Embed Size (px)
Citation preview

PHARMACOEPIDEMIOLOGY AND PRESCRIPTION
L. Bjerrum á J. Sùgaard á J. Hallas á J. Kragstrup
Polypharmacy: correlations with sex, age and drug regimen
A prescription database study
Received: 23 June 1997 /Accepted in revised form: 7 January 1998
Abstract Objective: To analyse the occurrence of mul-tiple drug use (polypharmacy, PP) in the population andto identify individuals particularly prone to PP.Methods: Data were derived from the Odense Pharma-coepidemiological Database (OPED) and covered allsubsidised prescriptions during 1994 presented by in-habitants in the county of Funen (n � 466 567). Thenumber of individuals concurrently using two to fourdrugs (minor PP) and ®ve or more drugs (major PP) wascalculated on a random day in 1994. Drugs were classi-®ed according to the Anatomical Therapeutical Chemical(ATC) classi®cation index. The main therapeutic class(second level of the ATC code) was used as an indicatorfor the type of health problem. A stepwise backwardslogistic regression was used to identify predictors ofmajor PP. Odds ratios were calculated for di�erent drugclasses, and the age and sex of all drug users.Results: On a random day, 8.3% of the population wereexposed to minor PP and 1.2% to major PP. The prev-alence of PP increased with age, and from the age of 70years, two thirds of all drug users were PP users. Drug usewas 50% more prevalent among women than men, butover the age of 70, the sexes did not di�er in the preva-lence of major PP. Many di�erent drug combinationswere found, and among major PP users (n � 5443), twothirds had their own unique drug regimen, di�erent fromall other drug users. Cardiovascular drugs and analgesicswere often involved in PP among the elderly, whileasthma drugs, psychotropic drugs and anti-ulcer drugs
were predominant among young individuals exposed toPP. The odds ratio (OR) for major PP was substantiallyincreased for individuals treated for cardiovascular dis-eases (OR, 4.5), anaemia (OR, 4.1) and respiratory dis-eases (OR, 3.6).Conclusions: PP is widespread in the population. Clini-cians and organisers who are responsible for quality as-surance programmes should intensify their surveillanceof the groups most prone to PP (the elderly and thoseusing analgesics or drugs for cardiovascular disease,anaemia, asthma and diabetes).
Key words Polypharmacy á Prescription database
Introduction
Simultaneous use of multiple drugs (polypharmacy, PP)has been associated with adverse drug reactions, medi-cation errors and an increased risk of hospitalisation [1].Treatment with two or three drugs may not result inmedication problems, but when the number of drugsexceeds four, studies have shown a signi®cant risk [2, 3].
Most reports of PP have been based on surveys ofpatients admitted to hospital departments [4±6] ornursing homes [7]. Our knowledge is sparse with respectto the prevalence of PP in the general population, theage and sex of PP users and the type of health problemtreated. The increased risk for PP users makes it desir-able to identify and keep such patients under intensi®edsurveillance [2]. The prescriber should be aware ofgroups with an increased prevalence of PP. Quality as-surance programmes aimed at reducing problems asso-ciated with PP are likely to be more e�ective if they focuson groups of patients at increased risk. A randomisedcontrolled trial that was aimed at improving prescribingpractice in primary care thus showed that generalpractitioners who received a letter identifying patientswho had been given ten or more prescriptions improvedprescribing practice and reduced the occurrence of PPcompared to the control group [8].
Eur J Clin Pharmacol (1998) 54: 197±202 Ó Springer-Verlag 1998
L. Bjerrum (&) á J. KragstrupResearch Unit of General Practice, Odense University,Winslùwparken 17, DK-5000 Odense, DenmarkTel. +45-66158696/3028; Fax +45-65911458;e-mail [email protected]
J. SùgaardCenter for Health and Social Policy,Odense University, Denmark
L. Bjerrum á J. HallasDepartment of Clinical Pharmacology, Odense University,Denmark

The purpose of this study was to analyse the occur-rence of PP in the population at large and to identifyindividuals particularly prone to PP. Furthermore, wewanted to investigate whether PP was associated withcertain drug regimens and to examine typical drugcombinations.
Materials and methods
Setting
Since 1990, prescription data from the county of Funen in Den-mark have been collected in the Odense PharmacoepidemiologicalDatabase (OPED), which has been described in detail earlier [9].The registry contains person-identi®able records of all prescriptionrefunds, and each record consists of a unique person-identi®er, thedate of prescription, codes for the pharmacy and the prescriber anda full account of what was purchased, including brand name, dis-pensed dose unit and quantity. The database does not contain in-formation about the prescribed doses or the indication for theprescription, nor does it contain data on drugs sold without aprescription (salicylates, paracetamol, ibuprofen, some anti-ulcerdrugs, antihistamines, laxatives and some antitussive remedies) oron prescription drugs not subsidised by the National Health In-surance (oral contraceptives, sedatives and hypnotics).
Data
The data were derived from the OPED and covered all prescrip-tions during 1993 and 1994 presented by inhabitants living in thecounty of Funen (n � 466 567 on 1 January 1994). Prescriptiondata for individuals aged less than 16 years were not included in theanalysis.
Analysis
Drugs were classi®ed according to the Anatomical TherapeuticChemical (ATC) classi®cation index [10] and di�erentiated to the®fth level of the ATC code (e.g. furosemide: C03CA01). We as-sumed that the use of a drug started on the day of purchase andcalculated the duration of treatment on an assumed daily intake ofone de®ned daily dose (DDD) [11]. Based on this calculation, thedrug regime on each day of the year was charted for all drug users.PP was de®ned as concurrent use of more than one prescribed drugand was classi®ed as minor PP when two to four drugs were usedand major PP when ®ve or more drugs were used on the examinedday. This method for identifying individuals subject to PP haspreviously been evaluated [12]. We calculated the point prevalenceof PP from the drug regimen on a random day in 1994 (1 April).The 1-year prevalence of PP was calculated from the number ofindividuals with one or more episodes of PP during 1994. Theincidence was estimated from the number of individuals with their®rst episode of PP during the last 3 months of 1994 (consideringthese to be incident cases of PP). The prevalence and incidence ofminor and major PP were calculated for various age-groups andboth sexes, and all drugs involved in PP were analysed. Utilisationpro®les were constructed for each main therapeutic drug class(second level of the ATC code), re¯ecting the degree of associationwith PP. The population of Funen (n � 466 567) was used as thedenominator for the calculation of prevalence and incidence.
Stepwise backwards logistic regression was used to identifypossible predictors for major PP among all drug users. The maintherapeutic class was used as an indicator for the type of healthproblem (e.g. purchase of angiotensin-converting enzyme inhibitorsas an indicator for treatment of a cardiovascular disease, purchaseof asthma drugs for a respiratory disease and purchase of anti-diabetic drugs for diabetes). The main therapeutic classes (ATC
code) included were gastrointestinal drugs (A01±09), anti-diabeticdrugs (A10), mineral supplements (A12), anti-thrombotic drugs(B01), anti-anaemic drugs (B03), cardiovascular drugs (C01±10),dermatological drugs (D01±11), genito urinary drugs and sexhormones (G01±04), thyroid drugs (H03), anti-infectious drugs(J01±07), anti-neoplastic and immunomodulating drugs (L01±03),anti-rheumatic drugs (M01±05), analgesics (N02), anti-epilepticdrugs (N03), anti-parkinsonian drugs (N04), psychotropic drugs(N05±06), anti-asthma drugs (R03) and eye and ear drugs (S01-S03). In order to estimate odds ratios of di�erent health problemsrelative to all health problems as such, we included the totalnumber of main therapeutic classes in the regression model. Inorder to avoid perfect co-linearity among the included predictors,one therapeutic class (nasal preparations, R01) was excluded. Thisclass was selected because it was a priori anticipated not to con-tribute above or below average to major PP. Subsequently, the leastsigni®cant main therapeutic classes were eliminated at each step ofthe stepwise backwards logistic regression until all included pre-dictors were statistically signi®cant at the 5% level. In order tominimise in¯ation of signi®cance by the search procedure, the totalnumber of prescriptions was randomly split in two sub-samples ofequal size (split half sample method). The search for signi®cantexplanatory variables using stepwise regression was carried outwith the one sub-sample (test sample), and the validation of theidenti®ed explanatory variables was based on the other sub-sample(validation sample).
Paradox database 4.5 and the statistical program SPSS, version7.0, were used to analyse data. A con®dence interval of 95% wasused.
The study was approved by the Regional Ethics Committee andthe Danish State Registry Board.
Results
In¯uence of age and sex on polypharmacy
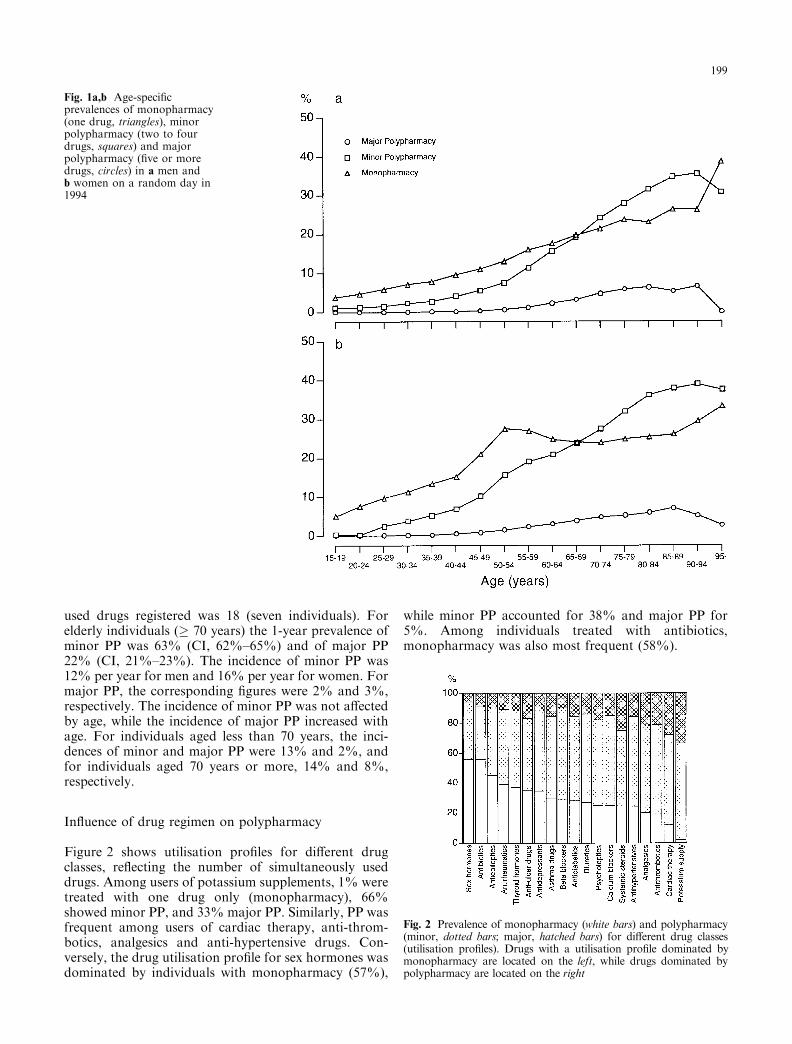
On 1 April 1994, 21.1% (CI, 21.0%±21.3%) of the studypopulation were drug users. Monopharmacy (treatmentwith only one drug) was observed for 11.6% (CI,11.5%±11.7%) of the population, minor polypharmacy(two to four drugs) for 8.3% (CI, 8.2%±8.4%) andmajor polypharmacy (®ve or more drugs) for 1.2% (CI,1.1%±1.3%). The age- and sex-speci®c prevalences ofdrug use are shown in Fig 1. The general trend was in-creased prevalence of PP with increasing age, but amongvery old individuals (³90 years of age) the prevalence ofPP decreased compared with the group aged 80±89 years(Chi-squared, P < 0.01). On average, the prevalence ofdrug use was approximately 50% higher for women thanfor men, but no statistically signi®cant di�erence in theprevalence of major PP was observed between men andwomen above 70 years of age. Among women, theprevalence of monopharmacy increased sharply betweenthe ages of 45 and 59. This increase was mainly due totreatment with sex hormones, which 11% of women inthis age-group used, compared with 1% in the age group35±44 years.
The 1-year prevalence of drug use was 57.8% (CI,57.3%±58.2%). Episodes of minor PP in 1994 wereobserved for 23.6% (CI, 23.2%±24.0%) and of major PPfor 5.1% (CI, 4.9%±5.3%). Episodes with a concurrentuse of ten or more drugs were observed for 3% (CI,2.8%±3.2%), and the maximal number of concurrently
198
used drugs registered was 18 (seven individuals). Forelderly individuals (� 70 years) the 1-year prevalence ofminor PP was 63% (CI, 62%±65%) and of major PP22% (CI, 21%±23%). The incidence of minor PP was12% per year for men and 16% per year for women. Formajor PP, the corresponding ®gures were 2% and 3%,respectively. The incidence of minor PP was not a�ectedby age, while the incidence of major PP increased withage. For individuals aged less than 70 years, the inci-dences of minor and major PP were 13% and 2%, andfor individuals aged 70 years or more, 14% and 8%,respectively.
In¯uence of drug regimen on polypharmacy
Figure 2 shows utilisation pro®les for di�erent drugclasses, re¯ecting the number of simultaneously useddrugs. Among users of potassium supplements, 1% weretreated with one drug only (monopharmacy), 66%showed minor PP, and 33% major PP. Similarly, PP wasfrequent among users of cardiac therapy, anti-throm-botics, analgesics and anti-hypertensive drugs. Con-versely, the drug utilisation pro®le for sex hormones wasdominated by individuals with monopharmacy (57%),
while minor PP accounted for 38% and major PP for5%. Among individuals treated with antibiotics,monopharmacy was also most frequent (58%).
Fig. 1a,b Age-speci®cprevalences of monopharmacy(one drug, triangles), minorpolypharmacy (two to fourdrugs, squares) and majorpolypharmacy (®ve or moredrugs, circles) in a men andb women on a random day in1994
Fig. 2 Prevalence of monopharmacy (white bars) and polypharmacy(minor, dotted bars; major, hatched bars) for di�erent drug classes(utilisation pro®les). Drugs with a utilisation pro®le dominated bymonopharmacy are located on the left, while drugs dominated bypolypharmacy are located on the right
199
Drug combinations involved in major polypharmacy
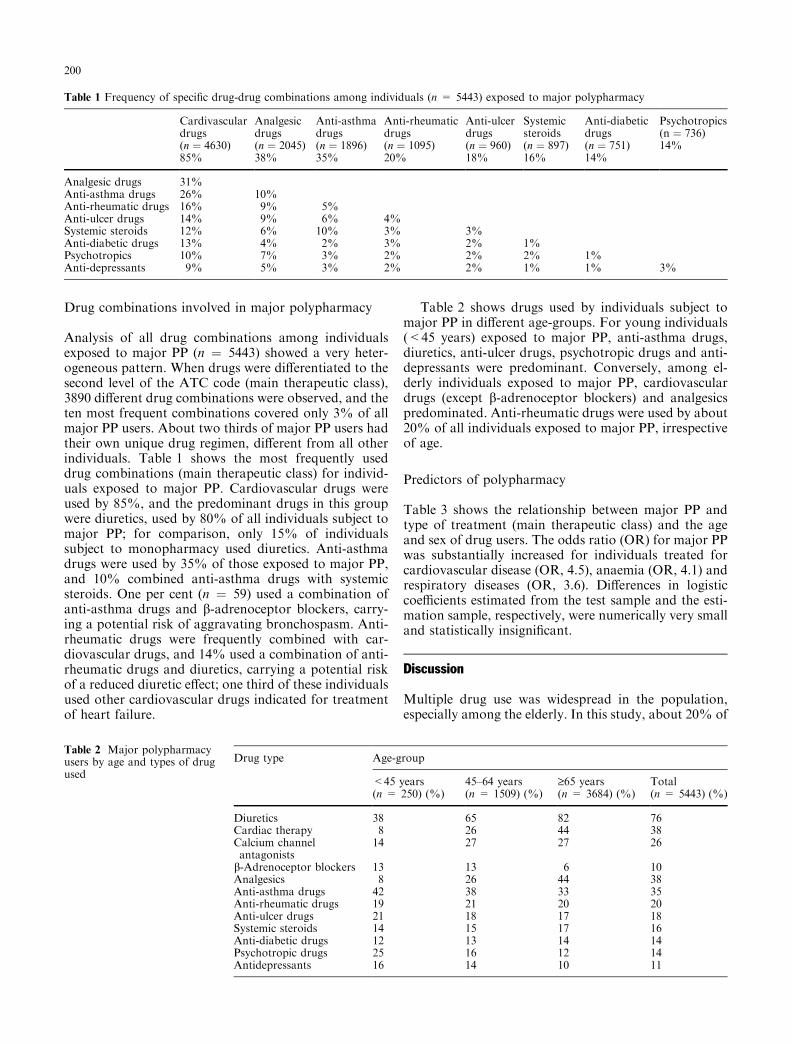
Analysis of all drug combinations among individualsexposed to major PP (n � 5443) showed a very heter-ogeneous pattern. When drugs were di�erentiated to thesecond level of the ATC code (main therapeutic class),3890 di�erent drug combinations were observed, and theten most frequent combinations covered only 3% of allmajor PP users. About two thirds of major PP users hadtheir own unique drug regimen, di�erent from all otherindividuals. Table 1 shows the most frequently useddrug combinations (main therapeutic class) for individ-uals exposed to major PP. Cardiovascular drugs wereused by 85%, and the predominant drugs in this groupwere diuretics, used by 80% of all individuals subject tomajor PP; for comparison, only 15% of individualssubject to monopharmacy used diuretics. Anti-asthmadrugs were used by 35% of those exposed to major PP,and 10% combined anti-asthma drugs with systemicsteroids. One per cent (n � 59) used a combination ofanti-asthma drugs and b-adrenoceptor blockers, carry-ing a potential risk of aggravating bronchospasm. Anti-rheumatic drugs were frequently combined with car-diovascular drugs, and 14% used a combination of anti-rheumatic drugs and diuretics, carrying a potential riskof a reduced diuretic e�ect; one third of these individualsused other cardiovascular drugs indicated for treatmentof heart failure.
Table 2 shows drugs used by individuals subject tomajor PP in di�erent age-groups. For young individuals(<45 years) exposed to major PP, anti-asthma drugs,diuretics, anti-ulcer drugs, psychotropic drugs and anti-depressants were predominant. Conversely, among el-derly individuals exposed to major PP, cardiovasculardrugs (except b-adrenoceptor blockers) and analgesicspredominated. Anti-rheumatic drugs were used by about20% of all individuals exposed to major PP, irrespectiveof age.
Predictors of polypharmacy
Table 3 shows the relationship between major PP andtype of treatment (main therapeutic class) and the ageand sex of drug users. The odds ratio (OR) for major PPwas substantially increased for individuals treated forcardiovascular disease (OR, 4.5), anaemia (OR, 4.1) andrespiratory diseases (OR, 3.6). Di�erences in logisticcoe�cients estimated from the test sample and the esti-mation sample, respectively, were numerically very smalland statistically insigni®cant.
Discussion
Multiple drug use was widespread in the population,especially among the elderly. In this study, about 20% of
Table 1 Frequency of speci®c drug-drug combinations among individuals (n = 5443) exposed to major polypharmacy
Cardivasculardrugs(n � 4630)85%
Analgesicdrugs(n � 2045)38%
Anti-asthmadrugs(n � 1896)35%
Anti-rheumaticdrugs(n � 1095)20%
Anti-ulcerdrugs(n � 960)18%
Systemicsteroids(n � 897)16%
Anti-diabeticdrugs(n � 751)14%
Psychotropics(n � 736)14%
Analgesic drugs 31%Anti-asthma drugs 26% 10%Anti-rheumatic drugs 16% 9% 5%Anti-ulcer drugs 14% 9% 6% 4%Systemic steroids 12% 6% 10% 3% 3%Anti-diabetic drugs 13% 4% 2% 3% 2% 1%Psychotropics 10% 7% 3% 2% 2% 2% 1%Anti-depressants 9% 5% 3% 2% 2% 1% 1% 3%
Table 2 Major polypharmacyusers by age and types of drugused
Drug type Age-group
<45 years(n = 250) (%)
45±64 years(n = 1509) (%)
³65 years(n = 3684) (%)
Total(n = 5443) (%)
Diuretics 38 65 82 76Cardiac therapy 8 26 44 38Calcium channelantagonists
14 27 27 26
b-Adrenoceptor blockers 13 13 6 10Analgesics 8 26 44 38Anti-asthma drugs 42 38 33 35Anti-rheumatic drugs 19 21 20 20Anti-ulcer drugs 21 18 17 18Systemic steroids 14 15 17 16Anti-diabetic drugs 12 13 14 14Psychotropic drugs 25 16 12 14Antidepressants 16 14 10 11
200

the total population were drug users, and about 10%were exposed to two or more drugs on a random day.
Estimates of the proportion of the population subjectto PP have shown some variation. In a community-basedinterview study from Australia, about 20% of individ-uals aged 60 years or more were taking three or moreprescription drugs on the day of the interview [13]. In astudy from general practice in London [14], 30% of theelderly (³75 years) were taking three or more prescrip-tion drugs. In our study, estimates of drug use werebased on drug purchase in the total population, and noton a selection of the elderly. Among people aged 70 yearsor more two thirds experienced episodes of minor PP andone ®fth episodes of major PP during one year. At arandom day, however, only about 5% of the elderly wereexposed to major PP. In a community-based study onself-reported use of prescription drugs in the UnitedStates [15] 10% of elderly (³65 years) reported regularlytaking ®ve or more drugs.
We used the number of DDD for each drug on theday of purchase to calculate the number of drugs in useon the study day, assuming a daily dose of 1 DDD.DDD is de®ned as the average maintenance dose per dayfor a drug used for its main indication [11]. However,some drugs are prescribed at dosages other than theDDD, and some drugs have no established DDD.Consequently, the estimates of drug use on the study daymay be biased, but this bias has a rather small e�ect onthe prevalence of PP [12]. Our study may, however,underestimate the total number of drugs taken by thepopulation, since we excluded non-prescription drugsand non-subsidised drugs. Studies of drug use in thepopulation have shown a highly signi®cant associationbetween use of prescription and non-prescription drugs[13, 16], and the real number of drugs used by any pa-tient may thus be higher than our estimate. For themajority of the inhabitants in Funen, prescription datawere limited to drugs with a general subsidy. However,for the inhabitants with the lowest income, all pre-scription drugs are subsidised, and for these individualsthe total drug regimen based on prescription drugs isregistered. Studies have shown extensive use of sedativesand hypnotics (non-subsidised drugs) in primary care,especially among older people [17], and the prevalence ofPP among these may thus be underestimated. Drugregimens classi®ed as monopharmacy may in fact be PP,and drug use classi®ed as minor PP (two to four drugs)
may have involved ®ve or more drugs. Thus the trueprevalence of PP in the population is likely to exceed ourestimate. This bias may be counteracted to some degreeby the fact that non-compliance is widespread in thepopulation, and much medication purchased may not betaken [18, 19].
We found a heterogeneous distribution of drug use inthe population. The prevalence of PP increased with age,and from the age of 70 years about two thirds of all drugusers were exposed to PP. The prevalence of PP amongvery old individuals (>90 years of age) was somewhatlower than among the elderly in general. Similarly,Helling et al. [20] found that the mean number of pre-scription drugs increased with age until the age of 85years for women and the age of 80 years for men, afterwhich the mean number of prescription drugs decreased.A plausible explanation for this might be that the veryelderly survivors are the most healthy individuals(``survival of the ®ttest''). Longitudinal studies indicate ahigher mortality rate among individuals subject tomultiple drug treatments [21]. A Swedish cohort study ofdrug users showed that individuals surviving after 82years used fewer drugs at the age of 70 and 75 comparedwith those who had died [22].
In most studies of PP, female sex and high age havebeen predictors of PP [23], but a few studies have notfound this relationship [24, 25]. We found a higherprevalence of drug use among women than men, and asimilar trend was observed for PP. Among the elderly,however, there were no di�erences between the sexes inthe prevalence of PP. This is in accordance with thestudy of age-related prescription patterns in generalpractice carried out by Nolan and O'Malley [23, 26],who found a steady increase in the proportion of mentaking prescription drugs, while the prescribing rates forwomen decreased from the age of 70 years; from thisage, there was no signi®cant di�erence between thesexes.
In general, the most important predictors for majorPP in this study concerned the health problems that werebeing treated. We used the drug class as a marker for thetype of health problem. This marker has also been usedin other studies of prescribing patterns and healthproblems [26, 27]. Drug users treated for cardiovasculardiseases, anaemia and respiratory diseases had about afour times higher risk for major PP than drug users ingeneral.
Polypharmacy may be caused by co-existing diseases,but it may also be the result of di�erent drugs being usedto treat the same disease. In our study, most major PPusers were treated with drugs from di�erent main ther-apeutic classes, indicating that multi-morbidity waspresent. Approximately 80% of individuals aged 65 ormore have at least one chronic health problem, andmulti-morbidity is prevalent among geriatric patients[23, 28, 29].
Our knowledge about the e�ects of combining a drugwith several other drugs is unsystematic and sparse.Indeed, some authors have stated that polypharmacy is
Table 3 Odds ratio for major polypharmacy
Predictors of polypharmacy Odds ratio 95% CI
Cardiovascular drugs 4.5 3.9±5.2Drugs for anaemia 4.1 2.7±6.1Asthma drugs 3.6 3.1±4.1Anti-diabetic drugs 1.7 1.4±2.0Analgesics 1.7 1.5±1.9Psychotropic drugs 1.2 1.1±1.5Age ³65 years 1.8 1.6±2.0Female sex 1.2 1.1±1.3
201

like an ``uncontrolled experiment'' with humans [30].This is illustrated in the present study, which showedthat most of the individuals exposed to major PP hadtheir own unique drug combination.
In this study, PP has been used simply to meanmultiple drug use. However, our data do not allow us todraw any conclusions about the justi®cation for PP. Formany patients, treatment with two to four drugs is ap-propriate and necessary, but when the number of si-multaneously used drugs increases to ®ve or more, thereis a pronounced risk of medication errors, especiallywhen the drugs have to be taken at di�erent times of theday [29, 31±33]. Patients may become confused and maymix up their drugs or forget to take essential drugs.Furthermore, PP poses a potential hazard to any patientthrough adverse drug reactions, drug±disease interac-tions and drug±drug interactions.
It may be concluded that PP is frequent in the pop-ulation. When treating individuals subject to PP, it isnecessary to keep them under special surveillance. Oth-erwise, there is an increased risk of health problemscaused by PP. Clinicians and organisers who are re-sponsible for quality assurance programmes aimed atreducing problems associated with PP should focus onthe groups that are most prone to PP (the elderly andthose being treated with drugs for cardiovascular dis-ease, anaemia, asthma, diabetes, mental illness andpain). There is a need to investigate the role of theprescriber in polypharmacy.
Acknowledgements This study was supported by SygekassernesHelsefond (grant no. 22/076-95), Praktiserende lñgers Uddannelseog udviklingsfond and Lundbeckfonden.
References
1. Colley CA, Lucas LM (1993) Polypharmacy: the cure becomesthe disease. J Gen Intern Med 8: 278±283
2. Stewart RB, Clu� LE (1972) A review of medication errors andcompliance in ambulant patients. Clin Pharmacol Ther 13:463±468
3. Bergman U, Wiholm BE (1981) Drug-related problems causingadmission to a medical clinic. Eur J Clin Pharmacol 20: 193±200
4. Bergman U, Wiholm BE (1981) Patient medication onadmission to a medical clinic. Eur J Clin Pharmacol 20: 185±191
5. McMillan DA, Harrison PM, Rogers LJ, Tong N, McLean AJ(1986) Polypharmacy in an Australian teaching hospital. Pre-liminary analysis of prevalence, types of drugs and associa-tions. Med J Aust 145: 339±342
6. Salzman C, van der Kolk BA (1979) Management of the ge-riatric patient in a general hospital. Psychotropic drugs andpolypharmacy in elderly patients in a general hospital. J GeriatrPsychiatry 12: 167±176
7. Daly MP, Lamy PP, Richardson JP (1994) Avoiding poly-pharmacy and iatrogenesis in the nursing home. Md Med J 43:139±144
8. Meyer TJ, Van Kooten D, Marsh S, Prochazka AV (1991)Reduction of polypharmacy by feedback to clinicians. J GenIntern Med 6: 133±136
9. Gaist D, Sorensen HT, Hallas J (1997) The Danish prescriptionregistries. Dan Med Bull 44: 445±448
10. Anonymous (1993) Guidelines for ATC classi®cation.WHO Collaborating Centre for Drug Statistics Methodol-ogy, Oslo
11. Dukes M (1993) Introduction. In: Dukes MNG (ed) Drugutilization studies: methods and uses. European Series no. 45.WHO Regional Publications, Geneva, pp 1±4
12. Bjerrum L, Rosholm JU, Hallas J, Kragstrup J (1997) Methodsfor estimating the occurrence of polypharmacy by means of aprescription database. Eur J Clin Pharmacol 53: 7±11
13. Simons LA, Tett S, Simons J, Lauchlan R, McCallum J,Friedlander Y et al (1992) Multiple medication use in the el-derly. Use of prescription and non-prescription drugs in anAustralian community setting. Med J Aust 157: 242±246
14. Ili�e S, Haines A, Gallivan S, Booro� A, Goldenberg E,Morgan P (1991) Assessment of elderly people in generalpractice. 2. Functional abilities and medical problems. Br J GenPract 41: 13±15
15. Lassila HC, Stoehr GP, Ganguli M, Seaberg EC, Gilby JE,Belle SH et al (1996) Use of prescription medications in anelderly rural population: the MoVIES Project. Ann Pharmac-other 30: 589±595
16. Kjùller M, Rasmussen N, Keiding L, Petersen H, Nielsen G(1995) [Health and disease in Denmark 1994] (in Danish).Dansk Institut for Klinisk Epidemiologi, Copenhagen
17. Bjerrum L, Christensen PB, Larsen PH (1993) [Prescription ofbenzodiazepines in general practice] (in Danish). Ugeskr La-eger 155: 315±319
18. Lassen LC (1989) Patient compliance in general practice. ScandJ Prim Health Care 7: 179±180
19. Beardon PH, McGilchrist MM, McKendrick AD, McDevittDG, MacDonald TM (1993) Primary non-compliance withprescribed medication in primary care. BMJ 307: 846±848
20. Helling DK, Lemke JH, Semla TP, Wallace RB, Lipson DP,Cornoni Huntley J (1987) Medication use characteristics in theelderly: the Iowa 65+ Rural Health Study. J Am Geriatr Soc35: 4±12
21. Incalzi RA, Gemma A, Capparella O, Terranova L, PorceddaP, Tresalti E et al (1992) Predicting mortality and length of stayof geriatric patients in an acute care general hospital. J Ger-ontol 47: M35±M39
22. Landahl S (1987) Drug treatment in 70±82-year-old persons: alongitudinal study. Acta Med Scand 221: 179±184
23. Nolan L, O'Malley K (1988) Prescribing for the elderly. II.Prescribing patterns: di�erences due to age. J Am Geriatr Soc36: 245±254
24. Gupta S, Rappaport HM, Bennett LT (1996) Polypharmacyamong nursing home geriatric Medicaid recipients. AnnPharmacother 30: 946±950
25. Castleden CM, Pickles H (1988) Suspected adverse drug reac-tions in elderly patients reported to the Committee on Safety ofMedicines. Br J Clin Pharmacol 26: 347±353
26. Nolan L, O'Malley K (1987) Age-related prescribing patternsin general practice. Compr Gerontol A 1: 97±101
27. Whitelaw FG, Nevin SL, Taylor RJ, Watt AH (1996) Mor-bidity and prescribing patterns for the middle-aged populationof Scotland. Br J Gen Pract 46: 707±714
28. LeSage J (1991) Polypharmacy in geriatric patients. Nurs ClinNorth Am 26: 273±290
29. Kroenke K (1985) Polypharmacy. Causes, consequences, andcure. Am J Med 79: 149±152
30. Stewart RB, Hale WE (1992) Acute confusional states in olderadults and the role of polypharmacy. Annu Rev Public Health13: 415±430
31. Siomopoulos V, Godbole A (1982) A survey among hospital-ized psychiatric patients. The perils of polypharmacy and co-pharmacy. IMJ 162: 430±433
32. Berndt S, Maier C, Schutz HW (1993) Polymedication andmedication compliance in patients with chronic non-malignantpain. Pain 52: 331±339
33. Honig PK, Cantilena LR (1994) Polypharmacy. Pharmacoki-netic perspectives. Clin Pharmacokinet 26: 85±90
202





























