Embed Size (px)
Citation preview

T
..
CALIFORNIA STATE UNIVEH.SI'.rY, NORTHP.IDGE
:PA'!TEN~~~ EDUCATION IN Z.>.:N VEBAN ,,
HOSPITAL HYPERTENSION CLINIC
A graduate project su~nitted in partial satisfaction of the requirements for the degree of Master of Public
Healt.h in
Community Heal t.h E:iucation
by
Nary Tentler ~

The gradua~e project of Mary Tentler and Linda Mcintosh .is Clf)l):ro·veCl!
~iay 197 G
l . .l

.. ·-··----·--~ ~--.- ~··---~~-->·- -· --~~~-~ __ ,_, -~---·-·-----~·-···-~
The authors extend warmest appreciation to:
Robert Iv1. Huff ·- f.irst for the opportunity t"o
.John ~r. Pod or
expertise as curriculum consultant.
L<:mni.n H. Glass &nd t;{alsed ll:..11-:h;s:teiO~D for
guidance aTid encouragement .
. i.:l .. i
I
i l
I ..
Jl.
III.,
.. <{,._.,
'l'l\BLE Cli~ CONTEN'I'S
Purpose cf the Study
Definition of Terms
~emographic Data
Ii~~L a.I~! ir1q {}r~L~n f.~ t.ttdyr i:.1 .. 2:k:.:l tt1e \/ e·t.e .. t· <-=tr! q
.l\d.rtli:n . .is:'::. X"~-~ t: i c.;.n l~()(J])~~.r a. ~·:i ~TE: S t.·u{:~:::r
}I_y !?G r.·t. 2:!.!. s J .. <.!C. ·;?D. t: i t~!·l t: F~t:.lu.t.:~;l ~ )_cJYt I) .r-·c)~l ;.: a.:.u L}l) j ·:::. (~ t. L \'t ~~ s.
-vii
vi
1.
1
2
3
3
5
,. 0
9
14
2] ..
28
23
31
33
36>

IV.
"f] ...
Eval ua t.ion
Recornmend.at:Lons for Lor;g-Term Ana_lysis and Evaluat:.on .
DISCUSSION .
EIBLIOG:t-'1\PHY •
APf'ENDICES
.A, HYPERTENSION~ Patient Questionnaire
B. IU~~~;ULTS OF HYP ERTENS IGN C'LINIC: PATIENT OUES 'IIONN~'\II<_E
f)E\/l~Ll).t>J:~D ..
v
37
4,.., ,,;_
44
47
47
48
l~9
51
55
6S
J
T ·r c·rp .,..J-1. ,,_) .J.. OF' TABLES
'I' able
I. Demographic Findinqs of Hypertension Clinic Ques-tionnaire ,
II. Ove:rviev.;r Class- Q·c.es·ticmnaire n~~sul ts
TV. Diet Class Questionnaire Results
Page
33
38
39
40

ABSTKsC'r
PATIENT EDUCA'T'ION IN A.N URBl,j')I
HOSPI'l'AL HYPKRTENSION CLINIC
by
M.ary 'l'en tlcr
a.nd
Linda Mcl.:lt.CBh
JV~a.st.e:r of Pnbl.:Lc Health
1~e purpose of the study ~as to design ~nd
Clinic Outpatients at Martin Luth~r King, Jr. General
physician crderz.
e\.l'aluaL]o.n tcels.
'
. f
The prog:ralTl was i.mplement.ed over a relat.:LveJ.y
short. period of time Eu1d because small sample 13izes pre·-
vailed, the decision o.:'3 to wheJchE~r or not the program ob-
jectives were met are necessarily partially S\~1jective.
The original hyr)othesis stat.:.ed in the Null form wa.s:
Increase in k·nov.;rledge and understanding of the condition of hypertension by the patient will not-. result in increased cmnp1.i;;mce with pllysic:ian orders.
Since pat..i.;;::nt. compliance J.s an extremely
difficult parameter to measure, this hypothesis can
neither be a.ccepted nor rejer:::ted until further .implemen-
t:a:~:i.on is compJ.eted and addi tiona.l data is obt.ainE;t.:i.
It was the authors feeling that because of the
~
a.I'1Ct ·t . •
rJ.~~··p~~r c.e:t1SJ.3J:::-l, x~:~.<::r:-2
conducted .

Statement of the Problem
Accordjng to ~ecent estinstes, approximately 25
1lion people in the
Stt.C'(~ :.
ti.t<2n .12 ~;;:~e:r c:er1-t: r~- f' ~., .J~ tJ.:~~at:rue.rrt. a~llt~ a de-
C!'J.i:"< 1:e con tro ."L •
m_j_}. .L i r)IL .e igttl~c1 Vole :rE~acJ1 tb.e c1.i.~:;t~r(~s s i !\ST cor1c:11JsicJ1: tl1at
close to 22 million people in the U.S. today have either
0£ these 22 mj_llion 1 at least S million are
.c ; __ , J_,.
circumstances (32:4~).
1
~ ' Ctl.S-
i I.

2
. Hypertensicm is often asympi:orr.at.ic. Couple with
th.is ·the fact~. that t:he dr:J.g;::; tisecT in t:he tr(:!s.·trnent of
blood pressure can cause unpleasant side
it can be seer: that. compl.iance ~.vi th physician orders to
patient feel worse is often difficult to ach1eve. 8(>IGe
of U<e other re:J.sons fer non-comp1iance a.~~e: lack of
patiel1t understan.dinq of ;r-.tJ.s ill. ness, J.ack of pat. ient.
awareness t.hat. treatment. must be continued th:roughout
'their 1i:fr::t:i.."ml3 and ·patient misuncJ.ers·candinq of 9hysician
directions (17:17).
It has been debated ~hether an increase in a
comitant behavior changa. Gntil !ecentlyr there were no
hard data to prove or disprove this. A::; more ressa:cc:h is
Health education has
p:::-oceedt=}d on this assrunpt.i.on a.nd :~n i97J l:::cu.i (in an un-
t.ient e<.Juca tion can ini}_::>.r<:::~ve pat.ieDt C(rr..-:p1ic.r;ce vli th
physician orders.
'.t'he Mas:t.i L. I,ut:her l<inq, JJ:. c::cner~1.1 Ho.spi t<:ll
(prior to th0 authors'
arriv2l) d~ew approximately 30 p~r cent of patients

3
This p:r:·oyram did not; nave
specified curriculum, objective:::;, o:r· evaluation t:ools.
It was the authors• intention to redesign and
implement. a hypertensjon p3tient education proJran' .. 'I' his
'Ih0 hypothesis of t!.'le s·tudy {st.ated in i:.he null
form) is:
of the ~cndition of hypertension by the patient
physician orders.
There ~re several fac~ors whic~ must be
The prosram was cond~ctea on a very
' . . consr.:ra.J.n cs duri.nr::r i:t1e implemer~i:a·-
Defini.tion of Tenns

4
--·· ······--···-----····-·-·- ---- ·--- -------------,
Diastolic blood pressure - the pressure of the blood on
the walls of the arteries when the heart is
relaxed.
Essential hypertension - high blood pressure without a
known. cause.
W:{pel .. te:ls.ion - hiqh b.lood pressure as identified by the
Mart.in Luther King, ~rr. General Hospital Hyper-
tension Clinic as 140/90 or above depending on
the aqe of the patient.
hypertension - h1gh blood pressure which 1
r1l3.s
a known cause.
Systolic blood pressure - the pressure of the blood on .: .( • .:.'.-o;''"J~
the ~-·Iall.s of t.he arterie~·:~,.,Xl~n the hea.::::t. is i:n.
ccn-tracticn.
II. LI'l'ERArro:t~E REVIEW
For purposes of health administration and health .- .•.·· .. ,_,·'- .• -
service area for Martin Luther K1ng, Jr. General Has-
pi tal"
The Southeast Region cons1sts of 154 census
tracts located in the South Central portion of Los
Angeles. Fifteen miles long· and e1<~~'TE1P mil.es wi.de f .i... t:
has a total population or 763,000 people. With 8,150
psopls per square mile it is not as densely populated as
the central part of Lcs Angeles. Of ~ie 763,000 people
in thn area, 303,470 f39. 6%) ax·•"! bl<::ck. 'I'he median f e::.m~
ily income is $7,754, well below the $10,970 for Lcs
r.,_ngc.~ les County .:~.s a whol•::.
1Xi thin the :region bl.a.c:-: :females outm:ur.J)e:r: b}.ack
fined 2.s )--15 years r.-.md 65 year::-: a.nd ciLdE~:c) compr.iseb 40
per cent of the population. The 8ducational level is
close "!:.C) h:l.gh school cornpL:;l:ic•n v,•i th t:he except.ion o.f the
6
~-···--·~- ··----~--·--·-·--·~·-·- -~······--·- ·--·-···~
' I
Because so many of the people in the u.s. who
are hypertensive are undetected, it has been extremely
difficult to estimate with accuracy the prevalence
Estil11a.tes by experl:s have· indicc}t'ed t'h.at as
rmmy as 25 million peopJe have: JJj.sTh blood p.ressure. For
reasons not yet understood, hypertension effects blacks
more ofte:n, and more seve:cely, than whi.-tes. Curry (4~2)
; has estimat.ed. t:hat om.~ black in four over the age of 18
has hype.rtension, or five million blacks in li.meri.ca t.oday.
Not only is hypertension more severe in blacks
generally; but it begins at a younger age, " . the
or mors t.imes g:ce;:d~.er in blacks E-H.Jed 25 ·to 4. 4 i:han wh.i tes
"Male sex, young age anct black race are all associated
ll)'?J?~:::rt:t.:·:..n.s ir.:)rl ( 16: 2 7 5) .
Tota.t. Black Popi..l1ntion 303,473
154,435
Blacks in S. E. Region with Hypertension 39,108

7
Research has shown no clear-cut data on the
causes of essential hypertension, but has rather offered
informa t.ion on factors which seem ·to contril)ut;:~, in some
people, in some ways, to elevations in blood pressure.
hypertension have been genetics, stress, obesity and
sodiur:t :l.r,t_a.ke. Srnoking .:n~d ,::;.xcessl\;e alcohol consump-
tion, w~--:;.ile not (":Onside:ced t.::cm.tr.ibu·tory to ·the etiology
of hypertension, have been kr.o;,·;n to .s::-::acerba.te ·the con-·
dition and are p:rominen·tly mE:~n t.ioneC!. in cont.rol proq::::-ams.
The role of genetics in hypertension
is unclear and the moBt t.hat can be said at p:t~esEmt is
that if a person has Oile or both parenta with hyperten-
·the disease t.han a person :,-~-:.-:>se parcm ts are no.rmot.ens:!. ve
(25:4). Hered:i. t·.y is :1ot. the only facto.1:, but seems t:o
cont.:r.-.ibu·te "ar,oc.t one-b.alf of i:~he ba.ck<;round for t.:he
developrnant of hypertension'' (31:106). The otter half 12
n.t-JC!E; s ·sa.ry F~L· h~~or~a~~~•'.)·l·l ~~ ........ .; -··_Ll_.~__._t.~-......t.-~w_._ · .... \...,
Stress,.. Stress ~s often m0ntiuned as one of the
contributory environmental factors in the etiology oi
high blood pressu~e. Da~a show that blood pressure var-
ies with socioeconomic stress, personal stress an~ life-
threat2ning situations (JB)

8
- --·······--· - -· ----·--··-~ ---·-·· -··-·---~--~~~---·-·------·----~~-- -··-~- .. -.... !
Kaplan states that increased blood pressure is
ing either a high or low standard of living and/or being
exposed to a rapidly changing life situation. It. is
·· :.s:.::Lfe·':t:::_:, ;;;ay, i .. heD,. ·drat people who have less control over
the stimuli :irnposed on them qenerally have higher blood
:t~'ressu~·~e.
Sodium Intak('. The relat.ionship bet,,·een socliulT>
int.ake and hyperb=nl:3ion is equivocal at best. It is gen-
e.:cctlly ac1mit.t.ed t.hat:: res·tricting dietary sodium int.:.ake
induce a decrease in blood pr~ssure, but the experts
t.o diffc~r on the importance of sodiuin consu:npti.on i1;.
the etiology of the disease. Dahl is one of the leading
proponents o.f the theoi:'y that people cLr-c: li teral1y po.1.son-
ing themselves with excessive salt iDtake. He has com-·
piled, sL,.ce. 1948; a 1.nassive body of data rela.t.in<;i to
:::~odiurr. an/i. h.i.gh blood press;xncO'. His data shbw nthat
(excessive) salt induces permanent and fatal hyperten-
sio.n '' :L:n rats 1 but he admits that evidence b'J ·the same
effect is u ;~;Jrc:u.:m.:::·tant:ial in ma.:-:11 ( 6: 2 42) . Wb.et:hcr or
not. excessive salt intake can be crn1sidered a causative
fc=~c·tor in hyrt:rt:ens:Lc:>n~ lm·rering of diet.a:cy sodiu:m intake
9
Obesity is anol.:.:her con tr.oversi.al
contributory factor that is under study. S·tamler states
that the association between obesity and hypertension is
"cons.istant and impressive, but. not powerful" {38: 22).
because only about one in four hypertensives is obese
(31:115). It .i.s, ho'!Jever, an aqgra.vaocing fac·1.:or because
'i.vhen obese hyper-tensives reduce, there is usually a con--
comitant reduction in blood pressuree
It can be seen that while the exact etiology of
esscmt:ial hypertension remains clouded, da:ta relative t.o
contributory factors is mounting. These data have led
to p~og£ess in the treatment and control of high blood
tinues to lead to a clearar understanding of the nature
ot hyp,:-)r t.ens ion and t~o form the 'bu.s is for educaticna.l
researchere and practitioners that untrc~ted hypertension
T~~ Veterans A5ministration Cooperative Study supplied
Il1/)T. ~? (:;\lid.t~l!.C!e t.O Sl.\rtJJC~rt the })E!lief th-fl t }1J."f:.1~~.'Ct~811Si.GTL
can be treated effectively. BotJ:l of t.he:.;c are landma.rk

10
studies that historically have provided the basis for the !
control of hypertension (29:301-310).
From 1949 to 1969 the National
Heart Institute of the United States Public Health Ser-
Massachusetts a prospective
study of the factors related to the development of Co!:'o··
nary Heat Disease (CHD) • In 1949 a total of 5,127 men
CJ.!1c1 ~ ... Jornen a.:;.red JG -62 years entered the study. These
volunteers did not have CHD and were classified according
to tho::.;e eha:r.:ttc·teristics believed to be important in
developing CHD (30:43).
The findinqs of Framingham link. hypert.Pnsi.on to
the development of c~rdicrJascular diseases. Angina,
coronary :Ln::,;uff:i.c:..en.cy,. myocardial i:1far.::::t:ion, and sudclEn
death were irnp=2ssively and distinctly £ound to be re-
lated to the l2vel of the systolic and diastolic blood
Hypertension \·las found tc rank befC~rc high
heart disease (30:51).
The lDcidence of Congestive Heart Failure (CHF)
as (!O-:ttJ:Ja:t:(-?.\.'1 to ~1<)r.tno-t.£~1-:.S i ~.res. ... In this study CHF \•las a
"leth<::l1 ph.e:;mmE~non, '' with only 50 per cent of t.he pcpula-
tion who de7eloped CHF surviving beyond five years
(. ] .. ·- ' t.••-l!:.)i<~-

11
'l'he Framingham study found that men w:t th the
highest. levels of blood pressure had tv:-o t.imes as great
a risk of de<..teloping heart disease and five times as
9Teat a :risk of deve1oping a stx:oke compared to normo·-
tensi\res" Hypertension ·;,,as found to increase the chances
o.f stroke even more in people below age 50 compar-ed to
those older than 50. Oldsr pormlaticns may have strokes
more frequent~ly bu-t hypertension is l>?.ss o£ a
t:he vascular disease that accompanies ag in.g.
factor than I
Framingham
found the incidence of s·troke is more than one and one
half ti1nes hig-her -with dias·tolic blood pressure levels
of 90-91~ as compa.rsd to 80-84 in ages 4.5--64 yearsi and
is three times as high with diastolic l(~Vc.Js of 100-l04rrt.'TI
Hg- (31:29r 3D, 36).
ini.tiat.ed a a-[:udy ::>n the value of ant.ih}rper·tensive drug
t.herapy 5n pr.svent.ing morbidity and mortality in mild to
moderab::>ly r;evEre for~-ns aJ: hy·pertens:i.cn. A prospective
Volunteer :c'Elle V-aterans Hos-
:t_)i·tal pa·t icmts 1.-;-ere dividr.::d .:Lni:.o two g-roups; those '.-V.:L th
mild to moJerate hyperLension indicated by a diastolic
blood p;:e~::;s;_n·e. a:.reraging ~')f) through 144 :inrn Hq. anc:i those
with moderately severe hypertension, indicated by a
diastolic blood prt'.::ssure averaging 115 ·through 129 mm Hg.
(10::~16).

12 .
In ·the moderately severe hypert:ensive group 143
patient.s wcre randomly assigned to either the experimen-
tal group, or the control g:coup. The patients in the
experimental group were given antihypertensive agen·ts,
whi.le .. t.hose .in the ·con:t..rol group were ·,gi:rreD.pJ .. a.cE:bos.
Twent.y-~>even (27) severe "complicating events 11 such as
myoca:t'dial infarc·tion, congestive heart failure and cere-
brovascular thrombosis {stroke) , developed in the cont.rol
. patients, as compared ·to t.wo 11 complicating C!Vent.s n in the
t.reatment group. In the con"crol group four patients
died, as a result of canliov·ascular diseases. When these
results >f'lere obt::lined approximately three years into the
All pa-·
tients .in the co:ntrc·l group were put on dru9 tlwrapy
(10: 1.19-120) •
In the second group of patients w.i·th mild Jco
moderate hypertension, 380 males were randomly assigned
to either the treatment.: q:r;oup 01~ p l<:tcebo group. 'l'he
results of this section of the study are:
(1) An estimated ri.sk of developing a morbid event
o:r cRrdiovascuJar complic.:<t.ion over a five-year
period was found to be reduced from 55 per cent
t.o 18 per cent by antihypertensive. t.rea.tment.
(2) Severe cardiov:.:Jscular complications resulted .1.n
thirty-five patients in the placebo group as
compa.:ced to ni:1e i.n t:Jte treatment group.

....... - .......... -------------------------·-··-·-·-·-··, i l
(3) ' j Ni.net.een deaths related to hypertension or I
atherosclerosis occurred in the placebo group, i
compared to eight in t.he treatment group. And
(4) Twenty placebo group patients developed
··· ,, ... J!-tc·rsiBtent diastolic levels of 125 mm Hg or
higher (9:1143).
'rhe overall effect:s of trea·tment ~·~ere not as
clrama·tic in t:tds second g:coup as in tb.e moderately severe
hypertensive group. "Trea.t.ment was mcs-l: effective in
preventing hypertensiVE~ complica'cions 1 and least effec-
tive in preventing atherosclero·tic complications." 'I'he
incidence of complica t.ions was no grea:ter in Blacks. In
fact~ in thE~ placebo group complications vwre low·er for
Blacks, 25.9 per cent COG0ared to 31 per cent (9:1150-
1151) •
Overall,. the results of the Veterans Administra-
tion Study leave litt.le doubt. that ar!tihypertensive drug
therapy is beneficial. Complications, such as congestive
heart failure, stroke, kidney deterioratio11, and neuro-
re-t.:Lnopat:hy lve:re elin.l.i:;·:ated or reduced in thE~ treatment
group (9:1152).
With the evidence gathered from both the Veterans
1\.dminist:.rat.ion C~ooperat:i.ve and ·the Framingham St1Jdies .:i.i:
has been shovm ·that hypert.ens ion should be controlled and
treated in ordf;!: to reduce the morhidi ty and mortali·ty
associated with"the disease. The authors will provide j ' '-•·--·-~-~--------~--~----··-.·· ·--·------··- -······ .. --~-~-- ____ _.. . ··- -·---·--·-~·-·----,·--------~· ~ ______ ,. ___ ~ .... ---..--1

14
evidence that· shmvs patient educat~io:h can 1ncrease
patient compliance. This increase in complJ.ance will
further reduce morbidity and mortality.
Factors in Patient Comoliance --·-----·------------;._----~·-·~--
Once a patient has been screened ·±-cf: hypertension ·-.
t.hf-~ next. step is referra.l to a hypertension t~eatment.
facilit.y. Rarsly do patients vd.th essential hyperh=m.sion
get over their condition, so essential hypertension is a
life long condition. This means the ·treatment: for hyp£-:r-
tension must be continued and monitored for the ent.ii·e
life of the liyperte.risivE: patient (31~ 66) ~
Tl1e cornp 1 ianCE:!
and continued monitoring through frequent clinic or of-
fice visits often is not achieved. Th<-;re are many reasons
for this noncompliance.
Finnerty exr-:-·lored some rE~asons for nonco;-ripliance
in t.he DisLcict c,£ Colunihia v>"here 71 per cent: of the pop-
1.;.lation w.Lth:Ln the LmJ.er. cii.::.y is black, 75 per cent of
645 deaths attributed to high blood pressure in 1965 were
low the aqe of 60 ;,..rere in blacks. A total of sixty clinic1
patients who missed two or more scheduled
appointments in a five week period ~ve:re intervim,red from
tl1f~ c:! 1 :i.ni(;s of th~e JJ.i. str i c:t (Jf: Col tliTtl)i .~ Gertt~:': al I-Jc)spi t:c:.1,
I ! I
15
VVcL.Shington Hospi-tal Center, CoJ. urnbia Hospital, and
Georgetown University Medical Center. At Distric·t of
Cohml'oia Hr)spi tal and ~'7asl1i:nton Hospital Cen·tcr clinics
the a~,re:r:age v1a:l. ting Jcime prior to an c;xamination by a
_doctor was 2.5 hours. After the examination, waiting
t~ime a.t the clirdc pharmacy was 1. 8 hours; averacJe t.i.me
spent with the physician was 7.5 minutes, and the patient
was e.xamined by a different physician on each V1.s1 t.
Many pad.entf3 were confused B.S to t.he seriousness of
hypertens1on; 44 per cent considered it equal to diabetes
in importance; 71 per cent consJ.dered it to be equal ·to
heart disease in importa.nce; 13 per cent_ thQught j_ t wzu3
equal to influenza; and 56 per cent recognized the need
for regular checkups.
According to Finnerty the model clinic should
concent·rate on redt1.ci.ng "\v'a.i ting t.irne, be ·p2.t it?nt· .. ·centered,
deveJ_op an effective patient-doc·tor relationship and be
oriented to patient education. Clinj.c dropouts were re-
duced by impJementing the abov-e .from ,12 per cent in 1966-
69 to 8 cerr:: in 1970·-71
Socio-cccr,Gmic <::~.nd other fac::..ors. Compliance in
! hypertension treatr:,,~nt seems to be the cc:xcept:ion rather
·than -the rule. Do:;:.·ot:hy ~'7att.;s says socio~econom:i.c factors
are rclc-cLed i:.o the ac~eptance Df medical ca:r·e by lov>' in···
The value placed on education, school

16
heaLth ~'JX.p;:~:cie::ncer family s·ta'bilityr and religiou.s
participation were highly correlated with specific
health knc.fviledge and acceptance of health care ( 4 0 z 4 2) .
Davis concurs that there are many factors that affect
the patient's age, sex, socio-
economic status, education; the doctor-patient relation-
ship~ and the medical regimen. Davis 1 revim·;r of ·the
lit.crat.ure on patient. compliance revc~aled t~hat: noncomp1.i-
ance can range f:cc'm JS-93 per: cent. Regardless of the
regimf.;:<:l prescribed a:nd illness involved, at least. 1/3 of
' pat,ients in rn.ost~ st.udies fc:tiled to comply ·.,vith ·the physi-
cian 1 s orders (8:11).
be treated for it.
Project in Ind1~s·try fron; 1967-1972 involved :10,000 ern-
r:.llo:let~s \V11o t.:v~::L"e re:~ct:;j_·vin\J trecltrneilt f~or h.~~.etr:·t }:J:coJJl~:rns ·J
females 1 6. 4 r~er cent of black males and. 21 per c:c::-nt of
black females were receiving trea~nent to control their
by_pc~r~teiiSi.ort ·~ On t..:he a.veraqe black •,:omen :r:ece:i_ve trea.t-
! ' "-'-·.'>···-~-·--·¥,.•-·~- ~·~·- - ~·-~~-n~ .. ~J
Doctor.-·Patient Helat.ionship and Communication. __ .._....,..~-----~--~-.. --.---·-=---···---~---~-~---·------·-·----
The Nat.ionnl High !3lood Pressure Education Program and
, "'1 .L!
·the Harri.s Poll of 1973 pointed out that the great major-
ity (77 per cent) of people that were not aware of their
.·t.<' .;, <·" · ;.hig.h .. b1ood p:r:0ssur·e hz:tvo had their blood p.r:asBI.JXe meas-
ured within the pasi 12 months. 'l'his points to the ·prob-
lem of poor com1n:_:micat:.ion by the doctor who initially
took the blood pn:~ssu.n.,~- or the lack of awareness by t.he
physician that. r:d .. 'jh' blood pr.essure shou.ld be treated.
For years experts told physicians that it was not advis-
able to treat..:. h.ype:cten.sion r.:;.ince the treatment. ~.vas worse
than the disease. 'I'his may indicate a need for medical
education to update this mistaken belief (38:46}.
'i'o impi:ovc compliar.:ce Freidson sugr:J<=~sts patients'
at.titud<3S regan3.ing medical care and physicians 1 atti-
t d ' .. -, ."'u es snc·u __ L(l be improved. Also, medical education should
include more information on patients and patient behav-
ior. The patients 1 attitudes about health and his re-
sponse to a physicia.n depends on many factors. Clement~;
say·s t.he p::~.ttents' feelings 2bout people in au.thori·ty,
and the patients 1 own past experiences Wlth physicians
are factors to be considered (40:16).
'I'here are gaps in doctor~ .. p<:ltic:;;nt corrrrnunic21t.ion
t.ha·t ccntribute to noncornpliance. Francis' study of 800
1 visits to Children's Hospital Los Angeles explore the
effect of ve:rbal commun.icat.ion bet\·leen doctor and patient
' 1..--------,~-~--~"""""""•~--------~---~----~----- ~---~--,~-- -~-- -~--- . ' . -· ·--~--- .. -~~----~------~---··· -·-----,.......... ..

18
... -·---·----·----·--· -- ·-·- ·-.. --............ ! i
on patient satisfaction and compliance to medical advice.
The results showed 24 per cent of patients to be grossly
dis:=.;atisfied, 38 per cent moderah'~.ly compliant and 11
per c.snt noncompliant. Reasons ci~ed for these results
we:.t'e the '.'Jack of warmth in i:he doctor-pa·tient relation--
ship and failure to ~eceive an explanation of the diag~
nos.is and cause of illness." Francis says there is a
significc-mt. relationship bet>,veen patient satisfact~ion
ar'd C"'"" .... ·l1.' ;:,r'C"' (, r: .• c-. 35) ! .J. '-"·''.!!·-· c •• -"" ..L::J.:> .•
Denial of condition. Another factor in patient
no:aconlpliance is the denial phenomenon. In the Peoples
Gas CornJ:;any Study, in the summe:r· of 1.969, middle acred
hypertensive men in Chicago were examined annually and
biennially over a ten year period and told of their
hypertension. But wh.en asked if they '11ere told of t.b.eir
hype:~t.ens:'Lon si.x per cent stated that they vJere never
made .:cda.re of their condition ( 3 8 : 4 8 , 9 3) •
For t.he hypertensive, as for ~:-:.ny person 'llfith c:.
health problem, to deny the existence of a condition, is
often possible. But ·the hyper:t.ensive has !nore diffi--
culty accepting ~he condition because there are no symp-
torr,s. Prom hL~ 1ivashingt-.on Heights Study, Suchman out·-
lines five s~eps that a patient must go through in order
to acc(~pt. a health proble.rn: " ( 1) decision that sorr.e~-
thing i.s wJ.:·on~;-··-sym:r;tom experience; C2) decision that

19
one is sick. and needs medical care-~assumption of a sick
role; (3) decision to seek care; (4) decision to transfer
con·t.rol -t:o the physician·---dependent patient role1 and
(5) the decision to relinguish the patien-t role--
Finnerty says developing an effective
doctor-patient relationship and patient education skills
could help t.:o counteract noncompliance. Bu·t, ''So many
practicing physicians are crisis-oriented, the sicker the
i patient, the more complica-ted the problem, -::he more the
doctors ar:e moti.vat.ed., Long t:e:t·.m :rou·tine care of hyper-
'censives offe:r.:s 1itt.le challenge." So the physician
shou1d be encouras;ed to dclr::s2te some of his responsibil.--·
i ties in t.he control of hypertensive :to the ·trt:d.ned nurse
or health worker (11:3).
More evidence that physicians 1 care of
hypertensives could be improved in order to increase com-
pliance is cited in the report prepared for the Michigan
Association for Regional Medical Programs. CulveJ:: in.-ter-:·
viewed 17 DeLco:i.t physicians in January, 1974 regarding
their Lreatment practices. An estimated 50 per cent
spent less than ten minutes per visit on patient educa-
tion. Another 50 per cenL said tho·t p<lt.ients vdJ.l do
whai: ·the doctor says without further inform.at:ion. I
! Eighty-eiqht per cent cf ·the physicians
i I
I I I
! L ------------·---., .. ------- ·-·-~---------·--------·········---------·· - ·-· -----· ·-·-·----- ----·-· ·····- .. ······~-------------·---·-·-···--·~----·--_)

20
v;;ould not allow anyone else to "educate 11 th~~ patient.
Sixty-five per cent routinely tell the patient their
blood pressure level. Only a small per cent felt it is
import<:mt for the patient to know the name of h.is medica.-
.tions.~ Cohen and Haw·kins intervieNed 60 randomly selec-
t.ed DE:t.ro.it physicians. One hundred per cent s~id they
inform a patient. ·when a diagnosis of hypertension is
made, and t-vhat a drug is used. fo·:e when they prescribe it.
Seventy~five per cent said they vJarn. patient.s about drug
side effects a.nd 29 per cent said they usually tell ·the
patient. the name of tl:,e drug (7:23.) . 'l'he findings cited above have implications for
professional education. 'l'he impori:::ance of p.:d:.ient. educa-
t . f . ~1on. as a :actor 1n reducing r:c)n.c8rnp liar1c..~E-~ ., JJe
stressed in medical and post-gra6uo.b~ educ;;,t.:i.on. Also,
the allocation of ten minutes by the physician for pa~
tient education seems rat,her inadequate,. Many physicians
may not be able to alloc~te adequate time for patient
educ;:J.tion. Since the 1'-LD. 1 s time is limited, physi-;:;ian~;
ta utilize the specialized skills of
a health educator to plan patient education programs.
Compliance and f~ruq t.he:t:apy. ----------------·- ------~~---~ - Noncor;q~1.iance
specific t.<) druq therapy has been studied. Bergm,::n1 and
Werner found t.h<3:t of the 8 3 per cent of pa tienb:; ¥?he said
! they were taking their medication only 50 per cent were i I i t ___ ......... _ ..................... _ .. _._, ____ ., __ ., _____ ,._- _ ...................................................... .
21
a~tually taking tl1eir oral penicillin for the txeatment
of a streptoccol throat infection. This was deteimined
'by urine checks and pill counts (40:20). Curtis found,
of a sample size of 26 t 60 per cen·t of elderly patients
•;,, ~'-A'- .. -·' r vJen:~<:.:takinq the.i:;:· medications incorrectly; less -than 50
per cent knew 1>1hy the· pills were prescribed. In
Sch-v,·artz' s stud~{ 3/5 of the patient population m.ade medi-
cat.ion errors, :mair1ly those of omission (40:21).
Preston and Miller also found noncompliance to
drug therapy in 25 pat.ients from an l' ... rmy Hospital~
Tuberculosis Follow-Up Clin~c. These V;v-o authors say
t:hat vjha·tev·er the reasons for noncompli.'3.nce a "
st.ron'J emph.:-:si.s needs to he plac<:~d on pat . .ient educat.ion
and ·that: :is dE::pendeni: in larcw measure upon the doctor-
patient relationship and mutual respect" (36:23).
In order to reduce noncompliance to hypertensive
treai:merd.: reqimer. mapy factors must be considered. For
<:~~:ample, :Ln a cl:Ln.ic set.ting· waiting t . .Lme should be
;;:;hort, a;:hl the doctor:-~patient. :celat:ion.ship and com.m1::'.nica-
tion ~ust be positive. Another factor in reducing non-
co~nplian,:;e is info:cminq the pa:tient about hypertension,
and ~JJha t r;art be done t.o control it.
Patient educat:ion can increase patient compliance
to tr·eat.ment regimen. Ir:.ui's study in Alexandria,

22
-- -·-··- ,_ ······--· ·- ------~-----.. ~----···- ·~···· ... --~ -·~ ···--·· -···--l
Vir':rinia in 1973 shmved that health education can achieve
at leu..st a 50 per cent improvement in adequately control~
ling blood pressures. His experimental study was part of
his I·:iaster' s thesis at ;rohn Hopkins Hospital, for ·v1hich
""Tnn:.L n1ceived the 1973 B.eryl ,J. Roberts Nemo:r::Lt.iJ. Award
for research i.n education. In this study physicians were
tutored in order to influence their hypertensive patients
·to comply with ·the medical regime:r1. The results of his
study are; First, patients became more knowledgeable
ab0ut ·their condit:ion, 2nd its complications; Second,
patient.:s became be·tLer informed on how ·to follow their
m,m t1~eatment; '['hird, patients adherence to drug ·therapy
became more reliable! and Fourth, pat-:ients blood pres··
su.ce improved ( 19 ; 51} •
Other studies that shm~r p<:c;.tient education can
increase compliance include tha c. of R.osenbE";rg. A multi-·
disciplinary approach was used for educating congestive
heart outpatients of a general hospital. After the pa-
tient education program th·8re t,vas an inc:rea::.>e in klK;',vl-
edge, a decrease in patients readmission to the hospital
and an increase in .patient compliance (20:62).
Clark 1 in 1972, cites patients' comp1lance vlit.h
the medical regimen of anticoagulant drug therapy after
r~~:cei ving an educational program. Also, t.he experimental
gr(YJP had an increase of knowledge about th8ir medica.-
i:iOl"i.S {20: 6.1) ~ i '~·--.~--~ ----~·-·-•-·----"n-·-~· e<- · • -·~~~~- ~·- --~·•·•_,·•·- --• •h·~~- • -• •-

23
In Lindeman' s study ·there was a decrease in
com:plications post-operatively for those pa t:.tcnts who
re.ceived p:r:e-operative education on what to expect as a
result of surgery, and what the patient can do to in-
l'""s a resuJ.t the.hospital stay vms
shorter and the general hospital performance was better
for the patient \vho received education (20~61).
Ave:cy studied thf:t utilization of emergency rooms
by Eaet BaJ.tin~ore 's inner city population who had acute
asthmatic at.:.-tacks. After an education program the con-··
trol group had twice as many emergency visits as did ·the
experimental group. Patients in the experimental group
' J.earn.ed to cope r,vith thc2ir asthrna, wit:h proper medica.ti.on
therapy (19:52).
Diabetics were given education in several phases
of 1.:heir se1f-man3.gement. in Bm\ren 1 s st.::ud.y. In 23 pa·-
tient~3 of t.he e]{perimental ~Troup overall knowled•:J€: and
skills 1 :.:,>;:;pscially in compliance vvi th dietary require·-
ments im?roved from 70 per cent to 95 per cent after an
ed'i..Lf::Gt t.~.ion p.t'()g·rc).ITt ~ The patients in the control group
however, regressed from 60 per cent to 40 ver cent com-
pliancc: >·Jit:.h diabet~.ic diet ther&Pl' (1~151-·159}.
'I'he Instit.ut~e of Hoscm,r spent severa.l years
evaluati~g the effects of various healt~ education pro-
grams. Zabo:!.ockaja, s program for Stag·e I Hy})ertensi.ve~>

24
cent attended the Institute of Moscow for regular
treatment. After one yea:r-, following an educational
program 64 per cent returned. Also peptic ulcer patients
were followed, after receiving education, and their com-
,,,_ '" _ pl_iance with follow up care increased from 4 7 p~r cent ' •'
Arustamova vJOrked with patient education
in cardiovascular diseases and found an increase from 35-
40 per cent to 95-98 per cent. Patie,nt.s complied wi,th
·the medic3.l reqimen, and observed dietary restrictions
{ 4 0: 6 0--61) •
Other Hypertension Patient Educ i1tT0n P iO-<ir ams---~-,~----···-- -·-----L------~-.·-
Before developing the hypertension patlent
education program at H-JTtin Luther Kin<J, Sr. General
Hospital Hypertension Clinic other hypertension patient
educat:icm programs were surveyed. The authors were
intereHb~c'i in prog~cams H1u.t v1ere not sv.ccessful as \·Ie,4.1
as p:c~)q:cc:nns that v;ere successful.
Mi.s.c>icn Hl11s,. Ca1i.forn:La developed a hypertensive pa···
Lien t ed-:.1c: at: ion pJ:~o~-JTar:l, Prior to the education program
knC'rllE'd.;e 1 att.i t~udes, aL<l health behavior relative to
compliance with the higl1 blood pressure ther~peutic reg-
1.n1e1t ~ llsing the que:;t.ionnaire aS a guide ·the ec1ucat.ion
pragrmn was designed with behavioral objectives, and pre
25
and post~ t.esting. Methods used .in inst.ruction included
individual and group instruction, and rap sessions,
visual aids and patient education packets or reading
materials were also utilized. A<::cording to the program
-: ,;- . , aut:hors the program was successful. PosJ.Ll.'ve }(<;J:havioral . ;~- -
changes did take place sac'l:1 as patients corr:ptyi~g with
clinic visit regime. drug therapy, and exercise plan.
Stat.istical info:rmation was not a1;:ail.;tbl.e (18).
At Tiburico Vasquez Nedica1 Center in Union City:
Califo:rn:La a detailed staff training program .,,.ras devel-
oped prior to the development of the hypertensive patient
education program. '1'he content outline gave more detail
on drug t.herii.py and lifes·tyle r.1od.ificat.ions than the
program conducted 2~ the Northeast Valley Health Corpora-
tion. Measurable objectlvss were nat available for the
patient program. Prt--:; and post t.esb::; we.re given, ho-:.·reve:c
evaluative information was not presented 1n the report
( 35) •
The Santa ClAra County Heart Association
. ~ \. . hypertenslon patlent educat1on progrmn, developed ln
December; 1974, incorporated pre and post testing, and
The content outline was mo:r:t::
tients' own ~cle ~n compliance. Evaluative infc~matlon
was not included in this Teport (r-' \ .) ) .
-. ~- -...... ··- ____ , ... ----··· -- -· - .. ~- . !

26
St. Mary's Hospital and Medical Center, in San
Francisco, California developed a "Model For Hypertension
Education In Ambulatc;ry Care." This ·was the most cornpre-
hensive report made available to these authors. The
patient t~ducation objectives, and .,~valuative tools ~Jere
not made available in this report. Interesting to note,
use of Yoga and Bio-Feedback were pointed out as
indicated for reducing stress (2).
The four programs mentioned above gave the
aut.hors an opportunity ·to survey r.vhat had been done in
hypertensive patient education. Each program stimulated
a nevl perspective for each of the five curricula devel-
oped for t.hs program at. the f.1a:rtin Luther King, Jr.
General Hospj_·t.:.:.l Hype:r·i:ension Clinic.
On a national level the National High Blood
Pressure Eclucation Program was revi<:o:-r.ved. •rhis program
of professional and public information was launched in
1972 in order ·to reduce t.he mo:r:bidit;y and mort.ali·ty n .. ~-
sul·ting from hypertens.iun in the United States. 'T'he
~.at __ ~o~.-.-~ .. 1 I.JJ.R~_i_.~',.l·t~.-~ r;f_- P .. ~c-.!·l+.h.- ~~-·-· t-~o ~an~r-~~en~ of Heal~h _, __ ._ ~·-'-~- - _' L c~· ~. -·- --··' _ ~- -!.J<c.:. J.Jt..;_ c- '-"·- 1.... ... - '-"' r
Education and Welfare agency that 12 ~esponsibls for the
coordinatfon of t~is program with ~he ~atianal Heart .,
c.l.nc~.
Lung Institute as the focal point.
The National Hi?h Blood Pressure Program offers
assistance to state and local hypertensive agencies by
offering through the Four Task.Forces: 1. a dc:ti:a base -

for retrieval of hypertensive research; 2. plan for
,, ..... _,
professional education; 3. plan for community education;
and. 4. resources and Impact assessmE-~nt to study the ef-·
feet of programs on health care systems (37).
:.~· 3\£ter r.evie\ving these few hypert.ens.:Lr~'~'. ;c;;cograms
in California and the National Program, the au·thors be..:.
came awarE: of t.he need for mon~ cornprehensive hyperten-
sio~1 pa.t:ient programs. 'Sine£~ many pro~rr-arns are not ·pub-
lished, i·t was difficult to determine hohr many programs
were impler:-1ented in California and Nationally. It: is
~.•be authors~ hope that more hypertension programs be
made available since thedisease effects 22 million
.Ame.r1 t=:ans,.

III. METHODS
Martin Luther
Kirtg, Jr. General Hospital, a 400 bed acute care facil-
it:y 1 opened i:tB doo:cs tJ.> the public in March, 1972. The
-' . • t 1" • 1' . ~ d- F h ou..::pat.l0\1 . il~~pertf.11Slon c .lnlc 't'7as !:un ed ~nroug an RHP
grant in October of 1973. The grant mandated physician
and nurse ·c:r.:-a.:Lnlng, and a health education component t.o
be i.n operation by :June 197 4. In t.he period between
Oct~obe:c ,. 19 7 3 and Ma:r ch , 19 7 4 , there ,,,Tas no pa:t ient ed u-
ca. t. i. c) l!. . . .
on an on-go;~g n~sl~.
In .Hare.!-., hedlth e':Iucati on. Gn a one·- to-one basls
was initiated in tlte hypertension clinic and also wit~
patients on the wards. A~ that time there was no spe0l-
fied for:nat or chrriculun .:>.nd r:o progr:am evaluat.ion. 0!1--
going during this time were needs assessment and develop-
rnent of teaching materials. In M~rch of 1975, organized
classes were imrlement2d after one and one-half years of
Classes were offered three
times per n-:ont:h d~::;penrl.:Lng on t:he ava:Llabilit:y of cla.ss-
At that tirne 1 course coritent consisted of an
28

29
t.he health educat.or or one of his ~.;pecially trained
co:rrununi·ty v10rkers. The other two classes taught in any
one month were chosen from the following: diet., drugs
(medications) , lifestyle modifications or blood pressure
taking. These classes were sometimes taught by the
health educator or community worker; or~ occasionally by
other hospi·tal staff as attempts \vere m.ade to draw
multidisciplinary support for the program.
The Hypertension
Clinic was organized with the following objectives:
1. 'l'o make availa_ble to patients the b.est current knowledge and ·te.chniques for diagnosis and treatmen·t of hypertension.
2. To provide diagnostic or therapeutic consultant servi.ce to otLer clinics, physicians and to ether health agencieo,> in t.he cornmtmi ty <
3. To develop efficient diagnostic evaluation procedures in order to a) Identify curable causes of
hYP'2rtension. b) Assess the effects of hypeitension,
particularly the extent of the associated target organ damage,
c} Make predictions concerning prognosis. 4. To develop systems which would assure
continuity of care of the hypeitensive patifmt.
5~ To develop educational tools and proce::;ses for providing adequate care and, thereby enable patieJits to make .soc·ial adj us !:ment.s and to assume respcmsibili ty for t.heir own care.
Patient eliqibilitv. - --~.._,._..,.._....,..__..~~·---~~·----;;.......~----··.=:lL-
Eligibility of patien-ts t.o
recej_ve ser~Jices :;.s determined bo:scd on specific medica.].
cr2.te:ria. document:ed in ·the operg.t.inq p:r:otccol for i:he

30
HYP'2rtension Clinic. These criteria include blood
pressure measurements! medical history regarding blood
pressure and medical evidence of target organ damage.
Screening of patient.s £or hypertension is performed
t:.hrm.:~qhout: the hospi·tal and in special com.TTiuni ty out-
.raach prog:co.ms. ·
Pat.ients v.Jha meet the above -eligibility
requirements may be referred direct.ly to the Hypertension
Clinic from a Local Health Depar-tment,. Martin. Luther
I<inq, ,Jr. Walk-In Clinic, and/or Emergency Room. Pa.-·
tients may be r_eferred indirectly by private practitioners
and by se1f-·referral, as from a corrrmunity hypertension
scree:rnng program.
Clinic personnel. ---··-------~----
The personnel who comprlse
t.he cJ.inic are: seven Physicians; t~1.'m Nurse Practi tion-
ers; five Licensed Nurses; a Medical Social Worker~ a
Nutritionist; a Health Educator; and Administrative and
C1.er:i.ca 1 E~taff.
Health E~ucation within the Clinic. The Martin
Luther King, Jr. Hypertension Clinic is education ori-
ented, as seen by one of the Clinic!s objectives:
To develop educational tools and processes for providing adequate care and thereby enable pa. tients to make social adj ust.:ml:',nts and to ass1.nne responsibi1i·ty for their own carE.:"

31
•rne Health Educa t.or is responsible for meeting ·the
above objec·tive. As par·t of the health team the Health
Educator works closely with the other health professionals
in accomplishing this objectiv·e. Howe~er, the Health Edu-
. . L catox- 1s a. so respon~ible for the educational need~ of the
Consu.'ller Heal t.h;
Diabetes: Tuberculosis;-and Arthritis. In addition Com-
m~nity Outreach in Hypertension education, screening,
n~:Eerral and follo~,,J-·up for· ·the South-East re<;_rion are a.lso
the responsibility of this Heal t_"h. Educator. Two Community
~ealth Workers, trained by the Health Educator, assist in
community outreach programs.
The Health Educator is respbnsible for many
aspects of education. Realizinq this,. the authors re-·
auested and \·:ere g-rar1·ted permission to participate as
graduate student field trainees in the hypertension
clinic in IV!.;;..y, 1975.
'l'"b.e au'chors proposed the redesign o:f the existing·
hypertension pci·L:!.ent ed1.:cation proqram. 'l:his ne~·I proq:r:am
i.nc~.uc1ed curricula, measurable program objecti \i'es and
eva1uatior..too1s.
•tbe design anC! implementation of any education
eva1ua.t.ion, but a needs i:tssessmen·t of the target popu_la.-
tton. 'The a1lt".hors design~~d and pre-t.ested a. patient
a.ssessmen.·l.: questionnaire on t.hirty Hypertension Clinic
patients. After revisions the questionnaire was admin~
istered to one hundred clinic patients.
Hypert:ensi.on Clinic· Questionnaire P..es.iift.-s-------·-·-------------------
The Hypertension Clinic Questionnaire was
32
desiqned by the authors to ident.ifv the Clinic population
demoq;:-,=~ph:Lc var:l.ables, quz~li t:y of care rece~ved in the
Clinic, and patient education needs. (See Appendices A
and B for Questionnairs and Complete Results.)
On<..:! hundred questionnaires -v:ere administered by
t.he "cwo C'omrnuni ty Health Workers in September and October,
19 7 5. A no:n-:candom sampling· t:echniq:uc \.Vas used.
':'he autho:cs v·!C:t:e conce~::ned about tl1e c:u.::tli ty of
tions wero directed at this concern.
tient~ were asked a~0ut waiting time to see a doctor, if
re.::v1 somet::·d_nq ;:bout high blood p:cE<3Sc.n:e and 84 per cent.
Even thuvgh a high per cent
87 per ce~t said they would like to learn more about high
bloo~ pressure ard 74 per cent were willing to attend

(
'
classes on high blood pressure.
Table I
De~ographic Findings of Hypertension Clinic Questionnaire
--··--···--·-··------··-------------·---- ---·--------------Dem0graphic Variable
Female Hale
Race
Black lvlexican -?\mer ican Asian Other
Years in School
0 - 6 years 7 9 years
10 ·- 12 years More than 12 years
D~ration of Clinic Attendance
Fi:rst tin1f= ., -· 6 ffi<)l11~11S .L
6 ~ ., ? .L~ mon·th.s
1 ') "''"' -· 24 months
Frequency·
54 41
8'/ 6 1 ... )
13 14 51 10
16 20 18 43
Percentage
---·----·-·--·---
57 43
90 6 1 .. .)
13 ., L!. J.. ~
53 20
16 21. 1.9 44
!L-fter making an asses::3ment. cf the needs of i:h•3
Clinic population, the following objectives were £orrnu-

1. To develop and implement a patient education
prot;rram for hypertension outpatieni:s at. ~1ar.tin
Luther King, Jr. General Hospital.
2. To develop a:nd implemen-t an effectivi?. patient
referral system to refer patients to the hyper-
tension educa ti.on proq.ram.
J. 'To increase patient. ccmp.liance wi ~:h physician
o:r:·ders ~,.;it.hin t.he Clin.:Lc.
4. 1'o develop evalua.tion tools to verify the
effectiveness of the education program.
C~r i cu.l U!~ Dev~ lor:~-~~2..-!:.:
34
The results of the clinic questionnaire were used
Also, after meeting with clinic health
professionals it. ~t?aE decided ·that five cu:rricul::t cr
teachins_;· modules (See Appendix C .for cnrricula) sho~1ld
be deve lopz~d.
Blood P:r-essnre." This class vvu.o:: designed to give a
The Health Educator
was the cont:ent spec.:i.:ot1ist and as3isted the <-:lutho:r:-3 1.n
developing the Gurric~lum. The Health Educator was also
the instrt.H.::t.o::r of th.~-s w.cdu1E ..

35
The next curriculum was "The Role of Drugs in the
Control of Hypertension." Originally it was the author:s!
intention to conEml t the Hospital pharmacist in develo;?-
ing this module. However, this was not possible because
::tbe .. phanna.ciBt was involved in implementing· a new mBdica·
tion refill system. ~he Health Educator served as the
content specialist and also agreed to teach this class.
Plans have been made to t.rain a nurse to teach this mod-
ul.e. The curricula was designed for patients to identify
tl::eir O'A7l1 prescribed antihypertensive drugs, t.he actions
and side effects associated with each drug.
H•rhe Role of Diet in ·the Control of High Blood
This module explains
'.'iil.Y ·::t sodium r•estricted d.iet is importa.nt. . It encouraqes
the atudfHlt to identify foocls high and lmv in sodium;
drug·s that con+_ain sodium.; and alternative 1mtJ sodium
sGa~3on.ing and rood preparing methods. The content ex-
pert.s ,.;ere ·t~e Hospital Dieticians. The class was de-
signed to b;;~ L:-1.ught by a dietician and a Home Economist.
The fou~th class was "~ifestyle Modifications in
the Control of High Blood Pressure." Effects of weight
control, smoking, alcohol, stress, rest and exercise are
':::'he pat.ients' expression and
discu;ssion of their C'l!Yl feelings about these modifica·-
tions is emphasized in this class. The Medical Social

36
Worker· conducts this class; and colla.bora.ted v.ri th the
authors in developing the curriculum.
The las·t class was "How to Take Your Own Blood
Pressu.re. 11 This class is designed to demonstrate how to
take blood pressures and requires a return demonstra·tion
on how to do ·this by the patient. The ins·truc·tor is the
Health Educator and/or the Conrmunity Health ~~Jorkers.
The first class is ta.uq.ht on a weekly basis,
every Monday. One of th..e four other classes 1 in order of
above discussion, is taught once a month on a Friday .
.Since the Overview class is taught weekly this allows a
patient to enter ·the ·whole program in any given we1~k, re-
ceivin9 a. basic overvie%' of high blood pressure, follmved
by more detailed classes on high blood pressure control.
I:mplementat.ion for the patient edncation prog-ram
was i.n·tended for lu.·te November but: due to the h.olidays in
November and December classes were re-schedl1led for
January. A minimal amou.n·t of insarvice education was
required since the instructors had assisted in the curric
ulum devclopntent and had previous teac:hin•J experience.
Ref ~!:_J:'a. J:..._§..ys t~.~~
~ssentially all patients from Martiri Luther King,
Jr. Hypertension Clinic are referred to the Health Educa-
tor for education either on an individual or group basis.
This is in accord.ance with the Clinic Protocol.. Since
37.
there were a.pproximo.teiy 2267 Clinic visits in 1975, r,,.rith
approximately 2 80 visits per month i·t would be imposs:i ble
for all these patients to be seen on an individual basis.
So these patients are referred to the Hypertension
such as in cases of language or educational barriers,
then the Health Educator would give individual instruc-
tion.
ThE~ Hypertension Clinic physicians refer all ne'll!"
p;:.;:tients and patients \vho have not ho.d previous hyperten-
sion education to the Overview Class. The Clinic nurses
are instructed to compl8te the referral form (See App€m-
dix D) and give the patient an appointment card for the
cla~=;s. 'l'he patient. is encoura,ged to attend the four
other classes, however it is not. required.
Evaluation
Inplementa·ti.on of the Hypertension Classes began
in Januc:~ry, ~, 0 .-y ._L:JtO.
January 22, 1976.
The Overvimv Class was held on
Sines this class was intended to be
qi ven on a weekly basis, on Nonc1ays, it. became necessary
for the Community Health Workers t.:o assist the Heal l:h
Educa'cor in teaching these cJ.a;;ses. On Janua:cy 19 and
J·anuary 26 the C'verview Cla.ssss '-'ren:: t~augr1.i: by the Cor:\-
nnmit.y Healt:h Workers, 'I'he questionnaires Y.ie.re not
distributed because it was believed that the Health

... ... ,;_ -.. ,.,·,:
38
li'Jorkers were still learning how t.o instruct according to
the curriculum, and the results would be questionable.
Due to other educational responsibilities this class was
given only twice in February by the Heal·th Educator.
(See Table II for Questionnaire Results.)
Table II
Overview Class Questionnaire Results
===-· ----=-...:::---.---=--===--------------=-------======= Pre Post
1/12/76
l. 2. 3. 4.
2/2/76
L 2. 3. 4 . 5. 6. 7 • 8.
2/23/76
l. 2.
4.
87 100
43 87
90 90 90 97
100 90 90 47
90 100
47 90
X = 84
lOO 100
87 80
100 90
100 100 100 100
60 67
100 100
67 70 --···-x -- 89
--M-------~,..·------~·---....... .-.--------··-·~·-·--r-··-·---.---_______ ;... _____ _
The. second ,:;J.a.ss, ''Ths: RoJ.e of Drugs i:n. the
Control of High Blood Press11re" was implemented on
January 9, 1976, and qive~ again on February 13, 1976.

Table III
"Drug" Class Questionnaire Results
1/ 9/76
l. 2.
2/13/76
4. 5. 6. 7.
·-----------
X ·~
Pre
20 20
0 80 40 20 40
37 X
Post
40 80
0 100 100
40 100
77%
"The Role of Die·t in the Control of Hi']"h Blood
39
Pressure" ~vas i:r:rplement2d on ,January 16 ·' 1976. The class
was not given in February because of scheduling changes
in the classes. it shoulcJ be mentioned here fhat the
dietician 1,vho t.c:tught the January clc:.s.s- ha.d somE; diffl.cul-
t:ies in covei.-in·~1 t.:h2 content. due to time GOI!St.ra.int.s,
i,e. 1 the class vias started late. Also, s1nc:r~ t.he qcLes--
nai:cc score is lower than tho average pre sco:;.<c~ t:.here i~s,___ __
some question as to the validity of this evaluation tool.
Further evaluation Ls needed. (See Table IV for
Ques·tionnc"tice Results.)

40
Table IV
Diet Class Questionnaire Results
------------
1/16/76
l. 2. '".:! '"'"
6.
----·--·--------··-----
Pre Post
J..n these first three classes ment.ioned above the
sample si~e of the questionnaire results is too small to
be g i .,r2n much im.por-c.ance. In order to have a valid sample
size~ for a s'cdtistical evaluation at least 30-50 question-
naires should be obtained
'l"he ne:{t cla~;;s, "Lifestyle Modifications in the
Control of Hiqh Blood Pressure" '\vas l!nplemented on
January 23, 1976. The only satisfactory way the authors
and class instru:ctor could fi.nd to evaluate this class
was by usinq sunj ecti ve measures. By referrin9 ·tb the
cnrricuJ.um. objectives (See Appendix C) ·the class instruc·-
tor can see that this class is ~ - ~ ~ a group process ln Whlch
the patisnts are encouraged to express their feelings
about the treatment regimen in the control. of high blood

41
pressurr-;. The authors witnessed that this class \vas
enthusiastically received by the patients on J·anuary 23.
There was participation in discussion by all the patients
present. The patients requested and received a second
.• sess.:Lon the fcllowing Heek. It vza.s felt by the instruc··-
tor, the Health Educator and the authors that the objec-
tives for the class had been met.
"How t:o 'l'ak.e Ycn.Jr Own Blood Pressure" was the
last class that was implerner.ted on February 6, 1976. The
two Community Health Workers instruct.ed the pat.ients on
how to take ·their own blood pressure. Family members
and friends of the patients V.7ere invited to attend t:b.is
class, as wsll as all other classes. In some cases the
patient ~ay not be able to learn this skill becaus~ of
problems in dexterity or hearing disabilities. Therefore
the patients' family or friend could assist the patient.
This class was well attanded and the patients requested
and receive~ another practice session in blood pressure
taking the follo~ing week.
Aft::.(!!" b;;ro months of program implementation it is
difficult to ~~ke anv clear cut evaluation of these
ord2r to have enough data to maks a valid evaluation.
Therefore the ori.ginal hypothesis:
"IncreasE: in knowledqe a.nd understanding
of the ccnd:it.ion o:E hypertension ·will not

42
result in increased compliance wi t.h
phys:Lcian orders. "
cannot be accepted or rejected until a longer period of
.implemen·tation takes place, with sufficient data obtained.
The relative effectiveness of educational
prog:carns such as this can best b•?. measured only after
long, continuous and closely monitored inplementation.
Rigorous statis·tical test:s of program effectiveness can
not be applied nor concJusions relative to increase in
patient compliance drawn, from the limited data yielded
durin9 only tv,'O months of implementation. 'l'here a.re , hm.v-
ever, :rec·onunendatio:rs which can be made for fut.u:ce, lcnq
term e1..ra.l ua.t ion of tnls pro~rra.m.
One of the main objectives of this program is
increaSed patient con~liance to physician orders. This
compliance is best: measured unobt.ru:siv8ly through checks
on the pc:ortient' s blood pressure r v;eight, smoJ.zi.n<:r beha,l-
iors, J.ift:-:~style rrtodifica·tir)u:o; J and Cl:i .. st~. 1\n in.i·tial pre-
education evaluation of blood pressure and weight meas-
u.rement plus diet. history and paticmt hi;;tory of the
:n;;;maining behaviox-.c-:; 1iJOuld estah1is:t bdseline data. It~
is recomrnended t.ha t the patient's blood pre.ssur:·e, weig·ht r.
and report of compliance in the other areas be taken
routinely on a monthly basis~ In this way, compliance

43
(or non-cornpliance) as witnessed by these para..'Tleters can
be checked over a shor-t term (six months) or over a
longer span of time (one or more years). Continued meas
ures should bP taken on patient's post-exposure as well
as on a cont:r:oi group.of patients matched for age, sex,
initial blood pressu:c.e and weight.
IV. DISCUSSION
During the course of implementation several other
·_programs and on-going· activities v.Tere taking place in the
' .. ,,. ·-- :Hosph.:al :that-should b(:. discussed. As of ,January ls·t;
I.os Angeles County Depart.ment of Health Services insti
tut.Eod a coraputerized billing system for all patient.s util
izing County services at fv1art.in Luther King, ,Jr. General
Hospital (and selected other clinics tl1roughout the
County}. The patient (at Martin Luther King, Jr. General
Hospital) is automatically billed $72.00/visit regardless
of the type or extent_of co.re they receive. This system
was instituted to increase_hospital revenues and third
, party ps.ymen t s . It. is obvious t.hat this syst:em would ef-
feet at.tenc1ance ::tt hospit:a.l run clinl.cs (i.e., the Hyper
tension Clinic) and it was indeed considered as a co~trib-
: utory factor ~o the decline in clini~ attendance. Because
patients are referred to classes through the clinic, a
decrease ir: clinic attendance would result in a drop in
the r:mrrilx:!r of peopJ. e referred and thrc:~r(~fo:ce actually at-
tending patient education classes.
During ·the planr.i.~·l,J and ear:ly implementation
stages of the program, a health education mural was
p~inted on ~he walls of th~ waiting room in the Hyperten-
sion Clinic. 'l'he mu:ra1 consis-ted of lar~)e p:Lct.oria1

45 .
representations of the main points stressed in
hypertenaion patient education: regul~r exerciser regular
check-ups, lm<'~ sodium diets, avoiding "junky" foods,
avoiding stress and smoking, continued taking of medica-
. tion. Although impossible ·to quantify, the .mura . .l most
probably had an effect on the states of knowledge of the
target population. The Clinic Health Educator admini-
stered a pre and post exposure questionnaire, but the
results have not been quant.ified .as y.et~
The clinic population was subjected to several
survey questionnaires during the planning of this program.
'Iwo surveys relating to t.he patient education program tvere
administerec} by the Health Edur;ator! s cmmnu:n.i ty wcrkers.
Th.e ac:ithors adrninis·ten-:;d a survey questionnaire to gat:her
data on patient's atti~udes toward the Clinic, Clinic
Personnel and wilLingness to attend classes. The ques-
tionnaire was pretested on 30 people and after revision,
\vas given to 100 morE:. Also circulating at that time was
a ho,:;pi ta.J. vvide questionr.aire on sick!.e cell anemia.. It
is easy to seer ther. .. , t.hat the clinic pa·tient populat:ion
was literally over-surveyed. It is well ·.vi thin t.he real.IT1
erfect ory patient re-
sponse to our questionnaire.
Since data \<Vere gathersd by the ·au·thors, a ne\<T,
more efficient appointineEi.: system has been insti-tuted.
An appcd.ntment clerk with poor patient rapport has been
replaced and the pharmacy has installed a computerized
pr:esc:cipt.ion refill system. All these changes have
shortened waiting times and made Clinic pai.:ients more
satisfied wi·th the service at the Clinic.
46
:r~ ,.,-a.iti:nq room education program has been
conducted sporadically in the Clinic for t.wo years. The
program consists of a film on hypertension shown to -!.;hose
; in the waiting room at the Clinic :Eollowed by a group
discussion lead by the ccnn::n:mity i•!orker. This program
was conducted monthly before ,January l, 1976, and is now
conducted on a daily basis. Since the mural was painted,
the mural also has been incorporated into ·the discussion
portion of the prograr.rt. Tht-3 community <tvor·kers do refer·-
rals for the patient education classes. A weight control
class, taught by a hospital dietician, also is conducted
one day each week.
As can be seen from the above discussion, there
are many concurrent education activities conducted in the
hospit:2:.l. The effects of these programs on the patients
have not b1~E::n evaluat.ed as 'Jet. As a result, it is dif-
ficult. to qua:1tify the effect: on the authors 1 pat.:i.ent
education ~lasses.

V. SUHM .. n..RY, CONCLUSIONS AND RECOV&1Ei~Dl1.rl'IONS
Approximately 22 rr.illion Americans have
. W.:lds::t.ecLed, untrea·ted or .inadequately treated lwperten-
s:Lon. Hlqh blood pressure is a leadinq cause of J.norbid-
H:y and mortali.t.y in the United States f as shm11 n by the
Pramingham and Veterans Ad.rninist::ea.tion Cooperative St;;<-
dies.
Essential hypertension is often asymptomatic.
It requires lifelong treatment. Patient comp:):iance in
regard tc drug therapy and modifications in diet and
lifestyle is often difficult to achieve.
•rhe e·tiology of csssntial hypert:ension rernains
u.ncJ~ea.r. Fa\::b::rs euch as sodi. um intake, genetics, stre.ss
and obesity have been shown to have contributory effects.
It was the authors intention to design and
implement a patient.: EJI-.1catL:m program at Hartin Lt1the:;::
King, Jr. Ge~eral Eospitsl Hypertension Clinic.
The authors
relat..i.or:.s:nip and patient ~:::ducati.on.
4.7

48
Other hypertension patient education programs in
California and the National High Blood Pressure Education
Program were reviewed in order to determine which pro-
grams were successful.
Prior to the authors' arrival, a patient-
education program was conduct.ed by the Clinic Health Edu--
cator. However, the program did not. have spr2cific cur-
ricula, measurZi.ble program obj ecti ve.s, and evalu~--i.tion
tools.
The authors conducted a needs assessment and
designed a comprehensive hypertension patient education
program. '.l'he program consis·ted of five separate teaching
modules complete '("7it~t objectives, curricula and evalua··-
tion tools. Course ccntent included modules dealing with
an overview of high blood pressure, diet, medications,
and in3truction in taking bleed pressure.
Concl-c.sions
Program implereentation was initiatad ~n January,
1976. Data v.Jo.s collecb::::d over a two l<tonth implementation
period. Sines the:~ p:rogra.m v-1as i::-nplemcnted over a rela--
ti vely short period of t.im.e and because small. sample.
program objectives were met arP necessarily partially
Stlbjec·::i'Ve.
49
The original. hypothesis, stated in the Null form,
was;
Increase in knowledge and understanding of the condition of hypertension by the patient will not result in increased patient compliance with physician orders.
l,atient cOJilpl.ianc.e ,is ... a. di£fix.:ul t parameter t.o
measure over so short a period of t:ime. As a result.: th0~
authors' hypothesis can neither be accepted nor rejected
~rlithout further implementation, data collection and
analysis.
The patient education program, a patient referral
system,. and evaluation t.ools were developed and imple-·
mented meeting the first, second, and fourth program· ob··
by increased compliance) , referral system and evaluation
t.ools can be mea2-ured only after a longer period of :i.m··~
plementation, ltliHl a significan·t number of pat.ient. partie-
i.pants.
Recommenda·tions
'I'he authors recommend t.hat the hypertension
pati<:orrt t'~ducat.ion program be continued in order i::.o gather
more data on the re lat.ionship bet.v-le.en pat.:i~::.n t t:;ducati·:m
and patient compliance. Revisicms a:ce recmm':lended i.n t.he
curricu1a as needed based on patient. feedback, dir:e: re-
sults of the curricu.la evaluation tools and input from
the moch.1le in::;tructors.

50
It is also recomrnendE::d t.hat ot.:her prog.rarns
directed at increasing the detection and control of high
blood pressure be implement.ed throughout the United
Statesr especially in urban areas, where incidence of
±:he disease is high.
The authors feel that the educational and
personal experience gained by working at Martin Luther
King, ,Jr. General Ho~rpit.al was an extremely posi·tive one.
T:i-1e ex;lerience of wr;:,:::.-ki:r~g in a. large, predominantly
Blackr urban county hospital added greatly to the
authors' personal and professional insight. I·t is hoped
the other graduate students will be encouraged to seek
out similar experiences.
BIBLIOGRAPHY
L Bowen, R. J. , et al. "Effect.s of Organized Instruction for Pa·tients With the Diagnosis o.f Diabet.es Nellitus;" Nursincr Research, 10:151--159, Sm;rrner , 19 61. ------------~-
2. Casebook on Hypertcnsiori anh· ··Edema, Seale and Cornpar:y, ·19 7 5. --------·-----
4.
5.
6.
., I •
B.
Curry, P. an~ Clinkenbeard, M. Hypertension _,.. o·"' ·1-r "' 1 • c .._. 1' m 11 1 "' t -: n ,.., I) '1 t: L. e nt ·-rr~·;:;;::;·-1·--:; a::;-:::-::;·~ \... l" ·~ . '--'···. '-' L. ···'~·~c. -'- ''1 c.-- ~ . ~·-'·'·!:· .... ... ~f:'- t
cia-:-rac5ounty -Heart.-1-\ssoci<?-tion, l97-4 .---
Curry, Chas. nHypertension: Number One Killer o-.c· America:::, Blacks,'' Hypertensi v·:-; PEttient, Bristol ~ .,. b ~r "' +- n. ~ ~ e· ,.. • r ~ 1 UlY8-:-;:::, 11 ;;;---;;_:;_U·-:,::;-}.---:::-y--P-0-::-1.-::- ·o " .l..-J(A..- ..... .1 o~-UJ~...L,~t vu_ ... a~!- \._..-<.~.._ 1 .i.'! tU.~-.Je ~ 'L.i., j;u £ 1
197').
Dahl, Le,Iis K. "Std.t 0.11d .H)tpertension," f.\.-rnerican ,J 0 urn ~L--~i c :1.:. in i ~~]. __ Nt; t~~)- ti ~;'Q. I 2 5 ; 2 31 ~-- 2-,rLr;--1§7 2 •
Da.vi s , 1'1i l tot' . "\Tariatiorls 1r1 Patiertt Corn_t)l:Lartce ~vit.l1 [)()C!'f.:ors Ord.ers:-. Ar;.a.lysis of C~tJll(Jr~IE~rlc~e .Bct;.;,"~~CTl S1
.. L~'1E.!]' ReS})()i1Ses an.d r~eS1J.l ts of }l;mr::·il-:Lc~cll
I:rr•.re::;ti<!,atinns r" l9~rr~~--of t':!:_edJ:~a}. E~;:':'~Ca._!_:':_?_~~,. 1, '1 • ~ ~ 'j u "' -, . .... _.....t..t>J ... L, ---·b-~.•
9. "Effects of Treatment on Morbidity ~n Hypertension: Results in Patients with Diastolic Blood Pressur2 flV.{=rasrirlg 90 1"tl11:-t)tlgl'l 114 ll1iTt ~dtJ r H ~r~~'~T~~.l ()_f __ ~~.b-.~~ ..
. ~1\.t.-rr!e~i·;_;an t•·1ed.:Lc;.11 i\SS()CiD.t.iOX1! 2l3!l143·-Jl.52, 'i~T1is-:--- ·-----------------·-----------
10. u :e~f ft-;:c:t:_s (J £ ~r-ceat.~r~c..J.: t ort :tv1oJ:"lJ i'J~i t~y· in Hy}Je~r--t~:: tls i()n; :.R(:)Sltl7s ir~- I: =::-t-t i.t.::.n.·l: ::-::: v:ri·t~l-l .D i\:tr:;;·tolic; Bl cJocl I~re~J s·~11~e
:;~~X~~~~~:~-~J~~;~~:K~;~~cl~~-2:~~, n~0;! ~~i~~~~i~--:~i-§-~]~~

12. Finnerty, Frank A .. ~ ,Jr. I et al. 11 HypE;rt.ension in the Inner City: .Analvsis of Clinic Dropouts,!; girc_:-!-lation, 47:73-75, 1973 .
. l3. F inne.rty ~ Fr a.nk A. r Jr ... ~ et .a l c II Hyr•cxt t~:r:s.ion in tl:~e. J. r1r1F2r City: DetE;ct.iori {.ti1:·d · ?·t"tl-.l.<?}iff~~l~~'P, u
_Circ~::.:!:~!:i:9Y1, 47:76-78.~ 1973.
14. Fodor f John rr. and Dalis I Gus 'I'. r.:rea--:l!-1:~-Instrl!_<..::'t_~_?.n_; ~teory and Application, Len nnd Febiger~ Philade1pn:Ccl,"-re"nn . , 19 7-.r:--
16.
.., -.t. I,
Francis, v., et al. "Gaps 1n ~actor-Patient Comr:mnical:iorl: Patients' Hesponse to i>'ledical hd'vice, n Nell England ~rournal of Hedicine, 280: r.;., h: ~ Q c.: 0 ~------------~--~--· -_,J_,, 1.-0.-·.
}.~reJ..::; 1 E(:J.-;,.JarG 'D" n .?-J.ge I P.a_ce !- SeY:: and Ot11ef:, Inct~ices of Risk i.1.1 Hypertension f" 1\merican Journal of .r'1edic ine! 55: 2 7 5-2 8 0 r 19 7 3 --=--------·--
Fj::: e i .s , 1~ (l "-"7 GtJ.~ ~!_ [; ~
}1.·v·~ert.(~11sion .. ~--'~ ..t£:;,. ----·-------~ ·---~ •··· •
D. c ~ T 19 73 ~
'l1he I"iio~J.er11 ~"ioJ.nacrement of ~\:l-:;·tera.t1S A_.2i8In.5_ st:rat~l()r:·;-t-\!tlS ~li rl~;t.~n t
19. G!>·?e:rt! !J ~ ~~J ·~ H 'l't~)~A!C;.J':(l cc~s·t-Be:ne~f it E'v;.:ll L1B. tior1S 0 f I-I,3t1.l tb. Ed.1JC~2-tiOl1 ~ !3cime COil':~f~l)t·.r:: .- .?·!et.ft(){'JS and
~~;~:l~;~~;i:: 1 ~~~~~hr¥-~¥~:E~~-:~~~1_2 __ i52~~o~~E.02.b~~, 2,
20. Gr0e~, L. W. a~2 FigQ-T~labonca, I. "S~ggestea Desi<JLS .:cL :::,_,-a.Lna·tion cf Pc..tiE.'nt Educ.Jt.ion Fi:·of;ran1s 1 ~ 1 ~i~~::~J-:_"!:~:_,_~q~-~-~at~i.~;r~ JYI~?l!_~~~f~~J)lls, 2:62 j· S(J!~.lr1g, ~L974~
22. }J(}.ri-:;.·:.1}~~; r t~.r-rlCSt .~ et.: al"' H sc~ci.oecolcl(rict:tl St:,L·2SSOr Areas and Black-W:tit2 Blood Pressure: Detroit," ~~.) 1J~~.:~~~:~-.-~ ~ S! ~f... C~1-:c ~?1:~.~:S::.~ ... .!2.~- s ~~-~.:~:. , 2 6 ~ !5 9 s ~- 6 11 1 19 7 3 .
23. Heart Facts 197 5, .America.n :Heart Association ---p -,Til")·;_.;-} .. _ at --.., Q -, .1
... C..\~t}; 1~~-c;:; -1 ..l,._.. _; •
53
24. Heyden, Siegfried, et al. "Elevated Blood Pressure Levels in Adolescents, Evans County, Georgia." cTournc.l of the Arner ica.n J'v1edical A~_:~O<;:~a t.io~ I 2 09: T6s3=I68~196-9.
1;;.; ,_Hypertension,'' Hypertensive Patit:'t\i:·, · Bristol Laboratories, 4, r9'7s. ·-------------
26. Huff~' Robert JVI. Hypertension Training Hanual, r-·Iart in r"u ther izing-;-Jr:--Gt:m;?!ra.l_Ifosi)i t.-a.T;-Hypertension Clinic, Los-Angeles, 1974.
27. l:I'uff, Robe:;:-t M. and Ashley, Hary. Cormmmity Health
28.
·vk>~kers -:n Hynt-::rt'"-nsion· r>. Trainin-:;-~~o,c.p=i ___ _ --=--:.:·:-- 1 ~, '. ...b. =tT-·-~---;~~-· ;-:_:.~~...:--~..,-1;--·:~l~ w ~ ;__~~~-·~~; ~ Con.su.rner ..tealth E~1.J.Cd.Cl0Lr c .. arle .. R. D~e"-
Postgraduate i'·1eaica1 School-·-Martin Luther King, Jr. GencT3.l Hospital, Los· Arlgeles, 197 4.
29. Kannel, W. B., et al. "Epidemiologic Assessment of t:hf~ Fole of Blood P;::-essun:~ · L~1. Strc;k.e-. TJ:e Fra.mingrte.J:,"t Stud/," ~~Tr.-:;urna1 of t::'\:0 .1\~r..erican Nedi·-- ..... , A"'~ (0.0: .~ ..:: :::1 +· .: " : ~ "";r:"""";:)o-·1-~::·.;:;-,-~~· .. -=-l~(i·;y·;r----------...... ---·.~--~~.:::-_._::: .::.OC -'-~::.:-::::_<?.::::::J ~ .L ., • .J . ,Lt. U 1 . -' , u •
30. Kannel, W. B., et al. "Blood Pressure and Risk of Coronc.ry Heart Disease: The Framiaghaw Stu.dy."
31,
32.
33.
D. ,· se ·~ .~ -, r• 0 .c the ,-q ... r•.,.. t ,. 6 . 4 ., ,... ~ .,, 9 ,- 9 ••. :::::_._:_'::::..:;'2_ :::_._:..___:;,_:~ ___ ::._~~~-! :J • .J- ~ .!. 1 -· 0 •
I<aplan, I\l'OJ:Tt1an .l'-1. Yo':tr Blood Pressure: The Host Deadly Hi9h. :v;:e;c:tC"CJm.Pr:ess~- New--York~ Ne~--York, 19 7 4 .--------
Maqer Robert F. Preporina Instructional . , --------·--·---=------------------------Ob1ectives, Fearon Publishers, Inc., Palo -Art'-,:::--;;·:, ll .. fc· rn l. ·~- 1 n '"''"~ '"'"" ..,.., I "-,.... Gt. - ... } - J. (...._ { _j~ __. ;.~ ......, •
34.
3 ~· :>.
36.
McPeak, Sunne and Flores, Kathy. Development of S·taff Traininq Program, Union cl ty f-Ieal th-Committee I Tlburico Vas<:iuez Hedical Clinic I Union City! California.
54 .
McPe~k. Sunne and Flores, Kathy. Patient Education M· .. '- _.,....· J.~ u ; •'"'. ~·- >-Ic=.~J.t'' c - .; t·:;:::-~--T.;l:--:;-:..:~-=-~~1 rL.on ~l .... y .ea h .. omrn.~ . .__e ... , _._)ur .... co Vasquez Medical Clinic, Union City, California.
Preston, D. F'. and Mil'ler,· .t·.·; L.··;.;·"~"l'hf'i 'l'nr.~er>culosis
Outpatients 1 Defection From 'l'herapy r II Arnerican Journa~ of Nedica.l Sc~~:I~S~_, 247:23, 19-64--.-----
37. F.eco~mnenda t.ions for a National Hiqh Blood Pressure ---·;::-.;-o·~ ·""L· ;;-s---;:-To---:;:;-::··1-£7'-:.'1 11c a{:: .; or·-;----P- 1 --, = De-n ar '--m-e·-;_,~-(- ·r-~I ,...,·~1-t ·n· l:" .. t- - 1._ ~) ....... ..._ -~~.(:t..J- .J\~!..,.. . \....-A . . _, . .J..C ... J.l r .r: r ~ L.. . _.-.1.J. \.... ). __ r c:a - . !
Educa·E.'io-:1~----Welfare, P'lmlica tion Number (NIH 7 5-S94:), 1973.
38. Stamler, .Jererr,ia.h, et al. Symposium: Hypertension in ·the Inner City I Moderri-Med[cir1e-PUJ::J]_ rcati 'o:rli3;· MTnnea.po 1 is ~'MTr;ne sot a· r 19 7 4 •
4 0. Young, r,n,a.:cj o:d.e A. C. r ef:~ a 1. "Review of Research and Studies Related to Health Education Pr~ctica· {1961-l:J66) Patient :Ed.uca'cion, n Healt~h ~:::~:!.<?..~:tj~ Moncqr.:.:.ohs, 26:4;::, 1968 •. ----~-

APPENDIX 'P.
HYPERTENSION
Patient Questionnaire
'i'Firs·t' Draft
1. Your Age:
.... £. .• Your Sex: .f\1 F
3. Numbc~r of Years in School
0-G 7-9
10-12 More than f2
4. · How long have you been coming to ·the clinic?
Fi:t~st time 1-3 Hont:hs 3-r. 5 }\•10J:1 tlt.S
6-12 J.'ilonths Over 12 Honths ---·
How lon~r do y0u vlai t to see the doc·t.or at -t:he clinic?
15-30 Minutes 1/2 hr . - l hr-.-----
1 hr. -· 1-1/2 hrs. _____ _ 1-l,/2 hrs - 2 hrs. -----·-
6. Hovl long .Jo yon ·wait. to get. your medica t.i.on at. ·the phar:rnac_y?
'1 I • a.
15-30 l"iinutes l/2 hr. - 1 hr·s-:-~_: __
1 hr. - 1-1/2 hrs. 1-1/2 hrs - 2 hrs.
I,. .. . . {nurse ) t-~,2>- ~ _,. • ne CL1.n:u:: (doctor) L-._a.t;::> me.
L.ik:.? ~'te/she is ·in a hurry Eous;h.Ly With indifference Gent.ly Wi.th ccncern
b. Do you ask questions of the doctor dr nurse?
Yes No
55

.. ~-
7. c. Are your questions answered to your satisfaction? Yes No
8 . Do you like the clinic? Yes No
9 . Does the clinic help you? Yes No
10 . po you have trouble making it to the clinic for .. _ ..... youT' a1?PD~i:nt."l"frents·? · .. ~J':es: No.·
Sometimes · -. - .. ·--· ---
11. Would you like to learn more .about your condition (High Blood Pressure)? Yes No
{If yes, please answer tf-12, #:l3r a.nd #14)
12. Would you be willing to attend classes on high
13.
blood pressure here at MLK? Yes No
Which day of 1:he ~veek is best~? ~~at time of the day?
14. Would you be willing to attend classes on high · blood pressure, \vhich talk about the following?
A. B. c.
Low Sodium Diet Your Medicines How .t.o t:c:.ke ycn1.:c BP
Ye~3
Yes. Yes
-·-- No 1~0
No
15. Have you ever read anything i'ibm1t high blood pressure? Yes -·-~ No ______ _
56
16. If you could make changes you do?
. +'' ln .. ne clinic, what would
'I'hank you for l:aking the t~ime to complet.e this questionnaire.

1. Your .P.ge:
2. Your Sex:
3. Your Race:
APPENDIX A
HYPERTENSION
Patient Qu~stionnaire
A. B. c. D. E.
Final Draft
Black Caucasian -Mexican A1ne:r.:rcan Asian ----Ot.her ·
4. Number of years in school: A. 0-6 B. 7-9 c. 10-12 __ _
n. Here tFla·n. 12
5. How long have you been coming to t.he ... . ·• ..... CJ.lDlC:
6·-12 Months
57
A. B.
First Time 1-6 Mon·ths ----· 12-24 Honths
G & fiov1 lcJng do ~tau ¥.1E\j_·t to see the doctor ai.: the clinj.c?
A. B~ c.
1.5- 30 rr,ins. l/2 - 1 hr. 1 . - 1-· 1 ;'" hr;,--··-~ ,.._, L... • ,;::) • _____.,..--...-
D. E .. · F .
1-1/2 - 2 hrs. 2 - 2-1/2 ----hrs. 2-1/2 ·-- ') hrs. ..J ·.--·--
7. How lonq do you. wait t:o g(~t. your medications at the pha.rmacy?
A. B. c.
15-:-·30 mins. 1/2 1 hr.
-...-~---
l - l-1/2 hrs :--=:~~~-·-
8. The clinic doctor t:cea t.s me:
A. B. c. D.
Like he is in a hurry n.oughly With inch ffl~rence G(-m·tly ··-----
D. 1:..1/2 ·- 2 E. 2 - 2-1/2 F. · 2·-1/2 - 3
hrs. _, __ __, .... hrs. ·
··-----~ ......... hrs.
E. With concern
F. Ot.her

58
9. The clinic nurse treats me:
A. B. c. D. E.
Like she is in a hurry Roughly With indifference Gently With concern
Yes No
F. Other
-(
11. Are your questions anm·1ered to your satisfaction'.?
Yes No
12. Do you like the clinic? Yes No I£ no, why? ----·
13, Does the clinic help you? Yes If no, why?
No
14.
15.
16.
17.
18.
Do you have trouble making it to the clinic for your appointment? Yes No Sometirnes If yes or sometime~-:-:reasons why~! -------- ~--
Have you e·v-er read anything about high blood pressure? Yes No Seen anything on T.V. about h'ighblood pressure·?
Yes No If yes, "''hat? ----------· Would you like to learn more (higb. blood pressure)? Yes
about your condition No
If nc, why? --,---------------·--···------·--(If yes, please answer 17, 18, 19.)
Would you be willing t.o a·t.tend classes on high pressure here at NLK? Yes ---~ No If no, why?
1vhich. da.y of the v-1eek is best fo-r· you·? What time of the day is best for you?
blood.
19. Would you bE:-; willing to attend classes on hi,:Jh blood pressure which talk about the fo~lowing:
.A. I.ow Sodium Diet B. Your Medications·--------C. How to take your own BP D. How to. live \.Vi th your HBP ___ _

20. If you c6uld make any changes in the clinic, what ·would they be?
59 .
Thank you for taking tht~ time ·to complete this questionna3_re.

APPENDIX B
RESULTS 01'~ HYPERTENSION CLINIC PATIENT QUES'l'ICll.\fNAIRE
1. Age X= 51.25 years Ages range from 17-97 years.
2. Sex
M F
f
41 54
%
43.2 56.8
Missing ~ases - 5 (Data not entered on questionnaire)
3. Race
Black Mexican-Amerjcan Aslan Other
Missing Cases - 3
4. Years in School
0·- 6 j!ears 7- 9 years
10-12 years Hore i:han 12 years
Missing Cases - 3
f
87 f)
1 3
f
13 14 51 19
5. Duration of Clinic Attendance
First time 1 6 months 6 - 12 months
12 ~ 24 months
Missing Cases - 3
16 20 1 '""" l.b
43
60
%
89.7 6.2 1
%
13.4 14.4 52.6 19.6
%
16.5 20.6. 18.6 44.3
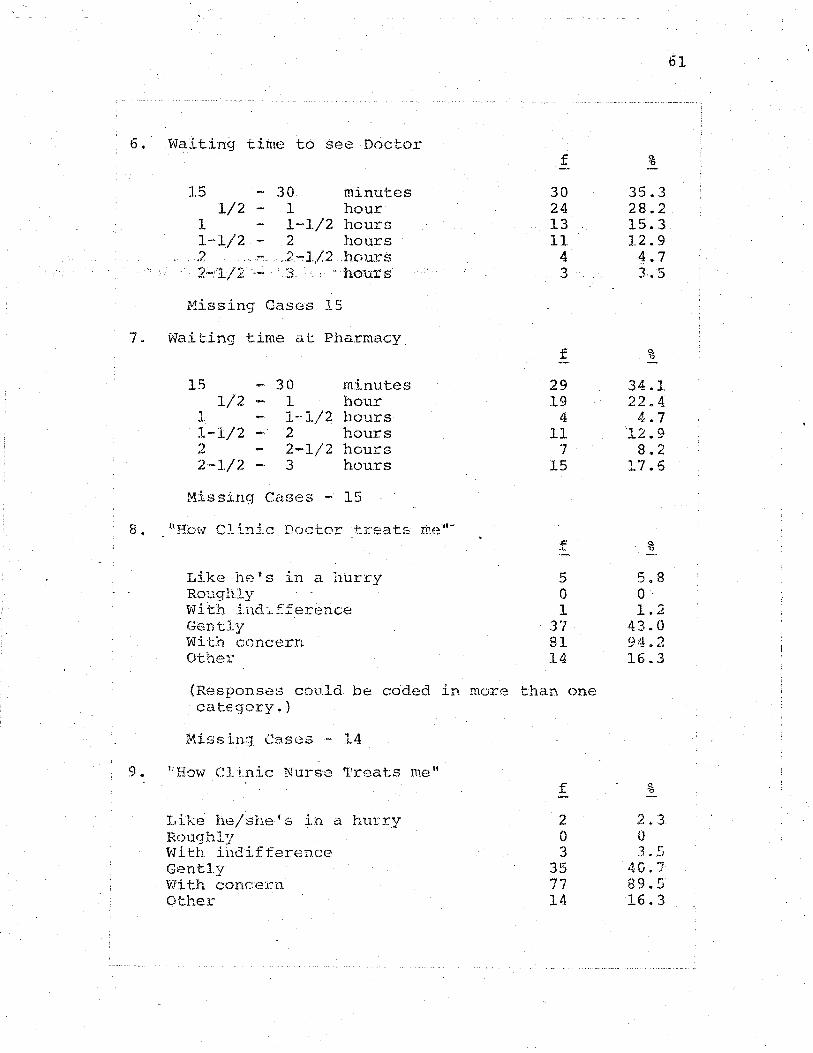
6.· Waiting time to see Doctor
15 - 30 minutes 1/2 - 1 hour
1 1-1/2 hours 1-1/2 - 2 hours
. .2 .. ·. .. . 2~1/2 .hours · · · 2-"1/2 · 3 ·. · · " hours
Missing Cases 15
7. Waiting time at Pharmacy
15
, .1.
1..,..1/2 -2 2·-1/2
30 1 1-1/2 2 2-1/2 3
minutes hour hours hours hours hours
Missing Cases - 15
8. 1'Ho\·l Clinic Doctor ·treats thE?"-
Like hets in a hurry Roughly Wi t"rt indif.ference Gently With ccncern Other
f
30 24 13 11
4 3
f
29 19
4 11
7 15
.{::
.) ....
5 0 1
. ., ·~ • .J I
81 14
(Responses could be c6ded in more than one ca te:gory. )
Missing Cases - 14
9. "How Clinic Nurse 'I'reat:s me 11
Like he/she's in a hurry Roughly With indifference Gently With concern Other
f
2 0 3
35 77 14
%
35.3 28.2 15.3 12.9
4.7 3.5
%
34.1 22.4 4.7
12.9 8.2
17.6
%
5.8 0 1 'j . ""'
43.0 94.2 16.3
%
2.3 0 3 ~.5
4G.7 89.5 16.3
61
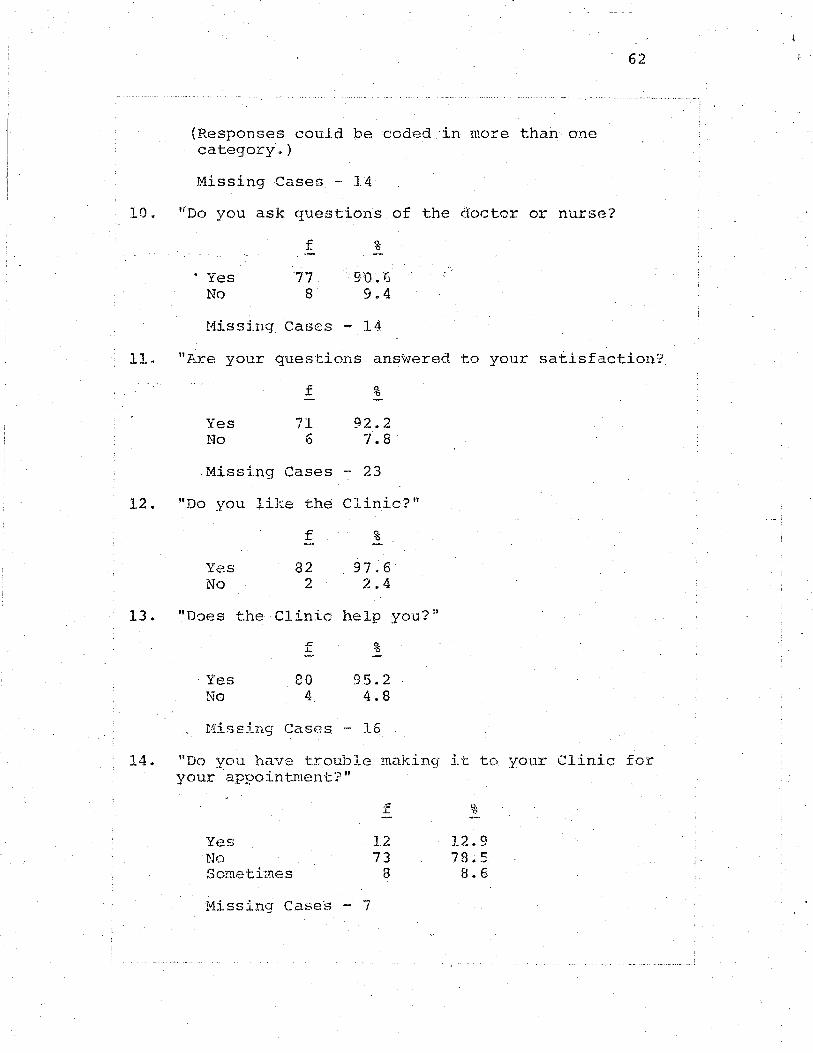
(Responses could be coded ·in more than one category".)
Missing Cases - 14
10. «oo you ask questions of the doctor or nurse?
· Yes No
f
77 8
%
9:0.6 9.4
Missing Cases - 14
62
11. "Are your questions ans~ered to your satisfaction?
12.
13.
Yes No
.Missing
f %
71 6
Cases -
92.2 7.8
23
"Do you like the Clinic?"
Yes No
"D-JeS the
Yes No
f %
82 97.6 2 2.4
Clinic help
f %
80 4
95.2 4.8
Missing Cases - 16
you?"
14. "Do you have trouble making it to your Clinic for your appointment'.?"
Yes No Sometimes
Missing Cases - 7
f
12 73
8
%
12.9 78.5 8.6
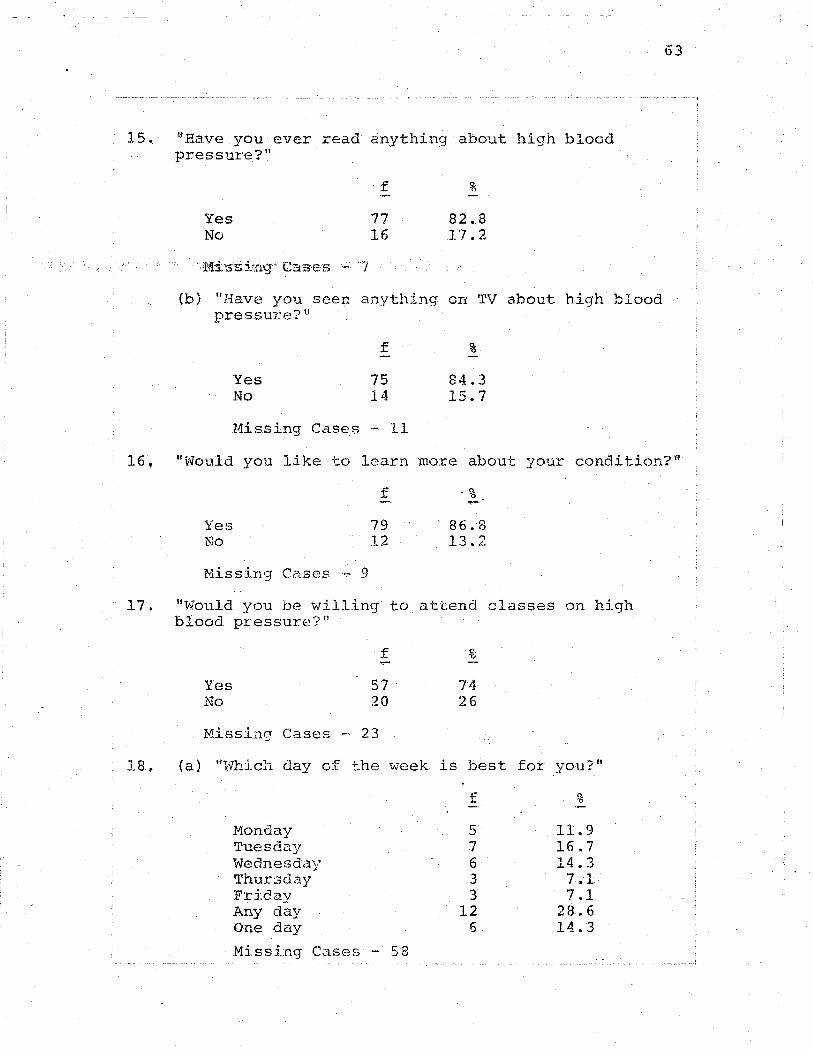
15 .. ~'Rave you ever read anything about high blood pressure? 11
f %
Yes 77 82.8 No 16 17.2
(b) nHave you seen anything on TV about high blood pressure?'-'
Yes No
f
75 14
Missing Cases - 11
%
84.3 15.7
63
16, "t:vould you like to learn more abou>c your condition?"
Yes No
Missing Cases ~ 9
f
79 12
86.8 13.2
17~ "Would you be willing to attend classes on high blood pressure?"
f (.', 'o ,_.
Yes 57 74 No 20 26
Missing Cases - 23
18. (a) "Hhich day o:f t.he week is best for you?"
Monday Tuesday Wednesday Thursday Friday Any day One day
Missing Cases - 58
f
5 7 6 3 3
12 6
%
11.9 16.7 14.3 7.1 7.1
28.6 14.3

{b} !'Wnat. time of day is best for you?"
.. .. ~· f %
AM 31 66.0 PM 13 27.7 Anytime 3 ~-4
19. "Would you be willing to attend classes on
Low Sodium diet Medica ·tions Blood Pressure taking Living with high blood pressure
f
19 20 23 30
20. I·f you could make any changes wha·t 'l.vould they be?
Comment No (;Orranent
Missing Cases - 3
f
35 62
lB - Waiting time too long a·t pharmacy and/or Clinic
8 - Comraents about staff, quality of care, ·and t.ime spen·t with patient.
64
APPENDIX C
Martin Luther King, Jr. General Hospital
Hypertension
Patient Education Program
Curricula Developed
by
Linda Mcintosh
and
Mary TentJer
Masters Degree Candidates
California State University, Northridge
In Collaboration with
Robert Huff, M.P.H.
Senior Health Educator Depart~ment of Hedicine
Charles R. Drew Postgraduate School of Medicine Martin Luther King, Jr. General Hospital
Los Angeles, California
NovembAr 1975 {Revised February 1976)
6.5

We gratefully acknowledge the advice and
encouragement of
and especially
consultant.
Linda Brown
Myrtis 'I'rc:.cey
Juanita Ed-vrards
Leondra Boone
Beverly Morgan
. Dieticians
Social Workers
Dr. John Fodor, California S·tate
•
66

67
Curriculum Module: High Blood Pressure Overview
Concept: High blood pressure is a leading cause of
I. OBJECTIVE: Following instruction, the student will
be able to define blood pressure; dis-
tinguishing between systolic and
diastolic blood pressure.
CONT.ENT: Motivational activity: Statistics -~------------------regarding the incidence of high blood
pressure in the U.S. and in Black
populations.
l. Function of the blood vessels in
determini~g blood pressure.
2. Definition of blood pressure.
3. Definition of the difference
bet.vreen systolic and diastolic
blood pressure.
l.El\Rt:Il\G OPPORTUNITIES:
Mntivational activity: Instruc·tor •~Jill
use a visual aid. to sh0w the incidence
and prevalence of hj_gh ~load pressure in
the U.S. and especially in Black popula-
+-' ~.lons.

68
1. Using the chalkboard, the instructor
will give an outline of the structure
and function of the arterial-venous
system ..
. ·. ,,2 .. . Tb.e j_nstructor will give a definition
of blood pressure.
3. The instructor ~,.;ill explain the
difference between systolic and
diastolic blood pressure.
II. OBJECTIVE: Following instruction, the student. \l'lill
be able to define high blood pressure,
discriminating between essential and
secondary hypertension.
CONTE1'i'f: 1. Definition of high blood pressure.
2. Definition of essential high blood
pressure.
3. Definition of secondary high blood
pressure.
LEl\FNil'-1G OPPORTUNITIES:
l~ Instructor will give a definition of
high blood pressure.
2~ Instructor will differentiate
between essential and secondary
high blood pressure by giving exam
ples of both types.

69 .
Concept; High b~ood pre_ssure can be controlled J?...Y
foll~wing the prescribed treatment regime.
III. OBJEC'l'IVE: Following instruction, the student will
be able to list at least three methods
o-f cc:mcu.:ul: for· high blood pressure.
CON'rEN'I·: 1. Methods for the control of high
blood pressure to include diet (low
sodium), medications and lifestyle
modifications.
2. Myths and misconceptions held by
the target group about hypertension.
LEARNING OPPORTUNITIES:
1. Instructor will discuss methods of
treat:nent and control of hig-;h blood
pressure.
2. Instructor will list on the
chalkboard and discuss common myt.hs
held regarding t.he controJ. of h.i<;rh
blood pressure. Inst.ructor v1ilJ.
call on volunteers t.o add· to the
list.
IV. OBJECTIVE; Following instruction, the student will
he able to lis·t a·t least three

CONTENT:
complications associated with
uncontrolled high blood pressure.
Complications and target organ damage
that can occur from untreated and un-
70
elude stroke, heart disease and kidney
disease.
LEARNING OPPORTUNITIES:
1. The instructor will discuss
complications that.can occur with
uncontrolled and/or untreated high
blood pressure to include heart
disease, kidney disease and stroke.
2. St.udent,s will be shm·m a film
cass.ette which emp~as izes the
treatment regime in the control of
high blood pressure and the compli
ca·tions associat:ed with uncont,.rolled
high blood pressure. Discussion
lead by the ins·tructor will follm-v
the film.
3. At the close of the lecture, the
students will be given a short
pest test of knowledge.
4. A question and answer period will
follow.
71 .
HESOURCES FOR'l'HIS CURRICULUM·
1. Kaplan, N.M., M.D. Your Blood Pressure: The .t.tlost
Deadlv High, Medcom Press, New York, 1974. ---------2. Modern Medical Pu.~licatior~s, Hypertension in the
3. The Hy_:eertens ion Handboo~, Merck, Sharp
and Dohme, West Point, Penn., 1974.
4. High Blood Pressure_f Professional Research 1 film
cassette, 17 minutes in length.
Handouts
1. Schedule of patient education classes
2. "Welcome to MLK, Jr. Gen; 1 Hospital Out:patient
Servicesn
3. .Pamphlet, "The more you kno;.; about high blood
pressure, the eas.ier it is to live \¥ith," Boehringer
Ingelheim Ltd., Elmsford, Ne~ York 10523
Expanded Con·t.ent Ou·t.line: · High Blood Pressure Overview
1. Pretest..
2. Statistics regarding high blood pressure in the
Uni t.ed Stat.es
A. High blood pressure is a leading cause of death
in the United States.
72
B. Tt,.,;enty four million people in the U.S. have high
blood pressure, but only 12 million know ·they
have it.
C. Only 3 million of these p~ople are receiving
treat-..ment.
D. Only about 1-1/2 million are receiving proper
treatmen-t.
E. For e·very one vJh.ite AmErican with high blood
pressure there are five Black Americans ·who have
it.
F. In L.A. , one White in nine ·but one Black in three
over t:he a.gt-::: of eight.een ha.ve high blood pressure.
G. Fo.:.:- every onE: h'hi te per son ~o~ho dies from high
blo;;:)d pressure 1 two Black people will die.
H. High 3lood Pr~ssurc ls a problem for all ages,
races and all types of people, rich and poor,
11 eas::l going" and "up t i.qh·t,"
3. Definition of high blocd pressure
A. EvsryonB has blood pressure

1. Blood c~rculates to all parts of the body.
2. Blood travels through blood vessels of
different sizes.
3. 'I'he heart ac·ts as a pump to keep the blood
circulating.
4. Each heartbeat pushes blood through the
vessels.
73
5. 'l'his pumping force creates a pressure of
blood against the inn~r wall of the vessels.
B. Blood pressure is a measure of this force.
1. Changes in blood pressure are caused by the
small arteries tightening up and relaxing,
si.rnilar to the vla.y the nozzle of a hose
works.
4. Two blood pressures are measured \•7hen the doctor
checks you.
A. Systolic is the first measure and the first
number you see when your blood pressure is
recorded.
1. The heart beats and the pr:essure on the walls
of the vessels is the highest.
2. 'l'his .i..s the larger: m.1F1ber in your blood
pressure reading.
B. Di<:tstolic is ·the second measure.
1. rrhe heart rests and the pressure on the walls
cf the vessels 1.s lower.

2. This is the smaller number o£ your reading.
C. An example of a blood pressure reading is:
120/80.
5. Definition of High Blood Pressure.
74
A~ When a pexson 1 .s.hloodpr.essure goes up and stays
that \vay, the condition is known as· high blood
pressure. The medical terms is 'hyper:t.ension' •
B. There are ·two t:ypes of high blood pressure.
1. The mos·t corruuon type is called essential or
primary hypertension.
a. Ninety per cen-t of people 'i-iho have high
blood pressure have this type.
b. We donlt know what causes this type, 'out
we do knm1 how to con tro 1 it.
2. The second type is called secondary
hype:t·tension.
a. vle do know the causes of this type.
b. 'I'his type can also b~ •created and
controlled.
6. Methods of Control
A. High blood pressure can be controlled.
B. ·control methods include medications prescribed by
you:r aoctor., chang-es in yot.'r diet and certain
changes in your lifestyle (quitting smoking,
learning to deal with stress).

c. Control programs must start as soon as possible
and be continued ·throughout your life.
D. You must stay on yo·ur diet and your medications
even though you feel just fine.
75
7. Complications associated with uncontrolled high blood
pressure
A. Even though your blood pressure is high, you may
not feel sick because high blood pressure usually
has no symptoms.
B .. In order to tell if you have high blood pressure,
you mus·t have your· blood pressure checked and
measured.
C. Uncontrolled high blood pressure can le~d to
·da."'naqe to the heart, ( strok.e, heart at.tack) ,
kidneys and brain (stroke).
8. Post test.

OVERVIEW
Name Date ---·-----
Please answer these questions by circling the letter
.nE:~xt to the ri9ht ansv·ler.
1. Hypertension is the same as
a) high blood p:r·essure.
b) too much blood
c) nervousness
d) tired blood
2. Untreated higt blood pressure can lead to
a) cancer·and leukemia
b) syphilis and gonorrhea
c) sickle cell anemia
d) heart: disease, kidney disease and stroke
Please fill in the blanks wi t.h the right answers.
3. Three ways to help control high blood pressure
are:
---·-----and
76 .
Please anS\Jer t.:.hese questions by circling T' if the :1l1S\•7er
is riqht or F' if the an.s·~.;er is wrong.
T F
T F
4. Blood pressure is the force against the walls
of the blood vessels.
5. Blood pressure is :r·ecorded in two ntm1bers,
for example 120/80.
77
T 6. The fi.:r:st number in a blood pressure reading
is called the systolic and the second is
called the diastolic.
T F 7. Secondary hyper-tension does not seem to be
caused by anything. ;._. __ ,.
F' 8. The person ~,lith high blood pressure u.sually
feels sick~
T F 9. Half of the people in the United States who
have hypertension don't knmv that they have
it.
T F 10. Eating garlic will cure high blood pressure.

78
Curriculum Modul~.:~~: the Role of Drugs in the Control of
kypertension
J... OBJECTIVE~ ~ollbwing instruction the studen~ will
J)e at/I.e to identify. the three categories
ot arugs arui their actions used in the
'treatment of hypertension.
C~~NTENT: 1. Review of hype.rtension.
~~ ~hree catego~ies of drugs are:
Eliuretics, vasodialators and nerve
blocking agents.
j. IIb\•T each type of drug func-tions on
'the body to loW•2r blood pressure.
' LEARNI?JG (lj::pgf{'i'U1:-lt•.i'IES:
1. The instruc'C:or wi l.l call on
voJ.unteer students for a definition
ef hypertension.
~~ ihe instructor will d~splay three
poster boards containing infarma-
tion relating to the three types of
d.:r-ugs ar~d ~.dll a isct.lSS t.he i:nforma-
-!::ion t:lerGon with the st.udents,
II. OBJEC'~.r'I\l1j; student: vl ill
b~ abls to ideptify side effects of
79
antihypertensive drugs.
CONTENT.: Side effects of antihypertensive drugs.
LEARNING OPPORTUNITIES:
1. The instructor will display and
discuss three posters. listing the
side effects of the drugs.
2. The instructor will then discuss the
importance of informing the doctor
of any intolerable side effects
rather than just stopping the
medication without informing the
doctor.
RESOURCES: 1. Drug Company Litera tun:.: CIBA;
lVJerck r Sharp a.nd Dohme.
2. Kaplan, N.M.r i'LD., Your Blood
Pressure: 'l'he Mos_t Deadly Higi::r
Medcom Press, Neli. York, 1974.
3. Drug Fact Sheets, abstracted from
11 A Model for Hypertension Education
in A.7nbu1a1:o:r:y Care," St. Hary' s
Hospi ta.l and Hedical Cen·ter, Scm
Francisco, California.
. . ... !

80
Expanded Content Outline-: The Role of Drugs in the
Control of Hypertension
1. Pretest.
2. Review of definition of hypertension.
3. · 'I'hree categories of antihypertensive d:cugs
A. Diuretics (water pills)
l. diuretics increase the loss of water and salt
in the urine
this reduces the amount of fluid in
circulation in the body.
3. examples of diuretics include:
Diuril, Hydrodiuril (Hydrochlorothiazide);
and Las~x (Furosemide).
B. J:-.ierve Blocking Agents (Clonidine hydroch1orid(:~,
!.•1e·thy.ldopa, Guanethidine)
1. Jchese drtlgs act to blocl~ tl1e nerve .impu.lses
to the muscles of the arteries.
2. this causes a reduction i~ the constriction
of the ·blood vess2ls .
. :) • the three most. frequently used are:
a. Clonidine Hydrochloride (Catapres) - used
in mild to moderate hypertension; may be
given with other nerve blocking agents
and diun::tics.
81
b~ Methyldopa (Aldomet) - used for patients
who were unsuccessful 'ilvith other drugs;
used for patients with kidney problems,
renal failure.
patients with moderate to severe hyper
tension; very strong and effectiver can
cause orthostatic hypotension.
C. Vasodilators (Hydralazine) {Apresoline)
1. works to lower blood pressure by acting on
the smooth muscles that make up the ~valls of
the arteries.
2. 'J:his drug can increase the heart rate a.nd
reverse the effects in lmvering the blood
pressure o _
3. Usually given in combination with a nerve
blocking aqent.
4. Side effects of drugs
1. loss of potassiu .. rn causing muscle weakness;
danger to the heart
2. loss of fluid results in reducing weight
3.. potassi~lliD supplernent (I<;Cl l-0·%, or dietary)
often given with these drugs
B. Nerve Blocking Agents

82
1. Catapres - dryness of mouth; drowsiness,
sedation.
2. Methyldopa - faintness, dizziness,
drowsiness, dryness of mouth
. '
ne?s, extreme weakness, impot.ence.
C. Vasodilators (Hydralazine)
Headaches, aching in the joints,. and
palpatat.ions.
5. If any side effects are experienced thr:m discuss them
with your doctoro He might want to change your med-
ication. But remember there is an adjustment period
for most drugs, so some may disappear~ ·
6. Hedication must be continued, in most ca.ses of
essential hypertension, for the rest of your life.
Do not stop taking pills, even if you feel better.
7. Post test.
DRUG
HOW DRUG
WORI<$ TO
BLOOD
PRESSURE
SJJ).E
EFFE~CTS
Martin Luther King, Jr. General Hospital
Hypertension Patient Education
DRUG FACT SHEE'r
D.iuretics (Water .. Pills)
Diuril (Chlorothiazide)
Dyazide
HydroDiuril {Hydrochlorothiazide)
Hygro·ton ( Chlorothal idone)
Lasix (Furosemide)
83
Diuretics lov1er ·blood pressure by helping the
kidneys get rid of salt (sodium) and r.-va·ter.
Diuretics :Lncrea.se the flmv of urine, sa yort
v.rill have to go to the bat.hroom more often.
T'he reduced amount of water circulating i!l
your body reduces the amount of work the
heart must do and this reduces the pressure
against the walls o:f the blood vessels. •rh,~
result is a lower blood prE::ssure.
Potassium, a mineral in the body, 1.s also·
lost when taking a diuretic. Your doctor
vd.ll want to take a blood test several times
a year to .be sure your pot.assimn level .is. not
too. low. If your potassium level is lmv your
doctor may order a pot.:assium 1:mpph;ment {or
•
84
KCl) or ask you to be sure to eat foods that
are high in potassium such as dried fruit,
bananas and oranges. Ii: you are ·taking
heart drugs (such as digitalis) replacing
potassium -is even .mo:re imp.o.rtx:n1±. .•
DRUG
liON DRUG
WORKS TO
I. OWER
BLOOD
PRESSURE
SIDE
EFFECTS
Martin Luther King, Jr. General Hospital
Hypertension Patient Education
DRUG FAC'l' SHEET
Nerve ,.Blocking Agent -
Ismelin (Guanethidine)
Ismelin lowers blood pressure by blocking
signals from the b:rain to the nerves which
control the small muscles around the blood
vessels. When,these muscles relax, more
blood flows through the vessels and t.he
blood pressure is ·lmvered.
Smr.e side effects of Ismelin m.ay be:
dizziness, fq.in·tness, diarrhea, dry mouth,
swelling, and an increase in Y.I~ight. Some
men may experier:>.ce impotence or reverse
ejaculation. Women are not sexually
effected,.
85
Since dizziness and faintness are major side
effect.:s some sugges,tions for reducing these
side effects are: 1) rnovin.g slowly when
getting up or lying down; 2) sitting dmvn to
do things instead of standing up; 3) avoid
heavy exercise; 4) raising the head of your
* * * *~':
bed; 5) avoid alcohol in large amounts; and
6) moving slowly when changing positions.
Ismelin interacts with other drugs. It is
important to understand that other drugs
86 '
may interfere with the effec"cs· of I·smelir..
Alcohol may lead to fainting by causing the
small blood vessels to enlarge. Many cold
and sinus drugs sold over the counter (with
out a prescription) may also interfere with
the effects of Ismelin. Check with your
doctor before taking any of these drugs.
YOU iv.'IAY HAVE SOJY'ill OF 'l'HESE SIDE EF:?EC'l'S
WHILF TAKING lSHEI.IN. {REMEMBER! NO'r
RVERYONE HAB SIDE EFFEC'l'S) IF THE SID!i:
EFFECTS BOTHBR You, DON' ·r J·usT sToP 'l1AKING
YOUR PILLS ! T.ALK 'I'O YOUR DOCTOR ABOUT IT,
HE .[v!J•.Y vn\N'I' TO CHANGE 'rfiE DOS~:U.GE OR PUT
YOU ON DIFF:E:RENT PIIJLS.

87
Martin Luth~r Ring, Jr. General Hospital
Hypertension Patient Education
DRUG FACT SHEET
.DRUG Nerve Blocking Ag.ent ·-
Aldomet (.f.iethyldopa or Alpha Methyldopa)
Hm'V DRUG Aldomet lov.rers blood pressure by blocking
NO.RKS 1'0 the nerve signals from the brain to the small
L0\'1ER nmscles ·that surround the blood Yessels.
BLOOD When these musclE's relax, more blood flows
PRESSURE throug·h the vessels and blood pressure is
lowered.
SIDE Aldomet may cause dro:vsiness, swelling in
EFFECTS the ankles, weight ga.in, dry mouth, diarrhea
or depression. Some men taking J.\ldome·t in
high doses may experience impotence. No-
men's sexual response is not effec·ted.
R~ely this drug can lead to anemia (.!];~!:_
Sickle Cell type) . This can shov1 up as
fatigue, chills, fever, dark or red ur~ne,
aching in the arms and legs.
***** YOU MAY HAVE SO.tviE OF THESE SIDE EFPEC'IS
WHILE 'l'AKING ALDOME'I' (REMEMBER! NO':L' EVERYONE
IF THE SIDE EFFECTS
88
BO'I'HER YOU 1 DON' •r JUST S'rOP TAKING YOUR
PILLS! TALK TO YOUR DOCTOR, HE ~1AY WANT
TO CHANGE 'I'HE DOSAGE OR PUT YOU ON DIFFERENT
PILLS.
• I
'I

89
Martin Luther King, Jr. General Hospital
Hypertension Patient Education
DRUG FACT SHEET
·DRUG
Catapres (Clonidine Hydrochloride)
HOW DRUG Catapres lowers.blood pressure by blocking
WORKS •ro signals from the brain to the nerves which
control the small muscles around th,:; blood
BLOOD vessels. When these muscles relax, more
PRESSURE blood flows through them and blood pressure
is lmvered.
SIDE Some side effects that may occur: are: dry
EFFECTS m~)ut::h, dr.mvsiness l .sedation, constipation r
dizzinesr::~ headaches and fat_.igue. Some of
these effects should decre.1.sa within a few
months.after you start taking Catapres.
Some men may experience impotenceo Women
are not effected sexually.
Alcohol interacts \vi th Ca·tapres causing a
greater sensitivity ·to the alcohol.
De not stop taking Catapres.
bra.j,.n disorders and "dea.th ha \te occurred when
90
p~tients suddenly stop taking this drug.
YOU HAY HAVE SOME OF THESE SIDE EFFECTS WHILE
TAKING CATAPRES (REMEMBER! NOT EVERYONE HAS
SIDE EFJ:<'ECTS). IF THE SIDE EFFECTS- BOTHER
YOU, DON 1 T ~JUST S"TOP TAKING YO\)R PILLS! T~..LK
TO YOUR DOCTOR, HE H.A.Y WANT TO CHl\.NGE THE
DOSAGE OR PUT YOU ON A DIFF'ERE~NT PII,L.

91
Martin Luther King, J:r. General Hospital
Hypertension Patient Education
DRUG F'l\C'!' SHEET
DRUG
Apresoiine (Hydralazine)
Hm•7 DRUG Apreso1ine \·mrks di.rect.ly on the small
WORKS TO rrn::.scles around the blood vessels causing
LOWER tb.em to relax and lowering the blood pres-
BLOOD sure. Usually· t~his . drug is t.aken iri combina-·
PRESSUFE tion with other antihypertensive drugs in
order to make it tno.re e.f fecti ve.
SIDE The most common side effec·ts of J.~presoline
EFFECTS are headaches, 'llhich usually wec.r off \vi thin
a week after you start taking t:hir.; 9-rug.
Headaches may return if ycur dosage is in-
creased, but should disappear with time.
o·ther side effects are: rapid heart beat,
chest pain when physically active, nausea,
loss of appetite 1 joint pain, and m.unbness
and tingling in the arms and legs.
***** YOU MAY Hl\.\lE SOME OF THESE SIDE EFI!'EC'rS \'iHII.:E
'.I'AKING APPJ~SOLINE. (REI:vm.l\IBER! NOT EVERYONE
Rl\S "SIDE EFFECTS) IF THE SIDE EFFECTS
BOTHER YOU, DON'T JUST STOP TAKING YOUR
PILLS! TAl.K TO YOUR DOC'I'OR ABOUT IT, HE
MAY ~vANT TO CHANGE THE DOSAGE OR PUT YOU ON
DIFFEREN'r PILLS.
92
QUESTIONNAIRE - DRUGS
DATE ·------~----------------------------
Please answer these questions by circling the letter
1. Which of t.he following is NOT a type o.f drug
used ir. the ·treatment of hypertension?
a) diuretic
b} an·ti.botic
c) nerve blocking agent
d) vasodilai:or
2. Diuretics help lo'\11.1er blood pressure by
93
a} reduci~g the amount of tva ter and sodiu:rt~ in the
body.
b) helping one to relax all over.
c) relaxing the muscles in the walls of the
blood vessels.
cl) blocking nerve messages to the blood vessels.
3. Nerve blocking agents help lower blood pressur-e
by
a) reducing the amount of tvater and sodiu.i1.1 in the
body.
b) helping one to relax all over.
C) relaxing the muscles in the walls of the
blood vessels.
d) blocking nerVE": messages to t.J1e blood vessels.

94
4. Vasodilatbrs help lower blood pressure by
a) reducing the amount of water and sodium in the
body.
b) helping one to relax all over.
>C) "re:laxing the lTillS.c.les . .in the ,walls the blood
vessels.
d) blocking nerve messages to the blood vessels.
5. Which of the following is NOT a side eff-ect of
an-tihypertensive drugs?
.a) Drowsiness, dizziness
b) Loss of potassium
c) toss of hearing
d"~ I l)ryness of mouth
e) Headaches

95
Curriculu.IG Nodule; The Role of Diet in the Control of
High Blocd Pressure
followinq a. diet lov1 in sodium ; ·, ' . .. ----~·--·-·----.._.;..,......_,... ____ ....-,~----~ ... --:-... ~----~·--"'""'" -~·-----~-
.... OBJEC'TIVE; Fo11mdng instructi.e:n the sb1dent will
be able to explain \vhy a sodium re-
stricted diet is irrport.ant'.
CON'rEN'I' : 1. Sodiu..rn is a nat.ural nutrient found
in foods.
2. Sodium holds water in the body.
3. Excess fluid in the body causes the
blo0n pressurr~ to :i.ncrea.se.
4. High blood prestmn~ can be reduced
if a low sodium diet is followed.
I.EAF.NING OPPOR'l'UNITIES ~
1. The instructor will explain the
effects of sodium on the body.
2. Thr3 instructor ,.,fill explain the
relationship bet.ween fluid n~b:m-
tion and the increase in blood
pressure.
II. Following instruction the student will
be able to iden·tify one food high in
sodium a.nd one food low in sodiu.'TI from
each of t.he four food grottps.
CON'l'.EN'l': 1. A balanced diet includes foods
from each of the four food groups
every day.
a. Milk and milk products
~b-.. Meat and meat subs·U. tutes
c. Fruits and vegetables
d. Breads and cereals
2. Examples of foods high in sodium
(bv food g-roup)
a. But·t:ermilk and cheese
96
b. Bolog·na; hot dogs, ham, canned
chili
c. Sauerkraut, pickles, canned
vegetables
d. Biscu.itsr cornbread, muffins,
crackers
3. Examples of foods low in sodi1,::m
(by food group)
a. Whole, lo"tlfa.t a.nd nonfat milk
b. Chicken, fresh pork, beef and
dried beans
c~ Fresh and canned fruits, fresh
vegetables, onions and
pota.t.oes.

1I1..
97
-d. Yeast breads, rice, grits,
macaroni, oatrneal, etc. (if
cooked without salt)
LEARNING OPPORTUNITIES
OBJECTIVE:
CONTENT;
, l_~ :r~h..e instructor will display a
poster/collage shovdng the four
food grOU?3·
2 § The inst.ructo:r ~vill (using t.he
poster) poi:r:.t out and give exar-np.les
of foods high and 1ow in sodimn.
3. The i~structor wiLl call on
voln.nt:eer ::::tuden·ts to give examples
of their favorite foods and instru6-
tor will identify whether they are
high or low· in sodium.
F'oJ.J.owing instruction the studt.mt ·will
be able to .ident,ify ::.:.t least t·v-:o sources
of diet.a:>:·y sodiu.TU and at least t:'i·JO non-
food sources of-sodium.
1. The great.est 21.rncu:r:.t of sodium
intake is in the form of table
salt (socliu..rr. chloride).
2. Bc:.king soda a:·HI baking powder are
both high in sodium.
3. Sodium preservat:i.ves are common in
lunch me&ts and other processed

98
foods.
4& Most condiments and many seasonings
contain salt.
5. Most. prepared, p.r.eserved and con
venience foods have salt and/or
sodium preservatives added.
6. Sodium is found in many non
prescription medications.
7. Toothpaste and mouthwash also
contain sodium.
LKZ\.RNING OPPORTUNITIES:
1. The instructor will have a display
of various medications and ~ill
distribute them among the students.
2. '!'he instructor will call on each
student to read the labels of the
medicat.ions and identify those :that
contain sodium and/or a warning
against use by persons with high
blood pr,8ssure.
3. The instructor will have a display
of various seasonings and will dis
trib;xte them to several of the
students. The students will be
asked to read the labels, identify-
ing those seasonings high, lmv, and

IV. OBJECTIVE:
CONT:El.JT:
99
wit.hout sodium.
4. The ins·tructor vtill identify Ot.ller
sources of sodium and hoT,r ·they are
used in the canning, preparing and
' :pre:-serving :foods .
Fo1lovving instruction the s·tudents •.vill
be able to identify· alternative lo;,.r
sodium. seasoning wid food preparing
methods~
Salt substitute (potassium
chloride) can be used a.t ·the table,
but not in cooking.
2. n Lj" tcSal t n (b:t ~orton) is not
in·tended for use in low sodium
diets.
3. Herbs, spices, and flavorings can
be used ·to add flavor to foods.
4. Fr.esh meat should be used to season
beans and vegetables instead of
salty meats and boullion.
5. Fresh onion, 9arlic and chili
peppers may be used freely.
I.EAHNING OPPORTUNITIES:
1. 'rhe ins·tru.ctor will distribute
samples of low sodium foods. A
discussio!1 '!Vill folh")vl abouJc the

RESOUF .. CES:
taste of these foods.
2. The instructor will call on
volunteer students to mention
their own favorite recipes and
100
· .. ~w.D.~ -then. e:i:'plain ho·.v these foods
can be prepared by reducing or
eliminating the sodium.
3. The instructor will distribute
some recipes to the class.
4. A question and a.nswer period will
conclude this session.
1. Ha::1douts £rom !-ILK Hospital
Dietician.
2 ~ I.ow Sodium Diets Can BE Deliciom~,
Fleisr...mann' s M.argarine, pamphlet.
3- Kaplan, Norman H., .H.D., Your Bloo4
Pressure: The Most Deadly High,
Medcom Press, New York, 1974.
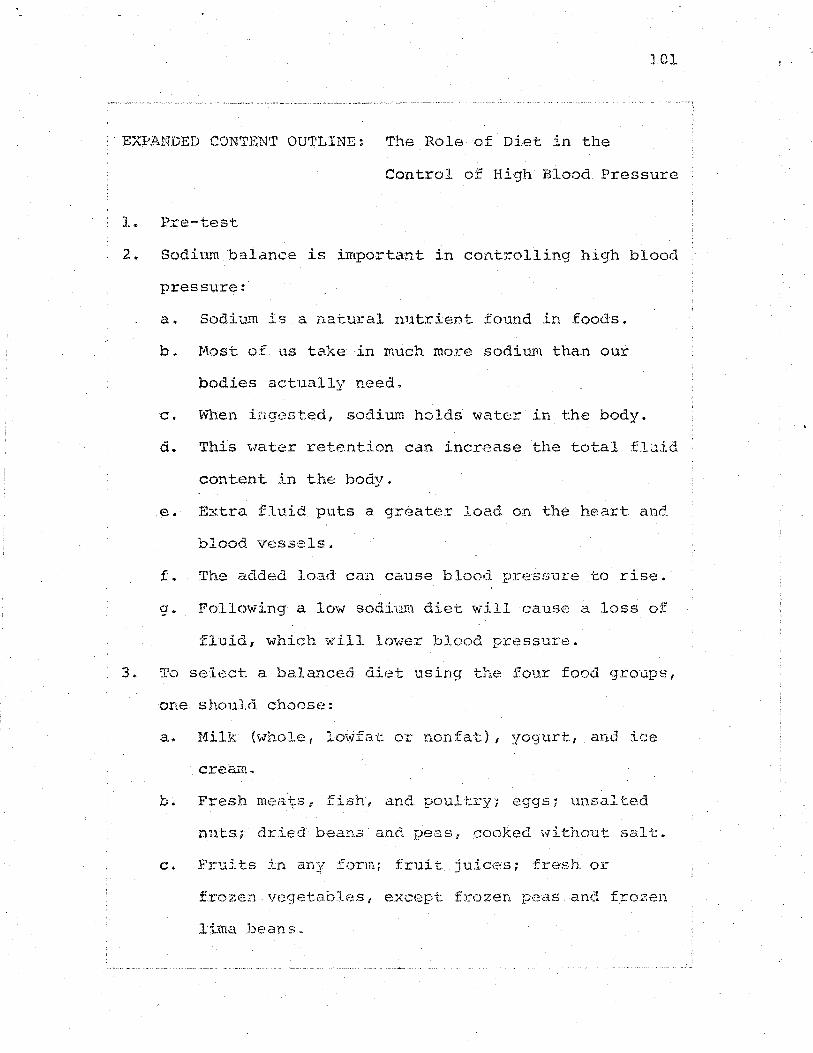
}01 1 '
EXPANDED COWrENT OU'l'LINE: The Role of Diet in the
Control of High Blood Pressure
1. Pre-test
2. SodiQ~ balance is important in controlling high blood
pressure:
a. Sodiu.-rn is a. nai::ural nutrient found in foods.
b. Host of us take in :much more sodium than our
bodies actually need.
c. lvhen ingested, sodium holds water in the body.
d. This \vater retention can increase the total fluid
content in the body.
e. Extra fluid puts a greater load on the heart and.
blood \resssls.
f. The added load can cause blood presf::lure to rise.
g ~ Following a low sodi·l!m diet w--ill caus.::; a loss of
fluid, which •A" ill lower blood pressure.
3. To select a balanced diet using the four food groups,
one should choose:
a. Hilk (whole, loi-'i'fat or nonfat:}, yoqurt, and ice
crea<11.
b. Fresh meats, fish, and poultry; eggs; unsalted
nuts; dried beans and peas, cooked without salt.
c. . - f . 1..n any :torm; .ru1. t. juices; fresh or
frozen vegetables, except frozen peas and frozen
lima. beans.
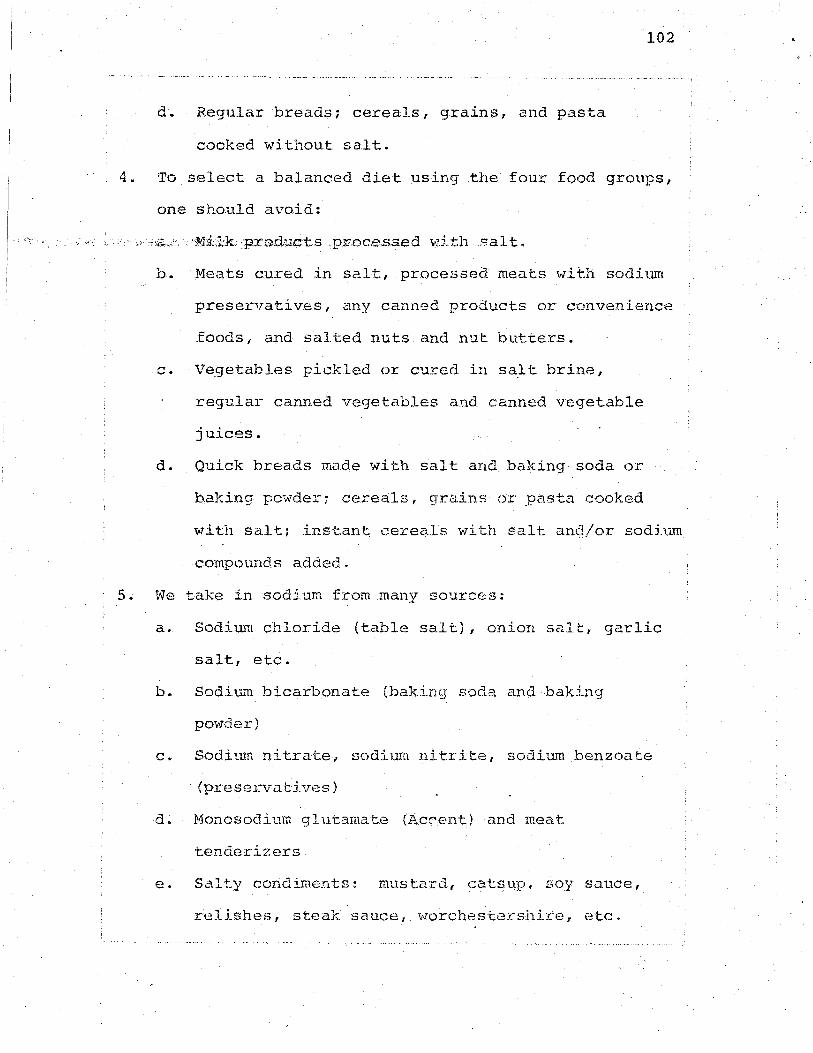
102 .
d. Regular breads; cereals, grains, and pasta
cooked without salt.
4. To select a balanced diet using the four food groups,
one should avoid:
b. Meats cured. in se.lt, processed mea·ts wit11 sodj_um
preservatives, any canned products or convenience
foods, and salted nuts and nut butters.
Vegetables pickled or cured in salt brine,
regular canned vegetables and canned vegetable
juices.
d. Quick breads made_with salt and baking soda or
baking powder7 cereals, grains or pasta cooked
with salt; inst:.ant cereals v1ith salt and/or sodium
compounds added.
5. We take in sodium from many sources:
a. Sodium chloride (table salt), onion salt, garlic
salt, etc.
b.. Sodiu..ll bicarbonate (baking soda and baking
pmvder)
c. Sodimn nitrate, sodium n.itri·te, sodium benzoa·te
(preservatives)
d. Monosodium glutamate (Accent) and meat
tenderizers
e. Salty condiments: mustard, catsup! soy sauce,
relishes, steak sauce, worchestershire, etc.
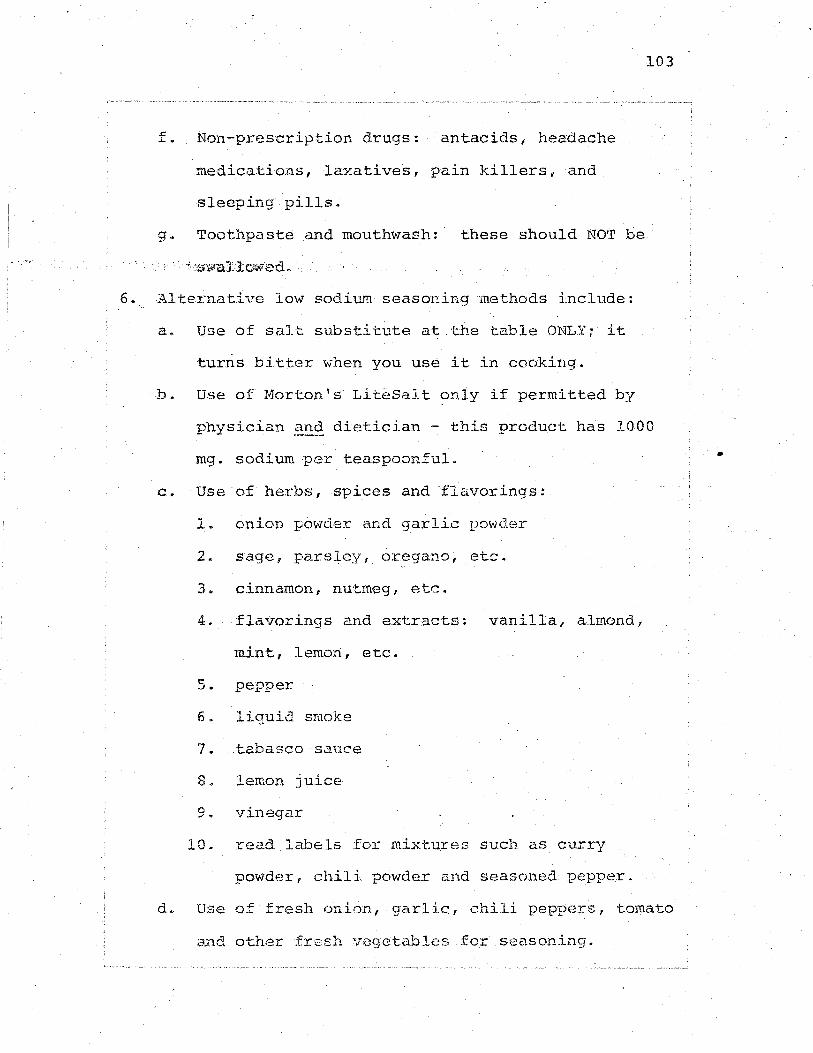
. -:' ~
6.
f. Non-prescription drugs: antacids, headache
medications, laxatives, pain killers, and
sleeping pills.
g~ Toothpaste and mouthwash: these should NO'r be
Alternative low sodium seasoning methods include:
a. Use of salt substitute at t:.he table ONLY; it
turns bitter when you use it in cooking.
103
b. Use of Morton 5 s LiteSalt oniy if permitted by
physician -~nd dietician - this product has 1000
mg. sodium per teaspoonful.
c. Use· of herbs, spices and ·flavorings:
1. onion powder and garlic povn:l.er
2. sage, parsley, oregano, etc.
3" cinnamon, nutrneg, etc.
4. flavorings and extracts! vanilla, almond,
mint, lemon, etc.
5. pepper
6. liquid smoke
7. tabasco sauce
8. lemon juice
9. vinegar
10. read labels for mixt.ures such as curry
powder, chili powder and seasoned pepper.
d. Use of fresh onion, garlic, chili peppers, tomato
and other fresh Vf.~ge·tables for sec.soning.
•

e~ Add a pinch of sugar to fresh vegetables when
cooking ta bring out the natural flavor.
7. Post test.
104

105
QUESTIONNAIRE - DIET . .
NA11E DATE
Please answer each question by circling the letter next
to the r:ight :answer .
1. Which of the following meats is allowed on a
low sodiun1 diet?
a) bacon
b) ham
c) pickled pig feet
d) chicken
2. Which of t:he following is allowed O!l a lov.r
sodium diet?
a) pickles
b) fresh fruit
c) olives
d) canned bse-::s
3. Which of ·the follo~tling ·milk products 1s allov-;ed
on a lo-r,..J sodimn diet?
a) Americaa cheese
b) buttermilk
c) Swiss cheese
d) whole milk -
4. h"'"!1ich o:f the following foods 1.s allowed on a
lmv sodium diet?
a) saltine crackers

b) biscuits
c) white bread
d) cornbread
5. Which of the following can be substituted for
a} onion salt
b) garlic powder
c) Adolph's Meat Tenderizer
d) monosodium glutamat.e
6. Wnich of the following terms best describes
hypertension?
a) nervousness
b) high blood pressure
c) ti:r-ed bl.ood
d) too much blood
106
Please ans•,v-er these questions by. circling 'I' if the
sta·tement is right or F if the statement. is wrong.
T F
F
T F
7. Reducing sodium in the die·t helps to lower
blood pressure.
8. .Labels on :non-prescription drugs will
indicate whether or not sodium is. contained
in the drug.
9. Beef bacon is allo•ded on a lmv sodi1.L'TI diet ..
T F 10. Using herbs to season foods .is allmV"ed on a
sodiu:m restrict.ed diet.
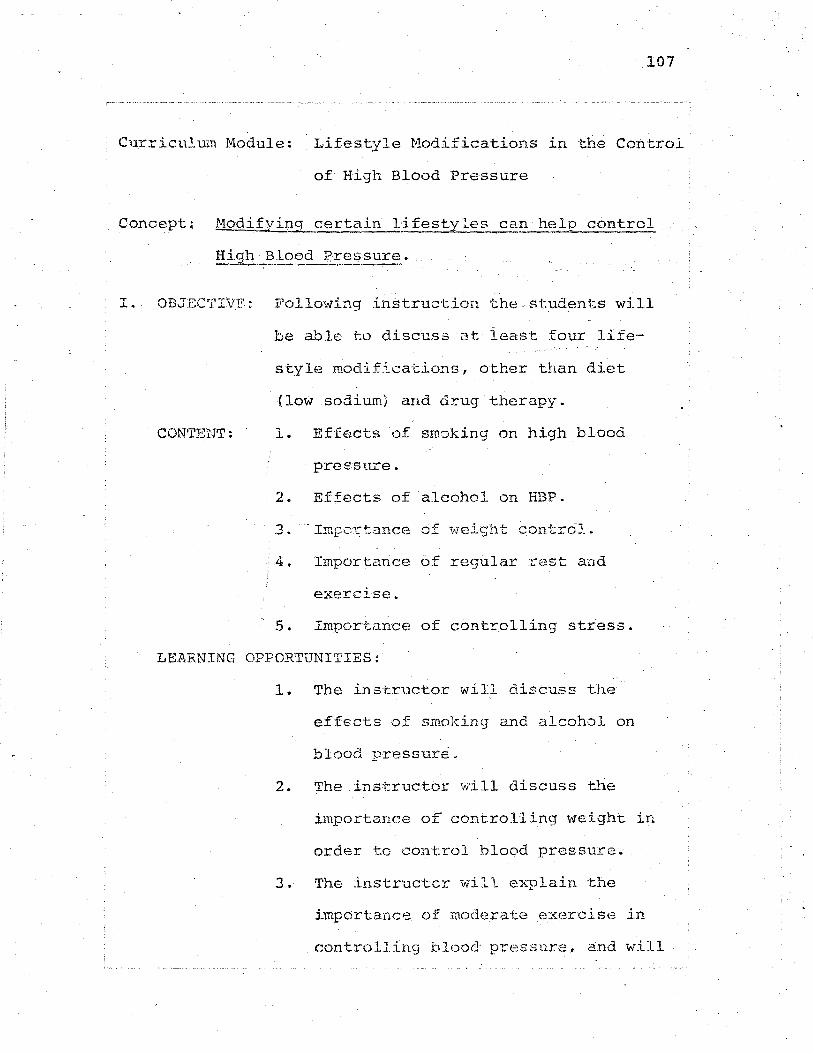
107
Curriculum Module: Lifestyle Nodificat.ion:S in ·the Control
of High Blood Pressure
Concept~ r·1oditying certain lifestyles can help control
Hiqh Blood Pressure. - ~.........,_...--.. -·--------
1. . OBJECTIVF: Following inst.ruction Jche. st.udents will
be able h) discuss at least four life-
style modifications, other than diet
(low sodium) and drug therapy.
CON'l'ENT: 1. Effects of smoking on high blood
pressure.
2. Effects of alcohol on HBP.
3. -- Imr)-C~t.ance of 1Neigl1t c.ontrOJ~ ~
4. Importance of regiJ.lar rest and
exercise.
5. Impor-tance of controlling stress.
LEARNING OPPORTUNITIES:
1. The instructor will discuss the
effects of smoking and alcohol on
blood pressure.
2. The instructor will discuss the
importance of controlling weight in
order to control blood pressure.
3. The .inst.ructcr "v'lill explain ·the
importance of moderate exercis(;; in
controlling blood pressure, and will
108
ask for volunteer students ·to give
personal examples. Instructor will
discuss the importance of adequate
rest.
4_,. The .in.structo.r 'irdll explain wha·t- is
meant by stress and will give exam-
ples of ho~¥ to control it. I.nstruc-:-
tor will also ask volunteer students
to share personal experiences regard-
ing s-tress in their: lives, and how
they are or are not able to control
it.
Concept; The-expression and discus~ion of feelings can
be helpful in patient acceptance C2L his_
condition.
I. OB,JECTIVE: F'ollowing instruction the students -will
CON'I:'ENT:
be able to exp-ress their feelinqs about
the lifestyl~ modifications and methods
necessary in the control of high blood
pressure.
, J..o Possible discussion topics:
Students express positive and negative
feelings about their high blood
pressure therapy.

109
-. ·~~---~~------------·-------~--~----------~
2. Students express their feelings about
daily drug dependence tc control high
blood pressure.
3. Students express feelings about:
.di.et . ., smokip.g .• and alocho-1, their
"pleasures in life" that must be
modified.
LE~ ... RNING OPPORTlJNI'I'IES:
RESOURCES:
1. The instructor will encourage the
students to express their feelings
about the p~rmanent changes and
treatments necessary in the control
of tlH:d.r high blood pressure. The
instructor will call on selected
students to express themselves on
specific changes that they have
found difficult.
1. Kaplan, N.M., M.D.~ Your Blood
Pressure: The ~-lost Deadly High,
Medcom Press, Ne1.v York; 1974.
2.. Personal Commu11ications \'litl1 !"Iedical
Social Worker.
110
Expanded Content Outline: T 'f t- 1 ·•,,f ri'f' . ' ~1 es_y e r~~l lCa~lOilS in the
Control of High Blood Pressure.
1. Effects of smoking on HBP:
A. Smoking has been linked to heart disease, lung
cancer 1 emphysema, and gas-trointestinal dis-
orders.
B ~ Tobacco contains a substance called nicot.ine.
C. Nicotine increases the heart rate and cons·tricts
the flow of blood. •
D. This causes the heart to work harder and blood
press~rre to rlse.
E. Even if :/ou can't stop sm9l:.:.ing completely cutting
down is helpful.
2. Effects of alcohol on HBP:
A. Alcohol in moderate amounts may sometimes reducE:
BP by releasing nervous tension, but alcohol
interfers with the effectiveness of your medi-
cations.
B. Alcohol is high in calories so if you are
watching your <;·might drinking can caw.se problems.
3. Importance of weight control
.A. Being ove~weiglYt can lead to HBP
B. Th,~ heart has to work harder to supply ·the extra
fat with the nutrients your body needs.
4. Importance of rest and exercise

11.1
A. Not getting enough rest can put added strain on
your heart causing your blood pressure to in
crease.
B. Getting regular rest is important in the control
of HBP.
C. Exercise should be regular and appropriate for
your age, sex, and general state of health.
1. Walking is a good form of exercise for a
hypertensive.
2. Other forms of exercise should be discussed
with your physician and tailored to your
needs.
5. ·Importance of controlling stress
A. Stress can include being worried, angry, up
tight, nervous.
B. Your heart~beats faster when you are under stress
and this causes your blood pressure to increase.
c. Hypertensives should try to avoid or reduce as
much stress as possible.
D. It is impol·tant for you to understand what
causes the stress in your life.
E. Everyone has different ways of handling their
stress. ~'IJ"'hat \vorks for one person may not work
for others.

112
Curriculum Module: How To Take Your Own Blood Pressure
Concept: The patient with hypertension can be an active
member of,the health care team in controlling
hypertension by learning how to take his mvn
blood pressure.
OBJECTIVE: Following instruction the students will be
able to take their own blood pressure ac
curately as witnessed by the instructor.
CONTENT: 1. Review of the definition of blood
pressure.
2. Equipment needed for taking blood
pressure.
3. Sounds associated with the measurement
·of blood pressure.
4. Procedure of taking blood pressure.
LEARNING· OPPORTUNITIES:
1. The instructor will call on volunteer
students to define blood pressure.
2. The instructor will display the equip
ment necessary in taking blood pressure 1
and will explain the functions of the
equipment.
3. The audio cassette tape will be played
for the students to hear the sounds that
they will listen for when taking blood
113
pressures. The instructor will explain
the significance of these sounds.
4. The instructor will demonstrate the
correct procedure of taking blood pres
sure on a volunteer student., pointing
out the appropriate steps to be taken
in the procedure.
5.~ Students will be placed into small
groups (3-4 persons per group) and will
be asked to practice taking blood pres
sures on each other.
6. The instructor, using a teaching (two
person) stethoscope will ask each stu
dent to take his own blood pressure
while the instructor monitors the
procedure.
RESOURCES: 1. American Heart Association Parnphle·t,
Recommendations for HUJ.11an Blood Pressure
Dete:_rmination By Sphymomanometers, 1967.
2. Merck Sharp and Dohme Pamphlet, Measuring
Blood Pressure, A Guide for Paramedical·
Personnel, 1974.
3. !1e:r:ck Sharp and Dohme Audio Cassette,
C~inical Significar.ce of. Sounds of
Korotk<Jff, 1972.
Expanded Con ten·t Outline: How To Take Your Own Blood
Pressure
1. Define blood pressure. Review factors that affect
blood pressure.
2. Equipment needed in taking l;>lood pressure
114
A. Stethoscope is needed for listening to the sounds
in blood pressure.
Approx~mate cost $13.
B. Sphymomanorneter is neede to determine the
measurement of the blood pressure. It consists
of:
1. compression bag enclosed in a cuff. Differ
ent sizes are available: average adult,
thin arm adults (also small children), and
large (obese) arm adults (also for thighs).
2. inflation bulb (pump)
3. manometer, two types: aneroid and mercury.
The aneroid should be checked and calibrated
yearly.
4. controlled exhaust valve to deflate the
system.
Approximate cost of aneroid $25, mercury
$35.
3. Sounds associated with the measurement of blood
pressure

115
A. Listen for when the·sounds first appear and when
they disappear.
B. There are actually five sounds in blood pressure,
but for the patient the first sound or systolic
and the last sound or diastolic are the most
important.
C. Tape will be played to give examples of these
sounds.
4. Procedure in taking blood pressure.
A. Person taking blood pressure should be able to
hear and see well.
B. Position patient or self - either sitting or
lying
1. sitting with arm resting on table, forearm
slightly bent, so cuff is at heart level.
2. lying with arm resting on bed.
c. Apply cuff
1. apply deflated cuff comfortably tight without
bulges to bare arm, one inch above the bend
in the arm.
2. the rubber bag that inflates the cuff should
cover the top and inside of the arm.
D. Positioning the stethoscope
1. ear pieces are placed comfortable in ears
2. the end part or bell is placed over the
brachial artery below cuff. Feel for strong

pulsation (artery) in the crease of arm,
little toward body.
E. Inflate cuff
1. feel for wrist (radial) pulse
2. close screw valve of rubber hand bulb
3. plli~P up cuff to point (number) where no
longer can feel wrist pulse beat.
4. note this number, but continue to inflate
20-30 mm higher than this point.
F. Deflate cuff
116
1. deflate cuff gradually (2 mm per heart beat)
open screw valve slowly
2. listen for first sound {systolic) and
remember the number
3. listen for the last sound (diastolic) and
remember the number
~h let. cuff deflate slowly, 10 nrrn lm,Jer than
last sound, then release screw valve
completely.
G. Should ~tJait 30 seconds before taking next blood
pressure.
H. Blood pressure may differ from left to right
arm. Left arm BP may be 10 nun higher than
right, record the higher number.
5. Practice session
Instructor supervises the students and checks each
students technique.





























