Embed Size (px)
Citation preview
CWM TAF UNIVERSITY HEALTH BOARD
AUDIT COMMITTEE MEETING
9 July 2018
A meeting of the Audit Committee will be held on Monday 9 July 2018, at
Ynysmeurig House, Navigation Park, Abercynon commencing at 9.00am.
DR CHRIS TURNER CHAIRMAN
PART ONE – CWM TAF UHB
AGENDA LEAD / ATTACHED
PART 1. PRELIMINARY MATTERS
1.1 Apologies for Absence
Chair/Oral
1.2 Welcome and Introductions
Chair/Oral
1.3 Declarations of Interest
Chair/Oral
1.4
Unconfirmed Minutes of the Audit Committee meeting
held on: 16 April 2018
8 May 2018 31 May 2018
Chair
Attachment
1.5 Action Log
Chair
Attachment
1.6 Matters arising not contained within the Action Log
Chair/Oral
PART 2. INTERNAL CONTROL AND RISK MANAGEMENT
2.1 Procurements and Scheme of Delegation Report
Director of Finance
Attachment
2.2 Audit Recommendations Tracker
Director of Governance /
Board Secretary
Attachment
2.3
Losses and Special Payments Report
Director of Finance
Attachment
2.4 Standards of Behaviour Report
Director of Governance /
Board Secretary
Attachment
1 Agenda - 9 July 2018
1 of 380Audit Committee - Part 1 9 July 2018-09/07/18
2.5 Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
Medical Director
Attachment
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the
Committee Terms of Reference)
Director of Governance /
Board Secretary
Attachment
PART 3. CHARITABLE FUNDS
3.1 Charitable Fund Balances as at 31 May 2018 Director of Finance
Attachment
PART 4. INTERNAL AUDIT Internal Audit
& Assurance
4.1 Internal Audit Progress Report Attachment
4.2 Directorate Review – ACT – Management Arrangements
Attachment
4.3 Directorate Review – ACT - Compliance Attachment
4.4 Health & Care Standards Attachment
4.5 Environmental Sustainability Reporting Attachment
4.6 Annual Quality Statement Attachment
4.7 JAG Accreditation – Follow Up Attachment
PART 5. EXTERNAL AUDIT
5.1 Wales Audit Office update Report Wales Audit Office
Attachment
5.2 Picture of Primary Care in Wales – National Report –
For Information Only
Wales Audit Office
Attachment
PART 6. ITEMS FOR INFORMATION
6.1
Committee Forward Work Plan 2018/19 Chair
Attachment
PART 7. ANY OTHER URGENT BUSINESS
7.1 Items for referral to other Committees
Oral/Chair
7.2 Close of Part 1 of the meeting – Date and time of
next meeting.
09.00am Monday 9 October 2018
Oral/Chair
In accordance with the provision of Section 1(2) of the Public Bodies (Admissions to Meetings) Act 1960 it has been resolved that representatives of the press and other members of the public are
excluded from the second part of the meeting on the grounds that it would be prejudicial to the public interest due to the confidential nature of the business transacted. This section of the meeting
is to be held in private session.
1 Agenda - 9 July 2018
2 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 1 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
CWM TAF UNIVERSITY HEALTH BOARD
‘UNCONFIRMED’ MINUTES OF THE MEETING OF THE AUDIT
COMMITTEE HELD ON 16 APRIL 2018, AT YNYSMEURIG HOUSE, ABERCYNON
PRESENT
Dr C Turner - Independent Member (Chair)
Mr P Griffiths - Independent Member Mrs M K Thomas - Independent Member (Vice Chair)
Mrs J Sadgrove - Independent Member
IN ATTENDANCE
Mr R Williams - Board Secretary / Director of
Corporate Services & Governance Mr H Evans - Head of Corporate Finance
Mr C Greenstock - Counter Fraud Manager, Cardiff & Vale Mr D Jones - Local Counter Fraud Specialist
Mr D Thomas - Wales Audit Office Mr G Lucey - Wales Audit Office
Mr S Webster - Director of Finance Mr P Dalton - Head of Internal Audit & Assurance
NHS Wales Shared Services Partnership (NWSSP) (in part)
Ms E Samways - Deputy Head of Internal Audit & Assurance NWSSP
Professor M Longley - UHB Chair (observing) Mr J Palmer - ‘Interim’ Chief Operating Officer
(in part)
Ms R Treharne - Deputy Chief Executive/Director of Planning & Performance (in part)
Mrs J Davies - Director of Workforce & Organisational Development (in part)
Mr S Lavender - NHS Wales Shared Services Partnership (NWSSP) – All Wales Post
Payment Verification Manager (In part) Ms S Jeremiah - NHS Wales Shared Services
Partnership (NWSSP) – Post Payment Verification Location Manager (In part)
Ms J Maunder - NHS Wales Shared Services Partnership (NWSSP) - Head of
Corporate Services (observing) Ms Z Ponting - Finance Trainee (Observing)
Miss E Walters - Committee Secretariat
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
1 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 2 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
AC/18/019 WELCOME AND INTRODUCTIONS
Dr C Turner, Chair, welcomed everyone to the meeting, particularly
Mr S Webster who had recently returned to Cwm Taf Health Board as Executive Director of Finance, Mr C Greenstock, LCFS Manager,
Cardiff & Vale UHB, who was in attendance to support the presentation of an update update on Local Counter Fraud issues and
Ms Z Ponting, Finance Trainee who was attending the meeting as an observer.
AC/18/020 APOLOGIES FOR ABSENCE
Apologies for absence had been received from Mrs S Utley, Wales
Audit Office.
AC/18/021 DECLARATIONS OF INTERESTS
Mrs J Dowden reinforced her previously declared interest, as a senior officer employee of Cardiff University in relation to the report being
considered by the Committee on the Research & Development Finance Policy.
AC/18/022 ‘UNCONFIRMED’ MINUTES OF THE AUDIT COMMITTEE MEETING HELD ON 15 JANUARY 2018.
The minutes of the meeting held on 15 January 2018, were
CONFIRMED as a true and accurate record.
AC/18/023 AUDIT COMMITTEE ACTION LOG
The Committee Action Log from the 15 January 2018 meeting was
reviewed by Members and the following was NOTED:
17/042 – Mr R Williams advised that work continued to be undertaken in relation to refinement of the Audit Recommendations
tracker and consideration had been given to including the original management response in the tracker (action log updated). Mr P
Griffiths advised that if too much information was included in the tracker, there may be a danger of losing track of what Directorates
said they would originally take forward and suggested that a balance was needed.
17/107 – Members NOTED that Follow up Outpatients Not Booked
(FUNB) remained under close scrutiny at the Quality, Safety & Risk Committee as well as Finance, Performance & Workforce Committee.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
2 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 3 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members NOTED that the Quality, Safety & Risk Committee
remained concerned in relation to whether any clinical harm was being caused by those patients who had experienced long waits and
had requested a further follow up report at the May meeting from the Chief Operating Officer. Members NOTED that the Wales Audit Office
would be developing an All Wales follow up report on Follow Ups Not Booked (FUNB) which would also include a focus on the related
clinical risks.
18/006 – Members NOTED that an internal review had been undertaken by Mr R Williams, Mr M Thomas and Mrs J Davies on the
related impacts of the Auditor General for Wales Public Interest Report. Members NOTED that the key action identified from the
review was linked primarily to the All Wales procurement approach in relation to Single Quotation Tenders (SQT). Mr R Williams advised
that the Director of Finance currently has to authorise a SQT prior to
submission to the Chief Executive. Mr R Williams advised that the changes being proposed by Procurement colleagues would need to be
reflected in the appropriate Health Board Financial Control Procedures.
18/012 – Members NOTED that an update on Clinical Audit was
scheduled to be presented to the May meeting of the Quality, Safety & Risk Committee and that work was being undertaken to align the
requirements within a refreshed Clinical Audit & Effectiveness Plan. Members NOTED that the Internal Audit review report would also be
submitted to the May Committee meeting to enable a related discussion to be held. Dr C Turner suggested that this matter remain
on the Audit Committee action log. Mrs M Thomas advised that discussions were also being held at the Quality Steering Group and
suggested that an update be provided at the next meeting (action
log updated).
Members RECEIVED and NOTED the Action Log.
AC/18/024 MATTERS ARISING
Page 7, 18/010 Charitable Funds Balances – Mr H Evans advised that in relation to the general purpose fund, some spend had now
been made against the fund. Mr H Evans advised that the fund needed to be used appropriately and all fund holders were being
encouraged to spend against the fund, which was specific to Prince Charles Hospital, which restricted how the fund could be used.
Dr C Turner expressed the importance of having a plan in place on how to spend against the fund in future and questioned whether a
reminder could be given to appropriate staff at Prince Charles
Hospital that this fund was in existence.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
3 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 4 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Mr S Webster questioned whether the fund had any alignment with
the extensive capital programme being progressed at Prince Charles Hospital.
Page 8, 18/012 Internal Audit & Assurance Reports – Mrs M
Thomas advised that the Internal Audit Review report in relation to JAG Accreditation – Endoscopy would be presented to the May
Quality, Safety & Risk Committee where the position, in relation to improvement actions, would be monitored.
PART 2. INTERNAL CONTROL AND RISK MANAGEMENT
AC/18/025 Scheme of Delegation
Mr H Evans presented the report which provided an update on the transactions approved as ‘exceptions’ within the Scheme of
Delegation for the period 1.12.17 to 28.2.18. The report also
provided an update on the work undertaken to improve Purchase to Pay processes and performance and highlighted other matters of
interest in relation to the application of financial control procedures and scheme of delegation.
Members NOTED that there were no engagements or contracts
entered into during the period, with 3 Single Tender Actions (STA) received for the period reported on. Members NOTED that additional
information was now being included in the report, to assist the Committee in understanding the context for each single tender
action.
A discussion was held in relation to SQT950, which related to the supply and fitting of light emitting diode (LED) lights at various sites
across the Health Board. Members NOTED that the scheme was
prioritised, as there were significant revenue savings associated with the scheme and that as it was too late to undertake a competitive
tender process, the Chief Executive agreed (on receipt of relevant advice from officers) to approve the STA on the basis that the Health
Board had previously used the company awarded with the contract. Dr C Turner advised that in relation to this particular matter, he had
been consulted by Mr M Thomas prior to the submission of the STA, where it was agreed that this was the best way forward and could be
seen as an invest to save opportunity.
Mr P Griffiths highlighted that there appeared to be an issue on an annual basis where there was a significant amount of non-recurring
money that needed to be spent in the latter end of the year and questioned whether any further forward planning could be
undertaken in relation to the tender process.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
4 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 5 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members AGREED to the principle of forward planning, if there was
previous procurement evidence available, and AGREED that the Committee wished to continue to receive the information and related
context behind each Single Tender Action (STA).
Members NOTED that there had been one contract requiring Ministerial approval during the reporting period.
Members NOTED that, following the request made at the January
meeting, procurement had provided an update in relation to maintenance contracts and the approach taken. Members NOTED
the process outlined within the report and advised that they were satisfied with the approach (action log updated).
Members NOTED that in relation to Purchase to Pay (P2P) draft
figures produced showed that the Health Board achieved the 95%
target for 2017/18 for the payment of non NHS invoices within 30 days. The accumulated position for the year was 95.3% compared
to a performance of 89.4% in 2016/17. Members NOTED that national work was being undertaken to introduce a No Purchase Order
(PO) No Pay Policy and that the Policy was being presented to the April Executive Board for approval prior to implementation.
Members NOTED that P2P performance would continue to be
monitored closely by the Finance, Performance & Workforce Committee and Dr C Turner advised that he would be happy for the
Audit Committee to continue to receive regular updates. Members NOTED that the Health Board compared well against other Health
Boards in relation to P2P performance and welcomed the positive improvement actions taken.
Members NOTED that the draft Financial Control Procedure (FCP) in relation to Medical Variable Pay was currently being reviewed by Mr
M Thomas and Mrs J Davies and it was NOTED that the final version would be presented to the May meeting of the Audit Committee
(added to the action log).
A discussion was held in relation to the Financial Control Procedure (FCP) for Private Patients. Members NOTED that at present the
Health Board invoiced patients directly for their hospital stay. Mr H Evans advised that a request had been received from a Consultant
Surgeon advising that he wished to be invoiced directly for the hospital costs so that he can present the patient with one invoice.
Members NOTED that even though this was outside of the current procedure it was being seen as less of a risk. Endorsement was now
being sought from the Committee to undertake a pilot of this
proposal.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
5 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 6 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Following discussion, Members suggested that consideration would
need to be given to putting a legal agreement in place and it was NOTED that this would need to be closely monitored through the
Debtors process. It was also suggested that a review was undertaken as to whether this had been undertaken at other Health Boards and
if so whether any learning could be adopted. Members AGREED to support the pilot project and looked forward to receiving progress
reports.
A discussion was held in relation to the FCP for Cash Management. Mr H Evans informed Committee that an error occurred on the last
working day of the year (Thursday 29 March 2018) in relation to the transfer of funds between Cwm Taf and WHSSC accounts, which did
not take place in time and resulted in the Cwm Taf accounts being overdrawn by £341k over the Easter weekend. Members NOTED
that this meant that the Health Board was in breach of the FCP and
that the Royal Bank of Scotland had contacted the Health Board, and whilst not concerned, they were required under relevant guidance to
inform HM Treasury. The Health Board had informed Welsh Government of the breach and provided assurance that year end
checklists were robust. Mr H Evans advised that consideration was now being given to setting up a BACS transfer as opposed to a manual
transfer, that would mitigate the potential for any similar occurrence. Members NOTED that the human error occurred as a result of extra
activity being undertaken and the area was overlooked on the day but detected the next working day (which followed a Bank Holiday
weekend period). Members NOTED that the Health Board received no financial penalty as the error was corrected on the first working
day.
Mr G Lucey, Wales Audit Office confirmed that this error would have
no implications on the end of year accounts and that even though the balance would be shown as overdrawn, a footnote would be included
in the report containing an explanation as to why the error occurred.
Mr H Evans provided Members with an update in relation to Continuing Healthcare (CHC) financial limits. Members NOTED that
as a result of the increasing costs of packages, with the most basic of packages now exceeding £30k, a review of limits needed to be
undertaken. Members NOTED that a discussion had been held with the Chief Executive on the proposal to increase the authorisation limit
to £45k. A discussion was held as to whether Members would be happy to accept the increase in limits to £45k. Mrs M Thomas advised
that she would be happy to accept an increase, as long as related controls procedures and monitoring remained in place.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
6 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 7 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Mrs J Sadgrove advised that she would have wished to have been
asked to consider a definitive proposal and would feel more comfortable with a proposition of a limit of no more than £45k.
Dr C Turner requested that an outcome of the discussions held with
the Chief Executive was confirmed at the next scheduled routine meeting of the Audit Committee meeting (added to the action log).
Members RECEIVED an update report which contained feedback on
the Single Tender Action for the Director of Finance vacancy – consultancy support. Following discussion, Members AGREED that
they were satisfied with the feedback and the outcomes contained within the report and NOTED the further work to be undertaken. Mr
R Williams AGREED to share the handover note developed by Mr S Wombwell with the Auditors (added to the action log).
Members RESOLVED to:
NOTE the transactions approved by exception within the Scheme of Delegation, for the period 1.12.17 to 28.2.18
NOTE the update regarding Purchase to Pay and that updates would continue to be received by the Audit
Committee; NOTE the development of a new Financial Control Procedure
(FCP) for Medical Variable Pay and AGREE to receive for approval at the May meeting;
ENDORSE the proposal to pilot an alternative method of invoicing for private patients that is outside of the current
FCP, subject to the safeguards discussed; NOTE the FCP breach on cash management arrangements
and the related corrective action proposed to mitigate any
recurrence; APPROVE that the Chief Executive and Director of Finance
have authority to implement appropriate new financial limits for authorising individual CHC placements and packages, up
to £45k for the Chair of the CHC panel; NOTE the report on feedback on the Single Tender Action
Director of Finance Vacancy – Consultancy support.
AC/18/027 RESEARCH & DEVELOPMENT FINANCE POLICY
Members NOTED Mrs J Sadgrove’s declared interest.
Mr S Webster presented Members with the report, which outlined the Welsh Government requirement for the Health Board to have a
Research & Development Finance policy and made reference to the
summary of the policy content and recommended its adoption.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
7 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 8 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members NOTED that the report identified the robust processes and
objectives that were currently in place.
Mrs M Thomas highlighted the importance of ensuring an Equality Impact Assessment was in place alongside the policy (added to the
action log).
Members RESOLVED to:
APPROVE the Research & Development Finance Policy.
AC/18/028 AUDIT RECOMMENDATIONS TRACKER
Mrs J Davies was in attendance for part of this item.
Mr R Williams presented the tracker report, which provided the
Committee with an updated on reported progress with implementation of Audit report recommendations.
Mr R Williams made Members aware of an error contained within the
report and advised that there were 16 internal audit recommendations outstanding as opposed to 14 identified within the report. Members
NOTED that 9 recommendations were overdue their original date for implementation, 6 of which related to the Occupational Health &
Wellbeing.
Mrs J Davies provided Members with an update in relation to the review undertaken into Occupational Health & Wellbeing and advised
that since the audit had been undertaken there had been a number of changes made within the department. Members NOTED that there
had been a significant turnover of staff within the department and a
separate review had been undertaken on staffing models. Mrs J Davies advised that since the audit, a new muscular skeletal (MSK)
model had been introduced with direct referrals being made into Physiotherapy. A Psychologist had also been appointed into the
service. Members NOTED that the majority of recommendations made were in relation to policies and protocols. Members NOTED
that there had been a significant increase in activity going into the department and there had also been some difficult operational issues
which had resulted in occupational health having to be provided to staff at short notice. Members NOTED that there had also been some
governance issues experienced within the department.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
8 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 9 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Dr C Turner advised that he recognised the pressures within the
system and questioned the likely timescales for improvement. Mrs J Davies advised that some of the systems and policies would be
implemented within the next month and that it was anticipated that the Service Level Agreement (SLA) would be finalised with ABMU
within the next two weeks.
Members NOTED that COHORT were also working with the Health Board to address the issues being experienced with pre-employment
screening. Dr C Turner suggested that a further update on progress was presented to the Audit Committee at the July meeting (added to
the action log).
Mrs J Davies advised that there had been a backlog of DATIX incidents which had all been cleared and the Health Board had achieved
Platinum and Gold Corporate Health Standard.
A discussion was held in relation to the timescales highlighted within
the tracker and it was suggested that moving forward, revised anticipated timescales need to be identified for recommendations that
have lapsed (added to the action log).
Mrs J Davies provided Members with an update in relation to the Health Board wide work being undertaken on the management of
Time off In Lieu (TOIL). Members NOTED that a holistic piece of work was being undertaken on TOIL and staff working additional hours.
Some temporary solutions had been agreed and put into place and work was being undertaken with Finance in relation to introducing
Financial Control Procedures in relation to TOIL. Dr C Turner thanked Mrs Davies for the update and advised that the Committee would
continue to monitor the position (added to the action log).
Mrs J Davies left the meeting at 10.37pm.
In relation to the outstanding Wales Audit Office recommendations,
Members NOTED that a plan was in place for scrutiny of the Outpatient Follow Ups Not Booked position to be undertaken by the
Finance, Performance & Workforce Committee and the Quality, Safety & Risk Committee.
A discussion was held in relation to the update received in relation to
CAMHS Data Quality. Mr R Williams advised that a discussion had been held with Mr A Lawrie who advised that the recommendation had
been delivered, even though the update did not appear to align with the recommendation and there now appeared to be issues in relation
to accommodation.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
9 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 10 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Mrs M Thomas advised that the Choice and Partnership Approach
(CAPA) model (performance) was being closely monitored by the Finance, Performance and Workforce Committee and Together for
Mental Health Partnership Board, clarification would be required in relation to the recommendation and response.
Mr P Griffiths questioned whether the Executive Team were regularly
being provided with the Audit Tracker for review. Mr R Williams advised that they do not receive the tracker unless they are being
asked for updates. Members NOTED that if there were issues in relation to any updates received the Executive would receive the
tracker by exception. Members NOTED that the position was improving and that the backlog of outstanding actions had reduced.
Mr P Dalton advised that Internal Audit were undertaking a review of some of the recommendations which had been closed throughout the
year.
Members RESOLVED to:
NOTE the report; ENDORSE the actions in place to monitor progress with all
outstanding Audit recommendations.
AC/18/029 POST PAYMENT VERIFICATION YEAR END REPORT
Mr S Lavender presented the report and advised Members that he had
now taken up post of All Wales Manager. Mr Lavender introduced his colleague, Ms S Jeremiah, who was now the Post Payment Verification
Manager for the Pontypool area.
Members NOTED that the aim of the report was to summarise the work undertaken by the Post Payment Verification (PPV) department
in accordance to the Welsh Government (WG) directions in respect of
General Medical Services (GMS), General Ophthalmic Services (GOS) and General Pharmaceutical Services (GPS).
Members NOTED that in relation to GMS, a successful training event
for GMS Practice Managers had been held which had a positive impact on the percentage of recoveries, which was reducing. Members
NOTED the programme was launched across Wales in October with a 63% uptake and that more engagement was being undertaken with
practices by telephone and email. Members NOTED that a request had been received from one Practice Manager for some 1-1 training
to be provided. Members NOTED that work was being undertaken to introduce a standard approach across Wales in relation to GOS3
claims being submitted by GOS contractors.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
10 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 11 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members NOTED that it had been identified that admin errors were
quite high and work was being undertaken to improve the position, recognising that it may take 1 or 2 cycles before an improvement was
seen.
Dr C Turner welcomed the report which was reasonably positive and advised that error rates were generally manageable. Dr Turner
advised that he was assured with the progress being made and that the Team were focussed on being proactive.
Mr P Griffiths questioned how Cwm Taf compared to the rest of Wales
in relation to error rates. Mr Lavender advised that, whilst all Wales comparators were available, he did not consider Cwm Taf UHB to be
an outlier on any of the reported performance indicators.
Mr P Griffiths made reference to the revisits undertaken to 2 opticians
and advised that both opticians were responsible for the highest error rates, even after the revisit had been undertaken. Mr S Lavender
explained the process which raise the error rate, support corrective action and that the practice would be given one year to show an
improvement and then a further two years to improve on their year of claims.
Mr S Webster advised that it would be helpful if a comparable picture
could be included in future reports. Members NOTED that permission would need to be received from other Health Board areas for their
data to be included (added to the action log).
A discussion was held in relation to GMS revisits and Mr S Webster sought clarity as to whether the practices who had error rates of over
10% had been revisited. Mr S Lavender advised that one practice
would have had an extended visit and the other practice with an error rate of 11.44% would trigger a revisit in a year’s time. Members
AGREED that it would be helpful if future reports could identify the difference between error rates two years prior and one year post the
revisits (added to the action log).
Members RESOLVED to: NOTE the report;
NOTE that the report would be refined further to include information on benchmarking and further detail on revisits.
Mr S Lavender and Ms S Jeremiah left the meeting at 11.00am.
AC/18/030 GENERAL DENTAL SERVICES CONTRACT MONITORING
Members RECEIVED and NOTED the report.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
11 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 12 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
AC/18/031 LOSSES AND SPECIAL PAYMENTS 01.12.17 – 28.02.18
Mr H Evans presented the report which provided the Committee with
an update on the losses and special payments made by UHB for the period 1 December 2017 to 28 February 2018, as required in Standing
Financial Instructions.
Members NOTED that there had been a substantial increase in medical negligence claims costs which related to one high value case.
Members NOTED that the number of live cases had increased substantially over the last few years and an exercise would be carried
out by Shared Services to try and close some cases which were still open.
Members NOTED that the net claim expenditure for the year was
£1.6m, which was higher than last year but similar to the two
previous years. Members NOTED that there had been a change in the Personal Injury discount rate which had been reflected in the
monthly costs.
Mr S Webster questioned whether a review was being undertaken on the areas of spend that had previously seen a downward trend but
were now increasing. Mr R Williams advised that the Concerns Panel had been re-established and discussions would be held on the areas
of concern. Members NOTED the intention to also re-establish the Claims Scrutiny Panel where close monitoring would be undertaken.
Mr R Williams AGREED to discuss the concerns raised with Mrs L Williams who was lead officer for both areas and would also ensure
that Mr J Hehir, Chair of both groups was made aware of the issues raised.
Members RESOLVED to: NOTE the report;
NOTE that a discussion would be held with Mrs L Williams to request that scrutiny of the Medical Negligence and Personal
Injury Claims, including costs, was undertaken by the Concerns Scrutiny and Claims Scrutiny Panel.
AC/18/032 CWM TAF UHB ‘DRAFT’ ACCOUNTABILITY REPORT 2017-2018
Mr R Williams presented the report, which Members NOTED was a
developing draft. Mr R Williams advised that a further discussion would be held with the Chief Executive in regards to the content of
the report, which would be circulated for comment. Members NOTED that the final draft would be presented to the Audit Committee
scheduled for the 8 May 2018.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
12 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 13 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members RESOLVED to:
NOTE the developing ‘draft’ accountability report for 2017/18.
AC/18/033 REVIEW AND UPDATE OF UHB STANDING ORDERS
Mr R Williams presented the report which provided Members with an update on the review of the Cwm Taf UHB’s standing orders and was
seeking approval from the Committee on the proposed changes. Mr Williams extended his thanks to Ms J Maunder for the work
undertaken in developing the report.
Members NOTED the summary of key changes contained within Appendix 1, which included:
Grammatical changes; The change in title of the Health Minister to Cabinet Secretary;
Reference made to the de-coupling of the Emergency
Ambulance Services Committee (EASC) and Welsh Health Specialised Services Committee (WHSSC) Governance
Framework; Reference made to the amalgamation of Corporate Risk
Committee and Quality & Safety Committee; Reference made to the interim change to Continuing Healthcare
authorisation levels, which would need to be reflected in the Scheme of Delegation.
Members NOTED that updated Terms of Reference for Committee meetings had been included, with the exception of Remuneration &
Terms of Service (RATS) Committee. Members NOTED that these would be updated and presented to the next RATS Committee
meeting.
Mrs M Thomas highlighted a point of accuracy in relation to Schedule
8 and advised that she was Chair of the Mental Health Act Monitoring Committee and not Mr M Jehu.
Members RESOLVED to:
NOTE the amendments to the Board’s Standing Orders; ENDORSE the updated Standing Orders and supporting
Schedules and the changes to the Schedule of additional delegations linked to the Standing Financial Instructions (SFIs),
for APPROVAL by the Board.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
13 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 14 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
PART 4. INTERNAL AUDIT
AC/18/034 INTERNAL AUDIT PROGRESS REPORT
Mr P Dalton, Head of Internal Audit & Assurance, presented the
Internal Audit & Assurance progress report. Since January 2018, Members NOTED that the following 6 reports had been finalised:
Performance Management, Monitoring & Reporting Limited
Governance arrangements for hosted bodies Reasonable
Risk Management Reasonable
IT Strategy Reasonable
Core Financial Systems Substantial
Scheme of Delegation Reasonable
Members NOTED that the report on Fire Safety had now been issued
and had been given a reasonable assurance rating. Members NOTED that the fieldwork in relation to Major Capital had now been
completed.
Members RESOLVED to:
NOTE the report.
AC/18/035 INTERNAL AUDIT & ASSURANCE AUDIT REPORTS
Performance Management, Monitoring & Reporting – Limited
Assurance
Ms R Treharne & Mr J Palmer were in attendance for this item.
Mr P Dalton presented the report and advised that the focus of the review was placed on Demand & Capacity reporting, particularly
within the Surgery & Therapies Directorates. The review had been given a limited assurance rating but it had been noted that the
approach to Demand & Capacity planning was developing and evolving. Members NOTED that an Assistant Director for Performance
& Information had recently been appointed which should improve the position. Ms R Treharne advised that Demand & Capacity planning
falls between Performance & Information and Operational Management.
Members NOTED that enhanced planning support and focus had been placed on demand & capacity planning over the last 4-5 years, with
yearly trajectories set which were being monitored by the Finance, Performance & Workforce Committee.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
14 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 15 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members NOTED that skilled staff were now in place to support the
process, with the most experienced staff being targeted to provide support in the most challenging areas. Ms R Treharne advised that
steps had been taken to improve monitoring processes.
A discussion was held in relation to the main areas of concern highlighted in the report. Members NOTED that monitoring of
Demand & Capacity Plans would now be undertaken at Clinical Business meetings and that Mr V Singh, Assistant Medical Director
had agreed to provide a clinical leadership role on demand & capacity planning. Mr J Palmer suggested that consideration would also need
to be given to including the Demand & Capacity planning activity being undertaken in the portfolio of the Director of Primary,
Community & Mental Health Services, in the follow up review moving forward.
Dr C Turner recognised the acceptance being given to the limited assurance rating and that a number of actions had been put into place
to improve the position, but questioned what likely improvement would have been made when the follow up review was undertaken.
Ms R Treharne advised that the position would vary by Directorate with some areas being more of a concern than others but there was
confidence that the position would improve moving forward.
Mrs M Thomas sought clarification on objective 4 outlined on page 9 of the report and questioned what outcome the auditors would be
expecting against the objective. Mr P Dalton advised that Internal Audit would require more evidence that Demand & Capacity planning
was being monitored through the Clinical Business meeting process.
Mr P Griffiths advised that the report was disappointing and
questioned whether focus on improvement was being placed across all specialities as opposed to Surgery & Therapies, which were the
focus of the review. Ms R Treharne advised that the report felt balanced enough to read across to all specialty areas and it had been
requested that a focus on Demand & Capacity planning is reviewed as part of all Directorate Reviews moving forward.
Members RESOLVED to:
NOTE the report
ACCEPT that the report was limited assurance; ADVISE the Board that the Committee had been provided with
assurance from Mr J Palmer and Ms R Treharne that the position should improve by the next follow up review.
Ms R Treharne left the meeting at 11.50am.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
15 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 16 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
IT Systems Strategy Review – Reasonable Assurance
Mr P Dalton presented the report, which was a review undertaken by
the IT specialist team. Members NOTED that the review focussed on the IT strategy and how it aligned with the IMTP and a reasonable
assurance rating had been given. Members NOTED that there had been two key findings from the review, one being a small portion of
strategy allocation had been deemed as protected and the other being the way costs and benefits had been presented within the appendices.
A discussion was held in relation to the capacity available to deliver
the strategy. Mr J Palmer advised that an action plan had been developed which had been taking risk levels into consideration and an
Assistant Director had been appointed which showed that progress was being made.
Members NOTED that there was no ring-fence available against the £17m and the strategy and the fundamental resource risk would need
to be considered as part of the Health Board’s overall prioritisation process.
Dr C Turner recognised that a significant amount of time had been
taken to develop the strategy and that there were concerns in relation to funding and resourcing. Dr C Turner advised that moving forward,
assurance would be required in relation to ensuring that priorities could be delivered when they were identified. Mr J Palmer advised
that the recent appointment of the Assistant Director would strengthen the Health Board’s capability in this.
Mr S Webster advised that significant investment would be required
in relation to digital technology and advised that costs and benefits
needed to be strongly identified within any Business Cases coming forward. It was also considered important that any opportunities to
align the digital technology agenda with the transformation agenda would be key.
Members RESOLVED to:
NOTE the report.
Welsh Ambulance Services Trust Report; Handover of Care at Emergency Departments – Limited Assurance
Mr R Williams advised that the report had been referred by the Chair
of the Welsh Ambulance Services Trust (WAST) Audit Committee, to
all Audit Committees in NHS Wales and was being presented for information and noting.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
16 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 17 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members NOTED that the report had not yet been shared with the
Emergency Ambulance Services Committee and the related process was questioned. Members NOTED that mixed feedback had been
received from Health Board Chief Operating Officers in relation to developing the related management response.
Mr J Palmer advised that this was a priority area for the Health Board
and that there was significant commitment in place to maintain handover performance. Members NOTED that all breaches of the 15
minute handover target were reviewed fully. Members NOTED that the Health Board had been approached by colleagues within other
Health Board areas to share examples of best practice.
Mrs J Sadgrove questioned whether the Health Board had any concerns in relation to the percentage of patients being conveyed to
hospital. Members NOTED that this featured predominantly in
discussions held at EAS Committee and was in the process of being evaluated. Mr J Palmer advised that consideration was being given
to appropriate admission avoidance approaches which should reduce the number of admissions.
Members RESOLVED to:
NOTE the report.
Risk Management – Reasonable Assurance
Ms E Samways presented the report which had been given a
reasonable assurance rating. Members NOTED that the review focussed on risk management processes within Ophthalmology and
Cancer Services, with 1 high, 2 medium and 2 low recommendations
made, mainly relating to Cancer services.
Members NOTED that there were concerns in relation to the low number of risks identified during the audit. Members NOTED that
within Ophthalmology, there was evidence to show that there had been a review of the risk register, but no evidence to show that the
risk register had been updated. Members NOTED that a few areas of good practice were also identified.
Mr P Griffiths questioned how the review within these two areas
compared against other areas within the Health Board. Mr R Williams advised that the two areas reviewed were selected as they featured
heavily in the Health Board’s main risk register. Members NOTED that previous Directorate Reviews had identified areas of good
practice in relation to risk management processes.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
17 of 380Audit Committee - Part 1 9 July 2018-09/07/18

Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 18 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Mr R Williams advised that risk management was being discussed as
part of the Clinical Business meeting process with DATIX being used more appropriately. Awareness raising was also being undertaken.
Members RESOLVED to:
NOTE the report; ACCEPT that further work was in progress.
Governance Arrangements with Hosted Bodies – Reasonable
Assurance
Ms E Samways presented the report which had been given a
reasonable assurance rating. Members NOTED that there had been 2 medium and 1 low rated recommendations made. Members
NOTED that there was concern raised around the lack of a Memorandum of Understanding (MOU) being in place and the poor
attendance seen at some Joint Committee meetings.
Dr C Turner questioned the difference in hosting arrangements
between EASC & WHSSC and those relating to the Imaging Academy. Mr R Williams advised that in relation to EASC and WHSSC, these
were statutory Joint Committees of the Seven Health Board in Wales, hosted via Cwm Taf UHB and that in relation to the National Imaging
Academy, the Health Board was only acting as host for the management of the building.
Mr R Williams advised that further action outlined within the
management response would be taken forward and that the Chief Executives had approved the Memorandum of Understanding (MOU),
but noted that no signed copy was in place at present.
Members RESOLVED to:
NOTE the report and ENDORSE the related management
response.
Core Financial Systems – Substantial Assurance
Ms E Samways presented the report which had been given a substantial assurance rating. Members NOTED that the focus of the
review can vary each year, with focus this year being placed on Cash
& Balance. Members NOTED that two low risk rated recommendations had been made. Mr P Griffiths questioned whether
the aged debt going back to 2008/2009 had now been cleared. Mr H Evans explained that this would have been a debt that would have
been paid in instalments.
Members RESOLVED to NOTE the report.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
18 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 19 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Scheme of Delegation Review – Reasonable Assurance
Ms E Samways presented the report which had been given a
reasonable assurance rating. Members NOTED that the review focussed on the application of the Scheme of Delegation, with 1
medium and 2 low risk rated recommendations made. Members NOTED that the medium recommendation related to the incorrect set
up of a member of staff which had gone unnoticed for a period of time and had now been rectified. Members NOTED that work was
being undertaken on training with the aim to have the Scheme of Delegation as one of the core competencies.
Members RESOLVED to:
NOTE the report.
AC/18/036 INTERNAL AUDIT PLAN 2018/19
Mr P Dalton presented the report which incorporated the Health Board’s two hosted bodies, EASC & WHSSC. Members NOTED that
the plan was risk based and engagement had been undertaken with all Executive Directors and Independent Members during the
development of the plan, and the plan had been developed following attendance at Committee meetings throughout the year.
Members NOTED that the work was spread out across 8 assurance
domains and supported the Health Board’s Annual Governance Statement. Members NOTED that detailed discussions had been held
with management, particularly in relation to Directorate Reviews. Discussions had been held in relation to increasing the days spent on
Directorate Reviews than in previous years and this was in the
process of being considered further. Mr S Webster advised that he would like to explore further the possibility with Internal Audit of
increasing the number of Directorate Reviews undertaken per year from 4 to 5 to ensure all were reviewed over a 3 year period.
Members RESOLVED to:
APPROVE the Internal Audit Plan for 2018/19;
APPROVE the Internal Audit Charter; NOTE the resource requirements.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
19 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 20 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
PART 3 CHARITABLE FUNDS
AC/18/037 CHARITABLE FUND BALANCES AS AT 28 FEBRUARY 2018
Mr H Evans presented the report which advised the Audit Committee of the activity and balances on charitable funds for the period 1
December 2017 to 28 February 2018.
Members NOTED that the balance at the end of February was £1.8m which was slightly less than the position reported in November.
Members NOTED that the number of low value funds was fairly active and discussions were constantly being held with fund holders on the
importance of utilising the fund.
Members NOTED that at one stage, investment was very close to the 20% threshold but since then the market conditions had deteriorated.
Members NOTED that the profit forecast for 2017/18 was currently
£61k.
Mr R Williams raised Members awareness of reported issues experienced at NHS Tayside in relation to the inappropriate use of
charitable funds.
Members RESOLVED to:
NOTE the report.
PART 5. EXTERNAL AUDIT
AC/18/038 WAO REVIEW OF NHS WALES INFORMATICS (NWIS) 2018
Mr D Thomas presented the report which had been published in
January. Members NOTED that all recommendations made within the report had been accepted by Welsh Government. Members
NOTED that a holding response had been received from Welsh Government and that a collective response had been received from
Mr Andrew Goodall.
Dr C Turner advised that it would be helpful to be made aware of the proposed next steps and actions required of the Health Board and for
clarity to be provided on related issues.
Mr D Thomas advised that holding to account arrangements would be undertaken via the Welsh Government’s Public Accounts Committee.
Mr J Palmer advised that there were as many challenges contained within the report for Welsh Government as there were for NWIS,
particularly in relation to resourcing.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
20 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 21 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members NOTED there would be substantial benefits in connecting
the patient record to the digital pathway.
Following discussion, Members NOTED that there were a number of issues to be resolved relating to the governance of NWIS and its
relationship with its host body and Welsh Government.
Members RESOLVED to:
NOTE the report.
AC/18/039 WALES AUDIT OFFICE UPDATE REPORT
Mr D Thomas presented the report which provided an update on the
performance work undertaken. Members NOTED that the suggested completion date for the review into Primary Care was May 2018 and
related to the phase 1 output. Members NOTED that the report
would be circulated to Members (added to the action log).
Members RESOLVED to:
NOTE the update. AC/18/040 DRAFT STRUCTURED ASSESSMENT REPORT 2017 AND
MANAGEMENT RESPONSE
Mr R Williams advised Members that the Wales Audit Office Annual
Report 2017 had already been received by the Board, but that the
Structured Assessment report had not been formally received by the Audit Committee, although it had been circulated to Members by
email.
Members NOTED the report was positive overall, with a deeper dive undertaken this year in relation to financial reporting. Members
NOTED that 7 recommendations had been made, which had all been accepted and contained within the management response. Members
NOTED that the timescales for completion against some of the recommendations looked challenging.
Mr P Griffiths advised that reference had been made within the report
that the Health Board had only achieved one out of two of its statutory targets.
Mr D Thomas advised that this was as a result of report sequencing
and would make sure this was made clearer in the final version of the report.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
21 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 22 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Mr D Thomas AGREED to seek clarity from Ms S Utley in relation to
the statement made on page 24 of the report regarding the Executive Team needing to have a better understanding of Independent
Members’ needs. Members NOTED that this may be in relation to the volume of information being received. Mr R Williams advised that
this may relate to the volume of information being presented to Members of the Quality, Safety & Risk Committee.
Members RESOLVED to;
NOTE the report
AC/18/041 WALES AUDIT OFFICE ANNUAL REPORT 2017
Mr D Thomas presented the report which provided a summary of the work undertaken during the year.
Mr C Greenstock raised concerns in relation to the statement made on page 14 & 15 of the report which stated that the Health Board had
not made effective use of the NFI to detect fraud and overpayments. Mr Greenstock advised that the Counter Fraud department did not
have access to payroll systems and there had been miscommunication with Shared Services. Mr Greenstock also shared
his disappointment that Wales Audit Office had not been more proactive in discussing the issues identified with Counter Fraud.
Mr Greenstock questioned whether the report could be amended prior
to being put into the public domain. Mr R Williams advised that as the report had been received by Board the report was already in
public.
Dr C Turner advised that he had discussed a number of concerns with
Mr M Thomas in relation to issues regarding timing and communication in relation to Counter Fraud matters and was now
assured that these issues would be corrected for the future. Mr D Thomas AGREED to consider the comments received.
Mr P Griffiths questioned whether it was possible to deliver the annual
audit letter and structured assessment by the end of the financial year. Mr D Thomas advised that the structured assessment needed
to be completed first prior to completion of the annual audit report.
Members RESOLVED to:
NOTE the report.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
22 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 23 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
AC/18/042 WALES AUDIT OFFICE ANNUAL AUDIT PLAN FOR 2018/19
Mr G Lucey presented the report which also included an update on
progress in relation to the Audit of the Accounts. Members NOTED that the Wales Audit Office would be issuing one Audit opinion which
would be reported within the ISA 260 at the May meeting of the Committee.
Members NOTED that performance audits would be undertaken in
relation to the Structured Assessment, alongside 2 All Wales thematic follow up reviews.
Members NOTED that as a result of efficiencies made, the audit fee
had reduced for 2018/19. Mr D Thomas confirmed that the Audit fee was exclusive of VAT.
Members RESOLVED to:
NOTE the report.
PART 6. ITEMS FOR INFORMATION
AC/18/043 Members received the following items for information;
Forward Work Plan 2017/18;
Wales Audit Office Review – Delivery of agreed management response progress dashboard – as at 31 March 2018.
Forward Work Plan 2017/18
Mr R Williams advised that the forward work plan would be amended to reflect discussions held today.
Wales Audit Office Review of Public Health Wales – Delivery of agreed management response progress dashboard – as at 31 March 2018.
Members NOTED that a request had been made by Public Health
Wales for the report to be shared with all Audit Committees and provided a summary of the list of key issues. Members NOTED that
a national follow up piece of work would be undertaken.
Mr R Williams advised that this could be included on the agenda for the July Audit Committee meeting where a discussion could be held
on progress being made against the local actions, aligned with the national update (added to the action log).
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
23 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 24 of 24 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
PART 7. ANY OTHER URGENT BUSINESS
AC/18/044 ITEMS FOR REFERRAL TO OTHER COMMITTEES
There were no Committee referrals made.
AC/18/045 AUDIT COMMITTEE MEMBERS TO MEET WITH THE AUDITORS
Members NOTED that Audit Committee members met with the Auditors in private, prior to the commencement of today’s meeting.
AC/18/046 CLOSE OF PART 1 OF THE MEETING – DATE AND TIME OF
NEXT MEETING:
In closing part 1 of the meeting, Members RESOLVED that in accordance with the provision of Section 1(2) of the Public Bodies
(Admissions to Meetings) Act 1960, that representatives of the press
and other members of the public are excluded from the second part of the meeting on the grounds that it would be prejudicial to the
public interest due to the confidential nature of the business transacted. This section of the meeting is to be held in private
session.
The next meeting of the Committee would be held at 14:00hrs on Tuesday 8 May 2018.
……………………………………………………….
Dr Chris Turner, Chair
Date ……………………………
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
24 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 1 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
CWM TAF UNIVERSITY HEALTH BOARD
‘UNCONFIRMED’ MINUTES OF THE MEETING OF THE AUDIT
COMMITTEE HELD ON 8 MAY 2018, AT YNYSMEURIG HOUSE, ABERCYNON
PRESENT
Dr C Turner - Independent Member (Chair)
Mr P Griffiths - Independent Member Mrs M K Thomas - Independent Member (Vice Chair)
Mrs J Sadgrove - Independent Member
IN ATTENDANCE
Mr R Williams - Board Secretary / Director of
Corporate Services & Governance Mr S Webster - Director of Finance
Mr H Evans - Head of Corporate Finance Mr S Davies - Director of Finance, WHSCC
Mr D Thomas - Wales Audit Office Mr G Lucey - Wales Audit Office
Mr J Herniman - Wales Audit Office Mr P Dalton - NHS Wales Shared Services
Partnership (NWSSP) – Head of Internal Audit & Assurance (in part)
Ms E Samways - NWSSP – Internal Audit & Assurance Ms D Varsani - Financial Accountant - Observing
Miss J Maunder - Observing/Committee Secretariat
AC/18/047 WELCOME AND INTRODUCTIONS
Dr C Turner, Chair, welcomed everyone to the meeting.
AC/18/048 APOLOGIES FOR ABSENCE
Apologies for absence were received from Ms S Utley, Wales Audit
Office (WAO) and Mr K Smith, Welsh Health Specialised Services Committee (WHSCC).
AC/18/049 DECLARATIONS OF INTEREST
There were no additional Declarations of Interests, other than those
previously notified.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
25 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 2 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
PART 2. INTERNAL CONTROL AND RISK MANAGEMENT
AC/18/050 ‘DRAFT 2017/2018 ANNUAL ACCOUNTS
2.1 WHSSC/EASC DRAFT 2017/18 ANNUAL ACCOUNTS
The Committee RECEIVED the Welsh Health Specialised Services
Committee (WHSCC)/Emergency Ambulance Services Committee (EASC) draft Annual Accounts for 2017/2018.
Mr S Davies, Director of Finance, WHSCC presented the covering
report and offered apologies for the late submission of the document.
Members NOTED the draft Annual Accounts Statement for 2017/2018, which provided assurance on the financial accounting
processes for both WHSSC and EASC.
Members NOTED that WHSCC were in a break even position and
additional funding had been allocated for strengthening the organ donation service.
Members NOTED that major investment had been made on stem cell
research, cochlear and Thoracic surgery and that high cost drugs accounted for a large proportion of the budget.
Members NOTED that a new contract had been agreed with North
Bristol NHS Trust to deliver specialised cardiac services, as Cardiff & Vale UHB were unable to provide the service.
Members NOTED that critical staff appointments had been made in
WHSCC and that the underspend on staffing budgets had decreased,
and in addition, the 95% compliance had been achieved against the Public Sector Pay Policy (PSPP) target.
Dr C Turner advised that it was important for members to review the
draft documents prior to final sign off on the 31 May 2018, and stated that it had been unfortunate that the report had not been
received on time as it gave members a limited amount of time to review the information contained within it.
Mrs M K Thomas stated that the reference to a decrease on page 5
of the report concerning Children & Adolescent Mental Health Services (CAMHS) out of area placements was moving in a positive
direction but that it remains an area of uncertainty.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
26 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 3 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
Members NOTED the creditors position and that WHSCC were
continuing to work with NHS England in resolving the related issues.
Mr P Griffiths stated that it was pleasing to see the zero end balance and queried if the Health Board’s three year Integrated Medium Term
Plan (IMTP) included the financial information for WHSCC. Mr S Davies advised that WHSSC had their own IMTP, which was approved
annually and only the Cwm Taf elements of its Specialised Services commissioning were reflected within its IMTP.
Mr P Griffiths queried what the repercussions were if the approved
expenditure outlined within the IMTP was exceeded and members NOTED that the change to net liabilities in year was based on activity
and reflected and managed through regular updates to the various Committees.
Members NOTED that the WHSCC budget was set and that variances were discussed with individual Health Boards to understand budget
flexibilities based on local pressures, that there was no flexibility to move expenditure year on year and that WHSCC were proactive in
managing financial risk.
Members NOTED that some of the narrative within the Welsh Government guidance required updating.
Dr C Turner thanked Mr S Davies and Mr Huw Evans for presenting
the information and encouraged members to feed any detailed comments back to them for inclusion in the final report.
Mr P Griffiths referred to significant variations year on year
concerning dental services and Mr S Webster advised that the Finance
team were reviewing the detail with primary care services and would report back to the next Committee.
Members NOTED that clinical negligence expenditure had reduced,
due to the impact of the change in discount rates in 2017, which would have been shown as clinical negligence and income in
2016/2017 when the NWSSP Legal & Risk Services team provided a broad estimate due to timing issues and that the actual quantum from
individual cases was now being included.
Dr C Turner advised that it was pleasing to note that a balanced
position had been achieved and thanked officers for achieving this position and advised that the document should be updated to reflect
the minor issues raised in preparation for the Audit Committee
meeting on 31 May 2018.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
27 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 4 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
Members RESOLVED to:
NOTE the Welsh Health Specialised Services Committee (WHSCC)/Emergency Ambulance Services Committee
(EASC) ‘draft’ Annual Accounts for 2017/2018
AC/18/051 CHIEF EXECUTIVE ‘DRAFT’ ACCOUNTABILITY REPORT
The Committee received the ‘draft’ Accountability report, which also included the remuneration report.
Mr R Williams presented the report and thanked everyone who had
provided feedback on the document. Members NOTED that feedback to date was constructive and generally positive, although it was noted
that external audit will review the developing draft further before it’s
finalised as there were a number of areas not completed for the draft report. Members were encouraged to send any additional comments
to Mr R. Williams to support developing the final report, which will include the ‘final’ Head of Internal Audit opinion for 2017/18.
Members RESOLVED to:
NOTE the ‘Draft’ Accountability Report
PART 3 INTERNAL AUDIT
AC/18/052 3.1 Internal Audit Progress Report
Members received the Internal Audit Progress Report.
Mr P Dalton, Head of Internal Audit & Assurance, presented the
Internal Audit & Assurance progress report, which covered the period since the last meeting up until May 2018.
Members NOTED that the ‘draft’ reports on compliance with the
Health and Care Standards framework and the management of major capital would be concluded in the coming week.
Members NOTED that a further de-brief meeting was scheduled for
11 May 2018, to discuss the individual directorate reviews.
Members NOTED that there had been a decrease in performance against the key performance indicator for management responses and
that this was being discussed with Mr R Williams to establish causal factors.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
28 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 5 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
Members NOTED that the percentage response rate to the Audit survey had decreased and that Dr C Turner and Mr R Williams were
discussing this with the internal audit team.
Mr R Williams advised that, if viewed subjectively, there might be a correlation between the assurance opinion and the internal audit
assessment rating.
Mrs J Sadgrove advised that following discussions on winter pressures at a previous Audit Committee meeting that it would be interesting to
assess if the response figure was better at the front end of the year. Mr S Webster agreed to review the information and assess where
delays were occurring.
Members RESOLVED to:
NOTE the report.
3.2 E-Rostering – Reasonable Assurance
Members received the e-rostering internal audit report.
Ms E Samways presented the report and advised that the focus of the review was based on nursing staff and the roll out of the e-rostering
system and to assess if the system was being used effectively.
Members NOTED that the report identified perceived inefficiencies of the automated roster process and that on one occasion the link
between the health roster system and the Electronic Staff Record
(ESR) was not inter-operable.
Mrs MK Thomas advised that it was important to be mindful that data entry was undertaken by ward managers, and there were issues
concerning protected time being made available to undertake administrative tasks, linked to staffing issues in those areas.
Members NOTED that the efficient use of staff rotas would be included
within the scope of the directorate reviews.
Mr P Griffiths sought clarification on how any concerns on management responses would be addressed and its was NOTED that
regular dialogue was held with colleagues in internal audit to discuss the quality of the management responses being provided and any
related concerns were raised with lead officers.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
29 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 6 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
Mr R Williams confirmed that the recommendations were captured on
the audit tracker and that an update on progress will be presented at the next meeting.
Members RESOLVED to:
NOTE the report and the related Management Response
3.3 Private & Overseas Patients – Limited Assurance
Members received the Private & Overseas Patients internal audit
report.
Ms E Samways presented the report, which was a review of arrangements in place for private patients treated on Health Board
sites and overseas patients who were possibly not entitled to free NHS
care.
Members NOTED that the report outlined a lack of executive leadership and that, whilst there was a Financial Control Procedure
(FCP) in place for private practice, there was no formal oversight of the process in place for overseas patients, due to the limited amount
of resource within the medical records team.
Ms E Samways advised that it had been identified that some medical records were not up to date and that a recommendation had been
made for a reconciliation between data sets. Members NOTED that all of the recommendations had been agreed and that Mr S. Webster
was named as the lead executive.
Members NOTED the need for improved awareness on process and
that Mr S Webster would provide an update on progress in addressing the recommendations at the next meeting following a whole process
review.
Members RESOLVED to:
NOTE the report and the related Management Response
3.4 Governance Arrangements with Local Authorities and Third Sector – Reasonable Assurance
Members received the internal audit report on Governance
Arrangements with Local Authorities and the Third Sector.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
30 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 7 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
Ms E Samways presented the report, which outlined the findings of
an audit of the governance arrangements in place for joint projects between the Health Board and Rhondda Cynon Taf Council and
Merthyr County Borough Council.
Members NOTED that there were appropriate risk registers in place. However, there were some minor issues concerning the monitoring
of risk, which were strengthened when the joint projects moved from business case proposals to delivery. Members also NOTED that there
was a need to ensure that business plans were in place linked to business cases and smart objectives.
Mr R Williams sought clarification on the link between organisational
risk and assurance as the management response implied that as the risk register had only been in place for a short time, there had been
insufficient time for the register to be fully integrated into directorate
work and that additional analysis was required to review evidence before finalising risk registers.
Members NOTED that risks had been captured on the Primary and
Community Care risk register and that some risks were being managed by the Local Authorities.
Members RESOLVED to:
NOTE the report and ENDORSE the related Management
Response
3.5 EASC WAO Follow Up Report – Reasonable Assurance
Members received the Emergency Ambulance Services Committee’s
(EASC’s) Wales Audit Office follow up report.
Ms E. Samways presented the report noting that the Audit Committee
had been kept appraised of the work of EASC throughout the year.
Members NOTED that action had been taken to address the twelve recommendations outlined within the report, and that three actions
required time to embed before being fully completed and that three were partially complete and progress was being monitored through
the audit tracker.
Dr C Turner expressed concern that the job description for the Chief Ambulance Services Commissioner (CASC) had not been finalised and
Mr R Williams explained that the focus of the job description had been updated to reflect the diverse portfolio of the role and was reportedly
with Welsh Government for approval.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
31 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 8 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
Members NOTED that a closure report was being submitted to the EASC meeting 15 May 2018 and that the advertisement to recruit a
new Chair for the Joint Committee has been advertised by Welsh Government.
Dr C Turner sought clarification on whether the report provided an
accurate reflection of the EASC position and Mr R Williams, in noting his interest as the Committee Secretary providing governance
support to EASC, confirmed that the report accurately reflected the position.
Members NOTED that the follow up audit review would be completed
by the end of May 2018 and would be presented to the next Audit Committee meeting.
Members RESOLVED to:
NOTE the report and the related Management Response
3.6 Fire Management – Reasonable Assurance
Members received the internal audit report on Fire Management. Mr
P Dalton presented the report which had been compiled by the Shared Services Capital team who had responsibility for monitoring
compliance with the legislative and regulatory framework for fire safety.
Members NOTED that one high risk recommendation had been
identified. Mr R Williams advised that he was the executive lead for fire safety and that he was broadly content with the report’s findings.
Mr Williams considered the report was reasonably balanced although
there had been frustrations with the inflexibilities of national software systems, which resulted in duplication of effort in undertaking local
Fire Risk Assessments in addition to those added to the National software. Members NOTED that, whilst the Board would continue to
raise matters associated with the national system and related software, it was not in a position to address directly the improvement
actions recommended.
Members RESOLVED to:
NOTE the report and ENDORSE the related Management Response.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
32 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 9 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
3.7 ‘Draft’ Head of Internal Audit Opinion and Annual Report
2017/18 – Reasonable Assurance
Members received the ‘draft’ Head of Internal Audit Opinion and Annual Report 2017/18. Mr P Dalton presented the report and
advised that the format was the same as in previous years. The report summarised results of the internal audit activity delivered
throughout 2017/18, which also included WHSCC and EASC. The internal audit team had reviewed topics across the eight domains, in
accordance with the Public Sector Internal Audit standards and the Head of Internal Audit Opinion (HIAO) was based on the work the
internal audit team had assessed throughout the year.
Members NOTED that the HIAO was a core requirement of the Annual Governance Statement led by a risk based audit plan and that the
overall draft Opinion was a ‘reasonable’ assurance rating.
Members NOTED that the internal audit team operated under an
external quality assessment (EQA) undertaken by the Chartered Institute of Internal Auditors (CIIA) every five years. This assessed if
the internal audit service provided to NHS Wales complied with the CIIAs International Standards and how it related to the financial
services code and the public sector standards (PSIAS). Members NOTED that the overall feedback indicated that internal audit were
complying with the 64 guiding principles of the International Standard and that a survey questionnaire was issued to Health
Boards, Trusts and hosted bodies seeking feedback on the internal audit function and a number of interviews were undertaken to gather
qualitative feedback to support the survey findings.
Dr C Turner advised that the report was positive and queried if the
final HIAO could be affected by the outstanding report on capital. Mr P Dalton advised that it was unlikely as the three out of the four
reports provided positive assurances.
Mr P Griffiths queried if it was possible to track the Health Board’s performance over the last few years to assess the impact the Audit
Committee had made on different areas of its systems of internal control. Members NOTED that the internal audit team could compile
the information, however risk profiles change over time and it would be difficult to make an objective assessment.
Mr R Williams advised that he had discussed trend analysis with Mr P
Dalton and that there was a need to focus the limited time available for audit work on the areas of greatest need.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
33 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 10 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
Members RESOLVED to:
NOTE the ‘Draft’ Head of Internal Audit Opinion and Annual
Report 2017/18 report
PART 4. EXTERNAL AUDIT
AC/18/053 WAO UPDATE ON PROGRESS WITH 2017/2018 ACCOUNTS AUDIT
Members received the report.
Mr G Lucey presented the report and members NOTED that all
financial audit work had been completed for 2017/18 and an independent examination of the Health Board’s charitable funds had
also been completed.
Members sought clarification on the underspend on dental,
particularly in light of our poor oral health profile and Mr S Webster agreed to provide an update at the next meeting. Members NOTED
that focus would now be placed on 2018/19 and the Wales Audit Office would present the Annual WAO plan to the May 2018 meeting.
Members RESOLVED to:
NOTE the update.
PART 5. ANY OTHER URGENT BUSINESS
AC/18/054 ITEMS FOR REFERRAL TO OTHER COMMITTEES
AC/18/056 AUDIT COMMITTEE MEMBERS TO MEET WITH THE AUDITORS
There was no requirement for members to meet in private with the Auditors on this occasion.
The next meeting of the Committee would be held on 31 May
2018 (to approve the Annual Accounts 2017-18) time to be confirmed.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
34 of 380 Audit Committee - Part 1 9 July 2018-09/07/18

Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 11 of 11 Audit Committee Meeting
Audit Committee 8 May 2018 9 July 2018
……………………………………………………. Dr Chris Turner, Chair
Date ……………………………
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
35 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 1 of 7 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
CWM TAF UNIVERSITY HEALTH BOARD
‘UNCONFIRMED’ MINUTES OF THE MEETING OF THE AUDIT
COMMITTEE HELD ON 31 MAY 2018, AT YNYSMEURIG HOUSE, ABERCYNON
PRESENT
Dr C Turner - Independent Member (Chair)
Mr P Griffiths - Independent Member Mrs M K Thomas - Independent Member (Vice Chair)
Mrs J Sadgrove - Independent Member
IN ATTENDANCE
Professor M Longley - UHB Chair
Mrs A Williams - Chief Executive Mr H Evans - Head of Corporate Finance
Mr G Lucey - Wales Audit Office Mr J Herniman - Wales Audit Office
Mr S Webster - Director of Finance Mr R Williams - Board Secretary / Director of
Corporate Services & Governance Professor V Harpwood - Chair, WHSSC
Ms S Lewis - Managing Director, WHSSC Mr S Davies - Director of Finance, WHSSC
Mr K Smith - Committee Secretary/Head of Corporate Services, WHSSC
Mr S Harrhy - Chief Ambulance Services Commissioner
Mr P Dalton - NHS Wales Shared Services
Partnership (NWSSP) – Head of Internal Audit & Assurance
Ms E Samways - NWSSP – Internal Audit & Assurance Ms R Treharne - Deputy Chief Executive/Director of
Planning & Performance Mr J Hehir - Independent Member
Cllr R Smith - Independent Member Mr M Jehu - Independent Member
Ms G Roberts - Head of Corporate Services Ms J Maunder - NHS Wales Shared Services
Partnership (NWSSP) - Head of Corporate Services
Ms E Russell - Graduate Trainee (Observing) Miss E Walters - Committee Secretariat
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
36 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 2 of 7 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
AC/18/057 WELCOME AND INTRODUCTIONS
Dr C Turner, Chair, welcomed everyone to the meeting.
Members NOTED that the Audit Committee had already had the
opportunity to receive and scrutinise the ‘draft’ annual accounts for 2017-18 along with the ‘draft’ accountability report and ‘draft’ Head
of Internal Audit Opinion in advance of today’s meeting. Members NOTED that the purpose of the meeting today was, subject to
scrutiny of the Accounts and related financial statement, that the Audit Committee make a recommendation to the University Health
Board to approve the Annual Accounts and related financial statements (including the Letter of Representation to the Auditors)
for 2017-18.
AC/18/058 APOLOGIES FOR ABSENCE
Apologies for absence had been received from Mr D Thomas and Mrs
S Utley, Wales Audit Office.
AC/18/059 DECLARATIONS OF INTERESTS
There were no additional Declarations of Interests, to those
previously notified.
AC/18/060 REPORT ON THE WELSH HEALTH SPECIALISED SERVICES
COMMITTEE (WHSSC)/EMERGENCY AMBULANCE SERVICES COMMITTEE (EASC) FINANCIAL ACCOUNTS 2017-18
Mr S Davies presented the report on the WHSSC/EASC Financial
Accounts for 2017-18.
Members NOTED that WHSSC achieved a break even position for
2017-18 which meant that there was neither a surplus nor a deficit and that all LHBs agreed to their financial share of the WHSSC outturn
position.
Members NOTED the key movements between 2016/17 and 2017/18, which included movements in the Annual Plan for
investment and the financial risk sharing outcome which related to the HRG4 pricing issues in England.
Members NOTED that in relation to performance, Welsh providers
had started to over-perform but at a much higher cost.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
37 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 3 of 7 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members NOTED the significant increase in investment made into
cancer drugs and Emergency Ambulance Services, the latter which related to the re-banding of paramedics from Band 5 to Band 6.
Members NOTED the positive performance achieved by WHSSC in
relation to compliance against the 95% target for the Public Sector Payment Policy.
Members NOTED that the increase in spend experienced in relation
to WHSSC structural staffing and that a large number of key vacancies had now been filled. Members NOTED that there had also
been a change in the way secondments were being reported in and out of the organisation, which had an impact on the reported position.
Members NOTED that a discussion had been held with Welsh Government in relation to this, where it was highlighted that an
amendment to the guidance for reporting of expenditure and income
would need to be undertaken.
Dr C Turner commended WHSSC colleagues on the solution found in relation to HRG4 issues and welcomed the clear set of accounts and
the resolution found in relation to secondment costs.
Members had no further specific comments relating to the accounts and thanked Mr S Davies for addressing the scrutiny issues raised in
the 8 May 2018 meeting.
Members RESOLVED to:
ENDORSE the final audited financial statements for the financial year ended 31 March 2018;
RECOMMEND their inclusion and publication unchanged in
the consolidated Cwm Taf Statutory Financial Statements.
AC/18/061 WHSSC ANNUAL GOVERNANCE STATEMENT FOR 2017-18
Mr K Smith presented the WHSSC Annual Governance Statement for 2017-18, which was addressed to Mrs A Williams, Chief Executive and
signed by Dr S Lewis, Managing Director of WHSSC.
Members NOTED that no significant governance issues had been identified and that the Integrated Commissioning Plan (ICP) had been
approved at the beginning of the financial year.
Dr S Lewis advised that she was pleased that the ICP had been approved in a timely manner and work continued internally in relation
to risk management processes.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
38 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 4 of 7 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Mr R Williams added that Audit Committee members had already had
the opportunity to review the statement and provide their comments to WHSSC.
Members RESOLVED to:
NOTE the report;
APPROVE the WHSSC Annual Governance Statement for 2017/18.
AC/18/062 EASC ANNUAL GOVERNANCE STATEMENT 2017-18
Mr R Williams advised that the EASC Annual Governance Statement
was considered and commented on at the March EAS Committee and advised that comments had also been received from Audit Committee
members.
Mr S Harrhy provided Members with an update in relation to the Wales
Audit Office report received on EASC Governance Arrangements. Members NOTED that the report was positive and contained 12
recommendations, each of which had been completed. Members NOTED that a report on progress was presented to the last EAS
Committee. Members NOTED that a response would be drafted to the Wales Audit Office confirming that all actions had been completed.
Members RESOLVED to:
NOTE the report; APPROVE the EASC Annual Governance Statement for 2017-
18.
AC/18/063 REPORT ON THE FINANCIAL ACCOUNTS OF THE CWM TAF UHB
FOR 2017/18
Mr H Evans presented Members with the audited Annual Accounts for the financial year ended 31 March 2018. Members NOTED that Audit
Committee had already had the opportunity to review the draft accounts at the meeting held on 8 May 2018.
Members NOTED that no fundamental changes had been made to
targets with the vast majority of changes being in relation to classification issues.
A discussion was held in relation to the reclassification of clinical
negligence liabilities and Members NOTED that there had been no change to the total liabilities or assets as a result of this amendment.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
39 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 5 of 7 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Mr H Evans explained the technical issue raised by Auditors since the
last meeting that related to the technical treatment of accounting for external secondments from WHSSC.
Dr C Turner recognised that the Health Board was pleased to have
achieved a breakeven position and extended his thanks to the Finance Team for the work undertaken.
Members RESOLVED to:
NOTE the report; Recommend that the Board APPROVE the Annual Accounts for
2017-18 together with the letter of representation to the Auditors.
AC/18/064 CWM TAF UHB ACCOUNTABILITY REPORT 2017/18
Mr R Williams presented Members with an update on matters developed since Members considered the draft report and confirmed
that minor corrections had been made to the Accountability report, which included the following:
Pensions comparison had been added to the report; An analysis of the breakdown of the Board had now been
included in the report; An error in relation to Professor D Mead’s end date of her term
of office had been corrected.
Mrs A Williams extended her thanks to Mr R Williams and the
Corporate Services Team for developing the report and also extended her thanks to Mr S Harrhy and Dr S Lewis and associated staff, for
their contribution. Mrs A Williams advised that the report was detailed and was an important document which provided assurance to the
Board and Welsh Government that governance controls were in place.
Mrs A Williams drew Members attention to the risks outlined within
the report that were currently being managed within the organisation and the reference made to changes that had been made to the risk
profile and risk register.
Dr C Turner advised that there should be no surprises contained within
the report that the Committee would not already be aware of and extended his thanks to Mr R Williams for producing the report.
Members RESOLVED to:
ENDORSE the accountability report and recommend that the Board APPROVE the report as part of its approval of the annual
accounts for 2017/18.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
40 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 6 of 7 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
AC/18/065 AUDIT OF THE FINANCIAL STATEMENTS (ISA 260) DRAFT
REPORT WHICH INCLUDES DRAFT LETTER OF REPRESENTATION
Mr G Lucey presented the report and advised that it was the intention
of the Auditor General for Wales to issue an unqualified opinion with no uncorrected misstatements of significance.
Members NOTED that all Audit work was now complete and Mr Lucey
extended his thanks to finance teams in the Health Board, EASC and WHSSC for the support provided. Members NOTED the amendments
contained within the report which were of a technical nature and that no corrections had been identified which affected the Health Board’s
overall three year financial duty surplus of £63k, as reported in the draft financial statements.
Members NOTED that included within the report was the unadjusted miss-statement alluded to earlier in the meeting by Mr S Davies and
that this had also been included in the letter of representation. Members NOTED that a typographical error had been identified within
the report and that this would be amended and reflected in the final version of the report.
Members RESOLVED to:
Recommend that the Board APPROVE the Annual Accounts and Financial Statements for 2017/18 together with the letter of
representation.
AC/18/067 HEAD OF INTERNAL AUDIT OPINION AND ANNUAL REPORT
2017/18
Mr P Dalton presented the report and advised that Members had
received a draft version of the report at the Audit Committee meeting held on 8 May 2018.
Members NOTED that the overall opinion remained as reasonable
assurance. Members NOTED that since the draft report was discussed at the Audit Committee on the 8 May, the Directorate
Review into Anaesthetics, Critical Care & Theatres (ACT) had been issued, and that the review into Capital Works at Prince Charles
Hospital (PCH) would require further field related work which would be undertaken during 2018/19. Members NOTED that discussions
were ongoing as to when in the year this review would be completed. Mrs A Williams advised that it may be helpful to connect the Internal
Audit review with the gateway review being undertaken in relation to the PCH Ground & First Floor Capital Development, which was being
planned for late summer, early September.
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
41 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item 1.4
‘Unconfirmed’ part 1 minutes Page 7 of 7 Audit Committee Meeting
Audit Committee 16 April 2018 9 July 2018
Members recognised that the plan was very challenging this year and
extended their thanks to Internal Audit & Directorate Teams for completing the reviews for Audit Committee.
Members RESOLVED to:
NOTE the update provided; NOTE that reasonable assurance had now been allocated.
AC/18/068 AUDIT ENQUIRIES CHECKLIST 2017/18
Mr R Williams advised that the checklist primarily focussed on counter
fraud and it was NOTED that Audit Committee members had previously provided comments on the content.
Members RESOLVED to:
NOTE the update.
AC/18/069 ANY OTHER URGENT BUSINESS
There was no other business to report.
AC/18/070 FINAL CLOSURE AND FUTURE MEETINGS
In closing the meeting, Dr C Turner extended his thanks to all Members for attending the meeting and to the Corporate Services
and Finance Departments for their contributory work.
The next meeting of the Committee would be held at 09:00hrs on Monday 9 July 2018.
………………………………………………………. Dr Chris Turner, Chair
Date ……………………………
1.4 Unconfirmed Minutes of the Audit Committee Meeting held on:
42 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda Item Number 1.5
Audit Committee Action Log Page 1 of 4 Audit Committee Meeting
9 July 2018
AUDIT COMMITTEE ACTION LOG FOLLOWING MEETING ON 16 APRIL 2018, 8 MAY 2018 & 31 MAY 2018
NO. MEETING
DATE
SUBJECT ACTION TIMESCALE RESPONSIBLE
OFFICER
STATUS AS AT
June 2018
17/130 11/09/
2017
Directorate
Review (Pathology)
Members agreed that the issue
of Time Off In Lieu (TOIL) which had featured within a number of
Directorate Governance
Reviews, be raised with the Director of Workforce & OD as
there was a concern that if allowed, there did not appear to
be a consistent UHB wide approach.
Mr M Thomas suggested that a
discussion needs to take place with Internal Audit in relation to
the balance of the Audit Plan with regards directorate reviews
with only 2 or 3 undertaken each year.
October
2017
Board
Secretary / Director of
Workforce & OD
Director of
Finance
Members noted at the
last meeting that issues in relation to TOIL had
been escalated to the
Director of Workforce & OD and that a standard
approach across the Health Board was being
taken forward.
Members noted that a
revised scope for Directorate Reviews was
being finalised with comments from the
Executive and this would be used in the 2018/19
Internal Audit Plan.
In progress – Follow up
meeting held with Internal Audit to agree
future scope of Directorate Reviews and
revised scope being applied to current
Directorate reviews likely to report in May 2018.
1.5 Action Log
43 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
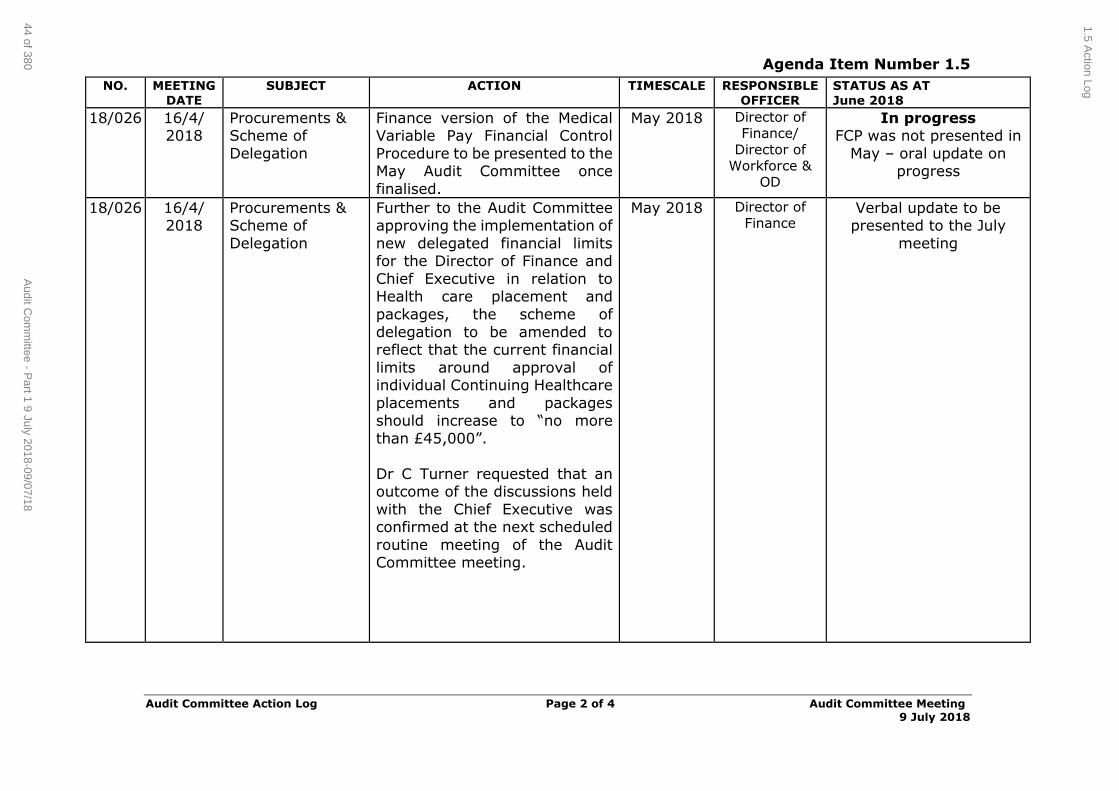
Agenda Item Number 1.5
Audit Committee Action Log Page 2 of 4 Audit Committee Meeting
9 July 2018
NO. MEETING
DATE
SUBJECT ACTION TIMESCALE RESPONSIBLE
OFFICER
STATUS AS AT
June 2018
18/026 16/4/ 2018
Procurements & Scheme of
Delegation
Finance version of the Medical Variable Pay Financial Control
Procedure to be presented to the May Audit Committee once
finalised.
May 2018 Director of Finance/
Director of Workforce &
OD
In progress FCP was not presented in
May – oral update on progress
18/026 16/4/ 2018
Procurements & Scheme of
Delegation
Further to the Audit Committee approving the implementation of
new delegated financial limits for the Director of Finance and
Chief Executive in relation to Health care placement and
packages, the scheme of
delegation to be amended to reflect that the current financial
limits around approval of individual Continuing Healthcare
placements and packages should increase to “no more
than £45,000”.
Dr C Turner requested that an outcome of the discussions held
with the Chief Executive was confirmed at the next scheduled
routine meeting of the Audit Committee meeting.
May 2018 Director of Finance
Verbal update to be presented to the July
meeting
1.5 Action Log
44 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
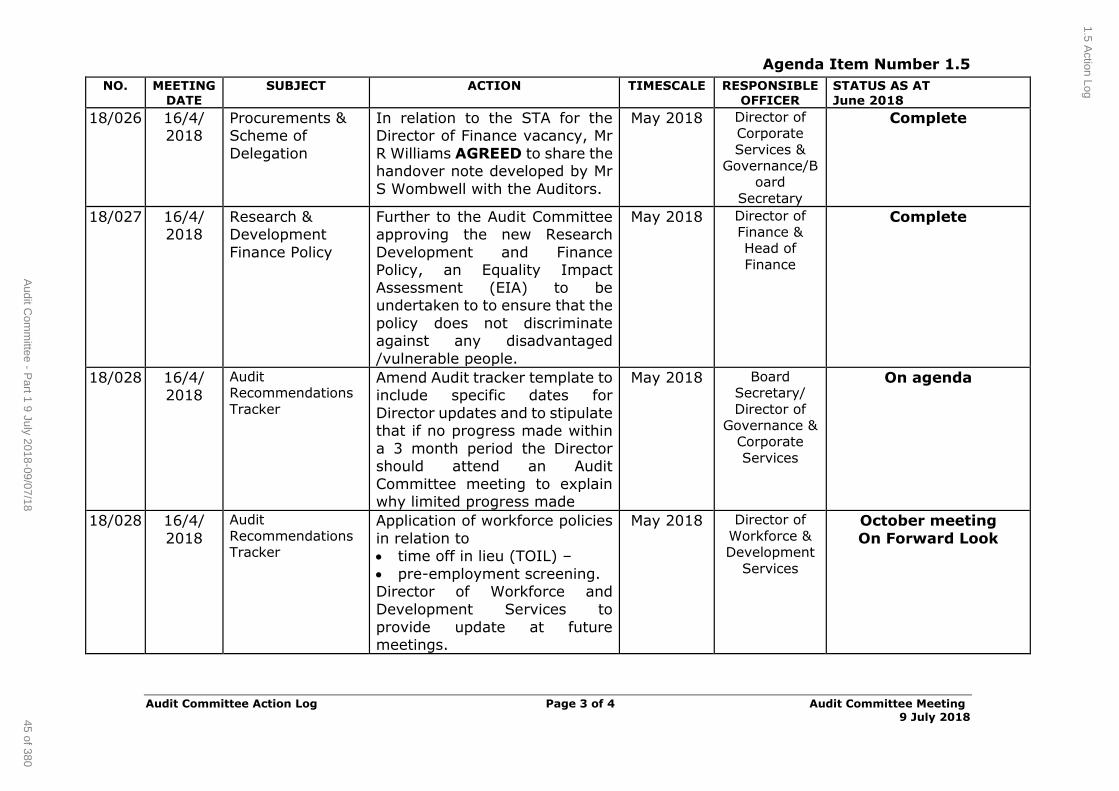
Agenda Item Number 1.5
Audit Committee Action Log Page 3 of 4 Audit Committee Meeting
9 July 2018
NO. MEETING
DATE
SUBJECT ACTION TIMESCALE RESPONSIBLE
OFFICER
STATUS AS AT
June 2018
18/026 16/4/ 2018
Procurements & Scheme of
Delegation
In relation to the STA for the Director of Finance vacancy, Mr
R Williams AGREED to share the handover note developed by Mr
S Wombwell with the Auditors.
May 2018 Director of Corporate
Services & Governance/B
oard
Secretary
Complete
18/027 16/4/ 2018
Research & Development
Finance Policy
Further to the Audit Committee approving the new Research
Development and Finance Policy, an Equality Impact
Assessment (EIA) to be undertaken to to ensure that the
policy does not discriminate against any disadvantaged
/vulnerable people.
May 2018 Director of Finance & Head of
Finance
Complete
18/028 16/4/ 2018
Audit Recommendations
Tracker
Amend Audit tracker template to include specific dates for
Director updates and to stipulate that if no progress made within
a 3 month period the Director should attend an Audit
Committee meeting to explain why limited progress made
May 2018 Board Secretary/
Director of Governance &
Corporate
Services
On agenda
18/028 16/4/
2018
Audit
Recommendations Tracker
Application of workforce policies
in relation to time off in lieu (TOIL) –
pre-employment screening. Director of Workforce and
Development Services to
provide update at future meetings.
May 2018 Director of
Workforce & Development
Services
October meeting
On Forward Look
1.5 Action Log
45 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
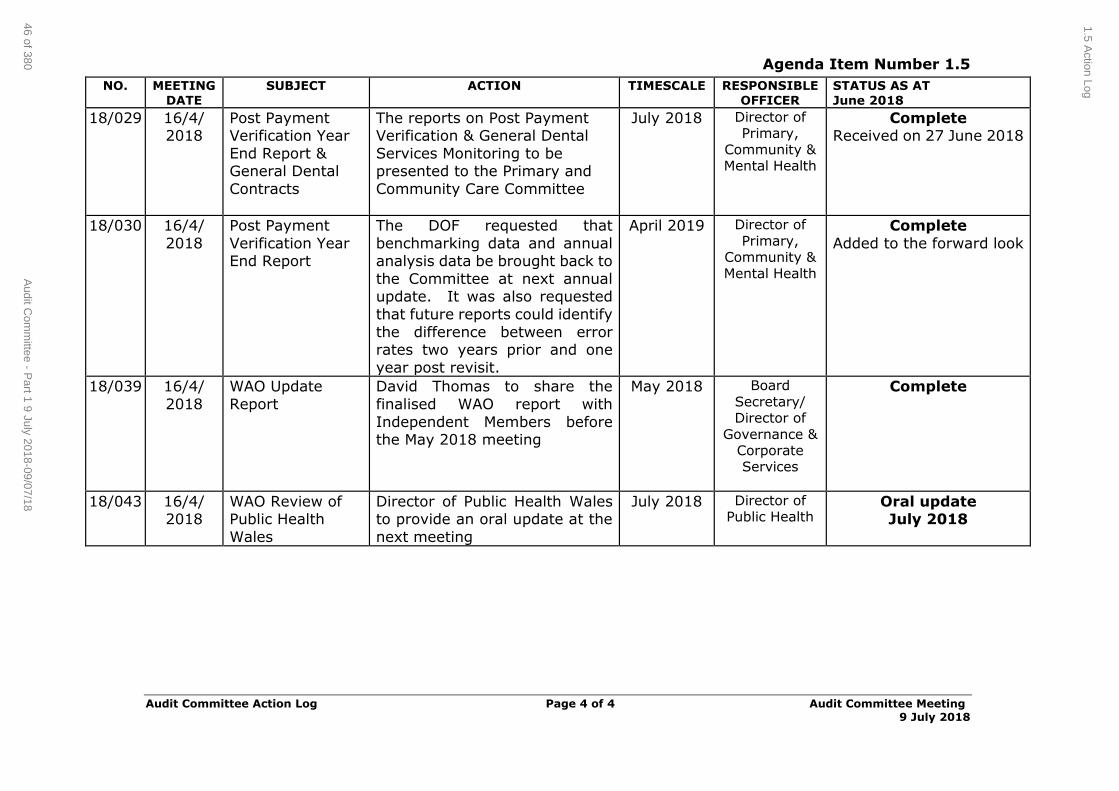
Agenda Item Number 1.5
Audit Committee Action Log Page 4 of 4 Audit Committee Meeting
9 July 2018
NO. MEETING
DATE
SUBJECT ACTION TIMESCALE RESPONSIBLE
OFFICER
STATUS AS AT
June 2018
18/029 16/4/ 2018
Post Payment Verification Year
End Report & General Dental
Contracts
The reports on Post Payment Verification & General Dental
Services Monitoring to be presented to the Primary and
Community Care Committee
July 2018 Director of Primary,
Community & Mental Health
Complete Received on 27 June 2018
18/030 16/4/
2018
Post Payment
Verification Year End Report
The DOF requested that
benchmarking data and annual analysis data be brought back to
the Committee at next annual update. It was also requested
that future reports could identify
the difference between error rates two years prior and one
year post revisit.
April 2019 Director of
Primary, Community &
Mental Health
Complete
Added to the forward look
18/039 16/4/
2018
WAO Update
Report
David Thomas to share the
finalised WAO report with
Independent Members before the May 2018 meeting
May 2018 Board
Secretary/ Director of
Governance & Corporate Services
Complete
18/043 16/4/ 2018
WAO Review of Public Health
Wales
Director of Public Health Wales to provide an oral update at the
next meeting
July 2018 Director of Public Health
Oral update July 2018
1.5 Action Log
46 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Scheme of Delegation Report Page 1 of 6 Audit Committee Meeting 9 July 2018
AGENDA ITEM 2.1
9 July 2018
Audit Committee Report
SCHEME OF DELEGATION REPORT
Executive Lead: Director of Finance
Author: Head of Finance (Financial Accounts, Capital & Systems)
Contact Details for further information: Huw Evans on 01443 443810 or [email protected]
Purpose of the Audit Committee Report
To report transactions approved as “exceptions” within the Scheme of
Delegation for the period 1.3.18 to 31.5.18;
To provide an update on the work undertaken to improve the Purchase to
Pay processes, in conjunction with the NHS Wales Shared Services Partnership (NWSSP); and
To highlight other matters of interest around the application of Financial Control Procedures and Scheme of Delegation.
Governance
Link to Health
Board Strategic Objective(s)
The Board’s overarching role is to ensure its Strategy
outlined within ‘Cwm Taf Cares’ 3 Year Integrated Medium Term Plan 2018-2021 and the related
organisational objectives aligned with the Institute of Healthcare Improvement's (IHI) ‘Triple Aim’ are being
progressed, these in summary are: To improve quality, safety and patient experience
To protect and improve population health To ensure that the services provided are accessible
and sustainable into the future
To provide strong governance and assurance To ensure good value based care and treatment for
our patients in line with the resources made available to the Health Board.
The main aim of this report is to improve governance and assurance.
Supporting evidence
N/A
Engagement – Who has been involved in this work?
NHS Wales Shared Services Partnership
2.1 Procurements and Scheme of Delegation Report
1 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Scheme of Delegation Report Page 2 of 6 Audit Committee Meeting 9 July 2018
Audit Committee Resolution to:
APPROVE √ ENDORSE √ DISCUSS NOTE √
Recommendation The Audit Committee is asked to:
a) NOTE the transactions approved by exception
within the Scheme of Delegation, for the period 1.3.18 to 31.5.18; and the All-Wales SQA/STA Documentation
b) NOTE the update regarding Purchase to Pay issues. c) APPROVE the change to the Scheme of Delegation
reflecting the new titles in the Patient Safety and Risk Directorate
Summarise the Impact of the Audit Committee Report
Equality and diversity
No specific impact
Legal implications No specific impact
Population Health No specific impact
Quality, Safety &
Patient Experience
No specific impact
Resources Assists in providing assurance that appropriate value for money is obtained where competitive
tenders have not been sought, and ensures resources are deployed according to set control
processes
Risks and Assurance Purchase to Pay processes are a key risk area for
the UHB, which has contributed to a failure to meet the prompt payment target of 95% non-NHS
invoices to be paid within 30 days in previous
years.
Health and Care
Standards
The 22 Health & Care Standards for NHS Wales
are mapped into the 7 Quality Themes: Staying Healthy; Safe Care; Effective Care;
Dignified Care; Timely Care; Individual Care; Staff & Resources.
Workforce No specific impact
Freedom of
information status
Open
2.1 Procurements and Scheme of Delegation Report
2 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Scheme of Delegation Report Page 3 of 6 Audit Committee Meeting 9 July 2018
SCHEME OF DELEGATION REPORT
1. SITUATION / PURPOSE OF REPORT
The purpose of the report is to:
To report transactions approved as “exceptions” within the Scheme
of Delegation for the period 1.3.18 to 31.5.18
To provide an update on the work undertaken to improve the Purchase to Pay processes, in conjunction with the NHS Wales
Shared Services Partnership (NWSSP) and
To highlight other matters of interest around the application of
Financial Control Procedures and Scheme of Delegation.
2. BACKGROUND
The following areas within the Scheme of Delegation may be considered contentious and therefore the Audit Committee may wish to be given the
opportunity to ask questions or request further information:
a) Engagement off contract of non-medical staff not paid via the payroll.
The Director of Workforce and Organisational Development (W&OD) and the Head of Procurement would need to confirm agreement prior to any
commitment.
b) Waiver of competitive tenders, as authorised by the Chief Executive.
c) Contracts requiring Ministerial approval (over £1m)
This report provides details of any such transactions within the period 1.3.18 to 31.5.18.
The report also provides an update on the Prompt Payment compliance for
2018-19
The report also highlights a small change required to the Scheme of
Delegation following a directorate restructure and change of titles
2.1 Procurements and Scheme of Delegation Report
3 of 380Audit Committee - Part 1 9 July 2018-09/07/18
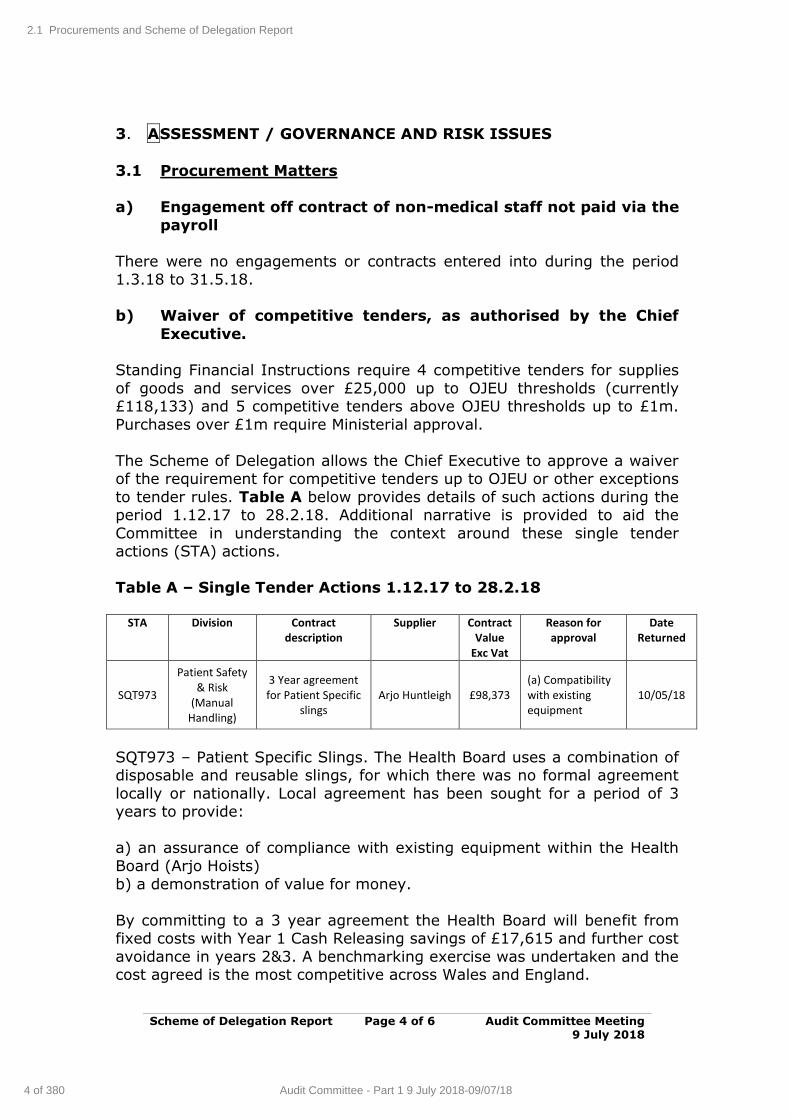
Scheme of Delegation Report Page 4 of 6 Audit Committee Meeting 9 July 2018
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
3.1 Procurement Matters
a) Engagement off contract of non-medical staff not paid via the
payroll
There were no engagements or contracts entered into during the period 1.3.18 to 31.5.18.
b) Waiver of competitive tenders, as authorised by the Chief
Executive.
Standing Financial Instructions require 4 competitive tenders for supplies
of goods and services over £25,000 up to OJEU thresholds (currently £118,133) and 5 competitive tenders above OJEU thresholds up to £1m.
Purchases over £1m require Ministerial approval.
The Scheme of Delegation allows the Chief Executive to approve a waiver of the requirement for competitive tenders up to OJEU or other exceptions
to tender rules. Table A below provides details of such actions during the period 1.12.17 to 28.2.18. Additional narrative is provided to aid the
Committee in understanding the context around these single tender actions (STA) actions.
Table A – Single Tender Actions 1.12.17 to 28.2.18
STA Division Contract
description Supplier Contract
Value Exc Vat
Reason for approval
Date Returned
SQT973
Patient Safety & Risk
(Manual Handling)
3 Year agreement for Patient Specific
slings Arjo Huntleigh £98,373
(a) Compatibility with existing equipment
10/05/18
SQT973 – Patient Specific Slings. The Health Board uses a combination of disposable and reusable slings, for which there was no formal agreement
locally or nationally. Local agreement has been sought for a period of 3 years to provide:
a) an assurance of compliance with existing equipment within the Health
Board (Arjo Hoists)
b) a demonstration of value for money.
By committing to a 3 year agreement the Health Board will benefit from fixed costs with Year 1 Cash Releasing savings of £17,615 and further cost
avoidance in years 2&3. A benchmarking exercise was undertaken and the cost agreed is the most competitive across Wales and England.
2.1 Procurements and Scheme of Delegation Report
4 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
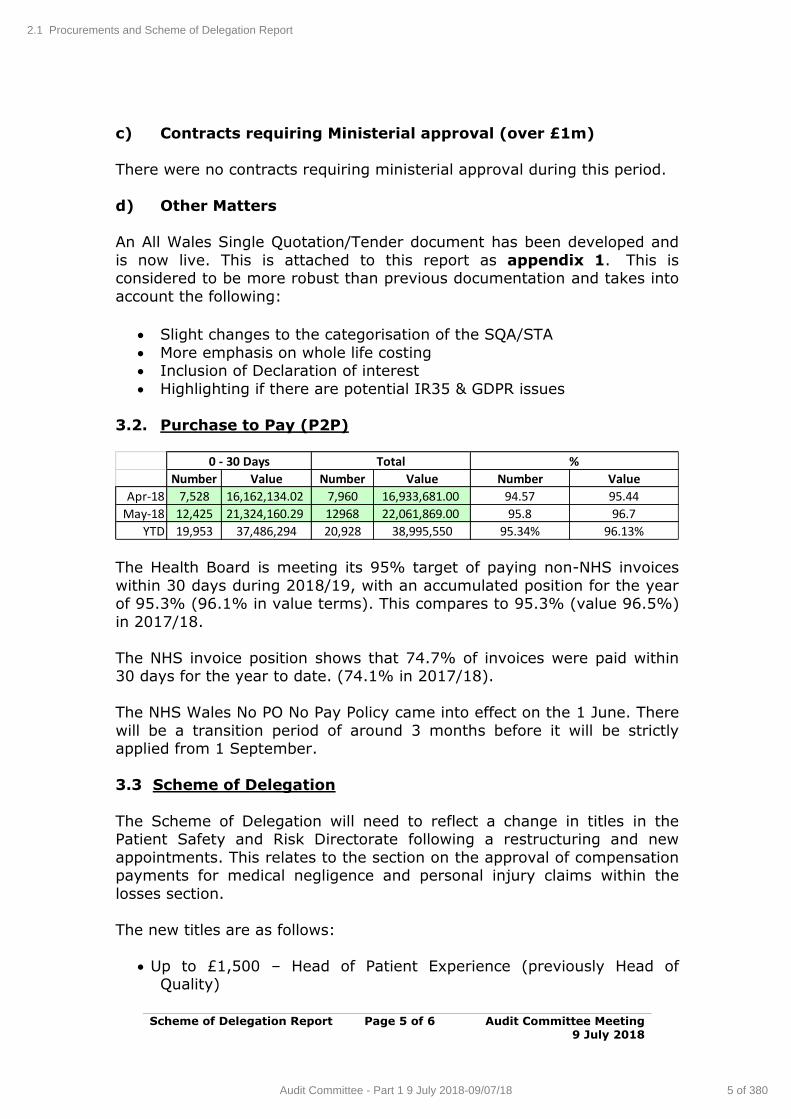
Scheme of Delegation Report Page 5 of 6 Audit Committee Meeting 9 July 2018
c) Contracts requiring Ministerial approval (over £1m)
There were no contracts requiring ministerial approval during this period.
d) Other Matters
An All Wales Single Quotation/Tender document has been developed and
is now live. This is attached to this report as appendix 1. This is considered to be more robust than previous documentation and takes into
account the following:
Slight changes to the categorisation of the SQA/STA
More emphasis on whole life costing Inclusion of Declaration of interest
Highlighting if there are potential IR35 & GDPR issues
3.2. Purchase to Pay (P2P)
Number Value Number Value Number Value
Apr-18 7,528 16,162,134.02 7,960 16,933,681.00 94.57 95.44
May-18 12,425 21,324,160.29 12968 22,061,869.00 95.8 96.7
YTD 19,953 37,486,294 20,928 38,995,550 95.34% 96.13%
0 - 30 Days Total %
The Health Board is meeting its 95% target of paying non-NHS invoices
within 30 days during 2018/19, with an accumulated position for the year of 95.3% (96.1% in value terms). This compares to 95.3% (value 96.5%)
in 2017/18.
The NHS invoice position shows that 74.7% of invoices were paid within 30 days for the year to date. (74.1% in 2017/18).
The NHS Wales No PO No Pay Policy came into effect on the 1 June. There
will be a transition period of around 3 months before it will be strictly applied from 1 September.
3.3 Scheme of Delegation
The Scheme of Delegation will need to reflect a change in titles in the Patient Safety and Risk Directorate following a restructuring and new
appointments. This relates to the section on the approval of compensation payments for medical negligence and personal injury claims within the
losses section.
The new titles are as follows:
Up to £1,500 – Head of Patient Experience (previously Head of Quality)
2.1 Procurements and Scheme of Delegation Report
5 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Scheme of Delegation Report Page 6 of 6 Audit Committee Meeting 9 July 2018
£1,500 - £5,000 – Head of Patient Experience (previously Assistant Director of Nursing and Quality)
£5,000 - £20,000 – Assistant Director Quality and Patient Experience (previously Assistant Director Quality Improvement and Clinical
Governance)
Titles of approvers above £20,000 remain unchanged
4. RECOMMENDATION
The Audit Committee is asked to:
a) NOTE the transactions approved by exception within the Scheme of Delegation, for the period 1.3.18 to 31.5.18; and
the All-Wales SQA/STA Documentation
b) NOTE the update regarding Purchase to Pay issues.
c) APPROVE the change to the Scheme of Delegation reflecting the new titles in the Patient Safety and Risk Directorate
Freedom of information status
Open
2.1 Procurements and Scheme of Delegation Report
6 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
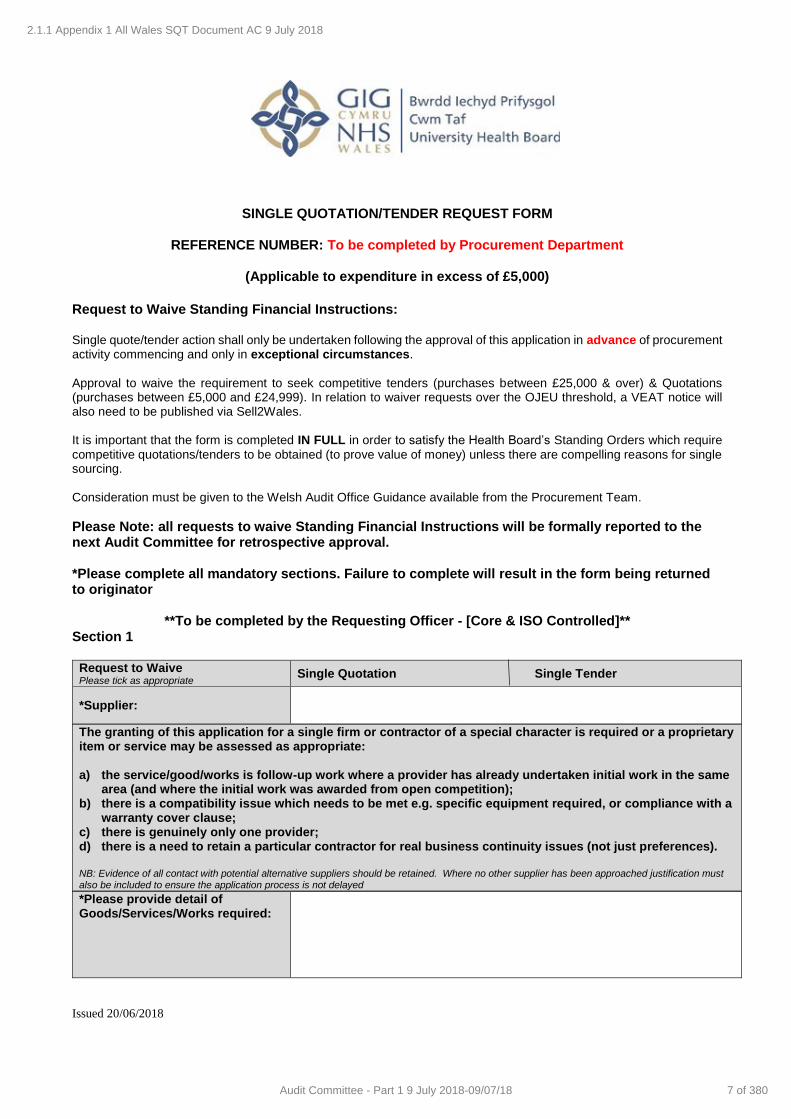
Issued 20/06/2018
SINGLE QUOTATION/TENDER REQUEST FORM
REFERENCE NUMBER: To be completed by Procurement Department
(Applicable to expenditure in excess of £5,000)
Request to Waive Standing Financial Instructions: Single quote/tender action shall only be undertaken following the approval of this application in advance of procurement activity commencing and only in exceptional circumstances. Approval to waive the requirement to seek competitive tenders (purchases between £25,000 & over) & Quotations (purchases between £5,000 and £24,999). In relation to waiver requests over the OJEU threshold, a VEAT notice will also need to be published via Sell2Wales. It is important that the form is completed IN FULL in order to satisfy the Health Board’s Standing Orders which require competitive quotations/tenders to be obtained (to prove value of money) unless there are compelling reasons for single sourcing. Consideration must be given to the Welsh Audit Office Guidance available from the Procurement Team.
Please Note: all requests to waive Standing Financial Instructions will be formally reported to the next Audit Committee for retrospective approval. *Please complete all mandatory sections. Failure to complete will result in the form being returned to originator
**To be completed by the Requesting Officer - [Core & ISO Controlled]** Section 1
Request to Waive Please tick as appropriate
Single Quotation Single Tender
*Supplier:
The granting of this application for a single firm or contractor of a special character is required or a proprietary item or service may be assessed as appropriate: a) the service/good/works is follow-up work where a provider has already undertaken initial work in the same
area (and where the initial work was awarded from open competition); b) there is a compatibility issue which needs to be met e.g. specific equipment required, or compliance with a
warranty cover clause; c) there is genuinely only one provider; d) there is a need to retain a particular contractor for real business continuity issues (not just preferences).
NB: Evidence of all contact with potential alternative suppliers should be retained. Where no other supplier has been approached justification must also be included to ensure the application process is not delayed
*Please provide detail of Goods/Services/Works required:
2.1.1 Appendix 1 All Wales SQT Document AC 9 July 2018
7 of 380Audit Committee - Part 1 9 July 2018-09/07/18
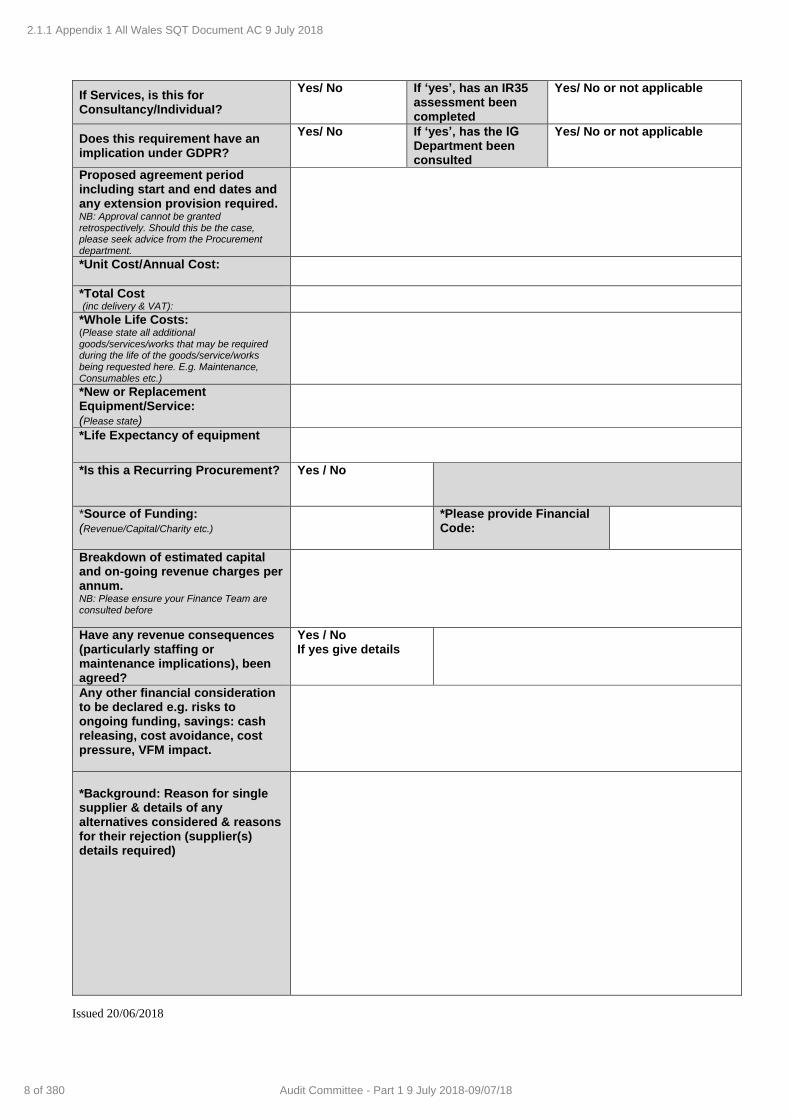
Issued 20/06/2018
If Services, is this for Consultancy/IndividuaI?
Yes/ No If ‘yes’, has an IR35 assessment been completed
Yes/ No or not applicable
Does this requirement have an implication under GDPR?
Yes/ No If ‘yes’, has the IG Department been consulted
Yes/ No or not applicable
Proposed agreement period including start and end dates and any extension provision required. NB: Approval cannot be granted retrospectively. Should this be the case, please seek advice from the Procurement department.
*Unit Cost/Annual Cost:
*Total Cost (inc delivery & VAT):
*Whole Life Costs: (Please state all additional goods/services/works that may be required during the life of the goods/service/works being requested here. E.g. Maintenance, Consumables etc.)
*New or Replacement Equipment/Service: (Please state)
*Life Expectancy of equipment
*Is this a Recurring Procurement?
Yes / No
*Source of Funding: (Revenue/Capital/Charity etc.)
*Please provide Financial Code:
Breakdown of estimated capital and on-going revenue charges per annum. NB: Please ensure your Finance Team are consulted before
Have any revenue consequences (particularly staffing or maintenance implications), been agreed?
Yes / No If yes give details
Any other financial consideration to be declared e.g. risks to ongoing funding, savings: cash releasing, cost avoidance, cost pressure, VFM impact.
*Background: Reason for single supplier & details of any alternatives considered & reasons for their rejection (supplier(s) details required)
2.1.1 Appendix 1 All Wales SQT Document AC 9 July 2018
8 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
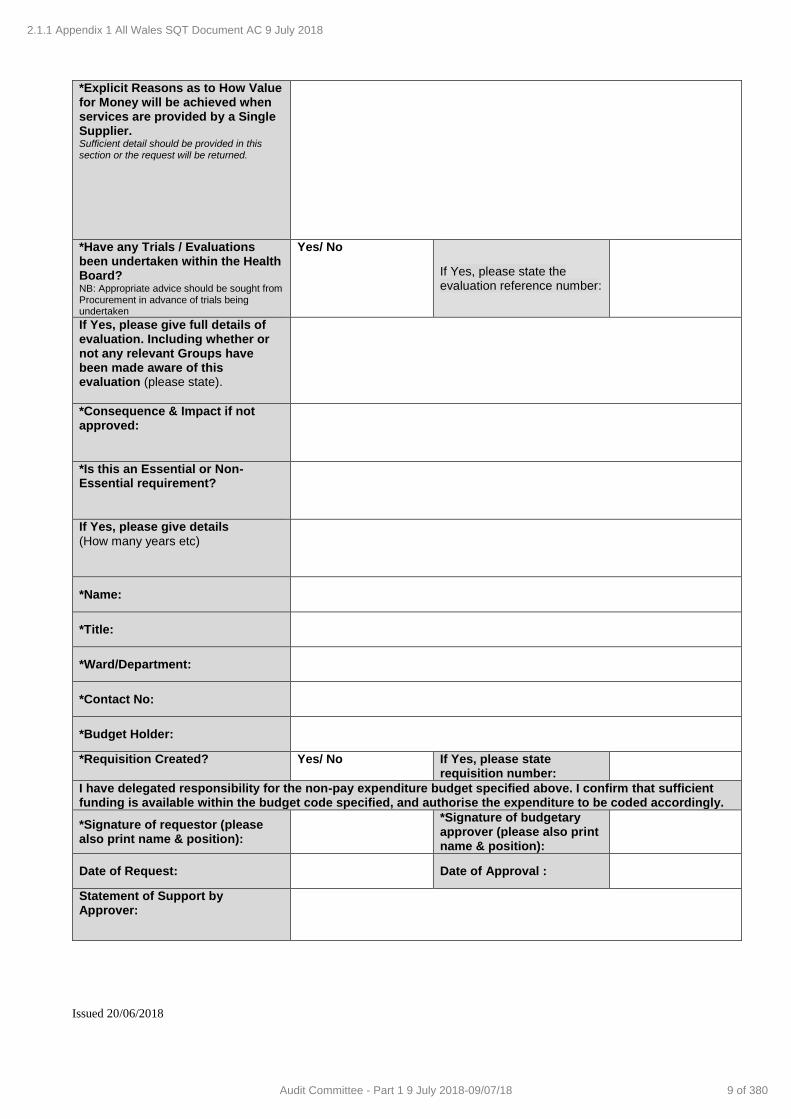
Issued 20/06/2018
*Explicit Reasons as to How Value for Money will be achieved when services are provided by a Single Supplier. Sufficient detail should be provided in this section or the request will be returned.
*Have any Trials / Evaluations been undertaken within the Health Board? NB: Appropriate advice should be sought from Procurement in advance of trials being undertaken
Yes/ No
If Yes, please state the evaluation reference number:
If Yes, please give full details of evaluation. Including whether or not any relevant Groups have been made aware of this evaluation (please state).
*Consequence & Impact if not approved:
*Is this an Essential or Non-Essential requirement?
If Yes, please give details (How many years etc)
*Name:
*Title:
*Ward/Department:
*Contact No:
*Budget Holder:
*Requisition Created? Yes/ No If Yes, please state requisition number:
I have delegated responsibility for the non-pay expenditure budget specified above. I confirm that sufficient funding is available within the budget code specified, and authorise the expenditure to be coded accordingly.
*Signature of requestor (please also print name & position):
*Signature of budgetary approver (please also print name & position):
Date of Request:
Date of Approval :
Statement of Support by Approver:
2.1.1 Appendix 1 All Wales SQT Document AC 9 July 2018
9 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Issued 20/06/2018
**Budget Approver to Complete** Section 2
Declaration of Interest The Health Board is obliged to ensure that all procurement processes are carried out in accordance with the public procurement rules and NHS Wales’s guidance. Where an employee is engaged in a procurement exercise a formal declaration is required to confirm that there is no potential interest which may give rise to a conflict.
Please confirm the following statements are correct:
1. Neither I, my family, friends, acquaintances or work colleagues involved in this process, will receive any benefit or gain (financial or otherwise, directly or indirectly) if the contract is awarded to any of the bidders involved in the process as they become known.
2a. I have no material interest in whether the contract is awarded or not.
2b. I am not in possession of any Additional Information in respect of the procurement process. (Save for the information in the ‘Additional Information box below)
3. I currently do not benefit in any way, financially or otherwise, including (but not limited to) the receipt of a grant or outside funding, that could influence my decision in respect of the procurement or any of the bidders involved in this process .
4.
I have not received hospitality (other than of a nominal value or that declared in the register of gifts and hospitality maintained by Corporate Management) or any material gifts, as outlined in the Trusts Standards of Behaviour Framework Policy http://howis.wales.nhs.uk/sitesplus/972/page/51681 from any of the bidders involved in the process.
5. I have read, understood and will abide by the NHS Guidance entitled "Standards of Business Conduct for NHS Staff" (DGM (93)84) and the Trust Standards of Behaviour Framework Policy. http://howis.wales.nhs.uk/sitesplus/972/page/51681
6.
By signing this declaration I understand that it is my responsibility that should my circumstance change or a new relationship be established in relation to any bidding organisation, I will consult with the Lead Procurement contact and am aware that I may be required to complete a new Declaration of Interest or be required to withdraw my participation.
7. I will keep the identities of the bidders, the content of the bids and procurement documents confidential.
I hereby certify that, to the best of my knowledge and belief, the statements set out above are correct. I understand that any failure on my part to declare an interest in a contract or otherwise to breach the rules and instructions mentioned above is a serious matter and could result in further legal or professional action being taken against me, including (but not limited to):
Exclusion from the current procurement exercise and future procurement activities
For Trust employees, it could result in disciplinary proceedings being initiated.
For non-employees of the Trust we reserve the right to report the matter to their relevant employing organisation and professional body as potential professional misconduct
Should the matter involve issues that are of a criminal nature e.g. fraud, bribery or corruption then the Trust will notify the appropriate authority to take any necessary action which may include prosecution.
Signature:
Signature:
Print Name:
Position:
Date:
2.1.1 Appendix 1 All Wales SQT Document AC 9 July 2018
10 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Issued 20/06/2018
Authorisation - [Section Non Core to be Amended in Line with Local Scheme of Delegation]
Section 3
Designation Signature Date Directorate Manager or equivalent Up to £25,000
Comments:
Assistant/Deputy Director Up to £50,000
Comments:
Executive Director Up to £100,000
Comments:
Please note Single Tender/Quotation Action requests cannot be processed unless supported by the above signatures, electronic signatures will NOT be accepted, unless accompanied by an e-mail trail to prove that the authorisation has been completed correctly.
Please now forward to Procurement Department
** For Procurement Department Completion Only**
Section 4
Procurement Advice (Delete or cross through as
appropriate)
Yes, the SQA or STA is an appropriate course
No, an alternative option can be pursued
No Option
Procurement Advice or Rejection Comments: (including any conditions/future actions):
Endorsed
Yes/No
Head of Procurement Signature:
Date:
2.1.1 Appendix 1 All Wales SQT Document AC 9 July 2018
11 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Issued 20/06/2018
** Director of Finance and/or Chief Executive Officer Approval** Section 5
Request Supported?
Yes/No
Supporting or Rejection Comments: (including any conditions/future actions):
Designation Signature Date
Mr Steve Webster Director of Finance
Mrs Allison Williams Chief Executive Officer
Notes:
Upon completion of this section, please forward to: Procurement Department
In the event that the Head of Procurement/Sourcing and Chief Executive do not authorise the request to waive the Standing Financial Instructions the budget holder will be advised immediately of the decision.
2.1.1 Appendix 1 All Wales SQT Document AC 9 July 2018
12 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Audit Recommendations Page 1 of 21 Audit Committee Meeting Tracker 9 July 2018
AGENDA ITEM 2.2
9 July 2018
Audit Committee Report
AUDIT RECOMMENDATIONS TRACKER
Executive Lead: Board Secretary / Director of Corporate Services
Author: Board Secretary / Director of Corporate Services
Contact Details for further information: Robert Williams, 01443 744800 or email [email protected]
Purpose of the Audit Committee Report
To update Audit Committee on reported progress with implementation of Audit report recommendations.
Governance
Link to Health
Board Strategic Objective(s)
The Board’s overarching role is to ensure its Strategy
outlined within ‘Cwm Taf Cares’ 3 Year Integrated Medium Term Plan 2018-2021 and the related
organisational objectives aligned with the Institute of Healthcare Improvement's (IHI) ‘Triple Aim’ are being
progressed, these in summary are: To improve quality, safety and patient experience.
To protect and improve population health. To ensure that the services provided are accessible
and sustainable into the future. To provide strong governance and assurance.
To ensure good value based care and treatment for our patients in line with the resources made available
to the Health Board.
This report focuses mainly on ensuring the Board
provides strong governance and assurance.
Supporting
evidence
Wales Audit Office Reports
Internal Audit Reports
Engagement – Who has been involved in this work?
Executive Director and Officer leads for each of the Wales Audit Office
(WAO) and Internal Audit (IA) reports have been involved in providing
updates on progress where appropriate.
2.2 Audit Recommendations Tracker
13 of 380Audit Committee - Part 1 9 July 2018-09/07/18
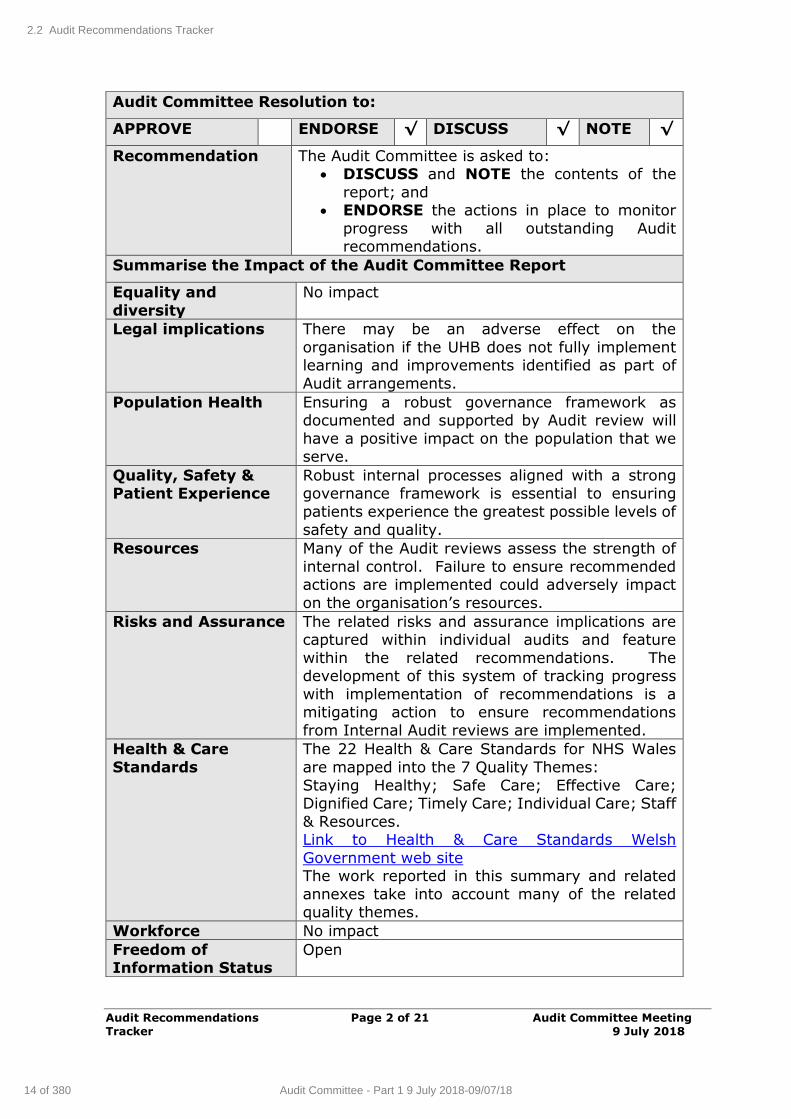
Audit Recommendations Page 2 of 21 Audit Committee Meeting Tracker 9 July 2018
Audit Committee Resolution to:
APPROVE ENDORSE √ DISCUSS √ NOTE √
Recommendation The Audit Committee is asked to: DISCUSS and NOTE the contents of the
report; and ENDORSE the actions in place to monitor
progress with all outstanding Audit recommendations.
Summarise the Impact of the Audit Committee Report
Equality and
diversity
No impact
Legal implications There may be an adverse effect on the
organisation if the UHB does not fully implement learning and improvements identified as part of
Audit arrangements.
Population Health Ensuring a robust governance framework as documented and supported by Audit review will
have a positive impact on the population that we serve.
Quality, Safety & Patient Experience
Robust internal processes aligned with a strong governance framework is essential to ensuring
patients experience the greatest possible levels of
safety and quality.
Resources Many of the Audit reviews assess the strength of
internal control. Failure to ensure recommended actions are implemented could adversely impact
on the organisation’s resources.
Risks and Assurance The related risks and assurance implications are captured within individual audits and feature
within the related recommendations. The development of this system of tracking progress
with implementation of recommendations is a mitigating action to ensure recommendations
from Internal Audit reviews are implemented.
Health & Care
Standards
The 22 Health & Care Standards for NHS Wales
are mapped into the 7 Quality Themes:
Staying Healthy; Safe Care; Effective Care; Dignified Care; Timely Care; Individual Care; Staff
& Resources. Link to Health & Care Standards Welsh
Government web site The work reported in this summary and related
annexes take into account many of the related quality themes.
Workforce No impact
Freedom of Information Status
Open
2.2 Audit Recommendations Tracker
14 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Audit Recommendations Page 3 of 21 Audit Committee Meeting Tracker 9 July 2018
AUDIT RECOMMENDATIONS TRACKER
1. SITUATION / PURPOSE OF REPORT
The main purpose of this report is to present an update to the Audit Committee
on reported progress with implementation of Audit report recommendations. This report relates to both internal and external audit review recommendations.
2. BACKGROUND / INTRODUCTION
Ensuring the organisation learns from and implements recommendations falling
out of Audit reports is an essential component of a strong organisational governance framework.
Tracking progress with implementation of Audit recommendations against agreed
timescales is also an important assurance tool to support the work of the Committee and to providing assurance into the Board.
It is also important to consider why implementation of some recommendations
has been delayed against the original agreed timescales and management response.
The attached summary table and supporting documents (Internal Audit –
Appendix 1) make reference to 5 of the 59 Internal Audit reports received by
the Audit Committee since April 2017, and 2* of the 23 Wales Audit Office reports received since January 2014 (including National reports). In relation to Internal
Audit, the summary table only references audit activity from April 2016 to date, as all pre April 2016 reports have reportedly been implemented (47 Audit
Reports).
A judgement on completion / partial completion has been made where progress is reported in this way.
Of the 59 Internal Audit report updates summarised and included in this report:
316 recommendations have been made; 289 recommendations have been reportedly implemented, although it is
important to note that some of these require ongoing action; 27 recommendations are reportedly outstanding; and of these
o 10 are overdue their original date for implementation (although a
number are partially implemented or related work is progressing). Of these, there is one categorised as a High Risk recommendation
(timescale June 2018).
Progress with reported completion of recommendations continues to improve and this update report focuses on the ‘overdue’ or ongoing recommendations
reported as outstanding within the updates sought from officer leads. A summary of updated actions against outstanding recommendations is attached
as Appendix 1a.
2.2 Audit Recommendations Tracker
15 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Audit Recommendations Page 4 of 21 Audit Committee Meeting Tracker 9 July 2018
Of the 23 Wales Audit Office reports (External Audit Appendix 2) covered within
the Audit Tracker:
174 recommendations have been made;
162 recommendations have reportedly been implemented, although it is important to note that some of these require ongoing action;
12 recommendations are outstanding (3 of which are overdue their originally agreed completion date and relate to Follow Up Outpatients Not
Booked), although it is important to note that some actions have taken place to progress implementation whilst some remain ongoing. Members
will note the close and ongoing scrutiny at Finance, Performance & Workforce Committee and Quality, Safety & Risk Committee on actions to
address the issues associated with Follow Up Outpatients Not Booked.
A summary of updated actions against outstanding recommendations is attached as Appendix 2a.
Members will note discussion regarding the follow up outpatient not booked review and related actions being reported through Quality, Safety & Risk
Committee (in May 2018) and Finance, Performance & Workforce Committee during the next quarter.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
Where there are actions outstanding within the tracker log, the related updates
are referenced below for consideration of the Audit Committee. The Audit Committee has agreed that where High and/or medium risk related
recommended actions fall outside a 6 months timescale, the lead Director (s) will be asked to present an update on the related reasons for the slippage in
timescales and intended action to address the recommendation to the Committee.
Members will note that at the last Committee meeting and in relation to ‘High’
risk actions outstanding associated with WAO Audit Reports, that the Director of Workforce & OD (Occupational Health & Well-Being) attended to discuss progress
and further action.
Since April’s meeting, further positive progress on implementation of management actions has been reported, with a further reduction overall in
outstanding actions in response to recommendations made.
2.2 Audit Recommendations Tracker
16 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Audit Recommendations Page 5 of 21 Audit Committee Meeting Tracker 9 July 2018
4. RECOMMENDATION
Members of the Audit Committee are asked to:
DISCUSS and NOTE this update report and the attached summary of
progress
ENDORSE the progress made to date and agree any related further actions, particularly relating to the High Risk recommendations, where
action has been significantly delayed beyond originally intended completion dates.
Freedom of Information Status
Open
2.2 Audit Recommendations Tracker
17 of 380Audit Committee - Part 1 9 July 2018-09/07/18
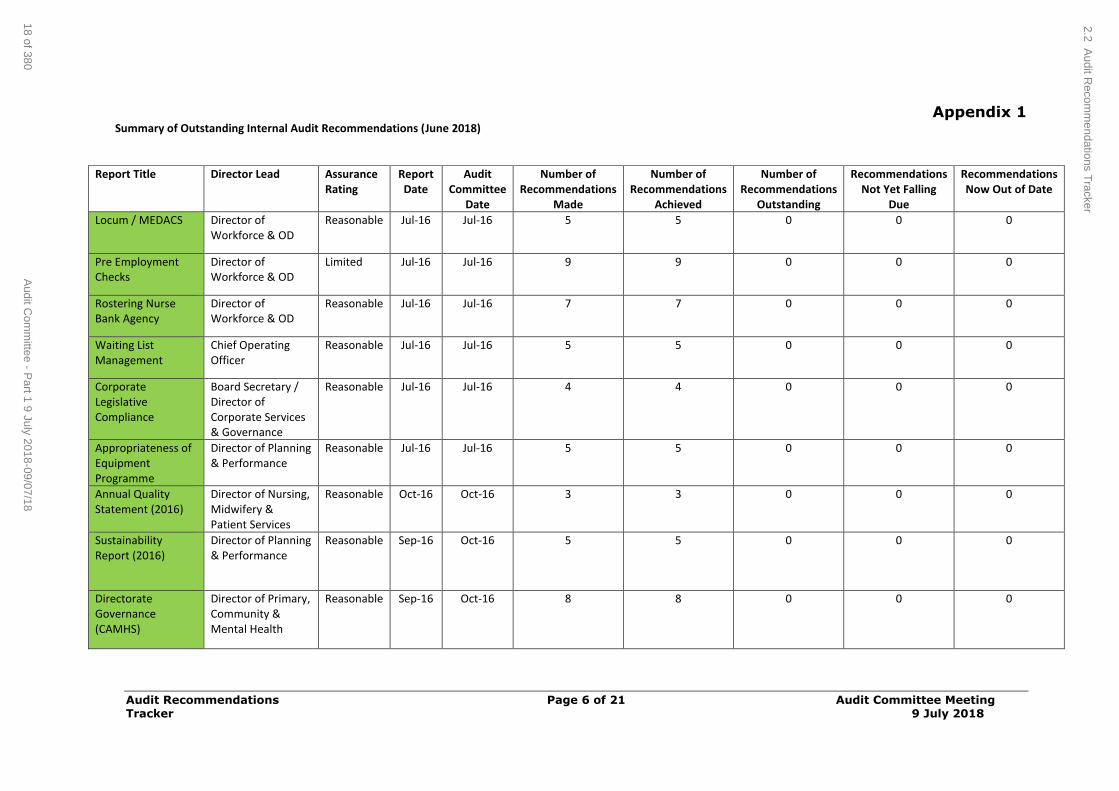
Audit Recommendations Page 6 of 21 Audit Committee Meeting Tracker 9 July 2018
Appendix 1 Summary of Outstanding Internal Audit Recommendations (June 2018)
Report Title Director Lead Assurance
Rating Report Date
Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
Locum / MEDACS Director of Workforce & OD
Reasonable Jul-16 Jul-16 5 5 0 0 0
Pre Employment Checks
Director of Workforce & OD
Limited Jul-16 Jul-16 9 9 0 0 0
Rostering Nurse Bank Agency
Director of Workforce & OD
Reasonable Jul-16 Jul-16 7 7 0 0 0
Waiting List Management
Chief Operating Officer
Reasonable Jul-16 Jul-16 5 5 0 0 0
Corporate Legislative Compliance
Board Secretary / Director of Corporate Services & Governance
Reasonable Jul-16 Jul-16 4 4 0 0 0
Appropriateness of Equipment Programme
Director of Planning & Performance
Reasonable Jul-16 Jul-16 5 5 0 0 0
Annual Quality Statement (2016)
Director of Nursing, Midwifery & Patient Services
Reasonable Oct-16 Oct-16 3 3 0 0 0
Sustainability Report (2016)
Director of Planning & Performance
Reasonable Sep-16 Oct-16 5 5 0 0 0
Directorate Governance (CAMHS)
Director of Primary, Community & Mental Health
Reasonable Sep-16 Oct-16 8 8 0 0 0
2.2 Audit R
ecomm
endations Tracker
18 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
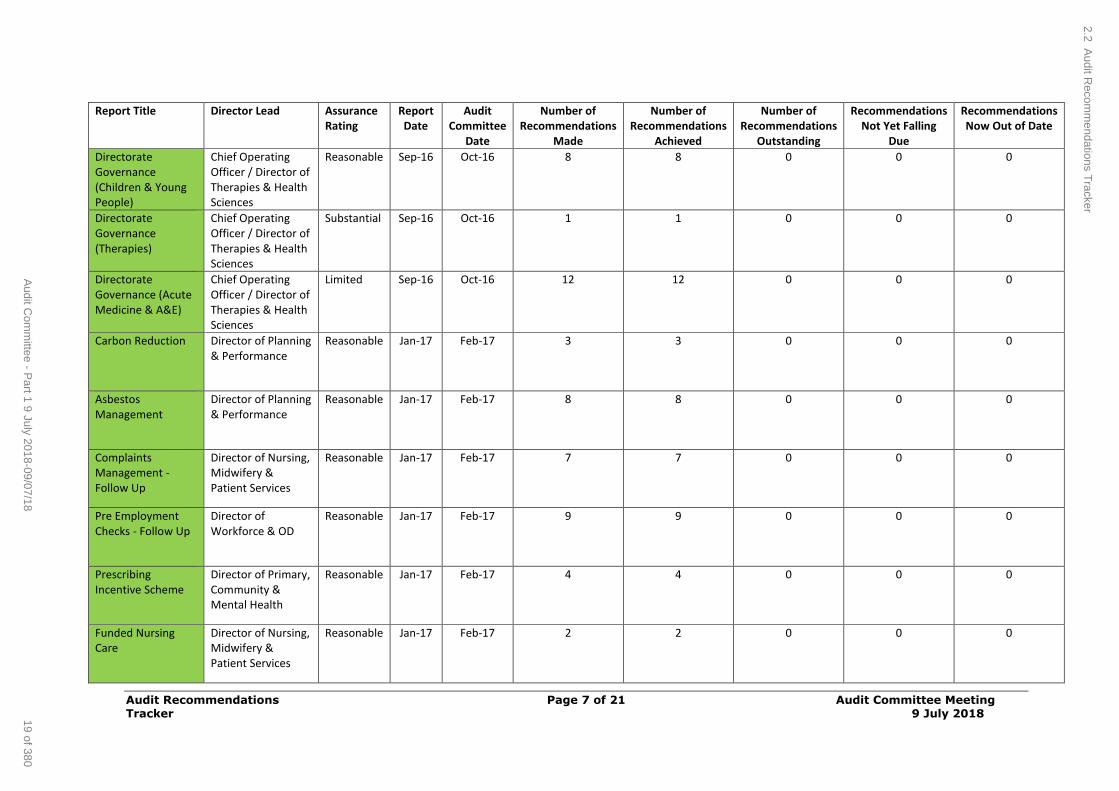
Audit Recommendations Page 7 of 21 Audit Committee Meeting Tracker 9 July 2018
Report Title Director Lead Assurance Rating
Report Date
Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
Directorate Governance (Children & Young People)
Chief Operating Officer / Director of Therapies & Health Sciences
Reasonable Sep-16 Oct-16 8 8 0 0 0
Directorate Governance (Therapies)
Chief Operating Officer / Director of Therapies & Health Sciences
Substantial Sep-16 Oct-16 1 1 0 0 0
Directorate Governance (Acute Medicine & A&E)
Chief Operating Officer / Director of Therapies & Health Sciences
Limited Sep-16 Oct-16 12 12 0 0 0
Carbon Reduction Director of Planning & Performance
Reasonable Jan-17 Feb-17 3 3 0 0 0
Asbestos Management
Director of Planning & Performance
Reasonable Jan-17 Feb-17 8 8 0 0 0
Complaints Management - Follow Up
Director of Nursing, Midwifery & Patient Services
Reasonable Jan-17 Feb-17 7 7 0 0 0
Pre Employment Checks - Follow Up
Director of Workforce & OD
Reasonable Jan-17 Feb-17 9 9 0 0 0
Prescribing Incentive Scheme
Director of Primary, Community & Mental Health
Reasonable Jan-17 Feb-17 4 4 0 0 0
Funded Nursing Care
Director of Nursing, Midwifery & Patient Services
Reasonable Jan-17 Feb-17 2 2 0 0 0
2.2 Audit R
ecomm
endations Tracker
19 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
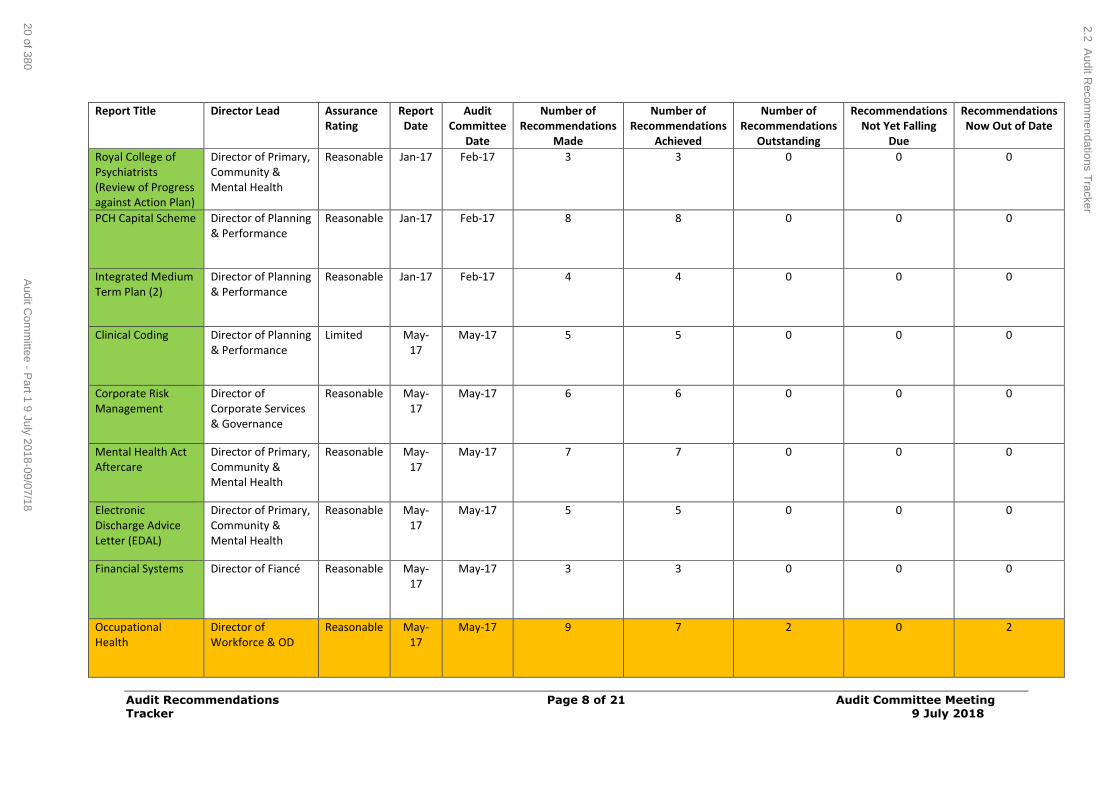
Audit Recommendations Page 8 of 21 Audit Committee Meeting Tracker 9 July 2018
Report Title Director Lead Assurance Rating
Report Date
Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
Royal College of Psychiatrists (Review of Progress against Action Plan)
Director of Primary, Community & Mental Health
Reasonable Jan-17 Feb-17 3 3 0 0 0
PCH Capital Scheme Director of Planning & Performance
Reasonable Jan-17 Feb-17 8 8 0 0 0
Integrated Medium Term Plan (2)
Director of Planning & Performance
Reasonable Jan-17 Feb-17 4 4 0 0 0
Clinical Coding Director of Planning & Performance
Limited May-17
May-17 5 5 0 0 0
Corporate Risk Management
Director of Corporate Services & Governance
Reasonable May-17
May-17 6 6 0 0 0
Mental Health Act Aftercare
Director of Primary, Community & Mental Health
Reasonable May-17
May-17 7 7 0 0 0
Electronic Discharge Advice Letter (EDAL)
Director of Primary, Community & Mental Health
Reasonable May-17
May-17 5 5 0 0 0
Financial Systems Director of Fiancé Reasonable May-17
May-17 3 3 0 0 0
Occupational Health
Director of Workforce & OD
Reasonable May-17
May-17 9 7 2 0 2
2.2 Audit R
ecomm
endations Tracker
20 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
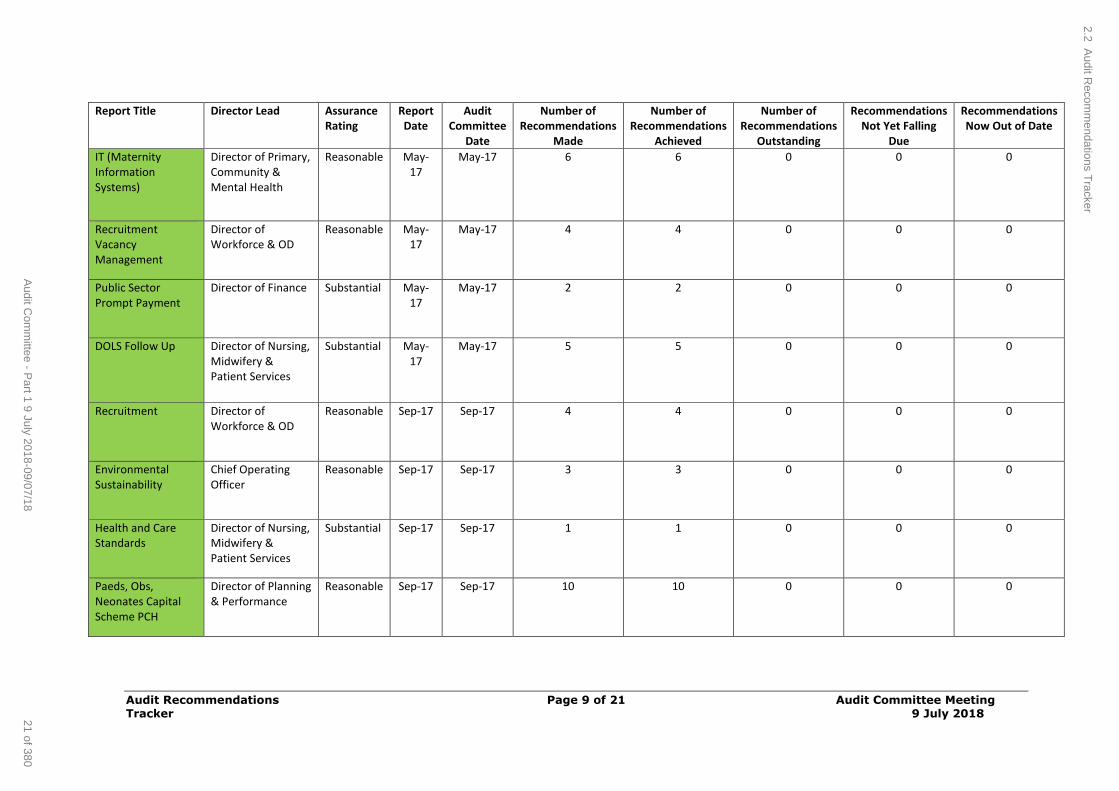
Audit Recommendations Page 9 of 21 Audit Committee Meeting Tracker 9 July 2018
Report Title Director Lead Assurance Rating
Report Date
Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
IT (Maternity Information Systems)
Director of Primary, Community & Mental Health
Reasonable May-17
May-17 6 6 0 0 0
Recruitment Vacancy Management
Director of Workforce & OD
Reasonable May-17
May-17 4 4 0 0 0
Public Sector Prompt Payment
Director of Finance Substantial May-17
May-17 2 2 0 0 0
DOLS Follow Up Director of Nursing, Midwifery & Patient Services
Substantial May-17
May-17 5 5 0 0 0
Recruitment Director of Workforce & OD
Reasonable Sep-17 Sep-17 4 4 0 0 0
Environmental Sustainability
Chief Operating Officer
Reasonable Sep-17 Sep-17 3 3 0 0 0
Health and Care Standards
Director of Nursing, Midwifery & Patient Services
Substantial Sep-17 Sep-17 1 1 0 0 0
Paeds, Obs, Neonates Capital Scheme PCH
Director of Planning & Performance
Reasonable Sep-17 Sep-17 10 10 0 0 0
2.2 Audit R
ecomm
endations Tracker
21 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
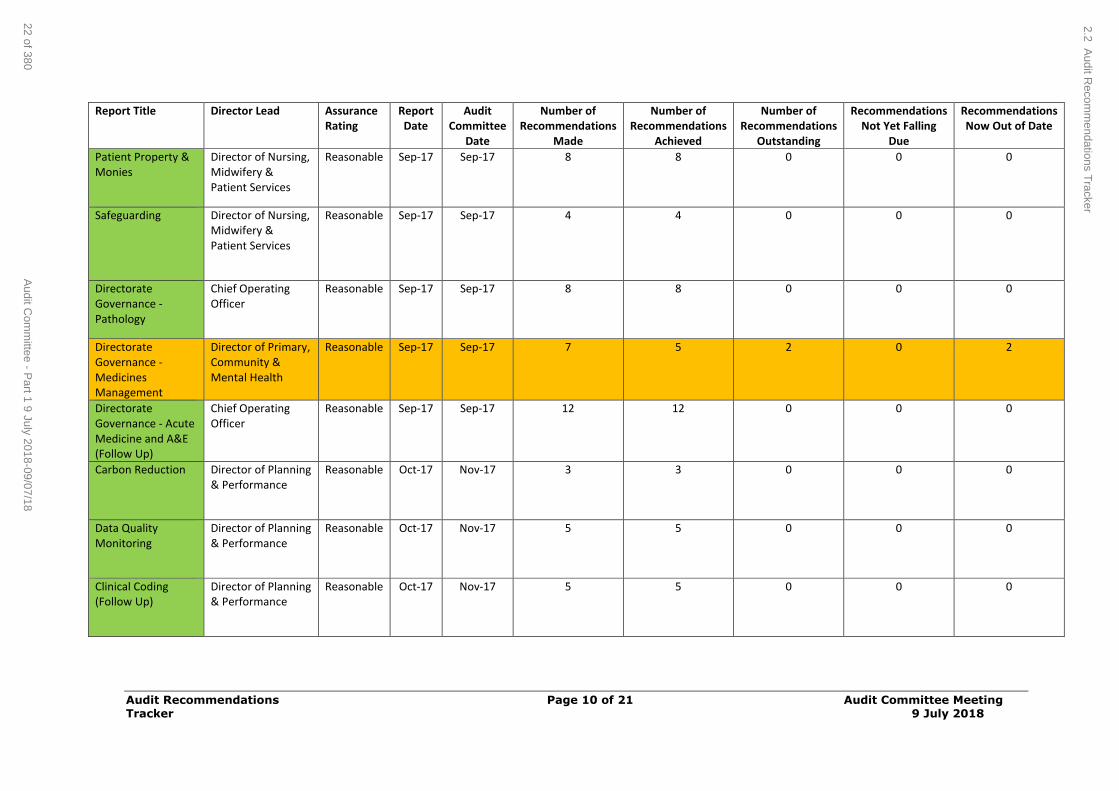
Audit Recommendations Page 10 of 21 Audit Committee Meeting Tracker 9 July 2018
Report Title Director Lead Assurance Rating
Report Date
Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
Patient Property & Monies
Director of Nursing, Midwifery & Patient Services
Reasonable Sep-17 Sep-17 8 8 0 0 0
Safeguarding Director of Nursing, Midwifery & Patient Services
Reasonable Sep-17 Sep-17 4 4 0 0 0
Directorate Governance - Pathology
Chief Operating Officer
Reasonable Sep-17 Sep-17 8 8 0 0 0
Directorate Governance - Medicines Management
Director of Primary, Community & Mental Health
Reasonable Sep-17 Sep-17 7 5 2 0 2
Directorate Governance - Acute Medicine and A&E (Follow Up)
Chief Operating Officer
Reasonable Sep-17 Sep-17 12 12 0 0 0
Carbon Reduction Director of Planning & Performance
Reasonable Oct-17 Nov-17 3 3 0 0 0
Data Quality Monitoring
Director of Planning & Performance
Reasonable Oct-17 Nov-17 5 5 0 0 0
Clinical Coding (Follow Up)
Director of Planning & Performance
Reasonable Oct-17 Nov-17 5 5 0 0 0
2.2 Audit R
ecomm
endations Tracker
22 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
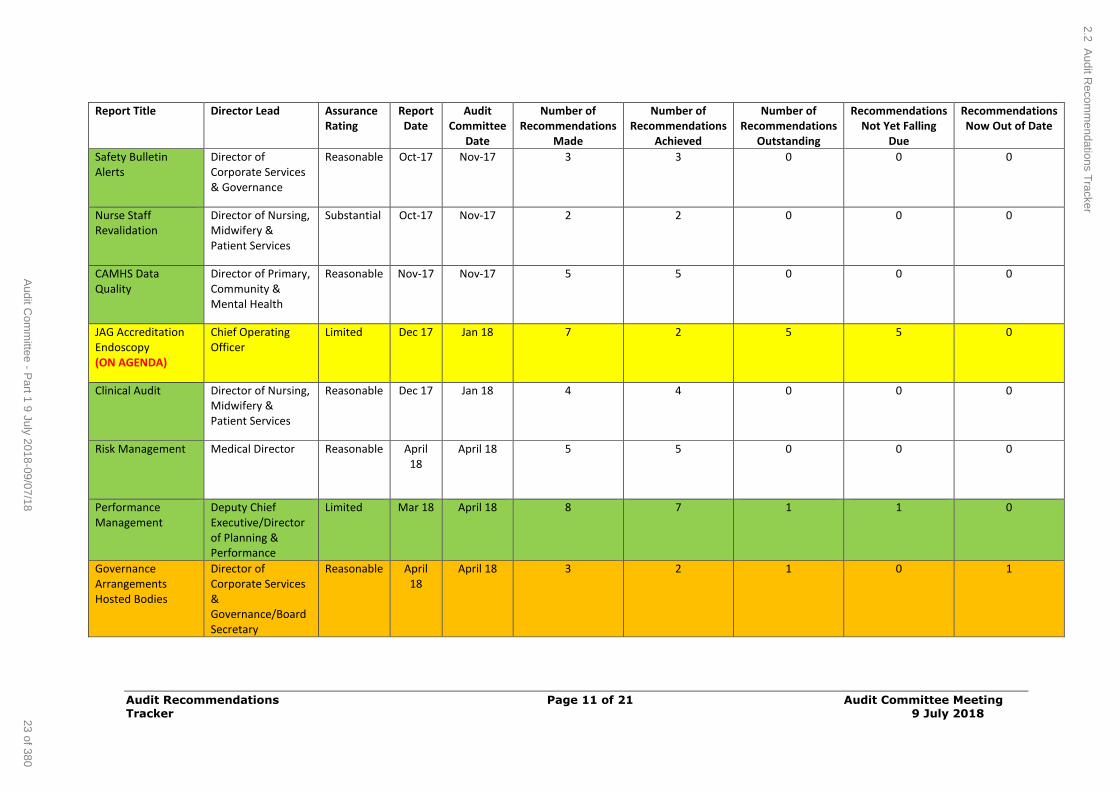
Audit Recommendations Page 11 of 21 Audit Committee Meeting Tracker 9 July 2018
Report Title Director Lead Assurance Rating
Report Date
Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
Safety Bulletin Alerts
Director of Corporate Services & Governance
Reasonable Oct-17 Nov-17 3 3 0 0 0
Nurse Staff Revalidation
Director of Nursing, Midwifery & Patient Services
Substantial Oct-17 Nov-17 2 2 0 0 0
CAMHS Data Quality
Director of Primary, Community & Mental Health
Reasonable Nov-17 Nov-17 5 5 0 0 0
JAG Accreditation Endoscopy (ON AGENDA)
Chief Operating Officer
Limited Dec 17
Jan 18
7 2 5 5 0
Clinical Audit Director of Nursing, Midwifery & Patient Services
Reasonable
Dec 17
Jan 18
4 4 0 0 0
Risk Management Medical Director Reasonable April 18
April 18 5 5 0 0 0
Performance Management
Deputy Chief Executive/Director of Planning & Performance
Limited Mar 18 April 18 8 7 1 1 0
Governance Arrangements Hosted Bodies
Director of Corporate Services & Governance/Board Secretary
Reasonable April 18
April 18 3 2 1 0 1
2.2 Audit R
ecomm
endations Tracker
23 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
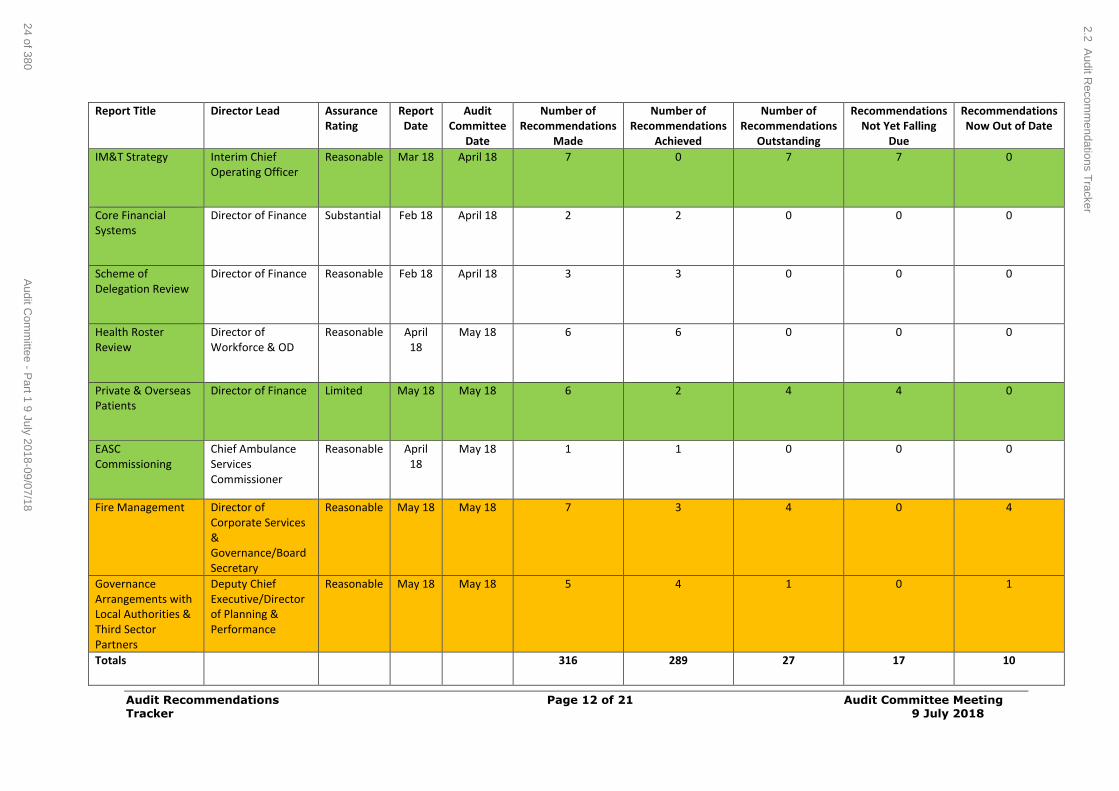
Audit Recommendations Page 12 of 21 Audit Committee Meeting Tracker 9 July 2018
Report Title Director Lead Assurance Rating
Report Date
Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
IM&T Strategy Interim Chief Operating Officer
Reasonable Mar 18 April 18 7 0 7 7 0
Core Financial Systems
Director of Finance Substantial Feb 18 April 18 2 2 0 0 0
Scheme of Delegation Review
Director of Finance Reasonable Feb 18 April 18 3 3 0 0 0
Health Roster Review
Director of Workforce & OD
Reasonable April 18
May 18 6 6 0 0 0
Private & Overseas Patients
Director of Finance Limited May 18 May 18 6 2 4 4 0
EASC Commissioning
Chief Ambulance Services Commissioner
Reasonable April 18
May 18 1 1 0 0 0
Fire Management Director of Corporate Services & Governance/Board Secretary
Reasonable May 18 May 18 7 3 4 0 4
Governance Arrangements with Local Authorities & Third Sector Partners
Deputy Chief Executive/Director of Planning & Performance
Reasonable May 18 May 18 5 4 1 0 1
Totals 316 289 27 17 10
2.2 Audit R
ecomm
endations Tracker
24 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
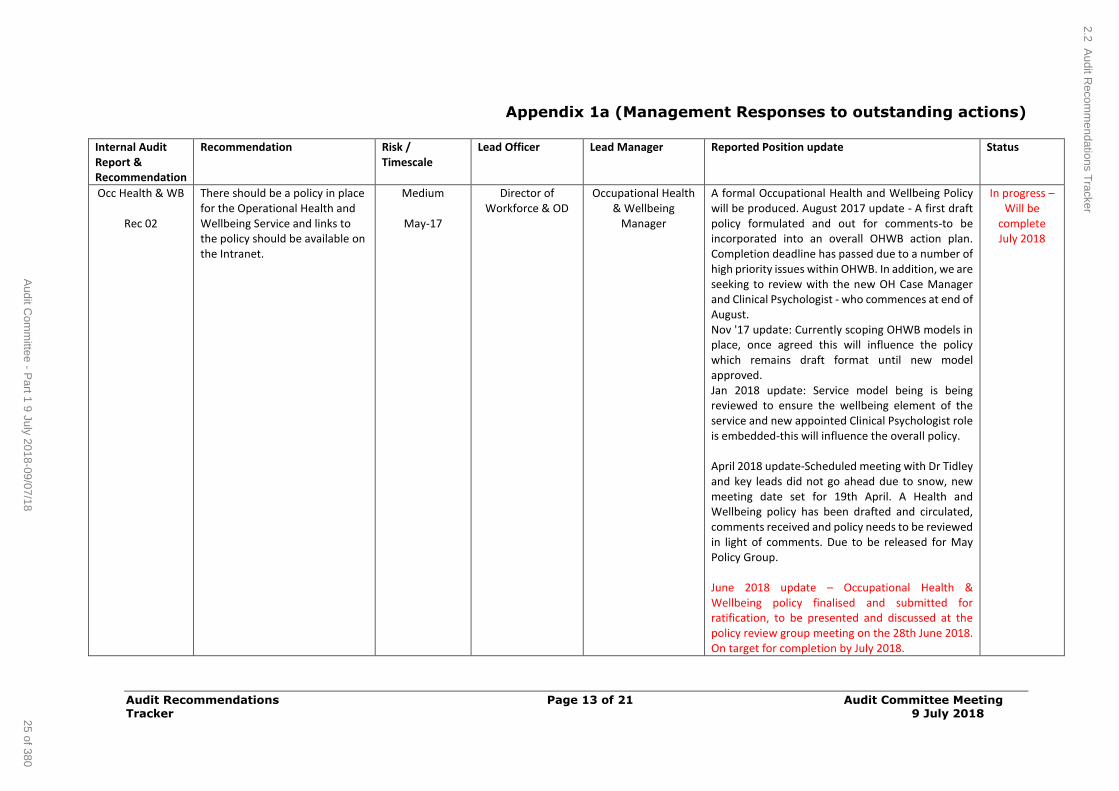
Audit Recommendations Page 13 of 21 Audit Committee Meeting Tracker 9 July 2018
Appendix 1a (Management Responses to outstanding actions)
Internal Audit Report & Recommendation
Recommendation Risk / Timescale
Lead Officer Lead Manager Reported Position update Status
Occ Health & WB
Rec 02
There should be a policy in place for the Operational Health and Wellbeing Service and links to the policy should be available on the Intranet.
Medium
May-17
Director of Workforce & OD
Occupational Health & Wellbeing
Manager
A formal Occupational Health and Wellbeing Policy will be produced. August 2017 update - A first draft policy formulated and out for comments-to be incorporated into an overall OHWB action plan. Completion deadline has passed due to a number of high priority issues within OHWB. In addition, we are seeking to review with the new OH Case Manager and Clinical Psychologist - who commences at end of August. Nov '17 update: Currently scoping OHWB models in place, once agreed this will influence the policy which remains draft format until new model approved. Jan 2018 update: Service model being is being reviewed to ensure the wellbeing element of the service and new appointed Clinical Psychologist role is embedded-this will influence the overall policy. April 2018 update-Scheduled meeting with Dr Tidley and key leads did not go ahead due to snow, new meeting date set for 19th April. A Health and Wellbeing policy has been drafted and circulated, comments received and policy needs to be reviewed in light of comments. Due to be released for May Policy Group. June 2018 update – Occupational Health & Wellbeing policy finalised and submitted for ratification, to be presented and discussed at the policy review group meeting on the 28th June 2018. On target for completion by July 2018.
In progress – Will be
complete July 2018
2.2 Audit R
ecomm
endations Tracker
25 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
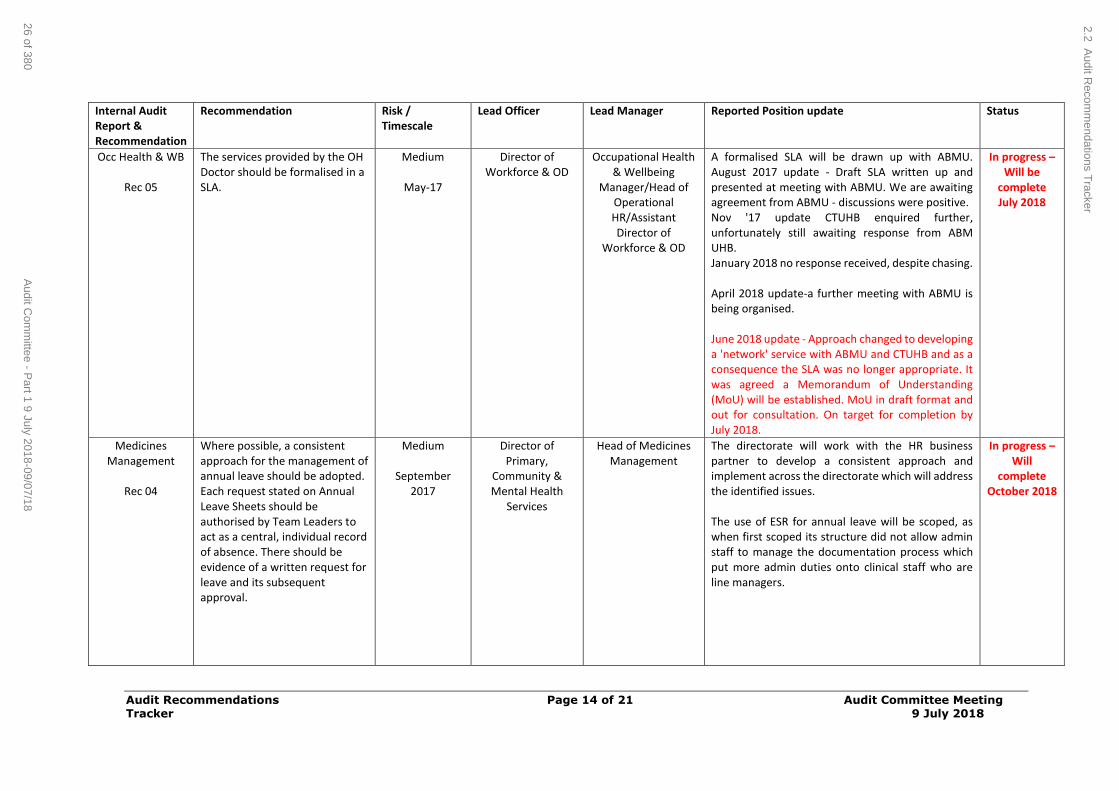
Audit Recommendations Page 14 of 21 Audit Committee Meeting Tracker 9 July 2018
Internal Audit Report & Recommendation
Recommendation Risk / Timescale
Lead Officer Lead Manager Reported Position update Status
Occ Health & WB
Rec 05
The services provided by the OH Doctor should be formalised in a SLA.
Medium
May-17
Director of Workforce & OD
Occupational Health & Wellbeing
Manager/Head of Operational HR/Assistant Director of
Workforce & OD
A formalised SLA will be drawn up with ABMU. August 2017 update - Draft SLA written up and presented at meeting with ABMU. We are awaiting agreement from ABMU - discussions were positive. Nov '17 update CTUHB enquired further, unfortunately still awaiting response from ABM UHB. January 2018 no response received, despite chasing. April 2018 update-a further meeting with ABMU is being organised. June 2018 update - Approach changed to developing a 'network' service with ABMU and CTUHB and as a consequence the SLA was no longer appropriate. It was agreed a Memorandum of Understanding (MoU) will be established. MoU in draft format and out for consultation. On target for completion by July 2018.
In progress – Will be
complete July 2018
Medicines Management
Rec 04
Where possible, a consistent approach for the management of annual leave should be adopted. Each request stated on Annual Leave Sheets should be authorised by Team Leaders to act as a central, individual record of absence. There should be evidence of a written request for leave and its subsequent approval.
Medium
September 2017
Director of Primary,
Community & Mental Health
Services
Head of Medicines Management
The directorate will work with the HR business partner to develop a consistent approach and implement across the directorate which will address the identified issues. The use of ESR for annual leave will be scoped, as when first scoped its structure did not allow admin staff to manage the documentation process which put more admin duties onto clinical staff who are line managers.
In progress – Will
complete October 2018
2.2 Audit R
ecomm
endations Tracker
26 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
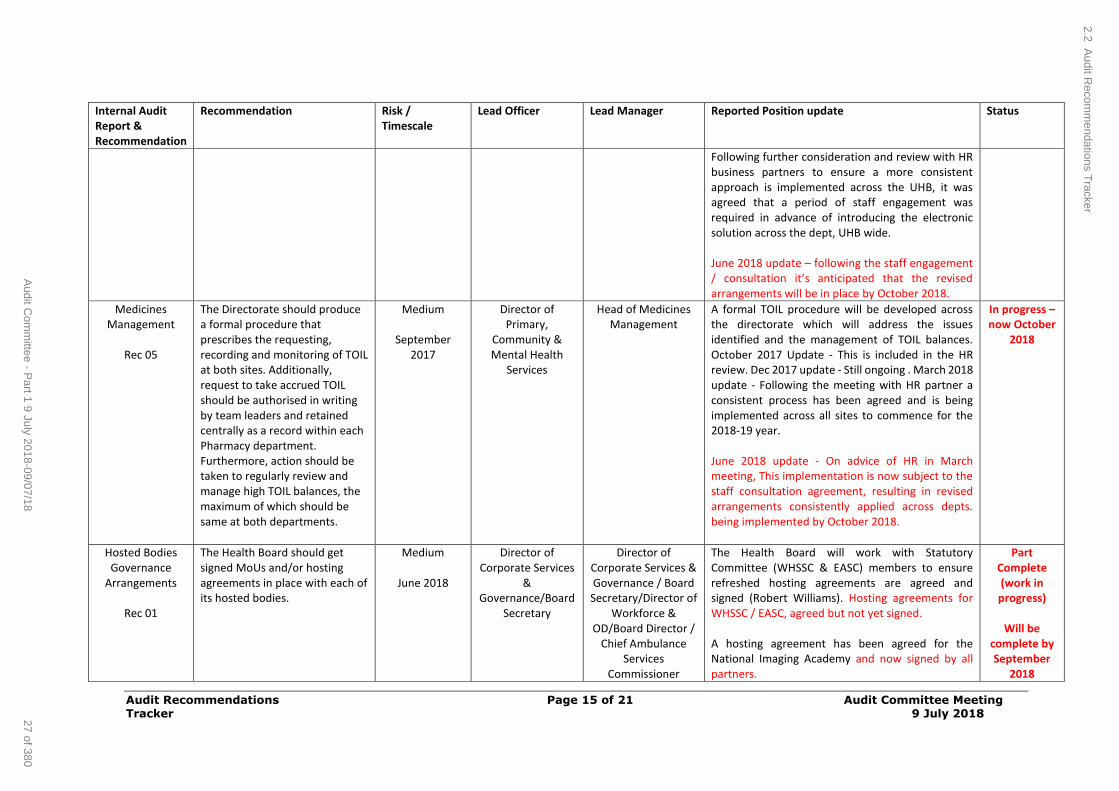
Audit Recommendations Page 15 of 21 Audit Committee Meeting Tracker 9 July 2018
Internal Audit Report & Recommendation
Recommendation Risk / Timescale
Lead Officer Lead Manager Reported Position update Status
Following further consideration and review with HR business partners to ensure a more consistent approach is implemented across the UHB, it was agreed that a period of staff engagement was required in advance of introducing the electronic solution across the dept, UHB wide. June 2018 update – following the staff engagement / consultation it’s anticipated that the revised arrangements will be in place by October 2018.
Medicines Management
Rec 05
The Directorate should produce a formal procedure that prescribes the requesting, recording and monitoring of TOIL at both sites. Additionally, request to take accrued TOIL should be authorised in writing by team leaders and retained centrally as a record within each Pharmacy department. Furthermore, action should be taken to regularly review and manage high TOIL balances, the maximum of which should be same at both departments.
Medium
September 2017
Director of Primary,
Community & Mental Health
Services
Head of Medicines Management
A formal TOIL procedure will be developed across the directorate which will address the issues identified and the management of TOIL balances. October 2017 Update - This is included in the HR review. Dec 2017 update - Still ongoing . March 2018 update - Following the meeting with HR partner a consistent process has been agreed and is being implemented across all sites to commence for the 2018-19 year. June 2018 update - On advice of HR in March meeting, This implementation is now subject to the staff consultation agreement, resulting in revised arrangements consistently applied across depts. being implemented by October 2018.
In progress – now October
2018
Hosted Bodies Governance
Arrangements
Rec 01
The Health Board should get signed MoUs and/or hosting agreements in place with each of its hosted bodies.
Medium
June 2018
Director of Corporate Services
& Governance/Board
Secretary
Director of Corporate Services & Governance / Board Secretary/Director of
Workforce & OD/Board Director /
Chief Ambulance Services
Commissioner
The Health Board will work with Statutory Committee (WHSSC & EASC) members to ensure refreshed hosting agreements are agreed and signed (Robert Williams). Hosting agreements for WHSSC / EASC, agreed but not yet signed. A hosting agreement has been agreed for the National Imaging Academy and now signed by all partners.
Part Complete (work in progress)
Will be
complete by September
2018
2.2 Audit R
ecomm
endations Tracker
27 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
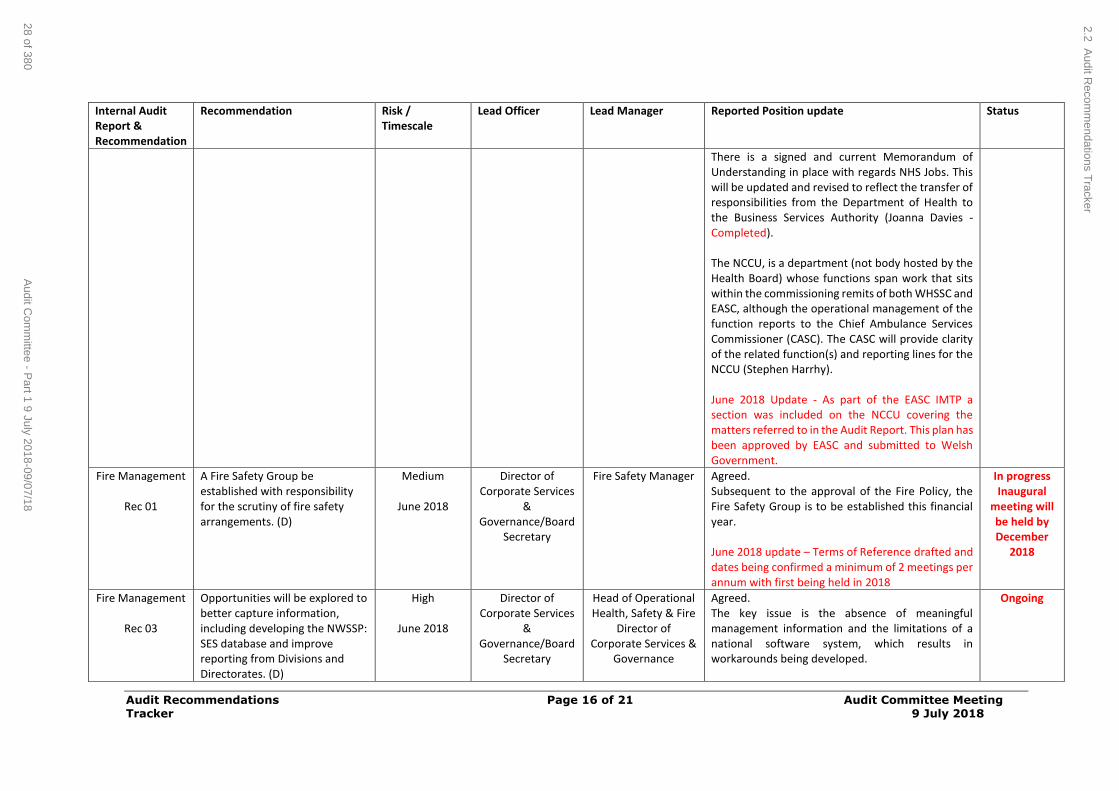
Audit Recommendations Page 16 of 21 Audit Committee Meeting Tracker 9 July 2018
Internal Audit Report & Recommendation
Recommendation Risk / Timescale
Lead Officer Lead Manager Reported Position update Status
There is a signed and current Memorandum of Understanding in place with regards NHS Jobs. This will be updated and revised to reflect the transfer of responsibilities from the Department of Health to the Business Services Authority (Joanna Davies - Completed). The NCCU, is a department (not body hosted by the Health Board) whose functions span work that sits within the commissioning remits of both WHSSC and EASC, although the operational management of the function reports to the Chief Ambulance Services Commissioner (CASC). The CASC will provide clarity of the related function(s) and reporting lines for the NCCU (Stephen Harrhy). June 2018 Update - As part of the EASC IMTP a section was included on the NCCU covering the matters referred to in the Audit Report. This plan has been approved by EASC and submitted to Welsh Government.
Fire Management
Rec 01
A Fire Safety Group be established with responsibility for the scrutiny of fire safety arrangements. (D)
Medium
June 2018
Director of Corporate Services
& Governance/Board
Secretary
Fire Safety Manager Agreed. Subsequent to the approval of the Fire Policy, the Fire Safety Group is to be established this financial year. June 2018 update – Terms of Reference drafted and dates being confirmed a minimum of 2 meetings per annum with first being held in 2018
In progress Inaugural
meeting will be held by December
2018
Fire Management
Rec 03
Opportunities will be explored to better capture information, including developing the NWSSP: SES database and improve reporting from Divisions and Directorates. (D)
High
June 2018
Director of Corporate Services
& Governance/Board
Secretary
Head of Operational Health, Safety & Fire
Director of Corporate Services &
Governance
Agreed. The key issue is the absence of meaningful management information and the limitations of a national software system, which results in workarounds being developed.
Ongoing
2.2 Audit R
ecomm
endations Tracker
28 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
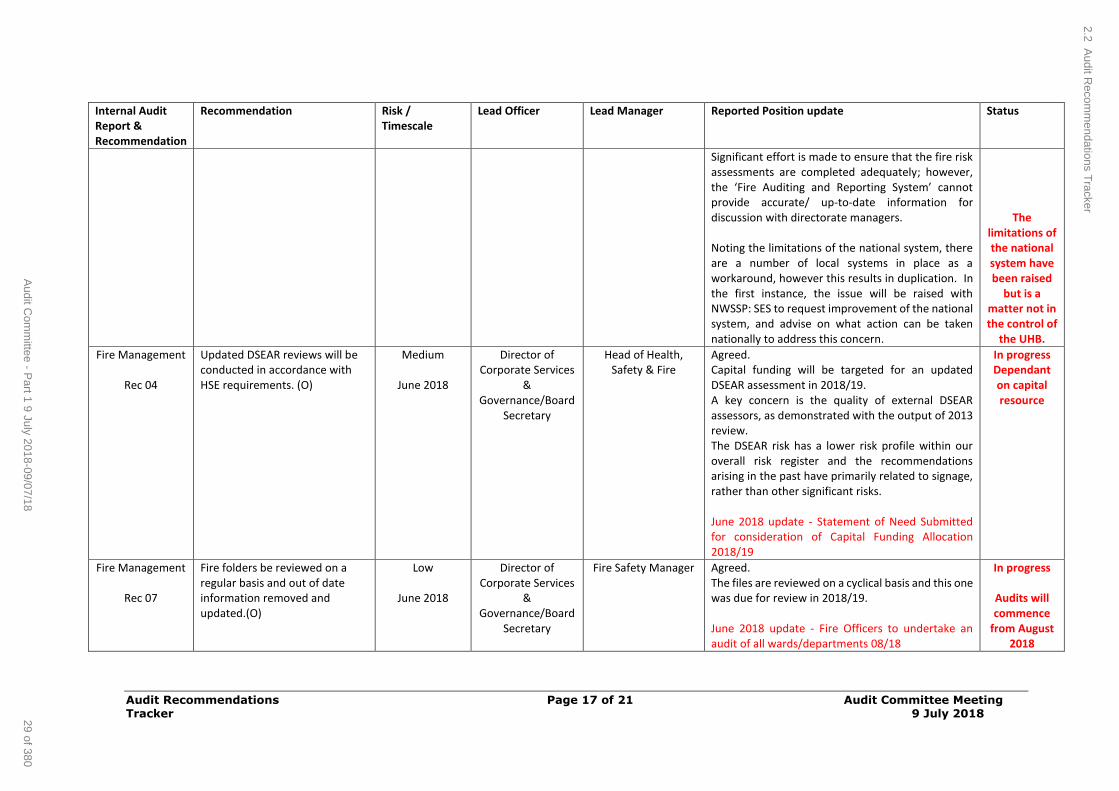
Audit Recommendations Page 17 of 21 Audit Committee Meeting Tracker 9 July 2018
Internal Audit Report & Recommendation
Recommendation Risk / Timescale
Lead Officer Lead Manager Reported Position update Status
Significant effort is made to ensure that the fire risk assessments are completed adequately; however, the ‘Fire Auditing and Reporting System’ cannot provide accurate/ up-to-date information for discussion with directorate managers. Noting the limitations of the national system, there are a number of local systems in place as a workaround, however this results in duplication. In the first instance, the issue will be raised with NWSSP: SES to request improvement of the national system, and advise on what action can be taken nationally to address this concern.
The limitations of the national system have been raised
but is a matter not in the control of
the UHB.
Fire Management
Rec 04
Updated DSEAR reviews will be conducted in accordance with HSE requirements. (O)
Medium
June 2018
Director of Corporate Services
& Governance/Board
Secretary
Head of Health, Safety & Fire
Agreed. Capital funding will be targeted for an updated DSEAR assessment in 2018/19. A key concern is the quality of external DSEAR assessors, as demonstrated with the output of 2013 review. The DSEAR risk has a lower risk profile within our overall risk register and the recommendations arising in the past have primarily related to signage, rather than other significant risks. June 2018 update - Statement of Need Submitted for consideration of Capital Funding Allocation 2018/19
In progress Dependant on capital resource
Fire Management
Rec 07
Fire folders be reviewed on a regular basis and out of date information removed and updated.(O)
Low
June 2018
Director of Corporate Services
& Governance/Board
Secretary
Fire Safety Manager Agreed. The files are reviewed on a cyclical basis and this one was due for review in 2018/19. June 2018 update - Fire Officers to undertake an audit of all wards/departments 08/18
In progress
Audits will commence
from August 2018
2.2 Audit R
ecomm
endations Tracker
29 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
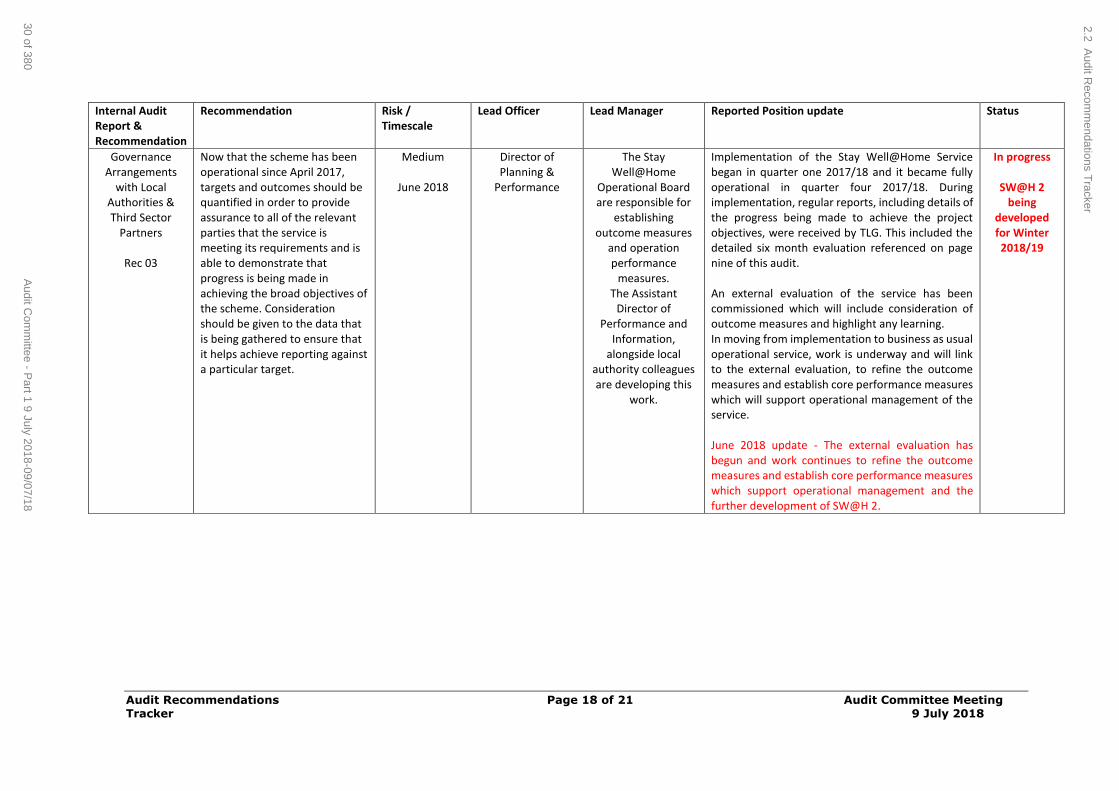
Audit Recommendations Page 18 of 21 Audit Committee Meeting Tracker 9 July 2018
Internal Audit Report & Recommendation
Recommendation Risk / Timescale
Lead Officer Lead Manager Reported Position update Status
Governance Arrangements
with Local Authorities & Third Sector
Partners
Rec 03
Now that the scheme has been operational since April 2017, targets and outcomes should be quantified in order to provide assurance to all of the relevant parties that the service is meeting its requirements and is able to demonstrate that progress is being made in achieving the broad objectives of the scheme. Consideration should be given to the data that is being gathered to ensure that it helps achieve reporting against a particular target.
Medium
June 2018
Director of Planning &
Performance
The Stay Well@Home
Operational Board are responsible for
establishing outcome measures
and operation performance
measures. The Assistant
Director of Performance and
Information, alongside local
authority colleagues are developing this
work.
Implementation of the Stay Well@Home Service began in quarter one 2017/18 and it became fully operational in quarter four 2017/18. During implementation, regular reports, including details of the progress being made to achieve the project objectives, were received by TLG. This included the detailed six month evaluation referenced on page nine of this audit. An external evaluation of the service has been commissioned which will include consideration of outcome measures and highlight any learning. In moving from implementation to business as usual operational service, work is underway and will link to the external evaluation, to refine the outcome measures and establish core performance measures which will support operational management of the service. June 2018 update - The external evaluation has begun and work continues to refine the outcome measures and establish core performance measures which support operational management and the further development of SW@H 2.
In progress
SW@H 2 being
developed for Winter 2018/19
2.2 Audit R
ecomm
endations Tracker
30 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
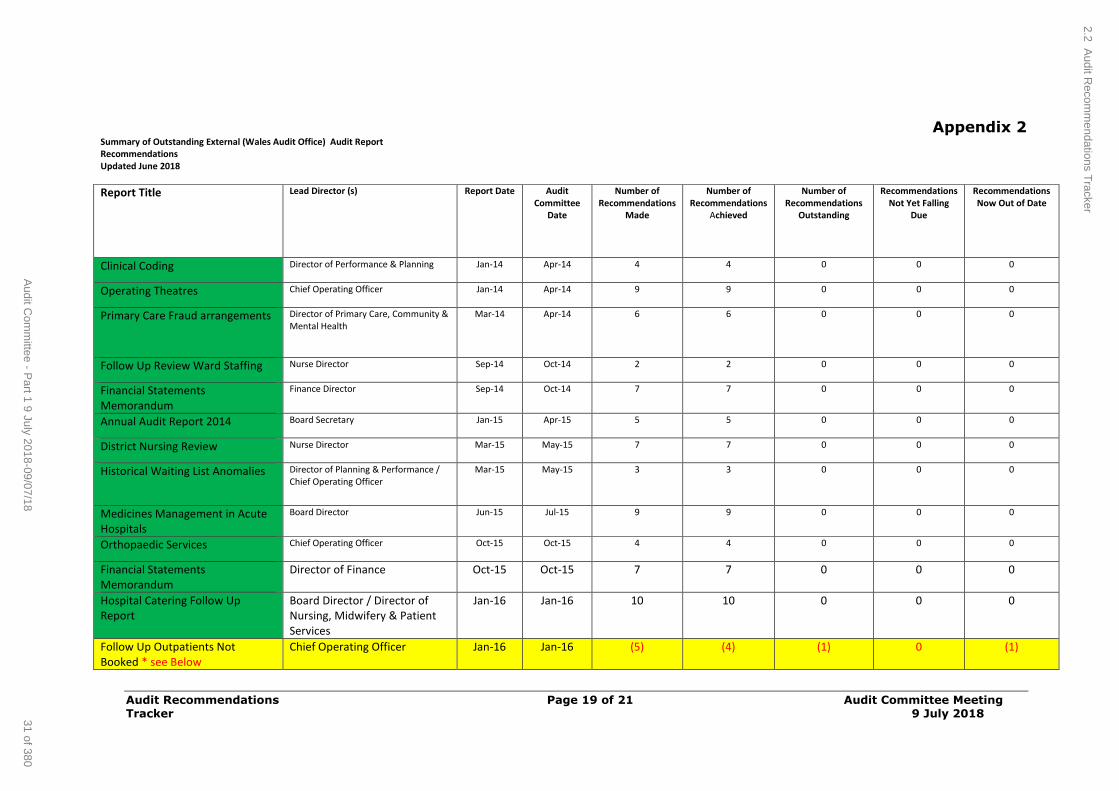
Audit Recommendations Page 19 of 21 Audit Committee Meeting Tracker 9 July 2018
Appendix 2 Summary of Outstanding External (Wales Audit Office) Audit Report Recommendations
Updated June 2018
Report Title Lead Director (s) Report Date Audit Committee
Date
Number of Recommendations
Made
Number of Recommendations
Achieved
Number of Recommendations
Outstanding
Recommendations Not Yet Falling
Due
Recommendations Now Out of Date
Clinical Coding Director of Performance & Planning Jan-14 Apr-14 4 4 0 0 0
Operating Theatres Chief Operating Officer Jan-14 Apr-14 9 9 0 0 0
Primary Care Fraud arrangements Director of Primary Care, Community & Mental Health
Mar-14 Apr-14 6 6 0 0 0
Follow Up Review Ward Staffing Nurse Director Sep-14 Oct-14 2 2 0 0 0
Financial Statements Memorandum
Finance Director Sep-14 Oct-14 7 7 0 0 0
Annual Audit Report 2014 Board Secretary Jan-15 Apr-15 5 5 0 0 0
District Nursing Review Nurse Director Mar-15 May-15 7 7 0 0 0
Historical Waiting List Anomalies Director of Planning & Performance / Chief Operating Officer
Mar-15 May-15 3 3 0 0 0
Medicines Management in Acute Hospitals
Board Director Jun-15 Jul-15 9 9 0 0 0
Orthopaedic Services Chief Operating Officer Oct-15 Oct-15 4 4 0 0 0
Financial Statements Memorandum
Director of Finance Oct-15 Oct-15 7 7 0 0 0
Hospital Catering Follow Up Report
Board Director / Director of Nursing, Midwifery & Patient Services
Jan-16 Jan-16 10 10 0 0 0
Follow Up Outpatients Not Booked * see Below
Chief Operating Officer Jan-16 Jan-16 (5) (4) (1) 0 (1)
2.2 Audit R
ecomm
endations Tracker
31 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
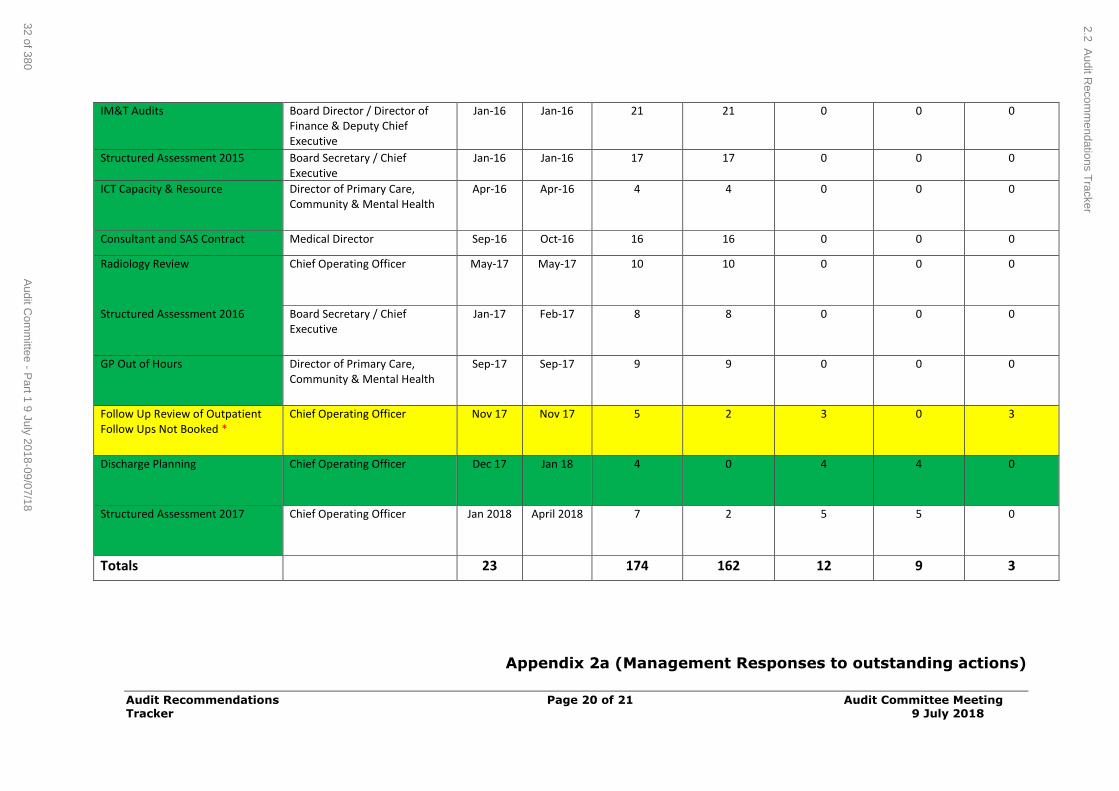
Audit Recommendations Page 20 of 21 Audit Committee Meeting Tracker 9 July 2018
IM&T Audits Board Director / Director of Finance & Deputy Chief Executive
Jan-16 Jan-16 21 21 0 0 0
Structured Assessment 2015 Board Secretary / Chief Executive
Jan-16 Jan-16 17 17 0 0 0
ICT Capacity & Resource Director of Primary Care, Community & Mental Health
Apr-16 Apr-16 4 4 0 0 0
Consultant and SAS Contract Medical Director Sep-16 Oct-16 16 16 0 0 0
Radiology Review Chief Operating Officer May-17 May-17 10 10 0 0 0
Structured Assessment 2016 Board Secretary / Chief Executive
Jan-17 Feb-17 8 8 0 0 0
GP Out of Hours Director of Primary Care, Community & Mental Health
Sep-17 Sep-17 9 9 0 0 0
Follow Up Review of Outpatient Follow Ups Not Booked *
Chief Operating Officer Nov 17
Nov 17 5 2 3 0 3
Discharge Planning Chief Operating Officer Dec 17
Jan 18 4 0 4 4 0
Structured Assessment 2017 Chief Operating Officer Jan 2018 April 2018 7 2 5 5 0
Totals 23 174 162 12 9 3
Appendix 2a (Management Responses to outstanding actions)
2.2 Audit R
ecomm
endations Tracker
32 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
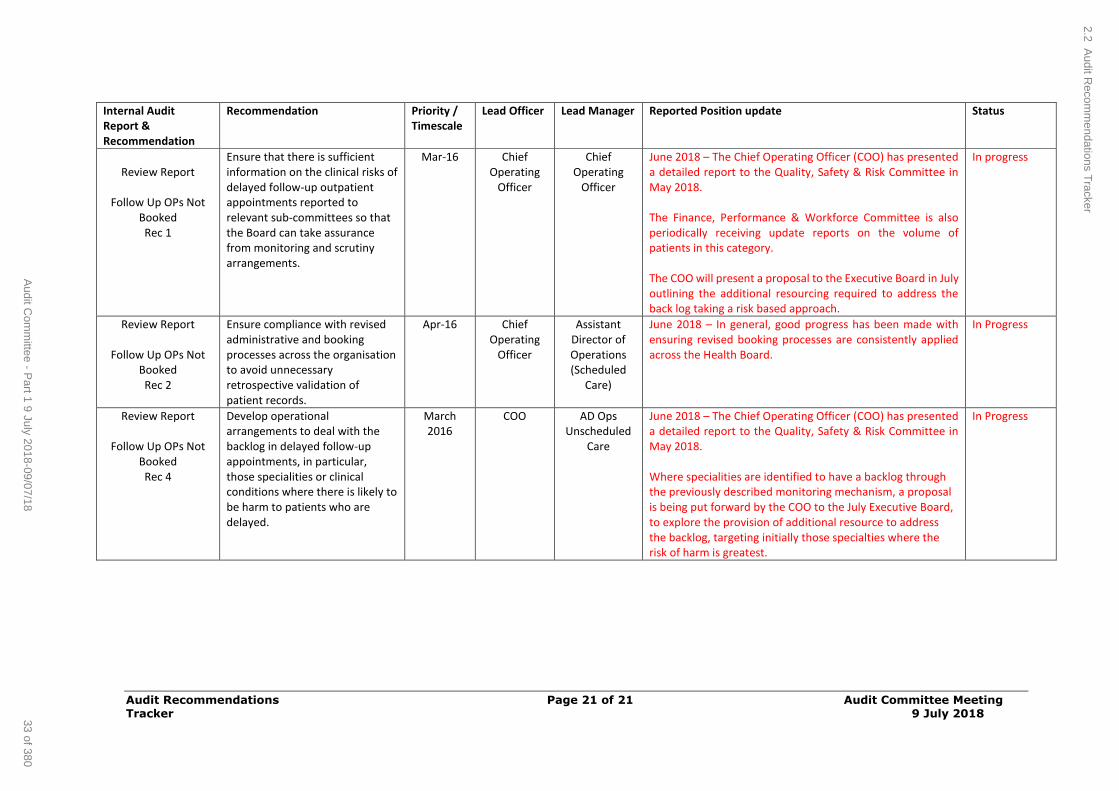
Audit Recommendations Page 21 of 21 Audit Committee Meeting Tracker 9 July 2018
Internal Audit Report & Recommendation
Recommendation Priority / Timescale
Lead Officer Lead Manager Reported Position update Status
Review Report
Follow Up OPs Not
Booked Rec 1
Ensure that there is sufficient information on the clinical risks of delayed follow-up outpatient appointments reported to relevant sub-committees so that the Board can take assurance from monitoring and scrutiny arrangements.
Mar-16 Chief Operating
Officer
Chief Operating
Officer
June 2018 – The Chief Operating Officer (COO) has presented a detailed report to the Quality, Safety & Risk Committee in May 2018. The Finance, Performance & Workforce Committee is also periodically receiving update reports on the volume of patients in this category. The COO will present a proposal to the Executive Board in July outlining the additional resourcing required to address the back log taking a risk based approach.
In progress
Review Report
Follow Up OPs Not Booked Rec 2
Ensure compliance with revised administrative and booking processes across the organisation to avoid unnecessary retrospective validation of patient records.
Apr-16 Chief Operating
Officer
Assistant Director of Operations (Scheduled
Care)
June 2018 – In general, good progress has been made with ensuring revised booking processes are consistently applied across the Health Board.
In Progress
Review Report
Follow Up OPs Not Booked Rec 4
Develop operational arrangements to deal with the backlog in delayed follow-up appointments, in particular, those specialities or clinical conditions where there is likely to be harm to patients who are delayed.
March 2016
COO
AD Ops Unscheduled
Care
June 2018 – The Chief Operating Officer (COO) has presented a detailed report to the Quality, Safety & Risk Committee in May 2018. Where specialities are identified to have a backlog through the previously described monitoring mechanism, a proposal is being put forward by the COO to the July Executive Board, to explore the provision of additional resource to address the backlog, targeting initially those specialties where the risk of harm is greatest.
In Progress
2.2 Audit R
ecomm
endations Tracker
33 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 1 of 16 Audit Committee Meeting 9 July 2018
AGENDA ITEM 2.3
9 July 2018
Audit Committee Report
LOSSES AND SPECIAL PAYMENTS 01.03.18 TO 31.05.18
Executive Lead: Director of Finance
Author: Financial Accountant
Contact Details for further information: Daxa Varsani on 01443
443808 or [email protected] or Huw Evans [email protected]
Purpose of the Audit Committee Report
To advise the Audit Committee on the losses and special payments made
by the UHB for the period 1st March 2018 to 31st May 2018, as required in Standing Financial Instructions.
Governance
Link to Health Board Strategic
Objective(s)
The Board’s overarching role is to ensure its Strategy outlined within ‘Cwm Taf Cares’ 3 Year Integrated
Medium Term Plan 2015-2018 and the related organisational objectives aligned with the Institute of
Healthcare Improvement's (IHI) ‘Triple Aim’ are being
progressed, these in summary are: To improve quality, safety and patient experience
To protect and improve population health To ensure that the services provided are accessible
and sustainable into the future To provide strong governance and assurance
To ensure good value based care and treatment for our patients in line with the resources made
available to the Health Board. The main aim of this report is to improve governance
and assurance.
Supporting evidence
N/A
Engagement – Who has been involved in this work?
NWSSP – legal services and Risk Pool
2.3 Losses and Special Payments Report
34 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 2 of 16 Audit Committee Meeting 9 July 2018
Audit Committee Resolution (insert √) To;
APPROVE ENDORSE DISCUSS NOTE √
Recommendation The Audit Committee is asked to: NOTE the losses and special payments incurred
for the period 1st March 2018 to 31st May 2018.
Summarise the Impact of the Audit Committee Report
Equality and
diversity
No specific impact
Legal implications Losses provided for are informed by legal advice where appropriate based on probability of a
successful claim
Population Health No specific impact
Quality, Safety &
Patient Experience
The majority of losses and special payments are as
a result of things going wrong and where quality, safety or patient experience may therefore have
been compromised.
Details of medical negligence and personal injury claims are provided quarterly to the Concerns
(Claims) Scrutiny Panel who subsequently reports to the Quality, Safety & Risk Committee
Resources The report highlights the resource impact of losses
both in expenditure and cash terms. It also highlights the level of provision within the balance
sheet for potential future payments.
Risks and Assurance Standing Financial Instructions require all losses to
be reported to the Audit Committee. This report is
therefore a key element of the governance process around losses and special payments.
Health and Care Standards
Standards for Health Services Reference Governance & Accountability Framework (1);
Workforce No specific impact
Freedom of information status
Open
2.3 Losses and Special Payments Report
35 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 3 of 16 Audit Committee Meeting 9 July 2018
LOSSES AND SPECIAL PAYMENTS 01.03.18 to 31.05.18
1. SITUATION / PURPOSE OF REPORT
This report advises the Audit Committee on the losses and special payments made by the UHB for the three month period from 1st March
2018 to 31st May 2018, as required in Standing Financial Instructions.
2. BACKGROUND
The report summarises the overall financial impact of losses in this
financial year and provides detail on individual payments for write-off.
The Health Board is liable for the first £25k of any Personal Injury or Medical Negligence claim (not including Redress cases), with amounts
over this being borne by the Welsh Risk Pool (WRP) managed by the NHS Wales Shared Services Partnership. For any “other” cases such as
Employment Matters or VER for example, the full cost of the loss is borne by the UHB. Where the WRP would be liable for a
reimbursement to the UHB then there will be timing differences
between payments being made and any reclaim from the Risk Pool. There is a strict protocol in place for reclaiming from the WRP.
In accounting for losses on claims, liability is recognised when legal
advice states that there is a probability in excess of 50% of the Health Board having to settle. The quantum of the claim, and associated
plaintiff costs are therefore recognised as “expenditure” at this point,
with the risk pool recovery element also being recognised. Other losses are recognised as and when they arise.
There is therefore a significant timing issue (which can be several
years) between expenditure being recognised within the Health Board’s accounts and cash payments being made. Write-off approval action is
only required for cash payments. This report highlights:
a) Amounts that have been charged to expenditure for which payments are yet to be made. These amounts are held within the
balance sheet as future amounts owing (or owed by the WRP) at the appropriate Balance Sheet date;
b) Amounts charged to expenditure during the current year
(together with income from the WRP), and which therefore has a
budgetary impact against the Health Board’s Revenue Resource Limit; and
c) Cash payments made during the period for which write-off action
is required, with details being provided within the appendices.
2.3 Losses and Special Payments Report
36 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
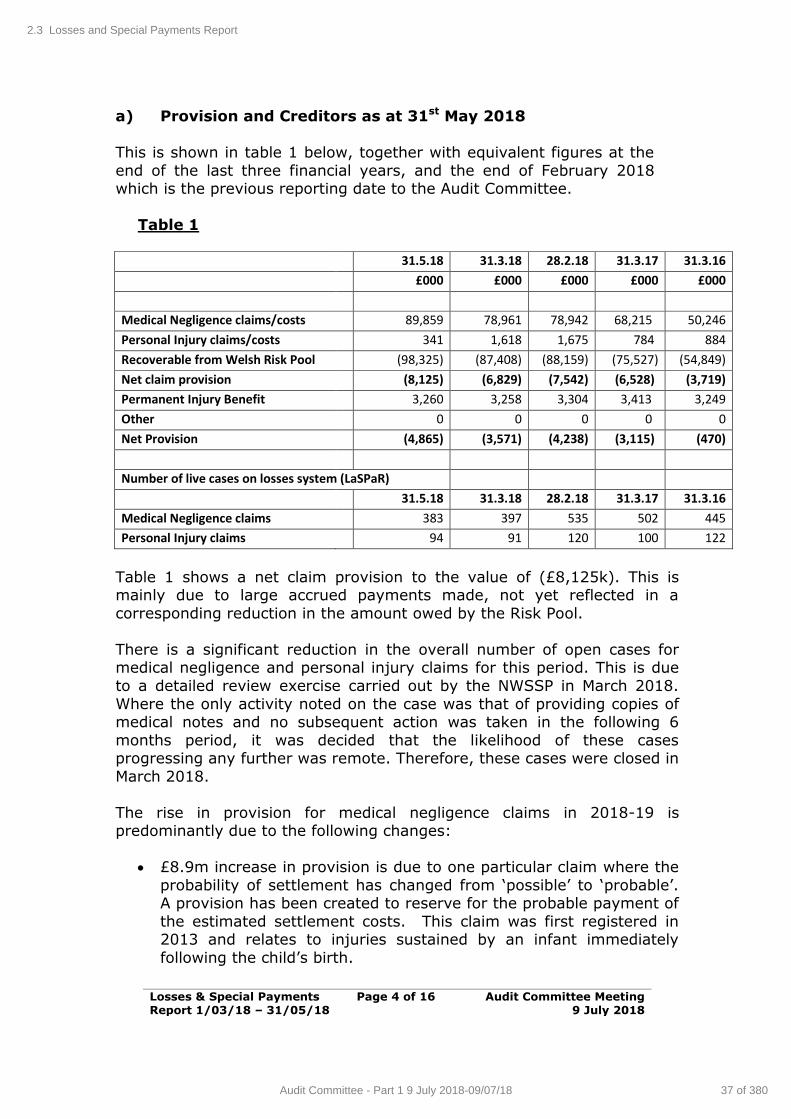
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 4 of 16 Audit Committee Meeting 9 July 2018
a) Provision and Creditors as at 31st May 2018
This is shown in table 1 below, together with equivalent figures at the
end of the last three financial years, and the end of February 2018 which is the previous reporting date to the Audit Committee.
Table 1
31.5.18 31.3.18 28.2.18 31.3.17 31.3.16
£000 £000 £000 £000 £000
Medical Negligence claims/costs 89,859 78,961 78,942 68,215 50,246
Personal Injury claims/costs 341 1,618 1,675 784 884
Recoverable from Welsh Risk Pool (98,325) (87,408) (88,159) (75,527) (54,849)
Net claim provision (8,125) (6,829) (7,542) (6,528) (3,719)
Permanent Injury Benefit 3,260 3,258 3,304 3,413 3,249
Other 0 0 0 0 0
Net Provision (4,865) (3,571) (4,238) (3,115) (470)
Number of live cases on losses system (LaSPaR)
31.5.18 31.3.18 28.2.18 31.3.17 31.3.16
Medical Negligence claims 383 397 535 502 445
Personal Injury claims 94 91 120 100 122
Table 1 shows a net claim provision to the value of (£8,125k). This is mainly due to large accrued payments made, not yet reflected in a
corresponding reduction in the amount owed by the Risk Pool.
There is a significant reduction in the overall number of open cases for medical negligence and personal injury claims for this period. This is due
to a detailed review exercise carried out by the NWSSP in March 2018.
Where the only activity noted on the case was that of providing copies of medical notes and no subsequent action was taken in the following 6
months period, it was decided that the likelihood of these cases progressing any further was remote. Therefore, these cases were closed in
March 2018.
The rise in provision for medical negligence claims in 2018-19 is predominantly due to the following changes:
£8.9m increase in provision is due to one particular claim where the
probability of settlement has changed from ‘possible’ to ‘probable’. A provision has been created to reserve for the probable payment of
the estimated settlement costs. This claim was first registered in 2013 and relates to injuries sustained by an infant immediately
following the child’s birth.
2.3 Losses and Special Payments Report
37 of 380Audit Committee - Part 1 9 July 2018-09/07/18
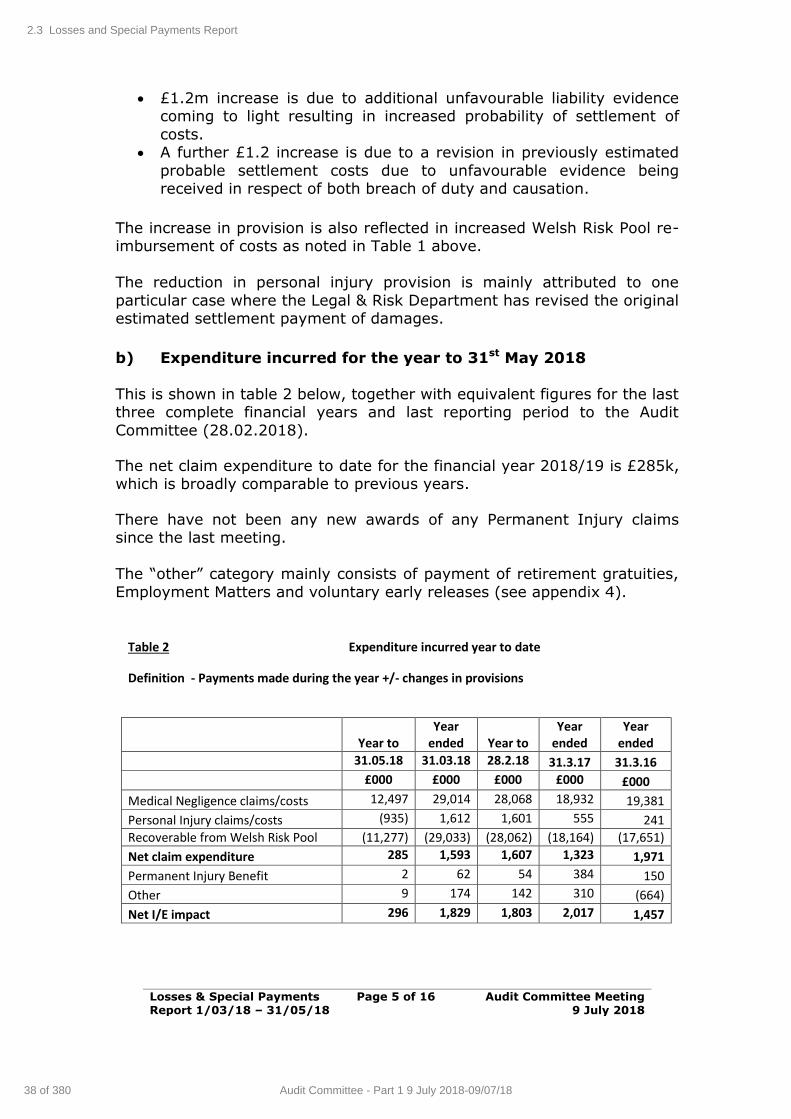
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 5 of 16 Audit Committee Meeting 9 July 2018
£1.2m increase is due to additional unfavourable liability evidence coming to light resulting in increased probability of settlement of
costs. A further £1.2 increase is due to a revision in previously estimated
probable settlement costs due to unfavourable evidence being received in respect of both breach of duty and causation.
The increase in provision is also reflected in increased Welsh Risk Pool re-imbursement of costs as noted in Table 1 above.
The reduction in personal injury provision is mainly attributed to one
particular case where the Legal & Risk Department has revised the original estimated settlement payment of damages.
b) Expenditure incurred for the year to 31st May 2018
This is shown in table 2 below, together with equivalent figures for the last three complete financial years and last reporting period to the Audit
Committee (28.02.2018).
The net claim expenditure to date for the financial year 2018/19 is £285k, which is broadly comparable to previous years.
There have not been any new awards of any Permanent Injury claims since the last meeting.
The “other” category mainly consists of payment of retirement gratuities,
Employment Matters and voluntary early releases (see appendix 4).
Table 2 Expenditure incurred year to date
Definition - Payments made during the year +/- changes in provisions
Year to
Year ended
Year to
Year ended
Year ended
31.05.18 31.03.18 28.2.18 31.3.17 31.3.16
£000 £000 £000 £000 £000
Medical Negligence claims/costs 12,497 29,014 28,068 18,932 19,381
Personal Injury claims/costs (935) 1,612 1,601 555 241
Recoverable from Welsh Risk Pool (11,277) (29,033) (28,062) (18,164) (17,651)
Net claim expenditure 285 1,593 1,607 1,323 1,971
Permanent Injury Benefit 2 62 54 384 150
Other 9 174 142 310 (664)
Net I/E impact 296 1,829 1,803 2,017 1,457
2.3 Losses and Special Payments Report
38 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
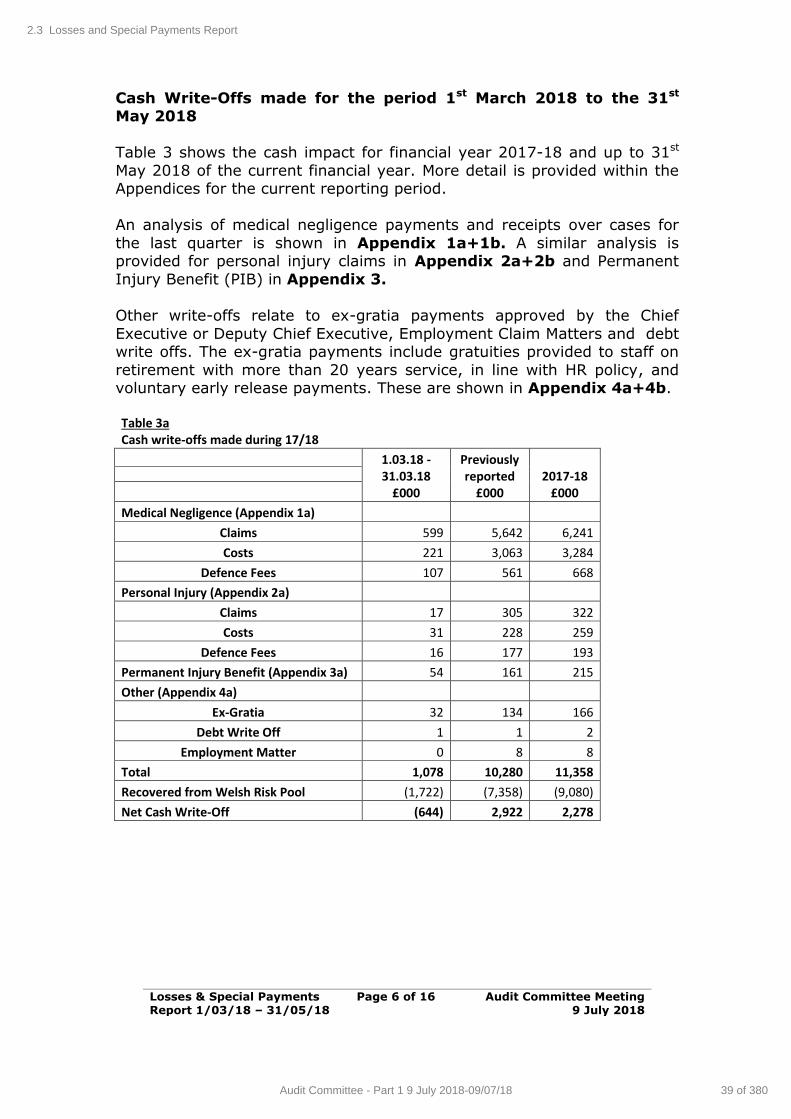
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 6 of 16 Audit Committee Meeting 9 July 2018
Cash Write-Offs made for the period 1st March 2018 to the 31st May 2018
Table 3 shows the cash impact for financial year 2017-18 and up to 31st
May 2018 of the current financial year. More detail is provided within the Appendices for the current reporting period.
An analysis of medical negligence payments and receipts over cases for
the last quarter is shown in Appendix 1a+1b. A similar analysis is provided for personal injury claims in Appendix 2a+2b and Permanent
Injury Benefit (PIB) in Appendix 3.
Other write-offs relate to ex-gratia payments approved by the Chief
Executive or Deputy Chief Executive, Employment Claim Matters and debt write offs. The ex-gratia payments include gratuities provided to staff on
retirement with more than 20 years service, in line with HR policy, and voluntary early release payments. These are shown in Appendix 4a+4b.
Table 3a Cash write-offs made during 17/18
1.03.18 -31.03.18
£000
Previously reported
£000 2017-18
£000
Medical Negligence (Appendix 1a) Claims 599 5,642 6,241
Costs 221 3,063 3,284
Defence Fees 107 561 668
Personal Injury (Appendix 2a) Claims 17 305 322
Costs 31 228 259
Defence Fees 16 177 193
Permanent Injury Benefit (Appendix 3a) 54 161 215
Other (Appendix 4a) Ex-Gratia 32 134 166
Debt Write Off 1 1 2
Employment Matter 0 8 8
Total 1,078 10,280 11,358
Recovered from Welsh Risk Pool (1,722) (7,358) (9,080)
Net Cash Write-Off (644) 2,922 2,278
2.3 Losses and Special Payments Report
39 of 380Audit Committee - Part 1 9 July 2018-09/07/18
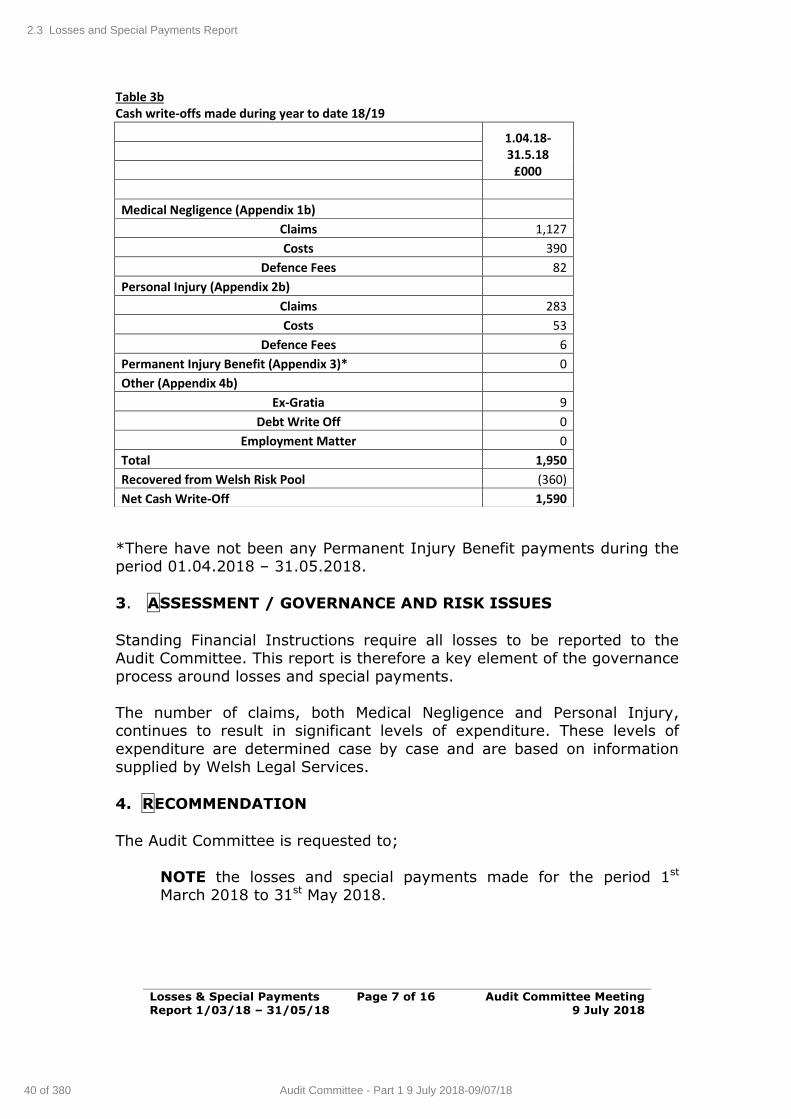
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 7 of 16 Audit Committee Meeting 9 July 2018
Table 3b Cash write-offs made during year to date 18/19
*There have not been any Permanent Injury Benefit payments during the period 01.04.2018 – 31.05.2018.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
Standing Financial Instructions require all losses to be reported to the Audit Committee. This report is therefore a key element of the governance
process around losses and special payments.
The number of claims, both Medical Negligence and Personal Injury, continues to result in significant levels of expenditure. These levels of
expenditure are determined case by case and are based on information supplied by Welsh Legal Services.
4. RECOMMENDATION
The Audit Committee is requested to;
NOTE the losses and special payments made for the period 1st March 2018 to 31st May 2018.
1.04.18-31.5.18
£000
Medical Negligence (Appendix 1b) Claims 1,127
Costs 390
Defence Fees 82
Personal Injury (Appendix 2b) Claims 283
Costs 53
Defence Fees 6
Permanent Injury Benefit (Appendix 3)* 0
Other (Appendix 4b) Ex-Gratia 9
Debt Write Off 0
Employment Matter 0
Total 1,950
Recovered from Welsh Risk Pool (360)
Net Cash Write-Off 1,590
2.3 Losses and Special Payments Report
40 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
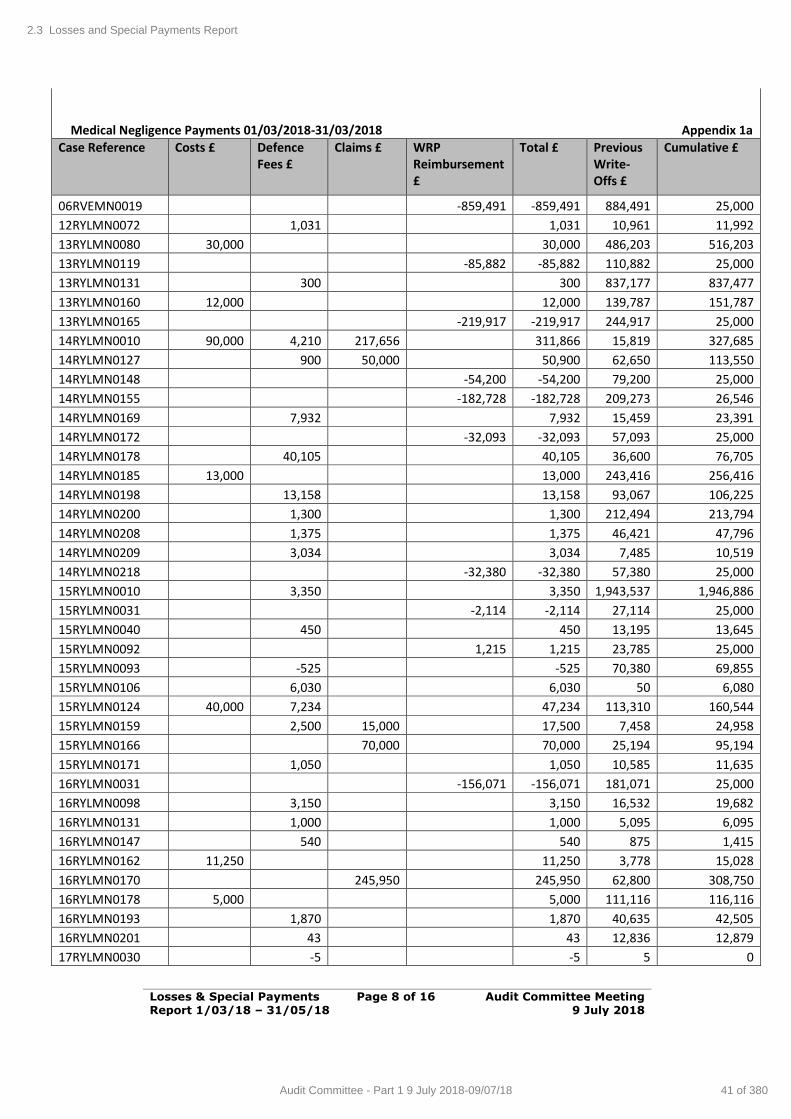
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 8 of 16 Audit Committee Meeting 9 July 2018
Medical Negligence Payments 01/03/2018-31/03/2018
Appendix 1a
Case Reference Costs £ Defence Fees £
Claims £ WRP Reimbursement £
Total £ Previous Write-Offs £
Cumulative £
06RVEMN0019 -859,491 -859,491 884,491 25,000
12RYLMN0072 1,031 1,031 10,961 11,992
13RYLMN0080 30,000 30,000 486,203 516,203
13RYLMN0119 -85,882 -85,882 110,882 25,000
13RYLMN0131 300 300 837,177 837,477
13RYLMN0160 12,000 12,000 139,787 151,787
13RYLMN0165 -219,917 -219,917 244,917 25,000
14RYLMN0010 90,000 4,210 217,656 311,866 15,819 327,685
14RYLMN0127 900 50,000 50,900 62,650 113,550
14RYLMN0148 -54,200 -54,200 79,200 25,000
14RYLMN0155 -182,728 -182,728 209,273 26,546
14RYLMN0169 7,932 7,932 15,459 23,391
14RYLMN0172 -32,093 -32,093 57,093 25,000
14RYLMN0178 40,105 40,105 36,600 76,705
14RYLMN0185 13,000 13,000 243,416 256,416
14RYLMN0198 13,158 13,158 93,067 106,225
14RYLMN0200 1,300 1,300 212,494 213,794
14RYLMN0208 1,375 1,375 46,421 47,796
14RYLMN0209 3,034 3,034 7,485 10,519
14RYLMN0218 -32,380 -32,380 57,380 25,000
15RYLMN0010 3,350 3,350 1,943,537 1,946,886
15RYLMN0031 -2,114 -2,114 27,114 25,000
15RYLMN0040 450 450 13,195 13,645
15RYLMN0092 1,215 1,215 23,785 25,000
15RYLMN0093 -525 -525 70,380 69,855
15RYLMN0106 6,030 6,030 50 6,080
15RYLMN0124 40,000 7,234 47,234 113,310 160,544
15RYLMN0159 2,500 15,000 17,500 7,458 24,958
15RYLMN0166 70,000 70,000 25,194 95,194
15RYLMN0171 1,050 1,050 10,585 11,635
16RYLMN0031 -156,071 -156,071 181,071 25,000
16RYLMN0098 3,150 3,150 16,532 19,682
16RYLMN0131 1,000 1,000 5,095 6,095
16RYLMN0147 540 540 875 1,415
16RYLMN0162 11,250 11,250 3,778 15,028
16RYLMN0170 245,950 245,950 62,800 308,750
16RYLMN0178 5,000 5,000 111,116 116,116
16RYLMN0193 1,870 1,870 40,635 42,505
16RYLMN0201 43 43 12,836 12,879
17RYLMN0030 -5 -5 5 0
2.3 Losses and Special Payments Report
41 of 380Audit Committee - Part 1 9 July 2018-09/07/18
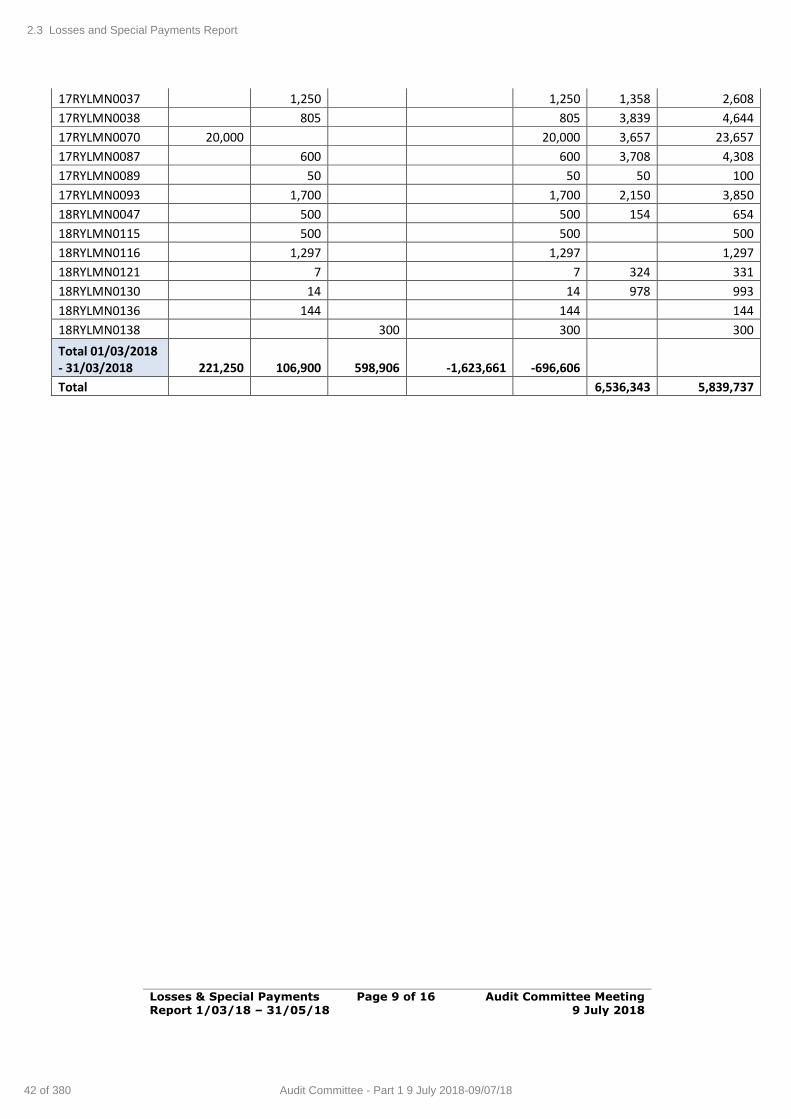
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 9 of 16 Audit Committee Meeting 9 July 2018
17RYLMN0037 1,250 1,250 1,358 2,608
17RYLMN0038 805 805 3,839 4,644
17RYLMN0070 20,000 20,000 3,657 23,657
17RYLMN0087 600 600 3,708 4,308
17RYLMN0089 50 50 50 100
17RYLMN0093 1,700 1,700 2,150 3,850
18RYLMN0047 500 500 154 654
18RYLMN0115 500 500 500
18RYLMN0116 1,297 1,297 1,297
18RYLMN0121 7 7 324 331
18RYLMN0130 14 14 978 993
18RYLMN0136 144 144 144
18RYLMN0138 300 300 300
Total 01/03/2018 - 31/03/2018 221,250 106,900 598,906 -1,623,661 -696,606
Total 6,536,343 5,839,737
2.3 Losses and Special Payments Report
42 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
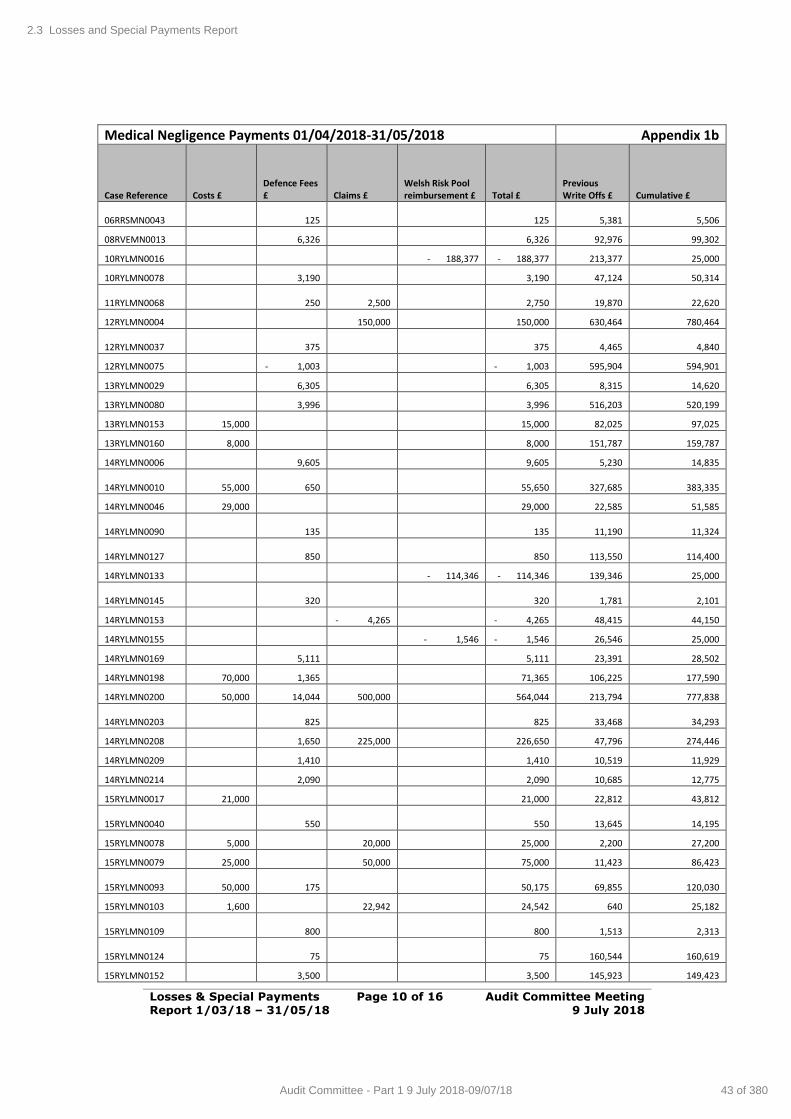
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 10 of 16 Audit Committee Meeting 9 July 2018
Medical Negligence Payments 01/04/2018-31/05/2018 Appendix 1b
Case Reference Costs £ Defence Fees £ Claims £
Welsh Risk Pool reimbursement £ Total £
Previous Write Offs £ Cumulative £
06RRSMN0043
125
125 5,381 5,506
08RVEMN0013 6,326 6,326 92,976 99,302
10RYLMN0016 - 188,377 - 188,377 213,377 25,000
10RYLMN0078 3,190 3,190 47,124 50,314
11RYLMN0068
250 2,500 2,750 19,870 22,620
12RYLMN0004 150,000 150,000 630,464 780,464
12RYLMN0037
375
375 4,465 4,840
12RYLMN0075 - 1,003 - 1,003 595,904 594,901
13RYLMN0029 6,305 6,305 8,315 14,620
13RYLMN0080 3,996 3,996 516,203 520,199
13RYLMN0153 15,000 15,000 82,025 97,025
13RYLMN0160 8,000 8,000 151,787 159,787
14RYLMN0006 9,605 9,605 5,230 14,835
14RYLMN0010 55,000
650 55,650 327,685 383,335
14RYLMN0046 29,000 29,000 22,585 51,585
14RYLMN0090
135
135 11,190 11,324
14RYLMN0127
850
850 113,550 114,400
14RYLMN0133 - 114,346 - 114,346 139,346 25,000
14RYLMN0145
320
320 1,781 2,101
14RYLMN0153 - 4,265 - 4,265 48,415 44,150
14RYLMN0155 - 1,546 - 1,546 26,546 25,000
14RYLMN0169 5,111 5,111 23,391 28,502
14RYLMN0198 70,000 1,365 71,365 106,225 177,590
14RYLMN0200 50,000 14,044 500,000 564,044 213,794 777,838
14RYLMN0203
825
825 33,468 34,293
14RYLMN0208 1,650 225,000 226,650 47,796 274,446
14RYLMN0209 1,410 1,410 10,519 11,929
14RYLMN0214 2,090 2,090 10,685 12,775
15RYLMN0017 21,000 21,000 22,812 43,812
15RYLMN0040
550
550 13,645 14,195
15RYLMN0078 5,000 20,000 25,000 2,200 27,200
15RYLMN0079 25,000 50,000 75,000 11,423 86,423
15RYLMN0093 50,000
175 50,175 69,855 120,030
15RYLMN0103 1,600 22,942 24,542 640 25,182
15RYLMN0109
800
800 1,513 2,313
15RYLMN0124
75
75 160,544 160,619
15RYLMN0152 3,500 3,500 145,923 149,423
2.3 Losses and Special Payments Report
43 of 380Audit Committee - Part 1 9 July 2018-09/07/18
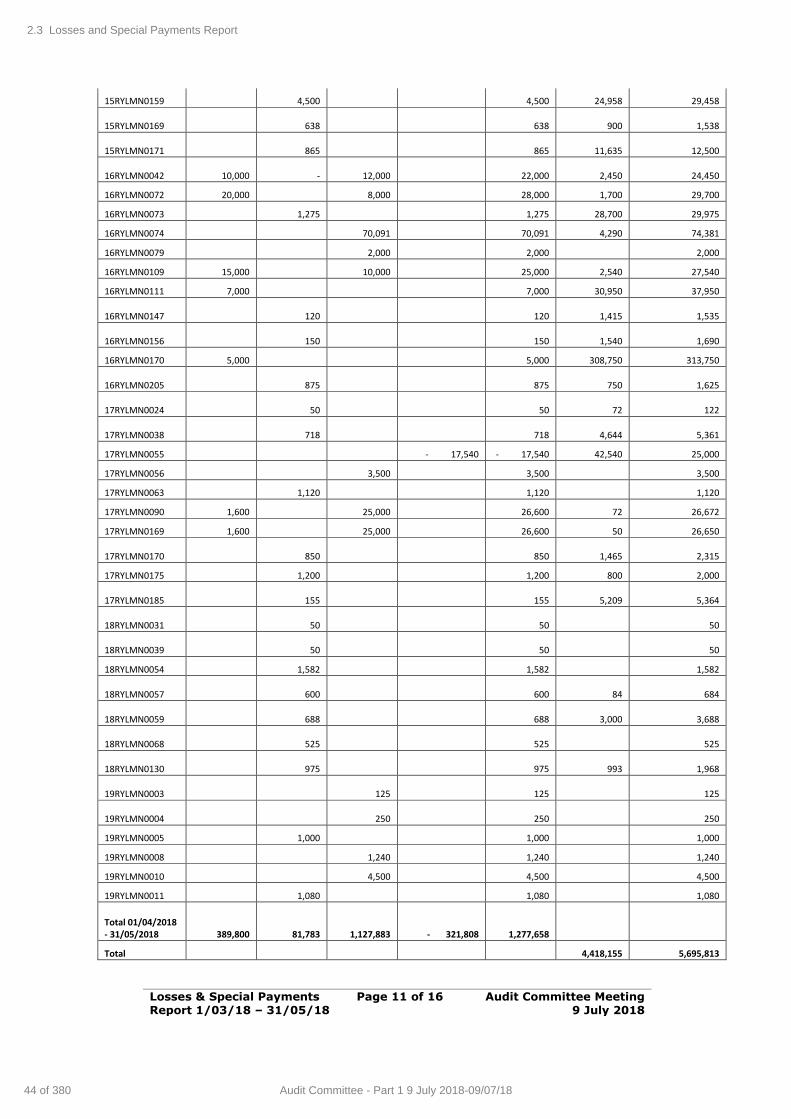
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 11 of 16 Audit Committee Meeting 9 July 2018
15RYLMN0159 4,500 4,500 24,958 29,458
15RYLMN0169
638
638 900 1,538
15RYLMN0171
865
865 11,635 12,500
16RYLMN0042 10,000
- 12,000 22,000 2,450 24,450
16RYLMN0072 20,000 8,000 28,000 1,700 29,700
16RYLMN0073 1,275 1,275 28,700 29,975
16RYLMN0074 70,091 70,091 4,290 74,381
16RYLMN0079 2,000 2,000 2,000
16RYLMN0109 15,000 10,000 25,000 2,540 27,540
16RYLMN0111 7,000 7,000 30,950 37,950
16RYLMN0147
120
120 1,415 1,535
16RYLMN0156
150
150 1,540 1,690
16RYLMN0170 5,000 5,000 308,750 313,750
16RYLMN0205
875
875 750 1,625
17RYLMN0024
50
50 72 122
17RYLMN0038
718
718 4,644 5,361
17RYLMN0055 - 17,540 - 17,540 42,540 25,000
17RYLMN0056 3,500 3,500 3,500
17RYLMN0063 1,120 1,120 1,120
17RYLMN0090 1,600 25,000 26,600 72 26,672
17RYLMN0169 1,600 25,000 26,600 50 26,650
17RYLMN0170
850
850 1,465 2,315
17RYLMN0175 1,200 1,200 800 2,000
17RYLMN0185
155
155 5,209 5,364
18RYLMN0031
50
50 50
18RYLMN0039
50
50 50
18RYLMN0054 1,582 1,582 1,582
18RYLMN0057
600
600 84 684
18RYLMN0059
688
688 3,000 3,688
18RYLMN0068
525
525 525
18RYLMN0130
975
975 993 1,968
19RYLMN0003
125
125 125
19RYLMN0004
250
250 250
19RYLMN0005 1,000 1,000 1,000
19RYLMN0008 1,240 1,240 1,240
19RYLMN0010 4,500 4,500 4,500
19RYLMN0011 1,080 1,080 1,080
Total 01/04/2018 - 31/05/2018 389,800 81,783 1,127,883 - 321,808 1,277,658
Total 4,418,155 5,695,813
2.3 Losses and Special Payments Report
44 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
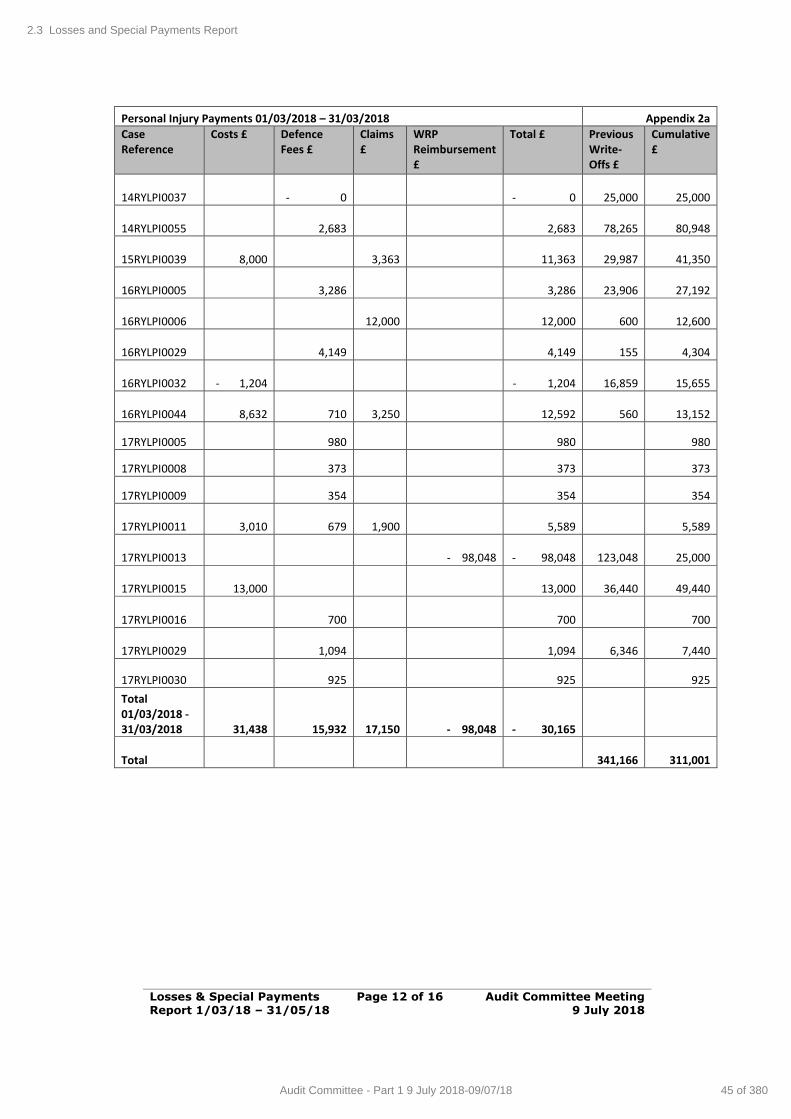
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 12 of 16 Audit Committee Meeting 9 July 2018
Personal Injury Payments 01/03/2018 – 31/03/2018 Appendix 2a
Case Reference
Costs £ Defence Fees £
Claims £
WRP Reimbursement £
Total £ Previous Write-Offs £
Cumulative £
14RYLPI0037 - 0 - 0
25,000 25,000
14RYLPI0055 2,683 2,683
78,265 80,948
15RYLPI0039 8,000
3,363 11,363
29,987 41,350
16RYLPI0005 3,286 3,286
23,906 27,192
16RYLPI0006
12,000 12,000
600 12,600
16RYLPI0029 4,149 4,149
155 4,304
16RYLPI0032 - 1,204 - 1,204
16,859 15,655
16RYLPI0044 8,632 710
3,250 12,592
560 13,152
17RYLPI0005 980 980 980
17RYLPI0008 373 373 373
17RYLPI0009 354 354 354
17RYLPI0011 3,010 679
1,900 5,589 5,589
17RYLPI0013 - 98,048 - 98,048
123,048 25,000
17RYLPI0015 13,000 13,000
36,440 49,440
17RYLPI0016 700 700 700
17RYLPI0029 1,094 1,094
6,346 7,440
17RYLPI0030 925 925 925
Total 01/03/2018 - 31/03/2018 31,438 15,932
17,150 - 98,048 - 30,165
Total
341,166 311,001
2.3 Losses and Special Payments Report
45 of 380Audit Committee - Part 1 9 July 2018-09/07/18
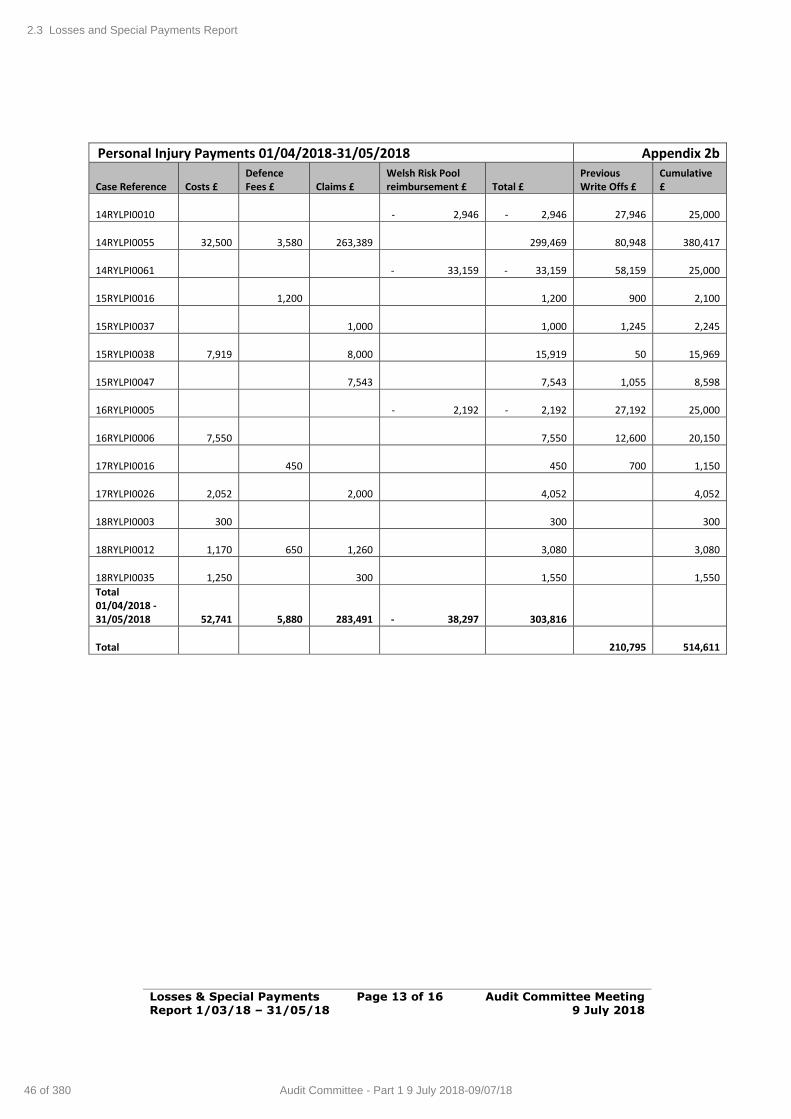
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 13 of 16 Audit Committee Meeting 9 July 2018
Personal Injury Payments 01/04/2018-31/05/2018 Appendix 2b
Case Reference Costs £ Defence Fees £ Claims £
Welsh Risk Pool reimbursement £ Total £
Previous Write Offs £
Cumulative £
14RYLPI0010 - 2,946 - 2,946
27,946
25,000
14RYLPI0055
32,500
3,580
263,389 299,469
80,948
380,417
14RYLPI0061 - 33,159 - 33,159
58,159
25,000
15RYLPI0016
1,200 1,200
900
2,100
15RYLPI0037
1,000 1,000
1,245
2,245
15RYLPI0038
7,919
8,000 15,919
50
15,969
15RYLPI0047
7,543 7,543
1,055
8,598
16RYLPI0005 - 2,192 - 2,192
27,192
25,000
16RYLPI0006
7,550 7,550
12,600
20,150
17RYLPI0016
450 450
700
1,150
17RYLPI0026
2,052
2,000 4,052
4,052
18RYLPI0003
300 300 300
18RYLPI0012
1,170
650
1,260 3,080
3,080
18RYLPI0035
1,250
300 1,550
1,550
Total 01/04/2018 - 31/05/2018
52,741
5,880
283,491 - 38,297 303,816
Total
210,795
514,611
2.3 Losses and Special Payments Report
46 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
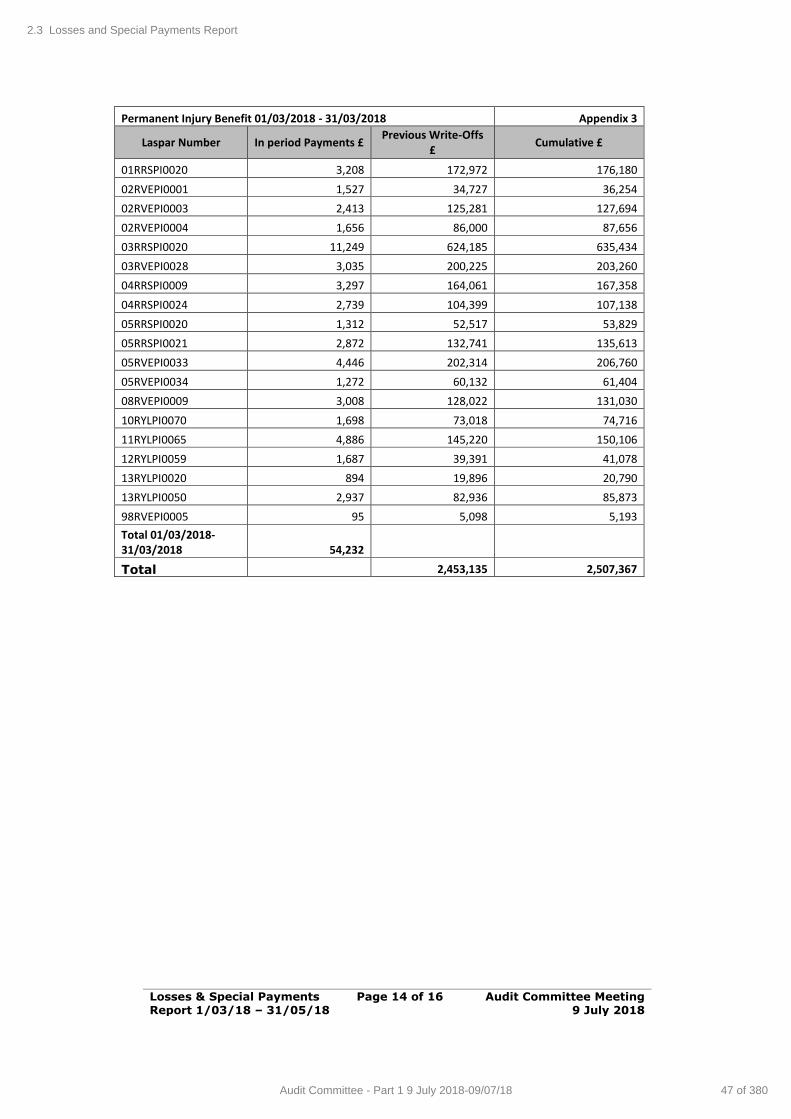
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 14 of 16 Audit Committee Meeting 9 July 2018
Permanent Injury Benefit 01/03/2018 - 31/03/2018 Appendix 3
Laspar Number In period Payments £ Previous Write-Offs
£ Cumulative £
01RRSPI0020 3,208 172,972 176,180
02RVEPI0001 1,527 34,727 36,254
02RVEPI0003 2,413 125,281 127,694
02RVEPI0004 1,656 86,000 87,656
03RRSPI0020 11,249 624,185 635,434
03RVEPI0028 3,035 200,225 203,260
04RRSPI0009 3,297 164,061 167,358
04RRSPI0024 2,739 104,399 107,138
05RRSPI0020 1,312 52,517 53,829
05RRSPI0021 2,872 132,741 135,613
05RVEPI0033 4,446 202,314 206,760
05RVEPI0034 1,272 60,132 61,404
08RVEPI0009 3,008 128,022 131,030
10RYLPI0070 1,698 73,018 74,716
11RYLPI0065 4,886 145,220 150,106
12RYLPI0059 1,687 39,391 41,078
13RYLPI0020 894 19,896 20,790
13RYLPI0050 2,937 82,936 85,873
98RVEPI0005 95 5,098 5,193
Total 01/03/2018-31/03/2018 54,232
Total 2,453,135 2,507,367
2.3 Losses and Special Payments Report
47 of 380Audit Committee - Part 1 9 July 2018-09/07/18
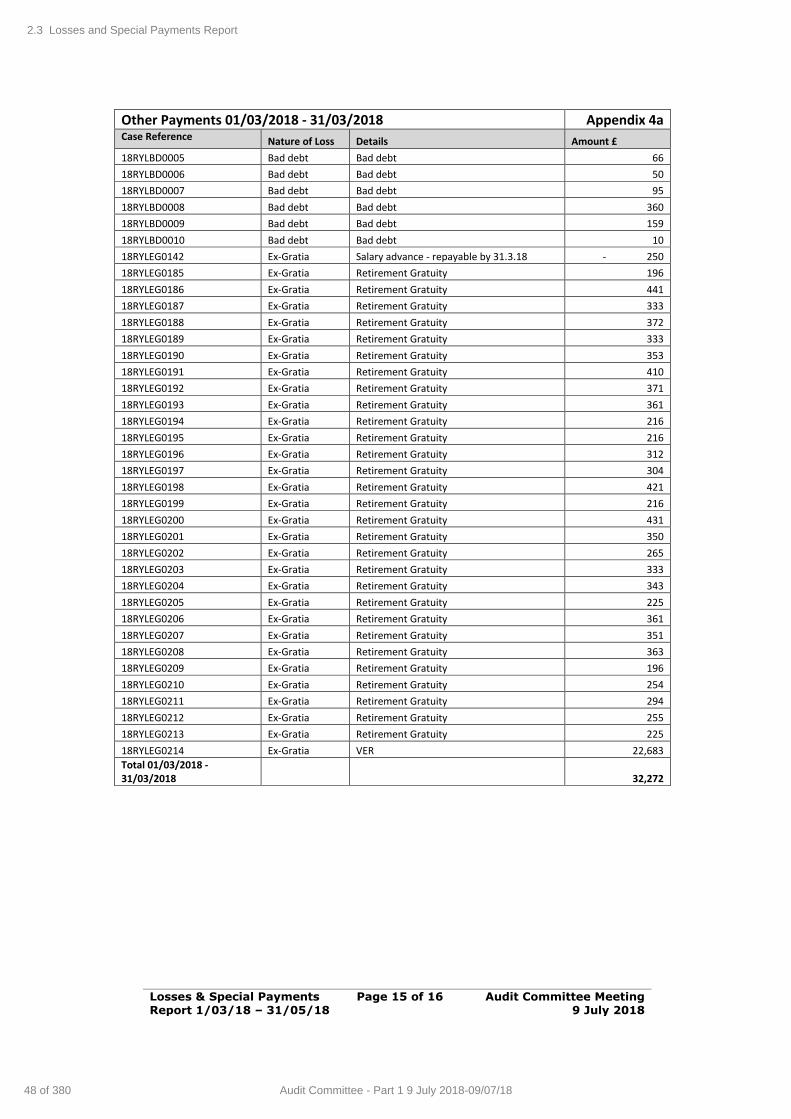
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 15 of 16 Audit Committee Meeting 9 July 2018
Other Payments 01/03/2018 - 31/03/2018 Appendix 4a Case Reference Nature of Loss Details Amount £
18RYLBD0005 Bad debt Bad debt 66
18RYLBD0006 Bad debt Bad debt 50
18RYLBD0007 Bad debt Bad debt 95
18RYLBD0008 Bad debt Bad debt 360
18RYLBD0009 Bad debt Bad debt 159
18RYLBD0010 Bad debt Bad debt 10
18RYLEG0142 Ex-Gratia Salary advance - repayable by 31.3.18 - 250
18RYLEG0185 Ex-Gratia Retirement Gratuity 196
18RYLEG0186 Ex-Gratia Retirement Gratuity 441
18RYLEG0187 Ex-Gratia Retirement Gratuity 333
18RYLEG0188 Ex-Gratia Retirement Gratuity 372
18RYLEG0189 Ex-Gratia Retirement Gratuity 333
18RYLEG0190 Ex-Gratia Retirement Gratuity 353
18RYLEG0191 Ex-Gratia Retirement Gratuity 410
18RYLEG0192 Ex-Gratia Retirement Gratuity 371
18RYLEG0193 Ex-Gratia Retirement Gratuity 361
18RYLEG0194 Ex-Gratia Retirement Gratuity 216
18RYLEG0195 Ex-Gratia Retirement Gratuity 216
18RYLEG0196 Ex-Gratia Retirement Gratuity 312
18RYLEG0197 Ex-Gratia Retirement Gratuity 304
18RYLEG0198 Ex-Gratia Retirement Gratuity 421
18RYLEG0199 Ex-Gratia Retirement Gratuity 216
18RYLEG0200 Ex-Gratia Retirement Gratuity 431
18RYLEG0201 Ex-Gratia Retirement Gratuity 350
18RYLEG0202 Ex-Gratia Retirement Gratuity 265
18RYLEG0203 Ex-Gratia Retirement Gratuity 333
18RYLEG0204 Ex-Gratia Retirement Gratuity 343
18RYLEG0205 Ex-Gratia Retirement Gratuity 225
18RYLEG0206 Ex-Gratia Retirement Gratuity 361
18RYLEG0207 Ex-Gratia Retirement Gratuity 351
18RYLEG0208 Ex-Gratia Retirement Gratuity 363
18RYLEG0209 Ex-Gratia Retirement Gratuity 196
18RYLEG0210 Ex-Gratia Retirement Gratuity 254
18RYLEG0211 Ex-Gratia Retirement Gratuity 294
18RYLEG0212 Ex-Gratia Retirement Gratuity 255
18RYLEG0213 Ex-Gratia Retirement Gratuity 225
18RYLEG0214 Ex-Gratia VER 22,683
Total 01/03/2018 - 31/03/2018 32,272
2.3 Losses and Special Payments Report
48 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
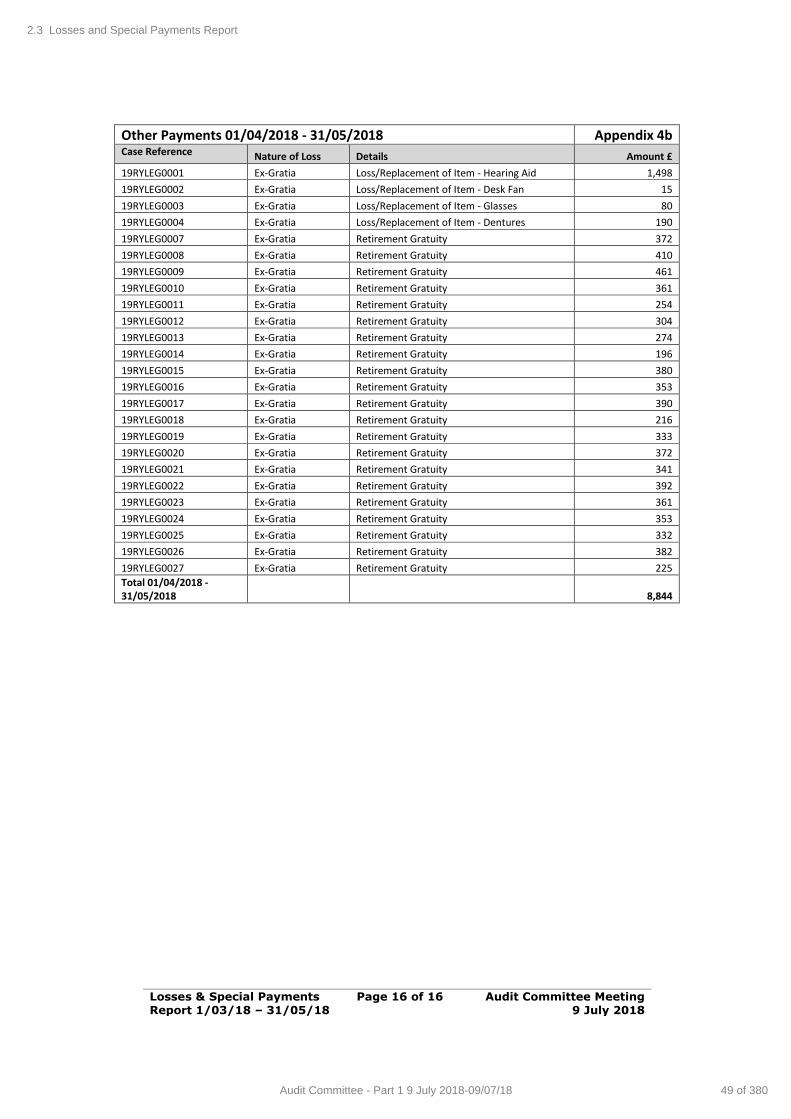
Losses & Special Payments Report 1/03/18 – 31/05/18
Page 16 of 16 Audit Committee Meeting 9 July 2018
Other Payments 01/04/2018 - 31/05/2018 Appendix 4b Case Reference Nature of Loss Details Amount £
19RYLEG0001 Ex-Gratia Loss/Replacement of Item - Hearing Aid 1,498
19RYLEG0002 Ex-Gratia Loss/Replacement of Item - Desk Fan 15
19RYLEG0003 Ex-Gratia Loss/Replacement of Item - Glasses 80
19RYLEG0004 Ex-Gratia Loss/Replacement of Item - Dentures 190
19RYLEG0007 Ex-Gratia Retirement Gratuity 372
19RYLEG0008 Ex-Gratia Retirement Gratuity 410
19RYLEG0009 Ex-Gratia Retirement Gratuity 461
19RYLEG0010 Ex-Gratia Retirement Gratuity 361
19RYLEG0011 Ex-Gratia Retirement Gratuity 254
19RYLEG0012 Ex-Gratia Retirement Gratuity 304
19RYLEG0013 Ex-Gratia Retirement Gratuity 274
19RYLEG0014 Ex-Gratia Retirement Gratuity 196
19RYLEG0015 Ex-Gratia Retirement Gratuity 380
19RYLEG0016 Ex-Gratia Retirement Gratuity 353
19RYLEG0017 Ex-Gratia Retirement Gratuity 390
19RYLEG0018 Ex-Gratia Retirement Gratuity 216
19RYLEG0019 Ex-Gratia Retirement Gratuity 333
19RYLEG0020 Ex-Gratia Retirement Gratuity 372
19RYLEG0021 Ex-Gratia Retirement Gratuity 341
19RYLEG0022 Ex-Gratia Retirement Gratuity 392
19RYLEG0023 Ex-Gratia Retirement Gratuity 361
19RYLEG0024 Ex-Gratia Retirement Gratuity 353
19RYLEG0025 Ex-Gratia Retirement Gratuity 332
19RYLEG0026 Ex-Gratia Retirement Gratuity 382
19RYLEG0027 Ex-Gratia Retirement Gratuity 225
Total 01/04/2018 - 31/05/2018 8,844
2.3 Losses and Special Payments Report
49 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Standards of Behaviour Policy Page 1 of 6 Audit Committee Meeting 9 July 2018
AGENDA ITEM 2.4
9 July 2018
Audit Committee Report
STANDARDS OF BEHAVIOUR
Executive Lead: Director of Corporate Services and Governance / Board
Secretary
Author: Head of Corporate Services
Contact Details for further information: Robert Williams, 01443 744800 or email [email protected]
Purpose of the Audit Committee Report
To provide the Audit Committee with information following receipt of the annual declarations of interest from Health Board staff and the Register of
Gifts and Hospitality for 2018-19.
Governance
Link to Health Board Strategic
Objective(s)
The Board’s overarching role is to ensure its Strategy outlined within ‘Cwm Taf Cares’ 3 Year Integrated
Medium Term Plan 2015-2018 and the related organisational objectives aligned with the Institute of
Healthcare Improvement's (IHI) ‘Triple Aim’ are being progressed, these in summary are:
To improve quality, safety and patient experience.
To protect and improve population health. To ensure that the services provided are
accessible and sustainable into the future. To provide strong governance and assurance.
To ensure good value based care and treatment for our patients in line with the resources made
available to the Health Board.
This report focuses mainly on providing strong governance & assurance.
Supporting evidence
Standards of Behaviour Policy Standing Orders
Engagement – Who has been involved in this work?
Board Members; All Senior Staff; Consultants in line with the
requirements of the Standards of Behaviour policy. This year for the first time, all staff at Band 8 or above have been asked to complete a
declaration, including nil interests.
2.4 Standards of Behaviour Report
50 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Standards of Behaviour Policy Page 2 of 6 Audit Committee Meeting 9 July 2018
Audit Committee Resolution to:
APPROVE ENDORSE √ DISCUSS √ NOTE √
Recommendation The Audit Committee is asked to: RECEIVE and NOTE the report and supporting
appendices in relation to the Health Board’s Standards of Behaviour Policy; and
NOTE the ongoing actions being taken to improve compliance and NOTE that an update
report will be provided at the next meeting.
Summarise the Impact of the Audit Committee Report
Equality and diversity
No specific impact identified all relevant staff required to complete
Legal implications No specific impact
Population Health No impact identified
Quality, Safety &
Patient Experience
Not related to patient care directly
Resources Online (intranet – SharePoint) requirement staff to access personally to complete.
Risks and Assurance Failure to declare relevant and material interests
could place Health Board staff in a position where a conflict of interest occurs. This could lead to
circumstances that would impact badly on the reputation of the Health Board and its
compliance with accepted standards of corporate governance.
Health & Care
Standards
Access to the Standards can be obtained from
the following link. www.wales.nhs.uk/siteplus/documents/1064/Eas
y%20Read%20Standards%20FINAL%20December%202010.pdf
Standard 1. Governance & Accountability.
Workforce No impact.
Freedom of
Information Status
Open
2.4 Standards of Behaviour Report
51 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Standards of Behaviour Policy Page 3 of 6 Audit Committee Meeting 9 July 2018
STANDARDS OF BEHAVIOUR
1. SITUATION / PURPOSE OF REPORT
To provide the Audit Committee with information following receipt of the annual
declarations of interest from Health Board staff and the Register of Gifts and Hospitality for the period starting from April 2018.
2. BACKGROUND / INTRODUCTION
The Health Board’s Standards of Behaviour Policy ensures that arrangements
are in place to support employees to act in a manner that upholds the Standards of Behaviour Framework as well as setting out specific arrangements
for the appropriate declarations of interests and acceptance / refusal and record of offers of Gifts, Hospitality or Sponsorship. The Policy also aims to capture
public acceptability of behaviours of those working in the public sector so that the Health Board can be seen to have exemplary practice in this regard.
Policy Review
Members will recall that the Standards of Behaviour Policy was reviewed in
2016 and approved for three years by the Audit Committee in July 2016.
The policy has been reviewed by the Head of Corporate Services comparing to best practice identified nationally. The following amendments are proposed:
Adding in the requirement for all staff at Agenda for Change Band 8 and above to complete a declaration (most for the first time)
Add the newly approved Intellectual Property Management Policy to those which should be considered alongside the current policy
Add the Special leave policy to link to time off for public duties.
Therefore, the information attached in the appendices supporting this report are against the UHB’s current Policy and supporting framework.
The process of undertaking an annual review of declarations of interest in accordance with the policy was traditionally resource intensive. During 2016 an
e-reporting system was introduced. The paper system has now been stopped and the following information provides progress to date.
Declarations of
Interest
2015 2016 2017 *2018 % age
inc/dec
Issued / targeted 338 403 684 834 22% inc
Returned ‘No Interests’ 136 216 440 252 30%
Returned with ‘declared
interests’
92 129 129 105 13%
Outstanding 110 58 115 477 57%
Compliance Rate 67% 86% 83%
*Note 2018 is currently in progress.
2.4 Standards of Behaviour Report
52 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Standards of Behaviour Policy Page 4 of 6 Audit Committee Meeting 9 July 2018
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
Declarations of Interest
As Members will be aware, the Standing Orders and Standards of Behaviour Policy of the Health Board set out the arrangements for Directors and other
senior staff to declare interests that are relevant and material to the business of the Health Board and any interests are entered into a Register that is available
for inspection by the public at the Health Board Offices. An annual review of recorded interests is conducted and all Directors are required to confirm their
entry in the Register.
There is also a requirement for staff to declare ‘relevant and material’ interests
held by their spouse or partner. This is because the pecuniary interest of one partner shall, if known to the other, be deemed to be also an interest of the
other and as such must be disclosed.
“Relevant interests” will include:
Directorships, including Non-Executive Directorships held in private companies or PLCs, with the exception of dormant companies;
Ownership or part-ownership, of private companies, businesses or consultancies likely or possibly seeking to do business with the Health
Board. This includes shareholdings, debentures or rights where the total nominal value is £5,000 or one hundredth of the total nominal value of
the issued share capital of the company or body, whichever is the less;
A personal or departmental interest in any part of the pharmaceutical / healthcare industry that could be perceived as having an influence on
decision making or on the provision of advice to members of the team; Sponsorship or funding from a known NHS supplier or associated
company/subsidiary; A position of authority in a charity or voluntary body in the field of health
and social care; Any other connection with a voluntary, statutory, charitable or private
body that could create a potential opportunity for conflicting interests; Employment by any other body where there could be a perceived or
actual conflict with NHS duties. This includes the undertaking of private practice.
Annual Review
All appropriate staff have been asked to complete their declaration by personal
email (including a nil return) and this year we have increased the number of staff targeted. This report details for the Audit Committee the nil returns
received, the number of outstanding declarations and the nature of any interests declared by Health Board Staff.
2.4 Standards of Behaviour Report
53 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Standards of Behaviour Policy Page 5 of 6 Audit Committee Meeting 9 July 2018
Health Board Returns
Under the Health Board Standing Orders, the Board Members are required to complete a declaration of interest annually and this was reported within the
approved Annual Report. For ease of reference, these are attached at
Appendix 1.
Nil Returns
Under the requirements of the Standards of Behaviour policy, senior staff are required to complete a declaration of interest annually which includes “Nil
Returns” and these are attached as Appendix 2.
Nature of Interests Declared
The nature of any interest declared by Health Board staff is set out in Appendix 3 and the Audit Committee is asked to consider this appendix and
confirm that it is content that no conflict of interest is apparent from the information received.
Outstanding Declarations
At the time of preparing this report, there remains a substantial number of declarations not returned despite having a 6 week window to complete their
individual declaration by 22 June. Most of those not returned are from clinical staff and some are from staff at Band 8 who have been asked for the first time
to complete a declaration of interest.
At the time of report there are 477 outstanding returns.
The lists of staff in each directorate who have not completed their declaration of interest have been sent back to the Directorate Manager and Clinical Director
for action; the Executive Director has also been a copy recipient. The staff have now been provided a last chance opportunity to complete their declarations
prior to further action by the directorates. An oral update on progress will be provided at the meeting.
Gifts, Hospitality and Sponsorship
Gifts A gift is an item of personal value, given by a third party e.g. a patient or a
supplier. The definition includes prizes in draws and raffles at sponsored events / conferences.
It is an offence to accept any money, gift or consideration as an inducement or reward from a person or organisation holding or seeking to hold a contract with
the Health Board. Such gifts should be refused and if they have already been received they should be returned clearly advising why they cannot be accepted.
2.4 Standards of Behaviour Report
54 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Standards of Behaviour Policy Page 6 of 6 Audit Committee Meeting 9 July 2018
The appropriate Director and the Director of Corporate Services / Board Secretary should be advised immediately.
Hospitality
Hospitality is where there is an offer of food, drinks, accommodation,
entertainment or entry into an event or function by a third party, regardless of whether provided during or outside normal working hours.
Employees in contact with contractors should be particularly mindful of
accepting any hospitality that might later be misconstrued as impacting on strict independence and impartiality.
Sponsorship
Sponsorship is sometimes provided by organisations to allow employees to attend conferences or working visits to view equipment. It may also include
sponsorship of posts and research and development.
No sponsorship should be accepted without the prior agreement of the appropriate Corporate / Clinical Director. A Gifts, Hospitality and Sponsorship
Form should also be completed prior to the acceptance of any sponsorship.
If sponsorship is inappropriately offered and / or declined this should also be
declared.
Attached at Appendix 4 is the Health Board Gifts, Hospitality and Sponsorship Register covering the period September 2017 – June 2018.
CONCLUSION
Further action will continue to be taken to increase the numbers of staff completing their annual declaration of interest form. Directorates will also
receive their own version of the register in order to be fully aware of any
interests held by their staff. An update report to confirm the position will be provided to the next Audit Committee. 4. RECOMMENDATION
Members of the Committee are asked to:
RECEIVE and NOTE the report and supporting appendices in relation to the
Health Board’s Standards of Behaviour Policy; and
NOTE the ongoing actions being taken to improve compliance and NOTE that an update report will be provided at the next meeting.
Freedom of
Information Status
Open
2.4 Standards of Behaviour Report
55 of 380Audit Committee - Part 1 9 July 2018-09/07/18
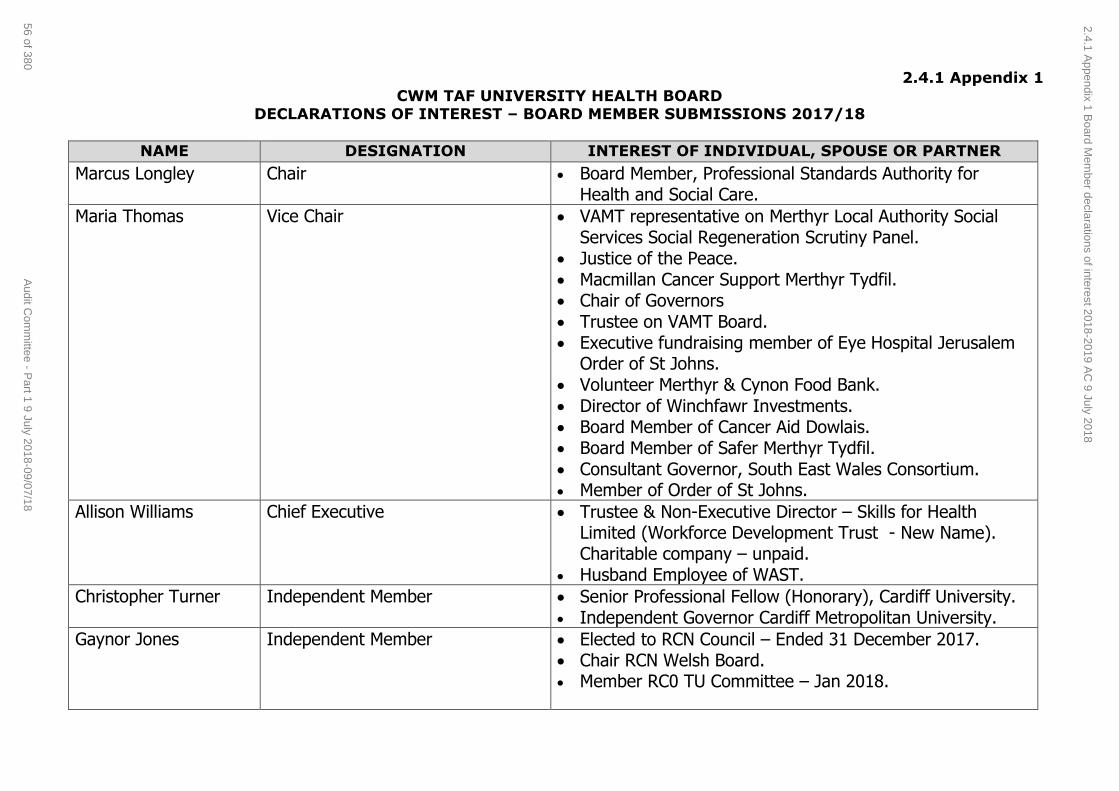
2.4.1 Appendix 1
CWM TAF UNIVERSITY HEALTH BOARD DECLARATIONS OF INTEREST – BOARD MEMBER SUBMISSIONS 2017/18
NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Marcus Longley Chair Board Member, Professional Standards Authority for Health and Social Care.
Maria Thomas Vice Chair VAMT representative on Merthyr Local Authority Social Services Social Regeneration Scrutiny Panel.
Justice of the Peace. Macmillan Cancer Support Merthyr Tydfil. Chair of Governors Trustee on VAMT Board. Executive fundraising member of Eye Hospital Jerusalem
Order of St Johns. Volunteer Merthyr & Cynon Food Bank. Director of Winchfawr Investments. Board Member of Cancer Aid Dowlais. Board Member of Safer Merthyr Tydfil. Consultant Governor, South East Wales Consortium. Member of Order of St Johns.
Allison Williams Chief Executive Trustee & Non-Executive Director – Skills for Health Limited (Workforce Development Trust - New Name). Charitable company – unpaid.
Husband Employee of WAST.
Christopher Turner Independent Member Senior Professional Fellow (Honorary), Cardiff University. Independent Governor Cardiff Metropolitan University.
Gaynor Jones Independent Member Elected to RCN Council – Ended 31 December 2017. Chair RCN Welsh Board. Member RC0 TU Committee – Jan 2018.
2.4.1 Appendix 1 B
oard Mem
ber declarations of interest 2018-2019 AC
9 July 2018
56 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
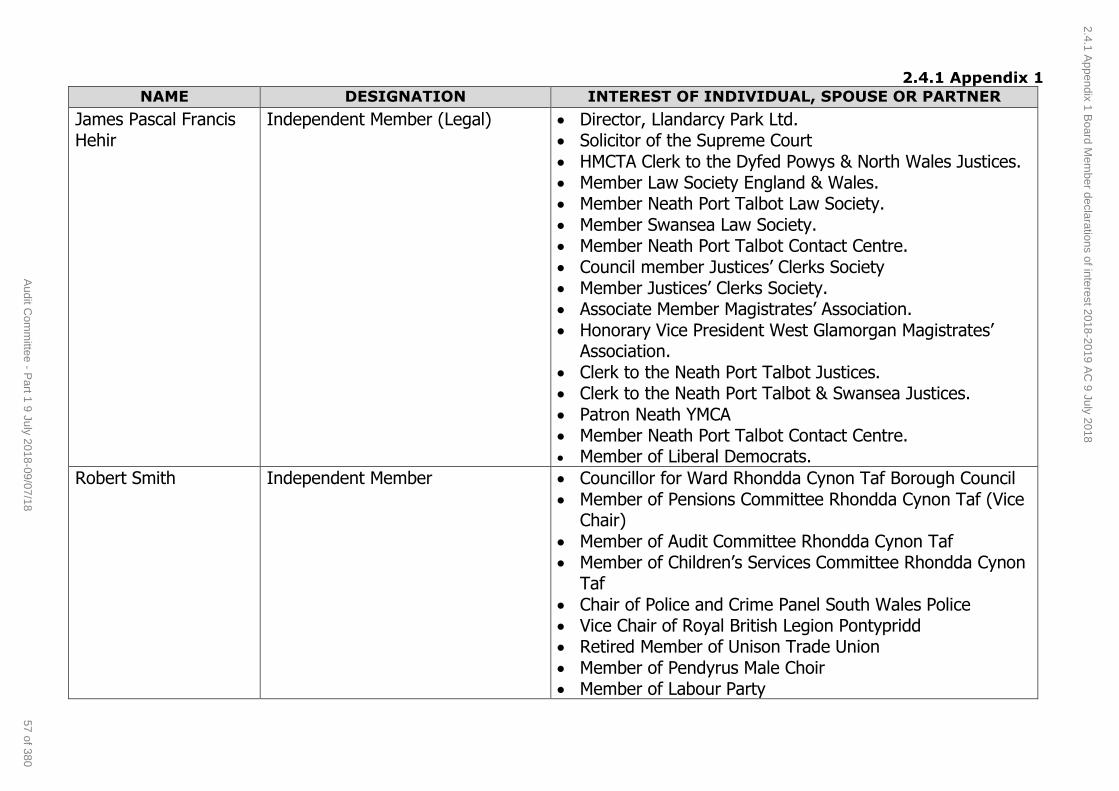
2.4.1 Appendix 1
NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
James Pascal Francis Hehir
Independent Member (Legal) Director, Llandarcy Park Ltd. Solicitor of the Supreme Court HMCTA Clerk to the Dyfed Powys & North Wales Justices. Member Law Society England & Wales. Member Neath Port Talbot Law Society. Member Swansea Law Society. Member Neath Port Talbot Contact Centre.
Council member Justices’ Clerks Society Member Justices’ Clerks Society. Associate Member Magistrates’ Association. Honorary Vice President West Glamorgan Magistrates’
Association. Clerk to the Neath Port Talbot Justices. Clerk to the Neath Port Talbot & Swansea Justices.
Patron Neath YMCA Member Neath Port Talbot Contact Centre. Member of Liberal Democrats.
Robert Smith Independent Member Councillor for Ward Rhondda Cynon Taf Borough Council Member of Pensions Committee Rhondda Cynon Taf (Vice
Chair) Member of Audit Committee Rhondda Cynon Taf Member of Children’s Services Committee Rhondda Cynon
Taf Chair of Police and Crime Panel South Wales Police Vice Chair of Royal British Legion Pontypridd Retired Member of Unison Trade Union Member of Pendyrus Male Choir Member of Labour Party
2.4.1 Appendix 1 B
oard Mem
ber declarations of interest 2018-2019 AC
9 July 2018
57 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
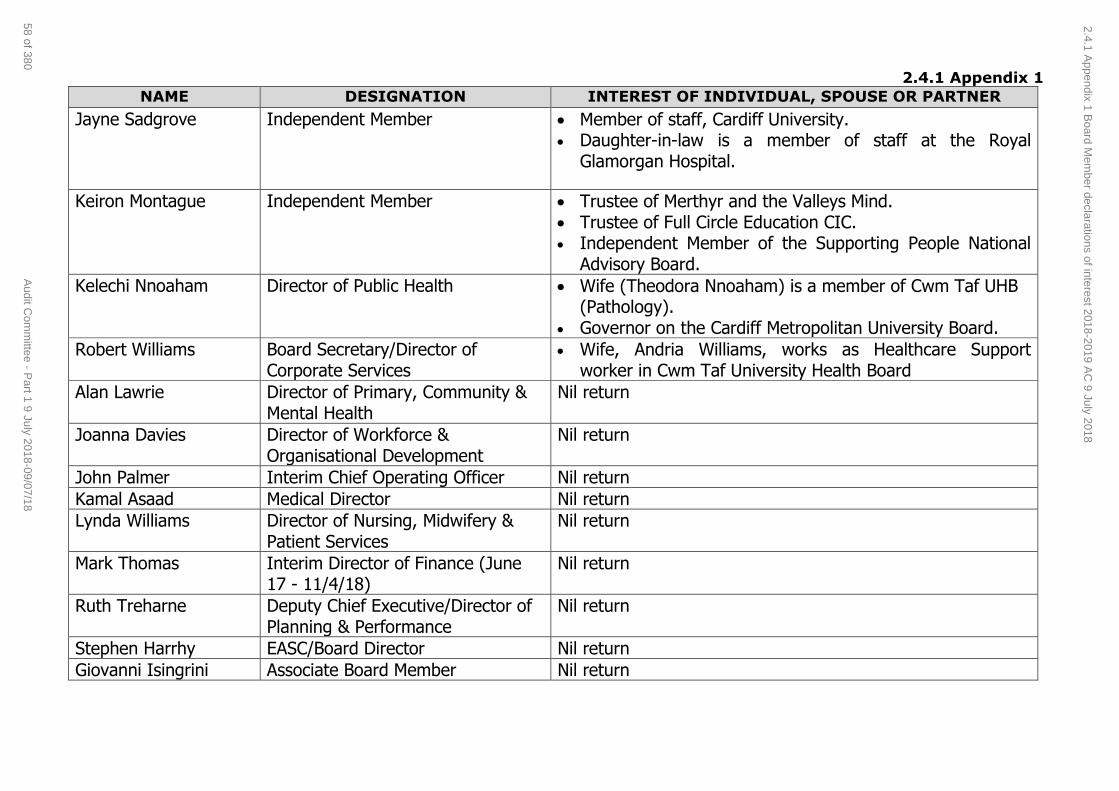
2.4.1 Appendix 1
NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Jayne Sadgrove Independent Member Member of staff, Cardiff University. Daughter-in-law is a member of staff at the Royal
Glamorgan Hospital.
Keiron Montague Independent Member Trustee of Merthyr and the Valleys Mind. Trustee of Full Circle Education CIC. Independent Member of the Supporting People National
Advisory Board.
Kelechi Nnoaham Director of Public Health Wife (Theodora Nnoaham) is a member of Cwm Taf UHB (Pathology).
Governor on the Cardiff Metropolitan University Board.
Robert Williams Board Secretary/Director of Corporate Services
Wife, Andria Williams, works as Healthcare Support worker in Cwm Taf University Health Board
Alan Lawrie Director of Primary, Community & Mental Health
Nil return
Joanna Davies Director of Workforce & Organisational Development
Nil return
John Palmer Interim Chief Operating Officer Nil return
Kamal Asaad Medical Director Nil return
Lynda Williams Director of Nursing, Midwifery & Patient Services
Nil return
Mark Thomas Interim Director of Finance (June 17 - 11/4/18)
Nil return
Ruth Treharne Deputy Chief Executive/Director of Planning & Performance
Nil return
Stephen Harrhy EASC/Board Director Nil return
Giovanni Isingrini Associate Board Member Nil return
2.4.1 Appendix 1 B
oard Mem
ber declarations of interest 2018-2019 AC
9 July 2018
58 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
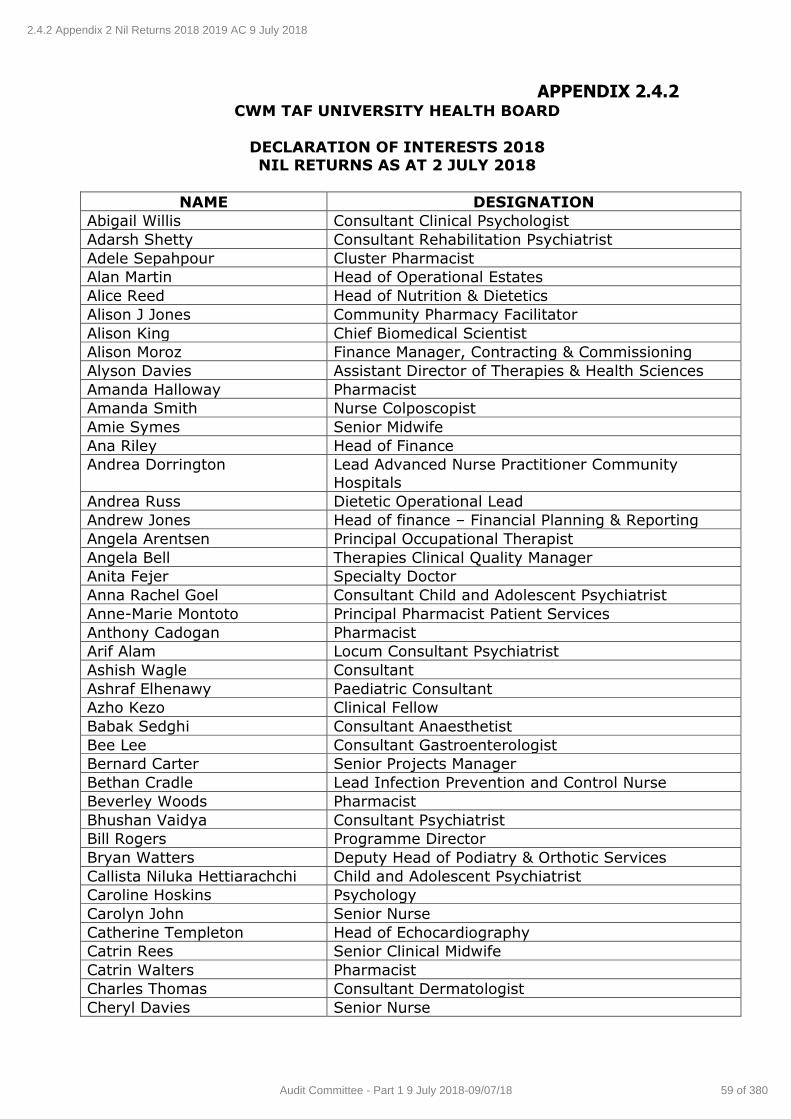
APPENDIX 2.4.2 CWM TAF UNIVERSITY HEALTH BOARD
DECLARATION OF INTERESTS 2018 NIL RETURNS AS AT 2 JULY 2018
NAME DESIGNATION
Abigail Willis Consultant Clinical Psychologist
Adarsh Shetty Consultant Rehabilitation Psychiatrist
Adele Sepahpour Cluster Pharmacist
Alan Martin Head of Operational Estates
Alice Reed Head of Nutrition & Dietetics
Alison J Jones Community Pharmacy Facilitator
Alison King Chief Biomedical Scientist
Alison Moroz Finance Manager, Contracting & Commissioning
Alyson Davies Assistant Director of Therapies & Health Sciences
Amanda Halloway Pharmacist
Amanda Smith Nurse Colposcopist
Amie Symes Senior Midwife
Ana Riley Head of Finance
Andrea Dorrington Lead Advanced Nurse Practitioner Community
Hospitals
Andrea Russ Dietetic Operational Lead
Andrew Jones Head of finance – Financial Planning & Reporting
Angela Arentsen Principal Occupational Therapist
Angela Bell Therapies Clinical Quality Manager
Anita Fejer Specialty Doctor
Anna Rachel Goel Consultant Child and Adolescent Psychiatrist
Anne-Marie Montoto Principal Pharmacist Patient Services
Anthony Cadogan Pharmacist
Arif Alam Locum Consultant Psychiatrist
Ashish Wagle Consultant
Ashraf Elhenawy Paediatric Consultant
Azho Kezo Clinical Fellow
Babak Sedghi Consultant Anaesthetist
Bee Lee Consultant Gastroenterologist
Bernard Carter Senior Projects Manager
Bethan Cradle Lead Infection Prevention and Control Nurse
Beverley Woods Pharmacist
Bhushan Vaidya Consultant Psychiatrist
Bill Rogers Programme Director
Bryan Watters Deputy Head of Podiatry & Orthotic Services
Callista Niluka Hettiarachchi Child and Adolescent Psychiatrist
Caroline Hoskins Psychology
Carolyn John Senior Nurse
Catherine Templeton Head of Echocardiography
Catrin Rees Senior Clinical Midwife
Catrin Walters Pharmacist
Charles Thomas Consultant Dermatologist
Cheryl Davies Senior Nurse
2.4.2 Appendix 2 Nil Returns 2018 2019 AC 9 July 2018
59 of 380Audit Committee - Part 1 9 July 2018-09/07/18
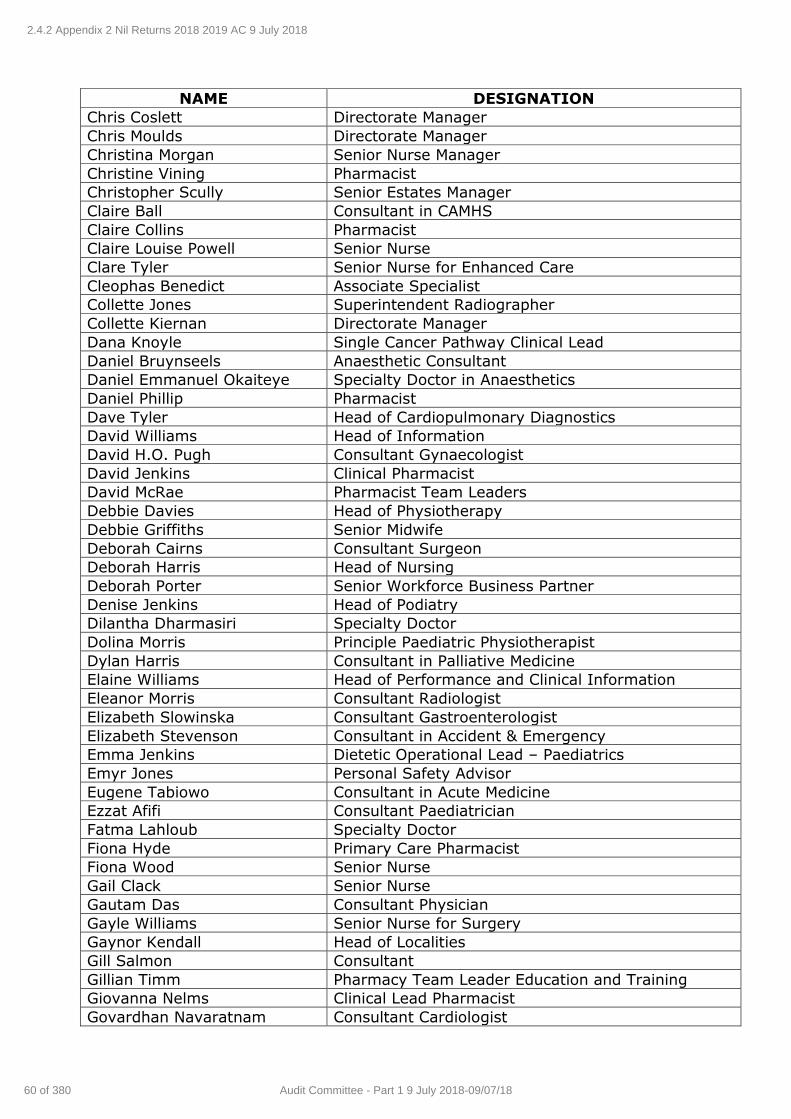
NAME DESIGNATION
Chris Coslett Directorate Manager
Chris Moulds Directorate Manager
Christina Morgan Senior Nurse Manager
Christine Vining Pharmacist
Christopher Scully Senior Estates Manager
Claire Ball Consultant in CAMHS
Claire Collins Pharmacist
Claire Louise Powell Senior Nurse
Clare Tyler Senior Nurse for Enhanced Care
Cleophas Benedict Associate Specialist
Collette Jones Superintendent Radiographer
Collette Kiernan Directorate Manager
Dana Knoyle Single Cancer Pathway Clinical Lead
Daniel Bruynseels Anaesthetic Consultant
Daniel Emmanuel Okaiteye Specialty Doctor in Anaesthetics
Daniel Phillip Pharmacist
Dave Tyler Head of Cardiopulmonary Diagnostics
David Williams Head of Information
David H.O. Pugh Consultant Gynaecologist
David Jenkins Clinical Pharmacist
David McRae Pharmacist Team Leaders
Debbie Davies Head of Physiotherapy
Debbie Griffiths Senior Midwife
Deborah Cairns Consultant Surgeon
Deborah Harris Head of Nursing
Deborah Porter Senior Workforce Business Partner
Denise Jenkins Head of Podiatry
Dilantha Dharmasiri Specialty Doctor
Dolina Morris Principle Paediatric Physiotherapist
Dylan Harris Consultant in Palliative Medicine
Elaine Williams Head of Performance and Clinical Information
Eleanor Morris Consultant Radiologist
Elizabeth Slowinska Consultant Gastroenterologist
Elizabeth Stevenson Consultant in Accident & Emergency
Emma Jenkins Dietetic Operational Lead – Paediatrics
Emyr Jones Personal Safety Advisor
Eugene Tabiowo Consultant in Acute Medicine
Ezzat Afifi Consultant Paediatrician
Fatma Lahloub Specialty Doctor
Fiona Hyde Primary Care Pharmacist
Fiona Wood Senior Nurse
Gail Clack Senior Nurse
Gautam Das Consultant Physician
Gayle Williams Senior Nurse for Surgery
Gaynor Kendall Head of Localities
Gill Salmon Consultant
Gillian Timm Pharmacy Team Leader Education and Training
Giovanna Nelms Clinical Lead Pharmacist
Govardhan Navaratnam Consultant Cardiologist
2.4.2 Appendix 2 Nil Returns 2018 2019 AC 9 July 2018
60 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
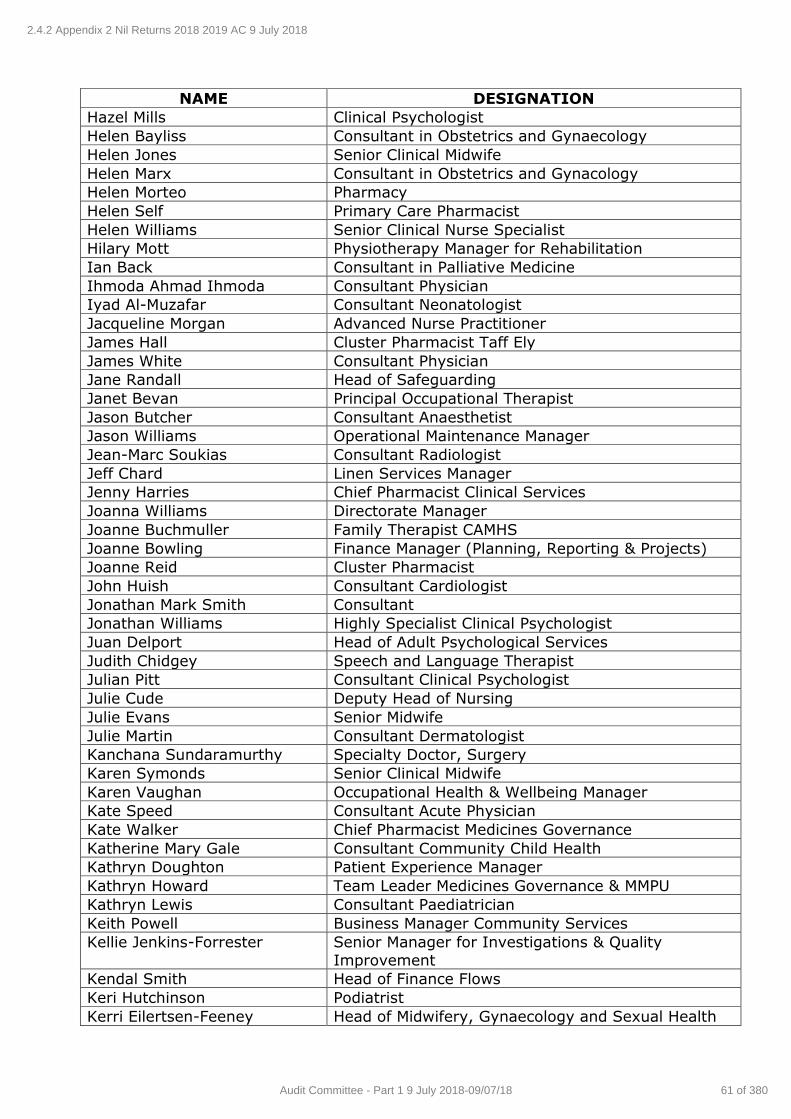
NAME DESIGNATION
Hazel Mills Clinical Psychologist
Helen Bayliss Consultant in Obstetrics and Gynaecology
Helen Jones Senior Clinical Midwife
Helen Marx Consultant in Obstetrics and Gynacology
Helen Morteo Pharmacy
Helen Self Primary Care Pharmacist
Helen Williams Senior Clinical Nurse Specialist
Hilary Mott Physiotherapy Manager for Rehabilitation
Ian Back Consultant in Palliative Medicine
Ihmoda Ahmad Ihmoda Consultant Physician
Iyad Al-Muzafar Consultant Neonatologist
Jacqueline Morgan Advanced Nurse Practitioner
James Hall Cluster Pharmacist Taff Ely
James White Consultant Physician
Jane Randall Head of Safeguarding
Janet Bevan Principal Occupational Therapist
Jason Butcher Consultant Anaesthetist
Jason Williams Operational Maintenance Manager
Jean-Marc Soukias Consultant Radiologist
Jeff Chard Linen Services Manager
Jenny Harries Chief Pharmacist Clinical Services
Joanna Williams Directorate Manager
Joanne Buchmuller Family Therapist CAMHS
Joanne Bowling Finance Manager (Planning, Reporting & Projects)
Joanne Reid Cluster Pharmacist
John Huish Consultant Cardiologist
Jonathan Mark Smith Consultant
Jonathan Williams Highly Specialist Clinical Psychologist
Juan Delport Head of Adult Psychological Services
Judith Chidgey Speech and Language Therapist
Julian Pitt Consultant Clinical Psychologist
Julie Cude Deputy Head of Nursing
Julie Evans Senior Midwife
Julie Martin Consultant Dermatologist
Kanchana Sundaramurthy Specialty Doctor, Surgery
Karen Symonds Senior Clinical Midwife
Karen Vaughan Occupational Health & Wellbeing Manager
Kate Speed Consultant Acute Physician
Kate Walker Chief Pharmacist Medicines Governance
Katherine Mary Gale Consultant Community Child Health
Kathryn Doughton Patient Experience Manager
Kathryn Howard Team Leader Medicines Governance & MMPU
Kathryn Lewis Consultant Paediatrician
Keith Powell Business Manager Community Services
Kellie Jenkins-Forrester Senior Manager for Investigations & Quality
Improvement
Kendal Smith Head of Finance Flows
Keri Hutchinson Podiatrist
Kerri Eilertsen-Feeney Head of Midwifery, Gynaecology and Sexual Health
2.4.2 Appendix 2 Nil Returns 2018 2019 AC 9 July 2018
61 of 380Audit Committee - Part 1 9 July 2018-09/07/18
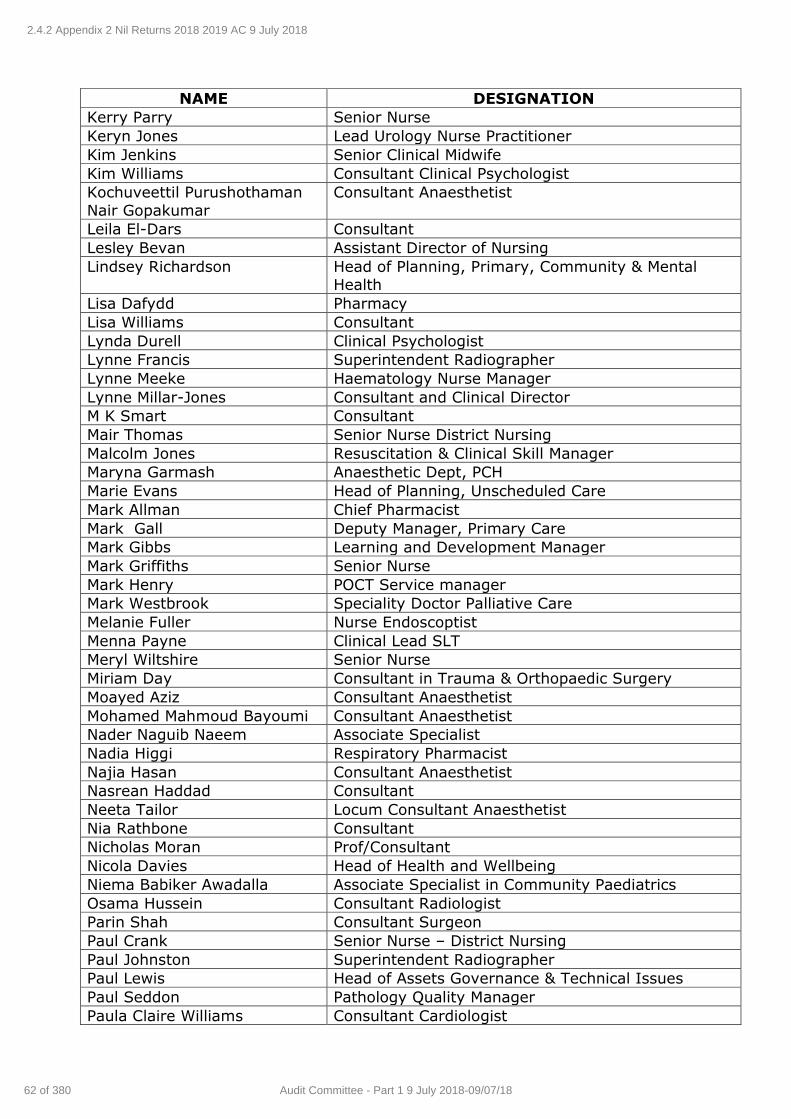
NAME DESIGNATION
Kerry Parry Senior Nurse
Keryn Jones Lead Urology Nurse Practitioner
Kim Jenkins Senior Clinical Midwife
Kim Williams Consultant Clinical Psychologist
Kochuveettil Purushothaman
Nair Gopakumar
Consultant Anaesthetist
Leila El-Dars Consultant
Lesley Bevan Assistant Director of Nursing
Lindsey Richardson Head of Planning, Primary, Community & Mental Health
Lisa Dafydd Pharmacy
Lisa Williams Consultant
Lynda Durell Clinical Psychologist
Lynne Francis Superintendent Radiographer
Lynne Meeke Haematology Nurse Manager
Lynne Millar-Jones Consultant and Clinical Director
M K Smart Consultant
Mair Thomas Senior Nurse District Nursing
Malcolm Jones Resuscitation & Clinical Skill Manager
Maryna Garmash Anaesthetic Dept, PCH
Marie Evans Head of Planning, Unscheduled Care
Mark Allman Chief Pharmacist
Mark Gall Deputy Manager, Primary Care
Mark Gibbs Learning and Development Manager
Mark Griffiths Senior Nurse
Mark Henry POCT Service manager
Mark Westbrook Speciality Doctor Palliative Care
Melanie Fuller Nurse Endoscoptist
Menna Payne Clinical Lead SLT
Meryl Wiltshire Senior Nurse
Miriam Day Consultant in Trauma & Orthopaedic Surgery
Moayed Aziz Consultant Anaesthetist
Mohamed Mahmoud Bayoumi Consultant Anaesthetist
Nader Naguib Naeem Associate Specialist
Nadia Higgi Respiratory Pharmacist
Najia Hasan Consultant Anaesthetist
Nasrean Haddad Consultant
Neeta Tailor Locum Consultant Anaesthetist
Nia Rathbone Consultant
Nicholas Moran Prof/Consultant
Nicola Davies Head of Health and Wellbeing
Niema Babiker Awadalla Associate Specialist in Community Paediatrics
Osama Hussein Consultant Radiologist
Parin Shah Consultant Surgeon
Paul Crank Senior Nurse – District Nursing
Paul Johnston Superintendent Radiographer
Paul Lewis Head of Assets Governance & Technical Issues
Paul Seddon Pathology Quality Manager
Paula Claire Williams Consultant Cardiologist
2.4.2 Appendix 2 Nil Returns 2018 2019 AC 9 July 2018
62 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
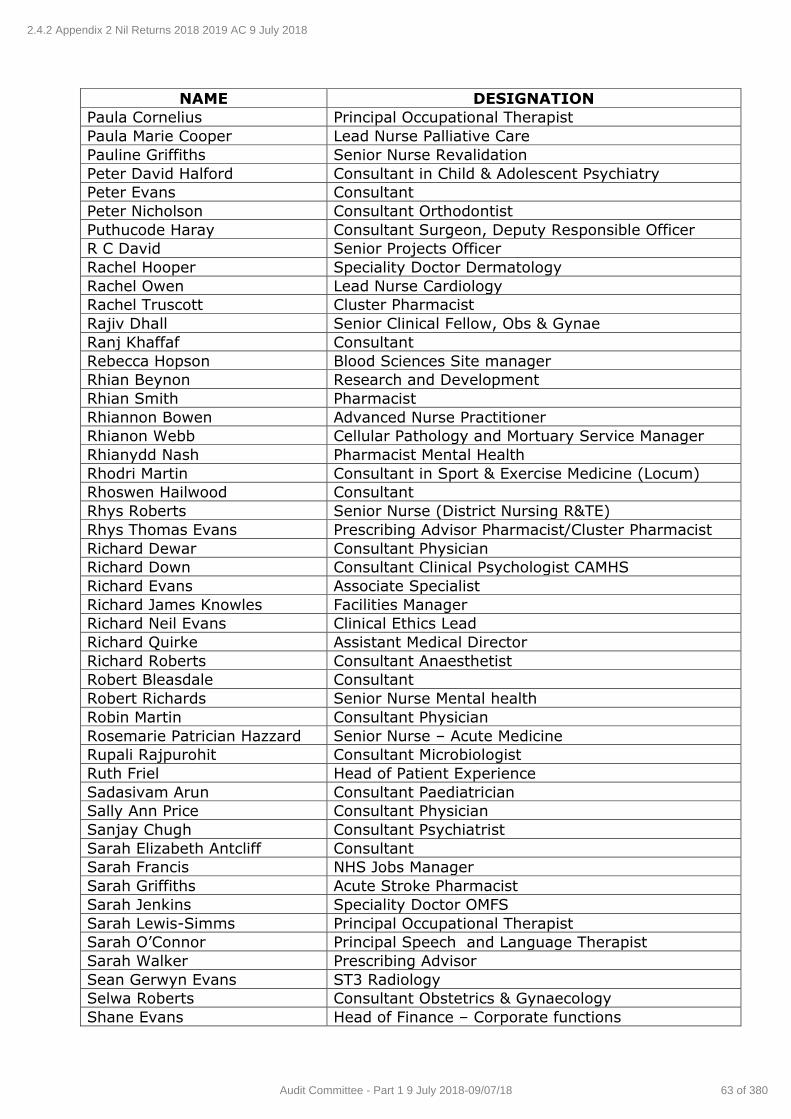
NAME DESIGNATION
Paula Cornelius Principal Occupational Therapist
Paula Marie Cooper Lead Nurse Palliative Care
Pauline Griffiths Senior Nurse Revalidation
Peter David Halford Consultant in Child & Adolescent Psychiatry
Peter Evans Consultant
Peter Nicholson Consultant Orthodontist
Puthucode Haray Consultant Surgeon, Deputy Responsible Officer
R C David Senior Projects Officer
Rachel Hooper Speciality Doctor Dermatology
Rachel Owen Lead Nurse Cardiology
Rachel Truscott Cluster Pharmacist
Rajiv Dhall Senior Clinical Fellow, Obs & Gynae
Ranj Khaffaf Consultant
Rebecca Hopson Blood Sciences Site manager
Rhian Beynon Research and Development
Rhian Smith Pharmacist
Rhiannon Bowen Advanced Nurse Practitioner
Rhianon Webb Cellular Pathology and Mortuary Service Manager
Rhianydd Nash Pharmacist Mental Health
Rhodri Martin Consultant in Sport & Exercise Medicine (Locum)
Rhoswen Hailwood Consultant
Rhys Roberts Senior Nurse (District Nursing R&TE)
Rhys Thomas Evans Prescribing Advisor Pharmacist/Cluster Pharmacist
Richard Dewar Consultant Physician
Richard Down Consultant Clinical Psychologist CAMHS
Richard Evans Associate Specialist
Richard James Knowles Facilities Manager
Richard Neil Evans Clinical Ethics Lead
Richard Quirke Assistant Medical Director
Richard Roberts Consultant Anaesthetist
Robert Bleasdale Consultant
Robert Richards Senior Nurse Mental health
Robin Martin Consultant Physician
Rosemarie Patrician Hazzard Senior Nurse – Acute Medicine
Rupali Rajpurohit Consultant Microbiologist
Ruth Friel Head of Patient Experience
Sadasivam Arun Consultant Paediatrician
Sally Ann Price Consultant Physician
Sanjay Chugh Consultant Psychiatrist
Sarah Elizabeth Antcliff Consultant
Sarah Francis NHS Jobs Manager
Sarah Griffiths Acute Stroke Pharmacist
Sarah Jenkins Speciality Doctor OMFS
Sarah Lewis-Simms Principal Occupational Therapist
Sarah O’Connor Principal Speech and Language Therapist
Sarah Walker Prescribing Advisor
Sean Gerwyn Evans ST3 Radiology
Selwa Roberts Consultant Obstetrics & Gynaecology
Shane Evans Head of Finance – Corporate functions
2.4.2 Appendix 2 Nil Returns 2018 2019 AC 9 July 2018
63 of 380Audit Committee - Part 1 9 July 2018-09/07/18
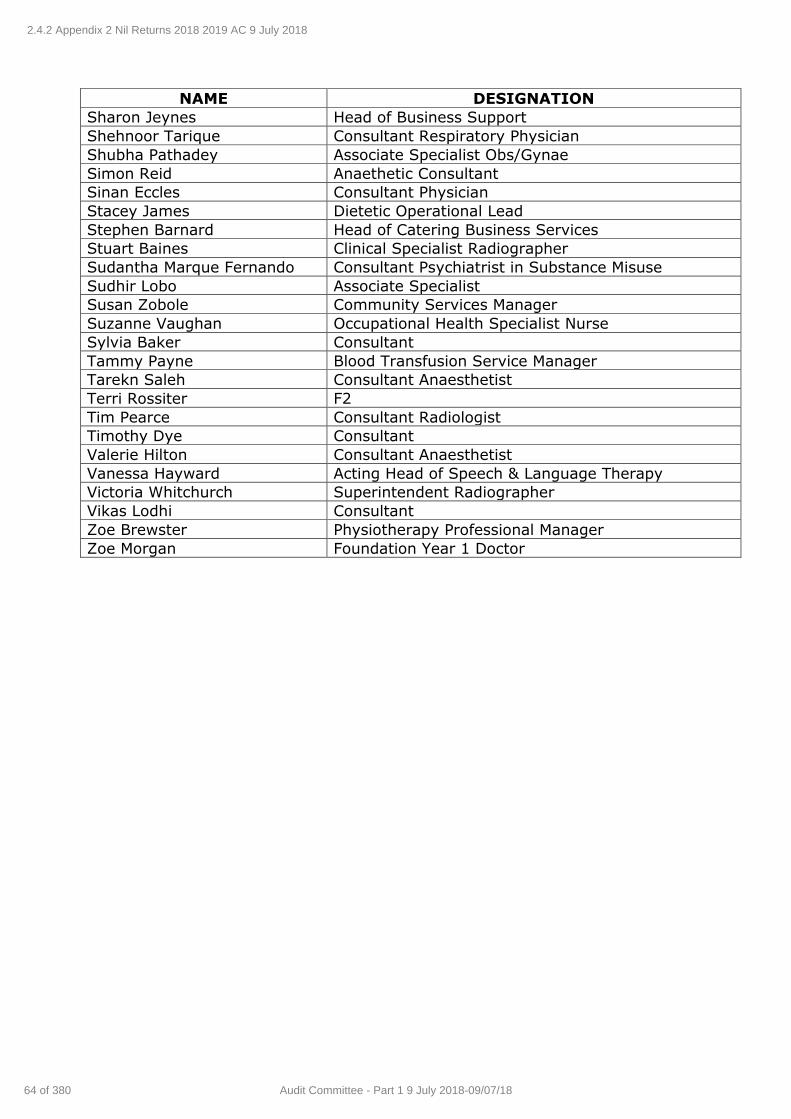
NAME DESIGNATION
Sharon Jeynes Head of Business Support
Shehnoor Tarique Consultant Respiratory Physician
Shubha Pathadey Associate Specialist Obs/Gynae
Simon Reid Anaethetic Consultant
Sinan Eccles Consultant Physician
Stacey James Dietetic Operational Lead
Stephen Barnard Head of Catering Business Services
Stuart Baines Clinical Specialist Radiographer
Sudantha Marque Fernando Consultant Psychiatrist in Substance Misuse
Sudhir Lobo Associate Specialist
Susan Zobole Community Services Manager
Suzanne Vaughan Occupational Health Specialist Nurse
Sylvia Baker Consultant
Tammy Payne Blood Transfusion Service Manager
Tarekn Saleh Consultant Anaesthetist
Terri Rossiter F2
Tim Pearce Consultant Radiologist
Timothy Dye Consultant
Valerie Hilton Consultant Anaesthetist
Vanessa Hayward Acting Head of Speech & Language Therapy
Victoria Whitchurch Superintendent Radiographer
Vikas Lodhi Consultant
Zoe Brewster Physiotherapy Professional Manager
Zoe Morgan Foundation Year 1 Doctor
2.4.2 Appendix 2 Nil Returns 2018 2019 AC 9 July 2018
64 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
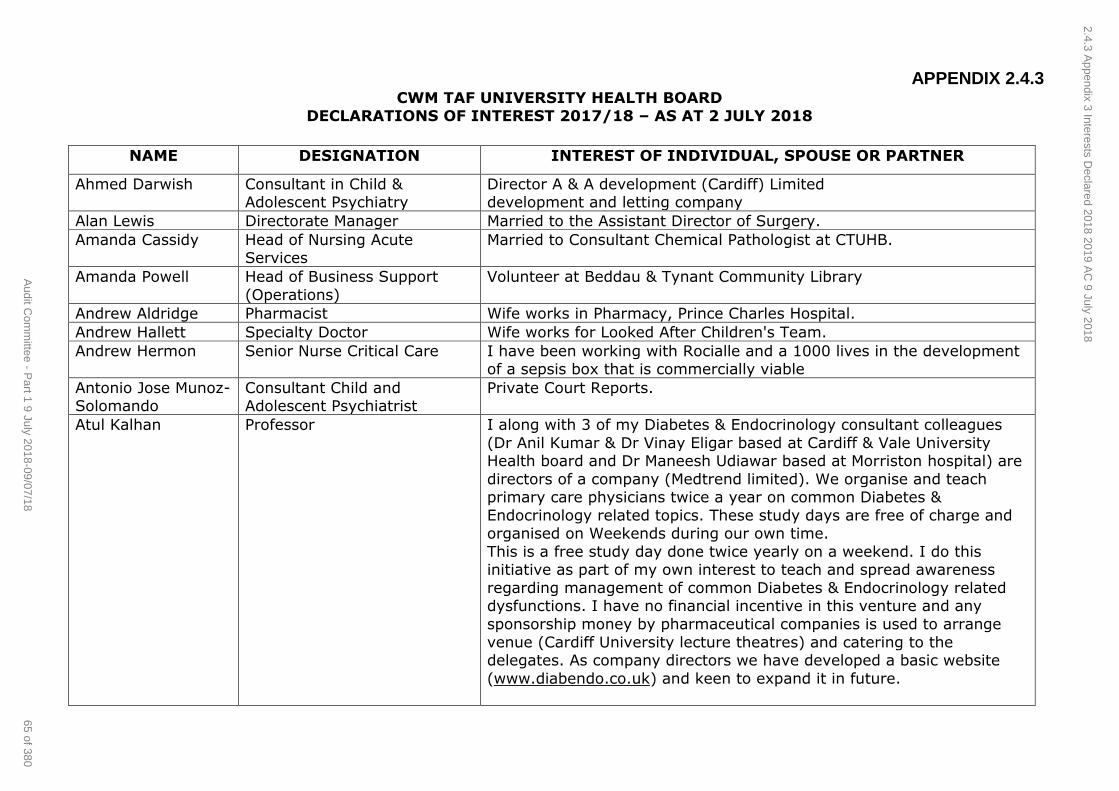
APPENDIX 2.4.3 CWM TAF UNIVERSITY HEALTH BOARD
DECLARATIONS OF INTEREST 2017/18 – AS AT 2 JULY 2018
NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Ahmed Darwish Consultant in Child & Adolescent Psychiatry
Director A & A development (Cardiff) Limited development and letting company
Alan Lewis Directorate Manager Married to the Assistant Director of Surgery.
Amanda Cassidy Head of Nursing Acute Services
Married to Consultant Chemical Pathologist at CTUHB.
Amanda Powell Head of Business Support
(Operations)
Volunteer at Beddau & Tynant Community Library
Andrew Aldridge Pharmacist Wife works in Pharmacy, Prince Charles Hospital.
Andrew Hallett Specialty Doctor Wife works for Looked After Children's Team.
Andrew Hermon Senior Nurse Critical Care I have been working with Rocialle and a 1000 lives in the development of a sepsis box that is commercially viable
Antonio Jose Munoz-Solomando
Consultant Child and Adolescent Psychiatrist
Private Court Reports.
Atul Kalhan Professor I along with 3 of my Diabetes & Endocrinology consultant colleagues
(Dr Anil Kumar & Dr Vinay Eligar based at Cardiff & Vale University Health board and Dr Maneesh Udiawar based at Morriston hospital) are
directors of a company (Medtrend limited). We organise and teach primary care physicians twice a year on common Diabetes &
Endocrinology related topics. These study days are free of charge and organised on Weekends during our own time.
This is a free study day done twice yearly on a weekend. I do this initiative as part of my own interest to teach and spread awareness
regarding management of common Diabetes & Endocrinology related dysfunctions. I have no financial incentive in this venture and any
sponsorship money by pharmaceutical companies is used to arrange
venue (Cardiff University lecture theatres) and catering to the delegates. As company directors we have developed a basic website
(www.diabendo.co.uk) and keen to expand it in future.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
65 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
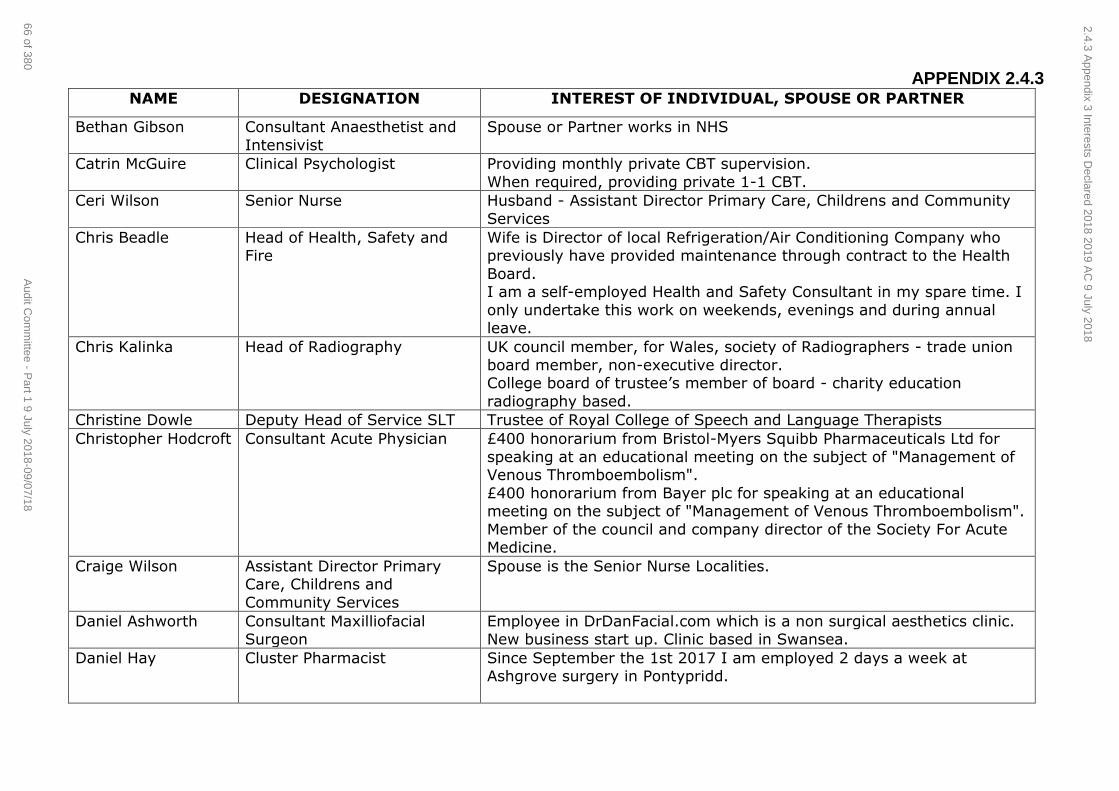
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Bethan Gibson Consultant Anaesthetist and
Intensivist
Spouse or Partner works in NHS
Catrin McGuire Clinical Psychologist Providing monthly private CBT supervision.
When required, providing private 1-1 CBT.
Ceri Wilson Senior Nurse Husband - Assistant Director Primary Care, Childrens and Community
Services
Chris Beadle Head of Health, Safety and Fire
Wife is Director of local Refrigeration/Air Conditioning Company who previously have provided maintenance through contract to the Health
Board. I am a self-employed Health and Safety Consultant in my spare time. I
only undertake this work on weekends, evenings and during annual leave.
Chris Kalinka Head of Radiography UK council member, for Wales, society of Radiographers - trade union
board member, non-executive director. College board of trustee’s member of board - charity education
radiography based.
Christine Dowle Deputy Head of Service SLT Trustee of Royal College of Speech and Language Therapists
Christopher Hodcroft Consultant Acute Physician £400 honorarium from Bristol-Myers Squibb Pharmaceuticals Ltd for
speaking at an educational meeting on the subject of "Management of Venous Thromboembolism".
£400 honorarium from Bayer plc for speaking at an educational meeting on the subject of "Management of Venous Thromboembolism".
Member of the council and company director of the Society For Acute Medicine.
Craige Wilson Assistant Director Primary Care, Childrens and
Community Services
Spouse is the Senior Nurse Localities.
Daniel Ashworth Consultant Maxilliofacial Surgeon
Employee in DrDanFacial.com which is a non surgical aesthetics clinic. New business start up. Clinic based in Swansea.
Daniel Hay Cluster Pharmacist Since September the 1st 2017 I am employed 2 days a week at Ashgrove surgery in Pontypridd.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
66 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
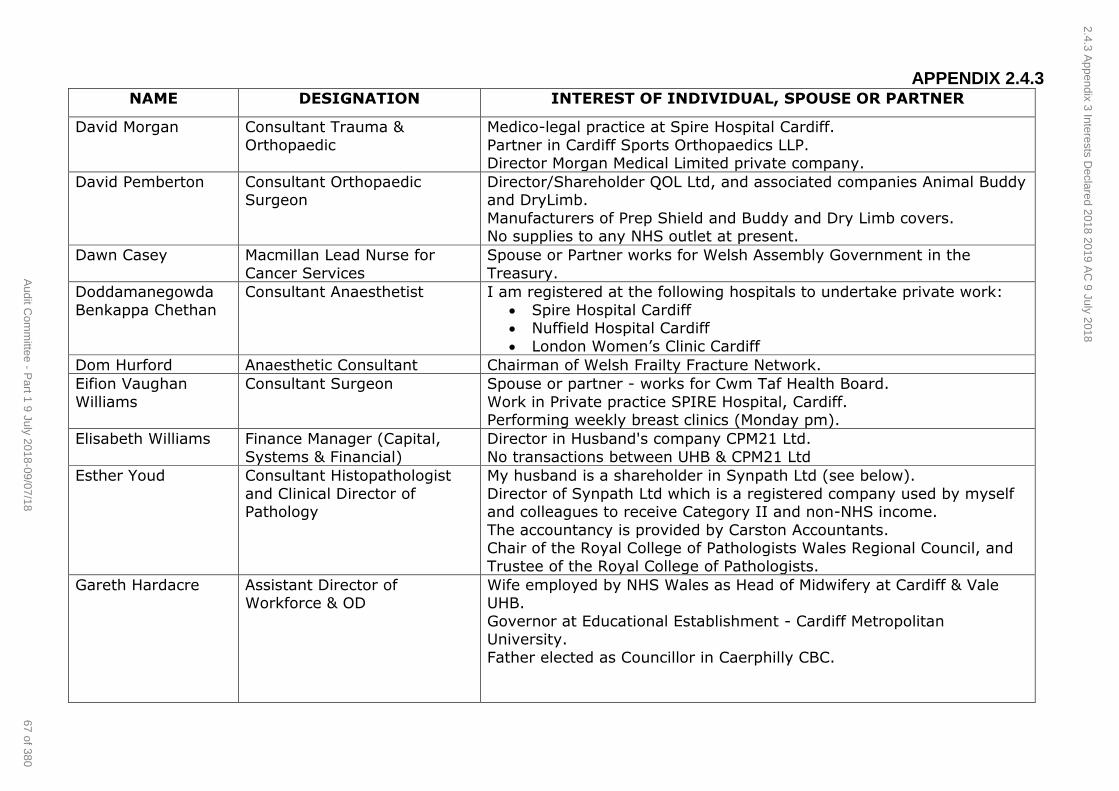
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
David Morgan Consultant Trauma &
Orthopaedic
Medico-legal practice at Spire Hospital Cardiff.
Partner in Cardiff Sports Orthopaedics LLP. Director Morgan Medical Limited private company.
David Pemberton Consultant Orthopaedic Surgeon
Director/Shareholder QOL Ltd, and associated companies Animal Buddy and DryLimb.
Manufacturers of Prep Shield and Buddy and Dry Limb covers. No supplies to any NHS outlet at present.
Dawn Casey Macmillan Lead Nurse for
Cancer Services
Spouse or Partner works for Welsh Assembly Government in the
Treasury.
Doddamanegowda
Benkappa Chethan
Consultant Anaesthetist I am registered at the following hospitals to undertake private work:
Spire Hospital Cardiff Nuffield Hospital Cardiff
London Women’s Clinic Cardiff
Dom Hurford Anaesthetic Consultant Chairman of Welsh Frailty Fracture Network.
Eifion Vaughan
Williams
Consultant Surgeon Spouse or partner - works for Cwm Taf Health Board.
Work in Private practice SPIRE Hospital, Cardiff. Performing weekly breast clinics (Monday pm).
Elisabeth Williams Finance Manager (Capital,
Systems & Financial)
Director in Husband's company CPM21 Ltd.
No transactions between UHB & CPM21 Ltd
Esther Youd Consultant Histopathologist
and Clinical Director of Pathology
My husband is a shareholder in Synpath Ltd (see below).
Director of Synpath Ltd which is a registered company used by myself and colleagues to receive Category II and non-NHS income.
The accountancy is provided by Carston Accountants. Chair of the Royal College of Pathologists Wales Regional Council, and
Trustee of the Royal College of Pathologists.
Gareth Hardacre Assistant Director of Workforce & OD
Wife employed by NHS Wales as Head of Midwifery at Cardiff & Vale UHB.
Governor at Educational Establishment - Cardiff Metropolitan University.
Father elected as Councillor in Caerphilly CBC.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
67 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
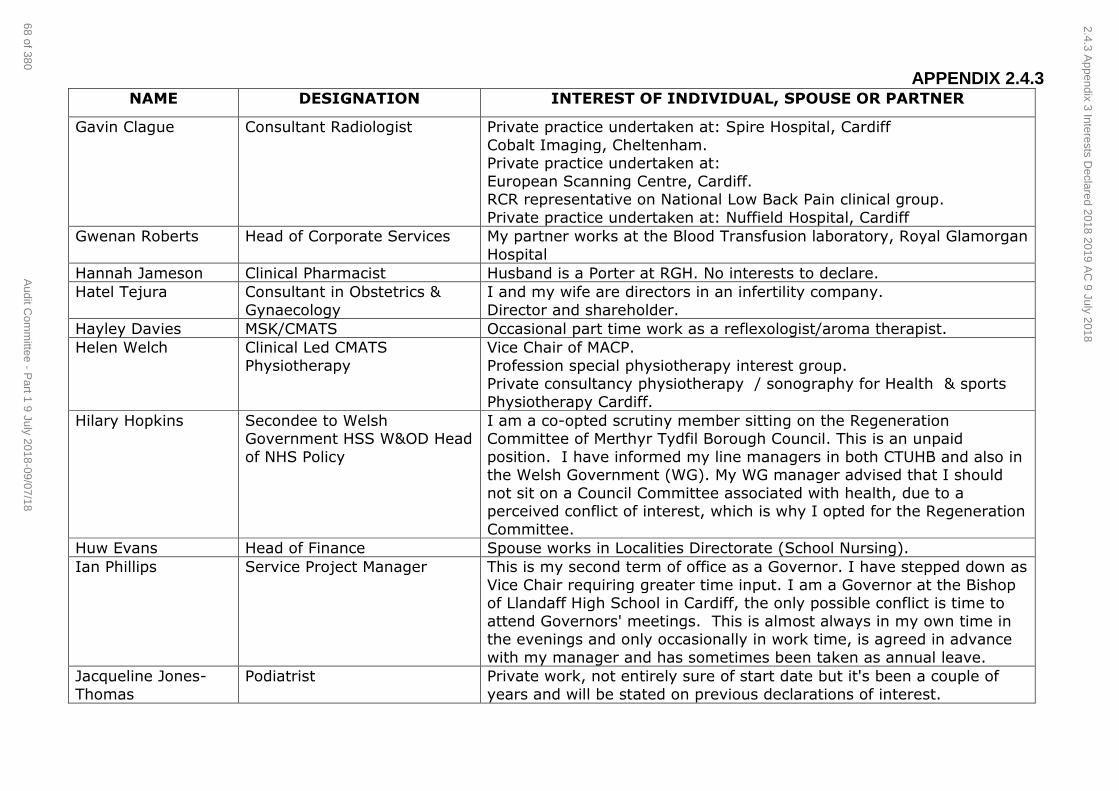
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Gavin Clague Consultant Radiologist Private practice undertaken at: Spire Hospital, Cardiff
Cobalt Imaging, Cheltenham. Private practice undertaken at:
European Scanning Centre, Cardiff. RCR representative on National Low Back Pain clinical group.
Private practice undertaken at: Nuffield Hospital, Cardiff
Gwenan Roberts Head of Corporate Services My partner works at the Blood Transfusion laboratory, Royal Glamorgan
Hospital
Hannah Jameson Clinical Pharmacist Husband is a Porter at RGH. No interests to declare.
Hatel Tejura Consultant in Obstetrics &
Gynaecology
I and my wife are directors in an infertility company.
Director and shareholder.
Hayley Davies MSK/CMATS Occasional part time work as a reflexologist/aroma therapist.
Helen Welch Clinical Led CMATS
Physiotherapy
Vice Chair of MACP.
Profession special physiotherapy interest group. Private consultancy physiotherapy / sonography for Health & sports
Physiotherapy Cardiff.
Hilary Hopkins Secondee to Welsh Government HSS W&OD Head
of NHS Policy
I am a co-opted scrutiny member sitting on the Regeneration Committee of Merthyr Tydfil Borough Council. This is an unpaid
position. I have informed my line managers in both CTUHB and also in the Welsh Government (WG). My WG manager advised that I should
not sit on a Council Committee associated with health, due to a perceived conflict of interest, which is why I opted for the Regeneration
Committee.
Huw Evans Head of Finance Spouse works in Localities Directorate (School Nursing).
Ian Phillips Service Project Manager This is my second term of office as a Governor. I have stepped down as
Vice Chair requiring greater time input. I am a Governor at the Bishop of Llandaff High School in Cardiff, the only possible conflict is time to
attend Governors' meetings. This is almost always in my own time in the evenings and only occasionally in work time, is agreed in advance
with my manager and has sometimes been taken as annual leave.
Jacqueline Jones-
Thomas
Podiatrist Private work, not entirely sure of start date but it's been a couple of
years and will be stated on previous declarations of interest.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
68 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
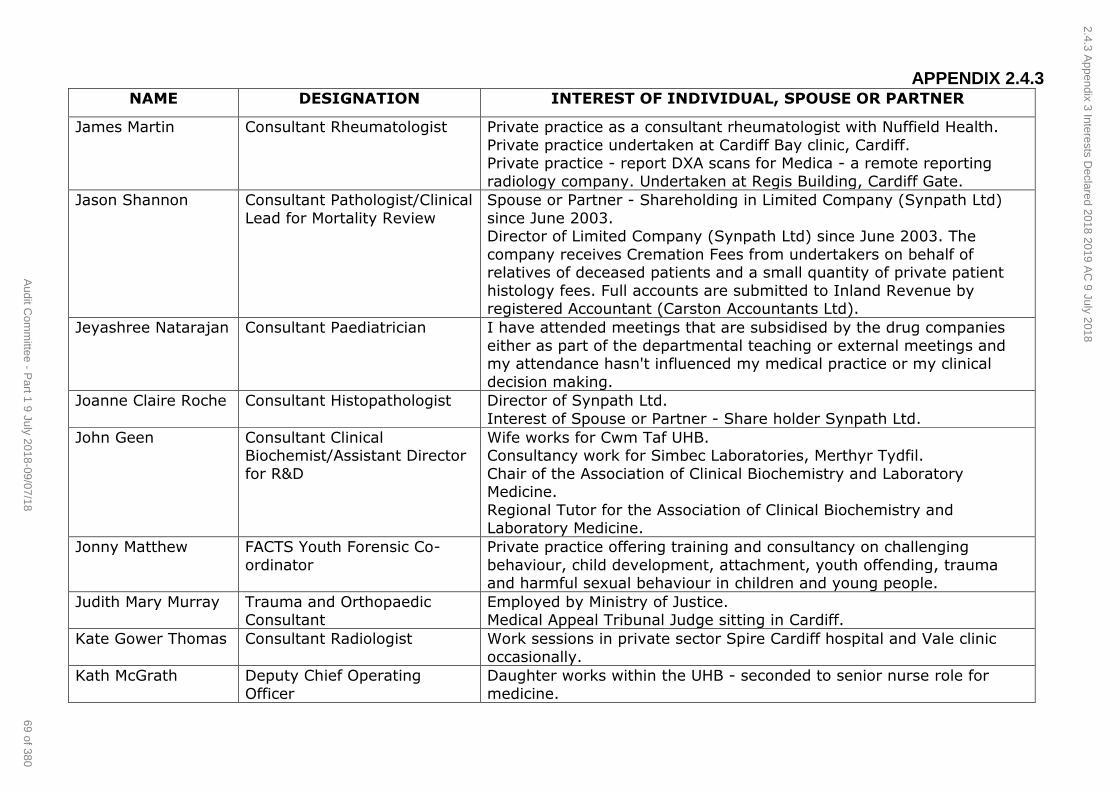
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
James Martin Consultant Rheumatologist Private practice as a consultant rheumatologist with Nuffield Health.
Private practice undertaken at Cardiff Bay clinic, Cardiff. Private practice - report DXA scans for Medica - a remote reporting
radiology company. Undertaken at Regis Building, Cardiff Gate.
Jason Shannon Consultant Pathologist/Clinical
Lead for Mortality Review
Spouse or Partner - Shareholding in Limited Company (Synpath Ltd)
since June 2003. Director of Limited Company (Synpath Ltd) since June 2003. The
company receives Cremation Fees from undertakers on behalf of relatives of deceased patients and a small quantity of private patient
histology fees. Full accounts are submitted to Inland Revenue by registered Accountant (Carston Accountants Ltd).
Jeyashree Natarajan Consultant Paediatrician I have attended meetings that are subsidised by the drug companies
either as part of the departmental teaching or external meetings and my attendance hasn't influenced my medical practice or my clinical
decision making.
Joanne Claire Roche Consultant Histopathologist Director of Synpath Ltd.
Interest of Spouse or Partner - Share holder Synpath Ltd.
John Geen Consultant Clinical Biochemist/Assistant Director
for R&D
Wife works for Cwm Taf UHB. Consultancy work for Simbec Laboratories, Merthyr Tydfil.
Chair of the Association of Clinical Biochemistry and Laboratory Medicine.
Regional Tutor for the Association of Clinical Biochemistry and Laboratory Medicine.
Jonny Matthew FACTS Youth Forensic Co-
ordinator
Private practice offering training and consultancy on challenging
behaviour, child development, attachment, youth offending, trauma and harmful sexual behaviour in children and young people.
Judith Mary Murray Trauma and Orthopaedic Consultant
Employed by Ministry of Justice. Medical Appeal Tribunal Judge sitting in Cardiff.
Kate Gower Thomas Consultant Radiologist Work sessions in private sector Spire Cardiff hospital and Vale clinic
occasionally.
Kath McGrath Deputy Chief Operating
Officer
Daughter works within the UHB - seconded to senior nurse role for
medicine.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
69 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
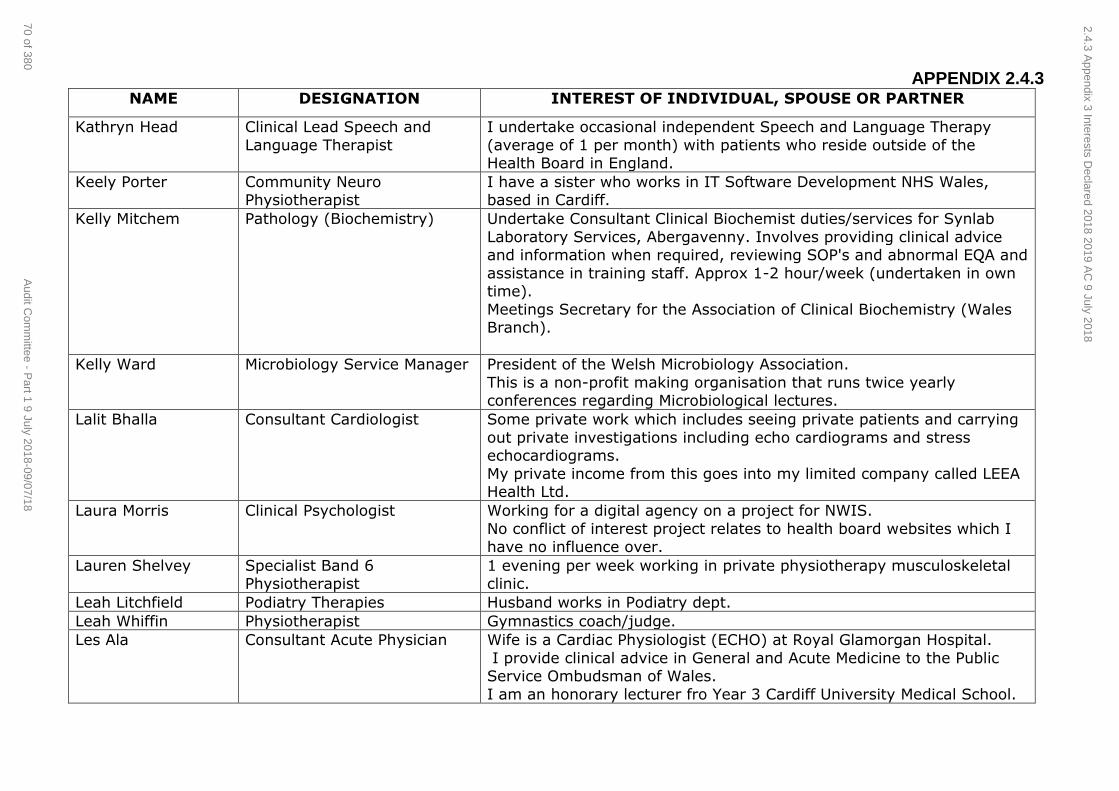
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Kathryn Head Clinical Lead Speech and
Language Therapist
I undertake occasional independent Speech and Language Therapy
(average of 1 per month) with patients who reside outside of the Health Board in England.
Keely Porter Community Neuro Physiotherapist
I have a sister who works in IT Software Development NHS Wales, based in Cardiff.
Kelly Mitchem Pathology (Biochemistry) Undertake Consultant Clinical Biochemist duties/services for Synlab
Laboratory Services, Abergavenny. Involves providing clinical advice and information when required, reviewing SOP's and abnormal EQA and
assistance in training staff. Approx 1-2 hour/week (undertaken in own time).
Meetings Secretary for the Association of Clinical Biochemistry (Wales Branch).
Kelly Ward Microbiology Service Manager President of the Welsh Microbiology Association.
This is a non-profit making organisation that runs twice yearly conferences regarding Microbiological lectures.
Lalit Bhalla Consultant Cardiologist Some private work which includes seeing private patients and carrying
out private investigations including echo cardiograms and stress echocardiograms.
My private income from this goes into my limited company called LEEA Health Ltd.
Laura Morris Clinical Psychologist Working for a digital agency on a project for NWIS.
No conflict of interest project relates to health board websites which I have no influence over.
Lauren Shelvey Specialist Band 6 Physiotherapist
1 evening per week working in private physiotherapy musculoskeletal clinic.
Leah Litchfield Podiatry Therapies Husband works in Podiatry dept.
Leah Whiffin Physiotherapist Gymnastics coach/judge.
Les Ala Consultant Acute Physician Wife is a Cardiac Physiologist (ECHO) at Royal Glamorgan Hospital.
I provide clinical advice in General and Acute Medicine to the Public Service Ombudsman of Wales.
I am an honorary lecturer fro Year 3 Cardiff University Medical School.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
70 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
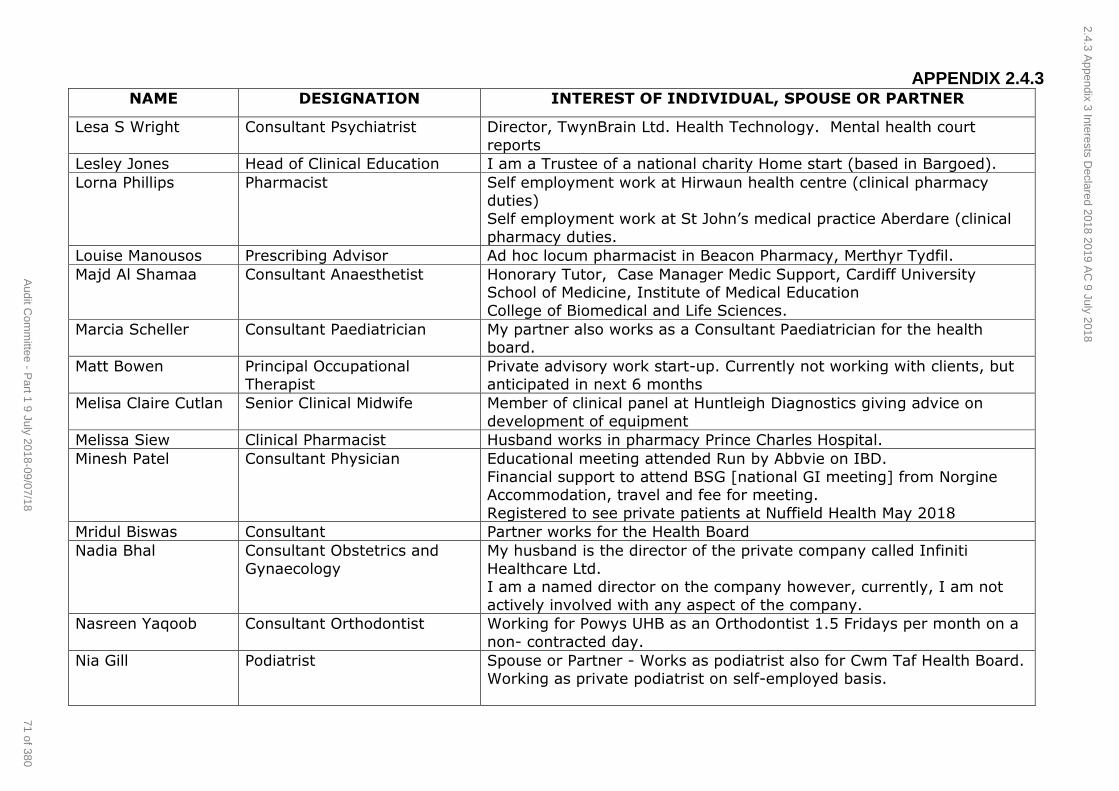
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Lesa S Wright Consultant Psychiatrist Director, TwynBrain Ltd. Health Technology. Mental health court
reports
Lesley Jones Head of Clinical Education I am a Trustee of a national charity Home start (based in Bargoed).
Lorna Phillips Pharmacist Self employment work at Hirwaun health centre (clinical pharmacy duties)
Self employment work at St John’s medical practice Aberdare (clinical
pharmacy duties.
Louise Manousos Prescribing Advisor Ad hoc locum pharmacist in Beacon Pharmacy, Merthyr Tydfil.
Majd Al Shamaa Consultant Anaesthetist Honorary Tutor, Case Manager Medic Support, Cardiff University School of Medicine, Institute of Medical Education
College of Biomedical and Life Sciences.
Marcia Scheller Consultant Paediatrician My partner also works as a Consultant Paediatrician for the health board.
Matt Bowen Principal Occupational Therapist
Private advisory work start-up. Currently not working with clients, but anticipated in next 6 months
Melisa Claire Cutlan Senior Clinical Midwife Member of clinical panel at Huntleigh Diagnostics giving advice on
development of equipment
Melissa Siew Clinical Pharmacist Husband works in pharmacy Prince Charles Hospital.
Minesh Patel Consultant Physician Educational meeting attended Run by Abbvie on IBD.
Financial support to attend BSG [national GI meeting] from Norgine Accommodation, travel and fee for meeting.
Registered to see private patients at Nuffield Health May 2018
Mridul Biswas Consultant Partner works for the Health Board
Nadia Bhal Consultant Obstetrics and
Gynaecology
My husband is the director of the private company called Infiniti
Healthcare Ltd. I am a named director on the company however, currently, I am not
actively involved with any aspect of the company.
Nasreen Yaqoob Consultant Orthodontist Working for Powys UHB as an Orthodontist 1.5 Fridays per month on a
non- contracted day.
Nia Gill Podiatrist Spouse or Partner - Works as podiatrist also for Cwm Taf Health Board. Working as private podiatrist on self-employed basis.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
71 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
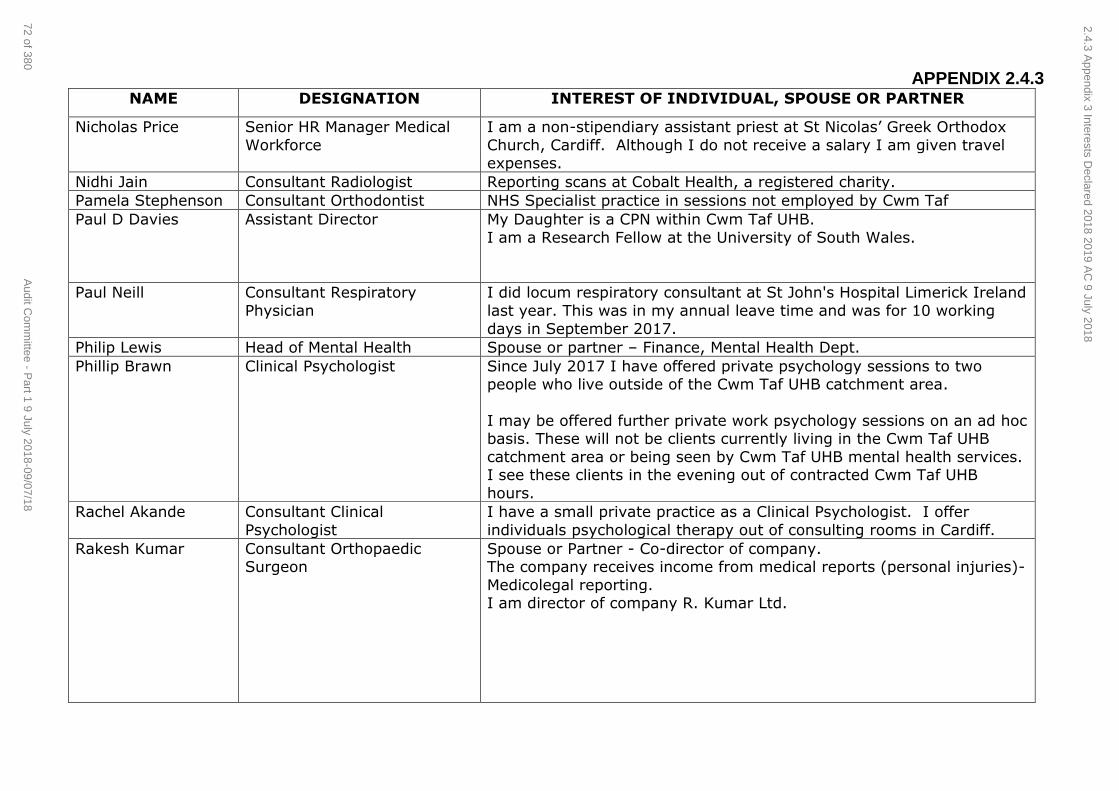
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Nicholas Price Senior HR Manager Medical
Workforce
I am a non-stipendiary assistant priest at St Nicolas’ Greek Orthodox
Church, Cardiff. Although I do not receive a salary I am given travel expenses.
Nidhi Jain Consultant Radiologist Reporting scans at Cobalt Health, a registered charity.
Pamela Stephenson Consultant Orthodontist NHS Specialist practice in sessions not employed by Cwm Taf
Paul D Davies Assistant Director My Daughter is a CPN within Cwm Taf UHB.
I am a Research Fellow at the University of South Wales.
Paul Neill Consultant Respiratory
Physician
I did locum respiratory consultant at St John's Hospital Limerick Ireland
last year. This was in my annual leave time and was for 10 working
days in September 2017.
Philip Lewis Head of Mental Health Spouse or partner – Finance, Mental Health Dept.
Phillip Brawn Clinical Psychologist Since July 2017 I have offered private psychology sessions to two people who live outside of the Cwm Taf UHB catchment area.
I may be offered further private work psychology sessions on an ad hoc basis. These will not be clients currently living in the Cwm Taf UHB
catchment area or being seen by Cwm Taf UHB mental health services. I see these clients in the evening out of contracted Cwm Taf UHB
hours.
Rachel Akande Consultant Clinical
Psychologist
I have a small private practice as a Clinical Psychologist. I offer
individuals psychological therapy out of consulting rooms in Cardiff.
Rakesh Kumar Consultant Orthopaedic Surgeon
Spouse or Partner - Co-director of company. The company receives income from medical reports (personal injuries)-
Medicolegal reporting. I am director of company R. Kumar Ltd.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
72 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
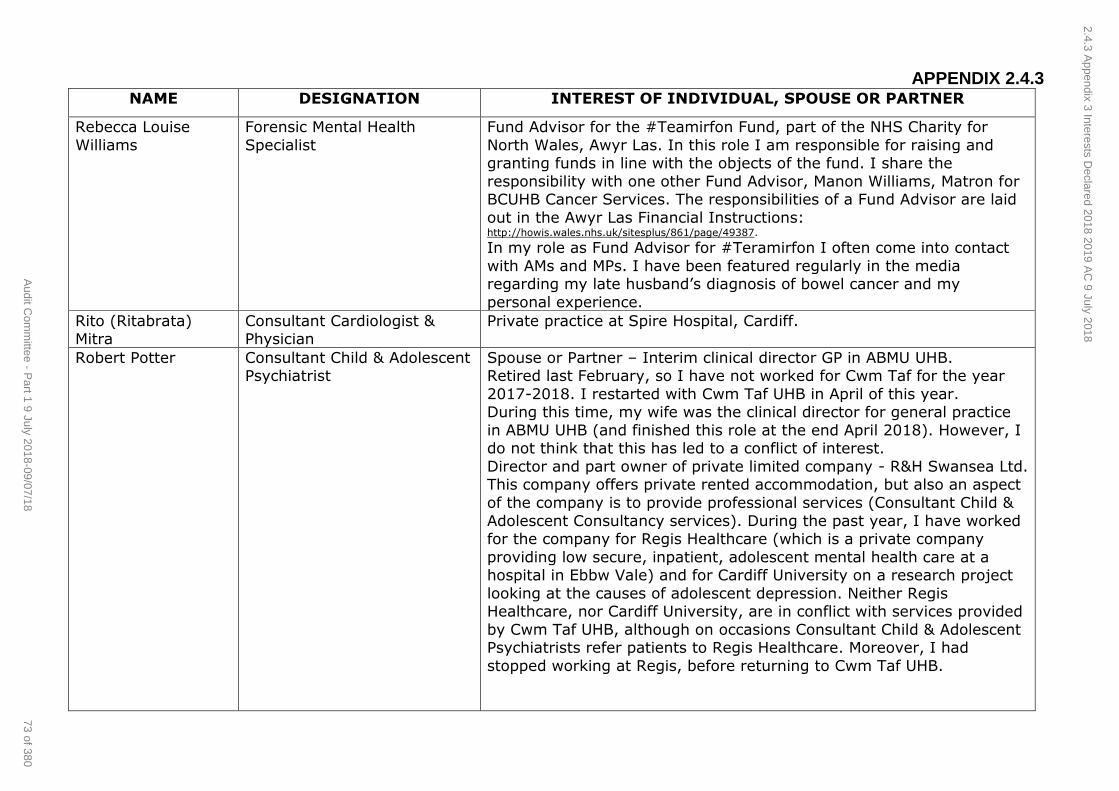
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Rebecca Louise
Williams
Forensic Mental Health
Specialist
Fund Advisor for the #Teamirfon Fund, part of the NHS Charity for
North Wales, Awyr Las. In this role I am responsible for raising and granting funds in line with the objects of the fund. I share the
responsibility with one other Fund Advisor, Manon Williams, Matron for BCUHB Cancer Services. The responsibilities of a Fund Advisor are laid
out in the Awyr Las Financial Instructions: http://howis.wales.nhs.uk/sitesplus/861/page/49387. In my role as Fund Advisor for #Teramirfon I often come into contact
with AMs and MPs. I have been featured regularly in the media regarding my late husband’s diagnosis of bowel cancer and my
personal experience.
Rito (Ritabrata) Mitra
Consultant Cardiologist & Physician
Private practice at Spire Hospital, Cardiff.
Robert Potter Consultant Child & Adolescent Psychiatrist
Spouse or Partner – Interim clinical director GP in ABMU UHB. Retired last February, so I have not worked for Cwm Taf for the year
2017-2018. I restarted with Cwm Taf UHB in April of this year. During this time, my wife was the clinical director for general practice
in ABMU UHB (and finished this role at the end April 2018). However, I do not think that this has led to a conflict of interest.
Director and part owner of private limited company - R&H Swansea Ltd. This company offers private rented accommodation, but also an aspect
of the company is to provide professional services (Consultant Child &
Adolescent Consultancy services). During the past year, I have worked for the company for Regis Healthcare (which is a private company
providing low secure, inpatient, adolescent mental health care at a hospital in Ebbw Vale) and for Cardiff University on a research project
looking at the causes of adolescent depression. Neither Regis Healthcare, nor Cardiff University, are in conflict with services provided
by Cwm Taf UHB, although on occasions Consultant Child & Adolescent Psychiatrists refer patients to Regis Healthcare. Moreover, I had
stopped working at Regis, before returning to Cwm Taf UHB.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
73 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
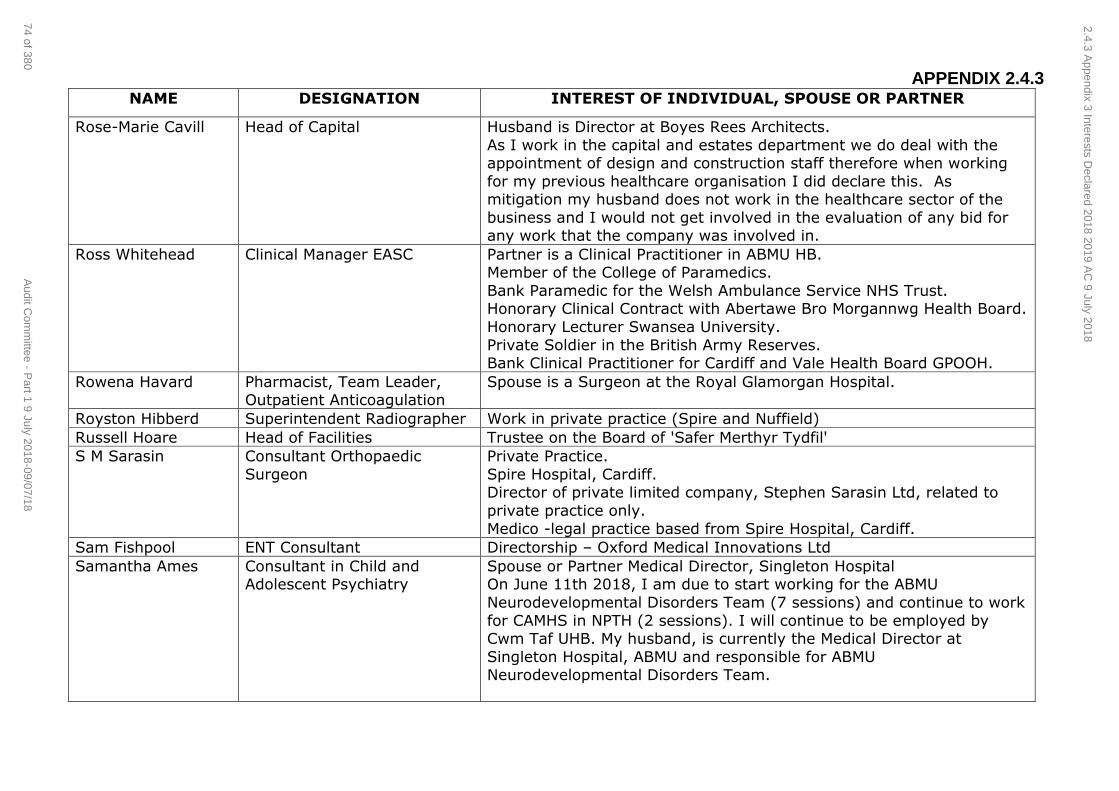
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Rose-Marie Cavill Head of Capital Husband is Director at Boyes Rees Architects.
As I work in the capital and estates department we do deal with the appointment of design and construction staff therefore when working
for my previous healthcare organisation I did declare this. As mitigation my husband does not work in the healthcare sector of the
business and I would not get involved in the evaluation of any bid for any work that the company was involved in.
Ross Whitehead Clinical Manager EASC Partner is a Clinical Practitioner in ABMU HB. Member of the College of Paramedics.
Bank Paramedic for the Welsh Ambulance Service NHS Trust. Honorary Clinical Contract with Abertawe Bro Morgannwg Health Board.
Honorary Lecturer Swansea University.
Private Soldier in the British Army Reserves. Bank Clinical Practitioner for Cardiff and Vale Health Board GPOOH.
Rowena Havard Pharmacist, Team Leader, Outpatient Anticoagulation
Spouse is a Surgeon at the Royal Glamorgan Hospital.
Royston Hibberd Superintendent Radiographer Work in private practice (Spire and Nuffield)
Russell Hoare Head of Facilities Trustee on the Board of 'Safer Merthyr Tydfil'
S M Sarasin Consultant Orthopaedic
Surgeon
Private Practice.
Spire Hospital, Cardiff. Director of private limited company, Stephen Sarasin Ltd, related to
private practice only.
Medico -legal practice based from Spire Hospital, Cardiff.
Sam Fishpool ENT Consultant Directorship – Oxford Medical Innovations Ltd
Samantha Ames Consultant in Child and Adolescent Psychiatry
Spouse or Partner Medical Director, Singleton Hospital On June 11th 2018, I am due to start working for the ABMU
Neurodevelopmental Disorders Team (7 sessions) and continue to work
for CAMHS in NPTH (2 sessions). I will continue to be employed by Cwm Taf UHB. My husband, is currently the Medical Director at
Singleton Hospital, ABMU and responsible for ABMU Neurodevelopmental Disorders Team.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
74 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
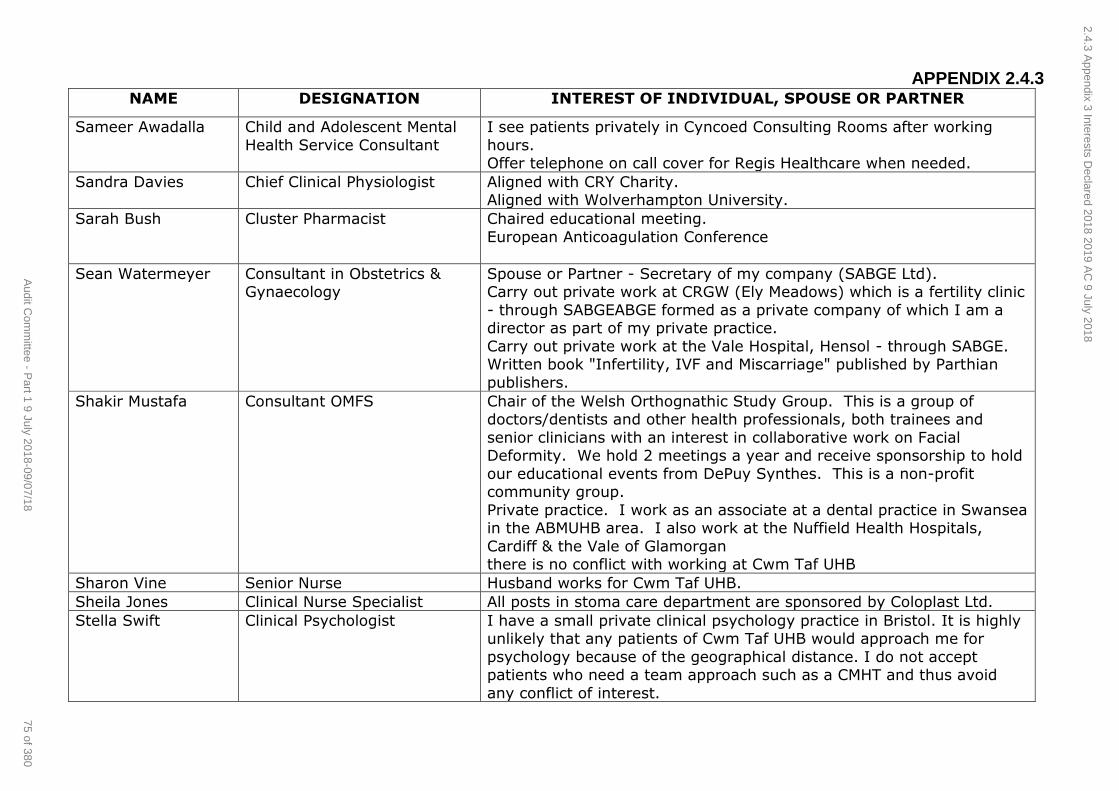
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Sameer Awadalla Child and Adolescent Mental
Health Service Consultant
I see patients privately in Cyncoed Consulting Rooms after working
hours. Offer telephone on call cover for Regis Healthcare when needed.
Sandra Davies Chief Clinical Physiologist Aligned with CRY Charity. Aligned with Wolverhampton University.
Sarah Bush Cluster Pharmacist Chaired educational meeting.
European Anticoagulation Conference
Sean Watermeyer Consultant in Obstetrics & Gynaecology
Spouse or Partner - Secretary of my company (SABGE Ltd). Carry out private work at CRGW (Ely Meadows) which is a fertility clinic
- through SABGEABGE formed as a private company of which I am a director as part of my private practice.
Carry out private work at the Vale Hospital, Hensol - through SABGE. Written book "Infertility, IVF and Miscarriage" published by Parthian
publishers.
Shakir Mustafa Consultant OMFS Chair of the Welsh Orthognathic Study Group. This is a group of doctors/dentists and other health professionals, both trainees and
senior clinicians with an interest in collaborative work on Facial Deformity. We hold 2 meetings a year and receive sponsorship to hold
our educational events from DePuy Synthes. This is a non-profit community group.
Private practice. I work as an associate at a dental practice in Swansea in the ABMUHB area. I also work at the Nuffield Health Hospitals,
Cardiff & the Vale of Glamorgan there is no conflict with working at Cwm Taf UHB
Sharon Vine Senior Nurse Husband works for Cwm Taf UHB.
Sheila Jones Clinical Nurse Specialist All posts in stoma care department are sponsored by Coloplast Ltd.
Stella Swift Clinical Psychologist I have a small private clinical psychology practice in Bristol. It is highly unlikely that any patients of Cwm Taf UHB would approach me for
psychology because of the geographical distance. I do not accept patients who need a team approach such as a CMHT and thus avoid
any conflict of interest.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
75 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
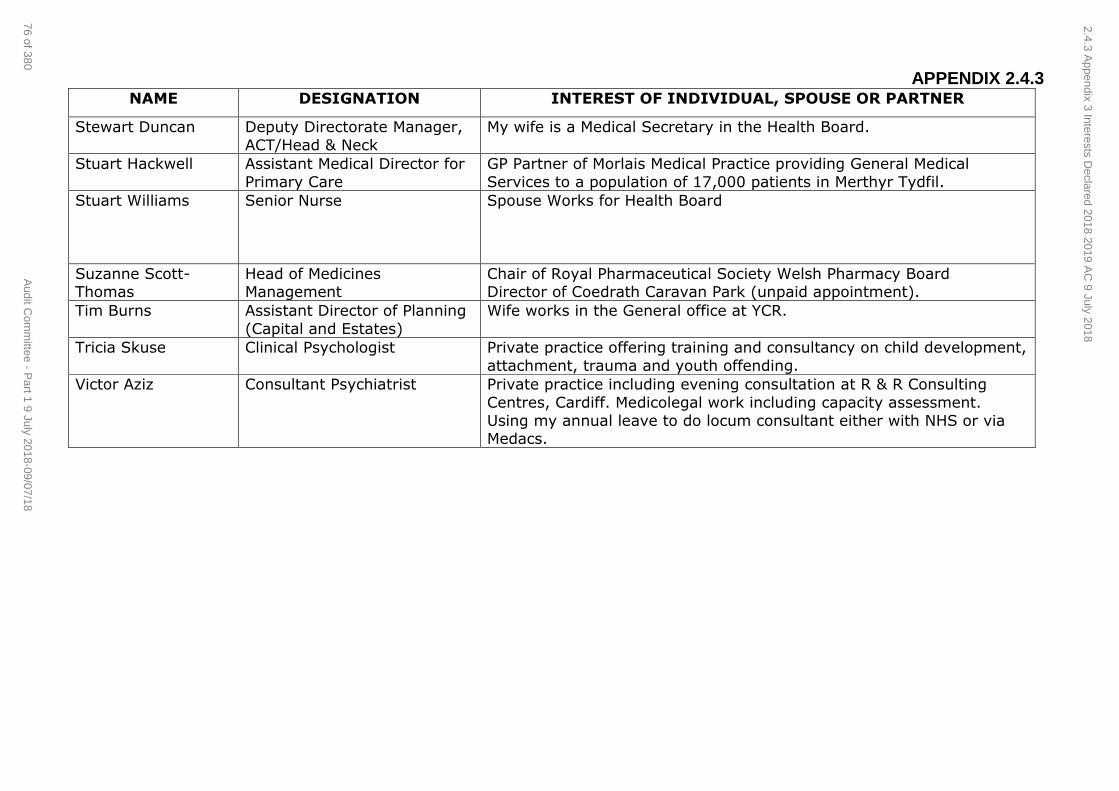
APPENDIX 2.4.3 NAME DESIGNATION INTEREST OF INDIVIDUAL, SPOUSE OR PARTNER
Stewart Duncan Deputy Directorate Manager,
ACT/Head & Neck
My wife is a Medical Secretary in the Health Board.
Stuart Hackwell Assistant Medical Director for
Primary Care
GP Partner of Morlais Medical Practice providing General Medical
Services to a population of 17,000 patients in Merthyr Tydfil.
Stuart Williams Senior Nurse Spouse Works for Health Board
Suzanne Scott-Thomas
Head of Medicines Management
Chair of Royal Pharmaceutical Society Welsh Pharmacy Board Director of Coedrath Caravan Park (unpaid appointment).
Tim Burns Assistant Director of Planning
(Capital and Estates)
Wife works in the General office at YCR.
Tricia Skuse Clinical Psychologist Private practice offering training and consultancy on child development,
attachment, trauma and youth offending.
Victor Aziz Consultant Psychiatrist Private practice including evening consultation at R & R Consulting
Centres, Cardiff. Medicolegal work including capacity assessment.
Using my annual leave to do locum consultant either with NHS or via Medacs.
2.4.3 Appendix 3 Interests D
eclared 2018 2019 AC
9 July 2018
76 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
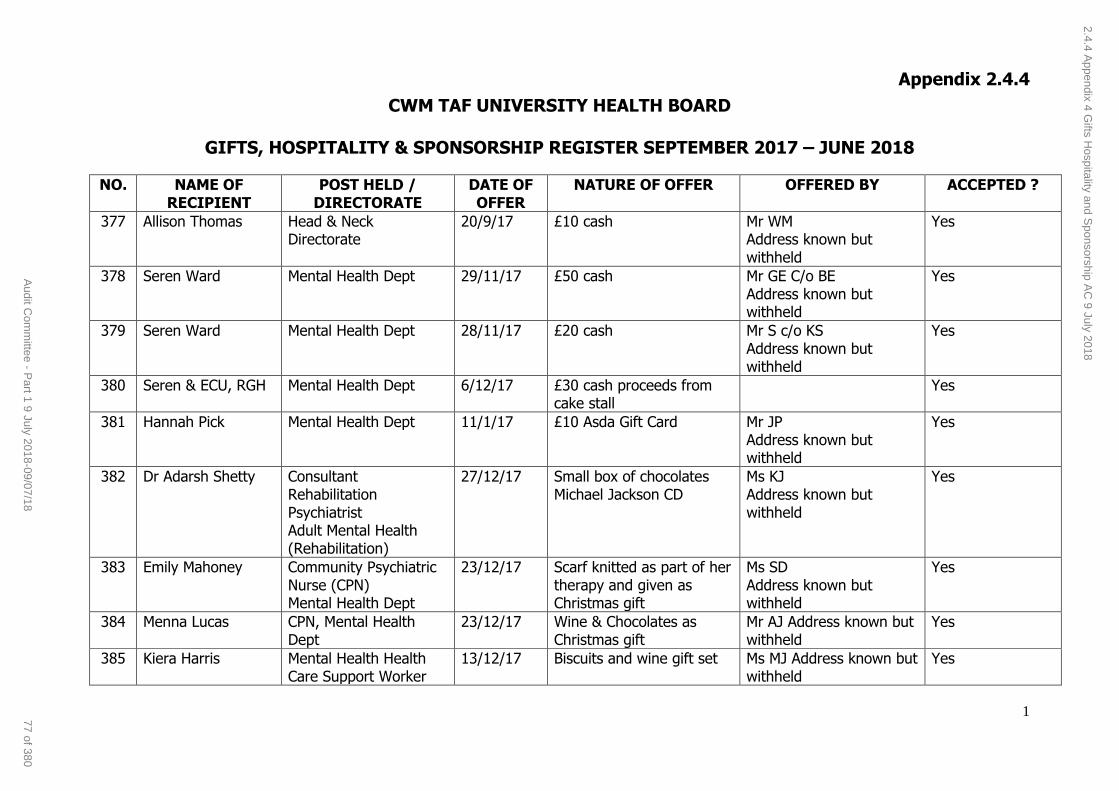
Appendix 2.4.4
1
CWM TAF UNIVERSITY HEALTH BOARD
GIFTS, HOSPITALITY & SPONSORSHIP REGISTER SEPTEMBER 2017 – JUNE 2018
NO. NAME OF RECIPIENT
POST HELD / DIRECTORATE
DATE OF OFFER
NATURE OF OFFER OFFERED BY ACCEPTED ?
377 Allison Thomas Head & Neck Directorate
20/9/17 £10 cash Mr WM Address known but withheld
Yes
378 Seren Ward Mental Health Dept 29/11/17 £50 cash Mr GE C/o BE Address known but withheld
Yes
379 Seren Ward Mental Health Dept 28/11/17 £20 cash Mr S c/o KS Address known but withheld
Yes
380 Seren & ECU, RGH Mental Health Dept 6/12/17 £30 cash proceeds from cake stall
Yes
381 Hannah Pick Mental Health Dept 11/1/17 £10 Asda Gift Card Mr JP Address known but withheld
Yes
382 Dr Adarsh Shetty Consultant Rehabilitation Psychiatrist Adult Mental Health (Rehabilitation)
27/12/17 Small box of chocolates Michael Jackson CD
Ms KJ Address known but withheld
Yes
383 Emily Mahoney Community Psychiatric Nurse (CPN) Mental Health Dept
23/12/17 Scarf knitted as part of her therapy and given as Christmas gift
Ms SD Address known but withheld
Yes
384 Menna Lucas CPN, Mental Health Dept
23/12/17 Wine & Chocolates as Christmas gift
Mr AJ Address known but withheld
Yes
385 Kiera Harris Mental Health Health Care Support Worker
13/12/17 Biscuits and wine gift set Ms MJ Address known but withheld
Yes
2.4.4 Appendix 4 G
ifts Hospitality and S
ponsorship AC
9 July 2018
77 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
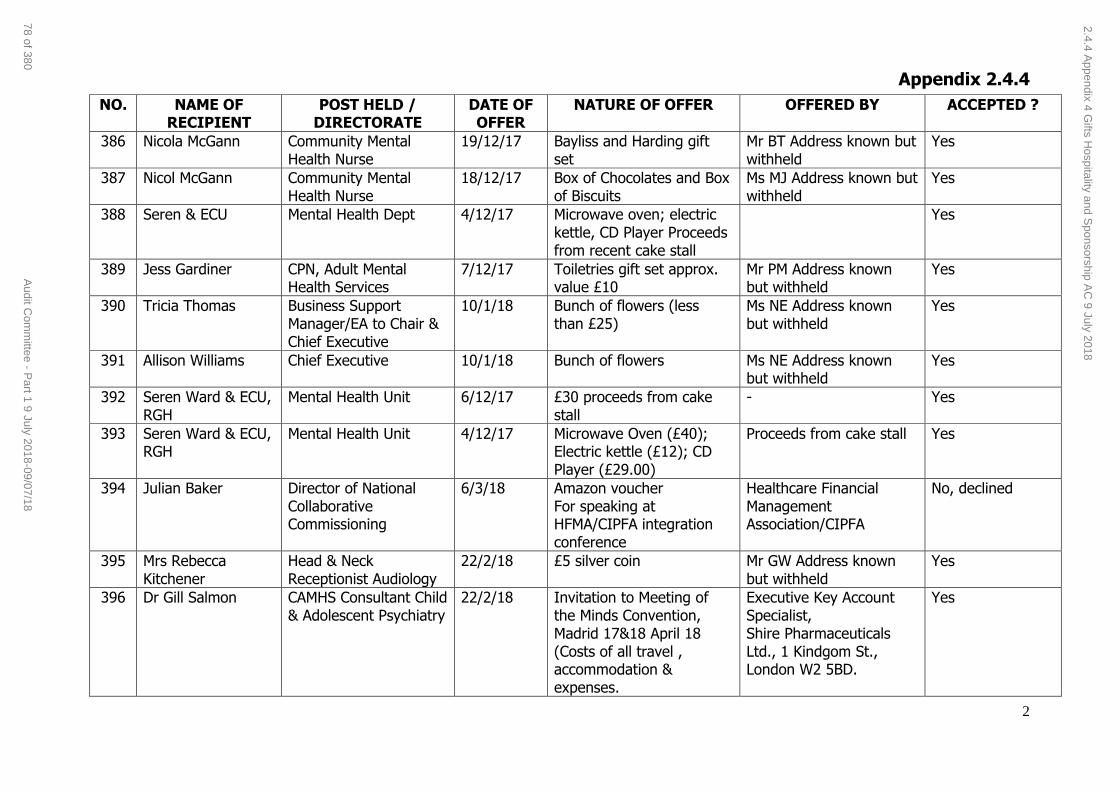
Appendix 2.4.4
2
NO. NAME OF RECIPIENT
POST HELD / DIRECTORATE
DATE OF OFFER
NATURE OF OFFER OFFERED BY ACCEPTED ?
386 Nicola McGann Community Mental Health Nurse
19/12/17 Bayliss and Harding gift set
Mr BT Address known but withheld
Yes
387 Nicol McGann Community Mental Health Nurse
18/12/17 Box of Chocolates and Box of Biscuits
Ms MJ Address known but withheld
Yes
388 Seren & ECU Mental Health Dept 4/12/17 Microwave oven; electric kettle, CD Player Proceeds from recent cake stall
Yes
389 Jess Gardiner CPN, Adult Mental Health Services
7/12/17 Toiletries gift set approx. value £10
Mr PM Address known but withheld
Yes
390 Tricia Thomas Business Support Manager/EA to Chair & Chief Executive
10/1/18 Bunch of flowers (less than £25)
Ms NE Address known but withheld
Yes
391 Allison Williams Chief Executive 10/1/18 Bunch of flowers Ms NE Address known but withheld
Yes
392 Seren Ward & ECU, RGH
Mental Health Unit 6/12/17 £30 proceeds from cake stall
- Yes
393 Seren Ward & ECU, RGH
Mental Health Unit 4/12/17 Microwave Oven (£40); Electric kettle (£12); CD Player (£29.00)
Proceeds from cake stall Yes
394 Julian Baker Director of National Collaborative Commissioning
6/3/18 Amazon voucher For speaking at HFMA/CIPFA integration conference
Healthcare Financial Management Association/CIPFA
No, declined
395 Mrs Rebecca Kitchener
Head & Neck Receptionist Audiology
22/2/18 £5 silver coin Mr GW Address known but withheld
Yes
396 Dr Gill Salmon CAMHS Consultant Child & Adolescent Psychiatry
22/2/18 Invitation to Meeting of the Minds Convention, Madrid 17&18 April 18 (Costs of all travel , accommodation & expenses.
Executive Key Account Specialist, Shire Pharmaceuticals Ltd., 1 Kindgom St., London W2 5BD.
Yes
2.4.4 Appendix 4 G
ifts Hospitality and S
ponsorship AC
9 July 2018
78 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
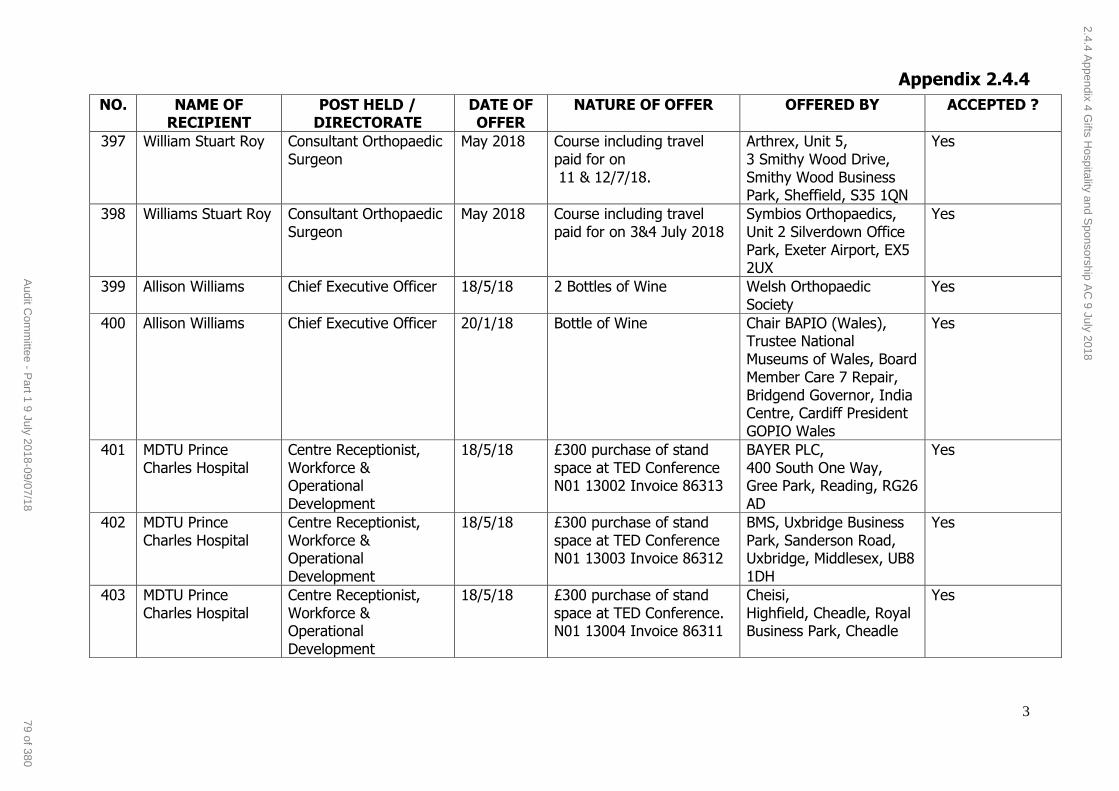
Appendix 2.4.4
3
NO. NAME OF RECIPIENT
POST HELD / DIRECTORATE
DATE OF OFFER
NATURE OF OFFER OFFERED BY ACCEPTED ?
397 William Stuart Roy Consultant Orthopaedic Surgeon
May 2018 Course including travel paid for on 11 & 12/7/18.
Arthrex, Unit 5, 3 Smithy Wood Drive, Smithy Wood Business Park, Sheffield, S35 1QN
Yes
398 Williams Stuart Roy Consultant Orthopaedic Surgeon
May 2018 Course including travel paid for on 3&4 July 2018
Symbios Orthopaedics, Unit 2 Silverdown Office Park, Exeter Airport, EX5 2UX
Yes
399 Allison Williams Chief Executive Officer 18/5/18 2 Bottles of Wine Welsh Orthopaedic Society
Yes
400 Allison Williams Chief Executive Officer 20/1/18 Bottle of Wine Chair BAPIO (Wales), Trustee National Museums of Wales, Board Member Care 7 Repair, Bridgend Governor, India Centre, Cardiff President GOPIO Wales
Yes
401 MDTU Prince Charles Hospital
Centre Receptionist, Workforce & Operational Development
18/5/18 £300 purchase of stand space at TED Conference N01 13002 Invoice 86313
BAYER PLC, 400 South One Way, Gree Park, Reading, RG26 AD
Yes
402 MDTU Prince Charles Hospital
Centre Receptionist, Workforce & Operational Development
18/5/18 £300 purchase of stand space at TED Conference N01 13003 Invoice 86312
BMS, Uxbridge Business Park, Sanderson Road, Uxbridge, Middlesex, UB8 1DH
Yes
403 MDTU Prince Charles Hospital
Centre Receptionist, Workforce & Operational Development
18/5/18 £300 purchase of stand space at TED Conference. N01 13004 Invoice 86311
Cheisi, Highfield, Cheadle, Royal Business Park, Cheadle
Yes
2.4.4 Appendix 4 G
ifts Hospitality and S
ponsorship AC
9 July 2018
79 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
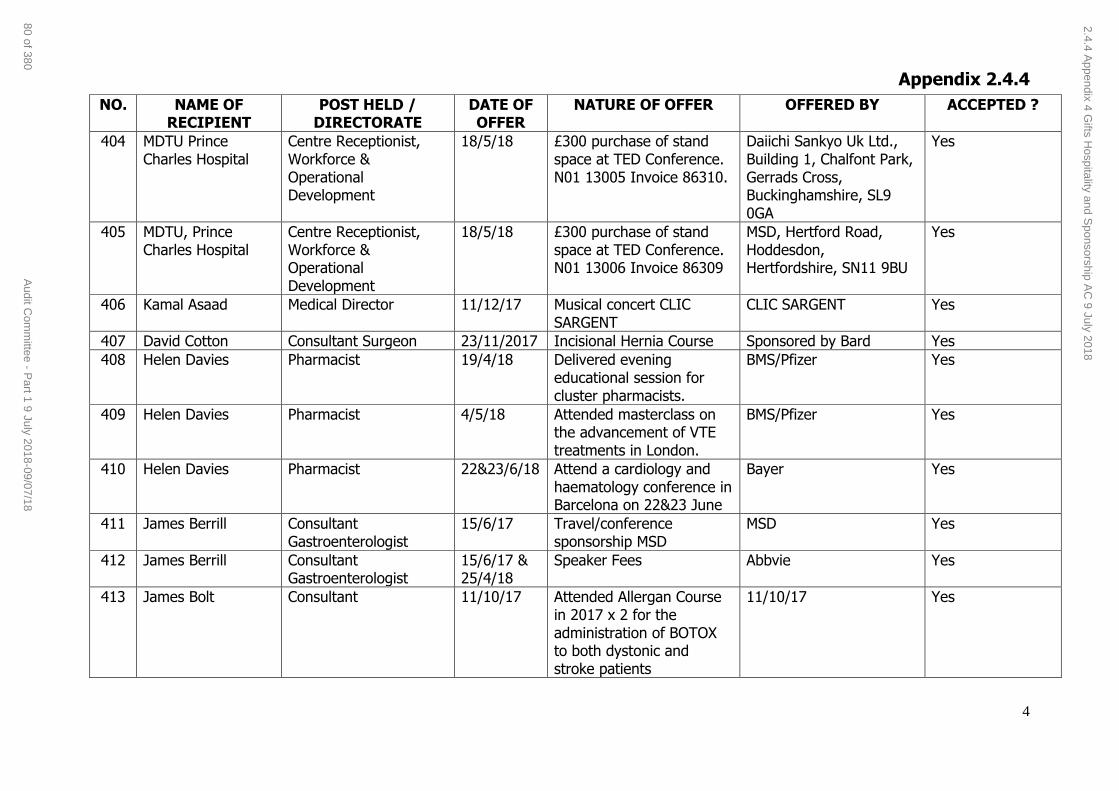
Appendix 2.4.4
4
NO. NAME OF RECIPIENT
POST HELD / DIRECTORATE
DATE OF OFFER
NATURE OF OFFER OFFERED BY ACCEPTED ?
404 MDTU Prince Charles Hospital
Centre Receptionist, Workforce & Operational Development
18/5/18 £300 purchase of stand space at TED Conference. N01 13005 Invoice 86310.
Daiichi Sankyo Uk Ltd., Building 1, Chalfont Park, Gerrads Cross, Buckinghamshire, SL9 0GA
Yes
405 MDTU, Prince Charles Hospital
Centre Receptionist, Workforce & Operational Development
18/5/18 £300 purchase of stand space at TED Conference. N01 13006 Invoice 86309
MSD, Hertford Road, Hoddesdon, Hertfordshire, SN11 9BU
Yes
406 Kamal Asaad Medical Director 11/12/17 Musical concert CLIC SARGENT
CLIC SARGENT Yes
407 David Cotton Consultant Surgeon 23/11/2017 Incisional Hernia Course Sponsored by Bard Yes
408 Helen Davies Pharmacist 19/4/18 Delivered evening educational session for cluster pharmacists.
BMS/Pfizer Yes
409 Helen Davies Pharmacist 4/5/18 Attended masterclass on the advancement of VTE treatments in London.
BMS/Pfizer Yes
410 Helen Davies Pharmacist 22&23/6/18 Attend a cardiology and haematology conference in Barcelona on 22&23 June
Bayer Yes
411 James Berrill Consultant Gastroenterologist
15/6/17 Travel/conference sponsorship MSD
MSD Yes
412 James Berrill Consultant Gastroenterologist
15/6/17 & 25/4/18
Speaker Fees Abbvie Yes
413 James Bolt Consultant 11/10/17 Attended Allergan Course in 2017 x 2 for the administration of BOTOX to both dystonic and stroke patients
11/10/17 Yes
2.4.4 Appendix 4 G
ifts Hospitality and S
ponsorship AC
9 July 2018
80 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
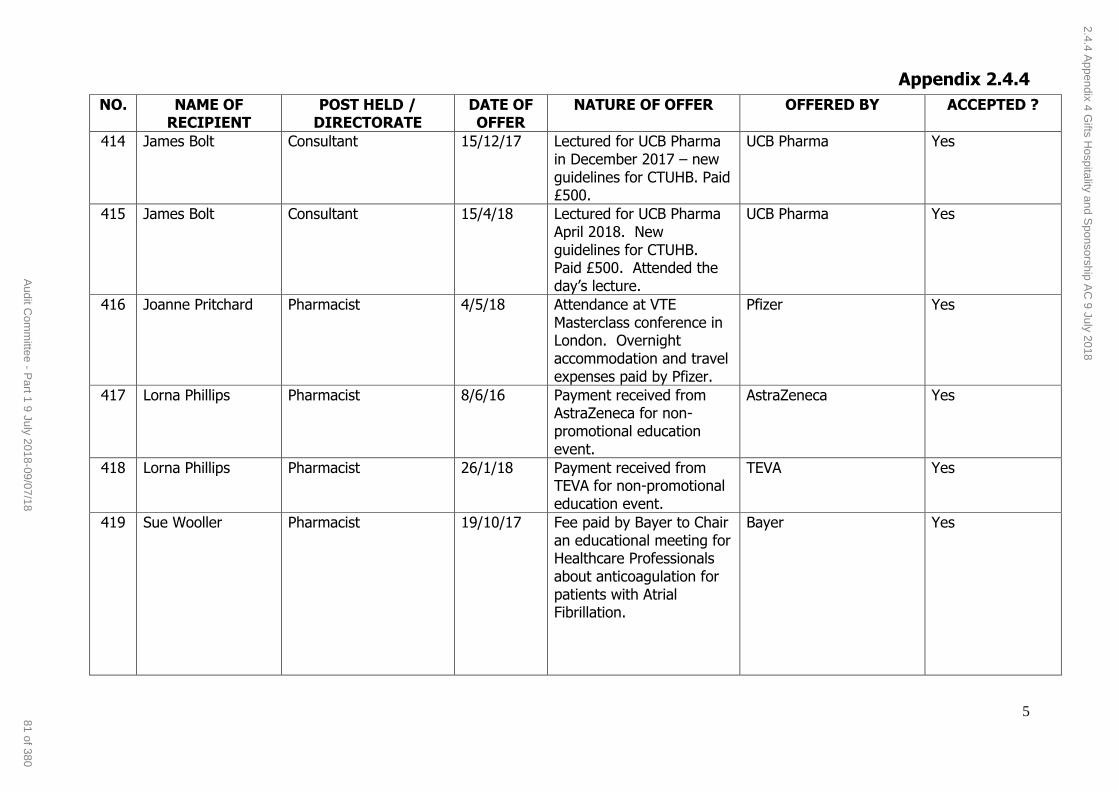
Appendix 2.4.4
5
NO. NAME OF RECIPIENT
POST HELD / DIRECTORATE
DATE OF OFFER
NATURE OF OFFER OFFERED BY ACCEPTED ?
414 James Bolt Consultant 15/12/17 Lectured for UCB Pharma in December 2017 – new guidelines for CTUHB. Paid £500.
UCB Pharma Yes
415 James Bolt Consultant 15/4/18 Lectured for UCB Pharma April 2018. New guidelines for CTUHB. Paid £500. Attended the day’s lecture.
UCB Pharma Yes
416 Joanne Pritchard Pharmacist 4/5/18 Attendance at VTE Masterclass conference in London. Overnight accommodation and travel expenses paid by Pfizer.
Pfizer Yes
417 Lorna Phillips Pharmacist 8/6/16 Payment received from AstraZeneca for non-promotional education event.
AstraZeneca Yes
418 Lorna Phillips Pharmacist 26/1/18 Payment received from TEVA for non-promotional education event.
TEVA Yes
419 Sue Wooller Pharmacist 19/10/17 Fee paid by Bayer to Chair an educational meeting for Healthcare Professionals about anticoagulation for patients with Atrial Fibrillation.
Bayer Yes
2.4.4 Appendix 4 G
ifts Hospitality and S
ponsorship AC
9 July 2018
81 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
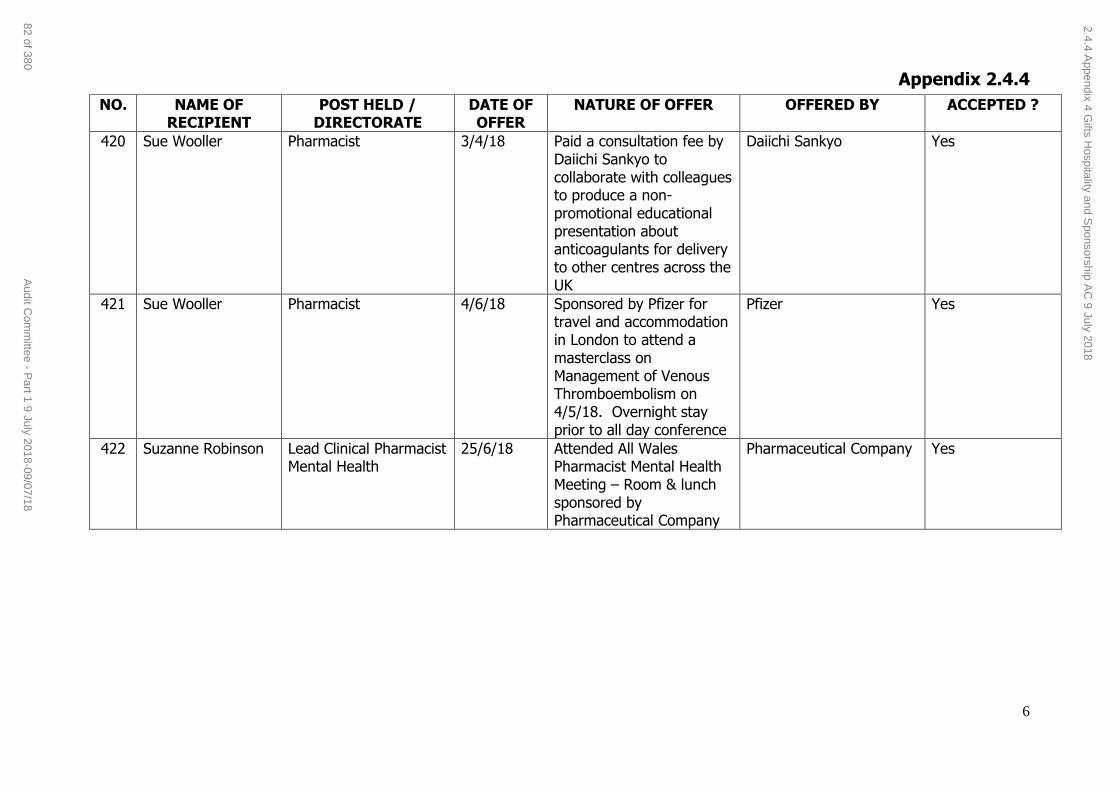
Appendix 2.4.4
6
NO. NAME OF RECIPIENT
POST HELD / DIRECTORATE
DATE OF OFFER
NATURE OF OFFER OFFERED BY ACCEPTED ?
420 Sue Wooller Pharmacist 3/4/18 Paid a consultation fee by Daiichi Sankyo to collaborate with colleagues to produce a non-promotional educational presentation about anticoagulants for delivery to other centres across the UK
Daiichi Sankyo Yes
421 Sue Wooller Pharmacist 4/6/18 Sponsored by Pfizer for travel and accommodation in London to attend a masterclass on Management of Venous Thromboembolism on 4/5/18. Overnight stay prior to all day conference
Pfizer Yes
422 Suzanne Robinson Lead Clinical Pharmacist Mental Health
25/6/18 Attended All Wales Pharmacist Mental Health Meeting – Room & lunch sponsored by Pharmaceutical Company
Pharmaceutical Company Yes
2.4.4 Appendix 4 G
ifts Hospitality and S
ponsorship AC
9 July 2018
82 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Clinical Audit Forward Plan Page 1 of 6 Audit Committee 9 July 2018
Agenda Item 2.5
9 July 2018
Audit Committee Report
FORWARD PLAN FOR CLINICAL AUDIT 2018 - 2019
Executive Lead: Medical Director
Authors: Head of Clinical Audit & Quality Informatics
and Clinical Audit and Effectiveness Manager
Contact Details for further information:
Mark Townsend, email: [email protected], Tel.: 01443 744800
Arlene Shenkorov, email: [email protected], Tel.: 01685 728416
Purpose of the Audit Committee Report
This Report has been developed to provide assurance to the Audit
Committee that a Clinical Audit Forward Plan for 2018-19 for Cwm Taf University Health Board (CTUHB) is in place along with the associated
Clinical Audit Operational Plan. This will ensure that robust evidence of the monitoring and escalation of audit compliance is in place, and that audit
outcomes are an integral part of the organisations continuous improvement programme of work.
Governance
Link to Health
Board Strategic Objective(s)
The Board’s key role is to ensure the Board’s IMTP and
its related Strategic Objectives are being progressed in relation to ensuring the provision of safe, effective,
high quality care.
Supporting
evidence
The Clinical Audit Forward Plan is based on the
following key publications: NHS Wales National Clinical Audit and Outcome
Review Plan National Institute of Health and Care Excellence
(NICE) Guidance
The Health & Care Standards (2015) All Wales Medicines Strategy Group publications
Welsh Risk Pool Management Standards Regional Cancer Strategy Network publications
Cwm Taf University Health Board’s Quality Strategy and Delivery Plan
1000 Lives Improvement
2.5 Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
83 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Clinical Audit Forward Plan Page 2 of 6 Audit Committee 9 July 2018
Engagement – Who has been involved in this work?
This Clinical Audit Forward Plan has been produced through engagement
with the Clinical Audit and Quality Improvement Operational Group and Directorate Clinical Audit Leads and is representative of all clinical
specialities within the Health Board. Each clinical audit has an assigned clinical lead.
The Clinical Audit Forward and Operational plans will be monitored for
compliance continuously and formally on a monthly basis by the Head of Clinical Audit and Quality Informatics and Clinical Audit and Effectiveness
Manager to ensure appropriate escalation where a deviation from plan is identified.
Compliance with the Clinical Audit Forward Plan will be reviewed and monitored on a quarterly basis through the Clinical Audit and Quality
Improvement Operational Group, and Quality Steering Group.
Clinical audit report findings will be released to support the organisation continuous improvement work and all learning outcomes will be reported
to an appropriate quality and governance forum within the Health Board.
Audit Committee Resolution (insert √) To;
APPROVE ENDORSE DISCUSS √ NOTE √
Recommendation The Audit Committee is asked to; DISCUSS and NOTE the Clinical Audit
Forward Plan for 2018 - 19
Summarise the Impact of the Health Board Report
Equality and diversity
Sets out the organisation ‘must do’ priority clinical audit activities for all clinical areas
including vulnerable patient groups (i.e. dementia care, learning disabilities) to enhance
the delivery of safe and effective care.
Legal implications There are no specific legal implications resulting
from this report.
Population Health Is required to meet the health needs of our changing population through the provision of
safe and effective care models to respond to patients reducing inequalities with the aim of
improving population outcomes.
Quality, Safety & Patient Experience
The Clinical Audit Forward Plan identifies all the clinical audit projects that must be undertaken
by CTUHB in 2018-19. It is essential that they are treated as priorities and that appropriate
resources are provided to support them. They form the core of the annual clinical audit
programme of work. The outcomes from this work will be used to improve the quality and
2.5 Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
84 of 380 Audit Committee - Part 1 9 July 2018-09/07/18

Clinical Audit Forward Plan Page 3 of 6 Audit Committee 9 July 2018
safety of care provided to our patients and to improve their experience.
Resources Resources to implement the forward plan will
require the resource of ‘Time’ of staff to collect the data to provide quality assurance and to
ensure that we put safe and effective care at the centre of everything we do.
Risks and Assurance Implementation of the forward plan will enable the health board to exercise arrangements to
compare practice against evidence-based care
standards to help mitigate risks and provide assurance.
Health and Care Standards
Standard 3.1 – Safe and Clinically Effective Care Standard 3.3 – Quality Improvement, Research
and Innovation.
Workforce Key workforce implication is time to participate in
quality improvement activities, including data collection and analysis to inform changes in
practice.
Freedom of
Information Status
Open
2.5 Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
85 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Clinical Audit Forward Plan Page 4 of 6 Audit Committee 9 July 2018
CLININCAL AUDIT FORWARD PLAN FOR 2018 - 19
1. SITUATION / PURPOSE OF REPORT
This report has been developed to provide assurance to the Audit Committee that a Clinical Audit Forward Plan 2018-19 for CTUHB is in place along with the
associated Clinical Audit Operational Plan. This will ensure that robust evidence of the monitoring and escalation of audit compliance is in place, and that audit
outcomes are an integral part of the organisations continuous improvement programme of work.
2. BACKGROUND / INTRODUCTION
The Plan has identified the projects the health board must participate in, for
example, the National Clinical Audit and Outcome Review Plan (NCAORP) which
have been designed to support the delivery of the NHS Wales Quality Delivery Plan and the Health and Care Standards for Wales. Information from these
national audits is also a central component for the implementation of a suite of Delivery Plans for NHS Wales.
Organisational internal local ‘must do’ audits are reflective of; clinical priorities;
patient and public experience initiatives; and compliance with regulatory requirements, e.g. audits with the aim of providing evidence of implementation
of NICE guidance, Cancer Standards, All Wales Medicines Strategy Group Guidance and Welsh Risk Management Standards.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
The Clinical Audit Forward Plan sets out a programme of prioritised continuous improvement activities, including clinical audit, and is designed to help to
embed the above principles into the everyday working practice of individuals and clinical teams to improve clinical outcomes for patients, through focused
and structured work.
The plan for 2018-19, is determined at both corporate and directorate level
based around priority categories established by the Healthcare Quality Improvement Programme (HQIP) and defined as:
1. External “must do” - Externally monitored audits that are driven
by commissioning and quality improvement are treated as the priority and appropriate resources are provided to support these.
Failure to participate or deliver on these externally driven audits may carry a penalty for the Health Board
2. Internal “must do” - Based on the classic criteria of high risk or
high profile identified by health board management. They may include national initiatives with health board-wide relevance but no
penalties exist for non participation. Many of these projects will
2.5 Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
86 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Clinical Audit Forward Plan Page 5 of 6 Audit Committee 9 July 2018
emanate from health board governance issues or high profile local initiatives.
In 2018-19, the programme of activities includes those priorities outlined within
the CTUHB Quality Strategy and Quality Delivery Plan, demonstrating the further developments made by the health board to align clinical audit with
quality improvement science which are an essential part of quality management for NHS Wales.
Risks
The planning process for clinical audit and continuous improvement priorities for each year starts in the January of the previous financial year, based on the
above prioritised categories. However, the NHS Wales National Clinical Audit and Outcome Review Plan (NCAORP) 2018-19, is not due for publication until
July 2018 and it is anticipated that some new national clinical audit projects, not currently included in this plan, will be added and commence in the later
part of 2018-19. To reflect this, the forward plan is a fluid, working document that provides an outline of work planned for the coming year, and can be added
to as priorities may change and fluctuate.
In respect of performance against the forward plan, including the NCAORP, the internal audit report of the Clinical Audit department received in January 2018
identified a key issue as a lack of a stand-alone annual clinical audit operational plan listing all clinical audit work to be carried out during 2017-18 and the lack
of clearly identified responsibilities and timeframes for completion of audit work
making it difficult to continuously monitor progress against the plan. This was highlighted against the 2017-18 plan when the deadline for submission of the
data for the National Joint Registry audit for 2015-16 was not achieved. Mitigating action has since been taken to ensure compliance with this national
audit. However, to improve monitoring against the national audit programme and to comply with the recommendations from the internal audit the Clinical
Audit Forward Plan for 2018-19 and operational plan include; evidence of compliance with the previous years forward plan; identified audit periods that
are monitored on a monthly and quarterly basis; information submission deadlines; and the date when the report or findings are planned for release.
In addition, due to vacancies and long-term sickness within the clinical audit
team the level of support offered for tier 3 and 4 level audits has been reduced to maintain the organisation national and local ‘must do’ priority audits,
ensuring that the Health Board participates fully in the national clinical audit
programme.
Governance
Welsh Government expects more robust scrutiny of health board actions to address national clinical audit and review findings hence a revised assurance
proforma has been introduced containing a ‘Part A’ which Welsh Health Boards must complete and return to Welsh Government within four weeks of
2.5 Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
87 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Clinical Audit Forward Plan Page 6 of 6 Audit Committee 9 July 2018
publication of NCAORP reports and, a ‘Part B’ which must be completed within three months. Part A will list the national findings and local implications the
organisation recognises they need to address and Part B details the actions and timescales for improvement. Where a financial or workforce recommendation is
identified there is a section requesting whether the issue is included in the Health Board Integrated Medium Term Plan.
A Key role of the Clinical Audit and Quality Improvement Operational Group is
to monitor progress against the forward plan. Issues identified and requiring attention will be brought to the attention of the respective Directorate
Integrated Governance Group and/or escalated to the Quality Steering Group.
Regular updates will be provided for the Quality and Safety Committee.
The CTUHB Clinical Audit Forward Plan 2018-19, is attached as Appendix 1.
4. RECOMMENDATION
The Audit Committee is asked to;
RECEIVE and NOTE the attached report.
Freedom of Information Status
Open
2.5 Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
88 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Knowing How Well
We Are Doing
Clinical Audit Forward Plan 2018-19
Standard 3.3:
Quality Improvement, Research and Innovation
Effective Care
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
89 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Page 2 of 16
Contents Page
1 Executive Summary 2
Standard 3.3: Quality Improvement, Research & Innovation
2 National Clinical Audit and Outcome Review Plan
3
3 NICE Guidance 9
4 Health Board Wide Audits 13
5 Welsh Risk Management Standards compliance audits
14
6 External Accreditation Scheme(s) 16
Executive Summary Clinical audit is a fundamental component of the organisations quality assurance process, based on transparency and candour. Quality assurance provides a systematic approach to maintaining consistently high quality by constantly measuring and reporting on effectiveness, highlighting the need for improvement and enabling the sharing of good practice. Cwm Taf University Health Board (CTUHB) is expected to participate in clinical audit as part of the requirements of Standard 3.3 of the Health and Care Standards 2015, which requires healthcare organisations to have a cycle of continuous quality improvement strategy that includes an audit and clinical effectiveness strategy and delivery plan.
All organisations in Wales are required as part of their Quality Strategy
to have an annual Clinical Audit Forward Plan in place which include
both national, and local audits that address their priorities.
The Clinical Audit Forward Plan identifies all the clinical audit projects
that must be undertaken by CTUHB in 2018-19. It is essential that they
are treated as priorities and that appropriate resources are provided
to support them. Failure to participate or deliver on these internal /
externally ‘must do’ audits may carry a penalty for the health board,
either financially, or in the form of a failed target, or non-compliance
with regulations. They form the core of the annual clinical audit
programme.
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
90 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Page 3 of 16
1. National Clinical Audit and Outcome Review Plan
The following National Clinical Audit and Outcomes Review Plan confirms the list of National Clinical Audits and Outcome Reviews which Cwm Taf University Health Board (CTUHB) are expected to participate in 2018-19 (when they provide the service). The Plan also confirms how the findings from audits and reviews will be used to measure and drive forward improvements in the quality and safety of healthcare services in Wales.
The agreed NHS Wales programme of audits includes the majority of audits currently supported by the National Clinical Audit and Patients Outcome Programme (NCAPOP) managed by the Healthcare Quality Improvement Partnership (HQIP). However, it also includes a number of other national or multi-organisational audits recognised by the National Clinical Audit and Outcome Review Advisory Committee as being essential. The programme is slowly being developed to be more inclusive of primary and community care.
As with previous reports, to ensure consistency, changes to the list of audits and reviews have been kept to a minimum, but some audits have now ended.
Measurement of Success Success is measured by year on year consideration of audit reports and in comparison, with other UK, European and International healthcare systems to determine how compliance with best practice and achievement of healthcare outcomes compares to national and international benchmarks.
The following key criteria will also be used for judging success:
100% participation, appropriate levels of case ascertainment and submission of complete data sets (where applicable) in the full programme of National Clinical Audits and Clinical Outcome Reviews.
Less variation between local services and measurable year on year improvements in performance to achieve the highest standards. Health board recognised as being above the audit “average” or within the top quartile for each audit and maintaining that level.
Improvements in the quality and safety of patient outcomes and experience brought about by learning and action arising from the findings of National Clinical Audit and Clinical Outcome Review reports.
The findings and recommendations from national clinical audit, outcome reviews and all other forms of reviews and assessments will be one of the principal mechanisms for assessing the quality and effectiveness of healthcare services provided by CTUHB.
Priority: External “must do” These audits are externally monitored and driven by commissioning and quality improvement and are treated as the priority, and therefore appropriate resources must be provided to support them. Failure to participate or deliver on these externally driven audits may carry a penalty for the health board.
Compliance Key
RED Cause for concern. Full compliance not achieved.
GREEN Audit completed, evidence of audit compliance provided.
BLUE Audit completed, assurance proforma completed by audit leads and signed off by Clinical Lead, Clinical Audit and Quality Improvement on behalf of the Medical Director (nominated executive)
% Score
The ‘Number’ of records audited ‘Out Of’ the total number of records that meet the audit criteria for the audit period.
* Compliance position as at 31st March 2018
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
91 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
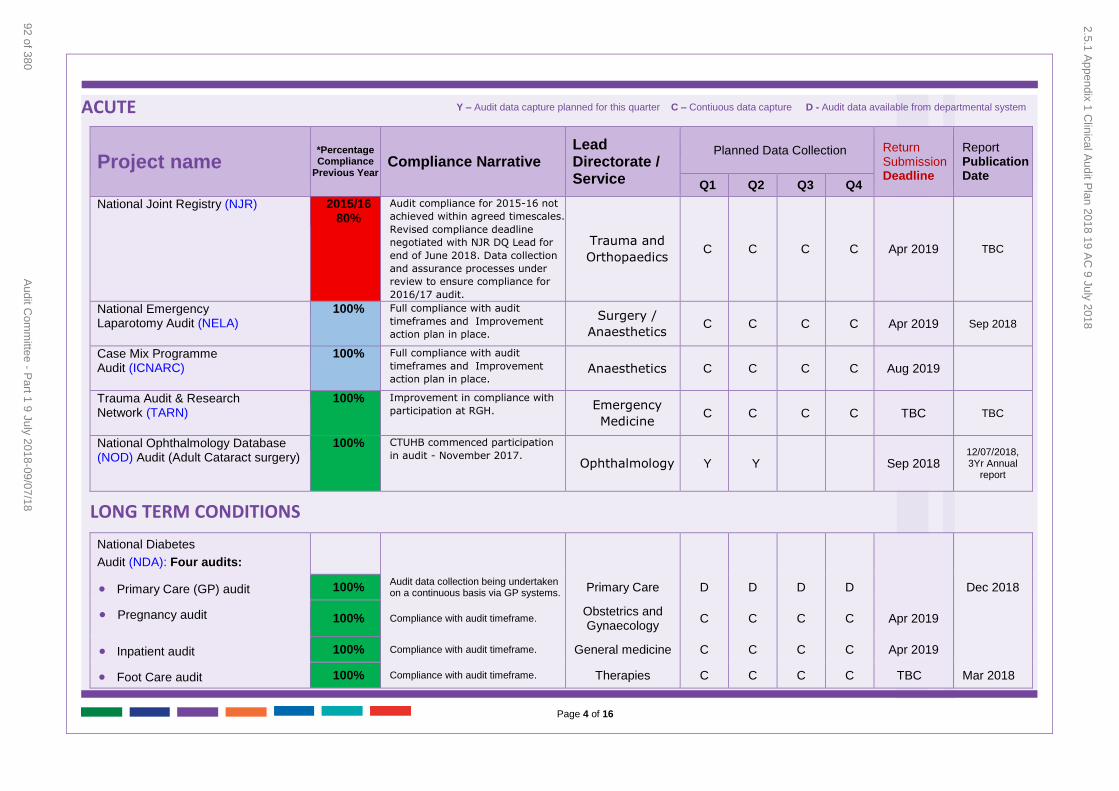
Page 4 of 16
ACUTE
Project name
*Percentage Compliance
Previous Year Compliance Narrative
Lead Directorate / Service
Planned Data Collection Return Submission Deadline
Report Publication Date
Q1 Q2 Q3 Q4
National Joint Registry (NJR) 2015/16 80%
Audit compliance for 2015-16 not
achieved within agreed timescales.
Revised compliance deadline
negotiated with NJR DQ Lead for
end of June 2018. Data collection
and assurance processes under
review to ensure compliance for
2016/17 audit.
Trauma and
Orthopaedics C C C C Apr 2019 TBC
National Emergency Laparotomy Audit (NELA)
100% Full compliance with audit
timeframes and Improvement
action plan in place.
Surgery /
Anaesthetics C C C C Apr 2019 Sep 2018
Case Mix Programme Audit (ICNARC)
100% Full compliance with audit
timeframes and Improvement
action plan in place. Anaesthetics C C C C Aug 2019
Trauma Audit & Research Network (TARN)
100% Improvement in compliance with
participation at RGH. Emergency
Medicine C C C C TBC TBC
National Ophthalmology Database (NOD) Audit (Adult Cataract surgery)
100% CTUHB commenced participation
in audit - November 2017. Ophthalmology Y Y Sep 2018
12/07/2018, 3Yr Annual
report
LONG TERM CONDITIONS
National Diabetes
Audit (NDA): Four audits:
Primary Care (GP) audit 100% Audit data collection being undertaken on a continuous basis via GP systems.
Primary Care D D D D Dec 2018
Pregnancy audit 100% Compliance with audit timeframe. Obstetrics and Gynaecology
C C C C Apr 2019
Inpatient audit 100% Compliance with audit timeframe. General medicine C C C C Apr 2019
Foot Care audit 100% Compliance with audit timeframe. Therapies C C C C TBC Mar 2018
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
92 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
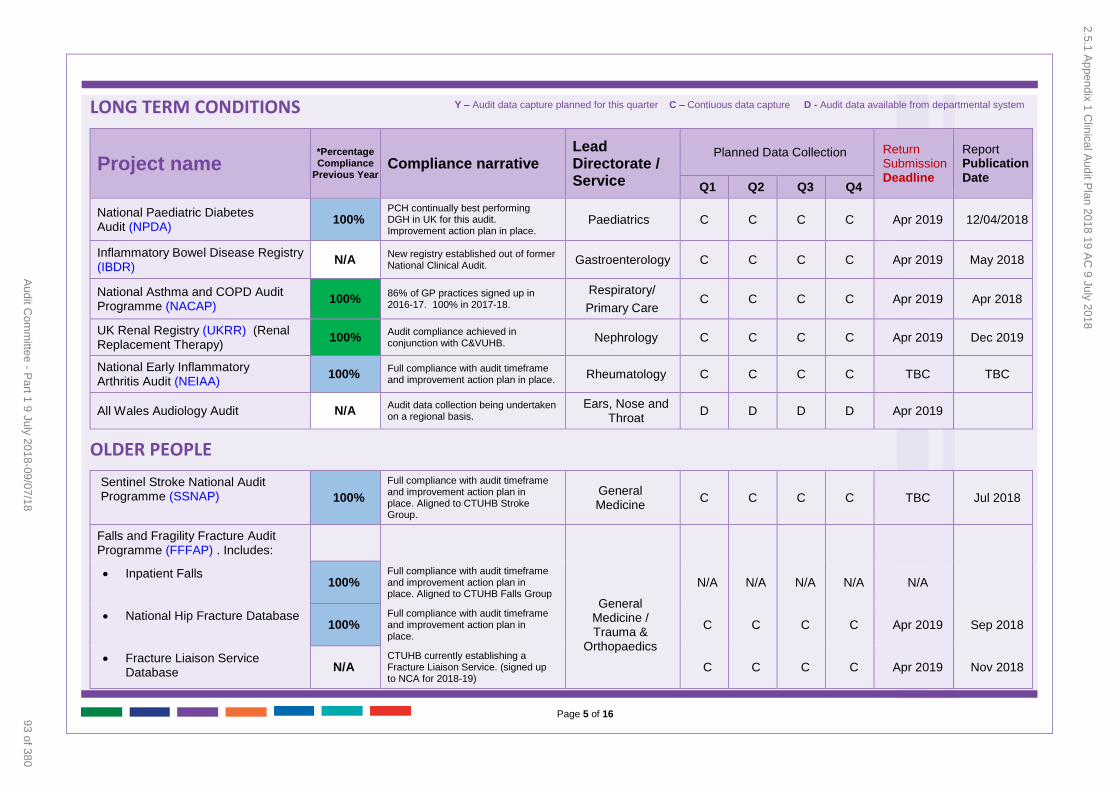
Page 5 of 16
LONG TERM CONDITIONS
Project name
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Data Collection Return Submission Deadline
Report Publication Date
Q1 Q2 Q3 Q4
National Paediatric Diabetes Audit (NPDA)
100% PCH continually best performing DGH in UK for this audit. Improvement action plan in place.
Paediatrics C C C C Apr 2019 12/04/2018
Inflammatory Bowel Disease Registry (IBDR)
N/A New registry established out of former National Clinical Audit.
Gastroenterology C C C C Apr 2019 May 2018
National Asthma and COPD Audit Programme (NACAP)
100% 86% of GP practices signed up in 2016-17. 100% in 2017-18.
Respiratory/
Primary Care C C C C Apr 2019 Apr 2018
UK Renal Registry (UKRR) (Renal Replacement Therapy)
100% Audit compliance achieved in conjunction with C&VUHB.
Nephrology C C C C Apr 2019 Dec 2019
National Early Inflammatory Arthritis Audit (NEIAA)
100% Full compliance with audit timeframe and improvement action plan in place.
Rheumatology C C C C TBC TBC
All Wales Audiology Audit N/A Audit data collection being undertaken on a regional basis.
Ears, Nose and Throat
D D D D Apr 2019
OLDER PEOPLE
Sentinel Stroke National Audit Programme (SSNAP) 100%
Full compliance with audit timeframe and improvement action plan in place. Aligned to CTUHB Stroke Group.
General Medicine
C C C C TBC Jul 2018
Falls and Fragility Fracture Audit Programme (FFFAP) . Includes:
Inpatient Falls 100%
Full compliance with audit timeframe and improvement action plan in place. Aligned to CTUHB Falls Group
General Medicine / Trauma &
Orthopaedics
N/A N/A N/A N/A N/A
National Hip Fracture Database 100%
Full compliance with audit timeframe and improvement action plan in place.
C C C C Apr 2019 Sep 2018
Fracture Liaison Service Database N/A
CTUHB currently establishing a Fracture Liaison Service. (signed up to NCA for 2018-19)
C C C C Apr 2019 Nov 2018
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
93 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
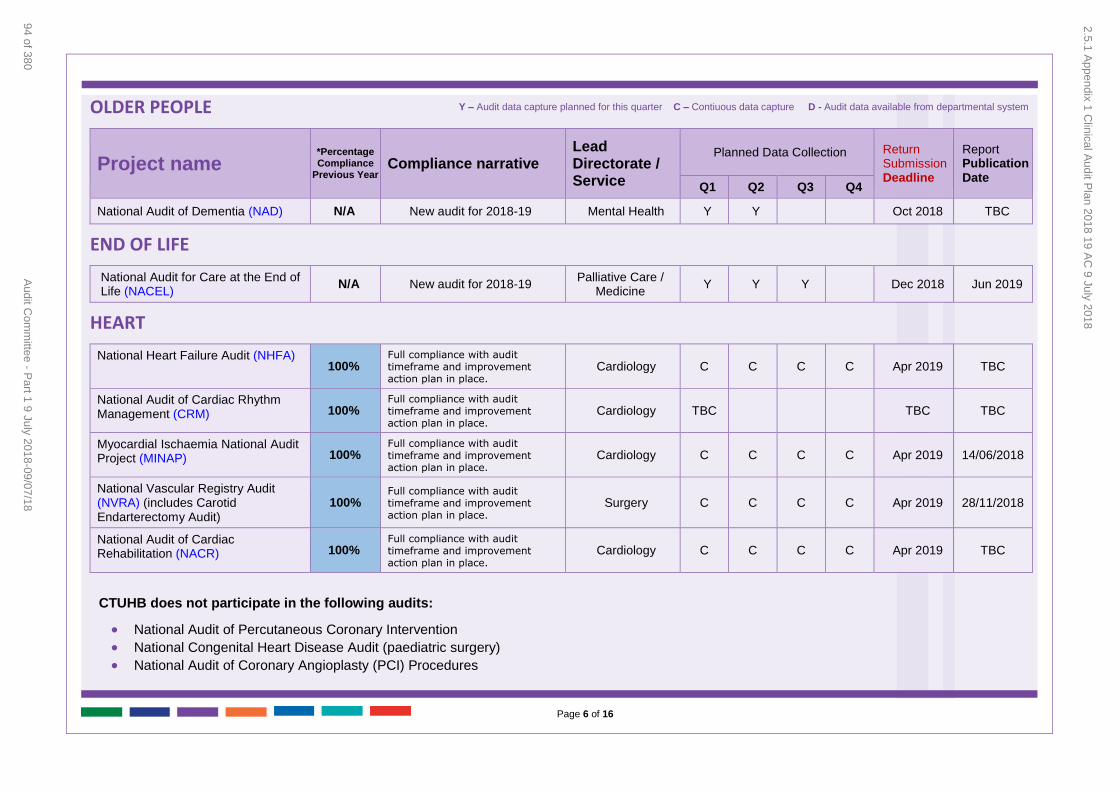
Page 6 of 16
OLDER PEOPLE
Project name
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Data Collection Return Submission Deadline
Report Publication Date
Q1 Q2 Q3 Q4
National Audit of Dementia (NAD) N/A New audit for 2018-19 Mental Health Y Y Oct 2018 TBC
END OF LIFE
National Audit for Care at the End of Life (NACEL)
N/A New audit for 2018-19 Palliative Care /
Medicine Y Y Y Dec 2018 Jun 2019
HEART
National Heart Failure Audit (NHFA) 100%
Full compliance with audit timeframe and improvement action plan in place.
Cardiology C C C C Apr 2019 TBC
National Audit of Cardiac Rhythm Management (CRM) 100%
Full compliance with audit timeframe and improvement action plan in place.
Cardiology TBC TBC TBC
Myocardial Ischaemia National Audit Project (MINAP) 100%
Full compliance with audit timeframe and improvement action plan in place.
Cardiology C C C C Apr 2019 14/06/2018
National Vascular Registry Audit (NVRA) (includes Carotid Endarterectomy Audit)
100% Full compliance with audit timeframe and improvement action plan in place.
Surgery C C C C Apr 2019 28/11/2018
National Audit of Cardiac Rehabilitation (NACR) 100%
Full compliance with audit timeframe and improvement action plan in place.
Cardiology C C C C Apr 2019 TBC
CTUHB does not participate in the following audits:
National Audit of Percutaneous Coronary Intervention
National Congenital Heart Disease Audit (paediatric surgery) National Audit of Coronary Angioplasty (PCI) Procedures
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
94 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
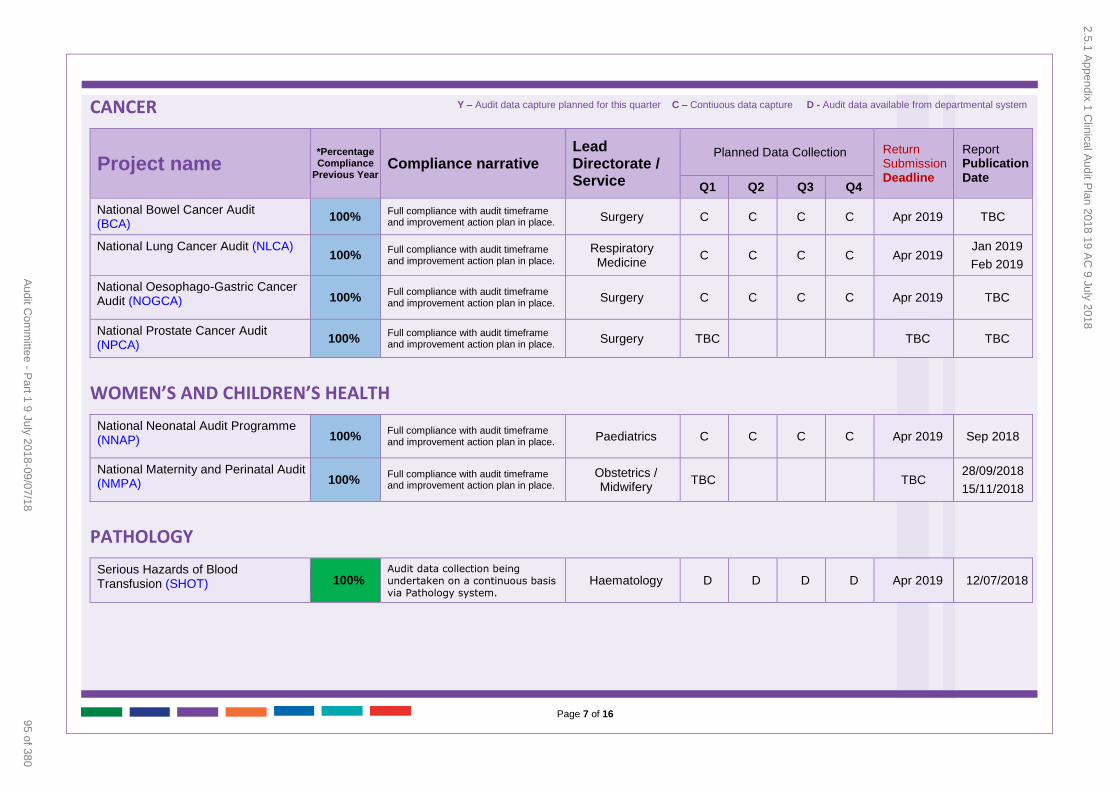
Page 7 of 16
CANCER
Project name
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Data Collection Return Submission Deadline
Report Publication Date
Q1 Q2 Q3 Q4
National Bowel Cancer Audit (BCA)
100% Full compliance with audit timeframe and improvement action plan in place. Surgery C C C C Apr 2019 TBC
National Lung Cancer Audit (NLCA) 100%
Full compliance with audit timeframe and improvement action plan in place.
Respiratory Medicine
C C C C Apr 2019 Jan 2019
Feb 2019
National Oesophago-Gastric Cancer Audit (NOGCA) 100%
Full compliance with audit timeframe and improvement action plan in place.
Surgery C C C C Apr 2019 TBC
National Prostate Cancer Audit (NPCA)
100% Full compliance with audit timeframe and improvement action plan in place.
Surgery TBC TBC TBC
WOMEN’S AND CHILDREN’S HEALTH
National Neonatal Audit Programme (NNAP) 100%
Full compliance with audit timeframe and improvement action plan in place.
Paediatrics C C C C Apr 2019 Sep 2018
National Maternity and Perinatal Audit (NMPA) 100%
Full compliance with audit timeframe and improvement action plan in place.
Obstetrics / Midwifery
TBC TBC 28/09/2018
15/11/2018
PATHOLOGY
Serious Hazards of Blood Transfusion (SHOT) 100%
Audit data collection being undertaken on a continuous basis via Pathology system.
Haematology D D D D Apr 2019 12/07/2018
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
95 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
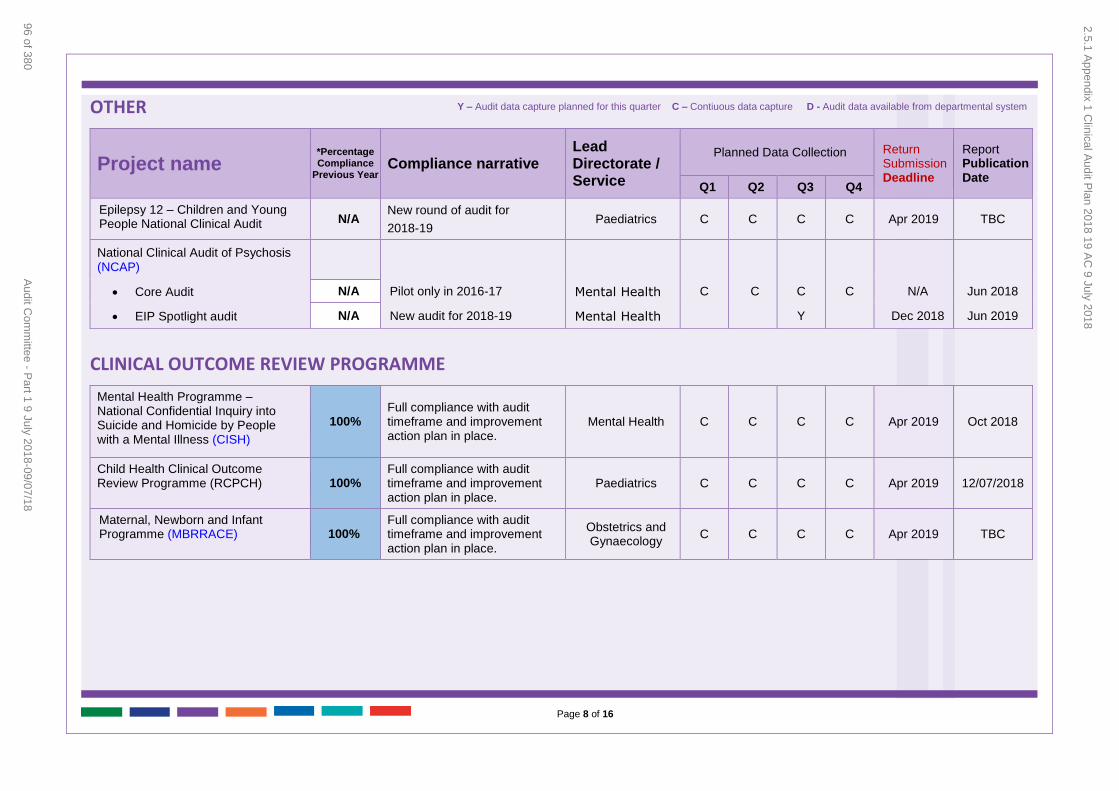
Page 8 of 16
OTHER
Project name
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Data Collection Return Submission Deadline
Report Publication Date
Q1 Q2 Q3 Q4
Epilepsy 12 – Children and Young People National Clinical Audit N/A
New round of audit for
2018-19 Paediatrics C C C C Apr 2019 TBC
National Clinical Audit of Psychosis (NCAP)
Core Audit N/A Pilot only in 2016-17 Mental Health C C C C N/A Jun 2018
EIP Spotlight audit N/A New audit for 2018-19 Mental Health Y Dec 2018 Jun 2019
CLINICAL OUTCOME REVIEW PROGRAMME
Mental Health Programme – National Confidential Inquiry into Suicide and Homicide by People with a Mental Illness (CISH)
100% Full compliance with audit timeframe and improvement action plan in place.
Mental Health C C C C Apr 2019 Oct 2018
Child Health Clinical Outcome Review Programme (RCPCH) 100%
Full compliance with audit timeframe and improvement action plan in place.
Paediatrics C C C C Apr 2019 12/07/2018
Maternal, Newborn and Infant Programme (MBRRACE) 100%
Full compliance with audit timeframe and improvement action plan in place.
Obstetrics and Gynaecology
C C C C Apr 2019 TBC
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
96 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
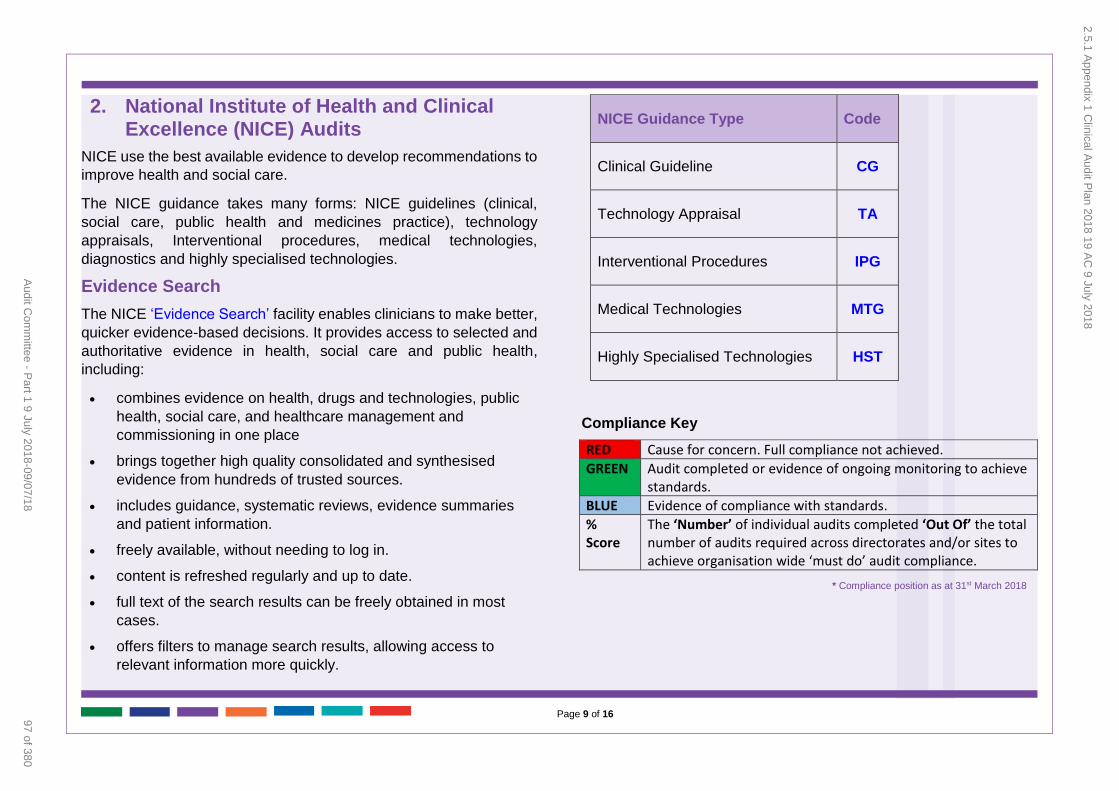
Page 9 of 16
2. National Institute of Health and Clinical Excellence (NICE) Audits
NICE use the best available evidence to develop recommendations to
improve health and social care.
The NICE guidance takes many forms: NICE guidelines (clinical,
social care, public health and medicines practice), technology
appraisals, Interventional procedures, medical technologies,
diagnostics and highly specialised technologies.
Evidence Search
The NICE ‘Evidence Search’ facility enables clinicians to make better,
quicker evidence-based decisions. It provides access to selected and
authoritative evidence in health, social care and public health,
including:
combines evidence on health, drugs and technologies, public
health, social care, and healthcare management and
commissioning in one place
brings together high quality consolidated and synthesised
evidence from hundreds of trusted sources.
includes guidance, systematic reviews, evidence summaries
and patient information.
freely available, without needing to log in.
content is refreshed regularly and up to date.
full text of the search results can be freely obtained in most
cases.
offers filters to manage search results, allowing access to
relevant information more quickly.
NICE Guidance Type Code
Clinical Guideline CG
Technology Appraisal TA
Interventional Procedures IPG
Medical Technologies MTG
Highly Specialised Technologies HST
Compliance Key
RED Cause for concern. Full compliance not achieved.
GREEN Audit completed or evidence of ongoing monitoring to achieve standards.
BLUE Evidence of compliance with standards.
% Score
The ‘Number’ of individual audits completed ‘Out Of’ the total number of audits required across directorates and/or sites to achieve organisation wide ‘must do’ audit compliance.
* Compliance position as at 31st March 2018
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
97 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
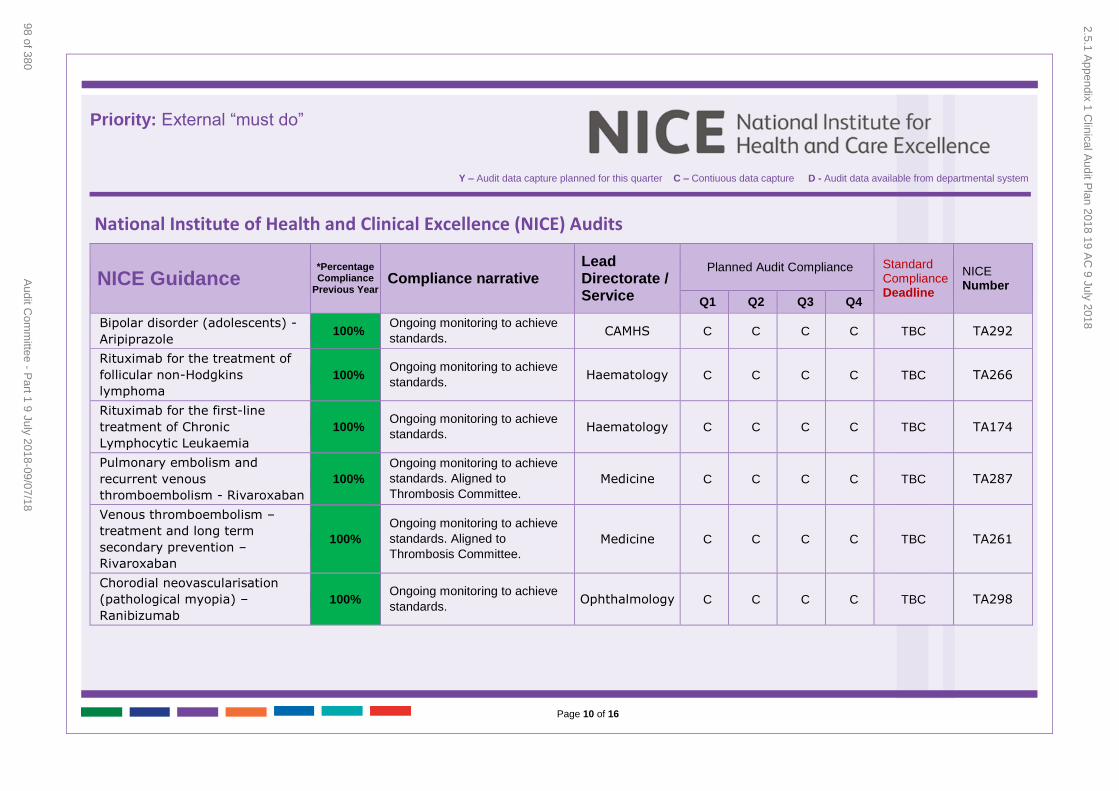
Page 10 of 16
Priority: External “must do”
National Institute of Health and Clinical Excellence (NICE) Audits
NICE Guidance
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Audit Compliance Standard Compliance Deadline
NICE Number
Q1 Q2 Q3 Q4
Bipolar disorder (adolescents) -
Aripiprazole 100%
Ongoing monitoring to achieve
standards. CAMHS C C C C TBC TA292
Rituximab for the treatment of
follicular non-Hodgkins
lymphoma
100% Ongoing monitoring to achieve
standards. Haematology C C C C TBC TA266
Rituximab for the first-line
treatment of Chronic
Lymphocytic Leukaemia
100% Ongoing monitoring to achieve
standards. Haematology C C C C TBC TA174
Pulmonary embolism and
recurrent venous
thromboembolism - Rivaroxaban
100%
Ongoing monitoring to achieve
standards. Aligned to
Thrombosis Committee.
Medicine C C C C TBC TA287
Venous thromboembolism –
treatment and long term
secondary prevention –
Rivaroxaban
100%
Ongoing monitoring to achieve
standards. Aligned to
Thrombosis Committee.
Medicine C C C C TBC TA261
Chorodial neovascularisation
(pathological myopia) –
Ranibizumab
100% Ongoing monitoring to achieve
standards. Ophthalmology C C C C TBC TA298
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
98 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
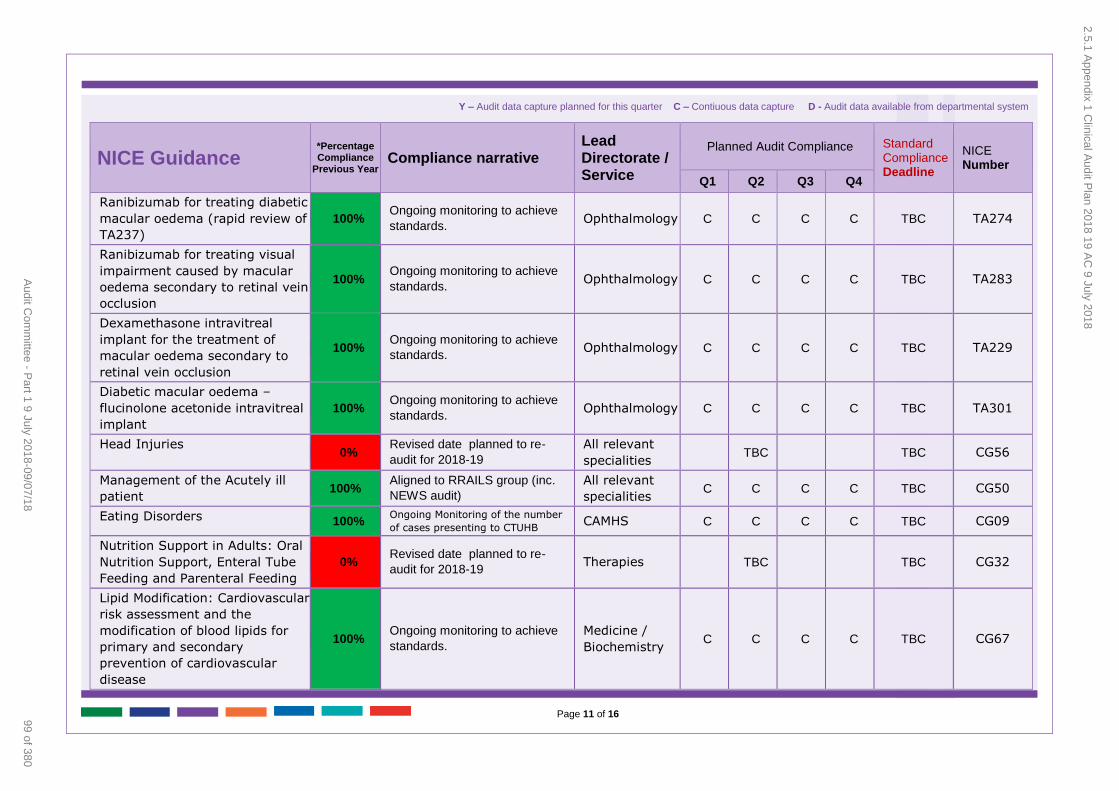
Page 11 of 16
NICE Guidance
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Audit Compliance Standard Compliance Deadline
NICE Number
Q1 Q2 Q3 Q4
Ranibizumab for treating diabetic
macular oedema (rapid review of
TA237)
100% Ongoing monitoring to achieve
standards. Ophthalmology C C C C TBC TA274
Ranibizumab for treating visual
impairment caused by macular
oedema secondary to retinal vein
occlusion
100% Ongoing monitoring to achieve
standards. Ophthalmology C C C C TBC TA283
Dexamethasone intravitreal
implant for the treatment of
macular oedema secondary to
retinal vein occlusion
100% Ongoing monitoring to achieve
standards. Ophthalmology C C C C TBC TA229
Diabetic macular oedema –
flucinolone acetonide intravitreal
implant
100% Ongoing monitoring to achieve
standards. Ophthalmology C C C C TBC TA301
Head Injuries 0%
Revised date planned to re-
audit for 2018-19
All relevant
specialities TBC TBC CG56
Management of the Acutely ill
patient 100%
Aligned to RRAILS group (inc.
NEWS audit)
All relevant
specialities C C C C TBC CG50
Eating Disorders 100% Ongoing Monitoring of the number
of cases presenting to CTUHB CAMHS C C C C TBC CG09
Nutrition Support in Adults: Oral
Nutrition Support, Enteral Tube
Feeding and Parenteral Feeding
0% Revised date planned to re-
audit for 2018-19 Therapies TBC TBC CG32
Lipid Modification: Cardiovascular
risk assessment and the
modification of blood lipids for
primary and secondary
prevention of cardiovascular
disease
100% Ongoing monitoring to achieve
standards.
Medicine /
Biochemistry C C C C TBC CG67
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
99 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
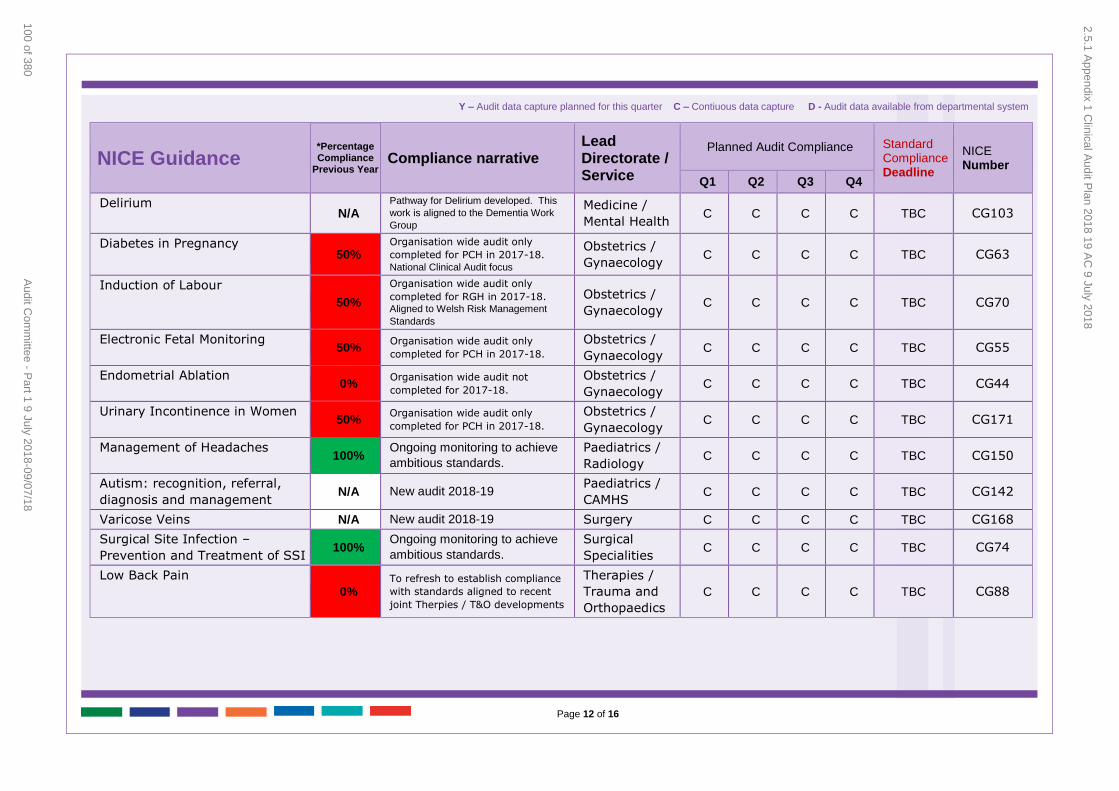
Page 12 of 16
NICE Guidance
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Audit Compliance Standard Compliance Deadline
NICE Number
Q1 Q2 Q3 Q4
Delirium N/A
Pathway for Delirium developed. This
work is aligned to the Dementia Work
Group
Medicine /
Mental Health C C C C TBC CG103
Diabetes in Pregnancy 50%
Organisation wide audit only
completed for PCH in 2017-18.
National Clinical Audit focus
Obstetrics /
Gynaecology C C C C TBC CG63
Induction of Labour
50%
Organisation wide audit only
completed for RGH in 2017-18. Aligned to Welsh Risk Management
Standards
Obstetrics /
Gynaecology C C C C TBC CG70
Electronic Fetal Monitoring 50%
Organisation wide audit only
completed for PCH in 2017-18. Obstetrics /
Gynaecology C C C C TBC CG55
Endometrial Ablation 0%
Organisation wide audit not
completed for 2017-18. Obstetrics /
Gynaecology C C C C TBC CG44
Urinary Incontinence in Women 50%
Organisation wide audit only
completed for PCH in 2017-18. Obstetrics /
Gynaecology C C C C TBC CG171
Management of Headaches 100%
Ongoing monitoring to achieve
ambitious standards.
Paediatrics /
Radiology C C C C TBC CG150
Autism: recognition, referral,
diagnosis and management N/A New audit 2018-19
Paediatrics /
CAMHS C C C C TBC CG142
Varicose Veins N/A New audit 2018-19 Surgery C C C C TBC CG168
Surgical Site Infection –
Prevention and Treatment of SSI 100%
Ongoing monitoring to achieve
ambitious standards.
Surgical
Specialities C C C C TBC CG74
Low Back Pain
0% To refresh to establish compliance
with standards aligned to recent
joint Therpies / T&O developments
Therapies /
Trauma and
Orthopaedics
C C C C TBC CG88
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
100 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
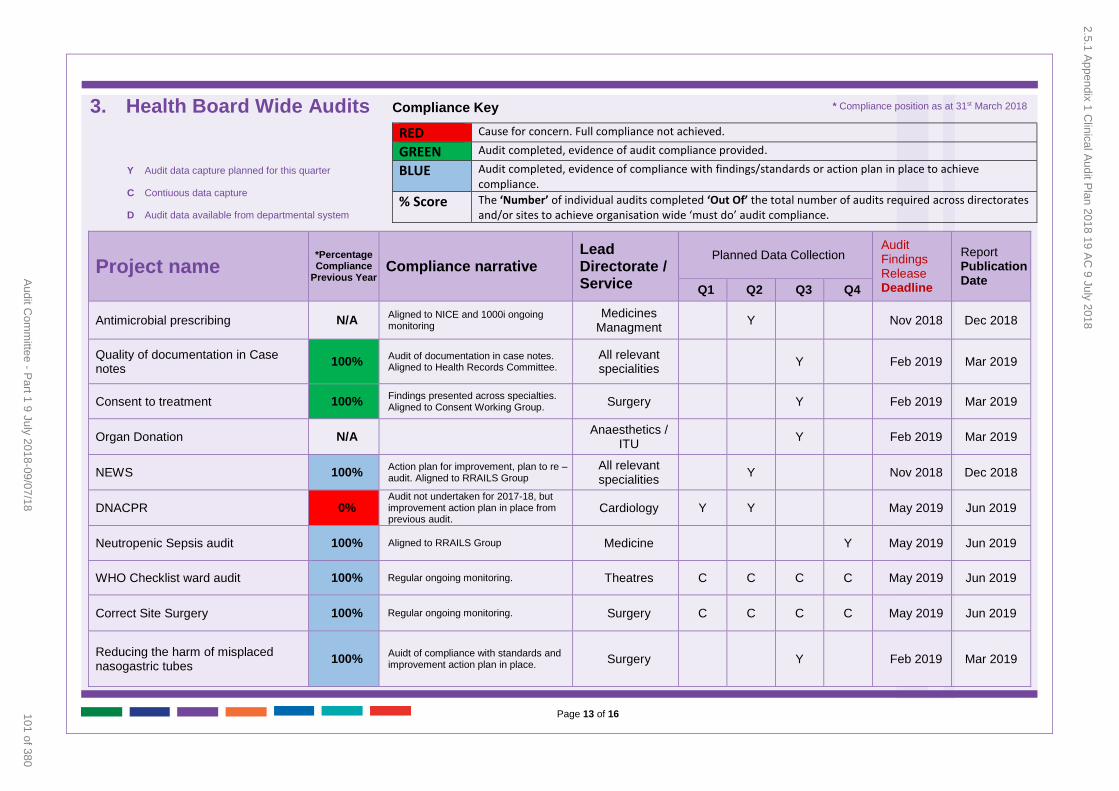
Page 13 of 16
3. Health Board Wide Audits
Compliance Key
RED Cause for concern. Full compliance not achieved.
GREEN Audit completed, evidence of audit compliance provided.
BLUE Audit completed, evidence of compliance with findings/standards or action plan in place to achieve compliance.
% Score The ‘Number’ of individual audits completed ‘Out Of’ the total number of audits required across directorates and/or sites to achieve organisation wide ‘must do’ audit compliance.
Project name
*Percentage Compliance
Previous Year Compliance narrative
Lead Directorate / Service
Planned Data Collection Audit Findings Release Deadline
Report Publication Date
Q1 Q2 Q3 Q4
Antimicrobial prescribing N/A Aligned to NICE and 1000i ongoing monitoring
Medicines Managment
Y Nov 2018 Dec 2018
Quality of documentation in Case notes
100% Audit of documentation in case notes. Aligned to Health Records Committee.
All relevant specialities
Y Feb 2019 Mar 2019
Consent to treatment 100% Findings presented across specialties. Aligned to Consent Working Group.
Surgery Y Feb 2019 Mar 2019
Organ Donation N/A Anaesthetics /
ITU Y Feb 2019 Mar 2019
NEWS 100% Action plan for improvement, plan to re –audit. Aligned to RRAILS Group
All relevant specialities
Y Nov 2018 Dec 2018
DNACPR 0% Audit not undertaken for 2017-18, but improvement action plan in place from previous audit.
Cardiology Y Y May 2019 Jun 2019
Neutropenic Sepsis audit 100% Aligned to RRAILS Group Medicine Y May 2019 Jun 2019
WHO Checklist ward audit 100% Regular ongoing monitoring. Theatres C C C C May 2019 Jun 2019
Correct Site Surgery 100% Regular ongoing monitoring. Surgery C C C C May 2019 Jun 2019
Reducing the harm of misplaced nasogastric tubes
100% Auidt of compliance with standards and improvement action plan in place.
Surgery Y Feb 2019 Mar 2019
* Compliance position as at 31st March 2018
Y Audit data capture planned for this quarter
C Contiuous data capture
D Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
101 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
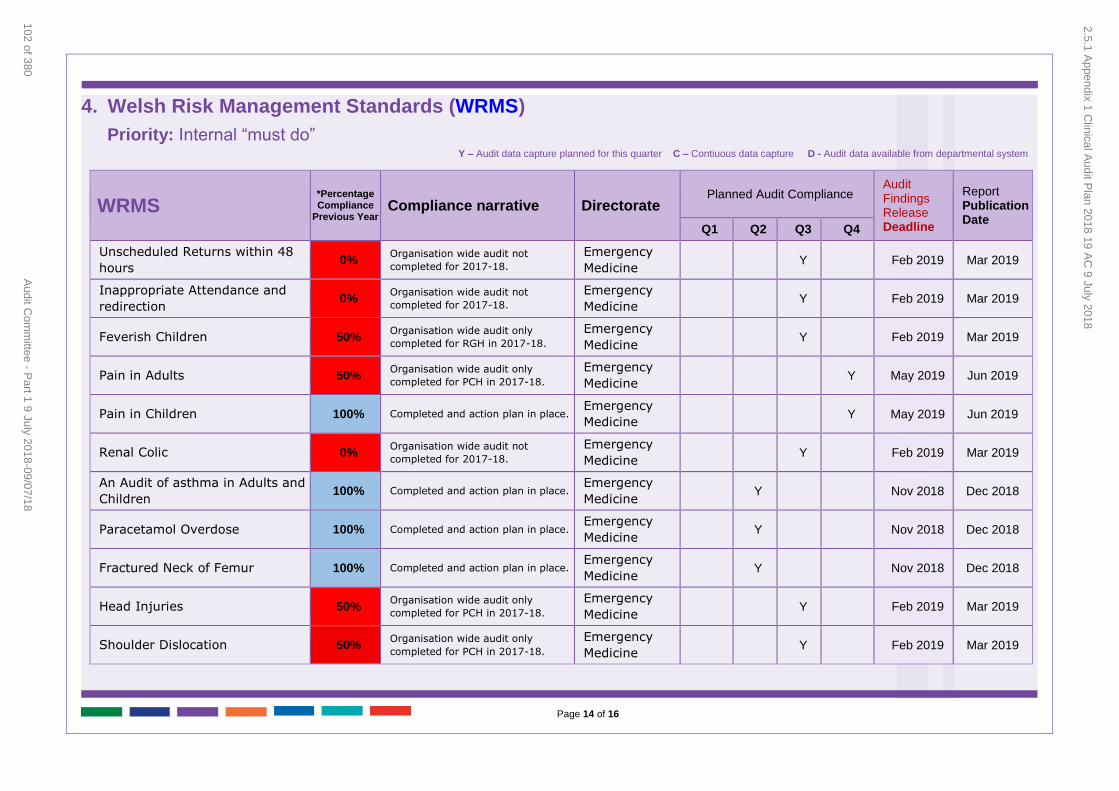
Page 14 of 16
4. Welsh Risk Management Standards (WRMS)
WRMS
*Percentage Compliance
Previous Year Compliance narrative Directorate
Planned Audit Compliance Audit Findings Release Deadline
Report Publication Date
Q1 Q2 Q3 Q4
Unscheduled Returns within 48
hours 0%
Organisation wide audit not
completed for 2017-18.
Emergency
Medicine Y Feb 2019 Mar 2019
Inappropriate Attendance and
redirection 0%
Organisation wide audit not
completed for 2017-18.
Emergency
Medicine Y Feb 2019 Mar 2019
Feverish Children 50% Organisation wide audit only
completed for RGH in 2017-18.
Emergency
Medicine Y Feb 2019 Mar 2019
Pain in Adults 50% Organisation wide audit only
completed for PCH in 2017-18.
Emergency
Medicine Y May 2019 Jun 2019
Pain in Children 100% Completed and action plan in place. Emergency
Medicine Y May 2019 Jun 2019
Renal Colic 0% Organisation wide audit not
completed for 2017-18.
Emergency
Medicine Y Feb 2019 Mar 2019
An Audit of asthma in Adults and
Children 100% Completed and action plan in place.
Emergency
Medicine Y Nov 2018 Dec 2018
Paracetamol Overdose 100% Completed and action plan in place. Emergency
Medicine Y Nov 2018 Dec 2018
Fractured Neck of Femur 100% Completed and action plan in place. Emergency
Medicine Y Nov 2018 Dec 2018
Head Injuries 50% Organisation wide audit only
completed for PCH in 2017-18.
Emergency
Medicine Y Feb 2019 Mar 2019
Shoulder Dislocation 50% Organisation wide audit only
completed for PCH in 2017-18.
Emergency
Medicine Y Feb 2019 Mar 2019
Priority: Internal “must do” Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
102 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
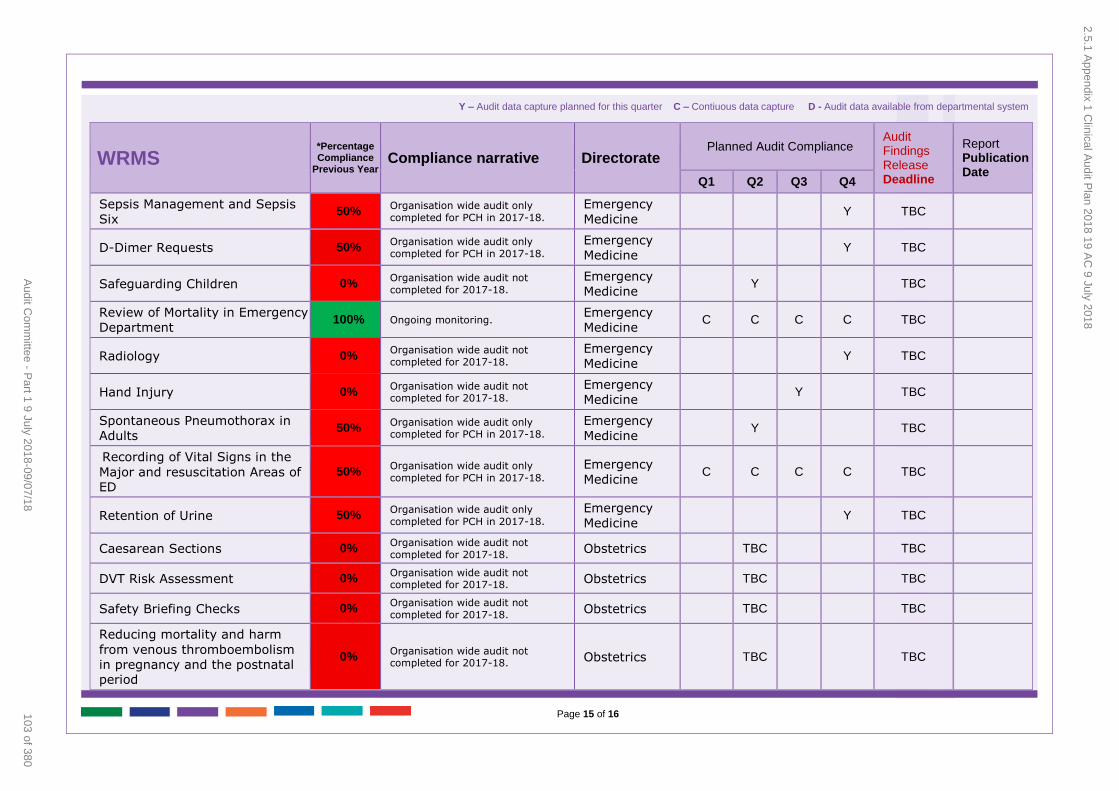
Page 15 of 16
WRMS
*Percentage Compliance
Previous Year Compliance narrative Directorate
Planned Audit Compliance Audit Findings Release Deadline
Report Publication Date
Q1 Q2 Q3 Q4
Sepsis Management and Sepsis
Six 50%
Organisation wide audit only completed for PCH in 2017-18.
Emergency
Medicine Y TBC
D-Dimer Requests 50% Organisation wide audit only completed for PCH in 2017-18.
Emergency
Medicine Y TBC
Safeguarding Children 0% Organisation wide audit not completed for 2017-18.
Emergency
Medicine Y TBC
Review of Mortality in Emergency
Department 100% Ongoing monitoring.
Emergency
Medicine C C C C TBC
Radiology 0% Organisation wide audit not completed for 2017-18.
Emergency
Medicine Y TBC
Hand Injury 0% Organisation wide audit not completed for 2017-18.
Emergency
Medicine Y TBC
Spontaneous Pneumothorax in
Adults 50%
Organisation wide audit only completed for PCH in 2017-18.
Emergency
Medicine Y TBC
Recording of Vital Signs in the
Major and resuscitation Areas of ED
50% Organisation wide audit only completed for PCH in 2017-18.
Emergency
Medicine C C C C TBC
Retention of Urine 50% Organisation wide audit only completed for PCH in 2017-18.
Emergency
Medicine Y TBC
Caesarean Sections 0% Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
DVT Risk Assessment 0% Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
Safety Briefing Checks 0% Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
Reducing mortality and harm
from venous thromboembolism
in pregnancy and the postnatal period
0% Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
103 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
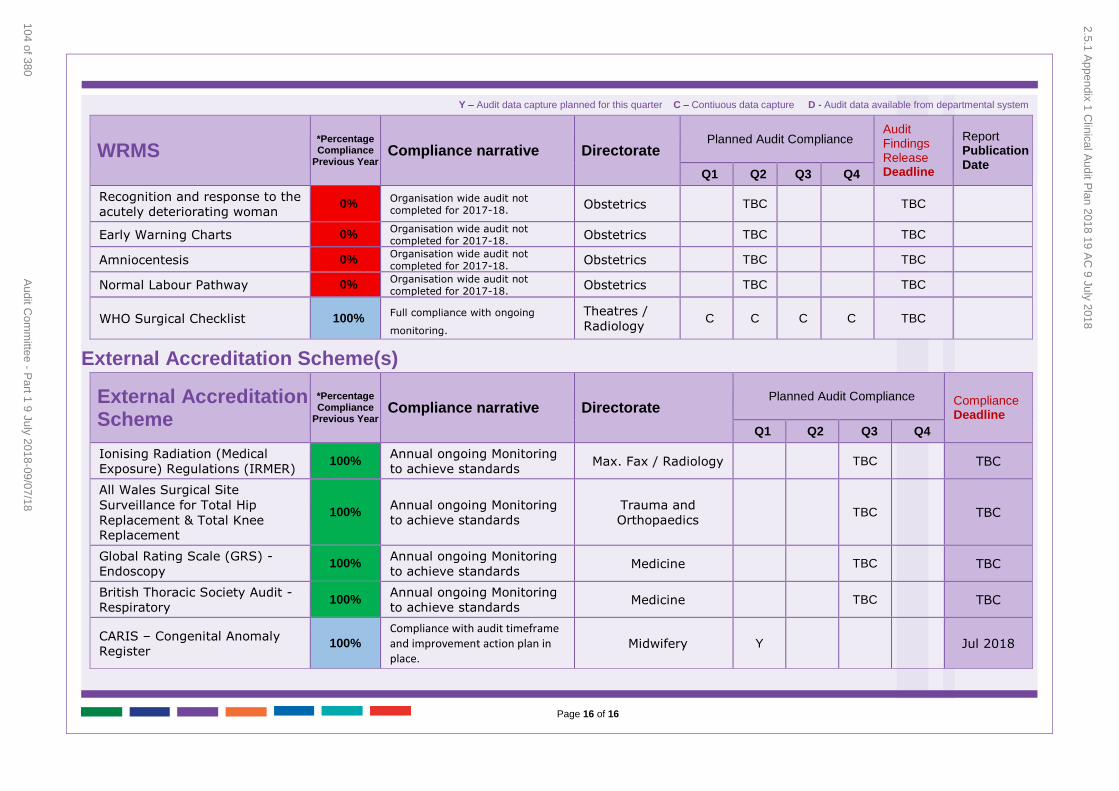
Page 16 of 16
WRMS
*Percentage Compliance
Previous Year Compliance narrative Directorate
Planned Audit Compliance Audit Findings Release Deadline
Report Publication Date
Q1 Q2 Q3 Q4
Recognition and response to the
acutely deteriorating woman 0%
Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
Early Warning Charts 0% Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
Amniocentesis 0% Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
Normal Labour Pathway 0% Organisation wide audit not completed for 2017-18.
Obstetrics TBC TBC
WHO Surgical Checklist 100% Full compliance with ongoing
monitoring.
Theatres /
Radiology C C C C TBC
External Accreditation Scheme(s)
External Accreditation Scheme
*Percentage Compliance
Previous Year Compliance narrative Directorate
Planned Audit Compliance Compliance Deadline
Q1 Q2 Q3 Q4
Ionising Radiation (Medical
Exposure) Regulations (IRMER) 100%
Annual ongoing Monitoring
to achieve standards Max. Fax / Radiology TBC TBC
All Wales Surgical Site
Surveillance for Total Hip
Replacement & Total Knee Replacement
100% Annual ongoing Monitoring
to achieve standards
Trauma and
Orthopaedics TBC TBC
Global Rating Scale (GRS) -
Endoscopy 100%
Annual ongoing Monitoring
to achieve standards Medicine TBC TBC
British Thoracic Society Audit -
Respiratory 100%
Annual ongoing Monitoring
to achieve standards Medicine TBC TBC
CARIS – Congenital Anomaly
Register 100%
Compliance with audit timeframe and improvement action plan in place.
Midwifery Y Jul 2018
Y – Audit data capture planned for this quarter C – Contiuous data capture D - Audit data available from departmental system
2.5.1 Appendix 1 C
linical Audit P
lan 2018 19 AC
9 July 2018
104 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 1 of 38
Audit Committee Meeting
9 July 2018
AGENDA ITEM 2.6
9 July 2018
Audit Committee Report
‘DRAFT’ AUDIT COMMITTEE ANNUAL REPORT 2017-2018
Executive Lead: Director of Corporate Services & Governance / Board Secretary
Author: Director of Corporate Services & Governance / Board Secretary
Contact Details for further information: Robert Williams 01443 744800 or
email [email protected]
Purpose of the Audit Committee Report
To purpose of this report is inform the Board of the work undertaken by the Audit Committee, and how it met its Terms of Reference during 2017-2018, and
to request that members of the Committee complete the self-assessment questionnaire to provide a view on the effectiveness of the Committee.
Governance
Link to Health Board Strategic
Objective(s)
The Board’s key role is to ensure its Strategy ‘Cwm Taf Cares’ and the related organisational objectives aligned with
the Institute of Healthcare Improvement’s (IHI) ‘Triple Aim’ are being progressed, these in summary align with:
– To improve quality, safety and patient experience. – To protect and improve population health.
– To ensure that the services provided are accessible
and sustainable into the future. – To provide strong governance and assurance.
– To ensure good value based care and treatment for our patients in line with the resources made available
to the Health Board. The report focuses on providing strong governance and
assurance.
Supporting
evidence
The work of the Audit Committee throughout 2017-2018
– web link http://cwmtaf.wales/how-we-work/audit-
committee/ NHS Audit Committee handbook
Head of Internal Audit Opinion and Annual Report 2017-2018 presented to the Audit Committee on 31 May 2018
Engagement – Who has been involved in this work?
Audit Committee Members, Internal and External Auditors
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
105 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 2 of 38
Audit Committee Meeting
9 July 2018
Audit Committee Resolution to:
APPROVE ENDORSE √ DISCUSS √ NOTE
Recommendation The Audit Committee is asked to:
DISCUSS and ENDORSE the draft Audit Committee Annual Report for 2017-2018 for approval by the
Health Board; ENDORSE the Terms of Reference for Board approval.
DISCUSS the attached self-assessment checklist at Appendix 3 for completion at the meeting.
Summarise the Impact of the Audit Committee Report
Equality and
diversity
No adverse equality and diversity issues have been
identified. The reports submitted to the Committee throughout the reporting period would have considered
the potential impact concerning equality and diversity for
each subject matter
Legal implications This report complies with the requirement to submit an
annual report to the Board through the Chair within 3 months of the end of the reporting year setting out its
activities during the year and detailing the results of a review of its performance and that of any sub-groups it
has established.
Population Health No impact.
Quality, Safety & Patient Experience
The Quality and accuracy of information presented to the Audit Committee is important to support and enable
them to make fully informed decisions. Informed decisions are more likely to impact favourably on the
quality, safety and experience of patients and staff.
Resources No impact.
Risks and Assurance
This report provides an assurance to the Board that the Audit Committee is effectively monitoring the risks
relating to the work of the Health Board.
Health & Care Standards
The Audit Committee annual report demonstrates compliance with the governance, leadership and
accountability overarching principle of the quality themes and the work of the Committee actively contributed
towards demonstrating compliance with all themes within the Health and Care Standards framework. Access to the
Standards can be obtained from the following link: http://www.wales.nhs.uk/sitesplus/documents/1064/247
29_Health%20Standards%20Framework_2015_E1.pdf
Workforce No impact.
Freedom of Information Status
Open
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
106 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 3 of 38
Audit Committee Meeting
9 July 2018
AUDIT COMMITTEE ‘DRAFT’ ANNUAL REPORT 2017-2018
1. SITUATION / PURPOSE OF REPORT
The purpose of this report is to highlight the activities and performance of the Audit Committee during 2017-2018 and to set out how it met its Terms of
Reference.
2. BACKGROUND / INTRODUCTION
The Chair of the Audit Committee is required to present an annual report
outlining the Audit Committee’s business throughout the financial year to the Health Board to provide an assurance on the monitoring and scrutiny
undertaken of CTUHB’s performance in relation to finance, risk and governance.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
The publication of the Annual report demonstrates compliance with the
Standing Orders, which stipulates that each Board Committee / Advisory Group is required to submit an annual report to the Board through the Chair within 3
months of the end of the reporting year setting out its activities during the year and detailing the results of a review of its performance and that of any sub-
groups it has established.
The Audit Committee Annual Report for 2017-2018 is presented at Appendix 1 for endorsement before submission to the Health Board on the 26 July 2018.
The revised Terms of Reference for the Audit Committee were received and endorsed by the Audit Committee in September 2017 and were subsequently
approved by the Board on November 2017. To ensure that there are effective governance arrangements in place for the Audit Committee the Terms of
reference are reviewed on an annual basis and are presented at Appendix 2 for approval. No material changes have been made to the document.
Members of the Audit Committee regularly review the effectiveness of the
Committee through open and honest discussion at each meeting and to support the feedback process all members are requested to complete the Audit
Committee Self-Assessment Checklist 2017-2018 (from the Audit Committee Handbook pages 53-63) presented for completion during the meeting at
Appendix 3.
A breakdown of the internal audits results presented to the Audit Committee
and the Board in 2017-2018 is presented at Appendix 4 for information.
A breakdown of the Audit results for the Hosted Bodies presented to the Audit Committee and the Board in 2017-2018 is presented at Appendix 5 for
information.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
107 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 4 of 38
Audit Committee Meeting
9 July 2018
4. RECOMMENDATION
The Audit Committee is asked to:
DISCUSS and ENDORSE the draft Audit Committee Annual Report for 2017-2018 for approval by the Health Board;
ENDORSE the Terms of Reference for Board approval. DISCUSS the attached self-assessment checklist at Appendix 3 for
completion at the meeting.
Freedom of
Information Status
Open
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
108 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 5 of 38
Audit Committee Meeting
9 July 2018
Appendix 1
Audit
Committee
Annual Report 2017-2018
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
109 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 6 of 38
Audit Committee Meeting
9 July 2018
AUDIT COMMITTEE ANNUAL REPORT 2017-2018
1. FOREWORD
As Chair of the Audit Committee, I am pleased to be able to commend to you
this annual report, which has been prepared for the attention of the Board and reviews the work of the Committee for the financial year 2017-2018.
During the year, I was ably supported by Mrs Maria Thomas, Mrs Jayne
Sadgrove and Mr John Hill-Tout, who provided considerable knowledge and wide-ranging experience to the Committee. I would also like to express my
gratitude to Mr John Hill-Tout whose tenure as an Independent Member ceased
in September 2017 for his stalwart contribution to the Audit Committee.
The Committee welcomed Mr Paul Griffiths as its new Independent Member in November 2017 who brings a wealth of financial and audit experience to the
Committee.
In 2017-2018, the Committee had a busy work programme and meetings were well attended with constructive dialogue and questioning by members and
attendees throughout. Indeed, a characteristic of the Committee’s work and its related meetings has been the willingness of all parties to raise issues,
acknowledge shortcomings and put forward positive suggestions to help bring about meaningful improvements to services, systems and day to day working
practices. This approach is to be welcomed and is very much appreciated by the Committee.
I would like to express my thanks to all the officers of the Committee who have supported and contributed to the work carried out and for their commitment in
meeting important targets and deadlines. I also wish to record my appreciation for the support and contribution given by the Internal Audit team at the NHS
Wales Shared Services Partnership (NWSSP) and by the Wales Audit Office (WAO).
Going forward, the Committee intends to continue to pursue a full programme
of work covering a wide range of topics and subject areas as part of its long term aim to help further strengthen the governance arrangements of the Health
Board.
Dr Chris Turner,
Chair of the Audit Committee Cwm Taf University Health Board (CTUHB)
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
110 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 7 of 38
Audit Committee Meeting
9 July 2018
2. INTRODUCTION
The Committee’s business cycle runs from the closure of the Annual Accounts in
one financial year to the next. This reflects its key role in the development and monitoring of the Governance and Assurance framework for Cwm Taf UHB,
which culminates in the production of the Annual Governance Statement.
The Terms of Reference for the Committee were reviewed in September 2017 and were formally approved by the Board in November 2017.
Members will be aware that all papers relating to the Committee (unless closed
or ‘in-committee’) are available on the Health Board website: http://cwmtaf.wales/how-we-work/audit-committee/
This report sets out the role and functions of the Audit Committee and
summarises the key areas of business undertaken during the year. In addition, the report sets out some of the key issues, which the Committee will be
focussing on over the next few years.
3. ROLE, MEMBERSHIP, ATTENDEES AND COMMITTEE ATTENDANCES
3.1 ROLE
The role of the Committee is to advise and assure the Board on whether there are effective arrangements in place – through the design and operation of the
Health Board system of assurance – to support it in its decision taking and in discharging the accountabilities for securing the achievement of the Health
Board objectives in accordance with the standards of good governance determined for the NHS in Wales.
The Organisation’s system of internal control has been designed to identify the
potential risks that could prevent Cwm Taf UHB achieving its aims and objectives. It evaluates the likelihood of the risks being realised, considers the
impact should they occur, and seeks to manage them efficiently, effectively and
economically. Where appropriate, the Committee will advise the Board and the Accountable Officer on where, and how, the assurance framework may be
strengthened and developed further.
The Committee’s Terms of Reference are reviewed annually and are included
within the Standing Orders for the Cwm Taf UHB.
3.2 MEMBERSHIP The membership of the Audit Committee comprises of four Independent
members, enabling the Committee to provide appropriate scrutiny and assurance to the Board independently of the management decision-making
processes.
A summary of the Independent membership during 2017-2018 is outlined in table 1 below:
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
111 of 380Audit Committee - Part 1 9 July 2018-09/07/18
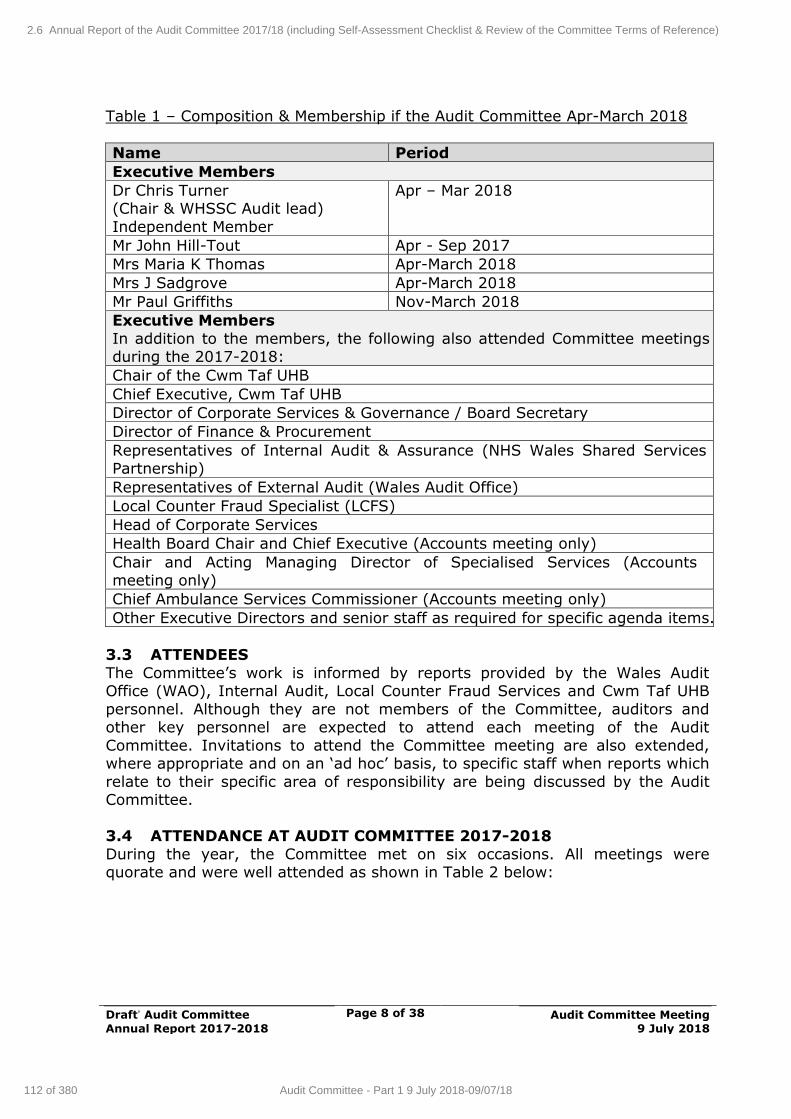
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 8 of 38
Audit Committee Meeting
9 July 2018
Table 1 – Composition & Membership if the Audit Committee Apr-March 2018
Name Period
Executive Members
Dr Chris Turner (Chair & WHSSC Audit lead)
Independent Member
Apr – Mar 2018
Mr John Hill-Tout Apr - Sep 2017
Mrs Maria K Thomas Apr-March 2018
Mrs J Sadgrove Apr-March 2018
Mr Paul Griffiths Nov-March 2018
Executive Members
In addition to the members, the following also attended Committee meetings during the 2017-2018:
Chair of the Cwm Taf UHB
Chief Executive, Cwm Taf UHB
Director of Corporate Services & Governance / Board Secretary
Director of Finance & Procurement
Representatives of Internal Audit & Assurance (NHS Wales Shared Services Partnership)
Representatives of External Audit (Wales Audit Office)
Local Counter Fraud Specialist (LCFS)
Head of Corporate Services
Health Board Chair and Chief Executive (Accounts meeting only)
Chair and Acting Managing Director of Specialised Services (Accounts meeting only)
Chief Ambulance Services Commissioner (Accounts meeting only)
Other Executive Directors and senior staff as required for specific agenda items.
3.3 ATTENDEES
The Committee’s work is informed by reports provided by the Wales Audit Office (WAO), Internal Audit, Local Counter Fraud Services and Cwm Taf UHB
personnel. Although they are not members of the Committee, auditors and other key personnel are expected to attend each meeting of the Audit
Committee. Invitations to attend the Committee meeting are also extended, where appropriate and on an ‘ad hoc’ basis, to specific staff when reports which
relate to their specific area of responsibility are being discussed by the Audit Committee.
3.4 ATTENDANCE AT AUDIT COMMITTEE 2017-2018
During the year, the Committee met on six occasions. All meetings were quorate and were well attended as shown in Table 2 below:
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
112 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
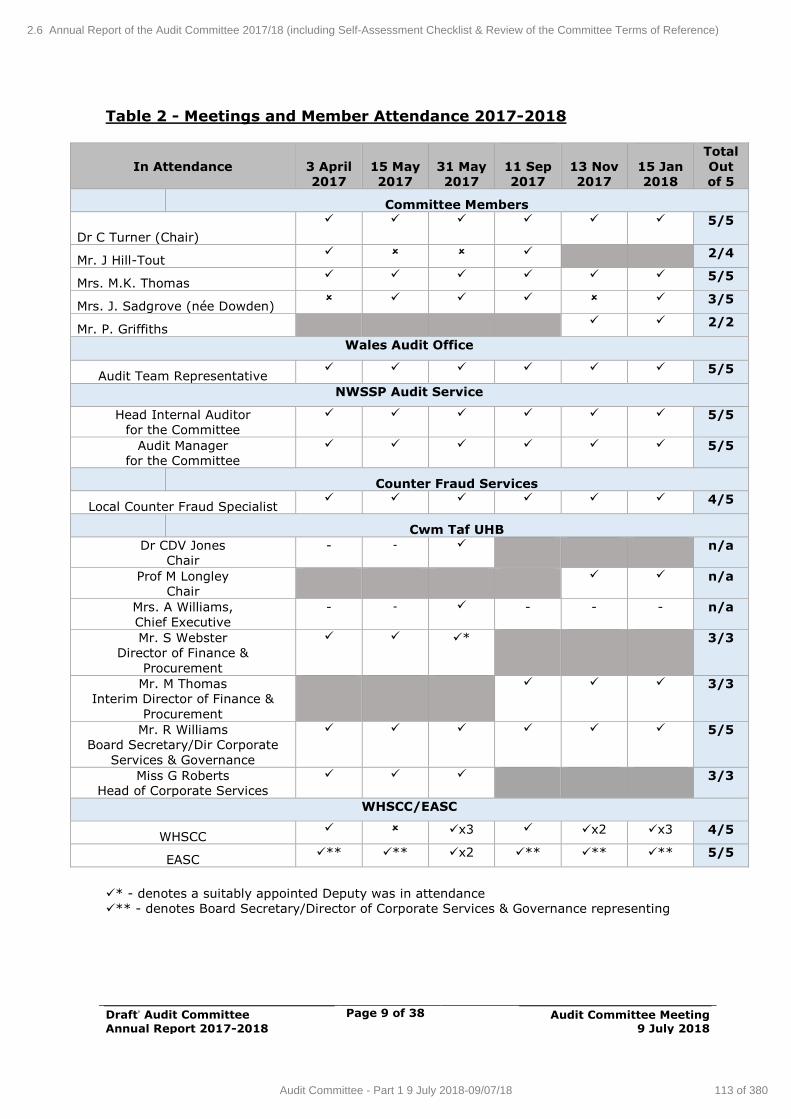
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 9 of 38
Audit Committee Meeting
9 July 2018
Table 2 - Meetings and Member Attendance 2017-2018
In Attendance
3 April
2017
15 May
2017
31 May
2017
11 Sep
2017
13 Nov
2017
15 Jan
2018
Total
Out
of 5
Committee Members
Dr C Turner (Chair)
5/5
Mr. J Hill-Tout 2/4
Mrs. M.K. Thomas 5/5
Mrs. J. Sadgrove (née Dowden) 3/5
Mr. P. Griffiths 2/2
Wales Audit Office
Audit Team Representative 5/5
NWSSP Audit Service
Head Internal Auditor
for the Committee
5/5
Audit Manager
for the Committee
5/5
Counter Fraud Services
Local Counter Fraud Specialist 4/5
Cwm Taf UHB
Dr CDV Jones
Chair
-
- n/a
Prof M Longley
Chair
n/a
Mrs. A Williams,
Chief Executive
-
- - -
-
n/a
Mr. S Webster
Director of Finance &
Procurement
* 3/3
Mr. M Thomas
Interim Director of Finance &
Procurement
3/3
Mr. R Williams
Board Secretary/Dir Corporate
Services & Governance
5/5
Miss G Roberts
Head of Corporate Services
3/3
WHSCC/EASC
WHSCC x3 x2 x3 4/5
EASC ** ** x2 ** ** ** 5/5
* - denotes a suitably appointed Deputy was in attendance
** - denotes Board Secretary/Director of Corporate Services & Governance representing
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
113 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 10 of 38
Audit Committee Meeting
9 July 2018
4. AUDIT COMMITTEE BUSINESS
The Audit Committee provides an essential element of the Health Board’s overall assurance framework. It has operated within its Terms of Reference in
accordance with the guidance contained within the NHS Wales Audit Committee Handbook.
The Audit Committee agenda broadly follows a standard format, comprising of
specific sections, which are outlined below:
4.1 MAIN AREAS OF AUDIT COMMITTEE ACTIVITY – PART 1 The agenda for each meeting followed a standard format, broken down into the
following 5 main parts:
1. Preliminary Matters
This included the apologies for absence, welcome and introductions, declarations of interest, receiving and approving the unconfirmed minutes of
the last meeting and receiving the action log.
2. Internal Control and Risk Management The following standard written reports were received by the Audit Committee
and considered accordingly: Counter Fraud updates
Local Counter Fraud Annual Report Organisational Risk Register
Procurement and payments report Audit Recommendations Tracker
Revised Scheme of Delegation
Losses and special payments report Audit Enquiries for those charged with Governance and Management
Draft Accountability Report Improving Purchase to Pay (P2P)
Post Payment Verification report Standards of Behaviour Policy
Audit Committee Annual Report 2016-2017 Board Assurance Framework
Completion of the 2016-2017 Committee Self-Assessment Questionnaire Procurements and Scheme of Delegation Report
Review the Audit Committee Terms of Reference Financial Control Procedures Review
3. Charitable Funds
Standard reports were received in respect of activity and balances held within
charitable funds. The Audit Committee plays a key role in overseeing the management of charitable funds to enable the Board to carry out its
responsibilities as Corporate Trustee to the Cwm Taf NHS Charitable Fund. In fulfilling this role, the Committee requested that management constantly review
the use of Funds and review those funds with little or no movement.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
114 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 11 of 38
Audit Committee Meeting
9 July 2018
During the year the Committee monitored progress with its managed investment fund to maximise the charitable income received, within agreed
ethical investment boundaries.
Charitable Fund balances were received at the meetings held on the 11 September 2017, 13 November 2017 and the 15 January 2018. Closure
reports for the Local Counter Fraud Service (LCFS) Pulmonary Hypertension Therapy (PHT) and the Home Parental Nutrition (HPN) projects were also
received at the meeting on the 17 November 2017.
4. Internal Audit NHS Wales Shared Services Partnership are the appointed internal auditors to
the Health Board and provide an update on progress against the internal audit
annual plan of business at each meeting together with finalised reports for each area that was subject to audit.
The Committee discussed concerns and sought assurance regarding some
internal audit reports being delayed beyond the timescales originally outlined within the 2016-2017 Internal Audit Plan.
Each report contained an assessment on the level of assurance provided.
Follow-up action was agreed for recommendations raised, which informed future audit plans.
5. External Audit
The Wales Audit Office (WAO) provide an Audit Position Statement at each meeting, summarising progress against its planned audit work.
4.2. MAIN AREAS OF AUDIT COMMITTEE ACTIVITY – PART 2 HOSTED BODIES
Welsh Health Specialised Services
Committee (WHSSC)
Emergency Ambulance Services
Committee (EASC)
As the host organisation, WHSSC and EASC (the latter established in April
2014) rely on Cwm Taf University Health Board (CTUHB) for its Audit Committee function, following a review and restructuring of its arrangements
during 2013.
To support the Audit Committee requirements for the both EASC and WHSCC the Health Board’s Audit Committee is separated into two parts, specifically Part
1 for Health Board business and Part 2 for the Hosted bodies. The relevant officers attend for the relevant components of the meeting.
Dr Chris Turner, Independent Member and Chair of the Health Board’s Audit Committee undertakes the role of the “Audit Lead” for WHSSC and reports all
matters relating to the audit function to the Joint Committee.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
115 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 12 of 38
Audit Committee Meeting
9 July 2018
The Director of Corporate Services and Governance / Board Secretary at Cwm Taf also attends both parts of the meetings.
The WHSSC and the EASC share the same external and internal audit teams
and Local Counter Fraud Services (LCFS) with Cwm Taf UHB. All these factors enable Cwm Taf UHB to take necessary assurances from the hosted bodies,
particularly in relation to the Accounts and the Annual Governance Statement and vice-versa for areas carried out by Cwm Taf on behalf of WHSSC/EASC as
part of its hosting responsibilities.
In March 2014, the Joint Committee’s approved the revised Governance and Accountability Framework for both WHSCC and EASC including the Standing
Orders. These were reviewed and updated during 2017/18.
The WAO undertook a national review of the Emergency Ambulance Services
Commissioning arrangements in 2017, which considered matters relating to governance. The WAO report on the “Review of Emergency Ambulance Services
Commissioning Arrangements”1 was published in July 2017 and all of the recommendations for EASC to implement to strengthen and develop its
governance and assurance framework have been completed.
4.3. WORK/ACTION LOG
In order to monitor progress and any necessary follow up action, in line with
recognised ‘house style’ templates a work log is maintained to capture all agreed actions from the Audit Committee and Joint Committees. This provides
an essential element of assurance both to the Committee and from the Committee to the Board.
5. INTERNAL AUDIT - OVERALL SUMMARY
In overall terms the Head of Internal Audit opinion, provided Reasonable
Assurance to the Board that arrangements to secure governance, risk
management and internal control are suitably designed and applied effectively in the following assurance domains:
Corporate Governance, Risk Management & Regulatory Compliance
Strategic Planning, Performance Management and Reporting Finance Governance and Management
Clinical Governance, Quality and Safety Information Governance and Information Technology (IT) security
Operational services and functional management Workforce management
Capital and Estates Management
1 WAO Report “Review of Emergency Ambulance Services Commissioning Arrangements”, July
6.22017
http://www.audit.wales/system/files/publications/review_emergency_ambulance_commissionin
g_arrangements_english.pdf
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
116 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
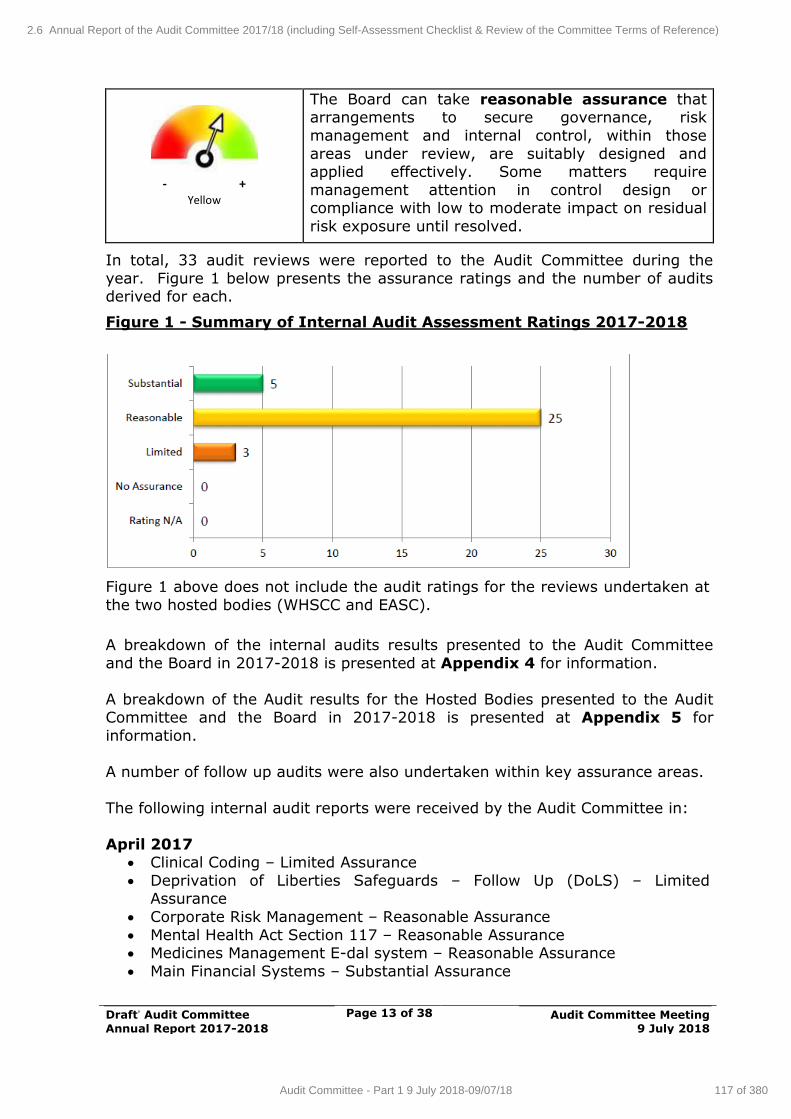
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 13 of 38
Audit Committee Meeting
9 July 2018
- +
Yellow
The Board can take reasonable assurance that arrangements to secure governance, risk
management and internal control, within those
areas under review, are suitably designed and applied effectively. Some matters require
management attention in control design or compliance with low to moderate impact on residual
risk exposure until resolved.
In total, 33 audit reviews were reported to the Audit Committee during the
year. Figure 1 below presents the assurance ratings and the number of audits derived for each.
Figure 1 - Summary of Internal Audit Assessment Ratings 2017-2018
Figure 1 above does not include the audit ratings for the reviews undertaken at
the two hosted bodies (WHSCC and EASC).
A breakdown of the internal audits results presented to the Audit Committee
and the Board in 2017-2018 is presented at Appendix 4 for information.
A breakdown of the Audit results for the Hosted Bodies presented to the Audit Committee and the Board in 2017-2018 is presented at Appendix 5 for
information.
A number of follow up audits were also undertaken within key assurance areas.
The following internal audit reports were received by the Audit Committee in:
April 2017 Clinical Coding – Limited Assurance
Deprivation of Liberties Safeguards – Follow Up (DoLS) – Limited Assurance
Corporate Risk Management – Reasonable Assurance
Mental Health Act Section 117 – Reasonable Assurance Medicines Management E-dal system – Reasonable Assurance
Main Financial Systems – Substantial Assurance
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
117 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 14 of 38
Audit Committee Meeting
9 July 2018
Occupational Health – Reasonable Assurance IT System Review – Maternity Information Technology System (MITS) –
Reasonable Assurance Recruitment Vacancy Management – Reasonable Assurance
May 2017
NHS Wales Shared Services Partnership – Audit & Assurance Services Progress Report
Public Sector Prompt Payments Audit – Substantial Assurance Draft Head of Internal Audit Opinion & Annual Report 2016-2017
September 2017
NHS Wales Shared Services Partnership – Audit & Assurance Services
Progress Report Recruitment Review – Reasonable Assurance
Annual Quality Statement – Substantial Assurance Environmental Sustainability Report – Reasonable Assurance
Health and Care Standards – Reasonable Assurance Paediatrics, Neonates & Obstetrics (Capital) Review – Reasonable
Assurance Patient’s monies and property – Reasonable Assurance
Safeguarding – Reasonable Assurance Deprivation of Liberties Safeguards 2nd Follow Up – Substantial Assurance
Directorate Review Pathology – Reasonable Assurance Directorate Review Medicines Management – Reasonable Assurance
Acute Medicine and A&E Directorate Follow Up – Reasonable Assurance
November 2017
NHS Wales Shared Services Partnership – Audit & Assurance Services Progress Report
Carbon Reduction Commitment Report – Reasonable Assurance Data Quality Monitoring Report – Reasonable Assurance
Clinical Coding – Follow up report – Reasonable Assurance Alerts/Safety Bulletins process – Reasonable Assurance
Nursing Staff Revalidation – Substantial Assurance Child and Adolescent Mental Health Services Data Quality review –
Reasonable Assurance
January 2017 NHS Wales Shared Services Partnership – Audit & Assurance Services
Progress Report Endoscopy Joint Accreditation Review – Limited Assurance
Clinical Audit – Reasonable Assurance
Welsh Risk Pool claims – Substantial Assurance
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
118 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 15 of 38
Audit Committee Meeting
9 July 2018
During 2017-2018, two audits were deferred: Primary Care Services – Clusters – following discussion with the Health
Board, it was greed to undertake an expanded approach to the planned review of the Anaesthetics, Critical Care and Theatres (ACT) directorate
and the Audit Committee agreed to defer the review until 2018-2019. Planned Preventative Maintenance – Following the Grenfell fire tragedy
there was an increased focus on fire safety work and Audit Committee agreed to defer the review until 2018-2019.
6. EXTERNAL AUDIT
6.1 Wales Audit Office (WAO)
The Wales Audit Office (WAO) provided a progress report at each meeting,
covering both probity and performance audits. The audit strategy, audit letters and statements of responsibilities were received and the ISA260 report was
approved as part of the Accounts approval process.
The following performance reports and management responses were also discussed during the year, with attendance from UHB Officers where considered
appropriate: Wales Audit Office (WAO) Progress Report (at each meeting)
Cwm Taf Audit enquiries letter 2017 Draft Audit Plan 2017
WAO Radiology Review Single Tender Actions
WAO Management Letter GP Out of Hours Review for Cwm Taf UHB
Review of Follow Up Outpatients – Assessment of Progress
Collaborative Arrangements for Managing Local Public Health Resources – Public Health Wales NHS Trust
Discharge Planning Report
6.2 Approval of the Annual Accounts
A special meeting of the Audit Committee was convened on 31 May 2017 to scrutinise the 2016-2017 Annual Accounts prior to approval by the Health
Board including the letter of representation to Auditors and the Annual Governance Statement. The 2016-2017 Annual Accounts were also scrutinised
and approved by the Board in June 2017. The meeting also scrutinised the Accounts and Statements for 2016-2017 from the Emergency Ambulance
Services Committee (EASC) and the Welsh Health Specialised Services Committee (WHSSC).
7. PRIVATE MEETING WITH AUDITORS
In line with recognised good practice, a private meeting was held on the 16 April 2017, between Audit Committee members, Internal Audit, External Audit
and the Local Counter Fraud Specialist. This provided an opportunity for free and frank discussion. No issues of concern arose from the meeting.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
119 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 16 of 38
Audit Committee Meeting
9 July 2018
8. LINKS WITH OTHER COMMITTEES
8.1 Other Sub Committees
The Audit Committee has close links with the Quality, Safety and Risk Committee and the three Committee Chairs meet with the Board Chair and Vice
Chair, along with Chairs of other Board Committees, to form the Integrated Governance Committee. The Integrated Governance Committee met on three
occasions during the period of this report, on the 5 April 2017, 2 August 2017 and the 6 December 2017. This ensured that the work of the three Committees
supported each other and avoided duplication of effort.
The minutes of all Audit Committee meetings were included in the public Health
Board papers and the Chair of the Audit Committee provided a report to the Board after each meeting.
9. LOCAL COUNTER FRAUD SERVICES
The work of the Local Counter Fraud Services is undertaken to help reduce and
maintain the incidence of fraud (and/or corruption) within Cwm Taf UHB to an absolute minimum.
Regular reports were received by the Committee to monitor progress against
the agreed Counter Fraud Plan.
As part of its work, the Counter Fraud Department has a regular annual
programme of raising fraud awareness within the Health Board for which a number of days are then allocated and included as part of an agreed Counter
Fraud Work-Plan which is signed off, by the Health Board’s Director of Finance & Procurement, on an annual basis.
As part of that planned area of work, regular fraud awareness sessions are
arranged and then held with various staff groups at which details on how and to who fraud can be reported are outlined.
In addition to this and in an attempt to promote an Anti-Fraud Culture within the Health Body, a quarterly newsletter is produced which is then available to
all staff on the Health Board’s Intranet and all successful prosecution cases are also publicised in order to obtain the maximum deterrent effect.
10. ASSURANCE TO THE BOARD
The Audit Committee provides an essential element of the overall governance
framework for the organisation and has operated within its Terms of Reference and in accordance with the guidance contained in the NHS Wales Audit
Committee Handbook.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
120 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 17 of 38
Audit Committee Meeting
9 July 2018
10.1 Internal Control & Risk Management - In addition to the audit reports dealt with by the Committee during the reporting period, a wide range of
internally generated ‘governance’ reports/papers were produced for consideration by the Audit Committee including, by way of example:
10.2 Annual Governance Statement - During 2016-2017, the Health Board
produced its Annual Governance Statement, which explains the processes and procedures in place to enable the Health Board to carry out its functions
effectively. The Statement was produced following a review of CTUHB’s governance arrangements undertaken by the Executive Board and the Board
Secretary/Director of Corporate Services & Governance. The Statement brings together all disclosures relating to governance, risk and control for the
organisation.
10.3 Tracking of Audit Recommendations - During the reporting period, the
Committee gave specific attention to the audit results relating to new areas of activity and to areas of general concern. Nevertheless, the Committee has
continued focus on the timely implementation of audit recommendations.
10.4 Audit Committee Effectiveness Survey - A confidential Committee Effectiveness Survey was undertaken in 2016-2017 to obtain feedback from
Committee members on potential areas for development.
The statements used in the survey were devised in accordance with the guidance outlined within the NHS Audit Committee Handbook.
11. CONCLUSION AND FORWARD LOOK
The Audit Committee in discharging its scrutiny and assurance role on behalf of the Board considers that on the basis of the risk based work completed by the
Committee during 2016-17, that there are effective measures in place and that there are no outstanding issues that the Audit Committee wishes
to bring to the attention of the Board.
The Directors have been held to account and have responded positively in dealing with any concerns raised by the Auditors and the Audit Committee.
The Health Board is required by Welsh Government to remain within the:
Revenue Resource Limit Capital Resource Limit
And both these targets were met.
Overall, the financial performance of the UHB represents a very significant achievement given the difficult financial environment in which the Health Board
operates. Substantial savings have been delivered and expenditure has been appropriately controlled within the Board’s objective of ensuring that the quality
of care is a central part of the financial plan.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
121 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 18 of 38
Audit Committee Meeting
9 July 2018
The Members welcome the continued progress made in the standard and quality of the reports that Officers present to the Committee and the
improvements made in the risk assessment ratings in the Internal Audit reports received.
This Annual Report will be supplemented by the annual self-assessment
questionnaire, which reviews the individual and collective function of the Committee against the NHS Audit Committee Handbook best practice guidance
and helps to inform the work of the Committee going forward.
The Committee is committed to continuing to develop its function and effectiveness and intends seeking further assurance in 2017-2018 in respect of:
Strengthening the reporting and monitoring of top organisational risks,
Fully enacting and utilising the Board Assurance Framework, Maintaining and strengthening the effectiveness of the Audit Tracker,
including seeking and implementing best practice, Discharging effectively the Board approved Committee Terms of
Reference, Reviewing the effectiveness of the application of the revised Standing
Orders and Scheme of Delegation, Monitoring the delivery of the Investment Strategy for Charitable Funds;
Improving the timeliness and completion of the Declarations of Interest forms for the organisation,
Ensuring all parties discharge their responsibilities appropriately as outlined within the Audit Charter,
Continue to strengthen processes and resources in place to prevent and respond to fraud activity.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
122 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 19 of 38
Audit Committee Meeting
9 July 2018
Appendix 2
AUDIT COMMITTEE TERMS OF REFERENCE
(Endorsed by the Audit Committee 11 September 2017 for approval at the Health Board meeting on 1 November 2017)
INTRODUCTION
The UHB’s standing orders provide that “The Board may and, where directed by the Welsh Government must, appoint Committees of the UHB either to
undertake specific functions on the Board’s behalf or to provide advice and
assurance to the Board in the exercise of its functions. The Board’s commitment to openness and transparency in the conduct of all its business extends equally
to the work carried out on its behalf by committees”.
In accordance with Standing Orders (and the UHB scheme of delegation), the Board shall nominate annually a committee to be known as the Audit
Committee. The detailed terms of reference and operating arrangements set by the Board in respect of this committee are set out below.
CONSTITUTION AND PURPOSE
The Board hereby resolves to establish a Committee of the Board to be known as the Audit Committee (The Committee).
The Committee is an independent member committee of the Board and has no
executive powers, other than those specifically delegated in these Terms of Reference. The Committee will function in accordance with the NHS Audit
Committee Handbook.
The Committee will also consider issues in respect of the roles and
responsibilities of Committees hosted by the UHB on behalf of NHS Wales as appropriate. These are the Welsh Health Specialised Services Committee and
the Emergency Ambulance Services Committee. The meeting will be split into two parts with Cwm Taf Health Board business and hosted Committee business
discussed and recorded separately.
The purpose of the Committee is to advise and assure the Board on whether effective arrangements are in place – through the design and operation of the
Health Board system of assurance – to support it in its decision taking and in discharging the accountabilities for securing the achievement of the Health
Board objectives in accordance with the standards of good governance determined for the NHS in Wales.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
123 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 20 of 38
Audit Committee Meeting
9 July 2018
SCOPE AND DUTIES
Internal Control and Risk Management
The Committee shall review the establishment and maintenance of an effective system of internal control and risk management. In particular, the Committee
will review the adequacy of:
all risk and control related disclosure statements (in particular the Annual Governance Statement), together with any accompanying Head of Internal
Audit statement, external audit opinion or other appropriate independent assurance, prior to endorsement by the Board;
the structures, processes and responsibilities for identifying and managing
key risks facing the organisation;
the Board Assurance Framework;
the policies for ensuring that there is compliance with relevant regulatory,
legal and code of conduct and accountability requirements.
the operational effectiveness of policies and procedures;
the policies and procedures for all work related to fraud and corruption as set out in the National Assembly for Wales Directions and as required by
NHS Protect and the Counter Fraud and Security Management Service.
proposed changes to the Standing Orders, Standing Financial Instructions and Financial Control Procedures;
the circumstances associated with each occasion where Standing Orders or
Standing Financial Instructions are waived.
The Committee will also:
Receive and determine action in response to the declaration of Board member and other officers interests in accordance with advice received from
the Director of Corporate Services & Governance / Board Secretary;
Approve individual cases for the write off of losses or making of special payments above the limits of delegation to the Chief Executive and officers;
Review all losses and special payments;
Retrospectively assure any purchase / expenditure above the delegated
financial limit of the Chief Executive.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
124 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 21 of 38
Audit Committee Meeting
9 July 2018
Internal Audit
The Committee shall:
consider the proposals for accessing internal audit services via a shared
services arrangement (where appropriate), the audit fee and any questions of resignation and dismissal;
review the internal audit programme, consider the major findings of internal
audit investigations, ensure co-ordination between the Internal and External Auditors and ensure all management responses to recommendations are
appropriate and timely;
ensure that the Internal Audit function is adequately resourced and has
appropriate standing within the organization;
assure itself that IA complies with the requirements of the public sector internal audit standards.
Monitor the timely implementation by management of agreed audit
recommendations.
Clinical Audit
Ensure where appropriate and in line with the Audit Committee Handbook
that the UHB has a Clinical Audit Programme in place and the outcomes of Clinical Audit provide internal assurance to the Board.
External Audit
The Committee shall consider the work carried out by key sources of external
assurance, in particular but not limited to the Health Board external auditors, is appropriately planned and co-ordinated and that the results of external
assurance activity complements and informs (but does not replace) internal assurance activity.
The Committee will:
from time to time, consider and make any necessary representations to the
Auditor General for Wales on his appointment of an engagement partner;
discuss with the External Auditor, in line with the agreed audit plan, before the audit commences, the nature and scope of the audit, and ensure
coordination, as appropriate, with other External Auditors in the local health
economy and with Internal Audit;
review External Audit reports, including value for money reports and annual audit letters, together with the management response;
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
125 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 22 of 38
Audit Committee Meeting
9 July 2018
Monitor the timely implementation by management of agreed audit
recommendations;
Receive a report from the Auditor General for Wales / Wales Audit Office on the results of his audit of the annual accounts before recommending
adoption of those accounts to the Accountable Officer and the Health Board.
Financial Reporting
The Committee shall review the annual financial statements before submission
to the Board, focusing particularly on: changes in, and compliance with, accounting policies and practices;
major judgemental areas;
significant adjustments resulting from the audit;
compliance with legal requirements;
review any material mis-statements identified during the Audit.
Charitable Funds
The Committee will:
Ensure that the UHB policies and procedures for charitable funds investments are followed and make decisions involving the sound investment
of charitable funds in a way that both preserves their capital value and
produces a proper return consistent with prudent investment and ensuring compliance with:
Trustee Act 2000 The Charities Act 1993
The Charities Act 2006 Terms of the fund’s governing documents
Annual Reporting to the Trustees
Receive at least twice per year reports for ratification from the Director of Finance on investment decisions and action taken through delegated powers
upon the advice of the UHB’s investment adviser if appropriate.
Oversee and monitor the functions performed by the Director of Finance and procurement as defined in Standing Financial Instructions.
Monitor the progress of any associated Charitable Appeal Funds.
Monitor and review the UHB scheme of delegation for Charitable Funds expenditure and set and reflect in Financial Control Procedures the approved
delegated limits for expenditure from Charitable Funds.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
126 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 23 of 38
Audit Committee Meeting
9 July 2018
AUTHORITY
The Committee is authorised by the Board to:
- investigate or have investigated any activity within its Terms of Reference and in performing these duties shall have the right, at all reasonable times,
to inspect any books, records or documents of the UHB. It can seek any information it requires from any employee and all employees are directed to
co-operate with any request made by the Committee;
- obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it
considers this necessary, subject to the Board’s budgetary and other requirements;
- by giving reasonable notice, require the attendance of any of the officers or
employees and auditors of the Board at any meeting of the Committee.
MEMBERSHIP
The Committee shall be appointed by the Board from amongst the Non-Officer
Members of the Health Board and shall consist of not less than 4 members.
The Committee may also co-opt additional independent external members from
outside the organisation to provide specialist skills, knowledge and experience.
The Health Board shall appoint the Chair of the Committee.
The Chair of the Health Board shall not be a member of the Committee.
The Director of Corporate Services & Governance / Board Secretary will determine the secretarial and support arrangements for the Committee.
The Director of Finance and appropriate Internal and External Audit
representatives shall normally attend meetings. However, at least once a year, the Committee will meet privately with the External and Internal Auditors
without any Executive Director or officer present. The opportunity to meet with
Auditors privately will be available at each meeting.
The Chief Executive and Chair shall be invited to attend at least annually to discuss the process for assurance that supports the Annual Governance
Statement and at the meeting to discuss the Accounts. The Director of Finance for WHSSC and Committee Secretary will normally attend the meetings of the
Audit Committee. The Director of Specialised and Tertiary Services and the Chair of the Welsh Health Specialised Services Committee shall be invited to
attend at least annually to discuss the process for assurance that supports the Annual Governance Statement and at the meeting to discuss the Accounts.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
127 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 24 of 38
Audit Committee Meeting
9 July 2018
The Emergency Ambulance Services Commissioner and the Chair of the Emergency Ambulance Services Committee shall be invited to attend at least
annually to discuss the process for assurance that supports the Annual Governance Statement and at the meeting to discuss the Accounts.
Other Directors may be invited to attend when the Committee is discussing
areas of risk or operation that are the responsibility of that Director.
The Health Board Local Counter Fraud Specialist will attend meetings of the Committee.
The Head of Internal Audit and the External Auditor shall have unrestricted
direct access to the Chair of the Committee.
Member Appointments
The membership of the Committee shall be determined by the Board, based on
the recommendation of the UHB Chair – taking account of the balance of skills and expertise necessary to deliver the Committee’s remit and subject to any
specific requirements or directions made by the Welsh Government.
The Independent Member who is the nominated Audit Lead for WHSSC and EASC must be a member of the Audit Committee.
The Board shall ensure succession planning arrangements are in place.
Support to Committee Members
The Director of Corporate Services & Governance / Board Secretary, on behalf of the Committee Chair, shall:
Arrange the provision of advice and support to committee members on any
aspect related to the conduct of their role; and
Co-ordinate the provision of a programme of organisational development for committee members.
COMMITTEE MEETINGS
Quorum A quorum shall be 2 Independent Members one of whom must be the Chair or
in the absence of the Chair, an Independent Member will be nominated to Chair the Committee.
Frequency of Meetings
Meetings shall be held not less than four times a year. The External Auditor or Head of Internal Audit may request a meeting if they consider that one is
necessary.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
128 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 25 of 38
Audit Committee Meeting
9 July 2018
The Committee will arrange meetings to fit in with key statutory requirements during the year consistent with the UHB’s annual plan of Board Business.
Withdrawal of Individuals in Attendance
The Committee may ask any or all of those who normally attend but who are not members to withdraw to facilitate open and frank discussion of particular
matters.
Circulation of Papers The Director of Corporate Services & Governance / Board Secretary will ensure
that all papers are distributed at least one calendar week in advance of the meeting.
REPORTING AND ASSURANCE ARRANGEMENTS
The Committee Chair shall:
report formally, regularly and on a timely basis to the Board on the
Committee’s activities. This includes verbal updates on activity, the submission of committee minutes and written reports.
bring to the Board’s specific attention any significant matters under
consideration by the Committee;
ensure appropriate escalation arrangements are in place to alert the UHB Chair, Chief Executive or Chairs of other relevant committees of any
urgent/critical matters that may affect the operation and/or reputation of the UHB.
The Committee shall provide a written, annual report to the Board on its work
in support of the Annual Governance Statement specifically commenting on the adequacy of the assurance arrangement, the extent to which risk management
is comprehensively embedded throughout the organisation, the integration of
governance arrangements and the appropriateness of self-assessment activity against relevant standards. The report will also record the results of the
Committees self-assessment and evaluation.
The Board may also require the Committee Chair to report upon the activities at public meetings or to community partners and other stakeholders, where this is
considered appropriate e.g. where the Committee’s assurance role relates to a joint or shared responsibility.
The Director of Corporate Services & Governance / Board Secretary, on behalf
of the Board, shall oversee a process of regular and rigorous self-assessment and evaluation of the Committee’s performance and operation.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
129 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 26 of 38
Audit Committee Meeting
9 July 2018
RELATIONSHIP WITH THE BOARD AND ITS COMMITTEES / GROUPS
The Chair of the Audit Committee and the Director of Finance as the Executive
Lead will meet with their counterparts on the Clinical Governance Committee, Corporate Risk Committee Finance & Performance Committee and the Mental
Health Act Monitoring Committee as part of the Integrated Governance Committee on a quarterly basis to plan the agenda and agree what issues are
being considered by each Committee and the timescales involved.
The Committee, through the Committee Chair and members, shall maximise cohesion and integration across all aspects of governance and assurance
through the:
joint planning and co-ordination of Board and Committee business; and
sharing of information, as appropriate.
The Committee shall embed the UHB’s corporate standards, priorities and
requirements, e.g. equality and human rights through the conduct of its business.
APPLICABILITY OF STANDING ORDERS TO COMMITTEE BUSINESS
The requirements for the conduct of business as set out in the UHB’s Standing Orders are equally applicable to the operation of the Committee, except in the
following areas:
Quorum
REVIEW
These Terms of Reference shall be adopted by the Audit Committee at its first
meeting and subject to review at least on an annual basis thereafter.
For review in July 2019.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
130 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
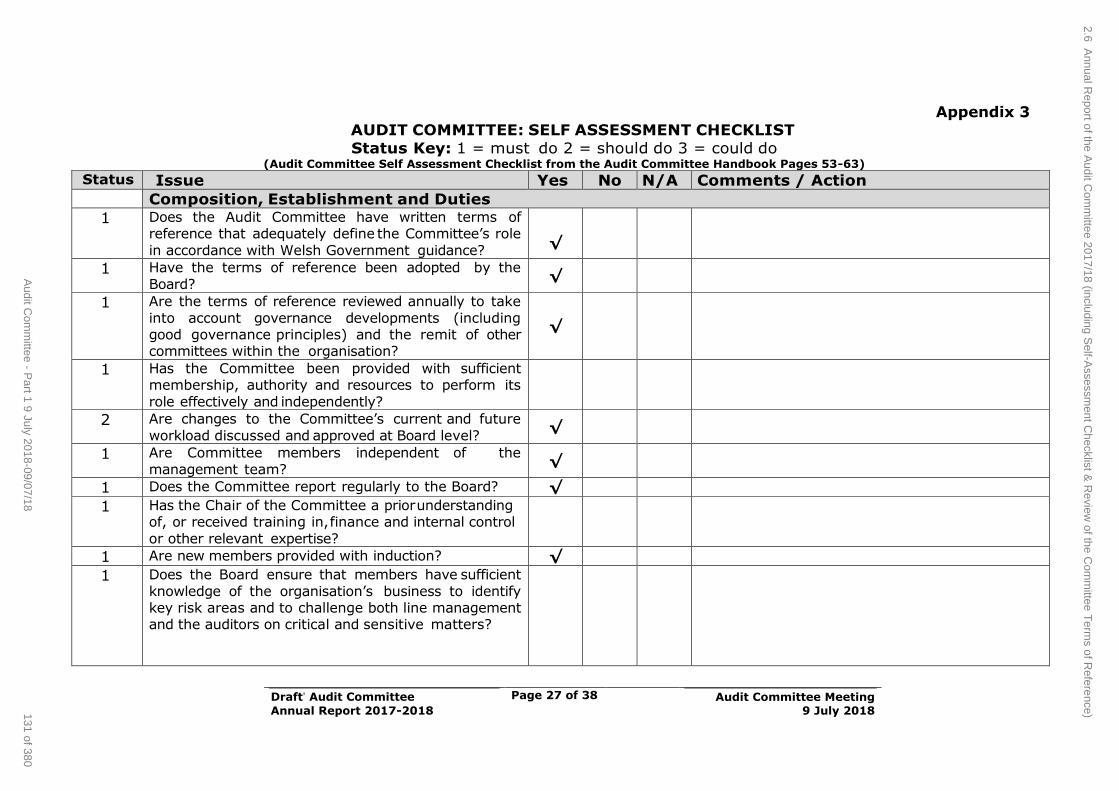
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 27 of 38
Audit Committee Meeting
9 July 2018
Appendix 3 AUDIT COMMITTEE: SELF ASSESSMENT CHECKLIST
Status Key: 1 = must do 2 = should do 3 = could do (Audit Committee Self Assessment Checklist from the Audit Committee Handbook Pages 53-63)
Status Issue Yes No N/A Comments / Action
Composition, Establishment and Duties
1 Does the Audit Committee have written terms of reference that adequately define the Committee’s role
in accordance with Welsh Government guidance?
√
1 Have the terms of reference been adopted by the
Board? √
1 Are the terms of reference reviewed annually to take
into account governance developments (including good governance principles) and the remit of other committees within the organisation?
√
1 Has the Committee been provided with sufficient membership, authority and resources to perform its
role effectively and independently?
2 Are changes to the Committee’s current and future
workload discussed and approved at Board level? √
1 Are Committee members independent of the
management team? √
1 Does the Committee report regularly to the Board? √
1 Has the Chair of the Committee a prior understanding of, or received training in, finance and internal control
or other relevant expertise?
1 Are new members provided with induction? √
1 Does the Board ensure that members have sufficient
knowledge of the organisation’s business to identify key risk areas and to challenge both line management and the auditors on critical and sensitive matters?
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)131 of 380
Audit C
omm
ittee - Part 1 9 July 2018-09/07/18
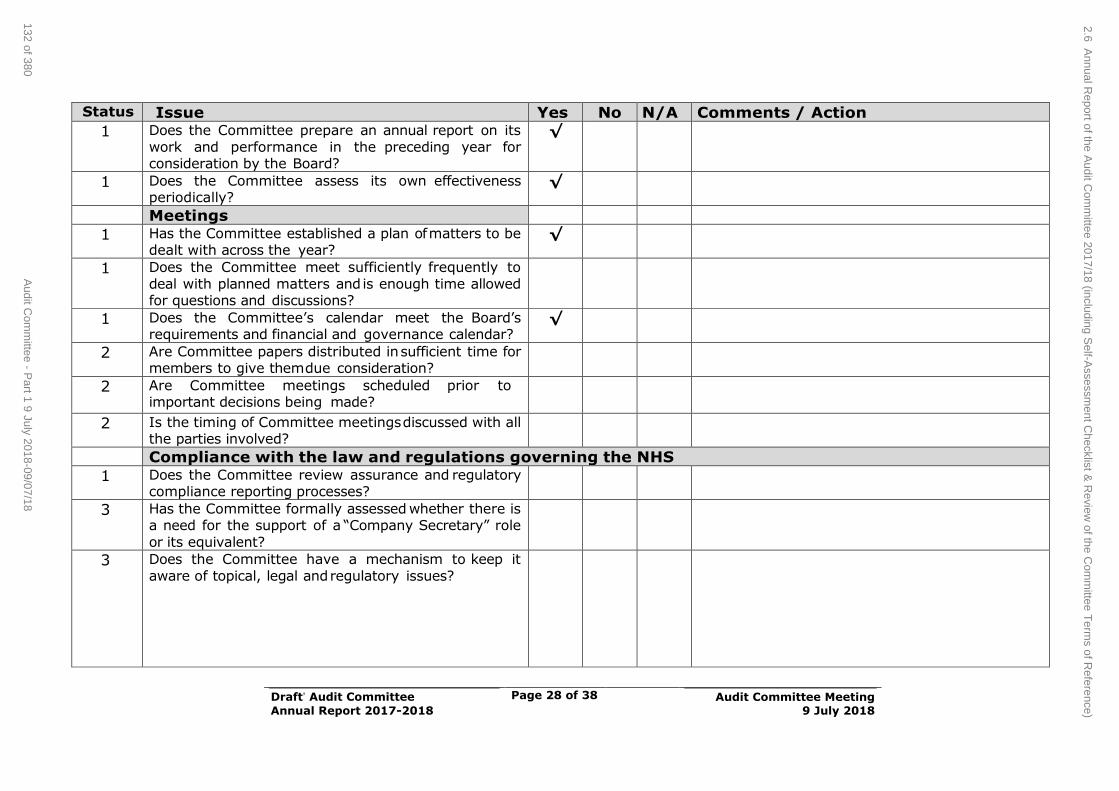
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 28 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action
1 Does the Committee prepare an annual report on its
work and performance in the preceding year for consideration by the Board?
√
1 Does the Committee assess its own effectiveness periodically?
√
Meetings
1 Has the Committee established a plan of matters to be dealt with across the year?
√
1 Does the Committee meet sufficiently frequently to
deal with planned matters and is enough time allowed for questions and discussions?
1 Does the Committee’s calendar meet the Board’s requirements and financial and governance calendar?
√
2 Are Committee papers distributed in sufficient time for members to give them due consideration?
2 Are Committee meetings scheduled prior to important decisions being made?
2 Is the timing of Committee meetings discussed with all the parties involved?
Compliance with the law and regulations governing the NHS
1 Does the Committee review assurance and regulatory compliance reporting processes?
3 Has the Committee formally assessed whether there is a need for the support of a “Company Secretary” role
or its equivalent?
3 Does the Committee have a mechanism to keep it
aware of topical, legal and regulatory issues?
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)
132 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
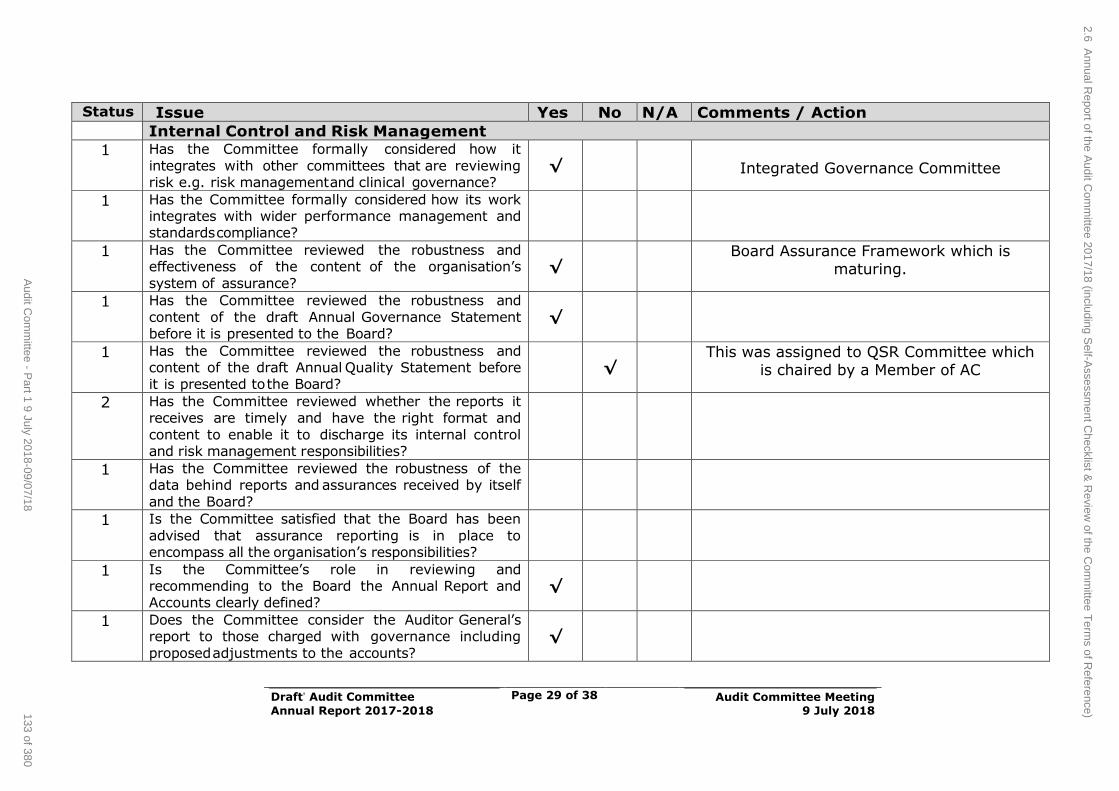
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 29 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action
Internal Control and Risk Management
1 Has the Committee formally considered how it
integrates with other committees that are reviewing risk e.g. risk management and clinical governance?
√
Integrated Governance Committee
1 Has the Committee formally considered how its work integrates with wider performance management and standards compliance?
1 Has the Committee reviewed the robustness and effectiveness of the content of the organisation’s
system of assurance? √
Board Assurance Framework which is maturing.
1 Has the Committee reviewed the robustness and
content of the draft Annual Governance Statement before it is presented to the Board?
√
1 Has the Committee reviewed the robustness and content of the draft Annual Quality Statement before it is presented to the Board?
√
This was assigned to QSR Committee which is chaired by a Member of AC
2 Has the Committee reviewed whether the reports it receives are timely and have the right format and
content to enable it to discharge its internal control and risk management responsibilities?
1 Has the Committee reviewed the robustness of the data behind reports and assurances received by itself
and the Board?
1 Is the Committee satisfied that the Board has been
advised that assurance reporting is in place to encompass all the organisation’s responsibilities?
1 Is the Committee’s role in reviewing and recommending to the Board the Annual Report and Accounts clearly defined?
√
1 Does the Committee consider the Auditor General’s report to those charged with governance including
proposed adjustments to the accounts? √
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)133 of 380
Audit C
omm
ittee - Part 1 9 July 2018-09/07/18
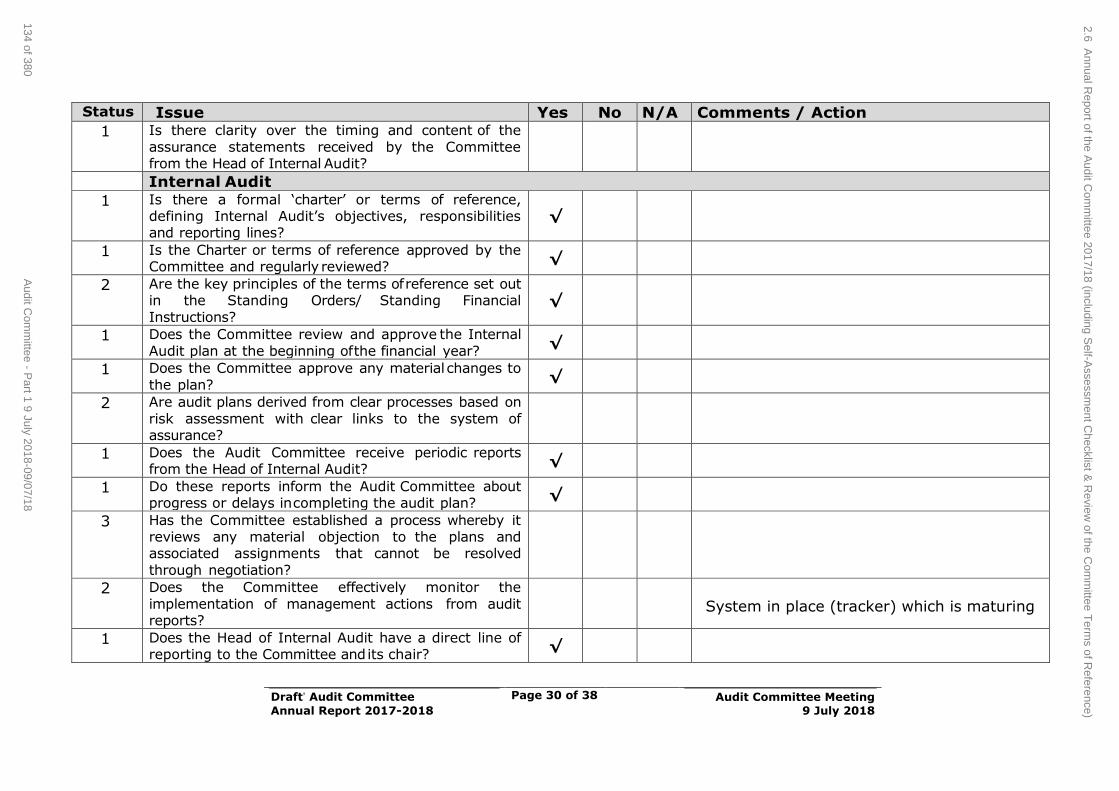
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 30 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action
1 Is there clarity over the timing and content of the
assurance statements received by the Committee from the Head of Internal Audit?
Internal Audit
1 Is there a formal ‘charter’ or terms of reference, defining Internal Audit’s objectives, responsibilities and reporting lines?
√
1 Is the Charter or terms of reference approved by the Committee and regularly reviewed?
√
2 Are the key principles of the terms of reference set out in the Standing Orders/ Standing Financial
Instructions? √
1 Does the Committee review and approve the Internal
Audit plan at the beginning of the financial year? √
1 Does the Committee approve any material changes to
the plan? √
2 Are audit plans derived from clear processes based on
risk assessment with clear links to the system of assurance?
1 Does the Audit Committee receive periodic reports from the Head of Internal Audit?
√
1 Do these reports inform the Audit Committee about progress or delays in completing the audit plan?
√
3 Has the Committee established a process whereby it reviews any material objection to the plans and associated assignments that cannot be resolved
through negotiation?
2 Does the Committee effectively monitor the
implementation of management actions from audit reports?
System in place (tracker) which is maturing
1 Does the Head of Internal Audit have a direct line of reporting to the Committee and its chair?
√
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)
134 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
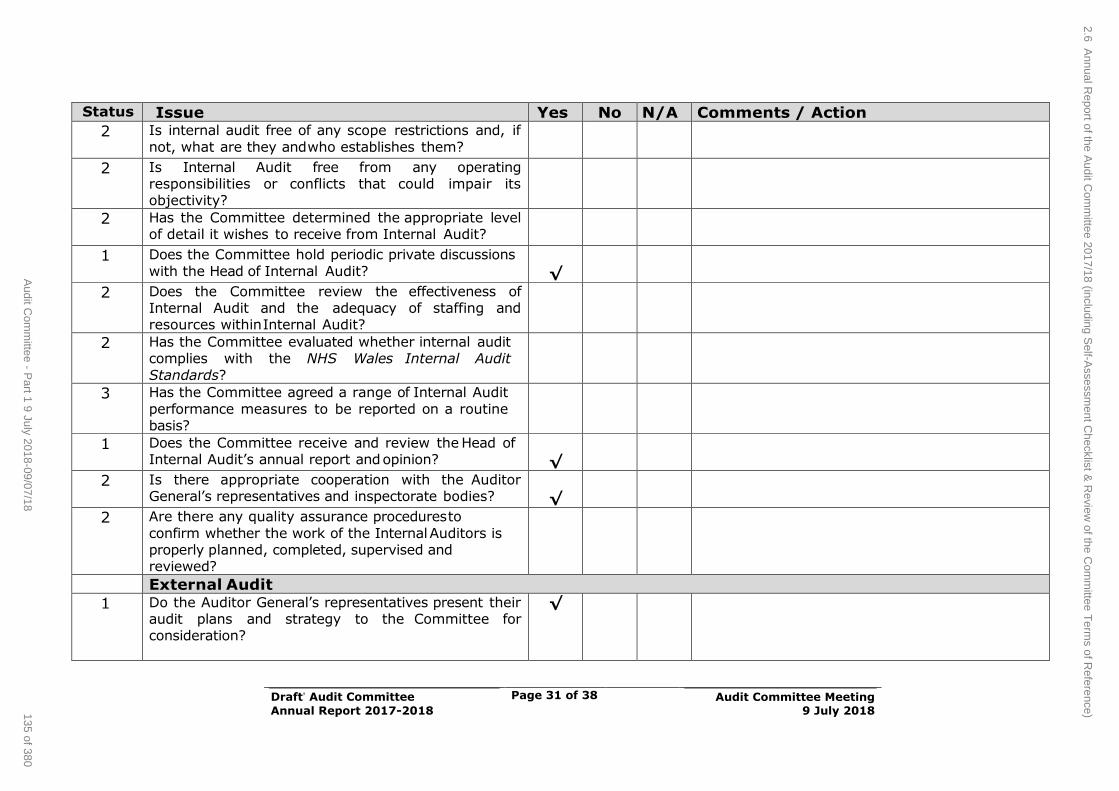
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 31 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action
2 Is internal audit free of any scope restrictions and, if
not, what are they and who establishes them?
2 Is Internal Audit free from any operating responsibilities or conflicts that could impair its objectivity?
2 Has the Committee determined the appropriate level of detail it wishes to receive from Internal Audit?
1 Does the Committee hold periodic private discussions
with the Head of Internal Audit?
√
2 Does the Committee review the effectiveness of Internal Audit and the adequacy of staffing and resources within Internal Audit?
2 Has the Committee evaluated whether internal audit complies with the NHS Wales Internal Audit
Standards?
3 Has the Committee agreed a range of Internal Audit
performance measures to be reported on a routine basis?
1 Does the Committee receive and review the Head of Internal Audit’s annual report and opinion?
√
2 Is there appropriate cooperation with the Auditor General’s representatives and inspectorate bodies?
√
2 Are there any quality assurance procedures to
confirm whether the work of the Internal Auditors is properly planned, completed, supervised and reviewed?
External Audit
1 Do the Auditor General’s representatives present their audit plans and strategy to the Committee for consideration?
√
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)135 of 380
Audit C
omm
ittee - Part 1 9 July 2018-09/07/18
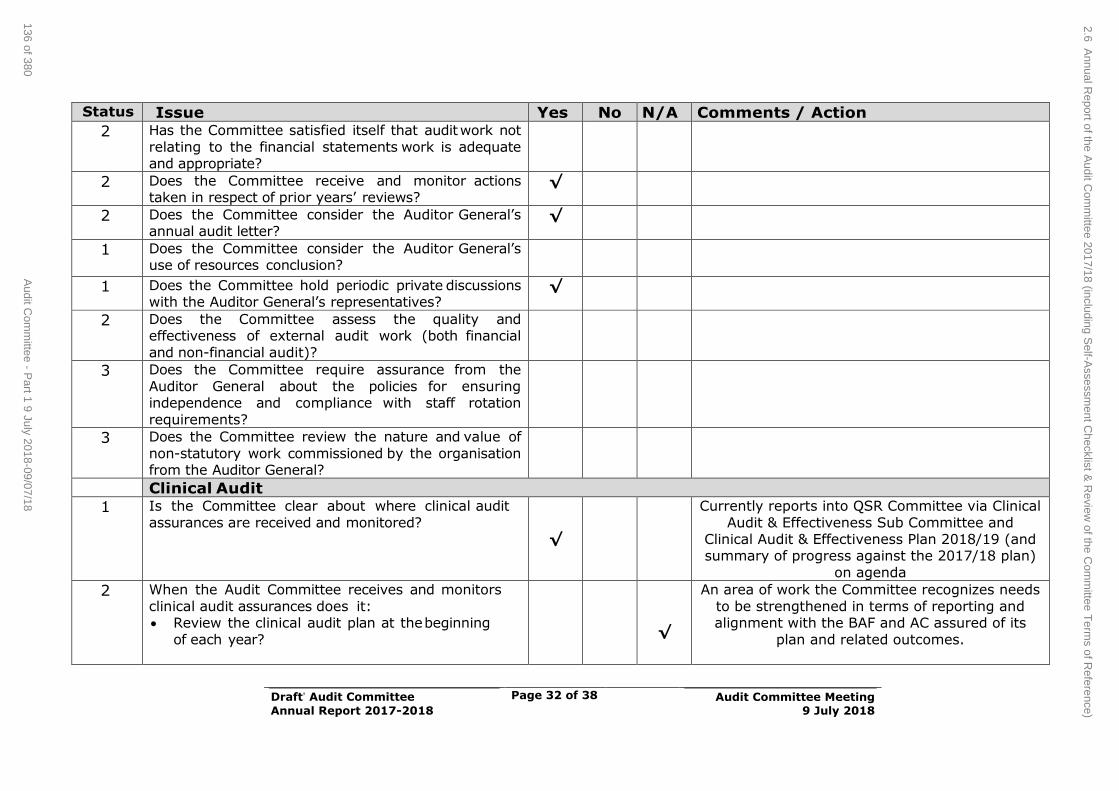
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 32 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action
2 Has the Committee satisfied itself that audit work not
relating to the financial statements work is adequate and appropriate?
2 Does the Committee receive and monitor actions taken in respect of prior years’ reviews?
√
2 Does the Committee consider the Auditor General’s annual audit letter?
√
1 Does the Committee consider the Auditor General’s use of resources conclusion?
1 Does the Committee hold periodic private discussions with the Auditor General’s representatives?
√
2 Does the Committee assess the quality and effectiveness of external audit work (both financial
and non-financial audit)?
3 Does the Committee require assurance from the
Auditor General about the policies for ensuring independence and compliance with staff rotation
requirements?
3 Does the Committee review the nature and value of
non-statutory work commissioned by the organisation from the Auditor General?
Clinical Audit
1 Is the Committee clear about where clinical audit
assurances are received and monitored?
√
Currently reports into QSR Committee via Clinical
Audit & Effectiveness Sub Committee and Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against the 2017/18 plan)
on agenda
2 When the Audit Committee receives and monitors
clinical audit assurances does it: Review the clinical audit plan at the beginning
of each year?
√
An area of work the Committee recognizes needs
to be strengthened in terms of reporting and alignment with the BAF and AC assured of its
plan and related outcomes.
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)
136 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
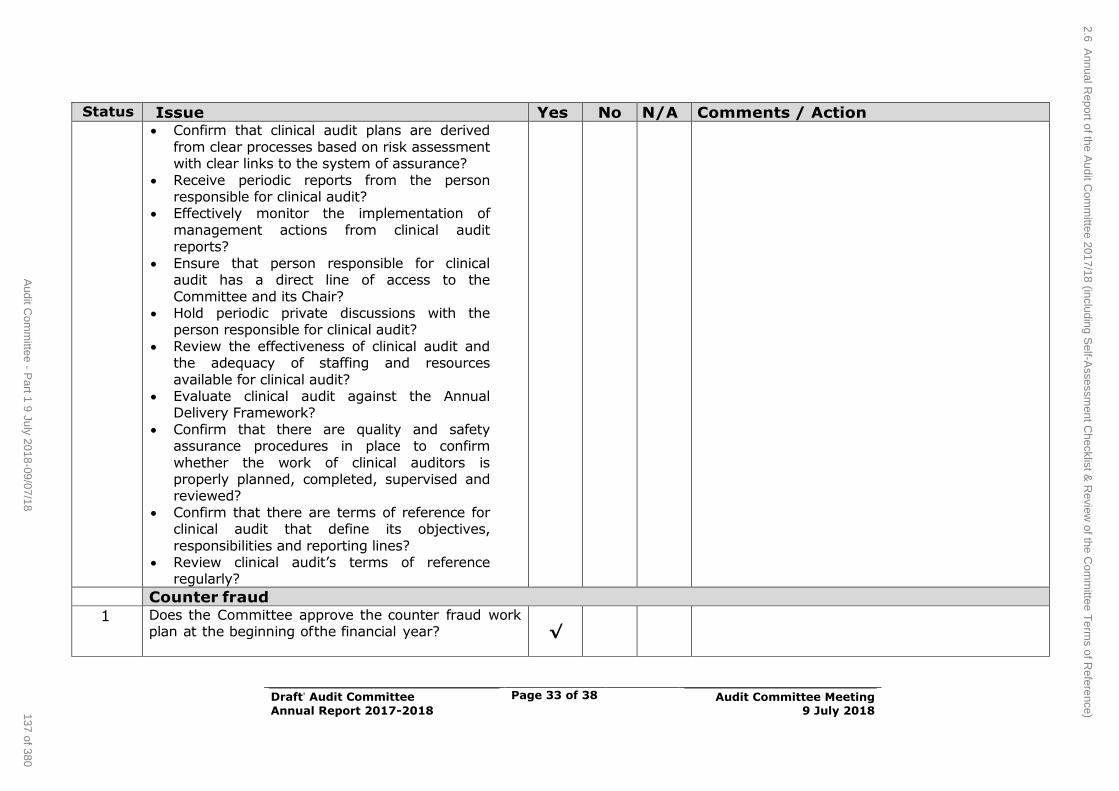
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 33 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action Confirm that clinical audit plans are derived
from clear processes based on risk assessment with clear links to the system of assurance?
Receive periodic reports from the person responsible for clinical audit?
Effectively monitor the implementation of
management actions from clinical audit reports?
Ensure that person responsible for clinical audit has a direct line of access to the
Committee and its Chair? Hold periodic private discussions with the
person responsible for clinical audit?
Review the effectiveness of clinical audit and the adequacy of staffing and resources
available for clinical audit? Evaluate clinical audit against the Annual
Delivery Framework?
Confirm that there are quality and safety assurance procedures in place to confirm
whether the work of clinical auditors is properly planned, completed, supervised and reviewed?
Confirm that there are terms of reference for clinical audit that define its objectives,
responsibilities and reporting lines? Review clinical audit’s terms of reference
regularly?
Counter fraud
1 Does the Committee approve the counter fraud work plan at the beginning of the financial year?
√
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)137 of 380
Audit C
omm
ittee - Part 1 9 July 2018-09/07/18
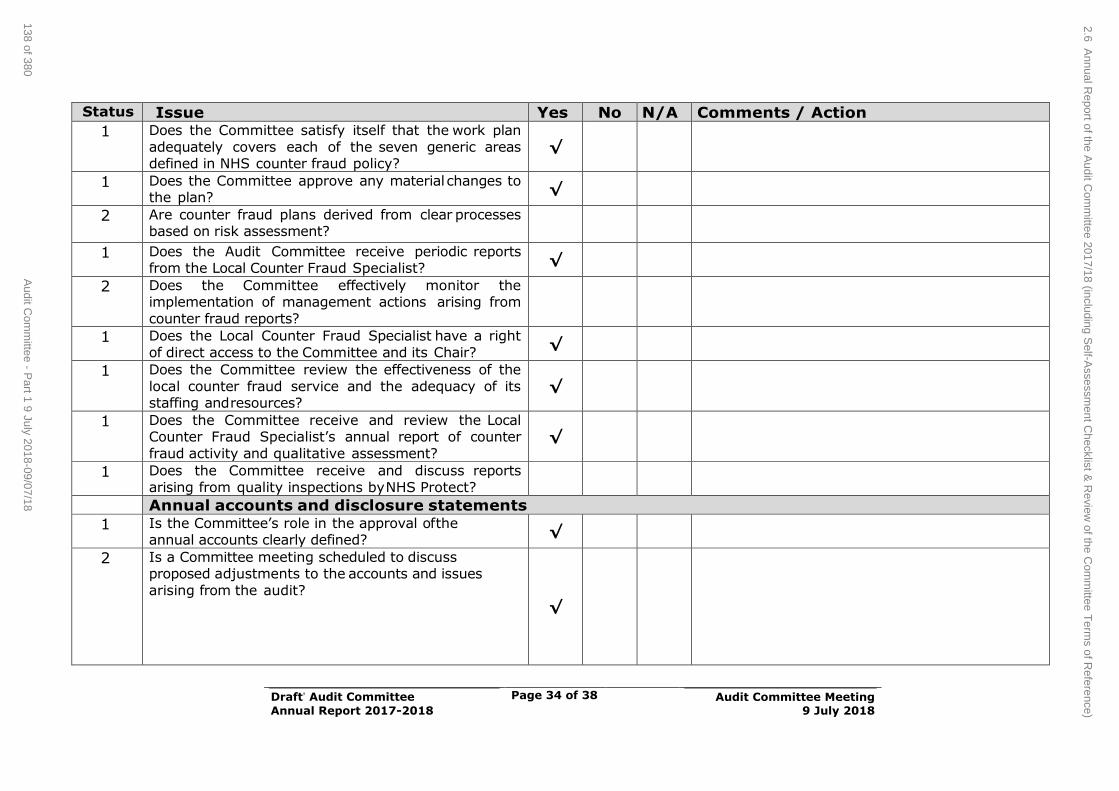
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 34 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action
1 Does the Committee satisfy itself that the work plan
adequately covers each of the seven generic areas defined in NHS counter fraud policy?
√
1 Does the Committee approve any material changes to the plan?
√
2 Are counter fraud plans derived from clear processes based on risk assessment?
1 Does the Audit Committee receive periodic reports from the Local Counter Fraud Specialist?
√
2 Does the Committee effectively monitor the implementation of management actions arising from
counter fraud reports?
1 Does the Local Counter Fraud Specialist have a right
of direct access to the Committee and its Chair? √
1 Does the Committee review the effectiveness of the
local counter fraud service and the adequacy of its staffing and resources?
√
1 Does the Committee receive and review the Local Counter Fraud Specialist’s annual report of counter
fraud activity and qualitative assessment? √
1 Does the Committee receive and discuss reports
arising from quality inspections by NHS Protect?
Annual accounts and disclosure statements
1 Is the Committee’s role in the approval of the annual accounts clearly defined?
√
2 Is a Committee meeting scheduled to discuss proposed adjustments to the accounts and issues
arising from the audit?
√
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)
138 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
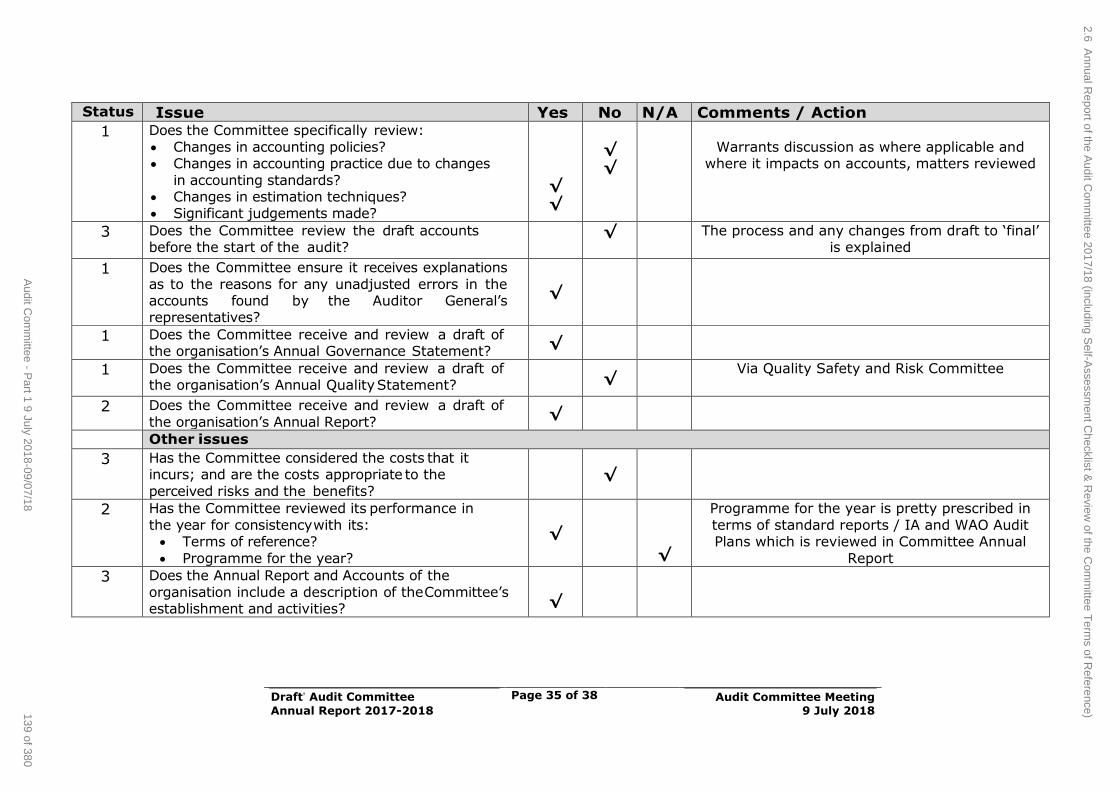
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 35 of 38
Audit Committee Meeting
9 July 2018
Status Issue Yes No N/A Comments / Action
1 Does the Committee specifically review:
Changes in accounting policies? Changes in accounting practice due to changes
in accounting standards? Changes in estimation techniques? Significant judgements made?
√
√
√
√
Warrants discussion as where applicable and where it impacts on accounts, matters reviewed
3 Does the Committee review the draft accounts before the start of the audit?
√ The process and any changes from draft to ‘final’ is explained
1 Does the Committee ensure it receives explanations
as to the reasons for any unadjusted errors in the accounts found by the Auditor General’s representatives?
√
1 Does the Committee receive and review a draft of the organisation’s Annual Governance Statement?
√
1 Does the Committee receive and review a draft of the organisation’s Annual Quality Statement?
√
Via Quality Safety and Risk Committee
2 Does the Committee receive and review a draft of
the organisation’s Annual Report? √
Other issues
3 Has the Committee considered the costs that it incurs; and are the costs appropriate to the
perceived risks and the benefits? √
2 Has the Committee reviewed its performance in
the year for consistency with its: Terms of reference?
Programme for the year?
√
√
Programme for the year is pretty prescribed in
terms of standard reports / IA and WAO Audit Plans which is reviewed in Committee Annual
Report
3 Does the Annual Report and Accounts of the
organisation include a description of the Committee’s establishment and activities?
√
2.6 Annual R
eport of the Audit C
omm
ittee 2017/18 (including Self-A
ssessment C
hecklist & R
eview of the C
omm
ittee Term
s of Reference)139 of 380
Audit C
omm
ittee - Part 1 9 July 2018-09/07/18
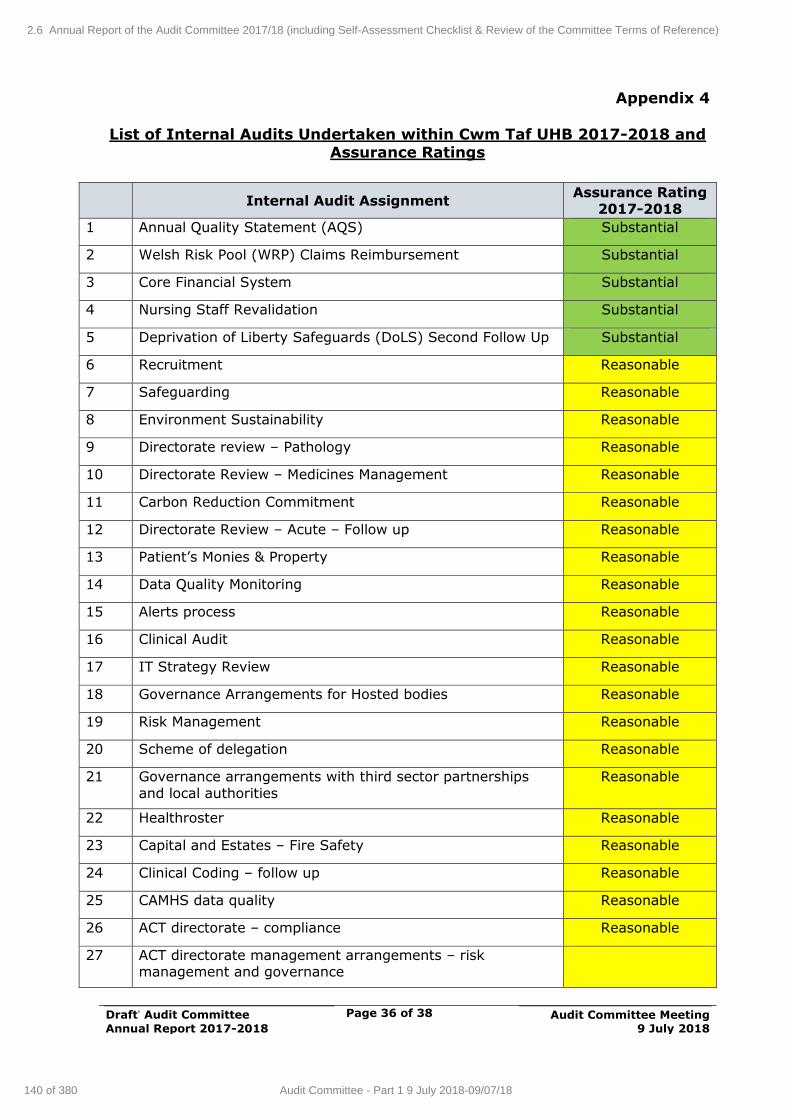
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 36 of 38
Audit Committee Meeting
9 July 2018
Appendix 4
List of Internal Audits Undertaken within Cwm Taf UHB 2017-2018 and Assurance Ratings
Internal Audit Assignment Assurance Rating
2017-2018
1 Annual Quality Statement (AQS) Substantial
2 Welsh Risk Pool (WRP) Claims Reimbursement Substantial
3 Core Financial System Substantial
4 Nursing Staff Revalidation Substantial
5 Deprivation of Liberty Safeguards (DoLS) Second Follow Up Substantial
6 Recruitment Reasonable
7 Safeguarding Reasonable
8 Environment Sustainability Reasonable
9 Directorate review – Pathology Reasonable
10 Directorate Review – Medicines Management Reasonable
11 Carbon Reduction Commitment Reasonable
12 Directorate Review – Acute – Follow up Reasonable
13 Patient’s Monies & Property Reasonable
14 Data Quality Monitoring Reasonable
15 Alerts process Reasonable
16 Clinical Audit Reasonable
17 IT Strategy Review Reasonable
18 Governance Arrangements for Hosted bodies Reasonable
19 Risk Management Reasonable
20 Scheme of delegation Reasonable
21 Governance arrangements with third sector partnerships
and local authorities
Reasonable
22 Healthroster Reasonable
23 Capital and Estates – Fire Safety Reasonable
24 Clinical Coding – follow up Reasonable
25 CAMHS data quality Reasonable
26 ACT directorate – compliance Reasonable
27 ACT directorate management arrangements – risk management and governance
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
140 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
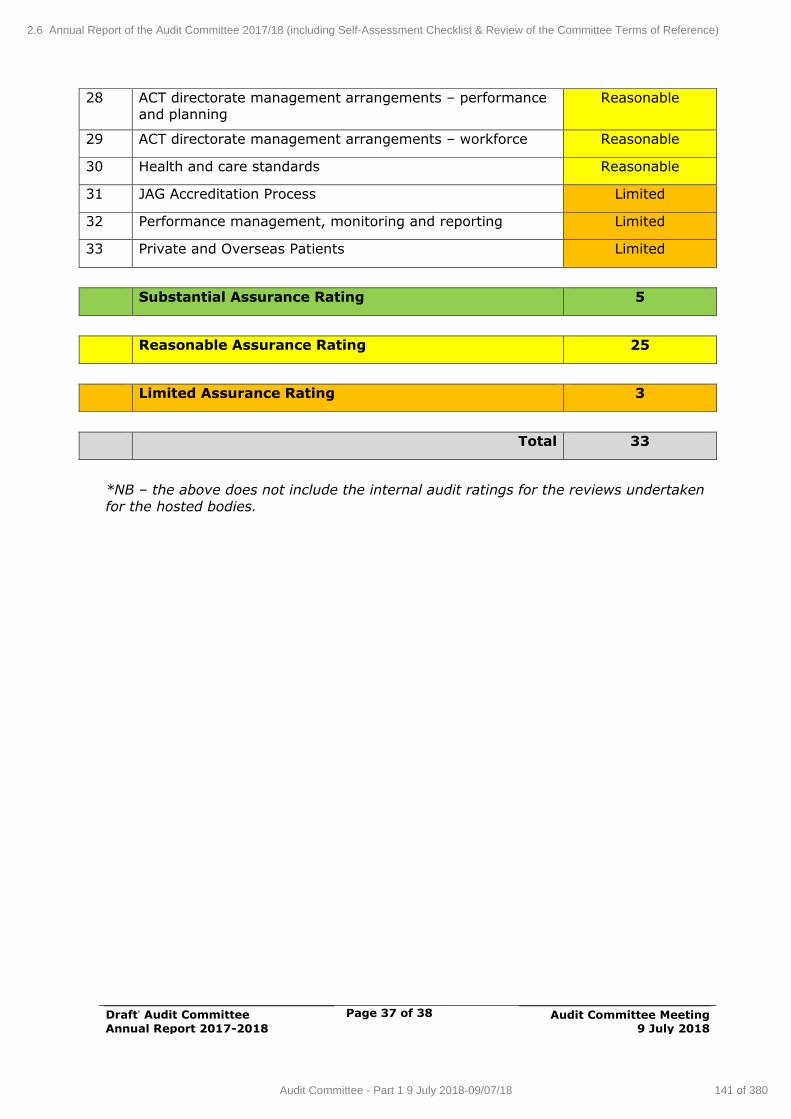
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 37 of 38
Audit Committee Meeting
9 July 2018
28 ACT directorate management arrangements – performance and planning
Reasonable
29 ACT directorate management arrangements – workforce Reasonable
30 Health and care standards Reasonable
31 JAG Accreditation Process Limited
32 Performance management, monitoring and reporting Limited
33 Private and Overseas Patients Limited
Substantial Assurance Rating 5
Reasonable Assurance Rating 25
Limited Assurance Rating 3
Total 33
*NB – the above does not include the internal audit ratings for the reviews undertaken
for the hosted bodies.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
141 of 380Audit Committee - Part 1 9 July 2018-09/07/18
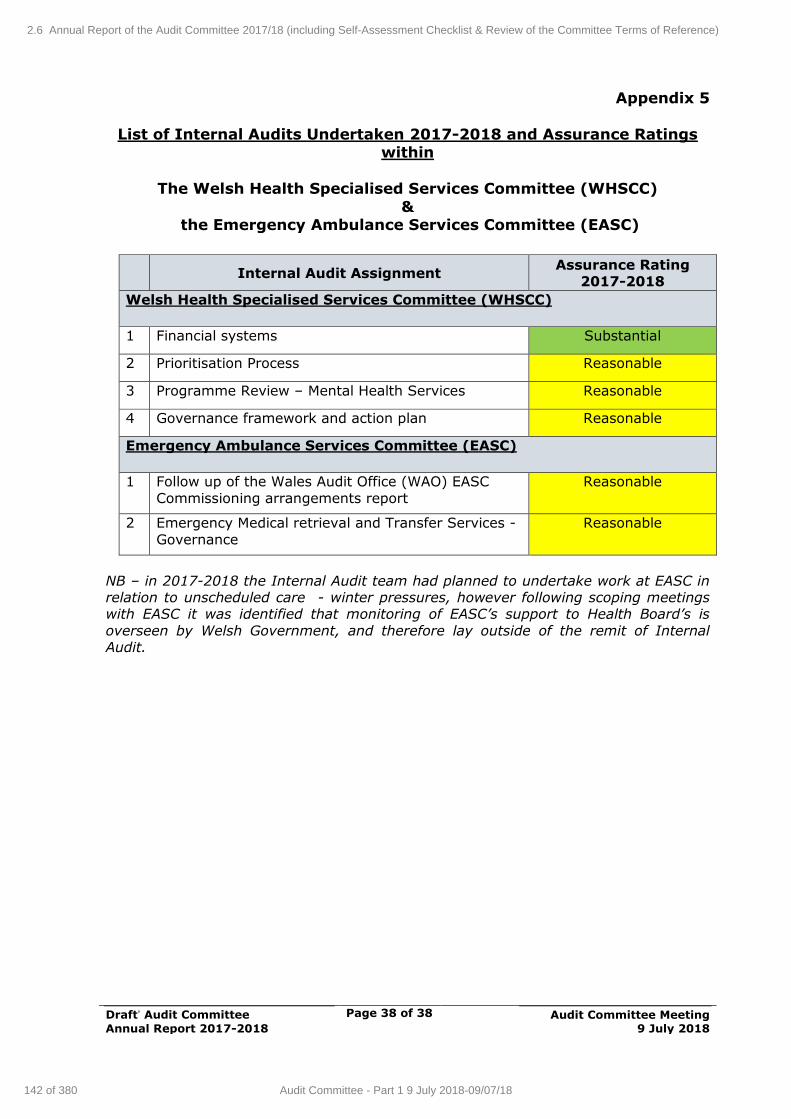
Cwm Taf University Health Board
Head of Internal Audit Opinion and Annual Report
Appendix D
Reports
Draft’ Audit Committee
Annual Report 2017-2018
Page 38 of 38
Audit Committee Meeting
9 July 2018
Appendix 5
List of Internal Audits Undertaken 2017-2018 and Assurance Ratings within
The Welsh Health Specialised Services Committee (WHSCC)
& the Emergency Ambulance Services Committee (EASC)
Internal Audit Assignment Assurance Rating
2017-2018
Welsh Health Specialised Services Committee (WHSCC)
1 Financial systems Substantial
2 Prioritisation Process Reasonable
3 Programme Review – Mental Health Services Reasonable
4 Governance framework and action plan Reasonable
Emergency Ambulance Services Committee (EASC)
1 Follow up of the Wales Audit Office (WAO) EASC
Commissioning arrangements report
Reasonable
2 Emergency Medical retrieval and Transfer Services -
Governance
Reasonable
NB – in 2017-2018 the Internal Audit team had planned to undertake work at EASC in relation to unscheduled care - winter pressures, however following scoping meetings with EASC it was identified that monitoring of EASC’s support to Health Board’s is
overseen by Welsh Government, and therefore lay outside of the remit of Internal Audit.
2.6 Annual Report of the Audit Committee 2017/18 (including Self-Assessment Checklist & Review of the Committee Terms of Reference)
142 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Charitable Funds Page 1 of 9 Audit Committee Meeting 9 July 2018
AGENDA ITEM 3.1
9 July 2018
Audit Committee Report
CHARITABLE FUNDS
Executive Lead: Director of Finance
Author: Head of Finance
Contact Details for further information: Huw Evans on 01443 443810 or [email protected]
Purpose of the Audit Committee Report
To advise the Audit Committee of the activity and balances on charitable funds for the period 1 March 2018 to 31 May 2018 and provides a
progress update on other matters of interest.
Governance
Link to Health
Board Strategic Objective(s)
The Board’s overarching role is to ensure its Strategy
outlined within ‘Cwm Taf Cares’ 3 Year Integrated Medium Term Plan 2015-2018 and the related
organisational objectives aligned with the Institute of
Healthcare Improvement's (IHI) ‘Triple Aim’ are being progressed, these in summary are:
To improve quality, safety and patient Experience
To protect and improve population health To ensure that the services provided are
accessible and sustainable into the future To provide strong governance and assurance
To ensure good value based care and treatment for our patients in line with the resources made
available to the Health Board. The main aim of this report is to improve governance
and assurance.
Supporting evidence
N/A
Engagement – Who has been involved in this work?
N/A
3.1 Charitable Funds Balances as at
1 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Charitable Funds Page 2 of 9 Audit Committee Meeting 9 July 2018
Audit Committee Resolution to:
APPROVE ENDORSE DISCUSS NOTE √
Recommendation The Audit Committee is requested to:
NOTE the contents of the report.
Summarise the Impact of the Audit Committee Report
Equality and diversity
There are no specific equality and diversity issues
Legal implications Charitable funds are required to be managed in accordance with charity legislation and
requirements of the Charity Commissioner.
Population Health No specific population health issues
Quality, Safety & Patient Experience
No specific quality, safety or patient experience issues
Resources Investment of surplus funds assists in
maximising income whilst safeguarding funds
Risks and Assurance The report is a key element of the charitable
funds governance and assurance process, and which enables Trustees’ to discharge their
responsibilities over the management of the
charitable fund.
Health and Care
Standards
The 22 Health & Care Standards for NHS Wales
are mapped into the 7 Quality Themes: Staying Healthy; Safe Care; Effective Care;
Dignified Care; Timely Care; Individual Care; Staff & Resources.
The work reported in this summary takes into account many of the related quality themes.
Workforce No specific workforce implications
Freedom of
Information Status
Open
3.1 Charitable Funds Balances as at
2 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Charitable Funds Page 3 of 9 Audit Committee Meeting 9 July 2018
CHARITABLE FUNDS
1. SITUATION / PURPOSE OF REPORT
To advise the Audit Committee of the activity and balances on charitable funds
for the period 1 March 2018 to 31 May 2018 and provides a progress update on other matters of interest.
2. BACKGROUND / INTRODUCTION
The previous report to the Audit Committee highlighted balances and transactions up to 28 February 2018. This report updates the position as at 31
May 2018 and provides further analysis over their use by both fund type and location. It will also highlight those funds with low balances and slow moving
funds with low levels of activity. An update is also provided on the investment performance.
BALANCES HELD BY THE CHARITABLE FUND
Balances held by the Charitable Fund as at 31 May 2018 are summarised in Appendices A1 (March 2018), and A2 (May 2018) analysed by fund type and
location. Income received and expenditure incurred during the period 1 March
to 31 March (A1) and 1 April to 31 May (A2) is also shown.
The balance at the end of May is £1.888m which is an increase of £6k since the last report (28.2.18).
These balances exclude the unrealised gain on investment referred to below.
LOW VALUE AND SLOW MOVING FUNDS
A listing of all funds below £1,000 as at 31 May 2018 is shown in Appendix B.
Actions agreed with fundholders and other relevant observations are included within the comments section.
It should be noted that certain funds with low balances are very active and are
being constantly used. This meets the objective of using funds for the
purposes intended rather than allowing balances to accumulate. Also shown therefore within Appendix B are those funds with higher balances where there
has been no expenditure activity during the previous six months, again with comments where appropriate.
3.1 Charitable Funds Balances as at
3 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Charitable Funds Page 4 of 9 Audit Committee Meeting 9 July 2018
INVESTMENT
The total units held remain at 783,307.83.
The market value at 31 May 2018 was £1.802m (a rise of £52k from the end
of February), compared to £1.5m invested (i.e. a surplus of £302k – 20.1%).
The Audit Committee previously decided that it will consider making a distribution of the capital to individual funds should the market value exceed
20% of cost (i.e. £1.8m). This threshold has now been reached, although clearly there is scope for reductions before year-end. It is proposed that this
be considered further at the January Audit Committee with a view to making a decision on distribution at that time (in readiness for year-
end)
Forecast income for 2018-19 is currently £62k – an income yield of 3.43%.
Actual income received for 2017-18 was £61k
A graphical presentation of the investment performance by week, along with a FTSE100 comparator, is shown in Appendix C.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
This report is a key element of the charitable funds governance and assurance process, and which enables Trustees’ to discharge their responsibilities over
the management of the charitable fund.
4. RECOMMENDATION
The Audit Committee is requested to:
NOTE the contents of the report.
Freedom of Information Status
Open
3.1 Charitable Funds Balances as at
4 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
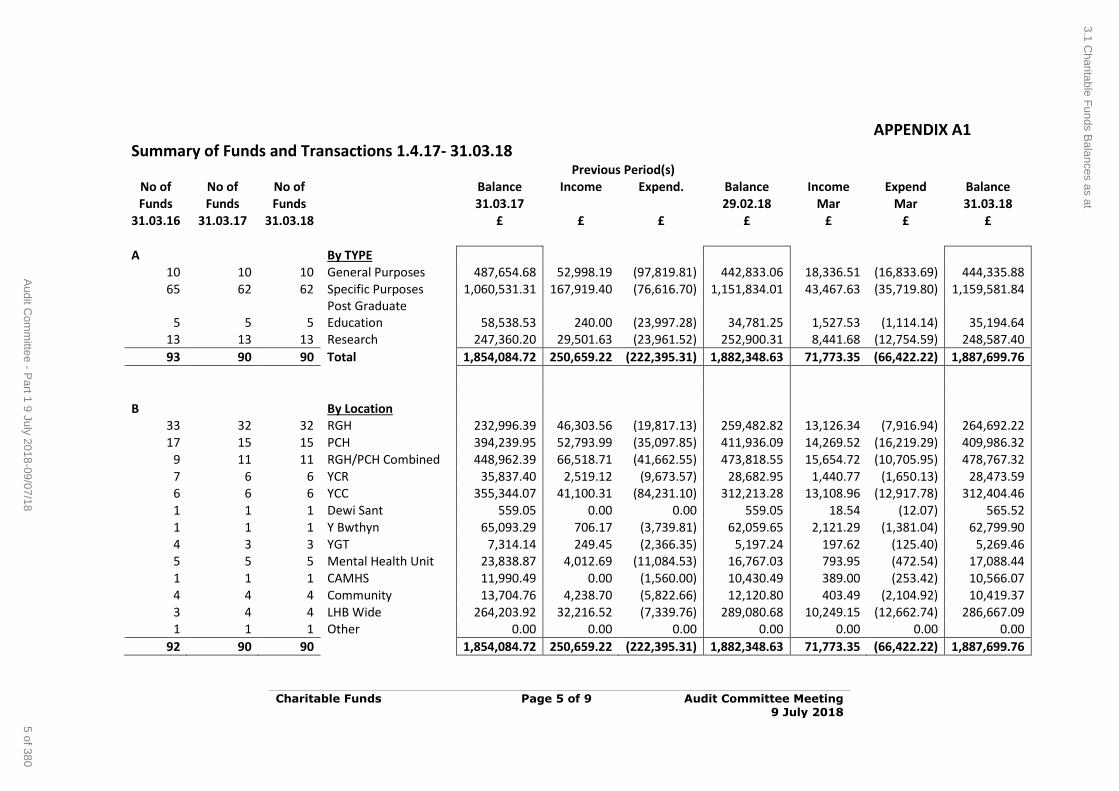
Charitable Funds Page 5 of 9 Audit Committee Meeting 9 July 2018
APPENDIX A1 Summary of Funds and Transactions 1.4.17- 31.03.18
Previous Period(s) No of No of No of
Balance Income Expend. Balance Income Expend Balance
Funds Funds Funds
31.03.17
29.02.18 Mar Mar 31.03.18 31.03.16 31.03.17 31.03.18
£ £ £ £ £ £ £
A
By TYPE
10 10 10 General Purposes 487,654.68 52,998.19 (97,819.81) 442,833.06 18,336.51 (16,833.69) 444,335.88 65 62 62 Specific Purposes 1,060,531.31 167,919.40 (76,616.70) 1,151,834.01 43,467.63 (35,719.80) 1,159,581.84
5 5 5 Post Graduate Education 58,538.53 240.00 (23,997.28) 34,781.25 1,527.53 (1,114.14) 35,194.64
13 13 13 Research 247,360.20 29,501.63 (23,961.52) 252,900.31 8,441.68 (12,754.59) 248,587.40
93 90 90 Total 1,854,084.72 250,659.22 (222,395.31) 1,882,348.63 71,773.35 (66,422.22) 1,887,699.76
B
By Location
33 32 32 RGH 232,996.39 46,303.56 (19,817.13) 259,482.82 13,126.34 (7,916.94) 264,692.22 17 15 15 PCH 394,239.95 52,793.99 (35,097.85) 411,936.09 14,269.52 (16,219.29) 409,986.32
9 11 11 RGH/PCH Combined 448,962.39 66,518.71 (41,662.55) 473,818.55 15,654.72 (10,705.95) 478,767.32 7 6 6 YCR 35,837.40 2,519.12 (9,673.57) 28,682.95 1,440.77 (1,650.13) 28,473.59 6 6 6 YCC 355,344.07 41,100.31 (84,231.10) 312,213.28 13,108.96 (12,917.78) 312,404.46 1 1 1 Dewi Sant 559.05 0.00 0.00 559.05 18.54 (12.07) 565.52 1 1 1 Y Bwthyn 65,093.29 706.17 (3,739.81) 62,059.65 2,121.29 (1,381.04) 62,799.90 4 3 3 YGT 7,314.14 249.45 (2,366.35) 5,197.24 197.62 (125.40) 5,269.46 5 5 5 Mental Health Unit 23,838.87 4,012.69 (11,084.53) 16,767.03 793.95 (472.54) 17,088.44 1 1 1 CAMHS 11,990.49 0.00 (1,560.00) 10,430.49 389.00 (253.42) 10,566.07 4 4 4 Community 13,704.76 4,238.70 (5,822.66) 12,120.80 403.49 (2,104.92) 10,419.37 3 4 4 LHB Wide 264,203.92 32,216.52 (7,339.76) 289,080.68 10,249.15 (12,662.74) 286,667.09 1 1 1 Other 0.00 0.00 0.00 0.00 0.00 0.00 0.00
92 90 90
1,854,084.72 250,659.22 (222,395.31) 1,882,348.63 71,773.35 (66,422.22) 1,887,699.76
3.1 Charitable F
unds Balances as at
5 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
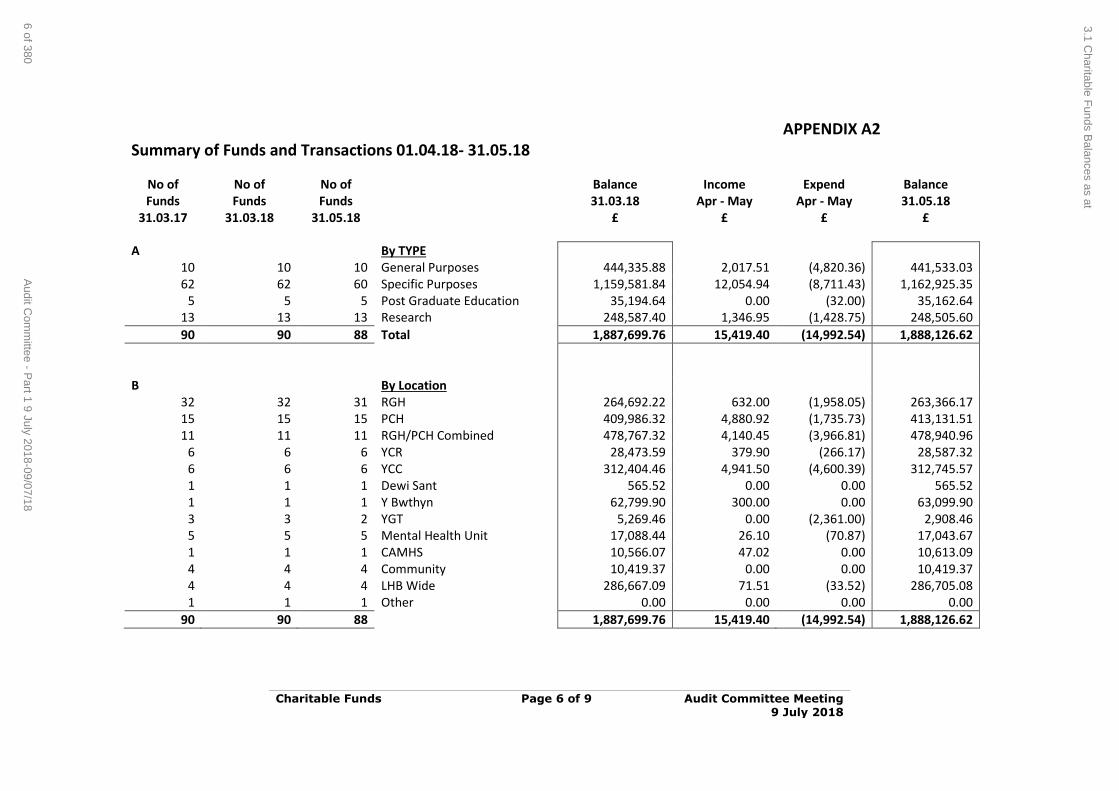
Charitable Funds Page 6 of 9 Audit Committee Meeting 9 July 2018
APPENDIX A2 Summary of Funds and Transactions 01.04.18- 31.05.18
No of No of No of
Balance Income Expend Balance Funds Funds Funds
31.03.18 Apr - May Apr - May 31.05.18
31.03.17 31.03.18 31.05.18
£ £ £ £
A
By TYPE
10 10 10 General Purposes 444,335.88 2,017.51 (4,820.36) 441,533.03 62 62 60 Specific Purposes 1,159,581.84 12,054.94 (8,711.43) 1,162,925.35
5 5 5 Post Graduate Education 35,194.64 0.00 (32.00) 35,162.64 13 13 13 Research 248,587.40 1,346.95 (1,428.75) 248,505.60
90 90 88 Total 1,887,699.76 15,419.40 (14,992.54) 1,888,126.62
B
By Location
32 32 31 RGH 264,692.22 632.00 (1,958.05) 263,366.17 15 15 15 PCH 409,986.32 4,880.92 (1,735.73) 413,131.51 11 11 11 RGH/PCH Combined 478,767.32 4,140.45 (3,966.81) 478,940.96
6 6 6 YCR 28,473.59 379.90 (266.17) 28,587.32 6 6 6 YCC 312,404.46 4,941.50 (4,600.39) 312,745.57 1 1 1 Dewi Sant 565.52 0.00 0.00 565.52 1 1 1 Y Bwthyn 62,799.90 300.00 0.00 63,099.90 3 3 2 YGT 5,269.46 0.00 (2,361.00) 2,908.46 5 5 5 Mental Health Unit 17,088.44 26.10 (70.87) 17,043.67 1 1 1 CAMHS 10,566.07 47.02 0.00 10,613.09 4 4 4 Community 10,419.37 0.00 0.00 10,419.37 4 4 4 LHB Wide 286,667.09 71.51 (33.52) 286,705.08 1 1 1 Other 0.00 0.00 0.00 0.00
90 90 88
1,887,699.76 15,419.40 (14,992.54) 1,888,126.62
3.1 Charitable F
unds Balances as at
6 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
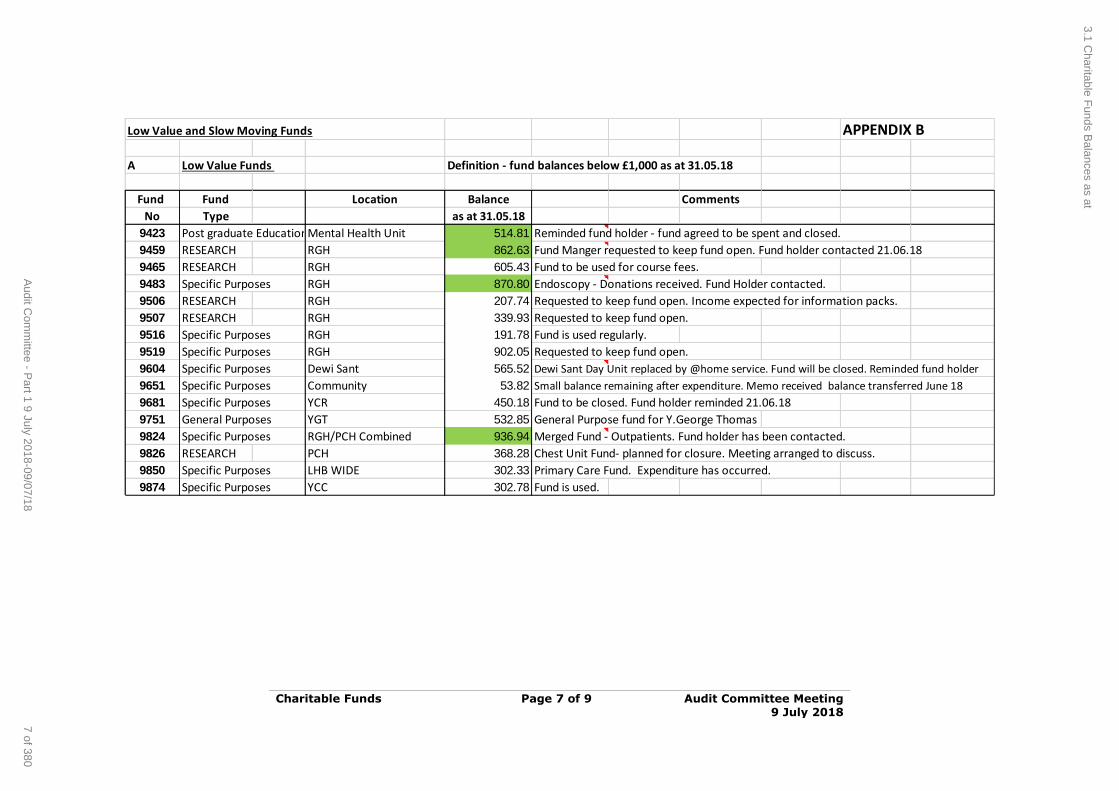
Charitable Funds Page 7 of 9 Audit Committee Meeting 9 July 2018
Low Value and Slow Moving Funds APPENDIX B
A Low Value Funds Definition - fund balances below £1,000 as at 31.05.18
Fund Fund Location Balance Comments
No Type as at 31.05.18
9423 Post graduate EducationMental Health Unit 514.81 Reminded fund holder - fund agreed to be spent and closed.
9459 RESEARCH RGH 862.63 Fund Manger requested to keep fund open. Fund holder contacted 21.06.18
9465 RESEARCH RGH 605.43 Fund to be used for course fees.
9483 Specific Purposes RGH 870.80 Endoscopy - Donations received. Fund Holder contacted.
9506 RESEARCH RGH 207.74 Requested to keep fund open. Income expected for information packs.
9507 RESEARCH RGH 339.93 Requested to keep fund open.
9516 Specific Purposes RGH 191.78 Fund is used regularly.
9519 Specific Purposes RGH 902.05 Requested to keep fund open.
9604 Specific Purposes Dewi Sant 565.52 Dewi Sant Day Unit replaced by @home service. Fund will be closed. Reminded fund holder
9651 Specific Purposes Community 53.82 Small balance remaining after expenditure. Memo received balance transferred June 18
9681 Specific Purposes YCR 450.18 Fund to be closed. Fund holder reminded 21.06.18
9751 General Purposes YGT 532.85 General Purpose fund for Y.George Thomas
9824 Specific Purposes RGH/PCH Combined 936.94 Merged Fund - Outpatients. Fund holder has been contacted.
9826 RESEARCH PCH 368.28 Chest Unit Fund- planned for closure. Meeting arranged to discuss.
9850 Specific Purposes LHB WIDE 302.33 Primary Care Fund. Expenditure has occurred.
9874 Specific Purposes YCC 302.78 Fund is used.
3.1 Charitable F
unds Balances as at
7 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
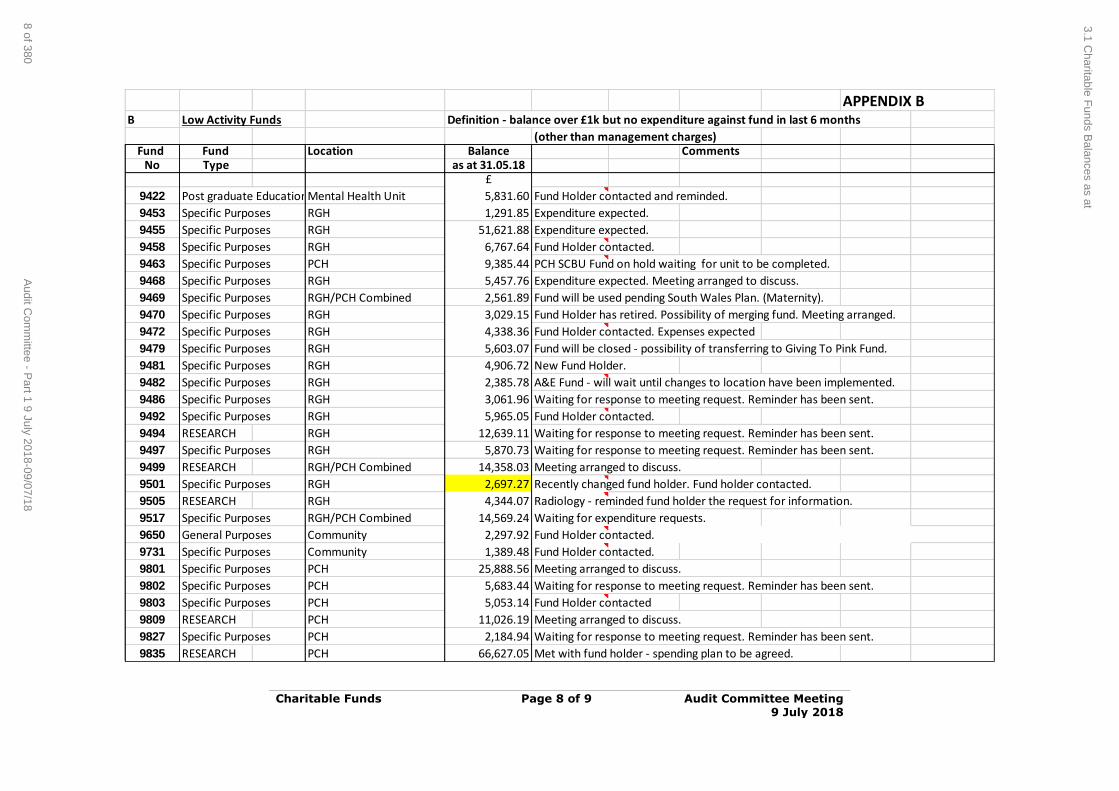
Charitable Funds Page 8 of 9 Audit Committee Meeting 9 July 2018
APPENDIX BB Low Activity Funds Definition - balance over £1k but no expenditure against fund in last 6 months
(other than management charges)Fund Fund Location Balance Comments
No Type as at 31.05.18£
9422 Post graduate EducationMental Health Unit 5,831.60 Fund Holder contacted and reminded.
9453 Specific Purposes RGH 1,291.85 Expenditure expected.
9455 Specific Purposes RGH 51,621.88 Expenditure expected.
9458 Specific Purposes RGH 6,767.64 Fund Holder contacted.
9463 Specific Purposes PCH 9,385.44 PCH SCBU Fund on hold waiting for unit to be completed.
9468 Specific Purposes RGH 5,457.76 Expenditure expected. Meeting arranged to discuss.
9469 Specific Purposes RGH/PCH Combined 2,561.89 Fund will be used pending South Wales Plan. (Maternity).
9470 Specific Purposes RGH 3,029.15 Fund Holder has retired. Possibility of merging fund. Meeting arranged.
9472 Specific Purposes RGH 4,338.36 Fund Holder contacted. Expenses expected
9479 Specific Purposes RGH 5,603.07 Fund will be closed - possibility of transferring to Giving To Pink Fund.
9481 Specific Purposes RGH 4,906.72 New Fund Holder.
9482 Specific Purposes RGH 2,385.78 A&E Fund - will wait until changes to location have been implemented.
9486 Specific Purposes RGH 3,061.96 Waiting for response to meeting request. Reminder has been sent.
9492 Specific Purposes RGH 5,965.05 Fund Holder contacted.
9494 RESEARCH RGH 12,639.11 Waiting for response to meeting request. Reminder has been sent.
9497 Specific Purposes RGH 5,870.73 Waiting for response to meeting request. Reminder has been sent.
9499 RESEARCH RGH/PCH Combined 14,358.03 Meeting arranged to discuss.
9501 Specific Purposes RGH 2,697.27 Recently changed fund holder. Fund holder contacted.
9505 RESEARCH RGH 4,344.07 Radiology - reminded fund holder the request for information.
9517 Specific Purposes RGH/PCH Combined 14,569.24 Waiting for expenditure requests.
9650 General Purposes Community 2,297.92 Fund Holder contacted.
9731 Specific Purposes Community 1,389.48 Fund Holder contacted.
9801 Specific Purposes PCH 25,888.56 Meeting arranged to discuss.
9802 Specific Purposes PCH 5,683.44 Waiting for response to meeting request. Reminder has been sent.
9803 Specific Purposes PCH 5,053.14 Fund Holder contacted
9809 RESEARCH PCH 11,026.19 Meeting arranged to discuss.
9827 Specific Purposes PCH 2,184.94 Waiting for response to meeting request. Reminder has been sent.
9835 RESEARCH PCH 66,627.05 Met with fund holder - spending plan to be agreed.
3.1 Charitable F
unds Balances as at
8 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
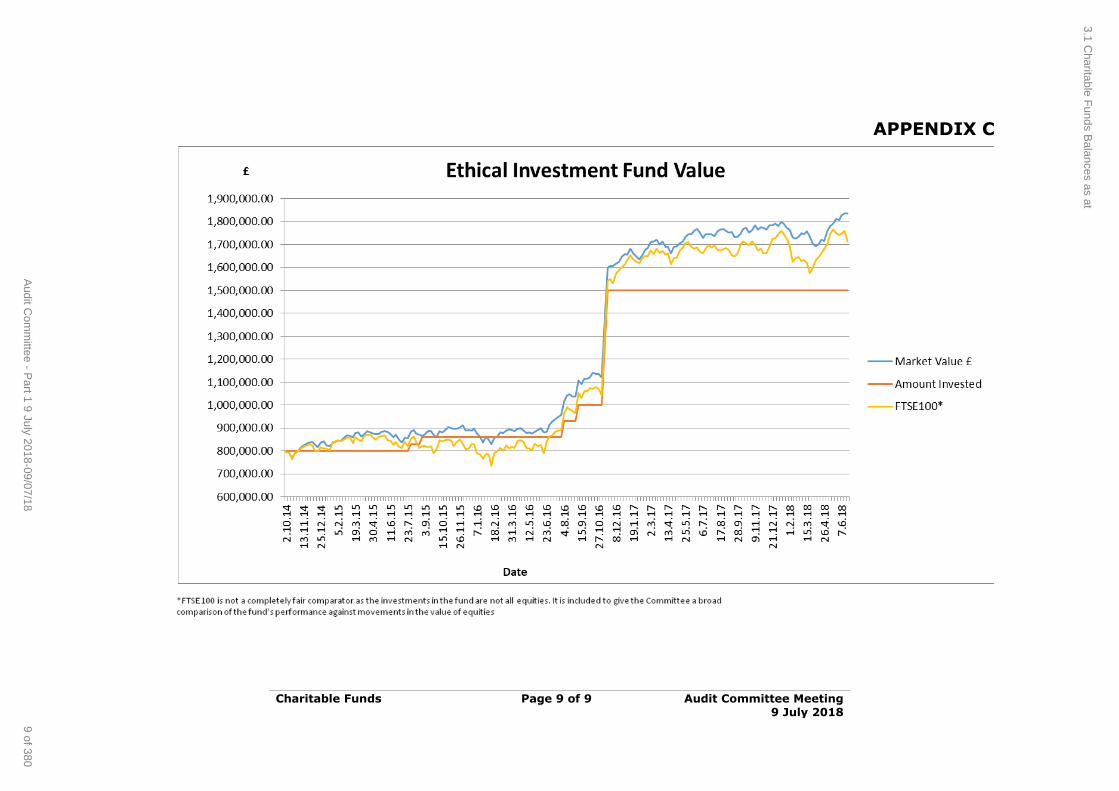
Charitable Funds Page 9 of 9 Audit Committee Meeting 9 July 2018
APPENDIX C
3.1 Charitable F
unds Balances as at
9 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Cwm Taf University Health Board
INTERNAL AUDIT PROGRESS REPORT
Audit Committee - July 2018
NHS Wales Shared Services Partnership
Audit and Assurance Services
4.1 Internal Audit Progress Report
1 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board Report Contents
Audit Committee - July 2018
NHS Wales Audit & Assurance Services
Contents
Page
1. Introduction 1
2. Outcomes from completed audit reviews 1
3. Delivery of the 2018/19 Internal Audit plan 2
4. Performance monitoring 2
Appendix A:
Table 1: Status of 2018/19 assignments
Please note:
This audit progress report has been prepared for internal use only. Audit & Assurance Services reports are prepared, in accordance with the Internal Audit Charter and the Annual Plan, approved by the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership – Audit and Assurance
Services, and addressed to Independent Members or officers including those designated as Accountable Officer. They are prepared for the sole use of the Cwm Taf University Local Health Board and no responsibility is taken by the Audit and Assurance Services Internal Auditors to any director or officer in their individual capacity, or to any third party.
4.1 Internal Audit Progress Report
2 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board Internal Audit Progress Report
Audit Committee - July 2018
NHS Wales Audit & Assurance Services Page | 1
1. Introduction
1.1. This progress report provides the Audit Committee (the ‘committee’) with the current position regarding the work undertaken by Internal
Audit as at 26 June 2018.
1.2. The report includes details of the progress made to date against
individual assignments along with details regarding the delivery of the
2017/18 plan, the 2018/19, and any required updates.
2. Outcomes from completed audit reviews
2.1 Since the May meeting of the committee 6 assignments have been finalised. Three are the final reports relating to the 2017/18
programme of work, and three relate to 2018/19. These are identified
in the table below along with the allocated assurance rating. The full versions of these reports are included in the committee’s papers as
separate items.
Assignments 2017/18 Assurance rating
Anaesthetics, Critical Care and Theatres (ACT)
directorate – management arrangements review:
Planning and performance
Workforce
Risk and governance
Reasonable
Reasonable
Reasonable
Anaesthetics, Critical Care and Theatres (ACT)
directorate – compliance review Reasonable
Health & Care standards Reasonable
Assignments 2018/19 Assurance rating
Sustainability reporting Substantial
Annual Quality statement Reasonable
JAG accreditation – follow up Reasonable
4.1 Internal Audit Progress Report
3 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
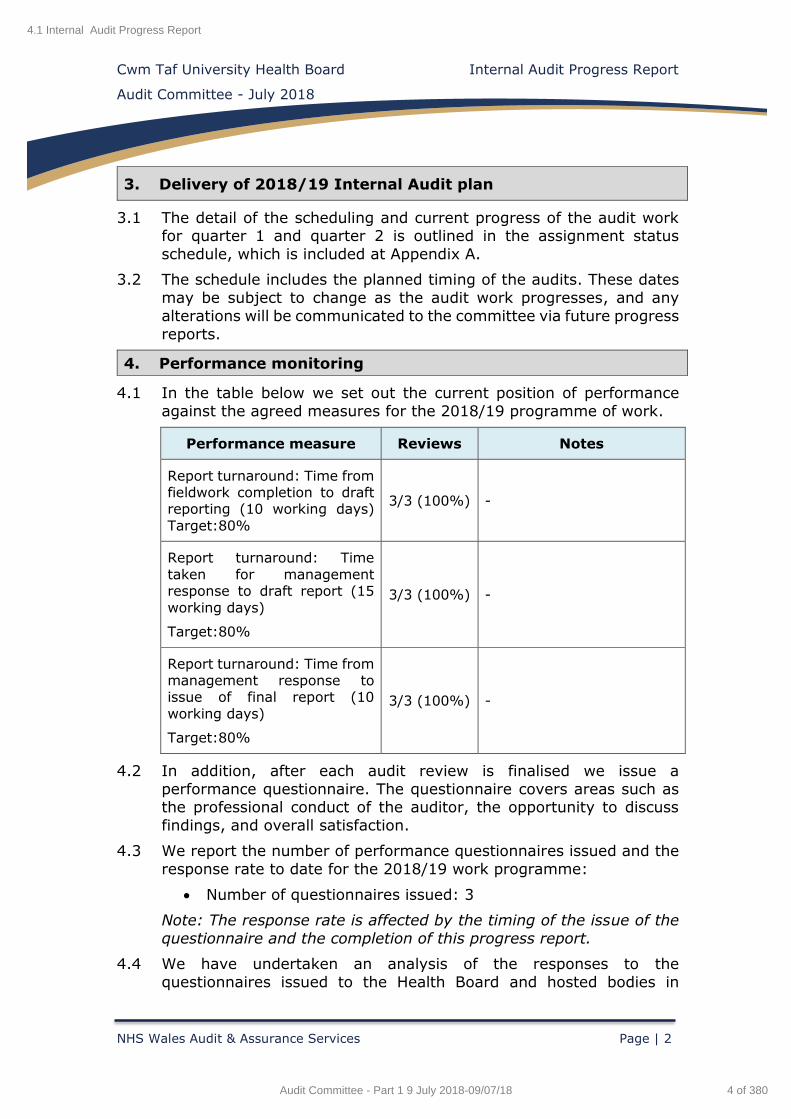
Cwm Taf University Health Board Internal Audit Progress Report
Audit Committee - July 2018
NHS Wales Audit & Assurance Services Page | 2
3. Delivery of 2018/19 Internal Audit plan
3.1 The detail of the scheduling and current progress of the audit work for quarter 1 and quarter 2 is outlined in the assignment status
schedule, which is included at Appendix A.
3.2 The schedule includes the planned timing of the audits. These dates
may be subject to change as the audit work progresses, and any
alterations will be communicated to the committee via future progress
reports.
4. Performance monitoring
4.1 In the table below we set out the current position of performance
against the agreed measures for the 2018/19 programme of work.
Performance measure Reviews Notes
Report turnaround: Time from fieldwork completion to draft reporting (10 working days)
Target:80%
3/3 (100%) -
Report turnaround: Time
taken for management response to draft report (15
working days)
Target:80%
3/3 (100%) -
Report turnaround: Time from management response to issue of final report (10
working days)
Target:80%
3/3 (100%) -
4.2 In addition, after each audit review is finalised we issue a
performance questionnaire. The questionnaire covers areas such as the professional conduct of the auditor, the opportunity to discuss
findings, and overall satisfaction.
4.3 We report the number of performance questionnaires issued and the
response rate to date for the 2018/19 work programme:
Number of questionnaires issued: 3
Note: The response rate is affected by the timing of the issue of the
questionnaire and the completion of this progress report.
4.4 We have undertaken an analysis of the responses to the
questionnaires issued to the Health Board and hosted bodies in
4.1 Internal Audit Progress Report
4 of 380Audit Committee - Part 1 9 July 2018-09/07/18
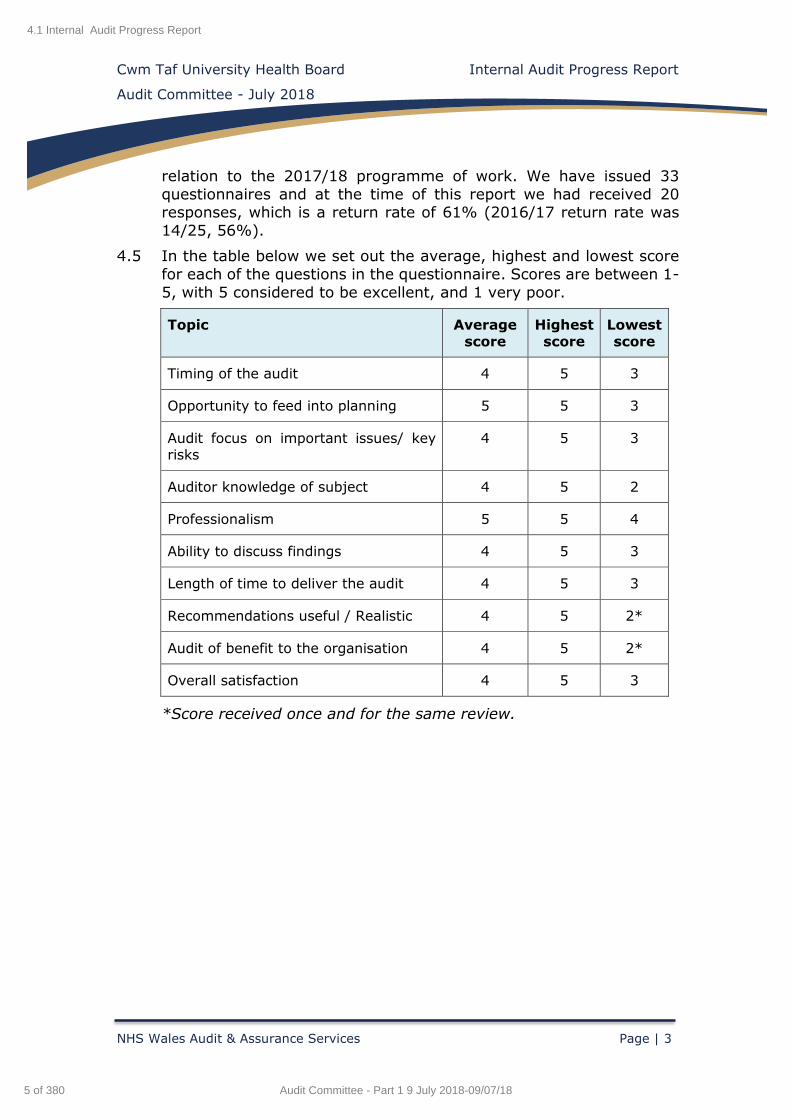
Cwm Taf University Health Board Internal Audit Progress Report
Audit Committee - July 2018
NHS Wales Audit & Assurance Services Page | 3
relation to the 2017/18 programme of work. We have issued 33
questionnaires and at the time of this report we had received 20 responses, which is a return rate of 61% (2016/17 return rate was
14/25, 56%).
4.5 In the table below we set out the average, highest and lowest score
for each of the questions in the questionnaire. Scores are between 1-
5, with 5 considered to be excellent, and 1 very poor.
Topic Average
score
Highest
score
Lowest
score
Timing of the audit 4 5 3
Opportunity to feed into planning 5 5 3
Audit focus on important issues/ key risks
4 5 3
Auditor knowledge of subject 4 5 2
Professionalism 5 5 4
Ability to discuss findings 4 5 3
Length of time to deliver the audit 4 5 3
Recommendations useful / Realistic 4 5 2*
Audit of benefit to the organisation 4 5 2*
Overall satisfaction 4 5 3
*Score received once and for the same review.
4.1 Internal Audit Progress Report
5 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
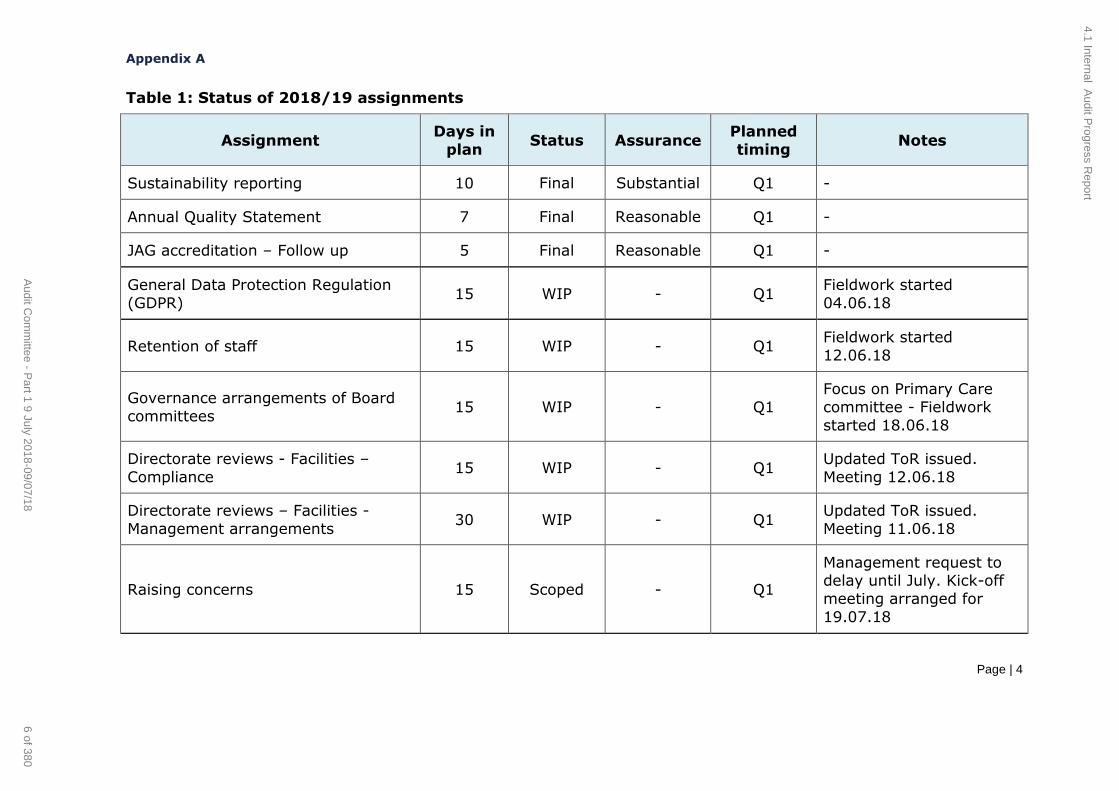
Appendix A
Page | 4
Table 1: Status of 2018/19 assignments
Assignment Days in
plan Status Assurance
Planned
timing Notes
Sustainability reporting 10 Final Substantial Q1 -
Annual Quality Statement 7 Final Reasonable Q1 -
JAG accreditation – Follow up 5 Final Reasonable Q1 -
General Data Protection Regulation
(GDPR) 15 WIP - Q1
Fieldwork started
04.06.18
Retention of staff 15 WIP - Q1 Fieldwork started
12.06.18
Governance arrangements of Board
committees 15 WIP - Q1
Focus on Primary Care
committee - Fieldwork
started 18.06.18
Directorate reviews - Facilities –
Compliance 15 WIP - Q1
Updated ToR issued.
Meeting 12.06.18
Directorate reviews – Facilities -
Management arrangements 30 WIP - Q1
Updated ToR issued.
Meeting 11.06.18
Raising concerns 15 Scoped - Q1
Management request to delay until July. Kick-off
meeting arranged for
19.07.18
4.1 Internal Audit P
rogress Report
6 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
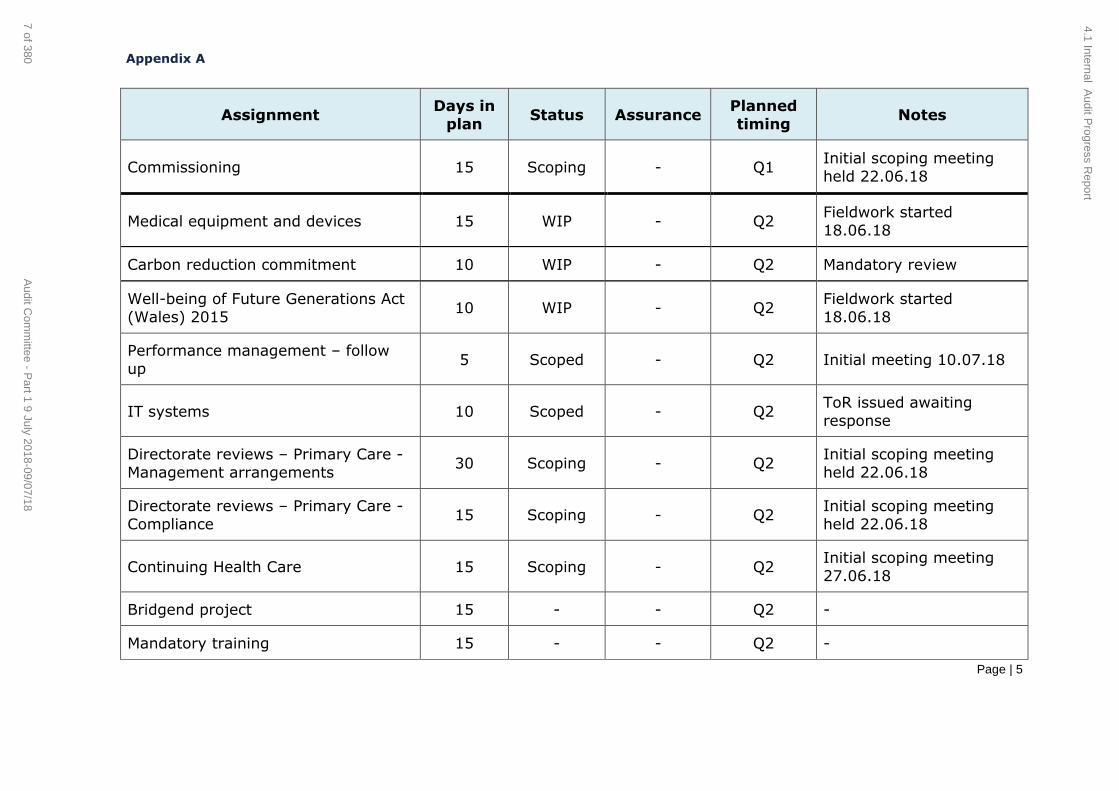
Appendix A
Page | 5
Assignment Days in
plan Status Assurance
Planned
timing Notes
Commissioning 15 Scoping - Q1 Initial scoping meeting
held 22.06.18
Medical equipment and devices 15 WIP - Q2 Fieldwork started
18.06.18
Carbon reduction commitment 10 WIP - Q2 Mandatory review
Well-being of Future Generations Act
(Wales) 2015 10 WIP - Q2
Fieldwork started
18.06.18
Performance management – follow
up 5 Scoped - Q2 Initial meeting 10.07.18
IT systems 10 Scoped - Q2 ToR issued awaiting
response
Directorate reviews – Primary Care -
Management arrangements 30 Scoping - Q2
Initial scoping meeting
held 22.06.18
Directorate reviews – Primary Care -
Compliance 15 Scoping - Q2
Initial scoping meeting
held 22.06.18
Continuing Health Care 15 Scoping - Q2 Initial scoping meeting
27.06.18
Bridgend project 15 - - Q2 -
Mandatory training 15 - - Q2 -
4.1 Internal Audit P
rogress Report
7 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
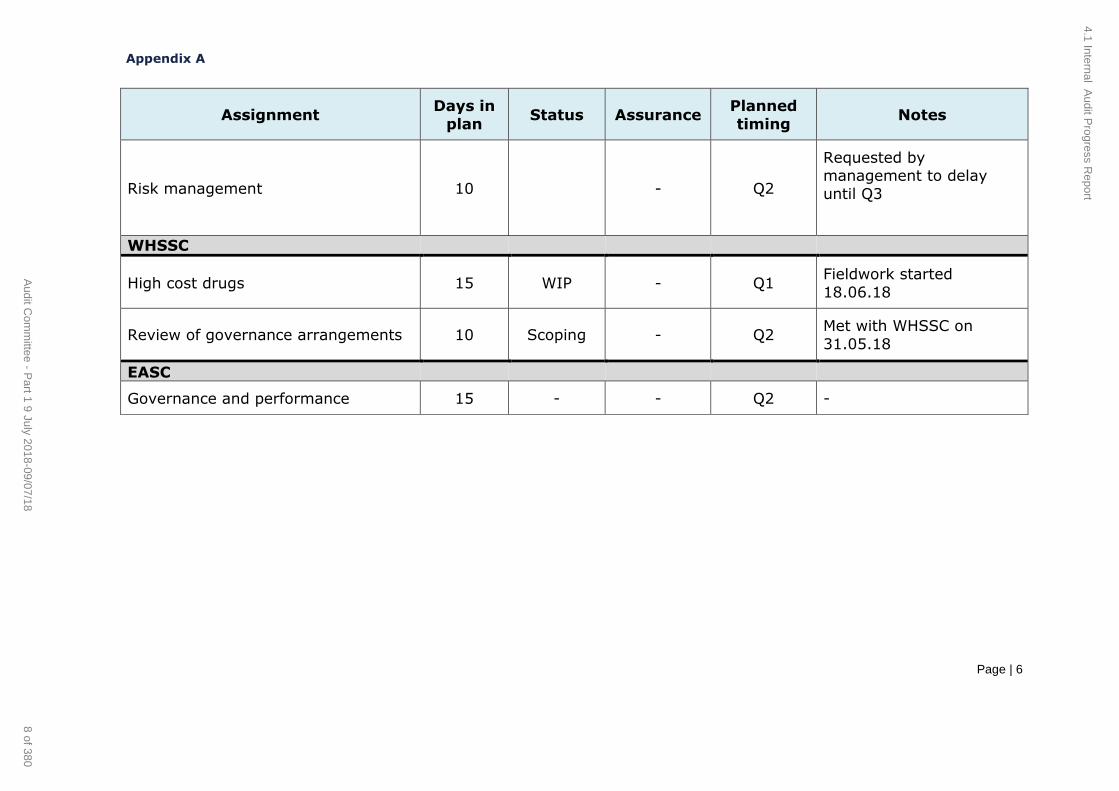
Appendix A
Page | 6
Assignment Days in
plan Status Assurance
Planned
timing Notes
Risk management 10 - Q2
Requested by management to delay
until Q3
WHSSC
High cost drugs 15 WIP - Q1 Fieldwork started
18.06.18
Review of governance arrangements 10 Scoping - Q2 Met with WHSSC on
31.05.18
EASC
Governance and performance 15 - - Q2 -
4.1 Internal Audit P
rogress Report
8 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review – Anaesthetics, Critical Care and Theatres (ACT)
Management Arrangements
Final Internal Audit Report
Cwm Taf University Health Board 2017/18
June 2018
NHS Wales Shared Services Partnership
Audit and Assurance Services
4.2 Directorate Review - ACT - Management Arrangements
9 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 2 of 56
Contents Page
1. Introduction and Background 3
2. Scope and Objectives 3
3. Associated Risks 5
Opinion and key findings
4. Overall Assurance Opinion 6
5. Assurance Summary 10
6. Summary of Audit Findings 11
7. Summary of Recommendations 15
Review reference: CTU-1718-20
Report status: Final Internal Audit Report
Fieldwork commencement: 8 February 2018 Fieldwork completion: 15 May 2018
Draft report issued: 29 May 2018 Management response received: 22 June 2018
Final report issued: 26 June 2018 Auditors: Elizabeth Vincent, Emma Samways
Executive sign off: John Palmer, Interim Chief Operating
Officer
Distribution: Deb Lewis, Assistant Director
Neil Cooper, Directorate Manager
Committee: Audit Committee
ACKNOWLEDGEMENT
NHS Wales Audit & Assurance Services would like to acknowledge the time and co-operation
given by management and staff during the course of this review.
Disclaimer notice - Please note:
This audit report has been prepared for internal use only. Audit & Assurance Services reports
are prepared, in accordance with the Internal Audit Charter and the Annual Plan, approved by
the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership – Audit
and Assurance Services, and addressed to Independent Members or officers including those
designated as Accountable Officer. They are prepared for the sole use of Cwm Taf University
Health Board and no responsibility is taken by the Audit and Assurance Services Internal Auditors
to any director or officer in their individual capacity, or to any third party.
Appendix A Appendix B
Management Action Plan Assurance opinion and action plan risk rating
4.2 Directorate Review - ACT - Management Arrangements
10 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 3 of 56
1. Introduction and Background
The review of the Anaesthetics, Critical Care and Theatres (ACT) directorate management arrangements was completed in line with the 2017/18
Internal Audit plan for Cwm Taf University Health Board (the 'Health Board'
or the 'organisation').
The relevant lead for the assignment is the Interim Chief Operation Officer.
As part of the Internal Audit programme, we have already reviewed the
governance arrangements for Pathology and Medicines management. During the year, we have worked with the Health Board’s management to
develop the scope of our directorate reviews. This, our final review includes
an expanded scope that means we now cover key objectives and risks in
relation to the directorate’s management arrangements for:
risk management and governance;
performance and planning; and
workforce.
In addition to this review of management arrangements within the
directorate, we have undertaken a separate review within the directorate to consider its compliance with the Health Board’s Scheme of Delegation
and Financial Control Procedures.
During 2017/18 the ACT directorate was restructured and elements of the
directorate, namely Outpatients and Medical Records, were moved and now form part of the Directorate of Medicine. The Directorate Manager changed
during September 2017.
2. Scope and Objectives
The overall objective of the audit was to evaluate and determine the
adequacy of the systems and controls in place in relation to governance, in order to provide assurance to the Health Board's Audit Committee that risks
material to the achievements of system's objectives are managed
appropriately.
The areas we sought to provide assurance on were:
Governance arrangements
Appropriate governance structures are in place including key
personnel and appropriate committees and groups.
Directorate policies and procedures are owned and are up to date.
Business partners’ arrangements are operating appropriately.
Reporting and monitoring processes are operating and are
appropriate.
There are appropriate mechanisms in place to ensure new legislative and regulatory information is received, disseminated and actioned on
a timely basis.
4.2 Directorate Review - ACT - Management Arrangements
11 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 4 of 56
Risk management
A risk management process is in place that ensures risks are appropriately identified, assessed, recorded and monitored. Risk
owners are identified for each risk and mitigation plans are in place
where appropriate.
Risks associated with demand and capacity are appropriately
captured.
Workforce management & service delivery
Annual leave is appropriately planned, requested, recorded and
authorised in line with the directorate’s policy.
Flexi-time and Time off in Lieu (TOIL) is appropriately recorded, monitored and managed in accordance with local procedures and
processes.
Sickness absence is appropriately recorded, monitored and managed
in accordance with the All Wales Sickness Management policy.
Staff and management appropriately complete PADRs in good time.
Staff complete mandatory training in line with specified timeframes.
Staff rosters are planned and approved in line with policy.
Systems are in place to ensure amendments to rosters that deviate from the template roster are appropriately reviewed and approved to
ensure optimum workforce deployment.
Consultant job plans are reviewed and agreed annually, and
monitored to ensure that clinical activity is delivered in line with the
agreed job plans.
Workforce planning arrangements exist to establish and plan for
known future changes to the directorate. For example, key staff due
to retire within three years.
Planning and performance
The directorate has appropriate arrangements in place to ensure that
its Integrated Medium Term Plan (IMTP) is in accordance with the Health Board’s corporate planning framework, including an
underpinning engagement plan to ensure directorate staff are
involved.
The directorate has an agreed planned approach, which has been appropriately scrutinised, to address its commitments as identified in
the Health Board’s IMTP.
The directorate has appropriate performance measures and key
performance indicators in place that cover service delivery and cross-cutting themes such as financial targets and workforce. These are
formally reviewed and reported on a regular basis with action plans
in place to address any issues.
4.2 Directorate Review - ACT - Management Arrangements
12 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 5 of 56
The directorate has appropriate recovery plans and mechanisms in
place, where required, in relation to both financial and non-financial activities. For example, should referral to treatment times begin to
show an adverse variance.
Demand and capacity plans are owned and used as ‘day to day’
business planning tools for managing the directorate.
Demand and capacity plans are monitored and reported to ensure
they remain fit for purpose.
Standards of conduct
Declarations of interest (or nil returns) are submitted for all relevant
staff and the directorate is aware of the declarations made.
Directorate specific objective
We also considered how good practice is captured and communicated between the directorate and other directorates so that shared
improvements to services can be made where appropriate.
3. Associated Risks
The potential risks considered in the review were as follows:
The directorate is not appropriately governed which could result in a
service that is not being delivered safely and effectively.
Services are not effectively planned.
Risks materialise as they have not been identified and / or addressed.
Reduced service provision / additional costs due to inappropriate or
unauthorised absence.
Staff performance is not effectively assessed and addressed.
Directorate objectives are not achieved as a result of demand and
capacity data failing to be properly used and monitored.
4.2 Directorate Review - ACT - Management Arrangements
13 of 380 Audit Committee - Part 1 9 July 2018-09/07/18

Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 6 of 56
OPINIONS AND KEY FINDINGS
4. Assurance Opinions
We are required to provide an opinion as to the adequacy and effectiveness of the system of internal control under review. Previous directorate reviews
have given one overall opinion for the scope of work covered as the objectives were considered in aggregate. However, as we have increased
the both the scope and number of objectives under each of the areas that align with assurance domains it is now more appropriate to report against
each of these domains individually. This review, focussing on management
arrangements, covers risk management and governance (which includes the objectives for standards of conduct and directorate specific),
performance and planning, and workforce, giving three separate opinions
relating to the relevant domain areas.
The opinions are based on the work performed as set out in the scope and objectives within this report. An assurance rating is provided describing the
effectiveness of the system of internal control in place to manage the
identified risks associated with the objectives covered in this review.
The overall level of assurance that can be assigned to a review is dependent on the severity of the findings as applied against the specific review
objectives and should therefore be considered in that context.
Risk management and governance
The level of assurance given as to the effectiveness of the system of internal control in place to manage the risks associated with risk management and
governance is reasonable assurance.
RATING INDICATOR DEFINITION
Reaso
nab
le
assu
ran
ce
The Board can take reasonable
assurance that arrangements to secure governance, risk management and
internal control, within those areas under review, are suitably designed and
applied effectively. Some matters require management attention in control
design or compliance with low to moderate impact on residual risk
exposure until resolved.
Governance Arrangements
There are two key governance groups within the directorate. The Clinical
Business Meeting (CBM) and the Directorate Integrated Governance Business Meeting (DIGBM). The DIGBM covers all aspects of the
directorate’s governance as opposed to there being separate groups for finance or quality, as we have seen in other directorates. In addition, we
understand that departmental meetings regularly occur across the
4.2 Directorate Review - ACT - Management Arrangements
14 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 7 of 56
directorate. Attendance was seen by Finance, Workforce and Planning
Business Partners at all CBM meetings reviewed, however, there was not
consistent attendance from the other Business Partners.
The directorate follows the Health Board's corporate policies and procedures. In addition, Hospital Sterilization and Decontamination Unit
(HSDU), Anaesthetics and Theatres on both sites also have polices that are more specific to the service. We found that Theatres at PCH had a number
of polices that needed to be reviewed.
The CBMs regularly receive workforce and finance performance reports.
However, the Directorate Manager's report, whose purpose is to ‘provide
the Director of Finance, Planning and the Chief Operating Officer with an overview of the directorate’s position in relation to Quality, Performance,
Risk & Finance’, was not on the meeting’s agenda between August 2017 to January 2018. It is unclear if a ‘verbal’ update was provided as an
alternative.
Risk Management
Our review of the risk register and minutes of the CBM and DIGBM meetings identified that risk does not appear to be regularly monitored at these
meetings. High risks in particular where not being reviewed in line with the Health Board’s risk scoring matrix and although evidence could be found
that discussions around the risk register were taking place at the directorate meetings, we found the same errors occurring each quarter they
were presented, which questioned the scrutiny of these reports.
Standards of Conduct
We understand through discussions with the Directorate Manager and
Directorate Support Manager that Declaration of Interest (DoI) requests are managed centrally by the Head of Corporate Services and the
directorate are not made aware of the returns made. As such, declarations and personal interests may not be taken into consideration. Going forward,
following the approval by Audit Committee to extend the range of staff required to complete a declaration to Band 8 and above, the directorate will
need to be clear as to who falls into this category. At present, they are not
requesting Speciality Doctors or Speciality Registrars to make a declaration.
4.2 Directorate Review - ACT - Management Arrangements
15 of 380 Audit Committee - Part 1 9 July 2018-09/07/18

Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 8 of 56
Performance and planning
The level of assurance given as to the effectiveness of the system of internal control in place to manage the risks associated with performance and
planning is reasonable assurance.
RATING INDICATOR DEFINITION
Reaso
nab
le
assu
ran
ce
The Board can take reasonable assurance that arrangements to secure
governance, risk management and internal control, within those areas
under review, are suitably designed and applied effectively. Some matters
require management attention in control
design or compliance with low to moderate impact on residual risk
exposure until resolved.
The directorate has used the Health Board’s Local Planning Framework to
develop its 2018/21 IMTP. The directorate has submitted its draft IMTPs to planning and performance in accordance with the Health Board’s timetable.
We note that the directorate failed to complete the section in the IMTP
appendix where details of the progress in achieving the 2017/18 key
deliverables is reported.
Progress of the development of the IMTP has been reported through the
directorate’s Directorate Integrated Governance Business Meeting.
The activity of the directorate is primarily driven by services to other areas of the Health Board, and as such, demand and capacity is largely driven by
the activity of other directorates. The directorate will begin recording and
reporting demand and capacity activity for Chronic Pain Service in 2018/19.
However, going forward, consideration will have to be given to the findings of the Internal Audit review of Performance Management - Demand and
Capacity Planning that was undertaken in March 2018 to ensure the directorate has the appropriate, robust mechanisms in place to ensure
effective monitoring of their demand and capacity plan.
4.2 Directorate Review - ACT - Management Arrangements
16 of 380Audit Committee - Part 1 9 July 2018-09/07/18

Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 9 of 56
Workforce
The level of assurance given as to the effectiveness of the system of internal control in place to manage the risks associated with workforce is reasonable
assurance.
RATING INDICATOR DEFINITION
Reaso
nab
le
assu
ran
ce
The Board can take reasonable assurance that arrangements to secure
governance, risk management and internal control, within those areas
under review, are suitably designed and applied effectively. Some matters
require management attention in control
design or compliance with low to moderate impact on residual risk
exposure until resolved.
An analysis of absence rates and training and PADR compliance rates was
undertaken for the directorate. The Hospital Sterilization and Decontamination Unit (HSDU) at Royal Glamorgan Hospital (RGH) and ITU
at Prince Charles Hospital (PCH) were the two areas subsequently chosen
for the workforce element of the review. HSDU at RGH is a decontamination
unit, which cleans and sterilizes theatre equipment.
Our workforce testing was split into seven key areas; annual leave, flexi-time and Time of in Lieu (TOIL), sickness management, PADRs, mandatory
training, staff rosters and consultant job plans. We identified examples in both departments where the monitoring and management was not in
accordance with policies. More comprehensive detail regarding these
findings are further on in the report.
No control testing was undertaken in relation to capturing and communication of good practice. Though it was observed through the CBM
and DIGBM meeting minutes that success stories and areas of recognition are discussed. It was also evident that the directorate have good
communication with other directorates as they are pivotal in helping other
achieve their Referral to Treatment (RTT) targets.
4.2 Directorate Review - ACT - Management Arrangements
17 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
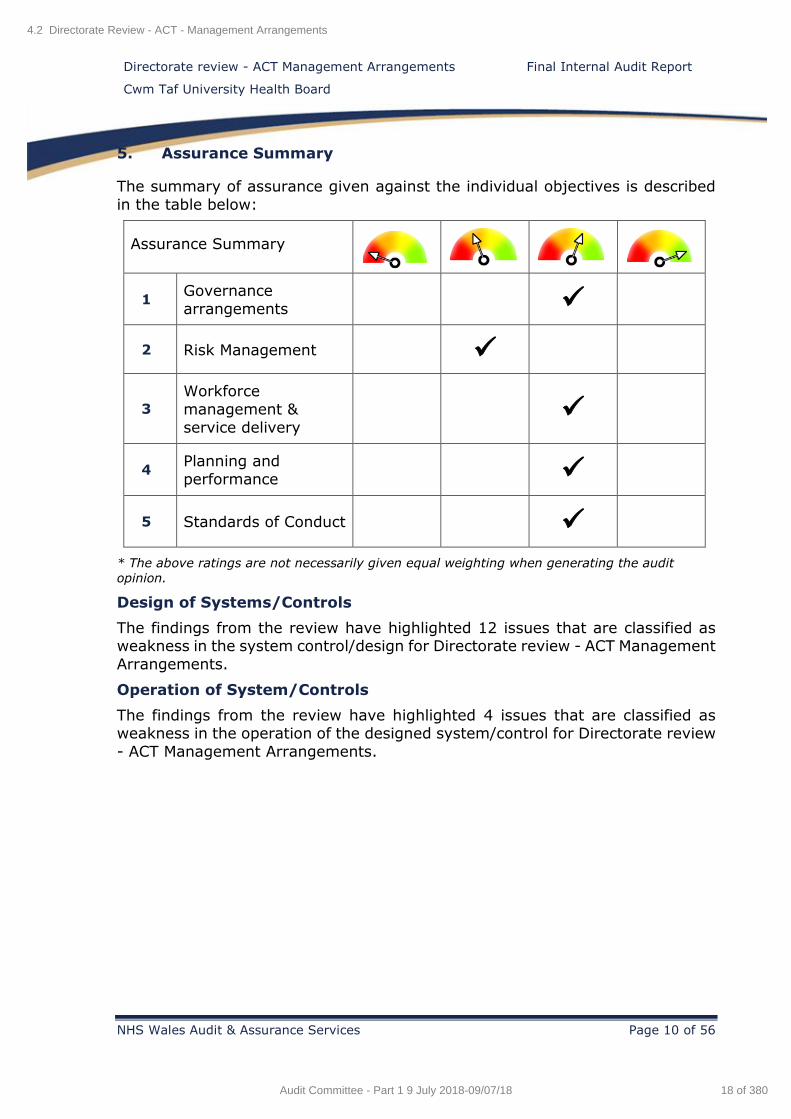
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 10 of 56
5. Assurance Summary
The summary of assurance given against the individual objectives is described
in the table below:
Assurance Summary
1 Governance
arrangements
2 Risk Management
3
Workforce
management &
service delivery
4 Planning and
performance
5 Standards of Conduct
* The above ratings are not necessarily given equal weighting when generating the audit
opinion.
Design of Systems/Controls
The findings from the review have highlighted 12 issues that are classified as weakness in the system control/design for Directorate review - ACT Management
Arrangements.
Operation of System/Controls
The findings from the review have highlighted 4 issues that are classified as weakness in the operation of the designed system/control for Directorate review
- ACT Management Arrangements.
4.2 Directorate Review - ACT - Management Arrangements
18 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 11 of 56
6. Summary of Audit Findings
In this section, we highlight areas of good practice that we identified during our review. We also summarise the findings made during our audit fieldwork. The
detailed findings are reported in the Management Action Plan (Appendix A).
Objective 1: Governance Arrangements
We note the following areas of good practice:
The Finance, Workforce and Planning Business Partners or
representatives attended all Clinical Business Meeting (CBM)
meetings that we reviewed.
The minutes of the directorate’s Integrated Governance Business
Meeting (DIGBM) are cross-referenced to the Health and Care
Standards.
The Hospital Sterilization and Decontamination Unit (HSDU) is ISO certified, and therefore externally assessed annually. Policies and
procedures are reviewed during this process and no issues have been
identified.
Between the CBM and DIGBM there was clear evidence that financial
and workforce performance is monitored.
We identified the following findings:
No terms of reference exist for the DIGBM group so we were unable
to establish the remit of the group, if the meetings were quorate, or
if they were held regularly enough.
There is no committee structure diagram in place that shows the link between the structure of the directorate and the key groups within
the directorate and how information flows between them.
Heads of Nursing have not attended any of the DIGBM meetings and
only a few CBM meetings that we reviewed.
Our review of the PCH Theatres policies and procedures identified that 12/15 policies that are out of date. Three of these policies have
not been reviewed since 2013 and 2014.
A small number of alerts received by the Health Board that are
relevant to the directorate did not appear to have been acted upon in
a timely manner.
Whilst there is evidence of some reporting in relation to the key service change / directorate priorities at both CBM and DIGBM, this
does not appear to be in a systematic way. The directorate managers’ report was not an item on the CBM agenda for the period August
2017 to January 2018.
Departmental mandatory training compliance data has not been
discussed during any of the DIGBM meetings minutes that we
reviewed.
4.2 Directorate Review - ACT - Management Arrangements
19 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 12 of 56
Objective 2: Risk Management
We identified the following findings:
The directorate has 12 risks categorised as high, three of which
according to DATIX records have not been reviewed since 2014.
Risks do not always have actions identified against them in DATIX.
Risks relating to Outpatients still feature on ACT risk register.
Outpatients has not been part of the directorate since mid-2017.
50% of the handlers that have a risk allocated to them on ACT risk
register no longer work for the directorate.
A review of the DIGBM meetings established that the risk register is
not a standing agenda item.
A review of the CBM meetings established that a report containing
risk data was presented for quarter one and two, but not for the latter part of the year. This report focusses on the high risks the directorate
currently has, however it does not contain basic information such as
when these risks were first created or last reviewed.
Objective 3 - Workforce & Service Delivery
We note the following areas of good practice:
Annual Leave
The process for booking annual leave within the ITU department is
well managed. We note that staff request annual leave months in advance, and it appears to be allocated fairly within the department.
Part way through the year management review outstanding leave to ensure staff are taking leave appropriately so as not to adversely
affect their wellbeing.
The annual leave dates for ITU that are shown on the roster system
(Health Roster) correspond to what is shown in ESR.
Sickness
HSDU use a ‘point of contact’ form to record the contact had with the
employee during their sickness, whereas ITU use the Human Resources ‘Sickness and Absence summary sheet’ to record sickness
episodes.
We identified the following findings:
Annual Leave
Reconciliations are not undertaken at the start of the year or at any
point in the year, between the ESR system and the systems used (Health Rostering or paper based) in the two areas where our testing
was carried out.
Both departments were calculating the annual leave entitlement
based on the incorrect number of bank holidays. Additionally, the
4.2 Directorate Review - ACT - Management Arrangements
20 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 13 of 56
annual leave entitlement was not adjusted for those who reduced
working hours during the year, or for those that were entitled to
additional leave due to years’ service.
We identified administration errors within HSDU in relation to running balances being incorrectly calculated on leave cards and leave cards
being continuously changing throughout the year, meaning a balance
could not be calculated.
We also note errors in relation to the recoding of leave within Health Rostering, where leave was recorded manually on the 'off duty'
(paper) roster but had not been transferred to the Health Roster
system. Furthermore the method of input of annual leave on Health Roster, means errors occur when the data is transferred to ESR,
resulting the ESR balance reporting incorrectly.
Flexi Leave and TOIL
There is no flexi time / TOIL policy in place within the directorate.
The ITU department at PCH use the Health Rostering system, which
has the facility to record hours as TOIL, however this function is not
being utilised.
Our testing at the HSDU department at the RGH identified a number
of operational errors in relation to record keeping.
Sickness
An out of date (January 2013) All Wales Sickness Policy was in use
at HSDU.
We identified errors in relation to completing self-certification and
Return to Work (RTW) forms in both areas we reviewed. We also
identified occasions when medical certificates were not always
obtained when required.
We noted instances whereby sickness triggers had been met and staff had not received the appropriate return to work / trigger interview
according to the sickness policy.
PADR's
A copy of the previous year’s PADR was not always retained in both
areas reviewed.
At the time of the audit both areas were not compliant with the Health Board target for PADR's. Out testing identified that not all staff had
been subjected to an annual PADR in 2017/18.
PADR documentation was not always completed fully and particularly
in HSDU no meaningful objectives had been set for staff. There were examples whereby the documentation was not signed by both the
manager and employee.
4.2 Directorate Review - ACT - Management Arrangements
21 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 14 of 56
Mandatory Training
Across the 11 core modules HSDU was reporting an average
compliance rate of 17% and ITU at PCH was 60%.
We identified that not all staff had updated ESR to reflect their Welsh
Language skills, which has an adverse effect on compliance rates.
Monitoring at a departmental level is not taking place to identify any
problem areas to identify reasons for non-compliance.
Staff Rostering
ITU at PCH are using the Health Rostering system and for a four week
period reviewed, the unit worked 32 out of 84 shifts under the
required template for qualified nurses and Health Care Support Workers (HSCW) staff. There was one instance when the unit
operated with five staff during the day shift instead of the
recommended eight.
There were occasions when the unit worked over the agreed template; 18 out of 84 shifts were over established by two staff, all
of which were day shifts.
Reasons for changes in the establishment are not recorded into the
Health Rostering system, therefore it was not possible to determine
the reasons behind the under / over establishment.
Consultant Job Plans
Out testing identified five of nine job plans where there was no
evidence that the plan had been signed-off by either the consultant, directorate manager or Clinical Director. These were recorded as
either 'in discussion' or 'locked down'.
One job plan the number of sessions for direct clinical care did not
fully reconcile to the information recorded on ESR.
Objective 4: Planning and Performance
We note the following areas of good practice:
The directorate has used the Local Planning Framework when developing its draft 2018/21 IMTP. The IMTP referenced all key areas
required, and the drafts of the IMTP were submitted to the Planning
and Performance department by the required deadlines.
The DIGBM group were kept up to date with the progress of drafting
the IMTP.
The performance measures applicable to the directorate are
referenced in the IMTP.
We identified the following finding:
The 2018/21 IMTP appendix contains a 2017/18 key deliverables
tracker, however this has not completed. Furthermore evidence
4.2 Directorate Review - ACT - Management Arrangements
22 of 380Audit Committee - Part 1 9 July 2018-09/07/18
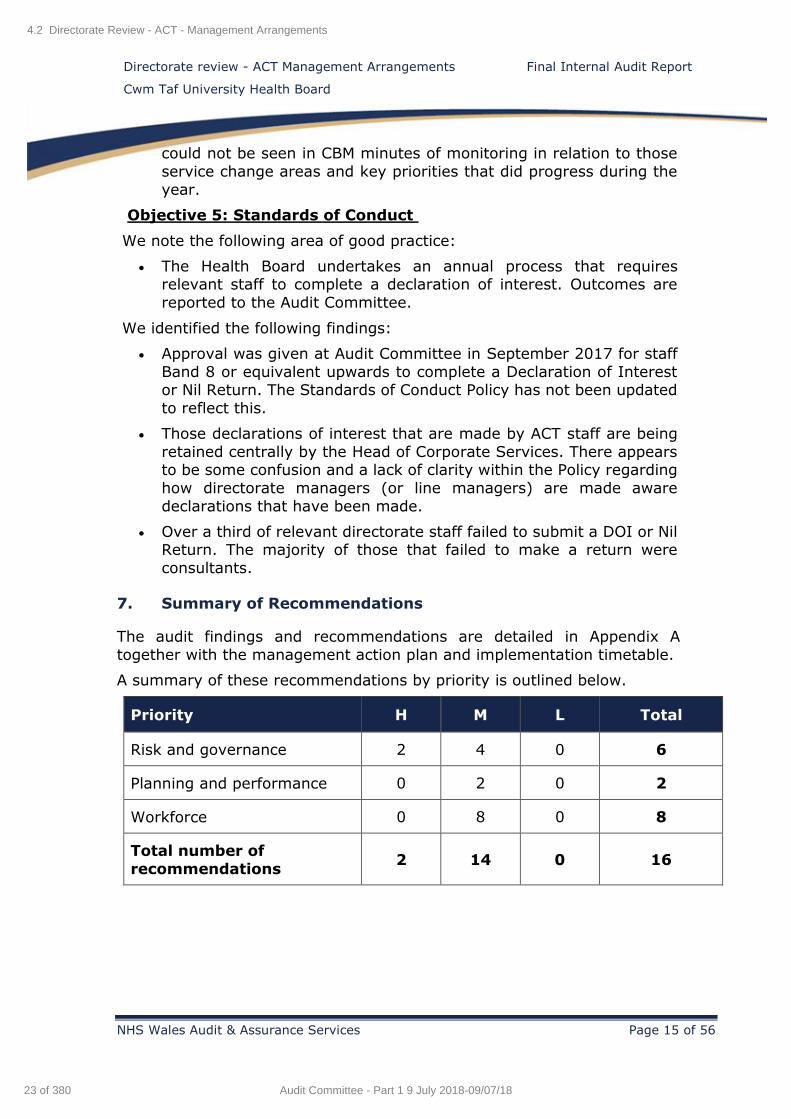
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 15 of 56
could not be seen in CBM minutes of monitoring in relation to those
service change areas and key priorities that did progress during the
year.
Objective 5: Standards of Conduct
We note the following area of good practice:
The Health Board undertakes an annual process that requires relevant staff to complete a declaration of interest. Outcomes are
reported to the Audit Committee.
We identified the following findings:
Approval was given at Audit Committee in September 2017 for staff
Band 8 or equivalent upwards to complete a Declaration of Interest or Nil Return. The Standards of Conduct Policy has not been updated
to reflect this.
Those declarations of interest that are made by ACT staff are being
retained centrally by the Head of Corporate Services. There appears to be some confusion and a lack of clarity within the Policy regarding
how directorate managers (or line managers) are made aware
declarations that have been made.
Over a third of relevant directorate staff failed to submit a DOI or Nil Return. The majority of those that failed to make a return were
consultants.
7. Summary of Recommendations
The audit findings and recommendations are detailed in Appendix A
together with the management action plan and implementation timetable.
A summary of these recommendations by priority is outlined below.
Priority H M L Total
Risk and governance 2 4 0 6
Planning and performance 0 2 0 2
Workforce 0 8 0 8
Total number of
recommendations 2 14 0 16
4.2 Directorate Review - ACT - Management Arrangements
23 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
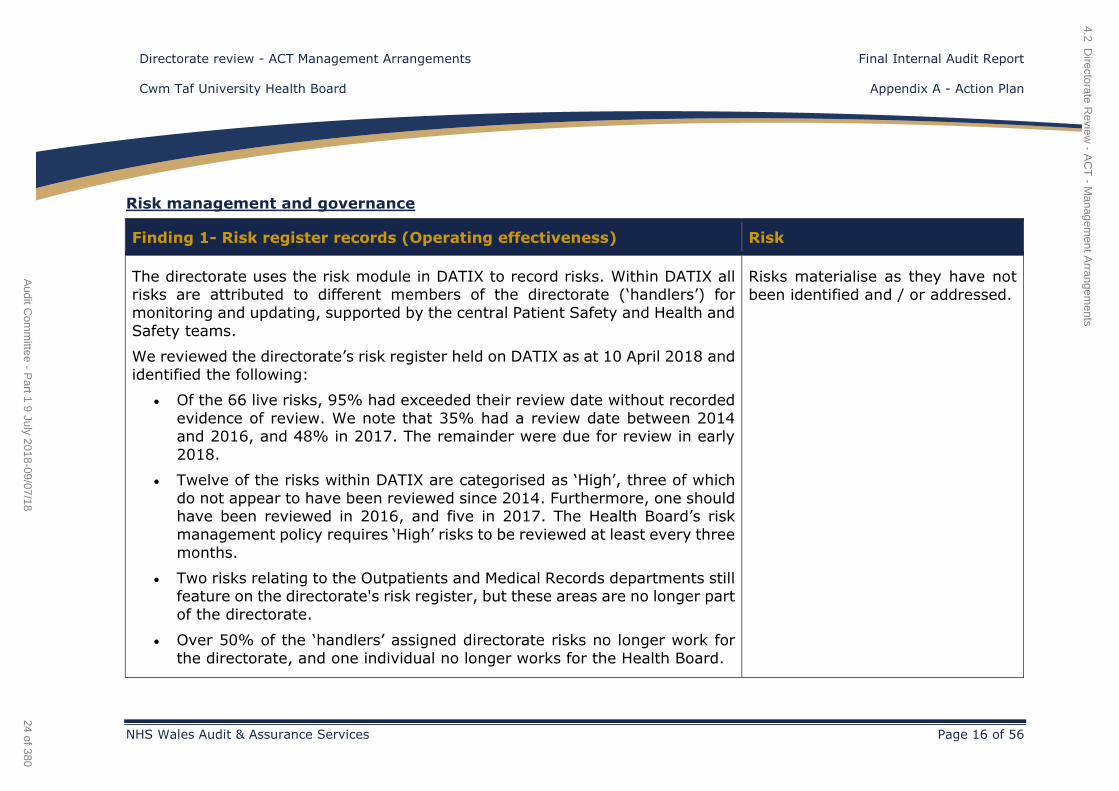
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 16 of 56
Risk management and governance
Finding 1- Risk register records (Operating effectiveness) Risk
The directorate uses the risk module in DATIX to record risks. Within DATIX all risks are attributed to different members of the directorate (‘handlers’) for
monitoring and updating, supported by the central Patient Safety and Health and
Safety teams.
We reviewed the directorate’s risk register held on DATIX as at 10 April 2018 and
identified the following:
Of the 66 live risks, 95% had exceeded their review date without recorded
evidence of review. We note that 35% had a review date between 2014 and 2016, and 48% in 2017. The remainder were due for review in early
2018.
Twelve of the risks within DATIX are categorised as ‘High’, three of which
do not appear to have been reviewed since 2014. Furthermore, one should have been reviewed in 2016, and five in 2017. The Health Board’s risk
management policy requires ‘High’ risks to be reviewed at least every three
months.
Two risks relating to the Outpatients and Medical Records departments still feature on the directorate's risk register, but these areas are no longer part
of the directorate.
Over 50% of the ‘handlers’ assigned directorate risks no longer work for
the directorate, and one individual no longer works for the Health Board.
Risks materialise as they have not
been identified and / or addressed.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
24 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
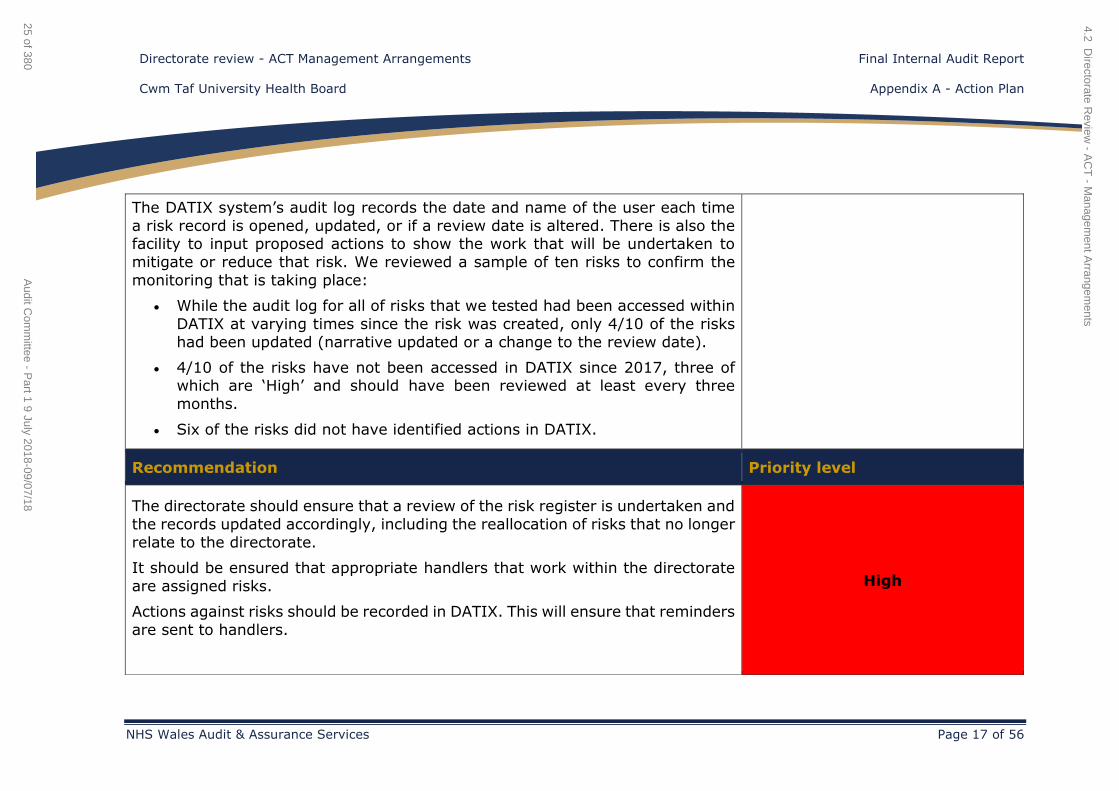
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 17 of 56
The DATIX system’s audit log records the date and name of the user each time
a risk record is opened, updated, or if a review date is altered. There is also the facility to input proposed actions to show the work that will be undertaken to
mitigate or reduce that risk. We reviewed a sample of ten risks to confirm the
monitoring that is taking place:
While the audit log for all of risks that we tested had been accessed within
DATIX at varying times since the risk was created, only 4/10 of the risks
had been updated (narrative updated or a change to the review date).
4/10 of the risks have not been accessed in DATIX since 2017, three of which are ‘High’ and should have been reviewed at least every three
months.
Six of the risks did not have identified actions in DATIX.
Recommendation Priority level
The directorate should ensure that a review of the risk register is undertaken and
the records updated accordingly, including the reallocation of risks that no longer
relate to the directorate.
It should be ensured that appropriate handlers that work within the directorate
are assigned risks.
Actions against risks should be recorded in DATIX. This will ensure that reminders
are sent to handlers.
High
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
25 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
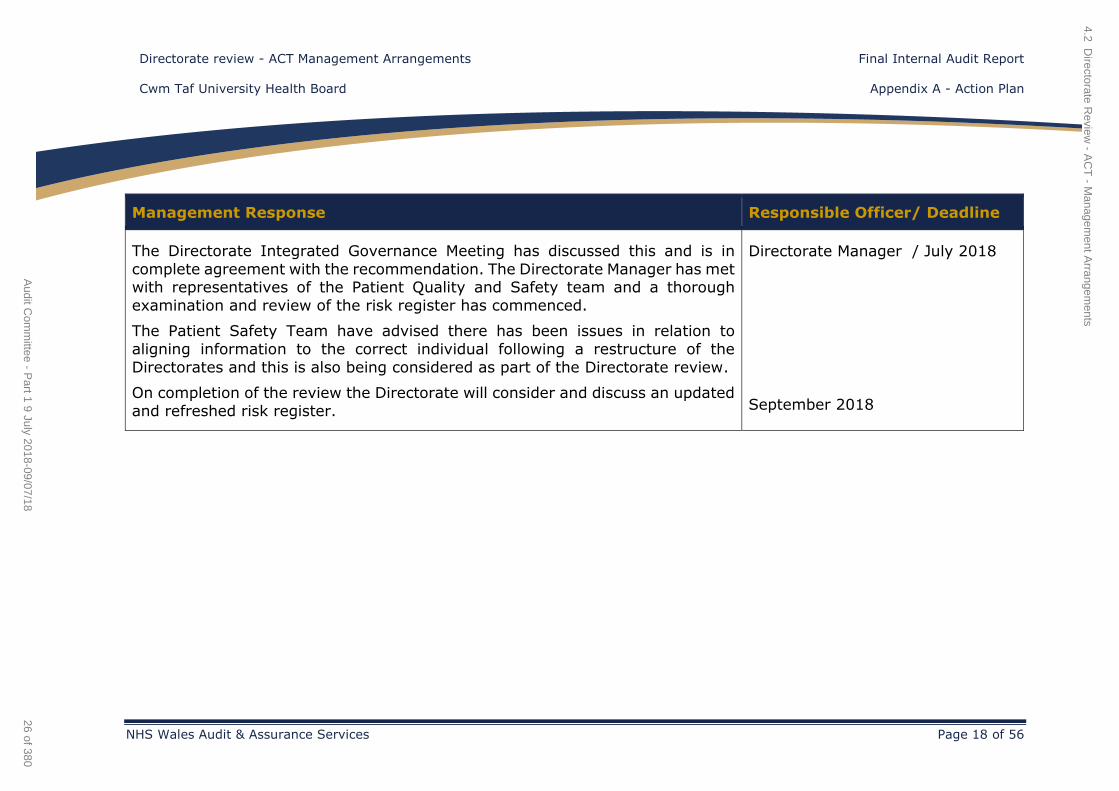
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 18 of 56
Management Response Responsible Officer/ Deadline
The Directorate Integrated Governance Meeting has discussed this and is in
complete agreement with the recommendation. The Directorate Manager has met with representatives of the Patient Quality and Safety team and a thorough
examination and review of the risk register has commenced.
The Patient Safety Team have advised there has been issues in relation to
aligning information to the correct individual following a restructure of the
Directorates and this is also being considered as part of the Directorate review.
On completion of the review the Directorate will consider and discuss an updated
and refreshed risk register.
Directorate Manager / July 2018
September 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
26 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 19 of 56
Finding 2 - Risk reporting (Operating effectiveness) Risk
Clinical Business Meeting (CBM)
While risk is discussed at the CBMs on a quarterly basis as part of the performance information section of the agenda, a more detailed review of risk
forms part of the Non Patient Safety Incidents, Risk and Claims report.
Our review of the CBM agendas confirmed that the Non Patient Safety Incidents,
Risk and Claims report was presented between May and October 2017. However, this report was not presented to the CBM between November 2017 and March
2018, although the reports were produced for this period (Quarter 3 and 4). We
note:
Risks awaiting approval are recorded separately in the report as they do
not feature on the risk register until they have been approved. Quarter 3 and 4 reported the same four risks in this status. Three of these risks have
been classified as potentially ‘high’ and should have been reviewed immediately. Furthermore, two of the handlers that had been assigned
these risks no longer work for the directorate.
Although the report identifies the number of high risks that are on the risk
register for the quarter, the date when the risk was first created and last reviewed is not included. Therefore, it is unclear how long a risk has been
on the register, and when it was last reviewed.
Risks materialise as they have not
been identified and / or addressed.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
27 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 20 of 56
Directorate Integrated Governance Business Meeting (DIGBM)
A risk register review is not a standing agenda item for the DIGBM. However, we can see from the minutes of the meeting that in May 2017 the Directorate
Manager at the time stated that the Patient Safety Manager was currently
updating the risk register as it was four years out of date. We also note that during the October 2017 meeting, it was highlighted that the risk register should
be reviewed regularly ‘especially as the Head of Nursing had retired’.
While there is some evidence of the risk and the risk register being discussed at
the CBM and DIGBM meetings, there does not appear to be the level of scrutiny
that we would expect.
Furthermore, there does not appear to be a named lead within the directorate with overall responsibility for monitoring the risk register. Whilst we understand
that the Directorate Manager reviews risks on DATIX on a regular basis we were
unable to confirm this from our sample of risks that we tested.
Recommendation Priority level
Proactive monitoring of risks should take place to ensure action is being taken in
a timely manner.
All actions taken, including amending the review date should be recorded in
DATIX.
Those potential risks awaiting approval should be allocated to current directorate
employees and assessed for inclusion on the register as a matter of urgency.
High
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
28 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 21 of 56
It should be ensured that the Non Patient Safety Incidents, Risk and Claims
report that contains the risk register is presented at each CBM meeting and if necessary at the DIGBM meetings in order for risks to be discussed in greater
detail.
The risk data contained in the report should be made more meaningful by including details of when the risk was first opened and when it was last reviewed.
Where is it obvious that the data contained within the report is inaccurate, action should be taken to remedy this. Basic errors in information, such as risks being
attributed to ex-employees, should not occur in consecutive reports.
Management Response Responsible Officer/ Deadline
The Directorate has a dedicated standing agenda item for patient safety and risk. The risk register will be attached with supporting papers and the key areas will
be discussed.
The key areas discussed at the Integrated Governance Meeting will be submitted
to the CBM as part of the Directorate Managers Report.
Directorate Manager/Head of
Nursing
July 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
29 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 22 of 56
Finding -3 - Declarations of Interest (Control design) Risk
In September 2017 the Audit Committee approved amendments to the Standards
of Behaviour Policy to incorporate the requirement for staff Band 8 and above to complete a declaration of interest. Reference was also made in the same Audit
Committee report to the requirement for ‘Nil Returns’. Neither of these points are
incorporated in the policy that is currently available to staff.
We reviewed the directorate’s declaration of interest returns to ensure relevant
staff within the directorate had submitted a Declaration of Interest (DoI) or a Nil Return for 2017/18. Based on the directorates’ interpretation of the policy
(Senior Managers, Nurse Managers and Consultants). For the directorate 31/52 returns were made in total. Of the 47 consultants within the directorate 29 had
completed their returns.
Those declarations of interest that are made by ACT staff are submitted and
retained centrally by the Head of Corporate Services. There appears to be some confusion, and a lack of clarity within the policy, regarding how line managers
are made aware of declarations that have been made by their staff, other than
to be provided with a list of outstanding returns.
The directorate is not appropriately
governed which could result in a service that is not being delivered
safely and effectively.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
30 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
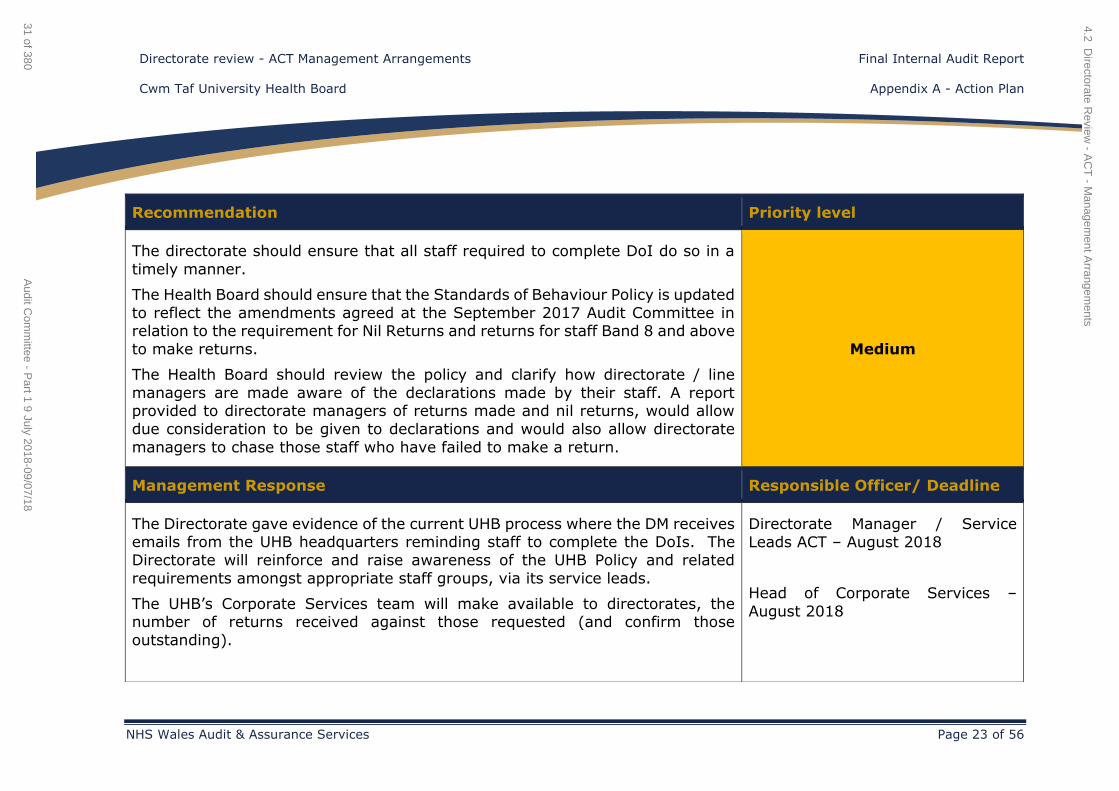
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 23 of 56
Recommendation Priority level
The directorate should ensure that all staff required to complete DoI do so in a
timely manner.
The Health Board should ensure that the Standards of Behaviour Policy is updated
to reflect the amendments agreed at the September 2017 Audit Committee in relation to the requirement for Nil Returns and returns for staff Band 8 and above
to make returns.
The Health Board should review the policy and clarify how directorate / line
managers are made aware of the declarations made by their staff. A report provided to directorate managers of returns made and nil returns, would allow
due consideration to be given to declarations and would also allow directorate
managers to chase those staff who have failed to make a return.
Medium
Management Response Responsible Officer/ Deadline
The Directorate gave evidence of the current UHB process where the DM receives emails from the UHB headquarters reminding staff to complete the DoIs. The
Directorate will reinforce and raise awareness of the UHB Policy and related
requirements amongst appropriate staff groups, via its service leads.
The UHB’s Corporate Services team will make available to directorates, the number of returns received against those requested (and confirm those
outstanding).
Directorate Manager / Service
Leads ACT – August 2018
Head of Corporate Services –
August 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
31 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 24 of 56
The UHB Policy is currently due for review and the report findings /
recommendation will be reviewed and considered further. It should be noted that all relevant staff not just those Band 8a and above, need to be aware of and
compliant with the Policy.
Board Secretary / Director of
Corporate Services & Governance -
August 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
32 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
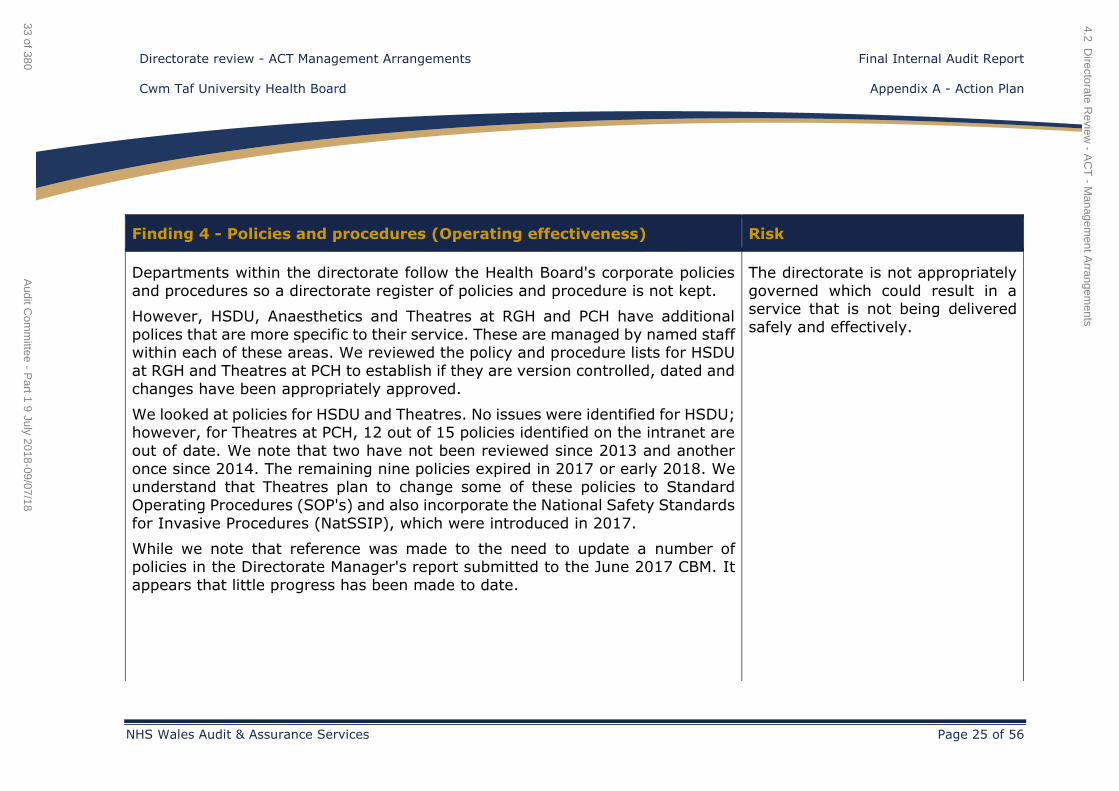
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 25 of 56
Finding 4 - Policies and procedures (Operating effectiveness) Risk
Departments within the directorate follow the Health Board's corporate policies
and procedures so a directorate register of policies and procedure is not kept.
However, HSDU, Anaesthetics and Theatres at RGH and PCH have additional
polices that are more specific to their service. These are managed by named staff within each of these areas. We reviewed the policy and procedure lists for HSDU
at RGH and Theatres at PCH to establish if they are version controlled, dated and
changes have been appropriately approved.
We looked at policies for HSDU and Theatres. No issues were identified for HSDU; however, for Theatres at PCH, 12 out of 15 policies identified on the intranet are
out of date. We note that two have not been reviewed since 2013 and another
once since 2014. The remaining nine policies expired in 2017 or early 2018. We understand that Theatres plan to change some of these policies to Standard
Operating Procedures (SOP's) and also incorporate the National Safety Standards
for Invasive Procedures (NatSSIP), which were introduced in 2017.
While we note that reference was made to the need to update a number of policies in the Directorate Manager's report submitted to the June 2017 CBM. It
appears that little progress has been made to date.
The directorate is not appropriately
governed which could result in a service that is not being delivered
safely and effectively.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
33 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
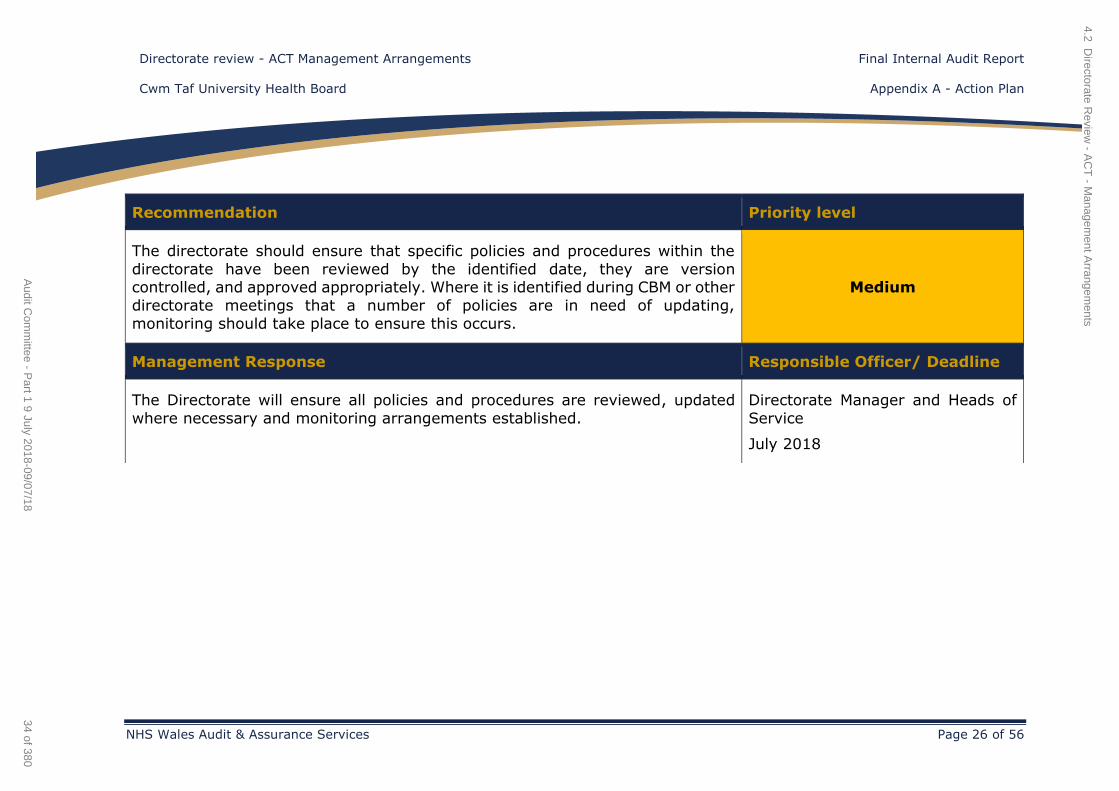
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 26 of 56
Recommendation Priority level
The directorate should ensure that specific policies and procedures within the
directorate have been reviewed by the identified date, they are version controlled, and approved appropriately. Where it is identified during CBM or other
directorate meetings that a number of policies are in need of updating,
monitoring should take place to ensure this occurs.
Medium
Management Response Responsible Officer/ Deadline
The Directorate will ensure all policies and procedures are reviewed, updated
where necessary and monitoring arrangements established.
Directorate Manager and Heads of
Service
July 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
34 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
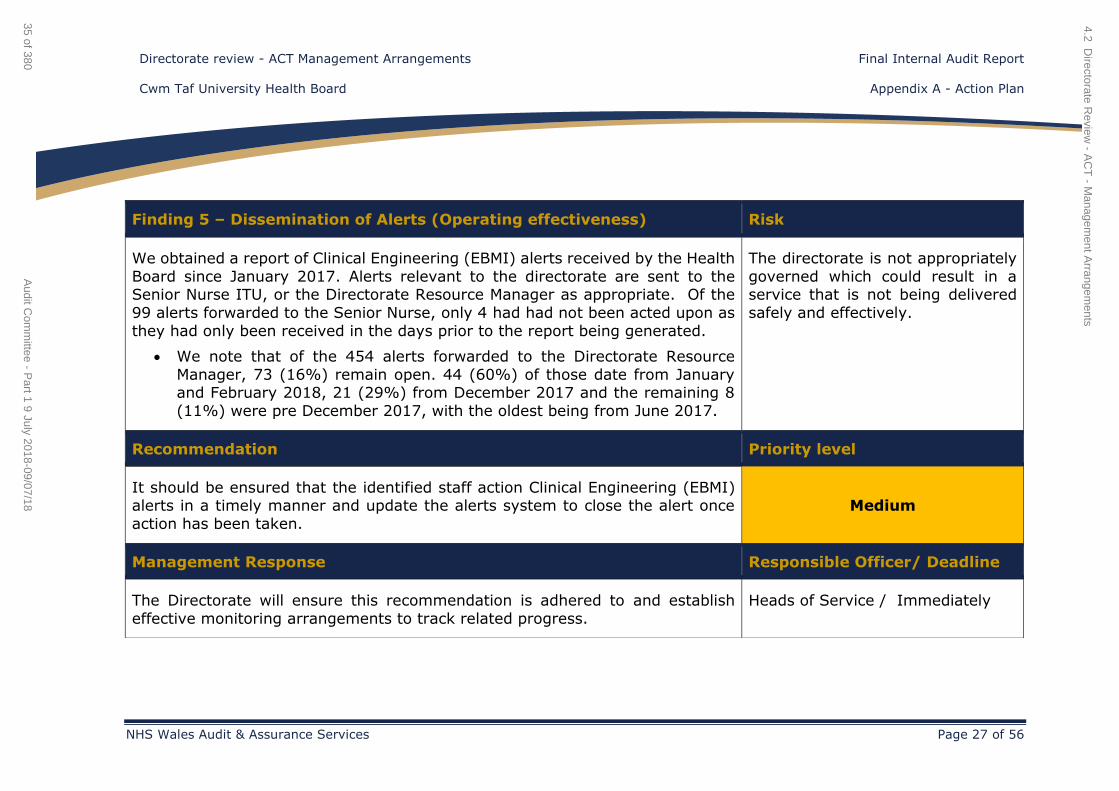
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 27 of 56
Finding 5 – Dissemination of Alerts (Operating effectiveness) Risk
We obtained a report of Clinical Engineering (EBMI) alerts received by the Health
Board since January 2017. Alerts relevant to the directorate are sent to the Senior Nurse ITU, or the Directorate Resource Manager as appropriate. Of the
99 alerts forwarded to the Senior Nurse, only 4 had had not been acted upon as
they had only been received in the days prior to the report being generated.
We note that of the 454 alerts forwarded to the Directorate Resource
Manager, 73 (16%) remain open. 44 (60%) of those date from January and February 2018, 21 (29%) from December 2017 and the remaining 8
(11%) were pre December 2017, with the oldest being from June 2017.
The directorate is not appropriately
governed which could result in a service that is not being delivered
safely and effectively.
Recommendation Priority level
It should be ensured that the identified staff action Clinical Engineering (EBMI) alerts in a timely manner and update the alerts system to close the alert once
action has been taken.
Medium
Management Response Responsible Officer/ Deadline
The Directorate will ensure this recommendation is adhered to and establish
effective monitoring arrangements to track related progress.
Heads of Service / Immediately
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
35 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
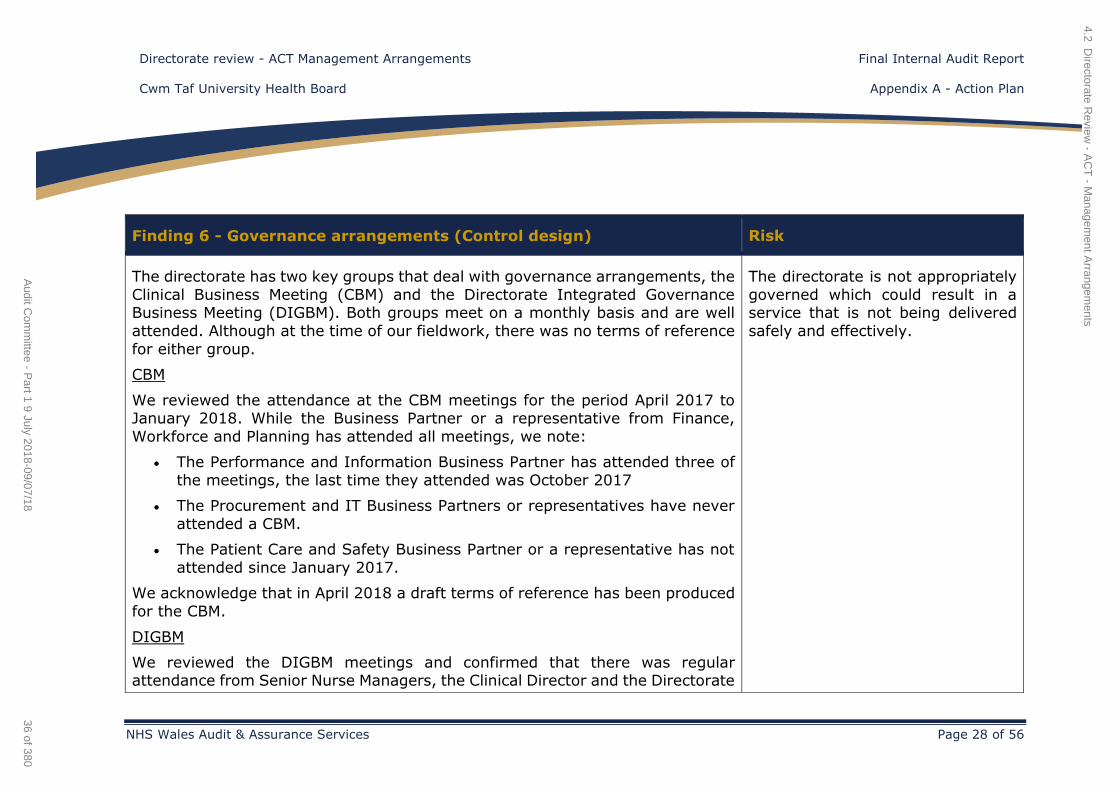
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 28 of 56
Finding 6 - Governance arrangements (Control design) Risk
The directorate has two key groups that deal with governance arrangements, the
Clinical Business Meeting (CBM) and the Directorate Integrated Governance Business Meeting (DIGBM). Both groups meet on a monthly basis and are well
attended. Although at the time of our fieldwork, there was no terms of reference
for either group.
CBM
We reviewed the attendance at the CBM meetings for the period April 2017 to January 2018. While the Business Partner or a representative from Finance,
Workforce and Planning has attended all meetings, we note:
The Performance and Information Business Partner has attended three of
the meetings, the last time they attended was October 2017
The Procurement and IT Business Partners or representatives have never
attended a CBM.
The Patient Care and Safety Business Partner or a representative has not
attended since January 2017.
We acknowledge that in April 2018 a draft terms of reference has been produced
for the CBM.
DIGBM
We reviewed the DIGBM meetings and confirmed that there was regular attendance from Senior Nurse Managers, the Clinical Director and the Directorate
The directorate is not appropriately
governed which could result in a service that is not being delivered
safely and effectively.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
36 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
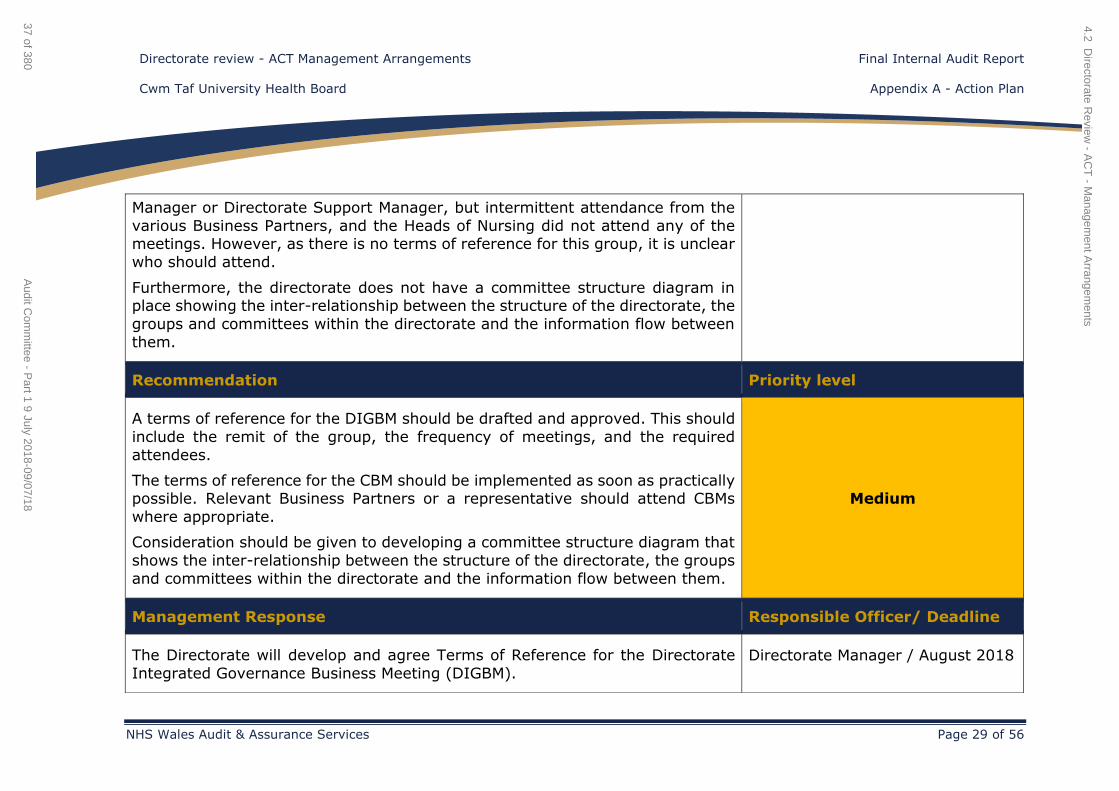
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 29 of 56
Manager or Directorate Support Manager, but intermittent attendance from the
various Business Partners, and the Heads of Nursing did not attend any of the meetings. However, as there is no terms of reference for this group, it is unclear
who should attend.
Furthermore, the directorate does not have a committee structure diagram in place showing the inter-relationship between the structure of the directorate, the
groups and committees within the directorate and the information flow between
them.
Recommendation Priority level
A terms of reference for the DIGBM should be drafted and approved. This should
include the remit of the group, the frequency of meetings, and the required
attendees.
The terms of reference for the CBM should be implemented as soon as practically possible. Relevant Business Partners or a representative should attend CBMs
where appropriate.
Consideration should be given to developing a committee structure diagram that
shows the inter-relationship between the structure of the directorate, the groups
and committees within the directorate and the information flow between them.
Medium
Management Response Responsible Officer/ Deadline
The Directorate will develop and agree Terms of Reference for the Directorate
Integrated Governance Business Meeting (DIGBM). Directorate Manager / August 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
37 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
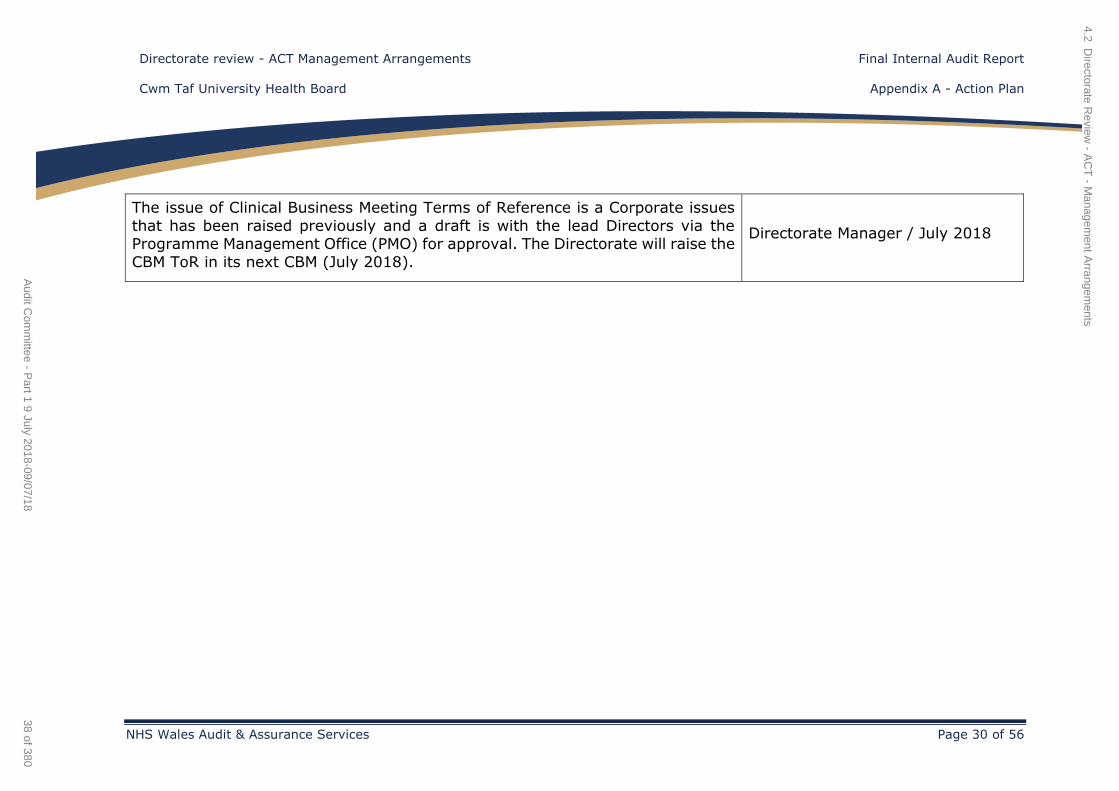
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 30 of 56
The issue of Clinical Business Meeting Terms of Reference is a Corporate issues
that has been raised previously and a draft is with the lead Directors via the Programme Management Office (PMO) for approval. The Directorate will raise the
CBM ToR in its next CBM (July 2018).
Directorate Manager / July 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
38 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 31 of 56
Planning and performance
Finding 7 - Tracking performance (Operating effectiveness) Risk
Within the appendices spreadsheet that accompanies the 2018/21 IMTP there is
a document called 'Directorate Progress Report'. It appears that this spreadsheet
is a tracker that should show the key deliverables for 2017/18, and RAG rate how these have been achieved. However in the draft IMTP submitted in March 2018
this particular spreadsheet is blank. The Directorate Manager confirmed that this tracker has never been completed, as an alternative a narrative report is included
in the main body of the IMTP.
We note that within the main body of the 2018/21 IMTP, Chapter 5 provides
information on Progress in Delivering the 2017/18 Plan. The content of the chapter mostly provides narrative details on the performance / achievements of
the key areas within the directorate such as Theatres, Chronic Pain, pre-assessment. However the link between the narrative here and the key service
changes (top five directorate priorities) that are listed in the 2017/20 IMTP are
not clear.
Services are not effectively
planned.
Recommendation Priority level
It should be ensured that all aspects of the IMTP template and appendices are
completed to allow the tracking of key service changes that the directorate is
trying to instigate.
Medium
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
39 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 32 of 56
Management Response Responsible Officer/ Deadline
The Directorate will ensure this recommendation is adhered to and establish
effective monitoring arrangements to track related progress aligned with the
IMTP processes.
Directorate Manager / March 2019
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
40 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 33 of 56
Finding 8 - Reporting and monitoring performance (Operating
effectiveness) Risk
There are a number of key areas where performance monitoring should occur, namely finance, workforce and key deliverables, and service change priorities
outlined in the IMTP. We reviewed agendas and action logs of the CBM and the agenda and minutes for the DIGBM to establish the level of monitoring taking
place. While we did not make any findings with regards to financial monitoring
we identified the following:
Service Change monitoring
A review of the IMTP for 2017/20 identifies the directorate priorities, including
the top five priorities that form the service change plan.
The CBM agendas contain a standing item called ‘Directorate Manager's Report’. The purpose of the report is to ‘provide the Director of Finance, Planning and the
Chief Operating Officer with an overview of the directorate’s position in relation to Quality, Performance, Risk & Finance’. As such, it is through this report that
the Directorate Manager should be reporting directorate’s progress against the
key priorities outlined in the IMTP.
For the period August 2017 to January 2018 directorate manager reports were not attached to the agenda, as such it is unclear if the Directorate Manager
submitted a report, or if verbal feedback was provided.
Our review of the Directorate Manager reports that were presented, along with
any other reports presented to CBM and the agenda and minutes of the DIGBM
identified that reference was made to the Pre-assessment business case and the
Services are not effectively
planned.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
41 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 34 of 56
24/7 Outreach service at PCH, which are two of the directorates top priorities
forming the service change plan.
However, as the Directorate Manager’s report was not on the agenda for the
period August to January, it is not possible to demonstrate fully how directorate
wide performance is being monitored against the priorities set out in the IMTP.
Workforce monitoring
We reviewed the agendas and papers of the CBM meetings, for nine meetings
covering the period April 2017 to January 2018 and note that:
A report on sickness was presented on four occasions.
A report on PADR compliance was presented at every meeting.
A report on Mandatory Training compliance rates was presented on eight
occasions.
We also note that the sickness reports to CBM are high level and the minutes of the DIGBM meetings confirmed that more detailed discussions by department
are undertaken at this meeting. Whilst we acknowledge that overall the directorate does not have a high sickness rate, there are departments within the
directorate that have higher rates than others do.
However, there was no evidence of mandatory training compliance at any of the
DIGBM meetings. As these meetings are attended by Heads of Department /
Service, then monitoring at department level should be taking place in order for
actions to filter down to department team meetings.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
42 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
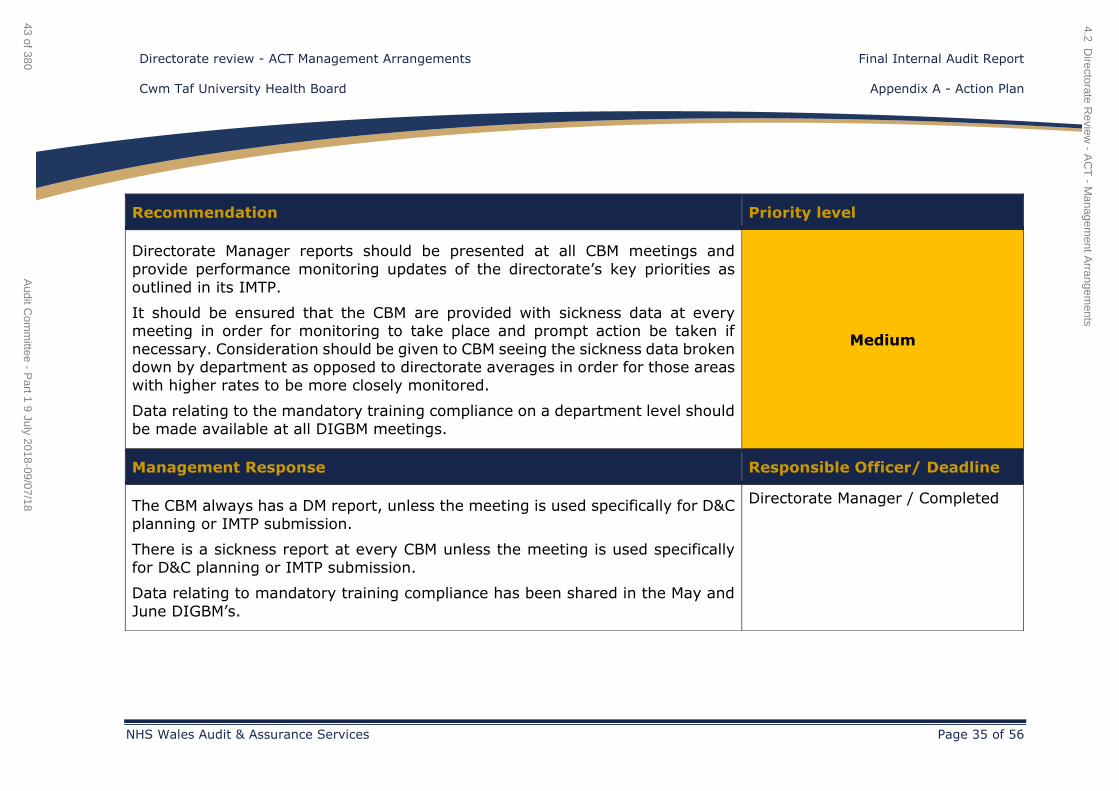
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 35 of 56
Recommendation Priority level
Directorate Manager reports should be presented at all CBM meetings and
provide performance monitoring updates of the directorate’s key priorities as
outlined in its IMTP.
It should be ensured that the CBM are provided with sickness data at every meeting in order for monitoring to take place and prompt action be taken if
necessary. Consideration should be given to CBM seeing the sickness data broken down by department as opposed to directorate averages in order for those areas
with higher rates to be more closely monitored.
Data relating to the mandatory training compliance on a department level should
be made available at all DIGBM meetings.
Medium
Management Response Responsible Officer/ Deadline
The CBM always has a DM report, unless the meeting is used specifically for D&C
planning or IMTP submission.
There is a sickness report at every CBM unless the meeting is used specifically
for D&C planning or IMTP submission.
Data relating to mandatory training compliance has been shared in the May and
June DIGBM’s.
Directorate Manager / Completed
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
43 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
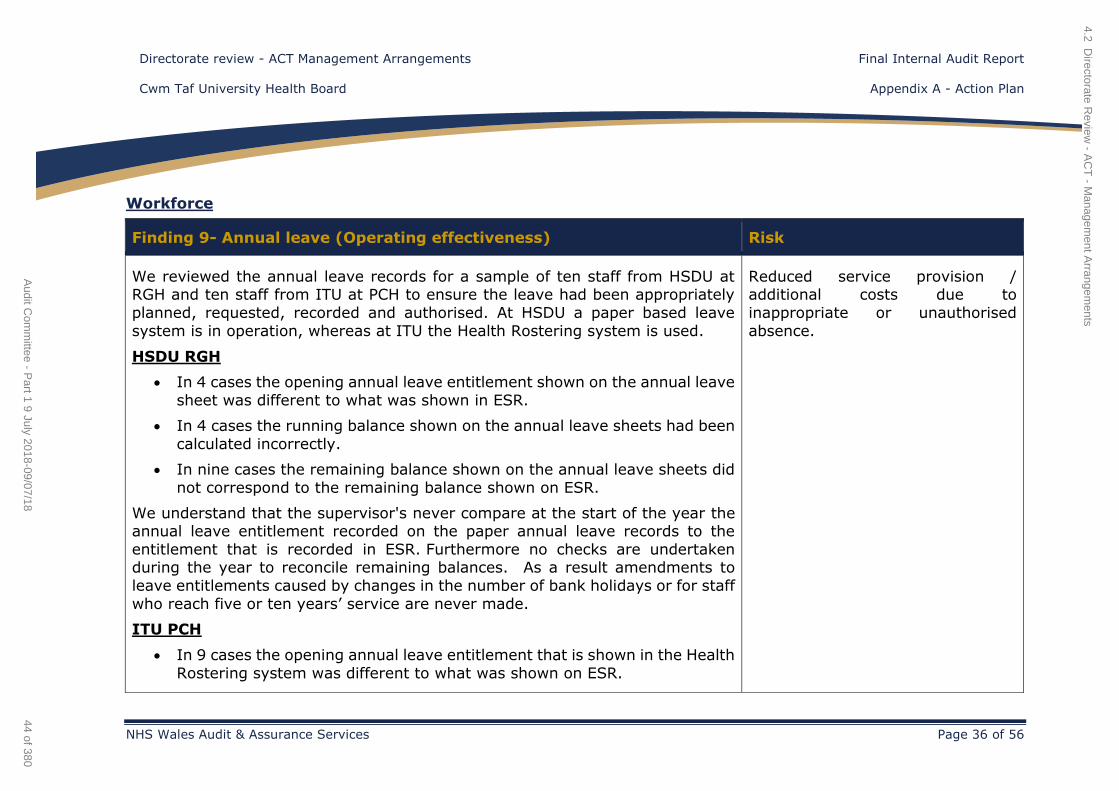
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 36 of 56
Workforce
Finding 9- Annual leave (Operating effectiveness) Risk
We reviewed the annual leave records for a sample of ten staff from HSDU at RGH and ten staff from ITU at PCH to ensure the leave had been appropriately
planned, requested, recorded and authorised. At HSDU a paper based leave
system is in operation, whereas at ITU the Health Rostering system is used.
HSDU RGH
In 4 cases the opening annual leave entitlement shown on the annual leave
sheet was different to what was shown in ESR.
In 4 cases the running balance shown on the annual leave sheets had been
calculated incorrectly.
In nine cases the remaining balance shown on the annual leave sheets did
not correspond to the remaining balance shown on ESR.
We understand that the supervisor's never compare at the start of the year the annual leave entitlement recorded on the paper annual leave records to the
entitlement that is recorded in ESR. Furthermore no checks are undertaken during the year to reconcile remaining balances. As a result amendments to
leave entitlements caused by changes in the number of bank holidays or for staff
who reach five or ten years’ service are never made.
ITU PCH
In 9 cases the opening annual leave entitlement that is shown in the Health
Rostering system was different to what was shown on ESR.
Reduced service provision / additional costs due to
inappropriate or unauthorised
absence.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
44 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
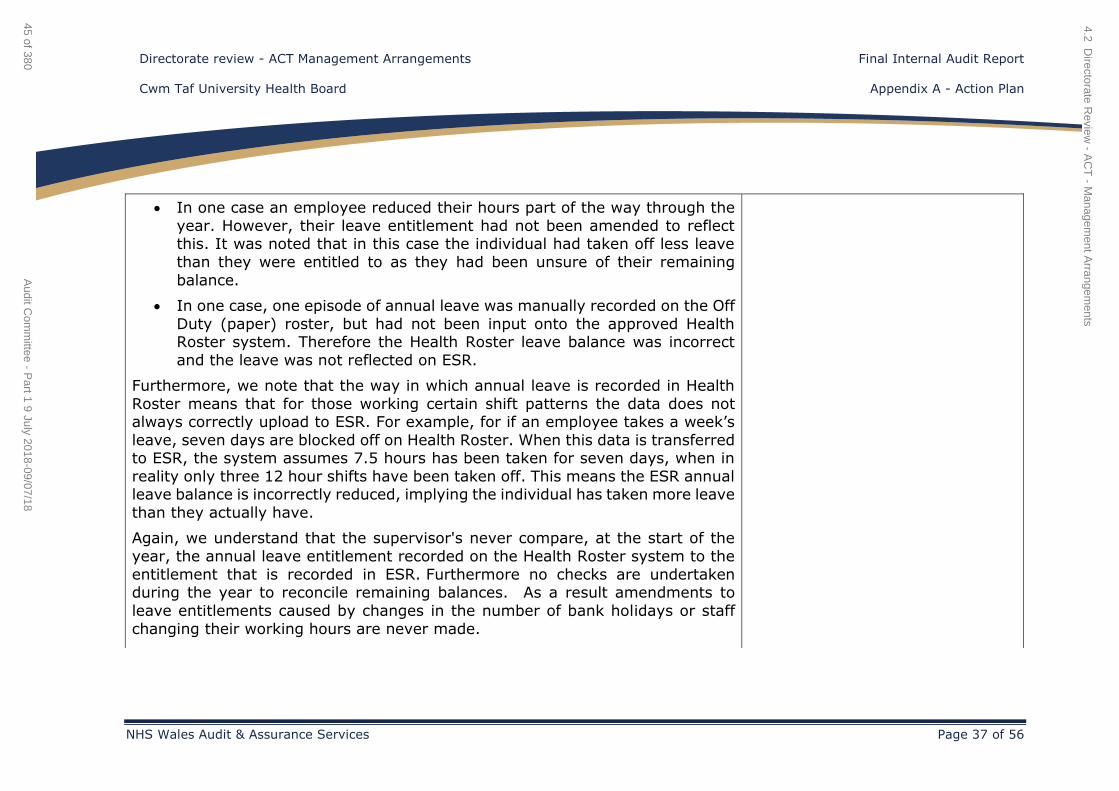
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 37 of 56
In one case an employee reduced their hours part of the way through the
year. However, their leave entitlement had not been amended to reflect this. It was noted that in this case the individual had taken off less leave
than they were entitled to as they had been unsure of their remaining
balance.
In one case, one episode of annual leave was manually recorded on the Off
Duty (paper) roster, but had not been input onto the approved Health Roster system. Therefore the Health Roster leave balance was incorrect
and the leave was not reflected on ESR.
Furthermore, we note that the way in which annual leave is recorded in Health
Roster means that for those working certain shift patterns the data does not always correctly upload to ESR. For example, for if an employee takes a week’s
leave, seven days are blocked off on Health Roster. When this data is transferred to ESR, the system assumes 7.5 hours has been taken for seven days, when in
reality only three 12 hour shifts have been taken off. This means the ESR annual leave balance is incorrectly reduced, implying the individual has taken more leave
than they actually have.
Again, we understand that the supervisor's never compare, at the start of the
year, the annual leave entitlement recorded on the Health Roster system to the
entitlement that is recorded in ESR. Furthermore no checks are undertaken during the year to reconcile remaining balances. As a result amendments to
leave entitlements caused by changes in the number of bank holidays or staff
changing their working hours are never made.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
45 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
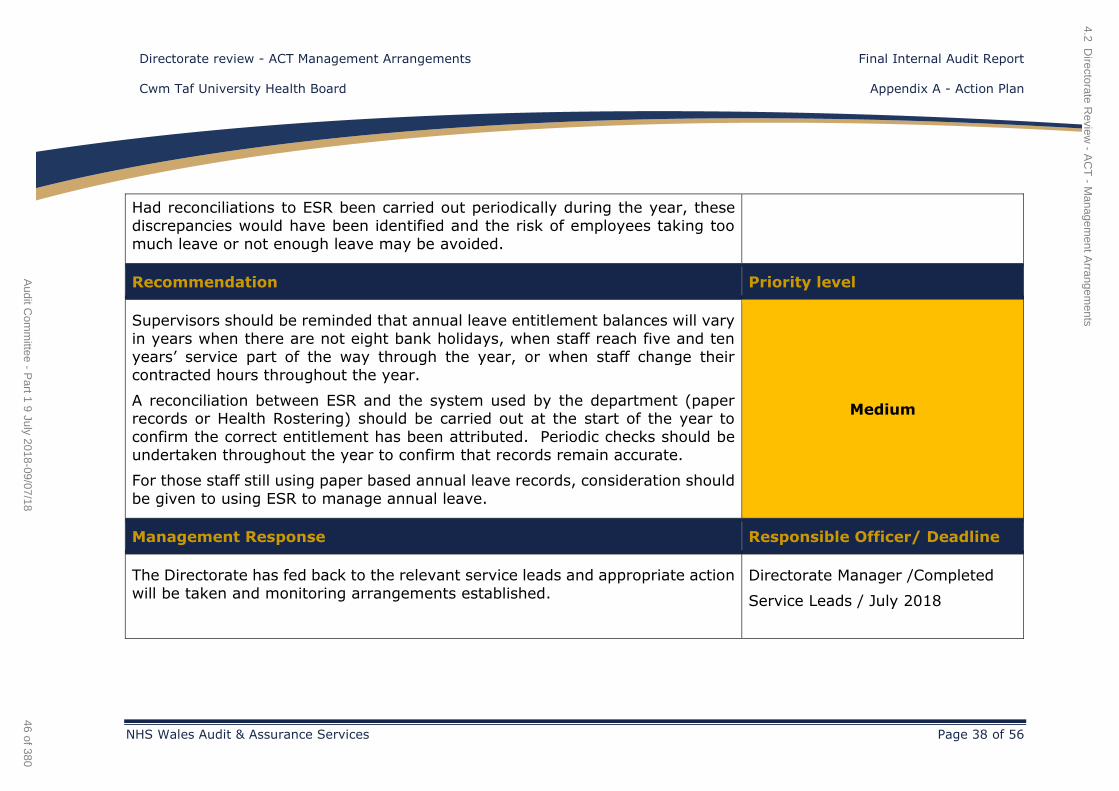
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 38 of 56
Had reconciliations to ESR been carried out periodically during the year, these
discrepancies would have been identified and the risk of employees taking too
much leave or not enough leave may be avoided.
Recommendation Priority level
Supervisors should be reminded that annual leave entitlement balances will vary
in years when there are not eight bank holidays, when staff reach five and ten
years’ service part of the way through the year, or when staff change their
contracted hours throughout the year.
A reconciliation between ESR and the system used by the department (paper records or Health Rostering) should be carried out at the start of the year to
confirm the correct entitlement has been attributed. Periodic checks should be
undertaken throughout the year to confirm that records remain accurate.
For those staff still using paper based annual leave records, consideration should
be given to using ESR to manage annual leave.
Medium
Management Response Responsible Officer/ Deadline
The Directorate has fed back to the relevant service leads and appropriate action
will be taken and monitoring arrangements established.
Directorate Manager /Completed
Service Leads / July 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
46 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
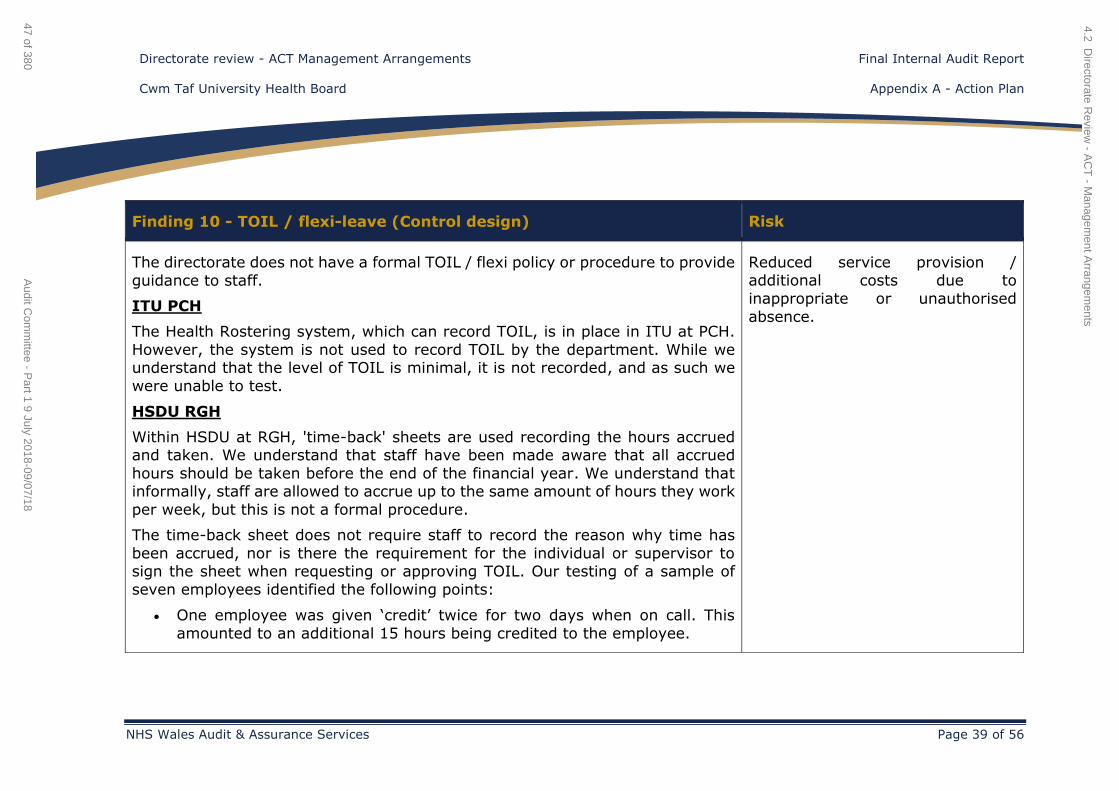
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 39 of 56
Finding 10 - TOIL / flexi-leave (Control design) Risk
The directorate does not have a formal TOIL / flexi policy or procedure to provide
guidance to staff.
ITU PCH
The Health Rostering system, which can record TOIL, is in place in ITU at PCH.
However, the system is not used to record TOIL by the department. While we understand that the level of TOIL is minimal, it is not recorded, and as such we
were unable to test.
HSDU RGH
Within HSDU at RGH, 'time-back' sheets are used recording the hours accrued and taken. We understand that staff have been made aware that all accrued
hours should be taken before the end of the financial year. We understand that informally, staff are allowed to accrue up to the same amount of hours they work
per week, but this is not a formal procedure.
The time-back sheet does not require staff to record the reason why time has
been accrued, nor is there the requirement for the individual or supervisor to sign the sheet when requesting or approving TOIL. Our testing of a sample of
seven employees identified the following points:
One employee was given ‘credit’ twice for two days when on call. This
amounted to an additional 15 hours being credited to the employee.
Reduced service provision / additional costs due to
inappropriate or unauthorised
absence.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
47 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
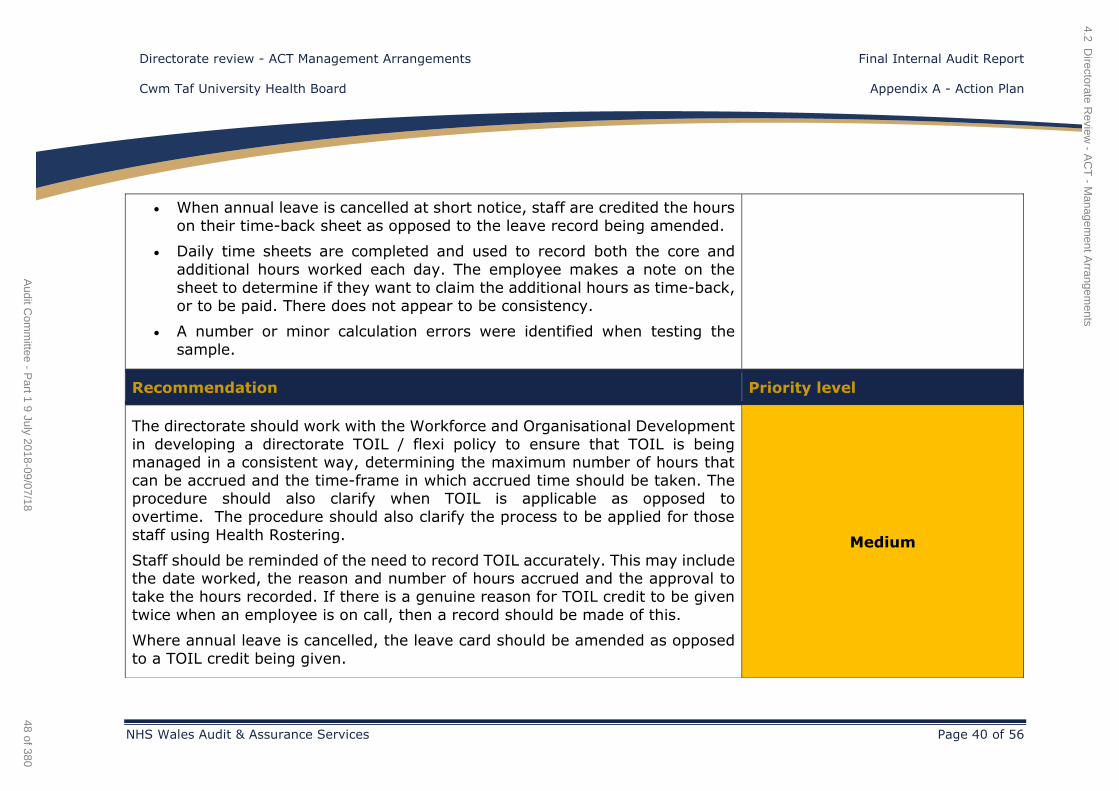
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 40 of 56
When annual leave is cancelled at short notice, staff are credited the hours
on their time-back sheet as opposed to the leave record being amended.
Daily time sheets are completed and used to record both the core and
additional hours worked each day. The employee makes a note on the
sheet to determine if they want to claim the additional hours as time-back,
or to be paid. There does not appear to be consistency.
A number or minor calculation errors were identified when testing the
sample.
Recommendation Priority level
The directorate should work with the Workforce and Organisational Development
in developing a directorate TOIL / flexi policy to ensure that TOIL is being managed in a consistent way, determining the maximum number of hours that
can be accrued and the time-frame in which accrued time should be taken. The procedure should also clarify when TOIL is applicable as opposed to
overtime. The procedure should also clarify the process to be applied for those
staff using Health Rostering.
Staff should be reminded of the need to record TOIL accurately. This may include the date worked, the reason and number of hours accrued and the approval to
take the hours recorded. If there is a genuine reason for TOIL credit to be given
twice when an employee is on call, then a record should be made of this.
Where annual leave is cancelled, the leave card should be amended as opposed
to a TOIL credit being given.
Medium
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
48 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 41 of 56
Management Response Responsible Officer/ Deadline
The Directorate has fed back to the relevant service leads and appropriate action
will be taken and monitoring arrangements established. Directorate Manager /Completed
Service Leads / July 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
49 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
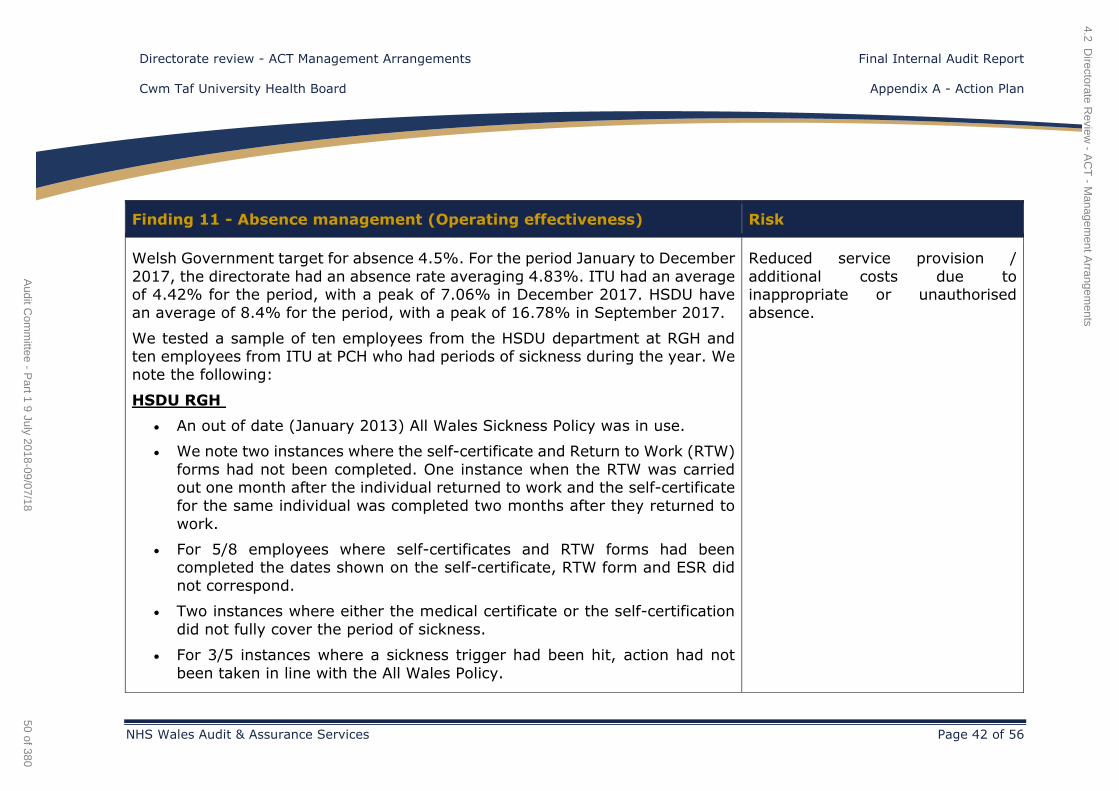
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 42 of 56
Finding 11 - Absence management (Operating effectiveness) Risk
Welsh Government target for absence 4.5%. For the period January to December
2017, the directorate had an absence rate averaging 4.83%. ITU had an average of 4.42% for the period, with a peak of 7.06% in December 2017. HSDU have
an average of 8.4% for the period, with a peak of 16.78% in September 2017.
We tested a sample of ten employees from the HSDU department at RGH and ten employees from ITU at PCH who had periods of sickness during the year. We
note the following:
HSDU RGH
An out of date (January 2013) All Wales Sickness Policy was in use.
We note two instances where the self-certificate and Return to Work (RTW)
forms had not been completed. One instance when the RTW was carried out one month after the individual returned to work and the self-certificate
for the same individual was completed two months after they returned to
work.
For 5/8 employees where self-certificates and RTW forms had been completed the dates shown on the self-certificate, RTW form and ESR did
not correspond.
Two instances where either the medical certificate or the self-certification
did not fully cover the period of sickness.
For 3/5 instances where a sickness trigger had been hit, action had not
been taken in line with the All Wales Policy.
Reduced service provision /
additional costs due to inappropriate or unauthorised
absence.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
50 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
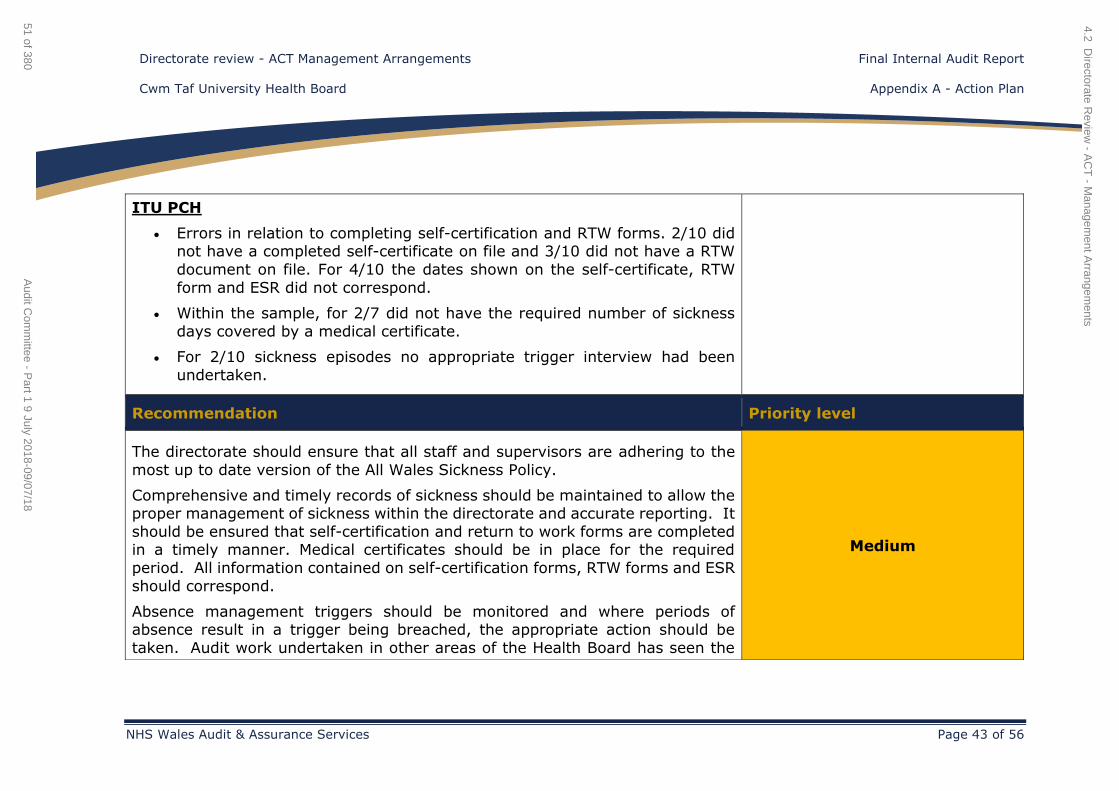
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 43 of 56
ITU PCH
Errors in relation to completing self-certification and RTW forms. 2/10 did not have a completed self-certificate on file and 3/10 did not have a RTW
document on file. For 4/10 the dates shown on the self-certificate, RTW
form and ESR did not correspond.
Within the sample, for 2/7 did not have the required number of sickness
days covered by a medical certificate.
For 2/10 sickness episodes no appropriate trigger interview had been
undertaken.
Recommendation Priority level
The directorate should ensure that all staff and supervisors are adhering to the
most up to date version of the All Wales Sickness Policy.
Comprehensive and timely records of sickness should be maintained to allow the proper management of sickness within the directorate and accurate reporting. It
should be ensured that self-certification and return to work forms are completed in a timely manner. Medical certificates should be in place for the required
period. All information contained on self-certification forms, RTW forms and ESR
should correspond.
Absence management triggers should be monitored and where periods of absence result in a trigger being breached, the appropriate action should be
taken. Audit work undertaken in other areas of the Health Board has seen the
Medium
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
51 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 44 of 56
use of sickness and absence summary sheets as a good practice tool for
monitoring absence.
Management Response Responsible Officer/ Deadline
The Directorate has fed back to the relevant service leads and appropriate action
will be taken and monitoring arrangements established.
Directorate Manager /Completed
Service Leads / July 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
52 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
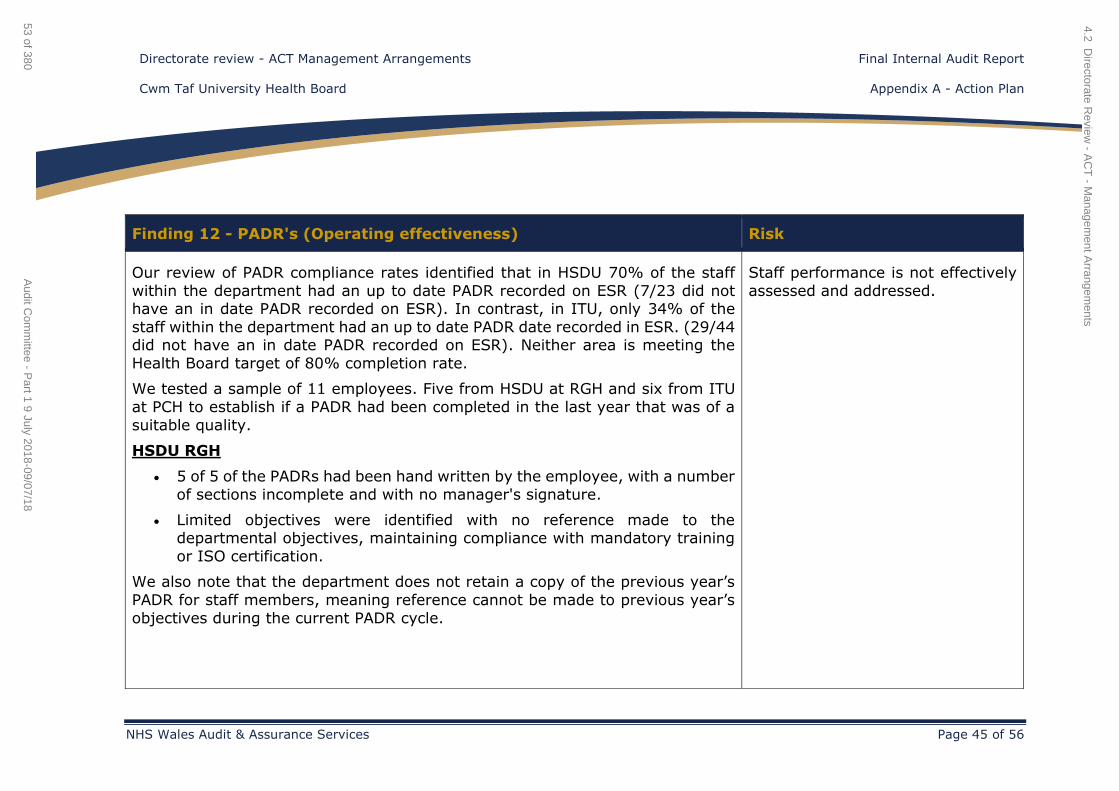
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 45 of 56
Finding 12 - PADR's (Operating effectiveness) Risk
Our review of PADR compliance rates identified that in HSDU 70% of the staff
within the department had an up to date PADR recorded on ESR (7/23 did not have an in date PADR recorded on ESR). In contrast, in ITU, only 34% of the
staff within the department had an up to date PADR date recorded in ESR. (29/44 did not have an in date PADR recorded on ESR). Neither area is meeting the
Health Board target of 80% completion rate.
We tested a sample of 11 employees. Five from HSDU at RGH and six from ITU
at PCH to establish if a PADR had been completed in the last year that was of a
suitable quality.
HSDU RGH
5 of 5 of the PADRs had been hand written by the employee, with a number
of sections incomplete and with no manager's signature.
Limited objectives were identified with no reference made to the departmental objectives, maintaining compliance with mandatory training
or ISO certification.
We also note that the department does not retain a copy of the previous year’s
PADR for staff members, meaning reference cannot be made to previous year’s
objectives during the current PADR cycle.
Staff performance is not effectively
assessed and addressed.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
53 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
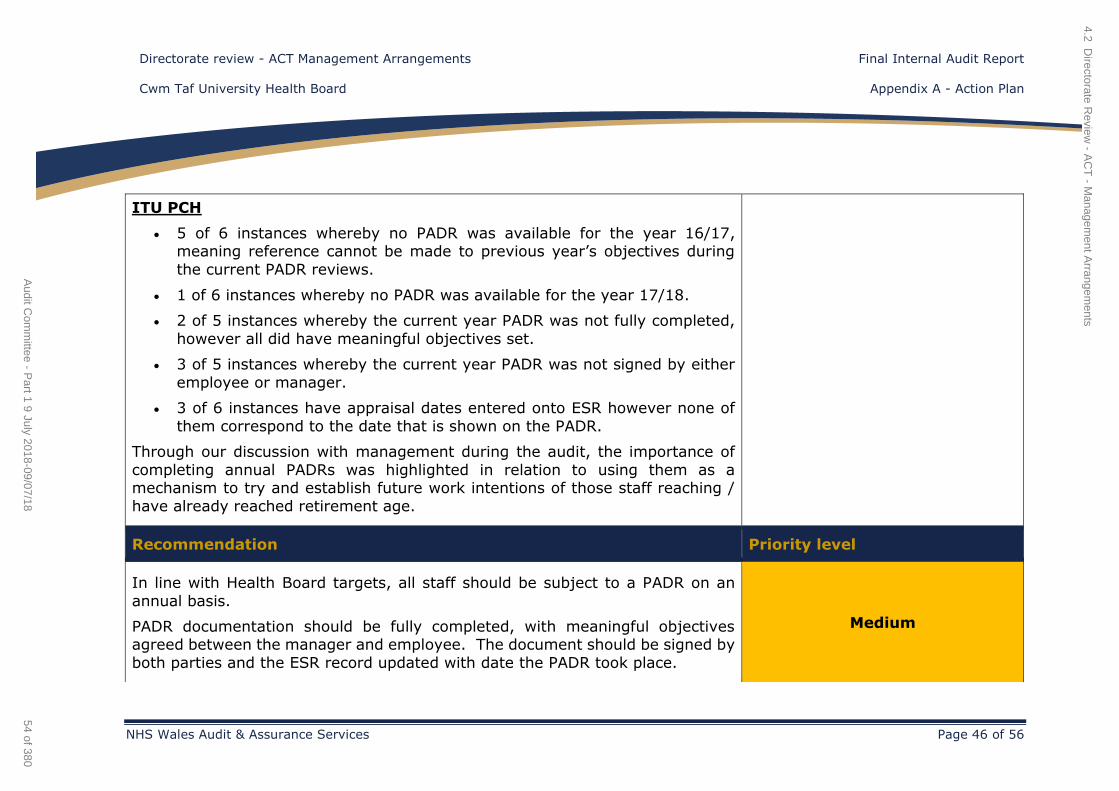
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 46 of 56
ITU PCH
5 of 6 instances whereby no PADR was available for the year 16/17, meaning reference cannot be made to previous year’s objectives during
the current PADR reviews.
1 of 6 instances whereby no PADR was available for the year 17/18.
2 of 5 instances whereby the current year PADR was not fully completed,
however all did have meaningful objectives set.
3 of 5 instances whereby the current year PADR was not signed by either
employee or manager.
3 of 6 instances have appraisal dates entered onto ESR however none of
them correspond to the date that is shown on the PADR.
Through our discussion with management during the audit, the importance of
completing annual PADRs was highlighted in relation to using them as a mechanism to try and establish future work intentions of those staff reaching /
have already reached retirement age.
Recommendation Priority level
In line with Health Board targets, all staff should be subject to a PADR on an
annual basis.
PADR documentation should be fully completed, with meaningful objectives agreed between the manager and employee. The document should be signed by
both parties and the ESR record updated with date the PADR took place.
Medium
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
54 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 47 of 56
Copies of previous PADRs should be retained and used by management
throughout the year to ensure staff are working towards agreed objectives and
used in the following years PADR to reflect on achievements during the year.
Management Response Responsible Officer/ Deadline
The Directorate commented that this has been a key feature of the CBM since
the introduction of the new Chief Operating Officer. The compliance rate was
shared at the June DIGBM and the Directorate Manager has directed the senior
team to improve compliance levels.
A review of ESR has taken place and there are a number of anomalies in relation to compliance and the Directorate is supporting a validation of the system.
Related improvements on performance are anticipated and the Directorate
Manager will monitor this via the Directorate and CBM process.
Directorate Manager / Completed
Heads of Service / August 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
55 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 48 of 56
Finding 13 - Workforce planning - Future staffing (Control design) Risk
As part of the IMTP planning process, workforce data is supplied to the directorate
by the Workforce Senior Business Partner. This data includes information on the profile of current staff including an analysis of those staff that are eligible to retire
in the near future.
While we acknowledge that legislation does not allow Health Board's to directly
ask when staff will retire, during our audit fieldwork we did not see evidence that the directorate is using current available staff data to consider future scenarios
where staff may retire so that appropriate contingency planning is in place when
staff advise that they plan to retire.
Services are not effectively
planned.
Recommendation Priority level
The directorate considers undertaking scenario planning for future retirements. Medium
Management Response Responsible Officer/ Deadline
Whilst noting the difficulties outlined above in confirming intended staff retirements to inform workforce planning and directorate IMTPs, where this is
known, this is factored into the Directorate’s IMTP narrative response.
Directorate Manager / Service Leads (Complete)
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
56 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 49 of 56
Finding 14 - Consultant job planning - Sign off of job plans (Operating
effectiveness) Risk
Consultant’s job plans are an annual agreement between the Health Board and the consultant setting out, amongst other things, what work the consultant does
for the Health Board, when and where the work is done, and how much time the
consultant is expected to be available for work.
The job plans cover a period of 42 weeks. At the time of our audit fieldwork there
were 42 consultants working within the ACT directorate. We tested a sample of nine 'live' job plans to confirm that the standard form had been used and had
been signed appropriately, and that the information on the form agreed to the
information held within the Health Board's ESR system. We identified that for:
5/9 job plans there was no evidence that the plan had been signed-off by either the consultant, directorate manager or clinical director. These were
recorded as either 'in discussion' or 'locked down'.
1/9 job plans the number of sessions for direct clinical care did not fully
reconcile to the information recorded on ESR.
Furthermore, the job plans within our sample had been 'live' for a number of
months. As such, we would expect these to be agreed either before or soon after
they become live.
Consultants have not agreed and signed-off job plans, which could
lead to changes to working commitments resulting in the
Health Board being unable to meet
short term demand.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
57 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 50 of 56
Recommendation Priority level
Management should work with consultants to ensure that job plans are signed
and agreed as soon as practically possible. Medium
Management Response Responsible Officer/ Deadline
The Directorate work closely with Consultant staff to ensure Job Planning is undertaken and implemented and will continue to work closely with the ESR team
to ensure this is captured effectively on related HB systems.
Directorate Manager/
Clinical Director August 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
58 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 51 of 56
Finding 15 - Mandatory training (Operating effectiveness) Risk
We tested mandatory training within HSDU at RGH and ITU at PCH. We note that
in February 2018 the HSDU department had an average completion rate of 17%
across the 11 core modules, and ITU had an average completion rate of 60%.
We tested a sample of five employees from each department. We note that none of the staff within the sample had completed all 11 core modules. While one
person at ITU had completed ten modules, in contrast two staff at HSDU had only
completed one module.
We understand that there is a Health Board requirement to update ESR with details of Welsh language skills. Three staff within HSDU, and two staff at ITU
had not updated ESR with this information.
As mentioned in recommendation 8 above, there have been no reports on mandatory training compliance to the DIGBMs, therefore it is unclear how
detailed monitoring at a department level is taking place, in order to ensure those departments with poor performance are targeted and help given to overcome
any barriers to completion that they are facing.
Recommendation Priority level
The directorate should ensure that all staff are provided with the opportunity to undertake their mandatory training and update ESR with their Welsh Language
skills. Monitoring at a departmental level should take place to identify any
Medium
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
59 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 52 of 56
problem areas and to establish reasons for non-compliance with a view to
providing support where necessary.
Management Response Responsible Officer/ Deadline
The Directorate will ensure this recommendation is taken forward and establish
effective monitoring arrangements to track related progress.
Directorate Manager Heads of
Service / August 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
60 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 53 of 56
Finding 16 - Rostering (Operating effectiveness) Risk
Our review of four weeks of rosters at ITU PCH identified that when the rosters
are first generated based on the current establishment, the unit was one qualified
nurse short for the majority of shifts.
The approved roster for the department is based on established staff contracted
hours with any shortfall in shifts offered to existing staff as overtime, or filled by agency staff. Due to vacancies, in March 2018, 37 shifts were filled using
overtime.
We reviewed the four-week roster for the period 12 February - 13 March 2018 to
establish if the worked roster varied to the agreed staffing template within the Health Roster system. During this period there were 84 shifts (28 days of early,
late and nights). Based on the agreed template the unit requires 7 qualified nurse and 1 Health Care Support Worker (HCSW) for both early and late shifts, but
only 7 qualified nurses during the night as HCSW are not required on weekends
or on night shifts. We found that:
Over the four-week period the unit worked 32 shifts (10 early, 12 late and 10 night shifts) where they were under staffed compared to the required
template for qualified nurses and HSCW staff.
We note one instance where the unit operated with five staff during the
day shift instead of the recommended eight, and a further five instances
(2 early, 2 late and 1 night shift) when the unit ran with six staff as opposed
to the required 8 during the day or 7 overnight / weekend.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
61 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 54 of 56
Further analysis identified that the unit also worked over staffed compared
to the agreed template. 18 shifts in total (7 early, 5 late and 6 night shifts) where they were over the agreed template. 5 out of 18 shifts were over
established by two, all of which were day shifts.
We were unable to establish from the Health Roster system the reasons for under/over establishing the unit during these shifts as the reasons were not
included on the system.
Recommendation Priority level
The directorate should explore its options going forward as to how it will sustainably manage wards where the current staffing levels fails to meet the
required establishment.
Where the unit is operating either above or below the agreed roster template, a
record should be made within the system to outline the key reasons in order for analysis and review to take place by the directorate and for continual problems
to be identified.
Medium
Management Response Responsible Officer/ Deadline
It is important to align the staffing requirement with the occupancy and acuity of patients on the Unit and it is recognised that some gaps against the template
staffing may be legitimate but should be recorded. As part of the Directorate Savings Plan this is a key area for change. The Directorate is working closely with
lead clinicians for ITU and Nurse Management to implement the correct
Directorate Manager, Head Of
Nursing / September 2018
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
62 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 55 of 56
establishment in line with the related UHB escalation arrangements.
4.2 Directorate R
eview - A
CT
- Managem
ent Arrangem
ents
63 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate review - ACT Management Arrangements Final Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit and Assurance Services Page 56 of 56
Appendix B - Assurance opinion and action plan risk rating
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact on residual risk exposure.
Reasonable assurance - The Board can take reasonable assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual risk exposure until
resolved.
Limited assurance - The Board can take limited assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
moderate impact on residual risk exposure until resolved.
No assurance - The Board can take no assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
high impact on residual risk exposure until resolved.
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
Priority
Level
Explanation Management
action
High
Poor key control design OR widespread non-
compliance with key controls.
PLUS
Significant risk to achievement of a system objective
OR evidence present of material loss, error or
misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve
efficiency or effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within Three
Months*
* Unless a more appropriate timescale is identified/agreed at the assignment.
4.2 Directorate Review - ACT - Management Arrangements
64 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate Review – Anaesthetics, Critical Care and Theatres (ACT) –
Compliance
Internal Audit Report
Cwm Taf University Health Board 2017/18
June 2018
NHS Wales Shared Services Partnership
Audit and Assurance Services
4.3 Directorate Review - ACT - Compliance
65 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 2 of 15
Contents Page
1. Introduction and Background 4
2. Scope and Objectives 4
3. Associated Risks 4
Opinion and key findings
4. Overall Assurance Opinion 5
5. Assurance Summary 6
6. Summary of Audit Findings 6
7. Summary of Recommendations 7
Review reference: CTU-1718-41
Report status: Internal Audit Report Fieldwork commencement: 19 March 2018
Fieldwork completion: 18 May 2018 Draft report issued: 25 May 2018
Management response received: 22 June 2018 Final report issued: 22 June 2018
Auditors: Jonathan Morris , Emma Samways
Executive sign off: John Palmer, Interim Chief Operating
Officer
Mark Thomas, Assistant Director Finance
Distribution: Deb Lewis, Assistant Director
Neil Cooper, Directorate Manager
Committee: Audit Committee
Appendix A
Appendix B
Management Action Plan
Assurance opinion and action plan risk rating
4.3 Directorate Review - ACT - Compliance
66 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 3 of 15
ACKNOWLEDGEMENT
NHS Wales Audit & Assurance Services would like to acknowledge the time and co-operation
given by management and staff during the course of this review.
Disclaimer notice - Please note:
This audit report has been prepared for internal use only. Audit & Assurance Services reports
are prepared, in accordance with the Internal Audit Charter and the Annual Plan, approved by
the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership – Audit
and Assurance Services, and addressed to Independent Members or officers including those
designated as Accountable Officer. They are prepared for the sole use of Cwm Taf University
Health Board and no responsibility is taken by the Audit and Assurance Services Internal Auditors
to any director or officer in their individual capacity, or to any third party.
4.3 Directorate Review - ACT - Compliance
67 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 4 of 15
1. Introduction and Background
The review of the Anaesthetics, Critical Care and Theatres (ACT) directorate’s compliance with key documents such as Standing Financial
Instructions, including the Scheme of Delegation, and Financial Control Procedures, was completed in line with the 2017/18 Internal Audit plan for
Cwm Taf University Health Board (the ‘Health Board’ or the ‘organisation’).
This review has taken place alongside a separate review of the
management arrangements in place within the directorate.
The relevant leads for the assignment were the Interim Director of Finance
and Interim Chief Operating Officer.
2. Scope and Objectives
The overall objective of the audit was to evaluate and determine the
adequacy of the systems and controls in place in relation to compliance with key documents, in order to provide assurance to the Health Board’s
Audit Committee that risks material to the achievement of the system’s
objectives are managed appropriately.
The areas that we will sought to provide assurance on were:
Awareness levels of key documents within the directorate. For
example, staff can access key documents and changes to them are
appropriately communicated.
The directorate’s compliance with the relevant elements of the
Scheme of Delegation.
The directorate’s compliance with relevant Financial Control
Procedures (FCPs).
We met with the Head of Corporate Finance and Assistant Director of Finance to
identify the FCPs most applicable to the directorate. We were advised that the
relevant FCPs were:
Capital Asset Register
Inventory of Non-capital Assets
Requisitioning Good and Services
Salaries and Wages
As such, our testing of FCPs focused on these areas.
3. Associated Risks
The potential risks considered in this review are as follows:
Inappropriate or unauthorised decisions are made if staff are unaware
of the relevant key documents.
Inappropriate or unauthorised decisions due to non-compliance with
legislation or corporate and operational policies.
4.3 Directorate Review - ACT - Compliance
68 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 5 of 15
OPINION AND KEY FINDINGS
4. Overall Assurance Opinion
We are required to provide an opinion as to the adequacy and effectiveness of
the system of internal control under review. The opinion is based on the work performed as set out in the scope and objectives within this report. An overall
assurance rating is provided describing the effectiveness of the system of internal control in place to manage the identified risks associated with the
objectives covered in this review.
The level of assurance given as to the effectiveness of the system of internal
control in place to manage the risks associated with established controls within
the ACT Directorate for compliance with key documents is reasonable assurance.
RATING INDICATOR DEFINITION
Reasonable assurance
The Board can take reasonable assurance that arrangements to secure governance,
risk management and internal control, within those areas under review, are
suitably designed and applied effectively. Some matters require management
attention in control design or compliance with low to moderate impact on residual
risk exposure until resolved.
Key staff within the directorate that we met had a sound understanding of the Financial Control Procedures and the elements of the Scheme of Delegation that
relate to them and know where to seek additional advice and support if
necessary.
Our testing identified that the directorate is mostly compliant with requirements set out in the FCP’s and the Scheme of Delegation. We did not identify any issues
in relation to the requisitioning of goods and services, but a small number of findings were identified when we tested the capital asset register and a minor
point was identified in relation to salaries and wages.
The directorate does not currently have any form of inventory of non-capital
assets.
At the current time, the management and oversight of the two store room
facilities may not be sufficient for the value of stock that is passing through
them.
The overall level of assurance that can be assigned to a review is dependent on
the severity of the findings as applied against the specific review objectives and
should therefore be considered in that context.
4.3 Directorate Review - ACT - Compliance
69 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
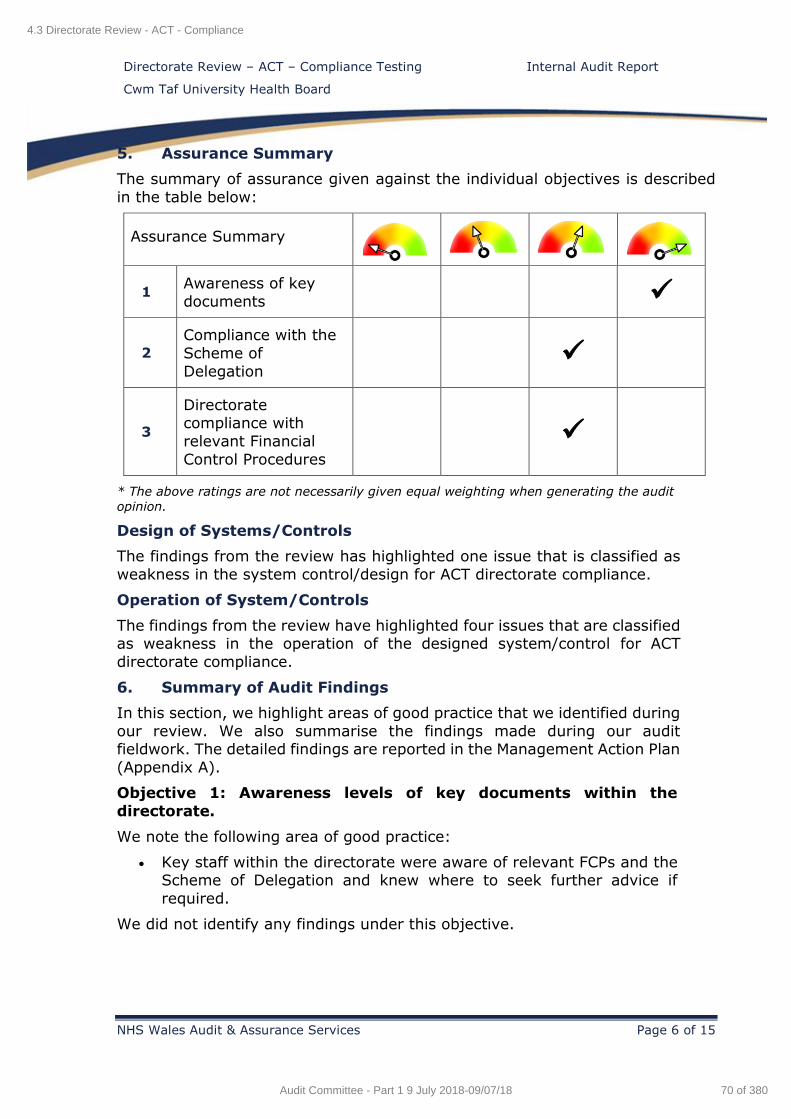
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 6 of 15
5. Assurance Summary
The summary of assurance given against the individual objectives is described
in the table below:
Assurance Summary
1 Awareness of key
documents
2
Compliance with the
Scheme of
Delegation
3
Directorate compliance with
relevant Financial
Control Procedures
* The above ratings are not necessarily given equal weighting when generating the audit
opinion.
Design of Systems/Controls
The findings from the review has highlighted one issue that is classified as
weakness in the system control/design for ACT directorate compliance.
Operation of System/Controls
The findings from the review have highlighted four issues that are classified as weakness in the operation of the designed system/control for ACT
directorate compliance.
6. Summary of Audit Findings
In this section, we highlight areas of good practice that we identified during
our review. We also summarise the findings made during our audit fieldwork. The detailed findings are reported in the Management Action Plan
(Appendix A).
Objective 1: Awareness levels of key documents within the
directorate.
We note the following area of good practice:
Key staff within the directorate were aware of relevant FCPs and the Scheme of Delegation and knew where to seek further advice if
required.
We did not identify any findings under this objective.
4.3 Directorate Review - ACT - Compliance
70 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 7 of 15
Objective 2: Compliance to relevant elements of the Scheme of
Delegation
We identified the following finding:
Given the value of items passing through the directorate’s two stores
facilities, there does not appear to be suitable controls in place.
Objective 3: Directorates compliance with relevant Financial
Control Procedures (FCPs)
We identified the following area of good practice:
The directorate has identified a clear hierarchy document showing
levels of authorising authority. This helps provide an enhanced
awareness across the directorate.
We identified the following findings:
A number of anomalies were identified whilst testing the Capital Asset Register including, an item that appeared on the register but had
been disposed of in 2011, incorrect serial numbers on the register and many assets without a serial number recorded, items identified
on site that did not appear on the register.
Clinical Engineering staff giving authorisation to dispose of assets and
remove from the register, as opposed to the Directorate Manager.
Lack of any Non-Capital Asset inventories within the directorate,
which is a requirement of FCP 11.
Additional hours paid could not always be reconciled to pay returns.
7. Summary of Recommendations
The audit findings and recommendations are detailed in Appendix A
together with the management action plan and implementation timetable.
A summary of these recommendations by priority is outlined below.
Priority H M L Total
Number of
recommendations 1 3 1 5
4.3 Directorate Review - ACT - Compliance
71 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 8 of 15
Finding 1 - Inventory of non-capital items (Operational effectiveness) Risk
The Financial Control Procedure for Inventory of Non-Capital Assets (FCP 11)
requires directorates to have and control an inventory of these assets. Items to include on the register should be valued at over £1,000 and have a useful life of
more than one year. Capital items, stock and consumable items should not be
included.
However, while we note that the directorate has assets that should be considered under this procedure, the directorate does not maintain an inventory of non-
capital assets.
Non-compliance with FCPs. Non –
capital assets are not held in a secure manner, not properly
maintained or utilised.
Recommendation Priority level
In accordance with Financial Control Procedure 11, an Inventory of Non-Capital
Assets should be complied for the ACT directorate. The register should be
maintained going forward.
High
Management Response Responsible Officer/ Deadline
The Directorate has discussed with the Capital team and Senior Nurse for
Theatres and an Equipment Register will be introduced.
Senior Nurse Theatres / September
2018
4.3 Directorate R
eview - A
CT
- Com
pliance
72 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 9 of 15
Finding 2 - Asset register verification (Operational effectiveness) Risk
We tested a sample of fourteen assets from the directorate’s asset register to
verify their existence and correct location within the directorate. We also identified and tested a sample of nine assets at various locations to verify them
back to the asset register. We note the following:
2/14 items (Haemofiltration unit and Ventilator) could not be located within the directorate at the time of our fieldwork. We understand that the
Haemofiltration unit had been condemned in 2011.
While the Ventilator was later traced by the department, we understand
that prior to our fieldwork it had been removed for maintenance and returned to a new place in the department. We note that no process is in
place to record the removal of the asset from the ward other than a note
in the 'handover' book.
1/14 items (Endovision 300 Camera) had an incorrect serial number recorded on the asset register. However, following our fieldwork, Clinical
Engineering have confirmed the correct serial number and unique EBME
number.
2/9 items (CYRO Machine Spembly Medical (RGH Outpatients) and Acupulze Lazer (PCH Theatres)) sighted during our testing did not appear
on the capital asset register.
As a general observation, we note that the columns on the capital asset register identifying serial and EBME numbers (Clinical Engineering reference) are often
not populated, with circa. 86% having no EBME reference. These identification
Ineffective identification, control
and reporting of company assets.
4.3 Directorate R
eview - A
CT
- Com
pliance
73 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 10 of 15
numbers help ensure that items are more easily found within the Health Board,
allowing effective maintenance.
Furthermore, the Capital Asset Register FCP requires directorates to verify their
capital asset register on a quarterly basis. When Finance send the quarterly
emails containing asset registers to directorates, they request that all items are
checked, but the FCP is silent on the level of coverage required.
We were able to confirm that the directorate is providing a return to Finance. However, given that our testing identified one asset that was condemned in 2011,
it appears that this asset has not been identified as missing on any of the
quarterly returns for over a six year period.
Recommendation Priority level
It should be ensured that when departments / wards are sent copies of their
asset register, that comprehensive checks are carried out to verify asset
existence and in reverse identify assets that are not recorded on the register.
To make the register as meaningful as possible consideration should be given to
including serial and EBME reference numbers.
Where assets are removed from the department / ward for servicing by Clinical Engineering a record should be made in order for the asset to be traced if needs
be.
Medium
4.3 Directorate R
eview - A
CT
- Com
pliance
74 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 11 of 15
Management Response Responsible Officer/ Deadline
The Directorate will raise this at the DIGBM and will request Heads of Service to
be vigilant with these recommendations.
Directorate Manager / Heads of
Service July 2018
4.3 Directorate R
eview - A
CT
- Com
pliance
75 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
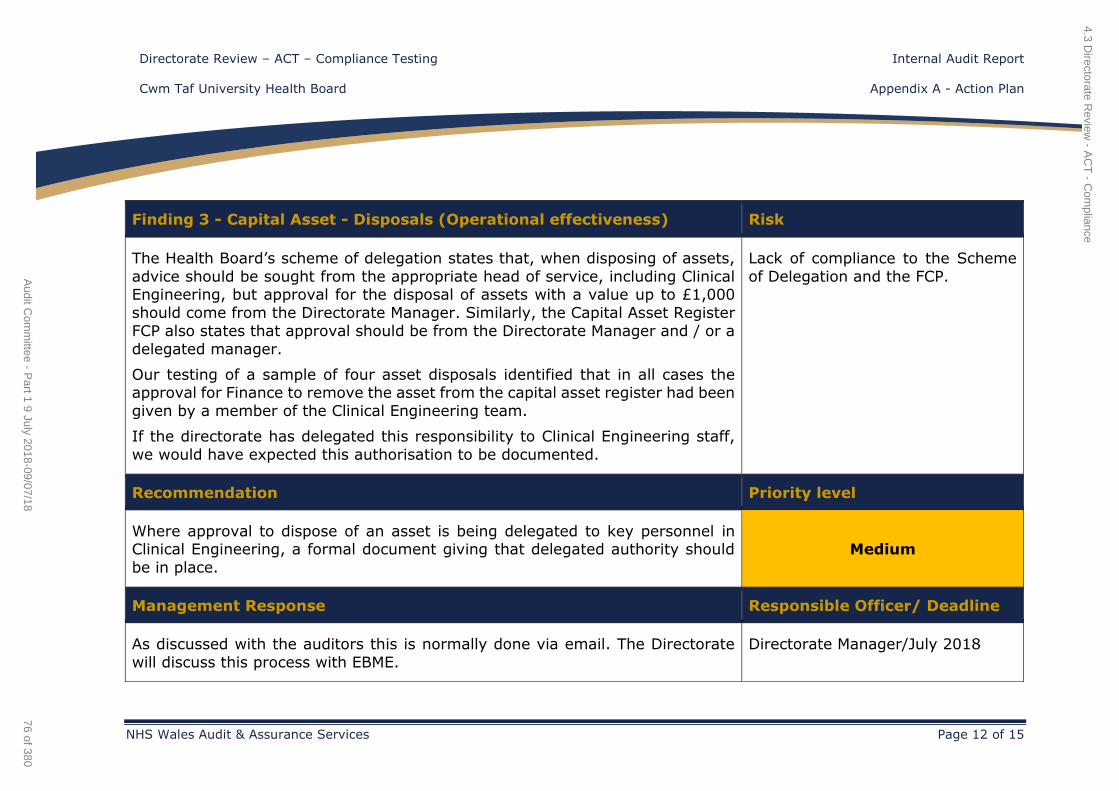
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 12 of 15
Finding 3 - Capital Asset - Disposals (Operational effectiveness) Risk
The Health Board’s scheme of delegation states that, when disposing of assets,
advice should be sought from the appropriate head of service, including Clinical Engineering, but approval for the disposal of assets with a value up to £1,000
should come from the Directorate Manager. Similarly, the Capital Asset Register
FCP also states that approval should be from the Directorate Manager and / or a
delegated manager.
Our testing of a sample of four asset disposals identified that in all cases the approval for Finance to remove the asset from the capital asset register had been
given by a member of the Clinical Engineering team.
If the directorate has delegated this responsibility to Clinical Engineering staff,
we would have expected this authorisation to be documented.
Lack of compliance to the Scheme
of Delegation and the FCP.
Recommendation Priority level
Where approval to dispose of an asset is being delegated to key personnel in Clinical Engineering, a formal document giving that delegated authority should
be in place.
Medium
Management Response Responsible Officer/ Deadline
As discussed with the auditors this is normally done via email. The Directorate
will discuss this process with EBME.
Directorate Manager/July 2018
4.3 Directorate R
eview - A
CT
- Com
pliance
76 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
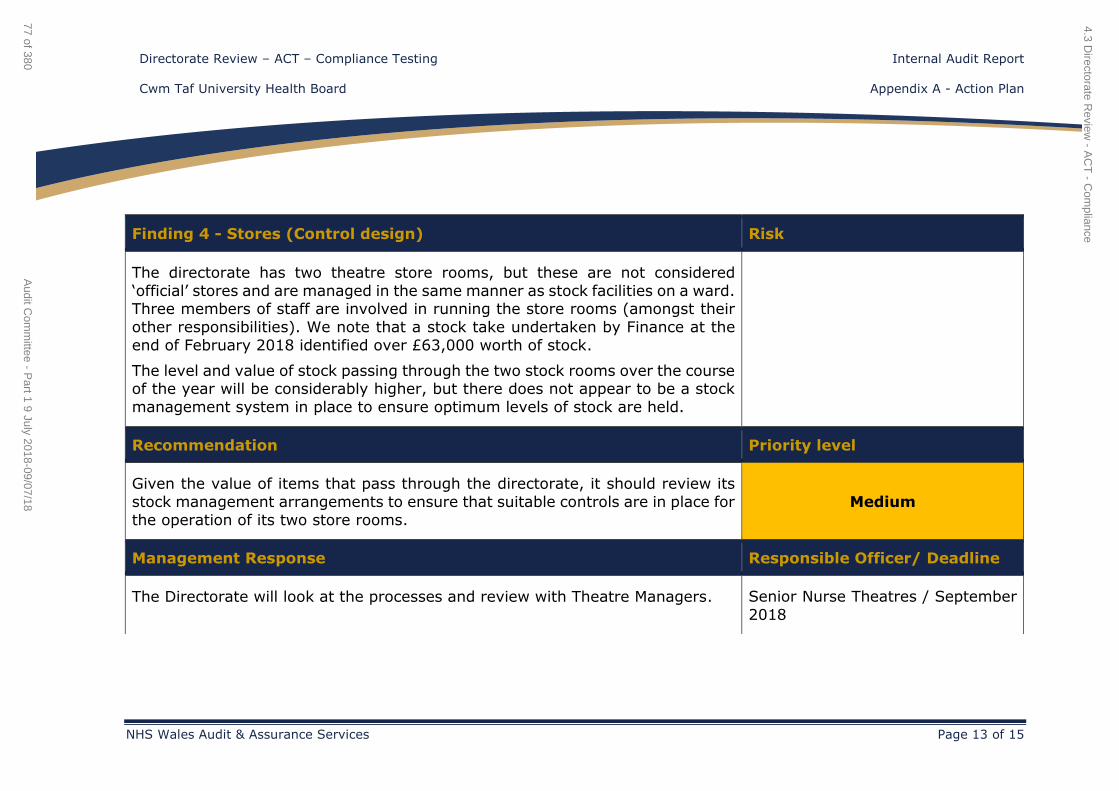
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 13 of 15
Finding 4 - Stores (Control design) Risk
The directorate has two theatre store rooms, but these are not considered
‘official’ stores and are managed in the same manner as stock facilities on a ward. Three members of staff are involved in running the store rooms (amongst their
other responsibilities). We note that a stock take undertaken by Finance at the
end of February 2018 identified over £63,000 worth of stock.
The level and value of stock passing through the two stock rooms over the course of the year will be considerably higher, but there does not appear to be a stock
management system in place to ensure optimum levels of stock are held.
Recommendation Priority level
Given the value of items that pass through the directorate, it should review its
stock management arrangements to ensure that suitable controls are in place for
the operation of its two store rooms.
Medium
Management Response Responsible Officer/ Deadline
The Directorate will look at the processes and review with Theatre Managers. Senior Nurse Theatres / September
2018
4.3 Directorate R
eview - A
CT
- Com
pliance
77 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
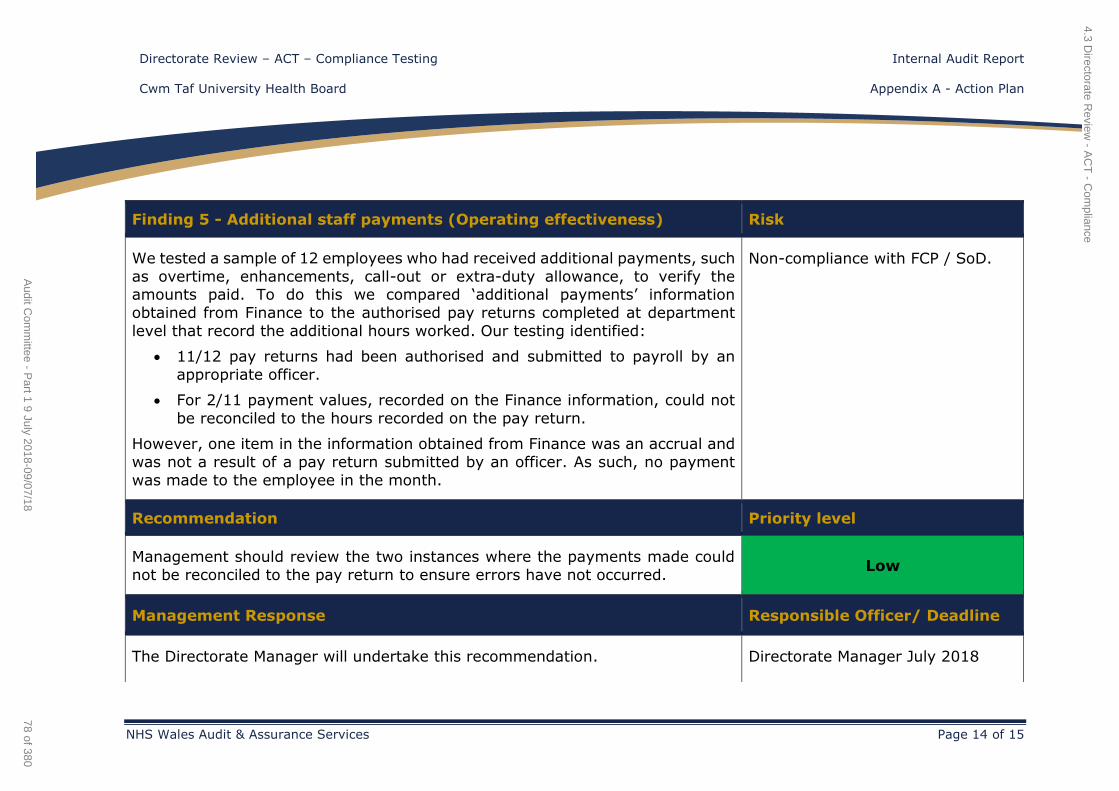
Directorate Review – ACT – Compliance Testing Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 14 of 15
Finding 5 - Additional staff payments (Operating effectiveness) Risk
We tested a sample of 12 employees who had received additional payments, such
as overtime, enhancements, call-out or extra-duty allowance, to verify the amounts paid. To do this we compared ‘additional payments’ information
obtained from Finance to the authorised pay returns completed at department
level that record the additional hours worked. Our testing identified:
11/12 pay returns had been authorised and submitted to payroll by an
appropriate officer.
For 2/11 payment values, recorded on the Finance information, could not
be reconciled to the hours recorded on the pay return.
However, one item in the information obtained from Finance was an accrual and
was not a result of a pay return submitted by an officer. As such, no payment
was made to the employee in the month.
Non-compliance with FCP / SoD.
Recommendation Priority level
Management should review the two instances where the payments made could
not be reconciled to the pay return to ensure errors have not occurred. Low
Management Response Responsible Officer/ Deadline
The Directorate Manager will undertake this recommendation. Directorate Manager July 2018
4.3 Directorate R
eview - A
CT
- Com
pliance
78 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Directorate Review – ACT – Compliance Testing Internal Audit Report
NHS Wales Audit and Assurance Services Page 15 of 15
Appendix B - Assurance opinion and action plan risk rating
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact on residual risk exposure.
Reasonable assurance - The Board can take reasonable assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual risk exposure until
resolved.
Limited assurance - The Board can take limited assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
moderate impact on residual risk exposure until resolved.
No assurance - The Board can take no assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
high impact on residual risk exposure until resolved.
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
Priority
Level
Explanation Management
action
High
Poor key control design OR widespread non-
compliance with key controls.
PLUS
Significant risk to achievement of a system objective
OR evidence present of material loss, error or
misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve
efficiency or effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within Three
Months*
* Unless a more appropriate timescale is identified/agreed at the assignment.
4.3 Directorate Review - ACT - Compliance
79 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Cwm Taf University Health Board
Health and Care Standards
Internal Audit Report
2017/18
June 2018
NHS Wales Shared Services Partnership
Audit and Assurance Services
4.4 Health & Care Standards
80 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Health and Care Standards Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 2 of 13
Contents Page
1. Introduction and Background 4
2. Scope and Objectives 4
3. Associated Risks 5
Opinion and key findings
4. Overall Assurance Opinion 5
5. Assurance Summary 6
6. Summary of Audit Findings 6
7. Summary of Recommendations 7
Review reference: CTU-1718-06
Report status: Final Internal Audit Report
Fieldwork commencement: 3 April 2018
Fieldwork completion: 30 April 2018
Draft report issued: 29 May 2018
Management response received: 14 June 2018
Final report issued: 15 June 2018
Auditors: Emma Samways, Stuart Bodman
Executive sign off: Lynda Williams, Director of Nursing,
Midwifery & Patient Services
Distribution: Alison Davies, Assistant Director Quality
and Patient Experience
Mark Townsend, Head of Clinical Audit &
Quality Informatics
Rebecca Thomas, Senior Nurse
Professional Standards & Quality
Improvement
Allison Thomas, Business Manager
Committee: Audit Committee
Appendix A Appendix B
Management Action Plan Assurance opinion and action plan risk rating
4.4 Health & Care Standards
81 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Health and Care Standards Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 3 of 13
ACKNOWLEDGEMENT
NHS Wales Audit & Assurance Services would like to acknowledge the time and co-operation
given by management and staff during the course of this review.
Disclaimer notice - Please note:
This audit report has been prepared for internal use only. Audit & Assurance Services reports
are prepared, in accordance with the Internal Audit Charter and the Annual Plan, approved by
the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership – Audit
and Assurance Services, and addressed to Independent Members or officers including those
designated as Accountable Officer. They are prepared for the sole use of Cwm Taf University
Health Board and no responsibility is taken by the Audit and Assurance Services Internal Auditors
to any director or officer in their individual capacity, or to any third party.
4.4 Health & Care Standards
82 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 4 of 13
1. Introduction and Background
The audit review of the Health and Care Standards was completed in line with the 2017/18 Internal Audit Plan for Cwm Taf University Health Board
(the 'Health Board').
The Health and Care Standards set out the Welsh Government's common
framework of standards to support the NHS and partner organisations in
providing effective, timely and quality services across all healthcare
settings.
They set out what the people of Wales can expect when they access health services and what part they themselves can play in promoting their own
health and wellbeing. They also set out the expectations for services and organisations, whether they provide or commission services for their local
citizens.
The Health and Care Standards came into force from April 2015 and
incorporate a revision of the 'Doing Well, Doing Better: Standards for Health
Services in Wales (2010)' and the 'Fundamental of Care Standards (2003)'.
The Health and Care Standards provide a consistent framework that enables health services to look across the range of their services in an
integrated way to ensure that all that they do is of the highest quality and that they are doing the right thing, in the right way, in the right place at
the right time and with the right staff.
The relevant lead for the assignment if the Director of Nursing, Midwifery
and Patient Care.
2. Scope and Objectives
The overall objective of this audit is to evaluate and determine the
adequacy of the systems and controls in place in relation to the Health and Care Standards. The review will seek to provide assurance to the Health
Board's Audit Committee that risks material to the achievement of the
system's objectives are managed appropriately.
The areas that the review sought to provide assurance on were:
Suitable oversight of the Health and Care Standards throughout the
Health Board is in place, with regular reporting at relevant
committees.
A process is in place for the preparation and completion of the self-assessments and these were completed in line with the Health
Board's prescribed timescales and are subject to formal sign-off.
Appropriate narrative, evidence and scoring is in place to support the
self-assessments.
The recommendation made in the previous Health and Care Standards
internal audit review was followed up during the course of this audit.
4.4 Health & Care Standards
83 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 5 of 13
3. Associated Risks
The potential risks considered in this review were as follows:
Insufficient governance and oversight of Health and Care Standards
throughout the Health Board.
Non-adherence to the relevant requirements of the Health and Care
Standards.
OPINION AND KEY FINDINGS
4. Overall Assurance Opinion
We are required to provide an opinion as to the adequacy and effectiveness of the system of internal control under review. The opinion is based on the
work performed as set out in the scope and objectives within this report. An overall assurance rating is provided describing the effectiveness of the
system of internal control in place to manage the identified risks associated
with the objectives covered in this review.
The level of assurance given as to the effectiveness of the system of internal control in place to manage the risks associated with the Health and Care
Standards process is Reasonable assurance.
RATING INDICATOR DEFINITION
Reasonable
assurance
The Board can take reasonable assurance that arrangements to
secure governance, risk management
and internal control, within those areas under review, are suitably designed
and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual
risk exposure until resolved.
There is both corporate and ward level awareness of the Health and Care Standards, with active engagement by ward staff to complete the annual
self-assessments, which forms part of the Health Board’s annual report.
Self-assessments are completed in line with the Health Board’s prescribed
timescales and are subject to review and sign-off by ward management.
However, we identified findings that require corporate and ward
management attention. These relate to the absence of formal written guidance for ward management in respect of the completion of self-
assessments, documentation of action planning and follow-ups arising from self-assessment audits, and provision of progress and process feedback to
ward management upon completion of the annual review.
The overall level of assurance that can be assigned to a review is dependent
on the severity of the findings as applied against the specific review
objectives and should therefore be considered in that context.
4.4 Health & Care Standards
84 of 380Audit Committee - Part 1 9 July 2018-09/07/18
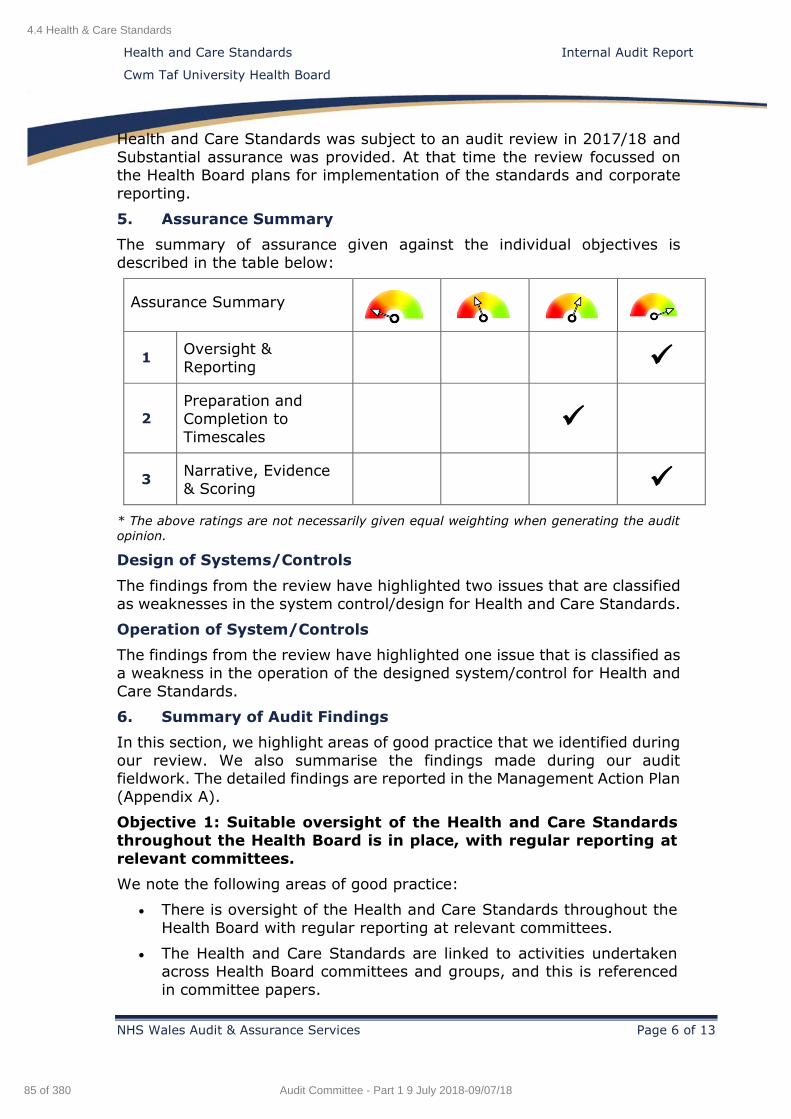
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 6 of 13
Health and Care Standards was subject to an audit review in 2017/18 and
Substantial assurance was provided. At that time the review focussed on the Health Board plans for implementation of the standards and corporate
reporting.
5. Assurance Summary
The summary of assurance given against the individual objectives is
described in the table below:
Assurance Summary
1 Oversight &
Reporting
2
Preparation and
Completion to
Timescales
3 Narrative, Evidence
& Scoring
* The above ratings are not necessarily given equal weighting when generating the audit
opinion.
Design of Systems/Controls
The findings from the review have highlighted two issues that are classified
as weaknesses in the system control/design for Health and Care Standards.
Operation of System/Controls
The findings from the review have highlighted one issue that is classified as
a weakness in the operation of the designed system/control for Health and
Care Standards.
6. Summary of Audit Findings
In this section, we highlight areas of good practice that we identified during
our review. We also summarise the findings made during our audit fieldwork. The detailed findings are reported in the Management Action Plan
(Appendix A).
Objective 1: Suitable oversight of the Health and Care Standards
throughout the Health Board is in place, with regular reporting at
relevant committees.
We note the following areas of good practice:
There is oversight of the Health and Care Standards throughout the
Health Board with regular reporting at relevant committees.
The Health and Care Standards are linked to activities undertaken across Health Board committees and groups, and this is referenced
in committee papers.
4.4 Health & Care Standards
85 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 7 of 13
We did not identify any findings under this objective.
Objective 2: A process is in place for the preparation and completion of the self-assessments and these were completed in
line with the Health Board's prescribed timescales and are subject
to formal sign-off.
We note the following good practice:
1. All ward self-assessments that we sampled were completed in line with the Health Board’s prescribed timescales and were subject to
review and sign-off by ward management.
We identified the following findings:
For the three wards that we tested, the ward managers and senior nurses were not aware of written guidance that is in place to support
them in the self-assessment process.
No recent training has been provided to support the use of the Health
and Care Monitoring System (HCMS) database in respect of the
Health and Care Standards module.
No action planning process is in place to support the identified
improvement actions that arise from the self-assessment process.
Objective 3: Appropriate narrative, evidence and scoring is in
place to support the self-assessments.
We note the following good practice:
1. Ward managers and staff that we met are actively engaged and
embrace the self-assessment exercise and process in place.
We did not identify any findings under this objective.
7. Summary of Recommendations
The audit findings and recommendations are detailed in Appendix A together
with the management action plan and implementation timetable.
A summary of these recommendations by priority is outlined below.
Priority H M L Total
Number of
recommendations 0 2 1 3
4.4 Health & Care Standards
86 of 380Audit Committee - Part 1 9 July 2018-09/07/18
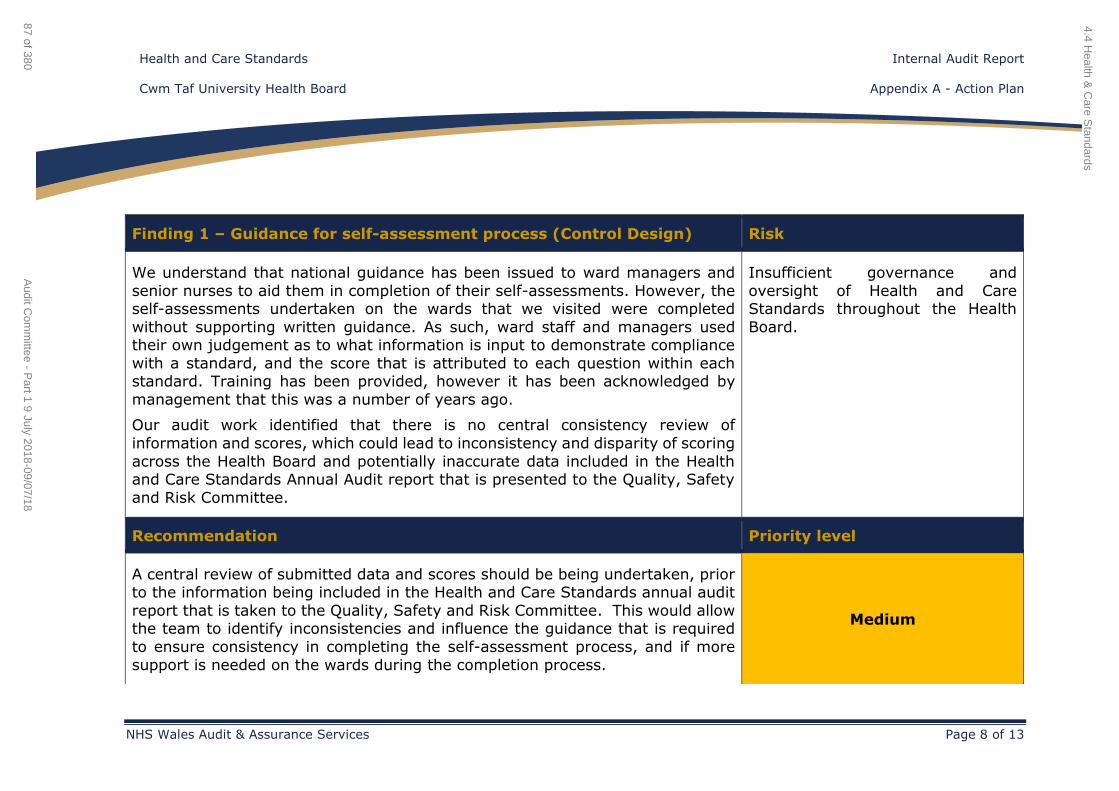
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 8 of 13
Finding 1 – Guidance for self-assessment process (Control Design) Risk
We understand that national guidance has been issued to ward managers and
senior nurses to aid them in completion of their self-assessments. However, the self-assessments undertaken on the wards that we visited were completed
without supporting written guidance. As such, ward staff and managers used their own judgement as to what information is input to demonstrate compliance
with a standard, and the score that is attributed to each question within each standard. Training has been provided, however it has been acknowledged by
management that this was a number of years ago.
Our audit work identified that there is no central consistency review of
information and scores, which could lead to inconsistency and disparity of scoring
across the Health Board and potentially inaccurate data included in the Health and Care Standards Annual Audit report that is presented to the Quality, Safety
and Risk Committee.
Insufficient governance and
oversight of Health and Care Standards throughout the Health
Board.
Recommendation Priority level
A central review of submitted data and scores should be being undertaken, prior to the information being included in the Health and Care Standards annual audit
report that is taken to the Quality, Safety and Risk Committee. This would allow the team to identify inconsistencies and influence the guidance that is required
to ensure consistency in completing the self-assessment process, and if more
support is needed on the wards during the completion process.
Medium
4.4 Health &
Care S
tandards
87 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
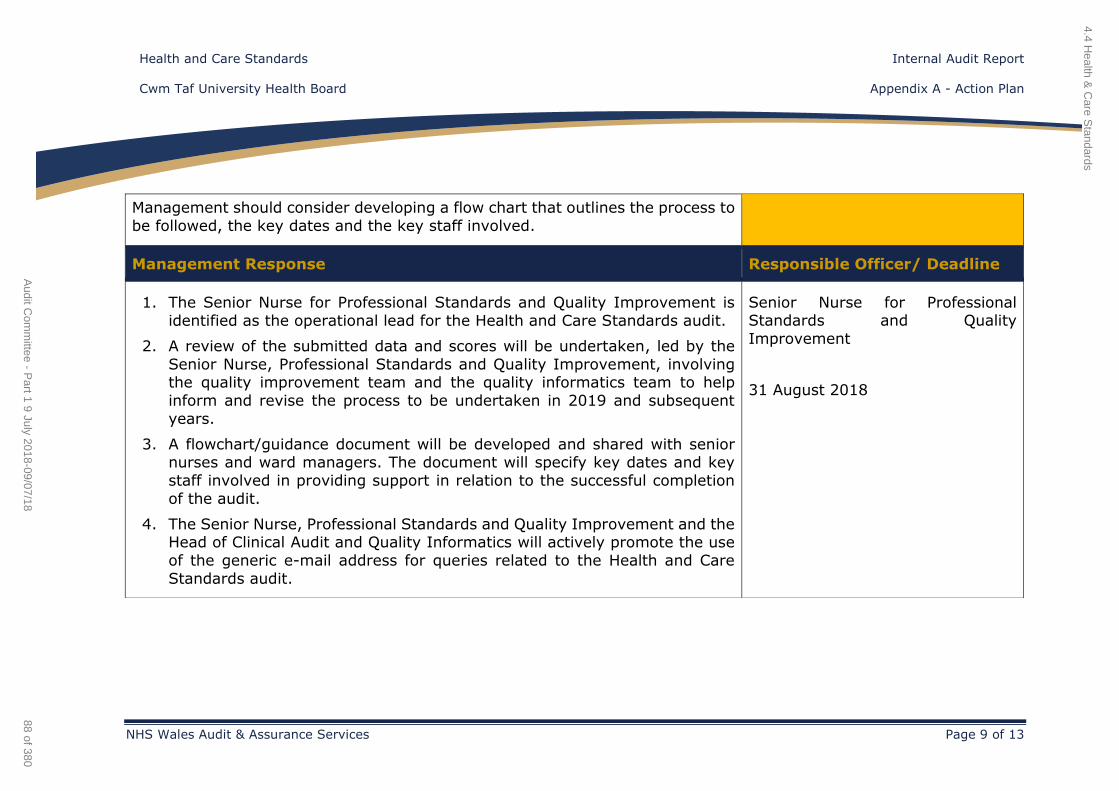
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 9 of 13
Management should consider developing a flow chart that outlines the process to
be followed, the key dates and the key staff involved.
Management Response Responsible Officer/ Deadline
1. The Senior Nurse for Professional Standards and Quality Improvement is
identified as the operational lead for the Health and Care Standards audit.
2. A review of the submitted data and scores will be undertaken, led by the
Senior Nurse, Professional Standards and Quality Improvement, involving the quality improvement team and the quality informatics team to help
inform and revise the process to be undertaken in 2019 and subsequent
years.
3. A flowchart/guidance document will be developed and shared with senior nurses and ward managers. The document will specify key dates and key
staff involved in providing support in relation to the successful completion
of the audit.
4. The Senior Nurse, Professional Standards and Quality Improvement and the Head of Clinical Audit and Quality Informatics will actively promote the use
of the generic e-mail address for queries related to the Health and Care
Standards audit.
Senior Nurse for Professional Standards and Quality
Improvement
31 August 2018
4.4 Health &
Care S
tandards
88 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
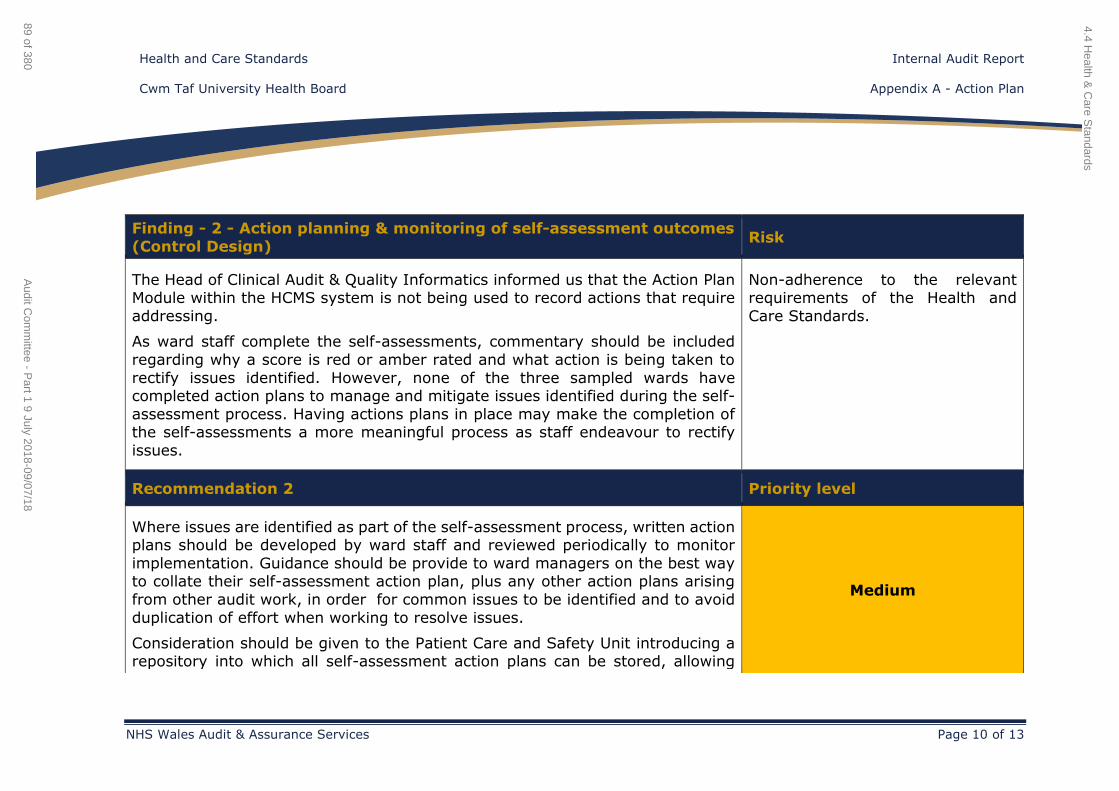
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 10 of 13
Finding - 2 - Action planning & monitoring of self-assessment outcomes
(Control Design) Risk
The Head of Clinical Audit & Quality Informatics informed us that the Action Plan Module within the HCMS system is not being used to record actions that require
addressing.
As ward staff complete the self-assessments, commentary should be included
regarding why a score is red or amber rated and what action is being taken to
rectify issues identified. However, none of the three sampled wards have completed action plans to manage and mitigate issues identified during the self-
assessment process. Having actions plans in place may make the completion of the self-assessments a more meaningful process as staff endeavour to rectify
issues.
Non-adherence to the relevant requirements of the Health and
Care Standards.
Recommendation 2 Priority level
Where issues are identified as part of the self-assessment process, written action plans should be developed by ward staff and reviewed periodically to monitor
implementation. Guidance should be provide to ward managers on the best way to collate their self-assessment action plan, plus any other action plans arising
from other audit work, in order for common issues to be identified and to avoid
duplication of effort when working to resolve issues.
Consideration should be given to the Patient Care and Safety Unit introducing a repository into which all self-assessment action plans can be stored, allowing
Medium
4.4 Health &
Care S
tandards
89 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
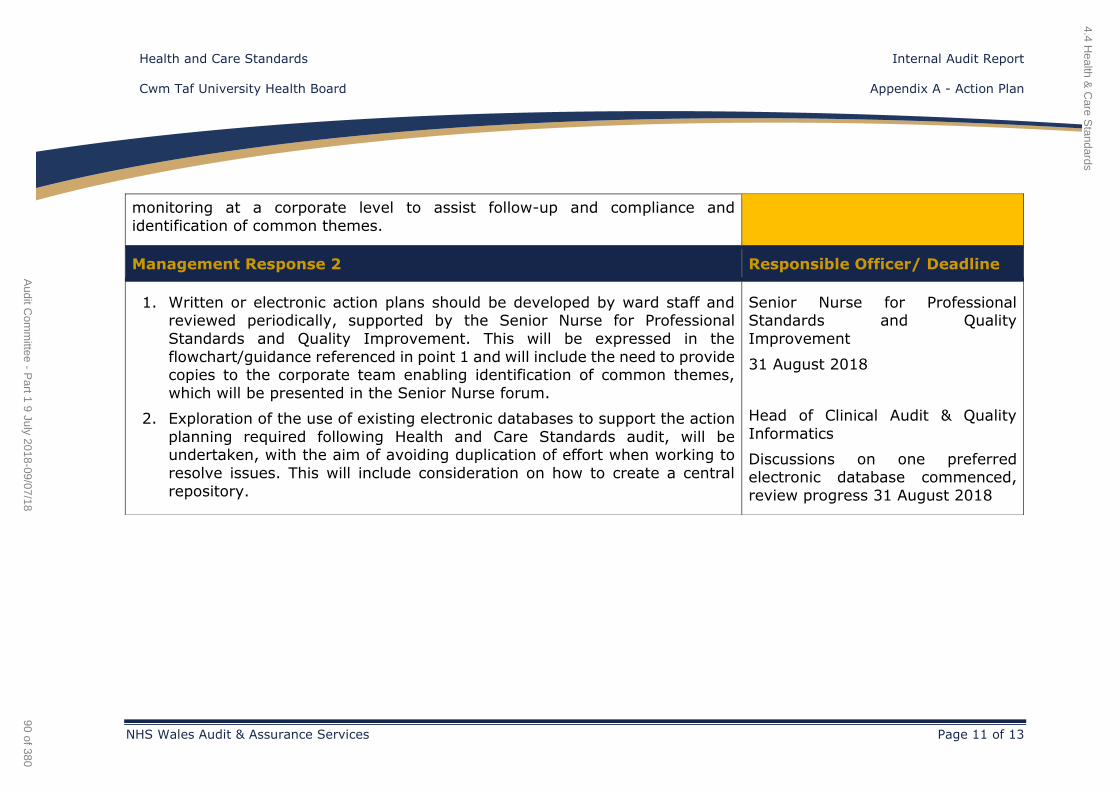
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 11 of 13
monitoring at a corporate level to assist follow-up and compliance and
identification of common themes.
Management Response 2 Responsible Officer/ Deadline
1. Written or electronic action plans should be developed by ward staff and reviewed periodically, supported by the Senior Nurse for Professional
Standards and Quality Improvement. This will be expressed in the
flowchart/guidance referenced in point 1 and will include the need to provide copies to the corporate team enabling identification of common themes,
which will be presented in the Senior Nurse forum.
2. Exploration of the use of existing electronic databases to support the action
planning required following Health and Care Standards audit, will be undertaken, with the aim of avoiding duplication of effort when working to
resolve issues. This will include consideration on how to create a central
repository.
Senior Nurse for Professional Standards and Quality
Improvement
31 August 2018
Head of Clinical Audit & Quality
Informatics
Discussions on one preferred electronic database commenced,
review progress 31 August 2018
4.4 Health &
Care S
tandards
90 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 12 of 13
Finding 3 - Feedback (Operating effectiveness) Risk
Whilst all three ward managers and staff that we met appear to actively embrace
and engage in the self-assessment process, all commented upon the absence of feedback provided at the completion of the process, which would aid
improvement to subsequent self-assessment exercises.
Non-adherence to the relevant
requirements of the Health and
Care Standards.
Recommendation 3 Priority level
The Patient Care and Safety Unit should provide feedback to ward management
on self-assessment outcomes to aid future planning and implementation
improvements.
Low
Management Response 3 Responsible Officer/ Deadline
Feedback to be presented at the Senior Nurse Forum following the completion of
the Health and Care Standards audit process, allowing for open and supportive discussions in order to enable improvement with subsequent self-assessment
audits.
Senior Nurse for Professional
Standards and Quality
Improvement
31 July 2018 and twice yearly
4.4 Health &
Care S
tandards
91 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
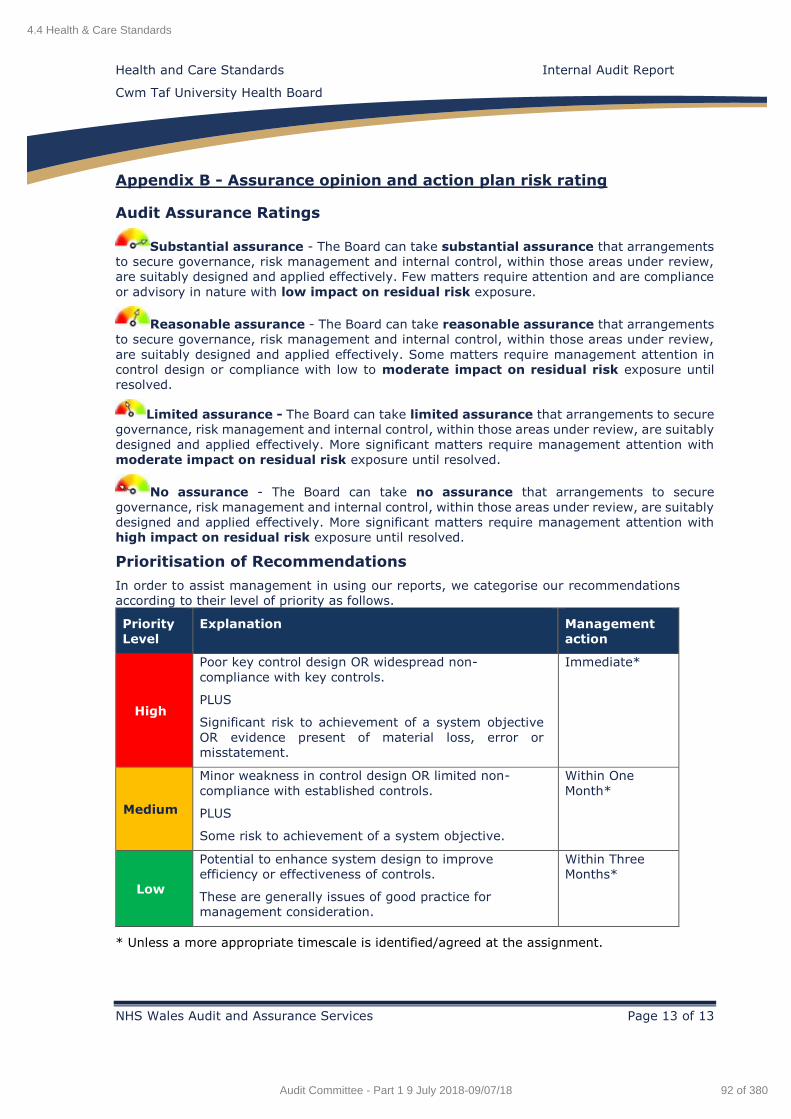
Health and Care Standards Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit and Assurance Services Page 13 of 13
Appendix B - Assurance opinion and action plan risk rating
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact on residual risk exposure.
Reasonable assurance - The Board can take reasonable assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual risk exposure until
resolved.
Limited assurance - The Board can take limited assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
moderate impact on residual risk exposure until resolved.
No assurance - The Board can take no assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
high impact on residual risk exposure until resolved.
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
Priority
Level
Explanation Management
action
High
Poor key control design OR widespread non-
compliance with key controls.
PLUS
Significant risk to achievement of a system objective
OR evidence present of material loss, error or
misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve
efficiency or effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within Three
Months*
* Unless a more appropriate timescale is identified/agreed at the assignment.
4.4 Health & Care Standards
92 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Environmental Sustainability reporting
Internal Audit Report
2018/19
Cwm Taf University Health Board
June 2018
NHS Wales Shared Services Partnership
Audit and Assurance Services
4.5 Environmental Sustainability Reporting
93 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Environmental Sustainability reporting Contents
Cwm Taf University Health Board
Audit and Assurance Services Page 2 of 8
Contents Page
1. Introduction and Background 3
2. Scope and Objectives 3
3. Associated Risks 4
Opinion and key findings
4. Overall Assurance Opinion 4
5. Assurance Summary 5
6. Summary of Audit Findings 6
7. Summary of Recommendations 7
Review reference: CTU-1819-35
Report status: Internal Audit Report
Fieldwork commencement: 5 June 2018 Fieldwork completion: 18 June 2018
Draft report issued: 19 June 2018 Management response received: 20 June 2018
Final report issued: 21 June 2018 Auditors: Emma Samways, Elizabeth Vincent
Executive sign off: John Palmer, Interim Chief Operating
Officer
Distribution: Russell Hoare, Acting Assistant Director
OSS
Committee: Audit Committee
ACKNOWLEDGEMENT NHS Wales Audit & Assurance Services would like to acknowledge the time and co-operation given by management and staff during the course of this review.
Disclaimer notice - Please note:
This audit report has been prepared for internal use only. Audit & Assurance Services reports are prepared,
in accordance with the Internal Audit Charter and the Annual Plan, approved by the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership – Audit and Assurance Services, and addressed to Independent Members or officers including those designated as Accountable Officer. They are prepared for the sole use of Cwm Taf University Health Board and no responsibility is
taken by the Audit and Assurance Services Internal Auditors to any director or officer in their individual capacity, or to any third party
Appendix A
Assurance opinion and action plan risk rating
4.5 Environmental Sustainability Reporting
94 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Environmental Sustainability reporting Internal Audit Report
Cwm Taf University Health Board
Audit and Assurance Services Page 3 of 8
1. Introduction and Background
Our review of Cwm Taf University Health Board’s (the ‘Health Board’) Environmental Sustainability reporting was completed in line with the
2018/19 Internal Audit Plan. The review sought to provide the Health Board with assurance regarding the process for the production and approval of
the Sustainability Report (the ‘report’).
The Government Financial Reporting Manual (the ‘FReM’) requires that entities falling within the scope of reporting under the Greening
Government commitments, and which are not exempted by the de minimis limit, or other exemptions under Greening Government (or other successor
policy), shall produce a sustainability report to be included within the Management Commentary in accordance with HM Treasury issued
Sustainability Reporting in the Public Sector guidance.
Wales is unique in the UK in having sustainable development as its central
organising principle. Sustainable reporting is an essential part of organisational governance in the public sector in Wales and the Welsh
Government’s aim is to enable integrated reporting.
From 2012/13 public bodies in Wales that report under the FReM and meet
the FReM de minimis limit have been required to produce a FReM sustainability report.
Guidance for the completion of sustainability reporting can be found on HM
Treasury website. The format within the IFRS NHS Wales 2017-18 Manual for Accounts provides a recommended structure for NHS Wales bodies
sustainability reports, including minimum requirements.
The 2013 Francis Report identified that Healthcare providers should be
required to have their quality accounts independently audited. Auditors should be given a wider remit enabling them to use their professional
judgement in examining the reliability of all statements in the accounts.
The relevant lead for the review is the interim Chief Operating Officer.
2. Scope and Objectives
The overall objective of the review was to assess the adequacy of
management arrangements for the production of the Sustainability Report within the Annual Report. The audit focussed upon the 2017/18 report. The
scope of the audit review was limited to the following aspects:
The Health Board has appropriate arrangements for the preparation,
approval and publication of the Sustainability Report including checks
to ensure compliance with relevant guidance.
The form and content of the report complies with the requirements
of guidance published by the Welsh Government.
Testing a sample of selected indicators to ensure the underpinning
data is robust and reliable, conforms to specified data quality standards and prescribed definitions, and is subject to appropriate
scrutiny and review.
4.5 Environmental Sustainability Reporting
95 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Environmental Sustainability reporting Internal Audit Report
Cwm Taf University Health Board
Audit and Assurance Services Page 4 of 8
Whether the information published within the report provides an
accurate and representative picture of the quality of services it
provides and the improvements it has committed to undertake.
3. Associated Risks
The potential risks considered in the review were as follows:
Reputational risk from non-compliance with Welsh Government
guidance and breach of key public disclosure reporting requirement
and lack of transparency.
Reputational risk that the published information does not present a fair and balanced picture to stakeholders of the performance in the
year.
Data quality risk that published information is either incomplete or
inaccurate due to a lack or failure of information governance controls overall or system controls over reported information for individual
data elements.
OPINION AND KEY FINDINGS
4. Overall Assurance Opinion
We are required to provide an opinion as to the adequacy and effectiveness
of the system of internal control under review. The opinion is based on the work performed as set out in the scope and objectives within this report.
An overall assurance rating is provided describing the effectiveness of the
system of internal control in place to manage the identified risks associated with the objectives covered in this review. The level of assurance given as
to the effectiveness of the system of internal control in place to manage the risks associated with the Environmental Sustainability reporting is
Substantial assurance.
RATING INDICATOR DEFINITION
Substantial Assurance
The Board can take substantial
assurance that arrangements to secure governance, risk management
and internal control, within those areas under review, are suitably designed
and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact
on residual risk exposure.
The audit identified that the Sustainability report for 2017/18 complies with
the required format set out in the HM Treasury guidelines and the information published within the report provides an accurate, fair and
consistent picture of the Health Board’s sustainability performance for 2017/18. Overall the controls in place to manage the risks associated with
the systems and processes tested within the review are of a sufficient
standard.
4.5 Environmental Sustainability Reporting
96 of 380Audit Committee - Part 1 9 July 2018-09/07/18
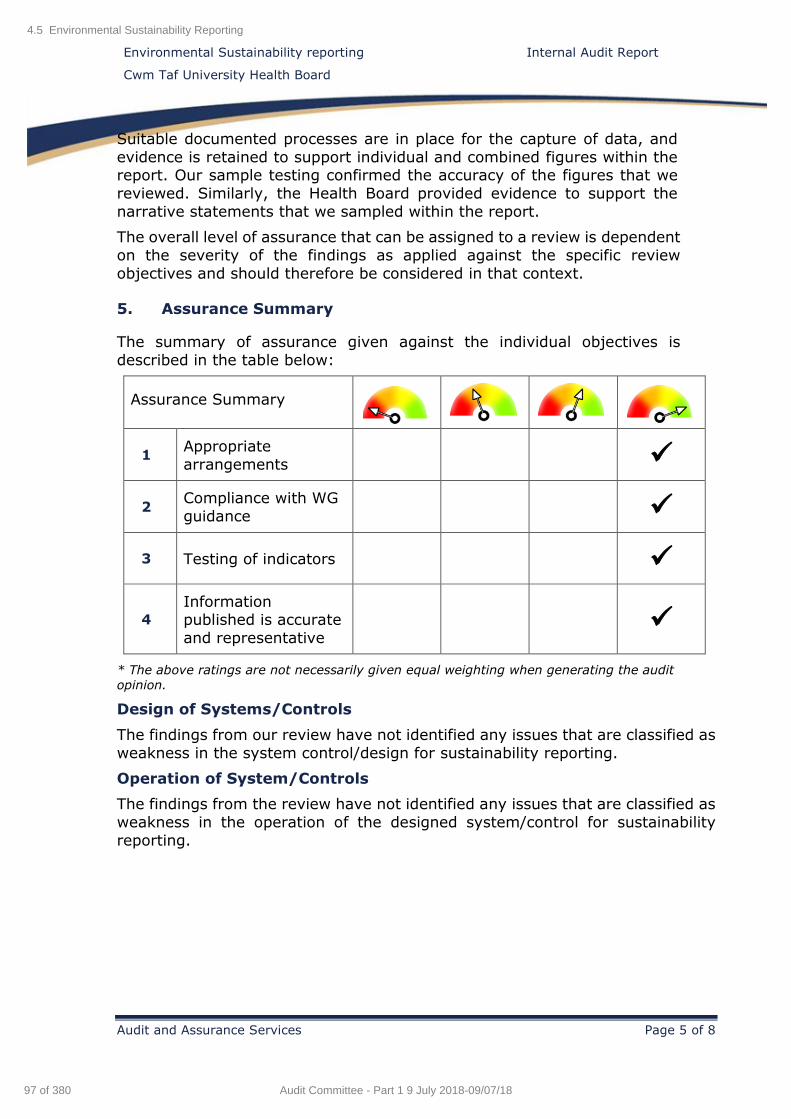
Environmental Sustainability reporting Internal Audit Report
Cwm Taf University Health Board
Audit and Assurance Services Page 5 of 8
Suitable documented processes are in place for the capture of data, and
evidence is retained to support individual and combined figures within the report. Our sample testing confirmed the accuracy of the figures that we
reviewed. Similarly, the Health Board provided evidence to support the
narrative statements that we sampled within the report.
The overall level of assurance that can be assigned to a review is dependent
on the severity of the findings as applied against the specific review
objectives and should therefore be considered in that context.
5. Assurance Summary
The summary of assurance given against the individual objectives is
described in the table below:
Assurance Summary
1 Appropriate
arrangements
2 Compliance with WG
guidance
3 Testing of indicators
4
Information published is accurate
and representative
* The above ratings are not necessarily given equal weighting when generating the audit
opinion.
Design of Systems/Controls
The findings from our review have not identified any issues that are classified as
weakness in the system control/design for sustainability reporting.
Operation of System/Controls
The findings from the review have not identified any issues that are classified as
weakness in the operation of the designed system/control for sustainability
reporting.
4.5 Environmental Sustainability Reporting
97 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Environmental Sustainability reporting Internal Audit Report
Cwm Taf University Health Board
Audit and Assurance Services Page 6 of 8
6. Summary of Audit Findings
As we did not identify any findings to be reported, in this section we highlight
areas of good practice that we identified during our review.
Objective 1: The Health Board has appropriate arrangements for preparation, approval and publication of the Sustainability Report
including checks to ensure compliance with relevant guidance.
We note the following areas of good practice:
Overall responsibility for preparing the report is devolved to the
Acting Assistant Director Operational Support Services. The report was drafted by the Facilities and Estates team, and coordinated by
the Facilities Compliance Manager.
The revised procedures for Sustainability reporting give clear
instructions on how the figures are entered into the report. In addition, the revised procedures describe the method to record,
monitor, and retain the data that is input.
There are well established systems in place for capturing the raw data
for inclusion in the report. The figures for electricity, gas, biomass, Combined Heat and Power (CHP) and water are obtained from the
energy consumption database (the TEAM database). The figures for waste and travel were obtained from the Facilities department’s
databases, which is consistent with last year.
Issues raised in previous years as a result of manual input for waste data have been minimised with the introduction of a new spreadsheet
to allow checking to take place.
We saw evidence that data and supporting narrative is validated at
the early stages of the production of the report before it is submitted
to us for review.
The final draft report (known as Version 5) was reviewed by the 'Head of Governance and Assets Estates' and the Acting Assistant Director
Operational Support Services.
We did not identify any findings under this objective.
Objective 2: The form and content of the report complies with the
requirements of guidance published by the Welsh Government.
We note the following areas of good practice:
The report details the environmental governance structure.
The format of the report is in accordance with the guidance contained
in the NHS Manual for Accounts.
The summary of performance within the report incorporates details
of initiatives and programmes and how the Health Board has achieved
against certain targets.
4.5 Environmental Sustainability Reporting
98 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Environmental Sustainability reporting Internal Audit Report
Cwm Taf University Health Board
Audit and Assurance Services Page 7 of 8
There is a summary of environmental performance which includes
key achievements during 2017/18, and key deliverables for 2018/19.
Commentary on other sustainability issues has been included, which
summarises the objectives and targets that have been agreed by the
Environmental Management Group to take forward as future projects.
We did not identify any findings under this objective.
Objective 3: Testing a sample of selected indicators to ensure the underpinning data is robust and reliable, conforms to specified data
quality standards and prescribed definitions, and is subject to
appropriate scrutiny and review.
We note the following areas of good practice:
We tested data on greenhouse gas emissions, and waste and use of
resources that was included within the Sustainability report. Our
testing confirmed the data back to supporting information.
In addition, we were able to confirm that combined figures within the report had been calculated correctly and were supported by
documentary evidence.
We did not identify any findings under this objective.
Objective 4: The information published within the report provides an accurate and representative picture of the quality of services it
provides and the improvements it has committed to undertake.
We note the following areas of good practice:
The report includes tables that show how the Health Board is
performing against the C02 emissions and water consumed targets.
As part of its governance arrangements the Health Board has devised
compliance scorecards, which detail legislative, statutory, and best
practice requirements relating to environmental activities.
As part of the ISO14001 programme the Health Board has developed a number of objectives and targets, which have been agreed by the
Environmental Management Group (EMG) and are now part of a three year delivery plan. The Health Board is compliant with ISO14001 for
the main acute sites; Royal Glamorgan Hospital and Prince Charles Hospital, and all community premises have been compliant since
December 2015.
7. Summary of Recommendations
There were no recommendations arising from this review.
4.5 Environmental Sustainability Reporting
99 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
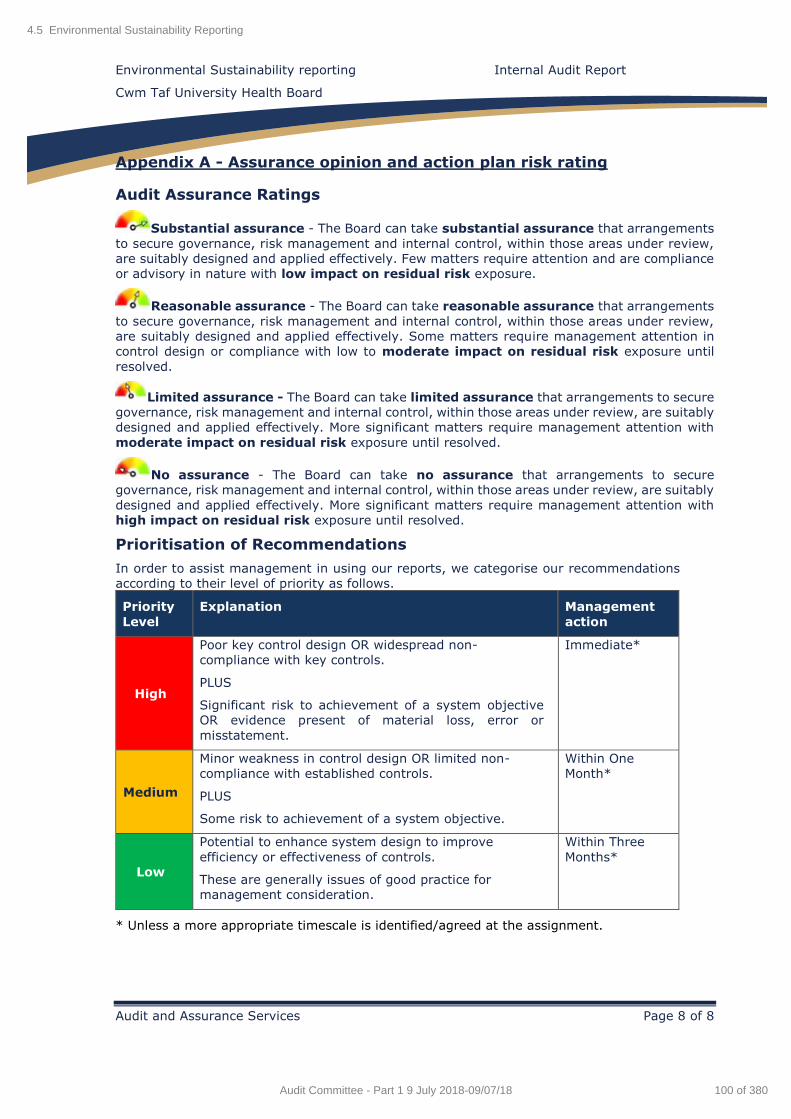
Environmental Sustainability reporting Internal Audit Report
Cwm Taf University Health Board
Audit and Assurance Services Page 8 of 8
Appendix A - Assurance opinion and action plan risk rating
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact on residual risk exposure.
Reasonable assurance - The Board can take reasonable assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual risk exposure until
resolved.
Limited assurance - The Board can take limited assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
moderate impact on residual risk exposure until resolved.
No assurance - The Board can take no assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
high impact on residual risk exposure until resolved.
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
Priority
Level
Explanation Management
action
High
Poor key control design OR widespread non-
compliance with key controls.
PLUS
Significant risk to achievement of a system objective
OR evidence present of material loss, error or
misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve
efficiency or effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within Three
Months*
* Unless a more appropriate timescale is identified/agreed at the assignment.
4.5 Environmental Sustainability Reporting
100 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement
Internal Audit Report
2018/19
Cwm Taf University Health Board
June 2018
NHS Wales Shared Services Partnership
Audit and Assurance Services
4.6 Annual Quality Statement
101 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 2 of 13
Contents Page
1. Introduction and Background 4
2. Scope and Objectives 4
3. Associated Risks 5
Opinion and key findings
4. Overall Assurance Opinion 5
5. Assurance Summary 6
6. Summary of Audit Findings 7
7. Summary of Recommendations 8
Review reference: CTU-1819-14
Report status: Internal Audit Report Fieldwork commencement: 2 May 2018
Fieldwork completion: 11 June 2018 Draft report issued: 14 June 2018
Management response received: 20 June 2018 Final report issued: 21 June 2018
Auditors: Emma Samways, Sian George
Executive sign off: Lynda Williams, Director of Nursing,
Midwifery and Patient Services
Distribution: Alison Davies, Assistant Director Quality
& Patient Experience;
Allison Thomas, Business Manager,
Quality & Safety;
Rebecca Thomas, Senior Nurse
Professional Standards and Quality.
Committee: Audit Committee
Appendix A
Appendix B
Management Action Plan
Assurance opinion and action plan risk rating
4.6 Annual Quality Statement
102 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 3 of 13
ACKNOWLEDGEMENT
NHS Wales Audit & Assurance Services would like to acknowledge the time and co-operation
given by management and staff during the course of this review.
Disclaimer notice - Please note:
This audit report has been prepared for internal use only. Audit & Assurance Services reports
are prepared, in accordance with the Internal Audit Charter and the Annual Plan, approved by
the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership – Audit
and Assurance Services, and addressed to Independent Members or officers including those
designated as Accountable Officer. They are prepared for the sole use of Cwm Taf University
Health Board and no responsibility is taken by the Audit and Assurance Services Internal Auditors
to any director or officer in their individual capacity, or to any third party.
4.6 Annual Quality Statement
103 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 4 of 13
1. Introduction and Background
The review of the Annual Quality Statement has been completed in line with the 2018/19 Internal Audit Plan. The review has sought to provide Cwm Taf
University Health Board (the 'UHB' or the 'Health Board') with assurance
regarding the process for the production of the Annual Quality Statement.
The Health Board is required to publish an Annual Quality Statement (AQS) reporting on the 2017/18 year, by 31 July 2018 in line with the annual
accounting and reporting timetable. The AQS is a statement from the UHB Board to the public. It provides an opportunity for the Health Board to let
its local population know, in an open and honest way, how it is doing to
ensure all its services are addressing local need and meeting high
standards.
The relevant lead for the assignment was the Director of Nursing, Midwifery
and Patient Services.
2. Scope and Objectives
The overall objective of this review was to assist the Health Board with
accuracy checking, including the triangulation of data and evidence, before
the publication of the AQS.
The scope was limited to assisting the Health Board to ensure that the AQS is accurate, complete and consistent with information reported to the UHB
Board over the period. In addition, we considered the Health Board's
compliance with Welsh Government guidance for 2017/18.
The main areas that the review has sought to provide assurance on are:
The timetable for the production and publication of the AQS is
appropriate.
There has been appropriate stakeholder engagement in the
production and review of the AQS.
Planned developments and stated challenges from the 2016/17 AQS
are appropriately reported within the 2017/18 AQS.
Performance indicators detailed in the AQS are accurate and can be validated back to source information. We will test a sample of
performance indicators detailed in the AQS.
Performance information and data within the AQS that demonstrates
2017/18 achievements and challenges is appropriate and consistent
with our knowledge of the Health Board.
The AQS is compliant with 2017/18 Welsh Government guidance.
4.6 Annual Quality Statement
104 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 5 of 13
3. Associated Risks
The potential risks considered in this review were as follows:
Failure to follow Welsh Government guidance.
The public is not clearly informed of any improvement and challenges experienced in the range of services being provided, as well as
improvement priorities for the forthcoming year; and
The information detailed in the Annual Quality Statement is
incomplete and / or incorrect.
OPINION AND KEY FINDINGS
4. Overall Assurance Opinion
We are required to provide an opinion as to the adequacy and effectiveness of the system of internal control under review. The opinion is based on the
work performed as set out in the scope and objectives within this report. An overall assurance rating is provided describing the effectiveness of the
system of internal control in place to manage the identified risks associated
with the objectives covered in this review.
The level of assurance given as to the effectiveness of the system of internal control in place to manage the risks associated with the Annual Quality
Statement is Reasonable assurance.
RATING INDICATOR DEFINITION
Reasonable assurance
The Board can take reasonable assurance that arrangements to
secure governance, risk management and internal control, within those areas
under review, are suitably designed and applied effectively. Some matters
require management attention in
control design or compliance with low to moderate impact on residual
risk exposure until resolved.
Our review of the AQS process focused on the ‘draft version four’ of the
statement, as this was the iteration available at the time of our audit fieldwork. As such, we were unable to comment on whether the document
had been written in a jargon free, clear language which is easily understood
by its audience, in accordance with Welsh Government guidance.
We were able to confirm that, in accordance with Welsh Government
guidance, the Health Board’s disclosure on Wales for Africa has been
included.
A timetable had been created for the development of the AQS, which set deadlines for the various tasks for the AQS to be completed by the given
publication date. When developing next year’s timetable it is important that
4.6 Annual Quality Statement
105 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
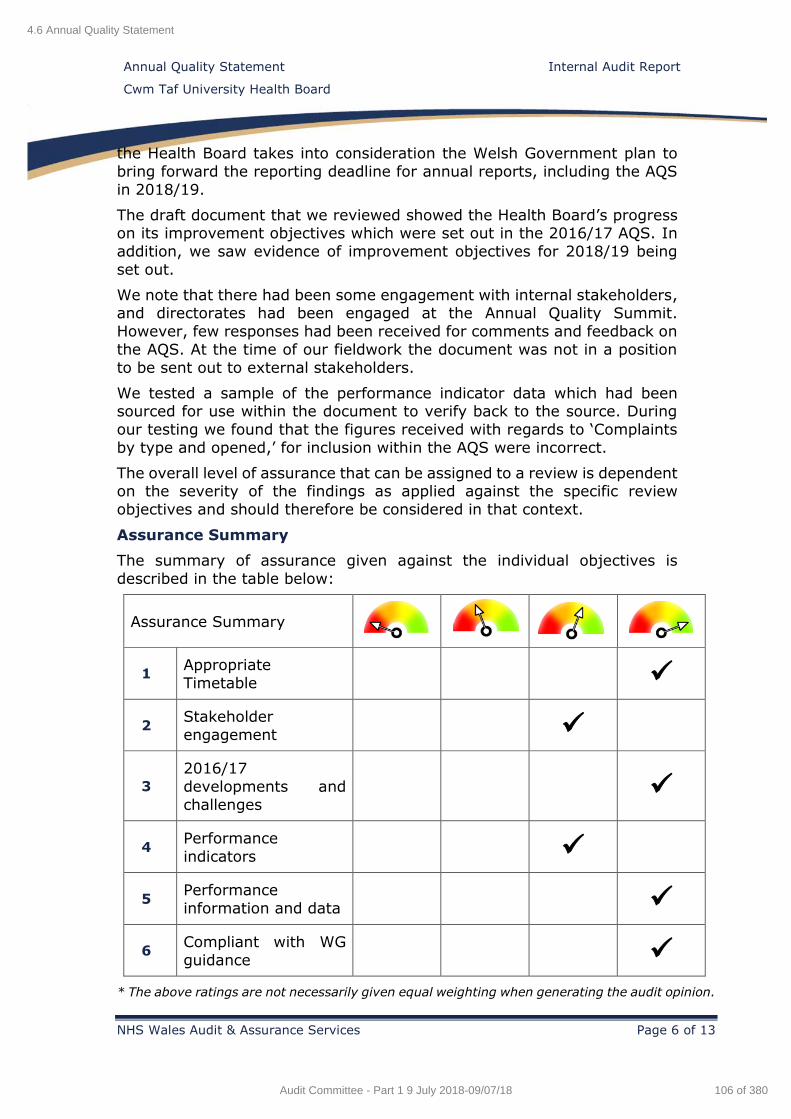
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 6 of 13
the Health Board takes into consideration the Welsh Government plan to
bring forward the reporting deadline for annual reports, including the AQS
in 2018/19.
The draft document that we reviewed showed the Health Board’s progress on its improvement objectives which were set out in the 2016/17 AQS. In
addition, we saw evidence of improvement objectives for 2018/19 being
set out.
We note that there had been some engagement with internal stakeholders, and directorates had been engaged at the Annual Quality Summit.
However, few responses had been received for comments and feedback on
the AQS. At the time of our fieldwork the document was not in a position
to be sent out to external stakeholders.
We tested a sample of the performance indicator data which had been sourced for use within the document to verify back to the source. During
our testing we found that the figures received with regards to ‘Complaints
by type and opened,’ for inclusion within the AQS were incorrect.
The overall level of assurance that can be assigned to a review is dependent on the severity of the findings as applied against the specific review
objectives and should therefore be considered in that context.
Assurance Summary
The summary of assurance given against the individual objectives is
described in the table below:
Assurance Summary
1 Appropriate
Timetable
2 Stakeholder
engagement
3
2016/17
developments and
challenges
4 Performance
indicators
5 Performance
information and data
6 Compliant with WG
guidance
* The above ratings are not necessarily given equal weighting when generating the audit opinion.
4.6 Annual Quality Statement
106 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 7 of 13
Design of Systems/Controls
We have not identified any issues that are classified as a weakness in the system
control/design for the Annual Quality Statement.
Operation of System/Controls
The findings from the review have highlighted two issues that are classified as a
weakness in the operation of the designed system/control for the Annual Quality
Statement.
5. Summary of Audit Findings
In this section, we highlight areas of good practice that we identified during our
review. We also summarise the findings made during our audit fieldwork. The
detailed findings are reported in the Management Action Plan (Appendix A).
Objective 1: The timetable for the production and publication of the
AQS is appropriate.
We note the following area of good practice:
A timetable has been created to set out the deadlines for the
development and completion of the AQS.
We did not identify any findings under this objective.
Objective 2: There has been appropriate stakeholder engagement
in the production and review of the AQS.
We note the following area of good practice:
Appropriate stakeholder engagement has been requested with
involvement of directorates at the Annual Quality Summit.
We identified the following findings:
Due to the short timescale given to internal stakeholders for their
comments and feedback on the AQS, there has not been enough time
for meaningful responses to be composed and returned for feedback.
At the time of our audit fieldwork no external stakeholder
engagement had taken place due to the document not being in a
refined state.
Objective 3: Planned developments and stated challenges from the
2016/17 AQS are appropriately reported within the 2017/18 AQS.
We note the following area of good practice:
Developments and challenges for 2017/18 have been referenced in
the AQS, and there are new challenges and objectives set for 2018/19 which do not repeat the previous year's challenges and
developments.
We did not identify any findings under this objective.
Objective 4: Performance indicators detailed in the AQS are
accurate and can be validated back to source information.
4.6 Annual Quality Statement
107 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page 8 of 13
We note the following area of good practice:
Performance indicators selected for the AQS are relevant to the
Health Board and appear to be of interest to the reader.
We identified the following finding:
During our verification of performance indicators we found that the
figures supplied in relation to complaints data were incorrect.
Objective 5: Performance information and data within the AQS that
demonstrates 2017/18 achievements and challenges is appropriate
and consistent with our knowledge if the Health Board.
We note the following area of good practice:
Performance information and data within the AQS demonstrates achievements and challenges during 2017/18 is appropriate and
consistent with our knowledge of the Health Board during the year.
We did not identify any findings under this objective.
Objective 6: The AQS is compliant with 2017/18 Welsh Government
guidance.
We note the following area of good practice:
The AQS in its current draft format is appropriately structured and
incorporates the Welsh Government’s requirement to include the
Health Board's Wales for Africa disclosure.
We did not identify any findings under this objective.
6. Summary of Recommendations
The audit findings and recommendations are detailed in Appendix A together
with the management action plan and implementation timetable.
A summary of these recommendations by priority is outlined below.
Priority H M L Total
Number of
recommendations 0 2 0 2
4.6 Annual Quality Statement
108 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 9 of 13
Finding - 1 – Checking performance indicators (Operating
effectiveness) Risk
The Patient Care and Safety Unit provided the Senior Nurse Professional Standards and Quality with a series of data for inclusion in the AQS. During our
verification of four sets of the data, for the complaints data we identified some significant differences between the data provided and the Datix system. These
were:
In relation to ‘Complaints by Type and Opened’, the original 2017/18 figure for ‘Admission/Transfer/Discharge’ was 335. However, our verification of the
information back to Datix identified that correct figure should be 26.
‘Complaints by Type and Opened’, the original 2017/18 figure for ‘Correct
Site Surgery’ was 75. However, our verification of the information back to
Datix identified that the correct figure should be 1.
The information detailed in the Annual Quality Statement is
incomplete and / or incorrect.
Recommendation Priority level
Figures should be verified by the contributor before submitting for inclusion
within the AQS to ensure that all information is correct for reporting. Medium
Management Response Responsible Officer/ Deadline
Email requests to the contributor for data to state categorically data range both in terms of dates and focus for figures to be received and included in the AQS.
Senior Nurse Professional Standards & Quality Improvement
4.6 Annual Q
uality Statem
ent
109 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 10 of 13
Data to be verified for accuracy prior to its submission for inclusion in the AQS.
A newly developed Editorial group will be responsible for reviewing the draft AQS
providing an additional level of quality assurance and scrutiny in terms of the data.
Senior Manager for Investigations
and Quality Improvement
Senior Nurse Professional
Standards & Quality Improvement
31st July 2018
4.6 Annual Q
uality Statem
ent
110 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
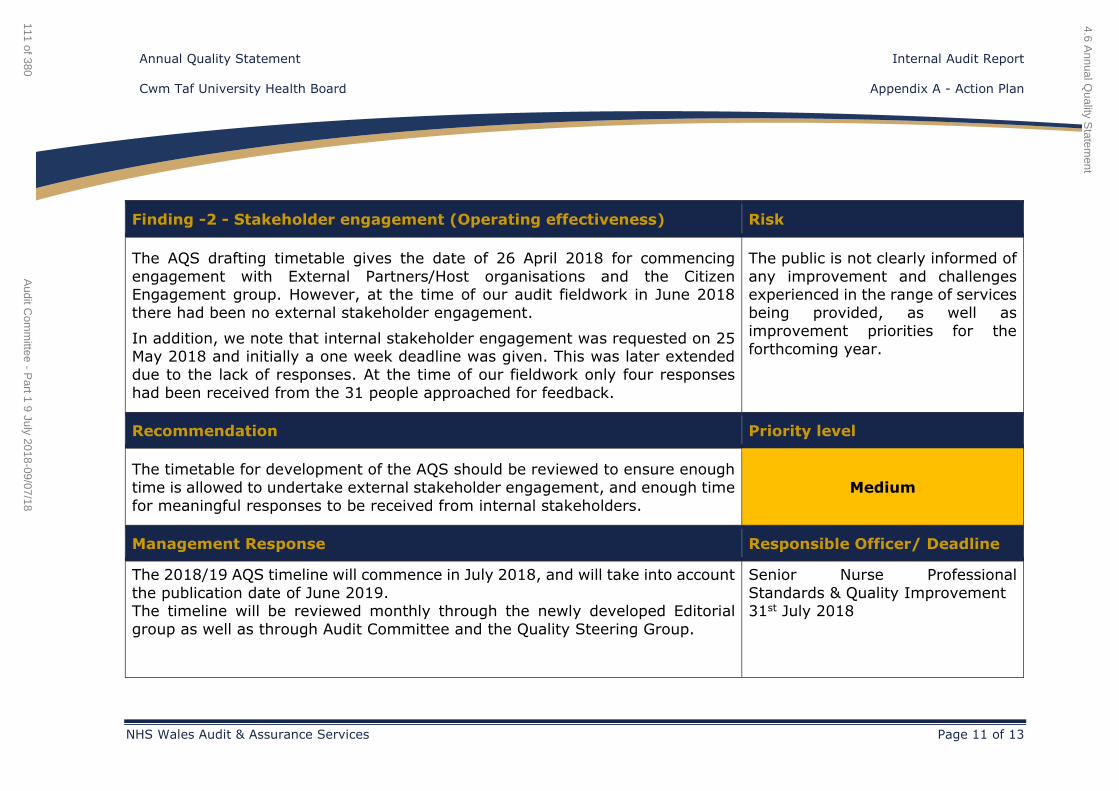
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 11 of 13
Finding -2 - Stakeholder engagement (Operating effectiveness) Risk
The AQS drafting timetable gives the date of 26 April 2018 for commencing
engagement with External Partners/Host organisations and the Citizen Engagement group. However, at the time of our audit fieldwork in June 2018
there had been no external stakeholder engagement.
In addition, we note that internal stakeholder engagement was requested on 25 May 2018 and initially a one week deadline was given. This was later extended
due to the lack of responses. At the time of our fieldwork only four responses
had been received from the 31 people approached for feedback.
The public is not clearly informed of
any improvement and challenges experienced in the range of services
being provided, as well as
improvement priorities for the
forthcoming year.
Recommendation Priority level
The timetable for development of the AQS should be reviewed to ensure enough
time is allowed to undertake external stakeholder engagement, and enough time
for meaningful responses to be received from internal stakeholders.
Medium
Management Response Responsible Officer/ Deadline
The 2018/19 AQS timeline will commence in July 2018, and will take into account
the publication date of June 2019. The timeline will be reviewed monthly through the newly developed Editorial
group as well as through Audit Committee and the Quality Steering Group.
Senior Nurse Professional
Standards & Quality Improvement 31st July 2018
4.6 Annual Q
uality Statem
ent
111 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
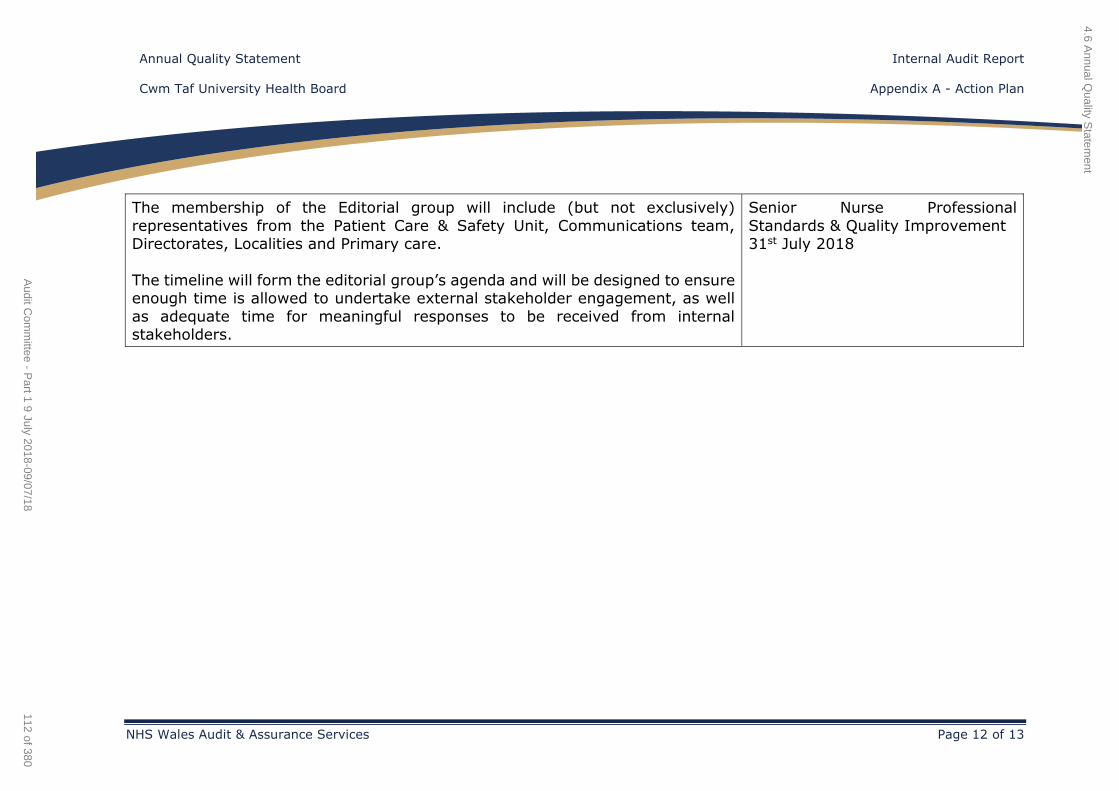
Annual Quality Statement Internal Audit Report
Cwm Taf University Health Board Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 12 of 13
The membership of the Editorial group will include (but not exclusively)
representatives from the Patient Care & Safety Unit, Communications team, Directorates, Localities and Primary care.
The timeline will form the editorial group’s agenda and will be designed to ensure enough time is allowed to undertake external stakeholder engagement, as well
as adequate time for meaningful responses to be received from internal stakeholders.
Senior Nurse Professional
Standards & Quality Improvement 31st July 2018
4.6 Annual Q
uality Statem
ent
112 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
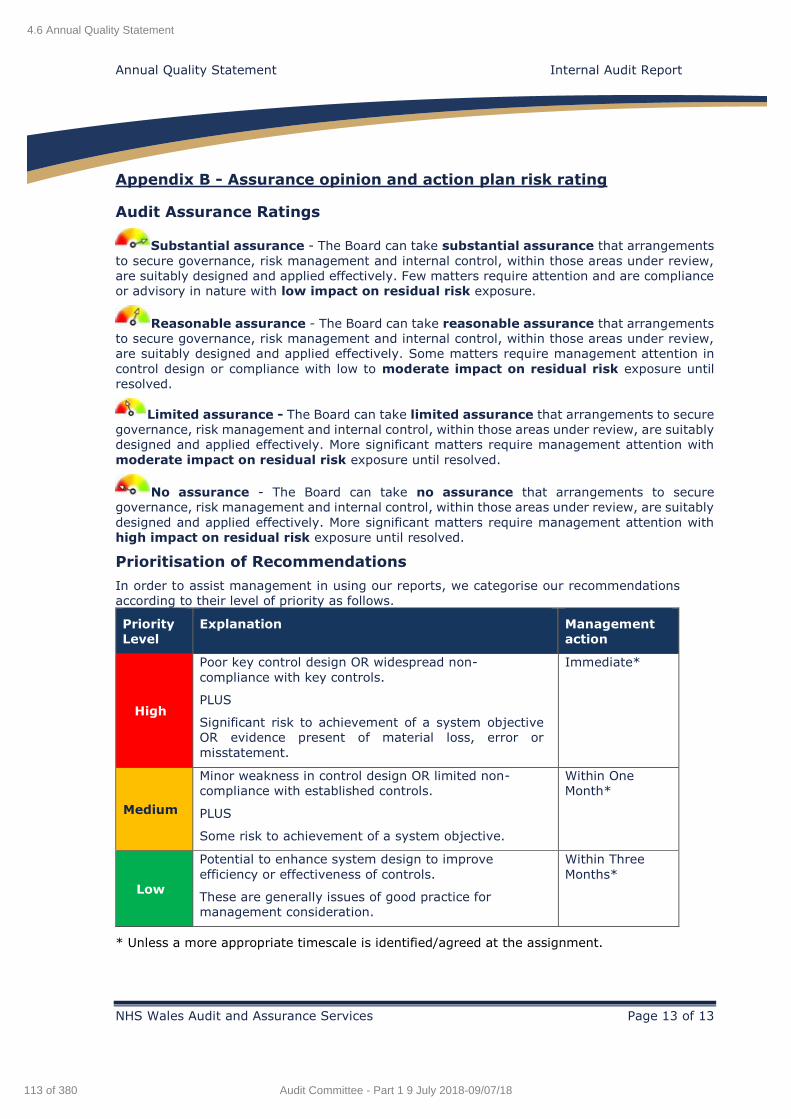
Annual Quality Statement Internal Audit Report
NHS Wales Audit and Assurance Services Page 13 of 13
Appendix B - Assurance opinion and action plan risk rating
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact on residual risk exposure.
Reasonable assurance - The Board can take reasonable assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual risk exposure until
resolved.
Limited assurance - The Board can take limited assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
moderate impact on residual risk exposure until resolved.
No assurance - The Board can take no assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
high impact on residual risk exposure until resolved.
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
Priority
Level
Explanation Management
action
High
Poor key control design OR widespread non-
compliance with key controls.
PLUS
Significant risk to achievement of a system objective
OR evidence present of material loss, error or
misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve
efficiency or effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within Three
Months*
* Unless a more appropriate timescale is identified/agreed at the assignment.
4.6 Annual Quality Statement
113 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy
Follow up
Internal Audit Report
2018/19
Cwm Taf University Health Board
Private and Confidential
NHS Wales Shared Services Partnership
Audit and Assurance Services
4.7 JAG Accreditation - Follow Up
114 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow Up Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page | 2
CONTENTS Page
1. Introduction 3
2. Scope and Objectives 3
3. Associated Risks 3
4. Opinion 5
5. Summary of audit findings 6
Review reference: CTU 1819_15
Report status: Final Fieldwork commencement: 4 June 2018
Fieldwork completion: 13 June 2018 Draft report issued: 15 June 2018
Management response received: 26 June 2018
Final report issued: Auditors:
26 June 2018 Emma Samways
Elizabeth Vincent Sian George
Executive sign off:
John Palmer- Interim Chief Operating Officer
Distribution:
Collette Kiernan – Directorate Manager,
Medicine, Outpatients and Medical Records
Committee: Audit Committee
Appendix A Appendix B
Original Action Plan and follow up position Assurance opinion and action plan risk rating
4.7 JAG Accreditation - Follow Up
115 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow Up Contents
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page | 3
Please note:
This audit report has been prepared for internal use only. Audit & Assurance Services
reports are prepared in accordance with the Internal Audit plan and Charter, approved by
the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership –
Audit and Assurance Services, and addressed to Independent Members or officers
including those designated as Accountable Officer. They are prepared for the sole use of
the Cwm Taf University Health Board and no responsibility is taken by the Audit and
Assurance Services Internal Auditors to any director or officer in their individual capacity,
or to any third party.
4.7 JAG Accreditation - Follow Up
116 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Internal Audit Report
Follow Up
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page | 4
1. Introduction
The follow-up review of Joint Advisory Group (JAG) Accreditation-
Endoscopy was completed in line with the 2018/19 Internal Audit plan for
Cwm Taf University Health Board (the ‘Health Board’).
The relevant lead for the assignment is the Chief Operating Officer.
The original Joint Advisory Group Accreditation Internal Audit report was
finalised in January 2018 and highlighted a total of seven issues which
resulted in an overall assurance rating of Limited Assurance.
2. Scope and objectives
The overall objective of this review was to provide the Health Board with assurance regarding the implementation of the agreed management
responses from the Joint Advisory Group Accreditation review that was
undertaken as part of our 2017/18 work programme.
The scope of this follow up review does not aim to provide assurance against the full review scope and objective of the original audit. The ‘follow-
up review opinion’ provides an assurance level against the implementation
of the agreed action plan only.
The main areas that this review sought to provide assurance on are:
Appropriate progress has been made with the implementation of the
agreed management responses within the agreed timescales.
Adequate evidence is available to support the level of progress that
has been made.
The actions implemented have effectively addressed the issues
highlighted during the original audit.
3. Associated risks
The potential risks considered in this review were as follows:
• Poor governance arrangements and a lack of oversight.
• Accreditation criteria not achieved and supporting evidence not
maintained.
• Services are not delivered in a safe and effective way.
• Reputational damage if accreditation status is not achieved.
4.7 JAG Accreditation - Follow Up
117 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Internal Audit Report
Follow Up
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page | 5
4. Opinion
This review considers all recommendations made (high, medium or low priority). This follow-up review does not aim to provide assurance against
the full review scope and objectives of the original audit. The ‘follow-up review opinion’ provides an assurance level against the implementation of
the agreed action plan only.
The Health Board has made progress towards implementing the agreed recommendations from the original review. More defined governance
arrangements are in place that provide the much needed managerial oversight. It is evident that a lot of work has taken place in drafting the
Operational Policy and to map out the current position and the future work necessary to achieve accreditation. However, the department is still in a
position where it is not collating the necessary evidence required to support
it submission for accreditation.
We consider two of the original four high priority findings to have been fully implemented, with one partially implemented and one, relating to the
retention of evidence on SharePoint, not yet implemented. There is demonstrable evidence of marked on-going progress of actions in respect
of the two medium priority findings and the one low priority finding.
The progress made against six of the seven original recommendations and agreed actions means that the level of assurance that can be given to
manage the risks associated with the Joint Advisory Group Accreditation
(Endoscopy) is Reasonable Assurance.
Reaso
nab
le
assu
ran
ce
- +
Yellow
Follow up - Some high and medium
level recommendations implemented and progress on the medium and low
level recommendations.
4.7 JAG Accreditation - Follow Up
118 of 380Audit Committee - Part 1 9 July 2018-09/07/18
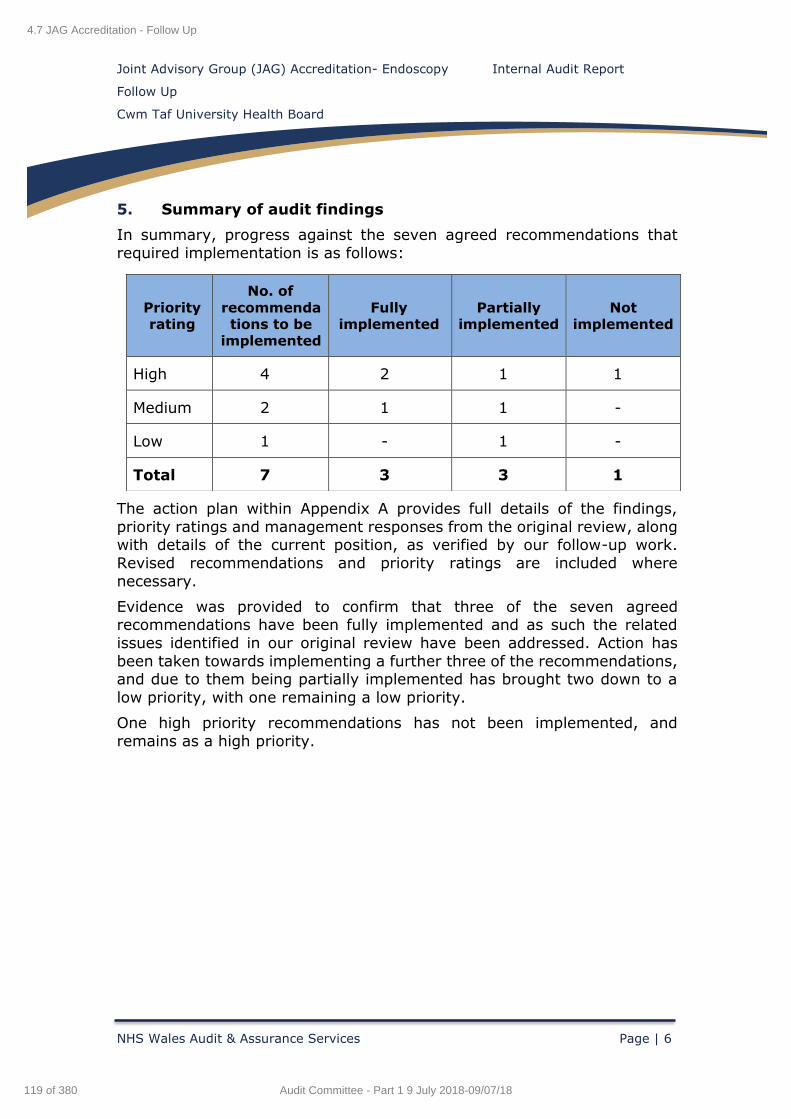
Joint Advisory Group (JAG) Accreditation- Endoscopy Internal Audit Report
Follow Up
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Page | 6
5. Summary of audit findings
In summary, progress against the seven agreed recommendations that
required implementation is as follows:
The action plan within Appendix A provides full details of the findings,
priority ratings and management responses from the original review, along with details of the current position, as verified by our follow-up work.
Revised recommendations and priority ratings are included where
necessary.
Evidence was provided to confirm that three of the seven agreed recommendations have been fully implemented and as such the related
issues identified in our original review have been addressed. Action has
been taken towards implementing a further three of the recommendations, and due to them being partially implemented has brought two down to a
low priority, with one remaining a low priority.
One high priority recommendations has not been implemented, and
remains as a high priority.
Priority rating
No. of
recommendations to be
implemented
Fully implemented
Partially implemented
Not implemented
High 4 2 1 1
Medium 2 1 1 -
Low 1 - 1 -
Total 7 3 3 1
4.7 JAG Accreditation - Follow Up
119 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
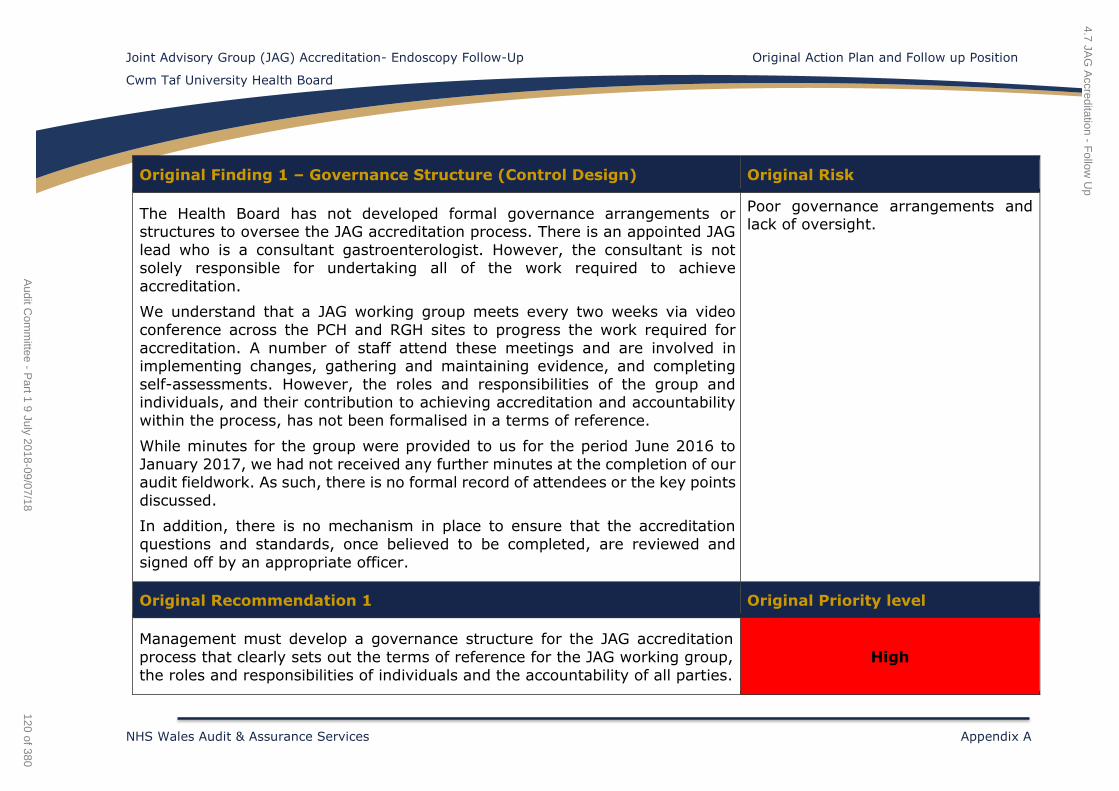
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Finding 1 – Governance Structure (Control Design) Original Risk
The Health Board has not developed formal governance arrangements or structures to oversee the JAG accreditation process. There is an appointed JAG
lead who is a consultant gastroenterologist. However, the consultant is not solely responsible for undertaking all of the work required to achieve
accreditation.
We understand that a JAG working group meets every two weeks via video
conference across the PCH and RGH sites to progress the work required for
accreditation. A number of staff attend these meetings and are involved in implementing changes, gathering and maintaining evidence, and completing
self-assessments. However, the roles and responsibilities of the group and individuals, and their contribution to achieving accreditation and accountability
within the process, has not been formalised in a terms of reference.
While minutes for the group were provided to us for the period June 2016 to
January 2017, we had not received any further minutes at the completion of our audit fieldwork. As such, there is no formal record of attendees or the key points
discussed.
In addition, there is no mechanism in place to ensure that the accreditation
questions and standards, once believed to be completed, are reviewed and
signed off by an appropriate officer.
Poor governance arrangements and lack of oversight.
Original Recommendation 1 Original Priority level
Management must develop a governance structure for the JAG accreditation
process that clearly sets out the terms of reference for the JAG working group,
the roles and responsibilities of individuals and the accountability of all parties.
High
4.7 JAG
Accreditation - F
ollow U
p
120 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
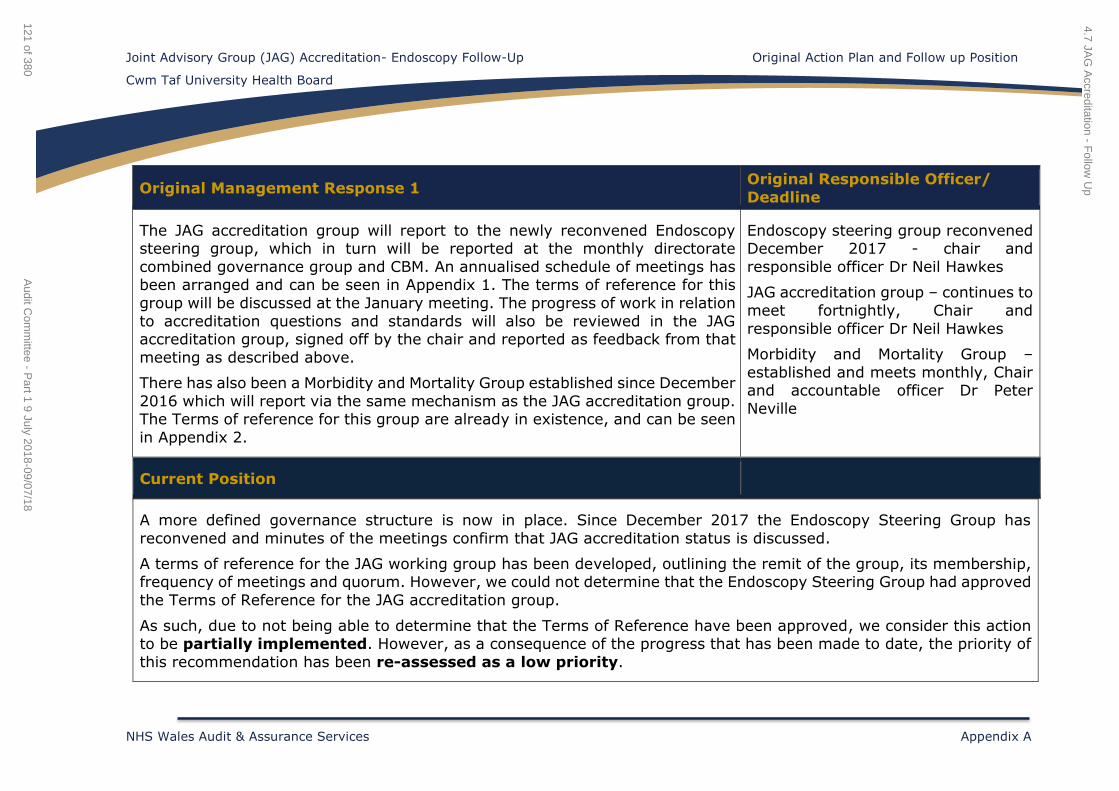
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Current Position
Original Management Response 1 Original Responsible Officer/
Deadline
The JAG accreditation group will report to the newly reconvened Endoscopy steering group, which in turn will be reported at the monthly directorate
combined governance group and CBM. An annualised schedule of meetings has been arranged and can be seen in Appendix 1. The terms of reference for this
group will be discussed at the January meeting. The progress of work in relation
to accreditation questions and standards will also be reviewed in the JAG accreditation group, signed off by the chair and reported as feedback from that
meeting as described above.
There has also been a Morbidity and Mortality Group established since December
2016 which will report via the same mechanism as the JAG accreditation group. The Terms of reference for this group are already in existence, and can be seen
in Appendix 2.
Endoscopy steering group reconvened December 2017 - chair and
responsible officer Dr Neil Hawkes
JAG accreditation group – continues to
meet fortnightly, Chair and
responsible officer Dr Neil Hawkes
Morbidity and Mortality Group –
established and meets monthly, Chair and accountable officer Dr Peter
Neville
A more defined governance structure is now in place. Since December 2017 the Endoscopy Steering Group has
reconvened and minutes of the meetings confirm that JAG accreditation status is discussed.
A terms of reference for the JAG working group has been developed, outlining the remit of the group, its membership, frequency of meetings and quorum. However, we could not determine that the Endoscopy Steering Group had approved
the Terms of Reference for the JAG accreditation group.
As such, due to not being able to determine that the Terms of Reference have been approved, we consider this action to be partially implemented. However, as a consequence of the progress that has been made to date, the priority of
this recommendation has been re-assessed as a low priority.
4.7 JAG
Accreditation - F
ollow U
p
121 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
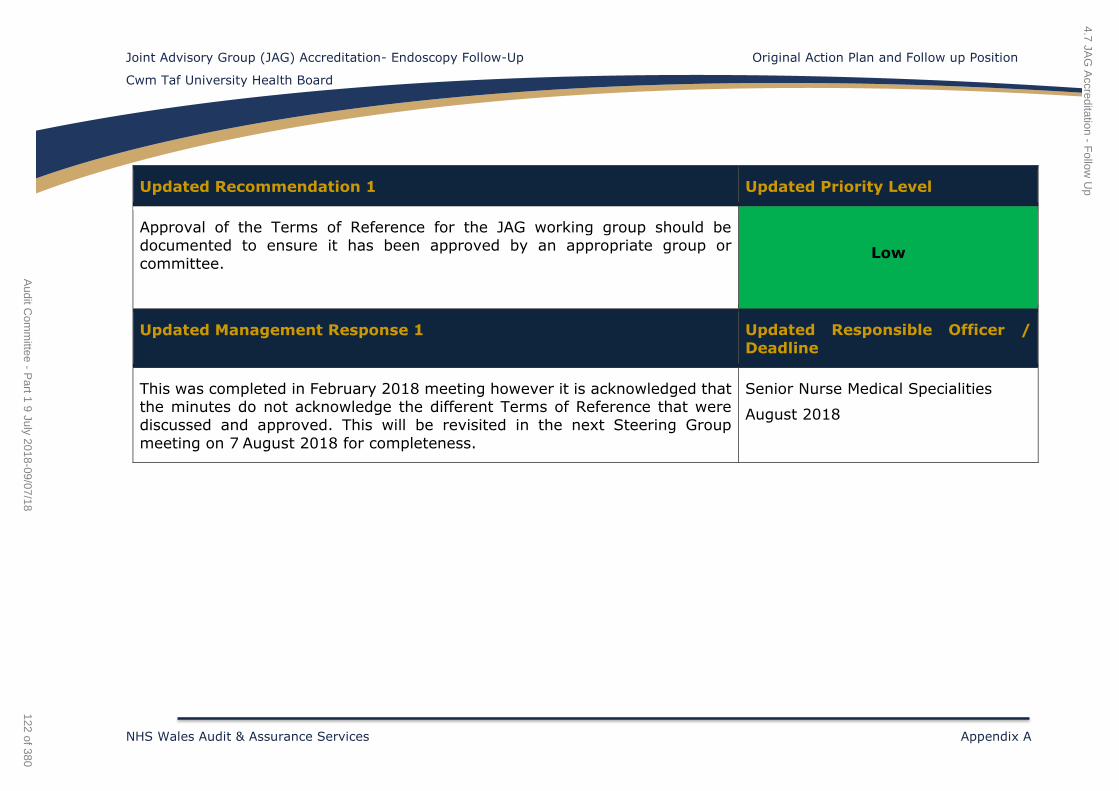
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Updated Recommendation 1 Updated Priority Level
Approval of the Terms of Reference for the JAG working group should be
documented to ensure it has been approved by an appropriate group or
committee.
Low
Updated Management Response 1 Updated Responsible Officer /
Deadline
This was completed in February 2018 meeting however it is acknowledged that the minutes do not acknowledge the different Terms of Reference that were
discussed and approved. This will be revisited in the next Steering Group
meeting on 7 August 2018 for completeness.
Senior Nurse Medical Specialities
August 2018
4.7 JAG
Accreditation - F
ollow U
p
122 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
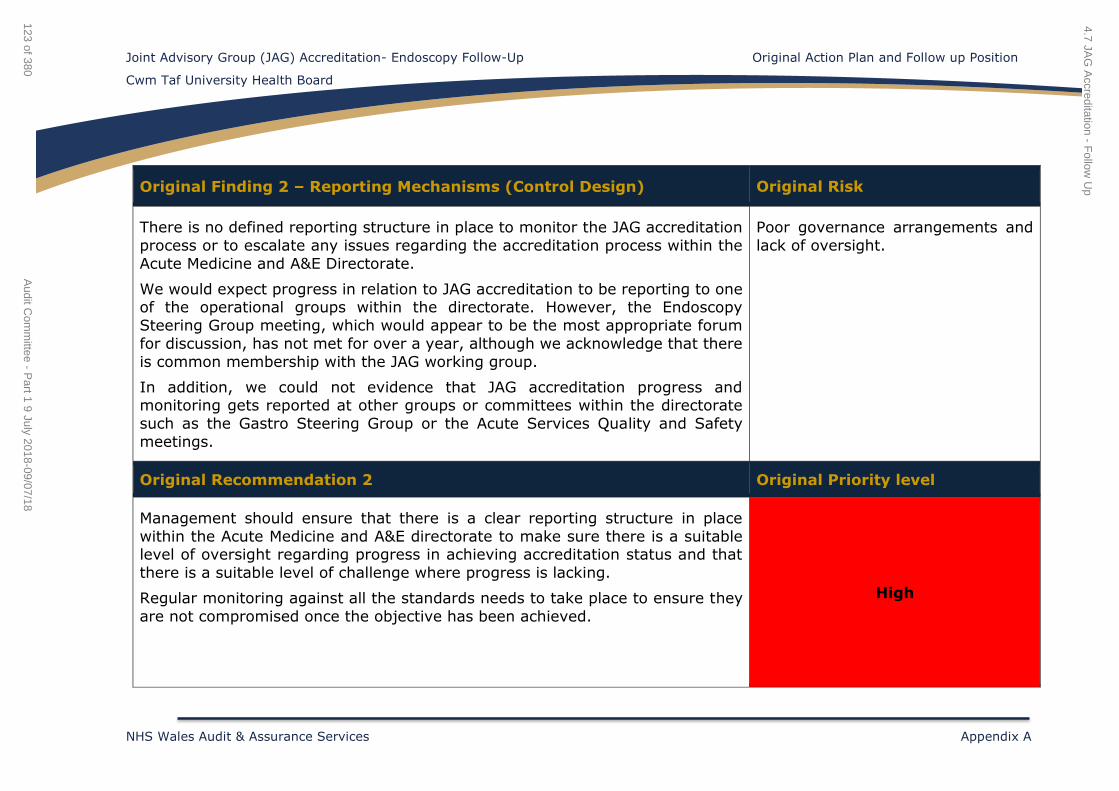
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Finding 2 – Reporting Mechanisms (Control Design) Original Risk
There is no defined reporting structure in place to monitor the JAG accreditation
process or to escalate any issues regarding the accreditation process within the
Acute Medicine and A&E Directorate.
We would expect progress in relation to JAG accreditation to be reporting to one of the operational groups within the directorate. However, the Endoscopy
Steering Group meeting, which would appear to be the most appropriate forum
for discussion, has not met for over a year, although we acknowledge that there
is common membership with the JAG working group.
In addition, we could not evidence that JAG accreditation progress and monitoring gets reported at other groups or committees within the directorate
such as the Gastro Steering Group or the Acute Services Quality and Safety
meetings.
Poor governance arrangements and
lack of oversight.
Original Recommendation 2 Original Priority level
Management should ensure that there is a clear reporting structure in place
within the Acute Medicine and A&E directorate to make sure there is a suitable level of oversight regarding progress in achieving accreditation status and that
there is a suitable level of challenge where progress is lacking.
Regular monitoring against all the standards needs to take place to ensure they
are not compromised once the objective has been achieved.
High
4.7 JAG
Accreditation - F
ollow U
p
123 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
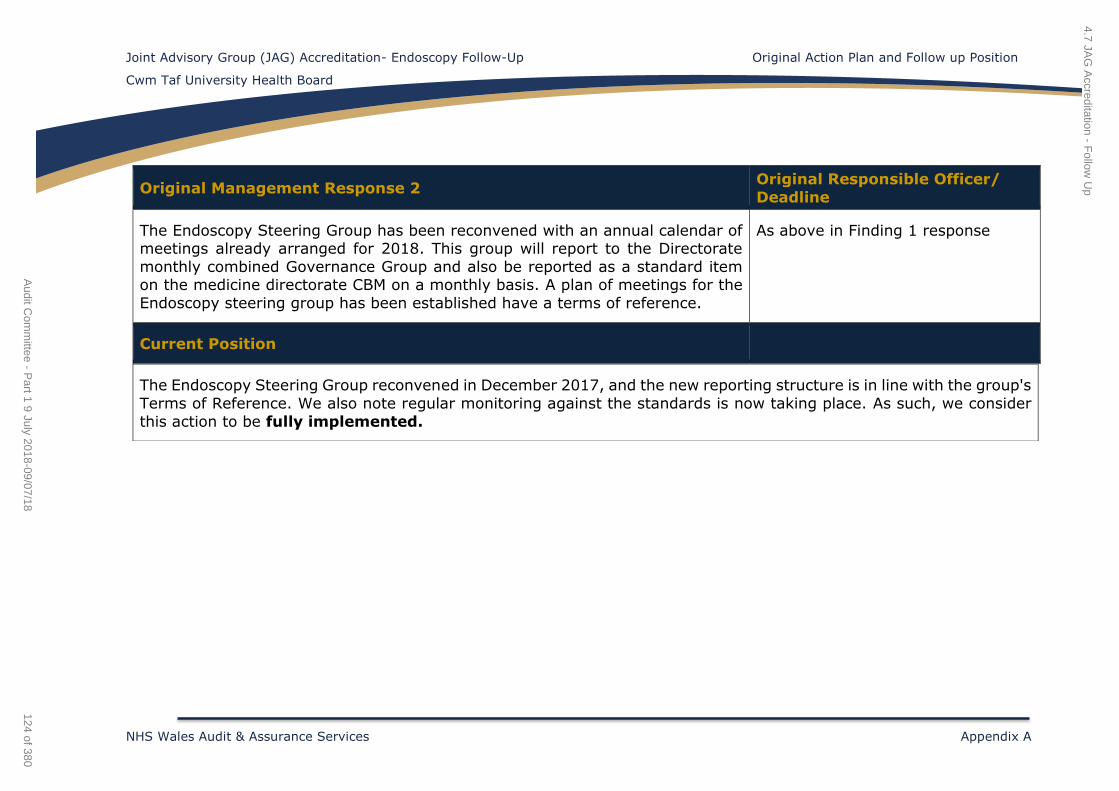
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Management Response 2 Original Responsible Officer/
Deadline
The Endoscopy Steering Group has been reconvened with an annual calendar of meetings already arranged for 2018. This group will report to the Directorate
monthly combined Governance Group and also be reported as a standard item on the medicine directorate CBM on a monthly basis. A plan of meetings for the
Endoscopy steering group has been established have a terms of reference.
As above in Finding 1 response
Current Position
The Endoscopy Steering Group reconvened in December 2017, and the new reporting structure is in line with the group's
Terms of Reference. We also note regular monitoring against the standards is now taking place. As such, we consider
this action to be fully implemented.
4.7 JAG
Accreditation - F
ollow U
p
124 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
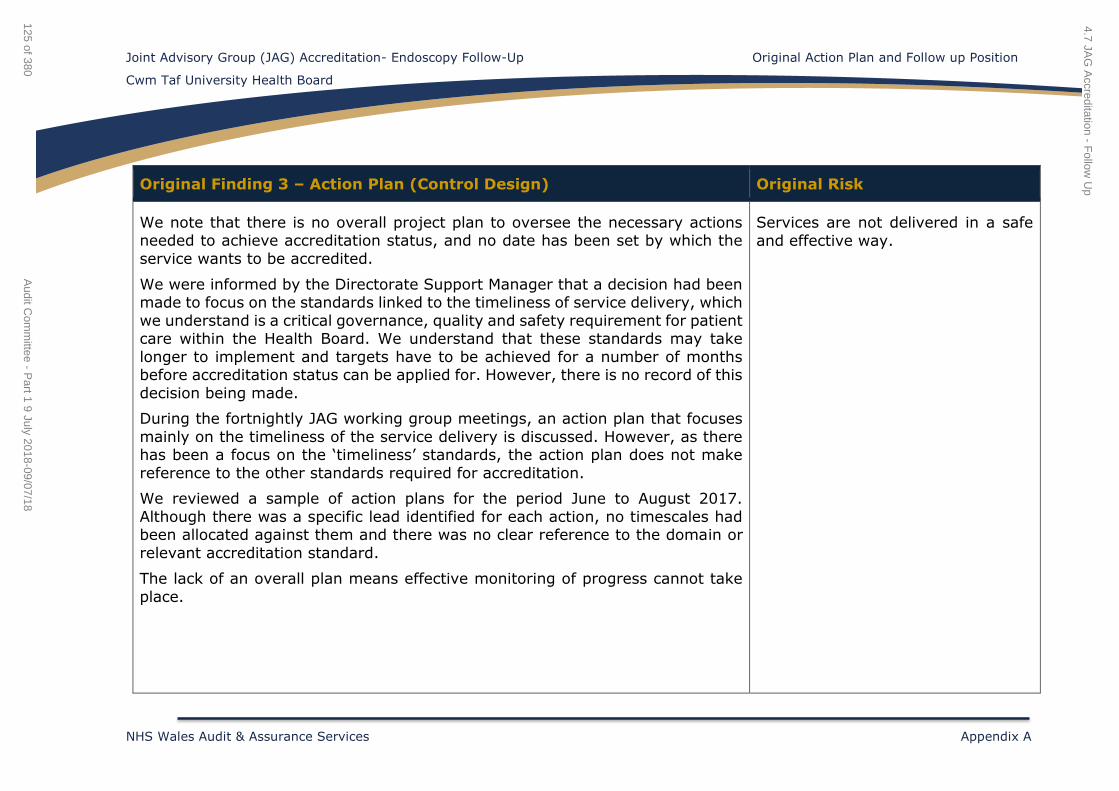
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Finding 3 – Action Plan (Control Design) Original Risk
We note that there is no overall project plan to oversee the necessary actions needed to achieve accreditation status, and no date has been set by which the
service wants to be accredited.
We were informed by the Directorate Support Manager that a decision had been made to focus on the standards linked to the timeliness of service delivery, which
we understand is a critical governance, quality and safety requirement for patient care within the Health Board. We understand that these standards may take
longer to implement and targets have to be achieved for a number of months before accreditation status can be applied for. However, there is no record of this
decision being made.
During the fortnightly JAG working group meetings, an action plan that focuses
mainly on the timeliness of the service delivery is discussed. However, as there has been a focus on the ‘timeliness’ standards, the action plan does not make
reference to the other standards required for accreditation.
We reviewed a sample of action plans for the period June to August 2017.
Although there was a specific lead identified for each action, no timescales had been allocated against them and there was no clear reference to the domain or
relevant accreditation standard.
The lack of an overall plan means effective monitoring of progress cannot take
place.
Services are not delivered in a safe
and effective way.
4.7 JAG
Accreditation - F
ollow U
p
125 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
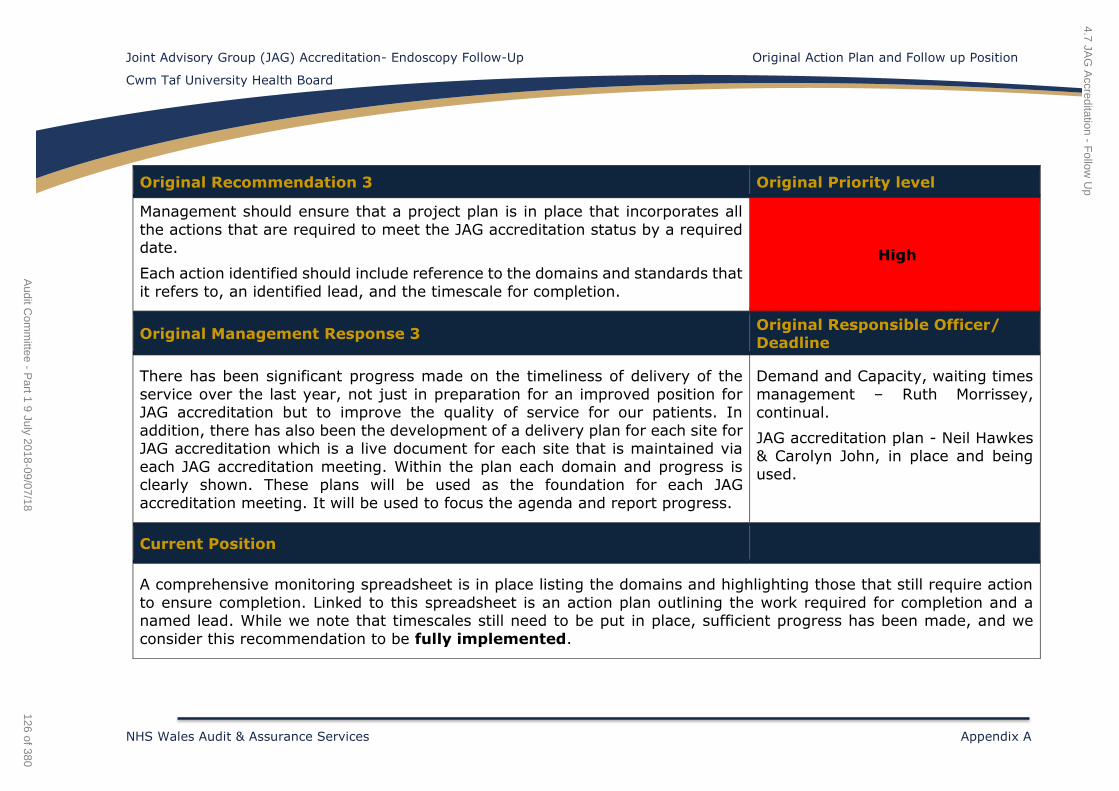
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Recommendation 3 Original Priority level
Management should ensure that a project plan is in place that incorporates all
the actions that are required to meet the JAG accreditation status by a required date.
Each action identified should include reference to the domains and standards that
it refers to, an identified lead, and the timescale for completion.
High
Original Management Response 3 Original Responsible Officer/ Deadline
There has been significant progress made on the timeliness of delivery of the
service over the last year, not just in preparation for an improved position for JAG accreditation but to improve the quality of service for our patients. In
addition, there has also been the development of a delivery plan for each site for JAG accreditation which is a live document for each site that is maintained via
each JAG accreditation meeting. Within the plan each domain and progress is clearly shown. These plans will be used as the foundation for each JAG
accreditation meeting. It will be used to focus the agenda and report progress.
Demand and Capacity, waiting times
management – Ruth Morrissey,
continual.
JAG accreditation plan - Neil Hawkes & Carolyn John, in place and being
used.
Current Position
A comprehensive monitoring spreadsheet is in place listing the domains and highlighting those that still require action
to ensure completion. Linked to this spreadsheet is an action plan outlining the work required for completion and a named lead. While we note that timescales still need to be put in place, sufficient progress has been made, and we
consider this recommendation to be fully implemented.
4.7 JAG
Accreditation - F
ollow U
p
126 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
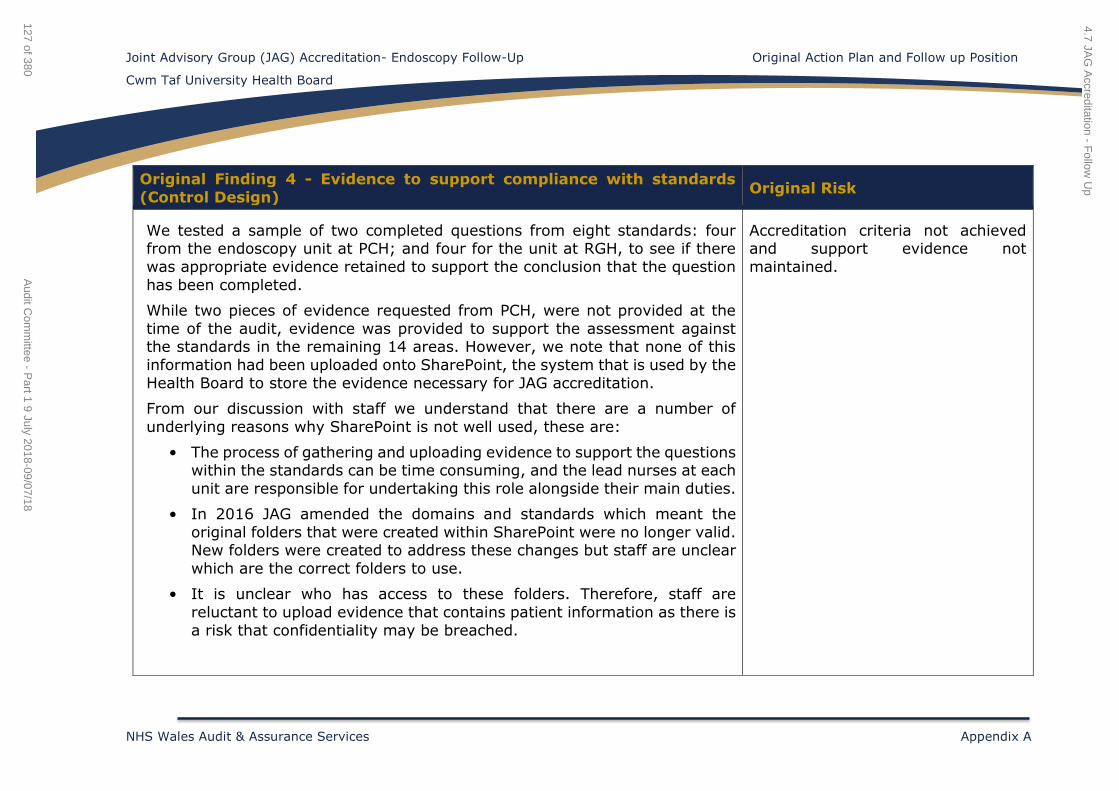
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Finding 4 - Evidence to support compliance with standards
(Control Design) Original Risk
We tested a sample of two completed questions from eight standards: four from the endoscopy unit at PCH; and four for the unit at RGH, to see if there
was appropriate evidence retained to support the conclusion that the question
has been completed.
While two pieces of evidence requested from PCH, were not provided at the
time of the audit, evidence was provided to support the assessment against the standards in the remaining 14 areas. However, we note that none of this
information had been uploaded onto SharePoint, the system that is used by the
Health Board to store the evidence necessary for JAG accreditation.
From our discussion with staff we understand that there are a number of
underlying reasons why SharePoint is not well used, these are:
• The process of gathering and uploading evidence to support the questions within the standards can be time consuming, and the lead nurses at each
unit are responsible for undertaking this role alongside their main duties.
• In 2016 JAG amended the domains and standards which meant the
original folders that were created within SharePoint were no longer valid. New folders were created to address these changes but staff are unclear
which are the correct folders to use.
• It is unclear who has access to these folders. Therefore, staff are
reluctant to upload evidence that contains patient information as there is
a risk that confidentiality may be breached.
Accreditation criteria not achieved and support evidence not
maintained.
4.7 JAG
Accreditation - F
ollow U
p
127 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
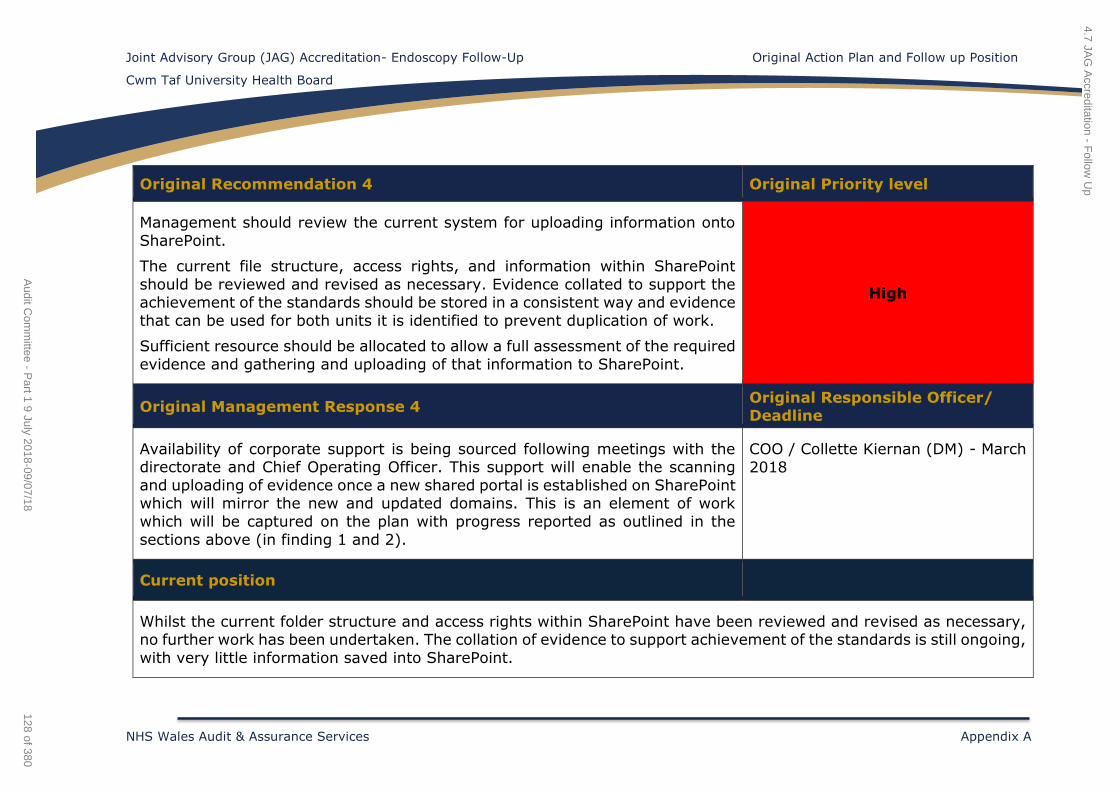
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Recommendation 4 Original Priority level
Management should review the current system for uploading information onto
SharePoint.
The current file structure, access rights, and information within SharePoint
should be reviewed and revised as necessary. Evidence collated to support the achievement of the standards should be stored in a consistent way and evidence
that can be used for both units it is identified to prevent duplication of work.
Sufficient resource should be allocated to allow a full assessment of the required
evidence and gathering and uploading of that information to SharePoint.
High
Original Management Response 4 Original Responsible Officer/ Deadline
Availability of corporate support is being sourced following meetings with the directorate and Chief Operating Officer. This support will enable the scanning
and uploading of evidence once a new shared portal is established on SharePoint which will mirror the new and updated domains. This is an element of work
which will be captured on the plan with progress reported as outlined in the
sections above (in finding 1 and 2).
COO / Collette Kiernan (DM) - March
2018
Current position
Whilst the current folder structure and access rights within SharePoint have been reviewed and revised as necessary, no further work has been undertaken. The collation of evidence to support achievement of the standards is still ongoing,
with very little information saved into SharePoint.
4.7 JAG
Accreditation - F
ollow U
p
128 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
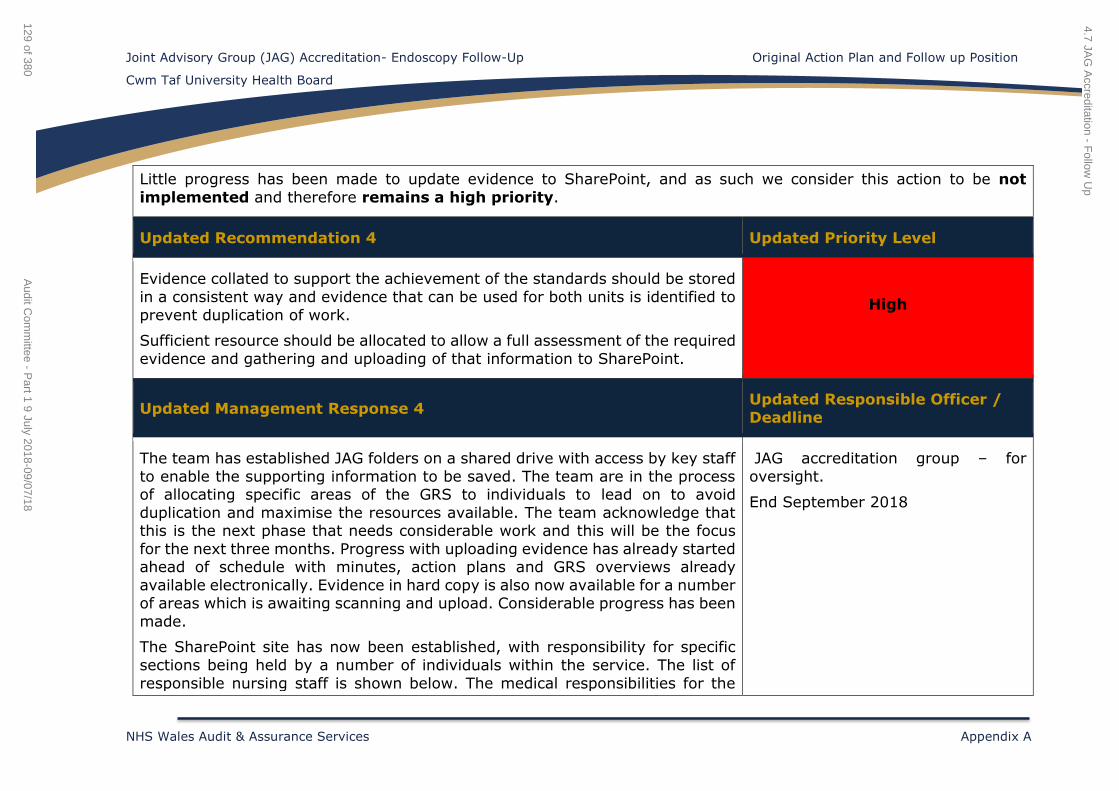
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Little progress has been made to update evidence to SharePoint, and as such we consider this action to be not
implemented and therefore remains a high priority.
Updated Recommendation 4 Updated Priority Level
Evidence collated to support the achievement of the standards should be stored
in a consistent way and evidence that can be used for both units is identified to
prevent duplication of work.
Sufficient resource should be allocated to allow a full assessment of the required
evidence and gathering and uploading of that information to SharePoint.
High
Updated Management Response 4 Updated Responsible Officer /
Deadline
The team has established JAG folders on a shared drive with access by key staff
to enable the supporting information to be saved. The team are in the process of allocating specific areas of the GRS to individuals to lead on to avoid
duplication and maximise the resources available. The team acknowledge that this is the next phase that needs considerable work and this will be the focus
for the next three months. Progress with uploading evidence has already started ahead of schedule with minutes, action plans and GRS overviews already
available electronically. Evidence in hard copy is also now available for a number of areas which is awaiting scanning and upload. Considerable progress has been
made.
The SharePoint site has now been established, with responsibility for specific
sections being held by a number of individuals within the service. The list of
responsible nursing staff is shown below. The medical responsibilities for the
JAG accreditation group – for
oversight.
End September 2018
4.7 JAG
Accreditation - F
ollow U
p
129 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
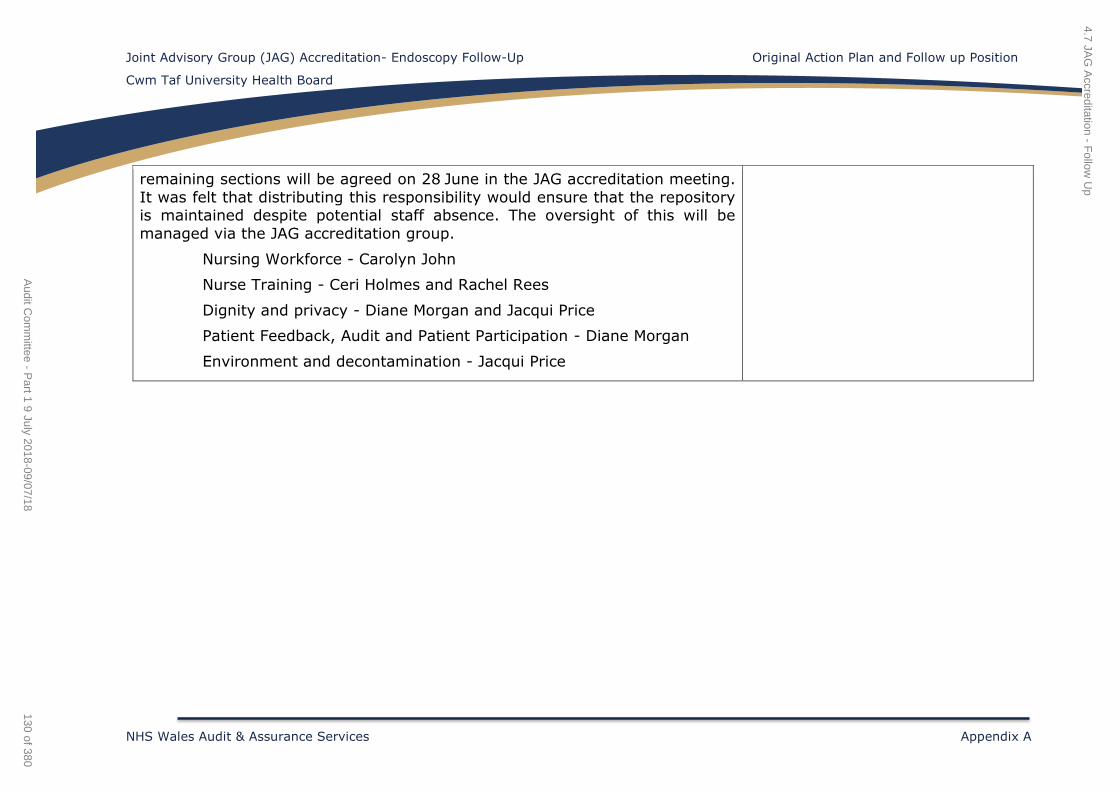
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
remaining sections will be agreed on 28 June in the JAG accreditation meeting.
It was felt that distributing this responsibility would ensure that the repository is maintained despite potential staff absence. The oversight of this will be
managed via the JAG accreditation group.
Nursing Workforce - Carolyn John
Nurse Training - Ceri Holmes and Rachel Rees
Dignity and privacy - Diane Morgan and Jacqui Price
Patient Feedback, Audit and Patient Participation - Diane Morgan
Environment and decontamination - Jacqui Price
4.7 JAG
Accreditation - F
ollow U
p
130 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Finding 5 - Scoring the GRS self-assessment (Operating
effectiveness) Original Risk
To obtain JAG accreditation the Health Board has to be able to demonstrate a minimum of one year participating in the Global Rating Scale (GRS) self-
assessment, and performing at the agreed GRS levels required for accreditation. Each GRS self-assessment is completed on-line via the JAG accreditation system.
Scoring is based on an A-D system, with grade ‘B’ being the minimum score
required for each question under a standard to achieve accreditation.
The PCH and RGH endoscopy units are not consistently maintaining the same
level of scoring when completing the GRS self-assessments. If the units are to achieve JAG accreditation status, there should be a continual improvement in
scores between each self-assessment. Our review of the last two self-
assessments undertaken by each unit identified:
PCH - Between April and October 2016
For 7 out of 19 standards the scoring level has remained the same.
• For 7 out of 19 standards the scoring level has improved.
• For 5 out of 19 standards the scoring level has decreased.
As at October 2016; 7 out of 19 had achieved the required scoring level of ‘B’
and above.
RGH – Between October 2016 - April 2017
• For 5 out of 19 standards the scoring level has remained the same.
• For 14 out of the 19 standards the scoring level had decreased. Nine of
these were originally scoring as an ‘A’ grade but have been downgraded to
‘D's’ and ‘C's’.
Services are not delivered in a safe
and effective way.
4.7 JAG
Accreditation - F
ollow U
p
131 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
As at April 2017 three out of 19 have achieved the scoring level of ‘B’.
As at October 2016 the endoscopy unit in PCH had achieved 37% of the standards
scoring a level ‘B’ and above, whereas in April 2017 RGH had only achieved 16%.
Original Recommendation 5 Original Priority level
Management should review and understand why the scoring rates have
decreased when comparing the GRS self-assessment to the previous
submissions.
Action plans should be created to address the short comings, which must include realistic timescales and persons' responsible. Failure to comply with the action
plan should be challenged by management.
Medium
Original Management Response 5 Original Responsible Officer/
Deadline
Self-evaluations that were submitted in October 2017 have been reviewed and compared and moving forward for the April 2018 submission there are plans that
each site will undertake the review independently and then this will be peer reviewed by the alternative acute site to ensure consistency in approach and to
give assurance prior to submission. The most recent review shows the deficits in each domain that are not at level B (the required standard) and therefore informs
the overall action plan for achieving accreditation. This review document can be
seen in Appendix 3.
In Place;
Dr Neil Hawkes – RGH
Dr Jo Hurley – PCH
Next Review April 2018
4.7 JAG
Accreditation - F
ollow U
p
132 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Current position
The monitoring of the achievement of each standard within each domain and any changes, is happening on a monthly basis and not just at the time of GRS submission. This monitoring is linked to the action plans that are produced and
these are discussed and monitored at the JAG steering group and Endoscopy Steering Group.
As such, we consider this action to be fully implemented.
4.7 JAG
Accreditation - F
ollow U
p
133 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Finding 6 – Operational policy (Operating effectiveness) Original Risk
An endoscopy operational policy is required to achieve JAG accreditation. In
September 2017 the directorate began drafting a policy document. We understand that the Health Board has identified that the policy will require
significant work to ensure that it meets the necessary standards for JAG
accreditation.
We understand that currently there is no timescale in place for the completion of
the review of this policy and its associated documents.
Services are not delivered in a safe
and effective way.
Original Recommendation 6 Original Priority level
Management must agree a timescale for the completion of the operational policy
review. Progress against the policy and the supporting appendices should be
discussed in the appropriate endoscopy working group or steering group.
Once policies and appendices have been updated they need to be appropriately
approved.
Medium
Original Management Response 6 Original Responsible Officer/ Deadline
The directorate now have a formalised action plan relating to the development
and completion of the operational policy. The plan gives structure and clarity around what is still required for completion of this significant document. This plan
can be seen in Appendix 4.
Action Plan is in place and significant
progress has been made. This work is led by Dr Jo Hurley, target
completion date February 2018.
4.7 JAG
Accreditation - F
ollow U
p
134 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Current position
The Operational Policy and supporting appendices have been drafted although final approval is still to take place as the
consultants within the directorate are required to read the policy and confirm their acceptance. This is due to take place
by the end of June 2018.
As such, we consider this action to be partially implemented. As a consequence of the progress that has been made
to date, the priority of this recommendation has been re-assessed as a low priority.
Updated Recommendation 6 Updated Priority Level
Review by the relevant consultants of the supporting appendices to the Operational Policy should be completed as soon as practically possible to allow
for final approval of the Operational Policy. Low
Updated Management Response 6 Updated Responsible Officer /
Deadline
Lead clinician is aware of the need to complete this piece of work as promptly as possible, with virtual agreement to be sought prior to the Gastro Strategy Group
meeting in July where this will be formally signed off (As Endoscopy steering
group is not scheduled until August).
Consultant Gastroenterologist
July 2018
4.7 JAG
Accreditation - F
ollow U
p
135 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Finding 7 – Completion of GRS self-assessments (Control
design) Original Risk
The Health Board currently completes GRS self-assessments every April and October although JAG guidance suggests quarterly returns. Within the GRS
system a clinical lead and nurse manager are set up to complete the self-
assessments at each site. However, we note that different people undertake the
self-assessments at the two sites leading to potential inconsistencies.
Furthermore, during our fieldwork we noted one instance where the six-monthly GRS self-assessment had not been completed as both the clinical lead and the
endoscopy nurse at PCH were not available. Given the lack of governance arrangements, there is no protocol in place to address this issue should both
leads be unavailable at the time the assessment needs to be completed.
Poor governance arrangements and a lack of oversight.
Original Recommendation 7 Original Priority level
Management should ensure that the GRS self-assessments are completed when
required and a protocol in place to address the problem should the appropriate
staff not be available to complete the assessments.
Furthermore, ensuring the same people undertake the assessments at both units provides the Health Board with an opportunity to remove inconsistencies across
the units.
Low
4.7 JAG
Accreditation - F
ollow U
p
136 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation- Endoscopy Follow-Up Original Action Plan and Follow up Position
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix A
Original Management Response 7 Original Responsible Officer/
Deadline
A plan has been put in place for cross site peer review of the GRS self-assessments prior to submission which should achieve improved consistency and
assurance across the Health Board.
Dr Jo Hurley and Dr Neil Hawkes. Will be delivered for April 2018
submission.
Current position
Whilst the practice of completing the GRS collectively has commenced to ensure consistency of scoring, a protocol has
not yet been developed to aid consistent completion should staff not be available.
As such, due to the lack of protocol for addressing the issues of staff not being able to complete the assessment, we
consider this action to be partially implemented. As a consequence of the progress that has been made to date, the
priority of this recommendation remains as a low priority.
Updated Recommendation 7 Updated Priority Level
A protocol should be put in place to address the problem should the appropriate
staff not be available to complete the GRS assessments. Low
Updated Management Response 7 Updated Responsible Officer /
Deadline
A protocol will be written, discussed and minuted at the next Endoscopy Steering
group meeting on 7 August 2018.
Senior Nurse Medical Specialties
August 2018
4.7 JAG
Accreditation - F
ollow U
p
137 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
Joint Advisory Group (JAG) Accreditation – Endoscopy Follow Up
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix B
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance
that arrangements to secure governance, risk management and internal control, within those areas under review, are suitably designed and applied
effectively. Few matters require attention and are compliance or advisory in
nature with low impact on residual risk exposure.
Follow up - All recommendations implemented and operating as expected.
Reasonable assurance - The Board can take reasonable assurance
that arrangements to secure governance, risk management and internal control, within those areas under review, are suitably designed and applied
effectively. Some matters require management attention in control design or
compliance with low to moderate impact on residual risk exposure until
resolved.
Follow up - All high level recommendations implemented and progress on the medium and low level recommendations.
Limited assurance - The Board can take limited assurance that
arrangements to secure governance, risk management and internal control, within those areas under review, are suitably designed and applied effectively.
More significant matters require management attention with moderate
impact on residual risk exposure until resolved.
Follow up - No high level recommendations implemented but progress on a majority of the medium and low recommendations.
No Assurance - The Board has no assurance that arrangements to
secure governance, risk management and internal control, within those areas under review, are suitably designed and applied effectively. Action is required
to address the whole control framework in this area with high impact on
residual risk exposure until resolved.
Follow up - No action taken to implement recommendations.
4.7 JAG Accreditation - Follow Up
138 of 380Audit Committee - Part 1 9 July 2018-09/07/18
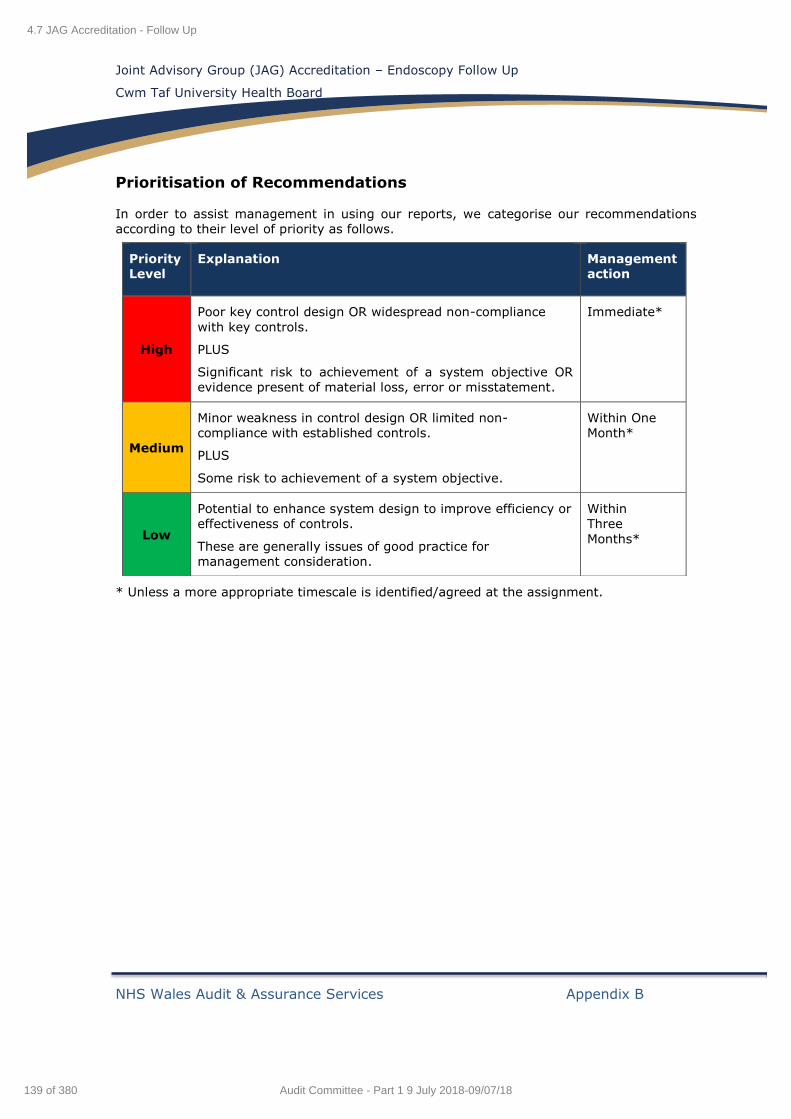
Joint Advisory Group (JAG) Accreditation – Endoscopy Follow Up
Cwm Taf University Health Board
NHS Wales Audit & Assurance Services Appendix B
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
* Unless a more appropriate timescale is identified/agreed at the assignment.
Priority
Level
Explanation
Management
action
High
Poor key control design OR widespread non-compliance
with key controls.
PLUS
Significant risk to achievement of a system objective OR
evidence present of material loss, error or misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve efficiency or
effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within
Three
Months*
4.7 JAG Accreditation - Follow Up
139 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Audit Committee Update – Cwm Taf University Health Board
Date issued: July 2018
Document reference: 123A2017
5.1 Wales Audit Office Update Report
1 of 380Audit Committee - Part 1 9 July 2018-09/07/18

This document has been prepared as part of work performed in accordance with statutory functions.
In the event of receiving a request for information to which this document may be relevant, attention
is drawn to the Code of Practice issued under section 45 of the Freedom of Information Act 2000.
The section 45 code sets out the practice in the handling of requests that is expected of public
authorities, including consultation with relevant third parties. In relation to this document, the Auditor
General for Wales and the Wales Audit Office are relevant third parties. Any enquiries regarding
disclosure or re-use of this document should be sent to the Wales Audit Office at
5.1 Wales Audit Office Update Report
2 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Contents
Page 3 of 10 - Audit Committee Update – Cwm Taf University Health Board
Summary report
About this document 4
Financial audit update 4
Performance audit update 5
NHS Related National Studies and Publications 7
Good Practice Exchange 8
5.1 Wales Audit Office Update Report
3 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Summary report
Page 4 of 10 - Audit Committee Update – Cwm Taf University Health Board
About this document
1 This document provides the Audit Committee of the Cwm Taf University Health
Board (the Health Board) with an update on current and planned Wales Audit
Office work. Financial and performance audit work is considered and information is
also provided on the Auditor General’s programme of national value-for-money
examinations.
Financial audit update
Exhibit 1: Financial audit update
Work area Progress Conclusions
Annual UHB Accounts 2017-18
Our audit of the 2017-18 financial statements is now complete. Our ‘Audit of
Financial Statements’ report was presented to the Audit Committee on 31 May which
summarised our findings. The accounts were certified by
the Auditor General for Wales on 6 June (with an unqualified audit opinion) and laid with the
National Assembly for Wales on 14 June.
Work complete.
Charitable Funds Accounts 2017-18
These financial statements are subject to an independent examination, rather than a full
audit. This work is scheduled to take
place over the autumn, allowing the accounts to be filed with the Charity Commission in advance of the
31 January 2019 deadline.
Work ongoing.
5.1 Wales Audit Office Update Report
4 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
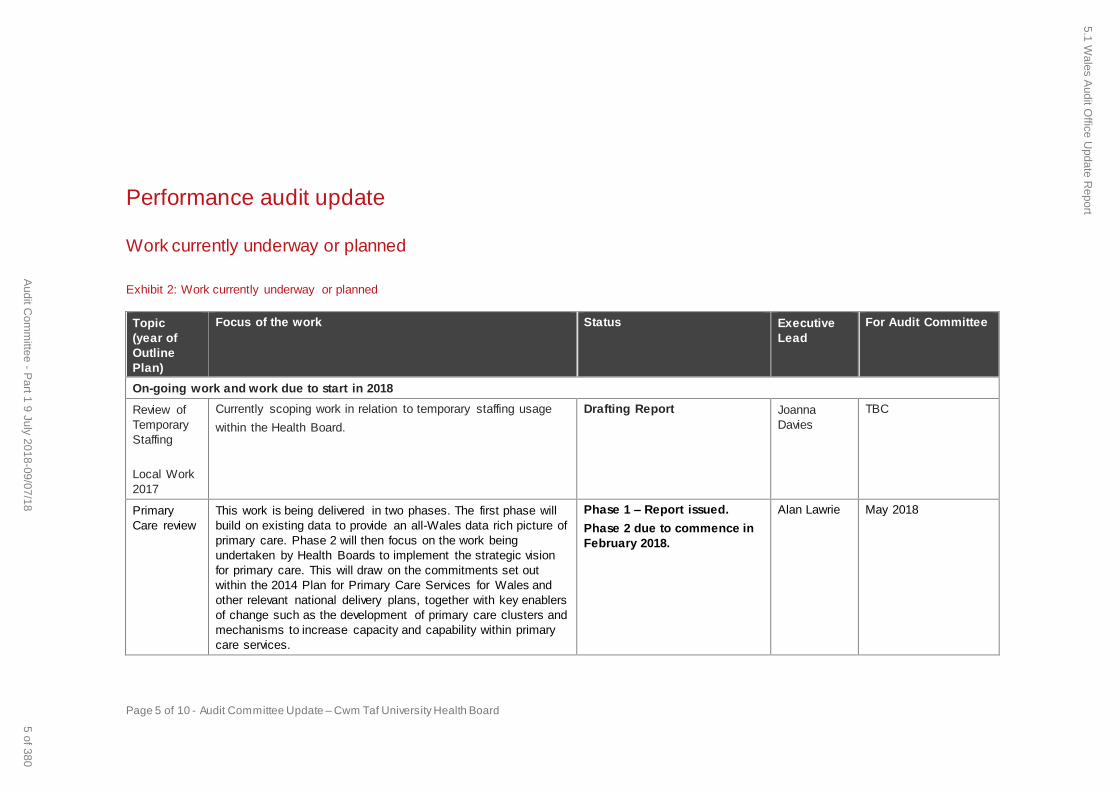
Page 5 of 10 - Audit Committee Update – Cwm Taf University Health Board
Performance audit update
Work currently underway or planned
Exhibit 2: Work currently underway or planned
Topic
(year of
Outline
Plan)
Focus of the work Status Executive
Lead
For Audit Committee
On-going work and work due to start in 2018
Review of
Temporary
Staffing
Local Work
2017
Currently scoping work in relation to temporary staffing usage
within the Health Board.
Drafting Report Joanna
Davies
TBC
Primary
Care review
This work is being delivered in two phases. The first phase will
build on existing data to provide an all-Wales data rich picture of
primary care. Phase 2 will then focus on the work being
undertaken by Health Boards to implement the strategic vision
for primary care. This will draw on the commitments set out
within the 2014 Plan for Primary Care Services for Wales and
other relevant national delivery plans, together with key enablers
of change such as the development of primary care clusters and
mechanisms to increase capacity and capability within primary
care services.
Phase 1 – Report issued.
Phase 2 due to commence in
February 2018.
Alan Lawrie May 2018
5.1 Wales A
udit Office U
pdate Report
5 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
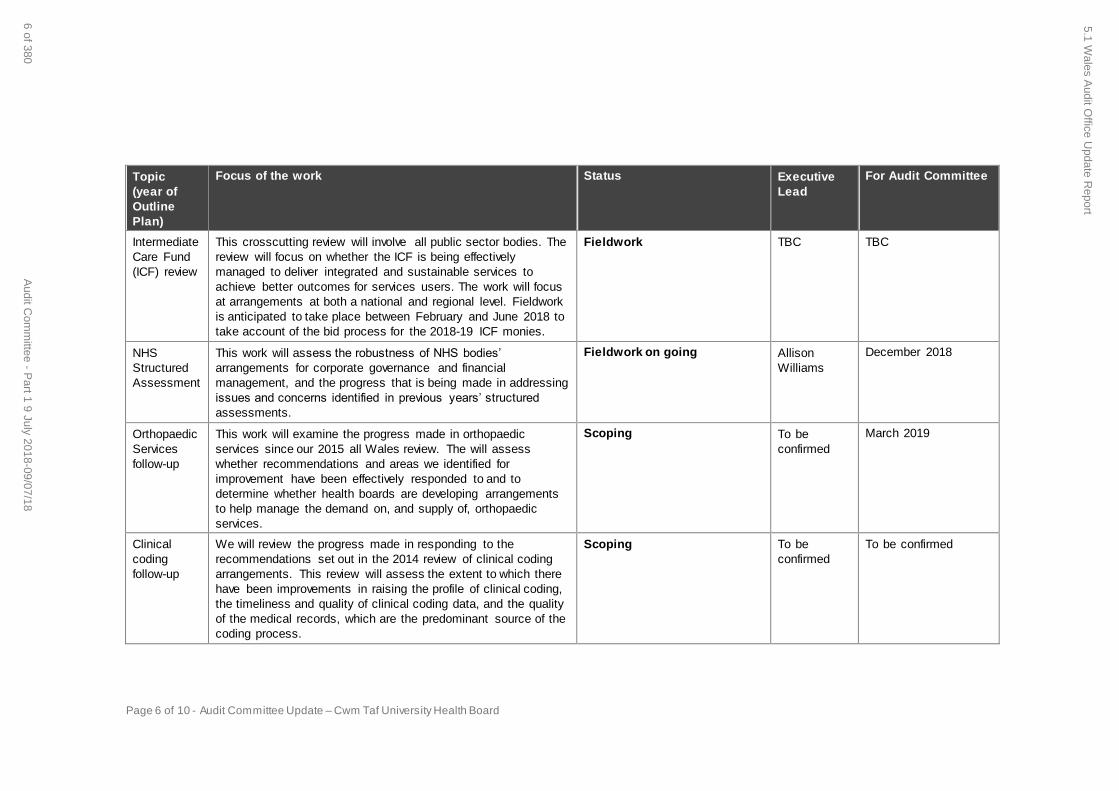
Page 6 of 10 - Audit Committee Update – Cwm Taf University Health Board
Topic
(year of
Outline
Plan)
Focus of the work Status Executive
Lead
For Audit Committee
Intermediate
Care Fund
(ICF) review
This crosscutting review will involve all public sector bodies. The
review will focus on whether the ICF is being effectively
managed to deliver integrated and sustainable services to
achieve better outcomes for services users. The work will focus
at arrangements at both a national and regional level. Fieldwork
is anticipated to take place between February and June 2018 to
take account of the bid process for the 2018-19 ICF monies.
Fieldwork TBC TBC
NHS
Structured
Assessment
This work will assess the robustness of NHS bodies’
arrangements for corporate governance and financial
management, and the progress that is being made in addressing
issues and concerns identified in previous years’ structured
assessments.
Fieldwork on going Allison
Williams
December 2018
Orthopaedic
Services
follow-up
This work will examine the progress made in orthopaedic
services since our 2015 all Wales review. The will assess
whether recommendations and areas we identified for
improvement have been effectively responded to and to
determine whether health boards are developing arrangements
to help manage the demand on, and supply of, orthopaedic
services.
Scoping To be
confirmed
March 2019
Clinical
coding
follow-up
We will review the progress made in responding to the
recommendations set out in the 2014 review of clinical coding
arrangements. This review will assess the extent to which there
have been improvements in raising the profile of clinical coding,
the timeliness and quality of clinical coding data, and the quality
of the medical records, which are the predominant source of the
coding process.
Scoping To be
confirmed
To be confirmed
5.1 Wales A
udit Office U
pdate Report
6 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
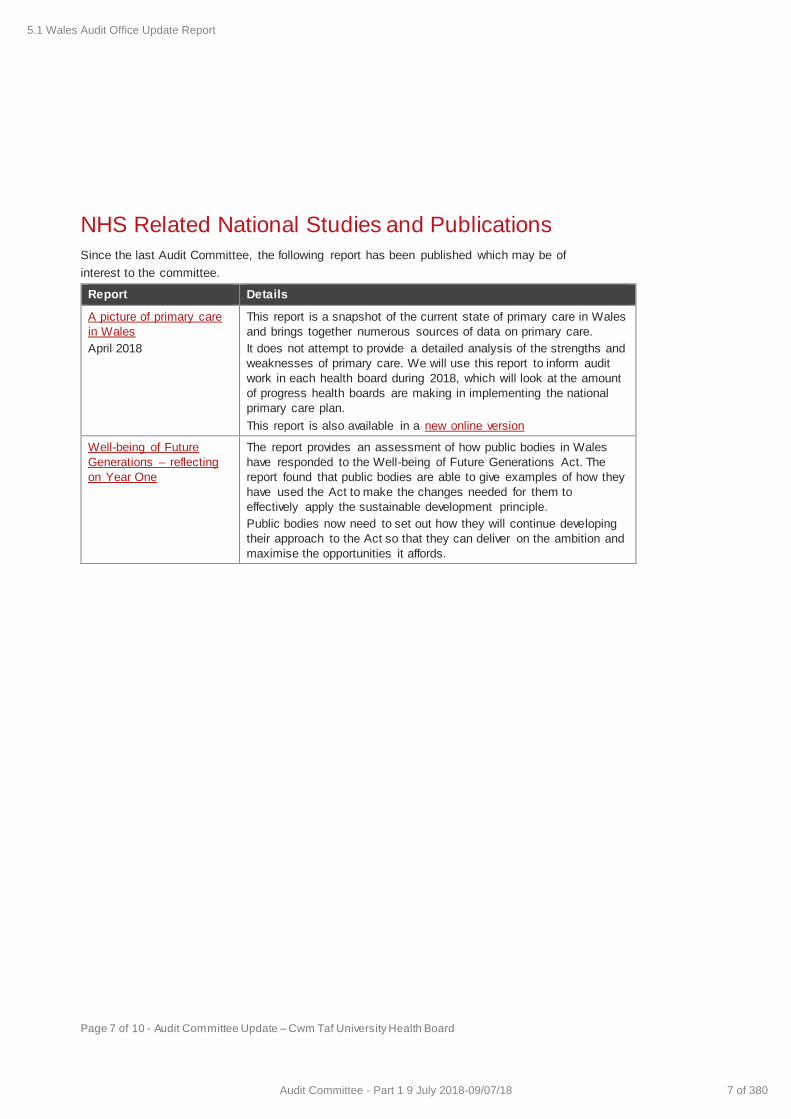
Page 7 of 10 - Audit Committee Update – Cwm Taf University Health Board
NHS Related National Studies and Publications
Since the last Audit Committee, the following report has been published which may be of
interest to the committee.
Report Details
A picture of primary care
in Wales
April 2018
This report is a snapshot of the current state of primary care in Wales
and brings together numerous sources of data on primary care.
It does not attempt to provide a detailed analysis of the strengths and
weaknesses of primary care. We will use this report to inform audit
work in each health board during 2018, which will look at the amount
of progress health boards are making in implementing the national
primary care plan.
This report is also available in a new online version
Well-being of Future
Generations – reflecting
on Year One
The report provides an assessment of how public bodies in Wales
have responded to the Well-being of Future Generations Act. The
report found that public bodies are able to give examples of how they
have used the Act to make the changes needed for them to
effectively apply the sustainable development principle.
Public bodies now need to set out how they will continue developing
their approach to the Act so that they can deliver on the ambition and
maximise the opportunities it affords.
5.1 Wales Audit Office Update Report
7 of 380Audit Committee - Part 1 9 July 2018-09/07/18
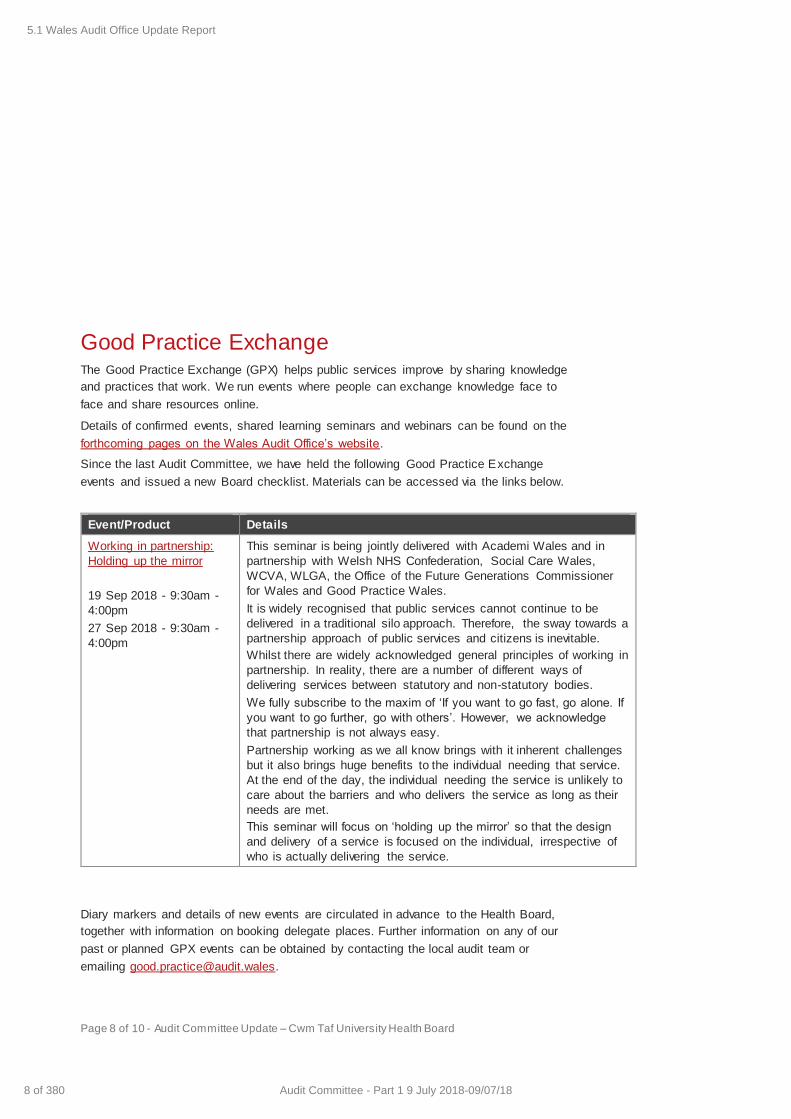
Page 8 of 10 - Audit Committee Update – Cwm Taf University Health Board
Good Practice Exchange
The Good Practice Exchange (GPX) helps public services improve by sharing knowledge
and practices that work. We run events where people can exchange knowledge face to
face and share resources online.
Details of confirmed events, shared learning seminars and webinars can be found on the
forthcoming pages on the Wales Audit Office’s website.
Since the last Audit Committee, we have held the following Good Practice Exchange
events and issued a new Board checklist. Materials can be accessed via the links below.
Event/Product Details
Working in partnership:
Holding up the mirror
19 Sep 2018 - 9:30am -
4:00pm
27 Sep 2018 - 9:30am -
4:00pm
This seminar is being jointly delivered with Academi Wales and in
partnership with Welsh NHS Confederation, Social Care Wales,
WCVA, WLGA, the Office of the Future Generations Commissioner
for Wales and Good Practice Wales.
It is widely recognised that public services cannot continue to be
delivered in a traditional silo approach. Therefore, the sway towards a
partnership approach of public services and citizens is inevitable.
Whilst there are widely acknowledged general principles of working in
partnership. In reality, there are a number of different ways of
delivering services between statutory and non-statutory bodies.
We fully subscribe to the maxim of ‘If you want to go fast, go alone. If
you want to go further, go with others’. However, we acknowledge
that partnership is not always easy.
Partnership working as we all know brings with it inherent challenges
but it also brings huge benefits to the individual needing that service.
At the end of the day, the individual needing the service is unlikely to
care about the barriers and who delivers the service as long as their
needs are met.
This seminar will focus on ‘holding up the mirror’ so that the design
and delivery of a service is focused on the individual, irrespective of
who is actually delivering the service.
Diary markers and details of new events are circulated in advance to the Health Board,
together with information on booking delegate places. Further information on any of our
past or planned GPX events can be obtained by contacting the local audit team or
emailing [email protected].
5.1 Wales Audit Office Update Report
8 of 380 Audit Committee - Part 1 9 July 2018-09/07/18

Page 9 of 10 - Audit Committee Update – Cwm Taf University Health Board
5.1 Wales Audit Office Update Report
9 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Wales Audit Office
24 Cathedral Road
Cardiff CF11 9LJ
Tel: 029 2032 0500
Fax: 029 2032 0600
Textphone.: 029 2032 0660
E-mail: [email protected]
Website: www.audit.wales
Swyddfa Archwilio Cymru
24 Heol y Gadeirlan
Caerdydd CF11 9LJ
Ffôn: 029 2032 0500
Ffacs: 029 2032 0600
Ffôn testun: 029 2032 0660
E-bost: [email protected]
Gwefan: www.archwilio.cymru
We welcome correspondence and telephone calls in Welsh and English. Rydym yn croesawu gohebiaeth a galwadau ffôn yn Gymraeg a Saesneg.
5.1 Wales Audit Office Update Report
10 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales
24 April 2018
Archwilydd Cyffredinol CymruAuditor General for Wales
5.2 Picture of Primary Care in Wales - National Report - For Information Only
11 of 380Audit Committee - Part 1 9 July 2018-09/07/18

A picture of primary care in Wales2
The Auditor General is independent of the National Assembly and government. He examines and certifies the accounts of the Welsh Government and its sponsored and related public bodies, including NHS bodies. He also has the power to report to the National Assembly on the economy, efficiency and effectiveness with which those organisations have used, and may improve the use of, their resources in discharging their functions.
The Auditor General also audits local government bodies in Wales, conducts local government value for money studies and inspects for compliance with the requirements of the Local Government (Wales) Measure 2009.
The Auditor General undertakes his work using staff and other resources provided by the Wales Audit Office, which is a statutory board established for that purpose and to monitor and advise the Auditor General.
© Auditor General for Wales 2018
You may re-use this publication (not including logos) free of charge in any format or medium. If you re-use it, your re-use must be accurate and must not be in a misleading context. The material must be acknowledged as Auditor General for Wales copyright and you must give the title of this publication. Where we have identified any third party copyright material you will need to obtain permission from the copyright holders concerned before re-use.
For further information, or if you require any of our publications in an alternative format and/or language, please contact us by telephone on 029 2032 0500, or email [email protected]. We welcome telephone calls in Welsh and English. You can also write to us in either Welsh or English and we will respond in the language you have used. Corresponding in Welsh will not lead to a delay.
Mae’r ddogfen hon hefyd ar gael yn Gymraeg.
I have prepared and published this report in accordance with the Government of Wales Act 1998.
The Wales Audit Office study team comprised Nigel Blewitt, Matthew Brushett, Stephen Lisle, Elaine Matthews and Emily Owen
under the direction of Dave Thomas.
Huw Vaughan ThomasAuditor General for Wales
Wales Audit Office24 Cathedral Road
CardiffCF11 9LJ
5.2 Picture of Primary Care in Wales - National Report - For Information Only
12 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales 3
Contents
Introduction 4What is primary care? 5What is the cost? 7What do patients think? 10What are the workforce issues? 15What is the plan to improve primary care? 22
5.2 Picture of Primary Care in Wales - National Report - For Information Only
13 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales4
Introduction
Primary care services play a vital role within the wider system of health and care in Wales. But services have come under increasing pressure from rises in demand and constraints in capacity, and it is recognised that changes need to be made to ensure that primary care services are sustainable and can play the key role that is required of them within the NHS in Wales.
This report is part of a suite of work we are undertaking on primary care services in Wales. It brings together numerous sources of data to provide a snapshot of primary care services. It is not intended to be a detailed evaluation of the strengths and weaknesses of primary care. Instead it sets out some key information on how current services are organised and highlights key issues which will be explored further as part our more detailed audit work at health boards.
During 2018 auditors will examine the progress health boards in Wales have made in implementing the national plan for primary care. A report will be produced for each health board, and a national summary of our findings will follow in early 2019.
We have already completed a separate and detailed review on GP Out of Hours Services, and reported our findings to health boards. A summary of these findings will be published in June 2018.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
14 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales 5
Primary care encompasses a wide range of services, typically delivered in the local community by general practitioners (GPs), pharmacists, dentists, optometrists and other healthcare professionals.
Definition of primary care- The definition in the national primary care plan in Wales is:
‘ Primary care is about those services which provide the first point of care, day or night for more than 90% of people’s contact with the NHS in Wales.’
‘ General practice is a core element of primary care: it is not the only element – primary care encompasses many more health services, including, pharmacy, dentistry, and optometry.’
‘ It is also – importantly – about coordinating access for people to the wide range of services in the local community to help meet their health and wellbeing needs.’
- Many GPs, pharmacists, dentists and optometrists work as independent contractors. Navigate to the workforce section of this report to find out more about their contracts with the NHS in Wales.
- Whilst this report aims to cover primary care in its broad sense, most of the publically available data in Wales focuses on general practice, which has consequently shaped the focus of some sections of this report.
What is primary care?
5.2 Picture of Primary Care in Wales - National Report - For Information Only
15 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales6
Why is primary care important?
First point of contactPrimary care is the first port of call for the majority of people who use health services.
Spending on primary careIn 2016-17, the NHS in Wales spent £1.39 billion on primary care, which is around a fifth of the total NHS spending in Wales.
Prevention and early interventionPrimary care is also important because of its focus on promoting well-being, early intervention and preventing people’s conditions from getting worse.
Coordinating carePrimary care has an important role in coordinating people's care. Primary care is the gateway to many other services.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
16 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
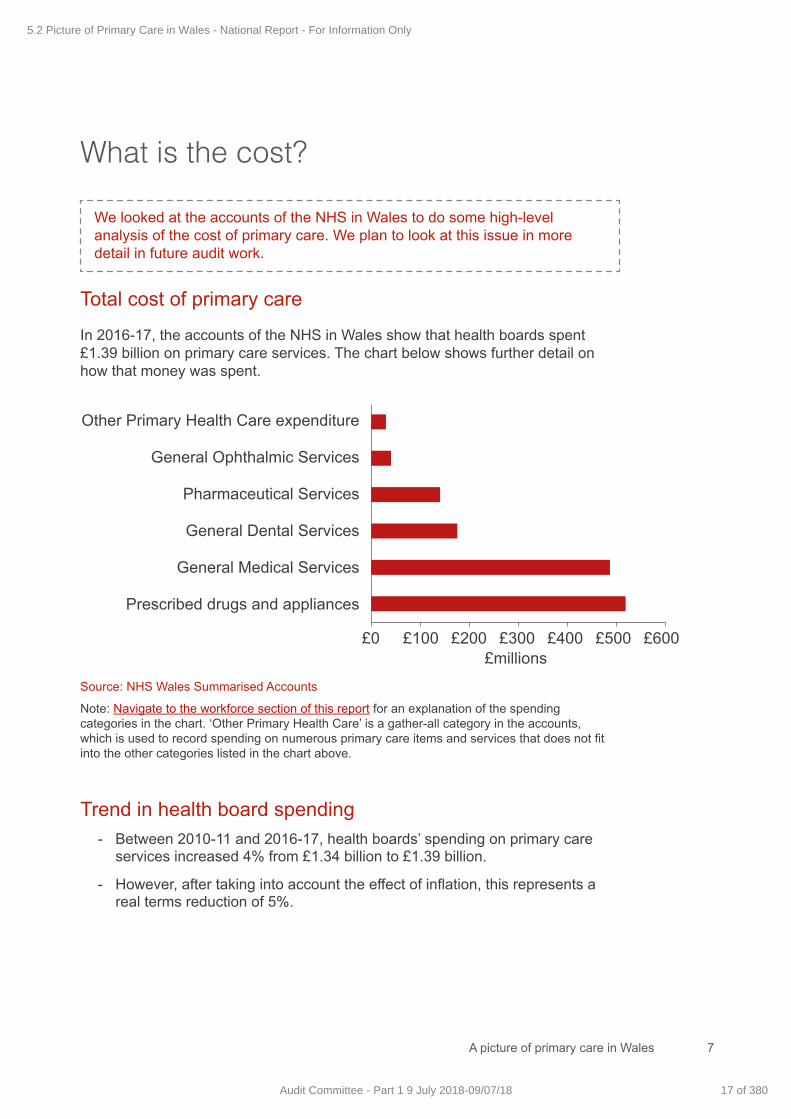
A picture of primary care in Wales 7
What is the cost?
We looked at the accounts of the NHS in Wales to do some high-level analysis of the cost of primary care. We plan to look at this issue in more detail in future audit work.
Total cost of primary care
In 2016-17, the accounts of the NHS in Wales show that health boards spent £1.39 billion on primary care services. The chart below shows further detail on how that money was spent.
Trend in health board spending- Between 2010-11 and 2016-17, health boards’ spending on primary care
services increased 4% from £1.34 billion to £1.39 billion.
- However, after taking into account the effect of inflation, this represents a real terms reduction of 5%.
Source: NHS Wales Summarised Accounts
Note: Navigate to the workforce section of this report for an explanation of the spending categories in the chart. ‘Other Primary Health Care’ is a gather-all category in the accounts, which is used to record spending on numerous primary care items and services that does not fit into the other categories listed in the chart above.
Other Primary Health Care expenditure
General Ophthalmic Services
Pharmaceutical Services
General Dental Services
General Medical Services
Prescribed drugs and appliances
£millions£0 £100 £200 £300 £400 £500 £600
5.2 Picture of Primary Care in Wales - National Report - For Information Only
17 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales8
Primary care spending as a proportion of total health board spending
- Between 2010-11 and 2016-17, total health board spending in Wales (Net Operating Costs) increased from £5.39 billion to £6.32 billion.
- However, over the same period, recorded spending on primary care as a percentage of total health board spending in Wales (Net Operating Cost) reduced from 25% to 22%.
- This would suggest that the shift in resources towards primary care that has been at the centre of much of the NHS policy in recent years is not being achieved. However, the picture is complicated by the fact that expenditure by health boards on primary care is not consistently categorised and as such it is likely that the figure recorded in the accounts does not represent the totality of primary care expenditure.
Funding from Welsh Government- The Welsh Government allocates money to local health boards to spend
on primary care services. In 2016-17, the allocation was around £887 million.
- This covers General Medical Services, Pharmaceutical Services, General Dental Services, the National Primary Care Fund, as well as funding for a range of optometry services and some aspects of primary care prescribing and dispensing.
- The allocation does not cover funding that community pharmacies receive indirectly as ‘retained purchase profit’. This is the profit that pharmacies retain when the NHS reimburses them for the costs of purchasing medicines.
- The allocation for General Medical Services is ring-fenced, meaning health boards should spend their entire allocation on General Medical Services. In 2016-17, the health boards spent 2.4% more than their allocation for the General Medical Services contract. However, not all of the General Dental Services allocation is ring-fenced and in 2016-17, health boards spent 6.4% less than their General Dental Services allocation.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
18 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales 9
Primary care premises- In October 2017, the NHS Wales directory showed there were 596
GP premises (including satellite practices), 428 dental practices, 448 private opticians and 717 pharmacies. Some of these properties are part of the NHS estate while others are privately owned.
- Our scoping work revealed some problems in Wales with a lack of physical space in current primary care buildings, such as GP practices and primary care health centres. This could make it more difficult to bring in new ways of working, such as introducing new clinics for physiotherapists, clinical pharmacists etc.
- Data is not available on the condition of the primary care estate so the costs of backlog maintenance are not known.
- In 2017, the Welsh Government announced a £68 million investment to build 11 new ‘hubs’ and GP centres, and improve 8 existing health centres, to be delivered by 2021.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
19 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales10
Patient surveys reveal positive views about GP services. But good data was not available for other services.
Patient experience: General Practice In the National Survey of Wales, around 10,000 people gave their views on GP appointments in 2016-17:
• 90% were satisfied with GP care.
• 96% felt treated with dignity and respect at their GP appointment.
• 86% felt they were given the information they needed at their appointment.
• 79% felt the GP knew all relevant information about the patient.
Patient experience: Dentistry, optometry and community pharmacy Many of these services carry out local surveys of patient experience but we were not able to find a collated picture of the results at an all Wales level.
What do patients think?
90%Satisfiedwith GP
care
5.2 Picture of Primary Care in Wales - National Report - For Information Only
20 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales 11
Quick and easy access • Better access to GP services has been a goal for many years. The current
Programme for Government continues to aim for improved ‘access to GP surgeries, making it easier to get an appointment’.
• Although there is no formal target, the Welsh Government expects patients with urgent needs to be seen at GP surgeries that day.
• The National Survey for Wales showed 62% of GP surgery patients found it easy or very easy to get an appointment at a convenient time. (38% found it difficult or very difficult.)
• The Older People’s Commissioner for Wales and Healthcare Inspectorate Wales have highlighted patient concerns about GP appointment systems…
Booking appointment impossible. Frustrating not being able to see same Dr, especially with ongoing medical condition.
Appointments – can get one for the day but getting a routine appointment ahead is difficult.
Appointment times not long enough. Feel rushed out of the door each time, so not all problems discussed.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
21 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales12
• The National Oral Health Plan for Wales highlights as a key issue ‘patchy access’ to NHS dentistry. A Welsh Government report from 2017 said access to NHS dental care has improved significantly in recent years but there are areas of Wales where access remains difficult and some where it has ‘slipped back’.
• The Prioritised Eye Care Plan describes progress improving access to eye care services in Wales. Actions have included new pathways to help patients access eye care closer to home, awareness raising and signposting, as well as training of primary care staff.
• Work is ongoing in Wales to look at the definition of ‘good access’. The national plan is for a multidisciplinary primary care team, so it will be important for patients to have good access to the appropriate member of that team. The new definition of ‘access’ may not mean access to appointments – it might mean access to email advice or on the telephone, or a home visit.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
22 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
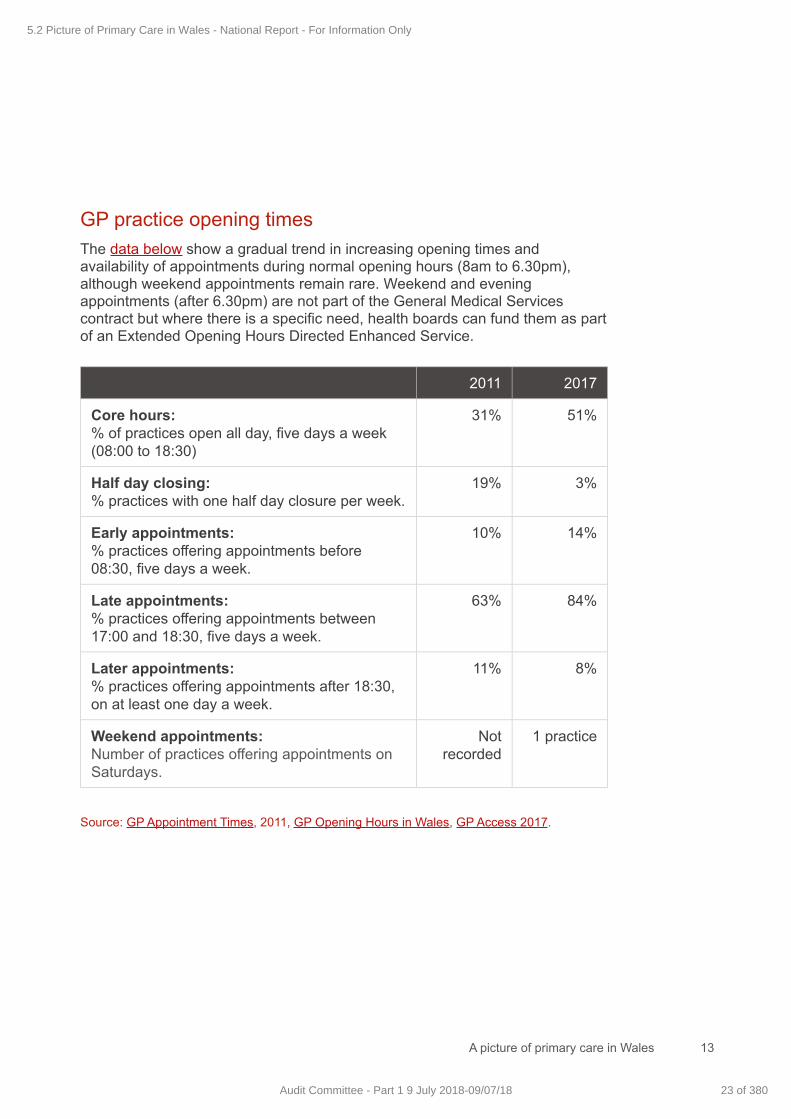
A picture of primary care in Wales 13
GP practice opening times The data below show a gradual trend in increasing opening times and availability of appointments during normal opening hours (8am to 6.30pm), although weekend appointments remain rare. Weekend and evening appointments (after 6.30pm) are not part of the General Medical Services contract but where there is a specific need, health boards can fund them as part of an Extended Opening Hours Directed Enhanced Service.
2011 2017
Core hours:% of practices open all day, five days a week (08:00 to 18:30)
31% 51%
Half day closing: % practices with one half day closure per week.
19% 3%
Early appointments: % practices offering appointments before 08:30, five days a week.
10% 14%
Late appointments: % practices offering appointments between 17:00 and 18:30, five days a week.
63% 84%
Later appointments: % practices offering appointments after 18:30, on at least one day a week.
11% 8%
Weekend appointments: Number of practices offering appointments on Saturdays.
Not recorded
1 practice
Source: GP Appointment Times, 2011, GP Opening Hours in Wales, GP Access 2017.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
23 of 380Audit Committee - Part 1 9 July 2018-09/07/18
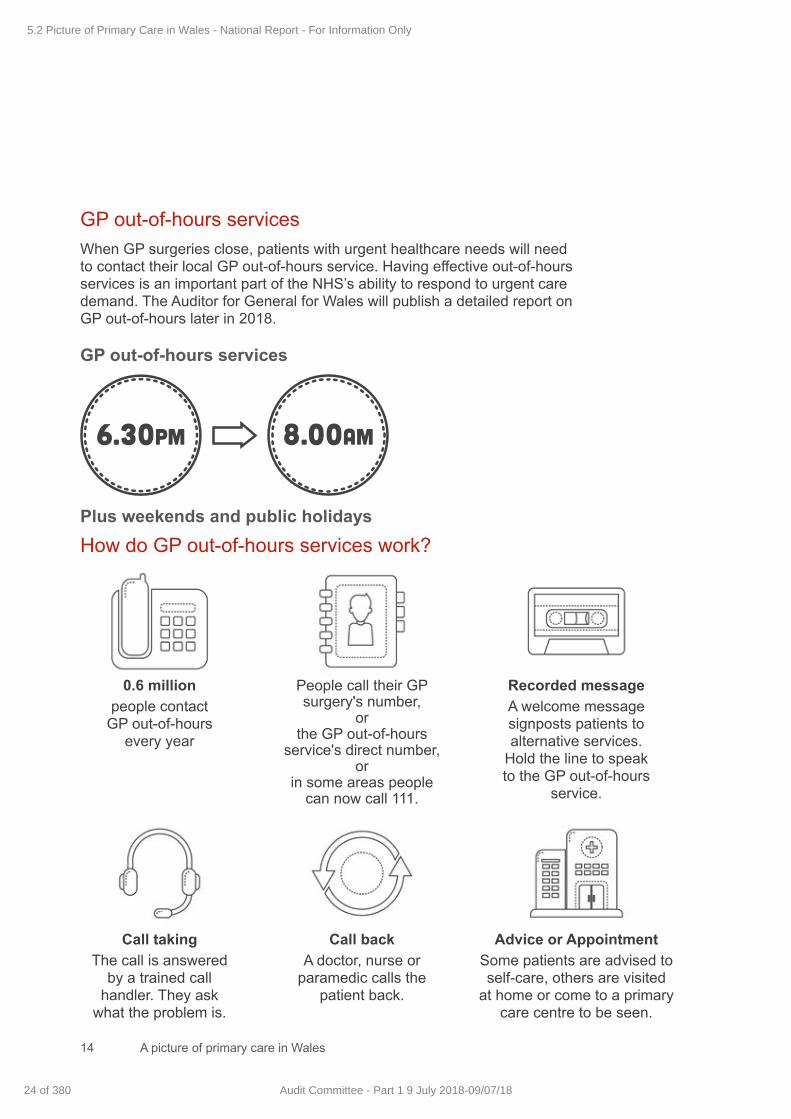
A picture of primary care in Wales14
GP out-of-hours services When GP surgeries close, patients with urgent healthcare needs will need to contact their local GP out-of-hours service. Having effective out-of-hours services is an important part of the NHS’s ability to respond to urgent care demand. The Auditor for General for Wales will publish a detailed report on GP out-of-hours later in 2018.
GP out-of-hours services
Plus weekends and public holidaysHow do GP out-of-hours services work?
6.30pm 8.00am
0.6 million people contact
GP out-of-hours every year
Call taking The call is answered
by a trained call handler. They ask
what the problem is.
Call back A doctor, nurse or
paramedic calls the patient back.
Advice or Appointment Some patients are advised to self-care, others are visited
at home or come to a primary care centre to be seen.
People call their GP surgery's number,
or the GP out-of-hours
service's direct number, or
in some areas people can now call 111.
Recorded messageA welcome message signposts patients to alternative services.
Hold the line to speak to the GP out-of-hours
service.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
24 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
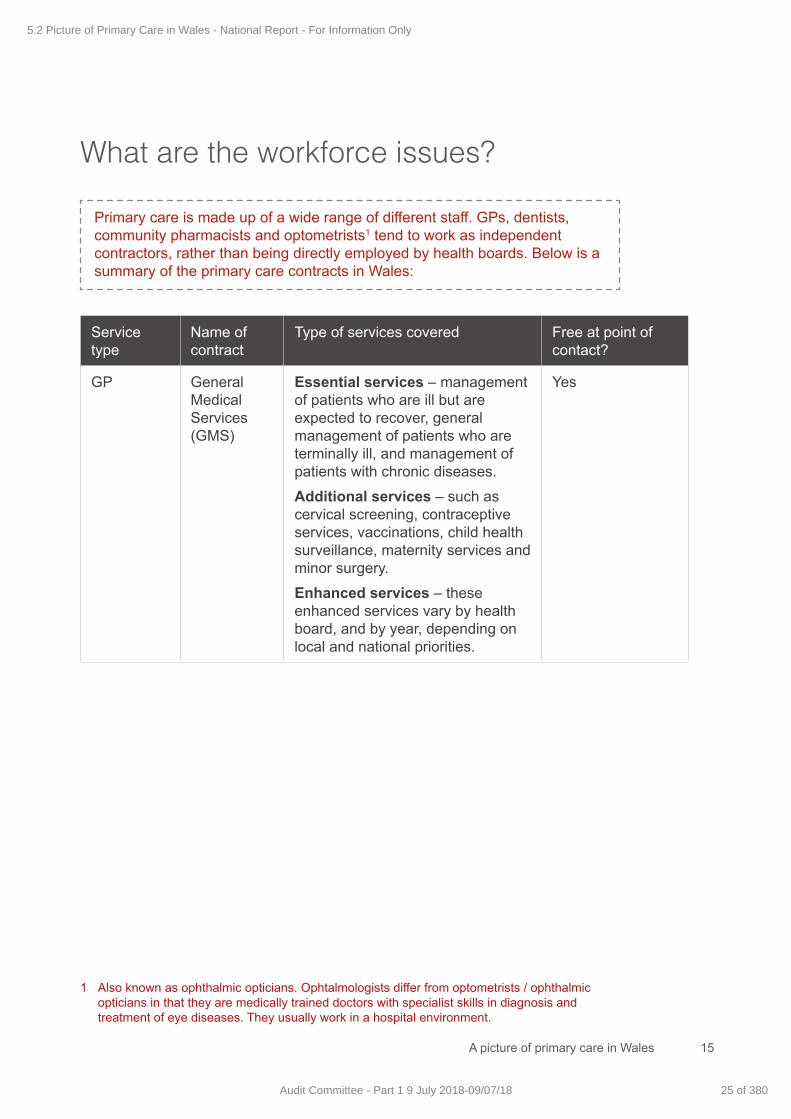
A picture of primary care in Wales 15
Primary care is made up of a wide range of different staff. GPs, dentists, community pharmacists and optometrists1 tend to work as independent contractors, rather than being directly employed by health boards. Below is a summary of the primary care contracts in Wales:
What are the workforce issues?
Service type
Name of contract
Type of services covered Free at point of contact?
GP General Medical Services (GMS)
Essential services – management of patients who are ill but are expected to recover, general management of patients who are terminally ill, and management of patients with chronic diseases. Additional services – such as cervical screening, contraceptive services, vaccinations, child health surveillance, maternity services and minor surgery.Enhanced services – these enhanced services vary by health board, and by year, depending on local and national priorities.
Yes
1 Also known as ophthalmic opticians. Ophtalmologists differ from optometrists / ophthalmic opticians in that they are medically trained doctors with specialist skills in diagnosis and treatment of eye diseases. They usually work in a hospital environment.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
25 of 380Audit Committee - Part 1 9 July 2018-09/07/18
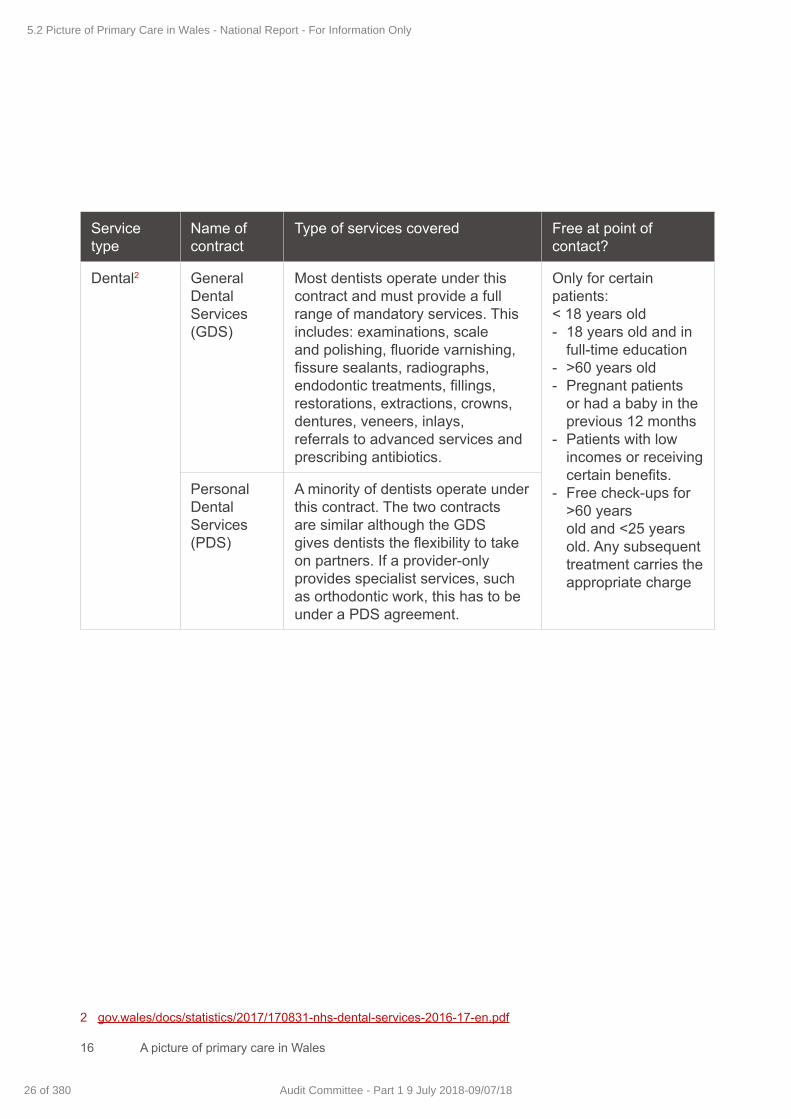
A picture of primary care in Wales16
Service type
Name of contract
Type of services covered Free at point of contact?
Dental2 General Dental Services (GDS)
Most dentists operate under this contract and must provide a full range of mandatory services. This includes: examinations, scale and polishing, fluoride varnishing, fissure sealants, radiographs, endodontic treatments, fillings, restorations, extractions, crowns, dentures, veneers, inlays, referrals to advanced services and prescribing antibiotics.
Only for certain patients:< 18 years old- 18 years old and in
full-time education- >60 years old - Pregnant patients
or had a baby in the previous 12 months
- Patients with low incomes or receiving certain benefits.
- Free check-ups for >60 years
old and <25 years old. Any subsequent treatment carries the appropriate charge
Personal Dental Services (PDS)
A minority of dentists operate under this contract. The two contracts are similar although the GDS gives dentists the flexibility to take on partners. If a provider-only provides specialist services, such as orthodontic work, this has to be under a PDS agreement.
2 gov.wales/docs/statistics/2017/170831-nhs-dental-services-2016-17-en.pdf
5.2 Picture of Primary Care in Wales - National Report - For Information Only
26 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
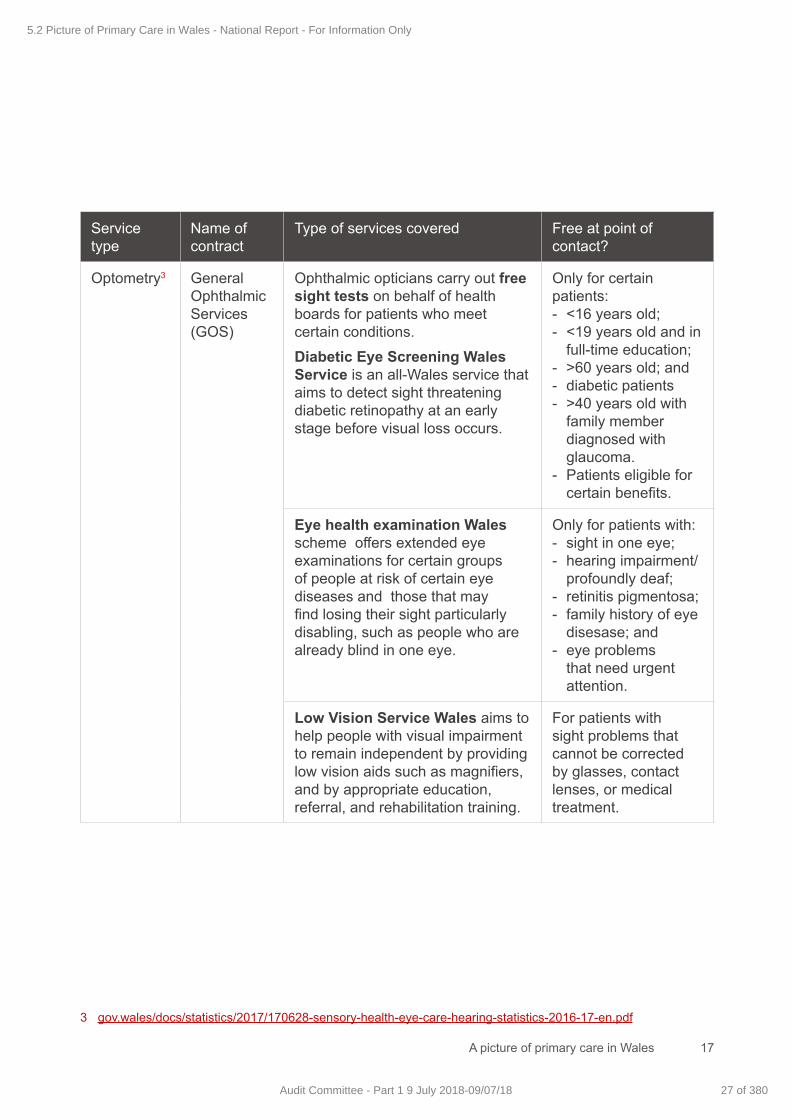
A picture of primary care in Wales 17
Service type
Name of contract
Type of services covered Free at point of contact?
Optometry3 General Ophthalmic Services (GOS)
Ophthalmic opticians carry out free sight tests on behalf of health boards for patients who meet certain conditions.Diabetic Eye Screening Wales Service is an all-Wales service that aims to detect sight threatening diabetic retinopathy at an early stage before visual loss occurs.
Only for certain patients:- <16 years old;- <19 years old and in
full-time education;- >60 years old; and- diabetic patients- >40 years old with
family member diagnosed with glaucoma.
- Patients eligible for certain benefits.
Eye health examination Wales scheme offers extended eye examinations for certain groups of people at risk of certain eye diseases and those that may find losing their sight particularly disabling, such as people who are already blind in one eye.
Only for patients with:- sight in one eye;- hearing impairment/
profoundly deaf;- retinitis pigmentosa;- family history of eye
disesase; and- eye problems
that need urgent attention.
Low Vision Service Wales aims to help people with visual impairment to remain independent by providing low vision aids such as magnifiers, and by appropriate education, referral, and rehabilitation training.
For patients with sight problems that cannot be corrected by glasses, contact lenses, or medical treatment.
3 gov.wales/docs/statistics/2017/170628-sensory-health-eye-care-hearing-statistics-2016-17-en.pdf
5.2 Picture of Primary Care in Wales - National Report - For Information Only
27 of 380Audit Committee - Part 1 9 July 2018-09/07/18
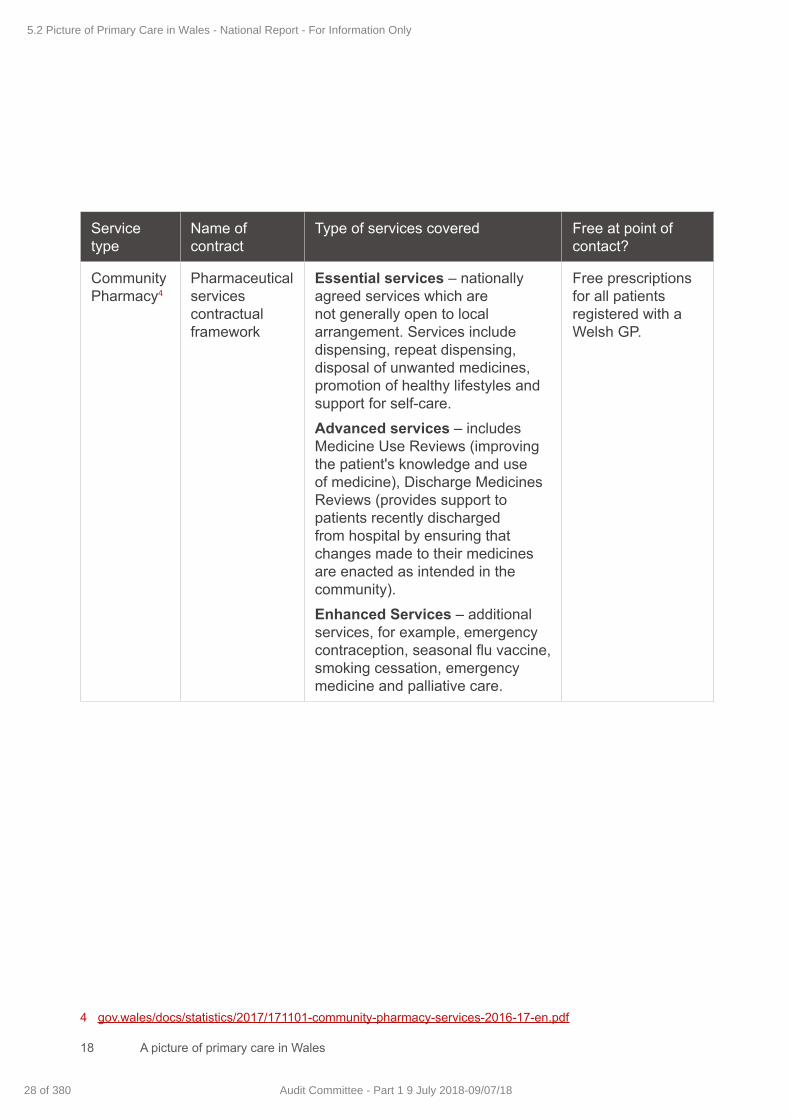
A picture of primary care in Wales18
Service type
Name of contract
Type of services covered Free at point of contact?
Community Pharmacy4
Pharmaceutical services contractual framework
Essential services – nationally agreed services which are not generally open to local arrangement. Services include dispensing, repeat dispensing, disposal of unwanted medicines, promotion of healthy lifestyles and support for self-care.Advanced services – includes Medicine Use Reviews (improving the patient's knowledge and use of medicine), Discharge Medicines Reviews (provides support to patients recently discharged from hospital by ensuring that changes made to their medicines are enacted as intended in the community).Enhanced Services – additional services, for example, emergency contraception, seasonal flu vaccine, smoking cessation, emergency medicine and palliative care.
Free prescriptions for all patients registered with a Welsh GP.
4 gov.wales/docs/statistics/2017/171101-community-pharmacy-services-2016-17-en.pdf
5.2 Picture of Primary Care in Wales - National Report - For Information Only
28 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
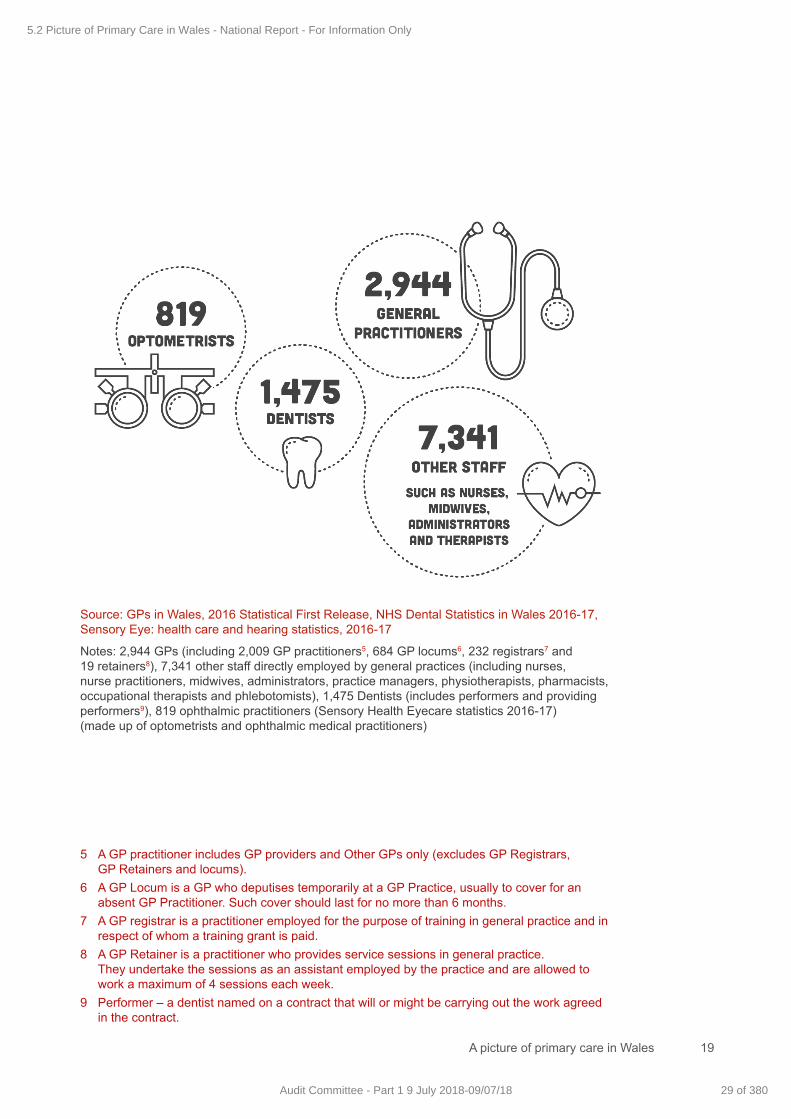
A picture of primary care in Wales 19
Source: GPs in Wales, 2016 Statistical First Release, NHS Dental Statistics in Wales 2016-17, Sensory Eye: health care and hearing statistics, 2016-17
Notes: 2,944 GPs (including 2,009 GP practitioners5, 684 GP locums6, 232 registrars7 and 19 retainers8), 7,341 other staff directly employed by general practices (including nurses, nurse practitioners, midwives, administrators, practice managers, physiotherapists, pharmacists, occupational therapists and phlebotomists), 1,475 Dentists (includes performers and providing performers9), 819 ophthalmic practitioners (Sensory Health Eyecare statistics 2016-17) (made up of optometrists and ophthalmic medical practitioners)
5 A GP practitioner includes GP providers and Other GPs only (excludes GP Registrars, GP Retainers and locums).
6 A GP Locum is a GP who deputises temporarily at a GP Practice, usually to cover for an absent GP Practitioner. Such cover should last for no more than 6 months.
7 A GP registrar is a practitioner employed for the purpose of training in general practice and in respect of whom a training grant is paid.
8 A GP Retainer is a practitioner who provides service sessions in general practice. They undertake the sessions as an assistant employed by the practice and are allowed to work a maximum of 4 sessions each week.
9 Performer – a dentist named on a contract that will or might be carrying out the work agreed in the contract.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
29 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales20
The Welsh Government’s Primary Care Workforce for Wales Plan stresses the importance of a multi-disciplinary team approach in primary care. Despite that, our research suggests the majority of primary care workforce data focuses on GPs.
The GP workforce • In 2016, there were 6.5 GPs per 10,000 population in Wales. The
equivalent figure in England was 6.4 per 10,000. The most up-to-date figures for Scotland are from 2015 and show that there were 8 GPs per 10,000 population.
• Between 2006 and 2016, the number of GP practitioners10 in Wales increased 7% to 2,009.
• Despite the increase in GP numbers, it is unclear if this has resulted in greater capacity. This is because we do not know which GPs are working full time or part time. Work is ongoing in Wales to improve this data.
• The number of female GP practitioners has increased by 55% since 2006. In 2016 women accounted for 52% of the GP practitioner workforce.
• The number of GPs under the age of 44 has increased by 15% between 2010 and 2016. GPs between the age of 45 and 54 have decreased by 8%. The greatest change has been in GPs over 65, having risen by 83% since 2006.
• Train Work Live is a national campaign launched in 2016 to promote Wales as an attractive place to work for GPs and other doctors. Navigate to the Train Work Live website for more details.
GP training• After medical school, potential GPs undertake a GP specialty training
programme. Competition for GP training places has reduced in Wales. In 2012, 1.5 applications were made for every training place. In 2016, there were 1.2 applications for every place.
• In recent years Wales has struggled to fill GP training places. In 2016, 75% of places were filled. But in 2017, the fill rate increased to 91%. New financial incentives to attract applications appear to have had a positive impact on fill rates in Ceredigion, North West Wales, Pembrokeshire and North East Wales.
10 Excluding registrars, retainers and locums.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
30 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales 21
Morale and job satisfaction• According to the BMA11 and the RCGP12 surveys, morale of GPs in Wales
is low. Survey respondents talked about an increasing workload, poor work-life balance, bureaucracy and financial pressures, particularly in partnerships.
• 95% of GPs in Wales feel that morale has gone down in past 5 years (93% Scotland, 94% NI) (RCGP).
• 61% of GPs in Wales say they do not have a good work life balance, with 58% saying it had got worse in the last year (BMA).
• The majority of GPs (82%) are worried about sustainability of their practice, with workload pressures and recruitment difficulties cited as the two main reasons for their concerns (BMA).
Pay and costs for GPs• For most GPs in Wales (those employed under the General Medical
Services contract) the average income before tax increased during the early 2000s but has since decreased slightly. This income rose from £65,007 in 2002-03 to £102,194 in 2005-06 but has since fallen to £93,400 in 2015-16 (UK £99,500).
• To become a partner, many GPs have to buy into the partnership. This cost may prevent some GPs becoming partners, and the number of GP partnerships in Wales has decreased from 496 in 2006 to 441 in 2016.
• An issue known as ‘last man standing’ is another barrier to buying into a partnership. This issue means that a single GP within a partnership can become financially liable for the practice and its property if all other partners retire.
• High indemnity costs for GPs is another barrier. Indemnity covers costs for medical negligence claims and investigations. The First Minister has announced plans13 to tackle the problem and part of the increased uplift in the General Medical Services contract has been given to act as a short-term help whilst a longer-term solution is found.
• In March 2018, a revised General Medical Services contract for 2018-19 was announced in Wales which included an interim 1% pay rise for GPs, a 1.4% increase in funding for expenses and funding to address rising indemnity costs.
11 BMA survey of General Practice, 201612 RCGP Survey of GPs in Devolved Nations, April 201613 First Minister Interview with BMJ, October 2016
5.2 Picture of Primary Care in Wales - National Report - For Information Only
31 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales22
Like other parts of the health system, primary care needs careful planning to help shape the way in which services are delivered. However, planning for primary care cannot be done in isolation and must instead be part of a whole system approach to the design and delivery of health and social care services.
Previous plans for primary care• NHS Wales has had plans for many years that stress the importance of
primary care. The plans aim to rebalance the system of care in Wales by moving resources towards primary and community care.
The Future of Primary Care (2001), A Question of Balance (2002), The Wanless Review (2003), Designed for Life (2005), Setting the Direction (2010), Our plan for a primary care service up to March 2018 (2014), Prosperity for All (2017)
• In 2001, the Future of Primary Care planned to reverse the ‘relative under-development of primary care in Wales’. The vision included team-based working, more integration and a greater focus on prevention.
• In 2017, the Welsh Government’s national strategy talks about the need to accelerate the shift towards moving care closer to patients’ homes.
What is the plan to improve primary care?
5.2 Picture of Primary Care in Wales - National Report - For Information Only
32 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales 23
The most recent plan for primary care• The most recent national primary care plan aims for a ‘social model’
that promotes physical, mental and social wellbeing, rather than just an absence of ill health. The plan has five priority areas:
Planning care locally The national plan says:
- health boards are responsible for identifying the needs of their population;
- this should be done at a community level;- the plan talks about more local autonomy for leadership,
collaboration and innovation; and- clusters are a key part of achieving this.
Improving access and quality The national plan says access to a high-quality primary care service is about:- information, advice and assistance to support and
motivate people to take responsibility for their own and their family’s health and wellbeing;
- diagnosis, investigation, treatment and continuity of care as close to home as possible.
- professionals working together as a coordinated team around the person;
- continuous improvement; and- openness and transparency.
Equitable accessThe national plan says:- equitable access to primary care is about a proactive,
proportionate and individual approach to improving the physical and mental health and wellbeing of individuals, families and communities.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
33 of 380Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales24
Planning to meet demand for primary care• The national primary care plan says ‘austerity is driving a wave of demand
into primary care on an unprecedented scale’. The plan also says that primary care is facing increasing and more complex demands due to an ageing population, and increases in long-term conditions.
• If health boards are to meet demand for, and improve access to, primary care, they need a good understanding of this demand. However, there are some fundamental issues with the data.
• The exact number of contacts that patients have with GP surgeries is not known at a national level because the data is held in the computer systems of individual GP practices and there are difficulties collating this information. Estimates range from 16 million14 to 23 million15 per year.
• There is better data in other parts of the primary care system, mainly because these services are paid depending on their activity:
- In 2016-17 the 716 community pharmacies in Wales dispensed 74.7 million prescription items to patients.
- In 2016-17, community optometrists performed eye tests on 776,827 people.
- In the two years up to 31 March 2017, more than 1.7 million people visited a dentist for NHS treatment.
A skilled local workforceThe national plan says:- primary care is fundamentally about trusted relationships
between people and professionals. We need to plan and build a workforce with the right numbers and mix of skills to meet the majority of people’s needs closer to home in flexible ways and flexible facilities.
Strong leadership The national plan says:- we need to strengthen and develop leadership at all
levels to deliver this plan to provide more care closer to home through primary care services.
14 Unscheduled Care Board, Ten High Impact Steps to Transform Unscheduled Care (USC), June 2011
15 BMA Cymru Wales presentation to National Primary Care Conference, November 2017
5.2 Picture of Primary Care in Wales - National Report - For Information Only
34 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
A picture of primary care in Wales 25
Changing the way we access servicesThe NHS in Wales is trying to change the way the public accesses primary care services. Traditionally, GPs have been the first port of call for people with healthcare needs, and have acted as a ‘gatekeeper’ to other services. In future, the aim is that patients’ will be able to access a wider range of healthcare professionals, depending on their needs. This will help ensure GP time is used to best effect in the context of growing demand for primary care services.
Innovation and a new model for primary care• The Welsh Government introduced the National Primary Care Fund in
2015-16 to encourage innovation and improvement.
The fund in 2016-17 was £41 million including £10 million for clusters and £3.8 million for pathfinders and pacesetters.
• Clusters are groups of neighbouring GP practices and partner organisations (such as the ambulance service, councils and third sector) which provide services for their local populations of between 30,000 and 50,000 people. Clusters have a key role in supporting local health needs assessments, allocating appropriate resources and forecasting the potential future demand on primary care.
• The pathfinders and pacesetters are a range of primary care projects, sponsored by Welsh Government, that aim to test elements of the primary care plan. This approach has produced some new ways of work that have been collated into the Transformational Model of Primary and Community Care.
• Key elements of the model include: sustainability in general practice, shared triage processes, multi-disciplinary teams working across practices, integrated working between health, social care and the third sector, improved access and a better informed public.
• The current approach to planning primary care is both ‘top-down’ (ie common priorities set out in the national plan) and ‘bottom-up’ (ie planning and innovation led by local practices and clusters). This means that there are various plans, at various levels, that need to make sense and complement one another.
5.2 Picture of Primary Care in Wales - National Report - For Information Only
35 of 380Audit Committee - Part 1 9 July 2018-09/07/18
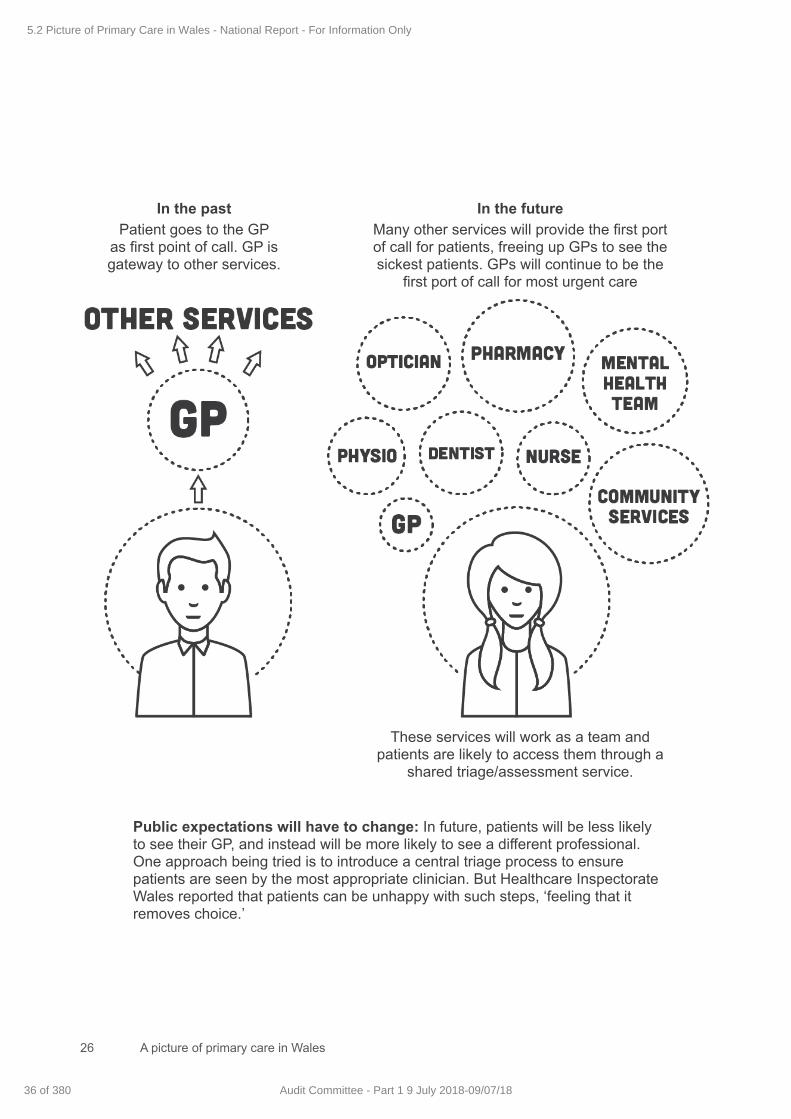
A picture of primary care in Wales26
In the past Patient goes to the GP
as first point of call. GP is gateway to other services.
In the future Many other services will provide the first port of call for patients, freeing up GPs to see the sickest patients. GPs will continue to be the
first port of call for most urgent care
These services will work as a team and patients are likely to access them through a
shared triage/assessment service.
Public expectations will have to change: In future, patients will be less likely to see their GP, and instead will be more likely to see a different professional. One approach being tried is to introduce a central triage process to ensure patients are seen by the most appropriate clinician. But Healthcare Inspectorate Wales reported that patients can be unhappy with such steps, ‘feeling that it removes choice.’
5.2 Picture of Primary Care in Wales - National Report - For Information Only
36 of 380 Audit Committee - Part 1 9 July 2018-09/07/18

A picture of primary care in Wales 27
5.2 Picture of Primary Care in Wales - National Report - For Information Only
37 of 380Audit Committee - Part 1 9 July 2018-09/07/18
Wales Audit Office
24 Cathedral Road
Cardiff CF11 9LJ
Tel: 029 2032 0500
Fax: 029 2032 0600
Textphone: 029 2032 0660
E-mail: [email protected]
Website: www.wao.gov.uk
Swyddfa Archwilio Cymru
24 Heol y Gadeirlan
Caerdydd CF11 9LJ
Ffôn: 029 2032 0500
Ffacs: 029 2032 0600
Ffôn Testun: 029 2032 0660
E-bost: [email protected]
Gwefan: www.wao.gov.uk
5.2 Picture of Primary Care in Wales - National Report - For Information Only
38 of 380 Audit Committee - Part 1 9 July 2018-09/07/18
Agenda item 6.1
Forward Work Plan Page 1 of 4 Audit Committee Meeting
9 July 2018
AUDIT COMMITTEE: FORWARD PLAN 2018/19
MEETING DATE – 9 JULY 2018
LEAD
Apologies for Absence Chair
Welcome and Introductions Chair
Declarations of Interest Chair
Unconfirmed Minutes of the previous Audit Committee meeting for accuracy and matters arising Chair
Action Log Board Secretary
INTERNAL CONTROL AND RISK MANAGEMENT
Procurements and Scheme of Delegation Report (to include an update on actions and progress relating to PSPP)
Director of Finance
Audit Recommendations Tracker Report Board Secretary
Losses and Special Payments Report Director of Finance
Clinical Audit & Effectiveness Plan 2018/19 (and summary of progress against 2017/18 plan) Medical Director
Local Counter Fraud Specialist update report (CLOSED ITEM) Director of Finance
CHARITABLE FUNDS
Charitable Fund Balances for last quarter Director of Finance
INTERNAL AUDIT & ASSURANCE
Head of Internal Audit Report Head of Internal Audit
Internal Audit Reports (any Limited or No assurance audit reports require the lead Executive
Director to be present – and at the discretion of the Committee Chair for any Reasonable Assurance Rated Report)
Head of Internal Audit
(Executive Leads as appropriate)
EXTERNAL AUDIT
WAO Progress report and any related external audit reviews Wales Audit Office lead
WAO Audit Reports (as per Annual Audit Plan 2017/18) Wales Audit Office lead
ITEMS FOR INFORMATION
Only items for information raised in advance with the Chair will be discussed Chair
Any other urgent Business Chair
OTHER ITEMS
Referrals to other Committees of the Board
Review of the Committee Forward Work Plan
Chair
Chair
6.1 Com
mittee F
orward W
ork Plan 2018/19
1 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
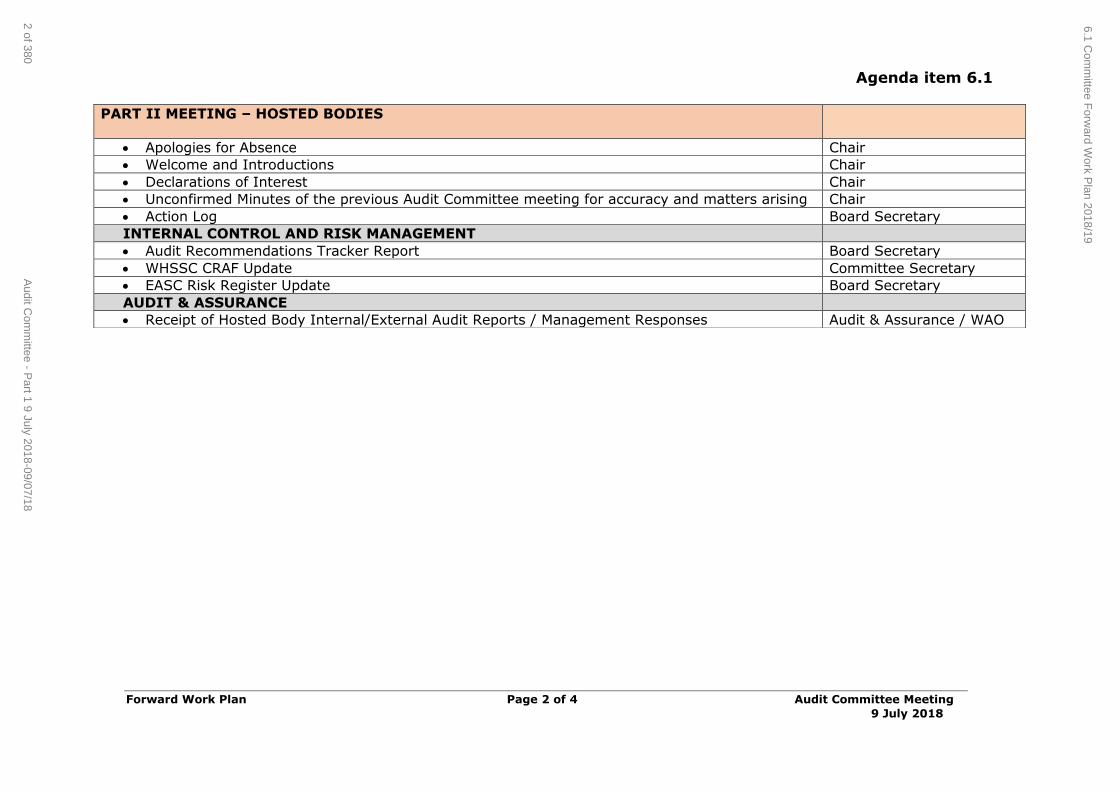
Agenda item 6.1
Forward Work Plan Page 2 of 4 Audit Committee Meeting
9 July 2018
PART II MEETING – HOSTED BODIES
Apologies for Absence Chair
Welcome and Introductions Chair
Declarations of Interest Chair
Unconfirmed Minutes of the previous Audit Committee meeting for accuracy and matters arising Chair
Action Log Board Secretary
INTERNAL CONTROL AND RISK MANAGEMENT
Audit Recommendations Tracker Report Board Secretary
WHSSC CRAF Update Committee Secretary
EASC Risk Register Update Board Secretary
AUDIT & ASSURANCE
Receipt of Hosted Body Internal/External Audit Reports / Management Responses Audit & Assurance / WAO
6.1 Com
mittee F
orward W
ork Plan 2018/19
2 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
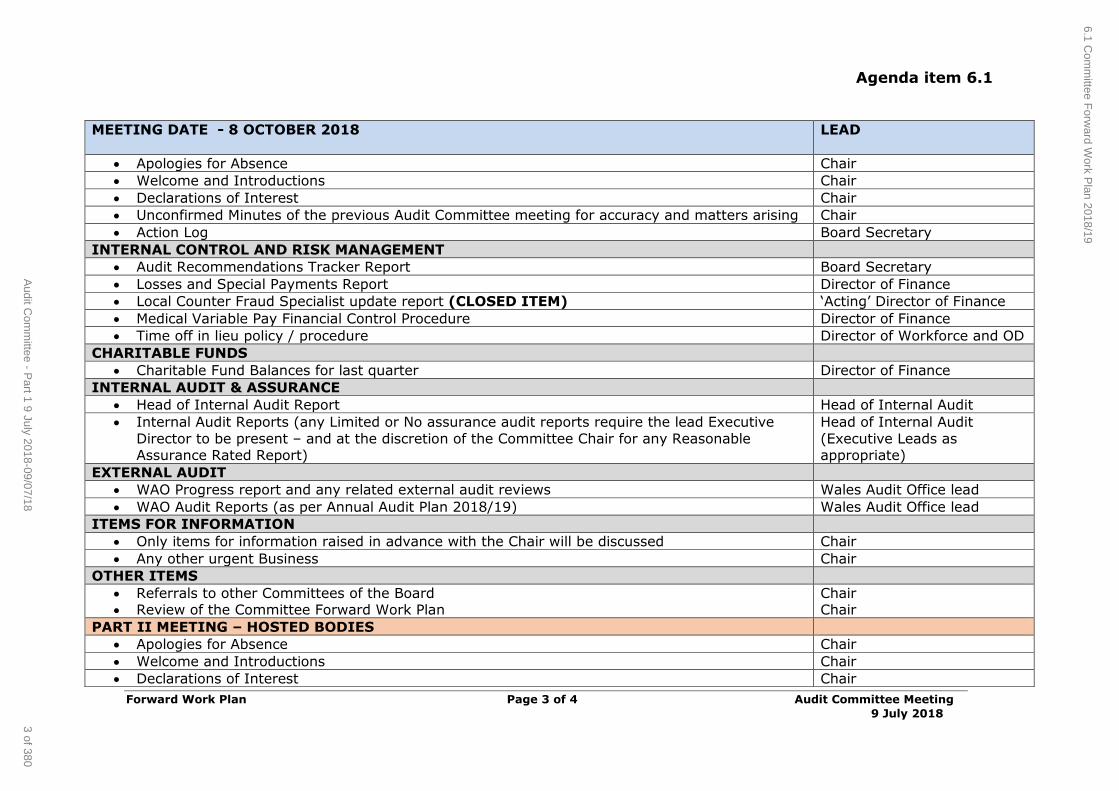
Agenda item 6.1
Forward Work Plan Page 3 of 4 Audit Committee Meeting
9 July 2018
MEETING DATE - 8 OCTOBER 2018
LEAD
Apologies for Absence Chair
Welcome and Introductions Chair
Declarations of Interest Chair
Unconfirmed Minutes of the previous Audit Committee meeting for accuracy and matters arising Chair
Action Log Board Secretary
INTERNAL CONTROL AND RISK MANAGEMENT
Audit Recommendations Tracker Report Board Secretary
Losses and Special Payments Report Director of Finance
Local Counter Fraud Specialist update report (CLOSED ITEM) ‘Acting’ Director of Finance
Medical Variable Pay Financial Control Procedure Director of Finance
Time off in lieu policy / procedure Director of Workforce and OD
CHARITABLE FUNDS
Charitable Fund Balances for last quarter Director of Finance
INTERNAL AUDIT & ASSURANCE
Head of Internal Audit Report Head of Internal Audit
Internal Audit Reports (any Limited or No assurance audit reports require the lead Executive
Director to be present – and at the discretion of the Committee Chair for any Reasonable Assurance Rated Report)
Head of Internal Audit
(Executive Leads as appropriate)
EXTERNAL AUDIT
WAO Progress report and any related external audit reviews Wales Audit Office lead
WAO Audit Reports (as per Annual Audit Plan 2018/19) Wales Audit Office lead
ITEMS FOR INFORMATION
Only items for information raised in advance with the Chair will be discussed Chair
Any other urgent Business Chair
OTHER ITEMS
Referrals to other Committees of the Board Review of the Committee Forward Work Plan
Chair Chair
PART II MEETING – HOSTED BODIES
Apologies for Absence Chair
Welcome and Introductions Chair
Declarations of Interest Chair
6.1 Com
mittee F
orward W
ork Plan 2018/19
3 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18
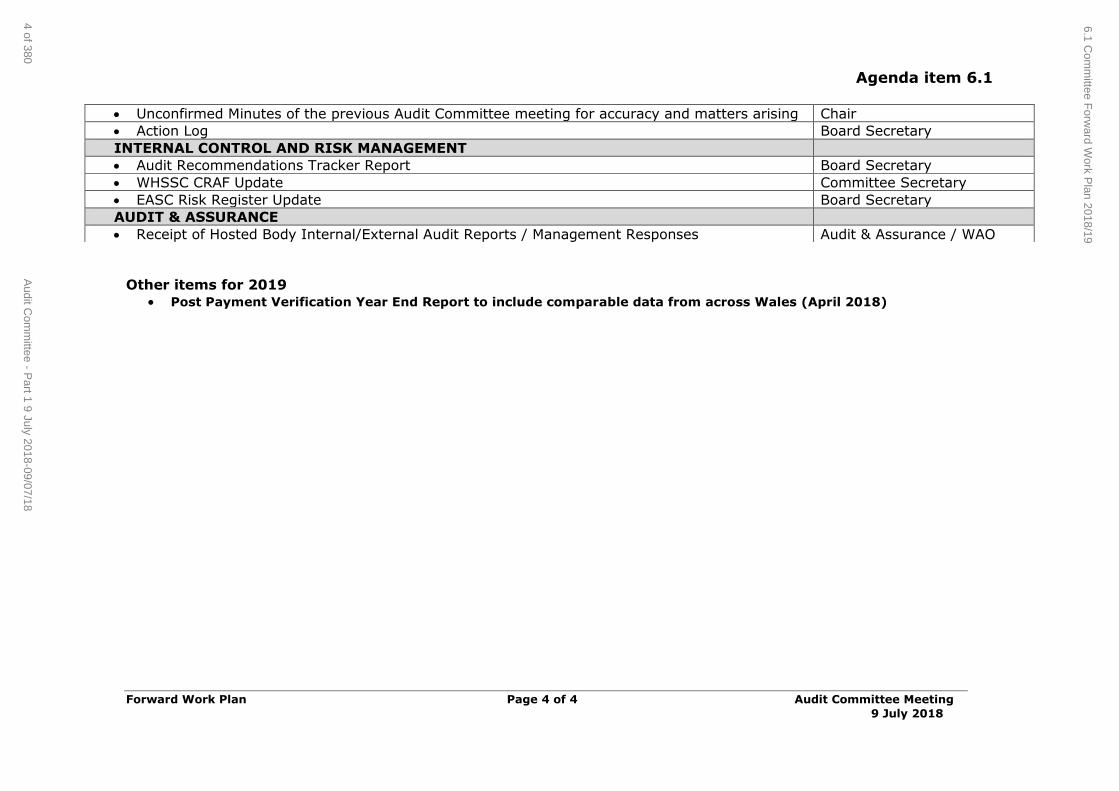
Agenda item 6.1
Forward Work Plan Page 4 of 4 Audit Committee Meeting
9 July 2018
Other items for 2019
Post Payment Verification Year End Report to include comparable data from across Wales (April 2018)
Unconfirmed Minutes of the previous Audit Committee meeting for accuracy and matters arising Chair
Action Log Board Secretary
INTERNAL CONTROL AND RISK MANAGEMENT
Audit Recommendations Tracker Report Board Secretary
WHSSC CRAF Update Committee Secretary
EASC Risk Register Update Board Secretary
AUDIT & ASSURANCE
Receipt of Hosted Body Internal/External Audit Reports / Management Responses Audit & Assurance / WAO
6.1 Com
mittee F
orward W
ork Plan 2018/19
4 of 380A
udit Com
mittee - P
art 1 9 July 2018-09/07/18