Embed Size (px)
Citation preview

25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC10.1146/annurev.med.54.101601.152442
Annu. Rev. Med. 2003. 54:343–69doi: 10.1146/annurev.med.54.101601.152442
Copyright c© 2003 by Annual Reviews. All rights reserved
MONOCLONAL ANTIBODY THERAPY FOR CANCER
Margaret von Mehren, Gregory P. Adams,and Louis M. WeinerDepartment of Medical Oncology, Fox Chase Cancer Center, 7701 Burholme Avenue,Philadelphia, Pennsylvania 19111; e-mail: [email protected],gp [email protected], [email protected]
Key Words immunoconjugate, immunotoxin, radioimmunotherapy,antibody-dependent cellular cytotoxicity
■ Abstract Monoclonal antibody therapy has emerged as an important therapeuticmodality for cancer. Unconjugated antibodies show significant efficacy in the treat-ment of breast cancer, non-Hodgkin’s lymphoma, and chronic lymphocytic leukemia.Promising new targets for unconjugated antibody therapy include cellular growth fac-tor receptors, receptors or mediators of tumor-driven angiogenesis, and B cell surfaceantigens other than CD20. Immunoconjugates composed of antibodies conjugated toradionuclides or toxins show efficacy in non-Hodgkin’s lymphoma. One immunocon-jugate containing an antibody and a chemotherapy agent exhibits clinically meaningfulantitumor activity in acute myeloid leukemia. Numerous efforts to exploit the abilityof antibodies to focus the activities of toxic payloads at tumor sites are under way andshow early promise. The ability to create essentially human antibody structures hasreduced the likelihood of host-protective immune responses that otherwise limit theduration of therapy. Antibody structures now can be readily manipulated to facilitateselective interaction with host immune effectors. Other structural manipulations thatimprove the selective targeting properties and rapid systemic clearance of immuno-conjugates should lead to the design of effective new treatments, particularly for solidtumors.
INTRODUCTION
The description of techniques for the production of monoclonal antibodies (MAb)by Kohler & Milstein 25 years ago led to the development of multiple reagentsemploying these structures. Antibodies, which initially were viewed as “target-ing missiles,” have proved much more complex in their targeting and biologicproperties than the field’s pioneers envisioned them. The ability to manipulate thegenes of antibodies with microbiologic techniques has allowed significant mod-ifications of these structures. Murine proteins can be readily transformed intohuman or humanized formats that are not readily recognized as foreign by the
0066-4219/03/0218-0343$14.00 343
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
344 VON MEHREN ¥ ADAMS ¥ WEINER
human immune system. In addition, novel antibody-based structures with multi-ple antigen recognition sites, altered size, or effector domains have been shownto influence the targeting ability of antibodies. Coupled with the identificationof appropriate cancer targets, antibody-based therapeutics are finding increasingapplications in cancer treatment, and they can be effective alone, in conjunctionwith chemotherapy or radiation therapy, or when conjugated to toxic moietiessuch as toxins, chemotherapy agents, or radionuclides. This review focuses onantibody-based agents with significant efficacy and novel approaches with clinicalpromise.
IMMUNOGLOBULIN STRUCTURE
IgG
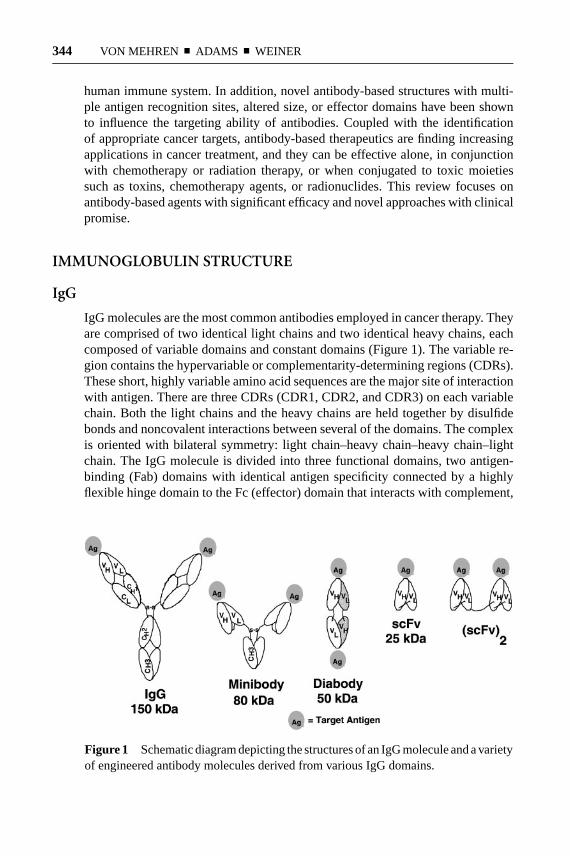
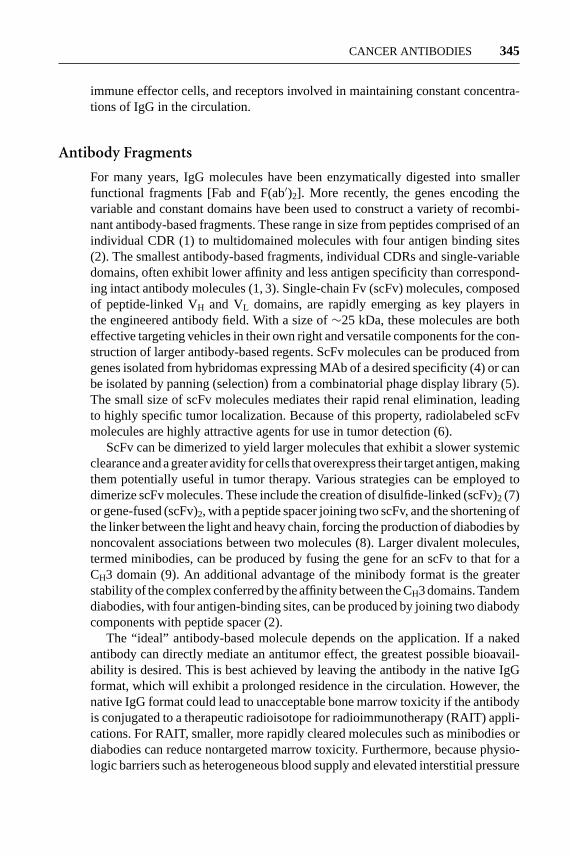
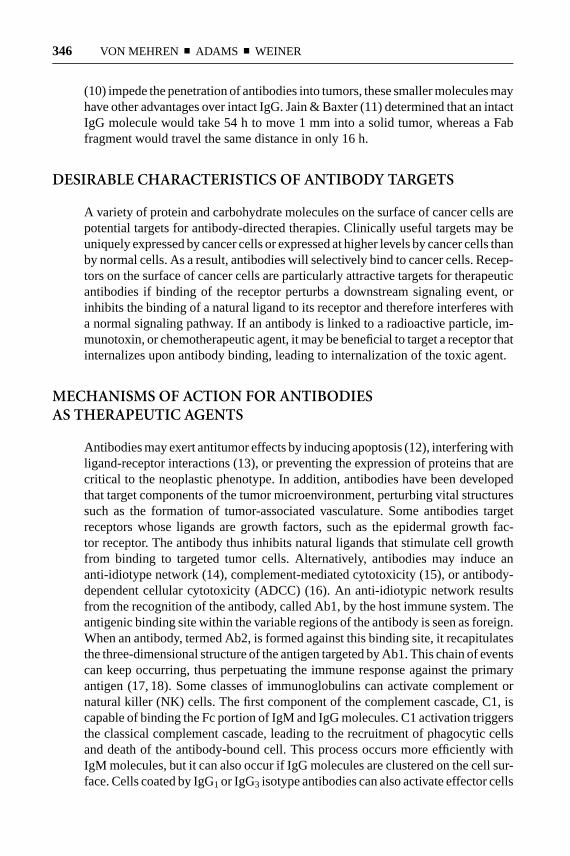
IgG molecules are the most common antibodies employed in cancer therapy. Theyare comprised of two identical light chains and two identical heavy chains, eachcomposed of variable domains and constant domains (Figure 1). The variable re-gion contains the hypervariable or complementarity-determining regions (CDRs).These short, highly variable amino acid sequences are the major site of interactionwith antigen. There are three CDRs (CDR1, CDR2, and CDR3) on each variablechain. Both the light chains and the heavy chains are held together by disulfidebonds and noncovalent interactions between several of the domains. The complexis oriented with bilateral symmetry: light chain–heavy chain–heavy chain–lightchain. The IgG molecule is divided into three functional domains, two antigen-binding (Fab) domains with identical antigen specificity connected by a highlyflexible hinge domain to the Fc (effector) domain that interacts with complement,
Figure 1 Schematic diagram depicting the structures of an IgG molecule and a varietyof engineered antibody molecules derived from various IgG domains.
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 345
immune effector cells, and receptors involved in maintaining constant concentra-tions of IgG in the circulation.
Antibody Fragments
For many years, IgG molecules have been enzymatically digested into smallerfunctional fragments [Fab and F(ab′)2]. More recently, the genes encoding thevariable and constant domains have been used to construct a variety of recombi-nant antibody-based fragments. These range in size from peptides comprised of anindividual CDR (1) to multidomained molecules with four antigen binding sites(2). The smallest antibody-based fragments, individual CDRs and single-variabledomains, often exhibit lower affinity and less antigen specificity than correspond-ing intact antibody molecules (1, 3). Single-chain Fv (scFv) molecules, composedof peptide-linked VH and VL domains, are rapidly emerging as key players inthe engineered antibody field. With a size of∼25 kDa, these molecules are botheffective targeting vehicles in their own right and versatile components for the con-struction of larger antibody-based regents. ScFv molecules can be produced fromgenes isolated from hybridomas expressing MAb of a desired specificity (4) or canbe isolated by panning (selection) from a combinatorial phage display library (5).The small size of scFv molecules mediates their rapid renal elimination, leadingto highly specific tumor localization. Because of this property, radiolabeled scFvmolecules are highly attractive agents for use in tumor detection (6).
ScFv can be dimerized to yield larger molecules that exhibit a slower systemicclearance and a greater avidity for cells that overexpress their target antigen, makingthem potentially useful in tumor therapy. Various strategies can be employed todimerize scFv molecules. These include the creation of disulfide-linked (scFv)2 (7)or gene-fused (scFv)2, with a peptide spacer joining two scFv, and the shortening ofthe linker between the light and heavy chain, forcing the production of diabodies bynoncovalent associations between two molecules (8). Larger divalent molecules,termed minibodies, can be produced by fusing the gene for an scFv to that for aCH3 domain (9). An additional advantage of the minibody format is the greaterstability of the complex conferred by the affinity between the CH3 domains. Tandemdiabodies, with four antigen-binding sites, can be produced by joining two diabodycomponents with peptide spacer (2).
The “ideal” antibody-based molecule depends on the application. If a nakedantibody can directly mediate an antitumor effect, the greatest possible bioavail-ability is desired. This is best achieved by leaving the antibody in the native IgGformat, which will exhibit a prolonged residence in the circulation. However, thenative IgG format could lead to unacceptable bone marrow toxicity if the antibodyis conjugated to a therapeutic radioisotope for radioimmunotherapy (RAIT) appli-cations. For RAIT, smaller, more rapidly cleared molecules such as minibodies ordiabodies can reduce nontargeted marrow toxicity. Furthermore, because physio-logic barriers such as heterogeneous blood supply and elevated interstitial pressure
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
346 VON MEHREN ¥ ADAMS ¥ WEINER
(10) impede the penetration of antibodies into tumors, these smaller molecules mayhave other advantages over intact IgG. Jain & Baxter (11) determined that an intactIgG molecule would take 54 h to move 1 mm into a solid tumor, whereas a Fabfragment would travel the same distance in only 16 h.
DESIRABLE CHARACTERISTICS OF ANTIBODY TARGETS
A variety of protein and carbohydrate molecules on the surface of cancer cells arepotential targets for antibody-directed therapies. Clinically useful targets may beuniquely expressed by cancer cells or expressed at higher levels by cancer cells thanby normal cells. As a result, antibodies will selectively bind to cancer cells. Recep-tors on the surface of cancer cells are particularly attractive targets for therapeuticantibodies if binding of the receptor perturbs a downstream signaling event, orinhibits the binding of a natural ligand to its receptor and therefore interferes witha normal signaling pathway. If an antibody is linked to a radioactive particle, im-munotoxin, or chemotherapeutic agent, it may be beneficial to target a receptor thatinternalizes upon antibody binding, leading to internalization of the toxic agent.
MECHANISMS OF ACTION FOR ANTIBODIESAS THERAPEUTIC AGENTS
Antibodies may exert antitumor effects by inducing apoptosis (12), interfering withligand-receptor interactions (13), or preventing the expression of proteins that arecritical to the neoplastic phenotype. In addition, antibodies have been developedthat target components of the tumor microenvironment, perturbing vital structuressuch as the formation of tumor-associated vasculature. Some antibodies targetreceptors whose ligands are growth factors, such as the epidermal growth fac-tor receptor. The antibody thus inhibits natural ligands that stimulate cell growthfrom binding to targeted tumor cells. Alternatively, antibodies may induce ananti-idiotype network (14), complement-mediated cytotoxicity (15), or antibody-dependent cellular cytotoxicity (ADCC) (16). An anti-idiotypic network resultsfrom the recognition of the antibody, called Ab1, by the host immune system. Theantigenic binding site within the variable regions of the antibody is seen as foreign.When an antibody, termed Ab2, is formed against this binding site, it recapitulatesthe three-dimensional structure of the antigen targeted by Ab1. This chain of eventscan keep occurring, thus perpetuating the immune response against the primaryantigen (17, 18). Some classes of immunoglobulins can activate complement ornatural killer (NK) cells. The first component of the complement cascade, C1, iscapable of binding the Fc portion of IgM and IgG molecules. C1 activation triggersthe classical complement cascade, leading to the recruitment of phagocytic cellsand death of the antibody-bound cell. This process occurs more efficiently withIgM molecules, but it can also occur if IgG molecules are clustered on the cell sur-face. Cells coated by IgG1 or IgG3 isotype antibodies can also activate effector cells

25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 347
via the binding of the terminal Fc portion of the antibody to Fc receptors, foundon NK cells, neutrophils, mononuclear phagocytes, some T cells, and eosinophils.ADCC occurs with the release of cytoplasmic granules containing perforins andgranzymes from these effector cells. This phenomenon can be amplified by con-structing bispecific antibodies that contain two binding domains, one that targetsa tumor antigen and one that targets the immunoglobulin Fc receptor on immuneeffector cells, thereby activating the effector cells for tumor lysis.
ANTIBODY LIMITATIONS
Initial clinical trials with MAb produced some striking antitumor effects (19),but most of the early experiences illustrated the obstacles to successful therapy(Table 1). Most of the MAb employed in early clinical trials were derived frommice, and patients exposed to them developed human antimouse antibody (HAMA)responses, which limited the number of treatments patients could safely receive(20). Molecular engineering techniques have overcome this obstacle by graftingcritical sequences in the human heavy-chain backbone onto the xenogeneic murineantibody structure, paring the interspecies differences and reducing the immuno-genicity of the resulting antibodies. Numerous techniques have further reducedimmunogenicity, and it is now possible to create fully human immunoglobulinswith limited capacity to induce HAMA. However, these approaches do not inhibitthe production of anti-idiotype antibodies (see previous section).
Some tumor antigens are shed or secreted. Antibodies that target these antigenswill bind their targets in the circulation, limiting the amount of unbound antibodyavailable to bind to tumor (21). Barriers that impede antibody distribution withintumors include (a) disordered tumor vasculature, (b) increased hydrostatic pressurewithin tumors and (c) heterogeneity of antigen distribution within tumors (11). Ithas been estimated that, due to these barriers, an IgG molecule will take 2 days totravel 1 mm and 7–8 months to travel 1 cm within a tumor. Estimates for a smallerantibody-based molecule, such as a Fab fragment, are 1 day to travel 1 mm and2 months to travel 1 cm. If antibodies do reach their targets, there is little evidence
TABLE 1 Obstacles to effective antibodytherapy
1. Immunogenicity of xenogeneic antibodies
2. Shedding of antigen into circulation
3. Disordered vasculature in tumors
4. Increased hydrostatic pressure in tumors
5. Heterogeneity of antigen on tumor surface
6. Limited numbers of effector cells at tumor
7. Immunosuppressive tumor microenvironment
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
348 VON MEHREN ¥ ADAMS ¥ WEINER
that they efficiently mediate ADCC in vivo. For this to occur, sufficient numbersof effector cells, such as macrophages, NK cells, or cytotoxic T cells, must bepresent in the tumor (22). Finally, many tumors are known to secrete compoundsthat downregulate the immune response (23, 24), or to have decreased effectorcells as a consequence of hypoxia (25). Despite these impediments, preclinical andclinical data with improved antibody-based molecules continue to demonstrate arole for antibody-based therapy as a component of the oncologic armamentarium.
ANTIBODY THERAPEUTICS
The ability to identify therapeutic targets and produce antibodies with limitedimmunogenicity has led to the production and testing of a host of agents, several ofwhich have demonstrated clinically important antitumor activity and have receivedFDA approval for treatment of cancer. We focus here on antibodies with provenefficacy, classified according to the tumor or antigen system that is targeted.
Hematologic Malignancy Antigens
B CELL ANTIGENS Initial studies employing antibodies directed against B celldeterminants showed that the passive administration of these antibodies led toclearance of circulating tumor cells and rare objective clinical responses (26). Ina series of landmark studies, Levy and colleagues prepared customized antibodiesreactive with a given lymphoma patient’s idiotype that was uniquely expressedon the surface of the malignant B cell clone. Each patient’s idiotype served as atumor-specific signature that could be targeted by a customized MAb. The pro-cedures for preparing such antibodies for each patient were laborious, but∼50%of treated patients experienced significant clinical responses, with some patientsachieving durable complete remissions (19). The addition of chemotherapy agents,interferon, or other cytokines did not appreciably improve treatment outcomes.Effective therapy had to overcome circulating lymphoma idiotype proteins thatdiverted antibodies from their cellular targets, and resistance to therapy resulted inpart from the emergence of idiotype-negative variants. The mechanisms underlyingresponses to these antibodies have not been completely elucidated but may includemechanisms such as ADCC (see below) and perturbation of signal transductionthrough idiotype engagement (27). Due to the immunosuppression of lymphomapatients, relatively few patients developed HAMA that interfered with repeatedtherapeutic antibody administration. This exciting approach was very cumbersome,as it required the generation of patient-customized reagents. These results couldnot be replicated using antibodies that recognize shared idiotypes expressed by alarge proportion of lymphoma patients (28). Despite this set of impediments, theseimportant observations have informed much of the subsequent work in this field.
CD52 The CAMPATH-1 antibody has specificity for CD52, a glycopeptide thatis highly expressed on T and B lymphocytes. It has been tested as a therapeutic
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 349
agent for chronic lymphocytic and promyelocytic leukemias, as well as othernon-Hodgkin’s lymphomas, and as a means to deplete T cells from allogeneic trans-plant grafts. Half of the patients with fludarabine-resistant chronic lymphocyticleukemia or B-prolymphocytic leukemia exhibited clinical responses toCAMPATH-1 (29). A larger phase II study reported a 42% response rate in pa-tients with relapsed or refractory chronic lymphocytic leukemia, but at the cost ofan increase in opportunistic infections and septicemia. CAMPATH-1 has also beenevaluated as first-line therapy for patients with chronic lymphocytic leukemia. Allpatients responded with loss of peripheral blood malignant lymphocytes. How-ever, patients with involvement of lymph nodes and/or spleen were less likely torespond completely. There was evidence of reactivation of cytomegalovirus in-fections. Subcutaneous administration of the antibody was found to be safe andeffective. A humanized version of the antibody (CAMPATH-1H) has been exten-sively tested.
In a phase II multicenter study of CAMPATH-1H in previously treated patientswith low-grade non-Hodgkin’s lymphomas, 50 patients with relapsed or refrac-tory disease were treated with 30 mg of CAMPATH-1H 3 times weekly for upto 12 weeks (30). Infection, anemia, and thrombocytopenia were common, andmyocardial infarction occurred in one patient with a prior history of angina andcongestive heart failure. The overall response rate was 20% (16% partial response,4% complete reponse). Responses were short in duration, with a median time toprogression of 4 months. Patients with mycosis fungoides responded more fre-quently and had a longer time to progression (10 months) than did patients withlow-grade non-Hodgkin’s lymphoma (4 months). Treatment was associated withreactivation of herpes simplex, oral candidiasis,pneumocystis cariniipneumonia,cytomegalovirus pneumonitis, pulmonary aspergillosis, disseminated tuberculo-sis, and seven cases of pneumonia and septicemia.
CAMPATH-1 has been used to deplete T cells from allogeneic transplant graftsin patients with hematologic malignancies (31, 32). The initial study suggestedthat the addition of CAMPATH-1 significantly decreased graft rejection and graft-versus-host disease compared with conventional therapy. However, the frequencyof graft rejection and graft failure was higher. A retrospective review of patientswith acute lymphocytic or acute myelogenous leukemia who underwent allogeneictransplantation with CAMPATH-1–purged marrow suggested no impact on thegraft-versus-leukemia effect, as there was no increase in leukemia relapse (33). Ad-ditionally, the incidence of Epstein-Barr virus (EBV)–related lymphoproliferativedisorders was decreased in allogeneic transplant patients who had T cell depletionwith CAMPATH-1 therapy compared with other methods of T cell depletion (e.g.,E-rosettes or other MAb) (34). CAMPATH-1 eliminated B cells within the graft,thus eliminating a potential reservoir of EBV or targets for subsequent infection.
CD20 The testing and evaluation of the chimeric anti-CD20 antibody, IDEC-C2B8, also known as rituximab, demonstrated impressive clinical responses.Rituximab is the first MAb to be approved by the FDA for use in human malignancy
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
350 VON MEHREN ¥ ADAMS ¥ WEINER
(35, 36). Rituximab is humanized and multiple doses can be safely administered.In vitro studies have demonstrated multiple mechanisms by which anti-CD20 an-tibodies lead to cell death: ADCC, complement-mediated lysis, and apoptosis thatis diminished by inhibitors of Lck and Fyn tyrosine kinases, calcium chelators,and caspase inhibitors (37).
In the phase I study to determine the maximum tolerated dose, patients with re-lapsed low-grade and intermediate/high-grade non-Hodgkin’s lymphoma receivedfour weekly infusions of rituximab (37). Thrombocytopenia and B cell lympho-cytopenia were observed. The lymphocytopenia persisted for 3–6 months. Six of18 patients, all of whom had low-grade lymphomas, demonstrated partial responses(33%). Phase II studies using the maximum tolerated dose, 375 mg/m2, confirmedthe efficacy of this therapy, demonstrating 46% and 48% response rates in twoseparate studies (38, 39). Although the numbers of circulating B cells were re-duced by therapy, there were no documented changes in serum immunoglobulinlevels. Bacterial and viral infections were seen in patients with relapsed indo-lent lymphomas, but in contrast to the CAMPATH-1 experience, treatment withrituximab did not result in significant morbidity due to infections. Patients withsmall-lymphocytic-B-cell lymphoma had lower response rates, probably relatedto the lesser expression of CD20 on these tumor cells.
Although phase I testing had not suggested significant activity in intermediate/high-grade lymphomas, a phase II trial evaluated rituximab in relapsing or refrac-tory diffuse large B cell lymphoma, mantle cell lymphoma, or other intermediate-or high-grade B cell non-Hodgkin’s lymphomas (40). The study randomized54 patients to either 8 weekly treatments of 375 mg/m2 intravenous rituximab or375 mg/m2 in week one followed by 7 weekly intravenous infusions of 500 mg/m2.Five complete responses and 12 partial responses were observed, for an overallresponse rate of 31%; there was no evidence of superiority of either treatment reg-imen. Patients with refractory disease and those with histologies other than diffuselarge B cell lymphoma appeared to have lower response rates. A novel use of rit-uximab has been reported for cutaneous B cell lymphoma; patients who receivedintralesional injections of the antibody showed partial clearing of nodules (41).
Rituximab has been tested in conjunction with chemotherapy (42). Preclinicaldata show that this antibody can sensitize chemotherapy-resistant cell lines to thecytotoxic effects of chemotherapy (43). Forty patients with low-grade or follicularB cell non-Hodgkin’s lymphoma were enrolled in the study. Thirty-five patientsreceived all six planned cycles of CHOP every 21 days, with six infusions ofrituximab at a dose of 375 mg/m2 given before, during, and after chemotherapy.Three patients did not complete treatment due to intercurrent infections (n = 2)and patient choice (n = 1), and two patients were withdrawn from the study prior totherapy. The overall response rate was 95% (38/40), with 55% complete responsesand 40% partial responses. Fewer complete responses were noted in patients withbulky disease. Median response duration and time to progression had not beenreached after 29+ months of follow-up. Seven of 8 patients who had initiallybeen positive for the bcl-2 translocation became negative for the translocation
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 351
by PCR assay after therapy; this has not been seen with CHOP chemotherapyalone (44). A preliminary analysis of a randomized study in elderly patients withdiffuse large-cell lymphoma comparing standard CHOP chemotherapy to CHOPwith rituximab demonstrated a 76% complete response rate in the combinationarm compared with 60% complete response rate in the chemotherapy arm withoutsignificant differences in toxicity between the two groups (40). Furthermore, theaddition of rituximab prolonged event-free survival and overall survival.
Rituximab also has been evaluated in conjunction with fludarabine in low-gradelymphomas. Significant leukopenias were associated with this combination, requir-ing a dose reduction in the fludarabine. An interim analysis after accruing 30 of the40 planned patients revealed a response rate of 93% with median response dura-tion of over 14 months. Cytogenetic responses were also observed in some patients(45). The significance of such responses is unclear. In a study of rituximab withCHOP chemotherapy in patients with mantle cell lymphoma, loss of a cytogeneticmarker was not associated with improved progression-free survival (46).
Another setting in which rituximab has been tested is following high-dosechemotherapy with autologous transplantation (47). Patients with at least a 75%reduction in tumor volume following CHOP chemotherapy underwent high-dosechemotherapy with stem cell transplantation. Two and six months following trans-plant, patients received four weekly treatments with rituximab. A preliminaryreport of this study describes four patients who have received one post-transplantcycle and eight who have received two post-transplant cycles. Two patients are re-ported with a partial response and another two patients with unconfirmed completeresponse.
Circulating CD20-positive cells, including lymphoma cells, may affect the ef-ficacy of rituximab. Peak levels of circulating antibody inversely correlate withpretreatment B cell counts as well as the bulk of tumor (38, 39). Greater numbersof peripheral lymphocytes and/or tumor bulk serve as an antigen sink, removingantibody from the circulation. For patients with bulky disease, a higher antibodydose or a greater number of cycles may be warranted, since patients with lowerserum rituximab concentrations have had statistically significant lower responserates. A dosage of eight cycles of weekly rituximab has been used safely in low-grade and follicular non-Hodgkin’s lymphoma (48). The efficacy of rituximab inchronic lymphocytic leukemia is clearly affected by lower circulative levels ofthe antibody. Initial studies revealed a 20% response rate. Chronic lymphocyticleukemia has lower antigen density than many lymphomas that express CD20, andthe cells circulate, acting as an antigen sink. A dose-escalation study demonstrateda clear dose-response relationship (49).
Rituximab therapy rarely selects for the emergence of an antigen-negative pop-ulation of tumor cells. At the present time, little is known about mechanisms ofresistance (49a). This phenomenon has been documented in a patient with a follic-ular mixed small- and large-cell lymphoma, who was treated with rituximab aftermultiple chemotherapy regimens (50). Approaches to overcome antigen-negativepopulations include combining rituximab with chemotherapy or with antibodies

25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
352 VON MEHREN ¥ ADAMS ¥ WEINER
targeting other antigens expressed by the lymphoma or leukemia being treated.For example, chronic lymphocytic leukemia expresses both CD20 and CD52.Studies are evaluating combination therapy with both rituxan and CAMPATH-1H(51). Other antigens that could target B cell lymphomas and leukemias includeCD22, which is expressed on pro-B and pre-B cell lymphomas, and the ma-jor histocompatability class II antigen, HLA-DR, found on B lymphocytes aswell as macrophages and dendritic cells. Epratuzumab, which targets CD22, andapolizumab, which targets a subset of HLA-DR molecules, are currently undergo-ing testing (52). Clearly these agents are candidates for combination therapy withrituximab.
In some patients with circulating blood tumor cells, rituximab therapy hasinduced an infusion-related syndrome characterized by fever, rigors, thrombocy-topenia, tumor lysis, bronchospasm, and hypoxemia, requiring discontinuationof the antibody infusion. Symptoms typically resolve with supportive care andpatients may continue further therapy without sequelae (53). Another case reportdocuments rapid tumor lysis in a patient with B cell chronic lymphocytic leukemiawith a pretreatment lymphocytosis of>100× 109/liter (54). Occasional severemucocutaneous reactions have been reported, some of which have been fatal.These present as paraneoplastic pemphigus, Stevens-Johnson syndrome, and toxicepidermal necrolysis (55).
Solid Tumor Antigens
HER-2/NEU HER-2/neu(c-erbB-2), a member of the epidermal growth factor re-ceptor (EGFR) family, has been targeted for antibody therapy because it is over-expressed on∼25% of breast cancers, as well as other adenocarcinomas of theovary, prostate, lung, and gastrointestinal tract. Trastuzumab (56, 57), also knownas Herceptin® and rhuMAb HER2, is a humanized antibody derived from 4D5, amurineMAb, which recognizes an epitope on the extracellular domain of HER-2/neu. A phase II trial in women with metastatic breast cancer reported an objec-tive response rate of 11.6%, with responses seen in the liver, mediastinum, lymphnodes, and chest wall. Patients received ten or more treatments with the antibody,and none developed an antibody response against trastuzumab. In a second phaseII study, 222 women with metastatic breast cancer were treated with 2 mg/kg oftrastuzumab weekly, with an objective response rate of 16% (56). The medianresponse duration was 9.1 months, with a median overall survival of 13 months,both of which are superior to outcomes reported for second-line chemotherapy inmetastatic disease. In each of these trials, about 30% of the patients had stable dis-ease, lasting more than 5 months. Overexpression of HER-2/neuthat is associatedwith gene amplification correlates with a clinical response to trastuzumab. Earlierstudies utilized variable criteria to define HER2 positivity that may account forthe differences in the response rates. The standard assay for determining HER2expression is the Hercept test. Breast tumors with 3+ expression by this assaycorrelate with gene overexpression; those with 2+ expression require testing by

25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 353
fluorescence in situ hybridization to confirm gene amplification. Intriguingly, pre-clinical studies have demonstrated decreased expression of vascular endothelialcell growth factor (VEGF) and vascular permeability factor with 4D5 therapy, sug-gesting that an antiangiogenesis mechanism may account for some of the clinicalimpact of this antibody (58). Trastuzumab continues to be evaluated clinically indiverse adenocarcinoma types.
A large, randomized phase III trial evaluating cytotoxic chemotherapy aloneand with trastuzumab has shown the efficacy of combination therapy (59). Patientsreceiving initial therapy for metastatic breast cancer were treated with cyclophos-phamide plus doxorubicin or epirubicin, or with paclitaxel if they had receivedan anthracycline in the adjuvant setting. Patients were randomized to receive thischemotherapy alone or in combination with weekly antibody therapy. Responserates for combination therapy with an anthracycline regimen increased from 43%to 52% with the addition of trastuzumab. Using a taxane regimen, response ratesincreased from 16% to 42% with the addition of trastuzumab. In addition, therewas evidence that the addition of trastuzumab to chemotherapy improved sur-vival at one year by 16% (60) and improved survival at 29 months by 25% (61).Myocardial dysfunction was observed more frequently in patients receiving dox-orubicin or epirubicin when trastuzumab was added. Therefore, trastuzumab is notrecommended in combination with anthracyclines.
Based on these clinical trial results, trastuzumab was approved by the FDAto treat women with metastatic breast cancer with HER-2/neu overexpression,given either alone or in combination with paclitaxel. Herceptin also has activity incombination with vinorelbine (62), docetaxel, cisplatin (63), and the combinationof gemcitabine and paclitaxel (64). In addition, breast cancer patients with lymphnode involvement whose cancers overexpress HER-2/neuare candidates for partic-ipation in a randomized phase III trial evaluating standard adjuvant chemotherapywith or without trastuzumab.
The use of Herceptin for breast cancer has been a therapeutic success. Al-though other adenocarcinomas may overexpress HER-2/neu, clinical trials havenot documented consistent therapeutic successes in other cancers. The Gyneco-logic Oncology Group evaluated Herceptin in patients with recurrent or refractoryovarian or primary peritoneal carcinoma (65). An overall response rate of 7.3% wasfound with a median treatment of 8 weeks and median progression-free interval of2 months. HER-2/neuhas also been found on prostate cancer and non–small-celllung cancer.
Epidermal Growth Factor Receptor
EGFR is overexpressed on many cancers. The receptor and its ligands, epidermalgrowth factor (EGF) and transforming growth factor–alpha (TGFα), act in an au-tocrine loop to stimulate the growth of breast cancer cells. In vitro, some anti-EGFRantibodies have been shown to inhibit the binding of the receptor ligands (66, 67).
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
354 VON MEHREN ¥ ADAMS ¥ WEINER
tyrosine kinases and inhibit growth of normal fibroblasts (68) as well as tumor cellsin culture (69). Also, combining anti-EGFR antibodies with cisplatin significantlydecreases the IC50 of cisplatin (70), and cures of established tumors have occurredwhen anti-EGFR antibodies are combined with cisplatin (71) or doxorubicin (72).Sequential treatment with topotecan followed by C225 (a chimerized version of theanti-EGFR antibody MAb225) in vitro leads to supra-additive growth inhibition inbreast, ovary, and colon cancer cell lines (73). C225 delivered simultaneously withradiation reduces phosphorylation of the EGFR and STAT-3, enhancing apoptosis(74). In vitro and in vivo studies suggest that anti-EGFR antibodies may lead toterminal differentiation of squamous cell carcinoma cells, with accumulation ofcells in G0–G1 phases of the cell cycle and expression of cell surface markers suchas involucrin and cytokeratin-10 (75).
MAb225 blocks in vitro phosphorylation of the EGFR and induces receptor in-ternalization, as occurs with binding of the natural ligand (76). However, receptorprocessing is slower with antibody engagement than with natural ligand engage-ment (77). Smaller bivalent F(ab′)2 and univalent Fab’ forms of this antibody alsoinhibit growth and decrease receptor phosphorylation, although the bivalent formis superior to the monovalent form (78). Since the smaller fragments lead to tumorregressions, the efficacy of antibody therapy is not dependent on ADCC, as thesesmaller fragments lack the Fc portion of the antibody required for ADCC. Rather,the efficacy of MAb225 is due to its ability to inhibit binding of the natural ligand,limit receptor phosphorylation and thus downstream signals, and induce receptorinternalization.
The chimeric form of MAb225, C225, has been evaluated in vitro and in vivo inhormone-sensitive and hormone-refractory prostate cancer (79). EGF is a strongchemoattractant for prostate cancer cells. Blocking the EGFR receptor with C225in vitro decreases migration of prostate cancer cells in a dose-dependent manner bydecreasing phosphorylation of the EGFR (80). C225 has also been shown to causecell cycle arrest and decrease proliferation of prostate cancer cells (81, 82). Thebinding of C225 to the EGFR results in multiple events that decrease proliferationand possibly metastatic potential in prostate cancer. It has also been shown toinhibit the expression of VEGF and vascular permeability factor, both of whichare involved in the induction of angiogenesis (59).
Phase I clinical trials of C225 alone or in combination with cisplatin have beenconducted in patients with cancers overexpressing EGFR (83). Skin toxicity inthe form of flushing, seborrheic dermatitis, and acneiform rash were observed atdoses higher than 100 mg/m2. The rash commonly presents on the head, neck,and trunk and resolves without scarring once the treatment has been discontinued(84). Epiglottitis resulting in severe shortness of breath was noted when C225was combined with cisplatin at 100 mg/m2, but not at 60 mg/m2 (83). Anotherphase I study, in which patients with recurrent head and neck cancer receivedcisplatin every three weeks and C225 weekly, found no such toxicity (85). Of the9 evaluable patients in that study, 2 patients previously treated with cisplatin hadcomplete responses and an additional 4 had partial responses. In addition, tumor
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 355
biopsies demonstrated a dose-dependent saturation of the EGFR and loss of EGFRtyrosine kinase activity following repeated doses of the antibody. Phase III trialsare now evaluating the impact of adding C225 to cisplatin in patients with recurrentor metastatic head and neck cancer and the benefit of adding C225 to radiationtherapy in patients with locally advanced head and neck cancer. Studies are alsoongoing in patients with non–small-cell lung cancer, who receive C225 along withvarious chemotherapy regimens including carboplatin and paclitaxel, gemcitabineand carboplatin, and docetaxel (84).
ABX-EGF, another antibody that targets EGFR, is also under clinical develop-ment. This antibody was produced in a transgenic mouse in which murine antibodygenes were inactivated and replaced by genes that encode the human sequences(86). The resulting fully human antibody has been shown to cause inhibition ofthe tyrosine phosphorylation of the receptor and internalization of the receptor.The inhibitory concentration of the antibody is lower than that of MAb225, theparent antibody of C225. Preclinical studies in animals have shown eradicationof EGFR tumors with ABX-EGF antibody therapy alone, whereas similar studieswith C225 have required the addition of chemotherapy to produce similar results(87). ABX-EGF is currently in clinical trials.
Ep-CAM (EGP-2/GA 733-2)
The 17-1A antibody, which recognizes Ep-CAM, has undergone extensive clinicaltesting, with some studies suggesting efficacy in colorectal carcinomas. The murineantibody has been replaced by a human chimeric construct that offers increasedmononuclear cell-mediated ADCC (88), a longer half-life, no development of hu-man antimouse antibody (HAMA), and radiolocalization to known sites of disease(89). Clinical trials have also incorporated cytokines because of in vitro data thatdemonstrate improved target cell killing by apoptosis with interferon-γ (90) andincreased ADCC with interferon-γ (91), GM-CSF (92, 93), the combination ofGM-CSF and interleukin (IL)-2 (94), IL-4 (95), and IL-8 (96). These studies haveformed the basis for clinical trials incorporating the antibody and cytokines suchas interferon-γ (97) and GM-CSF (98). Although these studies have shown ev-idence for cytokine immunomodulation, no consistent pattern of clinical benefithas emerged from therapy with these combinations.
The therapeutic use of 17-1A has also been shown to induce potentially effectiveanti-idiotypic antibodies (99–101), an effect that was increased by concomitanttherapy with GM-CSF (102), and to increase infiltration of macrophages and ofCD4+ and CD8+ T cells within tumors (103). Induction of T cells against anti-idiotypic epitopes has also been evaluated (104). Five of ten patients with anti-idiotypic antibodies were also found to have induction of EP-CAM antigen-specificT cells. Four of these patients showed a clinical response and their T cells demon-strated a proliferative response in vitro when stimulated with an anti-idiotypicantibody, in contrast to the six patients without evidence of T cells against anti-idiotypic epitopes.
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
356 VON MEHREN ¥ ADAMS ¥ WEINER
Initial phase I studies with 17-1A yielded promising results. Several studiesdemonstrated responses in patients with metastatic cancers of the gastrointesti-nal tract with only one intravenous dose of antibody. One patient received anintrahepatic infusion of autologous mononuclear cells mixed with 17-1A, whichresulted in regression of hepatic metastases. Antibody therapy was well toleratedwith mild nausea, vomiting, or diarrhea. Phase II studies in colon and pancreaticcancers were less encouraging (105, 106). Repeat-dose injections and combina-tions with cytokines to enhance effector cell number and activity did not result insignificant response rates, although in vitro assays of patient effector cells revealedincreased activity with cytokine therapy. Repeat-dose schedules with higher doseswere theorized to induce tolerance to the murine antibody, but this maneuver hadno significant impact on clinical response (106). Some trials reported evidenceof induction of anti-idiotypic antibodies, correlating with clinical response in onetrial. The overall lack of efficacy seen in these studies may have resulted from thelarge tumor burden or the associated immunosuppression in these patients withmetastatic disease.
The initial study evaluating 17-1A in the adjuvant setting suggested possibleefficacy. A phase III clinical trial of patients with lymph-node–positive colorectalcancer randomized patients to observation or therapy with 17-1A. The surgicalapproach was standardized and agreed to by all participating surgeons. All pa-tients were followed post-operatively in a similar manner, irrespective of treat-ment. Of 189 patients, 166 were evaluable for overall survival and disease-freesurvival. Therapy with 17-1A was well tolerated except for malaise, low-gradefevers and chills, and mild gastrointestinal discomfort. Four anaphylactic reactionswere treated without sequelae. At five years of follow-up, the death rate was 36%in the 17-1A group in contrast to 51% in the observation group, and the calculatedrecurrence rate was 48.7% versus 66.5% (107). At seven years the death rates were43% (17-1A) and 63% (observation), and the calculated recurrence rates were 52%and 68%, respectively, demonstrating a continued benefit in patients who received17-1A (108). Treatment with 17-1A was associated with a decreased incidenceof metastatic disease but did not alter the incidence of local failure. This shiftin failure pattern was felt to represent the ability of 17-1A to eradicate isolatedmetastatic cancer cells but not bulkier disease. Alternatively, altered vasculaturedue to surgery and scar tissue may have limited antibody diffusion to tumor cells.Another factor potentially accounting for the apparent lack of efficacy of 17-1Aon local control is that 11 patients in the observation group received pre- or post-operative radiation therapy alone or in combination with chemotherapy. This trialhas been criticized because of higher rates of recurrence and death in the controlarm than would be anticipated. However, it is intriguing because it demonstratesan effect of antibody-based therapy in the adjuvant setting of colorectal cancer.
Recent clinical trials were designed to confirm these results in stage II coloncancers and to test the value of adding 17-1A to standard chemotherapy in patientswith stage III disease. Therapy with antibody alone is unlikely to be effective in allpatients owing to the antigenic heterogeneity of cancer cells. Combining standard
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 357
adjuvant therapy with 17-1A would introduce therapies that have different mech-anisms of action, are cell-cycle–dependent and -independent, and allow death ofcancer cells irrespective of antigen expression patterns. A preliminary report ofthe phase III trial of 17-1A versus no therapy in the adjuvant setting revealed nodifference in overall survival in patients with stage II colorectal at a median followup of 13.4 months (109); a randomized study of chemotherapy with or without theantibody in patients with stage III disease has shown a minimal benefit of ques-tionable significance in a preliminary analysis. Overall survival was 81.6% forcombination therapy versus 78.9% for chemotherapy alone; this was not a statisti-cally significant difference. Irrespective of the final analyses of these large studies,the value of treating colorectal cancer patients with this antibody is unproven andlikely to be low.
Vascular Endothelial Growth Factor
Molecules that are selectively expressed in the tissue matrix surrounding tumorare potentially important targets for antibody therapy. The first of these targetsto be exploited resides in the vasculature that feeds tumor cells. Bevacizumab isa humanized MAb that blocks binding of the vascular endothelial growth factor(VEGF) to its receptor on vascular endothelium. VEGF is produced by manycancers to stimulate the growth of new blood vessels, and in some studies itsexpression at tumor sites is correlated with risk for metastases. A phase I clinicalstudy of bevacizumab tested doses of 0.1–10 mg/kg infused on days 1, 28, 35, and42 (110). No severe toxicities were found. At doses of 3–10 mg/kg, increases insystolic and diastolic blood pressure of>10 mm Hg were noted during therapy(110), and subsequent studies have confirmed that hypertension is a toxicity of thisagent (111). Two patients receiving 3 mg/kg experienced bleeding into their tumors.One patient with hepatocellular carcinoma bled into a previously undiagnosedbrain metastasis. Another patient with an extremity sarcoma and lung metastasesbled into the extremity mass and experienced hemoptysis.
In a phase II study of bevacizumab combined with carboplatin and paclitaxelin patients with non–small-cell lung cancer, 6 of 66 patients developed pulmonaryhemorrhage, 4 of whom died (112). Patients with squamous cell lung cancers andtumors with evidence of cavitation or squamous cell histology appeared to be athigher risk of hemoptysis. Interestingly, a study of bevacizumab and chemotherapyin metastatic colorectal cancer found an increase in thrombotic episodes as wellas hemorrhage. The incidence of thrombotic events was higher at the 5 mg/kgdose level than at the 10 mg/kg dose level. The majority of cases were deep venousthromboses, but one cerebral vascular accident and one pulmonary embolism werereported.
Clinical trials have suggested a therapeutic benefit from bevacizumab. Althoughthe phase I study demonstrated no objective responses, 12 of 23 patients hadstable disease during the trial (70 days) and an additional patient with renal cellcarcinoma experienced a minor response (110). A phase II study was conducted
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
358 VON MEHREN ¥ ADAMS ¥ WEINER
in 25 women whose metastatic breast cancer had progressed following at least oneanthracycline or taxane-based regimen. Clinical responses were noted at doses of3 mg/kg (n = 1/18) and 10 mg/kg (n = 2/17) (111). All responses were in lymphnodes or subcutaneous skin nodules. Bevacizumab has also been combined withchemotherapy in patients with non–small-cell lung cancer (113) and metastaticcolorectal cancer (114). The response rate and time to progression in patientswith lung cancer improved when carboplatin and paclitaxel were combined withbevacizumab at 10 mg/kg, but not at 5 mg/kg. A similar result was found in patientswith colorectal cancer receiving 5-fluorouracil and folinic acid plus bevacizumab,but the improved response rate was seen at the 5 mg/kg dose. Time to progressionimproved at the both 5 mg/kg and 10 mg/kg, but to a greater extent at 5 mg/kg.
RADIOIMMUNOTHERAPY
Radioimmunoconjugates
A tumor-specific antibody that does not alter tumor growth properties can be“armed” with a radioisotope to create a cytotoxic agent. Even antibodies that areeffective antitumor agents in an unconjugated state can have enhanced efficacywith the addition of a cytotoxic radioisotope. For example, although therapy withthe anti-CD20 MAb rituximab is associated with a significant antitumor effectin patients with non-Hodgkin’s lymphoma, significantly more patients exhibitcomplete responses when the90Y parent MAb Y2B8 is added to the treatmentprotocol (115). The recent availability of a panel of antibody-based constructs witha range of in vivo half-lives now makes it possible to select antibody/radioisotopecombinations with matched biologic and physical half-lives. This type of pairingenables the majority of the decay, and therefore cytotoxic emissions, to occurwhile the greatest quantity of labeled antibody is localized in the tumor. Williamset al. developed formulas, termed the imaging figure of merit (IFOM) and therapyfigure of merit (TFOM), to determine which isotopes best pair with a series ofantibodies and fragments based on the rate of MAb clearance, isotope half-life, andemission track length (116). This approach can be used to optimize the efficiencyand specificity of an imaging or treatment system.
Until recently, most RAIT studies employed131I, but improvements in labelingstrategies and the availability of large quantities of radiopharmaceutical-grade90Yhave enabled the study of90Y conjugates. Now, a wide variety of therapeuticradioisotopes are available for RAIT. They fall into two general categories, thosethat emit short–track-length (e.g., one cell length) alpha particles with a highlinear energy transfer (LET) and those that emit longer–track-length (e.g., 50 celllengths) beta particles with a low LET. Because the LET is a measure of the energydeposited along the track of the emitted particle, a high LET is associated with agreater probability of tumor cell death. This is in part dictated by the differencein the size of the particles. An alpha particle is equivalent to a helium nucleuswhereas a beta particle is an electron. Alpha particles tend to kill cells by causing
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 359
irreparable double-strand DNA breaks; beta particles lead to single-strand DNAbreaks.
Of the available beta-emitting radioisotopes,90Y (t1/2 = 64 h) is rapidly gainingdominance in most RAIT protocols owing to its ease of labeling and absence of agamma emission. The other commonly used radionuclide,131I (t1/2 = 8.02 days),requires a trained radiopharmacist and appropriately shielded/vented radiophar-macy because of its volatile nature. Other beta-emitting radioisotopes that haveshown promise for radioimmunotherapy include67Cu (t1/2 = 61.8 h) and177Lu(t1/2 = 6.73 days). There are also a number of alpha-emitting radioisotopes that arepotential partners with antibody-based molecules for RAIT. These include213Bi(t1/2 = 45 min), 212Bi (t1/2 = 61 min), and211At (t1/2 = 7.2 h). Whereas thehalf-life of 211At is compatible with the pharmacokinetics of several engineeredantibody-based molecules, the very short half-lives of the bismuth radioisotopeslimit their utility to the setting of disseminated disease or to pretargeted RAIT(described below).
Some clinical trials have demonstrated partial, short-lived clinical responses insome patients with advanced, solid tumors, but most of the significant advances inRAIT have occurred in the treatment of hematologic neoplasms. Lymphomas andleukemias remain the most sensitive tumor targets for RAIT, presumably becauseof their intrinsic sensitivity to radiation and the relatively good access of radioim-munoconjugates to the malignant cells that comprise these neoplasms. Patientswith hematologic neoplasms are also less likely to mount HAMA responses whenforeign MAbs are employed.
Radioimmunotherapy for Hematologic Malignancies
B-1 The CD20 antigen has been a very effective target for RAIT. Press and col-leagues used high, marrow-ablative doses of131I-B1 (tositumomab or Bexxar® )anti-CD20 RAIT in the setting of autologous bone marrow transplantation. In atotal of 42 patients with chemotherapy-refractory lymphomas, 24 exhibited MAbdistributions that were predictive of a favorable response and 19 received high-dose RAIT. Of the RAIT group, 84% exhibited a complete remission, and 11%had a partial remission (117). Many of the complete remissions observed with thisapproach have proven to be durable, with 62% exhibiting progression-free survivalat 2 years. Low-dose, non-myeloablative RAIT with131I-B1 has also proven effi-cacious, showing 50% response rates, with a median duration of 16.5 months, inpatients with chemotherapy-refractory B cell lymphoma (118, 119). Preliminarystudies have also shown that RAIT may be useful as a conditioning regimen prior tobone marrow transplantation in patients with acute myelogenous leukemia (120).
IBRITUMOMAB TIUXETAN Ibritumomab tiuxetan (Zevalin® ) is another MAb thattargets an epitope on the CD20 antigen that is distinct from the B1 epitope. Anotherdistinction between the ibritumomab trials and the tositumomab trials describedabove is that Ibritumomab employs90Y in place of131I. This antibody is the first,and to date only, MAb licensed for use in RAIT in the United States.
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
360 VON MEHREN ¥ ADAMS ¥ WEINER
A number of clinical trials have evaluated ibritumomab in over 230 patientswith relapsed or refractory low- or intermediate-grade non-Hodgkin’s lymphoma(reviewed in Reference 121). The most comprehensive study was a randomizedphase III trial that compared the safety and efficacy of a single dose of ibritumomabwith a standard treatment course of rituximab in 143 patients with low-grade, fol-licular or transformed non-Hodgkin’s lymphoma. In this trial, an overall responserate of 80% and a complete response rate of 30% was observed in the group treatedwith ibritumomab versus an overall response rate of 56% and a complete responserate of 16% in the group treated with rituximab (122).
LYM-1 Lym-1 is specific for a human leukocyte antigen (HLA-DR) expressedin >95% of B cell tumors. This murine MAb has not been humanized. In phaseI/II clinical trials, 131I-Lym-1 has shown significant antitumor activity. Low-dose,fractionated treatment of 30 patients (25 with non-Hodgkin’s lymphoma and 5with chronic lymphocytic leukemia) resulted in 3 complete responses and 14 partialresponses (123). When treated at the non-myeloablative maxiumum tolerated doseof 100 mCi/m2, 11 of 21 patients responded favorably (7 complete responses, 4partial responses) (124).
M195 The cell surface antigen CD33 is expressed on most myeloid leukemic blastsand leukemic progenitor cells. Its normal tissue expression is limited to committednormal myelomonocytic and erythroid progenitor cells and (at low levels) earlyhematopoietic stem cells. M195, a murine anti-CD33 MAb, has been used to de-liver therapeutic doses of131I in combination with busulfan or cyclophosphamideto eliminate disease before bone marrow transplantation (125). HuM195, a hu-manized version of M195, has been employed as a vehicle for the RAIT of acuteand chronic myelogenous leukemia. HuM195 RAIT resulted in minor responsesin 8 of 12 patients treated with90Y-conjugated Mab and 13 of 18 patients treatedwith 213Bi-conjugated Mab (126, 127). The213Bi studies were the first use of alphaparticles in RAIT.
Radioimmunotherapy of Solid Malignancies
Significantly less progress has been made in the treatment of solid malignancieswith RAIT. In most reported trials in patients with solid tumors (e.g., breast car-cinoma, colon carcinoma, ovarian carcinoma), RAIT is associated with, at best,stable disease. Although reports of a greater response do appear, their rarity givesthem the aura of an Elvis sighting. A phase II trial of 75 mCi/m2 of 131I-labeledCC49 MAb with interferon (to enhance target antigen expression) in patients withmetastatic prostate cancer reported minor radiographic responses and relief of pain(128). Similar results were reported for a phase I study of90Y-2IT-BAD-M170 inpatients with androgen-independent metastatic prostate cancer (129). In a recentphase I trial in patients with recurrent or persistent ovarian cancer, intraperitoneal177Lu-labeled CC49 MAb, plus interferon and Taxol® led to partial responses in 4 of17 treated patients and progression-free intervals in patients without measurable

25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 361
disease (130). Transient clinical responses were also observed in a phase I trial inmetastatic breast cancer patients treated with90Y-BrE-3 (131). Still, several newagents are currently undergoing clinical evaluation, many of which have novel char-acteristics (e.g., domain deletions or significant antitumor properties as a nakedMAb) that may translate into improved results.
Pretargeted Radioimmunotherapy
One new RAIT strategy recently examined in the clinic is pretargeted radioim-munotherapy (PRIT). PRIT differs from traditional RAIT in that the antibody andthe radioisotope are delivered to the tumor in separate steps. In the PRIT protocolsemployed to date, MAb-streptavidin (MAb-SA) or MAb-biotin (MAb-B) conju-gates were administered to the patient. After the MAb conjugate localized in the tu-mor, a clearing agent [e.g., a biotin–galactose–human serum albumin conjugateor streptavidin (SA)] is administered that binds to the circulating MAb conjugateand directs its clearance by the liver. After an additional 24 h, a biotin-chelate-90Ycomplex is administered that binds specifically to the MAb-SA or MAB-B-SAprelocalized in the tumor.
PRIT clinical trials have been performed in patients with glioma (132), coloncancer (133), prostate cancer, and non-Hodgkin’s lymphoma (134). Of 48 gliomapatients treated by PRIT at doses of 60–80 mCi/m2, 25% (12 patients) exhibiteda reduction in tumor mass ranging from>25% to 100%, with 8 responses lastinglonger than one year (132). In the PRIT treatment of patients with colon can-cer, 8% (2 of 25) of the patients treated with pretargeted NR-LU-10 MAb and110 mCi/m2 of 90Y-DOTA-biotin had a partial response, and 16% (4 of 25) exhib-ited stable disease. However, significant hematologic and nonhematologic toxic-ities (diarrhea) were reported (133). A companion trial directed against prostatecancer revealed similar toxicities (I. Horak, personal communication). Signifi-cantly more success was observed in the PRIT of non-Hodgkin’s lymphoma. Inthis trial, rituximab, which has antitumor properties in an unconjugated form, wasconjugated to SA as the first-step reagent. Six of seven patients treated with dosesof 30 or 50 mCi/m2 of 90Y-DOTA-biotin exhibited objective regressions, with onepartial response and three complete responses (134). The toxicities reported in thistrial were also less severe and were limited to grade I/II nonhematologic toxicityand transient grade III hematologic toxicity.
CONCLUSIONS
Therapeutic antibodies have made the transition from concept to clinical real-ity over the past two decades. Many are now being tested as adjuvant or first-linetherapies to assess their efficacy in improving or prolonging survival. Modified an-tibody structures, such as bispecific antibodies or smaller antibody fragments, haveyet to claim defined therapeutic roles, whereas radioimmunotherapy has clearlydemonstrated efficacy in some disease settings.
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
362 VON MEHREN ¥ ADAMS ¥ WEINER
The Annual Review of Medicineis online at http://med.annualreviews.org
LITERATURE CITED
1. Sivolapenko GB, Douli V, Pectasides D,et al. 1995. Breast cancer imaging withradiolabelled peptide from complemen-tarity-determining region of antitumor an-tibody.Lancet346:1662–66
2. Le Gall F, Kipriyanov SM, MoldenhauerG, Little M. 1999. Di-, tri- and tetramericsingle chain Fv antibody fragmentsagainst human CD19: effect of valency oncell binding.FEBS Lett.453:164–68
3. Ward ES, Gussow D, Griffiths AD, et al.1989. Binding activities of a repertoire ofsingle immunoglobulin variable domainssecreted fromEscherichia coli. Nature341:544–46
4. Huston JS, Levinson D, Mudgett-HunterM, et al. 1988. Protein engineering of an-tibody binding sites: recovery of specificactivity in an anti-digoxin single-chain Fvanalogue produced inE coli. Proc. Natl.Acad. Sci. USA85:5879–83
5. Marks JD, Hoogenboom HR, BonnertTP, et al. 1991. By-passing immuniza-tion. Human antibodies from V-gene li-braries displayed on phage.J. Mol. Biol.222:581–97
6. Begent RH, Verhaar MJ, Chester KA,et al. 1996. Clinical evidence of efficienttumor targeting based on single-chain Fvantibody selected from a combinatorial li-brary.Nat. Med.2:979–84
7. Adams GP, McCartney JE, Tai MS, et al.1993. Highly specificin vivo tumor tar-geting by monovalent and divalent formsof 741F8 anti-c-erbB-2 single-chain Fv.Cancer Res.53:4026–34
8. Holliger P, Prospero T, Winter G. 1993.“Diabodies”: small bivalent and bispecificantibody fragments.Proc. Natl. Acad. Sci.USA90:6444–48
9. Hu SSL, Raubitschek A, Sherman M,et al. 1996. Minibody: a novel engineeredanti-carcinoembryonic antigen antibodyfragment (single-chain Fv-CH3) which
exhibits rapid, high-level targeting ofxenografts.Cancer Res.56:3055–61
10. Jain RK. 1990. Physiological barriers todelivery of monoclonal antibodies andother macromolecules in tumors.CancerRes.(Suppl.) 50:814s–19s
11. Jain RK, Baxter LT. 1988. Mechanisms ofheterogeneous distribution of monoclonalantibodies and other macromolecules intumors: significance of elevated intersti-tial pressure.Cancer Res.48:7022–32
12. Trauth B, Klas C, Peters A, et al. 1989.Monoclonal antibody-mediated tumor re-gression by induction of apoptosis.Sci-ence245:301–5
13. Waldman T. 1991. Monoclonal antibod-ies in diagnosis and therapy.Science252:387–94
14. O’Connell M, Chen Z, Yang H, et al. 1989.Active specific immunotherapy with an-tiidiotypic antibodies in patients withsolid tumors.Semin. Surg. Oncol.5:441–47
15. Houghton A, Mintzer D, Cordon-CardoC, et al. 1985. Mouse monoclonal IgG3antibody detecting GD3 ganglioside: aphase I trial in patients with malignantmelanoma.Proc. Natl. Acad. Sci. USA82:1242–46
16. Steplewski Z, Lubeck M, Koprowski H.1983. Human macrophages armed withmurine immunoglobulin G2a antibodiesto tumors destroy human cancer cells.Sci-ence221:865–67
17. Lindenmann J. 1973. Speculations on Idsand homobodies.Ann. Immunol.124:171–84
18. Jerne N. 1974. Towards a network the-ory of the immune system.Ann. Immunol.125:373–89
19. Miller R, Maloney D, Warnke R, LevyR. 1982. Treatment of B-cell lymphomawith monocolonal anti-idiotype antibody.N. Engl. J. Med.306:517–22
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 363
20. Khazaeli M, Conry R, LoBuglio A. 1994.Human immune responses to monoclonalantibodies.J. Immunother.15:42–52
21. Peterson J, Couto J, Taylor M, Ceri-ani R. 1995. Selection of tumor-specificepitopes on target antigens for radioim-munotherapy of breast cancer.CancerRes.55:5847s–51s
22. Badger C, Anasetti C, Davis J, Bern-stein I. 1987. Treatment of malignancywith unmodified antibody.Pathol. Im-munopathol. Res.6:419–34
23. Holland G, Zlotnik A. 1993. Interleukin-10 and cancer.Cancer Invest.11:751–58
24. Norgaard P, Hougaard S, Poulsen H,Thomsen M. 1995. Transforming growthfactorβ and cancer.Cancer Treat. Rev.21:367–403
25. Lee J, Fenton BM, Koch CJ, et al. 1998.Interleukin 2 expression by tumor cells al-ters both the immune response and thetumor microenvironment.Cancer Res.58:1478–85
26. Nadler L, Stashenko P, Hardy R, et al.1980. Serotherapy of a patient with a mon-oclonal antibody directed against a humanlymphoma-associated antigen.CancerRes.40:3147–54
27. Vuist W, Levy R, Maloney D. 1994. Lym-phoma regression induced by monoclonalanti-idiotypic antibodies correlates withtheir ability to induce Ig signal transduc-tion and is not prevented by tumor expres-sion of high levels of bcl-2 protein.Blood83:899–906
28. Swisher E, Shawler D, Collins H, et al.1991. Expression of shared idiotypes inchronic lymphocytic leukemia and smalllymphocytic lymphoma.Blood77:1977–82
29. Bowen A, Zomas A, Emmett E, et al.1997. Subcutaneous CAMPATH-1H infludarabine-resistant/relapsed chroniclymphocytic and B-prolymphocytic leuk-aemia.Br. J. Haematol.96:617–19
30. Lundin J, Osterborg A, Brittinger G, et al.1998. CAMPATH-1H monoclonal anti-body in therapy for previously treated
low-grade non-Hodgkin’s lymphomas: aphase II multicenter study. EuropeanStudy Group of CAMPATH-1H Treat-ment in Low-Grade Non-Hodgkin’s Lym-phoma.J. Clin. Oncol.16:3257–63
31. Hale G, Zhang M, Bunjes D, et al. 1998.Improving the outcome of bone marrowtransplantation by using CD52 mono-clonal antibodies to prevent graft-versus-host disease and graft rejection.Blood92:4581–90
32. Naparstek E, Delukina M, Or R, et al.1999. Engraftment of marrow allograftstreated with Campath-1 monoclonal anti-bodies.Exp. Hematol.27:1210–18
33. Novitzky N, Thomas V, Hale G, Wald-mann H. 1999. Ex vivo depletion ofT cells from bone marrow grafts withCAMPATH-1 in acute leukemia: graft-versus-host disease and graft-versus-leukemia effect.Transplantation67:620–26
34. Hale G, Waldmann H. 1998. Risks of de-veloping Epstein-Barr virus–related lym-phoproliferative disorders after T-cell–depleted marrow transplants. CAMPATHUsers.Blood91:3079–83
35. Maloney D, Grillo-Lopez A, Bodkin D,et al. 1997. IDEC-C2B8: results of a phaseI multiple-dose trial in patients with re-lapsed non-Hodgkin’s lymphoma.J. Clin.Oncol.15:3266–74
36. Maloney D, Grillo-Lopez A, White C,1997. IDEC-C2B8 (Rituximab) anti-CD20 monoclonal antibody therapy inpatients with relapsed low-grade non-Hodgkin’s lymphoma.Blood90:2188–95
37. Shan D, Ledbetter J, Press O. 2000.Signaling events involved in anti-CD20–induced apoptosis of malignant humanB cells. Cancer Immunol. Immunother.48:673–83
38. McLaughlin P, Grillo-Lopez A, Link B,et al. 1998. Rituximab chimeric anti-CD20 monoclonal antibody therapy forrelapsed indolent lymphoma: half of pa-tients respond to a four-dose treatmentprogram.J. Clin. Oncol.16:2825–33
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
364 VON MEHREN ¥ ADAMS ¥ WEINER
39. Berinstein N, Grillo-L´opez A, WhiteC, et al. 1998. Association of serumRituximab (IDEC-C2B8) concentrationand anti-tumor response in the treat-ment of recurrent low-grade or follicu-lar non-Hodgkin’s lymphoma.Ann. On-col. 9:995–1001
40. Coiffier B, Haioun C, Ketterer N, et al.1998. Rituximab (anti-CD20 monoclonalantibody) for the treatment of patientswith relapsing or refractory aggressivelymphoma: a multicenter phase II study.Blood92:1927–32
41. Heinzerling L, Dummer R, Kempf W,et al. 2000. Intralesional therapy withanti–CD 20 monoclonal antibody ritux-imab in primary cutaneous lymphoma.Arch. Dermatol.136:374–78
42. Czuczman M, Grillo-L´opez A, WhiteC, et al. 1999. Treatment of patientswith low-grade B-cell lymphoma with thecombination of chimeric anti-CD20 mon-oclonal antibody and CHOP chemother-apy.J. Clin. Oncol.17:268–76
43. Demidem A, Lam T, Alas S, et al. 1997.Chimeric anti-CD20 (IDEC-C2B8) mo-noclonal antibody sensitizes a B cell lym-phoma cell line to cell killing by cyto-toxic drugs.Cancer Biother. Radiopharm.12:177–86
44. Gribben J, Freedman A, Woo S, et al.1991. All advanced stage non-Hodgkin’slymphomas with a polymerase chain reac-tion amplifiable breakpoint of bcl-2 haveresidual cells containing the bcl-2 rear-rangement at evaluation and after treat-ment.Blood78:3275–80
45. Czuczman M. 2002. Rituximab in combi-nation with CHOP or fludarabine in low-grade lymphoma.Semin. Oncol.20:36–40
46. Howard O, Gribben J, Neuberg D, et al.2002. Rituximab and CHOP inductiontherapy for newly diagnosed mantle-cell lymphoma: molecular complete re-sponses are not predictive of progression-free survival.J. Clin. Oncol.20:1288–94
47. Mangel J, Buckstein R, Imrie K, et al.
2002. Immunotherapy with rituximab fol-lowing high-dose therapy and autologousstem-cell transplantation for mantle celllymphoma.Semin. Oncol.29:56–69
48. Piro L, White C, Grillo-Lopez A, et al.1999. Extended rituximab (anti-CD20monoclonal antibody) therapy for re-lapsed or refractory low-grade or follic-ular non-Hodgkin’s lymphoma.Ann. On-col. 10:619–21
49. Keating M, O’Brien S. 2000. High-doserituximab therapy in chronic lymphocyticleukemia.Semin. Oncol.27:86–90
49a. Maloney DG, Smith B, Rose A. 2002. Rit-uximab: mechanisms of action and resis-tance.Semin. Oncol.29(1 Suppl. 2):2–9
50. Davis T, Czerwinski D, Levy R. 1999.Therapy of B-cell lymphoma with anti-CD20 antibodies can result in the loss ofCD20 antigen expression.Clin. CancerRes.5:611–15
51. Nabhan C, Rosen ST. 2002. Concep-tual aspects of combining rituximab andcampath-1H in the treatment of chroniclymphocytic leukemia.Semin. Oncol.29:75–80
52. Leonard J, Link B. 2002. Immunotherapyof non-Hodgkin’s lymphoma with hLL2(Epratuzumab, an anti-CD22 monoclonalantibody) and HuIDI0 (Apolizumab).Semin. Oncol.29:81–86
53. Byrd J, Waselenko J, Maneatis T, et al.1999. Rituximab therapy in hemato-logic malignancy patients with circulat-ing blood tumor cells: association with in-creased infusion-related side effects andrapid blood tumor clearance.J. Clin. On-col. 17:791–95
54. Jensen M, Winkler U, Manze O, et al.1998. Rapid tumor lysis in a patient withB-cell chronic lymphocytic leukemia andlymphocytosis treated with an anti-CD20monoclonal antibody (IDEC-C2B8, ritux-imab).Ann. Hematol.77:89–91
55. Grillo-Lopez A, Hedrick E, Rashford M,Benyunes M. 2002. Rituximab: ongoingand future clinical development.Semin.Oncol.29:102–12
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 365
56. Cobleigh M, Vogel C, Tripathy D, et al.1999. Multinational study of the effi-cacy and safety of humanized anti-HER2monoclonal antibody in women whohave HER2-overexpressing metastaticbreast cancer that has progressed afterchemotherapy for metastatic disease.J.Clin. Oncol.17:2639–48
57. Baselga J, Tripathy D, Mendelsohn J,et al. 1996. Phase II study of weekly in-travenous recombinant humanized anti-p185HER2 monoclonal antibody in pa-tients with HER2/neu-overexpressingmetastatic breast cancer.J. Clin. Oncol.14:737–44
58. Petit A, Rak J, Hung M, et al. 1997.Neutralizing antibodies against epidermalgrowth factor and ErbB-2/neu receptortyrosine kinases down-regulate vascularendothelial growth factor production bytumor cells in vitro and in vivo: angio-genic implications for signal transductiontherapy of solid tumors.Am. J. Pathol.151:1523–30
59. Slamon D, Leyland-Jones B, Shak S,et al. 2001. Use of chemotherapy plusa monoclonal antibody against HER2for metastatic breast cancer that overex-presses HER2.N. Engl. J. Med.344:783–92
60. Norton L, Slamon D, Leyland-Jones B.1999. Overall survival (OS) advantage tosimultaneous chemotherapy (CRx) plusthe humanized anti-HER2 monoclonalantibody Herceptin® (H) in HER2-over-expressing (HER2+) metastatic breastcancer (MBC).Proc. Am. Soc. Clin. On-col. 18:A127 (Abstr.)
61. Baselga J. 2001. Clinical trials ofHerceptin® (trastuzumab).Eur. J. Cancer37:S18–S24
62. Burstein HJ, Kuter I, Campos SM, et al.2001. Clinical activity of trastuzumaband vinorelbine in women with HER2-overexpressing metastatic breast cancer.J. Clin. Oncol.19:2722–30
63. Pegram M, Lipton A, Hayes D, et al.1998. Phase II study of receptor-en-
hanced chemosensitivity using re-combinant humanized anti-p185her2/neu
monoclonal antibody plus cisplatin inpatients with HER2/neu-overexpressingmetastatic breast cancer refractory tochemotherapy treatment.J. Clin. Oncol.16:2659–71
64. Miller KD, Sisk J, Ansari R, et al. 2001.Gemcitabine, paclitaxel, and trastuzumabin metastatic breast cancer.Oncology15:S38–S40
65. Bookman M, Darcy K, Clarke-PearsonD, et al. 2002. Evaluation of mono-clonal humanized anti-HER2 antibody(Trastuzumab, Herceptin) in patients withrecurrent or refractory ovarian or primaryperitoneal carcinoma with overexpressionof HER2: a phase II trial of the Gyneco-logic Oncology Group.J. Clin. Oncol.20:In press
66. Modjtahedi H, Komurasaki T, Toyoda H,Dean C. 1998. Anti-EGFR monoclonalantibodies which act as EGF, TGF alpha,HB-EGF, and BTC antagonists block thebinding of epiregulin to EGFR-expressingtumours.Int. J. Cancer75:310–16
67. Teramoto T, Onda M, Tokunaga A, AsanoG. 1996. Inhibitory effect of an anti-epidermal growth factor receptor anti-body on human gastric cancer.Cancer77:1639–45
68. Sato J, Kawamoto T, Le A, et al. 1983. Bi-ological effects in vitro of monoclonal an-tibodies to human epidermal growth fac-tor receptors.Mol. Biol. Med.1:511–29
69. Artega C, Corondo E, Osbore C. 1988.Blockade of the epidermal growth factorreceptor inhibits transforming growth fac-tor a–induced but not estrogen-inducedgrowth of hormone-dependent humanbreast cancer.Mol. Endocrinol.2:1064–69
70. Hoffman T, Hafner D, Ballo H, et al. 1997.Antitumor activity of anti-epidermalgrowth factor receptor monoclonal anti-bodies and cisplatin in ten human headand neck squamous cell carcinoma lines.Anticancer Res.17:4419–25
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
366 VON MEHREN ¥ ADAMS ¥ WEINER
71. Fan Z, Baselga J, Masui H, MendelsohnJ. 1993. Antitumor effect of anti-epi-dermal growth factor receptor monoclo-nal antibodies plus cis-diamminedi-chloroplatinum on well established A431cell xenografts.Cancer Res.53:4637–42
72. Baselga J, Norton L, Masui H, et al.1993. Antitumor effects of doxorubicin incombination with anti-epidermal growthfactor receptor monoclonal antibodies.J.Natl. Cancer Inst.85:1327–33
73. Ciardiello F, Bianco R, Damiano V,et al. 1999. Antitumor activity of sequen-tial treatment with topotecan and anti-epidermal growth factor receptor mono-clonal antibody C225.Clin. Cancer Res.5:909–16
74. Bonner J, Raisch K, Robert HT, et al.2000. Enhanced apoptosis with combina-tion C225/radiation treatment serves asthe impetus for clinical investigation inhead and neck cancers.J. Clin. Oncol.18(Suppl.):47s–53s
75. Modjtahedi H, Eccles S, Sandle J, et al.1994. Differentiation or immune destruc-tion: two pathways for therapy of squa-mous cell carcinomas with antibodiesto the epidermal growth factor receptor.Cancer Res.54:1695–701
76. Sunada H, Magun B, Mendelsohn J,MacLeod C. 1986. Monoclonal antibodyagainst the EGF receptor is internal-ized without stimulating receptor phos-phorylation.Proc. Natl. Acad. Sci. USA83:3825–28
77. Sunada H, Yu P, Peacock J, MendelsohnJ. 1990. Modulation of tyrosine serine andthreonine phosphorylation and intracellu-lar processing of the epidermal growthfactor receptor by anti-receptor mono-clonal antibody.J. Cell. Physiol.142:284–92
78. Fan Z, Masui M, Altas I, Mendel-sohn J. 1993. Blockade of the epider-mal growth factor receptor function bybivalent and monovalent fragments of225 anti-epidermal growth factor recep-
tor monoclonal antibodies.Cancer Res.53:4322–28
79. Prewett M, Rockwell R, Giorgio N, et al.1996. The biologic effects of C225, achimeric monoclonal antibody to theEGFR, on human prostate carcinoma.J.Immunother. Emphasis Tumor Immunol.19:419–27
80. Zolfaghari A, Djakiew D. 1996. Inhibitionof chemomigration of a human prostaticcarcinoma cell (TSU-pr1) line by inhibi-tion of epidermal growth factor receptorfunction.Prostate28:232–38
81. Peng D, Fan Z, Lu Y, et al. 1996. Anti-epidermal growth factor receptor mono-clonal antibody 225 up-regulatesp27KIP1 and induces G1 arrest in pro-static cancer cell line DU145.CancerRes.56:3666–69
82. Wu X, Rubin M, Fan Z, et al. 1996. In-volvement of p27KIP1 in G1 arrest me-diated by an anti-epidermal growth factorreceptor monoclonal antibody.Oncogene12:1397–403
83. Baselga J, Pfister D, Cooper M, et al. 2000.Phase I studies of anti-epidermal growthfactor receptor chimeric antibody C225alone and in combination with cisplatin.J. Clin. Oncol.18:909–14
84. Herbst R, Langer C. 2002. Epidermalgrowth factor receptors as a target for can-cer treatment: the emerging role of IMC-C225 in the treatment of lung and head andneck cancers.Semin. Oncol.29:27–36
85. Shin D, Donato N, Perez-Soler R, et al.2001. Epidermal growth factor receptor–targeted therapy with C225 and cisplatinin patients with head and neck cancer.Clin. Cancer Res.7:1204–13
86. Mendez M, Green L, Corvalan J, et al.1997. Functional transplant of megabasehuman immunoglobulin loci recapitulateshuman antibody response in mice.Nat.Genet.15:146–56
87. Yang X, Jia X, Corvalan J, et al. 1999.Eradication of established tumors by afully human monoclonal antibody to theepidermal growth factor receptor without
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 367
concomitant chemotherapy.Cancer Res.59:1236–43
88. Haga Y, Sivinski C, Woo D, TemperoM. 1994. Dose related comparison ofantibody-dependent cellular cytotoxicitywith chimeric and native monoclonal an-tibody 17-1A. Improved cytolysis of pan-creatic cancer cells with chimeric 17-1A.Int. J. Pancreatol.15:43–50
89. Meredith R, LoBuglio A, Plott W, et al.1991. Pharmacokinetics, immune respon-se, and biodistribution of iodine-131–labeled chimeric mouse/human IgG1 17-1A monoclonal antibody.J. Nucl. Med.32:1162–68
90. Takamuku K, Baba K, Aringa S, et al.1996. Apoptosis in antibody-dependentmonocyte-mediated cytotoxicity withmonoclonal antibody 17-1A againsthuman colorectal carcinoma cells: en-hancement with interferon gamma.Can-cer Immunol. Immunother.43:220–25
91. Reali E, Guiliani A, Spisani S, et al.1994. Interferon-gamma enhances mon-oclonal antibody 17-1A–dependent neu-trophil cytotoxicity toward colorectal car-cinoma cell line SW11-16.Clin. Immunol.Immunopathol.71:105–12
92. Ragnhammar P, Masucci G, Frodin J,et al. 1992. Cytotoxic functions of bloodmononuclear cells in patients with col-orectal carcinoma treated with mAb-17-1A and granulocyte/macrophage colonystimulating factor.Cancer Immunol. Im-munother.35:158–64
93. Ragnhammar P, Magnusson I, Masucci G,Mellstedt H. 1993. The therapeutic use ofthe unconjugated monoclonal antibodies(MAb) 17-1A in combination with GM-CSF in the treatment of colorectal carci-noma (CRC).Med. Oncol. Tumor Phar-macother.10:61–70
94. Masucci G, Ragnhammar P, Wersall P,Mellstedt H. 1990. Granulocyte-mono-cyte colony-stimulating factor augmentsthe interleukin-2 induced cytotoxic activ-ity of human lymphocytes in the absenceand presence of mouse or chimeric mon-
oclonal antibodies (mAb 17-1A).CancerImmunol. Immunother.31:231–35
95. Wersall P, Masucci G, Mellstedt H. 1991.Interleukin-4 augments cytotoxic capac-ity of lymphocytes and monocytes inantibody-dependent cellular cytotoxicity.Cancer Immunol. Immunother.33:45–49
96. Reali E, Spisani S, Gacili R, et al. 1995.IL-8 enhances antibody dependent cellu-lar cytotoxicity in human neutrophils.Im-munol. Cell Biol.73:234–38
97. Weiner L, Steplewski Z, Koprowski H,et al. 1986. Biologic effects of gamma in-terferon pre-treatment followed by mon-oclonal antibody 17-1A administration inpatients with gastrointestinal carcinoma.Hybridoma5:S65–77
98. Ragnhammar P, Fagerberg J, Frodin J,et al. 1993. Effect of monoclonal an-tibody 17-1A and GM-CSF in patientswith advanced colorectal carcinoma—long-lasting, complete remissions can beinduced.Int. J. Cancer53:751–58
99. Frodin J, Faxas M, Hagstrom B, et al.1991. Induction of anti-idiotypic (ab2)and anti-anti-idiotypic (ab3) antibodies inpatients treated with the mouse mono-clonal antibody 17-1A (ab1). Relation tothe clinical outcome—an important an-titumoral effector function?Hybridoma10:421–31
100. Hanzawa Y, Tsujisaki M, Tokuchi S,et al. 1992. Detection of xenogeneic anti-idiotypic antibodies specific to murinemonoclonal antibody 17-1A in patientswith gastrointestinal cancer.Tumour Biol.13:226–36
101. Fagerberg J, Frodin J, Wigzell H, Mell-stedt H. 1993. Induction of an immunenetwork cascade in cancer patients treatedwith monoclonal antibodies (ab1). I. Mayinduction of ab-1 reactive T cells and anti-anti-idiotypic antibodies (ab3) lead to tu-mor regression after mAb therapy?Can-cer Immunol. Immunother.37:264–70
102. Ragnhammar P, Fagerberg J, Frodin J-E, et al. 1995. Granulocyte/macrophage-colony–stimulating factor augments the
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
368 VON MEHREN ¥ ADAMS ¥ WEINER
induction of antibodies, especially anti-idiotypic antibodies to therapeutic mo-noclonal antibodies.Cancer Immunol.Immunother.40:367–75
103. Shetye J, Ragnhammar P, Liljefors M,et al. 1998. Immunopathology of meta-stases in patients of colorectal carcinomatreated with monoclonal antibody 17-1A and granulocyte macrophage colony–stimulating factor. Clin. Cancer Res.4:1921–29
104. Fagerberg J, Frodin J, Ragnhammar P,et al. 1994. Induction of an immune net-work cascade in cancer patients treatedwith monoclonal antibodies (ab1). II. Isinduction of anti-idiotype reactive T cells(T3) of importance for tumor responseto mAb therapy?Cancer Immunol. Im-munother.38:149–59
105. Sears H, Herlyn D, Steplewski Z, Ko-prowski H. 1985. Phase II clinical trialof a murine monoclonal antibody cy-totoxic for gastrointestinal adenocarci-noma.Cancer Res.45:5910–13
106. Weiner L, Harvey E, Padavic-Shaller K,et al. 1993. Phase II multicenter evalua-tion of prolonged murine monoclonal an-tibody 17-1a therapy in pancreatic carci-noma.J. Immunother.13:110–16
107. Reithmuller G, Schneider-Gadicke E,Schlimok G, et al. 1994. Randomised trialof monoclonal antibody for adjuvant ther-apy of resected Dukes’ C colorectal carci-noma. German Cancer Aid 17-1A StudyGroup.Lancet343:1177–83
108. Reithmuller G, Holz E, Schlimok G,et al. 1998. Monoclonal antibody therapyfor resected Dukes’ C colorectal cancer:seven-year outcome of a multicenter ran-domized trial.J. Clin. Oncol.16:1788–94
109. Dencausse Y, Hartung G, Sturm J,et al. 2001. Prospective randomized studyof adjuvant therapy with edrecolomab(Panorex)® of stage II colon cancer—interim analysis.Proc. Am. Soc. Clin. On-col. 21:A2198 (Abstr.)
110. Gordon M, Margolin K, Talpaz M, et al.2001. Phase I safety and pharmacokinetic
study of recombinant human anti-vascularendothelial growth factor in patients withadvanced cancer.J. Clin. Oncol.19:843–50
111. Sledge G, Miller K, Novotny W, et al.2000. A phase II trial of single agentrhuMAb VEGF (recombinant humanizedmonoclonal antibody to vascular endothe-lial cell growth factor) in patients with re-lapsed metastatic breast cancer.Proc. Am.Soc. Clin. Oncol.20:A5C (Abstr.)
112. Notovny W, Holmgren E, Griffing S,et al. 2001. Identification of squamouscell histology and central cavitary tu-mors as possible risk factors for pul-monary hemorrhage (PH) in patientswith advanced NSCLC receiving Beva-cizumab (B).Proc. Am. Soc. Clin. Oncol.21:A1318 (Abstr.)
113. DeVore R, Fehrenbacher L, Herbst R,et al. 2000. A randomized phase II trialcomparing RhuMAb VEGF (recombinanthumanized monoclonal antibody to vas-cular endothelial growth factor) plus car-boplatin/paclitaxel (CP) to CP alone in pa-tients with stage IIIB/IV NSCLC.Proc.Am. Soc. Clin. Oncol.20:A1896 (Abstr.)
114. Bergsland E, Hurwitz H, Fehrenbacher L,et al. 2000. A randomized phase II trialcomparing rhuMAb VEGF (recombinanthumanized monoclonal antibody to vas-cular endothelial cell growth factor) plus5-fluoruracil/leucovorin (FU/LV) in pa-tients with metastatic colorectal cancer.Proc. Am. Soc. Clin. Oncol.20:A939 (Ab-str.)
115. Witzig TE, White CA, Wiseman GA, et al.1999. Phase I/II trial of IDEC-Y2B8 ra-dioimmunotherapy for treatment of re-lapsed or refractory CD20 (+) B-cellnon-Hodgkin’s lymphoma.J. Clin. Oncol.17:3793–803
116. Williams LE, Liu A, Wu AM, et al. 1995.Figures of merit (FOMs) for imagingand therapy using monoclonal antibodies.Med. Phys.22:2025–27
117. Press OW, Eary JF, Appelbaum FR, et al.1993. Radiolabeled-antibody therapy of
25 Nov 2002 19:50 AR AR179-ME54-21.tex AR179-ME54-21.sgm LaTeX2e(2002/01/18)P1: IBC
CANCER ANTIBODIES 369
B-cell lymphoma with autologous bonemarrow support.N. Engl. J. Med.329:1219–24
118. Kaminski MS, Zasadny KR, FrancisIR, et al. 1993. Radioimmunotherapyof B-cell lymphoma with [131I] anti-B1(anti-CD20) antibody.N. Engl. J. Med.329:459–65
119. Kaminski MS, Zasadny KR, Francis IR,et al. 1996. Iodine-131–anti-B1 radioim-munotherapy for B-cell lymphoma.J.Clin. Oncol.14:1974–81
120. Caron PC, Scheinberg DA. 1993. Anti-CD33 monoclonal antibody M195 for thetherapy of myeloid leukemia.LeukemiaLymphoma11(Suppl. 2):1–6
121. White CA, Weaver RL, Grillo-L´opez AJ.2001. Antibody-targeted immunotherapyfor treatment of malignancy.Annu. Rev.Med.52:125–45
122. Witzig TE, Gordon LI, Cabanillas F,et al. 2002. Randomized controlled trialof yttrium-90–labeled ibritumomab tiux-etan radioimmunotherapy versus ritux-imab immunotherapy for patients withrelapsed or refractory low-grade, follicu-lar, or transformed B-cell non-Hodgkin’slymphoma.J. Clin. Oncol.20:2453–63
123. DeNardo GL, DeNardo SJ, Lamborn KR,et al. 1998. Low-dose, fractionated ra-dioimmunotherapy for B-cell malignan-cies using131I–Lym-1 antibody.CancerBiother. Radiopharm.13:239–54
124. DeNardo GL, DeNardo SJ, Goldstein DS,et al. 1998. Maximum-tolerated dose, tox-icity, and efficacy of131I–Lym-1 antibodyfor fractionated radioimmunotherapy ofnon-Hodgkin’s lymphoma.J. Clin. Oncol.16:3246–56
125. Jurcic JG, Caron PC, Nikula TK, et al.1995. Radiolabeled anti-CD33 mono-clonal antibody M195 for myeloidleukemias.Cancer Res.55(23 Suppl.):5908s–10s
126. Jurcic JG, Divgi CR, McDevitt MR,et al. 1998. Potential for myeloablation
with yttrium-90–HuM195 (anti-CD33):a phase I trial in advanced myeloidleukemias.Blood92:613A (Abstr.)
127. Jurcic JG, McDevitt MR, Sgouros G,et al. 1999. Phase I trial of targeted alphaparticle therapy for myeloid leukemiaswith bismuth-213–HuM195 (anti-CD33).Proc. Am. Soc. Clin. Oncol.18:7A(Abstr.)
128. Meredith RF, Khazaeli MB, Macey DJ,et al. 1999. Phase II study of interferon-enhanced131I-labeled high affinity CC49monoclonal antibody therapy in patientswith metastatic prostate cancer.Clin. Can-cer Res.5(Suppl.):3254s–58s
129. O’Donnell RT, DeNardo SJ, Yuan A,et al. 2001. Radioimmunotherapy with111In/90Y-2IT-BAD-m170 for metastaticprostate cancer.Clin. Cancer Res.7:1561–68
130. Meredith RF, Alvarez RD, PartridgeEE, et al. 2001. Intraperitoneal radioim-munochemotherapy of ovarian cancer: aphase I study.Cancer Biother. Radio-pharm.16:305–15
131. DeNardo SJ, Kramer EL, O’Donnell RT,et al. 1997. Radioimmunotherapy forbreast cancer using indium-111/yttrium-90 BrE-3: results of a phase I clinical trial.J. Nucl. Med.38:1180–85
132. Paganelli G, Grana C, Chinol M, et al.1999. Antibody-guided three-step therapyfor high grade glioma with yttrium-90 bi-otin. Eur. J. Nucl. Med.26:348–57
133. Knox SJ, Goris ML, Tempero M, et al.2000. Phase II trial of yttrium-90–DOTA-biotin pretargeted by NR-LU-10 antibody/streptavidin in patients withmetastatic colon cancer.Clin. Cancer Res.6:406–14
134. Weiden PL, Breitz HB, Press O, et al.2000. Pretargeted radioimmunotherapy(PRIT) for treatment of non-Hodgkin’slymphoma (NHL): initial phase I/II studyresults.Cancer. Biother. Radiopharm.15:15–29





























