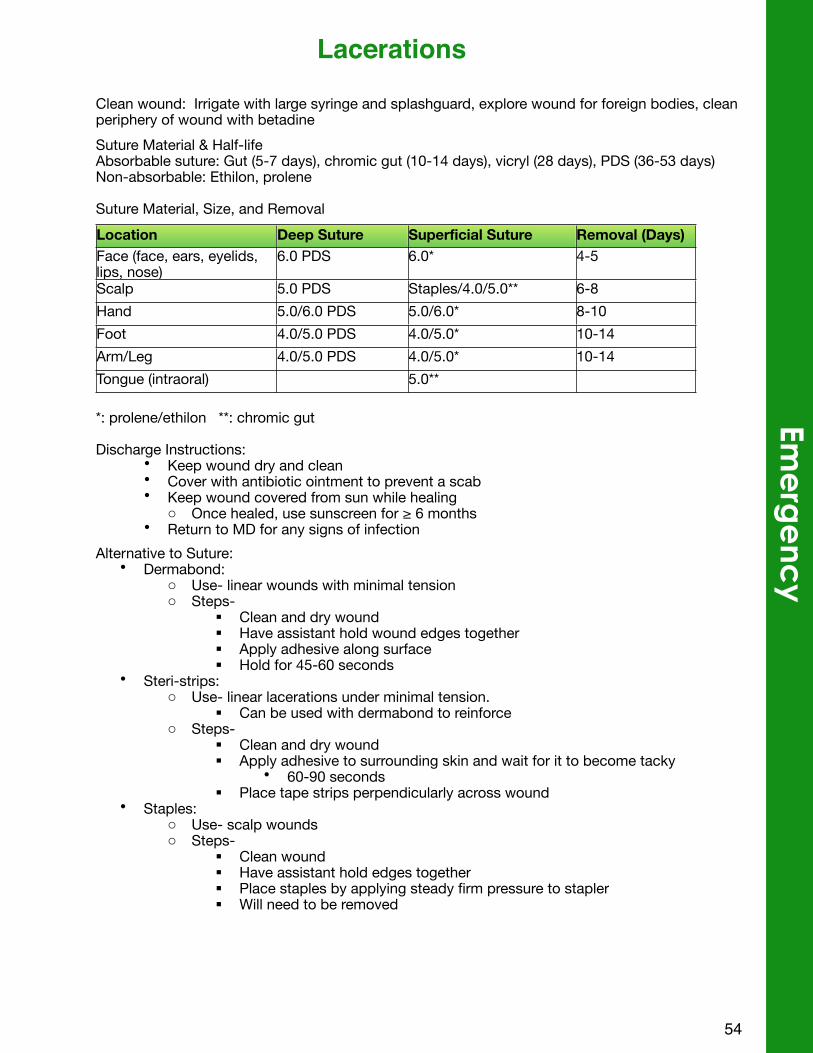
Clean wound: Irrigate with large syringe and splashguard, explore wound for foreign bodies, clean periphery of wound with betadineSuture Material & Half-lifeAbsorbable suture: Gut (5-7 days), chromic gut (10-14 days), vicryl (28 days), PDS (36-53 days)Non-absorbable: Ethilon, prolene
Suture Material, Size, and RemovalLocation Deep Suture Superficial Suture Removal (Days)Face (face, ears, eyelids, lips, nose)
6.0 PDS 6.0* 4-5
Scalp 5.0 PDS Staples/4.0/5.0** 6-8Hand 5.0/6.0 PDS 5.0/6.0* 8-10Foot 4.0/5.0 PDS 4.0/5.0* 10-14Arm/Leg 4.0/5.0 PDS 4.0/5.0* 10-14Tongue (intraoral) 5.0**
*: prolene/ethilon **: chromic gut
Discharge Instructions:• Keep wound dry and clean• Cover with antibiotic ointment to prevent a scab • Keep wound covered from sun while healing
o Once healed, use sunscreen for ≥ 6 months • Return to MD for any signs of infection
Alternative to Suture:• Dermabond:
o Use- linear wounds with minimal tensiono Steps-
! Clean and dry wound! Have assistant hold wound edges together! Apply adhesive along surface ! Hold for 45-60 seconds
• Steri-strips: o Use- linear lacerations under minimal tension.
! Can be used with dermabond to reinforceo Steps-
! Clean and dry wound! Apply adhesive to surrounding skin and wait for it to become tacky
• 60-90 seconds! Place tape strips perpendicularly across wound
• Staples: o Use- scalp woundso Steps-
! Clean wound! Have assistant hold edges together! Place staples by applying steady firm pressure to stapler! Will need to be removed
54
Eme
rge
ncy
Lacerations
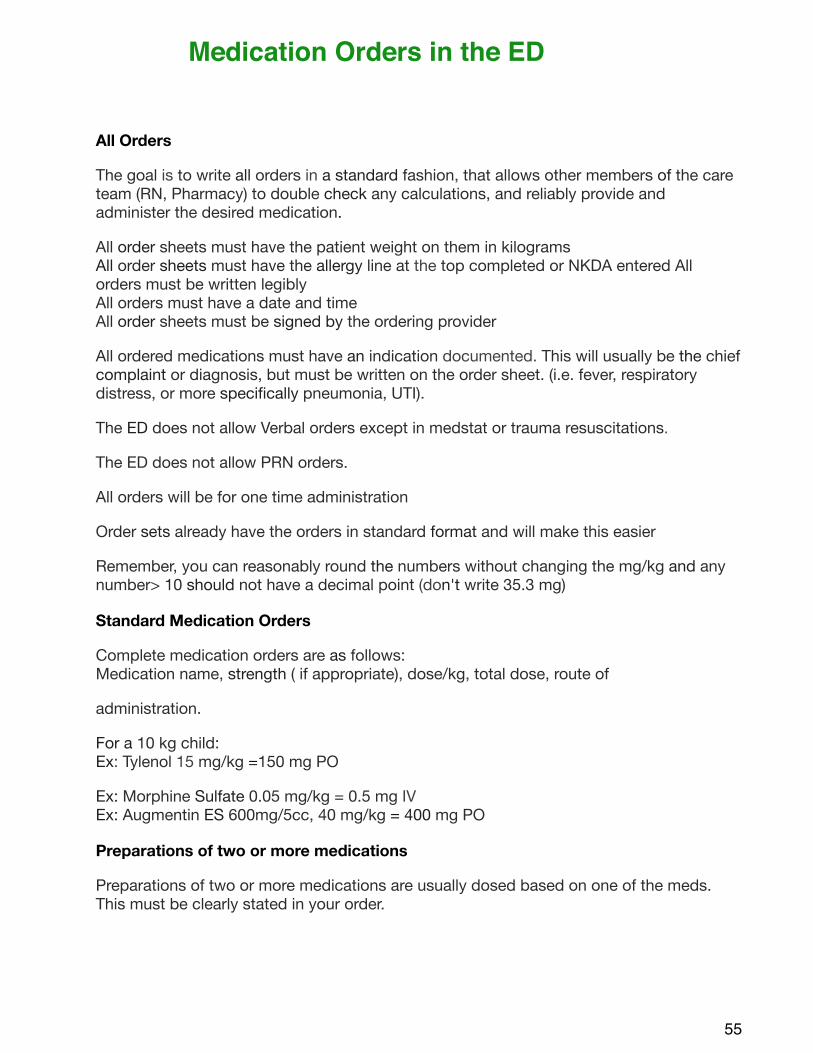
All Orders
The goal is to write all orders in a standard fashion, that allows other members of the care team (RN, Pharmacy) to double check any calculations, and reliably provide and administer the desired medication.
All order sheets must have the patient weight on them in kilogramsAll order sheets must have the allergy line at the top completed or NKDA entered All orders must be written legiblyAll orders must have a date and timeAll order sheets must be signed by the ordering provider
All ordered medications must have an indication documented. This will usually be the chief complaint or diagnosis, but must be written on the order sheet. (i.e. fever, respiratory distress, or more specifically pneumonia, UTI).
The ED does not allow Verbal orders except in medstat or trauma resuscitations.
The ED does not allow PRN orders.
All orders will be for one time administration
Order sets already have the orders in standard format and will make this easier
Remember, you can reasonably round the numbers without changing the mg/kg and any number> 10 should not have a decimal point (don't write 35.3 mg)
Standard Medication Orders
Complete medication orders are as follows:Medication name, strength ( if appropriate), dose/kg, total dose, route of
administration.
For a 10 kg child:Ex: Tylenol 15 mg/kg =150 mg PO
Ex: Morphine Sulfate 0.05 mg/kg = 0.5 mg IVEx: Augmentin ES 600mg/5cc, 40 mg/kg = 400 mg PO
Preparations of two or more medications
Preparations of two or more medications are usually dosed based on one of the meds. This must be clearly stated in your order.
55
Medication Orders in the ED
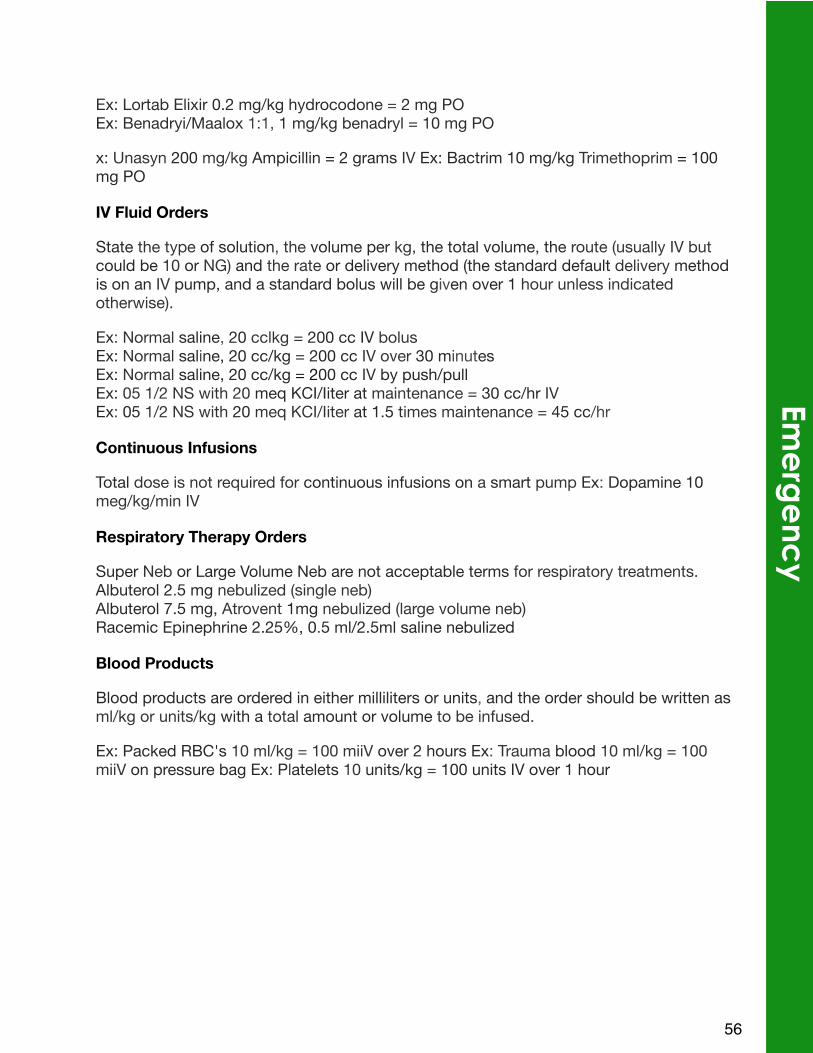
Ex: Lortab Elixir 0.2 mg/kg hydrocodone = 2 mg POEx: Benadryi/Maalox 1:1, 1 mg/kg benadryl = 10 mg PO
x: Unasyn 200 mg/kg Ampicillin = 2 grams IV Ex: Bactrim 10 mg/kg Trimethoprim = 100 mg PO
IV Fluid Orders
State the type of solution, the volume per kg, the total volume, the route (usually IV but could be 10 or NG) and the rate or delivery method (the standard default delivery method is on an IV pump, and a standard bolus will be given over 1 hour unless indicated otherwise).
Ex: Normal saline, 20 cclkg = 200 cc IV bolusEx: Normal saline, 20 cc/kg = 200 cc IV over 30 minutesEx: Normal saline, 20 cc/kg = 200 cc IV by push/pullEx: 05 1/2 NS with 20 meq KCI/Iiter at maintenance = 30 cc/hr IVEx: 05 1/2 NS with 20 meq KCI/Iiter at 1.5 times maintenance = 45 cc/hr
Continuous Infusions
Total dose is not required for continuous infusions on a smart pump Ex: Dopamine 10 meg/kg/min IV
Respiratory Therapy Orders
Super Neb or Large Volume Neb are not acceptable terms for respiratory treatments. Albuterol 2.5 mg nebulized (single neb)Albuterol 7.5 mg, Atrovent 1mg nebulized (large volume neb)Racemic Epinephrine 2.25%, 0.5 ml/2.5ml saline nebulized
Blood Products
Blood products are ordered in either milliliters or units, and the order should be written as ml/kg or units/kg with a total amount or volume to be infused.
Ex: Packed RBC's 10 ml/kg = 100 miiV over 2 hours Ex: Trauma blood 10 ml/kg = 100 miiV on pressure bag Ex: Platelets 10 units/kg = 100 units IV over 1 hour
56
Eme
rge
ncy
ResourcesVisit the Utah Pediatric Emergency Medicine Resident Canvas Page for links to education resources: learning modules, journal articles, links to EM podcasts and EM blogs.
• https://utah.instructure.com/courses/8974
Access the “PEM Topics” EverNote notebook for pediatric emergency medicine topics, guidelines, protocols, articles, and links to procedure videos, podcasts and blogs. Via your smartphone and/or tablet you can access a lot of helpful patent care information as you are seeing patients in the PCH ED (or anywhere with a WiFi network).
Contact Michael Miescier at [email protected] to gain access to Canvas Page or to “PEM Topics.”
57
58
Endocrinology
I. DEFINITION: A state of absolute or relative insulin deficiency resulting in hyperglycemia and metabolic acidosis accumulation of ketoacids in the blood (pH <7.3, serum bicarbonate <15).
II. CAUSES:
a. Initial presentation of type I DMb. A complication of established DM, usually precipitated by:
i. Intercurrent illness or infectionii. Missed insulin injections or inadequate dosage
iii. Stress (emotional, trauma, surgery, etc.)
III. CLASSIFICATION: Severity is estimated by the degree of acidosis (not the degree of hyperglycemia)
a. Moderate – Severe DKA: pH <7.2, HCO3<10, urine ketones: large, dehydration >10%
b. Mild – Moderate: pH 7.2-7.3, HCO3 10-15, urine ketones: mod-large
c. Ketosis: pH7.3-7.35, HCO3 15-18, urine ketones: small-large
IV. TREATMENT PLAN: Depends on the severity of DKA
a. Severe DKA: Requires IVF resuscitation and IV insulinb. Moderate DKA: May require IVF, but may often be managed with
subcutaneous insulinc. Mild DKA: PO hydration and subcutaneous insulin
V. MANAGEMENT OF SEVERE DKA:
a. Fluids
i. Initial volume expansion – Ringer’s lactate or NS bolus of 10-20mL/kg over the first 1-2 hours. Repeat only if there is evidence of CV instability (shock). Often this volume expansion results in a substantial reduction of the blood sugar.
ii. Insulin – Repeat BG at bedside before starting insulin therapy Insulin may be started after the initial fluid bolus. Insulin drip – 0.1units/kg/hr. 25 units regular insulin in 250mL NS. The aim is to reduce the BG gradually (about 50-100mg/dL/hr) to a level of 150-250 mg/dL so as to prevent hypoglycemia or acute changes in osmolarity. When the BG
60
Endo
crino
log
yDKA Guidelines
approaches 200mg/dL, dextrose should be added to the IV fluids. Except for situations of true hypoglycemia, do not decrease insulin below 0.08 units/kg/hr until the acidosis is resolved (bicarb>15, pH>7.3) since insulin is required to prevent ketogenesis and correct the acidodis. Instead of dextrose concentration in the IV fluids should be titrated up to 12.5% dextrose as required to maintain the blood glucose between 100 and 250 mg/dL.
iii. Fluid replacement- Make patient NPO (they usually have an ileus). Estimate the fluid deficit based on acute weight loss over a few weeks (preferred) or based on the physical exam varying from 5-15% body weight for mild to severe losses. Calculate fluid rate based on maintenance plus deficit replacement over 36 hours. This usually calculates to 1 ½ to 1 ¾ maintenance. In children who are very acidotic, very young (<age2), or hypernatremic, fluid replacement is over 48 hours (usually 1 ¼ to 1 ½ maintenance). Fluid intake should not exceed 4000 mL/m2/day (2x maintenance). If urine losses are excesive over the first 4-6 hours, these may need to be replaced. Keep track of ins and outs on flow sheet. No need for urinary catheter unless unconscious.
1. Sodium: Initial Na+ is frequently low. Reasons for this include:
a. Depletion from urinary losses/vomitingb. Hyperglycemia creates an osmotic dilution of extracellular
solutec. Hyperlipidemia displaces Na+ causing the serum Na+ to
be factitiously low.For each 100mg/dL increase in glucose above a 100mg/dL baseline, there is an expected decrease of 1.6mEq/L of Na+
Correction of the hyperglycemia and ketonemia will correct the laboratory hyponatremia. The Na+ deficit is 10mEq/kg for a child who is 10% dehydrated with a normal serum Na (after correction). Replacement is over 36 hours. Usually ½ - 2/3 NS is required after initial treatment with NS or LR. Follow the measured Na+ level; it should rise. A fall in Na+ during therapy is worrisome and requires re-evaluation.
61
2. Potassium: Very high urinary losses result in total body potassium depletion. Vomiting may contribute to hypokalemia. Acidosis causes a shift from intracellular to extracellular K+; therefore, while total body potassium is depleted, serum levels may be normal or high. K+ should not be given until the BUN and creatinine are known or urine output is assured. As acidosis is corrected, k+ is driven into the cells and there is usually a fall in serum K+. Potassium replacement may be in the form of KCl, KAcetate, or KPhos with 20-60mEq/L in the IV fluids. Giving half the K+ in the KPhos form helps replace the phosphorus deficit and decreases the chloride infusion. Abnormal serum K+ can be a cause of cardiac arrhythmia. Use cardiac monitoring if hyper- or hypokalemia is a concern.
3. Phosphorus: Like potassium, urinary losses result in significant depletion. Theoretically this might result in low red cell 2,3,DPG, causing a shift of the O2 dissociation curve to the left, and relative tissue hypoxia. No clinical problems resulting from low phosphorus have been described. Since a total body deficit is present some replacement is indicated and is achieved by replacing some of the potassium with K2PO4 (20mEq/L). Hypocalcemic tetany can occur with rapid or excessive phosphorus administration.
iv. Osmolarity – Calculated by 2(Na + K) + glucose/18 + BUN/2.8. Each 18mg/dL rise in BG results in a 1mOsm rise in osmolarity. If serum osmolarity is very high (>340), fluid deficit should be replaced even more gradually (over 48H). Hyperosmotic nonketotic come is different from DKA and should not be treated as outlined herein. It is rare in childhood.
v. Acid-base- Use of bicarbonate in children with DKA is almost never indicated. Theoretically improving the academia might improve myocardial contractility, insulin sensitivity, and the ventilator response to acidosis, BUT…
1. HCO3 + H ! H20 + CO2, and CO2 diffuses much more rapidly across the blood brain barrier than HCO3 which may yield paradoxical CNS acidosis.
62
Endo
crino
log
y
2. Rapid infusion of bicarbonate corrects acidosis and shifts the O2 dissociation curve to the left, decreasing O2 delivery to the tissues.
3. Rapid correction of acidosis will shirt K+ in to the cells and cause hypokalemia.
4. Kids generally have good hearts. During the management of DKA kids do not die from acidosis. They die from cerebral edema. Bicarbonate therapy may increase the risk of CNS acidosis and edema. Only in situations of extreme academia (pH<6.9) should bicarb administration be considered, and then only as a slow IV infusion.
vi. Monitoring
1. Flow sheet2. VS q1H. This should include careful neuro vitals. The most
serious complications of DKA are CNS events which may present with headache, irritability, or decreased level of consciousness. Be prepared to treat aggressively with IV mannitol (0.5-1g/kg), intubation, and hyperventilation, if necessary.
3. Accurate fluid intake and output. Weight qday.
4. Glucose q1 hour until stable, then q2 hours till off drip.5. VBG or bicarb for pH q2H until >7.2 then q4-6H until pH>7.36. Electrolytes, Ca q4-6H, BUN, Cr q24H7. Urine ketones initially, then qvoid until clear
vii. Clinical Course
1. Initially the BG drops, even before insulin is given. After insulin is initiated, BG should drop at 50-10mg/dL/hour.
2. During initial management with fluids and insulin, the pH may drop. This is due to reperfusion of peripheral tissue beds and washing of lactic acid in to the central circulation.
3. By 4-6 hours of therapy, the acidosis should be resolving. If it is not, check the pump, and consider re-making the drip. In 12-36 hours, DKA is generally resolved. Urine ketones may persist and
63
urine will be positive for glucose if BG >200. This is okay. When pH is >7.2 and bicarb is >12, may give po food and switch to SC insulin.
4. When bicarb is > 10 and vomiting has ceased, may use PO carbs to maintain blood sugar while on the insulin drip.
viii.Complications
1. CEREBRAL EDEMA!!! Headache, irritability, and decreased LOC are signs of cerebral edema. The risk is generally 6-24 hours into therapy for DKA. Herniation happens quickly. To avoid:
a. Monitor neuro vitals compulsively. Treat with mannitol (0.5-1g/kg over 30 minutes) before herniation occurs. Cut fluid rate, elevated head of the bed, and intubate if necessary. Hyperventilated until a pCO2 level of 25-27 mmHg is reached.
b. Give fluid judiciously and avoid free water loads. The children at greatest risk are those that are the sickest and the most dehydrated. A serum Na that is not rising appropriately suggests too much free water.
c. Cardiac arrhythmias – Secondary to electrolyte abnormalities. Watch shifts in K+ closely.
d. Hypocalcemic tetany – Phosphorus binds calcium, decreases serum ionized calcium, and may result in hypocalcemic tetany. Mg is often low and may contribute to the problem.
e. Respiratory failure – The children have severe metabolic acidosis. They are alive because of their compensatory increased respiration or hyperpnea. Nothing should be done to interfere with this drive to breathe- drugs which are respiratory depressants should NOT be used. If some sedation is needed (i.e. to place a central line), ketamine is a good choice. If intubation is necessary, a ventilator settings need to be adjusted so as to hyperventilate.
64
Endo
crino
log
y
VI. SUBCUTANEOUS INSULIN: Convert to subcutaneous insulin when the pH is >7.2, bicarb is >15, and the patient is ready and able to eat
a. Convert to subq basal-bolus insulin regimen. Basal insulin (Lantus) is gen once or twice daily and bolus insulin (Novolog or Humalog) is given with food intake (before meals and snacks). Convern to subq insulin before a meal.
b. If the patient is on an insulin drip, sstop the drip at the time the injection is given. T1/2 of IV insulin is 6 minutes. Stop any IV dextrose simultaneously unless hypoglycemia is a problem.
c. Insulin dose:
i. In a new diabetic child, begin with 0.5-1 unit/kg/day total daily insulin dose (TDD)
1. Use 0.5 units/kg/day for younger children and children not presenting with severe acidosis.
2. Use 1 unit/kg/day for teenagers and children who present in severe DKA
3. Give half the dose as basal insulin (Lantus) either in the morning before breakfast for young children or in the evening at bedtime for older children
4. Bolus insulin is given before meals as a carb dose to cover the carbohydrate intake with the addition of a correction dose if glucose is above target range.
a. Calculate a carb ratio: 500/TDD = grams of carbs covered by 1 unit of insulin
b. Calculate a correction dose (1800/TDD). This sit he mg/dL that glucose will be lowered in response to 1 unit of insulin.
ii. In an established diabetic – return to the normal home dose. DKA event may reflect a need for major revision in home insulin dose or management. This can be assessed by the response to the home dose.
d. Follow BGs – pre-meals, pre-bedtime snack, 2AM, and when hypoglycemia is suspected.
e. Diet – Order a carb counting diabetic diet. The children eat to their hunger. Snacks are allowed, but must be covered by insulin in most cases.
65
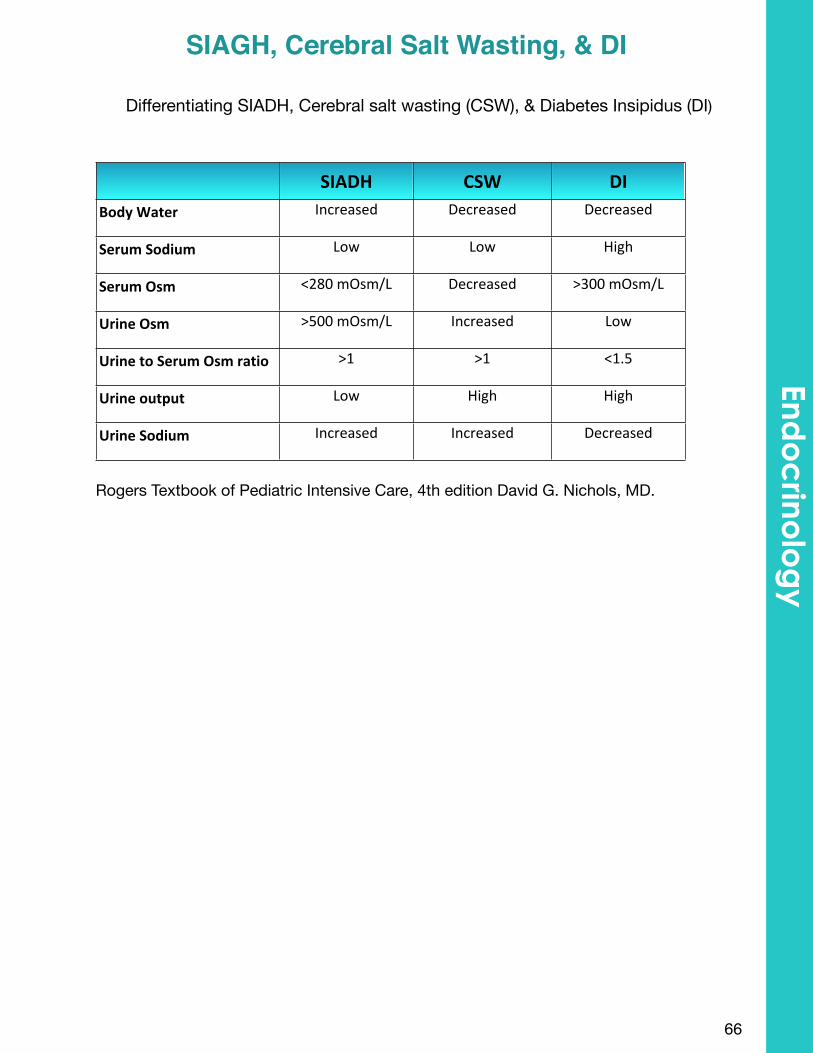
Differentiating SIADH, Cerebral salt wasting (CSW), & Diabetes Insipidus (DI)
SIADH CSW DIBody$Water Increased Decreased Decreased
Serum$Sodium Low Low High
Serum$Osm <2809mOsm/L Decreased >3009mOsm/L
Urine$Osm >5009mOsm/L Increased Low
Urine$to$Serum$Osm$ratio >1 >1 <1.5
Urine$output Low High High
Urine$Sodium Increased Increased Decreased
Rogers Textbook of Pediatric Intensive Care, 4th edition David G. Nichols, MD.
66
SIAGH, Cerebral Salt Wasting, & DIEnd
oc
rinolo
gy
68
Gastroenterology
I. DEFINITION OF CONSTIPATION: delay or difficulty in defecation present for more than two weeks
II. EVALUATION: Diagnosed based on History & Physical Exam
a. HISTORY: may include infrequent stooling associated with daytime intermittent crampy, often periumbilical abdominal pain, stool withholding, fecal soiling, toilet clogging, and dyschezia or hematochezia not associated with diarrhea
b. EXAMINATION: abdominal exam, visual exam of anus and perineum, digital rectal exam, neurologic findings, hydration status, pain status, ability to take oral fluids and medications, mental status
i. Constipation can be diagnosed on exam if there is a palpable fecal mass on abdominal exam and a large amount of stool present on d ig i ta l rectal exam
c. LABS: Optional: BMP, Celiac disease panel, TSH, UA
d. IMAGING: NO need to routinely order abdominal X-ray
i. Constipation is characterized by clinical symptoms.
Infant Home Bowel Clean-Out
1) For 7 days, an Infant glycerin suppository should be given once every 24 hours if a B.M is not passed spontaneously by the infant
2) Give one to four ounces a day of prune juice or pear juice to your infant as long as constipation continues
3) Avoid rice cereal feeding as long as constipation continues
Parents should be advised to call PCP promptly or seek medical attention if the infant becomes more constipated, especially if the constipation is associated with bloating or bilious vomiting.
70
Ga
stroe
ntero
log
yConstipation and Clean Outs
Child Home Bowel Clean-Out
1) One ounce per year of life up to 10 ounces bottle of magnesium citrate to drink over a 30 minute period. Best cold; it does not taste good.
2) Two to four hours after the magnesium citrate has been given, mix 238 gm of polyethylene glycol 3350 powder into one quart of any clear fluid (such as Gatorade®, Crystal Light® or water) and have the child drink all of this in four to six hours.
3) If stool is not clear after 24 hours, repeat steps (1) and (2) once more.
Once the initial clean-out of the bowel is complete the child should be started on a dailytreatment regimen of EITHER (choose JUST ONE OF THESE)
1) Polyethylene glycol 3350 powder, 17 grams (one capful) given in 6-8 oz of fluid at dinnertime
2) Lactulose (a prescription stool softener) 10-20 gms per day
3) One Ex-Lax® (sennoside) chewable tablet (generic OK) at dinner
4) One tablet bisacodyl at dinner
Daily routine should include:
1) Regular schedule of meals that include whole grains, vegetables, salads, fruits and nuts
2) Sit on toilet about 5-15 minutes after meals with feet supported and elbows on knees, twice a day,
3) 10 minutes each time. B.M.s can come easier after a meal and light activity such as a walk.
Goal of Maintenance Therapy: 1 to 2 mushy stools daily after meal stimulation
71
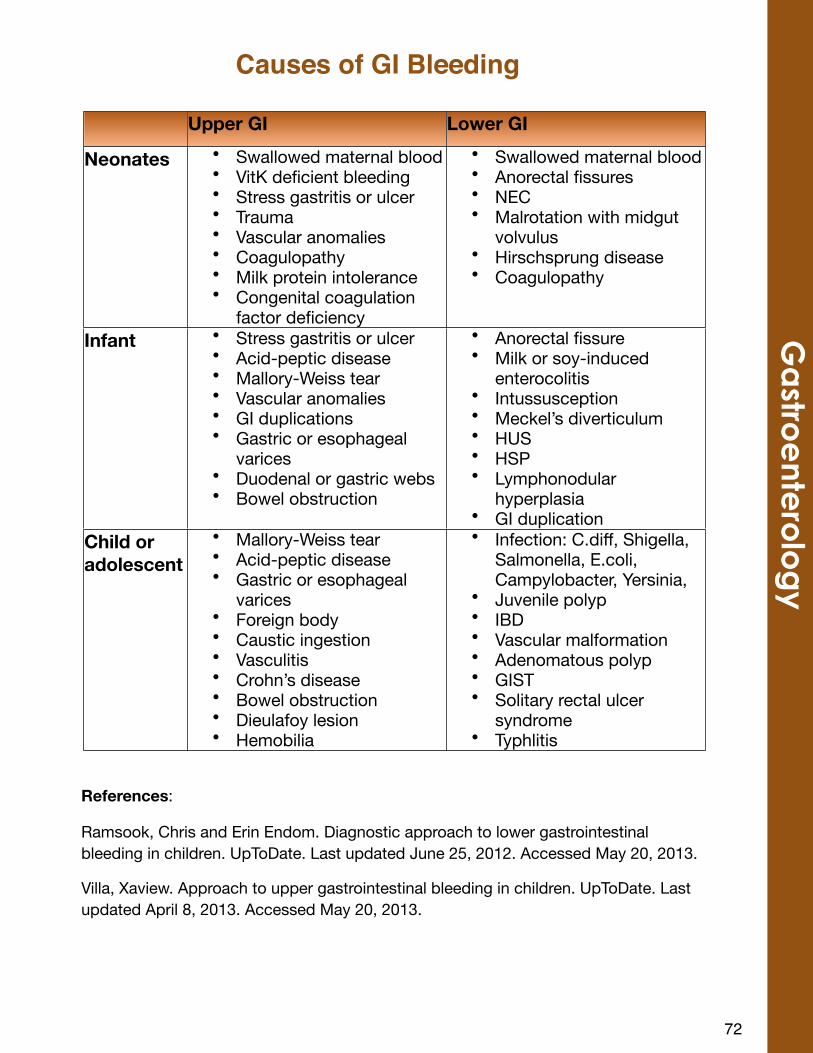
7253
Gastro
ente
rology
Upper GI Lower GI
Neonates • Swallowed maternal blood• VitK deficient bleeding• Stress gastritis or ulcer• Trauma• Vascular anomalies• Coagulopathy• Milk protein intolerance• Congenital coagulation
factor deficiency
• Swallowed maternal blood• Anorectal fissures• NEC• Malrotation with midgut
volvulus• Hirschsprung disease• Coagulopathy
Infant • Stress gastritis or ulcer• Acid-peptic disease• Mallory-Weiss tear• Vascular anomalies• GI duplications• Gastric or esophageal
varices• Duodenal or gastric webs• Bowel obstruction
• Anorectal fissure• Milk or soy-induced
enterocolitis• Intussusception• Meckel’s diverticulum• HUS• HSP• Lymphonodular
hyperplasia• GI duplication
Child or adolescent
• Mallory-Weiss tear• Acid-peptic disease• Gastric or esophageal
varices• Foreign body• Caustic ingestion • Vasculitis• Crohn’s disease• Bowel obstruction• Dieulafoy lesion• Hemobilia
• Infection: C.diff, Shigella, Salmonella, E.coli, Campylobacter, Yersinia,
• Juvenile polyp• IBD• Vascular malformation• Adenomatous polyp• GIST• Solitary rectal ulcer
syndrome• Typhlitis
Causes of GI Bleeding
References:
Ramsook, Chris and Erin Endom. Diagnostic approach to lower gastrointestinal bleeding in children. UpToDate. Last updated June 25, 2012. Accessed May 20, 2013.
Villa, Xaview. Approach to upper gastrointestinal bleeding in children. UpToDate. Last updated April 8, 2013. Accessed May 20, 2013.
Ga
stroe
ntero
log
y
74
Hematology/Oncology
• Always call the on call fellow or attending if you can’t figure something out. • We’d rather wake up in the middle of the night than to have an unpleasant surprise the next
AM• Preferred drug doses are on the Lahey drug card.
You should never feel compelled to write for chemotherapy Exception: Steroid dosing (after careful review of dosing with attending)
•No NSAIDS as they can cause platelet dysfunction in already thrombocytopenic patients •Sometimes ok for persistent fevers if not thrombocytopenic, but always ask first.
• All patients on chemo need Pneumocystis prophylaxis. Most common is Septra, bid on Mon/Tues. Others occasionally on dapsone (daily), pentamidine (monthly), or atovaquone (daily). Should be continued for all admits and start for all new dx unless otherwise instructed.
•Discharging the ICS patient: the earlier the DOADI is done, the better. *Let d/c planning know about major home needs early; may need a few days for insurance approval
• Primary Care Physiciano Not the primary oncologist, but their regular PCP (d/c info will be sent to their office)o Please include the medications that the patient is going home with in the DOADI
• Hematology clinic number and faxo Drop down list under clinic area on DOADI
• Home health care company name, phone, and faxo Can be found in discharge planning notes or previous discharge orders in Help2 OR
you can always ask Rachel or Tomokoo New diagnosis patients setup by Rachel or Tomoko (they will enter info into DOADI)
• Skilled Nursing visits as needed• Line care and supplies as needed
o Standing order form will also be sent with the DOADI; should be sent on all patients with central line/port (even if their ports is de-accessed) – needs signature from resident.
• Lab drawso Patients going home on Neuopogen/Neulasta or antibiotic duration based upon
ANC need CBC with diff every Monday and Thursday. Please include start date for labs.
• IV antibiotics with stop dateo Don’t send to outpatient pharmacy – IV orders have to be filled through home careo Usually until ANC >500 or for the full courseo Takes home care 4-6 hours to make; need to time medication
• TPN with stop dateo Usually until next clinic date or TBDo Takes home care 6 hours to make
• IV fluids with stop date
76
He
ma
tolo
gy/O
nco
log
yGeneral Hematology/Oncology Pearls
Mucositis – • Chemo impairs the ability of the mucosal lining to quickly regenerate. • Most commonly associated agents: methotrexate and anthracyclines. • Usually occurs while neutropenia and improves as ANC improves. • Exam:
o Can occur anywhere along the GI lining…even if you don’t see oral lesions. o All patients admitted with mucositis need visual inspection of peri-anal area.
• Treatment:o Can treat with pain meds or magic mouthwash (Maalox + Benadryl ±
lidocaine) o Have to wait for it to improve. o Need IVF or TPN if severe.
Pain – • Can be from chemo, tumor, etc. • Treatment: Narcotics
o Many patients will have a preference for a specific narcotic based on experience.
o Due to potential to mask fever, it is preferred to use narcotic only, not acetaminophen & narcotic combo.
Neuropathy – • Usually peripheral/stocking-glove pattern • Commonly associated agents: vincristine, less common with cisplatin, ifosfamide,
etc. • Presentation: ankle pain, foot drop, tripping. • Treatment: pain meds, PT, gabapentin.
• Cytopenias – (See neutropenia and transfusion info below) • Due to bone marrow suppression by chemo • GCSF: Figuring out who gets and who doesn’t get GCSF for neutropenia can be a
nightmare, it is both doc and protocol dependent. o If someone comes in on it and is neutropenic, continue it. o Otherwise, the attending will tell you who needs it started that wasn’t on it
before.
77
Common Chemotherapy Complications
Definitions: Fever: Single oral temperature ≥ 38.3°C OR sustained temperature ≥38.0°C for 1 hr.Neutropenia: ANC <500 cells/mm3 OR ANC expected to be <500 cells/mm3 within 48hrs.High risk neutropenia: Anticipated duration of neutropenia >7 days and profound neutropenia (ANC <100 cells/mm3. Alternatively, one of several validated scoring systems may be used (e. g. Ammann et al J ClinOncol 1010;28:2008-14)
Common pathogens:Although only 20-30% of patients will have a documented infection, all patients with fever and neutropenia should receive rapid (within 30-60 minutes of arrival) initiation of antibiotics after presentation, because they can rapidly decompensate. Empiric therapy provides broad spectrum anti bacterial therapy until culture results provide a guide to more narrow therapy. Patients are at risk for many potential pathogens.Gram-negative organisms are associated with high morbidity and mortality. Empiric regimens should always include coverage for Pseudomonas aeruginosa.
Initial evaluation:• Obtain at least two sets of blood cultures of appropriate volume for weight: All
lumens of CVC and consider simultaneous peripheral blood culture (especially if single lumen CVC). If no CVC obtain two blood cultures by venipuncture.
• Consider urinalysis and urine culture if recent or current Foley catheter.• Evaluate for early shock• CXR only if symptomatic (hypoxia, respiratory distress, cough or chest pain)
Treatment Notes:For clinically stable patients, the addition of vancomycin is not routinely recommended to empiric treatment of febrile neutropenia. In RCTs, addition of vancomycin to empiric therapy did not decrease duration of fever or mortality.
The following are reasons to add empiric vancomycin in clinically stable patients:o Radiographically documented pneumoniao Gram-positive bacteria in blood culture while awaiting identification and
susceptibilityo Catheter-related blood stream infection evidenced by cellulitis around
catheter entry site, or chills/rigors with infusion through central line lumeno Skin and soft-tissue infectiono Severe oral mucositisor recent exposure to high dose ARA-Cif using
ceftazidime
Modifications to initial regimen should be made if patient is colonized by resistant pathogens, e.g.if colonized by ESBLs, meropenem would be an appropriate empiric therapy, if known to be colonized by MRSA, vancomycin should be used empirically while awaiting cultures.
Concern for typhlitis requires anaerobic coverage. Piperacillin/tazobactam is adequate coverage if Clostridium difficile is not of concern. If cefepime is continued,
78
He
ma
tolo
gy/O
nco
log
yFever and Neutropenia
metronidazole 10 mg/kg/dose (max 500 mg) IV q8hrs should be added. Patients older than 1 year old with abdominal pain and distension or new onset diarrhea should be evaluated for C. difficile.
When concerned about viridans group Streptococcus due to mucositis or high dose ARA-C, piperacillin/tazobactam or cefepime have better activity against these organisms than ceftazidime.
Management of initial fever:Patient is clinically stable: If patient doesn’t meet criteria discussed above for therapy modifications, thenMonotherapy with antipseudomonal βlactam antibiotic
• Cefepime 50 mg/kg/dose (max 2 g) IV q 8hrsOR
• Piperacillin/tazobactam 75 mg/kg/dose (max 3 g) IV q6hrsOR
• SEVERE PENICILLIN ALLERGY: obtain allergy consult. Call ID or ASP for empiric therapy options
Patient is clinically unstableCombination therapy is indicated. Consider an ID consult.
• Antipseudomonal β-lactam antibiotic as described for clinically stable patient• PLUS vancomycin 20 mg/kg (max initial dose 2 g) IV q8 hrs (see vancomycin
dosing section for more information)• PLUS gentamicin 5 to 7.5 mg/kg IV q24hrs (see gentamicin dosing section for more
information)
Modifications to Antibacterial Therapy at > 24 to 72hrsPatient responding to therapy
• Discontinue double coverage for gram-negative organisms if initiated and no specific microbiological indication
• Discontinue vancomycin if initiated and no specific microbiologic indication
Patient clinically stable with continued fevers• No modifications necessary without specific microbiologic indication• Discontinue double coverage for gram-negative organisms if initiated and no
specific microbiological indication• Discontinue vancomycin if initiated and no specific microbiologic indication
Patient with persistent fevers who becomes clinically unstableCombination therapy is indicated. Consider an ID consult.
• Antipseudomonal β-lactam antibiotic as described for clinically stable patient• PLUS vancomycin 20 mg/kg (max initial dose 2 g) IV q8 hrs (see vancomycin
dosing section for more information)
79
• PLUS gentamicin 5 to 7.5 mg/kg IV q24hrs (see gentamicin dosing section for more information)
Cessation of Antibacterial TherapyTreat identified infections with appropriate durations as indicated by site of infection.
Discontinue empiric antibiotics in patients when all of the following criteria are met:• Negative blood cultures at 48hrs• Afebrile for at least 24hrs• Evidence of marrow recovery
o Often defined as ANC > 500 cells/mm3 for 2 consecutive days OR ANC > 1,000 cells/mm3 for 1 day
Empiric Antifungal UsePatients are categorized as high and low risk. The following patients are at high risk for invasive fungal infections when they have persistent fevers despite ≥96hrs of broad spectrum antibiotics and anticipated neutropenia of 10 or more days: AML, relapsed ALL, highly myelosupressive chemotherapy for other cancers, and BMT patients.
Add empiric antifungal therapy for neutropenic patients at high risk of invasive fungal disease if fevers persist without identified etiology after 96 hours or recur despite empiric broad spectrum antibiotics.
• Caspofungin 70 mg/m2/dose (max dose 70 mg) IV day 1 then 50 mg/m2/dose (max 50 mg) IV q24hrs
Consider adding empiric antifungal to regimen for patients for patients with persistent fever and neutropenia (as above) at low risk of invasive fungal disease.
• Caspofungin 70 mg/m2/dose (max dose 70 mg) IV day 1 then 50 mg/m2/dose (max 50 mg) IV q24hrs
IF SUSPECT ASPERGILLOSIS:Consult ID.
• Voriconazole o < 12yrs old: 9 mg/kg/dose IV q12hrs x 2 then 8 mg/kg/dose IV q12hrso 12yrs and greater: 6 mg/kg/dose IV q12hrs x 2 then 4 mg/kg/dose IV q12hrso Adjust dose based on trough concentrations using therapeutic drug
monitoring• PLUS Caspofungin 70 mg/m2/dose (max dose 70 mg) IV day 1 then 50 mg/m2/
dose (max 50 mg) IV q24hrs
IF SUSPECT OTHER FILAMENTOUS FUNGUS:Consult ID for recommendations
80
He
ma
tolo
gy/O
nco
log
y
Laboratory and Imaging notes• Consider twice weekly galactomannan (GM) in high-risk hospitalized patients.
Consider GM evaluation in BAL fluid and CSF to support diagnoses of pulmonary and CNS aspergillosis.
• Β-D-glucan monitoring is not recommended in children until further studies support its use.
• After 96hr of broad spectrum antibiotics, if high risk patient is still febrile, perform imaging for invasive fungal infection
o CT of lungs and targeted imaging of other clinically suspected areaso Consider CT of sinuses if 2 yrs old or greater
• If using voriconazole, please monitor trough concentrations. See voriconazole monitoring section of booklet.
References:Lerhnbecher T et al. Guideline for the management of fever and neutropenia in children with cancer and/orUndergoing hematopoietic stem-cell transplantation. J Clin Oncol. 2012 Sept 17. [Epub ahead of print]Freifeld AG et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. CID. 2011;52(4):e56-e93
81
• Fever and neutropenia (F&N) is a MEDICAL EMERGENCY o Most kids do not have bacteremia and do fine o Those who have bacteremia can quickly progress to sepsis/death due to
their immune-compromise.• Definitions:
o Fever = T>38.3 on any reading x1 or T>38.0 x2 more than 1 hour apart.o Neutropenia= ANC≤500
! In some circumstances, patients with fever may still be admitted with a higher ANC if it is known to be falling based on their recent chemo.
• Management:o Most of the time oral chemotherapy should be held when patients are
admitted with F&N. There are a few times when this is not true, but it is generally better to miss a dose than to give a dose in error.
• When called for a new fever:o Non-neutropenic patients need evaluation, blood culture, and ceftriaxone
(or equivalent coverage for central line if cephalosporin allergy). o Neutropenic patients need evaluation, blood culture, and ceftazidime. o Other evaluation such as VRP, urine, CXR, etc if specific symptoms warrant.
For heme/onc patients, ok to get blood culture only from central line, do not need peripheral. Rarely need fungal cultures, ask first.
o Add gentamicin if appears septic. Add gentamicin, metronidazole, or pip/tazo for abdominal concerns. Add vancomycin for patients with severe mucositis, concerning skin lesions, or recent exposure to high dose araC (most AML patients).
• When called for recurrent fever:o Repeat blood culture once every 24 hours. No changes needed if patient is
stable.o Persistent F&N (>5-7 days) should prompt eval for fungal disease
• Typhlitis: neutropenic colitis (usually around the cecum) o Often seen with F&N and abd pain. o Management:
! Broaden antibiotic coverage as above for GNR and Cdiff ! Make NPO ! Imaging to rule out perforation should be considered –different docs
prefer US vs CT.! Surgery consult if free air
82
Fever and Neutropenia Quick CardH
em
ato
log
y/Onc
olo
gy
Nosebleeds – (not usually life threatening but fits best here) • Treatment:
o Pressure ! Should be leaning forward with firm pressure just distal to the nasal
bone ! Hold pressure for a solid 15min without letting go to see if bleeding is
stopped o Afrin and amicar (see drug card for dosing) o ENT for packing
! Try other strategies first (including both drugs)! Most docs will want a neutropenic kid covered with antibiotics if they
have to be packed.
Hemorrhage:• Causes – severe refractory thrombocytopenia, invasion of tumor or fungus into
major blood vessels, post-op, coagulopathy/DIC, anti-coagulant overdose, etc. o Rarely in hemophilia, ITP, or routine chemotherapy induced
thrombocytopenia.• Management:
o Send stat coags ! Do NOT wait for the results before treating.
o Call for help:! Often need PICU transfer, particularly for pulmonary hemorrhage
(need intubated ASAP) ! Call surgery if something can be stitched.
o Replacement:! Specific factor replacements: available for hemophilia A (factor VIII
50U/kg), hemophilia B (factor IX 100U/kg), or von Willebrand’s (Humate P call for dosing).
! FFP, cryoprecipitate, platelets: as indicated • May benefit from continuous platelet infusion.
! pRBCs: Bleeding is always worse at a lower hct – transfuse RBC as well.
! Last effort: Activated factor VII will stop almost all bleeding (except in case of arterial erosion) but is insanely expensive. Dose is 90mcg/kg, but talk with attending first.
83
Life Threatening Hemorrhage
• Premedication for blood products:o Due to multiple exposures, many oncology patients have a history of transfusion
reactions and need premeds. o Sometimes hard to find easily in Help2 but most parents and nurses know.
• Order all blood products “per Heme/Onc protocol” o Means leukodepleted, irradiated, and CMV negative o Rarely there is a heme patient that only needs leukodepleted blood.
• Platelets: o Given for bleeding or prophylaxis when platelets <10, or platelets <25-50 in
patients with CNS hardware, or however high surgeons request them prior to OR.! New leukemia patients usually need plts to be 50-100 for line placement and
diagnostic LP. o Dosing: Use 1 pheresis unit for kids >15kg. For kids <15kg, use 10-15cc/kg.
• Should raise plt count by about 50K, but many onc patients don’t have that good of a response.
• pRBCs:• Given for symptomatic anemia or hct <23 (somewhat doc dependant). • Dosing: 12-15cc/kg should raise hct by 8-9%.
o New patients with acute presentation of severe anemia will need much smaller volume at much slower rate to prevent volume overload/cardiac failure.
• Transfusion reactions are common. Nurses monitor vitals more frequently during transfusions. If any concern about a reaction, STOP TRANSFUSION (most nurses will do before they call you).
o Hemolytic – actually very uncommon, usually due to blood bank or nursing error (blood given to wrong patient).
! Sx: back pain, fever, chills, hematuria, hypotension.! Rx: stop transfusion, aggressive hydration, blood bank to do work up to look
for cross-match error.o Allergic – very common in patients with multiple transfusion exposures, usually due
to patient antibodies to donor serum! Sx: usually urticaria & itching, can progress to cough/ laryngospasm/
bronchospasm! Rx: stop transfusion and give diphenhydramine, ok to resume if symptoms
resolve. Give steroids for mild/moderate airway symptoms and epi for anaphylactic symptoms.
o Febrile, non-hemolytic – not uncommon, usually from patient antibodies to donor WBC
! Sx: fever! Rx: stop transfusion, fever eval, give acetaminophen/diphenhydramine,
usually can finish transfusiono Transfusion related acute lung injury/transfusion associated circulatory
overload (TRALI/TACO) – uncommon in kids but cool acronyms! TRALI – donor antibodies against recipient WBC – dyspnea, hypoxia and
pulmonary infiltrates within 4hrs of transfusion. Usually self limited, support throughout duration, including intubation/vent if needed
! TACO – volume overload from rapid transfusion, diurese and monitor cardiac status
84
He
ma
tolo
gy/O
nco
log
yTransfusion Pearls
What is it?• HyperK+, hyperPO4-, hyperuricemia, hypoCa2+, fluid overload , and renal insufficiency • Caused by the rapid breakdown of tumor cells
When does it occur?• Most common in tumors with extremely high growth rate or very quick response to
chemotherapy. o Burkitt’s lymphoma & Tcell leukemia w/ very high WBC most commono Can happen in any leukemia, other lymphomas (usually lymphoblastic), or other
solid tumors (eg hepatoblastoma). o Leukemia with relatively normal WBC are still at risk (esp if they have hepatomegaly,
splenomegaly, or massive adenopathy)o Patients may actually present with TLS (particularly Burkitt’s) OR it can develop after
treatment is initiatedHow to treat/prevent in high risk patients
- Aggressive hydration – 125-200mL/m2/hr (125ml/m2/hr = 2x maintenance).o Fluids should NOT contain K+. Can lead to pulmonary edema, monitor respiratory
status.- Monitor urine output (seems simple, but often forgotten)
o You are giving a ton of fluid, they should be peeing a ton, at least 3mL/kg/hr.- Alkalinization of urine (allows for increased excretion of uric acid)
o D5-1/4 NS + 40meq NaHCO3/L with goal of urine pH 6.5-7.5. o If urine pH >7.5 need to decrease amt of bicarb in bag.
- Allopurinol – 100mg/m2/dose PO q8hr. Do not give IV ($$$$) . o Frequent lab monitoring – o Anywhere from q2hr to q12hr depending on pt’s risk. o Labs should include K, Phos, uric acid, Ca, and creatinine.
! LDH is not necessary. o BMP and CBC can usually be once daily.
Electrolyte imbalances:- Hypocalcemia – Do not treat unless symptomatic (and even then ask)
o It will increase the risk of phos precipitating in kidneys.- Hyperkalemia – Same as any other hyperkalemia –
o Increased IVF without K, ECG, furosemide, kayexalate, calcium gluconate, insulin/glucose, albuterol, etc. Check with pharmacist to make sure no K hiding in other meds.
- Hyperuricemia – o Can treat with rasburicase, 0.2mg/kg/dose (enzyme that converts uric acid to an
inactive and soluble metabolite)! Will usually decrease UA to 1 or less in a couple hours.
o Extremely expensive…always check with attending first!! Many reserve for a UA greater than 11 or 12
o Remind nurses that after rasburicase is given, UA needs sent on ice to prevent continued action of enzyme after sample drawn.
o Avoid in patients with G6PD deficiency – can cause severe hemolysis- Hyperphosphatemia –
o Want to avoid CaPO4 precipitationo Currently the most common cause of dialysis in TLS o Low phos diet (restrict dairy, cola, peanut butter, etc)o Phosphate binders such as amphogel and renagel
85
Tumor Lysis Syndrome
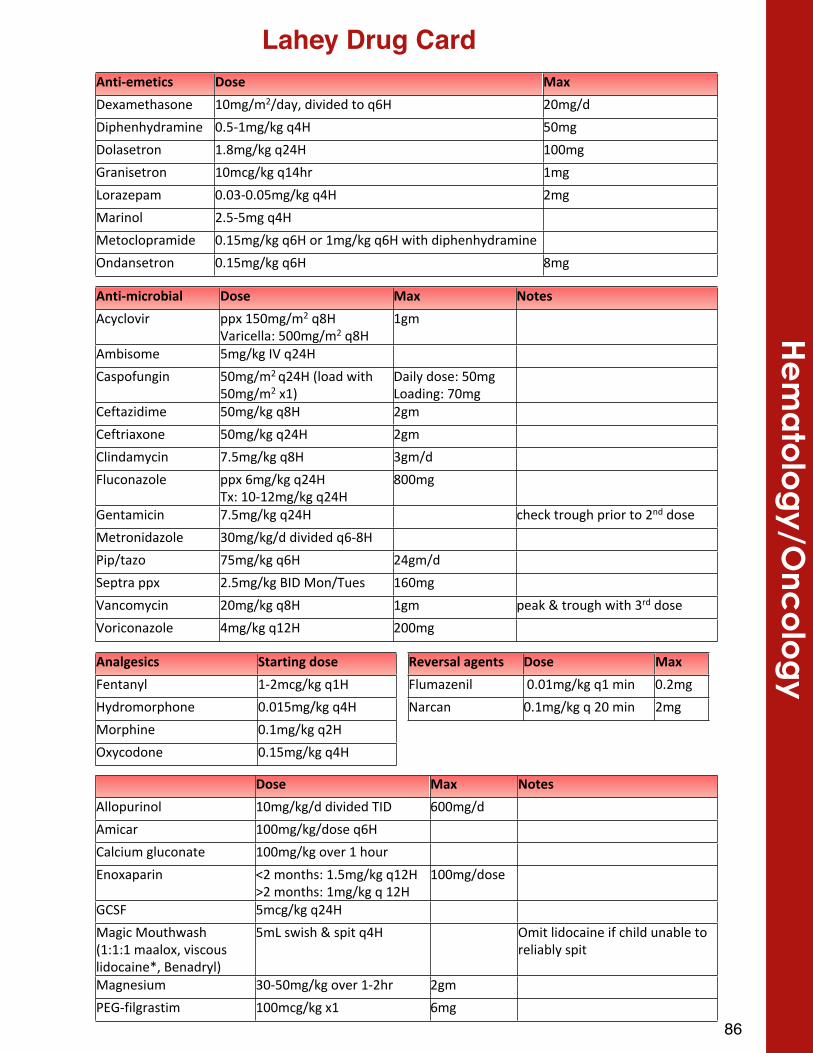
86
He
ma
tolo
gy/O
nco
log
yLahey Drug Card
AntiXmicrobial Dose Max NotesAcyclovir ppx#150mg/m2#q8H
Varicella:#500mg/m2#q8H1gm
Ambisome# 5mg/kg#IV#q24H
Caspofungin 50mg/m2#q24H#(load#with#50mg/m2#x1)
Daily#dose:#50mgLoading:#70mg
Ceftazidime 50mg/kg#q8H 2gm
Ceftriaxone 50mg/kg#q24H 2gm
Clindamycin 7.5mg/kg#q8H 3gm/d
Fluconazole ppx#6mg/kg#q24HTx:#10X12mg/kg#q24H
800mg
Gentamicin 7.5mg/kg#q24H# check#trough#prior#to#2nd#dose
Metronidazole 30mg/kg/d#divided#q6X8H
Pip/tazo 75mg/kg#q6H 24gm/d
Septra#ppx 2.5mg/kg#BID#Mon/Tues 160mg
Vancomycin# 20mg/kg#q8H 1gm peak#&#trough#with#3rd#dose
Voriconazole# 4mg/kg#q12H 200mg
Analgesics Starting$doseFentanyl 1X2mcg/kg#q1H
Hydromorphone 0.015mg/kg#q4H
Morphine 0.1mg/kg#q2H
Oxycodone# 0.15mg/kg#q4H
Reversal$agents Dose MaxFlumazenil #0.01mg/kg#q1#min 0.2mg
Narcan 0.1mg/kg#q#20#min 2mg
Dose Max NotesAllopurinol 10mg/kg/d#divided#TID 600mg/d
Amicar# 100mg/kg/dose#q6H
Calcium#gluconate 100mg/kg#over#1#hour
Enoxaparin# <2#months:#1.5mg/kg#q12H>2#months:#1mg/kg#q#12H
100mg/dose
GCSF 5mcg/kg#q24H
Magic#Mouthwash#(1:1:1#maalox,#viscous#lidocaine*,#Benadryl)
5mL#swish#&#spit#q4H Omit#lidocaine#if#child#unable#to#reliably#spit
Magnesium# 30X50mg/kg#over#1X2hr 2gm
PEGXfilgrastim 100mcg/kg#x1 6mg
AntiXemetics Dose MaxDexamethasone# 10mg/m2/day,#divided#to#q6H# 20mg/d
Diphenhydramine 0.5X1mg/kg#q4H# 50mg
Dolasetron 1.8mg/kg#q24H 100mg
Granisetron 10mcg/kg#q14hr 1mg
Lorazepam 0.03X0.05mg/kg#q4H 2mg
Marinol# 2.5X5mg#q4H
Metoclopramide# 0.15mg/kg#q6H#or#1mg/kg#q6H#with#diphenhydramine
Ondansetron 0.15mg/kg#q6H 8mg

88
Infectious Disease
Infectious Disease General Information General Rules
1. Consults. Notify us as soon as possible when you have a consult so that the patient has the best possible care. It is not acceptable to consult us for outpatient management on the day of discharge. When you do call, have a specific question you need addressed; if you don’t know the question, clarify it with the attending or senior resident before calling. If you don’t know the patient, please familiarize yourself with basic details about the case before calling
2. Informal or curbside consults. We are happy to answer questions but often cannot give specific advice regarding the management of your patient without formally seeing the patient. An acceptable informal question is one with a factual answer and lacks any identifying information about the patient, such as “Can influenza cause meningitis?” An inappropriate informal question is “Which antibiotic should I give this 3 year old patient who presented with fever and neck pain?”
3. Common courtesy. If we are consulting on a patient and the patient is not critically ill, we appreciate discussion about changes in antimicrobial therapy or further testing you are considering BEFORE the orders are submitted
4. Discharging patients on antibiotics. If a patient will follow up in Infectious Diseases clinic, please clarify the length of antimicrobial therapy needed before discharging the patient. In most cases the patient should remain on antibiotics until seen in follow up. The primary team needs to ensure that the patient has enough antibiotic once discharged
5. Antimicrobial stewardship. The stewardship team is an extension of the Infectious Diseases team and exists to help you optimize antimicrobial prescribing. Please feel free to be proactive and call the stewardship team with questions about antimicrobial agents on any patient
6. General antimicrobial dosing. If the patient is sick enough to be in the hospital, the patient deserves the maximum weight-based dose of antibiotics
7. Blood cultures. If a patient has a new positive blood culture, you need to repeat a blood culture before you start an antibiotic or change the antibiotic
8. Imaging. If renal function allows, always obtain contrast CT or MRI imaging when looking for infectious sources. Non-contrast imaging does not help detect infection.
9. Gram stains. They are operator-dependent and may be misleading. Never narrow antimicrobial coverage based solely on gram stain results
10. Susceptibilities. Use the hospital’s antibiogram (available on Germ Watch) as a starting point for selecting empiric antibiotics. The antibiogram is based on aggregate susceptibility data of common organisms
90
Infec
tious D
isea
se
ID References
• Red Book- Excellent resource for specific organisms and prophylaxis/infection control. Online access is available through the hospital
• The Sanford Guide- Excellent resource on antimicrobials and specific organisms • Nelson’s Pocket Book of Pediatric Antimicrobial Therapy-
Excellent resource for pediatric antimicrobial selection• UpToDate- Good starting point for most infections with review of recent
literature • Harriet Lane- Good starting point for common infections• The Yellow Card- Specific resource for febrile infant management•
Indications to Consult ID
• Anytime ID is expected to help with outpatient management, e.g. bone/joint infections, complicated pneumonia. Do not assume the patient’s primary provider will be comfortable managing outpatient IV antibiotics unless previously discussed with the provider
• Bacterial meningitis• Neonatal HSV infections• Serious infections is transplant/immunocompromised patients• Tuberculosis• HIV (including perinatal exposure)• Infections involving unusual organisms, e.g. Burkholderia, Gordonia, parasites• Concern for necrotizing fasciitis • Meningococcal infections• Persistent infections despite apparently adequate antibiotic coverage• Malaria• Toxic shock syndrome• Potential outbreak situations (multiple cases of same infection presenting at the same
time with a suspected common source)
Laboratory Tips
• PCH’s microbiology lab phone number is 662-2140. Please have the culture’s ascension number handy when you call. The lab can also answer questions about film array results or give updates on culture growth
• Please notify the microbiology lab about suspicion for organisms which can aerosolize so that the cultures can be properly handled. Such organisms include Bacillus anthracis (anthrax), Yersinia pestis (plague), Francisella tularensis (tularemia), Coccidioides, Histoplasma, and Brucella
• ARUPlab.com is a good resource for determining which laboratory tests to send. When ordering ARUP labs, include the ARUP lab number in the order.
• There is an on call ARUP microbiology fellow for questions about tests or special cultures. The fellow can be reached by pager through the University of Utah’s Smartweb
• When evaluating for acute EBV infection in a patient who is not immune compromised send an EBV antibody panel 1. In general, EBV PCR should only be used on immune compromised patients
91

• When evaluating for fungal bloodstream infections realize that a routine blood culture will detect Candida. A fungal blood culture is not needed for suspected Candida bloodstream infections
• When evaluating for pertussis send PCR or culture of nasal pharyngeal aspirate. Pertussis DFA has poor sensitivity
• When evaluating for HSV infection send PCR of suspicious skin lesions, blood, or CSF as indicated. Additionally swabs of the eyes, nose, and rectum can be sent for culture if HSV infection is suspected in a neonate
• When evaluating for pulmonary TB in a toddler or someone who cannot reliably produce sputum have respiratory therapy obtain a gastric aspirate for AFB smear and culture on three consecutive mornings. Serum quantiferon gold should only be ordered for patients > 5 years old, otherwise place a PPD
• When evaluating for diarrhea due to Yersinia specifically order stool to be cultured for Yersinia
92
Infec
tious D
isea
se
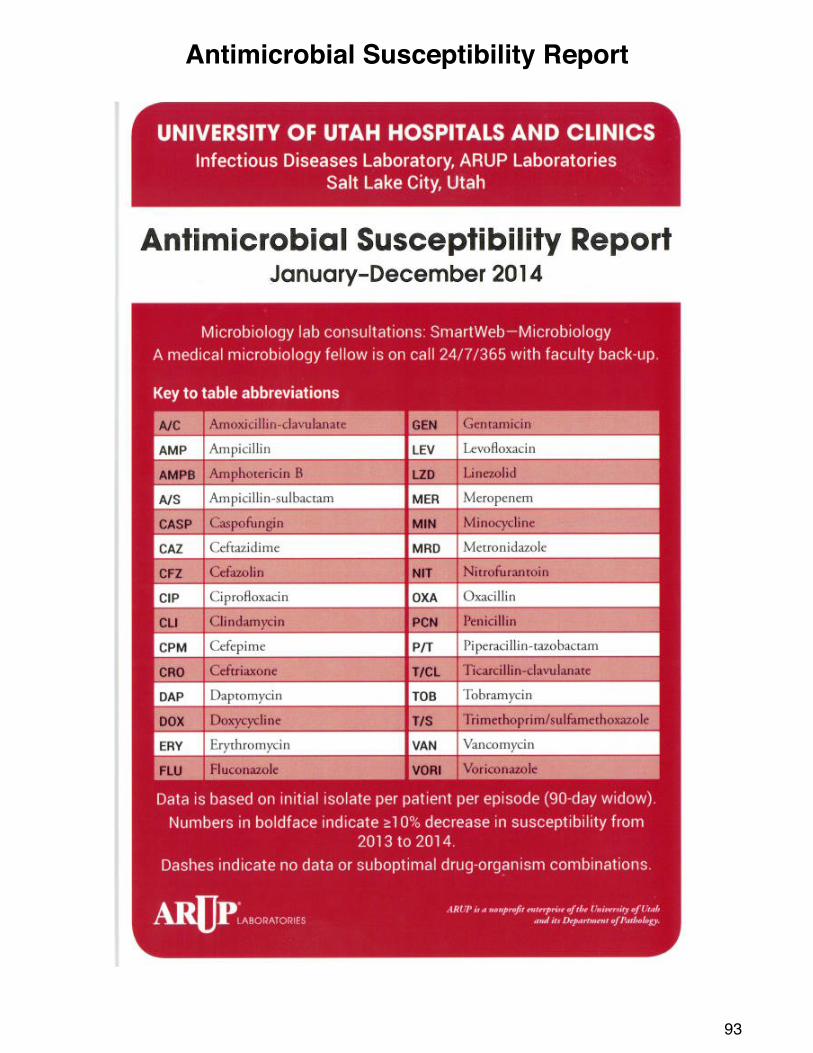
93
Antimicrobial Susceptibility Report
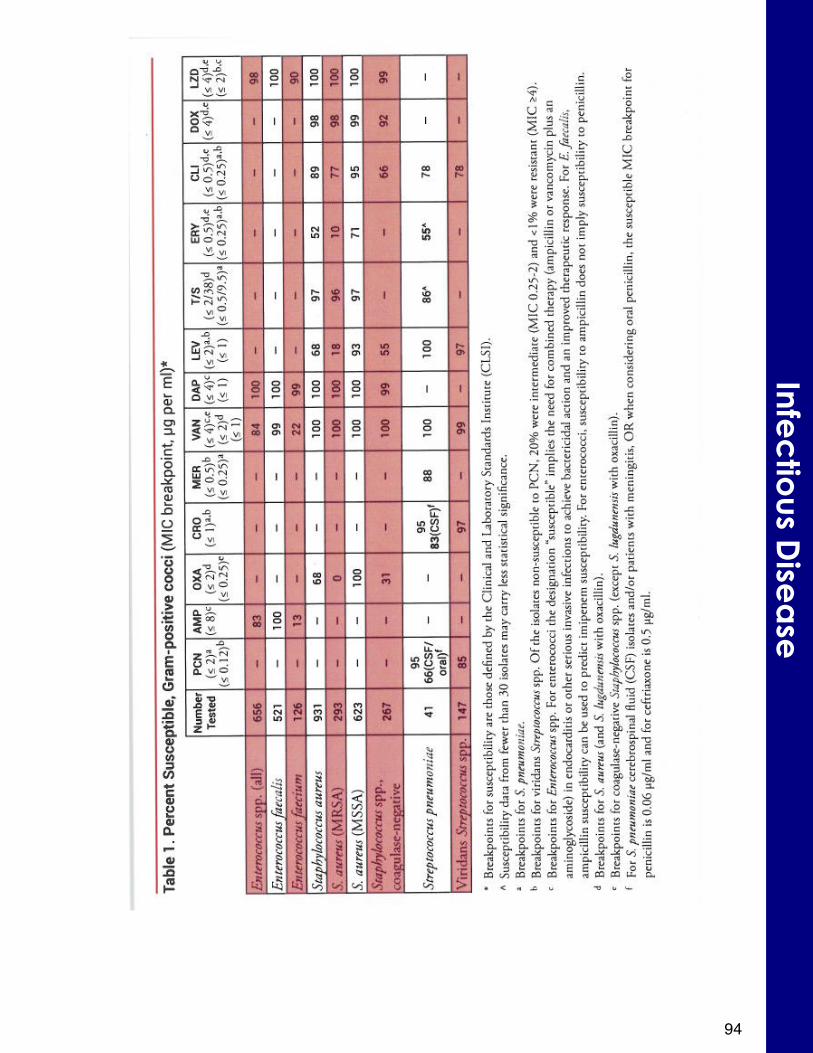
94
Infec
tious D
isea
se
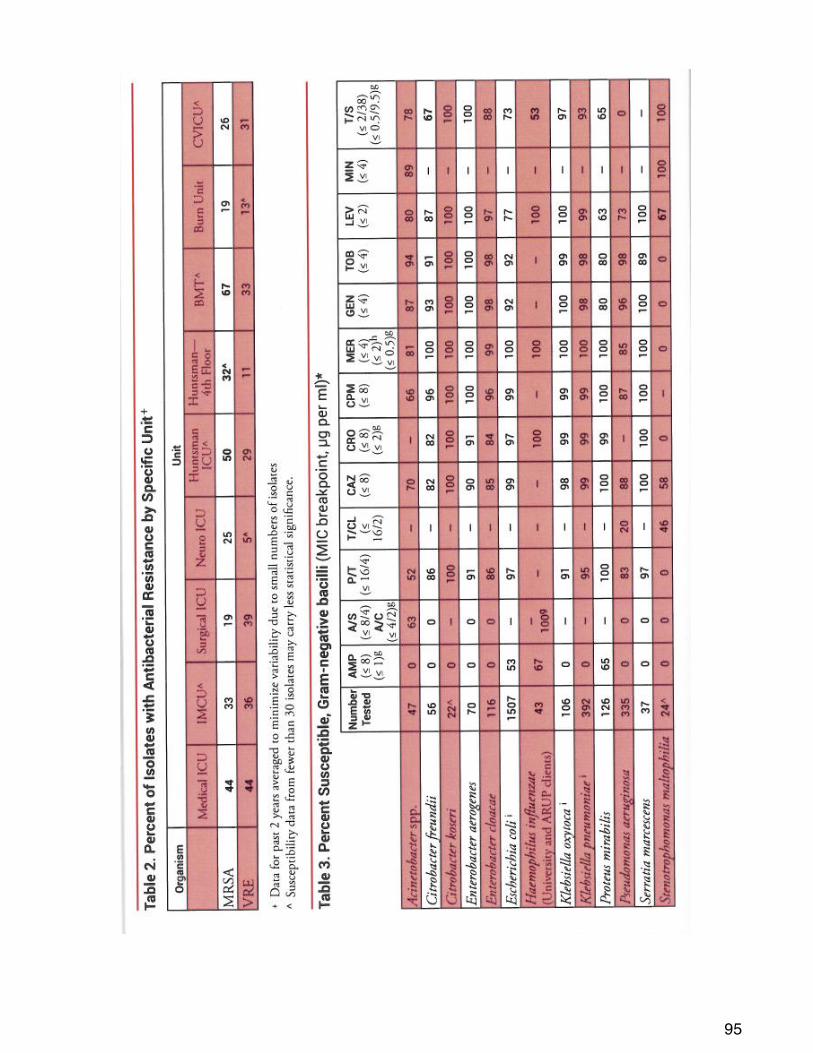
95
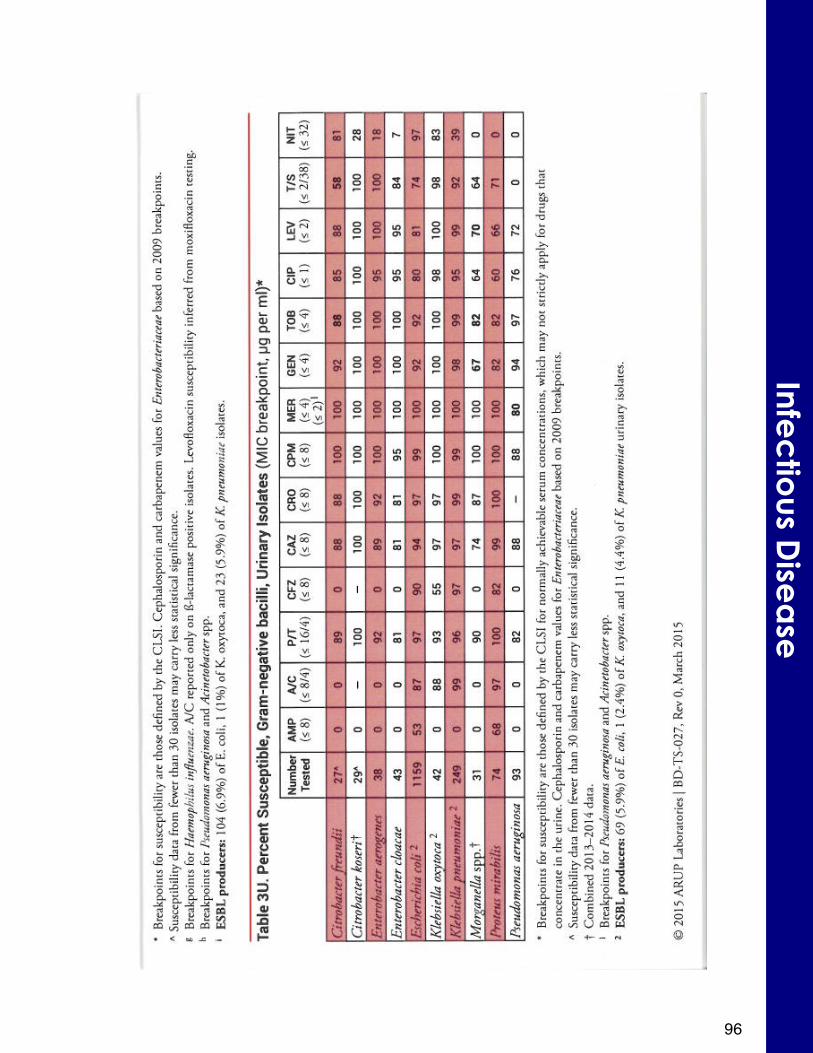
96
Infec
tious D
isea
se
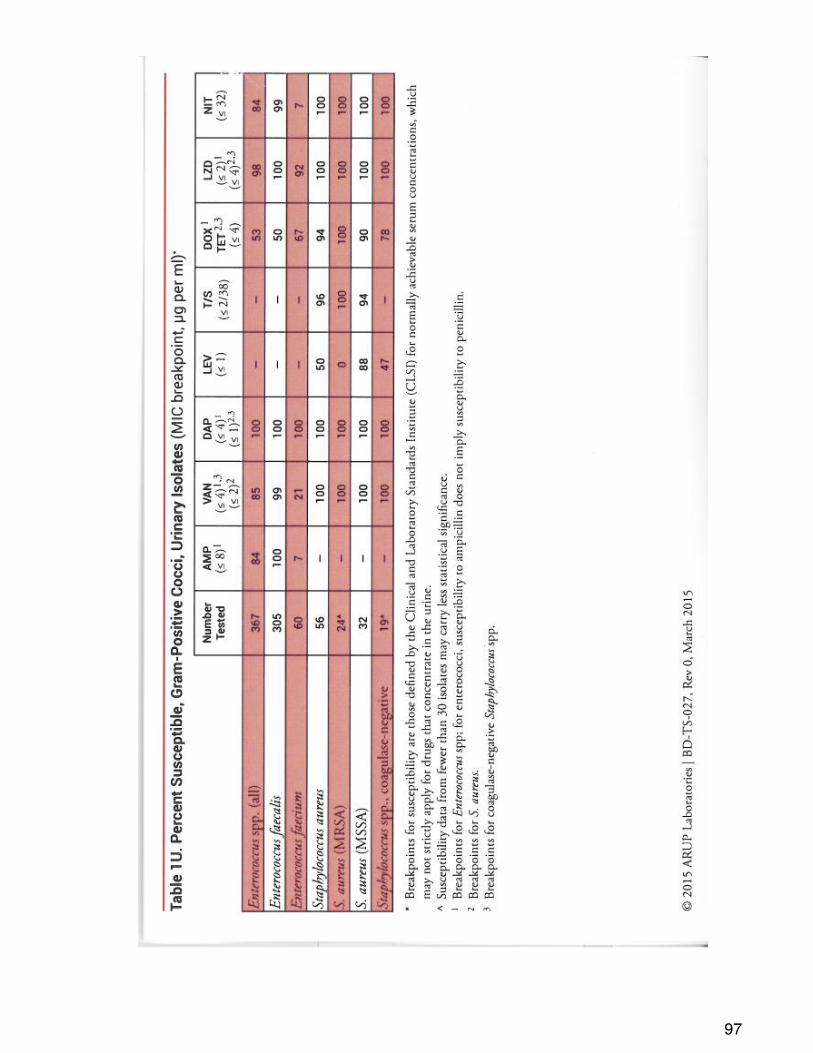
97
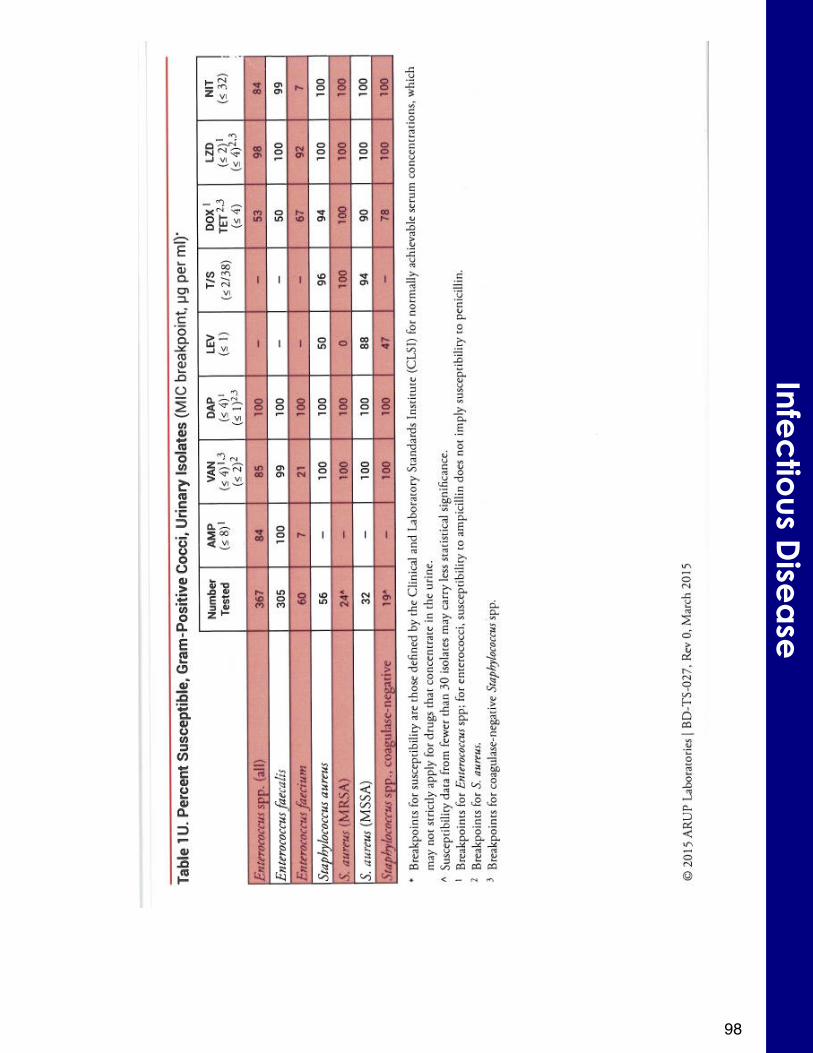
98
Infec
tious D
isea
se
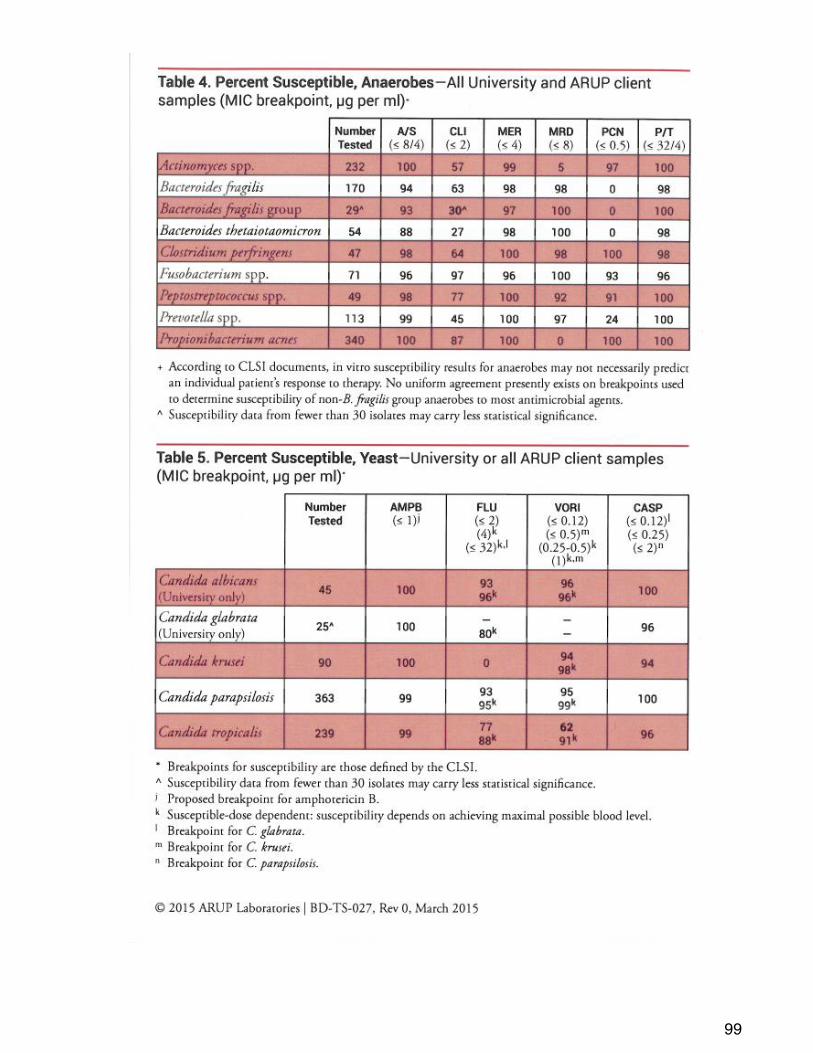
99
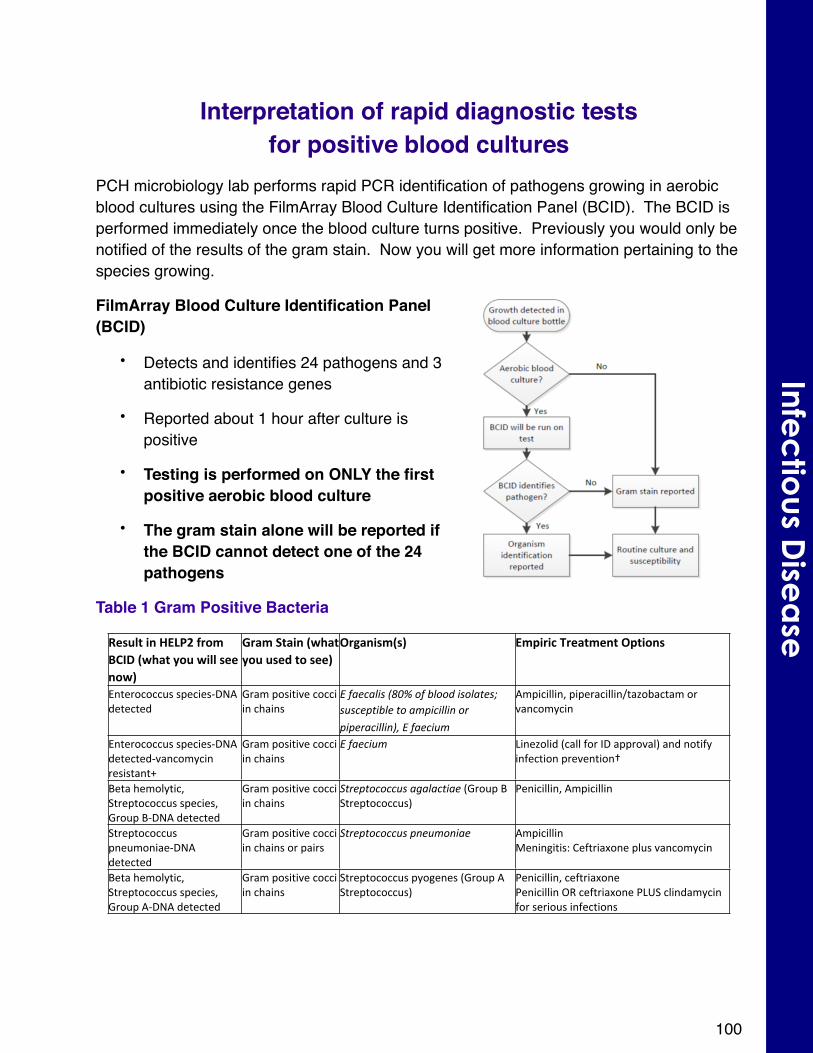
Interpretation of rapid diagnostic tests for positive blood cultures
PCH microbiology lab performs rapid PCR identification of pathogens growing in aerobic blood cultures using the FilmArray Blood Culture Identification Panel (BCID). The BCID is performed immediately once the blood culture turns positive. Previously you would only be notified of the results of the gram stain. Now you will get more information pertaining to the species growing.
FilmArray Blood Culture Identification Panel (BCID)
• Detects and identifies 24 pathogens and 3 antibiotic resistance genes
• Reported about 1 hour after culture is positive
• Testing is performed on ONLY the first positive aerobic blood culture
• The gram stain alone will be reported if the BCID cannot detect one of the 24 pathogens
Table 1 Gram Positive Bacteria
Result'in'HELP2'from'BCID'(what'you'will'see'now)
Gram'Stain'(what'you'used'to'see)
Organism(s) Empiric'Treatment'Options''
Enterococcus#speciesXDNA#detected
Gram#positive#cocci#in#chains
E"faecalis"(80%"of"blood"isolates;"susceptible"to"ampicillin"or"piperacillin),"E"faecium
Ampicillin,#piperacillin/tazobactam#or#vancomycin#
Enterococcus#speciesXDNA#detectedXvancomycin#resistant+
Gram#positive#cocci#in#chains
E"faecium Linezolid#(call#for#ID#approval)#and#notify#infection#prevention†
Beta#hemolytic,#Streptococcus#species,#Group#BXDNA#detected
Gram#positive#cocci#in#chains
Streptococcus"agalactiae#(Group#B#Streptococcus)
Penicillin,#Ampicillin
Streptococcus#pneumoniaeXDNA#detected#
Gram#positive#cocci#in#chains#or#pairs
Streptococcus"pneumoniae AmpicillinMeningitis:#Ceftriaxone#plus#vancomycin#
Beta#hemolytic,#Streptococcus#species,#Group#AXDNA#detected
Gram#positive#cocci#in#chains
Streptococcus#pyogenes#(Group#A#Streptococcus)
Penicillin,#ceftriaxonePenicillin#OR#ceftriaxone#PLUS#clindamycin#for#serious#infections
100
Infec
tious D
isea
se
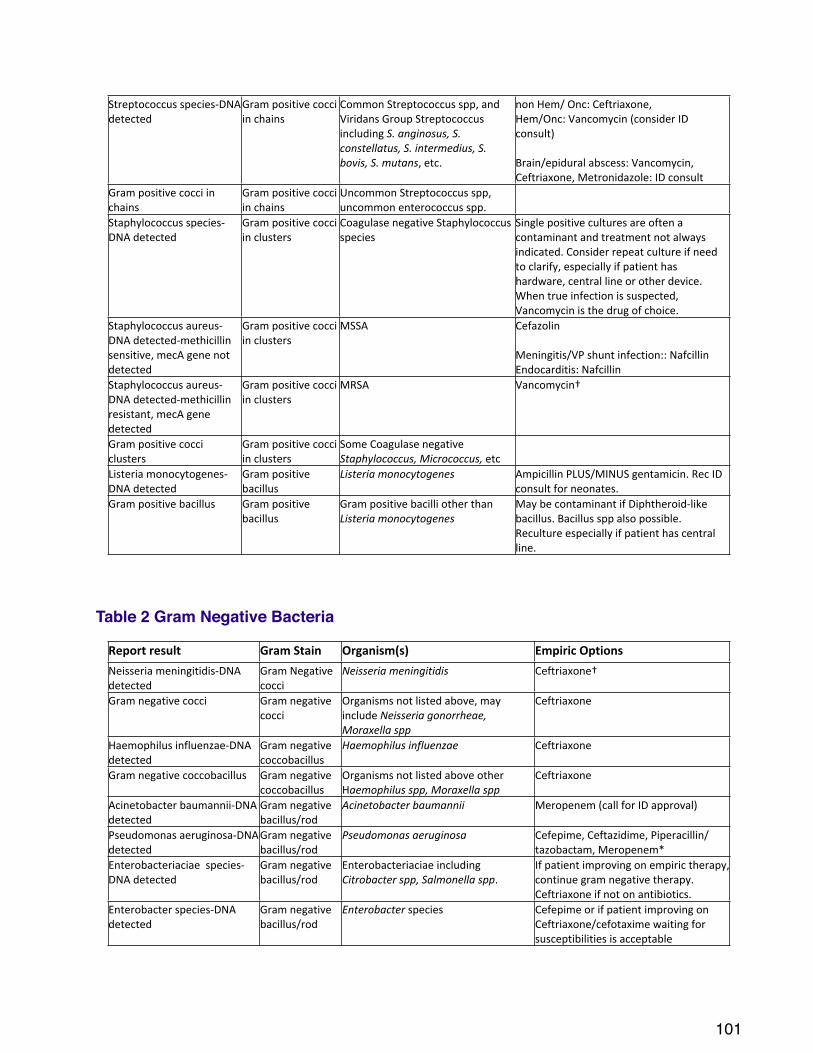
Streptococcus#speciesXDNA#detected
Gram#positive#cocci#in#chains
Common#Streptococcus#spp,#and#Viridans#Group#Streptococcus#including#S."anginosus,"S."constellatus,"S."intermedius,"S."bovis,"S."mutans,#etc.#
non#Hem/#Onc:#Ceftriaxone,#Hem/Onc:#Vancomycin#(consider#ID#consult)
Brain/epidural#abscess:#Vancomycin,#Ceftriaxone,#Metronidazole:#ID#consult
Gram#positive#cocci#in#chains
Gram#positive#cocci#in#chains
Uncommon#Streptococcus#spp,#uncommon#enterococcus#spp.
Staphylococcus#speciesXDNA#detected
Gram#positive#cocci#in#clusters
Coagulase#negative#Staphylococcus#species
Single#positive#cultures#are#often#a#contaminant#and#treatment#not#always#indicated.#Consider#repeat#culture#if#need#to#clarify,#especially#if#patient#has#hardware,#central#line#or#other#device.#When#true#infection#is#suspected,#Vancomycin#is#the#drug#of#choice.
Staphylococcus#aureusXDNA#detectedXmethicillin#sensitive,#mecA#gene#not#detected
Gram#positive#cocci#in#clusters
MSSA Cefazolin#
Meningitis/VP#shunt#infection::#Nafcillin#Endocarditis:#Nafcillin
Staphylococcus#aureusXDNA#detectedXmethicillin#resistant,#mecA#gene#detected
Gram#positive#cocci#in#clusters
MRSA Vancomycin†
Gram#positive#cocci#clusters
Gram#positive#cocci#in#clusters
Some#Coagulase#negative#Staphylococcus,"Micrococcus,#etc
Listeria#monocytogenesXDNA#detected
Gram#positive#bacillus
Listeria"monocytogenes Ampicillin#PLUS/MINUS#gentamicin.#Rec#ID#consult#for#neonates.
Gram#positive#bacillus Gram#positive#bacillus
Gram#positive#bacilli#other#than#Listeria"monocytogenes
May#be#contaminant#if#DiphtheroidXlike#bacillus.#Bacillus#spp#also#possible.##Reculture#especially#if#patient#has#central#line.
Table 2 Gram Negative Bacteria
Report'result Gram'Stain Organism(s) Empiric'OptionsNeisseria#meningitidisXDNA#detected
Gram#Negative#cocci
Neisseria"meningitidis Ceftriaxone†
Gram#negative#cocci Gram#negative#cocci
Organisms#not#listed#above,#may#include#Neisseria"gonorrheae,"Moraxella"spp
Ceftriaxone
Haemophilus#influenzaeXDNA#detected
Gram#negative#coccobacillus
Haemophilus"influenzae Ceftriaxone
Gram#negative#coccobacillus Gram#negative#coccobacillus
Organisms#not#listed#above#other#Haemophilus"spp,"Moraxella"spp
Ceftriaxone
Acinetobacter#baumanniiXDNA#detected
Gram#negative#bacillus/rod
Acinetobacter"baumannii Meropenem#(call#for#ID#approval)
Pseudomonas#aeruginosaXDNA#detected
Gram#negative#bacillus/rod
Pseudomonas"aeruginosa Cefepime,#Ceftazidime,#Piperacillin/tazobactam,#Meropenem*
Enterobacteriaciae##speciesXDNA#detected
Gram#negative#bacillus/rod
Enterobacteriaciae#including#Citrobacter"spp,"Salmonella"spp.#
If#patient#improving#on#empiric#therapy,#continue#gram#negative#therapy.#Ceftriaxone#if#not#on#antibiotics.
Enterobacter#speciesXDNA#detected
Gram#negative#bacillus/rod
Enterobacter#species Cefepime#or#if#patient#improving#on#Ceftriaxone/cefotaxime#waiting#for#susceptibilities#is#acceptable#
101
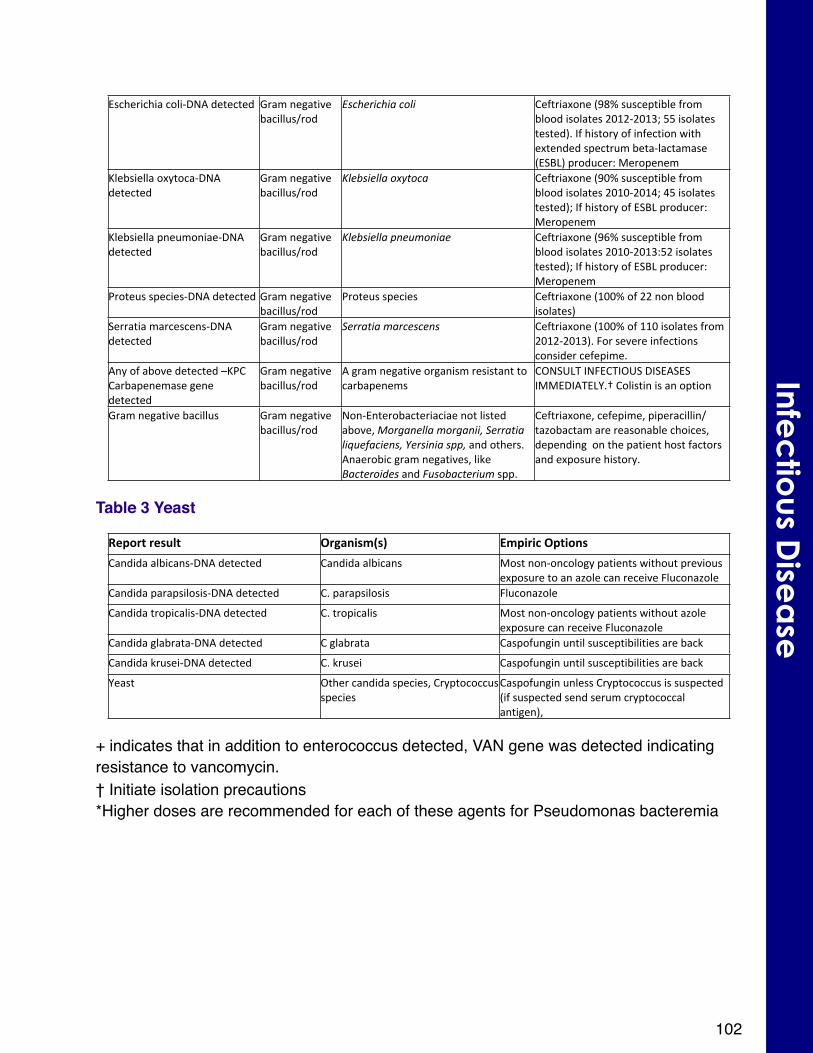
Escherichia#coliXDNA#detected Gram#negative#bacillus/rod
Escherichia"coli Ceftriaxone#(98%#susceptible#from#blood#isolates#2012X2013;#55#isolates#tested).#If#history#of#infection#with#extended#spectrum#betaXlactamase#(ESBL)#producer:#Meropenem
Klebsiella#oxytocaXDNA#detected
Gram#negative#bacillus/rod
Klebsiella"oxytoca Ceftriaxone#(90%#susceptible#from#blood#isolates#2010X2014;#45#isolates#tested);#If#history#of#ESBL#producer:#Meropenem
Klebsiella#pneumoniaeXDNA#detected
Gram#negative#bacillus/rod
Klebsiella"pneumoniae Ceftriaxone#(96%#susceptible#from#blood#isolates#2010X2013:52#isolates#tested);#If#history#of#ESBL#producer:#Meropenem
Proteus#speciesXDNA#detected Gram#negative#bacillus/rod
Proteus#species Ceftriaxone#(100%#of#22#non#blood#isolates)#
Serratia#marcescensXDNA#detected
Gram#negative#bacillus/rod
Serratia"marcescens Ceftriaxone#(100%#of#110#isolates#from#2012X2013).#For#severe#infections#consider#cefepime.
Any#of#above#detected#–KPC#Carbapenemase#gene#detected
Gram#negative#bacillus/rod
A#gram#negative#organism#resistant#to#carbapenems
CONSULT#INFECTIOUS#DISEASES#IMMEDIATELY.†#Colistin#is#an#option
Gram#negative#bacillus Gram#negative#bacillus/rod
NonXEnterobacteriaciae#not#listed#above,#Morganella"morganii,"Serratia"liquefaciens,"Yersinia"spp,#and#others.Anaerobic#gram#negatives,#like#Bacteroides"and"Fusobacterium#spp.
Ceftriaxone,#cefepime,#piperacillin/tazobactam#are#reasonable#choices,#depending##on#the#patient#host#factors#and#exposure#history.
Table 3 Yeast
Report'result Organism(s) Empiric'OptionsCandida#albicansXDNA#detected Candida#albicans Most#nonXoncology#patients#without#previous#
exposure#to#an#azole#can#receive#Fluconazole#Candida#parapsilosisXDNA#detected C.#parapsilosis Fluconazole
Candida#tropicalisXDNA#detected C.#tropicalis Most#nonXoncology#patients#without#azole#exposure#can#receive#Fluconazole
Candida#glabrataXDNA#detected C#glabrata Caspofungin#until#susceptibilities#are#back
Candida#kruseiXDNA#detected C.#krusei Caspofungin#until#susceptibilities#are#back
Yeast Other#candida#species,#Cryptococcus#species
Caspofungin#unless#Cryptococcus#is#suspected#(if#suspected#send#serum#cryptococcal#antigen),#
+ indicates that in addition to enterococcus detected, VAN gene was detected indicating resistance to vancomycin. † Initiate isolation precautions*Higher doses are recommended for each of these agents for Pseudomonas bacteremia
102
Infec
tious D
isea
se
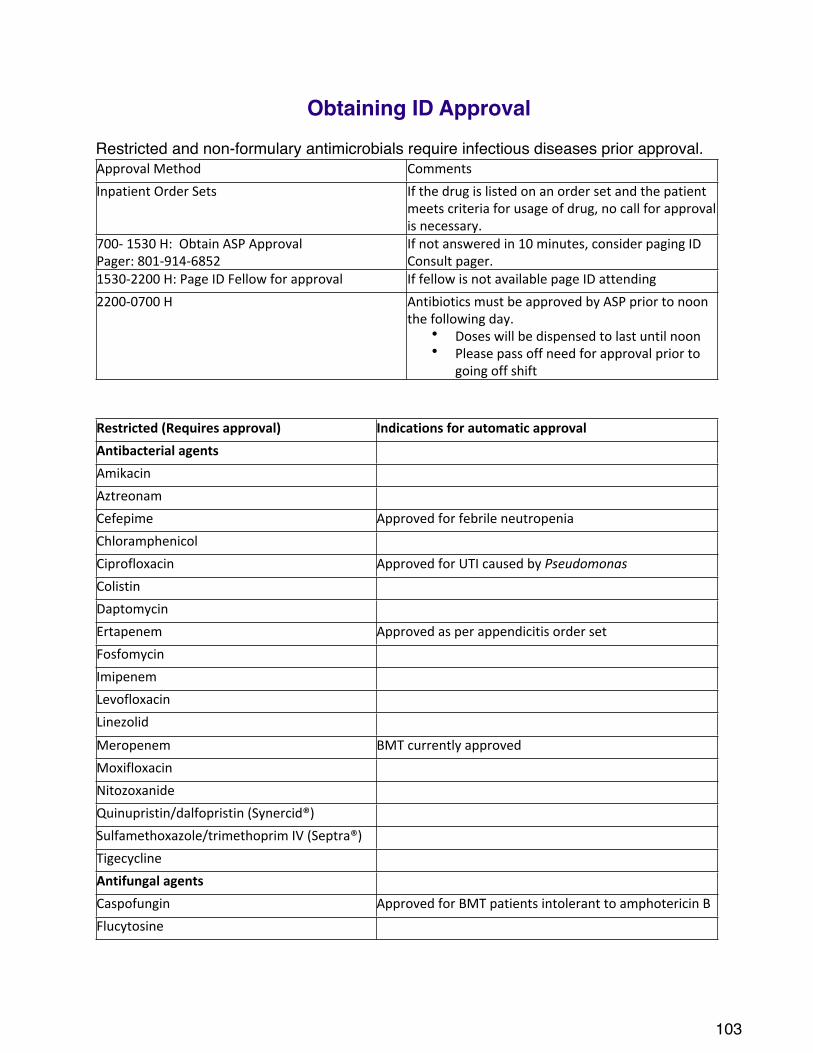
Obtaining ID ApprovalRestricted and non-formulary antimicrobials require infectious diseases prior approval. Approval#Method Comments
Inpatient#Order#Sets If#the#drug#is#listed#on#an#order#set#and#the#patient#meets#criteria#for#usage#of#drug,#no#call#for#approval#is#necessary.
700X#1530#H:##Obtain#ASP#ApprovalPager:#801X914X6852
If#not#answered#in#10#minutes,#consider#paging#ID#Consult#pager.
1530X2200#H:#Page#ID#Fellow#for#approval If#fellow#is#not#available#page#ID#attending
2200X0700#H Antibiotics#must#be#approved#by#ASP#prior#to#noon#the#following#day.
• Doses#will#be#dispensed#to#last#until#noon• Please#pass#off#need#for#approval#prior#to#
going#off#shift#
Restricted$(Requires$approval) Indications$for$automatic$approvalAntibacterial$agentsAmikacin
Aztreonam
Cefepime Approved#for#febrile#neutropenia
Chloramphenicol
Ciprofloxacin Approved#for#UTI#caused#by#PseudomonasColistin
Daptomycin
Ertapenem Approved#as#per#appendicitis#order#set#
Fosfomycin
Imipenem
Levofloxacin
Linezolid
Meropenem BMT#currently#approved
Moxifloxacin
Nitozoxanide
Quinupristin/dalfopristin#(Synercid®)
Sulfamethoxazole/trimethoprim#IV#(Septra®)
Tigecycline
Antifungal$agentsCaspofungin Approved#for#BMT#patients#intolerant#to#amphotericin#B
Flucytosine
103
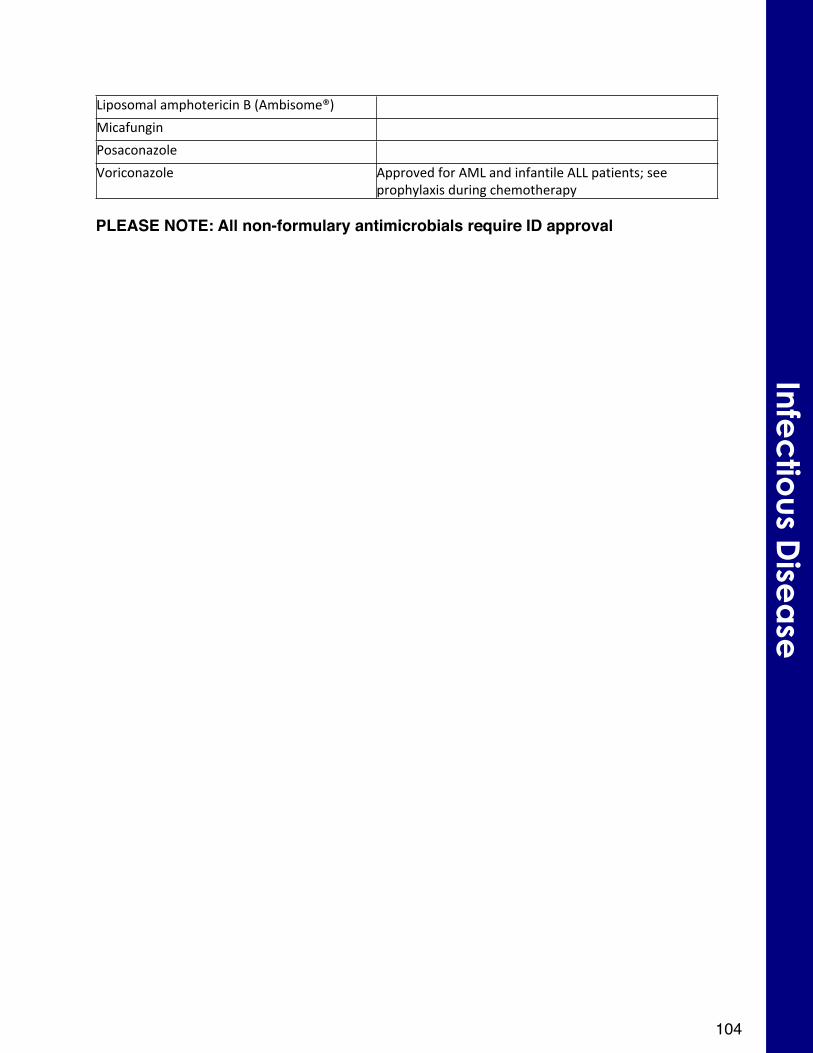
Liposomal#amphotericin#B#(Ambisome®)
Micafungin
Posaconazole
Voriconazole Approved#for#AML#and#infantile#ALL#patients;#see#prophylaxis#during#chemotherapy
PLEASE NOTE: All non-formulary antimicrobials require ID approval
104
Infec
tious D
isea
se
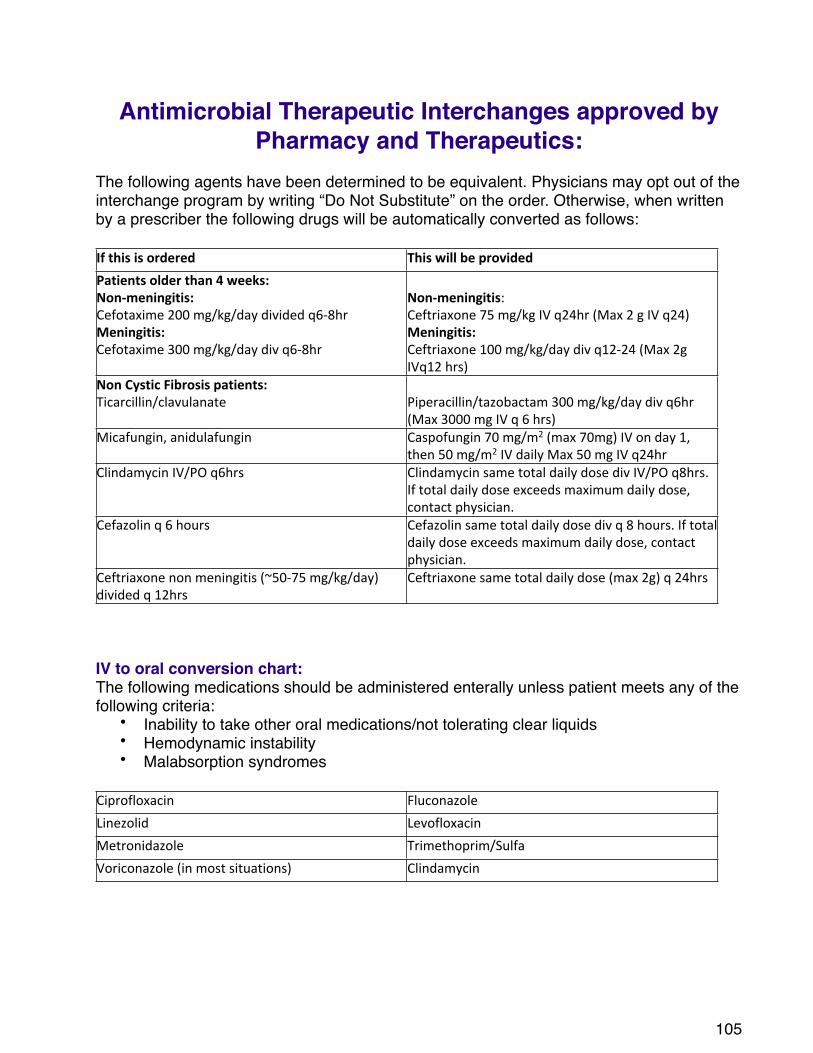
Antimicrobial Therapeutic Interchanges approved by Pharmacy and Therapeutics:
The following agents have been determined to be equivalent. Physicians may opt out of the interchange program by writing “Do Not Substitute” on the order. Otherwise, when written by a prescriber the following drugs will be automatically converted as follows:
If$this$is$ordered This$will$be$providedPatients$older$than$4$weeks:NonXmeningitis:Cefotaxime#200#mg/kg/day#divided#q6X8hrMeningitis:Cefotaxime#300#mg/kg/day#div#q6X8hr
NonXmeningitis:Ceftriaxone#75#mg/kg#IV#q24hr#(Max#2#g#IV#q24)#Meningitis:Ceftriaxone#100#mg/kg/day#div#q12X24#(Max#2g#IVq12#hrs)
Non$Cystic$Fibrosis$patients:Ticarcillin/clavulanate Piperacillin/tazobactam#300#mg/kg/day#div#q6hr#
(Max#3000#mg#IV#q#6#hrs)Micafungin,#anidulafungin Caspofungin#70#mg/m2#(max#70mg)#IV#on#day#1,#
then#50#mg/m2#IV#daily#Max#50#mg#IV#q24hrClindamycin#IV/PO#q6hrs Clindamycin#same#total#daily#dose#div#IV/PO#q8hrs.#
If#total#daily#dose#exceeds#maximum#daily#dose,#contact#physician.
Cefazolin#q#6#hours Cefazolin#same#total#daily#dose#div#q#8#hours.#If#total #daily#dose#exceeds#maximum#daily#dose,#contact#physician.
Ceftriaxone#non#meningitis#(~50X75#mg/kg/day)#divided#q#12hrs
Ceftriaxone#same#total#daily#dose#(max#2g)#q#24hrs
IV to oral conversion chart:The following medications should be administered enterally unless patient meets any of the following criteria:
• Inability to take other oral medications/not tolerating clear liquids• Hemodynamic instability• Malabsorption syndromes
Ciprofloxacin Fluconazole
Linezolid Levofloxacin
Metronidazole Trimethoprim/Sulfa
Voriconazole#(in#most#situations) Clindamycin
105
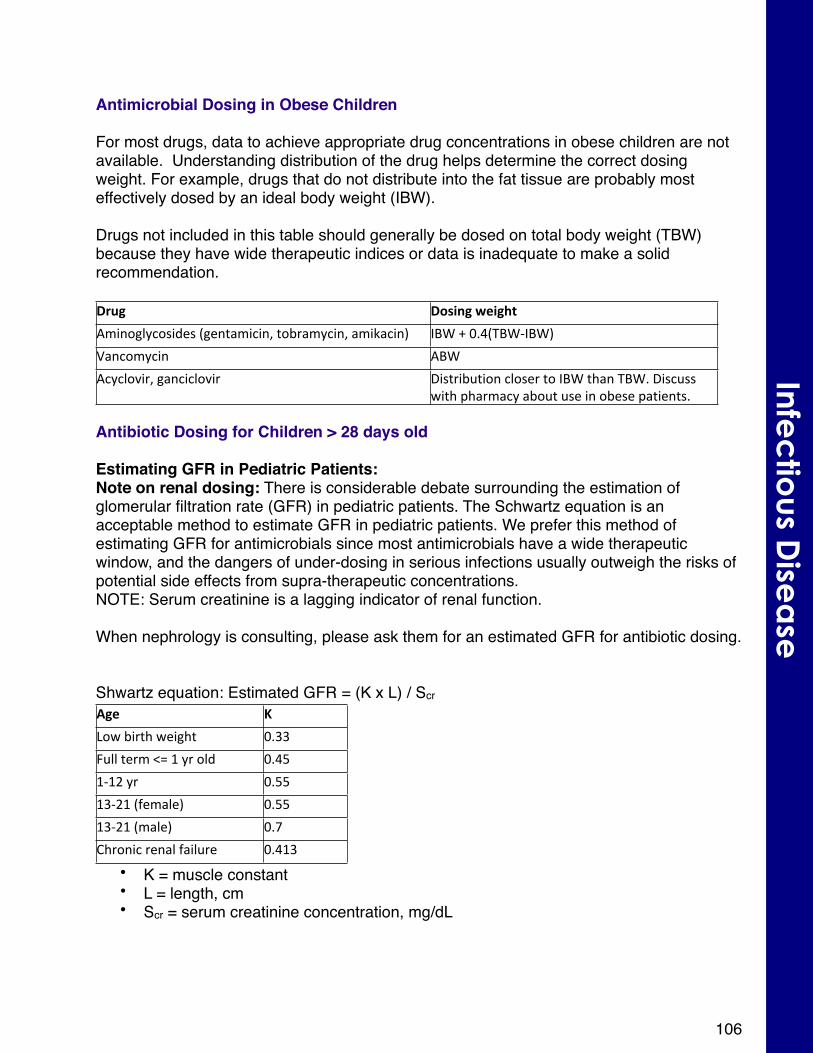
Antimicrobial Dosing in Obese Children
For most drugs, data to achieve appropriate drug concentrations in obese children are not available. Understanding distribution of the drug helps determine the correct dosing weight. For example, drugs that do not distribute into the fat tissue are probably most effectively dosed by an ideal body weight (IBW).
Drugs not included in this table should generally be dosed on total body weight (TBW) because they have wide therapeutic indices or data is inadequate to make a solid recommendation.
Drug Dosing$weightAminoglycosides#(gentamicin,#tobramycin,#amikacin) IBW#+#0.4(TBWXIBW)
Vancomycin ABW
Acyclovir,#ganciclovir Distribution#closer#to#IBW#than#TBW.#Discuss#with#pharmacy#about#use#in#obese#patients.
Antibiotic Dosing for Children > 28 days old
Estimating GFR in Pediatric Patients:Note on renal dosing: There is considerable debate surrounding the estimation of glomerular filtration rate (GFR) in pediatric patients. The Schwartz equation is an acceptable method to estimate GFR in pediatric patients. We prefer this method of estimating GFR for antimicrobials since most antimicrobials have a wide therapeutic window, and the dangers of under-dosing in serious infections usually outweigh the risks of potential side effects from supra-therapeutic concentrations. NOTE: Serum creatinine is a lagging indicator of renal function. When nephrology is consulting, please ask them for an estimated GFR for antibiotic dosing.
Shwartz equation: Estimated GFR = (K x L) / ScrAge KLow#birth#weight 0.33
Full#term#<=#1#yr#old 0.45
1X12#yr 0.55
13X21#(female) 0.55
13X21#(male) 0.7
Chronic#renal#failure 0.413
• K = muscle constant• L = length, cm• Scr = serum creatinine concentration, mg/dL
106
Infec
tious D
isea
se
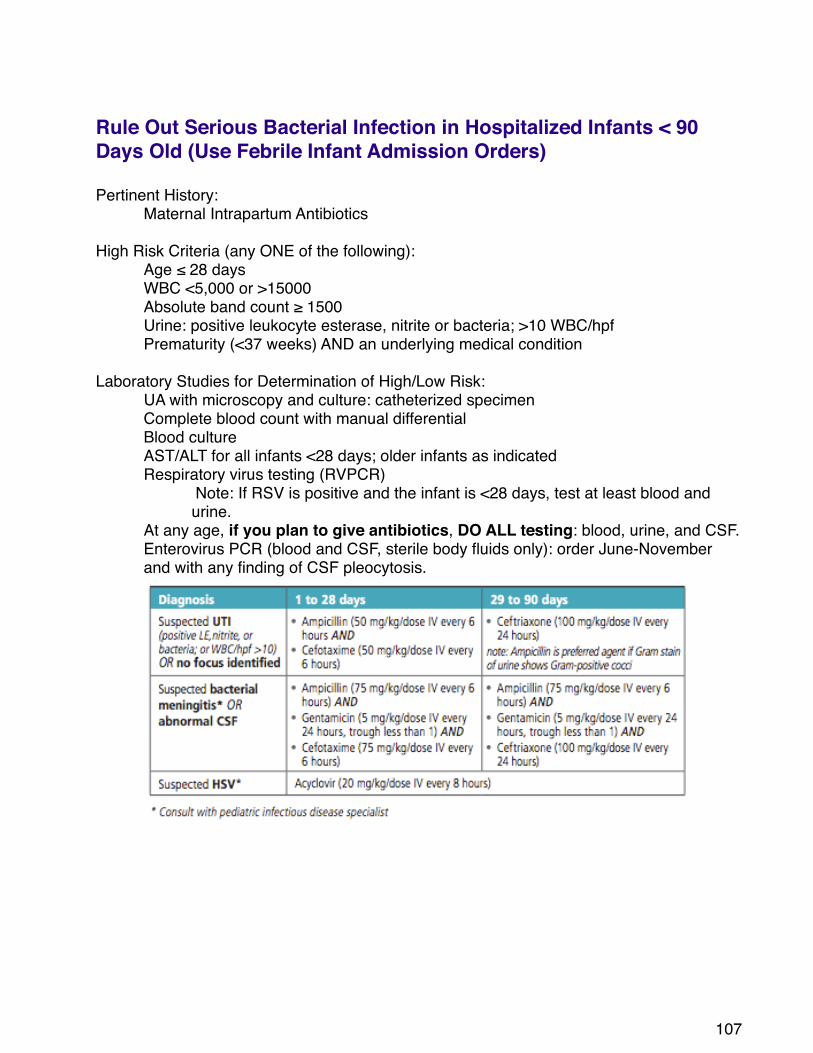
Rule Out Serious Bacterial Infection in Hospitalized Infants < 90 Days Old (Use Febrile Infant Admission Orders)
Pertinent History: ! Maternal Intrapartum Antibiotics
High Risk Criteria (any ONE of the following):! Age ≤ 28 days! WBC <5,000 or >15000! Absolute band count ≥ 1500! Urine: positive leukocyte esterase, nitrite or bacteria; >10 WBC/hpf! Prematurity (<37 weeks) AND an underlying medical condition
Laboratory Studies for Determination of High/Low Risk:! UA with microscopy and culture: catheterized specimen ! Complete blood count with manual differential ! Blood culture
AST/ALT for all infants <28 days; older infants as indicatedRespiratory virus testing (RVPCR)
Note: If RSV is positive and the infant is <28 days, test at least blood and urine.
At any age, if you plan to give antibiotics, DO ALL testing: blood, urine, and CSF.Enterovirus PCR (blood and CSF, sterile body fluids only): order June-November and with any finding of CSF pleocytosis.
107
Antimicrobial Choice:
When to Consider Discharge if Cultures are Negative:! Low Risk (As Defined Above): ! 24h! High Risk and + Viral Studies:! ! 24h! High Risk and – Viral Studies:! ! 36h
This tool is not intended to address neonatal HSV infection/see Febrile Infant CPM for more information. These recommendations do not indicate an exclusive course of treatment or procedure to be followed. Variations, taking into account individual circumstances, may be appropriate.
108
Infec
tious D
isea
se
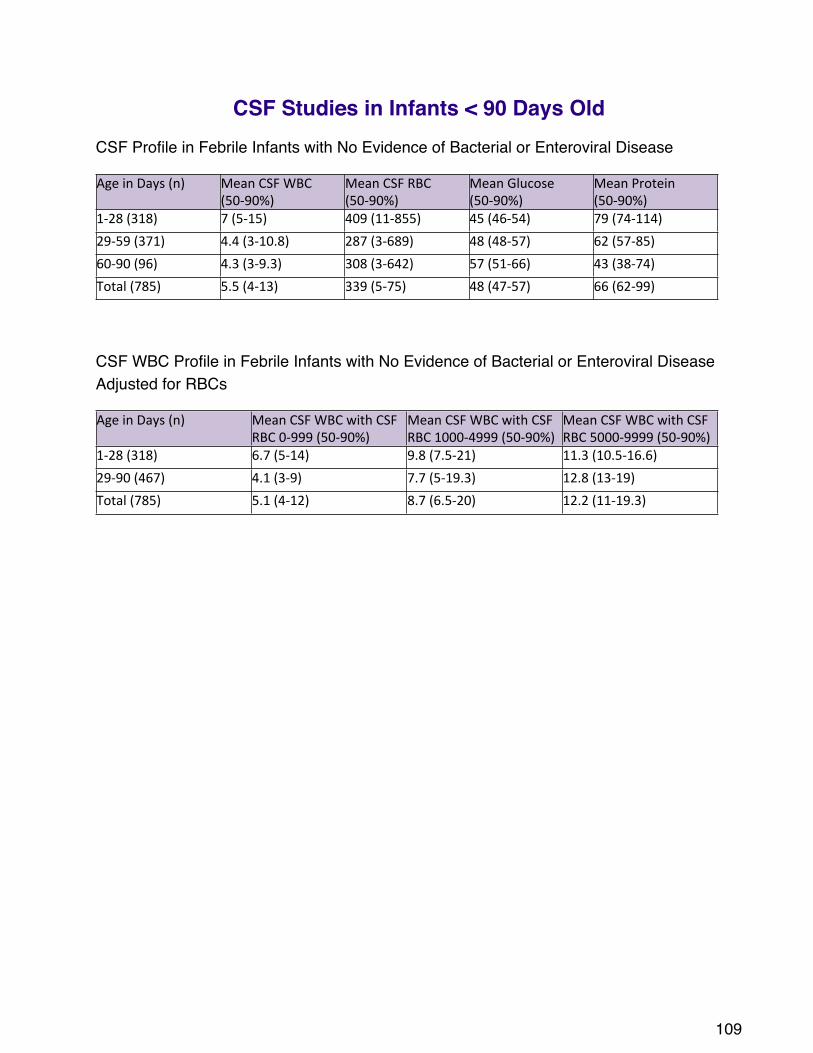
CSF Studies in Infants < 90 Days OldCSF Profile in Febrile Infants with No Evidence of Bacterial or Enteroviral Disease
Age#in#Days#(n) Mean#CSF#WBC#(50X90%)
Mean#CSF#RBC#(50X90%)
Mean#Glucose#(50X90%)
Mean#Protein#(50X90%)
1X28#(318) 7#(5X15) 409#(11X855) 45#(46X54) 79#(74X114)
29X59#(371) 4.4#(3X10.8) 287#(3X689) 48#(48X57) 62#(57X85)
60X90#(96) 4.3#(3X9.3) 308#(3X642) 57#(51X66) 43#(38X74)
Total#(785) 5.5#(4X13) 339#(5X75) 48#(47X57) 66#(62X99)
CSF WBC Profile in Febrile Infants with No Evidence of Bacterial or Enteroviral Disease Adjusted for RBCs
Age#in#Days#(n) Mean#CSF#WBC#with#CSF#RBC#0X999#(50X90%)
Mean#CSF#WBC#with#CSF#RBC#1000X4999#(50X90%)
Mean#CSF#WBC#with#CSF#RBC#5000X9999#(50X90%)
1X28#(318) 6.7#(5X14) 9.8#(7.5X21) 11.3#(10.5X16.6)
29X90#(467) 4.1#(3X9) 7.7#(5X19.3) 12.8#(13X19)
Total#(785) 5.1#(4X12) 8.7#(6.5X20) 12.2#(11X19.3)
109
Skin and Soft Tissue Infections (immunocompetent Host)Cutaneous abscess
Incision and drainage is primary treatment
When to consider adjuvant antibiotics: Severe/extensive disease (multiple lesions, large or deep abscess), rapid progression, associated cellulitis, systemic signs and symptoms of illness, area difficult to drain (face, hand, genitalia, etc), septic phlebitis, immunosuppression, lack of response to I&D alone. Antibiotic regimens: see purulent cellulitis (below)
Cellulitis in clinically stable patients:
Purulent Cellulitis: Purulent drainage or exudates without drainable abscessPathogens: Usually caused by Staphylococcus aureus (MRSA or MSSA)
Empiric Therapy:Oral: Clindamycin 13 mg/kg/dose (max dose 450 mg) po q 8 hr OR Trimethoprim/sulfamethoxazole 6 mg/kg/dose (max 160 – 320 mg = 1-2 DS tablets) po BID
IV: Clindamycin 13 mg/kg/dose (max dose 600 mg) IV q 8 hr (preferred when patient is clinically stable) OR Vancomycin 20 mg/kg/dose IV q 8 hr (target trough >= 10 )
Nonpurulent Cellulitis: No purulence or abscessPathogens: Usually caused by Streptococcus pyogenes (Group A Streptococcus)
Empiric Therapy:Oral: Cephalexin 12.5 mg/kg/dose (max dose 500 mg) po qid OR If Allergy: Clindamycin 13 mg/kg/dose (max dose 450 mg) po q 8 hr
IV: Cefazolin 33mg/kg /dose (max dose 2000 mg) IV q8hr OR IF Allergy: Clindamycin 13 mg/kg/dose (max dose 600 mg) IV q8 hr
Treatment Notes: • Beta hemolytic streptococci remain sensitive to beta lactams. Some isolates (10-20%) resistant to
clindamycin.• Elevate the affected extremity: Promotes gravity drainage of edema and hastens improvement• Improvement of erythema may take days in spite of adequate antibiotics
Oral SwitchWhen fever, warmth, edema have decreased substantially in uncomplicated cases consider switching to oral therapy.
Duration10 days of total therapy is generally adequate for uncomplicated cellulitis
References: Liu C et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of Methicillin-Resistant Staphylococcus aureus infections in adults and children. CID. 2011;52:1-38. Stevens DL et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. CID. 2005;41:1373-406.Lawrence HS, Nopper AJ. Superficial bacterial skin infections and cellulitis. In: Long SS et al. Principles and practice of pediatric infectious diseases, 4th edition. New York: Saunders ;2012:427-435.
110
Infec
tious D
isea
se
Bone and Joint Infection greater than 3 months oldObtain a blood culture prior to starting antibiotics. If patient is stable and drainage procedure/culture is planned, hold antibiotics until cultures are obtained.
Immunocompetent patient < 3 yrs of age immunized against H. fluPathogens: Staphylococcus aureus, Kingella kingae
Empiric therapy: •Preferred: Cefazolin 33 mg/kg/dose (max 2g) IV q 8hrs •Alternative: Clindamycin 13 mg/kg/dose (max 600 mg) IV q8 hrs (no activity against Kingella kingae)•Non-immunized: consider addition of H flu coverage: add Ceftriaxone 100 mg/kg/dose (max 4 g) IV q 24 hours to clindamycin
Immunocompetent patient >3 yrs of agePathogens: Staphylococcus aureus (mostly)
Empiric therapy:• Cefazolin 33 mg/kg (max 2 g) IV q 8hrs
OR • Clindamycin 13 mg/kg (max 600 mg) IV q 8hrs
CLINICAL NOTE: If the patient has been colonized with Methicillin resistant Staphylococcus aureus susceptible to clindamycin, consider empiric clindamycin
In Life-Threatening Disease, consider vancomycin (see dosing of vancomycin) +/- cefazolin 33 mg/kg/dose (max 2 g) IV q8hrs.
Patients with Sickle Cell DiseasePathogens: Staphylococcus aureus, Salmonella spp
Empiric Therapy:• Clindamycin 13 mg/kg (max 600 mg) IV q 8hrs! PLUS• Ceftriaxone 75 mg/kg/dose (max 2 g) IV q 24 hours
Sexually active patients
Add Ceftriaxone 75 mg/kg/dose to your empiric therapy to cover N.gonorrhoea. In this case, DO NOT use cefazolin as double cephalosporin therapy may cause more side effects.
Immunocompromized patients require broader coverage. Consult ID.
References:Gutierrez K. Osteomyelitis. In: Long SS et al. Principles and practice of pediatric infectious diseases, 4th edition. New York: Saunders ;2012:469-477. Gutierrez K. Infectious and inflammatory arthritis. In: Long SS et al. Principles and practice of pediatric infectious diseases, 4th edition. New York: Saunders ;2012:469-477.
111
Community Acquired Pneumonia: > 3 months old and Immunocompetent
Pathogens: Streptococcus pneumoniae
Empiric therapy: • Preferred, tolerating oral and not already received amoxicillin: amoxicillin 30 mg/kg/dose
(max 1 g) po tid• Preferred: Ampicillin 50 mg/kg/dose (max 2 g) IV q 6 hours • Allergy: Clindamycin 13 mg/kg/dose (max 600 mg) IV q8 hrs • Non-immunized for Haemophilus influenzae: consider ceftriaxone 75 mg/kg/dose (max 2 g)
IV q24 addition of H flu coverage. If blood culture is not positive, may transition back to amoxicillin oral. Oral amoxicillin is better than any other oral beta lactam
• Duration: 7-10 days of treatment
If atypical pneumonia is suspected/confirmedPathogens: Mycoplasma pneumoniae, Chlamydophila pneumoniae
Empiric therapy: azithromycin 10 mg/kg/dose (max 500 mg) po daily x 3 days
For more information refer to the care process model: https://intermountainhealthcare.org/ext/Dcmnt?ncid=522578601
112
Infec
tious D
isea
se
Lateral neck infections: > 3 months old and Immunocompetent
Pathogens: Staphylococcus aureus and Streptococcus pyogenes
Empiric therapy: • Clindamycin 13 mg/kg/dose (max 600 mg) IV/PO q 8 hours• Allergy: ampicillin/sulbactam 50 mg/kg/dose (max 2 g ampicillin) IV q 6 hours
Tailor antibiotics to culture/susceptibilities if available
For more information refer to the care process model
Suspected retropharyngeal abscess: > 3 months old and ImmunocompetentPathogens: Streptococcus pyogenes, anaerobes, Staphylococcus aureus
Empiric therapy: • Ampicillin/sulbactam 50 mg/kg/dose (max 2g ampicillin) IV q 6 hours
• Allergy: clindamycin 13 mg/kg/dose (max 600 mg) IV/PO q 8 hours
Tailor antibiotic to culture/susceptibility if available
For more information refer to care process models
113
Clostridium difficile infection (CDI)! Symptoms:
• Diarrhea that is severe (> 3 stools/day), prolonged (>5 days) or unexplained by other causes (viral, bacterial gastroenteritis, laxatives, oral contrast, etc.)
“Atypical” C difficile:• Little or no diarrhea• Ileus or Toxic megacolon• May resemble acute abdomen (abdominal pain, fever, elevated inflammatory
markers)• Unexplained neutrophilia without prominent abdominal symptoms• Cystic fibrosis with signs of inflammation and abdominal tenderness
! Testing:• Testing of children younger than one to two years of age should
generally be avoided, given the high rate of asymptomatic carriage in this age group and the relative rarity of severe C. difficile disease
• Only loose, watery, or semi-formed stool should be tested (exception for atypical disease with ileus).
• There is no indication for a Test of Cure at the end of therapy• Testing is not indicated in asymptomatic patients
! Treatment:• Discontinue therapy with the inciting antimicrobial agent(s) as soon as
possible• In mild cases without systemic signs, C. difficile-associated diarrhea often
resolves with discontinuation of the inducing antibiotic(s) and institution of supportive measures
• Relapse/reinfection rate 15% - 30% independent of drug• Response to treatment: with mild disease, clinical improvement in 24-48
hours, 4-6 days for resolution of diarrhea • The time to resolution of diarrhea might be shorter with vancomycin than with
metronidazole therapy
114
Infec
tious D
isea
se
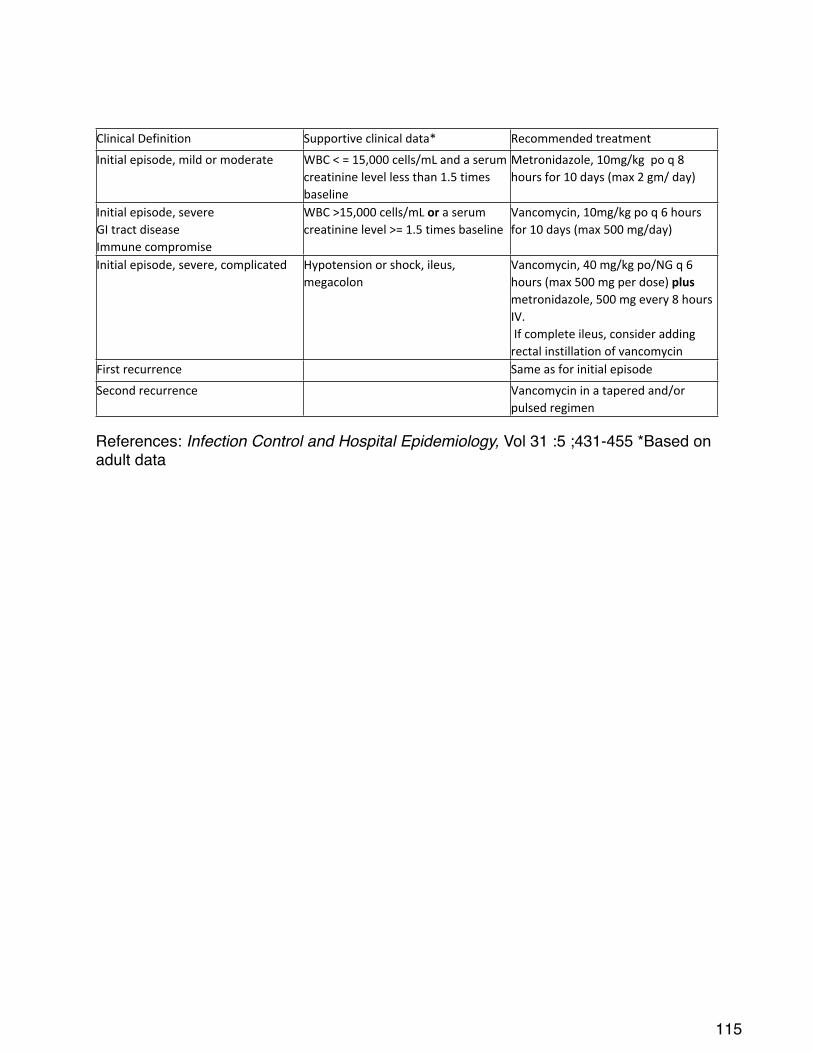
Clinical#Definition Supportive#clinical#data* Recommended#treatment
Initial#episode,#mild#or#moderate WBC#<#=#15,000#cells/mL#and#a#serum#creatinine#level#less#than#1.5#times#baseline
Metronidazole,#10mg/kg##po#q#8#hours#for#10#days#(max#2#gm/#day)
Initial#episode,#severeGI#tract#diseaseImmune#compromise
WBC#>15,000#cells/mL#or#a#serum#creatinine#level#>=#1.5#times#baseline
Vancomycin,#10mg/kg#po#q#6#hours#for#10#days#(max#500#mg/day)
Initial#episode,#severe,#complicated Hypotension#or#shock,#ileus,#megacolon
Vancomycin,#40#mg/kg#po/NG#q#6#hours#(max#500#mg#per#dose)#plus#metronidazole,#500#mg#every#8#hours#IV.#If#complete#ileus,#consider#adding#rectal#instillation#of#vancomycin
First#recurrence Same#as#for#initial#episode
Second#recurrence Vancomycin#in#a#tapered#and/or#pulsed#regimen
References: Infection Control and Hospital Epidemiology, Vol 31 :5 ;431-455 *Based on adult data
115
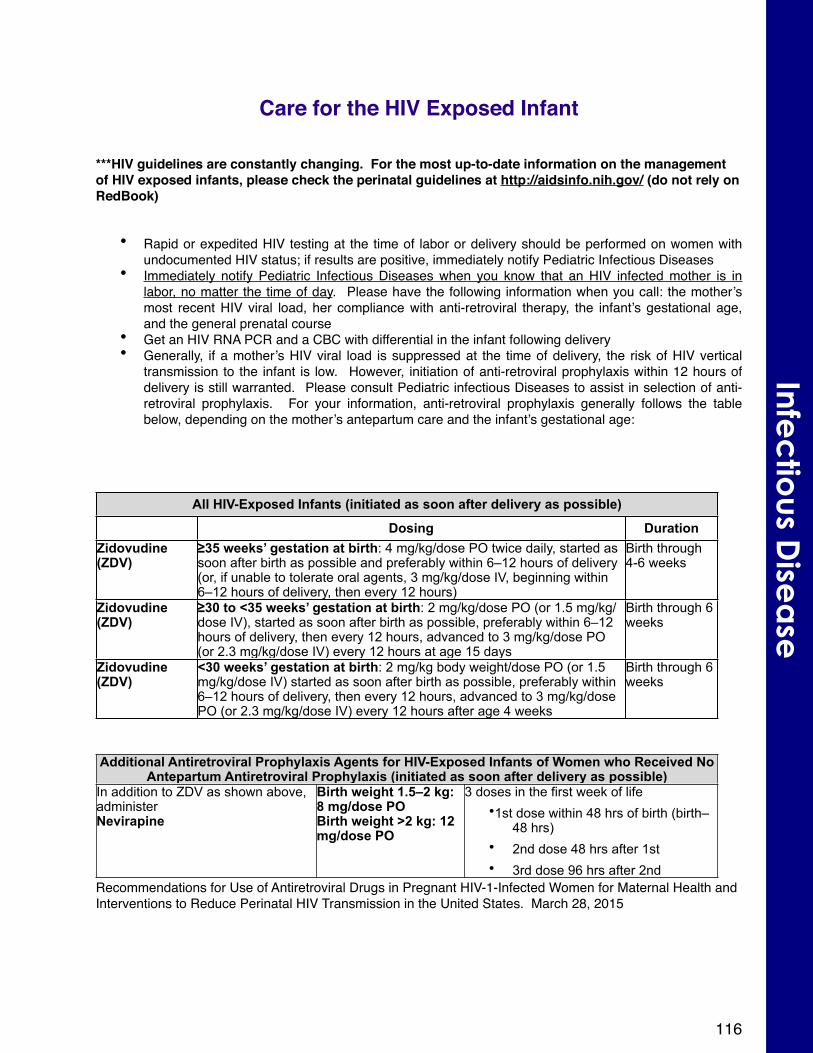
Care for the HIV Exposed Infant
***HIV guidelines are constantly changing. For the most up-to-date information on the management of HIV exposed infants, please check the perinatal guidelines at http://aidsinfo.nih.gov/ (do not rely on RedBook)
• Rapid or expedited HIV testing at the time of labor or delivery should be performed on women with undocumented HIV status; if results are positive, immediately notify Pediatric Infectious Diseases
• Immediately notify Pediatric Infectious Diseases when you know that an HIV infected mother is in labor, no matter the time of day. Please have the following information when you call: the mother’s most recent HIV viral load, her compliance with anti-retroviral therapy, the infant’s gestational age, and the general prenatal course
• Get an HIV RNA PCR and a CBC with differential in the infant following delivery• Generally, if a mother’s HIV viral load is suppressed at the time of delivery, the risk of HIV vertical
transmission to the infant is low. However, initiation of anti-retroviral prophylaxis within 12 hours of delivery is still warranted. Please consult Pediatric infectious Diseases to assist in selection of anti-retroviral prophylaxis. For your information, anti-retroviral prophylaxis generally follows the table below, depending on the mother’s antepartum care and the infant’s gestational age:
All HIV-Exposed Infants (initiated as soon after delivery as possible)All HIV-Exposed Infants (initiated as soon after delivery as possible)All HIV-Exposed Infants (initiated as soon after delivery as possible)
Dosing DurationZidovudine (ZDV)
≥35 weeks’ gestation at birth: 4 mg/kg/dose PO twice daily, started as soon after birth as possible and preferably within 6–12 hours of delivery (or, if unable to tolerate oral agents, 3 mg/kg/dose IV, beginning within 6–12 hours of delivery, then every 12 hours)
Birth through 4-6 weeks
Zidovudine (ZDV)
≥30 to <35 weeks’ gestation at birth: 2 mg/kg/dose PO (or 1.5 mg/kg/dose IV), started as soon after birth as possible, preferably within 6–12 hours of delivery, then every 12 hours, advanced to 3 mg/kg/dose PO (or 2.3 mg/kg/dose IV) every 12 hours at age 15 days
Birth through 6 weeks
Zidovudine (ZDV)
<30 weeks’ gestation at birth: 2 mg/kg body weight/dose PO (or 1.5 mg/kg/dose IV) started as soon after birth as possible, preferably within 6–12 hours of delivery, then every 12 hours, advanced to 3 mg/kg/dose PO (or 2.3 mg/kg/dose IV) every 12 hours after age 4 weeks
Birth through 6 weeks
Additional Antiretroviral Prophylaxis Agents for HIV-Exposed Infants of Women who Received No Antepartum Antiretroviral Prophylaxis (initiated as soon after delivery as possible)
Additional Antiretroviral Prophylaxis Agents for HIV-Exposed Infants of Women who Received No Antepartum Antiretroviral Prophylaxis (initiated as soon after delivery as possible)
Additional Antiretroviral Prophylaxis Agents for HIV-Exposed Infants of Women who Received No Antepartum Antiretroviral Prophylaxis (initiated as soon after delivery as possible)
In addition to ZDV as shown above, administerNevirapine
Birth weight 1.5–2 kg: 8 mg/dose POBirth weight >2 kg: 12 mg/dose PO
3 doses in the first week of life•1st dose within 48 hrs of birth (birth–
48 hrs)• 2nd dose 48 hrs after 1st• 3rd dose 96 hrs after 2nd
Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. March 28, 2015
116
Infec
tious D
isea
se
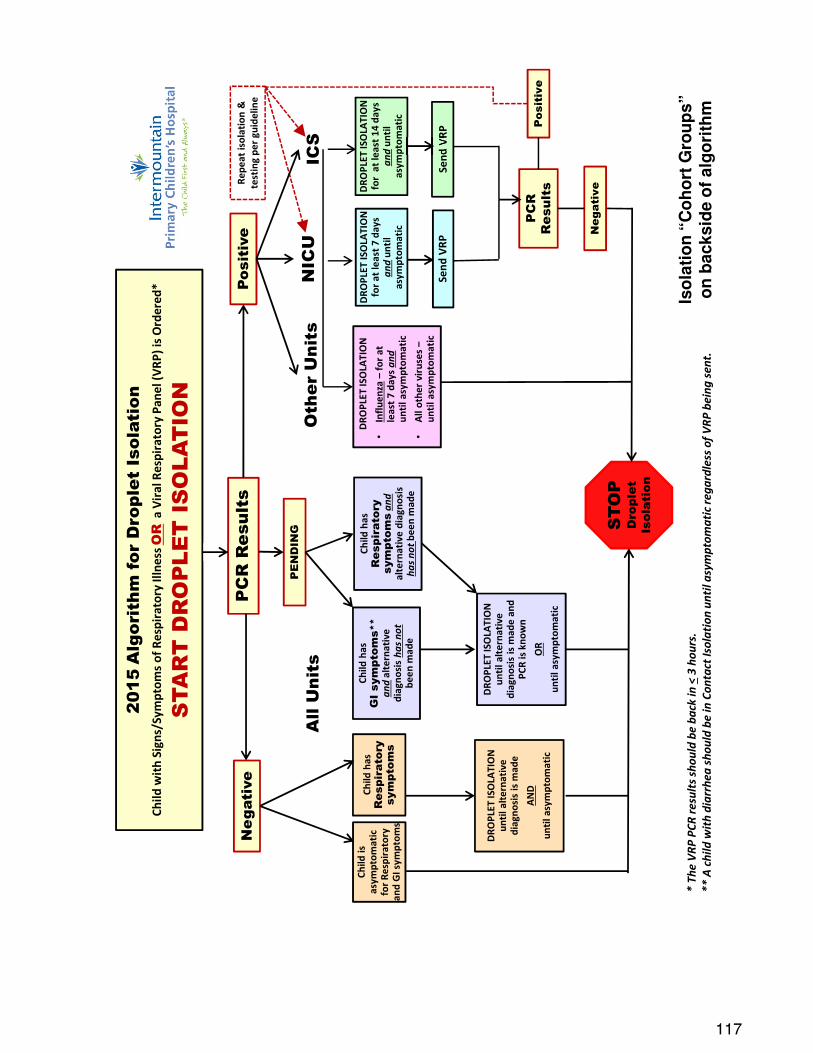
117
2015
Alg
orit
hm fo
r D
ropl
et I
sola
tion
Child
wit
h Si
gns/
Sym
ptom
s of
Res
pira
tory
Illn
ess O
Ra
Vir
al R
espi
rato
ry P
anel
(VRP
) is
Ord
ered
*
STA
RT
DR
OP
LET
IS
OLA
TIO
N
Child
has
GI
sym
ptom
s**
an
dal
tern
ativ
e di
agno
sis
has n
otbe
enm
ade
Child
has
R
espi
rato
ry
sym
ptom
san
dal
tern
ativ
e di
agno
sis
has n
ot b
een
mad
e
DRO
PLET
ISO
LATI
ON
un
til a
lter
nati
ve
diag
nosi
s is
mad
e an
d PC
R is
kno
wn
OR
unti
l asy
mpt
omat
ic
DRO
PLET
ISO
LATI
ON
fo
r at
leas
t 7 d
ays
and
unti
l as
ympt
omat
ic
Send
VRP
DRO
PLET
ISO
LATI
ON
fo
r a
t lea
st 1
4 da
ys
and
unti
l as
ympt
omat
ic
Send
VRP
PC
R R
esul
ts
ICS
NIC
U
Iso
lati
on
“C
oh
ort
Gro
up
s”
on
backsid
e o
f alg
ori
thm
Posi
tive
Neg
ativ
e
* Th
e VR
P PC
R re
sults
shou
ld b
e ba
ck in
<3
hour
s.**
A ch
ild w
ith d
iarr
hea
shou
ld b
e in
Con
tact
Isol
atio
n un
til a
sym
ptom
atic
rega
rdle
ss o
f VRP
bei
ng se
nt.
PC
RR
esul
ts
Child
is
asym
ptom
atic
fo
r Re
spir
ator
y an
d G
I sym
ptom
s
PE
ND
ING
DRO
PLET
ISO
LATI
ON
•In
fluen
za–
for
at
leas
t 7
days
and
unti
l asy
mpt
omat
ic
•A
ll ot
her
viru
ses
–un
til a
sym
ptom
atic
Oth
er U
nits
STO
PD
ropl
et
Isol
atio
n
All
Uni
ts
Child
has
R
espi
rato
ry
sym
ptom
s
DRO
PLET
ISO
LATI
ON
un
til a
lter
nati
ve
diag
nosi
s is
mad
e
AN
D
unti
l asy
mpt
omat
ic
Neg
ativ
e
Pos
itiv
e
Repe
at is
olat
ion
&
test
ing
per
guid
elin
e
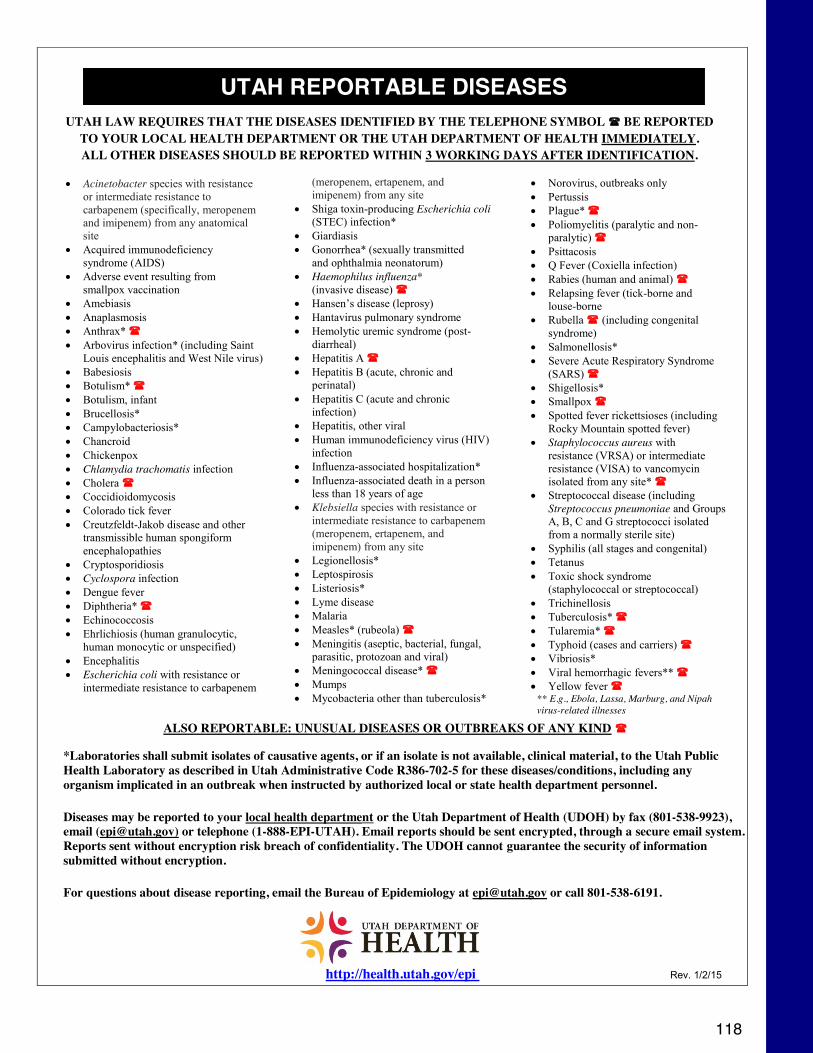
118
UTAH LAW REQUIRES THAT THE DISEASES IDENTIFIED BY THE TELEPHONE SYMBOL BE REPORTED TO YOUR LOCAL HEALTH DEPARTMENT OR THE UTAH DEPARTMENT OF HEALTH IMMEDIATELY. ALL OTHER DISEASES SHOULD BE REPORTED WITHIN 3 WORKING DAYS AFTER IDENTIFICATION.
ALSO REPORTABLE: UNUSUAL DISEASES OR OUTBREAKS OF ANY KIND
*Laboratories shall submit isolates of causative agents, or if an isolate is not available, clinical material, to the Utah Public Health Laboratory as described in Utah Administrative Code R386-702-5 for these diseases/conditions, including any organism implicated in an outbreak when instructed by authorized local or state health department personnel.
Diseases may be reported to your local health department or the Utah Department of Health (UDOH) by fax (801-538-9923), email ([email protected]) or telephone (1-888-EPI-UTAH). Email reports should be sent encrypted, through a secure email system. Reports sent without encryption risk breach of confidentiality. The UDOH cannot guarantee the security of information submitted without encryption.
For questions about disease reporting, email the Bureau of Epidemiology at [email protected] or call 801-538-6191.
http://health.utah.gov/epi Rev. 1/2/15
UTAH REPORTABLE DISEASES
x Acinetobacter species with resistance or intermediate resistance to carbapenem (specifically, meropenem and imipenem) from any anatomical site
x Acquired immunodeficiency syndrome (AIDS)
x Adverse event resulting from smallpox vaccination
x Amebiasis x Anaplasmosis x Anthrax* x Arbovirus infection* (including Saint
Louis encephalitis and West Nile virus) x Babesiosis x Botulism* x Botulism, infant x Brucellosis* x Campylobacteriosis* x Chancroid x Chickenpox x Chlamydia trachomatis infection x Cholera x Coccidioidomycosis x Colorado tick fever x Creutzfeldt-Jakob disease and other
transmissible human spongiform encephalopathies
x Cryptosporidiosis x Cyclospora infection x Dengue fever x Diphtheria* x Echinococcosis x Ehrlichiosis (human granulocytic,
human monocytic or unspecified) x Encephalitis x Escherichia coli with resistance or
intermediate resistance to carbapenem
x Norovirus, outbreaks only x Pertussis x Plague* x Poliomyelitis (paralytic and non-
paralytic) x Psittacosis x Q Fever (Coxiella infection) x Rabies (human and animal) x Relapsing fever (tick-borne and
louse-borne x Rubella (including congenital
syndrome) x Salmonellosis* x Severe Acute Respiratory Syndrome
(SARS) x Shigellosis* x Smallpox x Spotted fever rickettsioses (including
Rocky Mountain spotted fever) x Staphylococcus aureus with
resistance (VRSA) or intermediate resistance (VISA) to vancomycin isolated from any site*
x Streptococcal disease (including Streptococcus pneumoniae and Groups A, B, C and G streptococci isolated from a normally sterile site)
x Syphilis (all stages and congenital) x Tetanus x Toxic shock syndrome
(staphylococcal or streptococcal) x Trichinellosis x Tuberculosis* x Tularemia* x Typhoid (cases and carriers) x Vibriosis* x Viral hemorrhagic fevers** x Yellow fever
** E.g., Ebola, Lassa, Marburg, and Nipah virus-related illnesses
(meropenem, ertapenem, and imipenem) from any site
x Shiga toxin-producing Escherichia coli (STEC) infection*
x Giardiasis x Gonorrhea* (sexually transmitted
and ophthalmia neonatorum) x Haemophilus influenza*
(invasive disease) x Hansen’s disease (leprosy) x Hantavirus pulmonary syndrome x Hemolytic uremic syndrome (post-
diarrheal) x Hepatitis A x Hepatitis B (acute, chronic and
perinatal) x Hepatitis C (acute and chronic
infection) x Hepatitis, other viral x Human immunodeficiency virus (HIV)
infection x Influenza-associated hospitalization* x Influenza-associated death in a person
less than 18 years of age x Klebsiella species with resistance or
intermediate resistance to carbapenem (meropenem, ertapenem, and imipenem) from any site
x Legionellosis* x Leptospirosis x Listeriosis* x Lyme disease x Malaria x Measles* (rubeola) x Meningitis (aseptic, bacterial, fungal,
parasitic, protozoan and viral) x Meningococcal disease* x Mumps x Mycobacteria other than tuberculosis*

119
120
Neonatology

121
Cardiopulmonary status, urine output, and serum sodium values guide daily fluid
orders. Generally, fluids are ordered to start at 60-100 ml/kg/day, depending on
gestational age, and are increased daily by 20 ml/kg/day towards a maximum of 150
ml/kg/day. The daily caloric goal is 90 (TPN) or 120 Kcal/kg/day (enteral) or more if
not gaining. The weight gain goal is to regain birth weight by 7 (term) to 14 days
(preterm). Thereafter weekly weight gain should average about 15 g/kg/day for
infants < 2.0 kg and 20-30 g/day for infants > 2.0 kg.
Birth weight is used for reference until it is regained after which current weight or a
reference weight (estimated dry weight if edematous) is used. A higher caloric
intake or reference weight may be needed for some IUGR infants.
LINES:
UAC distance: (body weight (kg) x 3) + 9
HIGH PLACEMENT: T6-T8 (above celiac, SMA, and renal arteries) LOW
PLACEMENT: L3-L4
UVC distance: (UAC length/2) + 1
UVC PLACEMENT: In IVC, above the diaphragm, ideally around T9
Total Parenteral Nutrition (TPN)
Protein: Trophamine or Premasol (10% = 10 g/100 ml) are used for infants < 10 kg.
These solutions have AA essential for premature infants (aspartate, glutamate,
taurine, tyrosine) and lesser amounts of methionine, glycine, and phenylalanine. A
minimum of 1.5 g/kg/day and 40 Kcal/kg is needed to prevent a negative nitrogen
balance. Protein provides 4.0 Kcal/gm. Preterms need 3.5-4.5 g/kg/day (more if
younger gestation); term ~ 3.0 g/kg/day). Protein should be limited in renal failure.
Carbohydrate: 10% dextrose (10 gm/100ml) supplies 3.4 Kcal/g or 0.34 Kcal/ml.
Preterm glucose utilization varies from 5 to 8 mg/kg/min (term is 3 to 5 mg/kg/min).
The glucose infusion rate (GIR) in mg/kg/min = % glucose x (ml/kg/day) / 144. From
122
Ne
ona
tolo
gy
Fluids, Feedings and Electrolytes
this, the needed % glucose can be calculated depending on the desired fluid intake.
The GIR may be increased up to 8-10 mg/kg/min to improve caloric intake keeping
the maximum serum glucose < 140 mg/dl (practice varies).
Fat: intralipid (20% = 20 g/100 ml) is made from soybean oil, egg yolk phospholipids,
glycerin and water and is supplies essential FA (linoleic and linolenic) as well as
oleic, palmitic, and stearic FA. Fat provides 9 kcal/g or 2.2 Kcal/ml of 20% intralipid.
A minimum of 0.5 gm/kg/day is needed to prevent a deficiency of essential FA. A
normal lipid infusion rate of 0.5-3 gm/kg/day is calculated:
Desired gm/kg/day ÷ concentration (20 g/100 ml) x weight (kg) ÷ 24 (hr) = ml/hr
Carnitine: Plays an essential role in transferring long-chain FA across the
mitochondria for beta-oxidation. Infants < 32 weeks/1500 g are at risk for deficiency
due to ↓stores,
↓synthesis, and ↑lipid needs for growth. It is often added to TPN in the first week at
15 mg/kg/day particularly if hypertriglyceridemia is present.
123
Component kcal/kg/day calculations 2.0 kg premie receiving 10%
dextrose at 140 ml/kg/ day, 20% intralipid at 3 gm/kg/day, and
trophamine at 3 gm/kg/day:
Kcal/kg/day (carbohydrate) = 10 g/100 ml x 140 ml/kg/day x 3.4 kcal/g =
47.6 kcal/kg/ day
Kcal/kg/day (fat) = 30 ml/day x 2.2 kcal/ml / weight in kg = 33 kcal/kg/
day Kcal/kg/day (protein) = 3 g/kg/day x 4 kcal/g = 12 kcal/kg/day =
92.6 kcal/kg/day TOTAL
Protein/dextrose solutions are ordered on admission with infants <
1500 g or < 32 weeks starting on 2% Premasol + D10 via PIV or UVC
and 3.2% Premasol (NO glucose) via UAC, at total intake of 80-100 ml/
kg/d.Larger, older infants are started on D10 without protein at 60 ml/kg/
d. Glucose levels are checked hourly until stable and the GIR is
adjusted as needed to keep the glucose > 40. Depending on time of
birth, TPN orders may be initiated on either day 1 or 2 for all infants not
expected to achieve full enteral feedings within 48 hours. OInitial TPN
is generally written to provide 3 gm/kg protein and 1-2 gm/kg lipid with
% glucose based on GIR goal and fluid intake rate. Day 2 TPN orders
generally increase the GIR by 1 mg/kg/ min, protein to maximum intake
by gestation, and the lipid by 1 gm/kg/day. ELBW infants may return
abnormally high glucose and triglyceride levels even on minimal
intakes, so often are started low and advanced more slowly based on
tolerances. Daily labs are common for the initial 3-4 days while
increasing TPN content.
124
Ne
ona
tolo
gy
TPN monitoring and critical values (labs)
Glucose – The glucose should be checked daily until stable and while making changes in dextrose concentration. Thereafter, based on attending preference Hypoglycemia (< 40 g/dl) is managed with an IV bolus (2 ml/kg D10W) and an increase in the infusion rate (of 20 ml/kg) or % dextrose with a follow up glucose check within 30-60 minutes. Hyperglycemia (> 145 g/dl) is managed with a decrease in the infusion rate or % dextrose (never below 5%) with a follow up glucose check (less urgent). Insulin should only be used for hyperglycemia after discussing with the attending. The max % dextrose in a PIV is 12.5%, in a deep PICC or UAC is 15%, and in a central PICC or UVC above the diaphragm is 15-25%.
Electrolytes – Generally, electrolytes are checked as above and during periods of abnormal fluid intake or urine output. Periodic assessment may be indicated if growth is poor, unfortified breast milk is primary source of fluid intake and/or diuretic therapy is in use.
The underlying causes of critical values (Na < 125 or > 150 mEq/L, K < 3.0 or > 6.0) need prompt assessment, treatment, and followup (q1-4h) until trending towards normal.
Calcium/Phosphorus – Check about 12h after birth and daily until standard intake is achieved. When the serum Ca < 7 mg/dL or ionized Ca < 1.0 mmol/L and symptoms such as jitteriness, irritability, high-pitched cry, or for sure if seizures or tetany are present, give a calcium gluconate bolus of 100 mg/kg IV over 30 minutes.Assymptomatic hypocalcemia is managed with a continuous IV infusion of 200-600 mg/ kg/day, usually in TPN. When ordering, the CA:P ratio should be 1.3-1.7 to 1. Given the risk for osteopenia, preterm infants should have the maximum tolerated concentrations of Ca/P in their TPN.
125
Triglyceride – Check daily after starting IV lipids (preterms) until
standard intake is achieved and tolerance is demonstrated. The lipid
infusion rate may be increased for TG < 150 mg/dL, held for 150-200,
and generally stopped, then decreased if > 200 (practice varies and
there is no evidence to support any practice approach).
BUN/creatinine – Establish a baseline value by 2-3 days age. Assess
after 10-14 days age in preterm infants on unfortified breast milk, or any
preterm infants if weight gain is sub-optimal to access adequacy of
protein intake. Given above conditions, typically add additional protein if
BUN is < 10 to achieve BUN value of 10-15. Use caution in protein
supplementation if also on medications primarily eliminated through the
kidneys (gentamicin) or that affect kidney function (indomethacin).
Liver function – the propensity to develop cholestasis on long-term TPN
needs to be looked for beginning a week after starting TPN and weekly
thereafter while continuing TPN. TPN associated cholestasis appears
primarily related to the amount and/or type of lipid infused. Limiting lipid
to < 2 gm/kg/d and achieving a minimal amount of enteral feeding
(20-40 ml/lg/d) appear to be protective.
Trace elements – zinc, copper, manganese, chromium, selenium levels
are generally not checked unless very long term TPN is required.
Manganese and copper should be decreased if cholestasis develops.
Enteral feeding guidelines
Feedings may be delayed for significant birth depression, hypoxemic
conditions (PPHN), cardiovascular instability (shock, heart failure), or
congenital anomalies needing early surgical intervention, but otherwise
are generally initiated on day one or as soon as GI motility (bowel
sounds/stooling) is present. Breast milk is preferred and eventual
breast feeding needs to be actively encouraged and supported. For high
risk preterm populations (< 32 weeks), donor human milk (Medolac)
126
Ne
ona
tolo
gy
should be used if maternal breast milk is not available. Trophic feedings
of 20 ml/kg/day are typically started with feedings provided every 3
hours. Lower rates (i.e., 10 ml/kg/d) may be used for infants < 750 g with
feedings at intervals of every 6 hours. A feeding algorithm has been
developed for use in the U NICU and should be followed. Feedings are
usually advanced daily by 20 ml/kg/day (< 34 weeks) or 30-40 ml/kg/
day (> 34 weeks) (practice varies).
Central lines should be considered for removal and TPN discontinued
once a feeding volume of 100 ml/kg/day has been reached. For
premature infants breast milk typically requires fortification to either 22
or 24 Kcal/oz equivalent (occasionally even higher). Fortification may
be started between 80-150 ml/kg/d (this is attending dependent).
Developmentally, most preterm infants are ready to begin attempts at
PO feeding by 32 weeks gestation. We use a “cue-based” feeding
protocol for advancement to full PO feedings based on infant readiness
(as determined by the bedside RN). Infants > 34 weeks GA at birth
may be offered ad lib oral feedings while advancing on enteral feeding
volume.
Residuals – at the University NICU an algorithm is in place to determine
responses to (or not) of gastric residuals. More important than the
residual volume is the appearance (frankly bilious) or the presence of
clinical GI signs like abdominal distension, tenderness, or bloody stools.
Any of these GI symptoms or repeat large volume residuals may
warrant placing the infant NPO and obtaining an abdominal film (and
CBC/diff).
127
Respiratory StabilizationInfants with initial bradycardia or apnea at delivery should receive
positive pressure ventilation (PPV) with initial PIP of 20-26 and PEEP of
6 on 40% FiO2 giving a prolonged inspiratory time of 2-3 seconds for the
first 2-3 breaths, then continuing at 0.3-0.4 seconds and a rate of 40-60.
The PIP, PEEP, rate and/or SpO2 are then adjusted to bring the heart rate
up and achieve initial SpO2 of 85-95. When the HR and respirations are
normal, continued distress and FiO2 < 40% is best managed with CPAP;
if the FiO2 > 60%, intubation and surfactant therapy may be indicated. If
the FiO2 is between 40-60%, clinical & radiographic evaluation is
indicated to assist in determining a course of action.
Indications for intubation: (check end-tidal pCO2 to confirm intubation) 1-
Infant < 27 weeks gestation (prophylactic surfactant therapy)
1- Apnea despite 30 sec of PPV at resuscitation
2- HR < 100 and not increasing despite 30 sec of PPV at
resuscitation
3- FiO2 > 0.6 to maintain SpO2 > 85% on CPAP
4- Frequent or severe apnea and bradycardia on CPAP
5- Marked retractions on CPAP
6- Suspected airway obstruction (suction secretions)
7- Cardiovascular collapse (HR < 60 or shock )
8- Severe metabolic acidosis (arterial base deficit > -10)
9- Severe respiratory acidosis (arterial pCO2 > 65)
10- Certain congenital malformations: cong diaphragmatic hernia,
choanal atresia, etc.
11- Rescue surfactant therapy
128
Ne
ona
tolo
gy
Initial ventilator settings and adjustments:
1- Conventional (volume-targeted) Ventilator• Begin with VT of 5 ml/kg, PEEP of 6, and rate of 30 at the
same FiO2 needed with prior PPV.• Adjust VT (range 4-6 ml/kg) so that breath sounds are audible
in the apices
but slightly diminished in the bases. Chest excursion should be visible,
but not excessive.• Adjust Fi02 to maintain Sp02 within suggested parameters for
gestational age. • For FiO2 > 0.4 and moderate to severe retractions, increase
the PEEP (typically to no more than 8 cm H20 without further
consultation).• Adjust the rate to keep the arterial pC02 50-60 (art).
• Utilize blood gases, CXR, graphics, and serial exams to fine tune. . .
2- HFOV• Begin with the MAP set at ½ of the Neopuff PIP (MAP
generally 10-12 for smaller preterm infants, 13-18 for sicker,
larger infants. Increase if moderate to severe retractions are
present or until the Fi02 is decreasing while maintaining Sp02
within target range. Target inflation is a 9 rib expansion
without flattening of the diaphragms on the CXR.• Begin with the amplitude set at twice the MAP (amplitude
generally 20-28). Adjust to obtain adequate chest wall
movement (bounce) seen down to the
pelvic level without jiggling the lower extremities.
129
Ne
ona
tolo
gy
• Begin with a frequency of 10 Hz for premature infants and 8 Hz for term and
post-term infants.
While maintaining the SpO2 within target range, wean the FiO2 continuously until the FiO2
has dropped to < 0.30. This is especially necessary during resuscitation and during the
first 30-60 minutes after surfactant administration. Do not allow the SpO2 to go above 95%
without making an immediate decrease. If the SpO2 decreases below the lower target
range MAP may need to be increased again by 1-2 cm H2O. When the FiO2 has weaned to
< 0.30 on conventional support, wean mainly PIP or tidal volume (Vt) using the volume
monitor to maintain the Vt at 4-6 cc/kg and SpO2 within target range. Combine with
decreases of rate for an arterial pCO2 < 45, or with decreases of PEEP (if > 5) for SpO2 >
95%. If the FiO2 never weans to 0.4, adjust the PIP and PEEP after assessing lung
expansion by CXR. On HFO, wean the MAP by 0.5-1.0 cm H2O increments keeping the
SpO2 within target range. After surfactant, wean MAP by 1-2 cm H2O at least every 15
minutes or faster if the SpO2 is > 95%. If the FiO2 never weans to 0.4, assess lung
expansion by CXR and adjust MAP as indicated.
The guidelines above are oriented to management prior to blood gas availability. As soon
as arterial access is obtained, draw blood gases within 15-30 minutes of continuing
ventilator changes. The decision to make a change with any given blood gas value is
based on desired blood gas parameters. For example, to keep off mechanical ventilation,
one may accept a pCO2 of 45-60 (art) or 50-65 (cap). If on a ventilator, parameters of
50-60 (art) or 55-65 (cap) would facilitate weaning and minimize the potential for
barotrauma. If pulmonary hypertension is present, one may
130
Ne
ona
tolo
gy
desire a SpO2 > 95 (term) or 92-95 (preterm) while otherwise keeping SpO2
alarms set at 85-93 (< 29 weeks gestation) to minimize the risk for ROP.
For the abnormal values below, possible ventilator changes are listed
(practice varies):
abnormality Conv comment HFO comment
↑pCO2 ↑rate
↑PIP
↑PIP
and
PEEP
If#Vt#normal# IfVt#<4XXX6
If#Vt#<#4XXX6#and#FiO2#
>#0.4# and#CXR#<#9#
ribs#or#whiter
↑amp
↓Hz
If#CXR#>#9#ribs#or#
air#trapping#
present
↓pO2 ↑MAP Usually#↑PIP#and/or#PEEP# If#FiO2#
>#0.4#and/or#CXR
<#9#ribs#or#whiter
May#also#↑Ti#(aspira7on#or#
pneumonia# and# rate# <# 40)#May#
also#↑#rate#(if#↑pCO2)
↑MAP
131
On HFO, obtain a CXR early (within the first hour) even if line placement is
ongoing. Repeat within 1-2 hours of continuing MAP changes. If there are
no changes, repeat a CXR every 6-12 hours during the first 24 hours.. On
conventional ventilation, obtain a CXR after line placement, within 1-2 hours
of continuing PIP or PEEP changes in the first 24 hours, and at decreasing
intervals thereafter. After surfactant, with either ventilator, several rapid
changes may be made before a follow up CXR is ordered.
If a CXR shows hyperexpansion (> 10 rib expansion or showing flattening of
the diaphragm), the MAP (HFO) or PIP and/or PEEP (conventional) should
be weaned. Repeat a CXR within 1-2 hours. If hyperexpansion persists on
CXR or the infant does not tolerate decreases in pressure, consider
decreasing the frequency stepwise towards 6 (HFO) or rate (conventional)
or switching to another modality (HFO → conventional or HFJV).
High frequency jet ventilation (HFJV) may be used like HFO using a high
PEEP strategy for problems oxygenating or using a low MAP strategy for air
leak syndromes, which are the most common indications for HFJV use. In
general, the HFJV is initiated at a lower PIP (by 2) and a higher PEEP (by
2-3) as prior conventional settings with a rate of 360-420. A “background”
conventional ventilator may be used at a rate of 2-5 (to improve lung
inflation), but no backup rate should be used of air leak is present. For air
leaks, one simply weans PIP to reduce alveolar inflation (feeding the leak)
while keeping the PEEP up to avoid total atelectasis until the air leak has
resolved. The background PIP is usually kept 2 lower than the HFJV when
making changes to avoid interrupting jet breaths.
Extubation: Guidelines have been established to facilitate extubation as soon as
physiologically possible. Guidelines are based on the mode of ventilation as well as the
weight of the infant. The question should be asked at least daily in rounds for every infant
who is intubated as to whether they meet extubation criteria.
132
Ne
ona
tolo
gy
Apnea, bradycardia, and desaturations:
As indications for intubation, do NOT count events that occur as a result of
feeding, suctioning, handling or other iatrogenic situations such belatedly
finding the O2 disconnected or NCPAP prongs out, etc. Also do NOT count
events that feature only desaturation that readily responds to adjustments
in inspired oxygen or that requires no stimulation.
Frequent means more than 5 apneic or bradycardic events requiring mild-
moderate stimulation in the prior 6 hours, or unremitting events requiring
near constant stimulation in a shorter period of time (30-60 minutes). Severe
means more than 1 event requiring bag and mask ventilation in the prior 6
hours. Stimulation means tactile stimulation, not adjustments in inspired
oxygen. Stimulation is generally indicated if apnea or bradycardia (< 60-80)
is sustained > 20 seconds.
133
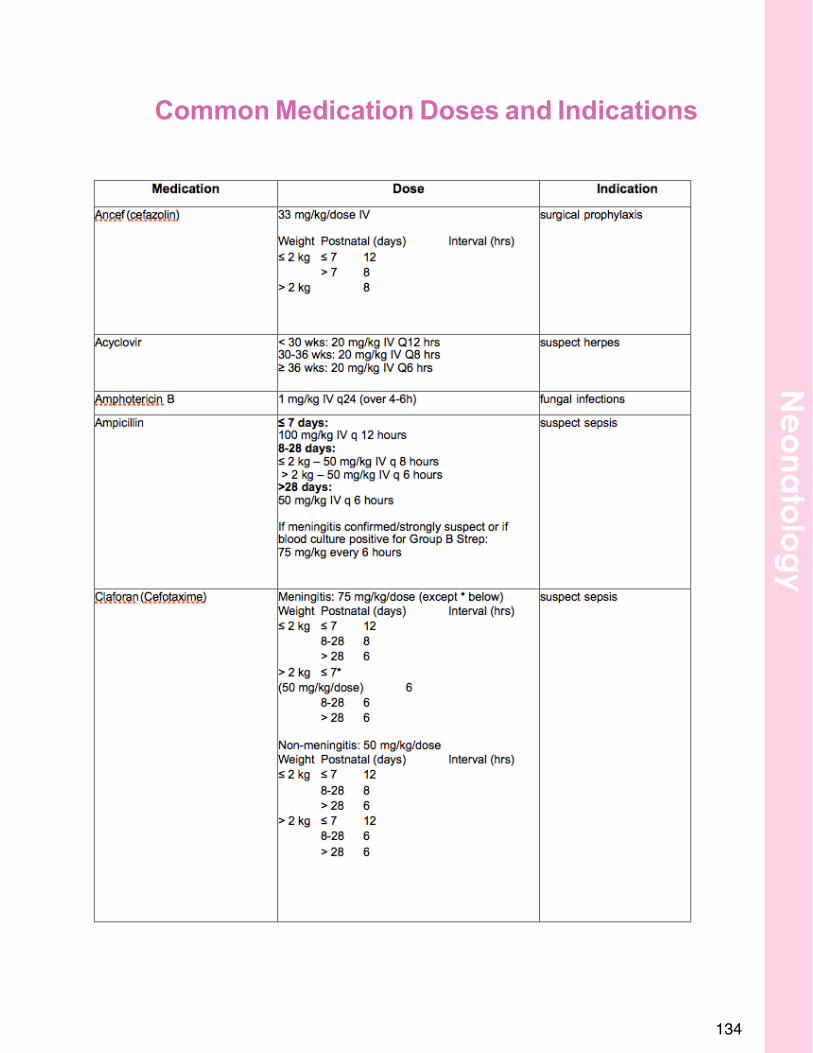
Common Medication Doses and Indications
134
Ne
ona
tolo
gy
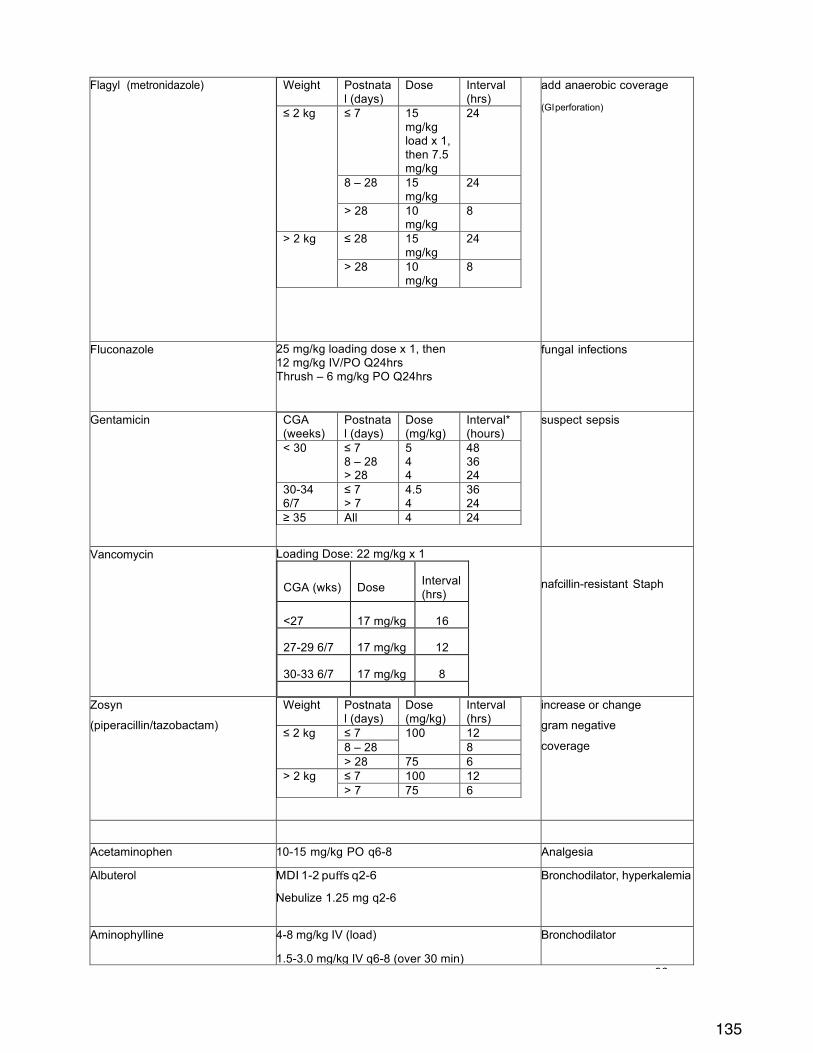
135
96 !
Flagyl (metronidazole) Weight Postnatal (days)
Dose Interval (hrs)
≤ 2 kg ≤ 7 15 mg/kg load x 1, then 7.5 mg/kg
24
8 – 28 15 mg/kg
24
> 28 10 mg/kg
8
> 2 kg ≤ 28 15 mg/kg
24
> 28 10 mg/kg
8
add anaerobic coverage
(GI perforation)
Fluconazole 25 mg/kg loading dose x 1, then 12 mg/kg IV/PO Q24hrs Thrush – 6 mg/kg PO Q24hrs
fungal infections
Gentamicin CGA (weeks)
Postnatal (days)
Dose (mg/kg)
Interval* (hours)
< 30 ≤ 7 8 – 28 > 28
5 4 4
48 36 24
30-34 6/7
≤ 7 > 7
4.5 4
36 24
≥ 35 All 4 24
suspect sepsis
Vancomycin Loading Dose: 22 mg/kg x 1
CGA (wks) Dose Interval (hrs)
<27 17 mg/kg 16
27-29 6/7 17 mg/kg 12
30-33 6/7 17 mg/kg 8
>33 6/7 17 mg/kg 6
nafcillin-resistant Staph
Zosyn
(piperacillin/tazobactam)
Weight Postnatal (days)
Dose (mg/kg)
Interval (hrs)
≤ 2 kg ≤ 7 100 12 8 – 28 8 > 28 75 6
> 2 kg ≤ 7 100 12 > 7 75 6
increase or change
gram negative
coverage
! !
Acetaminophen 10-15 mg/kg PO q6-8 Analgesia
Albuterol MDI 1-2 puffs q2-6
Nebulize 1.25 mg q2-6
Bronchodilator, hyperkalemia
Aminophylline 4-8 mg/kg IV (load)
1.5-3.0 mg/kg IV q6-8 (over 30 min)
Bronchodilator
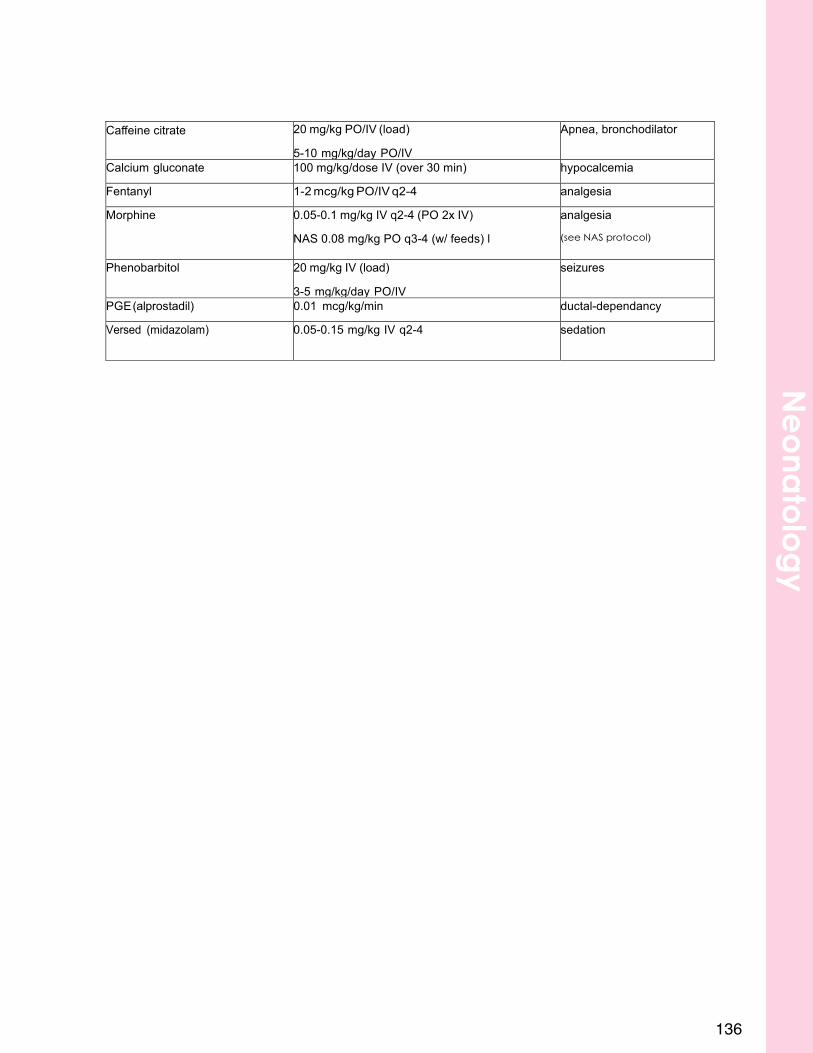
13697 !
Caeine citrate 20 mg/kg PO/IV (load)
5-10 mg/kg/day PO/IV
Apnea, bronchodilator
Calcium gluconate 100 mg/kg/dose IV (over 30 min) hypocalcemia
Fentanyl 1-2 mcg/kg PO/IV q2-4 analgesia
Morphine 0.05-0.1 mg/kg IV q2-4 (PO 2x IV)
NAS 0.08 mg/kg PO q3-4 (w/ feeds) l
analgesia
(see NAS protocol)
Phenobarbitol 20 mg/kg IV (load)
3-5 mg/kg/day PO/IV
seizures
PGE(alprostadil) 0.01 mcg/kg/min ductal-dependancy
Versed (midazolam) 0.05-0.15 mg/kg IV q2-4
sedation
Ne
ona
tolo
gy
138
Nephrology
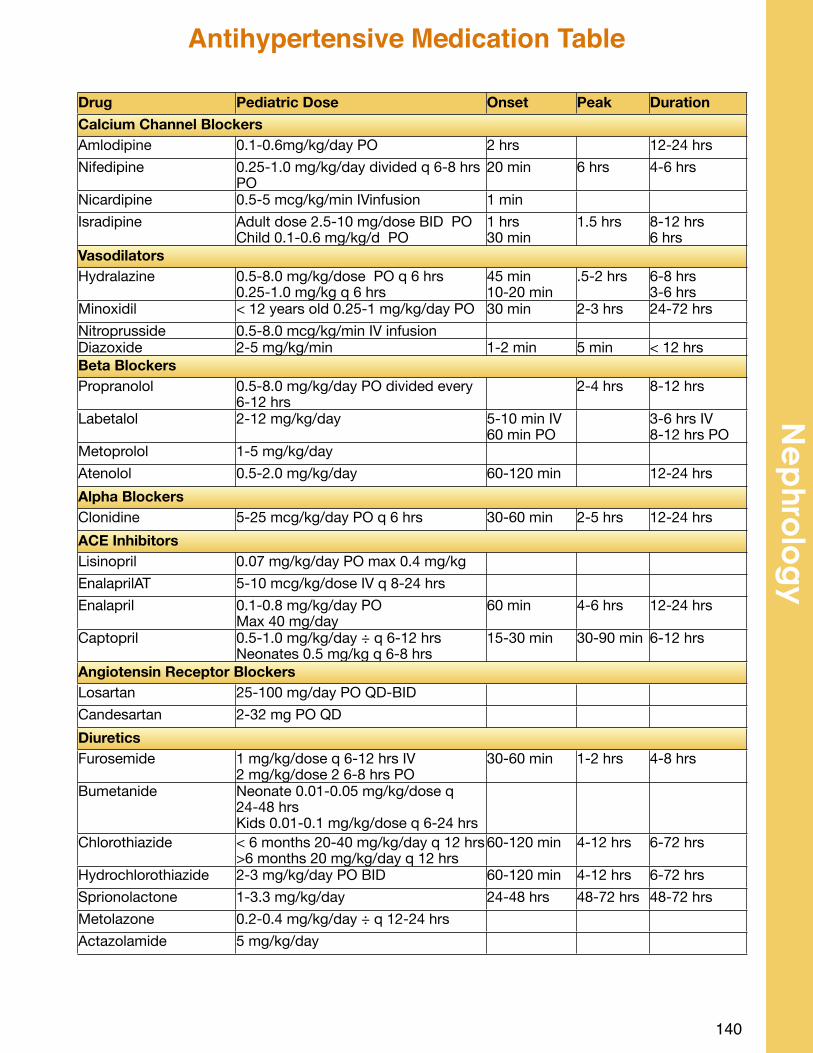
140
Ne
phro
log
yAntihypertensive Medication Table
Drug Pediatric Dose Onset Peak DurationCalcium Channel BlockersCalcium Channel BlockersCalcium Channel BlockersCalcium Channel BlockersCalcium Channel BlockersAmlodipine 0.1-0.6mg/kg/day PO 2 hrs 12-24 hrsNifedipine 0.25-1.0 mg/kg/day divided q 6-8 hrs
PO20 min 6 hrs 4-6 hrs
Nicardipine 0.5-5 mcg/kg/min IVinfusion 1 minIsradipine Adult dose 2.5-10 mg/dose BID PO
Child 0.1-0.6 mg/kg/d PO1 hrs30 min
1.5 hrs 8-12 hrs6 hrs
VasodilatorsVasodilatorsVasodilatorsVasodilatorsVasodilatorsHydralazine 0.5-8.0 mg/kg/dose PO q 6 hrs
0.25-1.0 mg/kg q 6 hrs45 min10-20 min
.5-2 hrs 6-8 hrs3-6 hrs
Minoxidil < 12 years old 0.25-1 mg/kg/day PO 30 min 2-3 hrs 24-72 hrsNitroprusside 0.5-8.0 mcg/kg/min IV infusionDiazoxide 2-5 mg/kg/min 1-2 min 5 min < 12 hrsBeta BlockersBeta BlockersBeta BlockersBeta BlockersBeta BlockersPropranolol 0.5-8.0 mg/kg/day PO divided every
6-12 hrs2-4 hrs 8-12 hrs
Labetalol 2-12 mg/kg/day 5-10 min IV60 min PO
3-6 hrs IV8-12 hrs PO
Metoprolol 1-5 mg/kg/dayAtenolol 0.5-2.0 mg/kg/day 60-120 min 12-24 hrsAlpha BlockersAlpha BlockersAlpha BlockersAlpha BlockersAlpha BlockersClonidine 5-25 mcg/kg/day PO q 6 hrs 30-60 min 2-5 hrs 12-24 hrsACE InhibitorsACE InhibitorsACE InhibitorsACE InhibitorsACE InhibitorsLisinopril 0.07 mg/kg/day PO max 0.4 mg/kgEnalaprilAT 5-10 mcg/kg/dose IV q 8-24 hrsEnalapril 0.1-0.8 mg/kg/day PO
Max 40 mg/day60 min 4-6 hrs 12-24 hrs
Captopril 0.5-1.0 mg/kg/day ÷ q 6-12 hrsNeonates 0.5 mg/kg q 6-8 hrs
15-30 min 30-90 min 6-12 hrs
Angiotensin Receptor BlockersAngiotensin Receptor BlockersAngiotensin Receptor BlockersAngiotensin Receptor BlockersAngiotensin Receptor BlockersLosartan 25-100 mg/day PO QD-BIDCandesartan 2-32 mg PO QDDiureticsDiureticsDiureticsDiureticsDiureticsFurosemide 1 mg/kg/dose q 6-12 hrs IV
2 mg/kg/dose 2 6-8 hrs PO30-60 min 1-2 hrs 4-8 hrs
Bumetanide Neonate 0.01-0.05 mg/kg/dose q 24-48 hrsKids 0.01-0.1 mg/kg/dose q 6-24 hrs
Chlorothiazide < 6 months 20-40 mg/kg/day q 12 hrs>6 months 20 mg/kg/day q 12 hrs
60-120 min 4-12 hrs 6-72 hrs
Hydrochlorothiazide 2-3 mg/kg/day PO BID 60-120 min 4-12 hrs 6-72 hrsSprionolactone 1-3.3 mg/kg/day 24-48 hrs 48-72 hrs 48-72 hrsMetolazone 0.2-0.4 mg/kg/day ÷ q 12-24 hrsActazolamide 5 mg/kg/day
Causes:• Transient: stress, fever, seizure, acute illness, dehydration, or vigorous exercise
o Shouldn’t be >2+• Orthostatic (postural): Increased urinary protein while upright; benign
o Not typically nephrotic range (pr/cr ration <3)• Persistent (6-12 months): nephrotic syndrome, AGN, tubulointerstitial nephritis,
SLE, DM, ATN, cystinosis, Dent’s syndrome, Wilson’s disease, Lowe’s syndrome, PCKD, mitochondrial disease, heavy metal poisoning
Often found on Dipstick:• Negative• Trace – between 15 and 30mg/dL protein• 1+ - between 30 and 100mg/dL protein• 2+ - between 100 and 300mg/dL protein• 3+ - between 300 and 1000mg/dL protein• 4+ - >1000mg/dL protein
Evaluation:• First morning urine protein/creatinine ratio
o Empty bladder before bedo No vigorous exercise x24H prior to sampleo Will be negative or markedly reduced for orthostatic proteinuriao Obtain weekly x3 to confirm proteinuria
• Exam: Check BP• Other labs to consider: RFP
Persistent Proteinuria Work-up:• History: edema, family history of hearing loss, hx of febrile UTI (scar), rash• Exam: Blood pressure• Labs: RFP, CBC, lipids• Imaging: Renal U/S• Additional work-up to be considered: C3, C4, ANA, ANCA, renal biopsy
141
Proteinuria
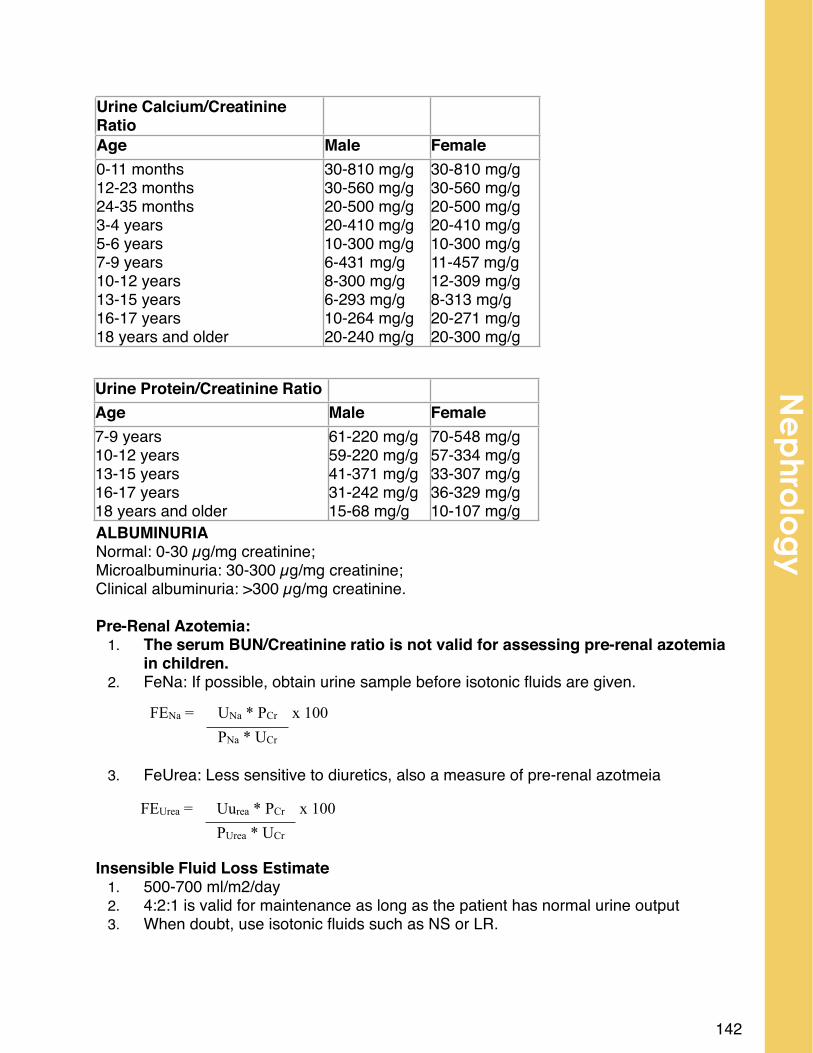
ALBUMINURIANormal: 0-30 µg/mg creatinine; Microalbuminuria: 30-300 µg/mg creatinine; Clinical albuminuria: >300 µg/mg creatinine. Pre-Renal Azotemia:
1. The serum BUN/Creatinine ratio is not valid for assessing pre-renal azotemia in children.
2. FeNa: If possible, obtain urine sample before isotonic fluids are given.
3. FeUrea: Less sensitive to diuretics, also a measure of pre-renal azotmeia
Insensible Fluid Loss Estimate1. 500-700 ml/m2/day2. 4:2:1 is valid for maintenance as long as the patient has normal urine output3. When doubt, use isotonic fluids such as NS or LR.
142
Urine Protein/Creatinine Ratio
Age Male Female 7-9 years10-12 years13-15 years16-17 years18 years and older
61-220 mg/g59-220 mg/g41-371 mg/g31-242 mg/g15-68 mg/g
70-548 mg/g57-334 mg/g33-307 mg/g36-329 mg/g10-107 mg/g
Urine Calcium/Creatinine Ratio
Age Male Female 0-11 months12-23 months24-35 months3-4 years5-6 years7-9 years10-12 years13-15 years16-17 years18 years and older
30-810 mg/g30-560 mg/g20-500 mg/g20-410 mg/g10-300 mg/g6-431 mg/g8-300 mg/g6-293 mg/g10-264 mg/g20-240 mg/g
30-810 mg/g30-560 mg/g20-500 mg/g20-410 mg/g10-300 mg/g11-457 mg/g12-309 mg/g8-313 mg/g20-271 mg/g20-300 mg/g
FEUrea = Uurea * PCr x 100 # PUrea * UCr #
FENa = UNa * PCr x 100 # PNa * UCr #
Ne
phro
log
y
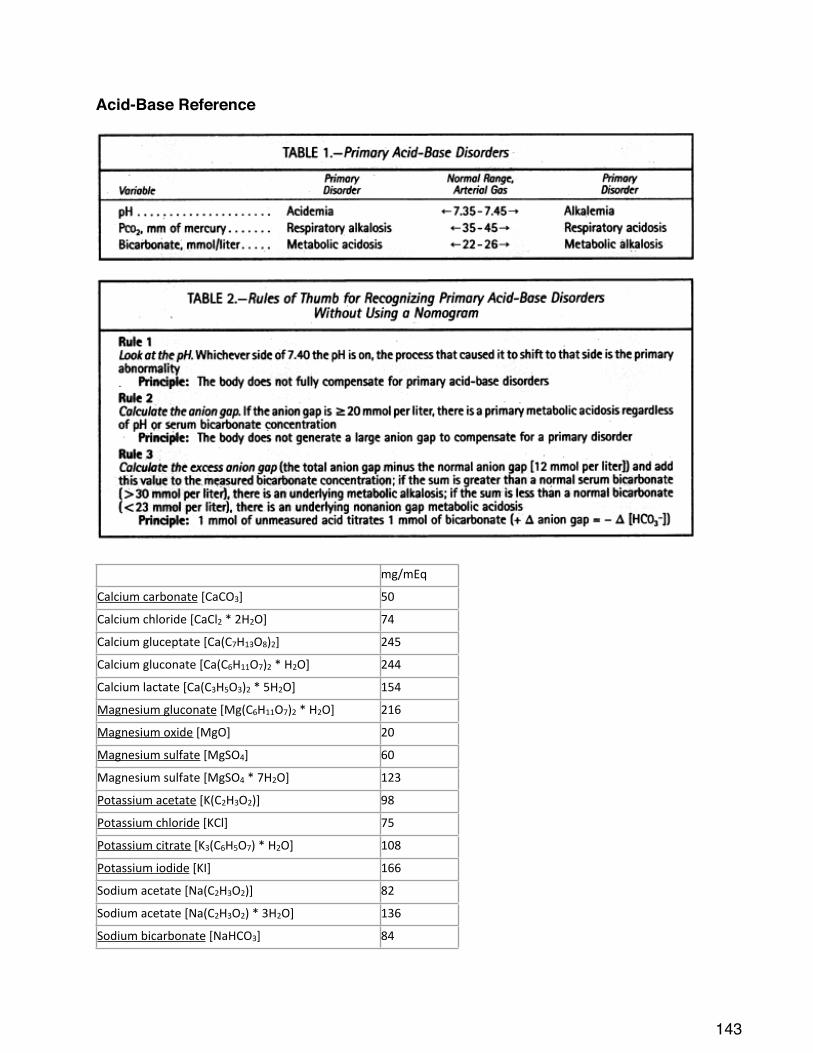
Acid-Base Reference
# mg/mEq#
Calcium#carbonate#[CaCO3]# 50
Calcium#chloride#[CaCl2#*#2H2O]# 74
Calcium#gluceptate#[Ca(C7H13O8)2]# 245
Calcium#gluconate#[Ca(C6H11O7)2#*#H2O]# 244
Calcium#lactate#[Ca(C3H5O3)2#*#5H2O]# 154
Magnesium#gluconate#[Mg(C6H11O7)2#*#H2O]# 216
Magnesium#oxide#[MgO]# 20
Magnesium#sulfate#[MgSO4]# 60
Magnesium#sulfate#[MgSO4#*#7H2O]# 123
Potassium#acetate#[K(C2H3O2)]# 98
Potassium#chloride#[KCl]# 75
Potassium#citrate#[K3(C6H5O7)#*#H2O]# 108
Potassium#iodide#[KI]# 166
Sodium#acetate#[Na(C2H3O2)]# 82
Sodium#acetate#[Na(C2H3O2)#*#3H2O]# 136
Sodium#bicarbonate#[NaHCO3]# 84
143
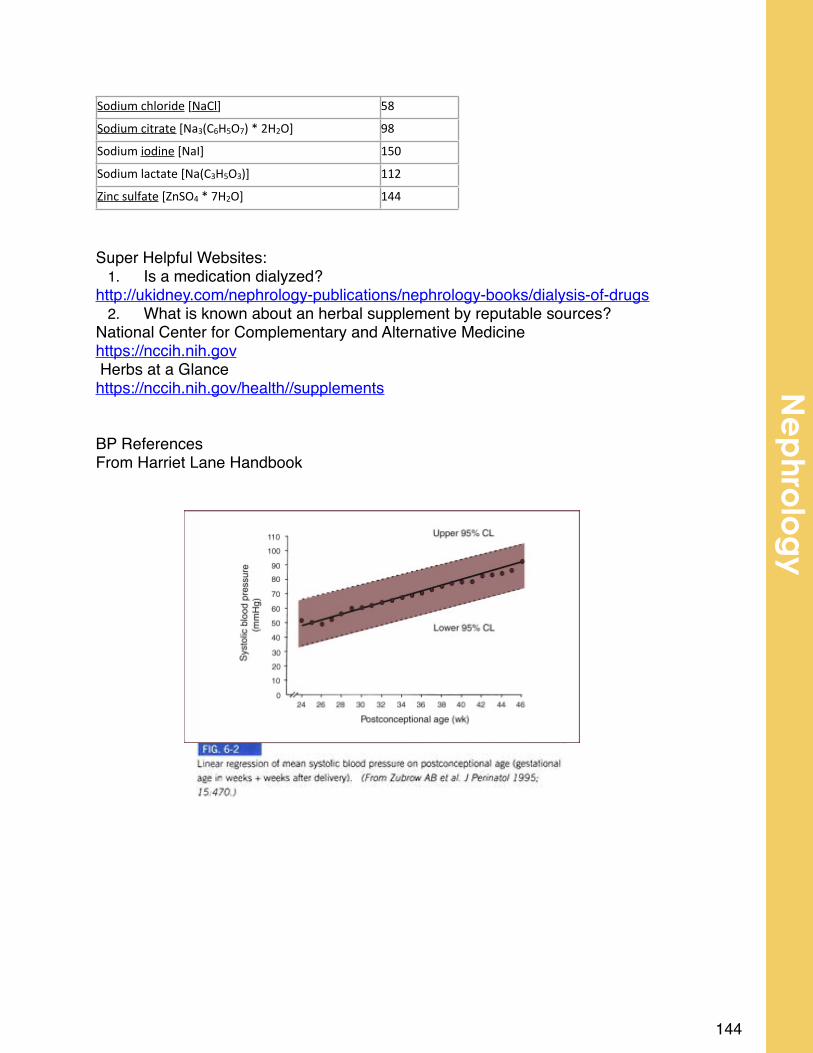
Sodium#chloride#[NaCl]# 58
Sodium#citrate#[Na3(C6H5O7)#*#2H2O]# 98
Sodium#iodine#[NaI]# 150
Sodium#lactate#[Na(C3H5O3)]# 112
Zinc#sulfate#[ZnSO4#*#7H2O]# 144
Super Helpful Websites:1. Is a medication dialyzed?
http://ukidney.com/nephrology-publications/nephrology-books/dialysis-of-drugs2. What is known about an herbal supplement by reputable sources?
National Center for Complementary and Alternative Medicinehttps://nccih.nih.gov Herbs at a Glancehttps://nccih.nih.gov/health//supplements BP ReferencesFrom Harriet Lane Handbook
144
Ne
phro
log
y
146
Neurology
Epidemiology/Pathophysiology• Parameters: 6 months to 6 years
o Simple Febrile Seizure: generalized, one seizure in 24 hour period, <15 minutes in duration
o Complex Febrile Seizure: Focal features, 2 or more seizures in 24 hour period, prolonged duration (>15 minutes)
• 2-5% of all children will have at least one febrile seizureClinical presentation: Generalized tonic clonic seizure in the setting of fever
Exam• Check for meningeal signs, other signs of infection, post-ictal paralysis• Lab/Studies: only as indicated by H&P• LP: all children concern for meningitis on other clinical grounds• EEG: not for simple febrile seizures, consider in complex FS or other concerns• Imaging: not for simple febrile seizures; yes if still encephalopathic at time of
eval.
Complications• Recurrent febrile seizure:
o After first febrile seizure, 30% risk of recurrenceo If 2nd simple febrile seizure, then 50% risk of 3rd febrile seizureo
• Epilepsy:o Only slightly greater than background risk: at 7 years:
estimated 1-5% will have epilepsy (vs. 0.5%)o Risk of epilepsy is not affected by number of febrile
seizures as such.o Risk of future epilepsy increases with number of complex
features
Course/Treatment• Antipyretics (even if scheduled) have not been proven to prevent febrile
seizures.• AEDs not routinely recommended
o Phenobarbital and valproic acid have both been shown effective in preventing febrile seizure recurrence, but not routinely recommended due to side effects.
148
Ne
urolo
gy
Simple Febrile Seizure
Epidemiology
Each year 25,000-40,000 children in the US will experience a first unprovoked seizure.
Clinical evaluation
• Describe the seizure (semiology=what the seizure looks like)o Generalized seizures (multiple types, all marked by synchronous, bilateral
brain involvement)• Absence: staring, unresponsive (Unconscious), brief (5-20 sec), frequent,
only minor subtle motor , automatisms -• can be confused with “complex partial seizure” but duration, post-
ictal features, frequency and EEG findings differ!• Myoclonic: rapid, shock-like jerks, typically maximal over head/neck/upper
extremities• Spasm: Longer than a myoclonic twitch, typically 1-2 seconds of forced
contraction (head, neck, trunk, extremities), most common in infants• Tonic: Prolonged (>10 seconds) of sustained whole body stiffening,
possibly followed by clonic jerking• Generalized Tonic Clonic (aka Grand Mal): tonic stiffening, followed by
rhythmic extremity jerkingo Focal seizure (highly variable in expression, depends on area of brain
involvement, starts within one hemisphere, may spread to generalized seizure): • “complex partial”, also known as staring or hypomotor seizure: absence of
major motor manifestations, prominent staring, inattentiveness, with automatisms (subtle, repetitive, semi-purposeful movements), alteration of consciousness; often some amnesia
• “simple partial”, also known as focal motor: rhythmic jerking, movements, with nearly preserved consciousness
• Other seizures types (visual, auditory, autonomic, etc) may be seen, although are less common.
• Look for differential diagnosis (breath-holding, syncope, GER)• Look for causes of seizure
o Exclude “provoking” factors, including hypoglycemia, ingestions, infection, trauma, etc. Seizures in these circumstances would not typically be considered epilepsy
Labs (As suggested by H&P)• Consider lytes, tox screen• LP if concerned for meningitis/encephalitis on clinical grounds.• EEG is indicated but not emergently.• Imaging: CT head emergently if persistent post-ictal paralysis or
encephalopathy. Otherwise, MRI as outpatient.
149
First Unprovoked Seizure
Complications• If one unprovoked seizure, ~50% will have recurrence (median 6 months)• If 2nd seizure: 72% will have 3rd seizure• If 3rd seizure: 81% will have 4th seizure
• Increased risk of recurrence if: remote symptomatic etiology (i.e., previously identified cause for unprovoked seizure such as brain malformation, prior brain injury, etc), abnormal EEG, asleep during first seizure, h/o febrile seizure, positive family history
• 10% will go on to have >10 seizures despite AEDsCourse/Treatment
• Treatment with AED is symptomatic and in general does not alter the natural history of the epilepsy
• Efficacy of an AED to prevent a second seizure is not 100%• Efficacy of an AED to prevent recurrent seizures is the same whether started
after the first seizure or the second or subsequent seizureo Starting AED after the first seizure does not prevent epilepsy
• Start an AED when the risk of a second seizure outweighs the AED side effects• Counsel patients:
o No swimming or bathing alone.o Wear a helmet for appropriate sports (skiing, skateboarding etc..).o Utah State Law says no driving until seizure free on stable AED dosing x3
months.• Information for parents:
o Camfield P, Camfield C. Special considerations for a first seizure in childhood and adolescence. Epilepsia. 2008.
!! Will it happen again?
!! How long do I have to wait for a recurrence?
!! Could my child die during a recurrence?
!! Could there be brain damage with a recurrence?
!! If medication treatment is delayed will there be any long-term change in the chance of a permanent remission?
!! Now that my child has had a seizure, how should his/her activities be restricted?
150
Ne
urolo
gy
Status Epilepticus
EPILEPSY
Definitions: Epilepsy= 2 unprovoked seizures in an individual (separated by >24 hours)
o May also be applied to individual with a single seizure AND with reasonable clinical history to suggest a high likelihood of future unprovoked seizures (presence of brain malformation, injury, genetic syndrome, etc)
Epidemiology/Pathophysiology! Lifetime risk of epilepsy is 1 in 26; 0.5-1% of all children carry
diagnosis of epilepsy
! Chance for remission of childhood epilepsy estimated at 50-60% (likelihood of “outgrowing it”), although ultimately dependent on underlying etiology
! Etiology: highly varied causes, broadly grouped as follows:• Symptomatic: known causative factor such as brain malformation,
metabolic syndrome, complex genetic syndrome (e.g. Angelman’s Syndrome, Dravet, etc) wherein seizures are a component or symptom of the underlying condition.
• Genetic Epilepsy: Formerly known as Idiopathic Epilepsy, now thought to be due to multiple genetic factors resulting in epilepsy in normally developing individuals
o Examples include Childhood Absence Epilepsy, Benign Rolandic Epilepsy, Juvenile Myoclonic Epilepsy
o Unknown: Everything else
Clinical presentation: Highly varied, dependent on underlying etiology and age of patient.o Electroclinical Syndrome: Take into account age of patient, type of
seizure, and EEG findings to better classify underlying epilepsy and to more accurately determine prognosis (as in Childhood Absence Epilepsy, Benign Rolandic Epilepsy, Juvenile Myoclonic Epilepsy)
Exam: often normal, but focal abnormalities (hemiparesis, asymmetric reflexes) may be seen in context of broader neurologic issues.
Complications: Epilepsy frequently (~50%) is associated with other neurocognitive issues such as developmental delay, mood dysregulation (depression/anxiety), migraines, and disrupted sleep.
151
Course/Treatment: After 2 seizures (or 1 with high risk of recurrence) initiate AED therapy…o Likelihood of seizure freedom after 1 AED started is ~50%o Likelihood of seizure freedom after 2 or 3 AEDs started is ~65%o 1/3 of all epilepsy is drug resistant (no significant gain from future AED
trials)
! When drug resistant, consider surgical evaluation (in focal epilepsy) and non-pharmaceutical options such as ketogenic diet and vagal nerve stimulator implantation
DefinitionsSeizures > 15 minutesSeries of seizures without regaining
consciousness in between Convulsive Status: generalized tonic-clonic (aka “grand mal” status) Epilepsia Partialis Continua (sustained focal seizure without impairment of consciousness)
Nonconvulsive Status:Absence Status (“petil mal” status) Complex partial Status
EtiologyFebrile seizureMedication noncompliance Infection (encephalitis, rotavirus) Metabolic derangement
Hypoglycemia Hypocalcemia Hyponatremia Hypomagnesemia
Trauma (NAT)Hypoxic-ischemic encephalopathy
Calculation for infants or children on Phenobarbital:Desired level-current level = dose in mg/kg IV
1. ABCs Airway: Suction Breathing: Provide O2
Intubation may be needed if seizures persist of hypoventilation occurs Cardiac: Assess perfusion
2. Drugs Lorazepam: 0.05 to 0.1 mg/kg IV Max Dose: 4 mg Midazolam: 0.2 mg IN via aerosol
152
Ne
urolo
gy
Max Dose: 10 mg Diazepam IV: 0.05 to 0.2 mg/kg Max Dose: 10 mg Diazepam (Diastat) PR 2 to 5 years: 0.5 mg/kg 6 to 11 years: 0.3 mg/kg 12 + years: 0.2 mg/kg Max Dose: 20 mg Phenobarbital: 10 to 20 mg/kg IV Fosphenytoin: 15 to 20 mg/kg IV Depacon (> 3 years of age): 10 to 20 mg/kg
Be prepared to intubate if the following are used Propofol: 1 mg/kg IV (Max = 40 mg as initial dose) Pentobarbital: 5 to 8 mg/kg IV
153
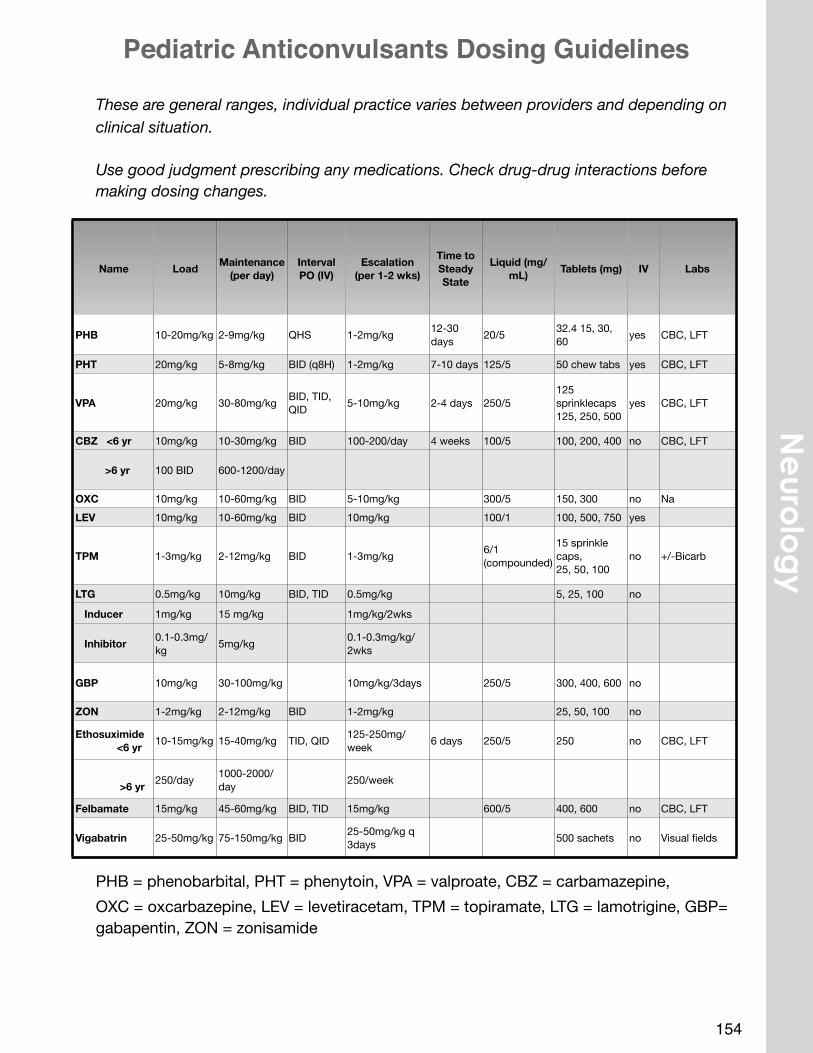
These are general ranges, individual practice varies between providers and depending on clinical situation.
Use good judgment prescribing any medications. Check drug-drug interactions before making dosing changes.
PHB = phenobarbital, PHT = phenytoin, VPA = valproate, CBZ = carbamazepine, OXC = oxcarbazepine, LEV = levetiracetam, TPM = topiramate, LTG = lamotrigine, GBP= gabapentin, ZON = zonisamide
154
Ne
urolo
gy
Pediatric Anticonvulsants Dosing Guidelines
Name Load Maintenance(per day)
IntervalPO (IV)
Escalation (per 1-2 wks)
Time to Steady State
Liquid (mg/mL) Tablets (mg) IV Labs
PHB 10-20mg/kg 2-9mg/kg QHS 1-2mg/kg 12-30 days 20/5 32.4 15, 30,
60 yes CBC, LFT
PHT 20mg/kg 5-8mg/kg BID (q8H) 1-2mg/kg 7-10 days 125/5 50 chew tabs yes CBC, LFT
VPA 20mg/kg 30-80mg/kg BID, TID, QID 5-10mg/kg 2-4 days 250/5
125 sprinklecaps125, 250, 500
yes CBC, LFT
CBZ <6 yr 10mg/kg 10-30mg/kg BID 100-200/day 4 weeks 100/5 100, 200, 400 no CBC, LFT
>6 yr 100 BID 600-1200/day
OXC 10mg/kg 10-60mg/kg BID 5-10mg/kg 300/5 150, 300 no NaLEV 10mg/kg 10-60mg/kg BID 10mg/kg 100/1 100, 500, 750 yes
TPM 1-3mg/kg 2-12mg/kg BID 1-3mg/kg 6/1 (compounded)
15 sprinkle caps, 25, 50, 100
no +/-Bicarb
LTG 0.5mg/kg 10mg/kg BID, TID 0.5mg/kg 5, 25, 100 no
Inducer 1mg/kg 15 mg/kg 1mg/kg/2wks
Inhibitor 0.1-0.3mg/kg 5mg/kg 0.1-0.3mg/kg/
2wks
GBP 10mg/kg 30-100mg/kg 10mg/kg/3days 250/5 300, 400, 600 no
ZON 1-2mg/kg 2-12mg/kg BID 1-2mg/kg 25, 50, 100 no
Ethosuximide <6 yr 10-15mg/kg 15-40mg/kg TID, QID 125-250mg/
week 6 days 250/5 250 no CBC, LFT
>6 yr 250/day 1000-2000/
day 250/week
Felbamate 15mg/kg 45-60mg/kg BID, TID 15mg/kg 600/5 400, 600 no CBC, LFT
Vigabatrin 25-50mg/kg 75-150mg/kg BID 25-50mg/kg q 3days 500 sachets no Visual fields
155
IV AnticonvulsantsHow to Choose
Less than 2 years old: PHB or LEV, never VPA2 years or older: LEV; see below for use of PHT, PHB and VPA
Problems with PHB: resp depression if already given benzos, bad cognitive and behavioral side effects in kids > 2years
Problems with PHT: if <5 years old serum levels will not remain consistent, PHT can be good for a one-time load to stop status in younger children
Problems with VPA: if there is an underlying metabolic error (causing their seizures) then VPA may cause fulminant liver failure
LEV is newly available in IV form. No standard practice yet.
Formula to adjust serum levels in the acute setting
IV load in mg = (change in serum concentration) x (kg) / *
* = coefficient reflecting volume of distribution
*PHB = 1 *PHT = 1 *VPA = 5
LEV does not require loading, can give 10-20mg/kg
Four Choices
Drug Loading Dose Acute SEs
fPHT 20mg/kg Rash, bradycardia
PHB 10-20mg/kg Resp depression
VPA 20mg/kg Hepatotoxicity
LEV 10 mg/kg BID* Psychosis
*no load, just start
Pediatric ED Patient with Headache, Concern for Migraine*
*Factors suggestive of Migraine Include: severe pain, decreased activity, nausea or vomiting, photo or phonophobia and family history of migraine. Do NOT Include patients with concern for stroke or with secondary HA (due to other cause such as meningitis, sinusitis, idiopathic intracranial hypertension). This guideline is for children ≥ 5 years, if child is younger discuss with pediatric neurologist.
ASK THE PATIENT:Does the patient have a Pediatric Neurologist? (If YES, check HELP2)
Check HELP2 – Is there a HA Action plan? (If YES, follow recommendations)
If NO, follow principles of acute migraine treatment
Control Nausea
Promote Sleep
Use anti-inflammatories
Avoid narcotics/opiates
STEP 1 Choose combination of anti-emetic, sedating antihistamine, anti-inflammatory (not all 3 needed for every patient) + hydration for all patients
ORAL OPTION: Ibuprofen 10 mg/kg (max. 800 mg), ondansetron 0.15 mg/kg (max 8 mg), diphenhydramine 1 mg/kg (max 50 mg) + oral hydration
IV OPTION(S): Ketorolac 0.5 mg/kg (max 30 mg), diphenhydramine 1 mg/kg (max 50 mg), antiemetic (prochlorperazine 0.15 mg/kg (max 10 mg), promethazine 0.5 mg/kg (max 25 mg), metoclopramide 0.1 mg/kg (max 10 mg), OR ondansetron (0.15 mg/kg (max 4 mg)), + IV hydration
OTHER Interventions in STEP 1: Allow patient to sleep, Minimize BP checks, alarms, place on CR monitor or Pulse ox to avoid waking patient for VS. Quiet room (lights off, TV off, no texting, phone calls, video games, visitors at minimum, door closed)
156
Ne
urolo
gy
Dihydroergotamine Administration PCH Procedure
PurposeTo describe the care of inpatient children and adolescents receiving DHE (dihydroergotamine) for vascular headaches. Early and aggressive treatment is important to prevent progression to chronic headaches.
ScopePrimary Children's Hospital
DefinitionsExclusion criteria/Contraindications -
• Has received the following medications in the proceeding 24 hours:• 5-HT1 agonists (“triptans”) medications: e.g., sumatriptan (Imitrex, Treximet),
frovatriptan (Frova), naratriptan (Amerge), rizatriptan (Maxalt), eletriptan (Relpax), zolmitriptan (Zomig), or almotriptan (Axert).
• Ergot alkaloids • Has discontinued MAO inhibitors within the last 2 weeks • Currently receiving anti retro-viral agents or macrolides (erythromycin, azithromycin,
clarithromycin, etc.). • Sensitivity to DHE or other ergot alkaloids. • Pregnancy: a pregnancy test should be obtained prior to DHE administration in
females of childbearing age. • Uncontrolled hypertension, ischemic heart disease, a history of myocardial
infarction, angina, coronary artery spasm, sepsis, peripheral vascular disease, hemiplegic or basilar migraine, severe hepatic or renal dysfunction, or following vascular surgery.
Procedure1. Review patient history prior to administering DHE for the above noted
contraindications. 2. Place patient on continuous cardiac monitoring.3. Check blood pressure before, and 15 minutes after, each dose of DHE. 4. Document the patient’s pain score (0=no headache to 10=worst headache ever)
before and after treatment, as well as other responses. 5. Observe for signs of severe vasoconstriction, such as numbness in fingers/toes,
chest pain, or muscle pain.
157
6. Place patient on “quiet” protocol (minimize visitors, no electronics or TV, maximize rest).
7. Ensure peripheral IV (PIV) is patent prior to each DHE dose. (Use a PICC for DHE administration only if PIV’s infiltrate.)
8. Administer an antiemetic 30 minutes before each DHE dose as ordered: a. Prior to DHE doses 1-3: Metoclopramide (Reglan®),prochlorperazine
(Compazine), or promethazine (Phenergan).b. Subsequent DHE doses: ondansetron should be used as pretreatment in
order to avoid extrapyramidal symptoms that can be seen with repeated doses of antidopaminergic meds.
9. Administration and Dosage 9.1 All patients should receive intravenous hydration of 20 ml/kg of NS before
beginning protocol.9.2 Administer antiemetic 30 minutes before DHE.9.3 Dilute doses of DHE in 25-50 ml of NS and infuse over 20 minutes using a
syringe pump.9.4 Administer a test dose of DHE. The test dosage of DHE is 0.01 mg/kg/dose
rounded to the nearest 0.1 mg, with a maximum test dose of 0.5 mg, or 1/2 that of the target dose (listed below). Onset of pain relief can begin almost immediately. Note: A test dose of DHE is recommended in all patients regardless of previous experience with the drug to observe for signs and symptoms of allergic reaction or potential side effects.
9.5 If DHE is tolerated without unacceptable adverse effects, the rest of the dose is given half an hour later.
9.6 Full dose of IV DHE is weight-based at 0.02 mg/kg/dose rounded to the nearest 0.1 mg, with a maximum dose of 1 mg. Doses are given every eight hours. If the patient has side effects from this dose, a lower dose may be used, or the patient can be switched to IV depacon.
9.7 Give the full dose every 8 hours until headache freedom, plus one additional dose, up to a maximum of 20 doses.
9.8. Continue antiemetic dosing 30 minutes before each DHE dose with antidopaminergic meds (first 3 doses) or ondansetron for subsequent doses. (as noted above).
10. All patients receive a minimum of 5 doses before deciding on unresponsiveness to DHE therapy (unless unacceptable adverse effects occur. These may include repeated emesis, diarrhea, excessive muscle cramping, oliguria suggesting renal insufficiency, or signs of myocardial ischemia). If there is any improvement in the patient’s headaches, the DHE is continued until the patient is headache free or unacceptable adverse effects occur.
158
Ne
urolo
gy
11. Upon admission, patients and their caretakers are informed that the headache can feel worse for the first few doses due to nausea/vomiting and anxiety.
ExceptionsNone
Primary SourcesColman, I et al. (2005) Parenteral (DHE) for Acute Migraine Headache: A Systematic Review of the Literature. Annals of Emergency Medicine. 45(4): 393-401.
El-Chammas et al (2013) Pharmacologic Treatment of Pediatric Headaches. JAMA Pediatr. 167(3): 250-258.
Kabbouche, MS, et al., 2008 Inpatient treatment of status migraine with dihydroergotamine in children and adolescents. Headache 49: 106-109.Linder, SL. Treatment of Childhood Headache with Dihydroergotamine Mesylate. Headache. 1994;34:578-580 Silberstein, SD & SH Kori. (2013) Dihydroergotamine: A Review of Formulation Approaches For the Acute Treatment of Migraine. CNS Drugs 27:385-394
Secondary MaterialsNelson, G, Bale, JF, and Kerr, LM. 2013. Inpatient Admission for Intravenous Dihydroergotamine Treatment of Migraine: Is it Worth the Headache. Presented at the Child Neurology Society Meeting, Austin, Texas.
Unpublished work of authorship. Copyright © Intermountain Health Care, Inc. (Intermountain Healthcare). All rights reserved.
Document Created: December2006
Subsequent Review Date(s): January2010; March 2014
Approver Name(s): Katy Welkie
Effective Date: March2011
Next Scheduled Review Date: February2014
Confidential and proprietary to Intermountain Health Care, Inc. If Intermountain Healthcare authorizes a person to access policies, procedures, and guidelines (PPGs), it also authorizes that person to disclose information from PPGs – not copies – but only as reasonably necessary for healthcare matters related to Intermountain Healthcare.
Reasonable efforts will be made to keep employees informed of policy changes; however, Intermountain Healthcare reserves the right in its sole discretion to amend, replace, and/or terminate this policy at any time.
Intermountain Healthcare is an At-Will Employer. The terms of this policy do not, either directly or indirectly, constitute any form of employment contract or other binding agreement between any employee and Intermountain.
Contact Intermountain Healthcare’s Legal Department for questions.
159
Division of Pediatric Neurology Steroid Protocol for Treatment of Childhood Neuroimmunological Diseases (ADEM, TM and ON)*
F. Filloux, MD (June 16, 2006)Agreed upon in Division of Pediatric Neurology, June 16, 2006.
• IV Methylprednisolone for 3 days• 15 mg/kg/day divided q6h up to max of 1 gm/day
• Oral steroid taper• Prednisone 1 mg/kg/day (or equivalent) up to maximum of 60 mg/day X 5
days• Then: 0.5 mg/kg/day, 0.25 mg/kg/day, then 0.1 mg/kg/day respectively for 2
days each, then stop.• Single AM dose
• Total duration of steroid therapy is 14 days
• Options:• Duration of IV MP can be adjusted between 3-5 days.• IV corticosteroid at equivalent dose can be substituted for oral prednisone in
case patient is unable to take PO meds; an equivalent taper should be carried out.
• GI prophylaxis with ranitidine (zantac) can be considered during corticosteroid administration.
• Any more substantive deviations to the protocol should be approved by attending pediatric neurologist on service at the time the decision is made.
*ADEM, acute disseminated encephalomyelitis; TM, transverse myelitis; ON, optic neuritis.
160
Ne
urolo
gy
Guillain Barré Syndrome (Acute Inflammatory Demyelinating Polyneuropathy; AIDP)
Epidemiology/Pathophysiology• Acute to sub-acute acquired autoimmune inflammation of the peripheral nerves: molecular
mimicry of an infectious agent presumably induces an immune response that inadvertently targets peripheral nervous tissue (usually myelin).
• Epidemiology: worldwide incidence ranges 0.4-4 cases/100,000 general population• Except for 1976 swine flu vaccine epidemic, 60% of cases are preceded by infection
(influenza, influenza-like illnesses, c. jejuni); other triggers include surgery, trauma, or malignancy such as lymphoma
• Differential diagnosis includes acute transverse myelitis, other spinal cord syndromes, other peripheral neuropathies, CIDP, myositis, rarely myasthenia gravis, conversion disorder.
• Variants: (axonal variants are seen more in Asian countries than US and tend to have incomplete recovery)
o AIDP (acute inflammatory demyelinating polyradiculoneuropathy, ie classic GBS): monophasic, demyelinating
o AMAN (acute motor axonal neuropathy)o AMSAN (acute motor sensory axonal neuropathy)o Fisher variant (ophthalmoplegia, ataxia, and areflexia); may have elevated Gq1b
ganglioside antibodyo Pharygeal-Brachial-Cervical variant (may have elevated Gq1b antibody; anti-Ta
antibody not clinically available)o Bickerstaff-Encephalitis
Clinical presentation: • Classically presents with rapidly ascending paralysis, areflexia, distal paresthesias• 50% of patients have bifacial weakness• 25% of patients have back pain or radicular pain
Exam• Distal > proximal weakness; motor > sensory dysfunction; autonomic dysfunction; areflexia
(or hyporeflexia); +/- eye findings without ptosisLab/Studies:
• LP: albuminocytologic dissociation (normal CSF WBC, elevated CSF protein; (~ 20% of children will have normal CSF early);
• EMG: o Slowed nerve conduction velocities, conduction block, temporal dispersion,
prolonged latencies, milder reduction in amplitude, and prolonged or absent f-waves;
o Needle EMG may show abnormal spontaneous firing or signs of reinnervation but may be normal if <10 days from onset.
o May help with DDx and to distinguish from transverse myelitis o May help assess severity/prognosis to help guide management (axonal involvement
often predicts incomplete recovery)
161
• Imaging: consider MRI spine with and w/o contrast to look for mass or demyelinating lesion; may see radicular (nerve root) enhancement in GBS
Complications• Watch for autonomic dysfunction: hyper- or hypotension, ileus, transient bladder dysfunction,
temperature instability, arrhythmia• Approximately 1 in 10 proceed to CIDP (chronic form); may rarely
need repeat IVIG vs steroid treatment for CIDP
• Some patients require ICU management, intubation.
• Predictors of slower recovery: severe weakness, rapid progression, cranial nerve deficits, ventilator requirement, axonal forms of GBS
Course/Treatment• IVIG 2g/kg divided over 2-4 days (2 day treatment may result in greater risk of side effects
such as headaches, vomiting, rash; a shorter, higher dose may be tolerated in order to shorten hospitalization).
• Monitor respiratory status (NIF, FVC daily or more); monitor for dysphagia.• Imminent respiratory failure when NIF (negative inspiratory force) of 15 cm H2O or FVC
15ml/kg. Therefore PICU consultation for NIF ≤ 20 cmH20 or FVC ≤ 20 ml/kg• Simple bedside FVC test in >5 year olds: have patient count (or do ABCs) as far as they can
in a single breath; for every count of 10 letters or numbers ~10ml/kg FVC; ie should be able to count to >20 in a single breath at rest.
• PT/OT/Rehab• Nadir typically reached by 1to 3weeks; recovery typically begins within a week of IVIG
162
Ne
urolo
gy
Neonatal Seizures BETSY OSTRANDER MD
Seizures in a neonate are usually a symptom of brain injury/insult rather than primary epilepsy. Try to identify the underlying cause at the same time as you are confirming and treating seizures.
Clinical presentation: In neonates, seizures tend to be of focal or multifocal. It is unusual to have a generalized seizure in a baby because of immature brain development. There is often electroclinical dissociation (clinical seizure not always accompanied by EEG correlate and electrographic seizure not always accompanied by clinical manifestations)
Distinguishing between Jitteriness and Seizure
Characteristic Seizure JitterinessCan it be elicited by external stimulus?
No Yes
Movement Irregular and jerky Symmetric fine tremorAssociated with increased HR?
Yes No
Associated with apnea? +/- NoCan movement be easily stopped?
No, self terminate Yes, by gentle bending/holding limb or making the baby suck on pacifier
Pathophysiology: • 80% of neonatal seizures are caused by one or more of the following:
o Strokeo Hypoxic ischemic encephalopathyo Infectiono Electrolyte abnormalities: hypoglycemia, hypocalcemia, hypomagnesemia
Diagnosis: Seizures in neonates can be difficult to identify clinically and most experts believe electrographic monitoring is essential to correctly diagnose and effectively treat seizures.
EEG monitoring can be initiated 24 hours a day, 7 days a week at PCH and UNICU. However, if there is strong clinical suspicion for seizure, you do not need to wait for EEG confirmation prior to initiating treatment.
Treatment: First line treatment in neonates• Phenobarbital 20mg/kg IV x 1, can give additional 10mg/kg x 1 if seizure persists. Monitor for
respiratory depression. Check PHB level prior to starting maintenance.• Second line treatments:
o Ativan 0.1 mg/kg x 1 (has a very long half life in neonates, between 24-40 hours)o Fosphenytoin 20mg/kg IV x 1
***** EEG monitoring cannot be performed in the well baby nursery *****
If you are worried that a neonate is having a seizure, this is an urgent issue. Contact the attending for the patient and discuss if transfer to the NICU is appropriate for further monitoring, evaluation and treatment.
163
ACUTE STROKE
BRANDON ZIELINSKI MD PHD, BETSY OSTRANDER MD
We should think about stroke when a patient has a sudden change in exam, consisting of:1. Unilateral face, arm, or leg weakness2. Facial Asymmetry3. Confusion and trouble speaking4. Dysarthria (slurred speech) or aphasia (not able to answer questions or name objects)
I. Resident to evaluate urgently, and if concern remains contact senior resident and team attending immediately. Obtain specific time of onset of the change in neurological exam.
II. If after evaluation, concern for stroke remains contact the pediatric neurology “on-call”. If using SmartWeb/text page, state clearly “This is <name and position>. I have a concern for an acute stroke in <bed number> with a time of onset at <time of onset>”. Expect a return within 5 minutes. (if no return, call neuro attending).
III. While awaiting callback, follow the stroke ABC’s (see also PCMC Med/Surg Stroke Admission Orderset):! a. Obtain vital signs, CR monitor & pulse ox; make NPO! b. Establish airway, ventilation! c. Oxygen supplementation prn to keep SaO2 >89% ! d. Restrict activity to bedrest, head of bed 30o ! e. Send STAT blood draw: CMP, iCa, Mg, P04, iSTAT glucose, CBC with diff, ! PT/INR, PTT, fibrinogen, tox screen! f. obtain STAT EKG! g. Establish venous access; PRN IV fluids to attain isotonic normovolemia (NS)! h. Blood pressure/perfusion: watch for hypotension, hypertension; treat as ! appropriate to goal MAP between 50%ile and 95%ile age norms.! i.Dextrose – establish normoglycemia at bedside & supplement glucose prn to ! goal blood glucose 65-100 mg/dl! j.Temperature: treat agressively prevent hyperthermia, goal temp <37.5o C! k. Call Radiology to discuss potential need for hyperacute imaging
IV. While awaiting head imaging, child neurology service to confirm time of onset, review exclusion criteria for tPA, and begin team/family discussions regarding potential risks/benefits of therapeutic options.
164
Ne
urolo
gy
Acute Stroke DDx
Common causes (in no particular order):
congenital heart disease 30%acquired heart disease (rheumatic fever)infection (bacterial meningitis, abscess, viral encephalitis)complicated migranousarterial dissectionvasculopathies 18 % (SLE, Kawasaki, hypersensitivity vasculitis, Takayasu arteritis)hypercoaguable states sickle cell dz (8% of by age 14 have a stroke)malignancies (metastatic neuroblastoma)chemotherapy cocaine usehemolytic uremic syndromethrombocytopeniaUncommon causes:Moyamoya fibromuscular dysplasiapolyarteritis nodosaEhlers-DanlosMarfan syndromeMELAS syndromespontaneous carotid artery dissectionneurofibromatosis
165
1. Neurofibromatosis type 1 (Mutation NF1 gene, 17q11.2; encodes neurofibromin)1. Diagnosis
a. Diagnostic Criteria:• Presence of café au lait spots (≥#6; ≥ 5 mm prepubertal; ≥ 15
mm postpubertal) and 1 or more of the following:• 2 or more neurofibromas
of any type or one or more plexiform neurofibromas
• axillary or inguinal freckling
• optic glioma• Lisch nodules (iris hamartomas; two or more)• Distinctive osseous lesion (sphenoid dysplsia,
pseudarthrosis) • First degree relative with NF-1
b. Definite diagnosis: two or more of the above criteriac. Diagnosis should be suspected in anyone with one of the above
(save +FHx) d. Since the manifestations are age dependent, it is difficult to
definitively diagnose younger children who lack a positive family history.
e. Genetic testing usually not necessary for diagnosis.2. Management in Childhood
a. Potential problems to anticipate:i. Developmental delayii. Macrocephalyiii. Neoplasiaiv. Neurofibromav. Optic nerve gliomavi. Other gliomasvii. Plexiform neurofibromaviii. Malignant peripheral nerve sheath tumorsix. Leukemiax. Moya-moya syndrome
b. Routine surveillance/managementi. Initial comprehensive and detailed history and PEii. Attention to FHx and history of subtle diagnostic features
listed aboveiii. Attention to BP, OFC, eye, skin, skeleton, cardiovascular
and neurological systems; palpate neck and limbs carefully.
iv. Annual comprehensive history and PE with attention to the above.
v. Ophthalmological exam at least yearly until age 6.vi. Developmental assessment and monitoringvii. Medical genetics consultation/genetic counseling
c. Other studies mostly based on clinical findings in the above.d. Imaging:
i. Controversial: Routine brain MRI not uniformly recommended by all experts
166
Ne
urolo
gy
Important Neurocutaneous Disorders
ii. If suspicion of visual problem or abnormal ophthalmologic exam" MRI brain (with and without contrast)
iii. Once obtained, subsequent brain MRI often needed due to discovery of subclinical lesions:
iv. Focal areas of high (T2) signal intensity (FASI) (previously known as “Unidentified bright objects;” (UBOs; not politically favored term). These are commonly identified on brain MRI and are usually of no clinical significance. Number or size of these does not correlated with clinical severity or features.
2. Tuberous sclerosis complex (TSC) [due to mutations in genes for hamartin (9q34; TSC1) or tuberin (16p13.3; TSC2)]
Multisystem disease with protean manifestations; autosomal dominant
Majority of cases are spontaneous mutations.
1. DiagnosisDiagnostic Criteria
a. Major featuresb. Hypomelanotic macules (≥#3, at least 5-mm diameter)c. Angiofibromas (≥#3) or fibrous cephalic plaqued. Ungual fibromas (≥#2)e. Shagreen patchf. Multiple retinal hamartomasg. Cortical dysplasias*h. Subependymal nodulesi. Subependymal giant cell astrocytomaj. Cardiac rhabdomyomak. Lymphangioleiomyomatosis (LAM)l. Angiomyolipomas (AML; ≥#2)
Minor featuresm. “Confetti” skin lesionsn. Dental enamel pits (≥#3)o. Intraoral fibromas (≥ 2)p. Retinal achromic patchq. Multiple renal cystsr. Nonrenal hamartomass. Definite diagnosis: Two major features or one major feature
with 2 or more minor features. (1 AML plus LAM alone is insufficient)Possible diagnosis: Either one major feature or 2 or more minor features2. Management
a. Potential problems to anticipate:i. Cardiac rhabdomyomas (may be clinically significant
pre-natally)ii. Infantile spasms, other epilepsy, developmental delay
and cognitive difficulties, neurobehavioral problems (TAND= Tuberous sclerosis associated neuropsychiatric disorders).
167
iii. Subependymal giant cell tumors (SEGA): 10% of children
iv. Retinal hamartomas (usually clinically silent)v. Skin lesions: depigmented macules (ash leaf spots),
facial angiofibromas (adenoma sebaceum), forehead plaques, shagreen patches.
vi. Renal hamartomas= angiomyolipomas (AML; typically become a problem after puberty)
vii. Pulmonary Lymphangiomyomatosis (LAM): primarily in women
b. Management and Surveillance:i. Initial comprehensive and detailed history and PEii. Attention to FHx and history of subtle diagnostic
features listed aboveiii. Attention to BP, OFC, eye, skin, cardiovascular and
neurological systems.iv. At least annual comprehensive history and PE with
attention to the above.v. Echocardiogram at least once- repeat as clinically
indicated nevery 1-3 years until rhabdomyomas involute. vi. Ophthalmological exam at least once.vii. Developmental assessment and monitoring/Screening
for TANDviii. Medical genetics consultation/genetic counseling
c. Surveillance:i. Echocardiogram: as aboveii. EKG every 3-5 years at least.iii. Brain MRI once diagnosis knowniv. Repeat every 1-3 years during childhoodv. Renal imaging once diagnosis known; repeat every 1-3
years depending on findings3. Treatment:
a. Symptomatic for epilepsyi. Vigabatrin specifically preferred for infantile spasms
(though toxicity and cost is a problem)b. Symptomatic for rhabdomyomas—usually improves with agec. SEGA
i. Surgery for acutely symptomatic (acute hydrocephalus; rare)
ii. mTOR inhibitors (sirolimus, everolimus) for growing SEGA
d. AMLi. mTOR inhibitorsii. Embolization if necessaryiii. Surgery if necessary.
3. Sturge-Weber Syndrome (SWS; Encephalofacial angiomatosis)
Association of facial port-wine stain with either 1) abnormal vasculature of the surface of the brain (leptomeningeal angioma), 2) glaucoma or 3) both.
• isolated intracranial variant: leptomeningeal angioma without skin or eye involvement• Most cases unilateral; about 15% bilateral
168
Ne
urolo
gy
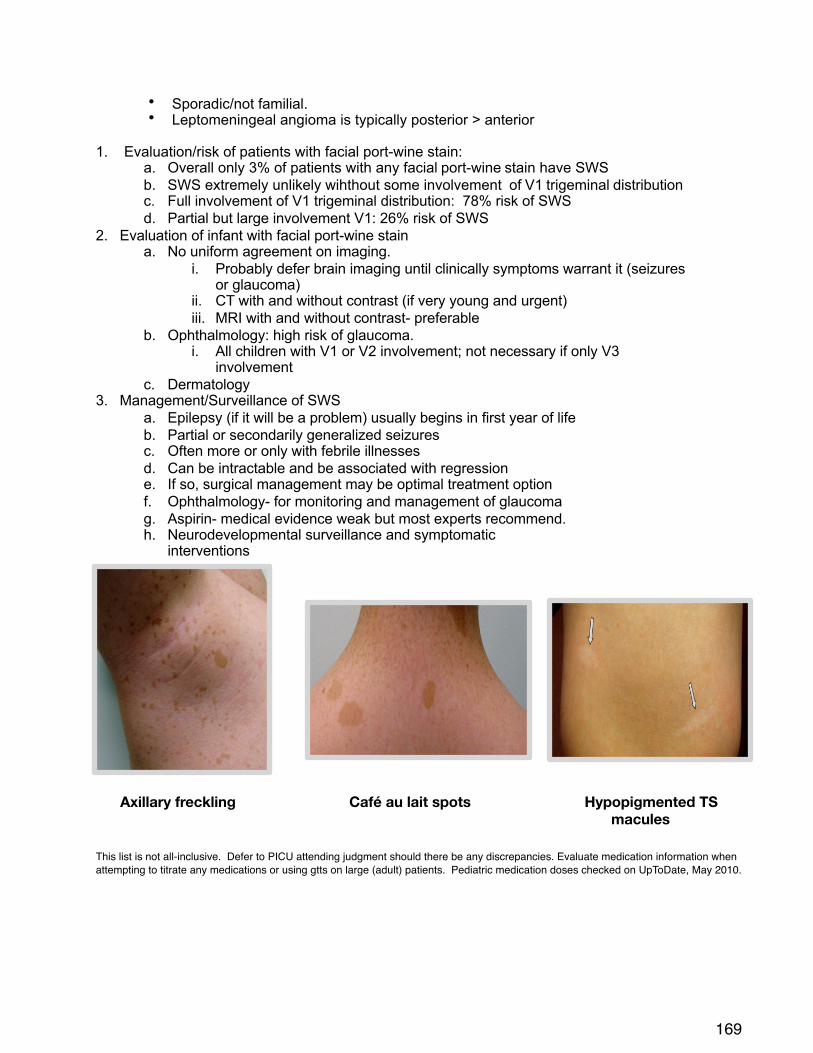
• Sporadic/not familial. • Leptomeningeal angioma is typically posterior > anterior
1. Evaluation/risk of patients with facial port-wine stain:a. Overall only 3% of patients with any facial port-wine stain have SWSb. SWS extremely unlikely wihthout some involvement of V1 trigeminal distributionc. Full involvement of V1 trigeminal distribution: 78% risk of SWSd. Partial but large involvement V1: 26% risk of SWS
2. Evaluation of infant with facial port-wine staina. No uniform agreement on imaging.
i. Probably defer brain imaging until clinically symptoms warrant it (seizures or glaucoma)
ii. CT with and without contrast (if very young and urgent)iii. MRI with and without contrast- preferable
b. Ophthalmology: high risk of glaucoma.i. All children with V1 or V2 involvement; not necessary if only V3
involvementc. Dermatology
3. Management/Surveillance of SWSa. Epilepsy (if it will be a problem) usually begins in first year of lifeb. Partial or secondarily generalized seizuresc. Often more or only with febrile illnessesd. Can be intractable and be associated with regressione. If so, surgical management may be optimal treatment optionf. Ophthalmology- for monitoring and management of glaucomag. Aspirin- medical evidence weak but most experts recommend. h. Neurodevelopmental surveillance and symptomatic
interventions# # #
Axillary freckling Café au lait spots Hypopigmented TS macules
This list is not all-inclusive. Defer to PICU attending judgment should there be any discrepancies. Evaluate medication information when attempting to titrate any medications or using gtts on large (adult) patients. Pediatric medication doses checked on UpToDate, May 2010.
169

170
Pediatric Intensive Care
SEDATIONGeneral#Principles:
1. Midazolam/lorazepam#offer#amnesia#and#sedation#but#NOT#pain#control#(include#fentanyl#or#morphine#for#analgesia)
2. If#a#patient#needs#increased#sedation,#bolus#with#a#new#higher#hourly#rate#and#then#increase#your#drip#accordingly#
a. For#example,#if#a#patient#was#on#fentanyl#1mcg/kg/hr,#bolus#with#2mcg/kg#and#increase#the#drip#to#2mcg/kg/hr
3. Ensure#that#any#patient#receiving#paralytic#medications#has#adequate#sedation4. Remember#that#many#sedation#drugs#cause#hypotension#and#decrease#respiratory#drive5. Remember#not#to#exceed#maximum#adult#doses,#particularly#in#older#children6. In#a#patient#is#ventilated#for#an#extended#period#of#time,#consider#transition#to#enteral#methadone/
enteral#lorazepam#via#NJ
BLOOD$PRODUCTS1. If#the#patient#is#not#actively#bleeding,#you#do#not#necessarily#need#to#correct#coags2. Dosing:#
a. PRBCs:#10X20mL/kg#over#2X4#hours#(may#need#to#follow#with#furosemide)b. Platelets:#10mL/kgc. FFP:#10mg/kgd. Cryoprecipitate:#1#unit/10kg#body#weight#(for#fibrogen#<100);#recheck#fibrinogen#after#
infusionXmay#need#second#dose#as#each#unit#of#cryo#has#variable#amount#of#fibrinogen
ELECTROLYTESGeneral#Principles:
1. Potassiuma. It#is#always#more#safe#to#have#a#potassium#level#that#is#slightly#low#instead#of#one#that#is#
high;#if#K#is#>3#be#cautious#about#replacement#b. ECG:##
i. HyperkalemiaX#peaked#T#wavesii. HypokalemiaX#flat/absent#T#waves#or#U#waves
c. K#replacement#for#hypokalemia:#consider#Kacetate#or#KCL#via#IV;#Kgluconate#or#KCl#orallyd. If#significant#hyperkalemia:
i. First,#calcium#gluconate#(50X100mg/kg)#for#cardiac#myocyte#stabilization#ii. Consider#albuterol,#sodium#bicarbonate,#insulin/glucose#per#pharmacy#protocol
INTUBATION1. Prepare,#preoxygenate,#premedicate
a. Meds:#Atropine,#fentanyl,#versed,#lidocaine,#etomidate#or#ketamine#(not#with#increased#ICP),#succinylcholine#or#rocuronium
2. Endotracheal#tube#size:#(age/4)#+#4a. Tube#length:#Number#at#teeth#=#tube#size#x#3
3. Oral#airway:#size#=#central#incisor#to#angle#of#jaw#(not#for#use#in#awake#patient)4. Nasal#airway:#size#=#tip#of#nose#to#ear#(can#use#in#awake#patient)
172
Ped
iatric
Critic
al C
are
PICU Pearls
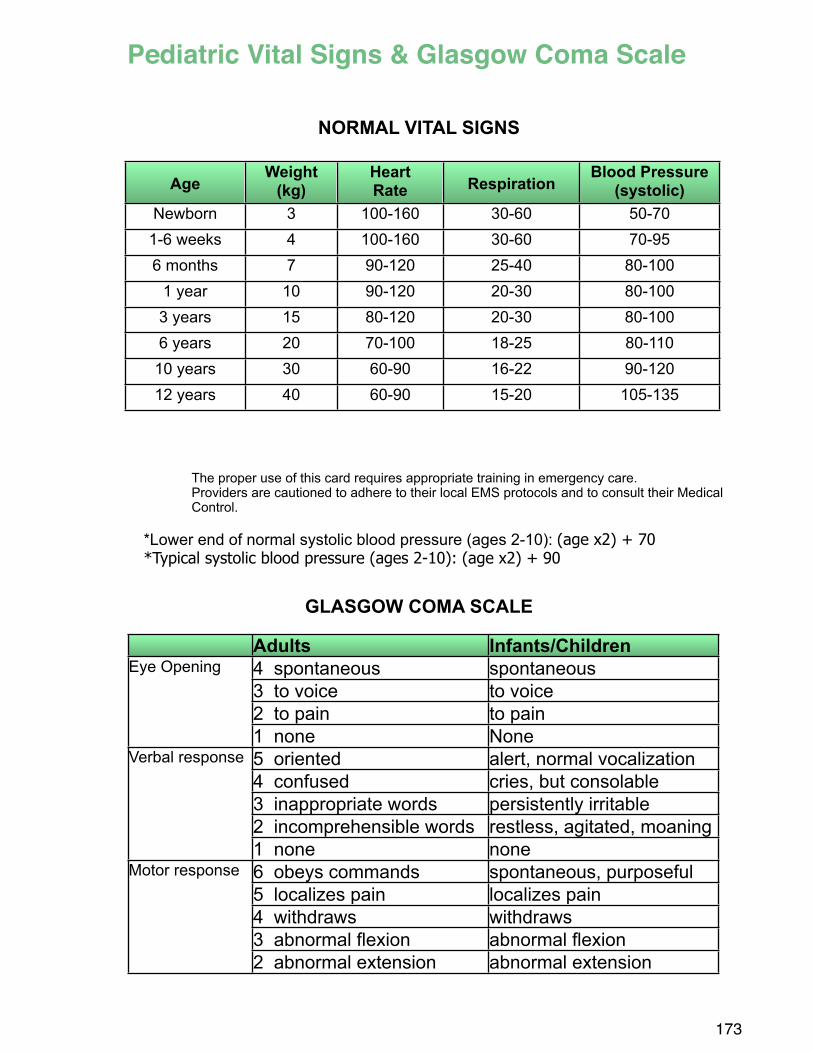
NORMAL VITAL SIGNS
The proper use of this card requires appropriate training in emergency care. Providers are cautioned to adhere to their local EMS protocols and to consult their Medical Control.
*Lower end of normal systolic blood pressure (ages 2-10): (age x2) + 70*Typical systolic blood pressure (ages 2-10): (age x2) + 90
GLASGOW COMA SCALE
173
Pediatric Vital Signs & Glasgow Coma Scale
Adults Infants/ChildrenEye Opening 4 spontaneous spontaneousEye Opening
3 to voice to voiceEye Opening
2 to pain to pain
Eye Opening
1 none NoneVerbal response 5 oriented alert, normal vocalizationVerbal response
4 confused cries, but consolableVerbal response
3 inappropriate words persistently irritable
Verbal response
2 incomprehensible words restless, agitated, moaning
Verbal response
1 none noneMotor response 6 obeys commands spontaneous, purposefulMotor response
5 localizes pain localizes painMotor response
4 withdraws withdraws
Motor response
3 abnormal flexion abnormal flexion
Motor response
2 abnormal extension abnormal extension
AgeWeight
(kg)HeartRate Respiration
Blood Pressure(systolic)
Newborn 3 100-160 30-60 50-701-6 weeks 4 100-160 30-60 70-956 months 7 90-120 25-40 80-100
1 year 10 90-120 20-30 80-1003 years 15 80-120 20-30 80-1006 years 20 70-100 18-25 80-110
10 years 30 60-90 16-22 90-12012 years 40 60-90 15-20 105-135
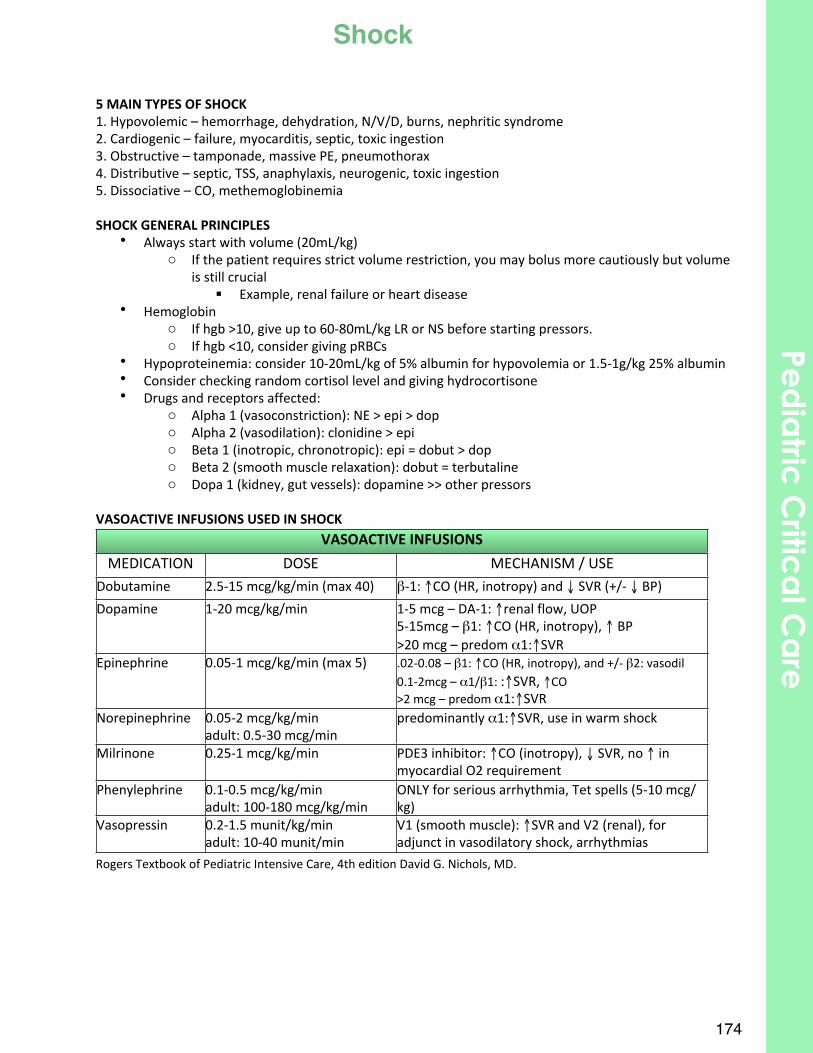
5$MAIN$TYPES$OF$SHOCK1.#Hypovolemic#–#hemorrhage,#dehydration,#N/V/D,#burns,#nephritic#syndrome2.#Cardiogenic#–#failure,#myocarditis,#septic,#toxic#ingestion3.#Obstructive#–#tamponade,#massive#PE,#pneumothorax4.#Distributive#–#septic,#TSS,#anaphylaxis,#neurogenic,#toxic#ingestion5.#Dissociative#–#CO,#methemoglobinemia
SHOCK$GENERAL$PRINCIPLES• Always#start#with#volume#(20mL/kg)#
o If#the#patient#requires#strict#volume#restriction,#you#may#bolus#more#cautiously#but#volume#is#still#crucial#
! Example,#renal#failure#or#heart#disease• Hemoglobin
o If#hgb#>10,#give#up#to#60X80mL/kg#LR#or#NS#before#starting#pressors.o If#hgb#<10,#consider#giving#pRBCs
• Hypoproteinemia:#consider#10X20mL/kg#of#5%#albumin#for#hypovolemia#or#1.5X1g/kg#25%#albumin#• Consider#checking#random#cortisol#level#and#giving#hydrocortisone• Drugs#and#receptors#affected:
o Alpha#1#(vasoconstriction):#NE#>#epi#>#dopo Alpha#2#(vasodilation):#clonidine#>#epio Beta#1#(inotropic,#chronotropic):#epi#=#dobut#>#dopo Beta#2#(smooth#muscle#relaxation):#dobut#=#terbutalineo Dopa#1#(kidney,#gut#vessels):#dopamine#>>#other#pressors
VASOACTIVE$INFUSIONS$USED$IN$SHOCKVASOACTIVE$INFUSIONSVASOACTIVE$INFUSIONSVASOACTIVE$INFUSIONS
MEDICATION DOSE MECHANISM9/9USEDobutamine 2.5X15#mcg/kg/min#(max#40) βX1:#↑CO#(HR,#inotropy)#and#↓#SVR#(+/X#↓#BP)#
Dopamine 1X20#mcg/kg/min 1X5#mcg#–#DAX1:#↑renal#flow,#UOP5X15mcg#–#β1:#↑CO#(HR,#inotropy),#↑#BP>20#mcg#–#predom#α1:↑SVR
Epinephrine 0.05X1#mcg/kg/min#(max#5) .02X0.08#–#β1:#↑CO#(HR,#inotropy),#and#+/X#β2:#vasodil0.1X2mcg#–#α1/β1:#:↑SVR,#↑CO>2#mcg#–#predom#α1:↑SVR
Norepinephrine 0.05X2#mcg/kg/minadult:#0.5X30#mcg/min
predominantly#α1:↑SVR,#use#in#warm#shock
Milrinone 0.25X1#mcg/kg/min PDE3#inhibitor:#↑CO#(inotropy),#↓#SVR,#no#↑#in#myocardial#O2#requirement
Phenylephrine 0.1X0.5#mcg/kg/minadult:#100X180#mcg/kg/min
ONLY#for#serious#arrhythmia,#Tet#spells#(5X10#mcg/kg)
Vasopressin 0.2X1.5#munit/kg/minadult:#10X40#munit/min
V1#(smooth#muscle):#↑SVR#and#V2#(renal),#for#adjunct#in#vasodilatory#shock,#arrhythmias
Rogers#Textbook#of#Pediatric#Intensive#Care,#4th#edition#David#G.#Nichols,#MD.
174
Ped
iatric
Critic
al C
are
Shock
Mechanical Ventilation:• PIP: Peak inspiratory pressure during respiratory cycle
o Adjust for good chest movement o Usually max around 30-35
• Tidal Volume (Tv): Volume of gas delivered during inspiration o Normal goal 5-6mL/kg
• Rate: number of breaths/minutes o Based on age and pCO2
• Positive end-expiratory pressure (PEEP): pressure maintained between inspiration and expiration that prevents alveolar collapse
o Physiologic PEEP = 3-5cm H20• Inspiratory Time (I time): length during breath cycle spent in inspiratory phase• Oxygenation: Measured by pO2 and saturation
o To improve: Increase PEEP or FiO2• Ventilation: Measured by pH and pCO2
o To improve: Increase PIP or Tv or increase rate
High Frequency Oscillatory Ventilation (HFOV): • Uncouples oxygenation and ventilation & keeps constant pressure in all areas of the lung• Settings:
o MAP: average pressure over entire respiratory cycle ! Somewhat like PEEP! Start at 3-5cm above MAP of conventional ventilator
o Amplitude (ΔP): determines volume delivered! Like PIP
o Hertz: Frequency! Like rate (1Hz = 60breath/minute)
• Signs: Chest wall vibration indicates Tvo Should have good “bounce” on chest into groin
• Oxygenation:o Assessed by: CXR (goal expansion of 9 ribs) & saturationo Improved by:
! Increase FiO2! Increase MAP
• Ventilation: o Assessed by blood gas
! Increase amplitude• Increases the displacement of the oscillating diaphragm ! increases
volume delivered to the patient ! Decrease frequency
• If amplitude is maximal…small changes in Hz translate to large CO2 changes
175
Ventilator Management
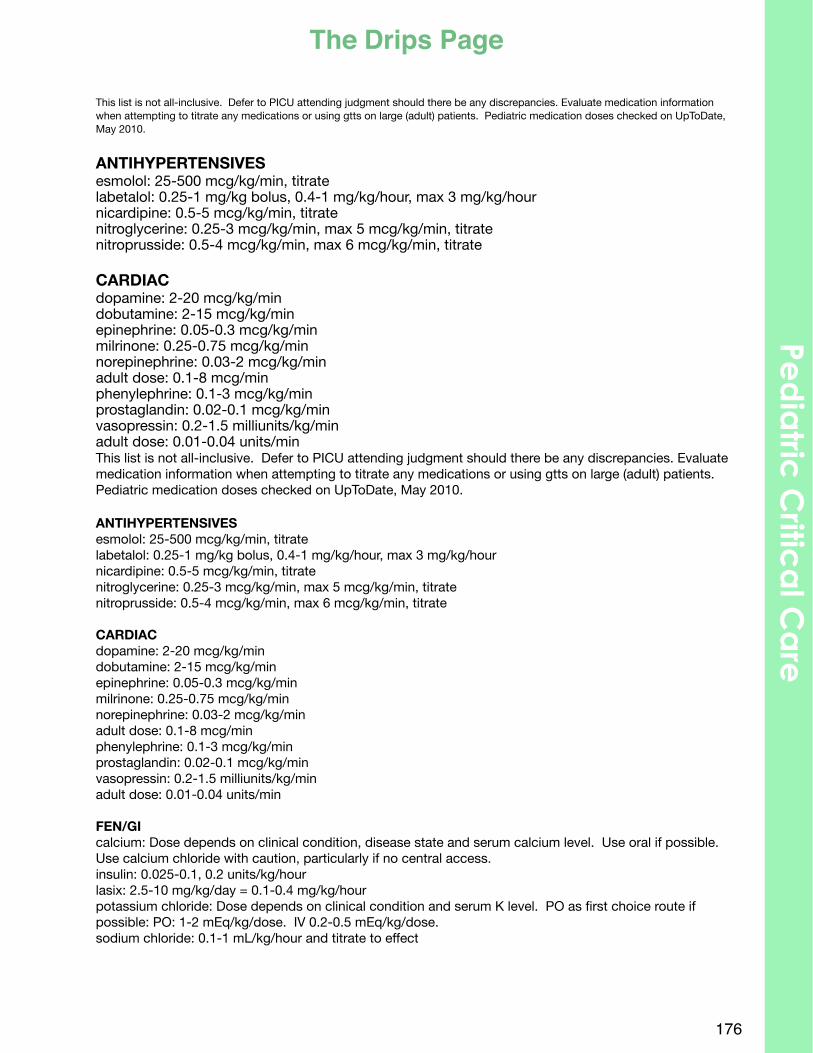
This list is not all-inclusive. Defer to PICU attending judgment should there be any discrepancies. Evaluate medication information when attempting to titrate any medications or using gtts on large (adult) patients. Pediatric medication doses checked on UpToDate, May 2010.
ANTIHYPERTENSIVESesmolol: 25‐500 mcg/kg/min, titratelabetalol: 0.25‐1 mg/kg bolus, 0.4‐1 mg/kg/hour, max 3 mg/kg/hournicardipine: 0.5‐5 mcg/kg/min, titratenitroglycerine: 0.25‐3 mcg/kg/min, max 5 mcg/kg/min, titratenitroprusside: 0.5‐4 mcg/kg/min, max 6 mcg/kg/min, titrate
CARDIACdopamine: 2‐20 mcg/kg/mindobutamine: 2‐15 mcg/kg/minepinephrine: 0.05‐0.3 mcg/kg/minmilrinone: 0.25‐0.75 mcg/kg/minnorepinephrine: 0.03‐2 mcg/kg/minadult dose: 0.1‐8 mcg/minphenylephrine: 0.1‐3 mcg/kg/minprostaglandin: 0.02‐0.1 mcg/kg/minvasopressin: 0.2‐1.5 milliunits/kg/minadult dose: 0.01‐0.04 units/minThis list is not all-inclusive. Defer to PICU attending judgment should there be any discrepancies. Evaluate medication information when attempting to titrate any medications or using gtts on large (adult) patients. Pediatric medication doses checked on UpToDate, May 2010.
ANTIHYPERTENSIVESesmolol: 25‐500 mcg/kg/min, titratelabetalol: 0.25‐1 mg/kg bolus, 0.4‐1 mg/kg/hour, max 3 mg/kg/hournicardipine: 0.5‐5 mcg/kg/min, titratenitroglycerine: 0.25‐3 mcg/kg/min, max 5 mcg/kg/min, titratenitroprusside: 0.5‐4 mcg/kg/min, max 6 mcg/kg/min, titrate
CARDIACdopamine: 2‐20 mcg/kg/mindobutamine: 2‐15 mcg/kg/minepinephrine: 0.05‐0.3 mcg/kg/minmilrinone: 0.25‐0.75 mcg/kg/minnorepinephrine: 0.03‐2 mcg/kg/minadult dose: 0.1‐8 mcg/minphenylephrine: 0.1‐3 mcg/kg/minprostaglandin: 0.02‐0.1 mcg/kg/minvasopressin: 0.2‐1.5 milliunits/kg/minadult dose: 0.01‐0.04 units/min
FEN/GIcalcium: Dose depends on clinical condition, disease state and serum calcium level. Use oral if possible. Use calcium chloride with caution, particularly if no central access.insulin: 0.025‐0.1, 0.2 units/kg/hourlasix: 2.5‐10 mg/kg/day = 0.1‐0.4 mg/kg/hourpotassium chloride: Dose depends on clinical condition and serum K level. PO as first choice route if possible: PO: 1-2 mEq/kg/dose. IV 0.2-0.5 mEq/kg/dose.sodium chloride: 0.1‐1 mL/kg/hour and titrate to effect
176
The Drips PagePe
dia
tric C
ritica
l Ca
re
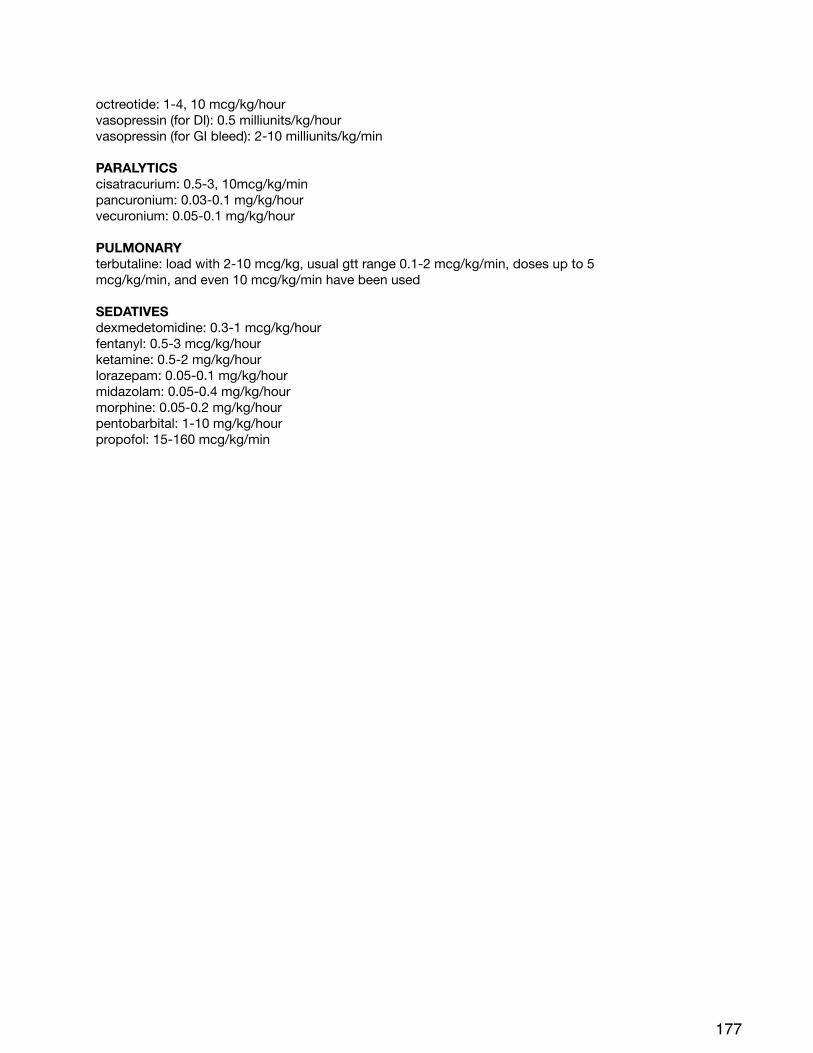
octreotide: 1‐4, 10 mcg/kg/hourvasopressin (for DI): 0.5 milliunits/kg/hourvasopressin (for GI bleed): 2‐10 milliunits/kg/min
PARALYTICScisatracurium: 0.5‐3, 10mcg/kg/minpancuronium: 0.03‐0.1 mg/kg/hourvecuronium: 0.05‐0.1 mg/kg/hour
PULMONARYterbutaline: load with 2‐10 mcg/kg, usual gtt range 0.1‐2 mcg/kg/min, doses up to 5mcg/kg/min, and even 10 mcg/kg/min have been used
SEDATIVESdexmedetomidine: 0.3‐1 mcg/kg/hourfentanyl: 0.5‐3 mcg/kg/hourketamine: 0.5‐2 mg/kg/hourlorazepam: 0.05‐0.1 mg/kg/hourmidazolam: 0.05‐0.4 mg/kg/hourmorphine: 0.05‐0.2 mg/kg/hourpentobarbital: 1‐10 mg/kg/hourpropofol: 15‐160 mcg/kg/min
177
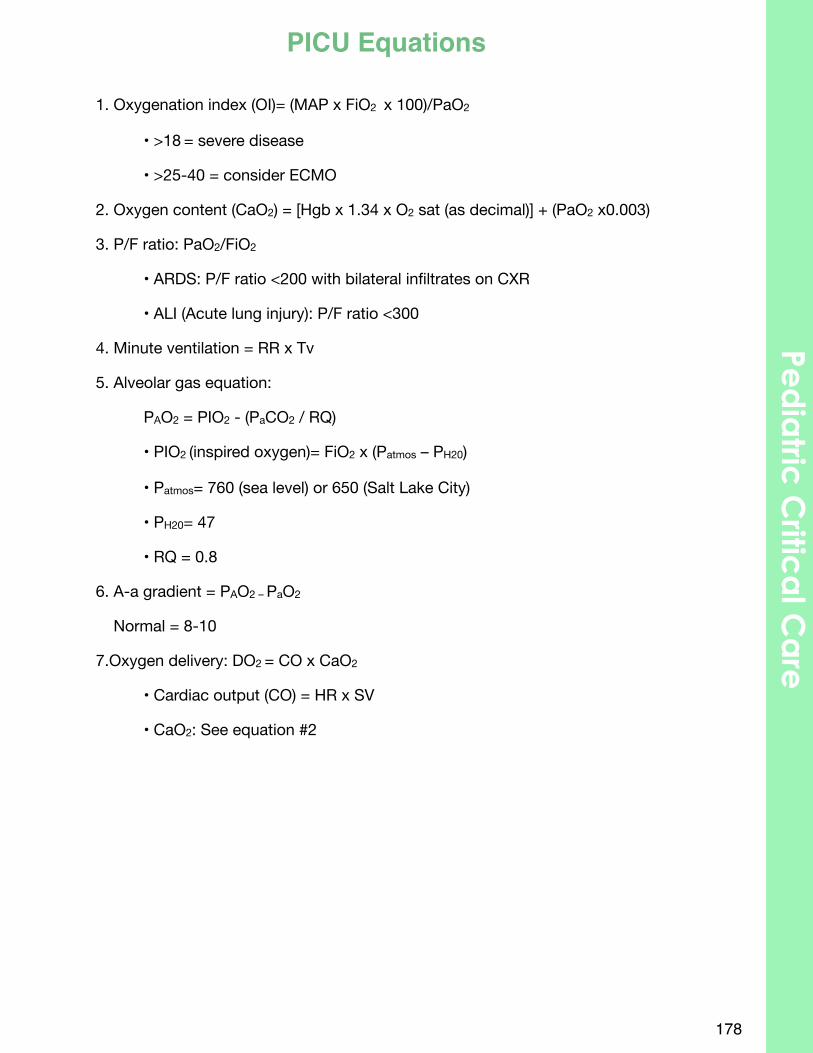
1. Oxygenation index (OI)= (MAP x FiO2 x 100)/PaO2
• >18 = severe disease
• >25-40 = consider ECMO
2. Oxygen content (CaO2) = [Hgb x 1.34 x O2 sat (as decimal)] + (PaO2 x0.003)
3. P/F ratio: PaO2/FiO2
• ARDS: P/F ratio <200 with bilateral infiltrates on CXR
• ALI (Acute lung injury): P/F ratio <300
4. Minute ventilation = RR x Tv
5. Alveolar gas equation:
PAO2 = PIO2 - (PaCO2 / RQ)
• PIO2 (inspired oxygen)= FiO2 x (Patmos – PH20)
• Patmos= 760 (sea level) or 650 (Salt Lake City)
• PH20= 47
• RQ = 0.8
6. A-a gradient = PAO2 – PaO2
Normal = 8-10
7.Oxygen delivery: DO2 = CO x CaO2
• Cardiac output (CO) = HR x SV
• CaO2: See equation #2
178
Ped
iatric
Critic
al C
are
PICU Equations

180
Primary Care
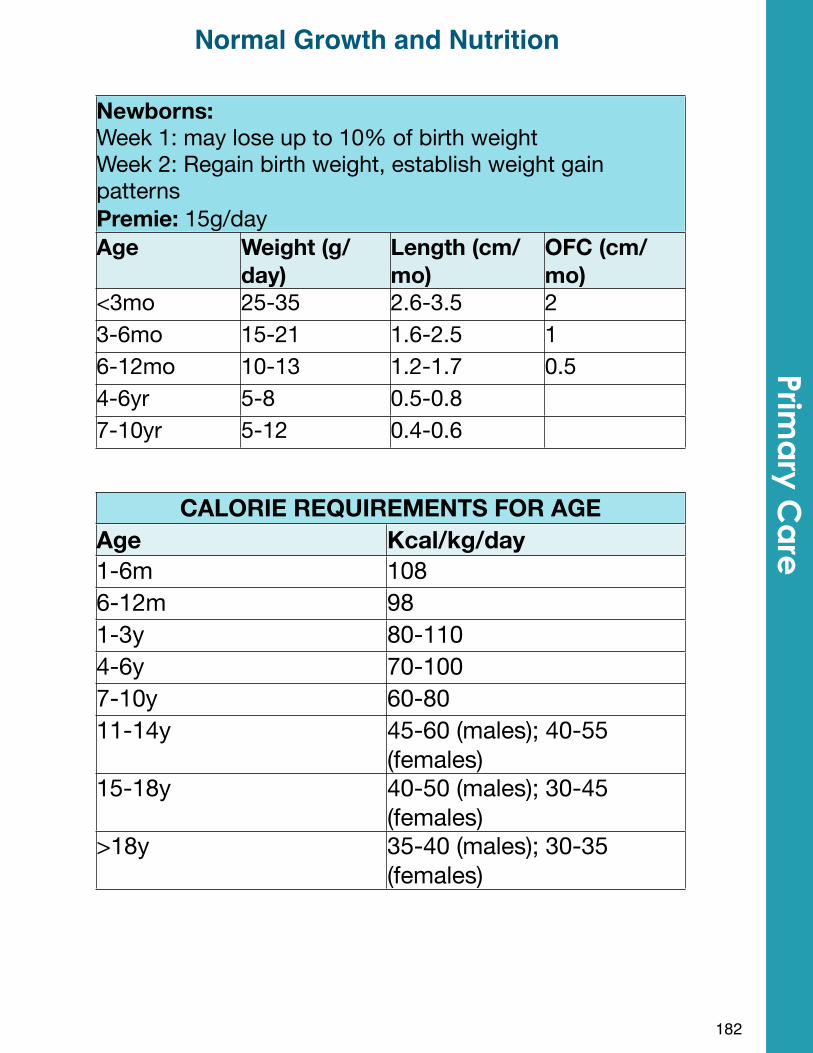
Newborns: Week 1: may lose up to 10% of birth weightWeek 2: Regain birth weight, establish weight gain patternsPremie: 15g/day
Newborns: Week 1: may lose up to 10% of birth weightWeek 2: Regain birth weight, establish weight gain patternsPremie: 15g/day
Newborns: Week 1: may lose up to 10% of birth weightWeek 2: Regain birth weight, establish weight gain patternsPremie: 15g/day
Newborns: Week 1: may lose up to 10% of birth weightWeek 2: Regain birth weight, establish weight gain patternsPremie: 15g/dayAge Weight (g/
day)Length (cm/mo)
OFC (cm/mo)
<3mo 25-35 2.6-3.5 23-6mo 15-21 1.6-2.5 16-12mo 10-13 1.2-1.7 0.54-6yr 5-8 0.5-0.87-10yr 5-12 0.4-0.6
CALORIE REQUIREMENTS FOR AGECALORIE REQUIREMENTS FOR AGEAge Kcal/kg/day1-6m 1086-12m 981-3y 80-1104-6y 70-1007-10y 60-8011-14y 45-60 (males); 40-55
(females)15-18y 40-50 (males); 30-45
(females)>18y 35-40 (males); 30-35
(females)
182
Prima
ry Ca
reNormal Growth and Nutrition
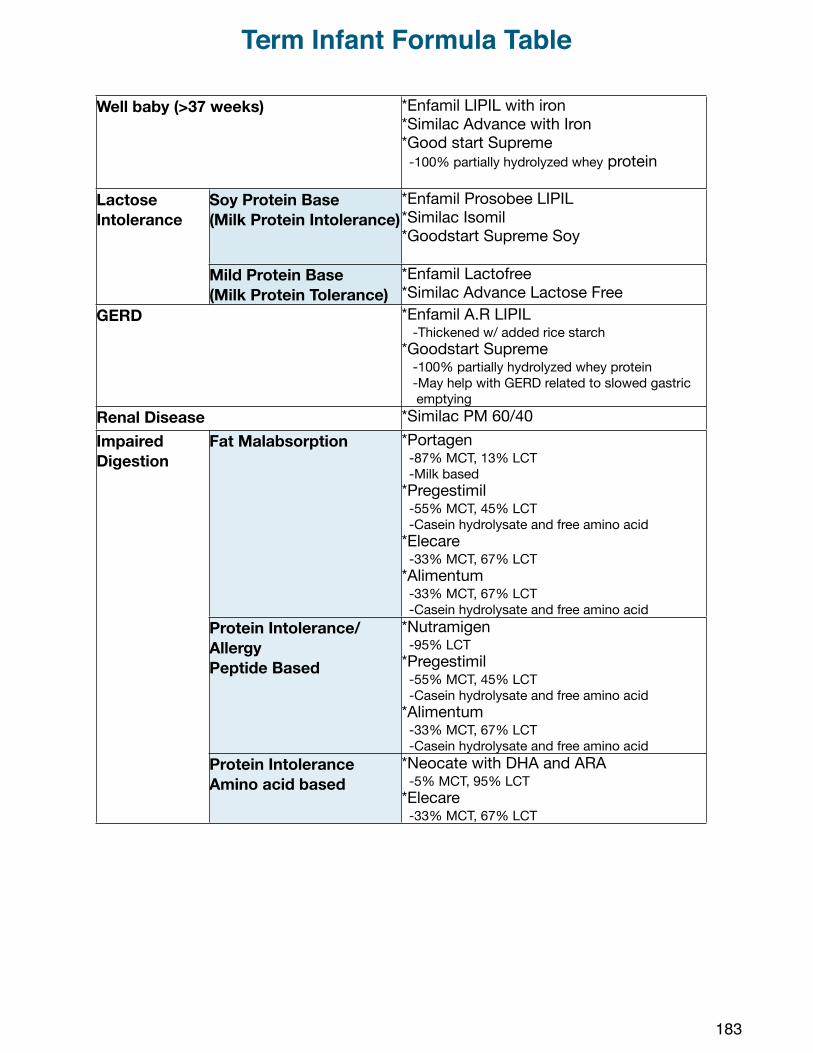
Well baby (>37 weeks)Well baby (>37 weeks) *Enfamil LIPIL with iron*Similac Advance with Iron*Good start Supreme -100% partially hydrolyzed whey protein
Lactose Intolerance
Soy Protein Base(Milk Protein Intolerance)
*Enfamil Prosobee LIPIL*Similac Isomil*Goodstart Supreme Soy
Lactose Intolerance
Mild Protein Base(Milk Protein Tolerance)
*Enfamil Lactofree*Similac Advance Lactose Free
GERDGERD *Enfamil A.R LIPIL -Thickened w/ added rice starch*Goodstart Supreme -100% partially hydrolyzed whey protein -May help with GERD related to slowed gastric emptying
Renal DiseaseRenal Disease *Similac PM 60/40Impaired Digestion
Fat Malabsorption *Portagen -87% MCT, 13% LCT -Milk based*Pregestimil -55% MCT, 45% LCT -Casein hydrolysate and free amino acid*Elecare -33% MCT, 67% LCT*Alimentum -33% MCT, 67% LCT -Casein hydrolysate and free amino acid
Impaired Digestion
Protein Intolerance/AllergyPeptide Based
*Nutramigen -95% LCT*Pregestimil -55% MCT, 45% LCT -Casein hydrolysate and free amino acid*Alimentum -33% MCT, 67% LCT -Casein hydrolysate and free amino acid
Impaired Digestion
Protein IntoleranceAmino acid based
*Neocate with DHA and ARA -5% MCT, 95% LCT*Elecare -33% MCT, 67% LCT
183
Term Infant Formula Table
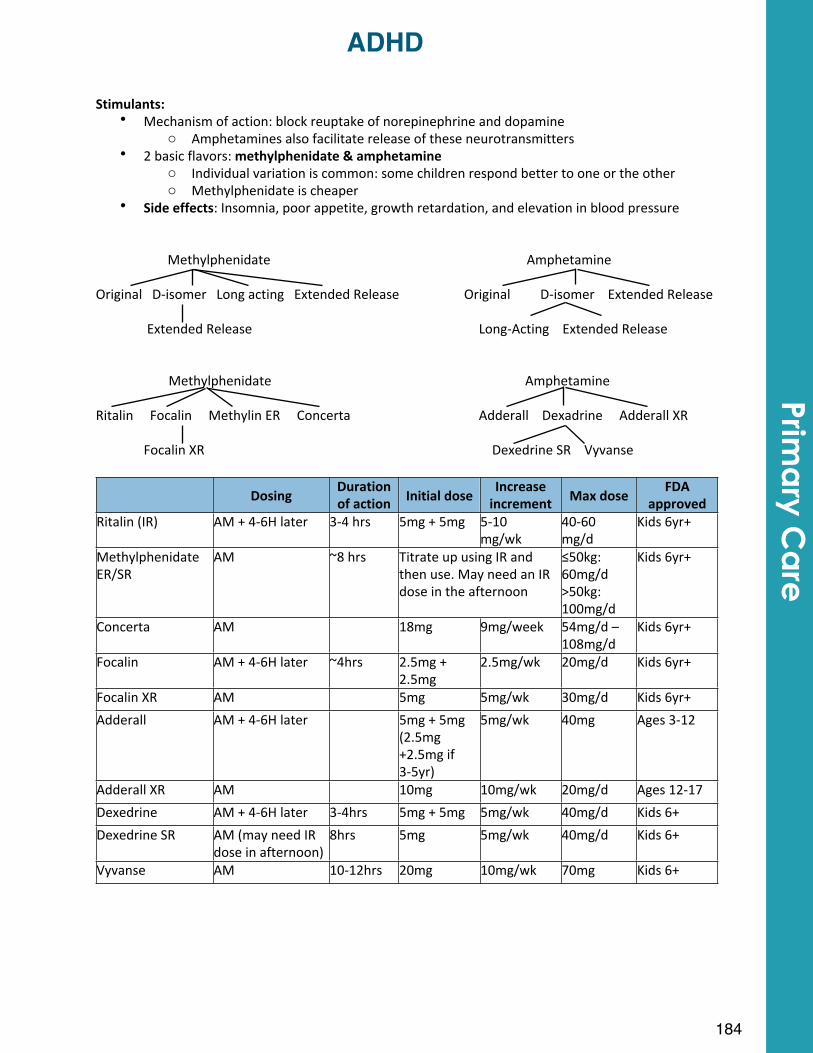
Stimulants:$• Mechanism#of#action:#block#reuptake#of#norepinephrine#and#dopamine
o Amphetamines#also#facilitate#release#of#these#neurotransmitters• 2#basic#flavors:#methylphenidate$&$amphetamine
o Individual#variation#is#common:#some#children#respond#better#to#one#or#the#othero Methylphenidate#is#cheaper
• Side$effects:#Insomnia,#poor#appetite,#growth#retardation,#and#elevation#in#blood#pressure
Methylphenidate# # # # # # Amphetamine
Original###DXisomer###Long#acting###Extended#Release# ##########Original#########DXisomer####Extended#Release
#Extended#Release# # # # # LongXActing####Extended#Release
######################Methylphenidate# # # # # ##############Amphetamine
Ritalin#####Focalin#####Methylin#ER#####Concerta## # # Adderall####Dexadrine#####Adderall#XR
# Focalin#XR# # # # # # ####Dexedrine#SR####Vyvanse
Dosing Duration$of$action Initial$dose Increase$
increment Max$dose FDA$approved
Ritalin#(IR) AM#+#4X6H#later# 3X4#hrs 5mg#+#5mg 5X10mg/wk
40X60mg/d
Kids#6yr+
Methylphenidate#ER/SR
AM# ~8#hrs Titrate#up#using#IR#and#then#use.#May#need#an#IR#dose#in#the#afternoon
Titrate#up#using#IR#and#then#use.#May#need#an#IR#dose#in#the#afternoon
≤50kg:#60mg/d>50kg:#100mg/d
Kids#6yr+
Concerta AM 18mg 9mg/week 54mg/d#–#108mg/d#
Kids#6yr+
Focalin AM#+#4X6H#later ~4hrs 2.5mg#+#2.5mg
2.5mg/wk 20mg/d Kids#6yr+
Focalin#XR AM 5mg 5mg/wk 30mg/d Kids#6yr+
Adderall AM#+#4X6H#later 5mg#+#5mg(2.5mg#+2.5mg#if#3X5yr)
5mg/wk 40mg Ages#3X12
Adderall#XR AM 10mg 10mg/wk 20mg/d Ages#12X17
Dexedrine AM#+#4X6H#later 3X4hrs 5mg#+#5mg 5mg/wk 40mg/d Kids#6+
Dexedrine#SR AM#(may#need#IR#dose#in#afternoon)
8hrs 5mg 5mg/wk 40mg/d Kids#6+
Vyvanse AM 10X12hrs 20mg 10mg/wk 70mg Kids#6+
184
ADHDPrim
ary C
are
Other$ADHD$meds:• Strattera:
o Mechanism of action: SNRIo Advantage: Can use when stimulants are contraindicated, doesn’t tend to cause
problems with appetite suppression and sleep disturbance, no known abuse potential
o Disadvantage: Usually takes longer to take effect than the stimulants• Alpha-2-adrenergic agonists: bind the receptor and inhibit further sympathetic output,
causing an anti-adrenergic effecto Clonidine:
! Advantage- Helps with more aggressive symptoms, cheap! Disadvantage- Side effects of sedation, hypotension, occasional dry mouth
and constipationo Guanfacine:
! Advantage- More selective alpha-2-adrenergic agonist than clonidine → less side effects
! Helps with aggressive symptoms ! Cheap (regular guanfacine… Intuniv is a newer long acting form that is
expensive)• Important Note: Best outcomes noted with medication + therapy
References:Stahl, Stephen M. The Prescriber’s Guide: 4th Edition. Cambridge University Press, 2011.Consumer Reports Health Evaluates: Best Buy Drugs for treating Attention-Deficit Hyperactivity Disorder. 2012. Online pdf. http://www.consumerreports.org/health/resources/pdf/best-buy-drugs/ADHDFinal.pdfPediatrics Review Education Program Self-Assessment 2011. American Academy of Pediatrics.
185
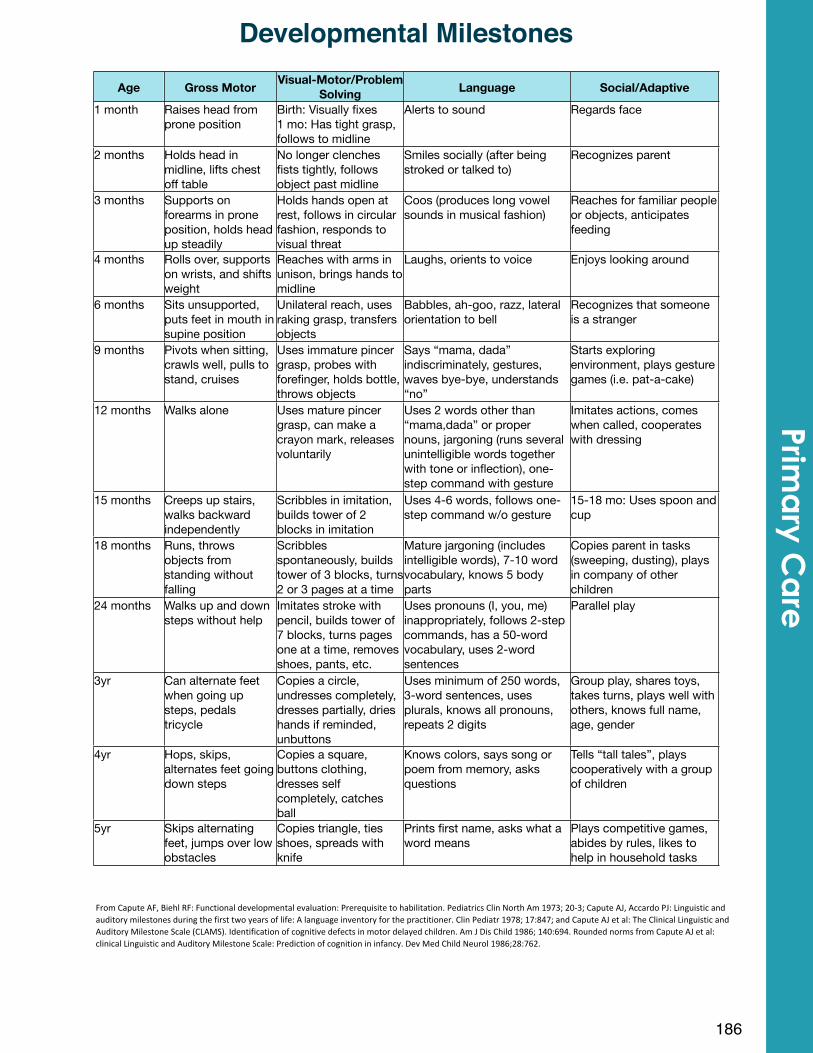
From%Capute%AF,%Biehl%RF:%Functional%developmental%evaluation:%Prerequisite%to%habilitation.%Pediatrics%Clin%North%Am%1973;%20E3;%Capute%AJ,%Accardo%PJ:%Linguistic%and%auditory%milestones%during%the%first%two%years%of%life:%A%language%inventory%for%the%practitioner.%Clin%Pediatr%1978;%17:847;%and%Capute%AJ%et%al:%The%Clinical%Linguistic%and%Auditory%Milestone%Scale%(CLAMS).%Identification%of%cognitive%defects%in%motor%delayed%children.%Am%J%Dis%Child%1986;%140:694.%Rounded%norms%from%Capute%AJ%et%al:%clinical%Linguistic%and%Auditory%Milestone%Scale:%Prediction%of%cognition%in%infancy.%Dev%Med%Child%Neurol%1986;28:762.
186
Developmental Milestones
Age Gross Motor Visual-Motor/Problem Solving Language Social/Adaptive
1 month Raises head from prone position
Birth: Visually fixes1 mo: Has tight grasp, follows to midline
Alerts to sound Regards face
2 months Holds head in midline, lifts chest off table
No longer clenches fists tightly, follows object past midline
Smiles socially (after being stroked or talked to)
Recognizes parent
3 months Supports on forearms in prone position, holds head up steadily
Holds hands open at rest, follows in circular fashion, responds to visual threat
Coos (produces long vowel sounds in musical fashion)
Reaches for familiar people or objects, anticipates feeding
4 months Rolls over, supports on wrists, and shifts weight
Reaches with arms in unison, brings hands to midline
Laughs, orients to voice Enjoys looking around
6 months Sits unsupported, puts feet in mouth in supine position
Unilateral reach, uses raking grasp, transfers objects
Babbles, ah-goo, razz, lateral orientation to bell
Recognizes that someone is a stranger
9 months Pivots when sitting, crawls well, pulls to stand, cruises
Uses immature pincer grasp, probes with forefinger, holds bottle, throws objects
Says “mama, dada” indiscriminately, gestures, waves bye-bye, understands “no”
Starts exploring environment, plays gesture games (i.e. pat-a-cake)
12 months Walks alone Uses mature pincer grasp, can make a crayon mark, releases voluntarily
Uses 2 words other than “mama,dada” or proper nouns, jargoning (runs several unintelligible words together with tone or inflection), one-step command with gesture
Imitates actions, comes when called, cooperates with dressing
15 months Creeps up stairs, walks backward independently
Scribbles in imitation, builds tower of 2 blocks in imitation
Uses 4-6 words, follows one-step command w/o gesture
15-18 mo: Uses spoon and cup
18 months Runs, throws objects from standing without falling
Scribbles spontaneously, builds tower of 3 blocks, turns 2 or 3 pages at a time
Mature jargoning (includes intelligible words), 7-10 word vocabulary, knows 5 body parts
Copies parent in tasks (sweeping, dusting), plays in company of other children
24 months Walks up and down steps without help
Imitates stroke with pencil, builds tower of 7 blocks, turns pages one at a time, removes shoes, pants, etc.
Uses pronouns (I, you, me) inappropriately, follows 2-step commands, has a 50-word vocabulary, uses 2-word sentences
Parallel play
3yr Can alternate feet when going up steps, pedals tricycle
Copies a circle, undresses completely, dresses partially, dries hands if reminded, unbuttons
Uses minimum of 250 words, 3-word sentences, uses plurals, knows all pronouns, repeats 2 digits
Group play, shares toys, takes turns, plays well with others, knows full name, age, gender
4yr Hops, skips, alternates feet going down steps
Copies a square, buttons clothing, dresses self completely, catches ball
Knows colors, says song or poem from memory, asks questions
Tells “tall tales”, plays cooperatively with a group of children
5yr Skips alternating feet, jumps over low obstacles
Copies triangle, ties shoes, spreads with knife
Prints first name, asks what a word means
Plays competitive games, abides by rules, likes to help in household tasks
Prima
ry Ca
re
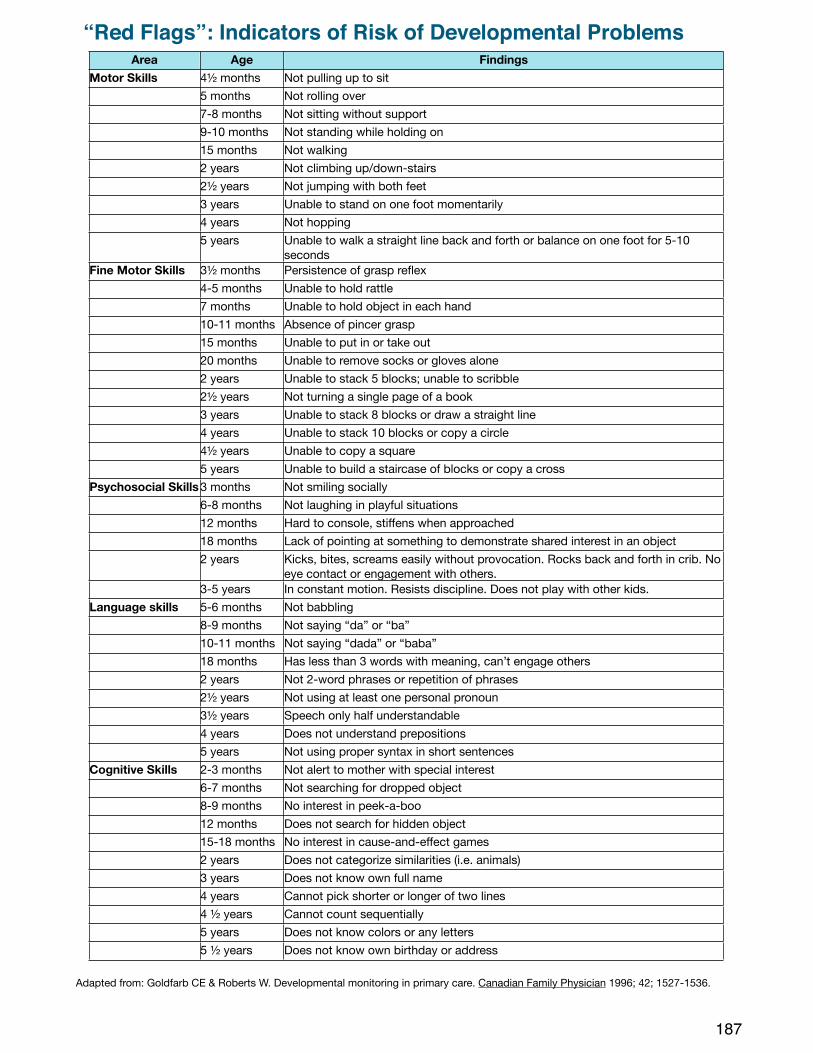
187
“Red Flags”: Indicators of Risk of Developmental ProblemsArea Age Findings
Motor Skills 4½ months Not pulling up to sit5 months Not rolling over7-8 months Not sitting without support9-10 months Not standing while holding on15 months Not walking2 years Not climbing up/down-stairs2½ years Not jumping with both feet3 years Unable to stand on one foot momentarily4 years Not hopping5 years Unable to walk a straight line back and forth or balance on one foot for 5-10
secondsFine Motor Skills 3½ months Persistence of grasp reflex
4-5 months Unable to hold rattle 7 months Unable to hold object in each hand10-11 months Absence of pincer grasp15 months Unable to put in or take out20 months Unable to remove socks or gloves alone2 years Unable to stack 5 blocks; unable to scribble2½ years Not turning a single page of a book3 years Unable to stack 8 blocks or draw a straight line4 years Unable to stack 10 blocks or copy a circle4½ years Unable to copy a square5 years Unable to build a staircase of blocks or copy a cross
Psychosocial Skills 3 months Not smiling socially6-8 months Not laughing in playful situations12 months Hard to console, stiffens when approached18 months Lack of pointing at something to demonstrate shared interest in an object2 years Kicks, bites, screams easily without provocation. Rocks back and forth in crib. No
eye contact or engagement with others.3-5 years In constant motion. Resists discipline. Does not play with other kids.
Language skills 5-6 months Not babbling8-9 months Not saying “da” or “ba” 10-11 months Not saying “dada” or “baba”18 months Has less than 3 words with meaning, can’t engage others2 years Not 2-word phrases or repetition of phrases 2½ years Not using at least one personal pronoun3½ years Speech only half understandable 4 years Does not understand prepositions5 years Not using proper syntax in short sentences
Cognitive Skills 2-3 months Not alert to mother with special interest6-7 months Not searching for dropped object8-9 months No interest in peek-a-boo12 months Does not search for hidden object15-18 months No interest in cause-and-effect games2 years Does not categorize similarities (i.e. animals)3 years Does not know own full name4 years Cannot pick shorter or longer of two lines4 ½ years Cannot count sequentially5 years Does not know colors or any letters5 ½ years Does not know own birthday or address
Adapted from: Goldfarb CE & Roberts W. Developmental monitoring in primary care. Canadian Family Physician 1996; 42; 1527-1536.
Common presentations:• Children: somatic complaints, psychomotor agitation, mood-congruent
hallucinations, school refusal, phobias/separation anxiety• Adolescents: Apathy/boredom, substance use, change in weight, sleep, & grades,
psychomotor retardation/hypersomnia, aggression/antisocial behavior, social withdrawal
Diagnosis: direct interview with patient/family using DSM-IV criteria• 5 or more symptoms >2 weeks and affect functioning
o At least 1 needs to depressed/irritable mood or anehodonia• Symptoms not explained by medical condition
Criteria: Depressed or irritable mood, Anhedonia, Appetite or weight change, Sleep disturbance, Psychomotor agitation or retardation. Loss of energy. Worthlessness or guilt, Poor concentration, Recurrent thoughts of death
Treatment:• All severity levels of depression:
o Supportive Management: active listening, reflectiono Psycho-education: Illness is NOT a weakness, stigma of mental health,o Address environmental factorso Safety planning
• Mild depression- CBT • Moderate to severe depression- CBT + antidepressant
Antidepresants: • 1st line – SSRI (fluoxetine, sertraline, citalopram, escitalopram)
o Black Box Warning: “Antidepressants may increase the risk of suicidal thinking and behavior in some children and adolescents with MDD”
• 2nd line – Another SSRI • 3rd line - venlafaxine, mirtazapine, buproprion, duloxetine
Treatment algorithm: • Follow-up: FDA recommends weekly for the first 4 weeks; then q2weeks until
recovery. • Titrate SSRI to effective dose:
o Reassess after 6-8 weeks: ! No improvement: Reassess diagnosis, Add therapy, Switch to
another SSRI! Partial Improvement – Increase med to max dose, add therapy,
explore poor adherence & comorbidities, consider augmentation! Improvement – Continue meds for 6-12 months after resolution
188
DepressionPrim
ary C
are
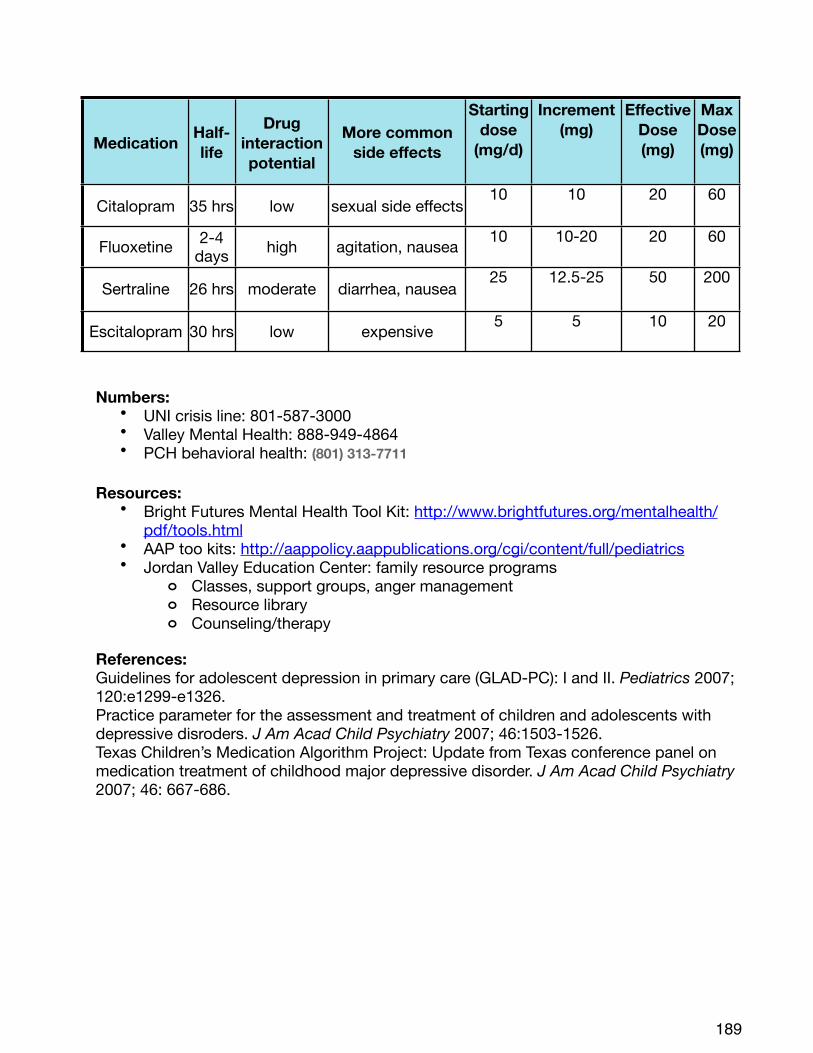
Numbers:• UNI crisis line: 801-587-3000• Valley Mental Health: 888-949-4864• PCH behavioral health: (801) 313-7711
Resources: • Bright Futures Mental Health Tool Kit: http://www.brightfutures.org/mentalhealth/
pdf/tools.html• AAP too kits: http://aappolicy.aappublications.org/cgi/content/full/pediatrics• Jordan Valley Education Center: family resource programs
o Classes, support groups, anger managemento Resource library o Counseling/therapy
References:Guidelines for adolescent depression in primary care (GLAD-PC): I and II. Pediatrics 2007; 120:e1299-e1326.Practice parameter for the assessment and treatment of children and adolescents with depressive disroders. J Am Acad Child Psychiatry 2007; 46:1503-1526.Texas Children’s Medication Algorithm Project: Update from Texas conference panel on medication treatment of childhood major depressive disorder. J Am Acad Child Psychiatry 2007; 46: 667-686.
189
Medication Half-life
Drug interaction potential
More common side effects
Starting dose
(mg/d)
Increment (mg)
Effective Dose (mg)
Max Dose (mg)
Citalopram 35 hrs low sexual side effects10 10 20 60
Fluoxetine 2-4 days high agitation, nausea 10 10-20 20 60
Sertraline 26 hrs moderate diarrhea, nausea25 12.5-25 50 200
Escitalopram 30 hrs low expensive 5 5 10 20
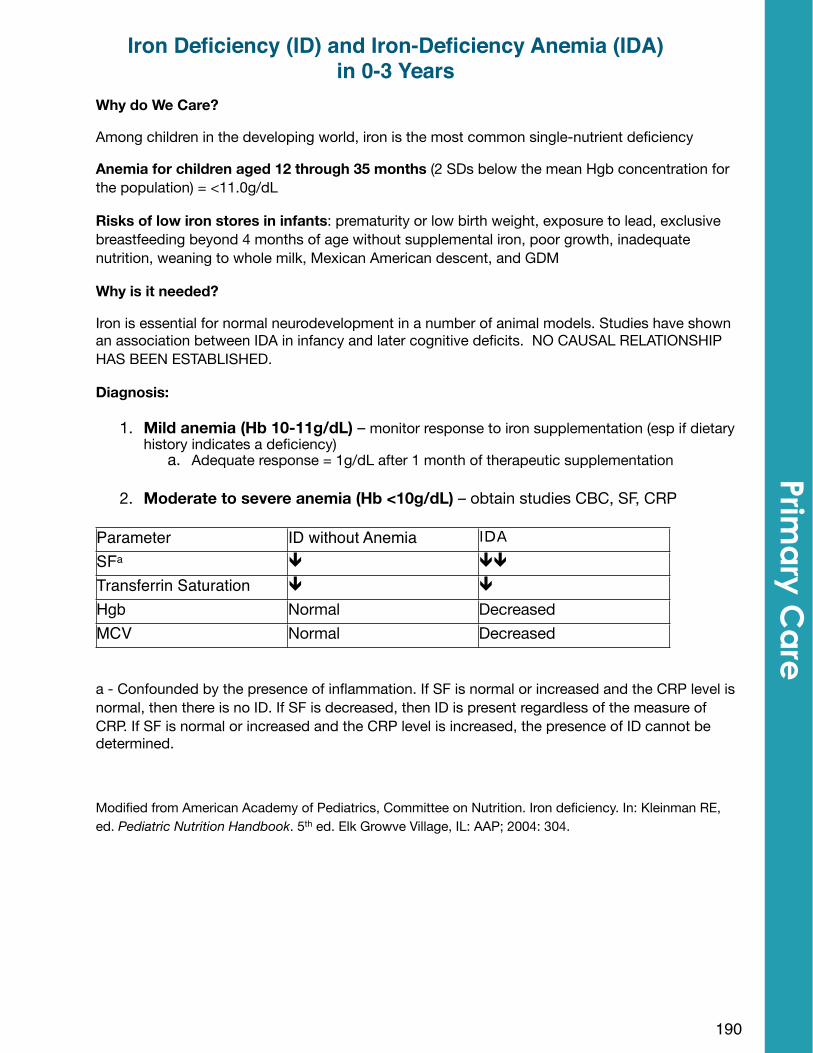
Why do We Care?
Among children in the developing world, iron is the most common single-nutrient deficiency
Anemia for children aged 12 through 35 months (2 SDs below the mean Hgb concentration for the population) = <11.0g/dL
Risks of low iron stores in infants: prematurity or low birth weight, exposure to lead, exclusive breastfeeding beyond 4 months of age without supplemental iron, poor growth, inadequate nutrition, weaning to whole milk, Mexican American descent, and GDM
Why is it needed?
Iron is essential for normal neurodevelopment in a number of animal models. Studies have shown an association between IDA in infancy and later cognitive deficits. NO CAUSAL RELATIONSHIP HAS BEEN ESTABLISHED.
Diagnosis:
1. Mild anemia (Hb 10-11g/dL) – monitor response to iron supplementation (esp if dietary history indicates a deficiency)
a. Adequate response = 1g/dL after 1 month of therapeutic supplementation
2. Moderate to severe anemia (Hb <10g/dL) – obtain studies CBC, SF, CRP
Parameter ID without Anemia
SFa " ""
Transferrin Saturation " "
Hgb Normal DecreasedMCV Normal Decreased
a - Confounded by the presence of inflammation. If SF is normal or increased and the CRP level is normal, then there is no ID. If SF is decreased, then ID is present regardless of the measure of CRP. If SF is normal or increased and the CRP level is increased, the presence of ID cannot be determined.
Modified from American Academy of Pediatrics, Committee on Nutrition. Iron deficiency. In: Kleinman RE, ed. Pediatric Nutrition Handbook. 5th ed. Elk Growve Village, IL: AAP; 2004: 304.
190
Iron Deficiency (ID) and Iron-Deficiency Anemia (IDA) in 0-3 Years
Prima
ry Ca
re
Iron requirements by Age:
Preterm infants – 2-4mg/kg/day orally Term infants (up to 6 months) – 0.27mg/day Term infants (6-12 months) – 11mg/dayToddlers (1-3 years) – 7mg/day
Prevention of ID & IDA:
Preterm infants (<37 weeks’ gestation): Should have an iron intake of 2mg/kg/d through 12 months of life
Term, breastfed infants: Iron supplementation of 1mg/kg/day at 4 months until appropriate iron-containing complementary foods have been introduced.
Term, partially breastfed infants: Treat as breastfed if >1/2 of their daily feedings are human milk
Term, formula fed infants: Iron needs met by standard infant formula.
Toddlers (1-3 years of age): Diet should include red meat, legumes, iron-fortified cereals, etc. Educate families that iron absorption is increased if consumed w/ VitC.
Screening:
Universal at 1 year: Hgb & assessment of risk factors
Selective Screening at any age: if risk factors identified
191
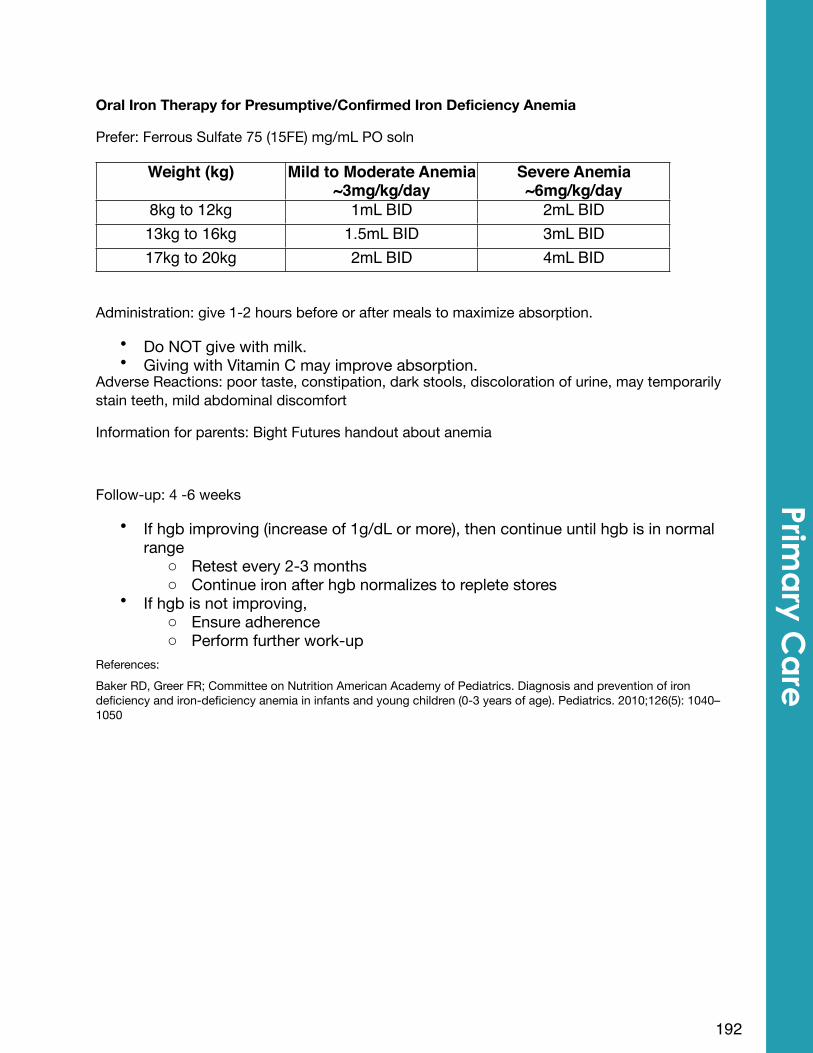
Oral Iron Therapy for Presumptive/Confirmed Iron Deficiency Anemia
Prefer: Ferrous Sulfate 75 (15FE) mg/mL PO soln
Weight (kg) Mild to Moderate Anemia~3mg/kg/day
Severe Anemia~6mg/kg/day
8kg to 12kg 1mL BID 2mL BID13kg to 16kg 1.5mL BID 3mL BID17kg to 20kg 2mL BID 4mL BID
Administration: give 1-2 hours before or after meals to maximize absorption.
• Do NOT give with milk. • Giving with Vitamin C may improve absorption.
Adverse Reactions: poor taste, constipation, dark stools, discoloration of urine, may temporarily stain teeth, mild abdominal discomfort
Information for parents: Bight Futures handout about anemia
Follow-up: 4 -6 weeks
• If hgb improving (increase of 1g/dL or more), then continue until hgb is in normal range
o Retest every 2-3 monthso Continue iron after hgb normalizes to replete stores
• If hgb is not improving, o Ensure adherenceo Perform further work-up
References: Baker RD, Greer FR; Committee on Nutrition American Academy of Pediatrics. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0-3 years of age). Pediatrics. 2010;126(5): 1040–1050
192
Prima
ry Ca
re
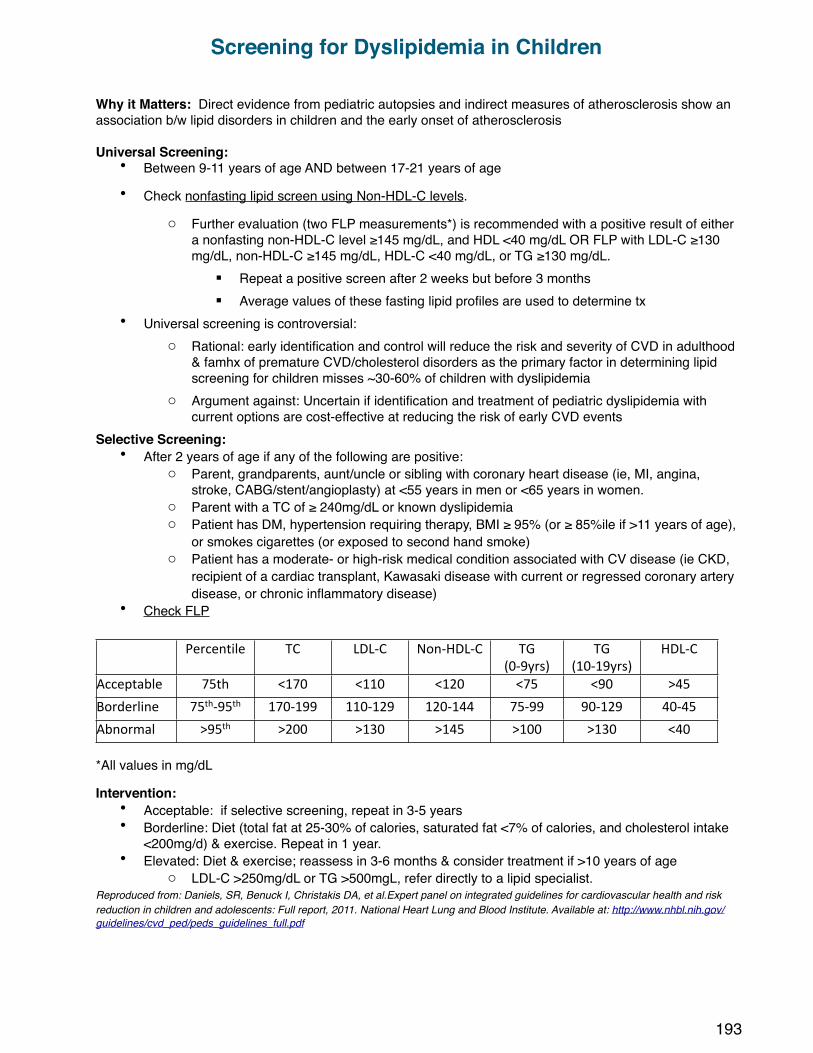
Why it Matters: Direct evidence from pediatric autopsies and indirect measures of atherosclerosis show an association b/w lipid disorders in children and the early onset of atherosclerosis
Universal Screening: • Between 9-11 years of age AND between 17-21 years of age
• Check nonfasting lipid screen using Non-HDL-C levels.
o Further evaluation (two FLP measurements*) is recommended with a positive result of either a nonfasting non-HDL-C level ≥145 mg/dL, and HDL <40 mg/dL OR FLP with LDL-C ≥130 mg/dL, non-HDL-C ≥145 mg/dL, HDL-C <40 mg/dL, or TG ≥130 mg/dL.
! Repeat a positive screen after 2 weeks but before 3 months! Average values of these fasting lipid profiles are used to determine tx
• Universal screening is controversial: o Rational: early identification and control will reduce the risk and severity of CVD in adulthood
& famhx of premature CVD/cholesterol disorders as the primary factor in determining lipid screening for children misses ~30-60% of children with dyslipidemia
o Argument against: Uncertain if identification and treatment of pediatric dyslipidemia with current options are cost-effective at reducing the risk of early CVD events
Selective Screening:• After 2 years of age if any of the following are positive:
o Parent, grandparents, aunt/uncle or sibling with coronary heart disease (ie, MI, angina, stroke, CABG/stent/angioplasty) at <55 years in men or <65 years in women.
o Parent with a TC of ≥ 240mg/dL or known dyslipidemiao Patient has DM, hypertension requiring therapy, BMI ≥ 95% (or ≥ 85%ile if >11 years of age),
or smokes cigarettes (or exposed to second hand smoke)o Patient has a moderate- or high-risk medical condition associated with CV disease (ie CKD,
recipient of a cardiac transplant, Kawasaki disease with current or regressed coronary artery disease, or chronic inflammatory disease)
• Check FLP
Percentile TC LDLXC NonXHDLXC TG(0X9yrs)
TG(10X19yrs)
HDLXC
Acceptable 75th <170 <110 <120 <75 <90 >45
Borderline 75thX95th 170X199 110X129 120X144 75X99 90X129 40X45
Abnormal >95th >200 >130 >145 >100 >130 <40
*All values in mg/dL
Intervention:• Acceptable: if selective screening, repeat in 3-5 years• Borderline: Diet (total fat at 25-30% of calories, saturated fat <7% of calories, and cholesterol intake
<200mg/d) & exercise. Repeat in 1 year. • Elevated: Diet & exercise; reassess in 3-6 months & consider treatment if >10 years of age
o LDL-C >250mg/dL or TG >500mgL, refer directly to a lipid specialist.Reproduced from: Daniels, SR, Benuck I, Christakis DA, et al.Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: Full report, 2011. National Heart Lung and Blood Institute. Available at: http://www.nhbl.nih.gov/guidelines/cvd_ped/peds_guidelines_full.pdf
193
Screening for Dyslipidemia in Children
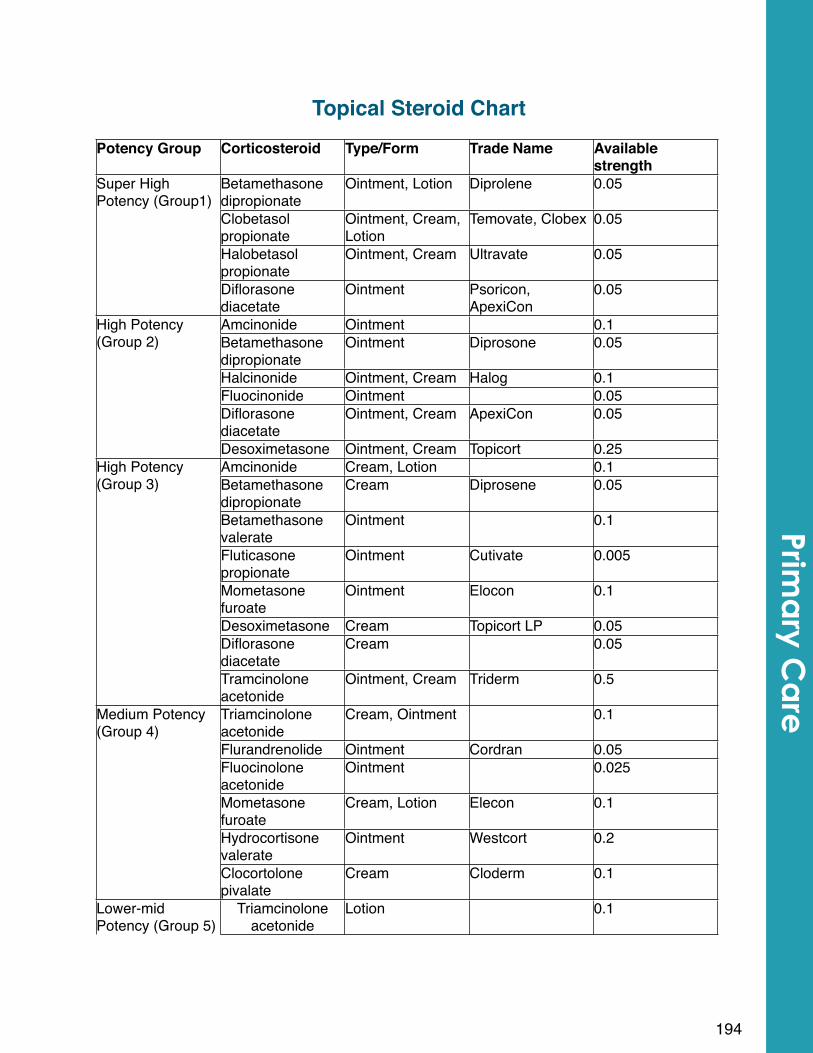
Topical Steroid ChartPotency Group Corticosteroid Type/Form Trade Name Available
strengthSuper High Potency (Group1)
Betamethasone dipropionate
Ointment, Lotion Diprolene 0.05Super High Potency (Group1)
Clobetasol propionate
Ointment, Cream, Lotion
Temovate, Clobex 0.05
Super High Potency (Group1)
Halobetasol propionate
Ointment, Cream Ultravate 0.05
Super High Potency (Group1)
Diflorasone diacetate
Ointment Psoricon, ApexiCon
0.05
High Potency (Group 2)
Amcinonide Ointment 0.1High Potency (Group 2) Betamethasone
dipropionateOintment Diprosone 0.05
High Potency (Group 2)
Halcinonide Ointment, Cream Halog 0.1
High Potency (Group 2)
Fluocinonide Ointment 0.05
High Potency (Group 2)
Diflorasone diacetate
Ointment, Cream ApexiCon 0.05
High Potency (Group 2)
Desoximetasone Ointment, Cream Topicort 0.25High Potency (Group 3)
Amcinonide Cream, Lotion 0.1High Potency (Group 3) Betamethasone
dipropionateCream Diprosene 0.05
High Potency (Group 3)
Betamethasone valerate
Ointment 0.1
High Potency (Group 3)
Fluticasone propionate
Ointment Cutivate 0.005
High Potency (Group 3)
Mometasone furoate
Ointment Elocon 0.1
High Potency (Group 3)
Desoximetasone Cream Topicort LP 0.05
High Potency (Group 3)
Diflorasone diacetate
Cream 0.05
High Potency (Group 3)
Tramcinolone acetonide
Ointment, Cream Triderm 0.5
Medium Potency (Group 4)
Triamcinolone acetonide
Cream, Ointment 0.1Medium Potency (Group 4)
Flurandrenolide Ointment Cordran 0.05
Medium Potency (Group 4)
Fluocinolone acetonide
Ointment 0.025
Medium Potency (Group 4)
Mometasone furoate
Cream, Lotion Elecon 0.1
Medium Potency (Group 4)
Hydrocortisone valerate
Ointment Westcort 0.2
Medium Potency (Group 4)
Clocortolone pivalate
Cream Cloderm 0.1
Lower-mid Potency (Group 5)
Triamcinolone acetonide
Lotion 0.1
194
Prima
ry Ca
re
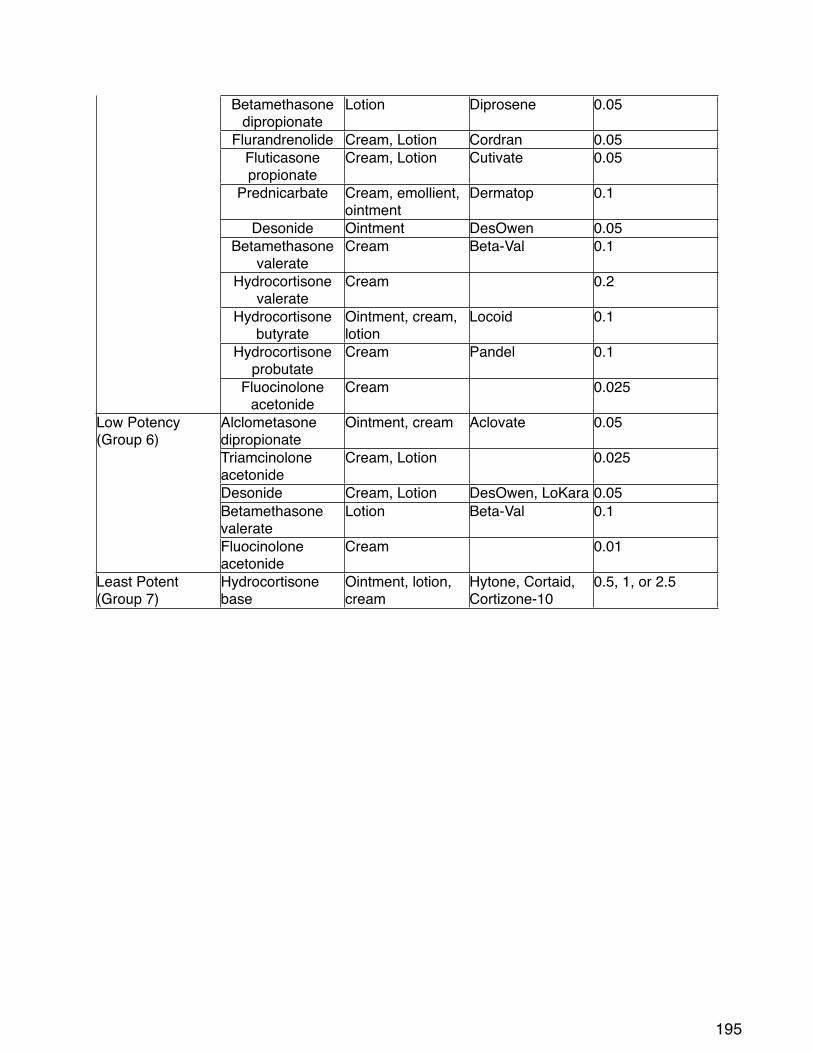
Lower-mid Potency (Group 5)
Betamethasone dipropionate
Lotion Diprosene 0.05
Lower-mid Potency (Group 5)
Flurandrenolide Cream, Lotion Cordran 0.05
Lower-mid Potency (Group 5)
Fluticasone propionate
Cream, Lotion Cutivate 0.05
Lower-mid Potency (Group 5)
Prednicarbate Cream, emollient, ointment
Dermatop 0.1
Lower-mid Potency (Group 5)
Desonide Ointment DesOwen 0.05
Lower-mid Potency (Group 5)
Betamethasone valerate
Cream Beta-Val 0.1
Lower-mid Potency (Group 5)
Hydrocortisone valerate
Cream 0.2
Lower-mid Potency (Group 5)
Hydrocortisone butyrate
Ointment, cream, lotion
Locoid 0.1
Lower-mid Potency (Group 5)
Hydrocortisone probutate
Cream Pandel 0.1
Lower-mid Potency (Group 5)
Fluocinolone acetonide
Cream 0.025
Low Potency (Group 6)
Alclometasone dipropionate
Ointment, cream Aclovate 0.05Low Potency (Group 6)
Triamcinolone acetonide
Cream, Lotion 0.025
Low Potency (Group 6)
Desonide Cream, Lotion DesOwen, LoKara 0.05
Low Potency (Group 6)
Betamethasone valerate
Lotion Beta-Val 0.1
Low Potency (Group 6)
Fluocinolone acetonide
Cream 0.01
Least Potent (Group 7)
Hydrocortisone base
Ointment, lotion, cream
Hytone, Cortaid, Cortizone-10
0.5, 1, or 2.5
195
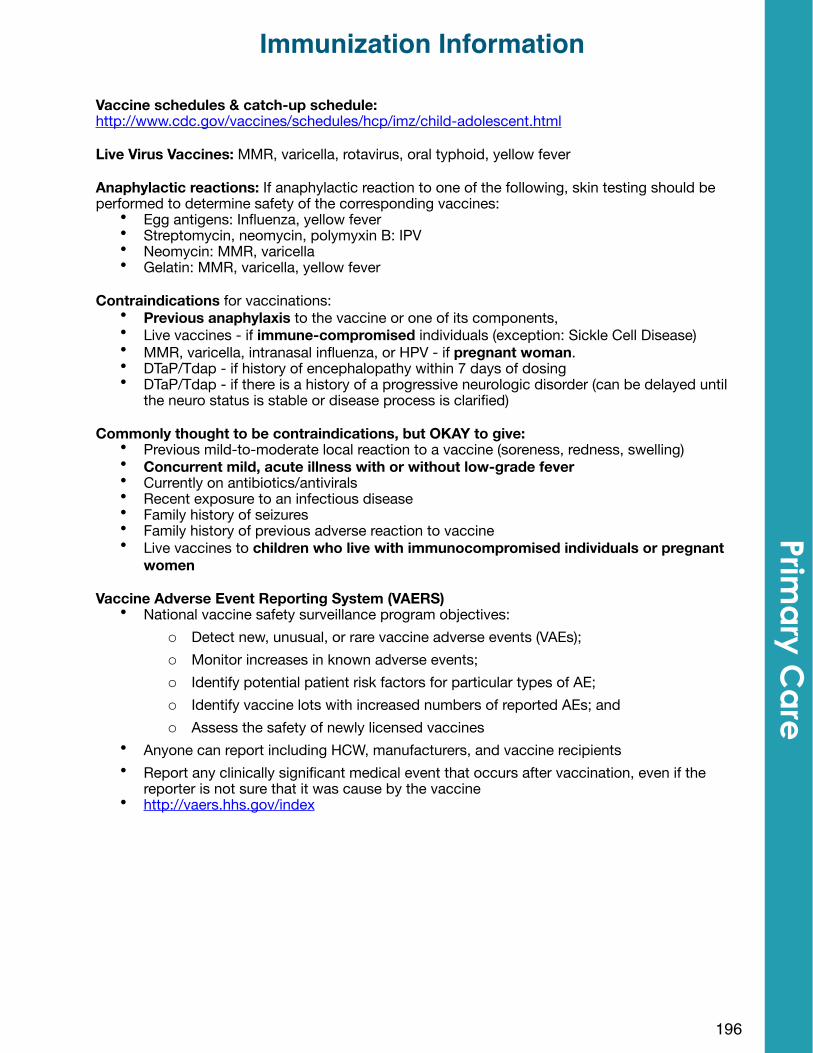
Vaccine schedules & catch-up schedule: http://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html
Live Virus Vaccines: MMR, varicella, rotavirus, oral typhoid, yellow fever
Anaphylactic reactions: If anaphylactic reaction to one of the following, skin testing should be performed to determine safety of the corresponding vaccines:
• Egg antigens: Influenza, yellow fever• Streptomycin, neomycin, polymyxin B: IPV• Neomycin: MMR, varicella• Gelatin: MMR, varicella, yellow fever
Contraindications for vaccinations: • Previous anaphylaxis to the vaccine or one of its components, • Live vaccines - if immune-compromised individuals (exception: Sickle Cell Disease)• MMR, varicella, intranasal influenza, or HPV - if pregnant woman. • DTaP/Tdap - if history of encephalopathy within 7 days of dosing• DTaP/Tdap - if there is a history of a progressive neurologic disorder (can be delayed until
the neuro status is stable or disease process is clarified)
Commonly thought to be contraindications, but OKAY to give:• Previous mild-to-moderate local reaction to a vaccine (soreness, redness, swelling)• Concurrent mild, acute illness with or without low-grade fever• Currently on antibiotics/antivirals• Recent exposure to an infectious disease• Family history of seizures• Family history of previous adverse reaction to vaccine• Live vaccines to children who live with immunocompromised individuals or pregnant
women
Vaccine Adverse Event Reporting System (VAERS)• National vaccine safety surveillance program objectives:
o Detect new, unusual, or rare vaccine adverse events (VAEs);o Monitor increases in known adverse events;o Identify potential patient risk factors for particular types of AE;o Identify vaccine lots with increased numbers of reported AEs; ando Assess the safety of newly licensed vaccines
• Anyone can report including HCW, manufacturers, and vaccine recipients• Report any clinically significant medical event that occurs after vaccination, even if the
reporter is not sure that it was cause by the vaccine• http://vaers.hhs.gov/index
196
Immunization Information Prim
ary C
are
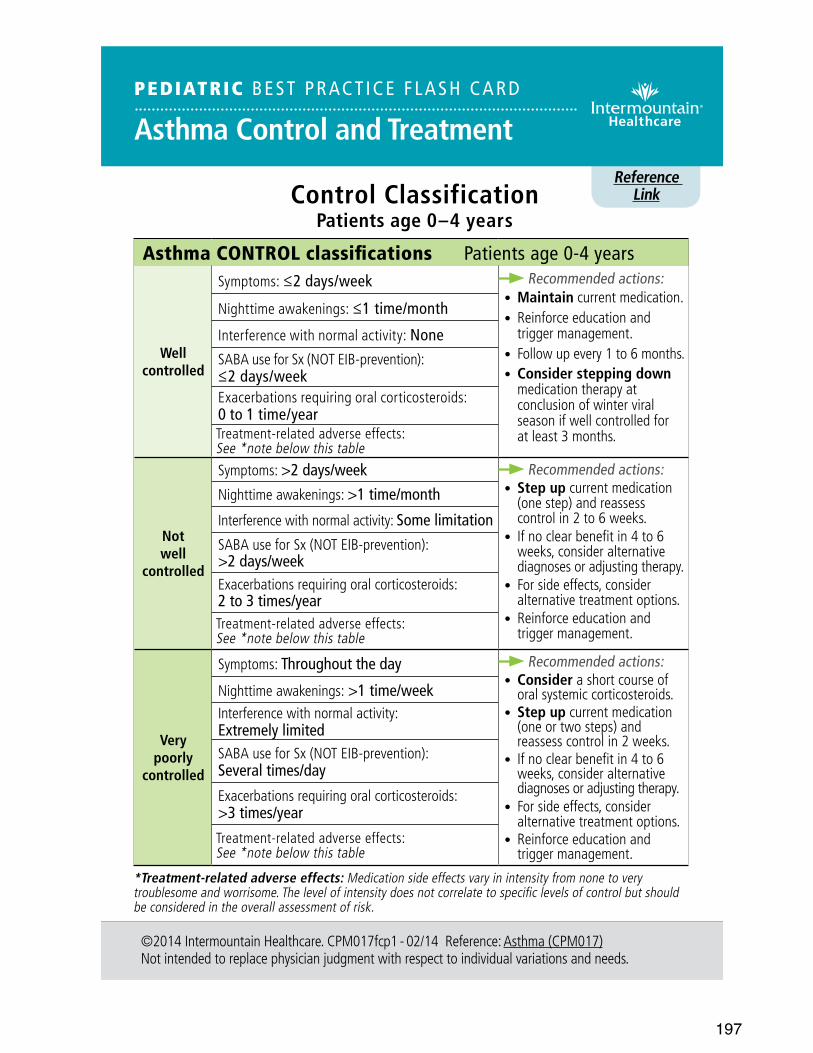
197
Reference Link
©2014 Intermountain Healthcare. CPM017fcp1 - 02/14 Reference: Asthma (CPM017)Not intended to replace physician judgment with respect to individual variations and needs.
Control ClassificationPatients age 0–4 years
PEDIATRIC BEST PRACT ICE F LASH CARD
Asthma Control and Treatment
Asthma CONTROL classifications Patients age 0-4 years
Well controlled
Symptoms: ≤2 days/week Recommended actions:• Maintain current medication.• Reinforce education and
trigger management.• Follow up every 1 to 6 months.• Consider stepping down
medication therapy at conclusion of winter viral season if well controlled for at least 3 months.
Nighttime awakenings: ≤1 time/month
Interference with normal activity: NoneSABA use for Sx (NOT EIB-prevention): ≤2 days/weekExacerbations requiring oral corticosteroids: 0 to 1 time/yearTreatment-related adverse effects: See *note below this table
Not well
controlled
Symptoms: >2 days/week Recommended actions:• Step up current medication
(one step) and reassess control in 2 to 6 weeks.
• If no clear benefit in 4 to 6 weeks, consider alternative diagnoses or adjusting therapy.
• For side effects, consider alternative treatment options.
• Reinforce education and trigger management.
Nighttime awakenings: >1 time/month
Interference with normal activity: Some limitationSABA use for Sx (NOT EIB-prevention): >2 days/weekExacerbations requiring oral corticosteroids: 2 to 3 times/yearTreatment-related adverse effects: See *note below this table
Very poorly
controlled
Symptoms: Throughout the day Recommended actions:• Consider a short course of
oral systemic corticosteroids.• Step up current medication
(one or two steps) and reassess control in 2 weeks.
• If no clear benefit in 4 to 6 weeks, consider alternative diagnoses or adjusting therapy.
• For side effects, consider alternative treatment options.
• Reinforce education and trigger management.
Nighttime awakenings: >1 time/weekInterference with normal activity: Extremely limitedSABA use for Sx (NOT EIB-prevention): Several times/dayExacerbations requiring oral corticosteroids: >3 times/yearTreatment-related adverse effects: See *note below this table
*Treatment-related adverse effects: Medication side effects vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
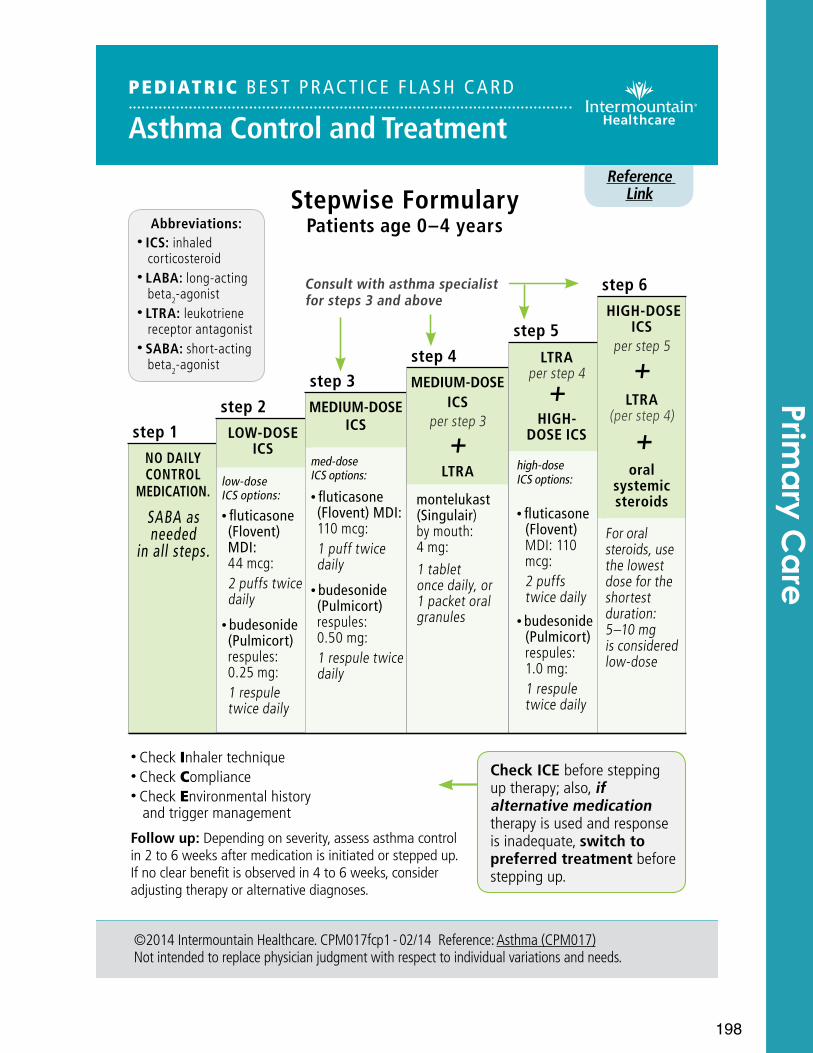
198
Reference Link
©2014 Intermountain Healthcare. CPM017fcp1 - 02/14 Reference: Asthma (CPM017)Not intended to replace physician judgment with respect to individual variations and needs.
PEDIATRIC BEST PRACT ICE F LASH CARD
Asthma Control and Treatment
Stepwise FormularyPatients age 0–4 years
step 1NO DAILY CONTROL
MEDICATION.
SABA as needed
in all steps.
step 2LOW-DOSE
ICS
low-dose ICS options:
• fluticasone (Flovent) MDI: 44 mcg: 2 puffs twice daily
• budesonide (Pulmicort) respules: 0.25 mg: 1 respule twice daily
step 3MEDIUM-DOSE
ICS
med-dose ICS options:
• fluticasone (Flovent) MDI: 110 mcg: 1 puff twice daily
• budesonide (Pulmicort) respules: 0.50 mg: 1 respule twice daily
step 4MEDIUM-DOSE
ICS per step 3
+ LTRA
montelukast (Singulair) by mouth: 4 mg: 1 tablet once daily, or 1 packet oral granules
step 5LTRA
per step 4 +
HIGH- DOSE ICS
high-dose ICS options:
• fluticasone (Flovent) MDI: 110 mcg: 2 puffs twice daily
• budesonide (Pulmicort) respules: 1.0 mg: 1 respule twice daily
step 6 HIGH-DOSE
ICS per step 5
+LTRA
(per step 4)
+oral
systemic steroids
For oral steroids, use the lowest dose for the shortest duration: 5–10 mg is considered low-dose
Abbreviations:• ICS: inhaled
corticosteroid• LABA: long-acting
beta2-agonist• LTRA: leukotriene
receptor antagonist• SABA: short-acting
beta2-agonist
Check ICE before stepping up therapy; also, if alternative medication therapy is used and response is inadequate, switch to preferred treatment before stepping up.
• Check Inhaler technique• Check Compliance• Check Environmental history and trigger management
Follow up: Depending on severity, assess asthma control in 2 to 6 weeks after medication is initiated or stepped up. If no clear benefit is observed in 4 to 6 weeks, consider adjusting therapy or alternative diagnoses.
Prima
ry Ca
re
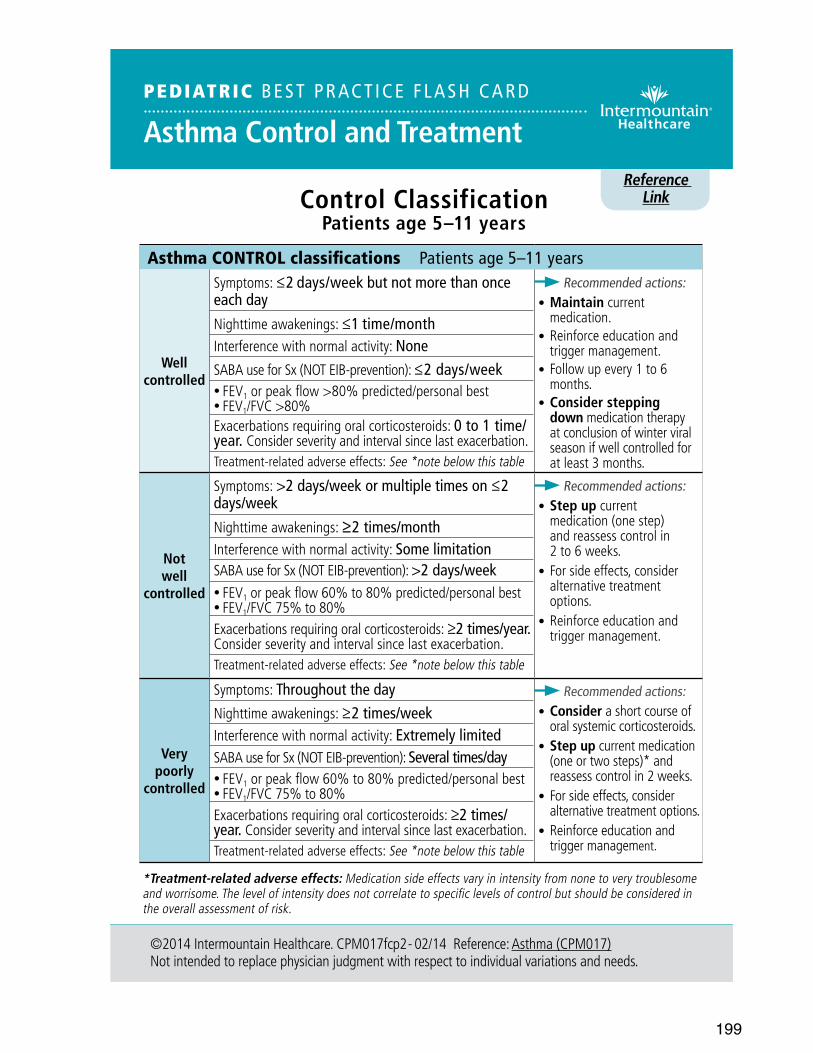
199
Reference Link
©2014 Intermountain Healthcare. CPM017fcp2 - 02/14 Reference: Asthma (CPM017)Not intended to replace physician judgment with respect to individual variations and needs.
Control ClassificationPatients age 5–11 years
PEDIATRIC BEST PRACT ICE F LASH CARD
Asthma Control and Treatment
Asthma CONTROL classifications Patients age 5–11 years
Well controlled
Symptoms: ≤2 days/week but not more than once each day
Recommended actions:• Maintain current
medication.• Reinforce education and
trigger management.• Follow up every 1 to 6
months.• Consider stepping
down medication therapy at conclusion of winter viral season if well controlled for at least 3 months.
Nighttime awakenings: ≤1 time/monthInterference with normal activity: NoneSABA use for Sx (NOT EIB-prevention): ≤2 days/week• FEV1 or peak flow >80% predicted/personal best • FEV1/FVC >80%Exacerbations requiring oral corticosteroids: 0 to 1 time/year. Consider severity and interval since last exacerbation.Treatment-related adverse effects: See *note below this table
Not well
controlled
Symptoms: >2 days/week or multiple times on ≤2 days/week
Recommended actions:• Step up current
medication (one step) and reassess control in 2 to 6 weeks.
• For side effects, consider alternative treatment options.
• Reinforce education and trigger management.
Nighttime awakenings: ≥2 times/monthInterference with normal activity: Some limitationSABA use for Sx (NOT EIB-prevention): >2 days/week• FEV1 or peak flow 60% to 80% predicted/personal best • FEV1/FVC 75% to 80%Exacerbations requiring oral corticosteroids: ≥2 times/year. Consider severity and interval since last exacerbation.Treatment-related adverse effects: See *note below this table
Very poorly
controlled
Symptoms: Throughout the day Recommended actions:• Consider a short course of
oral systemic corticosteroids.• Step up current medication
(one or two steps)* and reassess control in 2 weeks.
• For side effects, consider alternative treatment options.
• Reinforce education and trigger management.
Nighttime awakenings: ≥2 times/weekInterference with normal activity: Extremely limitedSABA use for Sx (NOT EIB-prevention): Several times/day• FEV1 or peak flow 60% to 80% predicted/personal best • FEV1/FVC 75% to 80%Exacerbations requiring oral corticosteroids: ≥2 times/year. Consider severity and interval since last exacerbation.Treatment-related adverse effects: See *note below this table
*Treatment-related adverse effects: Medication side effects vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
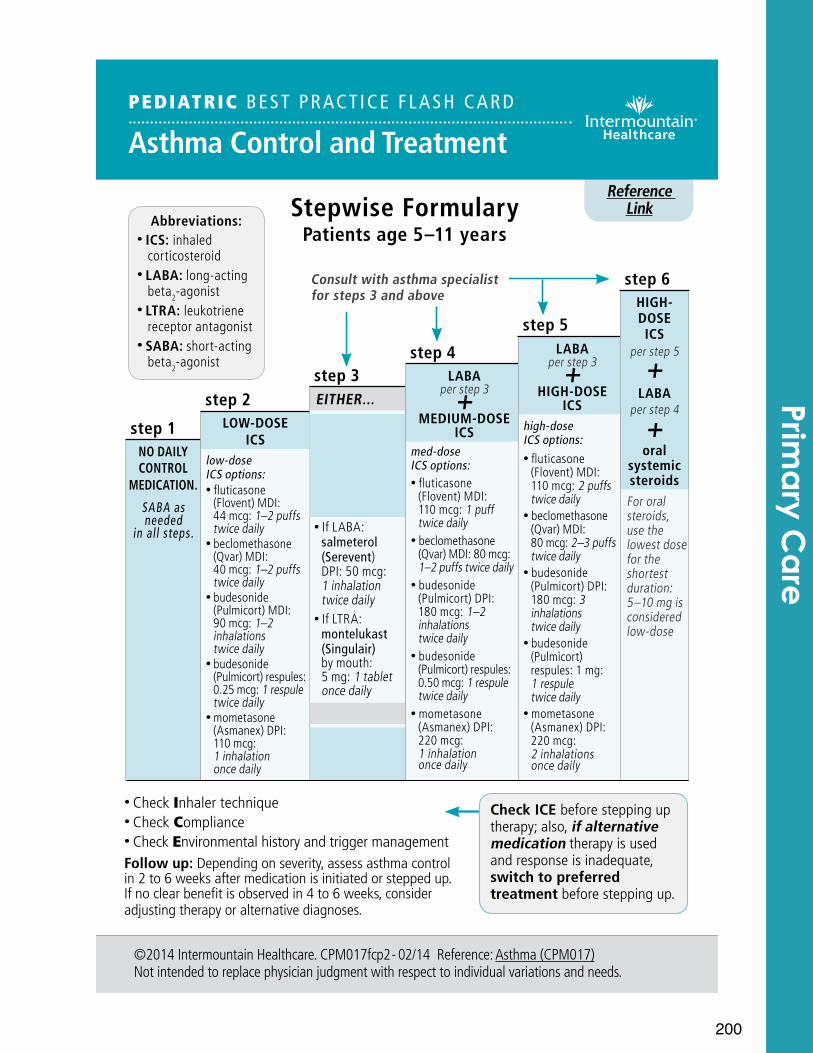
200
step 1NO DAILY CONTROL
MEDICATION.
SABA as needed
in all steps.
step 2LOW-DOSE
ICS low-dose ICS options:• fluticasone
(Flovent) MDI: 44 mcg: 1–2 puffs twice daily
• beclomethasone (Qvar) MDI: 40 mcg: 1–2 puffs twice daily
• budesonide (Pulmicort) MDI: 90 mcg: 1–2 inhalations twice daily
• budesonide (Pulmicort) respules: 0.25 mcg: 1 respule twice daily
• mometasone (Asmanex) DPI: 110 mcg: 1 inhalation once daily
step 3EITHER...
LOW-DOSE ICS
per step 2 +
either LABA or LTRA• If LABA:
salmeterol (Serevent) DPI: 50 mcg: 1 inhalation twice daily
• If LTRA: montelukast (Singulair) by mouth: 5 mg: 1 tablet once daily
OR...MEDIUM- DOSE ICSper step 4
Reference Link
©2014 Intermountain Healthcare. CPM017fcp2 - 02/14 Reference: Asthma (CPM017)Not intended to replace physician judgment with respect to individual variations and needs.
PEDIATRIC BEST PRACT ICE F LASH CARD
Asthma Control and Treatment
Stepwise FormularyPatients age 5–11 years
Abbreviations:• ICS: inhaled
corticosteroid• LABA: long-acting
beta2-agonist• LTRA: leukotriene
receptor antagonist• SABA: short-acting
beta2-agonist
Check ICE before stepping up therapy; also, if alternative medication therapy is used and response is inadequate, switch to preferred treatment before stepping up.
• Check Inhaler technique• Check Compliance• Check Environmental history and trigger managementFollow up: Depending on severity, assess asthma control in 2 to 6 weeks after medication is initiated or stepped up. If no clear benefit is observed in 4 to 6 weeks, consider adjusting therapy or alternative diagnoses.
step 4LABA
per step 3+MEDIUM-DOSE
ICS med-dose ICS options:• fluticasone
(Flovent) MDI: 110 mcg: 1 puff twice daily
• beclomethasone (Qvar) MDI: 80 mcg: 1–2 puffs twice daily
• budesonide (Pulmicort) DPI: 180 mcg: 1–2 inhalations twice daily
• budesonide (Pulmicort) respules: 0.50 mcg: 1 respule twice daily
• mometasone (Asmanex) DPI: 220 mcg: 1 inhalation once daily
step 5LABA
per step 3+HIGH-DOSE
ICS high-dose ICS options: • fluticasone
(Flovent) MDI: 110 mcg: 2 puffs twice daily
• beclomethasone (Qvar) MDI: 80 mcg: 2–3 puffs twice daily
• budesonide (Pulmicort) DPI: 180 mcg: 3 inhalations twice daily
• budesonide (Pulmicort) respules: 1 mg: 1 respule twice daily
• mometasone (Asmanex) DPI: 220 mcg: 2 inhalations once daily
step 6HIGH-DOSE ICS
per step 5
+
LABA per step 4
+oral
systemic steroidsFor oral steroids, use the lowest dose for the shortest duration: 5–10 mg is considered low-dose
Prima
ry Ca
re
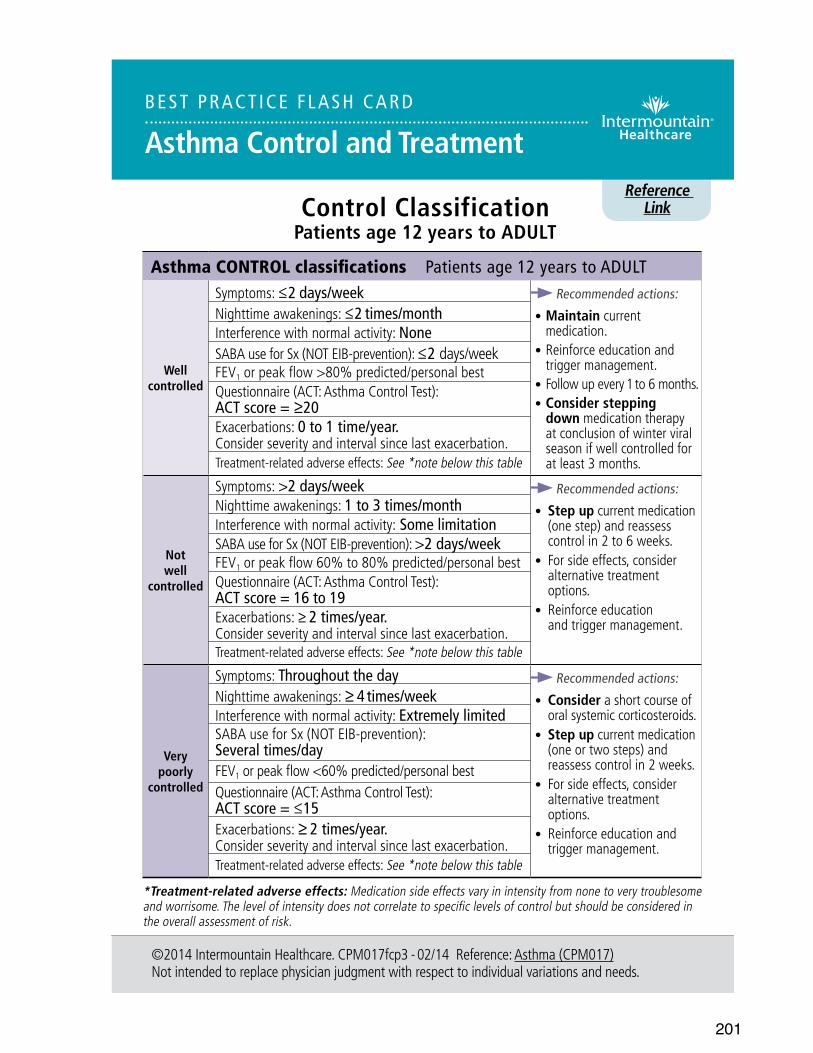
201
Reference Link
©2014 Intermountain Healthcare. CPM017fcp3 - 02/14 Reference: Asthma (CPM017)Not intended to replace physician judgment with respect to individual variations and needs.
Control ClassificationPatients age 12 years to ADULT
BE ST PRACT ICE F LASH CARD
Asthma Control and Treatment
Asthma CONTROL classifications Patients age 12 years to ADULT
Well controlled
Symptoms: ≤2 days/week Recommended actions:
• Maintain current medication.
• Reinforce education and trigger management.
• Follow up every 1 to 6 months.• Consider stepping
down medication therapy at conclusion of winter viral season if well controlled for at least 3 months.
Nighttime awakenings: ≤2 times/monthInterference with normal activity: NoneSABA use for Sx (NOT EIB-prevention): ≤2 days/weekFEV1 or peak flow >80% predicted/personal best Questionnaire (ACT: Asthma Control Test): ACT score = ≥20Exacerbations: 0 to 1 time/year. Consider severity and interval since last exacerbation.Treatment-related adverse effects: See *note below this table
Not well
controlled
Symptoms: >2 days/week Recommended actions:
• Step up current medication (one step) and reassess control in 2 to 6 weeks.
• For side effects, consider alternative treatment options.
• Reinforce education and trigger management.
Nighttime awakenings: 1 to 3 times/monthInterference with normal activity: Some limitationSABA use for Sx (NOT EIB-prevention): >2 days/weekFEV1 or peak flow 60% to 80% predicted/personal bestQuestionnaire (ACT: Asthma Control Test): ACT score = 16 to 19Exacerbations: ≥ 2 times/year. Consider severity and interval since last exacerbation.Treatment-related adverse effects: See *note below this table
Very poorly
controlled
Symptoms: Throughout the day Recommended actions:
• Consider a short course oforal systemic corticosteroids.
• Step up current medication (one or two steps) and reassess control in 2 weeks.
• For side effects, consider alternative treatment options.
• Reinforce education and trigger management.
Nighttime awakenings: ≥ 4 times/weekInterference with normal activity: Extremely limitedSABA use for Sx (NOT EIB-prevention): Several times/dayFEV1 or peak flow <60% predicted/personal bestQuestionnaire (ACT: Asthma Control Test): ACT score = ≤15Exacerbations: ≥ 2 times/year. Consider severity and interval since last exacerbation.Treatment-related adverse effects: See *note below this table
*Treatment-related adverse effects: Medication side effects vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk.
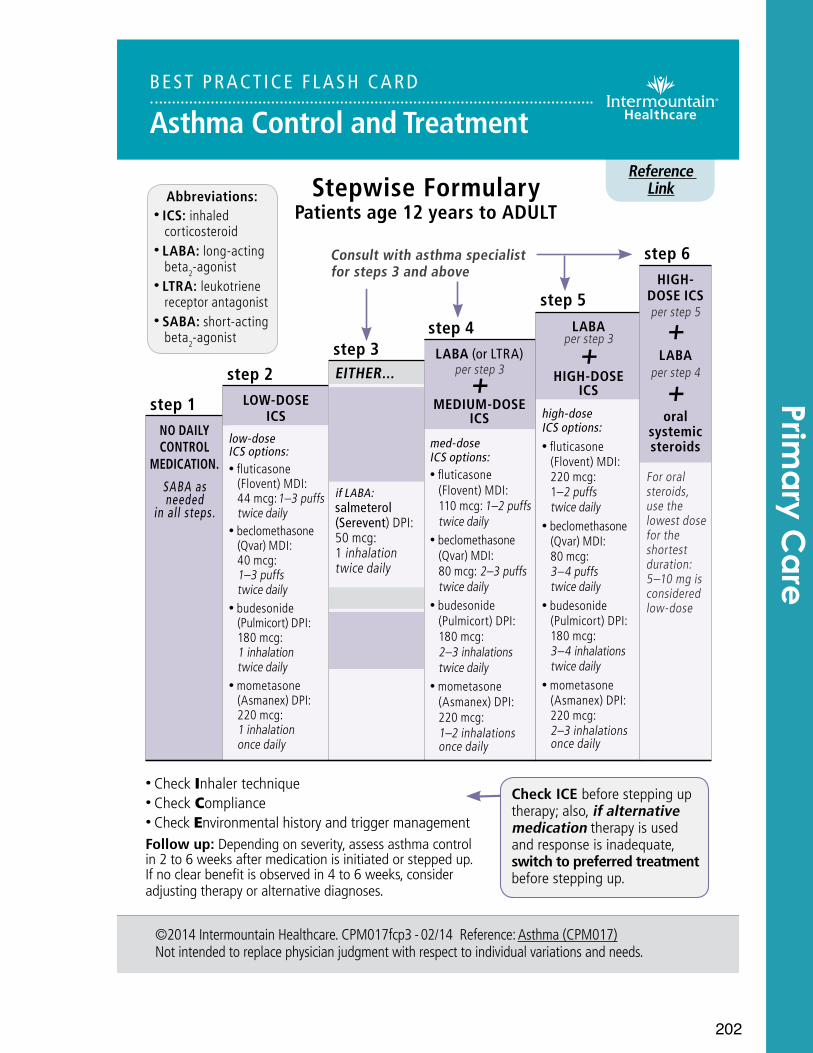
202
step 4LABA (or LTRA)
per step 3 +
MEDIUM-DOSE ICS
med-dose ICS options: • fluticasone
(Flovent) MDI:110 mcg: 1–2 puffs twice daily
• beclomethasone(Qvar) MDI: 80 mcg: 2–3 puffs twice daily
• budesonide(Pulmicort) DPI: 180 mcg:2–3 inhalations twice daily
• mometasone (Asmanex) DPI: 220 mcg: 1–2 inhalations once daily
step 1NO DAILY CONTROL
MEDICATION.
SABA as needed
in all steps.
step 2LOW-DOSE
ICS low-dose ICS options: • fluticasone
(Flovent) MDI: 44 mcg: 1–3 puffs twice daily
• beclomethasone (Qvar) MDI: 40 mcg: 1–3 puffs twice daily
• budesonide(Pulmicort) DPI:180 mcg:1 inhalation twice daily
• mometasone (Asmanex) DPI:220 mcg: 1 inhalation once daily
step 3EITHER...
LOW-DOSE ICS
per step 2
+ LABA (or LTRA)
if LABA: salmeterol (Serevent) DPI: 50 mcg: 1 inhalation twice daily
OR...MEDIUM-DOSE
ICS per step 4
step 5LABA
per step 3
+ HIGH-DOSE
ICS
high-dose ICS options: • fluticasone
(Flovent) MDI:220 mcg: 1–2 puffs twice daily
• beclomethasone(Qvar) MDI: 80 mcg:3–4 puffs twice daily
• budesonide(Pulmicort) DPI: 180 mcg:3–4 inhalations twice daily
• mometasone (Asmanex) DPI: 220 mcg: 2–3 inhalations once daily
Reference Link
©2014 Intermountain Healthcare. CPM017fcp3 - 02/14 Reference: Asthma (CPM017)Not intended to replace physician judgment with respect to individual variations and needs.
BEST PRACT ICE F LASH CARD
Asthma Control and Treatment
Stepwise FormularyPatients age 12 years to ADULT
Abbreviations:• ICS: inhaled
corticosteroid• LABA: long-acting
beta2-agonist• LTRA: leukotriene
receptor antagonist• SABA: short-acting
beta2-agonist
Check ICE before stepping up therapy; also, if alternative medication therapy is used and response is inadequate, switch to preferred treatment before stepping up.
• Check Inhaler technique• Check Compliance• Check Environmental history and trigger managementFollow up: Depending on severity, assess asthma control in 2 to 6 weeks after medication is initiated or stepped up. If no clear benefit is observed in 4 to 6 weeks, consider adjusting therapy or alternative diagnoses.
step 6HIGH-
DOSE ICS per step 5
+ LABA
per step 4
+ oral
systemic steroids
For oral steroids, use the lowest dose for the shortest duration: 5–10 mg is considered low-dose
Prima
ry Ca
re
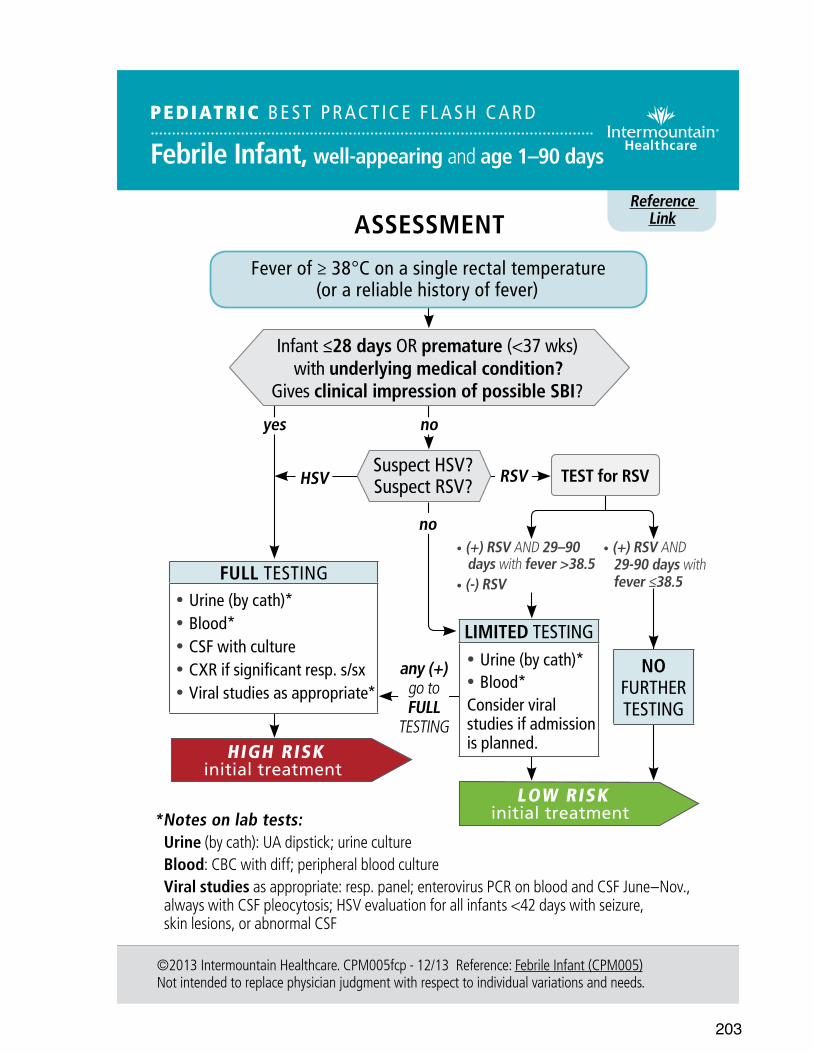
203
Reference Link
TEST for RSV
©2013 Intermountain Healthcare. CPM005fcp - 12/13 Reference: Febrile Infant (CPM005)Not intended to replace physician judgment with respect to individual variations and needs.
ASSESSMENT
• (+) RSV AND 29–90 days with fever >38.5• (-) RSV
noyes
PEDIATRIC BEST PRACT ICE F LASH CARD
Febrile Infant, well-appearing and age 1–90 days
Fever of ≥ 38°C on a single rectal temperature (or a reliable history of fever)
Infant ≤28 days OR premature (<37 wks) with underlying medical condition?
Gives clinical impression of possible SBI?
Suspect HSV? Suspect RSV? RSV
any (+) go to FULL
TESTING
• (+) RSV AND 29-90 days with fever ≤38.5
NO FURTHER TESTING
*Notes on lab tests:Urine (by cath): UA dipstick; urine cultureBlood: CBC with diff; peripheral blood cultureViral studies as appropriate: resp. panel; enterovirus PCR on blood and CSF June–Nov., always with CSF pleocytosis; HSV evaluation for all infants <42 days with seizure, skin lesions, or abnormal CSF
FULL TESTING • Urine (by cath)* • Blood* • CSF with culture • CXR if significant resp. s/sx • Viral studies as appropriate*
LIMITED TESTING • Urine (by cath)* • Blood*
Consider viral studies if admission is planned.HIGH RISK
initial treatment
HSV
no
LOW RISK initial treatment
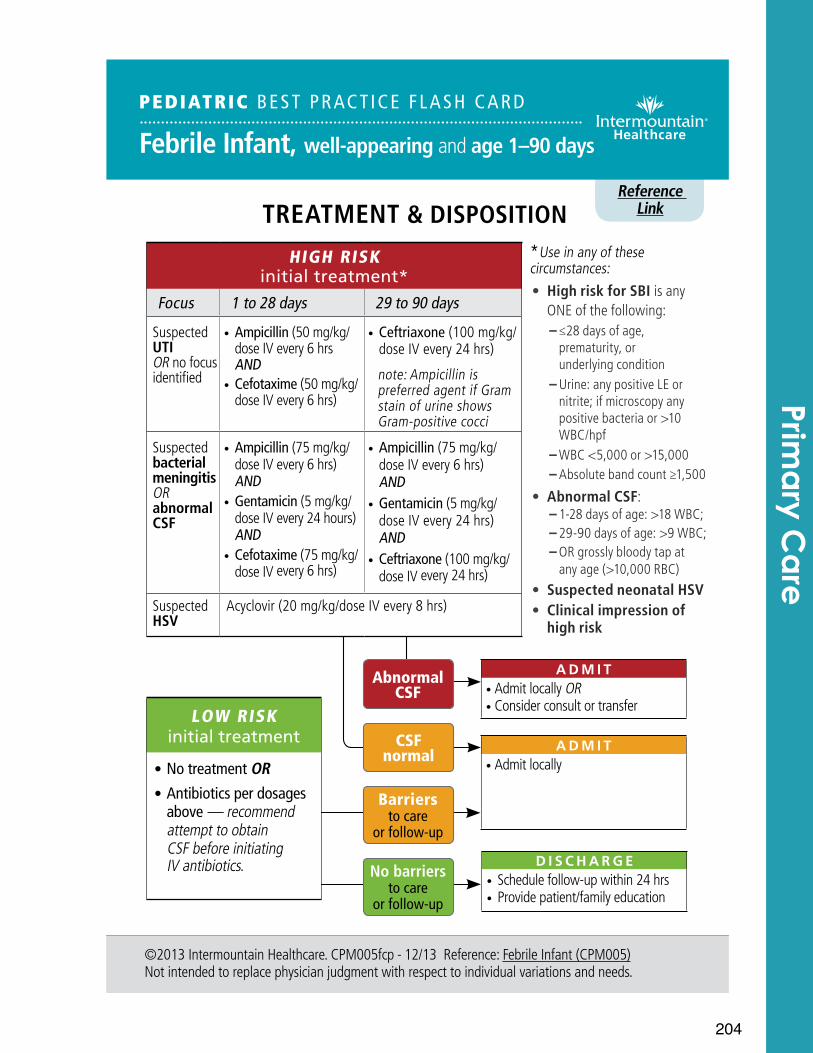
204
*Use in any of these circumstances:• High risk for SBI is any
ONE of the following: – ≤28 days of age, prematurity, or underlying condition – Urine: any positive LE or nitrite; if microscopy any positive bacteria or >10 WBC/hpf – WBC <5,000 or >15,000 – Absolute band count ≥1,500
• Abnormal CSF: – 1-28 days of age: >18 WBC; – 29-90 days of age: >9 WBC; – OR grossly bloody tap at any age (>10,000 RBC)
• Suspected neonatal HSV• Clinical impression of
high risk
No barriers to care
or follow-up
Abnormal CSF
Reference Link
©2013 Intermountain Healthcare. CPM005fcp - 12/13 Reference: Febrile Infant (CPM005)Not intended to replace physician judgment with respect to individual variations and needs.
TREATMENT & DISPOSITION
PEDIATRIC BEST PRACT ICE F LASH CARD
Febrile Infant, well-appearing and age 1–90 days
LOW RISKinitial treatment
• No treatment OR • Antibiotics per dosages above — recommend attempt to obtain CSF before initiating IV antibiotics.
ADM I T• Admit locally OR• Consider consult or transfer
HIGH RISK initial treatment*
Focus 1 to 28 days 29 to 90 days
Suspected UTI OR no focus identified
• Ampicillin (50 mg/kg/dose IV every 6 hrs AND
• Cefotaxime (50 mg/kg/dose IV every 6 hrs)
• Ceftriaxone (100 mg/kg/dose IV every 24 hrs)
note: Ampicillin is preferred agent if Gram stain of urine shows Gram-positive cocci
Suspected bacterial meningitis OR abnormal CSF
• Ampicillin (75 mg/kg/dose IV every 6 hrs) AND
• Gentamicin (5 mg/kg/dose IV every 24 hours) AND
• Cefotaxime (75 mg/kg/dose IV every 6 hrs)
• Ampicillin (75 mg/kg/ dose IV every 6 hrs) AND
• Gentamicin (5 mg/kg/ dose IV every 24 hrs) AND
• Ceftriaxone (100 mg/kg/dose IV every 24 hrs)
Suspected HSV
Acyclovir (20 mg/kg/dose IV every 8 hrs)
Barriers to care
or follow-up
CSF normal
ADM I T• Admit locally
D I S CHARGE• Schedule follow-up within 24 hrs• Provide patient/family education
Prima
ry Ca
re
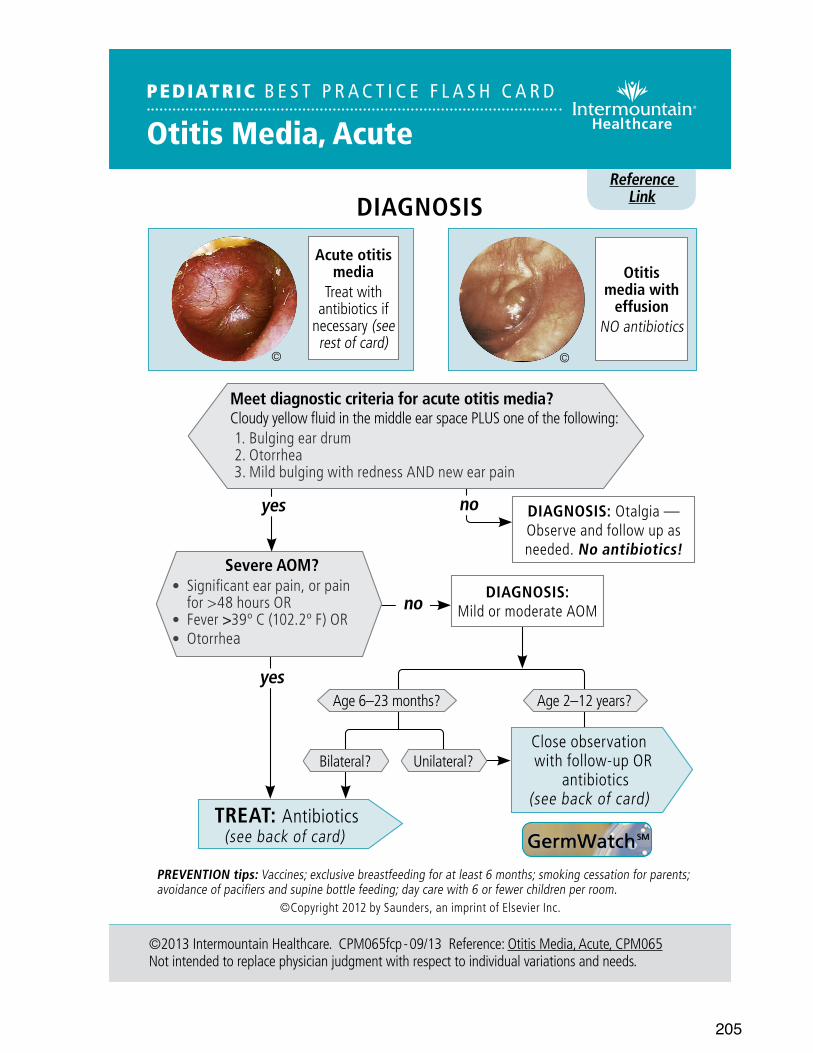
205
Reference Link
PEDIATRIC B E S T P R A C T I C E F L A S H C A R D
Otitis Media, Acute
©2013 Intermountain Healthcare. CPM065fcp - 09/13 Reference: Otitis Media, Acute, CPM065 Not intended to replace physician judgment with respect to individual variations and needs.
yes no DIAGNOSIS: Otalgia — Observe and follow up as needed. No antibiotics!
DIAGNOSIS
PREVENTION tips: Vaccines; exclusive breastfeeding for at least 6 months; smoking cessation for parents; avoidance of pacifiers and supine bottle feeding; day care with 6 or fewer children per room.
Acute otitis media
Treat with antibiotics if
necessary (see rest of card)
Otitis media with
effusionNO antibiotics
Severe AOM?• Significant ear pain, or pain
for >48 hours OR• Fever >39º C (102.2º F) OR• Otorrhea
Meet diagnostic criteria for acute otitis media?Cloudy yellow fluid in the middle ear space PLUS one of the following:1. Bulging ear drum2. Otorrhea3. Mild bulging with redness AND new ear pain
yes
noDIAGNOSIS:
Mild or moderate AOM
TREAT: Antibiotics (see back of card)
Unilateral?
Age 6–23 months? Age 2–12 years?
Close observation with follow-up OR
antibiotics (see back of card)
Bilateral?
©Copyright 2012 by Saunders, an imprint of Elsevier Inc.
© ©
GermWatch SM
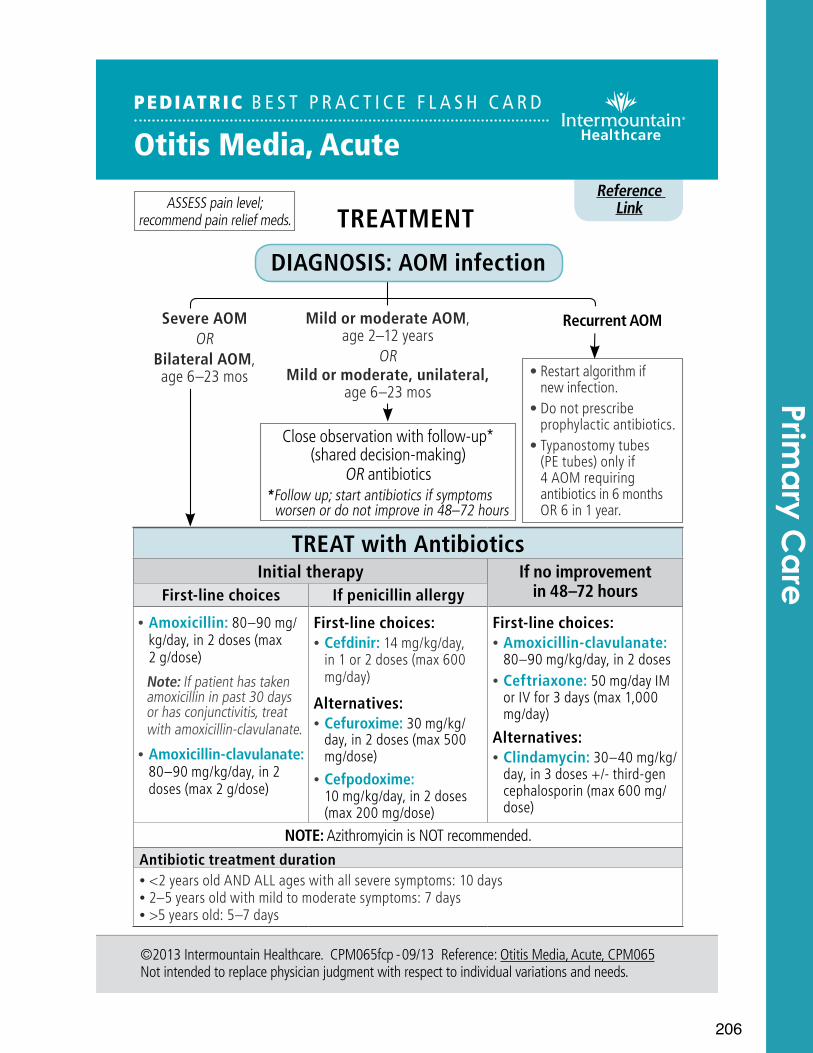
206
Reference LinkTREATMENT
PEDIATRIC B E S T P R A C T I C E F L A S H C A R D
Otitis Media, Acute
©2013 Intermountain Healthcare. CPM065fcp - 09/13 Reference: Otitis Media, Acute, CPM065Not intended to replace physician judgment with respect to individual variations and needs.
DIAGNOSIS: AOM infection
ASSESS pain level; recommend pain relief meds.
Mild or moderate AOM, age 2–12 years
OR Mild or moderate, unilateral,
age 6–23 mos
Close observation with follow-up* (shared decision-making)
OR antibiotics*Follow up; start antibiotics if symptoms
worsen or do not improve in 48–72 hours
• Restart algorithm if new infection.
• Do not prescribe prophylactic antibiotics.
• Typanostomy tubes (PE tubes) only if 4 AOM requiring antibiotics in 6 months OR 6 in 1 year.
Severe AOMOR
Bilateral AOM, age 6–23 mos
Recurrent AOM
TREAT with AntibioticsInitial therapy If no improvement
in 48–72 hoursFirst-line choices If penicillin allergy
• Amoxicillin: 80–90 mg/kg/day, in 2 doses (max 2 g/dose)
Note: If patient has taken amoxicillin in past 30 days or has conjunctivitis, treat with amoxicillin-clavulanate.
• Amoxicillin-clavulanate: 80–90 mg/kg/day, in 2 doses (max 2 g/dose)
First-line choices: • Cefdinir: 14 mg/kg/day, in 1 or 2 doses (max 600 mg/day)
Alternatives: • Cefuroxime: 30 mg/kg/day, in 2 doses (max 500 mg/dose)
• Cefpodoxime: 10 mg/kg/day, in 2 doses (max 200 mg/dose)
First-line choices: • Amoxicillin-clavulanate: 80–90 mg/kg/day, in 2 doses
• Ceftriaxone: 50 mg/day IM or IV for 3 days (max 1,000 mg/day)
Alternatives: • Clindamycin: 30–40 mg/kg/day, in 3 doses +/- third-gen cephalosporin (max 600 mg/dose)
NOTE: Azithromyicin is NOT recommended.Antibiotic treatment duration • <2 years old AND ALL ages with all severe symptoms: 10 days • 2–5 years old with mild to moderate symptoms: 7 days • >5 years old: 5–7 days
Prima
ry Ca
re
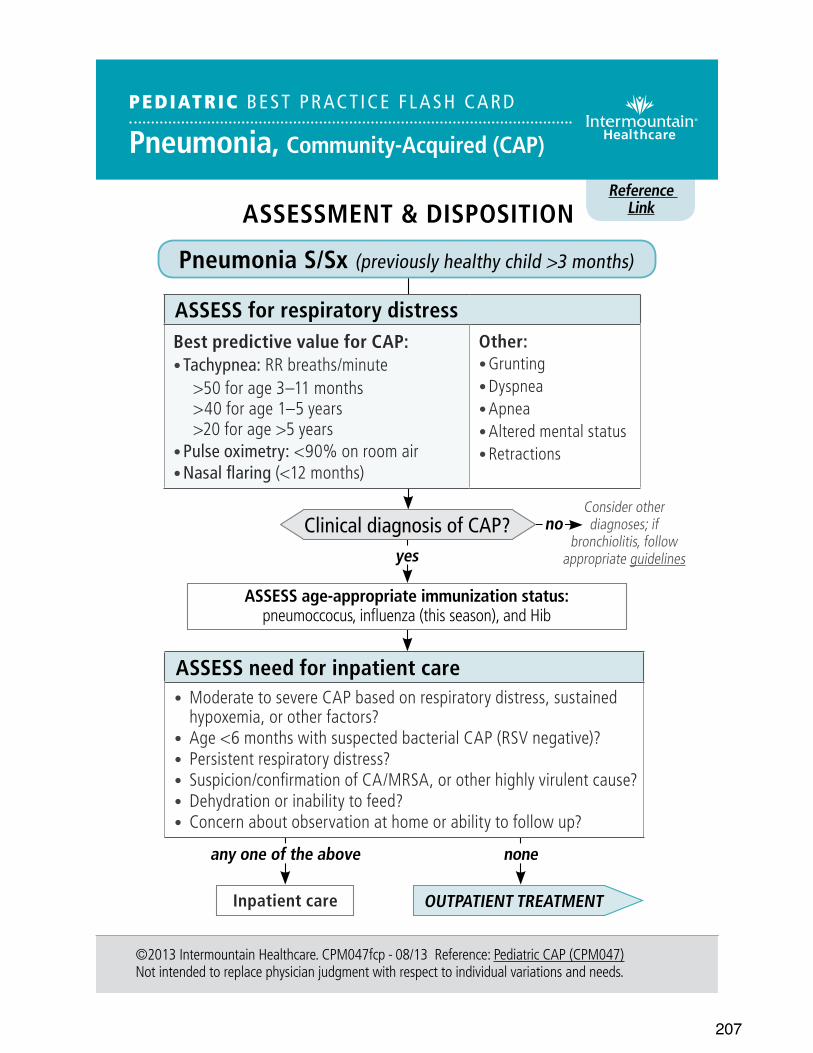
207
Reference Link
©2013 Intermountain Healthcare. CPM047fcp - 08/13 Reference: Pediatric CAP (CPM047)Not intended to replace physician judgment with respect to individual variations and needs.
ASSESSMENT & DISPOSITION
Consider other diagnoses; if
bronchiolitis, follow appropriate guidelines
no
yes
any one of the above
OUTPATIENT TREATMENT
PEDIATRIC BEST PRACT ICE F LASH CARD
Pneumonia, Community-Acquired (CAP)
Pneumonia S/Sx (previously healthy child >3 months)
ASSESS for respiratory distressBest predictive value for CAP:• Tachypnea: RR breaths/minute
>50 for age 3–11 months>40 for age 1–5 years>20 for age >5 years
• Pulse oximetry: <90% on room air• Nasal flaring (<12 months)
Other:• Grunting• Dyspnea• Apnea• Altered mental status• Retractions
Clinical diagnosis of CAP?
ASSESS age-appropriate immunization status: pneumoccocus, influenza (this season), and Hib
ASSESS need for inpatient care• Moderate to severe CAP based on respiratory distress, sustained
hypoxemia, or other factors?• Age <6 months with suspected bacterial CAP (RSV negative)?• Persistent respiratory distress? • Suspicion/confirmation of CA/MRSA, or other highly virulent cause?• Dehydration or inability to feed?• Concern about observation at home or ability to follow up?
Inpatient care
none
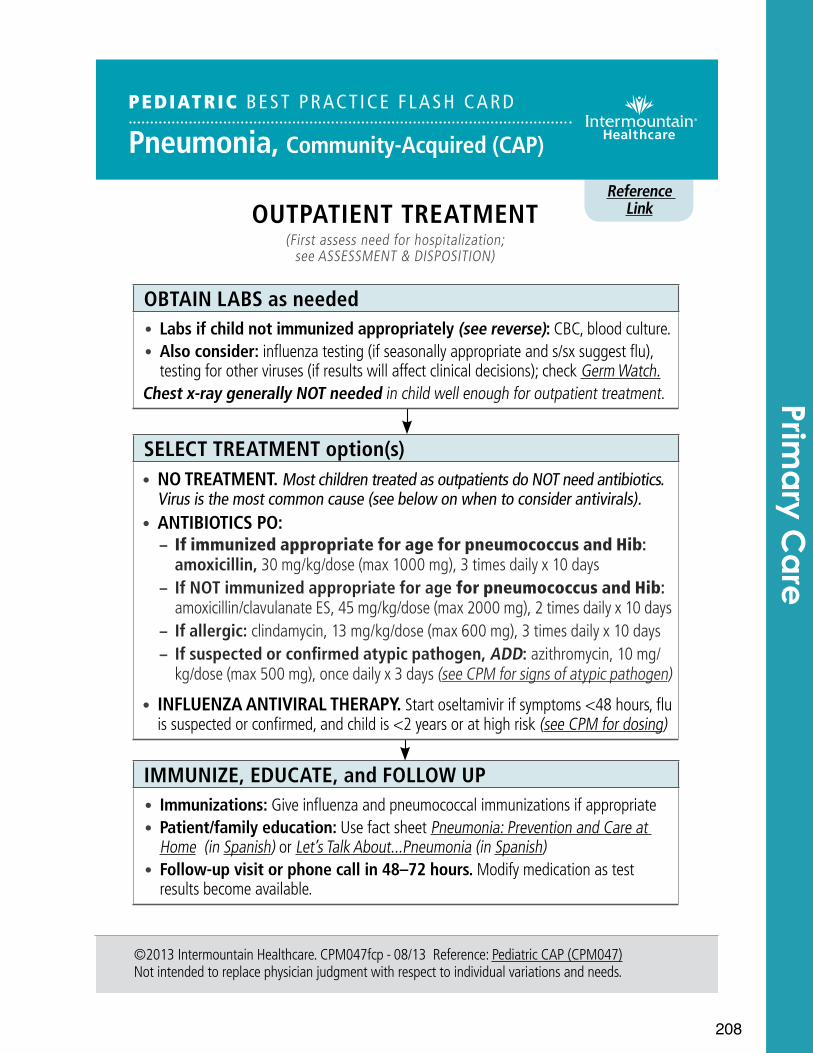
208
Reference Link
©2013 Intermountain Healthcare. CPM047fcp - 08/13 Reference: Pediatric CAP (CPM047)Not intended to replace physician judgment with respect to individual variations and needs.
OUTPATIENT TREATMENT (First assess need for hospitalization;
see ASSESSMENT & DISPOSITION)
OBTAIN LABS as needed• Labs if child not immunized appropriately (see reverse): CBC, blood culture.• Also consider: influenza testing (if seasonally appropriate and s/sx suggest flu),
testing for other viruses (if results will affect clinical decisions); check Germ Watch. Chest x-ray generally NOT needed in child well enough for outpatient treatment.
SELECT TREATMENT option(s)• NO TREATMENT. Most children treated as outpatients do NOT need antibiotics.
Virus is the most common cause (see below on when to consider antivirals).• ANTIBIOTICS PO:
– If immunized appropriate for age for pneumococcus and Hib: amoxicillin, 30 mg/kg/dose (max 1000 mg), 3 times daily x 10 days
– If NOT immunized appropriate for age for pneumococcus and Hib: amoxicillin/clavulanate ES, 45 mg/kg/dose (max 2000 mg), 2 times daily x 10 days
– If allergic: clindamycin, 13 mg/kg/dose (max 600 mg), 3 times daily x 10 days – If suspected or confirmed atypic pathogen, ADD: azithromycin, 10 mg/kg/dose (max 500 mg), once daily x 3 days (see CPM for signs of atypic pathogen)
• INFLUENZA ANTIVIRAL THERAPY. Start oseltamivir if symptoms <48 hours, flu is suspected or confirmed, and child is <2 years or at high risk (see CPM for dosing)
IMMUNIZE, EDUCATE, and FOLLOW UP• Immunizations: Give influenza and pneumococcal immunizations if appropriate• Patient/family education: Use fact sheet Pneumonia: Prevention and Care at
Home (in Spanish) or Let’s Talk About...Pneumonia (in Spanish)• Follow-up visit or phone call in 48–72 hours. Modify medication as test
results become available.
PEDIATRIC BEST PRACT ICE F LASH CARD
Pneumonia, Community-Acquired (CAP)
Prima
ry Ca
re
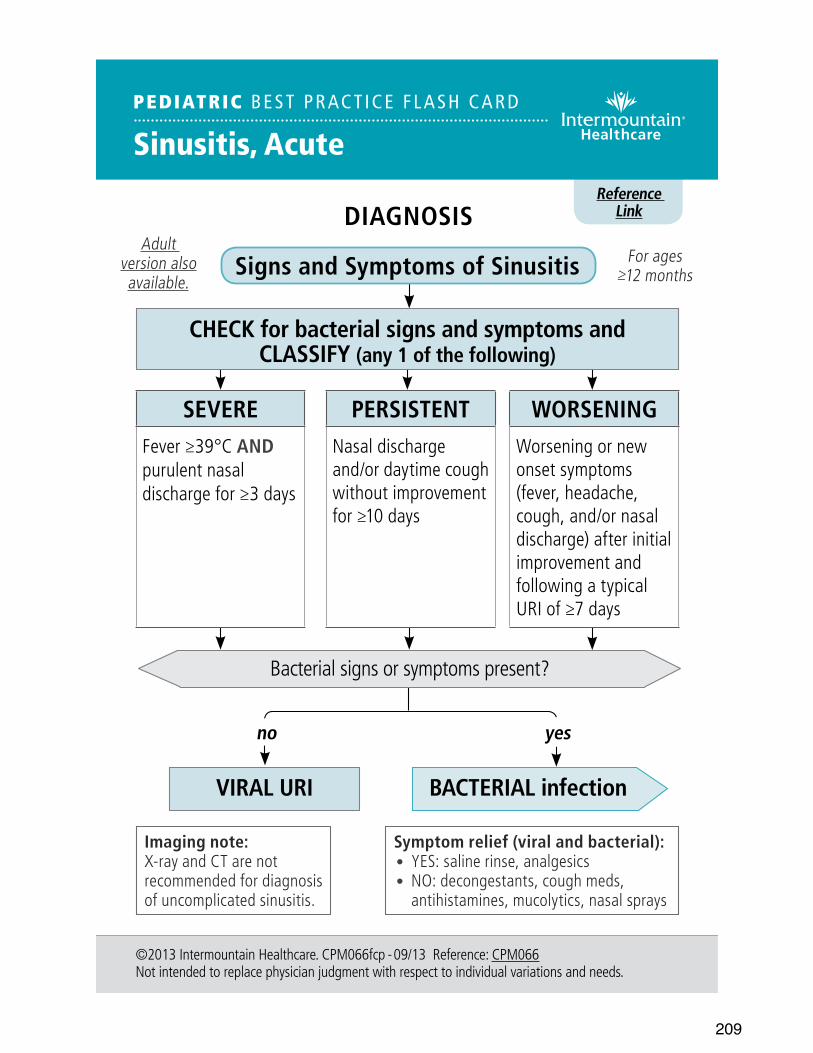
209
Reference Link
PEDIATRIC BEST PRACT ICE F LASH CARD
Sinusitis, Acute
©2013 Intermountain Healthcare. CPM066fcp - 09/13 Reference: CPM066Not intended to replace physician judgment with respect to individual variations and needs.
no yes
DIAGNOSIS
Signs and Symptoms of Sinusitis
BACTERIAL infection
Symptom relief (viral and bacterial):• YES: saline rinse, analgesics• NO: decongestants, cough meds,
antihistamines, mucolytics, nasal sprays
Adult version also available.
VIRAL URI
For ages ≥12 months
Imaging note: X-ray and CT are not recommended for diagnosis of uncomplicated sinusitis.
CHECK for bacterial signs and symptoms and CLASSIFY (any 1 of the following)
SEVEREFever ≥39°C AND purulent nasal discharge for ≥3 days
PERSISTENTNasal discharge and/or daytime cough without improvement for ≥10 days
WORSENINGWorsening or new onset symptoms (fever, headache, cough, and/or nasal discharge) after initial improvement and following a typical URI of ≥7 days
Bacterial signs or symptoms present?
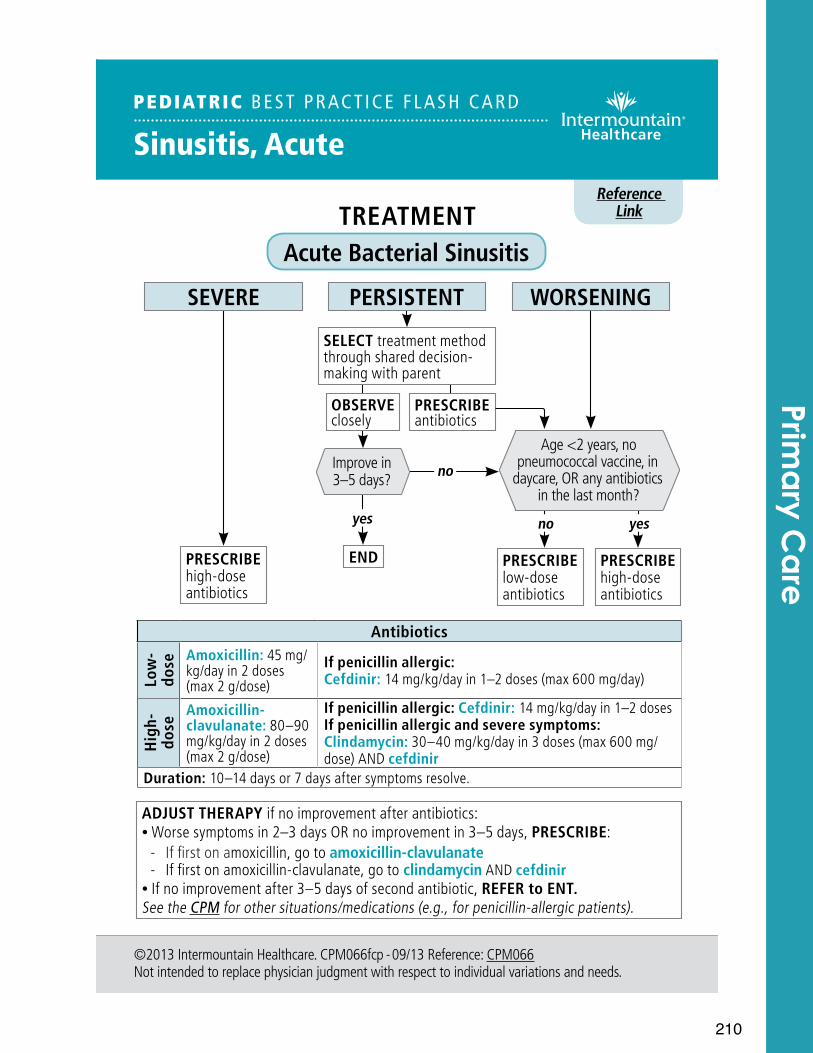
210
©2013 Intermountain Healthcare. CPM066fcp - 09/13 Reference: CPM066Not intended to replace physician judgment with respect to individual variations and needs.
TREATMENT Acute Bacterial Sinusitis
Reference Link
PEDIATRIC BEST PRACT ICE F LASH CARD
Sinusitis, Acute
Antibiotics
Low
- do
se Amoxicillin: 45 mg/kg/day in 2 doses (max 2 g/dose)
If penicillin allergic: Cefdinir: 14 mg/kg/day in 1–2 doses (max 600 mg/day)
Hig
h-
dose
Amoxicillin-clavulanate: 80–90 mg/kg/day in 2 doses (max 2 g/dose)
If penicillin allergic: Cefdinir: 14 mg/kg/day in 1–2 dosesIf penicillin allergic and severe symptoms: Clindamycin: 30–40 mg/kg/day in 3 doses (max 600 mg/dose) AND cefdinir
Duration: 10–14 days or 7 days after symptoms resolve.
PRESCRIBE high-dose antibiotics
PRESCRIBE antibiotics
SELECT treatment method through shared decision-making with parent
OBSERVE closely
yes
noImprove in 3–5 days?
END
no
Age <2 years, no pneumococcal vaccine, in
daycare, OR any antibiotics in the last month?
yes
PRESCRIBE low-dose antibiotics
PRESCRIBE high-dose antibiotics
ADJUST THERAPY if no improvement after antibiotics: • Worse symptoms in 2–3 days OR no improvement in 3–5 days, PRESCRIBE: - If first on amoxicillin, go to amoxicillin-clavulanate - If first on amoxicillin-clavulanate, go to clindamycin AND cefdinir
• If no improvement after 3–5 days of second antibiotic, REFER to ENT.See the CPM for other situations/medications (e.g., for penicillin-allergic patients).
SEVERE PERSISTENT WORSENING
Prima
ry Ca
re
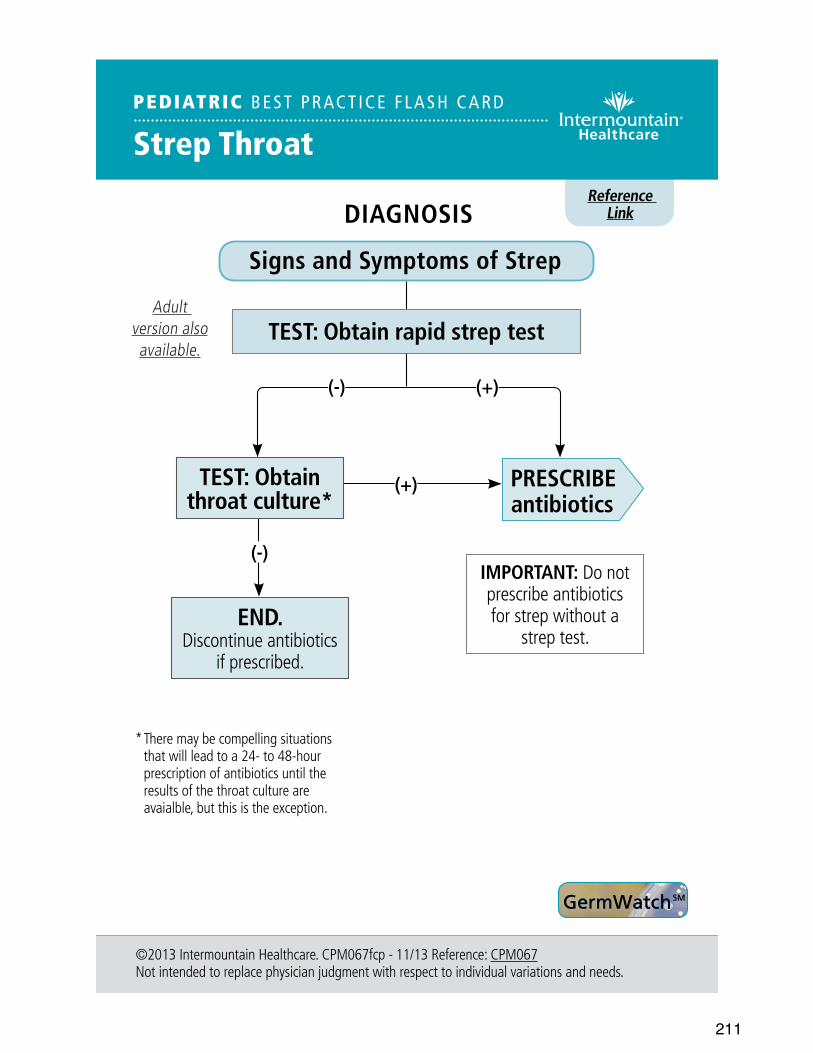
211
Reference Link
PEDIATRIC BEST PRAC T ICE F LASH CAR D
Strep Throat
©2013 Intermountain Healthcare. CPM067fcp - 11/13 Reference: CPM067 Not intended to replace physician judgment with respect to individual variations and needs.
DIAGNOSIS
Signs and Symptoms of Strep
TEST: Obtain rapid strep test
IMPORTANT: Do not prescribe antibiotics for strep without a
strep test.
GermWatch SM
PRESCRIBE antibiotics
(+)TEST: Obtain throat culture*
(-)
* There may be compelling situations that will lead to a 24- to 48-hour prescription of antibiotics until the results of the throat culture are avaialble, but this is the exception.
Adult version also available.
END. Discontinue antibiotics
if prescribed.
(+)(-)
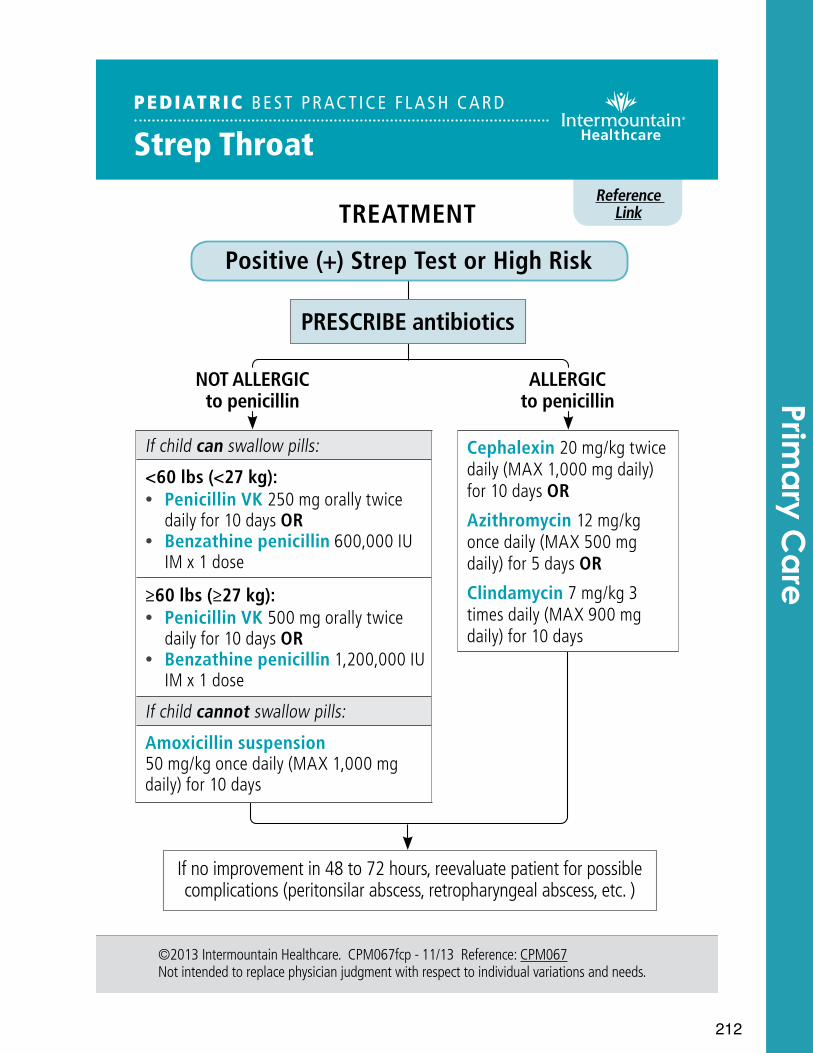
212
Reference Link
PEDIATRIC BEST PR ACT ICE F L A SH CARD
Strep Throat
©2013 Intermountain Healthcare. CPM067fcp - 11/13 Reference: CPM067Not intended to replace physician judgment with respect to individual variations and needs.
NOT ALLERGICto penicillin
ALLERGICto penicillin
TREATMENT
Positive (+) Strep Test or High Risk
If child can swallow pills:
<60 lbs (<27 kg): • Penicillin VK 250 mg orally twice
daily for 10 days OR • Benzathine penicillin 600,000 IU
IM x 1 dose
≥60 lbs (≥27 kg): • Penicillin VK 500 mg orally twice
daily for 10 days OR • Benzathine penicillin 1,200,000 IU
IM x 1 dose
If child cannot swallow pills:
Amoxicillin suspension 50 mg/kg once daily (MAX 1,000 mg daily) for 10 days
Cephalexin 20 mg/kg twice daily (MAX 1,000 mg daily) for 10 days OR
Azithromycin 12 mg/kg once daily (MAX 500 mg daily) for 5 days OR
Clindamycin 7 mg/kg 3 times daily (MAX 900 mg daily) for 10 days
PRESCRIBE antibiotics
If no improvement in 48 to 72 hours, reevaluate patient for possible complications (peritonsilar abscess, retropharyngeal abscess, etc. )
Prima
ry Ca
re

213
214
Pulmonary
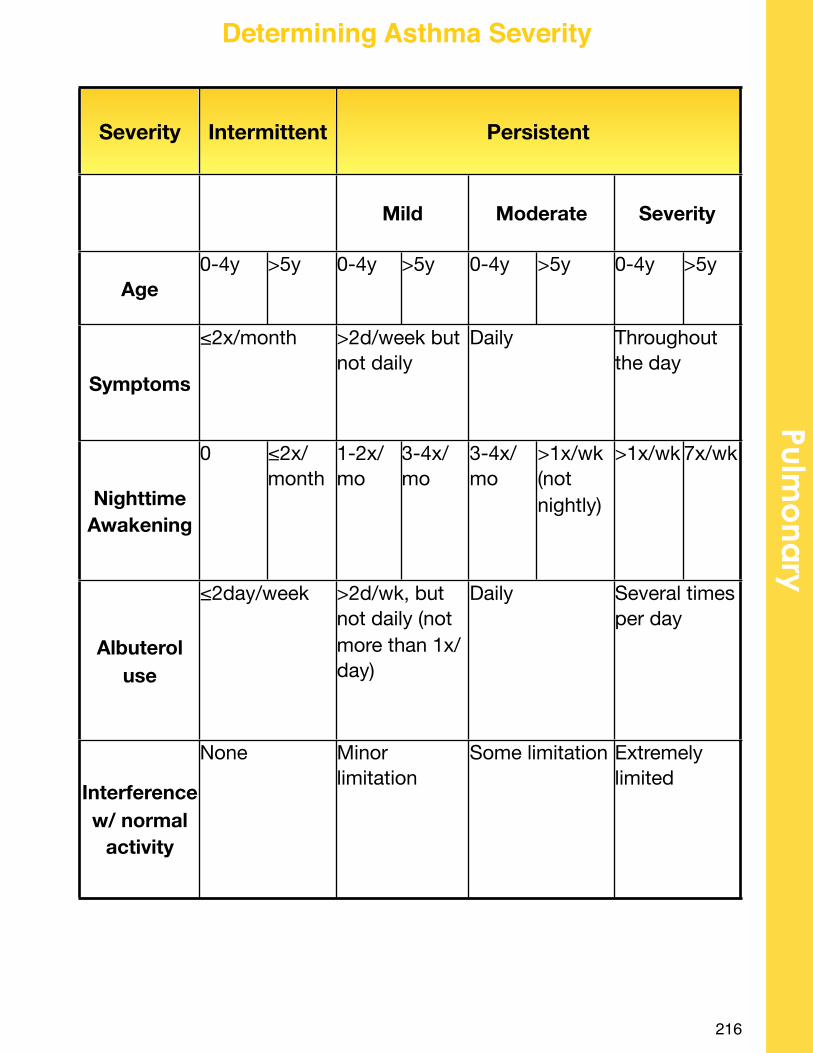
216
Pulmo
nary
Determining Asthma Severity
Severity IntermittentIntermittent PersistentPersistentPersistentPersistentPersistentPersistent
MildMild ModerateModerate SeveritySeverity
Age0-4y >5y 0-4y >5y 0-4y >5y 0-4y >5y
Symptoms
≤2x/month≤2x/month >2d/week but not daily>2d/week but not daily
DailyDaily Throughout the dayThroughout the day
Nighttime Awakening
0 ≤2x/ month
1-2x/ mo
3-4x/ mo
3-4x/ mo
>1x/wk (not nightly)
>1x/wk 7x/wk
Albuterol use
≤2day/week≤2day/week >2d/wk, but not daily (not more than 1x/day)
>2d/wk, but not daily (not more than 1x/day)
DailyDaily Several times per daySeveral times per day
Interference w/ normal
activity
NoneNone Minor limitationMinor limitation
Some limitationSome limitation Extremely limitedExtremely limited
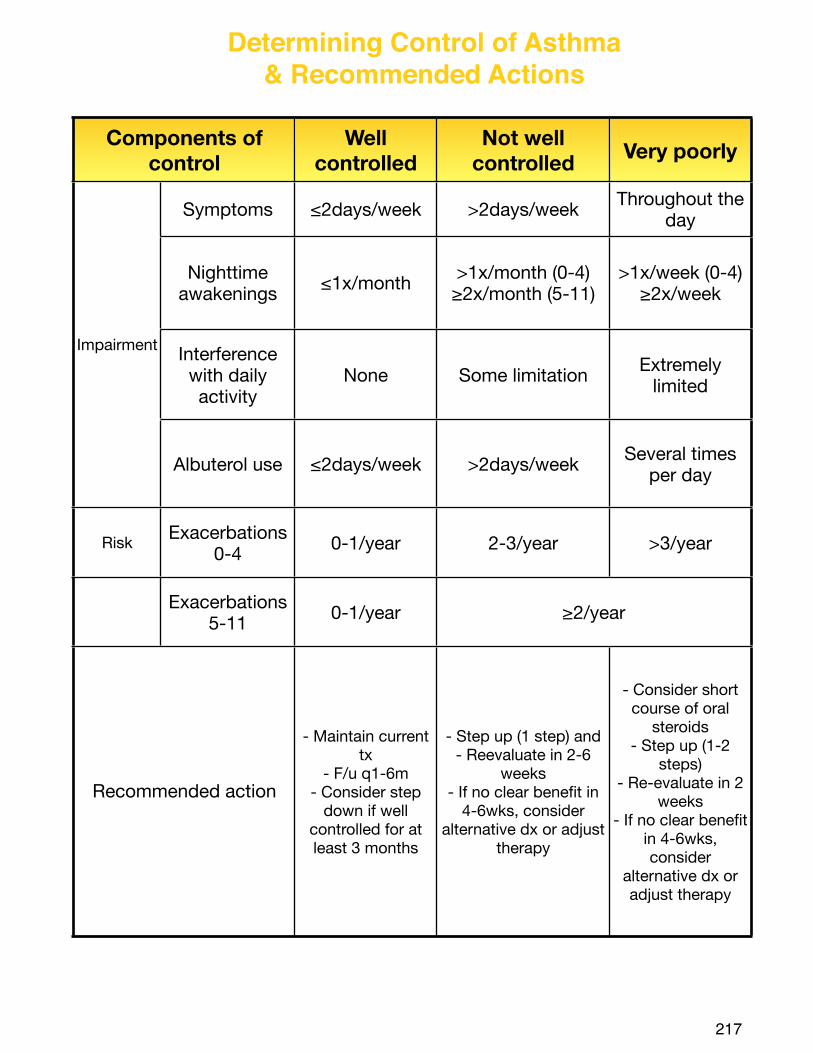
217
Determining Control of Asthma & Recommended Actions
Components of control
Components of control
Well controlled
Not well controlled Very poorly
Impairment
Symptoms ≤2days/week >2days/week Throughout the day
Impairment
Nighttime awakenings ≤1x/month >1x/month (0-4)
≥2x/month (5-11)>1x/week (0-4)
≥2x/week
Impairment Interference with daily activity
None Some limitation Extremely limited
Impairment
Albuterol use ≤2days/week >2days/week Several times per day
Risk Exacerbations 0-4 0-1/year 2-3/year >3/year
Exacerbations 5-11 0-1/year ≥2/year≥2/year
Recommended actionRecommended action
- Maintain current tx
- F/u q1-6m- Consider step
down if well controlled for at least 3 months
- Step up (1 step) and- Reevaluate in 2-6
weeks- If no clear benefit in
4-6wks, consider alternative dx or adjust
therapy
- Consider short course of oral
steroids- Step up (1-2
steps)- Re-evaluate in 2
weeks- If no clear benefit
in 4-6wks, consider
alternative dx or adjust therapy
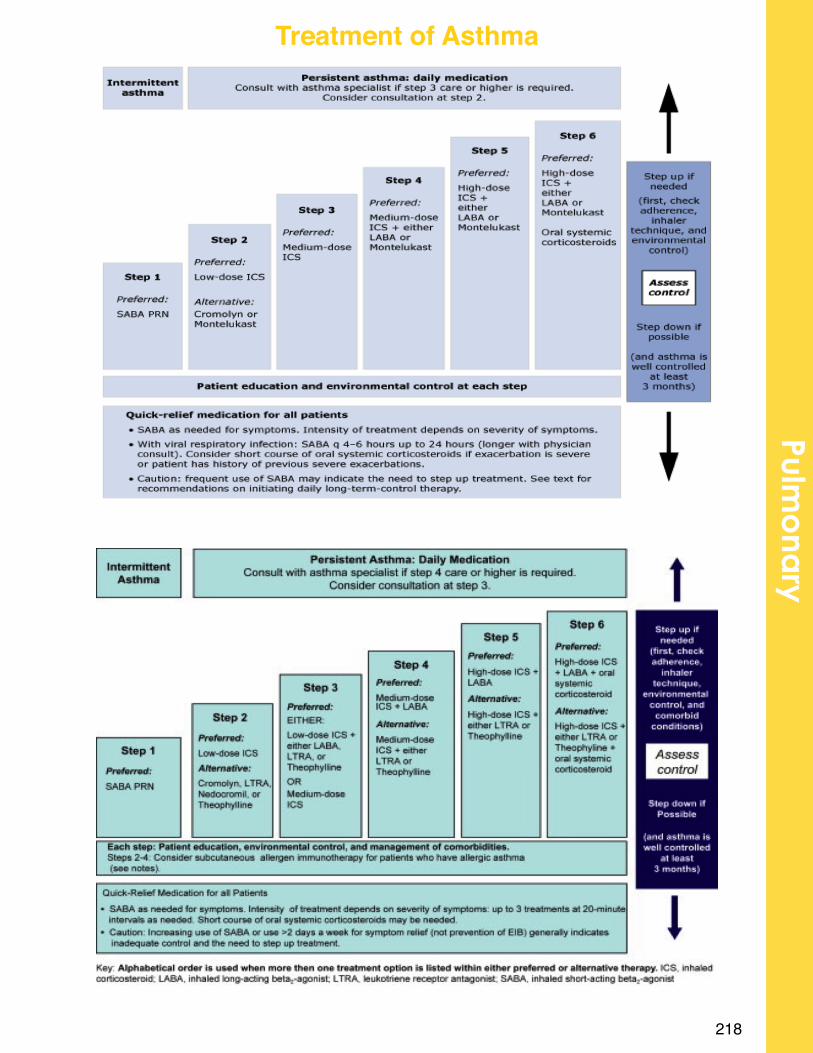
218
Pulmo
nary
Treatment of Asthma
220
Rheumatology
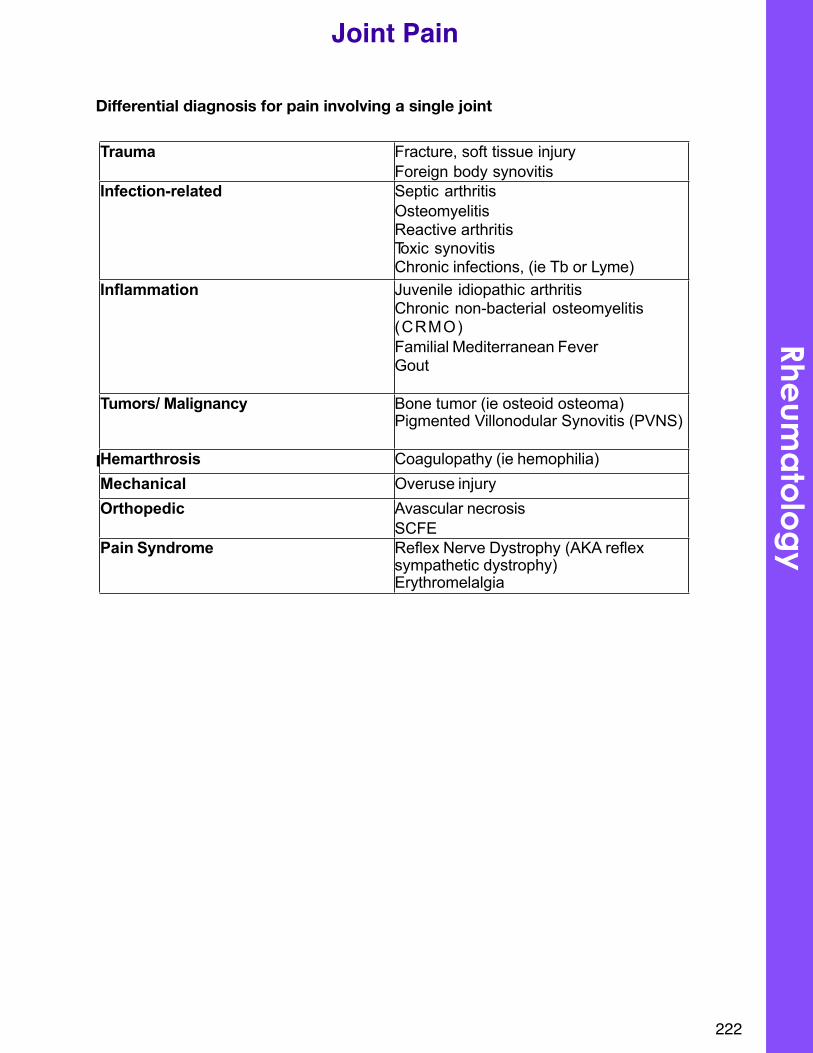
Differential diagnosis for pain involving a single joint
Differential diagnosis for pain involving multiple joints:
222
Joint Pain
Trauma Fracture, soft tissue injury Foreign body synovitis
Infection-related Septic arthritis Osteomyelitis Reactive arthritisToxic synovitisChronic infections, (ie Tb or Lyme)
Inflammation Juvenile idiopathic arthritisChronic non-bacterial osteomyelitis (CRMO)Familial Mediterranean FeverGout
Tumors/ Malignancy Bone tumor (ie osteoid osteoma)Pigmented Villonodular Synovitis (PVNS)
Hemarthrosis Coagulopathy (ie hemophilia)Mechanical Overuse injuryOrthopedic Avascular necrosis
SCFEPain Syndrome Reflex Nerve Dystrophy (AKA reflex
sympathetic dystrophy)Erythromelalgia
Rheum
ato
log
y
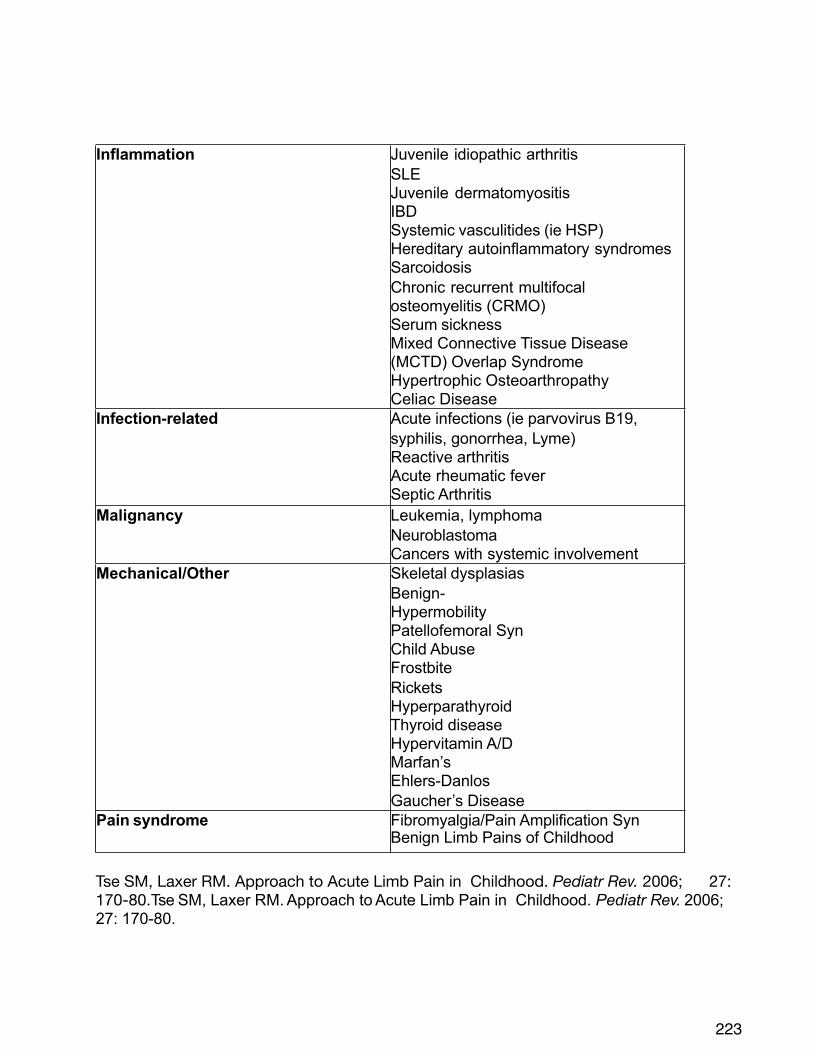
Tse SM, Laxer RM. Approach to Acute Limb Pain in Childhood. Pediatr Rev. 2006; 27: 170-80.Tse SM, Laxer RM. Approach to Acute Limb Pain in Childhood. Pediatr Rev. 2006; 27: 170-80.
223
Inflammation Juvenile idiopathic arthritis SLEJuvenile dermatomyositis IBDSystemic vasculitides (ie HSP) Hereditary autoinflammatory syndromes SarcoidosisChronic recurrent multifocal osteomyelitis (CRMO)Serum sicknessMixed Connective Tissue Disease (MCTD) Overlap SyndromeHypertrophic OsteoarthropathyCeliac Disease
Infection-related Acute infections (ie parvovirus B19, syphilis, gonorrhea, Lyme)Reactive arthritisAcute rheumatic feverSeptic Arthritis
Malignancy Leukemia, lymphoma NeuroblastomaCancers with systemic involvement
Mechanical/Other Skeletal dysplasiasBenign-HypermobilityPatellofemoral SynChild AbuseFrostbiteRicketsHyperparathyroidThyroid diseaseHypervitamin A/DMarfan’s Ehlers-Danlos Gaucher’s Disease
Pain syndrome Fibromyalgia/Pain Amplification SynBenign Limb Pains of Childhood
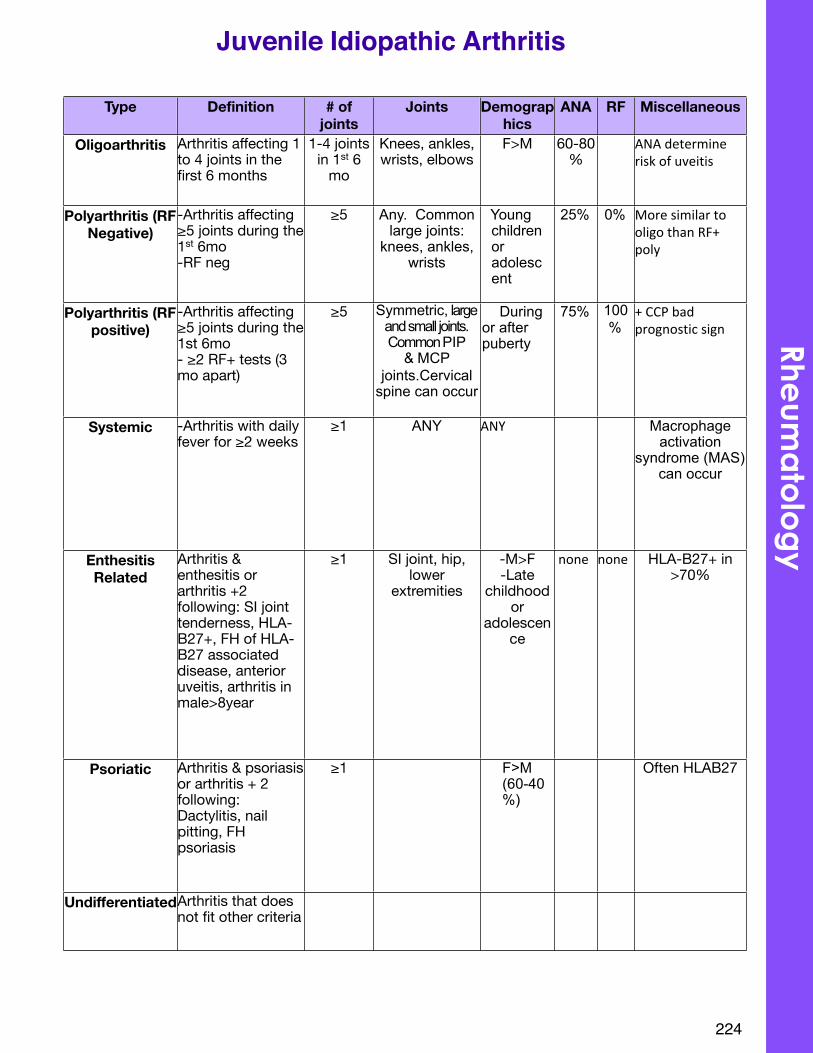
224
Juvenile Idiopathic Arthritis
Type Definition # of joints
Joints Demographics
ANA RF Miscellaneous
Oligoarthritis Arthritis affecting 1 to 4 joints in the first 6 months
1-4 joints in 1st 6
mo
Knees, ankles, wrists, elbows
F>M 60-80%
ANA#determine#risk#of#uveitis
Polyarthritis (RF Negative)
-Arthritis affecting ≥5 joints during the 1st 6mo-RF neg
≥5 Any. Common large joints:
knees, ankles, wrists
Young children or adolescent
25% 0% More#similar#to#oligo#than#RF+#poly
Polyarthritis (RF positive)
-Arthritis affecting ≥5 joints during the 1st 6mo- ≥2 RF+ tests (3 mo apart)
≥5 Symmetric, large and small joints. Common PIP
& MCP joints.Cervical
spine can occur
During or after puberty
75% 100%
+#CCP#bad#prognostic#sign
Systemic -Arthritis with daily fever for ≥2 weeks
≥1 ANY ANY Macrophage activation
syndrome (MAS) can occur
Enthesitis Related
Arthritis & enthesitis or arthritis +2 following: SI joint tenderness, HLA-B27+, FH of HLA-B27 associated disease, anterior uveitis, arthritis in male>8year
≥1 SI joint, hip, lower
extremities
-M>F-Late
childhood or
adolescence
#none none HLA-B27+ in >70%
Psoriatic Arthritis & psoriasis or arthritis + 2 following:Dactylitis, nail pitting, FH psoriasis
≥1 F>M (60-40%)
Often HLAB27
UndifferentiatedArthritis that does not fit other criteria
Rheum
ato
log
y
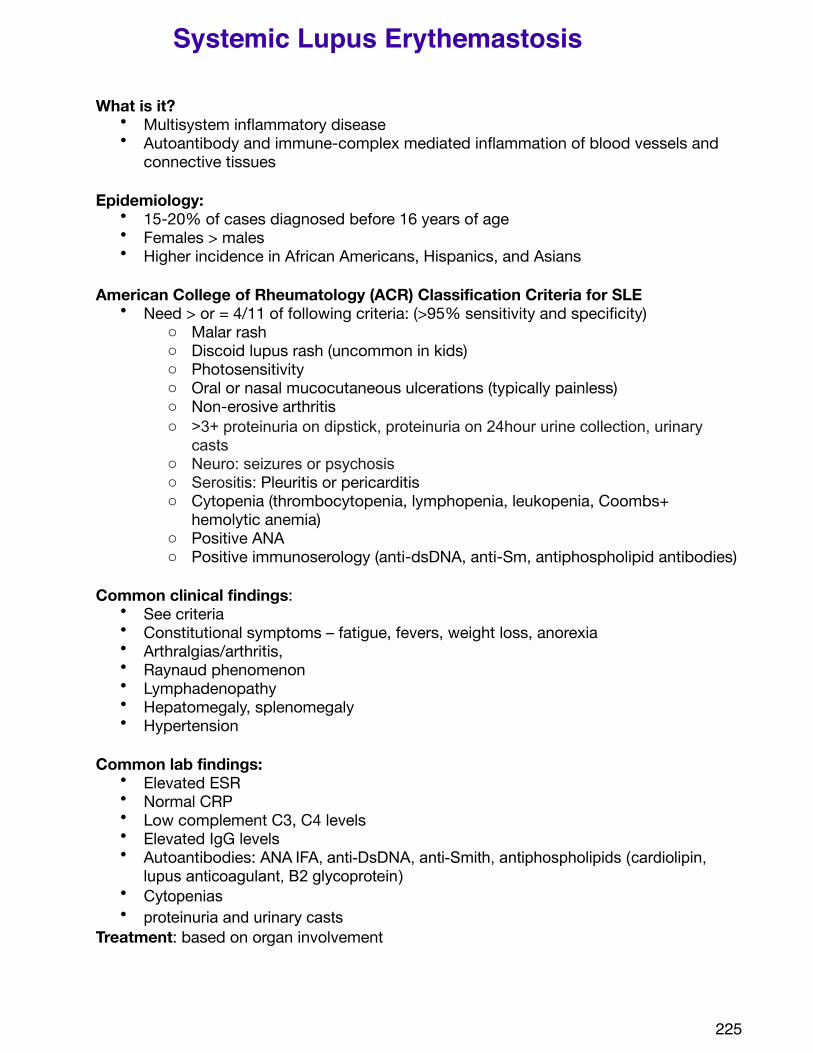
What is it? • Multisystem inflammatory disease • Autoantibody and immune-complex mediated inflammation of blood vessels and
connective tissues
Epidemiology:• 15-20% of cases diagnosed before 16 years of age• Females > males• Higher incidence in African Americans, Hispanics, and Asians
American College of Rheumatology (ACR) Classification Criteria for SLE• Need > or = 4/11 of following criteria: (>95% sensitivity and specificity)
o Malar rash o Discoid lupus rash (uncommon in kids)o Photosensitivityo Oral or nasal mucocutaneous ulcerations (typically painless)o Non-erosive arthritiso >3+ proteinuria on dipstick, proteinuria on 24hour urine collection, urinary
castso Neuro: seizures or psychosiso Serositis: Pleuritis or pericarditiso Cytopenia (thrombocytopenia, lymphopenia, leukopenia, Coombs+
hemolytic anemia)o Positive ANAo Positive immunoserology (anti-dsDNA, anti-Sm, antiphospholipid antibodies)
Common clinical findings:• See criteria• Constitutional symptoms – fatigue, fevers, weight loss, anorexia• Arthralgias/arthritis,• Raynaud phenomenon• Lymphadenopathy• Hepatomegaly, splenomegaly• Hypertension
Common lab findings:• Elevated ESR • Normal CRP• Low complement C3, C4 levels• Elevated IgG levels• Autoantibodies: ANA IFA, anti-DsDNA, anti-Smith, antiphospholipids (cardiolipin,
lupus anticoagulant, B2 glycoprotein)• Cytopenias• proteinuria and urinary casts
Treatment: based on organ involvement
225
Systemic Lupus Erythemastosis
• Hydroxychloroquineo Standard therapyo Decreases frequency and severity of disease flares
• Corticosteroidso Initial therapy o Pulse therapy used for severe nephritis, hematologic crisis, or CNS disease
• Azathioprineo Hematologic and renal manifestations
• Mycophenolate mofetilo Used for hematologic, renal, and CNS manifestations
• Cyclophosphamide/Cytoxano Used for severe renal and CNS manifestation
• Rituximabo Resistant thrombocytopenia
• Methotrexate• NSAIDs
Prognosis:• Relapsing and remitting course of disease
o Children have more active disease at presentation and over time o Children more likely to have active renal disease
• 10 year survival >90%• Most death related to infection, renal, cardiac, CNS, and pulmonary disease• Morbitiy related to disease and/or treatment:
o Children receive more intensive drug therapy and sustain more damage due to SLE
! Early onset of coronary artery disease! Bone disease – osteopenia, avascular necrosis! Malignancy
References:Benseler SM, Silverman ED. Systemic lupus erythematosus. Rheum Dis Clin North Am 2007; 33(3): 471-98.Hiraki LT, Benseler SM, Tyrrell PN, et al. Clnical and laboratory characteristics and long-term outcome of pediatric systemic lupus erythematosus: A longitudinal study. J Pediatr 2008; 152:550-6.Uptodate
226
Rheum
ato
log
y
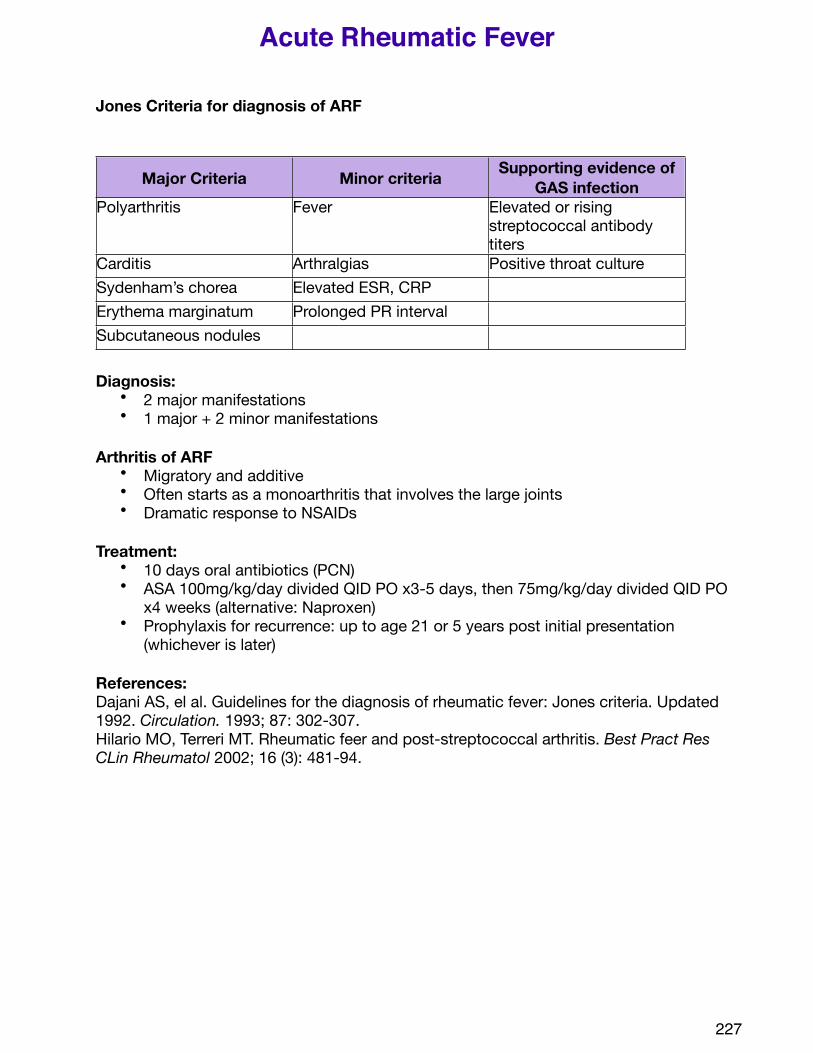
Jones Criteria for diagnosis of ARF
Major Criteria Minor criteria Supporting evidence of GAS infection
Polyarthritis Fever Elevated or rising streptococcal antibody titers
Carditis Arthralgias Positive throat cultureSydenham’s chorea Elevated ESR, CRPErythema marginatum Prolonged PR intervalSubcutaneous nodules
Diagnosis: • 2 major manifestations • 1 major + 2 minor manifestations
Arthritis of ARF• Migratory and additive• Often starts as a monoarthritis that involves the large joints• Dramatic response to NSAIDs
Treatment: • 10 days oral antibiotics (PCN)• ASA 100mg/kg/day divided QID PO x3-5 days, then 75mg/kg/day divided QID PO
x4 weeks (alternative: Naproxen)• Prophylaxis for recurrence: up to age 21 or 5 years post initial presentation
(whichever is later)
References:Dajani AS, el al. Guidelines for the diagnosis of rheumatic fever: Jones criteria. Updated 1992. Circulation. 1993; 87: 302-307.Hilario MO, Terreri MT. Rheumatic feer and post-streptococcal arthritis. Best Pract Res CLin Rheumatol 2002; 16 (3): 481-94.
227
Acute Rheumatic Fever
228
Toxicology
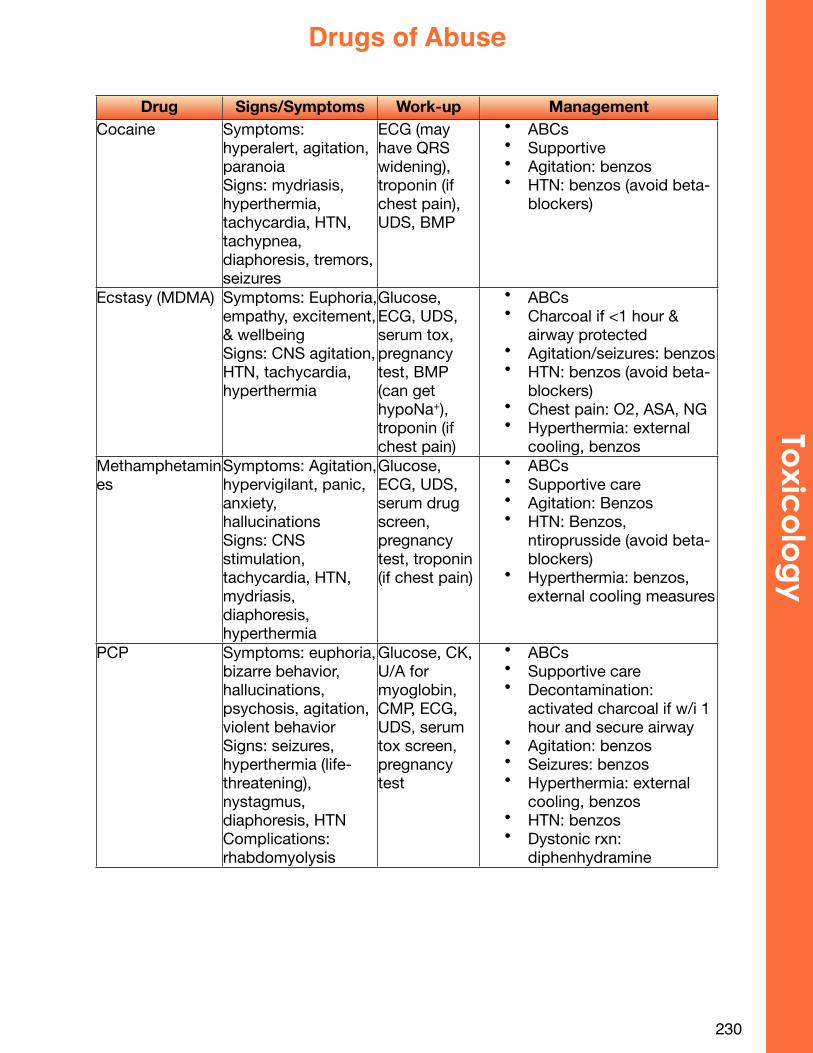
Drug Signs/Symptoms Work-up ManagementCocaine Symptoms:
hyperalert, agitation, paranoiaSigns: mydriasis, hyperthermia, tachycardia, HTN, tachypnea, diaphoresis, tremors, seizures
ECG (may have QRS widening), troponin (if chest pain), UDS, BMP
• ABCs• Supportive• Agitation: benzos• HTN: benzos (avoid beta-
blockers)
Ecstasy (MDMA) Symptoms: Euphoria, empathy, excitement, & wellbeingSigns: CNS agitation, HTN, tachycardia, hyperthermia
Glucose, ECG, UDS, serum tox, pregnancy test, BMP (can get hypoNa+), troponin (if chest pain)
• ABCs• Charcoal if <1 hour &
airway protected• Agitation/seizures: benzos• HTN: benzos (avoid beta-
blockers)• Chest pain: O2, ASA, NG• Hyperthermia: external
cooling, benzosMethamphetamines
Symptoms: Agitation, hypervigilant, panic, anxiety, hallucinationsSigns: CNS stimulation, tachycardia, HTN, mydriasis, diaphoresis, hyperthermia
Glucose, ECG, UDS, serum drug screen, pregnancy test, troponin (if chest pain)
• ABCs• Supportive care• Agitation: Benzos• HTN: Benzos,
ntiroprusside (avoid beta-blockers)
• Hyperthermia: benzos, external cooling measures
PCP Symptoms: euphoria, bizarre behavior, hallucinations, psychosis, agitation, violent behaviorSigns: seizures, hyperthermia (life-threatening), nystagmus, diaphoresis, HTNComplications: rhabdomyolysis
Glucose, CK, U/A for myoglobin, CMP, ECG, UDS, serum tox screen, pregnancy test
• ABCs• Supportive care• Decontamination:
activated charcoal if w/i 1 hour and secure airway
• Agitation: benzos• Seizures: benzos• Hyperthermia: external
cooling, benzos• HTN: benzos• Dystonic rxn:
diphenhydramine
230
Toxic
olo
gy
Drugs of Abuse
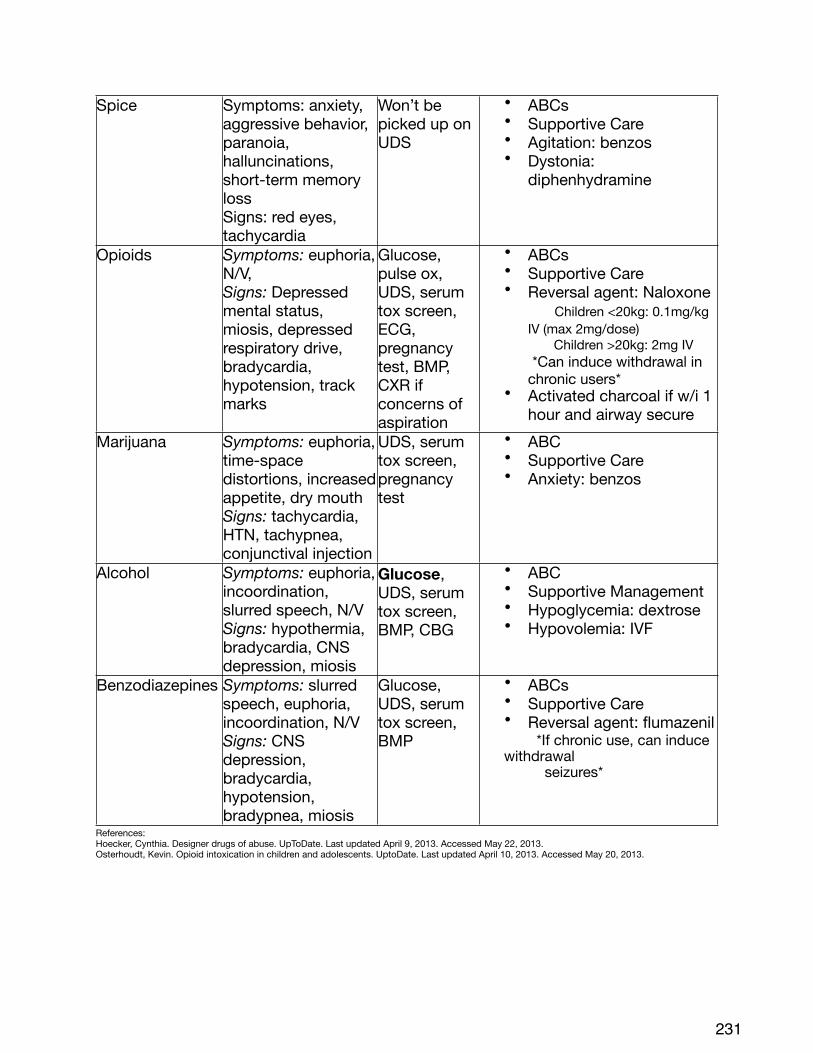
Spice Symptoms: anxiety, aggressive behavior, paranoia, halluncinations, short-term memory lossSigns: red eyes, tachycardia
Won’t be picked up on UDS
• ABCs• Supportive Care• Agitation: benzos• Dystonia:
diphenhydramine
Opioids Symptoms: euphoria, N/V, Signs: Depressed mental status, miosis, depressed respiratory drive, bradycardia, hypotension, track marks
Glucose, pulse ox, UDS, serum tox screen, ECG, pregnancy test, BMP, CXR if concerns of aspiration
• ABCs• Supportive Care• Reversal agent: Naloxone
Children <20kg: 0.1mg/kg IV (max 2mg/dose) Children >20kg: 2mg IV *Can induce withdrawal in chronic users*
• Activated charcoal if w/i 1 hour and airway secure
Marijuana Symptoms: euphoria, time-space distortions, increased appetite, dry mouthSigns: tachycardia, HTN, tachypnea, conjunctival injection
UDS, serum tox screen, pregnancy test
• ABC• Supportive Care• Anxiety: benzos
Alcohol Symptoms: euphoria, incoordination, slurred speech, N/VSigns: hypothermia, bradycardia, CNS depression, miosis
Glucose, UDS, serum tox screen, BMP, CBG
• ABC• Supportive Management• Hypoglycemia: dextrose• Hypovolemia: IVF
Benzodiazepines Symptoms: slurred speech, euphoria, incoordination, N/VSigns: CNS depression, bradycardia, hypotension, bradypnea, miosis
Glucose, UDS, serum tox screen, BMP
• ABCs• Supportive Care• Reversal agent: flumazenil *If chronic use, can induce withdrawal seizures*
References: Hoecker, Cynthia. Designer drugs of abuse. UpToDate. Last updated April 9, 2013. Accessed May 22, 2013. Osterhoudt, Kevin. Opioid intoxication in children and adolescents. UptoDate. Last updated April 10, 2013. Accessed May 20, 2013.
231
Toxic dose:
Child <12 years – 150mg/kg
Adolescents – 15g
Stages of Acetominophen Poisoning:
0-24 Hours- N/V, but may have no symptoms; LFTs normal
24-48 Hours- RUQ pain; LFTs may begin to rise
48-96 Hours- Peak of symptoms; AST >20,000, prolonged PT /INR
Death from hepatic failure of coagulopathy
4-14 days- Resolution of hepatic failure or progression to multi-organ failure
Management:• ABCs• Activated charcoal• Tylenol level (4H post-ingestion)
o Use Rummack Matthew Nomogram to determine if treatment is indicated
! if possible or probable hepatic toxicity• Call Poison Control Center: (800) 222-1222
• Use order set for tylenol/acetaminophen overdose• IV N-acetylcysteine: follow AST, ALT, PT, & PTT
232
Toxic
olo
gy
Tylenol
234
Wards
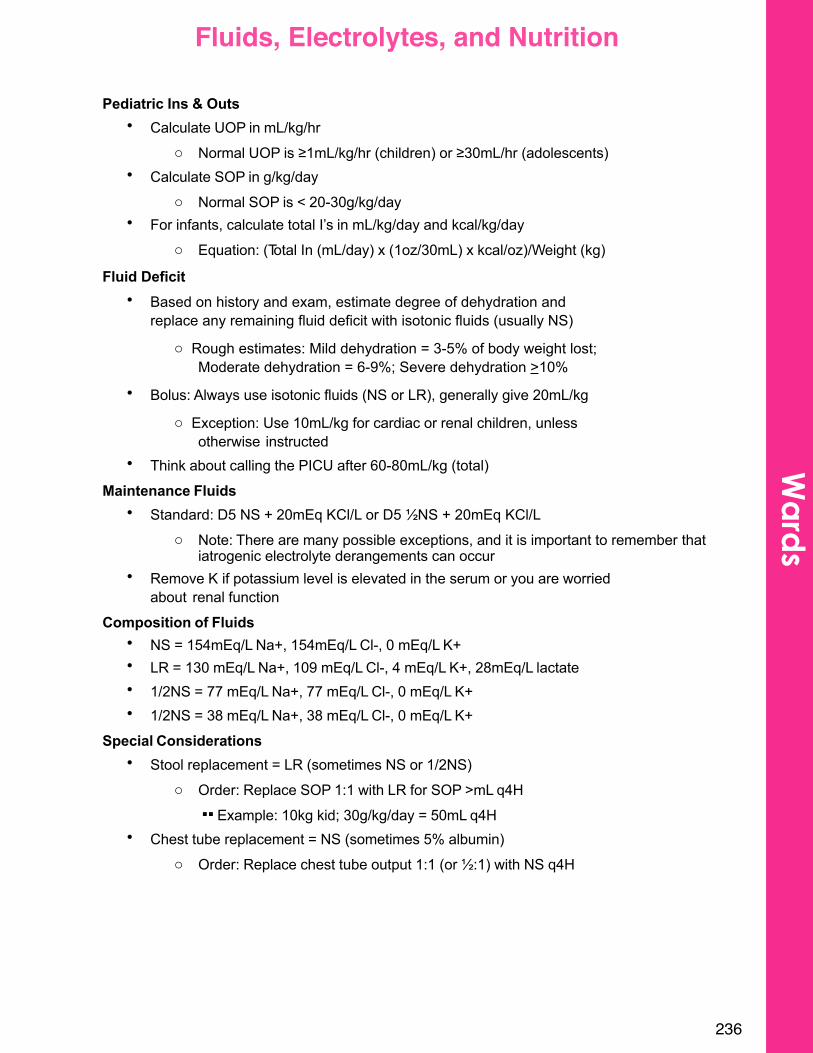
Pediatric Ins & Outs• Calculate UOP in mL/kg/hr
o Normal UOP is ≥1mL/kg/hr (children) or ≥30mL/hr (adolescents)• Calculate SOP in g/kg/day
o Normal SOP is < 20-30g/kg/day• For infants, calculate total I’s in mL/kg/day and kcal/kg/day
o Equation: (Total In (mL/day) x (1oz/30mL) x kcal/oz)/Weight (kg)
Fluid Deficit • Based on history and exam, estimate degree of dehydration and
replace any remaining fluid deficit with isotonic fluids (usually NS)
o Rough estimates: Mild dehydration = 3-5% of body weight lost; Moderate dehydration = 6-9%; Severe dehydration >10%
• Bolus: Always use isotonic fluids (NS or LR), generally give 20mL/kg
o Exception: Use 10mL/kg for cardiac or renal children, unless otherwise instructed
• Think about calling the PICU after 60-80mL/kg (total)
Maintenance Fluids• Standard: D5 NS + 20mEq KCl/L or D5 ½NS + 20mEq KCl/L
o Note: There are many possible exceptions, and it is important to remember that iatrogenic electrolyte derangements can occur
• Remove K if potassium level is elevated in the serum or you are worried about renal function
Composition of Fluids• NS = 154mEq/L Na+, 154mEq/L Cl-, 0 mEq/L K+• LR = 130 mEq/L Na+, 109 mEq/L Cl-, 4 mEq/L K+, 28mEq/L lactate• 1/2NS = 77 mEq/L Na+, 77 mEq/L Cl-, 0 mEq/L K+• 1/2NS = 38 mEq/L Na+, 38 mEq/L Cl-, 0 mEq/L K+
Special Considerations• Stool replacement = LR (sometimes NS or 1/2NS)
o Order: Replace SOP 1:1 with LR for SOP >mL q4H!! Example: 10kg kid; 30g/kg/day = 50mL q4H
• Chest tube replacement = NS (sometimes 5% albumin)o Order: Replace chest tube output 1:1 (or ½:1) with NS q4H
236
Wa
rds
Fluids, Electrolytes, and Nutrition
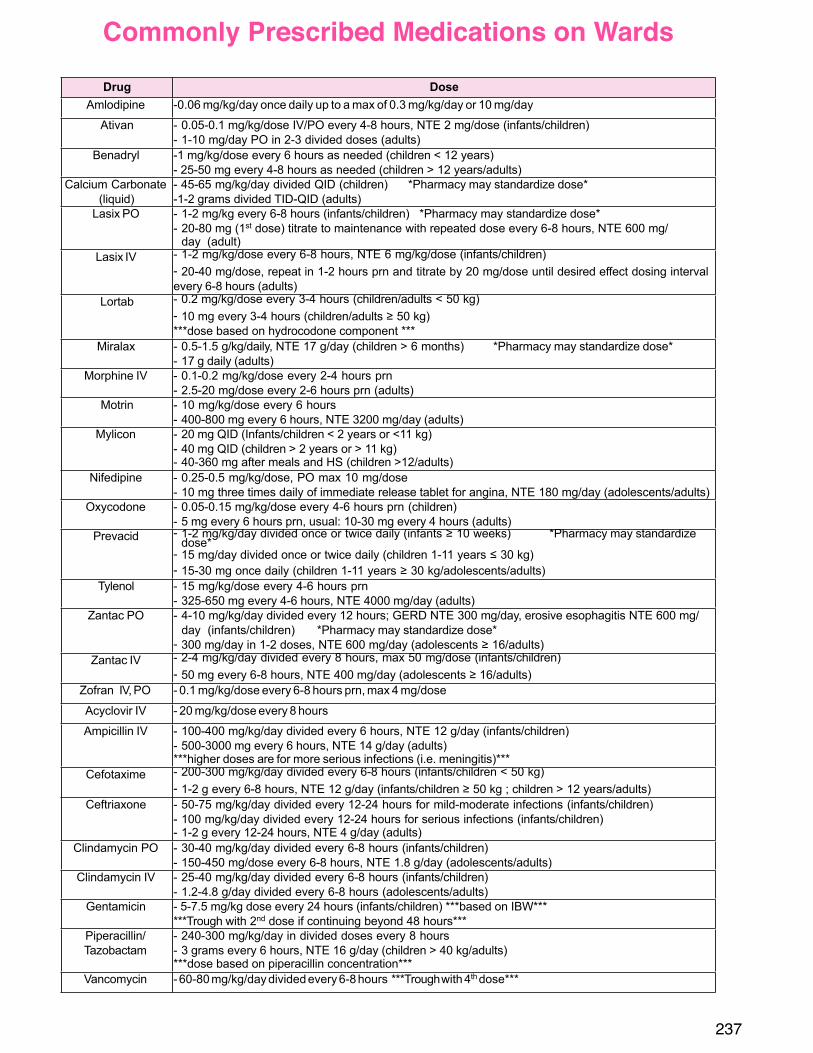
237
Commonly Prescribed Medications on Wards
Drug DoseAmlodipine -0.06 mg/kg/day once daily up to a max of 0.3 mg/kg/day or 10 mg/day
Ativan - 0.05-0.1 mg/kg/dose IV/PO every 4-8 hours, NTE 2 mg/dose (infants/children)- 1-10 mg/day PO in 2-3 divided doses (adults)
Benadryl -1 mg/kg/dose every 6 hours as needed (children < 12 years)- 25-50 mg every 4-8 hours as needed (children > 12 years/adults)
Calcium Carbonate (liquid)
- 45-65 mg/kg/day divided QID (children) *Pharmacy may standardize dose*-1-2 grams divided TID-QID (adults)
Lasix PO - 1-2 mg/kg every 6-8 hours (infants/children) *Pharmacy may standardize dose*- 20-80 mg (1st dose) titrate to maintenance with repeated dose every 6-8 hours, NTE 600 mg/
day (adult)Lasix IV - 1-2 mg/kg/dose every 6-8 hours, NTE 6 mg/kg/dose (infants/children)
- 20-40 mg/dose, repeat in 1-2 hours prn and titrate by 20 mg/dose until desired eect dosing intervalevery 6-8 hours (adults)
Lortab - 0.2 mg/kg/dose every 3-4 hours (children/adults < 50 kg)- 10 mg every 3-4 hours (children/adults 50 kg)***dose based on hydrocodone component ***
Miralax - 0.5-1.5 g/kg/daily, NTE 17 g/day (children > 6 months) *Pharmacy may standardize dose*- 17 g daily (adults)
Morphine IV - 0.1-0.2 mg/kg/dose every 2-4 hours prn- 2.5-20 mg/dose every 2-6 hours prn (adults)
Motrin - 10 mg/kg/dose every 6 hours- 400-800 mg every 6 hours, NTE 3200 mg/day (adults)
Mylicon - 20 mg QID (Infants/children < 2 years or <11 kg)- 40 mg QID (children > 2 years or > 11 kg)- 40-360 mg after meals and HS (children >12/adults)
Nifedipine - 0.25-0.5 mg/kg/dose, PO max 10 mg/dose- 10 mg three times daily of immediate release tablet for angina, NTE 180 mg/day (adolescents/adults)
Oxycodone - 0.05-0.15 mg/kg/dose every 4-6 hours prn (children)- 5 mg every 6 hours prn, usual: 10-30 mg every 4 hours (adults)
Prevacid - 1-2 mg/kg/day divided once or twice daily (infants 10 weeks) *Pharmacy may standardize dose*
- 15 mg/day divided once or twice daily (children 1-11 years 30 kg)- 15-30 mg once daily (children 1-11 years 30 kg/adolescents/adults)
Tylenol - 15 mg/kg/dose every 4-6 hours prn- 325-650 mg every 4-6 hours, NTE 4000 mg/day (adults)
Zantac PO - 4-10 mg/kg/day divided every 12 hours; GERD NTE 300 mg/day, erosive esophagitis NTE 600 mg/day (infants/children) *Pharmacy may standardize dose*
- 300 mg/day in 1-2 doses, NTE 600 mg/day (adolescents 16/adults)Zantac IV - 2-4 mg/kg/day divided every 8 hours, max 50 mg/dose (infants/children)
- 50 mg every 6-8 hours, NTE 400 mg/day (adolescents 16/adults)Zofran IV, PO - 0.1 mg/kg/dose every 6-8 hours prn, max 4 mg/dose
Acyclovir IV - 20 mg/kg/dose every 8 hours
Ampicillin IV - 100-400 mg/kg/day divided every 6 hours, NTE 12 g/day (infants/children)- 500-3000 mg every 6 hours, NTE 14 g/day (adults)***higher doses are for more serious infections (i.e. meningitis)***
Cefotaxime - 200-300 mg/kg/day divided every 6-8 hours (infants/children < 50 kg)- 1-2 g every 6-8 hours, NTE 12 g/day (infants/children 50 kg ; children > 12 years/adults)
Ceftriaxone - 50-75 mg/kg/day divided every 12-24 hours for mild-moderate infections (infants/children)- 100 mg/kg/day divided every 12-24 hours for serious infections (infants/children)- 1-2 g every 12-24 hours, NTE 4 g/day (adults)
Clindamycin PO - 30-40 mg/kg/day divided every 6-8 hours (infants/children)- 150-450 mg/dose every 6-8 hours, NTE 1.8 g/day (adolescents/adults)
Clindamycin IV - 25-40 mg/kg/day divided every 6-8 hours (infants/children)- 1.2-4.8 g/day divided every 6-8 hours (adolescents/adults)
Gentamicin - 5-7.5 mg/kg dose every 24 hours (infants/children) ***based on IBW******Trough with 2nd dose if continuing beyond 48 hours***
Piperacillin/ Tazobactam
- 240-300 mg/kg/day in divided doses every 8 hours- 3 grams every 6 hours, NTE 16 g/day (children > 40 kg/adults)***dose based on piperacillin concentration***
Vancomycin - 60-80 mg/kg/day divided every 6-8 hours ***Trough with 4th dose***
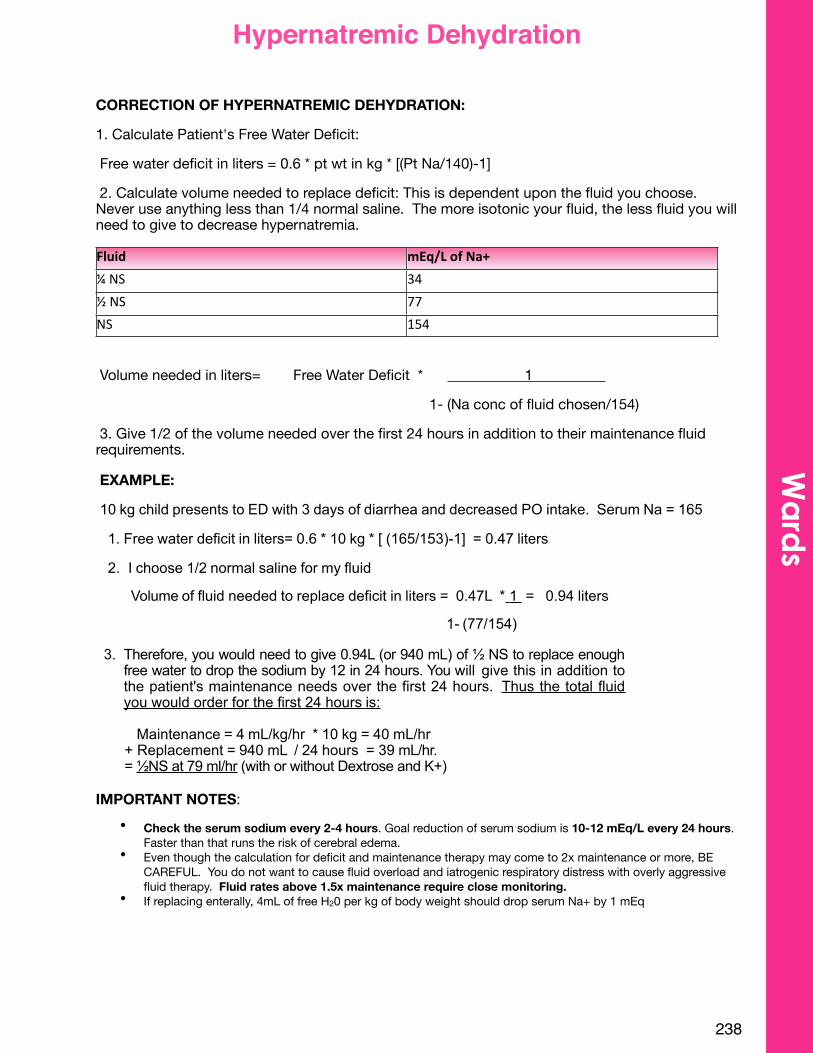
CORRECTION OF HYPERNATREMIC DEHYDRATION:
1. Calculate Patient's Free Water Deficit:
Free water deficit in liters = 0.6 * pt wt in kg * [(Pt Na/140)-1]
2. Calculate volume needed to replace deficit: This is dependent upon the fluid you choose. Never use anything less than 1/4 normal saline. The more isotonic your fluid, the less fluid you will need to give to decrease hypernatremia.
Fluid mEq/L$of$Na+¼#NS 34
½#NS 77
NS 154
Volume needed in liters= Free Water Deficit * 1
1- (Na conc of fluid chosen/154)
3. Give 1/2 of the volume needed over the first 24 hours in addition to their maintenance fluid requirements.
EXAMPLE:
10 kg child presents to ED with 3 days of diarrhea and decreased PO intake. Serum Na = 165
1. Free water deficit in liters= 0.6 * 10 kg * [ (165/153)-1] = 0.47 liters
2. I choose 1/2 normal saline for my fluid
Volume of fluid needed to replace deficit in liters = 0.47L * 1 = 0.94 liters
1- (77/154)
3. Therefore, you would need to give 0.94L (or 940 mL) of ½ NS to replace enough free water to drop the sodium by 12 in 24 hours. You will give this in addition to the patient's maintenance needs over the first 24 hours. Thus the total fluid you would order for the first 24 hours is:
Maintenance = 4 mL/kg/hr * 10 kg = 40 mL/hr + Replacement = 940 mL / 24 hours = 39 mL/hr.= ½NS at 79 ml/hr (with or without Dextrose and K+)
IMPORTANT NOTES:• Check the serum sodium every 2-4 hours. Goal reduction of serum sodium is 10-12 mEq/L every 24 hours.
Faster than that runs the risk of cerebral edema.• Even though the calculation for deficit and maintenance therapy may come to 2x maintenance or more, BE
CAREFUL. You do not want to cause fluid overload and iatrogenic respiratory distress with overly aggressive fluid therapy. Fluid rates above 1.5x maintenance require close monitoring.
• If replacing enterally, 4mL of free H20 per kg of body weight should drop serum Na+ by 1 mEq
238
Wa
rds
Hypernatremic Dehydration
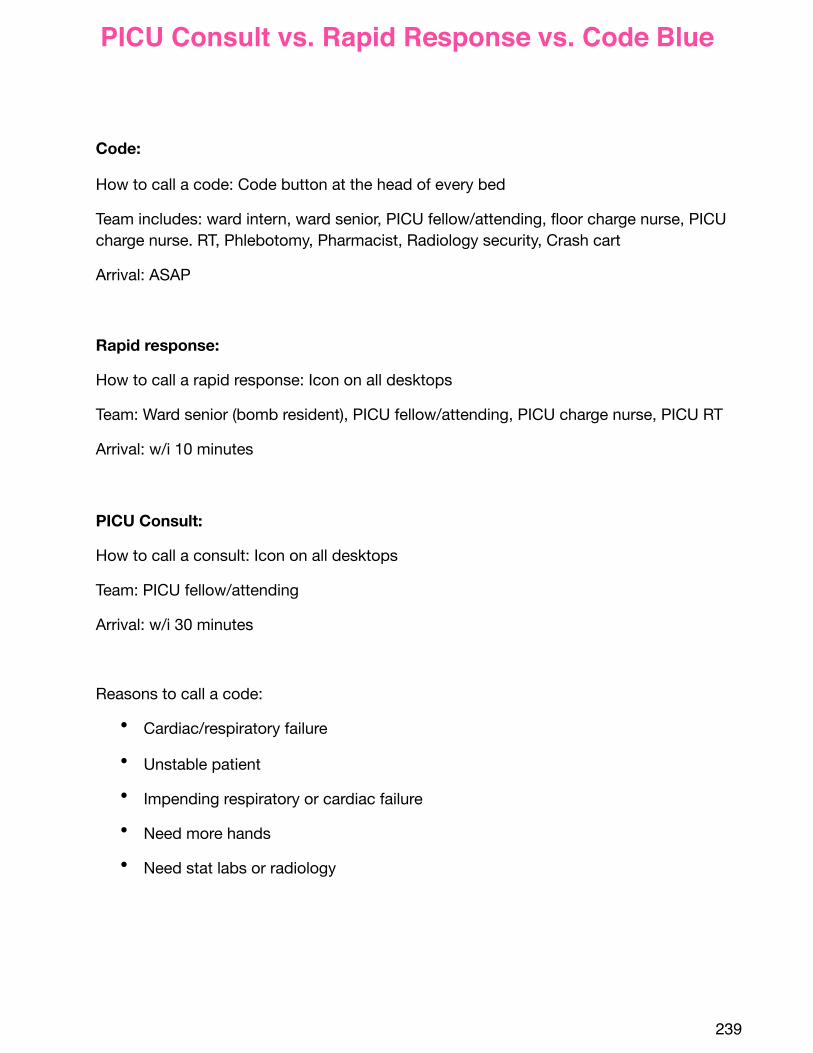
Code:
How to call a code: Code button at the head of every bed
Team includes: ward intern, ward senior, PICU fellow/attending, floor charge nurse, PICU charge nurse. RT, Phlebotomy, Pharmacist, Radiology security, Crash cart
Arrival: ASAP
Rapid response:
How to call a rapid response: Icon on all desktops
Team: Ward senior (bomb resident), PICU fellow/attending, PICU charge nurse, PICU RT
Arrival: w/i 10 minutes
PICU Consult:
How to call a consult: Icon on all desktops
Team: PICU fellow/attending
Arrival: w/i 30 minutes
Reasons to call a code:
• Cardiac/respiratory failure
• Unstable patient
• Impending respiratory or cardiac failure
• Need more hands
• Need stat labs or radiology
239
PICU Consult vs. Rapid Response vs. Code Blue
Fever without a source: Fever for ≤1 week without adequate explanation after a careful history and thorough physical exam
Fever of Unknown Origin:Fever >101° F (38.3° C) of ≥ 8 days’ duration without an apparent diagnosis after initial outpatient or hospital evaluation (includes a careful history and physical examination and initial laboratory testing)
Initial evaluation:
CBC with smearBlood cultureESR and CRPUrinalysis & urine cultureChest X-rayCMP+/- Tuberculin skin testing and HIV serology based on exposures
Causes:
• Infection:o Bacterial- Bacterial endocarditis, Bartonellahenslae, Brucellosis, Leptospirosis, liver
abscess, mastoiditis, osteomyelitis, pelvic abscess, perinephric abscess, pyelonephritis, Salmonellosis, sinusitis, subdiaphragmatic abscess, Tb, tularemia
o Viral- Adenovirus, arbovirus, CMV, hepatitis viruses, Enteroviruses, EBVo Chlamydial- Lymphogranulomavenereum, psittacosiso Rickettsial- Q fever, RMSFo Fungal- Blastomycosis, Histoplasmosis (disseminated)o Parasitic- Malaria, Toxoplasmosis
• Collagen Vascular Disease: JIV, polyarteritisnodosa, SLE• Malignancy: Hodgkin disease, leukemia/lymphoma, neuroblastoma• Miscellaneous: Central/nephrogenic DI, drug fever, ectodermal dysplasia, factitious fever,
familial dysautonomia, granulomatous colitis, HLH, infantile cortical hypostasis, Kawasaki Disease, Kikuchi-Fujimoto disease, pancreatitis, periodic fever, serum sickness, thyrotoxicosis, ulcerative colitis
• Unclassified: Sarcoidosis
References:
Lorin MI, Feigin RD. Fever without localizing signs and fever of unknown origin. In: Textbook of Pediatric Infectious Disease, 4thed. Feigin RD, Cherry JD, WB Saunders, Philadelphia 1998.
Palazzi, Debra L. Approach to the child with fever of uknown origin.UptoDate.Last updated: Jan 3, 2013.Accessed May 14, 2013.http://www.uptodate.com
240
Fever of Unknown OriginW
ard
s
242
Well Baby Nursery
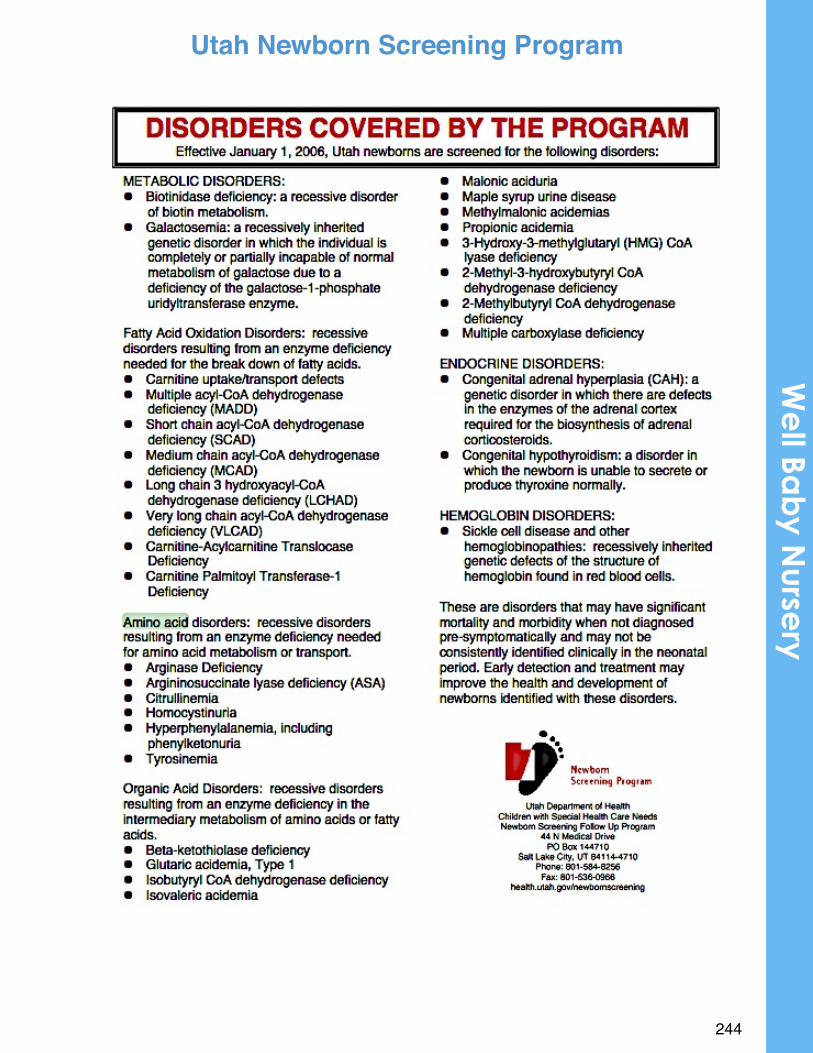
!
Newborn!Screening!Provider!Handbook!
244
We
ll Bab
y Nurse
ryUtah Newborn Screening Program
!
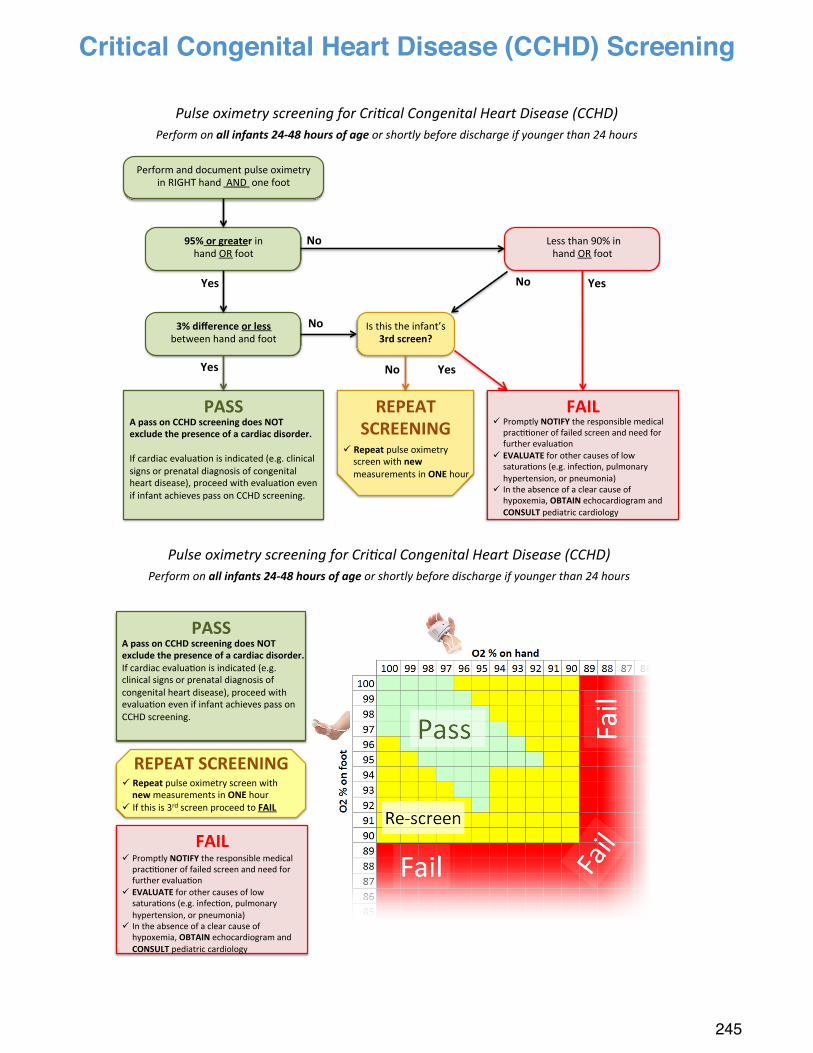
#############
###################
245
Critical Congenital Heart Disease (CCHD) ScreeningCritical(Congenital(Heart(Disease((CCHD)(Screening!(
((((((((((((( (
((((((((((((((((((( (
REPEAT&SCREENING&
PASS&!
FAIL&
95%&or&greater&in!!hand!OR!foot!
3%&difference&or&less!!between!hand!and!foot!
!
Yes&
Yes&
!Less!than!90%!in!!hand!OR!foot!
No&
Yes&No&
No& Is!this!the!infant’s!3rd&screen?&
Yes&No&
A&pass&on&CCHD&screening&does&NOT&exclude&the&presence&of&a&cardiac&disorder.&&If!cardiac!evalua;on!is!indicated!(e.g.!clinical!signs!or!prenatal!diagnosis!of!congenital!heart!disease),!proceed!with!evalua;on!even!if!infant!achieves!pass!on!CCHD!screening.!
! Repeat&pulse!oximetry!screen!with!new&measurements!in!ONE&hour!
! Promptly!NOTIFY!the!responsible!medical!prac;;oner!of!failed!screen!and!need!for!further!evalua;on!
! EVALUATE&for!other!causes!of!low!satura;ons!(e.g.!infec;on,!pulmonary!hypertension,!or!pneumonia)!
! In!the!absence!of!a!clear!cause!of!hypoxemia,!OBTAIN!echocardiogram!and!CONSULT&pediatric!cardiology!
Perform!and!document!pulse!oximetry!in!RIGHT!hand!!AND!!one!foot!
Pulse!oximetry!screening!for!Cri3cal!Congenital!Heart!Disease!(CCHD)!Perform!on!all#infants#24+48#hours#of#age!or!shortly!before!discharge!if!younger!than!24!hours!
PASS$!
FAIL$
A$pass$on$CCHD$screening$does$NOT$exclude$the$presence$of$a$cardiac$disorder.$If!cardiac!evalua-on!is!indicated!(e.g.!clinical!signs!or!prenatal!diagnosis!of!congenital!heart!disease),!proceed!with!evalua-on!even!if!infant!achieves!pass!on!CCHD!screening.!
! Repeat$pulse!oximetry!screen!with!new$measurements!in!ONE$hour!
! If!this!is!3rd!screen!proceed!to!FAIL$
! Promptly!NOTIFY!the!responsible!medical!prac--oner!of!failed!screen!and!need!for!further!evalua-on!
! EVALUATE$for!other!causes!of!low!satura-ons!(e.g.!infec-on,!pulmonary!hypertension,!or!pneumonia)!
! In!the!absence!of!a!clear!cause!of!hypoxemia,!OBTAIN!echocardiogram!and!CONSULT$pediatric!cardiology!
Pulse&oximetry&screening&for&Cri3cal&Congenital&Heart&Disease&(CCHD)&Perform&on&all#infants#24+48#hours#of#age&or&shortly&before&discharge&if&younger&than&24&hours!
REPEAT$SCREENING$
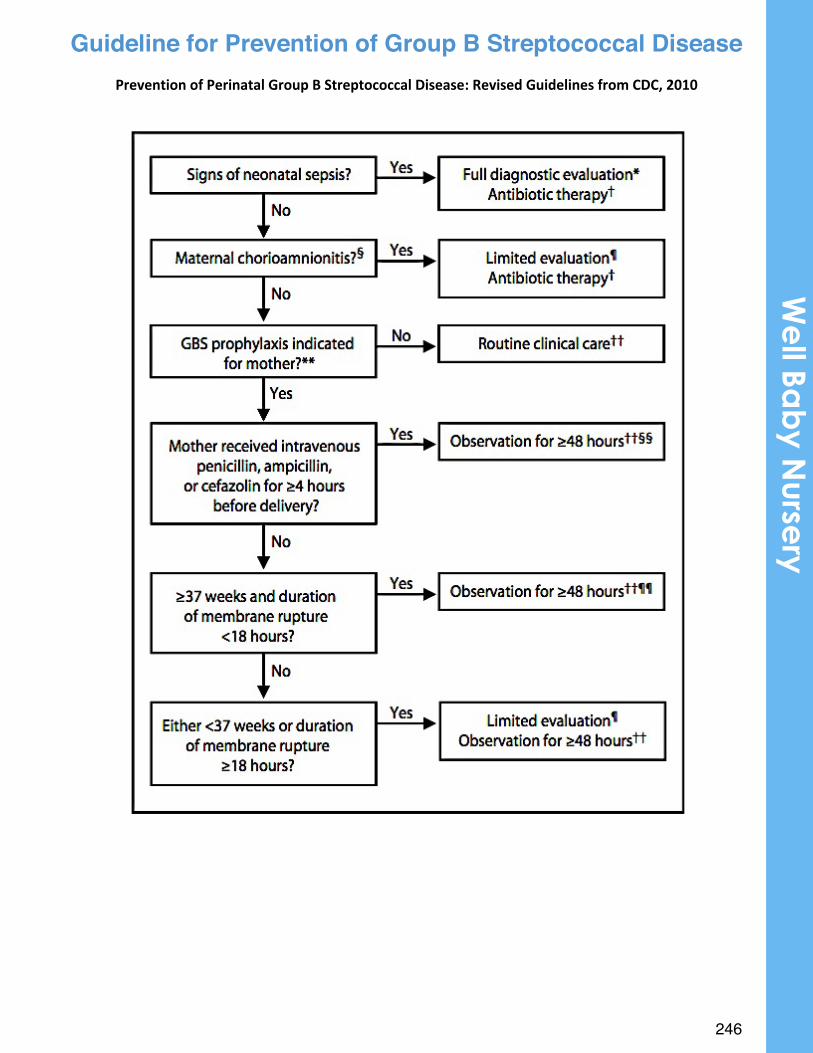
246
Guideline for Prevention of Group B Streptococcal Disease
!
Prevention)of)Perinatal)Group)B)Streptococcal)Disease:)Revised)Guidelines)from)CDC,)2010)
We
ll Bab
y Nurse
ry
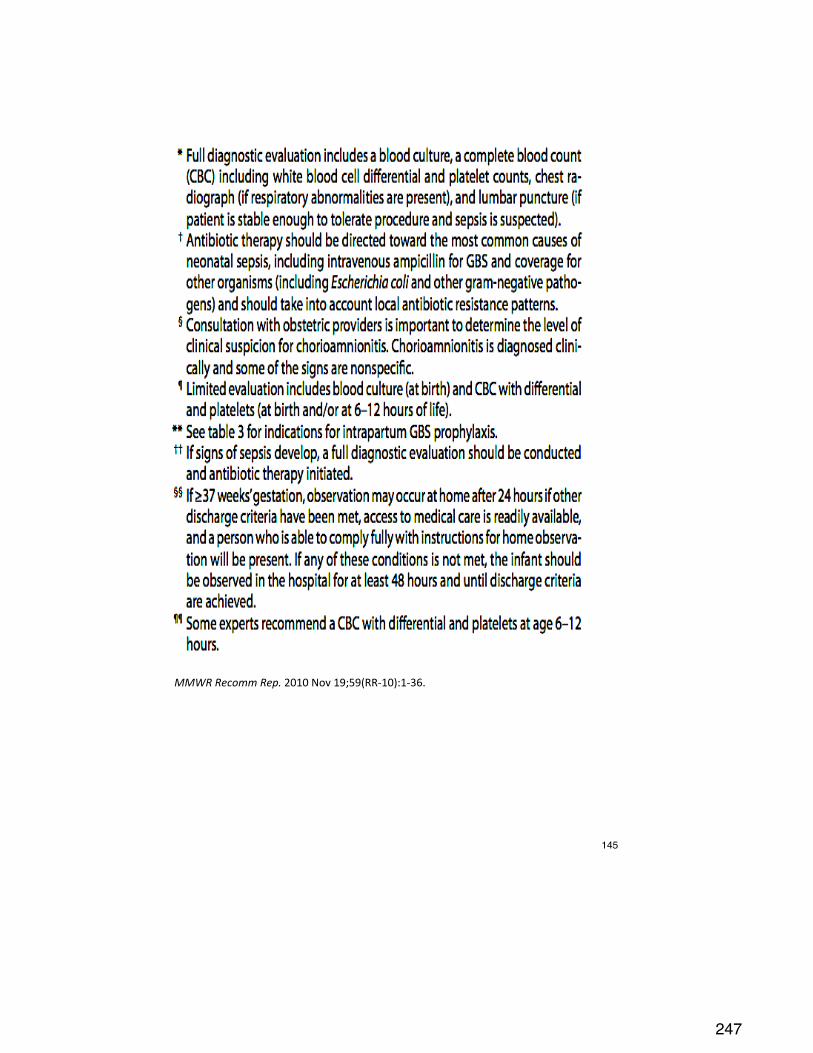
247
!
MMWR$Recomm$Rep.!2010!Nov!19;59(RR-10):1-36.!
145
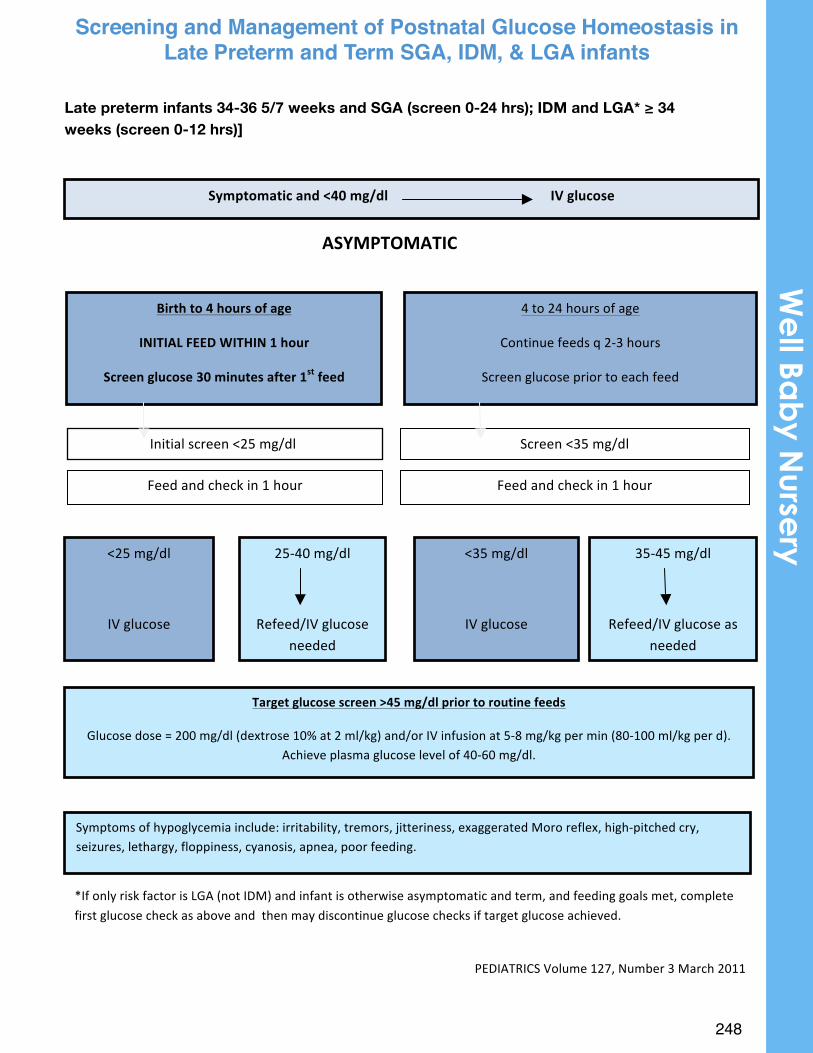
248
Screening(&(Management(of(Postnatal(Glucose(Homeostasis(in(Late(Preterm(and(Term(SGA,(IDM,(and(LGA(Infants(
(Late preterm infants 34-36 5/7 weeks and SGA (screen 0-24 hrs); IDM and LGA* ≥ 34 weeks (screen 0-12 hrs)]
(
!
ASYMPTOMATIC!
(
( (
( (
( ( (
( (
(
(
(
(
(
(
Symptomatic!and!<40!mg/dl!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!IV!glucose!
4(to(24(hours(of(age(
Continue(feeds(q(2B3(hours(
Screen(glucose(prior(to(each(feed(
Birth!to!4!hours!of!age!
INITIAL!FEED!WITHIN!1!hour!
Screen!glucose!30!minutes!after!1st!feed!
Screen(<35(mg/dl(Initial(screen(<25(mg/dl((
Feed(and(check(in(1(hour(Feed(and(check(in(1(hour(
35B45(mg/dl(
(
Refeed/IV(glucose(as(needed(
<35(mg/dl(
(
IV(glucose(
<25(mg/dl(
(
IV(glucose(
25B40(mg/dl(
(
Refeed/IV(glucose(needed(
Target!glucose!screen!>45!mg/dl!prior!to!routine!feeds!
Glucose(dose(=(200(mg/dl((dextrose(10%(at(2(ml/kg)(and/or(IV(infusion(at(5B8(mg/kg(per(min((80B100(ml/kg(per(d).((Achieve(plasma(glucose(level(of(40B60(mg/dl.((
Symptoms(of(hypoglycemia(include:(irritability,(tremors,(jitteriness,(exaggerated(Moro(reflex,(highBpitched(cry,(seizures,(lethargy,(floppiness,(cyanosis,(apnea,(poor(feeding.(
PEDIATRICS(Volume(127,(Number(3(March(2011(
(
*If(only(risk(factor(is(LGA((not(IDM)(and(infant(is(otherwise(asymptomatic(and(term,(and(feeding(goals(met,(complete(first(glucose(check(as(above(and((then(may(discontinue(glucose(checks(if(target(glucose(achieved.(
Screening and Management of Postnatal Glucose Homeostasis in Late Preterm and Term SGA, IDM, & LGA infants
We
ll Bab
y Nurse
ry
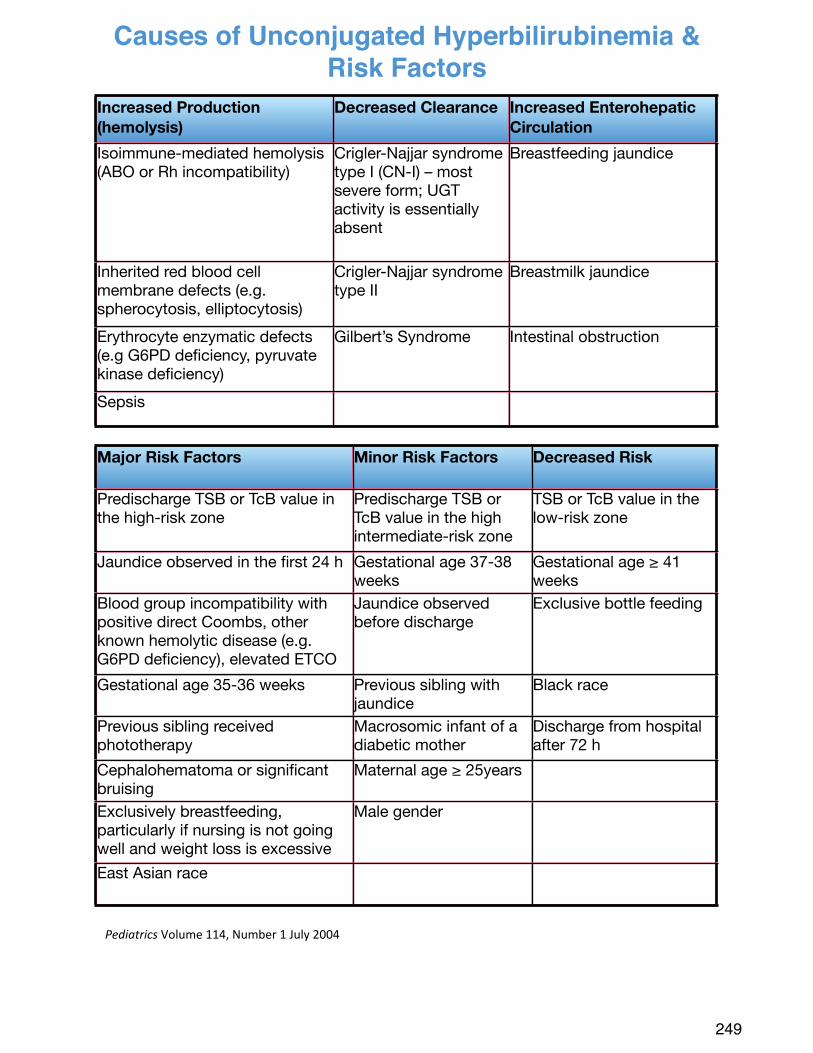
!Pediatrics!Volume!114,!Number!1!July!2004!!
249
Increased Production (hemolysis)
Decreased Clearance Increased Enterohepatic Circulation
Isoimmune-mediated hemolysis(ABO or Rh incompatibility)
Crigler-Najjar syndrome type I (CN-I) – most severe form; UGT activity is essentially absent
Breastfeeding jaundice
Inherited red blood cell membrane defects (e.g. spherocytosis, elliptocytosis)
Crigler-Najjar syndrome type II
Breastmilk jaundice
Erythrocyte enzymatic defects (e.g G6PD deficiency, pyruvate kinase deficiency)
Gilbert’s Syndrome Intestinal obstruction
Sepsis
Major Risk Factors Minor Risk Factors Decreased Risk
Predischarge TSB or TcB value in the high-risk zone
Predischarge TSB or TcB value in the high intermediate-risk zone
TSB or TcB value in the low-risk zone
Jaundice observed in the first 24 h Gestational age 37-38 weeks
Gestational age ≥ 41 weeks
Blood group incompatibility with positive direct Coombs, other known hemolytic disease (e.g. G6PD deficiency), elevated ETCO
Jaundice observed before discharge
Exclusive bottle feeding
Gestational age 35-36 weeks Previous sibling with jaundice
Black race
Previous sibling received phototherapy
Macrosomic infant of a diabetic mother
Discharge from hospital after 72 h
Cephalohematoma or significant bruising
Maternal age ≥ 25years
Exclusively breastfeeding, particularly if nursing is not going well and weight loss is excessive
Male gender
East Asian race
Causes of Unconjugated Hyperbilirubinemia & Risk Factors
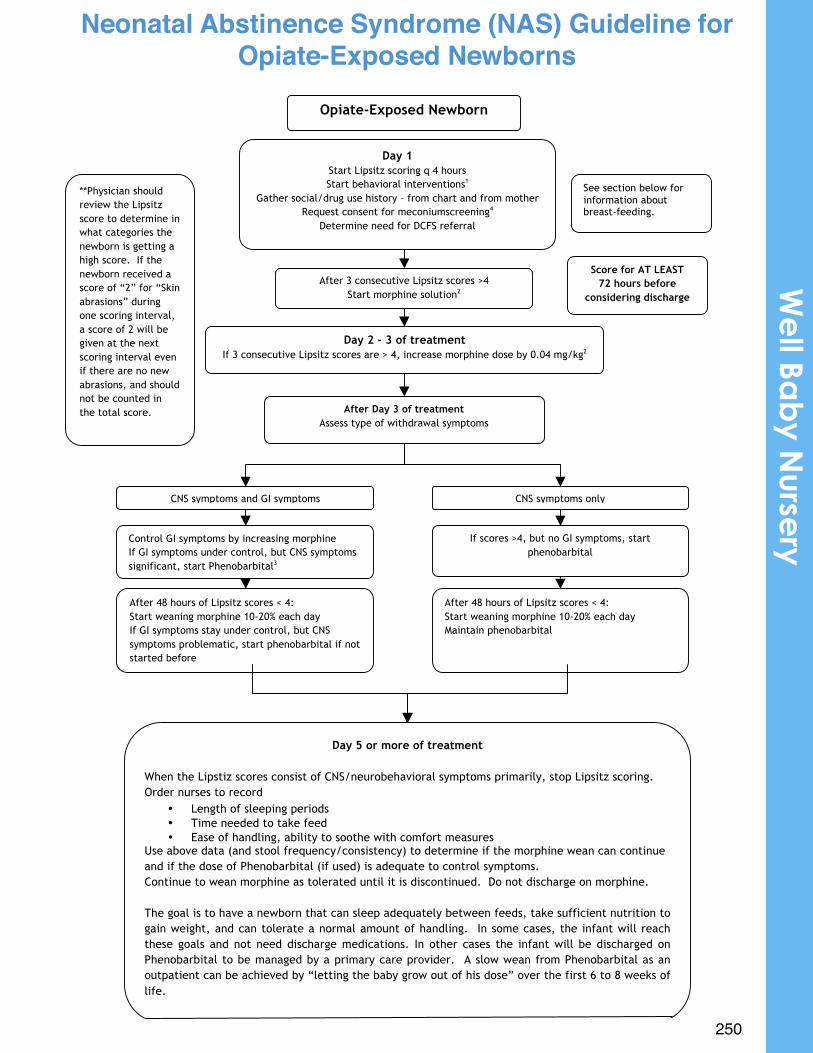
•
250
Neonatal(Abstinence(Syndrome((NAS)(Guideline(for(Opiate:Exposed(Newborns!(
(
Opiate-Exposed Newborn
Day 1 Start Lipsitz scoring q 4 hours Start behavioral interventions1
Gather social/drug use history – from chart and from mother Request consent for meconiumscreening4
Determine need for DCFS referral
(
After 3 consecutive Lipsitz scores >4 Start morphine solution2
(
Day 2 - 3 of treatment If 3 consecutive Lipsitz scores are > 4, increase morphine dose by 0.04 mg/kg2
((
CNS symptoms and GI symptoms( CNS symptoms only(
Control GI symptoms by increasing morphine If GI symptoms under control, but CNS symptoms significant, start Phenobarbital3
If scores >4, but no GI symptoms, start phenobarbital
After 48 hours of Lipsitz scores < 4: Start weaning morphine 10-20% each day If GI symptoms stay under control, but CNS symptoms problematic, start phenobarbital if not started before
(
After 48 hours of Lipsitz scores < 4: Start weaning morphine 10-20% each day Maintain phenobarbital(
Day 5 or more of treatment
When the Lipstiz scores consist of CNS/neurobehavioral symptoms primarily, stop Lipsitz scoring. Order nurses to record
• Length of sleeping periods • Time needed to take feed • Ease of handling, ability to soothe with comfort measures
Use above data (and stool frequency/consistency) to determine if the morphine wean can continue and if the dose of Phenobarbital (if used) is adequate to control symptoms. Continue to wean morphine as tolerated until it is discontinued. Do not discharge on morphine. The goal is to have a newborn that can sleep adequately between feeds, take sufficient nutrition to gain weight, and can tolerate a normal amount of handling. In some cases, the infant will reach these goals and not need discharge medications. In other cases the infant will be discharged on Phenobarbital to be managed by a primary care provider. A slow wean from Phenobarbital as an outpatient can be achieved by “letting the baby grow out of his dose” over the first 6 to 8 weeks of life. Identify a primary care provider and discuss case and follow-up plan prior to discharge.
After Day 3 of treatment Assess type of withdrawal symptoms(
Score for AT LEAST 72 hours before
considering discharge!
See section below for information about breast-feeding.
**Physician should review the Lipsitz score to determine in what categories the newborn is getting a high score. If the newborn received a score of “2” for “Skin abrasions” during one scoring interval, a score of 2 will be given at the next scoring interval even if there are no new abrasions, and should not be counted in the total score.
(
Neonatal Abstinence Syndrome (NAS) Guideline for Opiate-Exposed Newborns
We
ll Bab
y Nurse
ry
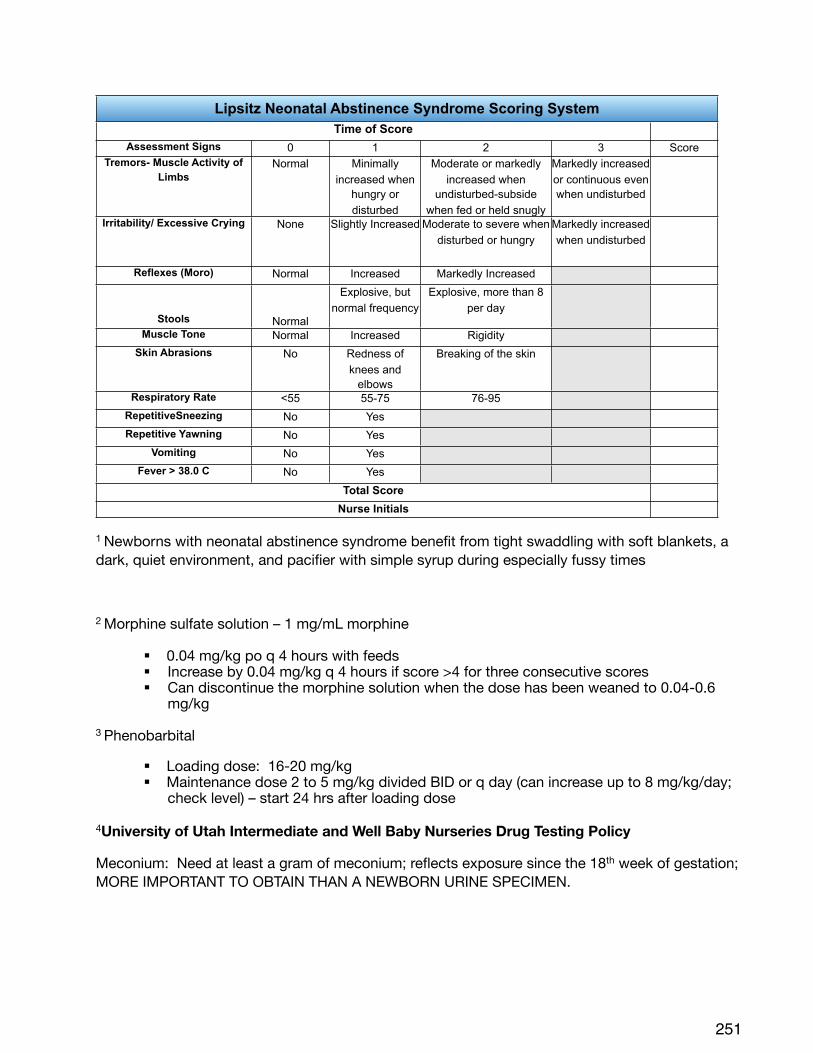
Lipsitz Neonatal Abstinence Syndrome Scoring SystemLipsitz Neonatal Abstinence Syndrome Scoring SystemLipsitz Neonatal Abstinence Syndrome Scoring SystemLipsitz Neonatal Abstinence Syndrome Scoring SystemLipsitz Neonatal Abstinence Syndrome Scoring SystemLipsitz Neonatal Abstinence Syndrome Scoring SystemTime of ScoreTime of ScoreTime of ScoreTime of ScoreTime of Score
Assessment Signs 0 1 2 3 ScoreTremors- Muscle Activity of
Limbs Normal Minimally
increased when hungry or disturbed
Moderate or markedly increased when
undisturbed-subside when fed or held snugly
Markedly increased or continuous even when undisturbed
Irritability/ Excessive Crying None Slightly Increased Moderate to severe when disturbed or hungry
Markedly increased when undisturbed
Reflexes (Moro) Normal Increased Markedly Increased
Stools Normal
Explosive, but normal frequency
Explosive, more than 8 per day
Muscle Tone Normal Increased RigiditySkin Abrasions No Redness of
knees and elbows
Breaking of the skin
Respiratory Rate <55 55-75 76-95RepetitiveSneezing No YesRepetitive Yawning No Yes
Vomiting No YesFever > 38.0 C No Yes
Total ScoreTotal ScoreTotal ScoreTotal ScoreTotal Score
Nurse InitialsNurse InitialsNurse InitialsNurse InitialsNurse Initials
1 Newborns with neonatal abstinence syndrome benefit from tight swaddling with soft blankets, a dark, quiet environment, and pacifier with simple syrup during especially fussy times
2 Morphine sulfate solution – 1 mg/mL morphine
! 0.04 mg/kg po q 4 hours with feeds! Increase by 0.04 mg/kg q 4 hours if score >4 for three consecutive scores! Can discontinue the morphine solution when the dose has been weaned to 0.04-0.6
mg/kg
3 Phenobarbital
! Loading dose: 16-20 mg/kg! Maintenance dose 2 to 5 mg/kg divided BID or q day (can increase up to 8 mg/kg/day;
check level) – start 24 hrs after loading dose
4University of Utah Intermediate and Well Baby Nurseries Drug Testing Policy
Meconium: Need at least a gram of meconium; reflects exposure since the 18th week of gestation; MORE IMPORTANT TO OBTAIN THAN A NEWBORN URINE SPECIMEN.
251
Testing meconium for substances of abuse on a newborn who IS NOT showing signs and symptoms of withdrawal: Written informed consent from mother/parent REQUIRED
Testing meconium for substances of abuse on a newborn who IS showing signs and symptoms of withdrawal: Written informed consent from mother/parent NOT REQUIRED
Implications
• If the maternal history is concerning for prenatal exposure to substances of abuse, then the mother should be asked to consent for newborn drug testing (meconium testing is the gold standard). It should be communicated to her that this information can be helpful in the management of her newborn.
• If the mother refuses to consent, it is permissible to collect the meconium, but not send it for testing.
• If the newborn becomes symptomatic with signs and symptoms of withdrawal, the meconium sample can be sent without maternal permission. Knowing the types of exposures the newborn has had can influence the treatment of withdrawal.
• If the newborn becomes symptomatic, this should be well-documented in the medical record.
This policy has been reviewed with Risk Management.
Breastfeeding
Mothers taking opiates may want to breastfeed. Most often it is safe to do so.
• Review the mother’s prenatal labs for contraindications to breastfeeding (e.g. HIV status)• Review mother’s history of use of drugs other than opiates
! If only taking opiates• Opiates will still be in breast milk but in much lower amounts than the newborn
received transplacentally. A 2007 study in Pediatrics found that concentrations of methadone in breast milk were low and not related to maternal dose. Studies have shown that possible methadone intake via breast milk by the infant (first month of life) ranges from 0.01 to 0.2 mg/day. The 2007 study found no relation between the plasma level of methadone in the breast feeding baby and the need for pharmacologic intervention. In other words, the amount of methadone obtained via breast milk is too low to count on to help with withdrawal symptomatology.
• Mothers using only opiates who want to breastfeed should be given accurate information and supported in their decision.
! If taking other drugs in addition to opiates• Must consider on a case-by-case basis for risk/benefit of breastfeeding
! SSRIs – most consider the risk of continued exposure to SSRIs to be much lower than the risk of negative outcomes from being parented by a depressed mother
! Cocaine, methamphetamine• Inform mothers that exposure to cocaine or methamphetamine
through breast milk is dangerous to the baby
252
We
ll Bab
y Nurse
ry
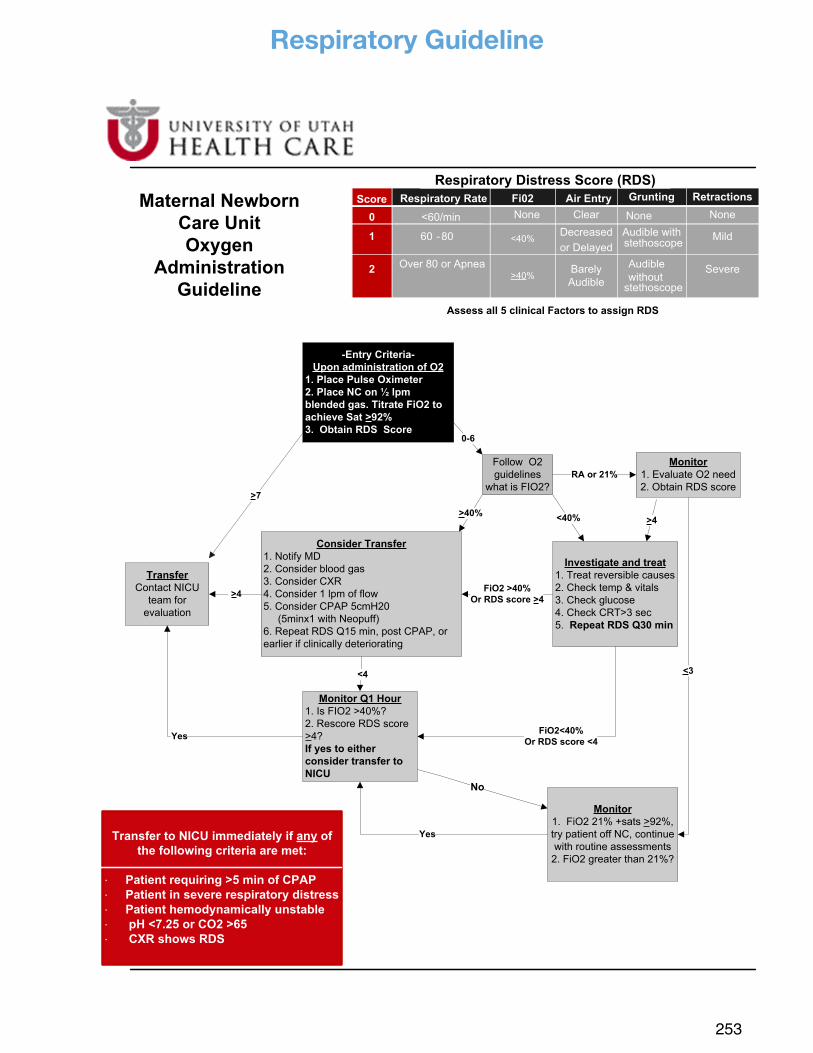
253
Respiratory Guideline
-Entry Criteria-Upon administration of O2
1. Place Pulse Oximeter2. Place NC on ½ lpm blended gas. Titrate FiO2 to achieve Sat >92% 3. Obtain RDS Score
TransferContact NICU
team for evaluation
Consider Transfer1. Notify MD2. Consider blood gas 3. Consider CXR 4. Consider 1 lpm of flow5. Consider CPAP 5cmH20 (5minx1 with Neopuff) 6. Repeat RDS Q15 min, post CPAP, or earlier if clinically deteriorating
>7
Investigate and treat1. Treat reversible causes2. Check temp & vitals3. Check glucose4. Check CRT>3 sec 5. Repeat RDS Q30 min
>4
Monitor Q1 Hour1. Is FIO2 >40%?2. Rescore RDS score >4? If yes to either consider transfer to NICU
FiO2 >40%Or RDS score >4
<4
FiO2<40%Or RDS score <4
Maternal Newborn Care Unit Oxygen
AdministrationGuideline
Yes
No
Transfer to NICU immediately if any of the following criteria are met:
! Patient requiring >5 min of CPAP! Patient in severe respiratory distress ! Patient hemodynamically unstable ! pH <7.25 or CO2 >65 ! CXR shows RDS
<40%
0-6
Follow O2 guidelines
what is FIO2?RA or 21%
<3
Monitor1. Evaluate O2 need2. Obtain RDS score
Monitor1. FiO2 21% +sats >92%, try patient off NC, continue with routine assessments
2. FiO2 greater than 21%?
>4
Yes
Page 1
>40%
Assess all 5 clinical Factors to assign RDS
Fi02
<40%
>40%
Score Respiratory Rate Air Entry Grunting Retractions
0 <60/min None Clear None None
1 60 -80 Decreasedor Delayed
Audible with stethoscope Mild
2 Over 80 or Apnea Barely Audible
Audible without
stethoscope
Severe
Respiratory Distress Score (RDS)
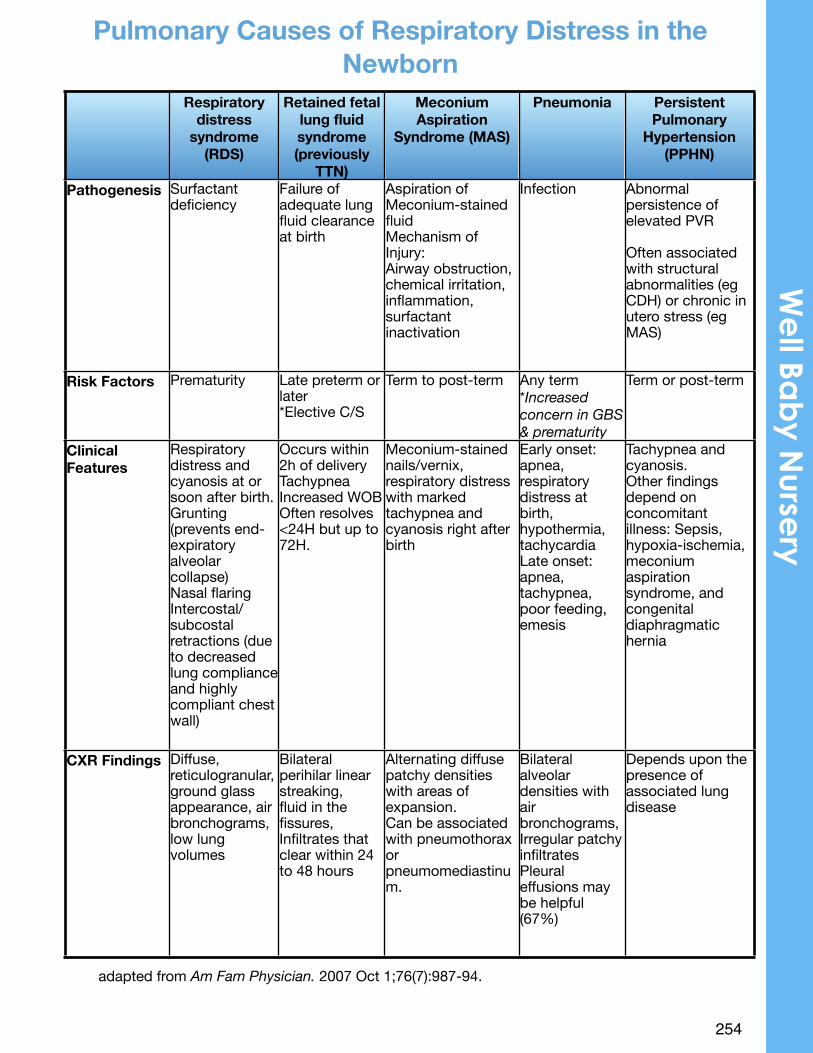
•
254
adapted from Am Fam Physician. 2007 Oct 1;76(7):987-94.
Respiratory distress
syndrome (RDS)
Retained fetal lung fluid syndrome (previously
TTN)
Meconium Aspiration
Syndrome (MAS)
Pneumonia Persistent Pulmonary
Hypertension (PPHN)
Pathogenesis Surfactant deficiency
Failure of adequate lung fluid clearance at birth
Aspiration of Meconium-stained fluid Mechanism of Injury:Airway obstruction, chemical irritation, inflammation, surfactant inactivation
Infection Abnormal persistence of elevated PVR
Often associated with structural abnormalities (eg CDH) or chronic in utero stress (eg MAS)
Risk Factors Prematurity Late preterm or later*Elective C/S
Term to post-term Any term*Increased concern in GBS & prematurity
Term or post-term
Clinical Features
Respiratory distress and cyanosis at or soon after birth. Grunting (prevents end-expiratory alveolar collapse) Nasal flaring Intercostal/subcostal retractions (due to decreased lung compliance and highly compliant chest wall)
Occurs within 2h of deliveryTachypneaIncreased WOBOften resolves <24H but up to 72H.
Meconium-stained nails/vernix, respiratory distress with marked tachypnea and cyanosis right after birth
Early onset: apnea, respiratory distress at birth, hypothermia, tachycardiaLate onset: apnea, tachypnea, poor feeding, emesis
Tachypnea and cyanosis.Other findings depend on concomitant illness: Sepsis, hypoxia-ischemia, meconium aspiration syndrome, and congenital diaphragmatic hernia
CXR Findings Diffuse, reticulogranular, ground glass appearance, air bronchograms,low lung volumes
Bilateral perihilar linear streaking,fluid in the fissures,Infiltrates that clear within 24 to 48 hours
Alternating diffuse patchy densities with areas of expansion.Can be associated with pneumothorax or pneumomediastinum.
Bilateral alveolar densities with air bronchograms,Irregular patchy infiltratesPleural effusions may be helpful (67%)
Depends upon the presence of associated lung disease
Pulmonary Causes of Respiratory Distress in the Newborn
We
ll Bab
y Nurse
ry





























