Embed Size (px)
Citation preview
PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Macy, Marisa]On: 15 January 2010Access details: Access Details: [subscription number 918633748]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
NHSA DialogPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t775653686
Keeping It “R-E-A-L” with Authentic AssessmentMarisa Macy a; Stephen J. Bagnato b
a Department of Education, Lycoming College, b Departments of Pediatrics and Psychology-in-Education, University of Pittsburgh Medical Center (UPMC),
Online publication date: 15 January 2010
To cite this Article Macy, Marisa and Bagnato, Stephen J.(2010) 'Keeping It “R-E-A-L” with Authentic Assessment', NHSADialog, 13: 1, 1 — 20To link to this Article: DOI: 10.1080/15240750903458105URL: http://dx.doi.org/10.1080/15240750903458105
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.
NHSA DIALOG, 13(1), 1–20Copyright C© 2010, National Head Start AssociationISSN: 1524-0754 print / 1930-9325 onlineDOI: 10.1080/15240750903458105
RESEARCH ARTICLES
Keeping It “R-E-A-L” with Authentic Assessment
Marisa MacyLycoming College, Department of Education
Stephen J. BagnatoUniversity of Pittsburgh Medical Center (UPMC), Departments of Pediatrics
and Psychology-in-Education
The inclusion of young children with disabilities has remained a function of the Head Start programsince its inception in the 1960s when the United States Congress mandated that children withdisabilities comprise 10% of the Head Start enrollment (Zigler & Styfco, 2000). Standardized, norm-referenced tests used to identify children with delays are problematic because (a) they have lowtreatment validity, (b) they are not universally designed or adaptable, (c) it is difficult to capture thereal life behaviors/skills of young children, (d) they do little to facilitate collaboration with parents,(e) they lack sensitivity to changes in the child’s development and learning, and (f) children withdisabilities are often excluded from group data. This study examined the use of an alternative approachthat uses early childhood authentic assessment to determine a young child’s eligibility for specialservices. Results of this study have implications for adopting authentic assessment practices.
Keywords: developmental delay, systems integration
The inclusion of young children with disabilities has remained a function of the Head Start pro-gram since its inception in the 1960s. The United States Congress mandated that children withdisabilities comprise 10% of the Head Start enrollment (Zigler & Styfco, 2000). Informal and for-mal types of assessment practices are used to determine children who are eligible for specializedservices (Bagnato, 2007; McLean, Bailey, & Wolery, 2004; National Association of School Psy-chologists, 2005; National Research Council, 2008). Informally, Head Start professionals observechildren on an ongoing basis as children participate in their early childhood programs. Profession-als note when children’s behavior and skills deviate from developmental expectations. Parents andcaregivers also contribute to understanding a young child’s development. Home visits and otheropportunities for collaboration allow Head Start programs to gather a holistic picture of children.
Correspondence should be addressed to Marisa Macy, Lycoming College, Department of Education, 700 CollegePlace, Williamsport, PA 17701. E-mail: [email protected]
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
2 MACY AND BAGNATO
Formally, professionals may incorporate the use of tools to screen children for delays in devel-opment and learning. An individual assessment may occur if a child’s academic or developmentalperformance is suspicious to a professional and parent, or a group of children may be screened.The Individuals with Disabilities Education Improvement Act of 2004 (IDEA) requires the imple-mentation of child-find efforts in order to locate young children who are eligible for services dueto delay or risk conditions. Screening tools offer a snapshot and are not comprehensive enoughto determine eligibility for IDEA services.
Eligibility assessments are used when enough data are collected to warrant an in-depth lookat a child’s development. Standardized, norm-referenced tests are the most widely used toolsto determine whether a child is eligible for IDEA services. This practice is a result of the factthat standardized, norm-referenced tests often contain standard scores that are required undermany state guidelines (Danaher, 2005; Shakelford, 2006). Standard deviation and percentagedelay are frequently used in order to identify the eligible population of young children; how-ever, several states make use of informed clinical opinion, which promotes more flexibility forchildren, their families, and professionals (Bagnato, McKeating-Esterle, Fevola, Bartalomasi, &Neisworth, 2008; Bagnato, Smith-Jones, Matesa, & McKeating-Esterle, 2006; Dunst & Hamby,2004; Shakelford, 2002). Informed clinical opinion, or clinical judgment, is often used by profes-sionals to understand a child’s special needs without having to administer formal tests to a child(Bagnato et al., 2006).
It is not unreasonable to assume that standardized, norm-referenced tests have been proven tobe reliable and valid. These tests have been in existence for several years and have widespread useamong professionals who believe them to have strong psychometric properties. A recent researchsynthesis examined the use of standardized, norm-referenced tests and established that few if anyof these tests are effective in determining eligibility for IDEA special services for young childrenwith disabilities (Bagnato, Macy, Salaway, & Lehman, 2007).
In addition to weak evidence supporting use of standardized, norm-referenced tests to identifyeligible young children with delays, the study (Bagnato et al., 2007) also pointed out severalflaws with using these tests for eligibility determination. First, most of the standardized, norm-referenced tests examined in Bagnato et al.’s (2007) study did not include children with disabilitiesin the standardization process. In addition, all of the standardized, norm-referenced tests lackeditem density and procedural flexibility, which are salient elements to assessing young childrenwith delays. The standardized, norm-referenced tests were also deficient in offering graduatedscoring options.
Another concern with using standardized, norm-referenced tests for eligibility determinationis that they do not inform treatment efforts or instruction. These tests can show the extent a child’sbehavior or skill is different from the norm, but they do not lay a foundation for the next steps inhelping the child reach his or her potential or supports she or he will need to be fully includedin a Head Start classroom. Differentiating children’s performances on a test is the main focus ofstandardized, norm-referenced tests, not necessarily what will occur after the test is over.
One of the basic tenets of IDEA is that assessment practices must be fair and nonbiased.Court cases have challenged the use of inappropriate assessments. Professional organizationslike the Division for Early Childhood (DEC) and the National Association for the Educationof Young Children (NAEYC) propose using multiple methods for collecting information aboutchildren. A promising alternative to standardized, norm-referenced testing is the use of authenticassessment, which promotes a natural context to best understand what a child can do. It is aform of assessment that favors events, materials, and individuals who are familiar to the child.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
AUTHENTIC ASSESSMENT 3
Real life conditions become the backdrop for children to apply what they know to a givensituation.
Head Start programs would benefit by having authentic eligibility assessments that link tocurriculum and instruction because children will enter their programs with meaningful informa-tion (Bagnato et al., 2007; Grisham-Brown, Hallam, & Pretti-Frontczak, 2008). Results from theauthentic assessment can be used to directly inform program planning, curriculum, instruction,and lesson plans. To implement authentic assessment, practitioners should pay close attention tothe R-E-A-L framework: roles, equipment, assessment tools, and location.
Role of data collector. Authentic assessment relies upon a team of people that consists of informedcaregivers such as parents, grandparents, and other family members as well as teachers, speechtherapists, and other professionals who are familiar with and have knowledge of the child’sskills and abilities (Bagnato & Neisworth, 1999; Guralnick, 2006). Effective teams havemutual respect for one another’s roles and expertise, ability to communicate with others,and openness to share assessment role responsibilities. Assessment responsibilities are sharedwhen (a) parents are considered central members of the team with valuable observationsand information to contribute (Meisels, Xue, Bickel, Nicholson, & Atkins-Burnett, 2001);(b) teachers and practitioners provide input (Dunst, 2002; Keilty, LaRocco, & Casell, 2009);and (c) the team relies upon the observations and evaluations of trained professionals such asoccupational and speech therapists, depending on the child’s need (Meisels, Bickel, Nicholson,Xue, & Atkins-Burnett, 2001).
Equipment and materials. Familiar equipment and materials are used to assess children using anauthentic assessment framework. Common toys or household items are examples of materialsthat children will recognize from their natural environments. When assessment includes theactual or authentic activity with companion materials, the child is operating under more usualconditions and has experience performing similar tasks. For example, assessing a child’sadaptive skills during snack with all the familiar accompanying utensils, food items, andfurniture can help to obtain an accurate assessment of the child’s true ability.
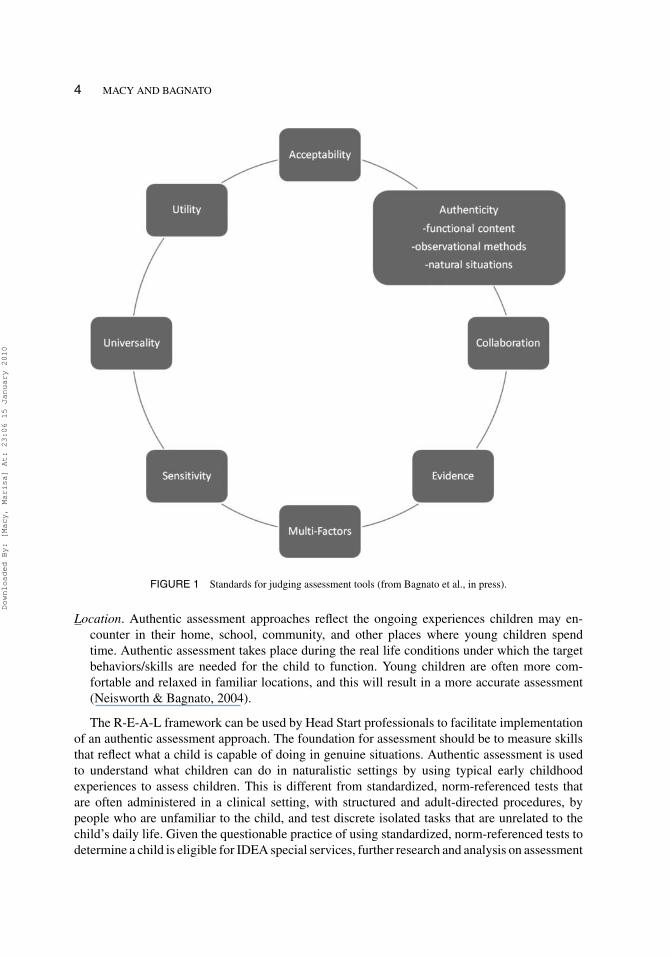
Assessment tools. Select authentic assessment tools that bring together interdisciplinary and in-teragency teams (Losardo & Notari-Syverson, 2001; Slentz & Hyatt, 2008). Curriculum-basedtools connect assessment to programming and intervention planning (Macy & Bricker, 2006).Curriculum-based assessments allow teams to gather information from various sources, in-cluding parents and teachers. Another benefit is that they can be used to monitor individual andgroup progress. Bagnato, Neisworth, and Pretti-Frontczak (in press) recommend eight qualitystandards for selecting assessment tools to include (a) acceptability—the social aspects of usinga tool; (b) authenticity—contextual factors (e.g., everyday situations); (c) collaboration—thetool can be easily incorporated into interdisciplinary teamwork; (d) evidence—the tool hasbeen found through research and practice to be valid, reliable, and useful; (e) multiple factors—used to gather information about a child (e.g., various methods, individuals, situations, andtime points); (f) sensitivity—the tool is sensitive to child performance; (g) universality—children with special needs can be accommodated; and (h) utility—the extent the tool is usefulto parents and professionals. These eight standards are illustrated in Figure 1. Approximately100 different authentic and standard, norm-referenced assessments were rated using the eightstandards by over 1,000 assessment users in an online study. Results from the online surveyindicated that users identified authentic assessment as meeting more of the eight standardsthan the standardized, norm-referenced tests.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
4 MACY AND BAGNATO
FIGURE 1 Standards for judging assessment tools (from Bagnato et al., in press).
Location. Authentic assessment approaches reflect the ongoing experiences children may en-counter in their home, school, community, and other places where young children spendtime. Authentic assessment takes place during the real life conditions under which the targetbehaviors/skills are needed for the child to function. Young children are often more com-fortable and relaxed in familiar locations, and this will result in a more accurate assessment(Neisworth & Bagnato, 2004).
The R-E-A-L framework can be used by Head Start professionals to facilitate implementationof an authentic assessment approach. The foundation for assessment should be to measure skillsthat reflect what a child is capable of doing in genuine situations. Authentic assessment is usedto understand what children can do in naturalistic settings by using typical early childhoodexperiences to assess children. This is different from standardized, norm-referenced tests thatare often administered in a clinical setting, with structured and adult-directed procedures, bypeople who are unfamiliar to the child, and test discrete isolated tasks that are unrelated to thechild’s daily life. Given the questionable practice of using standardized, norm-referenced tests todetermine a child is eligible for IDEA special services, further research and analysis on assessment
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
AUTHENTIC ASSESSMENT 5
alternatives is necessary. The purpose of this study was to examine the technical adequacy ofauthentic assessment measures.
METHOD
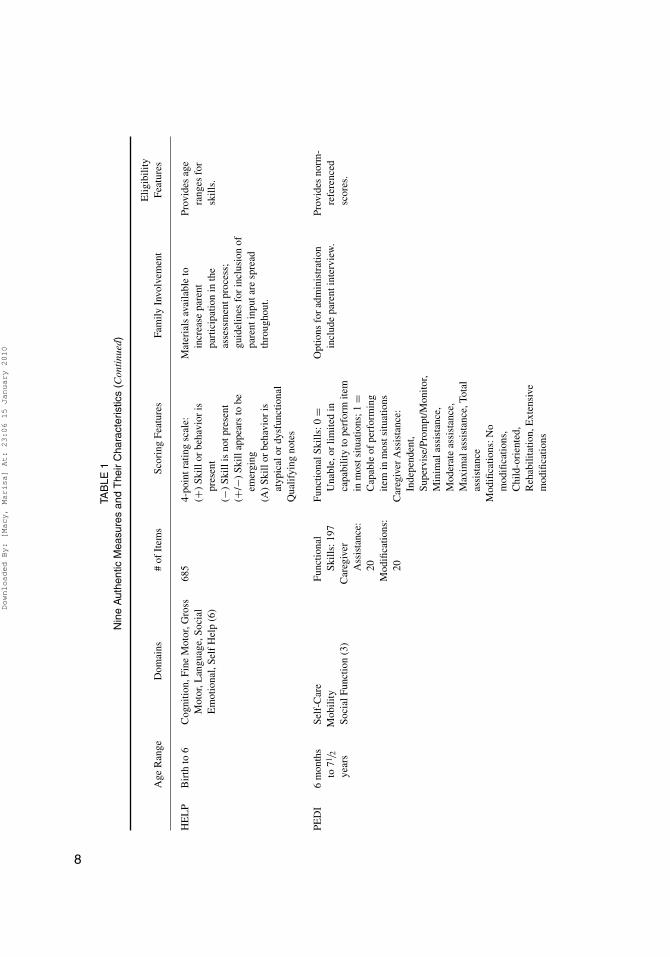
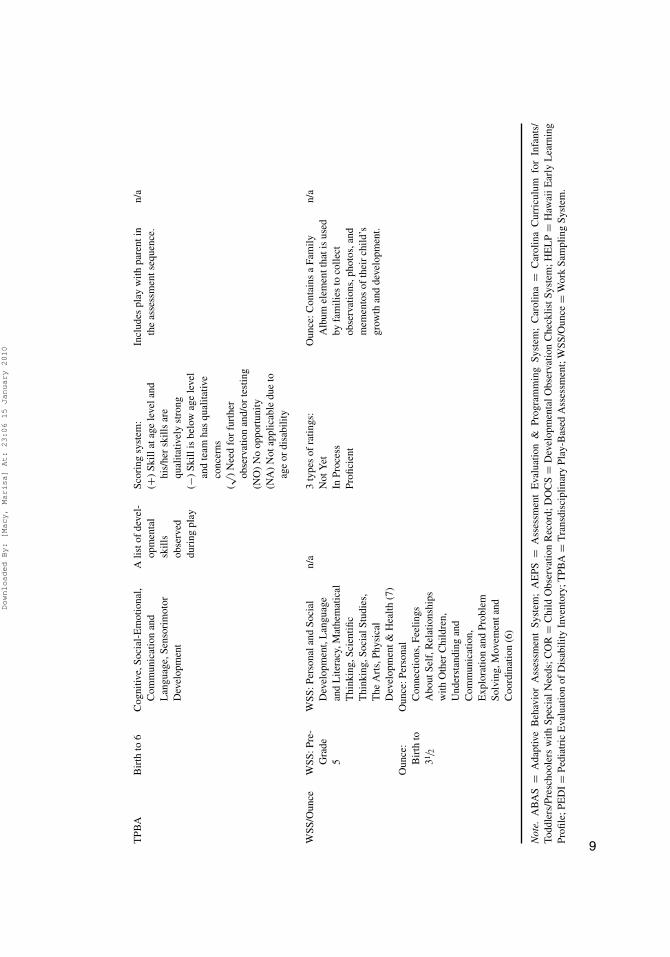
Nine authentic measures were chosen through a review of literature and surveys of practitionersinvestigating the most commonly used measures in preschool and early intervention settings(Bagnato, Neisworth, & Munson, 1997; Bagnato et al., in press; Pretti-Frontczak, Kowalski, &Brown, 2002). To be included in our review, the authentic measure needed to have publishedresearch available. Other authentic measures were considered for inclusion (like the Develop-mental Continuum from Teaching Strategies); however, we did not find published research onthese measures. The following nine authentic measures are included in the study:
� Adaptive Behavior Assessment System (ABAS),� Assessment Evaluation and Programming System (AEPS),� Carolina Curriculum for Preschoolers with Special Needs (Carolina),� Child Observation Record (COR),� Developmental Observation Checklist System (DOCS),� Hawaii Early Learning Profile (HELP),� Pediatric Evaluation of Disability Inventory (PEDI),� Transdisciplinary Play-Based Assessment (TPBA), and� Work Sampling System (WSS)/Ounce
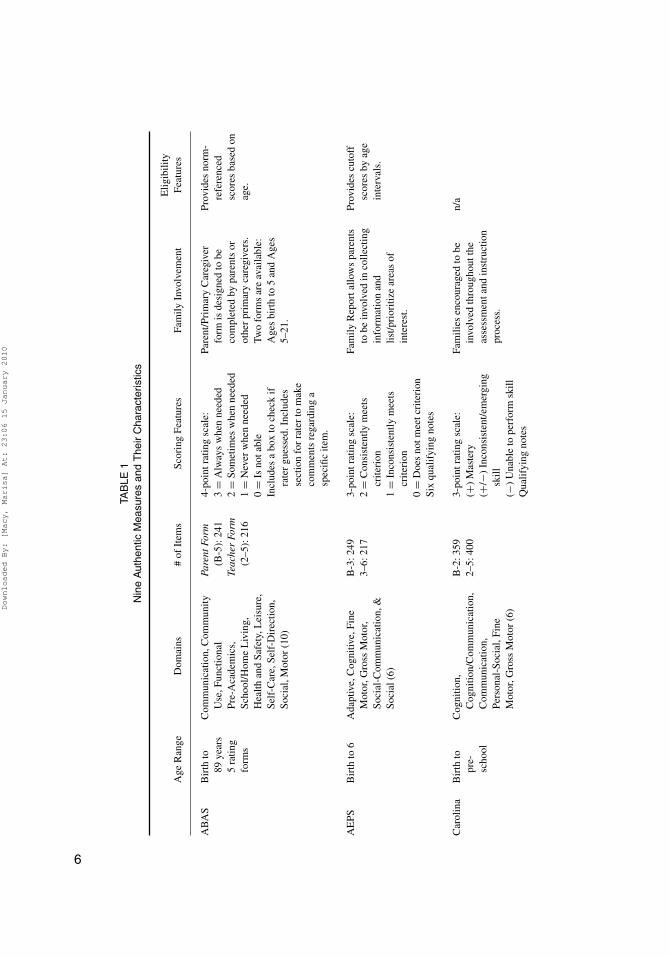
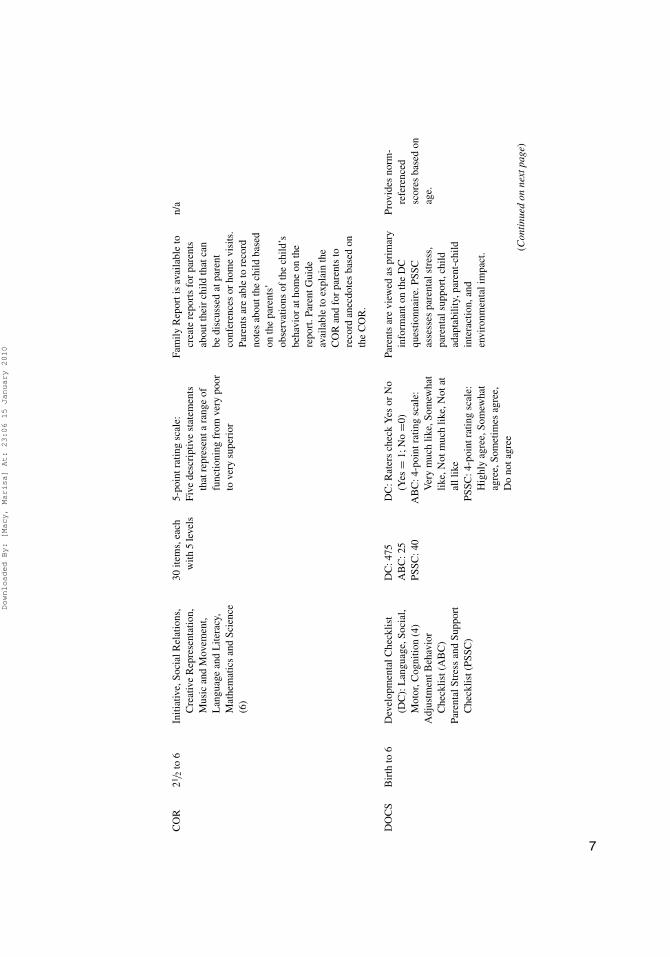
Some measures had multiple editions (i.e., AEPS, Carolina, ABAS, COR, and TPBA).Table 1 offers information about these measures.
Research studies on the identified authentic assessments (i.e., ABAS, AEPS, Carolina, COR,DOCS, HELP, PEDI, TPBA, and WSS/Ounce) were reviewed in this synthesis. Research char-acteristics fell into two categories: accuracy (reliability) and effectiveness (validity, utility).Accuracy refers to the extent to which a tool identifies young children with disabilities. Thisincludes reliability of the measure (e.g., consistency across test items and the use of cutoff scoresin order for the tool to precisely or accurately measure a skill or behavior). Examples of accuracyinclude test-retest reliability, interrater reliability, intrarater reliability, and interitem consistency.
Effectiveness refers to the extent to which a tool successfully identifies young children withdisabilities. This includes the validity of the measure (i.e., including to what extent does the toolmeasure what it was designed to measure) and how it relates significantly to similar measures.Examples of effectiveness include predictive validity, concurrent validity, construct validity, testfloors, and item gradients. The next section describes our strategy for searching the literature basefor research studies on the accuracy and effectiveness of authentic assessment measures.
Search Strategy
Search Terms. Relevant published research studies were identified using the followingsearch terms: authentic assessment, testing, early intervention, preschool, early childhood, eligi-bility, pediatrics, disabilities, handicap identification, and referral. More general terms of specialschools, state programs resource, centers, and evaluations were also used.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
TAB
LE1
Nin
eA
uthe
ntic
Mea
sure
san
dT
heir
Cha
ract
eris
tics
Elig
ibili
tyA
geR
ange
Dom
ains
#of
Item
sSc
orin
gFe
atur
esFa
mily
Invo
lvem
ent
Feat
ures
AB
AS
Bir
thto
89ye
ars
5ra
ting
form
s
Com
mun
icat
ion,
Com
mun
ityU
se,F
unct
iona
lPr
e-A
cade
mic
s,Sc
hool
/Hom
eL
ivin
g,H
ealth
and
Safe
ty,L
eisu
re,
Self
-Car
e,Se
lf-D
irec
tion,
Soci
al,M
otor
(10)
Pare
ntFo
rm(B
-5):
241
Teac
her
Form
(2–5
):21
6
4-po
intr
atin
gsc
ale:
Pare
nt/P
rim
ary
Car
egiv
erfo
rmis
desi
gned
tobe
com
plet
edby
pare
nts
orot
her
prim
ary
care
give
rs.
Two
form
sar
eav
aila
ble:
Age
sbi
rth
to5
and
Age
s5–
21.
Prov
ides
norm
-re
fere
nced
scor
esba
sed
onag
e.
3=
Alw
ays
whe
nne
eded
2=
Som
etim
esw
hen
need
ed1
=N
ever
whe
nne
eded
0=
Isno
tabl
eIn
clud
esa
box
toch
eck
ifra
ter
gues
sed.
Incl
udes
sect
ion
for
rate
rto
mak
eco
mm
ents
rega
rdin
ga
spec
ific
item
.
AE
PSB
irth
to6
Ada
ptiv
e,C
ogni
tive,
Fine
Mot
or,G
ross
Mot
or,
Soci
al-C
omm
unic
atio
n,&
Soci
al(6
)
B-3
:249
3–6:
217
3-po
intr
atin
gsc
ale:
Fam
ilyR
epor
tallo
ws
pare
nts
tobe
invo
lved
inco
llect
ing
info
rmat
ion
and
list/p
rior
itize
area
sof
inte
rest
.
Prov
ides
cuto
ffsc
ores
byag
ein
terv
als.
2=
Con
sist
ently
mee
tscr
iteri
on1
=In
cons
iste
ntly
mee
tscr
iteri
on0
=D
oes
notm
eetc
rite
rion
Six
qual
ifyi
ngno
tes
Car
olin
aB
irth
topr
e-sc
hool
Cog
nitio
n,C
ogni
tion/
Com
mun
icat
ion,
Com
mun
icat
ion,
Pers
onal
-Soc
ial,
Fine
Mot
or,G
ross
Mot
or(6
)
B-2
:359
3-po
intr
atin
gsc
ale:
Fam
ilies
enco
urag
edto
bein
volv
edth
roug
hout
the
asse
ssm
enta
ndin
stru
ctio
npr
oces
s.
n/a
2–5:
400
(+)
Mas
tery
(+/−
)In
cons
iste
nt/e
mer
ging
skill
(−)
Una
ble
tope
rfor
msk
illQ
ualif
ying
note
s
6
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
CO
R21
/ 2to
6In
itiat
ive,
Soci
alR
elat
ions
,C
reat
ive
Rep
rese
ntat
ion,
Mus
ican
dM
ovem
ent,
Lan
guag
ean
dL
itera
cy,
Mat
hem
atic
san
dSc
ienc
e(6
)
30ite
ms,
each
with
5le
vels
5-po
intr
atin
gsc
ale:
Five
desc
ript
ive
stat
emen
tsth
atre
pres
enta
rang
eof
func
tioni
ngfr
omve
rypo
orto
very
supe
rior
Fam
ilyR
epor
tis
avai
labl
eto
crea
tere
port
sfo
rpa
rent
sab
outt
heir
child
that
can
bedi
scus
sed
atpa
rent
conf
eren
ces
orho
me
visi
ts.
Pare
nts
are
able
tore
cord
note
sab
outt
hech
ildba
sed
onth
epa
rent
s’ob
serv
atio
nsof
the
child
’sbe
havi
orat
hom
eon
the
repo
rt.P
aren
tGui
deav
aila
ble
toex
plai
nth
eC
OR
and
for
pare
nts
tore
cord
anec
dote
sba
sed
onth
eC
OR
.
n/a
DO
CS
Bir
thto
6D
evel
opm
enta
lChe
cklis
t(D
C):
Lan
guag
e,So
cial
,M
otor
,Cog
nitio
n(4
)A
djus
tmen
tBeh
avio
rC
heck
list(
AB
C)
Pare
ntal
Stre
ssan
dSu
ppor
tC
heck
list(
PSSC
)
DC
:475
AB
C:2
5PS
SC:4
0
DC
:Rat
ers
chec
kY
esor
No
(Yes
=1;
No
=0)
AB
C:4
-poi
ntra
ting
scal
e:V
ery
muc
hlik
e,So
mew
hat
like,
Not
muc
hlik
e,N
otat
alll
ike
PSSC
:4-p
oint
ratin
gsc
ale:
Hig
hly
agre
e,So
mew
hat
agre
e,So
met
imes
agre
e,D
ono
tagr
ee
Pare
nts
are
view
edas
prim
ary
info
rman
ton
the
DC
ques
tionn
aire
.PSS
Cas
sess
espa
rent
alst
ress
,pa
rent
alsu
ppor
t,ch
ildad
apta
bilit
y,pa
rent
-chi
ldin
tera
ctio
n,an
den
viro
nmen
tali
mpa
ct.
Prov
ides
norm
-re
fere
nced
scor
esba
sed
onag
e.
(Con
tinu
edon
next
page
)
7
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
TAB
LE1
Nin
eA
uthe
ntic
Mea
sure
san
dT
heir
Cha
ract
eris
tics
(Con
tinu
ed)
Elig
ibili
tyA
geR
ange
Dom
ains
#of
Item
sSc
orin
gFe
atur
esFa
mily
Invo
lvem
ent
Feat
ures
HE
LP
Bir
thto
6C
ogni
tion,
Fine
Mot
or,G
ross
Mot
or,L
angu
age,
Soci
alE
mot
iona
l,Se
lfH
elp
(6)
685
4-po
intr
atin
gsc
ale:
Mat
eria
lsav
aila
ble
toin
crea
sepa
rent
part
icip
atio
nin
the
asse
ssm
entp
roce
ss;
guid
elin
esfo
rin
clus
ion
ofpa
rent
inpu
tare
spre
adth
roug
hout
.
Prov
ides
age
rang
esfo
rsk
ills.
(+)
Skill
orbe
havi
oris
pres
ent
(−)
Skill
isno
tpre
sent
(+/−
)Sk
illap
pear
sto
beem
ergi
ng(A
)Sk
illor
beha
vior
isat
ypic
alor
dysf
unct
iona
lQ
ualif
ying
note
s
PED
I6
mon
ths
to71
/ 2
year
s
Self
-Car
eM
obili
tySo
cial
Func
tion
(3)
Func
tiona
lSk
ills:
197
Car
egiv
erA
ssis
tanc
e:20
Mod
ifica
tions
:20
Func
tiona
lSki
lls:0
=U
nabl
e,or
limite
din
capa
bilit
yto
perf
orm
item
inm
osts
ituat
ions
;1=
Cap
able
ofpe
rfor
min
gite
min
mos
tsitu
atio
ns
Opt
ions
for
adm
inis
trat
ion
incl
ude
pare
ntin
terv
iew
.Pr
ovid
esno
rm-
refe
renc
edsc
ores
.
Car
egiv
erA
ssis
tanc
e:In
depe
nden
t,Su
perv
ise/
Prom
pt/M
onito
r,M
inim
alas
sist
ance
,M
oder
ate
assi
stan
ce,
Max
imal
assi
stan
ce,T
otal
assi
stan
ceM
odifi
catio
ns:N
om
odifi
catio
ns,
Chi
ld-o
rien
ted,
Reh
abili
tatio
n,E
xten
sive
mod
ifica
tions
8
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
TPB
AB
irth
to6
Cog
nitiv
e,So
cial
-Em
otio
nal,
Com
mun
icat
ion
and
Lan
guag
e,Se
nsor
imot
orD
evel
opm
ent
Alis
tof
deve
l-op
men
tal
skill
sob
serv
eddu
ring
play
Scor
ing
syst
em:
(+)
Skill
atag
ele
vela
ndhi
s/he
rsk
ills
are
qual
itativ
ely
stro
ng
Incl
udes
play
with
pare
ntin
the
asse
ssm
ents
eque
nce.
n/a
(−)
Skill
isbe
low
age
leve
lan
dte
amha
squ
alita
tive
conc
erns
(√ )N
eed
for
furt
her
obse
rvat
ion
and/
orte
stin
g(N
O)
No
oppo
rtun
ity(N
A)
Not
appl
icab
ledu
eto
age
ordi
sabi
lity
WSS
/Oun
ceW
SS:P
re-
Gra
de5
WSS
:Per
sona
land
Soci
alD
evel
opm
ent,
Lan
guag
ean
dL
itera
cy,M
athe
mat
ical
Thi
nkin
g,Sc
ient
ific
Thi
nkin
g,So
cial
Stud
ies,
The
Art
s,Ph
ysic
alD
evel
opm
ent&
Hea
lth(7
)
n/a
3ty
pes
ofra
tings
:N
otY
etIn
Proc
ess
Profi
cien
t
Oun
ce:C
onta
ins
aFa
mily
Alb
umel
emen
ttha
tis
used
byfa
mili
esto
colle
ctob
serv
atio
ns,p
hoto
s,an
dm
emen
tos
ofth
eir
child
’sgr
owth
and
deve
lopm
ent.
n/a
Oun
ce:
Bir
thto
31/ 2
Oun
ce:P
erso
nal
Con
nect
ions
,Fee
lings
Abo
utSe
lf,R
elat
ions
hips
with
Oth
erC
hild
ren,
Und
erst
andi
ngan
dC
omm
unic
atio
n,E
xplo
ratio
nan
dPr
oble
mSo
lvin
g,M
ovem
enta
ndC
oord
inat
ion
(6)
Not
e.A
BA
S=
Ada
ptiv
eB
ehav
ior
Ass
essm
ent
Syst
em;
AE
PS=
Ass
essm
ent
Eva
luat
ion
&Pr
ogra
mm
ing
Syst
em;
Car
olin
a=
Car
olin
aC
urri
culu
mfo
rIn
fant
s/To
ddle
rs/P
resc
hool
ers
with
Spec
ialN
eeds
;CO
R=
Chi
ldO
bser
vatio
nR
ecor
d;D
OC
S=
Dev
elop
men
talO
bser
vatio
nC
heck
listS
yste
m;H
EL
P=
Haw
aiiE
arly
Lea
rnin
gPr
ofile
;PE
DI=
Pedi
atri
cE
valu
atio
nof
Dis
abili
tyIn
vent
ory;
TPB
A=
Tra
nsdi
scip
linar
yPl
ay-B
ased
Ass
essm
ent;
WSS
/Oun
ce=
Wor
kSa
mpl
ing
Syst
em.
9
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
10 MACY AND BAGNATO
The nine authentic assessments (i.e., ABAS, AEPS, Carolina, COR, DOCS, HELP, PEDI,TPBA, and WSS/Ounce) were also included within the search. The search was done broadly inthe fields of psychology, developmental disabilities, special education, allied health fields (speechand language therapy, physical therapy, occupational therapy), and as early intervention.
Sources. The primary databases included the following sources: CINAHL, Cochrane Li-brary, Digital Dissertations, Ebsco Host, Education Resource Information Center (ERIC), GoogleScholar, Health Source, Illumina, Medline, Ovid/Mental Measurements Yearbook Buros, Psycho-logical Abstracts (PsycINFO), and Social Sciences Citation Index. Additionally, we conductedselective searches of unpublished masters’ theses and doctoral dissertations. Hand searches ofselect journals and ancestral searches were also conducted.
Selection Criteria. The study had to meet the following criteria for inclusion: (a) researchedone or more of the selected authentic assessment measures; (b) involved the evaluation of youngchildren with disabilities or at risk for developing a disability due to environmental or biologicalrisk conditions; (c) examined the accuracy or effectiveness of the measure at testing infants,toddlers, and preschool children with disabilities; and (d) disseminated in a scientific and scholarlypublication, which included dissertation and thesis studies. This research synthesis was conductedas part of literature reviews and syntheses conducted at the Tracking, Referral and AssessmentCenter for Excellence (Dunst, Trivette, & Cutspe, 2002).
RESULTS
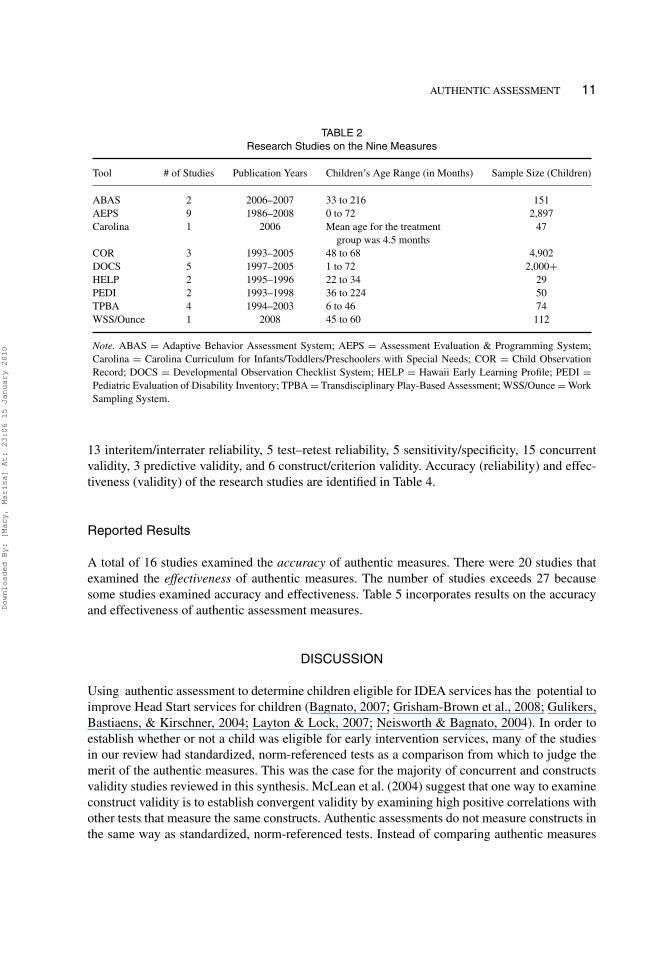
A total of 27 studies on authentic assessment were identified from the fields of child development,early intervention, psychology, special education, physical therapy, pediatrics, and behavioraldevelopment. The most studies were conducted on the AEPS. The following information ispresented in Table 2: total number of studies that met the inclusion criteria, years articles werepublished, age range included in the studies, and the total number of participants in study samples.
Participants
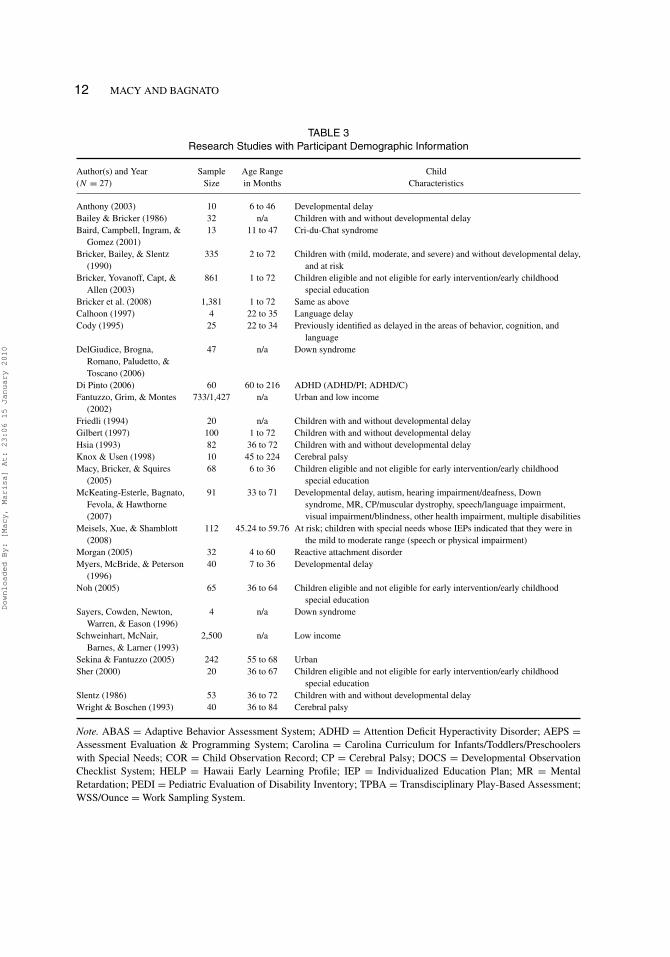
There were over 10,000 young children who participated in these research studies on authenticassessment. Children’s ages ranged from birth to 224 months. Children were identified withvarious disabilities, and there were several studies that included children without disabilitiesand children who were at risk for developing a disability. Table 3 shows child characteristicsthat include total sample size, mean age in months, age range in months, and child abilitycharacteristics.
Types of Studies
Each study reported in this synthesis examined some aspect of accuracy and/or effectivenessrelated to one or more of the authentic measures. We found the following types of studies:
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
AUTHENTIC ASSESSMENT 11
TABLE 2Research Studies on the Nine Measures
Tool # of Studies Publication Years Children’s Age Range (in Months) Sample Size (Children)
ABAS 2 2006–2007 33 to 216 151AEPS 9 1986–2008 0 to 72 2,897Carolina 1 2006 Mean age for the treatment
group was 4.5 months47
COR 3 1993–2005 48 to 68 4,902DOCS 5 1997–2005 1 to 72 2,000+HELP 2 1995–1996 22 to 34 29PEDI 2 1993–1998 36 to 224 50TPBA 4 1994–2003 6 to 46 74WSS/Ounce 1 2008 45 to 60 112
Note. ABAS = Adaptive Behavior Assessment System; AEPS = Assessment Evaluation & Programming System;Carolina = Carolina Curriculum for Infants/Toddlers/Preschoolers with Special Needs; COR = Child ObservationRecord; DOCS = Developmental Observation Checklist System; HELP = Hawaii Early Learning Profile; PEDI =Pediatric Evaluation of Disability Inventory; TPBA = Transdisciplinary Play-Based Assessment; WSS/Ounce = WorkSampling System.
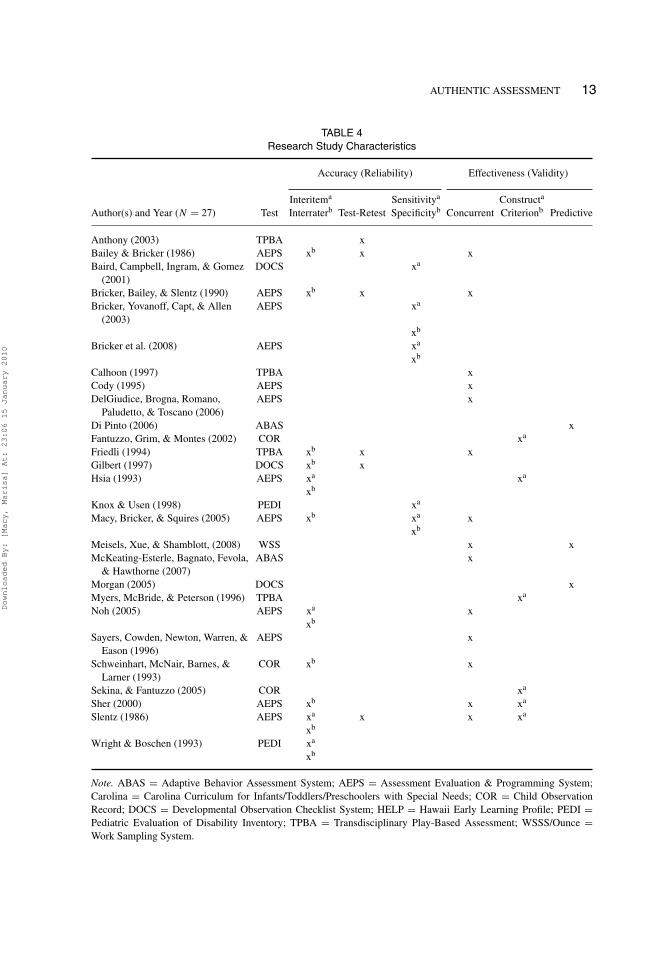
13 interitem/interrater reliability, 5 test–retest reliability, 5 sensitivity/specificity, 15 concurrentvalidity, 3 predictive validity, and 6 construct/criterion validity. Accuracy (reliability) and effec-tiveness (validity) of the research studies are identified in Table 4.
Reported Results
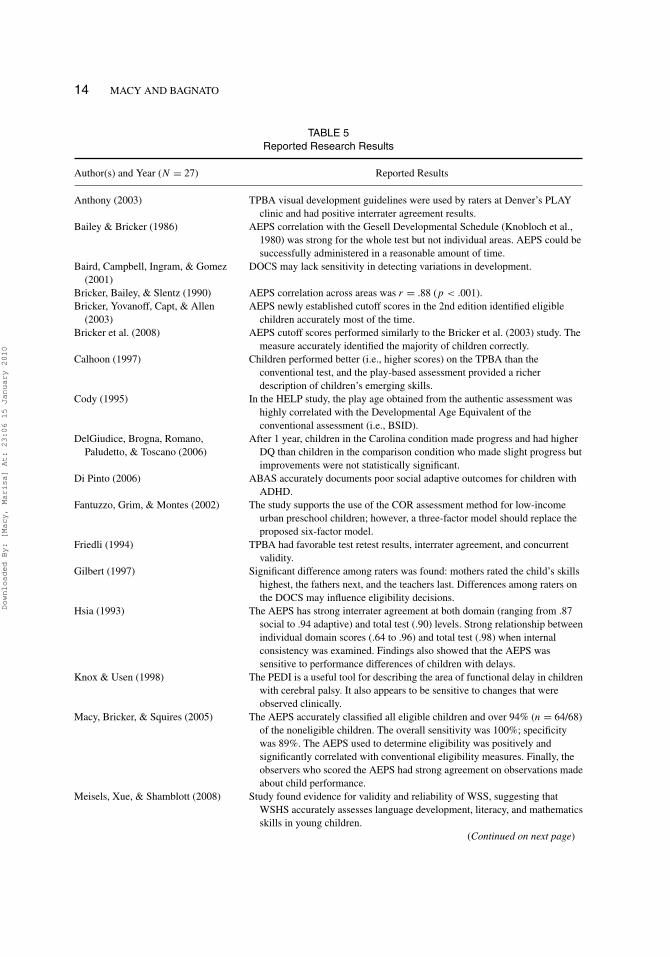
A total of 16 studies examined the accuracy of authentic measures. There were 20 studies thatexamined the effectiveness of authentic measures. The number of studies exceeds 27 becausesome studies examined accuracy and effectiveness. Table 5 incorporates results on the accuracyand effectiveness of authentic assessment measures.
DISCUSSION
Using authentic assessment to determine children eligible for IDEA services has the potential toimprove Head Start services for children (Bagnato, 2007; Grisham-Brown et al., 2008; Gulikers,Bastiaens, & Kirschner, 2004; Layton & Lock, 2007; Neisworth & Bagnato, 2004). In order toestablish whether or not a child was eligible for early intervention services, many of the studiesin our review had standardized, norm-referenced tests as a comparison from which to judge themerit of the authentic measures. This was the case for the majority of concurrent and constructsvalidity studies reviewed in this synthesis. McLean et al. (2004) suggest that one way to examineconstruct validity is to establish convergent validity by examining high positive correlations withother tests that measure the same constructs. Authentic assessments do not measure constructs inthe same way as standardized, norm-referenced tests. Instead of comparing authentic measures
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
12 MACY AND BAGNATO
TABLE 3Research Studies with Participant Demographic Information
Author(s) and Year Sample Age Range Child(N = 27) Size in Months Characteristics
Anthony (2003) 10 6 to 46 Developmental delayBailey & Bricker (1986) 32 n/a Children with and without developmental delayBaird, Campbell, Ingram, &
Gomez (2001)13 11 to 47 Cri-du-Chat syndrome
Bricker, Bailey, & Slentz(1990)
335 2 to 72 Children with (mild, moderate, and severe) and without developmental delay,and at risk
Bricker, Yovanoff, Capt, &Allen (2003)
861 1 to 72 Children eligible and not eligible for early intervention/early childhoodspecial education
Bricker et al. (2008) 1,381 1 to 72 Same as aboveCalhoon (1997) 4 22 to 35 Language delayCody (1995) 25 22 to 34 Previously identified as delayed in the areas of behavior, cognition, and
languageDelGiudice, Brogna,
Romano, Paludetto, &Toscano (2006)
47 n/a Down syndrome
Di Pinto (2006) 60 60 to 216 ADHD (ADHD/PI; ADHD/C)Fantuzzo, Grim, & Montes
(2002)733/1,427 n/a Urban and low income
Friedli (1994) 20 n/a Children with and without developmental delayGilbert (1997) 100 1 to 72 Children with and without developmental delayHsia (1993) 82 36 to 72 Children with and without developmental delayKnox & Usen (1998) 10 45 to 224 Cerebral palsyMacy, Bricker, & Squires
(2005)68 6 to 36 Children eligible and not eligible for early intervention/early childhood
special educationMcKeating-Esterle, Bagnato,
Fevola, & Hawthorne(2007)
91 33 to 71 Developmental delay, autism, hearing impairment/deafness, Downsyndrome, MR, CP/muscular dystrophy, speech/language impairment,visual impairment/blindness, other health impairment, multiple disabilities
Meisels, Xue, & Shamblott(2008)
112 45.24 to 59.76 At risk; children with special needs whose IEPs indicated that they were inthe mild to moderate range (speech or physical impairment)
Morgan (2005) 32 4 to 60 Reactive attachment disorderMyers, McBride, & Peterson
(1996)40 7 to 36 Developmental delay
Noh (2005) 65 36 to 64 Children eligible and not eligible for early intervention/early childhoodspecial education
Sayers, Cowden, Newton,Warren, & Eason (1996)
4 n/a Down syndrome
Schweinhart, McNair,Barnes, & Larner (1993)
2,500 n/a Low income
Sekina & Fantuzzo (2005) 242 55 to 68 UrbanSher (2000) 20 36 to 67 Children eligible and not eligible for early intervention/early childhood
special educationSlentz (1986) 53 36 to 72 Children with and without developmental delayWright & Boschen (1993) 40 36 to 84 Cerebral palsy
Note. ABAS = Adaptive Behavior Assessment System; ADHD = Attention Deficit Hyperactivity Disorder; AEPS =Assessment Evaluation & Programming System; Carolina = Carolina Curriculum for Infants/Toddlers/Preschoolerswith Special Needs; COR = Child Observation Record; CP = Cerebral Palsy; DOCS = Developmental ObservationChecklist System; HELP = Hawaii Early Learning Profile; IEP = Individualized Education Plan; MR = MentalRetardation; PEDI = Pediatric Evaluation of Disability Inventory; TPBA = Transdisciplinary Play-Based Assessment;WSS/Ounce = Work Sampling System.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
AUTHENTIC ASSESSMENT 13
TABLE 4Research Study Characteristics
Accuracy (Reliability) Effectiveness (Validity)
Interitema Sensitivitya Constructa
Author(s) and Year (N = 27) Test Interraterb Test-Retest Specificityb Concurrent Criterionb Predictive
Anthony (2003) TPBA xBailey & Bricker (1986) AEPS xb x xBaird, Campbell, Ingram, & Gomez
(2001)DOCS xa
Bricker, Bailey, & Slentz (1990) AEPS xb x xBricker, Yovanoff, Capt, & Allen
(2003)AEPS xa
xb
Bricker et al. (2008) AEPS xa
xb
Calhoon (1997) TPBA xCody (1995) AEPS xDelGiudice, Brogna, Romano,
Paludetto, & Toscano (2006)AEPS x
Di Pinto (2006) ABAS xFantuzzo, Grim, & Montes (2002) COR xa
Friedli (1994) TPBA xb x xGilbert (1997) DOCS xb xHsia (1993) AEPS xa xa
xb
Knox & Usen (1998) PEDI xa
Macy, Bricker, & Squires (2005) AEPS xb xa xxb
Meisels, Xue, & Shamblott, (2008) WSS x xMcKeating-Esterle, Bagnato, Fevola,
& Hawthorne (2007)ABAS x
Morgan (2005) DOCS xMyers, McBride, & Peterson (1996) TPBA xa
Noh (2005) AEPS xa xxb
Sayers, Cowden, Newton, Warren, &Eason (1996)
AEPS x
Schweinhart, McNair, Barnes, &Larner (1993)
COR xb x
Sekina, & Fantuzzo (2005) COR xa
Sher (2000) AEPS xb x xa
Slentz (1986) AEPS xa x x xa
xb
Wright & Boschen (1993) PEDI xa
xb
Note. ABAS = Adaptive Behavior Assessment System; AEPS = Assessment Evaluation & Programming System;Carolina = Carolina Curriculum for Infants/Toddlers/Preschoolers with Special Needs; COR = Child ObservationRecord; DOCS = Developmental Observation Checklist System; HELP = Hawaii Early Learning Profile; PEDI =Pediatric Evaluation of Disability Inventory; TPBA = Transdisciplinary Play-Based Assessment; WSSS/Ounce =Work Sampling System.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
14 MACY AND BAGNATO
TABLE 5Reported Research Results
Author(s) and Year (N = 27) Reported Results
Anthony (2003) TPBA visual development guidelines were used by raters at Denver’s PLAYclinic and had positive interrater agreement results.
Bailey & Bricker (1986) AEPS correlation with the Gesell Developmental Schedule (Knobloch et al.,1980) was strong for the whole test but not individual areas. AEPS could besuccessfully administered in a reasonable amount of time.
Baird, Campbell, Ingram, & Gomez(2001)
DOCS may lack sensitivity in detecting variations in development.
Bricker, Bailey, & Slentz (1990) AEPS correlation across areas was r = .88 (p < .001).Bricker, Yovanoff, Capt, & Allen
(2003)AEPS newly established cutoff scores in the 2nd edition identified eligible
children accurately most of the time.Bricker et al. (2008) AEPS cutoff scores performed similarly to the Bricker et al. (2003) study. The
measure accurately identified the majority of children correctly.Calhoon (1997) Children performed better (i.e., higher scores) on the TPBA than the
conventional test, and the play-based assessment provided a richerdescription of children’s emerging skills.
Cody (1995) In the HELP study, the play age obtained from the authentic assessment washighly correlated with the Developmental Age Equivalent of theconventional assessment (i.e., BSID).
DelGiudice, Brogna, Romano,Paludetto, & Toscano (2006)
After 1 year, children in the Carolina condition made progress and had higherDQ than children in the comparison condition who made slight progress butimprovements were not statistically significant.
Di Pinto (2006) ABAS accurately documents poor social adaptive outcomes for children withADHD.
Fantuzzo, Grim, & Montes (2002) The study supports the use of the COR assessment method for low-incomeurban preschool children; however, a three-factor model should replace theproposed six-factor model.
Friedli (1994) TPBA had favorable test retest results, interrater agreement, and concurrentvalidity.
Gilbert (1997) Significant difference among raters was found: mothers rated the child’s skillshighest, the fathers next, and the teachers last. Differences among raters onthe DOCS may influence eligibility decisions.
Hsia (1993) The AEPS has strong interrater agreement at both domain (ranging from .87social to .94 adaptive) and total test (.90) levels. Strong relationship betweenindividual domain scores (.64 to .96) and total test (.98) when internalconsistency was examined. Findings also showed that the AEPS wassensitive to performance differences of children with delays.
Knox & Usen (1998) The PEDI is a useful tool for describing the area of functional delay in childrenwith cerebral palsy. It also appears to be sensitive to changes that wereobserved clinically.
Macy, Bricker, & Squires (2005) The AEPS accurately classified all eligible children and over 94% (n = 64/68)of the noneligible children. The overall sensitivity was 100%; specificitywas 89%. The AEPS used to determine eligibility was positively andsignificantly correlated with conventional eligibility measures. Finally, theobservers who scored the AEPS had strong agreement on observations madeabout child performance.
Meisels, Xue, & Shamblott (2008) Study found evidence for validity and reliability of WSS, suggesting thatWSHS accurately assesses language development, literacy, and mathematicsskills in young children.
(Continued on next page)
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010

AUTHENTIC ASSESSMENT 15
TABLE 5Reported Research Results (Continued)
Author(s) and Year (N = 27) Reported Results
McKeating-Esterle, Bagnato, Fevola,& Hawthorne (2007)
ABAS-II is correlated with ratings of informed opinion when assessingchildren for early intervention.
Morgan (2005) Evidence supports the predictive validity of the DOCS-II in detecting RAD ina randomized sample.
Myers, McBride, & Peterson (1996) The overall mean number of days to complete the eligibility assessmentprocess took the group using the TPBA 22 days less than it took the groupusing a conventional test.
Noh (2005) The AEPS has satisfactory interrater reliability agreement in the cognitive andsocial domains. Strong relationship between individual domain scores anditems in the domains.
Sayers, Cowden, Newton, Warren, &Eason (1996)
When children’s scores increased on the gross motor domain of the HELP,they did the same for the PSI.
Schweinhart, McNair, Barnes, &Larner (1993)
The COR was found to be a psychometrically promising tool for theassessment of children’s development in developmentally appropriate earlychildhood programs. Also, the COR helped staff to understand earlychildhood development and curriculum and to prepare individualizededucation programs for their children.
Sekina, & Fantuzzo (2005) Univariate and multivariate results provide support for convergent anddivergent validity of the COR dimensions. Fifteen of the 18 variablesdifferentiated the three COR dimensions, particularly the COR Cognitiveand Social Engagement dimensions.
Sher (2000) Professionals using the AEPS were able to identify eligible children. Moderateinterrater reliability for the communication domain and high reliability forother domains.
Slentz (1986) Positive results of this study support the technical properties of the AEPS.Interrater agreement was very high at .94 for the entire test and ranged from.84 to .94 for the six domains. Results for two administrations of the AEPS(N = 18) revealed strong level of stability across time for the total test (.91),domain scores varied between high (fine motor .86, cognitive .91, socialcommunication .77) to moderate (social .50) to low stability (gross motor.07 and self-care .13). Internal consistency was strong for all domains exceptself-care. Concurrent validity was examined by comparing the AEPS withthe McCarthy (1972) and the Uniform Performance Assessment System(Haring, White, Edgar, Affleck, & Hayden, 1980) with mixed resultsranging from very weak to strong relationships between domains and scales.
Wright & Boschen (1993) Satisfactory information is provided to confirm the PEDI’s usefulness forclinical and research purposes with children with cerebral palsy.
Note. ABAS = Adaptive Behavior Assessment System; AEPS = Assessment Evaluation & Programming System;Carolina = Carolina Curriculum for Infants/Toddlers/Preschoolers with Special Needs; COR = Child ObservationRecord; DOCS = Developmental Observation Checklist System; HELP = Hawaii Early Learning Profile; PEDI =Pediatric Evaluation of Disability Inventory; TPBA = Transdisciplinary Play-Based Assessment; WSS/Ounce = WorkSampling System.
with other good examples of authentic and linked eligibility assessment, many of the studies inour review made comparisons with nonlinked eligibility tests. For example, in the Macy, Bricker,and Squires (2005) study, the AEPS (curriculum linked measure) was compared with the BattelleDevelopmental Inventory (not linked to curriculum).
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
16 MACY AND BAGNATO
Future research should continue not only to examine the accuracy and effectiveness of au-thentic measures but also to make comparisons using an external standard. Some examples ofexternal standards are (a) correct identification rates based on expert consensus, (b) the need forservices—service-based eligibility, and (c) probability of succeeding/progressing in Head Startor typical setting with typical peers without support services. Another area of research shouldstudy the effects of the initial eligibility assessment using authentic measures on child outcomesusing a longitudinal design. Cost–benefit studies need to be conducted on the use of authenticassessment practices used to determine children eligible for IDEA services. This type of evidencecould be helpful to policymakers when reauthorizing policies and updating eligibility assessmentguidelines.
Limitations
A number of authentic assessment measures are commercially available; however, we chose toexamine only these nine measures because they appeared most often in the professional literatureand by accounts from practitioners. Other authentic measures, like the Developmental Continuumfrom Teaching Strategies, were not included in this review because they did not meet our inclusioncriteria. For example, tools like the Developmental Continuum have conducted research studies;however, we were unable to locate these in journals and/or the databases we searched. Sometimespublishers maintain the results from studies for proprietary reasons and they are not available tothe public. The body of literature contained other publications related to authentic assessmentand we included only research studies that involved young children who were at risk or had adisability in the sample.
Authentic assessment can be used for designing a program for a child, creating interventions,and to evaluate the efficacy of a child’s individualized program. Not only does authentic as-sessment have potential to accurately identify children in need of services, it also has importantimplications beyond eligibility determination (Neisworth & Bagnato, 2004). Findings of thisstudy will help professionals to critically identify characteristics of authentic assessment researchfindings that influence the accurate and representative documentation of a young child’s earlyintervention eligibility assessment experience.
Head Start programs would benefit from an assessment approach that provides useful informa-tion linked to curriculum and instruction in order to serve children more efficiently. Additionally,an approach is needed that can monitor ongoing child performance (Downs & Strand, 2006;Grisham-Brown, Hallam, & Brookshire, 2006; Grisham-Brown et al., 2008; Hebbeler, Barton,& Mallik, 2008; Meisels, Liaw, Dorfman, & Nelson, 1995). Authentic assessment is a viable al-ternative to eligibility assessments that use standardized, norm-referenced tests (Bagnato, 2005,2007; Bagnato & Neisworth, 1992; Macy & Hoyt-Gonzales, 2007; McLean, 2005; Neisworth &Bagnato, 2004). An authentic assessment approach has growing support from early childhoodprofessional organizations (i.e., DEC and NAEYC) and from the literature base (Bagnato &Neisworth, 2005). The authentic assessment studies reported here in this research study are thefirst phase of research supporting the use of an authentic assessment approach for eligibilitydetermination. Although this foundation is a good start, more research is needed to continue toexplore authentic measures and approaches.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010

AUTHENTIC ASSESSMENT 17
REFERENCES
*Indicates studies used in the synthesis.**Indicates measures used in the synthesis.*Anthony, T. L. (2003). The inclusion of vision-development guidelines in the Transdisciplinary Play-Based Assessment:
A study of reliability and validity. Unpublished doctoral dissertation, University of Denver, Denver, CO.Bagnato, S. J. (2005). The authentic alternative for assessment in early intervention: An emerging evidence-based practice.
Journal of Early Intervention, 28, 17–22.Bagnato, S. J. (2007). Authentic assessment for early childhood intervention best practices: The Guilford school practi-
tioner series. New York: Guilford.Bagnato, S. J., Macy, M., Salaway, J., & Lehman, C. (2007). Research foundations for conventional tests and testing
to ensure accurate and representative early intervention eligibility. Pittsburgh, PA: TRACE Center for Excellencein Early Childhood Assessment, Early Childhood Partnerships, Children’s Hospital/University of Pittsburgh, U.S.Department of Education Office of Special Education Programs, and Orelena Hawks Puckett Institute.
Bagnato, S. J., McKeating-Esterle, E., Fevola, A. F., Bartalomasi, M., & Neisworth, J. T. (2008). Valid use of clinicaljudgment (informed opinion) for early intervention eligibility: Evidence-base and practice characteristics. Infants andYoung Children, 21, 334–348.
Bagnato, S. J., & Neisworth, J. T. (1992). The case against intelligence testing in early intervention. Topics in EarlyChildhood Special Education, 12, 1–20.
Bagnato, S. J., & Neisworth, J. T. (1999). Collaboration and teamwork in assessment for early intervention. ComprehensivePsychiatric Assessment of Young Children, 8, 347–363.
Bagnato, S. J., & Neisworth J. T. (2005). DEC recommended practices: Assessment. In S. Sandall, M. L. Hemmeter, B.J. Smith, & M. McLean (Eds.), DEC recommended practices (pp. 45–50). Longmont, CO: Sopris West.
Bagnato, S. J., Neisworth, J. T., & Munson, S. (1997). LINKing assessment and early intervention. Baltimore, MD:Brookes.
Bagnato, S. J., Neisworth, J. T., & Pretti-Frontczak, K. L. (in press). LINKing assessment and early intervention (4th ed.).Baltimore, MD: Brookes.
Bagnato, S. J., Smith-Jones, J., Matesa, M., & McKeating-Esterle, E. (2006). Research foundations for using clinicaljudgment (informed opinion) for early intervention eligibility determination. Cornerstones, 2(3), 1–14.
*Bailey, E., & Bricker, D. (1986). A psychometric study of a criterion-referenced assessment designed for infants andyoung children. Journal of the Division of Early Childhood, 10, 124–134.
*Baird, S. M., Campbell, D., Ingram, R., & Gomez, C. (2001). Young children with Cri-du-Chat: Genetic, developmental,and behavioral profiles. Infant-Toddler Intervention, 11, 1–14.
**Bricker, D. (Ed.). (1993). Assessment, evaluation, and programming system for infants and children (1st ed.). Baltimore,MD: Brookes.
**Bricker, D. (Ed.). (2002). Assessment, evaluation, and programming system for infants and children (2nd ed.).Baltimore, MD: Brookes.
*Bricker, D., Bailey, E., & Slentz, K. (1990). Reliability, validity, and utility of the Evaluation and Programming System:For infants and young children (EPS-I). Journal of Early Intervention, 14, 147–160.
*Bricker, D., Clifford, J., Yovanoff, P., Pretti-Frontczak, K., Waddell, M., Allen, D., et al. (2008). Eligibility determinationusing a curriculum-based assessment: A further examination. Journal of Early Intervention, 31, 3–21.
*Bricker, D., Yovanoff, P., Capt, B., & Allen, D. (2003). Use of a curriculum-based measure to corroborate eligibilitydecisions. Journal of Early Intervention, 26, 20–30.
*Calhoon, J. M. (1997). Comparison of assessment results between a formal standardized measure and a play-basedformat. Infant-Toddler Intervention: The Transdisciplinary Journal, 7, 201–214.
*Cody, D. A. (1995). Play assessment as a measure of cognitive ability in developmentally delayed preschoolers.Unpublished doctoral dissertation, George Mason University, Fairfax, VA.
Danaher, J. (2005). Eligibility policies and practices for young children under Part B of IDEA (NECTAC Notes No.15).Chapel Hill, NC: The University of North Carolina, FPG Child Development Institute, National Early ChildhoodTechnical Assistance Center.
*DelGiudice, E., Brogna, G., Romano, A., Paludetto, R., & Toscano, E. (2006). Early intervention for children with Downsyndrome in southern Italy: The role of parent-implemented developmental training. Infants & Young Children, 19,50–58.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010
18 MACY AND BAGNATO
*Di Pinto, M. (2006). The ecological validity of the Behavior Rating Inventory of Executive Functioning (BRIEF) inattention deficit hyperactivity disorder: Predicting academic achievement and social adaptive behavior in the subtypesof ADHD. Dissertation Abstracts International, 67(03), 1696B. (UMI No. 3209793)
Downs, A., & Strand, P. S. (2006). Using assessment to improve the effectiveness of early childhood education. Journalof Child and Family Studies, 15, 671–680.
Dunst, C. J. (2002). Family-centered practices: Birth through high school. Journal of Special Education, 36(3), 139–147.Dunst, C. J., Trivette, C. M., & Cutspe, P. A. (2002). An evidence-based approach to documenting the characteristics
and consequences of early intervention practices. Centerscope, 1(2), 1–6. Retrieved July 11, 2009, from http://www.evidencebasepractices.org/centerscope/centerscopevol1no2.pdf
Dunst, C. J., & Hamby, D. W. (2004). States’ Part C eligibility definitions account for differences in the percent-age of children participating in early intervention programs. Snapshots, 1(4). Retrieved July 12, 2009, fromhttp://www.tracecenter.info/products.php
*Fantuzzo, D., Grim, S., & Montes, G. (2002). Generalization of the Child Observation Record: A validity study fordiverse samples of urban, low-income preschool children. Early Childhood Research Quarterly, 17, 106–125.
*Friedli, C. (1994). Transdisciplinary play-based assessment: A study of reliability and validity. Unpublished doctoraldissertation, University of Colorado, Denver, CO.
*Gilbert, S. L. (1997). Parent and teacher congruency on variations of a screening assessment: An examination (ReportNo. H023B50009). Auburn, AL: Auburn University. (ERIC Document Reproduction Service No. ED413726)
Grisham-Brown, J., Hallam, R., & Brookshire, R. (2006). Using authentic assessment to evidence children’s progresstoward early learning standards. Early Childhood Education Journal, 34, 45–51.
Grisham-Brown, J., Hallam, R., & Pretti-Frontczak, K. L. (2008). Preparing Head Start personnel to use a curriculum-based assessment: An innovative practice in the “age of accountability.” Journal of Early Intervention, 30, 271–281.
Gulikers, T. M., Bastiaens, T. J., & Kirschner, P. A. (2004). A five-dimensional framework for authentic assessment.Educational Technology Research and Development, 52(3), 67–86.
Guralnick, M. J. (2006). Family influences on early development: Integrating the science of normative development,risk and disability, and intervention. In K. McCartney & D. Phillips (Eds.), Blackwell handbook of early childhooddevelopment (pp. 44–61). Malden, MA: Blackwell.
**Haley, S. M., Coster, W. J., Ludlow, L. H., Haltiwanger, J. T., & Andrellos, P. J. (1992). Pediatric Evaluation ofDisability Inventory (PEDI). Boston: New England Medical Center Hospitals, Inc.
**Harrison, P. L., & Oakland, T. (2003). Adaptive Behavior Assessment System-Second Edition. San Antonio, TX: ThePsychological Corporation.
Hebbeler, K., Barton, L. R., & Mallik, S. (2008). Assessment and accountability for programs serving young childrenwith disabilities. Exceptionality, 16, 48–63.
**High/Scope Educational Research Foundation. (2003). Preschool Child Observation Record–Second Edition. Ypsilanti,MI: High/Scope Press.
**Hresko, W. P., Miguel, S. A., Sherbenou, R. J., & Burton, S. D. (1994). Developmental Observation Checklist System.Austin, TX: PRO-ED.
*Hsia, T. (1993). Evaluating the psychometric properties of the Assessment, Evaluation, and Programming System forThree to Six Years: AEPS Test. Unpublished doctoral dissertation, University of Oregon, Eugene, OR.
Individuals with Disabilities Education Improvement Act, Pub. L. No. 108-446, 20 U.S.C. (2004).**Johnson-Martin, N. M., Attermeier, S. M., & Hacker, B. J. (2004). The Carolina curriculum for infants and toddlers
with special needs (3rd ed.). Baltimore, MD: Brookes.**Johnson-Martin, N. M., Hacker, B. J., & Attermeier, S. M. (2004). The Carolina curriculum for preschoolers with
special needs (2nd ed.). Baltimore, MD: Brookes.Keilty, B., LaRocco, D. J., & Casell, F. B. (2009). Early interventionists’ reports of authentic assessment methods through
focus group research. Topics in Early Childhood Special Education, 28, 244–256.*Knox, V., & Usen, Y. (1998). Clinical review of the Pediatric Evaluation of Disability Inventory. The British Journal of
Occupational Therapy, 63, 29–32.Layton, C. A., & Lock, R. H. (2007). Use authentic assessment techniques to fulfill the promise of No Child Left Behind.
Intervention in School & Clinic, 42, 169–173.**Linder, T. W. (1993). Transdisciplinary play-based assessment: A functional approach to working with young children.
Baltimore, MD: Brookes.Losardo, A., & Notari-Syverson, A. (2001). Alternative approaches to assessing young children. Baltimore, MD: Brookes.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010

AUTHENTIC ASSESSMENT 19
Macy, M., & Bricker, D. (2006). Practical applications for using curriculum-based assessment to create embedded learningopportunities for young children. Young Exceptional Children, 9(4), 12–21.
*Macy, M. G., Bricker, D. D., & Squires, J. K. (2005). Validity and reliability of a curriculum-based assessment approachto determine eligibility for part C services. Journal of Early Intervention, 28, 1–16.
Macy, M., & Hoyt-Gonzales, K. (2007). A linked system approach to early childhood special education eligibilityassessment. TEACHING Exceptional Children, 39(3), 40–44.
*McKeating-Esterle, E., Bagnato, S. J., Fevola, A., & Hawthorne, C. (2007). A comparison of clinical judgment (informedopinion) with performance-based assessment to document early intervention status. Unpublished master’s thesis,University of Pittsburgh, Pittsburgh, PA.
McLean, M. (2005). Using curriculum-based assessment to determine eligibility: Time for a paradigm shift? Journal ofEarly Intervention, 28, 23–27.
McLean, M., Bailey, D. B., & Wolery, M. (2004). Assessing infants and preschoolers with special needs (3rd ed.). UpperSaddle River, NJ: Pearson.
Meisels, S. J., Bickel, D. D., Nicholson, J., Xue, Y., & Atkins-Burnett, S. (2001). Trusting teachers’ judgments: A validitystudy of a curriculum-embedded performance assessment in kindergarten to grade 3. American Educational ResearchJournal, 38, 73–95.
**Meisels, S. J., Dombro, A. L., Marsden, D. B., Weston, D., & Jewkes, A. (2003). The Ounce Scale: An observationalassessment for infants, toddlers, and families. New York: Pearson Early Learning.
**Meisels, S. J., Jablon, J. R., Marsden, D. B., Dichtelmiller, M. L., & Dorfman, A. B. (2001). The Work Sampling System(4th ed.). New York: Pearson Early Learning.
Meisels, S. J., Liaw, F., Dorfman, A., & Nelson, R. F. (1995). The Work Sampling System: Reliability and validity of aperformance assessment for young children. Early Childhood Research Quarterly, 10, 277–296.
Meisels, S. J., Xue, Y., Bickel, D. D., Nicholson, J., & Atkins-Burnett, S. (2001). Parental reactions to authenticperformance assessment. Educational Assessment, 7, 61–85.
*Meisels, S. J., Xue, Y., & Shamblott, M. (2008). Assessing language, literacy, and mathematics skills with WorkSampling Head Start. Early Education and Development, 19, 963–981.
Morgan, F. T. (2005). Development of a measure to screen for reactive attachment disorder in children 0–5 years.Dissertation Abstracts International, 66(04), 2312B (UMI No. 3173576).
*Myers, C. L., McBride, S. L., & Peterson, C. A. (1996). Transdisciplinary, play-based assessment in early childhoodspecial education: An examination of social validity. Topics in Early Childhood Special Education, 16, 102–126.
National Association of School Psychologists. (2005). NASP position statement on early childhood assessment. Bethesda,MD: Author.
National Research Council. (2008). Early childhood assessment: Why, what, and how. Washington, DC: NationalAcademies Press.
Neisworth, J. T., & Bagnato, S. J. (2004). The mismeasure of young children: The authentic assessment alternative.Infants & Young Children, 17, 198–212.
*Noh, J. (2005). Examining the psychometric properties of the second edition of the Assessment, Evaluation, andProgramming System for three to six years: AEPS Test–Second Edition (3–6). Unpublished doctoral dissertation,University of Oregon, Eugene, OR.
**Parks, S., Furono, S., O’Reilly, K., Inatsuka, T., Hoska, C. M., & Zeisloft-Falbey, B. (1994). Hawaii early learningprofile (HELP). Palo Alto, CA: Vort.
Pretti-Frontczak, K., Kowalski, K., & Brown, R. D. (2002). Preschool teachers’ use of assessments and curricula: Astatewide examination. Exceptional Children, 69, 109–123.
*Sayers, L. K., Cowden, J. E., Newton, M., Warren, B., & Eason, B. (1996). Qualitative analysis of a pediatric strengthintervention on the developmental stepping movements of infants with Down syndrome. Adapted Physical ActivityQuarterly, 13, 247–268.
*Schweinhart, L. J., McNair, S., Barnes, H., & Larner, M. (1993). Observing young children in action to assess theirdevelopment: The High/Scope Child Observation Record study. Educational and Psychological Measurement, 53,445–454.
*Sekina, Y., & Fantuzzo, J. (2005). Validity of the Child Observation Record: An investigation of the relationship betweenCOR dimensions and social-emotional and cognitive outcomes for Head Start children. Journal of PsychoeducationalAssessment, 23, 242–261.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010

20 MACY AND BAGNATO
Shakelford, J. (2002). Informed clinical opinion (NECTAC Note No. 10). Chapel Hill, NC: The University of NorthCarolina, Frank Porter Graham Child Development Institute, National Early Childhood Technical Assistance Center.
Shakelford, J. (2006). State and jurisdictional eligibility definitions for infants and toddlers with disabilities under IDEA(NECTAC Note No. 21). Chapel Hill, NC: The University of North Carolina, Frank Porter Graham Child DevelopmentInstitute, National Early Childhood Technical Assistance Center.
*Sher, N. (2000). Activity-based assessment: Facilitating curriculum linkage between eligibility evaluation and interven-tion. Unpublished doctoral dissertation, University of Oregon, Eugene, OR.
*Slentz, K. (1986). Evaluating the instructional needs of young children with handicaps: Psychometric adequacy of theEvaluation and Programming System-Assessment Level II. Dissertation Abstracts International, 47 (11), 4072A.
Slentz, K. L., & Hyatt, K. J. (2008). Best practices in applying curriculum-based assessment in early childhood. In A.Thomas & J. Grimes (Eds.), Best practices in school psychology V (Vol. 2, pp. 519–534). Bethesda, MD: NationalAssociation of School Psychologists.
*Wright, F. V., & Boschen, K. (1993). The Pediatric Evaluation of Disability Inventory (PEDI) validation of a newfunctional assessment outcome instrument. Canadian Journal of Rehabilitation, 7, 41–42.
Zigler, E., & Styfco, S. J. (2000). Pioneering steps (and fumbles) in developing a federal preschool intervention. Topicsin Early Childhood Special Education, 20, 67–70.
Downloaded By: [Macy, Marisa] At: 23:06 15 January 2010





























