Embed Size (px)
Citation preview

DOCUMENTS ENCLOSED ARE SUBJECTTO THE PRIVACY ACT OF 1974
Contents shall not be disclosed, discussed, or shared withindividuals unless they have a direct need-to-know in theperformance of their official duties. Deliver this/thesedocument(s) directly to the intended recipient. DO NOT drop off with a third-party.
To be used onall documents
containing personalinformation
The enclosed document(s) may contain personal or privileged information and should be treatedas “For Official Use Only.” Unauthorized disclosure of this information may result in CIVIL andCRIMINAL penalties. If you are not the intended recipient or believe that you have received thisdocument(s) in error, do not copy, disseminate or otherwise use the information and contact the owner/creator or your Privacy Act officer regarding the document(s).
DD FORM 2923, SEP 2010
Privacy Act Data Cover Sheet
Privacy Act DataCover Sheet

Department of Naval Science
Femoyer Hall, Room 419
280 Stanger Street (0241)
Blacksburg, Virginia 24061
P: (540) 231-7883 F: (540) 231-4838
www.usnavy.vt.edu
✓ What follows is the “college program” application for new students. This application is for students NOT ON SCHOLARSHIP.
✓ If you have enrolled in the Corps of Cadets and desire to enroll in either Navy or Marine ROTC this is for you.
✓ Generally, it is completed at the beginning of the fall semester and has a DUE DATE of August 14th.
NOTICE****** NOTICE ****** NOTICE ****** NOTICE PLEASE REVIEW THESE FREQUENT MISTAKES AND GUIDANCE
BEFORE COMPLETING THIS PAPERWORK. ERRORS WILL REQUIRE THIS TO BE REACCOMPLISHED
Instructions:
✓ Download and SAVE the form package.
✓ OPEN the saved package and FILL-IN EACH FORM—BLUE BOXES ONLY. (If you “hover” over the blue block it will tell you what we need)
✓ DO NOT SIGN OR INITIAL ANY FORMS.

✓ USE dd mmm yyyy (12 FEB 2020)
FORMAT UNLESS IT
PREPOPULATES DIFFERENTLY
AUTOMATICALLY.
✓ Be careful to type in your FULL
NAME, include hyphens or
second middle or last names—
see full instructions.
✓ Next, complete the next 2 forms online at the following links:
• https://www.public.navy.mil/netc/NSTC/NSTC_Directives/forms_17/
NSTC%201533-101%20(07-16)%20-%20Drug%20Statement.pdf
• https://www.public.navy.mil/netc/NSTC/NSTC_Directives/forms_17/NSTC%201533-133%20(08-19)%20-%20NROTC%20College%20Program%20Application%20v2.pdf
✓ NOTE: If you get an error opening the

above forms; then download, save on your computer, and then open the form.
✓ PRINT ONE-SIDED ONLY ON WHITE PAPER.
✓ KEEP ALL FORMS IN ORDER OF PRINTING.
✓ CONTACT US WITH ANY QUESTIONS AT: (540) 231-1958 or 231-8525 [email protected] or [email protected]
(REMOVE THIS PAGE FROM PACKET—NOT NECESSARY TO PRINT OR INCLUDE—INSTRUCTIONS ONLY)

FOR OFFICIAL USE ONLY – PRIVACY SENSITIVE: ANY MISUSE OR UNAUTHORIZED
DISCLOSURE MAY RESULT IN BOTH CIVIL AND CRIMINAL PENALTIES
NROTC STUDENT INFORMATION SHEET -- FILLABLE
PRINT ONE-SIDED – DO NOT SIGN – READ INSTRUCTIONS
DEPARTMENT OF THE NAVY NAVAL RESERVE OFFICERS TRAINING CORPS
VIRGINIA POLYTECHNIC INSTITUTE AND STATE UNIVERSITY BLACKSBURG, VIRGINIA 24061
Name (as listed on birth document):
Last, First Full Middle Suffix
SSAN:
Projected/Actual Report Date to VT: Today’s Date:
Current Address:
Street:
Option:
(select)
City: State:
County:
VT Student ID#: VT School Email:
Date of Birth:
Gender: YYYY – MM - DD
Legal Resident State:
Passport Number: Exp:
Driver’s License#: REAL ID? (select) Are you a US citizen? (select) Do you hold dual citizenship? (select)
If NOT US citizen - What Country?
Race(select one): (select)
Ethnicity(select one): (select)
If Birth Certificate is Secure –
(uncopiable), list the following:
When will you be 18?
Full Name: DOB:
Certificate ID #: POB:
VERIFIED BY(for staff use):
BIRTH CERTIFICATE DRIVERS LICENSE SSAN CARD PASSPORT MUST PROVIDE CERTIFIED OR ORIGINAL DOCUMENTS
PersonalEmail:

FOR OFFICIAL USE ONLY – PRIVACY SENSITIVE: ANY MISUSE OR UNAUTHORIZED
DISCLOSURE MAY RESULT IN BOTH CIVIL AND CRIMINAL PENALTIES
(select)
NROTC STUDENT INFORMATION SHEET - CONTINUATION
Name:
Last Name
Last 4 SSAN:
JROTC Participation (select one) (select) Eagle Scout (select one)(select)
Have you ever been in the military? (select) DD368?
Have you been awarded a NROTC Scholarship? (select) OPMIS61?
Are You Currently Enrolled In Class? (select)
How Many Hours Are You Currently Enrolled?
Major:
Class Year:
(select) DoD ID# (if known):
Home Phone:
Cell Phone: Est. Graduation Date:
(Month/Year) Home Email:
HOME OF RECORD
Address1:
Address2:
City/COUNTY/State/Zip:
Country:
MEDICAL HEIGHT: (inches) WEIGHT: BLOOD TYPE:(select)
DO YOU HAVE A DoDMERB APPROVED PHYSICAL?
DODMERB
APPROVED BRANCH? APPROVAL DATE:
(within 90 days) SICKLE CELL:
SPORTS PHYSICAL: LAB TEST
(select) OTHER COLLEGES ATTENDED (list below) SAT/ACT SCORES:SAT COMP:
MATH:
VERBAL:
CORP OF CADETS Company: POSITION: ROOM:
2

FOR OFFICIAL USE ONLY – PRIVACY SENSITIVE: ANY MISUSE OR UNAUTHORIZED
DISCLOSURE MAY RESULT IN BOTH CIVIL AND CRIMINAL PENALTIES
NROTC STUDENT INFORMATION SHEET - CONTINUATION
Name:
Last Name
Last 4 SSAN:
Marital Status(select one) (select) (If Married/Spouse Name): Cell:
Are you a child of a military member? (select one)
If YES, Provide Name/Title/Rank/Relation below:
1.
2.
3. IF UNDER AGE 18, WHO WILL BE PRESENT FOR CONTRACT SIGNING? WHO?:
MOTHER’s (Guardian) Cell: (select) INFORMATION:
Name: Phone:
Street Address: City: State:
County: Country: Zip:
Email:
FATHER’s (Guardian) Cell:
INFORMATION:
Name: Phone:
Street Address: City: State:
County: Country: Zip:
Email:
3
STUDENT FILE INDEX
NAME (Last, First MI)
STATUS: Scholarship STA-21 / MECEP Navy
College Program SSOP/ USNR Marine Corps
NROTC Honor Code (NSTC 1533/121) – Original
NROTC Acceptance and Oath of Office (NSTC 1533/126) (Scholarship only)
Dependency Application/Record of Emergency Data (NAVPERS 1070/602) w/SGLI Election (SGLV 8286) - First and Third Copies
Copies of official correspondence originated at the unit and endorsements (LOA letters, probation letters, etc.)
Orders, or copies thereof, with all endorsements (less any LES)
Locally completed NROTC Scholarship/College Program Application
Check applicable: ____ NROTC 4-Year ASR Form (NSTC 1533/106) ____ NSTC - Controlled Scholarship Letter ____ NROTC College Program Application (NSTC 1533/133)
*Destroy Interviewer’s Appraisal Sheets
Drug and Alcohol Abuse Statement of Understanding (OPNAV 5350/1) - Original
NROTC Scholarship Service Agreement (NSTC 1533/135) or NROTC College Program Advanced Standing Service Agreement (NSTC 1533/127) - Original
Enlistment/Reenlistment Agreement(s) (DD Form 4)
- Agreement to Extend Enlistment (NAVPERS 1070/621)
Certificate of Release or Discharge from Active Duty (DD Form 214)
General Purpose Privacy Act Statement (OPNAV 5211/12)
Disclosure Accounting Form (OPNAV 5211/9)
Individual NROTC Education Program Cost (NSTC 1533/113) Original (Scholarship Only)
Birth Certificate (Certified to be a True Copy)
Certificate of Naturalization - May use Certificate of Proof of Citizenship of Foreign Born
Applicants for Enlisted (NAVMC 538) or Letter of Certification sighting Naturalization Papers
Tattoo screening form, Navy or Marine Corps as appropriate
IRR Notification statement (1/C Midshipman only)
FILE MUST BE REVIEWED ANNUALLY
__________________________________________________ Reviewed By Date
__________________________________________________ Reviewed By Date
__________________________________________________ Reviewed By Date
__________________________________________________ Reviewed By Date
__________________________________________________ Reviewed By Date
__________________________________________________ Reviewed By Date
__________________________________________________ Reviewed By Date
__________________________________________________ Reviewed By Date
FOR OFFICIAL USE ONLY NSTC 1533/128 (08-17)

NAVAL RESERVE OFFICERS TRAINING CORPS ACCEPTANCE AND OATH OFFICE
Privacy Act Statement
Authority: The authority to request this information is contained in: 5 USC § 301 (Authorizing Forms and Regulations) and 10 USC Sec. 2104, Subtitle A, Part III, Chapter 103 (Senior ROTC).
Principal Purpose(s): Used when administering the acceptance and oath of office for new Naval Reserve Officers Training Corps (NROTC) Midshipman.
Routine Purpose(s): Information you provide in this application is protected by the Privacy Act and will not be released outside the Department of Defense without your permission unless it comes within an exception to the Act or one of the routine uses in 32 CFR § 701.112,http://www.privacy.navy.mil and the routine uses set forth here.
Disclosure: Failure to provide the requested information may result in removal from the NROTC program and/or loss of scholarship benefits.
ACCEPTANCE
I,___________________________________________________________________________________,having been permanently
appointed as Midshipman, (USNR/USMCR) from the ___________________________________ day of
_______________________, ____________________ do accept such appointment.
__________________________________________________
APPOINTEE SIGNATURE
OATH OF OFFICE
I,___________________________________________________________________________________,having been appointed a midshipman, do solemnly swear (or affirm) that I will support and defend the Constitution of the United States against all enemies, foreign and domestic; that I will bear true faith and allegiance to the same; that I take this obligation freely, without any mental reservation or purpose of evasion; and that I will well and faithfully discharge the duties of office on which I am about to enter: So help me God. (Optional)
__________________________________________________
APPOINTEE SIGNATURE
Subscribed and sworn to before me this __________ day of ___________, ___________.
__________________________________________________
WITNESSING OFFICER PRINTED NAME
__________________________________________________
WITNESSING OFFICER SIGNATURE
NSTC 1533/126 (08-19)

DD FORM 93, JAN 2008 PREVIOUS EDITION IS OBSOLETE. Adobe Professional X
RECORD OF EMERGENCY DATA
PRIVACY ACT STATEMENT
AUTHORITY: 5 USC 552, 10 USC 655, 1475 to 1480 and 2771, 38 USC 1970, 44 USC 3101, and EO 9397 (SSN). PRINCIPAL PURPOSES: This form is used by military personnel and Department of Defense civilian and contractor personnel, collectively referred to as civilians, when applicable. For military personnel, it is used to designate beneficiaries for certain benefits in the event of the Service member's death. It is also a guide for disposition of that member's pay and allowances if captured, missing or interned. It also shows names and addresses of the person(s) the Service member desires to be notified in case of emergency or death. For civilian personnel, it is used to expedite the notification process in the event of an emergency and/or the death of the member. The purpose of soliciting the SSN is to provide positive identification. All items may not be applicable. ROUTINE USES: None. DISCLOSURE: Voluntary; however, failure to provide accurate personal identifier information and other solicited information will delay notification and the processing of benefits to designated beneficiaries if applicable.
INSTRUCTIONS TO SERVICE MEMBER
This extremely important form is to be used by you to show the names and addresses of your spouse, children, parents, and any other person(s) you would like notified if you become a casualty (other family members or fiance), and, to designate beneficiaries for certain benefits if you die. IT IS YOUR RESPONSIBILITY to keep your Record of Emergency Data up to date to show your desires as to beneficiaries to receive certain death payments, and to show changes in your family or other personnel listed, for example, as a result of marriage, civil court action, death, or address change.
INSTRUCTIONS TO CIVILIANS
This extremely important form is to be used by you to show the names and addresses of your spouse, children, parents, and any other person(s) you would like notified if you become a casualty. Not every item on this form is applicable to you. This form is used by the Department of Defense (DoD) to expedite notification in the case of emergencies or death. It does not have a legal impact on other forms you may have completed with the DoD or your employer.
IMPORTANT: This form is divided into two sections: Section 1 - Emergency Contact Information and Section 2 - Benefits Related
Information. READ THE INSTRUCTIONS ON PAGES 3 AND 4 BEFORE COMPLETING THIS FORM.
SECTION 1 - EMERGENCY CONTACT INFORMATION
1. NAME (Last, First, Middle Initial) 2. SSN
3a. SERVICE/CIVILIAN CATEGORY
ARMY NAVY MARINE CORPS
AIR FORCE
DoD
CIVILIAN
CONTRACTOR
b. REPORTING UNIT CODE/DUTY STATION
4a. SPOUSE NAME (If applicable) (Last, First, Middle Initial) b. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER
SINGLE DIVORCED WIDOWED
5. CHILDREN a. NAME (Last, First, Middle Initial)
b. RELATIONSHIP c. DATE OF BIRTH
(YYYYMMDD) d. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER
6a. FATHER NAME (Last, First, Middle Initial) b. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER
7a. MOTHER NAME (Last, First, Middle Initial) b. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER
8a. DO NOT NOTIFY DUE TO ILL HEALTH b. NOTIFY INSTEAD
9a. DESIGNATED PERSON(S) (Military only) b. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER
10. CONTRACTING AGENCY AND TELEPHONE NUMBER (Contractors only)
DD FORM 93 (BACK), JAN 2008
SECTION 2 - BENEFITS RELATED INFORMATION
11a. BENEFICIARY(IES) FOR DEATH GRATUITY
(Military only)
b. RELATIONSHIP c. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER d. PERCENTAGE
12a. BENEFICIARY(IES) FOR UNPAID PAY/ALLOWANCES (Military only) NAME AND RELATIONSHIP
b. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER c. PERCENTAGE
13a. PERSON AUTHORIZED TO DIRECT DISPOSITION (PADD) (Military only) NAME AND RELATIONSHIP
b. ADDRESS (Include ZIP Code) AND TELEPHONE NUMBER
14. CONTINUATION/REMARKS
15. SIGNATURE OF SERVICE MEMBER/CIVILIAN (Include rank, rate,
or grade if applicable)
16. SIGNATURE OF WITNESS (Include rank, rate, or grade
as appropriate)
17. DATE SIGNED
(YYYYMMDD)
DD FORM 93 (INSTRUCTIONS), JAN 2008
INSTRUCTIONS FOR PREPARING DD FORM 93
(See appropriate Service Directives for supplemental instructions for completion of this form at other than MEPS)
All entries explained below are for electronic or typewriter
completion, except those specifically noted. If a computer
or typewriter is not available, print in black or blue-black ink
insuring a legible image on all copies. Include "Jr.," "Sr.,"
"III" or similar designation for each name, if applicable.
When an address is entered, include the appropriate ZIP
Code. If the member cannot provide a current address,
indicate "unknown" in the appropriate item. Addresses
shown as P.O. Box Numbers or RFD numbers should
indicate in Item 14, "Continuations/Remarks", a street
address or general guidance to reach the place of
residence. In addition, the notation "See Item 14" should be
included in the item pertaining to the particular next of kin or
when the space for a particular item is insufficient. If the
address for the person in the item has been shown in a
preceding item, it is unnecessary to repeat the address;
however, the name must be entered. Those items that are
considered not applicable to civilians will be left blank.
ITEM 1. Enter full last name, first name, and middle initial.
ITEM 2. Enter social security number (SSN).
ITEM 3a. Service. Military: Mark X in appropriate block.
Civilian: Mark two blocks as appropriate. Examples: an
Army civilian would mark Army and either Civilian or
Contractor; a DoD civilian, without affiliation to one of the
Military Services, would mark DoD and then either Civilian or
Contractor as appropriate.
ITEM 3b. Reporting Unit Code/Duty Station. See Service
Directives.
ITEM 4a. Spouse Name. Enter last name (if different from
Item 1), first name and middle initial on the line provided. If
single, divorced, or widowed, mark appropriate block.
ITEM 4b. Address and Telephone Number. Enter the
"actual" address and telephone number, not the mailing
address. Include civilian title or military rank and service if
applicable. If one of the blocks in 4a is marked, leave blank.
ITEM 5a-d. Children. Enter last name (only if different from
Item 1) first name and middle initial, relationship, and date of
birth of all children. If none, so state. Include illegitimate
children if acknowledged by member or paternity/maternity
has been judicially decreed. Relationship examples: son,
daughter, stepson or daughter, adopted son or daughter or
ward. Date of birth example: 19950704. For children not
living with the member's current spouse, include address
and name and relationship of person with whom residing in
item 5d.
ITEM 6a. Father Name. Last name, first name and middle
initial.
ITEM 6b. Address and Telephone Number of Father. If
unknown or deceased, so state. Include civilian title or
military rank and service if applicable. If other than natural
father is listed, indicate relationship.
ITEM 7a. Mother Name. Last name, first name and middle
initial.
ITEM 7b. Address and Telephone Number of Mother. If
unknown or deceased, so state. Include civilian title or
military rank and service if applicable. If other than natural
mother is listed, indicate relationship.
ITEM 8. Persons Not to be Notified Due to Ill Health.
a. List relationship, e.g., "Mother," of person(s) listed in
Items 4, 5, 6, or 7 who are not to be notified of a casualty
due to ill health. If more than one child, specify, e.g.,
"daughter Susan." Otherwise, enter "None".
b. List relationship, e.g., "Father" or name and address of
person(s) to be notified in lieu of person(s) listed in item 8a.
If "None" is entered in Item 8a, leave blank.
ITEM 9a. This item will be used to record the name of the
person or persons, if any, other than the member's primary
next of kin or immediate family, to whom information on the
whereabouts and status of the member shall be provided if
the member is placed in a missing status. Reference 10
USC, Section 655. NOT APPLICABLE to civilians.
ITEM 9b. Address and telephone number of Designated
Person(s). NOT APPLICABLE to civilians.
ITEM 10. Contracting Agency and Telephone Number
(Contractors only). NOT APPLICABLE to military
personnel. Civilian contractors will provide the name of
their contracting agency and its telephone number.
Example: XYZ Electric, (703) 555-5689. The telephone
number should be to the company or corporation's
personnel or human resources office.
ITEM 11a. Beneficiary(ies) for Death Gratuity (Military
only). Enter first name(s), middle initial, and last name(s)
of the person(s) to receive death gratuity pay. A member
may designate one or more persons to receive all or a
portion of the death gratuity pay. The designation of a
person to receive a portion of the amount shall indicate the
percentage of the amount, to be specified only in 10 percent
increments, that the person may receive. If the member
does not wish to designate a beneficiary for the payment of
death gratuity, enter "None," or if the full amount is not
designated, the payment or balance will be paid as follows:
(1) To the surviving spouse of the person, if any;
(2) To any surviving children of the person and the
descendants of any deceased children by representation;
(3) To the surviving parents or the survivor of them;
(4) To the duly appointed executor or administrator of the
estate of the person;
(5) If there are none of the above, to other next of kin of the
person entitled under the laws of domicile of the person at
the time of the person's death.
The member should make specific designations, as it
expedites payment.

DD FORM 93 (INSTRUCTIONS) (BACK), JAN 2008
INSTRUCTIONS FOR PREPARING DD FORM 93
(Continued)
ITEM 11a. (Continued) Seek legal advice if naming a minor
child as a beneficiary. If a member has a spouse but
designates a person other than the spouse to receive all or a
portion of the death gratuity pay, the Service concerned is
required to provide notice of the designation to the spouse.
NOT APPLICABLE to civilians.
Item 11b. Relationship. NOT APPLICABLE to civilians.
ITEM 11c. Enter beneficiary(ies) full mailing address and
telephone number to include the ZIP Code. NOT
APPLICABLE to civilians.
ITEM 11d. Show the percentage to be paid to each person.
Enter 10%, 20%, 30%, up to 100% as appropriate. The sum
shares must equal 100 percent. If no percent is indicated and
more than one person is named, the money is paid in equal
shares to the persons named. NOT APPLICABLE to
civilians.
ITEM 12a. Beneficiary(ies) for Unpaid Pay/Allowance
(Military only). Enter first name(s), middle initial, last
name(s) and relationship of person to receive unpaid pay
and allowances at the time of death. The member may
indicate anyone to receive this payment. If the member
designated two or more beneficiaries, state the percentage
to be paid each in item 10c. If the member does not wish to
designate a beneficiary, enter "By Law." The member is
urged to designate a beneficiary for unpaid pay and
allowances as payment will be made to the person in order
of precedence by law (10 USC 2771) in the absence of a
designation. Seek legal advice if naming a minor child as
beneficiary. NOT APPLICABLE to civilians.
ITEM 12b. Enter beneficiary(ies) full mailing address and
telephone number to include the ZIP Code. NOT
APPLICABLE to civilians.
ITEM 12c. If the member designated two or more
beneficiaries, state the percentage to be paid each in this
section. The sum shares must equal 100 percent. NOT
APPLICABLE to civilians.
ITEM 13a. Enter the name and relationship of the Person
Authorized to Direct Disposition (PADD) of your remains
should you become a casualty. Only the following persons
may be named as a PADD: surviving spouse, blood relative
of legal age, or adoptive relatives of the decedent. If neither
of these three can be found, a person standing in loco
parentis may be named. NOT APPLICABLE to civilians.
ITEM 13b. Address and telephone number of PADD. NOT
APPLICABLE to civilians.
ITEM 14. Continuations/Remarks. Use this item for remarks
or continuation of other items, if necessary. Prefix entry with
the number of the item being continued; for example, 5/John
J./son/ 19851220/321 Pecan Drive, Schertz TX 78151. Also
use this item to list name, address, and relationship of other
persons the member desires to be notified. Other
dependents may also be listed. This block offers the
greatest amount of flexibility for the member to record other
important information not otherwise requested but
considered extremely useful in the casualty notification and
assistance process. Besides continuing information from
other blocks on this form, the member may desire to include
additional information such as: NOK language barriers,
location or existence of a Will, additional private insurance
information, other family member contact numbers, etc. If
additional space is required, attach a supplemental sheet of
standard bond paper with the information.
ITEM 15. Signature of Service Member/Civilian. Check and
verify all entries and sign all copies in ink as follows: First
name, middle initial, last name. Include rank, rate, or grade
if applicable. May be electronically signed (see DoD
Instruction 1300.18 for guidelines).
ITEM 16. Signature of Witness. Have a witness
(disinterested person) sign all copies in ink as follows: First
name, middle initial, last name. Include rank, rate, or grade
as appropriate. A witness signature is not required for
electronic versions of the DD Form 93 (see DoD Instruction
1300.18).
ITEM 17. Date the member or civilian signs the form. This
item is an ink entry and must be completed on all copies.

AUTHORIZATION RELEASE OF STUDENT INFORMATION
NROTCVPI FORM 1533/4 rev. Jan 2020
(Date)
From: MIDN
(Last, First MI) (SSN) (Student ID#)
To: Commanding Officer, NROTC Unit, Virginia Polytechnic
Institute and State University
Subj: RELEASE OF STUDENT INFORMATION; AUTHORIZATION FORM
1. I hereby give permission for release of any of my Virginia Polytechnic Institute and State University records to the Naval ROTC Unit, Virginia
Polytechnic Institute and State University (NROTC, VPI).
2. I hereby give permission for release of any information from my records in the Virginia Tech Corps of Cadets to the NROTC, VPI.
3. I hereby give permission for release of any information from my ROTC records to the Virginia Tech Corps of Cadets Commandant and
Commandant’s Staff.
4. I hereby give permission for the release of my hometown information (City, State) for the use of ceremonial and media purposes.
5. The Commanding Officer, Naval ROTC Unit, Virginia Polytechnic Institute and State University, is authorized to provide such information from my
university and Naval records as he deems necessary and appropriate to
the following personnel or agencies:
a. My Parents or Guardians
b. Agencies of the Navy Department
6. This authorization constitutes an exception to the Family Educational
Rights and Privacy Act 1974 and is limited to that period of time that I
am affiliated with the Naval Reserve Officers Training Corps Unit.
7. Such information as I desire released to any other persons or agencies
must be accompanied by my specific authorization.
(Signature)


Witness: SHALL be an active duty staff member attached to the unit.

UNITED STATES NAVY TATTOO SCREENING CERTIFICATE COMNAVCRUITCOMINST 1130.8 and 1131.2
NAME (Last, First, Middle, Jr., etc.) Date:
YES NO
Any "Yes" response to items 4, 5, 7, or 8 above is disqualifying, not authorized for Enlistment. Any "No" response to Item 6 is disqualifying, not authorized for Enlistment. NOTE: All questionable body markings, due to content, size, number, and/or location, shall be forwarded to NAVCRUITCOM for eligibility determination.
Applicant Signature Date DateRecruiter Signature
Describe all tattoos, brands, and/or body ornamentation (if applicable) on following page.
Explain tattoo, brand, and/or body ornamentation removal process, if applicable.
CO/XO/R-OPS/CMC/CR/EPDS Reviewing Comments:
NAVCRUIT 1130/104 (Rev 05-2016) For Official Use Only - Privacy Sensitive Page 1 0f 2
CO/XO/R-OPS/CMC/CR/EPDS Signature Typed Name/Title: Date:
N/A
1. Does the applicant/candidate have any tattoos/body art/branding?
2. Does the applicant/candidate have any tattoo/body art/brand visible behind the ears or on the neck
3. Has the applicant/candidate ever had any tattoo, body art or brand removed or covered?
N/A NO YES
4. Are any of the tattoos/body art/brands on the face (excluding cosmetic tattoos) or scalp?
5. Is there one or more tattoos larger than one inch on the neck or behind the ears, visible above the collar of a properly fitted crew neck t-shirt? (Excluding cosmetic tattoos)
6. If applicable, are cosmetic tattoos applied in good taste with natural color enhancement and of a conservative nature?
7. Are any of the tattoos/body art/branding representative of gang membership, advocate racial, ethnic, racial discrimination, sexism (including expressions of nudity), drug related, obscene, or are prejudicial to good order, discipline, and morale, or are of a nature to bring discredit upon the Navy? 8. Are any of the tattoos a result of a specific activity? (i.e., specifically an illegal activity or as a result of any violation of law (s))
Any "Yes" response above requires an enlistment eligibility determination by the NAVCRUITDIST CO (May be delegated to XO, R-OPS, CMC, CR, or EPDS when authorized "by direction" authority by the CO).
APPROVED DISAPPROVED

Documentation. The following depicts the location and description of the applicant's
body markings. Place number on body location and describe in corresponding blocks below
indicating content and size in inches (not required if no Tattoos):
FRONT VIEW BACK VIEW
1. 1.
2. 2.
3. 3.
4. 4.
5. 5.
6. 6.
7. 7.
8. 8.
9. 9.
10. 10.
Part V. Certification. I certify above body marking information is accurate.
(Name of Applicant) (Signature of Applicant) (Date)
(Name of Recruiting Rep) (Signature of Recruiting Rep) (Date)
UNITED STATES NAVY TATTOO SCREENING CERTIFICATE
NAVCRUIT 1130/104 (Rev 05/2016) Page 2 of 2
Example for above page: #1 Mickey Mouse 4 x 4 inches
#2 Quote: “live life” 1 x 6 inches
If you answered NO to item #6 on the previous form you
just disqualified yourself—go back and recheck it.
THERE ARE MORE PAGES AFTER THE
MARINE FORM—PLEASE SCROLL DOWN.
FOR MARINE OPTION ONLY:
COMPLETE THE ADDITIONAL
MARINE TATTOO FORM
(NEXT 4 PAGES)
NOTE: MARINES WILL COMPLETE BOTH
TATTOO FORMS.
(REMOVE THIS PAGE FROM PACKET—NOT NECESSARY TO
PRINT OR INCLUDE—INSTRUCTIONS ONLY)
USMC OFFICER TATTOO SCREENING FORM
Insert into MCRCO 1100.2A, Appendix O, Updated by MCRC FROST CALL 017-16
1
NAME_________________________________ L4 SSN_________________ DATE_____________
Part I: Purpose. The purpose of this form is to ensure that you disclose the full
extent of your tattoos, brands and/or body ornamentation. Refusal to complete the
form will result in termination of your enlistment processing.
1. Does the applicant currently have, or ever had any tattoos, brands, body
markings, or body ornamentation, or has the applicant ever had a tattoo, brand or
body ornamentation removed, concealed, covered or altered? (Initials in
appropriate block)
Y _____ N_____
Notes: If the answer to Question 1 is NO; move to Part II Certification Block of
this Screening Form. Questions 2 through 9 are not required. If the answer to
Question 1 is YES; complete Questions 2-9, then certify in Part II and forward for
Review.
2. Does applicant have body markings of any type that are exposed or partially
exposed while wearing the standard warm weather PT uniform (shorts & shirt)?
Y_____ N_____
3. Are any of the tattoos, brands or markings:
- on head or neck (above collarbone in front, above seventh [C7] cervical
[last] vertebrae in back or otherwise visible in open collar short sleeve khaki
shirt with white undershirt) or inside the mouth?
- on hands, elbows, knees, or fingers (with exception of wedding band tattoo–
not to exceed 3/8 of an inch), or within 2 inches of the wrists?
Y ____ N_____
4. Are any tattoos, markings or ornamentations exposed while wearing the standard
PT uniform:
- Larger than the individual wearers hand with fingers extended and joined?
- Band Tattoos, (cannot exceed 3 inches or the width of the individual’s four
fingers extended and joined, whichever is greater)?
- Single band tattoo on one finger (max width less than 3/8 of an inch)?
- Excessive Tattoos (combined coverage must be covered by the individual
wearers hand with their fingers extended and joined)?
Y _____N_____
5. Do any of the tattoos, markings etc., depict nudity, are they racist,
eccentric, offensive in nature, or express an association with conduct or
substances prohibited by the Marine Corps Drug policy, the UCMJ, to include tattoos
associated with illegal drugs, drug usage or paraphernalia?
Y _____N_____
6. Do any of the tattoos, brands or body ornamentation represent a gang membership
or extremist group, advocate racial, ethnic, or religious discrimination, obscene,
prejudicial to good order and discipline/morale or of a nature to discredit to the
Marine Corps?
Y______N______
7. Are any of the tattoos a result of a specific activity? (i.e. activity for
membership initiation, or as the result of any violation of law(s))?
Y _____N______
USMC OFFICER TATTOO SCREENING FORM
Insert into MCRCO 1100.2A, Appendix O, Updated by MCRC FROST CALL 017-16
2
NAME_________________________________ L4 SSN_________________ DATE_____________
8. Are there any body markings, ornamentation or mutilation (i.e. Tongue Splitting,
etc), Ornamental Body Piercing(s), Holes in Ear Lobes (large enough for light to
pass through opening), or Ornamental Implantations, (silicone implants on face,
horns on the forehead, etc).
Y______ N_____
Location(s) of an applicant’s current, removed, concealed, covered, or altered
tattoos, brands, markings, or ornamentation will be documented in Part IV of this
Screening Form. Removed, concealed, covered or altered tattoos need to be
annotated as such (i.e. removed) with full description of the original marking.
Part II: Certification. I have completely disclosed the full extent of my
tattoos, brands or body ornamentation to include those removed or altered.
_________________________________ ________________________________ _______
(Name of Candidate) (Signature) (Date)
“Applicant qualified in accordance with MCBul 1020 & Frost Call 017-16.”
_________________________________ ________________________________ ________
(Name of Certifying Officer) (Signature) (Date)
*Certifying Officer Comments:
___________________________________________________________________________________
___________________________________________________________________________________________________
* A Certifying Officer is a commissioned officer at the Recruiting Station, NROTC
Unit, USNA, or in the chain of command for enlisted Marines applying for a
Commissioning of Warrant officer Programs.
Part III: Reviewing.
a. If the applicant responded “Yes” to question 2, the tattoo must be reviewed
to determine eligibility. If the applicant responded “Yes” to questions 3-8, the
applicant is ineligible (with the exception to the wedding band tattoo authorized
on one finger) for commission.
b. Digital photos are required for all reviews. Photos not required of female
applicants with torso tattoos or male applicants with lower torso (below waist)
tattoos. Applicants may hand draw pictures of torso & lower torso tattoos
indicating size and location. Cross-check drawings with DD Form 2808 Medical
Examination, Block 37 documents for consistency. Under no circumstances will a
female applicant be photographed in less clothing than the standard warm weather
physical training uniform.
c. All questionable body markings in regards to content, size, number or
location will be forwarded to the appropriate authority for approval/review. Check
appropriate review authority:
[ ] Recruiting Districts. Review tattoos for applicants applying for the Platoon
Leaders Class, Officer Candidate Course, and Four Year Naval Reserve Officer
Training Scholarship programs.
USMC OFFICER TATTOO SCREENING FORM
Insert into MCRCO 1100.2A, Appendix O, Updated by MCRC FROST CALL 017-16
3
NAME_________________________________ L4 SSN_________________ DATE_____________
[ ] Marine Corps Recruiting Command. Review tattoos for applicants applying to all
other commissioning and Warrant Officer programs.
“Applicant is eligible for commissioning after review and adjudication in
accordance with MCBul 1020 & Frost Call 017-16.”
_____________________________________________________________________________
NAME/SIGNATURE OF REVIEWING OFFICER RANK BILLET
Part IV. Documentation. The following depicts the location and description of the
applicant’s Body Markings. Place number on body location and describe in blocks
below indicating content and size in inches:
FRONT VIEW BACK VIEW
1. ___________________________________ 1. __________________________________
2. ___________________________________ 2. __________________________________
3. ___________________________________ 3. __________________________________
4. ___________________________________ 4. __________________________________
5. ___________________________________ 5. __________________________________
6. ___________________________________ 6. __________________________________
USMC OFFICER TATTOO SCREENING FORM
Insert into MCRCO 1100.2A, Appendix O, Updated by MCRC FROST CALL 017-16
4
NAME_________________________________L4 SSN_________________DATE_____________
Part V. Certification. I certify above body marking information is accurate.
________________________________ ____________________________________ ____________
(Name of Candidate) (Signature) (Date)
“Applicant qualified in accordance with MCBul 1020 & Frost Call 017-16.”
_______________________________ ____________________________________ ____________
(Name of Certifying Officer) (Signature) (Date)
Part VI. Recertification. (Prior to Request for Appointment) I certify the
information previously given on Tattoo Screening Form remains the same. If any
change is indicated an addendum Tattoo Screening Form will be complete then
forwarded to the appropriate authority prior to the Request for Appointment.
1. Changes to this Tattoo Screening Form Y______ N _____
_________________________________ _______________________________ __________
(Name of Candidate) (Signature) (Date)
“Applicant is eligible for commissioning after review and adjudication in
accordance with MCBul 1020 & Frost Call 017-16.”
_____________________________________________________________________________
NAME/SIGNATURE OF REVIEWING OFFICER RANK BILLET

Witness: SHALL be an active duty staff member attached to the unit.
ONE LAST FORM—DIRECT DEPOSIT
THE NAVY PAYS EVERYONE BY
DEPOSITING FUNDS DIRECTLY INTO
YOUR CHECKING / SAVINGS.
EVERYONE NEEDS TO COMPLETE THIS
TO RECEIVE ANY REIMBURSEMENTS,
STIPENDS, BOOK PAYMENTS, OR TRAVEL
REIMBURSEMENT TO NAME A FEW.
YOU CAN SKIP COMPLETING SECTION 2
and 3, BUT WE MUST HAVE SECTION 1
COMPLETE (PLUS Account Number) AND
ROUTING NUMBER (Section 3).
NOTE: You can update or change this at any time.
(REMOVE THIS PAGE FROM PACKET—NOT NECESSARY TO
PRINT OR INCLUDE—INSTRUCTIONS ONLY)
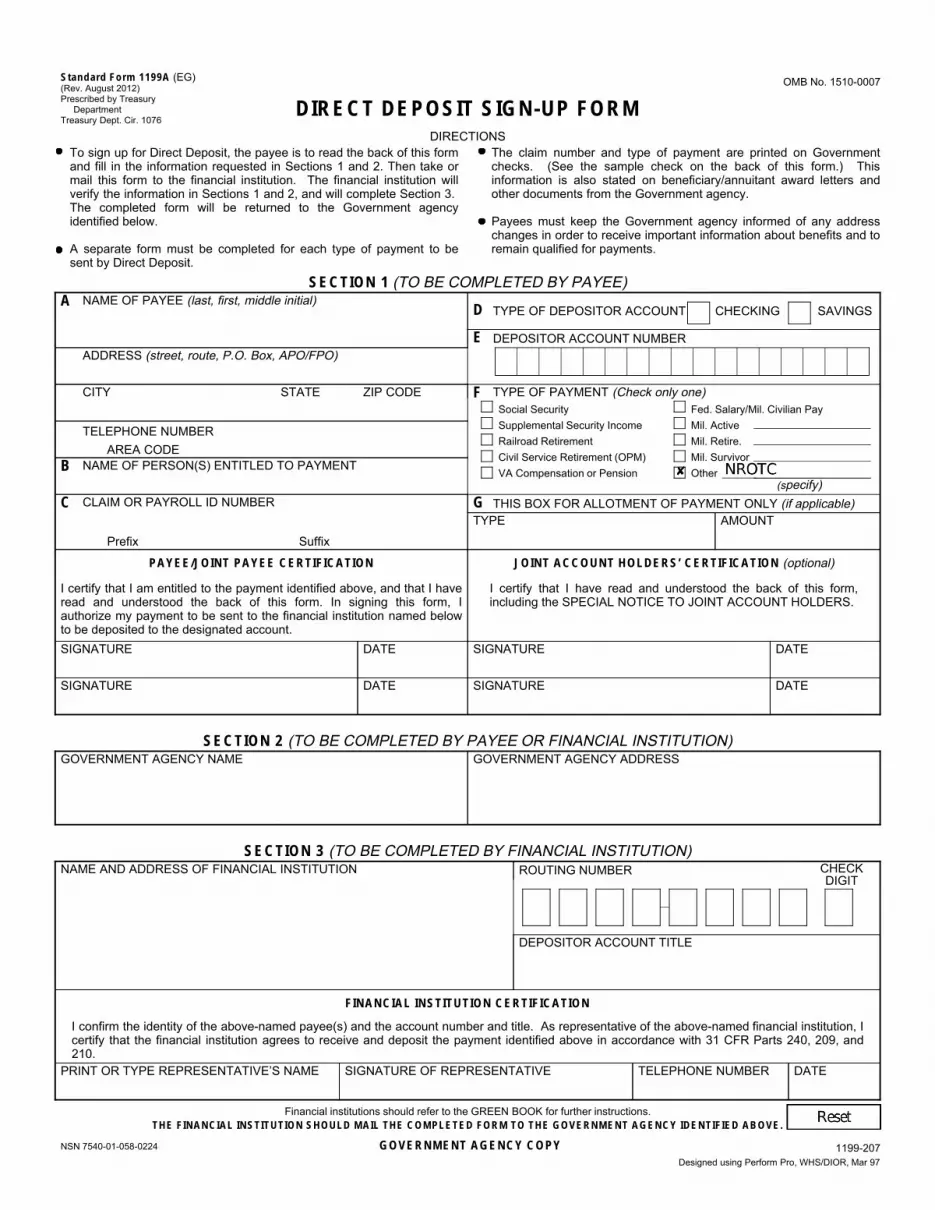
NSN 7540-01-058-0224 GOVERNMENT AGENCY COPY Designed using Perform Pro, WHS/DIOR, Mar 97
Standard Form 1199A (EG) OMB No. 1510-0007 (Rev. August 2012)Prescribed by Treasury
Department DIRECT DEPOSIT SIGN-UP FORM Treasury Dept. Cir. 1076
DIRECTIONS To sign up for Direct Deposit, the payee is to read the back of this form The claim number and type of payment are printed on Government and fill in the information requested in Sections 1 and 2. Then take or checks. (See the sample check on the back of this form.) This mail this form to the financial institution. The financial institution will information is also stated on beneficiary/annuitant award letters and verify the information in Sections 1 and 2, and will complete Section 3. other documents from the Government agency. The completed form will be returned to the Government agency identified below. Payees must keep the Government agency informed of any address
changes in order to receive important information about benefits and to A separate form must be completed for each type of payment to be remain qualified for payments.sent by Direct Deposit.
SECTION 1 (TO BE COMPLETED BY PAYEE) NAME OF PAYEE (last, first, middle initial) A
ADDRESS (street, route, P.O. Box, APO/FPO)
CITY STATE ZIP CODE
TELEPHONE NUMBER AREA CODE
NAME OF PERSON(S) ENTITLED TO PAYMENT B
CLAIM OR PAYROLL ID NUMBER C
Prefix Suffix
TYPE OF DEPOSITOR ACCOUNT D CHECKING SAVINGS
DEPOSITOR ACCOUNT NUMBER E
TYPE OF PAYMENT (Check only one) F Social Security Supplemental Security Income Railroad Retirement Civil Service Retirement (OPM) VA Compensation or Pension
Fed. Salary/Mil. Civilian Pay Mil. Active Mil. Retire. Mil. Survivor Other
(specify) THIS BOX FOR ALLOTMENT OF PAYMENT ONLY (if applicable) G
TYPE AMOUNT
PAYEE/JOINT PAYEE CERTIFICATION
I certify that I am entitled to the payment identified above, and that I have read and understood the back of this form. In signing this form, I authorize my payment to be sent to the financial institution named below to be deposited to the designated account.
JOINT ACCOUNT HOLDERS’ CERTIFICATION (optional)
I certify that I have read and understood the back of this form, including the SPECIAL NOTICE TO JOINT ACCOUNT HOLDERS.
SIGNATURE DATE
SIGNATURE DATE
SIGNATURE DATE
SIGNATURE DATE
SECTION 2 (TO BE COMPLETED BY PAYEE OR FINANCIAL INSTITUTION) GOVERNMENT AGENCY NAME GOVERNMENT AGENCY ADDRESS
SECTION 3 (TO BE COMPLETED BY FINANCIAL INSTITUTION) NAME AND ADDRESS OF FINANCIAL INSTITUTION ROUTING NUMBER CHECK
DIGIT
DEPOSITOR ACCOUNT TITLE
FINANCIAL INSTITUTION CERTIFICATION
I confirm the identity of the above-named payee(s) and the account number and title. As representative of the above-named financial institution, I certify that the financial institution agrees to receive and deposit the payment identified above in accordance with 31 CFR Parts 240, 209, and 210.
PRINT OR TYPE REPRESENTATIVE’S NAME SIGNATURE OF REPRESENTATIVE TELEPHONE NUMBER DATE
Financial institutions should refer to the GREEN BOOK for further instructions. THE FINANCIAL INSTITUTION SHOULD MAIL THE COMPLETED FORM TO THE GOVERNMENT AGENCY IDENTIFIED ABOVE.
1199-207

SF 1199A (Back)
BURDEN ESTIMATE STATEMENT
The estimated average burden associated with this collection of information is 10 minutes per respondent or recordkeeper, depending on individual circumstances. Comments concerning the accuracy of this burden estimate and suggestions for reducing this burden should be directed to the Financial Management Service, Records Management Branch, Room 135, 3700 East-West Highway, Hyattsville, MD 20782. THIS ADDRESS SHOULD ONLY BE USED FOR COMMENTS AND/OR SUGGESTIONS CONCERNING THE AMOUNT OF TIME SPENT TO COLLECT THIS DATA. DO NOT SEND THE COMPLETED PAPERWORK TO THE ADDRESS ABOVE FOR PROCESSING.
PRIVACY ACT NOTICE
Collection of the information in this Direct Deposit Sign-Up form is authorized by 5 U.S.C. § 552a, 31 U.S.C. § 3332(g), and Executive Order 9397 (November 22, 1943). Your social security number and the other information requested will allow the federal government to process your direct deposit. Your social security number is requested to ensure the accurate identification and retention of records pertaining to you and to distinguish you from other recipients of federal payments. This information will be disclosed to the Department of the Treasury and its fiscal and financial agents, and other federal agencies, as necessary to process your direct deposit. This information may also be disclosed to a court, congressional committee or another government agency as authorized or required to verify your receipt of federal payments. Although providing the requested information is voluntary, your direct deposit cannot be processed without it.
PLEASE READ THIS CAREFULLY
All information on this form, including the individual claim number, is required under 31 USC 3322, 31 CFR 209 and/or 210. The information is confidential and is needed to prove entitlement to payments. The information will be used to process payment data from the Federal agency to the financial institution and/or its agent. Failure to provide the requested information may affect the processing of this form and may delay or prevent the receipt of payments through the Direct Deposit/Electronic Funds Transfer Program.
INFORMATION FOUND ON CHECKS
Most of the information needed to complete boxes A and F in
Section 1 is printed on your government check:
A
F
Be sure that payee’s name is written exactly as it
appears on the check. Be sure current address is shown.
Type of payment is printed to the left of the amount.
Month Day Year
08 31 84
United States Treasury 15-51 000
KANSAS CITY, MO Check No.
0000 415785
Pay to
28 28
VA COMP
DOLLARS CTS
$****100 00 the order of JOHN DOE
123 BRISTOL STREET HAWKINS BRANCH TX 76543
A
F
NOT NEGOTIABLE ’:00000518’: 041571926"
SPECIAL NOTICE TO JOINT ACCOUNT HOLDERS
Joint account holders should immediately advise both the Government agency and the financial institution of the death of a beneficiary. Funds
deposited after the date of death or ineligibility, except for salary payments, are to be returned to the Government agency. The Government agency
will then make a determination regarding survivor rights, calculate survivor benefit payments, if any, and begin payments.
CANCELLATION
The agreement represented by this authorization remains in effect until cancelled by the recipient by notice to the Federal agency or by the death
or legal incapacity of the recipient. Upon cancellation by the recipient, the recipient should notify the receiving financial institution that he/she is doing so.
The agreement represented by this authorization may be cancelled by the financial institution by providing the recipient a written notice 30 days in
advance of the cancellation date. The recipient must immediately advise the Federal agency if the authorization is cancelled by the financial institution.
The financial institution cannot cancel the authorization by advice to the Government agency.
CHANGING RECEIVING FINANCIAL INSTITUTIONS
The payee’s Direct Deposit will continue to be received by the selected financial institution until the Government agency is notified by the payee that
the payee wishes to change the financial institution receiving the Direct Deposit. To effect this change, the payee will complete a new SF 1199A at the
newly selected financial institution. It is recommended that the payee maintain accounts at both financial institutions until the transition is complete, i.e.
after the new financial institution receives the payee’s Direct Deposit payment.
FALSE STATEMENTS OR FRAUDULENT CLAIMS
Federal law provides a fine of not more than $10,000 or imprisonment for not more than five (5) years or both for presenting a false statement or
making a fraudulent claim.
Department of Naval Science
Femoyer Hall, Room 419
280 Stanger Street (0241)
Blacksburg, Virginia 24061
P: (540) 231-7883 F: (540) 231-4838
www.liberalarts.vt.edu/rotc/navy/
MEDICAL/DENTAL RECORDS and MAINTENANCE
NOTICE****** NOTICE ****** NOTICE ****** NOTICE ERRORS WILL REQUIRE THIS TO BE
REACCOMPLISHED AND MAY DELAY THE ACTIVATION OF YOUR SCHOLARSHIP! ✓ All midshipmen (MIDN) whether or not on scholarship are required to have a
medical clearance to participate in NROTC. As a result, we build an official medical/dental record for everybody—this is especially helpful for college programmers who later are awarded scholarships. So, if you plan on applying for a scholarship, contact us about getting a DoDMERB physical—now.
✓ So, what is required? o An approved DoDMERB physical—this is forwarded to us by DoDMERB
when complete. NOTE: If your DoDMERB was completed for another service, such as the Naval Academy or the U.S. Air Force it needs to be transferred to NROTC—contact us for instructions;
o OR, an approved sports physical (can be completed by your doctor or at Schiffert Health Center on-campus at Virginia Tech https://www.healthcenter.vt.edu/appointments.html (NOTE: sports physicals generally should be within 90 days of the first day of school);
o AND, a sickle cell lab test (NOTE: if you have had this done previously bring us a copy of the results or you may schedule one at your local doctor or Schiffert Health Center);
o AND, record of immunizations.

✓ MIDN on scholarship are REQUIRED to have an approved DoDMERB physical qualification to activate their scholarship. If, your medical status is still PENDING you may participate in NROTC with an approved sports physical until such time as you are either qualified or waivered. You can then activate your scholarship, if otherwise still eligible. If there was a medical delay activating your scholarship you may be eligible to apply for retroactive tuition/fees.
✓ All MIDN require annual physical reviews to stay in the NROTC program. Annual reviews are also required to keep your DoDMERB active—up to 5 years. As a result you must complete an ANNUAL CERTIFICATE OF
PHYSICAL CONDITION each year; generally completed at the beginning of the fall semester. NOTE: If your annual review is older than 365 days after your previous review, your physical expires and those on scholarship will no longer receive tuition or stipends until such time as they are qualified again.
✓ Bottomline: No qualifying physical—no tuition/stipend.
✓ IF YOU ARE COMPLETING YOUR INITIAL FALL SEMESTER FORMS—COMPLETE
AND PRINT THIS FORM NOW.
✓ The ANNUAL CERTIFICATE OF PHYSICAL CONDITION (click on link to obtain form) can be submitted at any time if you have a CHANGE in medical/dental status. READ and COMPLETE this form carefully—contact us if you have any questions.
SELECTED INSTRUCTIONS: Today’s Date: select from drop-down ROTC Unit: VPI Unit 60 Rank/Class: MIDN/4C Birthdate: select from drop-down Since your last military physical examination have you had or been diagnosed with: “Yes” answers require explanation.

✓ Any “YES” answers require complete explanation and usually a copy of any medical records related to the condition for further review by the Navy Bureau of Medicine (BUMED).
✓ DO NOT WAIT ON COMPLETING YOUR REVIEW BECAUSE YOU DO NOT HAVE RECORDS—THEY CAN BE SUBMITTED LATE. The contents of medical records are restricted and secured or encrypted, as appropriate, in the NROTC unit. When sending us your records, do so securely.
EXAMPLE IN SECTION III: Item 7: Visited Dr. Brown at Schiffert Health Center, Blacksburg, Va in Feb 2020 for symptoms of a head cold (headache, sore throat, runny nose). The doctor prescribed a Zithromax Z-Pak anti-biotic for a sinus infection. The symptoms resolved after a week and a follow-up was not required (attached are copies of the doctors notes).
✓ You should be aware all “YES” answers on an annual review require a staff
review that may include further medical review by BUMED.
✓ How do I get a DoDMERB to qualify for a scholarship? See the HRA staff to assist in setting up a profile in DoDMETS. Then, go to the DoDMETS website https://www.dodmets.com/. A physical will be scheduled and once complete forwarded to DoDMERB for a determination.
✓ Most of the following forms ONLY require a name, SSAN or other header/footer. Follow the instructions on the date format.
✓ QUESTIONS?: Call us. We are generally in the office from 7:30 to 4:00 daily
(EST), which is 0730-1600, except federal holidays and weekends. Human Resources (HRA)
(540) 231-1958 or (540) 231-8525 [email protected] or [email protected]
NROTC STUDENT HEALTH RECORD INDEX NAME (Last, First, MI) SOCIAL SECURITY
NUMBER
The below listed forms are enclosed in the NROTC Student Health Record
LEFT SIDE – PART 1 RIGHT SIDE – PART II
☐ Record of Preventative Medicine and
Occupational Health ☐ Annual Certificates of Physical Condition
NSTC 1533/107, DD Form 2807-1, DD
Form 2807-2, NAVMED 6120/3
☐ Immunization Record SF601, CDC-731 ☐ Chronological Record of Medical Care SF
600
☐ Record of Occupational Exposure to
Ionizing Radiation NAVMED 6470/10
☐ Audiology
☐ Eye Exams
LEFT SIDE – PART III RIGHT SIDE – PART IV
☐ Report of Medical Examination DD Form
2351 or DD Form 2808 ☐ Electrocardiograph Record
☐ Anthropometric Data Record NAVMED
6410/9
Statement of Wearing Contact Lenses
NSTC 1533/103
☐ X-rays reports
☐ BUMED Waiver Letters/ Hospital
Records/Consults ☐ Laboratory Report
☐ Privacy Act Statement-Health Care
Records DD Form 2005 (signed)
☐ Record of Disclosure OPNAV 5211/9
HEALTH RECORD MUST BE REVIEWED ANNUALLY
REVIEWED BY DATE
REVIEWED BY DATE
REVIEWED BY DATE
REVIEWED BY DATE
REVIEWED BY DATE
PRIVACY ACT STATEMENT - HEALTH CARE RECORDS
This form is not an authorization or consent to use or disclose your health information.
1. AUTHORITY FOR COLLECTION OF INFORMATION INCLUDING SOCIAL SECURITY NUMBER (SSN):
10 U.S.C. 136, Under Secretary of Defense for Personnel and Readiness; 10 U.S.C. Chapter 55, Medical and Dental Care;
42 U.S.C. Chapter 32, Third Party Liability for Hospital and Medical Care; 32 CFR Part 199, Civilian Health and Medical
Program of the Uniformed Services (CHAMPUS); DoDI 6055.05, Occupational and Environmental Health (OEH); and
E.O. 9397 (SSN), as amended.
2. PRINCIPAL PURPOSES FOR WHICH INFORMATION IS INTENDED TO BE USED:
Information may be collected from you to provide and document your medical care; determine your eligibility for benefits
and entitlements; adjudicate claims; determine whether a third party is responsible for the cost of Military Health System
(MHS) provided healthcare and recover that cost; evaluate your fitness for duty and medical concerns which may have
resulted from an occupational or environmental hazard; evaluate the MHS and its programs; and perform administrative tasks
related to MHS operations and personnel readiness.
3. ROUTINE USES:
Information in your records may be disclosed to:
Private physicians and Federal agencies, including the Department of Veterans Affairs, Health and Human Services, and
Homeland Security (with regard to members of the Coast Guard), in connection with your medical care;
Government agencies to determine your eligibility for benefits and entitlements;
Government and nongovernment third parties to recover the cost of MHS provided care;
Public health authorities to document and review occupational and environmental exposure data; and
Government and nongovernment organizations to perform DoD-approved research.
Information in your records may be used for other lawful reasons which may include teaching, compiling statistical data, and
evaluating the care rendered. Use and disclosure of your records outside of DoD may also occur in accordance with 5 U.S.C.
552a(b) of the Privacy Act of 1974, as amended, which incorporates the DoD Blanket Routine Uses published at:
http://dpcld.defense.gov/privacy/SORNsIndex/BlanketRoutineUses.aspx.
Any protected health information (PHI) in your records may be used and disclosed generally as permitted by the HIPAA
Privacy Rule (45 CFR Parts 160 and 164), as implemented within DoD by DoD 6025.18-R. Permitted uses and disclosures of
PHI include, but are not limited to, treatment, payment, and healthcare operations.
4. WHETHER DISCLOSURE IS MANDATORY OR VOLUNTARY AND EFFECT ON INDIVIDUAL OF NOT PROVIDING INFORMATION:
Voluntary. If you choose not to provide the requested information, comprehensive health care services may not be possible,
you may experience administrative delays, and you may be rejected for service or an assignment. However, care will not be
denied.
This all inclusive Privacy Act Statement will apply to all requests for personal information made by MHS health care treatment
personnel or for medical/dental treatment purposes and is intended to become a permanent part of your health care record.
Your signature merely acknowledges that you have been advised of the foregoing. If requested, a copy of this form will be
furnished to you.
5. SIGNATURE OF PATIENT OR SPONSOR 6. SOCIAL SECURITY NUMBER OR
DOD IDENTIFICATION NUMBER
OF MEMBER OR SPONSOR
7. DATE (YYYYMMDD)
DD FORM 2005, JUN 2016 PREVIOUS EDITION IS OBSOLETE.

NROTC STUDENT DENTAL RECORD INDEX NAME (Last, First, MI) SOCIAL SECURITY
NUMBER
The below listed forms are enclosed in the NROTC Student Dental Record
LEFT SIDE RIGHT SIDE
☐ Unmounted radiographs in envelopes ☐ Record of Dental Care SF 603
☐ Sequential bite wing radiograph mounts
☐ Panographic or full mouth radiograph
☐ Report of Dental Exam DD Form 2480
☐ Privacy Act Statement-Health Care
Records
DD 2005 (signed)
☐ Record of Disclosure OPNAV 5211/9
DENTAL RECORD MUST BE REVIEWED ANNUALLY
REVIEWED BY DATE
REVIEWED BY DATE
REVIEWED BY DATE
REVIEWED BY DATE
REVIEWED BY DATE

PRIVACY ACT STATEMENT - HEALTH CARE RECORDS
This form is not an authorization or consent to use or disclose your health information.
1. AUTHORITY FOR COLLECTION OF INFORMATION INCLUDING SOCIAL SECURITY NUMBER (SSN):
10 U.S.C. 136, Under Secretary of Defense for Personnel and Readiness; 10 U.S.C. Chapter 55, Medical and Dental Care;
42 U.S.C. Chapter 32, Third Party Liability for Hospital and Medical Care; 32 CFR Part 199, Civilian Health and Medical
Program of the Uniformed Services (CHAMPUS); DoDI 6055.05, Occupational and Environmental Health (OEH); and
E.O. 9397 (SSN), as amended.
2. PRINCIPAL PURPOSES FOR WHICH INFORMATION IS INTENDED TO BE USED:
Information may be collected from you to provide and document your medical care; determine your eligibility for benefits
and entitlements; adjudicate claims; determine whether a third party is responsible for the cost of Military Health System
(MHS) provided healthcare and recover that cost; evaluate your fitness for duty and medical concerns which may have
resulted from an occupational or environmental hazard; evaluate the MHS and its programs; and perform administrative tasks
related to MHS operations and personnel readiness.
3. ROUTINE USES:
Information in your records may be disclosed to:
Private physicians and Federal agencies, including the Department of Veterans Affairs, Health and Human Services, and
Homeland Security (with regard to members of the Coast Guard), in connection with your medical care;
Government agencies to determine your eligibility for benefits and entitlements;
Government and nongovernment third parties to recover the cost of MHS provided care;
Public health authorities to document and review occupational and environmental exposure data; and
Government and nongovernment organizations to perform DoD-approved research.
Information in your records may be used for other lawful reasons which may include teaching, compiling statistical data, and
evaluating the care rendered. Use and disclosure of your records outside of DoD may also occur in accordance with 5 U.S.C.
552a(b) of the Privacy Act of 1974, as amended, which incorporates the DoD Blanket Routine Uses published at:
http://dpcld.defense.gov/privacy/SORNsIndex/BlanketRoutineUses.aspx.
Any protected health information (PHI) in your records may be used and disclosed generally as permitted by the HIPAA
Privacy Rule (45 CFR Parts 160 and 164), as implemented within DoD by DoD 6025.18-R. Permitted uses and disclosures of
PHI include, but are not limited to, treatment, payment, and healthcare operations.
4. WHETHER DISCLOSURE IS MANDATORY OR VOLUNTARY AND EFFECT ON INDIVIDUAL OF NOT PROVIDING INFORMATION:
Voluntary. If you choose not to provide the requested information, comprehensive health care services may not be possible,
you may experience administrative delays, and you may be rejected for service or an assignment. However, care will not be
denied.
This all inclusive Privacy Act Statement will apply to all requests for personal information made by MHS health care treatment
personnel or for medical/dental treatment purposes and is intended to become a permanent part of your health care record.
Your signature merely acknowledges that you have been advised of the foregoing. If requested, a copy of this form will be
furnished to you.
5. SIGNATURE OF PATIENT OR SPONSOR 6. SOCIAL SECURITY NUMBER OR
DOD IDENTIFICATION NUMBER
OF MEMBER OR SPONSOR
7. DATE (YYYYMMDD)
DD FORM 2005, JUN 2016 PREVIOUS EDITION IS OBSOLETE.