Embed Size (px)
Citation preview

Psychotherapy Research 10(2) 133-146, 2000 02000 Society for Psychotherapy Research
THE ~NFLUENCE OF INTERPERSONAL PROBLEMS AND S m O M SlWElWT ON THE DURATION AND OUTCOME OF SHORT-TERM PSYCHODYNAMIC qsYCHOTHERAPY
Henning Schauenburg Manfred Kuda Isa Sammet Micha Strack University of Göttingen
This naturaiistic outcome study investigated validity ~ p e c t s of the Inven- tory of Interpersonal Problems (IIP [Horowitz, Strauß, & Kordy, 19953). The sample consisted of 180 patients who received short-term psychody- namic psychotherapy for an average nurnber of 7.8 sessions and an aver- age duration of 3.4 months. Small changes in pre-post-measures irnply that the iiP is not to be recommended as an instnunent for outcome walu- ation in short-term psychotherapy, due to the traitlike character of its items. However, we showed by path analyses that a higher score on the affiliative dimension of the interpersonal circumplex goes along with a better treat- ment outcome. The influence of the dorninance dimension is gender spe- ciFic: male patients (who generally showed more dismissive and intro- verted behavior in *&is sample) received, if disrnissive and introyerted, a longer introductory therapy, whereafter they-in cases of high syrnptom load-were often referred to long-term treatrnent. Dominant male patients and, in general, female patients with high syrnptom scores, were referred faster, after only a few sessions. Results are discussed under aspects of adaptive therapist behavior.
Following a great number of quasi-experimental controiied comparative studies in psychotherapy (Grawe, Donati, & Beinauer, 1993), the call for natwalistic studies has been raised (e.g., Manz, Henningsen, & Rudolf, 1995). They are expected to shed light on everyday psychotherapy, that is to say, on the processes and results of thera- pies in different treaunent formats.
Severai assessment dunensions are generaily considered as relevant for evaluat- ing psychotherapy outcome: self- or expert evaluation, global assessments, indirect evaiuation by repeated measurement, and different fidds of functioning (symptoma- tology, everyday functioning, or interpersonal behavior). The use of standardized
Correspondence regading this anide should be addressed to Prof. Dr. med. Henning Schauenburg, Depmen t of Psychosomatics and Psychotherapy, University of Göttingen, Von Siebold-Sn. 5, Goningen, FRG. E-mail: HSCHAUEBPGWDG.DE.

134 SCHAUENBURG ET AL.
instruments to compare these dirnensions is quite useful, and the discussion about a "core batteryn of psychotherapeutic assessment methods has rnade good Progress (Strupp, Horowitz, & Ladxrt, 1998).
Questionnaires for the assessment of symptornatology and interpemnal change have been comparatively well established internationaily. Arnong them are the Symp- tom Checklist 9OR (SCL 90R; Derogatis, 1983; Franke, 1995), the Beck Depression Inventory (BDI; Hautzinger, Bailer, Worall, & Keller, 1995) and the Inventory of Interpersonal Problems (IIP; Horowitz, StrauR, & Kordy, 1995). Ail of thern are avail- able in a Gerrnan version.
We have reported before about the possibilities and potentials of SCL 90R to ascertain statistically and clinically relevant changes after psychotherapy (Schauenburg & Strack, 1999). This article treats the usefulness of applying the IiP. Because of its assessment of clinically relevant v h a l i t y aspects, the IIP is often used to comple- ment symptom questionnaires.
First, both the theoretical background of the questiomaire and the results of its application in psychotherapy research are described. This leads to our hypotheses for the prediction of outcome and process aspects. They were tested on a random sample of patients in psychodynamically oriented short-term psychotherapy.
BACKGROUND AND ASSUMPTiONS
INTERPERSONAL CIRCUMPLM MODELS
Sullivan's (1953) description of the fundamental interpersonality of human ex- perience and his conceptionalization of repetitive maladaptive relationship patterns has a long diagnostic tradition. The interpersonal concept is still an important con- struct in psychotherapy research. Interpersonal behavior is considered to be an im- portant predictor and outcome variable (e.g., Hoglend, 1993). .
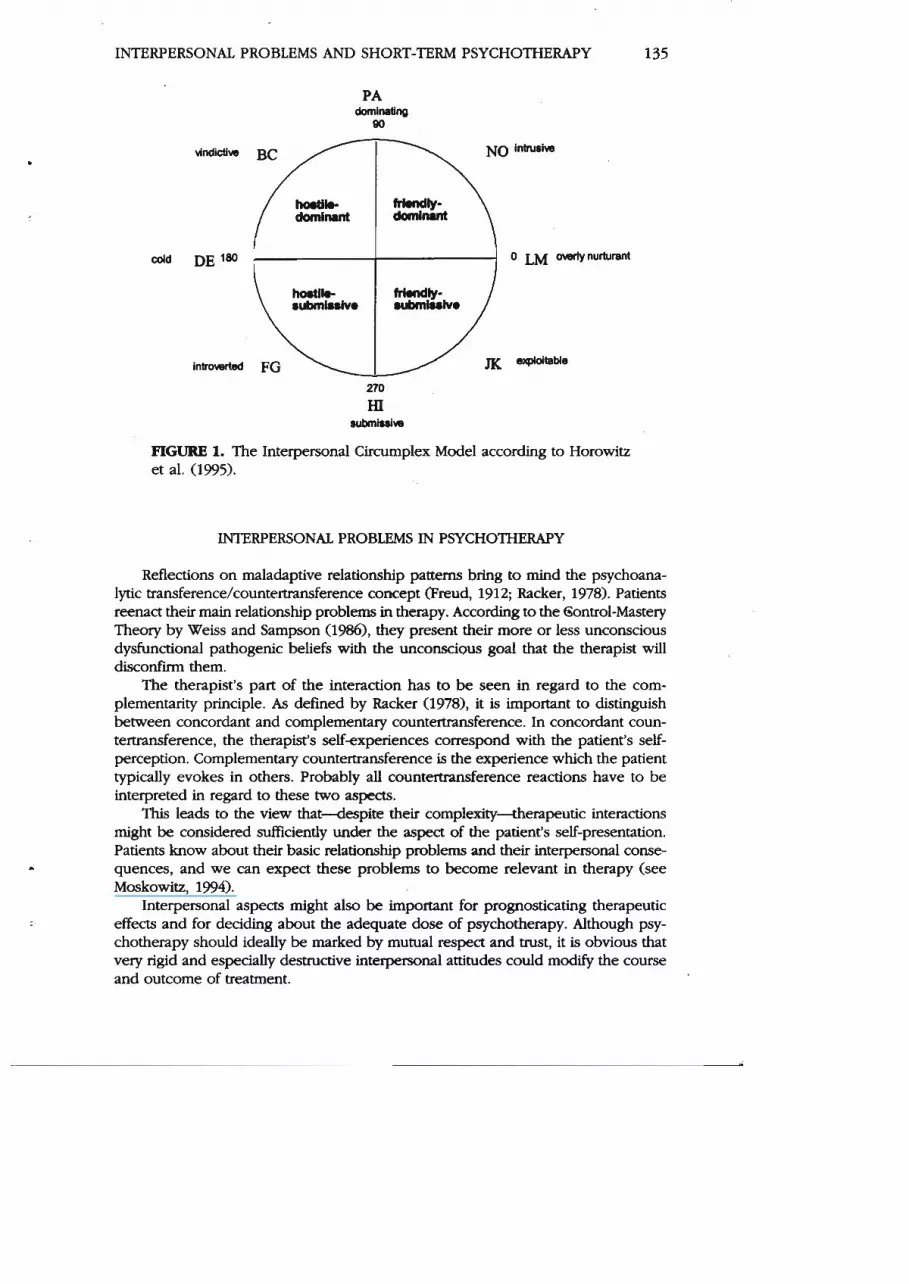
Among the many approaches to operationalize relevant interpersonal aspects of pemnality, the Interpersonal Circumplex Model (Leary, 1957; Kiesler, 1983, 1996; GifTord & OConnor, 1987; Wiggins, 1979; Wiggins & Broughton, 1991; Benjamin, 1993) takes a Special place. It shows interpersonal behavior in a two-dimensional space, which is created by the orthogonal axes "love-haten and "control-submission." Sirniliar behaviors are close to each other in the circle, while contrary behaviors face each other on opposite ends. Circular models have been validated in many ways. Extensive literature On the subject exists (Kiesler, 1996; Plutchik, 1998). Figure 1 shows a typical circumplex model, which is formed by the iterns of the IIP (Horowitz et al., 1995) described below.
A fundamental assumption of circumplex modeis is the complementarity of human behavior: certain behaviors and attitudes are overfrequently and non- randornly related to a particular response (e.g., submission induces dominance: See Kiesler, 1983; Strong et al,, 1988; Thompson, Hill, & Mahalik, 1991). Problem- atic behaviors and the response to them by others are often specifically linked and equally often experienced as an ever-rmrrent vicious cllcle. In the sense of com- plementarity, if behaviors often cause disappointing or injuring responses, the con- cerned persons dwelop a subjective dysfunctional knowledge of difficult interac- tion patterns. However, they are usually not able to understand the process by themselves.
INTERPERSONAL PROBLEMS AND SHORT-TERM PSYCHOTHERAPY 135
PIGURE 1. The Interpersonal Circumplex Model according to Horowitz et al. (1995).
INTERPERSONAL PROBLEMS IN PSYCHOTHERAPY
Reflections on maladaptive relationship Patterns bring to mind the psychoana- lytic transference/countertransference concept (Freud, 1912; Racker, 1978). Patients reenact their maui relationship problems in thmpy. According to the 6ontrol-Mastery Theory by Weiss and Sampson (1986), they present their more or less unconscious dysfunctional pathogenic beliefs with the unconscious goal that the therapist will d isconf i them.
The therapist's part of the interaction has to be seen in regard to the com- plementarity principle. As defined by Racker (1978), it is important to cüstinguish between concordant and complernentary countertransference. In concordant coun- tertransference, the therapist's seif-experiences correspond with the patient's self- perception. Complementary countertransference is the experience which the patient typically evokes in others. Probably ail countemansference reactions have to be interpreted in regard to these two aspects.
This leads to the view that-despite their complexity-therapeutic interactions might be considered sufftcientiy under the aspect of the patient's self-presentation. Patients know about their basic relationship problems arid their interpersonal conse- quences, and we can expect these problems to become relevant in therapy (see Moskowitz, 1994).
Interpersonal aspects rnight also be important for prognosticating therapeutic effects and for deciding about the adequate dose of psychotherapy. Although psy- chotherapy should ideally be rnarked by mutual respect and wust, it is obvious that very rigid and especiaily destructive interpersonal attitudes could modify the Course and outcome of treatment.

SCHAUENBURG ET AL.
To investigate these questions, a reliable and valid instrument to assess interper- sonal behavior is needed. The IIP is widely accepted for this purpose in Anglo-Saxon psychothefapy research.
OUTCOME PREDICTION
Studies using IIP found that therapy results can be predicted by differences on the affiiation axis, which means by nurturant versus hostile attitudes (Filak, Abeles, 82 Norquist, 1986; Horowitz, Rosenberg, & Bartholomew, 1993). The more the inter- personal problems of the patients rate as "overly numirant," the more they can profit from psychotherapy. However, the position on the dominance-subrnission axis was not correlated to outcome in the study af Filak et aL '(1986).
Horowitz et al. (1993) found that unselected psychotherapy patients showed rather little improvement after a psychotherapy of 2 0 4 0 sessions, if their main interper- sonal difficulties lay in the field of lacking intimacy and closeness (that is, too cold and introverted behavior).
Capreol and Alden (1933) described how patients with social phobia and lack of self-confidence, who perceived themselves as too cold and unfriendly, responded beaer to exposure therapy and less to psychodynamic therapy.
Also using IIP, Strauß and Hess (1993) studied haspitalized psychotherapy pa- tients in two different Settings. One setting was found to be less dective for patients with strongly dominant and cold behavior.
Eldredge, Locke, and Horowitz (1998) investigated psychotherapy outcome for patients with obesity. Those who described themselves as rather introverted had worse results concerning the change of their eating h a b . More weight Feduction was found for those whose interpersonal problems lay mostly in the field of vindictive behavior (BC). This means that an influence of the dominante axis on therapy results was demonstrated in contrast to the studies mentioned above.
Davies-Osterkamp, Strauß, and Schmitz (1996) showed diat patienas with "too expioitablen or "too subrnissiven behavior profit m r e from inpatient psychotherapy.
To conclude, the studies strongly support the facilitating effect of affiliative be- havior on therapy success, whereas the effect of dominant versus submissive behav- ior is less clear. Submissive styles seem to be a bit more promising for positive therapy outcomes, according to literature.
PREDICTION OF PROCESS ASPECTS
Schauenburg, Peknin, and Leibing (1995) studied distinaive subgroups of de- pressive patients. In the therapy sarnple, there were sigriificantly rnore patients with a rather "exploitablen localization (JK), whereas dominant-vindictive traits (BC and PA) prevailed in the healthy control group. Depression aside, this shows already that consulting behaviors are infiuenced by interpersonal aspects.
So far, there has been little research on the infiuence of interpersonal attitudes on the frequency of therapeutic contacts and on the duration of therapy. Meresman and Horowitz (1995) found that patients who desaibed themselves as rather sub- rnissive were treated longer. Patients who perceived thernselves as domineering had a greater tendency to drop out.
Furthermore, aspects of inkerpersonal dependency, as assessed by the dimen- sions of the circumplex model, might be relevant for psychotherapy. There is a con- tinuum of interpersonal dependency that ranges from "overly nurturant " (LM-pole,

INTERPERSONAL PROBLEMS AND SHORT-TERM PSYCHOTHERAPY 137
see Figure 11, over "too submissive" (pole HI), to "too introverted" (pole FG). The latter is more often connected with neuroticism and probably correlates with a greater need for therapy (Pincus & Gurtman, 1995).
The aforementioned findings show that the IIP allows the therapist to make predictions of therapy outcome and process aspects to a certain degree. Such stud- ies have usually been conducted with inpatient samples. Therefore, the instmment shall be tested on an outpatient sample in a naturalistic study.
DESIGN AND PURPOSE OF THE STüDY
The study was performed in an outpatient unit of the Deparunent of Psychoso- rnatics and Psychotherapy of the University Clinics of Göttingen, which provides psy- chotherapeutic treatrnent for students. The clientele derives mainly from middle-class families and is representative of psychotherapy patients concerning age and social class. The interventions comprise psychodynarnic crisis interventions, short-term psychothera- pies, and, within this Setting, clarifying treatrnent recornrnendations or referral to an outpatient long-term psychotherapy. Altogether, 57% of the patients were advised to seek ongoing therapy for different reasons. Most of them had personality disorders that could only be treated adequately in long-term therapy. For example, patients with severe depressive episodes needed longer psychotherapy to stabilize the initial relief of Symptoms than the outpatient clinic could offer. As found in a follow-up study, two- thirds of the patients had actually followed the given advice (Schauenburg et al., 1996).
The study was conceptualized as a pre-post-evaluation with a multivariate ap- proach. The purpose was the investigation of treatment decisions and psychotherapy results under naturalistic conditions.
The pre-post-assessment was performed in different dimensions, of which this article will only draw on Symptom severity and interpersonal problerns (see also Schauenburg, 2000).
QUESTIONS AND HYPOTHESES
After a short presentation of therapy outcomes, the following hypotheses will be tested on the basis of the findings described above: (1) Patients profit more from short-term psychotherapy when their interpersonal problems lie in the affiliative field of the circumplex at the begiming of therapy; and (2) patients with problems con- cerning submissiveness and negative affiliation (introversion) benefit less, stay in therapy longer, or are rather referred to long-term psychotherapy.
Because of the complex interdependencies of initial symptomatology, interper- sonal problems, duration of therapy, outcome, and referral, the hypotheses will be tested by pathanalytical methods.
METHOD
SAMPLE
The original sample consisted of 503 nonpreselected patients who came for a consultation to the psychotherapeutic outpatient unit between the end of 1W3 and the beginning of 1996. From those 451 patients who came more than once, 30 were still in therapy at the end of the study and 60 did not receive the questionnaires

138 SCHAUENBURG ET AL.
because they missed their appointments. Out of the remaining 355 patients, 175 cli- ents didn't return their questionnaires for different reasons that could not be clari- fied. The rate of returned questionnaires was 50.4%. 180 patients with complete forms were included into the final evaluation. Responding patients did not differ from nonresponding patients in their outset characteristics (SCL-scales, IIP-scales, Score of complaints [Effect size d < .12; t(488) < 1.2 and p > .201).
The questionnaires were passed out during the personal registration procedure, usually one week before the initial appointment. The intake interview was fol- lowed by a 15-minute case conference, at the end of which the eight participating therapists gave a consensual International Classification of Diseases (ICD) 10 di- agnosis. The final questionnaires were given in the last session. One-session con- tacts were excluded. The remaining sample was composed of crisis interventions, preappointed short-term psychotherapies, and longer diagnostic contacts (see Schauenburg, 1993).
Table 1 shows a description of the sample.
THERAPISTS
A total of eight therapists participated in the study. Table 2 shows their Sex and age, and their clinical psychotherapeutic experience in years, as well as the number of their cases and the average duration of their therapies. Due to job change, two therapists are represented with only a few cases. Most therapists considered them- selves to work mainly psychodynamically. One therapist saw himself as basically cognitive-behavioral but integrating psychodynamic elernents.
TABLE 1. Sample Characteristics (n = 180)
Females
Patients %
95 53
ICDlO diagnoses (multiple diagnoses possible) substance abuse 3 2 affective disorders 40 23 anxiety disorders 32 18 adjustment disorders 39 eating disorders 8 somatoform disorders
69 5 8 5
dissociative disorders 1 1 personality disorders 58 32
Duration of Symptoms up to 1 year 76 42 up to 5 years 59 32 up to 15 years 45 25
Recornrnendation for long-term therapy 103 57
Mean SD
Age (years) Duration of treatrnent (months) Number of sessions (minimum 2)
INTERPERSONAL PROBLEMS AND SHORT-TERM PSYCHOTHERAPY 139
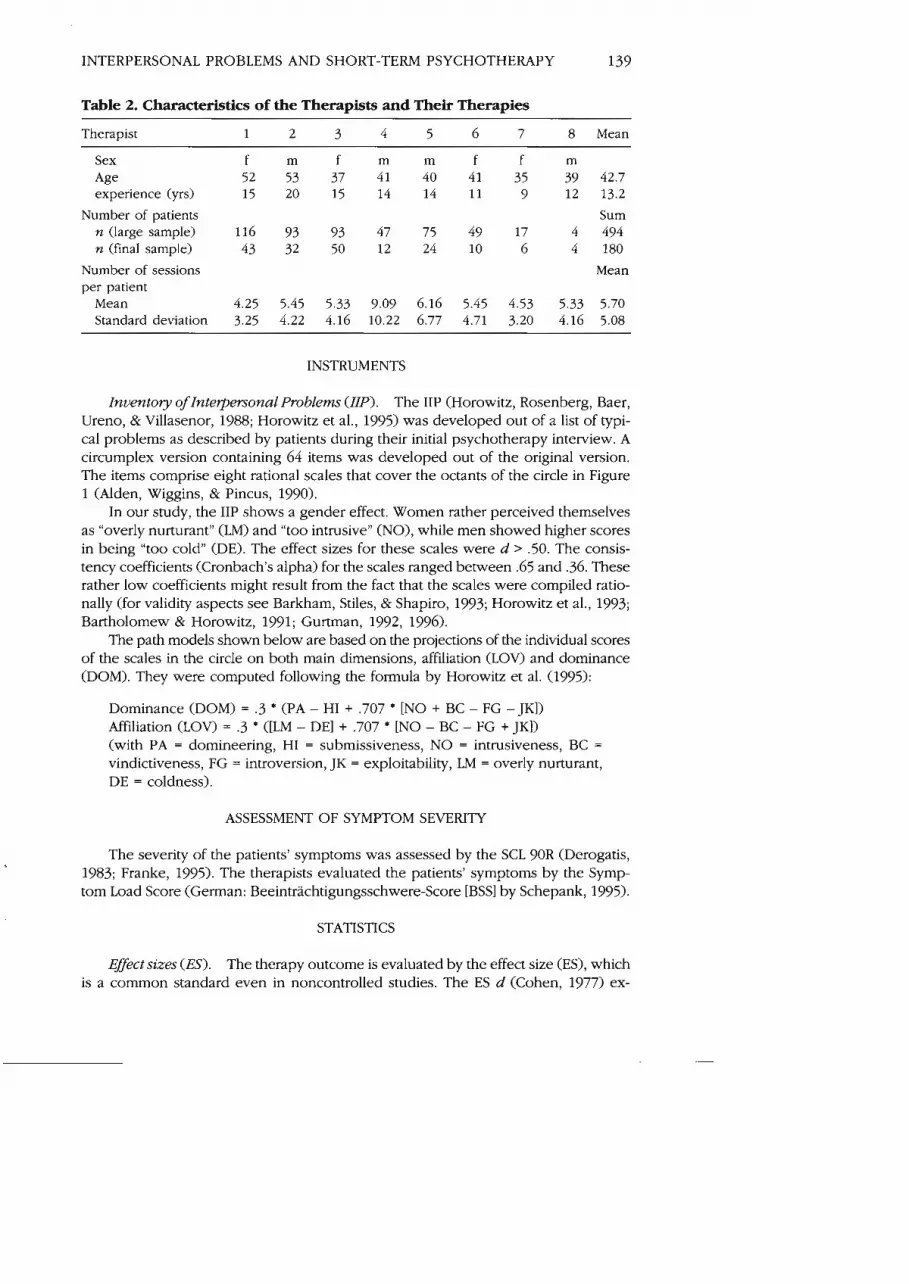
Table 2. Characteristics of the Therapists and Their Therapies
Therapist
Sex Age experience (yrs)
Number of patients n (large sample) n (fmal sample)
Number of sessions per patient
Mean Standard deviation
Mean
42.7 13.2
Sum 494 180
Mean
5.70 5.08
INSTRUMENTS
Inuentory of Intetpersonal Problems (IIP). The IIP (Horowitz, Rosenberg, Raer, Ureno, & Villasenor, 1988; Horowitz et al., 1995) was developed out of a list of typi- cal problems as described by patients during their initial psychotherapy interview. A circumplex version containing 64 items was developed out of the original version. The items comprise eight rational scales that Cover the octants of the circle in Figure 1 (Alden, Wiggins, & Pincus, 1990).
In our study, the IIP shows a gender effect. Women rather perceived themselves as "overly nurturant" (LM) and "too intrusive" (NO), while men showed higher scores in being "too cold" (DE). The effect sizes for these scales were d > .50. The consis- tency coefficients (Cronbach's alpha) for the scales ranged between .65 and .36. These rather low coefficients might result from the fact that the scales were compiled ratio- nally (for validity aspects See Barkham, Stiles, & Shapiro, 1993; Horowitz et al., 1993; Bartholomew & Horowitz, 1991; Gurtman, 1992, 1996).
The path models shown below are based on the projections of the individual scores of the scales in the circle on both main dimensions, affiliation (LOV) and dominance (DOM). They were computed following the forrnula by Horowitz et al. (1995):
Dominance (DOM) = .3 * (PA - H1 + .707 [NO + BC - FG - JKI) Affiliation (LOV) = .3 ([LM - DEI + .707 [NO - BC - FG + JK]) (with PA = domineering, H1 = submissiveness, NO = intrusiveness, BC =
vindictiveness, FG = introversion, JK = exploitability, LM = overly nurturant, DE = coldness).
ASSESSMENT OF SYMPTOM SEVERITY
The severity of the patients' symptoms was assessed by the SCL 90R (Derogatis, 1983; Franke, 1995). The therapists evaluated the patients' symptoms by the Symp tom Load Score (German: Beeinträchtigungsschwere-Score [BSSI by Schepank, 1995).
STATISTICS
Effectsizes (ES). The therapy outcome is evaluated by the effect size (ES), which is a cornmon Standard even in noncontrolled studies. The ES d (Cohen, 1977) ex-

SCHAUENBURG ET AL.
presses the average difference either between groups or between pre-post-values divided by the standard deviation (SD). If a control group is missing, it has to be determined which SD to use: the one of a standard sample, or of the prescores, or of pooled pre- and postscores of the sample (discussed by Hartmann & Herzog, 1995). The differences in the results depend on the respective characteristics of the sample and the instruments.
The skewedness to be assumed for symptom scores might cause a decrease in variance after therapy (the potential denominator of the quotient) such that an arti- ficial increase of the effect size Score d would result. Therefore, this study used the SD of the prevalues:
However, the mean values, the standard deviations, and the correlation of pre- and postvalues are fully documented here to allow alternative calculations or later meta- analyses (see Smith & Glass, 1977). According to the convention of Cohen (1977), effects are called weak, medium, or strong if effect sizes d are at least 0.2, 0.5, or 0.8 respec- tively. The corresponding scores for correlations are r = 0.1, r = 0.3, and r = 0.5.
Path analysis. Path analytical methods allow a synchronous investigation of in- terdependencies. In this case, initial symptom severity, the direction of interpersonal problerns, the duration of the intervention, and its outcome are analyzed. A path analysis consists of several simultaneously computed multiple regressions. Variables can be both criteria (dependent variables) and predictors for other variables. The pathcoef- ficients are computed from the correlation mauix, using the maximum likelihood es- tirnation. Standard errors allow tests against the t-distribution. The path-coefficients are to be interpreted similar to partial correlations. The fit of the model can be ex- pressed by different indices. We used: AGFI = Goodness of Fit = portion of reesti- mated covariances; RMR = Root Mean Square Residuals = portion of not reestirnated covariances. An AGFI > .9O and RMR < .10 could be considered quite good. Addition- ally, the PGFI = Parsimony Goodness of Fit Index will be shown, which is best for the least appropriate number of paths. The PGFI should exceed .20 (Backhaus, Erickson, Plinke, & Schuchard-Ficher, 1987). The computation was done using LISREL 8.03 (Jöreskog & Sörbom, 1993).
RESULTS
EFFECT SIZES
As documented in Table 3, the sample ( N = 180) shows an effect size of d = .67 for the General Severity Index (GSI) of the SCL WR. That is mainly due to the reduc- tion of the symptom load (PSDI), which is d = .82. The therapists' assessrnent of symptom load (BSS) shows a similar-sized effect of d = .81. So the accomplished change is on a moderate level, slightly beyond the global mean of d = .85 found by Smith and Glass (1977), and significantly below that one calculated by Grawe et al. (1993; d = 1.21) in his meta-analysis of controlled studies. If, following Grawe's advice, 0.10 is subtracted as an equivalent for the spontaneous remission to be expected in a control group, a pure treatment effect of about .50 (GSI), respectively .70 (BSS), remains. This average treatment effect is in accordance with what should be expected

INTERPERSONAL PROBLEMS AND SHORT-TERM PSYCHOTHERAPY 141
TABLE 3. Means and Effect Sizes
Pre-values Post-values Comparison ES
Mean SD Mean SD rtt diff SDdiff
GSI 1 .OO 0.50 0.65 0.50 .54 -0.35 0.48 .67 PST 44.0 15.0 34.7 17.7 .61 -9.3 15.2 .65 PSDI 1.95 0.51 1.53 0.48 .48 -0.42 0.50 .82 BSS 5.21 1.50 3.98 1.78 .61 -1.23 1.46 .8l IIP-G 12.5 3.94 12.32 3.44 .67 -0.18 0.35 .07
Note. GSI: Global Severiiy Index (SCL WR); PST: Number of Affirmed Symptoms (SCLWR); PSDI: Load of Affirrned Symptoms (SCL 9OR); BSS: therapist's evaluation of symptom load (Schepank, 1995); IIP-G: Global Sum Score of IIP; SD: standard deviation; rtt: Pre-Post-Correlation; diff: Pre-Post-Difference; ES d: Effect Size: n = 180.
from a short-term therapeutic service with its diagnostic interventions and respective referrals into ongoing therapy.
The IIP with an effect size of d = .07 in this sample of rather short interventions did not show significant change in the patients' interactional Patterns. There are dif- ferent possible interpretations for this result: Either the IIP is not suitable for measur- ing change, or the therapeutic interventions were inefficient. However, the most plau- sible explanation might be that the IIP assesses rather stable dimensions, which are mainly related to personal traits and, therefore, can hardly be influenced within a short-term treatment (Lueger, 1995).
OUTCOME PREDICTION
The central point of research is the impact of the patients' interpersonal charac- teristics on both outcome and duration of short-term psychodynamic therapy. The duration of the therapy was measured by months of treatment, as this variable showed better distribution characteristics than the number of sessions (correlation "months" and "number of sessions" r = .83). The correlation matrices for the path analysis turned out to be gender dependent (Chi-square(„, = 35.02; p = .03). This is reflected in dis- tinct paths for females and males.
In the path models shown in Figures 2 and 3, the pretreatment scores of the GSI and of both main dimensions of the IIP are represented on the left side. The arrows reflect their influence on duration, on therapy outcome, and on the recomrnenda- tion for long-term psychotherapy. Only significant interdependencies were included (t > 1.66). The high pre-post-correlation of symptom severity for females reveals that they show relatively less changes from high to low severity compared to males. The reverse case of deterioration is rare in general; it concerns less than 10% of the pa- tients (Schauenburg & Strack, 1999). It becomes clear that hypothesis 1 is confirmed for both genders (for females t = 2.41, for males t = 2.33). The more the scores are negative on the affiliation axis, the worse is therapy outcome. However, these cor- relations are not very strong and the effect sizes are small.
The dominance values in the IIP have no influence on the outcome of symptom scores. The gender-specific differences concern the influence of interpersonal domi- nance on the duration of therapy (hypothesis 2). For females, no influence of inter- personal dominance was found. When they stayed in the clinic for only a short time, they were referred into long-terrn therapy more often. This complies with the stan-

142 SCHAUENBURG ET AL.
Affiliation
Dominance
+.65
Duratlon (month)
Long-term therapy
FIGURE 2. Path model for the prediction of outcome and duration of treatment by initial symptom severity and interpersonal characteristics (n = 95 female patients). RMR, AGFI, PGFI are model fit indices (See p. 140).
Symptoms
GSI
Affiliation
Dominance
FIGURE 3. Path model for the prediction of outcome and duration of treatrnent by initial symptom severity and interpersonal characteristics (n = 85 male patients). RMR, AGFI, PGFI are model fit indices (see p. 140).

INTERPERSONAL PROBLEMS AND SHORT-TERM PSYCHOTHERAPY 143
dard model of short crisis interventions or diagnostic procedures. Females treated longer in this clinic receive a cornplete short-term therapy, which is why they did not have to be referred.
For rnales, the duration of therapy had no influence on therapy outcome or re- ferral. How long male clients stay in therapy is connected to a "too submissive" in- terpersonal style assessed by the IIP. This leads to the conclusion that males with low dominance values need longer internal treatment as a kind of compensation, in order to reach the same symptom reduction as dominant men. This fits quite well with the fact that the likelihood of being referred can be predicted rather by the initial symptom severity than by the severity remaining at the end of therapy. So the therapists knew that a longer treatrnent would be needed, but considered a longer preliminary treatment necessary to motivate and stabilize the patient for the "free therapy market."
DISCUSSION
The effect sizes of symptom change in this study were in the medium range. This was expected for patients mainly seen for the purpose of diagnosis and in prepara- tion for long-term treatment. As also expected, patients who considered their inter- personal behavior as too nurturant and too exploitable (high on the affiliation axis), could profit more from short-term therapy. Besides, the IIP showed a gender spe- cific irnpact: male patients get referrals even after longer therapy, so that the out- patient clinic treatment becomes a preliminary treatment. When having a rather "sub- missive-cold" attitude, as was more often found among them, they were not easily motivated to pursue long-term psychotherapy. Therapists possibly don't trust them to find a possibility for ongoing treatment by themselves. That means in fact that therapists adapt to their patients' self-evaluations.
Female patients who receive longer treatment don't get referrals as often. They receive real short-term therapies, completed within this outpatient therapy Format. This phenomenon can assurnably be explained by the higher motivation of fernales to use psychotherapy. Traditionally, the portion of women in psychotherapy is higher, as expected by the prevalence rates of disorders.
Aitogether, it becomes clear that prediction models with complex variables such as interpersonal problems, which are typical for heterogeneous samples in natural- istic studies, lead to differentiated (though not very strong) results.
Generally, the study confirms positive affiliation, which is behavior subjectively perceived as overly nurturant, to be an independent positive predictor of psycho- therapy outcome. Aspects of dominant behavior rather seemed to determine process Parameters, e.g., treatrnent duration and referral to ongoing therapy. It will have to be investigated in future studies whether the affiliation results imply that patients with a negative affiliation run into the risk of having their negative self-perception confmed in the therapy because of lack of success. Such a study would have to include other global and direct outcome rneasures.
The missing influence of the initial severity on the duration of therapy is known for short interventions (Svartberg & Stiles, 1991) and is probably connected to global remoralization processes as described by Howard, Lueger, Maling, and Martinovich (1993) in their theory of psychotherapy phases (see also Lueger, 1995). This initial relief is Seen for many patients who begin psychotherapy after a long period of hesitation and fears, and then usually find helpful support.

144 SCHAUENBTJRG ET AL.
But it must not be overlooked that the part of variance explained by the IIP is com- paratively small. In our opinion, this has to do with the fact that therapists adjust their therapeutic strategies to the interpersonal experience of their patients, in the sense of adapting their treatment. They do not and should not let thernselves be induced by their patients to rejecting interactions in the sense of a complementary aaing out. This paradox is a basic problem of every outcome study that tries to use Person and interac- tion variables as predictors, because interactional or dyadic aspects are difficult to as- sess. Besides, the chronicity of the disorders or Symptoms might play a role for the interpersonal interaction Patterns. Although the duration of the symptoms is not corre- lated with the localization in the circumplex, the presence of a personality disorder tends to have a gender-specific effect women with a personality disorder had lower scores on the affiliation axis, whde males had a little higher scores (Multiple Analysis of Vari- ance [MANOVAI, interaction effect gender personality disorder F[1,177I3 3 . 2 2 ; ~ = .08). The gender-specific effect of the dominance localization remains untouched by this.
The purpose of our work was to demonstrate the usefulness of an instrument that is based on interpersonal circumplex models and is capable of assessing clini- cally relevant aspects when applied routinely. The Inventory of Interpersonal Prob- lems is, in our opinion, not suited as an outcome instmment for shorter therapies, at least with the present instmction, since it is developed to measure traits that can only be changed over a long period of time. But it is very useful for predictive pur- poses in psychotherapy outcome research. Interpersonal behavior has an effect on the process and perspective of psychotherapy that is independent of other influences. Further studies will have to investigate whether primary interpersonal styles are less important in inpatient or long-term outpatient treatments, and also, if effects can be shown on other aspects of the process, like the dropout rate.
REFERENCES
Alden, L. E., Wiggins, J. S., & Pincus, A. L. (1990). Consuuction of circurnplex scales for the inven- tory of interpersonal problems. J Personal As- Ses, 55, 521-536.
Backhaus, W., Erickson, B., Plinke, W., & Schuchard-Ficher, B. (1987). Multiuariate Analysemethoden, 4. Auflage. Springer, Berlin, Heidelberg, New York.
Barkham, M., Stiles, W. B., & Shapiro, D. A. (1993). The shape of change in psychotherapy: Longi- tudinal assessrnent of personal problems. JCon- sul Clin Psychol, 61, 667477.
Bartholomew, K . , & Horowitz, L. M. (1991). At- tachment styles among young adulrs: A test of a four-category model. J Personal Soc Psychol, 61, 226244.
Benjamin, L. S. (1993). Intetpmonal diagnosis of petsonality disorders. New York: Guilford Press.
Capreol, M. J., & Alden, L. E. (1993). Avoidant personality disorder. Interpersonal problerns as predictors of treatrnent response. Behavior Therapy, 24, 357-376.
Cohen, J. (1977). Statisticalpouietanalysis for the behauioral sciences. New York: Academic Press.
Davies-Osterkarnp, S., Strauß, B. M., & Schmitz, N.
(1996). Interpersonal problerns as predictors of syrnptom-related treatment outcome. Psycho- therapy Research, 6, 164-176.
Derogatis, L. R. (1983). Administration, scoring andprocedures manual. Towson, MD: Clinical Psychometrie Research.
Eldredge, K. L., Locke, K. D., & Horowitz, L. M. (1998). Patterns of interpersonal problems as- sociated with binge eating disorder. J Eating Disorh, 23 (4, 385389.
Filak, J., Abeles, N., & Norquist, S. (1986). Clients' pretherapy interpersonal attitudes and psycho- therapy outcorne. ProJessional Psychology, Re- search und Practice, 1 7, 217-222.
Franke, G. (1995). SCL-90-R. Die Symptom-Check- liste von Derogatis. Göttingen: Beltz Test.
Freud, S. (1912). Zur Dynamik der Übertragung. Gesammelte Werke Bd. W I 1912, 363374.
Gifford, H . , & O'Connor, B. (1987). The interper- sonal circurnplex as a behavior map. ]Personal Social Psychol, 52, 10 19-1026.
Grawe, K., Donati, R., & Bernauer, F. (1994). m h o - thempie im Wandel. Von der Konfwion m r h - fession. Göningen: Hogrefe.
Gurtman, M. B. (1992). Constmct validity of in-

INTERPERSONAL PROBLEMS AND SHORT-TERM PSYCHOTHERAPY 145
terpersonal personality measures: The interper- sonal circumplex as a nomological net. JPer- sonal Social Psychol, 63, 105-118.
Gurtman, M. B. (1996). Interpersonal prob- lems and the psychotherapy context: The con- struct validity of the Inventory of Interpersonal Problems. Psychological Assesmenl, 8, 241- 255.
Hartmann, A., & Herzog, T. (1995). Varianten der effektstärkenberechnung in meta-analysen: Kommt es zu variablen ergebnissen? Z Klin P~ycbol, 24, 337-343.
Hautzinger, M., Bailer, M., Worall, H., & Keller, F. (1995). Beck-Depressions-Inventar - BDI. Testhandbuch. Bern: Hans Huber.
Hoglend, P. (1993). Suitability for brief dynamic psychotherapy: psychodynarnic variables as pre- dictors of outcome. Acta Psychiatr Scand, 88, 104110.
Horowitz, L. M., Rosenberg, S. E., Baer, B. A., Ureno, G., & Villasenor, V. S. (1988). Inventory of interpersonal problems: Psychometric prop- erties and clinical applications. J Consult Clin Psychol, 56, 885-4392,
Horowitz, L. M., Rosenberg, S. E., & Bartholomew, K. (1993). Interpersonal problems, attachment styles and outcome in brief dynamic psycho- therapy. J Consult Clin Psychol, 61, 549-560.
Horowirz, L., Strauß, B., Kordy, H. (1995). Das Inventar zur Erfassung interpersoneller Problem+IIP. Weinheim: Beltz Testverlag.
Howard, K. I,, Lueger, R. J., Maling, M. S., & Martinovich, 2. (1993). A phase model of psycho- therapy outcome: Causa1 mediation of change. J Consult Clin Psychol, 61, 678-685.
Jöreskog, K. G., & Sörbum, D. (1993). DOS-LISREL 8.03: Analysis of Linear Stmctural Relationships. Chicago: Scientific Software International, Inc.
Kiesler, D. J. (1983). The 1982 interpersonal circle: A taxonomy for cornplementarity in human transactions. Psychol Rev, 90, 185211.
Kiesler, D. J . (1996). Contemporary interpersonal rheory and research. New York: Wiley.
Leary, T. (1957). Interpersonal Diagnosis of Per- sonality. New York: The Ronald Press Co.
Lueger, R. J. (1995). Ein Phasenmodell der Veränderung in der Psychotherapie. Psycho- therapeut, 40, 267.
Manz, R., Henningsen, C., & Rudolf, G. (1995). Methodische und statistische Aspekte der Therapieevaluation am Beispiel der Berliner Therapiestudie. Psychoiher Psychosom Med Psychol, 45, 52-59.
Meresrnan,J. F., Horowitz, L. M., & Bein, E. (1995). The treatment assignment, dropout, and out- come of depressed patients who somaticize. Psychotherapy Research, 5 , 245-257.
Moskowitz, D. S. (1994). Cross-situational gener- ality and the interpersonal circumplex. J Per- sonal Soc Psychol, 66, 921-933.
Pincus, A. L., Gurtman, M. B. (1995). The three faces of interpersonal dependency: structural analyses of self-report dependency measures. J Personal SocMl Psychol, 69, 744758.
Plutchik, R., & Conte, H. R. (1998). Circumplex models ofpersonality und emotions. Washing- ton, DC: American Psychological Press.
Racker, H. (1978). tibertragung und Gegenüber- tragung. München: Reinhard.
Schauenburg, H. (1993). Erfahrungen mit der Diagnostik nach ICD-10 in einer psychotherapeu- tischen Ambulanz für Studierende. W. Schneider, H. J. Freyberger, A. Muhs, & G. Schüßler (Eds.) Diagnostik und Kkmijibtion nach ICD-I0 (pp. 237-2471, Kap. V; hrsg. V. Göttingen: Vanden- hoeck & Ruprecht.
Schauenburg, H. (2000). Bindungstheoretische und interpersonelle Aspekte kunerpsychothera- peutischer Interuentionen. Frankfurt: VAS.
Schauenburg, H., Pekrun, G., & Leibing, E. (1995). Diagnostik interpersonaler Probleme bei depressiven Stömngen. Z Klin Psychol Psy- chopath Psychoth, 43, 200-21 3.
Schauenburg, H., & Strack, M. (1999). Measuring psychotherapeutic change with the SCL-90-R. Psychother Psychosom, 68, 199-206.
Schepank, H. (1995). Der Beeinträchtigungs- schwerescmBSS, Handanweisung. GöRingen: Belrz.
Smith, M. L., & Glass, G. V. (1977). meta-analysis of psychotherapy outcome studies. Am Psy- chologist, 32, 752-760.
Strauß, B . , & Hess, H. (1993). Interpersonale Prob- leme, interpersonale Orientierung und Behand- lungserfolg nach stationärer Gruppenpsycho- therapie. Psycbotber Psychosom Med Psychol, 43, 82-92.
Strong, S. R., Hills, H. I,, Kilmanin, C. T., De Vries, H., Lanier, K., Nelson, B. N., Strickland, D., & Meyer 111, C. W. (1988). The dynamic relations among interpersonal behaviors: A test of complementarity and anticomplementariry. J Personal Social Psychol, 54, 79E-810.
Stnipp, H. H., Horowitz, L. M., Lambert, M. J. (1998). Measuring Patient changes in mood, anxiety und personality disorders-towards a core battety. Washington, DC: American Psy- chological Association.
Sullivan, H. (1953). B e intetpersonal theory of psrchiatry. New York: Norton.
Svartberg, M., & Stiles, T. C. (1991). Comparative effects of short-term psychodynamic psycho- therapy: A meta-analysis. JConsult Clin Psychol, 59, 704-714.
Thompson, B. J., Hill, C. E., & Mahalik, J. R. (1991). A test of the complementarity hypoth- eses in the interpersonal theory of psycho- therapy: Multiple case comparisons. Psycho- therapy, 28, 572-579.
Weiss, J., & Sampson, H. (1986). Thepsycho-

SCHAUENBURG ET AL.
analytic process Theory, clinical observation domain. J Personal Social Psychol, 3 7, 395- und empirical research. New York: Guilford 412. Press. Wiggins, J. S., & Broughton, R. (1991): A geomet-
Wiggins, J. S. (1979). A psychological taxonomy ric taxonomy of personality scales. EumpJPer- of trait-descriptive terms: The interpersonal sonal, 5, 343-365.
Zusammenfassung In einer naturalistischen Ergebnisstudie wurden Aspekte der Validität des Inventars zur Erfassung interpersonaler Probleme (IIP, Horowitz et al.) untersucht. Die Stichprobe bestand aus 180 Patienten, die eine psychodynamische Kurzzeitpsychotherapie mit durchschnittlich 7.8 Sitzungen und einer mittleren Dauer von 3.4 Monaten erhielten. Sehr geringe Veränderungen im Prä-Post-Vergleich implizieren, dass das IIP nicht als Evaiuationsinstmment zur Erfassung von Kurzzeitpsychotherapieeffekten empfohlen werden kann, da die Items sich auf überdauernde Eigenschaften beziehen. Mit Hilfe von Pfadanalysen konnten wir zeigen, dass ein höherer Wert auf der Zuneigungsdimension des interpersonalen Circumplex mit besseren Therapieergebnissen einhergeht. Der Einfluss der Dominanzdimension dagegen erwies sich als geschlechtsabhängig. Männliche Patienten, die insgesamt abweisenderes und introvertierteres Verhalten beschreiben, erhielten-wenn sie abweisend und introvertiert w a r e n d i n e längere ,Ein- führungsbehandlung", nach der sie-im Falle ausgeprägter Symptomatik-oftmals einer Langzeit- psychotherapie zugewiesen wurden. .Dominanten männliche Patienten und weibliche Patienten mit hohen Symptomwerten wurden rascher, nach nur wenigen Sitzungen überwiesen. Die Ergebnisse werden unter dem Aspekt adaptiven Therapeutenverhaltens diskutiert.
&um€ Cette etude naturaliste de resultats a investigue des aspects de validite de I'lnventaire de Problemes Interpersonnels (IIP, Horowitz et al.). L'echantillon etait compose de 180 patients recevant en moyenne 7.8 kances de psychotherapie psychodynamique breve durant 3.4 mois en moyenne. Des changements peu importants dans les mesures pre-post impliquent que I'IIP n'est pas i2 recommander en tant qu'instrument d'evaluation des Kisultats dans Une psychothkrapie b*e, vu que ses items mesurent des traits plut6t stables. Nous avons cependant pu montrer par Une analyse des coefficients de direction (path analysis) qu'un score eleve dans la dimension affiliative du circumplexe interpemmel allait de pair avec un meilleur ksultat du traitement. L'influence de la dimension . dominance . depend du sexe : des pa- tients miles qui, dans cet echantillon, montrent en general un comportement plus dedaigneux er introverti, ont btneficie d'une therapie - introductive plus longue avant d'etre, en cas de charge symptomatique irnportante, transmis pour un traitement 3 long terme. Des patients . dominants . et en gtneral des patientes avec un taux de syrnptornes haut ktaient transmis plus rapidement, apres quelques seances. Les resultats sont discutes SOUS I'aspea d'une attitude adaptative du therapeute.
Resumen Este estudio naturalista de resultados investig6 algunos aspectos de la validez del Inventario de Problemas Interpersonales IIP (Horowitz et al.). La muestra estuvo constituida por ciento ochenta pacientes que recibieron psicoterapia psicodinimica breve con un promedio de 7.8 sesiones y una duracion tambien promedio de 3.4 meses. Las escasas vaiaciones entre las mediciones pre-post indican que la IIP no es recomendable para evaluar resultados de psicoterapia a corto plazo, debido al caricter de rasgos de sus items. Sin embargo, pudimos mostrar, por medio de anilisis de pasos, que un puntaje mis alto en la dimensi6n afdiativa del complejo interpersonal corre parejo con la mejoria del tratamiento. La influencia de la dirnensi6n "dominancia" esta ligada al genero: los pacientes masculinos, que en esta muestra generalmente registran un componamiento m5s displicente e introvertido, recibieron una terapia mis larga "introductorian, luego de la cual -en caso de una gran carga de sintomas-se los denv6 a tratamiento a largo plazo. Los pacientes masculinos "dominantes" y, en general, las pacientes femeninas con puntajes altos e n sintomas se derivaron mis ripido, luego de u m s pocas sesiones. Se discuten los resultados de la actinid adaptativa del terapeuta.
Received February 2, 1999 R d i o n received May 21, 1999
Accepted May 26, 1999





























