Embed Size (px)
Citation preview

Brrtrsh Jourd of Plasm Surgery (1995). 48. 533-539 0 1995 The Bntish Assocdon of Plastic Surgeons
Internal mammary vessels : a reliable recipient system for free flaps in breast reconstruction
M. Ninkovid, H. Anderl, L. Hefel, A. Schwabegger and G. Wechselberger
University Clinic for Plastic and Reconstructive Surgery, Innsbruck, Austria
SUMMAR Y. In breast reconstruction with a free flap following mastectomy, the recipient vessels most widely used are in the axillary system, which limits flap movement and flexibility in breast shaping. In addition, scarring and fibrosis can make dissection of the vessels difficult.
We have performed 22 breast reconstructions using a free transverse rectus abdominis myocutaneous (TRAM) flap anastomosed to the internal mammary (thoracic) vessels. There has been no flap failure. The surgical techniques and the advantages and limitations of the internal mammary system are presented and the internal mammary vessels compared with the axillary vessels as a recipient vascular system.
Current methods of autogenous tissue reconstruction of the female breast include the free or conventional transverse rectus abdominis myocutaneous (TRAM) flap,“l latissimus dorsi flap,l’-l8 gluteal free flap,1g-22 lateral transverse thigh flap,23 superficial inferior epi- gastric flap24 and groin flap. 15, 25 Free flap breast reconstruction offers several advantages over con- ventional flaps and has become a routinely performed technique.2-6s 26
The difficulties involved in microsurgical techniques of breast reconstruction are much more associated with the recipient vessels, especially in irradiated patients, than with the donor vessels.2-5,1s122 The recipient vessels most commonly used are the thoraco- dorsal vessels.lmll For optimum flap positioning and anastomosis to the thoracodorsal artery and vein, long flap pedicles or even vein grafts are required.
In our experience, the use of axillary vessels as the recipient system limits the flap movement required to achieve greater medial projection, ptosis, and ideal breast symmetry. In secondary breast reconstruction, scar formation and fibrosis in the axilla make dis- section of the vessels difficult.
During the past 3 years, we have performed breast reconstructions with TRAM flaps anastomosed to the internal mammary vessels. Based on the results of our anatomical studies as well as the clinical findings, we came to conclude that this recipient vascular system is far superior to others with regard to breast position and natural ptosis.
Methods
Between March 1992 and June 1994,22 delayed breast reconstructions were performed with free TRAM flaps. The interval between mastectomy and recon- struction ranged from 8 months to 5 years (average 34 months). The mean age of the patients was 46 years, with the youngest being 3 1 and the oldest 64 years old. 82 % of the patients had undergone modified radical
mastectomy, 9 % subcutaneous mastectomy and 9 % radical mastectomy (Table 1). Whenever possible, 2 units of autologous blood were collected pre- operatively for possible transfusion.
Surgical technique
The day before surgery, the flap design is outlined with the patient in a standing position, so that the infra- mammary line can be determined. The TRAM flap has the shape of a horizontal ellipse just above the pubic hair line inferiorly and remaining below the umbilical level superiorly. This design ensures better contouring of the abdominal wall and allows the horizontal scar to be placed very distally, similar to a standard abdominoplasty. The small vertical scar resulting from incision around the umbilicus is nearly invisible.
On the same day, colour Doppler ultrasound is performed to detect the number (two or three) and location of the main perforators of the epigastric artery as well as the size and location of the internal mammary vessels. Based on these findings, the area where the big perforators are localized is chosen as the donor site. Two operating teams work simultaneously on the donor and recipient sites. The TRAM flap is elevated in a standard approach, beginning laterally and including a very small piece of the rectus abdominis muscle. The pedicle must be dissected as long as possible.
Dissection of the recipient vascular system
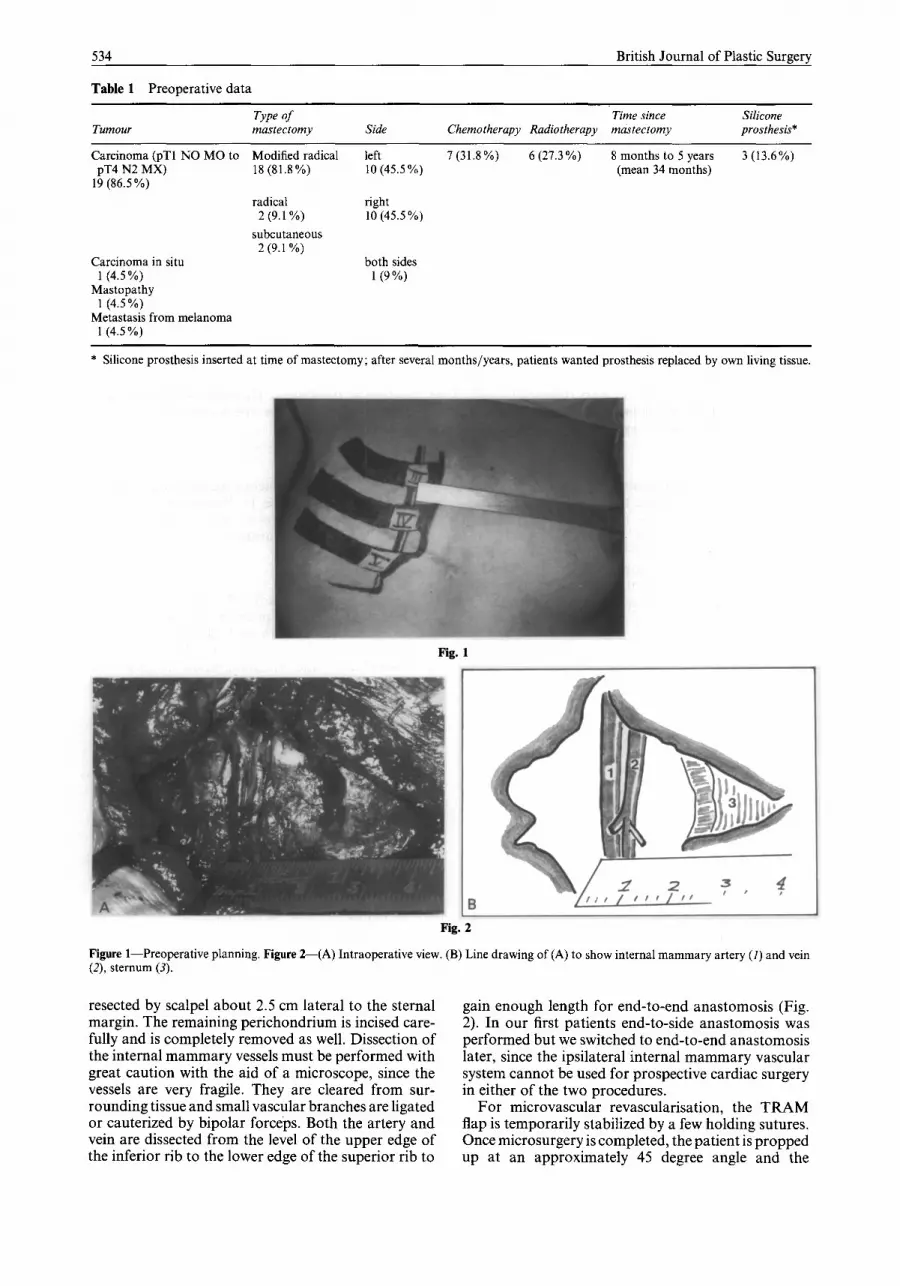
The scar tissue resulting from the mastectomy is excised for histological examination and the chest skin flaps are elevated. After elevation of the superior and inferior skin flaps, the costal cartilages of the 3rd, 4th or 5th rib are identified (Fig. 1). Which rib is selected for resection depends on the findings of colour Doppler ultrasound, in particular the level of the vessels with the largest diameter. After dissection of the perichondrium, a 2 cm piece of costal cartilage is
533
534
Table 1 Preoperative data
British Journal of Plastic Surgery
Tumour Type of mastectomy Side
Time since Silicone Chemotherapy Radiotherapy mastectomy prosthesis*
Carcinoma (pT1 NO MO to pT4 N2 MX)
19 (86.5 %)
Carcinoma in situ 1 (4.5 %)
Mastopathy 1 (4.5%)
Metastasis from melanoma 1 (4.5%)
Modified radical 18 (81.8%)
left 7 (31.8%) 6 (27.3 %) 8 months to 5 years 3 (13.6%) 10 (45.5 %) (mean 34 months)
radical 2 (9.1%)
subcutaneous 2 (9.1%)
right 10 (45.5 %)
both sides 1 (9%)
* Silicone prosthesis inserted at time of mastectomy; after several months/years, patients wanted prosthesis replaced by own living tissue.
Fig. 1
Fig. 2
Figure l-Preoperative planning. Figure 2-(A) Intraoperative view. (B) Line drawing of (A) to show internal mammary artery (I) and vein (2), sternum (3).
resected by scalpel about 2.5 cm lateral to the sternal margin. The remaining perichondrium is incised care- fully and is completely removed as well. Dissection of the internal mammary vessels must be performed with great caution with the aid of a microscope, since the vessels are very fragile. They are cleared from sur- rounding tissue and small vascular branches are ligated or cauterized by bipolar forceps. Both the artery and vein are dissected from the level of the upper edge of the inferior rib to the lower edge of the superior rib to
gain enough length for end-to-end anastomosis (Fig. 2). In our first patients end-to-side anastomosis was performed but we switched to end-to-end anastomosis later, since the ipsilateral internal mammary vascular system cannot be used for prospective cardiac surgery in either of the two procedures.
For microvascular revascularisation, the TRAM flap is temporarily stabilized by a few holding sutures. Once microsurgery is completed, the patient is propped up at an approximately 45 degree angle and the
Internal mammary vessels for free flaps
Fig. 3
Fig. 4
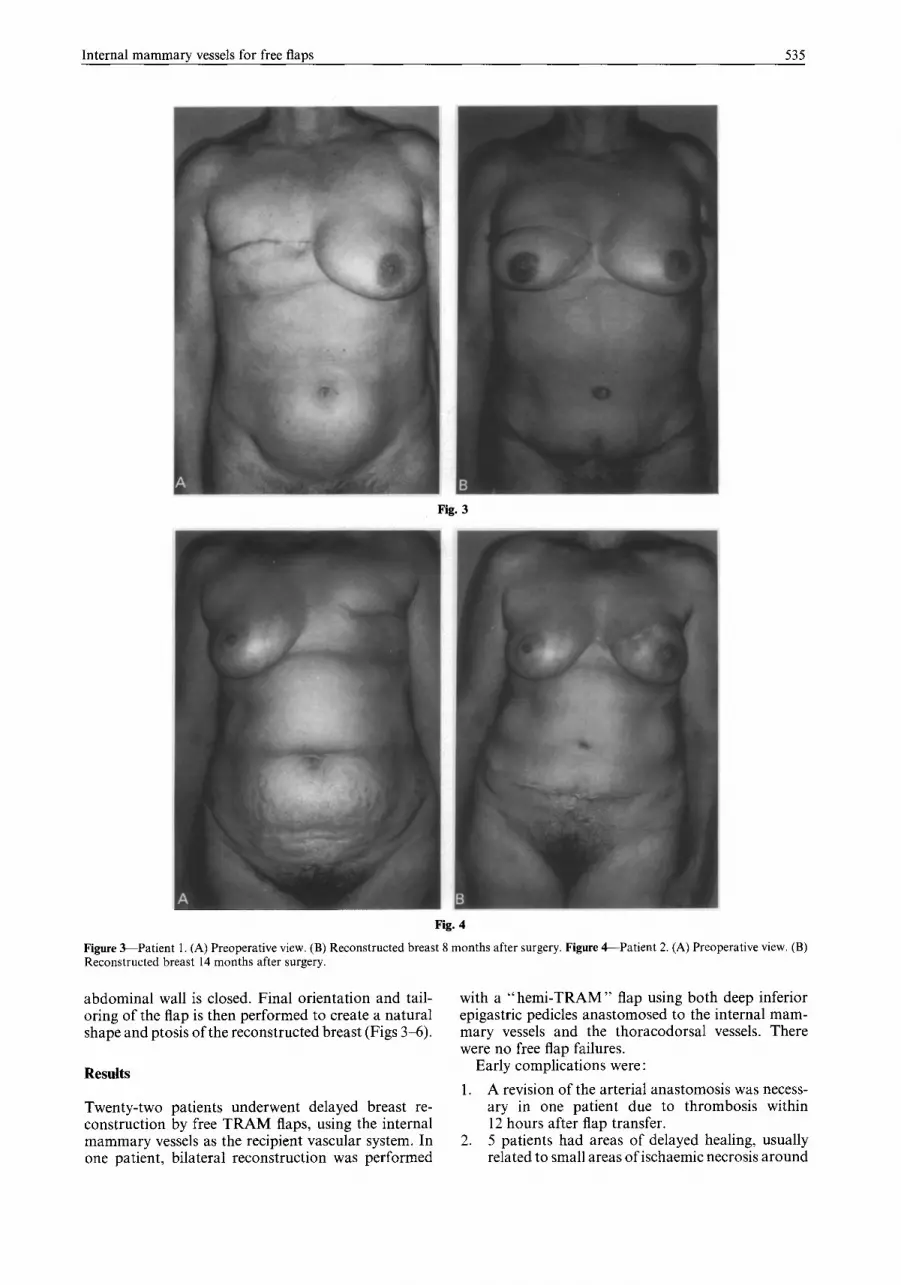
Figure S-Patient 1. (A) Preoperative view. (B) Reconstructed breast 8 months after surgery. Figure &Patient 2. (A) Preoperative view. (B) Reconstructed breast 14 months after surgery.
abdominal wall is closed. Final orientation and tail- oring of the flap is then performed to create a natural shape and ptosis of the reconstructed breast (Figs 3-6).
Results
Twenty-two patients underwent delayed breast re- construction by free TRAM flaps, using the internal mammary vessels as the recipient vascular system. In one patient, bilateral reconstruction was performed
with a “hemi-TRAM” flap using both deep inferior epigastric pedicles anastomosed to the internal mam- mary vessels and the thoracodorsal vessels. There were no free flap failures.
Early complications were : 1. A revision of the arterial anastomosis was necess-
ary in one patient due to thrombosis within 12 hours after flap transfer.
2. 5 patients had areas of delayed healing, usually related to small areas of ischaemic necrosis around
536 British Journal of Plastic Surgery
Fig. 5
Fig. 6
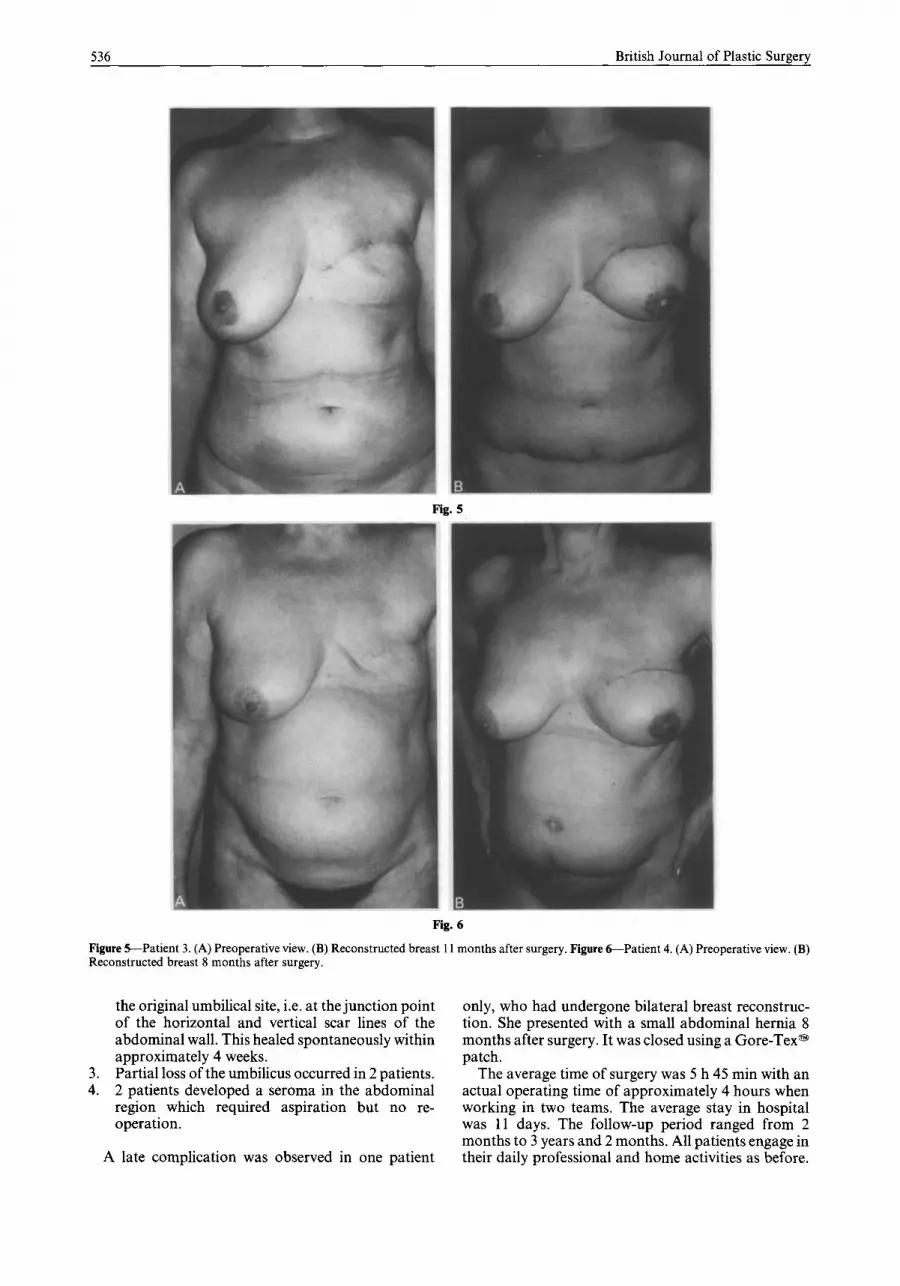
Figure S-Patient 3. (A) Preoperative view. (B) Reconstructed breast 11 months after surgery. Figure &Patient 4. (A) Preoperative view. (B) Reconstructed breast 8 months after surgery.
the original umbilical site, i.e. at the junction point only, who had undergone bilateral breast reconstruc- of the horizontal and vertical scar lines of the tion. She presented with a small abdominal hernia 8 abdominal wall. This healed spontaneously within months after surgery. It was closed using a Gore-Tex@’ approximately 4 weeks. patch.
3. Partial loss of the umbilicus occurred in 2 patients. The average time of surgery was 5 h 45 min with an 4. 2 patients developed a seroma in the abdominal actual operating time of approximately 4 hours when
region which required aspiration but no re- working in two teams. The average stay in hospital operation. was 11 days. The follow-up period ranged from 2
months to 3 years and 2 months. All patients engage in A late complication was observed in one patient their daily professional and home activities as before.

Internal mammary vessels for free flaps
Table 2 Details of patients illustrated
537
Case Initials Age (years) Tumour
1 (Fig. 3) K.H. 51 PT AM, 2 (Fig. 4) T.M. 43 PTP& 3 (Fig. 5) Z.J. 43 PT&M, 4 (Fig. 6) S.I. 52 PT AM,
TYPO of mastectomy, side
modified radical, right
modified radical, left
modified radical, left
modified radical, left
Chemotherapy Radiotherapy
no no
yes yes no no
no no
Time since mastectomy
2 years 6 months
5 years
2 years
3 years
Details about the patients illustrated in Figures 3-6 are given in Table 2. No reduction mammoplasty was performed on the opposite side, since all the patients insisted on leaving their healthy breast untouched.
Discussion
A new approach to breast reconstruction began in the 1970s with the rediscovery of the latissimus dorsi myocutaneous flap”-” used together with a silicone prosthesis. Although early results were good, longer follow-up has revealed problems such as capsular contractures, malposition, inappropriate size and very often aesthetically inadequate results. As pointed out by De Mey et al., the rate of these late complications is 30 %.l8 Using extended latissimus dorsi flaps, some authorsl’x l7 attempted to eliminate these problems caused by the prosthesis. However, this technique creates a longer scar in the back and more complications at the donor site.
In recent years, more interest has been given to breast reconstruction by free flaps.‘-‘ja 15, lgmz5 The gluteus maximus myocutaneous free flap was first reported by Fujino et a1.1g~20 In spite of adequate reconstruction of the breast mound, in most patients the position of the breast was too high on the chest due to a short vascular pedicle. Other free transfers performed included the groin flap with silicone breast prosthesis,15, 25 the contralateral latissimus dorsi flap,15 and the inferior gluteal free flap.”
The first “free abdominoplasty flap” described by Holmstrom in 1979 was a composite myocutaneous flap based on the inferior epigastric vessels.’ Soon after this, the transverse rectus abdominus myocutaneous island (TRAM) flap became the most popular method of autogenous reconstruction. Hartrampf et a1.,8 Scheflan and Dinner93 lo presented very good results using conventional pedicled TRAM flaps. Many other authors emphasized the advantages of free TRAM flapsl-‘j The problem most commonly associated with pedicled TRAM flaps is flap ischaemia, manifested as fat necrosis and/or partial skin necrosis.2m6
In breast reconstruction with a free flap the selection of suitable recipient vessels remains one of the most critical decisions for the surgeon. In our experience this selection should be based on:
1. The time of breast reconstruction
When using a free flap in immediate breast recon- struction, the recipient vessels in the axilla have already been dissected and are ready for anastomosis. In cases planned for free TRAM flap reconstruction, Grotting
recommended “maintaining the superior rectus muscle pedicled until the adequacy of the recipient vessels has been verified”.5 In late reconstruction we have often found these vessels to be heavily scarred, small, vulnerable and unsuitable for microvascular surgery.
2. The length of the free pap pedicle and the recipient artery
The length of the flap pedicle and the recipient vessels determine the flexibility of flap positioning and tissue moulding and thus the possibility of achieving ad- equate breast projection and symmetry. Using micro- anastomoses to the axillary system, the “freedom of movement” of the free flap is very often limited. Due to the extensive range of movements of the shoulder, sufficient length of the pedicle is essential to prevent its disruption.
3. The diameter and site of the recipient vessels
After radiotherapy, the vessels in the axilla tend to be small and surrounding fibrosis makes dissection very difficult. When using the thoracodorsal artery proxi- mal to the branches to the serratus anterior muscle in order to preserve the blood supply of the latissimus dorsi muscle,14 the portion of the rectus muscle included in the free TRAM flap usually cannot be placed just beneath the point of maximum projection of the breast mound. Therefore the medial contour of the reconstructed breast cannot be matched to the opposite breast.
In 1980, Harashinaz5 recognized the possibility of using the internal mammary vessels as recipient vessels by using a free groin flap for breast reconstruction. In 1983, ShawZ1 presented excellent results of breast reconstruction with superior gluteal free flaps. Out of 10 cases, 7 had the internal mammary artery as the recipient artery and in 4 cases internal mammary veins were used as recipient veins. In other patients, he used vein grafts to the axilla or mobilised the cephalic vein from the middle of the upper arm. On several occasions, he found that the internal mammary vein instead of being one large vessel consisted of two smaller veins, making an anastomosis much more risky or impossible. He dissected the internal mam- mary artery and vein after resection of the 5th costal cartilage. In 1989, Paletta et al. reported the same experience with the internal mammary vessels during the application of four inferior gluteal free flaps for breast reconstruction.22
Our anatomical studies revealed that the internal mammary artery and veins commonly had large

538 British Journal of Plastic Surgery
calibres and that their location in the 3rd or 4th intercostal space was very consistent. In each case colour Doppler ultrasound (Toshiba SSA-270 HG, Linear 7.5 MHz Picker CS 192 PQ Hitachi) was used preoperatively to determine the exact location and calibre of the internal mammary artery and comitant veins as well as the location and number of the main perforators of the TRAM flap. Depending on the results of ultrasound examination, we resected the cartilage of the 3rd, 4th (mostly), or 5th rib to mobilize the internal mammary artery and vein. Due to this procedure, we had no difficulty in finding an adequate vein and artery for microvascular anastomosis in any of the 22 patients. Knowing the location and number of perforators simplifies the decisions about which side and which part of the rectus muscle it would be better to take. In 8 1.8 % (18 cases) we dissected the TRAM flap based on the ipsilateral vascular system. This means that only on the reconstructed side were the recipient internal mammary and deep inferior epi- gastric donor vessels used, leaving the contralateral vascular system intact in case it should be required for future cardiac surgery.
The advantages of the internal mammary vascular system over the axillary vascular system are :
Consistent location (mean 15.35 mm lateral to the margin of the sternum). Large calibre (artery mean diameter 1.87 mm; vein mean diameter 1.97 mm). Easy preparation after the resection of costal cartilage. Maximum “freedom of flap movement” to achieve the best projection and medial contour of the reconstructed breast. No changes after radiotherapy and no scarring or fibrosis. Exact localization of vessels by preoperative colour Doppler ultrasound examination. Negative pressure in vein supports venous drainage of the flap. The risk of pedicle damage is decreased in cases having secondary reshaping of the breast, espe- cially by flap reinsertion to form the anterior axillary fold.
The disadvantages of the internal mammary vas- cular system versus the axillary vascular system are :
1. Thin and fragile vein wall. 2. Difficulties during microsurgery because of res-
piration. 3. Risk of pneumothorax. 4. The internal mammary artery cannot be used in
cardiac surgery after TRAM flap transfer (but other options exist).
In our 22 patients the problem of pneumothorax never occurred. With careful technique, perforation of the pleura can be avoided. Should the pleura be punctured, careful closure of the wound under positive airway pressure followed by the introduction of a catheter with a water seal is required. After the lung has expanded entirely, the catheter may be removed.”
Breast reconstruction is an aesthetically critical procedure and should be performed to match the
opposite breast in shape, contour, and position. Breast reconstruction with a free flap can achieve this goal. The selection of suitable recipient vessels is most important for successful free tissue transfer. In our opinion, the internal mammary vessels should be the recipient vascular system of choice for delayed breast reconstruction. For immediate reconstruction pro- cedures, however, the axillary vascular system is still to be preferred.
Acknowledgement The authors would like to thank Dr Berresheim Ulrike for her assistance in translating the manuscript.
This paper was presented in part at the 7th Congress, European Section, International Confederation for Plastic, Reconstructive and Aesthetic Surgery, Berlin, Germany, June 1993.
References 1. Holmstrijm H. The free abdominoplasty flap and its use in
breast reconstruction. Stand J Plast Reconstr Surg 1979; 13: 423-7.
2. Arnei ZM, Smith RW, Eder E, Solinc M, KersniE M. Breast reconstruction by the free lower transverse rectus abdominis musculocutaneous flap. Br J Plast Surg 1988; 41: 50&5.
3. Arnei ZM, Bajec J, Bardsley FA, Scamp T, Webster MHC. Experience with 50 free TRAM flap breast reconstructions. Plast Reconstr Surg 1991; 87: 47&82.
4. Arnei ZM, Scamp T. The bipedicled free TRAM flap. Br J Plast Surg 1992; 45: 2148.
5. Grotting CJ, Urist MM, Maddox AW, Vasconez OL. Con- ventional TRAM flap versus free microsurgical TRAM flap for immediate breast reconstruction. Plast Reconstr Surg 1989; 83: 82844.
6. Schusterman AM, Kroll SS, Weldon EM. Immediate breast reconstruction: why the free TRAM over the conventional TRAM flap? Plast Reconstr Surg 1992; 90: 255-61.
7. Robbins TH. Post-mastectomy breast reconstruction using a rectus abdominis musculocutaneous island flap. Br J Plast Surg 1981; 34: 28690.
8. Hartrampf CR, Scheflan M, Black PW. Breast reconstruction with a transverse abdominal island flap. Plast Reconstr Surg 1982; 69: 21624.
9. Scheflan M, Dinner M. The transverse abdominal island flap: part I. indications, contraindications, results, and com- plications. Ann Plast Surg 1983; 10: 1,24-36.
10. Scheflan M, Dinner M. The transverse abdominal island flap: part II. surgical technique. Ann Plast Surg 1983: 10: 2, 12&9.
11. Harashina T, Sone K, Inoue T, Fukuzumi S, Enomoto K. Augmentation of circulation of pedicled transverse rectus abdominis musculocutaneous flaps by microvascular surgery. Br J Plast Surg 1987; 40: 367-70.
12. Olivari N. The latissimus flap. Br J Plast Surg 1976; 29: 1268. 13. Schneider WJ, Hill HL Jr, Brown RG. Latissimus dorsi
myocutaneous flap for breast reconstruction. Br J Plast Surg 1977; 30: 277-81.
14. Maxwell GP, McGibbon MB, Hoopes JE. Vascular con- siderations in the use of a latissimus dorsi myocutaneous flap after a mastectomy with an axillary dissection. Plast Reconstr Surg 1979; 64: 771-80.
15. Serafin D, Voci EV, Georgiade GN. Microsurgical composite tissue transplantation: indications and technical con- siderations in breast reconstruction following mastectomy. Plast Reconstr Surg 1982; 70: 2434.
16. Marshall DR, Anstee EJ, Stapleton MJ. Soft tissue recon- struction of the breast using an extended composite latissimus dorsi myocutaneous flap. Br J Plast Surg 1984; 37: 361-8.
17. Papp C, Zanon E, McGraw J. Breast volume replacement using the de-epithelialized latissimus dorsi myocutaneous flap. Eur J Plast Surg 1988; 11: 12&5.
18. De Mey A, Lejour M, Declety A, Meythiaz AM. Late results and current indications of latissimus dorsi breast re- constructions. Br J Plast Surg 1991; 44: 14.

Internal mammary vessels for free flaps 539
19. Fujino T, Harashina T, Aoyagi F. Reconstruction for aplasia of the breast and pectoral region by microvascular transfer of a free flap from the buttock. Plast Reconstr Surg 1975; 56: 178-81.
20. Fujino T, Harashina T, Enomoto K. Primary breast recon- struction after a standard radical mastectomy by a free flap transfer. Plast Reconstr Surg 1976; 58: 3714.
21. Shaw WW. Breast reconstruction by superior gluteal micro- vascular free flaps without silicone implants. Plast Reconstr Surg 1983; 72: 490-9.
22. Paletta EC, Bostwick III J, Nahai F. The inferior gluteal free flap in breast reconstruction. Plast Reconstr Surg 1989; 84: 875-85.
23. Elliott LF, Beegle PH, Hartrampf CR. The lateral transverse thigh free flaps: an alternative for autogenous-tissue breast reconstruction, Plast Reconstr Surg 1990; 85: 169981.
24. Volpe AG, Rothkopf MD, Walton LR. Versatile superficial inferior epigastric flap for breast reconstruction. Ann Plast Surg 1994; 32: 113-7.
25. Harashina T, Imai T, Nakajima H, Fujino T. Breast re- construction with microsurgical free composite tissue trans- plantation Br J Plast Surg 1980; 33: 30-7.
26. Tuominen HP, Asko-Seljavaara S, Svartling NE. Cutaneous blood flow in the free TRAM flap. Br J Plast Surg 1993; 46: 665-9.
27. Converse, JM. Transplantation of bone. In: Converse JM, ed. Reconstructive plastic surgery. 2nd ed. Philadelphia: WB Saunders, 1977: 337-8.
The Authors
Milomir Ninkovif, MD Hans Anderl, MD Ludwig Hefel, MD Anton Schwabegger, MD Gottfried Wechselberger, MD
Universititsklinik fur Plastische und Wiederherstellungschirurgie, Anichstrage 35, 6020 Innsbruck, Austria.
Correspondence to: Milomir Ninkovic, Universitatsklinik fur Plastische und Wiederherstellungschirurgie, Anichstrage 35, 6020 Innsbruck, Austria.
Paper received 4 August 1994. Accepted 22 June 1995, after revision.





























