Embed Size (px)
Citation preview

EARLY DENTINE EROSION ASSESSMENT WITH NON-INVASIVE METHOD
MADIHA HABIB
FACULTY OF DENTISTRY UNIVERSITY OF MALAYA
KUALA LUMPUR
2018
Univers
ity of
Mala
ya

EARLY DENTINE EROSION ASSESSMENT WITH
NON-INVASIVE METHOD
MADIHA HABIB
THESIS SUBMITTED IN FULFILMENT OF THE
REQUIREMENTS FOR THE DEGREE OF DOCTOR OF
PHILOSOPHY
FACULTY OF DENTISTRY
UNIVERSITY OF MALAYA
KUALA LUMPUR
2018
Univers
ity of
Mala
ya
ii
UNIVERSITY OF MALAYA
ORIGINAL LITERARY WORK DECLARATION
Name of Candidate: MADIHA HABIB
Matric No: DHA140014
Name of Degree: DOCTOR OF PHILOSOPHY
Title of Thesis: EARLY DENTINE EROSION ASSESSMENT WITH NON-
INVASIVE METHOD
Field of Study: RESTORATIVE DENTISTRY
I do solemnly and sincerely declare that:
(1) I am the sole author/writer of this Work;
(2) This Work is original;
(3) Any use of any work in which copyright exists was done by way of fair
dealing and for permitted purposes and any excerpt or extract from, or
reference to or reproduction of any copyright work has been disclosed
expressly and sufficiently and the title of the Work and its authorship have
been acknowledged in this Work;
(4) I do not have any actual knowledge nor do I ought reasonably to know that
the making of this work constitutes an infringement of any copyright work;
(5) I hereby assign all and every rights in the copyright to this Work to the
University of Malaya (“UM”), who henceforth shall be owner of the
copyright in this Work and that any reproduction or use in any form or by any
means whatsoever is prohibited without the written consent of UM having
been first had and obtained;
(6) I am fully aware that if in the course of making this Work I have infringed
any copyright whether intentionally or otherwise, I may be subject to legal
action or any other action as may be determined by UM.
Candidate’s Signature Date:
Subscribed and solemnly declared before,
Witness’s Signature Date:
Name:
Designation:
Univers
ity of
Mala
ya

iii
EARLY DENTINE EROSION ASSESSMENT WITH NON-INVASIVE
METHOD
ABSTRACT
Non-invasive assessment of early dentine erosion is required for clinical validation of
therapeutic strategies aiming to reduce or arrest the progression of this condition. The
purpose of this thesis was to seek a non-invasive method suitable for monitoring early
dentine erosion progression with the ultimate goal of using this tool in clinical trials
involving dentine erosion. To achieve this purpose, this thesis aimed to first assess the
potential of optical coherence tomography (OCT) for monitoring early dentine erosion
progression, second, to assess the potential of surface roughness as a method for
measuring early dentine erosion progression in simulated intraoral conditions and
finally to assess if OCT is a sensitive tool to detect early dentine erosion and monitor its
progression in simulated intraoral conditions by correlating OCT data with surface
roughness data. Root dentine samples were first immersed in 0.3% citric acid for a total
of 30 minutes. Measurements with OCT and field-emission scanning electron
microscopy (FE-SEM) were obtained at varying erosion intervals. Integrated OCT
intensity changes were compared with FE-SEM observations. Next, root dentine
samples were subjected to a cycling erosion challenge with 0.3% citric acid for 10
minutes, three times a day interspersed with periods of simulated salivary
remineralisation for three days. Measurements with OCT and non-contact profilometry
were obtained on every cycling day. Fractional change of average roughness and
bearing curve parameters was compared with fractional change of surface loss and FE-
SEM observations. Finally, fractional change of integrated OCT intensity was compared
with fractional change of roughness parameters and FE-SEM observations. Integrated
OCT intensity was able to monitor the progression of early dentine erosion for 30
Univers
ity of
Mala
ya

iv
minutes with a detection threshold of two minutes from baseline. Mean percentage
change in integrated OCT intensity exhibited linear pattern (R2 = .99) with erosion
interval. Integrated OCT intensity changes corresponded with FE-SEM observations.
Average roughness (fRa1) and bearing curve parameters namely core roughness (fRk),
peak roughness (fRpk) and valley roughness (fRvk) were able to longitudinally measure
the progression of early dentine erosion as opposed to fractional change of surface loss.
FE-SEM images supported the surface roughness results. Integrated OCT intensity was
able to longitudinally measure early dentine erosion for three days in simulated intraoral
conditions with a detection threshold of day one from baseline measurement. Fractional
change of integrated OCT intensity correlated moderately but significantly with fRk and
fRa1 (r = .428 and .394 respectively) and showed a weak but significant correlation with
fRpk and fRvk (r = .300 and .217 respectively). Integrated OCT intensity changes
corresponded with ultrastructural changes of early eroded dentine. These studies
suggested that OCT and surface roughness parameters are suited for monitoring the
progression of in vitro early dentine erosion non-invasively and could be possible tools
for monitoring early dentine erosion progression in clinical trials.
Keywords: Early dentine erosion, non-invasive methods, monitoring.
Univers
ity of
Mala
ya

v
EARLY DENTINE EROSION ASSESSMENT WITH NON-INVASIVE METHOD
ABSTRAK
Penilaian yang bukan invasif terhadap hakisan dentine yang awal diperlukan untuk
pengesahan klinikal terhadap strategi terapeutik yang bertujuan untuk mengurangkan
atau memberhentikan perkembangan keadaan ini. Tujuan tesis ini adalah untuk mencari
kaedah pengimejan bukan invasif yang sesuai untuk memantau perkembangan hakisan
dentine awal dengan matlamat menggunakan alat ini dalam ujian klinikal yang
melibatkan hakisan dentine. Untuk mencapai tujuan ini, tesis ini bermatlamat untuk
pertama sekali, menilai potensi tomografi koheren optik (OCT) untuk memantau
progressi erosi dentine yang awal. Kedua, ia bertujuan untuk menilai potensi parameter
kekasaran permukaan untuk memantau perkembangan hakisan dentine awal dalam
keadaan intraoral bersimulasi. Akhir sekali, ia bertujuaan untuk menilai potensi OCT
untuk memantau perkembangan hakisan dentine awal dalam keadaan simulasi intraoral.
Pertama, sampel akar dentine direndam dalam 0.3% asid sitrik selama 30 minit.
Pengukuran menggunakan OCT dan mikroskop elektron pengimbasan-emisi lapangan
(FE-SEM) diperolehi berdasarkan pelbagai tempoh hakisan. Perubahan intensiti OCT
yang bersepadu dibandingkan dengan perubahan ketumpatan mineral dan pemerhatian
FE-SEM. Seterusnya, sampel akar dentine dikenakan cabaran pengitaran hakisan
dengan 0.3% asid sitrik selama 10 minit, tiga kali sehari secara berselang dengan
tempoh remineralisasi saliva bersimulasi selama 3 hari. Pengukuran dengan OCT dan
profilometri tanpa hubungan diperolehi pada setiap hari pengitaran. Perubahan
fraksional pada purata kekasaran dan parameter lengkungan galas dibandingkan dengan
perubahan fraksional kehilangan permukaan dan pemerhatian FE-SEM. Akhir sekali,
perubahan fraksional terhadap intensiti OCT yang berintegrasi dibandingkan dengan
perubahan fraksional parameter kekasaran dan pemerhatian FE-SEM. Intensiti OCT
yang berintegrasidapat memantau perkembangan hakisan dentine awal selama 30 minit
Univers
ity of
Mala
ya
vi
dengan ambang pengesanan selama dua minit dari garis dasar. Perubahan peratusan min
dalam ketumpatan OCT menunjukkan corak linear (R2 = .99) dengan jarak pengesan
hakisan masing-masing. Perubahan intensiti OCT yang berintergrasi berpadanan dengan
pemerhatian FE-SEM. Parameter purata kekasaran (fRa1) dan lengkung galas
terutamanya kekasaran teras (fRk), kekasaran puncak (fRpk) dan kekasaran lembah
(fRvk) dapat memantau perkembangan hakisan dentine awal bertentangan dengan
perubahan fraksional kehilangan permukaan. Imej FE-SEM menyokong keputusan
kekasaran permukaan. Keamatan OCT yang berintegrasi dapat mengukur hakisan
dentine awal secara mendadak selama 3 hari dalam keadaan simulasi intraoral dengan
ambang pengesanan hari pertama dari pengukuran baseline. Perubahan fraksional
intensiti OCT berintegrasi berkorelasi secara sederhana tetapi secara signifikan dengan
fRk dan fRa1 (r = .428 dan .394 masing-masing) dan menunjukkan korelasi yang lemah
tetapi signifikan dengan fRpk dan fRvk (r = .300 dan .177). Perubahan intensiti OCT
berintegrasi sesuai dengan perubahan ultrastruktur dentine yang terhakis awal. Kajian-
kajian ini mencadangkan bahawa parameter OCT dan permukaan kekasaran adalah
sesuai untuk memantau perkembangan in vitro awal hakisan dentine yang bukan invasif
dan berkemungkinan untuk menjadi calon untuk memantau perkembangan hakisan awal
dentine dalam ujian klinikal.
Kata kunci: Hakisan dentine awal, kaedah bukan invasif, memantau perkembangan.
Univers
ity of
Mala
ya

vii
ACKNOWLEDGEMENTS
I am grateful first and foremost to Almighty Allah for making this possible for me
and for everything else.
I would like to express my earnest thanks to my main supervisor, Associate Professor
Dr. Chew Hooi Pin. She has been both an advisor and a mentor. I am truly grateful to
her for the trust she showed in hiring me and for the freedom of decision making during
this journey. She has inspired me in many ways both at a personal and professional
level.
I am grateful to my co-supervisor Dr. Christian Zakian for his arduous efforts in
designing the Matlab programme and for his insights in the analysis part of the study. I
am indebted to him for introducing me to experimental part of research.
I am grateful to Professor Alex Fok and his research team for the use of micro-CT
and scanning electron microscopy in University of Minnesota. My research would not
have been possible without their efforts and input.
Thank you my co-workers and friends in the lab and entire HIR-team for all the
support. I am grateful to Ali for all the troubleshooting. Many thanks to the entire lab
staff especially madam Zarina for facilitating my work in many ways.
I am grateful to University of Malaya for the High Impact Research scholarship and
for the use of many generous resources both at national and international level.
I am grateful to Professor Prabhakaran for showing me this path and to Lakshmi for
introducing me to him.
I owe everything in my life to my mother and father who made me who I am today.
Words cannot express my gratitude for all the selfless and ceaseless support they have
given me throughout my life. Thanks to my brother and sister for their moral support
and love.
Lastly, I would like to thank my husband and son for their encouragement and
unconditional support. I am very fortunate to have you both in my life. Mansoor, I can
never thank you enough for being my pillar of strength throughout this journey. Rayyan,
I love you the most.
This thesis is dedicated to my late father Dr. Habib Ullah Malik, my mother Dr.
Zahida Habib, Mansoor and Rayyan.
Univers
ity of
Mala
ya
viii
TABLE OF CONTENTS
Abstract ....................................................................................................................... iii
Abstrak ......................................................................................................................... v
Acknowledgements ..................................................................................................... vii
Table of Contents ....................................................................................................... viii
List of Figures ............................................................................................................ xvi
List of Tables ............................................................................................................ xxv
List of Symbols and Abbreviations ........................................................................ xxviii
List of Appendices .................................................................................................... xxx
CHAPTER 1: INTRODUCTION............................................................................... 1
1.1 Background and research problem ....................................................................... 1
1.2 Research purpose and questions ........................................................................... 7
1.3 Aims and objectives ............................................................................................. 8
1.4 Significance and scope ......................................................................................... 9
1.5 Thesis structure .................................................................................................. 10
CHAPTER 2: LITERATURE REVIEW ................................................................. 12
2.1 Process of dental erosion .................................................................................... 12
2.1.1 Terminology and definitions ................................................................. 12
2.1.2 Prevalence and incidence of erosion ...................................................... 14
2.1.3 Etiology of dental erosion ..................................................................... 17
2.1.4 Chemical factors ................................................................................... 18
2.1.5 Biological factors .................................................................................. 22
2.1.5.1 Saliva. .................................................................................... 22
2.1.5.2 Pellicle ................................................................................... 24
Univers
ity of
Mala
ya

ix
2.1.6 Behavioral factors ................................................................................. 26
2.1.7 Structural and histopathological aspects of dentine erosion ................... 27
2.2 Clinical assessment ............................................................................................ 30
2.2.1 Diagnosis .............................................................................................. 30
2.2.2 Indices .................................................................................................. 32
2.2.3 Assessment of progression rate ............................................................. 34
2.3 Assessment techniques of dentine erosion .......................................................... 36
2.3.1 Quantitative assessment ........................................................................ 36
2.3.1.1 Surface microhardness ............................................................ 36
2.3.1.2 Nanohardness ......................................................................... 38
2.3.1.3 Surface profilometry ............................................................... 39
2.3.1.4 Chemical analysis of dissolved minerals ................................. 42
2.3.1.5 Atomic force microscopy........................................................ 44
2.3.1.6 Microradiography ................................................................... 45
2.3.1.7 Quantitative light induced florescence .................................... 48
2.3.1.8 Optical coherence tomography ............................................... 49
2.3.1.9 Optical specular and diffuse reflection .................................... 53
2.3.2 Qualitative assessment .......................................................................... 53
2.3.2.1 Scanning electron microscopy ................................................ 53
2.3.3 Conclusion ............................................................................................ 55
CHAPTER 3: MONITORING OF EARLY DENTINE EROSION WITH
OPTICAL COHERENCE TOMOGRAPHY .......................................................... 56
3.1 Introduction ....................................................................................................... 56
3.1.1 Principle of OCT imaging ..................................................................... 57
3.1.2 Assessment of demineralisation with OCT ............................................ 60
3.1.3 Aim....................................................................................................... 64
Univers
ity of
Mala
ya

x
3.2 Materials and Methods ....................................................................................... 65
3.2.1 Pilot studies .......................................................................................... 65
3.2.1.1 Sample preparation ................................................................. 65
3.2.1.2 Speed of agitation ................................................................... 67
3.2.1.3 Drying time of eroded dentine ................................................ 68
3.2.1.4 Reduction of specular reflection ............................................. 69
3.2.1.5 Determination of early erosion before step change .................. 70
3.2.1.6 Protocol verification ............................................................... 72
3.2.1.7 Removal of smear layer .......................................................... 74
3.2.1.8 Effect of smear layer removal on OCT intensity ..................... 76
3.2.1.9 Assessment of early dentine erosion with Micro-CT: .............. 77
3.2.2 Experimental design .............................................................................. 83
3.2.3 OCT ...................................................................................................... 83
3.2.3.1 Sample preparation ................................................................. 83
3.2.3.2 Erosion challenge ................................................................... 85
3.2.3.3 Measurements with OCT ........................................................ 87
3.2.3.4 Data processing ...................................................................... 89
3.2.3.5 Trend of backscattered intensity ............................................. 91
3.2.3.6 Parameters for intensity analysis ............................................. 91
3.2.3.7 Comparison by effect size ....................................................... 94
3.2.4 FE-SEM ................................................................................................ 94
3.2.4.1 Sample Preparation:................................................................ 94
3.2.4.2 Erosion challenge ................................................................... 96
3.2.4.3 Imaging .................................................................................. 97
3.2.5 Statistical Analysis: ............................................................................... 98
3.3 Results. .............................................................................................................. 99
Univers
ity of
Mala
ya

xi
3.3.1 OCT ...................................................................................................... 99
3.3.1.1 Trend of backscattered intensity ............................................. 99
3.3.1.2 Outcomes measures .............................................................. 110
3.3.1.3 Comparison of effect size ..................................................... 125
3.3.2 FE-SEM .............................................................................................. 127
3.4 Discussion ....................................................................................................... 130
3.4.1 OCT .................................................................................................... 131
3.4.2 FE-SEM .............................................................................................. 135
3.5 Conclusions ..................................................................................................... 138
CHAPTER 4: MONITORING OF EARLY DENTINE EROSION WITH
SURFACE ROUGHNESS ...................................................................................... 140
4.1 Introduction ..................................................................................................... 140
4.1.1 Roughness parameters ......................................................................... 141
4.1.1.1 Average roughness ............................................................... 141
4.1.1.2 Bearing area curve ................................................................ 143
4.1.2 Aim..................................................................................................... 147
4.2 Materials and Methods ..................................................................................... 149
4.2.1 Experimental design ............................................................................ 149
4.2.2 Profilometry ........................................................................................ 149
4.2.2.1 Sample preparation ............................................................... 149
4.2.2.2 Erosive pH-cycling ............................................................... 150
4.2.2.3 Measurements with Profilometry .......................................... 152
4.2.2.4 Data extraction ..................................................................... 156
4.2.2.5 Calculation of fractional change ........................................... 162
4.2.2.6 Comparison of effect size ..................................................... 163
4.2.3 FE-SEM .............................................................................................. 164
Univers
ity of
Mala
ya
xii
4.2.3.1 Erosive pH-cycling ............................................................... 164
4.2.3.2 Imaging ................................................................................ 165
4.2.4 Statistical Analysis .............................................................................. 165
4.3 Results. ............................................................................................................ 166
4.3.1 Profilometry ........................................................................................ 166
4.3.1.1 Average roughness: .............................................................. 166
4.3.1.2 Bearing area curve parameters .............................................. 169
4.3.1.3 Tissue loss ............................................................................ 181
4.3.2 FE-SEM .............................................................................................. 182
4.4 Discussion ....................................................................................................... 184
4.4.1 Profilometry ........................................................................................ 185
4.4.1.1 Average roughness ............................................................... 185
4.4.1.2 Bearing area curve parameters .............................................. 186
4.4.1.3 Tissue loss ............................................................................ 188
4.4.2 FE-SEM .............................................................................................. 189
4.5 Conclusions ..................................................................................................... 191
CHAPTER 5: MONITORING OF EARLY DENTINE EROSION WITH
OPTICAL COHERENCE TOMOGRAPHY IN A SIMULATED INTRAORAL
CONDITION…...…………………………………………………………………….193
5.1 Introduction ..................................................................................................... 193
5.1.1 Cycling and non-cycling models ......................................................... 195
5.1.2 Erosion pH-cycling models ................................................................. 195
5.1.3 Substrate ............................................................................................. 196
5.1.4 Polishing and sample preparation ........................................................ 198
5.1.5 Demineralising agent .......................................................................... 199
5.1.6 Remineralising agent ........................................................................... 200
Univers
ity of
Mala
ya

xiii
5.1.7 Time ................................................................................................... 203
5.1.8 Environment ....................................................................................... 204
5.1.9 Temperature ........................................................................................ 205
5.1.10 Timing of measurement ...................................................................... 205
5.1.11 Recommendations / Conclusions ......................................................... 206
5.1.12 Aim..................................................................................................... 207
5.2 Materials and Methods ..................................................................................... 208
5.2.1 Pilot study ........................................................................................... 208
5.2.2 Experimental design ............................................................................ 210
5.2.3 OCT .................................................................................................... 210
5.2.3.1 Measurements with OCT ...................................................... 210
5.2.3.2 Data processing .................................................................... 212
5.2.3.3 Trend of backscattered intensity ........................................... 213
5.2.3.4 Parameters for intensity analysis ........................................... 213
5.2.3.5 Comparison by effect size ..................................................... 215
5.2.3.6 Correction with reference ..................................................... 216
5.2.4 FE-SEM .............................................................................................. 217
5.2.5 Comparison with surface roughness .................................................... 217
5.2.5.1 Calculation of fractional change in intensity ......................... 217
5.2.5.2 Correlation ........................................................................... 218
5.2.6 Statistical Analysis .............................................................................. 218
5.3 Results. ............................................................................................................ 219
5.3.1 OCT .................................................................................................... 219
5.3.1.1 Trend of backscattered intensity ........................................... 219
5.3.1.2 Outcome measures ............................................................... 229
5.3.1.3 Comparison by effect size ..................................................... 240
Univers
ity of
Mala
ya

xiv
5.3.1.4 Correction with reference ..................................................... 240
5.3.2 FE-SEM .............................................................................................. 246
5.3.3 Comparison with surface roughness findings ....................................... 249
5.3.3.1 Fractional change in intensity, fR (I(23µm : 58µm)) ..................... 249
5.3.3.2 Relationship between fR and fRa1 ......................................... 250
5.3.3.3 Relationship between fR and fRk .......................................... 251
5.3.3.4 Relationship between fR and fRpk ......................................... 252
5.3.3.5 Relationship between fR and fRvk ......................................... 253
5.3.3.6 Relationship between fR and fMR1 ...................................... 254
5.3.3.7 Relationship between fR and fMR2 ...................................... 255
5.3.3.8 Significance of difference between correlation coefficients of
fRa and fRk ........................................................................... 257
5.3.3.9 Correlation on day one ......................................................... 257
5.3.3.10 Correlation on day two ......................................................... 257
5.3.3.11 Correlation on day three ....................................................... 258
5.4 Discussion ....................................................................................................... 260
5.4.1 OCT .................................................................................................... 262
5.4.2 FE-SEM .............................................................................................. 267
5.4.3 Comparison with surface roughness findings ....................................... 269
5.5 Conclusions ..................................................................................................... 272
CHAPTER 6: CONCLUSIONS ............................................................................. 274
6.1 Summary and conclusions................................................................................ 274
6.1.1 Aim 1 .................................................................................................. 275
6.1.2 Aim 2 .................................................................................................. 277
6.1.3 Aim 3 .................................................................................................. 279
6.2 Contribution to research ................................................................................... 282
Univers
ity of
Mala
ya

xv
6.3 Limitations of this study .................................................................................. 283
6.4 Future work ..................................................................................................... 284
References ................................................................................................................ 285
List of Publications and Papers Presented ................................................................. 309
Appendix .................................................................................................................. 311
Univers
ity of
Mala
ya

xvi
LIST OF FIGURES
Figure 1.1: Research framework. ............................................................................... 11
Figure 2.1: Salivary factors associated with the control of dental erosion in enamel and
dentine (Buzalaf et al., 2012a). .................................................................................... 26
Figure 3.1: Stereomicroscope image of a root dentine sample used for exploratory
work. The sample was sectioned 1 mm below the cemento-enamel junction. The
demineralisation window was covered with blue adhesive tape. It has been highlighted
by a red box. ............................................................................................................... 67
Figure 3.2: OCT B-scans of root dentine samples taken with SS-OCT at (a) baseline
measurement and (b) after 24 hours of erosive challenge. White line at the center
indicates the border between the reference and eroded areas. The transparent arrows
indicate the backscattered intensity (demineralisation) at the surface of eroded dentine
sample. Minimal increase in backscattered intensity was observed in the B-scan after 24
hours of erosion challenge (b) in comparison to the intensity observed in the B-scan at
baseline measurement (a). ........................................................................................... 67
Figure 3.3: Box plots represent the OCT data acquired after 20 seconds and 10 minutes
of air-drying. ............................................................................................................... 69
Figure 3.4: OCT B-scans of root dentine samples before and after tilting. (a) high
specular reflection was observed in the B-scan of the sample before tilting. Arrows
indicate columnar artefacts of specular reflection (b) OCT B-scan taken after the sample
was tilted at 20 degrees at a plane perpendicular to beam was devoid of specular
reflection..................................................................................................................... 70
Figure 3.5: OCT B-scans of a sample taken at (a) baseline and (b) after 10 minutes of
exposure to hydrochloric acid. Step change (circled in red) was observed at the junction
of reference and eroded areas after 10 minutes of HCL exposure. ............................... 71
Figure 3.6: OCT B-scans of a dentine sample at (a) baseline (b) after 30 minutes of
erosion challenge and (c) after 60 minutes of erosion challenge. White line at the center
indicates the border between the reference and eroded areas. The transparent arrows
indicate the backscattered intensity (demineralisation) at the surface of eroded dentine
sample. No step change was observed at the border between reference and eroded areas
in the OCT B-scan even after 60 minutes of erosion challenge (c). .............................. 72
Figure 3.7: Mean integrated intensity of the reference and eroded areas at different
erosion time points. Arrows indicate the intensity fluctuations in the eroded area. ....... 74
Figure 3.8: Stereomicroscope images of a sample taken after polishing, pre-EDTA
ultrasonication, post-EDTA treatment, post EDTA ultrasonication taken at
Univers
ity of
Mala
ya

xvii
magnification of 1x (1a-1d) 1.6x (2a-2d) 2.5x (3a-3d) respectively. Dentine surface
appeared to be clearer after a combination of ultrasonication and EDTA treatment ..... 75
Figure 3.9: shows (a) sound dentine covered with smear layer (b) Dentine with smear
layer removed by 10 % EDTA treatment for 3 minutes pre- and post ultrasonication.
The dentinal tubules became patent after the smear layer removal without any obvious
gross changes in dentine morphology. ......................................................................... 76
Figure 3.10: shows (a) mean integrated intensity of the reference area of the samples at
various erosion time points. (b) mean integrated intensity of the eroded area of the
samples at various erosion time points. ....................................................................... 77
Figure 3.11: Micro-CT images of samples eroded for (a) 2 minutes, (b) 25 minutes and
(c) 30 minutes. No obvious difference in contrast was observed between the reference
and eroded areas of these samples. .............................................................................. 82
Figure 3.12: Experimental design of the study. ........................................................... 83
Figure 3.13: Sample preparation (a) root of premolar tooth (b) coronal view of root (c)
root sectioned along the long axis buccolingually into two halves (d & e) each half of
root considered as one sample (f) prepared sample. ..................................................... 85
Figure 3.14: Apparatus used for erosion challenge. A beaker containing citric acid
(pH=3.2) was placed on a magnetic stirrer device. A stir bar was added in the solution
(circled in red). The root dentine samples were suspended in the beaker as shown in the
figure. The temperature of citric acid and speed of agitation was controlled by the
magnetic stirrer. .......................................................................................................... 87
Figure 3.15: OCT equipment and repositioning jig. .................................................... 89
Figure 3.16: Data processing of OCT C-scan images (a) graphic user interface (GUI) of
Matlab programme for uploading and processing of data (b) aligned surface view of one
C-scan of one time point. Green and red selections represent the regions of interest
selected for reference and eroded areas respectively (c) mean depth-resolved intensity
profile (A-scan) for the reference and eroded areas represented by green and red plots
respectively (d) data from mean A-scan for one C-scan of one time points exported to
excel files separately for reference and eroded areas.................................................... 90
Figure 3.17: Illustration of the calculation of decay of intensity between optical depths
of 23 µm and 58 µm. Figure shows the mean depth-resolved intensity profile (A-scan)
of the first 120 µm for the eroded area of the sample. Each line plot represents the OCT
intensity (a.u) plotted in optical depth (µm) for all 20 samples at each measurement time
point. The longer black arrow represents the intensity at an optical of 23 µm and shorter
black arrow represents the intensity at 58 µm. The red arrow shows the decay of
intensity between 23 µm and 58 µm. ........................................................................... 92
Univers
ity of
Mala
ya

xviii
Figure 3.18: Illustration of the calculation of integrated intensity from an optical depth
of 23 µm to an optical depth of 58 µm. Figure shows the mean depth-resolved intensity
profile (A-scan) of the first 120 µm for the eroded area of the sample. Each line plot
represents the OCT intensity (a.u) plotted in optical depth (µm) for all 20 samples at
each measurement time point. The longer black arrow represents the intensity at an
optical of 23 µm and shorter black arrow represents the intensity at 58 µm. The red
arrow shows the integrated intensity between 23 µm and 58 µm. Z is the differential
distance between two physical depths. ........................................................................ 93
Figure 3.19: Prepared root dentine sample for FE-SEM imaging. The blue rectangle
indicates the window prepared on the sample. The left half of the window (reference
area) was kept covered with red nail varnish during erosion challenges while the right
half of the window (eroded area) was exposed to erosion challenge ............................ 96
Figure 3.20: Mean depth-resolved intensity profile (A-scan) of the first 120 µm for the
reference area of the sample. Each line plot represents OCT intensity (a.u) plotted in
optical depth (µm) for all 20 samples at each measurement time point. Red, blue and
green dotted lines represent the superficial optical depths chosen for the analysis.
Plateau of intensity is shown by black dotted line. The error bars represent standard
deviation. .................................................................................................................. 101
Figure 3.21: Mean depth-resolved intensity profile (A-scan) of the first 120 µm for the
eroded area of the sample. Each line plot represents OCT intensity (a.u) plotted in
optical depth (µm) for all 20 samples at each measurement time point. Red, blue and
green dotted lines represent the superficial optical depths chosen for the analysis.
Plateau of intensity is shown by black dotted line. The error bars represent standard
deviation. .................................................................................................................. 101
Figure 3.22: Representative OCT A-scans of one sample at (a) baseline measurement
(b) 2 minutes (c) 4 minutes (d) 6 minutes (e) 8 minutes (f) 10 minutes (g) 12 minutes (h)
14 minutes (i) 16 minutes (j) 20 minutes (k) 25 minutes (l) 30 minutes. Each A-scan
shows the OCT intensity (a.u) plotted in optical depth (µm). The red text box indicates
the OCT intensity at a depth of 23 µm. The chart title of each A-scan indicates the time
interval for which the A-scan was plotted. The increase in intensity at 23 µm is obvious
with time. .................................................................................................................. 102
Figure 3.23: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious. .......................................................................................................... 104
Figure 3.24: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
Univers
ity of
Mala
ya

xix
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious. .......................................................................................................... 105
Figure 3.25: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious. .......................................................................................................... 106
Figure 3.26: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious. .......................................................................................................... 107
Figure 3.27: Representative OCT B-scans of a sample at (a) baseline measurement (b)
2 minutes (c) 4 minutes (d) 6 minutes (e) 8 minutes (f) 10 minutes (g) 12 minutes (h) 14
minutes (i) 16 minutes (j) 20 minutes (k) 25 minutes and (l) 30 minutes. A composite
slab was used as reference as shown by the red arrow in the figure. Transparent arrows
indicate the backscattered intensity at the surface of eroded area. .............................. 108
Figure 3.28: Mean decay of intensity of reference and eroded areas at various erosion
intervals between superficial optical depth of 5 µm and intensity plateau at 58 µm. .. 111
Figure 3.29: Mean decay of intensity of reference and eroded areas at various erosion
intervals between superficial optical depth of 11 µm and intensity plateau at 58 µm. 112
Figure 3.30: Mean decay of intensity of reference and eroded areas at various erosion
intervals between superficial optical depth of 23 µm and intensity plateau at 58 µm. 113
Figure 3.31: Mean integrated intensity of reference and eroded areas at various erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 5
µm to the intensity plateau at 58 µm. ........................................................................ 118
Figure 3.32: Mean integrated intensity of reference and eroded areas at various erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 11
µm to the intensity plateau at 58 µm. ........................................................................ 119
Figure 3.33: Mean integrated intensity of reference and eroded areas at various erosion
intervals. The intensity was integrated from superficial optical depth of 23 µm to the
intensity plateau at 58 µm. ........................................................................................ 120
Figure 3.34: Mean percentage change in integrated intensity of eroded area for intensity
integrated from superficial optical depth of 23 µm to the intensity plateau at 58 µm. . 121
Univers
ity of
Mala
ya

xx
Figure 3.35: Best fit regression line of backscattered intensity change with erosion
interval...................................................................................................................... 122
Figure 3.36: FE-SEM micrographs (2000x) of eroded areas (a-g) of samples treated
with citric acid for 2, 4, 8, 12, 16, 25 and 30 minutes. ............................................... 127
Figure 3.37: FE-SEM images showing the interface between the reference and eroded
areas of samples eroded for 8 minutes (1a, 1b), 12 minutes (2a, 2b), 16 minutes (3a, 3b),
25 minutes (4a, 4b) and 30 minutes (5a, 5b). ............................................................. 128
Figure 3.38: Cross-section of a sample eroded for 25 minutes at (a) 400x (b) 1000x and
(c) 2000x. ................................................................................................................. 129
Figure 4.1: Three different surfaces having similar Ra values. (a) The first profile has
sharp peaks, (b) the second deep valleys and (c) the third has neither (Bewoor &
Kulkarni, 2009) ......................................................................................................... 143
Figure 4.2: Generation of bearing area curve from roughness profile. Modified from
(Field et al., 2010). Bearing length or tp is the sum of lengths of individual plateaus (L1,
L2), divided by the total assessment length (L) .......................................................... 144
Figure 4.3: Bearing area curve parameters (1) Maximum height (2) Peak area defined
(3) 40% of minimum slope (4) Valley area (5) Minimal height (Infinitefocus, 2009). 145
Figure 4.4: Experimental design of the study ........................................................... 149
Figure 4.5: Photograph of profilometry equipment ................................................... 152
Figure 4.6: 3D model of image captured and displayed by live viewer ..................... 154
Figure 4.7: Repositioning of samples at different measurement time points. (a) custom-
made sample holder pasted on paper (b) sample holder pasted on the stage during
scanning (c) close up of sample-holder with the sample snugly fitted inside .............. 155
Figure 4.8: 3D images acquired by profilometry at the junction of reference and eroded
areas (a) Baseline image (b) Day one image (c) Day two image (d) Day three image 155
Figure 4.9: Measurement of Ra5 (a) Measurement area drawn on the image and its
associated roughness profile displayed (b) Five measurement areas drawn on the image
for calculation of Ra5. Each measurement area was 43 microns wide and was composed
of 100 points. Ra5 was an average of five such areas. ................................................. 158
Figure 4.10: A single measurement area drawn on the image for the calculation of Ra1.
The measurement area was 344 microns wide and was composed of 800 points. ....... 159
Figure 4.11: (a) Roughness profile generated from the single measurement area (b) Ra1
values exported to excel sheet ................................................................................... 159
Univers
ity of
Mala
ya

xxi
Figure 4.12: shows (a) bearing area curve generated from the measurement area (b)
values for bearing area curve parameters automatically exported to excel sheets ....... 160
Figure 4.13: Measurement of tissue loss. Green line represents reference measurement
line and red line represents eroded measurement line. Delta z values are given at the
bottom of the image .................................................................................................. 162
Figure 4.14: Fractional change in average roughness of reference and eroded areas of
fRa5 (a) and fRa1 (b) with erosion interval. ................................................................. 169
Figure 4.15: Fractional change in average core roughness (fRk) of reference and eroded
areas with erosion interval......................................................................................... 170
Figure 4.16: Fractional change in average peak roughness (fRpk) of reference and
eroded areas with erosion interval. ............................................................................ 171
Figure 4.17: Fractional change in average valley roughness (fRvk) of reference and
eroded areas with erosion interval. ............................................................................ 172
Figure 4.18: Fractional change in proportion of profile peaks (fMR1) of reference and
eroded areas with erosion interval. ............................................................................ 173
Figure 4.19: Fractional change in proportion of profile valleys (fMR2) of reference and
eroded areas with erosion interval ............................................................................. 174
Figure 4.20: Representative profiles (a) and bearing area curves (b) of a sample at
baseline measurement. The excel sheets show the values of Ra and bearing area curve
parameters. ............................................................................................................... 177
Figure 4.21: Representative profiles (a) and bearing area curves (b) of a sample after
one day of cycling erosion challenge. The excel sheets show the values of Ra and
bearing area curve parameters. .................................................................................. 178
Figure 4.22: Representative profiles (a) and bearing area curves (b) of a sample after
two days of cycling erosion challenge. The excel sheets show the values of Ra and
bearing area curve parameters. .................................................................................. 179
Figure 4.23: Representative profiles (a) and bearing area curves (b) of a sample after
three days of cycling erosion challenge. The excel sheets show the values of Ra and
bearing area curve parameters. .................................................................................. 180
Figure 4.24: Fractional change in surface loss (fΔZ) with erosion interval. ............... 181
Figure 4.25: FE-SEM micrographs (1000x) of the root dentine samples. a-c show the
reference areas of samples subjected to erosion challenge for one - three days at 1000x.
d-f show the eroded areas of samples subjected to erosion challenge for one - three days
at 1000x .................................................................................................................... 183
Univers
ity of
Mala
ya

xxii
Figure 5.1: OCT B-scans of a root dentine sample at (a) baseline, (b) after three days of
cycling erosion challenge. Red line at the center indicates the border between the
reference and eroded areas. The arrows indicate the backscattered intensity
(demineralisation) at the surface of eroded dentine sample. No visible step change was
discerned at the border between the reference and eroded areas. ................................ 209
Figure 5.2: Experimental design of the study............................................................ 210
Figure 5.3: Illustration of the calculation of decay of intensity between optical depths of
23 µm and 58 µm. Figure shows the mean depth-resolved intensity profile (A-scan) of
the first 120 µm for the eroded area of the sample. Each line plot represents the OCT
intensity (a.u) plotted in optical depth (µm) for all 20 samples at each measurement time
point. The longer black arrow represents the intensity at an optical of 23 µm and shorter
black arrow represents the intensity at 58 µm. The red arrow shows the decay of
intensity between 23 µm and 58 µm. ......................................................................... 214
Figure 5.4: Illustration of the calculation of integrated intensity from an optical depth of
23 µm to an optical depth of 58 µm. Figure shows the mean depth-resolved intensity
profile (A-scan) of the first 120 µm for the eroded area of the sample. Each line plot
represents the OCT intensity (a.u) plotted in optical depth (µm) for all 20 samples at
each measurement time point. The longer black arrow represents the intensity at an
optical of 23 µm and shorter black arrow represents the intensity at 58 µm. The red
arrow shows the integrated intensity between 23 µm and 58 µm. Z is the differential
distance between two physical depths. ...................................................................... 215
Figure 5.5: Mean depth-resolved intensity profile (mean A-scan) of the first 120 µm for
the reference area of the sample. Each line plot represents the OCT intensity (a.u)
plotted in optical depth (µm) for all 20 samples at each measurement time point. Red,
blue and green dotted lines represent the superficial optical depths chosen for the
analysis. Plateau of intensity is shown by black dotted line. The error bars represent
standard deviation. .................................................................................................... 221
Figure 5.6: Mean depth-resolved intensity profile (mean A-scan) of the first 120 µm for
the eroded area of the sample. Each line plot represents the OCT intensity (a.u) plotted
in optical depth (µm) for all 20 samples at each measurement time point. Red, blue and
green dotted lines represent the superficial optical depths chosen for the analysis.
Plateau of intensity is shown by black dotted line. The error bars represent standard
deviation. .................................................................................................................. 222
Figure 5.7: Representative OCT A-scans of one sample (a - d). Each A-scan shows the
OCT intensity (a.u) plotted in optical depth (µm). The red text box indicates the OCT
intensity at a depth of 23 µm. The chart title of each A-scan indicates the time interval
for which the A-scan was plotted. The increase in intensity at 23 µm is obvious with
time. ......................................................................................................................... 223
Univers
ity of
Mala
ya

xxiii
Figure 5.8: Representative A-scans of a sample at (a) baseline time point and b) after
three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious. .......................................................................................................... 224
Figure 5.9: Representative A-scans of a sample at (a) baseline time point and b) after
three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious. .......................................................................................................... 225
Figure 5.10: Representative A-scans of a sample at (a) baseline time point and b) after
three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious. .......................................................................................................... 226
Figure 5.11: Representative A-scans of a sample at (a) baseline time point and b) after
three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious. .......................................................................................................... 227
Figure 5.12: Representative OCT B-scans of one sample at (a) baseline measurement
(b) day one (c) day two and (d) day three of cycling erosion challenge. Transparent
arrows indicate the backscattered intensity at the surface of eroded area. .................. 228
Figure 5.13: Mean decay of intensity of reference and eroded areas at cycling erosion
intervals between superficial optical depth of 5 µm and intensity plateau at 58 µm. .. 231
Figure 5.14: Mean decay of intensity of reference and eroded areas at cycling erosion
intervals between superficial optical depth of 11 µm and intensity plateau at 58 µm. 232
Figure 5.15: Mean decay of intensity of reference and eroded areas at cycling erosion
intervals between superficial optical depth of 23 µm and intensity plateau at 58 µm. 233
Figure 5.16: Mean integrated intensity of reference and eroded areas at cycling erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 5
µm to the intensity plateau at 58 µm. ........................................................................ 235
Univers
ity of
Mala
ya

xxiv
Figure 5.17: Mean integrated intensity of reference and eroded areas at different
cycling erosion intervals. The backscattered intensity was integrated from superficial
optical depth of 11 µm to the intensity plateau at 58 µm............................................ 237
Figure 5.18: Mean integrated intensity of reference and eroded areas at cycling erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 23
µm to the intensity plateau at 58 µm. ........................................................................ 238
Figure 5.19: Corrected integrated intensity for the reference and eroded areas for
outcome measures (a) I(5µm : 58µm) (b) I(11µm : 58µm) and (c) I(23µm : 58µm). ......................... 242
Figure 5.20: Corrected decay of intensity for the reference and eroded areas for
outcome measures (a) I58µm / I5µm (b) I58µm / I11µm and (c) I58µm / I23µm. ........................ 243
Figure 5.21: Comparison of OCT outcome measures of decay of intensity and
integrated intensity with FE-SEM micrographs (a) The ‘decay of intensity’ outcome
measures plotted in time (b) the ‘integrated intensity’ outcome measures plotted in time
(c) FE-SEM image of sound dentine (d-f) FE-SEM images taken after day one, day two
and day three of cycling erosion challenge respectively............................................. 247
Figure 5.22: Comparison of OCT outcome measure with FE-SEM micrographs (a)
OCT outcome measure of integrated intensity I(23µm : 58µm) plotted in time (b) FE-SEM
image of sound dentine (c-e) FE-SEM images taken after day one, day two and day
three of cycling erosion challenge respectively .......................................................... 248
Figure 5.23: Fractional change in integrated intensity with baseline (fR) of reference
and eroded areas at cycling erosion intervals. The backscattered intensity was integrated
from superficial optical depth of 23 µm to the intensity plateau at 58 µm .................. 250
Figure 5.24: Relationship between fR and fRa .......................................................... 251
Figure 5.25: Relationship between fR and fRk .......................................................... 252
Figure 5.26: Relationship between fR and fRpk ......................................................... 253
Figure 5.27: Relationship between fR and fRvk ......................................................... 254
Figure 5.28: Relationship between fR and fMR1 ...................................................... 255
Figure 5.29: Relationship between fR and fMR2 ...................................................... 256
Univers
ity of
Mala
ya

xxv
LIST OF TABLES
Table 3.1: Specifications of OCS1300SS Swept Source OCT..................................... 59
Table 3.2: OCT parameters and their outcome measures defined. ............................. 110
Table 3.3: Results of repeated measures ANOVA analysis for reference and eroded
areas of outcome measures of decay of intensity. ...................................................... 114
Table 3.4: Post hoc comparisons of all erosion time points with baseline, for the eroded
area of outcome measures of decay of intensity. ........................................................ 114
Table 3.5: Post hoc comparisons of consecutive erosion intervals for the eroded area of
outcome measures of decay of intensity. ................................................................... 115
Table 3.6: Mean and standard deviation (given in brackets) for the eroded area of
outcome measures of decay of intensity. ................................................................... 116
Table 3.7: Results of repeated measures ANOVA analysis for reference and eroded
areas of outcome measures of integrated intensity. .................................................... 122
Table 3.8: Post hoc comparisons of all erosion time points with baseline for the eroded
area of outcome measures of integrated intensity....................................................... 123
Table 3.9: Post hoc comparisons of consecutive erosion intervals for the eroded area of
all outcome measures for integrated intensity. ........................................................... 124
Table 3.10: Mean and standard deviation (given in brackets) for the eroded area of all
outcome measures for integrated intensity. ................................................................ 125
Table 3.11: Comparison of effect sizes of outcome measures used for analysis. ....... 126
Table 4.1: Description of roughness parameters ....................................................... 145
Table 4.2: Calculation methods for surface roughness parameters used in the study.
RaL* was only explored in the pilot study .................................................................. 156
Table 4.3: Results for generalized estimating equations (GEE) for reference and eroded
areas of fRa1 and fRa5................................................................................................. 167
Table 4.4: Post-hoc comparisons of erosion intervals for the eroded areas of fRa1 and
fRa5 ........................................................................................................................... 168
Table 4.5: Effect size comparison of all outcome measures ...................................... 174
Table 4.6: Results for generalized estimating equations (GEE) for reference and eroded
areas of bearing area curve parameters. ..................................................................... 175
Univers
ity of
Mala
ya

xxvi
Table 4.7: Results for repeated measures ANOVA for reference and eroded areas of
MR2. ........................................................................................................................ 175
Table 4.8: Post hoc comparisons of erosion intervals for the eroded areas of bearing
area curve parameters................................................................................................ 176
Table 4.9: Results for generalized estimating equations (GEE) for fΔZ .................... 181
Table 4.10: Fractional change in average roughness, bearing area curve parameters and
surface loss with respect to baseline values given at different time points. Standard
deviations are within brackets. Values in bold denote a significant effect. ................. 182
Table 5.1: OCT parameters and their outcome measures defined. ............................. 229
Table 5.2: Results of repeated measures ANOVA analysis for reference and eroded
areas of outcome measures of decay of intensity. ...................................................... 233
Table 5.3: Post hoc comparisons for the eroded area of outcome measures for decay of
intensity. ................................................................................................................... 234
Table 5.4: Mean and standard deviation (given in brackets) for the eroded area of
outcome measures for decay of intensity ................................................................... 234
Table 5.5: Results of repeated measures ANOVA analysis for reference and eroded
areas of all outcome measures for integrated intensity. .............................................. 238
Table 5.6: Post hoc comparisons for the eroded area of outcome measures for integrated
intensity. ................................................................................................................... 239
Table 5.7: Mean and standard deviation (given in brackets) for the eroded area of
outcome measures for integrated intensity. ................................................................ 239
Table 5.8: Comparison of effect sizes of all outcome measures used for analysis. .... 240
Table 5.9: Results of repeated measures ANOVA analysis for corrected data of
outcome measures of decay of intensity and integrated intensity. .............................. 243
Table 5.10: Post hoc comparisons for the eroded area of outcome measures of corrected
decay of intensity. ..................................................................................................... 244
Table 5.11: Post hoc comparisons for the eroded area of outcome measures of corrected
integrated intensity. ................................................................................................... 244
Table 5.12: Mean and standard deviation (given in brackets) for the corrected eroded
area of outcome measures of decay of intensity. ........................................................ 245
Univers
ity of
Mala
ya

xxvii
Table 5.13: Mean and standard deviation (given in brackets) for the corrected eroded
area of outcome measures of integrated intensity....................................................... 245
Table 5.14: Overall relationship between fractional change of OCT outcome measure
(fR) and fractional change of each surface roughness outcome measure .................... 256
Table 5.15: Relationship between fractional change of OCT outcome measure (fR) and
fractional change of surface roughness outcome measures at each time point (day). .. 259
Univers
ity of
Mala
ya

xxviii
LIST OF SYMBOLS AND ABBREVIATIONS
3D : 3-dimensional
A-scan : Depth-resolved intensity profile
BEWE : Basic Erosive Wear Index
D : Decay of intensity
db : Decibel
FE-SEM : Field emission scanning electron microscopy
f : Fractional change
HA : Hydroxyapatite
I : OCT backscattered intensity
I5 : Intensity at a depth of 5 micrometers from tooth-air interface
I11 : Intensity at a depth of 11 micrometers from tooth-air interface
I23 : Intensity at a depth of 23 micrometers from tooth-air interface
I58 : Intensity at a depth of 58 micrometers from tooth-air interface
MR1 : Proportion of profile peaks
MR2 : Proportion of profile valleys
Micro-CT : Micro-computed tomography
OCT : Optical coherence tomography
R : Integrated intensity
Ra : Average roughness
Rk : Core roughness
Rpk : Peak roughness
Rvk : Valley roughness
RaL : Average roughness measured by 5 measurement lines
Ra1 : Average roughness measured by a single measurement area
Univers
ity of
Mala
ya

xxix
Ra5 : Average roughness measured by 5 measurement areas
ΔZ : Surface loss
Univers
ity of
Mala
ya

xxx
LIST OF APPENDICES
Appendix A: Classification of correlation coefficient……………………………... 311
Appendix B: Raw data of surface roughness measurements………………………. 312
Appendix C: Raw data for integrated intensity…………………………………….. 318
Appendix D: Raw data for integrated intensity in simulated intraoral conditions…. 322
Appendix E: Other research activities during candidature………………………… 324
Univers
ity of
Mala
ya
1
CHAPTER 1: INTRODUCTION
1.1 Background and research problem
Dental erosion has been defined as a chemical process that involves the dissolution
of enamel and dentine by acids not derived from bacteria when the surrounding aqueous
phase is undersaturated with respect to tooth mineral (Larsen, 1990). There is evidence
that the prevalence of erosion is growing steadily especially in younger age groups
(Jaeggi & Lussi, 2014). This could be associated with the increase in consumption of
dietary acids which are the main sources of extrinsic erosion (Lussi et al., 2004;
Moazzez et al., 2000). Intrinsic sources of erosion, on the other hand, include those
conditions or habits which expose the dentition to gastric acid by reflux or vomiting
(Johansson et al., 2012).
Initial exposure to acid results in a partial dissolution of mineral or early stage
surface softening (Arends & Tencate, 1981) reaching a few micrometers into enamel or
dentine (Cheng et al., 2009b; Finke et al., 2000; Vanuspong et al., 2002). At this stage,
these acid-softened tissues are remineralisable (Attin et al., 2000; Attin et al., 2001) but
also susceptible to mechanical wear or continued acid attack leading to irreversible
substance loss (Shellis & Addy, 2014; Wiegand et al., 2009) which may be a painful
experience for the patient and require extensive restorative treatment. Timely diagnosis
and appropriate preventive measures are therefore imperative in arresting and reversing
these early erosion lesions by non-operative means and contributing to a better quality
of life for the patient.
Diagnosis of dental erosion is currently limited to subjective interpretation of clinical
inspection because a tool for detection and specific quantification of dental erosion is
absent in routine clinical practice (Ganss & Lussi, 2006). Exposed dentine is diagnosed
on the basis of colour and luster differences from enamel and the diagnosis is not yet
Univers
ity of
Mala
ya

2
validated. In fact, it was found that the accuracy of the diagnosis of exposed dentine in
comparison to the histological findings was poor (Ganss et al., 2006). Accurate
diagnosis of exposed dentine is important for the therapeutic decision making in case of
erosion and for the assessment of progression rate (Ganss & Lussi, 2014).
Contrary to the popular belief, dentine is often exposed in the initial stages of
erosion for instance at the cervical area where the enamel covering is relatively thin
(Ganss et al., 2013) or in cases of cupped cusps in the coronal area (Ganss et al., 2014).
Moreover, gingival recession can also result in loss of cementum which makes the
exposed dentine surfaces prone to dentine erosion (West et al., 2014).Therefore, early
diagnosis of not only enamel erosion but also dentine erosion is imperative and dentine
too should be considered as an important target tissue for anti-erosion strategies (Ganss
et al., 2013).
The effects of anti-erosion strategies for dentine erosion have been investigated
previously (Poggio et al., 2017; Sales-Peres et al., 2007; Steiner-Oliveira et al., 2010).
However, these studies have been conducted mostly in the in vitro and in situ settings
and provide variable and to some extent inconclusive results (Canadian Advisory Board
on Dentin, 2003). This could be attributed to the lack of standardisation in the study
designs especially in terms of erosive parameters employed (Young & Tenuta, 2011).
Moreover, erosion is a multifactorial phenomenon (Lussi & Carvalho, 2014) and the
intraoral conditions, especially the interaction between the saliva and erosive agent or
treatment product is difficult to fully simulate extraorally. Hence, the results of the in
vitro and in situ studies are difficult to extrapolate and generalise to clinical situations.
Additionally, the histology of dentine erosion might differ under experimental or in
vivo conditions (Ganss et al., 2014). Likewise, the efficacy of interventions investigated
for dentine erosion might vary in experimental and clinical conditions. For example in
Univers
ity of
Mala
ya

3
vitro or in situ erosion in dentine results in the formation of a histological feature
marked by a demineralised layer of organic material on the surface (Ganss et al.,
2009b). The fate of this organic matrix is not clear clinically but as it can be digested by
collagenases (Ganss et al., 2004) and proteolytic enzymes (Schlueter et al., 2010), it can
be assumed that it does not survive in vivo (Ganss et al., 2014) and the anti-erosive
effect of fluoride was indeed found less in the absence of organic matrix (Ganss et al.,
2004). Therefore, it is increasingly important to evaluate the efficacies of treatment
modalities meant for treating early dentine erosion in clinical trials.
Clinical trials evaluating the anti-caries products are simpler as compared to those
evaluating the efficacy of anti-erosion products. The reason is that the efficacy of anti-
caries treatments can be confidently assessed in case of cavitated carious lesions. The
erosive wear facet, on the other hand, is characterised by overlapping of wear processes
clinically. Although the effect of erosion is mostly dominant (Addy & Shellis, 2006), it
is difficult to ascertain the degree to which the wear lesion was facilitated by erosion.
The interventions meant to reduce erosion would not be effective if administered for
lesions where erosion had played little or no role. The only cohort of patients where one
would be confident of involvement of erosion would be the patients with confirmed
gastroesophageal reflux disease. However, the erosive wear observed in such patients is
moderate to severe (Moazzez & Bartlett, 2014). For testing the efficacy of interventions
in reducing or preventing early dentine erosion, it would be more reasonable to recruit
patients with gingival recession. However, from an ethical viewpoint, the amount of
erosion induced would have to be clinically small and reversible (Huysmans et al.,
2011). Subsequently, instruments employed in such trials would have to be sensitive
enough to detect and monitor the subtle alterations associated with early
demineralisation over the period of therapy.
Univers
ity of
Mala
ya
4
Monitoring of early dentine erosion over the period of therapy is necessary to
investigate the efficacies of treatment products, ascertain whether therapy is required,
and for the decision making regarding the restoration of worn teeth (Ganss & Lussi,
2014). A suitable method for monitoring of erosion progression should allow for the
exact quantification of erosion. (Schlueter et al., 2005). Monitoring of erosion has
previously been attempted by comparison of sequential study casts or clinical
photographs over time. These methods although suitable for clinical decision making
regarding the restoration of erosive wear, are not sensitive enough to measure exactly
the small changes in surface loss over the period of therapy. Hence, they cannot be
applied for the assessment of effects of preventive measures or the rate of erosive wear
(Azzopardi et al., 2000). Likewise, the currently used tooth wear indices are not
sensitive enough to be employed for longitudinal monitoring of the effect of
interventions (Bardsley, 2008).
Additionally, review of the literature reveals that it is difficult to find an appropriate
method for longitudinal or in vivo assessment of early-stage dentine erosion. Firstly, the
currently used analytical methods in spite of many advantages could be invasive (such
as microradiography), involve destructive measurement effects (such as microhardness,
nanohardness) or require time-consuming sample preparation (such as scanning electron
microscopy, atomic force microscopy) and hence their use is mostly limited to in vitro
assessments. Secondly, the shrinkage-prone nature of exposed organic matrix of dentine
might limit the use of certain techniques (such as surface profilometry) for its
assessment. Finally, due to histological differences between the two tissues, most
methods while applicable for enamel assessment might not be suitable for dentine
assessment (Schlueter et al., 2011). Currently, transverse microradiography is
considered a gold standard technique for determination of mineral content for
assessment of demineralisation and remineralisation in vitro (Hamba et al., 2012).
Univers
ity of
Mala
ya
5
However, it is not suitable for in vivo assessments because of extended X-ray exposure
times and destructive sample preparation (Ganss et al., 2005) whereas longitudinal
microradiography was found to have limited applicability in studies of dentine erosion
(Ganss et al., 2009b).
The two quantitative methods most commonly used to assess dental erosion are
surface profilometry and microhardness (Schlueter et al., 2011). Surface microhardness
is suitable for the measurement of early enamel erosion (Attin, 2006), but not for
dentine erosion because the elastic nature of dentine causes the indentations to shrink
after indentation (Herkstroter et al., 1989). In addition to this, the need to be site-
specific in the indenting process as intertubular and peritubular dentine have distinctly
different hardness values (Kinney et al., 1996) makes surface nanohardness a time
consuming and a non-feasible method for longitudinal erosion study designs.
Profilometry has been used extensively for the assessment of dentine erosion and has
been employed to a limited extent in the in vivo settings (West et al., 1998; Whitehead
et al., 1997). The parameter commonly used for assessment for erosion with
profilometry is surface loss appearing as a step change between the sound and
demineralised surfaces. Although suitable for assessment of advanced stages, it might
not be applicable for initial stages of erosion which do not result in bulk surface loss.
Moreover, assessment of dentine erosion with profilometry (both contact and non-
contact profilometry) may not be accurate because of the organic component of dentine
which forms a layer on the surface of the eroded dentine and interferes with the mineral
loss measurement. Therefore, it has been recommended that organic matrix be removed
from the dentine samples before performing measurements with profilometry (Ganss et
al., 2009b; Ganss et al., 2007). Removal of organic matrix will make profilometry a
Univers
ity of
Mala
ya

6
destructive technique and render it non-suitable for application in longitudinal or in vivo
studies.
Surface roughness measurements with profilometry most commonly in the form of
roughness average (Ra) seem to be useful for assessing early erosion (Schlueter et al.,
2011) and bearing area curve parameters could yield extra information in this regard
(Field et al., 2013). However, this is poorly explored for early dentine erosion. If surface
roughness parameters could be validated for early dentine erosion assessment, then this
non-invasive technique can be applied for assessment of early dentine erosion in vitro
and in vivo studies. Moreover, this method could have the potential of being used to
validate the use of other non-invasive optical techniques.
Another sensitive technique suitable for longitudinal assessment of erosion involves
the quantification of minerals released from dental hard tissues as a result of erosion
process (Hjortsjo et al., 2009). However, the in vivo applicability of this method is
limited because the presence of salivary calcium can interfere with the analysis
(Schlueter et al., 2011).
Optical techniques are non-invasive and could be potentially applicable for clinical
monitoring of early dentine erosion. Quantitative light induced fluorescence while
validated for assessment of enamel demineralisation (Ablal et al., 2009; Chew et al.,
2014; Elton et al., 2009; Pretty et al., 2003, 2004) was found to have limited
applicability for dentine demineralisation (Banerjee & Boyde, 1998). An optical
reflectometer based on the principle of specular reflection measurement was
successfully used for the measurement of early enamel erosion (Carvalho et al., 2016;
Rakhmatullina et al., 2013; Rakhmatullina et al., 2011) but little is known about its
potential for the assessment of dentine erosion.
Univers
ity of
Mala
ya
7
Another non-invasive optical technique which has the potential of evaluating initial
stages of erosion because of its capability of measuring small dimensional changes on
tooth surfaces is optical coherence tomography (OCT) (Chan et al., 2014). While
validated for both early and advanced erosion in enamel (Austin et al., 2017; Chew et
al., 2014; Wilder-Smith et al., 2009), it has only been assessed for dentine erosion
recently (De Moraes et al., 2017). However, only the advanced dentine erosion after the
appearance of surface loss in the OCT images was assessed. Little is known about the
applicability of this method for assessment of early dentine erosion.
As noted above, the problem is that currently the clinical validation of anti-erosion
strategies for preventing early dentine erosion is lacking because of the non-availability
of an in vivo monitoring tool. Although OCT and surface roughness measurements with
profilometry seem to be suitable methods for this task, their sensitivity and potential for
monitoring early dentine erosion have not been investigated previously.
1.2 Research purpose and questions
In view of the research problem discussed immediately above, the purpose of this
thesis was to seek a non-invasive technique suitable for monitoring of early dentine
erosion progression with the ultimate aim of developing it into a tool for clinical trials
involving dentine erosion.
This research purpose was guided by the following research questions,
1. Can optical coherence tomography be used to detect and monitor early dentine
erosion progression?
2. Can surface roughness measurements with profilometry be used to detect and
monitor early dentine erosion progression?
Univers
ity of
Mala
ya

8
1.3 Aims and objectives
These research questions were investigated by the following aims,
Aim 1: To assess the potential of optical coherence tomography in monitoring the
progression of in vitro early dentine erosion
In order to achieve this aim, the research objectives were as follows;
1. To explore the potential of OCT for measuring early dentine erosion and the
quantum.
2. To identify an optimum outcome measure for measuring early dentine erosion.
3. To identify the detection threshold of OCT for measuring early dentine erosion.
4. To compare the OCT backscattered intensity changes of early eroded dentine
with ultrastructural changes.
Aim 2: To assess the potential of surface roughness as a method for longitudinally
measuring in vitro early dentine erosion in simulated intraoral conditions.
In order to achieve this aim, the research objectives were as follows;
1. To explore the use of surface roughness parameters for measuring early dentine
erosion in simulated intraoral conditions.
2. To identify the most sensitive surface roughness parameter for measuring early
dentine erosion in simulated intraoral conditions.
3. To identify the detection threshold of surface roughness parameters for
measuring early dentine erosion in simulated intraoral conditions.
4. To compare the changes of surface roughness parameters in early dentine
erosion with surface ultrastructural changes.
Univers
ity of
Mala
ya

9
Aim 3: To assess if optical coherence tomography is a sensitive tool to detect early
dentine erosion and monitor its progression in simulated intraoral conditions by
correlating OCT data with the surface roughness data.
In order to achieve this aim, the research objectives were as follows;
1. To explore the potential of OCT for measuring early dentine erosion and the
quantum in simulated intraoral conditions.
2. To identify the optimum outcome measure for measuring early dentine erosion
in simulated intraoral conditions.
3. To identify the detection threshold of OCT for early dentine erosion in simulated
intraoral conditions.
4. To compare the OCT backscattered intensity changes of early eroded dentine in
simulated intraoral conditions with surface ultrastructural changes.
5. To compare the OCT backscattered intensity changes of early eroded dentine in
simulated intraoral conditions with surface roughness measurements.
1.4 Significance and scope
This thesis sought to evaluate the suitability of OCT and surface roughness
measurements with profilometry for the longitudinal assessment of early dentine erosion
progression. As no previous study in the existing literature has sought to accomplish
this, the scope of this thesis is innovative. If these methods become available for
monitoring early dentine erosion progression non-invasively, this would enable the
testing of anti-erosion management strategies in clinical trials. It is hoped that it will
serve to eliminate the inevitable variability encountered in the in vitro and in situ study
designs and the efficacies of anti-erosion management strategies would then be assessed
Univers
ity of
Mala
ya

10
more accurately. Effective prevention of dentine erosion progression in the early stages
would save the patients from expensive and extensive restorative treatments.
Development of such an in vivo tool would therefore be a significant contribution to
scientific and clinical research.
A long term benefit would be the use of OCT as a chair-side diagnostic tool for
assessment of early dentine erosion. However, this would require further investigation
which is beyond the scope of this thesis.
1.5 Thesis structure
This thesis has 6 chapters and this chapter is the first. The general body of literature
relevant to this area of research is reviewed in depth in chapter 2 of this thesis. Chapters
3, 4 and 5 deal with the specific investigation of research aims 1, 2 and 3 respectively.
Chapter 6 summarises the most important conclusions drawn in relation to all aims and
includes recommendations for future research. The research framework of this study is
given in Figure 1.1.
Univers
ity of
Mala
ya

11
Figure 1.1: Research framework.
Univers
ity of
Mala
ya
12
CHAPTER 2: LITERATURE REVIEW
This chapter reviews the process of dental erosion and various etiological and risk
factors affecting its outcome. The challenges faced in the clinical assessment of dentine
erosion have been described. In the end, the most frequently employed tools for dental
erosion are presented and critically evaluated regarding their suitability for assessment
of early dentine erosion.
2.1 Process of dental erosion
2.1.1 Terminology and definitions
Erosive wear or erosive tooth wear is a term used to describe the progressive loss of
dental hard tissues by a combination of chemical and mechanical processes. The
mechanical processes are mainly abrasion and attrition. Abrasion is the mechanical
tooth wear resulting from interaction of teeth with other foreign materials, the most
common being tooth brushing. Attrition is the mechanical wear resulting from action of
opposing teeth. Erosion on the other hand refers to demineralisation of dental hard
tissues from chemical action of acids (Shellis & Addy, 2014). Sometimes, a fourth
process called abfraction is included in erosive tooth wear. Abfraction has been
described as the loss of tooth tissue by the stresses induced by abnormal occlusal
biomechanical loading on cervical enamel and dentine at a location away from loading
(Sarode & Sarode, 2013) . However due to lack of appropriate clinical evidence, it is
still considered very much as a theoretical concept (Michael et al., 2009).
It is important to note that tooth wear per se is actually a physiological process and
the term tooth wear would not always refer to pathological wear although it is very
challenging to draw a distinction between both (Schlueter et al., 2012). In fact, physical
Univers
ity of
Mala
ya

13
loss of tooth tissue takes place throughout the duration of a person’s life by erosion and
mechanical wear. For instance, tooth brushing when performed vigorously is the most
common cause of abrasion but it is also an indispensable part of oral health care regime
(Shellis & Addy, 2014). Moreover, consumption of less abrasive diet by Western
population has been considered a causative or exacerbating factor for many dental
problems due to failure of development of attritional occlusion (Kaifu et al., 2003).
Dental erosion by definition is a chemical process that involves the dissolution of
enamel and dentine by acids not derived from bacteria when the surrounding aqueous
phase is undersaturated with respect to tooth mineral (Larsen, 1990). The term
‘softening’ was first employed to describe the loss of structural integrity and mechanical
strength in dental hard tissues followed by acid attack (Koulourides, 1968). Dental
erosion was then described as the chemical process involving softening of enamel and
dentine and erosive wear as the accelerated, pathological wear of dental hard tissues
resulting from the combination of mechanical factors like abrasion and attrition with
softened enamel and dentine (Huysmans et al., 2011). However, tooth tissue loss can
also result exclusively in case of prolonged erosive challenges for instance as a result of
continued vomiting (Lussi & Carvalho, 2014) and is also achieved in experimental
models investigating erosion. Therefore, the term ‘erosion’ was later described as
having a softening phase as well as any surface loss resulting solely from the
continuation of erosive challenge without intervention of any mechanical forces (Shellis
et al., 2011).
From this discussion, it appears that dental erosion can be thought of having two
main phases: Early phase which has been termed as softening phase and a later phase
which involves surface loss due to prolonged acid challenge. This early stage surface
softening or superficial partial dissolution of mineral (Arends & Tencate, 1981) can
Univers
ity of
Mala
ya

14
reach a few micrometers into enamel or dentine (Cheng et al., 2009b; Finke et al.,
2000; Vanuspong et al., 2002). At this stage, this surface can be remineralised or
progress to irreversible tooth structure loss as a result of exposure to prolonged acid
challenge. Enamel softening has been investigated extensively (Cheng et al., 2009b;
Rios et al., 2006). However, limited data is available on softening stage of dentine
erosion.
In this thesis, the terms “dentine softening” and “early dentine erosion” will be used
interchangeably to describe the early stage softening of dentine and primary substance
loss induced by the action of acids before the occurrence of any tooth tissue loss causing
a step change between the eroded and reference areas of sample. The pathophysiology
of this phase will be discussed in more detail in the subsequent sections of the thesis.
2.1.2 Prevalence and incidence of erosion
There is some evidence that the presence of erosion is growing steadily in children.
The prevalence of erosion increased from the time of UK children’ dental health survey
in 1993 to a study involving 4-year old to 18-year-olds in 1996/1997 and a trend
towards a higher prevalence of erosion was observed in children aged 3.5 to 4.5 (Nunn
et al., 2003). Additionally, the prevalence of erosion was assessed in a sample of 987
preschool children (aged 2-5 years) and only primary maxillary incisors were examined.
It was found that 31% of children had evidence of erosion and 13% of children
exhibited dentine and/or pulpal involvement. (Al-Malik et al., 2002). 1,949 Preschoolers
(aged 3-5 years) were examined in China and 5.7% showed signs of erosion on their
primary maxillary incisors. 4.9% of children had their lesions confined to enamel and
0.9% showed involvement of dentine and/or pulp (Luo et al., 2005). More recently, it
was shown that out of 967 children (aged 3 - 4 years), 51.6% had at least one tooth
Univers
ity of
Mala
ya

15
affected by erosive tooth wear. However, 93.9% of lesions were confined to enamel. In
this study, palatal surfaces of upper incisors and occlusal surfaces of lower molar were
examined (Murakami et al., 2011). A higher dentine involvement was found in 5 year
old Irish children. Of the 202 children examined, 21% showed dentine involvement out
of a total of 47% children showing evidence of erosion in primary maxillary incisors.
Interestingly, an association of low-economic status and frequency of fruit squash and
carbonated drink consumption and dentine erosion was found (Harding et al., 2003).
Similarly, another study conducted in rural Switzerland showed that 48% of total 42
children (aged five to nine) showed dentine involvement. Another study examined 463
children (aged two to seven) and found that the prevalence of erosion increased with
increasing age and 13.2 % of children showed dentine involvement with an overall
prevalence of 32%. It is apparent that data from different studies is difficult to compare
because of different sample size and tooth surfaces examined.
Incidence data on tooth erosion among adolescents is rare. The progression of
erosion was assessed in 1308 adolescents at the age of 12 years and two years later. The
incidence of enamel and dentine lesions rose from 5% to 13% and 2% to 9% in two
years respectively. 12% of adolescents without any evidence of erosion developed this
condition in two years of time and a total of 27% of children developed new and
advanced lesions during the study period (Dugmore & Rock, 2003). Another
longitudinal study showed an increased erosion incidence of 24% over a period of 1.5
years with the increase in deep enamel or dentinal erosion from 1.8% to 13.3% (El Aidi
et al., 2008). In 55 adults (aged 26-30years and 46-55 years), the progression of erosion
was assessed over a period of 6 years and no active therapy was given although the
participants were informed about the risk of erosive tooth wear. The results indicated a
distinct progression of erosion on facial and occlusal surfaces. The incidence of occlusal
erosive lesion with dentine involvement rose from 3% to 8% and 8% to 26% in people
Univers
ity of
Mala
ya

16
aged 26-30 years and 46-50 years at the time of first examination (Lussi & Schaffner,
2000).
Dentine hypersensitivity is a common condition and current evidence supports that it
is tooth wear phenomenon (Addy, 2005). Epidemiological studies conducted on dentine
hypersensitivity provides variable data which ranges between 1.34% (Bamise et al.,
2007) to 98% (Chabanski et al., 1997). Interestingly, this prevalence was found to be
higher in patients with periodontal problems ranging from 60% to 98% possibly as a
result of gingival recession associated with periodontal disease, periodontal therapy or
surgery (Mantzourani & Sharma, 2013). Peak incidence of dentine hypersensitivity has
been reported to occur between third and fourth decade of life (Rees, 2000) and in
general, the prevalence of dentine sensitivity is higher in women as compared to men
(Splieth & Tachou, 2013) .
Review of the literature reveals that overall the prevalence data concerning erosion
are not homogeneous. However, a trend for more increasing rate of erosion in younger
age groups is clearly observed which can compromise the child’s dentition and may
require expansive and repeated restorations (Lussi et al., 2006). Therefore, there is a
need to minimise the risk of erosion by early diagnosis and appropriate therapy. The
comparison of different studies in terms of their outcomes is challenging because of the
different scoring systems, sample size and examiners employed in the studies (Jaeggi &
Lussi, 2014) and an immediate standardisation is required in this regard to render the
comparison of prevalence studies possible.
Univers
ity of
Mala
ya

17
2.1.3 Etiology of dental erosion
The etiology of dental erosion is conventionally categorised into extrinsic and
intrinsic factors (Johansson et al., 2012). Any of the acidic products that we consume in
the form of acidic drinks and foodstuff (Cheng et al., 2009a) are considered extrinsic
factors. Also included in this category are the inborn acids that are inhaled or consumed
as a result of regular and continued exposure to acidic environment such as by acid
factory workers (Amin et al., 2001; Johansson et al., 2005) or by professional wine
tasters (Mulic et al., 2011). These factors constitute occupational-related erosion.
Although less investigated, consumption of acidic medications (Bahal & Djemal, 2014;
Lussi et al., 2012) and use of low pH oral hygiene products (Pontefract et al., 2001;
Pretty et al., 2003) have also been known to cause erosion.
Intrinsic factors on the other hand include all those diseases and habits that expose
the teeth to the acidic stomach contents (Johansson et al., 2012). The destruction caused
by intrinsic factors would be expected to be severe as compared to that caused by
extrinsic erosion as the pH and titratability of gastric acid in higher than dietary acids
(Moazzez & Bartlett, 2014). The acid reaches the oral cavity by means of reflux,
recurrent vomiting or regurgitation. Intrinsic causes of somatic origin include
gastroesophageal reflux disease and alcohol consumption (Manarte et al., 2009) .
Pregnancy has also been associated with dental erosion mainly because of unusual
eating habits, vomiting and increased reflux (Moazzez & Bartlett, 2014). Eating
disorders of psychosomatic origin like anorexia nervosa and bulimia (Mehler &
Andersen, 2017) have also been liked to tooth erosion. Sometimes, erosion occurs
without any obvious identifiable cause and is known as Idiopathic erosion (Koch et al.,
2017). In this case an erosion-like pathology is observed as the result of exposure to
acids of unknown sources.
Univers
ity of
Mala
ya

18
Like dental caries, dental erosion is a multifactorial condition. In addition to the
etiological factors explained above, dental erosion results from cumulative interaction
of many other factors. These factors can be categorised as biological, chemical and
behavioral factors.
2.1.4 Chemical factors
Dietary acids are the most dominant cause of dental erosion especially in children
and adolescents (Murakami et al., 2011). The erosive potential of these acids is
modulated by certain parameters inherent to them. It is important to note that the pH of
the acidic drinks is not the only chemical factor determining their erosive potential and
many studies have shown the profound effect of titratable acidity, buffering capacity,
mineral content and calcium-chelation potential of the drinks on their erosive potential
(Jensdottir et al., 2005; West et al., 2001). All these factors constitute the chemical
factors affecting dental erosion.
The critical pH is the pH value at which the solution is just saturated with respect to
dental hard tissues and no dissolution or precipitation of mineral is expected to occur.
During an erosion challenge a solution comes in contact with dental hard tissues. If the
pH of the solution is less than critical pH, it will lead to dissolution of enamel or
dentine. Conversely, if the solution pH is higher than critical pH, it will result in the
precipitation of mineral. Therefore, pH is a crucial factor determining the erosive
potential of solutions (Dawes, 2003). However, it is important to know that unlike
caries, there is no fixed ‘critical pH’ value for erosion. In the case of dental caries, the
critical pH is calculated from the plaque which has a fixed amount of calcium and
phosphate, although it might still vary among individuals. Dental erosion however is the
dissolution of dental hard tissues in the absence of plaque. Hence the critical pH values
Univers
ity of
Mala
ya

19
of enamel and dentine as previously calculated from plaque for dental caries cannot be
extrapolated to erosion. For dental erosion, the pH of the erosive solution itself will
determine the degree of dissolution of tissues which will further depend on the
concentration of mineral constituents of the erosive solution (Lussi & Carvalho, 2014).
The erosive potential of sixty different agents was tested in a study and it was found that
the critical pH values ranged between 3.9 and 6.5 (Lussi et al., 2012). Below the pH of
3.9, erosion will take place irrespective of the mineral status of the solution although the
concentration of minerals is still expected to modulate the rate of dissolution (Lussi &
Carvalho, 2014).
The most important minerals in this context are calcium and phosphate. These salts
determine the erosive potential of acidic drinks by controlling their degree of saturation
with respect to tooth mineral. The dissolution of dental hard tissues will not occur when
the erosive agent is oversaturated with respect to tooth mineral. If it is slightly
undersaturated with respect to tooth mineral, superficial initial demineralisation will
occur until the levels of mineral increase in the fluid layer adjacent to dental hard
tissues. There will result in a local rise in pH and further demineralisation will not take
place. However, swishing of the drink by the patient will increase the dissolution
process because the renewal of ions will readily take place in the solution next to tooth
surface. The addition of calcium and phosphate has been known to decrease the erosive
potential of acidic drinks in dentine (Scaramucci et al., 2011). However, it is important
to understand that the erosion cannot be eliminated completely by the addition of these
salts and only its progression can be retarded to some extent (Lussi & Jaeggi, 2006).
Fluoride is known to form fluorapatite or fluorhydroxyapatite which is more resistant
to dissolution as compared to hydroxyapatite. Therefore, modification of erosive
potential of acidic beverages by addition of fluoride has also been investigated. It was
Univers
ity of
Mala
ya

20
found that fluoride was unable to reduce enamel erosion (Larsen & Richards, 2002). On
the other hand, a significant correlation between erosive potential of drinks and their
fluoride content was found (Mahoney et al., 2003) and it was concluded that in low
concentrations fluoride content of beverages might not exhibit any protection against
enamel softening because the erosion challenge induced by these drinks is severe
(Mahoney et al., 2003). High concentrations of fluoride may be detrimental for health
and thus cannot be added in drinks (Lussi & Jaeggi, 2006). Erosive mineral loss can be
inhibited by intensive fluoridation in erosion softened dentine (Ganss et al., 2001).
However, it was found that the presence of organic matrix is essential for the fluoride
treatment to be effective (Ganss et al., 2004).
In dentine, the chemical events leading to erosion are mainly similar but are rendered
more complex by the presence of organic matrix. The organic matrix once exposed has
been known to protect the dentine from dissolution. It prevents the demineralising agent
from penetrating deeper into the dentine and at the same time prevents the ions from
diffusing out. Degradation of this matrix would increase the demineralisation process. It
can be degraded by Matrix metalloproteinases (MMPs) that are proteolytic enzymes
present in saliva and dentine. Matrix metalloproteinase (MMP) inhibitors reduce the
degradation of organic matrix of dentine and hence reduce erosion in dentine (Buzalaf
et al., 2012b). The effect of adding green tea, a natural matrix metalloproteinase (MMP)
inhibitor in soft drinks was tested in a study and it was postulated that supplementation
of soft drinks with green tea extract might be a method to reduce their erosive potential
against dentine (Barbosa et al., 2011).
Another factor affecting the erosive potential is the chelating property of certain
acids. In this regard, citric acid being the main ingredient of acidic drinks should be
considered. Citric acid has the ability to directly attack the tooth surface by the
Univers
ity of
Mala
ya
21
production of hydrogen ions and also to bind with calcium through its anion. The H+ ion
binds with carbonate and/or phosphate resulting in dissolution of mineral. The citrate
anion indirectly promotes dissolution of minerals by forms complexes with calcium in
the saliva and reducing its degree of supersaturation with respect to tooth mineral or
directly promotes dissolution by removal of calcium from the crystals. Therefore, acids
with chelating properties like citric acid promote demineralisation through dual
mechanisms and as such are more detrimental to the tooth surfaces (Featherstone &
Lussi, 2006; Meurman & Ten Cate, 1996).
In addition, the ability of the acidic food or drink to adhere to the tooth surface and
its potential to be displaced by the film of saliva will also affect the overall erosive
potential (Lussi & Jaeggi, 2006). It was shown that various beverages differed in their
ability to stick to enamel surface which was calculated based on their thermodynamic
properties like surface tension and contact angle of liquid with tooth surface. (Ireland et
al., 1995). The beverages also differed in terms of their degree of displacement by the
saliva. The authors concluded that longer the fluid is in contact with the tooth surface,
the greater will be the intensity of the erosion challenge and drinks with greater ability
to stick to tooth surface as compared to saliva will not be displaced easily by the action
of saliva. Also important in this regard is the buffering capacity of the acidic food. The
higher the buffering capacity of an acidic food or beverage the greater will be the
dissolution because more mineral ions will be required to inactivate it and it will take
saliva longer to neutralise the acid. Different solutions have different buffering
capacities. For instance 124 mmol/l of base is needed to neutralise the pH of orange
juice in contrast to just 34 mmol/l of base required to raise the pH of degassed coca cola
(Zero & Lussi, 2005).
Univers
ity of
Mala
ya

22
In conclusion, the effect of all chemical factors must be taken into account while
determining the erosive potential of acidic drinks or food. It is felt that less work has
been done to explore the erosive potential of food stuff as compared to acidic drinks and
further work is required in this regard. Importantly, there is no fixed critical pH value
for dissolution of dental hard tissues in relation to process of erosion. Moreover, it is felt
that the reported values of these chemical factors in erosion protocols vary immensely
and an immediate standardisation is required in this regard to be able to compare the
findings of different erosion studies.
2.1.5 Biological factors
The biological factors affecting erosion include saliva, acquired pellicle, type and
structure of dental substrate, dental and oral anatomy, occlusion and physiological tooth
movements (Hara et al., 2006b).
2.1.5.1 Saliva
Saliva is the most important biological factor because of its ability to dilute,
neutralise and remove the acids from the oral cavity, form dental pellicle, slow down the
demineralisation and enhance remineralisation with its organic and inorganic
components (Meurman & Ten Cate, 1996). The extent to which saliva modulates the
process of erosion can be judged by the reduction of enamel erosion by the order of 10
times in an in situ study as compared to its similar in vitro counterpart (West et al.,
1998). Also important is the association of low salivary flow rate (Alghilan et al., 2015)
and low buffering capacity (Lussi & Schaffner, 2000) with increased erosion.
Univers
ity of
Mala
ya
23
Before the erosion challenge, the salivary flow is increased by the sight and smell of
food (Keesman et al., 2016). With the increased salivary flow, a favorable environment
is created for prevention and minimisation of initial erosion attack by the increase in
organic and inorganic components of saliva. Inorganic components include calcium and
phosphate which are responsible for maintaining tooth mineral integrity and bicarbonate
ion or hydrogen carbonate is responsible for the buffering capacity of saliva (Buzalaf et
al., 2012a).
Erosive challenge in the form of acidic foodstuff or drinks entering the oral cavity
further increases the salivary flow and output. Three droplets of 4% citric acid applied
to the tongue every 5 minutes increased the salivary flow rate to about 1.87 ml/min
which was significantly higher than unstimulated salivary flow rate of 0.3ml/min
(Engelen et al., 2003). Other factors associated with the salivary flow rate are
mastication (Yeh et al., 2000), stimulation of the mechanoreceptive neurons in gingiva
(Inenaga et al., 2009) and variation in salivary secretion by different salivary glands
(Engelen et al., 2003). Increase in salivary flow rate enhances its ability to neutralise
and remove the acid challenge from the oral cavity and increases its buffering capacity
as the amount of bicarbonate ions in the saliva increases (Lussi & Schaffner, 2000).
Of all the salivary parameters mentioned above, only its flow rate and buffering
capacity have been directly associated with the process of erosion (Zero & Lussi, 2005).
Therefore, the tests for measuring stimulated and unstimulated salivary flow rates and
buffering capacity of saliva are indicators of susceptibility of individuals to dental
erosion (Hara et al., 2006b). The organic components of saliva include various proteins
and glycoproteins and their main role in the process of erosion is exerted through the
formation of pellicle.
Univers
ity of
Mala
ya

24
2.1.5.2 Pellicle
The salivary pellicle is a protein based bacteria-free layer readily formed on the tooth
surfaces after its removal by tooth brushing with dentifrice, chemical dissolution or
prophylaxis (Hara et al., 2006b). It is composed of mucins, glycoproteins and proteins
including several enzymes (Hannig et al., 2005). It was shown that this layer forms in
two distinct stages. The initial stage was detectable after only 2 - 3 minutes after being
exposed to the environment of oral cavity and 30 minutes later reached a thickness 3
times greater as compared to the initial thickness and was maintained for the next 10
hours (Skjorland et al., 1995).
The protection of enamel against erosion by pellicle formation has been investigated
many times (Hannig et al., 2004; Nekrashevych et al., 2004). Only limited data is
available for its effects on dentine erosion and due to differences in composition and
histology of both tissues, protective effect of pellicle might differ for both tissues. The
protective effect of saliva was found greater for enamel erosion as compared to dentine
erosion in an in situ study conducted over a period of 14 days and the protective effect
of pellicle formed in situ was greater for both tissues as compared to that offered by in
vitro storage in saliva (Hall et al., 1999). It was found that the pellicle formed in situ for
120 minutes on dentine eroded for 5 minutes with HCL (pH 2.3) provided limited
protection. Although, it resulted in significantly reduced calcium loss in pellicle coated
dentine samples however thickness of demineralised dentinal surface was similar in
pellicle-coated and pellicle-free dentine samples. (Hannig et al., 2007). In contrast to
this, pellicle formed for two hours was not effective in reducing dentine softening
induced by orange juice (pH = 3.8) for 10, 20 and 30 minutes (Hara et al., 2006a).
The pellicle provides protection against enamel erosion by acting as a diffusion
barrier or a perm-selective membrane thus preventing the contact between tooth surface
Univers
ity of
Mala
ya

25
and acids (Hannig & Balz, 2001) which results in dissolution of hydroxyapatite
(Lendenmann et al., 2000). In dentine, however it was suggested that dentinal pellicle
works like an ion permeable membrane rather than a barrier (Hannig et al., 2007).
Dentine is more soluble and porous than enamel and therefore demineralises at a faster
rate and this prevents the pellicle from acting as a diffusion barrier. It was suggested
that perhaps protective effect of pellicle for dentine could be enhanced by allowing the
pellicle to mature for longer periods of time (Hara et al., 2006a) which will increase its
acid-resistance by the structural modelling with enzymes (Hannig et al., 2005; Yao et
al., 2001).
To summarise, saliva is the most important biological factor affecting the
progression of erosion (Figure 2.1) and enhancement of its protective effects can be
utilised for the prevention and retardation of the process of erosion in cases of mild
erosion challenges. The protective effect of pellicle on enamel erosion is established but
further investigation is required for dentine erosion in this regard. Information gained
from in vitro and in situ studies seems to be contradicting and should be verified
through clinical trials. This will only be possible with the development of non-invasive
tools which can be employed in clinical trials.
Univers
ity of
Mala
ya

26
Figure 2.1: Salivary factors associated with the control of dental erosion in enamel and
dentine (Buzalaf et al., 2012a).
2.1.6 Behavioral factors
Behavioral factors also play a vital role in modulating the process of erosion during
and after and erosion challenge. The most important factors to be considered in this
regard are those habits or lifestyles that increase the contact time of acidic food or
drinks with the tooth surface predisposing it to demineralisation. Excessive and frequent
consumption of soft drinks (Johansson et al., 2002), acidic food juices (Kunzel et al.,
2000) and acidic candies (Carvalho et al., 2017) are included in this category (Kunzel
et al., 2000). The manner in which acidic food is consumed such as by swallowing,
gulping and whether or not a straw is employed will determine which teeth come in
contact with the acidic challenge and also affect the clearance of acidic food / drinks
from the oral cavity (Cheng et al., 2009a; Zero & Lussi, 2006). In addition, the habit of
holding drink in the mouth lowering the pH (Johansson et al., 2004) and drinking acidic
beverages at night when salivary flow is absent (Hamasha et al., 2014) can increase the
risk for erosion.
Healthier lifestyle choices involve regular exercise and consumption of more fruits
and vegetables. Exercise though beneficial for the overall health can increase the risk of
dental erosion (Zero & Lussi, 2006). For instance athletes may be prone to risk of dental
erosion because of frequent consumption of acidic sports drinks, fruit juices and other
carbonated and uncarbonated acidic drinks led by increased energy demands in an
overall dehydrated state with low salivary flow rate (Sirimaharaj et al., 2002). Vigorous
exercise can also induce gastroesophageal reflux in normal subjects (Herregods et al.,
2016). Healthy diets contain more fruits and vegetables. A lactovegetarian diet
Univers
ity of
Mala
ya

27
containing acidic foods has been associated with dental erosion (Staufenbiel et al.,
2015). On the other hand, unhealthy food choices can also cause dental erosion. For
instance, excessive alcohol consumption (Manarte et al., 2009) and use of illegal
designer drugs like ‘ecstasy’ (3,4-methylenedioxy-methamphetamine) have been
associated with dental erosion (Brand et al., 2008).
To summarise, it appears that several habits or lifestyle choices may contribute
significantly to increasing the risk for erosion. Changes in lifestyles via patient
education would be necessary to prevent and retard the progression of dental erosion.
Therefore, it is important for the clinicians to have a thorough understanding of these
factors for appropriate treatment planning. Moreover, there is a need to take into
account the various behavioural factors affecting erosion like those related to drinking
habits of individuals, while designing erosion protocols and interpreting of outcomes.
2.1.7 Structural and histopathological aspects of dentine erosion
Dentine is mainly composed of bulk dentine and dentinal tubules. Bulk dentine is in
turn composed of peritubular and intertubular dentine. The peritubular dentine
surrounds the dentinal tubules and intertubular dentine. The intertubular dentine is
further composed of collagen fibrils and interfibrillar compartments. (Zijp & Bosch,
1993). The peritubular dentine is more mineralised (at least 40%) (Gulabivala & Ng,
2014) and harder than intertubular dentine (Kinney et al., 1996).
Enamel and dentine are different in terms of structure and composition. Dentine is
softer and less brittle than enamel (Scheid & Weiss, 2012). The inorganic component of
dentine is lower (45 vol%), organic component is higher (33 vol%) and amount of
water is considerably higher than enamel (by 22vol%) (Nanci & Cate, 2008). The
Univers
ity of
Mala
ya

28
mineral component in dentine exists in the form of a non-stoichiometric hydroxyapatite
(Ganss et al., 2014) but these crystals are smaller in size in dentine (50 nm x 20 nm x
5nm) as compared to enamel where the crystals are 10 times larger (Abou Neel et al.,
2016). Because of the smaller size and greater solubility of these crystals, the dentine
crystals are dissolved over a shorter distance leaving a narrow zone of partially
demineralised dentine between the demineralised dentine and the sound dentine
(Amaechi, 2015).
When enamel is exposed to an erosive agent, the mineral is partially dissolved and
the roughness of enamel surfaces is increased (Nekrashevych & Stosser, 2003). The
surface structure of eroded enamel closely resembles typical etching pattern
(Eisenburger et al., 2004). This etched or partially demineralised surface is marked by
reduced hardness and is called the early stage softening of erosion (Arends & Tencate,
1981). The loss of hardness progresses with continued acid exposure and makes enamel
susceptible to physical wear (Wiegand et al., 2007) .
When the dentine is exposed to acids, the mineral component of peritubular and
intertubular area is readily dissolved while the organic portion remains intact (Lussi et
al., 2011). Initially the mineral loss occurs at the border between the peritubular and
intertubular dentine. The peritubular dentine is lost and the diameter of dentinal tubules
increases. Subsequently, the intertubular dentine demineralises with the exposure of
organic matrix (Schlueter et al., 2011). Initially, the peritubular and intertubular dentine
recede at comparable rates. However, after the first minute, the intertubular dentine
recedes more slowly while the peritubular dentine continues to dissolve at a linear rate
(Kinney et al., 1995). The demineralised dentine appears rougher at this stage as
compared to the sound dentine (Toledano et al., 2014).
Univers
ity of
Mala
ya

29
It appears that organic matrix is already exposed in early stages of dentine erosion.
Dentine was etched with low pH citric acid and maleic acid (pH 0.7, 1.4) for 30 seconds
and it was found that it resulted in exposure of the complex dentine collagen fibril
network mixed with crystals and debris particularly on the peritubular and intertubular
dentine. (Breschi et al., 2002). The thickness of this organic matrix increases with
increasing erosion time and eventually a fully demineralised zone of collagen matrix
appears. Immediately below this zone of collagen matrix partially demineralised dentine
of roughly constant mineral density is present until sound or fully demineralised dentine
is reached (Kinney et al., 1995). However, this partially demineralised zone is not
always present (Lussi et al., 2011).
This organic matrix has a few important properties in relation to dentine erosion
(Ganss et al., 2014). Firstly, when it reaches a specific thickness, all chemical processes
become diffusion controlled and the process of demineralisation is retarded (Ganss et
al., 2009b; Hara et al., 2005). Secondly, organic matrix is resistant to abrasive forces
(Ganss et al., 2007). Finally, the presence of this organic matrix might interfere with the
quantification of mineral loss in dentine (Schlueter et al., 2011). The level of this
organic tissue remains at the same level as that of adjacent sound tissue as long as it is
kept hydrated but rapidly undergoes shrinkage when exposed to air (Ganss et al., 2007).
Importantly, the histology of dentine erosion in the oral cavity is not clearly
understood. Clinically, dentinal lesions appear hard and shiny but in vitro experiments
show they are resilient and dull. The fate of the organic matrix in vivo is also unclear. It
is assumed because of the presence of proteolytic enzymes (Schlueter et al., 2010) and
collagenases (Tjaderhane et al., 2015) in the oral cavity, organic matrix is digested as
soon as the mineral is dissolved and does not survive. In the absence of organic matrix,
Univers
ity of
Mala
ya

30
the erosion process in dentine would also be surface controlled rather diffusion
controlled. (Ganss et al., 2014).
In short, dentine erosion is different from enamel erosion histologically. Exposure of
dentine to acids result in loss of mineral while organic matrix persists on the surface
leading to formation of a three-zoned tissue with demineralised layer on the surface,
partially demineralised dentine in the middle and sound dentine on the inner side.
Unlike enamel, there is no bulk surface loss in dentine (Ganss et al., 2009b). As a
result, the analytical methods which are applicable for assessment of enamel might not
be suitable for dentine erosion (Schlueter et al., 2011) and will need to be re-assessed
for dentine. The complex histology of dentine and in particular the clinical outcome of
organic matrix needs to be investigated further through clinical studies.
2.2 Clinical assessment
2.2.1 Diagnosis
Early diagnosis of dental erosion is important. To date a clinical device for definitive
diagnosis of dental erosion is lacking in routine clinical practice. Therefore, dentists are
fully dependent on the recognition of clinical appearance for the diagnosis of dental
erosion. Most dentists count the early changes of erosive tooth wear a part of the
physiological process occurring within normal limits and do not start any preventive
therapy at this stage. Consequently, the erosive wear is allowed to progress and is only
diagnosed in later stages when the irreversible tissue loss has occurred and altered the
appearance of the teeth. The ‘early’ signs of erosive wear include smooth silky-glazed
sometimes dull appearing enamel, presence of intact enamel along the gingival margin
and change in color, cupping and grooving on occlusal surfaces. However it is
important to note that by the time these signs become apparent, some tissue loss has
Univers
ity of
Mala
ya

31
already taken place. (Lussi & Carvalho, 2014). Moreover, it is difficult to determine the
exact cause of tooth wear (erosion, abrasion or attrition) which is important from the
view point of timely delivery of preventive measures required to retard the progression
of this condition.
It is very challenging to determine if dentine is exposed or not (Ganss et al., 2006)
and it is important to note that dentine is often exposed in the initial stages of erosion
for instance at the cervical area where the enamel covering is relatively thin (Ganss et
al., 2013) or in cases of cupped cusps in the coronal area (Ganss et al., 2014). The
exposed dentine has a yellowish or brownish appearance and is different from enamel in
terms of luster (Ganss et al., 2006). In the root area, the dentine is exposed by gingival
recession followed by loss of cementum. It was previously found that even the earliest
detectable exposures of root dentine were devoid of cementum (Bevenius et al., 1994)
which suggests that cementum is lost rapidly after root exposure occurs. Causes of
gingival recession include vigorous tooth brushing with improper tooth brushing
technique, periodontal diseases or its treatment (Jati et al., 2016) .
The effect of extrinsic acids from dietary and environmental sources on the dentine
surface would be to initiate and localise dentine hypersensitivity (West et al., 2014)
which might be the first clinical symptom experienced by the patient. Erosion and
gingival recession were found to be the most common causes of dentine hypersensitivity
(Canadian Advisory Board on Dentin, 2003). The exposed dentine either has open
dentinal tubules or is covered by a smear layer composed of oral debris such as calcium
or toothpaste ingredients (West et al., 2014). Removal of this smear layer can take place
by the action of acidic dietary compounds containing organic acids and is accelerated
with brushing after the exposure of dentine to dietary acids (Pinto et al., 2010) . The
progression of dentine erosion can be retarded by institution of appropriate preventive
Univers
ity of
Mala
ya
32
therapy at this stage. However if the erosion process is allowed to proceed it will result
in irreversible mineral loss and require expansive rehabilitation procedures.
It should be borne in mind that dental erosion is a multifactorial condition and a
thorough knowledge of the etiological and risk factors affecting it would be essential for
definitive diagnosis of this condition. Complete diagnosis would therefore require a
though history of the patient with respect to general health, diet, habits, lifestyle,
occupation along with assessment of salivary quantity and quality (Ganss & Lussi,
2006). Moreover, timely diagnosis of not only enamel but also dentine is essential to
arrest the progression of erosive wear by the appropriate preventive measures.
2.2.2 Indices
An ideal index is the one which is simple to understand and use, is clear in its scoring
criteria and is demonstrably reproducible. Over the years many indices have been
introduced for the epidemiological and clinical assessment of erosive wear (Bardsley,
2008). Most of these indices originated from indices published by Eccles (Eccles, 1979)
and Smith and Knight (Smith & Knight, 1984) and combine both qualitative and
quantitative criteria for scoring.
The original index of Eccles classified lesions as early, small and advanced thus
allowing room for wide interpretation (Eccles, 1978). However, later this index was
expanded and description of the grading criteria was included (Eccles, 1979). This idea
was taken one step further and a tooth wear index was proposed to measure and monitor
multifactorial tooth wear. (Smith & Knight, 1984) It was a comprehensive scoring
method which allowed for the scoring of all four visible surfaces (buccal, cervical,
lingual and occlusal-incisal). However, the etiology of wear was not taken into
Univers
ity of
Mala
ya
33
consideration in this index. This tooth wear index was modified to study erosive wear in
the primary and young secondary dentitions (Millward et al., 1994). The cervical
surfaces were not included in the scoring. Later, a qualitative scoring method with listed
diagnostic criteria and a four-scale grading of severity of erosion related to degree of
dentine involvement was introduced (Linkosalo & Markkanen, 1985) This index was
later modified to score labial, lingual and occlusal surfaces of all teeth except the third
molars (Lussi et al., 1991) It is important to remember that indices have been mainly
used as part of epidemiological studies to evaluate prevalence of erosive wear in
population samples rather than for individual assessment (Azzopardi et al., 2000).
Most indices include the diagnostic criteria of quantification of hard tissue loss as
well as the differentiation of dental erosion from abrasion and attrition. Mainly two
criteria are employed for the estimation of tissue loss. The size of the area affected is
calculated in proportion to the sound surface and the depth of defect is estimated by the
criterion of dentine being affected or not. In this way the dentine exposure becomes
related to the tissue loss which might not be always be true as dentine could be exposed
in early stages of erosion. Moreover, the visual assessment of exposed dentine can
prove to be challenging as changes in anatomical form, luster or color assumed to be
easily seen makes this criterion yet to be validated (Ganss & Lussi, 2014). The accuracy
and consistency of visual diagnosis of exposed dentine was investigated (Ganss et al.,
2006). The authors found that the accuracy of the diagnosis of exposed dentine (in
comparison to the histological findings) was poor. Only 65% of areas with exposed
dentine, 88 % of areas with enamel present and 67% of all areas examined had been
diagnosed correctly. Moreover, dentine exposure was not related to significant amounts
of tissue loss. This finding was also found in another study involving primary teeth (Al-
Malik et al., 2001). Dentine was exposed in all cases of cupping or grooving if only
minor tissue loss had occurred. This would suggest that dentine is involved in initial
Univers
ity of
Mala
ya

34
stages of erosion and if cupping is related to dentinal exposure the current grading of
early and advanced occlusal lesions have to be revised. Also, the criterion of ‘dentine
affected or not’ should be reassessed keeping in view the problems encountered in
diagnosing exposed dentine correctly. It is important to note that diagnosing exposed
dentine is important for therapeutic approach in case of erosion or as a prognostic factor
with respect to the progression of wear.
To address these issues, another system for scoring ‘Basic Erosive Wear Index’ was
introduced (Bartlett et al., 2008). It was designed to grade the lesions irrespective of
whether and to what extent the dentine was exposed and aimed to provide a simple
scoring method for use in general practice. In each sextant, the most severely affected
surface is recorded with a four level score. The cumulative score is then associated with
the clinical management of the condition. This index allows the comparison of the
studies and it is hoped that in time it will lead to the development of an internationally
accepted and standardised index.
To summarise, it appears that to date there is no single index which is sensitive
enough to be employed for the clinical staging and longitudinal monitoring of dental
erosion and erosive wear. Moreover, there is a need to regulate the use of these indices
to allow for the comparison between different study-outcomes.
2.2.3 Assessment of progression rate
The clinical signs of erosion progression include frosty appearance and absence of
extrinsic staining. Clinical monitoring of erosion progression is important for
ascertaining the need for treatment, to test the efficacy of preventive measures and/or
Univers
ity of
Mala
ya

35
treatment products and for the decision making regarding the restoration of worn teeth
(Ganss & Lussi, 2014).
A suitable method for monitoring of erosion progression should firstly allow for the
exact quantification of erosion. As the amount of tissue loss that can be induced
clinically should be reversible and small, so the method should be sensitive enough to
measure it. In addition, it should be simple to perform and cost effective (Schlueter et
al., 2005).
One of the challenges of quantification of erosive loss over time is the absence of
stable reference areas as the references areas chosen on tooth surface are liable to
undergo changes with time. The macroscopic estimation of erosion progression has
been performed by usingsequential study casts and photographs. These methods
although inaccurate are sufficient for assisting in clinical decision making regarding the
restoration of erosive wear. However, they are not sensitive enough to measure the
small changes in erosive loss and cannot be applied for the assessment of efficacy of
preventive measures or to assess the rate of erosive wear (Azzopardi et al., 2000).
Moreover, they may be difficult to apply in general dental practice (Bartlett et al.,
2005).
For the quantification of tooth tissue loss, optical methods which generate and
superimpose images of consecutive study casts, surface mapping methods which
generate superimposed 3 D images by usingnull contact stylus Profiler (Pesun et al.,
2000) or 3-D optical scanner (Dai et al., 2015) and electroconductive replicas
(Chadwick & Mitchell, 2001) have been used. These methods are however time
consuming and require extensive equipment. To resolve this issue, a simple approach of
using metal markers on the tooth surface to act as reference areas for profilometric
measurements was used (Schlueter et al., 2005) It was later applied in a clinical trial
Univers
ity of
Mala
ya

36
(Sundaram et al., 2007) to assess the efficacy of bonding agent on dentine wear.
Although this method measured the wear difference between control and resin-coated
dentine surface but it was complicated by the loss of metal discs and changing control
surface height.
All these methods of monitoring erosion employ study casts which are less accurate
and time consuming. Therefore, a non-invasive method which could be applied directly
in the oral cavity would be ideal. Optical coherence tomography and ultrasound are non-
invasive techniques and might prove to be useful in this regard (Ganss & Lussi, 2014).
2.3 Assessment techniques of dentine erosion
Dental erosion can be thought of having two main phases: The early phase which is
marked by softening and later phase which is characterised by the tissue loss resulting
from continued acid exposure resulting in a step change. The choice of the method for
assessment of erosion would be mainly guided by the phase of erosion and the dental
hard tissue being investigated. Over the years many techniques have been introduced for
the assessment of dental erosion. This section will provide an overview of the most
frequently applied methods for investigation of dental erosion and special emphasis will
be placed on their suitability for investigation of dentine erosion particularly the erosion
softening stage.
2.3.1 Quantitative assessment
2.3.1.1 Surface microhardness
Surface microhardness has been extensively used for the assessment of dental
erosion. The effect of an erosive agent would be to cause the tooth substance to get
Univers
ity of
Mala
ya

37
softened or lose its hardness. An indentation made in the softened tissue will easily
penetrate it and reach a greater length as compared to the sound tissue. Using this
principle, an indent is made by microhardness diamond tip in enamel or dentine. Two
types of indenters namely Knop hardness with a rhomboidal shape and Vickers indenter
with a tetra-pyramidal shape can be employed for this purpose. Knoop indenter is
considered more sensitive to early changes of erosion. After making an indentation, the
degree of hardness is then calculated by the length and load of the indentation
(Schlueter et al., 2011) Hardness has been shown to correlate very well with the loss of
mineral induced by the processes of demineralisation (Lippert & Lynch, 2014). Apart
from its usefulness in assessment of erosion softening stage, microhardness has also
been employed for the differentiation of erosion potential of erosion causing beverages
(Lussi et al., 2000).
Microhardness may have a potential of being used for in vivo assessments. The accuracy
of using microhardness on natural surfaces could be limited as flat and polished surfaces
have been recommended for finer indents (Schlueter et al., 2011). Microhardness was
successfully used for assessment of natural surfaces recently. However, the tests were
performed on incisors which have a relatively flatter profile as compared to other teeth
(Chew et al., 2014).
Microhardness is a gold standard assessment technique for the investigation of softening
stage of enamel (Shellis et al., 2011) and was able to detect enamel erosion after a few
minutes of erosion challenge (Hara et al., 2006a). Dentine as opposed to enamel is a
highly elastic tissue. The indentations made in demineralised dentine with a load of 500
gram for 10 seconds were unstable and reversed by about 30% within the first 24 hours
(Herkstroter et al., 1989). Therefore, it has been recommended that indentations in
dentine be measured after 24 hours for the indentations applied with forces as high as
Univers
ity of
Mala
ya

38
500 grams. However, this arrangement would not be feasible for longitudinal study
designs where the measurements may have to be repeated within 24 hours depending on
the study protocol. For lower forces, no clear cut instructions have been given. This
indicates that microhardness might have limited applicability in assessment of early
dentine erosion.
2.3.1.2 Nanohardness
Nanohardness uses the same principle of indentation as microhardness but at a
smaller scale. It typically employs a Berkovich diamond tip which can apply smaller
loads in order of nanonewtons to millinewtons. A load is applied to the substrate which
is being investigated. The substrate is then allowed to relax by reducing the load slowly.
A displacement or load curve is then generated by the continuous measurement of load
and displacement throughout this process. This curve then gives information about
various mechanical properties of that substrate (Attin & Wegehaupt, 2014; Schlueter et
al., 2011).
The ability of nanohardness to create nano-scale indentation makes it a very sensitive
tool. This suggests its applicability in assessment of softening stage of erosion in
enamel and dentine. It can measure hardness, fracture toughness, Young’s modulus,
creep and energy of the test substrate. For the erosion studies, parameters of importance
would be hardness and young’s module of elasticity. Young’s modulus has been
claimed to be a more sensitive parameter than hardness (Attin & Wegehaupt, 2014;
Barbour & Rees, 2004; Schlueter et al., 2011) and might be useful in assessment of
softening stage of erosion. In enamel, it has been reported to detect erosion only after
two seconds of erosion challenge (White et al., 2010).
Univers
ity of
Mala
ya

39
Nanohardness seems to be a more suitable tool than microhardness for assessment of
dentine erosion. Dentine has a complex structure composed of microstructures and each
component has a distinct hardness and elastic modulus value. The size of microhardness
indenter is larger than microstructures of dentine and so it gives only a composite
average of hardness and elastic properties of peritubular dentine, intertubular dentine
and tubular orifices. Nanohardness, because of its smaller size can allow the
measurement of properties of peritubular and intertubular dentine separately rather than
giving only a composite average. This gives a more accurate picture of material
properties of dentine as it eliminates the possibility of competing effects of tubular
morphology and density (Kinney et al., 1996).
However, as each microstructure of dentine has a distinct hardness value, the indent
has to be made at the same component at every measurement. This is especially
important if several measurements are to be taken for instance in a longitudinal study
design. Therefore, for visual control, a combination of atomic force microscopy and
nanoindentation has been proposed for visual control (Schlueter et al., 2011). With
nanohardness, dentine can be measured in hydrated conditions which is an added
advantage (Angker & Swain, 2006). Moreover, nanohardness has the ability to be used
on unpolished, native surfaces and so might have the potential of being employed in the
in vivo conditions (Attin & Wegehaupt, 2014; Schlueter et al., 2011). However, the need
to indent specifically at the same dentinal component repeatedly would be time-
consuming and non-feasible for longitudinal studies.
2.3.1.3 Surface profilometry
Surface profilometry has become the standard technique for quantification of tissue loss
in erosion-related research. After being established for use in in vitro and in situ erosion
Univers
ity of
Mala
ya

40
studies, it was further adopted for in vivo research (Pintado et al., 1997; Sundaram et al.,
2007). With profilometry, the advanced stages of erosion can be quantified by
measuring loss of dental hard tissue between treated and non-treated areas or early
stages of erosion could be assessed by means of surface roughness parameters
(Schlueter et al., 2011).
A two or three dimensional profile of the specimen is generated by using a contact or
non-contact measuring device. Contact stylus profilometry is an older and more
established technique which measures the tissue loss directly by traversing the surface
with a diamond or steel tipped stylus. The advantage of using this technique is the large
vertical range (2 to 250 µm) which becomes possible because of the intimate contact of
the stylus with the tissue (Field et al., 2010). However, the stylus can also damage the
surface of the specimen by producing scratches as deep as 10-25 nm as measured
previously by atomic force microscopy (Beyer et al., 2012). This disadvantage of
contact profilometer can be overcome by using non-contact profilometers. Non-contact
profilometry uses coaxial white light to perform the measurements instead of a contact
stylus. A light spot typically below 100 µm diameter is directed at the specimen surface.
The surface is profiled by measuring the deflection of light spot on CCD camera by
using triangulation sensor or the profile is recorded by using confocal principle (white
light) (Rodriguez et al., 2009). The vertical range for white light profilometry varies
from 300 µm to 10 mm. With this vertical range, measurement of deep erosion pits and
curved natural surfaces is possible. However flattening of samples increases the
sensitivity and accuracy of measurements. (Schlueter et al., 2011). Using flat samples,
tissue loss of about 0.5 µm could be consistently measured with profilometry (Hara &
Zero, 2008; Hooper et al., 2003).
Univers
ity of
Mala
ya
41
Profilometry has been used in combination with ultrasonication to measure the depth
of softening of enamel (Eisenburger et al., 2000) and dentine (Vanuspong et al., 2002).
The softened enamel surface was removed with ultrasonication and the resulting lesion
depth was measured with profilometry. The same methodology was later applied for
assessment of softening of dentine (Vanuspong et al., 2002) and it was found that
softening zone for dentine was thinner and plateaued in depth at approximately 2 µm at
similar exposure time for enamel (two hours). Interestingly, it was more resistant to
removal and required an extended periods of time of ultrasonication as compared to
enamel. The depth of softening varied with the pH of the citric acid employed.
Softening produced by two hours of erosion increased to 2 µm from pH 2.54 to pH 3.2
and decreased at higher pH values after that. Using similar methodology, it was shown
that this softened zone was susceptible to removal by abrasive action of tongue (Gregg
et al., 2004).
Profilometry has been thoroughly validated for assessment of enamel erosion (Ganss
et al., 2005) and has been used as a gold-standard method for comparison of other
techniques (Hall et al., 1997). Dentine erosion however has a complex histology and
assessment of dentine erosion with profilometry requires a few considerations. Erosion
in dentine results in centripetal loss of peritubular dentine and intertubular dentine until
zone of fully demineralised collagen layer appears on surface which is thick and stable
when hydrated (Kinney et al., 1995). This histological feature indicates that there is no
bulk tissue loss and if mineral loss is the target criterion, it can be difficult to quantify in
the presence of this structure on the surface (Ganss et al., 2009b) . The other target
criterion could be the measurement of level or loss of organic matrix from the surface
which is especially of interest when evaluating degradation of organic matrix by
enzymes. Dentine when demineralised, is prone to shrinkage (Zhang et al., 2009) and
profilometry measurements will reveal a step height difference between treated and
Univers
ity of
Mala
ya

42
non-treated areas which will be absent in controlled moisture conditions. This step does
not represent the true mineral loss or surface level of organic matrix. Similar problems
will be encountered when using a contact profilometry because the mechanical stylus
would cave in the organic matrix to an unknown extent. Therefore, it is critical to scan
dentine samples while wet. However, most profilometry systems are not designed to
scan wet samples and therefore it is recommended that samples be kept wet until before
scanning (Attin et al., 2009; Ganss et al., 2007) or that the drying time be standardised
to 10 minutes to allow for the organic matrix to undergo shrinkage (Steiner-Oliveira et
al., 2010).
Profilometry measurements of eroded dentine in the presence of organic matrix are
not solely related to mineral loss. To resolve this issue, it was recommended that
organic matrix be removed from the dentine samples before performing measurements
with profilometry (Ganss et al., 2009b; Ganss et al., 2007). However, removal of
organic matrix will make profilometry a destructive technique and therefore non-
suitable for application in longitudinal studies. Profilometry is capable of quantifying
erosion by surface roughness parameters (Schlueter et al., 2011) which are reviewed in
chapter 4 of this thesis.
2.3.1.4 Chemical analysis of dissolved minerals
The effect of acid on dental hard tissues is to cause the release of minerals like
calcium and phosphate from dental hard tissues. Quantification of these ions is a well-
established and sensitive technique for assessment of erosion or its treatment (Hjortsjo
et al., 2009). Calcium analysis can be carried out by using ion-selective electrode or
atomic absorption spectroscopy. Ion selective electrode (Hara & Zero, 2008) may be
subject to error because of needing a specific environmental pH to work precisely or by
Univers
ity of
Mala
ya

43
complexation of calcium with certain acid (Attin et al., 2005a) Atomic absorption
spectroscopy is a reliable method for analysis of calcium and has been employed for
assessment of both enamel and dentine erosion (Wiegand et al., 2008) However,
disadvantages of this technique include intensive preparation of solution, the need of
solution to exceed a volume of 100 µl and risk of errors due to contamination (Attin &
Wegehaupt, 2014).
Small amounts of solution i-e 10 µl can be utilised for analysis of both calcium and
phosphate ions by calorimetric methods. The minimum detectable and quantifiable
concentration for calcium was found to be 12.4 µmol/l depending on the acid employed
by using Arsenazo III calorimetric method (Attin et al., 2005a) and 1.9 µl to 9 µ mol/l
for phosphate by using Malachite green procedure (Attin et al., 2005b). The Malachite
green procedure was found to be a reliable method whereas the precision of Arsenazo
III may not be the same with all acids (Attin & Wegehaupt, 2014). Importantly, no
sample preparation is required for these methods. In fact, prepared samples might show
increased concentration of mineral because of presence of smear layer. Not only have
these methods been employed in in vitro and in situ studies but also in vivo (Young et
al., 2006). The presence of saliva in vivo can however cause problems with the analysis
(Schlueter et al., 2011).
In short, chemical analysis of dissolved minerals are a set of well establish
techniques which are easy to administer. However, they have to be combined with other
techniques since they do not provide any structural information. They are very sensitive
to early changes in erosion (Attin & Wegehaupt, 2014) and might prove useful for the
assessment of early dentine erosion.
Iodide permeability test involves the immersion of enamel samples in potassium
iodide. The iodide is recovered by Millipore prefilter paper discs. The amount of iodide
Univers
ity of
Mala
ya

44
recovered from enamel gives information about the pore volume and hence the
demineralisation and remineralisation status of enamel (Attin & Wegehaupt, 2014).
Although this method is sensitive to detection of early stages of demineralisation and
remineralisation in enamel, it is not suitable for assessment of dentine erosion
(Schlueter et al., 2011).
2.3.1.5 Atomic force microscopy
Atomic force microscope (AFM) belongs to the family of scanning probe
microscopies and combines the properties of scanning tunneling microscope and the
stylus profilometer (Yang et al., 2018) . A sharp tip attached to a flexible cantilever
moves on the sample and tracks the surface features. Two main modes of AFM are
being used in erosion studies are contacting mode and tapping mode. The tapping mode
is less damaging to the surface of fragile samples as no actual contact is established
between the tip and the sample during scanning. The contacting mode of atomic force
microscopy is similar to stylus profilometry. However it appears that AFM is a better
tool than profilometry in terms of its much higher resolution and imaging capability.
Additionally, AFM provides quantitative information on the surface roughness and step
height difference between the reference and eroded areas at an atomic level which
suggests it usefulness for assessment of early erosion. When compared with scanning
electron microscopy, AFM provides a better qualitative analysis as no sample
preparation is required. Moreover, the scanning can take place in ambient conditions,
air, liquid and vacuum and longitudinal measurements are possible. In spite of all these
advantages, the scanning of AFM is very time-consuming and only a small area can be
scanned at a time. Scan size of < 0.5 X 0.5 mm2
can a employed and it can take up to 60
minutes to scan this area. Several scans have to be taken to make sure that the scanning
Univers
ity of
Mala
ya
45
area is representative of the whole sample (Barbour & Rees, 2004). This might make
AFM non-feasible for longitudinal study designs.
AFM has been used for the assessment of early erosion on native surfaces of enamel
(Cheng et al., 2009b; Finke et al., 2000). Dentine demineralisation has also been
assessed by using atomic force microscopy and it was found that average roughness (Ra)
was significantly different from baseline measurement after only 20 seconds of etching
with 32% phosphoric acid (Ma et al., 2009). In an in situ study, it was found that
dentine demineralised by 10 vol% citric acid for 15 seconds followed by immersion in
6.5vol% sodium hypochlorite for 100 - 200 seconds could be visualised at a level at
which single collagen fibres could be recognised (Habelitz et al., 2002). More recently,
topographical and numerical analysis of dentine surface was performed by AFM to
evaluate the efficacy of a new formulation toothpaste for the prevention of dentine
erosion (Poggio et al., 2014).
It appears that AFM is highly suitable for the assessment of early dentine erosion
because of its ability to qualify and quantify erosion at an atomic level in real time on
native surfaces. However, the time consumed in scanning and its ability to scan only a
small area might limit its usefulness for longitudinal studies.
2.3.1.6 Microradiography
Microradiography is a method that quantifies the mineral loss in dental hard tissues
by the measurement of attenuation of x-rays passing through these tissues (Attin &
Wegehaupt, 2014). A couple of approaches can be used to calculate the mineral mass.
One method is by using X-ray detectors which enable the counting of photons when
appropriate mass attenuation coefficient is known (Anderson & Elliott, 2000). Another
Univers
ity of
Mala
ya

46
approach is by using X-ray sensitive photographic plates or films which calculate
mineral mass by means of gray values acquired by photographic density measurements
calibrated using an aluminium step wedge (Cochrane et al., 2014).
For dental research, microradiography has been categorised as transverse or contact
microradiography (TMR) dealing with assessment of thin sections approximately 200
microns in thickness, longitudinal microradiography (LMR) used for analysing thicker
sections than TMR which are 4 mm in thickness (Joshi et al., 2016) and wavelength-
dependent microradiography for quantification of mineral in whole teeth (Thomas et al.,
2006). Microradiography has mainly been used for assessment of dental caries but has
also been adopted for assessment of mineral loss in erosion studies.
Transverse microradiography has been the most commonly used type of
microradiography been used in dental research. It has been known to calculate both the
lesion depth as well as integrated mineral loss over the depth of lesion (Ablal et al.,
2009; Amaechi & Higham, 2001a, 2001b). However, the tissue loss has to exceed 20
microns for it to be detectable by the microradiography system. For the assessment of
surface softening alone, this equipment is not sensitive enough as 5 - 10 microns of the
edge of tissue samples prepared for TMR can become fuzzy (Attin & Wegehaupt,
2014).
A correlation between transverse microradiography and profilometry was established
and it was shown that transverse microradiography could be used to measure the
mineral loss in both enamel and dentine for erosion challenge of less than 1 hour (Hall
et al., 1997) A correlation between microradiography and chemical analysis of
hydroxyapatite solution was also found (Margolis et al., 1999). Since then it has been
used as a gold standard against which the newer techniques are validated (Elton et al.,
2009; Pretty et al., 2004). The fact that extensive specimen preparation is still required
Univers
ity of
Mala
ya

47
for the analysis makes transverse microradiography inappropriate for longitudinal study
designs.
To overcome this disadvantage of transverse microradiography, longitudinal
microradiography (LMR) was introduced. Sample slices thicker than that used for
transverse microradiography could be prepared for LMR. Moreover, the samples could
be non-destructively analysed multiple times. Therefore this technique can be applied in
longitudinal studies and pH-cycling models of erosion. However, increase in thickness
of sample compromises the sensitivity of the technique. As a result, this method is
unable to measure the minor changes in mineral and might have limited applicability in
studies investigating early erosion (Attin & Wegehaupt, 2014).
It is important to note that for dentine, thicker samples of 800 microns have to be
prepared in contrast to enamel samples for which the recommended thickness is 400
microns which might further compromise the sensitivity of this technique. This could be
the reason why LMR was found to have limited applicability for dentine as the detection
limit for dentine was adjusted to 50 microns which amounts to 25 microns of mineral
loss. In contrast to dentine, mineral loss greater than 20 microns could be reliably
measured in enamel. Interestingly, the organic matrix, due to its low X-ray absorption
property did not affect the LMR measurements significantly in dentine leading to the
conclusion that removal of organic matrix would be unnecessary when LMR is
employed (Ganss et al., 2009a; Ganss et al., 2005; Ganss et al., 2009b). However,
because of having low detection threshold for mineral loss, LMR is not suitable for the
assessment of early dentine erosion.
Univers
ity of
Mala
ya

48
2.3.1.7 Quantitative light induced florescence
Quantitative light induced florescence (QLF) is an optical method that was
developed for the longitudinal analysis of early demineralisation in enamel caries (Van
Der Veen & De Josselin De Jong, 2000). The fundamental principle of QLF is described
elsewhere in detail (Angmar-Mansson & Ten Bosch, 2001) Basically, the fluorophores
mainly located at the dentine-enamel junction and underlying dentine, produce natural
florescence of tooth when the tooth is illuminated by filtered blue-violet light. In
demineralised tissue, the mineral content is altered leading to higher scattering and less
absorption of light. Therefore, less light is able to reach the fluorophores decreasing the
intensity of florescence issuing from the demineralised tissue as a result of which the
demineralised tissue appears darker as compared to the surrounding fluorescent sound
tissue. The outcome measure used is the average difference in the fluorescence intensity
[ΔF (%)] of the lesion and the sound area which is calculated by the system software
(Attin & Wegehaupt, 2014) .
Major advantage of QLF for erosion studies would be the non-destructive imaging
and its potential for longitudinal assessment of erosion in in vivo studies. QLF has been
employed for the assessment of enamel erosion in a few studies (Ablal et al., 2009;
Elton et al., 2009; Pretty et al., 2003, 2004) A weak poor correlation was found between
QLF and TMR for measuring the depth of wear but it was concluded that QLF was
reliable for measuring the shallow erosive lesions. It was shown that QLF was able to
detect demineralisation after only 10 minutes of erosive challenge induced by orange
juice (pH = 3.8) in enamel and was suitable for monitoring of early enamel erosion
(Chew et al., 2014). The influence of demineralisation on the fluorescent properties
of dentine was investigated in an in vitro study. ΔF of carious lesions in dentine
measured by micro-Raman spectroscope was correlated with mineral loss profiles of
same lesions by using microradiography and a linear correlation was found between the
Univers
ity of
Mala
ya

49
fluorescence scans and mineral loss (Van Der Veen et al., 1996). On the contrary; the
fluorescence measured by QLF issuing from carious dentine was not found to be linked
to demineralisation which suggests that QLF might not be suitable for assessment of
dentine demineralisation. (Banerjee & Boyde, 1998). For dentine erosion, however the
applicability of QLF remains to be tested.
2.3.1.8 Optical coherence tomography
Optical coherence tomography (OCT) is a non-invasive optical imaging modality
which is based on interference between signals received from the object under
investigation and a local reference and is capable of producing cross-sectional real-time
imaging (Podoleanu, 2012). Basically, OCT is an extension of a technique called low-
coherence interferometry initially used for in vivo assessment of axial length of eye
(Fercher et al., 1988). OCT is comparable to ultrasound because both methods provide
cross-sectional images of tissues by measuring the echo time delay of backscattered
wavelength. However, OCT uses infrared light waves in comparison to ultrasound
which uses sound waves. The use of light waves as a medium by OCT makes it possible
for it to be non-contact for the patient whereas ultrasound needs a transducing medium
such as water along its path to conduct the sound waves. Moreover, OCT provides high
resolution imaging about 10-100 times higher than conventional ultrasound (Joiner &
Van Der Kogel, 2016).
OCT was first presented for in vivo cross-sectional imaging of eye tissues (Huang et
al., 1991). Since then it has been used for the investigation of many aspects of medicine
and dentistry. Its non-invasive, real-time and near-histological imaging makes it highly
suitable for medical imaging. Its main applications in medicine have been in areas of
ophthalmology (Abdolrahimzadeh et al., 2016; Hangai et al., 2007), gastroenterology
Univers
ity of
Mala
ya

50
(Desai et al., 2016; Tsai et al., 2014) and dermatology (Olsen et al., 2016; Von
Braunmuhl et al., 2016).
In dentistry, the use of OCT was first reported in 1998 (Colston et al., 1998). A novel in
vivo optical coherence tomography system was developed for the assessment of oral
hard tissues using which the first in vivo images of oral cavity were presented. Since
then OCT has been used in many fields of dentistry. OCT can be used as a non-invasive
method for high definition visualisation of periodontal structures, calculus and gingival
sulcus which could aid in the early detection of active periodontal disease before bone
loss and help identify the causative factors (Park et al., 2017). Visualisation of soft
tissues in the oral cavity would additionally aid in early diagnosis of soft tissue lesions
including oral tumors (Lee et al., 2012). Recent research in orthodontics has focused on
using OCT for the assessment of demineralisation near the orthodontic bracket base
(Nee et al., 2014), its prevention (Pithon et al., 2015) and for evaluating the enamel
damage after debonding (Leao Filho et al., 2015). However, the principal tissue
evaluated in this regard has only been enamel.
In cariology, numerous applications of OCT have been reported in the recent years.
Of paramount clinical importance is the detection of incipient caries in an attempt to
stabilize and remineralize it. OCT can non-invasively and non-destructively assess early
demineralisation in dental hard tissues (Holtzman et al., 2014; Kang et al., 2010). In
contrast, the conventionally employed X-rays expose the patients to unnecessary
radiation and are unable to detect early demineralisation. Researchers have evaluated
the ability of OCT to detect dental caries on occlusal surfaces (Simon et al., 2017) and
more challenging proximal surfaces (Shimada et al., 2014). Moreover, the potential of
OCT to monitor remineralisation was evaluated (Jones et al., 2006b) and the research is
on-going in this regard. The efficacy of anti-caries agents such as fluoride and different
Univers
ity of
Mala
ya

51
lasers in arresting caries has also been investigated using OCT (Hsu et al., 2008;
Manesh et al., 2009). OCT can additionally detect microleackage and gap formation in
the composite restorations (Nazari et al., 2013). Accurate refractive index of dental hard
tissues would play an important role in the clinical diagnosis of caries as it affects the
light scattering. An attempt was made to understand the impact of different structural
orientations of enamel and dentine structures on the refractive indices of these tissues
and it was found that unlike enamel, refractive index in dentine varies with structural
orientation (Hariri et al., 2012). Moreover, the remaining dentine thickness during caries
removal has been measured using OCT from the viewpoint of preventing accidental
pulp exposures (Majkut et al., 2015).
Since optical coherence tomography is capable of measuring small dimensional
changes non-destructively on tooth surfaces, it appears to be an ideal tool for monitoring
tooth erosion (Chan et al., 2013). When the dental hard tissues get demineralised, they
exhibit increased porosity. This alters the optical property of the tissues resulting in
increased backscattering of light at the surface with reduced depth of penetration in
comparison to sound tissues. Therefore, the eroded areas reflect more light intensity at
the surface in the OCT images. This is the basis on which the sound tissues are
distinguished from the demineralised tissues in case of erosion. On the other hand, the
remineralised areas can be distinguished as having reduced signal intensity as compared
to eroded areas in the OCT images (Attin & Wegehaupt, 2014; Huysmans et al., 2011).
Use of optical coherence tomography for assessment of enamel erosion was first
tested in a double-blind randomised clinical trial and erosive loss in GORD patients
before and after therapy of proton pump inhibitors was measured (Wilder-Smith et al.,
2009). The intensity of backscattered light in treatment area was significantly reduced
as compared to reference area as hypothesized. The OCT was further validated for early
Univers
ity of
Mala
ya

52
enamel erosion in an in vitro study (Chew et al., 2014). Authors were able to detect
demineralisation in enamel after 10 minutes of erosion challenge and the OCT findings
were compared with surface microhardness. This study was followed by a clinical study
in which SS-OCT successfully detected orange juice-induced-demineralisation in
comparison to mineral water rising in enamel of 30 volunteers (Austin et al., 2017).
Recently, OCT was employed for diagnosing and monitoring erosion progression in
dentine (De Moraes et al., 2017).This study aimed to assess the progression of erosive
lesions after irradiation with Nd:YAG laser (Neodymium-doped Yttrium Aluminum
Garnet) and topical fluoride application. The authors were able to measure the amount
of tooth tissue loss over the 20 days of erosive cycle, before and after treatments, and
monitor dentine demineralisation progression with optical coherence tomography.
However, advanced stage dentine erosion was targeted in this study as the criteria set
for development of erosion was visibility of erosive lesions in the OCT images
indicating that bulk tissue loss had taken place. A limitation of this study was that
findings of OCT were not compared with any other qualitative or quantitative
technique.
Because of the histological differences in the enamel and dentine, the information
gathered from studies on enamel erosion cannot be always applicable for dentine
erosion. Therefore, it is felt that further research is needed to assess the applicability of
OCT for measuring early dentine erosion progression. Moreover, there is a need to
develop appropriate algorithms for performing quantitative analysis and for this purpose
optimum outcome measures need to be identified for monitoring erosion progression in
dentine. At the same time, it would be useful if the findings of OCT are compared with
other appropriate qualitative and quantitative reference methods. Optical coherence
tomography is further reviewed in chapter 3 of this thesis.
Univers
ity of
Mala
ya

53
2.3.1.9 Optical specular and diffuse reflection
An optical spectrometer can record specular or diffuse reflection at different
wavelengths and therefore characterise the eroded surface. A reflectometer based on this
principle was successfully used for the measurement of enamel erosion (Rakhmatullina
et al., 2011). It was later developed into a portable optical device and more recently a
Table-top device (Carvalho et al., 2016; Rakhmatullina et al., 2013). These methods
were found suitable for assessment of early enamel erosion and were validated against
calcium loss, surface roughness and hardness measurements. However, these methods
have been only tested for enamel and little is known about their potential for assessment
of dentine.
2.3.2 Qualitative assessment
2.3.2.1 Scanning electron microscopy
Scanning electron microscopy (SEM) is an established technique for qualification of
ultrastructural changes in demineralised tissues. Two main types of scanning electron
microscopy have been used for assessment of dental erosion. The conventional SEM
requires the samples to be coated with gold or other particles like carbon in order to
avoid charging effects. Further, the high vacuum used in the conventional SEM might
cause drying artefacts. This means that the samples cannot be used in longitudinal study
designs. These shortcomings of conventional SEM can be addressed by using
environmental SEM (ESEM). Environment SEM uses a low vacuum which means that
the samples do not need to be dried or coated with any material (Schlueter et al., 2011).
However, the resolution of ESEM is lower as compared to SEM (Attin & Wegehaupt,
2014).
Univers
ity of
Mala
ya

54
In dentine, the process of erosion would result in opening of dentinal tubules which
can then be scored according to its degree. It is believed that ESEM would especially
prove to be useful for qualification of eroded dentine. In eroded dentine, the organic
matrix undergoes considerable shrinkage under dry conditions. Therefore, it is desirable
to keep the dentine samples as hydrated as possible while imaging. ESEM which
allows the samples to be imaged after being dried with air only can be used to assess the
structural alterations following the process of erosion in dentine samples when being
only air-dried (Meurman et al., 1991) However, care should be exercised in drying the
samples as no technique can fully prevent the shrinkage of organic matrix in
demineralised dentine (Carvalho et al., 1996). To assess the sub surface effects of
erosion, the samples have to be fractured or sectioned. In enamel this technique is of
limited value since the fractured enamel surface is irregular. In dentine however, the
linear or areal extent of structural effects can be visualised at the junction of sound and
eroded dentine in fractured and polished sections (Schlueter et al., 2010).
It appears that both of the techniques are suitable for assessment of structural
changes induced by early erosion and ESEM might prove to be more suitable for
imaging erosion softened dentine. Although they provide a subjective and qualitative
assessment, but the fact they allow the visualisation of erosion induced ultrastructural
changes make them a valuable supporting tool when used in combination with
quantitative methods for early erosion studies. Moreover, both techniques can be used
for imaging of native surfaces.
SEM and ESEM have also been used in combination with Energy dispersive X-ray
spectroscopy (EDX, also known as EDS). In EDX, X-rays are emitted when electron
beam comes in contact with the sample surface and causes the atoms and ions in the top
few micrometres of the surface to become excited. These X-rays when analysed give
Univers
ity of
Mala
ya
55
information about the distribution of elements like Calcium, phosphate, stannous or
fluoride within the sample (Barbour & Rees, 2004). EDX was used in in combination
with scanning electron microscopy for the investigation of mechanism of action of tin
containing fluorides for dentine erosion (Ganss et al., 2010). Recent studies also report
the use of EDX for dentine erosion (Flury et al., 2013; Wang et al., 2016).
2.3.3 Conclusion
Review of the literature reveals that overall the assessment of dentine erosion is
challenging because of its complex histology. Although a number of techniques have
been proposed for the qualification and quantification of dental erosion in dentine
however, no single technique in isolation is able to satisfy all the requirements for the
assessment of early dentine erosion. Hence, a combination of techniques is usually
employed for its assessment. However, using a combination of methods is non-feasible
because of specialist and time consuming nature of these techniques. Although good
enough for laboratory experiments, a method which can be used in clinical trials for
direct measurements for monitoring and as a chair side tool is lacking. Optical methods
seem to have the greatest potential in this regard but their validation is lacking for
assessment of early dentine erosion. The next three chapters deal with the qualitative
and quantitative assessment of early dentine erosion with non-invasive methods.
Univers
ity of
Mala
ya

56
CHAPTER 3: MONITORING OF EARLY DENTINE EROSION WITH
OPTICAL COHERENCE TOMOGRAPHY
This chapter details the assessment of early eroded dentine with optical coherence
tomography (OCT) and qualitative assessment with field-emission scanning electron
microscopy (FE-SEM). The findings of OCT were compared with FE-SEM
observations.
3.1 Introduction
Gingival recession is a common occurrence in adults and elderly population leading
to the subsequent exposure of root dentine that is prone to dental erosion (West et al.,
2014). Dental erosion is a chemical process that involves the dissolution of enamel and
dentine by acids not derived from bacteria when the surrounding aqueous phase is
undersaturated with respect to tooth mineral (Larsen, 1990). Initial exposure to acids
results in a partial dissolution of mineral or early stage surface softening of dentine
(Vanuspong et al., 2002). At this stage, dentine is prone to remineralisation (Attin et al.,
2001) or irreversible tooth structure loss by mechanical wear or continued acid
challenge (Shellis & Addy, 2014; Wiegand et al., 2009). Accurate diagnosis at this stage
followed by institution of appropriate management strategies can help to arrest or
reverse these lesions by non-surgical means.
Efficacies of management strategies proposed for dentine erosion have been explored
through a substantial number of in vitro and lesser number of in situ studies (Chiga et
al., 2016; Hannas et al., 2016). However, the multifactorial nature of the erosion process
(Lussi & Jaeggi, 2008) makes the information extracted from these studies inconclusive
and unsafe to extrapolate into clinical settings. Importantly, the in vitro or in situ erosion
in dentine results in formation of a histological feature marked by a demineralised layer
of organic material on the surface (Ganss et al., 2009b). The clinical fate of this organic
Univers
ity of
Mala
ya
57
matrix is not clear, but as it can be digested by collagenases (Ganss et al., 2004) and
proteolytic enzymes (Schlueter et al., 2010), it can be assumed that it does not survive in
vivo (Ganss et al., 2014). The presence and absence of this layer of organic matrix on
eroded dentine could affect the efficacy of anti-erosion treatments (Ganss et al., 2004).
Therefore, clinical validation of the therapeutic methods proposed for reducing dentine
erosion is imperative before implementing them in clinical practice.
Clinical validation of these interventions can only be performed if non-invasive
analytical tools sensitive to early stages of dentine erosion become available. Analytical
techniques being currently used for assessment of dentine erosion are either invasive
(such as microradiography) or require sample preparation (such as scanning electron
microscopy) because of which their use is restricted to in vitro and in situ settings (Attin
& Wegehaupt, 2014). Hence a device which can detect and monitor the progression of
early eroded dentine in a clinical setting would prove to be advantageous in this regard.
One such device is optical coherence tomography which can provide non-invasive
cross-sectional imaging of dental hard tissues at near histological resolution.
3.1.1 Principle of OCT imaging
OCT works on the principle of low-coherence interferometry and uses a device
called white light Michelson interferometer. Non-invasive light and biomedical optics
are combined to provide cross-sectional imaging of internal biological structure in real
time at near histological resolution thus providing microstructural details of tissues up
to 3 mm in depth from the surface. Briefly, near-infrared light from a low coherence
source is split by a fiber-optic splitter into a sample beam and reference beam. Sample
beam passes through the imaging probe and is incident on the sample being imaged. It is
then attenuated by the optical properties of the sample tissue during its forward and
Univers
ity of
Mala
ya

58
reverse course through the sample resulting in either backscattering or absorption of
light. Light backscattered from the sample and reference arm are combined again at the
splitter. The light then passes through the photodetector and is directed to the OCT
monitor (Gimbel, 2008) (Huang et al., 1991). The net difference of the two recombined
echo time delays of the sample beam and the reference beam is then recorded as
interference profile. The backscattered intensity information in the form of reflectivity
profile in depth can then be extracted from this interference profile (Gabriele et al.,
2011).
There are two main types of OCT, time domain OCT (TD-OCT) and spectral domain
OCT (SD-OCT). SD-OCT has the advantage of elimination of need for depth scanning
over TD-OCT in which it is carried out by mechanical means. SD-OCT is further
categorised into two methods (1) Spectrometer-based (SB-OCT) and (2) Swept source-
based (SS-OCT). Each method has its own advantages and disadvantages. SS-OCT, the
OCT system employed in this thesis combines the properties of rapidly sweeping a
narrow linewidth laser through a broad optical bandwidth. This enables a reduced signal
to noise ratio because of an immediate depth scan calculation by Fourier-transform
(Drexler & Fujimoto, 2008; Podoleanu, 2012).
Significant key parameters determining the functioning of an OCT system include
central wavelength, axial and lateral resolution and imaging depth etc. The
specifications of the OCT system used in this study are given in the table 3.1 below,
Univers
ity of
Mala
ya
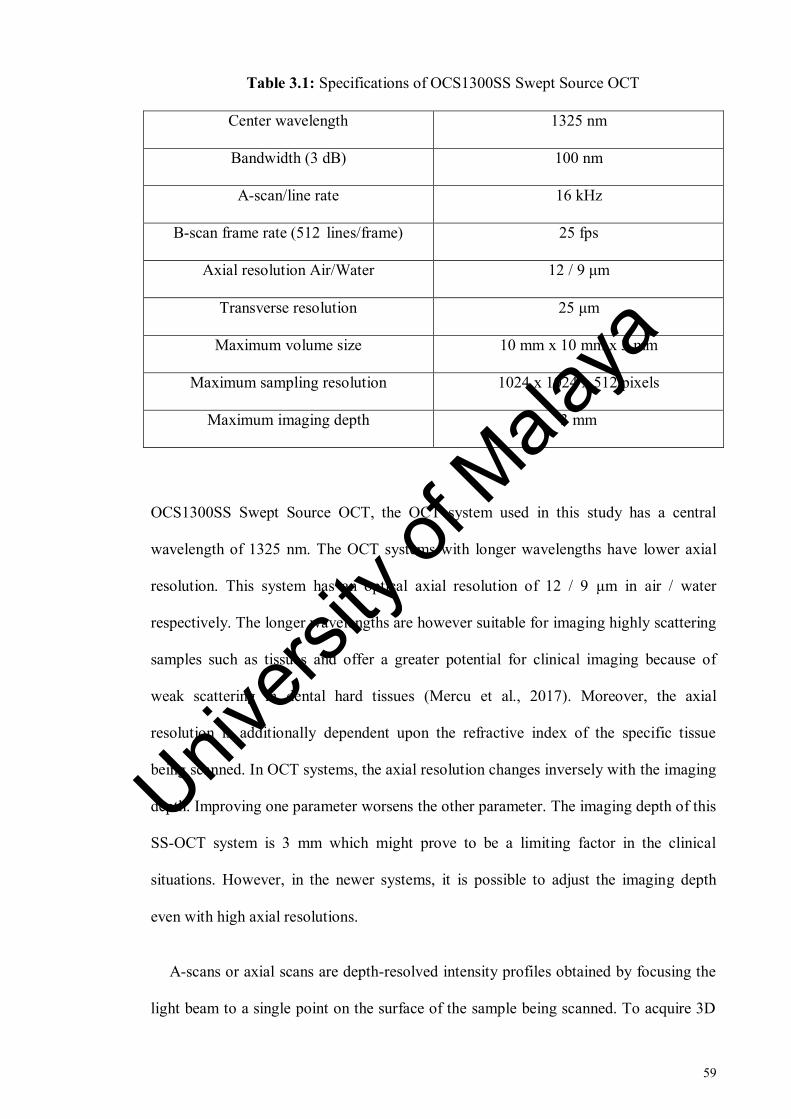
59
Table 3.1: Specifications of OCS1300SS Swept Source OCT
Center wavelength 1325 nm
Bandwidth (3 dB) 100 nm
A-scan/line rate 16 kHz
B-scan frame rate (512 lines/frame) 25 fps
Axial resolution Air/Water 12 / 9 μm
Transverse resolution 25 μm
Maximum volume size 10 mm x 10 mm x 3 mm
Maximum sampling resolution 1024 x 1024 x 512 pixels
Maximum imaging depth 3 mm
OCS1300SS Swept Source OCT, the OCT system used in this study has a central
wavelength of 1325 nm. The OCT systems with longer wavelengths have lower axial
resolution. This system has an optical axial resolution of 12 / 9 μm in air / water
respectively. The longer wavelengths are however suitable for imaging highly scattering
samples such as tissues and offer a greater potential for clinical imaging because of
weak scattering in dental hard tissues (Mercu et al., 2017). Moreover, the axial
resolution is additionally dependent upon the refractive index of the specific tissue
being scanned. In OCT systems, the axial resolution changes inversely with the imaging
depth. Improving one parameter worsens the other parameter. The imaging depth of this
SS-OCT system is 3 mm which might prove to be a limiting factor in the clinical
situations. However, in the newer systems, it is possible to adjust the imaging depth
even with high axial resolutions.
A-scans or axial scans are depth-resolved intensity profiles obtained by focusing the
light beam to a single point on the surface of the sample being scanned. To acquire 3D
Univers
ity of
Mala
ya

60
images, the OCT imaging system is equipped with scanning means to scan the object
both in depth and transversally. As a result, different scan planes can be created
depending on the scanning order and scanning direction. Collection of multiple A-scans
by scanning linearly across the tissue gives rise to one B-scan or longitudinal scan. Each
B-scan has a depth axis and lateral or angular axis. A-scan or line rate determines the
speed with which a B-scan is collected. A-scan rate in turn is related to the sensitivity of
the equipment. A higher A-scan rate results in lower sensitivity of the system. For
Swept-Source OCT systems, the A-scan rate is determined by the sweep speed of the
swept laser source. OCS1300SS Swept Source OCT has an axial scan rate of 16 kHz
with a sensitivity of 100 dB. When the OCT beam is scanned transversally over the
target tissue, T-scans or en-face scans are produced which generate a reflectivity profile
in angular or lateral position. Collection of many T-scans in transverse plane gives rise
to C-scans or transverse slice scans. Different transversal slices are obtained from
different depths (Podoleanu, 2005).
3.1.2 Assessment of demineralisation with OCT
Optical coherence tomography has been used for both the qualitative and quantitative
evaluation of dental caries. Dental erosion is different from dental caries in terms of
being a ‘surface’ or ‘near-surface’ phenomenon rather than a subsurface process (Lussi
& Carvalho, 2014). The backscattered light intensity is therefore expected to present
differently for both processes.
The process of demineralisation causes the loss of mineral from dental hard tissues.
The demineralised dental tissues hence become porous and the pores created differ from
each other in terms of size and shape. Therefore, the structural organisation of the
demineralised tissue becomes complex in comparison to sound tissue. The light
Univers
ity of
Mala
ya
61
travelling through demineralised tissue undergoes two types of interactions. One
interaction is with the regular components of tissue that results in scattering. The other
would be the interaction of light with the newly formed pores which results in (1)
increased intensity of backscattered light because of the change in refractive index and
(2) increased depth of penetration of light in the porous tissue. End result of this would
be the increased backscattering of light received by the OCT system which can then be
qualified or quantified through the OCT images. In the sound tissues, where the pores
are absent, the light only interacts with the regular components of the tissue which
results in less light being transferred to the OCT system as compared to demineralised
tissue. This is the basis on which OCT is able to differentiate the sound tissue from the
demineralised tissues. For dental erosion, this technique is used to quantify the increase
in backscattered intensity at the surface which in turn gives information about the
surface porosity and also the depth of penetration of the region of interest which is
reduced when surface scattering occurs (Huysmans et al., 2011; Wilder-Smith et al.,
2009).
For dentine, the passage of light would be expected to be increasingly complex
because of the presence of organic matrix. However, it was found that dentinal tubules
were the main structures responsible for dentine and organic matrix contributed little to
the overall scattering. Further, both scattering and absorption of light were greater in
dentine as compared to enamel (Zijp & Bosch, 1993).
Use of optical coherence tomography for the assessment of dental erosion was first
tested in a double-blind randomised clinical trial. The erosive loss in GORD (gastro-
esophageal reflux disease) patients before and after therapy with proton pump inhibitors
was measured (Wilder-Smith et al., 2009). The intensity of backscattered light in the
treatment area was significantly reduced as compared to reference area as hypothesized.
Univers
ity of
Mala
ya

62
Although the study was limited to assessment of advanced dental erosions only, it
served to validate OCT as a reliable tool for quantification of dental erosion which had
not been done before. The erosive loss was assessed by measuring the change in enamel
thickness with respect to dentino-enamel junction (DEJ). However, using DEJ as a
reference could prove to be complicated in the presence of saliva or in the case of
erosion-induced roughening or subsurface demineralisation. Irregular boundary of DEJ
can further complicate the analysis (Chan et al., 2013; Chan et al., 2014).
OCT was further validated for monitoring of early enamel erosion in an in vitro
study (Chew et al., 2014). Surface softening stage of enamel erosion before the
occurrence of any surface loss reducing enamel height was targeted in this study.
Authors were able to detect demineralisation in enamel after 10 minutes of erosion
challenge and the OCT findings were compared with surface microhardness. Only 2D
imaging (with B-scans) was employed in this study. The accurate repositioning of B-
scans can be challenging and could result in higher standard deviation. The parameter
used in this study was decay of intensity between two optical depths. One optical depth
was located near the surface and the other optical depth at the intensity plateau where
the backscattered intensity was almost constant. Mean percentage of difference in ratio
of exposed area and ratio of reference area was used as the outcome measure. High
specular reflection near the tooth surface can mask the OCT signal (Chan et al., 2015)
and a systematic way of finding a cut-off level to address the specular reflection by use
of this outcome measure was proposed in this study. In another recent clinical study,
Fresnel reflections near the surface were avoided by using a custom algorithm to
analyse all A-scan profiles instead of using data up to a specific depth. SS-OCT system
used in this study was able to detect statistically significant increase in the OCT signal
post orange juice rinsing in comparison to water rinsing (Austin et al., 2017).
Univers
ity of
Mala
ya

63
A reference area is needed in erosion studies to address the issues of systematic
errors and biological variability among the samples. This reference area is expected to
remain unchanged during the erosion challenges and instrumental measurements at
different measurement time points. The reliability of erosion-induced changes in the
eroded area can then be assessed by comparing the results against this constant
reference. Application of acid-resistant varnish and adhesive tape over the reference
area is common practice in erosion studies. A disadvantage of these methods is that they
cannot be used in the clinical settings. Dentino-enamel junction (DEJ) and CO2 laser
were tested as possible reference methods for erosion studies using OCT (Chan et al.,
2013). It was found that using DEJ can be unreliable in the case of roughness and
subsurface demineralisation. A subablative CO2 laser because of being non-invasive
has a potential of being used in clinical studies and its use as a reference was tested
previously (Chan et al., 2014). The authors however used a pH-cycling model of six
and 12 days indicating that erosion induced was rather aggressive. It implies that this
laser is only applicable in clinical studies investigating advanced erosion and the
usefulness of this subablative laser therefore needs to be explored for early stages of
erosion. A sturdy non-toxic material which can be applied on the tooth surfaces
clinically would be feasible and for this purpose, the use of composites has been
suggested (Chan et al., 2014). Another such material would be the bonding agent which
has the potential of being applied in the in vivo protocols.
Root dentine has been assessed with OCT only in a few studies. The percentage
reflectivity loss in relation to demineralisation on root surfaces was quantified and it
was shown that there was a linear correlation between % reflectivity loss and mineral
loss measured with microradiography (Amaechi et al., 2004). However the
measurement of reflectivity loss could be questionable as the lesion reflectivity would
be expected to increase not decrease with demineralisation. Therefore, the integrated
Univers
ity of
Mala
ya
64
reflectivity was calculated instead of reflectivity loss to assess root dentine caries and
inhibition potential of fluoride for root caries, and a positive correlation was found
between integrated reflectivity and integrated mineral loss (Lee et al., 2009) .
A recent study employed OCT for diagnosing and monitoring erosive wear
progression in dentine (De Moraes et al., 2017). This study aimed to assess the
progression of erosive lesions after irradiation with Nd:YAG laser (Neodymium-doped
Yttrium Aluminum Garnet) and topical fluoride application. Bovine root dentine
samples were exposed to citric acid (pH = 2.3) for a total of 20 days. The authors were
able to measure the amount of tooth tissue loss over 20 days of erosive cycle, before and
after treatments. The dentine demineralisation progression could be monitored with
optical coherence tomography. However, advanced stage dentine erosion was targeted
in this study as the criteria for development of erosion was visibility of erosive lesions
in the OCT images indicating that bulk tissue loss had taken place. To date, the early
stage of dentine erosion before bulk surface loss has not been assessed with OCT.
3.1.3 Aim
The aim of this study was to assess the potential of optical coherence tomography
(OCT) in monitoring the progression of in vitro early dentine erosion.
In order to achieve this aim, the research objectives were as follows;
1. To explore the potential of OCT for measuring early dentine erosion and the
quantum.
2. To identify an optimum outcome measure for measuring early dentine erosion.
3. To identify the detection threshold of OCT for measuring early dentine erosion.
Univers
ity of
Mala
ya

65
4. To compare the OCT backscattered intensity changes of early eroded dentine
with ultrastructural changes.
The null hypotheses tested were as follows;
1. OCT is not able to detect early dentine erosion in vitro.
2. OCT is not able to measure early dentine erosion progression in vitro.
3.2 Materials and Methods
3.2.1 Pilot studies
Several pilot studies were performed in order to design and test the protocol before
conducting the main experiment. Most of these pilot studies are also applicable to the
research aims discussed in the subsequent chapters 4 and 5. A brief account of these
experiments is given below.
3.2.1.1 Sample preparation
The objective of this pilot study was to identify a suitable sample preparation of root
dentine for the main experiment. Three extracted sound human premolars were
sectioned 1 mm below the cemento-enamel junction using slow-speed microtome
cutting machine (Micracut 125, Metkon Instruments Inc., Bursa, Turkey) and roots were
embedded in self-curing acrylic resin with the sectioned surface facing upwards. The
dentine surface was polished in a water-cooled rotating grinding / polishing machine
(Buehler, USA) under running water to create a flat and smooth surface. A
demineralisation window was created by using a non-residue adhesive tape and bonding
agent as shown in Figure 3.1. The polished dentine surfaces, except for the
Univers
ity of
Mala
ya
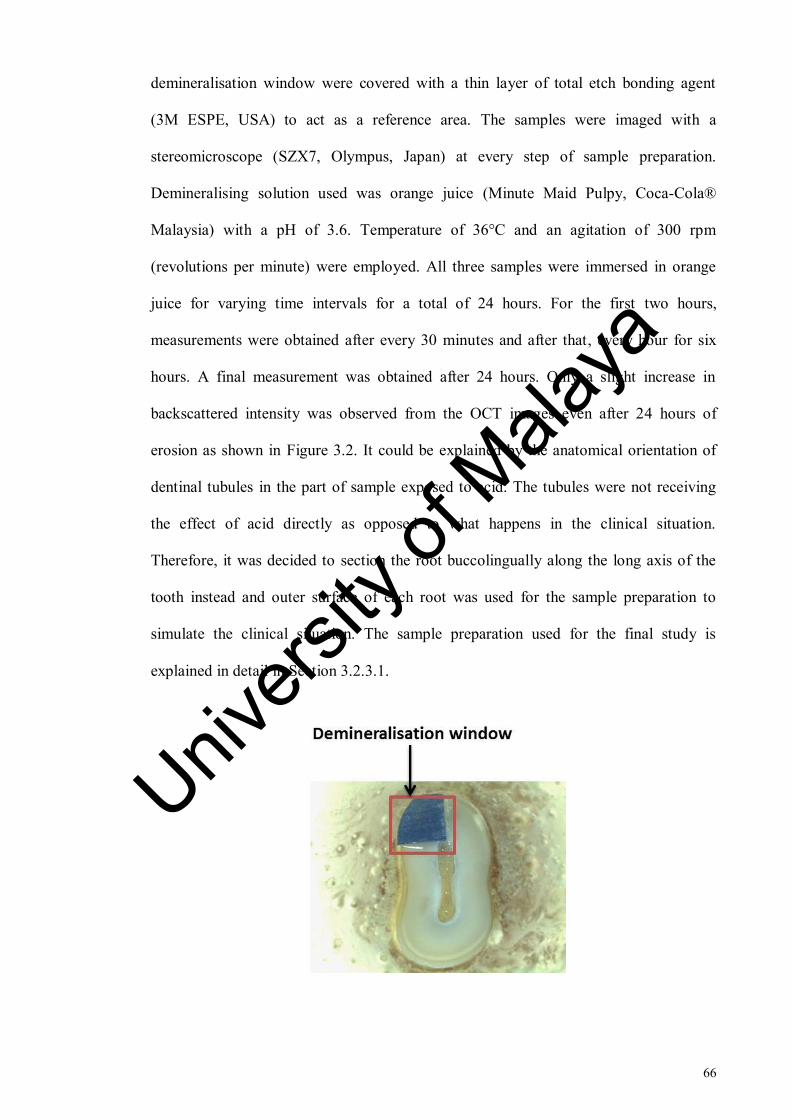
66
demineralisation window were covered with a thin layer of total etch bonding agent
(3M ESPE, USA) to act as a reference area. The samples were imaged with a
stereomicroscope (SZX7, Olympus, Japan) at every step of sample preparation.
Demineralising solution used was orange juice (Minute Maid Pulpy, Coca-Cola®
Malaysia) with a pH of 3.6. Temperature of 36°C and an agitation of 300 rpm
(revolutions per minute) were employed. All three samples were immersed in orange
juice for varying time intervals for a total of 24 hours. For the first two hours,
measurements were obtained after every 30 minutes and after that, every hour for six
hours. A final measurement was obtained after 24 hours. Only a slight increase in
backscattered intensity was observed from the OCT images even after 24 hours of
erosion as shown in Figure 3.2. It could be explained by the anatomical orientation of
dentinal tubules in the part of sample exposed to acid. The tubules were not receiving
the effect of acid directly as opposed to what happens in the clinical situation.
Therefore, it was decided to section the root buccolingually along the long axis of the
tooth instead and outer surface of each root was used for the sample preparation to
simulate the clinical situation. The sample preparation used for the final study is
explained in detail in Section 3.2.3.1.
Univers
ity of
Mala
ya

67
Figure 3.1: Stereomicroscope image of a root dentine sample used for exploratory
work. The sample was sectioned 1 mm below the cemento-enamel junction. The
demineralisation window was covered with blue adhesive tape. It has been highlighted
by a red box.
Figure 3.2: OCT B-scans of root dentine samples taken with SS-OCT at (a) baseline
measurement and (b) after 24 hours of erosive challenge. White line at the center
indicates the border between the reference and eroded areas. The transparent arrows
indicate the backscattered intensity (demineralisation) at the surface of eroded dentine
sample. Minimal increase in backscattered intensity was observed in the B-scan after 24
hours of erosion challenge (b) in comparison to the intensity observed in the B-scan at
baseline measurement (a).
3.2.1.2 Speed of agitation
To simulate the swishing of the drink within the oral cavity in clinical erosion, the
samples are stirred in erosion experiments. The objective of this pilot study was to
determine the optimum speed of stirring for the main experiment. A magnetic stirrer
Univers
ity of
Mala
ya

68
(RCT basic, IKA, Germany) (Figure 3.14) was employed and five root dentine samples
were immersed in 0.3% citric acid solution (A&C American Chemicals Ltd., North
Carolina, USA). The experiment was performed at a constant temperature of 36°C. A
magnetic stirrer is a laboratory device used for stirring a ‘stir bar’ added in the liquid by
employing a magnetic field. The solution is stirred as a result of it.
The speed of solution was increased from 20 rpm (revolutions per minute) to 700
rpm. Lower range of agitation was based on the speed at which the solution was being
stirred uniformly and higher range was based on the speed which the samples did not
move vigorously. The objective was to mimic the intraoral environment in the advent of
clinical erosion challenge when the drink swishes around the teeth whereas the teeth
remain stable. A speed of 300 rpm at a constant temperature of 36 °C was identified as
the optimum stirring speed at which the samples remained stable while the solution was
being stirred uniformly.
3.2.1.3 Drying time of eroded dentine
In a previous OCT validation study, the enamel samples were dried for 20 seconds
before scanning with OCT (Chew et al., 2014). This experiment aimed to assess
whether 20 seconds could also be suitable for drying the dentine samples before OCT
scanning. Five root dentine samples eroded in 0.3% citric acid (A&C American
Chemicals Ltd., North Carolina, USA) for 30 minutes were dried for 20 seconds and
then dried for 10 min. Samples were scanned with OCT at baseline, after 20 seconds
and 10 minutes of drying. Images were analysed with a programme written in Matlab
(The MathWorks, Inc., USA). Between baseline and 20 seconds, OCT signal remained
constant. However, some difference in OCT intensity was observed between 20 seconds
and 10 minutes of dehydration of samples as shown in the Figure 3.3. Based on this
Univers
ity of
Mala
ya

69
experiment, it was decided to restrict drying time of dentine samples to 20 seconds
before scanning them with OCT.
Figure 3.3: Box plots represent the OCT data acquired after 20 seconds and 10
minutes of air-drying.
3.2.1.4 Reduction of specular reflection
Strong specular reflections were observed in the OCT images while scanning and it
was decided that the specimens would be tilted to avoid mirror reflections from the
surface of specimen on the OCT image. The objective of this pilot study was to identify
the optimum tilting angulation and tilting plane to reduce the specular reflection to the
maximum from the OCT images. Tilting was performed 1) on a plane parallel to the
beam and 2) and on a plane perpendicular to the beam. It was found that the specular
reflection reduced significantly if the root dentine specimens were titled at a plane
perpendicular to the beam. In order to identify the tilting angulation, the samples were
tilted at various angles starting from five degrees to 40 degrees. It was found that the
Univers
ity of
Mala
ya
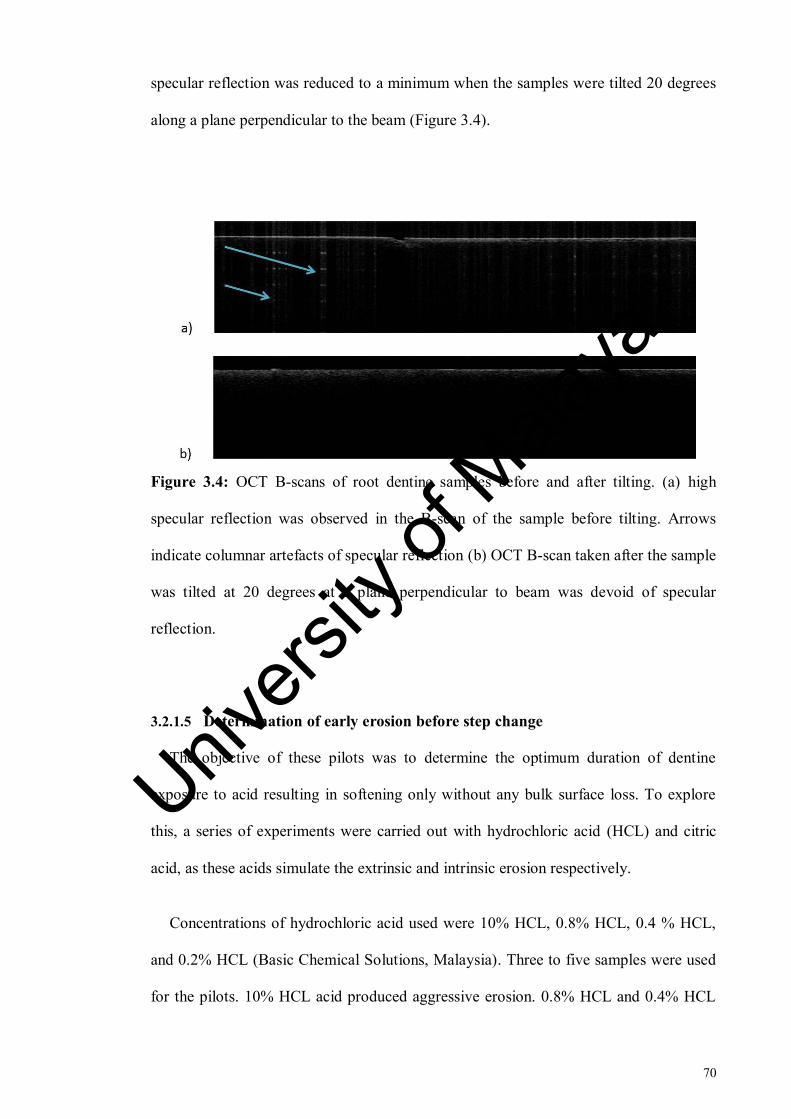
70
specular reflection was reduced to a minimum when the samples were tilted 20 degrees
along a plane perpendicular to the beam (Figure 3.4).
Figure 3.4: OCT B-scans of root dentine samples before and after tilting. (a) high
specular reflection was observed in the B-scan of the sample before tilting. Arrows
indicate columnar artefacts of specular reflection (b) OCT B-scan taken after the sample
was tilted at 20 degrees at a plane perpendicular to beam was devoid of specular
reflection.
3.2.1.5 Determination of early erosion before step change
The objective of these pilots was to determine the optimum duration of dentine
exposure to acid resulting in softening only without any bulk surface loss. To explore
this, a series of experiments were carried out with hydrochloric acid (HCL) and citric
acid, as these acids simulate the extrinsic and intrinsic erosion respectively.
Concentrations of hydrochloric acid used were 10% HCL, 0.8% HCL, 0.4 % HCL,
and 0.2% HCL (Basic Chemical Solutions, Malaysia). Three to five samples were used
for the pilots. 10% HCL acid produced aggressive erosion. 0.8% HCL and 0.4% HCL
Univers
ity of
Mala
ya

71
also resulted in a step change in the OCT images after 10 minutes of erosion challenge
(Figure 3.5). 0.2% HCL did not result in a step change after 10 minutes.
Figure 3.5: OCT B-scans of a sample taken at (a) baseline and (b) after 10 minutes of
exposure to hydrochloric acid. Step change (circled in red) was observed at the junction
of reference and eroded areas after 10 minutes of HCL exposure.
0.3% citric acid (A&C American Chemicals Ltd., North Carolina, USA) (pH = 3.2)
was used for used for this experiment. Samples were immersed in citric acid for 60
minutes and measurements with OCT were taken 10 minutes stepwise. Exposed surface
(eroded) could clearly be distinguished from baseline measurement as well as the
reference surface after only 10 minutes. Surface backscattering increased consistently
up to 40 min and then showed a decline at 50 min and 60 minutes of erosion. However
no step change was observed in the OCT images as shown in Figure 3.6.
Univers
ity of
Mala
ya
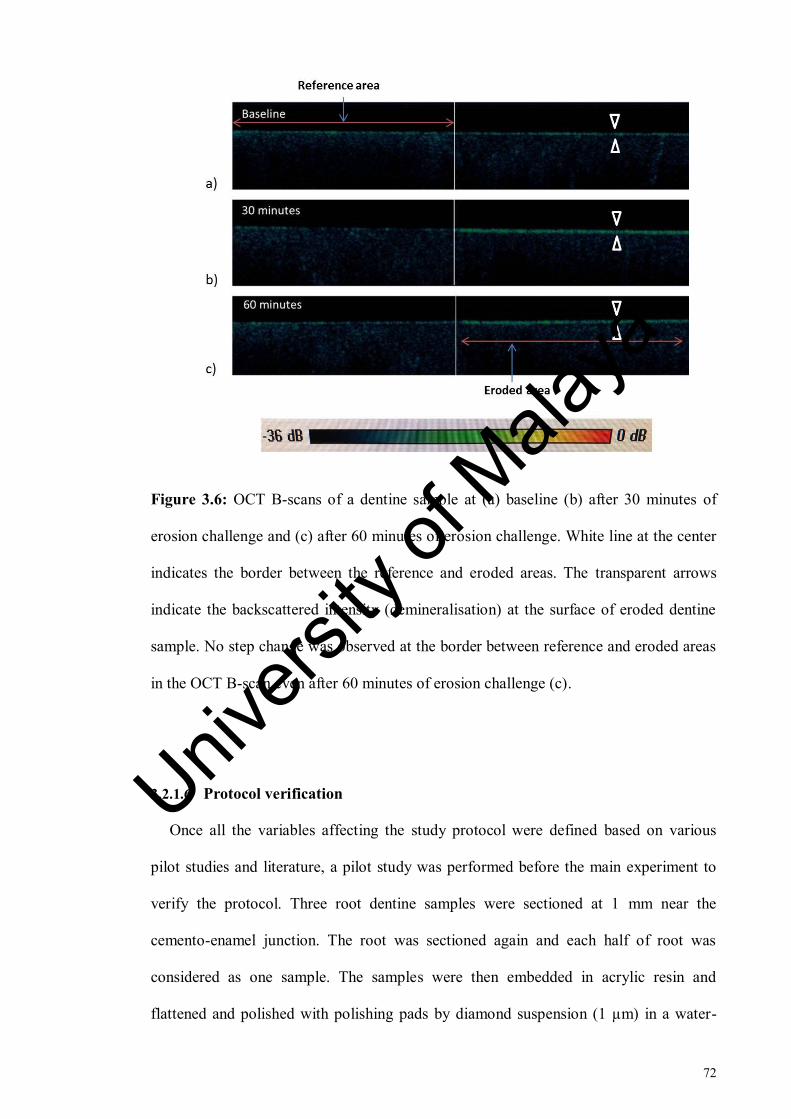
72
Figure 3.6: OCT B-scans of a dentine sample at (a) baseline (b) after 30 minutes of
erosion challenge and (c) after 60 minutes of erosion challenge. White line at the center
indicates the border between the reference and eroded areas. The transparent arrows
indicate the backscattered intensity (demineralisation) at the surface of eroded dentine
sample. No step change was observed at the border between reference and eroded areas
in the OCT B-scan even after 60 minutes of erosion challenge (c).
3.2.1.6 Protocol verification
Once all the variables affecting the study protocol were defined based on various
pilot studies and literature, a pilot study was performed before the main experiment to
verify the protocol. Three root dentine samples were sectioned at 1 mm near the
cemento-enamel junction. The root was sectioned again and each half of root was
considered as one sample. The samples were then embedded in acrylic resin and
flattened and polished with polishing pads by diamond suspension (1 µm) in a water-
Univers
ity of
Mala
ya

73
cooled rotating grinding/polishing machine (Buehler, USA). A window was created on
the sample with an adhesive tape and half of the window was covered with adhesive
tape to act as reference surface. Baseline scanning was performed with OCT. The
samples were then immersed in 0.3 % citric acid (pH 3.2) (A&C American Chemicals
Ltd., North Carolina, USA) and measurements with OCT were taken every two minutes
for the first 16 minutes and then again at 20, 25 and 30 minutes post-demineralisation.
The temperature of the solution was kept constant at 36°C and the speed of agitation
was kept constant at 300 rpm throughout the experiment. After being removed from
acid, the samples were rinsed with deionised water and air dried for 20 seconds. By
using a programme written in Matlab (The MathWorks, Inc., USA), all the images were
aligned horizontally with respect to the tooth-air interface and each aligned image
consisted of a reference and an eroded area (See Figure 3.16 and Section 3.2.3.4 for
details). Regions of interest were selected on each aligned image in the reference and
eroded sections of the image. A-scans were then generated from the regions of interest
selected for both the reference and eroded areas and intensity values were exported
automatically to excel sheets. Integrated intensity was calculated as the sum of pixels
intensities from a superficial optical depth of 23 µm to an optical depth of 58 µm. 58
µm was chosen because at this depth, no further changes in intensity were observed.
(See Section 3.2.3.5 and equation 3.2 for details). The plot is given in the Figure 3.7.
Plot showed that the intensity in the eroded area exhibited fluctuations with time
interval and remained almost constant from baseline measurement to 30 minutes. The
similarity in the intensity fluctuations in the reference and eroded areas suggested that
these were merely instrumental variations in time and the erosion induced was below
the detection threshold of the instrument employed. It was assumed that the presence of
smear layer on the surface had reduced the permeability of dentinal tubules to acid,
Univers
ity of
Mala
ya

74
resulting in very low surface scattering. Therefore, it was decided to conduct another
pilot study and remove the smear layer from the samples.
Figure 3.7: Mean integrated intensity of the reference and eroded areas at different
erosion time points. Arrows indicate the intensity fluctuations in the eroded area.
3.2.1.7 Removal of smear layer
The aim of this pilot study was to assess whether the smear layer was to be removed
by ultrasonication alone or that it would require the use of an agent. The samples were
prepared and polished as described before in Section 3.2.1.6. Samples were imaged with
stereomicroscope (SZX7, Olympus, Japan) at the magnifications of 1x, 1.6x and 2.5x.
The samples were then ultrasonicated with distilled water for 50 seconds. Post-
ultrasonication, the samples were imaged again with stereomicroscope (SZX7,
Olympus, Japan). EDTA is commonly used for removal of smear layer and its chelating
action is used to disintegrate the smear layer and open up the dentine tubules (Serper &
Calt, 2002). Other than the chemical removal of smear layer, ultrasonication has also
been shown to remove smear layer and smear plugs from dentinal tubules(Violich &
Chandler, 2010) . The samples were treated with 10% EDTA for 3 minutes, imaged
with stereomicroscopy and then ultrasonicated for 50 seconds. The imaging was
repeated again. One of the samples was additionally imaged with field-emission
Univers
ity of
Mala
ya
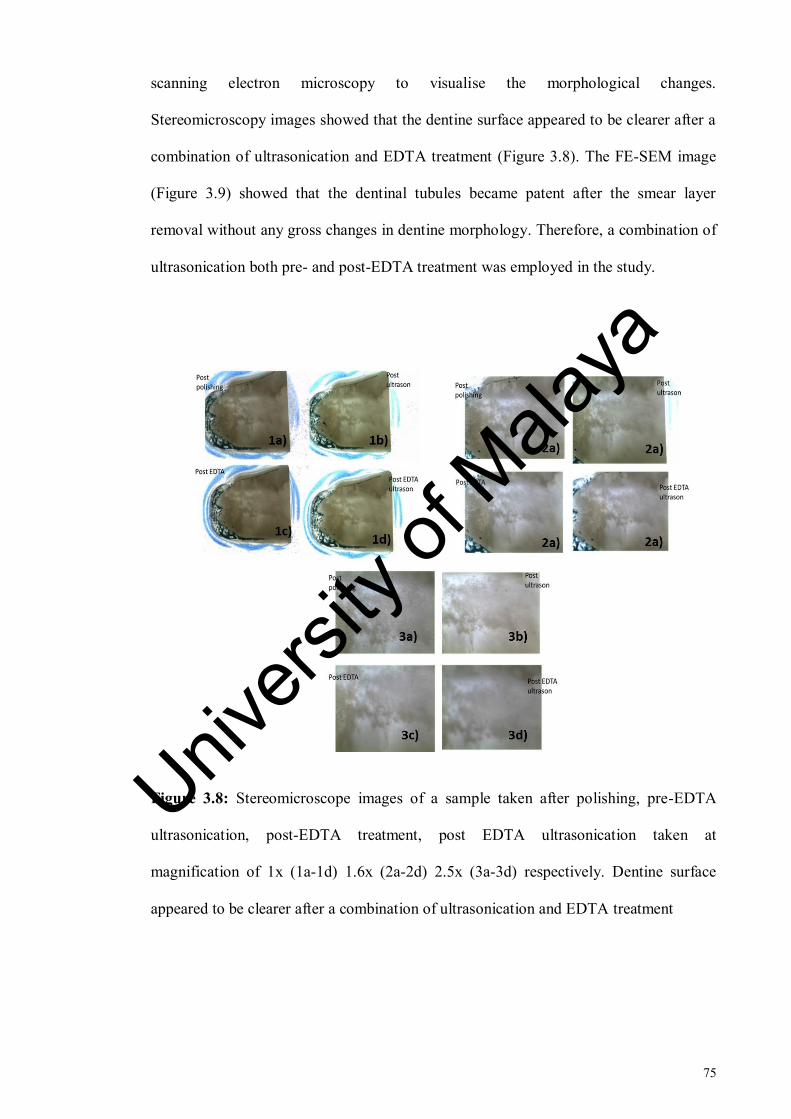
75
scanning electron microscopy to visualise the morphological changes.
Stereomicroscopy images showed that the dentine surface appeared to be clearer after a
combination of ultrasonication and EDTA treatment (Figure 3.8). The FE-SEM image
(Figure 3.9) showed that the dentinal tubules became patent after the smear layer
removal without any gross changes in dentine morphology. Therefore, a combination of
ultrasonication both pre- and post-EDTA treatment was employed in the study.
Figure 3.8: Stereomicroscope images of a sample taken after polishing, pre-EDTA
ultrasonication, post-EDTA treatment, post EDTA ultrasonication taken at
magnification of 1x (1a-1d) 1.6x (2a-2d) 2.5x (3a-3d) respectively. Dentine surface
appeared to be clearer after a combination of ultrasonication and EDTA treatment
Univers
ity of
Mala
ya

76
Figure 3.9: shows (a) sound dentine covered with smear layer (b) Dentine with smear
layer removed by 10 % EDTA treatment for 3 minutes pre- and post ultrasonication.
The dentinal tubules became patent after the smear layer removal without any obvious
gross changes in dentine morphology.
3.2.1.8 Effect of smear layer removal on OCT intensity
The objective of this pilot was to assess the effect of smear layer removal on the
OCT backscattered intensity using the previously employed erosion protocol. Five pre-
molars were prepared and demineralised as described before in Section 3.2.1.7.
However, before inducing demineralisation, smear layer was removed from the samples
by a combination of 50-second ultrasonication before and after treatment with 10%
EDTA solution.
A programme written in Matlab (The MathWorks, Inc., USA) was used for the
intensity analysis as described above (Section 3.2.1.6) and data was plotted. The plot for
the eroded area showed that there was a net increase in erosion from baseline to 30
minutes as shown in Figure 3.10, b). Hence it was decided to remove the smear layer in
the final study. The intensity changes in the reference area as shown in Figure 3.10, a)
suggested that a different reference be used since the residue left by adhesive tape could
be the cause of these fluctuations in intensity. Therefore, it was decided to employ a
Univers
ity of
Mala
ya

77
reference material rather than protecting reference area with adhesive tape during
erosion challenge.
Figure 3.10: shows (a) mean integrated intensity of the reference area of the samples at
various erosion time points. (b) mean integrated intensity of the eroded area of the
samples at various erosion time points.
3.2.1.9 Assessment of early dentine erosion with Micro-CT:
Microradiography is a gold standard technique for determination of mineral content
for assessment of demineralisation and remineralisation in vitro (Hamba et al., 2012).
However, it requires destructive sample preparation and results are inferred from very
thin sections of samples. Longitudinal microradiography has limited applicability in
studies of dentine erosion (Ganss et al., 2009b). Micro-CT is well-known technology
Univers
ity of
Mala
ya

78
with the most notable advantage of offering high resolution and non-destructive 3D
cross-sectional imaging which makes it applicable for in vitro longitudinal studies. This
pilot study aimed to assess if micro-CT is a suitable technique to be employed for
assessment of early dentine erosion.
(a) Sample preparation
Fourteen root dentine samples were prepared from seven intact upper or lower
human premolars. The teeth were collected and disinfected as described in Section
3.2.3.1. An ultrasonic scaler (Peizon® Master 400 Switzerland) was employed to
remove the hard deposits and soft tissues from the teeth. After scaling, the crowns were
sectioned horizontally 1 mm below the cemento-enamel junction using slow speed
microtome cutting machine (Micracut 125, Metkon Instruments Inc., Bursa, Turkey)
under copious water irrigation and discarded. Next, the roots were sectioned
longitudinally in the buccolingual direction. Each half of root was considered as one
sample. Resin blocks with dimensions of 30 x 20 x 15 mm were prepared with acrylic
resin (Quick Mount 2 Epoxy resin, Ace Technologies Inc., Arizona) and each sample
was attached to a separate resin block with a removable adhesive material (Tack-it,
Faber Castel, Malaysia) with external part of the root facing the surface. Samples were
ground flat with 600-grit silicon carbide paper (Struers Inc., Ohio, USA) followed by
polishing with polishing pads (8-inch Micropad polishing pad PSA, Pace® technologies,
Arizona) using diamond suspension (1 µm) in a water-cooled rotating
grinding/polishing machine (Buehler, USA) which removed the cementum.
The smear layer was removed from the surface of dentine by a combination of
EDTA and ultrasonication as explained in Section 3.2.3.1. A window with dimensions
of 5 x 3 mm was created on the surface of each sample by using red nail varnish
Univers
ity of
Mala
ya

79
(Revlon, USA). Additionally, the nail varnish was applied on the left half of the window
to create a reference and an eroded area. The reference surface was kept covered with
nail varnish (Revlon, USA) during erosion challenges. After the erosion challenge was
completed, the varnish was removed from the reference surface carefully with acetone
(Sigma-Aldrich, St. Louis, Missouri, USA). A bur mark was made with fissure bur at
the lower end of the window on the reference side of the sample to aid in identification
of reference area in micro-CT images. The prepared sample is shown in Figure 3.19.
(b) Erosion challenge
The prepared samples were suspended in a beaker containing 0.3% citric acid (pH =
3.2) (A&C American Chemicals Ltd., North Carolina, USA) on a movable stand with
wires and plastic clips. The temperature and speed of the solution were controlled by
placing the beakers on a magnetic stirrer (IKA RCT basic, Germany). A magnetic stirrer
is a laboratory device used for stirring a ‘stir bar’ added in the liquid by employing a
magnetic field. The solution is stirred as a result of it. The temperature of the solution
was kept constant at 36°C and the speed was kept constant at 300 rpm during the
experiment (See Figure 3.14).
The samples were not eroded longitudinally and so each sample was eroded for a
defined period of time. Two samples were eroded each for 2, 4, 8, 12, 16, 25 and 30
minutes. After being removed from the beaker containing acid, the samples were rinsed
with deionised water and dried with dental syringe for 20 seconds. The dental syringe
was kept at a distance of 10 cm from the samples. Citric acid was renewed after every
time point. The reference surface was kept covered with nail varnish (Revlon, USA)
during erosion challenges.
Univers
ity of
Mala
ya

80
(c) Measurements with Micro-CT
Micro-CT scanning of the root dentine samples took place in Minnesota Dental
Research for Biomaterials and Biomechanics (MDRCBB) School of Dentistry,
University of Minnesota. To transport the samples, each sample was attached to a
separate resin block with a removable adhesive material (Tack-it, Faber Castel,
Malaysia) with external part of the root facing the surface. Each sample attached to its
resin block was then placed in a separate container. In order to retain humidity, a wet
towel was placed at the bottom of the container avoiding any contact between the towel
and the sample surface (Francescut et al., 2006). Each resin block with the sample was
wrapped in moist gauze and placed in a separate aluminum packet. Fourteen packets
were prepared and placed in one aluminum bag which was air vacuumed. It was then
placed in a thermocol box which was sealed and couriered to reach MDRCBB School of
Dentistry, University of Minnesota for micro-CT scanning.
A high-resolution desktop micro-CT system (HMX-XT 225, X-tek system United
Kingdom) was used to scan the specimens. It had a resolution of 8 µm. Each sample
was placed on the stage inside the Micro-CT chamber using a plastic holder. Scanning
was performed using X-rays produced with tube voltage of 95 kV, tube current of 90
µA, exposure time of 708 m/s with 720 projections and 4 frames per projection. A total
of 14 dentine samples with two samples eroded for 2, 4, 8, 12, 16, 25 and 30 minutes
were scanned. Each sample was kept moist with wet cotton during scanning. Total
scanning time for each sample was 34 minutes. Each tooth was rotated at 360 degrees.
The distances from the x-ray source to the sample and to the detector were 65 and 972
mm respectively. Data was acquired as DICOM image stack for reconstruction of the
3D image of pixel resolution of 8 x 8 µm2 with isotropic voxel sizes of 8 x 8 x 8 µm
3.
Univers
ity of
Mala
ya

81
To minimise ring artefacts, air calibration of the detector was carried out prior to each
scanning. Averaging of 128 frames was applied in the acquisition phase to improve the
signal-to-noise ratio (SNR). The reconstruction of volume data was attempted using the
software CT Pro 3D (Nikon metrology, Inc., Brighton, MI, USA).
(d) Data processing and conclusions
The area of the sample which could be visualised in the DICOM files was the cut
surface of the root sample from where the crown had been sectioned from the root. The
area of interest however was located on the outer surface of the coronal portion of the
root sample. Therefore, a software programme 3D-Doctor (Able Software Corp., USA)
was employed to get the desired orientation of the image to be able to select and analyse
the regions of interest. These 3D images were uploaded in Image J programme (Wayne
Rasband, National Institute of Health, Bethesda, USA). Each image consisted of
approximately 500 micro-CT slices. Demineralised areas appear radiolucent in the
micro-CT images (Espigares et al., 2015). However, in this study visually no apparent
gray scale differences were observed between the sound dentine in the reference and
demineralised dentine in the eroded sides of each sample. Even the samples eroded for
30 minutes showed similar contrast in the reference and eroded areas (Figure 3.11).
Issues of beam hardening and shadow artefacts can sometimes make the detection and
characterisation of lesions with small mineral loss difficult (Espigares et al., 2015). This
coupled with the fact that amount of demineralisation induced in this study was very
low could be the reason that eroded areas did not appear distinct in terms of contrast
from the reference areas in the micro-CT images. Therefore, it could be concluded that
micro-CT had insufficient sensitivity to detect early dentine erosion induced in this
study.
Univers
ity of
Mala
ya

82
Figure 3.11: Micro-CT images of samples eroded for (a) 2 minutes, (b) 25 minutes and
(c) 30 minutes. No obvious difference in contrast was observed between the reference
and eroded areas of these samples.
Univers
ity of
Mala
ya
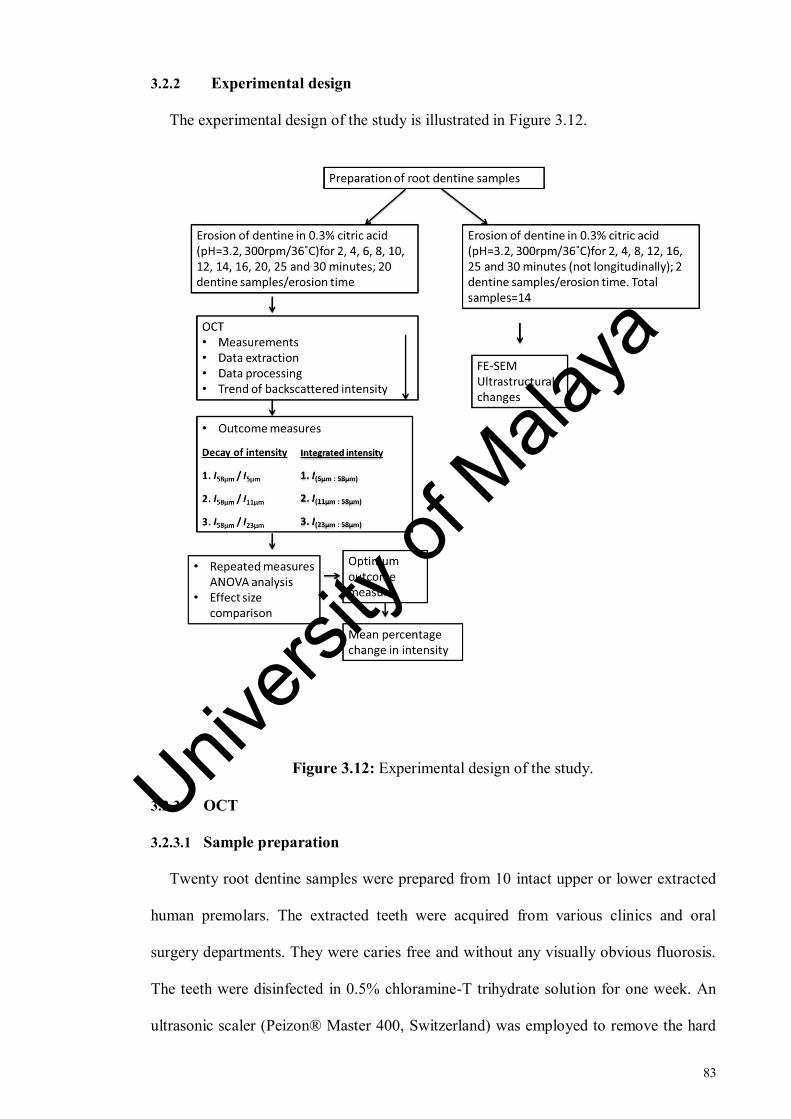
83
3.2.2 Experimental design
The experimental design of the study is illustrated in Figure 3.12.
Figure 3.12: Experimental design of the study.
3.2.3 OCT
3.2.3.1 Sample preparation
Twenty root dentine samples were prepared from 10 intact upper or lower extracted
human premolars. The extracted teeth were acquired from various clinics and oral
surgery departments. They were caries free and without any visually obvious fluorosis.
The teeth were disinfected in 0.5% chloramine-T trihydrate solution for one week. An
ultrasonic scaler (Peizon® Master 400, Switzerland) was employed to remove the hard
Univers
ity of
Mala
ya
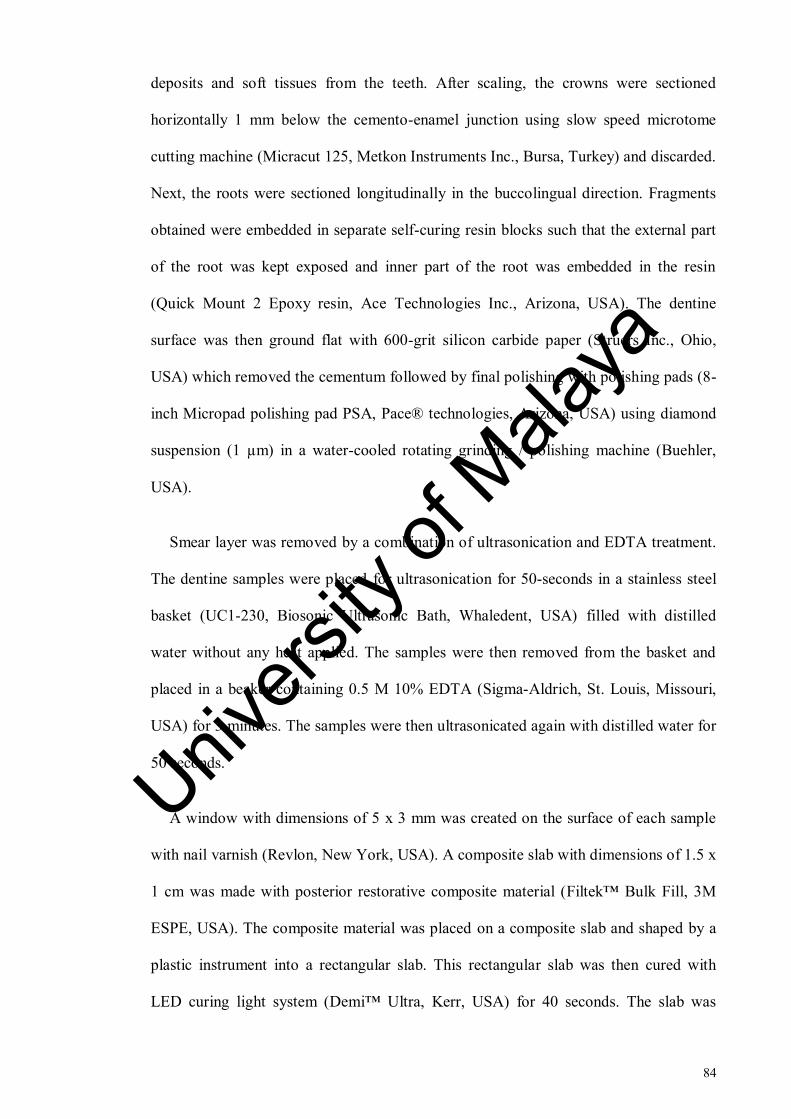
84
deposits and soft tissues from the teeth. After scaling, the crowns were sectioned
horizontally 1 mm below the cemento-enamel junction using slow speed microtome
cutting machine (Micracut 125, Metkon Instruments Inc., Bursa, Turkey) and discarded.
Next, the roots were sectioned longitudinally in the buccolingual direction. Fragments
obtained were embedded in separate self-curing resin blocks such that the external part
of the root was kept exposed and inner part of the root was embedded in the resin
(Quick Mount 2 Epoxy resin, Ace Technologies Inc., Arizona, USA). The dentine
surface was then ground flat with 600-grit silicon carbide paper (Struers Inc., Ohio,
USA) which removed the cementum followed by final polishing with polishing pads (8-
inch Micropad polishing pad PSA, Pace® technologies, Arizona, USA) using diamond
suspension (1 µm) in a water-cooled rotating grinding / polishing machine (Buehler,
USA).
Smear layer was removed by a combination of ultrasonication and EDTA treatment.
The dentine samples were placed for ultrasonication for 50-seconds in a stainless steel
basket (UC1-230, Biosonic Ultrasonic Bath, Whaledent, USA) filled with distilled
water without any heat applied. The samples were then removed from the basket and
placed in a beaker containing 0.5 M 10% EDTA (Sigma-Aldrich, St. Louis, Missouri,
USA) for 3 minutes. The samples were then ultrasonicated again with distilled water for
50 seconds.
A window with dimensions of 5 x 3 mm was created on the surface of each sample
with nail varnish (Revlon, New York, USA). A composite slab with dimensions of 1.5 x
1 cm was made with posterior restorative composite material (Filtek™ Bulk Fill, 3M
ESPE, USA). The composite material was placed on a composite slab and shaped by a
plastic instrument into a rectangular slab. This rectangular slab was then cured with
LED curing light system (Demi™ Ultra, Kerr, USA) for 40 seconds. The slab was
Univers
ity of
Mala
ya

85
flattened until it reached a diameter of 0.3 mm and polished with 1200-grit silicon
carbide paper (Struers Inc., Ohio, USA) in a water-cooled rotating grinding / polishing
machine (Buehler, USA). This slab was then used as a reference (Figure 3.13).
Figure 3.13: Sample preparation (a) root of premolar tooth (b) coronal view of root (c)
root sectioned along the long axis buccolingually into two halves (d & e) each half of
root considered as one sample (f) prepared sample.
3.2.3.2 Erosion challenge
Samples were scanned with OCT to acquire 3D images for baseline measurements.
Composite slab was placed on the left side of each sample while scanning the sample
with OCT. The samples were then suspended in a beaker containing 0.3% citric acid
(pH = 3.2) (A&C American Chemicals Ltd., North Carolina, USA) on a movable stand
with wires and plastic clips. A movable stand was used in order to facilitate the
immersion and removal of all samples simultaneously at the beginning or end of erosion
Univers
ity of
Mala
ya

86
challenge to standardise the acid exposure time. Five samples were suspended in 500 ml
of citric acid (A&C American Chemicals Ltd., North Carolina, USA) at one time. The
temperature and speed of the solution were controlled by placing the beakers on a
magnetic stirrer (RCT basic, IKA, Germany). A magnetic stirrer is a laboratory device
used for stirring a ‘stir bar’ added in the liquid by employing a magnetic field. The
solution is stirred as a result of it. The temperature of the solution was kept constant at
36°C and the speed was kept constant at 300 rpm during the erosion challenge
throughout the experiment as shown in the figure 3.14.
After two minutes of erosion challenge, the samples were removed from the beaker
and rinsed with deionised water. With rinsing, the erosion process is expected to be
slowed down or stopped (Lussi & Hellwig, 2014) which helps to avoid any variation in
the acid exposure time during measurements. The samples were then dried with dental
syringe for 20 seconds. The dental syringe was kept at a distance of 10 cm from the
samples. The samples were then scanned again with OCT.
The samples were immersed in citric acid for a total time period of 30 minutes but
they were removed from the acid after every two minutes for the first 16 minutes, then
after 20, 25 and 30 minutes exposure to acid followed by rinsing, drying and scanning
with OCT. Similar protocol of rinsing with deionised water and drying was used at all
time points. Citric acid was renewed after every erosion challenge. Univers
ity of
Mala
ya

87
Figure 3.14: Apparatus used for erosion challenge. A beaker containing citric acid
(pH=3.2) was placed on a magnetic stirrer device. A stir bar was added in the solution
(circled in red). The root dentine samples were suspended in the beaker as shown in the
figure. The temperature of citric acid and speed of agitation was controlled by the
magnetic stirrer.
3.2.3.3 Measurements with OCT
A commercially available OCT system (OCS1300SS Thorlabs Ltd., USA) was used
to capture three dimensional OCT data of the exposed window of the dentine samples.
This OCT system has a high-speed frequency swept laser centered at 1325nm. It has a
transverse resolution of 11 µm and an axial resolution of 9 µm in air according to the
manufacturer. This axial resolution would correspond to about 6 µm in dentine as the
refractive index of dentine is 1.54. The probing head was mounted with the beam facing
downwards. The probe was set at a distance of 1 cm from the sample surface, with the
scanning beam oriented at 0˚ to the surface. The samples were placed on a translational
stage perpendicular to the probe. The stage was fixed with a custom made jig (Figure
3.15) that enabled the samples to be repositioned to the same position and alignment
Univers
ity of
Mala
ya

88
during different measuring time points. This jig was also capable of tilting the samples
to a certain angle to reduce the specular reflection.
The Thorlabs OCT capturing software was used for capturing the images and
controlling the OCT settings and the light beam. The transverse resolution of the X-axis
was set at 1024 pixels in 5 mm and Y-axis at 96 pixels in 2 mm. The axial resolution of
the Z-axis was set at 512 pixels in 3 mm in air or 1.9 mm in dentine (refractive index of
dentine is 1.54). With these settings a total of 96 B-scans were generated for each 3D
image. The (x, y) coordinate of the light beam for each sample was recorded for
replication at consecutive measuring time points. Other parameters such as brightness
and contrast were kept constant for all samples. The inbuilt ruler within the system
software was used for standardising the height of each image and also for repositioning
the reference composite slab. Background noise was removed before the acquisition of
each image.
Each resin-mounted sample was removed from its container (containing deionised
water) immediately before imaging and dried with dental syringe for 20 seconds at a
distance of 10 cm. In order to ensure the repeatability of the OCT scan at various time
points, the specimens were placed at the same orientation as accurately as possible.
After adjusting all the system settings in the B-scan mode, a 3D scan was performed for
the pre-determined area of interest containing both the reference and eroded area within
the exposed window on each sample. All the samples were tilted at 20° to reduce the
specular reflection from the surface of the specimen on the OCT image (Chan et al.,
2015).
The composite slab was placed manually on the left side of the sample during
scanning at each time point. Therefore, each OCT 3D scan had composite slab on the
left side and eroded area on the right side. A bur mark was made on the anterior end of
Univers
ity of
Mala
ya

89
the reference slab to aid in repositioning of slab. Further, an inbuilt ruler within the
Thorlabs OCT software was used to mark the border between the reference and the
eroded side of the image. X and y coordinates of the ruler were recorded and same
values were employed for repositioning in the subsequent scanning.
Figure 3.15: OCT equipment and repositioning jig.
3.2.3.4 Data processing
A program was written in MATLAB (The MathWorks, Inc., USA) to load the OCT
C scan (3D scan) images and analyse the changes of the backscattered light intensity in
time. C scans of each measuring time point of each sample were aligned to reach a
horizontal surface corresponding to the tooth-air interface. Each aligned image
consisted of a reference and an eroded area. Regions of interest were selected on each
aligned image in the reference and eroded sections of the image. Each region of interest
was restricted to 10,500 A-scans in order to standardise the area being analysed. In
Univers
ity of
Mala
ya

90
order to standardise the analysis, all 12 time points of each sample were aligned in a
similar manner and identical regions of interest were loaded for them. A-scans were
then generated from the regions of interest selected for both the reference and eroded
areas and intensity values were exported automatically to excel sheets. Figure 3.16 (a-d)
shows the main steps of data processing through Matlab programme.
Figure 3.16: Data processing of OCT C-scan images (a) graphic user interface (GUI) of
Matlab programme for uploading and processing of data (b) aligned surface view of one
C-scan of one time point. Green and red selections represent the regions of interest
selected for reference and eroded areas respectively (c) mean depth-resolved intensity
profile (A-scan) for the reference and eroded areas represented by green and red plots
respectively (d) data from mean A-scan for one C-scan of one time points exported to
excel files separately for reference and eroded areas.
Univers
ity of
Mala
ya

91
3.2.3.5 Trend of backscattered intensity
In the excel programme, the values of each A-scan generated for the reference or
eroded area of each 3D OCT image was further reduced to single values by averaging
the intensity per pixel. Once the A-scans were averaged for all the samples for each time
point, a mean A-scan was then generated and the standard deviation was also calculated
from the averaged intensity per pixel. The data for the reference and eroded areas was
separately plotted to observe and compare the main trend of backscattered intensity in
both areas.
3.2.3.6 Parameters for intensity analysis
(a) Decay of intensity
Two parameters, ‘decay of intensity’ and ‘integrated intensity’ were employed for
the analysis. Decay of intensity calculates the relationship of the attenuation of
backscattered light between two optical depths of an OCT mean A-scan. It had been
employed in a previous study for the monitoring of early enamel erosion with OCT
(Chew et al., 2014). Integrated intensity had been shown to correlate with the integrated
mineral loss (volume % mineral × µm) ΔZ, in the previous studies (Jones et al., 2006a;
Ngaotheppitak et al., 2005).
The first parameter ‘decay of intensity’ or D is represented by the function below,
𝐷 =𝐼𝑝𝑙𝑎𝑡𝑒𝑎𝑢
𝐼𝑠𝑢𝑝𝑒𝑟𝑓𝑖𝑐𝑖𝑎𝑙
(3.1)
Iplateau is the intensity at an optical depth at which the A-scans had reached a plateau
and were assumed not to be affected further by the erosive challenge. It was observed at
58 µm (physical depth = 38 µm) for this study. Isuperficial is the intensity near the surface
located immediately below the tooth-air interface. For this study, three optical depths 5
Univers
ity of
Mala
ya
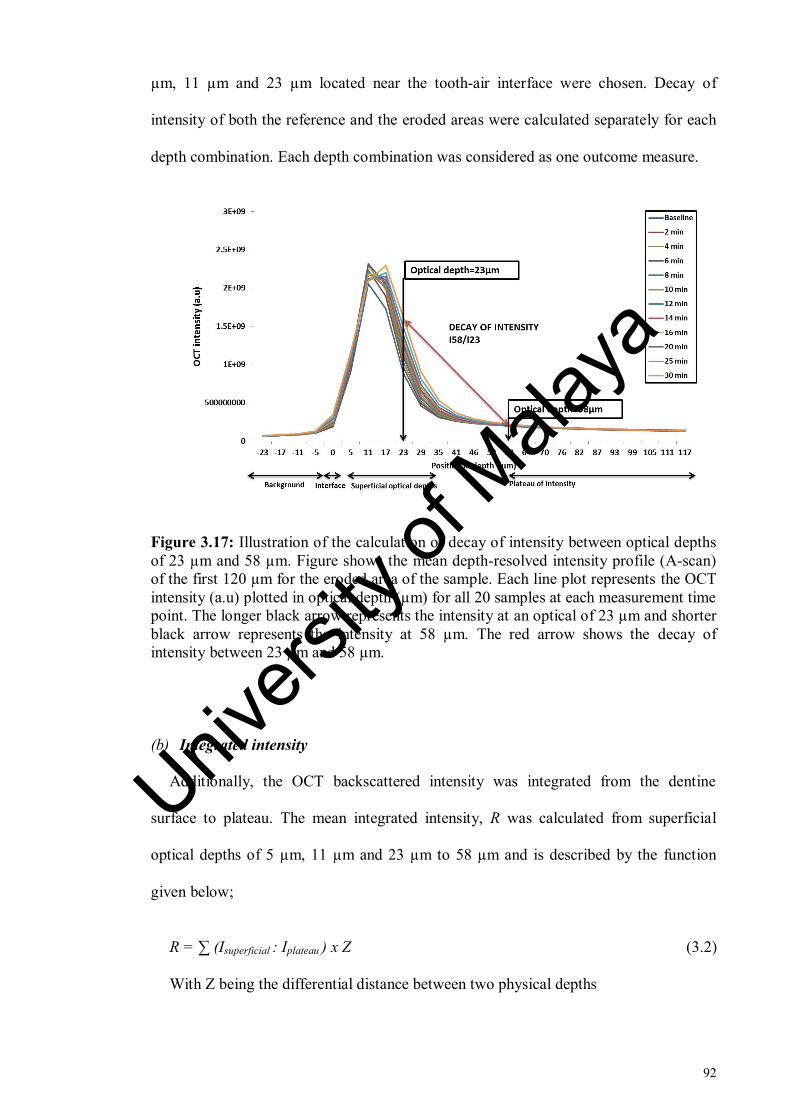
92
µm, 11 µm and 23 µm located near the tooth-air interface were chosen. Decay of
intensity of both the reference and the eroded areas were calculated separately for each
depth combination. Each depth combination was considered as one outcome measure.
Figure 3.17: Illustration of the calculation of decay of intensity between optical depths
of 23 µm and 58 µm. Figure shows the mean depth-resolved intensity profile (A-scan)
of the first 120 µm for the eroded area of the sample. Each line plot represents the OCT
intensity (a.u) plotted in optical depth (µm) for all 20 samples at each measurement time
point. The longer black arrow represents the intensity at an optical of 23 µm and shorter
black arrow represents the intensity at 58 µm. The red arrow shows the decay of
intensity between 23 µm and 58 µm.
(b) Integrated intensity
Additionally, the OCT backscattered intensity was integrated from the dentine
surface to plateau. The mean integrated intensity, R was calculated from superficial
optical depths of 5 µm, 11 µm and 23 µm to 58 µm and is described by the function
given below;
R = ∑ (Isuperficial : Iplateau ) x Z (3.2)
With Z being the differential distance between two physical depths
Univers
ity of
Mala
ya

93
Integrated intensity of both the reference and the eroded areas were calculated
separately for each depth combination. Each depth combination was considered as one
outcome measure.
Figure 3.18: Illustration of the calculation of integrated intensity from an optical depth
of 23 µm to an optical depth of 58 µm. Figure shows the mean depth-resolved intensity
profile (A-scan) of the first 120 µm for the eroded area of the sample. Each line plot
represents the OCT intensity (a.u) plotted in optical depth (µm) for all 20 samples at
each measurement time point. The longer black arrow represents the intensity at an
optical of 23 µm and shorter black arrow represents the intensity at 58 µm. The red
arrow shows the integrated intensity between 23 µm and 58 µm. Z is the differential
distance between two physical depths.
Further, percentage change in integrated intensity of the eroded area during a
particular time point from baseline time point of eroded area was calculated. ΔR for
each measurement time point is represented by the formula:
∆𝑅(𝑡) = 100 ∗ [𝑅𝐸(𝑡) − 𝑅𝐸(𝑡0)
𝑅𝐸(𝑡0)]
(3.3)
Where RE is mean integrated intensity of the eroded area, 𝑡0 is the baseline time point
and t is the specific measurement time point.
Univers
ity of
Mala
ya

94
The mean percentage change in backscattered intensity was plotted with erosion
interval and line fitting was performed with Microsoft Office Excel® 2010 programme
to observe the trend of ΔR with time. The validity and significance of model was
assessed by R2
value.
3.2.3.7 Comparison by effect size
Effect size is a quantitative measure of strength of a phenomenon. In order to identify
the most suitable outcome measure for analysis, the outcome measures of both
parameters were compared in terms of their effect size to assess their strength. The
effect sizes of all outcome measures were compared by partial eta square values
generated by SPSS, version 22 (IBM SPSS Statistics 22.0 Inc., USA) as part of repeated
measures ANOVA analysis.
3.2.4 FE-SEM
3.2.4.1 Sample Preparation:
Fourteen root dentin samples were prepared from seven intact upper or lower human
premolars. The teeth were collected and disinfected in a similar manner as described in
Section 3.2.3.1. An ultrasonic scaler (Peizon® Master 400 Switzerland) was employed
to remove the hard deposits and soft tissues from the teeth. After scaling, the crowns
were sectioned horizontally 1 mm below the cemento-enamel junction using slow speed
microtome cutting machine (Micracut 125, Metkon Instruments Inc., Bursa, Turkey)
under copious water irrigation and discarded. Next, the roots were sectioned
longitudinally in the buccolingual direction. Each half of root was considered as one
sample. Resin blocks with dimensions of 30 x 20 x 15 mm were prepared with acrylic
Univers
ity of
Mala
ya

95
resin (Quick Mount 2 Epoxy resin, Ace Technologies Inc., Arizona) and each sample
was attached to a separate resin block with a removable adhesive material (Tack-it,
Faber Castel, Malaysia) with external part of the root facing the surface. The fragments
were not embedded in the resin because the presence of resin can act as a confounding
factor during micro-CT scanning as previously determined from a pilot study. Samples
were ground flat with 600-grit silicon carbide paper (Struers Inc., Ohio, USA) which
removed the cementum followed by polishing with polishing pads (8-inch Micropad
polishing pad PSA, Pace® technologies, Arizona) using diamond suspension (1 µm) in a
water-cooled rotating grinding/polishing machine (Buehler, USA).
The smear layer was removed from the surface of dentine by a combination of
EDTA and ultrasonication as explained in Section 3.2.3.1. A window with dimensions
of 5 x 3 mm was created on the surface of each sample with red nail varnish (Revlon,
USA). Additionally, the nail varnish was applied on the left half of the window to create
a reference and an eroded area. The reference surface was kept covered with nail
varnish (Revlon, USA) during erosion challenges. After the erosion challenge was
completed, the varnish was removed from the reference surface carefully with acetone
(Sigma-Aldrich, St. Louis, Missouri, USA). A bur mark was made with fissure bur at
the lower end of the window on the reference side of the sample to aid in identification
of reference area in micro-CT images. The prepared sample is shown in Figure 3.19.
Univers
ity of
Mala
ya

96
Figure 3.19: Prepared root dentine sample for FE-SEM imaging. The blue rectangle
indicates the window prepared on the sample. The left half of the window (reference
area) was kept covered with red nail varnish during erosion challenges while the right
half of the window (eroded area) was exposed to erosion challenge
3.2.4.2 Erosion challenge
The prepared samples were suspended in a beaker containing 0.3% citric acid (pH =
3.2) (A&C American Chemicals Ltd., North Carolina, USA) on a movable stand with
wires and plastic clips. The temperature and speed of the solution were controlled by
placing the beakers on a magnetic stirrer (IKA RCT basic, Germany). A magnetic stirrer
is a laboratory device used for stirring a ‘stir bar’ added in the liquid by employing a
magnetic field. The solution is stirred as a result of it. The temperature of the solution
Univers
ity of
Mala
ya

97
was kept constant at 36°C and the speed was kept constant at 300 rpm during the
experiment as shown in the figure 3.14.
The samples were not eroded longitudinally and so each sample was eroded for a
defined period of time. Two samples were eroded each for 2, 4, 8, 12, 16, 25 and 30
minutes. After being removed from the beaker containing acid, the samples were rinsed
with deionised water and dried with dental syringe for 20 seconds. The dental syringe
was kept at a distance of 10 cm from the samples. Citric acid was renewed after every
time point. The reference surface was kept covered with nail varnish (Revlon, USA)
during erosion challenges.
3.2.4.3 Imaging
High magnification imaging of the surface of dentine samples was performed with
field emission scanning electron microscopy (FE-SEM) to assess the erosion-associated
surface alterations. Two samples exposed to erosion challenge for 2, 4, 8, 12, 16, 25 and
30 minutes (total fourteen samples) were scanned with field emission scanning electron
microscope (FE-SEM; FEI, Quanta 200F, United Kingdom).
Moisture loss within dentine can lead to additional alterations of the surface and
collapse of organic matrix (Attin & Wegehaupt, 2014), therefore, the samples were
dried for only 20 seconds with dental syringe before imaging. The images were captured
at a magnification of 1000x and 2000x at an accelerating voltage of 10 kv. Six images
were obtained in total for each sample. Three images were obtained at a magnification
of 1000x and the other three at a magnification of 2000x. One image was obtained at the
reference side of each sample with healthy dentine, second image was taken at the
Univers
ity of
Mala
ya

98
eroded side of each sample and the third image was taken at the middle of the sample at
the junction of reference surface and the eroded surface.
Additionally, a cross-section of a sample eroded for 25 minutes was obtained to
assess if the demineralisation induced had resulted in a step change between the
reference and eroded areas. The root dentine sample was embedded in epoxy resin and
sectioned at the border between the reference and eroded areas by Isomet™ diamond
saw (Buehler, Lake Bluff, IL, USA) in a transverse plane. The sectioned surfaces were
polished increasingly with sandpapers up to 1200 grits, and then fine polished by a
series of napped cloth impregnates with alumina pastes, finishing with a grain size of
0.1 µm. Imaging was performed at three levels of magnifications i-e 400x, 1000x and
2000x. The sample was air-dried before imaging.
3.2.5 Statistical Analysis:
Statistical data analysis was performed with SPSS, version 22 (IBM SPSS Statistics
22.0 Inc., USA). The level of significance was set at p < 0.05. Shapiro-Wilk test and
skewness were assessed to check the assumption of normality. Outliers were removed
from the data if present. One-way repeated measures ANOVA was performed with post
hoc multiple comparisons. A Bonferroni-Holm correction was performed to reduce risk
of type 1 errors in multiple comparisons using Holm-Bonferroni correction calculator
(Gaetano, 2013). The Bonferroni-Holm correction is a modification of conventionally
used Bonferroni correction. Bonferroni correction addresses the familywise error rates
for multiple comparisons but lacks statistical power. Bonferroni Holm correction not
only addresses the familywise error rates for multiple comparisons but offers more
statistical power at the same time with similar ease of calculation (Mclaughlin &
Sainani, 2014).
Univers
ity of
Mala
ya

99
3.3 Results
3.3.1 OCT
3.3.1.1 Trend of backscattered intensity
Mean A-scan curve generated from reference (Figure 3.20) and eroded areas (Figure
3.21) showed that initially the light travelled for a certain distance in air without
changing (background intensity, Ibackground). The intensity started to increase from the
tooth-air interface (intensity at interface, Iinterface) observed at approximately at 0 µm,
increased below the interface (Intensity at surface, Isurface) until it reached the maximum
intensity value at approximately 11 µm (maximum intensity, Imax). From Imax onwards,
the intensity then proceeded to decline (Intensity drop, Idrop) until it reached a point
where no further changes in intensity were observed (Intensity plateau, Iplateau). Iplateau
was identified at an optical depth of 58 µm, translated to a physical depth of 38 µm as
the refractive index of the dentine is 1.54 (Natsume et al., 2011).
Each line graph in mean A-scan of reference and eroded area represented the
averaged intensity of all samples for each time point (Figure 3.20 & Figure 3.21). Line
graphs in the mean A-scan of reference area (Figure 3.20) showed little separation at
various depths suggesting that little or no changes in intensity had occurred over time in
the reference area. The mean A-scan of eroded area (Figure 3.21) however showed
separation between line graphs indicating the erosion interval related shift in intensity
from baseline measurement to increasing erosion intervals. Moreover, the line plots in
the eroded area were arranged in increasing order of intensity from baseline
measurement to 30 minutes except for plots of 6 and 10 minutes which were almost
indistinguishable. With the scanning resolution of 512 pixels in 1.90 mm in the z-axis,
there were approximately 21 depth points in the first 120 µm of mean A-scans. The
minimal optical separation of the two adjacent points was about six microns amounting
to 3.8 µm of physical separation.
Univers
ity of
Mala
ya
100
The standard deviation of all samples at each optical depth for every measurement
time point was calculated by using function STDEV (C1 : C20) in Microsoft excel
where C is the intensity of one sample at an optical depth. The error bars in the Figure
3.20 and Figure 3.21 represent the standard deviation. The mean A-scans showed that
the near the surface there was very high variation in the intensity among the samples
and from an optical depth of 23 µm (translated to physical depth of 15 µm) onwards, the
intensity became relatively stable as shown by lower values of standard deviation.
Figure 3.27 shows the representative OCT B-scans of one sample taken at baseline
and increasing erosion intervals. The increase in backscattered intensity signal at the
surface of the eroded side of the sample was evident as the erosion interval progressed.
These representative B-scans were selected because they represent frame 50 of every 3
D image and so were located right in the center of the 96 B scans.
Univers
ity of
Mala
ya

101
Figure 3.20: Mean depth-resolved intensity profile (A-scan) of the first 120 µm for the
reference area of the sample. Each line plot represents OCT intensity (a.u) plotted in
optical depth (µm) for all 20 samples at each measurement time point. Red, blue and
green dotted lines represent the superficial optical depths chosen for the analysis.
Plateau of intensity is shown by black dotted line. The error bars represent standard
deviation.
Figure 3.21: Mean depth-resolved intensity profile (A-scan) of the first 120 µm for the
eroded area of the sample. Each line plot represents OCT intensity (a.u) plotted in
optical depth (µm) for all 20 samples at each measurement time point. Red, blue and
green dotted lines represent the superficial optical depths chosen for the analysis.
Plateau of intensity is shown by black dotted line. The error bars represent standard
deviation.
Univers
ity of
Mala
ya

102
Figure 3.22: Representative OCT A-scans of one sample at (a) baseline measurement
(b) 2 minutes (c) 4 minutes (d) 6 minutes (e) 8 minutes (f) 10 minutes (g) 12 minutes (h)
14 minutes (i) 16 minutes (j) 20 minutes (k) 25 minutes (l) 30 minutes. Each A-scan
shows the OCT intensity (a.u) plotted in optical depth (µm). The red text box indicates
the OCT intensity at a depth of 23 µm. The chart title of each A-scan indicates the time
interval for which the A-scan was plotted. The increase in intensity at 23 µm is obvious
with time.
Univers
ity of
Mala
ya

103
Figure 3.22 Continued
Univers
ity of
Mala
ya

104
Figure 3.23: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious.
Univers
ity of
Mala
ya

105
Figure 3.24: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious. Univers
ity of
Mala
ya

106
Figure 3.25: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious.
Univers
ity of
Mala
ya

107
Figure 3.26: Representative A-scans of a sample at (a) baseline time point and b) after
30 minutes of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to 30 minutes of erosion (b) at 23
µm is obvious.
Univers
ity of
Mala
ya

108
Figure 3.27: Representative OCT B-scans of a sample at (a) baseline measurement (b)
2 minutes (c) 4 minutes (d) 6 minutes (e) 8 minutes (f) 10 minutes (g) 12 minutes (h) 14
minutes (i) 16 minutes (j) 20 minutes (k) 25 minutes and (l) 30 minutes. A composite
slab was used as reference as shown by the red arrow in the figure. Transparent arrows
indicate the backscattered intensity at the surface of eroded area.
Univers
ity of
Mala
ya
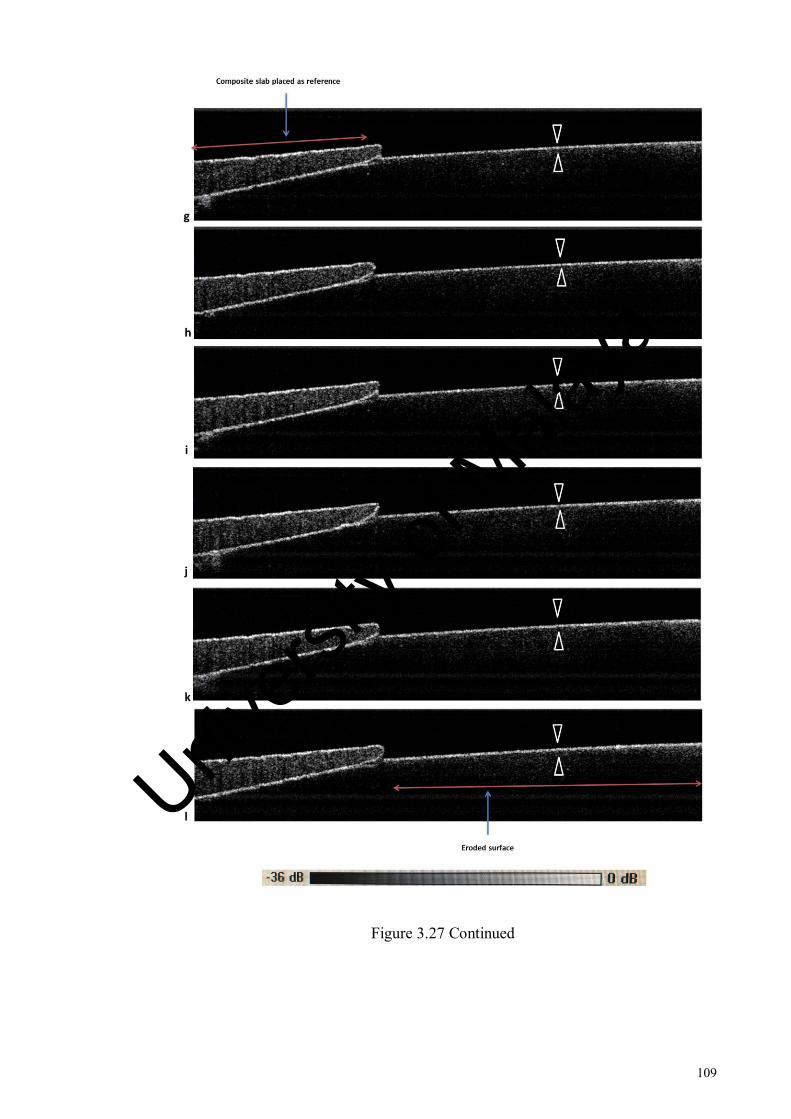
109
Figure 3.27 Continued
Univers
ity of
Mala
ya

110
3.3.1.2 Outcomes measures
OCT parameters and their outcome measures have been summarised in the Table 3.2.
Table 3.2: OCT parameters and their outcome measures defined.
Parameters Symbol Equation Outcome measures
Decay of
intensity
D D = 𝐼𝑝𝑙𝑎𝑡𝑒𝑎𝑢
𝐼𝑠𝑢𝑝𝑒𝑟𝑓𝑖𝑐𝑖𝑎𝑙
I58µm / I5µm
I58µm / I11µm
I58µm / I23µm
Integrated
intensity R
R = ∑ Isuperficial : Iplateau ) x Z
I(5µm : 58µm)
I(11µm : 58µm)
I(23µm : 58µm)
Mean %
Integrated
intensity
ΔR
∆𝑅(𝑡) = 100 ∗ [𝑅𝐸(𝑡) − 𝑅𝐸(𝑡0)
𝑅𝐸(𝑡0)]
Where R = I(23µm : 58µm)
Mean % I(23µm : 58µm)
Shapiro-Wilk test and skewness values showed that the data was normally distributed
for the outcome measures I58µm / I5µm, I58µm / I11µm, I(5µm : 58µm), I(11µm : 58µm) and I(23µm :
58µm). Data for I58µm / I23µm did not confirm to a normal distribution. Hence, analysis for
I58µm / I23µm was performed after logarithmic transformation to a normal distribution.
One-way repeated measures ANOVA was performed and Mauchly’s test was used to
evaluate the sphericity assumption. If sphericity was not met, the adjusted F-value of the
Greenhouse-Geisser correction was considered.
Mean and standard deviation (given in brackets) for the eroded area of outcome
measures of decay of intensity and integrated intensity are given in Table 3.6 and Table
3.10 respectively.
Univers
ity of
Mala
ya

111
(a) I58µm / I5µm
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (2 = 148.6, p < 0.0001) and eroded areas, (
2 = 196.37, p < 0.0001).
Therefore, the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA analysis showed that there was a significant
effect of erosion interval on OCT backscattered intensity of both the reference,
(F(2.61,46.9) = 17.2, p < 0.0001, η2=.489) and eroded areas (F(3.01,54.2) = 8.88, p < 0.0001,
η2 = .331) as shown in table 3.3.
Post hoc comparisons for the eroded area showed that the mean intensity values of
all time points were significantly different with respect to their baseline intensity values
(table 3.4). However, significant differences were only observed among consecutive
time points between baseline and 4 minutes as shown in table 3.5. Data plot is given in
Figure 3.28.
Figure 3.28: Mean decay of intensity of reference and eroded areas at various erosion
intervals between superficial optical depth of 5 µm and intensity plateau at 58 µm.
Univers
ity of
Mala
ya

112
(b) I58µm / I11µm
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (2 =206.5, p < 0.0001) and eroded areas (
2 = 215.9, p < 0.0001). Therefore,
the adjusted F-values of the Greenhouse-Geisser correction were considered. One-way
repeated measures ANOVA analysis showed that there was a significant effect of
erosion interval on the OCT backscattered intensity of both the reference, (F(2.1,40.06) =
15.7, p < 0.0001, η2
= .53) and the eroded areas, (F(2.6,49.5) = 6.49, p = 0.001, η2
= .255)
(table 3.3).
Post hoc comparisons for the eroded area showed that mean intensity values of only
4 minutes were significantly different to their baseline intensity values (table 3.4).
However, no significant differences were observed among any of the consecutive time
points (table 3.5). Data plot is given in Figure 3.29.
Figure 3.29: Mean decay of intensity of reference and eroded areas at various erosion
intervals between superficial optical depth of 11 µm and intensity plateau at 58 µm.
Univers
ity of
Mala
ya

113
(c) I58µm / I23µm
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference and (2 = 220.27, p < 0.0001) eroded areas (
2 = 181.82, p < 0.0001).
Therefore, the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA analysis (table 3.3) showed that there was a
significant effect of erosion interval on the OCT backscattered intensity of both the
reference (F(2.05, 36.9) = 12.1, p < 0.0001, η2
= .403) and the eroded areas (F (3.008, 54.1) =
57.2, p < 0.0001, η2 = .761).
Post hoc comparisons for the eroded area showed that mean intensity values of all
time points were significantly different with respect to their baseline values (p<0.05)
given in table 3.4. Significant differences in mean intensity values were observed
between consecutive time intervals between baseline and 6 minutes of erosion duration
(table 3.5). Plot is given in Figure 3.30.
Figure 3.30: Mean decay of intensity of reference and eroded areas at various erosion
intervals between superficial optical depth of 23 µm and intensity plateau at 58 µm.
Univers
ity of
Mala
ya

114
Table 3.3: Results of repeated measures ANOVA analysis for reference and eroded
areas of outcome measures of decay of intensity.
Outcome
measure
Reference area Eroded area
Mean
square
F-statistic p-value Mean
square
F-statistic p-value
I58µm / I5µm .005 17.242 <0.0001 .006 8.886 <.0001
I58µm / I11µm .001 15.751 <0.0001 .002 6.496 .001
I58µm / I23µm .021 12.161 <0.0001 .309 57.261 <.0001
Table 3.4: Post hoc comparisons of all erosion time points with baseline, for the eroded
area of outcome measures of decay of intensity.
Time (I) Time(J) Mean difference (I-J)
I58µm / I5µm I58µm / I11µm I58µm / I23µm
Baseline 2min .012** .006 .032**
Baseline 4min .019** .007* .057***
Baseline 6min .022*** .007 .078***
Baseline 8min .020** .004 .093***
Baseline 10min .025*** .005 .121***
Baseline 12min .030*** .006 .143***
Baseline 14min .029*** .004 .151***
Baseline 16min .031*** .002 .161***
Baseline 20min .030*** -.002 .173***
Baseline 25min .031*** -.005 .195***
Baseline 30min .030*** -.008 .214***
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Univers
ity of
Mala
ya
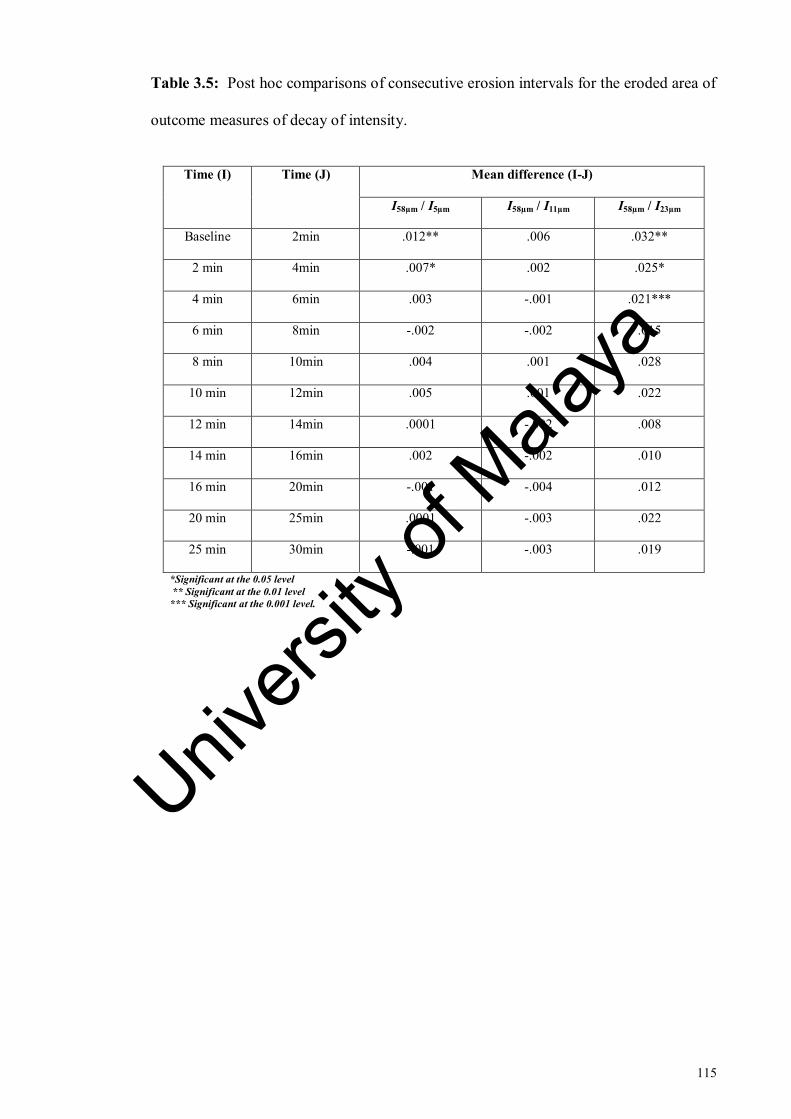
115
Table 3.5: Post hoc comparisons of consecutive erosion intervals for the eroded area of
outcome measures of decay of intensity.
Time (I) Time (J) Mean difference (I-J)
I58µm / I5µm I58µm / I11µm I58µm / I23µm
Baseline 2min .012** .006 .032**
2 min 4min .007* .002 .025*
4 min 6min .003 -.001 .021***
6 min 8min -.002 -.002 .015
8 min 10min .004 .001 .028
10 min 12min .005 .001 .022
12 min 14min .0001 -.002 .008
14 min 16min .002 -.002 .010
16 min 20min -.001 -.004 .012
20 min 25min .0001 -.003 .022
25 min 30min -.001 -.003 .019
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Univers
ity of
Mala
ya

116
Table 3.6: Mean and standard deviation (given in brackets) for the eroded area of
outcome measures of decay of intensity.
Time point
Outcome measure
I58µm / I5µm I58µm / I11µm I58µm / I23µm
Baseline .213
(.054)
.099
(.028)
0.226
(0.058)
2 minutes .201
(.056)
.093
(.028)
0.21
(0.059)
4 minutes .194
(.051)
.091
(.027)
0.198
(0.053)
6 minutes .191
(.052)
.092
(.029)
0.188
(0.049)
8 minutes .193
(.057)
.094
(.03)
0.183
(0.051)
10 minutes .189
(.053)
.094
(.03)
0.172
(0.049)
12 minutes .184
(.048)
.093
(.027)
0.162
(0.041)
14 minutes .184
(.049)
.095
(.028)
0.159
(0.039)
16 minutes .182
(.045)
.097
(.029)
0.154
(0.034)
20 minutes .183
(.045)
.101
(.03)
0.151
(0.038)
25 minutes .182
(.044)
.104
(.03)
0.143
(0.035)
30 minutes .183
(.041)
.107
(.028)
0.136
(0.028)
Univers
ity of
Mala
ya

117
(d) I(5µm : 58µm)
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (reference, 2 = 192.22, p < 0.0001) and eroded areas (
2 = 196.92, p <
0.0001). Therefore, the adjusted F-values of the Greenhouse-Geisser correction were
considered. One-way repeated measures ANOVA analysis showed that there was a
significant effect of erosion interval on OCT backscattered intensity for the eroded area
(F(3.2, 61.8) = 16.6, p < 0.0001, η2
= .467) whereas no significant effect of erosion interval
on OCT backscattered intensity was found for the reference area (F(3.03, 57.6) = 2.2, p =
0.092, η2 = .106) as shown in Table 3.7.
Post hoc comparisons for the eroded area showed that mean intensity values of all
time points were significantly different with respect to their baseline intensity values (p
< 0.05) (Table 3.8). Significant differences were observed among consecutive time
points from baseline to 6 minutes of erosion challenge (Table 3.9). Data plots for
reference and eroded areas are given in Figure 3.31
Univers
ity of
Mala
ya

118
Figure 3.31: Mean integrated intensity of reference and eroded areas at various erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 5
µm to the intensity plateau at 58 µm.
(e) I(11µm : 58µm)
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (reference, 2 = 193.209, p < 0.0001) and eroded areas (
2 = 200.914, p <
0.0001). Therefore, the adjusted F-values of the Greenhouse-Geisser correction were
considered. One-way repeated measures ANOVA analysis showed that there was a
significant effect of erosion interval on backscattered intensity of the eroded area (F(3.1,
59.4) = 16.7, p < 0.0001, η2
= .468) whereas no significant effect of erosion interval was
found on backscattered intensity in the reference area (F(2.97, 56.4) = 2.148, p = 0.105, η2
=
.102) as shown in Table 3.7.
Post hoc comparisons for the eroded area showed that mean intensity of all erosion
intervals was significantly different with respect to their baseline intensity values (Table
3.8). However, significant differences in mean intensity values among consecutive time
points were only observed from baseline to 6 minutes of erosion challenge (Table 3.9).
Data plots for reference and eroded areas are given in Figure 3.32. Univers
ity of
Mala
ya
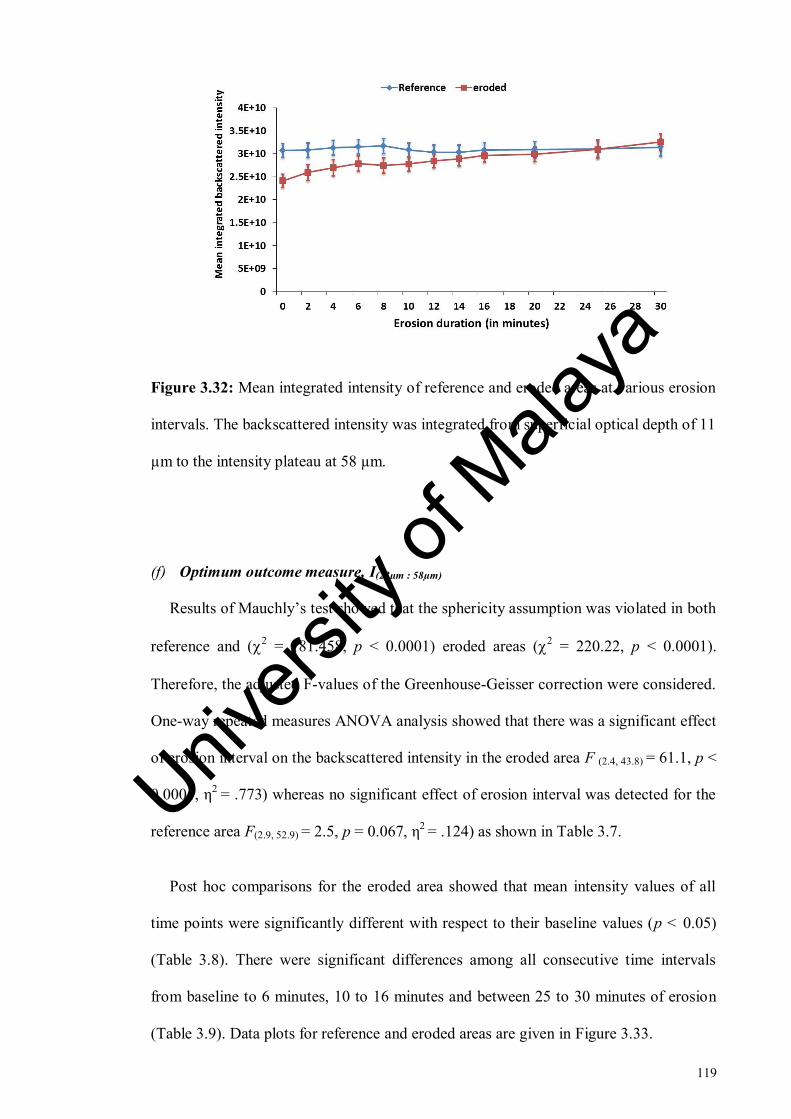
119
Figure 3.32: Mean integrated intensity of reference and eroded areas at various erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 11
µm to the intensity plateau at 58 µm.
(f) Optimum outcome measure, I(23µm : 58µm)
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference and (2 = 181.458, p < 0.0001) eroded areas (
2 = 220.22, p < 0.0001).
Therefore, the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA analysis showed that there was a significant effect
of erosion interval on the backscattered intensity in the eroded area F (2.4, 43.8) = 61.1, p <
0.0001, η2
= .773) whereas no significant effect of erosion interval was detected for the
reference area F(2.9, 52.9) = 2.5, p = 0.067, η2 = .124) as shown in Table 3.7.
Post hoc comparisons for the eroded area showed that mean intensity values of all
time points were significantly different with respect to their baseline values (p < 0.05)
(Table 3.8). There were significant differences among all consecutive time intervals
from baseline to 6 minutes, 10 to 16 minutes and between 25 to 30 minutes of erosion
(Table 3.9). Data plots for reference and eroded areas are given in Figure 3.33.
Univers
ity of
Mala
ya

120
Figure 3.33: Mean integrated intensity of reference and eroded areas at various erosion
intervals. The intensity was integrated from superficial optical depth of 23 µm to the
intensity plateau at 58 µm.
(g) Mean % I(23µm : 58µm)
Results of Mauchly’s test showed that the sphericity assumption was violated (2 =
217.879, p < 0.0001). Therefore, the adjusted F-values of the Greenhouse-Geisser
correction were considered. One-way repeated measures ANOVA analysis showed that
there was a significant main effect of erosion interval on the backscattered intensity F
(2.3, 42.2) = 66.683, p < 0.0001, η2 = .787) as shown in Table 3.7.
Post hoc comparisons showed that mean percentage of integrated intensity of all time
points were significantly different with respect to their baseline values (p < 0.05) (Table
3.8). There were significant differences among all consecutive time intervals from
baseline to 6 minutes, 10 to 16 minutes and between 25 to 30 minutes of erosion (Table
3.9). Data plot is given in Figure 3.34.
Univers
ity of
Mala
ya

121
Almost 20% erosion occurred in the first 10 minutes, 40% by 20 minutes and 60 %
by 30 minutes. Interestingly, almost 17% of erosion occurred in the first 6 minutes.
Figure 3.34: Mean percentage change in integrated intensity of eroded area for intensity
integrated from superficial optical depth of 23 µm to the intensity plateau at 58 µm.
Moreover, a linear line was fitted to the data for ΔR as shown in the Figure 3.35. ΔR
was related to the erosion interval by the equation given below,
𝑦 = 2.17𝑥 + 1.46 (3.8)
Where y is the mean percentage change in backscattered intensity and x is the erosion
interval.
R2 = 0.995 showed that this equation was statistically significant with 99%
confidence interval.
Univers
ity of
Mala
ya

122
Figure 3.35: Best fit regression line of backscattered intensity change with erosion
interval.
Table 3.7: Results of repeated measures ANOVA analysis for reference and eroded
areas of outcome measures of integrated intensity.
Outcome
measure
Reference area Eroded area
Mean
square
F-statistic p-value Mean
square
F-statistic p-value
I(5µm : 58µm) 1.83E+19 2.248 .092 4.29E+20 16.640 <.0001
I(11µm : 58µm) 1.43E+19 2.148 .105 3.59E+20 16.720 <.0001
I(23µm : 58µm) 2.87E+18 2.55 .067 2.68E+20 61.183 <.0001
Mean %
I(23µm : 58µm)
- - - 3.18E+04 66.683 <.0001
Univers
ity of
Mala
ya

123
Table 3.8: Post hoc comparisons of all erosion time points with baseline for the eroded
area of outcome measures of integrated intensity.
Time (I) Time (J)
Mean difference (I-J)
I(5µm : 58µm) I(11µm : 58µm) I(23µm : 58µm)
Mean %
I(23µm : 58µm)
Baseline 2min -2.096E+9** -1.805E+9** -0.397E+9** -6.164***
Baseline 4min -3.326E+9*** -2.860E+9*** -0.864E+9*** -10.981***
Baseline 6min -4.328E+9*** -3.743E+9*** -1.453E+9*** -16.745***
Baseline 8min -3.804E+9*** -3.306*** -1.544E+9*** -18.355***
Baseline 10min -4.130E+9*** -3.644*** -1.878E+9*** -23.102***
Baseline 12min -4.939E+9*** -4.341E+9*** -2.424E+9*** -27.794***
Baseline 14min -5.448E+9*** -4.792E+9*** -2.818E+9*** -32.436***
Baseline 16min -6.282E+9*** -5.526E+9*** -3.343E+9*** -37.517***
Baseline 20min -6.545E+9*** -5.780E+9*** -3.834E+9*** -43.163***
Baseline 25min -7.713E+9*** -6.864E+9*** -4.620E+9*** -51.679***
Baseline 30min -9.448E+9*** -8.449E+9*** -5.903*** -63.070***
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Univers
ity of
Mala
ya

124
Table 3.9: Post hoc comparisons of consecutive erosion intervals for the eroded area of
all outcome measures for integrated intensity.
Time (I) Time (J)
Mean difference (I-J)
I(5µm : 58µm) I(11µm : 58µm) I(23µm : 58µm)
Mean %
I(23µm : 58µm)
Baseline 2min -2.096E+9** -1.805E+9** -0.397E+9** -6.164***
2min 4min -1.231E+9** -1.055E+9** -0.467E+9*** -4.816***
4min 6min -1.001E+9* -0.882E+9* -0.588E+9*** -5.764***
6min 8min 0.524E+9 0.437E+9 -0.090E+9 -1.610
8min 10min 0.325E+9 0.338E+9 -0.334E+9 -4.747
10min 12min -0.809E+9 0.696E+9 0.334E+9* -4.692*
12min 14min -5.091E+9 -0.450E+9 -0.393E+9** -4.641***
14min 16min -0.834E+9 -0.734E+9 -0.525E+9** -5.081***
16min 20min -0.263E+9 -0.254E+9 -0.490E+9 -5.646
20min 25min -1.166E+9 -1.084E+9 -0.786E+9 -8.515
25min 30min -1.735E+9 -1.084E+9 -1.283E+9* -11.391**
Univers
ity of
Mala
ya
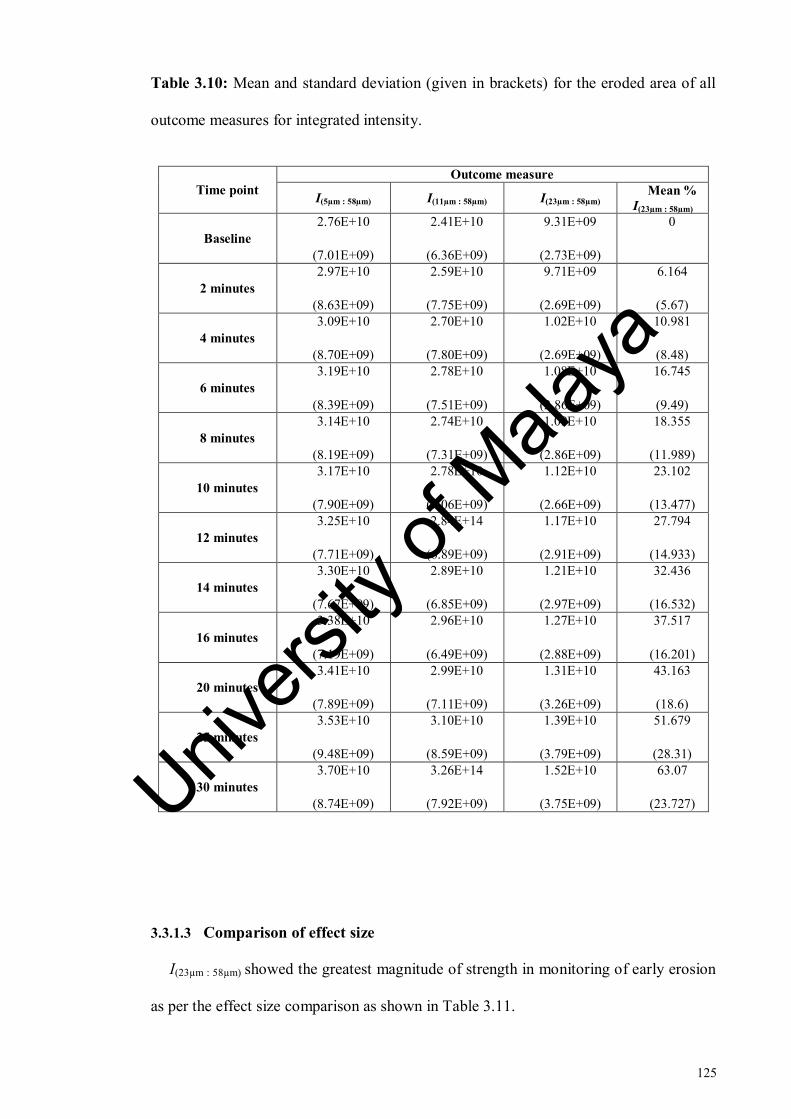
125
Table 3.10: Mean and standard deviation (given in brackets) for the eroded area of all
outcome measures for integrated intensity.
Time point
Outcome measure
I(5µm : 58µm) I(11µm : 58µm) I(23µm : 58µm) Mean %
I(23µm : 58µm)
Baseline
2.76E+10
(7.01E+09)
2.41E+10
(6.36E+09)
9.31E+09
(2.73E+09)
0
2 minutes
2.97E+10
(8.63E+09)
2.59E+10
(7.75E+09)
9.71E+09
(2.69E+09)
6.164
(5.67)
4 minutes
3.09E+10
(8.70E+09)
2.70E+10
(7.80E+09)
1.02E+10
(2.69E+09)
10.981
(8.48)
6 minutes
3.19E+10
(8.39E+09)
2.78E+10
(7.51E+09)
1.08E+10
(2.86E+09)
16.745
(9.49)
8 minutes
3.14E+10
(8.19E+09)
2.74E+10
(7.31E+09)
1.09E+10
(2.86E+09)
18.355
(11.989)
10 minutes
3.17E+10
(7.90E+09)
2.78E+10
(7.06E+09)
1.12E+10
(2.66E+09)
23.102
(13.477)
12 minutes
3.25E+10
(7.71E+09)
2.84E+14
(6.89E+09)
1.17E+10
(2.91E+09)
27.794
(14.933)
14 minutes
3.30E+10
(7.67E+09)
2.89E+10
(6.85E+09)
1.21E+10
(2.97E+09)
32.436
(16.532)
16 minutes
3.38E+10
(7.19E+09)
2.96E+10
(6.49E+09)
1.27E+10
(2.88E+09)
37.517
(16.201)
20 minutes
3.41E+10
(7.89E+09)
2.99E+10
(7.11E+09)
1.31E+10
(3.26E+09)
43.163
(18.6)
25 minutes
3.53E+10
(9.48E+09)
3.10E+10
(8.59E+09)
1.39E+10
(3.79E+09)
51.679
(28.31)
30 minutes
3.70E+10
(8.74E+09)
3.26E+14
(7.92E+09)
1.52E+10
(3.75E+09)
63.07
(23.727)
3.3.1.3 Comparison of effect size
I(23µm : 58µm) showed the greatest magnitude of strength in monitoring of early erosion
as per the effect size comparison as shown in Table 3.11.
Univers
ity of
Mala
ya

126
Table 3.11: Comparison of effect sizes of outcome measures used for analysis.
Parameter Outcome measure Effect size
Decay of intensity
I58µm / I5µm 0.331
I58µm / I11µm 0.255
I58µm / I23µm 0.761
Integrated intensity
I(5µm : 58µm) 0.467
I(11µm : 58µm) 0.468
I(23µm : 58µm) 0.773
Univers
ity of
Mala
ya
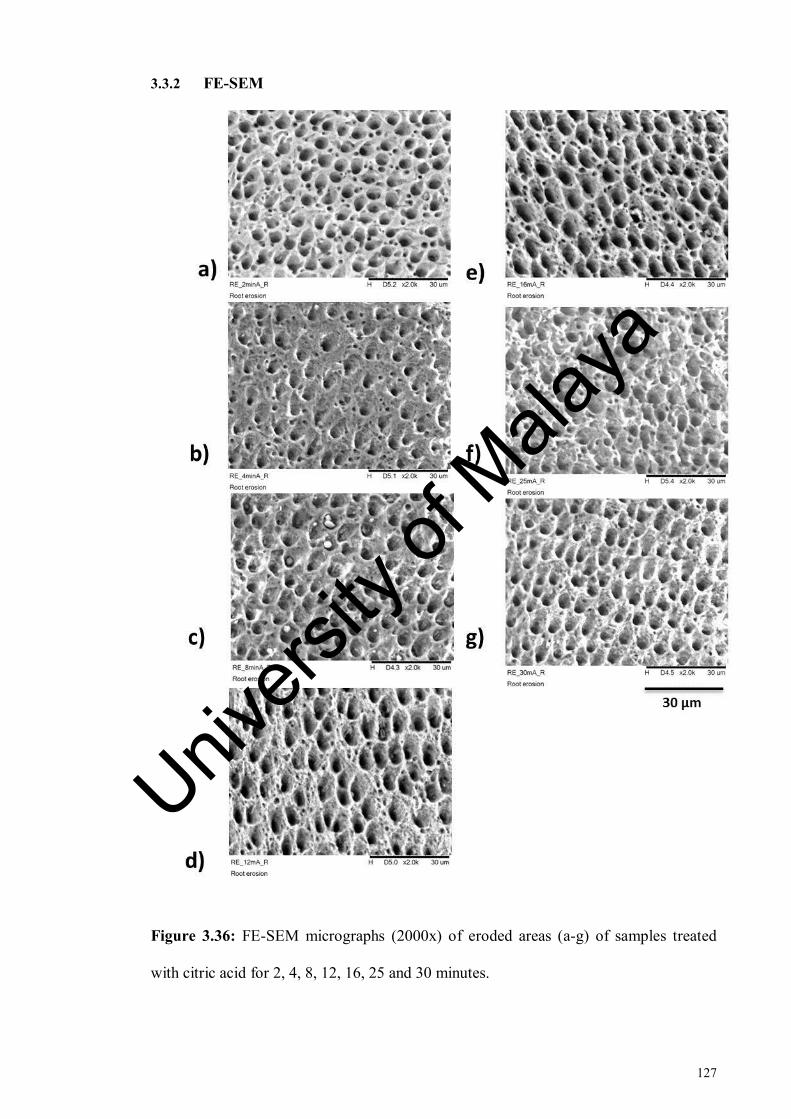
127
3.3.2 FE-SEM
Figure 3.36: FE-SEM micrographs (2000x) of eroded areas (a-g) of samples treated
with citric acid for 2, 4, 8, 12, 16, 25 and 30 minutes.
Univers
ity of
Mala
ya

128
Figure 3.37: FE-SEM images showing the interface between the reference and eroded
areas of samples eroded for 8 minutes (1a, 1b), 12 minutes (2a, 2b), 16 minutes (3a, 3b),
25 minutes (4a, 4b) and 30 minutes (5a, 5b).
FE-SEM images given in Figure 3.36 (a-g) showed the ultrastructural changes of
dentine surface associated with progression of erosion from two to 30 minutes. The
sound dentine (reference areas of same samples) in comparison given in Figure 3.37
(1a-7a) exhibited standard pattern of evenly distributed circular dentinal tubule lumen.
From two to eight minutes, the changes were limited to peritubular dentine as shown in
Figure 3.36 (a-c). Image d (Figure 3.37) representing 12 minutes of erosion showed
marked porosities in the inter-tubular area as compared to the preceding images
Univers
ity of
Mala
ya
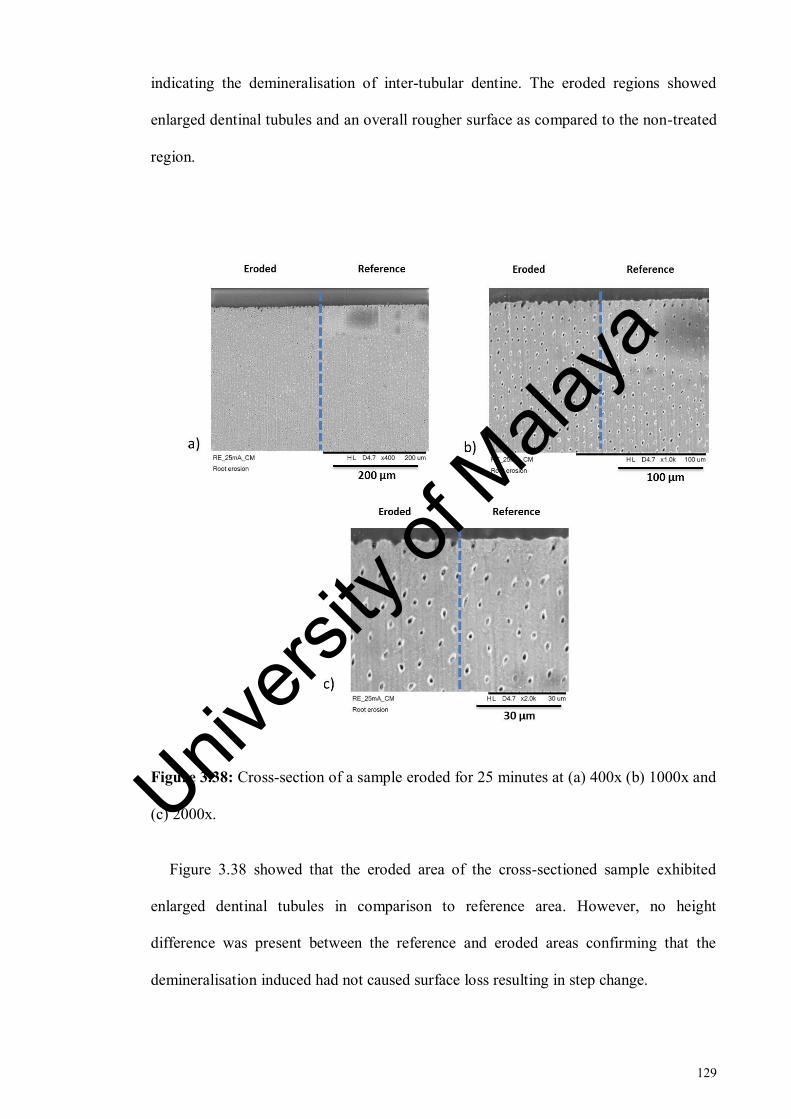
129
indicating the demineralisation of inter-tubular dentine. The eroded regions showed
enlarged dentinal tubules and an overall rougher surface as compared to the non-treated
region.
Figure 3.38: Cross-section of a sample eroded for 25 minutes at (a) 400x (b) 1000x and
(c) 2000x.
Figure 3.38 showed that the eroded area of the cross-sectioned sample exhibited
enlarged dentinal tubules in comparison to reference area. However, no height
difference was present between the reference and eroded areas confirming that the
demineralisation induced had not caused surface loss resulting in step change.
Univers
ity of
Mala
ya

130
3.4 Discussion
This study aimed to assess the applicability of optical coherence tomography for
monitoring the progression of early dentine erosion in vitro. As early stage dentine
erosion was targeted in this study, therefore the demineralisation induced was small,
involving surface-softening only without any evidence of surface loss as ascertained
from FE-SEM images.
A series of pilot studies were performed to determine the optimum duration of
demineralisation required to produce early stage dentine erosion before bulk surface
loss. Citric acid was used instead of commercially available soft drinks to avoid any
potential problems due to variation between the batches in terms of acid concentration
or pH (Shellis et al., 2011). The concentration and pH of the citric acid were kept
similar to that of a commercially available orange juice (Austin et al., 2010; Chiga et al.,
2016) and 10 minutes of erosion was adopted to mimic the consumption of a can of
soda or juice (Faller et al., 2011). Temperature of 36°C was employed to simulate the
intraoral temperature (Shellis et al., 2011). Speed of agitation was pre-determined in a
pilot study. Before the execution of main experiment, the protocol was verified by
performing pilot studies.
Reference area not subjected to erosive challenge is needed in erosion studies to
minimise any systematic errors or biological variability. Previous studies have
employed acid-resistant varnish (Fried et al., 2002), dentino-enamel junction, CO2 laser
(Chan et al., 2013), sub-ablative laser (Chan et al., 2014) and bonding agent to protect
reference areas in erosion-related OCT research. This reference area is expected to
remain unchanged over time against which the changes in the eroded area could be
reliably measured. Use of robust materials like composite would be more applicable for
in vivo research (Chan et al., 2014) and therefore a composite slab was used as a
Univers
ity of
Mala
ya

131
reference in this study. Sectioning of dentine samples creates a smear layer or smear
plugs which can clog the dentinal tubules reducing the permeability of dentine (Ghazali,
2003; Prati et al., 2003). Minimal increase in backscattered intensity was observed in
the OCT images of dentine samples covered with smear layer when eroded in citric acid
for 30 minutes in a pilot study (Section 3.2.1.6). Therefore, to be able to effectively
observe the OCT backscattered intensity changes with erosion interval, it was decided
to remove the smear layer from the root dentine samples before the induction of
demineralisation. The protocol of smear layer removal was adjusted based on pilot
studies and finalised at using a combination of weak chelating agent EDTA in low
concentration and ultrasonication, without significantly affecting the surface
morphology of dentine samples which was confirmed from FE-SEM images. Specular
reflection has been known to mask the information near the tooth-air interface (Fried et
al., 2002). In this study, the issue of specular reflection was addressed by the use of a
custom-made jig attached to the OCT stage which allowed the samples to be inclined to
a certain angle. The samples were inclined at 20 degrees perpendicular to the OCT
beam which effectively reduced the specular reflection from the images. Moreover, the
jig also allowed the samples to be correctly repositioned to the same alignment during
different measurement time points.
3.4.1 OCT
For this study, two different parameters were assessed to determine their potential in
detecting and monitoring the early dentine erosion over time. The first parameter ‘decay
of intensity’ was employed for this study because it has been used to monitor the
progression of early enamel erosion effectively (Chew et al., 2014). However, because
of histological differences between enamel and dentine, the possibility of same
Univers
ity of
Mala
ya

132
parameter of analysis not being applicable for dentine remained. Therefore another
parameter ‘integrated intensity’ was also used for the analysis. Integrated intensity had
been shown to correlate with the integrated mineral loss ΔZ, in the previous studies
involving dental caries (Jones et al., 2006a; Ngaotheppitak et al., 2005).
The outcome measures or depth combinations were selected based on the OCT
backscattered intensity trend observed from mean A-scans. Initially, exploration of data
was performed and many outcome measures were assessed with the both parameters.
Different outcome measures showed different results. In order to standardise the
analysis, it was decided to choose a depth at a subsurface level where the OCT intensity
signal had become constant and did not show any further changes. This depth was
named plateau of intensity. To find an optimal superficial depth to attain maximal
sensitivity of OCT, three superficial depths 5 µm, 11 µm and 23 µm located
immediately below the tooth-air interface were selected for data analysis and
comparison. Their relationship with plateau was assessed by using both ‘decay of
intensity’ and ‘integrated intensity’. The selection of optimum outcome measure was
based on the 1) trend of OCT backscattered intensity 2) repeated measures ANOVA
analysis 3) effect size comparison for assessing the magnitude of strength of outcome
measures and 4) comparison with FE-SEM observations as later discussed in Section
3.4.2
With decay of intensity, significant effect of erosion interval on OCT backscattered
intensity of the reference area was found by all outcome measures employed. Therefore,
the significant differences in backscattered intensity of the eroded area could not be
considered reliable. I58µm / I5µm and I58µm / I23µm were able to monitor intensity changes
for all erosion intervals from baseline whereas I58µm / I11µm was only able to monitor 4
minutes of erosion from baseline. However, with decay of intensity none of the three
Univers
ity of
Mala
ya

133
outcome measures employed was able to detect or monitor intensity between
consecutive erosion intervals beyond 6 minutes of erosion.
In contrast, for integrated intensity, no significant effect of erosion interval on
backscattered intensity of the reference areas was found by all three outcome measures
rendering the outcomes of this parameter for the eroded area more reliable. The
intensity integrated from the first two superficial optical depths I5µm and I11µm to plateau
were sensitive to intensity changes for the initial two to six minutes of erosion challenge
only. I(23µm : 58µm) was the only outcome measure which was able to monitor intensity
changes between consecutive time intervals from baseline to 30 minutes of erosion
challenge. The plotted data for I(23µm : 58µm) showed net increase in intensity from
baseline measurement to 30 minutes of erosion challenge. However, significant
differences were observed between consecutive time points from baseline measurement
to 6 minutes, from six to 12 minutes, from 12 to 16 minutes and from 16 to 30 minutes
of erosion challenge. The results were in line with the trend of intensity observed from
the mean A-scans at this depth where plots of 6 and 10 minutes were indistinguishable
and separation between time points was evident at this depth (23 µm). These
observations were further confirmed by effect size comparison of the outcome
measures. The outcome measure, I(23µm : 58µm) had the largest effect size which indicated
that it had the greatest magnitude of strength in monitoring the early dentine erosion in
comparison to other outcome measures.
At the tooth-air interface, specular reflection is very strong and could be 20dB higher
than OCT backscattered intensity (Fried et al., 2002). . This could lead to scattering
information being masked at or immediately below the tooth-air interface. With both
parameters, the outcome measures near the tooth-air interface did not monitor erosion
beyond 6 minutes of erosion challenge. It could be the result of these outcome measures
Univers
ity of
Mala
ya
134
being influenced by the much stronger specular reflection at superficial optical depths.
Moreover, the mean A-scans for the reference and eroded areas also showed that the
standard deviation near the surface and Imax was very high (Figure 3.20 & Figure 3.21)
which further strengthened this assumption.
The OCT system used in this study (OCS1300SS Thorlabs Ltd., USA) has an axial
resolution of 9 µm in air corresponding to about 6 µm (physical depth) in dentine with
refractive index of dentine being 1.54. Therefore, demineralisation below 6 µm is not
expected to be detected by this OCT system. The plot in Fig 3.21 showed that using this
OCT system, differences in demineralisation over time were detected at about 23 µm
from the surface. This depth would be translated to about 15 µm of physical depth.
Therefore, demineralisation was detected well within the axial optical resolution of this
SS-OCT system however very close to its resolution limit. The earlier depths near the
surface were most probably confounded by the specular reflection. However, the
resolution and penetration depth in the oral cavity will be affected by the presence of
calculus, stain or plaque on the teeth surfaces as well the presence of moisture in the
oral cavity (Park et al., 2013).
Cut-off depths by the exclusion of variety of distances from the surface for different
specimens were identified previously in order to minimise the specular reflection
(Amaechi et al., 2001). In the view of the study results and observation of mean A-
scans, the statistical cut-off depth for monitoring of early dentine erosion would be 23
µm from the tooth-air interface. This is consistent with the statistical cut-off depth of 20
µm determined for monitoring of early enamel erosion previously (Chew et al., 2014).
This is the first study, to the best of our knowledge to examine the ability of OCT for
early stage dentine erosion assessment before the occurrence of any bulk tissue loss
marked by step change. Only one other recent study had examined potential of OCT for
Univers
ity of
Mala
ya

135
dentine erosion but only the advanced stages of dentine erosion after the appearance of
surface loss in the OCT images were explored and only a qualitative analysis was
performed (De Moraes et al., 2017).
This study is a significant step forward since the study findings indicated that
monitoring of erosion progression in root dentine over time was possible with OCT.
This could be used in future for clinical monitoring of progression or regression of early
dentine erosion for testing of treatments products over the period of time. An optimum
outcome measure for the longitudinal monitoring of early dentine erosion was identified
which is currently lacking in literature. Early stage erosion which can be reversed would
have to be induced in clinical trials using healthy subjects (Huysmans et al., 2011). This
study revealed that using the current study protocol, OCT can be employed for
monitoring of dentine erosion starting as early as two minutes. OCT intensity changes
over time (quantum) identified in this study can help in designing the future study
protocols in which the periods of constant intensity can be skipped and measurements
can be taken at fewer intervals. However, a pH-cycling model of erosion was not
applied in this study as the presence of remineralisation step between periods of erosion
challenge could complicate the interpretation of final results. Therefore it was unclear
whether OCT had the potential of being applied to clinical conditions. This was
attempted later and is detailed in chapter 5 of this thesis.
3.4.2 FE-SEM
Scanning electron microscopy (SEM) is a commonly employed method for
qualification of morphological changes in eroded dentine. One of the drawbacks of
conventional SEM is high-vacuum imaging which causes loss of water in biological
samples. Demineralised dentine is prone to shrinkage when dehydrated (Zhang et al.,
Univers
ity of
Mala
ya

136
2009). For this reason, environmental SEM has been recommended for its assessment
(Attin & Wegehaupt, 2014). It allows the samples to be imaged in low-vacuum
conditions thus minimising drying defects. Moreover, environmental SEM as opposed
to conventional SEM does not need any prior metallisation which makes it more
suitable for longitudinal study designs. In this study Field emission scanning electron
microscopy (FE-SEM) was employed to assess the erosion-related surface alterations in
dentine and scanning was performed in low vacuum conditions which did not dehydrate
the samples. The samples were not coated with any metal and were only air-dried before
imaging.
The reference area of each sample was protected with acid-resistant varnish during
the challenges and was not expected to exhibit any demineralisation-associated changes
on surface whereas eroded area of each sample was exposed to citric acid and was
expected to exhibit morphological changes related to erosion. The OCT mean A-scans
extracted for the reference area showed that the backscattered intensity was constant
over time as indicated by the minimal separation between line plots representing various
time points. Mean A-scans for the eroded area showed erosion interval related shift in
backscattered intensity as indicated by the separation of line graphs at various depths.
The FE-SEM images confirmed these findings. The reference areas of the samples
showed the standard pattern of sound dentine without any signs of demineralisation in
comparison to the eroded areas of the same samples which showed signs of progressing
demineralisation with increasing erosion interval.
Repeated measures ANOVA analysis for decay of intensity showed that there were
significant differences in the OCT intensity in the reference area for all outcome
measures employed. Moreover, with this parameter, none of the three outcome
measures employed was able to detect or monitor intensity over consecutive erosion
Univers
ity of
Mala
ya
137
intervals beyond 6 minutes of erosion. In contrast, the reference areas of the samples in
the FE-SEM images did not appear to be demineralised and the eroded areas of the
samples showed progression of erosion. Therefore, SEM images confirmed that decay
of intensity was not suitable for assessment of early dentine erosion within the
limitation of this study protocol.
There were no significant differences in the OCT backscattered intensity over time in
the references areas with integrated intensity. This could be confirmed from the FE-
SEM images. Moreover, I(23µm : 58µm) was the only outcome measure which was able to
monitor intensity changes between consecutive time intervals from baseline to 30
minutes of erosion challenge and showed net increase in intensity from baseline
measurement to 30 minutes of erosion challenge. The suitability of this outcome
measure I(23µm : 58µm) for longitudinal monitoring of early eroded dentine was further
confirmed by FE-SEM images showing signs of progressing erosion with increasing
erosion interval.
OCT outcome measure I(23µm : 58µm) showed an initial increase in backscattered
intensity from baseline measurement to the first 6 minutes of erosion. This could be the
result of the initial rapid dissolution of peritubular dentine as observed in the FE-SEM
images showing 2, 4 and 8 minutes of demineralisation as previously reported (Kinney
et al., 1995). Between 6 and 10 minutes, the OCT intensity remained constant and OCT
could not monitor the erosion progression between these time points. The backscattered
intensity increased from 12 minutes onwards. The increase in OCT backscattered
intensity on the surface of demineralised dentine is associated with increased porosities
which develop as a result of mineral loss (Huysmans et al., 2011). The FE-SEM images
for 12 minutes of erosion showed demineralised intertubular dentine with increased
porosities as previously reported (Meurman et al., 1991). Although there was an
Univers
ity of
Mala
ya

138
increase in backscattered intensity between from 16 to 25 minutes, the changes were not
significantly different. Overall these intensity fluctuations could be attributed to the
changes in the porosity, in structural phase (organic versus mineral-organic) and optical
properties in the demineralised area as previously observed (Natsume et al., 2011)
It has been emphasised that some verification of absence of substance loss should be
given for the protocols dealing with initial erosion (Shellis et al., 2011). One sample
eroded for 25 minutes was embedded in epoxy resin and cross-sectioned in a transverse
plane to see if there was any step change at the border between the reference and eroded
areas. No obvious changes in height were present between reference and eroded areas
confirming the absence of substance loss.
3.5 Conclusions
Within the limitations of the current study design, the following conclusions were
drawn from the study findings,
1. OCT was able to measure early dentine erosion up to 30 minutes. The quantum
of OCT for measuring early dentine erosion varied with different outcome
measures. I(23µm : 58µm) showed significant changes in the first three 2-minute
intervals (0-6 minutes) but not in the subsequent three 2-minute intervals (6-12
minutes). However, in the subsequent eighteen minutes (12-30 minutes), I(23µm :
58µm) detected significant 2-minutes interval change only up to 16 minutes and
significant changes were detected in the consecutive time intervals only between
25 and 30 minutes for the next 14 minutes (16-30 minutes).
2. Integrated intensity was more suitable and sensitive than decay of intensity for
measuring in vitro early dentine erosion. I(23µm : 58µm) was the most sensitive
Univers
ity of
Mala
ya
139
outcome measure for measuring in vitro early dentine erosion. OCT outcome
measure ΔR showed a linear pattern (R2 = 0.995) as goodness of fit model for
measuring in vitro early dentine erosion.
3. The in vitro early dentine erosion detection threshold of OCT varied with
different outcome measures. With I(23µm : 58µm), the detection threshold was 2
minutes of erosion challenge from baseline measurement.
4. FE-SEM images supported the results of OCT backscattered intensity analysis .
With I(23µm : 58µm), continuous increase in backscattered intensity in relation to
incubation time in acid was obvious during erosion progression. The eroded
regions of FE-SEM showed gradually enlarging dentinal tubules with increasing
erosion intervals.
The null hypotheses one and two were rejected as shown below;
1. OCT was able to detect early dentine erosion with a detection threshold of two
minutes from baseline measurement.
2. OCT was able to measure the progression of early dentine erosion up to 30
minutes in vitro.
Univers
ity of
Mala
ya

140
CHAPTER 4: MONITORING OF EARLY DENTINE EROSION WITH
SURFACE ROUGHNESS
This chapter details the profilometric assessment of early eroded dentine in simulated
intraoral environment both with conventional and novel parameters and its qualitative
assessment using field emission scanning electron microscopy.
4.1 Introduction
It is a challenging task to find a suitable method for quantification and monitoring of
early dentine erosion because of the complex histology of these lesions. Surface
microhardness is suitable for the measurement of early enamel erosion (Attin, 2006) but
not for dentine erosion. This could be attributed to the elastic nature of dentine which
causes the indentations to shrink by about 30% within 24 hours after indentation
(Herkstroter et al., 1989). In addition to this, as intertubular and peritubular dentine have
distinctly different hardness values (Kinney et al., 1996) the need to be site-specific in
the indenting process makes surface nanohardness a time consuming and non-feasible
method for longitudinal erosion study designs.
Surface profilometry has been used extensively for the quantification of dental
erosion (Aykut-Yetkiner et al., 2014; Borges et al., 2014; Charone et al., 2014). This
method has been described in more detail in Section 2.3.1.3 of this thesis. The
parameter commonly used is the amount of tissue loss in the form of a step between the
reference and eroded areas (Borges et al., 2014; Paepegaey et al., 2013). However,
initial dental erosion is not marked by bulk surface loss (Young & Tenuta, 2011) and it
is speculated that this parameter might not be effective in measuring the early stages of
erosion.
Univers
ity of
Mala
ya

141
Moreover, measurement of tissue loss in eroded dentine is rendered complicated by
the presence of organic matrix and it has been recommended that organic matrix be
removed from the dentine samples before performing measurements with profilometry
(Ganss et al., 2009b; Ganss et al., 2007). However, the need to remove organic matrix
from dentine samples makes profilometry a destructive technique and therefore non-
suitable for application in longitudinal or in vivo studies. Besides being able to provide
information on height differences between two areas, surface profilometry can also
quantify the surface roughness of dental hard tissues with surface roughness parameters.
Preliminary work has shown that surface roughness parameters seem to be useful for
assessing early erosion (Field et al., 2013; Schlueter et al., 2011).
4.1.1 Roughness parameters
Roughness parameters, depending upon their functionality have normally been
categorised into four groups. These groups are height parameters, amplitude parameters,
spacing parameters and hybrid parameters (Grzesik, 2016). Out of these, amplitude
parameters are the most important in describing the surface topography of a surface and
measure surface characteristics of surface deviations (Gadelmawla et al., 2002). The
most commonly used amplitude parameter in relation to dentistry is surface roughness
average (Ra) (Kukiattrakoon et al., 2011).
4.1.1.1 Average roughness
Ra, the average mean roughness, is defined as the absolute average deviation of
roughness irregularities from the mean line of a sampling length (Gadelmawla et al.,
2002). The mean line is that section through the profile that cuts off equal areas above
Univers
ity of
Mala
ya

142
and below it. It is the mean of the absolute values of the deviations of the profile
(Darvell, 2009). Ra is described by the equation given as follows:
𝑅𝑎 = 1
𝑛∑|𝑦𝑖|
𝑛
𝑖=1
(4.1)
Where n is the number of points at which height measurements are made and 𝑦𝑖 is
the vertical distance from the mean line to the ith data point.
Although Ra is the most commonly reported surface roughness parameter in dentistry
and engineering (Kukiattrakoon et al., 2011), there are a few downsides of reporting Ra
value in isolation. While Ra value furnishes basic information about the relative
departures from the mean line, still it fails to distinguish between these asperities and
valleys in terms of their slopes, sizes, direction or shapes and does not take into account
the frequency of their occurrence. As a result, it is possible to have the same Ra values
for two surfaces with widely different profiles (Rîpă et al., 2003) (Figure 4.1). Other
drawbacks include the inability of Ra value to give any information regarding the
textural characteristics of wear, rate of wear, susceptibility or resistance of a surface
towards future wear or its potential to hold fluids (Field et al., 2010). It is felt that the
description of such surfaces with Ra value alone would be incomplete and more
sophistical parameters could describe such surfaces more efficiently. Univers
ity of
Mala
ya

143
Figure 4.1: Three different surfaces having similar Ra values. (a) The first profile has
sharp peaks, (b) the second deep valleys and (c) the third has neither (Bewoor &
Kulkarni, 2009)
4.1.1.2 Bearing area curve
The bearing area curve or Abott-Firestone curve is obtained by plotting the
cumulative distribution of the lengths of individual plateaus, normalised by the total
assessment length against the sample height (Field et al., 2010). In order to obtain the
bearing area curve from surface profile, a parallel line is drawn at a distance from a
reference line. This parallel line is called the bearing line. Then the length of each
material intercept along this line is calculated and these lengths are summed up. The
proportion of this sum to the total length is then calculated and is called the bearing
length (tp) (figure 4.2). The same procedure is repeated along a number of bearing lines
starting from the highest peak to the lowest valley and the bearing length ratio
(fractional land length) as a function of height of each slice is plotted in the form of a
curve (Bhushan, 2013). The calculation of the bearing area curve from a roughness
profile is shown in Figure 4.2
Univers
ity of
Mala
ya

144
Figure 4.2: Generation of bearing area curve from roughness profile. Modified from
(Field et al., 2010). Bearing length or tp is the sum of lengths of individual plateaus (L1,
L2), divided by the total assessment length (L)
Bearing curve parameters have basically being described in relation to load carrying
surfaces. Peak roughness, Rpk has been described as the top portion of the surface which
will be worn when another surface comes in contact with it. Core roughness, Rk is the
working part of the surface. After the initial running-in period this part of the surface
will carry the load and influence the overall performance of the engine. Valley
roughness, Rvk is the lowest part of the surface that can retain the fluids. Proportion of
peaks, MR1 represents the bearing ratio at which Rpk and Rk meet and forms the upper
part of the core roughness profile. Proportion of valleys, MR2 is the bearing ratio at
which Rvk and Rk meet and represent the lower limit of the core roughness profile
(Menezes et al., 2013). A brief description of the parameters explored in this study in
given in Table 4.1 (Field et al., 2013).
Univers
ity of
Mala
ya

145
Table 4.1: Description of roughness parameters
Parameter Description
Ra
Arithmetic average of all deviations of the profile
from the mean line
Rpk Height of the material peaks
Rk Height of the material core
Rvk Depth of the material valleys
MR1 Proportion of peaks within the sample
MR2 Proportion of valleys within the sample
Figure 4.3: Bearing area curve parameters (1) Maximum height (2) Peak area defined
(3) 40% of minimum slope (4) Valley area (5) Minimal height (Infinitefocus, 2009)
Univers
ity of
Mala
ya

146
Figure 4.3 shows the algorithm for the extraction of bearing curve parameters from
bearing curve. A line segment representing 40% material ratio is fitted in the curve
starting from extreme left point. This is shown by blue line fitting into the red bearing
area curve in the Figure 4.3. The slope of this line matching with the bearing curve
gives an equivalent straight line. This equivalent straight line is extended to meet the
vertical lines drawn at 0% and 100% and difference in height denotes the parameter Rk.
Horizontal lines are drawn to meet the bearing curve at MR1 and MR2. Rpk and Rvk are
represented by the shaded grey areas located above and below the Rk respectively
(Management Association, 2012). .
It has been suggested that bearing area curve parameters can be used to describe
many complex surfaces that cannot be described adequately by simple parameters like
Ra. Among such surfaces are multi-processed surfaces which are treated by more than
one distinct surface processes (Bacova & Draganovska, 2004; Pawlus & Grabon, 2008).
One process may act to remove peaks and the second process may introduce a finer
texture into the resulting plateaus while the deeper valleys may remain unchanged at the
same time. An example of such surfaces is ‘multi-stratified’ surfaces. The assessment of
these surfaces is notoriously difficult as they are negatively skewed (Field et al., 2010;
Whitehouse, 2010). Interestingly, eroded or eroded / abraded surfaces could also be
included in this category. During an erosion challenge, the acid challenge is interspersed
with salivary remineralisation or abrasion (Young & Tenuta, 2011) and the resulting
surfaces could be considered as multi-processed or multi-stratified. Therefore, it could
be assumed that bearing area curve would have the ability of explaining such surfaces
better than other basic surface roughness parameters like Ra. Moreover, tooth wear is
known to occur in two phases, a primary phase described as ‘running-in’ phase followed
by secondary phase called ‘steady-state wear’ (Kaidonis et al., 1998) and bearing area
curve might have a potential of assessing such bi-phasic processes (Field et al., 2010).
Univers
ity of
Mala
ya

147
Bearing curve parameters were successfully employed for the in vivo qualification
and monitoring of changes in enamel surface induced by erosion over a period of 3
months via silicon models. (Whitehead et al., 1997). Moreover, 3D bearing curve
parameters were employed to characterise the topography of native enamel surface with
active erosive wear. (Las Casas et al., 2008). Recently, the usefulness of bearing curve
for evaluation of early enamel erosion was shown in a pilot study and a comparison was
drawn between bovine and human enamel characteristics at baseline and post-erosion
challenge (Field et al., 2013).
Importantly, all of these studies employed enamel as the tissue of interest and the
usefulness of bearing curve parameters for assessment of dentine erosion has not been
evaluated previously. Because of the histopathological differences between enamel and
dentine erosion, the applicability of methods need to be re-assessed for dentine. The
present study therefore sought to achieve the following aim,
4.1.2 Aim
To assess the potential of surface roughness as a method for longitudinally measuring in
vitro early dentine erosion in simulated intraoral conditions.
Research Objectives
In order to achieve this aim, the following research objectives were defined.
1. To explore the use of surface roughness parameters for measuring early dentine
erosion in simulated intraoral conditions.
Univers
ity of
Mala
ya

148
2. To identify the most sensitive surface roughness parameter for measuring early
dentine erosion in simulated intraoral conditions.
3. To identify the detection threshold of surface roughness parameters for
measuring early dentine erosion in simulated intraoral conditions.
4. To compare the changes of surface roughness parameters in early dentine erosion
with surface ultrastructural changes.
The null hypotheses tested were as follows:
1. Surface roughness parameters cannot be used to measure early dentine erosion
progression in simulated intraoral conditions.
2. There is no difference of the sensitivity of Ra and bearing curve parameters in
measuring early dentine erosion in simulated intraoral conditions.
Univers
ity of
Mala
ya
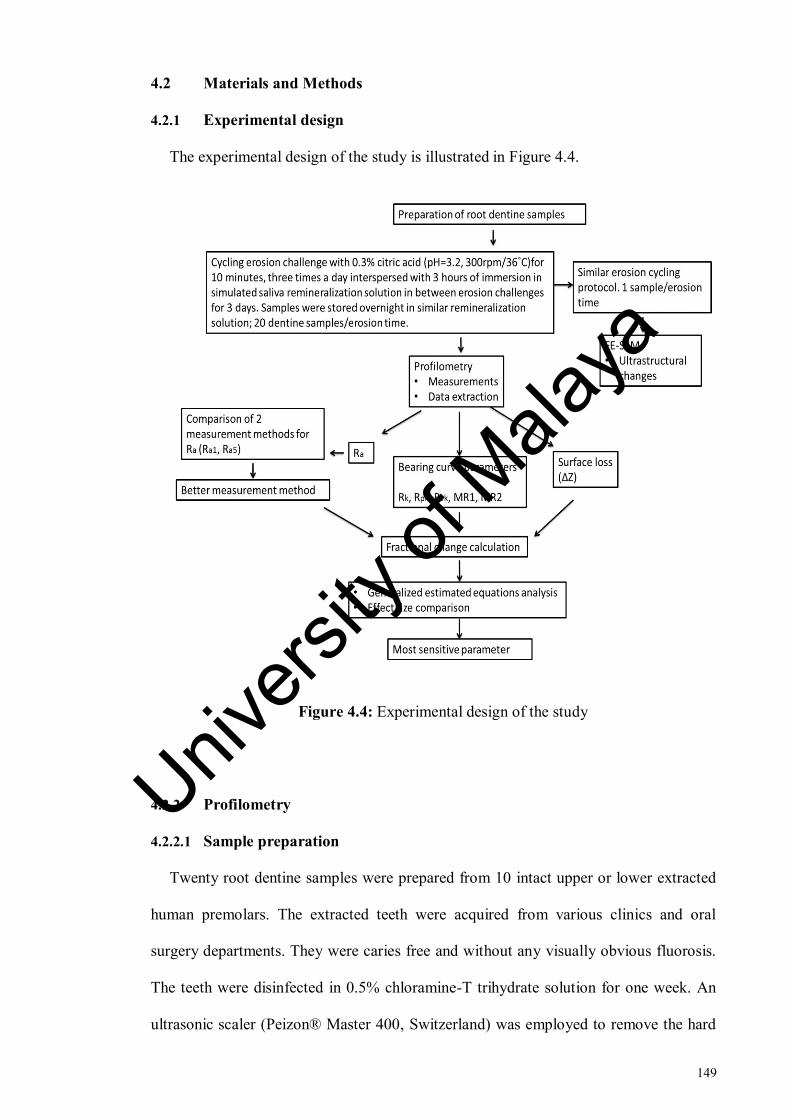
149
4.2 Materials and Methods
4.2.1 Experimental design
The experimental design of the study is illustrated in Figure 4.4.
Figure 4.4: Experimental design of the study
4.2.2 Profilometry
4.2.2.1 Sample preparation
Twenty root dentine samples were prepared from 10 intact upper or lower extracted
human premolars. The extracted teeth were acquired from various clinics and oral
surgery departments. They were caries free and without any visually obvious fluorosis.
The teeth were disinfected in 0.5% chloramine-T trihydrate solution for one week. An
ultrasonic scaler (Peizon® Master 400, Switzerland) was employed to remove the hard
Univers
ity of
Mala
ya

150
deposits and soft tissues from the teeth. After scaling, the crowns were sectioned
horizontally 1 mm below the cemento-enamel junction using slow speed microtome
cutting machine (Micracut 125, Metkon Instruments Inc., Bursa, Turkey) and discarded.
Next, the roots were sectioned longitudinally in the buccolingual direction. Fragments
obtained were embedded in separate self-curing methyl methacrylate resin blocks such
that the external part of the root was kept exposed and inner part of the root was
embedded in the resin (Quick Mount 2 Epoxy resin, Ace Technologies Inc., Arizona).
The dentine surface was then ground flat with 600-grit silicon carbide paper (Struers
Inc., Ohio, USA) which removed the cementum followed by final polishing with
polishing pads (8-inch Micropad polishing pad PSA, Pace® technologies, Arizona)
using diamond suspension (1 µm) in a water-cooled rotating grinding / polishing
machine (Buehler, USA). The samples were prepared in a flat plane as parallel to the
base of the sample as possible to ensure the surface could be scanned by the
profilometer.
A window with dimensions of 5 x 3 mm was created with non-residue adhesive tape
(3M, United States) on the surface of each sample. Left half of the window was kept
covered with the adhesive tape during the cycling erosion challenges to act as a
reference surface. Middle of the window was marked with a permanent marker on the
resin at the top and bottom part of the each resin embedded sample. This step was
carried out to aid in the identification of the reference and eroded areas in baseline and
subsequent measurements.
4.2.2.2 Erosive pH-cycling
Samples were scanned with a non-contact profilometry (Alicona InfiniteFocus®
Optical 3D Measurement Device G4f, Austria) to acquire images for baseline
Univers
ity of
Mala
ya

151
measurements. The reference area of each sample was covered with non-residue
adhesive tape (3M, United States). The samples were then suspended in a beaker
containing 0.3% citric acid (pH = 3.2) (A&C American Chemicals Ltd., North Carolina,
USA) on a movable stand with wires and plastic clips. Five samples were suspended in
500 ml of citric acid (A&C American Chemicals Ltd., North Carolina, USA) at one
time. The temperature and speed of the solution were controlled by placing the beakers
on magnetic stirrer (RCT basic, IKA, Germany). A magnetic stirrer is a laboratory
device used for stirring a ‘stir bar’ added in the liquid by employing a magnetic field.
The solution is stirred as a result of it (Figure 3.14). The temperature of the solution was
kept constant at 36°C and the speed was kept constant at 300 rpm during the erosion
phase of the cycling throughout the experiment. Temperature of 36°C was employed to
mimic the intraoral temperature. A pilot study was conducted to verify the speed at
which the samples did not move while the solution remained stirred homogeneously as
discussed in Section 3.2.1.2 of Chapter 3. After 10 minutes of erosion challenge,
samples were removed from the beaker and rinsed with deionised water. 10 minutes of
erosion was adopted to mimic the consumption of a can of soda or juice (Faller et al.,
2011). Following this, each sample was stored in a separate plastic container containing
simulated saliva remineralisation solution and kept in incubator at 36°C for 3 hours. The
remineralisation solution (A&C American Chemicals Ltd., North Carolina, USA)
contained 8.38 Millimolar (mM) KCl, 0.29 mM MgCl2.6H2O, 1.13 mM CaCl2.2H2O,
4.62 mM K2HPO4, 2.40 mM KH2PO4, 0.022 ppm fluoride and the pH was adjusted to
7.2 using KOH. After storage in simulated saliva remineralisation solution, samples
were then removed from their respective bottles, dried with dental syringe for 20
seconds at a distance of 10 cm and tapes were reapplied on the reference areas of each
sample. This alternating episode of demineralisation and remineralisation was repeated
three times in one cycling day. At the end of each cycling day, the samples were stored
Univers
ity of
Mala
ya

152
overnight (8 hours) in similar remineralisation solution. Citric acid was renewed after
every exposure and remineralisation solution was refreshed after every 24 hours. This
cycling erosive challenge was repeated for a total of three consecutive days. After every
cycling day, measurements were obtained with both optical coherence tomography and
non-contact profilometry. This chapter details the non-contact profilometric
measurements of these samples whereas the OCT measurements of these samples have
been detailed in chapter 5.
4.2.2.3 Measurements with Profilometry
After every cycling day, a non-contact profilometry device (Alicona InfiniteFocus®
Optical 3D Measurement Device G4f, Austria) in combination with bespoke
measurement software (IFM software) was employed for scanning the samples. Figure
4.5 shows the profilometry equipment used in the experiment.
Figure 4.5: Photograph of profilometry equipment
Univers
ity of
Mala
ya

153
The calibration of the IFM system of the device was performed by the manufacturer
using a gauge block set, alicona calibration tool (known as IF-CalibrationTool), PTB
depth adjustment standard and PTB micro contour standard (known as IF-
VerificationTool) (Infinitefocus, 2009). This equipment uses coaxial white light to
perform the measurements instead of a contact stylus. Each resin-mounted sample was
removed from its container (containing remineralisation solution) before imaging and
tape covering the reference area was removed from the surface of each sample. One
sample at a time was placed on the motorised profilometer stage such that the
experimental surface was parallel to the horizontal plane. A custom-made sample holder
was attached to an A-4 paper which in turn was taped to the stage throughout the study
period as shown in the Figure 4.7. Repositioning of samples at various measurement
time points was achieved by placing the sample in this sample holder. The coaxial white
light was provided by a light source delivered through a beam splitter to a series of
objectives with fixed magnification. The objective lens of 20x magnification was used
for imaging of samples. At this magnification, a lateral resolution of 0.5 µm and a
vertical resolution of ≤100 nm could be achieved. The maximum vertical imaging range
was 100 mm. An area of 0.7 x 0.5 mm (711.46 x 539.73 µm) composed of 1624 x 1232
points was selected for scanning for each image. The sampling distance was kept at
438.09 x 438.09 nm. The stage calibrated itself by moving to the reference position
automatically at startup. The border between the reference and eroded areas for each
sample was identified by using live 3D view function which gives a preview of the
image before capturing. Before capturing the image, a capture range was specified by
using stage control to select a lower bound and an upper bound which represent
different z positions of the stage. Following this, the 3D model of the image was
captured and displayed within an image viewer as shown in the Figure 4.6. Once
captured, the images were then saved for further analysis.
Univers
ity of
Mala
ya
154
Figure 4.6: 3D model of image captured and displayed by live viewer
Non-contact profilometers fail to scan surfaces with steep slopes and highly curved
features. Therefore, each sample was scanned before baseline imaging to ensure that the
surface was smooth and flat. Samples were allowed to dry for 10 minutes before
obtaining measurements in order to address any possible interference by organic
matrix.(Steiner-Oliveira et al., 2010). A total of three images were captured for each
time point for all samples. First image was captured at the reference area, second at the
eroded area and third at the junction between the reference and the eroded areas as
shown in Figure (4.8).
Univers
ity of
Mala
ya

155
Figure 4.7: Repositioning of samples at different measurement time points. (a) custom-
made sample holder pasted on paper (b) sample holder pasted on the stage during
scanning (c) close up of sample-holder with the sample snugly fitted inside
Figure 4.8: 3D images acquired by profilometry at the junction of reference and eroded
areas (a) Baseline image (b) Day one image (c) Day two image (d) Day three image
Univers
ity of
Mala
ya

156
Table 4.2: Calculation methods for surface roughness parameters used in the study.
RaL* was only explored in the pilot study
Parameter Symbol Calculation method
Average roughness RaL* Calculated by an average of 5
measurement lines.
Ra5 Calculated by an average of 5
measurement areas.
Ra1 Calculated from a single measurement area
Core roughness Rk
Calculated from a single measurement area
Peak roughness Rpk
Valley roughness Rvk
Proportion of peaks MR1
Proportion of valleys MR2
4.2.2.4 Data extraction
The saved files were then opened and analysed with the profile analysis software
(IFM 2.1.5 software). The IFM software utilises EN/ISO standards for surface
roughness measurement. Utilising this software, the measurements conform to
ISO4287/ISO4288/. The 3D profile was first activated and levelled using a best-fit
plane. For the roughness measurement, the form of the 3D image was removed. Next,
the extraction parameters were selected and roughness filter was applied to separate the
roughness and waviness from the overall form. A cut-off wavelength of 80 and a profile
length of 500 µm were chosen. Next a red measurement line or area was drawn over the
image at the desired location and values for the parameters were then calculated.
Univers
ity of
Mala
ya

157
(a) Ra
Ra has most commonly been reported as an average of five separately made
measurements rather than a single area. It is believed that a single area that covers most
of the image will be better representative of the overall roughness value. In this study,
Ra was measured with both methods and a comparison was drawn between the both to
find the best method.
For the first method, five measurement areas were drawn on each image and Ra5
value was recorded for each area. One measurement area could be drawn at a time. The
profile viewer displayed the roughness profile of the measurement area as shown in the
Figure 4.9 (a). The Ra5 value for the selected region was recorded. Each measurement
area was composed of 100 points with a width of 43 microns. Next, another
measurement area at a distance of approximately 50 µm from the first area was drawn
on the image. In this manner, five measurement areas were drawn as shown in the
Figure 4.9 (b). Data was entered manually in Microsoft Excel programme. An average
value of Ra5 was calculated as a mean of values recorded from five measurement areas
at every time point. Average Ra5 values were calculated in this manner for both the
reference and eroded images of each sample at every time point.
Univers
ity of
Mala
ya
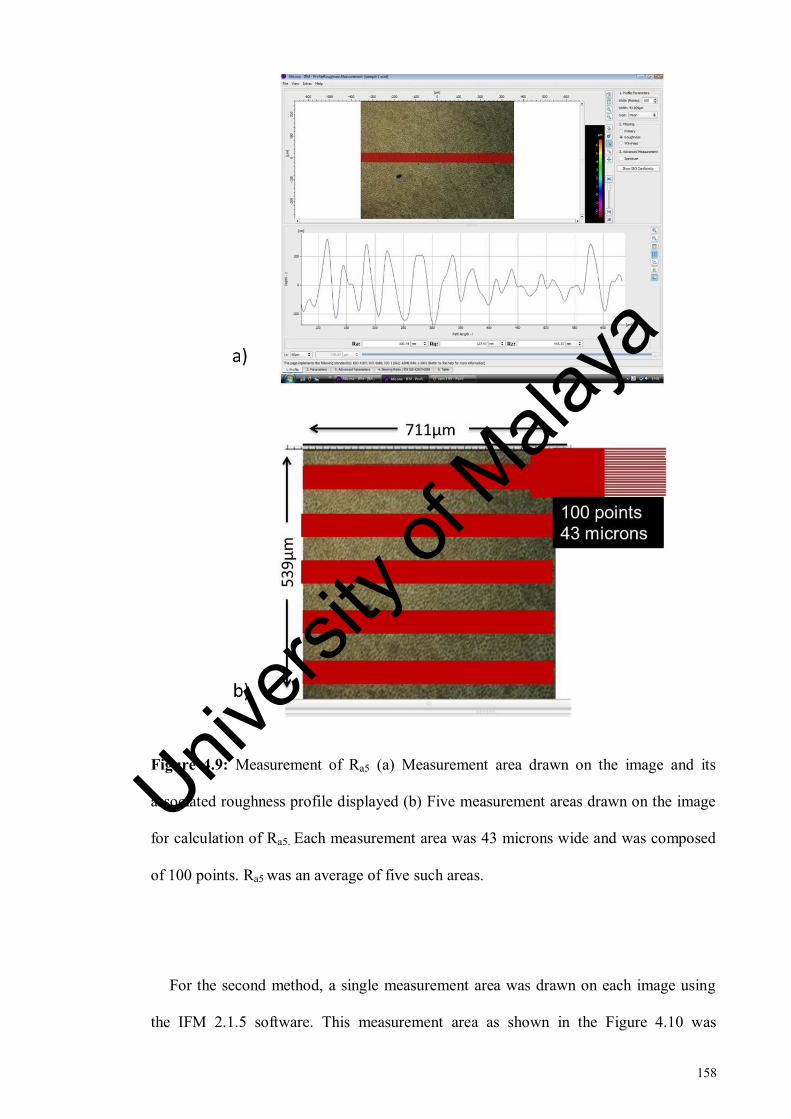
158
Figure 4.9: Measurement of Ra5 (a) Measurement area drawn on the image and its
associated roughness profile displayed (b) Five measurement areas drawn on the image
for calculation of Ra5. Each measurement area was 43 microns wide and was composed
of 100 points. Ra5 was an average of five such areas.
For the second method, a single measurement area was drawn on each image using
the IFM 2.1.5 software. This measurement area as shown in the Figure 4.10 was
Univers
ity of
Mala
ya

159
composed of 800 points and had a width of 334 microns. Average roughness values
(Ra1) were then extracted and exported to Microsoft Excel Programme as shown in
Figure 4.11. The data was measured and exported for both reference and eroded images
of every time point for each sample.
Figure 4.10: A single measurement area drawn on the image for the calculation of Ra1.
The measurement area was 344 microns wide and was composed of 800 points.
Figure 4.11: (a) Roughness profile generated from the single measurement area (b) Ra1
values exported to excel sheet
Univers
ity of
Mala
ya
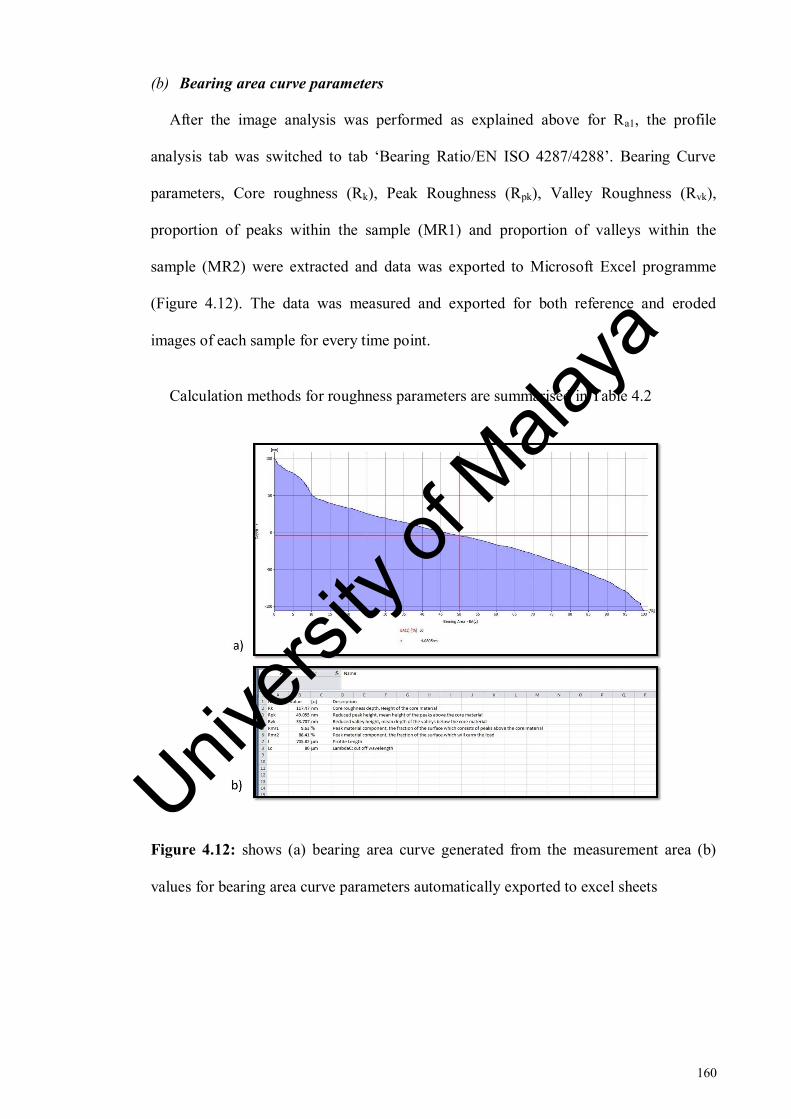
160
(b) Bearing area curve parameters
After the image analysis was performed as explained above for Ra1, the profile
analysis tab was switched to tab ‘Bearing Ratio/EN ISO 4287/4288’. Bearing Curve
parameters, Core roughness (Rk), Peak Roughness (Rpk), Valley Roughness (Rvk),
proportion of peaks within the sample (MR1) and proportion of valleys within the
sample (MR2) were extracted and data was exported to Microsoft Excel programme
(Figure 4.12). The data was measured and exported for both reference and eroded
images of each sample for every time point.
Calculation methods for roughness parameters are summarised in Table 4.2
Figure 4.12: shows (a) bearing area curve generated from the measurement area (b)
values for bearing area curve parameters automatically exported to excel sheets
Univers
ity of
Mala
ya

161
(c) Tissue loss measurement
Tissue loss (ΔZ) of each time point was measured for all samples using the IFM
2.1.5 software. Image taken at the junction of both reference and challenged areas at
each time point was selected for the analysis. Figure 4.13 shows the measurement of the
Z differences between the reference and eroded areas. A profile line was drawn from the
reference area to the eroded area. A green measurement line was positioned on the
reference area and another red measurement line was positioned on the eroded area
along the profile path as shown in Figure 4.13. A small circle on the profile path in the
image viewer indicated correspondence between the measurement line and the position
on the profile path in the image viewer. The vertical distance of these measurement
lines was calculated as tissue loss (ΔZ). At a time only one profile line could be
measured. Following the similar procedure, a total of three measurements at a distance
of 200 µm were made and ΔZ values were recorded. To standardise the measurements,
the reference measurement line was positioned at 100 µm and eroded measurement line
was positioned at 500 µm on the x-axis for all the time points of all samples. The data
was then transferred manually to excel programme and a mean of three measurements
was calculated for each time point for all samples.
Univers
ity of
Mala
ya

162
Figure 4.13: Measurement of tissue loss. Green line represents reference measurement
line and red line represents eroded measurement line. Delta z values are given at the
bottom of the image
4.2.2.5 Calculation of fractional change
The mean data of each parameter was normalised for the reference area (fPR) and
eroded area (fPE) by using the function given below:
𝑓𝑃𝑅 =𝑃𝑅 (𝑡)
𝑃𝑅(𝑡𝑜)
(4.1)
where fPR is the fraction of reference area of each parameter with its baseline, PR (t)
is each time point for the reference area and PR (to) is the baseline time point for the
reference area.
𝑓𝑃𝐸 =𝑃𝐸 (𝑡)
𝑃𝐸(𝑡𝑜)
(4.2)
Univers
ity of
Mala
ya

163
where fPE is the fraction of eroded area of each parameter with its baseline, PE(t) is
the erosive challenge time point for the eroded area and PE (to) is the baseline time point
for the eroded area.
And ΔZ was normalised by the following function:
𝑓𝛥𝑍 =𝛥𝑍(𝑡)
𝛥𝑍(𝑡𝑜)
(4.3)
where fΔZ is the fraction of Z difference with its baseline, ΔZ (t) is the Z difference
at each time point and ΔZ (to) is the Z difference at baseline time point.
4.2.2.6 Comparison of effect size
The effect size and Cohen’s d of all parameters was calculated for each outcome
measure by using means and standard deviations of baseline and day three of the eroded
group. The effect size was computed by using an online calculator (Becker, 2000)
employing the formula given below (Cohen, 2013) ,
Cohen′s d =M1−M2
σpooled. (4.4)
Where M1 and M2 are the means of day three and baseline measurements respectively
and
σpooled = √[(σ1
2 + σ22)
2]
(4.5)
Univers
ity of
Mala
ya

164
4.2.3 FE-SEM
4.2.3.1 Erosive pH-cycling
Another four root dentine samples were prepared from intact human premolar teeth.
The teeth collection and disinfection, the sample preparation was performed as
previously described (Section 4.2.2.1). Three samples were suspended in a beaker
containing 300 ml of 0.3% citric acid (pH = 3.2) (A&C American Chemicals Ltd.,
North Carolina, USA) on a movable stand with wires and plastic clips. The temperature
and speed of the solution were controlled by placing the beakers on a magnetic stirrer
(RCT basic, IKA, Germany). A magnetic stirrer is a laboratory device used for stirring a
‘stir bar’ added in the liquid by employing a magnetic field. The solution is stirred as a
result of it. The temperature of the solution was kept constant at 36°C and the speed was
kept constant at 300 rpm during the erosion phase of the cycling throughout the
experiment as shown in the figure 3.14. After 10 minutes of erosion challenge, samples
were removed from the beaker and rinsed in deionised water. Following this, each
sample was stored in a separate plastic container containing remineralisation solution
(A&C American Chemicals Ltd., North Carolina, USA) and kept in incubator at 36°C
for 3 hours. The samples were then removed from the bottles, dried with dental syringe
for 20 seconds at a distance of 10 cm and tapes were reapplied on the reference areas of
each sample. This alternating episode of demineralisation and remineralisation was
repeated three times during one cycling day. Citric acid was renewed after every
exposure and remineralisation solution was changed after every 24 hours. This cycling
erosive challenge was repeated for a total of three consecutive days. At the end of the
every cycling day, one of the three samples was removed from cycling and was stored
in incubator. Therefore, after three consecutive days of cycling, four representative
samples were imaged with FE-SEM. They included one sound sample which had not
undergone any erosion challenge and was representative of samples at baseline
Univers
ity of
Mala
ya

165
scanning. Three samples, each of which had undergone cycling erosion challenge for
one, two and three cycling days respectively.
4.2.3.2 Imaging
High magnification imaging of the surface was performed to assess the surface
alterations brought about by the cycling erosion challenge using scanning electron
microscopy (SEM). Imaging was performed for four prepared specimens one for each
time point (baseline, day one , day two and day three) using a Field Emission Scanning
Electron Microscope (FESEM; FEI, Quanta 200F, United Kingdom).
As moisture loss within dentine can lead to alterations of the surface and collapse of
organic matrix (Attin & Wegehaupt, 2014), therefore, the samples were dried for only
20 seconds with dental syringe before imaging. The images were captured at
magnifications of 1000x and 2000x and at an accelerating voltage of 10 kv. Six images
were obtained in total for each sample. Three images were obtained at each
magnification. One image was obtained at the reference side of the sample with healthy
dentine, second image at the eroded side of the sample and the third image was taken at
the middle of the sample containing both reference surface and the eroded surface.
4.2.4 Statistical Analysis
Statistical data analysis was performed with SPSS, version 22 (IBM SPSS Statistics
22.0 Inc., USA). The level of significance was set at p < 0.05. Shapiro-Wilk test and
skewness values were assessed to check the assumption of normality. Outcome measure
used was the fraction of the roughness parameter values of each time point with baseline
values (fRa1, fRk, fRpk, fRvk, fMR1, fMR2, fΔZ) to account for the biological variation
Univers
ity of
Mala
ya

166
among samples. The data was not normally distributed for fRa1, fRk, fRpk, fRvk,
fMR1and fΔZ. Therefore, Generalized estimating equations was performed with post
hoc multiple comparisons. A Bonferroni-Holm correction within SPSS, version 22
(IBM SPSS Statistics 22.0 Inc., USA) was performed to reduce risk of type 1 errors in
multiple comparisons. Sample 13 was identified as outlier and was removed from the
data of all parameters. Data for fMR2 assumed normal distribution and hence was
analysed using one-way repeated measures ANOVA.
4.3 Results
4.3.1 Profilometry
4.3.1.1 Average roughness:
Generalized estimating equations showed that the effect of erosion interval on the
fRa1 (Ra calculated from a single large area) of the eroded area was statistically
significant (Wald2
= 72.695, p < 0.0001) whereas no significant effect of erosion
interval was detected on fRa1 of the reference area (Wald2
= 4.18, p = 0.243).
There was a significant effect of erosion interval on fRa5 (Ra calculated from five
areas) of both reference (Wald2
= 32.744, p < 0.0001) and eroded areas (Wald2
=
69.702, p < 0.0001) (Table 4.3).
Univers
ity of
Mala
ya

167
Table 4.3: Results for generalized estimating equations (GEE) for reference and eroded
areas of fRa1 and fRa5
Area
fRa5 fRa1
Wald Chi-
Square
Degrees
of
freedom
p-value
Wald Chi-
Square
Degrees of
freedom
p-value
Reference 32.744 3 <0.0001 4.180 3 0.243
Eroded 69.702 3 <0.0001 72.695 3 <0.0001
Post hoc comparisons for fRa5 showed that eroded average roughness values of all
time points were significantly different with respect to their baseline roughness values
and significant differences were observed between day one - day two and between day
two - day three roughness values.
Eroded average roughness values (fRa1) of day two and day three were significantly
different with respect to their baseline roughness values whereas fRa1 failed to detect
any significant differences in roughness values between baseline and day 1. Moreover,
fRa1 detected significant difference between day one and day two roughness values only
(Table 4.4).
Univers
ity of
Mala
ya

168
Table 4.4: Post-hoc comparisons of erosion intervals for the eroded areas of fRa1 and
fRa5
Time (I) Time (J)
Mean difference (I-J)
fRa5 fRa1
Baseline Day 1 .099* -.0751
Baseline Day 2 -.1138* -.4370***
Baseline Day 3 -.3170*** -.6569***
Day 1 Day 2 -.2137*** -.3619**
Day 2 Day 3 -.2031*** -.2199
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Although, fRa5 was able to detect differences in roughness values between more time
points than fRa1 but the fact that changes in its reference area were also significant made
the findings of fRa5 unreliable. Hence, it was decided to employ fRa1 (single large area)
for further analysis in this study. Data plots for both fRa5 and fRa1 are given in Figure
4.14.
Univers
ity of
Mala
ya
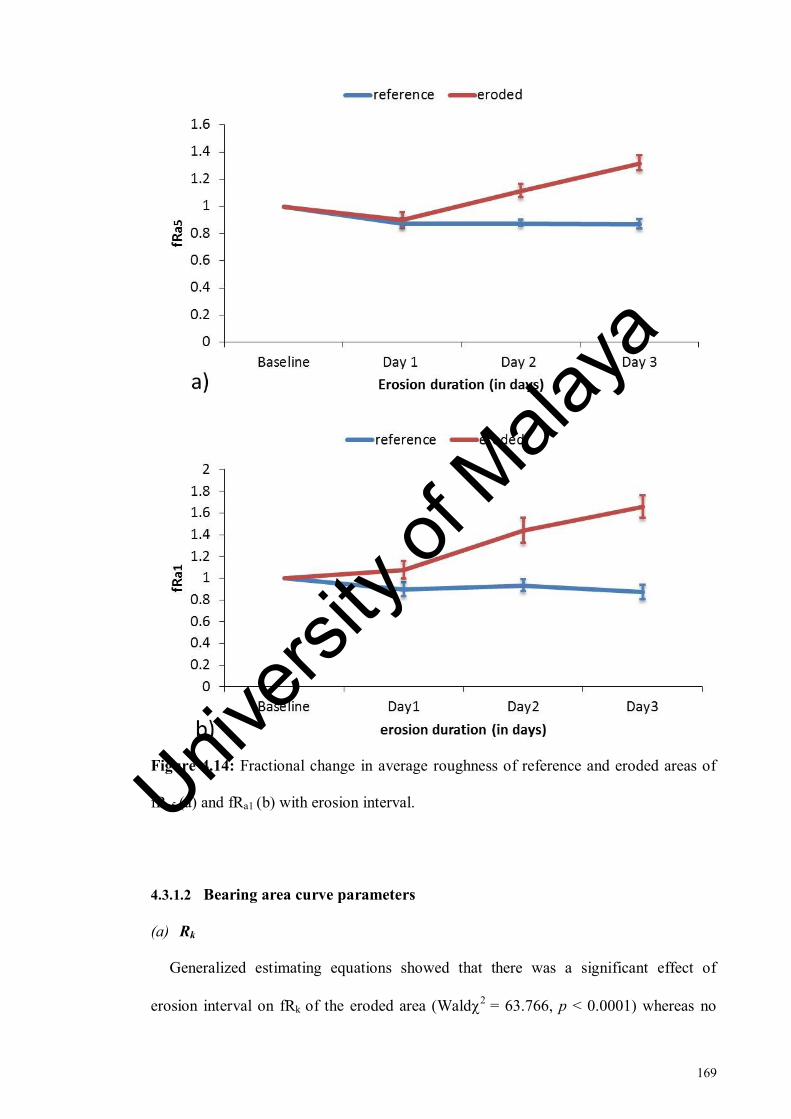
169
Figure 4.14: Fractional change in average roughness of reference and eroded areas of
fRa5 (a) and fRa1 (b) with erosion interval.
4.3.1.2 Bearing area curve parameters
(a) Rk
Generalized estimating equations showed that there was a significant effect of
erosion interval on fRk of the eroded area (Wald2
= 63.766, p < 0.0001) whereas no
Univers
ity of
Mala
ya
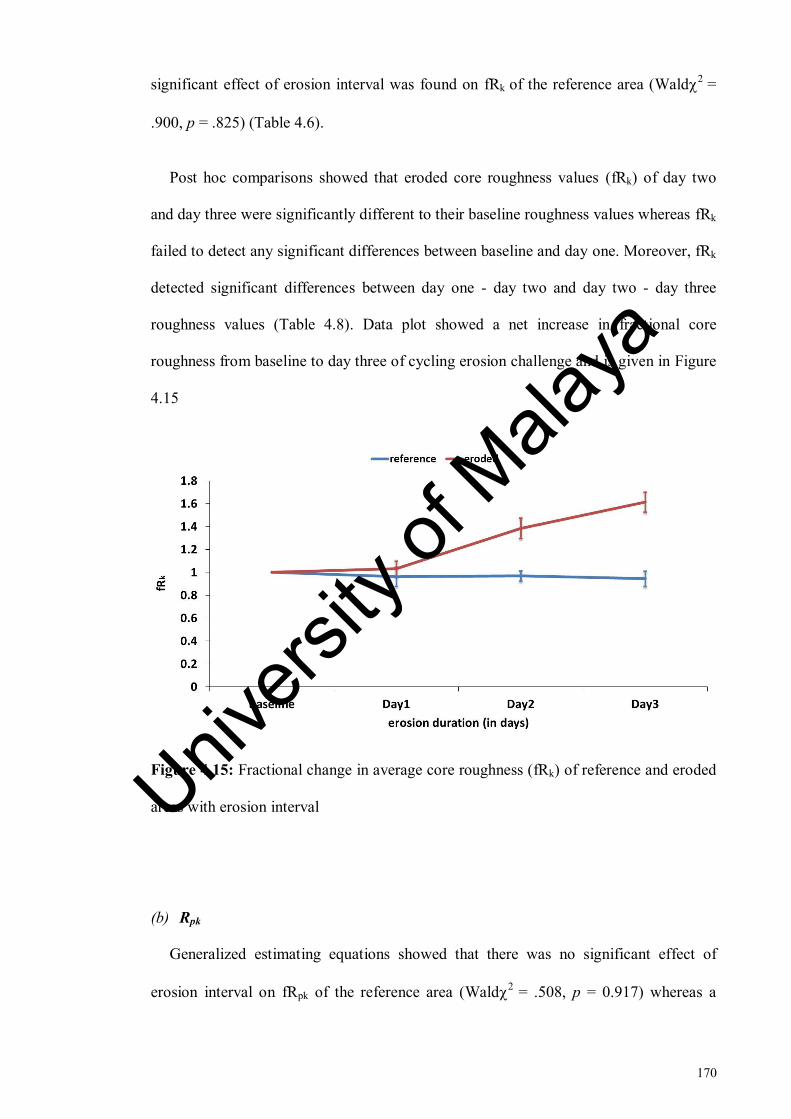
170
significant effect of erosion interval was found on fRk of the reference area (Wald2
=
.900, p = .825) (Table 4.6).
Post hoc comparisons showed that eroded core roughness values (fRk) of day two
and day three were significantly different to their baseline roughness values whereas fRk
failed to detect any significant differences between baseline and day one. Moreover, fRk
detected significant differences between day one - day two and day two - day three
roughness values (Table 4.8). Data plot showed a net increase in fractional core
roughness from baseline to day three of cycling erosion challenge and is given in Figure
4.15
Figure 4.15: Fractional change in average core roughness (fRk) of reference and eroded
areas with erosion interval
(b) Rpk
Generalized estimating equations showed that there was no significant effect of
erosion interval on fRpk of the reference area (Wald2
= .508, p = 0.917) whereas a
Univers
ity of
Mala
ya
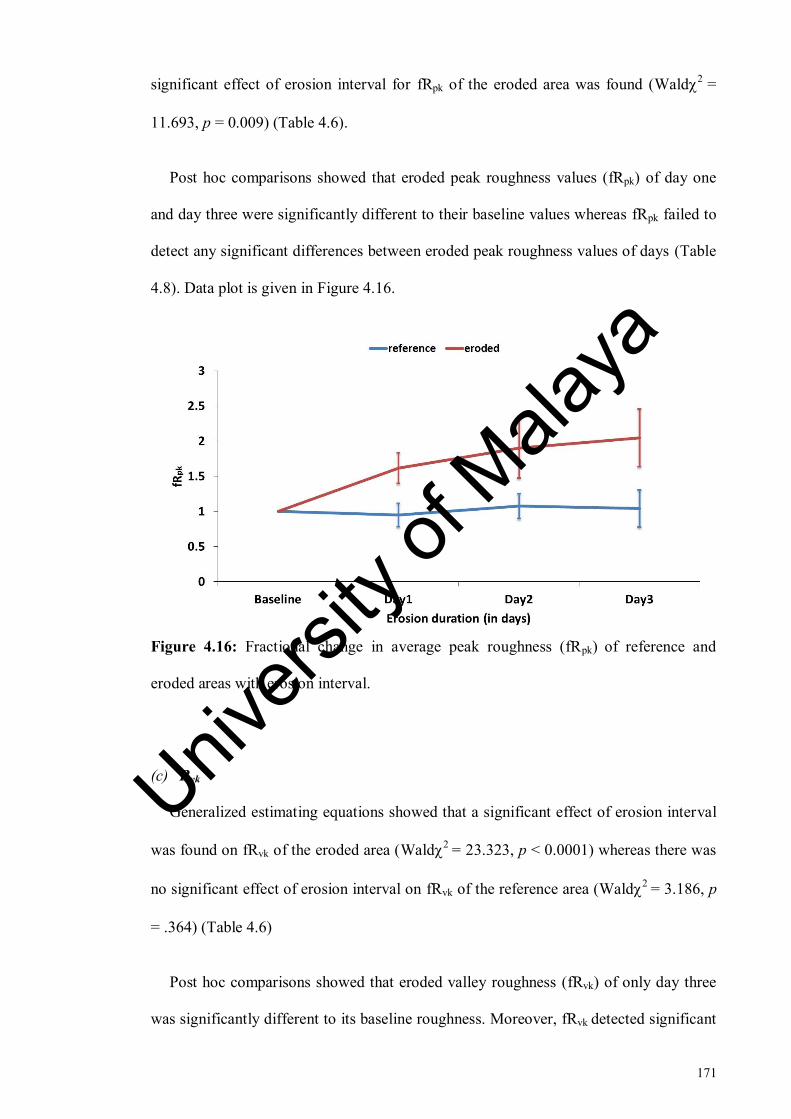
171
significant effect of erosion interval for fRpk of the eroded area was found (Wald2
=
11.693, p = 0.009) (Table 4.6).
Post hoc comparisons showed that eroded peak roughness values (fRpk) of day one
and day three were significantly different to their baseline values whereas fRpk failed to
detect any significant differences between eroded peak roughness values of days (Table
4.8). Data plot is given in Figure 4.16.
Figure 4.16: Fractional change in average peak roughness (fRpk) of reference and
eroded areas with erosion interval.
(c) Rvk
Generalized estimating equations showed that a significant effect of erosion interval
was found on fRvk of the eroded area (Wald2
= 23.323, p < 0.0001) whereas there was
no significant effect of erosion interval on fRvk of the reference area (Wald2
= 3.186, p
= .364) (Table 4.6)
Post hoc comparisons showed that eroded valley roughness (fRvk) of only day three
was significantly different to its baseline roughness. Moreover, fRvk detected significant
Univers
ity of
Mala
ya

172
differences between day two and day three roughness values (Table 4.8). Data plot is
given in Figure 4.17.
Figure 4.17: Fractional change in average valley roughness (fRvk) of reference and
eroded areas with erosion interval.
(d) MR1
Generalized estimating equations showed that there was no significant main effect of
erosion interval on fMR1 of eroded area (Wald2
= 2.785, p = 0.426) whereas a
significant effect of erosion interval was detected for the reference area (Wald2
=
11.234, p = 0.011) (Table 4.6). Data plot is given in Figure 4.18.
Univers
ity of
Mala
ya

173
Figure 4.18: Fractional change in proportion of profile peaks (fMR1) of reference and
eroded areas with erosion interval.
(e) MR2
Mauchly’s test showed that the assumption of sphericity was not violated for
reference (2 = 5.872, p = .320) and eroded areas (
2 = 2.826, p =.727).
One-way repeated measures ANOVA showed that there was no significant effect of
erosion interval on fMR2 of both the reference (F(3) =.188, p = .904, η2
= .01) and
eroded areas (F(3) = .240, p = .868, η2
= .013) (Table 4.7). Data plot is given in Figure
4.19.
Univers
ity of
Mala
ya
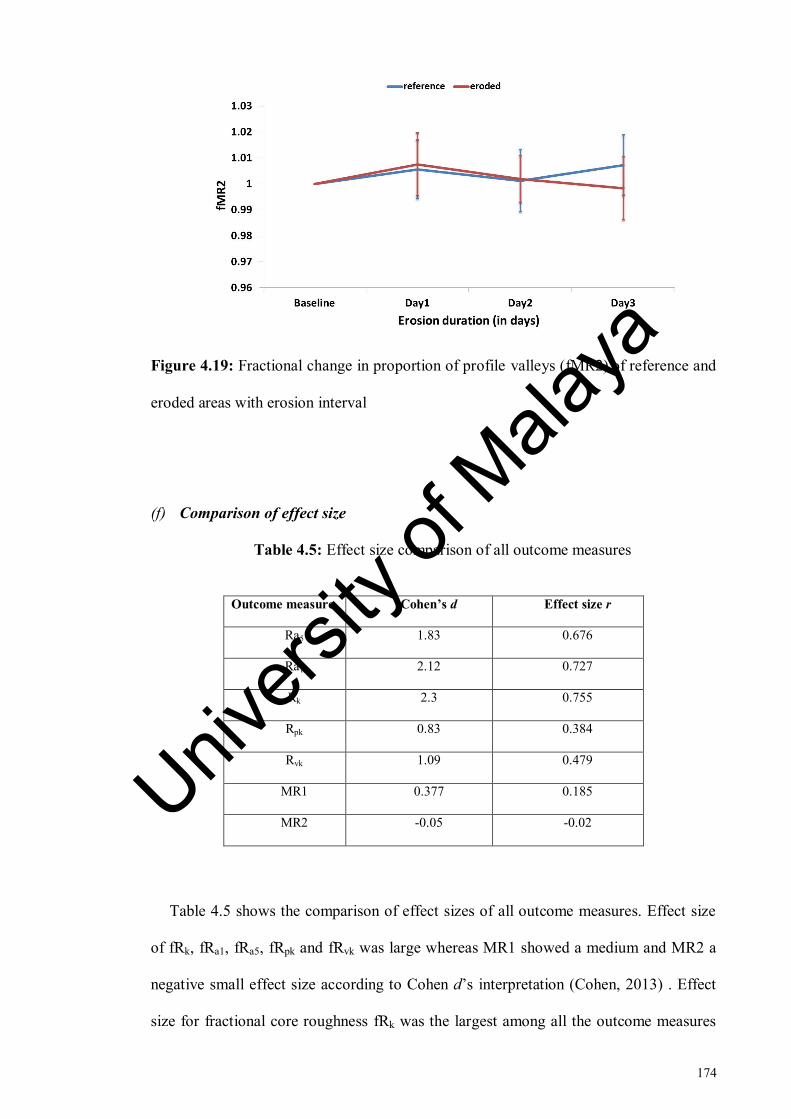
174
Figure 4.19: Fractional change in proportion of profile valleys (fMR2) of reference and
eroded areas with erosion interval
(f) Comparison of effect size
Table 4.5: Effect size comparison of all outcome measures
Outcome measure Cohen’s d Effect size r
Ra5 1.83 0.676
Ra1 2.12 0.727
Rk 2.3 0.755
Rpk 0.83 0.384
Rvk 1.09 0.479
MR1 0.377 0.185
MR2 -0.05 -0.02
Table 4.5 shows the comparison of effect sizes of all outcome measures. Effect size
of fRk, fRa1, fRa5, fRpk and fRvk was large whereas MR1 showed a medium and MR2 a
negative small effect size according to Cohen d’s interpretation (Cohen, 2013) . Effect
size for fractional core roughness fRk was the largest among all the outcome measures
Univers
ity of
Mala
ya

175
with r = 0.755, d = 2.3 followed by effect size of r = 0.727, d = 2.12 for fractional
average roughness fRa1. Moreover, fRa1 showed a larger effect size as compared to fRa5
(r = 0.676, d = 1.83).
Table 4.6: Results for generalized estimating equations (GEE) for reference and eroded
areas of bearing area curve parameters.
Outcome
measure
Reference Eroded
Wald Chi-
Square
Degrees of
freedom
p-value
Wald Chi-
Square
Degrees
of
freedom
p-value
fRk .900 3 0.825 63.766 3 <0.0001
fRpk .508 3 0.917 11.693 3 0.009
fRvk 3.186 3 0.364 23.323 3 <0.0001
fMR1 11.234 3 0.011 2.785 3 0.426
Table 4.7: Results for repeated measures ANOVA for reference and eroded areas of
MR2.
Outcome
measure
Reference Eroded
Mean
square
F-statistic p-value
Mean
square
F-statistic p-value
fMR2 <0.0001 0.188 0.904 <0.0001 0.240 0.868
Univers
ity of
Mala
ya

176
Table 4.8: Post hoc comparisons of erosion intervals for the eroded areas of bearing
area curve parameters.
Time (I) Time (J)
Mean difference (I-J)
fRk fRpk fRvk
Baseline Day 1 -.0306 -.6148* -.0338
Baseline Day 2 -.3851*** -.8993 -.1965
Baseline Day 3 -.6128*** -1.0465* -.8816**
Day 1 Day 2 -.3545*** -.2845 -.1627
Day 2 Day 3 -.2277** -.1473 -.6851*
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Univers
ity of
Mala
ya

177
Figure 4.20: Representative profiles (a) and bearing area curves (b) of a sample at
baseline measurement. The excel sheets show the values of Ra and bearing area curve
parameters.
Univers
ity of
Mala
ya
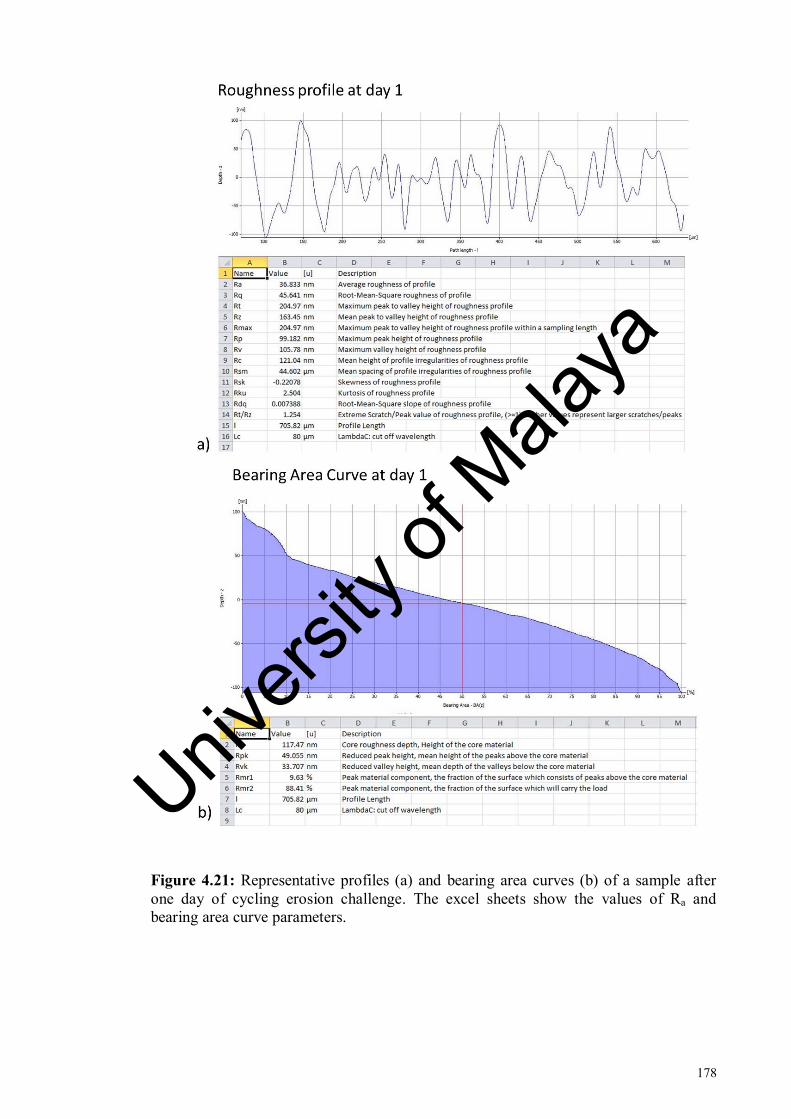
178
Figure 4.21: Representative profiles (a) and bearing area curves (b) of a sample after
one day of cycling erosion challenge. The excel sheets show the values of Ra and
bearing area curve parameters.
Univers
ity of
Mala
ya

179
Figure 4.22: Representative profiles (a) and bearing area curves (b) of a sample after
two days of cycling erosion challenge. The excel sheets show the values of Ra and
bearing area curve parameters.
Univers
ity of
Mala
ya

180
Figure 4.23: Representative profiles (a) and bearing area curves (b) of a sample after
three days of cycling erosion challenge. The excel sheets show the values of Ra and
bearing area curve parameters.
Univers
ity of
Mala
ya

181
4.3.1.3 Tissue loss
Generalized estimating equations showed that no main significant effect of erosion
interval on fΔZ was detected (2
= 4.036, p = 0.258) as shown in the Table 4.9. Data
plot is given in Figure 4.24.
Table 4.9: Results for generalized estimating equations (GEE) for fΔZ
Outcome measure Wald Chi-Square Degrees of freedom p-value
fΔZ 4.036 3 0.258
Figure 4.24: Fractional change in surface loss (fΔZ) with erosion interval.
Univers
ity of
Mala
ya

182
Table 4.10: Fractional change in average roughness, bearing area curve parameters and
surface loss with respect to baseline values given at different time points. Standard
deviations are within brackets. Values in bold denote a significant effect.
Time
Point
fRa1 fRa5 fRk fRpk fRvk fMR1 fMR2 fΔZ
Day 1
1.08
(0.3)
0.9
(0.23)
1.03
(0.29)
1.61
(0.95)
1.034
(0.61)
1.16
(0.51)
1.007
(0.05)
-1.2
(6.35)
Day 2
1.44
(0.5)
1.11
(0.21)
1.39
(0.38)
1.89
(1.86)
1.20
(0.49)
1.06
(0.35)
1.001
(0.04)
2.41
(13.67)
Day 3
1.66
(0.44)
1.31
(0.24)
1.61
(0.37)
2.04
(1.78)
1.88
(1.14)
1.07
(0.30)
0.998
(0.05)
-0.29
(4.9)
4.3.2 FE-SEM
FE-SEM images showed that dentine surface in the eroded sides of the samples
(Figure 4.25, d-f), showed an overall rougher appearance. The sound dentine in contrast
was fairly smooth (Figure 4.25, a-c). Eroded side of day one image (Figure 4.25, d)
showed that the surface was partially covered with smear layer but in contrast to the
reference surface (Figure 4.25, a), the dentinal tubules were opened in patches. In day
two image (Figure 4.25, e), the border between the peritubular and intertubular dentine
was demineralised and dentinal tubules were slightly widened as compared to dentinal
tubules in day one image. In day three image (Figure 4.25, f) the dentinal tubules were
further widened. The intertubular dentine appeared to be demineralised although the
peritubular dentine was still intact in most of the tubules. Acid erosion mediated
Univers
ity of
Mala
ya

183
increase in roughness of dentine surface was observed from day one image to day three
image (Figure 4.25, d-f).
Figure 4.25: FE-SEM micrographs (1000x) of the root dentine samples. a-c show
the reference areas of samples subjected to erosion challenge for one - three days at
Univers
ity of
Mala
ya

184
1000x. d-f show the eroded areas of samples subjected to erosion challenge for one -
three days at 1000x
4.4 Discussion
This study investigated the utility of surface roughness parameters for assessment of
early dentine erosion in a clinically relevant model. Traditionally employed parameter
tissue loss (ΔZ) was also measured. Based on the findings, the original null hypothesis
was rejected and it was concluded that surface roughness parameters can be used for
monitoring the progression of early dentine erosion whereas measurement of tissue loss
was not found suitable for its assessment. Moreover, use of bearing area curve enabled
the monitoring of early dentine erosion with sensitive parameters providing a deeper
understanding of overall erosion process which could not be attained by reporting Ra
value alone.
For this study, a pH-cycling model of erosion was employed where erosion
challenges with citric acid were interspersed with periods of simulated salivary
remineralisation. The remineralisation solution employed had a composition similar to
artificial saliva but without methyl p-hydroxybenzoate and sodium carboxymethyl
cellulose. This solution was shown to be more effective than artificial saliva in
remineralising early eroded enamel previously (Amaechi & Higham, 2001b) and was
therefore adopted for this study. Stylus profilometry has the potential of damaging the
specimen surface by producing scratches as deep as 10-25 nm as measured previously
by atomic force microscopy (Beyer et al., 2012). Therefore, a non-contact profilometry
was employed for performing the measurements. It is known that the use of flat samples
increases the accuracy and sensitivity of profilometry (Schlueter et al., 2011). Therefore
the samples were flattened and polished before imaging. The flatness of the samples
Univers
ity of
Mala
ya

185
was further assessed in the baseline scan before scanning. It is critical to reposition a
specimen correctly when monitoring small erosive surface alterations (Attin, 2006).
Hence, a custom made jig was employed to ensure correct repositioning of the samples
at various measurement time points.
4.4.1 Profilometry
4.4.1.1 Average roughness
Ra is traditionally extracted as a line profile through an area and is commonly
reported as an average of several line profiles (Gomez-Lopez, 2012). However, single
line profiles are not representative of the roughness of the entire image as the overall
value may be affected by a single atypical peak or valley (Leach, 2014; Moazzez et al.,
2014). Therefore, it was decided to select areas rather than measurement lines in order
to increase the accuracy of the extraction method of Ra. Although extracted from the
same surface, multiple measurements are known to result in a range of significantly
different Ra values (Wichern & Rasp, 2005). To solve this problem, 3D parameters have
been used (Moazzez et al., 2014). 2D Ra is still the most commonly reported form of
surface roughness in dentistry (Kukiattrakoon et al., 2011) and was therefore employed
in this study. It is felt that a single large area that covers most of the image will be better
representative of the overall roughness value rather than small multiple areas.
Therefore, Ra was measured with 1) a single large measurement area (Ra1) and 2) five
small measurement areas (Ra5) and a comparison was drawn between both measurement
techniques to find the most suitable method. Generalised estimating equation analysis
showed that fRa5 of eroded area was able to monitor roughness over time but the fact
that changes in roughness of its reference area were also significant made the findings
of fRa5 unreliable. Moreover, fRa1 showed a larger effect in monitoring of early dentine
Univers
ity of
Mala
ya

186
erosion as compared to fRa5 as shown by its greater effect size value. Based on these
findings, fRa1 was found most suitable and was employed for further analysis in this
study.
4.4.1.2 Bearing area curve parameters
Bearing area curve can be used to characterise surfaces having different functional
properties at different depths (De Chiffre et al., 2000) called multi-stratified surfaces.
Assessment of multi-stratified surfaces can prove to be challenging and measurement of
these surfaces by simple parameters like Ra might not yield sufficient information (Field
et al., 2010). Dentine erosion likewise is not a simple surface process and its assessment
is a challenging task because of the presence of its organic content. Therefore, same set
of profilometric data was used to extract bearing area curve parameters in adjunct to
average roughness to assess their potential and sensitivity for monitoring of early
dentine erosion.
Results showed that fRpk was most sensitive for detection of early dentine erosion
with detection sensitivity of day one from baseline. fRpk represents the height of the
material peaks or the area which comes in contact with the acidic solution first which
explains its ability to detect erosion by the first day of cycling erosion challenge.
An erosion model is expected to exhibit deeper valleys. The deeper valleys are
expected to result from natural tendency of fluids to deposit in these areas (Las Casas et
al., 2008). The findings of this study supported this assumption. fRvk value, representing
the depth of material valleys was significantly different by day three of erosion
challenge. This would indicate that the valleys had become deeper by the pooling of
citric acid in these areas by third day of cycling erosion challenge. It could be
Univers
ity of
Mala
ya
187
speculated that this acid entrapment might be followed by more aggressive erosion in
case of continued acid challenge. However, it is important to bear in mind that a pH-
cycling model was employed for this study and every erosion challenge was
accompanied by simulated salivary remineralisation of 3 hours. In addition, the samples
were immersed in remineralisation solution overnight. Therefore, significant increase in
valley depths could also be attributed to the pooling of remineralisation solution in these
areas which could aid in resisting demineralisation in the later stages after day three of
erosion. These speculations need further investigation in a prolonged cycling erosion
protocol.
Fraction change in average roughness (fRa1) and fraction change in core roughness
(fRk) showed similar results for the eroded group with detection sensitivity of two days
from baseline. However, unlike fRk, fRa1 was not able to monitor erosion in advanced
stages between day two and day three. Effect size comparison between all roughness
parameters showed that fRk had the greatest effect size and hence could be considered
most effective in monitoring the progression of early erosion in dentine. This could
suggest the possibility of Ra being replaced by a more effective parameter like Rk in
future.
Fractional change in proportion of profile peaks (fMR1) and fractional change in
proportion of profile valleys (fMR2) were not sensitive enough to detect and monitor
early dentinal erosion. The amount of demineralisation induced in this study was
perhaps too low to have brought about a significantly different increase or decrease in
the total number of peaks or valleys between cycling days. At the same time, lesser
degree of remineralisation would be expected from the remineralisation solution
simulating saliva utilised in this study as compared to what would be expected to occur
by a treatment product. It is speculated that MR1 might be more suitable for evaluation
Univers
ity of
Mala
ya

188
of more aggressive erosion in dentine and MR2 might be used for investigation of
efficacy of treatment products or remineralising agents for dentine erosion but this area
undoubtedly requires further investigation. For this particular protocol, these
parameters did not prove to be effective for monitoring early dentine erosion
progression.
4.4.1.3 Tissue loss
Dentine when demineralised is prone to shrinkage (Zhang et al., 2009) and
profilometric measurements of dried eroded dentine will reveal a step height difference
between reference and eroded areas which is absent otherwise in controlled moisture
conditions (Ganss et al., 2009b). This step height does not represent the true mineral
loss or surface level of organic matrix (Schlueter et al., 2011) and it was recommended
that dentine samples be kept wet until measurements are performed (Attin et al., 2009;
Ganss et al., 2007). However, the profilometry system used in this study like most other
systems did not allow the samples to be profiled under wet or moist conditions. This is
because profiling of wet samples can create artifacts by parts of light being reflected by
the water (Attin et al., 2009). The effect of ambient drying on eroded dentine was
assessed and it was found that drying effects reached a plateau after 10 minutes (Ganss
et al., 2007). Therefore, samples were air dried for 10 minutes to standardise the organic
matrix shrinkage for this study as previously employed (Steiner-Oliveira et al., 2010).
Moreover, ΔZ like all other parameters was reported as fractional change with respect to
its baseline measurement (fΔZ) which could address any step height difference between
the reference and eroded areas if present at baseline measurement due to drying.
Tissue loss appearing in the form of a step change between the reference and eroded
areas is conventionally measured by profilometry (Borges et al., 2014; Charone et al.,
Univers
ity of
Mala
ya

189
2014; Paepegaey et al., 2013). However, the initial stage dental erosion is not expected
to produce a step change (Young & Tenuta, 2011) and it is speculated that this
parameter might not be effective in measuring the early stages of erosion. The results of
this study confirmed this assumption and tissue loss was not able to detect or monitor
the early dentinal erosion. This is in accordance with the previous study where non-
contact profilometry was not able to detect changes in surface loss before the digestion
of organic matrix. However, after the removal of organic matrix the mineral loss values
increased (Ganss et al., 2009b). Removal of organic matrix would render non-contact
profilometry a destructive method restricting its use for longitudinal studies and for
clinical trials. Monitoring of early dentine erosion with surface roughness parameters
would be more suitable in this regard.
4.4.2 FE-SEM
FE-SEM images were obtained to visualise the morphological changes in eroded
dentine in comparison to sound dentine in the reference areas. Moreover, the effect of
erosion in time could be visualised by comparing samples eroded for different erosion
intervals. For this study, a field-emission scanning electron microscopy (FE-SEM) was
employed which allowed the samples to be imaged after air-drying only without any
sample preparation or metallisation.
The sound dentine in reference areas of all samples showed a smooth surface covered
with smear layer (Figure 4.25, a-c). Treatment with citric acid resulted in exposure of
dentinal tubules which could be seen in day one image of eroded area (Figure 4.25, d).
However, the tubules were seen partially or completely occluded in the day one image.
It would be tempting to assume that the tubules were occluded with smear plug
remnants due to the partial removal of smear layer by citric acid. However, it is
Univers
ity of
Mala
ya

190
important to bear in mind that a cycling model of erosion was employed for this study
and tubular occlusion observed in the images could also be the result of deposition of
mineral by remineralising solution used in this study. A previous study reported that
artificial saliva deposited mineral on eroded dentine and dentinal tubules were occluded
or partially occluded as result of it (Vanuspong et al., 2002) however authors found that
this deposit was lost after ultrasonication . This is in accordance with our study and it
could be speculated that at day one, the dentinal tubules were opened as a result of
exposure to citric acid. But then the samples were immersed for 3 hours in
remineralising solution after every erosion challenge and overnight. This partially
occluded the opened dentinal tubules as a result of deposition of mineral. However, this
deposit can be assumed to be partially or completely removed with every erosion
challenge until the effect of erosion induced overcame the effect of remineralisation and
deposition of mineral with remineralisation solution could offer little protection. In day
two image of eroded area ((Figure 4.25, d), demineralisation of peritubular dentine at
the border between the peritubular and intertubular dentine was obvious and dentinal
tubules were slightly widened in comparison to reference dentine and eroded dentine in
day one image. In day three image (Figure 4.25, f) the dissolution of peritubular dentine
was obvious and dentine tubules were observed to be further widened as a result of it.
The intertubular dentine appeared to be demineralised and the overall surface appeared
roughened and porous in day three image (Figure 4.25, e) as previously reported
(Meurman et al., 1991).
All the surface roughness parameters except for fMR1 and fMR2 showed an increase
in roughness from baseline to day three of cycling erosion. This was confirmed by the
FE-SEM images which showed considerable roughening on the surface of dentine
especially at day three. This is in line with the previous studies which reported that
Univers
ity of
Mala
ya
191
dentine surface becomes rougher when eroded (Azzopardi et al., 2004; Meurman et al.,
1991; Mirkarimi & Toomarian, 2012).
Surface profilometry has the potential of being employed in clinical studies as shown
previously (West et al., 1998; Whitehead et al., 1997). Use of parameters sensitive to
early changes in erosion process would aid in the assessment of early dentine erosion
and its proposed treatment strategies in clinical trials. Also, the in vivo capability of this
method would make it a potential quantitative reference method to validate the findings
of newer non-invasive techniques in erosion studies. Based on our findings, it is
recommended that a combination of bearing area curve parameters Rpk and Rk be used
for the longitudinal monitoring of early dentine erosion within the limitation of the
current model. Rpk is most suitable for assessment of early erosion challenge and Rk for
monitoring of subsequent erosion challenges between day one- day two and day two –
day three. Rvk might aid in testing the efficacy of anti-erosion treatment products and/or
development of any remineralisation-associated resistance.
4.5 Conclusions
Within the limitations of the current study design, the following conclusions were
drawn from the study findings,
1. Average surface roughness, fRa1 and bearing area curve parameters, fRk (core
roughness), fRpk (peak roughness) and fRvk (valley roughness) were able to
detect and longitudinally measure early dentine erosion. fMR1, fMR2
(Fractional change in proportion of profile peaks and profile valleys
respectively) and fΔZ (surface loss) were not able to detect and measure early
dentine erosion.
Univers
ity of
Mala
ya

192
2. fRk showed the greatest magnitude of strength in measuring early dentine
erosion as determined by its largest effect size.
3. The early dentine erosion detection threshold of surface roughness varied with
different parameters. fRpk showed a detection threshold of day one from baseline
measurement. fRk and fRa1 were able to detect erosion by day two from baseline
measurement. fRvk showed a detection threshold of day three from baseline
measurement.
4. FE-SEM images supported the surface roughness results. FE-SEM images of the
eroded areas of samples showed increase in overall roughness of dentine surface
during erosion progression. Continuous rise of roughness shown by fRa1, fRk,
fRpk and fRvk in relation to the incubation time in acid was obvious.
The null hypotheses were rejected as shown below,
1. Surface roughness parameters fRpk, fRk, fRa1 and fRvk can be used to measure
early dentine erosion progression for three days in simulated intraoral conditions.
2. Bearing curve parameters fRpk and fRk are more sensitive than fRa1 in measuring
early dentine erosion in simulated intraoral conditions.
Univers
ity of
Mala
ya

193
CHAPTER 5: MONITORING OF EARLY DENTINE EROSION WITH
OPTICAL COHERENCE TOMOGRAPHY IN A SIMULATED INTRAORAL
CONDITION
This chapter describes the assessment of early eroded dentine with optical coherence
tomography (OCT) in a simulated intraoral environment and is a continuation of the
study conducted in chapter 4. Same samples were employed in both studies for
comparison purposes. Therefore, the findings of optical coherence tomography were
compared with the surface roughness measurements made with profilometry and
ultrastructural changes acquired with field-emission scanning electron microscopy (FE-
SEM). An introduction to the research purpose is followed by a review of various
conditions necessary for modelling simulated intraoral environment in erosion studies.
5.1 Introduction
Researchers investigate real-world phenomena by creating simulation study models
which enables them to explain the various aspects of those phenomena (Nersessian,
2009). Over the years, extensive research has been carried out to investigate dental
erosion using different study models.
Ideally it is desirable to conduct clinical trials to evaluate the erosion process and its
subsequent prevention. However, due to various challenges encountered in measuring
erosion in the in vivo settings (Attin, 2006) as well as the ethical considerations
involved in the induction of significant levels of erosion clinically (Huysmans et al.,
2011), a number of in vitro and in situ models have been developed and used.
In vitro models are important in erosion studies because they aid in understanding the
process of erosion, help in assessment of measurement techniques and efficacies of the
Univers
ity of
Mala
ya

194
proposed treatment strategies for arresting the progression of erosion. In these models
tightly standardised experimental conditions can be implemented, the effect of variables
can be examined individually or in combination and precise measurement techniques
can be employed to assess the alterations in dental hard tissues caused by the process of
erosion. These models are relatively inexpensive and can be performed in shorter
periods of time (West et al., 2011). Well designed in vitro models provide valuable data
that closely matches with the clinical situation without the fear of causing any harmful
effects to individuals.
Dental erosion is known to interact with the other aspects of tooth wear, which are
attrition and abrasion and it is hard to separate them clinically. Therefore the interaction
of these three processes has been studied widely with in vitro studies in order to
determine the role of each process in the net outcome of wear and their interaction with
each other. Depending on the objective of a study, each component has been studied
either individually or in combination by the help of in vitro or in situ studies (Paepegaey
et al., 2013). During the initial stages of erosive wear, softening caused by initial acid
attack makes the tooth surface vulnerable to mechanical wear. Hence it is important to
understand the process of erosion independently in order to be able to control the
progression of this condition.
OCT showed the potential of monitoring the progression of early dentine erosion as
discussed in chapter 3 of this thesis. However, the potential of OCT in monitoring the
progression of early dentine erosion in simulated erosion conditions was unknown. The
simulated oral environment was created by adopting a cycling model of erosion.
Univers
ity of
Mala
ya

195
5.1.1 Cycling and non-cycling models
The term ‘cycling’ has been used interchangeably in erosion studies to mean either
erosion models in which the acid challenges are interspersed with periods of exposure to
remineralising medium or models with cyclic alternation of erosion with abrasion or
attrition (Addy & Shellis, 2006). The former cycling models have been used to mimic
the intraoral conditions where the erosion process is modulated by the presence of saliva
while the latter cycling models attempt to mimic the clinical interaction between the
mechanical wear processes of attrition and abrasion with erosion. The scope of this
review is the former and in order to differentiate it from the latter, the term ‘pH-cycling’
will be used henceforth and by non pH-cycling models, we mean the erosion models
that do not have a remineralisation phase and only involve the exposure of the substrate
to acid challenges. The primary aim of these pH-cycling models is to simulate the
natural repair process that takes place in the oral cavity during erosion challenges
(Shellis et al., 2011) as results attained from non pH-cycling models, arguably, could
not be extrapolated into the clinical scenario.
Review of literature reveals that there is lack of consistency in the design of erosion
models that makes the comparison of different study outcomes difficult. Although the
use of pH-cycling in dental erosion studies has repeatedly been recommended in the
literature (Shellis et al., 2011; Young & Tenuta, 2011) especially when the phenomenon
of remineralisation related to dental erosion is to be investigated (West et al., 2011),
currently there are no guidelines or consensus as to when and how it should be used.
5.1.2 Erosion pH-cycling models
Generally the in vitro erosion pH-cycling models can be classified into
demineralisation or remineralisation models depending on the loss or gain of minerals
Univers
ity of
Mala
ya
196
occurring in the erosion challenge or treatment respectively. Demineralisation models
are usually employed to analyse the loss of mineral in sound substrate under erosive
conditions or to assess the degree of further demineralisation of lesions which were
already eroded. Remineralisation models deal with the assessment of mineral gain in
eroded lesions as a result of application of different treatment products (Buzalaf et al.,
2010) or assess the ability of various treatment formulations in increasing the resistance
of sound tooth substrate against the initiation and progression of acid induced damage
(Faller et al., 2011; Yamashita et al., 2013). Cycling can be brought about either by
transferring samples manually between the erosive and remineralising media or
automated set-ups such as the artificial mouth models (Attin et al., 2003; Attin et al.,
2005c) which enable intermittent episodes of demineralisation and remineralisation to
be performed more efficiently and meticulously.
The erosion pH-cycling model is made up of a demineralising and a remineralising
arm. Each of these two arms by itself comprises of three components, the de- or
remineralising agent, the time factor and the environment (stirring). Previous
comprehensive reviews had addressed the factors related to demineralising arm in detail
such as for in vitro Erosion / Abrasion studies (West et al., 2011; Wiegand & Attin,
2011; Young & Tenuta, 2011) , however the remineralising arm has been less reviewed.
5.1.3 Substrate
Generally, samples of enamel (Faller et al., 2011; Murakami et al., 2009), or dentine
(Cruz et al., 2012; Karlinsey et al., 2011; Wang et al., 2013) obtained from bovine
incisors, human premolars and third molars have been used as substrates in pH-cycling
erosion studies. Sometimes both enamel and dentine samples have also been assessed in
the same experiment (Piekarz et al., 2008; Scaramucci et al., 2011) which probably
Univers
ity of
Mala
ya

197
offers greater advantage since it aids in making comparisons between these dental hard
tissues simultaneously.
Moreover, sound substrate is usually employed in the in vitro erosion studies which
can then be subjected to a variety of artificially induced erosive challenges depending
on the protocol. This explains the frequent use of human premolars or third molars
which extracted for orthodontic or surgical purposes respectively are available in
relatively conserved state. However, the fact that partially erupted or impacted teeth can
be more porous and hence more susceptible to demineralisation than other permanent
teeth, should be taken into account during comparison of different studies (Buzalaf et
al., 2010).
Primary teeth have rarely been employed in pH-cycling erosion studies probably
because of the difficulty in acquiring them, and the smaller area they present for
handling during experiments (Buzalaf et al., 2010). The erosion rates in primary enamel
as compared to permanent enamel have been reported to be higher by some authors
(Hunter et al., 2000a) whereas others did not find any significant differences (Addy &
Shellis, 2006; Hunter et al., 2000b; Lippert et al., 2004b). However, this conflicting data
may have arisen because substrates of different developmental and post-eruptive ages
were employed in these experiments. Hence, while selecting primary teeth for erosion
experiments, special consideration should be paid to their developmental ages as it is
known to affect the progression of the erosion rate (Murakami et al., 2009).
Ideally, it is preferable to use human teeth in erosion experiments from the
perspective of clinical relevance, but due to the ethical issues involved and difficulties
posed in acquiring sound human teeth, bovine teeth have also been frequently used.
Somewhat inconsistent outcomes have been drawn from the studies investigating and
comparing human and bovine teeth (Yassen et al., 2011). Moreover, bovine teeth have
Univers
ity of
Mala
ya
198
been known to exhibit greater porosity and as a result greater response to erosion
challenge (Wang et al., 2012) . In spite of this, bovine teeth have been considered as
acceptable substitutes for human teeth in erosion experiments (Venasakulchai et al.,
2010; Young & Tenuta, 2011).
5.1.4 Polishing and sample preparation
Although natural surfaces of teeth from the viewpoint of clinical relevance would
make ideal substrates for erosion experiments, yet polished samples have been used in
majority of erosion studies mainly because most of the methods available currently for
measurement of dental erosion (such as profilometry, surface microhardness,
nanohardness) require sample preparation and polishing for maximum precision. But it
should also be considered that during the intraoral erosion challenge, the outer surface
of the natural teeth gets removed by the effect of acid, producing smooth polished
surfaces (Attin, 2006) and the use of polished substrate also aids in reducing the
experimental time by abolishing the more variable natural surface (Young & Tenuta,
2011). However, the fact that polished enamel is more susceptible to erosion than
natural enamel should be taken into consideration while interpreting the study outcomes
(Ganss et al., 2000; Lippert et al., 2004a).
Further, a number of factors need to be considered while preparing the samples for
erosion studies. Structural variations in erosive lesions in enamel specimens prepared
from the same as well as different teeth have been observed (Meurman & Frank, 1991).
This problem can be minimised by random distribution of samples. Additionally, as
radicular dentine has shown to be less susceptible to the effect of acid as compared to
coronal dentine, samples from crown and root dentine should never be combined during
an experiment (Ganss et al., 2000).
Univers
ity of
Mala
ya

199
5.1.5 Demineralising agent
The source of acid causing dental erosion could either be extrinsic or intrinsic in
origin. Extrinsic sources are mainly from food and beverage such as soft drinks, citrus
fruit juices and pickles and less frequently, from occupational exposure to acid vapour
in battery factories or in wine tasters. Intrinsic factors are those chronic diseases or
habits that cause frequent regurgitation of acidic stomach contents. These include
gastroesophageal reflux disease (GORD), eating disorders, chronic vomiting and
rumination (Johansson et al., 2012). Therefore, these acids had been employed as
demineralising agents in erosion studies either in pure form or as inherent acids in soft
drinks (Cheng et al., 2009a). Citric acid being the main inherent acid in acidic beverages
had most frequently been employed for induction of erosion challenge in pH-cycling
erosion models. The other less frequently used acids are phosphoric acid, hydrochloric
acid and maleic acid (Addy, 2005; Addy & Hunter, 2003; Faller et al., 2011). Acids in
inherent form have the advantage of providing more realistic testing but at the same
time are known to vary between batches in terms of pH, concentration and buffering
capacity of the formulation. This could produce variation in the data especially in the
cycling models where the demineralising agent is to be used several times during the
study and standardisation of its formulation is critical. On the other hand, plain acids (in
pure form) are far easier to formulate, reproduce and produce consistent responses
throughout the study (Shellis et al., 2011). Therefore, it is felt that when it comes to
prolonged cycling in erosion pH-cycling models, it is better to use an acid in pure form
rather than a commercial acidic drink.
Further, the inclusion of a standard acid solution for assessment of the employed
methodology has been recommended. The pH and concentration of acid which also
determine the buffering capacity of the acid should fall in clinically relevant ranges
Univers
ity of
Mala
ya

200
according to the type of erosion challenge being simulated (Shellis et al., 2011; Young
& Tenuta, 2011).
5.1.6 Remineralising agent
Dental erosion is a multifactorial condition and involves an interplay of biological,
chemical and behavioural factors (Lussi & Jaeggi, 2008). Saliva is the most important
biological factor affecting dental erosion and influences the rate and progression of
dental erosion through the properties of salivary clearance, pellicle formation, buffering
capacity and its ability to remineralise the eroded tissues by the provision of various
minerals necessary for remineralisation of tissues (Buzalaf et al., 2012a). These
characteristics make the incorporation of saliva in pH-cycling models necessary where
simulation of clinical erosion is critical. The medium used for interim storage of
samples in pH-cycling models can be human natural saliva or simulated salivary fluids
such as artificial saliva and remineralisation solution.
Natural saliva is composed mainly of organic and inorganic components. The
inorganic components include a variety of minerals that play a vital in the process of
erosion. Acid challenge leads to demineralisation and softening of dental hard tissues
and salivary calcium and phosphate serve to remineralise these tissues. They act as
common ions to the tooth mineral and aid in maintenance of tooth integrity by slowing
down the rate of mineral dissolution after an erosive challenge. Moreover, substantial
enhancement of remineralisation is known to occur in the presence of fluoride ions.
Bicarbonate is linked to the buffering capacity of saliva which plays an important role in
neutralisation and buffering of dietary acids (Al-Malik et al., 2002; Buzalaf et al.,
2012a). Neutralisation of acids by saliva directly affects the amount of mineral lost from
dental hard tissues during an erosion challenge. The longer it takes for saliva to buffer
Univers
ity of
Mala
ya
201
the incoming dietary acids, the more mineral loss occurs from the tooth structure (Lussi
et al., 2011).
The storage medium employed in erosion studies should ideally be able to replicate
the intraoral salivary functions modulating the process of erosion. That is why various
recipes of artificial saliva and remineralisation solutions employed in erosion studies
have incorporated the electrolyte component of natural saliva.
The organic component of natural saliva is mainly composed of salivary proteins and
glycoproteins. The main role these proteins play in the process of erosion is through the
formation of pellicle. Pellicle is a protein-based bacteria-free layer formed on the
surfaces of teeth immediately after brushing with dentifrice, prophylaxis or chemical
dissolution (Hara et al., 2006b; Moazzez et al., 2014). It is known to adhere to the tooth
surfaces and provides protection against dental erosion by acting as a perm-selective
membrane hampering the contact of acid with tooth surface, thus preventing dissolution
of dental hard tissues. However, it has also been claimed to reduce the remineralisation
process overall although it might encourage some subsurface remineralisation (Hara et
al., 2006b; Young & Tenuta, 2011). Salivary proteins such as proline-rich proteins,
statherin and histatins play an important role in the formation of salivary pellicle. In
addition, salivary mucins have been known to contribute greatly to provide protection
against enamel erosion by the formation of the acquired pellicle. It is important to note
that the recipes of artificial saliva and remineralisation media do not have an organic
component and hence cannot be expected to allow the adequate formation of salivary
pellicle (Lussi & Carvalho, 2014; Smith & Knight, 1984). Therefore, it is
recommended that if the effect of pellicle is to be investigated in pH-cycling models,
then either natural saliva is to be used or organic component be added to the artificial
storage media.
Univers
ity of
Mala
ya

202
The other important function of salivary proteins is the formation of complexes with
minerals. Statherin and proline-rich proteins are known to bind and prevent the
precipitation of calcium phosphate thus allowing the saliva to maintain its state of
supersaturation with respect to calcium and phosphate salts (Buzalaf et al., 2012a) . This
could lead to greater remineralisation in the in vitro models as compared to in vivo
models. This is because salivary proteins are usually lacking in artificial storage media
employed in the in vitro models. Moreover, some salivary proteins are known to bind
calcium. Recipes of artificial saliva and remineralisation solutions used in erosion pH-
cycling models are based on mineral composition of natural saliva and lack salivary
proteins. Hence, there is always a chance that these artificially formulated solutions
might exhibit too high a degree of supersaturation due to precipitation of calcium
phosphate salts. It has therefore been recommended that the concentration of calcium in
artificial saliva and remineralisation mediums be adjusted accordingly (Shellis et al.,
2011).
Although, exposure of samples to natural saliva in erosion experiments would be the
ideal case scenario, it can also pose a set of problems. Firstly the experiment might
require saliva in large quantities, the collection of which might prove to be quite time
consuming and tedious. Moreover, early decomposition or alteration of natural saliva in
erosion experiments, risk of cross-infection and high intra- / inter-sample variability are
some of the challenges encountered while using natural saliva. Therefore, the use of
artificial saliva has been considered acceptable (West et al., 2011; Wiegand & Attin,
2011).
However, it was shown that a remineralisation solution was better at remineralising
early eroded enamel lesions as compared to artificial saliva (Amaechi & Higham,
2001b) The remineralisation solution used in the study had the same composition as that
Univers
ity of
Mala
ya

203
of artificial saliva with the exception of methyl p-hydroxybenzoate and sodium
carboxymethyl cellulose. The former acts as a preservative whereas the latter is added to
increase the viscosity of artificial saliva to simulate natural saliva. Sodium
carboxymethyl cellulose (CMC) had also been shown to limit the remineralisation
potential of artificial saliva (Ionta et al., 2014). This decrease in remineralisation
potential of artificial saliva had been attributed to the property of CMC to form
complexes with calcium and phosphate ions as well as causing an increase in viscosity
thereby reducing the diffusion rate of solution. Therefore, a properly formulated
remineralisation solution or artificial saliva containing calcium, phosphate and fluoride
in appropriate concentrations at a neutral pH but without CMC could also be used in the
erosion pH-cycling models instead of natural saliva (Amaechi & Higham, 2001b).
5.1.7 Time
The duration of erosion challenge should be in a clinically relevant range. An erosion
challenge of ten minutes has been adopted by researchers to simulate the effect of
extrinsic erosion as it represents the time frame of consumption of a can of soft drink or
juice (Faller et al., 2011) whereas erosion protocols with erosion challenge of five
minutes have mimicked the erosion challenge in individuals at high risk for dental
erosion (Cruz et al., 2012) such as patients with eating disorders involving repeated
vomiting (Schlueter et al., 2010).
It is important to note that for simulation of initial erosion, shorter acid challenges
should be induced to prevent the occurrence of bulk tissue loss keeping in consideration
that erosion caused must always be detectable by the method chosen to measure erosion
(Young & Tenuta, 2011).
Univers
ity of
Mala
ya

204
5.1.8 Environment
Generally, the erosive agents are stirred at a particular rate during erosion
experiments. This is to simulate the swishing of the drink or acid within the oral cavity
in clinical erosion. An increase in agitation of the drink will aid in renewing the solution
on the surface of the layer of liquid lying adjacent to the tooth, thus causing it to become
under saturated with respect to tooth mineral, thereby increasing the dissolution process
of dental hard tissues (Lussi & Jaeggi, 2006). Also, the agitation rate influences the
dissolution rate of tissues by altering the thickness of diffusion layer. Usually an
increase in agitation will decrease the thickness of this layer and also the degree of
saturation at the tooth-tissue interface. Agitation can be achieved with a calibrated
stirrer, rotary mixer, orbital shaker or a chamber pumping the solution at a particular
rate (Barbour et al., 2011; Shellis et al., 2011; West et al., 2011). As stirring rate is
known to greatly influence the outcome of the erosion experiments (Young & Tenuta,
2011) therefore it is recommended that it should be clearly reported in publications in
terms of revolution rate / minute instead of just gentle or continuous agitation.
Moreover, in order to fully simulate the intraoral situation, the stirring rate should be the
value at which the samples do not move whereas the solution remains uniformly stirred
at all times during the experiment. This will help mimic the clinical situation where
drink swishes around the teeth whereas the teeth remain stable.
Since saliva remains stimulated only for short periods clinically when the acid enters
the oral cavity, therefore stirring of storage medium for longer periods should be
avoided. However for in vitro models involving short-term exposures to saliva, (Panich
& Poolthong, 2009) the saliva could be stirred mimicking the intraoral situation where
teeth are exposed to saliva stimulated by the acid challenge.
Univers
ity of
Mala
ya

205
5.1.9 Temperature
Temperature also affects the erosion rate significantly and hence should be controlled
with a water bath, incubator or calibrated devices. Usually the temperature of the
erosive agent is kept constant at 36˚C, mimicking the intraoral temperature or 37˚C,
simulating the body temperature. Since body temperature is known to vary
geographically, a constant temperature of 25˚C has also been suggested. In general,
erosion has been known to increase with increasing temperature (Shellis et al., 2011;
West et al., 2011).
5.1.10 Timing of measurement
In the erosion studies aiming to ascertain the overall changes induced in enamel or
dentine by erosion challenge or by various treatment strategies (Attin et al., 2003; Faller
et al., 2011), the measurements are obtained at the beginning and end of pH-cycling.
However, in monitoring protocols where the progression of loss or gain of mineral is to
be assessed for example to validate new instruments for monitoring of enamel or
dentine erosion or for monitoring of efficacy of treatment products, the measurements
have to be obtained at regular intervals such as after every cycling day.
In this case, it remains questionable whether to obtain measurements directly after
erosion challenge or the next day after the samples had been stored in saliva overnight.
Because clinically the teeth always get exposed to saliva after erosion challenge, it only
makes more sense if the measurements are obtained at the end of one complete erosion
cycle which would include overnight storage in saliva as well. Therefore it is
recommended that the measurements be obtained after the completion of erosion cycle
(including overnight salivary storage) in erosion cycling models.
Univers
ity of
Mala
ya

206
5.1.11 Recommendations / Conclusions
1. It is advisable to employ pH-cycling in erosion studies as these models simulate the
clinical erosion challenge more closely.
2. The experimental details of various parameters employed should be clearly
reported.
3. In order to mimic the intraoral erosion challenge, stirring rate should be the value at
which the samples do not move whereas the solution remains uniformly stirred at
all times during the experiment.
4. Stirring of saliva for longer periods should be avoided; however saliva can be
stirred in models involving short term exposures to saliva after acid challenge.
5. It is better to use a pure (plain) acid for prolonged pH-cycling in erosion models in
order to keep the formulation of acid standardised throughout cycles.
6. Both artificial saliva and remineralisation media can be used in erosion cycling
models instead of natural saliva.
7. If the effect of pellicle is to be investigated in cycling models, then either natural
saliva be used or organic component be added to the artificial storage media.
8. Greater remineralisation is expected to occur in in vitro models as compared in vivo
settings if artificial storage media have been used instead of natural saliva (As in
vivo some salivary proteins inhibit calcium phosphate).
9. The concentration of calcium in artificial saliva and remineralisation solution is to
be adjusted keeping in consideration that certain salivary proteins bind calcium in
vivo.
10. It is advisable to remove sodium carboxymethyl cellulose from the artificial saliva
formulations as it had been shown to limit the remineralisation potential of artificial
saliva.
Univers
ity of
Mala
ya

207
11. Erosion cycle would be incomplete without overnight storage in saliva; therefore it
is recommended that measurements be obtained on the next morning in erosion
cycling models.
5.1.12 Aim
As a necessary step before the clinical trials, this study aimed to assess if optical
coherence tomography is a sensitive tool to detect early dentine erosion and monitor its
progression in simulated intraoral conditions (using salivary simulated remineralisation
solution) by correlating OCT data with surface roughness data.
In order to achieve this aim, the research objectives were as follows;
1. To explore the potential of OCT for measuring early dentine erosion and the
quantum in simulated intraoral conditions.
2. To identify the optimum outcome measure for measuring early dentine erosion
in simulated intraoral conditions.
3. To identify the detection threshold of OCT for early dentine erosion in simulated
intraoral conditions.
4. To compare the OCT backscattered intensity changes of early eroded dentine in
simulated intraoral conditions with surface ultrastructural changes.
5. To compare the OCT backscattered intensity changes of early eroded dentine in
simulated intraoral conditions with surface roughness measurements.
The null hypotheses tested were as follows;
1. OCT is not able to detect early dentine erosion in simulated intraoral conditions.
Univers
ity of
Mala
ya

208
2. OCT is not able to measure the progression of early dentine erosion in simulated
intraoral conditions.
3. There is no correlation between profilometric surface roughness measurements
and OCT backscattered changes.
5.2 Materials and Methods
5.2.1 Pilot study
A pilot study was performed before the execution of the main experiment. The
objective of this pilot study was to determine the optimum duration of dentine exposure
to acid, producing early dentine erosion without any bulk surface loss. Three root
dentine samples were prepared and polished as explained before (Section 4.2.2.1). The
samples were immersed in 0.3% citric acid (pH = 3.2) (A&C American Chemicals Ltd.,
North Carolina, USA) for 10 minutes three times a day for three days. The temperature
of the solution was kept constant at 36°C and the speed of citric acid was kept constant
at 300 revolutions per minute (rpm) during the erosion phase of the cycling throughout
the experiment. In between erosive challenges and overnight, the samples were stored in
remineralisation solution (A&C American Chemicals Ltd., North Carolina, USA). After
three days of cycling erosion challenge, no visible step change was discerned in the
OCT images as shown in the Figure 5.1. Univers
ity of
Mala
ya

209
Figure 5.1: OCT B-scans of a root dentine sample at (a) baseline, (b) after three days of
cycling erosion challenge. Red line at the center indicates the border between the
reference and eroded areas. The arrows indicate the backscattered intensity
(demineralisation) at the surface of eroded dentine sample. No visible step change was
discerned at the border between the reference and eroded areas.
Univers
ity of
Mala
ya

210
5.2.2 Experimental design
The experimental design of the study is illustrated in Figure 5.2.
Figure 5.2: Experimental design of the study.
5.2.3 OCT
5.2.3.1 Measurements with OCT
Same 20 root dentine samples were used for the experiments described in chapter 4
and chapter 5. Therefore the details of the sample preparation and erosive pH-cycling
Univers
ity of
Mala
ya
211
have been previously described (Section 4.2.2.1 and Section 4.2.2.2 respectively). After
measurements with non-contact profilometry were performed (detailed in chapter 4), a
commercially available OCT system (OCS1300SS Thorlabs Ltd., USA) was used to
capture three dimensional OCT data of the exposed window of the dentine samples.
This OCT system has a high-speed frequency swept laser centered at 1325 nm. It has a
transverse resolution of 11 µm and an axial resolution of 9 µm in air according to the
manufacturer. This axial resolution would correspond to about 6 µm in dentine as the
refractive index of dentine is 1.54. The probing head was mounted with the beam facing
downwards. The probe was set at a distance of 1 cm from the sample surface, with the
scanning beam oriented at 0 degrees to the sample surface. The samples were placed on
a translational stage perpendicular to the probe. The stage was fixed with a custom
made jig that enabled the samples to be repositioned to the same position and alignment
during the different measuring time points. This jig was also capable of tilting the
samples to a certain angle to reduce the specular reflection.
The Thorlabs OCT capturing software was used for capturing the images and
controlling the OCT settings and the light beam. The transverse resolution of the X-axis
was set at 1024 pixels in 5 mm and Y-axis at 96 pixels in 2 mm as for the previous
study (chapter 3). The axial resolution of the Z-axis was set at 512 pixels in 3 mm in air
or 1.9 mm in dentine (refractive index of dentine is 1.54) . With these settings a total of
96 B-scans were generated for each 3D image. The (x, y) coordinate of the light beam
for each sample was recorded for replication at consecutive measuring time points.
Other parameters such as brightness and contrast were kept constant for all samples.
The inbuilt ruler within the system software was used to standardise the height of each
image. Background noise was removed before the acquisition of each image.
Univers
ity of
Mala
ya

212
Each resin-mounted sample was removed from its container (containing
remineralisation solution) immediately before scanning and dried with dental syringe
for 20 seconds at a distance of 10 cm. In order to ensure the repeatability of the OCT
scan at various time points, the specimens were placed at the same orientation as
accurately as possible. After adjusting all the system settings in the B-scan mode, a 3D
scan was performed for the pre-determined area of interest containing both the reference
and eroded area within the exposed window on each sample. All the samples were tilted
at 20 degrees to reduce the specular reflection from the surface of the specimen on the
OCT image.
The measurements with OCT were performed at baseline and repeated at the end of
every cycling day including the overnight storage in remineralisation solution (A&C
American Chemicals Ltd., North Carolina, USA) for a total of three consecutive days.
5.2.3.2 Data processing
A program was written in MATLAB (The MathWorks, Inc., USA) to load the OCT
C scan (3D scan) images and analyse the changes of the backscattered light intensity in
time. C scans of each sample from different measuring time points were aligned to
reach a horizontal surface corresponding to the tooth-air interface. Each aligned image
consisted of a reference and an eroded area. Regions of interest were selected on each
aligned image in the reference and eroded sections of the image. Each region of interest
was restricted to 7500 A-scans in order to standardise the area being analysed. In order
to standardise the analysis further, all four time points of each sample were aligned in a
similar manner and identical regions of interest were loaded for them. A-scans were
then generated from the regions of interest selected for both the reference and eroded
areas and intensity values were exported automatically to excel sheets.
Univers
ity of
Mala
ya
213
5.2.3.3 Trend of backscattered intensity
In the excel programme, the values of each A-scan generated for the reference or
eroded area of each 3D OCT image was further reduced to single values by averaging
the intensity per pixel. Once the A-scans were averaged for all the samples for each time
point, a mean A-scan was then generated and the standard deviation was also calculated.
The data for the reference and eroded areas was separately plotted to observe and
compare the main trend of backscattered intensity in both areas.
5.2.3.4 Parameters for intensity analysis
(a) Decay of intensity
Two parameters, ‘decay of intensity’ and ‘integrated intensity’ were employed for
the analysis. Again, the decay of intensity or D is represented by the function below,
𝐷 =𝐼𝑝𝑙𝑎𝑡𝑒𝑎𝑢
𝐼𝑠𝑢𝑝𝑒𝑟𝑓𝑖𝑐𝑖𝑎𝑙
(5.1)
Iplateau is the intensity at an optical depth at which the A-scans had reached a plateau
and were assumed not to be affected further by the erosive challenge. It was observed at
58 µm (physical depth = 38 µm) for this study. The Isuperficial is the intensity near the
surface located immediately below the tooth-air interface. For this study, three optical
depths 5 µm, 11 µm and 23 µm below the tooth-air interface were chosen. Decay of
intensity or D of both the reference and the eroded areas were calculated separately for
each depth combination. Each depth combination was considered as one outcome
measure.
Univers
ity of
Mala
ya

214
Figure 5.3: Illustration of the calculation of decay of intensity between optical depths of
23 µm and 58 µm. Figure shows the mean depth-resolved intensity profile (A-scan) of
the first 120 µm for the eroded area of the sample. Each line plot represents the OCT
intensity (a.u) plotted in optical depth (µm) for all 20 samples at each measurement time
point. The longer black arrow represents the intensity at an optical of 23 µm and shorter
black arrow represents the intensity at 58 µm. The red arrow shows the decay of
intensity between 23 µm and 58 µm.
(b) Integrated intensity
Additionally, the OCT backscattered intensity was integrated from the dentine
surface to plateau. The mean integrated intensity, R was calculated from superficial
optical depths of 5 µm, 11 µm and 23 µm to 58 µm and is described by the function
below;
R = ∑ (Isuperficial : Iplateau ) x Z (5.2)
With Z being the differential distance between the two physical depths
Univers
ity of
Mala
ya
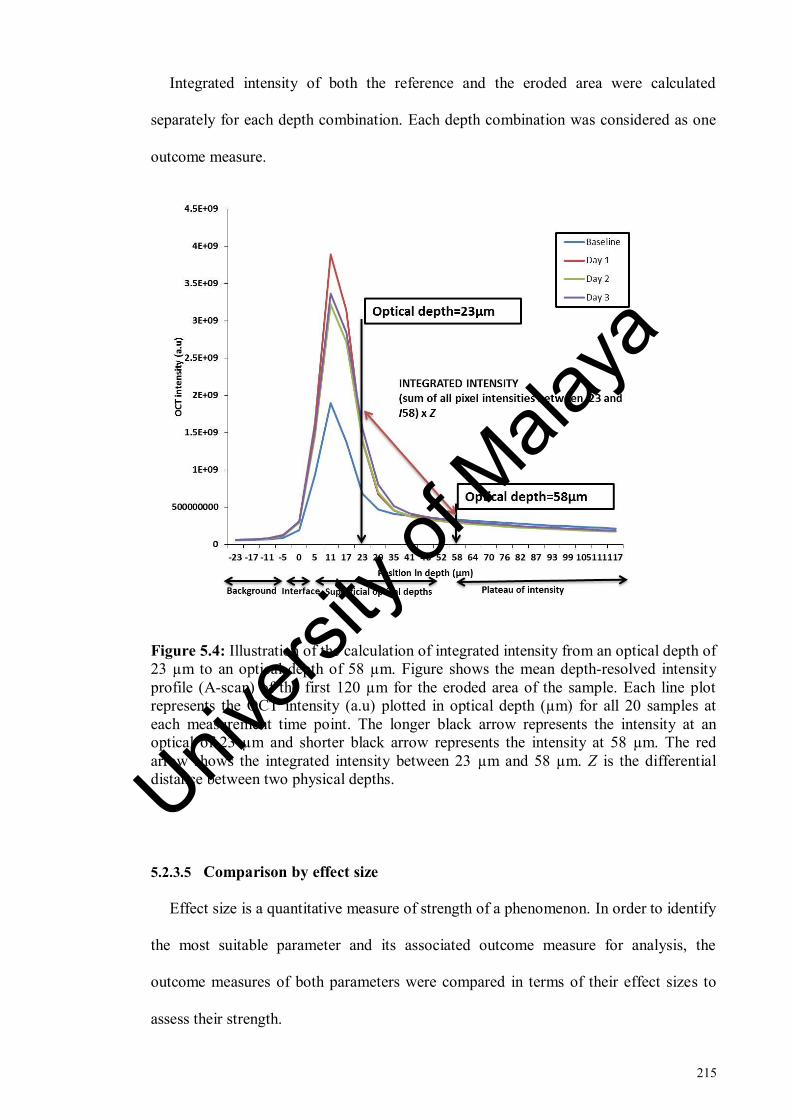
215
Integrated intensity of both the reference and the eroded area were calculated
separately for each depth combination. Each depth combination was considered as one
outcome measure.
Figure 5.4: Illustration of the calculation of integrated intensity from an optical depth of
23 µm to an optical depth of 58 µm. Figure shows the mean depth-resolved intensity
profile (A-scan) of the first 120 µm for the eroded area of the sample. Each line plot
represents the OCT intensity (a.u) plotted in optical depth (µm) for all 20 samples at
each measurement time point. The longer black arrow represents the intensity at an
optical of 23 µm and shorter black arrow represents the intensity at 58 µm. The red
arrow shows the integrated intensity between 23 µm and 58 µm. Z is the differential
distance between two physical depths.
5.2.3.5 Comparison by effect size
Effect size is a quantitative measure of strength of a phenomenon. In order to identify
the most suitable parameter and its associated outcome measure for analysis, the
outcome measures of both parameters were compared in terms of their effect sizes to
assess their strength.
Univers
ity of
Mala
ya

216
The effect size of all outcome measures were compared by partial eta square values
generated by SPSS, version 22 (IBM SPSS Statistics 22.0 Inc., USA) as part of repeated
measures ANOVA analysis.
5.2.3.6 Correction with reference
In order to assess the stability of outcome measures (depth combinations) and to
identify any instrumental variations in time, the data for each outcome measure was
corrected for eroded area at each time point with the function given below:
𝐷𝑎𝑡𝑎𝐸 𝑐𝑜𝑟𝑟𝑒𝑐𝑡𝑒𝑑(𝑡) = 𝐷𝑎𝑡𝑎𝐸𝑎𝑏𝑠𝑜𝑙𝑢𝑡𝑒(𝑡)/𝑘(𝑡)
(5.3)
Where 𝐷𝑎𝑡𝑎𝐸 𝑐𝑜𝑟𝑟𝑒𝑐𝑡𝑒𝑑(𝑡) = corrected data for eroded area of the outcome
measure, (t) is the erosion time point, Data E absolute = absolute data of eroded area of
outcome measure and k (t) is the correction factor calculated by the equation below,
𝑘(𝑡) =𝐷𝑎𝑡𝑎𝑅𝑎𝑏𝑠𝑜𝑙𝑢𝑡𝑒(𝑡)
𝐷𝑎𝑡𝑎𝑅𝑎𝑏𝑠𝑜𝑙𝑢𝑡𝑒(𝑡0)
(5.4)
Where 𝐷𝑎𝑡𝑎𝑅𝑎𝑏𝑠𝑜𝑙𝑢𝑡𝑒(𝑡) is the absolute data of the reference area at each time
point and 𝐷𝑎𝑡𝑎𝑅 𝑎𝑏𝑠𝑜𝑙𝑢𝑡𝑒(𝑡0) is the absolute data of the reference area at baseline time
point.
Univers
ity of
Mala
ya

217
5.2.4 FE-SEM
Same root dentine samples were used for the experiments described in chapter 4 and
chapter 5. Therefore, details for FE-SEM imaging and erosive pH-cycling have been
previously described in Section 4.2.3.1 and Section 4.2.3.2 of chapter 4 of this thesis.
5.2.5 Comparison with surface roughness
Same samples were used for pH cycling in chapter 4 and chapter 5. A comparison
between the OCT findings (section 5.3.1.2, f) and surface roughness findings (section
4.3.1) was made in this chapter.
5.2.5.1 Calculation of fractional change in intensity
In order to compare the findings of OCT with surface roughness, fractional change
for the reference and eroded area of the optimum OCT outcome measure was calculated
by the function given below,
f𝑅𝑅 =𝑅𝑅 (𝑡)
𝑅𝑅(𝑡𝑜)
(5.5)
fRR is the fraction of reference area of OCT outcome measure with its baseline, RR(t)
is each time point for the reference area and RR (to) is the baseline time point for the
reference area.
f𝑅𝐸 =𝑅𝐸 (𝑡)
𝑅𝐸(𝑡𝑜)
(5.6)
Univers
ity of
Mala
ya

218
fRE is the fraction of eroded area of each parameter with its baseline, RE(t) is the
erosive challenge time point for the eroded area and RE (to) is the baseline time point for
the eroded area.
5.2.5.2 Correlation
The significance and strength of the relationship between fractional change of the
optimum OCT outcome measure (fR) and fractional change of surface roughness
outcome measures, average roughness (fRa1), core roughness (fRk), peak roughness
(fRpk), valley roughness (fRvk), proportion of peaks (fMR1) and proportion of valleys
(fMR2) was determined by using correlation analysis. Firstly, overall relationship was
determined between fR and each of the surface roughness outcome measures. Moreover,
the correlation was also performed on a day by day basis for each of the surface
roughness outcome measure with fR of OCT.
5.2.6 Statistical Analysis
Statistical data analysis was performed with SPSS, version 22 (IBM SPSS Statistics
22.0 Inc., USA). The level of significance was set at p < 0.05. Shapiro-Wilk test and
skewness were assessed to check the assumption of normality. Outliers were removed
from the data if present. One-way repeated measures ANOVA was performed with post
hoc multiple comparisons. A Bonferroni-Holm correction was performed to reduce risk
of type 1 errors in multiple comparisons using Holm-Bonferroni correction calculator
(Gaetano, 2013).
Univers
ity of
Mala
ya

219
Pearson correlation coefficient test was performed to determine the relationship of fR
with fRa, fRk, fRpk, fRvk, fMR1 and fMR2. The table used for the interpretation of
correlation has been added in Appendix A.
5.3 Results
5.3.1 OCT
5.3.1.1 Trend of backscattered intensity
Mean A-scan curve generated from both reference and eroded areas showed that
initially the light travelled for a certain distance in air without changing (background
intensity, Ibackground). The intensity of light started to increase from approximately 0 µm
at the tooth-air interface, increased below the interface (Intensity at surface, Isurface) until
it reached the maximum intensity value at approximately 11 µm (maximum intensity,
Imax). From Imax onwards, the intensity then proceeded to decline at 23 µm (Intensity
drop, Idrop) until it reached a point where no further changes in intensity were observed
(plateau of intensity, Iplateau).
Each line graph in mean A-scan of reference and eroded area represented the
averaged intensity of all samples for each time point. At a depth of 23 µm, a juncture
between the line plots of all days was observed and the intensity of day three was
observed to be at a higher level than other two line plots whereas it was located at a
lower intensity level than day one intensity at more superficial depths. Moreover at this
depth, the line plots of day one and day two were almost indistinguishable from each
other.
The line graphs of all time points in the mean A-scan of reference area (Figure 5.5)
adhered to one intensity range suggesting that little changes in intensity had occurred
Univers
ity of
Mala
ya

220
over time in the reference area. At the area of maximum intensity (11 µm), separation
between time points was observed even in the mean A-scan of the reference area. The
mean A-scan of eroded area in Figure 5.6 however showed clear separation between
line graphs representing each time point indicating the erosion interval related shift in
intensity from baseline to increasing erosion intervals. The baseline line plot showed a
huge separation from the remaining days at all superficial optical depths. With the
scanning resolution of 512 pixels in 1.90 mm in the z-axis, there were approximately 21
depth points in the first 120 µm. The minimal optical separation of the two adjacent
points was about six microns amounting to 3.8 µm of physical separation.
The standard deviation of samples relative to the mean intensity at each optical depth
was calculated and the error bars in the Figure 5.5 and Figure 5.6 represent the standard
deviation. Similar to what was observed in chapter 3, the mean A-scans showed that the
near the surface there was very high variation in the intensity among the samples and
from an optical depth of 23 µm onwards, the intensity became relatively stable as shown
by lower values of standard deviation.
Also, it was estimated that from an optical depth of 58 µm (translated to physical
depth of 38 microns) onwards the intensity had reached a plateau and did not appear to
be affected by the cycling erosive challenge anymore. The refractive index of the
dentine is 1.54 (Natsume et al., 2011) therefore, these optical depths were translated to
physical depths of 15 µm and 38 µm respectively.
The OCT B-scans of one sample taken at baseline, day one, day two and day three of
cycling erosion challenge are shown in Figure 5.12. The increase in backscattered
intensity signal at the surface of the eroded side of the sample was evident as the erosion
interval progressed. These representative B-scans were selected because they represent
frame 50 of every 3 D image and so were located right in the center of the 96 B scans.
Univers
ity of
Mala
ya

221
Figure 5.5: Mean depth-resolved intensity profile (mean A-scan) of the first 120 µm for
the reference area of the sample. Each line plot represents the OCT intensity (a.u)
plotted in optical depth (µm) for all 20 samples at each measurement time point. Red,
blue and green dotted lines represent the superficial optical depths chosen for the
analysis. Plateau of intensity is shown by black dotted line. The error bars represent
standard deviation.
Univers
ity of
Mala
ya
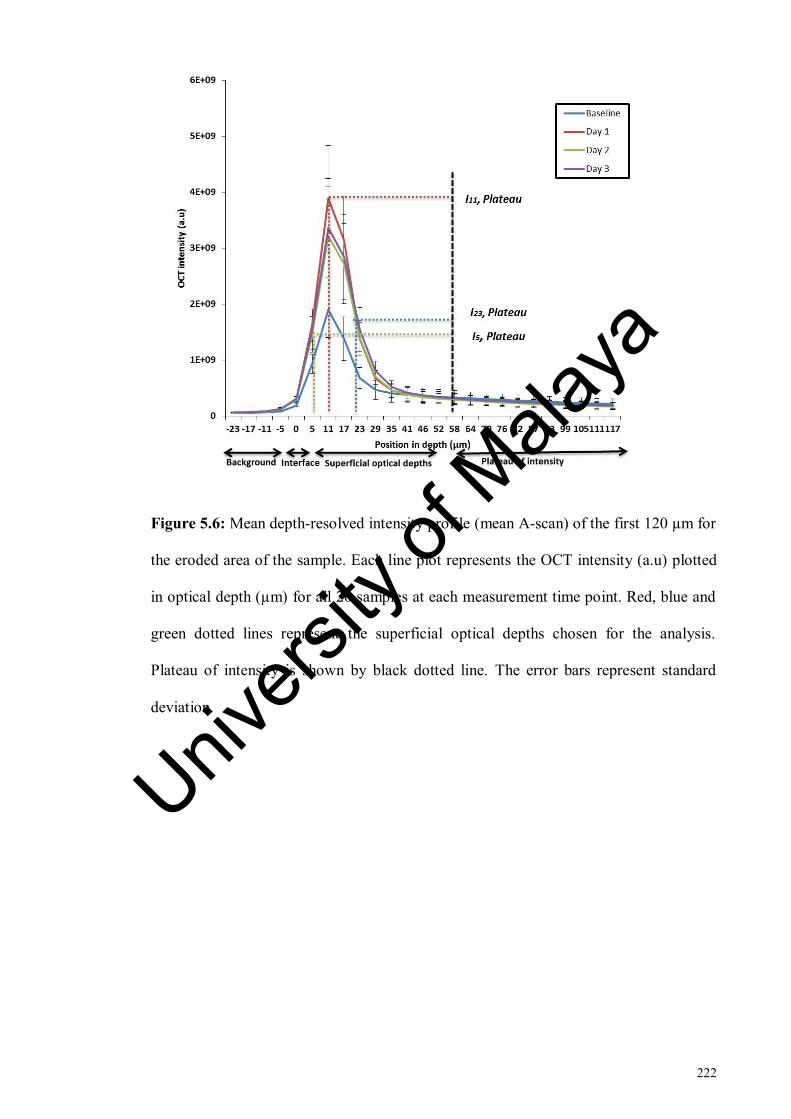
222
Figure 5.6: Mean depth-resolved intensity profile (mean A-scan) of the first 120 µm for
the eroded area of the sample. Each line plot represents the OCT intensity (a.u) plotted
in optical depth (µm) for all 20 samples at each measurement time point. Red, blue and
green dotted lines represent the superficial optical depths chosen for the analysis.
Plateau of intensity is shown by black dotted line. The error bars represent standard
deviation.
Univers
ity of
Mala
ya

223
Figure 5.7: Representative OCT A-scans of one sample (a - d). Each A-scan shows the
OCT intensity (a.u) plotted in optical depth (µm). The red text box indicates the OCT
intensity at a depth of 23 µm. The chart title of each A-scan indicates the time interval
for which the A-scan was plotted. The increase in intensity at 23 µm is obvious with
time.
Univers
ity of
Mala
ya

224
Figure 5.8: Representative A-scans of a sample at (a) baseline time point and b) after
three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious.
Univers
ity of
Mala
ya

225
Figure 5.9: Representative A-scans of a sample at (a) baseline time point and b) after
three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious. Univers
ity of
Mala
ya

226
Figure 5.10: Representative A-scans of a sample at (a) baseline time point and b)
after three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious.
Univers
ity of
Mala
ya
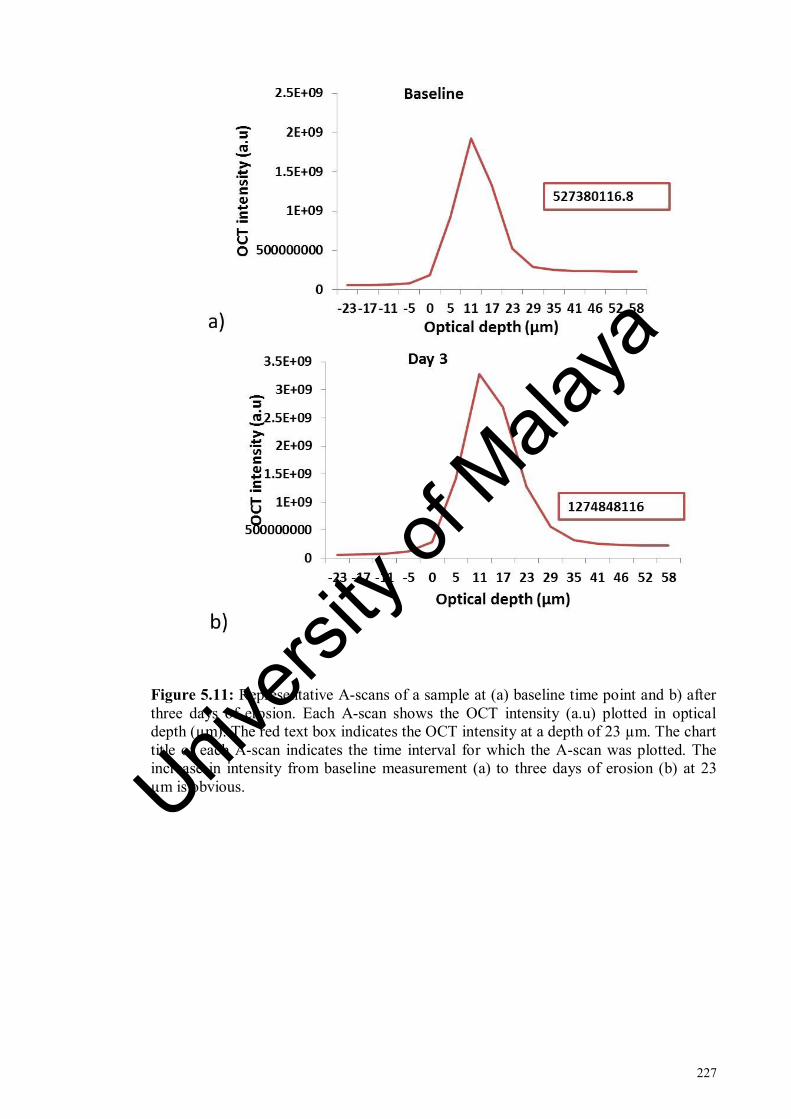
227
Figure 5.11: Representative A-scans of a sample at (a) baseline time point and b) after
three days of erosion. Each A-scan shows the OCT intensity (a.u) plotted in optical
depth (µm). The red text box indicates the OCT intensity at a depth of 23 µm. The chart
title of each A-scan indicates the time interval for which the A-scan was plotted. The
increase in intensity from baseline measurement (a) to three days of erosion (b) at 23
µm is obvious. Univers
ity of
Mala
ya

228
Figure 5.12: Representative OCT B-scans of one sample at (a) baseline measurement
(b) day one (c) day two and (d) day three of cycling erosion challenge. Transparent
arrows indicate the backscattered intensity at the surface of eroded area.
Univers
ity of
Mala
ya

229
5.3.1.2 Outcome measures
OCT parameters and their outcome measures have been summarised in the Table 5.1.
Table 5.1: OCT parameters and their outcome measures defined.
Parameters Symbol Equation Outcome measures
Decay of
intensity
D D = 𝐼𝑝𝑙𝑎𝑡𝑒𝑎𝑢
𝐼𝑠𝑢𝑝𝑒𝑟𝑓𝑖𝑐𝑖𝑎𝑙
I58µm / I5µm
I58µm / I11µm
I58µm / I23µm
Integrated
intensity R
R = ∑ Isuperficial : Iplateau ) x Z
I(5µm : 58µm)
I(11µm : 58µm)
I(23µm : 58µm)
Fractional
Integrated
intensity with
baseline
fR
f𝑅𝐸 =𝑅𝐸 (𝑡)
𝑅𝐸(𝑡𝑜)
f (I(23µm : 58µm))
Data correction
for eroded area
DataE
corrected
𝐷𝑎𝑡𝑎𝐸 𝑐𝑜𝑟𝑟𝑒𝑐𝑡𝑒𝑑
= 𝐷𝑎𝑡𝑎𝐸𝑎𝑏𝑠𝑜𝑙𝑢𝑡𝑒(𝑡)/𝑘(𝑡)
Corrected I58µm / I5µm
Corrected I58µm / I11µm
Corrected I58µm / I23µm
Corrected I(5µm : 58µm)
Corrected I(11µm : 58µm)
Corrected I(11µm : 58µm)
Shapiro-Wilk test and skewness values showed that the data was normally distributed
for the outcome measures I58µm / I5µm, I58µm / I11µm and I58 µm / I23 µm, I(5µm : 58µm), I(11µm :
58µm) and I(23µm : 58µm). One-way repeated measures ANOVA, with Bonferroni-Holm
correction were performed and Mauchly’s test was used to evaluate the sphericity
assumption. If sphericity was not met, the adjusted F-value of the Greenhouse-Geisser
correction was considered.
Univers
ity of
Mala
ya

230
Mean and standard deviations for eroded areas of I58µm / I5µm, I58µm / I11µm and I58µm /
I23µm are given in Table 5.4 and for eroded areas of I(5µm : 58µm), I(11µm : 58µm) and I(23µm :
58µm) in Table 5.7.
(a) I58µm / I5µm
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (2 = 11.414, p = .04) and eroded areas (
2 = 49.536, p < 0.0001). Therefore,
the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA showed that there was a significant effect of
erosion interval on backscattered intensity in the eroded area (F (1.2, 22.05) = 88.3, p <
0.0001, η2
= .831) whereas no significant effect was found on intensity in the reference
area (F (2.3, 42.07) = 1.13, p = 0.337, η2 = .337) as shown in Table 5.2.
Post hoc comparisons for the eroded area showed that the mean intensity values of
all days were significantly different with respect to their baseline intensity values.
However, significant differences were only observed between day one and day two
intensity values as shown in Table 5.3. Data plot is given in Figure 5.13.
Univers
ity of
Mala
ya

231
Figure 5.13: Mean decay of intensity of reference and eroded areas at cycling erosion
intervals between superficial optical depth of 5 µm and intensity plateau at 58 µm.
(b) I58µm / I11µm
Results of Mauchly’s test showed that the sphericity assumption was violated in
both reference (2 =11.788, p = 0.038) and eroded areas (
2 = 70.734 p < 0.0001).
Therefore, the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA showed that there was a significant effect of
erosion interval on backscattered intensity in the eroded area (F (1.1, 19.8) = 64.573, p <
0.0001, η2
= .782) whereas no significant effect of erosion interval on intensity was
observed in the reference area (F (2.1, 38.2) = 1.43, p = 0.251, η2
= .07) as shown in Table
5.2.
Post hoc comparisons for the eroded area showed that the mean intensity values of
all days were significantly different with respect to their baseline intensity values.
Univers
ity of
Mala
ya
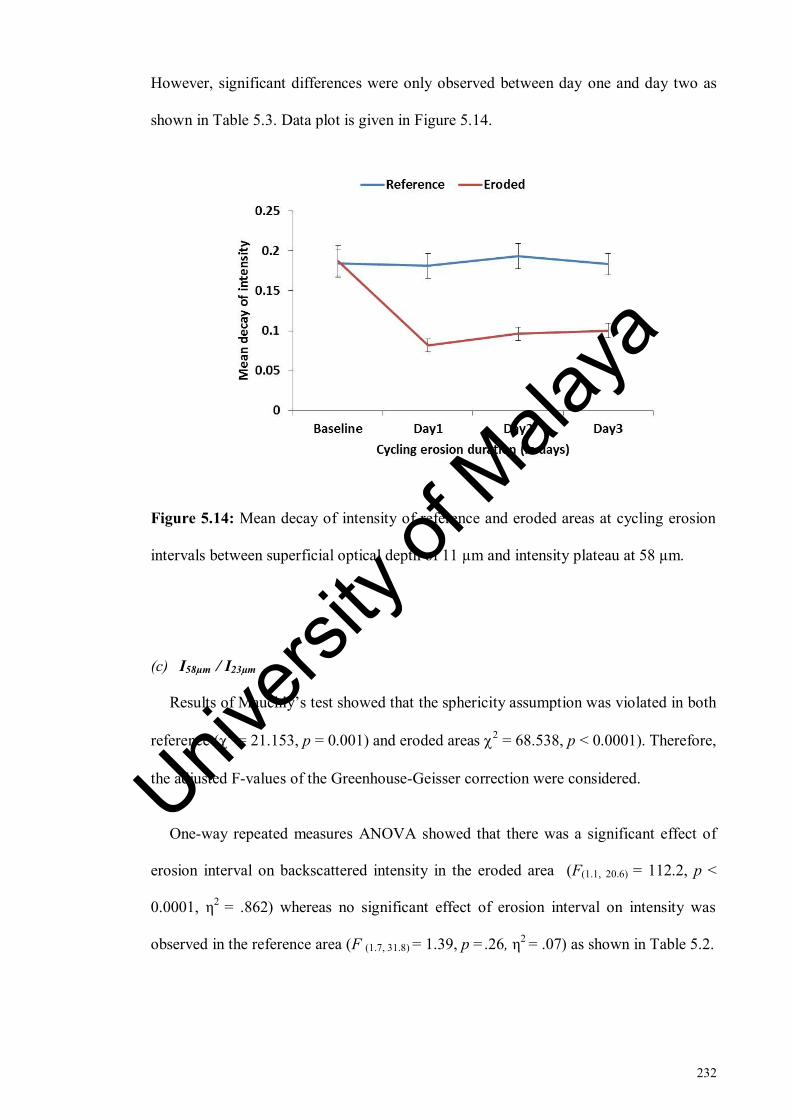
232
However, significant differences were only observed between day one and day two as
shown in Table 5.3. Data plot is given in Figure 5.14.
Figure 5.14: Mean decay of intensity of reference and eroded areas at cycling erosion
intervals between superficial optical depth of 11 µm and intensity plateau at 58 µm.
(c) I58µm / I23µm
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (2 = 21.153, p = 0.001) and eroded areas
2 = 68.538, p < 0.0001). Therefore,
the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA showed that there was a significant effect of
erosion interval on backscattered intensity in the eroded area (F(1.1, 20.6) = 112.2, p <
0.0001, η2
= .862) whereas no significant effect of erosion interval on intensity was
observed in the reference area (F (1.7, 31.8) = 1.39, p =.26, η2 = .07) as shown in Table 5.2.
Univers
ity of
Mala
ya

233
Post hoc comparisons for the eroded area showed that the mean intensity values of
all days were significantly different with respect to their baseline intensity values.
However, no significant differences were observed between days as shown in Table 5.3.
Data plot is given in Figure 5.15.
Figure 5.15: Mean decay of intensity of reference and eroded areas at cycling erosion
intervals between superficial optical depth of 23 µm and intensity plateau at 58 µm.
Table 5.2: Results of repeated measures ANOVA analysis for reference and eroded
areas of outcome measures of decay of intensity.
Outcome
measure
Reference area Eroded area
Mean
square
F-statistic p-value
Mean
square
F-statistic p-value
I58µm / I5µm .002 1.135 .337 .257 88.380 <.0001
I58µm / I11µm .001 1.432 .251 .099 64.573 <.0001
I58µm / I23µm .006 1.395 .261 .909 112.268 <.0001
Univers
ity of
Mala
ya
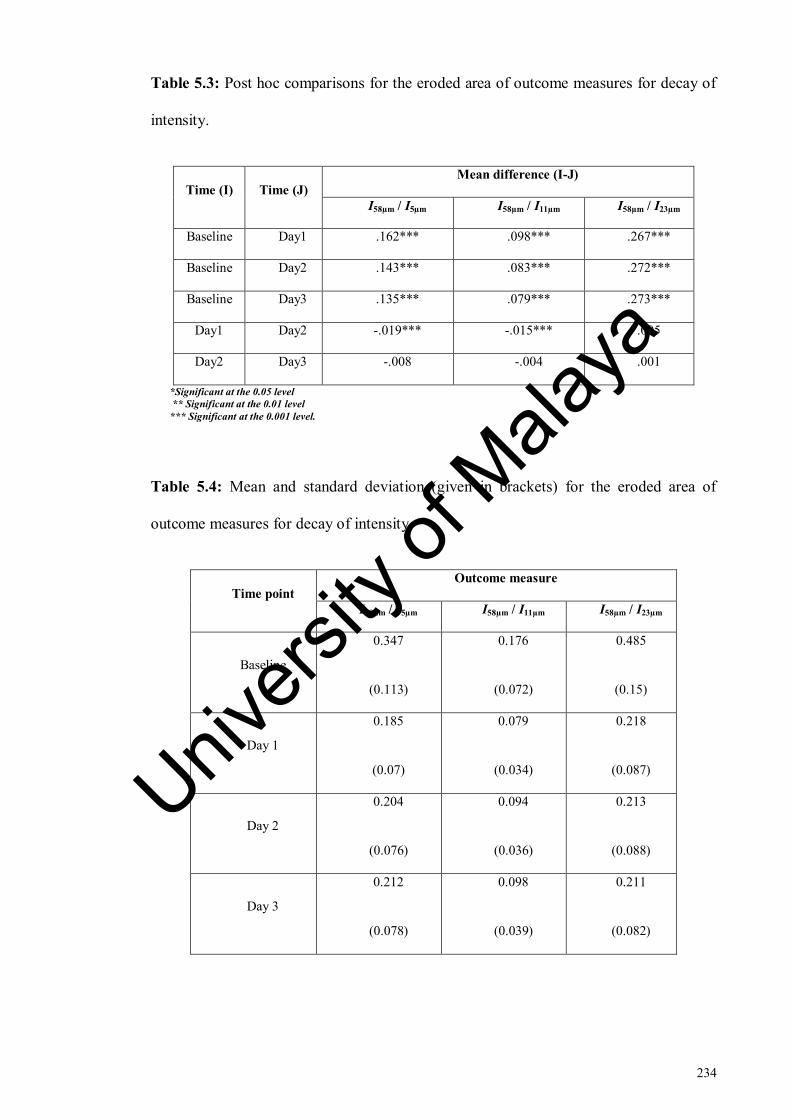
234
Table 5.3: Post hoc comparisons for the eroded area of outcome measures for decay of
intensity.
Time (I) Time (J)
Mean difference (I-J)
I58µm / I5µm I58µm / I11µm I58µm / I23µm
Baseline Day1 .162*** .098*** .267***
Baseline Day2 .143*** .083*** .272***
Baseline Day3 .135*** .079*** .273***
Day1 Day2 -.019*** -.015*** .005
Day2 Day3 -.008 -.004 .001
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Table 5.4: Mean and standard deviation (given in brackets) for the eroded area of
outcome measures for decay of intensity
Time point
Outcome measure
I58µm / I5µm I58µm / I11µm I58µm / I23µm
Baseline
0.347
(0.113)
0.176
(0.072)
0.485
(0.15)
Day 1
0.185
(0.07)
0.079
(0.034)
0.218
(0.087)
Day 2
0.204
(0.076)
0.094
(0.036)
0.213
(0.088)
Day 3
0.212
(0.078)
0.098
(0.039)
0.211
(0.082)
Univers
ity of
Mala
ya

235
(d) I(5µm : 58µm)
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (2 =25.447, p < 0.0001) and eroded areas (
2 = 25.049 p < 0.0001).
Therefore, the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA showed that there was a significant effect of
erosion interval on backscattered intensity in the eroded area (F(1.6, 30.08) = 100.1, p <
0.0001, η2
= .848) whereas no significant effect of erosion interval on intensity was
observed in the reference area (F(1.5, 27.4) = 3.5, p = 0.055, η2
= .163) as shown in Table
5.5.
Post hoc comparisons for the eroded area showed that the mean intensity values of
all days were significantly different with respect to their baseline intensity values.
Moreover, significant differences were observed between all days as shown in Table
5.6. Data plot is given in Figure 5.16.
Figure 5.16: Mean integrated intensity of reference and eroded areas at cycling erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 5
µm to the intensity plateau at 58 µm.
Univers
ity of
Mala
ya

236
(e) I(11µm : 58µm)
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (2 = 27.008, p < 0.0001) and eroded areas (
2 = 24.560, p < 0.0001).
Therefore, the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA showed that there was a significant effect of
erosion interval on backscattered intensity in the eroded area (F (1.6, 30.5) = 99.403, p <
0.0001, η2
= .847) whereas no significant effect of erosion interval on intensity was
observed in the reference area (F (1.4, 26.8) = 3.2, p = 0.069, η2
= .151) as shown in Table
5.5.
Post hoc comparisons for the eroded area showed that the mean intensity values of
all days were significantly different with respect to their baseline intensity values.
Moreover, significant differences were observed between all days as shown in Table
5.6. Data plot is given in Figure 5.17
Univers
ity of
Mala
ya

237
Figure 5.17: Mean integrated intensity of reference and eroded areas at different
cycling erosion intervals. The backscattered intensity was integrated from superficial
optical depth of 11 µm to the intensity plateau at 58 µm.
(f) Optimum outcome measure, I(23µm : 58µm)
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (2 = 20.618, p<0.001) and eroded areas (
2 = 22.900, p<0.0001). Therefore,
the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA showed that there was a significant effect of
erosion interval on backscattered intensity in the eroded area (F(1.6, 30.5) =39.183, p <
0.0001, η2
= .673) whereas no significant effect of erosion interval on intensity was
observed in the reference area (F(1.5, 26.8) =1.509, p = 0.236, η2
= .07) as shown in Table
5.5.
Post hoc comparisons for the eroded area showed that the mean intensity values of
all days were significantly different with respect to their baseline intensity values.
Univers
ity of
Mala
ya

238
Moreover, significant differences were observed between day two and day three as
shown in Table 5.6. Data plot is given in Figure 5.18
Figure 5.18: Mean integrated intensity of reference and eroded areas at cycling erosion
intervals. The backscattered intensity was integrated from superficial optical depth of 23
µm to the intensity plateau at 58 µm.
Table 5.5: Results of repeated measures ANOVA analysis for reference and eroded
areas of all outcome measures for integrated intensity.
Outcome
measure
Reference area Eroded area
Mean
square
F-statistic p-value
Mean
square
F-
statistic
p-value
I(5µm : 58µm) 4.273E+19 3.507 0.055 2.632E+21 100.105 <0.0001
I(11µm : 58µm) 3.312E+19 3.207 0.069 1.976E+21 99.403 <0.0001
I(23µm : 58µm) 3.539E+18 1.509 0.236 1.602E+20 39.183 <0.0001
fR(I(23µm : 58µm)) 0.03 1.77 0.193 2.057 33.039 <0.0001
Univers
ity of
Mala
ya
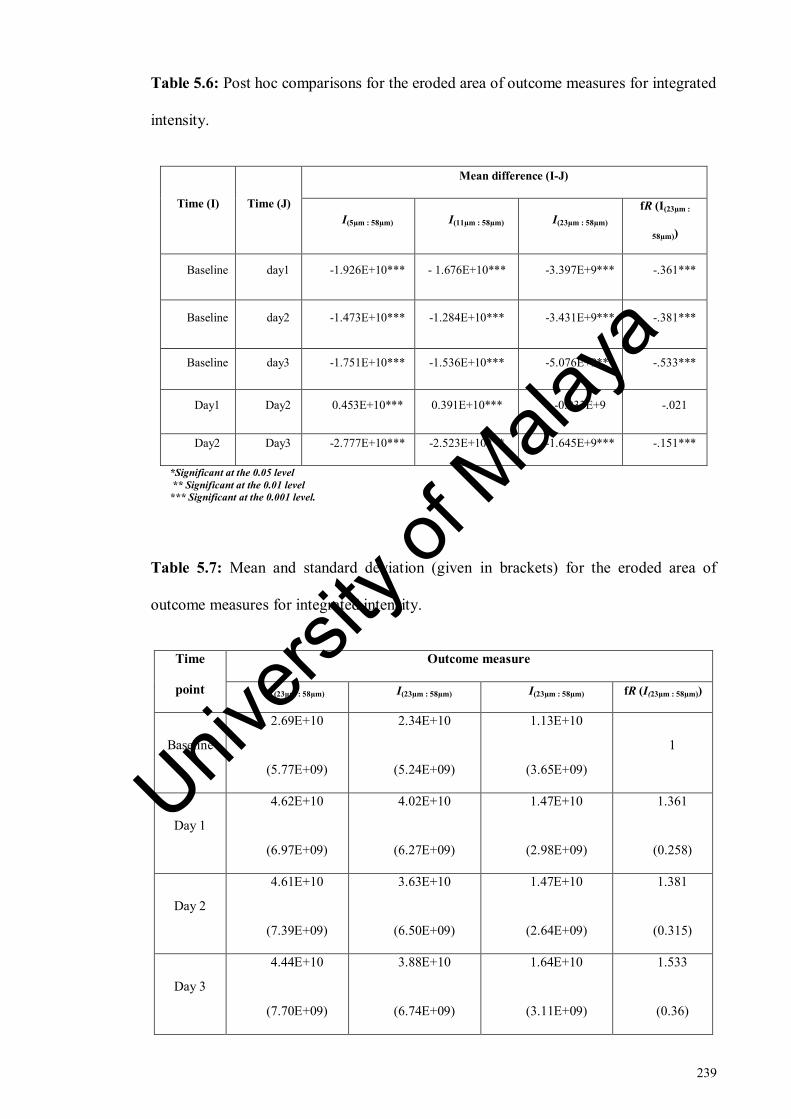
239
Table 5.6: Post hoc comparisons for the eroded area of outcome measures for integrated
intensity.
Time (I) Time (J)
Mean difference (I-J)
I(5µm : 58µm) I(11µm : 58µm) I(23µm : 58µm)
fR (I(23µm :
58µm))
Baseline day1 -1.926E+10*** - 1.676E+10*** -3.397E+9*** -.361***
Baseline day2 -1.473E+10*** -1.284E+10*** -3.431E+9*** -.381***
Baseline day3 -1.751E+10*** -1.536E+10*** -5.076E+9*** -.533***
Day1 Day2 0.453E+10*** 0.391E+10*** -0.033E+9 -.021
Day2 Day3 -2.777E+10*** -2.523E+10*** -1.645E+9*** -.151***
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Table 5.7: Mean and standard deviation (given in brackets) for the eroded area of
outcome measures for integrated intensity.
Time
point
Outcome measure
I(23µm : 58µm) I(23µm : 58µm) I(23µm : 58µm) fR (I(23µm : 58µm))
Baseline
2.69E+10
(5.77E+09)
2.34E+10
(5.24E+09)
1.13E+10
(3.65E+09)
1
Day 1
4.62E+10
(6.97E+09)
4.02E+10
(6.27E+09)
1.47E+10
(2.98E+09)
1.361
(0.258)
Day 2
4.61E+10
(7.39E+09)
3.63E+10
(6.50E+09)
1.47E+10
(2.64E+09)
1.381
(0.315)
Day 3
4.44E+10
(7.70E+09)
3.88E+10
(6.74E+09)
1.64E+10
(3.11E+09)
1.533
(0.36)
Univers
ity of
Mala
ya

240
5.3.1.3 Comparison by effect size
The effect sizes of all outcome measures were assessed to find the most sensitive
parameter and outcome measure. I58µm / I23µm was the most powerful outcome measure
as per the effect size comparison as shown in Table 5.8.
Table 5.8: Comparison of effect sizes of all outcome measures used for analysis.
Parameter Outcome measure
Effect size
(partial eta square value)
Decay of intensity
I58µm / I5µm 0.831
I58µm / I11µm 0.782
I58µm / I23µm 0.862
Integrated intensity
I(5µm : 58µm) 0.848
I(11µm : 58µm) 0.847
I(23µm : 58µm) 0.673
5.3.1.4 Correction with reference
Shapiro-Wilk test and skewness values showed that the data was normally distributed
for all the outcome measures for both ‘decay of intensity’ and ‘integrated intensity’.
One-way repeated measures ANOVA was performed and Mauchly’s test was used to
evaluate the sphericity assumption.
Mauchly’s test showed that assumption of sphericity was violated for corrected data
for all outcome measures (p < 0.05). Therefore, the adjusted F-value of the Greenhouse-
Geisser correction was considered. One-way repeated measures ANOVA showed that
there was a significant effect of erosion interval on backscattered intensity for all the
Univers
ity of
Mala
ya

241
outcome measures (p < 0.0001). F-values and p-values are given in Table 5.9.
Therefore, post hoc comparisons with Holm-Bonferroni correction were performed to
ascertain where the differences had occurred.
Post hoc comparisons for corrected I58µm / I5µm and corrected I58µm / I11µm showed that
after correction, no significant differences were detected between days as opposed to
their absolute outcome measures where significant differences had been observed
between day one and day two values. Corrected I58µm / I23µm showed that mean intensity
values between day one - day two became statistically significant whereas no significant
differences had been observed in the absolute I58µm / I23µm previously.
Results for corrected I(5µm : 58µm) and corrected I(11µm : 58µm) showed that after day one,
intensity became constant as opposed to their absolute outcome measures where
intensity values were significantly different between all days.
I(23µm : 58µm) was the only outcome measure which showed similar results for corrected
and absolute values showing that it was the most stable outcome measure. Detailed
results are given in Tables 5.10-5.11.
Figures 5.19 (a-c) and 5.20 (a-c) show the corrected integrated intensity and
corrected decay of intensity respectively for the reference and eroded areas for all
outcome measures plotted in time. The reference areas in all plots achieved a horizontal
line in time against which the intensity changes in the eroded area were evaluated. Mean
and standard deviations are given in Tables 5.12 and 5.13.
Univers
ity of
Mala
ya

242
Figure 5.19: Corrected integrated intensity for the reference and eroded areas for
outcome measures (a) I(5µm : 58µm) (b) I(11µm : 58µm) and (c) I(23µm : 58µm).
Univers
ity of
Mala
ya

243
Figure 5.20: Corrected decay of intensity for the reference and eroded areas for
outcome measures (a) I58µm / I5µm (b) I58µm / I11µm and (c) I58µm / I23µm.
Table 5.9: Results of repeated measures ANOVA analysis for corrected data of
outcome measures of decay of intensity and integrated intensity.
Parameter Outcome measure Mean square F-statistic p-value
Corrected decay
of intensity
I58µm / I5µm .252 55.669 <.0001
I58µm / I11µm .101 46.629 <.0001
I58µm / I23µm .990 97.883 <.0001
Corrected
integrated
intensity
I(5µm : 58µm) 3.671E+21 86.030 <.0001
I(11µm : 58µm) 2.743E+21 84.540 <.0001
I(23µm : 58µm) 1.402E+20 30.430 <.0001
Univers
ity of
Mala
ya

244
Table 5.10: Post hoc comparisons for the eroded area of outcome measures of corrected
decay of intensity.
Time (I) Time (J)
Mean difference (I-J)
Corrected
I58µm / I5µm
Corrected
I58µm / I11µm
Corrected
I58µm / I23µm
Baseline day1 .164*** .101*** .285***
Baseline day2 .160*** .095*** .299***
Baseline day3 .138*** .083*** .296***
Day1 Day2 -.004 -.006 .014*
Day2 Day3 -.026 -.012 -.003
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Table 5.11: Post hoc comparisons for the eroded area of outcome measures of corrected
integrated intensity.
Time (I) Time (J) Mean difference (I-J)
Corrected I(5µm :
58µm)
Corrected I(11µm :
58µm)
Corrected
I(23µm : 58µm)
Baseline Day1 -2.134E+10*** -1.871E+10*** -3.267E+9***
Baseline Day2 -1.924E+10*** -1.681E+10*** -3.667E+9***
Baseline Day3 -2.108E+10*** -1.860E+10*** -5.337E+9***
Day1 Day2 0.210E+10 0.189E+10 -0.400E+9
Day2 Day3 -0.184E+10 -0.179E+10 -1.669E+9**
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Univers
ity of
Mala
ya
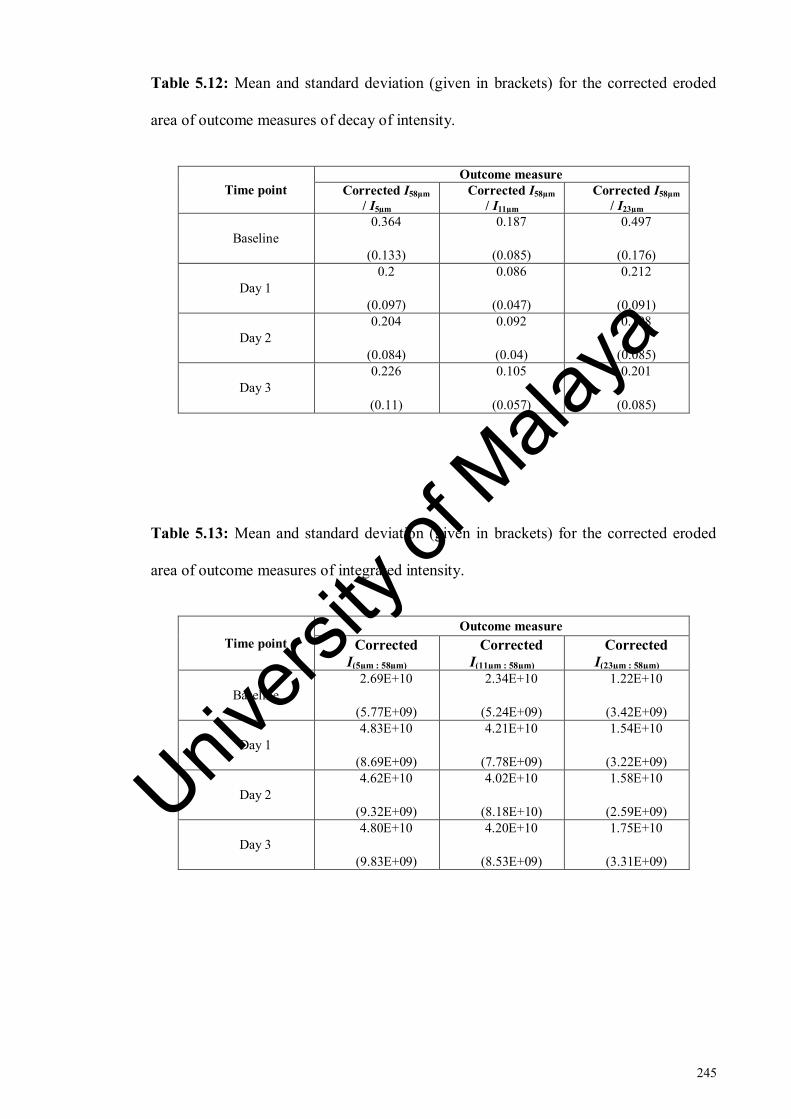
245
Table 5.12: Mean and standard deviation (given in brackets) for the corrected eroded
area of outcome measures of decay of intensity.
Time point
Outcome measure
Corrected I58µm
/ I5µm
Corrected I58µm
/ I11µm
Corrected I58µm
/ I23µm
Baseline
0.364
(0.133)
0.187
(0.085)
0.497
(0.176)
Day 1
0.2
(0.097)
0.086
(0.047)
0.212
(0.091)
Day 2
0.204
(0.084)
0.092
(0.04)
0.198
(0.085)
Day 3
0.226
(0.11)
0.105
(0.057)
0.201
(0.085)
Table 5.13: Mean and standard deviation (given in brackets) for the corrected eroded
area of outcome measures of integrated intensity.
Time point
Outcome measure
Corrected
I(5µm : 58µm)
Corrected
I(11µm : 58µm)
Corrected
I(23µm : 58µm)
Baseline
2.69E+10
(5.77E+09)
2.34E+10
(5.24E+09)
1.22E+10
(3.42E+09)
Day 1
4.83E+10
(8.69E+09)
4.21E+10
(7.78E+09)
1.54E+10
(3.22E+09)
Day 2
4.62E+10
(9.32E+09)
4.02E+10
(8.18E+10)
1.58E+10
(2.59E+09)
Day 3
4.80E+10
(9.83E+09)
4.20E+10
(8.53E+09)
1.75E+10
(3.31E+09)
Univers
ity of
Mala
ya

246
5.3.2 FE-SEM
Figure 5.21 shows the comparison of OCT outcome measures with FE-SEM
observations. FE-SEM image representing day one of erosion (Figure 5.21, d) showed
the opened dentinal tubules after the partial removal of smear layer. This phenomenon
was detected by both decay of intensity and integrated intensity. However, after day
one, the intensity of all outcome measures of decay of intensity and I(5µm : 58µm) and I(11µm
: 58µm) of integrated intensity remained almost constant. In the FE-SEM images (Figure
5.21, c-f), the progression of erosion was evident especially in day three image (Figure
5.21, f). Therefore, results for decay of intensity and integrated intensity of the first two
superficial depths were not in accordance with the FE-SEM micrographs.
When compared to FE-SEM micrographs, it is clear that only I(23µm : 58µm) was able to
detect and monitor day three of erosion as shown in the Figure 5.22. Figure 5.22, a)
showed that the intensity between day one and day two was almost constant. From the
FE-SEM images representing day one and day two of cycling erosion, (Figure 5.22, c &
d) it could be observed that the erosion-associated changes were limited to peritubular
dentine. It can be speculated that the overall porosity level was not affected much until
the acid challenge demineralised the intertubular dentine as observed in day three image
of FE-SEM (Figure 5.22, f). Hence, this change was not detected with OCT.
Univers
ity of
Mala
ya
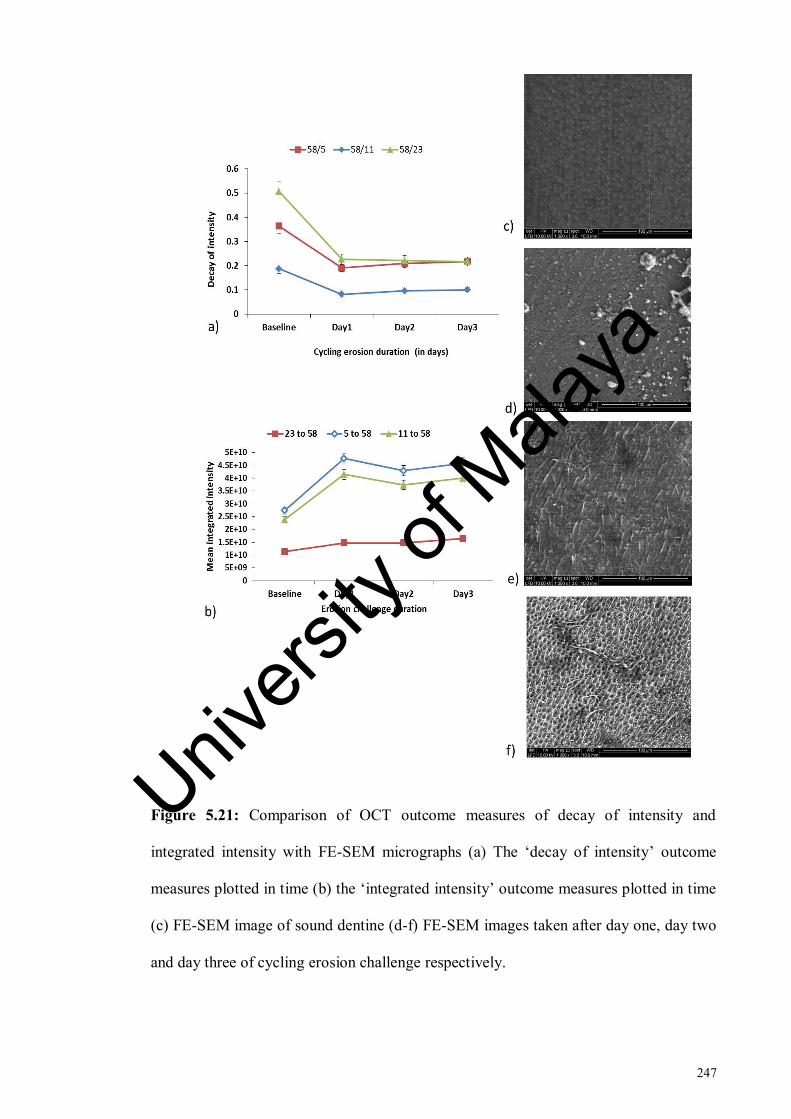
247
Figure 5.21: Comparison of OCT outcome measures of decay of intensity and
integrated intensity with FE-SEM micrographs (a) The ‘decay of intensity’ outcome
measures plotted in time (b) the ‘integrated intensity’ outcome measures plotted in time
(c) FE-SEM image of sound dentine (d-f) FE-SEM images taken after day one, day two
and day three of cycling erosion challenge respectively.
Univers
ity of
Mala
ya
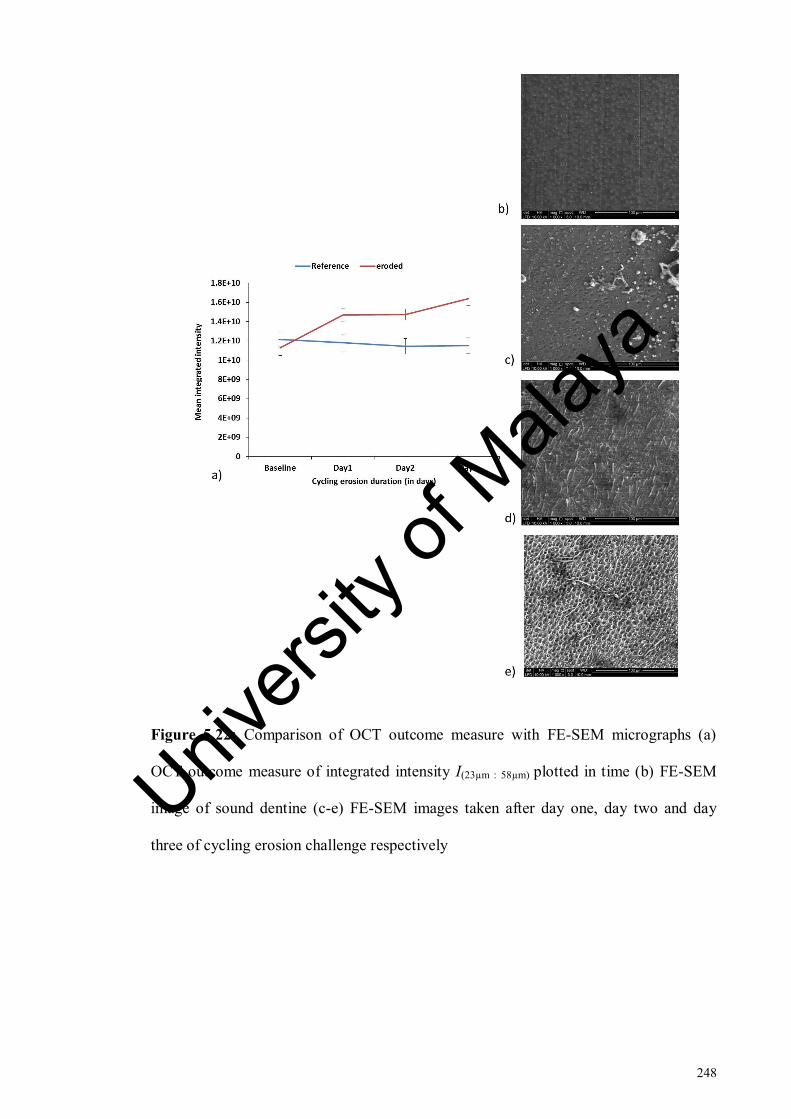
248
Figure 5.22: Comparison of OCT outcome measure with FE-SEM micrographs (a)
OCT outcome measure of integrated intensity I(23µm : 58µm) plotted in time (b) FE-SEM
image of sound dentine (c-e) FE-SEM images taken after day one, day two and day
three of cycling erosion challenge respectively
Univers
ity of
Mala
ya

249
5.3.3 Comparison with surface roughness findings
5.3.3.1 Fractional change in intensity, fR (I(23µm : 58µm))
Results of Mauchly’s test showed that the sphericity assumption was violated in both
reference (reference, 2 = 26.975, p<0.0001) and eroded area (
2 = 33.08, p<0.0001).
Therefore, the adjusted F-values of the Greenhouse-Geisser correction were considered.
One-way repeated measures ANOVA showed that there was a significant effect of
erosion interval on backscattered intensity in the eroded area (F (1.4, 28.25) = 33.03,
p<0.0001, η2
= .635) whereas no significant effect of erosion interval on intensity was
observed in the reference area (F (1.5, 29.4) = 1.77, p = .193, η2
= .08) as shown in Table
5.5.
Post hoc comparisons for the eroded area showed that the mean intensity values of
all days were significantly different with respect to their baseline intensity values.
Moreover, significant differences were observed between day two and day three as
shown in Table 5.6. Data plot is given in Figure 5.23
Univers
ity of
Mala
ya

250
Figure 5.23: Fractional change in integrated intensity with baseline (fR) of reference
and eroded areas at cycling erosion intervals. The backscattered intensity was integrated
from superficial optical depth of 23 µm to the intensity plateau at 58 µm
5.3.3.2 Relationship between fR and fRa1
Significance and level of relationship between OCT outcome measure fR (fractional
change in I(23µm : 58µm)) and fractional change in surface roughness outcome measures,
average roughness (fRa1), core roughness (fRk), peak roughness (fRpk), valley roughness
(fRvk), proportion of peaks (fMR1) and proportion of valleys (fMR2) was determined by
Pearson correlation coefficient test. Overall difference and correlation between fR and
surface roughness outcome measures is stated in Table 5.14
Pearson correlation coefficient test showed that there was a significant relationship
between fR of OCT and fRa1 (p<0.0001). Pearson coefficient of r = 0.428 showed a
moderate positive relationship between the two variables. A linear function was fitted to
the variable relationship with a R2 value of 0.161 as shown in Figure 5.24
Univers
ity of
Mala
ya

251
Figure 5.24: Relationship between fR and fRa
5.3.3.3 Relationship between fR and fRk
Pearson correlation coefficient test showed that there was a significant relationship
between fR of OCT and fRk (p<0.0001). Pearson coefficient of r = .394 showed a
moderate positive relationship between the two variables. A linear function was fitted to
the variable relationship with a R2 value of 0.156 as shown in Figure 5.25
Univ
ersity
of M
alaya

252
Figure 5.25: Relationship between fR and fRk
5.3.3.4 Relationship between fR and fRpk
Pearson correlation coefficient test showed that there was a significant relationship
between fR of OCT and fRpk (p = 0.001). However, Pearson coefficient of r = 0.300
showed a weak positive relationship between the two variables. A linear function was
fitted to the variable relationship with a R2 value of 0.068 as shown in Figure 5.26
Univers
ity of
Mala
ya

253
Figure 5.26: Relationship between fR and fRpk
5.3.3.5 Relationship between fR and fRvk
Pearson correlation coefficient test showed that there was a significant relationship
between fR of OCT and fRpk (p = .019). However, Pearson coefficient of r = 0.217
showed a weak positive relationship between the two variables. A linear function was
fitted to the variable relationship with R2 value of 0.047 as shown in Figure 5.27
Univers
ity of
Mala
ya

254
Figure 5.27: Relationship between fR and fRvk
5.3.3.6 Relationship between fR and fMR1
Pearson correlation coefficient test showed that there was a significant relationship
between fR of OCT and fMR1 (p = 0.036). However, Pearson coefficient of r = 0.192
showed a weak positive relationship between the two variables. A linear function was
fitted to the variable relationship with a R2 value of 0.037 as shown in Figure 5.28
Univers
ity of
Mala
ya

255
Figure 5.28: Relationship between fR and fMR1
5.3.3.7 Relationship between fR and fMR2
Pearson correlation coefficient test showed that the relationship between fR of OCT
and fMR2 was not significant (p = 0.180). Pearson coefficient of r = -.123showed a
weak negative relationship between the two variables. A linear function was fitted to the
variable relationship with a R2 value of 0.015 as shown in Figure 5.29
Univ
ersity
of M
alaya
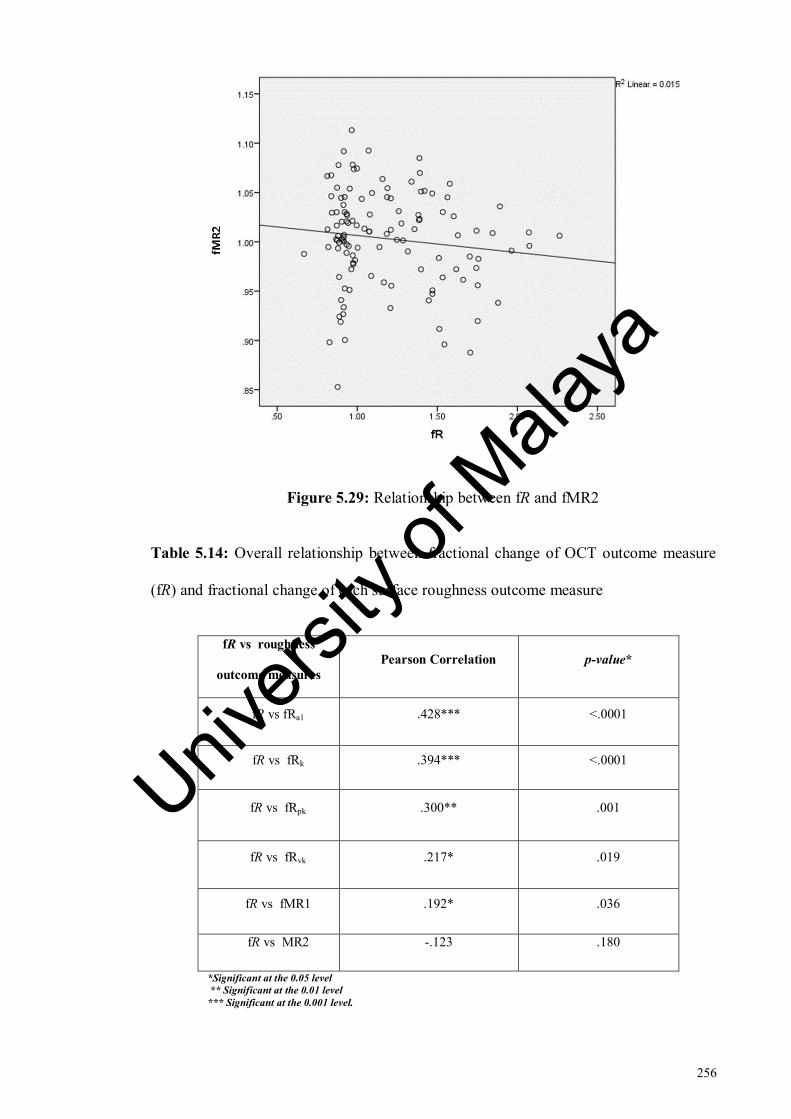
256
Figure 5.29: Relationship between fR and fMR2
Table 5.14: Overall relationship between fractional change of OCT outcome measure
(fR) and fractional change of each surface roughness outcome measure
fR vs roughness
outcome measures
Pearson Correlation p-value*
fR vs fRa1 .428*** <.0001
fR vs fRk .394*** <.0001
fR vs fRpk .300** .001
fR vs fRvk .217* .019
fR vs fMR1 .192* .036
fR vs MR2 -.123 .180
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Univers
ity of
Mala
ya

257
5.3.3.8 Significance of difference between correlation coefficients of fRa and fRk
fRa1 showed the highest Pearson correlation coefficient with r = 0.428 closely
followed by fRk with r = 0.394. In order to assess whether the difference between the
two correlation coefficients was significant, Fisher r-to-z transformation was used by
using an online calculator (Soper, 2017).
The Z-value was 0.17 and the p-value was 0.86 showing that there was no
statistically significant difference between the two Pearson correlation coefficients.
5.3.3.9 Correlation on day one
By day one, only fRpk showed a significant relationship with fR (p < 0.003).
Moreover, a moderate positive relationship was found between fRpk and fR (r = .457).
The relationship between fR and all other surface roughness parameters was not
significant. A weak positive Pearson correlation was present between fR and fRa1, fRk,
fRvk and fMR1 whereas a weak negative relationship was found between fR and fMR2
(Table 5.15)
5.3.3.10 Correlation on day two
On day two, Pearson correlation coefficient test showed that fRa1 showed a moderate
positive relationship with fR indicated by r = .320 which was significant (p = .047).
Similarly, fRk also showed a moderate positive relationship with fR as indicated by r =
0.347 which was significant (p = 0.03). Although both surface roughness parameters
showed similar relationship with fR, however the correlation coefficient was slightly
higher for fRk as compared to fRa1.
Univers
ity of
Mala
ya
258
The relationship between fR and all other surface roughness parameters was not
significant on day two. A weak positive Pearson correlation was present between fR and
fRa, fRk, fRvk and fMR1 whereas a weak negative relationship was found between fR
and fMR2. Detailed results are given in Table 5.15.
5.3.3.11 Correlation on day three
On day three, the correlation coefficients of both fRa1 and fRk became higher and
showed a strong positive relationship with fR as indicated by r = 0.578 for fRa1 vs fR
and r = .556 for fRk vs fR. Moreover, the relationship of both fRa1 and fRk was highly
significant by day three (p<0.0001). fRvk also showed a moderate positive relationship
with fR with r = 0.337 which was significant (p = .039). A moderate positive
relationship between fR and fMR1 was found as indicated by r = .444 which was
significant (p = .004).
fRpk showed a weak positive relationship with fR which was not significant. As on
day one and day two, fMR2 showed a weak negative relationship with fR which was not
significant either (Table 5.15).
Univers
ity of
Mala
ya

259
Table 5.15: Relationship between fractional change of OCT outcome measure (fR) and
fractional change of surface roughness outcome measures at each time point (day).
Day fR vs roughness
outcome measures
Pearson correlation p-value
Day 1 fR vs fRa1 .261 .108
fR vs fRk .114 .489
fR vs fRpk .457** .003
fR vs fRvk .079 .632
fR vs fMR1 .182 .260
fR vs fMR2 -.146 .369
Day 2 fR vs fRa1 .320* .047
fR vs Rk .347* .030
fR vs Rpk .225 .169
fR vs Rvk .137 .404
fR vs MR1 .038 .816
fR vs MR2 -.144 .374
Day 3 fR vs Ra1 .578*** <0.0001
fR vs Rk .556*** <0.0001
fR vs Rpk .224 .135
fR vs Rvk .337* .039
fR vs MR1 .444** .004
fR vs MR2 -.094 .564
*Significant at the 0.05 level
** Significant at the 0.01 level
*** Significant at the 0.001 level.
Univers
ity of
Mala
ya

260
5.4 Discussion
The purpose of this study was to assess whether OCT could be used to monitor the
progression of early dentine erosion in simulated intraoral environment. The OCT
backscattered intensity changes of early eroded dentine were compared with
ultrastructural changes and surface roughness measurements.
A laboratory cycling erosion model was employed in this study to replicate the main
chemical and biological conditions related to extrinsic dental erosion. All the variables
of this study protocol were chosen as much as practically possible to mimic the key
processes occurring in the oral cavity leading to early dentine erosion. In this relation a
literature search was conducted to review the pH-cycling erosion models and the most
frequently employed clinically relevant variables were tabulated and considered.
Observations from previously performed pilot studies explained in chapter 3 were also
taken into account.
Citric acid was used instead of commercially available soft drinks to avoid any
inconsistency in the formulation among the batches which can be problematic in studies
with multiple exposures to acid (Shellis et al., 2011). The concentration and pH of the
citric acid was kept similar to that of a commercially available orange juice (Austin et
al., 2010; Chiga et al., 2016; Eisenburger et al., 2001) and 10 minutes of erosion was
adopted to mimic the consumption of a can of soft drink or juice beverage (Faller et al.,
2011). Temperature of 36°C was employed to simulate the intraoral temperature
(Shellis et al., 2011). The speed of agitation was pre-determined in a pilot study to
mimic the swishing of drink around the teeth at which the samples did not move while
the solution remained stirred homogeneously.
Many formulations of artificial saliva are available and have been used to simulate
the effect of natural saliva in erosion studies (Alexandria et al., 2017; Scaramucci et al.,
Univers
ity of
Mala
ya
261
2011). It was shown that a remineralisation solution was better at remineralising early
eroded enamel lesions as compared to artificial saliva (Amaechi & Higham, 2001b).
This remineralisation solution had the same composition as that of artificial saliva with
the exception of methyl p-hydroxybenzoate and sodium carboxymethyl cellulose.
Sodium carboxymethyl cellulose has been known to limit remineralisation potential of
saliva by forming complexes with calcium and phosphate ions as well as causing an
increase in viscosity (Ionta et al., 2014). Keeping this in view, a remineralisation
solution of similar composition was used in this study. It is felt that overinclusion of
variables in the same protocol can render the interpretation of results difficult.
Previously, the presence of pellicle was speculated to mask the OCT backscattered
intensity on early eroded enamel (H.P.Chew, 2013). Therefore, to keep the effect of
variables to minimum, the organic portion of saliva was not included in the
remineralisation solution at this point.
As dentine is naturally protected by a smear layer in the oral cavity (Cummins,
2009), therefore smear layer was not removed from dentine samples in this study. Each
root was sectioned in a buccolingual direction ensuring that the direction of acid attack
on the dentine samples was similar to that occurring in vivo. Although it is not possible
to use adhesive tape as reference in vivo, the reference surface was still covered with
non-residue adhesive tape during the erosion challenges so that natural surface of the
same tooth could be used as reference for more realistic comparisons during the data
analysis. Moreover, the samples had to be embedded in the resin to aid in repositioning
although the resin cannot be used in vivo conditions.
A pilot study was performed to determine the optimum duration of dentine exposure
to acid resulting in early dentine erosion without any bulk surface loss. After three days
of cycling erosion challenge, no visible step change was discerned in the OCT images.
Univers
ity of
Mala
ya

262
Therefore, the cycling erosion protocol was limited to three cycling days with 0.3%
citric acid three times a day interspersed with periods of simulated salivary
remineralisation of 3 hours in between the erosion challenges followed by overnight
immersion in remineralisation solution.
5.4.1 OCT
Mean depth profiles for the reference and eroded areas of all samples were plotted up
to a depth of 120 µm to observe the general intensity trend. Mean A-scan for the
reference area showed that little changes in intensity had occurred over time. In
contrast, mean A-scan for the eroded area showed erosion interval related shift in
backscattered intensity indicated by the separation of line graphs representing erosion
intervals. The most remarkable separation between line graphs in the eroded area was
observed at a depth of 11 µm (Imax) from tooth-air interface. The intensity increased at
day one at this depth and then dropped back. This could be the effect of smear plugs or
surface deposits of mineral on the surface of dentine (Figure 5.21, d). However, the
surface variation was very high at this depth (shown by high standard deviation) both in
the reference and eroded areas and became relatively moderate at 23 µm (Idrop). Similar
intensity trends had been observed in mean A-scans extracted from the non-pH-cycling
experiment in chapter 3. This could be the result of previously observed phenomenon of
very strong reflection at the tooth surface which can interfere with assessment of early
demineralisation (Lee et al., 2009). Although an attempt was made to minimise the
effect of specular reflection to some extent by inclining the samples to 20 degrees
perpendicular to the OCT beam by a custom made jig, however it was obvious that
complete elimination of this surface reflection was not possible.
Univers
ity of
Mala
ya

263
It would be almost impossible to monitor erosion in early stages solely based on
visual detail contained in OCT images. Therefore, it was important to identify
parameters that could non-subjectively discriminate eroded tissues from sound tissues
and allow the monitoring of erosion over time. The parameters used by other
researchers in OCT-associated research are spectral peak ratio analysis (Sowa et al.,
2007), peak intensity (Bakhsh et al., 2011), area under the curve (Louie et al., 2010) and
attenuations (Mandurah et al., 2013). Previously, two parameters ‘decay of intensity’
and ‘integrated intensity’ were employed to assess the potential of OCT in longitudinal
monitoring of early dentine erosion described in chapter 3. Results had shown that
integrated intensity was more suitable for the analysis. However, the erosion protocol
for this study differed from the previous study by the inclusion of salivary
remineralisation step and intact smear layer. A possibility remained that same parameter
might not prove to be as effective for monitoring of dentinal demineralisation for this
study. Hence, the sensitivity of both parameters was again tested for this study.
A fixed depth value of 200 µm was employed previously and statistically significant
correlations were found between the integrated intensity value and demineralisation
periods (Fried et al., 2002). The demineralisation was induced up to 14 pH-cycling days
as the objective was to simulate artificial caries rather than erosion. In this study, the
demineralisation was induced for three cycling days only and hence a comparatively
more superficially located fixed subsurface optical depth of 58 µm was employed. At
this subsurface depth, the OCT intensity signal had become constant and did not show
any further changes and was called plateau of intensity. To find an optimal superficial
depth to attain maximal sensitivity of OCT, three superficial depths 5 µm, 11 µm and 23
µm located immediately below the tooth-air interface were selected for data analysis
and comparison. Their relationship with plateau of intensity was assessed by using both
parameters. The selection of optimum outcome measure was based on 1) trend of
Univers
ity of
Mala
ya
264
backscattered intensity of mean A-scans 2) repeated measures ANOVA analysis for
sensitivity and 3) effect size comparison for assessing the magnitude of strength of
outcome measures 4) comparison with FE-SEM images (Section 5.4.2) and 5) data
correction with respect to reference.
All outcome measures for decay of intensity were able to monitor OCT backscattered
intensity between each cycling day and baseline measurement. I58µm / I5µm and I58µm /
I11µm were able to monitor dentine demineralisation between day one and day two only
whereas I58µm / I23µm was not able to monitor demineralisation between days. With
integrated intensity, all outcome measures were able to monitor mean backscattered
intensity between each cycling day and baseline measurement. I(5µm : 58µm) and I(11µm :
58µm) were able to monitor mean intensity values between all days. However, I(23µm : 58µm)
was able to monitor intensity from baseline to day one and day two to day three.
The effect size comparison showed that I58µm / I23µm had the greatest magnitude of
strength in monitoring early dentine erosion for this study. It was important to take into
consideration the overall intensity trend of each outcome measure. With decay of
intensity, the intensity is expected to decrease with increasing erosion intervals(Chew et
al., 2014). Unexpectedly, for I58µm / I5µm and I58µm / I11µm day one intensity values of
0.185 and 0.079 increased to .212 and .098 at day three respectively. For I58µm / I23µm, the
intensity was constant after day one of cycling erosion challenge. With integrated
intensity, the backscattered intensity is expected to increase with increasing erosion
intervals. For eroded areas of I(5µm : 58µm) and I(11µm : 58µm) , backscattered intensity at day
one was 4.62E+10 and 4.02E+10 respectively and decreased to 4.44E+10 and 3.88E+10
at day three respectively. For I(23µm : 58µm) the intensity value increased from 1.47E+10 at
day one to 1.64E+10 at day three. It could be ascertained that the first two superficial
depths with either parameter were not able to detect erosion-related intensity change at
Univers
ity of
Mala
ya

265
day three while I(23µm : 58µm) was the only outcome measure to show net increase in
erosion from baseline to day three of cycling erosion challenge. This could be
confirmed from the FE-SEM images as discussed in Section 5.4.2. In the previous study
(chapter 3), I(23µm : 58µm) was identified as the optimum outcome measure for monitoring
of demineralisation in dentine. Moreover, the surface variation in intensity at superficial
depths of I5 and I11 was evident in the mean A-scans.
In order to assess the stability of outcome measures and to identify any instrumental
variations in time, the data for each outcome measure was corrected for eroded area at
each time point by dividing the absolute data of eroded area at each time point by a
correction factor. This correction factor was derived from the absolute data of reference
area. The corrected values were then plotted and statistically analysed. A comparison
was then drawn between the corrected and absolute outcome measures. Corrected I58µm /
I5µm and corrected I58µm / I11µm showed that after correction no statistically significant
differences were detected between days as opposed to their absolute outcome measures
where significant differences had been observed between day one and day two intensity
values. Similarly, corrected I(5µm : 58µm) and corrected I(11µm : 58µm) showed that after day
1, intensity became constant as opposed to their absolute outcome measures where
intensity values were significantly different between all days. Corrected I58µm / I23µm
showed that mean intensity values between day one and day two became statistically
significant whereas it was not significantly different in the absolute I58 µm / I23 µm. I(23µm :
58µm) was the only outcome measure which showed statistically similar results for
corrected and absolute values indicating that it was the most stable outcome measure.
Based on the findings it could be suggested that I(23µm : 58µm) was the optimum
outcome measure for monitoring of early dentine erosion. The statistically determined
cut off depth was therefore 23 µm for this study. This showed that OCT used in this
Univers
ity of
Mala
ya

266
study was most sensitive to the demineralisation activity that occurs at this depth. At the
tooth-air interface, the specular reflection is very strong and could be 20dB higher than
OCT backscattered intensity. This could lead to scattering information being masked at
or immediately below the tooth-air interface (Fried et al., 2002). Apparently,
backscattered intensity of the superficial layers located next to tooth-air interface was
influenced by the much higher specular reflection at these depths. The optical depth of
23 µm could be translated to its physical depth, 15 µm measured from the tooth-air
interface. This would imply that the erosion-linked demineralisation had occurred all the
way into this depth for this study. This concurs with the findings in chapter 3 and
previously reported statistical depth for early enamel erosion (Chew et al., 2014)
This is the first study, to the best of our knowledge to assess the potential of OCT in
measuring the progression of early dentine erosion in simulated oral conditions. Only
one other recent study has examined potential of OCT for dentine erosion but only the
advanced stages of dentine erosion after the appearance of surface loss in the OCT
images were explored in that study (De Moraes et al., 2017). Importantly, pH-cycling
model of erosion was not employed in that study and only a qualitative analysis was
performed.
Within the limitations of this study, it could be established that OCT would very
likely have the ability to longitudinally monitor the progression of early dentine erosion.
With the OCT set up used in this study and the outcome measure selected, it was
possible to measure erosion by day one of cycling erosion challenge and monitoring
was possible between day one and day three of erosion whereas monitoring from
baseline measurement was possible at all cycling days. With this study it was possible
to develop an in vitro model to monitor early dentine erosion with OCT which can
potentially be translated to an in vivo setting. This information could provide a blueprint
Univers
ity of
Mala
ya

267
for testing of treatments products for dentine erosion over the period of time in a clinical
study.
A statistical comparison of non pH-cycling study in chapter 3 and cycling erosion
study explained in this chapter cannot be made as both studies were conducted under
different experimental and acidic challenge conditions. The cumulative erosion induced
was 30 minutes in the non pH-cycling study in chapter 3 as compared to 90 minutes for
this study. The FE-SEM images however showed that the day-three of erosion induced
in the pH cycling was not more aggressive than 30 minutes of erosion induced earlier.
Moreover, the estimated physical depth of demineralisation was 15 µm for both studies.
It could be because of two reasons. A cycling model was employed in this study and
samples were immersed in remineralisation solution for considerable periods of time
which could have offered some degree of remineralisation and resistance against
erosion. Absence of salivary proteins is further expected to have increased the
remineralisation potential of this remineralisation solution (Shellis et al., 2011).
Additionally, as opposed to non pH-cycling study the smear layer was not removed
from the samples before the induction of demineralisation. Both these factors could
have resulted in lesser erosion in this study as would be expected otherwise in a non-
cycling erosion model.
5.4.2 FE-SEM
FE-SEM micrographs served to confirm the OCT findings. Corrected data for I5µm
and I11µm with both parameters showed that the intensity became constant after day one
and I58µm / I23µm was able to monitor erosion between day one and day two only. FE-
SEM images clearly showed that the effects of acid challenge were more pronounced on
day three as compared to day two. Therefore, the intensity trend shown by these
Univers
ity of
Mala
ya
268
outcome measures was not in accordance with the ultrastructural changes as observed in
SEM images. I(23µm : 58µm) on the other hand was the only outcome measure which was
able to monitor intensity from baseline to day one and day two to day three and showed
a net increase in backscattered intensity from baseline to day three which was in line
with the FE-SEM observations. Hence FE-SEM observations further confirmed I(23µm :
58µm) as the optimum outcome measure for the monitoring of early dentine erosion under
the conditions of this study protocol.
The FE-SEM images showed that the effects of acid challenge in the eroded areas of
all samples were evident in comparison to reference areas which appeared smooth.
These observations were in line with those made from mean A-scans. Mean A-scans for
the eroded area showed erosion interval related shift in backscattered intensity as
indicated by the separation of line graphs at various depths in comparison to reference
area which showed little changes in intensity over time. The sequence of events of
dentine erosion observed from the FESEM images from day one to day three of cycling
erosion were similar to those previously reported (Meurman et al., 1991) (Kinney et al.,
1995). One day of cycling erosion challenge resulted in opening of dentinal tubules.
Day two image showed dissolution at the border of peritubular and intertubular dentine
with slight widening of tubules. Day three image showed that the dissolution of
peritubular dentine had taken place. The intertubular dentine was attacked and showed a
roughened and porous surface.
In comparison to the sound dentine, the day one image showed that treatment with
citric acid resulted in exposure of dentinal tubules. The image also showed that the
tubules were partially or completely occluded and there were white spots on the surface.
This could have resulted because of incomplete removal of smear layer from dentine
surface or from mineral deposition (formation of CaF) due to immersion of dentine
Univers
ity of
Mala
ya

269
samples in salivary simulated remineralisation solution as previously observed
(Vanuspong et al., 2002). In a previous study, dentine was exposed to remineralisation
solution for 20 days after being demineralised for six days. PS-OCT images showed the
presence of an intact mineralized layer on the remineralised dentine surface. However,
the overall effect of remineralisation of dentine was reduction in integrated intensity in
the remineralised region in comparison to the demineralized region (Manesh et al.,
2009). The remineralisation induced in this our study was part of a pH cycling regime
only which lasted only for three days. Therefore, it could be speculated that the effect of
these surface deposits would not affect the OCT scattering to the same extent or cause a
reduction in the integrated intensity if at all.
It is known that demineralised dentine becomes porous after the removal of
peritubular dentine (Kinney et al., 1995) (Meurman et al., 1991). OCT was not able to
monitor dentine demineralisation between day one and day two of cycling erosion
challenge. This could be attributed to the almost similar porosity status between day one
and day two as ascertained from the FE-SEM images. On day three images, the
peritubular dentine dissolved and intertubular dentine with increased porosities became
visible which was detected with OCT.
5.4.3 Comparison with surface roughness findings
Process of erosion in dentine results in creation of porosities and increased surface
roughness (Meurman et al., 1991). OCT quantifies erosion by the increase in porosity of
demineralised tissues which brings about a change in reflected backscattered intensity
as compared to sound tissues (Huysmans et al., 2011) whereas increase in erosion-
associated surface roughness can be measured by surface roughness parameters. This
Univers
ity of
Mala
ya

270
would suggest that both of these methods would have the potential of quantifying early
dentine erosion.
In order to compare the findings of OCT with surface roughness measurements,
fractional change, fR for the reference and eroded area of the optimum OCT outcome
measure I(23µm : 58µm) was calculated. Repeated measures ANOVA followed by post hoc
comparisons (Table 5.6) showed that the sensitivity of fR was exactly similar to that to
I(23µm : 58µm). Significance and level of relationship between OCT outcome measure fR
and surface roughness parameters fRa1, fRk, fRpk, fRvk, fMR1 and fMR2 were examined
by Pearson correlation coefficient test. Pearson correlation coefficient test showed that
there was a significant and moderate positive relationship between fR of OCT with fRa1
and fRk. The correlation coefficient of fRa1 (0.428) was higher as compared to fRk
(0.394), however, it was found that there was no statistically significant difference
between the two correlation coefficients.
Moreover, there was a significant weak positive relationship between fR of OCT and
fRpk, fRvk and fMR1. The relationship between fR of OCT and fMR2 was however
weak negative and not statistically significant. This would mean that an increase in OCT
backscattered intensity would result in a lower value for fMR2. This correlation could
be of value in testing of treatment products for erosion. OCT backscattered intensity
would decrease as a result of remineralisation (Manesh et al., 2009). On the other hand
as a result of remineralisation, the profile will be expected to become smoother with
resultant increase in proportion of valleys and MR2 value. However, it warrants further
investigation.
By day one, only fRpk showed a significant moderate positive relationship with fR.
The relationship between fR and all other surface roughness parameters was weak
positive and not statistically significant. This is in accordance with the surface
Univers
ity of
Mala
ya
271
roughness findings (chapter 4) where only fRpk was able to detect dentine
demineralisation by day one from baseline measurement. This would imply that fRpk is
most suited for monitoring of earliest stage of dentine erosion.
On day two, both fRa1 and fRk showed a significant and moderate positive
relationship with fR. The relationship between fR and all other surface roughness
outcome measures was weak positive and not statistically significant. This finding is
also in line with the surface roughness results (chapter 4) where both fRa1 and fRk were
able to monitor erosion by day two whereas Rpk was not able to monitor erosion at day
two from baseline. As would be expected, the correlation coefficients of fRa1 and fRk
with fR became higher and highly significant on day three as compared to day two. By
day three, fRvk was significantly different from baseline value (chapter 4) and also
showed a significant and moderate positive relationship with fR on day three. Although
fMR1 did not show any significantly different results on any of the days (chapter 4), it
still showed a significant and moderate positive relationship with fR on day three. This
would indicate that fMR1 may have a potential of monitoring erosion in more advanced
stages of dentine erosion.
Based on the correlation findings, it could be suggested that fRpk was well-suited to
compare the findings of OCT at day one of erosion from baseline measurement and fRa1
and fRk could be used for comparing the findings of OCT in the more advanced stages
of early dentine erosion. However, fRa1 was not able to monitor erosion between day
two and day three which could be accomplished with fRk. Hence, within the limits of
current study protocol, it could be suggested that a combination of fRpk and fRk are
suitable for comparing the findings of OCT in longitudinal monitoring of early dentine
erosion.
Univers
ity of
Mala
ya
272
In chapter 4, it was shown that surface roughness parameters can be employed for
longitudinal monitoring of early dentine erosion in simulated oral conditions.
Particularly, inclusion of bearing curve parameters provided extra information and
sensitive parameters for its monitoring. This study proves that OCT has the potential of
being employed for early dentine demineralisation in intraoral simulated conditions.
With both methods, day one of demineralisation could be detected and monitored. OCT
was not able to monitor erosion between day one and day two which was possible with
bearing area curve. However, OCT has additional advantage over profilometry in being
non-invasive and can be applied directly in clinical trials. Profilometry requires the use
of indirect impression technique which can cause inaccurate measurements.
5.5 Conclusions
Within the limitations of the current study design, the following conclusions were
drawn from the study findings,
1. OCT was able to measure early dentine erosion for three days in simulated
intraoral conditions. The quantum of OCT for measuring early dentine erosion in
simulated intraoral conditions varied with different outcome measures. I(23µm :
58µm) showed significant changes between baseline - day 1 and between day one -
day three of cycling erosion challenge.
2. Integrated intensity was more suitable and sensitive than decay of intensity for
measuring in vitro early dentine erosion in simulated intraoral conditions. I(23µm :
58µm) was the most sensitive outcome measure for measuring in vitro early
dentine erosion in simulated intraoral conditions.
Univers
ity of
Mala
ya

273
3. The simulated intraoral early dentine erosion detection threshold of OCT varied
with different outcome measures. With I(23µm : 58µm), the detection threshold was
one day of cycling erosion challenge from baseline measurement.
4. FE-SEM images supported the results of OCT backscattered intensity analysis .
With I(23µm : 58µm), a net increase of backscattered intensity in relation to
incubation time in acid was observed during erosion progression. The eroded
regions of FE-SEM showed gradually enlarging dentinal tubules and increase in
roughness of dentine surface with increasing erosion intervals.
5. OCT outcome measure fR (fI(23µm : 58µm)) showed a significant and moderate
positive relationship with surface roughness outcome measures fRa1 and fRk.
With fRpk, fRvk and fMR1, fR showed a weak positive but significant
relationship. With fMR2, fR showed a weak negative relationship which was not
significant.
6. On day one, OCT outcome measure fR showed a moderate positive and
significant relationship with fRpk. On day two, fR showed a moderate positive
and significant relationship with fRk and fRa1. On day three, fR showed a
significant and moderate positive relationship with fRk, fRa1, fRvk and fMR1.
The null hypotheses were rejected as shown below;
1. OCT was able to detect early dentine erosion with a detection sensitivity of one
pH-cycling day from baseline.
2. OCT was able to measure the progression of early dentine erosion for three days
in simulated intraoral conditions.
3. OCT backscattered intensity changes were correlated with surface roughness
measurements.
Univers
ity of
Mala
ya

274
CHAPTER 6: CONCLUSIONS
6.1 Summary and conclusions
Longitudinal monitoring of early dentine erosion in an in vivo setting is desirable to
evaluate the performance of anti-erosion interventions more accurately as various in
vitro and in situ studies provide contradictory results. Such in vivo studies can only be
materialised by the development of non-invasive methods sensitive to early
demineralisation. The purpose of this thesis was to seek a non-invasive tool which could
be used for detection and monitoring of early dentine erosion in clinical trials to
evaluate the efficacies of treatment strategies meant to reduce the progression of dentine
erosion.
Such a tool is expected to possess a few qualities. It should be a non-destructive and
non-invasive method which is sensitive to early demineralisation and is able to quantify
erosion over time. Review of literature revealed that the currently employed methods do
not meet these criteria. Of the optical methods used in erosion research, optical
coherence tomography (OCT) seemed to be the potential tool for this task. While tested
previously for enamel erosion and advanced staged dentine erosion, its potential in the
assessment of early dentine erosion remained to be tested. Therefore, the first study of
this thesis aimed to assess the applicability of OCT for detection and monitoring of
early dentine erosion. Thirty minutes of erosion was induced in a non pH-cycling model
to assess the potential and the detection capacity of this instrument.
Surface profilometry has been used extensively for the assessment of dentine erosion
and has been employed to a limited extent in the in vivo settings. However, the
conventionally used parameter, surface loss may not be suitable for assessment of early
stage of dentine erosion which is not expected to result in bulk surface loss.
Additionally, in order to compare the findings of newer non-invasive techniques in vivo
Univers
ity of
Mala
ya

275
and in vitro, sensitive and quantitative reference methods are needed. Therefore, the
second study aimed at assessing the potential of surface roughness parameters, in
particular the bearing area curve parameters for monitoring of early dentine erosion in
simulated intraoral conditions.
The potential of OCT to monitor early dentine erosion and its detection capacity had
been identified in chapter 3. Subsequent course of action was to perform an in situ or an
in vivo validation study or proceed with an in vitro study with a simulated intraoral
environment. It was felt that sufficient information about the clinical situation could not
be derived from the first study (chapter 3) and variables like simulated salivary
remineralisation and presence of smear layer could potentially affect the OCT
outcomes. Moreover, from a non-cycling model it is difficult to predict the amount of
erosion that could be induced and monitored in clinical situation. Therefore, it was
decided to evaluate the potential of OCT for monitoring early dentine erosion in
simulated intraoral conditions before testing this tool in more expensive in situ or in
vivo studies.
This multi-aimed study was divided into three main chapters and had the following
aims,
6.1.1 Aim 1
To assess the potential of optical coherence tomography (OCT) in monitoring the
progression of in vitro early dentine erosion
The null hypotheses tested were as follows;
1. OCT is not able to detect early dentine erosion in vitro.
2. OCT is not able to measure early dentine erosion progression in vitro.
Univers
ity of
Mala
ya

276
In order to test these null hypotheses, 20 root dentine samples were subjected to 30
minutes of erosion with 0.3% citric acid and measurements were obtained with OCT at
0, 2, 4, 6, 8, 10, 12, 14, 16, 20, 25 and 30 minutes. A composite slab was used as a
reference during the measurements. Another 14 root dentine samples were imaged with
field emission scanning electron microscopy (FE-SEM) but not longitudinally after 2, 4,
8, 12, 16, 25 and 30 minutes of erosion challenge with similar citric acid. The OCT data
was extracted and processed using a bespoke software programme developed with
MATLAB (The MathWorks, Inc., USA). The OCT data was subsequently analysed
using two parameters ‘decay of intensity’ (D) and ‘integrated intensity’ (R) and their
related outcome measures. The findings of OCT were then compared with
ultrastructural changes.
Based on the data collected and analysed (please refer Sections 3.2 and 3.3), null
hypotheses one and two were rejected as shown below;
1. OCT was able to detect early dentine erosion with a detection threshold of two
minutes from baseline measurement.
2. OCT was able to measure the progression of early dentine erosion up to 30
minutes in vitro.
Following the rejection of the above null hypotheses, further conclusions were drawn
from the study findings;
1. OCT was able to measure early dentine erosion up to 30 minutes. The quantum
of OCT for measuring early dentine erosion varied with different outcome
measures. I(23µm : 58µm) showed significant changes in the first three 2-minutes
intervals (0-6 minutes) but not in the subsequent three 2-minute intervals (6-12
minutes). However, in the subsequent eighteen minutes (12-30 minutes), I(23µm :
Univers
ity of
Mala
ya

277
58µm) detected significant 2-minutes interval change only up to 16 minutes and
significant changes were detected in the consecutive time intervals only between
25 and 30 minutes for the next 14 minutes (16-30 minutes).
2. Integrated intensity was more suitable and sensitive than decay of intensity for
measuring in vitro early dentine erosion. I(23µm : 58µm) was the most sensitive
outcome measure for measuring in vitro early dentine erosion. OCT outcome
measure ΔR showed a linear pattern (R2 = 0.995) as goodness of fit model for
monitoring of in vitro early dentine erosion.
3. The in vitro early dentine erosion detection threshold of OCT varied with
different outcome measures. With I(23µm : 58µm), the detection threshold was 2
minutes of erosion challenge from baseline measurement.
4. FE-SEM images supported the results of OCT backscattered intensity analysis.
With I(23µm : 58µm), continuous increase in backscattered intensity in relation to
incubation time in acid was obvious during erosion progression. The eroded
regions of FE-SEM showed gradually enlarging dentinal tubules with increasing
erosion intervals.
6.1.2 Aim 2
To assess the potential of surface roughness as a method for longitudinally
measuring in vitro early dentine erosion in simulated intraoral conditions.
The null hypotheses tested were as follows:
1. Surface roughness parameters cannot be used to measure early dentine erosion
progression in simulated intraoral conditions.
Univers
ity of
Mala
ya
278
2. There is no difference of the sensitivity of Ra and bearing curve parameters in
measuring early dentine erosion in simulated intraoral conditions.
20 root dentine samples were subjected to a cycling erosion challenge with 0.3%
citric acid for 10 minutes three times a day interspersed with 3-hour long periods of
simulated salivary remineralisation and overnight storage with a remineralisation
solution for three days. Measurements were obtained with non-contact profilometry
after every cycling day. Moreover, three samples were additionally prepared for FE-
SEM imaging using similar demineralisation and remineralisation conditions.
Traditionally used parameter Ra and bearing curve parameters were extracted and
analysed. Different measurement methods for Ra extraction were explored. Moreover,
another conventionally employed parameter, surface loss was also measured.
Based on the data collected and analysed (please refer Sections 4.2 and 4.3), null
hypotheses one and two were rejected as shown below;
1. Surface roughness parameters fRa1, fRpk, fRk and fRvk (fractional change of
average roughness, peak roughness, core roughness and valley roughness
respectively) can be used to measure early dentine erosion progression for three
days in simulated intraoral conditions.
2. Bearing curve parameters fRpk and fRk are more sensitive than fRa1 in measuring
early dentine erosion in simulated intraoral conditions.
Following the rejection of the above null hypotheses, further conclusions were
drawn from the study findings;
1. Average surface roughness, fRa1 and bearing area curve parameters, fRk (core
roughness), fRpk (peak roughness) and fRvk (valley roughness) were able to
detect and longitudinally measure early dentine erosion. fMR1, fMR2
Univers
ity of
Mala
ya

279
(Fractional change in proportion of profile peaks and profile valleys
respectively) and fΔZ (surface loss) were not able to detect and measure early
dentine erosion.
2. fRk showed the greatest magnitude of strength in measuring early dentine
erosion as determined by its largest effect size.
3. The early dentine erosion detection threshold of surface roughness varied with
different parameters. fRpk showed a detection threshold of day one from baseline
measurement. fRk and fRa1 were able to detect erosion by day two from baseline
measurement. fRvk showed a detection threshold of day three from baseline
measurement.
4. FE-SEM images supported the surface roughness results. FE-SEM images of the
eroded areas of samples showed increase in overall roughness of dentine surface
during erosion progression. Continuous rise of roughness shown by fRa1, fRk,
fRpk and fRvk in relation to the incubation time in acid was obvious.
6.1.3 Aim 3
To assess if optical coherence tomography is a sensitive tool to detect early dentine
erosion and monitor its progression in simulated intraoral conditions by correlating
OCT data with the surface roughness data.
The null hypotheses tested were as follows;
1. OCT is not able to detect early dentine erosion in simulated intraoral conditions.
2. OCT is not able to measure the progression of early dentine erosion in simulated
intraoral conditions.
Univers
ity of
Mala
ya

280
3. There is no correlation between profilometric surface roughness measurements
and OCT backscattered changes.
As opposed to chapter 3, root dentine samples were eroded in a pH-cycling erosion
model and smear layer was kept intact on the samples. Literature reviewed for the
cycling erosion models helped in molding the design of this study. 20 root dentine
samples (same as employed in chapter 4) were subjected to a cycling erosion challenge
for three days with 0.3% citric acid, three times a day interspersed with periods of
simulated salivary remineralisation of 3 hours in between the erosion challenges
followed by overnight immersion in similar remineralisation solution. The OCT
measurements were obtained at the end of each cycling day. The OCT data was
extracted and processed using a bespoke software programme developed with
MATLAB (The MathWorks, Inc., USA). The data was further analysed using two
parameters ‘decay of intensity’ (D) and ‘integrated intensity’ (R) and their related
outcome measures. The OCT findings were compared with those of surface roughness
and with the ultrastructural changes.
Based on the data collected and analysed (please refer Sections 5.2 and 5.3), null
hypotheses one, two and three were rejected as shown below;
1. OCT was able to detect early dentine erosion with a detection sensitivity of one
pH-cycling day from baseline
2. OCT was able to measure the progression of early dentine erosion for three days
in simulated intraoral conditions.
3. OCT backscattered intensity changes were correlated with surface roughness
measurements.
Following conclusions could be drawn from the study findings,
Univers
ity of
Mala
ya

281
1. OCT was able to measure early dentine erosion for three days in simulated
intraoral conditions. The quantum of OCT for measuring early dentine erosion in
simulated intraoral conditions varied with different outcome measures. I(23µm :
58µm) showed significant changes between baseline - day one and between day
one - day three of cycling erosion challenge.
2. Integrated intensity was more suitable and sensitive than decay of intensity for
measuring in vitro early dentine erosion in simulated intraoral conditions. I(23µm :
58µm) was the most sensitive outcome measure for longitudinal monitoring of in
vitro early dentine erosion in simulated intraoral conditions.
3. The simulated intraoral early dentine erosion detection threshold of OCT varied
with different outcome measures. With I(23µm : 58µm), the detection threshold was
one day of cycling erosion challenge from baseline measurement.
4. FE-SEM images supported the results of OCT backscattered intensity analysis .
With I(23µm : 58µm), a net increase of backscattered intensity in relation to
incubation time in acid was observed during erosion progression. The eroded
regions of FE-SEM showed gradually enlarging dentinal tubules and increase in
roughness of dentine surface with increasing erosion intervals.
5. OCT outcome measure fR (fI(23µm : 58µm)) showed a significant and moderate
positive relationship with surface roughness outcome measures fRa1 and fRk.
With fRpk, fRvk and fMR1, fR showed a weak positive but significant
relationship. With fMR2, fR showed a weak negative relationship which was not
significant.
6. On day one, OCT outcome measure fR showed a moderate positive and
significant relationship with fRpk. On day two, fR showed a moderate positive
and significant relationship with fRk and fRa1. On day three, fR showed a
significant and moderate positive relationship with fRk, fRa1, fRvk and fMR1.
Univers
ity of
Mala
ya

282
6.2 Contribution to research
The findings made in this thesis make original contributions to the existing
literature on assessment of early dentine erosion. The research contribution of this
study, within its limitations can be summed as,
1. To the best of author’s knowledge, OCT was employed for the first time for
early dentine erosion assessment (before any visible bulk surface loss). The
immediate impact of this research would be the use of this tool for the clinical
validation of management strategies meant to prevent or reduce erosion
progression in dentine. A long term impact would be the use of OCT as a non-
contact chairside tool in routine clinical practice for diagnosing dentine erosion
which to date is dependent on subjective clinical diagnosis.
2. To the best of author’s knowledge, novel bearing curve parameters were used for
the first time as a method for early dentine erosion assessment in simulated
intraoral conditions. This method could be used in the in vivo settings (by
indirect impression technique) for monitoring of early dentine erosion and also
as a quantitative reference method for validation of other newer non-invasive
techniques.
3. The methodologies employed in this study are expected to provide a blueprint
for assessment of early dentine erosion in vivo as;
1. A novel bespoke algorithm developed in Matlab (The Math works, Inc., USA)
for the OCT research under HIR UM.C / 625 / 1 / HIR / MOHE /_Dent_/1 for
OCT data processing with a Graphic Unit interface (GUI) has been used for the
analysis of OCT data. This software was designed by Dr. Christian Zakian
(research collaborator for HIR and co-supervisor for this project).
Univers
ity of
Mala
ya

283
2. An optimum outcome measure has been established for assessment of early
dentine erosion with OCT.
3. An optimum cut-off depth for exclusion of surface effects of specular reflection
for assessment of early dental erosion has been defined in this study.
6.3 Limitations of this study
The limitations of this study are as follows,
1. Use of flat and polished dentine samples in the study. Polished samples were
used in this study to achieve a standardised sample surface and minimize the
natural variability of tooth surface as a new tool (OCT) was being employed.
Moreover, polished samples were required as they increase the accuracy of
profilometry imaging.
2. Absence of organic portion of saliva in the salivary simulated remineralisation
solution. The organic portion of saliva contains salivary enzymes and proteins
which could have an overall impact on salivary remineralisation in vivo. The
organic portion of saliva was not added at this point to keep the effect of
variables to a minimum as potential of a new tool (OCT) was being assessed.
3. Use of adhesive tape to cover reference surfaces in pH-cycling study which
cannot be employed in clinical settings. The reference surface was covered with
non-residue adhesive tape during the erosion challenges so that natural surface of
the same tooth could be used as a reference for more realistic comparisons during
the data analysis.
Univers
ity of
Mala
ya

284
6.4 Future work
This study within its limitations establishes fundaments and is expected to present a
gateway for future research protocols aimed at non-invasive in vivo assessment of early
dentine erosion for the clinical validation of treatment strategies related to its timely
management.
In this direction, future research could aim at,
1. Detection and monitoring of early dentine erosion with OCT using natural
dentine samples instead of polished samples.
2. Assessment of early dentine erosion with polarised sensitive optical coherence
tomography to avoid specular reflection near the tooth-air interface.
3. Assessment of efficacies of anti-erosion products for early dentine erosion with
OCT in vitro or in situ.
4. Assessment of early dentine erosion with OCT and bearing curve parameters in a
clinical trial.
Univers
ity of
Mala
ya

285
REFERENCES
Abdolrahimzadeh, S., Piraino, D. C., Scavella, V., Abdolrahimzadeh, B., Cruciani, F.,
Gharbiya, M., & Recupero, S. M. (2016). Spectral domain optical coherence
tomography and B-scan ultrasonography in the evaluation of retinal tears in
acute, incomplete posterior vitreous detachment. BMC Ophthalmology, 16, 60.
Ablal, M. A., Kaur, J. S., Cooper, L., Jarad, F. D., Milosevic, A., Higham, S. M., &
Preston, A. J. (2009). The erosive potential of some alcopops using bovine
enamel: An in vitro study. Journal of Dentistry, 37(11), 835-839.
Abou Neel, E. A., Aljabo, A., Strange, A., Ibrahim, S., Coathup, M., Young, A. M.,
Bozec, L., & Mudera, V. (2016). Demineralization-remineralization dynamics in
teeth and bone. International Journal of Nanomedicine, 11, 4743-4763.
Addy, M. (2005). Tooth brushing, tooth wear and dentine hypersensitivity--are they
associated? International Dental Journal, 55(4 Suppl 1), 261-267.
Addy, M., & Hunter, M. L. (2003). Can tooth brushing damage your health? Effects on
oral and dental tissues. International Dental Journal, 53 Suppl 3, 177-186.
Addy, M., & Shellis, R. P. (2006). Interaction between attrition,abrasion and erosion in
tooth wear. Monographs in Oral Science, 20, 17-31.
Al-Malik, M. I., Holt, R. D., & Bedi, R. (2002). Erosion, caries and rampant caries in
preschool children in Jeddah, Saudi Arabia. Community Dentistry and Oral
Epidemiology, 30(1), 16-23.
Al-Malik, M. I., Holt, R. D., Bedi, R., & Speight, P. M. (2001). Investigation of an
index to measure tooth wear in primary teeth. Journal of Dentistry, 29(2), 103-
107.
Alexandria, A. K., Vieira, T. I., Pithon, M. M., da Silva Fidalgo, T. K., Fonseca-
Goncalves, A., Valenca, A. M., Cabral, L. M., & Maia, L. C. (2017). In vitro
enamel erosion and abrasion-inhibiting effect of different fluoride varnishes.
Archives of Oral Biology, 77, 39-43.
Alghilan, M. A., Cook, N. B., Platt, J. A., Eckert, G. J., & Hara, A. T. (2015).
Susceptibility of restorations and adjacent enamel/dentine to erosion under
different salivary flow conditions. Journal of Dentistry, 43(12), 1476-1482.
Amaechi, B. T. (2015). Dental Erosion and Its Clinical Management: Springer
International Publishing.
Amaechi, B. T., & Higham, S. M. (2001a). Eroded enamel lesion remineralization by
saliva as a possible factor in the site-specificity of human dental erosion.
Archives of Oral Biology, 46(8), 697-703.
Amaechi, B. T., & Higham, S. M. (2001b). In vitro remineralisation of eroded enamel
lesions by saliva. Journal of Dentistry, 29(5), 371-376.
Univers
ity of
Mala
ya

286
Amaechi, B. T., Higham, S. M., Podoleanu, A. G., Rogers, J. A., & Jackson, D. A.
(2001). Use of optical coherence tomography for assessment of dental caries:
Quantitative procedure. Journal of Oral Rehabilitation, 28(12), 1092-1093.
Amaechi, B. T., Podoleanu, A. G., Komarov, G., Higham, S. M., & Jackson, D. A.
(2004). Quantification of root caries using optical coherence tomography and
microradiography: A correlational study. Oral Health & Preventive Dentistry,
2(4), 377-382.
Amin, W. M., Al-Omoush, S. A., & Hattab, F. N. (2001). Oral health status of workers
exposed to acid fumes in phosphate and battery industries in Jordan.
International Dental Journal, 51(3), 169-174.
Anderson, P., & Elliott, J. C. (2000). Rates of mineral loss in human enamel during in
vitro demineralization perpendicular and parallel to the natural surface. Caries
Research, 34(1), 33-40.
Angker, L., & Swain, M. V. (2006). Nanoindentation: Application to dental hard tissue
investigations. Journal of Materials Research, 21(8), 1893-1905.
Angmar-Mansson, B., & ten Bosch, J. J. (2001). Quantitative light-induced fluorescence
(QLF): a method for assessment of incipient caries lesions. Dento Maxillo
Facial Radiology, 30(6), 298-307.
Arends, J., & Tencate, J. M. (1981). Tooth enamel remineralization. Journal of Crystal
Growth, 53(1), 135-147.
Attin, T. (2006). Methods for assessment of dental erosion. Monographs in Oral
Science, 20, 152-172.
Attin, T., Becker, K., Hannig, C., Buchalla, W., & Hilgers, R. (2005a). Method to detect
minimal amounts of calcium dissolved in acidic solutions. Caries Research,
39(5), 432-436.
Attin, T., Becker, K., Hannig, C., Buchalla, W., & Wiegand, A. (2005b). Suitability of a
malachite green procedure to detect minimal amounts of phosphate dissolved in
acidic solutions. Clinical Oral Investigations, 9(3), 203-207.
Attin, T., Becker, K., Roos, M., Attin, R., & Paque, F. (2009). Impact of storage
conditions on profilometry of eroded dental hard tissue. Clinical Oral
Investigations, 13(4), 473-478.
Attin, T., Buchalla, W., Gollner, M., & Hellwig, E. (2000). Use of variable
remineralization periods to improve the abrasion resistance of previously eroded
enamel. Caries Research, 34(1), 48-52.
Attin, T., Buchalla, W., & Putz, B. (2001). In vitro evaluation of different
remineralization periods in improving the resistance of previously eroded bovine
dentine against tooth-brushing abrasion. Archives of Oral Biology, 46(9), 871-
874.
Univers
ity of
Mala
ya

287
Attin, T., Meyer, K., Hellwig, E., Buchalla, W., & Lennon, A. M. (2003). Effect of
mineral supplements to citric acid on enamel erosion. Archives of Oral Biology,
48(11), 753-759.
Attin, T., & Wegehaupt, F. J. (2014). Methods for assessment of dental erosion.
Monographs in Oral Science, 25, 123-142.
Attin, T., Weiss, K., Becker, K., Buchalla, W., & Wiegand, A. (2005c). Impact of
modified acidic soft drinks on enamel erosion. Oral Diseases, 11(1), 7-12.
Austin, R. S., Haji Taha, M., Festy, F., Cook, R., Andiappan, M., Gomez, J., Pretty, I.
A., & Moazzez, R. (2017). Quantitative Swept-Source Optical Coherence
Tomography of Early Enamel Erosion in vivo. Caries Research, 51(4), 410-418.
Austin, R. S., Rodriguez, J. M., Dunne, S., Moazzez, R., & Bartlett, D. W. (2010). The
effect of increasing sodium fluoride concentrations on erosion and attrition of
enamel and dentine in vitro. Journal of Dentistry, 38(10), 782-787.
Aykut-Yetkiner, A., Wiegand, A., Ronay, V., Attin, R., Becker, K., & Attin, T. (2014).
In vitro evaluation of the erosive potential of viscosity-modified soft acidic
drinks on enamel. Clinical Oral Investigations, 18(3), 769-773.
Azzopardi, A., Bartlett, D. W., Watson, T. F., & Sherriff, M. (2004). The surface effects
of erosion and abrasion on dentine with and without a protective layer. British
Dental Journal, 196(6), 351-354; discussion 339.
Azzopardi, A., Bartlett, D. W., Watson, T. F., & Smith, B. G. (2000). A literature
review of the techniques to measure tooth wear and erosion. The European
Journal of Prosthodontics and Restorative Dentistry, 8(3), 93-97.
Bacova, V., & Draganovska, D. (2004). Analyses of the quality of blasted surfaces.
Materials Science, 40(1), 125-131.
Bahal, P., & Djemal, S. (2014). Dental erosion from an excess of vitamin C. Case
Reports in Dentistry, 2014, 485387.
Bakhsh, T. A., Sadr, A., Shimada, Y., Tagami, J., & Sumi, Y. (2011). Non-invasive
quantification of resin–dentin interfacial gaps using optical coherence
tomography: Validation against confocal microscopy. Dental Materials, 27(9),
915-925.
Bamise, C. T., Olusile, A. O., Oginni, A. O., & Dosumu, O. O. (2007). The prevalence
of dentine hypersensitivity among adult patients attending a Nigerian teaching
hospital. Oral Health & Preventive Dentistry, 5(1), 49-53.
Banerjee, A., & Boyde, A. (1998). Autofluorescence and mineral content of carious
dentine: scanning optical and backscattered electron microscopic studies. Caries
Research, 32(3), 219-226.
Barbosa, C. S., Kato, M. T., & Buzalaf, M. A. (2011). Effect of supplementation of soft
drinks with green tea extract on their erosive potential against dentine.
Australian Dental Journal, 56(3), 317-321.
Univers
ity of
Mala
ya

288
Barbour, M. E., Lussi, A., & Shellis, R. P. (2011). Screening and prediction of erosive
potential. Caries Research, 45 Suppl 1, 24-32.
Barbour, M. E., & Rees, J. S. (2004). The laboratory assessment of enamel erosion: A
review. Journal of Dentistry, 32(8), 591-602.
Bardsley, P. F. (2008). The evolution of tooth wear indices. Clinical Oral
Investigations, 12 Suppl 1, S15-S19.
Bartlett, D., Ganss, C., & Lussi, A. (2008). Basic Erosive Wear Examination (BEWE):
A new scoring system for scientific and clinical needs. Clinical Oral
Investigations, 12 Suppl 1, S65-S68.
Bartlett, D. W., Palmer, I., & Shah, P. (2005). An audit of study casts used to monitor
tooth wear in general practice. British Dental Journal, 199(3), 143-145.
Becker, L. A. (2000). Effect size calculators.
Bevenius, J., Lindskog, S., & Hultenby, K. (1994). The micromorphology in vivo of the
buccocervical region of premolar teeth in young adults. A replica study by
scanning electron microscopy. Acta Odontologica Scandinavica, 52(6), 323-334.
Bewoor, A. K., & Kulkarni, V. A. (2009). Metrology and Measurement: Tata McGraw-
Hill Education.
Beyer, M., Reichert, J., Sigusch, B. W., Watts, D. C., & Jandt, K. D. (2012).
Morphology and structure of polymer layers protecting dental enamel against
erosion. Dental Materials, 28(10), 1089-1097.
Bhushan, B. (2013). Introduction to Tribology: Wiley.
Borges, A. B., Scaramucci, T., Lippert, F., Zero, D. T., & Hara, A. T. (2014). Erosion
protection by calcium lactate/sodium fluoride rinses under different salivary
flows in vitro. Caries Research, 48(3), 193-199.
Brand, H. S., Dun, S. N., & Amerongen, A. V. N. (2008). Ecstasy (MDMA) and oral
health. British Dental Journal, 204(2), 77-81.
Breschi, L., Gobbi, P., Mazzotti, G., Falconi, M., Ellis, T. H., & Stangel, I. (2002). High
resolution SEM evaluation of dentin etched with maleic and citric acid. Dental
Materials, 18(1), 26-35.
Buzalaf, M. A., Hannas, A. R., & Kato, M. T. (2012a). Saliva and dental erosion.
Journal of Applied Oral Science, 20(5), 493-502.
Buzalaf, M. A., Hannas, A. R., Magalhaes, A. C., Rios, D., Honorio, H. M., & Delbem,
A. C. (2010). pH-cycling models for in vitro evaluation of the efficacy of
fluoridated dentifrices for caries control: Strengths and limitations. Journal of
Applied Oral Science, 18(4), 316-334.
Univers
ity of
Mala
ya
289
Buzalaf, M. A., Kato, M. T., & Hannas, A. R. (2012b). The role of matrix
metalloproteinases in dental erosion. Advances in Dental Research, 24(2), 72-
76.
Canadian Advisory Board on Dentin, H. (2003). Consensus-based recommendations for
the diagnosis and management of dentin hypersensitivity. The Journal of the
Canadian Dental Association, 69(4), 221-226.
Carvalho, R. M., Yoshiyama, M., Brewer, P. D., & Pashley, D. H. (1996). Dimensional
changes of demineralized human dentine during preparation for scanning
electron microscopy. Archives of Oral Biology, 41(4), 379-386.
Carvalho, T. S., Baumann, T., & Lussi, A. (2016). A new hand-held optical
reflectometer to measure enamel erosion: Correlation with surface hardness and
calcium release. Scientific Reports, 6, 25259.
Carvalho, T. S., Schmid, T. M., Baumann, T., & Lussi, A. (2017). Erosive effect of
different dietary substances on deciduous and permanent teeth. Clinical Oral
Investigations, 21(5), 1519-1526.
Chabanski, M. B., Gillam, D. G., Bulman, J. S., & Newman, H. N. (1997). Clinical
evaluation of cervical dentine sensitivity in a population of patients referred to a
specialist periodontology department: A pilot study. Journal of Oral
Rehabilitation, 24(9), 666-672.
Chadwick, R. G., & Mitchell, H. L. (2001). Conduct of an algorithm in quantifying
simulated palatal surface tooth erosion. Journal of Oral Rehabilitation, 28(5),
450-456.
Chan, K. H., Chan, A. C., Darling, C. L., & Fried, D. (2013). Methods for Monitoring
Erosion Using Optical Coherence Tomography. Proceedings of SPIE--the
International Society for Optical Engineering, 8566, 856606.
Chan, K. H., Chan, A. C., Fried, W. A., Simon, J. C., Darling, C. L., & Fried, D. (2015).
Use of 2D images of depth and integrated reflectivity to represent the severity of
demineralization in cross-polarization optical coherence tomography. Journal of
Biophotonics, 8(1-2), 36-45.
Chan, K. H., Tom, H., & Fried, D. (2014). Monitoring the inhibition of erosion by a
CO2 laser with OCT. Proceedings of SPIE--the International Society for Optical
Engineering, 8929, 89290F.
Charone, S., Cardoso Cde, A., Kato, M. T., Ducati, P., Fukushima, R., Gennaro, G.,
Magalhaes, A. C., & Buzalaf, M. A. (2014). The effect of mouthwashes
containing biguanides on the progression of erosion in dentin. BMC Oral
Health, 14, 131.
Cheng, R., Yang, H., Shao, M. Y., Hu, T., & Zhou, X. D. (2009a). Dental erosion and
severe tooth decay related to soft drinks: A case report and literature review.
Journal of Zhejiang University-Science B, 10(5), 395-399.
Univers
ity of
Mala
ya
290
Cheng, Z. J., Wang, X. M., Cui, F. Z., Ge, J., & Yan, J. X. (2009b). The enamel
softening and loss during early erosion studied by AFM, SEM and
nanoindentation. Biomedical Materials, 4(1), 015020.
Chew, H. P., Zakian, C. M., Pretty, I. A., & Ellwood, R. P. (2014). Measuring initial
enamel erosion with quantitative light-induced fluorescence and optical
coherence tomography: An in vitro validation study. Caries Research, 48(3),
254-262.
Chiga, S., Toro, C. V., Lepri, T. P., Turssi, C. P., Colucci, V., & Corona, S. A. (2016).
Combined effect of fluoride varnish to Er:YAG or Nd:YAG laser on
permeability of eroded root dentine. Archives of Oral Biology, 64, 24-27.
Cochrane, N. J., Iijima, Y., Shen, P., Yuan, Y., Walker, G. D., Reynolds, C., MacRae,
C. M., Wilson, N. C., Adams, G. G., & Reynolds, E. C. (2014). Comparative
study of the measurement of enamel demineralization and remineralization using
transverse microradiography and electron probe microanalysis. Microscopy and
Microanalysis, 20(3), 937-945.
Cohen, J. (2013). Statistical Power Analysis for the Behavioral Sciences (2 ed.): Taylor
& Francis.
Colston, B. W., Sathyam, U. S., DaSilva, L. B., Everett, M. J., Stroeve, P., & Otis, L. L.
(1998). Dental OCT. Optics Express, 3(6), 230-238.
Cruz, J. B., Lenzi, T. L., Tedesco, T. K., Guglielmi, C. D. B., & Raggio, D. P. (2012).
Eroded dentin does not jeopardize the bond strength of adhesive restorative
materials. Brazilian Oral Research, 26(4), 306-312.
Cummins, D. (2009). Dentin hypersensitivity: From diagnosis to a breakthrough therapy
for everyday sensitivity relief. The Journal of Clinical Dentistry, 20(1), 1-9.
Dai, N., Hu, J., & Liu, H. (2015). 3D Simulation Modeling of the Tooth Wear Process.
PLoS One, 10(8), e0134807.
Darvell, B. W. (2009). Materials Science for Dentistry: Elsevier Science.
Dawes, C. (2003). What is the critical pH and why does a tooth dissolve in acid? The
Journal of the Canadian Dental Association, 69(11), 722-724.
De Chiffre, L., Lonardo, P., Trumpold, H., Lucca, D. A., Goch, G., Brown, C. A., Raja,
J., & Hansen, H. N. (2000). Quantitative Characterisation of Surface Texture.
CIRP Annals - Manufacturing Technology, 49(2), 635-652.
de Moraes, M. C., Freitas, A. Z., & Aranha, A. C. (2017). Progression of erosive lesions
after Nd:YAG laser and fluoride using optical coherence tomography. Lasers In
Medical Science, 32(1), 1-8.
Desai, A. P., Tyberg, A., Kedia, P., Smith, M. S., Martinez, G., Zamarripa, F.,
Schneider, Y., Bertani, H., Frazzoni, M., Casas, F., Khanna, L. G., Lambroza,
A., Kumta, N. A., Khan, A., Sharaiha, R. Z., Salgado, S., Gaidhane, M., Sethi,
A., & Kahaleh, M. (2016). Optical coherence tomography (OCT) prior to peroral
Univers
ity of
Mala
ya

291
endoscopic myotomy (POEM) reduces procedural time and bleeding: A
multicenter international collaborative study. Surgical Endoscopy, 30(11), 5126-
5133.
Drexler, W., & Fujimoto, J. G. (2008). Optical Coherence Tomography: Technology
and Applications: Springer Berlin Heidelberg.
Dugmore, C. R., & Rock, W. P. (2003). The progression of tooth erosion in a cohort of
adolescents of mixed ethnicity. International Journal of Paediatric Dentistry,
13(5), 295-303.
Eccles, J. D. (1978). The treatment of dental erosion. Journal of Dentistry, 6(3), 217-
221.
Eccles, J. D. (1979). Dental erosion of nonindustrial origin. A clinical survey and
classification. The Journal of Prosthetic Dentistry, 42(6), 649-653.
Eisenburger, M., Addy, M., Hughes, J. A., & Shellis, R. P. (2001). Effect of time on the
remineralisation of enamel by synthetic saliva after citric acid erosion. Caries
Research, 35(3), 211-215.
Eisenburger, M., Hughes, J., West, N. X., Jandt, K. D., & Addy, M. (2000).
Ultrasonication as a method to study enamel demineralisation during acid
erosion. Caries Research, 34(4), 289-294.
Eisenburger, M., Shellis, R. P., & Addy, M. (2004). Scanning electron microscopy of
softened enamel. Caries Research, 38(1), 67-74.
El Aidi, H., Bronkhorst, E. M., & Truin, G. J. (2008). A longitudinal study of tooth
erosion in adolescents. Journal of Dental Research, 87(8), 731-735.
Elton, V., Cooper, L., Higham, S. M., & Pender, N. (2009). Validation of enamel
erosion in vitro. Journal of Dentistry, 37(5), 336-341.
Engelen, L., de Wijk, R. A., Prinz, J. F., van der Bilt, A., & Bosman, F. (2003). The
relation between saliva flow after different stimulations and the perception of
flavor and texture attributes in custard desserts. Physiology & Behavior, 78(1),
165-169.
Espigares, J., Sadr, A., Hamba, H., Shimada, Y., Otsuki, M., Tagami, J., & Sumi, Y.
(2015). Assessment of natural enamel lesions with optical coherence
tomography in comparison with microfocus x-ray computed tomography.
Journal of Medical Imaging (Bellingham, Wash.), 2(1), 014001.
Faller, R. V., Eversole, S. L., & Tzeghai, G. E. (2011). Enamel protection: A
comparison of marketed dentifrice performance against dental erosion.
American Journal of Dentistry, 24(4), 205-210.
Featherstone, J. D., & Lussi, A. (2006). Understanding the chemistry of dental erosion.
Monographs in Oral Science, 20, 66-76.
Univers
ity of
Mala
ya

292
Fercher, A. F., Mengedoht, K., & Werner, W. (1988). Eye-length measurement by
interferometry with partially coherent light. Optics Letters, 13(3), 186-188.
Field, J., German, M., & Waterhouse, P. (2013). Using bearing area parameters to
quantify early erosive tooth surface changes in enamel: A pilot study. Journal of
Dentistry, 41(11), 1060-1067.
Field, J., Waterhouse, P., & German, M. (2010). Quantifying and qualifying surface
changes on dental hard tissues in vitro. Journal of Dentistry, 38(3), 182-190.
Finke, M., Jandt, K. D., & Parker, D. M. (2000). The Early Stages of Native Enamel
Dissolution Studied with Atomic Force Microscopy. Journal of Colloid and
Interface Science, 232(1), 156-164.
Flury, S., Koch, T., Peutzfeldt, A., Lussi, A., & Ganss, C. (2013). The effect of a tin-
containing fluoride mouth rinse on the bond between resin composite and
erosively demineralised dentin. Clinical Oral Investigations, 17(1), 217-225.
Francescut, P., Zimmerli, B., & Lussi, A. (2006). Influence of different storage methods
on laser fluorescence values: A two-year study. Caries Research, 40(3), 181-
185.
Fried, D., Xie, J., Shafi, S., Featherstone, J. D., Breunig, T. M., & Le, C. (2002).
Imaging caries lesions and lesion progression with polarization sensitive optical
coherence tomography. Journal of Biomedical Optics, 7(4), 618-627.
Gabriele, M. L., Wollstein, G., Ishikawa, H., Kagemann, L., Xu, J., Folio, L. S., &
Schuman, J. S. (2011). Optical coherence tomography: History, current status,
and laboratory work. Investigative Ophthalmology & Visual Science, 52(5),
2425-2436.
Gadelmawla, E. S., Koura, M. M., Maksoud, T. M. A., Elewa, I. M., & Soliman, H. H.
(2002). Roughness parameters. Journal of Materials Processing Technology,
123(1), 133-145.
Gaetano, J. (2013). Holm-Bonferroni Sequential Correction: An EXCEL Calculator
(1.1) [Microsoft Excel Workbook]. .
Ganss, C., Hardt, M., Blazek, D., Klimek, J., & Schlueter, N. (2009a). Effects of
toothbrushing force on the mineral content and demineralized organic matrix of
eroded dentine. European Journal of Oral Sciences, 117(3), 255-260.
Ganss, C., Hardt, M., Lussi, A., Cocks, A. K., Klimek, J., & Schlueter, N. (2010).
Mechanism of action of tin-containing fluoride solutions as anti-erosive agents
in dentine - An in vitro tin-uptake, tissue loss, and scanning electron microscopy
study. European Journal of Oral Sciences, 118(4), 376-384.
Ganss, C., Klimek, J., & Lussi, A. (2006). Accuracy and consistency of the visual
diagnosis of exposed dentine on worn occlusal/incisal surfaces. Caries
Research, 40(3), 208-212.
Univers
ity of
Mala
ya

293
Ganss, C., Klimek, J., Schaffer, U., & Spall, T. (2001). Effectiveness of two fluoridation
measures on erosion progression in human enamel and dentine in vitro. Caries
Research, 35(5), 325-330.
Ganss, C., Klimek, J., & Schwarz, N. (2000). A comparative profilometric in vitro study
of the susceptibility of polished and natural human enamel and dentine surfaces
to erosive demineralization. Archives of Oral Biology, 45(10), 897-902.
Ganss, C., Klimek, J., & Starck, C. (2004). Quantitative analysis of the impact of the
organic matrix on the fluoride effect on erosion progression in human dentine
using longitudinal microradiography. Archives of Oral Biology, 49(11), 931-
935.
Ganss, C., & Lussi, A. (2006). Diagnosis of erosive tooth wear. Monographs in Oral
Science, 20, 32-43.
Ganss, C., & Lussi, A. (2014). Diagnosis of erosive tooth wear. Monographs in Oral
Science, 25, 22-31.
Ganss, C., Lussi, A., & Klimek, J. (2005). Comparison of calcium/phosphorus analysis,
longitudinal microradiography and profilometry for the quantitative assessment
of erosive demineralisation. Caries Research, 39(3), 178-184.
Ganss, C., Lussi, A., Scharmann, I., Weigelt, T., Hardt, M., Klimek, J., & Schlueter, N.
(2009b). Comparison of calcium analysis, longitudinal microradiography and
profilometry for the quantitative assessment of erosion in dentine. Caries
Research, 43(6), 422-429.
Ganss, C., Lussi, A., & Schlueter, N. (2014). The histological features and physical
properties of eroded dental hard tissues. Monographs in Oral Science, 25, 99-
107.
Ganss, C., Schlueter, N., Hardt, M., von Hinckeldey, J., & Klimek, J. (2007). Effects of
toothbrushing on eroded dentine. European Journal of Oral Sciences, 115(5),
390-396.
Ganss, C., Schulze, K., & Schlueter, N. (2013). Toothpaste and erosion. Monographs in
Oral Science, 23, 88-99.
Ghazali, F. B. (2003). Permeability of dentine. Malaysian Journal of Medical Sciences,
10(1), 27-36.
Gimbel, C. (2008). Optical coherence tomography diagnostic imaging. General
Dentistry, 56(7), 750-757; quiz 758-759, 768.
Gomez-Lopez, V. M. (2012). Decontamination of Fresh and Minimally Processed
Produce: Wiley.
Gregg, T., Mace, S., West, N. X., & Addy, M. (2004). A study in vitro of the abrasive
effect of the tongue on enamel and dentine softened by acid erosion. Caries
Research, 38(6), 557-560.
Univers
ity of
Mala
ya
294
Grzesik, W. (2016). Advanced Machining Processes of Metallic Materials: Theory,
Modelling, and Applications: Elsevier Science.
Gulabivala, K., & Ng, Y. L. (2014). Endodontics E-Book: Elsevier Health Sciences.
H.P.Chew. (2013). Novel Assessments of Early Enamel Erosion. (Doctor of
Philosophy), University of Manchester, Manchester, UK.
Habelitz, S., Balooch, M., Marshall, S. J., Balooch, G., & Marshall, G. W., Jr. (2002).
In situ atomic force microscopy of partially demineralized human dentin
collagen fibrils. Journal of Structural Biology, 138(3), 227-236.
Hall, A. F., Buchanan, C. A., Millett, D. T., Creanor, S. L., Strang, R., & Foye, R. H.
(1999). The effect of saliva on enamel and dentine erosion. Journal of Dentistry,
27(5), 333-339.
Hall, A. F., Sadler, J. P., Strang, R., de Josselin de Jong, E., Foye, R. H., & Creanor, S.
L. (1997). Application of transverse microradiography for measurement of
mineral loss by acid erosion. Advances in Dental Research, 11(4), 420-425.
Hamasha, A. A., Zawaideh, F. I., & Al-Hadithy, R. T. (2014). Risk indicators associated
with dental erosion among Jordanian school children aged 12-14 years of age.
International Journal of Paediatric Dentistry, 24(1), 56-68.
Hamba, H., Nikaido, T., Sadr, A., Nakashima, S., & Tagami, J. (2012). Enamel lesion
parameter correlations between polychromatic micro-CT and TMR. Journal of
Dental Research, 91(6), 586-591.
Hangai, M., Ojima, Y., Gotoh, N., Inoue, R., Yasuno, Y., Makita, S., Yamanari, M.,
Yatagai, T., Kita, M., & Yoshimura, N. (2007). Three-dimensional imaging of
macular holes with high-speed optical coherence tomography. Ophthalmology,
114(4), 763-773.
Hannas, A. R., Kato, M. T., Cardoso Cde, A., Magalhaes, A. C., Pereira, J. C.,
Tjaderhane, L., & Buzalaf, M. A. (2016). Preventive effect of toothpastes with
MMP inhibitors on human dentine erosion and abrasion in vitro. Journal of
Applied Oral Science, 24(1), 61-66.
Hannig, C., Becker, K., Hausler, N., Hoth-Hannig, W., Attin, T., & Hannig, M. (2007).
Protective effect of the in situ pellicle on dentin erosion - an ex vivo pilot study.
Archives of Oral Biology, 52(5), 444-449.
Hannig, C., Hannig, M., & Attin, T. (2005). Enzymes in the acquired enamel pellicle.
European Journal of Oral Sciences, 113(1), 2-13.
Hannig, M., & Balz, M. (2001). Protective properties of salivary pellicles from two
different intraoral sites on enamel erosion. Caries Research, 35(2), 142-148.
Hannig, M., Fiebiger, M., Guntzer, M., Dobert, A., Zimehl, R., & Nekrashevych, Y.
(2004). Protective effect of the in situ formed short-term salivary pellicle.
Archives of Oral Biology, 49(11), 903-910.
Univers
ity of
Mala
ya

295
Hara, A. T., Ando, M., Cury, J. A., Serra, M. C., Gonzalez-Cabezas, C., & Zero, D. T.
(2005). Influence of the organic matrix on root dentine erosion by citric acid.
Caries Research, 39(2), 134-138.
Hara, A. T., Ando, M., Gonzalez-Canbezas, C., Cury, J. A., Serra, M. C., & Zero, D. T.
(2006a). Protective effect of the dental pellicle against erosive challenges in situ.
Journal of Dental Research, 85(7), 612-616.
Hara, A. T., Lussi, A., & Zero, D. T. (2006b). Biological factors. Monographs in Oral
Science, 20, 88-99.
Hara, A. T., & Zero, D. T. (2008). Analysis of the erosive potential of calcium-
containing acidic beverages. European Journal of Oral Sciences, 116(1), 60-65.
Harding, M. A., Whelton, H., O'Mullane, D. M., & Cronin, M. (2003). Dental erosion in
5-year-old Irish school children and associated factors: a pilot study. Community
Dental Health, 20(3), 165-170.
Hariri, I., Sadr, A., Shimada, Y., Tagami, J., & Sumi, Y. (2012). Effects of structural
orientation of enamel and dentine on light attenuation and local refractive index:
an optical coherence tomography study. Journal of Dentistry, 40(5), 387-396.
Herkstroter, F. M., Witjes, M., Ruben, J., & Arends, J. (1989). Time dependency of
microhardness indentations in human and bovine dentine compared with human
enamel. Caries Research, 23(5), 342-344.
Herregods, T. V., van Hoeij, F. B., Oors, J. M., Bredenoord, A. J., & Smout, A. J.
(2016). Effect of Running on Gastroesophageal Reflux and Reflux Mechanisms.
The American Journal of Gastroenterology, 111(7), 940-946.
Hjortsjo, C., Jonski, G., Thrane, P. S., Saxegaard, E., & Young, A. (2009). The effects
of acidic fluoride solutions on early enamel erosion in vivo. Caries Research,
43(2), 126-131.
Holtzman, J. S., Ballantine, J., Fontana, M., Wang, A., Calantog, A., Benavides, E.,
Gonzalez-Cabezas, C., Chen, Z., & Wilder-Smith, P. (2014). Assessment of
early occlusal caries pre- and post-sealant application--an imaging approach.
Lasers in Surgery and Medicine, 46(6), 499-507.
Hooper, S., West, N. X., Pickles, M. J., Joiner, A., Newcombe, R. G., & Addy, M.
(2003). Investigation of erosion and abrasion on enamel and dentine: A model in
situ using toothpastes of different abrasivity. Journal of Clinical Periodontology,
30(9), 802-808.
Hsu, D. J., Darling, C. L., Lachica, M. M., & Fried, D. (2008). Nondestructive
assessment of the inhibition of enamel demineralization by CO2 laser treatment
using polarization sensitive optical coherence tomography. Journal of
Biomedical Optics, 13(5), 054027.
Huang, D., Swanson, E. A., Lin, C. P., Schuman, J. S., Stinson, W. G., Chang, W., Hee,
M. R., Flotte, T., Gregory, K., Puliafito, C. A., & et al. (1991). Optical
coherence tomography. Science, 254(5035), 1178-1181.
Univers
ity of
Mala
ya

296
Hunter, M. L., West, N. X., Hughes, J. A., Newcombe, R. G., & Addy, M. (2000a).
Erosion of deciduous and permanent dental hard tissue in the oral environment.
Journal of Dentistry, 28(4), 257-263.
Hunter, M. L., West, N. X., Hughes, J. A., Newcombe, R. G., & Addy, M. (2000b).
Relative susceptibility of deciduous and permanent dental hard tissues to erosion
by a low pH fruit drink in vitro. Journal of Dentistry, 28(4), 265-270.
Huysmans, M. C., Chew, H. P., & Ellwood, R. P. (2011). Clinical studies of dental
erosion and erosive wear. Caries Research, 45 Suppl 1, 60-68.
Inenaga, K., Inangaki, T., Hosokawa, R., & Ono, K. (2009). Parotid salivary secretion
induced by stimulation of periodontal regions with toothbrush in humans. The
Journal of Medical Investigation, 56 Suppl, 277.
InfiniteFocus, A. (2009). IFM Manual: Alicona Imaging GmbH.
Ionta, F. Q., Mendonca, F. L., de Oliveira, G. C., de Alencar, C. R., Honorio, H. M.,
Magalhaes, A. C., & Rios, D. (2014). In vitro assessment of artificial saliva
formulations on initial enamel erosion remineralization. Journal of Dentistry,
42(2), 175-179.
Ireland, A. J., McGuinness, N., & Sherriff, M. (1995). An investigation into the ability
of soft drinks to adhere to enamel. Caries Research, 29(6), 470-476.
Jaeggi, T., & Lussi, A. (2014). Prevalence, incidence and distribution of erosion.
Monographs in Oral Science, 25, 55-73.
Jati, A. S., Furquim, L. Z., & Consolaro, A. (2016). Gingival recession: its causes and
types, and the importance of orthodontic treatment. Dental press journal of
orthodontics, 21(3), 18-29.
Jensdottir, T., Bardow, A., & Holbrook, P. (2005). Properties and modification of soft
drinks in relation to their erosive potential in vitro. Journal of Dentistry, 33(7),
569-575.
Johansson, A. K., Johansson, A., Stan, V., & Ohlson, C. G. (2005). Silicone sealers,
acetic acid vapours and dental erosion: A work-related risk? Swedish Dental
Journal, 29(2), 61-69.
Johansson, A. K., Lingstrom, P., & Birkhed, D. (2002). Comparison of factors
potentially related to the occurrence of dental erosion in high- and low-erosion
groups. European Journal of Oral Sciences, 110(3), 204-211.
Johansson, A. K., Lingstrom, P., Imfeld, T., & Birkhed, D. (2004). Influence of
drinking method on tooth-surface pH in relation to dental erosion. European
Journal of Oral Sciences, 112(6), 484-489.
Johansson, A. K., Omar, R., Carlsson, G. E., & Johansson, A. (2012). Dental erosion
and its growing importance in clinical practice: From past to present.
International Journal of Dentistry, 2012, 632907.
Univers
ity of
Mala
ya

297
Joiner, M. C., & van der Kogel, A. (2016). Basic Clinical Radiobiology, Fifth Edition:
Taylor & Francis.
Jones, R. S., Darling, C. L., Featherstone, J. D., & Fried, D. (2006a). Imaging artificial
caries on the occlusal surfaces with polarization-sensitive optical coherence
tomography. Caries Research, 40(2), 81-89.
Jones, R. S., Darling, C. L., Featherstone, J. D., & Fried, D. (2006b). Remineralization
of in vitro dental caries assessed with polarization-sensitive optical coherence
tomography. Journal of Biomedical Optics, 11(1), 014016.
Joshi, M., Joshi, N., Kathariya, R., Angadi, P., & Raikar, S. (2016). Techniques to
Evaluate Dental Erosion: A Systematic Review of Literature. Journal of Clinical
and Diagnostic Research, 10(10), Ze01-ze07.
Kaidonis, J. A., Richards, L. C., Townsend, G. C., & Tansley, G. D. (1998). Wear of
human enamel: A quantitative in vitro assessment. Journal of Dental Research,
77(12), 1983-1990.
Kaifu, Y., Kasai, K., Townsend, G. C., & Richards, L. C. (2003). Tooth wear and the
"design" of the human dentition: A perspective from evolutionary medicine.
American Journal of Physical Anthropology, Suppl 37, 47-61.
Kang, H., Jiao, J. J., Lee, C., Le, M. H., Darling, C. L., & Fried, D. (2010).
Nondestructive Assessment of Early Tooth Demineralization Using Cross-
Polarization Optical Coherence Tomography. IEEE Journal of Selected Topics
in Quantum Electronics, 16(4), 870-876.
Karlinsey, R. L., Mackey, A. C., Schwandt, C. S., & Walker, T. J. (2011). SEM
evaluation of demineralized dentin treated with professional-strength NaF
topical pastes. American Journal of Dentistry, 24(6), 357-362.
Keesman, M., Aarts, H., Vermeent, S., Hafner, M., & Papies, E. K. (2016).
Consumption Simulations Induce Salivation to Food Cues. PLoS One, 11(11),
e0165449.
Kinney, J. H., Balooch, M., Haupt, D. L., Jr., Marshall, S. J., & Marshall, G. W., Jr.
(1995). Mineral distribution and dimensional changes in human dentin during
demineralization. Journal of Dental Research, 74(5), 1179-1184.
Kinney, J. H., Balooch, M., Marshall, S. J., Marshall, G. W., Jr., & Weihs, T. P. (1996).
Hardness and Young's modulus of human peritubular and intertubular dentine.
Archives of Oral Biology, 41(1), 9-13.
Koch, G., Poulsen, S., Espelid, I., & Haubek, D. (2017). Pediatric Dentistry: A Clinical
Approach: Wiley.
Koulourides, T. (1968). Experimental Changes of Mineral Density. In R. Harris (Ed.),
Art and Science of Dental Caries Research (pp. 355-378). New York: Academic
Press.
Univers
ity of
Mala
ya

298
Kukiattrakoon, B., Hengtrakool, C., & Kedjarune-Leggat, U. (2011). Effect of acidic
agents on surface roughness of dental ceramics. Dental Research Journal, 8(1),
6-15.
Kunzel, W., Cruz, M. S., & Fischer, T. (2000). Dental erosion in Cuban children
associated with excessive consumption of oranges. European Journal of Oral
Sciences, 108(2), 104-109.
Larsen, M. J. (1990). Chemical events during tooth dissolution. Journal of Dental
Research, 69 Spec No, 575-580; discussion 634-576.
Larsen, M. J., & Richards, A. (2002). Fluoride is unable to reduce dental erosion from
soft drinks. Caries Research, 36(1), 75-80.
Las Casas, E. B., Bastos, F. S., Godoy, G. C. D., & Buono, V. T. L. (2008). Enamel
wear and surface roughness characterization using 3D profilometry. Tribology
International, 41(12), 1232-1236.
Leach, R. (2014). Fundamental Principles of Engineering Nanometrology: Elsevier
Science.
Leao Filho, J. C., Braz, A. K., de Araujo, R. E., Tanaka, O. M., & Pithon, M. M. (2015).
Enamel Quality after Debonding: Evaluation by Optical Coherence
Tomography. Brazilian dental journal, 26(4), 384-389.
Lee, C., Darling, C. L., & Fried, D. (2009). Polarization-sensitive optical coherence
tomographic imaging of artificial demineralization on exposed surfaces of tooth
roots. Dental Materials, 25(6), 721-728.
Lee, C. K., Chi, T. T., Wu, C. T., Tsai, M. T., Chiang, C. P., & Yang, C. C. (2012).
Diagnosis of oral precancer with optical coherence tomography. Biomedical
Optics Express, 3(7), 1632-1646.
Lendenmann, U., Grogan, J., & Oppenheim, F. G. (2000). Saliva and dental pellicle--a
review. Advances in Dental Research, 14, 22-28.
Linkosalo, E., & Markkanen, H. (1985). Dental erosions in relation to lactovegetarian
diet. Scandinavian Journal of Dental Research, 93(5), 436-441.
Lippert, F., & Lynch, R. J. M. (2014). Comparison of Knoop and Vickers surface
microhardness and transverse microradiography for the study of early caries
lesion formation in human and bovine enamel. Archives of Oral Biology, 59(7),
704-710.
Lippert, F., Parker, D. M., & Jandt, K. D. (2004a). In vitro
demineralization/remineralization cycles at human tooth enamel surfaces
investigated by AFM and nanoindentation. Journal of Colloid and Interface
Science, 280(2), 442-448.
Lippert, F., Parker, D. M., & Jandt, K. D. (2004b). Susceptibility of deciduous and
permanent enamel to dietary acid-induced erosion studied with atomic force
microscopy nanoindentation. European Journal of Oral Sciences, 112(1), 61-66.
Univers
ity of
Mala
ya

299
Louie, T., Lee, C., Hsu, D., Hirasuna, K., Manesh, S., Staninec, M., Darling, C. L., &
Fried, D. (2010). Clinical Assessment of Early Tooth Demineralization Using
Polarization Sensitive Optical Coherence Tomography. Lasers in Surgery and
Medicine, 42(10), 738-745.
Luo, Y., Zeng, X. J., Du, M. Q., & Bedi, R. (2005). The prevalence of dental erosion in
preschool children in China. Journal of Dentistry, 33(2), 115-121.
Lussi, A., & Carvalho, T. S. (2014). Erosive tooth wear: A multifactorial condition of
growing concern and increasing knowledge. Monographs in Oral Science, 25, 1-
15.
Lussi, A., & Hellwig, E. (2014). Risk assessment and causal preventive measures.
Monographs in Oral Science, 25, 220-229.
Lussi, A., Hellwig, E., Zero, D., & Jaeggi, T. (2006). Erosive tooth wear: Diagnosis,
risk factors and prevention. American Journal of Dentistry, 19(6), 319-325.
Lussi, A., & Jaeggi, T. (2006). Chemical factors. Monographs in Oral Science, 20, 77-
87.
Lussi, A., & Jaeggi, T. (2008). Erosion--diagnosis and risk factors. Clinical Oral
Investigations, 12 Suppl 1, S5-S13.
Lussi, A., Jaeggi, T., & Zero, D. (2004). The role of diet in the aetiology of dental
erosion. Caries Research, 38 Suppl 1, 34-44.
Lussi, A., Kohler, N., Zero, D., Schaffner, M., & Megert, B. (2000). A comparison of
the erosive potential of different beverages in primary and permanent teeth using
an in vitro model. European Journal of Oral Sciences, 108(2), 110-114.
Lussi, A., Megert, B., Shellis, R. P., & Wang, X. (2012). Analysis of the erosive effect
of different dietary substances and medications. British Journal of Nutrition,
107(2), 252-262.
Lussi, A., & Schaffner, M. (2000). Progression of and risk factors for dental erosion and
wedge-shaped defects over a 6-year period. Caries Research, 34(2), 182-187.
Lussi, A., Schaffner, M., Hotz, P., & Suter, P. (1991). Dental erosion in a population of
Swiss adults. Community Dentistry and Oral Epidemiology, 19(5), 286-290.
Lussi, A., Schlueter, N., Rakhmatullina, E., & Ganss, C. (2011). Dental erosion--an
overview with emphasis on chemical and histopathological aspects. Caries
Research, 45 Suppl 1, 2-12.
Ma, S., Cai, J., Zhan, X., & Wu, Y. (2009). Effects of etchant on the nanostructure of
dentin: An atomic force microscope study. Scanning, 31(1), 28-34.
Mahoney, E., Beattie, J., Swain, M., & Kilpatrick, N. (2003). Preliminary in vitro
assessment of erosive potential using the ultra-micro-indentation system. Caries
Research, 37(3), 218-224.
Univers
ity of
Mala
ya
300
Majkut, P., Sadr, A., Shimada, Y., Sumi, Y., & Tagami, J. (2015). Validation of Optical
Coherence Tomography against Micro-computed Tomography for Evaluation of
Remaining Coronal Dentin Thickness. Journal of Endodontics, 41(8), 1349-
1352.
Management Association, I. R. (2012). Industrial Engineering: Concepts,
Methodologies, Tools, and Applications: Concepts, Methodologies, Tools, and
Applications: Engineering Science Reference.
Manarte, P., Manso, M. C., Souza, D., Frias-Bulhosa, J., & Gago, S. (2009). Dental
erosion in alcoholic patients under addiction rehabilitation therapy. Medicina
Oral Patologia Oral Y Cirugia Bucal, 14(8), e376-383.
Mandurah, M. M., Sadr, A., Shimada, Y., Kitasako, Y., Nakashima, S., Bakhsh, T. A.,
Tagami, J., & Sumi, Y. (2013). Monitoring remineralization of enamel
subsurface lesions by optical coherence tomography. Journal of Biomedical
Optics, 18(4), 046006.
Manesh, S. K., Darling, C. L., & Fried, D. (2009). Nondestructive assessment of dentin
demineralization using polarization-sensitive optical coherence tomography after
exposure to fluoride and laser irradiation. Journal of Biomedical Materials
Research Part B: Applied Biomaterials, 90(2), 802-812.
Mantzourani, M., & Sharma, D. (2013). Dentine sensitivity: Past, present and future.
Journal of Dentistry, 41 Suppl 4, S3-S17.
Margolis, H. C., Zhang, Y. P., Lee, C. Y., Kent, R. L., Jr., & Moreno, E. C. (1999).
Kinetics of enamel demineralization in vitro. Journal of Dental Research, 78(7),
1326-1335.
McLaughlin, M. J., & Sainani, K. L. (2014). Bonferroni, Holm, and Hochberg
corrections: fun names, serious changes to p values. American academy of
Physical Medicine and Rehabilitation, 6(6), 544-546.
Mehler, P. S., & Andersen, A. E. (2017). Eating Disorders: A Guide to Medical Care
and Complications: Johns Hopkins University Press.
Menezes, P. L., Nosonovsky, M., Ingole, S. P., Kailas, S. V., & Lovell, M. R. (2013).
Tribology for Scientists and Engineers: From Basics to Advanced Concepts:
Springer New York.
Mercu, T. V., Popescu, S. M., Scrieciu, M., Amarascu, M. O., Vatu, M., Diaconu, O.
A., Osiac, E., & Ghelase, S. M. (2017). Optical coherence tomography
applications in tooth wear diagnosis. Romanian Journal of Morphology and
Embryology, 58(1), 99-106.
Meurman, J. H., Drysdale, T., & Frank, R. M. (1991). Experimental erosion of dentin.
Scandinavian Journal of Dental Research, 99(6), 457-462.
Meurman, J. H., & Frank, R. M. (1991). Progression and surface ultrastructure of in
vitro caused erosive lesions in human and bovine enamel. Caries Research,
25(2), 81-87.
Univers
ity of
Mala
ya

301
Meurman, J. H., & ten Cate, J. M. (1996). Pathogenesis and modifying factors of dental
erosion. European Journal of Oral Sciences, 104(2 ( Pt 2)), 199-206.
Michael, J. A., Townsend, G. C., Greenwood, L. F., & Kaidonis, J. A. (2009).
Abfraction: Separating fact from fiction. Australian Dental Journal, 54(1), 2-8.
Millward, A., Shaw, L., Smith, A. J., Rippin, J. W., & Harrington, E. (1994). The
distribution and severity of tooth wear and the relationship between erosion and
dietary constituents in a group of children. International Journal of Paediatric
Dentistry, 4(3), 151-157.
Mirkarimi, M., & Toomarian, L. (2012). Effect of green tea extract on the treatment of
dentin erosion: An in vitro study. Journal of Dentistry (Tehran), 9(4), 224-228.
Moazzez, R., & Bartlett, D. (2014). Intrinsic causes of erosion. Monographs in Oral
Science, 25, 180-196.
Moazzez, R., Smith, B. G., & Bartlett, D. W. (2000). Oral pH and drinking habit during
ingestion of a carbonated drink in a group of adolescents with dental erosion.
Journal of Dentistry, 28(6), 395-397.
Moazzez, R. V., Austin, R. S., Rojas-Serrano, M., Carpenter, G., Cotroneo, E., Proctor,
G., Zaidel, L., & Bartlett, D. W. (2014). Comparison of the possible protective
effect of the salivary pellicle of individuals with and without erosion. Caries
Research, 48(1), 57-62.
Mulic, A., Tveit, A. B., Hove, L. H., & Skaare, A. B. (2011). Dental erosive wear
among Norwegian wine tasters. Acta Odontologica Scandinavica, 69(1), 21-26.
Murakami, C., Bönecker, M., Corrêa, M. S. N. P., Mendes, F. M., & Rodrigues, C. R.
M. D. (2009). Effect of fluoride varnish and gel on dental erosion in primary and
permanent teeth. Archives of Oral Biology, 54(11), 997-1001.
Murakami, C., Oliveira, L. B., Sheiham, A., Nahas Pires Correa, M. S., Haddad, A. E.,
& Bonecker, M. (2011). Risk indicators for erosive tooth wear in Brazilian
preschool children. Caries Research, 45(2), 121-129.
Nanci, A., & Cate, A. R. T. (2008). Ten Cate's Oral Histology: Development, Structure,
and Function: Mosby Elsevier.
Nangolo, C., & Musingwini, C. (2011). Empirical correlation of mineral commodity
prices with exchange-traded mining stock prices. Journal of the Southern
African Institute of Mining and Metallurgy, 111(7), 459-468.
Natsume, Y., Nakashima, S., Sadr, A., Shimada, Y., Tagami, J., & Sumi, Y. (2011).
Estimation of lesion progress in artificial root caries by swept source optical
coherence tomography in comparison to transverse microradiography. Journal
of Biomedical Optics, 16(7), 071408.
Nazari, A., Sadr, A., Shimada, Y., Tagami, J., & Sumi, Y. (2013). 3D assessment of
void and gap formation in flowable resin composites using optical coherence
tomography. The journal of adhesive dentistry, 15(3), 237-243.
Univers
ity of
Mala
ya
302
Nee, A., Chan, K., Kang, H., Staninec, M., Darling, C. L., & Fried, D. (2014).
Longitudinal monitoring of demineralization peripheral to orthodontic brackets
using cross polarization optical coherence tomography. Journal of Dentistry,
42(5), 547-555.
Nekrashevych, Y., Hannig, M., & Stosser, L. (2004). Assessment of enamel erosion and
protective effect of salivary pellicle by surface roughness analysis and scanning
electron microscopy. Oral Health & Preventive Dentistry, 2(1), 5-11.
Nekrashevych, Y., & Stosser, L. (2003). Protective influence of experimentally formed
salivary pellicle on enamel erosion. An in vitro study. Caries Research, 37(3),
225-231.
Nersessian, N. J. (2009). How do engineering scientists think? Model-based simulation
in biomedical engineering research laboratories. Topics in cognitive science,
1(4), 730-757.
Ngaotheppitak, P., Darling, C. L., & Fried, D. (2005). Measurement of the severity of
natural smooth surface (interproximal) caries lesions with polarization sensitive
optical coherence tomography. Lasers in Surgery and Medicine, 37(1), 78-88.
Nunn, J. H., Gordon, P. H., Morris, A. J., Pine, C. M., & Walker, A. (2003). Dental
erosion -- changing prevalence? A review of British National childrens' surveys.
International Journal of Paediatric Dentistry, 13(2), 98-105.
Olsen, J., Themstrup, L., De Carvalho, N., Mogensen, M., Pellacani, G., & Jemec, G. B.
(2016). Diagnostic accuracy of optical coherence tomography in actinic
keratosis and basal cell carcinoma. Photodiagnosis and Photodynamic Therapy.
Paepegaey, A. M., Barker, M. L., Bartlett, D. W., Mistry, M., West, N. X., Hellin, N.,
Brown, L. J., & Bellamy, P. G. (2013). Measuring enamel erosion: A
comparative study of contact profilometry, non-contact profilometry and
confocal laser scanning microscopy. Dental Materials, 29(12), 1265-1272.
Park, J. Y., Chung, J. H., Lee, J. S., Kim, H. J., Choi, S. H., & Jung, U. W. (2017).
Comparisons of the diagnostic accuracies of optical coherence tomography,
micro-computed tomography, and histology in periodontal disease: an ex vivo
study. Journal of Periodontal & Implant Science, 47(1), 30-40.
Park, K. J., Schneider, H., & Haak, R. (2013). Assessment of interfacial defects at
composite restorations by swept source optical coherence tomography. Journal
of Biomedical Optics, 18(7), 076018.
Pawlus, P., & Grabon, W. (2008). The method of truncation parameters measurement
from material ratio curve. Precision Engineering-Journal of the International
Societies for Precision Engineering and Nanotechnology, 32(4), 342-347.
Pesun, I. J., Olson, A. K., Hodges, J. S., & Anderson, G. C. (2000). In vivo evaluation
of the surface of posterior resin composite restorations: a pilot study. The
Journal of Prosthetic Dentistry, 84(3), 353-359.
Univers
ity of
Mala
ya

303
Piekarz, C., Ranjitkar, S., Hunt, D., & McIntyre, J. (2008). An in vitro assessment of the
role of Tooth Mousse in preventing wine erosion. Australian Dental Journal,
53(1), 22-25.
Pintado, M. R., Anderson, G. C., DeLong, R., & Douglas, W. H. (1997). Variation in
tooth wear in young adults over a two-year period. The Journal of Prosthetic
Dentistry, 77(3), 313-320.
Pinto, S. C., Batitucci, R. G., Pinheiro, M. C., Zandim, D. L., Spin-Neto, R., &
Sampaio, J. E. (2010). Effect of an acid diet allied to sonic toothbrushing on root
dentin permeability: an in vitro study. Brazilian dental journal, 21(5), 390-395.
Pithon, M. M., Dos Santos, M. J., Andrade, C. S., Leao Filho, J. C., Braz, A. K., de
Araujo, R. E., Tanaka, O. M., Fidalgo, T. K., Dos Santos, A. M., & Maia, L. C.
(2015). Effectiveness of varnish with CPP-ACP in prevention of caries lesions
around orthodontic brackets: an OCT evaluation. European journal of
orthodontics, 37(2), 177-182.
Podoleanu, A. G. (2005). Optical coherence tomography. The British Journal of
Radiology, 78(935), 976-988.
Podoleanu, A. G. (2012). Optical coherence tomography. Journal Of Microscopy,
247(3), 209-219.
Poggio, C., Gulino, C., Mirando, M., Colombo, M., & Pietrocola, G. (2017). Preventive
effects of different protective agents on dentin erosion: An in vitro investigation.
Journal of Clinical and Experimental Dentistry, 9(1), e7-e12.
Poggio, C., Lombardini, M., Vigorelli, P., Colombo, M., & Chiesa, M. (2014). The role
of different toothpastes on preventing dentin erosion: An SEM and AFM
study(R). Scanning, 36(3), 301-310.
Pontefract, H., Hughes, J., Kemp, K., Yates, R., Newcombe, R. G., & Addy, M. (2001).
The erosive effects of some mouthrinses on enamel. A study in situ. Journal of
Clinical Periodontology, 28(4), 319-324.
Prati, C., Montebugnoli, L., Suppa, P., Valdre, G., & Mongiorgi, R. (2003).
Permeability and morphology of dentin after erosion induced by acidic drinks.
Journal of Periodontology, 74(4), 428-436.
Pretty, I. A., Edgar, W. M., & Higham, S. M. (2003). The erosive potential of
commercially available mouthrinses on enamel as measured by Quantitative
Light-induced Fluorescence (QLF). Journal of Dentistry, 31(5), 313-319.
Pretty, I. A., Edgar, W. M., & Higham, S. M. (2004). The validation of quantitative
light-induced fluorescence to quantify acid erosion of human enamel. Archives
of Oral Biology, 49(4), 285-294.
Rakhmatullina, E., Bossen, A., Bachofner, K. K., Meier, C., & Lussi, A. (2013). Optical
pen-size reflectometer for monitoring of early dental erosion in native and
polished enamels. Journal of Biomedical Optics, 18(11), 117009.
Univers
ity of
Mala
ya

304
Rakhmatullina, E., Bossen, A., Hoschele, C., Wang, X., Beyeler, B., Meier, C., & Lussi,
A. (2011). Application of the specular and diffuse reflection analysis for in vitro
diagnostics of dental erosion: correlation with enamel softening, roughness, and
calcium release. Journal of Biomedical Optics, 16(10), 107002.
Rees, J. S. (2000). The prevalence of dentine hypersensitivity in general dental practice
in the UK. Journal of Clinical Periodontology, 27(11), 860-865.
Rios, D., Honorio, H. M., Magalhaes, A. C., Buzalaf, M. A., Palma-Dibb, R. G.,
Machado, M. A., & da Silva, S. M. (2006). Influence of toothbrushing on
enamel softening and abrasive wear of eroded bovine enamel: An in situ study.
Brazilian Oral Research, 20(2), 148-154.
Rîpă, M., Tomescu, L., Hapenciuc, M., & Crudu, I. (2003). Tribological
characterisation of surface topography using Abbott-Firestone curve. ANNALS,
24, 26.
Rodriguez, J. M., Curtis, R. V., & Bartlett, D. W. (2009). Surface roughness of
impression materials and dental stones scanned by non-contacting laser
profilometry. Dental Materials, 25(4), 500-505.
Sales-Peres, S. H., Pessan, J. P., & Buzalaf, M. A. (2007). Effect of an iron mouthrinse
on enamel and dentine erosion subjected or not to abrasion: An in situ/ex vivo
study. Archives of Oral Biology, 52(2), 128-132.
Sarode, G. S., & Sarode, S. C. (2013). Abfraction: A review. Journal of Oral and
Maxillofacial Pathology, 17(2), 222-227.
Scaramucci, T., Hara, A. T., Zero, D. T., Ferreira, S. S., Aoki, I. V., & Sobral, M. A.
(2011). In vitro evaluation of the erosive potential of orange juice modified by
food additives in enamel and dentine. Journal of Dentistry, 39(12), 841-848.
Scheid, R. C., & Weiss, G. (2012). Woelfel's Dental Anatomy: Wolters
Kluwer/Lippincott Williams & Wilkins Health.
Schlueter, N., Ganss, C., De Sanctis, S., & Klimek, J. (2005). Evaluation of a
profilometrical method for monitoring erosive tooth wear. European Journal of
Oral Sciences, 113(6), 505-511.
Schlueter, N., Hara, A., Shellis, R. P., & Ganss, C. (2011). Methods for the
measurement and characterization of erosion in enamel and dentine. Caries
Research, 45 Suppl 1, 13-23.
Schlueter, N., Hardt, M., Klimek, J., & Ganss, C. (2010). Influence of the digestive
enzymes trypsin and pepsin in vitro on the progression of erosion in dentine.
Archives of Oral Biology, 55(4), 294-299.
Schlueter, N., Jaeggi, T., & Lussi, A. (2012). Is dental erosion really a problem?
Advances in Dental Research, 24(2), 68-71.
Serper, A., & Calt, S. (2002). The demineralizing effects of EDTA at different
concentrations and pH. Journal of Endodontics, 28(7), 501-502.
Univers
ity of
Mala
ya

305
Shellis, R. P., & Addy, M. (2014). The interactions between attrition, abrasion and
erosion in tooth wear. Monographs in Oral Science, 25, 32-45.
Shellis, R. P., Ganss, C., Ren, Y., Zero, D. T., & Lussi, A. (2011). Methodology and
models in erosion research: Discussion and conclusions. Caries Research, 45
Suppl 1, 69-77.
Shimada, Y., Nakagawa, H., Sadr, A., Wada, I., Nakajima, M., Nikaido, T., Otsuki, M.,
Tagami, J., & Sumi, Y. (2014). Noninvasive cross-sectional imaging of
proximal caries using swept-source optical coherence tomography (SS-OCT) in
vivo. Journal of Biophotonics, 7(7), 506-513.
Simon, J. C., Kang, H., Staninec, M., Jang, A. T., Chan, K. H., Darling, C. L., Lee, R.
C., & Fried, D. (2017). Near-IR and CP-OCT imaging of suspected occlusal
caries lesions. Lasers in Surgery and Medicine, 49(3), 215-224.
Sirimaharaj, V., Brearley Messer, L., & Morgan, M. V. (2002). Acidic diet and dental
erosion among athletes. Australian Dental Journal, 47(3), 228-236.
Skjorland, K. K., Rykke, M., & Sonju, T. (1995). Rate of pellicle formation in vivo.
Acta Odontologica Scandinavica, 53(6), 358-362.
Smith, B. G., & Knight, J. K. (1984). An index for measuring the wear of teeth. British
Dental Journal, 156(12), 435-438.
Soper, D. S. (2017). Significance of the Difference between Two Correlations
Calculator [Software].
Sowa, M. G., Popescu, D. P., Werner, J., Hewko, M., Ko, A. C., Payette, J., Dong, C.
C., Cleghorn, B., & Choo-Smith, L. P. (2007). Precision of Raman
depolarization and optical attenuation measurements of sound tooth enamel.
Analytical and Bioanalytical Chemistry, 387(5), 1613-1619.
Splieth, C. H., & Tachou, A. (2013). Epidemiology of dentin hypersensitivity. Clinical
Oral Investigations, 17 Suppl 1, S3-8.
Staufenbiel, I., Adam, K., Deac, A., Geurtsen, W., & Gunay, H. (2015). Influence of
fruit consumption and fluoride application on the prevalence of caries and
erosion in vegetarians--a controlled clinical trial. Eur J Clin Nutr, 69(10), 1156-
1160.
Steiner-Oliveira, C., Nobre-dos-Santos, M., Zero, D. T., Eckert, G., & Hara, A. T.
(2010). Effect of a pulsed CO2 laser and fluoride on the prevention of enamel
and dentine erosion. Archives of Oral Biology, 55(2), 127-133.
Sundaram, G., Wilson, R., Watson, T. F., & Bartlett, D. (2007). Clinical measurement
of palatal tooth wear following coating by a resin sealing system. Operative
Dentistry, 32(6), 539-543.
Thomas, R. Z., Ruben, J. L., de Vries, J., ten Bosch, J. J., & Huysmans, M. C. (2006).
Transversal wavelength-independent microradiography, a method for
Univers
ity of
Mala
ya

306
monitoring caries lesions over time, validated with transversal
microradiography. Caries Research, 40(4), 281-291.
Tjaderhane, L., Buzalaf, M. A., Carrilho, M., & Chaussain, C. (2015). Matrix
metalloproteinases and other matrix proteinases in relation to cariology: the era
of 'dentin degradomics'. Caries Research, 49(3), 193-208.
Toledano, M., Osorio, E., Cabello, I., & Osorio, R. (2014). Early dentine
remineralisation: Morpho-mechanical assessment. Journal of Dentistry, 42(4),
384-394.
Tsai, T. H., Lee, H. C., Ahsen, O. O., Liang, K., Giacomelli, M. G., Potsaid, B. M., Tao,
Y. K., Jayaraman, V., Figueiredo, M., Huang, Q., Cable, A. E., Fujimoto, J., &
Mashimo, H. (2014). Ultrahigh speed endoscopic optical coherence tomography
for gastroenterology. Biomedical Optics Express, 5(12), 4387-4404.
van der Veen, M. H., & de Josselin de Jong, E. (2000). Application of quantitative light-
induced fluorescence for assessing early caries lesions. Monographs in Oral
Science, 17, 144-162.
van der Veen, M. H., Tsuda, H., Arends, J., & ten Bosch, J. J. (1996). Evaluation of
sodium fluorescein for quantitative diagnosis of root caries. Journal of Dental
Research, 75(1), 588-593.
Vanuspong, W., Eisenburger, M., & Addy, M. (2002). Cervical tooth wear and
sensitivity: Erosion, softening and rehardening of dentine; effects of pH, time
and ultrasonication. Journal of Clinical Periodontology, 29(4), 351-357.
Venasakulchai, A., Williams, N. A., Gracia, L. H., & Rees, G. D. (2010). A
comparative evaluation of fluoridated and non-fluoridated mouthrinses using a
5-day cycling enamel erosion model. Journal of Dentistry, 38 Suppl 3, S21-29.
Violich, D. R., & Chandler, N. P. (2010). The smear layer in endodontics - a review.
International Endodontic Journal, 43(1), 2-15.
von Braunmuhl, T., Hartmann, D., Tietze, J. K., Cekovic, D., Kunte, C., Ruzicka, T.,
Berking, C., & Sattler, E. C. (2016). Morphologic features of basal cell
carcinoma using the en-face mode in frequency domain optical coherence
tomography. Journal of the European Academy of Dermatology and
Venereology, 30(11), 1919-1925.
Wang, C., Li, Y., Wang, X., Zhang, L., Tiantang, & Fu, B. (2012). The enamel
microstructures of bovine mandibular incisors. The Anatomical Record, 295(10),
1698-1706.
Wang, W., Xie, Q., Xu, T., Wang, Q., Malmstrom, H. S., & Ren, Y. F. (2013). Fluoride
release and anti-erosive effects of dentifrices containing PVM/MA copolymers.
Journal of Dentistry, 41(2), 148-154.
Wang, Z., Maezono, H., Shen, Y., & Haapasalo, M. (2016). Evaluation of Root Canal
Dentin Erosion after Different Irrigation Methods Using Energy-dispersive X-
ray Spectroscopy. Journal of Endodontics.
Univers
ity of
Mala
ya

307
West, N., Seong, J., & Davies, M. (2014). Dentine hypersensitivity. Monographs in
Oral Science, 25, 108-122.
West, N. X., Davies, M., & Amaechi, B. T. (2011). In vitro and in situ erosion models
for evaluating tooth substance loss. Caries Research, 45 Suppl 1, 43-52.
West, N. X., Hughes, J. A., & Addy, M. (2001). The effect of pH on the erosion of
dentine and enamel by dietary acids in vitro. Journal of Oral Rehabilitation,
28(9), 860-864.
West, N. X., Maxwell, A., Hughes, J. A., Parker, D. M., Newcombe, R. G., & Addy, M.
(1998). A method to measure clinical erosion: the effect of orange juice
consumption on erosion of enamel. Journal of Dentistry, 26(4), 329-335.
White, A. J., Yorath, C., ten Hengel, V., Leary, S. D., Huysmans, M. C., & Barbour, M.
E. (2010). Human and bovine enamel erosion under 'single-drink' conditions.
European Journal of Oral Sciences, 118(6), 604-609.
Whitehead, S. A., Lo, L. Y., Watts, D. C., & Wilson, N. H. (1997). Changes of surface
texture of enamel in vivo. Journal of Oral Rehabilitation, 24(6), 449-453.
Whitehouse, D. J. (2010). Handbook of Surface and Nanometrology, Second Edition (2
ed.): CRC Press.
Wichern, C. M., & Rasp, W. (2005). Measuring and quantifying the surface-roughness
anisotropy of modeled and industrially produced surfaces. In M. Geiger, J.
Duflou, H. J. J. Kals, B. Shirvani & U. P. Singh (Eds.), Sheet Metal 2005 (Vol.
6-8, pp. 573-580).
Wiegand, A., & Attin, T. (2011). Design of erosion/abrasion studies--insights and
rational concepts. Caries Research, 45 Suppl 1, 53-59.
Wiegand, A., Bliggenstorfer, S., Magalhaes, A. C., Sener, B., & Attin, T. (2008).
Impact of the in situ formed salivary pellicle on enamel and dentine erosion
induced by different acids. Acta Odontologica Scandinavica, 66(4), 225-230.
Wiegand, A., Kuhn, M., Sener, B., Roos, M., & Attin, T. (2009). Abrasion of eroded
dentin caused by toothpaste slurries of different abrasivity and toothbrushes of
different filament diameter. Journal of Dentistry, 37(6), 480-484.
Wiegand, A., Wegehaupt, F., Werner, C., & Attin, T. (2007). Susceptibility of acid-
softened enamel to mechanical wear--ultrasonication versus toothbrushing
abrasion. Caries Research, 41(1), 56-60.
Wilder-Smith, C. H., Wilder-Smith, P., Kawakami-Wong, H., Voronets, J., Osann, K.,
& Lussi, A. (2009). Quantification of dental erosions in patients with GERD
using optical coherence tomography before and after double-blind, randomized
treatment with esomeprazole or placebo. The American Journal of
Gastroenterology, 104(11), 2788-2795.
Univers
ity of
Mala
ya

308
Yamashita, J. M., Torres, N. M., Moura-Grec, P. G., Marsicano, J. A., Sales-Peres, A.,
& Sales-Peres, S. H. (2013). Role of arginine and fluoride in the prevention of
eroded enamel: An in vitro model. Australian Dental Journal, 58(4), 478-482.
Yang, W., Liu, X., Lu, W., & Guo, X. (2018). Influence of probe dynamic
characteristics on the scanning speed for white light interference based AFM.
Precision Engineering, 51, 348-352.
Yao, Y., Grogan, J., Zehnder, M., Lendenmann, U., Nam, B., Wu, Z., Costello, C. E., &
Oppenheim, F. G. (2001). Compositional analysis of human acquired enamel
pellicle by mass spectrometry. Archives of Oral Biology, 46(4), 293-303.
Yassen, G. H., Platt, J. A., & Hara, A. T. (2011). Bovine teeth as substitute for human
teeth in dental research: A review of literature. Journal of Oral Science, 53(3),
273-282.
Yeh, C. K., Johnson, D. A., Dodds, M. W., Sakai, S., Rugh, J. D., & Hatch, J. P. (2000).
Association of salivary flow rates with maximal bite force. Journal of Dental
Research, 79(8), 1560-1565.
Young, A., & Tenuta, L. M. (2011). Initial erosion models. Caries Research, 45 Suppl
1, 33-42.
Young, A., Thrane, P. S., Saxegaard, E., Jonski, G., & Rolla, G. (2006). Effect of
stannous fluoride toothpaste on erosion-like lesions: An in vivo study. European
Journal of Oral Sciences, 114(3), 180-183.
Zero, D. T., & Lussi, A. (2005). Erosion--chemical and biological factors of importance
to the dental practitioner. International Dental Journal, 55(4 Suppl 1), 285-290.
Zero, D. T., & Lussi, A. (2006). Behavioral factors. Monographs in Oral Science, 20,
100-105.
Zhang, D., Mao, S., Lu, C., Romberg, E., & Arola, D. (2009). Dehydration and the
dynamic dimensional changes within dentin and enamel. Dental Materials,
25(7), 937-945.
Zijp, J. R., & Bosch, J. J. (1993). Theoretical model for the scattering of light by dentin
and comparison with measurements. Applied Optics, 32(4), 411-415.
Univers
ity of
Mala
ya
309
LIST OF PUBLICATIONS AND PAPERS PRESENTED
Habib M., Zakian C.M., H.P. Chew. Longitudinal monitoring of early dentine erosion
with surface roughness, oral presentation at 28th Annual Scientific Meeting,
International Association for Dental Research (IADR) South East Asia and 25th Annual
Scientific Meeting South East Asia Association for dental education, 11th
- 14th
August
2014, IADR-SEA Division (International)
Habib M., Zakian C.M., H.P. Chew. Longitudinal monitoring of early dentine erosion
with bearing curve, oral and poster Presentation at 62nd
Congress of the European
Organisation for Caries Research (ORCA), Brussels Belgium, 2nd
- 5th
July, 2015
(International)
Univers
ity of
Mala
ya

310
Publication submitted to Journal of Applied Optics
Assessing surface characteristics of eroded dentine with optical
coherence tomography: a preliminary in vitro validation study
KUAN MING LEE,1,† MADIHA HABIB,2,† YIH MIIN LIEW,3,* CHRISTIAN ZAKIAN,4
NGIE MIN UNG,5 HOOI PIN CHEW2, 6,*
1 Department of Biomedical Imaging, Faculty of Medicine, University of Malaya, Kuala Lumpur 50603,
Malaysia 2 Department of Restorative Dentistry, Faculty of Dentistry, University of Malaya, Kuala Lumpur 50603,
Malaysia
3 Department of Biomedical Engineering, Faculty of Engineering, University of Malaya, Kuala Lumpur
50603, Malaysia
4 R&D Department, Kevork Instruments, S.A. de C.V., 66450, San Nicolás de los Garza, N.L.Mexico
5 Clinical Oncology Unit, Faculty of Medicine, University of Malaya, Kuala Lumpur 50603, Malaysia
6 Minnesota Dental Research Center for Biomaterials and Biomechanics, University of Minnesota,
Minneapolis 55435, US
*Corresponding author: [email protected] and [email protected]
†Both authors contributed equally to this manuscript.
Received XX Month XXXX; revised XX Month, XXXX; accepted XX Month XXXX; posted XX Month XXXX (Doc. ID XXXXX); published XX Month XXXX
We conducted the first pilot study to investigate using attenuation coefficient from OCT
backscattered signal as a measure of surface roughness changes in eroded dentine. Ten human
premolar root samples were subject to citric acid treatment before scanning by OCT. The extracted
relative attenuation coefficient (μR) from backscattered OCT signal was shown to increase with the
duration of acid challenge. Validated against roughness measurements (rSa) from scanning electron
microscopy (SEM) scans, μR is significantly correlated with rSa indicative of severity of erosion (p
< 0.01, r = 0.9195). We conclude that OCT attenuation coefficient of the immediate sub-surface in
eroded dentine can be a surrogate measure for its surface roughness, of which has been shown to be
able distinguish erosion from other wear processes. © 2015 Optical Society of America
Univers
ity of
Mala
ya





























