Embed Size (px)
Citation preview

Interpersonal Dependency and Depression: A Meta-Analytic Review
_________________________
A Dissertation
Presented to the Faculty
of
The Gordon F. Derner
School of Psychology
Adelphi University
____________________________
In Partial Fulfillment
Of the Requirement for the Degree
Doctor of Philosophy
____________________________
Alyssa M. Deitchman, M.A.
2020

2
Committee Members
Committee Chair…………………………………………….………Robert F. Bornstein, Ph.D.
Member………………………………………………………………Kate Szymanski, Ph.D.
Member………………………………………………………………Michael T. Moore, Ph.D.
Member………………………………………………………………Mary Cortina, Ph.D.
3
Acknowledgements
I want to first thank the members of my dissertation committee, Dr. Robert Bornstein, Dr.
Michael Moore, Dr. Kate Szymanski, and Dr. Mary Cortina, for their support of this project. I
want to particularly extend my utmost gratitude to my research mentor, Dr. Robert Bornstein,
without whom none of this work would be possible. Dr. Bornstein has provided with me
pervasive and unrelenting encouragement since we began working together at the start of my
Ph.D. program in 2014. He went above and beyond his responsibility as my mentor in that he
supported me through unprecedented times that challenged my ability to perform in my graduate
program. Despite these challenges, he refused to give up on me. At times, his encouragement
was the sole vehicle through which I maintained the momentum that brought me here today.
Dr. Michael Moore was also of particular support beyond just the scope of the current
project. Through our endeavors in clinical supervision, coursework, and research, I knew I could
count on Dr. Moore for prompt, sincere, and enthusiastic support, which was a pillar of comfort
and safety in my time at Derner. Dr. Kate Szymanski also represented a source of strength,
support, and warmth in the sometimes challenging world of academia. She has always been
generous with her knowledge and encouragement to me as a student. It was an honor to learn
from all of you. Next, I would like to give special thanks to Dr. Mary Cortina, for serving as an
outside reader on this project. It is that kind of generosity and enthusiasm for supporting students
that makes being an Adelphi student a special gift. I would also like to give special thanks to Dr.
Adam Natoli and Dr. Bernard Gorman, both of whom provided invaluable feedback on this
project.
Next, I would like to thank my family: my father, mother, and brother, grandmother, and
the Santarsiero’s. The love, patience, and kindness with which you have treated me has made
4
me the person I am today and I am grateful for all of you. While both my parents are extremely
intelligent and insightful people, neither of their life circumstances allowed for them to graduate
from college. I am hopeful that my academic journey has given them something of which they
are proud. I would also like to share thanks to the amazing guidance counselors and teachers at
Locust Valley High School who inspired my love of learning at an early age. Next, I would like
to thank the Big Guy Foundation and New York University’s scholarship awards, which enabled
me to attend the college of my dreams at little to no cost, which I could never have afforded
otherwise. I am forever indebted for the opportunity that opened so many doors for me and
shaped the person and scholar I am today.
I would also like to thank my amazing partner, my husband, Jelle Welagen, who
provides me with a beautiful life full of love, inspiration, laughter, and genuine support of my
well-being and career. I cannot count the amount of pots of coffee made or take-out meals
consumed together as I worked my way through this project – and there is no one with whom I
would have rather spent those times. Of note, we also spend most of our first year of marriage
surviving quarantining together during a pandemic – and it was surprisingly smooth-sailing,
which I believe is a testament to our strong bond and natural friendship. I would like to thank
my best friend, Erin Fitzgerald, who has checked in with me multiple times daily during this
process and who provides a friendship so strong, it feels more like family. I would also like to
thank my friends Cassie Williams, Nicole Auditore, Samantha Maurice, Brit Lippman, Shira
Spiel, Kahlen Kim, and Divya Robin. Lastly, I would like to thank my neighbors and community
around Hopewell, New Jersey, who have also been cheering me on during this challenging
process. I consider myself extremely fortunate to have this kind of positivity and light in my life.
Thank you to all.

5
Table of Contents
List of Tables…………………………………….…………………….…………….6
List of Figures…………………………………………………………………….….7
Abstract ……………………………………………………………………………...8
Chapter I: Personality and Psychopathology ………………………….…………….9-12
Chapter II: Interpersonal Dependency ………………………………………………13-29
Chapter III: Depression………………………………………………………………30-49
Chapter IV: Dependency and Depression……………………………………………50-60
Chapter V: Present Study ……………………………………………………………61-62
Chapter VI: Methodology………………………………………………………….…63-72
Chapter VII: Results………………………………………………………………….73-84
Chapter VIII: Discussion………………………………………………….………….85-95
Chapter IX: Conclusion……………………………………………………………….96-97
References………………………………………………………………………….…98-116
Appendix I: Statistical Formulas……………………………………………………...117
Appendix II: Summary of Data from Meta-Analysis Articles ….……………………118-129
Appendix III: References for Articles Included in Meta-Analysis……………………130-143

6
List of Tables
1 The Cognitive, Motivational, Affective and Behavioral Manifestations of
Depression and Dependency 55
2 Location of Study 81-82
3 Type of Sample 82
4 Type of Depression Measure 83
5 Type of Dependency Measure 84

7
List of Figures
1 PRISMA Diagram 75
2 Forest Plot of Effect Sizes 77
3 Funnel Plot of Effect Sizes (r) Against Standard Error 79

8
Abstract
Although considerable research has been conducted examining the relationship between
interpersonal dependency and depression, the body of literature reveals mixed and sometimes
conflicting results. These mixed findings suggest that meta-analytic review of the dependency—
depression literature might clarify the overarching link between the two constructs, and variables
that moderate this link. The current study uses a random-effects meta-analysis to address this
issue, using articles from PubMed, Google Scholar, and PsychNet, with inclusion based on their
use of a measure or index of depression and a measure or index of interpersonal dependency. 105
studies met inclusion criteria. Based on a review of the literature in this area, it is hypothesized
that meta-analysis will reveal a small to medium positive effect size between dependency and
depression. It was hypothesized that several variables may moderate the dependency-depression
link including: gender, type of dependency measure, type of depression measure, location of
sample, and type of sample. Results from this study confirm the first hypothesis, such that an
overall Pearson correlation of r = .32 was obtained. The variables identified as potential
moderators had minimal impact on the magnitude of the effect sizes found. This research fills a
crucial gap in the literature and can help inform diagnostic screenings about markers and
vulnerabilities of depression, resulting in more accurate diagnosis and more nuanced treatment of
depressive disorders.
Keywords: depression, dependency, dependent personality, meta-analysis, systematic review

9
Chapter I: Personality and Psychopathology
Personality and psychopathology are universally recognized features of the human
experience that transcend time and culture (Anderson & Bienvenu, 2011). Personality can best
be understood as an individual’s distinctive patterns of thinking, behaving, and feeling across the
lifespan (Thomas & Chess, 1977); an individual’s personality is relatively stable over time, is to
some degree heritable, and plays an imperative role in each individual’s unique life course
(Anderson & Beinvenu, 2011). Psychopathology is a dense yet wide-ranging field that refers to
the study of abnormalities in both intra- and interpersonal functioning, including cognitive
processes, perception, affect, and behavior.
Nosological systems, such as the Diagnostic Statistical Manual, (DSM), describe and
characterize psychopathology via psychiatric diagnosis. However, prior to the development of
such systems, the Hippocratean Humoral theory of personality and psychopathology (which will
be elaborated on in a later section), prevailed until Freud and other scholars proposed theories
that linked disturbances in sexual development to later psychopathology (Anderson & Bienvenu,
2011). Modern research on the link between personality and psychopathology was spearheaded
in part by Widiger (e.g., Widiger, 1999, 2009, 2011) who suggested that personality and
psychopathology are inextricably linked in a variety of ways, such that they cannot entirely be
considered unique constructs. Millon (2011) and others generally subscribe to Widiger’s
conceptualization of the essential links between personality and psychopathology.
Widiger (2011) posited that personality and psychopathology can relate to each other in
at least three ways: (1) personality and psychopathology can influence the presentation of each
other, in what is considered a pathoplastic relationship; (2) personality and psychopathology can
share the same underlying etiology, categorized as a spectrum relationship, or (3) personality and

10
psychopathology can play causal roles in the etiology of one another. Each of these
relationships, including both their theoretical and clinical implications, will be delineated in an
effort to better understand the link between these constructs.
Pathoplastic relationships are bidirectional in nature, such that they can potentially
influence the affective, cognitive, and behavioral presentations of each other. For instance,
psychopathology can vary in symptomatic manifestation based on an individual’s personality
structure. In the same way, the presentation of personality traits can be influenced by underlying
psychopathology (Widiger, 2011; Millon, 2011; Farmer, 2000; Widiger & Samuel, 2005). When
the pathoplastic effect of personality on psychopathology was considered, Widiger utilized an
anecdote of a patient with an eating disorder. He explained that this patient could likely be
characterized as having a highly conscientious and achievement-striving personality that in turn
drives the eating disorder behavior. In contrast, the pathoplastic effect of psychopathology on
personality was illustrated by studies that demonstrated fluctuations in an individual’s self-
attributed personality characteristics based on the presence and severity of psychopathology
(Widiger, 2011).
In contrast to the pathoplastic theory, the spectrum model conceptualizes personality and
psychopathology along the same dimension, or spectrum, of functioning (Samuel & Widiger,
2008; Widiger & Trull, 2007). In this way, “All personality disorders may in fact be
maladaptive variants of general personality traits, and some personality disorders could be early
onset, chronic, and pervasive variants of other mental disorders” (Widiger, 2011, p. 104).
Ironically, support for this perspective lies in the lack of literature that examines how personality
traits contribute to the onset of actual personality disorders; Widiger (2011) argued that this lack
of empirical investigation implies a consensus that personality and personality disorders lie along

11
the same continuum. To further support this perspective, Widiger (2011) explained how
obsessive-compulsive personality disorder (OCPD) can be theoretically conceptualized as
maladaptive conscientiousness as defined by the five-factor model (FFM).
Arguably of primary concern to both clinicians and researchers, is the etiological or
causal relationship between personality and psychopathology, which Widiger (2011) and others
(e.g., World Health Organization, 1992; McLean & Gallop, 2003; Widiger, 2009) described as
bidirectional in nature. Widiger (2011) elaborated, “One’s characteristic way of thinking, feeling,
behaving, and relating to others can…result in the development of a mental disorder, just as a
severe or chronic mental disorder can contribute to fundamental changes to personality” (p. 105).
The causal impact of psychopathology on personality seems obvious: It is unsurprising that an
individual just diagnosed with a mental disorder would see themselves and the world around
them differently, which would lead to changes in affect, behavior, and other features of
personality. Additionally, consider the ways in which the symptomatic manifestations of
posttraumatic stress disorder would impact an individual’s personality presentation both
internally and externally.
The other side of the etiological relationship theory is the way in which personality
impacts, or is conducive to the development of psychopathology, which is an area of robust
empirical investigation (Widiger, 2011). The central tenet of this perspective is that premorbid
personality traits can increase potential vulnerability to stressful life events, which can in turn
manifest as psychopathology. This model emphasizes the interaction between an individual’s
environment and baseline personality characteristics in the development of psychopathology.
Widiger highlighted the ways in which neuroticism is predictive of a multiplicity of mental

12
illnesses, such as mood disorders, eating disorders, anxiety, and substance abuse, among others
(see Malouff & Schutte, 2005).
Widiger’s (2011) review of the various relationships (i.e., pathoplastic, spectrum, and
etiological), between personality and psychopathology synthesizes a vast body of literature
across disciplines and theoretical orientations (Anderson & Bienvenu, 2011). This understanding
of the various ways in which personality and psychopathology are interrelated provides the
conceptual foundation for the current investigation of interpersonal dependency and depression.

13
Chapter II: Interpersonal Dependency
Defining Dependency as a Construct
Due to the fact that dependency research has been conducted across various theoretical
perspectives, it has been difficult for psychologists to agree upon a universally applicable
definition of dependency as a construct. Early dependency literature demonstrates researchers’
attempts to provide a working definition of dependency. For example, Hirschfeld et al. (1977)
explained dependency as “a complex of thoughts, beliefs, feelings and behaviors which revolve
around the need to associate closely with, interact with, and rely upon valued other people” (p.
610). Other definitions (e.g., Disney, 2013; Bornstein, 2005, Bornstein, Porcelli, Huprich, &
Markova, 2009, Bornstein, 2012) described it as essentially a proclivity to depend on others
excessively, especially when it is unwarranted (i.e., when autonomous functioning is possible).
Over time, researchers were able to delineate the underlying components of dependency via the
utilization of correlational and factor-analytic techniques. These components included self-
reports of: “passivity, suggestibility, interpersonal compliance, conflict-avoidance, pessimism,
self-doubt, emotional reliance on others, lack of social self-confidence, conformity, help seeking,
and need for approval” (Bornstein, 1993, p. 18).
Bornstein (1993, 2012a) offers a comprehensive definition of dependency that
synthesizes the ways in which the literature describes and understands dependency as a
construct. He describes it primarily as a type of personality trait or feature that can be broken
down across four domains of functioning. First, there is a motivational component, which
consists of a strong desire for “guidance, approval, and support from others” (Bornstein, 1993, p.
19). Secondly, dependency manifests itself in the cognitive domain, such that the dependent
individual has a fixed perception of the self as both powerless and ineffectual. Next, there is an

14
affective component, such that the dependent individual will experience both anxiety and fear
when prompted to act independently, especially in the context of being evaluated by others.
Lastly, there is a behavioral component that translates in the dependent individual consistently
seeking help, emotional support, direction, and reassurance from others, as well as a tendency to
yield to others in interpersonal scenarios. However, this most modern conceptualization will be
further examined in a later section of this paper, as it reflects the Cognitive/Interactionist
perspective (Bornstein, 2012b).
History of Dependency
Given the fact that humans are innately social beings, it is no surprise that the
investigation of interpersonal dependency dates back to the origins of psychology. Dependency
has been one of the most studied personality constructs in the past 50 years, but remains largely
misunderstood (Bornstein, Languirand, Geiselman, Creighton, West, Gallagher & Eisenhart,
2003). For instance, dependency is wrought with negative connotations by mental health
professionals and laypeople, evident in the research literature and in colloquial language alike.
Dependency is typically associated with passivity, acquiescence, and immaturity (Millon, 1981).
In fact, the term dependency was derived from the Latin dependere, which translates as “to be
suspended or hang down” (Bornstein, 2005). Therefore, it can be seen from the earliest definition
of the term that there is an inherent pejoration that permeates the definition itself. In her work,
Ainsworth (1972) noted that dependency in adults implies immaturity; Siegel (1988) asserted
“Dependency is devalued and pathologized. It is linked with symbiosis, weakness, passivity,
immaturity and is attributed to women, children, and persons perceived as inadequately
functioning” (Siegel, 1988, p. 113). Later research emphasized the importance of distinguishing
“normal” (i.e., contextually appropriate) dependency from “pathological” (i.e., maladaptive

15
and/or inflexible) dependency. This shift in the literature underscores the idea that some
expressions of dependency are normal and even adaptive (Bornstein, 2012a).
Studies that examine the adaptive aspects of dependency can be grouped into three
overarching areas: 1) adherence to medical and psychotherapeutic regimens, 2) increased
sensitivity to interpersonal cues, and 3) strong academic performance. First, the dependent
person is inclined to rely on authority figures for support and guidance, resulting in rigorous
compliance with both medical and psychotherapeutic regimes (Bornstein, 2012a). Several studies
that have investigated this phenomenon suggest that not only do dependent individuals have
more positive attitudes about physicians and therapists, but they seek treatment more quickly
than do nondependent individuals following the onset of symptoms (Bornstein, 1994; Geurtzen
et al., 2018). Next, because of their high motivation to develop and maintain close relationships
with others, interpersonal sensitivity and more specifically, sensitivity to interpersonal cues, is an
important skill for the dependent person to possess. Experimental studies in this area
demonstrated that dependent individuals are indeed more sensitive than nondependent
individuals to detect and respond to warm versus cold treatment by a research confederate (see,
e.g., Masling, O’Neill, & Katkin, 1982). Lastly, three disparate sets of findings demonstrate the
ways in which high levels of dependency are associated with strong academic performance
across elementary school, high school, and college students (Bornstein, 1994). The various
maladaptive and adaptive aspects of dependency confirm that it is a complex and nuanced
construct at risk for misinterpretation due to longstanding clinical lore. Recognizing the polarity
of the ways in which researchers associate dependency with pathology and adaptation, is
important to delineate prior to deepening the examination of its historical roots.

16
The study of interpersonal dependency traces back to the early works of Freud within the
formation of psychoanalytic theory. Freud (1905) first loosely conceptualized the notion of
interpersonal dependency within his Three Contributions to the Theory of Sexuality, but later
described dependency as being related to either frustration or overgratification during the oral
phase of psychosexual development. As a result of these early conceptualizations, researchers
examined the epigenesis of dependency via the empirical examination of the relationship
between feeding in infancy and the later development of dependent personality traits and
behaviors (Bornstein, 1993). Though each study in this area tested unique hypotheses, some
overarching trends emerged in the literature such that these hypotheses can be synthesized in
more general terms. For instance, researchers hypothesized that heightened dependency
behaviors in childhood or adulthood result from “(1) either a very long (i.e., ‘overgratifying’) or
very brief (i.e., ‘frustrating’) nursing period; (2) a rigid (as opposed to flexible) feeding schedule;
(3) bottle feeding rather than breastfeeding; and (4) ‘severe’ (i.e., abrupt) weaning” (Bornstein,
1993, p. 35).
Most of the research that examined the relationship between infantile weaning and the
development of dependency-related behavior was conducted throughout the 1940s, 1950s, and
1960s. The overarching approach utilized by these studies involved the analysis of weaning
behaviors from the mother (i.e., breast vs. bottle feeding, consistency of adhering to a feeding
schedule, and duration of feeding), combined with the assessment of both childhood or adult
levels of dependency (Bornstein, 1992). A seminal and comprehensive study in this area was
conducted by Sears et al. (1953), who utilized multiple measures of dependent behavior to assess
a mixed-sex sample of young school children. The results of the study conducted by Sears et al.
(1953) were promising, in that they found a difference in level of dependent behavior between

17
male and female elementary school students when assessing the relationship between the rigidity
of feeding schedule and the onset of teacher-specific dependency (Sears et al., 1953). However,
when a follow-up study (Sears, Rau. & Alpert, 1965) was conducted on a larger scale by the
same set of researchers, they did not find a relationship between infantile feeding and
dependency. The results of these and other studies are therefore mixed, which highlighted both
the need for further investigation and the potential presence of methodological issues within the
studies’ design that implicated their clarity. For example, the data were often collected based on
the mothers’ retroactive accounts of feeding and weaning processes under operationalizations
(i.e., rigidity of feeding schedule), that are largely subjective and therefore difficult to assess in a
generalizable and accurate manner.
As dependency research evolved, the focus shifted from the specificity of weaning, to the
overall quality of the infant-caregiver relationship and its subsequent impact on the development
of dependency. As a result of this shift in focus and subsequent shift in methodology, more
consistent data from a multiplicity of studies were produced. For example, Finney (1961)
conducted an early study that found significantly positive correlations between the ratings of the
measure of maternal protectiveness and the scores on the measures that assessed the child’s
dependency retroactively. Later studies (i.e., Hatfield et al., 1967; Murphy, 1962; Gordon &
Tegtemeyer, 1983) obtained similar findings that further reinforce the idea that paternal
behaviors have a significant impact on the development of dependency-related attitudes and
behaviors.
More specifically, studies conducted in later years were able to delineate the impact of
parenting style on later dependency. The results of a multitude of studies conducted in this area
corroborated the hypothesis that parental overprotectiveness and authoritarianism are ultimately

18
associated with increased dependency in children and adults (see Bornstein, 1992 for a review).
In fact, the results are highly consistent across a variety of populations (i.e., with respect to
culture, socioeconomic status, and level of education) and via the utilization of a diverse array of
methodological approaches. Therefore, the link between authoritarian parenting style and the
development of dependency appears to be generalizable. Modern research has further explored
the dynamic between authoritarian parenting and the onset of dependent behaviors. Bornstein
(1992) synthesizes the findings such that it can best be understood as a transactional process
between child and caregiver. He explained,
Parental overprotectiveness and authoritarianism may serve simultaneously to reinforce
dependent behaviors in children of both sexes and to prevent the child from developing
independent, autonomous behaviors (because the parents do not permit the child to
engage in the kinds of trial-and-error learning that is involved in developing a sense of
independence and mastery during childhood) (p. 7).
As current research reflects, increased dependency can best be understood as a by-
product of overprotective and/or authoritarian parenting that manifests across various domains of
functioning. While this understanding stems from the results of various empirical investigations,
different schools of thought reflect diverse ways of conceptualizing dependency as a trait and
personality style.
Psychoanalytic Perspective
When examining dependency from a classical psychoanalytic perspective, its etiology is
linked to Freud’s oral phase of psychosexual development (Bornstein, 1993, 2005, 2011). As
noted, the classical psychoanalytic model of dependency emphasizes the importance of either
frustration or overgratification during the oral stage of development, which is believed to

19
manifest as “oral fixation” (Freud, 1905). Therefore, the dependent person will “remain
dependent on others for nurturance and support and….continue to exhibit behaviors in adulthood
that reflect the oral stage of development” (Bornstein, 1992, p. 4).
Abraham (1927) extended and elaborated upon Freud’s original conceptualization of
dependency as reflecting either overgratification or frustration in the oral phase of development,
such that he delineated and compared the traits of individuals who were products of one or the
other end of the spectrum. For example, he explained how infants who were overgratified in the
oral phase are intrinsic optimists; others (i.e., Goldman-Eisler, 1948) added to this notion by
describing these individuals as “sociable, nurturant, extroverted, and ambitious” (Bornstein,
1993, p. 3). On the contrary, individuals who experienced frustration in the oral phase of
development were thought to be pessimistic and prone to depression and a pervasive need for
reassurance from others (Sandler & Dare, 1970). While subsequent research attempted to
empirically evaluate these hypotheses, the results were ultimately inconclusive (Bornstein, 1993;
2006). Later psychoanalytic investigations of dependency did not divide dependency into these
two categories, and instead conceptualized it as a unitary dimension or trait of personality.
The classical psychoanalytic perspective on dependency, which centers around an
unresolved preoccupation with orality, comes with the following implications. First, because all
human beings must navigate the oral phase of development, some degree of dependency will be
universal in personality development. Next, the psychoanalytic perspective suggests that most of
these processes occur outside conscious awareness, with ego defenses moderating the emotional
discomfort that manifests as a result of unresolved dependency needs. Because there is usually a
high degree of ambivalence around dependency-related issues the individual’s dependency needs
will often be expressed or manifested indirectly (Bornstein, 2005).
20
Object Relational Perspective
The object relational perspective on dependency occurred as a natural evolution of the
classical psychoanalytic conceptualization. The relational model centers around an examination
of the emergence of the self and the relationship (i.e., internalization versus separation) that
occurs between the self and others, or objects. Therefore, this approach shifted the emphasis
from the biological gratification of the infant to the socialization of the infant by the caregiver
(Bornstein, 1993). Specifically, object relations theory focuses on the impact of internal
representations of the self and others and the dynamics that occur between them. Thus, this
theoretical conceptualization differed from classical psychoanalytical modes of thinking such
that it emphasizes the impact of social interaction on the formation of personality, instead of
focusing primarily on biological factors and psychosexual development.
While this approach de-emphasizes the importance of biological influences such as
feeding and weaning, it is similar to the classical psychoanalytic perspective in that it highlights
the importance of early dynamics in the infant-caregiver relationship on personality formation
and the potential development of psychopathology. The underlying mechanisms of the object
relational perspective involve the processes of the internalization of self and object
representations (Klein, 1963; Kohut, 2013). The first object that is internalized is the infant’s
primary caregiver via the caretaking interaction, which is thought to shape following interactions
with others (Kohut, 2013). These mental representations of both the self and others are initially
shaped in infancy and early childhood; ultimately maturation and a successful developmental
trajectory requires a successful process of separation-individuation from primary caregivers.
Therefore, in accordance with the key tenets of the overall approach, the object relational
perspective on dependency examined the transactional social exchange between mother and

21
child that either promoted or hindered the development of the self in relation to a “selfobject
matrix” (Kohut, 2013, p. 52). More specifically, Kohut presented the idea that as humans, we
are inevitably born into a self-object matrix wherein we each strive for autonomy via the use of a
selfobject to facilitate regulation of affect (Kohut, 2013). In other words, we do not become
autonomous beings as a result of our internal resources, but through the ongoing transactional
experiences with other selfobjects that comprise the matrix. Kohut (2013) delineated this process
when he explained,
I am referring to the claim that a move from dependence (symbiosis) to independence
(autonomy) is an impossibility and that the developmental moves of normal
psychological life must be seen in the changing nature of the relationships between the
self and its selfobjects-not as a replacement of selfobjects by love objects, not as a move
from narcissism to object love. (p. 52).
In sum, the object relations perspective on dependency highlights the impact of the early
caregiving experience on the development of dependent (and eventually autonomous) behaviors
via the internalization of self and object representations. As mentioned earlier, the infant’s early
introjection (i.e., internalization), of the caregiver object based on their social interactions lays
the blueprint for functioning in later relationships with others (Klein, 1975). Klein elaborated
that the process of introjection was largely an unconscious defense mechanism used to defend
against the anxiety and frustrations of the infant’s inner world. For example, through introjection,
the infant attempts to internalize or introject features of the external “good object” to defend
against elements of a “bad object” (Klein, 1975). Projective identification is another defense
mechanism used by the infant to protect the infant and his/her good objects from an external bad
object (Klein, 1975). In summation, the infant’s introjection and projective identification

22
processes that involve both good and bad object representation set the frame for later social
interaction and eventual dependency or autonomy.
Social Learning Perspective
Social learning theory posits that human beings acquire patterns of social behavior from
their interactions with others (Bandura, 1971). As Bandura (1971) elaborated, “In the social
learning view, man is neither driven by his inner forces nor buffeted helplessly by environmental
influences. Rather, psychological functioning is best understood in terms of a continuous
reciprocal interaction between behavior and its controlling conditions” (p. 2). In this respect
social learning theory appears somewhat similar to the object relations perspective, such that
both emphasize the importance of the reciprocal, transactional exchange between the individual
and his/her social environment. Therefore, the underlying mechanisms inherent in both the object
relational and social learning theories involve cognitive processes rather than biological drives as
emphasized by classic psychoanalytic theory.
More specifically, social learning theory emphasizes the cognitive acquisition of
information from external resources that become interpreted, internalized, and acted out
behaviorally. The process of social knowledge acquisition, as portrayed by Bandura (1971)
involves a multi-step process: learning by direct experience, modeling, observational learning,
and cognitive reinforcement (i.e., via the informative functions, the motivational functions, and
the cognitive mediation effects), among others that are imperative to the integration and
assimilation of social learning. When understanding the phenomenon of dependency from a
social learning perspective, many of the aforementioned tenets apply. For instance, social
learning theory highlights the importance of both modeling and cognitive reinforcement in the
development of behaviors associated with dependency (i.e., Bandura, 1977). Considering these

23
underlying mechanisms that lead to the development of dependency-related attitudes and
behaviors, there is an implicit understanding that dependent behaviors,
…[are] exhibited because they are rewarded, were rewarded, or-at the very least-are
perceived by the dependency person as likely to bring rewards…therefore, individual
differences in childhood and adult dependency result from variations in the degree to
which passive, dependent behavior was reinforced by the primary caregiver during
infancy and early childhood (Bornstein, 1992, p. 5).
Although social learning theory’s early conceptualization of dependency has its roots in
drive theory, as proposed by Hull (1943) and Mowrer (1956), wherein dependency was
operationalized as a drive that was acquired to reduce the emotional discomfort associated with
primary drives (e.g., hunger), as a result of the evolution of the empirical and theoretical
investigation of dependency from the social learning perspective, the emphasis shifted from the
impact of conditioned responses to an increased emphasis on the resulting cognitive paradigms.
For example, modern theorists from the social learning perspective conceptualize dependency
via an attributional style “in which a person perceives him- or herself as powerless, helpless, and
unable to influence the outcome of events in a positive way” (Bornstein, 1992, p. 5). As a result
of these mechanisms, cognitive distortions in the processing of interpersonal information only
heighten the dependent individual’s schemas or core beliefs about their own perceived
ineffectiveness (Bornstein, 1992; 2011).
Cognitive-Behavioral Perspective
The Cognitive Behavioral model highlights the role of our thought patterns, (particularly
automatic thoughts), in the formation of cognitive schemas that subsequently inform the
emotional and behavioral domains of functioning (Beck, 1991). Beck (1991) elaborated, “Each

24
of the psychological systems (cognition, affect, motivation) is interconnected so that changes in
one system may produce changes in other systems” (p. 371). Therefore, it is unsurprising that
this model of dependency overlaps with the Social Learning perspective, such that both
orientations emphasize how dependency-related thoughts, feelings, and behaviors are initially
formed and later reinforced by the environment (e.g., in the social transactional exchange
between child and caregiver). Cognitive schemas that involve low self-esteem, anxiety around
interpersonal situations, and chronic indecisiveness, are conceptualized as underlying
mechanisms in the etiology and exacerbation of dependency (Beck, 1991).
A proposed Cognitive Behavioral intervention for excessive dependency involves four
stages: active guidance, enhancement of self-esteem, promotion of autonomy, and relapse
prevention (Overholser & Fine, 1994). These steps are congruent with the orientation’s
theoretical conceptualization of dependency, such that they emphasize the role of negative
schemas regarding the self in the formation (and subsequent intervention) of dependency-related
thoughts, feelings, and behaviors. This treatment model conceptualizes dependent individuals as
being low in assertiveness and unable to express or even be consciously aware of feelings of
anger (Overholser & Fine, 1994). Therefore, they will behave passively in their interpersonal
dynamics, which will manifest in others treating them in ways that are congruent with these
behaviors, which further reinforces the schema of the self as ineffectual, passive, and weak
(Overholser & Fine, 1994; Beck, 1991).
In line with other theoretical models, the Cognitive Behavioral perspective delineates
developmental antecedents that contribute to the onset of dependency, such as parenting style
(i.e., overprotective and authoritarian), childhood temperament, and physical health problems
(Overholser, 1997). From these developmental antecedents, maladaptive views or schemas about
25
the self and other are created and further reinforced from the social exchanges in the
environment. For example, the self will be viewed negatively (i.e., low self-esteem, a proclivity
for self-criticism, and low self-reinforcement), and social interaction will trigger feelings of
anxiety that are thought to manifest in poor social cue recognition, attachment problems, and
overly submissive/compliant behavior. As a result of these negative views of both the self and
other, negative affect emerges (i.e., depression or anxiety), which one will likely attempt to
combat through reinforcing dependency-related behaviors and interactions with caregivers
(Overholser, 1997).
Cognitive/Interactionist Perspective
The Cognitive/Interactionist orientation regarding dependency incorporates and builds
upon the contributions of the aforementioned theoretical antecedents. Bornstein (2011) describes
the model of dependency as manifesting across four distinct domains: the cognitive domain (i.e.,
self-perception as powerless), the motivational domain (i.e., a desire to forge and maintain close
relationships with nurturant figures), the affective domain (i.e., fear of rejection/abandonment),
and the behavioral domain (i.e., the utilization of strategies to promote and reinforce dependency
cycles). From this perspective, the etiology of dependency from which all other manifestations
derive is the individual’s helpless self-concept.
The perception of the self as helpless and ineffectual comes to fruition as the direct result
of overprotective/authoritarian parenting, coupled with gender role socialization and cultural
beliefs surrounding achievement versus relatedness (Bornstein, 2012b). This is the key
component of dependency around which all manifestations occur. For example, this belief
creates and reinforces the motivational component of dependency. Holding this belief will create
a strong need to seek out relationships with prospective caregivers, which further manifests

26
behaviorally as acting in ways that maintain and reinforce the dependency feedback loop.
Furthermore, the affective response, (though varying based on individual differences and many
factors), emerges as a result of the initial cognitive beliefs around the self as ineffectual and in
need of guidance.
From the Cognitive/Interactionist (C/I) model, dependency is therefore operationalized as
“proactive, goal-driven, and guided by beliefs and expectations regarding the self, other people,
and the self-other interactions” (Bornstein, 2012b, p. 125). As a result, individual differences in
dependency-related beliefs and behaviors can be adaptive or maladaptive. For instance, this
model highlights the adaptive aspects of dependency that include enhanced social abilities, in
tact impulse control and emotion regulation, as well as the incorporation of more mature, rather
than immature, defense mechanisms (Bornstein, 2012b). Because this theoretical
conceptualization parallels overall trends in broader personality research (Bornstein, 2012b), the
maladaptive aspects of dependency are also highlighted, but are best understood as a result of
several complex and underlying mechanisms that are moderated by many factors.
Assessing Dependency
Because interpersonal dependency is a key aspect of the human experience, with
important clinical implications, it has been empirically assessed and evaluated cross a wide range
of disciplines for many years. For instance, a thorough review of the literature conducted in 1993
concluded there were more than 35 unique measures of dependency developed since the 1940s
(Bornstein, 1993). More recent sources estimate the existence of approximately 50 unique
measures of dependency (Disney, 2013). Measures of dependency can be categorized into two
overarching categories: first, via the use of content: (i.e., measures of interpersonal dependency
versus oral dependency) and secondly, via format (i.e., self-report or performance based)

27
(Bornstein, 1992). These types of measures fall within 4 methodological approaches: “objective
interpersonal, objective oral, projective interpersonal, and projective oral” (Bornstein, 1993, p.
22; Bornstein, 2005). Having said that, it is no surprise that the interpersonal measures of
dependency utilize an objective format and the oral measures of dependency tend to be
projective (i.e., performance-based) in nature. The objective methodological approaches, in
contrast, directly ask participants to reflect upon their dependent behaviors, thoughts and beliefs.
Performance-based measures of dependency require participants to respond to
purposefully ambiguous stimuli, such as inkblots or drawings. Participants’ responses are then
coded for dependent content (i.e., the Thematic Apperception Test dependency scale, Kagan &
Mussen, 1956) or specifically oral dependent content (i.e., Masling et al.’s [1967] Rorschach
Oral Dependency (ROD) scale). When it comes to the utilization of performance-based measures
to assess dependency, the ambiguity of the stimuli is an inherent strength, as it minimizes the
potential for bias inherent in self-report measures. However, performance-based measures only
yield a single, more global measure of dependency, which does not allow for the differentiation
dependency-related orality with orality centered around a preoccupation with oral activities in
general (e.g., eating, food, etc.). Because the ROD is more frequently utilized in the dependency
literature than is the TAT dependency scale (Bornstein, 2005), this review will only synthesize
the utilization and properties of the ROD.
Masling et al.’s (1967) ROD scale (which has since been integrated into Rorschach
Performance Assessment System, (R-PAS) and renamed the Oral Dependent Language [ODL]
Scale; see Meyer et al., 2011) is the most commonly utilized performance-based measure to
assess dependency. The ROD asks individuals to write down several responses of what they see
on the 10 Rorschach cards. The written descriptions are then coded and scored for oral

28
dependency using a two-category system. First, dependent imagery is coded, which may
manifest in seeing images explicitly related to dependent behavior (i.e. figures demonstrating
dependency-related behaviors, incidents of helplessness, or images of caregiver figures. The
second category involves the analysis of oral imagery, which typically involves food and other
orally-related activities (i.e., eating, kissing and other activities involving the mouth). Following
the coding procedure, participants are then granted one point per dependency-related responses,
which yield results ranging from 0 to 25, with higher scores suggesting higher levels of oral
dependency at large. Due to the lexical nature of the coding procedures, interrater reliability
scores are quite high, with scores of approximately 90% (Bornstein & Masling, 1985).
In contrast to performance-based measures of dependency, objective measures of
dependency require subjects to introspect and respond directly to specific prompts regarding
their beliefs, attitudes, and behaviors around dependency. Many of these self-report style
questionnaires utilize a true-false format or a Likert-style scale format. Generally speaking,
objective measures of dependency also have high-face validity, even when faced with the
inevitable effects of the limitations of self-report data. A commonly used objective measure of
interpersonal dependency was created by Hirschfeld, Klerman, Gough, Barrett, Korchin, and
Chodoff’s (1977) Interpersonal Dependency Inventory (IDI). The IDI is a 48-item self-report
inventory designed to measure thoughts, feelings, and behaviors associated with dependency.
There are 3 subscales that comprise the IDI: Emotional Reliance on Others, Lack of Social Self-
Confidence, and Assertion of Autonomy.
Other commonly utilized objective measures of interpersonal dependency include the
dependency subscale on the Depressive Experience Questionnaire (DEQ; Welkowitz, Lish, &
Bond, 1985). The DEQ is comprised of 66 rationally constructed items that are designed to
29
sample experiences reported by depressed individuals, but not actual symptoms of depression. In
this way the DEQ is generally regarded as a measure of premorbid disposition. The DEQ is
comprised of three subscales: Dependency, Self-Criticism, and Efficacy. For the purposes of the
current study, only the Dependency subscale will be used in calculating effect sizes. The test-
retest reliabilities for the Dependency subscale ranged from .81, (week 5) to .89, (week 13;
Nietzel & Harris, 1990). Next, is the Sociotropy-Autonomy Scale (SAS; Beck et al., 1983). The
SAS has 2 unique subscales: Sociotropy (i.e., dependency) and Autonomy (i.e., individuation).
The former subscale was measured to have a coefficient alpha of .93, while the latter was
measured at .83 (Beck et al., 1983).
Lastly, pathological levels of dependency can also be assessed using the diagnostic
criteria for Dependent Personality Disorder (DPD) in the Diagnostic Statistical Manual of Mental
Disorders (DSM). In clinical situations, structured clinical interviews based on the current
assessment regulations of the current DSM. However, the diagnostic criteria for DPD has
evolved since its original inception in the DSM-III (APA, 1980). The current (i.e., DSM-5)
diagnostic criteria for DPD include criteria such as: difficulty making simple decisions without
reassurance from others, a pervasive fear of risking disapproval, feeling vulnerable and
incomplete when alone, as well as an obsessional preoccupation with being left alone and feeling
unable to take care of oneself (APA, 2013). Because DPD occurs comorbidly with a plethora of
disorders (e.g., depression, eating disorders, etc.), the diagnostic criteria have evolved to better
capture the core features of pathological dependency (Bornstein, 2012a).

30
Chapter III: Depression
Defining Depression as a Construct
Depression can best be conceptualized as either a trait or state phenomenon. In the former
context, depression may manifest itself in a form of personality pathology known as Depressive
Personality Disorder (DPD). The diagnostic criteria for DPD was first elucidated in the DSM, 2nd
Edition (DSM-II; APA, 1968), and has since been a source of debate, such that its characteristics
overlap with both clinical mood disorders as well as other personality disorders. The DSM-IV
(APA, 1994) defined DPD as “A pervasive pattern of depressive cognitions and behaviors
beginning by early adulthood and occurring in a variety of contexts” (Huprich, 2009, p. 43).
Some of the diagnostic criteria included: a persistent mood of dejection, a self-concept centered
around feelings of worthlessness that involve harsh self-criticism, a predisposition to worry, an
overarching negative and pessimistic view of the world, as well as a predisposition to feel guilt
or remorse (APA, 1994). The DSM-IV-TR (APA, 2000) categorized DPD in Appendix B as an
area that required further examination and the current edition of the DSM (DSM-5) does not
include DPD as its own diagnosis but is instead considered an Unspecified Personality Disorder
(APA, 2013).
Depression as a state, unlike a trait, involves both cognitive and somatic symptoms
(Huprich, 2009). Clinical state depression takes many forms and is salient in a multitude of
psychiatric diagnoses including: disruptive mood dysregulation disorder, major depressive
disorder (MDD); bipolar disorder, persistent depressive disorder (formerly known as Dysthymic
Disorder), premenstrual dysphoric disorder, substance / medication-induced depressive disorder,
depressive disorder due to another medical condition, other specified depressive disorder, and
unspecified depressive disorder (APA, 2013). In addition to the cognitive and intrapsychic

31
symptoms as described above, clinical depression manifests in the physiological domain via the
following symptoms: sleep disturbances (i.e., insomnia or hypersomnia), general aches and
pains, weight gain or loss, and changes in appetite (Estroff-Marano, 2001). Additionally, clinical
state depression involves a complex and pervasive set of emotional manifestations, including:
reduction in gratification, loss of emotional attachments, chronic crying spells, and loss of
positive affect (Beck & Alford, 2009).
History and Evolution of its Conceptualization
The history and evolution of the conceptualization of depression and its etiology are
complex. The first scholarly investigation of depression, (what was then called melancholia or
melancholy depending on the context), dates back to the works of Aristotle and Hippocrates.
Aristotle’s conceptualization of melancholia was more romantic than it was pathologizing: He
noted the frequent correlation between the melancholic temperament and high intelligence found
in famous scholars, artists, and physicians (Jouanna et al., 2004). Aristotle’s notions of
depression were challenged by the Hippocratean and Galenian pathology-driven understanding
of its etiology and symptoms but were later corroborated by Renaissance academics’
perspectives on the subject. Therefore, its history and evolution highlight the mixed and often
conflicting perspectives on depression, its etiology, and its symptoms.
The Hippocratic accounts of depression conceptualized it as a disease of the body that
resulted from an imbalance in one of the body’s four fluids, or ‘humors,’ which consisted of:
phlegm, blood, yellow bile, and black bile (Radden, 2002). Melancholia resulted from an excess
of black bile in certain regions of the body, such as the spleen or gallbladder (Radden, 2002).
The humoral theory was pervasive in Ancient medicine and originated from the work of

32
Hippocrates, which was later elaborated upon by the Ancient Roman physician, Galen of
Pergamum (Radden, 2002).
Though many physicians and scientists subscribed to the Humoral theory well into the
19th century, some philosophers, laypeople, and even members of the medical community of the
Medieval era conceptualized depression as being a disease of the soul, rather than of the body
that manifested from demon possession or a lack of faith (Radden, 2002). The emphasis on
Christianity in the discussion of depression paralleled the larger political and social climate of
that era. In spite of this notable shift, the Humoral theory persevered and was further advanced
within the medical and scientific community. Medieval scholars whose works furthered the
understanding of melancholia’s origins include, but are not limited to, Cassian and Avicenna; the
former understood depression as a symptom that stemmed from a lack of faith, while the latter
furthered the humoral theory when he differentiated the different types of depression based on
the location of the black bile within the organs (Radden, 2002).
The humoral theory held a pervasive impact on the medical investigation of depression
until the 19th century, during which time Virchow’s study of cellular pathology among many
other advancements in neuroanatomy resulted in a clearer definition of and differentiation
between depressive disorders (Diethelm, 1975). The German Psychiatrist Emil Kraepelin’s
(1883) categorization and elaborate clinical descriptions of various mental disorders laid the
foundation for the modern DSM. Kraepelin’s most notable contribution to the discussion of
depression came through his work that separated manic-depressive insanity from a “mood or
affective disorder” (Radden, 2002, Chapter 24, p. 3). Kraepelin described as “melancholia
simplex,” as a milder and more common form of the illness from which many suffered, whereas
“melancholia gravis” included the more severe type of melancholia that involved the presence of

33
auditory and hallucinatory delusions, (e.g., what is now referred to as MDD with psychotic
features). Kraepelin’s nosological system delineated several more types of melancholia and
described their symptoms in great detail. Additionally, Kraepelin was among the first to identify
genetic or biological correlates of depression.
Kraepelin’s system of psychiatry and conceptualization of depression laid the foundation
for more modern theories on its symptomology and etiology. Sigmund Freud’s psychoanalytic
perspective highlighted the role of the unconscious and of mourning on the onset of depressive
symptomology. Many perspectives both furthered and diverted from Freud’s impactful
perspective throughout the history of psychiatry, including the object relational, cognitive
behavioral, and biological perspectives. Modern day clinicians, regardless of their theoretical
orientation, generally attribute depression to a combination of both biological and environmental
conditions that manifests in a variety of cognitive, psychological, and physiological symptoms
(Radden, 2002). The following sections elucidate the perspectives of the various schools of
thought on the etiology and symptomatic manifestation of depression.
Psychoanalytic Perspective
Early twentieth century Freudian theory, which emphasized the role of libidinal drives
and unconscious conflicts, stood in stark contrast to the advances in science and medicine laid
forth by Kraepelin and other Western psychiatrists and physicians (Radden, 2002). However,
Freud’s conceptualization of melancholy via loss highlighted an important shift in understanding
depression. Freud’s model laid the foundation for others (i.e., Kleinian, Object Relational, and
Self-Psychological approaches) in the understanding of the etiology and conceptualization of
depression.

34
Freud’s seminal work on depression is considered to be Mourning and Melancholia
(1917). Freud developed a comparative system between the “normative” grief and sadness that
accompanied the loss of a loved one, and the more clinically severe condition of melancholia. In
the latter condition, “dispirited mood states and self-hatred” (Radden, 2002, p. 3) are some of the
many embedded pathological components. Freud’s Mourning and Melancholia also introduced
concepts such as projective identification and introjection, which are now well-established
concepts within object relational and self-psychological perspectives.
The important Freudian contribution in the context of the history of the etiology of
depression was his way of reframing the underlying mechanisms through which symptoms
manifested. For instance, his emphasis on loss and mourning as the key underlying etiology of
melancholy represented a shift from thinking of it as a bodily state of imbalance. As such, Freud
explained that depression, specifically, involved the loss of a loved “object,” most typically
understood to be the mother. The loss described in this writing does not refer to an actual loss via
death, but the loss via a certain detachment, or an inability to meet the infant’s needs (Radden,
2002; Freud, 1917). The perceived loss manifests in self-blame and rage that becomes
internalized and results in the symptomatic manifestation of depression (Radden, 2002).
However, the rage that was directed inward (i.e., the process of introjection) is rejected by the
individual because it is so difficult to tolerate. As a result, the rage and discontent become
projected into the other person or object. Freud emphasized the fact that all of these processes
occurred below the individual’s conscious perception (Freud, 1917).
Modern psychodynamic conceptualizations of depression are rooted within Freud’s
theory on loss and mourning. The Psychodynamic Diagnostic Manual, 2nd Edition, (PDM-2,
2017) describes the internal experiences of depressive disorders using the following domains:

35
affective states (i.e. anaclitic or introjective); cognitive patterns (propensity toward guilt,
fantasies of loss of approval, low self-regard, suicidal ideas); somatic states (loss of sexual
interest, physical irritability, headaches, muscle pains, substance abuse); and relationship patterns
(increased dependency or hostility, and feelings of being unworthy).
When disentangling the depressive disorders, the PDM-2 (2017) elaborates that PDD
involves chronic depressive symptoms marked by both cognitive and physical symptomatic
manifestations. Given the multifactorial etiology of PDD, the psychosocial or environmental
triggers that are thought to worsen the condition, and the long-term persistence of symptoms, it is
considered difficult to treat with psychopharmacology alone and is best treated using an
approach that integrates psychotherapeutic treatment.
The PDM-2 (2017) conceptualizes MDD using a highly medicalized definition that
emphasizes the physiological impacts and deficit in various domains of functioning, noting that,
MDD is not just a form of extreme sadness. It is a disorder that affects both brain and
body, including cognition, behavior, the immune system, and the peripheral nervous
system. Unlike transient sadness, MDD is considered a disorder because it interferes with
ordinary functioning in work, school, or relationships (p. 183).
The above conceptualization shies away from traditional psychoanalytic notions of depression,
while a later section, entitled Subjective Experiences of Depression includes more traditional
psychoanalytic conceptualizations, including the separation of anaclitic versus introjective
depression. Additionally, the PDM-2 includes a discussion of pathological views of the self and
its impact on personality pathology from an overarching, modern psychodynamic perspective,
such that it includes theories rooted in object relational and interpersonal orientations.
Object Relational Perspective

36
The object relational perspective on depression extended the works of Freud by
attempting to answer several of the questions posited by his Mourning and Melancholia (Lubbe,
2011). For instance, Freud was unable to distinguish why the gradual detachment of libido within
normative grief resulted in extraordinary emotional pain while the patient simultaneously
demonstrated “forbearance in absorbing the degree of suffering” (Lubbe, 2011, p. 25).
Additionally, he postulated the difference in symptomatic manifestation between conscious and
unconscious loss (Freud, 1917, p. 245). Lastly, he was unable to understand why only certain
depressive patients experienced the upward highs of mania. While many scholars have
contributed to the development of the object relational perspective on depression by addressing
these questions, the works of Karl Abraham and Melanie Klein stand out.
Karl Abraham’s (1924) theory of depression disentangled depression from obsessional
neurosis, and provided an alternative understanding of the utility of mania in the context of a
depressed patient. Abraham utilized Freud’s psychosexual phases of development to frame his
discussion, deconstructing the underlying mechanisms (i.e., unconscious meanings) of
depression. For instance, he described mania as being a natural by-product of the alleviation of
depression (Lubbe, 2011). As such, he postulated that when mania does not occur after the
resolution of a depressed episode, it was repressed. Abraham also posited that depression and
mania have the same etiology, which he described as a “hostile expulsion and hostile
incorporation of the lost object” (Lubbe, 2011, p. 22). Abraham’s conceptualization of mania as
well as the role of object love and loss are embedded within Melanie Klein’s theory on
depression.
Melanie Klein believed there were both conscious and unconscious loss processes that
manifested in depressive symptomology. Furthermore, she attributed the extraordinary pain of

37
which Freud spoke to not only the actual object loss, but to the loss of the internal representation
of the object (Lubbe, 2011; Klein, 1940). Like many psychoanalytic theorists, Klein emphasized
the role of narcissism in depressive illness; her theory of narcissism in depression was elaborated
in her theory of the paranoid-schizoid versus the depressive position. In the paranoid-schizoid
position, the infant creates and internalizes both good and bad objects through what she deemed
narcissistic processes that occur both externally and internally (Klein, 1940). When a negative
event occurs with the good object, that event becomes split off and projected into the bad object
(Lubbe, 2011). In the depressive position, the infant is mourning the loss of the object and/or
existing in a state of fear or anxiety of losing the love of the object (Klein, 1940).
Therefore, the object relations position on depression emphasizes a deficit in the ability to
form healthy internal representations of others, resulting in interpersonal frustrations that
manifest in depressive symptomology. Therefore, this perspective understands the etiology of
depression via the processes of the introjection, projection or projective identification of
problematic love objects, which Klein deemed largely unavoidable (Lubbe, 2011). In fact, Klein
posited that depression was a natural byproduct of the transition from narcissism to object love
that takes place throughout both infantile and adolescent development (Lubbe, 2011). Therefore,
depression as defined by an object relational perspective was not deemed as pathogenic relative
to other perspectives.
Biological Perspective
The biological approach to understanding depression involves several factors that have
been examined in the fields of psychiatry, biology and neurology. Biological theories emphasize
the roles of neurotransmitters, neuroplasticity, and endocrinology, as well as genetic factors in
the development of depression.

38
Goodwin and Jamison’s (1990) Manic-Depressive Illness is regarded as the “gold
standard” for the neurochemical theories relating to depression (Radden, 2002). Goodwin and
Jamison (1990) delineated the neurobiological underpinnings of both disorders, emphasizing the
interactions between neurotransmitters, receptors, and other components of the central nervous
system (CNS; Goodwin & Jamison, 1990). Specifically, they discussed three systems that have
been theorized to be impacted by a manic-depressive or unipolar depressive illness, monoamine
neurotransmitters, neuropeptides, and electrolytes. However, the specific neuronal systems in
which monoamines are the primary neurotransmitters have been investigated for their role in
mood disorder etiology since the 1960’s (e.g., the Catecolamine Hypothesis [1965] suggested
depression resulted from a deficiency in norepinephrine).
In addition to the role of neurotransmitters, the modern concept of neuroplasticity plays
an important role in understanding depression. The process of neuroplasticity refers to the brain’s
ability to reorganize itself through the formation of connections between neurons as a result of
new experiences; therefore, neuroplasticity is the avenue through which the formation of
memories and the process of learning occur (Nemade, 2018). The brain’s neuronal networks and
their connections are responsive to the individual’s environment. For instance, stress or negative
experiences can result in the cessation of functioning of certain receptors. As a result, the brain’s
messages may be sent and received in an impaired manner that can produce a negative mood
(Nemade, 2018; Brunoni, Lopes, & Fregni, 2008).
Neurotransmitters are just one of many chemical agents that serve as messengers in the
body and are implicated in the onset of depression. Hormones within the endocrine system
communicate with the nervous system via the hypothalamus, a complex brain structure
responsible for many human functions, including regulating blood pressure, appetite, immune

39
responses, body temperature, and circadian rhythms (Nemade, 2018). The hypothalamus is
intimately involved with depression, such that it is responsible for releasing hormones in
response to stress that manifest in decreased mood. Many studies have demonstrated that
depressed individuals have a higher concentration of stress hormones than normal controls
(Brunomi, Lopes, & Fregni, 2008). The thyroid and adrenal glands, as well as testosterone and
estrogen are also implicated in depression.
In addition to neurotransmitters and hormones, the genetics of an individual play a role in
the development of depression. Recent reviews revealed the heritability of depression based on a
multitude of twin studies is roughly 40% to 50% (Levinson, 2006; Beck & Alford, 2009).
However, the genetics of depression likely involve environmental influences that trigger its
genetic expression via gene-environment interactions (Levinson, 2006). More specifically, most
studies on the genetic influence on depression focus on functional polymorphisms, DNA
sequence variations that impact both the expression and functioning of the gene itself, in the
specific brain regions (i.e., loci) that encode mostly serotonin and dopamine receptors (Levinson,
2006).
Modern research has also focused on brain imaging techniques to glean insight into the
regions and their functioning relevant to the expression of depression. For example, noninvasive
techniques that range from Computed Axial Tomography (CAT) to Functional Magnetic
Resonance Imaging (fMRI) have demonstrated that individuals with depression have structural
and functional neurological differences when compared to normal controls (Nemade, Reiss, &
Dombeck, 2017). In sum, the biology of depression involves a multitude of complex and
multifactorial systems that are influenced by environmental triggers (i.e., gene-environment
interactions).

40
Cognitive Behavioral Perspective
Beck and Alford’s (2009) Depression: Causes and Treatment elucidates the overarching
cognitive behavioral perspective on the development of depression. In accordance with the
macro-level cognitive behavioral orientation, depression is thought to result from negative
cognitions about the self and others (Beck & Alford, 2009). From this perspective, an
individual’s self-concept and ideas about others are formed by early experiences with other
people and the world at large. Once a particular self-concept is formed, particularly consisting of
negative attributes, (i.e., perceiving oneself as incapable, unlovable, or inept), it becomes further
solidified through reinforcement from the environment (Beck & Alford, 2009). Once this
concept becomes ‘structuralized’ (Beck & Alford, 2009, p. 246), it is permanently internalized as
a cognitive structure called a schema.
An individual’s self-concept is inextricably linked to one’s self-esteem, which plays a
fundamental role in intra- and inter-personal functioning. The role of low self-esteem induced
from a negative self-concept plays a role of central importance in the development of depression.
For instance, a negative self-concept manifests in a constellation of pervasively and persistently
negative attitudes about the self, the world, and the future (Beck & Alford, 2009; Beck, Rush,
Shaw, & Emery, 1979).
The particular depressive constellation is comprised of an inter-connected network of
negative attitudes, that are typically generalizations about the self that may include thoughts such
as “I am dumb and people don’t like me,” (Beck & Alford, 2009, p. 246) coupled with negative
value judgments about those particular attributes. An additional component of a depressive
constellation regarding the self involves a pervasive propensity toward shame and/or self-blame.
Another group of attitudes within the “predepressive constellation” consists of negative

41
expectations and overall pessimistic view of the future (Beck & Alford, 2009, p. 247). When
these negative attitudes become triggered by external events, they manifest symptomatically as
the hopelessness that is characteristic of depression. Beck and Alford provide a formulaic and
cumulative series of internal events that occurs when an individual’s depressive constellation is
activated that ultimately results in the painful symptoms of depression.
From this perspective, the individual must possess a pre-existing constellation of self-
defeating attitudes about the self, the world, and others, that becomes activated by external
events. Even if an individual is predisposed to depression given this vulnerability, the onset of
clinical depression depends upon external conditions such as, in milder cases, everyday stress, or
in more severe cases, trauma.
Current Diagnostic Criteria
The current diagnostic criteria for depressive disorders are found in the most recent
edition of the DSM (DSM-5; APA, 2013). For the purposes of the current review, the diagnostic
criteria for MDD will be delineated to provide a more nuanced understanding of its symptoms
and the diagnostic process. In order to meet criteria for MDD, five (or more) of the following
symptoms must be present during one two-week period that underscore a marked difference
from previous or baseline functioning. These include: (1) Depressed mood most of the day on a
majority of days indicated by either self-report or observations of others; (2) Markedly
diminished interest or pleasure in all or almost all activities; (3) Significant weight gain or loss;
(4) Insomnia or hypersomnia most, if not all days; (5) Psychomotor agitation or retardation; (6)
Persistent fatigue or loss of energy; (7) Feelings of worthlessness or excessive guilt; (8)
Diminished ability to think and/or concentrate in addition to indecisiveness; and (9) Recurrent

42
thoughts of death, and/or recurrent suicidal ideation with or without a specific plan or attempt for
completing suicide (APA, 2013, p. 160-161).
In addition to meeting at least five of the above criteria, in order to be diagnosed with
MDD, differential diagnosis must be made, such that the occurrence of the episode cannot be
explained by any of the following: schizoaffective disorder, schizophrenia, schizophrenia
spectrum (and other psychotic disorders), and bipolar disorders (i.e. the individual must never
had experienced a hypomanic or manic episode). Lastly, the depressive episode must not be
attributed to physiological and psychological impacts of substances or other medications (APA,
2013).
Prevalence and Cost of Depression
MDD is the leading cause of disability in the U.S. among those aged 15 to 44 (Anxiety
and Depression Association of America, 2017). In fact, more than 15 million American adults,
roughly 7% of the U.S. population, are diagnosed with MDD in a given year. MDD can develop
at any age, however, the median age of onset is in one’s early 30s. It is more prevalent in women
than it is in men (APA, 2013; Beck & Alford, 2009). While there are many risks associated with
untreated depression, the most dangerous risk is suicide. In fact, two-thirds of all suicides are
associated with a depressive disorder (Kessler, 2012). Every year, approximately 45,000 people
die by suicide (American Foundation for Suicide Prevention, 2018) and these rates are
increasing.
While other metaphorical ‘costs’, correlates, and comorbidities will be elaborated upon in
a later section, depression has presented the U.S. with a significant financial burden. According
to multiple sources of data within the last several years (i.e., Greenberg, 2015; Kessler, 2012;

43
Insel, 2008; Levinson, 2006), depressive disorders cost American society an upwards of $210
billon per year. Specifically, researchers found that:
For every dollar spent treating depression, an additional $4.70 is spent on direct and
indirect costs of related illnesses, and another $1.90 is spent on a combination of reduced
workplace productivity and the economic costs associated with suicide directly linked to
depression (Greenberg, 2015, p. 2).
Greenberg’s (2015) most recent study found that the rising societal and financial burden
of depression stems from a combination of population growth, the increased rate at which
individuals are being diagnosed (in part due to changing attitudes regarding mental illness), as
well as higher treatment costs per patient. He also noted the care that individuals do receive is
usually not of the highest quality, such that people are often being prescribed antidepressants and
not necessarily following through with psychotherapeutic treatment concurrently (Greenberg,
2015).
Correlates and Comorbidities of Depression
Given the rising prevalence of depression in the U.S., it is important for researchers and
clinicians to delineate both the correlates and comorbidities of depression to provide more
nuanced diagnoses and subsequent effective, targeted treatment. Birnbaum et al.’s (2010) review
delineated several correlates and comorbidities for depression that influence the psychosocial
and biological domains of functioning.
Birnbaum et al. (2010) elaborated on the psychosocial impairments associated with
MDD, such as the empirically documented correlation of early-onset mental disorders with the
early termination of education. More specifically, his review found that MDD is associated with
approximately 60% elevated odds of failure to complete education post a High School level.

44
MDD is also associated with impairments in marital timing and stability, such that a pre-marital
history of MDD predicted increased likelihood of divorce (Jorm et al., 2003; Kessler, Walters, &
Forthofer, 1998). Additionally, a number of studies have revealed the correlation between MDD
and negative parenting behaviors that manifest in maladaptive interactions shown to interfere
with infantile affect regulation and subsequent child development (Tronick & Reck, 2009;
Wilson & Durbin, 2010). In terms of financial success, individuals diagnosed with MDD will
earn a substantially lower lifetime income than people without MDD (Birnbaum et al., 2010).
MDD is also associated with physiological correlates, including a wide variety of
physical disorders, such as asthma, arthritis, cancer, cardiovascular disease, diabetes, and
hypertension among others (Birnbaum et al., 2010). As a predictive risk factor, the presence of
MDD leads to an increased likelihood of diagnosis of these disorders, replete with their
associated financial burdens, symptoms, and increased mortality risk (Birnbaum et al., 2010,
Tronick & Reck, 2009), A number of mechanisms have been provided to understand the link
between MDD and these disorders; several studies involve poor health behaviors associated with
MDD, including substance abuse, obesity, and low compliance with medical and
psychotherapeutic treatment (Birnbaum et al., 2010).
Many empirical studies have examined comorbid psychiatric illnesses that occur
alongside depressive disorders. These studies have found that anxiety disorders (i.e., generalized
anxiety disorder and panic disorder) occur most frequently with depressive disorders (Rush,
Zimmerman, Wisniewski, Fava, Hollon, Warden, Biggs, Shores-Wilson, Shelton, Luther,
Thomas & Trivedi, 2005; Gotlib & Hamlin, 2002). The presence of an anxiety disorder or
anxious features within MDD complicate treatment efficacy, such that both sets of symptoms
tend to be more severe (Gotlib & Hamlin, 2002). As mentioned earlier, substance abuse,

45
particularly alcohol abuse, is especially common in the MDD population. In fact, mood disorders
are the most common psychiatric comorbidities among individuals with substance use issues
(Quello, Brady & Sonne, 2005). MDD also occurs within a variety of personality disorders and
posttraumatic stress disorder (Gotlib & Hamlin, 2002).
The above data clearly demonstrate that MDD is commonly occurring and incredibly
burdensome across multiple domains of functioning. Due to the many comorbidities and
correlates of MDD, multimethod assessment involving dual-diagnostic procedures must be taken
to provide the most effective course of treatment.
Assessing Depression
Acquiring appropriate and effective treatment starts with the correct assessment
techniques. A thorough assessment of depression must include appropriate measures for
quantifying symptoms and associated risks. With this in mind, Gotlib and Hammen (2002) list
the following goals or processes for the assessment of depression, including: (1) screening; (2)
diagnosis and classification; (3) description of problem areas and symptoms; (4) case formation
and clinical hypothesis testing; (5) treatment planning; (6) prediction of behavior, and (7)
outcome evaluation (p. 62).
Screening for depression in clinical settings involves administration of one or more well-
validated questionnaires, and/or diagnostic interviewing associated with the concurrent DSM-5.
The Structured Clinical Interview for DSM-5 (SCID-5; APA, 2013). is a semi-structured
interview protocol administered by a mental health clinician used to assess whether an
individual’s symptoms meet criteria for a psychiatric disorder. However, there are also more
nuanced measures, both clinician-rated and self-report that hone in on the specific symptoms of
depression. While there are upwards of 50 measures that have been created and utilized in the

46
assessment of depression, only some of the most frequently utilized in the more current literature
will be discussed.
An example of a frequently utilized clinician-rated depression measure in both research
and clinical settings is the Hamilton Rating Scale for Depression (HRSD, Hamilton, 1960), a
highly reliable and well-validated scale that has been utilized frequently since its inception
(Gotlib & Hammen, 2002). The HRSD is a 21-item measure that takes approximately 10 minutes
to complete after the administration of a 30-minute interview. While it is largely clinician-rated,
the patient is required to respond to questions concerning depressive symptoms during a certain
time-period. Nine items utilize 5-point likert style scales (ranged 0-4) representing rising levels
of severity. The remaining eight items utilize 3-point scales (ranged 0-2), which also represent
rising levels of severity. Interrater reliability coefficients for the HRSD are strong, reported to be
at least .84, while its internal consistency was reported to range between .45-.78 (Gotlib &
Hammen, 2002).
A widely-used self-report measure of depression is the Beck Depression Inventory (BDI;
Beck, Ward, Mendelson, Mock & Erbaugh, 1961). However, there have been developments
since its original inception and is now in its second edition (BDI-II, 1996). The BDI-II is a 21-
item self-report inventory that measures the severity of depression in both adolescents and adults
(i.e. ages 13 and over) and adheres to the diagnostic criteria of depression found in the DSM – 4th
edition (DSM-IV; APA, 1994). Each question is anchored on a 4-point Likert-scale, ranged 0-3,
the higher scores indicating higher levels of depression. The retest reliability of the BDI-II over
an interval of 6 months was found to be .93, while the internal consistency (alpha) was .92
(Wang & Gorenstein, 2013). Further research suggests that the BDI-II has a strong positive
correlation to the HRSD (r = .71).

47
The Zung Self-Rating Depression Scale (SDS; Zung, 1965) is also a widely utilized self-
report depression measure. The SDS is a 30-item questionnaire that was specifically constructed
to target the affective, cognitive, and behavioral symptoms of depression (Gotlib & Hammen,
2002). Each item presents dichotomous (i.e., one positive and one negative) feelings, behaviors,
or thoughts, to which respondents must respond how much each statement resonates with them
as of the last several days. Responses are ranked using a 4-point Likert-type scale (ranging from
1-4), with 4 representing the maximum severity (i.e. “I feel this way most of the time”). A 1987
factor analysis derived three factors, including: depressed mood, loss of self-esteem, and
irritability and agitation (Kivelae & Pashkala, 1987). The SDS possesses solid psychometric
properties, such that the internal consistency was found to be .82 and the split-half reliability was
.79 (Gotlib & Hammen, 2002),
The Carroll Rating Scale for Depression Revised, (CRS-R; Carroll, 1998) is a self-report
instrument that closely parallels the contents of the HRSD (Gotlib & Hammen, 2002). The CRS-
R is a 61-item self-report questionnaire that was designed to be highly compatible with the
DSM-IV diagnostic criteria of depression (Carroll, 1998). The scale is designed to have a
maximum score of 61, with participants prompted to either “yes” or “no” to self-descriptive
items relating to affect, cognition, and behavior characteristic of depressive disorders. Carroll
(1998) reported that the psychometric properties for the CRS-R are strong, such that the internal
consistency in the form of split-half reliability coefficients was found to be .87 (Gotlib &
Hammen, 2002, p. 75). Additionally, Carroll (1998) reported that the CRS-R correlated r = .86
with the BDI. Additionally, the CRS-R was highly related to the HRSD from a self-report and
not clinician-rated perspective.

48
The Hamilton Depression Inventory (HDI; Reynolds & Kobak, 1995) is a self-report
version of the original HRSD (Hamilton, 1960). The full-scale version of the HDI is comprised
of 23 items that are evaluated using 38 total questions, with some items consisting of several
questions, that are ultimately weighted to produce a single score. There is a melancholia subscale
that is derived to evaluate all melancholic features of depressive disorders as specified by the
DSM-IV diagnostic criteria of MDD (Gotlib & Hammen, 2002). Reynolds and Kobak (1995), in
the HDI manual, provide normative data that revealed internal consistency between .90 to .90,
and retest reliability of .95 over a one-week period (Reynolds & Kobak, 1995). The HDI was
also found to be an instrument with high validity, such that it correlates at r = .94 with clinician-
ratings of the HRSD (Gotlib & Hammen, 2002). Lastly, its convergent validity was also strong
such that it correlates highly with the BDI (r = .93; Gotlib & Hammen, 2002).
Finally, the Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977)
is a 20-item self-report questionnaire that was largely developed to trace the change in symptom
severity over time from as a research instrument (Gotlib & Hammen, 2002). The items were
specifically derived from multiple measures of depression, such as the BDI, Zung SDS, and the
depression scale of the Minnesota Multiphasic Personality Inventory, to best capture depressive
symptomology in ways that were proven to be psychometrically sound and effective.
Respondents were asked to rank how much a statement described their feelings, attitudes, or
behaviors within the past week, on a 4-point Likert-type scale (ranging from 0-3). The potential
total scores range from 0 to 60. Radloff (1977) provided both descriptive norms and
psychometric properties based on both community and psychiatric populations. The internal
(consistency coefficient) alphas were revealed to be .85 for the community sample and .90 for

49
the psychiatric sample (Radloff, 1977). Additionally, CES-D scores correlated highly with other
measures of depression, such as the HRSD, BDI, and Zung SDS.
Dysthymia as a Depressive Disorder
Dysthymia, or persistent depressive disorder, has many symptomatic overlaps with major
depressive disorder. They are closely related constructs, both in theoretical etiology, as well as
symptomatic manifestations. Because of their similarities across cognitive, motivational,
affective, and behavioral components, dysthymia will be included in the literature search and
data collection process for potential inclusion in the current meta-analysis.
50
Chapter IV: Dependency and Depression
Dependency and Psychopathology
The relationship between dependency and psychopathology is complex, such that
dependency can be either a predictor or consequence of psychopathology (Bornstein, 1993;
2005). The existing research that examined dependency as a risk factor in depression is plagued
by the same methodological limitations as the literature on personality and psychopathology in
general, and the body of literature that establishes correlational relationships between
dependency and psychopathology is more robust than the literature that examines dependency as
a causal factor (Bornstein, 2005). In spite of these limitations, there is evidence that supports the
theory that dependency can be predictive of depression. Both of these relationships will be
explored using the existing body of literature.
Dependency as a Risk Factor
Evidence supports the theory that dependency, especially when coupled with life stress,
predicts (i.e., through statistical methodology) depression (Bornstein, 1993, 2005; Auerbach, Ho,
& Kim, 2014). Dependency was also predictive of tobacco usage (Bornstein, 1993), and
increased levels of maladaptive dependency are associated with domestic violence and child
abuse (Bornstein, 2012; Kane & Bornstein, 2016). Additionally, maladaptive dependency (i.e.,
DPD) was proven to be a strong correlate of suicide attempts as well as self-harm behaviors
when compared to other psychological conditions (Bolton, Belik, Enns, Cox, & Sareen, 2008;
Bornstein & O’Neill, 2000). Evidence of dependency association regarding the development of
psychopathologies that are orally-involved is mixed (Bornstein, 1996); future research should
attempt to dismantle the underlying mechanisms of psychopathology, including the potential
causal role of dependent beliefs, attitudes, and behaviors.

51
Dependency as a Correlate/Consequence
Findings suggest that DPD is associated with a plethora of psychological impairments,
including personality disorders, anxiety disorders, mood disorders, eating disorders, and
substance use (Disney, 2013; Bornstein, 2005). Studies have demonstrated overlap between DPD
and other personality disorders (PDs), but more specifically with the other Cluster C disorders as
specified by the various versions of the DSM. However, as some have noted, this could highlight
issues of discriminant validity among the cluster C disorders (Blashfield & Breen, 1989;
Bornstein, 1995). For instance, there is significant overlap, (e.g., a strong correlation), between
dependent and avoidant PDs (AVPD; Disney, 2013). A study conducted by Bachrach et al.
(2012) found a correlation of r = .66 between the symptoms of DPD and those of AVPD.
Literature that examined the symptomatic overlaps between DPD and AVPD emphasized the
similarities in the manifestation of social behaviors while the underlying motivations for the
styles of interpersonally relating are disparate (Disney, 2013).
In addition to correlations with Cluster C disorders, there is a well-established
relationship between DPD and certain Cluster B disorders, especially borderline and histrionic
PDs. In fact, evidence suggests that borderline personality disorder (BPD) involves underlying
intense dependency needs (Bornstein, Becky-Matero, Winarick, & Reichman, 2010). The DSM-
IV (APA, 1994) and DSM-IV-TR (APA, 2000) highlighted multiple overlaps in the symptoms
between the disorders and even listed as DPD as a rule-out in differential diagnosis for BPD
(Bornstein et al., 2010). Moreover, multiple theoretical frameworks (i.e., classical
psychoanalytic, object relational, interpersonal, cognitive behavioral) have noted links between
the underpinnings of these PDs. For example, Kernberg (1975, p. 145) emphasized the role of
“conflictual pathological dependency” in the onset and symptomatic manifestation of BPD

52
(Bornstein et al., 2010). A multiplicity of studies (e.g.., Nunberg et al., 1991; Oldham et al.,
1992; Blais, McCann, Benedic, & Norman, 1997) found moderate to strong positive correlations
between BPD and DPD (i.e., r = .30 – .40). However, it is important to note two important
findings from this body of literature: Several variables moderate the relationship between BPD
and DPD, and healthy levels of trait rather than state dependency do not correlate as strongly to
symptoms associated with BPD (Bornstein et al., 2010). Variables that moderate the relationship
between BPD and DPD include, but are not limited to, measures of BPD and DPD, type of
sample (i.e., clinical or nonclinical), and gender (Bornstein et al., 2010).
Given that DPD has historically been classified as a Cluster C PD, it is perhaps
unsurprising that it shows significant overlap with a variety of anxiety disorders, such as several
specific phobias and obsessive-compulsive disorder (OCD). Similar to other findings on
comorbidities of DPD, these correlations are likely due in part to similarities in the underlying
mechanisms and etiologies of these disorders. For example, Bienvenu and Brandes (2005)
suggest that the overlap can be explained by the high levels of neuroticism that are found in both
DPD and anxiety disorders. Early literature revealed somewhat mixed findings, with effect sizes
ranging from r = .10 – .60 (Bornstein, 1993); a more recent meta-analysis on 89 studies clarified
the relationship between anxiety disorders and dependency such that it revealed an overall effect
size of r = .11, with a combined Z of 8.686 (p < .0001), and a fail-safe N of 2,389 (Ng &
Bornstein, 2005, p. 397). Though this effect size can be considered small, the other statistical
values suggest that the link between DPD and anxiety disorders is likely a reliable one (Ng &
Bornstein, 2005). Researchers have also found a correlation between hoarding behaviors and
DPD (Disney, 2013). Studies examining links between specific phobias (e.g., school phobia) and
DPD revealed mixed findings (Disney, 2013; Bornstein, 1993).

53
DPD has also shown associations with a variety of eating disorders (Disney, 2013;
Bornstein, 1993; 2005). For example, a study with a large sample of individuals with a
diagnosable eating disorder (i.e., 182 individuals with anorexia and 112 with bulimia), revealed
comorbidity with DPD of 37.4% and 45.5% respectively (Loas et al., 2002). A plethora of earlier
studies (e.g.., Bornstein & Greenberg, 1991; Jacobson & Robins, 1989; Yager et al.) corroborate
these findings such that they found moderate to large correlations between DPD and both
anorexia and bulimia. The existing literature supports the hypothesis that moderators, such as
gender and stressful life events, moderate the dependency-eating disorders relationship
(Bornstein, 1993).
Lastly, DPD shows a positive correlation with substance use, particularly alcoholism
(Bornstein, 1995; Disney, 2013; Loas et al., 2005; The psychoanalytic conceptualization of
dependency, which emphasizes oral frustration or gratification, would support the theory that
individuals with DPD would likely suffer from alcoholism rather than cocaine or opiate abuse
given its oral component (Bornstein, 1993). However, there are somewhat mixed findings in this
area: Loranger (1996) actually found a significantly lower risk of substance abuse among
psychiatric patients diagnosed with DPD than among patients with other PDs. In an attempt to
clarify the hypothesized link and inconclusive findings, Echeburua, de Medina, and Aizpiri
(2009) found that DPD was the most commonly diagnosed PD in an alcohol/no cocaine group
(i.e., 31.3%) when compared to the alcohol and cocaine group combined (16.1%). This particular
finding was consistent with their (2013) results, which demonstrated that DPD was the most
common PD diagnosis in a sample of 30 inpatient alcohol-dependent individuals (Disney, 2013).
Dependency and Depression
Theoretical Links

54
The links between dependency and depression are prolific and pervasive across a variety
of theoretical orientations. In an effort to delineate these various links, the classical
psychoanalytic perspective on dependency (operationalized as the concept of orality) in the
context of depression will be considered. Then, the components of both dependency and
depression as constructs (the former operationalized from an interactionist perspective and the
latter from a diagnostic perspective as conveyed by the DSM), will be deconstructed to
extrapolate the theoretical links between them. Finally, Joiner and Metalsky’s (1995)
interpersonal model of depression will be discussed in light of the dependency-depression link.
The role of orality (i.e., oral dependency) in the etiology and symptomatic manifestation
of depression has been a topic of scholarly pursuit among psychoanalytic theorists since its
inception in the late 19th century (Bornstein, Poynton, & Masling, 1985). Abraham (1927),
among others, noted the changes in appetite associated with depression as being rooted in orality.
Accordingly, he argued that depression resulted in regression to the oral phase in Freud’s
psychosexual phases of development. Fenichel (1945) supported this theory when he explained
how a refusal to eat was a hallmark symptom of melancholia. He went on to note that this oral
deprivation is predictive of a particularly pessimistic or sadistic attitude that will negatively
implicate the patient’s desire and ability to engage in self-care, therefore allocating those
activities to the likes of others, (i.e., increased dependency). In fact, most psychoanalytic
conceptualizations of depression emphasize the role of oral processes (i.e., deprivation or
overgratification) in its etiology and symptomatic manifestation (see, e.g., Blatt, 1974).
However, the study conducted by Bornstein et al. (1985) highlighted the levels of complexity
involved in the depression-orality/dependency relationship. They found that dependency is “less

55
a factor in depression than is a personality constellation marked by egocentrism, immaturity, fear
of rejection, helplessness, and lack of integration” (Bornstein et al., 1985, p. 241).
To further clarify the theoretical links between dependency and depression, their modern
conceptualizations will be deconstructed and compared to extrapolate theoretical and conceptual
overlaps. The Cognitive/Interactionist model proposed by Bornstein (2011) will be used as a
framework to drive this discussion. Therefore, the following table [Table 1] deconstructs both
dependency and depression into their cognitive, motivational, affective, and behavioral
components using Bornstein’s (2011) article and Beck and Alford’s (2009) book on depression.
Table 1. Cognitive, Motivational, Affective and Behavioral Attributes of Depression and Dependency
Construct Cognitive Motivational Affective Behavioral
Depression • Negative
self-schema
usually
involving
feelings of
worthlessness
and being
unlovable
• Regressive
and self-
punitive
wishes –
desires to
escape, hide,
or die
• Specific
alteration in
mood:
sadness,
loneliness
and apathy
• Vegetative
changes:
anorexia,
insomnia,
loss of libido
• Changes in
activity level:
retardation or
agitation
Dependency • Schema of
the self as
helpless,
ineffectual,
vulnerable,
and weak
• Strong desire
to create and
maintain
nurturing and
supportive
relationships
• Fears of
abandonment
and negative
evaluation
• Strategies
aimed at
facilitating
relationships
Based on the information presented in Table 1, there are both overlaps and discrepancies
across these domains of functioning between depression and dependency. Most notably, both
constructs involve similar underlying cognitive manifestations that involve a negative self-
concept. The self-schema involved in depression centers around ideas of the self as unworthy
and unlovable, and worthless, while the self-schema involved in dependency identifies the self as

56
helpless, vulnerable, and ineffectual. The ways in which these self-concepts could overlap are
numerous, involving both bidirectional and causal relationships. For instance, one could argue
that seeing oneself as weak could manifest in feelings of hopelessness and worthlessness, and
vice versa. These perceptions of self-concept could also present themselves in causal ways. A
negative self-schema could most certainly elicit negative affect and other depressive symptoms.
The motivational aspects of dependency and depression initially appear to differ, but the
opposite could be also argued. They are dissimilar at face-value in that depression manifests in a
desire to escape or hide, while dependency manifests in a desire to do the opposite, which is to
reach out and seek nurturance through interpersonal interactions. However, the regressive
wishes in depression can, in some individuals, manifest in the motivation to seek nurturance and
support through primary caregivers (Beck & Alford, 2009). Individual differences involving
personality and temperament moderate this relationship (Beck & Alford, 2009).
As Table 1 shows, the affective components involved in depression and dependency are
not entirely dissimilar. The affective components of dependency, including a fear of
abandonment and of negative evaluation, are associated with high levels of anxiety. There is an
abundance of evidence that suggests anxiety and depression occur comorbidly as often as in 60%
of cases (Cameron, 2007). It can be argued that the relationship between these affective
components can also occur bidirectionally or in a causal fashion.
Lastly, the behavioral components of depression and dependency often manifest
differently. The behaviors of a depressed individual stem from an underlying loss of motivation
and interest in engaging in activities s/he used to find enjoyable (Beck & Alford, 2009). In this
way, the behavioral characteristics of depression are passive and reactive in nature, whereas the
behavioral characteristics inherent in dependency are generally proactive and goal-directed

57
(Beck & Alford, 2009; Beck, 1991). A depressed person tends to isolate, while many dependent
people actively seek out connections with others.
Joiner and Metalsky’s (1995) investigation evaluated and extended Coyne’s (1976)
interpersonal theory of depression. Specifically, Coyne postulated that the interpersonal attitudes
and behaviors of depressed individuals produce a type of interpersonal dynamic that may
facilitate rejection from others. Joiner and Metalsky (1995) elaborated on this hypothesis when
they suggested that these depressed individuals will likely engage in pervasive reassurance
seeking, which in turn would manifest in negative interpersonal interactions that could
exacerbate their pre-existing depression and dependency yearnings.
Overview of Findings
A literature review on the relationship between dependency and depression (including
MDD and dysthymic disorder) was conducted and revealed a multitude of correlational studies
that found small to moderate positive effect sizes (Bornstein, 1993, 2005; Disney, 2013). This
small to moderate effect size appears relatively constant across subject groups or populations
(e.g., clinical, nonclinical, children, men, and women). However, as this review will demonstrate,
the dependent-depression relationship has several moderators that manifest in mixed and
sometimes conflictual data.
The magnitude of the relationship between dependency and depression is stronger in men
than in women suggesting that gender moderates the dependency-depression relationship
(Bornstein, 1993, 2006; Mongrain & Leather, 2006, Sanathara, Gardner, Prescott et al., 2003).
For example, Blatt, Quinlan, Chevron, McDonald, and Zuroff’s (1982) study found that men in
their sample (both patients and normal controls) had dependency-depression correlations of
r=.34, and r=.31 (p<.001) respectively, while women in the sample (patients and normal

58
controls) had dependency-depression correlations of r=.20 and r=.24 (p<.001). Smith, O’Keefe,
and Jenkins (1988) revealed similar findings but with a smaller magnitude, such that the
dependency-depression correlation for females was reported at r=.08, while the correlation
among men was reported at r=.10 (p<.01). Additionally, Sanathara et al. (2003) found that
higher interpersonal dependency scores in males were significantly more predictive of lifetime
MDD when compared to females.
The type of dependency measure used in studies has also been found to moderate the
relationship between depression and dependency, such that the dependency subscale of the
Depressive Experiences Questionnaire (DEQ) revealed smaller effect sizes than those associated
with the Interpersonal Dependency Inventory (IDI). The same moderating relationship applies to
the type of depression measure being utilized. For instance, the Beck Depression Inventory
(BDI) found larger effect sizes than a study that used the Zung Depression Scale (SDS; Zung,
1965). Additionally, where studies were conducted influenced the magnitude of the effect size in
the relationship between dependency and depression. For instance, a study conducted on working
community members in Japan revealed a larger effect size than that found in U.S. samples
(Takagishi, Sakatara, & Kitamura, 2011).
In an early attempt to clarify the body of literature, a meta-analysis (Nietzel & Harris,
1990) analyzed dependency, depression, achievement, and autonomy; their analysis of the
dependency-depression relationship revealed mean correlations that ranged from r=.19 to r=.33.
Another study conducted by Luyten, Sabbe, Blatt, Meganck, Jensen, De Grave, Maes, and
Corveleyn (2007) revealed that both men and women with MDD had elevated levels of
dependency compared to normal controls, r = .20. These scores corroborate Bornstein’s (1993)
initial assessment of the dependency-depression relationship.

59
Some in this area have reported correlations between dependency and depression that
differ from those in the aforementioned studies. For instance, a study conducted by Schulte,
Mongrain, and Flora (2008) revealed a correlation coefficient of r = .64, such that all dependency
subscales of a particular measure (except connectedness and love) were significantly correlated
with past episodes of depression. Another study found a correlation of r = .41 between a self-
report measure of depression and a self-report measure of dependency among hospitalized
adolescents (Fehon, Grilo, & Martino, 1997). A study that examined depression and sociotropy
in undergraduate students revealed the same correlation of r = .41 (Sato & McCann, 2000), while
a study of 466 community adults in Japan revealed a correlation of r = .55 between depression
and dependency. Lastly, Smith, Hewitt, Flett, and Harvey (2003) found a correlation of r = .44
between depression and dependency in 70 psychiatric patients. Although these studies represent
a minority in the context of the larger body of literature, they underscore the range of the effect
sizes among the data.
Call for a Meta-Analytic Understanding
Research needs to dismantle the components of dependency to further isolate the specific
mechanisms that contribute to the development of depressive mood disorders, as it has yet to
establish a causational understanding of the link between these constructs. There is currently a
lack of synthesized, corroborating data upon which to draw broader, overarching conclusions
about the dependency-depression relationship. For instance, there is an unusually large range of
the magnitude of effect sizes in the literature, which underscores its inconsistency. Moreover,
Nietzel and Harris’ (1990) meta-analysis is nearly 30 years old, and included only the 21 articles
that were found in the published literature at that time. Since that time there have been dozens of
additional studies that examine the relationship between these constructs have been conducted,

60
necessitating a current meta-analysis to synthesize all the current available data. This study
proposes the conduction of a meta-analysis that will fill this crucial gap in the literature and will
ultimately inform both research and clinical practice.
The current study is guided by the following question: What is the overall magnitude of
the dependency-depression relationship and what are the variables that moderate this relationship
and to what extent?

61
Chapter V: Present Study
Overview
Despite the burgeoning body of literature that empirically investigates the dependency-
depression relationship, only one prior meta-analysis was conducted nearly thirty years ago
(Nietzel & Harris, 1990) and is therefore not representative of the state of the contemporary
literature. With the prevalence of depressive disorders increasing, it will be important to further
investigate the underlying mechanisms, particularly factors such as interpersonal dependency,
which is not typically involved in diagnostic screening for depressive disorders. Therefore, a
meta-analysis that examines the dependency-depression relationship can inform clinical practice
allowing clinicians to understand, assess, and treat depressive disorders in a more nuanced and
effective way.
Hypotheses
Consistent with the findings of Nietzel & Harris’ (1990) meta-analysis, the current study
hypothesizes that meta-analysis will reveal a small to moderate positive effect size between
dependency and depression. A second set of less definitive hypotheses are that variables such as
type of depression measure, type of dependency measure, gender, type of sample (i.e., clinical vs.
nonclinical), and location of sample, will moderate the dependency-depression relationship. We
expect the dependency—depression effect size to be larger in clinical than nonclinical samples,
and larger in women than in men.
The aforementioned variables were selected based on an overview of findings in the
dependency-depression literature. As a later section will elaborate, Nietzel and Harris’ (1990)
meta-analysis revealed variation between effect sizes across self-report, performance-based
measures, and interview techniques. Additional findings from various studies identified some

62
degree of variation in effect sizes across the other variables selected for analysis, including
gender, age, and location of the sample (see Disney, 2013; Mongrain & Leather, 2006; Sanathara
et al., 2003).

63
Chapter VI: Methodology
Systematic Review of the Literature
A systematic review of the literature on the relationship between interpersonal
dependency and depression facilitated the thorough interpretation and synthesis of the available
research to date. According to Petticrew and Roberts (2006), a systematic literature review is a
multi-step and comprehensive method of interpreting a substantial body of information. A
systematic review allows for the identification of areas of uncertainty, and highlights where little
research has been done. Petticrew and Roberts’ (2006) approach lends well to research in which
studies produce conflicting or mixed results. Given that the current state of the dependency-
depression literature is mixed, this approach is most appropriate for the data involved in the
current study.
Petticrew and Roberts’ (2006) approach to systematic reviews in meta-analyses involves
a multi-step process as follows: (1) The researcher must clearly delineate the guiding research
question the study seeks to address as well as develop hypotheses the review will test; (2) The
types of studies that are required to answer the research questions and address the hypothesis
must be determined; (3) A thorough and highly systematized search of the literature must be
conducted in order to locate the required studies; (4) Once the results of the literature search have
been compiled, they must be screened utilizing specific inclusion and exclusion criteria; (5) The
included studies must be critically appraised; (6) The studies must be synthesized, such that the
heterogeneity of the studies’ findings is assessed; and lastly (7) The findings of the review must
be disseminated appropriately.
Description of Methods Used in Primary Research

64
The most common methods used in the dependency-depression literature involve the
application of statistical analysis to various self-report questionnaires of both dependency and
depression. Sometimes, however, interview-based diagnostic screening based the DSM is
utilized for assessing depressive disorders. In this context, it is important to note that
questionnaire and interview-based dependency and depression measures assess explicit, rather
than implicit components of each construct. In addition, all studies included in the current meta-
analysis utilized measures that assessed dependency and depression either prospectively or cross-
sectionally.
A number of studies incorporated multiple methods of measuring both dependency and
depression. The benefits of multimethod assessment are vast, such that it facilitates a more
comprehensive and reliable pool of data from which to draw more accurate conclusions
(Hopwood & Bornstein, 2014) On the negative side, however, a majority of the studies utilized
correlational methods to assess the general relationship between dependency and depression,
which limits the extent to which causation and the underlying mechanisms of the relationship
occur. An additional limitation is that many studies included in the current review utilize
undergraduate students as their sample, which may limit the generalizability of their findings.
Approximately 75% of studies included in this review were conducted in the United States,
whereas the remaining 25% were conducted internationally, but reported in English.
Criteria for Inclusion and Exclusion of Studies
In order for a study to be included in the meta-analysis, it must meet the following
detailed set of criteria:
1.) Studies must contain at least one measure or index of interpersonal dependency or
utilize the diagnostic criteria of DPD in the DSM.

65
2.) Studies are required to utilize at least one measure or index of a depressive disorder,
specifically, MDD or PDD. Studies that assess populations with other mood or
personality disorders in which depressive symptomology is present will not be
included (e.g., studies that examined populations with a bipolar diagnosis will not be
included, even if data were obtained in a depressive rather than hypomanic or manic
state).
3.) Quantitative and descriptive data regarding the relationship between dependency and
depression, (i.e. mean, standard deviations, p values, etc.) must be reported for a
study to be included, so that an effect size can be derived.
4.) Studies must be published in a peer-reviewed source.
5.) Studies must be conducted and results must be reported in English.
Search Strategy for Identification of Studies
Search Terms for Identification of Applicable Studies
The following search terms or keywords were utilized in various pairings when exploring
and collecting the dependency-depression research. Regarding depression, the following search
terms were used: “depressed”, “depression”, “depressive”, “dysthymic”, “dysthymia”, and
“mood disorder”. The following search terms were used to describe dependency: “dependent”,
“dependent personality”, “dependency”, “oral”, “orality”, “sociotropy”, “sociotropic”, and
“anaclitic”. All possible pairwise combinations were utilized in the search for applicable studies
throughout the literature.
Electronic Databases Utilized
The electronic databases utilized to collect literature included: PsychNet, PubMed, and
MedLine. PubMed and MedLine were accessed in order to collect psychiatric literature about the

66
dependency-depression relationship that may have been excluded from using PsychNet. Google
Scholar and Google.com were also searched using the above keywords.
Reference Lists
An exhaustive review of the reference lists of each of the studies included in this current
review was conducted to determine eligibility and applicability of related studies for potential
inclusion in this review.
Conducting and Documenting the Search Selection Process
A thorough account of all searches and resulting data collection as well as storage of data
was created and updated throughout the process to document all searches. The account includes
all of the following information: (1) Time periods searched; (2) Databases or websites utilized;
(3) Number of hits per search; and (4) Key words utilized. The majority of studies were found
and included through the Adelphi University Library system. Studies were saved and maintained
in an electronic application, Notability. Duplicate PDF files were created and stored in a separate
electronic folder. The PRISMA (2009) system (including the checklist and flowchart) was
utilized to systematically sort through and solidify the literature to be included in the current
review [see Figure 1 in the Results Chapter].
Identifying Moderating Variables
In all meta-analyses, it is imperative to raise questions regarding what factors contribute
to the range of effect sizes within the universe of data. The search for and identification of
moderating variables is crucial to the meta-analytic process by providing important insights into
the nature of the relationship between the two constructs of interest (Rosenthal & DiMatteo,
2001). The process of identifying moderating variables in a meta-analysis is inquisitive and not
confirmatory (Rosenthal & DiMatteo, 2001). The coding procedure for data collection shed light

67
on relationships between effect sizes and certain variables being examined that are hypothesized
to moderate the dependency-depression relationship, including: type of depression measure, type
of dependency measure, gender, type of sample (i.e., clinical vs. nonclinical), age and location of
sample.
Coding Procedure
Coding took place for all studies that met inclusion criteria. A single excel spreadsheet
was used to record pertinent data regarding the studies. The following raw information was
recorded per each individual study: bibliographic details (author and publication date), sample
type, sample size, percentage of female participants, depression measure, dependency measure,
effect size(s), p value, a synthesis of overall findings (sections of results and discussion section),
and effect size calculation method.
Inter-rater Reliability
To assess for and ensure the validity of the data being coded, processes to analyze inter-
rater reliability (IRR) was utilized. In addition to the author, a trained research assistant (i.e., a
recent graduate of a Ph.D. program in Clinical Psychology) will code each of the included
studies using the coding procedure described above. The resulting variance between coders will
be analyzed. Specifically, an IRR analysis seeks to identify the extent to which the variance of
the observed scores stems from variance in the true scores once the variance due to measurement
errors among the coders has been accounted for (Hallgreen, 2012). Cohen’s (1960) kappa and
related kappa variants was used when computing IRR. The Kappa statistic measures the
observed degree of corroboration between coders for a collection of nominal ratings that account
for the agreement that would be estimated due to chance, which ultimately produced a

68
standardized index of overall IRR that can be applied across the included studies (Hallgreen,
2012).
Statistical Analysis
Random-Effects Meta-Analysis
Determining the meta-analysis model (i.e., random or fixed-effects) involves
consideration of many factors. According to Hedges and Vevea (1998), the decision lies in the
researcher’s assumption of the heterogeneity versus homogeneity of the effect sizes within their
data based on the characteristics of the universe of studies. For meta-analyses in which
homogeneity can be assumed, it is more appropriate to conduct a fixed-effects model (Hedges &
Vevea, 1998). In contrast, when heterogeneity is assumed, a random-effects model should be
utilized. Random-effects models involve the premise that assumptive generalizations about
features of the data (i.e. population size, statistical method used, effect size computation), cannot
be applied because the data are highly heterogeneous.
In the context of the dependency-depression literature, a random-effects model would be
most appropriate due to the differences in research methodology, statistical analysis, and
demographic characteristics of the population. Therefore, this project utilized a random-effects
model to best suit the nature of the universe of data in the current analysis.
Effect Size Computation
Whatever statistical model of analysis was used in each study was converted into a
correlation coefficient, r value, to demonstrate the magnitude of the relationship between
dependency and depression measures. The correlation coefficient is the most straightforward
method to convey both the overall strength and magnitude of the dependency-depression

69
relationship. Outcome statistical effect size conversion and calculation processes were
conducted utilizing the below meta-analytic formulas outlined by Rosenthal (1991, pp. 59-81).
For studies that report t, F, or other statistics, such conversion formulas including
Hedges’ g and Cohen’s d will be utilized to determine the standardized mean difference
regarding the effect size estimate (Rosenthal, 1991). These procedures involve a pooling and
averaging system that centers around combining mean effect sizes across multiple studies to
produce an overall average (Littell et al., 2008). The formulas can be found in Appendix B of
this document.
Several logistical measures were effectuated to account for studies that reported multiple
effect sizes. For instance, when a study reports effect sizes per subscale of a measure, these
effect sizes will be averaged to calculate an overall effect size for the depression-dependency
interaction. Additionally, when a study reports separate effect sizes in women and men, these
scores will also be averaged to produce an overall effect size per the study. Lastly, when effect
sizes are reported across multiple time points, they are averaged to produce an overall effect size.
Of note, all studies included in Nietzel & Harris’ (1990) meta-analysis were coded and therefore
included in the current analysis.
Combined Z
The Stouffer method of combining standard normal deviations (Zs) was used to quantify
the levels of significance for combined studies. Rosenthal (1991) elaborated on the statistical
mechanisms of deriving this variable for generalized application in meta-analyses as the
following to facilitate a normal approximation of the binominal distribution that would apply
well to even smaller samples. The formula is as follows:

70
Z = 2P – N / N, where P represents the number of positive effect sizes obtained and N
represents the sum of both positive and negative effect sizes obtained (Rosenthal, 1991, p. 113).
In this way, the combined Z value is used to capture both the magnitude of the r in
addition to the total number of participants that were included to compute it. For instance, even
if an r value is the same across two studies, when the combined Z value is greater, it indicates a
higher degree of confidence in the overall relationship. Therefore, the statistical significance of
the observed dependency-depression link is not based on the r value, but the combined Z value
that has been identified. In accordance, the resulting p value will decrease as the combined Z
value increases.
Accounting for Publication Bias
The Fail-Safe N variable was derived to address the file-drawer sampling issue in
research (Bornstein, 2005; Rosenthal, 1979, 1991). Rosenthal (1991) among others (i.e.
Schuessler & Bakan, 1968; McNemar, 1960; Smart, 1964; & Sterling, 1959) elaborated that
journals typically publish only studies that report statistically significant results, “while the file
drawers back at the lab are filled with the 95% of studies that show nonsignificant (e.g., p > .05)
results” (Rosenthal, 1991, p. 104).
Combatting or at least accounting for the file-drawer problem in meta-analytic projects
involves a statistical process to first determine whether or not the universe of data is susceptible
to publication sampling bias. First, one must calculate the number of studies that average null
results (i.e., r = 0.00) that must be included in the “file drawer” before the overall probability of a
type I error can be manipulated into any desired level of significance (Rosenthal, 1991, p. 104).
In other words, it represents a theoretical estimate of how many studies with an effect size of
zero would need to exist to render the obtained effect size not statistically significant. The fail-

71
safe N is calculated by adding the Z scores of each available effect size, squaring this result,
dividing the resulting figure by an appropriate constant (i.e., Z = 1.645, Rosenthal, 1991, p. 104),
and finally subtracting the number of effect sizes used to calculate it, which Rosenthal labels as
the K value. The resulting number represents the fail-safe N, which helps more accurately depict
the robustness of an observed dependency-depression relationship (Rosenthal, 1991, p. 104).
Additionally, Duval and Tweedie’s (2000) funnel plot was utilized as a way to assess the
symmetry of the dispersion of effect sizes across standard error. When these values are plotted
and inversed and the distribution of data is symmetrical, it resembles a funnel or a normal
distribution curve. If the plot of the data appears to be asymmetrical, a “trim and fill” method of
adjusting the reported effect sizes to become more symmetrical needs to be implemented (Duval
& Tweedie, 2000). The funnel plot and option to include the trim and fill method adds an
additional assessment of potential publication bias in the distribution of data.
Assessing for Heterogeneity
The Q-Statistic, (Hedges & Olkin, 2014) sometimes called Cochran’s Q is another
comprehensive way of assessing heterogeneity in meta-analyses. The Q-statistic is calculated as
the weighted sum of the squares of differences between the study effects of an individual study
and the cumulative effect across studies (Gavaghan, Moore, McQay, 2000). It is frequently
utilized in random-effects meta-analyses to determine the degree of variability in effect sizes. In
essence, this value was calculated to delineate the extent of the variance both between and within
levels of various moderators (Moore & Fresco, 2012; Borenstein, 2009).
Additional statistics, such as the Omnibus Test of Model Coefficients were used in
comparison to the Q-statistics to confirm or disconfirm the need for a random-effects model.
The statistic τ was calculated to assess for the heterogeneity of effect sizes, while τ² was

72
calculated to find the between-study variance. Lastly, the I2 statistic was calculated to determine
the percentage of variation across studies that is due specifically to heterogeneity rather than by
chance.

73
Chapter VII: Results
Research Questions, Hypotheses, and Literature Search
The current meta-analysis investigated the following questions:
1. What is the overarching relationship between interpersonal dependency and depression?
2. Which variables moderate the relationship between interpersonal dependency and
depression and to what extent?
It was first hypothesized that the current meta-analysis would reveal a small to medium
overall positive effect size between dependency and depression. Second, we hypothesized that
variables such as the type of depression measure, type of dependency measure, gender, type of
sample, (e.g., clinical vs. nonclinical), as well as location of sample, might moderate the
dependency-depression relationship. The only moderators for which we had specific hypotheses
were gender and sample type; the other moderator analyses were exploratory. Specifically, we
expected the dependency-depression effect size to be larger in clinical than nonclinical samples,
and larger in women than in men. These hypotheses were established following a thorough
review of both the theoretical and empirical literature.
The initial search of databases yielded 208 potential studies for inclusion based on all
possible pairwise combinations of the search terms that were utilized to capture the entire
universe of data that investigated this subject. The PRISMA diagram in Figure 1 provides more
detail regarding the inclusion and exclusion of data that occurred in arriving at the final 105
studies that met criteria for inclusion. The 103 studies that were excluded from the final analysis
were omitted for one or more of the following reasons:
1.) Studies that were literature reviews rather than original empirical investigations.
2.) Studies that assessed for both measures of dependency and depression but did not report

74
on the relationship between the two constructs.
3.) Studies that quantitatively assessed only one of the two constructs, (e.g., depression but
not dependency).
4.) Studies that did not provide sufficient data from which to compute an effect size.
5.) Studies that were not available in English.
6.) Studies that utilized statistical methodology that was not translatable to a computable
effect size.
7.) Studies that were duplicates.
A detailed summary of the data for each of the 105 studies included in the analysis can be
found in Appendix III. However, it is important to delineate several summarizing factors about
the data. First, the 105 studies included in the current analysis were conducted in many countries
in addition to the United States, including Canada, Taiwan, Israel, and The Netherlands. These
studies investigated the dependency-depression relationship among clinical, (i.e., psychiatric
inpatients and outpatients), and nonclinical samples (community adults and university students).
The sample sizes ranged from 27 to 7174.

75
PRISMA 2009 Flow Diagram
"Relationship of depedency and achievement/autonomy to depression ".
Figure 1. PRISMA Flow Diagram of Study Selection Procedure
Records identified through database searching
(n = 335)
Scre
enin
g In
clu
ded
El
igib
ility
Id
enti
fica
tio
n
Additional records identified through other sources
(n = 8)
Records after duplicates removed (n = 271)
Records screened (n = 208)
Records excluded (n = 50)
Full-text articles assessed for eligibility
(n = 158)
Full-text articles excluded, with reasons
(n = 40)
Studies included in qualitative synthesis
(n = 118)
Studies included in quantitative synthesis
(meta-analysis) (n = 105)

76
The studies included in the current analysis utilized 23 unique measures of depression and 22
unique measures of dependency, using varying assessment methods (e.g., self-report vs.
clinician-assessed). The mean age of the samples included in the analysis ranged from 10 to 80
years. Additionally, there was significant variation in the demographic characteristics of the
various samples of the studies that were included for analysis, particularly in the area of
socioeconomic status, race and ethnicity, as well as education. The percentage of females in
samples ranged from 0-100. Therefore, the universe of data appeared to be highly heterogeneous
in nature. A forest plot of the studies and their effect sizes can be found in Figure 2 below.

77
Figure 2. Forest Plot of Effect Sizes

78
Inter-Rater Reliability in Data Coding
To assess reliability in data coding a second rater (a recent Ph.D. graduate in Clinical
Psychology), unaware of the initial rater’s judgments, coded all relevant variables for a
subsample of 40 studies. Cohen’s (1960) Kappa statistic was calculated using SPSS for each
moderator; Pearson’s correlation was used to assess reliability for the dependency-depression
effect size. These analyses revealed a kappa of 1 (perfect agreement between the two coders),
across the following domains: Type of Dependency Measure, Type of Depression Measure, Type
of Sample, (e.g., outpatient, inpatient, community, or university students), Location of Sample,
Percentage of Female Participants, and Mean age. The correlation between the two raters’ coding
of dependency-depression effect size was .82, an acceptable level of agreement.
Assessing for Publication Bias
The current analysis investigated the potential impact of publication bias via two
methods: Rosenthal’s (1991) Fail-Safe-N, as well as a funnel plot analysis (Duval & Tweedy,
2000). Fail-Safe N results are described in the ensuing sections. The funnel plot analysis,
summarized in Figure 3, suggested that the dispersion of effect sizes and standard error was
largely symmetrical in nature.
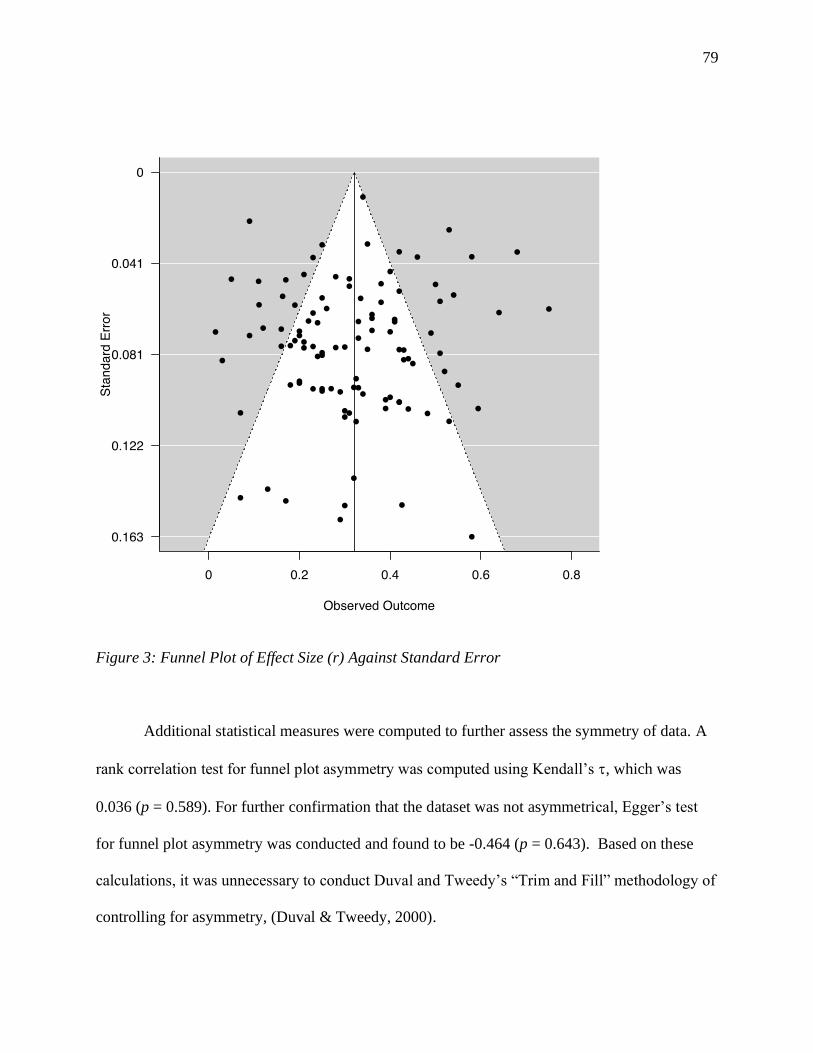
79
Figure 3: Funnel Plot of Effect Size (r) Against Standard Error
Additional statistical measures were computed to further assess the symmetry of data. A
rank correlation test for funnel plot asymmetry was computed using Kendall’s , which was
0.036 (p = 0.589). For further confirmation that the dataset was not asymmetrical, Egger’s test
for funnel plot asymmetry was conducted and found to be -0.464 (p = 0.643). Based on these
calculations, it was unnecessary to conduct Duval and Tweedy’s “Trim and Fill” methodology of
controlling for asymmetry, (Duval & Tweedy, 2000).

80
Heterogeneity
Cochrane’s Q for a test of Residual Heterogeneity was found to be 738.115 (p < 0.001),
which was significantly higher than the Q value for the Ombinus test of Model Coefficients
458.623 (p < 0.001), suggesting a random-effects model would be most appropriate given the
characteristics of the data. Additionally, several residual heterogeneity estimates were calculated.
τ² was 0.017, representing variance between studies. The heterogeneity within the universe of
effect sizes was 0.132, as indicated by τ. The I² statistic assessing the percentage of variation
across studies that is due exclusively to heterogeneity alone rather than chance was 84.6%,
indicating a high level of heterogeneity. These results confirm the necessity of utilizing a
random-effects model to accommodate the heterogeneity of studies included in the current
analysis.
Overall Dependency-Depression Relationship
An overall effect size reflecting the weighted average of the individual effect sizes that
were converted to Pearson’s correlation coefficient was calculated using conversion formulas
found in the Method section as well as Appendix II. The overall effect size r was found to be .32,
p < .001, with a Combined Z score of 21.415, revealing a small to medium positive relationship
between dependency and depression, confirming our hypothesis. The Fail-Safe N associated with
this overall effect size was 101,712, suggesting that it is highly unlikely that unpublished
nonsignificant results are responsible for the significant relationship obtained.
Moderators
Several potential moderators were examined, including: gender (operationalized as
percentage of female participants in a sample), age, location of study, type of depression

81
measure, type of sample, (e.g., clinical vs. nonclinical), and type of dependency measure. These
results are described below.
The literature suggests that dependent traits and behaviors are generally higher in females
than in males, which is postulated to be linked to sociocultural constructs such as gender norms,
(Blatt, 1974; Bornstein, 1993; Disney, 2013; see also Bornstein, 2006; Mongrain & Leather,
2006, Sanathara et al., 2003). Pearson’s correlation was calculated between percentage of
females in the study and overall effect size, which revealed a small to medium correlation of .26,
(p < 0.001). The larger the percentage of women in a study, the larger the dependency-depression
relationship. Similarly, the correlation between mean age of sample and overall effect size was
found to be .23 (p < 0.001): The older the sample, the stronger the dependency-depression link.
Table 2 summarizes results regarding location of study in relation to effect size. As this
table shows, Asia had the largest effect size relative to other locales. However, it is important to
note that only 2 effect sizes from Asia were included in the current meta-analysis. The other
locations revealed effect sizes that were close to each other, with the United States representing
the second largest effect size. These results indicate that the relationship between dependency
and depression is generally consistent despite potential cultural impacts on the experience and
expression of dependency and depression.
Table 2: Location of Study
Study
Location
Number of
Effect
Sizes
Combined
Effect Size
(r)
Combined
Z
p Fail-Safe N
U.S. 84 .34 16.869 <.001 43,145
Canada 20 .27 13.285 <.001 1,196
Asia 2 .51 5.523 <.001 134
Europe 15 .28 7.433 <.001 2,324

82
Israel 4 .28 2.865 0.004 148
Australia 1 .25 1.64 <.05 ---
When considering characteristics of the samples, it is important to investigate the
possibility that overall severity of depression within a sample might impact the link between
dependency and depression. The type of samples in the universe of data included combinations
of inpatients, outpatients, university students, and community members; we hypothesized that
inpatients would show the largest effect sizes, and community adults and university students
would show the smallest effect sizes. The results of this analysis are summarized in Table 3. Our
results indicate that type of sample actually accounts for little variation in the effect sizes. There
was no difference in effect size between inpatients and outpatients, and these effect sizes
represented slightly smaller effect sizes when compared to other populations, contrary to our
initial hypotheses. University students and effect sizes within the ‘other’ category, (i.e., studies
that pooled effect sizes across multiple types of samples), were found to have the largest effect
sizes, at r = .31 and r = .36, respectively.
Table 3: Type of Sample
Sample
Type
Number of
Effect
Sizes
Combined
Effect Size
(r)
Combined
Z
p Fail-Safe N
Community 25 .29 10.281 <.001 6,388
Inpatient 7 .25 4.122 <.001 137
Outpatient 15 .25 8.630 <.001 2026
Other 23 .36 9.791 <.001 4544
University 56 .31 17.682 <.001 24,317
Note. Studies within the ‘Other’ category include those that pooled effect sizes across multiple
sample types.

83
Other characteristics of the studies that were examined included the types of measures
used to assess depression and dependency. These results are summarized in Tables 4 and 5. As
Table 4 shows, type of depression measure had minimal impact on the observed dependency-
depression link (although studies in the Other category had a larger effect size when compared to
self-report and interviews as individual measures). However, because studies in the Other
category were pooled across different types of measures, it is difficult to draw more specific
conclusions from these results.
Table 4: Type of Depression Measure
Measure
Type
Number of
Effect
Sizes
Combined
Effect Size
(r)
Combined
Z
p Fail-Safe N
Self-
Report
89 .32 18.070 <.001 62,159
Interview 13 .29 5.206 <.001 331
Other 24 .39 10.642 <.001 2696
Note. Studies within the ‘Other’ category include those that utilized a combination of self-report
and interview methods.
Finally, the effect of the type of dependency measure was analyzed, with the expectation
that performance-based dependency measures would yield smaller effect sizes than self-report
and interview measures (see Bornstein, 1995, 2005). As Table 5 shows, performance-based
measures of dependency, (i.e., the Rorschach Oral Dependency Scale) were associated with a
slightly smaller effect size than self-report measures, a finding that is consistent with the
literature on cross-method test score relationships.

84
Table 5: Type of Dependency Measure
Measure
Type
Number of
Effect
Sizes
Combined
Effect Size
(r)
Combined
Z
p Fail-Safe N
Self-Report 115 .32 20.424 <.001 83,255
Performance-
Based
3 .27 2.455 <.001 30
Other 8 .30 6.787 <.001 512
Note. Studies within the ‘Other’ category include those that utilized a combination of self-report
and interview methods, in addition to measures that could not be included in either the self-report
or performance-based categories.

85
Chapter VIII: Discussion
Summary of Findings
The current meta-analysis revealed a small to medium effect size, r = .32, between
interpersonal dependency and depression that was consistent across several moderators,
including gender, location, and age. A random-effects model was applied to a dataset of a total of
105 studies (total number of participants = 30,824) to account for the high degree of
heterogeneity among the data. Funnel plot analysis indicated that the observed effect size was a
reasonable estimate of the actual effect sizes; Fail-Safe N revealed that it would take over
100,000 unpublished studies averaging zero effect size to render the observed relationship
nonsignificant. Therefore, it can be concluded with confidence that dependency and depression
levels are positively related.
Perhaps most important, the current results affirm the consistency of the small to medium
positive correlation between dependency and depression across several variables. For example,
regardless of whether the sample population consisted of inpatients, outpatients, or university
students, the magnitude of the effect size remained consistent. The location of the population did
not influence the dependency-depression relationship, reaffirming the consistency of the
relationship across culture. As expected, measures that assessed implicit dependency revealed a
slightly smaller effect size when compared to self-report measures of dependency, findings
which are congruent to the larger body of literature.
Fit with Previous Research
The theoretical links between dependency and depression were explored in a previous
chapter. As noted, the psychoanalytic conceptualization emphasizes the causal role of early
experiences (including oral dependency) in the onset of depressogenic thoughts, feelings,

86
attitudes, and behavior, while cognitive approaches highlight the development of schemas about
the self as being helpless and ineffectual as a potential risk factor for depression. Despite these
theoretical differences in the etiology of depression, the empirical literature suggests that
interpersonal dependency and the depressive disorders are linked constructs, both conceptually
and experientially (e.g., both dependency and depression are associated with feelings of
helplessness, and lack of agency). The results of the current meta-analysis corroborate this link.
To best understand the ways in which the current investigation fits with prior research, it
is important to revisit the results obtained from Nietzel and Harris’ (1990) meta-analysis on
interpersonal dependency, autonomy/achievement, and depression. The authors provide
theoretical context for the study, including the idea that dependency is one of the many pathways
to the development of depression by describing anaclitic depression (Spitz, 1946) as well as the
specificity hypothesis (Robins & Block, 1988). In short, the authors illustrate the myriad ways in
which interpersonal dependency represents a vulnerability marker for the onset of depressive
disorders. The results from their meta-analysis revealed an overall effect size of r = .28,
suggesting a small to medium positive relationship between dependency and depression. Our
meta-analytic investigation found an effect size within the same range, very close to that of the
earlier analysis, corroborating Nietzel and Harris’ findings.
While Nietzel and Harris’ (1990) meta-analysis is illuminating and especially relevant to
this work, it is also helpful to compare the results of the current investigation to individual
studies across several time points, research methodologies, and sample characteristics. First,
many individual studies found small-medium effect sizes between dependency and depression.
For instance, Allen, Horne, and Trinder (1996) performed a cross-sectional study to evaluate trait
measures of sociotropy and autonomy as predictive of immediate emotional responses to
87
imagery conditions that depicted interpersonal rejection and failure to achieve. They ultimately
found that sociotropy was indeed a vulnerability factor to dysphoric responses, with r = .25. In
additional support of the small-medium correlation between dependency and depression,
Sprohge et al. (2002) found an effect in the same range when they utilized the ROD in two types
of samples in comparison to levels of depression. O’Neill and Bornstein (1991) examined links
between the ROD and BDI in a sample of psychiatric inpatients and found a correlation of r =
.29, furthering the observation that dependency-depression relationship is consistent across
implicit and explicit measures. Additionally, Abi-Habib and Luyten (2014) also found an effect
size of r = .25 when they evaluated the correlation between self-report measures of both
dependency and depression in a sample of community members in Belgium.
As is true for many psychological phenomena, not all individual studies yielded results
that mirrored those of the universe of data. For example, Shahar et al. (2004), found an effect
size of r = 0.15 when they calculated the correlation between the BDI and DEQ on a sample of
198 university students. Hirschfeld et al. (1989) empirically evaluated various personality traits
associated with the onset of major depression in a clinical and non-clinical sample and identified
interpersonal dependency as a risk factor, with a small effect size (r = .05). In an earlier study
conducted by the same lead researcher, an effect size of r = .07 was found when obtained among
recovered and unrecovered outpatients with depression (Hirschfeld et al., 1983). Similarly, a few
studies found medium to large effect sizes linking dependency and depression. For example,
Schulte, Mongrain, and Flora (2008) found unhealthy dependence to be a significant predictor of
recurrences of major depressive episodes, with an effect size of r = .64. Similar results were
obtained by Birtchnell, Deahl, and Fallowski, (1991), when they analyzed the relationship of
scores on self-report measures for both dependency and depression; they found a correlation (r)

88
of .68 between these two measures in a sample comprised of 424 inpatients and community
controls.
Theoretical Implications
In addition to understanding the ways in which the findings of the current study fit within
the empirical literature, it is important to explore the theoretical implications of these findings in
the context of dependency and depression as separate but related constructs. The findings of the
current systematic review have several implications regarding theories of personality and
psychopathology. In particular, the implications of this study for Beck’s cognitive vulnerability
model (e.g., Persons, Miranda, & Perloff, 1991) and Hewitt and Flett’s specific vulnerability
hypothesis, sometimes called the specificity hypothesis (Hewitt, Flett, & Ediger, 1996) are worth
examining. Additionally, the ways in which the current investigation has implications regarding
the constructs of both anaclitic and introjective depression warrant attention.
Hewitt and Flett (see Hewitt et al., 1996) created a model to extrapolate the underlying
mechanisms of perfectionistic dimensions in relation to the development of depression as an
extension of Blatt and Zuroff’s (1992) vulnerability hypothesis. Their model categorized
perfectionistic dynamics into three unique personality configurations: self-oriented perfectionism
(SOP), other-oriented perfectionism (OOP), and socially prescribed perfectionism (SPP; see
Sherry et al., 2003). SOP is an intrapersonal dimension, while OOP and SPP are hypothesized to
be interpersonal in nature, therefore relating to dependency yearnings, attitudes, and behaviors.
The model postulates that these interpersonal dimensions, (e.g., OOP and SPP), have a direct
influence on depression via exposure to ego-threatening events, in that such events are viewed as
important and therefore potentially stress-inducing. Specifically, these events prime stringent

89
self-expectations and trigger intense self-criticism within these interpersonal perfectionistic
configurations.
According to Hewitt and Flett’s specific vulnerability hypothesis, interpersonally derived
perfectionistic beliefs play a causal role in the exacerbation of depressive attitudes, behaviors,
and beliefs, and ultimately, symptoms. The findings of the current analysis that verify the
pervasiveness of the dependency-depression relationship provide indirect support for the specific
vulnerability hypothesis, though these correlational data cannot account for underlying causal
mechanisms. Research beyond the scope of the current review has been conducted to confirm
the specificity hypothesis by applying targeted research methodology that evaluates moderating
and mediating processes (see Zuroff & Mongrain, 1987; Fresco, Sampson, Craighead & Koons,
2001; Desmet, Vanheule, & Veraeghe, 2006; Adams, Abela, Auerbach, & Skitch, 2009).
The findings of this review also have implications for Beck’s (1996) cognitive
vulnerability model. Beck’s model (e.g., Beck, 1976; Persons, Miranda, & Perloff, 1991)
describes the role of cognitive schemas that involve dysfunctional beliefs about the self and
others in the onset of depressive disorders. More specifically, Beck and colleagues hypothesized
that perfectionistic attitudes, such as unrealistic standard-setting and fear of negative evaluation,
are intrinsically linked to dependent attitudes, which involve the desire to please others, and
receive admiration, acceptance, and validation from others’ approval (Sherry et al., 2003). As a
result of these internalized attitudes, the individual is at increased risk for the development of
affective disturbance, particularly depression. The results of the current investigation support
Beck’s model in a similar way that it supported the specific vulnerability hypothesis, indirectly
but not conclusively.

90
Finally, our results implicate Blatt’s (1974) conceptualizations of anaclitic and
introjective depression, which categorized depression into two subtypes denoting the
configurations of personality traits that create vulnerability to affective disturbance. The state of
anaclitic depression is “characterized by feelings of helplessness and weakness, by fears of being
abandoned, and by wishes to be cared for, loved, and protected” (Blatt, D’Afflitti, & Quinlan,
1976, p. 383). Therefore, anaclitic depression is directly associated with dependency longings
and characteristics. In contrast, introjective depression is described as the state of feeling intense
inadequacy, guilt, and even worthlessness (Blatt et al., 1976). While the two states involve
seemingly disparate etiologies, both involve personality dimensions that are similar to those
described in the aforementioned frameworks (i.e., the specific vulnerability hypothesis and the
cognitive vulnerability model). The findings in the current investigation provide support for
Blatt’s construct of anaclitic depression by demonstrating that dependency and depression
covary in a variety of participant groups.
In an effort to further contextualize Blatt’s theory regarding anaclitic depression in
relation to dependency, causal links between anaclitic traits and depression will be explored.
First, the anaclitic state involves intense fears of abandonment from others that stem from the
aforementioned perception of oneself as weak and helpless. Therefore, individuals with anaclitic
traits tend to show elevated levels of dependency compared to individuals with introjective traits.
As a result of this personality organization, Blatt (1974) and others, (e.g., Beck 1983; Clark et al,
1999), suggest that these individuals are more susceptible to life events that affect their
relationships with important events. Kopala-Sibley and Zuroff (2010) elaborate, noting that:
The beliefs of vulnerable individuals may influence the meaning assigned to an
event. If the meaning of an event has negative implications about the person in

91
question, negative automatic thoughts, cognitive errors, and negative appraisals
may follow and precipitate depressive symptoms. (p. 271).
Therefore, anaclitic mood states in which dependency needs are inherent represent a
causal mechanism for the onset of depressive thoughts, feelings, attitudes, and behaviors.
Implications for Intervention
The current diagnostic criteria for various depressive disorders emphasize somatic and
affective disturbance in lieu of describing its implications for and connections with interpersonal
functioning. Given the finding that the dependency-depression link is pervasive and consistent
across a spectrum of variables, these results suggest that it would be useful to assess for
characteristics of heightened dependency in assessment of depressive disorders. For example, in
structured clinical interviewing, clinicians can ask about an individual’s desire for approval and
validation from others, reassurance-seeking behaviors, and their tendency to ask others for
support or assistance when autonomous functioning is possible. Nuance can be added to this line
of inquiry by incorporating tenets of Bornstein’s (2012) Cognitive/Interactionist perspective on
dependency by assessing for the specific motivational, affective, behavioral, and cognitive
manifestations of dependency. By revising diagnostic criteria to include salient aspects of
interpersonal functioning, more targeted and edifying clinical information can be obtained. The
said shift in diagnostics would facilitate more efficacious screening for depressive disorders. As
Table 5 suggests, a variety of self-report and performance-based measures of interpersonal
dependency may be helpful in illuminating dependency-related antecedents and correlates of
depression.
The current findings would also facilitate more nuanced psychotherapeutic treatment of
depressive disorders that could improve therapeutic outcomes. If working within a

92
psychoanalytic and/or relational framework, the clinician can use the therapeutic alliance (e.g.,
exploring transference and countertransference) as an exclusive avenue through which to explore
dependency traits or behaviors that are attributable in part to the patient’s symptomatic
manifestation of depression. Bornstein (2005) elaborated on the ways in which the dependent
patient’s transference can be thoroughly explored as a means to treat dependency-related issues.
Specifically, he delineates common transference patterns among dependent patients, including
idealization, possessiveness, and projective identification. Idealization refers to the patient’s
denial of the therapist’s own imperfections, while possessiveness involves the patient’s feelings
of jealousy and a lack of desire to share the therapist with others. Lastly, projective
identification can occur wherein the patient unconsciously mimics the therapist’s mannerisms.
All of the aforementioned transferences can be explored in the treatment in addition to the
therapist using his or her own countertransference as clinical information regarding the patient’s
dependency needs.
When applying a cognitive-behavioral approach, treatment for depression can involve
exploration of the depressed patient’s helpless self-schema, and promotion of self-schemas that
involve autonomy and independence. By applying the current findings to treatment, the clinician
is able to conceptualize the patient’s affective disturbance as one manifestation of the schema of
the self as helpless and ineffectual, which exacerbates depressive experiences. The clinician will
be better able to explore the dysfunctional attitudes and automatic dependency-related thought
patterns in relation to the patient’s intrapersonal experience of depression. More specifically,
when observing this phenomenon via Bornstein’s (2012) C/I conceptualization of interpersonal
dependency, altering the self-schemas associated with increased dependency would in turn be

93
expected to effect changes across the motivational, behavioral, and affective responses which
foster depressogenic thoughts.
Limitations of Current Review
While the present findings have noteworthy implications for understanding the
overarching dependency-depression relationship, several methodological limitations are worth
noting. For example, many studies combined various types of samples (e.g., clinical and non-
clinical) within their analysis, which necessitated the inclusion of a relatively ambiguous ‘other’
category for analysis. The same obscuring phenomenon applies to other moderators found in this
review, such as type of depression measure and type of dependency measure. For instance,
many studies utilized multiple measures of each construct in their analysis, without reporting
separate outcomes for each measure. While multimethod assessment has its clear merits, it
implicated the calculation of some effect sizes in a limiting way, such that these effect sizes also
had to be grouped into an ‘other’ category for analysis and interpretation.
There were additional unresolved issues that originate from individual studies within the
dataset, such as a lack of reporting important demographic characteristics about their samples.
For example, many studies did not include the average age of their sample, therefore limiting the
generalizability of the statistics found when age was examined as a potential moderating
variable. Additionally, information regarding other characteristics of the samples, such as race,
ethnicity, socioeconomic status, and obtained education level was inconsistently reported among
studies. Therefore, conclusions about the impact of more specific demographic variables on the
dependency-depression relationship cannot be made. Studies typically did not report separate
effect sizes for women and men when mixed-sex samples were examined, limiting the
conclusions that could be drawn regarding sex differences in the magnitude of the dependency-

94
depression relationship. Lastly, the present review only evaluated dependency in light of unipolar
and not bipolar depression.
Future Directions
The current review facilitates the development of future directions for the literature
regarding the dependency-depression relationship. For instance, the potential impact of culture,
race, and ethnicity in the link between dependency and depression should be examined from a
culturally competent and theoretically informed perspective (Feldman & Masalha, 2007;
Satterwhite & Luchner, 2016). Literature has documented the impact of these variables on
dependency and depression as individual, but not overlapping constructs. Therefore, an
empirical investigation of these issues would be particularly informative and essential for
understanding the complexities of intersectionality and the marginalization of identities in
relation to the development of psychopathology. Findings from an investigation of race and
ethnicity in relation to the dependency-depression relationship would be particularly useful in the
current sociocultural and sociopolitical climate of the United States, and elsewhere.
An additional area of exploration could include more focused investigation of the impact
of type of dependency measure (e.g., implicit vs explicit) on the magnitude of the dependency-
depression relationship. The incorporation of theories regarding the impact of unconscious
dependency strivings in relation to depressive attributes should be foundational to future work in
this area. The literature in its current state mostly relies on self-report measures, which are
vulnerable to many potential reporting errors due to a multitude of factors, including
introspective limitations, self-presentation effects, and the potential for internalized stigma and
defense mechanisms to confound self-reports (see Lilienfeld & Fowler, 2006). The utilization of

95
implicit measures could potentially reveal more accurate information regarding the dependency-
depression relationship, less strongly affected by self-presentation confounds.
Another topic for further study is how best to conceptualize the relationships between
various personality dimensions and depression. As Nietzel and Harris (1990) explain, many of
the studies in this universe of data describe personality characteristics, (e.g., dependency and
autonomy/achievement) as predispositions to depression, but causal mechanisms remain unclear.
While their meta-analytic investigation included far fewer studies than the present analysis, this
limitation of the data remains relatively unchanged 30 years later. Some studies have attempted
to address this gap in the literature (e.g., Calvete, 2011; Nusslock, Shackman, Harmon-Jones,
Alloy, Coan, & Abramson, 2011), but further investigation is required before drawing definitive
conclusions regarding causal links between interpersonal dependency and depression.

96
Chapter IX: Conclusion
Several distinct objectives and research questions guided the current systematic review.
First, we aimed to better understand the overarching association between dependency and
depression through meta-analytic procedures. A meta-analytic approach was warranted to
address the mixed and sometimes conflicting findings regarding the dependency-depression
relationship. The current investigation also aimed to understand the potential impact of
moderating variables on the dependency-depression relationship, such as age, gender, sample
location, type of sample, (e.g., clinical vs. non-clinical), and type of measures used to assess
dependency and depression. Lastly, the current review summarized theories regarding the
etiology of dependency and depression as both individual and inextricably linked constructs in
conjunction with findings from the empirical literature to provide context for our meta-analytic
results.
The results from the meta-analysis revealed a small to moderate positive correlation
between dependency and depression using a dataset of 105 studies that are highly heterogeneous
with respect to measure and sample. While certain variables were hypothesized to contribute to
variation in the magnitude of the effect size for the dependency-depression relationship, our
results reveal a high level of consistency, with little variation. Of note, implicit measures of
dependency revealed a relatively smaller effect size when compared to explicit (self-report)
measures, confirming our hypothesis. Considered separately, many studies included in this
review provided empirical support for several theories regarding the etiology of depressive
disorders, specifically, personality dimensions that centered around the desire for approval and
validation from others. These studies complement our meta-analytic results by providing a
nuanced exploration of these theories, while in the context of the current meta-analysis, they

97
provide further support for the existence of a positive association between dependency and
depression.
Our findings contribute to the growing body of literature that aims to extrapolate the
underlying mechanisms of psychopathology, particularly in the area of personality
predispositions. For instance, the heterogeneous and occasionally conflicting data on the
investigation of the dependency-depression link necessitated the clarity that accompanies meta-
analytic procedures, therefore successfully filling a gap in the literature. Our results corroborate
and extend the results obtained from a seminal meta-analytic review (Nietzel & Harris, 1990),
with a much larger number of studies. While causal inferences cannot be made from our results,
meta-analytic techniques can play an impactful role in the development of new research
regarding the dependency-depression relationship, in addition to providing a highly reliable
synthesis of the available evidence.
In addition to the value of the present review with regard to the dependency-depression
link, it has important implications for policy and public health at large by enriching our
understanding of depressive disorders. Depressive disorders are a significant global health issue
that contributes substantially to increased mortality and economic burden (Greenburg, 2015). By
conceptualizing the etiology and course of depression through the lens of interpersonal
dependency, diagnostic criteria and interventions may eventually be more nuanced, targeted, and
effective.

98
References
Abi-Habib, R., & Luyten, P. (2013). The role of Dependency and Self-Criticism in the relationship
between anger and depression. Personality and Individual Differences, 55(8), 921-925.
doi:10.1016/j.paid.2013.07.466
Abraham, K. (1927). The influence of oral eroticism on character formation. In C.A.D. Bryan & A.
Strachey (Eds.). Selected papers on psycho-analysis (p. 393-406). London: Hogarth Press.
Adams, P., Abela, J. R., Auerbach, R., & Skitch, S. (2009). Self-criticism, dependency, and stress
reactivity: An experience sampling approach to testing Blatt and Zuroff’s (1992) theory of
personality predispositions to depression in high-risk youth. Personality and Social Psychology
Bulletin, 35(11), 1440-1451. doi:10.1177/0146167209343811
Ainsworth, M. D. (1972). Attachment and dependency: A comparison. In J. L. Gewirtz (Eds.).
Attachment and Dependency. (pp. 97-137). Washington, DC: Winston.
Allen, N. B., Horne, D. J., & Trinder, J. (1996). Sociotropy, autonomy, and dysphoric emotional
responses to specific classes of stress: A psychophysiological evaluation. Journal of Abnormal
Psychology, 105(1), 25-33. doi:10.1037/0021-843x.105.1.25
American Foundation for Suicide Prevention. (n.d.). Retrieved from https://afsp.org/
American Psychiatric Association. Diagnostic and statistical Manual of Mental Disorders: 3rd ed.
(1980). Washington: D.C.,
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed.
(1994). Washington, D.C.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5.
(2013). Arlington, VA:

99
Andersen, A. M., & Bienvenu, O. J. (2011). Personality and psychopathology. International Review of
Psychiatry, 23(3), 234-247. doi:10.3109/09540261.2011.588692
Anxiety and Depression Association of America: Facts & Statistics. (n.d.). Retrieved from
https://adaa.org/about-adaa/press-room/facts-statistics
Auerbach, R. P., Ho, M. R., & Kim, J. C. (2014). Identifying Cognitive and Interpersonal Predictors of
Adolescent Depression. Journal of Abnormal Child Psychology, 42(6), 913-924.
doi:10.1007/s10802-013-9845-6
Bachrach, N., Croon, M.A., & Bekker, M. J. (2012). Factor structure of self-reported clinical disorders
and personality disorders: A review of the existing literature and a factor analytical study.
Journal of Clinical Psychology, 68(6), 645–660. http://dx.doi.org/10.1002/jclp.21841.
Bandura, A. (1971). Behavior therapy from a social learning perspective. Proceedings of the XIXth
International Congress of Psychology. London, England.
Bandura, A. (1977). Social learning theory. Englewood Cliffs: Prentice-Hall.
Beck, A. T. (1961). An Inventory for Measuring Depression. Archives of General Psychiatry, 4(6), 561.
doi:10.1001/archpsyc.1961.01710120031004
Beck, A. T. (1967). Depression: Clinical, experimental, and theoretical aspects. New York: Harper and
Row. Republished as: Beck, A. T. (1970). Depression: Causes and treatment. Philadelphia:
University of Pennsylvania Press.
Beck, A. T., Rush, A., Shaw, B., & Emery, G. (1979). Cognitive Therapy of Depression. New York The
Guilford Press.
Beck, A.T., Epstein, N., Harrison, R.P., & Emery, G. (1983). Development of the Sociotropy-
Autonomy Scale: A measure of personality factors in depression. Unpublished manuscript,
University of Pennsylvania, Philadelphia.

100
Beck, A. T. (1991). Cognitive therapy: A 30-year retrospective. American Psychologist, 46(4), 368-375.
doi:10.1037//0003-066x.46.4.368
Beck, A. T., & Alford, B. A. (2009). Depression: causes and treatments. Philadelphia: University of
Pennsylvania Press.
Bienvenu, O. J., & Brandes, M. (2005). The interface of personality traits and anxiety
disorders. Primary Psychiatry, 12(3), 35-39.
Birnbaum, H. G., Kessler, R. C., Kelley, D., Ben-Hamadi, R., Joish, V. N., & Greenberg, P. E. (2010).
Employer burden of mild, moderate, and severe major depressive disorder: Mental health
services utilization and costs, and work performance. Depression and Anxiety, 27(1), 78-89.
doi:10.1002/da.20580
Birtchnell, J., Deahl, M., & Falkowski, J. (1991). Further exploration of the relationship between
depression and dependence. Journal of Affective Disorders, 22(4), 221-233. doi:10.1016/0165-
0327(91)90068-4
Blashfield, R. K., & Breen, M. J. (1989). Face validity of the DSM-III-R personality disorders. The
American Journal of Psychiatry, 146(12), 1575–1579.
Blais, M.A., McCann, J.T., Benedict, K.B., & Norman, D.K. (1997). Toward an empirical/theoretical
grouping of the DSM-III-R personality disorders. Journal of Personality Disorders, 11, 191-198.
Blatt, S.J. (1974). Levels of object representation in anaclitic and introjective depression. Psychoanalytic
Study of the Child, 29, 107-157.
Blatt, S. J., D'Afflitti, J. P., & Quinlan, D. M. (1976). Experiences of depression in normal young adults.
Journal of Abnormal Psychology, 85, 383-389.
Blatt, S. J., D'Afflitti, J. P., & Quinlan, D. M. (1979). Depressive experiences questionnaire.
Unpublished manual, Yale University, New Haven, CT.

101
Blatt, S. J., & Quinlan, D.M., Chevron, E.S., McDonald, C., & Zuroff, D. (1982). Dependency and self-
criticism: Psychological dimensions of depression. Journal of Consulting and Clinical
Psychology, 50(1), 113-124. doi:10.1037/0022-006x.50.1.113
Bolton, J. M., Belik, S., Enns, M. W., Cox, B. J., & Sareen, J. (2008). Exploring the correlates of suicide
attempts among individuals with major depressive disorder: Findings from the National
Epidemiologic Survey on Alcohol and Related Conditions. Journal of Clinical Psychiatry, 69,
1139–1149. http://dx.doi.org/10.4088/JCP.v69n071.
Borenstein, M. (2009). Introduction to meta-analysis. Chichester: Wiley.
Bornstein, R. F., & Masling, J. M. (1985). Orality and latency of volunteering to serve as experimental
subjects: A replication. Journal of Personality Assessment, 49(3), 306-310.
Bornstein, R. F., Poynton, F. G., & Masling, J. (1985). Orality and depression: An empirical
study. Psychoanalytic Psychology, 2(3), 241-249. http://dx.doi.org/10.1037/0736-9735.2.3.241
Bornstein, R. F., & Greenberg, R. P. (1991). Dependency and Eating Disorders in Female Psychiatric
Inpatients. The Journal of Nervous and Mental Disease, 179(3), 148-152.
doi:10.1097/00005053-199103000-00006
Bornstein, R. F. (1992). The dependent personality: Developmental, social, and clinical
perspectives. Psychological Bulletin, 112(1), 3-23.
Bornstein, R. F. (1993). The dependent personality. New York: Guilford Press.
Bornstein, R. F. (1994). Dependency as a social cue: A meta-analytic review of research on the
dependency–helping relationship. Journal of Research in Personality,28(2), 182-213.
doi:10.1006/jrpe.1994.1015
Bornstein, R. F. (1995). Active dependency. Journal of Nervous and Mental Disease, 183(2), 64–77.
http://dx.doi.org/10.1097/00005053-199502000-00002.

102
Bornstein, R. F., & Oneill, R. M. (2000). Dependency and suicidality in psychiatric inpatients. Journal
of Clinical Psychology, 56(4), 463. doi:10.1002/(sici)1097-4679(200004)56:43.3.co;2-x
Bornstein, R. F., Languirand, M. A., Geiselman, K. J., Creighton, J. A., West, M. A., Gallagher, H. A.,
& Eisenhart, E. A. (2003). Construct Validity of the Relationship Profile Test: A Self-Report
Measure of Dependency-Detachment. Journal of Personality Assessment, 80(1), 64-74.
doi:10.1207/s15327752jpa8001_15
Bornstein, R. F. (2005). The dependent patient: A practitioner's guide. Washington, DC: American
Psychological Association.
Bornstein, R. F., Porcerelli, J. H., Huprich, S. K., & Markova, T. (2009). Construct Validity of the
Relationship Profile Test: Correlates of Overdependence, Detachment, and Healthy Dependency
in Low Income Urban Women Seeking Medical Services. Journal of Personality
Assessment, 91(6), 537-544. doi:10.1080/00223890903228406
Bornstein R. F., Becker-Matero N., Winarick D. J., & Reichman A. L. (2010). Interpersonal dependency
in borderline personality disorder: clinical context and empirical evidence. Journal of
Personality Disorders. 24: 109-127.
Bornstein, R. F. (2011). An interactionist perspective on interpersonal dependency. Current Directions
in Psychological Science, 20(2), 124-128. doi:10.1177/0963721411403121
Bornstein, R. F. (2012a). Illuminating a neglected clinical issue: Societal costs of interpersonal
dependency and dependent personality disorder. Journal of Clinical Psychology, 68, 766- 781.
Bornstein RF. (2012b). From dysfunction to adaptation: An interactionist model of dependency Annual
Review of Clinical Psychology. 8: 291-316. DOI: 10.1146/annurev-clinpsy-032511-143058
Brunoni, A. R., Lopes, M., & Fregni, F. (2008). A systematic review and meta-analysis of clinical
studies on major depression and BDNF levels: Implications for the role of neuroplasticity in

103
depression. International Journal of Neuropsychopharmacology, 11(8), 1169-1180.
doi:10.1017/s1461145708009309
Cameron, O. (2007, December 01). Understanding Comorbid Depression and Anxiety. Retrieved from
http://www.psychiatrictimes.com/anxiety/understanding-comorbid-depression-and-anxiety
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological
Measurement, 20, 37-46.
Coyne, J. C. (1976). Toward an Interactional Description of Depression. Psychiatry, 39(1), 28-40.
doi:10.1080/00332747.1976.11023874
Cloninger, C. R. (1987). A systematic method for clinical description and classification of personality
variants. Archives of General Psychiatry, 44, 573–588.
Desmet, M., Vanheule, S., & Verhaeghe, P. (2006). Dependency, self-criticism, and the symptom
specificity hypothesis in a depressed clinical sample. Social Behavior and Personality: An
International Journal, 34(8), 1017-1026. doi:10.2224/sbp.2006.34.8.1017
Diethelm, O. (1975). The evolution of the concept of depression. In F.F. Flach & S.C. Draghi (Eds.),
The Nature and Treatment of Depression. NY: John Wiley & Sons, pp. 11-27.
Disney, K. L. (2013). Dependent personality disorder: A critical review. Clinical Psychology
Review,33(8), 1184-1196. doi:10.1016/j.cpr.2013.10.001
Echeburua, E., De Medina, R. B., & Aizpiri, J. (2009). Personality disorders among alcohol-dependent
patients manifesting or not manifesting cocaine abuse: A comparative pilot study. Substance Use
and Misuse, 44(7), 981-999.
Estroff-Marano, H. (2001, July 1). Depression Doing the Thinking. Retrieved from
https://www.psychologytoday.com/us/articles/200107/depression-doing-the-thinking

104
Facts & Statistics. (n.d.). Retrieved April 21, 2017, from https://www.adaa.org/about-adaa/press-
room/facts-statistics
Farmer, R. F. (2000). Issues in the assessment and conceptualization of personality disorders. Clinical
Psychology Review, 20(7), 823-851. doi:10.1016/s0272-7358(99)00014-8
Fehon, D. C., Grilo, C. M., & Martino, S. (1997). A comparison of dependent and self-critically
depressed hospitalized adolescents. Journal of Youth and Adolescence, 29(1), 93-106.
Fenichel, O. (1945). The psychoanalytic theory of neurosis. New York: Norton.
Finney, J.C. (1961) Some maternal influences on children’s personality and character. Genetic
Psychology Monographs, 63, 199-278.
Fredricks, R. (n.d.). Biology of Depression - Neuroplasticity and Endocrinology. Retrieved September
13, 2018, from https://www.gracepointwellness.org/5-depression-depression-related-
conditions/article/13000-biology-of-depression-neuroplasticity-and-endocrinology
Fresco, D. M., Sampson, W. S., Craighead, L. W., & Koons, A. N. (2001). The relationship of
sociotropy and autonomy to symptoms of depression and anxiety. Journal of Cognitive
Psychotherapy, 15(1), 17-31. doi:10.1891/0889-8391.15.1.17
Freud, S. (1905). Three Essays on Sexuality and Other Works. Standard Edition of the complete
psychological works of Sigmund Freud (S.E.), 7, 125-245.
Freud, S. (1917). Mourning and melancholia. S.E., 14, 243-258.
Funtowicz, M. N., & Widiger, T. A. (1999). Sex bias in the diagnosis of personality disorders: An
evaluation of DSM-IV criteria. Journal of Abnormal Psychology, 108(2), 195-201.
Gavaghan, D. J., Moore, A. R., & Mcquay, H. J. (2000). An evaluation of homogeneity tests in meta-
analyses in pain using simulations of individual patient data. Pain, 85(3), 415-424.
doi:10.1016/s0304-3959(99)00302-4

105
Geurtzen, N., Keijsers, G. P., Karremans, J. C., & Hutschemaekers, G. J. (2018). Patients’ care
dependency in mental health care: Development of a self-report questionnaire and preliminary
correlates. Journal of Clinical Psychology, 74(7), 1189-1206. doi:10.1002/jclp.22574
Goldman-Eisler, F. (1948). Breast-feeding and character formation. Journal of Personality, 17, 83-103.
Goodwin, F., & Jamison, K. R. (1990). Manic Depressive Illness. In Radden, J. (Ed)., The nature of
melancholy: from Aristotle to Kristeva (chapter 31). NY: Oxford University Press.
Gordon, M. & Tegtemeyeyer, P.E. (1983). Oral dependent content in children’s Rorschach protocols.
Perceptual and Motor Skills, 57, 1163-1168.
Gotlib, I. H., & Hammen, C. L. (2002). Handbook of depression. NY: Guilford Press.
Greenberg, P. E. (2015, February 25). The Growing Economic Burden of Depression in the U.S.
Retrieved from https://blogs.scientificamerican.com/mind-guest-blog/the-growing-economic-
burden-of-depression-in-the-u-s/
Hallgren, K. A. (2012). Computing inter-rater reliability for observational data: An overview and
tutorial. Tutorials in Quantitative Methods for Psychology, 8(1), 23-34.
doi:10.20982/tqmp.08.1.p023
Hamilton, M. (1960). Hamilton Rating Scale for Depression. PsycTESTS Dataset. doi:10.1037/t04100-
000
Hatfield, J.S., Ferguson, P.E., Rau, L. & Alpert, R. (1967) Mother-child interaction and the socialization
process. Child Development, 38, 365-414
Hedges, L. V., & Vevea, J. L. (1998). Fixed- and random-effects models in meta-analysis.
Psychological Methods, 3(4), 486-504. doi:10.1037//1082-989x.3.4.486
Hedges, L. V., & Olkin, I. (2014). Statistical Methods for Meta-Analysis. Saint Louis: Elsevier Science.
106
Hewitt, P. L., Flett, G. L., & Ediger, E. (1996). Perfectionism and depression: Longitudinal assessment
of a specific vulnerability hypothesis. Journal of Abnormal Psychology, 105(2), 276-280.
doi:10.1037/0021-843x.105.2.276
Hirschfeld, R. M., Klerman, G. L., Gouch, H. G., Barrett, J., Korchin, S. J., & Chodoff, P. (1977). A
Measure of Interpersonal Dependency. Journal of Personality Assessment, 41(6), 610-618.
doi:10.1207/s15327752jpa4106_6
Hirschfeld, R. M., Klerman, G. L., Lavori, P., Keller, M. B., Pamela, G., & Coryell, W. (1989).
Premorbid personality assessments of first onset of major depression. Archives of General
Psychiatry, 46(4), 345. doi:10.1001/archpsyc.1989.01810040051008
Hopwood, C. J., & Bornstein, R. F. (2014). Multimethod clinical assessment. NY: Guilford Press.
Hull, C. L. (1943). Principles of behavior: An introduction to behavior theory. New York: Appleton-
Century-Crofts.
Huprich, S. K. (2009). What Should Become of Depressive Personality Disorder in DSM-V? Harvard
Review of Psychiatry, 17(1), 41-59. doi:10.1080/10673220902735694
Insel, T. R. (2008). Assessing the Economic Costs of Serious Mental Illness. American Journal of
Psychiatry, 165(6), 663-665. doi:10.1176/appi.ajp.2008.08030366
Jacobson, R., & Robins, C. J. (1989). Social dependency and social support in bulimic and nonbulimic
women. International Journal of Eating Disorders, 8(6), 665-670. doi:10.1002/1098-
108x(198911)8:63.0.co;2-7
Joiner, T. E., & Metalsky, G. I. (1995). A prospective test of an integrative interpersonal theory of
depression: A naturalistic study of college roommates. Journal of Personality and Social
Psychology, 69(4), 778-788. doi:10.1037/0022-3514.69.4.778

107
Jouanna, J., Allies, N., & Eijk, P. V. (2012). Greek medicine from Hippocrates to Galen: Selected
papers. Leiden: Brill.
Kagan, J. & Mussen, P. (1956) Dependency themes on the TAT and group conformity. Journal of
Consulting Psychology, 20, 29-32.
Kane F. A., Bornstein R. F. (2016). Beyond passivity: Dependency as a risk factor for intimate partner
violence. Personality and Mental Health. DOI:10.1002/pmh.1322
Kendler, K. S., Prescott, C. A., Myers, J., & Neale, M. C. (2003). The Structure of Genetic and
Environmental Risk Factors for Common Psychiatric and Substance Use Disorders in Men and
Women. Archives of General Psychiatry, 60(9), 929. doi:10.1001/archpsyc.60.9.929
Kernberg, O.F. (1975). Borderline conditions and pathological narcissism. New York: Jason Aronson.
Kessler, R. C., Walters, E. E., & Forthofer, M. S. (1998). The Social Consequences of Psychiatric
Disorders, III: Probability of Marital Stability. American Journal of Psychiatry, 155(8), 1092-
1096. doi:10.1176/ajp.155.8.1092
Kessler, R. C. (2012). The Costs of Depression. Psychiatric Clinics of North America, 35(1), 1-14.
doi:10.1016/j.psc.2011.11.005
Kivelae, S., & Pahkala, K. (1987). Factor structure of the Zung Self-Rating Depression Scale among a
depressed elderly population. International Journal of Psychology, 22, 289-300.
Klein, M. (1940). Mourning and its relation to manic-depressive states. International Journal of
Psychoanalysis, 21, 125-153.
Klein, M. (1963). The psychoanalysis of children. London: Hogarth Press.
Kohut, H., Goldberg, A., & Stepansky, P. E. (2013). How does analysis cure? Chicago: University of
Chicago Press.

108
Kraepelin, E. (1883). Compendium of Psychiatry: For the use of Students and Physicians. Von Dr.
Docent an der Universität, Leipzig. Leipzig: Abel
Levinson, D. F. (2006). The Genetics of Depression: A Review. Biological Psychiatry, 60(2), 84-92.
doi:10.1016/j.biopsych.2005.08.024
Lilienfeld, S. O., & Fowler, K. A. (2006). The Self-Report Assessment of Psychopathy: Problems,
Pitfalls, and Promises. In C. J. Patrick (Ed.), Handbook of psychopathy (p. 107–132). The
Guilford Press.
Littell, J. H., Corcoran J., & Pillai, V. (2008). Systematic reviews and meta-analysis. New York: Oxford
University Press.
Lingiardi, V., & McWilliams, N. (2017). Psychodynamic diagnostic manual: PDM-2. NY: Guilford
Press.
Loas, G., Atger, F., Perdereau, F., Verrier, A., Guelfi, J., Halfon, O., et al. (2002). Comorbidity of
dependent personality disorder and separation anxiety disorder in addictive disorders and in
healthy subjects. Psychopathology, 35(4), 249–253. http://dx.doi.org/10.1159/000063830.
Loas, G., Guilbaud, O., Perez-Diaz, F., Verrier, A., Stephan, P., Lang, F., . . . Jeammet, P. (2005).
Dependency and suicidality in addictive disorders. Psychiatry Research, 137(1-2), 103-111.
doi:10.1016/j.psychres.2004.06.022
Loranger, A. W. (1996). Dependent personality disorder: Age, sex, and axis I comorbidity. Journal of
Nervous and Mental Disease, 184(1), 17–21. http://dx.doi.org/ 10.1097/00005053-199601000-
00004.
Lubbe, T. (2011). Object relations in depression: A return to theory. London: Routledge.
Luyten, P., Sabbe, B., Blatt, S. J., Meganck, S., Jansen, B., Grave, C. D., . . . Corveleyn, J. (2007).
Dependency and self-criticism: relationship with major depressive disorder, severity of

109
depression, and clinical presentation. Depression and Anxiety, 24(8), 586-596.
doi:10.1002/da.20272
Malouff, J. M., Thorsteinsson, E. B., & Schutte, N. S. (2005). The Relationship Between the Five-Factor
Model of Personality and Symptoms of Clinical Disorders: A Meta-Analysis. Journal of
Psychopathology and Behavioral Assessment, 27(2), 101-114. doi:10.1007/s10862-005-5384-y
Masling, J., Rabie, L., & Blondheim, S. H. (1967). Obesity, level of aspiration, and Rorschach and TAT
measures of oral dependence. Journal of Consulting Psychology, 31(3), 233-239.
doi:10.1037/h0020999
Masling, J., Oneill, R., & Katkin, E. S. (1982). Autonomic arousal, interpersonal climate, and
orality. Journal of Personality and Social Psychology, 42(3), 529-534. doi:10.1037/0022-
3514.42.3.529
McKay, K. (2018, January 26). The History of Depression. Retrieved from
https://www.artofmanliness.com/articles/the-history-of-depression/
Mclean, L. M., & Gallop, R. (2003). Implications of Childhood Sexual Abuse for Adult Borderline
Personality Disorder and Complex Posttraumatic Stress Disorder. American Journal of
Psychiatry,160(2), 369-371. doi:10.1176/appi.ajp.160.2.369
McNemar, Q. (1960). At random: Sense and nonsense. American Psychologist, 15(5), 295-300.
http://dx.doi.org/10.1037/h0049193
Meyer, G. J, Finn, S. E., Eyde, L. D., Kay G. G., Moreland, K. L., Dies, R. R…Read, G. M. (2001).
Psychological testing and psychological assessment: A review of evidence and issues. American
Psychologist, 56(2), 128-165
Millon, T. (1981). Disorders of Personality: DSM-III: Axis II. New York: Wiley.

110
Millon, T. (2011). Disorders of personality: Introducing a DSM/ICD spectrum from normal to
abnormal. Hoboken, NJ: Wiley.
Mongrain, M., & Leather, F. (2006). Immature dependence and self-criticism predict the recurrence of
major depression. Journal of Clinical Psychology, 62(6), 705-713. doi:10.1002/jclsp.20263
Moore, M. T., & Fresco, D. M. (2012). Depressive realism: A meta-analytic review. Clinical
Psychology Review, 32(6), 496-509. doi:10.1016/j.cpr.2012.05.004
Mowrer, O. H. (1956). Two-factor learning theory reconsidered, with special reference to secondary
reinforcement and the concept of habit. Psychological Review, 63(2), 114-128.
http://dx.doi.org/10.1037/h0040613
Murphy, L.B. (1962). The widening world of childhood. New York: Basic Books.
Nemade, R. (n.d.). Biology of Depression - Neurotransmitters. Retrieved September 13, 2018, from
https://www.gracepointwellness.org/5-depression-depression-related-conditions/article/12999-
biology-of-depression-neurotransmitters
Nemade, R., Staats Reiss, N., & Dombeck, M. (n.d.). Biology of Depression - Genetics and Imaging.
Retrieved September 13, 2018, from https://www.gracepointwellness.org/5-depression-
depression-related-conditions/article/13001-biology-of-depression-genetics-and-imaging
Ng, H. M., & Bornstein, R. F. (2005). Comorbidity of dependent personality disorder and anxiety
disorders: A meta-analytic review. Clinical Psychology: Science and Practice, 12, 395–406.
Nietzel, M. (1990). Relationship of dependency and achievement/autonomy to depression. Clinical
Psychology Review, 10(3), 279-297. doi:10.1016/0272-7358(90)90063-g
Nurberg, H.G., Raskin, M., Levine, P.E., Pollack, S., Stegel, O., & Prince, R. (1991). The comorbidity
of borderline personality disorder and other DSM-III-I Axis II personality disorders. American
Journal of Psychiatry, 148, 1371-1377.

111
Oldham, J.M., Skodol, A.E., Kellman, H.D., Hyler, S.E., Rosnick, L., & Davies, M. (1992). Diagnosis
of DSM-III-R personality disorders by two structured interviews: Patterns of comorbidity.
American Journal of Psychiatry, 149. 213-220.
Oneill, R. M., & Bornstein, R. F. (1991). Orality and depression in psychiatric inpatients. Journal of
Personality Disorders, 5(1), 1-7. doi:10.1521/pedi.1991.5.1.1
Overholser, J. C., & Fine, M. A. (1994). Cognitive-behavioral treatment of excessive interpersonal
dependency: A four-stage psychotherapy model. Journal of Cognitive Psychotherapy, 8(1), 55-
70.
Overholser, J. C. (1997). Treatment of Excessive Interpersonal Dependency: A Cognitive-Behavioral
Model. Journal of Contemporary Psychotherapy, 27(4), 283-301.
Petticrew, M., & Roberts, H. (2006). Systematic reviews in the social sciences: A practical guide.
Oxford: Blackwell Publishing.
Sanathara, V. A., Gardner, C. O., Prescott, C. A., & Kendler, K. S. (2003). Interpersonal dependence
and major depression: Aetiological inter-relationship and gender differences. Psychological
Medicine, 33(5), 927-931. doi:10.1017/s0033291703007542
Sears, R. R., Rau, L., & Alpert, R. (1965). Identification and child rearing. Stanford: Stanford
University Press.
Schuessler, K., & Bakan, D. (1968). On Method: Toward a Reconstruction of Psychological
Investigation. American Sociological Review, 33(4), 669. doi:10.2307/2092486
Schulte, F.S., Mongrain, M., & Flora, D.B. (2008). Healthy and unhealthy dependence: Implications for
depression. British Journal of Clinical Psychology, 47(3), 341-353.

112
Sherry, S. B., Hewitt, P. L., Flett, G. L., & Harvey, M. (2003). Perfectionism dimensions, perfectionistic
attitudes, dependent attitudes, and depression in psychiatric patients and university
students. Journal of Counseling Psychology, 50(3), 373-386. doi:10.1037/0022-0167.50.3.373
Smith, T. W., Okeeffe, J. L., & Jenkins, M. (1988). Dependency and Self-Criticism: Correlates of
Depression or Moderators of the Effects of Stressful Events? Journal of Personality
Disorders,2(2), 160-169. doi:10.1521/pedi.1988.2.2.160
Quello, S., Brady, K., & Sonne, S. (2005). Mood Disorders and Substance Use Disorder: A Complex
Comorbidity. Science and Practice Perspectives, 3(1), 13-21. doi:10.1151/spp053113
Radden, J. (2002). The nature of melancholy: from Aristotle to Kristeva. New York, NY: Oxford
University Press.
Radloff, L. S. (1977). The CES-D Scale. Applied Psychological Measurement, 1(3), 385-401.
doi:10.1177/014662167700100306
Reynolds, W. M., & Kobak, K. A. (1995). Reliability and validity of the Hamilton Depression
Inventory: A paper-and-pencil version of the Hamilton Depression Rating Scale Clinical
Interview. Psychological Assessment, 7(4), 472-483. http://dx.doi.org/10.1037/1040-
3590.7.4.472
Rosenthal, R. (1979) The ‘file drawer’ problem and tolerance for null results. Psychological Bulletin,
86, 638-641
Rosenthal, R. (1990) Meta-analytic procedures for social research (2nd ed). Thousand Oaks, CA: Sage.
Rosenthal, R., & Dimatteo, M. R. (2001). Meta-analysis: Recent developments in quantitative methods
for literature reviews. Annual Review of Psychology, 52(1), 59-82.
doi:10.1146/annurev.psych.52.1.59

113
Rush, A. J., Zimmerman, M., Wisniewski, S. R., Fava, M., Hollon, S. D., Warden, D., . . . Trivedi, M.
H. (2005). Comorbid psychiatric disorders in depressed outpatients: Demographic and clinical
features. Journal of Affective Disorders, 87(1), 43-55. doi:10.1016/j.jad.2005.03.005
Samuel, D., & Widiger, T. (2008). A meta-analytic review of the relationships between the five-factor
model and DSM-IV-TR personality disorders: A facet level analysis. Clinical Psychology
Review, 28(8), 1326-1342. doi:10.1016/j.cpr.2008.07.002
Sandler, J., & Dare, C. (1970). The psychoanalytic concept of orality. Journal of Psychodynamic
Research, 14, 211-222.
Sato, T., & McCann, D. (2000). Sociotropy-autonomy and the beck depression Inventory. European
Journal of Psychological Assessment, 16(1), 66-76. doi:10.1027//1015-5759.16.1.66
Satterwhite, A. K., & Luchner, A. F. (2016). Exploring the relationship among perceived
resilience, dependency, and self-criticism: The role of culture and social support. North
American Journal of Psychology, 18(1), 71–84.
Schuessler, K., & Bakan, D. (1968). On method: Toward a reconstruction of psychological
investigation. American Sociological Review, 33(4), 669. doi:10.2307/2092486
Sears, R.R., Whiting, J.W.M., Nowlis, V., & Sears, P.S. (1953) Some childrearing antecedents of
aggression and dependency in young children. Genetic Psychology Monographs, 47, 135-236
Siegel, R. J. (1988). Women’s "dependency" in a male-centered value system. Women and
Therapy,7(1), 113-123. doi:10.1300/j015v07n01_09
Smart, R. G. (1964). The importance of negative results in psychological research. Canadian
Psychologist/Psychologie Canadienne, 5a(4), 225-232. doi:10.1037/h0083036

114
Smith, T. W., Okeeffe, J. L., & Jenkins, M. (1988). Dependency and self-criticism: Correlates of
depression or moderators of the effects of stressful events? Journal of Personality
Disorders, 2(2), 160-169. doi:10.1521/pedi.1988.2.2.160
Sprohge, E., Handler, L., Plant, D. D., & Wicker, D. (2002). A Rorschach study of oral dependence in
alcoholics and depressives. Journal of Personality Assessment, 79(1), 142-160.
doi:10.1207/s15327752jpa7901_09
Sterling, T.D. (1959). Publication decisions and their possible effects on inferences drawn from tests of
significance – or vice versa. Journal of the American Statistical Association, 54, 30-34.
Takagishi, Y., Satara, M., & Kitamura, T. (2011). Effects of self-esteem on state and trait components of
interpersonal dependency and depression in the workplace. Journal of Clinical Psychology,
67(9), 918-926.
The catecholamine hypothesis of affective disorders: A review of supporting evidence. 1965 [classical
article]. (1995). The Journal of Neuropsychiatry and Clinical Neurosciences, 7(4), 524-533.
doi:10.1176/jnp.7.4.524
Thomas, A., & Chess, S. (1977). Temperament and development. Oxford, England: Brunner/Mazel.
Tronick, E., & Reck, C. (2009). Infants of depressed mothers. Harvard Review of Psychiatry, 17(2),
147-156. doi:10.1080/10673220902899714
Wang, Y., & Gorenstein, C. (2013). Psychometric properties of the Beck Depression Inventory-II: a
comprehensive review. Revista Brasileira de Psiquiatria, 35(4), 416-431. doi:10.1590/1516-
4446-2012-1048
Welkowitz, J., Lish, J. D., & Bond, R. N. (1985). The Depressive Experiences Questionnaire: Revision
and validation. Journal of Personality Assessment, 49(1), 89-94.
doi:10.1207/s15327752jpa4901_17

115
Widiger, T. A., Verheul, R. & Vanden Brink, W. (1999). Personality and psychopathology. In L.A.
Pervin & O.P. John (Eds), Handbook of Personality, Second Edition (pp. 347–366). NY:
Guilford Press.
Widiger, T. A., & Samuel, D. B. (2005). Evidence-based assessment of personality
disorders. Personality Disorders: Theory, Research, and Treatment, S(1), 3-17.
doi:10.1037/1949-2715.s.1.3
Widiger, T. A., & Trull, T. J. (2007). Plate tectonics in the classification of personality disorder: Shifting
to a dimensional model. American Psychologist, 62(2), 71-83. doi:10.1037/0003-066x.62.2.71
Widiger, T. A., & Mullins-Sweatt, S. N. (2009a). Five-factor model of personality disorder: A proposal
for DSM-V. Annual Review of Clinical Psychology, 5(1), 197-220.
doi:10.1146/annurev.clinpsy.032408.153542
Widiger T. A. (2009b). Neuroticism. In Leary M. R., & Hoyle R. H. (Eds). Handbook of individual
differences in social behavior. NY: Guilford Press., 129-46.
Widiger, T. A. (2011). Personality and psychopathology. World Psychiatry,10(2), 103-106.
doi:10.1002/j.2051-5545.2011.tb00024.x
Widiger, T. A. (2012). Future directions of personality disorder. Oxford Handbooks Online.
doi:10.1093/oxfordhb/9780199735013.013.0038
Wilson S., & Durbin C.E. (2010). Effects of paternal depression on fathers' parenting behaviors: a meta-
analytic review. Clinical Psychology Review, 30:167–80.
World Health Organization. (1992). The ICD-10 classification of mental and behavioural disorders:
Clinical descriptions and diagnostic guidelines. Geneva: World Health Organization.

116
Yager, J., Landsverk, J., Edelstein, C. K., & Hyler, S. E. (1989). Screening for Axis II personality
disorders in women with bulimic eating disorders. Psychosomatics, 30(3), 255-262.
doi:10.1016/s0033-3182(89)72269-6
Zung, W. W. (1965). Self-Rating Depression Scale in an outpatient clinic. Archives of General
Psychiatry, 13(6), 508. doi:10.1001/archpsyc.1965.01730060026004
Zuroff, D. C., & Mongrain, M. (1987). Dependency and self-criticism: Vulnerability factors for
depressive affective states. Journal of Abnormal Psychology, 96(1), 14-22. doi:10.1037/0021-
843x.96.1.14

117
Appendix A: Statistical Formulas
Hedges’ g utilizes the pooled estimate of standard deviation, which can be calculated as:
Cohen’s d produces the pooled sample standard deviation, using:

Appendix B: Summary of Data from Meta-Analysis Articles
Study Mean
Age
%
Female
Sample
Size
(N)
Depression
Measure
Dependency
Measure
Sample
Location
Sample Type Effect Size
( r )
p
Hirschfeld
et al. (1977)
29 59 400 Symptoms
Checklist
(SCL-90)
Interpersonal
Dependency
Inventory (IDI)
U.S. Inpatient 0.42, 0.48 <0.0001
Blatt et al.
(1982)
34.05 61.2 459 Zung
Depression
Scale (ZDS),
Beck
Depression
Inventory
(BDI)
Depressive
Experiences
Questionnaire
(DEQ)
U.S. Outpatient and
University
0.28, 0.27
0.23
<0.001
Hirschfeld
et al. (1983)
31.1 65.7 88 Schedule for
Affective
Disorders and
Schizophrenia
(SADS)
IDI U.S. Inpatient and
Outpatient
0.07 .3491
Hammen et
al. (1985)
N/A 71 94 BDI, SADS-L Sociotropy
Autonomy
Scale (SAS)
U.S. University
Students
0.52 <0.0001
Bornstein,
Poyton, &
Masling
(1985)
N/A 0 417 DEQ Rorschach Oral
Dependency
(ROD)
U.S. University
Students
0.11 <0.05
Welkowitz,
Lish, &
Bond
(1985)
N/A 58 131 BDI DEQ U.S. University
Students
0.43 <0.0001
Zuroff &
Mongrain
NA 56.2 300 Multiple Affect
Adjective
DEQ U.S. University
Students
0.50 <0.001
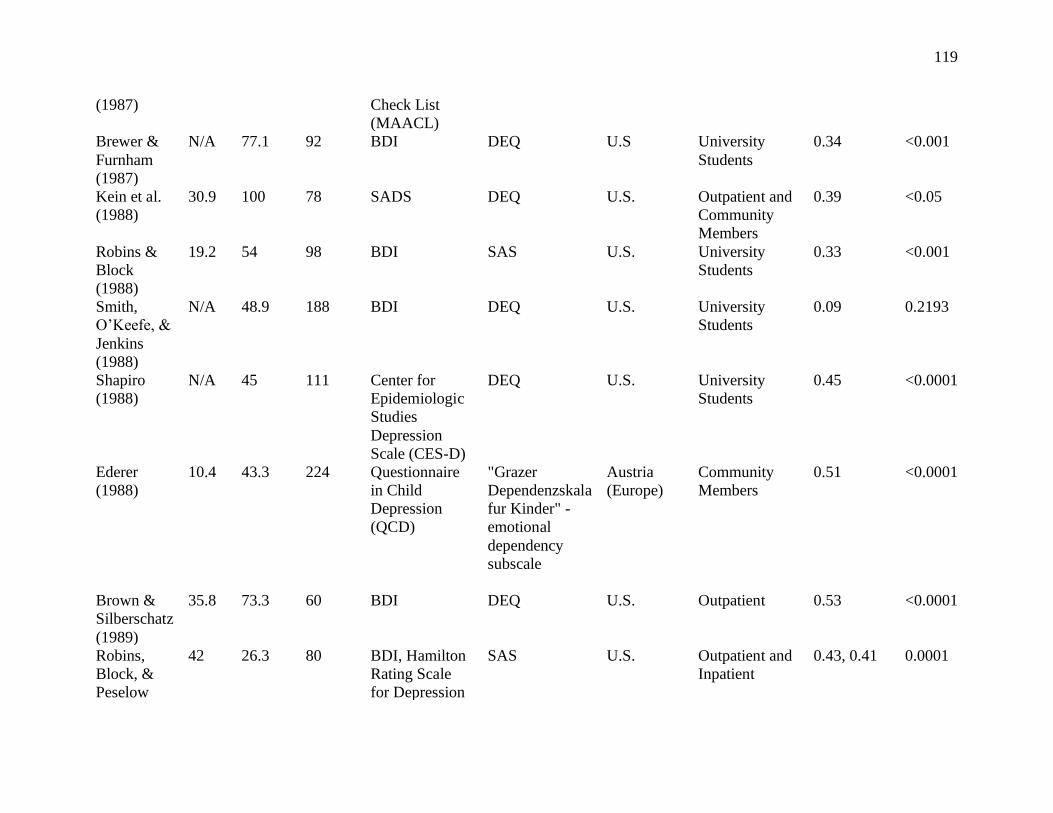
119
(1987) Check List
(MAACL)
Brewer &
Furnham
(1987)
N/A 77.1 92 BDI DEQ U.S University
Students
0.34 <0.001
Kein et al.
(1988)
30.9 100 78 SADS DEQ U.S. Outpatient and
Community
Members
0.39 <0.05
Robins &
Block
(1988)
19.2 54 98 BDI SAS U.S. University
Students
0.33 <0.001
Smith,
O’Keefe, &
Jenkins
(1988)
N/A 48.9 188 BDI DEQ U.S. University
Students
0.09 0.2193
Shapiro
(1988)
N/A 45 111 Center for
Epidemiologic
Studies
Depression
Scale (CES-D)
DEQ U.S. University
Students
0.45 <0.0001
Ederer
(1988)
10.4 43.3 224 Questionnaire
in Child
Depression
(QCD)
"Grazer
Dependenzskala
fur Kinder" -
emotional
dependency
subscale
Austria
(Europe)
Community
Members
0.51 <0.0001
Brown &
Silberschatz
(1989)
35.8 73.3 60 BDI DEQ U.S. Outpatient 0.53 <0.0001
Robins,
Block, &
Peselow
42 26.3 80 BDI, Hamilton
Rating Scale
for Depression
SAS U.S. Outpatient and
Inpatient
0.43, 0.41 0.0001

120
(1989) (HRSD)
Hirschfeld
et al. (1989)
37.3 438 SADS IDI U.S. Community
Members
0.05 .3191
Hammen,
Ellicott, &
Gitlin
(1989)
N/A 77.7 27 Diagnostic
Statistical
Manual, 3rd
edition, Text
Revised,
(DSM-III-TR)
SAS U.S. Outpatient 0.58 0.0015
Block &
Peselow
(1989)
42 26.3 80 SADS, HRSD SAS U.S. Outpatient and
Inpatient
0.42 0.0001
Mongrain
& Zuroff
(1989)
N/A N/A 275 BDI DAS, DEQ,
Anaclitic and
Introjective Life
Event Scales,
Anaclitic and
Introjective
Dysfunctional
Attitude Scales
Canada University
Students
0.19 <.10
Robins 1
(1990)
41 N/A 124 SADS SAS U.S. Outpatient and
Inpatient
0.42 0.0045
Robins 2
(1990)
41 N/A 82 BDI SAS U.S. University
Students
0.26 0.1
O’Neil &
Bornstein
(1991)
33.2 50 40 BDI ROD U.S. Inpatient 0.29 0.0695
Robins &
Luyten
(1991)
44.12 74 50 DSM-III-TR SAS U.S. Inpatient 0.32 <0.05
Birtchnell,
Deahl, &
N/A N/A 424 Depression
Screening
Self-Rating
Questionnaire,
U.S. Community
Members and
0.68 <0.001

121
Falowski
(1991)
Instrument,
(DSI)
(SRQ); IDI Inpatient
Overholser
(1991)
N/A N/A 43 DSM-III-TR,
Inventory of
Depressive
Symptomology,
(IDS)
IDI,
Dysfunctional
Attitude Scales
(DAS)
U.S.
Inpatient 0.30 0.0506
Franche &
Dobson
(1992)
N/A N/A 60 BDI IDI, DEQ U.S. Outpatient and
Community
Members
0.59 0.01
Segal et al.
(1992)
38.8 84.3 51 SADS, BDI DAS Canada Community
Members
0.13 0.36
Bagby et al.
(1992)
35.32 65.9 47 BDI, DSM-III-
TR, SADS
DEQ Canada Outpatient 0.17 0.2533
Rude &
Burnham
(1993)
N/A 72.4 421 BDI DEQ, SAS,
DAS
U.S. University
Students
0.17 <0.05
Mongrain
& Zuroff
(1994)
N/A 50 152 Positive and
Negative Affect
Mood Scales
DEQ U.S. University
Students
0.28 <0.0001
Lakey &
Ross (1994)
N/A 69.2 133 BDI, SADS DEQ U.S. University
Students
0.42 <0.0001
Bagby et al.
(1994)
36.6 N/A 74 HRSD DEQ Canada Outpatient 0.325 0.0047
Moore &
Blackburn
(1994)
40 61 118 SADS, BDI SAS U.S. Outpatient and
Inpatient
0.44 <0.001
Gilbert,
Allan, &
Trent
(1995)
32 74.6 79 BDI SAS U.S University
Students and
Outpatient
0.55 <0.001
Haaga et al.
(1995)
19.8 80 115 BDI, Inventory
to Diagnose
SAS U.S. University
Students
0.51 <0.05

122
Depression
(IDD)
Alford &
Gerrity
(1995)
N/A 62.5 112 BDI SAS U.S. University
Students
0.20 0.0345
Allen,
Horne, &
Trinder
(1996)
21.77 50 100 Self-Rating
Depression
Scale
SAS Australia University
Students
0.25 <.05
Veiel
(1996)
41 66 205 IDD, DSM-III Succourance’
scale of the
German
adaptation of
the Personality
Research Form
Germany Inpatient 0.12 0.0866
Alden &
Bieling
(1996)
19.6 100 107 BDI DEQ, Inventory
of Interpersonal
Problems –
Circumplex,
(IIP-C)
U.S. University
Students
0.325 0.0006
Moore &
Blackburn
(1996)
40 61 119 HRSD, BDI SAS U.S. Outpatient and
Inpatient
0.75 <0.0001
Fehon,
Grillo, &
Martino
(1997)
15.8 57 194 BDI DEQ-A
(Adolescent)
U.S. Inpatient 0.41 0.001
Zaretsky et
al. (1997)
40.4 58.4 142 DSM-III-TR,
HRSD
DAS U.S. Community
Members
0.25 0.003
Allen et al.
(1997)
80 70 80 DSM-III-TR,
HRSD
SAS U.S. Outpatient 0.35, 0.27
0.0051
Robins et
al. (1997)
39.8 59 103 DSM-IV, BDI,
SCL
SAS Canada Outpatient 0.23 0.0194

123
Brewin &
Firth-
Cozens
(1997)
22.4 39.6 318 Self-Rating
Depression
Scale (SRDS),
SCL
DEQ England University
Students
0.07, 0.11 <0.0001
Clark et al.
(1997)
36.57 52 2067 BDI, HRSD SAS U.S. Outpatient 0.09 0.6993
Sato &
McCann
(1997)
20.1 84 652 BDI SAS U.S. University
Students
0.42 <0.0001
Flett et al.
(1997)
19.8 52.8 176 CES-D SAS Canada University
Students
0.36 <0.01
Loas et al.
(1998)
21.54 84.2 202 BDI IDI U.S. University
Students
0.33 <0.0001
Rosenfarb
et al. (1998)
38.5 100 118 DSM-III, BDI DEQ U.S. Outpatient and
Community
Members
0.43 <0.0001
Fairbrother
& Moretti
(1998)
N/A N/A 68 BDI SAS Canada Outpatient and
Community
Members
0.48 <0.0001
Sato &
McCann
(1998)
20.9 75.4 652 BDI SAS, SAS,
Self-Construal
Scale (SCS)
Canada University
Students
0.42, 0.11 <0.0001
Zuroff et al.
(1999)
35 70 142 BDI, SCL DAS U.S. Outpatient 0.35 <0.0001
Sato &
McCann
(2000)
19.65 76,4 293 BDI SAS U.S. University
Students
0.42 0.05
Sato &
McCann
(2000)
20.18 52.5 255 BDI SAS U.S. University
Students
0.20 0.05
Rector et al.
(2000)
N/A 67 109 BDI DEQ U.S. Outpatient 0.18 0.01
Priel & 23 64.3 182 CES-D DEQ Israel University 0.20 0.0068

124
Shahar
(2000)
Students
Harkness &
Luther
(2001)
37.3 100 74 DSM-IV,
HRSD, BDI
Life Events and
Difficulties
Scale (LEDS) –
Dependent
Events
U.S. Community
Members
0.44 <0.0001
Beck et al.
(2001)
18.1 70 167 CES-D SAS U.S. University
Students
0.40 <0.01
Bieling &
Alden
(2001)
NA 70.7 82 DSM-III, BDI SAS Canaa Outpatient and
Community
0.30 Ns
Fresco et al.
(2001)
N/A 69.2 78 BDI SAS U.S. University
Students
0.30 <0.0076
Sprohge et
al. (2002)
32.3 52 146 DSM-III-TR ROD U.S. Outpatient and
University
Students
0.25 <0.0023
Raghavan,
Le, &
Berenbaum
(2002)
28.2 100 39 DSM-IV SAS U.S. Community
Members
0.43 <0.01
Sherry et al.
(2003)
36.1 N/A 350 BDI DAS Canada Outpatient,
Inpatient, and
University
Students
0.44, 0.18 <0.0001
Huprich et
al. (2004)
19.2 75 141 BDI, DSM-IV Dependent
Personality
Style Scale
(DPSS)
U.S. University
Students
0.24 0.0042
Besser &
Priel (2004)
69.64 51.5 237 CES-D DEQ Israel Community
Members
0.54 0.0001
Shahar et
al. (2004)
19.9 54 198 BDI DEQ U.S. University
Students
0.15 <0.05

125
Speranza et
al. (2004)
N/A N/A 1084 BDI DEQ, IDD France Outpatient 0.66, 0.44 <0.05
Mongrain
& Leather
(2006)
N/A 75 158 CES-D DEQ U.S. University
Students
0.23 0.001
Abela et al.
(2006)
N/A 86.3 102 BDI DEQ Canada Community
Members
0.25 0.05
Desmet et
al. (2006)
39.45 71.8 163 BDI DEQ Belgium Outpatient 0.16 0.0413
Allen et al.
(2006)
13.34 51.7 143 Childhood
Depression
Inventory
(CDI)
Emotional
dependency
upon closet
friend – 8-
minute
interaction,
observed
adolescent
autonomy and
relatedness with
peers, 8-minute
task
U.S. Community
members
0.03 0.7221
Westmas,
Ferrence, &
Wild
(2006)
41 56 210 CES-D SAS Canada Community
Members
0.24 <0.01
McBride,
Zuroff, &
Bagby
(2006)
N/A 84.8 151 BDI DEQ Canada University
Students
0.3 <0.0001
Cogswell,
Alloy, &
Spasojevic
(2006)
N/A 65 168 BDI, SADS DEQ U.S. University
Students
0.21 0.0063

126
Shih (2006) 19.08 50.5 99 DSM-IV, BDI SAS U.S. University
Students
0.32 <0.05
Mongrain
&
Blackburn
(2006)
N/A 67 97 IDD, DSM-IV,
CES-D
SAS Canada University
Students
0.29 0.0040
Frewen &
Dozois
(2006)
18.51 76 188 BDI SAS Canada University
Students
0.41 <0.001
Luyten et
al. (2007)
N/A 70.8 890 BDI DEQ U.S. Inpatient,
Outpatient,
Community, &
University
Students
.34, 0.25,
.0.40, 0.26,
0.27. 0.26,
0.19, 0.11,
0.28, 0.17,
0.19, 0.30
0.0175
Schulte,
Mongrain,
& Flora
(2008)
29.95 62.5 152 CES-D DEQ U.S. University
Students
0.64 0.001
Abu-Kaf &
Priel (2008)
22.33 68.8 192 CES-D DEQ Israel University
Students
0.20 <0.001
Vliegen &
Luyten
(2008)
N/A 100 299 BDI DEQ Belgium Outpatient and
Community
0.25 0.01
Permuy,
Merino, &
Fernandez-
Rey (2009)
21.26 86.8 164 BDI SAS U.S. University
Students
0.33 <0.05
Adams et
al. (2009)
10.6 45 49 CDI Children’s DEQ
(CDEQ)
Canada Community
Members
0.07 Ns
Cantazaro
& Wei
19.45 62 424 SDS DEQ, SAS U.S. University
Students
0.28 0.01

127
(2010)
Kopala-
Sibley &
Zuroff
(2010)
20.17 52.9 172 BDI DEQ U.S. University
Students
0.19 0.05
Campos,
Besser, &
Blatt (2010)
36.39 50 200 CES-D DEQ Portugal Community
Members
0.16 <0.05
Takagishi,
Sakata, &
Kitamura
(2011)
N/A 34.1 466 Hopkins
Symptom
Check List
(HSCL)
IDI Japan Community
Members
0.58 <0.0001
Calvete
(2011)
15.86 52 853 Youth Self-
Report
Adolescent
Cognitive Style
Questionnaire
(ACSQ);
Sociotropy
Scale for
Adolescents
Spain Community
Members
0.35 <0.0001
Sutton et al.
(2011)
16.9 69 550 Mood and
Anxiety
Symptom
Questionnaire
(MASQ); IDD
DAS, SAS U.S. Community
Members
0.46 <0.01
Nusslock et
al. (2011)
20.23 N/A 110 BDI, SADS SAS, DAS,
DEQ
U.S. Community
Members
0.20 0.0362
Liu et al.
(2012)
19.39 89 84 BDI DEQ Taiwan University
Students
0.39 0.01
Gonzales &
Jenkins
(2012)
N/A 54.4 217 BDI DEQ U.S. University
Students
0.36 0.01
Huprich,
Rosen, &
35.49 50.7 7174 Outcome
Questionnaire
Relationship
Profile Test
U.S. Outpatient 0.34 <0.0001

128
Kiss (2013) (OQ) (RPT)
Abi-Habib
& Luyten
(2013)
32.21 58.3 253 BDI DEQ Belgium Community
Members
0.26 <0.001
Kopala-
Sibley et al.
(2014)
12.57 42,7 241 CDI DEQ-A U.S. Community
Members
0.23 <0.001
Brewer &
Olive
(2014)
23 71 217 CES-D IDI England Community
Members
0.22 0.0011
Auberach,
Ho, & Kim
(2014)
13.99 59.2 157 CES-D,
Children’s
Depressive
Expereinces
Questionnaire,
(CDEQ)
ACSQ,
Adolescent Life
Events
Qsetionnaire-
Revised
(ALEQ)
Canada Community
Members
0.21 <0.05
Campos,
Mesquita,
Besser, &
Blatt (2014)
21.5 100 101 CES-D DEQ, ROD Portugal University
Students
0.27 0.0063
Casalin et
al. (2014)
29 63 281 BDI DEQ The
Netherlands
Community
Members
0.31 <0.001
Campos et
al. (2014)
16.4 49.4 346 CDI DEQ Portugal Community
Members
0.38 <0.01
Dinger et
al. (2015)
36.9 N/A 283 BDI DEQ Germany Inpatient and
Outpatient
0.11 0.05
Sturbman et
al. (2015)
20.02 71.8 163 CES-D DEQ U.S. University
Students
0.18 0.0215
Chui et al.
(2015)
37.5 61 149 HRSD DEQ U.S. Community
Members
0.39 0.04
Denckla,
Cosedine,
&
19 72 85 SCL RPT U.S. University
Students
0.40 <0.0001

129
Bornstein
(2016)
Shahar et
al. (2017)
54.84 N/A 428 CES-D SAS Israel Community
Members
0.40 <0.0001
Appendix C: References of Studies Included in Meta-Analysis
Abela, J. R., Webb, C. A., Wagner, C., Ho, M. R., & Adams, P. (2006). The role of self-criticism,
dependency, and hassles in the course of depressive Illness: A Multiwave Longitudinal
Study. Personality and Social Psychology Bulletin, 32(3), 328-338.
doi:10.1177/0146167205280911
Abi-Habib, R., & Luyten, P. (2013). The role of Dependency and Self-Criticism in the relationship
between anger and depression. Personality and Individual Differences, 55(8), 921-925.
doi:10.1016/j.paid.2013.07.466
Abu-Kaf, S., & Priel, B. (2008). Dependent and self-critical vulnerabilities to depression in two different
cultural contexts. Personality and Individual Differences, 44(3), 689-700.
doi:10.1016/j.paid.2007.10.002
Adams, P., Abela, J. R., Auerbach, R., & Skitch, S. (2009). Self-criticism, dependency, and stress
reactivity: An experience sampling approach to testing Blatt and Zuroff’s (1992) theory of
personality predispositions to depression in high-risk youth. Personality and Social Psychology
Bulletin, 35(11), 1440-1451. doi:10.1177/0146167209343811
Alden, L. E., & Bieling, P. J. (1996). Interpersonal Convergence of Personality Constructs in Dynamic
and Cognitive Models of Depression. Journal of Research in Personality, 30(1), 60-75.
doi:10.1006/jrpe.1996.0004
Alford, B. A., & Gerrity, D. M. (1995). The specificity of sociotropy-autonomy personality dimensions
to depression vs. Anxiety. Journal of Clinical Psychology, 51(2), 190-195. doi:10.1002/1097-
4679(199503)51:23.0.co;2-s

131
Allen, J. P., Insabella, G., Porter, M. R., Smith, F. D., Land, D., & Phillips, N. (2006). A social-
interactional model of the development of depressive symptoms in adolescence. Journal of
Consulting and Clinical Psychology, 74(1), 55-65. doi:10.1037/0022-006x.74.1.55
Allen, N. B., Horne, D. J., & Trinder, J. (1996). Sociotropy, autonomy, and dysphoric emotional
responses to specific classes of stress: A psychophysiological evaluation. Journal of Abnormal
Psychology, 105(1), 25-33. doi:10.1037/0021-843x.105.1.25
Allen, N. B., Ames, D., Layton, T., Bennetts, K., & Kingston, K. (1997). The relationship between
sociotropy/autonomy and patterns of symptomatology in the depressed elderly. British Journal of
Clinical Psychology, 36(1), 121-132. doi:10.1111/j.2044-8260.1997.tb01235.x
Bagby, R., Cox, B. J., Schuller, D. R., Levitt, A. J., Swinson, R. P., & Joffe, R. T. (1992). Diagnostic
specificity of the dependent and self-critical personality dimensions in major depression. Journal
of Affective Disorders, 26(1), 59-63. doi:10.1016/0165-0327(92)90035-5
Bagby, M. R., Schuller, D. R., Parker, J. D., Levitt, A., Joffe, R. T., & Shafir, S. M. (1994). Major
depression and the self-criticism and dependency personality dimensions. American Journal of
Psychiatry, 151(4), 597-599. doi:10.1176/ajp.151.4.597
Bekker, M. H., & Croon, M. A. (2010). The roles of autonomy-connectedness and attachment styles in
depression and anxiety. Journal of Social and Personal Relationships, 27(7), 908-923.
doi:10.1177/0265407510377217
Besser, A., & Priel, B. (2005). Interpersonal relatedness and self-definition In late adulthood depression:
Personality predispositions, and protective factors. Social Behavior and Personality: An
International Journal, 33(4), 351-382. doi:10.2224/sbp.2005.33.4.351
Bieling, P.J., Alden, L.E. (2001). Sociotropy, autonomy, and the interpersonal model of depression: An
integration. Cognitive Therapy and Research, 25(2), 167-184.

132
Birtchnell, J., Deahl, M., & Falkowski, J. (1991). Further exploration of the relationship between
depression and dependence. Journal of Affective Disorders, 22(4), 221-233. doi:10.1016/0165-
0327(91)90068-4
Blatt, S. J., Quinlan, D. M., Chevron, E. S., Mcdonald, C., & Zuroff, D. (1982). Dependency and self-
criticism: Psychological dimensions of depression. Journal of Consulting and Clinical
Psychology, 50(1), 113-124. doi:10.1037/0022-006x.50.1.113
Bornstein, R. F., Poynton, F. G., & Masling, J. (1985). Orality and depression: An empirical
study. Psychoanalytic Psychology, 2(3), 241-249. doi:10.1037/0736-9735.2.3.241
Brewer, G., & Olive, N. (2014). Depression in men and women: Relative rank, interpersonal
dependency, and risk-taking. Evolutionary Behavioral Sciences, 8(3), 142-147.
doi:10.1037/h0097761
Brewin, C. R., & Furnham, A. (1987). Dependency, self-criticism and depressive attributional
style. British Journal of Clinical Psychology, 26(3), 225-226. doi:10.1111/j.2044-
8260.1987.tb01350.x
Brewin, C. B., & Firth-Cozens, J. (1997). Dependency and self-criticism as predictors of depression in
young doctors. Journal of Occupational Health Psychology, 2(3), 242-246. doi:10.1037/1076-
8998.2.3.242
Brown, J. D., & Silberschatz, G. (1989). Dependency, self-criticism, and depressive attributional
style. Journal of Abnormal Psychology, 98(2), 187-188. doi:10.1037/0021-843x.98.2.187
Calvete, E. (2010). Integrating Sociotropy, Negative Inferences and Social Stressors as Explanations for
the Development of Depression in Adolescence: Interactive and Mediational
Mechanisms. Cognitive Therapy and Research, 35(5), 477-490. doi:10.1007/s10608-010-9320-4

133
Campos, R. C., Besser, A., & Blatt, S. J. (2010). The mediating role of self-criticism and dependency in
the association between perceptions of maternal caring and depressive symptoms. Depression
and Anxiety, 27(12), 1149-1157. doi:10.1002/da.20763
Campos, R. C., Besser, A., Morgado, C., & Blatt, S. J. (2013). Self-criticism, dependency, and
adolescents externalising and internalising problems. Clinical Psychologist, 18(1), 21-32.
doi:10.1111/cp.12024
Campos, R. C., Mesquita, I., Besser, A., & Blatt, S. J. (2014). Neediness and depression in
women. Bulletin of the Menninger Clinic, 78(1), 16-33. doi:10.1521/bumc.2014.78.1.16
Cantazaro, A., & Wei, M. (2010). Adult Attachment, Dependence, Self-Criticism, and Depressive
Symptoms: A Test of a Mediational Model. Journal of Personality. doi:10.1111/j.1467-
6494.2010.00645.x
Casalin, S., Luyten, P., Besser, A., Wouters, S., & Vliegen, N. (2014). A longitudinal cross-lagged study
of the role of parental self-criticism, dependency, depression, and parenting stress in the
development of child negative affectivity. Self and Identity, 13(4), 491-511.
doi:10.1080/15298868.2013.873076
Chui, H., Zilcha-Mano, S., Dinger, U., Barrett, M. S., & Barber, J. P. (2016). Dependency and self-
criticism in treatments for depression. Journal of Counseling Psychology, 63(4), 452-459.
doi:10.1037/cou0000142
Cogswell, A., Alloy, L. B., & Spasojevic, J. (2006). Neediness and Interpersonal Life Stress: Does
Congruency Predict Depression? Cognitive Therapy and Research, 30(4), 427-443.
doi:10.1007/s10608-006-9052-7
Clark, D.A., Steer, R.A., Haslam, N., Beck, A.T., & Brown, G.K. (1997). Cognitive Therapy and
Research, 213), 267-283.

134
Denckla, C. A., Consedine, N. S., & Bornstein, R. F. (2016). Self-compassion mediates the link between
dependency and depressive symptomatology in college students. Self and Identity, 16(4), 373-
383. doi:10.1080/15298868.2016.1264464
Desmet, M., Vanheule, S., & Verhaeghe, P. (2006). Dependency, self-criticism, and the symptom
specificity hypothesis in a depressed clinical sample. Social Behavior and Personality: An
International Journal, 34(8), 1017-1026. doi:10.2224/sbp.2006.34.8.1017
Dinger, U., Barrett, M. S., Zimmermann, J., Schauenburg, H., Wright, A. G., Renner, F., . . . Barber, J.
P. (2014). Interpersonal problems, dependency, and self-criticism in major depressive
disorder. Journal of Clinical Psychology, 71(1), 93-104. doi:10.1002/jclp.22120
Ederer, E. (1988). Dysthymia, psychosocial dependency, and self-esteem in ten-year-old boys and girls:
An empirical contribution to clinical personality research. Studia Psychologica, 30(3), 227-235.
Fairbrother, N., & Moretti, M. (1998). Sociotropy, autonomy, and self-discrepancy: Status in depressed,
remitted depressed, and control participants. Cognitive Therapy and Research, 22(3). 279-296.
Fehon, D. C., Grilo, C. M., & Martino, S. (2000). A comparison of dependent and self-critically
depressed hospitalized adolescents. Journal of Youth and Adolescence, 29(1), 93-106.
doi:10.1023/a:1005125322629
Flett, G.L., Hewitt, P.L., Garshowitz, M., & Martin, T.R. (1997). Canadian Journal of Behavioral
Science, 29(1), 28-37.
Franche, R., & Dobson, K. (1992). Self-criticism and interpersonal dependency as vulnerability factors
to depression. Cognitive Therapy and Research, 16(4), 419-435. doi:10.1007/bf01183166
Fresco, D. M., Sampson, W. S., Craighead, L. W., & Koons, A. N. (2001). The relationship of
sociotropy and autonomy to symptoms of depression and anxiety. Journal of Cognitive
Psychotherapy, 15(1), 17-31. doi:10.1891/0889-8391.15.1.17

135
Frewen, P. A., & Dozois, D. J. (2006). Social, achievement, and control dimensions of personality-life
event vulnerability to depression. Cognitive Therapy and Research, 30(1), 1-17.
doi:10.1007/s10608-006-9008-y
Haaga, D. A., Fine, J. A., Terrill, D. R., Stewart, B. L., & Beck, A. T. (1995). Social problem-solving
deficits, dependency, and depressive symptoms. Cognitive Therapy and Research, 19(2), 147-
158. doi:10.1007/bf02229691
Hammen, C., Marks, T., Mayol, A., & Demayo, R. (1985). Depressive self-schemas, life stress, and
vulnerability to depression. Journal of Abnormal Psychology, 94(3), 308-319. doi:10.1037/0021-
843x.94.3.308
Hammen, C., Ellicott, A., & Gitlin, M. (1989). Vulnerability to specific life events and prediction of
course of disorder in unipolar depressed patients. Canadian Journal of Behavioural Science /
Revue Canadienne Des Sciences Du Comportement, 21(4), 377-388. doi:10.1037/h0079841
Harkness, K. L., & Luther, J. (2001). Clinical risk factors for the generation of life events in major
depression. Journal of Abnormal Psychology, 110(4), 564-572. doi:10.1037/0021-
843x.110.4.564
Hirschfeld, R.M., Klerman, G.L., Gough, H.G., Barrett, J., Korchin, S.J., & Chodoff, P. (1977). Journal
of Personality Assessment, 41(6), 610-618.
Hirschfeld, R. M., Klerman, G. L., Lavori, P., Keller, M. B., Pamela, G., & Coryell, W. (1989).
Premorbid personality assessments of first onset of major depression. Archives of General
Psychiatry, 46(4), 345. doi:10.1001/archpsyc.1989.01810040051008
Huprich, S.K., Clancy, C., Bornstein, R.F., Nelson-Gray, R.O. (2004). Do dependency and social skills
combine to predict depression? Linking two diatheses in mood disorder research. Individual
Differences Research, 2(1). 2-16.

136
Gonzáles, D.A., & Jenkins, S.R. (2012). Dependency and depression: Mediation and moderation by
interpersonal problems. Paper presented at the120th meeting of the American Psychological
Association Convention, Orlando, Florida.
Hirschfeld, R. M., Klerman, G. L., Clayton, P. J., Keller, M. B., McDonald-Scott, P., & Barbara, L. H.
(1983). Assessing personality: Effects of the depressive state on trait measurement. American
Journal of Psychiatry, 140(6), 695-699. doi:10.1176/ajp.140.6.695
Huprich, S.K., Clancy, C., Bornstein, R.F., & Nelson-Gray, R.O. (2004). Do dependency and social
skills combine to predict depression? Linking two diatheses in mood disorders research.
Individual Differences Research, 2(1), 2-16.
Huprich, S., Rosen, A., & Kiss, A. (2013). Manifestations of interpersonal dependency and depressive
subtypes in outpatient psychotherapy patients. Personality and Mental Health, 7(3), 223-232.
doi:10.1002/pmh.1222
Klein, D. N., Harding, K., Taylor, E. B., & Dickstein, S. (1988). Dependency and self-criticism in
depression: Evaluation in a clinical population. Journal of Abnormal Psychology, 97(4), 399-
404. doi:10.1037/0021-843x.97.4.399
Klein, D. N., Harding, K., Taylor, E. B., & Dickstein, S. (1988). Dependency and self-criticism in
depression: Evaluation in a clinical population. Journal of Abnormal Psychology, 97(4), 399-
404. doi:10.1037/0021-843x.97.4.399
Kopala-Sibley, D. C., & Zuroff, D. C. (2010). Proximal predictors of depressive symptomatology:
Perceived losses in self-worth and interpersonal domains and introjective and anaclitic mood
states. Cognitive Behaviour Therapy, 39(4), 270-282. doi:10.1080/16506073.2010.501810
Kopala-Sibley, D. C., Zuroff, D. C., Hankin, B. L., & Abela, J. R. (2015). The development of self-
criticism and dependency in early adolescence and their role in the development of depressive

137
and anxiety symptoms. Personality and Social Psychology Bulletin, 41(8), 1094-1109.
doi:10.1177/0146167215590985
Lakey, B., & Ross, L. T. (1994). Dependency and self-criticism as moderators of interpersonal and
achievement stress: The role of initial dysphoria. Cognitive Therapy and Research, 18(6), 581-
599. doi:10.1007/bf02355670
Liu, E. T., Chen, W., Tsai, L., Wu, M., & Hong, C. (2012). Interpersonal mechanisms in the
relationships between dependency/self-criticism and depressive symptoms in taiwanese
undergraduates: A prospective study. Journal of Social and Clinical Psychology, 31(9), 972-
1006. doi:10.1521/jscp.2012.31.9.972
Loas, G., Verrier, A., Gayant, C., & Guelfi, J. D. (1998). Depression and dependency: Distinct or
overlapping constructs? Journal of Affective Disorders, 47(1-3), 81-85. doi:10.1016/s0165-
0327(97)00121-3
Luyten, P., Sabbe, B., Blatt, S. J., Meganck, S., Jansen, B., Grave, C. D., . . . Corveleyn, J. (2007).
Dependency and self-criticism: Relationship with major depressive disorder, severity of
depression, and clinical presentation. Depression and Anxiety, 24(8), 586-596.
doi:10.1002/da.20272
Mcbride, C., Zuroff, D. C., Bacchiochi, J., & Bagby, R. M. (2006). Depressive Experiences
Questionnaire: Does It Measure Maladaptive And Adaptive Forms Of Dependency? Social
Behavior and Personality: An International Journal, 34(1), 1-16. doi:10.2224/sbp.2006.34.1.1
Mongrain, M., & Zuroff, D. C. (1989). Cognitive Vulnerability to Depressed Affect in Dependent and
Self-Critical College Women. Journal of Personality Disorders, 3(3), 240-251.
doi:10.1521/pedi.1989.3.3.240

138
Mongrain, M., & Zuroff, D. C. (1995). Motivational and affective correlates of Dependency and Self-
Criticism. Personality and Individual Differences, 18(3), 347-354. doi:10.1016/0191-
8869(94)00139-j
Mongrain, M., & Blackburn, S. (2005). Cognitive vulnerability, lifetime risk, and the recurrence of
major depression in graduate students. Cognitive Therapy and Research, 29(6), 747-768.
doi:10.1007/s10608-005-4290-7
Mongrain, M., & Leather, F. (2006). Immature dependence and self-criticism predict the recurrence of
major depression. Journal of Clinical Psychology, 62(6), 705-713. doi:10.1002/jclp.20263
Moore, R. G., & Blackburn, I. (1994). The relationship of sociotropy and autonomy to symptoms,
cognition and personality in depressed patients. Journal of Affective Disorders, 32(4), 239-245.
doi:10.1016/0165-0327(94)90087-6
Moore, R. G., & Blackburn, I. (1996). The stability of sociotropy and autonomy in depressed patients
undergoing treatment. Cognitive Therapy and Research, 20(1), 69-80. doi:10.1007/bf02229244
Nusslock, R., Shackman, A. J., Harmon-Jones, E., Alloy, L. B., Coan, J. A., & Abramson, L. Y. (2011).
Cognitive vulnerability and frontal brain asymmetry: Common predictors of first prospective
depressive episode. Journal of Abnormal Psychology, 120(2), 497-503. doi:10.1037/a0022940
O’neill, R. M., & Bornstein, R. F. (1991). Orality and depression in psychiatric inpatients. Journal of
Personality Disorders, 5(1), 1-7. doi:10.1521/pedi.1991.5.1.1
Overholser, J. C. (1991). Categorical Assessment of the Dependent Personality Disorder in Depressed
Inpatients. Journal of Personality Disorders, 5(3), 243-255. doi:10.1521/pedi.1991.5.3.243
Permuy, B., Merino, H., & Fernandez-Rey, J. (2010). Adult attachment styles and cognitive
vulnerability to depression in a sample of undergraduate students: The mediational roles of

139
sociotropy and autonomy. International Journal of Psychology, 45(1), 21-27.
doi:10.1080/00207590903165059
Priel, B., & Shahar, G. (2000). Dependency, self-criticism, social context and distress: Comparing
moderating and mediating models. Personality and Individual Differences, 28(3), 515-525.
doi:10.1016/s0191-8869(99)00116-6
Raghavan, C., Le, H.N., & Berenbaum, H. (2002). Predicting dysphoria and hostility using the diathesis-
stress model of sociotropy and autonomy in a contextualized stress setting. Cognitive Therapy
and Research, 26(2), 231-244.
Robins, C.J., Bagby, M.R., Rector, N.A., Lynch, T.R., & Kennedy, S.H. (1997). Sociotropy, autonomy,
and patterns of symptoms in patients with major depression: A comparison of dimensional and
categorical approaches. Cognitive Therapy and Research, 21(3). 285-300.
Rector, N.A., Bagby, M., Segal, Z.V., Joffe, R.T., & Levitt, A. (2000). Self-criticism and dependency in
depressed patients treated with cognitive therapy or pharmacotherapy. Cognitive Therapy and
Research, 24(5), 571-584.
Robins, C. J., & Block, P. (1988). Personal vulnerability, life events, and depressive symptoms: A test of
a specific interactional model. Journal of Personality and Social Psychology, 54(5), 847-852.
doi:10.1037/0022-3514.54.5.847
Robins, C. J., Block, P., & Peselow, E. D. (1989). Relations of sociotropic and autonomous personality
characteristics to specific symptoms in depressed patients. Journal of Abnormal
Psychology, 98(1), 86-88. doi:10.1037/0021-843x.98.1.86
Robins, C. J., Block, P., & Peselow, E. D. (1989). Relations of sociotropic and autonomous personality
characteristics to specific symptoms in depressed patients. Journal of Abnormal
Psychology, 98(1), 86-88. doi:10.1037/0021-843x.98.1.86

140
Robins, C. J. (1990). Congruence of personality and life events in depression. Journal of Abnormal
Psychology, 99(4), 393-397. doi:10.1037/0021-843x.99.4.393
Robins, C. J., & Luten, A. G. (1991). Sociotropy and autonomy: Differential patterns of clinical
presentation in unipolar depression. Journal of Abnormal Psychology, 100(1), 74-77.
doi:10.1037/0021-843x.100.1.74
Rosenfarb, I. S., Becker, J., Khan, A., & Mintz, J. (1998). Dependency and self-criticism in bipolar and
unipolar depressed women. British Journal of Clinical Psychology, 37(4), 409-414.
doi:10.1111/j.2044-8260.1998.tb01398.x
Sato, T., & Mccann, D. (1997). Vulnerability factors in depression: The facets of sociotropy and
autonomy. Journal of Psychopathology and Behavioral Assessment, 19(1), 41-62.
doi:10.1007/bf02263228
Sato, T., & Mccann, D. (1998). Individual differences in relatedness and individuality: An exploration of
two constructs. Personality and Individual Differences, 24(6), 847-859. doi:10.1016/s0191-
8869(98)00020-8
Sato, T., & Mccann, D. (2000). Sociotropy-Autonomy and the Beck Depression Inventory. European
Journal of Psychological Assessment, 16(1), 66-76. doi:10.1027//1015-5759.16.1.66
Schulte, F. S., Mongrain, M., & Flora, D. B. (2008). Healthy and unhealthy dependence: Implications
for major depression. British Journal of Clinical Psychology, 47(3), 341-353.
doi:10.1348/014466508x299682
Segal, Z. V., Shaw, B. F., Vella, D. D., & Katz, R. (1992). Cognitive and life stress predictors of relapse
in remitted unipolar depressed patients: Test of the congruency hypothesis. Journal of Abnormal
Psychology, 101(1), 26-36. doi:10.1037/0021-843x.101.1.26

141
Shahar, G., Lerman, S. F., Topaz, M., Brill, S., Shalev, H., & Rudich, Z. (2017). Depressive personality
vulnerability in chronic physical pain: Centrality of sociotropy. Journal of Personality, 86(6),
907-918. doi:10.1111/jopy.12365
Shapiro, J. P. (1988). Relationships between Dimensions of Depressive Experience and Evaluative
Beliefs about People in General. Personality and Social Psychology Bulletin, 14(2), 388-400.
doi:10.1177/0146167288142016
Sherry, S. B., Hewitt, P. L., Flett, G. L., & Harvey, M. (2003). Perfectionism dimensions, perfectionistic
attitudes, dependent attitudes, and depression in psychiatric patients and university
students. Journal of Counseling Psychology, 50(3), 373-386. doi:10.1037/0022-0167.50.3.373
Shih, J. H. (2006). Sex Differences in Stress Generation: An Examination of Sociotropy/Autonomy,
Stress, and Depressive Symptoms. Personality and Social Psychology Bulletin, 32(4), 434-446.
doi:10.1177/0146167205282739
Smith, T. W., Okeeffe, J. L., & Jenkins, M. (1988). Dependency and self-criticism: Correlates of
depression or moderators of the effects of stressful events? Journal of Personality
Disorders, 2(2), 160-169. doi:10.1521/pedi.1988.2.2.160
Speranza, M., Corcos, M., Stéphan, P., Loas, G., Pérez-Diaz, F., Lang, F., . . . Jeammet, P. (2004).
Alexithymia, Depressive Experiences, and Dependency in Addictive Disorders. Substance Use
& Misuse, 39(4), 551-579. doi:10.1081/ja-120030058
Sprohge, E., Handler, L., Plant, D. D., & Wicker, D. (2002). A Rorschach Study of Oral Dependence in
Alcoholics and Depressives. Journal of Personality Assessment, 79(1), 142-160.
doi:10.1207/s15327752jpa7901_09
Sturman, E. D., Rose, S., Mckeighan, K. M., Burch, J., & Evanico, K. (2015). Personality and the
generation of defeat, involuntary subordination, and depression. Canadian Journal of

142
Behavioural Science / Revue Canadienne Des Sciences Du Comportement, 47(1), 47-58.
doi:10.1037/a0036896
Sutton, J. M., Mineka, S., Zinbarg, R. E., Craske, M. G., Griffith, J. W., Rose, R. D., . . . Mor, N. (2010).
The relationships of personality and cognitive styles with self-reported symptoms of depression
and anxiety. Cognitive Therapy and Research, 35(4), 381-393. doi:10.1007/s10608-010-9336-9
Takagishi, Y., Sakata, M., & Kitamura, T. (2011). Effects of self-esteem on state and trait components
of interpersonal dependency and depression in the workplace. Journal of Clinical
Psychology, 67(9), 918-926. doi:10.1002/jclp.20815
Viel, H.O.F. (1996). Gender differences in the role of interpersonal dependency in depression.
Interpersonal factors in the origin and course of affective disorders. 168-189.
Vliegen, N., & Luyten, P. (2008). The role of Dependency and Self-Criticism in the relationship
between postpartum depression and anger. Personality and Individual Differences, 45(1), 34-40.
doi:10.1016/j.paid.2008.02.015
Welkowitz, J., Lish, J. D., & Bond, R. N. (1985). The depressive experiences questionnaire: Revision
and validation. Journal of Personality Assessment, 49(1), 89-94.
doi:10.1207/s15327752jpa4901_17
Westmaas, J. L., Ferrence, R., & Wild, T. C. (2006). Autonomy (vs. sociotropy) and depressive
symptoms in quitting smoking: Evidence for trait-congruence and the role of gender. Addictive
Behaviors, 31(10), 1744-1760. doi:10.1016/j.addbeh.2005.12.013
Zaretsky, A. E., Fava, M., Davidson, K. G., Pava, J. A., Matthews, J., & Rosenbaum, J. F. (1997). Are
Dependency and Self-Criticism Risk Factors for Major Depressive Disorder? The Canadian
Journal of Psychiatry, 42(3), 291-297. doi:10.1177/070674379704200307

143
Zuroff, D. C., & Mongrain, M. (1987). Dependency and self-criticism: Vulnerability factors for
depressive affective states. Journal of Abnormal Psychology, 96(1), 14-22. doi:10.1037/0021-
843x.96.1.14
Zuroff, D. C., Blatt, S. J., Sanislow, C. A., Bondi, C. M., & Pilkonis, P. A. (1999). Vulnerability to
depression: Reexamining state dependence and relative stability. Journal of Abnormal
Psychology, 108(1), 76-89. doi:10.1037/0021-843x.108.1.76





























