Embed Size (px)
Citation preview

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/authorsrights
Author's personal copy
Complementary Therapies in Medicine (2013) 21, 364—378
Available online at www.sciencedirect.com
j ourna l ho me pa g e: www.elsev ierhea l th .com/ journa ls /c t im
Profile of the complementary and alternativemedicine workforce across Australia, New Zealand,Canada, United States and United Kingdom
Matthew J. Leach ∗
School of Nursing & Midwifery, University of South Australia, North Terrace, Adelaide, South Australia 5000, AustraliaAvailable online 23 May 2013
KEYWORDSCensus;Complementary andalternative medicine;Health services;Workforce
SummaryBackground: Despite the expressed demand for complementary and alternative medicine (CAM)services in developed countries, little is known about the CAM workforce in terms of supply andcomposition.Objective: To describe the CAM workforce across five developed countries to better informhealth workforce and health services planning, and perchance, inform debate on future publichealth and primary care policy.Methods: Data from the Australian, New Zealand, Canadian, UK and US Censuses of popula-tion were interrogated for information pertaining to the size and characteristics of the CAMworkforce. This was supplemented by other population-level workforce data where available.Results: The quality and availability of population-level data on the CAM workforce vary sub-stantially across nations. Of the nine CAM disciplines explored, massage therapy consistentlycomprised the largest portion of the CAM workforce, followed closely by chiropractic. Disci-plines in shortest supply were homoeopathy in Australia, traditional Chinese medicine in NewZealand, and naturopathy in the US. Across the broader CAM workforce, practitioners weretypically female, aged ≥40 years, worked within a primary care setting, held a vocational orhigher education level qualification, worked full-time, and earned <$1000 gross per week.Conclusions: This work has helped shape current understandings of the CAM workforce. In doingso, it will help to inform the training and continuing education needs of the evolving CAMworkforce, and further, ensure the provision of a competent CAM workforce to service theneeds of consumers. Addressing the many limitations of existing data sources will assist inmeeting these needs.© 2013 Elsevier Ltd. All rights reserved.
IntroductionComplementary and alternative medicine (CAM) representsa diverse range of health-related therapies and interven-
∗ Tel.: +61 8 8302 2846; fax: +61 8 8302 2168.E-mail address: [email protected]
tions that are largely considered to be outside the realmof Western medicine. Consumer interest in complementaryand alternative medicines and CAM services has increasedover the past decade. Recent data indicate that a large pro-portion of the population of developed countries,1 includingAustralia (52—69% of those surveyed),2,3 Canada (59—60%),4
the United States (62%),5 Singapore (76%)6 and Japan (50%),7
0965-2299/$ — see front matter © 2013 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.ctim.2013.04.004

Author's personal copy
Profile of the CAM workforce 365
have used CAM at least once over a twelve-month period.Over the same period of time, close to twelve percent ofCanadian adults,8 sixteen percent of US adults,9 twenty-sixpercent of English adults,10 and twenty-three11 to forty-fourpercent of Australians3 had consulted a CAM practitioner,with massage being the most commonly used service.
Even though a comparatively greater proportion of thepopulation of developed countries visit Western medicalpractitioners (i.e. >77%) than CAM practitioners,12,13 thereis surprisingly little difference in the total number and costof visits between groups, at least in Australia. For instance,in 2005, Australian adults made an estimated 69.2 millionvisits to CAM practitioners, at an estimated cost of AU$1.73billion. In the same year, there were approximately 68.9 mil-lion consults with Western medical practitioners, at a totalcost of AU$1.6 billion.3 In the US, the out-of pocket costsfor CAM services are far less than Western medical care. In2007, US adults made 354.2 million visits to CAM practition-ers, at an estimated out-of-pocket cost of US$11.9 billion14;the out-of-pocket cost of Western physician services in thesame year was $US46.8 billion.15 These data provide clearevidence of expressed demand for CAM services in developedcountries, which is not too dissimilar from the expresseddemand for Western medical services.
There are several explanations for the increasing useof complementary medicines and CAM services across theglobe.2,9 Earlier studies have suggested that consumer dis-satisfaction with Western medicine may be a leading reasonfor CAM use1; however, more recent reports indicate that anaspiration for active health-care participation, greater dis-ease chronicity and severity, holistic health-care beliefs, andan increase in health-awareness behaviour are more likelyto be associated with CAM use.16—18 These transformationsin consumer attitude and health behaviour have paralleledchanges in the way many CAM specialties practice.19 Thissuggests that complementary medicines and CAM servicesare addressing unmet needs in health care.
Despite the increasing demand and need for CAM servicesin developed countries, little is known about the CAM work-force in terms of supply and composition; and apart froma few workforce surveys, which are hampered by narrowscope, limited data, poor response rates, and/or moderate-sized convenience samples,20—23 little has been published inthe public domain. Without knowledge of the compositionof the CAM workforce, it is difficult to (1) understand thediversity and characteristics of the CAM workforce, (2) meetthe training and continuing education needs of the evolvingCAM workforce, and (3) ensure the provision of a compe-tent CAM workforce to service the needs of consumers. Inrecognising these concerns, this article describes the CAMworkforce across five developed countries in order to bet-ter inform health workforce and health services planning,and perchance, inform debate on future public health andprimary care policy.
Methods
Geographical regions were limited to organisation for eco-nomic cooperation and development (OECD) countries asthe increasing demand for CAM is largely reported in thesedeveloped nations. Of these countries, only those that pro-vided publicly accessible census data on the CAM workforce
were considered. Five countries were selected: Australia,New Zealand, Canada, United Kingdom and the UnitedStates.
The CAM workforce was defined as any health service notconsidered a core component of Western medicine, nursingor allied health,24 and delivered in any industry of employ-ment. This included, but was not limited to, system-basedtherapies (e.g. naturopathy, herbal medicine, traditionalChinese medicine [TCM], acupuncture, homoeopathy) andmanipulative therapies (e.g. chiropractic, osteopathy andmassage therapy). Diagnostic techniques (e.g. iridology,kinesiology) were excluded.
Census data were acquisitioned by request where possi-ble (e.g. Australia and New Zealand), and where requestsfor data were not feasible or cost-prohibitive (e.g. UK,US and Canada), data were sourced from the websites ofeach census administrator. Data from the 2006 AustralianBureau of Statistics Census of Population and Housing, 2006Statistics New Zealand Census of Population and Dwellings,2006 Statistics Canada Census of Population, 2001 UK Officefor National Statistics Census, and the 2000 US CensusBureau Census of Population and Housing were interro-gated for information pertaining to the size of the CAMworkforce, as well as key characteristics of the workforce,such as age, sex, primary discipline, highest level of edu-cation attained, industry of employment, hours workedper week, and gross weekly income. These five popula-tion censuses were selected as they employed similar studymethods, used comparable survey items, and provided high-quality data that were highly representative of each nationalpopulation (Table 1). Where possible, census informationwas supplemented by workforce data reported by otherpertinent sources where the publication date closely approx-imated the census date of the selected country. While morerecent censuses have been conducted across four of thefive selected countries (i.e. Australia, Canada, UK and US),detailed occupation data were not publicly available fromany of these censuses during the conduct of the project.
Available data were analysed descriptively using fre-quencies and percentages. Workforce populations wereconverted to patient-provider ratios to allow for interna-tional comparisons. General/family practitioner populationdata were included as a point of reference only.
Results
Quality of CAM workforce data
The Australian and New Zealand Census of population pro-vided the most comprehensive population-level data on theCAM workforce; although, data were only available for sevendistinct CAM disciplines (Table 1). The Canadian Census ofpopulation provided data for most fields of interest, butonly for chiropractors and general practitioners. Data forall other CAM occupations were reported in aggregate formwith other non-CAM occupations and were not useful foroccupation-specific workforce planning. US population cen-sus data were limited, with data available for only few fieldsof interest for chiropractors and massage therapists; data formost fields had to be sourced from workforce surveys. Datafor all other occupations were reported in aggregate form

Author's personal copy366
M.J.
Leach
Table 1 Quality of CAM workforce data derived from population censuses.
Census Year conducted Description of Census Data available Notes
Australian Bureau ofStatistics Census ofPopulation andHousing
2006 The Australian census is aself-administered questionnairecomprising 60 closed/free textquestions. It is administered nationallyto every home in Australia, every 5years.In 2006, the Australian census achieveda response rate of 97%.
- Reports demographic data (i.e. gender, age,highest qualification held, hours worked perweek in all jobs, gross weekly income, industryof employment) for each of the followingprimary occupations: osteopath, chiropractor,naturopath, homoeopath, acupuncturist,traditional Chinese medicine practitioner,massage therapist and general medicalpractitioner.- Data for herbalists, aromatherapists,iridologists and reflexologists are reported inaggregate form (under ‘natural remedyconsultant’) and cannot be separated.
Detailed occupation data fromthe 2011 census were notavailable as at 30th Sep 2012.
Statistics Canada Censusof Population
2006 The Canadian census is aself-administered questionnaire, whichis distributed in two main forms. Theshort form comprises 8 closed/free textquestions, and is distributed to 80% ofthe Canadian population. The long formcomprises 61 closed/free text questions,and is distributed to 20% of thepopulation. The census is administerednationally to every home in Canada,every 5 years.In 2006, the Canadian census achieved aresponse rate of 97%.
- Reports demographic data (i.e. gender, age,highest qualification held, hours of paid workper week in all jobs, gross annual income,industry of employment) for each of thefollowing primary occupations: chiropractorsand general practitioners.- Data for other professional occupations (e.g.naturopath, osteopath, podiatrist andorthoptist) are reported in aggregate form andcannot be separated.
Detailed occupation data fromthe 2011 census were notavailable as at 30th Sep 2012.
Statistics New ZealandCensus of Populationand Dwellings
2006 The New Zealand (NZ) census is aself-administered questionnairecomprising 47 closed/free textquestions. It is administered nationallyto every home in NZ, every 5 years.In 2006, the NZ census achieved aresponse rate of 98%.
- Reports demographic data (i.e. gender, age,highest qualification held, hours worked perweek in all jobs, gross annual income, industryof employment) for each of the followingprimary occupations: osteopath, naturopath,herbalist, homoeopath, acupuncturist,traditional Chinese medicine practitioner,massage therapist, general practitioner andother CAM provider.
The next census is scheduledfor 2013
UK Office for NationalStatistics (OFN) Census
2001 The UK census is a self-administeredquestionnaire comprising 44 closed/freetext questions. It is administerednationally to every home in England andWales, every 10 years.In 2001, the UK census achieved aresponse rate of 98%.
- Data for ‘therapists not elsewhere classified’(i.e. acupuncturist, dietician, masseur,orthoptist, osteopath and psychotherapist) arereported in aggregate form and cannot beseparated.- Does not report income or qualification datafor occupation groups.
Detailed occupation data fromthe 2011 census were notavailable as at 30th Sep 2012.

Author's personal copy
Profile of the CAM workforce 367
US
Cens
us
Bure
au
Cens
usof
Popu
lati
on
and
Hou
sing
2000
The
US
cens
us
is
a
self
-adm
inis
tere
dqu
esti
onna
ire,
whi
ch
is
dist
ribu
ted
intw
o
mai
n
form
s.
The
shor
t
form
com
pris
es
7
clos
ed/f
ree
text
ques
tion
s,an
d
is
dist
ribu
ted
to
100%
of
the
US
popu
lati
on.
The
long
form
com
pris
es
53cl
osed
/fre
e
text
ques
tion
s,
and
isdi
stri
bute
d
to
17%
of
the
popu
lati
on.
The
cens
us
is
adm
inis
tere
d
nati
onal
ly
toev
ery
hom
e
in
the
US,
ever
y
10
year
s.In
2001
,
the
US
cens
us
achi
eved
are
spon
se
rate
of
67%.
-
Repo
rts
dem
ogra
phic
data
(i.e
.
gend
er,
age
and
gros
s
annu
al
inco
me)
for
the
follo
win
gpr
imar
y
occu
pati
ons:
chir
opra
ctor
s
and
mas
sage
ther
apis
ts.
-
Dat
a
for
gene
ral p
ract
itio
ners
are
aggr
egat
edw
ith
phys
icia
ns
and
surg
eons
and
cann
ot
bese
para
ted.
-
Dat
a
for
CAM
prac
titi
oner
s
are
aggr
egat
edw
ith
‘oth
er
heal
th
diag
nosi
ng
and
trea
ting
prac
titi
oner
s’
(i.e
.
acup
unct
uris
t,
natu
ropa
th,
hypn
othe
rapi
st)
and
‘oth
er
heal
thca
repr
acti
tion
ers
and
tech
nica
l wor
kers
’
(i.e
.tr
adit
iona
l Chi
nese
herb
alis
t,
podi
atri
st)
and
cann
ot
be
sepa
rate
d.
Det
aile
d
occu
pati
on
data
from
the
2010
cens
us
wer
e
not
publ
icly
avai
labl
e
as
at
30th
Sep
2012
.
with other non-CAM occupations and thus, were not use-ful for occupation-specific workforce planning. Data derivedfrom the UK census were insufficient for the purposes ofCAM workforce planning due to the way data were codedand aggregated; subsequently, all UK data had to be sourcedfrom workforce surveys. Population-level data for the herbalmedicine workforce could not be sourced for any country.
Size of the CAM workforce
The collective CAM workforce was relatively smaller thanthe general practitioner workforce in Australia (19,401 vs.29,920) and New Zealand (3495 vs. 4011) in 2006, but com-paratively larger in the US (189,855 vs. 86,848) in 2000(Table 2). The most prevalent CAM occupation, which hadthe greatest number of providers per head of population,was massage therapy; this was followed by ‘other’ CAM disci-plines and naturopathy in Australia and New Zealand, and bychiropractic and osteopathy in the US. Disciplines in shortestsupply were homoeopathy in Australia, traditional Chinesemedicine in New Zealand, and naturopathy in the US. Apartfrom massage therapy and acupuncture, and chiropractic inAustralia, Canada and the US, provider-population ratios foreach discipline were generally inconsistent across countries.
Gender composition
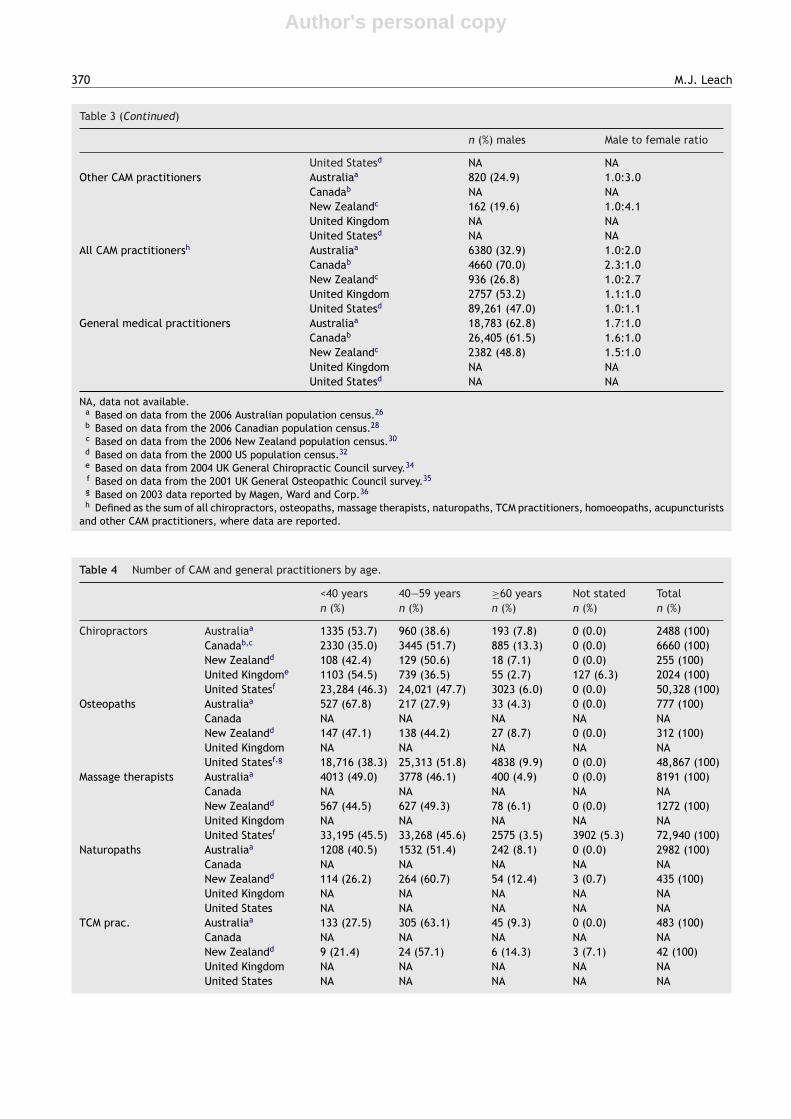
The gender composition of each CAM discipline was largelyconsistent across countries where data were available(Table 3). Chiropractic in all countries but the UK, andosteopathy in the US, were clearly male dominant, with amale to female ratio of at least 2.1 to 1. Traditional Chi-nese medicine was only slightly dominated by males, witha minimum male to female ratio of 1.4 to 1; not dissimi-lar to general practice, where male to female ratios rangedbetween 1.5 and 1.7. Female dominance was particularlyevident for occupations such as massage therapy, natur-opathy and homoeopathy, where there were at least threefemale practitioners to every male. The ratio of males tofemales in osteopathy (in Australia and New Zealand) andacupuncture was almost 1 to 1.
Age distribution
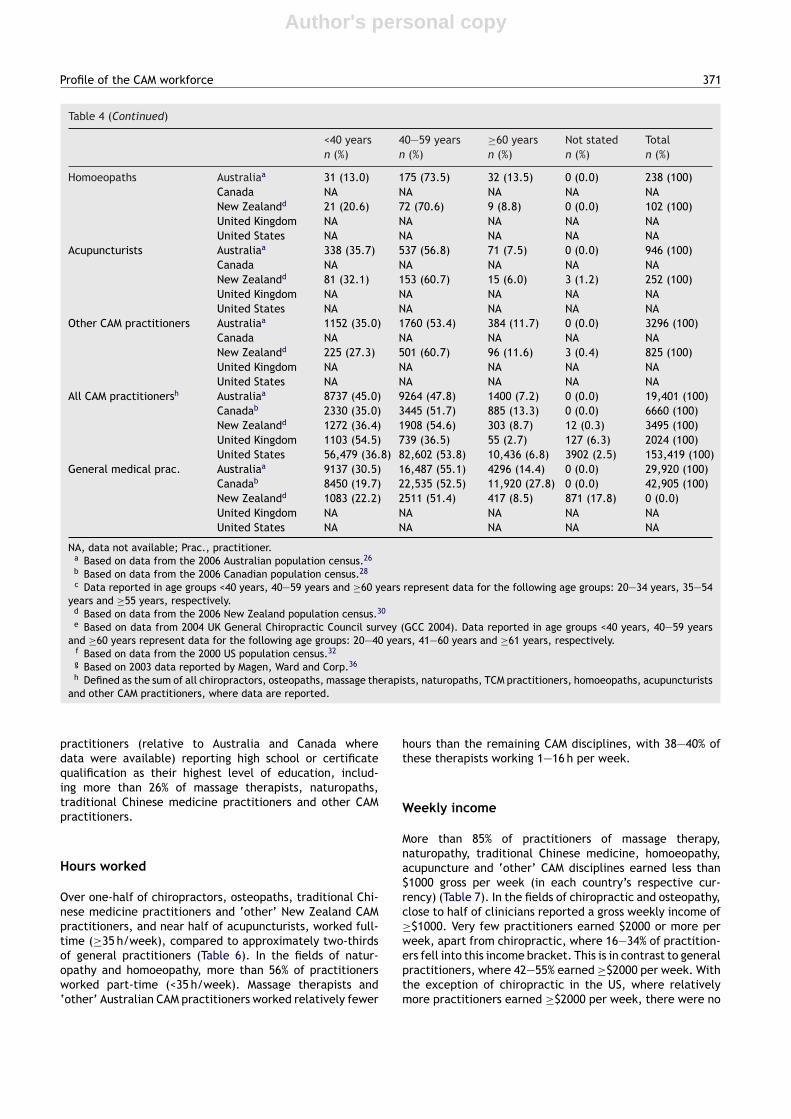
The distribution of practitioners across the three age groups,for each CAM discipline, was similar between countries(Table 4). Across the nine CAM disciplines, 35—55 percentof practitioners were aged under 40 years, and less than 15percent were aged 60 years or older. Approximately two-thirds of practitioners of acupuncture, traditional Chinesemedicine, naturopathy and other CAM disciplines were aged40 years or over; which is comparable to general practice.Homoeopathy was the oldest workforce, with more than 79%of practitioners aged ≥40 years. For massage therapy andchiropractic, the distribution of practitioners aged <40 yearsand ≥40 years was similar. Osteopathy demonstrated vari-able distribution across countries; in Australia, close to 68%of osteopaths were <40 years of age, compared to the US,where around two thirds of clinicians were aged ≥40 years;

Author's personal copy
368 M.J. Leach
for New Zealand, the proportion of practitioners aged <40years and ≥40 years was similar.
Educational attainment
Most practitioners of chiropractic, osteopathy and acupunc-ture held a Bachelor degree or postgraduate degree astheir highest level of education, which was comparableto general practice (Table 5). For traditional Chinesemedicine practitioners, close to half possessed a Bachelor
degree qualification. Massage therapists and other CAMpractitioners reported the lowest level of education, withmost holding a qualification no higher than a Diplomaor Advanced Diploma. Over half of naturopaths held astheir highest qualification a Diploma, Advanced Diplomaor Bachelor degree. Most homoeopathic practitioners alsopossessed a Diploma, Advanced Diploma or Bachelor degreequalification, though proportions did vary across countries,with 53% of New Zealand homoeopaths holding a Bachelordegree, compared to 37% of Australian homoeopaths. Bycontrast, New Zealand had a greater proportion of CAM
Table 2 Number of CAM and general practitioners by country, across all industries of employment.
Population PPR
Chiropractors Australiaa 2488 1:7980Canadab 6660 1:4747New Zealandc 255 1:15,796United Kingdom 2024e 1:29,206United Statesd 50,330 1:5464
Osteopaths Australiaa 777 1:25,554Canadab NA NANew Zealandc 312 1:12,910United Kingdom 3161f 1:18,701United Statesd 48,678g 1:5781
Massage therapists Australiaa 8191 1:2424Canadab NA NANew Zealandc 1272 1:3167United Kingdom NA NAUnited Statesd 72,940 1:3858
Naturopaths Australiaa 2982 1:6658Canadab NA NANew Zealandc 435 1:9260United Kingdom NA NAUnited Statesd 3679h 1:76,494
TCM practitioners Australiaa 483 1:41,108Canadab NA NANew Zealandc 42 1:95,904United Kingdom NA NAUnited Statesd NA NA
Homoeopaths Australiaa 238 1:83,426Canadab NA NANew Zealandc 102 1:39,490United Kingdom NA NAUnited Statesd NA NA
Acupuncturists Australiaa 946 1:20,989Canadab NA NANew Zealandc 252 1:15,984United Kingdom NA NAUnited Statesd 14,228i 1:19,779
Other CAM practitioners Australiaa 3296 1:6024Canadab NA NANew Zealandc 825 1:4882United Kingdom NA NAUnited Statesd NA NA
All CAM practitionersk Australiaa 19,401 1:1023Canadab 6660 1:4747New Zealandc 3495 1:1153United Kingdom 5185 1:11,400United Statesd 189,855 1:1482

Author's personal copy
Profile of the CAM workforce 369
Table 2 (Continued)
Population PPR
General medical practitioner Australiaa 29,920 1:664Canadab 42,605 1:737New Zealandc 4011 1:1004United Kingdom 28,802l 1:2052United Statesd 86,848j 1:3240
NA, data not available; PPR, provider-population ratio.a Based on 2006 Australian population data25 and data from the 2006 Australian population census.26
b Based on 2006 Canadian population data27 and data from the 2006 Canadian population census.28
c Based on 2006 New Zealand population data29 and data from the 2006 New Zealand population census.30
d Based on 2000 US population data31 and data from the 2000 US population census.32
e Based on 2004 UK population data33 and data reported by the 2004 UK General Chiropractic Council.34
f Based on 2001 UK population data33 and data reported by the 2001 UK General Osteopathic Council.35
g Based on 2003 data reported by Magen, Ward and Corp.36
h Based on 2000 data reported by Hough, Dower and O.Neill.23
i Based on 2000 data reported by the US National Acupuncture Foundation.37
j Based on 2000 data reported by Salsberg and Forte.38
k Defined as the sum of all chiropractors, osteopaths, massage therapists, naturopaths, TCM practitioners, homoeopaths, acupuncturistsand other CAM practitioners, where data are reported.
l Based on 2001 data for England only, reported by Office for National Statistics.46
Table 3 Number of CAM and general practitioners by gender.
n (%) males Male to female ratio
Chiropractors Australiaa 1675 (67.3) 2.1:1.0Canadab 4660 (70.0) 2.3:1.0New Zealandc 177 (69.4) 2.3:1.0United Kingdom 1113 (55.0)e 1.2:1.0United Statesd 39,311 (78.1) 3.6:1.0
Osteopaths Australiaa 401 (51.6) 1.1:1.0Canadab NA NANew Zealandc 165 (52.9) 1.1:1.0United Kingdom 1644 (52.0)f 1.1:1.0United Statesd 36,211 (74.0)g 2.9:1.0
Massage therapists Australiaa 2041 (24.9) 1.0:3.0Canadab NA NANew Zealandc 195 (15.3) 1.0:5.5United Kingdom NA NAUnited Statesd 13,739 (18.8) 1.0:4.3
Naturopaths Australiaa 626 (21.0) 1.0:3.8Canadab NA NANew Zealandc 66 (15.2) 1.0:5.6United Kingdom NA NAUnited Statesd NA NA
TCM practitioners Australiaa 284 (58.8) 1.4:1.0Canadab NA NANew Zealandc 24 (57.1) 1.6:1.0United Kingdom NA NAUnited Statesd NA NA
Homoeopaths Australiaa 58 (24.4) 1.0:3.1Canadab NA NANew Zealandc 12 (11.8) 1.0:7.3United Kingdom NA NAUnited Statesd NA NA
Acupuncturists Australiaa 475 (50.2) 1.0:1.0Canadab NA NANew Zealandc 135 (53.6) 1.2:1.0United Kingdom NA NA
Author's personal copy
370 M.J. Leach
Table 3 (Continued)
n (%) males Male to female ratio
United Statesd NA NAOther CAM practitioners Australiaa 820 (24.9) 1.0:3.0
Canadab NA NANew Zealandc 162 (19.6) 1.0:4.1United Kingdom NA NAUnited Statesd NA NA
All CAM practitionersh Australiaa 6380 (32.9) 1.0:2.0Canadab 4660 (70.0) 2.3:1.0New Zealandc 936 (26.8) 1.0:2.7United Kingdom 2757 (53.2) 1.1:1.0United Statesd 89,261 (47.0) 1.0:1.1
General medical practitioners Australiaa 18,783 (62.8) 1.7:1.0Canadab 26,405 (61.5) 1.6:1.0New Zealandc 2382 (48.8) 1.5:1.0United Kingdom NA NAUnited Statesd NA NA
NA, data not available.a Based on data from the 2006 Australian population census.26
b Based on data from the 2006 Canadian population census.28
c Based on data from the 2006 New Zealand population census.30
d Based on data from the 2000 US population census.32
e Based on data from 2004 UK General Chiropractic Council survey.34
f Based on data from the 2001 UK General Osteopathic Council survey.35
g Based on 2003 data reported by Magen, Ward and Corp.36
h Defined as the sum of all chiropractors, osteopaths, massage therapists, naturopaths, TCM practitioners, homoeopaths, acupuncturistsand other CAM practitioners, where data are reported.
Table 4 Number of CAM and general practitioners by age.
<40 years 40—59 years ≥60 years Not stated Totaln (%) n (%) n (%) n (%) n (%)
Chiropractors Australiaa 1335 (53.7) 960 (38.6) 193 (7.8) 0 (0.0) 2488 (100)Canadab,c 2330 (35.0) 3445 (51.7) 885 (13.3) 0 (0.0) 6660 (100)New Zealandd 108 (42.4) 129 (50.6) 18 (7.1) 0 (0.0) 255 (100)United Kingdome 1103 (54.5) 739 (36.5) 55 (2.7) 127 (6.3) 2024 (100)United Statesf 23,284 (46.3) 24,021 (47.7) 3023 (6.0) 0 (0.0) 50,328 (100)
Osteopaths Australiaa 527 (67.8) 217 (27.9) 33 (4.3) 0 (0.0) 777 (100)Canada NA NA NA NA NANew Zealandd 147 (47.1) 138 (44.2) 27 (8.7) 0 (0.0) 312 (100)United Kingdom NA NA NA NA NAUnited Statesf,g 18,716 (38.3) 25,313 (51.8) 4838 (9.9) 0 (0.0) 48,867 (100)
Massage therapists Australiaa 4013 (49.0) 3778 (46.1) 400 (4.9) 0 (0.0) 8191 (100)Canada NA NA NA NA NANew Zealandd 567 (44.5) 627 (49.3) 78 (6.1) 0 (0.0) 1272 (100)United Kingdom NA NA NA NA NAUnited Statesf 33,195 (45.5) 33,268 (45.6) 2575 (3.5) 3902 (5.3) 72,940 (100)
Naturopaths Australiaa 1208 (40.5) 1532 (51.4) 242 (8.1) 0 (0.0) 2982 (100)Canada NA NA NA NA NANew Zealandd 114 (26.2) 264 (60.7) 54 (12.4) 3 (0.7) 435 (100)United Kingdom NA NA NA NA NAUnited States NA NA NA NA NA
TCM prac. Australiaa 133 (27.5) 305 (63.1) 45 (9.3) 0 (0.0) 483 (100)Canada NA NA NA NA NANew Zealandd 9 (21.4) 24 (57.1) 6 (14.3) 3 (7.1) 42 (100)United Kingdom NA NA NA NA NAUnited States NA NA NA NA NA
Author's personal copy
Profile of the CAM workforce 371
Table 4 (Continued)
<40 years 40—59 years ≥60 years Not stated Totaln (%) n (%) n (%) n (%) n (%)
Homoeopaths Australiaa 31 (13.0) 175 (73.5) 32 (13.5) 0 (0.0) 238 (100)Canada NA NA NA NA NANew Zealandd 21 (20.6) 72 (70.6) 9 (8.8) 0 (0.0) 102 (100)United Kingdom NA NA NA NA NAUnited States NA NA NA NA NA
Acupuncturists Australiaa 338 (35.7) 537 (56.8) 71 (7.5) 0 (0.0) 946 (100)Canada NA NA NA NA NANew Zealandd 81 (32.1) 153 (60.7) 15 (6.0) 3 (1.2) 252 (100)United Kingdom NA NA NA NA NAUnited States NA NA NA NA NA
Other CAM practitioners Australiaa 1152 (35.0) 1760 (53.4) 384 (11.7) 0 (0.0) 3296 (100)Canada NA NA NA NA NANew Zealandd 225 (27.3) 501 (60.7) 96 (11.6) 3 (0.4) 825 (100)United Kingdom NA NA NA NA NAUnited States NA NA NA NA NA
All CAM practitionersh Australiaa 8737 (45.0) 9264 (47.8) 1400 (7.2) 0 (0.0) 19,401 (100)Canadab 2330 (35.0) 3445 (51.7) 885 (13.3) 0 (0.0) 6660 (100)New Zealandd 1272 (36.4) 1908 (54.6) 303 (8.7) 12 (0.3) 3495 (100)United Kingdom 1103 (54.5) 739 (36.5) 55 (2.7) 127 (6.3) 2024 (100)United States 56,479 (36.8) 82,602 (53.8) 10,436 (6.8) 3902 (2.5) 153,419 (100)
General medical prac. Australiaa 9137 (30.5) 16,487 (55.1) 4296 (14.4) 0 (0.0) 29,920 (100)Canadab 8450 (19.7) 22,535 (52.5) 11,920 (27.8) 0 (0.0) 42,905 (100)New Zealandd 1083 (22.2) 2511 (51.4) 417 (8.5) 871 (17.8) 0 (0.0)United Kingdom NA NA NA NA NAUnited States NA NA NA NA NA
NA, data not available; Prac., practitioner.a Based on data from the 2006 Australian population census.26
b Based on data from the 2006 Canadian population census.28
c Data reported in age groups <40 years, 40—59 years and ≥60 years represent data for the following age groups: 20—34 years, 35—54years and ≥55 years, respectively.
d Based on data from the 2006 New Zealand population census.30
e Based on data from 2004 UK General Chiropractic Council survey (GCC 2004). Data reported in age groups <40 years, 40—59 yearsand ≥60 years represent data for the following age groups: 20—40 years, 41—60 years and ≥61 years, respectively.
f Based on data from the 2000 US population census.32
g Based on 2003 data reported by Magen, Ward and Corp.36
h Defined as the sum of all chiropractors, osteopaths, massage therapists, naturopaths, TCM practitioners, homoeopaths, acupuncturistsand other CAM practitioners, where data are reported.
practitioners (relative to Australia and Canada wheredata were available) reporting high school or certificatequalification as their highest level of education, includ-ing more than 26% of massage therapists, naturopaths,traditional Chinese medicine practitioners and other CAMpractitioners.
Hours worked
Over one-half of chiropractors, osteopaths, traditional Chi-nese medicine practitioners and ‘other’ New Zealand CAMpractitioners, and near half of acupuncturists, worked full-time (≥35 h/week), compared to approximately two-thirdsof general practitioners (Table 6). In the fields of natur-opathy and homoeopathy, more than 56% of practitionersworked part-time (<35 h/week). Massage therapists and‘other’ Australian CAM practitioners worked relatively fewer
hours than the remaining CAM disciplines, with 38—40% ofthese therapists working 1—16 h per week.
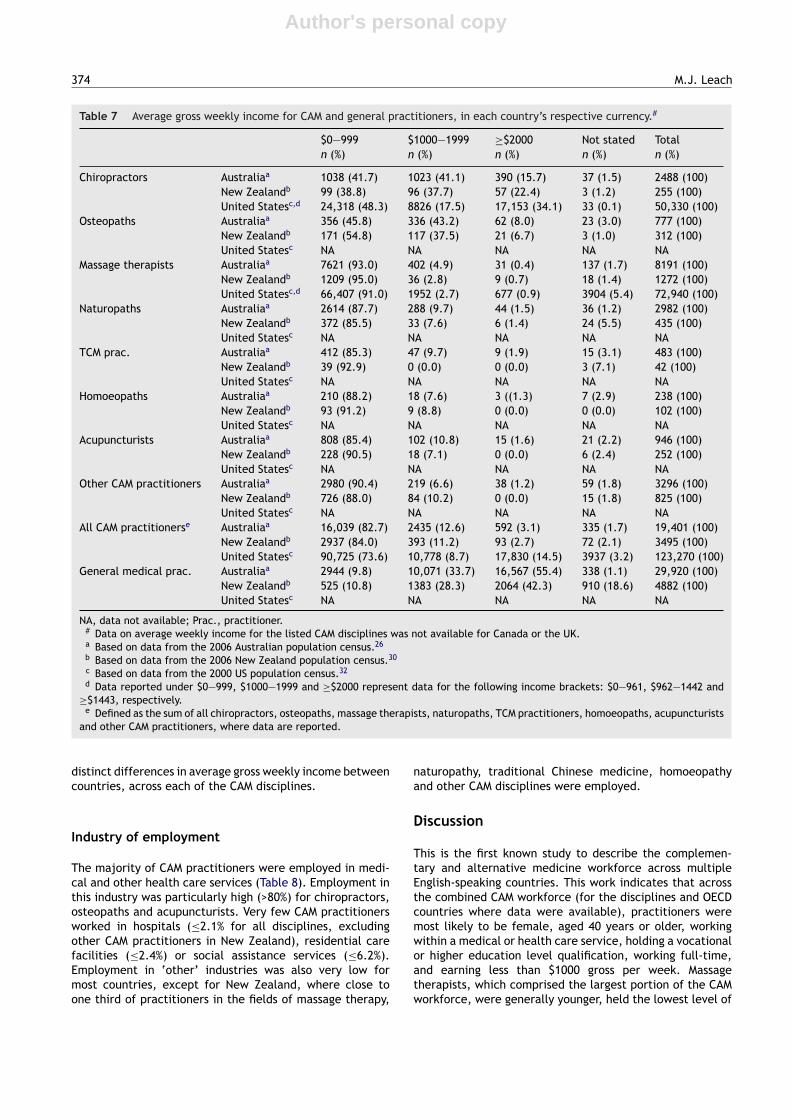
Weekly income
More than 85% of practitioners of massage therapy,naturopathy, traditional Chinese medicine, homoeopathy,acupuncture and ‘other’ CAM disciplines earned less than$1000 gross per week (in each country’s respective cur-rency) (Table 7). In the fields of chiropractic and osteopathy,close to half of clinicians reported a gross weekly income of≥$1000. Very few practitioners earned $2000 or more perweek, apart from chiropractic, where 16—34% of practition-ers fell into this income bracket. This is in contrast to generalpractitioners, where 42—55% earned ≥$2000 per week. Withthe exception of chiropractic in the US, where relativelymore practitioners earned ≥$2000 per week, there were no

Author's personal copy372
M.J.
Leach
Table 5 Highest level of education attained for CAM and general practitioners.#
High school orcertificate
Diploma oradvanceddiploma
Bachelor degree Graduatediploma orcertificate
Postgrad.degree
No qualif. ornot stated
Total
n (%) n (%) n (%) n (%) n (%) n (%) n (%)
Chiropractors Australiaa 66 (2.6) 119 (4.8) 1129 (45.4) 61 (2.5) 1023 (41.1) 90 (3.6) 2488 (100)Canadab 65 (1.0) 470 (7.1) 2835 (42.6) 960 (14.4) 2320 (34.8) 10 (0.2) 6660 (100)New Zealandc 9 (3.6) 3 (1.2) 180 (70.6) 60 (23.5) 3 (1.2) 255 (100)
Osteopaths Australiaa 9 (1.2) 89 (11.5) 304 (39.1) 15 (1.9) 340 (43.8) 20 (2.6) 777 (100)Canadab NA NA NA NA NA NA NANew Zealandc 21 (6.7) 99 (31.7) 81 (26.0) 108 (34.6) 3 (1.0) 312 (100)
Massage therapists Australiaa 2261 (27.6) 4030 (49.2) 1075 (13.1) 109 (1.3) 101 (1.2) 615 (7.5) 8191 (100)Canadab NA NA NA NA NA NA NANew Zealandc 489 (38.4) 459 (36.1) 171 (13.4) 45 (3.5) 108 (8.5) 1272 (100)
Naturopaths Australiaa 300 (10.1) 1272 (42.7) 1042 (34.9) 72 (2.4) 80 (2.7) 216 (7.2) 2982 (100)Canadab NA NA NA NA NA NA NANew Zealandc 114 (26.2) 162 (37.2) 99 (22.8) 30 (6.9) 30 (6.9) 435 (100)
TCM prac. Australiaa 43 (8.9) 77 (15.9) 234 (48.4) 7 (1.5) 80 (16.6) 42 (8.7) 483 (100)Canadab NA NA NA NA NA NA NANew Zealandc 15 (35.7) 3 (7.1) 21 (50.0) 0 (0.0) 3 (7.1) 42 (100)
Homoeopaths Australiaa 0 (0.0) 123 (51.7) 88 (37.0) 3 (1.3) 12 (5.0) 12 (5.0) 238 (100)Canadab NA NA NA NA NA NA NANew Zealandc 6 (5.8) 24 (23.5) 54 (52.9) 15 (14.7) 3 (2.9) 102 (100)
Acupuncturists Australiaa 31 (3.2) 208 (22.0) 506 (53.5) 15 (1.6) 129 (13.6) 57 (6.0) 946 (100)Canadab NA NA NA NA NA NA NANew Zealandc 42 (16.7) 15 (6.0) 147 (58.3) 36 (14.3) 12 (4.8) 252 (100)
Other CAM practitioners Australiaa 1027 (31.2) 1031 (31.3) 605 (18.4) 162 (4.9) 142 (4.3) 329 (9.9) 3296 (100)Canadab NA NA NA NA NA NA NANew Zealandc 288 (34.9) 228 (27.6) 168 (20.4) 81 (9.8) 60 (7.3) 825 (100)
All CAM practitionersd Australiaa 1476 (8.6) 6949 (40.5) 4983 (29.1) 444 (2.6) 1907 (11.1) 1381 (8.1) 19,401 (100)Canadab 65 (1.0) 470 (7.1) 2835 (42.6) 960 (14.4) 2320 (34.8) 10 (0.2) 6660 (100)New Zealandc 984 (28.2) 993 (28.4) 921 (26.4) 375 (10.7) 222 (6.4) 3495 (100)
General medical prac. Australiaa 305 (1.1) 125 (0.4) 21,585 (72.1) 580 (1.9) 5818 (19.4) 1507 (5.0) 29,920 (100)Canadab 80 (0.2) 315 (0.7) 34,800 (81.1) 190 (0.4) 7480 (17.4) 40 (0.1) 42,905 (100)New Zealandc 96 (2.0) 27 (0.6) 1287 (26.4) 2598 (53.2) 874 (17.9) 4882 (100)
NA, data not available; Prac., practitioner.# Highest level of education data for the listed CAM disciplines was not available for the US or UK.a Based on data from the 2006 Australian population census.26
b Based on data from the 2006 Canadian population census.28
c Based on data from the 2006 New Zealand population census.30
d Defined as the sum of all chiropractors, osteopaths, massage therapists, naturopaths, TCM practitioners, homoeopaths, acupuncturists and other CAM practitioners, where data arereported.

Author's personal copyProfile
of
the
CAM
workforce
373
Table 6 Number of hours worked per week by CAM and general practitioners.#
0 h 1—16 h 17—34 h ≥35 h Not stated Totaln (%) n (%) n (%) n (%) n (%) n (%)
Chiropractors Australiaa 62 (2.5) 246 (9.9) 787 (31.6) 1354 (54.4) 39 (1.6) 2488 (100)Canadab,d 160 (2.4) 420 (6.3) 2710 (40.7) 3340 (50.2) 30 (0.5) 6660 (100)New Zealandc 0 (0.0) 9 (3.5) 78 (30.6) 156 (61.2) 12 (4.7) 255 (100)
Osteopaths Australiaa 28 (3.6) 90 (11.6) 188 (24.2) 453 (58.3) 18 (2.3) 777 (100)Canadab NA NA NA NA NA NANew Zealandc 0 (0.0) 33 (10.6) 90 (28.9) 174 (55.8) 15 (4.8) 312 (100)
Massage therapists Australiaa 309 (3.8) 3102 (37.9) 2660 (32.5) 1932 (23.6) 188 (2.3) 8191 (100)Canadab NA NA NA NA NA NANew Zealandc 0 (0.0) 486 (38.2) 405 (31.8) 315 (24.8) 66 (5.2) 1272 (100)
Naturopaths Australiaa 100 (3.4) 737 (24.7) 946 (31.7) 1134 (38.0) 65 (2.2) 2982 (100)Canadab NA NA NA NA NA NANew Zealandc 0 (0.0) 114 (26.2) 141 (32.4) 156 (35.9) 24 (5.5) 435 (100)
TCM prac. Australiaa 14 (2.9) 61 (12.6) 123 (25.5) 274 (56.7) 11 (2.3) 483 (100)Canadab NA NA NA NA NA NANew Zealandc 0 (0.0) 9 (21.4) 6 (14.3) 24 (57.1) 3 (7.1) 42 (100)
Homoeopaths Australiaa 12 (5.0) 83 (34.9) 79 (33.2) 54 (22.7) 10 (4.2) 238 (100)Canadab NA NA NA NA NA NANew Zealandc 0 (0.0) 30 (29.4) 33 (32.4) 39 (38.2) 0 (0.0) 102 (100)
Acupuncturists Australiaa 17 (1.8) 167 (17.7) 290 (30.7) 458 (48.4) 14 (1.5) 946 (100)Canadab NA NA NA NA NA NANew Zealandc 0 (0.0) 39 (15.5) 69 (27.4) 129 ((51.2) 15 (6.0) 252 (100)
Other CAM practitioners Australiaa 151 (4.6) 1320 (40.0) 898 ((27.2) 836 (25.4) 91 (2.8) 3296 (100)Canadab NA NA NA NA NA NANew Zealandc 0 (0.0) 147 (17.8) 204 (24.7) 444 (53.8) 30 ((3.6) 825 (100)
All CAM practitionerse Australiaa 693 (3.6) 5806 (29.9) 5971 (30.8) 6495 (33.5) 436 (2.3) 19,401 (100)Canadab 160 (2.4) 420 (6.3) 2710 (40.7) 3340 (50.2) 30 (0.5) 6660 (100)New Zealandc 0 (0.0) 867 (24.8) 1026 (29.4) 1437 (41.1) 165 (4.7) 3495 (100)
General medical prac. Australiaa 1100 (3.7) 1871 (6.3) 5222 (17.5) 21,300 (71.2) 427 (1.4) 29,920 (100)Canadab,d 1475 (3.4) 1675 (3.9) 7305 (17.0) 32,080 (74.8) 370 (0.9) 42,905 (100)New Zealandc 0 (0.0) 240 (4.9) 756 (15.5) 2805 (57.5) 1081 (22.1) 4882 (100)
NA, data not available; Prac., practitioner.# Data on number of hours worked for the listed CAM disciplines was not available for the US or UK.a Based on data from the 2006 Australian population census.26
b Based on data from the 2006 Canadian population census.28
c Based on data from the 2006 New Zealand population census.30
d Data reported under 1—16 h, 17—34 h and ≥35 h represent data for the following groups: 1—19 h, 20—39 h and ≥40 h, respectively.e Defined as the sum of all chiropractors, osteopaths, massage therapists, naturopaths, TCM practitioners, homoeopaths, acupuncturists and other CAM practitioners, where data are
reported.
Author's personal copy
374 M.J. Leach
Table 7 Average gross weekly income for CAM and general practitioners, in each country’s respective currency.#
$0—999 $1000—1999 ≥$2000 Not stated Totaln (%) n (%) n (%) n (%) n (%)
Chiropractors Australiaa 1038 (41.7) 1023 (41.1) 390 (15.7) 37 (1.5) 2488 (100)New Zealandb 99 (38.8) 96 (37.7) 57 (22.4) 3 (1.2) 255 (100)United Statesc,d 24,318 (48.3) 8826 (17.5) 17,153 (34.1) 33 (0.1) 50,330 (100)
Osteopaths Australiaa 356 (45.8) 336 (43.2) 62 (8.0) 23 (3.0) 777 (100)New Zealandb 171 (54.8) 117 (37.5) 21 (6.7) 3 (1.0) 312 (100)United Statesc NA NA NA NA NA
Massage therapists Australiaa 7621 (93.0) 402 (4.9) 31 (0.4) 137 (1.7) 8191 (100)New Zealandb 1209 (95.0) 36 (2.8) 9 (0.7) 18 (1.4) 1272 (100)United Statesc,d 66,407 (91.0) 1952 (2.7) 677 (0.9) 3904 (5.4) 72,940 (100)
Naturopaths Australiaa 2614 (87.7) 288 (9.7) 44 (1.5) 36 (1.2) 2982 (100)New Zealandb 372 (85.5) 33 (7.6) 6 (1.4) 24 (5.5) 435 (100)United Statesc NA NA NA NA NA
TCM prac. Australiaa 412 (85.3) 47 (9.7) 9 (1.9) 15 (3.1) 483 (100)New Zealandb 39 (92.9) 0 (0.0) 0 (0.0) 3 (7.1) 42 (100)United Statesc NA NA NA NA NA
Homoeopaths Australiaa 210 (88.2) 18 (7.6) 3 ((1.3) 7 (2.9) 238 (100)New Zealandb 93 (91.2) 9 (8.8) 0 (0.0) 0 (0.0) 102 (100)United Statesc NA NA NA NA NA
Acupuncturists Australiaa 808 (85.4) 102 (10.8) 15 (1.6) 21 (2.2) 946 (100)New Zealandb 228 (90.5) 18 (7.1) 0 (0.0) 6 (2.4) 252 (100)United Statesc NA NA NA NA NA
Other CAM practitioners Australiaa 2980 (90.4) 219 (6.6) 38 (1.2) 59 (1.8) 3296 (100)New Zealandb 726 (88.0) 84 (10.2) 0 (0.0) 15 (1.8) 825 (100)United Statesc NA NA NA NA NA
All CAM practitionerse Australiaa 16,039 (82.7) 2435 (12.6) 592 (3.1) 335 (1.7) 19,401 (100)New Zealandb 2937 (84.0) 393 (11.2) 93 (2.7) 72 (2.1) 3495 (100)United Statesc 90,725 (73.6) 10,778 (8.7) 17,830 (14.5) 3937 (3.2) 123,270 (100)
General medical prac. Australiaa 2944 (9.8) 10,071 (33.7) 16,567 (55.4) 338 (1.1) 29,920 (100)New Zealandb 525 (10.8) 1383 (28.3) 2064 (42.3) 910 (18.6) 4882 (100)United Statesc NA NA NA NA NA
NA, data not available; Prac., practitioner.# Data on average weekly income for the listed CAM disciplines was not available for Canada or the UK.a Based on data from the 2006 Australian population census.26
b Based on data from the 2006 New Zealand population census.30
c Based on data from the 2000 US population census.32
d Data reported under $0—999, $1000—1999 and ≥$2000 represent data for the following income brackets: $0—961, $962—1442 and≥$1443, respectively.
e Defined as the sum of all chiropractors, osteopaths, massage therapists, naturopaths, TCM practitioners, homoeopaths, acupuncturistsand other CAM practitioners, where data are reported.
distinct differences in average gross weekly income betweencountries, across each of the CAM disciplines.
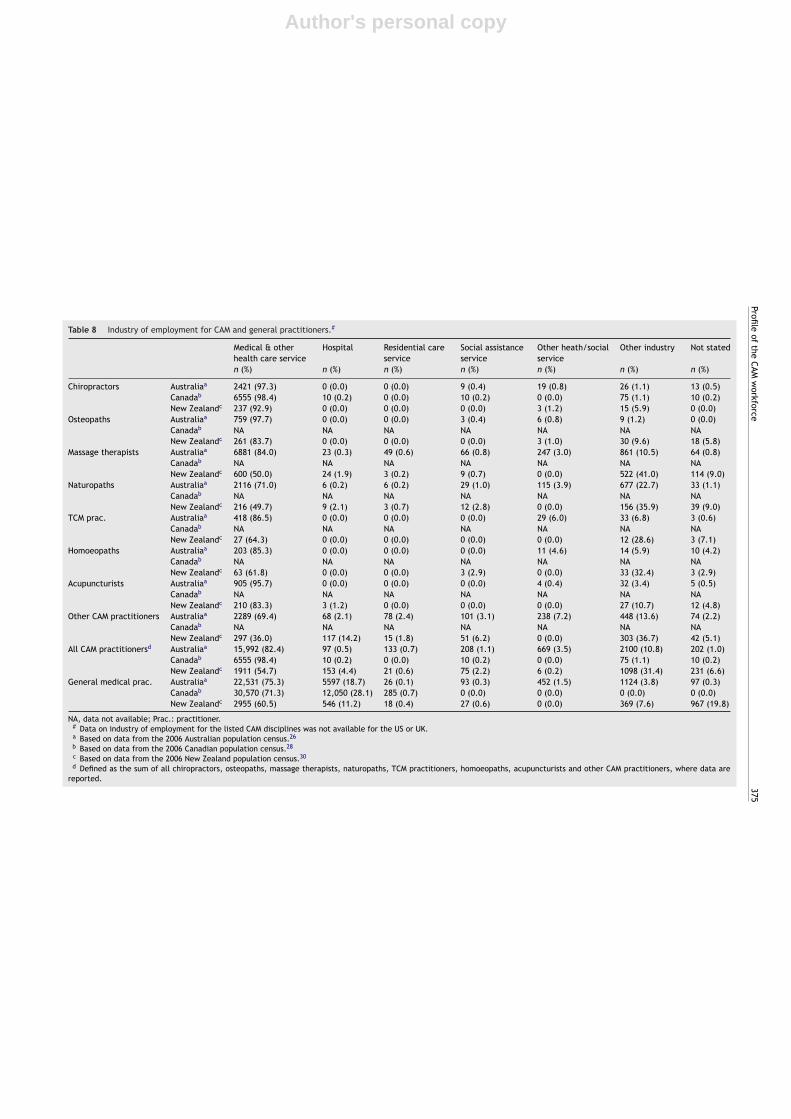
Industry of employment
The majority of CAM practitioners were employed in medi-cal and other health care services (Table 8). Employment inthis industry was particularly high (>80%) for chiropractors,osteopaths and acupuncturists. Very few CAM practitionersworked in hospitals (≤2.1% for all disciplines, excludingother CAM practitioners in New Zealand), residential carefacilities (≤2.4%) or social assistance services (≤6.2%).Employment in ‘other’ industries was also very low formost countries, except for New Zealand, where close toone third of practitioners in the fields of massage therapy,
naturopathy, traditional Chinese medicine, homoeopathyand other CAM disciplines were employed.
Discussion
This is the first known study to describe the complemen-tary and alternative medicine workforce across multipleEnglish-speaking countries. This work indicates that acrossthe combined CAM workforce (for the disciplines and OECDcountries where data were available), practitioners weremost likely to be female, aged 40 years or older, workingwithin a medical or health care service, holding a vocationalor higher education level qualification, working full-time,and earning less than $1000 gross per week. Massagetherapists, which comprised the largest portion of the CAMworkforce, were generally younger, held the lowest level of
Author's personal copyProfile
of
the
CAM
workforce
375
Table 8 Industry of employment for CAM and general practitioners.#
Medical & otherhealth care service
Hospital Residential careservice
Social assistanceservice
Other heath/socialservice
Other industry Not stated
n (%) n (%) n (%) n (%) n (%) n (%) n (%)
Chiropractors Australiaa 2421 (97.3) 0 (0.0) 0 (0.0) 9 (0.4) 19 (0.8) 26 (1.1) 13 (0.5)Canadab 6555 (98.4) 10 (0.2) 0 (0.0) 10 (0.2) 0 (0.0) 75 (1.1) 10 (0.2)New Zealandc 237 (92.9) 0 (0.0) 0 (0.0) 0 (0.0) 3 (1.2) 15 (5.9) 0 (0.0)
Osteopaths Australiaa 759 (97.7) 0 (0.0) 0 (0.0) 3 (0.4) 6 (0.8) 9 (1.2) 0 (0.0)Canadab NA NA NA NA NA NA NANew Zealandc 261 (83.7) 0 (0.0) 0 (0.0) 0 (0.0) 3 (1.0) 30 (9.6) 18 (5.8)
Massage therapists Australiaa 6881 (84.0) 23 (0.3) 49 (0.6) 66 (0.8) 247 (3.0) 861 (10.5) 64 (0.8)Canadab NA NA NA NA NA NA NANew Zealandc 600 (50.0) 24 (1.9) 3 (0.2) 9 (0.7) 0 (0.0) 522 (41.0) 114 (9.0)
Naturopaths Australiaa 2116 (71.0) 6 (0.2) 6 (0.2) 29 (1.0) 115 (3.9) 677 (22.7) 33 (1.1)Canadab NA NA NA NA NA NA NANew Zealandc 216 (49.7) 9 (2.1) 3 (0.7) 12 (2.8) 0 (0.0) 156 (35.9) 39 (9.0)
TCM prac. Australiaa 418 (86.5) 0 (0.0) 0 (0.0) 0 (0.0) 29 (6.0) 33 (6.8) 3 (0.6)Canadab NA NA NA NA NA NA NANew Zealandc 27 (64.3) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 12 (28.6) 3 (7.1)
Homoeopaths Australiaa 203 (85.3) 0 (0.0) 0 (0.0) 0 (0.0) 11 (4.6) 14 (5.9) 10 (4.2)Canadab NA NA NA NA NA NA NANew Zealandc 63 (61.8) 0 (0.0) 0 (0.0) 3 (2.9) 0 (0.0) 33 (32.4) 3 (2.9)
Acupuncturists Australiaa 905 (95.7) 0 (0.0) 0 (0.0) 0 (0.0) 4 (0.4) 32 (3.4) 5 (0.5)Canadab NA NA NA NA NA NA NANew Zealandc 210 (83.3) 3 (1.2) 0 (0.0) 0 (0.0) 0 (0.0) 27 (10.7) 12 (4.8)
Other CAM practitioners Australiaa 2289 (69.4) 68 (2.1) 78 (2.4) 101 (3.1) 238 (7.2) 448 (13.6) 74 (2.2)Canadab NA NA NA NA NA NA NANew Zealandc 297 (36.0) 117 (14.2) 15 (1.8) 51 (6.2) 0 (0.0) 303 (36.7) 42 (5.1)
All CAM practitionersd Australiaa 15,992 (82.4) 97 (0.5) 133 (0.7) 208 (1.1) 669 (3.5) 2100 (10.8) 202 (1.0)Canadab 6555 (98.4) 10 (0.2) 0 (0.0) 10 (0.2) 0 (0.0) 75 (1.1) 10 (0.2)New Zealandc 1911 (54.7) 153 (4.4) 21 (0.6) 75 (2.2) 6 (0.2) 1098 (31.4) 231 (6.6)
General medical prac. Australiaa 22,531 (75.3) 5597 (18.7) 26 (0.1) 93 (0.3) 452 (1.5) 1124 (3.8) 97 (0.3)Canadab 30,570 (71.3) 12,050 (28.1) 285 (0.7) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)New Zealandc 2955 (60.5) 546 (11.2) 18 (0.4) 27 (0.6) 0 (0.0) 369 (7.6) 967 (19.8)
NA, data not available; Prac.: practitioner.# Data on industry of employment for the listed CAM disciplines was not available for the US or UK.a Based on data from the 2006 Australian population census.26
b Based on data from the 2006 Canadian population census.28
c Based on data from the 2006 New Zealand population census.30
d Defined as the sum of all chiropractors, osteopaths, massage therapists, naturopaths, TCM practitioners, homoeopaths, acupuncturists and other CAM practitioners, where data arereported.

Author's personal copy
376 M.J. Leach
education, worked the least number of hours and earnedthe lowest income relative to other disciplines. By contrast,chiropractors and osteopaths held the highest level of edu-cation, worked the longest hours and earned the highestincome, compared with most other CAM disciplines.
The CAM workforce collectively contained a high propor-tion of female practitioners relative to male practitioners(i.e. 54% vs. 46%). This is not dissimilar to the patternobserved within the mainstream health workforce acrossfour of the five included countries, where more thanseventy-one percent of practitioners were female.25,28,29,32
The proportion of females in female-dominant occupations(i.e. >60% female) was also similar between the CAM andmainstream health workforce (at least in Australia and NewZealand). For instance, for the female-dominant disciplinesof massage therapy, naturopathy and homoeopathy, morethan seventy-nine percent of practitioners were female;likewise, across the female-dominant professions of nurs-ing, physiotherapy, dietetics, social work, speech therapyand occupational therapy, more than 80% of clinicians werefemale.39 For the fields of chiropractic, osteopathy, TCM andacupuncture, which collectively comprise seventy-four per-cent male practitioners, this was similar to the fields ofdentistry, optometry and general practice, where approx-imately 58% of practitioners were male.25 Further researchmay help in understanding the reasons for these gender dif-ferences across CAM disciplines.
Many fields of CAM, such as acupuncture, naturopathy,TCM and homoeopathy, were characterised by an olderworkforce. This is consistent with the age profile of manymainstream health occupations, namely dentistry, nursingand general practice.25,28,29,32 Several factors may explainthe older age profile of these CAM disciplines: it is proba-ble that the older age profile reflects the high number ofmature-age students entering CAM courses or programs40;it also may be indicative of high rates of retention inthese disciplines.39 These same factors may also explainthe relatively younger age profile of massage therapistsand chiropractors across the selected countries, as well asosteopaths in Australia. It is difficult to determine how thisolder workforce and/or potentially low retention rates willimpact on the future supply of CAM practitioners withoutfirst understanding CAM workforce demand; unfortunately,this work has yet to be done.
Three occupations (i.e. chiropractic, osteopathy andacupuncture) demonstrated a higher level of education rel-ative to other CAM disciplines. This may be because eachof these occupations are statutory regulated (includingacupuncture and TCM in Australia), and as such, minimumtraining requirements for board certification or registrationare clearly stipulated. On the other hand, no assurance canbe given that these qualifications are related to these CAMdiscipline areas; it is possible that the high levels of educa-tion could, in some cases, be related to other fields or prioroccupations.
For most of the other CAM occupations, the highest qual-ification held was a Diploma or Advanced Diploma (withthe exception of homoeopathy in New Zealand, for whichmost practitioners held a Bachelor degree). Several rea-sons can be given for the relatively lower education levelof these disciplines. First, neither of these occupations isstatutory regulated (at least in Australia and New Zealand
where data were available). Second, membership of perti-nent Australian/New Zealand CAM professional associationsonly requires a Diploma/Advanced Diploma as a minimumtraining requirement. Third, Bachelor degrees for many ofthese disciplines have only emerged recently.41 Given thatthese conditions are likely to vary across countries, it isprobable that the highest qualifications held by CAM practi-tioners in other countries will vary. It also infers that changesin the regulation of CAM disciplines (i.e. introduction oflicensing or statutory regulation) may drive improvementsin the education level of practitioners.
Most CAM practitioners in Australia, Canada and NewZealand had worked full-time (≥35 h a week) in the yearof the population census (i.e. 2006). The disciplines thatlargely comprised a part-time workforce, such as natur-opathy, homoeopathy and massage therapy, were alsofemale-dominant occupations. This is not surprising asfemale practitioners work on average fewer hours per weekthan their male counterparts; one reason being to care foryounger children.42,43 The older age profile of naturopa-thy and homoeopathy also may have contributed to thehigher proportion of practitioners working part-time in thesefields.42 The association between increasing female partici-pation in the workforce, an ageing workforce, and the risingnumber of medical practitioners working part-time, lendssupport to these assertions.42
Much of the CAM workforce earned less than $1000gross per week. Practitioners earning equal to or greaterthan $1000 per week (i.e. chiropractors and osteopaths)were typically in male-dominant occupations, held a higher-education qualification, and worked full-time. While each ofthese factors is likely to contribute to the higher weeklyincome of these disciplines, another consideration is theduration of the patient consultation. Relative to other CAMdisciplines (e.g. naturopathy, herbalism, acupuncture andmassage therapy), which typically provide consultations of40—60 min duration,10,44 chiropractic and osteopathic con-sultations are generally of shorter length, often less than20 min duration; similar to Western physicians.44 This poten-tially allows for greater patient throughput, and hence,higher turnover.
Complementary and alternative medicine services inAustralia and New Zealand, and possibly Canada, werelargely delivered through primary care settings. Very fewservices were provided through secondary or tertiary healthcare settings, such as hospitals and residential care facili-ties. Given that patients attending CAM services are in manycases self-referred,10,44 CAM practitioners may be for manyconsumers the first point of contact with the health care sys-tem, and in such cases, may be the patient’s primary careprovider. There are concerns, however, that the low levelof education of some practitioners, as well as the absenceof appropriate regulatory and quality standards for practicefor some CAM disciplines,45 could mean that some clini-cians may not have the necessary competencies to deliverappropriate and effective primary care. Tighter regulationof several CAM disciplines, including the stipulation of min-imum training requirements, may help to safeguard thoseconsumers who choose to use CAM practitioners as primarycare providers.
While this work has provided some insights into thebroader CAM workforce, it has highlighted two major issues

Author's personal copy
Profile of the CAM workforce 377
with using census data for the assessment of CAM workforcesupply, and more generally, health workforce planning. Thefirst issue is that few data sources provide comprehensivelow-level data on the characteristics of the CAM workforce,with the exception of the Australian Bureau of Statistics Cen-sus of Population and Housing and Statistics New ZealandCensus of Population and Dwellings. As illustrated in Table 1,most sources only capture limited data on age, gender andincome, with few reporting on hours worked, highest quali-fication held, and industry of employment.
The second issue relates to the paucity of data foreach distinct discipline area, particularly herbalism. Thismay be attributed in part to the way CAM disciplines arecategorised, with each country utilising different occupa-tional classification systems to code occupations; despiteeach census questionnaire recording occupation in free-textform. As a result, many data sources had grouped distinctCAM disciplines (e.g. herbalists) with often unrelated occu-pations (e.g. podiatry); such data is unlikely to be of anyuse to either discipline. Similarly, many data providers col-lapsed data from multiple CAM occupations into broader,often meaningless categories (e.g. other healthcare practi-tioners), which has little value in health workforce planning.
Even though census data from each of the selectedcountries is trustworthy, reliable and highly representativeof each nation’s population, the data quality issues afore-mentioned limit the conclusions that can be made aboutthe CAM workforce across these countries. Furthermore,because much of the US and UK data were derived fromsources other than the census, it is possible that method-ological differences between data sources could contributein part to the differences observed between countries.
These data quality issues draw attention to the need formore comprehensive data on the CAM workforce, includ-ing specific details on each distinct CAM discipline. Furtherexploration of the CAM workforce beyond the five selectedcountries is also recommended, as distinct cultural, polit-ical and social differences between countries are likely tohave a notable impact on the profile of the CAM workforce.Many of these issues could be addressed through the imple-mentation of a comprehensive CAM workforce survey, or byrevising the way CAM disciplines are coded and reported inpopulation censuses. This work is a call for that research.
Conclusion
This work has broadened understanding of the CAM work-force across Australia, Canada, New Zealand, UnitedKingdom and United States. One insight gained from thiswork was the notable differences between disciplines inincome, hours worked and education level. Whilst differ-ences in the former may be attributed to the gender profileof the discipline and the duration of the patient consul-tation, the latter is expected to be driven by disparateregulatory and training requirements across disciplines. Theimplementation of tighter regulation is one strategy thatmay help to raise the education level of many CAM practi-tioners, and in so doing, ensure the provision of a competentCAM workforce to service the needs of consumers; it mayalso serve to safeguard consumers who use CAM practitionersas primary care providers. Although the quality of available
data somewhat limits the conclusions that can be made, itdoes emphasise the need for better quality data on the CAMworkforce, including the provision of comprehensive data oneach distinct CAM discipline; it also highlights the need forgreater understanding of CAM workforce demand in order tobetter inform the training and continuing education needsof the evolving CAM workforce.
Conflict of interest statement
None declared.
References
1. Leach MJ. Public, nurse and medical practitioner attitude andpractice of natural medicine. Complementary Therapies inNursing and Midwifery 2004;10:13—21.
2. MacLennan AH, Myers SP, Taylor AW. The continuing use ofcomplementary and alternative medicine in South Australia:costs and beliefs in 2004. Medical Journal of Australia2006;184:27—31.
3. Xue CCL, Zhang AL, Lin PHV, Da Costa C, Story DF. Comple-mentary and alternative medicine use in Australia: a nationalpopulation-based survey. Journal of Alternative and Comple-mentary Medicine 2007;13:643—50.
4. Quan H, Lai D, Johnson D, Verhoef M, Musto R. Complemen-tary and alternative medicine use among Chinese and whiteCanadians. Canadian Family Physician 2008;54:1563—9.
5. Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complemen-tary and alternative medicine use among adults: United States,2002. Seminars in Integrative Medicine 2004;2:54—71.
6. Lim MK, Sadarangani P, Chan HL, Heng JY. Complementary andalternative medicine use in multiracial Singapore. Complemen-tary Therapies in Medicine 2005;13:16—24.
7. Hori S, Mihaylov I, Vasconcelos JC, McCoubrie M. Patterns ofcomplementary and alternative medicine use amongst outpa-tients in Tokyo, Japan. BMC Complementary and AlternativeMedicine 2008;8:14—23.
8. Metcalfe A, Williams J, McChesney J, Patten SB, Jette N. Useof complementary and alternative medicine by those with achronic disease and the general population — results of anational population based survey. BMC Complementary andAlternative Medicine 2010;10:58.
9. Su D, Li L. Trends in the use of complementary and alternativemedicine in the United States: 2002—2007. Journal of HealthCare for the Poor and Underserved 2011;22:296—310.
10. Hunt KJ, Coelho HF, Wider B, Perry R, Hung SK, Terry R,et al. Complementary and alternative medicine use in England:results from a national survey. International Journal of ClinicalPractice 2010;64:1496—502.
11. Lin V, Bensoussan A, Myers S, McCabe P, Cohen M, Hill S, et al.The practice and regulatory requirements of naturopathy andwestern herbal medicine. Melbourne: State of Victoria Depart-ment of Human Services; 2006.
12. Hurwitz EL, Chiang LM. A comparative analysis of chiroprac-tic and general practitioner patients in North America: findingsfrom the joint Canada/United States survey of health, 2002—03.BMC Health Services Research 2006;6:49.
13. Knox SA, Harrison CM, Britt HC, Henderson JV. Estimating preva-lence of common chronic morbidities in Australia. MedicalJournal of Australia 2008;189:66—70.
14. Nahin RL, Barnes PM, Shussman BJ, Bloom B. Costs if comple-mentary and alternative medicine (CAM) and frequency of visitsto CAM practitioners: United States, 2007. National Health
Author's personal copy
378 M.J. Leach
Statistics Reports, No. 18. Hyattsville. Maryland: National Cen-tre for Health Statistics; 2009.
15. Centers for Medicare and Medicaid Services. Nationalhealth expenditures by source of funds and type ofexpenditure: calendar years 2004—2010. Baltimore,MD: Department of Health & Human Services; 2010.http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/tables.pdf [accessed 12.03.12].
16. Busato A, Donges A, Herren S, Widmer M, Marian F. Health sta-tus and health care utilisation of patients in complementaryand conventional primary care in Switzerland-an observationalstudy. Family Practice 2006;23:116—24.
17. Robinson A, Chesters J, Cooper S. People’s choice: comple-mentary and alternative medicine modalities. ComplementaryHealth Practice Review 2007;12:99—119.
18. Sirois FM, Purc-Stephenson RJ. Consumer decision factorsfor initial and long-term use of complementary and alter-native medicine. Complementary Health Practice Review2008;13:3—20.
19. Leach MJ. Clinical decision making in complementary and alter-native medicine. Sydney, Australia: Churchill Livingstone; 2010.
20. Bensoussan A, Myers SP, Wu SM, O’Connor K. Naturopathicand western herbal medicine practice in Australia — a work-force survey. Complementary Therapies in Medicine 2004;12:17—27.
21. Hale A. National survey of naturopaths, herbalists and acupunc-turists. Macarthur, New South Wales: School of Behavioural andCommunity Health Sciences, Faculty of Health Sciences, Uni-versity of Sydney; 2002.
22. Davis MA, Davis AM, Luan J, Weeks WB. The supply and demandof chiropractors in the United States from 1996 to 2005. Alter-native Therapies in Health and Medicine 2009;15:36—40.
23. Hough HJ, Dower C, Neill OEH. Profile of a profession:naturopathic practice. San Francisco: Center for the HealthProfessions, University of California; 2001.
24. National Center for Complementary and AlternativeMedicine (NCCAM). What is CAM?. Maryland: NCCAM;2011. http://nccam.nih.gov/health/whatiscam/ [accessed01.03.12].
25. Australian Bureau of Statistics (ABS). CDATA online. Canberra:ABS; 2012. http://www.abs.gov.au/CDATAOnline [accessed24.03.12].
26. Australian Bureau of Statistics (ABS). 2006 Census of populationand housing: customised data report. Brisbane: InformationConsultancy Services; 2012.
27. Statistics Canada. Population and dwelling counts, for Canada,provinces and territories, 2006 and 2001 censuses. Cat. No. 97-550-XWE2006002. Ottawa: Statistics Canada; 2008.
28. Statistics Canada. Occupation — national occupational clas-sification for statistics 2006 (720C), sex (3) and selecteddemographic, cultural, labour force, educational and incomecharacteristics (273) for the population 15 years and over ofCanada, provinces, territories, census metropolitan areas andcensus agglomerations, 2006 census. Ottawa: Statistics Canada;2008.
29. Statistics New Zealand. Quick stats New Zealand. Christchurch:Statistics New Zealand; 2009. http://www.stats.govt.nz/census/census-outputs/quickstats/snapshotplace2.htm?id=9999999&type=region [accessed 16.07.11].
30. Statistics New Zealand. 2006 census of population anddwellings: customised data report. Christchurch: Statistics NewZealand; 2012.
31. United States Census Bureau. Population estimates. Wash-ington, District of Columbia: United States Census Bureau;2011. http://www.census.gov/popest/national/national.html[accessed 15.02.12].
32. United States Census Bureau. EEO residence data results fortotal US, by occupation. Retrieved from Census 2000 EEOdata tool. Washington, District of Columbia: United StatesCensus Bureau; 2000. http://www.census.gov/cgi-bin/broker[accessed 14.02.12].
33. Office for National Statistics. Population estimates forUK, England and Wales, Scotland and Northern Ireland,population estimates timeseries 1971 to current year.Newport, South Wales: Office for National Statistics; 2011.http://www.ons.gov.uk/ons/rel/pop-estimate/population-estimates-for-uk–england-and-wales–scotland-and-northern-ireland/population-estimates-timeseries-1971-to-current-year/index.html [accessed 05.07.12].
34. General Chiropractic Council (GCC). Consulting the pro-fession: a survey of UK chiropractors. London: GCC; 2004.http://www.gcc-uk.org/files/link file/ConsultTheProfession.pdf [accessed 06.07.12].
35. General Osteopathic Council. Snapshot survey 2001. Lon-don: GOC; 2001. http://www.osteopathy.org.uk/uploads/survey2snapshot survery results 2001.pdf [accessed 06.07.12].
36. Magen MS, Ward D, Corp S. Osteopathic workforce study.In: Swartwout JE, editor. Compendium of osteopathicworkforce studies. 2004. http://www.tst.do-online.org/pdf/lcl optirepworkstudycompenium.pdf [accessed 15.08.12].
37. National Acupuncture Foundation. Acupuncture and Orientalmedicine state laws and regulations. Washington: NationalAcupuncture Foundation; 2005.
38. Salsberg ES, Forte GJ. Trends in the physician workforce,1980—2000. Health Affairs 2002;21:165—73.
39. Leach MJ, Segal L, May E. Lost opportunities forAustralia’s workforce? Medical Journal of Australia 2010;193:167—72.
40. Princetonreview.com. The Princeton review. Fra-mingham, MA: TPR Education IP Holdings; 2012.http://www.princetonreview.com [accessed 19.08.12].
41. Evans S. The story of naturopathic education in Australia. Com-plementary Therapies in Medicine 2000;8:234—5.
42. Australian Bureau of Statistics (ABS). Selected health occupa-tions: Australia, 2006. Cat. No. 4819.0. Canberra: ABS; 2006.
43. Productivity Commission. Australia’s health workforce:Productivity Commission research report. Canberra:Commonwealth of Australia; 2005. http://www.pc.gov.au/ data/assets/pdf file/0003/9480/healthworkforce.pdf[accessed 15.06.12].
44. Cherkin DC, Deyo RA, Sherman KJ, Hart LG, Street JH, HrbekA, et al. Characteristics of visits to licensed acupuncturists,chiropractors, massage therapists, and naturopathic physi-cians. Journal of the American Board of Family Practice2002;15:463—72.
45. Wardle J, Adams J, Magalhaes RJS, Sibbritt D. Distribution ofcomplementary and alternative medicine (CAM) providers inrural New South Wales, Australia: a step towards explaininghigh CAM use in rural health? Australian Journal of Rural Health2011;19:197—204.
46. Office for National Statistics. General and personal medicalservices, England — 1999—2009. Newport, South Wales:Office for National Statistics; 2011. http://data.gov.uk/dataset/general and personal medical services england[accessed 07.01.13].




























