Embed Size (px)
Citation preview
MOOD DISORDERS 0193-953>(/96 $0.00 + .20
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER
John C. Markowitz, MD
In the past 20 years, psychotherapy research has demonstrated the efficacy of time-limited, active talking treatments for acute major depression. Both cognitive behavioral therapy (CBT)s and interpersonal psychotherapy (IPT)32 have shown efficacy in comparative clinical trials, both of them demonstrating superiority to placebo and, to varying degrees, holding their own in comparison to antidepressant medication.s,
Yet major depression, it may be argued, is a heterogeneous disorder with a relatively high placebo response rate. How does such focused psychotherapy perform in the face of chronic depression?
For most of this century, chronic depression was considered a temperamental or character disorder, that is, depressive personality dis-
Its preferred treatment was felt to be psychotherapy, and it generally was considered to have a poor progn~sis .~ In 1980, however, a key act of the authors of DSM-I11 was to reconceptualize chronic depression as dysthymic disorder, as an affective syndrome rather than a personality disorder. This nosologic shift encouraged successful trials of antidepressant pharmacotherapy'j, 12, 25, 27, 36, 37, 59, for dysthymic disor- der. As psychotherapy trials have not been as quick to follow, medica-
Presented in part at the NIMH Workshop on Subsyndromal Mood Disorders: Dysthy- mia and Cyclothymia, Bethesda, MD, April 1993; and at the 146th Annual Meeting of the American Psychiatric Association, San Francisco, CA, May 1993; and at the NIMH Work- shop on the Effectiveness and Cost of Psychotherapy, Tyson's Comer, VA, January 1994.
Portions of text adaptedfrom Markowitz JC: Psychotherapy of dysthymia. Am J Psychia- try 151:1114-1121, 1994; 0 1994, American Psychiatric Association; with permission.
Supported in part by grant MH-19069 from the National Institute of Mental Health.
From the Department of Psychiatry, Come11 University Medical College, Payne Whitney Clinic, The New York Hospital-Cornell Medical Center, New York, New York
THE PSYCHIATRIC CLINICS OF NORTH AMERICA
VOLUME 19 * NUMBER 1 - MARCH 1996 133
134 MARKOWITZ
tion should for now be considered the de facto treatment of choice for chronic depression.
In 1984, shortly after the reclassification of dysthymic disorder, Weissman and AkiskaF5 proposed research on psychotherapeutic ap- proaches to dysthymic disorder. Noting that only "indirect" evidence existed for psychotherapeutic efficacy in chronic depression, they en- couraged trials to assess short-term interpersonal, cognitive, and behav- ioral therapies, either alone or in combination with medi~at ion.~~ Since then, diagnosis has been honed with greater precision in DSM-III-R (dysthymia) and DSM-IV (back to dysthymic di~order) .~ The high preva- lence,3°* 66 and comorbiditp 66 of dysthymic disorder are better understood. Indeed, the damage dysthymic disorder deals to quality of life and social and occupational functioning appears to out- weigh that of major depres~ion,6~ although the latter receives far more research attention. Dysthymic disorder should no longer be considered "subsyndromal" but a major public health problem.
Clinicians are becoming increasingly aware of controlled clinical trials demonstrating the efficacy of antidepressant medication for many dysthymic patients.6, 12, 25, 27, 36, 37, 59, 63 There have been few controlled psychotherapy trials for dysthymic disorder. Yet dysthymic patients are known to make frequent use of mental health services,66 and it is com- monly assumed that they comprise substantial proportions of many, if not most, psychotherapeutic practices.
As medication can so effectively treat dysthymic disorder, what is the rationale for antidysthymic psychotherapy? Roughly half of dysthy- mic patients do not respond to antidepressant medication. Others de- velop intolerable side effects, or hypomania,' or simply refuse medica- tion. Pregnancy and other medical conditions may be relative contraindications to medication. About 3% of American adults have dysthymic disorder.30, 66 Dysthymic individuals frequently use mental health many visiting nonpsychiatrists who cannot prescribe medication. Thus, despite the ascendancy of antidepressant medication as a quasi-standard treatment for this condition, antidysthymic psycho- therapy remains potentially important. The limitations of antidepressant medication and the treatment preferences of patients and therapists argue for the development of effective psychotherapeutic interventions. Moreover, dysthymic disorder offers a research challenge to psychoth5r- apeutic efficacy because of its low placebo response rate.36
This article reviews outcome research on dysthymic disorder that used psychotherapy either alone or in combination with antidepressant medication. The author searched the literature using a computerized data base and checking selections under "chronic depression," "dysthymia," "dysthymic disorder," and "psychotherapy" from Ex- cerpta Medica: Psychiatry (Database on CD-ROM) (Silverplatter Version 3.1 1, Amsterdam, Elsevier Science Publishers, 1980-1993). This review includes all studies that reported psychotherapy treatment outcome for dysthymic patients excepting studies of late-life chronic major depres- sion. Distinctions to keep in mind for this literature include those be-
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 135
tween "pure" dysthymic disorder (i.e., occurring without meeting crite- ria for a major depressive episode) and "double depression" (major depression superimposed on dysthymic disorder), early versus late onset of dysthymic disorder, full versus partial remission, and treatment with psychotherapy alone versus combined pharmaco/p~ychotherapy.~~, 42
The author believes that "pure" dysthymic disorder and "double depre~sion,"~~ which differ in number of symptoms while sharing insidi- ous onset and chronicity, are more alike than different. Although Weiss- man and Akiskal argued that late-onset chronic depression-essentially unresolved acute depression-might have a better prognosis, most stud- ies have addressed early-onset dysthymic disorder. (This article does not address the former syndrome, which DSM-IV4 discriminates as chronic major depression.)
PSYCHOTHERAPY STUDIES
Akiskal, in 1980, cited Donald Klein, MD, and "[referring] clinicians' beliefs" in claiming that chronic depression not only responded poorly to pharmacotherapy but that "various forms of psychotherapy [were] equally disappointing" (reference 3, p. 778). This comment appears to reflect the general view of psychotherapy with long depressed, hopeless, masochistic, self-sabotaging patients, albeit such pessimism is hard to find explicit in the literature. A recent description of masochistic charac- ter, whose author distinguishes it from but says it often overlaps with dysthymic disorder, expresses this clinical sentiment:
They are the patients who unconsciously provoke their therapists either to give up on them, or sadistically abuse them with premature and unempathic interpretations, or pejoratively dismiss them with the misdiagnosis of borderline personality disorder or passive aggressive personality disorder. . . . But whatever the unconscious motives may be in an individual case, the final behavioral outcome is the achievement of what Theodor Reik (1941) called "victory through defeat," and often the defeat is a failed psychiatric treatment.56
Prior to beginning our own psychotherapy research on dysthymic disorder, we assessed clinical opinion to determine whether the progno- sis was universally believed to be so grim. We surveyed 43 clinicians and researchers about their experience in treating forms of chronic depression. Thirty-two (74%) responded, including 25 (58%) who com- pleted our questionnaires. They reported a mean 70.7% rate of improve- ment among patients treated either with some form of psychotherapy alone, or combined psychopharmacotherapy.46 This impressionistic find- ing contradicted the apparently prevailing opinion of a bleak prognosis.
The few psychotherapy studies of dysthymic disorder generally suffer from methodologic weakness, small sample size, or both. The reader should weigh psychotherapeutic efficacy in these studies against
136 MARKOWITZ
the low placebo response rate of dysthymic patients, which is less than 15% for doubly depressed and probably in the range of 19% to 24% for “pure” dysthymic patients.25, 63 Among methodologic issues are the number of treating psychotherapists involved, the generalizabil- ity of their technique, the use of adherence monitoring, and the charac- teristics of the patient population (e.g., inclusion of prior treatment failures). Readers also should note the studies’ definitions of response and length of follow-up.
Psychodynamic Psychotherapy and Psychoanalysis
The recent psychoanalytic literature pays meager attention to de- pression generally, and to dysthymic disorder in parti~u1ar.l~. 28, 56,
Because psychoanalysts have not focused on diagnostic issues, their work rarely differentiates acute and chronic forms of depression. The best work (e.g., references 5 and 11) has provided rich insights about depressed patients, suggested interpersonal techniques, but offered no outcome data. In the 1970s, some authors iterated the historical con- tention that psychodynamic psychotherapy was the treatment of choice for chronic depre~sion.~, 14, 28 Unfortunately, there has been no published psychodynamic research on dysthymic disorder, no treatment manuals or trials. Recent reviews of supportive dynamic psychotherapy do not mention dysthymic 54 Hence although psychotherapists con- tinue to prescribe long-term psychodynamic therapy for dysthymic pa- tients, there is no evidence that either short- or long-term psychody- namic treatment benefits such patients. We as dysthymia treatment researchers hear, admittedly from a selected sample of psychodynamic treatment failures, that years of such treatment often have provided insights about depression, but little relief from it.
One potential difficulty with a psychoanalytically oriented approach to dysthymic disorder involves the confusion of chronic mood state with personality trait. In dysthymic disorder of insidious early onset, whose chronicity is often as long as the patient can recall, personality trait and chronic mood disorder easily can be confused by both patient and therapist. Dysthymic patients are the first to attribute their problems to a personality defect. Using a conflictual rather than a medical model of psychopathology, psychoanalytically oriented therapists may tend to “blame the victim” by agreeing to assign the patient responsibility for his or her mood disorder.16 Analytic abstinence and neutrality also may be contraindicated for patients whose outlooks are distorted by a chronically depressed mood. They instead may need active support, even therapeutic cheerleading, to balance their perspective.
Cognitive-Behavioral Therapy
Cognitive behavioral therapy (CBT) is a structured, time-limited psychotherapy developed by Beck and colleagues.8 Its efficacy in the
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 137
treatment of acute major depression has been demonstrated in multiple clinical trials. The CBT therapist focuses on the “automatic” negative thoughts that depressed patients report about themselves, their situa- tions, and their future. Patients learn, in rational discussions with their therapists and through written and behavioral homework assignments, to modify irrationally negative thoughts. As they do, their depression improves.
Several cognitive approaches have been tested in treating dysthymic patients (Table 1). Gonzalez and colleaguesz2 treated 113 patients with 12 2-hour individual or group sessions of a skills-training-oriented psy- choeducational approach over 2 months, with follow-up sessions at 1 and 6 months after the acute treatment. They found that subjects having acute major depression, according to Research Diagnostic Criteria (RDC)158 were more likely to recover (75%) than those with (chronic) intermittent depression (43%) or ”double depression” (27%). Recovery was defined as 8 weeks essentially symptom-free, with a rating of 1 or 2 on the Longitudinal Interval Follow-up Evaluation (LIFE).55 Follow-up varied between 1 and 3 years. The number of therapists is unstated.
De Tong et all7 treated 30 unmedicated inpatients who met DSM-I11 criteria for both dysthymic disorder and major depression (i.e., double depression) and whose family histories were negative for mood disor- der. A 2- to 3-month trial of combined activity scheduling, social compe- tence training, and cognitive restructuring yielded a higher response rate (60%) than either cognitive restructuring alone (30%) or waiting list
Table 1. REPORTS OF COGNITIVE-BEHAVIORAL THERAPY FOR DYSTHYMIC DISORDER
Number of Response Follow-up Study Subjects Treatment Intensity (“h) (Months) Remarks
Gonzalez et aIz2
de Jong et all9
Fennel1 & Teasdalelg
Harpin et aIz4
Stravynski et
McCul lo~gh~~
Mercier et a149
aP2
TOTALS
28 dysthymic
26 double 10 double
5
6
6
20
8 dysthmic 7 double -
116
12 2-hr sesssionsl8 weeks
2-3 months inpatient
20 sessions/l 2 weeks
20 sessions/l 0 weeks
15 sessions + 25 mg TCA
14-44 C-BASP sessions
12-1 6 sessions
43
27 60*
20
33
67
50
38 43
41 -
12 Individual or group
36 RDC criteria psychotherapy
6 DSM-Ill criteria CR and waiting
list comparisons - RDC criteria
HAM-D 23 + 17 6 HAM-D26+ 16
Waiting list control 6 DSM-Ill criteria
24 DSM-Ill criteria
6 DSM-Ill criteria
HAM-D 24 + 9
9 remitted at 2 yrs
Double = double depression; RDC = Research Diagnostic Criteria; CR = cognitive restructuring:
*Three early dropouts omitted from outcome analysis. From Markowitz JC: Psychotherapy of dysthymia. Am J Psychiatry 151:1114-1121, 1994, 0 1994,
TCA = tricyclic antidepressant; C-BASP = Cognitive-Behavioral Analysis System of Psychotherapy.
American Psychiatric Association; with permission.
138 MARKOWITZ
status (10%). Response was defined as meeting two of the following three criteria: post-treatment Beck Depression Inventory (BDI)7 score of less than or equal to 14 or a greater than or equal to 50% reduction from pretreatment BDI, and a greater than or equal to 50% reduction from pretreatment on two infrequently used treatment scales. The analyses omitted three early dropouts from the two active treatments. Follow-up of a subsample (n = 14) at 6 months suggested stable treatment effects. This study is idiosyncratic in its use of inpatients, its specification of a negative family history of depression (suggesting a nonmood disorder), and its outcome measurements.
Fennel1 and Teasdale19 treated five subjects who met RDC for major depressive disorder. They had Hamilton Depression Rating Scale (HAM- D)23 scores of at least 15 (mean HAM-D = 23), BDI scores of at least 20 (mean BDI = 31), and a duration of depression ranging from 18 months (less than the 2-year temporal criterion for dysthymic disorder) to 16 years. These subjects had failed to respond to an (undefined) "adequate trial" of antidepressant medication. Therapists with 3 months of CBT training provided patients with 20 sessions over 4 months. Improve- ments were "modest": mean HAM-D score fell from 22.8 to 17.4 and BDI from 30.8 to 21.4. Only one subject clearly improved (BDI 5 9). The authors attributed lack of improvement to the chronicity of the patients' depressions.
Harpin et alZ4 identified 12 subjects whose chronic depression aver- aged 18 years in duration, who had an intake HAM-D score of greater than or equal to 20, and who had failed an (unspecified) exposure to antidepressant medication. Subjects were assigned alternately to 10 weeks of twice weekly CBT or to a waiting list control. Therapy focused on the remediation of interpersonal difficulties; subjects also received 25 mg [sic] of tricyclic antidepressant medication daily. The six subjects receiving active treatment had a significant ( t = 2.37, df = 5, P < 0.05) fall in HAM-D from 26.0 2 6.4 to 16.3 2 14.6, whereas the mean waiting list HAM-D did not change. Because of the small sample size, the between group difference in HAM-D change score was not statistically significant; and the mean final HAM-D of 16 suggests limited clinical benefit as well. At 6-month follow-up, subjects who had received active treatment still had lowered anxiety, but HAM-D scores no longer dif- fered significantly from pretreatment. Two of six treated patients showed major pre- to post-treatment improvement on the HAM-D, and one maintained this at the 6-month follow-up, whereas no control subjects improved.
Using 15 hourly sessions of CBT, Stravynski et aP2 treated six patients clinically diagnosed as having DSM-I11 dysthymic disorder. Two additional dysthymic subjects were excluded for comorbid narcis- sistic and dependent personality disorders. Independent raters noted "significant improvement" at termination and at 6-month follow-up: HAM-D fell from 23.7 f 2.6 to 9.3 f 1.8 post-treatment and 8.5 f 9.8 at 6 months, and BDI fell from 26.3 2 3.1 to 11.7 * 4.5 post-treatment and 10.9 f 8.9 at 6 months. Four subjects no longer met criteria for
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 139
dysthymic disorder at the end of treatment. The authors suggested that the responders had had dysthymic disorder with a discrete onset defined by a precipitating life event.
McC~l lough~~ described 10 cases of DSM-I11 dysthymic disorder treated with his manualized Cognitive-Behavioral Analysis System of Psychotherapy in 14 to 44 weekly sessions; the mean length was 31 2 9.3 sessions. Eight had double depression (J. McCullough, personal communication, April 1993). All reached termination criteria, which were defined by BDI and Rotter Locus of Control Scale scores of less than or equal to 10. Nine cases remained in remission 2 years later. Of an original cohort of 20, 4 did not complete therapy and the remaining 6 were unavailable for follow-up; following the author's methodology, their data were not evaluated (J. McCullough, personal communication, May 1993).
Mercier and colleagues49 used a 12- to 16-week trial of standard CBT to treat 15 DSM-I11 dysthymic patients among a sample of patients with atypical depression. Three of eight subjects with dysthymic disor- der alone and three of seven with double depression responded. All responders had been depressed for at least 7 years. Response upon completing CBT was defined as a Clinical Global Im~ress ion~~ score of 1 to 2 (very much or much improved), indicating a major reduction in the psychopathologic condition and no need for additional treatment. Of all the depressed subjects who remitted during CBT, 69% maintained improvement over a 6-month follow-up that included 4 preplanned booster sessions. The authors do not report the rate of sustained remis- sion among the subset of dysthymic patients.
In summary, the literature contains seven reports of cognitive be- havioral treatments of dysthymic patients. Most treated small, idiosyn- cratic samples (e.g., inpatients, varying degrees of antidepressant nonre- sponse) and used varying outcome measures. None monitored therapist adherence to the psychotherapy protocol, and most 39, 49, 62
reflect the work of a single therapist. Most studies did include some degree of follow-up assessment, an appropriate consideration for treat- ment of a chronic disorder. If the results have not been dramatic, they do indicate that some dysthymic patients respond to brief cognitive therapies. The cumulative Pesponse rate of 41% (Table 1) indeed ap- proaches the level of efficacy reported in controlled trials of antidepres- sant medi~a t ion .~~ Because of the scarcity of evidence, however, such hopeful conclusions must be considered preliminary.
Interpersonal Therapy
Interpersonal therapy (IPT), like CBT, is a time-limited, manualized, psychotherapy that has demonstrated efficacy in controlled clinical trials for outpatient major depression32 and an increasing range of other diag- n o s e ~ . ~ ~ The IPT therapist helps the patient recognize links between mood and current interpersonal experiences, focusing the therapy on
140 MARKOWJTZ
one of four interpersonal problem areas: grief, role dispute, role transi- tion, or interpersonal deficits.’ Depression is explained as a medical illness rather than a personality defect, and the patient is given the sick
IPT has shown benefit for treatment of acute depression32 as well as prophylaxis against recurrent major depression.20
The NIMH Treatment of Depression Collaborative Research Pro- gram*s, 57 focused on major depression but did include subjects with “double depression” (RDC-defined major depression plus chronic minor depression or intermittent depressive disorder). Of 71 (29.8%) subjects with double depression randomized to treatment with IPT, CBT, imipra- mine, or placebo, 43 (26.7%) completed the trial. Exploratory analyses found double depression to be associated with greater initial depressive severity, to predict poorer placebo response, and to predict higher symp- tom severity at termination and incomplete response across treatment condition^.^^ Thus chronicity and severity of mood disorder appeared to predict poorer outcome, albeit not lack of improvement, in standardized treatments for major depression.
Interpersonal approaches have been suggested to treat dysthymic disorder2, 13, 21, 26, 65 in recognition of the interpersonal difficulties dysthy- mic patients encounter. Researchers at Cornell have developed a manual that adapts IPT to dysthymic disorder (IPT-D).44 Among its adaptations is the use of the formal diagnosis of dysthymic disorder in the therapy as a novel form of interpersonal role transition: that is, a transition for a patient who has previously seen him- or herself as character disordered to the recognition of the problem as chronic depression, and a subse- quent movement from dysthymic disorder into euthymia. Another ob- servation is the need to meet the patient’s pessimism with an equal and opposite optimism. Therapists are regularly supervised and monitored for treatment adherence.
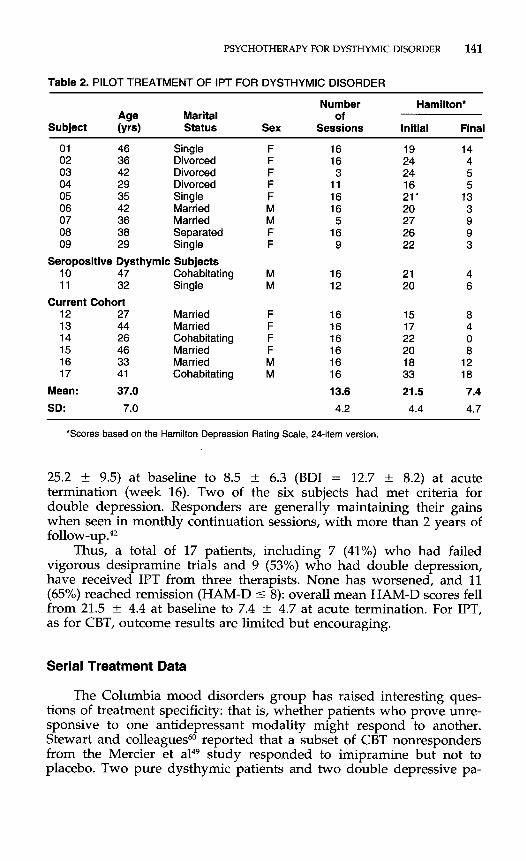
Pilot data include three small series of subjects (Table 2). In the first, Mason et a148 treated nine dysthymic subjects with IPT: five women who failed to respond to a vigorous DMI trial, and four subjects who refused medication. Mean age was 37 f 5.4 (SD) years; most reported protracted dysthymic disorder (mean duration 22.4 +- 18.9 years, omitting the first 5 years of life). Seven met criteria for double depression. Subjects re- ceived 12.0 ? 4.9 sessions of IPT (range, 3-16). Initial HAM-D scores foF the group averaged 19.4 ? 5.0. Scores fell for all subjects; mean HAM- D at termination was 7.4 ? 3.8. When compared in a quasi-experimental design to randomly chosen dysthymic subjects treated with DMI, IPT response and medication response were equivalent.
A separate project using IPT to treat depressed HIV-seropositive individuals included two dysthymic subjects. These white gay men, ages 47 and 32 years, reported lifelong depression. Despite the added stress of HIV infection, they improved on HAM-D from a mean score of 20.5 at intake to 5.0 at termination of IPT (12 and 16 sessions, re~pectively).~~
We are continuing to test the efficacy of IPT-D with additional therapists. Two therapists have thus far completed treatment on six subjects, producing drops in HAM-D scores from 20.8 +- 6.4 (BDI =
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 141
Table 2. PILOT TREATMENT OF IPT FOR DYSTHYMIC DISORDER
Number Hamilton* Age Marital of
Subject (yrs) Status Sex Sessions Initial Final
01 46 Single 02 36 Divorced 03 42 Divorced 04 29 Divorced 05 35 Single 06 42 Married 07 36 Married 08 38 Separated 09 29 Single
Seropositive Dysthymic Subjects 10 47 Cohabitating 1 1 32 Single
12 27 Married 13 44 Married 14 26 Cohabitating 15 46 Married 16 33 Married 17 41 Cohabitating
Current Cohort
Mean: 37.0
SD: 7.0
M M
16 16 3
1 1 16 16 5 16 9
16 12
16 16 16 16 16 16 13.6
4.2
19 14 24 4 24 5 16 5 21 - 13 20 3 27 9 26 9 22 3
21 4 20 6
15 8 17 4 22 0 20 8 18 12 33 18 21.5 7.4
4.4 4.7
'Scores based on the Hamilton Depression Rating Scale, 24-item version.
25.2 2 9.5) at baseline to 8.5 k 6.3 (BDI = 12.7 k 8.2) at acute termination (week 16). Two of the six subjects had met criteria for double depression. Responders are generally maintaining their gains when seen in monthly continuation sessions, with more than 2 years of
Thus, a total of 17 patients, including 7 (41%) who had failed vigorous desipramine trials and 9 (53%) who had double depression, have received IPT from three therapists. None has worsened, and 11 (65%) reached remission (HAM-D 5 8): overall mean HAM-D scores fell from 21.5 * 4.4 at baseline to 7.4 2 4.7 at acute termination. For IPT, as for CBT, outcome results are limited but encouraging.
follow-up .42
Serial Treatment Data
The Columbia mood disorders group has raised interesting ques- tions of treatment specificity: that is, whether patients who prove unre- sponsive to one antidepressant modality might respond to another. Stewart and colleagues60 reported that a subset of CBT nonresponders from the Mercier et a149 study responded to imipramine but not to placebo. Two pure dysthymic patients and two double depressive pa-
142 MARKOWITZ
tients who failed CBT responded when randomly assigned to imipra- mine, whereas two double depressive patients randomized to placebo again failed to respond (J. Stewart, personal communication, April 1993).
The lone responder in the Fennel1 and Teasdale study19 and two psychotherapy responders treated by Harpin and c011eagues~~ had been pre-selected as medication nonresponders, although details of medica- tion trials unfortunately were not specified. In our studies, seven nonre- sponders to a 10-week trial of high-dosage desipramine improved with IPT. Although these numbers are small indeed, their results imply that medication and psychotherapy may serve complementary purposes in treating differing subpopulations of dysthymic patients.68
Combined Treatment Studies
Combined treatment studies are still more scarce. In an open trial, Miller et also found that two of four treatment-refractory inpatients with DSM-I11 double depression responded to the combination of either CBT or social skills training (SST) and assorted psychotropic medications (antidepressants as well as neuroleptic agents in two cases). Following a fortnight of inpatient assessment, patients received 5 days per week of psychotherapy, with an average of 28 sessions over 22 weeks.
Becker et aP lo reported preliminary results on 39 mildly symptom- atic dysthymic subjects who were assigned randomly to either SST or crisis-supportive psychotherapy and to nortriptyline or placebo. Patients received 16 weekly sessions followed by 2 biweekly sessions. Initial 17- item HAM-D mean score was 10.9, declining to 4.5 at termination. Self- report and clinician ratings showed significant improvement for all four treatment conditions.
Waring et a P described 12 women meeting RDC for dysthymia who were randomized to 10 weeks of cognitive marital or supportive therapy, and to doxepin (maximum 150 mg/d) or atropine placebo. All patients improved (mean HAM-D pretreatment score: 14.5; post- treatment score: 7.1; P = 0.003). Final results have not been reported for either the studies by Becker et a1 or Waring et al.
The conclusions of the 1987 NIMH Workshop on Combined Medica- tion and Psychotherapy in Depressions1 were that finding differences between antidepressant effects of psycho- and pharmacotherapy was difficult because of the small sample sizes in most reported studies, and because each treatment singly was so effective. Patients with chronip depression were deemed an ideal treatment population for differentiat- ing combined and mode-specific treatment benefits of antidepressant therapies. Despite this call to action, the studies still remain to be done.
DISCUSSION
To date there have been no large, systematic controlled clinical trials of the psychotherapy for dysthymic disorder. Data from open trials
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 143
are promising but meager. There are many similarities in symptom profile and course between dysthymic disorder and major depression that becomes chronic. As major depression already has been shown to respond to antidepressant psychotherapy, a reasonable case can be made for testing the efficacy of psychotherapy in patients with dysthymic disorder. If, as antidepressant medication trials suggest, dysthymic pa- tients are more difficult patients than those with acute major depression, the more reason to seek clinical tools to treat them.
The limited available evidence suggests that, contrary to intuition, brief psychotherapies may effectively treat chronic mood disorder. In our experience, an advantage of brief focal psychotherapy is the pressure it puts on both patient and therapist to work actively and to maintain high treatment expectations. Diagnostic data corroborate the psychoana- lytic perception that “masochism” is common among dysthymic pa- tients: we found that 35% of 34 dysthymic patients met SCID-I1 criteria for self-defeating personality disorder.47 The question is whether such features imply a bad prognosis, and whether they represent a trait or chronic state. It would be unsurprising if longer-term therapists, daunted by the grinding chronicity and fatalistic pessimism of dysthymic pa- tients, were unwittingly to collude with the dysthymiaI6 by setting lower psychotherapeutic goals, thereby achieving lesser or slower results. Ther- apeutic optimism, a medical model of mood disorder, a ”here and now” focus on current issues, and the leverage of time-limited therapy may help to jostle patients out of their dysthymic rut. Once relieved of mood disorder, many dysthymic patients experience a great release, a second lease on life.
CLINICAL RECOMMENDATIONS
Current evidence supports the use of antidepressant medication as a first-line treatment for dysthymic disorder. Psychotherapy may prove a useful adjunct to rnedi~ation.~~ Psychotherapy, despite the limited availability of efficacy data, may, nonetheless, offer a reasonable monoth- erapy, particularly for patients who previously have not received mood- targeted psychotherapy or who refuse medication. Should dysthymic disorder fail to improve after months of aggressive psychotherapeutic treatment, however, antidepressant medication again should be consid- ered. With the help of an established therapeutic alliance and recognition that psychotherapy is not alleviapg symptoms, a patient who pre- viously has refused medication may be willing to try it.
Suggestions for Antidysthymic Psychotherapy
Use of Time-limited, Manualized Psychotherapy
Beyond its therapeutic advantages, brief psychotherapy has eco- nomic benefits compared with longer-term therapies and it allows com-
144 MARKOWITZ
parison with pharmacologic interventions. At least three brief therapies for dysthymic disorder have been codified in manuals: C-BA!~JP,~~ SST,’O and IPT.@ Standard CBT, for which a manual exists to treatment acute depression: appears to have some efficacy for dysthymic disorder as well. The latter three approaches have been used in studies that circum- scribed time and frequency of sessions.
Interpersonal Focus
A theme emerging from the studies reviewed in this article is that psychotherapies aimed at dysthymic disorder attack the interpersonal difficulties that are a hallmark of the disorder. Interpersonal difficulties are obviously the focus of IPT, but the behavioral description of Harpin et alZ4 also conforms with an interpersonal approach: It provides social skills training in “interpersonal themes,” including ”refusing unreason- able requests, expressing positive feelings to another.” That treatment protocol involved significant others in cases where ”the goal of training was to improve the interpersonal interaction and communication be- tween the subject and significant other.” Social skills training9 also emphasizes interpersonal behavior and social perception. Although us- ing different language and a different conceptual approach, McCul- l o ~ g h ~ ~ also focuses on “person’ x person2 interaction” as “the basic subject matter for psychotherapy” (reference 38, p 9).
This shared focus of treatments reflects the salience of interpersonal difficulties in dysthymic disorder and the need to address them in antidysthymic psychotherapy. Group or family therapies might also help dysthymic patients to work on interpersonal issues.
Serial Design
Initial controlled treatment trials should compare efficacy of psycho- therapy with a standard reference treatment, that is, antidepressant medication, and to a placebo or other control condition. Because psycho- therapy and medication may treat different dysthymic populations, non- responders to either active treatment might be crossed over productively to an open trial of the alternative treatment.
Continuation and Maintenance Treatment
The chronicity of dysthymia and the general risk of relapse and recurrence for mood disorders argue for providing some form of ongo- ing treatment to maintain acute gains in responsive patients. In this respect, psychotherapy probably does not differ from pharmacotherapy for dysthymic disorder. Our limited experience suggests that dysthymic patients who remit in IPT greatly appreciate monthly continuation ses- sions. They use the time following acute treatment to consolidate IPT treatment gains and to build confidence in new attitudes and patterns
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 145
of behavior. The need for ongoing treatment could be tested in a ran- domized discontinuation study.
Combined Treatment Trials
From a formal vantage point it is premature to compare combined with single-modality therapy when the efficacy of psychotherapy for dysthymic patients has not yet been demonstrated conclusively. Yet even if psychotherapy alone should not show utility for dysthymic patients, it might still augment the benefits of antidepressant medication for medication responder~ .~~ “Post-dysthymic” medication responders approach but may not attain community levels of social and vocational functioning, at least acutely.35 They may no longer appear personality- disordered (our first two IPT-D responders ceased to meet SCID-I1 criteria for personality disorders as well as for SCID-P DSM-111-R dysthy- mia); yet, not knowing how to act socially, they may need and greatly benefit from p~ychotherapy.~~
Combined pharmaco/psychotherapy may prove optimal for many dysthymic patients. Psychotherapy has the advantage of empowering patients to prove to themselves that they can control their mood and their environment. Medication may provide faster relief and may offer surer prophylaxis against recurrence (see reference 20).
Follow-up Assessments
Because dysthymic disorder is by definition chronic, acute treatment outcome may be less meaningful than repeated assessment of sustained outcome over a follow-up of 6 months or longer. Follow-up assessment, therefore, should be included in antidysthymic outcome research.
Psychotherapy research of dysthymic disorder has received rela- tively little funding. This partly reflects the relatively late development of research psychotherapies, which initially focused on acute depression. Dysthymic disorder itself has had a slippery reputation: although chronic suffering over decades may equal or outweigh the pain of more severe but briefer major depressi~n?~ many clinicians seem to have judged dysthymic disorder with suspicion, considering it a ”soft” diag- nosis. The diagnostic system is biased by a tyranny of the acute, defining ”major” depression by the severity of its current symptoms while rele- gating severity of duration to the ”subsyndromal.” Yet paradoxically, chronicity of symptoms may daunt psychotherapists who treat dysthy- mic disorder more than acute severity does.
Perhaps too great attentionfias been paid to the distinction between pure dysthymic disorder and double depression. (This is, admittedly, an area of some controversy.) Some studies (e.g., reference 9) have foun- dered in the pursuit of ”pure” dysthymic patients. Yet the DSM-IV field trials found that 79% of dysthymic patients eventually develop a major depression, qualifying for ”double depres~ion.”~~ What may be a largely artifactual difference in severity criteria34 could hold less prognostic and
146 MARKOWITZ
diagnostic importance than the chronicity of the mood disorder. The distinction between ”pure” dysthymic disorder and “double” depres- sion should not be a barrier to research, although studies should control for their presence.
Given the public health significance of dysthymic disorder and the availability of treatment technology, the time is ripe to answer Weissman and Akiskal’s proposal for antidysthymic psychotherapy trials.
SUMMARY
The psychotherapy of dysthymic disorder has received too little serious attention and funding. Impressive advances in the pharmaco- therapy of dysthymic disorder should not obscure the need for psy- chosocial treatment for the high proportion of patients who do not respond to medication. Despite the dearth of psychotherapy outcome studies in this area, such data that do exist suggest that relatively brief, focal, antidepressant psychotherapies may successfully treat many patients with lifelong mood disorders. Maintenance therapy probably is indicated to ensure the persistence of treatment gains.
References
7 8.
9.
10.
11.
12.
13.
1. Akiskal H S Subaffective disorders: Dysthymic, cyclothymic and bipolar I1 disorders in the “borderline” realm. Psychiatr Clin North Am 42546, 1981
2. Akiskal HS: Towards a definition of dysthymia: Boundaries with personality and mood disorders. In Burton SW, Akiskal HS (eds): Dysthymic Disorder. London, Gaskell, 1990,
3. Akiskal HS, Rosenthal TL, Haykal RF, et al: Characterological depressions: Clinical and sleep EEG findings separating ”subaffective dysthymias” from “character spectrum disorders.” Arch Gen Psychiatry 37777-783, 1980
4. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disor- ders, ed 4. Washington, American Psychiatric Association, 1994
5. Arieti S, Bemporad J: Severe and Mild Depressions. New York, Basic Books, 1978 6. Bakish D, Lapierre YD, Weinstein R, et al: Ritanserin, imipramine and placebo in the
pp 1-12
treatment of dysthymic disorder. J Clin Psychopharmacol 13:409414, 1993 . Beck A T Depression Inventory. Philadelphia, Center for Cognitive Therapy, 1978 , Beck AT, Rush AJ, Shaw BF, Emery G: Cognitive Therapy of Depression. New York,
Guilford, 1979 Becker RE, Heimberg RG: Dysthymia: Preliminary results of treatment with social skills training, crisis supportive psychotherapy, nortriptyline, and placebo [unpublished manuscript] Becker RE, Heimber RG, Bellack A S Social Skills Training Treatment for Depression. New York, Pergamon, 1987 Bemporad J: Psychotherapy of the depressive character. J Am Acad Psychoanal 4:347- 372, 1976 Bersani G, Pozzi F, Marini S, et al: 5-HT2 receptor antagonism in dysthymic disorder: A double-blind placebo controlled study with ritanserin. Acta Psychiatr Scand 83244- 248, 1991 Cassano GB, Perugi G, Maremmani I, Akiskal HS: Social adjustment in dysthymia. In Burton SW, Akiskal HS (eds): Dysthymic Disorder. London, Gaskell, 1990, pp 78-85
PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 147
14. Chodoff P: The depressive personality: A critical review. Arch Gen Psychiatry 25:666- 673, 1972
15. Cohen MB, Baker G, Cohen RA, et al: An intensive study of twelve cases of manic- depressive psychosis. Psychiatry 17103-137, 1954
16. Cooper AM: Will neurobiology influence psychoanalysis? Am J Psychiatry 1421395- 1402, 1985
17. de Jong R, Treiber R, Henrich G: Effectiveness of two psychological treatments for inpatients with severe and chronic depressions. Cognitive Therapy Research 10:645- 663, 1986
18. Elkin I, Shea MT, Watkins JT, et al: National Institute of Mental Health treatment of depression collaborative research program: General effectiveness of treatments. Arch Gen Psychiatry 46:971-982, 1989
19. Fennel1 MJV, Teasdale JD. Cognitive therapy with chronic, drug-refractory depressed outpatients: A note of caution. Cognitive Therapy Research 6:455460, 1982
20. Frank E, Kupfer DJ, Perel JM, et al: Three-year outcomes for maintenance therapies in recurrent depression. Arch Gen Psychiatry 471093-1099, 1990
21. Goldberg DP, Bridges KW: Epidemiological observations on the concept of dysthymic disorder. In Burton SW, Akiskal HS (eds): Dysthymic Disorder. London, Gaskell, 1990, p 104
22. Gonzalez LR, Lewinsohn PM, Clarke GN: Longitudinal follow-up of unipolar de- pressives: An investigation of predictors of relapse. J Consult Clin Psycho1 53:461- 469, 1985
23. Hamilton M: A rating scale for depression. J Neurol Neurosurg Psychiatry 25:56-62, 1960
24. Harpin RE, Liberman RP, Marks I, et al: Cognitive-behavior therapy for chronically depressed patients: A controlled pilot study. J Nerv Ment Dis 170295-301, 1982
25. Hellerstein D, Yanowitch P, Rosenthal J: A randomized double-blind study of fluoxe- tine versus placebo in treatment of dysthymia. Am J Psychiatry 150:1169-1175, 1993
26. Hirschfeld RMA: Personality and dysthymia. In Burton SW, Akiskal HS (eds): Dysthy- mic Disorder. London, Gaskell, 1990, p 75
27. Howland RH: Pharmacotherapy of dysthymia. J Clin Psychopharmacol 1~83-92,1991 28. Jacobson E: Depression. New York, International Universities Press, 1971 29. Keller MB, Lavori PW, Endicott J, et al: "Double depression": Two-year follow-up. Am
J Psychiatry 140:689-694, 1983 30. Kessler RC, McGonagle KA, Zhao S, et al: Lifetime and 12-month prevalence of DSM-
111-R psychiatric disorders in the United States: Results from the National Comorbidity study. Arch Gen Psychiatry 51:8-19, 1994
31. Klerman GL, Weissman MM (eds): New Applications of Interpersonal Psychotherapy. Washington, American Psychiatric Press, 1993
32. Klerman GL, Weissman MM, Rounsaville BJ, Chevron ES: Interpersonal Psychotherapy of Depression. New York, Basic Books, 1984
33. Klerman GL, Weissman MM, Markowitz J, et al: Medication and psychotherapy. In Bergin AE, Garfield SL (eds): Handbook of Psychotherapy and Behavior Change, ed 4. New York, John Wiley and Sons, 1994, pp 734-782
34. Kocsis JH, Frances AJ: A critical discussion of DSM-I11 dysthymic disorder. Am J Psychiatry 144:1534-1542, 1987
35. Kocsis JH, Frances AJ, Voss C, et al: Imipramine and social-vocational adjustment in chronic depression. Am J Psychiatry 145:997-999, 1988
36. Kocsis JH, Frances AJ, Voss C, et al: Imipamine treatment for chronic depression. Arch Gen Psychiatry 45253-257, 1988
37. Kocsis JH, Thase ME, Koran L, et al: Pharmacotherapy for "pure" dysthymia: Sertraline vs. imipramine vs. placebo. Eur Neuropsychopharmacol4:204, 1994
38. McCullough JP: The Manual for Therapists Treating the Chronic Depressions and Using the Cognitive-Behavioral Analysis System of Psychotherapy. Richmond, VA, Virginia Commonwealth University, 1992
39. McCullough JP: Psychotherapy for dysthymia: A naturalistic study of ten patients. J Nerv Ment Dis 179:734-740, 1991
40. McCullough JP, Klein DN, Shea MT, Miller I: Review of DSM-IV mood disorder data
148 MARKOWITZ
in the field trials. Presented at the 100th Meeting of the American Psychological Association, Washington, DC, September 1992
41. McGlashan T (ed): The Documentation of Clinical Psychotropic Drug Trials. Rockville, MD, National Institute of Mental Health, 1973
42. Markowitz JC: Psychotherapy of dysthymia. Am J Psychiatry 151:1114-1121, 1994 43. Markowitz JC: Psychotherapy of the post-dysthymic patient. Journal of Psychotherapy
Practice and Research 2157-163, 1993 44. Markowitz JC, Klerman GL: Manual for Interpersonal Therapy of Dysthymic Disorder,
ed 2.1. New York, Cornell University Medical College, 1993 45. Markowitz JC, Klerman GL, Perry S Interpersonal psychotherapy of depressed HIV-
seropositive outpatients. Hosp Community Psychiatry 43:885-890, 1992 46. Markowitz JC, Moran ME, Kocsis JH: Does psychotherapy treat chronic depression?
Paper presented at the 146th Annual Meeting of the American Psychiatric Association, New York, May 1990
47. Markowitz JC, Moran ME, Kocsis JH, Frances AJ: Prevalence and comorbidity of dysthymic disorder among psychiatric outpatients. J Affect Dis 24:63-71, 1992
48. Mason BJ, Markowitz J, Klerman GL: IPT for dysthymic disorder. In Klerman GL, Weissman MM (eds): New Applications of Interpersonal Therapy. Washington, Ameri- can Psychiatric Press, 1993, pp 225-264
49. Mercier MA, Stewart JW, Quitkin FM A pilot sequential study of cognitive therapy and pharmacotherapy of atypical depression. J Clin Psychiatry 53166170, 1992
50. Miller IW, Bishop SB, Norman WH, Keitner G I Cognitive/behavioural therapy and pharmacotherapy with chronic, drug-refractory depressed inpatients: A note of opti-
51. NIMH Workshop on Combined Medication and Psychotherapy in Depression [con-
52. Parsons T Illness and the role of the physician: A sociological perspective. Am J
53. Rockland LH: A review of supportive psychotherapy, 19861992. Hosp Community
54. Rockland LH: Supportive Therapy. New York, Basic Books, 1989 55. Shapiro R, Keller M: Longitudinal Interval Follow-up Evaluation (LIFE). Boston, Mas-
sachusetts General Hospital, 1979 56. Simons RC: Psychoanalytic contributions to psychiatric nosology: Forms of masochistic
behavior. J Am Psychoanal Assoc 35:583408, 1987 57. Sotsky SM, Glass DR, Shea MT, et al: Patient predictors of response to psychotherapy
and pharmacotherapy: Findings in the NIMH treatment of depression collaborative research program. Am J Psychiatry 148:997-1008, 1991
58. Spitzer RL, Endicott J, Robins E: Research Diagnostic Criteria (RDC) for a Selected Group of Functional Disorders, ed 3. New York, New York State Psychiatric Institute, Biometrics Research, 1978
59. Stewart JW, McGrath PJ, Quitkin FM: Relevance of DSM-I11 depressive subtype and chronicity of antidepressant efficacy in atypical depression. Arch Gen Psychiatry
60. Stewart JW, Mercier MA, Agosti V, et al: Imipramine is effective after unsuccessful cognitive therapy: Sequential use of cognitive therapy and imipramine in depressed outpatients. J Clin Psychopharmacol 13:114-119, 1993
61. Stone L: Psychoanalytic observations on the pathology of depressive illness: Selected spheres of ambiguity or disagreement. J Am Psychoanal Assoc 34:329-362, 1986
62. Stravynski A, Shahar A, Verreault R A pilot study of the cognitive treatment of dysthymic disorder. Behav Psychother 4:369-372, 1991
63. Versiani M: Pharmacotherapy of dysthymia: A controlled study of imipramine, moclo- bemide or placebo. Neuropsychopharmacology 10298, 1994
64. Waring EM, Chamberlaine CH, McCrank EW, et al: Dysthymia: A randomized study of cognitive marital therapy and antidepressants. Can J Psychiatry 3396-99, 1988
65. Weissman MM, Akiskal HS: The role of psychotherapy in chronic depressions: A proposal. Compr Psychiatry 25:23-31, 1984
66. Weissman MM, Leaf PJ, Bruce ML, Florio L The epidemiology of dysthymia in five
I mism. Behav Psychother 13:320-327, 1985
vened by Prien R, Hirschfeld RMA]. Washington, September 1987
Orthopsychiatry 21:452460, 1951
Psychiatry 44:1053-1060, 1993
46:1080-1087, 1989

PSYCHOTHERAPY FOR DYSTHYMIC DISORDER 149
communities: Rates, risks, comorbidity, and treatment. Am J Psychiatry 145:81!%819, 1988
67. Wells KB, Burnam MA, Rogers W, et al: The course of depression in adult outpatients: Results from the medical outcomes study. Arch Gen Psychiatry 49:788-794, 1992
68. Wright JH, Thase ME: Cognitive and biological therapies: A synthesis. Psychiatr Ann 22451458,1992
Address reprint requests to John C. Markowitz, MD
Cornell University Medical College 445 East 68th Street, Suite 3K
New York, NY 10021





























