Embed Size (px)
Citation preview
Female Urethral Catheterisation
Learning Outcomes
By the end of the session you will be able to:
• Apply ANTT to performing female catheterisation
• Gain an understanding of the female anatomy
• Identify indications and contraindications for
catheterisation
• Understand equipment used
• Describe associated care and documentation
• Reduce the risk and manage inoculation injuries
Protocols and Competency
• Guides and protects practice
• Supports update of knowledge
• Act within your limitations
• Supervised Practice must be documented in your clinical
procedural passport until graduation
• Keep clinical procedural passport in your portfolio as
evidence of clinical supervision and practice
Aseptic Non Touch Technique (ANTT)
ANTT is a framework which maintains Asepsis in order to protect
patients from potentially harmful organisms.
“Key Parts must only come into contact with other aseptic Key
parts or Key Sites” (www.antt.co.uk)
Asepsis is achieved by:
• Hand decontamination
• Non touch technique
• Sterile equipment
• Cleaning equipment/site until aseptic
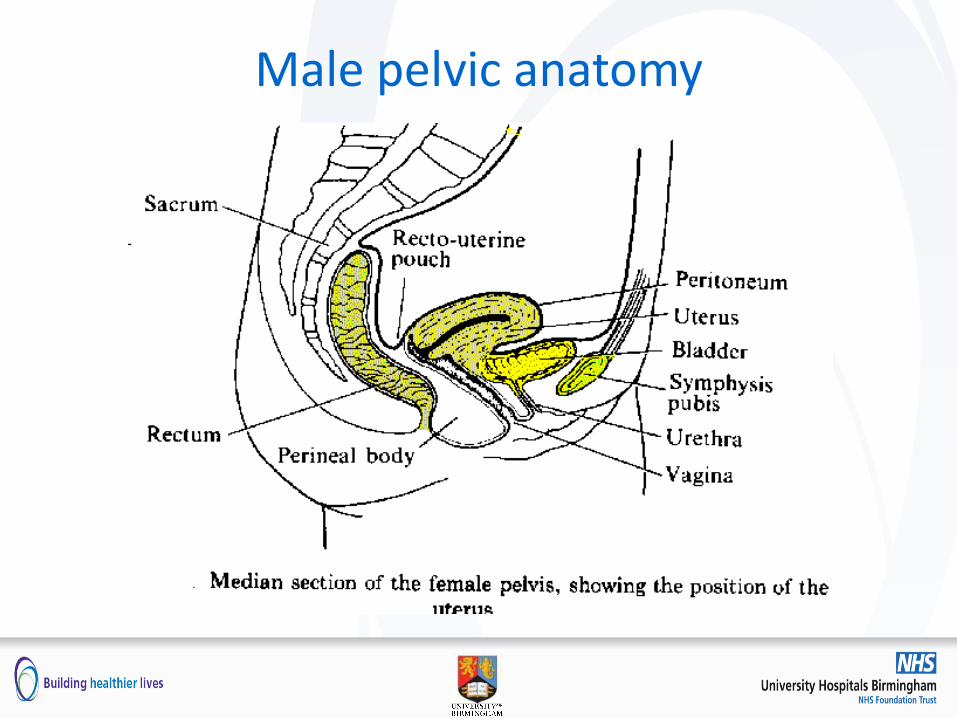
Male pelvic anatomy
Indications
• Retention
• Accurate measurement of output
• Drainage prior to or during surgery/ investigations
• Enable bladder function tests
• Installation of bladder irrigation or intravesical drugs
• Dilatation of stricture
• Management of urinary incontinence when all other methods
inappropriate / unsuccessful
Contraindications and Limitations
• Contraindications
– Patient refusal
– Do not catheterise recorded
– Patients under 16
• Limitations
– Difficult catheterisation or false passage
– Ill defined or oedematous genitals
– Pelvic trauma
– Maximum 1 attempt before referral
Preparing the Patient
• Indication
• Confirm patient identity and allergies
• Gain consent and explain procedure
• Assess genitalia
• Soap and water wash
• Chaperone
• Psychological implications
Catheter sizing
• Two lengths: Female 22-26cm Standard 40-44cm • Charriere size: Measurement of external diameter of the
catheter Or: French Gauge (Fg) or French (F)
• One Charriere unit is 0.33mm:
• 12Ch = 4mm and a 16Ch = 5.3mm diameter
• Ch determines fluid drained
• Larger the Ch greater the risk of trauma
• Balloon sizes
Catheter Materials
• Polyvinylchloride (PVC)
– Used for intermittent self catheterisation
– Sometimes post surgery
– Crack easily
– Easy bacterial attachment
– Single use only
Catheter Materials
• Latex
– Coated with Polytetrafluoroethylene (PTFE) to
produce a smooth outer surface
– Decreased incidence of irritation to urethral mucosa
and encrustation
– Up to 4 weeks insitu: Teflon deteriorates
Catheter Materials
• Silicone
– Latex free
– Walls of the catheter thinner so internal channel equal to larger size E.g. 12Ch = 14Ch
– Time insitu up to 12 weeks
– Balloon material can allow diffusion
– Not as flexible
– Sometimes balloon doesn’t deflate fully or ridges form
Documentation
• Insertion and ongoing care record
• Time and date of insertion / removal date
• Indication for catheter
• Material used: length and size of catheter
• Charriere size and balloon infil
• Lot number and expiry
• Difficulties during the catheterisation
• Residual urine / colour / dip stick
• Fluid Balance
Urinary Catheter Insertion & Ongoing Care Record
Urinary Catheter Insertion & Ongoing Care Record
Catheter Management
• Change catheter bag every 5-7 days
• Keep catheter bag below bladder
• Maintaining a closed system
• G strap or CliniFix
• Bladder washouts
• Education on cleaning
• Obtaining samples
• Changing of catheter
Discharge Planning
• Education
• District Nurse, G.P involvement
• Catheter & Equipment TTO
• Charter Healthcare
• Documentation
Trial without catheter (TWOC)
• Risk assess for need for additional PPE – e.g. goggles /
visor
• Best completed first thing in the morning
• Ensure balloon completely deflated
• Patient to produce urine sample
Catheter Removal If Balloon Fails To Deflate
• Do not pull the catheter
– risk of urethral stricture
– severe trauma
• Use a different syringe
• Check if patient is constipated
• Milking catheter
• Never cut the valve
• Record rationale e.g. - catheter left in whilst waiting to relieve constipation
Cessation of Drainage
• Mechanical obstruction
– Kinked tubing
– Occlusion of tubing by G strap
• Bag higher than the level of bladder
• Is the patient constipated?
• Encrustation
• Urethral spasm
• Dehydration or renal failure
• If none of the above consider blockage
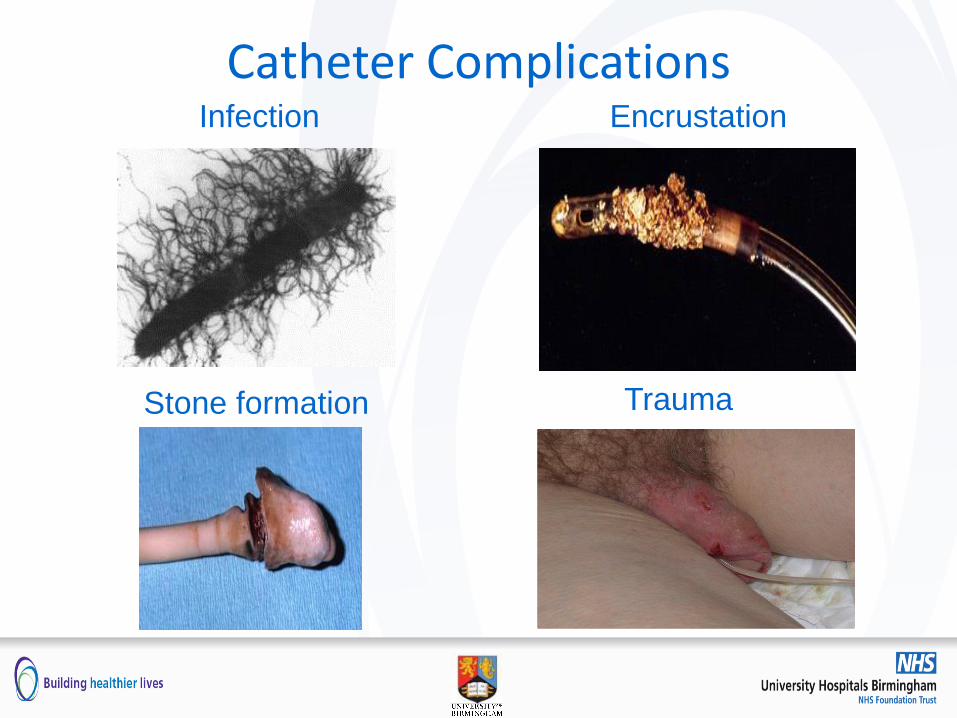
Catheter Complications Infection Encrustation
Stone formation Trauma
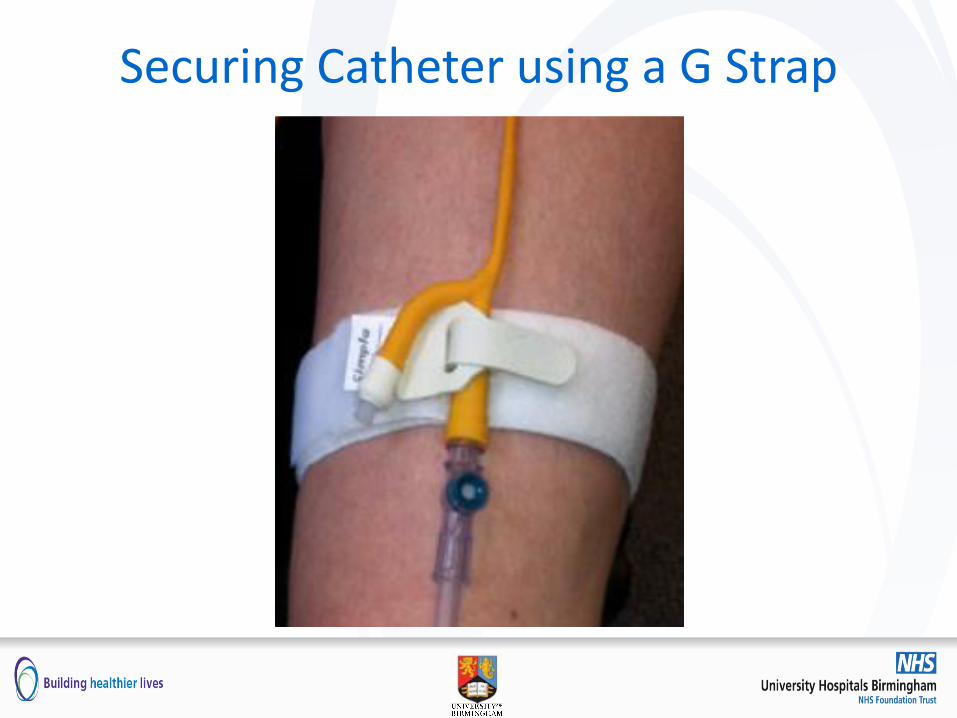
Securing Catheter using a G Strap
Inoculation Injuries
• What is an Inoculation Injury?
– Definition:
Any incident where somebody’s blood or body fluids
could contaminate your blood or mucous membranes
How Can Inoculation Injuries Occur?
• Sharps
• Splashes
• Bites
• Scratches
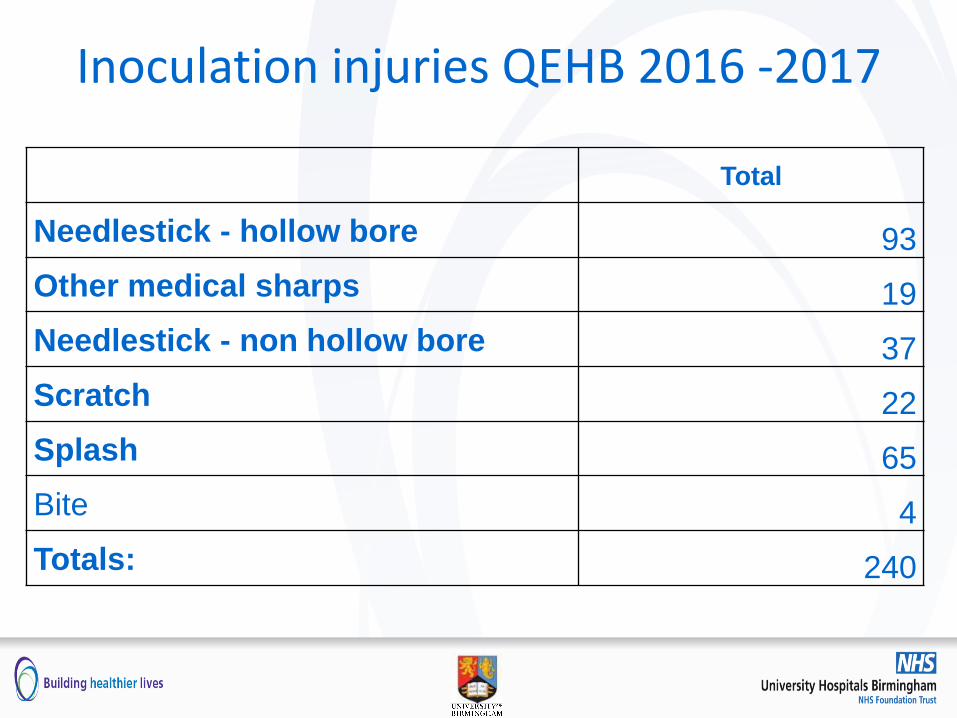
Inoculation injuries QEHB 2016 -2017
Total
Needlestick - hollow bore 93
Other medical sharps 19
Needlestick - non hollow bore 37
Scratch 22
Splash 65
Bite 4
Totals: 240
Total incidents requiring post exposure prophylaxis
• 1 Staff Member required prophylactic treatment for HIV
post inoculation injury
• There were 6 high risk inoculation injuries in 2016 –
2017
Reducing the Risk
• Wear clean non-sterile gloves and apron
– Risk assess for other PPE
• Do not re-sheathe needles
• Dispose sharps at the point of care
• Dispose of syringes and needles as a single unit
• Do not overfill sharps containers
• Use temporary closure device on sharp bins
• Dispose of your own clinical waste
First Aid Treatment for Inoculation Injury
• Bleed and wash with warm running water and cover
• Splash or bite injury irrigate with water
• Report incident to your Manager and complete incident form
• Contact Occupational Health Hub
• Out of hours report to Emergency Department
– Leave a message on the Occupational Health dedicated
answer phone on X17170 with your contact details
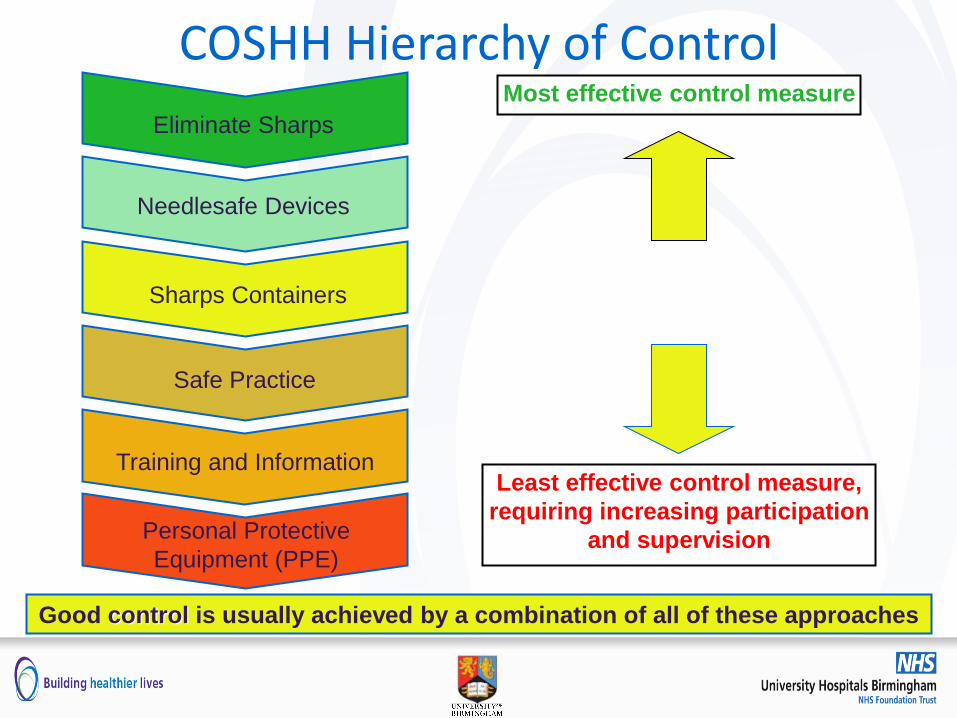
COSHH Hierarchy of Control Most effective control measure
Least effective control measure,
requiring increasing participation
and supervision
Good control is usually achieved by a combination of all of these approaches
Personal Protective
Equipment (PPE)
Training and Information
Safe Practice
Sharps Containers
Needlesafe Devices
Eliminate Sharps

Any Questions?
Learning Outcomes
You are now able to:
• Apply ANTT to performing female catheterisation
• Understand of the female anatomy
• Identify indications and contraindications for
catheterisation
• Understand equipment used
• Describe associated care and documentation
• Reduce the risk and manage inoculation injuries




























