Embed Size (px)
Citation preview

Provider-type and Heart Failure Hospitalizations
A Research Grant Proposal
Presented to the faculty of the School of Nursing
California State University, San Marcos
Submitted in partial satisfaction of the requirements for the degree of
MASTER OF SCIENCE
in
Nursing
Family Nurse Practitioner
by
Maria Cecilia C. Jamito
SPRING 2017

ii

iii

iv

v
Abstract
of
Provider-type and Heart Failure Hospitalizations
by
Maria Cecilia C. Jamito
This grant proposal seeks funding for the collection of data that may provide a groundwork of information as to differences in outpatient care of heart failure patient by the physician vs. nurse practitioner. Results of previous research in primary care settings have shown that as compared to physicians, nurse practitioners have provided the same quality care, if not better, to patients and have effectively prevented unnecessary hospitalizations.
Physicians and nurse practitioners come from differing educational backgrounds, with the first going through four years of medical school and another four years of residency and potentially a fellowship, with the latter obtaining experience as a registered nurse and a bachelor’s degree prior to completing two to three years of graduate school. With the need for nurse practitioners steadily increasing as the baby boomer population ages, there is a need for research in the work and care given by nurse practitioners, with comparisons to the traditional providers—physicians.
The study will look to see if a model nationwide healthcare organization that places physicians and NPs on an almost equal playing field in outpatient care will show if NPs provide the same if not better, outpatient heart failure management.
Statement of Problem
Heart failure is just one chronic disease managed by physicians and nurse practitioners, and if managed poorly, results in exacerbations and recurrent hospitalizations which require the administration of intravenous diuretics and closer monitoring of the patient. This in turn, results in a decreased quality of life for the patient, as well as a burden of costs on the patient and nation as a whole. Exacerbations of heart failure are widely considered to be preventable, so a closer look may give some insight as to the efficacy of heart failure management relative to a particular provider-type.

vi

vii
ACKNOWLEDGEMENTS
Thank you to my supportive friends and family for helping me through the turbulent ups and downs I experienced in my three years of grad school. I can’t imagine having gotten as far as I have without you
all by my side. Special thanks to Dr. Denise Boren, Dr. Linnea Axman, and Lindsey Sheets for your guidance, and my mom Lyn, dad Jun, sister Marie, and boyfriend Francisco for all of your love!

viii

ix

Running head: PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
1
Provider-type and Heart Failure Hospitalizations
Chapter One: Introduction Background and Significance
Heart failure is a “complex clinical syndrome” that results from an abnormal structure or
dysfunction of either the filling of the ventricles with blood or the ejection of the blood (Yancy et
al., 2013). Shortness of breath (dyspnea) and fatigue are the main clinical manifestations of heart
failure which limit one’s tolerance for exercise, and the retention of fluid, which can potentially
lead to congestion in the lungs and organs in the abdomen or thorax (Yancy et al., 2013)
Heart failure is a preventable disease – patients have the ability to control their blood
pressure, diet, and other vascular risk factors (Delgado-Passler & McCaffrey, 2006). Patients
frequently need to be hospitalized when heart failure is exacerbated, but hospitalization is also
considered largely preventable (Delgado-Passler & McCaffrey, 2006).
Unplanned hospital admissions place a tremendous strain on healthcare systems
throughout the world, and have costly repercussions (Busby, Purdy, & Hollingworth, 2015).
This budget issue is ever-increasing, with a 13% increase in hospital bed days in the USA
between 2000 and 2009 (Busby et al., 2009). Unfortunately, and perhaps more grave, are the
serious health implications of the need for increased unplanned hospital admissions. The
increases may be a result of a mixture of the following: patient populations growing more
acutely ill, suboptimal primary care prevention and follow-up, non-compliance, and/or
inadequate care during the hospital stay.
Three critical factors of heart failure care include patient and family education, support,
and involvement (Yancy et al., 2013, p. e295). Per the American Heart Association (Yancy et
al., 2013, p. e295), a likely cause of the United States’ high rates of re-hospitalization and

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
2
mortality in heart failure patients within 30 days is the “failure to understand and follow a
detailed and often nuanced plan of care.”
Heart failure is associated with a decreased health-related quality of life. Heart failure
“significantly decreases health-related quality of life, especially in the areas of physical
functioning and vitality” (Yancy et al., 2013). Lack of a post-hospital discharge improvement in
health-related quality of life is a strong predictor of a patient’s readmission to the hospital and
mortality (Yancy et al., 2013). Additionally, heart failure risk factors and subsequent
concomitant conditions such as diabetes mellitus, metabolic syndrome (consisting of abdominal
adiposity, hyperlipidemia, hypertension, and fasting hyperglycemia), and atherosclerotic diseases
further decrease heart failure patients’ health-related quality of life (Yancy et al., 2013). Hence,
it is imperative that primary care providers make the effort to educate and improve patient
outcomes during clinic encounters.
Heart failure has a staggering financial burden. In the United States, the numbers of
unplanned hospital admissions (and subsequent readmissions) for heart failure and heart failure
exacerbation are astounding. Heart failure is the primary diagnosis in over 1 million
hospitalizations every year, with patients at a high risk for all-cause re-hospitalization, and a
readmission rate of 25% within one month (Yancy et al., 2013, p. e248). Additionally, over half
of the $30 billion+ spent annually on heart failure in the United States is spent on
hospitalizations (Yancy et al., 2013, p. e248). Since 2012, the Centers for Medicare & Medicaid
Services have “reduced payments to inpatient prospective payment system hospitals with excess
readmissions” (David, Britting, & Dalton, 2015). Therefore, it is prudent and imperative that
care should be taken to decrease hospital admissions and readmissions in the heart failure
population.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
3
The Problem
Per Yancy et al. (2013), one in five Americans will be older than 65 years of age by the
year 2050. Because the prevalence of heart failure is highest in those 65 years of age and older,
“the number of Americans with heart failure is expected to significantly worsen in the future”
(Yancy et al., 2013). In 2043, 6.3 million veterans are projected to be 65 years of age and older
(U.S. Department of Veterans Affairs [VA], 2015c). However, perhaps more alarming is the
steadily increasing numbers of baby boomer veterans getting older now – a whopping 9.8 million
veterans were 65 years of age and older in 2013 (VA, 2015c). Because of this, action must also
be taken now to improve both the health-related quality of life for this sample of patients, while
also lessen the financial burden of the disease.
Purpose of the Research
The purpose of this study is to determine if outpatient heart failure care provider-type
(physician or NP) has an impact on numbers of heart failure exacerbation
admissions/readmissions.
Implications for Nursing Practice/Policy/Research
Among those caring for heart failure patients are physicians (MDs/DOs) and mid-level
providers, which include nurse practitioners (NPs) and physician assistants (PAs). Worldwide,
substitution of physicians by nurse practitioners in primary care has become commonplace as a
result of physician shortages “and the need for high-quality, affordable care, especially for
chronic and multi-morbid patients” (Martínez-González et al., 2014). However, despite the
national shortage of primary care physicians, disagreement exists as to NPs role in the leadership
of clinical practice (Buerhaus, DesRoches, Dittus, & Donelan, 2015). Therefore, it is important
to examine the impact that nurse practitioners have in outpatient care.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
4
Research Question
In adult patients receiving heart failure care at a major military medical center in southern
California, is there a difference in the number of hospitalizations for heart failure exacerbation
based on provider-type?
Hypothesis
Although physician and NP education and training differ, NPs will either have the same
numbers or lower rates of patients with heart failure exacerbation admissions. This will be
attributed to the different approach that NPs take in caring for their patients through Lydia Hall’s
Care, Cure, Core Theory.
Research Variables
The dependent variable in the study is the unplanned hospital admission related to heart
failure exacerbations. The independent variables studied were outpatient care provided by
physicians and outpatient care provided by nurse practitioners.
Conceptual Model
Lydia Hall’s Care, Cure, and Core Theory. The theory shows the importance of nursing
interventions – in this case, advance practice nursing, on the care of heart failure patients.
Assumptions of Hall’s Care, Cure, and Core Theory (Wayne, 2014):
1. The motivation and energy necessary for healing exist within the patient, rather
than in the healthcare team.
2. The three aspects of nursing should not be viewed as functioning independently
but as interrelated.
3. The three aspects interact, and the circles representing them change size,
depending on the patient’s total course of progress.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
5
Importance of the Research
Research is needed that will examine the impact of NP care on patient and utilization
outcomes (David et al., 2015), especially with heart failure exacerbation admission and
readmissions. An association between primary care provider type and unplanned hospital
admissions for heart failure exacerbation can aid in supporting potential initiatives that either
improve access/quality to primary care, or develop alternatives to hospital admissions (Busby et
al., 2015). Decreased hospital admissions means decreased costs, and would demonstrate
improved control of patients’ heart failure.
An unplanned hospitalization for heart failure exacerbation is costly for both patients’
health and hospitals’ budgets. A closer look at patients’ primary care provider-type may aid in
determining what, if anything, a certain provider-type may be doing that leads to less
hospitalizations. Because many admissions for conditions cared for and addressed in
ambulatory/primary care are preventable (Busby et al., 2015), it is important to look at the
practice characteristics of primary care providers, and see what best-practice is in treatment and
maintenance of heart failure. The Veterans Health Administration (VHA), an organization of the
VA, is a prime health care system to study due to its relatively expansive use of NPs,
“unparalleled national system of coded data,” and “the high burden of chronic disease in its
population” (Morgan, Abbott, McNeil, & Fisher, 2012). NPs employed by the U.S. Department
of the Navy are also ideal to study, as they are considered to be “licensed independent
practitioners that function in an expanded and specialized area of nursing and possess the
knowledge and clinical skills required to accept and provide services to patients requiring
primary care management” (“BUMEDINST 6550.10B,” 2015).

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
6
Chapter Two: Literature Review
Introduction
Research articles were identified through PubMed, Cumuluative Index to Nursing and
Allied Health Literature (CINAHL), SAGE Journals, the Cochrane Database of Systematic
Reviews, and ScienceDirect databases. Literature search terms included “primary care,”
“unplanned hospital admissions,” “heart failure exacerbation,” and “ambulatory care.” The
search was limited to English language, peer-reviewed articles with full-text available.
Previous research exists on heart failure admission rates and the acute care nurse
practitioner (David et al., 2015), but research is lacking with respect to care of these patients by
primary care NPs. Even withstanding, David et al.’s (2015) research on the cardiac acute care
nurse practitioner’s role in decreasing 30-day readmissions is a step in the right direction. In a
retrospective 2-group comparative study, David et al. (2015) evaluated the outcomes of 185
cardiovascular intensive care patients with either ST- or non-ST-segment elevation myocardial
infarction or heart failure in an urban medical center. The patients were either treated by a
medical team and cardiac acute care NP (n = 109) or the medical team alone (consisting of only
physicians) (n = 76). The findings of the study were impressive:
• Those who received care from a medical team with a NP were readmitted
approximately 50% less often than those who received care from a medical team
without a NP
• 30-day hospital readmission (p = .11) and 30-day return rates to the emergency
department (p = .21) were both significantly lower in treatment teams that
included a NP.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
7
“The [VHA] has been a frontrunner in the use of [NPs and PAs],” with the two
professions providing approximately 30% of all primary care encounters (Morgan et al., 2012).
The VHA is the U.S.’s largest integrated health system and “is a leader in primary care
innovation” (Morgan et al., 2012). As will be described further in the “Major Variables
Defined” section, both VHA primary care NPs and Department of the Navy NPs (civilian or
military) function similarly to physicians. The prominence of NPs in the VHA and in Navy
Medicine brings about a need for an analysis as to the impact of NP care of both patient and
utilization outcomes (e.g., decreased heart failure exacerbation admissions and readmissions).
A systematic review by Laurant et al. (2005), through The Cochrane Collaboration,
gleaned 4253 potentially relevant studies, and reduced the review to 16 relevant studies that met
inclusion criteria regarding the substitution of physicians by nurses in the primary care setting.
The studies suggested that with appropriate training, nurses in primary care can provide care as
high of a quality as primary care doctors and their patients can achieve equally optimal health
outcomes.
Though a systematic review of 24 randomized clinical trials (RCTs) by Martínez-
González et al. (2014), analysis “showed that NPs had a positive effect in reducing all-cause
admissions to [the] hospital (RRs 0.74, 95% CI 0.62 to 0.89),” estimates increased with non-
urgent, on-going care (primary care) visits with lengthened follow-up episodes of at least 12
months and in large RCTs (N>200).
Mundinger et al. (2000) conducted a randomized clinical trial of 1316 patients with no
regular source of care, with random enrollment and initial primary care appointments with either
a NP (n = 806) or physician (n = 510). The setting for the study occurred at four community-
based primary care clinics with 17 physicians and one primary care clinic with seven nurse

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
8
practitioners at an urban, academic medical center (Mundinger et al., 2000). The aim of the
study was compare outcomes for these patients in a setting where nurse practitioners and
physicians practiced with the same degree of independence. The results of the study generally
showed support for NP care:
• Patients’ health status: no significant differences at six months (p = .92)
• Physiologic test results for diabetics or asthmatics: no significant differences (p =
.82, p = .77, respectively)
• Diastolic blood pressure in hypertensive patients: Statistically significantly lower
for NP patients (82 vs. 85 mmHg; p = .04)
• Health services utilization after six months or one year: no significant differences
• Satisfaction ratings after initial appointment: no differences (p = .88 for overall
satisfaction)
Major Variables Defined
Physician. Physicians are also known as doctors of medicine [MDs] or doctors of
osteopathy [DOs]) and have little-to-no restrictions on medical practice. They diagnose and treat
illnesses and injuries (Bureau of Labor Statistics [BLS], 2014b). Their medical training is a
rigorous and a long drawn-out process. They complete four years of medical school after
obtaining a bachelor’s degree, receive either a doctoral or professional degree upon graduation.
After graduation, they are matched into an internship, residency, or fellowship for three to eight
years of on-the-job training before being able to fully practice independently as an attending
physician.
Title 38 United States Code (U.S.C., also called the Code of Laws of the U.S.A.)
mandates that the VA is required to assist in training resident physicians, as well as other health

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
9
professional trainees, to optimize the quality of care provided to Veterans under the VA health
care system (VA, 2015b). In 2014 alone, the VA’s Graduate Medical Education (GME) program
consisted of 41,223 medical residents, 22,931 medical students, and 311 fellows – all of which
received their clinical training at a VA facility (VA, 2015b). Additionally, 135 of 141 allopathic-
accredited (also known as “western medicine,” which MDs fall under) medical schools and 30
out of 40 osteopathic medical schools (which ODs fall under) have affiliation agreements with
the VA (VA, 2015b). Because the VHA is a teaching organization that relies heavily upon
resident physicians that continuously rotate through primary care (among other specialties), they
will be considered physicians in the study.
Through their GME program, a southern California Naval Medical Center has also
provided physicians opportunities for internships, residencies, and fellowships for the past 70
years and trains these physicians to provide care for active and prior military patients and their
families (“GME – Internal Medicine Residency,” 2017). In the prospective study, care provided
by physicians, whether they be interns, residents, or attendings in a primary care setting that
precedes an admission for heart failure exacerbation will be included, and will be one of the two
independent variables.
Nurse practitioner. Nurse practitioners are registered nurses (RN) with graduate- or
doctoral-level training. The minimum degree required of nurse practitioners is a master’s
degree, which is a two- to three-year long program post-bachelor’s degree (BLS, 2014a). A
residency is not required to practice, and is uncommon. In the United States, each state has its
own jurisdiction over their nurse practitioners’ scope of practice – some states are more or less
restrictive than others. In states where their licensure and scope of practice is restricted, nurse
practitioners are considered mid-level practitioners, outranked by physicians. VHA primary care

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
10
NPs function more as substitutes for physicians, rather than as complements (Morgan et al.,
2012). VHA primary care NPs are typically responsible for managing their own patients, can
prescribe medications, place orders, and can sign documentation without physician co-signatures
(Morgan et al., 2012). As stated earlier, the Department of the Navy employs NPs that act as
independent providers in primary care, whose clinical judgment are theirs alone, without
supervision by a physician (“BUMEDINST 6550.10B,” 2015). Care provided by nurse
practitioners in a primary care setting, preceding or following an admission for heart failure
exacerbation will be included in the study, and will be the other of the two independent variables.
Primary care. The American Academy of Family Physicians (AAFP), the national
association of family physicians, provided definitions of primary care and their own descriptions
of those who provide primary care. Per the AAFP (2015), primary care is care provided by those
with specific training and skills in comprehensive initial visits, as well as ongoing care for
anyone with undiagnosed signs, symptoms, or health concerns. The AAFP’s stance on providing
primary care is that non-physician primary care providers “may meet the needs of specific
patients,” and they should only practice collaboratively with physicians, who retain the “ultimate
responsibility” of the patient (AAFP, 2015). Beliefs such as this are another justification for the
need for this study. The organization is against allowing NPs to take the reins in caring for
primary care patients, and insists on maintaining a hierarchy of providers. Research must be
conducted in an effort to provide evidence-based support for the role of the nurse practitioner.
Heart failure. The World Health Organization has assigned the diagnosis of heart
failure the code I50 under the current version of International Classification of Diseases, version
10-Clinical Modification (ICD-10-CM; Centers for Medicare & Medicaid Services [CMS],
n.d.b) and 428 under the previous version, ICD-9-CM (CMS, n.d.a). This standardized code is

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
11
used internationally to refer to heart failure. Only patients with an I50 code on their problem
lists will be included in the study. The number of heart failure exacerbation hospital admissions
for a particular patient will be tallied and categorized under either care from primary care NPs or
primary care physicians.
Veteran. There are numerous criteria for what qualifies someone as a Veteran that can
receive VA or military healthcare, but for simplicity’s sake, a veteran is someone who served in
the U.S. military. Male veterans are much more prevalent than female veterans; the VA (2015c)
reported that in 2013 there were 20.2 million men in the total of 22.2 million living U.S.
veterans. (This means that women made up only 2.2 million of the veteran population.).
There may be a link between veterans, post-traumatic stress disorder, and heart disease –
making this population all the more important to study. In a study of 281 pairs of twins who
served in the military during the Vietnam War, those who were diagnosed with PTSD were more
than twice as likely to develop heart disease than those that did not (23% vs. 9%) (Kuehn, 2013).
Theoretical Framework/Conceptual Model
According to nursing theorist Lydia Hall, the patient consists of three aspects: the person,
the body, and the disease (Parker & Smith, 2010). Per Hall, medicine (e.g., physicians) is
responsible for pathology and treatment, but the area of person is “sadly neglected” (Parker &
Smith, 2010). An expert nurse “must know how to modify the care depending on the pathology
and treatment while considering the patient’s unique needs and personality” (Parker & Smith,
2010). Hall’s Care, Cure, and Core Model stands to represent the nature of nursing, with three
overlapping circles that change in size according to a patient’s phase of healing (Parker & Smith,
2010).

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
12
Care. Hall suggested that providing intimate bodily care to patients (i.e., activities of
daily living such as bathing, feeding, toileting, etc.) is an aspect that belongs entirely to nursing
(Parker & Smith, 2010). This is just one example of “care;” building rapport through an
interpersonal relationship is perhaps a more overarching use of the term. The model holds that
the patient as a person (in addition to his/her body) will respond to the physical/comforting care
provided by the nurse. The care circle is predominant during the evaluation and follow-up phase
– where primary care nurse practitioners carry out their therapeutic interventions and teaching.
Cure. This is the area of the nursing process that is shared with physicians (medicine).
Interventions of a medical/surgical nature that are performed by nurses fall under this circle.
These can include tasks such as measuring intake and output as a bedside nurse, to diagnosing
and prescribing medications as a nurse practitioner. This portion of the circle is largest during
the acute care phase, or when patients are hospitalized for heart failure exacerbations.
Core. This area of nursing is shared with other helping professions, and emphasizes the
“social, emotional, spiritual, and intellectual needs of the patient in relation to family, institution,
community, and the world” (Parker & Smith, 2010). The core is based on the therapeutic use of
oneself and the social sciences (Parker & Smith, 2010). With the aid of nurses’ comfort and the
provision of intimate bodily care, the patient will comfortably be able to introspectively explore
the core of his or her being. Questions answered that will rapidly progress one towards healing
and rehabilitation include who a person is, where that person is and where they want to go, and
whether or not they will accept help in getting there (Parker & Smith, 2010). All-in-all, this
framework can be an explanation for the high quality of care provided by NPs, despite having a
shorter education and less training compared to physicians.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
13
Summary. Using Lydia Hall’s Care, Cure, and Core Model, the professional nurse (and
nurse practitioner) provides care that assists the patient in learning to reach the core of his or her
difficulties, and sees him or her through the cure (Parker & Smith, 2010). Through this nursing
process, the patient has the potential to learn from his or her illness, and may even emerge
healthier than they were prior (Parker & Smith, 2010). Despite the differences in schooling and
training, nurse practitioners’ unknowing application of the nursing process as described Lydia
Hall’s Care, Cure, and Core Model helps to bring their quality of care up to par with that of
physicians’.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
14
Chapter Three: Methodology
Introduction
With the high rates of heart failure in the U.S., and the shift towards increased utilization
of NPs in primary care, it is pertinent that research be conducted on the impact that NPs have on
patient outcomes and quality of life. This is especially true because of the known lower health-
related quality of life associated with repeated hospital admissions for heart failure exacerbation.
Differences in training and education may or may not be a factor in numbers of admissions, and
this study aims to find out just that. If the research shows that NP care results in either the same
outcomes as physicians, or perhaps even more so if NP care results in less admissions, further
evidence in support of the role of the NP will be added to the body of knowledge. With more
evidence is the potential for changes in either state policy on NP scope of practice, and also
providing funding for hiring more NPs nationwide.
Research Question
In adult patients receiving heart failure care at a major military medical center in southern
California, is there a difference in the number of hospitalizations for heart failure exacerbation
based on provider-type?
Hypothesis. Although physician and NP education and training differ, primary care NPs
will either have the same numbers or lower rates of patients with heart failure exacerbation
admissions. This will be attributed to the different approach that NPs take in caring for their
patients through Lydia Hall’s Care, Cure, Core Theory.
Null hypothesis (H0). There will not be a difference in the number of heart failure
exacerbation admissions after care from either a primary care physician or primary care NP.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
15
Alternative hypothesis (HA). There will be a statistically significant difference in the
number of heart failure exacerbation admissions after care from either a primary care physician
or primary care NP.
Identification of Setting
Because the same patients commonly seek care in both the VA system and in military
hospitals, where NPs practice primary care independent of a physician, an argument can be made
for the setting of the research study to be in either healthcare system. The VHA might have
ample data, as it is “the United States’ largest integrated health care system consisting of 150
medical centers, [and] nearly 1,400 community-based outpatient clinics (CBOCs)” (VA, 2015a).
Although the VHA is at first glance an obvious choice due to the entire patient population
consisting of veterans, the researcher will opt for studying heart failure patients at a southern
California military hospital instead. (The reason for this will be explained further in the “Chapter
Four: Grants Elements” section.) This study will not be inclusive of all nationwide military
facilities, as it would require extensive time and research, although it could provide valuable
information for a future study. Southern California is an ideal location to study patients, due to
the concentration of numerous military bases in the region, and its diverse patient population.
Additionally, the hospital’s mission is aligned with that of the researcher’s: to “[provide] the
safest, highest quality patient-centered medical care for [the] veterans” (Naval Medical Center
San Diego [NMCSD], 2016). The medical center reports having received more than 1.2 million
outpatient visits and having admitted more than 19,000 patients in 2014 alone (Naval Medical
Center San Diego, 2016).
PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
16
Research Design
A non-experimental, retrospective longitudinal study will be completed on outpatient
care encounter data from a major military hospital in southern California. A follow-up study as a
type of longitudinal design is preferred, because clinical data will be collected at more than one
point in time over an extended period on the same patients (Polit & Beck, 2012, p. 187). A
limitation of archival research is that patients may have been admitted to civilian hospitals for
heart failure exacerbation, and this is likely not recorded in the military electronic chart. Another
limitation of the design in that looking backwards in time in a patient’s chart may very likely
show changes in provider type throughout the continuum of care.
Population and Sample
A moderate effect size of 0.30 will be used, as there is a lack of previous research on this
particular topic. The significance level will be .05, with a power of 0.80. After inputting the
aforementioned values into the computer software G*Power 3.1, a total sample size of 352
(n=352) was determined, with 176 patients in each group (Faul, Erdfelder, Lang, & Buchner,
2009). The total degrees of freedom are 350 (n – 2) and the critical value for the t-statistic (which
will determine whether the null hypothesis will be rejected) is 1.960. Attrition will not be
accounted for, as the data will be obtained from retrospective chart reviews, and will be collected
via quota sampling. Quota sampling is a semi-purposive sampling method (Polit & Beck, 2012,
p. 279). Data collection will conclude once data on 176 patients who meet criteria for both
groups are collected. A confidence interval will be set at 95%, because per Polit & Beck (2012),
it is richer and more powerful in clinical application than p values alone.
Demographic variables include physicians, nurse practitioners, and veteran patients.
Inclusion criteria for providers include those treating patients in outpatient with a title of MD,

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
17
OD, or NP. Exclusion criteria for providers are any physician assistants, as they are neither
physicians nor nurse practitioners. Inclusion criteria for the patients include those with ICD-9-
CM and ICD-10-CM codes for heart failure, those receiving outpatient heart failure care from
either an NP, MD/OD at a major military center in southern California, and those that have had
at least one heart failure exacerbation hospital admission. Exclusion criteria for patients include
heart failure patients with no prior heart failure exacerbation admissions.
Measurement Methods
A tool will be made in the form of a Microsoft Excel worksheet that will list the number
of individual patients’ hospitalizations for heart failure exacerbation and will include their
outpatient care provider type. This data will then be transferred to SPSS 22, a statistical analysis
software. The independent variables of physician care and NP care are considered to have a
nominal level of measurement, while the dependent variable of numbers of heart failure
exacerbation admissions (per patient) are a ratio level of measurement.
In the study, the number of hospitalizations a patient has will be operationalized by
merely counting the number of heart failure exacerbation admissions a patient has. NP care and
physician care will be operationalized by looking at signed provider notes and looking at those
providers’ credentials/titles.
Data Collection Process
Chart reviews of the patients’ electronic health records will provide the data necessary for
this study. As stated before, data will be collected retrospectively, and will follow individual
patients’ records from their first heart failure exacerbation to their most recent. In order to
collect the most recent and relevant information, quota sampling will occur in a reverse
chronological order – meaning that data will be collected starting at the current time and going

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
18
backwards. Data will be kept on an Excel document that will be saved on a password-protected
laptop. Because the data will contain personally identifiable information, and is needed to
backtrack and verify the researchers’ work prior to finalization of reports, care will be taken so
that the information is deleted as soon as analysis is complete. Additionally, patients’
confidentiality will be protected by ensuring that personally identifiable information is not
accessible to anyone outside of the research team, and that the team is trained on the Health
Insurance Portability and Accountability Act of 1996 (HIPAA), a federal law protecting patient
information.
Coding
Numeric codes have been assigned to represent the grouping variables (1 = outpatient
care from physicians and 2 = outpatient care from NPs). These codes will be used in both Excel
and SPSS. Scoring not does apply to this study and therefore will be omitted.
Data Analysis
A two-tailed independent t test will be performed, in order to compare the means of the
grouping/independent variables (outpatient care of heart failure patients by physicians vs. NPs),
and to detect any differences between the two (Kellar & Kelvin, 2013, p. 98). The data will meet
all of the necessary assumptions, due to the following:
1. The grouping variable is dichotomous (care by physicians and care by NPs)
2. The data points (each heart failure exacerbation hospitalization) are independent
of one another.
3. Data are normally distributed.
4. The number of hospital admissions is a ratio variable.
PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
19
Bias
Selective deposit and selective survival are two biases that will be considered when
controlling for threats to internal validity. Selective deposit can result when patients’ health
records or documents are not the complete set of record, but are instead selectively retained
based on criteria that could potentially bias the complete set (Polit & Beck, 2012, p. 742).
Selective survival is a bias that may occur when selected patients’ records are not a complete set
of records because of a non-random method of maintaining them (Polit & Beck, 2012, p. 742).
For this study, data will be selectively handpicked from nationwide military electronic health
records based on inclusion criteria. In an attempt to curb selection bias while also attempting to
collect the most recent or relevant data (especially with regards to provider-care), patients will be
selected by going backwards in time, and stop upon fulfillment of the quota/sample size (176
patients who received primary care from a physician, and 176 patients who received primary
care from a nurse practitioner).
Ethical Considerations
Ethical issues for consideration are relevant to the sample of patients. Veterans are a
potentially vulnerable population because of the following (deLanda, 2010):
1) Their history of obeying orders from their superiors & making sacrifices for the
benefit of others
2) The disparities in their access to other health care – some may not have access
due to their socioeconomic status
3) Active duty may have contributed to psychological issues (e.g. posttraumatic
stress disorder [PTSD])

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
20
Therefore, careful, intentional and conscientious protection of these patients’ health information
will be protected at all times. As described earlier, they will be safeguarded through the research
design. Only data that exists as a result of standard care will be included – there is no
intervention in the form of an experiment and only prior data will be collected. The researchers
will use patient identifiers such as full name and birthday to access the record, but these details
will be deleted prior to removal of data collection sheets from the clinic site. Permission will be
requested and received to remotely access patient records, and research will be completed on a
password-protected computer.
Summary
As discussed earlier, active duty may have contributed to psychological issues such as
PTSD. Additionally, there may be a link between veterans, post-traumatic stress disorder, and
heart disease. Therefore, the cardiac health of our veteran population, and any factors
contributing to better health outcomes should be studied.
Possible limitations of the study may include patient and/or family members’
undetermined involvement and compliance/non-compliance with their care. This study will
solely be looking at provider type, and with the data collected, will attempt to identify any
differences in heart failure patient outcomes. Additionally, the study does not account for
changes in provider – the data will be collected according to who initially cared for the patient.
As discussed earlier, heart failure as a condition is a complex syndrome, with other highly likely
co-morbidities such as diabetes. This study will only be looking heart failure, and future studies
that include information on co-morbidities and patient involvement in their care can be further
stratified and assessed. Furthermore, the sample will only include veteran patients in southern
California. Lastly, most veterans in general are male (VA, 2015c), therefore data will heavily

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
21
consist of male patients with a poor representation of women (approximately a 10:1 ratio).
However, because gaps in the literature still show a need for any research on the impact of NPs
on heart failure exacerbation, the study will still be beneficial in the care of the heart failure
patient.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
22
Chapter Four: Grant Elements
Grants Considered and Chosen
Three grants were considered for funding of the proposed research: VA Research;
American Heart Association (AHA) Institutional Research Enhancement Award (AIREA); and
the TriService Nursing Research Program.
At first glance, VA Research was initially considered to be the best pick as far as where
to receive funding, as the funding would directly benefit the sample patients in the study.
However, upon further inquiry, the principal investigator (PI) would not be eligible for
application with just a master’s degree. Rather, a VA-employed doctorally-prepared nurse
clinician/scientist would have to hold the title of PI. Potentially, this doctorally-prepared nurse
could serve as PI while the applicant is relegated to assistant investigator (AI), but with the
timeline required of the study and little time to find an available VA-employed nurse
clinician/scientist with a doctorate, the author has opted instead to be the PI herself.
The AHA has provides various awards for different research purposes. Their Mentored
Clinical and Population Research Award allows funding for “all clinical and population research
broadly related to cardiovascular disease and stroke” (AHA, 2016). Their required focus appears
to be an easy fit for the purpose of this study, however the funding per year does not cover the
proposed budget and timeline. Although applications from VA employees will be accepted,
because the VA institution in itself will only allow doctorally-prepared VA nurse scientists to
serve as PIs in any VA-related project, the feasibility of this grant is additionally reduced.
Lastly, per the AHA restrictions for applying, if the research is to be performed at a military
hospital (a federal institution), the researcher’s application will face a high probability of being
rejected.
PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
23
The TriService Nursing Research Program (TSNRP) is the most ideal organization from
which to apply for a grant, as it offers an Exploratory Research Award, and would be likely to
support nurse practitioner research at the intended clinical site, a southern California military
hospital. Research priorities for the TSNRP include “description and evaluation of the military
nursing competencies necessary to sustain a patient from [a] health event through the continuum
of care” (Uniformed Services University of the Health Sciences, 2016c). The TriService
Nursing Research Group (TSNR Group)’s origins lie in the informal meetings held by
doctorally-prepared Army, Navy, and Air Force Nurses at the Association of Military Surgeons
of the U.S. convention in 1988 (Uniformed Services University of the Health Sciences, 2016a).
The TSNRP continues to promote military nursing research and the participation of doctorally-
prepared nurses in that research, as there very “few, if any, doctorally prepared nurse researchers
[that] participate as investigators in other [Department of Defense] medical research,
development, test, and evaluation programs” (Uniformed Services University of the Health
Sciences, 2016a). The TSNRP Exploratory Research award is intended for “preparatory
investigations that may lead to larger studies that follow from advancements made by this work”
and awards $150,000 per year for up to 2 years. Additionally, investigators can range from
novice to experienced, will have a mentor that is either an active, reserve, or retired nurse officer,
and allows the researcher to generate preliminary data or show feasibility of research before
applying for a larger grant award (Uniformed Services University of the Health Sciences,
2016b).

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
24
Budget Total: $119,678
Personnel cost. Maria Jamito, MSN, RN will serve as Principal Investigator (PI) on this
research project. Ms. Jamito will receive her Master’s in Nursing with a focus on specializing as
a family nurse practitioner in May 2017. She has five years of experience as a registered nurse–
all of which have been working with veterans within the VA San Diego Healthcare System. She
will be responsible for the overall direction of the study, including presenting the study to the
Institutional Review Board, forming a research team and leading their meetings on a regular
basis, overseeing the study budget, and preparing progress reports. She will devote 50% of her
time to this project, while maintaining part-time work as a nurse practitioner. Based upon San
Diego average salaries for a nurse practitioner and principal investigators, the salary requested
for Ms. Jamito will be $48,000 plus fringe benefits of 26% ($12,480), which total $60,480 for
the year-long study (Indeed, 2016).
The two research assistants (RA’s) for this study are to be determined. The ideal
candidates are those who are bachelor-prepared, with experience in either nursing, heart failure,
or working with electronic health records. They will be responsible for (a) collection of data as
assigned by the PI, (b) verify the accuracy and validity of data entered in databases, and (c) will
provide assistance to the PI with preparation of reports, manuscripts, and presentations
(PayScale, 2016). Based on Glassdoor (2016)’s estimation of research assistants’ salaries in San
Diego, the requested salaries of each research assistant will be $12,000 with fringe benefits of
26% ($3,120), totaling to $15,120 per RA for the year-long study. They each will devote 50% of
their time to this project.
Consultant costs. Dr. Linnea Axman, DrPH, MSN, FNP-BC, FAANP, will provide
guidance and support in quantitative methodology and analysis, including but not limited to

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
25
computer-assisted quantitative analysis. Dr. Axman is a family nurse practitioner and professor
who recently moved to Chicago, IL, from San Diego, CA, and has a wealth of experience in
military nursing and research. She will provide 20 hours of consultation for this one-year study.
Total cost is $3000 ($150 x 20 hours).
Major equipment. Three laptop computers and a printer are needed to create reports,
and store and analyze data. USB flash drives will be needed to back up data from the laptop hard
drives. Total cost is estimated at $1325 ($400 Dell laptop x 3 laptops; $80 printer; $15 32gb
USB flash drive x 3).
Materials/supplies/consumables. General office supplies and copy paper will be
needed during the study. General office supplies include writing supplies, staplers, and printer
ink are estimated at $500 for the 1-year study. Copy paper will be needed for forms,
correspondence, and transcribed data, which includes draft/final reports. The estimated expense
for copy paper is $150 ($30/case x 5 cases). Total cost is estimated at $650.
Software. Microsoft Office and IBM SPSS 22 are software programs that will be needed
for the collection, storage, and statistical analysis of data. One subscription of Microsoft Office
365 Home can be downloaded onto up five PCs or devices, which will be enough to cover the
three laptops requested. The Office suite will be used for creation of the manuscript, any reports,
presentations, and contains the Excel software which will hold the collected data for transfer into
SPSS 22. SPSS 22 is a statistical software product for data management and analysis. The Base
version of SPSS 22 for Windows will suffice for the purposes of this research study. Total cost
is estimated at $1269.99 ($99.99 for 1-year subscription of Microsoft Office 365 Home 2016,
$1170.00 for 1-year subscription of SPSS 22).
PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
26
Travel costs. (Average estimates for flights, hotel accommodations, and rental cars were
obtained from Expedia.com.) The PI will travel to Denver, CO to present their findings at the
American Association of Nurse Practitioners (AANP) 2018 National Conference on June 26-July
1, 2018. Total cost is estimated at $1645 ($250/night for hotel stay x 5 nights, $340/round-trip
ticket, $45/day for one rental car x 5 days).
The study consultant, Dr. Axman, will travel to San Diego, CA from Chicago, IL 2 times
during the 1-year study. The consultant will meet with the project team members to discuss
computer-assisted content analysis. Total cost is $1960 ($500 round-trip flights from Chicago to
San Diego x 2 round-trip flights; $200/night for a hotel in San Diego x 4 nights, $40 rental
car/day x 4 days).
Facilities and administrative costs. Facilities and administrative consortium/contractual
costs will be about 19%, or $19108.
Grand total. The total budget requested comes out to $119,678.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
27

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
28
PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
29
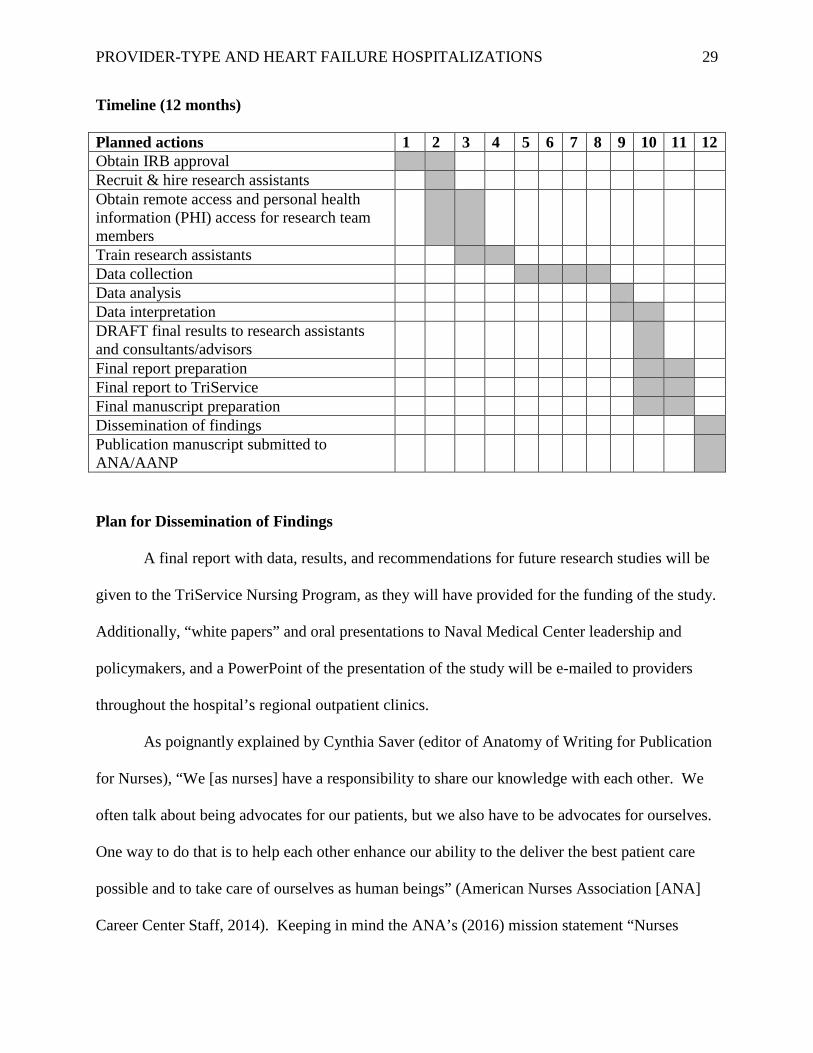
Timeline (12 months)
Planned actions 1 2 3 4 5 6 7 8 9 10 11 12 Obtain IRB approval Recruit & hire research assistants Obtain remote access and personal health information (PHI) access for research team members
Train research assistants Data collection Data analysis Data interpretation DRAFT final results to research assistants and consultants/advisors
Final report preparation Final report to TriService Final manuscript preparation Dissemination of findings Publication manuscript submitted to ANA/AANP
Plan for Dissemination of Findings
A final report with data, results, and recommendations for future research studies will be
given to the TriService Nursing Program, as they will have provided for the funding of the study.
Additionally, “white papers” and oral presentations to Naval Medical Center leadership and
policymakers, and a PowerPoint of the presentation of the study will be e-mailed to providers
throughout the hospital’s regional outpatient clinics.
As poignantly explained by Cynthia Saver (editor of Anatomy of Writing for Publication
for Nurses), “We [as nurses] have a responsibility to share our knowledge with each other. We
often talk about being advocates for our patients, but we also have to be advocates for ourselves.
One way to do that is to help each other enhance our ability to the deliver the best patient care
possible and to take care of ourselves as human beings” (American Nurses Association [ANA]
Career Center Staff, 2014). Keeping in mind the ANA’s (2016) mission statement “Nurses

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
30
advancing our profession to improve health for all,” the research team will publish a manuscript
for submission to the ANA, so that nurses without an advanced degree will be motivated to
improve upon their care of heart failure patients, and further their education for the continued
progression of the nursing practice. Additionally, a manuscript will be submitted to the AANP
for printing in their journal, for widespread distribution to nurse practitioners.
Additionally, as explained earlier in the costs section, the primary investigator plans on
presenting the study with results in the form of posters and oral presentations in national
meetings including but not limited to the AANP National Conference in late June 2018. The
AANP organization is the largest full-service national professional membership organization for
NPs of all specialties (AANP, 2016). The AANP’s mission is aligned with that of the
researcher’s – to empower nurse practitioners to advance quality care through either practice,
education, advocacy, research, and leadership (AANP, 2016). The researcher’s hope is that by
sharing the results of the study with NPs in attendance, they will be encouraged to take
ownership in providing optimal care to heart failure patients, and begin a related research study
of their own in the field. This study in and of itself will not be enough on its own to encourage
policymakers to provide more support for expansion of the nurse practitioner scope of practice
and independence, but can serve as a foundational and supportive research study for it in the
future.

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
31
References
American Academy of Family Physicians. (2015). Primary care. Retrieved from
http://www.aafp.org/about/policies/all/primary-care.html#1
American Association of Nurse Practitioners. (2016). About AANP: AANP mission & values.
Retrieved from https://www.aanp.org/about-aanp
American Heart Association. (2016). Mentored Clinical and Population Research Award.
Retrieved from
https://professional.heart.org/professional/ResearchPrograms/ApplicationInformation/UCM_443
302_Mentored-Clinical-and-Population-Research-Award.jsp
American Nurses Association. (2016). About ANA. Retrieved from
http://www.nursingworld.org/FunctionalMenuCategories/AboutANA
American Nurses Association Career Center Staff. (2014). How to boost your nursing career by
getting published. Retrieved from http://nursingworld.org/Content/Resources/Boost-
Your-Nursing-Career.html
Buerhaus, P. I., DesRoches, C. M., Dittus, R., & Donelan, K. (2015). Practice characteristics or
primary care nurse practitioners and physicians. Nursing Outlook, 63(2), 144-153.
doi:10.1016/j.outlook.2014.08.008
Bureau of Labor Statistics. (2014a). Nurse anesthetists, nurse midwives, and nurse practitioners.
In Occupational Outlook Handbook, 2014-15 Edition (Healthcare). Retrieved from
http://www.bls.gov/ooh/healthcare/nurse-anesthetists-nurse-midwives-and-nurse-
practitioners.htm
Bureau of Labor Statistics. (2014b). Physicians and surgeons. In Occupational Outlook
Handbook, 2014-15 Edition (Healthcare). Retrieved from

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
32
http://www.bls.gov/ooh/healthcare/nurse-anesthetists-nurse-midwives-and-nurse-
practitioners.htm
Busby, J., Purdy, S., & Hollingworth, W. (2015). A systematic review of the magnitude and
cause of geographic variation in unplanned hospital admission rates and length of stay for
ambulatory care sensitive conditions. BMC Health Services Research, 15(324), 1-15.
doi:10.1186/s12913-015-0964-3
Centers for Medicare & Medicaid Services. (n.d.a). ICD-9 code lookup. Retrieved from
https://www.cms.gov/medicare-coverage-database/staticpages/icd-9-code-lookup.aspx
Centers for Medicare & Medicaid Services. (n.d.b). ICD-10 code lookup. Retrieved from
https://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx
David, D., Britting, L., & Dalton, J. (2015). Cardiac acute care nurse practitioner and 30-day
readmission. Journal of Cardiovascular Nursing, 30(3), 248-255.
doi:10.1097/JCN.0000000000000147
deLanda, B. (2010). Vulnerable populations and human subjects review. [PDF document].
Retrieved from
http://humansubjects.stanford.edu/education/2010_10_Vulnerable_Populations.pdf
Delgado-Passler, P., & McCaffrey, R. (2006). The influences of postdischarge management by
nurse practitioners on hospital readmission for heart failure. Journal of the American
Academy of Nurse Practitioners, 18(4), 154-160. doi:10.1111/j.1745-7599.2006.00113.x
Department of the Navy Bureau of Medicine and Surgery. (2015). BUMED INSTRUCTION
6550.10B: Utilization guidelines for nurse practitioners and certified nurse midwives.
Retrieved from
http://www.med.navy.mil/directives/ExternalDirectives/6550.10B%20with%20CH-1.pdf

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
33
Faul, F., Erdfelder, E., Lang, A., & Buchner, A. (2009). G*Power 3.1 [computer software].
Düsseldorf, Germany: Heinrich Heine University of Düsseldorf.
Glassdoor. (2016). Research assistant salaries in San Diego, CA. Retrieved from
https://www.glassdoor.com/Salaries/san-diego-research-assistant-salary-
SRCH_IL.0,9_IM758_KO10,28.htm
Human Resources and Services Administration. (2016). HRSA-17-067 Advanced Nursing
Education Workforce (ANEW) program. Retrieved from
http://www.grants.gov/web/grants/view-opportunity.html?oppId=289064
IBM Corp. (2013). IBM SPSS Statistics (Version 22) [Software]. Available from
https://www.csusm.edu/fshd/cougarapps
Indeed. (2016). Principal investigator salary in San Diego, CA. Retrieved from
http://www.indeed.com/salary/q-Principal-Investigator-l-San-Diego,-CA.html
Kellar, S. P., & Kelvin, E. A. (2013). Munro’s statistical methods for health care research.
Philadelphia, PA: Wolters Kluwer Health | Lippincott, Williams, & Wilkins.
Kuehn, B. M. (2013). PTSD doubles heart risk for veterans. The Journal of the American
Medical Association, 310(8), 787. doi: 10.1001/jama.2013.276613
Laurant, M., Reeves, D., Hermens, R., Braspenning, J., Grol, R., & Sibbald, B. (2005).
Substitution of doctors by nurses in primary care. Cochrane Database of Systematic
Reviews, 2005(2), 1-41. doi:10.1002/14651858.CD001271.pub2
Martínez-González, N. A., Djalali, S., Tandjung, R., Huber-Geismann, F., Markun, S., Wensing,
M., & Rosemann, T. (2014). Substitution of physicians by nurses in primary care: A
systematic review and meta-analysis. BMC Health Services Research, 14(214), 1-17.
doi:10.1186/1472-6963-14-214

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
34
Morgan, P. A., Abbott, D. H., McNeil, R. B., & Fisher, D. A. (2012). Characteristics of primary
care office visits to nurse practitioners, physician assistants and physicians in United
States Veterans Health Administration facilities, 2005 to 2010: A retrospective cross-
sectional analysis. Human Resources for Health, 10(42), 1-8. doi:10.1186/1478-4491-10-
42
Mundinger, M. O., Kane, R. L., Lenz, E. R., Totten, A. M., Tsai, W.-Y., Cleary, P. D., …
Shelanski, M. L. (2000). Primary care outcomes in patients treated by nurse practitioners
or physicians: A randomized trial. The Journal of the American Medical Association,
283(1). Retrieved from http://jama.jamanetwork.com/article.aspx?articleid=192259
Naval Medical Center San Diego. (2016). Why NMCSD. Retrieved from
http://www.med.navy.mil/sites/nmcsd/pages/visitors/why.aspx
Parker, M. E., & Smith, M. C. (2010). Nursing theories and nursing practice (3rd ed.).
Philadelphia, PA: F.A. Davis Co.
PayScale. (2016). Research assistant, medical salary (United States): Job description for
research assistant, medical. Retrieved from
http://www.payscale.com/research/US/Job=Research_Assistant,_Medical/Salary
Polit, D. F., & Beck, C. T. (2012). Nursing research: Generating and assessing evidence for
nursing practice. Philadelphia: Wolters Kluwer.
Uniformed Services University of the Health Sciences. (2016a). TriService Nursing Research
Program. Retrieved from https://www.usuhs.edu/content/triservice-nursing-research-
program
Uniformed Services University of the Health Sciences. (2016b). TriService Nursing Research
Program: Application instructions. Retrieved from

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
35
https://www.usuhs.edu/sites/default/files/media/tsnrp/pdf/2016-application-
instructions.pdf
Uniformed Services University of the Health Sciences. (2016c). What is fundable?. Retrieved
from https://www.usuhs.edu/tsnrp/research-priorities
U.S. Department of Veterans Affairs. (2015a). About VHA. Retrieved from
http://www.va.gov/health/aboutvha.asp
U.S. Department of Veterans Affairs. (2015b). Medical and dental education program. Retrieved
from http://www.va.gov/oaa/GME_default.asp
U.S. Department of Veterans Affairs. (2015c). Veteran population. Retrieved from
http://www.va.gov/vetdata/Veteran_Population.asp
Wayne, G. (2014). Lydia E. Hall’s Care, Cure, Core Theory. Retrieved from
http://nurseslabs.com/lydia-e-halls-care-cure-core-theory/
Yancy, C. W., Jessup, M., Bozkurt, B., Butler, J., Casey, D. E., Drazner, M. H., … Wilkoff, B.
L. (2013). 2013 ACCF/AHA guideline for the management of heart failure: A report of
the American College of Cardiology Foundation/American Heart Association Task Force
on Practice Guidelines. Circulation, 128(16), e240-e327. doi:
10.1161/CIR.0b013e31829e8776

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
36
Appendix A: Instrument
This is a self-made Excel document with data on fictitious patients, with their numbers of heart
failure admissions and a code for their provider-type, with “1” = physician and “2” = NP
PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
37
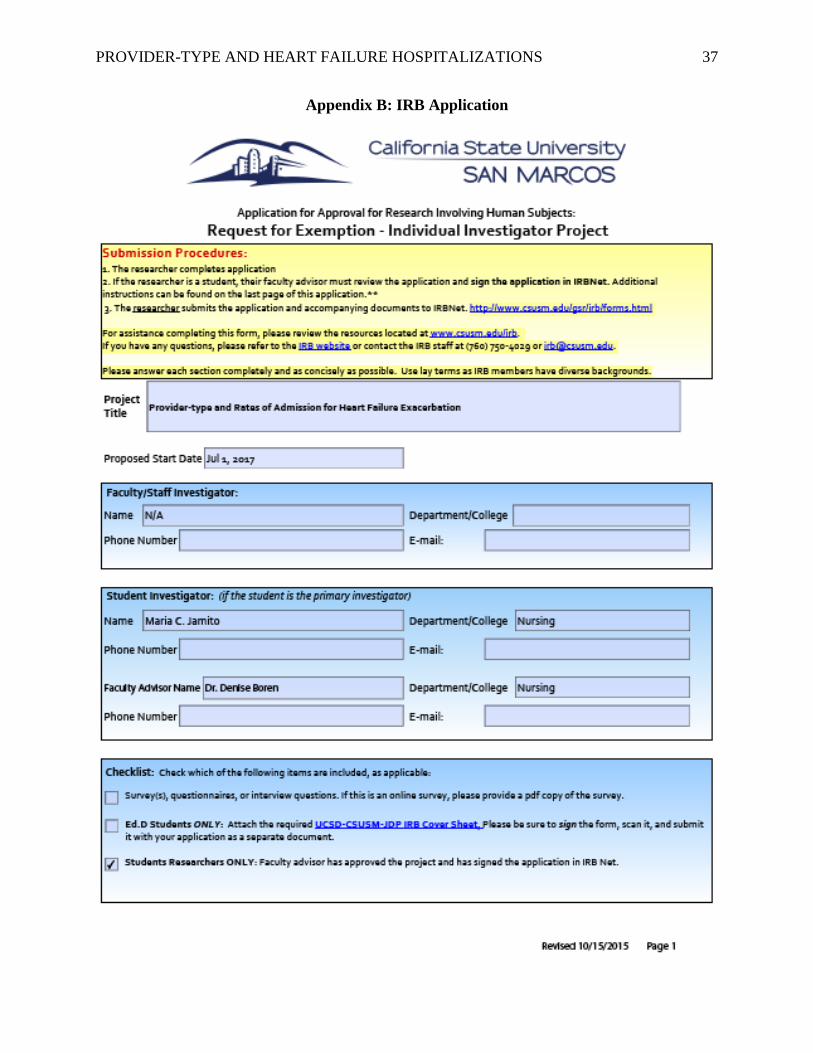
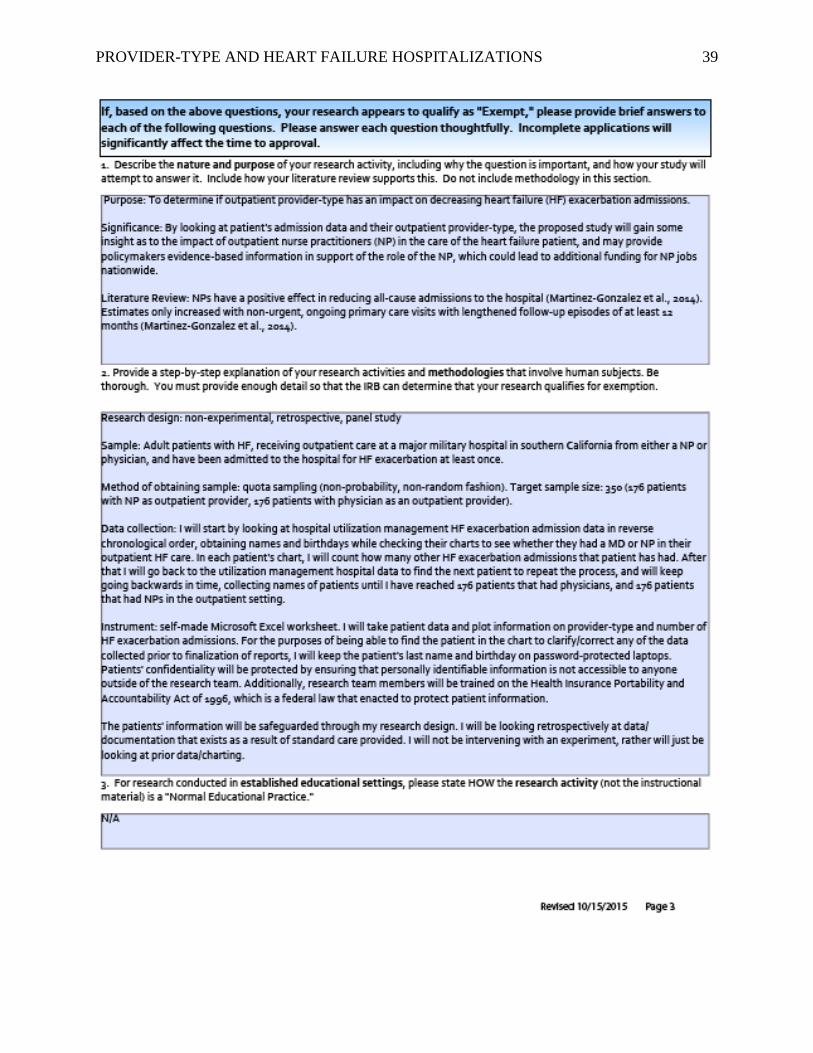
Appendix B: IRB Application

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
38
PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
39

PROVIDER-TYPE AND HEART FAILURE HOSPITALIZATIONS
40





























