Embed Size (px)
Citation preview

A
I
m
opaIIo
©
K
1
wwvmdsii
1d
Available online at www.sciencedirect.com
Digestive and Liver Disease 40 (2008) 240–247
Alimentary tract
Interleukin-13 mucosal production in Helicobacter pylori-relatedgastric diseases
B. Marotti a, A. Rocco a, P. De Colibus a, D. Compare a, G. de Nucci a,S. Staibano b, F. Tatangelo d, M. Romano c, G. Nardone a,∗
a Department of Clinical and Experimental Medicine, Gastroenterology Unit, University of Naples “Federico II”, Italyb Department of Biomorphological and Functional Sciences, Pathology Unit, University of Naples “Federico II”, Naples, Italy
c Department of Medicine, Gastroenterology, Second University of Naples, Naples, Italyd Pathology Unit, Cancer Institute of Naples, Pascale Foundation, Italy
Received 17 July 2007; accepted 26 November 2007Available online 19 February 2008
bstract
A shift from Th1 (IFN-�) towards Th2 (IL-4)-type immune response was found in patients with gastric cancer and dysplasia. Recently,L-13 has been described as a central mediator of Th2-dominant immune response in different inflammatory diseases.
Aim and Methods. to analyse, by Enzyme-Linked-Immuno-SPOT (ELISPOT) assay and immunohistochemistry, the IL-13 production ofononuclear cells obtained from gastric biopsies of 19 H. pylori-negative subjects and 23 H. pylori-positive patients.Results. By ELISPOT, we did not find any significant variation of the spot range number of IL-13, IL-4 and IFN-� secreting cells, irrespective
f H. pylori status. After antigenic exposition, the spot range for IL-13, IL-4 and IFN-� significantly increased (p < .0001) only in H. pylori-ositive patients. A prevalent Th1 (IFN-�) immunoresponse was observed in 2/23 cases with active gastritis, while a prevalent Th2 (IL-13nd IL-4) was detected in 5/23 cases all with atrophic chronic gastritis of whom two with intestinal metaplasia. By immunohistochemistry,L-13, IL-4 and IFN-� were detectable in all cases directly related to the inflammatory infiltrate. In the two cases with intestinal metaplasia,
L-13 and IL-4 were localised in both inflammatory and epithelial cells. This immunopattern was confirmed in selected additional 10 casesf H. pylori-positive chronic atrophic gastritis with intestinal metaplasia and 10 cases of intestinal type gastric cancer.Conclusion. These preliminary results suggest that IL-13 could be implicated in the different outcome of H. pylori infection.2007 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
eywords: Helicobacter pylori; Gastric carcinogenesis; IL-13; Local immune response; Th2; ELISPOT assay
gltaioM(
. Introduction
Helicobacter pylori (H. pylori) is one of the mostidespread infectious agent affecting more than 50% of theorld’s population [1,2]. Although almost all infected indi-iduals develop from moderate to severe inflammation, theajority of these people remain asymptomatic, a minority
evelops symptomatic gastritis or peptic ulcer disease and a
maller subset develops gastric malignancies [3,4]. The clin-cal outcome of the infection depends on a number of factors,ncluding environmental factors, age at the time of infection,∗ Corresponding author. Tel.: +39 081 7464293; fax: +39 081 7464293.E-mail address: [email protected] (G. Nardone).
R4daoo
590-8658/$30 © 2007 Editrice Gastroenterologica Italiana S.r.l. Published by Elseoi:10.1016/j.dld.2007.11.021
enotype of the bacterium, host genetic susceptibility, andocal immune response [5–9]. Colonisation of the human gas-ric mucosa with H. pylori is associated with a complex localnd systemic immune response. However, H. pylori-relatedmmune reaction seems to contribute to the mucosal pathol-gy rather than being able to eliminate the infection [10–20].any studies have demonstrated a predominant Th1 response
IFN-�-mediated) in H. pylori-positive patients but recently,en et al. found a shift from Th1 (IFN-�) towards Th2 (IL-)-type immune response in patients with gastric cancer and
ysplasia. These authors suggested that the near completebsence of IFN-� production from the mucosa at the marginsf the tumour might be a critical factor in promoting growthf neoplastic cells [21]. Recently IL-13, functionally simi-vier Ltd. All rights reserved.

d Liver
lm
atebsc
rig
2
2
rPoewbai
emdtIa
sgi
lUt
2
tfifieiwncr
2
bmwCTsmtsaw
2
gtiutc11tHse
2
I4Mu(oacmcGr2ec5Tb
B. Marotti et al. / Digestive an
ar to its homologue IL-4, has been described as a centralediator of Th2-dominant immune response [22].Enzyme-Linked-Immuno-SPOT (ELISPOT) technique is
highly sensitive procedure that allows the ex vivo iden-ification of cells actively secreting cytokines [23–25]. Bynumerating dynamically the number of secreting cells, atasal level and after specific antigenic stimulation, ELISPOThows a sensitivity and specificity up to 200 times greater thanonventional ELISA [26–28].
The aim of the study was to dissect out the gastric immuneesponse to H. pylori infection by ELISPOT assay, focus-ng on IL-13 production of mononuclear cells isolated fromastric biopsies.
. Patients and methods
.1. Subjects
We enrolled 58 subjects (32 men; age range 26–63 years)eferred to our Endoscopic Unit for dyspeptic symptoms.atients who had previous H. pylori infection or had presencef anti-H. pylori antibodies or were treated successfully withradicating therapy were excluded. Furthermore, patientsho had taken antibiotics, histamine-2 receptor antagonists,ismuth, proton pump inhibitors, steroids or non-steroidalnti-inflammatory drugs in the last month were not includedn the study.
At least 12 biopsy specimens were taken during upperndoscopy in the gastric body, angulus and antrum. Further-ore, serum samples were collected from each patient to
etermine anti-H. pylori and anti-CagA antibodies (Helori-est IgG Chromo, Helori CTX IgG, Eurospital SpA, Trieste,talia). H. pylori status was evaluated according to rapid ure-se test (RUT), histology and serology.
In addition, we retrospectively selected from our endo-copic and pathological files 10 cases of chronic atrophicastritis with complete intestinal metaplasia and 10 cases ofntestinal type gastric cancer.
The study was performed in accordance with the guide-ines of the Institutional Ethics Committee of Federico IIniversity of Naples. Informed consent for personal data and
issue utilisation was obtained from all patients.
.2. Histopathological diagnosis
The histopathological diagnosis was done on hema-oxylin and eosin stained sections obtained from formalinxed, paraffin-embedded gastric mucosa samples. Modi-ed Giemsa stain was used for H. pylori identification. Inach biopsy sample, the presence of H. pylori, grade ofnflammation, glandular atrophy and intestinal metaplasia
as diagnosed and classified according to the up-dated Syd-ey system [29]. Intestinal metaplasia and gastric cancer werelassified according to Jass and Filipe, and Lauren’s criteria,espectively [30,31].2U(S
Disease 40 (2008) 240–247 241
.3. Isolation of mucosal cells
Mucosal cells were isolated from a pool of at least fiveiopsy specimens collected, in each patient, from antralucosa as previously described [32]. Briefly, biopsy samplesere treated with 600 U of collagenase IX (Sigma–Aldricho. St. Louis, MO, USA) under stirring agitation for 3–4 h.he mucosal cells were separated from the undigested tis-ue by cell strainer system and re-suspended in RPMI 1640edium, with 2 mM l-glutamine, 1% penicillin, 1% strep-
omycin, 1% nonessential amino acids and 10% foetal calferum heat-inactivated (BioWittaker, Cambrex). The numbernd viability of the cells were evaluated by a Burker chamberith nigrosine staining.
.4. Gastric antigenic extract
Gastric antigenic extract (GAE) was obtained from antralastric mucosa of each patient, irrespective of H. pylori sta-us. Briefly, at least three gastric biopsies were collectedn sterile buffer phosphate (PBS) and incubated for 3–4 hnder constant high stirring agitation. The mixture was fil-ered on the cell strainer system and the undigested tissue andells debris were separated by centrifugation at 2000 rpm for0 min. The suspension was centrifuged at 13,500 rpm for5 min, re-suspended in PBS, and then was measured spec-rophotometrically at OD560 [17]. The presence/absence of. pylori in the GAE was evaluated by modified Giemsa
taining performed on glass slides prepared with aliquots ofach sample.
.5. Cytokine specific ELISPOT assay
The number of mucosal cells secreting IL-13, IL-4 andFN-� was evaluated by ELISPOT technique using IL-13, IL-, IFN-� specific anti-human antibodies (Endogen, WoburnA, USA), as previously described [26]. Briefly, individ-
al wells of nitrocellulose bottomed 96 well millititre platesMAHA 4550 Millipore, Eschborn, Germany) were coatedvernight at 4 ◦C with 1.25 �g/ml of purified polyclonalnti-IL-13, polyclonal anti-IL-4 and monoclonal anti-IFN-�,lone 2G1, and then, blocked for 3 h. Subsequently, 2 × 105
ucosal cells from each patient was incubated in dupli-ate and in parallel, with (a) medium, (b) 100 �l of its ownAE (OD560: 0.2), (c) 10 �g/ml E. coli lipopolysaccha-
ide (LPS), (d) 3 �g/ml phytohemagglutinin (PHA) and (e).5 �g/ml H. pylori antigens strain 49503 (Meridian Life Sci-nce, Inc.). H. pylori antigens, LPS and PHA were used asontrol stimulants. After 40–42 h of incubation at 37 ◦C and% CO2, plates were extensively washed with PBS/0.05%ween20 and incubated for 2 h with 1.25 �g/ml of specificiotinylated antibody (anti-IL-13, clone 5A2; anti-IL-4, clone
5D2; anti-IFN-�, clone B1335 (Endogen, Woburn MA,SA). Thereafter, plates were washed, and streptavidin-HRPEndogen, Woburn MA, USA) was added for 1 h incubation.pots were developed by adding 3-amino-9-ethylcarbazole
2 d Liver Disease 40 (2008) 240–247
abGB
2
fatitstp4aMdUwewic(abrw
2
Mtpms
3
pjofit
(
Table 1Clinical and histological characteristics of the studied population
H. pylori-negative H. pylori-positiveNo. 19 No. 23N (%) N (%)
Sex (M/F) 11/8 14/9Age (range) 26–44 26–58IgG anti-H. pylori – 23 (100)IgG anti-CagA – 16 (69)Inflammatory infiltrate −/+ 23 (100)AAI
gmwapo
InnIs
b(tccf0F
drii(ficm
IC
Ingt
42 B. Marotti et al. / Digestive an
nd IL-13, IL-4 and IFN-� secreting cells were countedy an immunospot image analyser (A.EL.VIS, Hannover,ermany) and blindly at a stereomicroscope (Leica GZ6,uffalo, NY) by two separate observers (BM and PD).
.6. Immunohistochemistry
For each biopsy, 4-�m thick serial sections were cutrom paraffin blocks, mounted on acid-cleaned glass slides,nd heated at 55 ◦C for 60 min. Slides were re-hydrated,hen the endogenous peroxidase activity was inhibited byncubation with 3% H2O2 in methanol (20 min at roomemperature). To reduce non-specific background staining,lides were incubated with 5% goat serum (15 min at roomemperature). Finally, slides were incubated with the appro-riate primary antiserum in a moist chamber overnight at◦C (anti-IL-13, dilution 1:150; anti-IL-4, dilution 1:150nd anti-IFN-�, clone 2G1, dilution 1:100; Endogen, WoburnA, USA). The avidin–biotin–peroxidase complex proce-
ure (ABC standard, Vector Laboratories, Burlingame, CA,SA) was then performed. Peroxidase activity was detectedith diaminobenzidine as the substrate according to Hsu
t al. [33]. Finally, sections were weakly counterstainedith Harris’s hematoxylin and mounted. The intensity of
mmunopositivity for all the antibodies was graded as 0 (<5%ell with positive staining), 1 (5–30%), 2 (30–60%) and 3>60%). The histological and immunohistochemical evalu-tion was performed on all biopsy samples independentlyy two pathologists (AR and SS). After the independenteview, each case was evaluated jointly and disagreementsere resolved by consensus.
.7. Statistical analysis
Data were analysed using the SPSS package for Windows.ann–Whitney U-test was used to estimate significances of
he mean difference in the secreting cell number in the studyopulation; the Wilcoxon matched pairs test was used to esti-ate significances of the mean difference before and after
timulation. P < 0.05 was taken as level of significance.
. Results
The clinical and histological characteristics of the studiedopulation are summarised in Table 1. Sixteen out of 58 sub-ects enrolled in the study were excluded since the numberf mucosal cells isolated from biopsy specimens was insuf-cient for ELISPOT analysis. According to H. pylori status,
he population was grouped in:
(a) 19 H. pylori-negative: RUT and histology negative;absence of anti-H. pylori and anti-CagA serum antibod-
ies;b) 23 H. pylori-positive: RUT and histology positive; pres-ence of anti-H. pylori. Sixteen of those (69%) hadanti-CagA serum antibodies.
cfca
ctivity – 18 (80)trophy – 5 (22)
ntestinal metaplasia – 2 (9)
In the H. pylori-negative group, all subjects had normalastric mucosa with a minimal infiltration of lymphocytes andonocytes in the lamina propria. In H. pylori-positive cases,e found active non-atrophic chronic gastritis in 18/23 (80%)
nd a moderate degree of gastric atrophy in the remaining fiveatients associated with complete intestinal metaplasia in twof these (Table 1).
At basal level, we found a spot range number of IL-13,L-4 and IFN-� higher in H. pylori-positive than H. pylori-egative, but the differences were not significant (H. pylori-egative vs. H. pylori-positive; IL-13: 4–22 vs. 5–116, p 0.16;L-4: 3–20 vs. 1–87, p 0.22; IFN-�: 4–18 vs. 9–80, p 0.25ecreting cells; Figs. 1 and 2).
After GAE stimulation, the cytokines’ spot range num-er significantly increased only in H. pylori-positive patientsIL-13: from 5–116 to 4–220, p < .0001; IL-4: from 1–87o 9–356, p < .0001; IFN-�: from 9–80 to 10–350 secretingells, p < .0001; Figs. 1 and 2). None of H. pylori-negativeases significantly responded to GAE stimulation (IL-13:rom 4–22 to 3–55; p 0.07, IL-4: from 3–20 to 8–95, p.08; and IFN-�: from 4–18 to 10–27 secreting cells, p 0.06;igs. 1 and 2).
The analysis of Th type response after GAE stimulationemonstrated in H. pylori-positive cases a balanced Th1/Th2esponse (increase of IL-13, IL-4 and IFN-� secreting cells)n 16/23 (69%), a Th1 response (increase of IFN-� secret-ng cells) in 2/23 (9%) and a predominant Th2 responseincrease of IL-13 and IL-4 secreting cells) in the remainingve patients (Table 2). Interestingly, these five patients hadhronic atrophic gastritis associated with complete intestinaletaplasia in two of them.At basal level and post-GAE stimulation, the number of
L-13, IL-4 and IFN-� secreting cells did not correlate withagA positivity.
By immunohistochemistry, all cytokines (IL-13, IL-4 andFN-�) were detectable in gastric mucosa of both H. pylori-egative subjects and H. pylori-positive patients. In bothroups, the immunostaining was localised in the inflamma-ory cells but it was scattered and faint in H. pylori-negative
ases and strong and definite in H. pylori-positive cases (e.g.or IL-13: Fig. 3A). Interestingly, in two H. pylori-positiveases with intestinal metaplasia, an intense staining for IL-13nd IL-4 was observed in both inflammatory and epithelial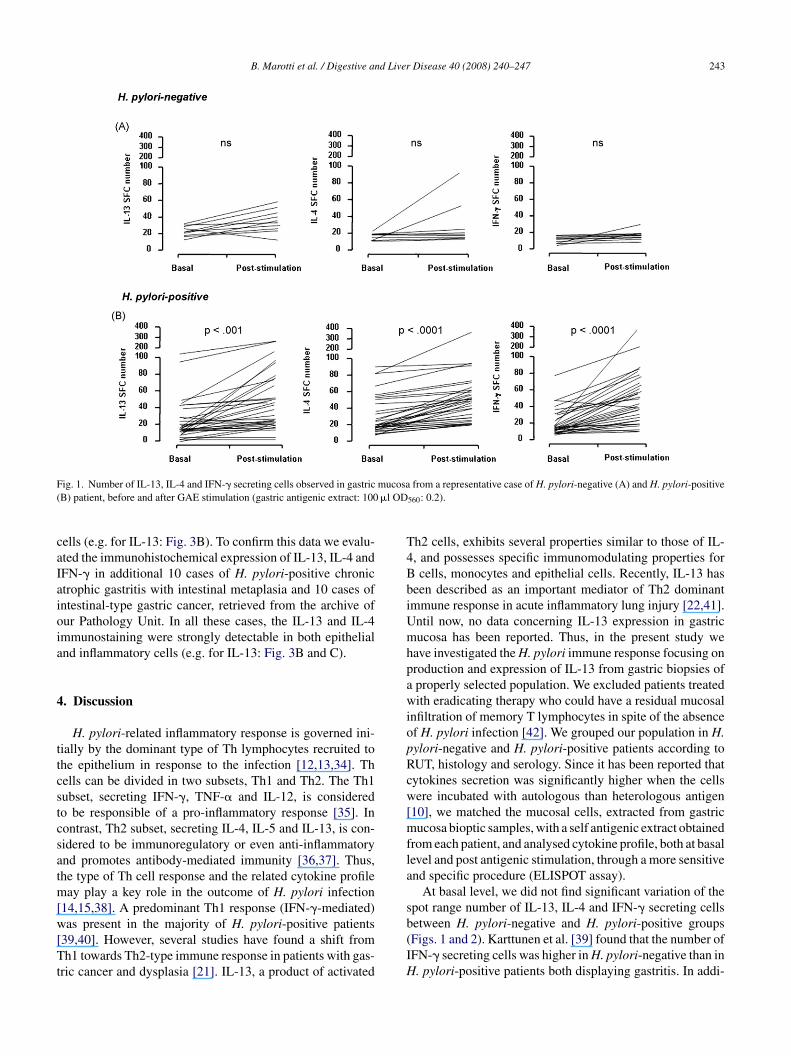
B. Marotti et al. / Digestive and Liver Disease 40 (2008) 240–247 243
F mucosa( �l OD
caIaioia
4
ttcstcsatm[w[Tt
T4BbiUmhpawiopRcw[mfla
s
ig. 1. Number of IL-13, IL-4 and IFN-� secreting cells observed in gastricB) patient, before and after GAE stimulation (gastric antigenic extract: 100
ells (e.g. for IL-13: Fig. 3B). To confirm this data we evalu-ted the immunohistochemical expression of IL-13, IL-4 andFN-� in additional 10 cases of H. pylori-positive chronictrophic gastritis with intestinal metaplasia and 10 cases ofntestinal-type gastric cancer, retrieved from the archive ofur Pathology Unit. In all these cases, the IL-13 and IL-4mmunostaining were strongly detectable in both epithelialnd inflammatory cells (e.g. for IL-13: Fig. 3B and C).
. Discussion
H. pylori-related inflammatory response is governed ini-ially by the dominant type of Th lymphocytes recruited tohe epithelium in response to the infection [12,13,34]. Thells can be divided in two subsets, Th1 and Th2. The Th1ubset, secreting IFN-�, TNF-� and IL-12, is consideredo be responsible of a pro-inflammatory response [35]. Inontrast, Th2 subset, secreting IL-4, IL-5 and IL-13, is con-idered to be immunoregulatory or even anti-inflammatorynd promotes antibody-mediated immunity [36,37]. Thus,he type of Th cell response and the related cytokine profile
ay play a key role in the outcome of H. pylori infection14,15,38]. A predominant Th1 response (IFN-�-mediated)
as present in the majority of H. pylori-positive patients39,40]. However, several studies have found a shift fromh1 towards Th2-type immune response in patients with gas-
ric cancer and dysplasia [21]. IL-13, a product of activated
b(IH
from a representative case of H. pylori-negative (A) and H. pylori-positive
560: 0.2).
h2 cells, exhibits several properties similar to those of IL-, and possesses specific immunomodulating properties forcells, monocytes and epithelial cells. Recently, IL-13 has
een described as an important mediator of Th2 dominantmmune response in acute inflammatory lung injury [22,41].ntil now, no data concerning IL-13 expression in gastricucosa has been reported. Thus, in the present study we
ave investigated the H. pylori immune response focusing onroduction and expression of IL-13 from gastric biopsies ofproperly selected population. We excluded patients treatedith eradicating therapy who could have a residual mucosal
nfiltration of memory T lymphocytes in spite of the absencef H. pylori infection [42]. We grouped our population in H.ylori-negative and H. pylori-positive patients according toUT, histology and serology. Since it has been reported thatytokines secretion was significantly higher when the cellsere incubated with autologous than heterologous antigen
10], we matched the mucosal cells, extracted from gastricucosa bioptic samples, with a self antigenic extract obtained
rom each patient, and analysed cytokine profile, both at basalevel and post antigenic stimulation, through a more sensitivend specific procedure (ELISPOT assay).
At basal level, we did not find significant variation of thepot range number of IL-13, IL-4 and IFN-� secreting cells
etween H. pylori-negative and H. pylori-positive groupsFigs. 1 and 2). Karttunen et al. [39] found that the number ofFN-� secreting cells was higher in H. pylori-negative than in. pylori-positive patients both displaying gastritis. In addi-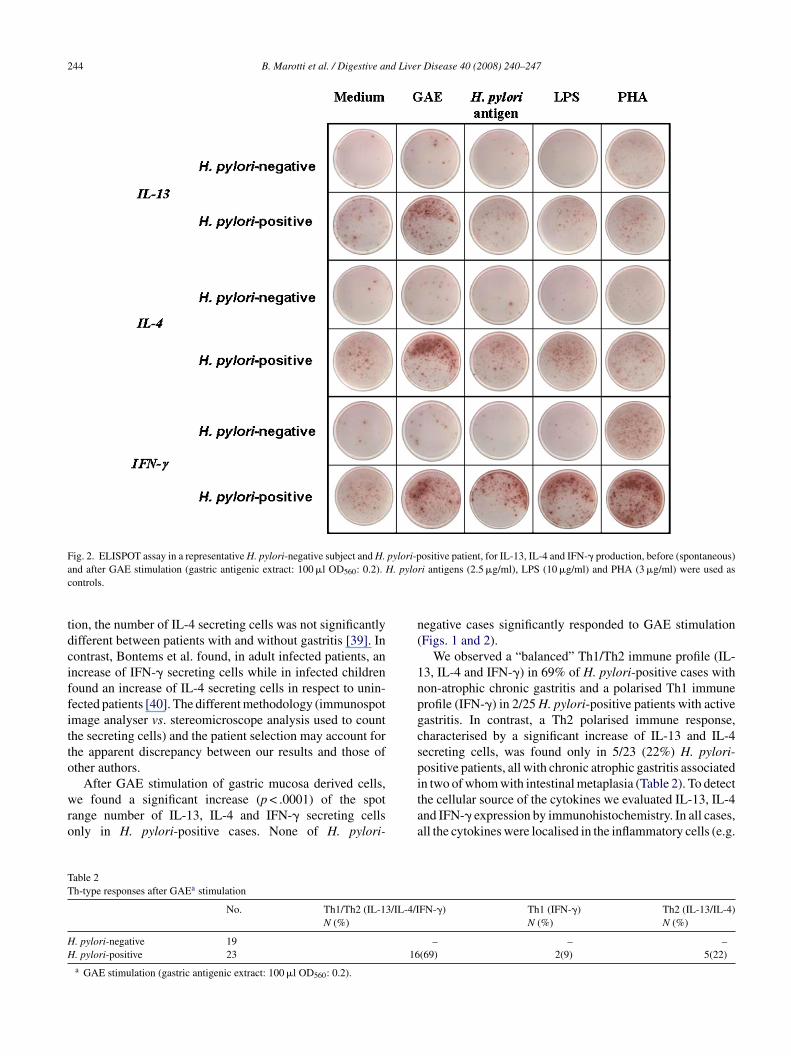
244 B. Marotti et al. / Digestive and Liver Disease 40 (2008) 240–247
Fig. 2. ELISPOT assay in a representative H. pylori-negative subject and H. pylori-positive patient, for IL-13, IL-4 and IFN-� production, before (spontaneous)a H. pyloc
tdciffitto
wro
n(
1npgcspi
TT
HH
nd after GAE stimulation (gastric antigenic extract: 100 �l OD560: 0.2).ontrols.
ion, the number of IL-4 secreting cells was not significantlyifferent between patients with and without gastritis [39]. Inontrast, Bontems et al. found, in adult infected patients, anncrease of IFN-� secreting cells while in infected childrenound an increase of IL-4 secreting cells in respect to unin-ected patients [40]. The different methodology (immunospotmage analyser vs. stereomicroscope analysis used to counthe secreting cells) and the patient selection may account forhe apparent discrepancy between our results and those ofther authors.
After GAE stimulation of gastric mucosa derived cells,
e found a significant increase (p < .0001) of the spotange number of IL-13, IL-4 and IFN-� secreting cellsnly in H. pylori-positive cases. None of H. pylori-
taa
able 2h-type responses after GAEa stimulation
No. Th1/Th2 (IL-13/IL-4/IN (%)
. pylori-negative 19
. pylori-positive 23 16a GAE stimulation (gastric antigenic extract: 100 �l OD560: 0.2).
ri antigens (2.5 �g/ml), LPS (10 �g/ml) and PHA (3 �g/ml) were used as
egative cases significantly responded to GAE stimulationFigs. 1 and 2).
We observed a “balanced” Th1/Th2 immune profile (IL-3, IL-4 and IFN-�) in 69% of H. pylori-positive cases withon-atrophic chronic gastritis and a polarised Th1 immunerofile (IFN-�) in 2/25 H. pylori-positive patients with activeastritis. In contrast, a Th2 polarised immune response,haracterised by a significant increase of IL-13 and IL-4ecreting cells, was found only in 5/23 (22%) H. pylori-ositive patients, all with chronic atrophic gastritis associatedn two of whom with intestinal metaplasia (Table 2). To detect
he cellular source of the cytokines we evaluated IL-13, IL-4nd IFN-� expression by immunohistochemistry. In all cases,ll the cytokines were localised in the inflammatory cells (e.g.FN-�) Th1 (IFN-�) Th2 (IL-13/IL-4)N (%) N (%)
– – –(69) 2(9) 5(22)
B. Marotti et al. / Digestive and Liver
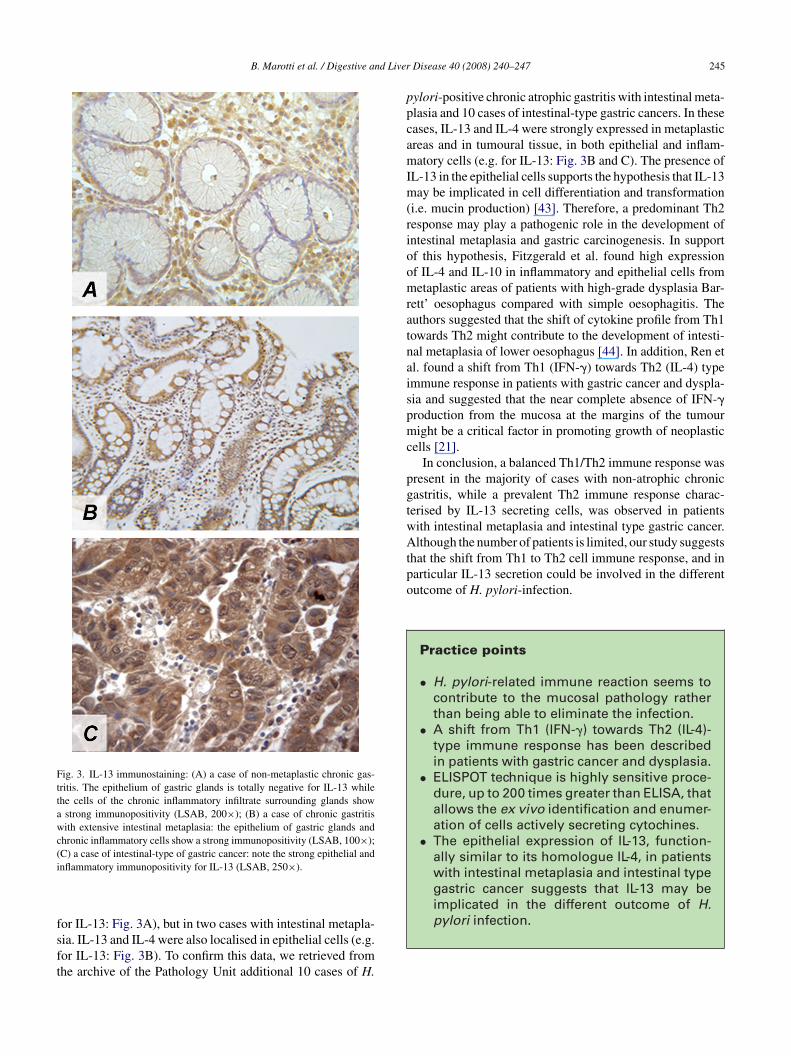
Fig. 3. IL-13 immunostaining: (A) a case of non-metaplastic chronic gas-tritis. The epithelium of gastric glands is totally negative for IL-13 whilethe cells of the chronic inflammatory infiltrate surrounding glands showa strong immunopositivity (LSAB, 200×); (B) a case of chronic gastritiswith extensive intestinal metaplasia: the epithelium of gastric glands andchronic inflammatory cells show a strong immunopositivity (LSAB, 100×);(C) a case of intestinal-type of gastric cancer: note the strong epithelial andi
fsft
ppcamIm(rioomratnaispmc
pgtwAtpo
pylori infection.
nflammatory immunopositivity for IL-13 (LSAB, 250×).
or IL-13: Fig. 3A), but in two cases with intestinal metapla-
ia. IL-13 and IL-4 were also localised in epithelial cells (e.g.or IL-13: Fig. 3B). To confirm this data, we retrieved fromhe archive of the Pathology Unit additional 10 cases of H.Disease 40 (2008) 240–247 245
ylori-positive chronic atrophic gastritis with intestinal meta-lasia and 10 cases of intestinal-type gastric cancers. In theseases, IL-13 and IL-4 were strongly expressed in metaplasticreas and in tumoural tissue, in both epithelial and inflam-atory cells (e.g. for IL-13: Fig. 3B and C). The presence of
L-13 in the epithelial cells supports the hypothesis that IL-13ay be implicated in cell differentiation and transformation
i.e. mucin production) [43]. Therefore, a predominant Th2esponse may play a pathogenic role in the development ofntestinal metaplasia and gastric carcinogenesis. In supportf this hypothesis, Fitzgerald et al. found high expressionf IL-4 and IL-10 in inflammatory and epithelial cells frometaplastic areas of patients with high-grade dysplasia Bar-
ett’ oesophagus compared with simple oesophagitis. Theuthors suggested that the shift of cytokine profile from Th1owards Th2 might contribute to the development of intesti-al metaplasia of lower oesophagus [44]. In addition, Ren etl. found a shift from Th1 (IFN-�) towards Th2 (IL-4) typemmune response in patients with gastric cancer and dyspla-ia and suggested that the near complete absence of IFN-�roduction from the mucosa at the margins of the tumouright be a critical factor in promoting growth of neoplastic
ells [21].In conclusion, a balanced Th1/Th2 immune response was
resent in the majority of cases with non-atrophic chronicastritis, while a prevalent Th2 immune response charac-erised by IL-13 secreting cells, was observed in patientsith intestinal metaplasia and intestinal type gastric cancer.lthough the number of patients is limited, our study suggests
hat the shift from Th1 to Th2 cell immune response, and inarticular IL-13 secretion could be involved in the differentutcome of H. pylori-infection.
Practice points
• H. pylori-related immune reaction seems tocontribute to the mucosal pathology ratherthan being able to eliminate the infection.
• A shift from Th1 (IFN-�) towards Th2 (IL-4)-type immune response has been describedin patients with gastric cancer and dysplasia.
• ELISPOT technique is highly sensitive proce-dure, up to 200 times greater than ELISA, thatallows the ex vivo identification and enumer-ation of cells actively secreting cytochines.
• The epithelial expression of IL-13, function-ally similar to its homologue IL-4, in patientswith intestinal metaplasia and intestinal typegastric cancer suggests that IL-13 may beimplicated in the different outcome of H.

246 B. Marotti et al. / Digestive and Liver
Research agenda
• To confirm the role of IL-13 in “in vitro” and“in vivo” models of gastric cancer
• To use IL-13 as a target for new therapeuticstrategy in patients with pre-cancerous and
CN
A
eIr
2
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[31] Lauren P. The two histological main types of gastric carcinoma: diffuse
cancerous lesions.
onflict of interest statementone declared.
cknowledgements
We thank Dr. Carmen Gianfrani (Institute of Food Sci-nce, CNR-AV, Italy) for ELISPOT analyser (Immunospotmage Analyser, A.EL.VIS, Hannover, Germany) and criticaleview of the manuscript.
This work was supported by Grants from MIUR, PRIN004.
eferences
[1] Blanchard TG, Czinn SJ. Helicobacter pylori acquisition and transmis-sion: where does it all begin? Gastroenterology 2001;121:483–5.
[2] Blaser MJ. Helicobacter pylori and gastric disease. Br Med J1998;316:1507–10.
[3] Kuipers EJ, Thijs JC, Festen HPM. The prevalence of Helicobacterpylori in peptic ulcer disease. Aliment Pharmacol Ther 1995;9:59–69.
[4] Forman D, Newell DG, Fullerton F, Yarnell JW, Stacey AR, Wald N,et al. Association between infection with Helicobacter pylori and riskof gastric cancer: evidence from a prospective investigation. Br Med J1991;302:1302–5.
[5] Moss SF, Blaser MJ. Mechanisms of disease: inflammation and theorigins of cancer. Nat Clin Pract Oncol 2005;2:90–7.
[6] Nguyen TN, Barkun AN, Fallone CA. Host determinants of Heli-cobacter pylori infection and its clinical outcome. Helicobacter1999;4:185–97.
[7] Nardone G, Rocco A, Malfertheiner P. Helicobacter pylori and molec-ular events in precancerous gastric lesions. Aliment Pharmacol Ther2004;20:261–70.
[8] Holck S, Norgaard A, Bennedson M. Gastric mucosal cytokineresponses in Helicobacter pylori-infected patients with gastritis andpeptic ulcers. Association with inflammatory parameters and bacteriaload. FEMS Immunol Med Microbiol 2003;36:175–80.
[9] Naito Y, Yoshikawa T. Molecular and cellular mechanisms involvedin Helicobacter pylori-induced inflammation and oxidative stress. FreeRadic Biol Med 2002;33:323–36.
10] Jakob B, Birkholz S, Schneider T, Duchmann R, Zeitz M, Stallmach A.Immune response to autologous and heterologous Helicobacter pyloriantigens in humans. Microsc Res Technol 2001;53:419–24.
11] Meyer F, Keith TW, Stephen PJ. Modulation of innate cytokine responseby products of Helicobacter pylori. Infect Immun 2000;68:6265–72.
12] Crabtree JE. Immune and inflammatory response to Helicobacter pyloriinfection. Scand J Gastroenterol 1996;215:3–10.
13] Genta RM. The immunobiology of Helicobacter pylori gastritis. SeminGastrointest Dis 1997;8:2–11.
[
Disease 40 (2008) 240–247
14] D’Elios MM, Amedei A, Del Prete G. Helicobacter pylori antigen-specific T-cell responses at gastric level in chronic gastritis, pepticulcer, gastric cancer and low-grade mucosa-associated lymphoid tissue(MALT) lymphoma. Microbes Infect 2003;5:723–30.
15] D’Elios MM, Manghetti M, Almerigogna F, Amedei A, Costa F,Burroni D, et al. Different cytokine profile and antigen-specificity reper-toire in Helicobacter pylori-specific T cell clones from the antrum ofchronic gastritis patients with or without peptic ulcer. Eur J Immunol1997;27:1751–5.
16] Stromberg E, Lundgren A, Edebo A, Lundin S, Svennerholm AM, Lind-holm C. Increased frequency of activated T-cells in the Helicobacterpylori-infected antrum and duodenum. FEMS Immunol Med Microbiol2003;36:159–68.
17] Bamford KB, Fan X, Crowe SE, Leary JF, Gourley WK, LuthraGK, et al. Lymphocytes in the human gastric mucosa during Heli-cobacter pylori have a T helper cell 1 phenotype. Gastroenterology1998;114:482–92.
18] Luzza F, Parrello T, Sebkova L, Pensabene L, Imeneo M, Mancuso M,et al. Expression of proinflammatory and Th1 but not Th2 cytokines isenhanced in gastric mucosa of Helicobacter pylori infected children.Dig Liver Dis 2001;33:14–20.
19] Lindholm C, Quiding-Jarbrink M, Lonroth H, Hamlet A, SvennerholmAM. Local cytokine response in Helicobacter pylori-infected subjects.Infect Immun 1998;66:5964–71.
20] Tanahashi T, Kita M, Kodama T, Yamaoka Y, Sawai N, Ohno T, etal. Cytokine expression and production by purified Helicobacter pyloriurease in human gastric epithelial cells. Infect Immun 2000;68:664–71.
21] Ren Z, Pang G, Clancy R, Li LC, Lee CS, Batey R, et al. Shift of thegastric T-cell response in gastric carcinoma. J Gastroenterol Hepatol2001;16:142–8.
22] Minty A, Chalon P, Derocq JM, Dumont X, Guillemot JC, Kaghad M, etal. Interleukin-13 is a new human lymphokine regulating inflammatoryand immune response. Nature 1993;362:248.
23] Kouwenhoven M, Ozenci V, Teleshova N, Hussein Y, Huang YM, Euse-bio A, et al. Enzyme-Linked Immunospot Assay provide a sensitivetool for detection of cytokine secretion by monocytes. Clin Diagn LabImmunol 2001;8:1248–57.
24] Power CA, Grand CL, Ismail N, Peters NC, Yurkowski DP, BretscherPA. A valid ELISPOT assay for enumeration of ex vivo, antigen-specific. IFN �-producing T cells. J Immun Methods 1999;227:99–107.
25] Carol M, Lambrechts A, Van Gossum A, Libin M, Goldman M,Mascara-Lemone F. Spontaneous secretion of interferon-� and inter-leukin 4 by human intraepithelial and lamina propria gut lymphocytes.Gut 1998;42:643–9.
26] Fujihashi K, McGhee JR, Beagley KW, McPherson DT, McPher-son SA, Huang CM. Cytokine-specific ELISPOT assay. Single cellanalysis of IL-2, IL-4 and IL-6 producing cells. J Immun Methods1993;160:181–9.
27] Czerkinsky CC, Nilsson LA, Nygren H, Ouchterlony O, TarkowskiA. A solid-phase enzyme-linked immunospot (ELISPOT) assay forenumeration of specific antibody-secreting cells. J Immun Methods1983;65:109.
28] Hauer AC, Bajaj-Elliott M, Williams CB, Walker-Smith JA, MacDon-ald TT. An analysis of interferon-�, IL-4, IL-5 and IL-10 production byELISPOT and quantitative reverse transcriptase-PCR in human Peyer’spatches. Cytochine 1998;10:627–34.
29] Dixon MF, Genta MR, Yardley JH, Correa P. Classification and gradingof gastritis. Am J Surg Pathol 1996;20:1161–81.
30] Jass JR, Filipe MI. The mucin profiles of normal gastric mucosa, intesti-nal metaplasia and its variants and gastric carcinoma. Histochem J1981;13:931–9.
and so-called intestinal-type carcinoma. Acta Pathol Microbiol Scand1965;64:31–49.
32] Gianfrani C, Troncone R, Mugione P, Casentini E, De Pascale M,Faruolo C, et al. Celiac disease association with CD8+ T cell responses:

d Liver
[
[
[
[
[
[
[
[
[
[
[
sia into ciliated epithelia in airway epithelial cell culture. Allergol Int
B. Marotti et al. / Digestive an
identification of a novel gliadin-derived HLA-A2-restricted epitome. JImmunol 2003;170:2719–26.
33] Hsu SM, Raine L, Fanger H. Use of avidin–biotin–peroxidase com-plex (ABC) in immunoperoxidase technique: a comparison betweenABC and unlabeled antibody (PAP) procedures. J Histochem Cytochem1981;29:577–80.
34] Tarkkanen J, Kosunen TU, Saksela E. Contact of lymphocytes withHelicobacter pylori augments natural killer cell activity and inducesproduction of gamma interferon. Infect Immun 1993;61:3012–6.
35] Haeberle HA, Kubin M, Bamford KB, Garofalo R, Graham DY, El-Zaatari F, et al. Differential stimulation of interleukin-12 (IL-12) andIL-10 by live and killed Helicobacter pylori in vitro and associationof IL-12 production with gamma interferon-producing T cells in thehuman gastric mucosa. Infect Immun 1997;65:4229–35.
36] Bergman M, Del Prete G, van Kooyk Y, Appelmelk B. Helicobacterpylori phase variation, immune modulation and gastric autoimmunity.
Nat Rev Microbiol 2006;4:151–9.37] Abbas AK, Murphy KM, Sher A. Functional diversity of helper Tlymphocytes. Nature 1996;383:787–93.
38] Taylor DE. Third international workshop on pathogenesis and hostresponse in Helicobacter pylori infections. Helicobacter 1998;3:303–4.
[
Disease 40 (2008) 240–247 247
39] Karttunen R, Karttunen T, Ekre HP, MacDonald TT. Interferon gammaand interleukin 4 secreting cells in the gastric antrum in Helicobacterpylori positive and negative gastritis. Gut 1995;36:341–5.
40] Bontems P, Robert F, Van Gossum A, Cadranel S, Mascart F. Heli-cobacter pylori modulation of gastric and duodenal mucosal T cellcytokine secretions in children compared with adults. Helicobacter2003;8:216–26.
41] Lentsch AB, Czermak BJ, Jordan JA, Ward PA. Regulationof acute inflammatory injury by endogenous IL-13. J Immunol1999;162:1071–6.
42] Tepes B, Kavcic B, Zaletel LK, Gubina M, Ihan A, Poljak M, et al. Twoto four-year histological follow-up of gastric mucosa after Helicobacterpylori eradication. J Pathol 1999;188:24–9.
43] Kondo M, Tamaoki J, Takeyama K, Isono K, Kawatani K, Izumo T,et al. Elimination of IL-13 reverses established goblet cell metapla-
2006;55(3):329–36.44] Fitzgerald RC, Abdalla S, Onwuegbusi BA, Sirieix P, Saeed IT,
Burnham WR, et al. Inflammatory gradient in Barrett’s oesophagus:implication for disease complications. Gut 2002;51:316–22.





























