Embed Size (px)
Citation preview
Ealing Borough Council Democratic Services Officer: Town Hall Lee Teasdale New Broadway Direct Line: 020 8825 7919 London W5 2BY Fax: 020 8825 6909 Email: [email protected]
Health and Wellbeing Board
Venue:The Liz Cantell Room, Town Hall, New Broadway, Ealing, W5 2BY
Date and Time: Tuesday, 18 September 2018 at 18:00
MEMBERSHIP: Councillors: Julian Bell (Chair), Joy Morrissey (Non-Voting), Yvonne Johnson, Peter Mason and Binda Rai. Clinical Commissioning Group: Dr Mohini Parmar (Vice-Chair), Dr Raj Chandok, Mark Easton and Tessa Sandall. Lay Members: Tim Spilsbury (Healthwatch) and Andy Roper (ECN). Service Director: Judith Finlay (Executive Director Children & Adults’ LBE) and Wendy Meredith (Director, Public Health) Health Providers (Non-voting): Sid Datta (GP Federation), Dame Jacqueline Doherty (NWL Hospitals Trust), Professor Tim Orchard (Imperial College Healthcare Trust), Sarah Rushton (West London Mental Health Trust), and David Searle (Hillingdon Hospital Trust).
Page 1 of 324
AGENDA
Open to Public and Press
1 Apologies for Absence
2 Urgent Matters
3 Declarations of Interest
4 Matters to be Considered in Private
5 Minutes
To approve as a correct record the minutes of the meeting held on 17 July 2018.
Minutes Arising from the Meeting of 17 July 2018 5 - 20
6 Oral Health Progress Report on Pilot 21 - 30
7 Progress Report on Ealing Standard 31 - 48
8 Update on progress in relation to Special Education Needs
Disability Reforms
49 - 82
9 CQC Report-Review of Health Services for Children Looked
After and Safeguarding (CLAS) in Ealing
83 - 158
10 Ealing Market Position Statement 159 - 204
11 Winter Preparedness 205 - 216
12 Joint response to LGA Green Paper consultation 217 - 320
13 HWBB forward plan 2018-2019 321 - 324
14 Date of Next Meeting
The next meeting will be held on 27 November 2018.
Page 2 of 324

Paul Najsarek
Chief Executive
Page 3 of 324
Page 4 of 324
Health and Wellbeing Board – 17 July 2018
1
HEALTH AND WELLBEING BOARD MEETING
MINUTES
Tuesday 17 July 2018 PRESENT: Members (Councillors – Voting): Paul Driscoll - Councillor substituting for the Cabinet Portfolio Holder
for Health and Adults Services Yvonne Johnson - Cabinet Portfolio Holder – Children and Young People Peter Mason - (Nominated Chair) Cabinet Portfolio Holder – Housing,
Planning and Transformation Members (Councillors – Non-Voting): Joy Morrissey - Shadow Portfolio Holder, Health and Wellbeing and
Housing Clinical Commissioning Group: Tessa Sandall - Managing Director, Ealing CCG Dr Vijay Tailor - Ealing CCG, substituting for Dr Mohini Parmar, Board
Vice Chair Service Director: Judith Finlay - Executive Director of Children and Adults’ Services, LBE Health Providers (Non-voting): Sarah Rushton - West London Mental Health Trust Also Present: Dr Rubinder Bains - Consultant in Public Health, LBE Mystica Burridge - Area Manager, Healthwatch Ealing Kim Carey - Interim Director, Adults Services, LBE Judith Cosaitis - Community Safety Manager (Health), London Fire
Brigade Jillian Robson - Fire Safety Project Officer (Health), London Fire Brigade Lee Teasdale - Democratic Services Officer, LBE Lauren Walker - Fire, Safe and Well, Regional Manager Valerie Wilson - Mental Health Commissioning Manager, Ealing CCG At the commencement of the meeting the Democratic Services Officer announced that due to a sudden family bereavement, Councillor Julian Bell, the Board Chair would be unable to attend the meeting. The Vice-Chair was substituted at the meeting, requiring the nomination of a Board Member to Chair the meeting. Councillor Peter Mason received a nomination for Chair – upon the vote of the Board, Councillor Mason was duly elected as the Chair for this meeting only. Upon taking the Chair, Councillor Mason and the Board expressed their sincere condolences and well wishes to Councillor Bell and his family.
Page 5 of 324
Health and Wellbeing Board – 17 July 2018
2
1. Apologies for Absence (Agenda Item 1) Apologies were received from Councillor Julian Bell (Board Chair and Leader of the Council, LBE). Councillor Binda Rai (Cabinet Portfolio Holder for Health and Adults Services) was substituted at the meeting by Councillor Paul Driscoll. Dr Mohini Parmar (Vice-Chair and Chair of Ealing CGG) was substituted at the meeting by Dr Vijay Tailor.
2. Urgent Matters (Agenda Item 2) There were none.
3. Matters to be Considered in Private (Agenda Item 3) There were none.
4. Declarations of Interest (Agenda Item 4) There were none.
5. Minutes of the meeting of 29 May 2018 (Agenda Item 5)
Resolved: That, subject to the above amendment, the minutes of the meeting of 29 May 2018 be agreed as a true and correct record.
6. Implementation Report on ‘Fire, Safe and Well’ (Agenda Item 6) The Chair invited Lauren Walker (Fire, Safe and Well, Regional Manager), Judith Cosaitis (Community Safety Manager (Health), London Fire Brigade) and Jillian Robson (Fire Safety Project Officer (Health), London Fire Brigade), to present a report to the Board updating it on the progress of London Fire Brigade’s (LFB) ‘Fire, Safe and Well’ pilot. The pilot had been running in Ealing since December 2017, and the report aimed to identify early successes and challenges arising from the visits undertaken so far, with a focus upon the referral pathways that contributed to the Board’s objectives. The ‘Fire, Safe and Well’ visits built upon LFB’s ‘Home Fire Safety Visit’ model. It did this by harnessing the unique access that LFB had to the homes of the most vulnerable in society, with a new emphasis placed on promoting better health and wellbeing outcomes, as well as traditional fire safety interventions. This model aligned with the direction of travel for fire and rescue services across England. Two Community Safety Advisors had been delivering visits with Ealing residents since December 2017, and would continue to do so until March 2019. The outcomes
Page 6 of 324

Health and Wellbeing Board – 17 July 2018
3
from the pilots, being held across five London boroughs, would inform how LFB develops home intervention in future, across all London boroughs. Three key health priorities were being addressed during visits – smoking cessation, falls prevention and winter warmth/fuel poverty. The Ealing Fire Safe, and Well working group had identified additional local priorities of atrial fibrillation and social isolation. Pathways had been developed to enable the Community Safety Advisors to make referrals for beneficiaries of ‘Fire, Safe and Well’ visits into a range of local Ealing services that supported the priorities. They also undertook signposting to a range of local organisations including Age UK and Neighbourly Care. Over 350 visits had been completed across the five pilot boroughs so far, with 80% of visits having resulted in at least one onward referral to a partner agency. Formal evaluation was yet to commence, but anecdotal feedback had indicated that visits were being well received. In Ealing there had been some difficulties with the channels of communication being used to send onward referrals to partner services. The falls pathway had been suspended since February 2018 as it had not been possible to establish an efficient means of sending falls risk information to GPs, in order that they may make a further referral to the falls prevention service. Atrial fibrillation testing had been identified by Ealing CCG as a local priority, and was already running as a pathway in Merton. The pathway was yet to be established in Ealing due to challenges agreeing an appropriate means of sending test results to GPs, and in receiving feedback from GPs in order to evaluate the benefits of the intervention and inform the project evaluation. These difficulties were affecting the impact and reach of the pilot. NHSmail addresses had recently secured for use by the Community Safety Advisors, which would assist in overcoming some of the communications issues, and the project team were keen to push forward in re-establishing the falls pathway and establishing an atrial fibrillation pathway. Support was sought from the Ealing working group and Health and Wellbeing Board members to ensure that the pathways were fit for purpose, efficient, and resulted in meaningful outcomes. The Chair thanked the London Fire Brigade officers for the report and invited Board Members to comment and ask questions. Questions Tessa Sandall stated that there needed to clear agreement on the best approach around pathways, and with that in mind, it would be best the liaise through the working group on the right approach. There was a definite keenness to support to the atrial fibrillation pathway, though it was noted that there would be complexities in the borough in terms of GP relationships, given the 76 separate practices currently in operation.
Page 7 of 324
Health and Wellbeing Board – 17 July 2018
4
Dr Tailor stated that more energy needed to be put into getting Atrial Fibrillation pathways off the ground, this could happen by initiating it within a few specific networks first such as Acton. Councillor Johnson advised that an elderly resident in her ward had recently passed away as a result of smoke inhalation. Could work take place with registered social landlords to liaise around contacts for vulnerable elderly residents in their properties? It was felt that this was a helpful suggestion - LFB needed to be quite targeted due to finite resources, but officers would look into pursuing this. Sarah Rushton asked if contact had been made with Community Mental Health teams. West London Mental Health Trust had quite chaotic service users, with a considerably higher than average prevalence of smokers. Had any conversations taken place? It was advised that LFB officers were looking at discharge process pathways in terms of referring people leaving Mental Health settings into the ‘Fire Safe and Well’ programme. Work was definitely taking place with teams in this sphere. Sarah Rushton advised that she would help with further links where needed. Judith Finlay advised that Councillors were in the process of a scrutiny review through the Health and Adults’ Services Scrutiny Committee looking at falls prevention. Resolved: That (i) the Fire, Safe and Well project update be received;
(ii) the support for the Fire, Safe and Well project be re-affirmed by the Board;
and (iii) London Fire Brigade representatives be asked to explore possibilities around
liaising with Landlords to contact vulnerable residents in their properties.
7. Integrated Care Update (Agenda Item 7) Kim Carey (Interim Director of Adults Services) and Tessa Sandall (Managing Director, Ealing CCG) provided an update to the Board on Health and Social Care Integration in Ealing. Including updates on:
Better Care Fund Reporting Timetable
Care Home work update
iMPOWER progress report It was advised that the BCF Reporting Timetable for 2018/19 had now been released. The first submission date was 20 July 2018. An enhancement had been made on the previous year with the incorporation of the improved BCF reporting into a single template rather than having to submit two separate reports. Completed reports would be brought to the Board for noting throughout the year.
Page 8 of 324
Health and Wellbeing Board – 17 July 2018
5
As part of the North-West London Sustainability and Transformation Plan (STP), health and social care were working together to improve outcomes for older people. A key focus for the work to improve care for older people was around enhancing the care provided in care homes. One of the elements of the support for care home staff was to develop a training programme to help in spotting the early warning signs of those they cared for becoming unwell. A new guide called ‘Is My Resident Well’ and the associated training programme was being rolled out to care homes across North West London to support these care workers. Across North West London 40 clinical staff had been trained during June on how to use the guide and provided with a training programme to go on and train care home staff and carers. The aim was to have 40% of care homes in North West London using the guide by the end of 2018/19. In Ealing, the training would be provided to staff in 17 care homes that provided care for up to 1137 residents. The training would be delivered by Meadow House Hospice. The reviewing of case files by iMPOWER had generated a number of potential opportunities to reduce the number of unplanned admissions where people were known to both health and to social care. The reviews identified a number key interfaces between parts of the health and social care system where better communication could have changed the outcome for patients. To progress this, all partners would come together to explore case examples and work up detailed and timely plans to improve the way people were supported without the need for a hospital admission. The intention was to generate plans that would deliver quick wins, feed into the winter planning cycle and embed culture change across the interfaces. This would provide an opportunity to build on the success in addressing delayed transfers of care. Resolved: That (i) the BCF reporting timetable for 2018/19 and the inclusion of the iBCF
reporting into a single report and submission be noted;
(ii) the work with care homes in Ealing be noted; and (iii) the work being undertaken by iMPOWER to reduce the avoidable demand
across the health and social care interface as part of the Better Lives programme be noted.
8. Mental Health Update
(Agenda Item 8) The Chair invited Tessa Sandall (Managing Director, Ealing CCG), Sarah Rushton (West London Mental Health Trust) and Valerie Wilson (Mental Health Commissioning Manager, Ealing CCG) to present a paper to the Board updating them on the first year of implementation of the Mental Health Strategy, highlighting issues raised and the next steps for the year ahead.
Page 9 of 324
Health and Wellbeing Board – 17 July 2018
6
It was advised that throughout 2018, the Board’s priority would be to oversee the delivery of the Mental Health Strategy’s action plan. Which meant:
Promoting continued joint operational working and information sharing
Building strong partnerships in commissioning
Ensuring the best possible use could be made of scarce resources for the benefit of Ealing residents.
Five broad outcomes had been agreed upon, these were: Outcome 1: Prevention and Wellbeing for the whole population: including reducing stigma and social isolation; identifying mental health needs earlier; addressing the links between physical and mental health; suicide prevention. Outcome 2: Better outcomes and support for people with common mental health needs: including those with long term physical health conditions; better access to primary care. Outcome 3: New model of care for people with serious and long term mental health needs: including crisis response; community based support; primary care; early intervention; carer support. Outcome 4: Working better together: health, social care, housing, police and communities; adults and children; substance misuse, alcohol and mental health; learning disabilities and mental health; criminal justice. Outcome 5: Reaching all our communities: geographical; age; BAME; LGBT; class. Equality of access and treatment; reducing suicide; reducing restraint; carers. It was stated that the Strategy was ambitious, meaning that some targets would fall into 2019/20 – apart from this the Partnership Board was happy with progress being made. All agencies were collaborating well to best deliver the common aims of the West London Mental Health Local Services Transformation Programme. Six key workstreams had been established that were all clinically led. All trusts and CCGs in North West London had signed up to the new model of care for people with serious and long term mental health needs, and the case for change had been based on a series of national, regional and local factors, with a key aim of helping patients to spend less time in acute settings, with more support being provided in community settings. Locally, the agencies had aligned their work to drive implementation of the model of care, with good progress having been made so far. Examples of the progress made include the Single Point of Access (SPA) helpline, which had been launched in 2016. Patients and carers could call the helpline 24/7 for help or advice in a crisis from trained mental health advisors and clinicians. GPs and colleagues from the police also used the number to make referrals and seek advice.
Page 10 of 324
Health and Wellbeing Board – 17 July 2018
7
A Crisis Assessment and Treatment Team (CATT) had also been established in 2016. This provided fast and responsive assessment and care. The CATT could visit people in their homes, where possible and where patients felt more comfortable with this, or they could come to a clinician. There were strict standards in place for responding to emergency referrals within 4 hours and urgent cases within 24 hours. Inpatient pathway improvement work had taken place and helped in significantly improving bed utilisation within the acute adult’s inpatient bed base and reduced the need for patients to be sent to out of the area or private mental health beds to zero. The bed occupancy rate had been sustained below the recommended occupancy rates since Autumn 2017. Each of the transformation workstream steering groups and the Transformation Board had service user and carer representatives in attendance, these worked alongside officers as true partners and played an important part in all the stages of transformation. Ealing Recovery House (provided by Rethink) had been established as an alternative to traditional inpatient ward settings. This was a true partnership between the Trust and Rethink. Immediate challenges remained at a local, London and national level. The most pressing issue was that of workforce shortages. There was a national shortage of certain clinical staff which impacted adversely on plans. At a more localised level, the cost of living in West London also made it hard to attract some staff. Going forwards it would be vital to sustain the system flow and make sure that the quality of delivery was consistently right at every level, ahead of a probable CQC report in the Autumn of 2018. Questions Councillor Johnson referenced concerns around children being placed in adult hospitals with mental issues due to a lack of provision for younger people. Was this an issue in Ealing? Was there adequate provision for issues such as eating disorders? It was advised that the level of provision currently available depended on what the issue was. There were very few CAHMS beds available in North West London, there was however, a very strong eating disorder service. Work was taking place to develop some NHS beds for adolescents, which was a really welcome step. This meant though in the meantime that there has been some need to use private sector providers - with the unfortunate side effect that some of these were not close to home, and private sector providers would not provide assessment over the weekend period. Children 16 years and younger would usually always stay on a paediatric ward, however, sometimes 17-18-year olds did have to be placed in an adult bed for a very short time with high level safeguarding always in place in such situations. Following such scenarios, officers would always write up reports based on the specific incident to learn from it in future.
Page 11 of 324
Health and Wellbeing Board – 17 July 2018
8
A member of the public expressed concerns about mental health issues in relation to maternity. This was a particular issue at Hillingdon Hospital, where it was stated that no one knew who held the responsibilities for post-natal depression. Within North West London, what kind of psychiatric analysis was made for pregnant and post-partum women? Was there a cohesive programme in place to address these very serious mental health issues? It was advised that this had been a primary consideration when setting up the perinatal service. A system had been arranged for all hospitals where Ealing women delivered, with linked pathways created to see them afterwards in other settings more convenient to them. The logistics were arguably more complex since moving services from Ealing Hospital, but officers reviewed the pathways carefully and midwives were fully conversant in their knowledge of how to access and refer to relevant services. Dr Tailor agreed that it was important to ensure a cohesive programme for this. It was a leading cause of death in women of child bearing age and the identification of any women at risk was vital. There was a 24-hour access line for mental health services, and whilst there was not an individual unit in Ealing, private sector facilities were used to ensure that mothers and babies were not separated, as it was paramount at this time to ensure that they were kept together for bonding. Perinatal services were in place to identify at the earliest possible stage any issues during the ante-natal period. Close consideration was also given to potential early trigger warnings, such as domestic violence, drug and alcohol abuse, past history of post-natal depression etc to make sure that the right support at the right time was available. The member of the public stated that it was important to find out the outcomes arising from this work. It was advised that a benefits realisation paper had been taken to the Health and Adults’ Services Scrutiny Committee and was available online. This paper had evidenced that the pathways in place were working. The Chair made reference to London’s Section 136 Pathway launched by the Mayor in 2016. Was this being worked up? It was stated that the interface was working reasonably well in Ealing but there was always room for improvement. Regular meetings took place between the West London Mental Health Trust and the Metropolitan Police to go through data in detail. The Law had been changed to create tighter turnaround times for seeing people referred through Section 136. Out of hours now had a four-hour target which was incredibly difficult to meet. There was definitely more that needed to be worked on in the system to get it right. The Chair then made reference to ongoing workforce issues. The Council had set a target for delivering 2500 genuinely affordable homes. With this in mind, officers and cabinet members would have lots of conversations on what this could deliver for the NHS and other public-sector partners. Resolved: That (i) the one-year update on the Ealing Mental Health Strategy be received; and
Page 12 of 324
Health and Wellbeing Board – 17 July 2018
9
(ii) the update on the West London Mental Health Local Services Transformation
be received.
9. Healthwatch Ealing Progress Report (Agenda Item 9) Mystica Burridge (Area Manager, Healthwatch Ealing) was invited to provide an update to Board Members of the progress of Healthwatch Ealing from April 2017 to March 2018 and the priorities of the service moving forward. One key highlight was the implementation of the digital feedback centre which had been successfully embedded within Healthwatch Ealing service delivery. Since launching in September 2017, Healthwatch Ealing had received over 3000 individual patient experiences and produced two full quarterly reports. The number of experiences collected and the current growth in feedback placed Healthwatch Ealing as the second highest nationally in terms of collecting patient experiences. Healthwatch Ealing had a dedicated programme of Enter and View visits planned six months in advance, after the initial recruitment and training phase of Enter and View authorised representatives. 13 such visits had been conducted with a target of between 20-24 visits for the upcoming year. Over the year, Healthwatch Ealing had researched GP access across the borough by speaking to 2,500 people about access, opening times and utilisation of 111. Various hard to reach groups had been targeted and there had been efforts to speak to commuters. A community services report had also been produced that spoke to 217 patients of all community health services to establish themes and trends across provision as opposed to specific service reviews. The Service was in the process of liaising with CAMHS to understand individual experiences of eating disorder provision through in-depth case studies. Questions Councillor Johnson complemented the work of Healthwatch Ealing over the year, stating that it was good to see the number of volunteers getting involved. A member of the public made reference to a survey that took place in Hillingdon regarding the experience of Ealing women using maternity services, the outcomes from which had not been very positive. She requested that Healthwatch Ealing look at their experience, and the problems seen with transport and long waits amongst other issues. Tessa Sandall advised that the Hillingdon Healthwatch survey had taken place around 12 months ago. Following on from the negative feedback received, the CCG had worked with them to instigate improvements. She advised that she would locate the reports advising on actions taken since then. Resolved: That (i) the Healthwatch Ealing progress report be received; and
Page 13 of 324
Health and Wellbeing Board – 17 July 2018
10
(ii) the CCG be asked to provide reports advising on actions taken to improve services at Hillingdon Hospital over the past 12 months for the Board’s information.
10. Ealing CCG Business Plan 18-19
(Agenda Item 10) Tessa Sandall introduced a report outlining NHS Ealing CCG’s 18/19 Business Plan priorities within the context of delivering the North-West London (NWL) Sustainability and Transformation Plan (STP). NHS Ealing CCG’s clinical and senior management team had refined the CCG’s local priorities and ensured that its Business Plan aligned work programmes across the collaborative and locally to the NWL objectives and areas of focus. The Business Plan reflected locally led, prioritised, projects and programmes that sat outside of the ‘Business as Usual’ (BAU) work of the CCG. Ealing CCG also worked in partnership with the NWL Strategy and Transformation Team to deliver NWL-wide projects and programmes, however as they were led and resourced at a NWL level these were not included in the Ealing Business Plan. The Business Plan also reflected the CCG’s priorities in terms of increasing capacity within the health and social care system and delivery of financial sustainability in 18/19. Questions Councillor Johnson asked for further detail about how the CCG was aiming to ensure financial sustainability. It was advised that as with all areas of the public sector, the CCG was faced with a very challenging environment and was being monitored very closely in the delivery of its savings. An £18m savings target was in place, which would be a real challenge to meet, especially in the face of growing demand and acuity of needs. Difficult decisions were having to be made in relation to this. Close work was taking place with the 76 GP practices in the borough to improve outcomes out-of-hospital and ensure that robust care plans were in place. ECCG was investing where it could into the right areas to ensure future sustainability. Close work was taking place on admissions where the patient could have been better cared for out of the hospital. Where they were admitted unnecessarily there were risks around the need for more rehabilitation as a consequence, therefore officers were trying to reduce instances of this. Revised guidelines around blocked catheter work had been signed off, with the London Ambulance Service in place to provide a professional service on this in a set amount of time, which could prevent up to 1300 unnecessary admissions each year. Investment had also been made into a community cardiology service, which was consultant led outside of the hospital setting. This had multiple benefits of delivering savings and being better for the patient. The Chair referred to the local hospital outline business case – where did the CCG stand currently in terms of developing the model?
Page 14 of 324
Health and Wellbeing Board – 17 July 2018
11
It was advised that the frailty model of care was being worked on. This had started as a pilot with colleagues in the Trust to develop a frailty front end service at Ealing Hospital. Unfortunately, it had taken place at a time when staffing capacity was very low, and they were not able to continue running the service, so work had been taking place on looking at how best to work around this. Patients had been visited in their own homes to work with them to understand their needs when they returned to the hospital. The CCG was trying to get to a place of coherent out-of-hospital care. It was important to understand that patients did not just use Ealing Hospital, so work on making sure that pathways across North West London Trusts were strong was critical. The Chair then made reference to the quality outcomes framework review and the estate. Would One Public Estate be realised? It was advised that each year the CCG had small scale improvement grants they could apply for. These were usually for around a maximum of 200k. Currently ECCG was supporting a number of practices to put in bids. ECCG had also asked for support around hubs in Acton and Greenford, and were currently waiting to hear the outcomes on. There was absolute cognisance of the need to improve the estate in general practice. The Chair then asked for further details around plans for winter resilience. It was advised that the winter resilience action plans were not fully in place for 18/19 yet but these were in the process of being considered. There was a much-reduced winter resilience budget that had to be taken account of. Work was currently taking place with iMPOWER on finding quicker wins before the winter period. The ECCG would look to bring the plans to the Board before winter. The Chair stated that the Board would welcome this and suggested that the plans be brought to the September meeting. Resolved: That (i) the CCG Business Plan for 18/19 be noted; and
(ii) the CCG winter resilience action plan be added to the forward plan for the
September 2018 meeting of the Board.
11. Update on Delayed Transfers of Care (Agenda Item 11) A report was provided updating the Board on progress around Delayed Transfers of Care (DTOC) performance. The key messages arising from the figures were:
Ealing borough had progressed well and had been noted nationally as producing some of the greatest improvements in reducing DTOC
Significant developments within local mental health services had supported improvement which had led to freeing up significant acute mental health bed
Page 15 of 324
Health and Wellbeing Board – 17 July 2018
12
occupancy to support patients getting the right care at times of crisis, with reported acute bed occupancy at the low 80% values, where previously occupancy was at 100%
Continued progress had been seen across acute providers and the good practice that had been implemented with mental health was being rolled out to acute processes.
Work was ongoing to continually improve and the next steps included:
Undertaking a joint review with the mental health trust partner of current delayed pathways. This would feed into the next iteration of the DTOC plan.
Reviewing the mental health rehabilitation bed pathway to support further improvements in patient flow.
Jointly review the operational process to further implement the processes adopted with mental health services.
Teams continuing to build relationships where the population was treated in wider hospital trusts outside of North-West London to support a fast transfer back into local community health and social care services when required.
Questions Councillor Driscoll noted the dramatic improvements that had been made and asked how these could be sustained so that this now remained the expected standard level of performance. It was advised that the work with partners in reducing occupancy rate was paying off – huge amounts of work had been undertaken by the trust to identify and support discharge team work on getting patients back home. The aim was to ensure that this was done in a sustainable way. A huge amount of process mapping had been undertaken. Initial work had been targeting long stayers and then sustainability had to be embedded. Sarah Rushton advised that processes had been in place where the local authority were not fully engaged. A piece of work right through the system had been undertaken on this. Processes were now embedded for all and drawn out in a clear way making them more sustainable. Kim Carey stated that it had been useful learning that could now be applied to acute partners. Throughput was now higher. Councillor Joy Morrissey asked for a walk through of the acute bed process. What type of care were they in? Were these largely those with long term mental health needs? It was advised that a small number had highly complex needs, and whilst their numbers were small, their stays were significant. It was about recognising who they were and making the right decision for their needs with appropriate flagging between
Page 16 of 324
Health and Wellbeing Board – 17 July 2018
13
partners. It was important to ensure that these people were not pointlessly sent somewhere that could not deal with their needs. Kim Carey advised that for many housing was an issue. So that needed to be flagged as well. It was also important to manage expectation, so that people did not have an automatic expectation of alternative housing provision just because they had been in hospital. Councillor Joy Morrissey made further reference to the housing support. Was this through the Trust or the Council? It was advised that there was a fund through Supporting People, there was someone in place effectively employed by the Council but liaising very closely with mental health teams. The Chair stated that essentially there appeared to be two broad cohorts – those with high level mental health needs, and elderly patients with complex needs. It was clear that housing situations needed to be looked at more broadly to understand what is happening in the system. Councillor Johnson asked if there was a typical age range for those with the most complex needs. It was advised that they tended to be older, from 40s and upwards. They were also more likely to be men. The Chair stated that overall, this was a really good news story, and deserved the congratulations of the Board. Resolved: That (i) the update on delayed transfers of care be noted; and
(ii) the Board be minded to express its congratulations for the achievements in
reducing the level of DTOC to date.
12. Stop Smoking Consultation Outcomes (Agenda Item 12) The Executive Director of Children, Adults and Public Health advised the Board that the Stop Smoking Service consultation outcomes had been submitted to Cabinet for the meeting on 10 July 2018. The report set out the results of the consultation exercise that took place from 19 February to 24 April 2018 relating to the proposal to end the Stop Smoking Services from April 2019. The proposal had been agreed by the Cabinet, and was subsequently called in by the Conservative Group, to be heard at the Overview and Scrutiny Committee meeting of 2 August 2018. Part of the recommendations from the Cabinet stated that officers were to review the ceasing of the service closely and look at possibilities around creating a smaller more targeted service. Public Health officers would work closely with the CCG about possibilities around this.
Page 17 of 324
Health and Wellbeing Board – 17 July 2018
14
Questions Councillor Johnson stated that overall in recent years the prevalence of smoking had reduced significantly, however, it was appreciated that there were communities that needed to be targeted as they contained a much higher than average amount of heavy smokers. Tessa Sandall stated that ECCG noted where the consultation had got to, but officers were well aware of the fact that the CCG was strongly against this move. The importance of keeping a close watch on the potential consequences was reemphasised. The CCG had done a cost analysis and it was expected that cost pressures would be seen through non-elective admissions. It was highly unlikely that the CCG could contribute towards any financial assistance. But work would take place with Public Health on how they might target funding. A member of the public noted concern about how the decision may impact upon child mortality. Teenage smoking during pregnancy remained common and it was important not to be blasé about this risk. The Executive Director of Children and Adults’ Services stated that this was partly why a targeted service was being planned – pregnant mothers would be one of the key targets. Infant mortality was a reducing trend, and work continued with schools on teenage pregnancy. Dr Rubinder Bains (Consultant in Public Health) advised that a public health colleague has been looking directly at teenage smoking and pregnancy related issues in Northolt, which was the area of the borough where this was statistically the most prevalent. She advised that the outcomes of the report arising from this could be shared with the Board. Dr Tailor agreed that the money available needed to be used in the areas where it would have the biggest impact. With mental health patients being another key demographic to target. With this in mind, a uniform targeting approach would be beneficial. The Chair stated that given the financial pressures all areas of the public sector were being placed under, it was an unfortunate fact that there would not always be agreement around uncomfortable decisions. He stated that many of the biggest impacts in smoking reduction in recent years had come through large scale national programmes, such as the banning of smoking ban inside public houses. Sarah Rushton stated that there needed to be real evaluation of the impact around a year after implementation of the decision – looking at the changes seen and the costs to health that could be attributed to the lack of the service. Resolved: That (i) the report updating the Board on the findings of the Stop Smoking Service
consultation on the proposal to cease the service be noted;
(ii) the report arising from the public health study of teenage pregnancy and smoking in Northolt be shared with the Board; and
Page 18 of 324
Health and Wellbeing Board – 17 July 2018
15
(iii) the concerns raised by Board Members regarding the proposed ceasing of the
service be noted.
13. HWBB Forward Plan 2018-2019 (Agenda Item 13) The Chair asked that the Panel note the Forward Plan, and suggest any amendments where required. It was advised that the Stop Smoking Service Consultation item needed to be removed from the September 2018 agenda. It was asked that following on from Item 10 of the Agenda, that an item on winter resilience be added to the agenda for September 2018. Resolved: That, subject to the above amendments, the updated Health and Wellbeing Board Forward Plan 2018-2019 be noted by the Board.
14. Date of Next Meeting (Agenda Item 14) The next meeting of the Panel would be held on 18 September 2018.
Councillor Peter Mason Nominated Chair in absence of Chair and Vice-Chair.
The meeting ended at 7:50pm.
Page 19 of 324

Page 20 of 324
1
Contains Confidential or Exempt Information
NO
Title Oral Health Progress Report on Pilot
Responsible Officer(s) (EDG Officers only)
Author(s) Louise Taylor, Claire Robertson (PHE), Kelly Nizzer (NHS England)
Portfolio(s) Cllr Binda Rai and Cllr Yvonne Johnson
For Consideration By Health & Wellbeing Board
Date to be Considered 18th September 2018
Implementation Date if Not Called In
N/A
Affected Wards “All” Keywords/Index Child Oral Health
Purpose of Report: The purpose of this report is to give an update on Child Oral Health work in Ealing.
1. Recommendations HWBB are asked to note the recent improvements in children’s oral health and to note the progress in delivering the oral health improvement plan/link to appropriate strategy.
2. Reason for Decision and Options Considered N/A
3. Key Implications The implications of doing no oral health work with children and young people in Ealing will lead to an increase in numbers of children with tooth decay, and wider implications including ability to sleep, eat, speak, play and socialise with other children. Poor oral health also has wider impacts at school and for families if a child misses school or when a parent must take time off work if their child needs dental treatment.
Often dental treatment for young children (such as extractions of decayed teeth) may only be done under general anaesthetic, which is both distressing for the families concerned and expensive. Dental extractions are currently the number one reason why children are admitted for a general anaesthetic in England.
Report for: ACTION/INFORMATION Item Number: 6
Page 21 of 324
2
The financial impact of dental disease is significant. Although largely preventable, tooth
decay remains the most common oral disease affecting children and young people. Treating
oral diseases within the NHS costs £3.4 billion annually in England.
4. Financial Not Applicable. The funding for the Oral Health promoter comes directly from NHS England to the Community Dental Service as part of a bigger contract in place with the provider. We are exploring possible funding opportunities for future funding of the Supervised Tooth Brushing Programme.
5. Legal
N/A 6. Value For Money
N/A.
7. Sustainability Impact Appraisal N/A
8. Risk Management
Poor oral health may be indicative of dental neglect and wider safeguarding issues. Dental neglect is defined as “the persistent failure to meet a child’s basic oral health needs, likely to result in the serious impairment of a child’s oral or general health or development”.
9. Community Safety
N/A
10. Links to the 3 Key Priorities for the Borough By seeking to ensure good child oral health in Ealing we are addressing the council’s key priority of making it a healthy borough by enabling our children to have good oral health.
11. Equalities, Human Rights and Community Cohesion
Page 22 of 324
3
N/A 12. Staffing/Workforce and Accommodation implications: In terms of staffing the Public Health Specialist oversees the workload of the oral health promoter and works on other elements of the oral health programme in Ealing along with obesity and physical activity (which has overlap with risk factors). There are no accommodation implications.
13. Property and Assets N/A.
14. Any other implications: N/A
15. Consultation
16. Timetable for Implementation
The action plan work is ongoing, with the exception of the supervised tooth brushing programme which ended in June 2018.
17. Appendices
Appendix 1: Progress Report on Children’s Oral Health in Ealing
18. Background Information
1. JSNA (2017) Child Oral Health: Ealing https://www.ealing.gov.uk/downloads/download/4545/joint_strategic_needs_assessment_jsna_2017
2. PHE. Delivering better oral health: an evidence-based toolkit for prevention, Third
edition. 2014.
3. PHE. Commissioning better oral Health. 2014.
4. Oral Health Survey of 5 Year Old Children (2017) is published here:
http://www.nwph.net/dentalhealth/
Page 23 of 324
4
Consultation (Mandatory)
Name of consultee
Post held Date sent to
consultee
Date response received
Comments appear in
paragraph:
Internal
e.g. Paul Najsarek Executive Director
e.g. Helen Harris Director, Legal Services e.g. 5. Legal
e.g. Ross Brown Director, Finance e.g. 4. Financial
e.g. Julian Bell Leader / Cabinet Member for:
External
eg voluntary organisation
Report History
Decision type: Urgency item?
For information No
Report no.: Louise Taylor, Public Health Specialist: [email protected]
Page 24 of 324
Appendix 1: Progress Report on Children’s Oral Health in Ealing
1. Background Despite improvements in children’s oral health over the past 30 years, tooth decay remains a significant public health problem and is the most common oral disease affecting children and young people in England, yet it is largely preventable by reducing the amount and frequency of sugar in the diet and optimising exposure to fluoride.
Poor oral health can affect children’s and young people’s ability to sleep, eat, speak, play and socialise with other children. Other impacts include pain, infections, poor diet, and impaired nutrition and growth.
Poor oral health also has wider impacts at school and for families if a child misses school or when a parent must take time off work if their child needs dental treatment.
Often dental treatment for young children (such as extractions of decayed teeth) may only be done under general anaesthetic, which is both distressing for the families concerned and expensive. Dental extractions are currently the number one reason why children are admitted for a general anaesthetic in England. Poor oral health shares the same common risks as many other chronic diseases, and any action to reduce these risks (particularly sugars in the diet) has the potential to improve oral as well as general health. Tooth decay as with other health inequalities shows that 5-year-old children living in areas with higher Index of Multiple Deprivation (IMD) scores display higher numbers of decayed, missing (due to decay) and filled teeth (dmft).
There is also a financial impact of dental disease to an individual and the local health services which can be significant.
2. Summary of key data related to children’s oral health
Levels of tooth decay:
• Looking at 2017 data Ealing children have shown some improvement from the previous survey in their levels of tooth decay with 30.7% of 5-year-old children experiencing tooth decay (compared to the 2015 data where Ealing children had the highest child tooth decay rates in London with 39% of 5 year old children having experienced dental decay), but this is still greater than the London (25.7%) and England (23.3%) averages.
Child hospital admissions and extractions: Dental decay is the most common reason for non-emergency hospital admissions in children aged over 1 year.
• The total number of child hospital admissions for Ealing resident children in 2016/17 was 644. Dental Decay remains the top cause for child hospital admissions in Ealing for 1-18 year olds and 5-9 year olds and is the borough with the highest overall number of admissions for dental decay in London.
• Children aged 1-18 years in Ealing have the second highest rate across London for hospital tooth extractions; double that for England with 83% of these for children under 10 years old (2015/16).
Page 25 of 324
Access and uptake of dental services: Individuals and families may access primary care dental services where ever they wish and are not constrained to access care within the borough where they reside or are registered with a GP.
• Uptake of dental services for children (1-17 years) in Ealing is better than the average for London.
• In the 24 months to September 2016, 52,709 child patients (defined as patients under 18 on the last day of the 24 month period) were seen in the borough of Ealing which accounted for 29.9% of all patients seen in that time period.
• Ealing resident child uptake rates for NHS dentistry vary by ward across the borough, with the highest rates in the wards of Northfield, Southall Green and Southall Broadway, and the lowest in Southfield, Ealing Broadway, Hanger Hill and Northolt West End.
Fluoride varnish: There is strong evidence to support the application of fluoride varnish (FV) at least twice a year for children over 3 years of age and 3-4 times for those at higher risk of tooth decay.
• In Ealing, there has been a year on year increase in the proportion of child (3-17 years) NHS courses of treatment with a fluoride varnish application from 2010 to 2016, by child resident postcode. The FV rate for children with an Ealing resident postcode in the 24 months before September 2016 was 39% which was an increase from 30.2% in 2014.
• Despite this increase there is a great deal of variation in rates of FV application for children resident across the borough, with the highest rates in children residing in Southall Broadway (52.3%), Northolt Mandeville (51.2%) and Dormers Wells (50%) compared to the lowest rates for those children resident in Ealing Broadway (24.8%) and Elthorne (26.2%).
For more information see the oral health JSNA (2017)
https://www.ealing.gov.uk/downloads/download/4545/joint_strategic_needs_assessment_jsn
a_2017
3. Current Interventions & Assets This section summarises the key oral health activities in the period 2016-2018.
➢ Ealing children and young people’s oral health action ➢ Ealing Children & Young people multi-agency oral health steering group ➢ Children’s Oral health JSNA document ➢ An annual oral health promotion campaign ➢ Oral Health Promoter for Ealing
➢ Oral Health MECC type training programme a resource pack, a universal training package
➢ An advanced training programme
➢ ‘Healthy teeth, Healthy Smiles Ealing’ leaflets
➢ ‘Now You Have Teeth’ Programme
➢ UNICEF baby friendly accreditation ➢ Communication of key messages ➢ A pilot supervised tooth brushing programme ➢ Starting Well
Page 26 of 324
1. There is an Ealing children and young people’s oral health action plan (2017-2020) which has been developed to address childrens oral health in the borough and aligns with national guidance for local authorities in Commissioning Better Oral Health (2014), and includes the recommendations of the evidence-based “North West London Child Oral Health Improvement Strategy (2011-16) across the three overarching priority areas: Integration of oral health with other Public Health and Children’s Programmes, Increasing children’s exposure to fluoride (both fluoride toothpaste and fluoride varnish) and Making oral health everybody’s business and making every contact count.
2. An Ealing Children & Young people multi-agency oral health steering group is now in place which meets quarterly to discuss and direct activity being undertaken across the borough.
3. In addition to the action plan a Children’s Oral health JSNA document has been produced (2017) with the support of PHE and includes a series of recommendations
4. An annual oral health promotion campaign is held to promote National Smile week.
5. The Oral Health Promoter for Ealing is working across children’s centres and schools providing oral health workshops and training sessions with the aim of educating families, professionals and all others around the key activities they should be undertaking to achieve good oral health, raising the profile of oral health and encouraging and empowering families to register with a dentist and to attend regularly.
6. Building capacity in the wider professional workforce by: Providing training to key health and non-health professionals in a sustainable fashion in order to embed oral health within all children’s services and health promotion activities. Ensuring that children across Ealing receive consistent appropriate oral health advice from health and non-health professionals surrounding diet, tooth brushing, exposure to fluoride and supporting making every contact count (http://makingeverycontactcount.co.uk/). Embedding oral health as part of the specification for the wider workforce involved in delivering the 0-19 integrated healthy child programme. The new service specification will include specific reference to oral health to ensure that staff will be expected to discuss oral health with families.
7. We successfully secured one off funding from health Education North West London (HENWL) to run an Oral Health MECC type training programme which the oral health promoter and PHE has been assisting with the delivery of, and this has included the development of a resource pack, a universal training package aimed at all health and non-health professionals including School Nurses, Health Visitors, Early Years and children’s centre staff, other professionals and groups working with families such as nurseries, childminders and foster carers. This training aims to ensure that oral health becomes everybody’s business and support the “making every contact count” movement. An advanced training programme will then be offered to those individuals who would like to become Oral Health Champions.
8. Following a common risk factor approach through: Aligning with the current local obesity strategy to maximise reach and impact. Support the ambition that all Ealing primary and secondary schools sign up to the sugar smart project as supported by the Ealing Healthy Weight, Healthy Lives Strategy 2016-2019. Ealing is implementing a borough wide Sugar Smart campaign, implementing the model developed by Sustain and the Jamie Oliver Food Foundation to raise awareness of the risks of high levels of sugar consumption, and to promote alternatives (http://sugarsmartuk.org), this ties in with the evidence around the introduction of healthy food and drink policies. Identifying and supporting healthy policies in childhood and family settings which support reducing sugar consumption.
Page 27 of 324
9. Developing children’s centres as an oral health promoting setting with some key performance indicators
10. Work has been undertaken to promote the ‘Healthy teeth, Healthy Smiles Ealing’ leaflets (available at children’s centres, primary and junior schools), which aim to encourage registering with and regularly attending a dentist, promote fluoride varnish application and provide advice on diet and tooth-brushing. Also, “bottle to cup packs” are being disseminated to encourage the transition of children away from drinking from bottles to using cups.
11. Ealing will continue to support the ‘Now You Have Teeth’ project at Health Visitor clinics for child progress checks and children’s centres. This is a collaborative outreach programme delivered by young dentists to encourage parents to take their children to the dentist by the age of one year.
12. Further work is being undertaken across the borough to achieve UNICEF baby friendly accreditation which will contribute to oral health through messaging around breastfeeding.
13. Further communication of key messages will be undertaken across the borough at available opportunities such as in the family information service leaflet, the local voluntary sector health newsletter and using social media and a variety of other communication methods.
14. Increasing exposure to fluoride by: Empowering parents and carers to seek dental check-ups and request fluoride varnish application for their children. Include a brief intervention on oral health to be delivered during existing child progress checks, within the Health Visitor service specification.
15. Work with our collaborative partners to: Support the development of oral health promoting dental practices in Ealing in collaboration with NHS England. Support GPs and practice nurses to provide brief interventions on oral health, to support making every contact count and develop a prompt on their patient record software to facilitate this. Identify sugar ambassadors in the council who can champion “sugar smart” within council directorates.
16. Explore novel interventions to increase service utilisation such as: Assessing the feasibility of sending out birthday cards to families to prompt dental check-ups.
17. A pilot supervised tooth brushing programme has been running successfully in Ealing for the last year and targeted a number of primary schools and nurseries across the borough and engaged with over 4,200 children aged 3-5 across 36 schools and nurseries (please see Box 2 below).
18. Starting Well: Ealing was identified in 2016 as one of the 13 worst areas in England for child oral health and is now contributing to the Starting Well National Programme Board and its programme implementation in the Borough of Ealing (please see box 3 below).
Box 2: Supervised Toothbrushing Programme
The programme involves an oral health promoter engaging with the school and seeking parental consent for the children to participate in the supervised toothbrushing programme. Parents are then invited to a workshop session where they have an opportunity to learn about key aspects of good oral health.
Staff within the school setting are then trained in the delivery of a practical supervised toothbrushing programme in the school, and are supported in the implementation of the programme. Each child is given their own toothbrush and on a daily basis all children in a classroom brush their teeth. Children are also given a toothbrush and toothpaste to take home with them.
Page 28 of 324
Summary of initial qualitative results of supervised toothbrushing programme:
Early feedback from the participating schools has been very positive, with schools reporting that children are enjoying the programme and families are engaged with the process, and are feeding back that they are toothbrushing at home.
Local dental practices have fed back that families have been registering and coming into the dental practices as a result. 4 of the primary schools have also expressed a desire to roll out the programme across the whole school and details have been provided about the available resources that would be required to support each school going forward.
Unfortunately, funding has now ended at the end of June 2018, so we are unable to continue with this evidence based programme.
Box 3: Starting Well
Following the local launch in September 2017, NHSE London has commissioned 12 practices to join the scheme in Acton, Southall and Northolt & Greenford where there is a high level of socio economic deprivation and large ethnic diversity. Practices participate on a voluntary basis and are funded for the initiatives at various levels.
Starting Well 13 in Ealing went live in January 2018, and 12 practices have signed up to be an advanced preventive practice, with practice prevention oral health champions, the undertaking of audits, and reaching out to early years settings and families with young children to make a difference in the child decay rates and healthy eating in the borough.
The team has produced and printed a wealth of evidence based resources for practices all of which has been signed off by local/national comms and has been distributed to all practices involved.
Evidence-based training and resources have now been provided to all practices by the collaborative from Public Health England, NHSE, Whittington Health (the local community dental services provider) and HEE on a range of topics from communication, behaviour change, and clinical management of young children, together with clinical skills training by consultants in paediatric dentistry.
There is a support network group which began meeting monthly and has now moved to every two months. The support network consists of NHSE, representation from the Local Dental Committee, CCG, Local Council Public Health Team, Children’s Centres, Community Dental Services, Local Dental Network Chair and Public Health England.
The contract is in place for 2 years at this point and will be reviewed at 6 months and 12 months as well as monitoring the monthly audit.
Many of the resources produced in Ealing are being used in other Starting Well programmes nationally.
Starting Well Practice teams have offered oral health advice and signposting to dental services at the Southall Parade earlier this year, and the NHS 70 parkrun on the 9th June as well as at more local events currently being held.
4. Next steps
In addition to the activity listed above please also refer to the 2017 Oral Health JSNA chapter: https://www.ealing.gov.uk/downloads/download/4545/joint_strategic_needs_assessment_jsna_2017
Page 29 of 324

Page 30 of 324
1
Contains Confidential or Exempt Information
NO (If yes, state to which paragraph of the Access to Information Rules the exemption relates)
Title Progress Report on Ealing Standard Mobilisation and Delivery
Responsible Officer(s)
Author(s) Neha Unadkat, Deputy Managing Director, ECCG
Portfolio(s)
For Consideration By Health and Wellbeing Board
Date to be Considered
Implementation Date if Not Called In
N/A
Affected Wards
Keywords/Index
Purpose of Report: This report is a summary of progress against delivery of the Ealing Primary Care Standards contract which is a single 3.5 year wrap around contract for primary care in Ealing. The contract consists of a set of 23 standards with key performance indicators which practices are asked to deliver against working with other local practices in Ealing to ensure population coverage for all 23 standards.
1. Recommendations The Health and Wellbeing Board are asked to note the progress against mobilisation and delivery of the Ealing Standard Contract. 2. Reason for Decision and Options Considered This report provides an update on progress of the delivery of the Ealing Standard which will have an impact on outcomes on the health of the local population.
3. Key Implications The Ealing standard is a contract developed by Ealing CCG to commission a set of 23 standards of care from Ealing General Practices. The length of the contract is 3.5 years with the first standard – Access commencing as of 1st October 2017. The remaining standards commenced on the 1st April 208, when the Out of Hospital came to an end.
Report for: ACTION/INFORMATION Item Number: 7
Page 31 of 324
2
The Ealing standard business case was approved by Ealing Governing Body in public in July 2017. Progress report covers:
Context
Principles of the Business Case
Expected Benefits from the contract
The 23 standards
The Contract
The Access standard
Workforce
Engagement with practices
Contract management process at both Practice and Network level
Population Coverage
IT templates
Business Intelligence 4. Financial The funding for this contract comes from Ealing CCG’s core budget and the Primary Care Delegated Budget and has been agreed for the term of the contract. 5. Legal Not applicable
5. Value For Money
Value for Money is set out in the Business Case available on the Ealing CCG Governing Body Papers. This does not form a part of this report.
6. Sustainability Impact Appraisal
Not applicable
8. Risk Management The CCG holds a comprehensive risk register. All risks are monitored under the risk register and risks are managed by the Primary Care Commissioning Committee 9. Community Safety None
10. Links to the 3 Key Priorities for the Borough The council’s administration has three key priorities for Ealing. They are:
Good, genuinely affordable homes
Opportunities and living incomes
Page 32 of 324
3
A healthy and great place
This programme of work directly links to priority 3 – A health and great place.
11. Equalities, Human Rights and Community Cohesion The business case available on the CCG Website includes a comprehensive EQIA which was prepared prior to submission to the GB. 12. Staffing/Workforce and Accommodation implications: Workforce is considered in the report directly. 13. Property and Assets
If the report does not involve property, please state that there are no property implications.
Not Applicable
14. Any other implications: Not Applicable 15. Consultation Not Applicable 16. Timetable for Implementation The contract was let in October 2017 and is for a period of 3.5years. 17. Appendices Health and Wellbeing Board Paper Ealing Standard September 2018 18. Background Information
(This is a statutory requirement – please include the public documents referred to in writing the report, officer research and advice documents which Members or Members of the Public may request from the report author)
Page 33 of 324
4
Consultation (Mandatory)
Name of consultee
Post held Date sent to
consultee
Date response received
Comments appear in
paragraph:
Internal
External
Report History
Decision type: Urgency item?
For information
No
Report no.: Report author and contact for queries:
Neha Unadkat, Deputy Managing Director, Ealing CCG [email protected] 0208 280 8119
Page 34 of 324

The Ealing Standard
HWBBSeptember 2018
Page 35 of 324
Ealing Primary Care Standard - Context
The new Ealing Standard is a single 3.5 year wrap around contract for primary care that asks practices to deliver a set of 23 standards with key performance indicators.
The investment to primary care includes:
• Available NHS England investment that has not been otherwise allocated to fund changes in the core contract, changes in rents and rates reimbursements and demographic changes.
• All existing discretionary CCG funding for services, including winter resilience, LIS schemes and the Out of Hospital services
• Reinvestment of the PMS premium• Investment of a further £923k of discretionary CCG funding offset by
savings in the acute setting system
2Page 36 of 324
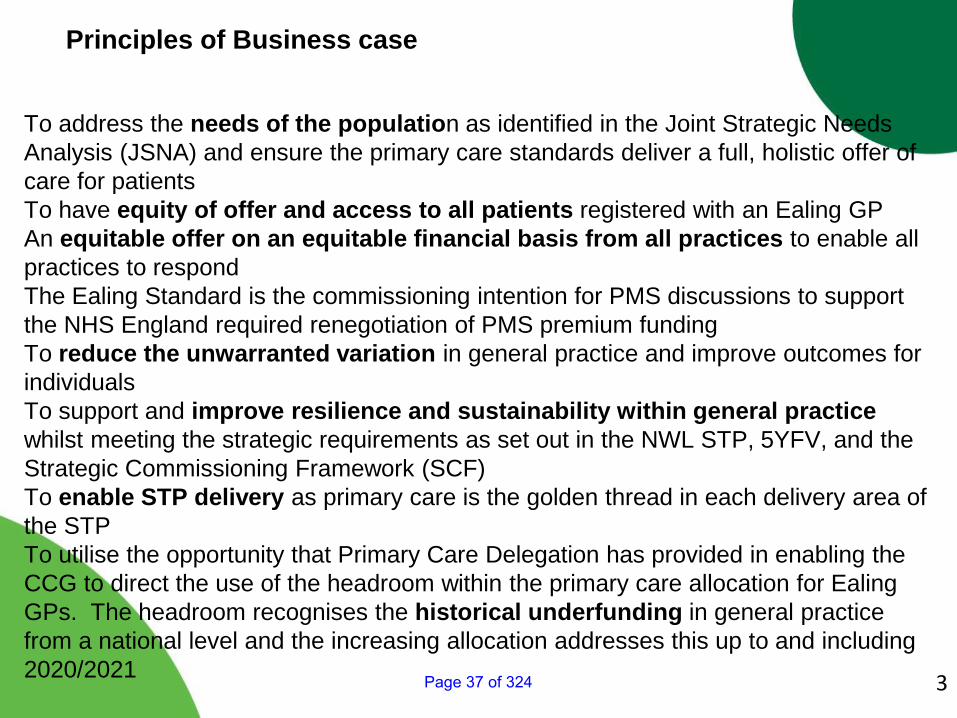
Principles of Business case
To address the needs of the population as identified in the Joint Strategic Needs Analysis (JSNA) and ensure the primary care standards deliver a full, holistic offer of care for patientsTo have equity of offer and access to all patients registered with an Ealing GP An equitable offer on an equitable financial basis from all practices to enable all practices to respond The Ealing Standard is the commissioning intention for PMS discussions to support the NHS England required renegotiation of PMS premium fundingTo reduce the unwarranted variation in general practice and improve outcomes for individualsTo support and improve resilience and sustainability within general practice whilst meeting the strategic requirements as set out in the NWL STP, 5YFV, and the Strategic Commissioning Framework (SCF)To enable STP delivery as primary care is the golden thread in each delivery area of the STP To utilise the opportunity that Primary Care Delegation has provided in enabling the CCG to direct the use of the headroom within the primary care allocation for Ealing GPs. The headroom recognises the historical underfunding in general practice from a national level and the increasing allocation addresses this up to and including 2020/2021 3Page 37 of 324
Benefits Realisation
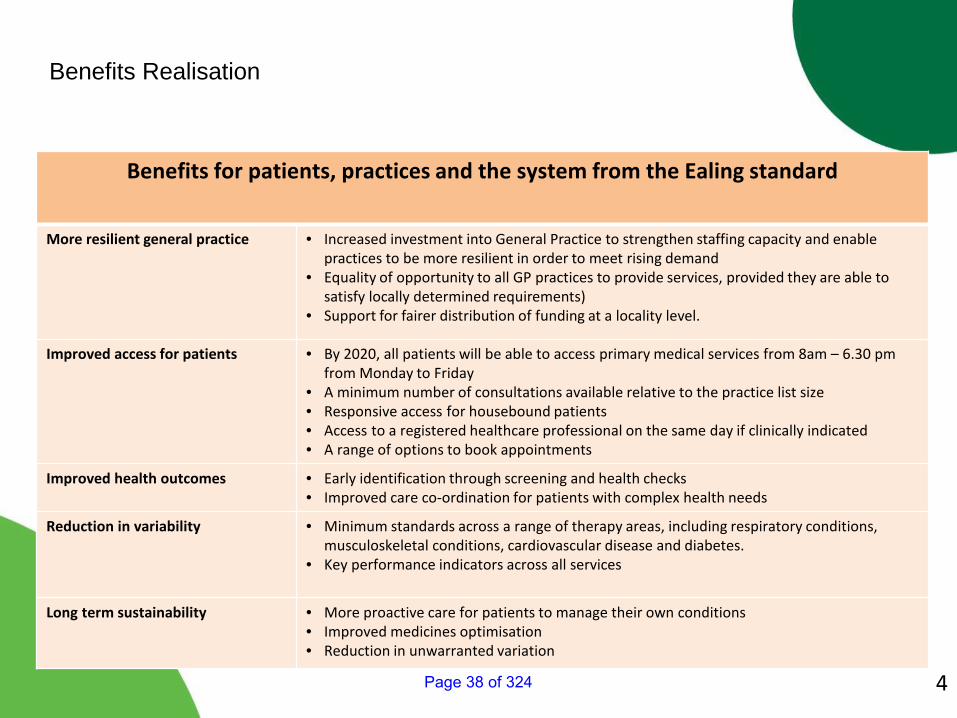
Benefits for patients, practices and the system from the Ealing standard
More resilient general practice • Increased investment into General Practice to strengthen staffing capacity and enable practices to be more resilient in order to meet rising demand
• Equality of opportunity to all GP practices to provide services, provided they are able to satisfy locally determined requirements)
• Support for fairer distribution of funding at a locality level.
Improved access for patients • By 2020, all patients will be able to access primary medical services from 8am – 6.30 pm from Monday to Friday
• A minimum number of consultations available relative to the practice list size• Responsive access for housebound patients• Access to a registered healthcare professional on the same day if clinically indicated• A range of options to book appointments
Improved health outcomes • Early identification through screening and health checks• Improved care co-ordination for patients with complex health needs
Reduction in variability • Minimum standards across a range of therapy areas, including respiratory conditions, musculoskeletal conditions, cardiovascular disease and diabetes.
• Key performance indicators across all services
Long term sustainability • More proactive care for patients to manage their own conditions• Improved medicines optimisation • Reduction in unwarranted variation
4Page 38 of 324
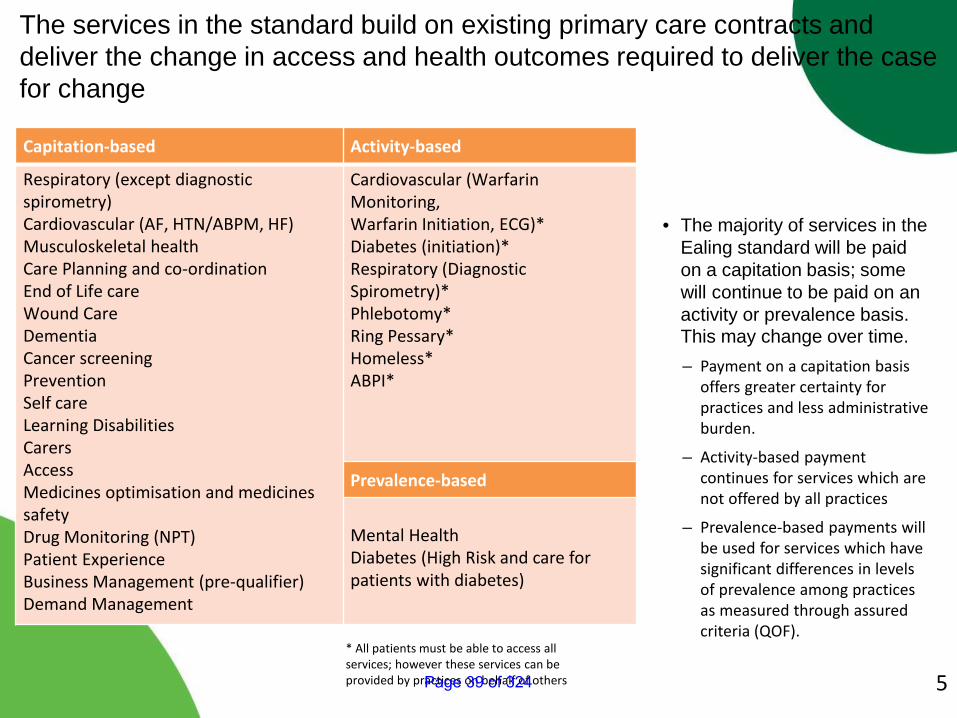
Capitation-based Activity-based
Respiratory (except diagnostic spirometry)Cardiovascular (AF, HTN/ABPM, HF)Musculoskeletal healthCare Planning and co-ordinationEnd of Life careWound CareDementia Cancer screeningPreventionSelf careLearning DisabilitiesCarersAccess Medicines optimisation and medicines safetyDrug Monitoring (NPT)Patient ExperienceBusiness Management (pre-qualifier)Demand Management
Cardiovascular (Warfarin Monitoring,Warfarin Initiation, ECG)*Diabetes (initiation)*Respiratory (Diagnostic Spirometry)*Phlebotomy*Ring Pessary*Homeless*ABPI*
Prevalence-based
Mental Health Diabetes (High Risk and care for patients with diabetes)
* All patients must be able to access all services; however these services can be provided by practices on behalf of others
The services in the standard build on existing primary care contracts and deliver the change in access and health outcomes required to deliver the case for change
• The majority of services in the Ealing standard will be paid on a capitation basis; some will continue to be paid on an activity or prevalence basis. This may change over time.– Payment on a capitation basis
offers greater certainty for practices and less administrative burden.
– Activity-based payment continues for services which are not offered by all practices
– Prevalence-based payments will be used for services which have significant differences in levels of prevalence among practices as measured through assured criteria (QOF).
5Page 39 of 324
Progress on the Mobilisation of the Ealing Standard – Contract
All 76 practices have signed the contract for the Ealing Standard and are progressing with delivery.
• The CCG and Londonwide LMC worked closely over several months to develop the contract
• The CCG extended the Heads of Terms originally signed in September 2017 to the end of May 18 to enable on going delivery pending completion of the contract
• The contract was released to practices on 20th April 2018• All 76 practices have signed the contract and are progressing with full delivery
Page 40 of 324
Progress on the Mobilisation of the Ealing Standard – Access – Part 1
All 76 practices have signed the contract for the Ealing Standard and are progressing with delivery.
The Access standard started 1st October 2017 across all practices which meant:• Practices began to explore ways to achieve the target of 100/1000 appointments
per weighted patient as of October 2017. • All Practices provided additional capacity during winter• A number of practices have employed additional workforce in order to deliver
additional capacity• This coincided with the changes in the National Contract where practices could
not claim for Extended Hours Enhanced Services, if they were closed half a day during the week.
• Only 24 (32%) practices are now closed half day per week, compared to 43 (57%) in April 2017. One of the ambitions of this contract is that by April 2020, all patients will be able to access primary medical services 8-6.30 Monday to Friday.
• We are working with practices to reduce the number of practices closing during core hours
• In order to compare the number of appointments offered to each practice, the CCG has worked to establish a template for how practices should use their appointment system, which is being mobilised at practice level at present.
Page 41 of 324
• The solution to access in Primary Medical Services, does not rely on the contract alone, but also being able to retain and recruit a variety of workforce to man the clinics for the additional hours.
• The funding associated with the Ealing Standard contract gives practices the confidence to recruit to a variety of posts substantively or commit to longer term contracts, which helps to attract and retain staff in the local area. The commissioning approach previously committed funding on an annual basis and therefore practices were reluctant to recruit for longer periods of time.
• In addition, Ealing Community Education Provider Network (CEPN) which is hosted by Ealing CCG, has run a number of courses for staff in primary care to upskill the existing and new workforce, again creating an additional incentive of training for staff and improving staff satisfaction as they feel valued and supported. The feedback has been extremely positive.
• Since 2016, the CEPN has run 368 courses for various clinical and non-clinical staff, with 8,138 attendees to date (individuals attend more than one training course).
• The training ranges from Clinical courses, such as ECGs, to customer service. • A National workload tool has also been launched to support practices to
understand their workforce utilisation. These tools were piloted in a number of Ealing Practices.
Progress on the Mobilisation of the Ealing Standard – Access Part 2
Page 42 of 324
Practices are also exploring new and innovative ways to increase access, e.g. telephone triage/appointment, or Online access to appointments etc.
Engagement:
• Since before the business case was approved, Ealing CCG has worked closely with its members and the LMC to co-produce the 23 Standards of care
• The contract is an evolution of the Out of Hospital Contract, which was let across Inner NWL CCGs
• The engagement included, co-production workshops, drop-in sessions, paper based reviews and challenge sessions. The approval process also included a review by an independent panel to ensure the funding being applied to the contract would deliver value for money.
• Following GB approval of the business case, the CCG established a mobilisation steering group, which was chaired by a Lay Member of the CCG Governing Body
• Regular update reports have also been presented to the Primary Care Commissioning Committee in the public part of the meeting.
• In addition, a communication was sent to the PPG groups in practices to explain the contract.
Page 43 of 324
Contract Management:
Practice Meetings• Since the start of the contract, 72 of the 76 practices have been visited by
the team at the CCG.The meeting is an opportunity to:• clarify any issues, • ensure all the standards are being provided for either at the practice or a
practice close by, • resolve any issues, • support the practice with any issues with referring patients to other services, • remind the practice of training opportunities, • review activity and performance against the contract, • resolve finance queries etc.
The team intend to meet each practice at least 3 times a year at the practice as a part of the contract management approach
If the practice requires additional support, the team would visit the practice more often
Page 44 of 324
Contract Management:
Network Meetings
Part of the contract is for practices to work together to find solutions and ensure population coverage. E.g. it may not be appropriate for all practices to provide Anticoagulation services, as the volume of patients to monitor may be small (in a small practice) and national training competencies suggest that a practice has to monitor a certain number of patients to maintain a level of competency. Therefore some services are provided by a practice on behalf of a few small local practices.
The CCG therefore encourages networks to meet quarterly or more frequently if they prefer at which they ensure population coverage, work to find solutions to support each other, share good practice or think through new models of care.
Page 45 of 324
Population coverage – as of April 2018:
• All 76 practices are delivering the capitated and prevalence based standards to their own patients
• Practices have identified those activity based standards they are providing for their own patients and on behalf of colleagues across their networks
• We have coverage for all Standards across all 7 networks with practices working collaboratively to ensure delivery.
IT and Business Intelligence
IT Templates• There are two systems that GPs in Ealing use. 74 practices use SystmOne and 2
practices use EMIS Web• For each standard and for each system, a template has been created to collate all
the information relevant to that standard. • The template acts as a reminder to the individual clinician on the requirements of
the standard, but also captures the information required to monitor the contract. • Each template has been developed with each clinical lead to ensure the accuracy of
the template and that it supports clinical conversations with patients.Page 46 of 324
IT and Business Intelligence contd.
Business Intelligence• In parallel, the CCG business intelligence team have worked with our clinical leads to
create dashboards that help practices understand progress against each standard, but also support payment and achievement against the KPIs.
• The first draft of the dashboard was released to practices in August. The data is still being checked for accuracy to ensure the information being collated out of systems is robust.
To ensure that the information being collated from the systems is accurate and the information being shared is consistent practice to practice, a number of iterations have been published of the IT template.
In addition the BI team have released Data Quality Reports, which practices can run directly in the system and check on a real time basis how they are performing.
Training and support has been available to all practices.
The templates for EMIS practices have not yet been published.
Page 47 of 324
Conclusion
The CCG has worked very closely with practices to mobilise the Ealing Standard
This is a complex programme with potentially a lot of positive impact on outcomes for Ealing registered patients.
It is essential that the programme focusses not only on the delivery of the contract itself, but also the support to practices in recruiting and retaining a variety of workforce to deliver core services as well as this contract as well as using the IT systems to full effect.
Future papers will provide an update on progress against the delivery of the contract.
Page 48 of 324
1
Contains Confidential or Exempt Information
NO
Title Update on progress in relation to Special Educational Needs & Disability Reforms
Responsible Officer(s) Judith Finlay - Executive Director of Adults, Children and Public Health Tessa Sandall, Managing Director Ealing CCG
Author(s) Natasha Patten – Designated Clinical Officer for SEND, Ealing and Hounslow CCGs. John Miller – Head of Special Educational Needs and Disabilities and Principal Educational Psychologist
Portfolio(s) Cllr Yvonne Johnson – Cabinet Member for Schools and Children’s Services
For Consideration By Health & Wellbeing Board
Date to be Considered 18th September 2018
Implementation Date if Not Called In
N/A
Affected Wards All
Keywords/Index Children & young people with special educational needs & disabilities
Purpose of Report: The purpose of this report is to provide an update on the local implementation of the Special Educational Needs and Disabilities (SEND) reforms to the members of the Health and Wellbeing Board.
1. Recommendations
i. To note progress made with the SEND Strategic plan and updated Self-
Evaluation ii. To update on preparation for the joint CQC / Ofsted SEND local area inspection
2. Reason for Decision and Options Considered
The report provides members of the Health and Well Bring Board the opportunity to comment on the progress made in implementing the SEND Reforms and
Report for: ACTION/INFORMATION
Item Number: 8
Page 49 of 324
2
consider preparations for the area inspection following the last update report presented in March 2018.
3. Key Implications On the 1st September 2014 the Children and Families Act came into effect. The
Act placed new duties on local authorities, schools and clinical commissioning
groups, on the delivery of services and support for disabled children and young
people and those with Special Educational Needs (SEN). A revised Code of
Practice for SEN & Disability (SEND) was published in 2015. The age range for
statutory education, health and care assessments has been extended to cover
the age range 0-25 years. The previous Statement covered young people until
they left school at age 16 or 19. Those attending college had a Learning
Disability Assessment (LDA). The timeframe for the statutory education, health
and care needs assessment has been reduced from 26 to 20 weeks.
On 1st April 2015 new duties for the provision of support to young people with
SEN in youth custody came into effect. Further statutory guidance on supporting
pupils with medical needs in schools was published in December 2015
3.1 Key principles of the reforms include:
The vision that all children and young people can succeed, no matter what
their background. Aspirations for children and young people will be raised
through an increased focus on life outcomes, including employment and
greater independence.
Early identification of a child’s special educational needs and disabilities with
support routinely put in place quickly, and information for parents to inform
them what services they can reasonably expect to be provided.
Children and young people and their parents or carers will be fully involved in
decisions about their support and what they want to achieve.
Those with more complex needs will have an integrated assessment and
where appropriate, a single Education, Health and Care plan for their support
from education, health and social care.
Local authorities and their local health partners work together to implement the
new arrangements and jointly plan and commission services for children and
young people aged 0 to 25 years who have special educational needs or are
disabled.
3.2 Governance arrangements in Ealing
Arrangements for the local implementation of the SEND reforms are
overseen by the 0 to 25 SEND and Inclusion Executive Board, chaired
by the Local Authority’s Director of Children and Families. The Clinical
Commissioning Group’s (CCG) Deputy Managing Director for Service Redesign and the Designated Clinical Officer for SEND are members
of this Board. Following a recent refresh of the SEND Strategy there
Page 50 of 324
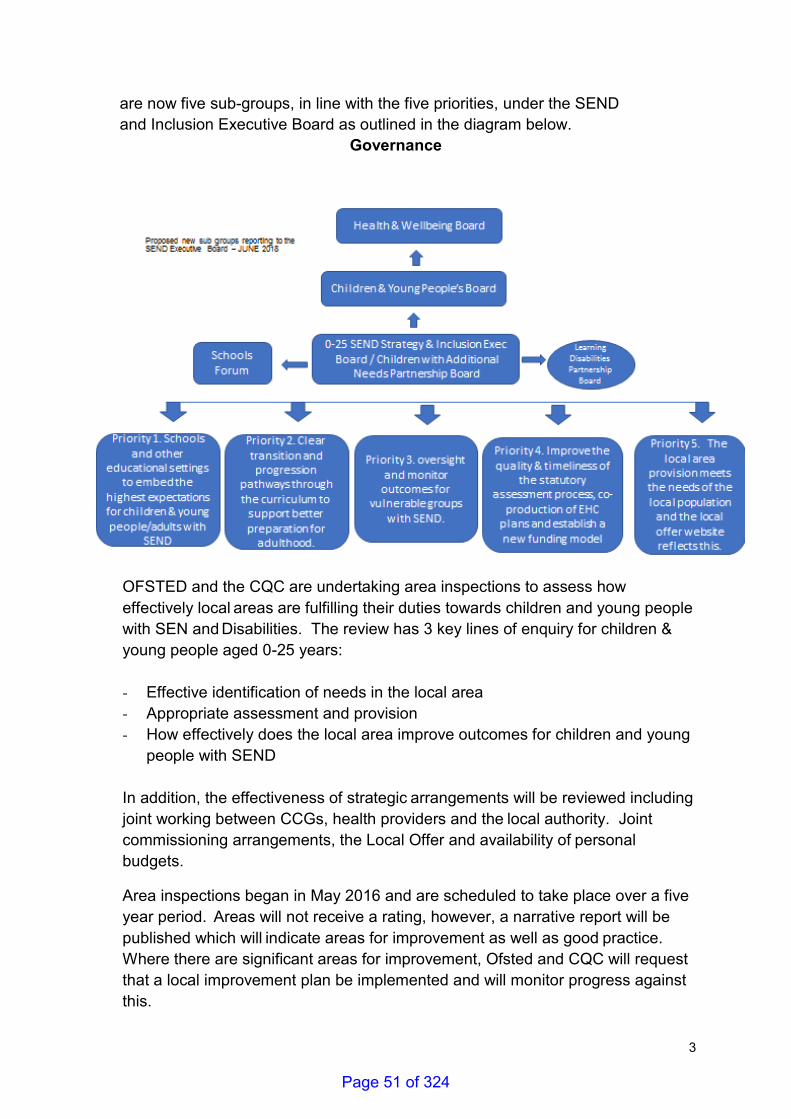
3
are now five sub-groups, in line with the five priorities, under the SEND
and Inclusion Executive Board as outlined in the diagram below.
Governance
OFSTED and the CQC are undertaking area inspections to assess how
effectively local areas are fulfilling their duties towards children and young people
with SEN and Disabilities. The review has 3 key lines of enquiry for children &
young people aged 0-25 years:
- Effective identification of needs in the local area
- Appropriate assessment and provision
- How effectively does the local area improve outcomes for children and young
people with SEND
In addition, the effectiveness of strategic arrangements will be reviewed including
joint working between CCGs, health providers and the local authority. Joint
commissioning arrangements, the Local Offer and availability of personal
budgets.
Area inspections began in May 2016 and are scheduled to take place over a five
year period. Areas will not receive a rating, however, a narrative report will be
published which will indicate areas for improvement as well as good practice.
Where there are significant areas for improvement, Ofsted and CQC will request
that a local improvement plan be implemented and will monitor progress against
this.
Page 51 of 324
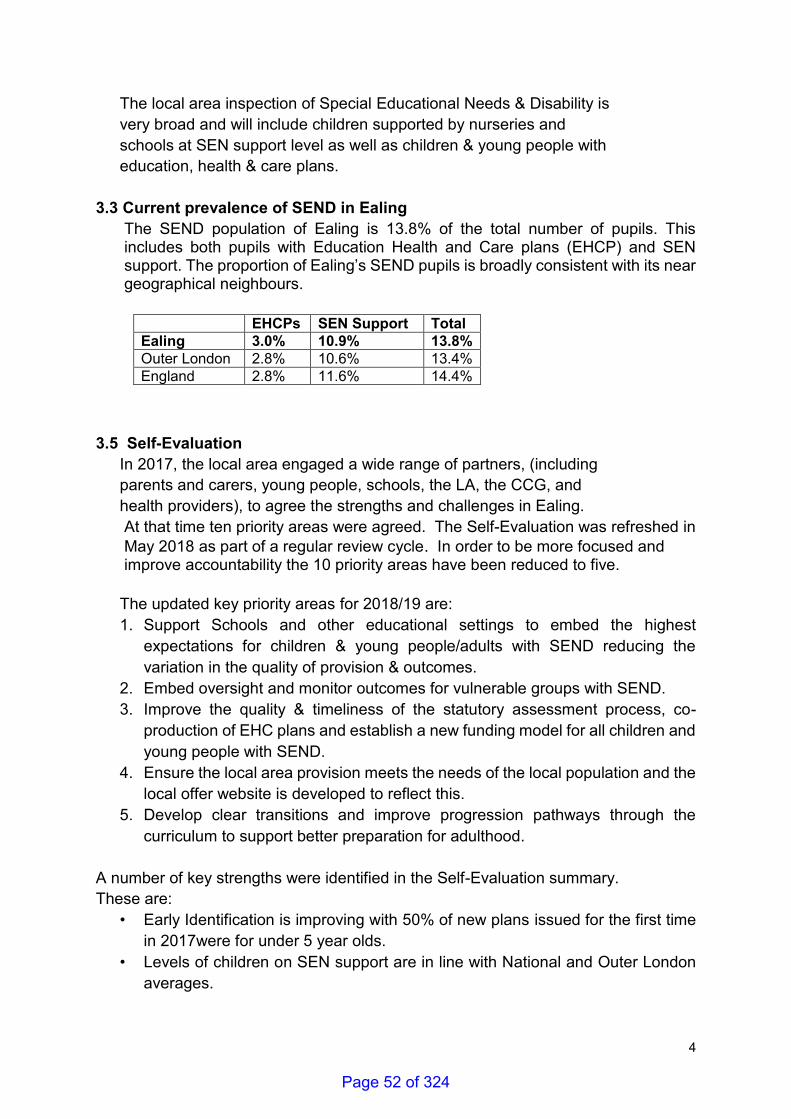
4
The local area inspection of Special Educational Needs & Disability is
very broad and will include children supported by nurseries and
schools at SEN support level as well as children & young people with
education, health & care plans.
3.3 Current prevalence of SEND in Ealing
The SEND population of Ealing is 13.8% of the total number of pupils. This includes both pupils with Education Health and Care plans (EHCP) and SEN support. The proportion of Ealing’s SEND pupils is broadly consistent with its near geographical neighbours.
3.5 Self-Evaluation
In 2017, the local area engaged a wide range of partners, (including
parents and carers, young people, schools, the LA, the CCG, and
health providers), to agree the strengths and challenges in Ealing.
At that time ten priority areas were agreed. The Self-Evaluation was refreshed in
May 2018 as part of a regular review cycle. In order to be more focused and improve accountability the 10 priority areas have been reduced to five.
The updated key priority areas for 2018/19 are:
1. Support Schools and other educational settings to embed the highest
expectations for children & young people/adults with SEND reducing the
variation in the quality of provision & outcomes.
2. Embed oversight and monitor outcomes for vulnerable groups with SEND.
3. Improve the quality & timeliness of the statutory assessment process, co-
production of EHC plans and establish a new funding model for all children and
young people with SEND.
4. Ensure the local area provision meets the needs of the local population and the
local offer website is developed to reflect this.
5. Develop clear transitions and improve progression pathways through the
curriculum to support better preparation for adulthood.
A number of key strengths were identified in the Self-Evaluation summary.
These are:
• Early Identification is improving with 50% of new plans issued for the first time
in 2017were for under 5 year olds.
• Levels of children on SEN support are in line with National and Outer London
averages.
EHCPs SEN Support Total
Ealing 3.0% 10.9% 13.8%
Outer London 2.8% 10.6% 13.4%
England 2.8% 11.6% 14.4%
Page 52 of 324
5
• Ealing uses its network of children centres, which are all judged to be good or
outstanding, to place young children with additional needs from the age of 2
onwards depending on need. The children centres offer supports a range of
multiagency services - allowing early identification and early help through to
specialist provision for children with profound and complex needs.
• Early Start has a specialist SEND team who provide consultancy and direct
support to families of young children as their needs emerge, enabling effective
early identification and support. Good links are made between the mandated
health checks. These are used to signpost families to appropriate services such
as specialist parenting classes, SLT led group sessions and more intensive
home learning support. The Early Years Placement Panel offers young children
with emerging SEND timely access to appropriate provision.
• Good progress is being made with co-production and participation in SEND
planning, For example termly meetings with Ealing Parent Carer Forum (EPCF)
creates a forum for the CCG and LA to become aware of parental issues arising
through the PCF.
• Ealing Mencap’s Power Group gives young people with SEND the chance to develop ideas and contribute to the planning of services to meet their social,
emotional and independence needs.
• Joint commissioning arrangements between LA and CCG are in place. There
are robust integrated arrangements in place via Section.75 agreements for
Early Start, ESCAN & the Community Team for People with Learning
Disabilities.
• Increase in communication and cooperation between ESCAN’s therapy
services and the EPCF, regularly delivering joint workshops for parents and
working together to develop better communication with parents as well as a
better understanding of each other’s perspectives. • The Building My Future project is being co-produced with and supported by
parents via the Ealing Parent Community Forum.
• We have a strong commitment to mediation; the number of disputes leading to
appeals or tribunals is low. This is a positive outcome for families.
3.6 Updates / Progress since March 2018:
Work is taking place to update the Joint Strategic Needs Assessment (JSNA) in
relation to SEND by the Council’s Public Health Service. It is intended to bring
together the JSNA into one chapter. It is anticipated that a first draft will be
completed by the end of December 2018. The scope of the JSNA will cover three
core areas: identifying SEND; assessing and meeting need and improving
outcomes. Areas of focus will include transition into adulthood and vulnerable
groups within SEND. It is anticipated that this chapter will highlight any current
gaps and will offer recommendations for the health and wellbeing board.
Page 53 of 324
6
One of the issues raised out of the self-evaluation was long waiting lists for a
diagnostic assessment for Autism. A review of the Autism assessment pathway
was completed between March and June 2018. The findings of the work were
ratified in a multi-agency feedback session in July, with agreement to establish
four task and finish groups to develop improvement plans. Action plans are in
process of being developed and will be fed into the Autism Board on 13th
September 2018, where they will be monitored.
A new Local Offer website was launched on 2nd July 2018. This updated website
is more user friendly and contains more information.
Local Authorities are required to undertake and complete the statutory Education,
Health and Care assessment within 20 weeks. Challenges in meeting this Key
Performance Indicator (KPI) across the whole system still remain. There is a
detailed action plan in place to improve the KPI of meeting the 20 week
timescale, which is being rigorously monitored by senior managers on a
fortnightly basis.
Schools have a duty to meet the needs of pupils in schools with medical
conditions. Public Health led a multiagency working group across health and
education to develop and consult on a policy ‘Supporting pupils at schools with medical conditions’ which is planned to be launched in the Autumn Term 2018. In order for this policy to support the whole range of medical needs which
may be experienced by children in schools and offer a graduated approach to
include universal and specialist services available, the Designated Clinical Officer
for SEND and Children’s Continuing Care Manager will be providing supporting
documentation for more complex health needs which will be taken to the CCG for
approval in October 2018.
A review of SEND provision has been undertaken and stakeholders views
obtained on: supporting local schools to meet the needs of pupils with SEND;
providing more places in Additionally Resourced Provision attached to
mainstream school (ARPS) and better preparation for adulthood. The
conclusions of the review have been analysed and in general there is support for
more places in ARPs which will underpin SEND strategy moving forward.
Proposals will be considered to extend the age range to Springhallow to 19 to
provide more local and cost effective provision for children with Autism. This
links with the SEND strategy and five priorities.
The DfE funded Building My Future Project is now operational and taking referral
since June 2018. The BMF project model aims to prevent school breakdown for
young people aged 11-25 years who have a learning difficulty and behaviour that
challenges or mental health issues, and who may be at risk at exclusion.
Page 54 of 324
7
4. Financial Education provision for children and young people with SEND is funded by the
local authority through the High Needs Block of the Dedicated Schools Grant.
For 2018-19 the Council’s HNB is £52.9m before deductions for places funded for Ealing residents by the Education Skills and Funding Agency.
The increased child population in Ealing has had a significant impact on the number of children and young people requiring statutory education, health and care assessments. In 2013 there were 1631 statutory plans and in 2016/17 there were
2055 statutory plans, representing a 26% increase over a 3 year period. There was a
further increase in 2017 to 2,022. Based on past trends, the number of EHCPs is projected to increase to 2,350 in the next 5 years.
Like most London local authorities, Ealing is facing significant pressures on its
High Needs Block. The projected growth on the HNB is £2.2m in 2018-19 and a
further £2.1m in 2019-20.
For 2018-19, the Schools Forum, a group consisting of representatives of head
teachers and governors, agreed to transfer £1.2m from the mainstream schools
funding block towards these pressures. In doing so, it asked the LA and partner
agencies to undertake thorough review of high needs spending.
The CCG and LA provide specialist services funding for Ealing Service for
Children with Additional Need, (ESCAN) and Community Team for People with
Learning Disabilities, (CTPLD). In addition, there is a range of other health
provision funded by CCG for example Speech and Language Therapy and
Specialist School Nursing.
The CCG is also working with partners to improve access and provision for
children and young people with mental health needs via the CAMHS
Transformation programme. This includes our focus on the development of a
North West London CAMHS model of care, within a Children and Young
People’s Emotional Wellbeing and Mental Health service Delivery Framework, which will result in a revised Tier 3 Service Specification in year.
5. Legal
Special educational needs and disabilities statutory provision is set out
in the Children and Families Act 2014. This seeks to improve services
for vulnerable children and young people (0 to 25) and to support
families. The Act and the associated major reform programme are
underpinned by the Special Educational Needs and Disability (SEND)
Code of Practice and a set of SEND Regulations.
Page 55 of 324
8
6. Value For Money
A key part of managing the pressures in high needs is to ensure that the provision is as cost effective as possible.
7. Sustainability Impact Appraisal None
8. Risk Management
Progress on implementing the SEND reforms is considered and reviewed at the
SEND and Inclusion Executive Board. There would be a risk to the local area’s reputation if the outcome of the SEND inspection was poor. Financial
pressures are reviewed as part of the Council’s budget monitoring setting and monitoring processes
9. Community Safety Not applicable.
10. Links to the 6 Priorities for the Borough
The Future Ealing Priorities that are relevant to children & young people with
SEND are:
Children and young people fulfil their potential
Children and young people grow up safe from harm
Residents are physically and mentally healthy, active and independent
The CCG’s business plan outlines key priorities and projects linked to the Sustainability and Transformation Plan (STP). The SEND Health action plan sits
under the strategic objective ‘Eliminating unwarranted variation and improving long term condition management’ in this plan. The CAMHS Transformation plan sits under strategic objective of ‘Improving outcomes for children and adults with mental health needs’ and forms the local plan for the North West London
children and young people’s mental health and transformation plan
11. Equalities, Human Rights and Community Cohesion
This report concerns a number of groups – children; young people with additional
needs and disabilities; parent and young carers. Schools and services are
required to make reasonable adjustments for children in line with the Equality Act
2010. An EIA was not necessary as this is an update report.
Page 56 of 324
9
12. Staffing/Workforce and Accommodation implications: The Designated Clinical Officer for SEND has carried out three workshops with
CAMHS to improve their knowledge and understanding of responsibilities in
relation to the SEND Reforms. Briefing sessions with other health and social
care staff have also been carried out to improve understanding and improve
processes for engagement with the reforms.
13. Property and Assets
Not applicable.
14. Any other implications: Not applicable.
15. Consultation
In line with best practice of engaging with service users and a key principle in the implementation of the SEND reforms, engagement is ongoing in the borough. There are several examples of this including:
A workshop was held on 17th January 2017 with health, education, care, voluntary sector agencies, parents and young people representatives to contribute to the development of, and priority setting for the SEND Action Plan.
Representatives from the Parent Carer Forum (PCF) are on the SEND Executive Board and subgroups. PCF representatives have also been involved in specific projects in the borough e.g. co-producing outcomes pilot.
ESCAN meet termly with the PCF where issues are highlighted and resolutions sought. The Designated Clinical Officer for SEND (DCO) also attends this meeting.
Send Provision review included a range of views from stakeholders including parents and carers.
16. Timetable for Implementation
Time scales for actions are outlined in the SEND & Inclusion Strategic Plan (see
appendix). The Local Authority and CCG will be given 5 days notice for the local
area SEND Review. Reviews occur during term-time only and take place over a
week.
17. Appendices
Draft SEND & Inclusion Strategic Plan 2018-19
18. Background Information
Report submitted to Health and Wellbeing Board in July 2016: SEN and
Disability – Ealing’s Inclusion Strategy for children and young people aged 0-25,
and in March 2018: Update on progress in relation to Special Educational
Needs & Disability Reforms
Page 57 of 324
10
Consultation (Mandatory)
Name of consultee
Post held Date sent to
consultee
Date response received
Comments appear in
paragraph:
Internal
Debbie Grey AD ESCAN 23 August 2018
28 August 2018
3.6
Vaish Madden Public Health consultant 28 August 2018
28 August 2018
3.6
Bethan Loveless Public Health Registrar 24 August 2018
28 August 2018
3.6
External
Report History
Decision type: Urgency item?
EITHER: Key decision OR Non-key decision OR For information (delete as applicable)
Yes / No (delete as applicable) [Is it a general or special urgency key decision, which was not included in the Forward Plan with at least one month’s notice ?] If yes, set out the reasons both why the item was not included and why a decision cannot be deferred.
Report no.: Report author and contact for queries:
Natasha Patten – Designated Clinical Officer for SEND, Ealing and Hounslow CCGs. John Miller – Head of Special Educational Needs and Disabilities and Principal Educational Psychologist
Page 58 of 324
DRAFT
Achieving Excellence & Raising Expectations
Every child and young person has the greatest possible opportunity to be the best they can be, to be happy and have
choice and control over their support to lead the life they have chosen
SEND & Inclusion Strategic Plan 2018-19
Building communities that benefit everybody through collaboration, communication, cohesion
Updated August 2018
Page 59 of 324
2
Introduction
The SEN and Inclusion Strategy ‘Achieving Excellence & Raising Expectations’ is a 3 year strategy 2015-18 with three strategic priorities and an
action plan setting out actions and success criteria. Early in 2017 key stakeholders across the local area met to agree what the key strengths and
challenges were as part of the local area self-assessment of special educational needs and disability provision.
This action plan merges the 2015-2018 strategy plan with the 5 priorities arising from the local area self- assessment (2018). It is a strategic
document designed to enable the SEND Executive Board to monitor and drive improvements in SEN & Disability services across the local area.
There may be other action plans, specific to individual organisations/services that sit below this document.
The SEN and Inclusion strategy ‘Achieving Excellence & Raising Expectations’ will align with this action plan until 2019.
Since 2014 there have been significant changes nationally in the education landscape with:
- An increasing number of academies and free schools and increasing autonomy in schools.
- A new curriculum and new assessment system
- Confirmation that the recommendations in the Rochford Review on assessment and reporting of progress for children and young people with
SEND will be implemented.
- Schools Funding Reforms - from April 2018 most Dedicated Schools Grant funds will be delegated directly to schools and only the High
Needs Block (HNB) will come to the local authority with less flexibility for transferring funding between funding blocks.
-
Locally demand for statutory education, health & care assessments has increased in line with the population increase and nationally it is recognised
that there are still challenges in the system and local areas for example:
The Council for Disabled Children (CDC) published two significant reports: ‘Understanding the Needs of Disabled Children with Complex Needs or
Life-Limiting Conditions’ and ‘These Are Our Children’ a review of agencies responses to children & young people with disabilities/Autism and
Page 60 of 324
3
behaviour that challenges. The latter report identifies Ealing Service for Children With additional needs for its innovative Intensive Therapeutic
Short-Breaks, (ITSBS) service model to enable children and young people’s needs to be met locally.
In June 2017 Children’s Services were successful in the DfE innovation bid of £1.6M to fund the ‘Building my Future’ (BMF) project. BMF will build
on the ITSBS model to target young people aged 11-25 years with a learning difficulty, mental health issues and behaviour that challenges. The
cohort will largely be in mainstream schools at SEN support level or with an EHCP. BMF is important for our strategy as we have identified a high
number of exclusions within the project target group.
Strategically across the council via Future Ealing the intention is to focus on what matters to residents; to concentrate on the outcomes. Under
Future Ealing, we are looking to strengthen employment opportunities for young adults with SEND through a more co-ordinated approach. A
number of council services are involved in the employability agenda and together aim to expand pathways to employment and sustained
employment for young people with SEND.
The 3 strategic key themes set for 2015-18 remain into 2019:
A. Young people to be included in all aspects of their lives enjoy the experience and achieve well.
B. Improve outcomes for children and young people with SEND and their families
C. Preparing for adulthood and employment
The previous action plan 2015-18 is now closed down and the revised version will be in operation 2018-19.
This revised action plan sets out:
o The 5 priorities agreed in March 2018 following the self-evaluation workshop in February.
o The actions needed in 2018/19 to achieve the 5 priorities
Page 61 of 324
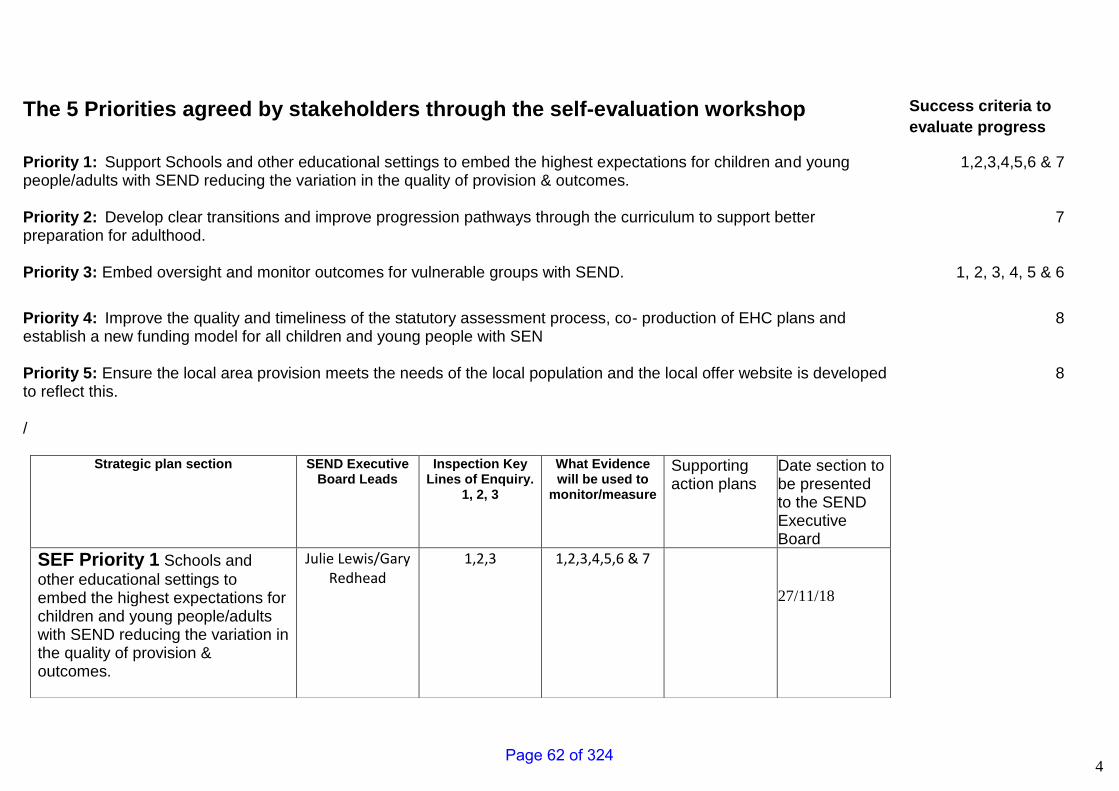
4
The 5 Priorities agreed by stakeholders through the self-evaluation workshop
Success criteria to
evaluate progress
Priority 1: Support Schools and other educational settings to embed the highest expectations for children and young people/adults with SEND reducing the variation in the quality of provision & outcomes.
1,2,3,4,5,6 & 7
Priority 2: Develop clear transitions and improve progression pathways through the curriculum to support better preparation for adulthood.
7
Priority 3: Embed oversight and monitor outcomes for vulnerable groups with SEND. 1, 2, 3, 4, 5 & 6
Priority 4: Improve the quality and timeliness of the statutory assessment process, co- production of EHC plans and establish a new funding model for all children and young people with SEN
8
Priority 5: Ensure the local area provision meets the needs of the local population and the local offer website is developed to reflect this. /
Strategic plan section SEND Executive Board Leads
Inspection Key Lines of Enquiry.
1, 2, 3
What Evidence will be used to
monitor/measure
Supporting action plans
Date section to be presented to the SEND Executive Board
SEF Priority 1 Schools and
other educational settings to embed the highest expectations for children and young people/adults with SEND reducing the variation in the quality of provision & outcomes.
Julie Lewis/Gary Redhead
1,2,3 1,2,3,4,5,6 & 7
27/11/18
8
Page 62 of 324
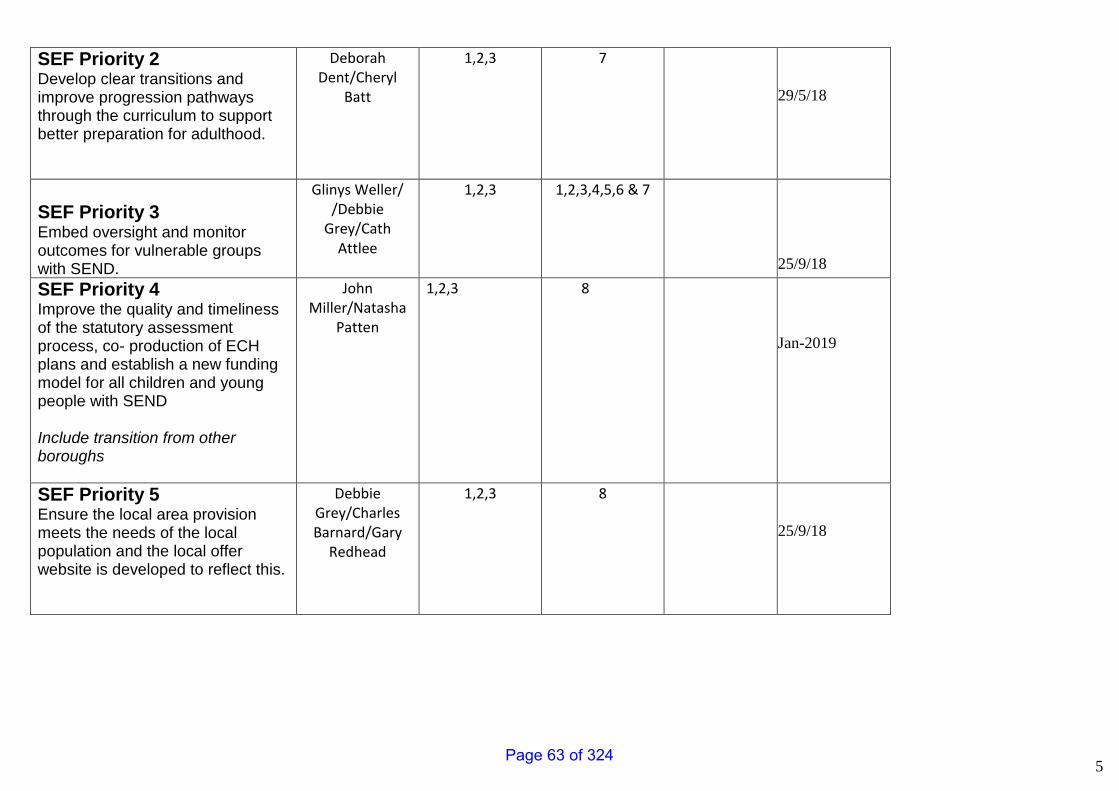
5
SEF Priority 2 Develop clear transitions and improve progression pathways through the curriculum to support better preparation for adulthood.
Deborah Dent/Cheryl
Batt
1,2,3 7
29/5/18
SEF Priority 3 Embed oversight and monitor outcomes for vulnerable groups with SEND.
Glinys Weller/ /Debbie
Grey/Cath Attlee
1,2,3 1,2,3,4,5,6 & 7
25/9/18
SEF Priority 4 Improve the quality and timeliness of the statutory assessment process, co- production of ECH plans and establish a new funding model for all children and young people with SEND Include transition from other boroughs
John Miller/Natasha
Patten
1,2,3 8
Jan-2019
SEF Priority 5 Ensure the local area provision meets the needs of the local population and the local offer website is developed to reflect this.
Debbie Grey/Charles Barnard/Gary
Redhead
1,2,3 8
25/9/18
Page 63 of 324
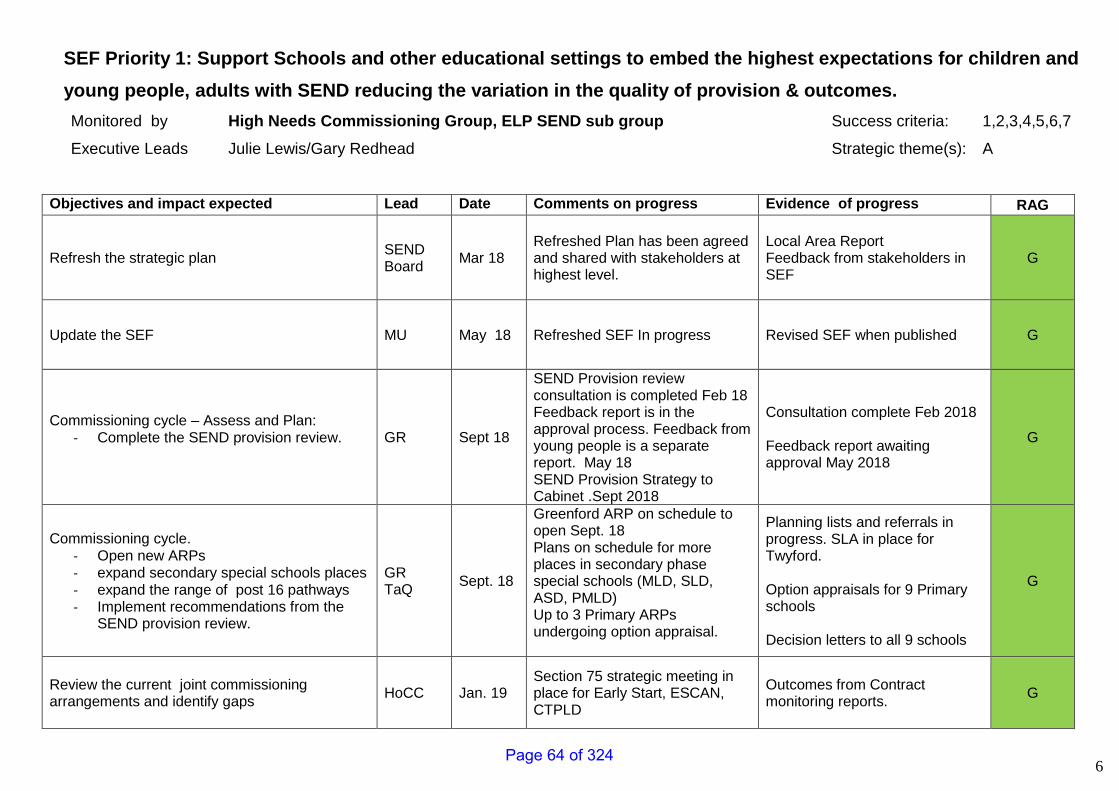
6
SEF Priority 1: Support Schools and other educational settings to embed the highest expectations for children and
young people, adults with SEND reducing the variation in the quality of provision & outcomes.
Monitored by High Needs Commissioning Group, ELP SEND sub group Success criteria: 1,2,3,4,5,6,7
Executive Leads Julie Lewis/Gary Redhead Strategic theme(s): A
Objectives and impact expected Lead Date Comments on progress Evidence of progress RAG
Refresh the strategic plan SEND Board
Mar 18
Refreshed Plan has been agreed and shared with stakeholders at highest level.
Local Area Report Feedback from stakeholders in SEF
G
Update the SEF MU May 18 Refreshed SEF In progress Revised SEF when published G
Commissioning cycle – Assess and Plan: - Complete the SEND provision review.
GR Sept 18
SEND Provision review consultation is completed Feb 18 Feedback report is in the approval process. Feedback from young people is a separate report. May 18 SEND Provision Strategy to Cabinet .Sept 2018
Consultation complete Feb 2018 Feedback report awaiting approval May 2018
G
Commissioning cycle. - Open new ARPs - expand secondary special schools places - expand the range of post 16 pathways - Implement recommendations from the
SEND provision review.
GR TaQ
Sept. 18
Greenford ARP on schedule to open Sept. 18 Plans on schedule for more places in secondary phase special schools (MLD, SLD, ASD, PMLD) Up to 3 Primary ARPs undergoing option appraisal.
Planning lists and referrals in progress. SLA in place for Twyford. Option appraisals for 9 Primary schools Decision letters to all 9 schools
G
Review the current joint commissioning arrangements and identify gaps
HoCC Jan. 19 Section 75 strategic meeting in place for Early Start, ESCAN, CTPLD
Outcomes from Contract monitoring reports.
G
Page 64 of 324
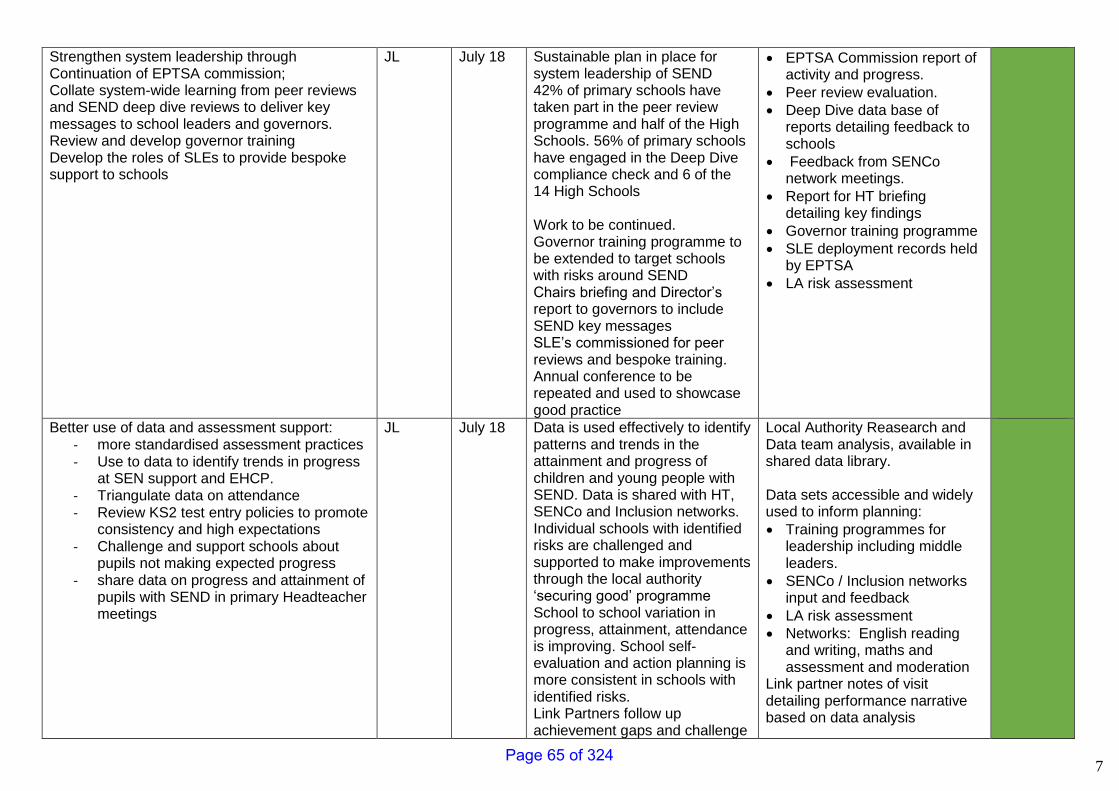
7
Strengthen system leadership through Continuation of EPTSA commission; Collate system-wide learning from peer reviews and SEND deep dive reviews to deliver key messages to school leaders and governors. Review and develop governor training Develop the roles of SLEs to provide bespoke support to schools
JL July 18 Sustainable plan in place for system leadership of SEND 42% of primary schools have taken part in the peer review programme and half of the High Schools. 56% of primary schools have engaged in the Deep Dive compliance check and 6 of the 14 High Schools Work to be continued. Governor training programme to be extended to target schools with risks around SEND Chairs briefing and Director’s report to governors to include SEND key messages SLE’s commissioned for peer reviews and bespoke training. Annual conference to be repeated and used to showcase good practice
• EPTSA Commission report of activity and progress.
• Peer review evaluation.
• Deep Dive data base of reports detailing feedback to schools
• Feedback from SENCo network meetings.
• Report for HT briefing detailing key findings
• Governor training programme
• SLE deployment records held by EPTSA
• LA risk assessment
Better use of data and assessment support: - more standardised assessment practices - Use to data to identify trends in progress
at SEN support and EHCP. - Triangulate data on attendance - Review KS2 test entry policies to promote
consistency and high expectations - Challenge and support schools about
pupils not making expected progress - share data on progress and attainment of
pupils with SEND in primary Headteacher meetings
JL July 18 Data is used effectively to identify patterns and trends in the attainment and progress of children and young people with SEND. Data is shared with HT, SENCo and Inclusion networks. Individual schools with identified risks are challenged and supported to make improvements through the local authority ‘securing good’ programme School to school variation in progress, attainment, attendance is improving. School self-evaluation and action planning is more consistent in schools with identified risks. Link Partners follow up achievement gaps and challenge
Local Authority Reasearch and Data team analysis, available in shared data library. Data sets accessible and widely used to inform planning:
• Training programmes for leadership including middle leaders.
• SENCo / Inclusion networks input and feedback
• LA risk assessment
• Networks: English reading and writing, maths and assessment and moderation
Link partner notes of visit detailing performance narrative based on data analysis
Page 65 of 324
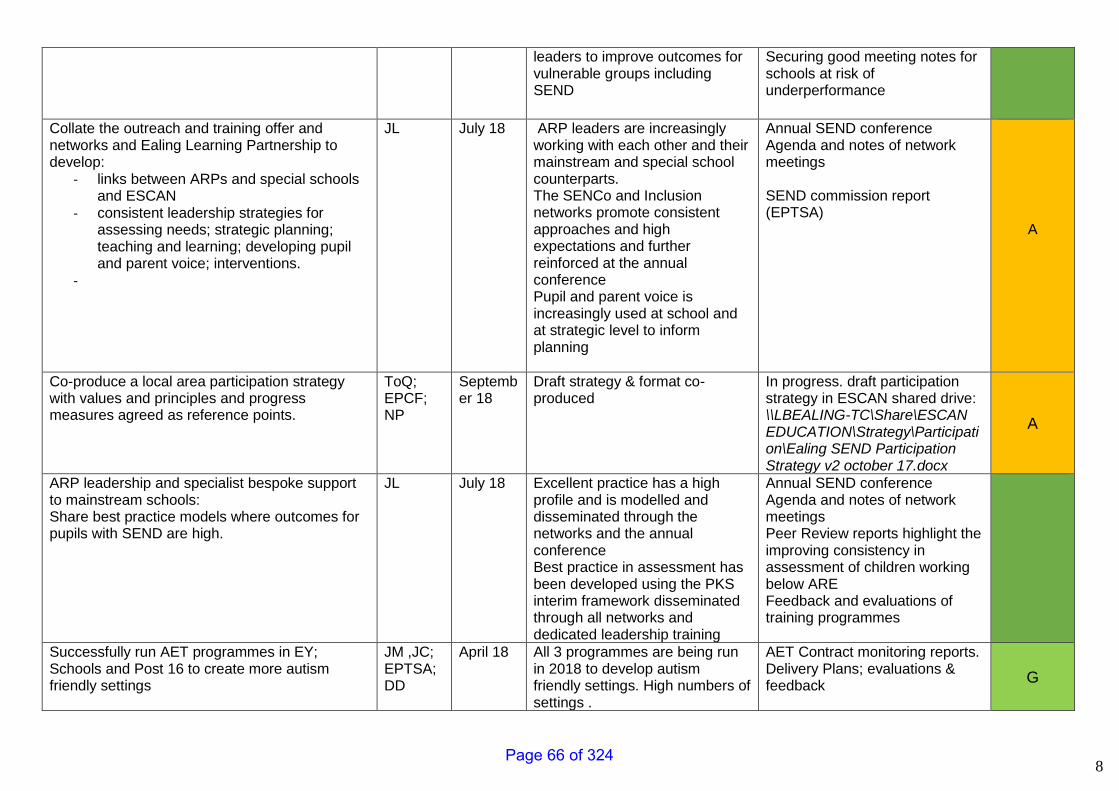
8
leaders to improve outcomes for vulnerable groups including SEND
Securing good meeting notes for schools at risk of underperformance
Collate the outreach and training offer and networks and Ealing Learning Partnership to develop:
- links between ARPs and special schools and ESCAN
- consistent leadership strategies for assessing needs; strategic planning; teaching and learning; developing pupil and parent voice; interventions.
-
JL July 18 ARP leaders are increasingly working with each other and their mainstream and special school counterparts. The SENCo and Inclusion networks promote consistent approaches and high expectations and further reinforced at the annual conference Pupil and parent voice is increasingly used at school and at strategic level to inform planning
Annual SEND conference Agenda and notes of network meetings SEND commission report (EPTSA)
A
Co-produce a local area participation strategy with values and principles and progress measures agreed as reference points.
ToQ; EPCF; NP
September 18
Draft strategy & format co-produced
In progress. draft participation strategy in ESCAN shared drive: \\LBEALING-TC\Share\ESCAN EDUCATION\Strategy\Participation\Ealing SEND Participation Strategy v2 october 17.docx
A
ARP leadership and specialist bespoke support to mainstream schools: Share best practice models where outcomes for pupils with SEND are high.
JL July 18 Excellent practice has a high profile and is modelled and disseminated through the networks and the annual conference Best practice in assessment has been developed using the PKS interim framework disseminated through all networks and dedicated leadership training
Annual SEND conference Agenda and notes of network meetings Peer Review reports highlight the improving consistency in assessment of children working below ARE Feedback and evaluations of training programmes
Successfully run AET programmes in EY; Schools and Post 16 to create more autism friendly settings
JM ,JC; EPTSA; DD
April 18 All 3 programmes are being run in 2018 to develop autism friendly settings. High numbers of settings .
AET Contract monitoring reports. Delivery Plans; evaluations & feedback
G
Page 66 of 324
9
- EY programme combines programmes previously run by early year’s services & therapy services into one model.
- Schools programme rolled out successfully.
- Post 16 programmes being run on sub-regional basis – aiming to link up with WLC.
Page 67 of 324
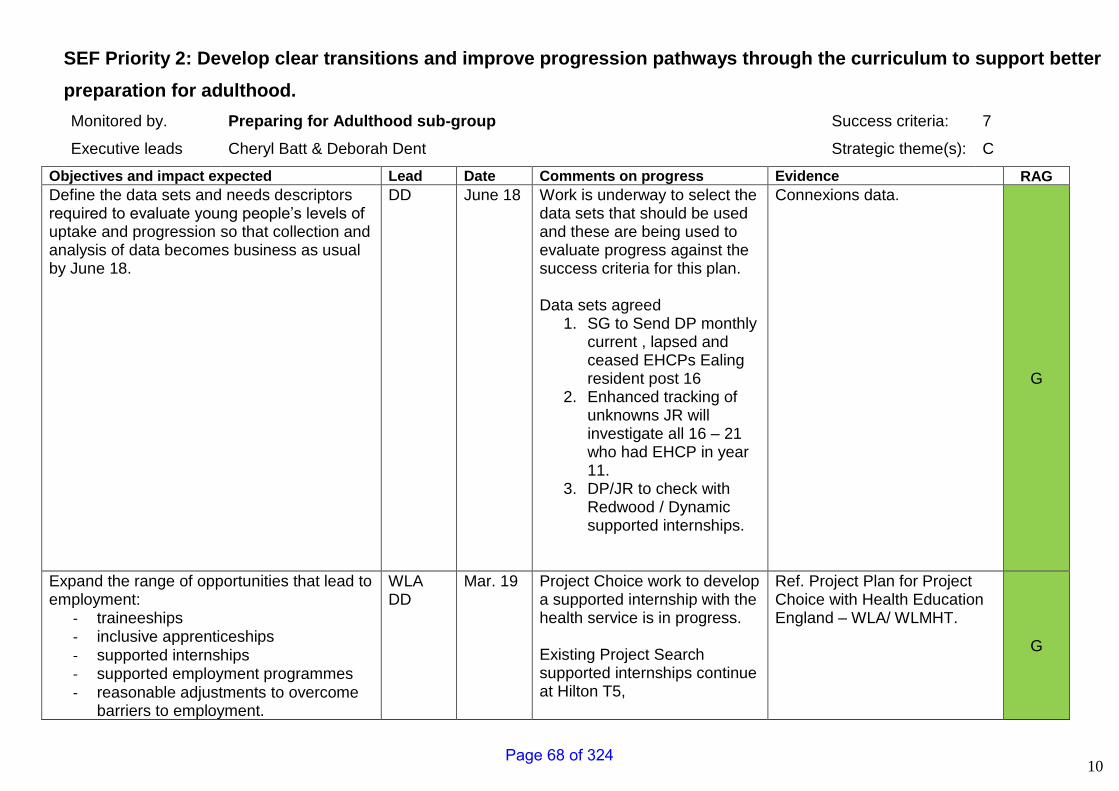
10
SEF Priority 2: Develop clear transitions and improve progression pathways through the curriculum to support better
preparation for adulthood.
Monitored by. Preparing for Adulthood sub-group Success criteria: 7
Executive leads Cheryl Batt & Deborah Dent Strategic theme(s): C
Objectives and impact expected Lead Date Comments on progress Evidence RAG
Define the data sets and needs descriptors required to evaluate young people’s levels of uptake and progression so that collection and analysis of data becomes business as usual by June 18.
DD June 18 Work is underway to select the data sets that should be used and these are being used to evaluate progress against the success criteria for this plan. Data sets agreed
1. SG to Send DP monthly current , lapsed and ceased EHCPs Ealing resident post 16
2. Enhanced tracking of unknowns JR will investigate all 16 – 21 who had EHCP in year 11.
3. DP/JR to check with Redwood / Dynamic supported internships.
Connexions data.
G
Expand the range of opportunities that lead to employment:
- traineeships - inclusive apprenticeships - supported internships - supported employment programmes - reasonable adjustments to overcome
barriers to employment.
WLA DD
Mar. 19 Project Choice work to develop a supported internship with the health service is in progress. Existing Project Search supported internships continue at Hilton T5,
Ref. Project Plan for Project Choice with Health Education England – WLA/ WLMHT.
G
Page 68 of 324
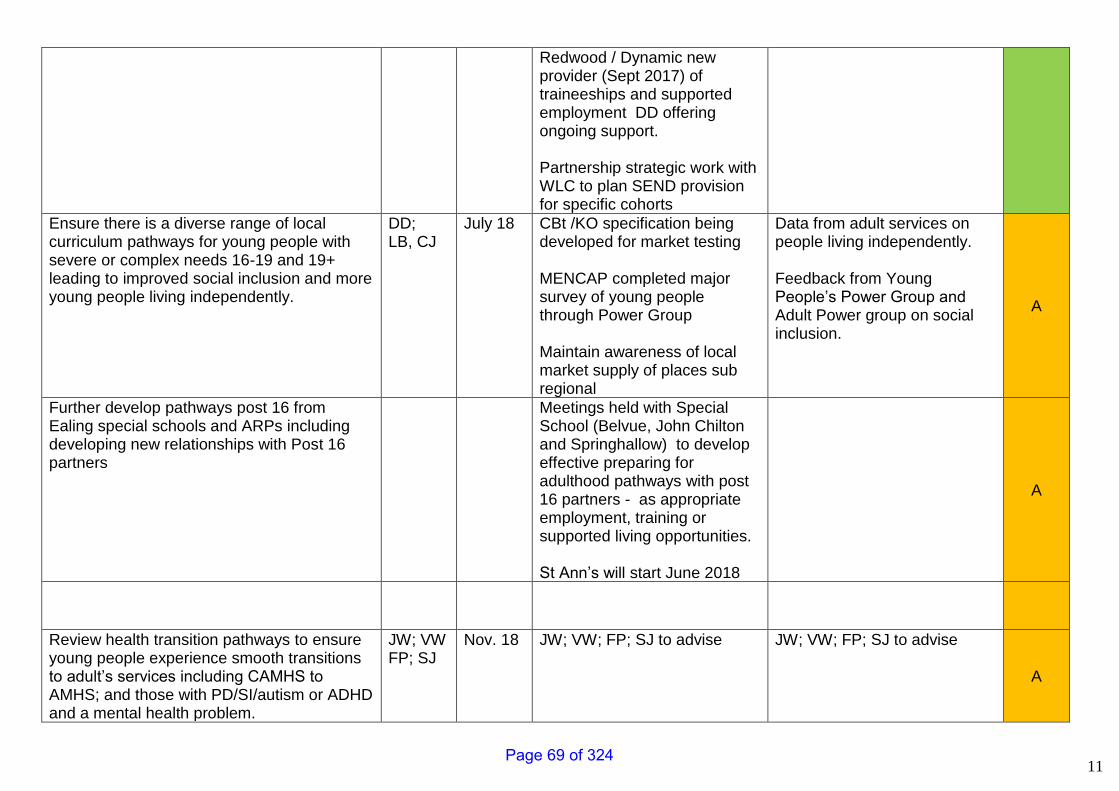
11
Redwood / Dynamic new provider (Sept 2017) of traineeships and supported employment DD offering ongoing support. Partnership strategic work with WLC to plan SEND provision for specific cohorts
Ensure there is a diverse range of local curriculum pathways for young people with severe or complex needs 16-19 and 19+ leading to improved social inclusion and more young people living independently.
DD; LB, CJ
July 18 CBt /KO specification being developed for market testing MENCAP completed major survey of young people through Power Group Maintain awareness of local market supply of places sub regional
Data from adult services on people living independently. Feedback from Young People’s Power Group and Adult Power group on social inclusion.
A
Further develop pathways post 16 from Ealing special schools and ARPs including developing new relationships with Post 16 partners
Meetings held with Special School (Belvue, John Chilton and Springhallow) to develop effective preparing for adulthood pathways with post 16 partners - as appropriate employment, training or supported living opportunities. St Ann’s will start June 2018
A
Review health transition pathways to ensure young people experience smooth transitions to adult’s services including CAMHS to AMHS; and those with PD/SI/autism or ADHD and a mental health problem.
JW; VW FP; SJ
Nov. 18 JW; VW; FP; SJ to advise JW; VW; FP; SJ to advise
A
Page 69 of 324
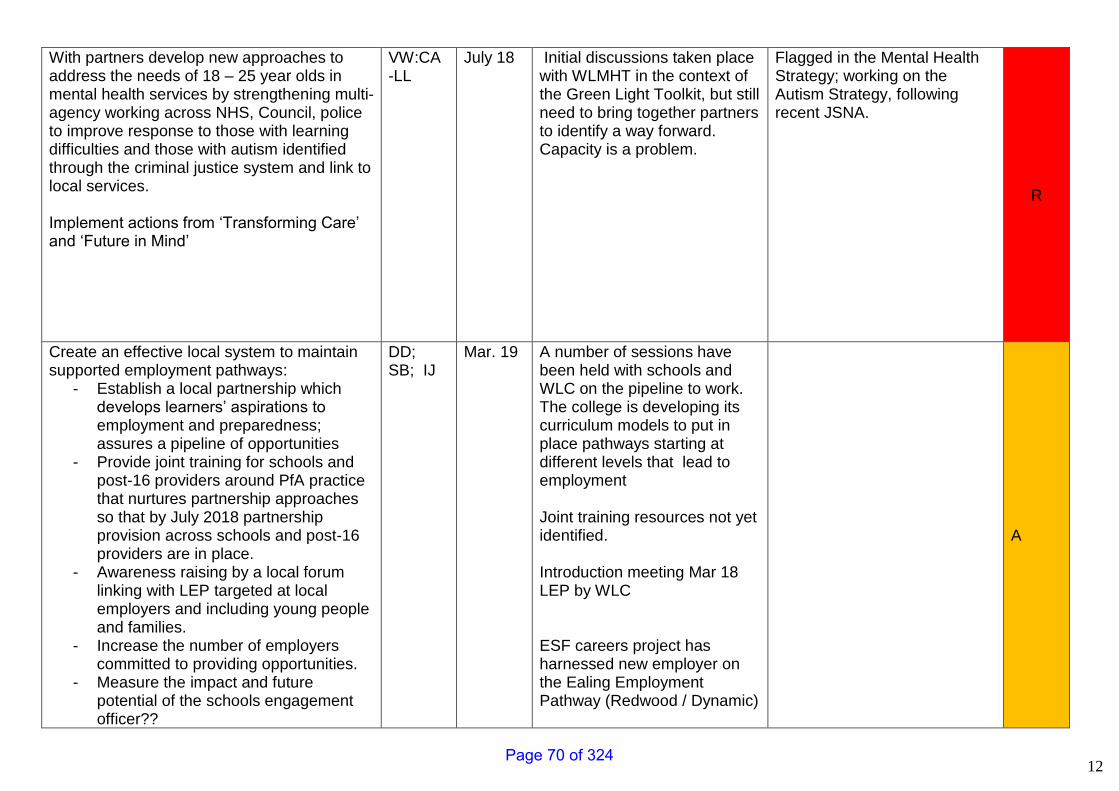
12
With partners develop new approaches to address the needs of 18 – 25 year olds in mental health services by strengthening multi-agency working across NHS, Council, police to improve response to those with learning difficulties and those with autism identified through the criminal justice system and link to local services. Implement actions from ‘Transforming Care’ and ‘Future in Mind’
VW:CA -LL
July 18 Initial discussions taken place with WLMHT in the context of the Green Light Toolkit, but still need to bring together partners to identify a way forward. Capacity is a problem.
Flagged in the Mental Health Strategy; working on the Autism Strategy, following recent JSNA.
R
Create an effective local system to maintain supported employment pathways:
- Establish a local partnership which develops learners’ aspirations to employment and preparedness; assures a pipeline of opportunities
- Provide joint training for schools and post-16 providers around PfA practice that nurtures partnership approaches so that by July 2018 partnership provision across schools and post-16 providers are in place.
- Awareness raising by a local forum linking with LEP targeted at local employers and including young people and families.
- Increase the number of employers committed to providing opportunities.
- Measure the impact and future potential of the schools engagement officer??
DD; SB; IJ
Mar. 19 A number of sessions have been held with schools and WLC on the pipeline to work. The college is developing its curriculum models to put in place pathways starting at different levels that lead to employment Joint training resources not yet identified. Introduction meeting Mar 18 LEP by WLC ESF careers project has harnessed new employer on the Ealing Employment Pathway (Redwood / Dynamic)
A
Page 70 of 324
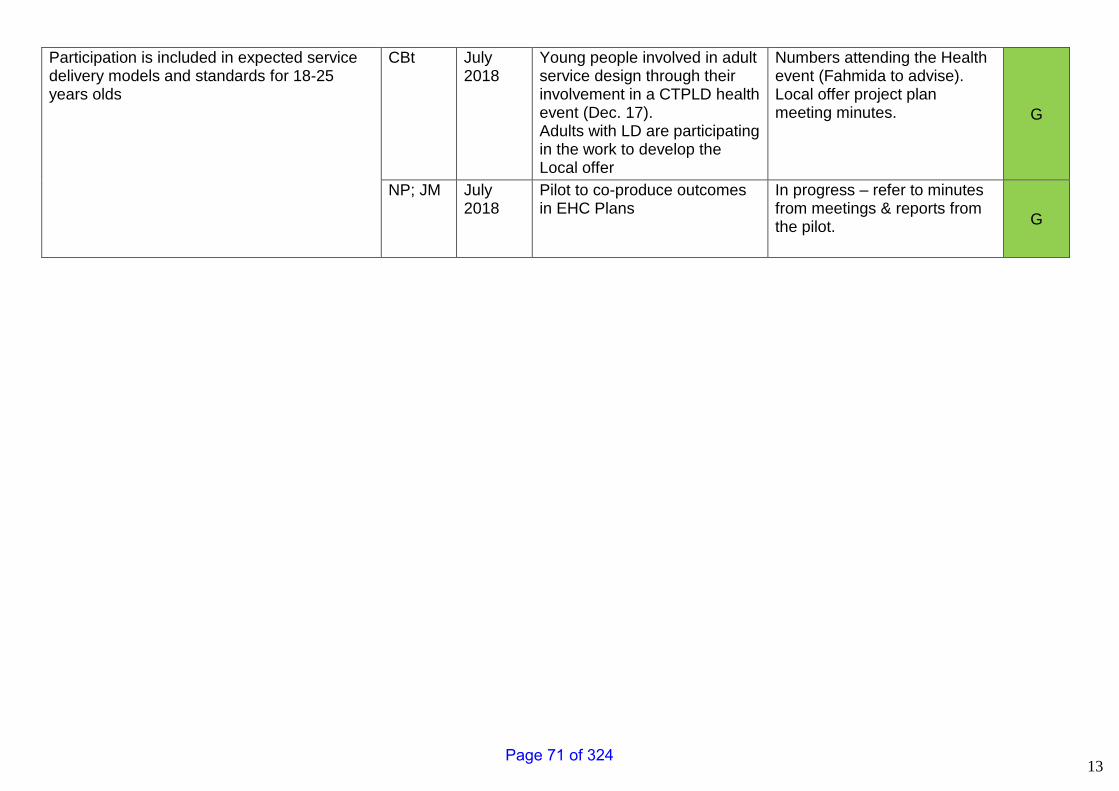
13
Participation is included in expected service delivery models and standards for 18-25 years olds
CBt July 2018
Young people involved in adult service design through their involvement in a CTPLD health event (Dec. 17). Adults with LD are participating in the work to develop the Local offer
Numbers attending the Health event (Fahmida to advise). Local offer project plan meeting minutes. G
NP; JM July 2018
Pilot to co-produce outcomes in EHC Plans
In progress – refer to minutes from meetings & reports from the pilot.
G
Page 71 of 324
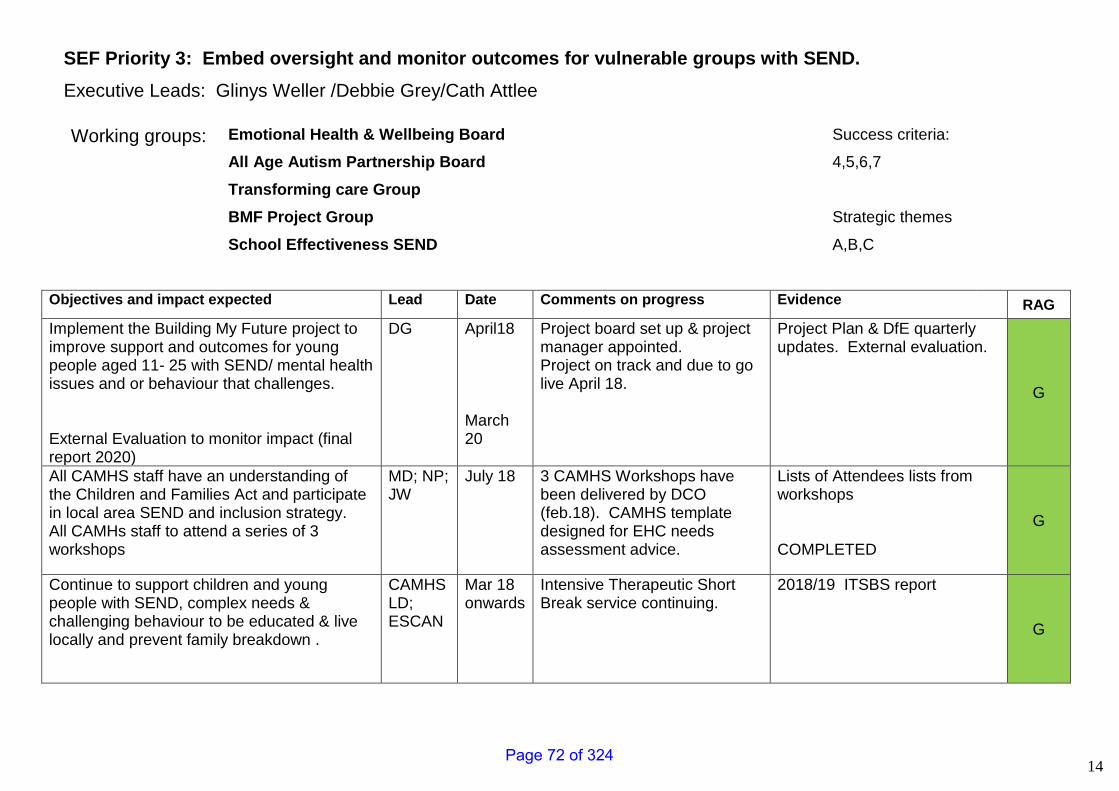
14
SEF Priority 3: Embed oversight and monitor outcomes for vulnerable groups with SEND.
Executive Leads: Glinys Weller /Debbie Grey/Cath Attlee
Working groups:
Emotional Health & Wellbeing Board
All Age Autism Partnership Board
Transforming care Group
BMF Project Group
School Effectiveness SEND
Success criteria:
4,5,6,7
Strategic themes
A,B,C
Objectives and impact expected Lead Date Comments on progress Evidence RAG
Implement the Building My Future project to improve support and outcomes for young people aged 11- 25 with SEND/ mental health issues and or behaviour that challenges. External Evaluation to monitor impact (final report 2020)
DG April18 March 20
Project board set up & project manager appointed. Project on track and due to go live April 18.
Project Plan & DfE quarterly updates. External evaluation.
G
All CAMHS staff have an understanding of the Children and Families Act and participate in local area SEND and inclusion strategy. All CAMHs staff to attend a series of 3 workshops
MD; NP; JW
July 18 3 CAMHS Workshops have been delivered by DCO (feb.18). CAMHS template designed for EHC needs assessment advice.
Lists of Attendees lists from workshops COMPLETED
G
Continue to support children and young people with SEND, complex needs & challenging behaviour to be educated & live locally and prevent family breakdown .
CAMHS LD; ESCAN
Mar 18 onwards
Intensive Therapeutic Short Break service continuing.
2018/19 ITSBS report
G
Page 72 of 324
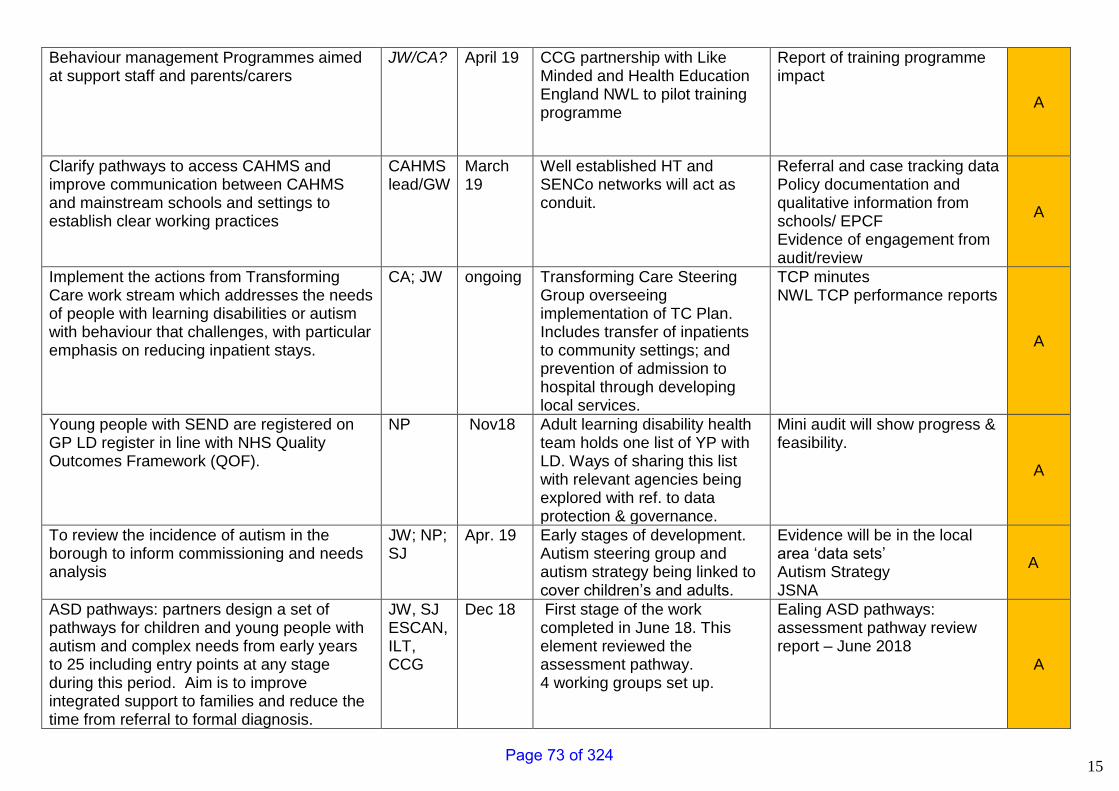
15
Behaviour management Programmes aimed at support staff and parents/carers
JW/CA? April 19 CCG partnership with Like Minded and Health Education England NWL to pilot training programme
Report of training programme impact
A
Clarify pathways to access CAHMS and improve communication between CAHMS and mainstream schools and settings to establish clear working practices
CAHMS lead/GW
March 19
Well established HT and SENCo networks will act as conduit.
Referral and case tracking data Policy documentation and qualitative information from schools/ EPCF Evidence of engagement from audit/review
A
Implement the actions from Transforming Care work stream which addresses the needs of people with learning disabilities or autism with behaviour that challenges, with particular emphasis on reducing inpatient stays.
CA; JW ongoing Transforming Care Steering Group overseeing implementation of TC Plan. Includes transfer of inpatients to community settings; and prevention of admission to hospital through developing local services.
TCP minutes NWL TCP performance reports
A
Young people with SEND are registered on GP LD register in line with NHS Quality Outcomes Framework (QOF).
NP Nov18 Adult learning disability health team holds one list of YP with LD. Ways of sharing this list with relevant agencies being explored with ref. to data protection & governance.
Mini audit will show progress & feasibility.
A
To review the incidence of autism in the borough to inform commissioning and needs analysis
JW; NP; SJ
Apr. 19
Early stages of development. Autism steering group and autism strategy being linked to cover children’s and adults.
Evidence will be in the local area ‘data sets’ Autism Strategy JSNA
A
ASD pathways: partners design a set of pathways for children and young people with autism and complex needs from early years to 25 including entry points at any stage during this period. Aim is to improve integrated support to families and reduce the time from referral to formal diagnosis.
JW, SJ ESCAN, ILT, CCG
Dec 18 First stage of the work completed in June 18. This element reviewed the assessment pathway. 4 working groups set up.
Ealing ASD pathways: assessment pathway review report – June 2018 A
Page 73 of 324
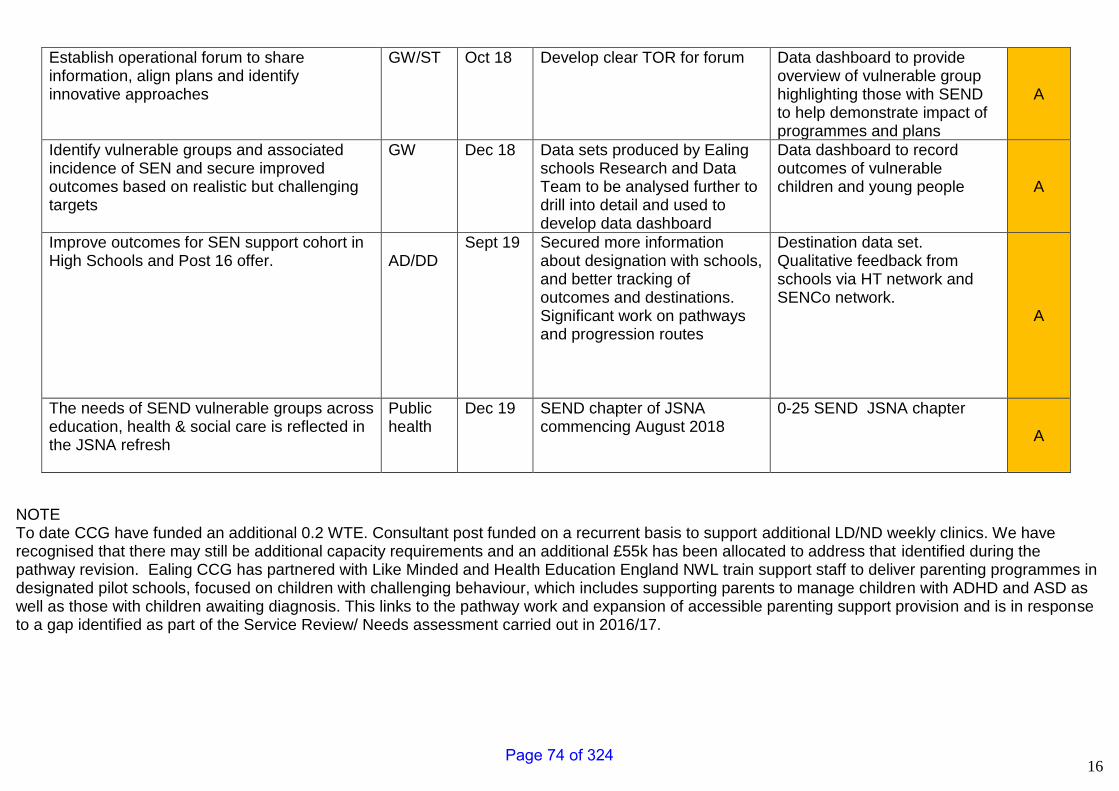
16
Establish operational forum to share information, align plans and identify innovative approaches
GW/ST Oct 18 Develop clear TOR for forum Data dashboard to provide overview of vulnerable group highlighting those with SEND to help demonstrate impact of programmes and plans
A
Identify vulnerable groups and associated incidence of SEN and secure improved outcomes based on realistic but challenging targets
GW Dec 18 Data sets produced by Ealing schools Research and Data Team to be analysed further to drill into detail and used to develop data dashboard
Data dashboard to record outcomes of vulnerable children and young people A
Improve outcomes for SEN support cohort in High Schools and Post 16 offer.
AD/DD
Sept 19
Secured more information about designation with schools, and better tracking of outcomes and destinations. Significant work on pathways and progression routes
Destination data set. Qualitative feedback from schools via HT network and SENCo network.
A
The needs of SEND vulnerable groups across education, health & social care is reflected in the JSNA refresh
Public health
Dec 19
SEND chapter of JSNA commencing August 2018
0-25 SEND JSNA chapter
A
NOTE To date CCG have funded an additional 0.2 WTE. Consultant post funded on a recurrent basis to support additional LD/ND weekly clinics. We have recognised that there may still be additional capacity requirements and an additional £55k has been allocated to address that identified during the pathway revision. Ealing CCG has partnered with Like Minded and Health Education England NWL train support staff to deliver parenting programmes in designated pilot schools, focused on children with challenging behaviour, which includes supporting parents to manage children with ADHD and ASD as well as those with children awaiting diagnosis. This links to the pathway work and expansion of accessible parenting support provision and is in response to a gap identified as part of the Service Review/ Needs assessment carried out in 2016/17.
Page 74 of 324
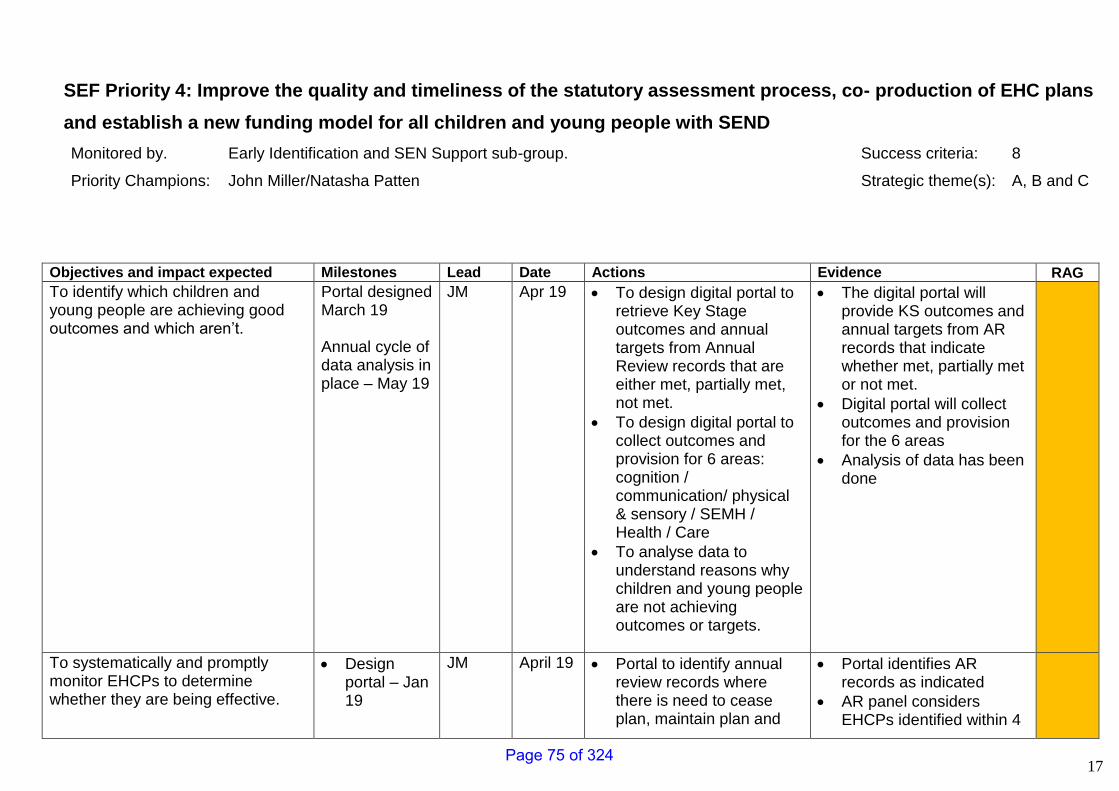
17
SEF Priority 4: Improve the quality and timeliness of the statutory assessment process, co- production of EHC plans
and establish a new funding model for all children and young people with SEND
Monitored by. Early Identification and SEN Support sub-group. Success criteria: 8
Priority Champions: John Miller/Natasha Patten Strategic theme(s): A, B and C
Objectives and impact expected Milestones Lead Date Actions Evidence RAG
To identify which children and young people are achieving good outcomes and which aren’t.
Portal designed March 19 Annual cycle of data analysis in place – May 19
JM Apr 19 • To design digital portal to retrieve Key Stage outcomes and annual targets from Annual Review records that are either met, partially met, not met.
• To design digital portal to collect outcomes and provision for 6 areas: cognition / communication/ physical & sensory / SEMH / Health / Care
• To analyse data to understand reasons why children and young people are not achieving outcomes or targets.
• The digital portal will provide KS outcomes and annual targets from AR records that indicate whether met, partially met or not met.
• Digital portal will collect outcomes and provision for the 6 areas
• Analysis of data has been done
To systematically and promptly monitor EHCPs to determine whether they are being effective.
• Design portal – Jan 19
JM April 19 • Portal to identify annual review records where there is need to cease plan, maintain plan and
• Portal identifies AR records as indicated
• AR panel considers EHCPs identified within 4
Page 75 of 324
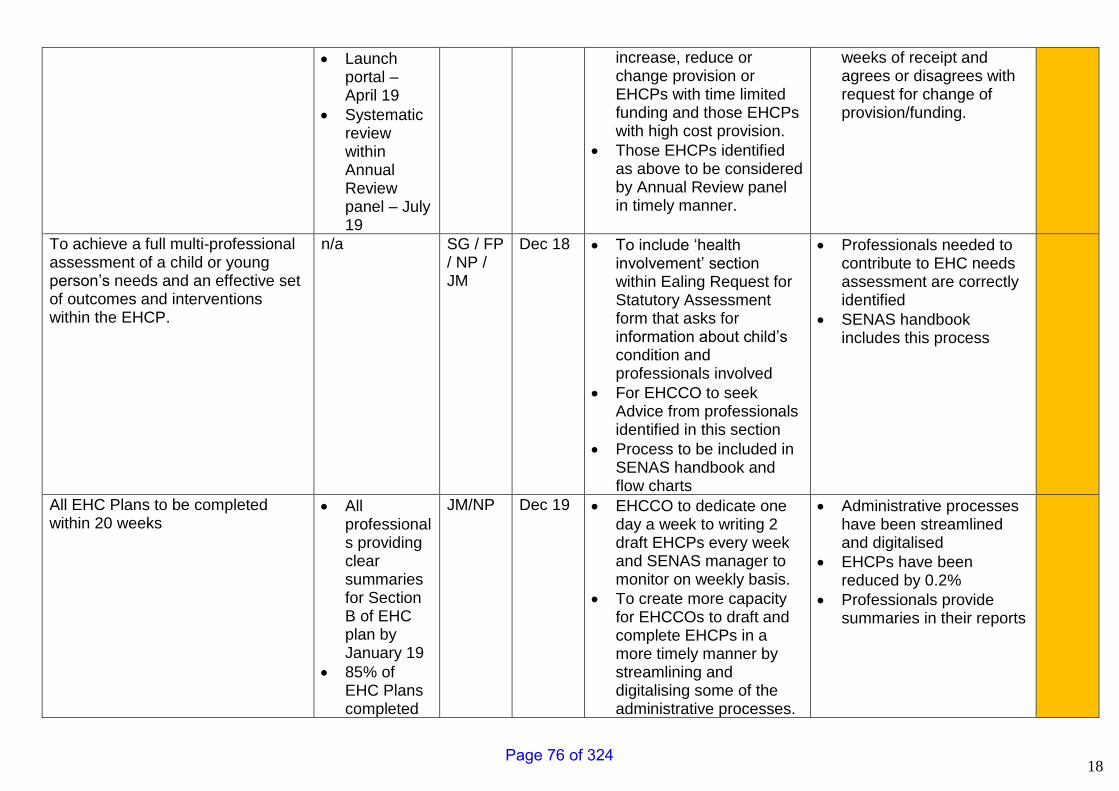
18
• Launch portal – April 19
• Systematic review within Annual Review panel – July 19
increase, reduce or change provision or EHCPs with time limited funding and those EHCPs with high cost provision.
• Those EHCPs identified as above to be considered by Annual Review panel in timely manner.
weeks of receipt and agrees or disagrees with request for change of provision/funding.
To achieve a full multi-professional assessment of a child or young person’s needs and an effective set of outcomes and interventions within the EHCP.
n/a SG / FP / NP / JM
Dec 18 • To include ‘health involvement’ section within Ealing Request for Statutory Assessment form that asks for information about child’s condition and professionals involved
• For EHCCO to seek Advice from professionals identified in this section
• Process to be included in SENAS handbook and flow charts
• Professionals needed to contribute to EHC needs assessment are correctly identified
• SENAS handbook includes this process
All EHC Plans to be completed within 20 weeks
• All professionals providing clear summaries for Section B of EHC plan by January 19
• 85% of EHC Plans completed
JM/NP Dec 19 • EHCCO to dedicate one day a week to writing 2 draft EHCPs every week and SENAS manager to monitor on weekly basis.
• To create more capacity for EHCCOs to draft and complete EHCPs in a more timely manner by streamlining and digitalising some of the administrative processes.
• Administrative processes have been streamlined and digitalised
• EHCPs have been reduced by 0.2%
• Professionals provide summaries in their reports
Page 76 of 324
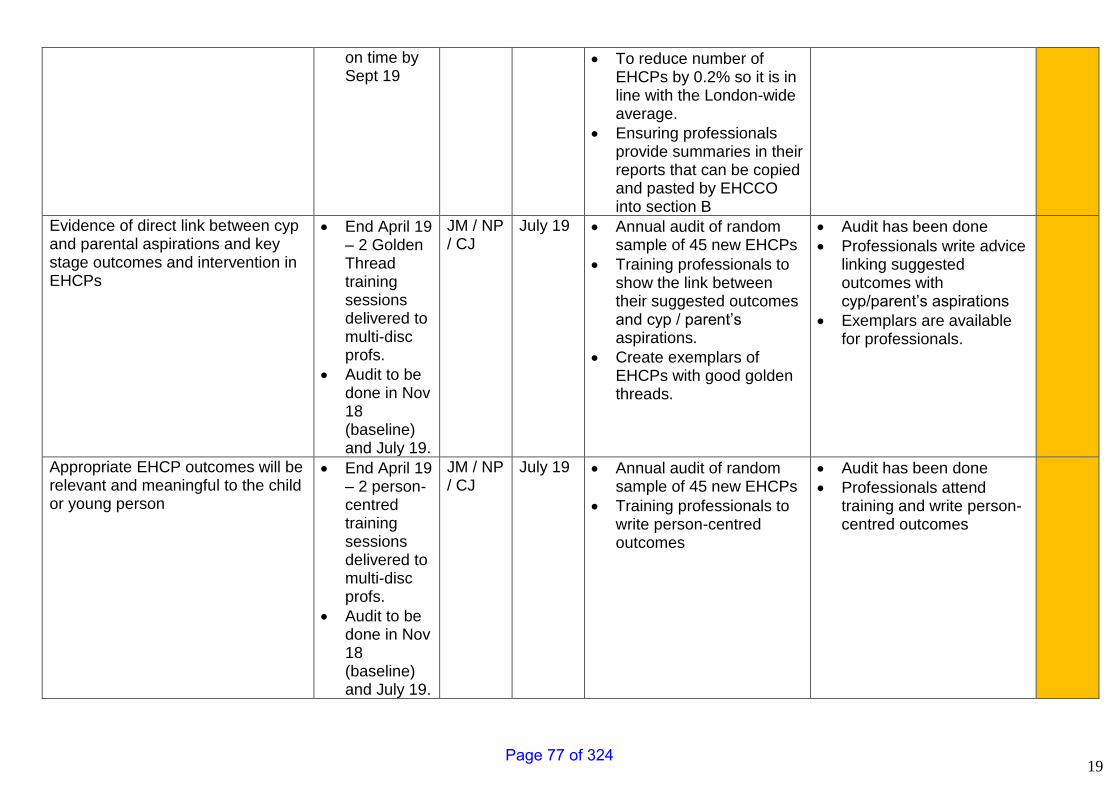
19
on time by Sept 19
• To reduce number of EHCPs by 0.2% so it is in line with the London-wide average.
• Ensuring professionals provide summaries in their reports that can be copied and pasted by EHCCO into section B
Evidence of direct link between cyp and parental aspirations and key stage outcomes and intervention in EHCPs
• End April 19 – 2 Golden Thread training sessions delivered to multi-disc profs.
• Audit to be done in Nov 18 (baseline) and July 19.
JM / NP / CJ
July 19 • Annual audit of random sample of 45 new EHCPs
• Training professionals to show the link between their suggested outcomes and cyp / parent’s aspirations.
• Create exemplars of EHCPs with good golden threads.
• Audit has been done
• Professionals write advice linking suggested outcomes with cyp/parent’s aspirations
• Exemplars are available for professionals.
Appropriate EHCP outcomes will be relevant and meaningful to the child or young person
• End April 19 – 2 person-centred training sessions delivered to multi-disc profs.
• Audit to be done in Nov 18 (baseline) and July 19.
JM / NP / CJ
July 19 • Annual audit of random sample of 45 new EHCPs
• Training professionals to write person-centred outcomes
• Audit has been done
• Professionals attend training and write person-centred outcomes
Page 77 of 324
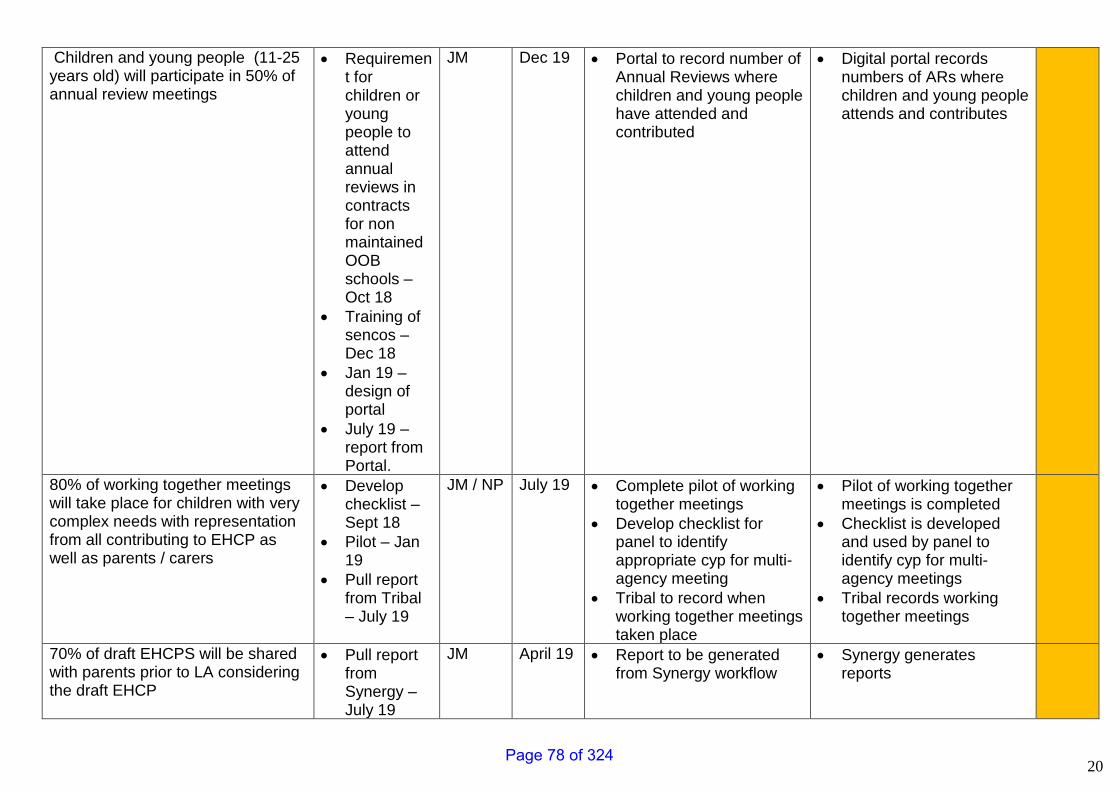
20
Children and young people (11-25 years old) will participate in 50% of annual review meetings
• Requirement for children or young people to attend annual reviews in contracts for non maintained OOB schools – Oct 18
• Training of sencos – Dec 18
• Jan 19 – design of portal
• July 19 – report from Portal.
JM Dec 19 • Portal to record number of Annual Reviews where children and young people have attended and contributed
• Digital portal records numbers of ARs where children and young people attends and contributes
80% of working together meetings will take place for children with very complex needs with representation from all contributing to EHCP as well as parents / carers
• Develop checklist – Sept 18
• Pilot – Jan 19
• Pull report from Tribal – July 19
JM / NP July 19 • Complete pilot of working together meetings
• Develop checklist for panel to identify appropriate cyp for multi-agency meeting
• Tribal to record when working together meetings taken place
• Pilot of working together meetings is completed
• Checklist is developed and used by panel to identify cyp for multi-agency meetings
• Tribal records working together meetings
70% of draft EHCPS will be shared with parents prior to LA considering the draft EHCP
• Pull report from Synergy – July 19
JM April 19 • Report to be generated from Synergy workflow
• Synergy generates reports
Page 78 of 324

21
Page 79 of 324
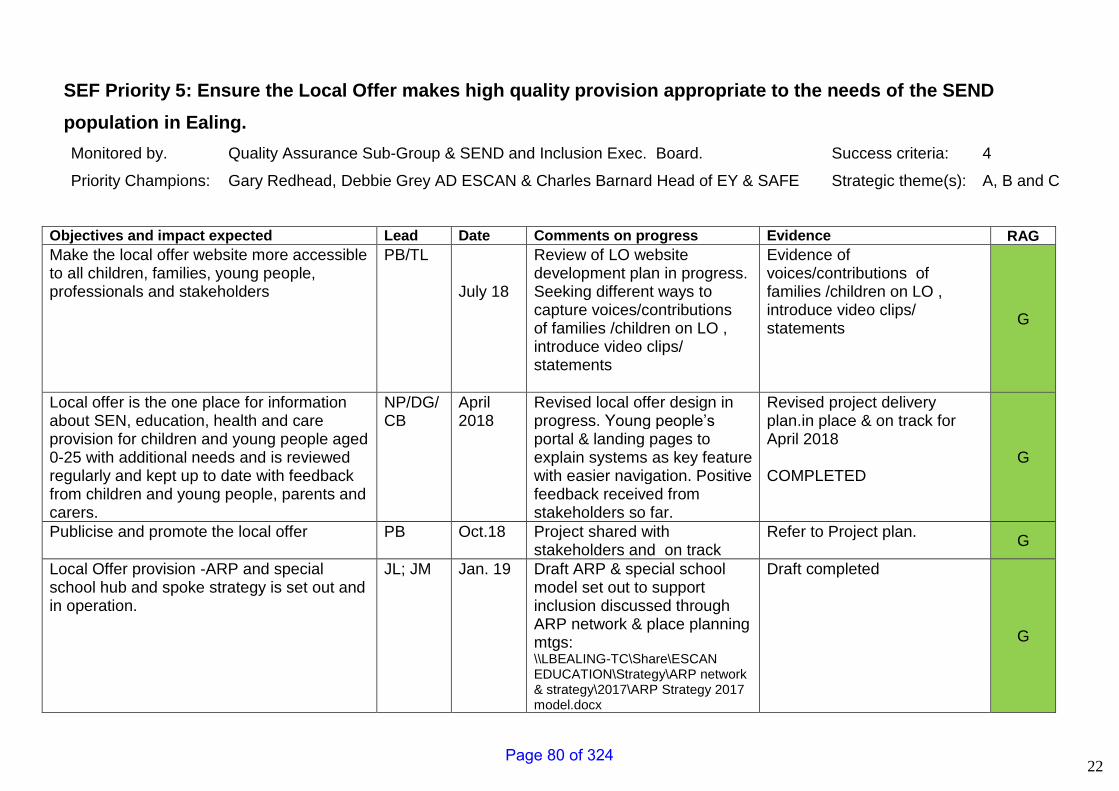
22
SEF Priority 5: Ensure the Local Offer makes high quality provision appropriate to the needs of the SEND
population in Ealing.
Monitored by. Quality Assurance Sub-Group & SEND and Inclusion Exec. Board. Success criteria: 4
Priority Champions: Gary Redhead, Debbie Grey AD ESCAN & Charles Barnard Head of EY & SAFE Strategic theme(s): A, B and C
Objectives and impact expected Lead Date Comments on progress Evidence RAG
Make the local offer website more accessible to all children, families, young people, professionals and stakeholders
PB/TL July 18
Review of LO website development plan in progress. Seeking different ways to capture voices/contributions of families /children on LO , introduce video clips/ statements
Evidence of voices/contributions of families /children on LO , introduce video clips/ statements
G
Local offer is the one place for information about SEN, education, health and care provision for children and young people aged 0-25 with additional needs and is reviewed regularly and kept up to date with feedback from children and young people, parents and carers.
NP/DG/CB
April 2018
Revised local offer design in progress. Young people’s portal & landing pages to explain systems as key feature with easier navigation. Positive feedback received from stakeholders so far.
Revised project delivery plan.in place & on track for April 2018 COMPLETED
G
Publicise and promote the local offer PB Oct.18 Project shared with stakeholders and on track
Refer to Project plan. G
Local Offer provision -ARP and special school hub and spoke strategy is set out and in operation.
JL; JM Jan. 19 Draft ARP & special school model set out to support inclusion discussed through ARP network & place planning mtgs: \\LBEALING-TC\Share\ESCAN EDUCATION\Strategy\ARP network & strategy\2017\ARP Strategy 2017 model.docx
Draft completed
G
Page 80 of 324
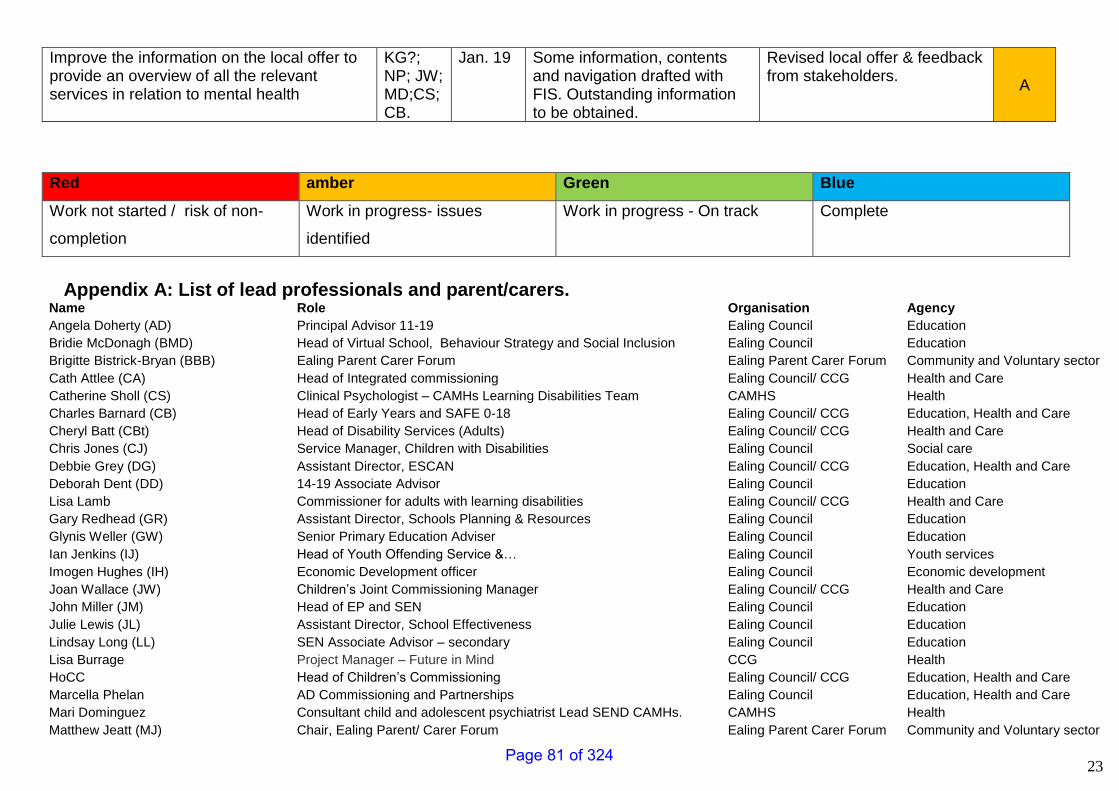
23
Improve the information on the local offer to provide an overview of all the relevant services in relation to mental health
KG?; NP; JW; MD;CS; CB.
Jan. 19 Some information, contents and navigation drafted with FIS. Outstanding information to be obtained.
Revised local offer & feedback from stakeholders.
A
Red amber Green Blue
Work not started / risk of non-
completion
Work in progress- issues
identified
Work in progress - On track Complete
Appendix A: List of lead professionals and parent/carers.
Name Role Organisation Agency
Angela Doherty (AD) Principal Advisor 11-19 Ealing Council Education
Bridie McDonagh (BMD) Head of Virtual School, Behaviour Strategy and Social Inclusion Ealing Council Education
Brigitte Bistrick-Bryan (BBB) Ealing Parent Carer Forum Ealing Parent Carer Forum Community and Voluntary sector
Cath Attlee (CA) Head of Integrated commissioning Ealing Council/ CCG Health and Care
Catherine Sholl (CS) Clinical Psychologist – CAMHs Learning Disabilities Team CAMHS Health
Charles Barnard (CB) Head of Early Years and SAFE 0-18 Ealing Council/ CCG Education, Health and Care
Cheryl Batt (CBt) Head of Disability Services (Adults) Ealing Council/ CCG Health and Care
Chris Jones (CJ) Service Manager, Children with Disabilities Ealing Council Social care
Debbie Grey (DG) Assistant Director, ESCAN Ealing Council/ CCG Education, Health and Care
Deborah Dent (DD) 14-19 Associate Advisor Ealing Council Education
Lisa Lamb Commissioner for adults with learning disabilities Ealing Council/ CCG Health and Care
Gary Redhead (GR) Assistant Director, Schools Planning & Resources Ealing Council Education
Glynis Weller (GW) Senior Primary Education Adviser Ealing Council Education
Ian Jenkins (IJ) Head of Youth Offending Service &… Ealing Council Youth services
Imogen Hughes (IH) Economic Development officer Ealing Council Economic development
Joan Wallace (JW) Children’s Joint Commissioning Manager Ealing Council/ CCG Health and Care
John Miller (JM) Head of EP and SEN Ealing Council Education
Julie Lewis (JL) Assistant Director, School Effectiveness Ealing Council Education
Lindsay Long (LL) SEN Associate Advisor – secondary Ealing Council Education
Lisa Burrage Project Manager – Future in Mind CCG Health
HoCC Head of Children’s Commissioning Ealing Council/ CCG Education, Health and Care
Marcella Phelan AD Commissioning and Partnerships Ealing Council Education, Health and Care
Mari Dominguez Consultant child and adolescent psychiatrist Lead SEND CAMHs. CAMHS Health
Matthew Jeatt (MJ) Chair, Ealing Parent/ Carer Forum Ealing Parent Carer Forum Community and Voluntary sector
Page 81 of 324
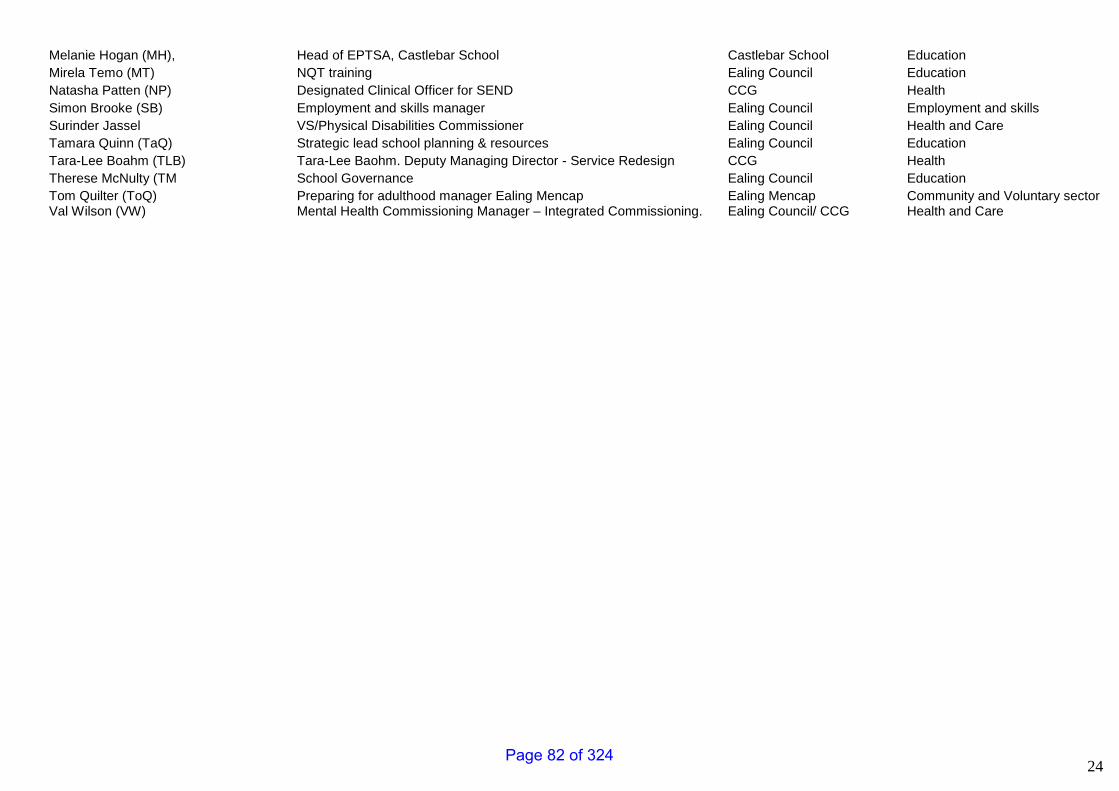
24
Melanie Hogan (MH), Head of EPTSA, Castlebar School Castlebar School Education
Mirela Temo (MT) NQT training Ealing Council Education
Natasha Patten (NP) Designated Clinical Officer for SEND CCG Health
Simon Brooke (SB) Employment and skills manager Ealing Council Employment and skills
Surinder Jassel VS/Physical Disabilities Commissioner Ealing Council Health and Care
Tamara Quinn (TaQ) Strategic lead school planning & resources Ealing Council Education
Tara-Lee Boahm (TLB) Tara-Lee Baohm. Deputy Managing Director - Service Redesign CCG Health
Therese McNulty (TM School Governance Ealing Council Education
Tom Quilter (ToQ) Preparing for adulthood manager Ealing Mencap Ealing Mencap Community and Voluntary sector Val Wilson (VW) Mental Health Commissioning Manager – Integrated Commissioning. Ealing Council/ CCG Health and Care
Page 82 of 324
1
Contains Confidential or Exempt Information
NO
Title CQC Report-Review of Health Services for Children Looked After and Safeguarding (CLAS) in Ealing
Responsible Officer(s) (EDG Officers only) N/A - Ealing CCG
Author(s) Ann Coles – Designated Nurse Safeguarding Children – Ealing CCG
Portfolio(s) Children
For Consideration By Health and Wellbeing Board
Date to be Considered 18th September 2018
Implementation Date if Not Called In
N/A
Affected Wards All
Keywords/Index Safeguarding Children and Looked After Children
Purpose of Report: On the 13th June 2018 the Care Quality Commission (CQC) published their review of Ealing health services for Children Looked After and Safeguarding. The CQC review took place over five days: 12th- 16th March 2018. This report to the Ealing Health and Wellbeing Board is to provide information about the Review, to acknowledge the positive findings and to confirm that Ealing CCG has worked with our partners to develop and submit an action plan to the CQC; to address areas for improvement. Including the single and multi-agency plans for monitoring progress against the action plan.
1. Recommendations
The Health and Wellbeing Board; is asked to note the CQC CLAS Review Report and associated Action Plan. The Action Plan was submitted to the CQC on 11th July 2018. The Board is also asked to note that Ealing Local Authority/Public Health are progressing a separate Action Plan to address the 10 points for consideration that the CQC raised for the attention of Ealing Local Authority. These points relate to Local Authority commissioned health services. The current (30th August 2018) draft of the Local Authority Action Plan is submitted alongside the CQC Action Plan for information to the H&WBB.
Report for: INFORMATION Item Number: 9
Page 83 of 324
2
2. Reason for Decision and Options Considered The focus of the CLAS Review, was on the experiences and outcomes for children within the geographical area of Ealing and reports on the performance of health providers serving the area, including the Clinical Commissioning Group; assessed by the CQC Team during the review period. The review was conducted under Section 48 of the Health and Social Care Act 2008 which permits CQC to review the provision of healthcare and the functions of NHS England and Clinical Commissioning Groups. The CQC report did not provide a rating, but made 20 recommendations for improvements, relation to the NHS commissioned health organisations involved in the review. The CQC report found lots of good practice and some of the feedback the CQC received from young people and families was very rewarding and demonstrated that we should be rightly proud of the services that we provide to children and families in the borough. However, as you would expect there is always room for improvement and Ealing CCG have been working with our partners to develop and progress an action plan; which was submitted to the CQC within the required 20 working days from publication of the report. Where the CQC Team found areas for improvement in services provided by the NHS, but commissioned by the local authority; the CQC documented their intention to write to the Local Authority/public health team to bring the 10 issues to their attention.
3. Key Implications The findings of the review support the work and priorities of the H&WB Board, ensuring that all key organisations work better together to improve health and well-being.
4. Financial
a) Financial impact on the budget - no financial implications.
5. Legal
No legal implications
6. Value For Money
Report for information – N/A
Page 84 of 324
3
7. Sustainability Impact Appraisal N/A
8. Risk Management
No risks identified.
9. Community Safety None
10. Links to the 3 Key Priorities for the Borough CLAS report findings link to: - A healthy and great place The council’s administration has three key priorities for Ealing. They are: Good, genuinely affordable homes
Opportunities and living incomes
A healthy and great place
11. Equalities, Human Rights and Community Cohesion
The review was conducted under Section 48 of the Health and Social Care Act 2008 which permits the CQC to review the provision of healthcare and the exercise of functions of both NHS England and Clinical Commissioning Groups. Effective Safeguarding and patient safety are managed through quality service provision. Accordingly equality and diversity issues are considered at all levels and benchmarked against the Equality Act 2010.
12. Staffing/Workforce and Accommodation implications:
None
13. Property and Assets
No property implications.
14. Any other implications: N/A
15. Consultation
No consultation. The review was conducted under Section 48 of the Health and Social Care Act 2008 which permits CQC to review the provision of healthcare and the functions of NHS England and Clinical Commissioning Groups.
Page 85 of 324
4
Give a summary of the consultation methodology used e.g. How you decided who to consult and draw up the sample, what method of consultation, efforts to involve hard to reach groups, and how many responded overall.
16. Timetable for Implementation
N/A Please include a simple timetable to show the stages and deadlines for implementing the recommendations – preferably as a table – and include a list of measurable aims and outcomes with the date by which they should be achieved.
17. Appendices
If appendices are essential to the understanding of the report, list titles here. Please ensure that appendices have proper titles. Appendix 1: CQC Report - Review of Health Services for Children Looked After and Safeguarding (CLAS) in Ealing – Dated 13th June 2018 Appendix 2: CQC CLAS Action Plan – V5 – Dated 11.07.2018 Appendix 3: Ealing LA Draft Action Plan – Version date 30.08.2018
18. Background Information
(This is a statutory requirement – please include the public documents referred to in writing the report, officer research and advice documents which Members or Members of the Public may request from the report author) Appendix 1: Report published by the CQC and available on the CQC website - https://www.cqc.org.uk/publications/themed-inspection/child-safeguarding-and-looked-after-children-inspection-programme#PublishedReports
Page 86 of 324
5
Consultation
Name of consultee
Post held Date sent to
consultee
Date response received
Comments appear in
paragraph:
Internal
External
Report History
Decision type: Urgency item ?
For information
No History of Governance and Reporting Report/Action Plan has been submitted to, discussed and noted at the following: 20th June 2018 - Ealing CCG – Quality and Patient Safety Committee (Report) 28th June 2018 - Ealing Safeguarding Children Board (Report) 18th July 2018 - Ealing CCG – Quality and Patient Safety Committee (Action Plan) 18th July 2018 - Ealing CCG – Governing Body (Report) Monitoring At CQC level, the Action Plan will now be considered by the inspection team and progress will be followed up through CQC’s regional compliance team. At CCG, local level, progress against the Action Plan will be overseen by the Ealing CCG Quality and Safety Committee and taken through the provider organisations respective Clinical Quality Group / Contract Monitoring Groups, to monitor progress against the agreed actions. The Report and both Action plans will have multi agency oversight via the ESCB/Safeguarding Children Partnership arrangements
Page 87 of 324

6
Report no: 1 Report author and contact for queries:
Ann Coles – Designated Nurse Safeguarding Children For Ealing CCG: Managing Director – Tessa Sandall
Page 88 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 1 of 47
Review of health services for
Children Looked After and Safeguarding in
Ealing
Page 89 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 2 of 47
Children Looked After and Safeguarding
The role of health services in Ealing
Date of review: 12th March 2018 to 16th March 2018
Date of publication: 13th June 2018
Name(s) of CQC inspector: Daniel Carrick Sue Knight Elizabeth Fox Jeffery Boxer Nikki Holmes
Provider services included: London North West University Healthcare NHS Trust (LNWUH)
Change, Grow, Live (CGL) Recovery Interventions Service Ealing (RISE).
West London Mental Health Trust (WLMHT)
Greenbrook Healthcare (Ealing Urgent Care Centre – Located at Ealing Hospital site)
CCGs included: NHS Ealing CCG
NHS England area: London
CQC region: London
CQC Deputy Chief Inspector, Primary Medical Services and Integrated Care:
Ursula Gallagher
Page 90 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 3 of 47
Contents
Summary of the review 4 About the review 4 How we carried out the review 5 Context of the review 5 The report 7 What people told us 8
The child’s journey 11 Early help 11 Children in need 19 Child protection 24 Looked after children 31
Management 35 Leadership & management 35 Governance 39 Training and supervision 42
Recommendations 45
Next steps 47
Page 91 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 4 of 47
Summary of the review
This report records the findings of the review of health services in safeguarding and looked after children services in Ealing. It focuses on the experiences and outcomes for children within the geographical boundaries of the local authority area and reports on the performance of health providers serving the area including Clinical Commissioning Groups (CCGs) and Local Area Teams (LATs). Where the findings relate to children and families in local authority areas other than Ealing, cross-boundary arrangements have been considered and commented on. Arrangements for the health-related needs and risks for children placed out of area are also included.
About the review
The review was conducted under Section 48 of the Health and Social Care Act 2008 which permits CQC to review the provision of healthcare and the exercise of functions of NHS England and Clinical Commissioning Groups.
• The review explored the effectiveness of health services for looked after children and the effectiveness of safeguarding arrangements within health for all children.
• The focus was on the experiences of looked after children and children and their families who receive safeguarding services.
• We looked at:
o the role of healthcare providers and commissioners.
o the role of healthcare organisations in understanding risk factors, identifying needs, communicating effectively with children and families, liaising with other agencies, assessing needs and responding to those needs and contributing to multi-agency assessments and reviews.
o the contribution of health services in promoting and improving the health and wellbeing of looked after children including carrying out health assessments and providing appropriate services.
• We also checked whether healthcare organisations were working in accordance with their responsibilities under Section 11 of the Children Act 2004. This includes the statutory guidance, Working Together to Safeguard Children 2015.
• Where we found areas for improvement in services provided by NHS but commissioned by the local authority then we will bring these issues to the attention of the local public health team in a separate letter.
Page 92 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 5 of 47
How we carried out the review
We used a range of methods to gather information both during and before the visit. This included document reviews, interviews, focus groups and visits. Where possible we met and spoke with children and young people. This approach provided us with evidence that could be checked and confirmed in several ways. We tracked a number of individual cases where there had been safeguarding concerns about children. This included some cases where children were referred to social care and also some cases where children and families were not referred, but where they were assessed as needing early help and received it from health services. We also sampled a spread of other such cases. Our tracking and sampling also followed the experiences of looked after children to explore the effectiveness of health services in promoting their well-being. In total, we took into account the experiences of 49 children and young people.
Context of the review
The Ealing Joint Strategic Needs Analysis of 2017 notes that the population of Ealing has risen from 292,800 in 1996 to 343,000 in 2015. Ealing has a higher proportion of males and females aged 0-9 years and 25-44 years compared to England. Ealing is the third largest London borough in terms of population, after Barnet (379,700) and Croydon (379,000). At 61 persons per hectare, Ealing is also the third most densely populated borough in Outer London (after Brent and Waltham Forest). Between 2001 and 2015, Ealing’s population of 0-15 year olds increased by 23.1% (from 59,700 to 73,500). In the same time period, the number of 0-15 year olds increased by 21.8% across London and by 5.1% across England. In 2016 there were 88,000 children and young people aged 0 to nine years in Ealing. The rate of children in care has been consistently lower than the England average for the last four years. In 2016 there were 370 children from Ealing in care. There were 426,086 people registered with 79 GP practices in Ealing in April 2016. This is larger than the number of residents in Ealing (343,000 according to 2015 mid-year estimates). The main reason for this difference is registration of people from abroad (e.g. visiting relatives, au pairs), who then leave and are not deregistered. In addition, some people will attend GP surgeries who are not picked up by the national census. Out of the 426,086 registered patients, 49% (206,900) were aged 15-44.
Page 93 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 6 of 47
The population of government maintained schools in Ealing is ethnically diverse, with 83% of pupils classified as being of minority ethnic origin (this proportion has remained unchanged for the last four years). 84% of primary school pupils (compared to 30% nationally) and 82% of high school pupils (compared to 27% nationally) are from an ethnic minority. 30% of pupils are white, 29% Asian or Asian British, 16% black or black British, 8% from mixed backgrounds and 16% of other ethnic heritage. The ethnic composition of schools in Ealing varies. The proportion of children of minority ethnic origin ranges from 50% to 100% between schools. The most common ethnic groups in Ealing’s school population are white British (15%), Indian (14%), Eastern European (10%), Somali (8%), Pakistani (7%), Asian Other (7%), Afghan (4%), Arab Other (4%) and black Caribbean (4%). Whilst the white British population remains the largest group it continues to fall in numbers. There was a 2.7% increase in the overall school population in the year to January 2016; over the same period the number of white British pupils in Ealing state 14 funded schools reduced by 129. The Eastern European population continues to grow steadily. There are now 5,344 Eastern European pupils, an increase of 325 (6.5%) in the last year. The Indian population has also increased by almost 500 (7%) since last year to 7,540. In the year ending 31 March 2016 in Ealing, there were 296 children aged 0-17 who were subject of a child protection plan. This represents a rate of 36.4 per 10,000 children, which is lower than both the London (37.9) and national (43.1) rates. Traveller groups have frequented Ealing for many years. Department of Environment 'caravan counts' consistently record Ealing as having one of the largest traveller populations in the Greater London area. These figures do not include the large and unrecognised 'hidden' traveller communities who, due to a deficit in caravan site provision and rapid evictions from roadside encampments, live in other forms of accommodation. The total traveller population in Ealing is estimated to be in excess of 2,000 individuals at certain times of the year. Currently, traveller groups resorting to, or residing in, the borough are largely from the following traditional communities: Travellers of Irish heritage, East European Roma and English, European and international circus and fairground travellers. Since the break-up of political systems in Eastern Europe, some Roma families have travelled to Ealing. They now constitute the second largest gypsy traveller group in the borough. Roma families have a very strong allegiance to their traditions, which can be traced back to northern India and ancient Persia (modern Iran and Iraq). Their first language is Roma, and their second language is generally that of their point of departure e.g. Polish, Czech, Slovak, Albanian, Romanian or any of the languages of the former Yugoslavia. Ealing performs worse than London and England in both measures of homeless published in the Public Health Outcomes Framework. In Ealing, the rate of homeless households living in temporary accommodation is significantly higher than in London and more than five times the England average. Most (90.2%) of Ealing residents are registered with a GP practice that is a member of NHS Ealing CCG Clinical Commissioning Group (CCG). There are some Ealing residents that are registered with GP’s that are a part of further CCG’s but these are much lower in number. NHS Ealing CCG had a headline rating of good in the CCG Assurance Annual Assessment 2016/17.
Page 94 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 7 of 47
Ofsted published a report on 26th August 2016 following their Inspection of services for children in need of help and protection; children looked after and care leavers and review of the effectiveness of the Local Safeguarding Children Board (LSCB). The reports overall findings were:
1. Children who need help and protection: Good 2. Children Looked After and achieving permanence: Good
2.1 Adoption Performance: Good 2.2 Experiences and progress of care leavers: Outstanding
3. Leadership, management and governance: Good
Commissioning and planning of most health services for children are carried out by Ealing CCG and Ealing Local Authority
Acute hospital services are provided by a range of hospitals, including London North West University Hospital NHS Trust (LNWUH) Urgent Care services at Ealing Hospital are provided by Greenbrook Healthcare Specialist Ophthalmology services are provided by Moorefield’s Eye Hospital on the Ealing Hospital site
Community based services are provided by London North West University Hospital NHS Trust (LNWUH)
Child and Adolescent Mental Health Services (CAMHS) are provided by West London Mental Health Trust
Specialist facilities are: Adult and Young People’s Substance Misuse Services provided by Change, Grow, Live
The last inspection of health services for Ealing’s children took place in May 2011 as a joint inspection, with Ofsted, of safeguarding and looked after children’s services. Recommendations from that inspection are covered in this review.
The report
This report follows the child’s journey reflecting the experiences of children and young people or parents/carers to whom we spoke, or whose experiences we tracked or checked. A number of recommendations for improvement are made at the end of the report.
Page 95 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 8 of 47
What people told us
We spoke with young people looked after in Ealing. When asked about the service they receive one young person told us; “Health services are very good – I always get what I need. If something is wrong with my health I get referred and get seen really quickly. I last saw my GP a few months ago and that was fine – no problems.” They went on to say; “I have never had to wait for any health appointment The most I have had to wait is two months to be seen (for an eye complaint) when I needed to go to hospital but that was because the earlier appointment they gave was when I was on my holidays so they put it back for me. I am very happy with my health appointments, never had to complain and everyone is very nice.” We asked them about the health assessment process. They said; “My last health assessment with the nurse was half an hour. I felt listened to and I think I was able to make a good contribution. They asked me about all kinds of things, like school, not just about my health. They listened to me then read it all back with me and explained everything and if I didn’t agree with anything I could change it.” They went on to say; “Been to one appointment with CAMHS and they were really nice, they really listened to me and let me talk and explain how I was feeling. They were very patient with me.” We then went on to speak with the young person’s allocated social worker. They told us; “I will just reiterate what you have been told, when they have their review (health assessment) all their appointments are made and they are always seen really quickly. For CAMHS, they know when they need to speak to someone and they are really responsive to their needs.” They went on to say; “We all work really closely together, the foster carers, the young person and the health services. There is really good multi-disciplinary working and good robust processes for children and young people’s health here in Ealing. Young people are listened to in their health assessments and so I would say that they are an important part of the planning process.”
Page 96 of 324

Review of Health services for Children Looked After and Safeguarding in Ealing Page 9 of 47
We spoke with another Looked After young person. They told us; “I have been a looked after young person since I was six years old. I have always felt that my social workers have been kind, and that the looked after children’s team have been kind too. If I have worries or concerns there are people that I can talk to, I know they will support me and listen. The Looked After Children team have made sure I can speak to other young people in my situation. That is important as they really understand what I have gone through.” We then spoke with the young person’s foster carer. They told us; “Health services in Ealing are good. I feel really listened to. As a long term foster carer as well, I feel well supported and like services really want what is best for the child. I have challenged the looked after team at times, when I haven’t agreed with a course of action, but feel that they listen to my point of view and are committed to reaching solutions and conclusions that are in the best interests of the children in my care.” We spoke with one Ealing Foster Carer about the support they get to undertake their role. They told us; “When I have fostered babies the midwife and health visitor are always there to give me advice, I just have to call them. We are supported very well and the training I have had has been very good.” They went on to tell us; “I had a baby with lots of problems; they became very unwell and I needed to do CPR. The ambulance service were so good and the hospital too. I was very pleased I had my first aid training from foster training.” When asked about the health assessment process they told us, “The doctors fully assess the children and they listen to what I have to say as they know I care for the baby and know how they are. You only have to ask and they explain everything to you.” We spoke with other foster carers. They told us; “Health staff are open and friendly and work well together to be flexible. I don’t have any problems getting any health support for Looked After Children (LAC). The LAC nurse is good and includes me in things; I attend some of the sessions for the health assessments if needed. I have good communication with the LAC nurse and get a say in when and where appointments are.” They went on to say; “Sometimes if a child (LAC) doesn’t want to engage, they [services] discharge them. It would be better if they were more flexible and patient too.”
Page 97 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 10 of 47
Another foster carer told us; “My health visitor, GP and LAC nurse are all really good. I can contact them by telephone, text and email and they always get back to me quickly. I have meetings with the LAC nurse every six months. I haven’t had any problems with any health services and there isn’t anything I would change. Maybe the time for speech therapy is too long for some people but I don’t need it for my [foster] baby who is doing really well.” We spoke with a young person attending the Ealing UCC with their mother. They told us; “It’s nice here, there is lots of space. The nurse spoke to me and not my mum which was good.” When asked if they felt safe they told us; “Yes, it’s all OK. We are sitting here I think to see a doctor next. (They had been directed to wait for a short time in the adult area). It’s busy round there (the paediatric waiting area) but we should be seen soon. It’s OK here.” We also spoke with an expectant mother at the Northwick Park maternity unit. They told us; “I am very satisfied with my midwife; I have no worries or complaints. My only problem has been depression, it was worst in my first trimester. I was referred to a specialist midwife and I felt free to call anytime I needed. She is an amazing person, every time I saw her I felt better straight away. She also referred me (to the perinatal mental health team) to see what the next steps would be. She arranged talking therapy for me. It is a very nice service for depressed people and I really appreciate the help I get. She is like my angel.”
Page 98 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 11 of 47
The child’s journey
This section records children’s experiences of health services in relation to safeguarding, child protection and being looked after.
1. Early help
1.1 Health input (provided by London North West University Healthcare NHS Trust (LNWUH)) at the Ealing Multi-Agency Safeguarding Hub (MASH)1 is respected well by multi-agency partners we spoke with who also work at the MASH. Daily meetings take place within the MASH to discuss new cases referred for consideration by the team, and once a case has been presented at the MASH meeting, feedback is given within a maximum of 24 hours and a plan of action agreed of how best to progress the case. If a case is considered as urgent (red) then it will be referred directly to the Multi-Agency Safeguarding Team (MAST) for more urgent attention, generally within four hours. During our review we were party to a more expanded weekly multi-agency meeting and saw how, once a case has been presented by one of the partner agencies, then those other partners will immediately share their own information regarding the case discussed which can disclose, for example; siblings, significant adults or other important information which can aid the decision making process. One case discussion we observed led to an initial ‘amber’ rating being raised to ‘red’ which meant the case was immediately referred to the MAST team for their interventions to take place. This ensured that children and young people identified as potentially at risk were protected at the earliest opportunity. 1.2 Children and young people missing from home are also discussed at the MASH. Where a young person remains missing after 72 hours the case will automatically be referred to the MAST if the case has not already been rated ‘red’. This means that all available resources are directed to ensure the safety of those particular vulnerable young people.
1 The Ealing MASH is a model for managing and responding to referrals received by Ealing Children’s Integrated Response Service (ECIRS (the single point of entry for all referrals where there is a need for support, or where there are specific concerns about the welfare of a child or young person)). The MASH is a multi-agency team of professionals who work together to share information within a secure environment to support better decision-making on cases. By bringing representatives of different agencies together, more information is available in relation to each case, meaning a more sound assessment of risk can be made. This will ultimately result in better decisions being made, leading to better outcomes for children and young people.
Page 99 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 12 of 47
1.3 There is a well-designed paediatric Emergency Department (ED) at Northwick Park Hospital (as provided by LNWUH) which allows children and young people attending the unit to wait and be seen away from adult attenders. This means that those young people do not routinely have contact with adult attenders who might cause them distress. The paediatric waiting area is also well equipped for children to be easily observed by clinical practitioners at all times during their attendance. This enables those practitioners to respond swiftly should a child’s condition deteriorate, but it also allows them to observe the interactions between those young people and their accompanying adult(s) and act on any concerns accordingly. 1.4 A standardised electronic triage form is used Northwick Park paediatric ED for all children and young people attending the unit. The form also contains an inbuilt safeguarding screening tool. The discharge process from the ED cannot be completed until the screening tool is completed. In all the records examined we saw that this tool had been completed well. There is also a clear flagging system to alert clinicians and staff when a child has safeguarding concerns already identified. 1.5 When a child presents at the Northwick Park ED and is known to social care, is looked after, or when onward referrals to other services are known to have been made, a health visitor liaison form is completed which alerts the health visiting and school nursing services of the child’s attendance. This then allows community services to provide ongoing and additional support when needs have been identified to children, young people and their families. A health visitor liaison form is also completed when a child has presented at the ED on three or more occasions within a six month period. This ensures that community services are aware of multiple attendances and are attuned to emerging risks and needs. 1.6 The paediatric liaison team at Northwick Park Hospital comprises of three health visitors and one full time administrator. The paediatric liaison team screen all under 18 attendances at the hospital and since the recent closure of the designated ED department at Ealing hospital, all of their daily UCC attendances to ensure that any child that presents at the Ealing UCC have had their needs adequately met. 1.7 Where children and young people receive care and support from the Ealing Urgent Care Centre (UCC), then paediatric liaison are informed remotely so that appropriate information sharing can take place. Paediatric liaison then feed back to the UCC on a weekly basis requesting, for example, missing information. Paediatric liaison will also suggest a referral to children’s social care if one has not already been made and this can then be actioned by UCC practitioners. 1.8 The use of alerts on patient casualty cards at the Northwick Park ED is effective. Clinicians and staff are easily able to identify when a child is vulnerable and has safeguarding concerns already noted. This is also the case in the adult ED, and we saw examples of how these alerts had prompted practitioners to enquire if the patient had parental responsibility and also to assess the impact that substance misuse, poor mental health and domestic abuse may have on children and other family members associated with the patient.
Page 100 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 13 of 47
1.9 Currently, both paper and electronic patient records are in use in the ED at Northwick Park Hospital. Whilst there is a dedicated team of administrative staff that upload paper files and documents onto the electronic records, we heard that during busy periods there may be a delay in doing so, resulting in some patient records not being completed in a timely way. For example, we heard that when a CAMH assessment has been completed on the ED, a paper copy of the assessment is provided which should be uploaded onto the patient’s electronic record. However, this is not always undertaken in a timely way, resulting in potential delays in meeting the needs of children and young people. We could also not be assured that those paper records might not be mislaid before being uploaded to the electronic record which would result in those records remaining incomplete. (Recommendation 2.1) 1.10 At the Ealing UCC provided by Greenbrook Healthcare, we saw that there is a dedicated paediatric waiting and treatment area away from that used by adults. Those attending the unit are directed to a separate reception area where demographic details are taken before being asked to wait in the paediatric waiting area. The young person will then be seen by a nurse who will assess the nature of the attendance and continue adding information on the SystmOne electronic patient record system, including the associated safeguarding template. Information obtained includes full patient details, details of any accompanying adults, GP details and, if known, allocated social worker details. Once a decision has been taken as to whether care and support can be provided by GPs at the UCC, then the child or young person will undergo further medical assessment. Before being discharged from the unit the electronic safeguarding element of the assessment must be completed before the discharge can be completed. Should the young person require additional support and care, then they will be directed to an appropriate ED where that additional support over and above what can be offered by a GP will be provided. If any safeguarding concernes have been identified, including issues of self-harm, unaccompanied young people or if there are suspicions regarding the accompanying adult, then transfer will take place automatically by ambulance to further ensure their safety.
In one case examined we saw how an adult male had presented at the Northwick Park adult ED under the influence of alcohol stating that he had also taken an overdose. The clinician completing his triage assessment exercised professional curiosity and ascertained that the he was the father of two young children. As a result, a health visitor referral form was completed, ensuring that the school nurses attached to the children’s school were made aware of their father’s attendance and presentation at the ED. This enabled community services to monitor the risks that might have potentially been posed to his children. A social care referral was also made, and the case was discussed at the weekly ‘safety net’ meeting held on the ED, where it was identified that a referral to adult drug and alcohol services was also appropriate to further support the patient.
Page 101 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 14 of 47
1.11 Although the UCC generally does not provide care to children and young people over and above that which can be provided by a GP at an individual GP practice, there is a paediatric trained nurse on duty 24 hours per day, seven days per week as well as duty GPs. This ensures the medical needs of children and young people are met and vulnerabilities can be identified at the earliest opportunity. 1.12 The patient champion role at the Ealing Hospital UCC is a patient support role (including children and young people) to direct attenders to care and support that might be more appropriate to their needs as opposed to attendance at an ED or at the UCC. Young people for example, can be signposted to receive support from the Kidscape ZAP anti-bullying workshops or the Stem4 teenage mental health workshops. The patient champion practitioner is also pro-active in liaising with such groups allowing them to promote their service offer by undertaking regular presentations at the UCC. 1.13 LNWUH midwives at Northwick Hospital provide supportive and personalised maternity care to women living in and around Ealing. There is a team of specialist safeguarding midwives – The Jade Team, for perinatal mental health, teenage pregnancy, Female Genital Mutilation (FGM) and also for vulnerable women. This means that those identified vulnerable expectant mothers will receive targeted support to ensure not only their own safety but also that of their unborn child. 1.14 Expectant women and post-natal mothers in Ealing who experience mental health problems are being better supported through the perinatal mental health service. We saw good links with the newly established perinatal mental health service. The named midwife attends the weekly multi-disciplinary meeting to discuss new referrals and there are joint clinics held by the consultant obstetrician, consultant psychiatrist, perinatal mental health nurse and specialist midwife for vulnerable women. This leads to a coordinated assessment and package of care tailored to individual women with mental health needs during their pregnancy and for up to 12 months after birth. 1.15 The Early Start Ealing2 (ESE) service (Health Visiting) comprises of the Family Nurse Partnership3 (FNP) covering the whole of the Ealing Borough, and three health visiting teams working geographically across the locality. The health visiting service has clear and effective systems to identify and support children and families who would benefit from early help.
2 Early Start Ealing is a service for families - pregnant mums, expectant dads, parents, babies and children up to the age of five; bringing together workers from children's centres, early years, health and other specialist services. 3 The Family Nurse Partnership is a preventative programme for first time young parents. The programmes primary focus is improving the health and wellbeing of the child and mother in pregnancy, supporting parents understanding of their child's development and encouraging parents to fulfil their aspirations for their baby and themselves.
Page 102 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 15 of 47
The teams are co-located with the local authority’s ESE teams along with Ealing social workers. The locality leads and Early Start practitioners have access to Framework-I (the social care electronic records system) which means that multi-agency information can, where appropriate, be shared more easily between multi-agency partners.
1.16 We also saw a good use of the varied skill mix amongst the ESE teams comprising of; specialist health visitors (for families with complex needs), health visitors, community staff nurses, community nursery nurses, early start workers and health visiting assistants. This means children and their families can benefit from easy access to early help from a diverse skill mix. 1.17 Health visitors across Ealing ensure the full implementation of the healthy child programme4. Assessments are undertaken by health visitors at various stages following on from the birth of the child up to age five when handover to the school nurse service takes place. The healthy child programme aims to ensure that every child in Ealing gets the good start they need to lay the foundations of a healthy life. It is also an opportunity for health professionals to undertake checks to ensure the child and family are safeguarded. 1.18 School nursing in Ealing provides part of the integrated 0-19 service and is commissioned by Ealing Local Authority and services are provided by LNWUH. The current school nursing team is comprised of community nursery nurses, qualified school nurses and staff nurses. 1.19 There is an allocated school nurse in each primary and secondary mainstream school in Ealing, and they have effective and well embedded relationships with schools which can facilitate the early identification of need. However, due to a reduction in school nurse numbers, the school ‘drop-in’ service is no longer offered across Ealing. This means that the opportunity for children and young people to flag concerns and seek support in an environment where they feel comfortable has been diminished. This matter will be bought to the attention of Public Health commissioners. 1.20 Children who attend the Northwick Park Hospital ED are notified to the Ealing school nurse team by paediatric liaison and this is an effective process. However, we heard that ED notifications from other hospitals that serve the Ealing population, such as the Hillingdon Hospital, are not swiftly screened. This is due to other ED’s not triaging referrals in the same way as at Northwick Park Hospital. At present, the school nurse team have a three month backlog of ‘out-of-Borough’ ED referrals which need to be screened. We were advised that this is due to the sheer volume of ED notifications and a reduction in staffing capacity within the school nurse team. This matter will be bought to the attention of Public Health commissioners.
4 The Healthy Child Programme for the early life stages focuses on a universal preventative service, providing families with a programme of screening, immunisation, health and development reviews, supplemented by advice around health, wellbeing and parenting.
Page 103 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 16 of 47
1.21 The CAMHS service provided by West London Mental Health Trust (WLMHT) is a strong contributor into Ealing’s multi-agency early help offer to vulnerable children and young people. CAMHS practitioners are deployed to local authority area teams that provide early help services and enhance the support provided to children and young people and their families. These teams include the MAST, the Supportive Action for Families in Ealing5 (SAFE) teams, ‘Brighter Futures’6, the Looked After Children team and the Ealing Service for Children with Additional Needs (ESCAN). CAMHs also support the behavioural support teams who provide an in-reach service to schools for children who are at risk of failing education. The extensive reach of the WLMHT CAMHS service into the early help arrangements across Ealing ensures that emotional wellbeing and mental health needs are central to plans and interventions for children and young people who require additional or targeted support. 1.22 The single point of access into the WLMHT CAMHS service utilises a weekly multi-disciplinary team allocation meeting involving a senior CAMHS consultant and a clinician from the SAFE team. All new referrals into the service are directed to either one of the community CAMHS services or to the SAFE team. In this way, young people are offered support by the most appropriate service without delay. 1.23 There is a strong think child approach in the adult mental health team provided by WLMHT. Practitioners consider children who are associated with adult clients at the time they access the service through the trust’s single point of contact by the use of a templated risk assessment in the electronic patient record system. This alerts all practitioners to the client’s family make up. Risk assessments are updated frequently and whenever there are changes in a client’s situation, such as when they disclose they have entered into a new relationship. This provides an at-a-glance picture of the current or changing risk at any given time and enables better oversight by team managers.
5 SAFE gives information, advice and help to children and families to access the appropriate services and support to help before a manageable problem becomes bigger and more difficult to resolve. The team is made up of psychologists, therapists, counsellors, pupil/ school workers, family workers and other experts. SAFE also have links with other support groups and services in Ealing to ensure those children and families are supported in the area in which they live.
6 Ealing’s Brighter Futures Intensive Engagement Model is a complex, whole system intervention that was launched in June 2015. Its implementation was intended to support and enable the children’s social care workforce to build effective, consistent relationships with adolescents, families, communities and carers, and to use those successful relationships to bring about positive change, particularly those young people living at the edge of care.
Page 104 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 17 of 47
1.24 Ealing RISE (Recovery Interventions Service Ealing, provided by a consortium of Change Grow Live, Central & North West London NHS Mental Health Trust and Build on Belief and commissioned by Ealing Borough Council) is a drug and alcohol intervention service offering a community based support treatment and rehabilitation service for adult substance users. The service has an open referral system whereby people can ‘self-refer’ into the service or be referred by professionals. They operate from two hubs in Southall and West Ealing, share care with nine GP practices and also have a 24 hour crisis telephone service. 60% of referrals made into the service are ‘self-referrals’. 1.25 Ealing RISE practitioners make good use of the electronic client record system to comprehensively capture risk and maintain a chronology of safeguarding events. In records examined we saw that there was good consistency in the way that those records were maintained which means they are kept up-to-date with information held by the team in relation to clients using services and, on the whole, children and young people in their care. 1.26 Although Ealing RISE substance misuse services electronic client records are good; those same records did evidence a lack of professional curiosity and responsive multi-disciplinary and multi-agency information sharing. This is true of both the adult substance misuse service and the young person’s service. This is a missed opportunity to improve and build a comprehensive knowledge base regarding children and young people in the care of adult service users who can lead sometimes chaotic lifestyles which put those vulnerable young people at risk. A multi-agency approach to information sharing is integral to managing risk and the safety of vulnerable children and young people. This matter will be bought to the attention of Public Health commissioners.
In one record examined within adult substance misuse services we saw how a young person who was looked after and in the care of a children’s home disclosed to her case worker that she may be pregnant. Although this conversation was recorded in the electronic record there was no evidence of any discussion regarding the appropriateness of the relationship and also no subsequent conversation with the young person’s allocated social worker or carers to check on the young person’s safety. In another case examined we saw how a service user who also had a young child in their care had disclosed their concerns of being at risk from their ex-partner following a court non molestation order being granted. Although there was clear advice given on action to take to enhance their own and their child’s safety by the Ealing RISE practitioner, there was no recorded contact with the social worker to share those disclosed concerns.
Page 105 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 18 of 47
1.27 The LNWUH Genito Urinary Medicine (GUM) services and Contraception and Sexual Health (CASH) services provide flexible ‘drop in’ services without appointment to meet the needs of young people up to age 20 in Ealing who wish to seek advice regarding contraception and other sexual health advice. The CASH service provide dedicated young people’s services twice per week at times to suit young people not having to miss education. 1.28 Both the CASH and GUM clinics are provided by practitioners who, on the whole, have provided care and support to the young people of Ealing for many years thus being well placed to recognise their individual needs well. 1.29 Although the GUM and CASH service do not ‘hold cases’ in relation to their clients due to the nature of the service offer, we saw that the assessment process prompts practitioners to identify any safeguarding issues that might be relevant. We examined assessment documentation that prompts practitioners to ask sometimes difficult questions and we were further assured that those practitioners expand on the document by way of professional curiosity whilst still building and maintaining good working relationships with their clients.
Page 106 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 19 of 47
2. Children in need
2.1 The paediatric liaison team also maintains oversight of paediatric attendances at nearby hospitals such as Hillingdon (provided by The Hillingdon Hospital NHS Foundation Trust) and the Chelsea and Westminster urgent care centre. This enables them to them to identify if a child from Ealing is making multiple attendances at various sites, and can also help identify cases of Child Sexual Exploitation (CSE), and instances where a child may be involved in county line enterprises7.
2.2 The Paediatric liaison has good links with community services in Ealing and ensures that all vulnerable children are provided with support in the community. Paediatric liaison have well embedded links with the young person’s substance misuse team, and regularly make onward referrals to them for ongoing support in cases where it has been identified that a child or young person has been attended to ED due to drug and alcohol misuse. 2.3 Children who present at Northwick Park ED who are under 16 years of age will be seen on in paediatric ED. However, once a child reaches 16 they are triaged and treated within the adult ED and adult wards. Children who are looked-after of this age group are also not eligible to be treated on a paediatric ward, unless they have a recognised learning disability. Children aged 16 to 18 are not given the option to articulate where they would feel most comfortable to be seen, and therefore have little input into this element of their care and treatment once they reach their 16th birthday. Adult wards can be anxiety provoking for some young people especially those who are vulnerable. (Recommendation 2.2) 2.4 The ‘Jack’s Place’ paediatric ward at Northwick Park Hospital is well equipped to provide care and support to children and young people of varying ages. There are two nurse stations which allow staff good observation to the entire ward at all times. There is also a separate section for babies, infants and younger children and a purposely designed adolescent room, which affords those older children and young people who are required to stay on the ward privacy and space. 2.5 When a child is transferred from the paediatric ED to the paediatric ward and safeguarding concerns have been identified, a full individual risk assessment and comprehensive handover is undertaken. In addition to this, upon admission to the ward, all children are subject to an ‘activities of daily living assessment’ (a medical and social care assessment) which provides the child or young person with a further opportunity to discuss issues that may be of concern to them that they might not have been comfortable discussing on the ED, for example if an adult was present at the time.
7 County lines, or ‘going country’ means groups or gangs using young people or vulnerable adults to carry and sell drugs across county boundaries, including London boroughs and beyond. It is a tactic used by groups or gangs to facilitate the selling of drugs in an area outside of the area they live, reducing their risk of detection.
Page 107 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 20 of 47
2.6 Ealing travelling communities are served well by a named health visitor to provide them with specific care and support that best suits their chosen lifestyles. This means that children within those communities can be provided with services that ensures the safe delivery of care to them so that they are less likely to miss out on services provided. 2.7 School nurses are delivering the National Child Measurement Programme (NCMP) and are issuing a school entry health needs assessment for all children who start school. However, we heard that when health needs assessments are not returned, no standard response or proactive follow up of families is in place. Due to commissioning arrangements, no additional health and needs questionnaire is offered at other key stages. This hinders the early identification of emerging and unmet health needs in school aged children. This matter will be bought to the attention of Public Health commissioners. 2.8 LNWUH school nursing links with the LNWUH health visiting team are strong, and the co-location of school nursing and health visiting teams facilitates the effective and timely sharing of information and concerns. Health visitors and school nurses are both using the same electronic record system, which ensures that the child’s health and social history is easily accessible to the school nurse and can be used effectively to support a child who is transitioning from an early years setting into school. 2.9 Health visitors and school nurses routinely hold face to face handover meetings when a child with health needs or safeguarding concerns is transitioning to the school nursing service. This ensures that the school nurse is well informed of the child’s risks and vulnerabilities and can continue to provide good continuity of care and support once transition is complete. 2.10 School nurses are not provided with any training or support from CAHMs to assist them in their engagement with children and young people who have emotional wellbeing needs. School nurse practitioners report that when referrals are made to CAMHs, children are waiting for significant lengths of time until they can access support and therefore there are delays in their needs being met. Waiting times are exacerbated by school nurses not referring into CAMHs directly, but by referring the child to the GP who then requests to see the child at their practice in order to complete a CAHMs referral. This matter will be bought to the attention of Public Health commissioners.
2.11 Young people who elect to attend colleges to pursue their education are no longer able to access support from the school nursing service. Therefore, the school nursing offer is not equitable to all young people aged 16-19 as the school nurse service is not extended to them. This matter will be bought to the attention of Public Health commissioners.
Page 108 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 21 of 47
2.12 Children schooled at home or who have disengaged from education also does not currently receive any school nursing support. As school nurses are not commissioned to support children not currently in mainstream education, the opportunity to assess if the child’s parent is misusing their right to home educate to conceal risk and vulnerability, is missed. This matter will be bought to the attention of Public Health commissioners. 2.13 Throughout our review of the records of children and young people receiving a service from WLMHT CAMH, we noted that the voice of the child was clearly evidenced and recorded. Records examined were child focused and prominently described the wishes and feelings of the child or young person in a way that demonstrated that they were actively involved in their own support planning. 2.14 Practitioners from the WLMHT CAMH service play an active role in supporting children in need in Ealing. In cases examined, we saw that CAMHs practitioners attend child in need meetings and actively contribute information and carry out activity agreed as part of the child in need plan. As with early help, this ensures that children’s emotional wellbeing and mental health are viewed as part of the bigger picture of need and lead to better, more meaningful child in need plans. However, in those records examined, it was not always clearly recorded what had been discussed at those child in need meetings or what the agreed actions were. Records were inconsistent and child in need plans were not always uploaded to the electronic patient record system. This means that other users of the record may not have a clear picture of their role in supporting a child due to the variability in the detail of the information. (Recommendation 4.1) 2.15 Children and young people who have self- harmed and attend emergency departments that serve Ealing, benefit from a clear case management pathway where WLMHT CAMHs provide care and support. Children and young people up to and including the age of 15 who attend the acute hospitals where there is a paediatric ED and children’s ward with CAMH services provided by WLMHT CAMHs, are seen by a CAMHS clinician during the day. Children who attend those served EDs out-of-hours or at weekends will be seen by a CAMHS duty psychiatric registrar who has access to a consultant by telephone. The registrar is supported by an out-of-hours mental health nurse. Both these resources are rostered to work and so they are not on-call and this means that children and young people are seen in a timely way. Assessments were seen to be comprehensive and child focused and, where appropriate, support discharge to community services. 2.16 Young people aged 16 to 18 who taken to the Ealing hospital UCC and are in mental health distress are seen and assessed by the WLMHT hospital psychiatric liaison team, supported by CAMHS staff or the out-of-hours CAMHS practitioners at West Middlesex Hospital. This is primarily an adult team. However, our review of records showed that assessments are detailed and child/young person focused and that they also support effective discharge to the community CAMHS service.
Page 109 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 22 of 47
2.17 Children and young people who present at the paediatric ED at Northwick Park Hospital may be transferred to the paediatric assessment unit (PAU) for up to 24 hours whilst they wait for a CAMHs assessment from the out of hours CAMHs team provided by Central and North West London Foundation Trust (CNWLFT). However, we heard from practitioners on the ward that out of hours CAMHs assessments are often delayed. Staff on the paediatric ward told us that there have been recent cases where a child has been admitted to the ward over the weekend as they had to wait until Monday for a CAMHs assessment to be completed. This impacts on the capacity on the paediatric ward, and in some cases (for example where self-harm is a presenting factor) the child will require one to one constant observation to minimise the risk of further incidents of harm which might impact on workload. (Recommendation 6.1) 2.18 A newly developed transitions protocol has been implemented for children and young people who will require support from the WLMHT adult mental health service on transition from CAMHs. The protocol is aimed at enabling some flexibility when the young person reaches 18 in relation to a gradual hand-over of their care plan. In the WLMHT adult mental health service, we examined two cases and noted that the system is effective in ensuring the young person’s precise needs are well understood and clear plans made for a graduated hand-over of care from CAMHs to adult mental health. 2.19 Children who are referred for assessments for Autistic Spectrum Disorder/Condition (ASD/C) or Attention Deficit Hyperactivity Disorder (ADHD) are currently subjected to long waiting times for assessment. However, once admitted to the waiting list, children and young people are offered a range of services that will meet behavioural needs or support them with managing anxieties whilst awaiting further assessment and therapeutic interventions. This includes; the SAFE team, family support workers from the early help teams, the behavioural support team and sensory support from the integrated therapies service. Young people who develop an acute psychiatric need are prioritised for early neurodevelopmental assessment. 2.20 Women who experience mental ill-health during or following pregnancy are supported by a dedicated, well-resourced perinatal mental health team provided by WLMHT. Whilst there are challenges in relation to the six different birth units supported by the team, a robust pathway ensures that the service is consistent for all sites. 2.21 Where a woman is identified during pregnancy as requiring additional support, a multi-disciplinary team meets at 32 weeks pregnancy, comprising a perinatal mental health nurse and midwife and often including the health visitor and a member of the mental health recovery team. The team agrees a joint perinatal mental health plan that covers the antenatal and perinatal period and the plan is kept under review. This ensures a holistic view of the woman’s care is taken and any impact on the baby is well understood and planned for.
Page 110 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 23 of 47
2.22 Both GP practices visited in Ealing were seen to have effective arrangements in place to manage and follow-up children who are identified as vulnerable or at risk. This activity is coordinated by regular multi-disciplinary team meetings involving the GPs, practice nurse’s, midwives, health visitors and district nurses. School nurses tend not to attend due to capacity issues but both practices liaise with school nurse teams on a case by case basis if appropriate. We saw a number of examples where those multi-disciplinary meetings had helped the practice to coordinate activity to ensure children were kept safe.
In another case examined we saw that adult mental health practitioners have a clear understanding of safeguarding thresholds and make appropriate referrals to children's social care whenever there is a risk of harm to a child associated with an adult client. We saw that a woman who had a young son had been assaulted by her male partner (the client of the service) and that there were additional risks in relation to alcohol misuse that placed the child at greater risk. The practitioner recognised the risk and ensured a referral was made straight away to children's social care. The practitioner also went on to support the woman’s wish to make a complaint to the police. The practitioner’s advocacy of the woman in this case in this case ensured that both she and her child were protected.
In one of the cases we examined, we saw that a woman who had given birth during a weekend was identified as experiencing acute mental ill-health whilst still on the birth unit. After an initial assessment by the WLMHT Crisis and Assessment Team over the weekend, the perinatal mental health nurse completed a comprehensive assessment on the following Monday and identified a number of social factors, including domestic abuse that added to the risk of the mother’s mental health and her ability to care for her new born baby. We noted an exceptionally detailed and well-reasoned formulation of risk resulting in the mother ultimately being admitted, with her baby, to a mother and baby unit under a section of the Mental Health Act where her needs could be better assessed and met. At the point of her discharge sometime later, the perinatal mental health nurse compiled a comprehensive plan that outlined clear relapse indicators and a plan for mother, her supporters and associated health professionals to ensure risks were identified early and mother and baby were kept safe.
Page 111 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 24 of 47
3. Child protection
3.1 We heard that whilst the alert systems on casualty cards and the triage system used within the ED at Northwick Park Hospital are effective in highlighting risk, if a child has just recently become subject to a child protection plan or looked after, the alert may not show immediately on the child’s record. LNWUH Trust is aware that timely and effective sharing of information across health and social care is vital in aiding the identification of vulnerable children and young people and required to protect them from further harm. There is a plan to implement the Child Protection Information system (CP-IS). CP-IS will connect local authority social care systems with systems used in unscheduled care settings such as ED departments at Northwick Park and Ealing Hospital and also the UCC, notifying practitioners with immediacy when a child has become subject to a child protection plan or has been given looked after status. However, the CP-IS system cannot be implemented until the current electronic patient record system (Symphony) is upgraded. (Recommendation 2.3) 3.2 There is a clear did not wait policy in place within Northwick Park ED. When a child was bought into ED but did not wait to be triaged, or to be seen by a clinician post triage assessment, a letter is generated and sent to the child’s GP to inform them. A health visitor referral form is also completed, alerting their health visitor or school nurse of their attendance so further assessment and contact can be made with the child in the community and thus better ensure their safety and wellbeing. 3.3 In cases where the child is thought to have a serious medical condition or injury and may be at significant risk of harm as a result of not seeing a medical practitioner, Northwick Park ED practitioners will call the police and social care will be notified. Checks will be carried out as a priority to ensure that the child is safe, well and able to receive the medical treatment that they may need. A similar, effective system is also in place at the Greenbrook UCC at Ealing Hospital to ensure the safety of vulnerable children who attend the unit but did not wait to be seen. 3.4 In some cases, older young people who present with mental health concerns are placed on adult wards at Northwick Park Hospital. We were advised that individual risk assessments would be undertaken to mitigate any risk to those young people, but at the time of the review we could not be assured that the reasons and rationale for such decisions were being appropriately documented within patient records. (Recommendation 2.4)
Page 112 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 25 of 47
3.5 There is significant variation in the way referrals are being made into social care by practitioners at Northwick Park Hospital. We were advised that due to the Ealing social care e-mail address not being secure, acute staff have been advised to make referrals via fax, which is breach of the hospital’s information governance policy. Referrals can be made securely via ‘Egress Switch’ secure email, but updates from social care can only be received if the sender has created a receiver account, and updates are not being sent to a central location or safeguarding team. This means that if the receiver is absent from their place of work pertinent safeguarding information may not feature in the patient record. This issue has been flagged on the Trust’s risk register with an action plan in place. However, practitioners we spoke with were inconsistent in their understanding of referral processes. (Recommendation 3.1) 3.6 At Ealing Hospital’s UCC, we saw how that paediatric liaison will, on receiving attendance information, suggest that a referral is made to children’s social care if considered appropriate and one has not yet already been made. We examined one case where on initial examination the GP did not make a referral to social care but paediatric liaison suggested later that one be made. Although the reasons for a referral not having been made in the first instance was explained to us during our review, there was nothing written in the client notes on SystmOne that explained the GPs decision making rationale. It is important that, when making such decisions, then the reasons for them are clearly explained. In this instance the referral was rejected by social care. (Recommendation 5.1) 3.7 Expectant women in Ealing benefit from a comprehensive risk assessment when booking their pregnancy which is revisited at regular intervals throughout the pregnancy by midwives both at Northwick Park Hospital and in the community. In records examined we saw that questions pertaining to the increased risk of domestic abuse during pregnancy are also asked and the answers recorded accordingly. 3.8 Expectant women who disclose domestic abuse and/or violence are supported well through close links with the Independent Domestic Violence Advisors (IDVA) who offer support and guidance where domestic abuse is indicated. This also supports early identification of risk to children and young people who might witness and be affected by such domestic abuse.
We heard an example of a 15 year old boy who presented in paediatric ED as being aggressive due to his poor mental health. Due to his presentation, it was assessed that he could not be placed on the paediatric assessment unit due to the risk posed to other children and young people, so he was admitted to an adult ward to receive care and support. Managers we spoke with expressed their concern and frustration about the delay in accessing the CAMHs out of hour’s service and the impact that this delay has on the wellbeing of children and young people.
Page 113 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 26 of 47
3.9 We saw that there is good information sharing between GPs and the maternity service. We were further advised that the majority of midwifery bookings come from GPs in the first instance. The booking referrals template used by GPs is also used to highlight concern regarding medical or social vulnerability so that midwives will be aware of any concerns when interacting with vulnerable women. 3.10 Unborn children are generally safeguarded well by midwives. However, records examined contained variable chronologies of significant events and copies of child protection plans to protect the new born infant were also not visible in those records. This was also highlighted in one case we tracked where a mother and baby on a child protection plan for emotional abuse were discharged home without a discharge planning meeting or social worker being made aware of the birth. This incident was raised within the Trust and has been investigated. However, from those records examined we could not be assured that systems put in place are robust enough to ensure that risk of similar incidents occurring is appropriately mitigated. (Recommendation 2.5) 3.11 Good arrangements are in place to ensure timely follow up of those expectant women who do not attend their antenatal appointments as arranged. Midwives are tenacious in ensuring women are seen regularly during the antenatal period, therefore protecting the health of the woman and the unborn child. 3.12 Health assessments, care planning and review arrangements are well targeted within the Ealing LNWUH health visiting service. They were seen to be child centred, and recognise the diversity of children and their families’ needs. We were informed and also examined evidence of families’ ethnicity and language clearly documented with the targeted allocation of appropriate members of the multi-lingual skill mix team to support those families. 3.13 In cases where a child is at risk of disengaging from their school, the LNWUH school nurse will offer to conduct a home visit. Some home visits are carried out jointly with social care or a health visiting practitioner and this facilitates the school nurse to see the child in their home environment and offer the opportunity to identify additional concerns that may not have been apparent by seeing the child in a school setting. In some of the cases we examined, we saw that the offer of home visits was evident in the child’s health record. 3.14 If a child has been identified as a Child in Need or is on a Child Protection Plan but has no presenting health needs, the LNWUH school nurse will not keep them on their active caseloads due to a revision of the Safeguarding Children School Nursing Pathway. This cohort of children are now placed onto an inactive caseload which is not regularly subject to audit or regular review, and therefore the school nurse may not be aware of safeguarding updates or changes in the child’s circumstances.
Page 114 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 27 of 47
The change in the safeguarding pathway means that school nurses do not have oversight of all children who are at significant risk of harm due to the inactive caseload not being effectively audited or reviewed regular intervals. This matter will be bought to the attention of Public Health Commissioners. 3.15 In cases where a child moves out of borough, LNWUH school nurses have a clear protocol in place to ensure that the child’s needs, risks and vulnerabilities are clearly articulated to the school nursing service in the area where the child is relocating to. A standardised transfer form, containing clear summaries and chronologies, is consistently completed and shared. This increases the likelihood of the child continuing to be robustly safeguarded in their new area. 3.16 LNWUH school nurses are not using a standardised CSE identification tool when exploitation has been identified as a possibility. Whilst they are attending CSE strategy meetings to discuss cases where CSE may be a concern, the use of a standardised screening tool where risk is being considered may assist school nurses in the early identification of need, and enable them to provide a more proactive as opposed to reactive response and also support any referral to children’s social care. This matter will be bought to the attention of Public Health Commissioners. 3.17 WLMHT CAMHS practitioners are generally clear about child protection thresholds and make detailed referrals to the children's social care single front door, the Ealing Children’s Integrated Response Service (ECIRS). Most records we examined showed a good level of detail in referrals although there was no routine use of an assessment model or framework which would enhance the analysis of risk factors. The understanding of thresholds was not always consistent. (Recommendation 4.2)
In one of the tracked cases we examined we saw how the school nurse knew the child in the case but had removed them from her active case load due to the child having no presenting physical health concerns, despite the child being subject to a child protection plan. The child’s mother had raised concerns with regard to her child being sexually active with a significantly older person and that the young person might be at risk of exploitation. The School nurse had no prior knowledge of the child’s involvement with CAMHs and had not been made aware of the new risks the child was exposed to due to the child no longer being proactively monitored on the school nurse active caseload.
Page 115 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 28 of 47
3.18 There is no routine use of risk assessment tools for CSE within WLMHT CAMHs. In two cases examined we saw that potentially exploitative situations were correctly identified and referrals made, largely due to the diligence and professional curiosity of the staff members. However, the use of an established assessment tool would support practitioners to fully explain the risks arising from a young person’s situation and enable wider risks to be understood and informed decisions made. For example, in one case examined we saw that a key piece of information that was known about the perpetrator was not provided on the referral document. This was a missed opportunity to ensure children's social care and the CSE team were aware of key intelligence. (Recommendation 3.2) 3.19 WLMHT CAMHS practitioners routinely attend child protection conferences and provide information to enable the conference decision making process. CAMHS practitioners also attend core group meetings and ensure the child or young person’s mental health needs are foremost when measuring progress against plans. However, as with child in need plans, records of conferences are not routinely uploaded to the electronic patient record system and the level of detail in the record’s progress notes is inconsistent. This means that other users of the record may not be clear about the current child protection plan, a particular risk if the care co-ordinator is on leave or if the case gets handed over to another practitioner. (Recommendation 4.1 as at 2.14 above) 3.20 Child protection referrals made by WLMHT CAMHS practitioners are not always uploaded on to the electronic patient record system. This was the case for two of the three cases we tracked in CAMHS. Although the nature of the referral was outlined in each case within the progress notes, the absence of a clear record of referrals made means that the record is incomplete and there is no surety about the extent of the information passed at the point of referral. (Recommendation 4.1 as at 2.14 and 3.19 above)
In one case we examined, we saw how a young person of primary school age was previously being supported on a child in need plan. The young person’s anxiety and behaviour rapidly deteriorated following a child in need meeting and their suicidal thoughts and verbalisation of those thoughts also escalated. Within a number of weeks it became clear that the young person was at significant risk of self-harm with their parents not being able to control their outbursts. In this case the young person’s clinical needs had been managed and a placement was found to keep them safe while their mental health needs were assessed. However, during this period of escalation, the young person’s social worker was not informed of their deteriorating condition and there was no child protection referral made. This was despite the practitioner having clinical supervision during this period.
Page 116 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 29 of 47
3.21 WLMHT adult mental health practitioners routinely attend all child in need, child protection and core group meetings relating to children of their clients. Reports are submitted to the child protection conference chair in advance of the meeting and are also shared with parents. In cases examined we saw that reports are not always submitted in the same format, but are nonetheless detailed and analytical, enabling the conference to make good decisions about children subject of child protection plans. 3.22 A lack of a single standardised template and guidance on how to complete this is hindering practitioners within Ealing RISE substance misuse services to effectively analyse risk to inform case conference reports, although the service can access the multiagency case conference report template that does facilitate risk assessment. Although information is being shared, and in the majority of cases examined showed practitioner involvement in statutory meetings, there is room for improvement in the quality and consistency of reports submitted to inform the decision making process. This matter will be bought to the attention of Public Health commissioners. 3.23 Adult substance misusers who have responsibility for the care of children and young people must agree to a home visit from Ealing RISE practitioners, however in some cases due to risk concerns an unannounced visit may take place. This is so that practitioners can assure themselves of the home environment and subsequent safety of those children service user care. It is also a requirement that those service users prescribed a substance substitute such as methadone, must agree to the fitting of a ‘safe box’ so that medication can be stored safely out of the reach of vulnerable young people. Safe storage boxes are also offered no non prescribed clients. This is checked at subsequent home visits to ensure compliance. 3.24 Both GP practices we visited were confident in how to refer a child or family to children’s social care via email to the ECIRS. In records reviewed, we examined detailed safeguarding referrals which clearly articulated risk. This means that the decision making process at the ECIRS and the MASH will be well informed.
In one tracked case we examined we saw how the client electronic record contained appropriate ‘flags’ to highlight to the practitioner that there were safeguarding concerns and the safeguarding template had been completed. There was evidence of discussions held with social services but not with associated health partners, in this particular case midwifery services. Although the Ealing RISE practitioner did attend case discussions, we saw that reports submitted were not analytical and detailed in relation to recognised concerns. They were more of a chronology of contacts between practitioner and service user. This means that had that practitioner not been able to attend the conference meetings in person then the conference might not have had full access to important information.
Page 117 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 30 of 47
3.25 Where CSE risk is considered, GPs are not using appropriate tools to further identify risk and therefore strengthen referrals made to children’s social care. This means we cannot be assured of practitioners identifying some important safeguarding concerns as the approach to undertaking risk assessment is too variable. There is an over-reliance on professional curiosity with decisions not underpinned by the use of available screening tools. (Recommendation 1.1) 3.26 Both GP practices visited had appropriate processes in place to ensure that reports written in response to requests for information sharing for child protection conferences and core group meetings were responded to appropriately and those seen in patient’s records were detailed in nature so as to inform the decision making process. Where the GP practice had received child protection conference minutes, these were uploaded onto the patient’s record and appropriate flags updated on electronic patient records. 3.27 In both GP practices visited we saw that the details regarding adults accompanying a child to a GP appointment is not consistently recorded and needs strengthening to include full names and relationships. For example, recording simply ‘mum’ or ‘dad’ as opposed to recording their full details is insufficient, particularly if the person accompanying the child is not a patient at the same practice and their own records are not linked to the child’s. This is important not only to ascertain who has parental or carer responsibility for a child or young person and therefore able to consent to treatment, but in a fractured family with complex dynamics, the recording of names is as relevant as the reported relationship. (Recommendation 1.2)
Page 118 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 31 of 47
4. Looked after children
4.1 The Looked After Children’s health service in Ealing is provided by LNWUH. We saw that there are effective processes in place to meet the health needs of Looked After Children in Ealing through services provided. All initial health assessments of children and young people taken into the care of the London Borough of Ealing are undertaken by a team of appropriately qualified paediatricians and associated specialist doctors in line with intercollegiate guidance and best practice. 4.2 Initial health assessments reviewed were seen to contain appropriate and adequate information to inform the reader of the child or young person’s needs when first becoming looked after and, where appropriate, demonstrated the ‘voice of the child’ to show that they had been involved in the assessment process. 4.3 Ealing looked after children placed ‘in borough’ receive timely access to Review Health Assessments. The LNWUH Looked After Children’s nurses have changed their availability to 8am-6pm to offer additional flexibility to children and young people in their care, especially those not wishing to interrupt their school day. This was in response to service user feedback about the service. 4.4 Overall, review health assessments we examined undertaken by the Looked After Children’s nurse specialist were seen to contain detail that ensured care plans were SMART and support the child’s health needs being met. 4.5 Review health assessments examined also demonstrated that consent was routinely sought and in some cases those consenting young people had signed their assessment to demonstrate this. We also saw a consistent approach to raise and discuss internet safety within all review health assessments seen. 4.6 Some records seen within the Looked After Children service demonstrated that, where issues were identified, they were not always explored further to measure any impact or if additional support might be required. In one record examined we saw how the young person was noted as being underweight and that this was a worry to their carer. However, there could have been greater exploration of their physical activity and possible impact on their physical activity against food intake in preparation for the referral offered to be assessed by a dietician. (Recommendation 2.6) 4.7 LMWUH Looked After Children nurses are not using a local or national CSE tool to support exploration of CSE where it is indicated as a possible risk. The use of such screening tools, especially where a referral is made to children’s social care, might strengthen that referral and thus support the decision making process. Practitioners we spoke with articulated well how they would escalate concerns in relation to CSE but did not use tools to support this. (Recommendation 3.2 as at 3.18 above)
Page 119 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 32 of 47
4.8 The LNWUH Looked After Children team have established processes to support a consistent standard of care for Ealing children placed out of the borough. Service level agreements are established with the area undertaking the review and an information pack is issued by the Ealing Looked After Children team outlining guidance and expectation of the area undertaking the review health assessment. The last review health assessment is also shared with the receiving area. This is further supported by rigorous quality assurance by the Looked After Children lead community paediatrician of all out of borough review health assessments. We heard how this has led, in consultation with the allocated social worker, to children being brought back to Ealing for their review health assessment if it is felt their needs are not being adequately assessed or met elsewhere. 4.9 All unaccompanied asylum seeking children receive a comprehensive initial health assessment by LNWUH clinicians who have received additional training in relation to assessing the holistic health needs of this vulnerable cohort of LAC young people. 4.10 One unaccompanied asylum seeking child’s initial health assessment we examined captured well the voice of the child and the impact of experiences they had been exposed to. The emotional health and wellbeing of the child was assessed through the use of the evidence based ‘Impact of Events Scale’8. We noted in another case reviewed that, although the young person reported feeling ‘normal,’ the tool assisted the practitioner in objectively identifying the risk of Post-Traumatic Stress Disorder. This work is ensuring unaccompanied asylum seeking children receive timely help to address emotional trauma they may have experienced.
8 The Impact of Events Scale is a widely used screening tool measuring children at risk for post-traumatic stress symptoms, and is designed to be used in children aged eight years and over. It has been applied in a variety of cultures as post-traumatic stress symptoms in children are more similar than they are different from one culture to the other.
In one case examined we saw how a young person placed in care had been the subject of neglect. It was correctly identified by the Looked After Children nurse that the young person’s behaviours were likely to place them at risk of being sexually exploited. The nurse raised this with the young person’s social worker and challenged them when they felt that their views regarding the case were not being given due consideration and, following being provided with advice and guidance in supervision on how to progress the case, the young person was subsequently placed in a setting that would provide them with a sense of increased safety. However, the approach in this particular case would have been enhanced by the use of available CSE screening tools to better articulate those risks already identified.
Page 120 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 33 of 47
4.11 The LNWUH Looked After Children team engage well with care leavers and seek to ensure their health needs are met as they move into adulthood. When leaving care, young people receive a comprehensive summary of their health history which was developed in association and in consultation with the care leaver’s councils. Another outcome of liaison with care leavers is for Looked After Children health clinics being run in the Local Authority Horizons Centre9. Young people are also directed to the comprehensive information contained on the NHS GO app10. 4.12 The LNWUH CASH service has developed good relationships with the Looked After Children service, recognising well the additional vulnerabilities of this particular cohort of young people. Although the CASH service provides confidential care and support to young people in Ealing, if a young person requests, then a member of the Looked After Children’s team will accompany them to a CASH clinic to provide support. This means that those vulnerable young people are supported well to obtain appropriate care which they might not otherwise choose to do. Where a young person is known to be Looked After attends a drop-in clinic they are ‘fast tracked’ to a consultation with a practitioner to better assure engagement with them.
9 Ealing Horizons Centre is part of Ealing social services leaving care programme in partnership with Ealing Youth and Connexions Service. The centre offers young people in care and those who have recently left care a 'safe space' where they can share experiences, seek information, help and advice in order to plan and prepare for independent living. The centre also promotes inclusion through programmes of social education, personal development, and recreational activities in an informal and relaxed environment. 10 NHS Go is a free to download health app designed for young people by young Londoners. It gets its information directly from the data that fuels NHS Choices but is organised differently, with topics and articles that appeal to young people. It is an up-to-date resource relating to issues that might affect young people as they are taking greater responsibility for their own health.
An unaccompanied asylum seeking young person had undertaken a long solo journey to the UK from their own country. As part of the initial health assessment the paediatrician sensitively explored if any sexual harm had come to the young person during the journey, and it was disclosed that this was the case. Following on from the disclosure, we saw how a high level of liaison between clinicians was undertaken to identify the right services to manage the young person’s physical health needs and further to support them to access them. The disclosure also led to the paediatrician advocating for the young person who then shared the distress caused to them by living in supported lodging in close proximity to members of the opposite sex not known to them. Joint discussions with the local authority led to more appropriate accommodation being found where the young person then felt safe.
Page 121 of 324

Review of Health services for Children Looked After and Safeguarding in Ealing Page 34 of 47
4.13 The Ealing CCG Named GP for safeguarding children has developed a Looked After Children information pack. This has been distributed to GPs across Ealing informing them of the definition of a Looked After Child, the demographic of Looked After Children in Ealing, the additional risks posed to Looked After Children and their responsibilities in relation to informing the health assessment process. The pack, including the LNWUH ‘Rainbow Guidance’ is also sent to any out of Borough GPs undertaking an Ealing child’s LAC Health Assessment. Use of this guidance was evident in both Initial and review health assessments seen during our review.
Page 122 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 35 of 47
Management
This section records our findings about how well led the health services are in relation to safeguarding and looked after children.
5.1 Leadership and management
5.1.1 Health access to multiple health electronic systems and also social care electronic records at the MASH, with the facility to also update those records, is a positive step to ensure the safety of vulnerable children, young people and families. Having such access enables the health practitioner at the MASH to be able to maintain full and detailed records and also undertake accurate checks on children, young people and families of concern. Information sharing protocols ensure that as electronic systems develop as planned then such access will continue. 5.1.2 There is strong, visible leadership and management within the ED at Northwick Park Hospital. The head of safeguarding children has been in post for 12 months and has successfully integrated the safeguarding team in Ealing with the neighbouring boroughs of Harrow and Brent, to ensure that the teams work together in a co-ordinated way to safeguard children and young people who may be transient across Boroughs. The move from silo working has resulted in greater information sharing, along with a consistent approach to safeguarding which has been adopted across sites. This means that if a child from Ealing presents at ED’s in neighbouring boroughs then they are more likely to receive equitable standards of care. 5.1.3 Joint strategic work is ongoing to improve the health of Looked After Children through the Ealing Looked After Children Wellbeing Project. Data has, for example, identified that more Looked After Children are obese than those not Looked After. The CCG Looked After Children leads are working with Public Health and the local authority to set up initiatives that give Looked After Children free access to local fitness facilities, foster carers access to dietetic advice and also a CAMHS psychologist up-skilling Looked After Children’s nurses regarding the underlying issues that may be associated with overeating to support discussion in health assessments. This collective approach recognises the complexity of weight management and is taking a multi-agency approach to tackling the problem for an already vulnerable group of children.
Page 123 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 36 of 47
5.1.4 A joint project to produce a Foster Carers Handbook is currently in final draft. This has been created in conjunction with looked after young people and foster carers but has yet to be published. We had access to a draft copy of the handbook and saw that it contains relevant information that will be of use to foster carers in Ealing and that it contains material that evidences co-production with those service users and carers. 5.1.5 There is a strong collaborative approach to audit from the Looked After Children service provider and Designated Doctor in Ealing and these are working towards improving outcomes for children and young people. A well-developed action plan is in place for the Looked After Children service which this forms part of the annual report. Evidence of work seen demonstrated that it had progressed well over the year. An example of ongoing work is an audit to assess whether transition planning was robust for young people placed out of borough leaving care. This then led to focused care planning on the health needs of a number young people in readiness for them moving to adult health services. 5.1.6 There are some recognised capacity issues within the health visiting service. We were informed that one of the three teams in Ealing has reached a critical staffing level with a 40% practitioner vacancy rate. This is currently on the LNWUH risk register and steps have taken to mitigate risk including, for example, part time health visitors currently undertaking additional ‘bank’ hours to manage the shortfall. LNWUH is also planning to utilise the use of appropriately trained agency staff. We were given assurances all bank or agency staff are, and continue to be trained at level three safeguarding children training as recommended by intercollegiate guidance. 5.1.7 Management oversight and review supports the effective tracking of risks to children and improvements in child health outcomes within the LNWUH health visiting service. The health visiting teams have a robust duty and triage system with good managerial oversight of all referrals made to children’s social care and also of notifications and requests for information coming into the service.
This means risks to children are effectively tracked and appropriate plans and interventions can be put into place in a timely manner to improve outcomes for children. 5.1.8 One of the locality leads for the LNWUH school nursing service is a non-clinician from a social care background. We heard how she has worked well to ensure that school nurses are not only completing clinical assessments, but are taking an holistic, ‘think family’ approach when engaging with the children and young people of Ealing. She is also able to access local authority records which further support school nurses in being able to quickly and efficiently obtain additional information concerning the child to support their own risk assessment and decision making processes.
Page 124 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 37 of 47
5.1.9 Partnership working between WLMHT and children's social care is well developed at both strategic and operational levels. Vulnerable adolescent panels with leaders from the WLMHT CAMHS and children's social care meet regularly to discuss individual cases where there are complexities that have led to delays in the progress in those cases, whether due to processes or availability of resources. The purpose of these panels is to ensure that where progress is delayed then the reasons are dealt with at an operational management level and that work continues to provide good outcomes for young people.
5.1.10 Partnership boards have recently been set up between the CAMHS and the local authority at executive level. These panels are intended to improve multi-agency pathways and to agree programmes to implement changes that would lead to systemic improvements. For example, the most recent board discussion relates to improvements in the way that children and young people with Special Educational Needs and Disabilities (SEND) are facilitated to gain access to services; this latest discussion is very recent and so at the time of our inspection we are unable to say whether this has yet made an impact. 5.1.11 Within WLMHT there is good management oversight of safeguarding children activity in relation to children who are associated with clients of the adult mental health service. There are daily ‘zoning’ team meetings where all cases that have complex features or specific risk factors are discussed and any additional activity required by the care co-ordinators is triggered. Clients who have access to children and where there are safeguarding concerns are discussed at the Monday zoning meeting and this ensures any risks are discussed fully and action taken in a timely way to mitigate those risks. In the cases we sampled in the East recovery team, we noted that action that had been agreed at the zoning meetings had been taken including referrals to children's social care. 5.1.12 Managers in the WLMHT adult mental health service also have a clear picture of children and families of clients where there are safeguarding concerns, including children who are referred to children's social care and children who are the subject of child in need or child protection plans. A ‘safeguarding referral map’ database is updated with all new information about children. This is used to trigger discussion at the daily zoning meetings and also to provide the WLMHT safeguarding team with monthly data returns. This eliminates the risk of children and young people of clients being overlooked and is evidence of the strong think child approach reported in early help above. 5.1.13 In both the WLMHT CAMHs and adult mental health services, referrals to children's social care are not routinely copied to the trust safeguarding team at the point of referral. Instead, a monthly return is required by each service team which enables the safeguarding team to gather data about the nature and extent of referrals. In the absence of any formal means of sampling cases, this system is not sufficiently robust to enable proactive monitoring of the nature and quality of referrals by the safeguarding team. (Recommendation 4.3)
Page 125 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 38 of 47
5.1.14 CGL substance misuse services have been responsive in their review of the GP shared care option for clients following a small number of patient deaths. A deep dive audit of those clients who receive shared care has led to recommendations to improve the offer. As part of the subsequent action plan, a review of safeguarding risk indicators for these clients is being revisited. This is an ongoing piece of work within the Ealing RISE service with the aim to improve the shared care package on offer.
Page 126 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 39 of 47
5.2 Governance
5.2.1 The Central London, West London, Hammersmith and Fulham, Hounslow and Ealing Clinical Commissioning Groups collaborative (CWHHE) provided a Savile Report to provide assurance regarding arrangements and practices in place to protect vulnerable people following on from the Lampard ‘lessons learnt’ report of 2015 and subsequent NHS investigations. This especially relates to safeguarding, access to patients and listening to and acting on patient concerns. Current practice in Ealing was examined and strengthened where required to ensure that the safeguarding team across the CWHHE collaborative are assured that robust and evidence based procedures are in place to protect vulnerable children and young people and that governing bodies are kept up-to-date and informed. We saw that practice in relation to the report and its findings are regularly reviewed. 5.2.2 The theme of the November 2017 Ealing Safeguarding Children Board (ESCB) conference was to promote an understanding of domestic abuse and the effect it has on children, adolescents, families and the elderly in Ealing. The conference bought together professionals from across the Ealing partnership including; social care, the police, health and the private and voluntary sector with the objective to share experiences and responsibilities, learn from domestic homicide reviews and serious case reviews and work together across the partnership. We saw that feedback following on from the conference was overall positive with partners describing feeling empowered and encouraged to share the experience with colleagues in their respective workplaces. This means that those delegates in attendance at the conference better understood and could share with colleagues the importance of identifying and reporting domestic abuse to protect not only those people subject to the abuse but also those witnessing it. 5.2.3 This first CWHHE joint safeguarding report dated January 2018 provides an updated position on the key safeguarding activity within the main provider trusts which CWHHE commissioned during quarter one 2017-18 into one document. This approach is envisaged to develop over time to reflect the views of those CCGs to ensure required strategic content and local reflection. In addition, the report highlights key issues in relation to multi-agency working and compliance with the Children Act, Care Act and other CCG requirements in respect to NHS England. Future reporting could include (depending on trending issues) safeguarding supervision, Ealing Violence Against Women and Girls (VAWG) and looked after children progress. The report also provides assurances that Ealing CCG is compliant with the duties and responsibilities placed on it by existing legislation, guidance and frameworks to ensure children and young people are supported by practitioners who are suitable trained to recognise and report safeguarding concerns.
Page 127 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 40 of 47
5.2.4 The Out Of Borough Looked After Children Transition Review dated July 2017 recognises the CCGs statutory responsibility to support Ealing Local Authority to ensure that Ealing’s Looked After Children’s health needs are met irrespective of where the child or young person is placed, including those placed out of Ealing. The review aimed to identify all Looked After Children who were in their last years of being in care and placed ‘out of borough’ to establish if their health needs were being met. It also seeks to identify those children and young people Looked After who had been assessed as requiring SEND provision to assess if their health needs were being met and that appropriate transition planning had or was taking place. The report identified that there was strong evidence to show that, for example, just under a quarter of 17 year olds placed out of borough required SEND provision and further that just under half of all 17 year olds placed out of borough lived with a mental health, behavioural or developmental disorder. As a result of the findings contained within the report, the Designated Doctor for Looked After Children identified a need to work with the Looked After Children’s team to ensure appropriate transition referrals were made where they had not been, that young people placed out of the Ealing area do not wait longer for a CAMH assessment than those placed in the Ealing area and that those young people requiring SEND provision would be reviewed with greater scrutiny to ensure appropriate transition planning was in place. 5.2.5 WLMHT has well-established and responsive governance arrangements for safeguarding that provides good accountability and generally good oversight of safeguarding activity. There are safeguarding children leads for each of the localities that serve each of the three West London Boroughs and for the specialist forensic and high security hospital services. This includes a dedicated safeguarding lead for CAMHs and adult mental health services provided by the trust in Ealing. The safeguarding leads work closely with the operational managers and the teams to support their safeguarding activity, develop safeguarding practice and promote a safeguarding culture. The visibility and influence of the safeguarding leads and the strong safeguarding culture was evident in our interviews with managers and practitioners and in the strength of the ‘child’s voice’ in the records we reviewed.
5.2.6 The WLMHT safeguarding team is led by a medical director of safeguarding children and vulnerable adults. The safeguarding team is resourced with a named nurse, named doctor, safeguarding children advisor, practice development lead and business support staff. However, given the size of the trust’s geographical footprint and the population it serves, it is unclear if the team has sufficient capacity to carry out a quality monitoring role on live cases. For example, there is currently no dynamic system of monitoring the quality of referrals to children's social care with a reliance on monthly returns to provide management information. (Recommendation 4.3 as at 5.1.13 above) 5.2.7 There is a strong culture of learning and the sharing of learning at all levels within Greenbrook Care and this is shared across all of their Urgent Care sites including that at Ealing. This ensures that practitioners delivering care and support to vulnerable children and young people are aware of their associated roles and responsibilities.
Page 128 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 41 of 47
5.2.8 Commissioners across Ealing effectively consider learning from both local and national serious case reviews. Ealing safeguarding children board action plans seen were detailed and clearly focussed on the findings from those serious case reviews and what actions are to be implemented to negate further risk. However, where, for example, risk assessment tools were reviewed and amended in line with report findings, there is more to do to ensure that those tools are used effectively by practitioners in there interactions with children and young people where risk is identified. The use of screening tools, such as when CSE is indicated, is too variable. Robust oversight and quality assurance measures would better ensure those tools readily available are used effectively. (Recommendation 3.2 as at 3.18 and 4.7 above) 5.2.9 In one GP practice we visited we saw that the use of alerts on the SystmOne electronic patient record was effective in identifying children and young people with safeguarding concerns. This also included the recognition of the risks posed by, and vulnerabilities of, adults within the household with appropriate linking of information between parent and children’s records. However, this was not seen to be as strong in the second GP practice visited and it was recognised that the use of alerts could be strengthened. Better governance procedures would ensure a more standardised approach to the use of alerts across GPs in Ealing. (Recommendation 1.3) 5.2.10 There is more to do by leaders and managers to ensure continuity of both understanding and implementation of methods to refer cases of concern to children’s social care. Too many practitioners across multi-disciplinary services in Ealing have a different understanding of the referral route; be it by email, fax or delivered by hand in person. This is particularly important as Ealing shares its borders with other London boroughs that might have different methods in which way a referral should be made. (Recommendation 3.3) 5.2.11 There is variance in the way that safeguarding teams across providers in Ealing are made aware of referrals made to children’s social care and thus maintain oversight of both the quality of those referrals and their effectiveness in influencing the decision making process. Too often we heard and saw variations in the quality of referrals made to social care and we heard how practitioners making those referrals are not given feedback on either the quality of that referral or any eventual outcome. (Recommendation 3.3 as at 5.2.10 above)
Page 129 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 42 of 47
5.3 Training and supervision
5.3.1 The LNWUH target for level three safeguarding children and adults training is 90%, but currently 80% of staff who are required to be trained to level three in accordance with intercollegiate guidance have completed this training. Leaders at Northwick Park Hospital are aware that regular audits and data cleansing needs to be undertaken in order for them to form an accurate picture of exactly what percentage of staff require training commensurate to their roles, as there is a cohort of staff and clinicians highlighted as requiring training who are no longer with the Trust, are on sick or maternity leave. This means that current data cannot be accurately relied upon and as such the 80% figure might be inaccurate in the positive or negative. (Recommendation 2.7) 5.3.2 Within LNWUH there are two full time Named Nurse posts (one acute and one community), linked to Ealing borough based services. One of these posts is currently vacant and this has impacted on the ability to provide regular 1:1 structured safeguarding supervision within acute settings, although 1:1 advice and guidance can be requested and is provided as required. 5.3.3 Group safeguarding supervision is provided on a three monthly basis at the Northwick Park ED, and this has been successful in developing practitioner’s knowledge base and safeguarding competencies which ensure that they are able to effectively identify and respond to safeguarding concerns. In addition to group supervision, weekly ‘Safety Net’ meetings are held in Northwick Park ED and are attended by the Named Nurse, Named Doctor, ED nursing staff and consultants. Outside agencies such as the young person’s drug and alcohol service also attend on a regular basis. During these meetings, cases that have presented at the ED during the previous week are discussed. Good practice is highlighted and shared, and cases are screened to ascertain if any further action is required. These meetings also provide an opportunity for peer support and reflection. 5.3.4 Safeguarding supervision is regularly provided to all LNWUH school nurses, Family Nurse Partnership practitioners and Health Visitors. One to one child protection supervision is provided on a quarterly basis and group supervision is provided every six weeks. Group supervision provides a forum to discuss more complex and challenging cases and receive peer support and guidance. This ensures that staff are well supported and that their safeguarding practice is subject to regular scrutiny and challenge.
Page 130 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 43 of 47
5.3.5 WLMHT have made significant inroads in ensuring that CAMHS staff and relevant staff in the adult mental health service have all received relevant training to recognise and report children and young people’s vulnerabilities and safeguarding concerns. At the time of the trust inspection in November 2016, the compliance rates of training at level three and level three specialist of the relevant guidance were around 60%. This has now improved and, at the time of our inspection, the numbers of staff who are up-to-date with level three or level three specialist training varies between 80% and 90% (against a trust target of 90%), although the figures are slightly skewed in some teams due to the lower numbers of staff in those teams. 5.3.6 WLMHT have a well-developed system for monitoring training compliance and so we are assured that they remain on trajectory to deliver relevant safeguarding training to their key staff groups. This means that children and young people using CAMHS or clients of the adult mental health service who have access to children are supported for by staff with the appropriate safeguarding competencies. 5.3.7 There is a multi-layered supervision model in use in the WLMHT CAMHs service. One-to-one clinical supervision is offered to all staff. All of a staff member’s cases are routinely reviewed at each clinical supervision and this ensures those cases of concern are properly discussed. In addition, complex and high risk cases are discussed at weekly team meetings. Lastly, reflective practice sessions are also arranged by the trust’s safeguarding team and these are open for all staff members to attend and to discuss cases of concern. 5.3.8 WLMHT practitioner attendance at reflective practice sessions is not mandatory and data supplied by the trust shows that attendance is variable from session to session. The absence of discrete safeguarding supervision can lead to an overly clinical focus to cases where there are complex safeguarding features and this was evident in one case we examined. (Recommendation 4.4) 5.3.9 Managers in the WLMHT adult mental health service run a weekly safeguarding clinic. Practitioners can book single or multiple 15 minute slots during the day to discuss safeguarding cases of concern that might require additional support and guidance or to help with their thinking around particular issues. Other team members and agency staff are invited to attend these clinic slots to enable a multi-disciplinary or multi-agency discussion of the issue. A strength of the system is that clients themselves are also invited so that they are involved in the discussions and can add their views on the issues or the solutions and this leads to better outcomes for children and young people. 5.3.10 As with CAMHs, adult mental health practitioners also receive regular scheduled clinical supervision during which all safeguarding cases are discussed and any further actions are agreed. As well as being noted on client’s records, the outcome of supervision sessions are noted on the daily zoning meeting template which ensures that actions can be tracked.
Page 131 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 44 of 47
5.3.11 There is a good training offer to practitioners within the LNWUH CASH and GUM services to ensure they are qualified to meet the needs of vulnerable young people in their care. Practitioners who are involved in any one-to-one work with young people are trained to level three safeguarding in line with intercollegiate guidance. Healthcare assistants are also trained to the same level recognising the important contribution they play in the safeguarding. 5.3.12 The supervision model within the CASH service would be strengthened by the addition of structured, mandatory safeguarding supervision. The current practice is fragmented and relies heavily of practitioners seeking advice and guidance from the safeguarding team as and when required. This means that those same practitioners might be providing care to a young person without recognising risk that might be better identified within more formal, recorded safeguarding supervision. (Recommendation 2.8)
Page 132 of 324
Review of Health services for Children Looked After and Safeguarding in Ealing Page 45 of 47
Recommendations
1. Ealing CCG should:
1.1 Ensure GPs use recognised screening tools to assist the safeguarding process where vulnerability is identified.
1.2 Ensure that GPs are thoroughly recording the details of accompanying adults when children attend a consultation.
1.3 Ensure that GP practices across the Borough manage the use of alerts on
electronic patient records to provide consistency in the way that those records are managed.
2. London North West University Healthcare NHS Trust should:
2.1 Prioritise the amalgamation of paper records and electronic records so that
potential risk can be identified on those electronic records at the earliest opportunity and that those electronic records are complete.
2.2 Provide young people aged 16 to 18 the opportunity to be seen in either the
paediatric ED or the adult ED according to their own needs and wishes.
2.3 Expedite the upgrading of patient electronic records systems at Northwick
Park ED to ensure the implementation of CP-IS can be undertaken at the earliest opportunity.
2.4 Implement methods to ensure that when young people are admitted to adult
wards when in mental health distress or for any other reasons then those reasons must be clearly documented to provide an accountable audit trail.
2.5 Ensure that patient records are appropriately maintained and complete and
contain up-to-date information to inform practitioner interactions with vulnerable pregnant women and unborn children.
2.6 Ensure that practitioners explore need and evidence those explorations by
recording those explorations in client records. More robust quality assurance of records will also assure leaders of the quality of such work.
2.7 Ensure that there are systems in place at the earliest opportunity to assure
themselves of the accuracy of training records in line with intercollegiate guidance and provider targets.
Page 133 of 324
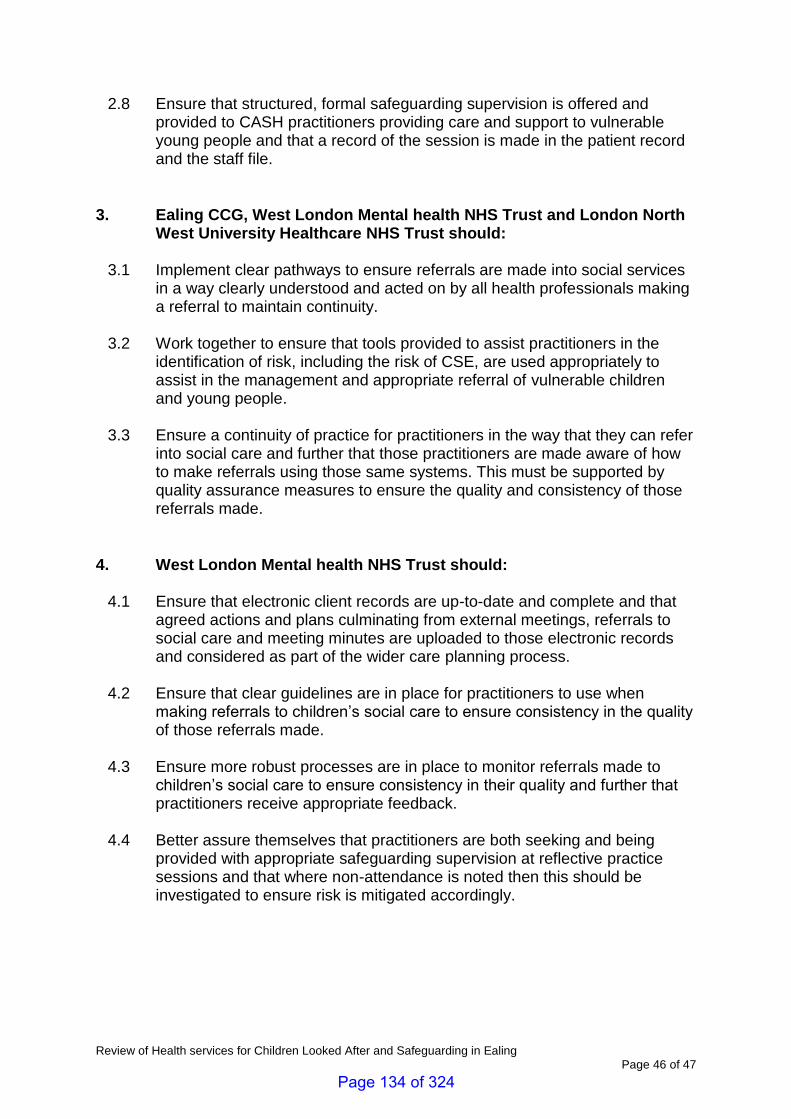
Review of Health services for Children Looked After and Safeguarding in Ealing Page 46 of 47
2.8 Ensure that structured, formal safeguarding supervision is offered and provided to CASH practitioners providing care and support to vulnerable young people and that a record of the session is made in the patient record and the staff file.
3. Ealing CCG, West London Mental health NHS Trust and London North
West University Healthcare NHS Trust should:
3.1 Implement clear pathways to ensure referrals are made into social services in a way clearly understood and acted on by all health professionals making a referral to maintain continuity.
3.2 Work together to ensure that tools provided to assist practitioners in the identification of risk, including the risk of CSE, are used appropriately to assist in the management and appropriate referral of vulnerable children and young people.
3.3 Ensure a continuity of practice for practitioners in the way that they can refer into social care and further that those practitioners are made aware of how to make referrals using those same systems. This must be supported by quality assurance measures to ensure the quality and consistency of those referrals made.
4. West London Mental health NHS Trust should:
4.1 Ensure that electronic client records are up-to-date and complete and that
agreed actions and plans culminating from external meetings, referrals to social care and meeting minutes are uploaded to those electronic records and considered as part of the wider care planning process.
4.2 Ensure that clear guidelines are in place for practitioners to use when making referrals to children’s social care to ensure consistency in the quality of those referrals made.
4.3 Ensure more robust processes are in place to monitor referrals made to
children’s social care to ensure consistency in their quality and further that practitioners receive appropriate feedback.
4.4 Better assure themselves that practitioners are both seeking and being
provided with appropriate safeguarding supervision at reflective practice sessions and that where non-attendance is noted then this should be investigated to ensure risk is mitigated accordingly.
Page 134 of 324
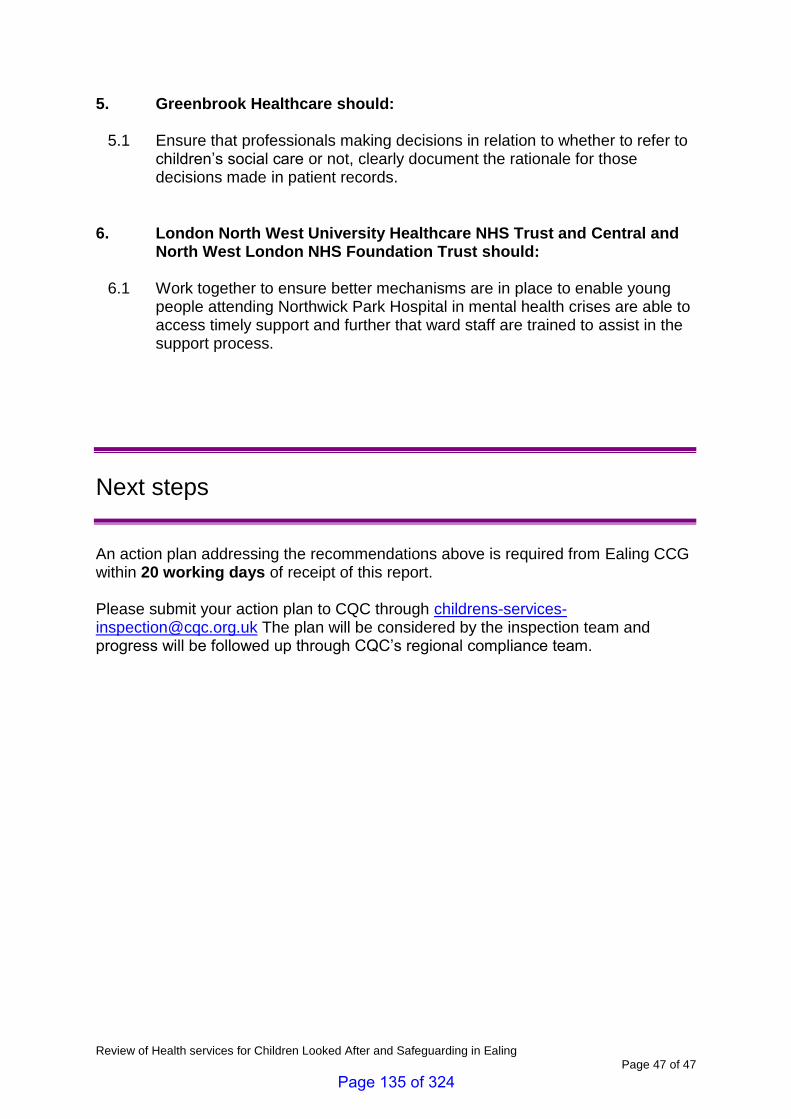
Review of Health services for Children Looked After and Safeguarding in Ealing Page 47 of 47
5. Greenbrook Healthcare should:
5.1 Ensure that professionals making decisions in relation to whether to refer to children’s social care or not, clearly document the rationale for those decisions made in patient records.
6. London North West University Healthcare NHS Trust and Central and
North West London NHS Foundation Trust should:
6.1 Work together to ensure better mechanisms are in place to enable young people attending Northwick Park Hospital in mental health crises are able to access timely support and further that ward staff are trained to assist in the support process.
Next steps
An action plan addressing the recommendations above is required from Ealing CCG within 20 working days of receipt of this report. Please submit your action plan to CQC through [email protected] The plan will be considered by the inspection team and progress will be followed up through CQC’s regional compliance team.
Page 135 of 324

Page 136 of 324
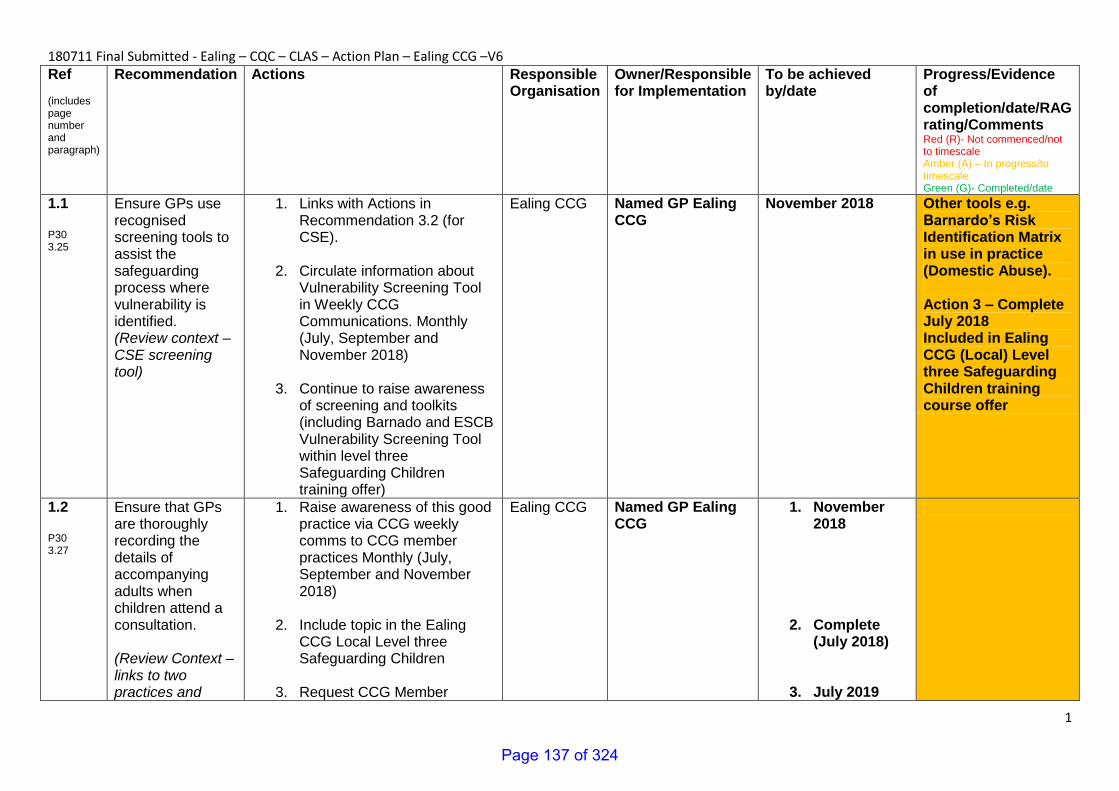
1
180711 Final Submitted - Ealing – CQC – CLAS – Action Plan – Ealing CCG –V6 Ref (includes page number and paragraph)
Recommendation Actions Responsible Organisation
Owner/Responsible for Implementation
To be achieved by/date
Progress/Evidence of completion/date/RAG rating/Comments Red (R)- Not commenced/not to timescale Amber (A) – In progress/to timescale Green (G)- Completed/date
1.1 P30 3.25
Ensure GPs use recognised screening tools to assist the safeguarding process where vulnerability is identified. (Review context – CSE screening tool)
1. Links with Actions in Recommendation 3.2 (for CSE).
2. Circulate information about
Vulnerability Screening Tool in Weekly CCG Communications. Monthly (July, September and November 2018)
3. Continue to raise awareness
of screening and toolkits (including Barnado and ESCB Vulnerability Screening Tool within level three Safeguarding Children training offer)
Ealing CCG Named GP Ealing CCG
November 2018 Other tools e.g. Barnardo’s Risk Identification Matrix in use in practice (Domestic Abuse). Action 3 – Complete July 2018 Included in Ealing CCG (Local) Level three Safeguarding Children training course offer
1.2 P30 3.27
Ensure that GPs are thoroughly recording the details of accompanying adults when children attend a consultation. (Review Context – links to two practices and
1. Raise awareness of this good practice via CCG weekly comms to CCG member practices Monthly (July, September and November 2018)
2. Include topic in the Ealing CCG Local Level three Safeguarding Children
3. Request CCG Member
Ealing CCG Named GP Ealing CCG
1. November 2018
2. Complete (July 2018)
3. July 2019
Page 137 of 324
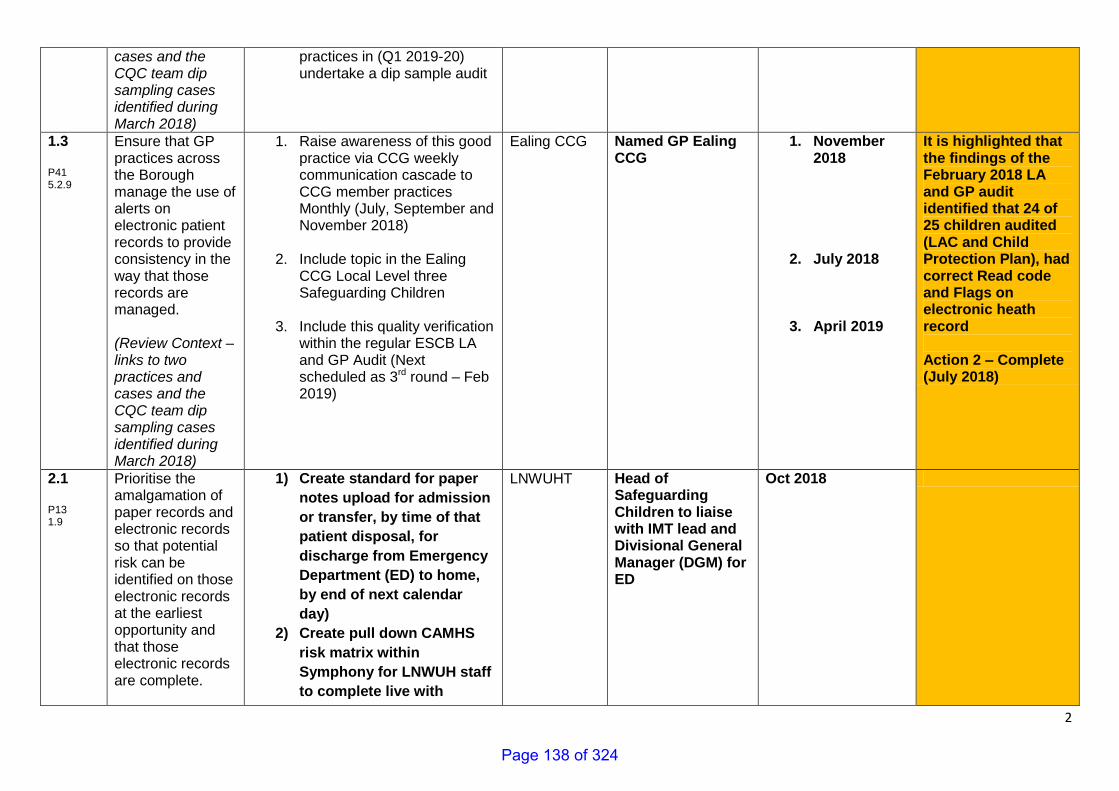
2
cases and the CQC team dip sampling cases identified during March 2018)
practices in (Q1 2019-20) undertake a dip sample audit
1.3 P41 5.2.9
Ensure that GP practices across the Borough manage the use of alerts on electronic patient records to provide consistency in the way that those records are managed. (Review Context – links to two practices and cases and the CQC team dip sampling cases identified during March 2018)
1. Raise awareness of this good practice via CCG weekly communication cascade to CCG member practices Monthly (July, September and November 2018)
2. Include topic in the Ealing CCG Local Level three Safeguarding Children
3. Include this quality verification within the regular ESCB LA and GP Audit (Next scheduled as 3rd round – Feb 2019)
Ealing CCG Named GP Ealing CCG
1. November 2018
2. July 2018
3. April 2019
It is highlighted that the findings of the February 2018 LA and GP audit identified that 24 of 25 children audited (LAC and Child Protection Plan), had correct Read code and Flags on electronic heath record Action 2 – Complete (July 2018)
2.1 P13 1.9
Prioritise the amalgamation of paper records and electronic records so that potential risk can be identified on those electronic records at the earliest opportunity and that those electronic records are complete.
1) Create standard for paper
notes upload for admission
or transfer, by time of that
patient disposal, for
discharge from Emergency
Department (ED) to home,
by end of next calendar
day)
2) Create pull down CAMHS
risk matrix within
Symphony for LNWUH staff
to complete live with
LNWUHT Head of Safeguarding Children to liaise with IMT lead and Divisional General Manager (DGM) for ED
Oct 2018
Page 138 of 324
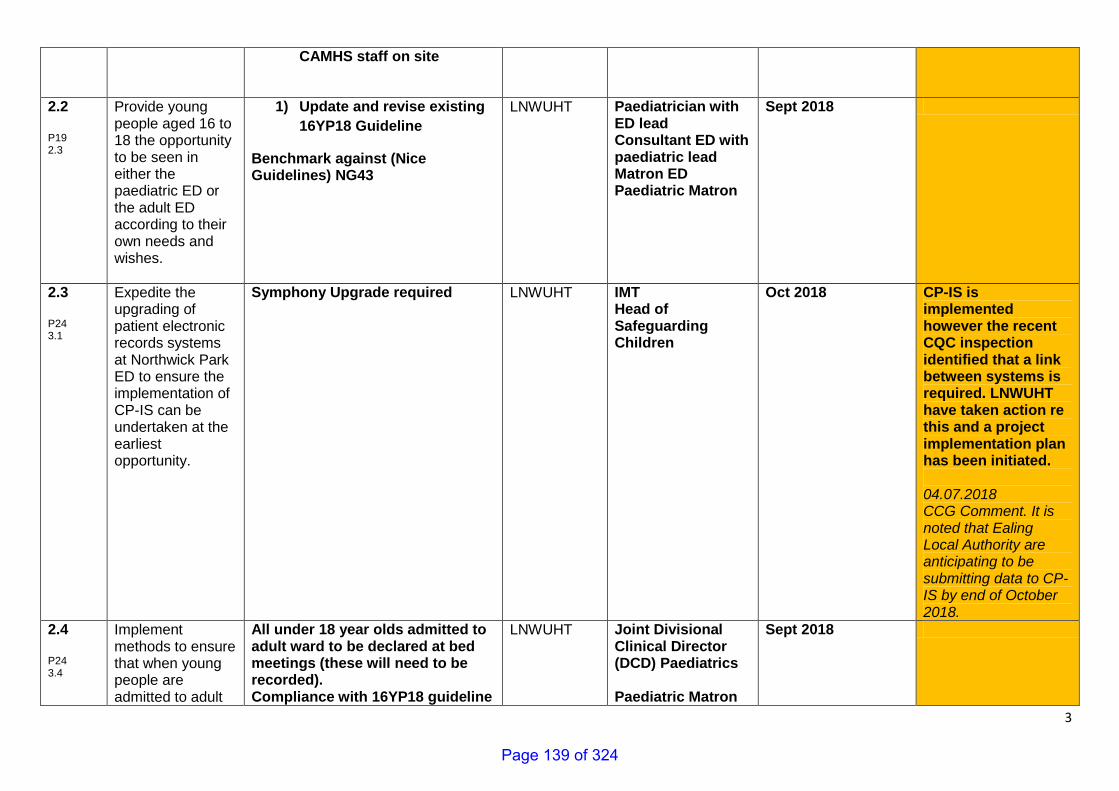
3
CAMHS staff on site
2.2 P19 2.3
Provide young people aged 16 to 18 the opportunity to be seen in either the paediatric ED or the adult ED according to their own needs and wishes.
1) Update and revise existing
16YP18 Guideline
Benchmark against (Nice Guidelines) NG43
LNWUHT Paediatrician with ED lead Consultant ED with paediatric lead Matron ED Paediatric Matron
Sept 2018
2.3 P24 3.1
Expedite the upgrading of patient electronic records systems at Northwick Park ED to ensure the implementation of CP-IS can be undertaken at the earliest opportunity.
Symphony Upgrade required LNWUHT IMT Head of Safeguarding Children
Oct 2018 CP-IS is implemented however the recent CQC inspection identified that a link between systems is required. LNWUHT have taken action re this and a project implementation plan has been initiated. 04.07.2018 CCG Comment. It is noted that Ealing Local Authority are anticipating to be submitting data to CP-IS by end of October 2018.
2.4 P24 3.4
Implement methods to ensure that when young people are admitted to adult
All under 18 year olds admitted to adult ward to be declared at bed meetings (these will need to be recorded). Compliance with 16YP18 guideline
LNWUHT Joint Divisional Clinical Director (DCD) Paediatrics Paediatric Matron
Sept 2018
Page 139 of 324
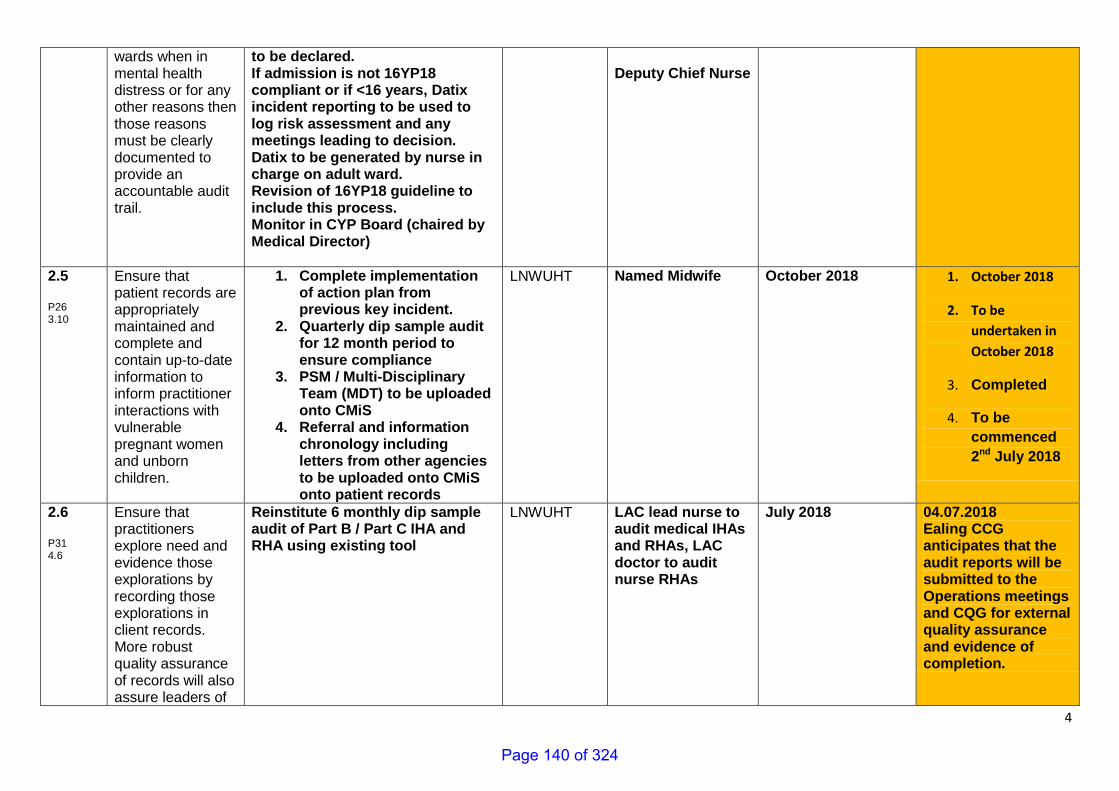
4
wards when in mental health distress or for any other reasons then those reasons must be clearly documented to provide an accountable audit trail.
to be declared. If admission is not 16YP18 compliant or if <16 years, Datix incident reporting to be used to log risk assessment and any meetings leading to decision. Datix to be generated by nurse in charge on adult ward. Revision of 16YP18 guideline to include this process. Monitor in CYP Board (chaired by Medical Director)
Deputy Chief Nurse
2.5 P26 3.10
Ensure that patient records are appropriately maintained and complete and contain up-to-date information to inform practitioner interactions with vulnerable pregnant women and unborn children.
1. Complete implementation of action plan from previous key incident.
2. Quarterly dip sample audit for 12 month period to ensure compliance
3. PSM / Multi-Disciplinary Team (MDT) to be uploaded onto CMiS
4. Referral and information chronology including letters from other agencies to be uploaded onto CMiS onto patient records
LNWUHT Named Midwife October 2018 1. October 2018
2. To be
undertaken in
October 2018
3. Completed
4. To be
commenced
2nd July 2018
2.6 P31 4.6
Ensure that practitioners explore need and evidence those explorations by recording those explorations in client records. More robust quality assurance of records will also assure leaders of
Reinstitute 6 monthly dip sample audit of Part B / Part C IHA and RHA using existing tool
LNWUHT LAC lead nurse to audit medical IHAs and RHAs, LAC doctor to audit nurse RHAs
July 2018 04.07.2018 Ealing CCG anticipates that the audit reports will be submitted to the Operations meetings and CQG for external quality assurance and evidence of completion.
Page 140 of 324
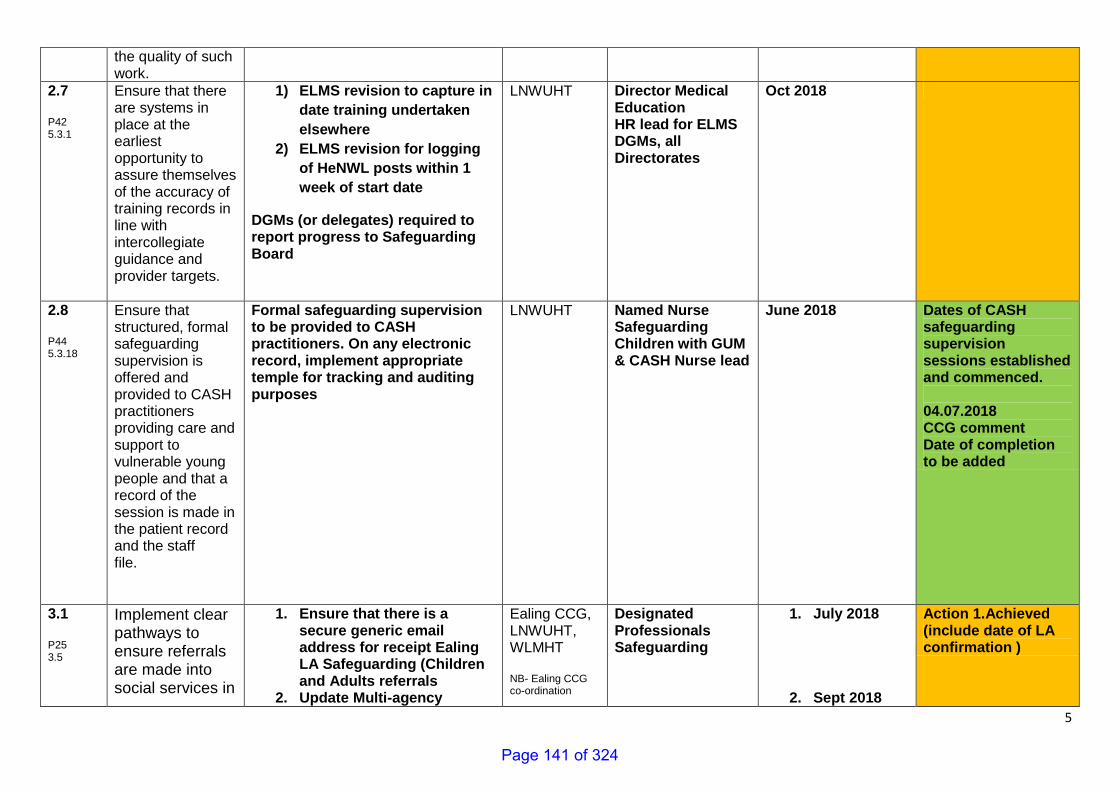
5
the quality of such work.
2.7 P42 5.3.1
Ensure that there are systems in place at the earliest opportunity to assure themselves of the accuracy of training records in line with intercollegiate guidance and provider targets.
1) ELMS revision to capture in
date training undertaken
elsewhere
2) ELMS revision for logging
of HeNWL posts within 1
week of start date
DGMs (or delegates) required to report progress to Safeguarding Board
LNWUHT Director Medical Education HR lead for ELMS DGMs, all Directorates
Oct 2018
2.8 P44 5.3.18
Ensure that structured, formal safeguarding supervision is offered and provided to CASH practitioners providing care and support to vulnerable young people and that a record of the session is made in the patient record and the staff file.
Formal safeguarding supervision to be provided to CASH practitioners. On any electronic record, implement appropriate temple for tracking and auditing purposes
LNWUHT Named Nurse Safeguarding Children with GUM & CASH Nurse lead
June 2018 Dates of CASH safeguarding supervision sessions established and commenced. 04.07.2018 CCG comment Date of completion to be added
3.1 P25 3.5
Implement clear pathways to ensure referrals are made into social services in
1. Ensure that there is a secure generic email address for receipt Ealing LA Safeguarding (Children and Adults referrals
2. Update Multi-agency
Ealing CCG, LNWUHT, WLMHT NB- Ealing CCG co-ordination
Designated Professionals Safeguarding
1. July 2018
2. Sept 2018
Action 1.Achieved (include date of LA confirmation )
Page 141 of 324
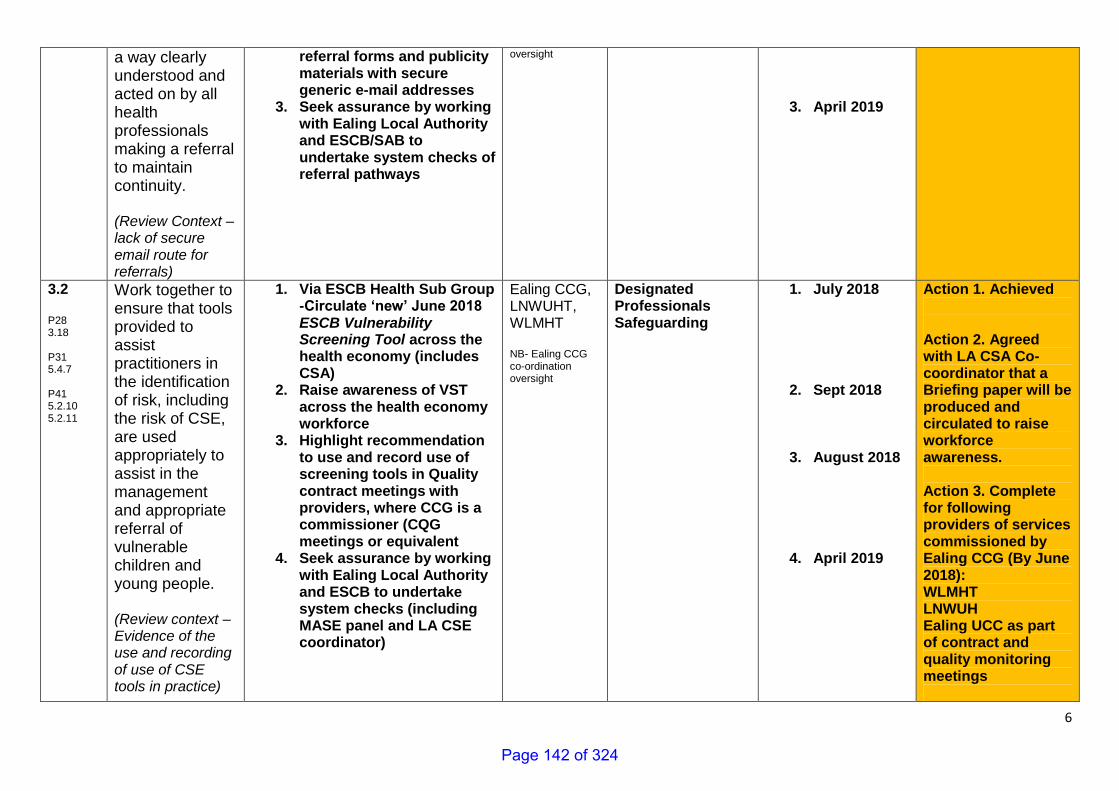
6
a way clearly understood and acted on by all health professionals making a referral to maintain continuity. (Review Context – lack of secure email route for referrals)
referral forms and publicity materials with secure generic e-mail addresses
3. Seek assurance by working with Ealing Local Authority and ESCB/SAB to undertake system checks of referral pathways
oversight
3. April 2019
3.2 P28 3.18 P31 5.4.7 P41 5.2.10 5.2.11
Work together to ensure that tools provided to assist practitioners in the identification of risk, including the risk of CSE, are used appropriately to assist in the management and appropriate referral of vulnerable children and young people. (Review context – Evidence of the use and recording of use of CSE tools in practice)
1. Via ESCB Health Sub Group -Circulate ‘new’ June 2018 ESCB Vulnerability Screening Tool across the health economy (includes CSA)
2. Raise awareness of VST across the health economy workforce
3. Highlight recommendation to use and record use of screening tools in Quality contract meetings with providers, where CCG is a commissioner (CQG meetings or equivalent
4. Seek assurance by working with Ealing Local Authority and ESCB to undertake system checks (including MASE panel and LA CSE coordinator)
Ealing CCG, LNWUHT, WLMHT NB- Ealing CCG co-ordination oversight
Designated Professionals Safeguarding
1. July 2018
2. Sept 2018
3. August 2018
4. April 2019
Action 1. Achieved
Action 2. Agreed with LA CSA Co-coordinator that a Briefing paper will be produced and circulated to raise workforce awareness.
Action 3. Complete for following providers of services commissioned by Ealing CCG (By June 2018): WLMHT LNWUH Ealing UCC as part of contract and quality monitoring meetings
Page 142 of 324
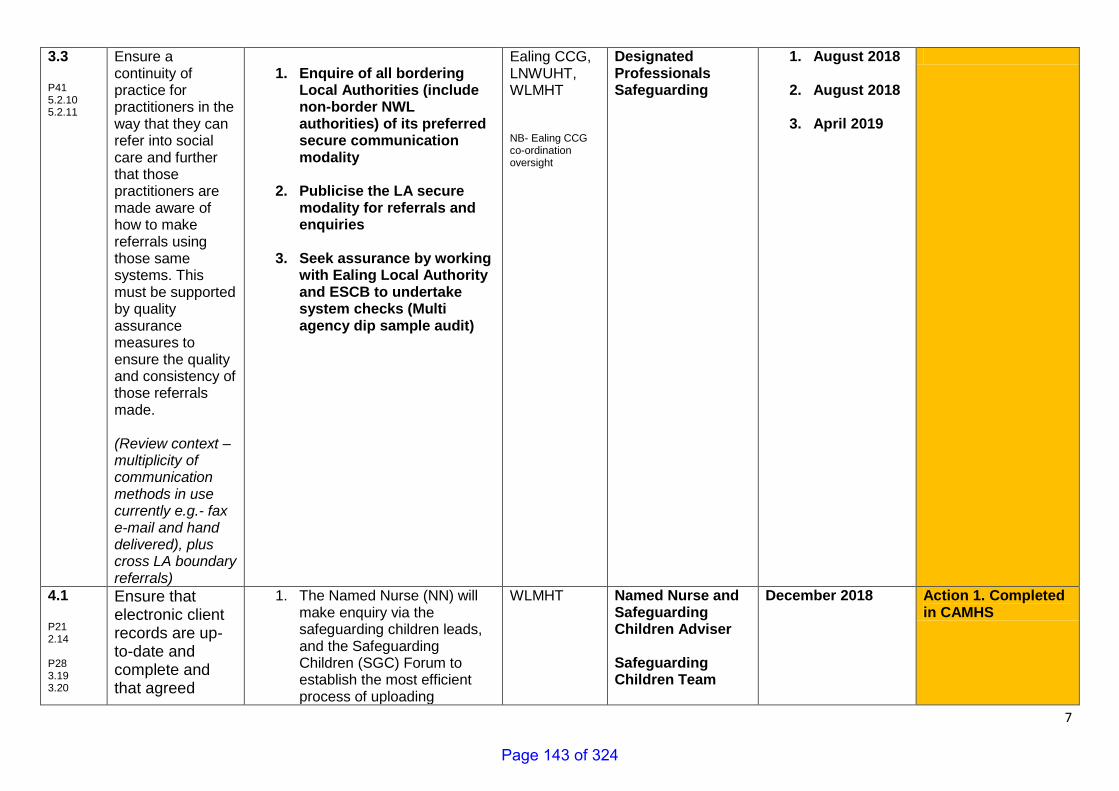
7
3.3 P41 5.2.10 5.2.11
Ensure a continuity of practice for practitioners in the way that they can refer into social care and further that those practitioners are made aware of how to make referrals using those same systems. This must be supported by quality assurance measures to ensure the quality and consistency of those referrals made. (Review context – multiplicity of communication methods in use currently e.g.- fax e-mail and hand delivered), plus cross LA boundary referrals)
1. Enquire of all bordering
Local Authorities (include non-border NWL authorities) of its preferred secure communication modality
2. Publicise the LA secure modality for referrals and enquiries
3. Seek assurance by working with Ealing Local Authority and ESCB to undertake system checks (Multi agency dip sample audit)
Ealing CCG, LNWUHT, WLMHT NB- Ealing CCG co-ordination oversight
Designated Professionals Safeguarding
1. August 2018
2. August 2018
3. April 2019
4.1 P21 2.14 P28 3.19 3.20
Ensure that electronic client records are up-to-date and complete and that agreed
1. The Named Nurse (NN) will make enquiry via the safeguarding children leads, and the Safeguarding Children (SGC) Forum to establish the most efficient process of uploading
WLMHT Named Nurse and Safeguarding Children Adviser Safeguarding Children Team
December 2018 Action 1. Completed in CAMHS
Page 143 of 324
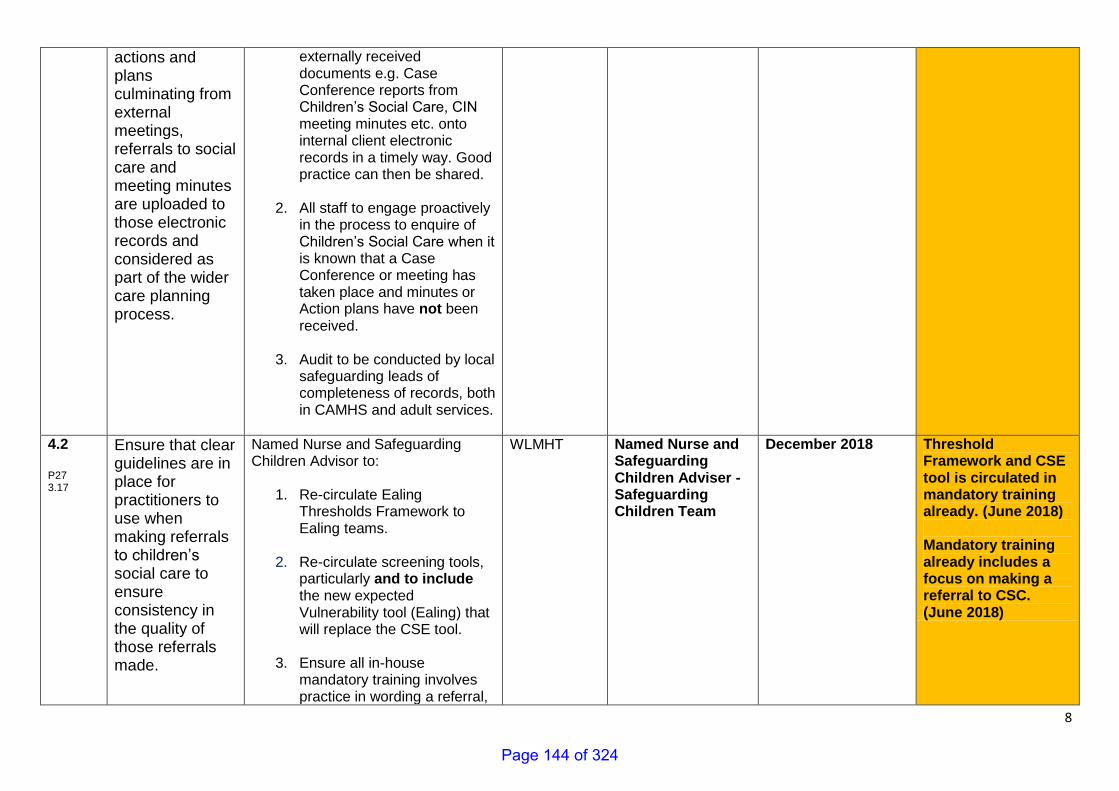
8
actions and plans culminating from external meetings, referrals to social care and meeting minutes are uploaded to those electronic records and considered as part of the wider care planning process.
externally received documents e.g. Case Conference reports from Children’s Social Care, CIN meeting minutes etc. onto internal client electronic records in a timely way. Good practice can then be shared.
2. All staff to engage proactively in the process to enquire of Children’s Social Care when it is known that a Case Conference or meeting has taken place and minutes or Action plans have not been received.
3. Audit to be conducted by local
safeguarding leads of completeness of records, both in CAMHS and adult services.
4.2 P27 3.17
Ensure that clear guidelines are in place for practitioners to use when making referrals to children’s social care to ensure consistency in the quality of those referrals made.
Named Nurse and Safeguarding Children Advisor to:
1. Re-circulate Ealing Thresholds Framework to Ealing teams.
2. Re-circulate screening tools, particularly and to include the new expected Vulnerability tool (Ealing) that will replace the CSE tool.
3. Ensure all in-house
mandatory training involves practice in wording a referral,
WLMHT Named Nurse and Safeguarding Children Adviser - Safeguarding Children Team
December 2018 Threshold Framework and CSE tool is circulated in mandatory training already. (June 2018)
Mandatory training already includes a focus on making a referral to CSC. (June 2018)
Page 144 of 324
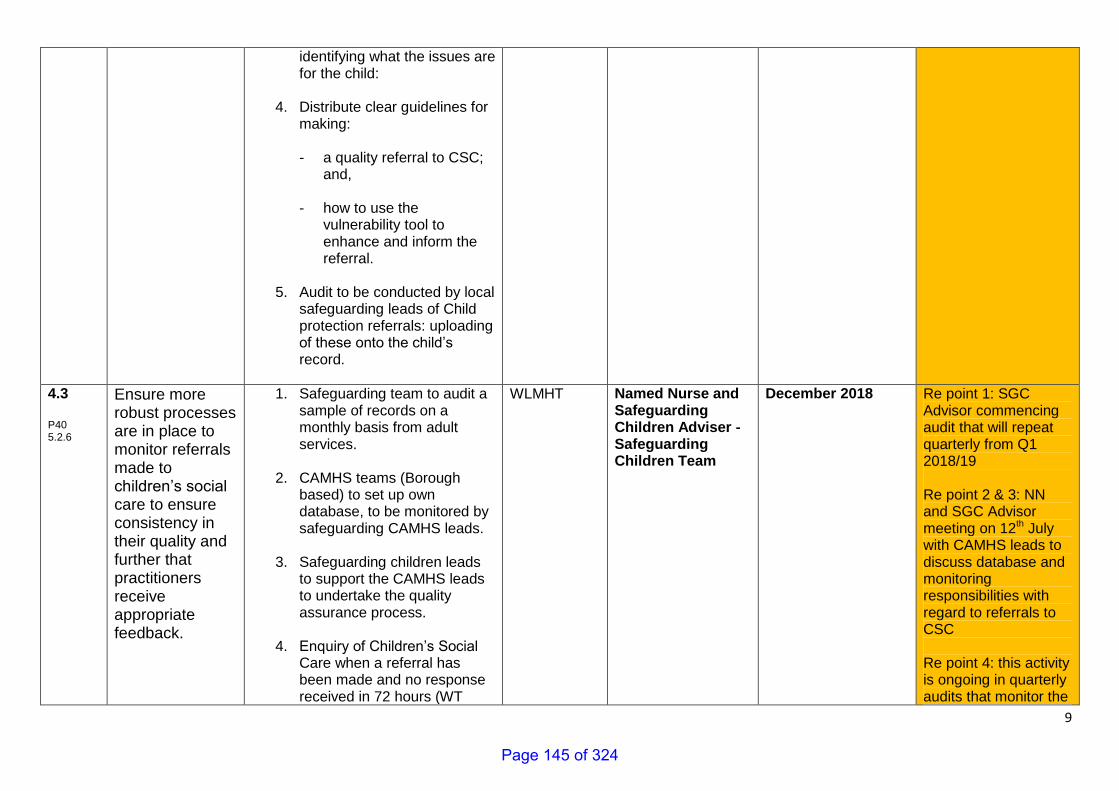
9
identifying what the issues are for the child:
4. Distribute clear guidelines for
making: - a quality referral to CSC;
and,
- how to use the vulnerability tool to enhance and inform the referral.
5. Audit to be conducted by local
safeguarding leads of Child protection referrals: uploading of these onto the child’s record.
4.3 P40 5.2.6
Ensure more robust processes are in place to monitor referrals made to children’s social care to ensure consistency in their quality and further that practitioners receive appropriate feedback.
1. Safeguarding team to audit a sample of records on a monthly basis from adult services.
2. CAMHS teams (Borough
based) to set up own database, to be monitored by safeguarding CAMHS leads.
3. Safeguarding children leads
to support the CAMHS leads to undertake the quality assurance process.
4. Enquiry of Children’s Social
Care when a referral has been made and no response received in 72 hours (WT
WLMHT Named Nurse and Safeguarding Children Adviser - Safeguarding Children Team
December 2018 Re point 1: SGC Advisor commencing audit that will repeat quarterly from Q1 2018/19 Re point 2 & 3: NN and SGC Advisor meeting on 12th July with CAMHS leads to discuss database and monitoring responsibilities with regard to referrals to CSC Re point 4: this activity is ongoing in quarterly audits that monitor the
Page 145 of 324
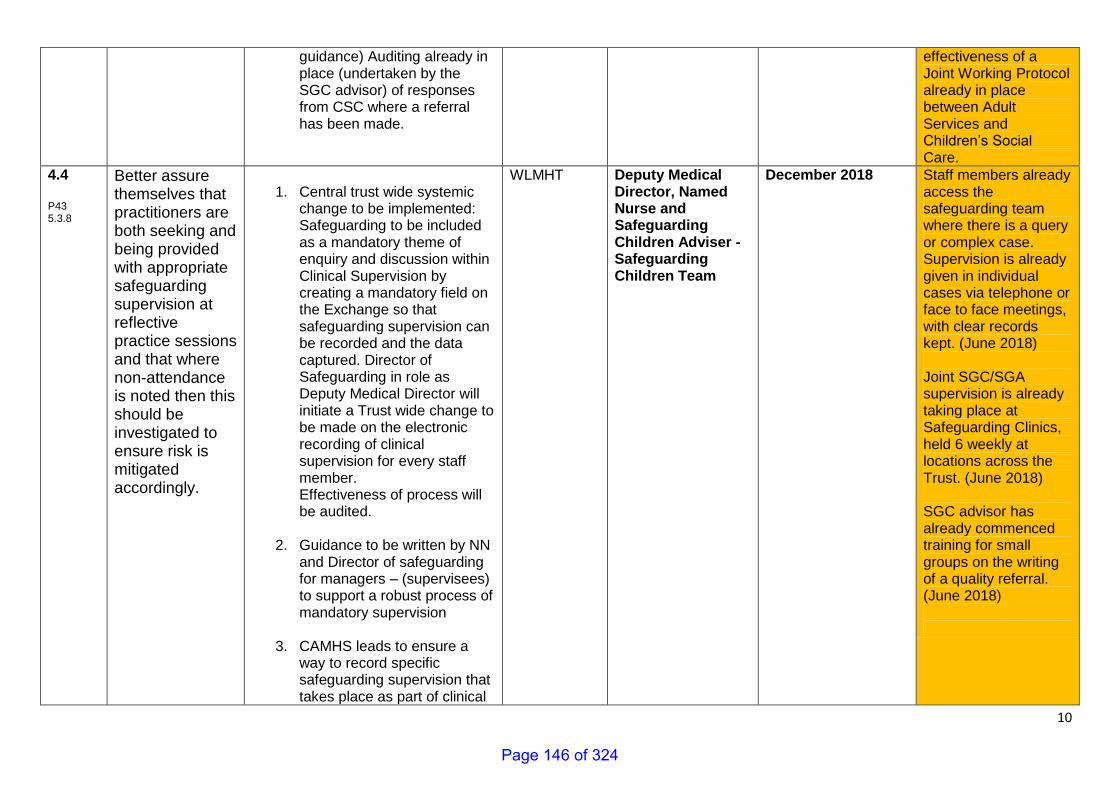
10
guidance) Auditing already in place (undertaken by the SGC advisor) of responses from CSC where a referral has been made.
effectiveness of a Joint Working Protocol already in place between Adult Services and Children’s Social Care.
4.4 P43 5.3.8
Better assure themselves that practitioners are both seeking and being provided with appropriate safeguarding supervision at reflective practice sessions and that where non-attendance is noted then this should be investigated to ensure risk is mitigated accordingly.
1. Central trust wide systemic
change to be implemented: Safeguarding to be included as a mandatory theme of enquiry and discussion within Clinical Supervision by creating a mandatory field on the Exchange so that safeguarding supervision can be recorded and the data captured. Director of Safeguarding in role as Deputy Medical Director will initiate a Trust wide change to be made on the electronic recording of clinical supervision for every staff member. Effectiveness of process will be audited.
2. Guidance to be written by NN and Director of safeguarding for managers – (supervisees) to support a robust process of mandatory supervision
3. CAMHS leads to ensure a
way to record specific safeguarding supervision that takes place as part of clinical
WLMHT Deputy Medical Director, Named Nurse and Safeguarding Children Adviser - Safeguarding Children Team
December 2018 Staff members already access the safeguarding team where there is a query or complex case. Supervision is already given in individual cases via telephone or face to face meetings, with clear records kept. (June 2018) Joint SGC/SGA supervision is already taking place at Safeguarding Clinics, held 6 weekly at locations across the Trust. (June 2018) SGC advisor has already commenced training for small groups on the writing of a quality referral. (June 2018)
Page 146 of 324
11
supervision.
4. Safeguarding Children Advisor to undertake supervision with CAMHS teams on a quarterly basis as additional assurance.
5. Safeguarding Children Policy to be updated by the NN
5.1 P25 3.6
Ensure that professionals making decisions in relation to whether to refer to children’s social care or not, clearly document the rationale for those decisions made in patient records.
To be disseminated to all clinicians by email & weekly blog. Has been discussed in daily huddles by lead GP. Lead GP to audit notes to ensure compliance in 3 months
Greenbrook Ealing UCC Safeguarding Lead Doctor and Nurse Across Greenbrook sites: Medical Director
September 2018
EUCC BLOG 28.6.18 (2).docx
6.1 P22
Work together to
ensure better
1. Improve awareness of the Mental Health Crisis Pathway:
LNWUHT, CNWL
Associate Director of Safety and Safeguarding
1 & 2 Sept 2018
Training dates being agreed to coincide with team meetings
Page 147 of 324
12
2.17 mechanisms are
in place to
enable young
people attending
Northwick Park
Hospital in
mental health
crises are able to
access timely
support and
further that ward
staff are trained
to assist in the
support process.
Crib sheet of contact details for in hours and OOH’s for CAMHS liaison assessments
CAMHS Out of Hours Team to have a nurse based in Hillingdon or NPH to improve response times.
develop guidance to support roles and responsibilities for ward staff and CAMHS teams that includes the escalation guidance
monitoring of partnership working via standing item on the monthly meeting between Urgent Care, CAMHS Psychiatry, Hub Manager, ED Manager
2. ED staff training – Service Manager will deliver training to junior medics and nurses in team meetings to clarify their roles and what support these patients need.
3. NHS Ealing CCG will work with lead commissioners (Brent CCG for LNWUH
CNWL Head of Safeguarding LNWUHT
3 December 2018
as far as possible. Ealing CCG are seek assurance of arrangements across sites all five paediatric service commissioned sites
Page 148 of 324
13
Acute and Harrow CCG for CNWL CAMHS) and providers as part of system assurance.
Organisational sign off: CCG – Managing Director, Chief Nurse /Director of Quality and Ealing CCG Clinical Lead Children LNWUH – Interim Chief Nurse/Deputy Chief Nurse WLMHT – Medical Director Greenbrook – Medical Director CNWL – Exec Director of Safeguarding
Page 149 of 324
Page 150 of 324
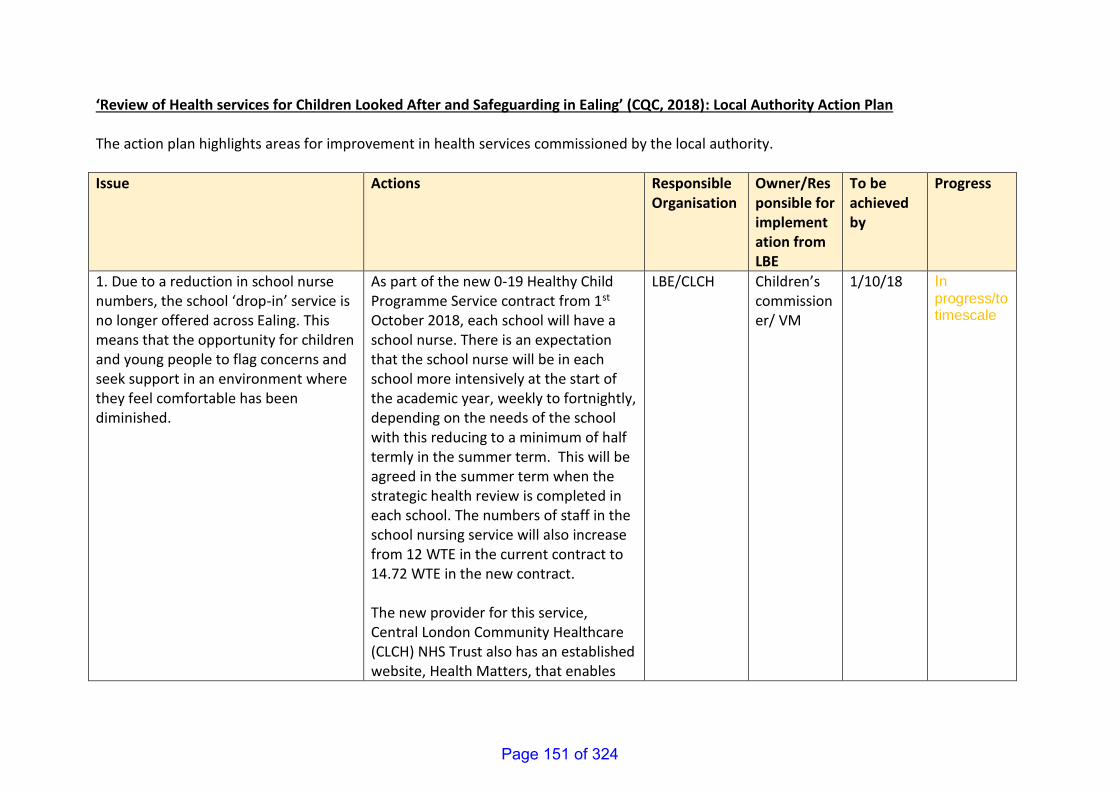
‘Review of Health services for Children Looked After and Safeguarding in Ealing’ (CQC, 2018): Local Authority Action Plan The action plan highlights areas for improvement in health services commissioned by the local authority.
Issue Actions Responsible Organisation
Owner/Responsible for implementation from LBE
To be achieved by
Progress
1. Due to a reduction in school nurse numbers, the school ‘drop-in’ service is no longer offered across Ealing. This means that the opportunity for children and young people to flag concerns and seek support in an environment where they feel comfortable has been diminished.
As part of the new 0-19 Healthy Child Programme Service contract from 1st October 2018, each school will have a school nurse. There is an expectation that the school nurse will be in each school more intensively at the start of the academic year, weekly to fortnightly, depending on the needs of the school with this reducing to a minimum of half termly in the summer term. This will be agreed in the summer term when the strategic health review is completed in each school. The numbers of staff in the school nursing service will also increase from 12 WTE in the current contract to 14.72 WTE in the new contract. The new provider for this service, Central London Community Healthcare (CLCH) NHS Trust also has an established website, Health Matters, that enables
LBE/CLCH Children’s commissioner/ VM
1/10/18 In progress/to timescale
Page 151 of 324
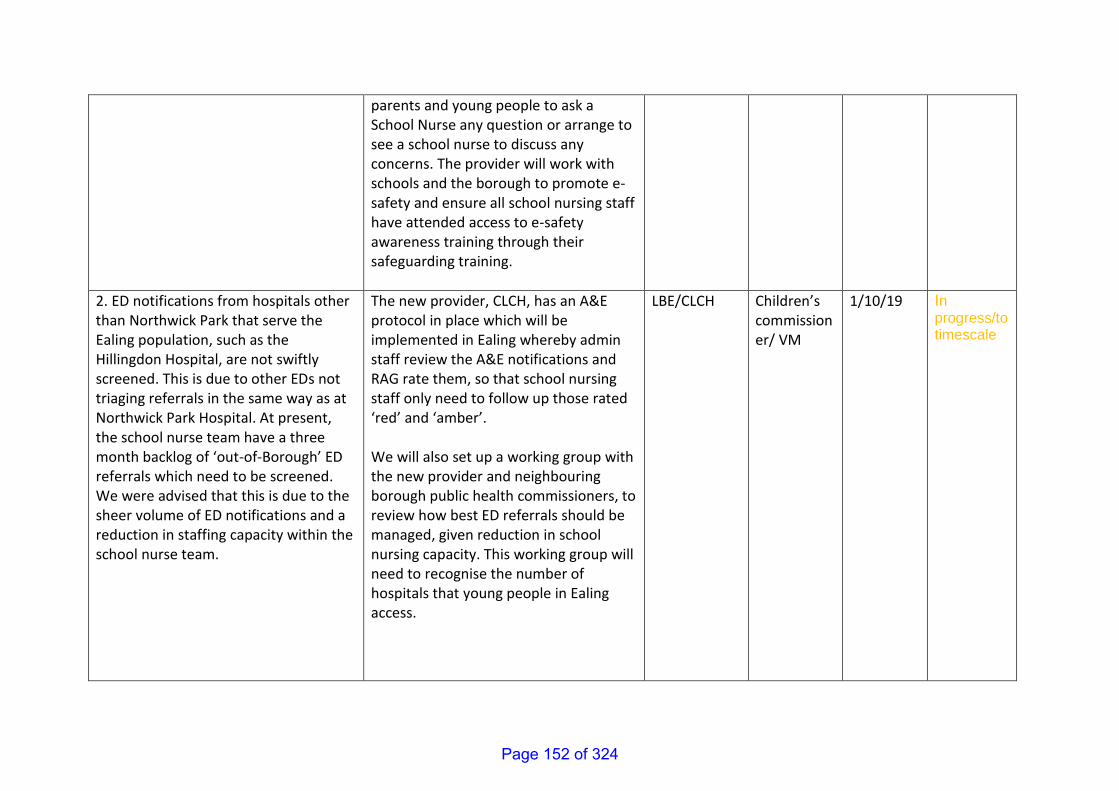
parents and young people to ask a School Nurse any question or arrange to see a school nurse to discuss any concerns. The provider will work with schools and the borough to promote e-safety and ensure all school nursing staff have attended access to e-safety awareness training through their safeguarding training.
2. ED notifications from hospitals other than Northwick Park that serve the Ealing population, such as the Hillingdon Hospital, are not swiftly screened. This is due to other EDs not triaging referrals in the same way as at Northwick Park Hospital. At present, the school nurse team have a three month backlog of ‘out-of-Borough’ ED referrals which need to be screened. We were advised that this is due to the sheer volume of ED notifications and a reduction in staffing capacity within the school nurse team.
The new provider, CLCH, has an A&E protocol in place which will be implemented in Ealing whereby admin staff review the A&E notifications and RAG rate them, so that school nursing staff only need to follow up those rated ‘red’ and ‘amber’. We will also set up a working group with the new provider and neighbouring borough public health commissioners, to review how best ED referrals should be managed, given reduction in school nursing capacity. This working group will need to recognise the number of hospitals that young people in Ealing access.
LBE/CLCH Children’s commissioner/ VM
1/10/19 In progress/to timescale
Page 152 of 324
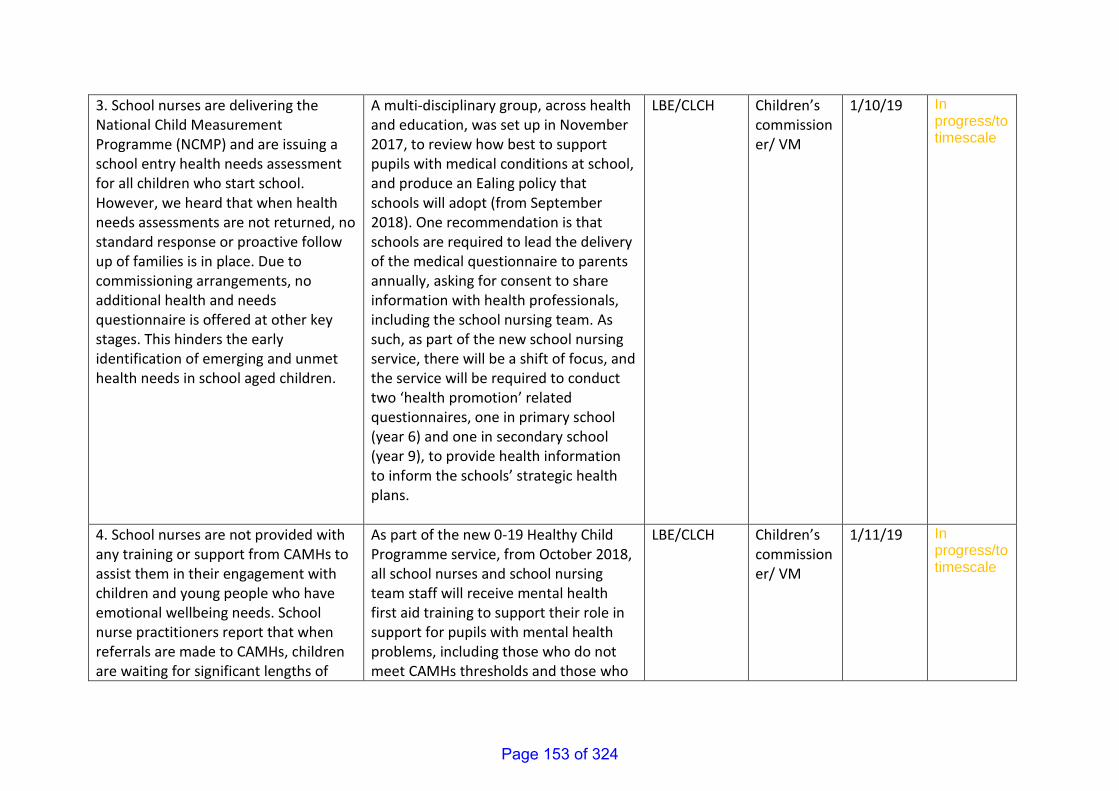
3. School nurses are delivering the National Child Measurement Programme (NCMP) and are issuing a school entry health needs assessment for all children who start school. However, we heard that when health needs assessments are not returned, no standard response or proactive follow up of families is in place. Due to commissioning arrangements, no additional health and needs questionnaire is offered at other key stages. This hinders the early identification of emerging and unmet health needs in school aged children.
A multi-disciplinary group, across health and education, was set up in November 2017, to review how best to support pupils with medical conditions at school, and produce an Ealing policy that schools will adopt (from September 2018). One recommendation is that schools are required to lead the delivery of the medical questionnaire to parents annually, asking for consent to share information with health professionals, including the school nursing team. As such, as part of the new school nursing service, there will be a shift of focus, and the service will be required to conduct two ‘health promotion’ related questionnaires, one in primary school (year 6) and one in secondary school (year 9), to provide health information to inform the schools’ strategic health plans.
LBE/CLCH Children’s commissioner/ VM
1/10/19 In progress/to timescale
4. School nurses are not provided with any training or support from CAMHs to assist them in their engagement with children and young people who have emotional wellbeing needs. School nurse practitioners report that when referrals are made to CAMHs, children are waiting for significant lengths of
As part of the new 0-19 Healthy Child Programme service, from October 2018, all school nurses and school nursing team staff will receive mental health first aid training to support their role in support for pupils with mental health problems, including those who do not meet CAMHs thresholds and those who
LBE/CLCH Children’s commissioner/ VM
1/11/19 In progress/to timescale
Page 153 of 324
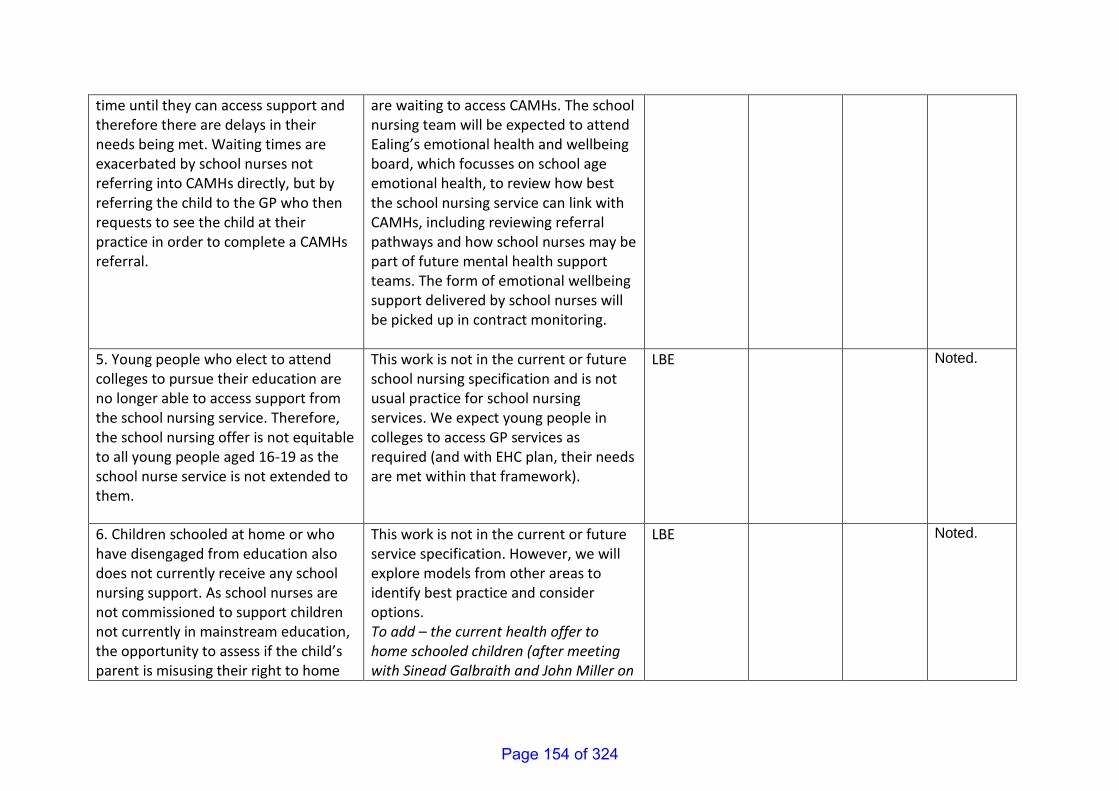
time until they can access support and therefore there are delays in their needs being met. Waiting times are exacerbated by school nurses not referring into CAMHs directly, but by referring the child to the GP who then requests to see the child at their practice in order to complete a CAMHs referral.
are waiting to access CAMHs. The school nursing team will be expected to attend Ealing’s emotional health and wellbeing board, which focusses on school age emotional health, to review how best the school nursing service can link with CAMHs, including reviewing referral pathways and how school nurses may be part of future mental health support teams. The form of emotional wellbeing support delivered by school nurses will be picked up in contract monitoring.
5. Young people who elect to attend colleges to pursue their education are no longer able to access support from the school nursing service. Therefore, the school nursing offer is not equitable to all young people aged 16-19 as the school nurse service is not extended to them.
This work is not in the current or future school nursing specification and is not usual practice for school nursing services. We expect young people in colleges to access GP services as required (and with EHC plan, their needs are met within that framework).
LBE Noted.
6. Children schooled at home or who have disengaged from education also does not currently receive any school nursing support. As school nurses are not commissioned to support children not currently in mainstream education, the opportunity to assess if the child’s parent is misusing their right to home
This work is not in the current or future service specification. However, we will explore models from other areas to identify best practice and consider options. To add – the current health offer to home schooled children (after meeting with Sinead Galbraith and John Miller on
LBE Noted.
Page 154 of 324
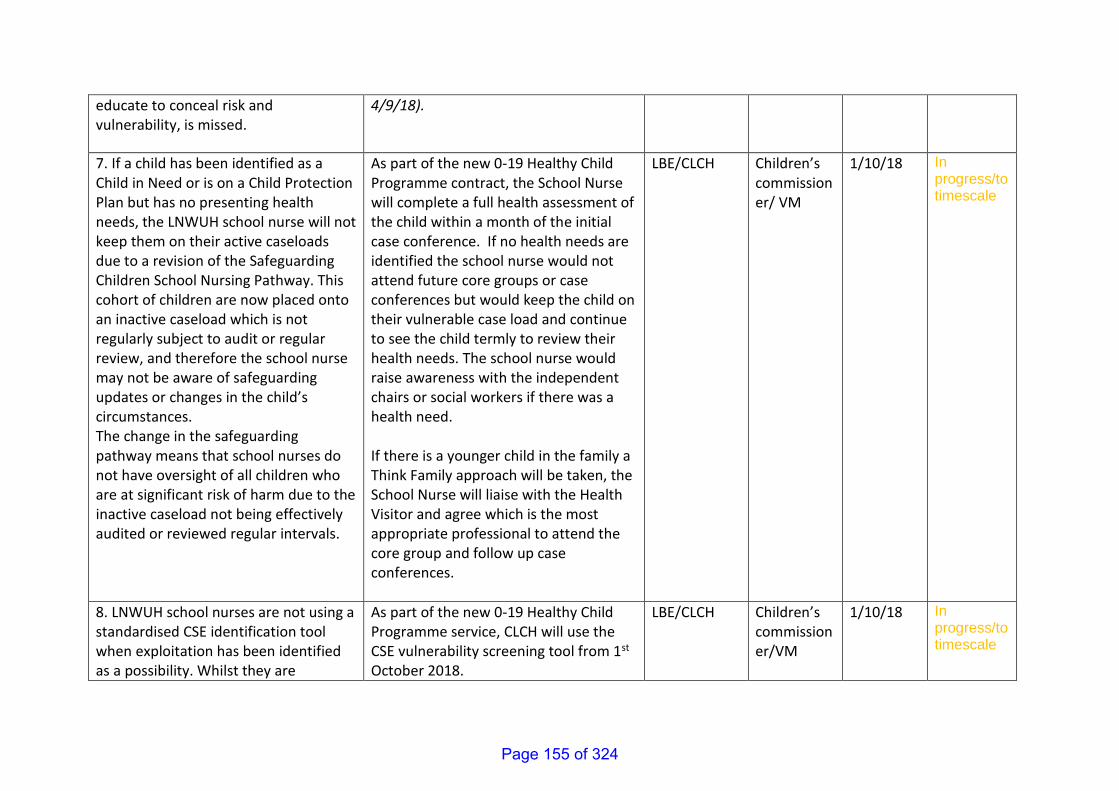
educate to conceal risk and vulnerability, is missed.
4/9/18).
7. If a child has been identified as a Child in Need or is on a Child Protection Plan but has no presenting health needs, the LNWUH school nurse will not keep them on their active caseloads due to a revision of the Safeguarding Children School Nursing Pathway. This cohort of children are now placed onto an inactive caseload which is not regularly subject to audit or regular review, and therefore the school nurse may not be aware of safeguarding updates or changes in the child’s circumstances. The change in the safeguarding pathway means that school nurses do not have oversight of all children who are at significant risk of harm due to the inactive caseload not being effectively audited or reviewed regular intervals.
As part of the new 0-19 Healthy Child Programme contract, the School Nurse will complete a full health assessment of the child within a month of the initial case conference. If no health needs are identified the school nurse would not attend future core groups or case conferences but would keep the child on their vulnerable case load and continue to see the child termly to review their health needs. The school nurse would raise awareness with the independent chairs or social workers if there was a health need. If there is a younger child in the family a Think Family approach will be taken, the School Nurse will liaise with the Health Visitor and agree which is the most appropriate professional to attend the core group and follow up case conferences.
LBE/CLCH Children’s commissioner/ VM
1/10/18 In progress/to timescale
8. LNWUH school nurses are not using a standardised CSE identification tool when exploitation has been identified as a possibility. Whilst they are
As part of the new 0-19 Healthy Child Programme service, CLCH will use the CSE vulnerability screening tool from 1st October 2018.
LBE/CLCH Children’s commissioner/VM
1/10/18 In progress/to timescale
Page 155 of 324
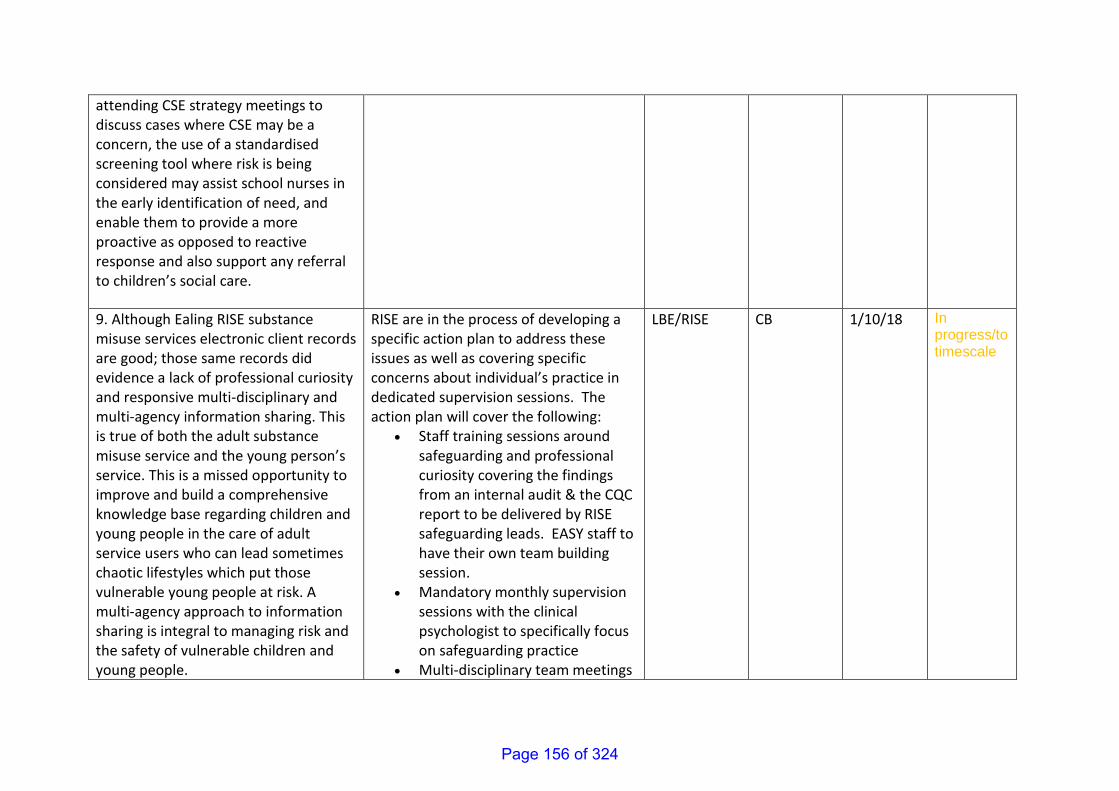
attending CSE strategy meetings to discuss cases where CSE may be a concern, the use of a standardised screening tool where risk is being considered may assist school nurses in the early identification of need, and enable them to provide a more proactive as opposed to reactive response and also support any referral to children’s social care.
9. Although Ealing RISE substance misuse services electronic client records are good; those same records did evidence a lack of professional curiosity and responsive multi-disciplinary and multi-agency information sharing. This is true of both the adult substance misuse service and the young person’s service. This is a missed opportunity to improve and build a comprehensive knowledge base regarding children and young people in the care of adult service users who can lead sometimes chaotic lifestyles which put those vulnerable young people at risk. A multi-agency approach to information sharing is integral to managing risk and the safety of vulnerable children and young people.
RISE are in the process of developing a specific action plan to address these issues as well as covering specific concerns about individual’s practice in dedicated supervision sessions. The action plan will cover the following:
• Staff training sessions around safeguarding and professional curiosity covering the findings from an internal audit & the CQC report to be delivered by RISE safeguarding leads. EASY staff to have their own team building session.
• Mandatory monthly supervision sessions with the clinical psychologist to specifically focus on safeguarding practice
• Multi-disciplinary team meetings
LBE/RISE
CB 1/10/18 In progress/to timescale
Page 156 of 324
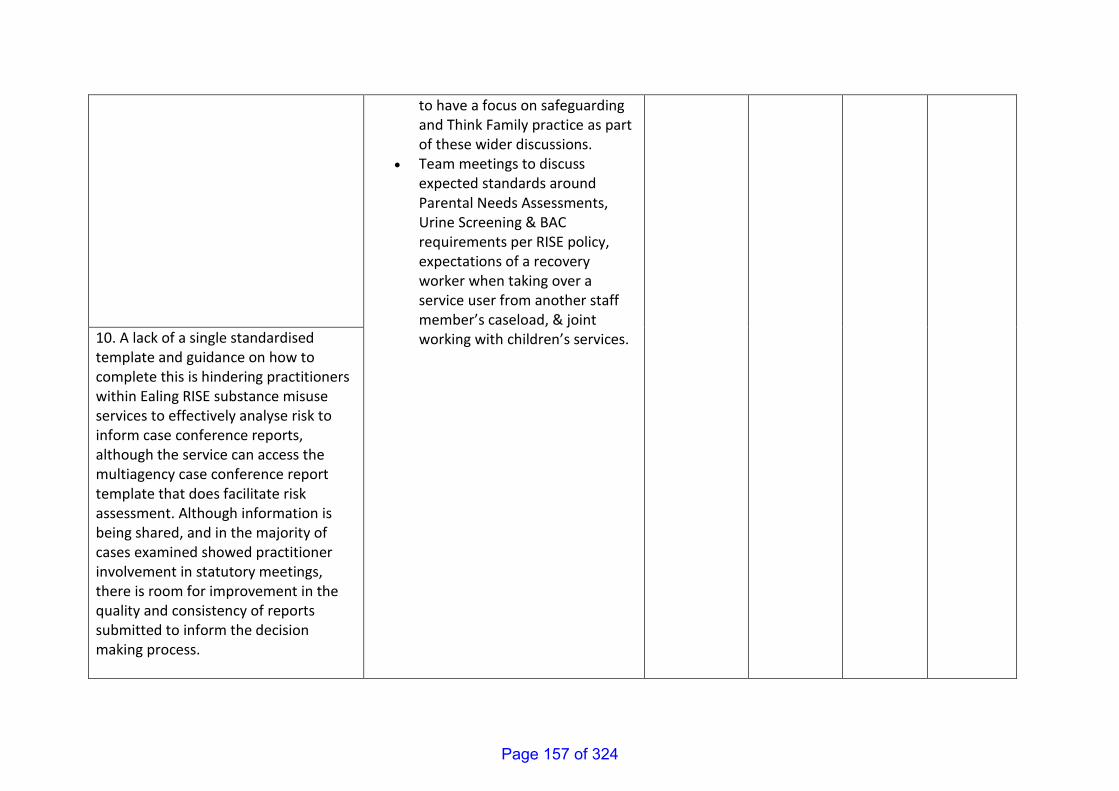
to have a focus on safeguarding and Think Family practice as part of these wider discussions.
• Team meetings to discuss expected standards around Parental Needs Assessments, Urine Screening & BAC requirements per RISE policy, expectations of a recovery worker when taking over a service user from another staff member’s caseload, & joint working with children’s services.
10. A lack of a single standardised template and guidance on how to complete this is hindering practitioners within Ealing RISE substance misuse services to effectively analyse risk to inform case conference reports, although the service can access the multiagency case conference report template that does facilitate risk assessment. Although information is being shared, and in the majority of cases examined showed practitioner involvement in statutory meetings, there is room for improvement in the quality and consistency of reports submitted to inform the decision making process.
Page 157 of 324
Page 158 of 324
1
Contains Confidential or Exempt Information
NO
Title Ealing Market Position Statement 2018-19
Responsible Officer(s) Judith Finlay
Author(s) Gordon Crighton
Portfolio(s) Cllr Rai
For Consideration By Health and Wellbeing Board (HWB)
Date to be Considered 18th September 2018
Implementation Date if Not Called In
N/A
Affected Wards All
Keywords/Index Commissioning, Social Care, Market,
Purpose of Report: The purpose of the report is to inform H&WB members of publication of the Children’s & Adults Market Position Statement for 2018-19
1. Recommendations
Members are asked to note annual publication of Ealing’s Market Position Statement (MPS) for 2018-19
2. Reason for Decision and Options Considered
Ealing’s Market Position Statement (MPS) is aimed at our local (and sub-regional) social care market – its produced and circulated to all care providers working with Ealing’s Children’s & Adults’ Services. It also provides the market with key information on changes in demand and need, and the future commissioning opportunities relevant to the provision of adults’ social care and children’s services in the borough. The MPS in effect assists our local care market with their own business planning and development.
3. Key Implications
There are no key implications for the Council from the MPS itself – rather the statement sets out the challenges and opportunities that are likely to impact our local children’s and adults’ services care providers in the coming year.
Report for: ACTION/INFORMATION Item Number: 10
Page 159 of 324
2
4. Financial
a) Financial impact on the budget (mandatory)
There is no direct financial impact from the MPS itself – the service opportunities and developments detailed in the report are accounted for in our budget setting arrangements for this financial year.
Year 1(state year) Year 2(state year) Year 3(state year)
Capital £000
Capital £000
Capital £000
Addition
- - -
Reduction (-)
- - -
Year 1(state year) Year 2(state year) Year 3(state year)
*Revenue £000
Revenue £000
Revenue £000
Addition
- - -
Reduction (-)
- - -
b) Financial background (optional) Not applicable
5. Legal
Section 5 of the Care Act 2014 introduced new regulations for Councils in regard to market shaping and the commissioning of adult care and support. These duties includes:
promoting quality services, including through workforce development and remuneration and ensuring appropriately resourced care and support
supporting sustainability
ensuring choice
designing strategies that meet local needs
engaging with providers and local communities
understanding the market and facilitating the development of the market
securing supply in the market and assuring its quality through contracting Ealing’s MPS is an integral component of effectively engaging with the care market to build and maintain high quality and sustainable care services for borough residents.
The MPS has also been developed to incorporate the drive for the greater integration of health and social care services.
Page 160 of 324
3
In addition, Sections 3, 6 and 7 of the Care Act 2014 requires that local authorities must carry out their care and support responsibilities with the aim of joining-up the services provided or other actions taken with those provided by the NHS and other health-related services – in particular:
local authorities must carry out their care and support responsibilities with the aim of promoting greater integration with NHS and other health-related services
local authorities and their relevant partners must cooperate generally in performing their functions related to care and support; and, supplementary to this,
in specific individual cases, local authorities and their partners must cooperate in performing their respective functions relating to care and support and carers wherever they can
6. Value For Money
The requirements to secure best value for the Council are detailed throughout the MPS document
7. Sustainability Impact Appraisal As highlighted in Section 5 of this report, the MPS is an integral component of the Council’s approach (and duty) to build and maintain a sustainable local care market.
8. Risk Management
There are no identified risks pertaining to the publication of the MPS
9. Community Safety None
10. Links to the 3 Key Priorities for the Borough The MPS in particular supports the following borough priorities:
Opportunities and living incomes
A healthy and great place
11. Equalities, Human Rights and Community Cohesion
An EAA is not required for the MPS itself – separate EAA’s have been undertaken (as appropriate) for the developments and service opportunities set out in the MPS document.
12. Staffing/Workforce and Accommodation implications None
Page 161 of 324
4
13. Property and Assets There are no property implications
14. Any other implications
None 15. Consultation
Consultation was undertaken with Childrens’ and Adults’ commissioners; the local Providers Forums and the Registered Managers Network.
16. Timetable for Implementation Not applicable
17. Appendices Ealing’s MPS for 2018-19
18. Background Information
The Care Act 2014
Commissioning for Better Outcomes: A Route Map – University of Birmingham
Page 162 of 324
5
Consultation (Mandatory)
Name of consultee
Post held Date sent to
consultee
Date response received
Comments appear in
paragraph:
Internal
Kim Carey Director Adults Services 04/09/18
Chuhr Nijjar Senior Contracts Lawyer
Jumoke Adebisi Senior Finance Business Partner
Cllr Rai Portfolio Holder
External
Report History
Decision type: Urgency item?
EITHER: Key decision OR Non-key decision OR For information (delete as applicable)
No
Report no.:
Gordon Crighton Ext. 7632
Page 163 of 324

Page 164 of 324
Page 1 of 39
Market Position Statement
For health, social care and children’s services providers working with Ealing
2018 – 2019
Children’s & Adults Services
Page 165 of 324
Ealing Market Position Statement 2018-19 Page 2 of 39
Contents
Part 1 - Purpose of the Market Position Statement
What is a market position statement? 3 Who is the market position statement for? 3 The Context: Future Ealing, Brighter Futures and Better Lives 3 What does this mean for providers? 6 Commissioning standards and quality assurance 6 Sub-regional market management via the West London Alliance 7 CarePlace 7 Achievements and successes 2017-18 8
Part 2 - Developments and market opportunities 2018-19 Service developments and opportunities 9 Workforce development 10 Provider engagement 11
Part 3 - Service area profiles
Children and young people 12 Looked after children (LAC) 14 Older adults 16 Physical disabilities and sensory impairment 18 Learning disabilities 19 Autism spectrum disorders 21 Mental health (including forensic services) 24 Substance misuse 27 Support for carers 29 Housing related support 31 Direct payments 32 Voluntary and community sector grants 2018-19 34
Glossary 36
Page 166 of 324
Ealing Market Position Statement 2018-19 Page 3 of 39
Part 1 - Purpose of the Market Position Statement
What is a market position statement? Ealing’s Market Position Statement (MPS) sets out the key changes that are likely to impact our local service providers in the coming year, giving information on changes in demand and future opportunities relevant to the provision of health, social care and children’s services in the borough. Ealing’s MPS is updated annually and is available to download online at www.ealing.gov.uk. Although primarily a Council document, we have included reference to health and wellbeing services where these are jointly commissioned with Ealing Clinical Commissioning Group.
Who is the market position statement for? Ealing’s MPS is targeted at providers of health, social care and children’s services across the private, not-for-profit, voluntary and statutory sectors. It is anticipated that these markets will change significantly over the next few years as a result of ongoing policy and population changes, and in light of the continued financial pressures faced by statutory agencies. In this context, commissioners recognise that service providers are an important source of intelligence as to the capacity and resilience of our markets. Consequently, we will work closely with both commissioned and grant funded service providers to utilise their knowledge and experience in thinking more creatively and innovatively about the delivery of future service models and solutions that can best respond to the anticipated changes within our marketplaces.
The Context - Future Ealing
‘Future Ealing’ is the Council's strategic plan and sets out nine outcomes which the Council wishes to achieve:
• a strong, diverse and fair community
• an environmentally friendly borough
• keeping young people safe
• a growing economy, creating jobs and opportunities
• helping residents to stay active, healthy and independent
• more affordable housing
• helping young people to achieve their potential
• a clean and great place to live
• reducing crime and helping residents to feel safe These outcomes can only be achieved by the Council in partnership with the people who live and work in the borough, including all those who provide services. They therefore provide the context for all council departments in our relationship with the market. These outcomes are combined with those of the NHS in the Ealing Health and Wellbeing Strategy which identifies measures which the Council and NHS can take together to reduce health inequalities and increase wellbeing. These are informed by a rolling analysis of data captured in the Joint Strategic Needs Assessment (JSNA) which presents a picture of the changing population and profile of the borough and forecasts future needs. These documents are available on the Council's website.
Page 167 of 324
Ealing Market Position Statement 2018-19 Page 4 of 39
Ealing Joint Strategic Needs Assessment can be downloaded at: https://www.ealing.gov.uk/downloads/download/4545/joint_strategic_needs_assessment NHS priorities are also reflected in the North-West London Sustainability and Transformation Plan which is available on the Clinical Commissioning Group's website: http://www.ealingccg.nhs.uk/about-us/our-plans
Brighter Futures Brighter futures (BF) is a programme of innovation and service transformation in children and family services, that has been rolled out in Children’ Services since 2015. The programme combines a model of intensive multi-agency support to children and families, enhanced and evidence based training, a focus on fostering recruitment and a redesign of preventative services. It is a whole system transformation of Ealing’s approach to supporting young people and their families in and on the edge of care as well as transforming our early intervention and prevention offer to reduce demand in social care. The focus is on enabling our workforce to build consistent effective relationships with children, young people, families, communities and carers and use those successful relationships to drive better outcomes. The programme aims to improve outcomes for the most vulnerable children and families by: 1. Preventing children from coming into contact with the social care system 2. Reducing the numbers of children currently in the social care system 3. Delivering better value for money and better outcomes for children currently in the care system In achieving these three objectives, BF also aims to enable the development of a more efficient, effective and financially sustainable service for vulnerable children and families in the borough. Key outcomes of Brighter Futures, in partnership with providers is to:
• Increase in number of looked after children who return home safely and quickly
• Fewer young people become looked after and long distance residential placements
• Children and young people who are looked after will be in local, well supported, less expensive, stable, foster care placements, with only a small number in residential care
• Outcomes for young people will improve on all indicators (improved educational attainment and placement stability, reduction in substance use, offending behaviour and early parenthood)
What does Brighter Futures mean for Providers? We want providers to work in partnership with children and family multi-agency approach. Work will vary and is based on the needs of individual children and families. We want to work with providers to increase and improve local support services and supporting local foster care recruitment and foster carers.
Better Lives1 The continuing rise in demand and cost continues to present a significant challenge to the delivery of services within current funding levels. Because of these pressures the Council recognises the need to transform the way we work to give even greater emphasis to reflecting strength-based and outcomes-based approaches to support people to live independently for as long as possible, whilst
1 A full report on the Better Lives programme can be found in the March 2018 Cabinet papers at http://ealing.cmis.uk.com/ealing/committees
Page 168 of 324
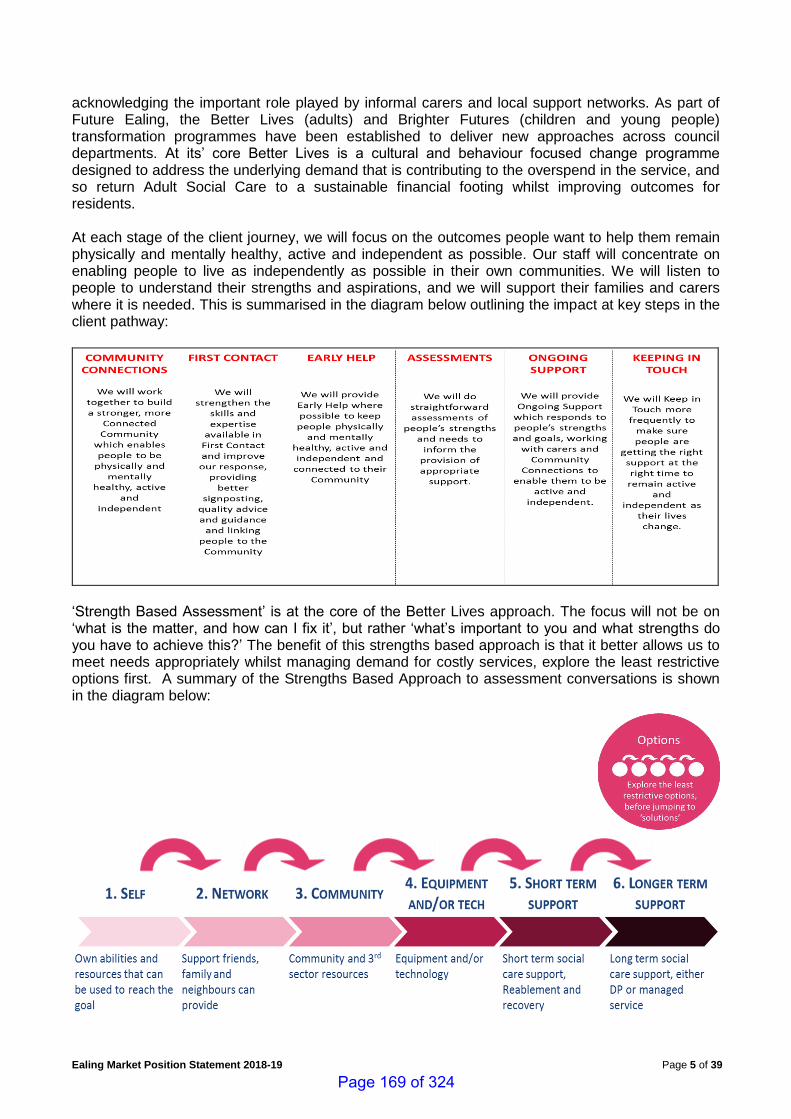
Ealing Market Position Statement 2018-19 Page 5 of 39
acknowledging the important role played by informal carers and local support networks. As part of Future Ealing, the Better Lives (adults) and Brighter Futures (children and young people) transformation programmes have been established to deliver new approaches across council departments. At its’ core Better Lives is a cultural and behaviour focused change programme designed to address the underlying demand that is contributing to the overspend in the service, and so return Adult Social Care to a sustainable financial footing whilst improving outcomes for residents. At each stage of the client journey, we will focus on the outcomes people want to help them remain physically and mentally healthy, active and independent as possible. Our staff will concentrate on enabling people to live as independently as possible in their own communities. We will listen to people to understand their strengths and aspirations, and we will support their families and carers where it is needed. This is summarised in the diagram below outlining the impact at key steps in the client pathway:
‘Strength Based Assessment’ is at the core of the Better Lives approach. The focus will not be on ‘what is the matter, and how can I fix it’, but rather ‘what’s important to you and what strengths do you have to achieve this?’ The benefit of this strengths based approach is that it better allows us to meet needs appropriately whilst managing demand for costly services, explore the least restrictive options first. A summary of the Strengths Based Approach to assessment conversations is shown in the diagram below:
Page 169 of 324
Ealing Market Position Statement 2018-19 Page 6 of 39
During 2017-18 the Council has been working with front line staff and managers to embed this approach to working; we have streamlined the assessment and review forms and given greater emphasis to monitoring outcomes and enabling people to move towards more independent living, wherever possible. In January, we wrote to service providers setting out the aims of the Better Lives programme and explaining what it will mean and how we would like to work together to implement these aims. We have sent you a survey asking about your knowledge of this approach and what support you would welcome to take it forward in your organisation. We had a good response to the survey. The key points made were: [xxx] and we will be taking these into account in the coming year. We have also been presenting our plans to provider forums and, at their invitation, visited a number of organisations to talk through details of the programme. If you would like us to come to your organisation contact us at:
What does Better Lives mean for Providers? We want providers to also focus on outcomes and strengths-based service delivery to meet the changing needs of people in their care. The approach will, of course, vary depending on the client cohort for whom you are caring, and for each individual within that cohort, but the principle of identifying outcomes and implementing plans to achieve those outcomes, should apply for everyone. We want to work with you to develop strengths-based services, where these are not already in place. Some of your staff have already taken up the offer of training in Motivational Interviewing and Making Every Contact Count. We want to explore how we can further develop the training offer for providers with your input. You can find out more about Strength-Based Working through the following link: https://www.scie.org.uk/care-act-2014 Our commissioners will be improving service specifications and contract terms to be clear about what we want to be provided and how we will monitor services in relation to setting and delivering outcomes for our residents. We recognise that outcomes for someone on a recovery pathway through different levels of support will be different from those for someone with a deteriorating condition or approaching the end of their life.
Commissioning standards and quality assurance Ealing’s commissioning approach and procurement practice aims to incorporate the following core standards2:
1. Person-centred, strength-based and focused on outcomes
2. Promote health and wellbeing for all 3. Delivers social value
4. Co-produces with local people, networks and communities 5. Promotes positive engagement with providers
6. Promotes equality
7. Well-led by local authorities
8. Demonstrates a ‘whole systems’ approach 9. Actively uses evidence about what works
10. Ensures the diversity, sustainability and quality of the market 11. Provides value for money
12. Develops the workforce
The provision of high quality services is ever more important, particularly at a time when the financial pressures on public services are increasing. We believe that our providers share our
2 Commissioning for Better Outcomes: A Route Map – University of Birmingham
Page 170 of 324
Ealing Market Position Statement 2018-19 Page 7 of 39
commitment to high quality services and we want to work with them achieve to translate this into practice that makes a real difference to people’s lives. Consequently, the focus on quality will be a central feature of our engagement with providers throughout the coming year. To underpin our commitment to the quality agenda - Ealing Council, Ealing Clinical Commissioning Group (ECCG) and the Care Quality Commission (CQC) operate a Joint Quality Information & Assurance Panel to share market intelligence and better co-ordinate joint agency responses to quality related matters and / or concerns. Ealing Healthwatch has also joined this Panel and this has helped inform their programme of Enter and View Visits and service surveys. • Local adult social care provider information can be found at:
https://www.careplace.org.uk/Information/Ealingproviders
• Quality improvement service provider guides can be found at: http://www.careimprovementworks.org.uk/
• A Quality Matters Guide is also available at the Gov.UK website:
https://www.gov.uk/government/publications/adult-social-care-quality-matters The council also wishes to ensure that adult self-funders buying their own care and support have the same assurances on quality. Our Adults’ Placements and Brokerage Teams will, as requested, assist self-funders in navigating the care and support market.
Sub-regional market management (via the West London Alliance) The West London Alliance (WLA) continues to be an effective sub-regional hub for implementing cross-borough procurement arrangements for both children’s and adults’ services across North West London.
• Children’s Services - there is a wide-ranging children’s programme coordinated by the WLA, which involves 9 local authorities working together on a range of issues, examples of which are:
o Joint provider forums o A joint contract for independent fostering and semi-independent accommodation o A residential children’s home managers network
• Adult’s social care commissioners via the WLA have: o Developed sub-regional procurement projects with neighbouring authorities including the
Dynamic Purchasing System (DPS) for Care Homes and Supported Living Placements. o Introduced an e-brokerage solution for care home, supported living and domiciliary care
referrals o Established a North-West London Market Management Working Group to oversee
improved integrated working between the boroughs and the NHS
• As part of the London Consortium led by the London Borough of Hammersmith & Fulham, Ealing commissioned a new Community Equipment Service from April 2019
CarePlace
The West London Alliance boroughs jointly commission the online care and support platform CarePlace. The system provides accessible online information, advice and a real-time directory of care and support resources.
Page 171 of 324
Ealing Market Position Statement 2018-19 Page 8 of 39
Health, social care and children’s services providers are actively encouraged to place details of their services (at no cost to the provider) on the CarePlace system via the following link:
www.careplace.org.uk
Achievements and successes 2017-18 Our achievements and successes in 2017-18 included: Children's Services:
• Developed a ‘Local Offer’ website for Ealing – you can view the website at: https://www.ealingfamiliesdirectory.org.uk/kb5/ealing/directory/localoffer.page?localofferchannel=0
• Procured an Information and Advice Service for the 0-25 years old population
• Secured funding for a young person’s substance outreach worker to work with hard to reach groups
• Recommissioned transport for children and young people with additional needs
• Established young carers support within the wider Carers' Support Service
• Secured 2 years funding for a Building My Futures programme – supporting vulnerable young people, aged 11-25 with a learning difficulty or disability who have behaviour that challenges and / or mental health issues.
• Added new domiciliary care providers to the short-breaks summer holiday programme for children aged 16-18 years old.
Adults’ Services:
• Procured a new Ealing Healthwatch Service
• Procured a new Carers' Support Service (including support for young carers)
• Implemented a new Dynamic Purchasing System (DPS) for Support at Home - incorporating personal care, complex care and reablement service categories
• Procured a new Community Equipment Service (as part of a London-wide Consortium)
• Secured DCLG funding for an Access to Employment project
Page 172 of 324
Page 9 of 39
Part 2 - Developments and Market Opportunities 2018-19
Service developments and opportunities
Children's Services’ will:
• Recommission a Health Visiting and School Nursing Service
• Commission a Tier 2 mental health service
• Open the DPS for Domiciliary Care for Children and Young People aged 0-25
• Undertake a review of children’s short breaks provision in the borough
• There is noted demand for: o local foster carer placements for older young people in their teens. o high quality local residential care for teenagers o high quality local semi-independent accommodation o domiciliary care for children with challenging behaviour o accessible transport with passenger assistance
Adults’ Services’ will:
• Develop an enhanced health in care homes model of care in partnership with the WLA and NHS
• Open further rounds of the Dynamic Purchasing Systems (DPS) for: o Care Home and Supported Living Placements o Support at Home (Homecare) o Residential Rehabilitation, Detoxification and Structured Day-care Providers o Advocacy Services The DPS opportunities can be accessed be the London Tenders Portal at: https://procontract.due-north.com/Opportunities/Index?p=2241eb95-058a-e511-80f7-000c29c9ba21&v=1
• Recommission day centre transport via the Council's new Transport Hub
• Procure a care and support service for adults with learning disabilities with complex needs and significant challenging behaviour
• Explore options to increase the number of residential and nursing dementia beds for respite and short-stay purposes
• Establish education, training and employment support for substance misusers
• Increase the capacity of the Ealing women’s complex needs service
• Develop a service specification for the integrated community drug and alcohol treatment service
• Develop the Personal Assistant (PA) market for direct payment users to ensure they have
access to a reliable and skilled workforce
• Develop new flexible home-based ‘services’ to support carers using direct payments to
purchase their own support
• Actively engage with the market to embed strength-based working practices
The following opportunities will be available for both adult & children's service providers:
• We plan to recommission specialist substance misuse services for adults and young people
• There will be an opportunity for eligible organisations and service providers to bid for Voluntary Sector Grant funding for the period 2019-2023; including for a Specialist Advice Service.
Page 173 of 324

Ealing Market Position Statement 2018-19 Page 10 of 39
Workforce Development The Council and CCG are aware of the challenges faced by many providers in recruiting and retaining staff to work in West London. We are keen to work with providers to help with workforce development opportunities. Children’s Services: In the main, children’s services providers are expected to take the initiative in this area either working individually or collectively across the Central and West London sectors. A voluntary sector safeguarding project is funded to provide information, advice and training on issues around safeguarding. Adults Services: Are fully committed to providing professional development opportunities for care and support staff from across the private, voluntary and independent sectors. This includes care homes, homecare agencies, voluntary groups and carers organisations. Our criteria for registration is that providers must be either based in Ealing or have a contract to provide care and support services on Ealing Council’s behalf. As well as ‘classroom’ style training Ealing also offers access online e-Learning courses via the Council’s e-Learning website. The ‘general’ adult social care courses offered for 2018-19 are as follows:
• Safeguarding Adults Level 1 - Raising a Concern
• Introduction to the Mental Capacity Act
• Working with Clients Who Lack Capacity
• Introduction to Dementia
• Learning Disability Awareness
• Autism Awareness
• Challenging Behaviour - Learning Disabilities
• Boundaries and Good Practice in Adult Care
• Level 2 Award - Promoting Dignity in Care
• Level 2 Award - End of Life Care Awareness The general courses are at an introductory level and intermediate level and aimed primarily at unqualified staff. Care Certificate related courses offered for 2018-19 are as follows:
• Level 2 Award - Duty of Care
• Level 2 Award - Person Centred Care and Support
• Level 2 Award - Effective Communication
• Level 2 Award - Food Safety, Nutrition and Hydration
• Level 2 Award - Infection Control and Prevention The Care Certificate is an identified set of standards that health and social care workers adhere to in their daily working life. Designed with the non-regulated workforce in mind, the Care Certificate gives everyone the confidence that workers have the same introductory skills, knowledge and behaviours to provide compassionate, safe and high quality care and support. All the adult social care courses remain free of charge for 2018-19
Page 174 of 324
Ealing Market Position Statement 2018-19 Page 11 of 39
Ealing’s Training & Development Team can be contact at [email protected] or on 020 8825 8780. The LNW CCG Collaborative has commissioned (via My Home Life) a ‘NW London Leadership and Professional Support Programme for Care Home Managers’ working with Older Adults in North-West London. The programme consists of a four-day workshop followed by monthly action learning sets and a completion day. Trained professional facilitators will support Managers and / or their Deputies to lead on the development of their care home practices and settings that embed a culture that is person-centred, relational, dignified and compassionate. Further details on the programme can be obtained from My Home Life at [email protected] Providers can also make use of online workforce tools to assist them in developing their workforce including. Skills for Care currently offer the following online tools:
• Skills for Care – Workforce Capacity Planning Tool http://www.skillsforcare.org.uk/Standards/Care-Act/Workforce-capacity-planning/Workforce-capacity-planning-model/Workforce-capacity-planning-model.aspx
• Skills for Care – Workforce Readiness Tool https://www.snapsurveys.com/wh/surveylogin.asp?k=141137934094
Provider Engagement 2018-19 Ealing works with a wide range of service providers to ensure regular engagement on both operational and strategic issues, and welcome the involvement of all service providers in this process. Children’s & Adults’ Services will engage with service providers throughout 2018-19 through the following facilitated forums and events:
• Children’s Residential Care Provider Forum
• Ealing Care Home Provider Forum
• Learning Disabilities Provider Forum
• Mental Health Provider Forum
• Ealing Homecare Provider Forum
• Ealing Information and Advice Provider Network
• Ealing Registered Managers Network As part of its Better Lives programme, Adults Services, also plan to run a series of ‘challenge and innovation’ sessions throughout the year with providers - details of which will be circulated to service providers in due course.
Page 175 of 324
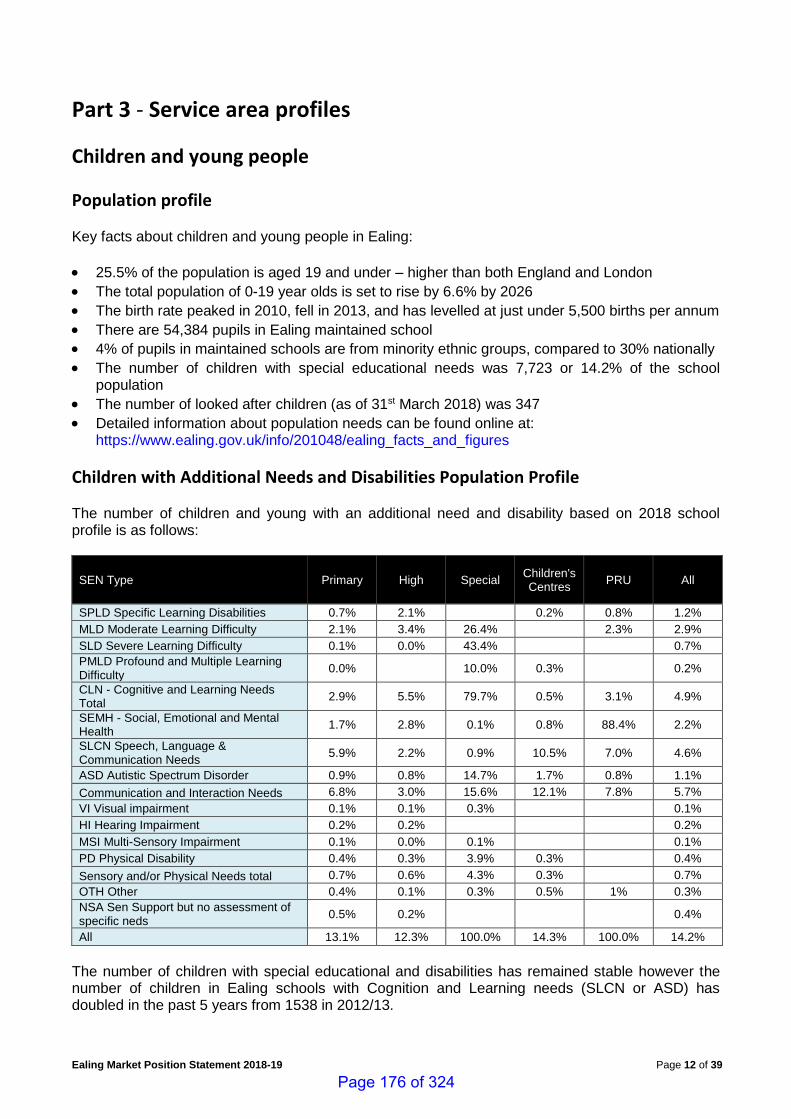
Ealing Market Position Statement 2018-19 Page 12 of 39
Part 3 - Service area profiles
Children and young people
Population profile Key facts about children and young people in Ealing:
• 25.5% of the population is aged 19 and under – higher than both England and London
• The total population of 0-19 year olds is set to rise by 6.6% by 2026
• The birth rate peaked in 2010, fell in 2013, and has levelled at just under 5,500 births per annum
• There are 54,384 pupils in Ealing maintained school
• 4% of pupils in maintained schools are from minority ethnic groups, compared to 30% nationally
• The number of children with special educational needs was 7,723 or 14.2% of the school population
• The number of looked after children (as of 31st March 2018) was 347
• Detailed information about population needs can be found online at: https://www.ealing.gov.uk/info/201048/ealing_facts_and_figures
Children with Additional Needs and Disabilities Population Profile The number of children and young with an additional need and disability based on 2018 school profile is as follows:
SEN Type Primary High Special Children's Centres
PRU All
SPLD Specific Learning Disabilities 0.7% 2.1% 0.2% 0.8% 1.2%
MLD Moderate Learning Difficulty 2.1% 3.4% 26.4% 2.3% 2.9%
SLD Severe Learning Difficulty 0.1% 0.0% 43.4% 0.7%
PMLD Profound and Multiple Learning Difficulty
0.0% 10.0% 0.3% 0.2%
CLN - Cognitive and Learning Needs Total
2.9% 5.5% 79.7% 0.5% 3.1% 4.9%
SEMH - Social, Emotional and Mental Health
1.7% 2.8% 0.1% 0.8% 88.4% 2.2%
SLCN Speech, Language & Communication Needs
5.9% 2.2% 0.9% 10.5% 7.0% 4.6%
ASD Autistic Spectrum Disorder 0.9% 0.8% 14.7% 1.7% 0.8% 1.1%
Communication and Interaction Needs 6.8% 3.0% 15.6% 12.1% 7.8% 5.7%
VI Visual impairment 0.1% 0.1% 0.3% 0.1%
HI Hearing Impairment 0.2% 0.2% 0.2%
MSI Multi-Sensory Impairment 0.1% 0.0% 0.1% 0.1%
PD Physical Disability 0.4% 0.3% 3.9% 0.3% 0.4%
Sensory and/or Physical Needs total 0.7% 0.6% 4.3% 0.3% 0.7%
OTH Other 0.4% 0.1% 0.3% 0.5% 1% 0.3%
NSA Sen Support but no assessment of specific neds
0.5% 0.2% 0.4%
All 13.1% 12.3% 100.0% 14.3% 100.0% 14.2%
The number of children with special educational and disabilities has remained stable however the number of children in Ealing schools with Cognition and Learning needs (SLCN or ASD) has doubled in the past 5 years from 1538 in 2012/13.
Page 176 of 324
Ealing Market Position Statement 2018-19 Page 13 of 39
Current demand profile Ealing Service for Children with Disabilities social work team at the end of 2017-18 had 390 children registered. In 2017-18 over 2.7 million was spent on Community Short Break Packages and direct payments, for 340 children and young people with disabilities. Community short break includes: domiciliary care provision in the home and community, overnight care, day time and holiday short break activities such as afterschool school clubs and holiday clubs. There are currently 20 Domiciliary Care providers on the Councils Dynamic Purchasing list with 38 Providers used in total. In 2017-18, over 77,000 hour of domiciliary care was purchased by the council for over 160 individual children and young people. Packages of care are tailored to meet a wide range of needs. 70% of care packages are for children & young people with physical and or learning disabilities and 30% are for very complex health needs and behaviour that challenges. Of the 30%, approximately one third require specialist health care and behaviour support. In addition to domiciliary care short breaks provision, community based short breaks and resources are commissioned such as specialist play and holiday clubs. Residential short breaks were provided to 21 children and young people at a cost of £430k. Residential short break services cater primarily for children with most complex needs. These may include children who require assistance with moving and personal care, children who require invasive clinical procedures and those with behaviour that challenges. There are 11 children & young people with complex needs who are in full time residential placements. The total spend last year was £1.7million with the social care contribution being £994,000 and health & education making up the remainder.
What do we plan to change or extend? During 2018-19 we would welcome provider involvement with the following: • Explore options to increase the number of local based, community short break and respite
provision • Develop Domiciliary Care provision to meet ongoing need • Work will continue to develop innovative approaches to supporting children & young people to
remain at home with their families as an alternative to residential care where this is the best option. This will require high quality, dedicated support staff to work with parents and carers.
Page 177 of 324
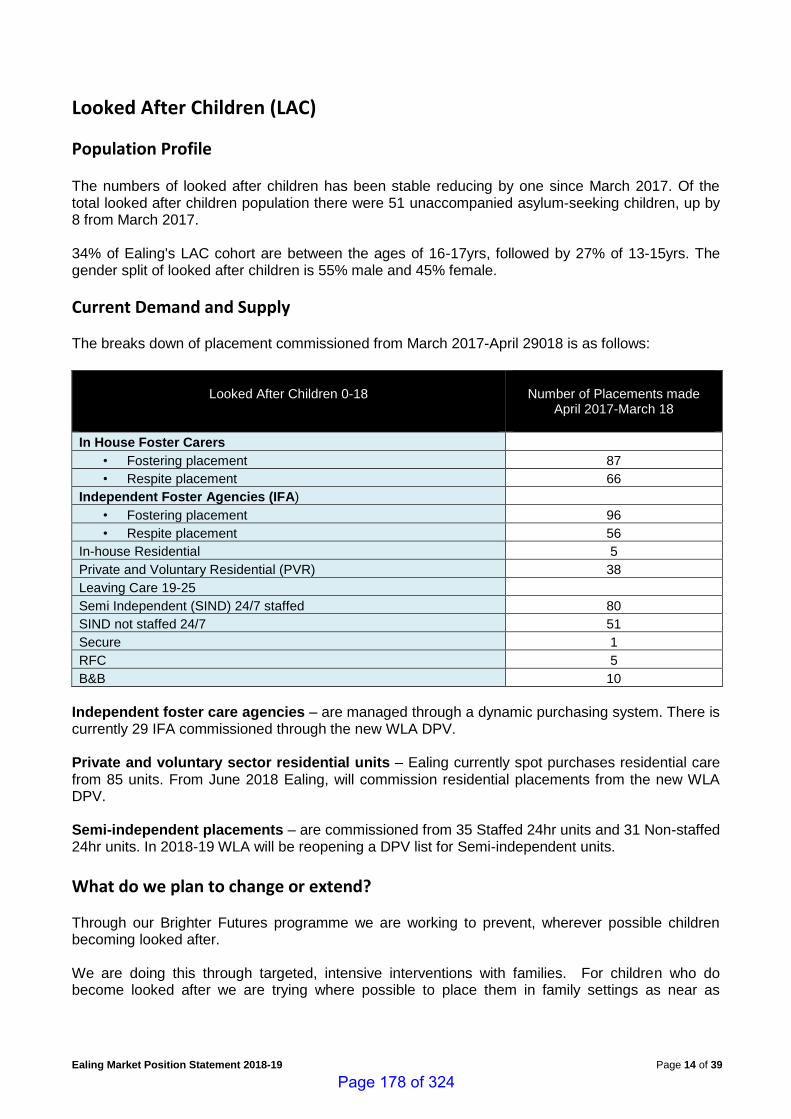
Ealing Market Position Statement 2018-19 Page 14 of 39
Looked After Children (LAC)
Population Profile The numbers of looked after children has been stable reducing by one since March 2017. Of the total looked after children population there were 51 unaccompanied asylum-seeking children, up by 8 from March 2017. 34% of Ealing's LAC cohort are between the ages of 16-17yrs, followed by 27% of 13-15yrs. The gender split of looked after children is 55% male and 45% female.
Current Demand and Supply The breaks down of placement commissioned from March 2017-April 29018 is as follows:
Looked After Children 0-18
Number of Placements made
April 2017-March 18
In House Foster Carers • Fostering placement 87
• Respite placement 66
Independent Foster Agencies (IFA) • Fostering placement 96
• Respite placement 56
In-house Residential 5
Private and Voluntary Residential (PVR) 38
Leaving Care 19-25
Semi Independent (SIND) 24/7 staffed 80
SIND not staffed 24/7 51
Secure 1
RFC 5
B&B 10
Independent foster care agencies – are managed through a dynamic purchasing system. There is currently 29 IFA commissioned through the new WLA DPV. Private and voluntary sector residential units – Ealing currently spot purchases residential care from 85 units. From June 2018 Ealing, will commission residential placements from the new WLA DPV. Semi-independent placements – are commissioned from 35 Staffed 24hr units and 31 Non-staffed 24hr units. In 2018-19 WLA will be reopening a DPV list for Semi-independent units.
What do we plan to change or extend? Through our Brighter Futures programme we are working to prevent, wherever possible children becoming looked after. We are doing this through targeted, intensive interventions with families. For children who do become looked after we are trying where possible to place them in family settings as near as
Page 178 of 324

Ealing Market Position Statement 2018-19 Page 15 of 39
possible to their home area. We know, though, that we shall have an ongoing need for some residential care for looked after children. There is ongoing demand for: • Local and high quality foster care placements with a focus for older young people in their teens • High quality local residential care for teenagers
Page 179 of 324
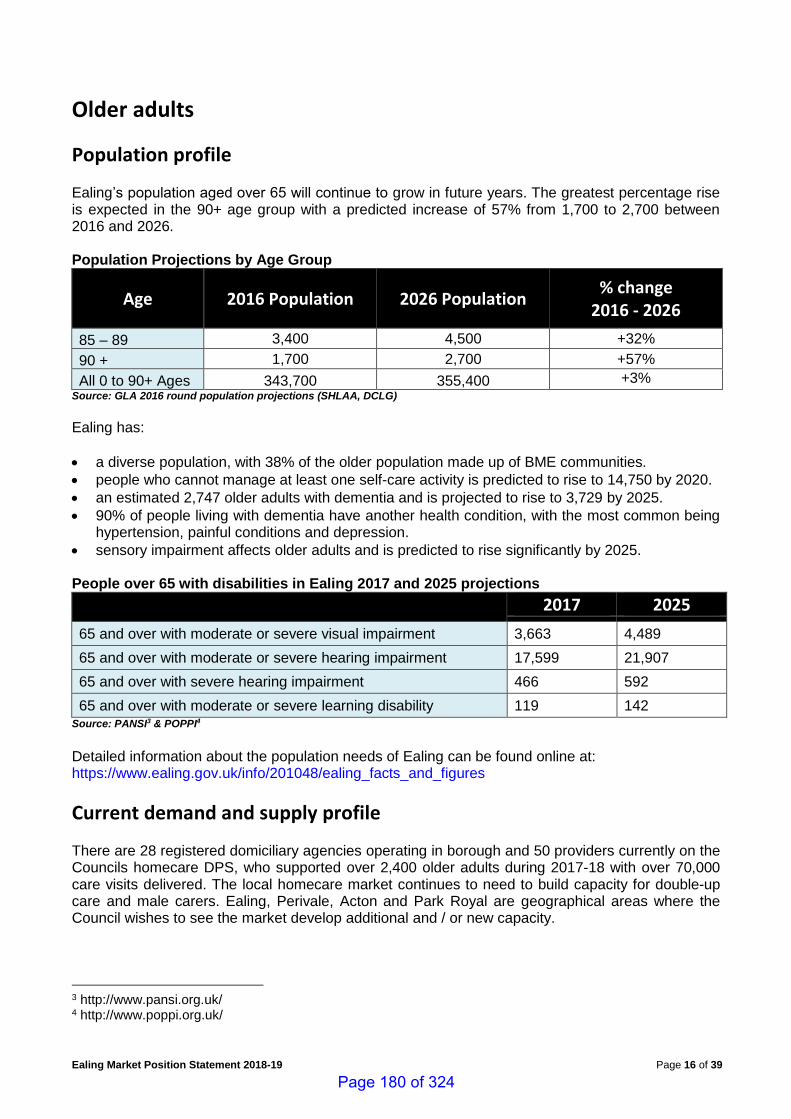
Ealing Market Position Statement 2018-19 Page 16 of 39
Older adults
Population profile Ealing’s population aged over 65 will continue to grow in future years. The greatest percentage rise is expected in the 90+ age group with a predicted increase of 57% from 1,700 to 2,700 between 2016 and 2026. Population Projections by Age Group
Age 2016 Population 2026 Population % change
2016 - 2026
85 – 89 3,400 4,500 +32%
90 + 1,700 2,700 +57%
All 0 to 90+ Ages 343,700 355,400 +3% Source: GLA 2016 round population projections (SHLAA, DCLG)
Ealing has:
• a diverse population, with 38% of the older population made up of BME communities.
• people who cannot manage at least one self-care activity is predicted to rise to 14,750 by 2020.
• an estimated 2,747 older adults with dementia and is projected to rise to 3,729 by 2025.
• 90% of people living with dementia have another health condition, with the most common being hypertension, painful conditions and depression.
• sensory impairment affects older adults and is predicted to rise significantly by 2025.
People over 65 with disabilities in Ealing 2017 and 2025 projections
2017 2025
65 and over with moderate or severe visual impairment 3,663 4,489
65 and over with moderate or severe hearing impairment 17,599 21,907
65 and over with severe hearing impairment 466 592
65 and over with moderate or severe learning disability 119 142 Source: PANSI3 & POPPI4
Detailed information about the population needs of Ealing can be found online at: https://www.ealing.gov.uk/info/201048/ealing_facts_and_figures
Current demand and supply profile There are 28 registered domiciliary agencies operating in borough and 50 providers currently on the Councils homecare DPS, who supported over 2,400 older adults during 2017-18 with over 70,000 care visits delivered. The local homecare market continues to need to build capacity for double-up care and male carers. Ealing, Perivale, Acton and Park Royal are geographical areas where the Council wishes to see the market develop additional and / or new capacity.
3 http://www.pansi.org.uk/ 4 http://www.poppi.org.uk/
Page 180 of 324
Ealing Market Position Statement 2018-19 Page 17 of 39
There are 53 registered care homes in the borough offering 1,653 beds (of which 955 are nursing beds). Most local in-borough referrals to care homes were for people with dementia. There is a noted need for dementia placements to support residents with challenging needs. The need for residential and nursing dementia beds remains high, particularly for respite and short-stay. People who are placed in residential care are now more likely to have complex care needs. In terms of placement activity Adults Services commissioned (both in and outside Ealing) 332 permanent nursing placements and 300 permanent residential placements in 2017-18. In addition to this, 372 older adults were also provided with either short-term or respite care placements during the year. There are two extra-care schemes providing 75 self-contained flats in the borough. We expect demand for this service model to grow in future years. Consequently, we continue to be open to discussions with service providers as to how extra-care capacity can be developed in the borough to meet new demand. Adults Services also provides up to 100 places per day at the Michael Flanders Centre, a dedicated day service for older adults with dementia.
What do we plan to change or extend? During 2018-19 we would welcome provider involvement with the following: • Explore options to increase the number of residential and nursing dementia beds for respite and
short-stay purposes.
• Develop a new Older People's Housing Strategy to ensure that the housing needs of frail older people and those with dementia are met in the future
• Develop an end of life crisis management pathway
• Establish Dementia Friendly Communities and a Dementia Friends' Network
Page 181 of 324
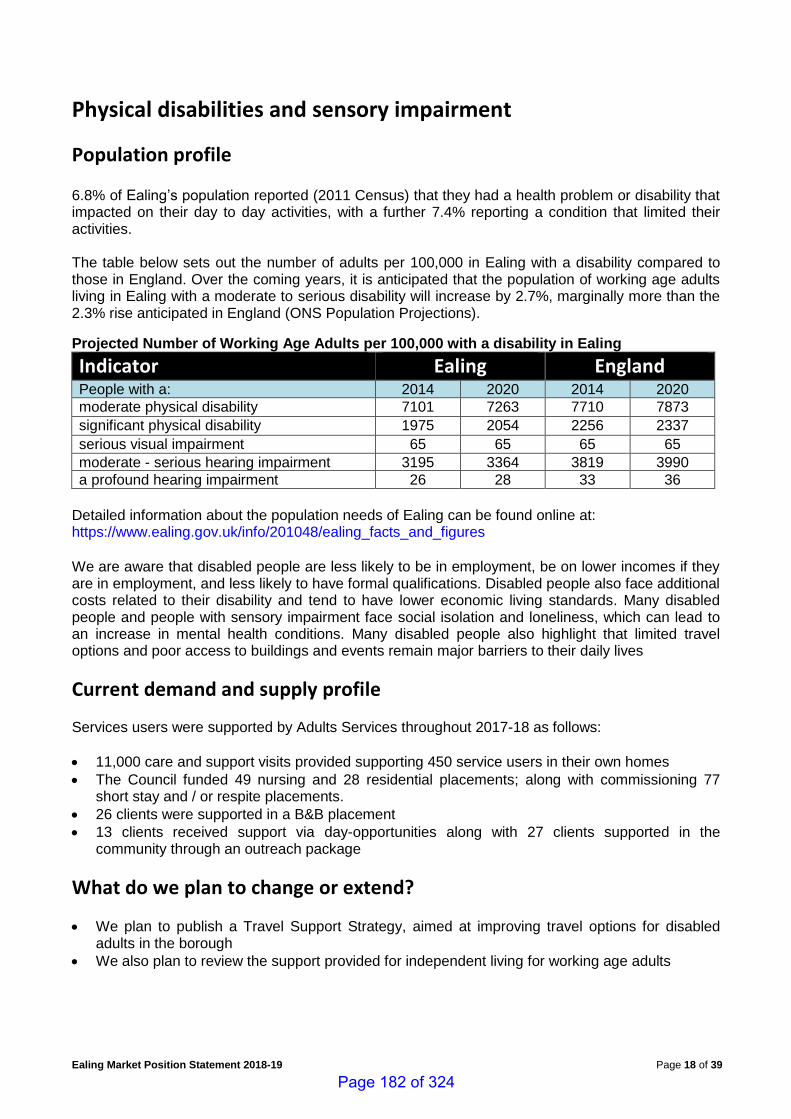
Ealing Market Position Statement 2018-19 Page 18 of 39
Physical disabilities and sensory impairment
Population profile 6.8% of Ealing’s population reported (2011 Census) that they had a health problem or disability that impacted on their day to day activities, with a further 7.4% reporting a condition that limited their activities. The table below sets out the number of adults per 100,000 in Ealing with a disability compared to those in England. Over the coming years, it is anticipated that the population of working age adults living in Ealing with a moderate to serious disability will increase by 2.7%, marginally more than the 2.3% rise anticipated in England (ONS Population Projections).
Projected Number of Working Age Adults per 100,000 with a disability in Ealing
Indicator Ealing England People with a: 2014 2020 2014 2020
moderate physical disability 7101 7263 7710 7873
significant physical disability 1975 2054 2256 2337
serious visual impairment 65 65 65 65
moderate - serious hearing impairment 3195 3364 3819 3990
a profound hearing impairment 26 28 33 36
Detailed information about the population needs of Ealing can be found online at: https://www.ealing.gov.uk/info/201048/ealing_facts_and_figures We are aware that disabled people are less likely to be in employment, be on lower incomes if they are in employment, and less likely to have formal qualifications. Disabled people also face additional costs related to their disability and tend to have lower economic living standards. Many disabled people and people with sensory impairment face social isolation and loneliness, which can lead to an increase in mental health conditions. Many disabled people also highlight that limited travel options and poor access to buildings and events remain major barriers to their daily lives
Current demand and supply profile Services users were supported by Adults Services throughout 2017-18 as follows:
• 11,000 care and support visits provided supporting 450 service users in their own homes
• The Council funded 49 nursing and 28 residential placements; along with commissioning 77 short stay and / or respite placements.
• 26 clients were supported in a B&B placement
• 13 clients received support via day-opportunities along with 27 clients supported in the community through an outreach package
What do we plan to change or extend?
• We plan to publish a Travel Support Strategy, aimed at improving travel options for disabled adults in the borough
• We also plan to review the support provided for independent living for working age adults
Page 182 of 324
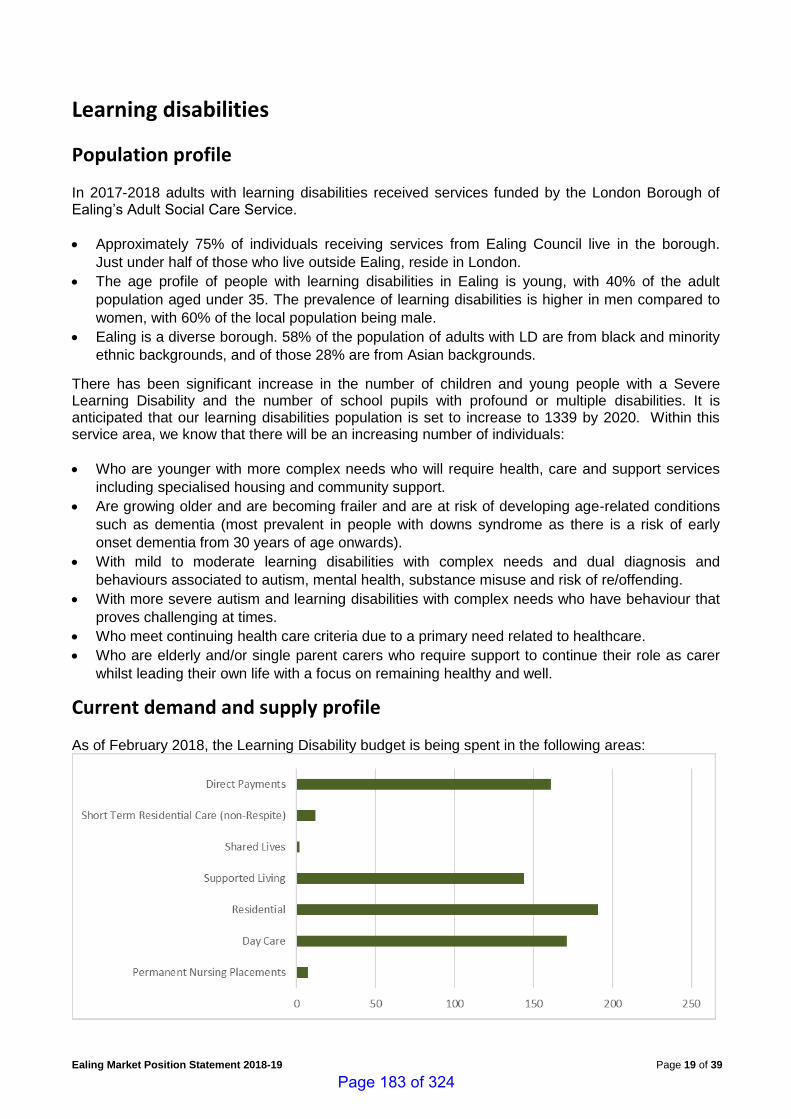
Ealing Market Position Statement 2018-19 Page 19 of 39
Learning disabilities
Population profile In 2017-2018 adults with learning disabilities received services funded by the London Borough of Ealing’s Adult Social Care Service.
• Approximately 75% of individuals receiving services from Ealing Council live in the borough.
Just under half of those who live outside Ealing, reside in London.
• The age profile of people with learning disabilities in Ealing is young, with 40% of the adult
population aged under 35. The prevalence of learning disabilities is higher in men compared to
women, with 60% of the local population being male.
• Ealing is a diverse borough. 58% of the population of adults with LD are from black and minority
ethnic backgrounds, and of those 28% are from Asian backgrounds.
There has been significant increase in the number of children and young people with a Severe Learning Disability and the number of school pupils with profound or multiple disabilities. It is anticipated that our learning disabilities population is set to increase to 1339 by 2020. Within this service area, we know that there will be an increasing number of individuals:
• Who are younger with more complex needs who will require health, care and support services
including specialised housing and community support.
• Are growing older and are becoming frailer and are at risk of developing age-related conditions
such as dementia (most prevalent in people with downs syndrome as there is a risk of early
onset dementia from 30 years of age onwards).
• With mild to moderate learning disabilities with complex needs and dual diagnosis and
behaviours associated to autism, mental health, substance misuse and risk of re/offending.
• With more severe autism and learning disabilities with complex needs who have behaviour that
proves challenging at times.
• Who meet continuing health care criteria due to a primary need related to healthcare.
• Who are elderly and/or single parent carers who require support to continue their role as carer
whilst leading their own life with a focus on remaining healthy and well.
Current demand and supply profile As of February 2018, the Learning Disability budget is being spent in the following areas:
Page 183 of 324
Ealing Market Position Statement 2018-19 Page 20 of 39
In addition to the above service profile Ealing Council supported 112 homecare service users with a learning disability in 2017-18 providing over 2000 visits; along with 89 service users who received outreach support in the community. Detailed information about the population needs of Ealing can be found online at: https://www.ealing.gov.uk/info/201048/ealing_facts_and_figures
What do we plan to change or extend? Providers are requested to respond to the diverse and complex needs of service users who meet the Transforming Care definition by ensuring that their workforce has the right skills and expertise to support the following LD cohorts:
• autism and behaviour that may challenge
• mental health support needs
• people who display anti-social, risky or offending behaviour
• people who misuse drugs and alcohol
• people who display harmful sexual behaviour During 2018-19 we will be working closely with providers to develop further options for community provision of care for people with complex needs and challenging behaviour. We will continue to review current placements to monitor agreed outcomes, and where appropriate, support service users to move to more independent living.
Page 184 of 324
Ealing Market Position Statement 2018-19 Page 21 of 39
Autism spectrum disorders (ASD)
Population profile
Current demand and supply profile Data about the number of people living with autism is available from several different sources. The latest information is included in the Autism Joint Strategic Needs Assessment published in 2017. You can view this at www.ealing.gov.uk/jsna We know how many people living with a) ASD and b) ASD plus a Learning Disability have received a service from London Borough of Ealing. For those who have serious and enduring mental health needs as well as living with ASD we know how many have had an assessment/treatment from an integrated mental health team. We also know how many people receive treatment for mental health needs and have both a Learning Disability and live with ASD. What we don’t know is how many people are living with ASD but not accessing any services or treatment for their condition.
Estimated prevalence
The most recent prevalence study of autism in the UK was commissioned by the Department of Health and published by the NHS Information Centre (now NHS Digital)5. Applying this estimate to the population of Ealing6 would indicate that there are approximately 3,780 (95% confidence interval 1,030 – 6,530) people living with ASD in the borough. Studies suggest that the prevalence of ASD maybe be higher among children and young people. For example, the Centres for Disease Control and Prevention in the USA estimate a prevalence of ASD among children and young people of 1.46% (95% confidence interval 0.82 – 2.46%)7. People of all nationalities and cultural, religious and social backgrounds live with autism, although it appears to affect more men than women. Recent studies have reported an increased prevalence, leading to an increased demand for diagnostic and support services. The reason for this increase is not fully understood.
Prevalence of ASD recorded in the Ealing School Census
According to the Ealing Spring School Census 2017, there were 7388 children and young people resident in Ealing who were recorded as living with ASD in state schools in Ealing (including children’s centres, primary/secondary schools and special schools). This represents 1.5% of all children and young people in Ealing state schools who live in the borough (738 out of 49,197 pupils in total). Of these 738 children and young people, 504 had living with ASD listed as their primary need whilst a further 234 had ASD classified as a secondary need9. Based on the School Census, over the last five years the number of children and young people in Ealing schools recorded as living with ASD has increased by 57% (Figure 1). Possible reasons for this rise could include families with children
5 The NHS Information Centre, Community and Mental Health Team, Brugha, T. et al (2012). Estimating the prevalence of autism spectrum conditions in adults: extending the 2007 Adult Psychiatric Morbidity Survey. Leeds: NHS Information Centre for Health and Social Care 6 2015 Greater London Authority Population Projection – SHLAA based 7 https://www.cdc.gov/ncbddd/autism/data.html (accessed on 09/02/2017) 8 An additional 57 children who were non-Ealing residents were recorded in the Ealing Spring School Census as having an ASD; making a total of 795 with an ASD in Ealing state schools.
Page 185 of 324
Ealing Market Position Statement 2018-19 Page 22 of 39
and young people living with ASD being attracted to Ealing to attend specialist schools (specialist provision has increased in recent years). It may be that as awareness of ASD rises among schools and parents, the number of children and young people put forward for a diagnosis has increased. Finally, it may be that recording of ASD by schools has improved over the time period.
Prevalence of ASD among people with a learning disability
Recent research by the Learning Disabilities Observatory indicates that around 20-30% of people with Learning Disabilities (LD) live with an ASD2. At October 2016, the top registered specific condition for adults with LD in receipt of services commissioned by London Borough of Ealing was autism, followed by other physical Illness, epilepsy, physical impairment and sensory impairment10. There were 149 people with LD identified as living with autism (including eight clients with Asperger’s Syndrome) who were eligible for support from London Borough of Ealing. Of these, 105 were male and 41 were female. When the snapshot was taken, 47 clients were using services outside of the borough (mainly in residential care). The majority of people (58%) with LD who also live with ASD are aged 18-34 years (Figure 2). The ethnicity profile of people with LD who also live with ASD is similar to that of all people with LD in Ealing; around half are White, a quarter Asian/Asian British and a sixth Black/Black British (Figure 3). Prevalence of mental health and/or challenging behaviour in local population of adults living with ASD and a learning disability. The needs of people with learning disabilities living with autism can be particularly complex, with many having a co-existing mental illness and/or challenging behaviour and often needing psychiatric or psychological interventions. This cohort is more likely to be at risk of admission to inpatient mental health services. At November 2016, 78% of adults with learning disabilities placed in assessment and treatment (commissioned by NHS Ealing CCG) also had a diagnosis of autism.
Projections of the number of adults with ASD
Projecting Adult Needs and Service Information (PANSI) and Projecting Older People Population Information (POPPI) are databases designed for analysing population data and projecting numbers into the future. With a focus on people aged 18-64 (PANSI) and people aged 65 and over (POPPI), figures from the Census 2011 are applied to Office for National Statistics population projections to give estimated numbers. Projections of the number of adults living with ASD are available from 2016 to 2030. These indicate a small, gradual increase in the number of adults living with ASD in Ealing. However, we have already seen that the number of children and young people in Ealing schools living with ASD has increased by 54% since 2012. Given this sharp increase in the number of diagnoses among children and young people, it seems logical that the increase will follow through to the adult population as these young people become adults. Whilst it is possible that some young adults living with ASD may be able to live independently, this increase is likely to have implications for the demand on services from this group.
Number of adults receiving an ASD assessment and/or treatment
West London Mental Health Trust (WLMHT) provides assessments and treatment to children and young people living with ASD, whether or not they also have mental health needs. Adults who live with an ASD and who are being treated by mental health services will have needs associated with their autism addressed and reasonable adjustments made to support their access to treatments. In the period 2015-16, 44 people were given an assessment by WLMHT and 126 received treatment for their mental health condition.
10 Source: London Borough of Ealing Adults Performance & Management Team, 2016
Page 186 of 324
Ealing Market Position Statement 2018-19 Page 23 of 39
The majority of those who received an assessment and/or treatment were male. The majority were also aged below 18 years old.
What do we plan to change or extend? There are areas we have identified where we need to explore solutions and focus on improvement. Work has already started on these areas but we need to do more.
• There is a need to ensure that providers delivering support and education to children and young people living with autism are adequately trained. This includes staff working in schools, SEND Coordinators and community based services such as domiciliary care.
• Access to information and signposting for recently diagnosed children and young people is a gap highlighted by parents.
• Transition into adulthood is a stressful time for many people living with autism. Support for young people is limited as they approach adulthood.
• The lack of specialist post-16 education facilities for young people living with autism who don’t have a moderate or severe LD has been highlighted as a gap by families.
• Adults who live with autism but do not have a learning disability or a mental health need are at risk of falling between services and not having their needs met, as many would not be eligible for social care support. This is a particular risk for people who are not diagnosed until adulthood and for whom there is no published care pathway. For individuals who do not meet the adult social care eligibility criteria, post diagnostic support both immediately and in the long term is limited to services provided by the voluntary sector.
• There is a shortage of affordable housing in Ealing that is suitable and safe for adults living with autism and challenging needs, particularly the cohort who struggle to share space with others due to the frequency and intensity of the challenging behaviour they exhibit and the risks they present to themselves and others. This often results in vulnerable people being placed out of borough away from their families and social networks.
• We will be looking to increase specialist residential respite service for adults with learning disabilities and autism who have challenging behaviour and live at home
• There is a need to ensure that all providers delivering support to children, young people and adults living with autism and challenging behaviour have the right skills and expertise to work collaboratively with local clinicians to implement services which are compliant with the recently published NICE guidelines.
Page 187 of 324
Ealing Market Position Statement 2018-19 Page 24 of 39
Mental health (including forensic services)
Population profile Mental health and wellbeing are part of everyone’s life, impacting on physical health, opportunities, feelings, behaviour and life expectancy. Everyone struggles with their mental health and wellbeing from time to time, through life events such as bereavement, loss and unemployment. For some of us, mental ill health seriously disrupts our lives. Many of us seek help and support. Estimates suggest that at some point in our lives, one in four of us will experience mental health difficulties severe enough to seek help. At any one time, at least one in ten of us will be living with common mental health needs – depression, anxiety, Obsessive Compulsive Disorder (OCD). At least one in a hundred of us will experience one or more psychotic episodes, experiencing the world differently, often as terrifying and dangerous to us or our loved ones. Many people recover from these experiences, some will live with them for their whole lives and will be severely disabled by them and by the associated stigma. For detailed data about prevalence of mental health needs in Ealing see the Mental Health Chapter of the Ealing Joint Strategic Needs Assessment (JSNA). Headlines are that in Ealing:
• 40,484 adults (all ages) are estimated by NHSE to be living with a common mental health need;
• Only 15,369 of these were registered with their GP as having depression in 2015/16 (lower than London and England);
• 4,576 people were registered with their GP as having psychoses in 2015/1611 (lower than England, similar to London);
• These numbers are predicted to rise over the next five years by approximately 0.4% per year;12 • On average, there are 20 people discharged from secure forensic services and are supported in
the community in Ealing each year. Many people with mental health needs also have hazardous substance use (drugs and alcohol). Prevalence of hazardous substance use amongst psychiatric inpatients is estimated at between 22% and 44%, and during 2015/16, 30% of Ealing’s new presentations for alcohol treatment and 29% of new presentations for drug treatment were receiving care from mental health services for reasons other than substance use.
Services and spending Most mental health services in Ealing are commissioned by the Ealing NHS Clinical Commissioning Group (ECCG) and are provided by the West London Mental Health NHS Trust, which has a single point of access (SPA) for all adult mental health services. This includes inpatient and urgent care; integrated community teams (Recovery Teams) supporting those with the most complex needs; an Early Intervention in Psychosis service; a Primary Care Mental Health Team supporting people with a range of mental health needs under the care of their GP; and national forensic services commissioned by NHS England. The Trust also provides Improving Access to Psychological Therapies (IAPT), a Vocational Support service and a Recovery College.
11 Source: HSCIC, QOF data 2015/16 12 Source: PANSI, 2014
Page 188 of 324

Ealing Market Position Statement 2018-19 Page 25 of 39
Other services commissioned include Supported Housing (164 individual places in 16/17) which is currently commissioned through several block contracts; Supported Living and Residential Care Homes (approximately 340 places) mostly individually commissioned through the DPS; support and care at home (60 people in 2016/17). The Council with ECCG supports a range of third sector organisations providing peer support, help finding and staying in work, counselling and other talking treatments, practical support with accessing housing and financial help, and challenging loneliness, stigma and social exclusion. The majority of these are grant-funded and the process for this is currently being reviewed with a view to procuring and funding services differently from 2019. ECCG and Ealing Council invest over £50 million per year in adult mental health. £40 million of this is for NHS services outlined above. £10 million is on supported living, residential care, nursing care, community and voluntary sector services and counselling. In Ealing, if a person has been detained under a section of the Mental Health Act and is assessed as having ongoing needs for care and support to remain out of hospital after discharge, they may be eligible for section 117 aftercare. This is the responsibility of the NHS and the Local Authority. In Ealing, there is a 50:50 agreement for funding s117 aftercare for new people. This can include a variety of services which support a person to live safely out of hospital, including support at home, supported living and residential care. These needs must be regularly reviewed to make sure they are still current and the support is appropriate.
How we want services to develop and opportunities for 2018-19 The Ealing Mental Health and Wellbeing Strategy 2017-21 outlines a vision for developing mental health services by shifting resources away from the most intensive services and towards more preventative and enabling services focusing on the outcomes people want to achieve and their own personal recovery. Resources are limited: we are interested in working with providers to make the best of what we have, providing good quality services for the people who need them and value for money. We want to support services which will provide what people want and need, and which will also save public money, such as:
• Services which will reduce, delay or prevent people’s need for social care, and which will reduce inappropriate use of health services, including emergency departments;
• Innovative ideas to provide more opportunities for people to live well with severe and enduring mental health needs, supporting people to recover and find what they need within their communities. This should include improving people’s access to financial, legal and housing support;
• Projects focusing on helping people to improve and maintain their mental health;
• New ways to improve access to Talking Therapies, especially integrated services for people with long term physical health needs, older people and those from BAME backgrounds;
• Enabling support and care at home – more support to develop or regain skills in looking after ourselves, and less ‘doing for’;
• Services supporting people with common mental health needs to become better connected with their local community support services;
• Services to help people with Autism and people with ADHD who do not have a diagnosed Learning Disability to live well in the community13;
• Supported living for people with complex and multiple needs, including involvement with the criminal justice system, hazardous substance use, physical health difficulties, focusing on recovery and achieving personal goals and ambitions;
13 See Autism chapter
Page 189 of 324
Ealing Market Position Statement 2018-19 Page 26 of 39
• ‘Step down’ accommodation and floating support for people when they are able to be more independent, so that people in higher support services can be supported to move on, making higher support available to those most in need;
We are keen to work with providers who will:
• Focus on outcomes with people o increasing independence, individual and community resilience, o improve people’s chances of getting and staying in employment o increase opportunities to contribute to society and communities (geographical and
interest based).
• Set up partnerships and/or consortia, planning together to provide across a range of needs, working closely with the NHS, third sector, private business and the local authority.
• Develop service models which are co-produced with the people who will benefit from them We encourage providers to take part in the Mental Health Providers’ Forum and the Registered Managers’ Network if relevant. We encourage providers to join the appropriate Dynamic Purchasing System for the services they plan to deliver.
Page 190 of 324
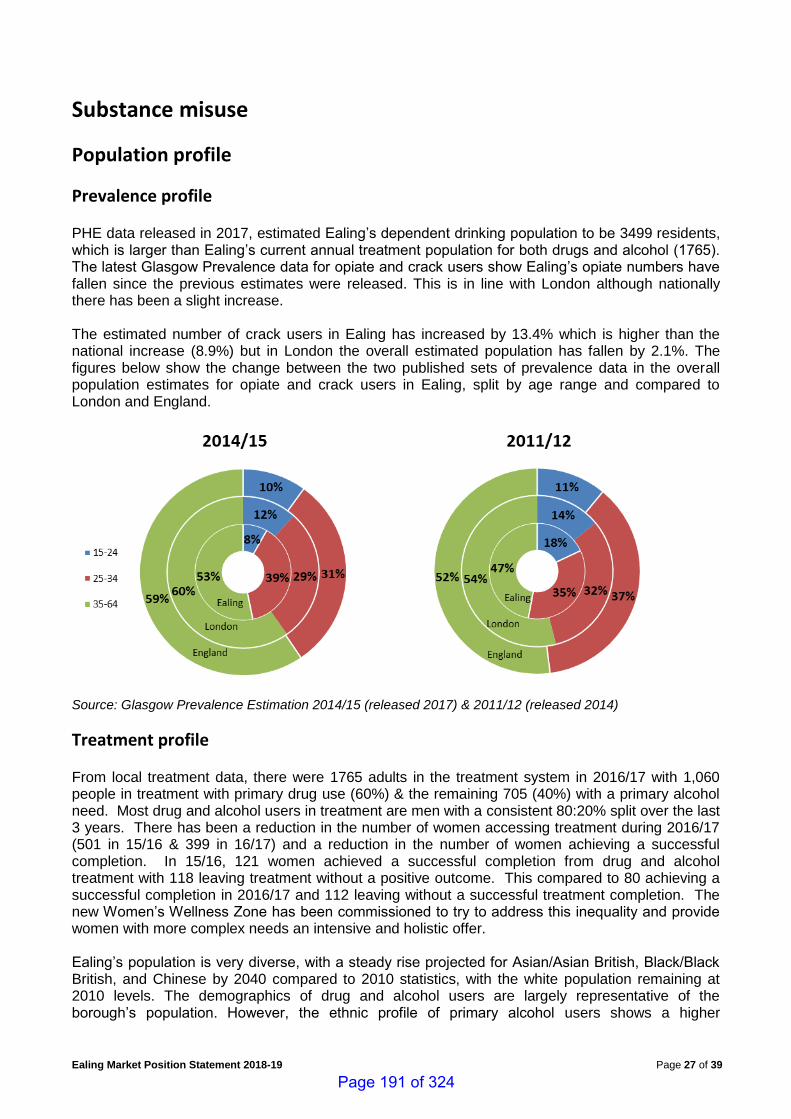
Ealing Market Position Statement 2018-19 Page 27 of 39
Substance misuse
Population profile
Prevalence profile PHE data released in 2017, estimated Ealing’s dependent drinking population to be 3499 residents, which is larger than Ealing’s current annual treatment population for both drugs and alcohol (1765). The latest Glasgow Prevalence data for opiate and crack users show Ealing’s opiate numbers have fallen since the previous estimates were released. This is in line with London although nationally there has been a slight increase. The estimated number of crack users in Ealing has increased by 13.4% which is higher than the national increase (8.9%) but in London the overall estimated population has fallen by 2.1%. The figures below show the change between the two published sets of prevalence data in the overall population estimates for opiate and crack users in Ealing, split by age range and compared to London and England.
Source: Glasgow Prevalence Estimation 2014/15 (released 2017) & 2011/12 (released 2014)
Treatment profile From local treatment data, there were 1765 adults in the treatment system in 2016/17 with 1,060 people in treatment with primary drug use (60%) & the remaining 705 (40%) with a primary alcohol need. Most drug and alcohol users in treatment are men with a consistent 80:20% split over the last 3 years. There has been a reduction in the number of women accessing treatment during 2016/17 (501 in 15/16 & 399 in 16/17) and a reduction in the number of women achieving a successful completion. In 15/16, 121 women achieved a successful completion from drug and alcohol treatment with 118 leaving treatment without a positive outcome. This compared to 80 achieving a successful completion in 2016/17 and 112 leaving without a successful treatment completion. The new Women’s Wellness Zone has been commissioned to try to address this inequality and provide women with more complex needs an intensive and holistic offer. Ealing’s population is very diverse, with a steady rise projected for Asian/Asian British, Black/Black British, and Chinese by 2040 compared to 2010 statistics, with the white population remaining at 2010 levels. The demographics of drug and alcohol users are largely representative of the borough’s population. However, the ethnic profile of primary alcohol users shows a higher
Page 191 of 324
Ealing Market Position Statement 2018-19 Page 28 of 39
proportion from the white populations, accounting for 59% compared to 47% in the total population. There is a greater representation of heroin and other opiate use among the Asian populations. In 2016/17, 30% of the combined treatment population were White British; 38% Asian/Asian British; 7% White other; & 3% White Irish. The adult treatment population is getting older with the 55+ cohort of drug users in treatment increasing year on year. 70% of the alcohol treatment cohort is over 40. RISE is seeing an increase in physical health problems with rises in COPD as well as an increase in alcohol-related brain damage including Wernicke-Korsakoffs syndrome and alcohol-related dementia. In 2016-17 RISE supported 242 substance misusers living with their own or other people’s children (12% of the treatment population) and a further 436 parents whose children were not living with them (21% of the treatment population).
Current demand and supply profile Ealing currently commissions RISE to deliver an integrated drug and alcohol community based treatment system. RISE is a consortium led by CGL, with clinical services provided by CNWL, peer recovery support delivered by Build on Belief, and some specialist courses offered by Intuitive Thinking Skills. This contract continues until March 31st 2020. Ealing’s DPS for Residential Rehabilitation, Detoxification and Structured Day-care Providers is used by the Social Work Substance Misuse team in Adult Services to provide placements for service users requiring more intensive support in addition to input from RISE. Funding pressures will continue to be an issue for these interventions. Placements are likely to be shorter, with suppliers encouraged to provide positive treatment outcomes more creatively and in less time. This means tapered treatment plans, aftercare support back in the community, and more effective joined up working with the community drug and alcohol treatment service (RISE) to ensure seamless care packages. The community integrated drug and alcohol treatment system (RISE) has been reduced by 33% and the specialist criminal justice team has been subsumed into the generic recovery teams after the DIP MOPAC funding ended. Ealing has worked with local CJ partners to use available resources as effectively as possible but there remain issues with the continuity of care pathway between some prisons and the community.
What do we plan to change or extend? We plan to:
• Establish education, training and employment support for substance misusers through a WLA
project
• Increase the capacity of Ealing women’s complex needs service, Women’s Wellness Zone
• Develop a service specification for the integrated community drug and alcohol treatment service
• Open further rounds of Ealing’s Dynamic Purchasing Systems (DPS) for Residential
Rehabilitation, Detoxification and Structured Day-care Providers
Page 192 of 324
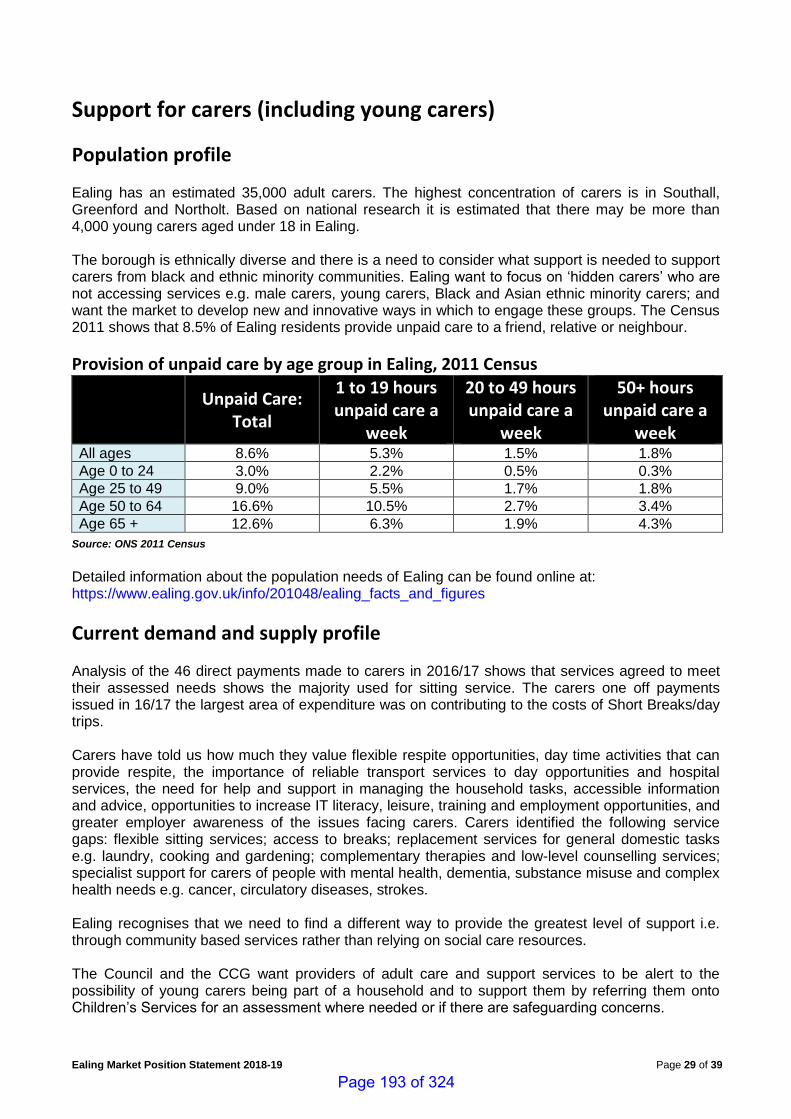
Ealing Market Position Statement 2018-19 Page 29 of 39
Support for carers (including young carers)
Population profile Ealing has an estimated 35,000 adult carers. The highest concentration of carers is in Southall, Greenford and Northolt. Based on national research it is estimated that there may be more than 4,000 young carers aged under 18 in Ealing. The borough is ethnically diverse and there is a need to consider what support is needed to support carers from black and ethnic minority communities. Ealing want to focus on ‘hidden carers’ who are not accessing services e.g. male carers, young carers, Black and Asian ethnic minority carers; and want the market to develop new and innovative ways in which to engage these groups. The Census 2011 shows that 8.5% of Ealing residents provide unpaid care to a friend, relative or neighbour.
Provision of unpaid care by age group in Ealing, 2011 Census
Unpaid Care: Total
1 to 19 hours unpaid care a
week
20 to 49 hours unpaid care a
week
50+ hours unpaid care a
week All ages 8.6% 5.3% 1.5% 1.8%
Age 0 to 24 3.0% 2.2% 0.5% 0.3%
Age 25 to 49 9.0% 5.5% 1.7% 1.8%
Age 50 to 64 16.6% 10.5% 2.7% 3.4%
Age 65 + 12.6% 6.3% 1.9% 4.3%
Source: ONS 2011 Census
Detailed information about the population needs of Ealing can be found online at: https://www.ealing.gov.uk/info/201048/ealing_facts_and_figures
Current demand and supply profile Analysis of the 46 direct payments made to carers in 2016/17 shows that services agreed to meet their assessed needs shows the majority used for sitting service. The carers one off payments issued in 16/17 the largest area of expenditure was on contributing to the costs of Short Breaks/day trips. Carers have told us how much they value flexible respite opportunities, day time activities that can provide respite, the importance of reliable transport services to day opportunities and hospital services, the need for help and support in managing the household tasks, accessible information and advice, opportunities to increase IT literacy, leisure, training and employment opportunities, and greater employer awareness of the issues facing carers. Carers identified the following service gaps: flexible sitting services; access to breaks; replacement services for general domestic tasks e.g. laundry, cooking and gardening; complementary therapies and low-level counselling services; specialist support for carers of people with mental health, dementia, substance misuse and complex health needs e.g. cancer, circulatory diseases, strokes. Ealing recognises that we need to find a different way to provide the greatest level of support i.e. through community based services rather than relying on social care resources. The Council and the CCG want providers of adult care and support services to be alert to the possibility of young carers being part of a household and to support them by referring them onto Children’s Services for an assessment where needed or if there are safeguarding concerns.
Page 193 of 324
Ealing Market Position Statement 2018-19 Page 30 of 39
What do we plan to change or extend? We plan to:
• Implement a new Carers' Strategy and action plan
• Develop new flexible home-based ‘services’ to support carers using direct payments to purchase their own support.
Page 194 of 324
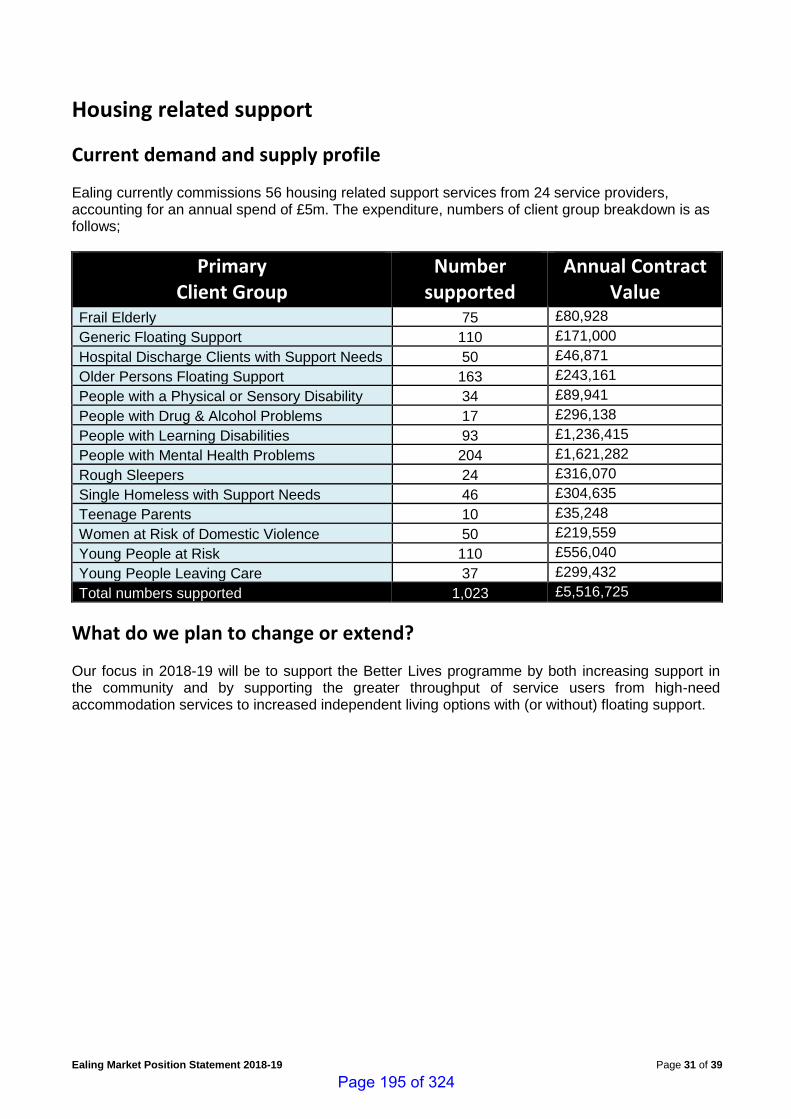
Ealing Market Position Statement 2018-19 Page 31 of 39
Housing related support
Current demand and supply profile Ealing currently commissions 56 housing related support services from 24 service providers, accounting for an annual spend of £5m. The expenditure, numbers of client group breakdown is as follows;
Primary Client Group
Number supported
Annual Contract Value
Frail Elderly 75 £80,928
Generic Floating Support 110 £171,000
Hospital Discharge Clients with Support Needs 50 £46,871
Older Persons Floating Support 163 £243,161
People with a Physical or Sensory Disability 34 £89,941
People with Drug & Alcohol Problems 17 £296,138
People with Learning Disabilities 93 £1,236,415
People with Mental Health Problems 204 £1,621,282
Rough Sleepers 24 £316,070
Single Homeless with Support Needs 46 £304,635
Teenage Parents 10 £35,248
Women at Risk of Domestic Violence 50 £219,559
Young People at Risk 110 £556,040
Young People Leaving Care 37 £299,432
Total numbers supported 1,023 £5,516,725
What do we plan to change or extend? Our focus in 2018-19 will be to support the Better Lives programme by both increasing support in the community and by supporting the greater throughput of service users from high-need accommodation services to increased independent living options with (or without) floating support.
Page 195 of 324
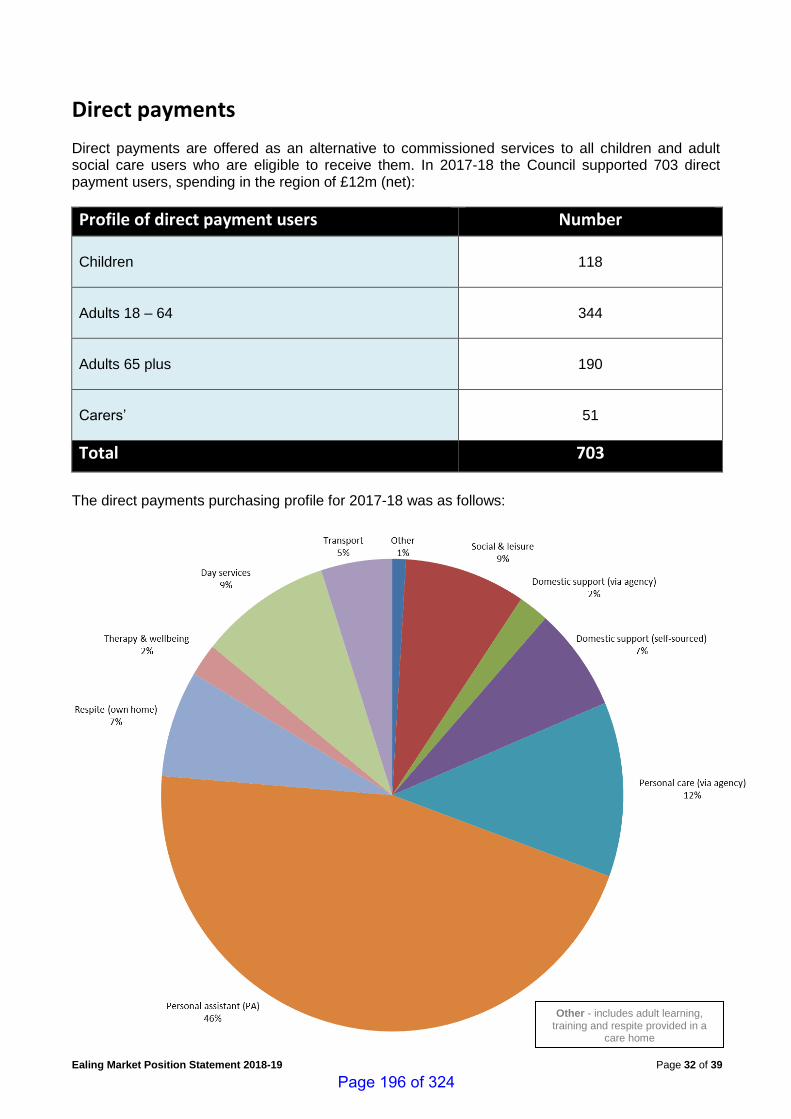
Ealing Market Position Statement 2018-19 Page 32 of 39
Direct payments
Direct payments are offered as an alternative to commissioned services to all children and adult social care users who are eligible to receive them. In 2017-18 the Council supported 703 direct payment users, spending in the region of £12m (net):
Profile of direct payment users Number
Children
118
Adults 18 – 64
344
Adults 65 plus
190
Carers’
51
Total 703
The direct payments purchasing profile for 2017-18 was as follows:
Other - includes adult learning, training and respite provided in a
care home
Page 196 of 324
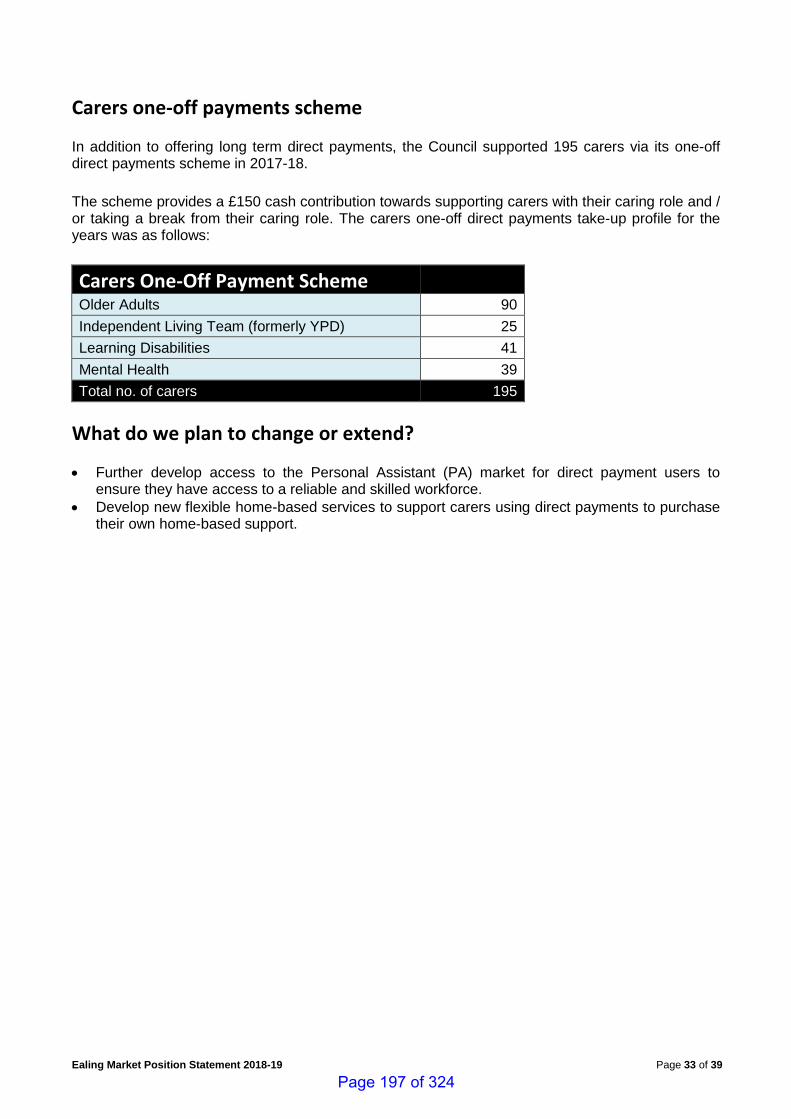
Ealing Market Position Statement 2018-19 Page 33 of 39
Carers one-off payments scheme In addition to offering long term direct payments, the Council supported 195 carers via its one-off direct payments scheme in 2017-18.
The scheme provides a £150 cash contribution towards supporting carers with their caring role and / or taking a break from their caring role. The carers one-off direct payments take-up profile for the years was as follows:
Carers One-Off Payment Scheme Older Adults 90
Independent Living Team (formerly YPD) 25
Learning Disabilities 41
Mental Health 39
Total no. of carers 195
What do we plan to change or extend?
• Further develop access to the Personal Assistant (PA) market for direct payment users to ensure they have access to a reliable and skilled workforce.
• Develop new flexible home-based services to support carers using direct payments to purchase their own home-based support.
Page 197 of 324
Ealing Market Position Statement 2018-19 Page 34 of 39
Voluntary & community sector grants 2018-19
Children’s The children’s grant programme comprises of Ealing Council and Ealing CCG funding totalling £459,556 per annum up to 2018-19.
The children’s grant priorities for funding up to 2018-19 are:
• Young carers support
• Support for children and families experiencing specific forms of disadvantage
• Safeguarding
• Information, advice and support for families with a child with a disability or special educational needs or complex health needs
• Community short breaks for children with a disability or special educational needs or complex health needs
• Support for children affected by domestic violence.
Adults The health and social care grant funding priorities have been designed to underpin the Council’s Care Act duties and to underpin drive towards the integration of health and social care.
The adult grant funded services (and lead agencies) for 2018-19 are:
• Travel Buddy Project - Ealing Mencap
• Improving Health & Housing Outcomes for People with Learning Disabilities and Autism - Certitude
• Mental Health Support Service - CAPE
• Community Activities for Older People - Neighbourly Care
• Support for Individuals with Asperger Syndrome - National Autistic Society
• The Restore Plus Project - Age UK Ealing
• Borough-wide Befriending Scheme - Neighbourly Care
• Ealing Disability Unite Project - Southall Day Centre
• Call & Care Service - Dementia Concern
• Short-term Respite Breaks for Carers of Adults with Learning Disabilities - Certitude
• Short Breaks / Respite - The Asian Health Agency
• Counselling Services - Ealing Abbey Counselling Consortium
• Ealing Specialist Advice Service – Consortia led by Ealing Mencap
• Ealing Cares - Southall Community Alliance
• Support Planning & Brokerage - Certitude
Allocation 2018-19
CCG and Council contribution £459,556
Allocation 2018-19
CCG and Council contribution £1,906m
Page 198 of 324
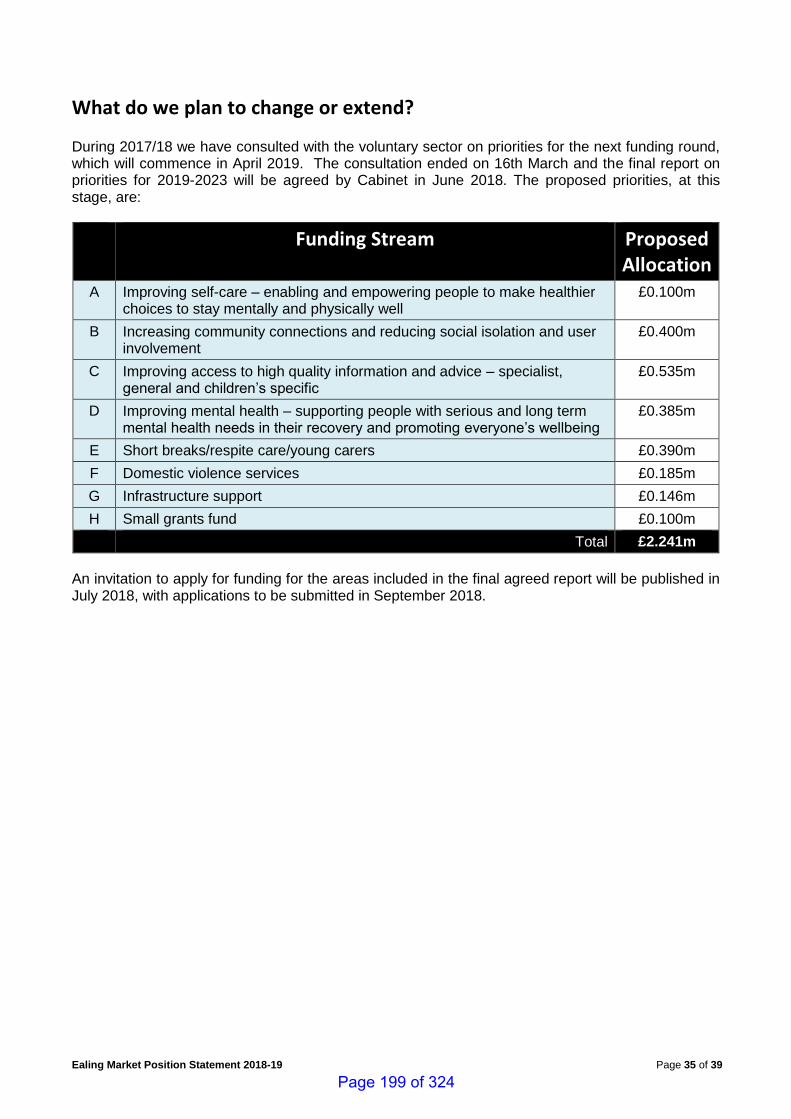
Ealing Market Position Statement 2018-19 Page 35 of 39
What do we plan to change or extend? During 2017/18 we have consulted with the voluntary sector on priorities for the next funding round, which will commence in April 2019. The consultation ended on 16th March and the final report on priorities for 2019-2023 will be agreed by Cabinet in June 2018. The proposed priorities, at this stage, are:
Funding Stream Proposed Allocation
A Improving self-care – enabling and empowering people to make healthier choices to stay mentally and physically well
£0.100m
B Increasing community connections and reducing social isolation and user involvement
£0.400m
C Improving access to high quality information and advice – specialist, general and children’s specific
£0.535m
D Improving mental health – supporting people with serious and long term mental health needs in their recovery and promoting everyone’s wellbeing
£0.385m
E Short breaks/respite care/young carers £0.390m
F Domestic violence services £0.185m
G Infrastructure support £0.146m
H Small grants fund £0.100m
Total £2.241m
An invitation to apply for funding for the areas included in the final agreed report will be published in July 2018, with applications to be submitted in September 2018.
Page 199 of 324
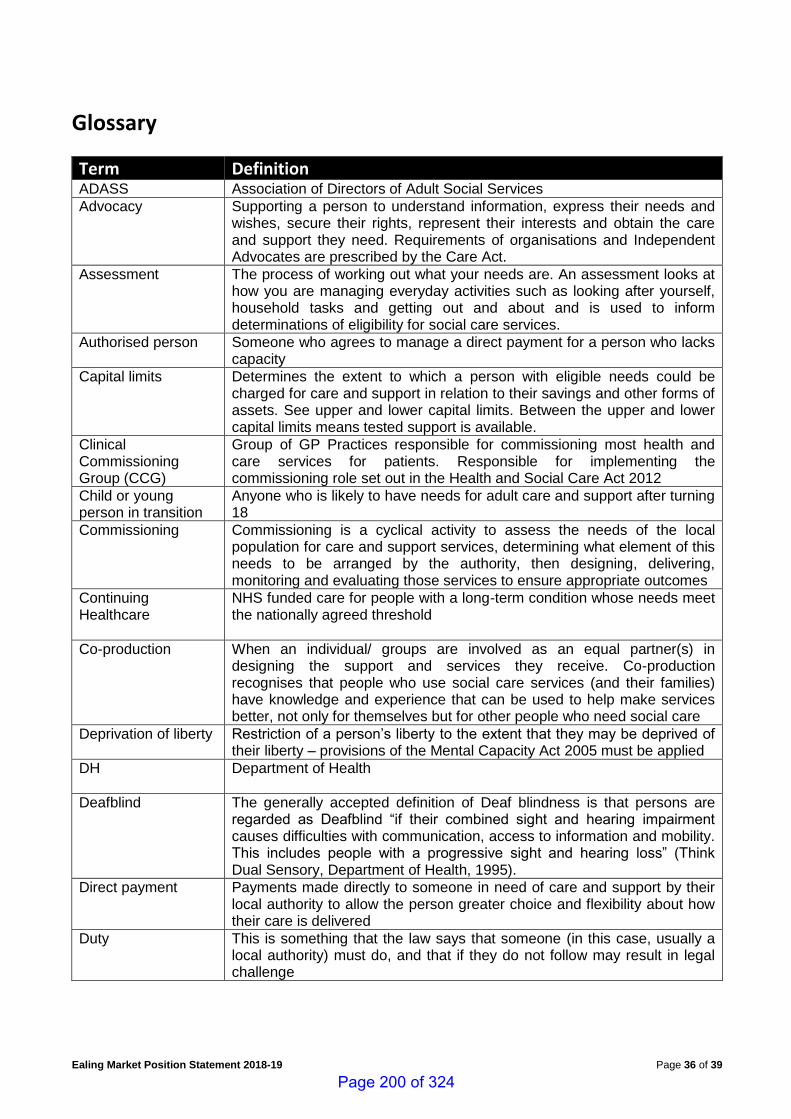
Ealing Market Position Statement 2018-19 Page 36 of 39
Glossary
Term Definition ADASS Association of Directors of Adult Social Services
Advocacy
Supporting a person to understand information, express their needs and wishes, secure their rights, represent their interests and obtain the care and support they need. Requirements of organisations and Independent Advocates are prescribed by the Care Act.
Assessment
The process of working out what your needs are. An assessment looks at how you are managing everyday activities such as looking after yourself, household tasks and getting out and about and is used to inform determinations of eligibility for social care services.
Authorised person Someone who agrees to manage a direct payment for a person who lacks capacity
Capital limits Determines the extent to which a person with eligible needs could be charged for care and support in relation to their savings and other forms of assets. See upper and lower capital limits. Between the upper and lower capital limits means tested support is available.
Clinical Commissioning Group (CCG)
Group of GP Practices responsible for commissioning most health and care services for patients. Responsible for implementing the commissioning role set out in the Health and Social Care Act 2012
Child or young person in transition
Anyone who is likely to have needs for adult care and support after turning 18
Commissioning Commissioning is a cyclical activity to assess the needs of the local population for care and support services, determining what element of this needs to be arranged by the authority, then designing, delivering, monitoring and evaluating those services to ensure appropriate outcomes
Continuing Healthcare
NHS funded care for people with a long-term condition whose needs meet the nationally agreed threshold
Co-production When an individual/ groups are involved as an equal partner(s) in designing the support and services they receive. Co-production recognises that people who use social care services (and their families) have knowledge and experience that can be used to help make services better, not only for themselves but for other people who need social care
Deprivation of liberty Restriction of a person’s liberty to the extent that they may be deprived of their liberty – provisions of the Mental Capacity Act 2005 must be applied
DH
Department of Health
Deafblind The generally accepted definition of Deaf blindness is that persons are regarded as Deafblind “if their combined sight and hearing impairment causes difficulties with communication, access to information and mobility. This includes people with a progressive sight and hearing loss” (Think Dual Sensory, Department of Health, 1995).
Direct payment Payments made directly to someone in need of care and support by their local authority to allow the person greater choice and flexibility about how their care is delivered
Duty This is something that the law says that someone (in this case, usually a local authority) must do, and that if they do not follow may result in legal challenge
Page 200 of 324
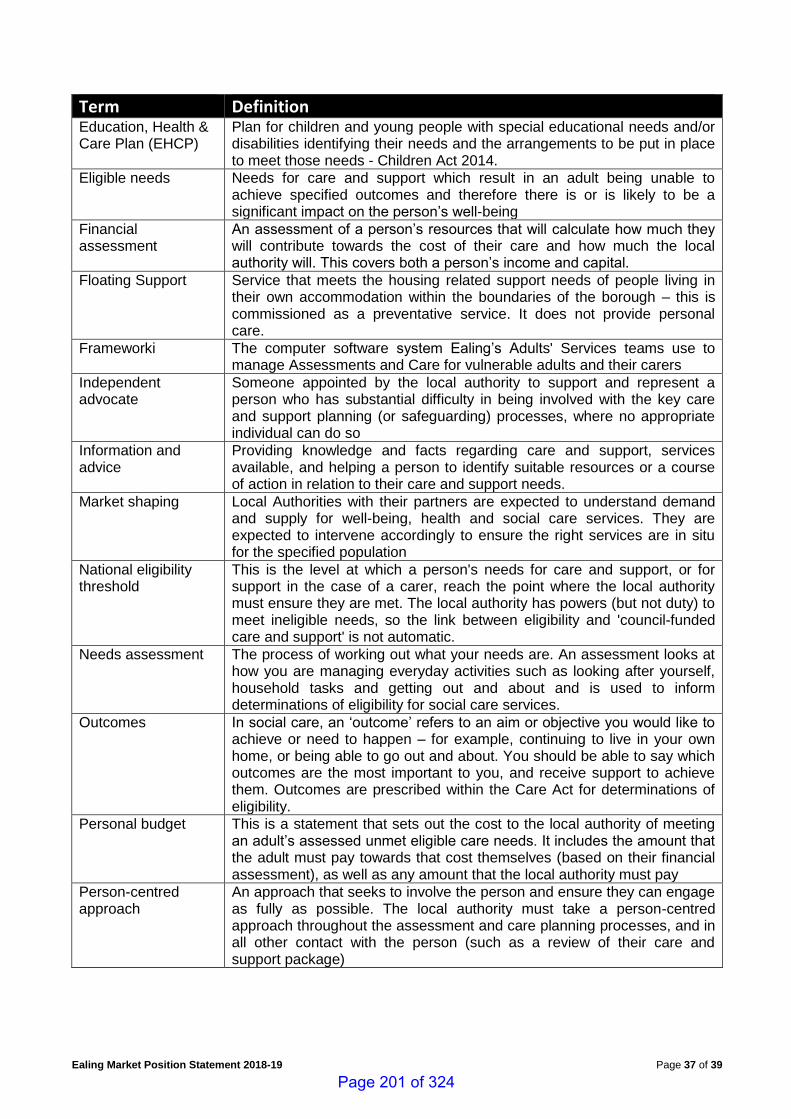
Ealing Market Position Statement 2018-19 Page 37 of 39
Term Definition Education, Health & Care Plan (EHCP)
Plan for children and young people with special educational needs and/or disabilities identifying their needs and the arrangements to be put in place to meet those needs - Children Act 2014.
Eligible needs Needs for care and support which result in an adult being unable to achieve specified outcomes and therefore there is or is likely to be a significant impact on the person’s well-being
Financial assessment
An assessment of a person’s resources that will calculate how much they will contribute towards the cost of their care and how much the local authority will. This covers both a person’s income and capital.
Floating Support Service that meets the housing related support needs of people living in their own accommodation within the boundaries of the borough – this is commissioned as a preventative service. It does not provide personal care.
Frameworki The computer software system Ealing’s Adults' Services teams use to manage Assessments and Care for vulnerable adults and their carers
Independent advocate
Someone appointed by the local authority to support and represent a person who has substantial difficulty in being involved with the key care and support planning (or safeguarding) processes, where no appropriate individual can do so
Information and advice
Providing knowledge and facts regarding care and support, services available, and helping a person to identify suitable resources or a course of action in relation to their care and support needs.
Market shaping Local Authorities with their partners are expected to understand demand and supply for well-being, health and social care services. They are expected to intervene accordingly to ensure the right services are in situ for the specified population
National eligibility threshold
This is the level at which a person's needs for care and support, or for support in the case of a carer, reach the point where the local authority must ensure they are met. The local authority has powers (but not duty) to meet ineligible needs, so the link between eligibility and 'council-funded care and support' is not automatic.
Needs assessment The process of working out what your needs are. An assessment looks at how you are managing everyday activities such as looking after yourself, household tasks and getting out and about and is used to inform determinations of eligibility for social care services.
Outcomes In social care, an ‘outcome’ refers to an aim or objective you would like to achieve or need to happen – for example, continuing to live in your own home, or being able to go out and about. You should be able to say which outcomes are the most important to you, and receive support to achieve them. Outcomes are prescribed within the Care Act for determinations of eligibility.
Personal budget This is a statement that sets out the cost to the local authority of meeting an adult’s assessed unmet eligible care needs. It includes the amount that the adult must pay towards that cost themselves (based on their financial assessment), as well as any amount that the local authority must pay
Person-centred approach
An approach that seeks to involve the person and ensure they can engage as fully as possible. The local authority must take a person-centred approach throughout the assessment and care planning processes, and in all other contact with the person (such as a review of their care and support package)
Page 201 of 324
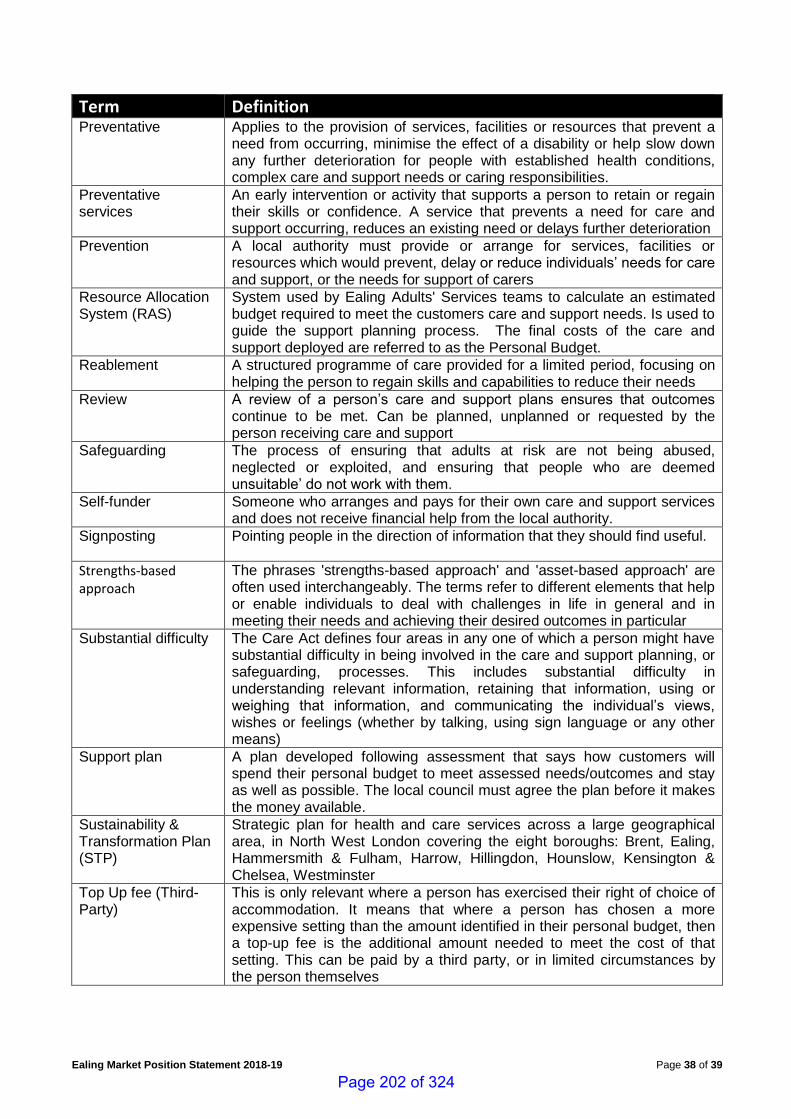
Ealing Market Position Statement 2018-19 Page 38 of 39
Term Definition Preventative Applies to the provision of services, facilities or resources that prevent a
need from occurring, minimise the effect of a disability or help slow down any further deterioration for people with established health conditions, complex care and support needs or caring responsibilities.
Preventative services
An early intervention or activity that supports a person to retain or regain their skills or confidence. A service that prevents a need for care and support occurring, reduces an existing need or delays further deterioration
Prevention A local authority must provide or arrange for services, facilities or resources which would prevent, delay or reduce individuals’ needs for care and support, or the needs for support of carers
Resource Allocation System (RAS)
System used by Ealing Adults' Services teams to calculate an estimated budget required to meet the customers care and support needs. Is used to guide the support planning process. The final costs of the care and support deployed are referred to as the Personal Budget.
Reablement A structured programme of care provided for a limited period, focusing on helping the person to regain skills and capabilities to reduce their needs
Review A review of a person’s care and support plans ensures that outcomes continue to be met. Can be planned, unplanned or requested by the person receiving care and support
Safeguarding The process of ensuring that adults at risk are not being abused, neglected or exploited, and ensuring that people who are deemed unsuitable’ do not work with them.
Self-funder Someone who arranges and pays for their own care and support services and does not receive financial help from the local authority.
Signposting
Pointing people in the direction of information that they should find useful.
Strengths-based approach
The phrases 'strengths-based approach' and 'asset-based approach' are often used interchangeably. The terms refer to different elements that help or enable individuals to deal with challenges in life in general and in meeting their needs and achieving their desired outcomes in particular
Substantial difficulty The Care Act defines four areas in any one of which a person might have substantial difficulty in being involved in the care and support planning, or safeguarding, processes. This includes substantial difficulty in understanding relevant information, retaining that information, using or weighing that information, and communicating the individual’s views, wishes or feelings (whether by talking, using sign language or any other means)
Support plan A plan developed following assessment that says how customers will spend their personal budget to meet assessed needs/outcomes and stay as well as possible. The local council must agree the plan before it makes the money available.
Sustainability & Transformation Plan (STP)
Strategic plan for health and care services across a large geographical area, in North West London covering the eight boroughs: Brent, Ealing, Hammersmith & Fulham, Harrow, Hillingdon, Hounslow, Kensington & Chelsea, Westminster
Top Up fee (Third-Party)
This is only relevant where a person has exercised their right of choice of accommodation. It means that where a person has chosen a more expensive setting than the amount identified in their personal budget, then a top-up fee is the additional amount needed to meet the cost of that setting. This can be paid by a third party, or in limited circumstances by the person themselves
Page 202 of 324
Ealing Market Position Statement 2018-19 Page 39 of 39
Term Definition Transition assessment
An assessment of a child or young person, young carer or child’s carer that will inform a transition plan to receive care and support from Adults Services.
Transition plan A statutory requirement for young people and carers if they are likely to need care and support when they turn 18
Wellbeing Wellbeing is a broad concept, and it is described as relating to the following areas in particular: personal dignity (including treatment of the individual with respect); physical and mental health and emotional wellbeing; protection from abuse and neglect; control by the individual over day-to-day life (including over care and support provided and the way it is provided); participation in work, education, training or recreation; social and economic wellbeing; domestic, family and personal relationships; suitability of living accommodation; the individual’s contribution to society
WLA West London Alliance (WLA) is a partnership between 8 Boroughs: Ealing, Brent, Harrow, Hounslow, Barnet, Hillingdon, Hammersmith & Fulham, Kensington & Chelsea, Westminster
Page 203 of 324

Page 204 of 324
1
Contains Confidential or Exempt Information
NO
Title Ealing – Winter Preparedness 2018
Responsible Officer(s) Tessa Sandall – Managing Director, Ealing CCG
Author(s) Usha Prema – Assistant Director Unplanned Care, Ealing CCG
Portfolio(s) Cllr Binda Rai – Health and Adult Social Care
For Consideration By Health and Well Being Board
Date to be Considered 18 September 2018
Implementation Date if Not Called In
N/A
Affected Wards All
Keywords/Index
Purpose of Report:
The purpose of this report is to inform the Health and Well Being Board on the preparation underway for winter 2018/19 in partnership with all key stakeholders. Resilience planning is considered all year round and not just for winter; however, additional planning goes in to winter.
This year there is also an emphasis on NWL STP system wide winter preparations to provide consistent quality and patient experience during the winter months for those people who need urgent and emergency service.
The key focus will be on the following key areas to ensure system flow:
Admission Avoidance
Care Homes
Community/Primary Care
Community Bedded Resource
Delivery of the 4-hour A&E target
Efficiency In-Hospital Flow from Front Door to Discharge
Social Care – Market Flexibility/Urgent Response
Whole System: Communications to all stakeholders, public/patient, carers
Report for: ACTION/INFORMATION
Item Number: 11
Page 205 of 324
2
1. Recommendations
The Board is asked:
To note the responsibilities of all partner agencies in the Ealing local health economy for winter planning and management of emergency services during high demand, especially periods of cold weather periods.
To note the arrangements being made for winter planning as partners working together jointly agreeing the best use of resources, their mobilisation and co-ordination to deliver agreed priorities at NWL STP system level as well as Ealing local delivery.
To note all partner agencies commitment to work collaboratively in the improvement and sustainability and delivery of the A&E performance, whilst maintaining quality and safety of service.
To note in addition to the services described below and the services resilience planning business as usual throughout year, the following table summarises additional key winter priorities.
a. Primary Care/GP Access
During winter months – Clinical consultations of an additional 5 face to face consultations per 1000 weighted patients per week
Direct appointment booking in-hours from NHS 111 service to reduce attendances at Urgent Care Centres for primary care need
Prioritise and increase utilisation of appointments available at 3 Ealing GP Extended Access Hubs
b. London Ambulance Service – to ensure the new LAS protocol to District Nursing Service is fully implemented and utilised to reduce conveyances to hospital, especially for catheter management issues.
c. Reducing length of stay – London North West University Healthcare NHS Trust – to reduce from 255 to 189 long stay patients’ length of stay (LoS) patients discharged per month by December 2018. See Home First – Discharge to Assess below to support discharge pathway simplification and to expedite discharges in timely way.
d. Workforce for all services: to ensure rotas are matched to demand and seasonally adjusted where required to ensure operational resilience heading into and throughout winter.
e. Care Homes: CCG and local authority to working in partnership
Page 206 of 324
3
with key care homes in Ealing to ensure acceptance of returning residents 7 days a week and new residents to minimise delays in discharges across winter period.
f. Communications and Engagement Plan across NWL, linked to any London wide and National messages to access appropriate services in the community such as NHS 111, pharmacy, etc. Local messages to vulnerable groups via local Healthwatch/ECVS
g. Flu immunisation/Pneumonia To commence flu/pneumococcal immunisation from Sept 18 or as soon as vaccines are available, particularly targeting vulnerable patient groups, including care homes and front line staff.
h. Social Care: To ensure proactive engagement in discharge planning and expediting discharges as appropriate, working with care agencies to ensure timely provision of care.
2. Reason for Decision and Options Considered The London North West University Healthcare Trust (LNWUHT) A&E Delivery Board will provide oversight and strong, proactive and effective leadership of organisations during the winter period and will be crucial to the delivery of safe and high quality services during the challenging winter period. This leadership will include members of the Board assuring themselves as local leaders throughout the winter that their organisation is delivering in line with plans and is working well in partnership with other providers and commissioners. Members include Senior Executive level representatives from LNWUHT, CCGs (Ealing, Brent and Harrow), Social Services (Ealing, Brent and Harrow), Community Services providers from the three CCGs, Urgent Care Centres (UCC), London Ambulance Service (LAS), other local providers, NHS England (NHSE) and NHS Improvement (NHSI). The Delivery Board is Chaired by Dame Jacqueline Docherty, Chief Executive Officer, and LNWUHT.
3. Background Resilience Planning and Delivery
Resilience planning is considered to be all year round, taking into consideration specific surges/demand around bank holidays during the year, including Christmas and New Year. All providers are expected to take these into consideration when planning for additional resource at such times of pressure. Winter planning has been informed by national winter requirements for 2018/19, lessons from 2017/18 and two local workshops held in July 2018.
Whole Systems Integrated Resilience Workshop
Page 207 of 324
4
o This workshop focussed on the Health and Social Care joint ambition and opportunity to reduce non-elective ‘potentially avoidable’ admissions for over 65year olds.
LNWUHT – held winter workshop with Ealing, Harrow and Brent key stakeholders.
o This workshop focussed on the patient flow within the hospital,
particularly the pressures on inpatient beds, flow into community beds and support from the system to discharge patients into the community. The need to ensure from the hospital perspective for ease of operational management to ensure there is one set of criteria and one point of access for community services.
A Whole Systems Resilience Group was set up to take forward the key items from the two workshops above for winter preparedness in the first instance. The first meeting was held on 10 August 2018. The Group will continue to meet to implement the plans, ensure delivery and monitor the impact during winter months.
Winter planning is also informed by the letter from NHSE/I June 2018 from
Pauline Phillips, National Director of Urgent and Emergency Care:
prioritising reducing patients who are long stayers in hospital, achieve better outcomes for patients stays over 7 days, and 21 plus days by further increasing the volume of discharges
Implement effective demand management schemes that support longer term sustainable change
The following describes some of the new services and/or improvements to support attendance/admission avoidance and ensure efficient flow through the hospital system and back to patient home. Throughout September/October further planning and implementation meetings are taking place locally and NWL STP level with system partners to further refine winter proposals and ensure implementation.
Lessons from 2017/18 The key lessons from 2017/18 also being incorporated into the winter plans for
2018/19 are as follows:
Workforce – staff rota to commence as early as possible and to build in an additional capacity for additional demand during winter months
To ensure robust plans and contingencies for short notice staff sickness absence, both nursing and clinical staff. For example on the 2nd January 2018, experienced nursing staff shortage. Northwick Park was short of 28 nurses and Ealing Hospital were down 16 nurses. The shortages impacted on the ability to discharge patients causing blocks to the flow of patients in the system.
Page 208 of 324
5
This applies not only to staff in hospitals, but also across the system and all services, such as NHS 111, LAS, Primary Care, and community services.
Ensure senior staff support on site at Ealing Hospital 7 days a week.
4. Reducing Long Stays in Hospital Potentially Avoidable Admissions In July the Whole Systems Resilience Workshop agreed with the ambition to reduce potentially avoidable admissions by 20%. Aligning with the initiative launched by Pauline Philips (National director of urgent and emergency care) in June 2018: “…a new national ambition to lower bed occupancy by reducing the number of long stay patients (and long stay bed days) in acute hospitals by 25% and to ask you to work with your system partners to deliver on this ambition.” “By reducing the number of long stay patients in hospital we will collectively reduce bed occupancy to increase safe flow through the system, greatly improving the working and care environment, reducing A&E crowding and enabling patients to be treated consistently in the right bed by clinical teams with the right skills.”
This needs to be delivered whilst holding and/or reducing the length of stay for all other patients and reducing bed occupancy to manageable levels by December 2018. Home First – Discharge to Assess This was one of the key areas being monitored through the Better Care Fund (BCF) in 17/18. Ealing developed through joint working with providers and taking into account the 8 High Impact Change Model. The key area developed was Home First/Discharge to Assess. The pilot commenced in June 2017, following the Medway Model with Pathway 1, and was rolled out with some additional resources over the winter months of 2017/18. The model is as follows:
Pathway 0 – The patient no longer has any additional needs
Pathway 1 – The patient has some additional needs that can be safely met at home
Pathway 2 – The patient is unable to return home immediately. The discharge may need more planning due to complex needs or the patient may need an intermediate care bed for a short period of time
Pathway 3 – The patient has complex needs and is unable to return home
Pathway simplification from the current 17 discharge pathways to the above 3 pathways has commenced and is being embedded as business as usual by the end of September 2018. Planning for Pathway 2/3, more complex discharges
Page 209 of 324
6
have commenced with a workshop on 28th August 2018 with key health and social care partners. It is envisaged this will be piloted for winter. Systems and processes are already in place to monitor daily, weekly and monthly delayed transfers of care (DTOCs), by patient with health and social care with appropriate escalation processes in place to unblock any barriers for timely discharges. Ealing CCG and Ealing Social Services with LNWUHT at Ealing Hospital monitor the long stayers on a weekly basis. These are patients who have stayed beyond their discharge dates: more than 7, 14 and 21 days. This was introduced during winter of 2017, and has remained and embedded as best practice. During winter there are North West London (NWL) system wide daily calls to monitor and support system flow, expediting patient transfers across the system, escalating to senior management of each organisation.
5. Demand Management Schemes in out of hospital services to reduce management of flows into emergency care NHS 111 Online NHS 111 Online went live in August in Ealing, Hounslow, Brent and Harrow via www.111.nhs.uk. Patients are now able to go on line with their issues and be sign posted to appropriate services based on clinical need. NHS 111 can also now if clinically appropriate are able to directly book an appointment for patients in an Extended Primary Care Access Centre, described below. NWL Integrated Urgent Care (IUC) programme has also commenced implementation of direct booking during practice opening hours, starting with Hounslow. There is a roll out plan for rest of CCGs in NWL by December, with Ealing being planned next. Extended Primary Care Access Centre Ealing CCG commissioned additional primary care appointments with a GP and/or Nurse at three hubs: Sunrise Medical Centre, Elmbank Surgery and Florence Road Surgery. The appointments are available seven days a week, including bank holidays, 6.30pm – 8.00pm during weekdays and 8am to 8pm at weekends. London Ambulance Service (LAS)
A paramedic or other health professional is based in the control room to operate a ‘Hear & Treat’/‘See & Treat’ model, thus avoiding either an ambulance call out or a conveyance to hospital.
Page 210 of 324
7
To reduce conveyances to hospitals, NWL LAS Protocol with Rapid Response Services has been in place and promoted through awareness raising activities with ambulance crews since November 2017. This has continuously been promoted and will again be accelerated between ambulance crews and rapid response services in each CCG. In Ealing, the Home ward rapid response service continues to work with the LAS, and will be exploring opportunities to shadow LAS crews to build relationships and understanding of the respective services. New this year, NWL LAS Protocol with District Nursing Services also went live on the 16th July 2018. The protocol will improve the management of patients in the community, preventing hospital conveyances to A&E and non-elective admissions. Urgent Care Centre (UCC) Ealing Hospital has a co-located UCC and the Patient Champion role supports re-direction of patients back into primary/community care as appropriate. The role also provides patient support to register with a GP practice, book appointments in practice hours or directly book into GP Extended Access Hubs. The Patient Champion also provides signposting and information to other services in the community.
6. Care Homes
To support care homes, particularly nursing homes, Ealing CCG continues to commission an enhanced primary care services, provided by the Argyle Care Home Service. Since 2013, they have led on flu vaccinations for all the nursing home residents under their care and also offered the vaccinations to staff in the homes. It is planned Argyle Care Home Service will commence flu vaccination programme at the beginning of autumn, including pneumococcal vaccinations for targeted vulnerable groups. More specifically this year, as part of supporting and reducing long stayers in hospital, Ealing CCG and Ealing Social Services have commenced early work on the following guidance from NHSE and NHSI:
care homes accept admissions (discharges from hospital) seven days a week;
for new residents until 5pm and returning residents up until 8pm
7. Other In-Hospital schemes to improve flow from front door
LNWUHT have been focusing on delivering transformational improvements in patient flow from front door to discharges at the back door at both sites. Some of the key areas are as follows:
ED floor – UCC to A&E referral times and relationships, managing overnight demand and performance of the A&E 4hour target.
Red to Green Days – to ensure patient progress to timely discharge date
Page 211 of 324
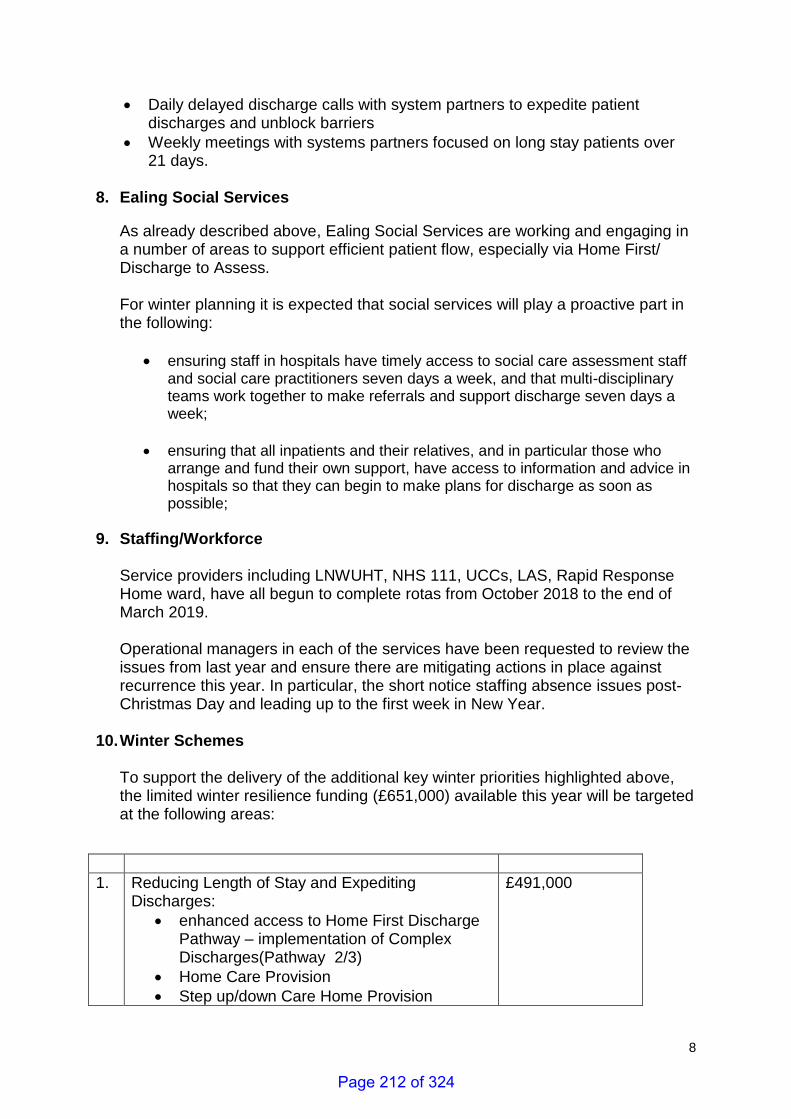
8
Daily delayed discharge calls with system partners to expedite patient discharges and unblock barriers
Weekly meetings with systems partners focused on long stay patients over 21 days.
8. Ealing Social Services
As already described above, Ealing Social Services are working and engaging in a number of areas to support efficient patient flow, especially via Home First/ Discharge to Assess. For winter planning it is expected that social services will play a proactive part in the following:
ensuring staff in hospitals have timely access to social care assessment staff and social care practitioners seven days a week, and that multi-disciplinary teams work together to make referrals and support discharge seven days a week;
ensuring that all inpatients and their relatives, and in particular those who arrange and fund their own support, have access to information and advice in hospitals so that they can begin to make plans for discharge as soon as possible;
9. Staffing/Workforce
Service providers including LNWUHT, NHS 111, UCCs, LAS, Rapid Response Home ward, have all begun to complete rotas from October 2018 to the end of March 2019. Operational managers in each of the services have been requested to review the issues from last year and ensure there are mitigating actions in place against recurrence this year. In particular, the short notice staffing absence issues post-Christmas Day and leading up to the first week in New Year.
10. Winter Schemes To support the delivery of the additional key winter priorities highlighted above, the limited winter resilience funding (£651,000) available this year will be targeted at the following areas:
1. Reducing Length of Stay and Expediting Discharges:
enhanced access to Home First Discharge Pathway – implementation of Complex Discharges(Pathway 2/3)
Home Care Provision
Step up/down Care Home Provision
£491,000
Page 212 of 324
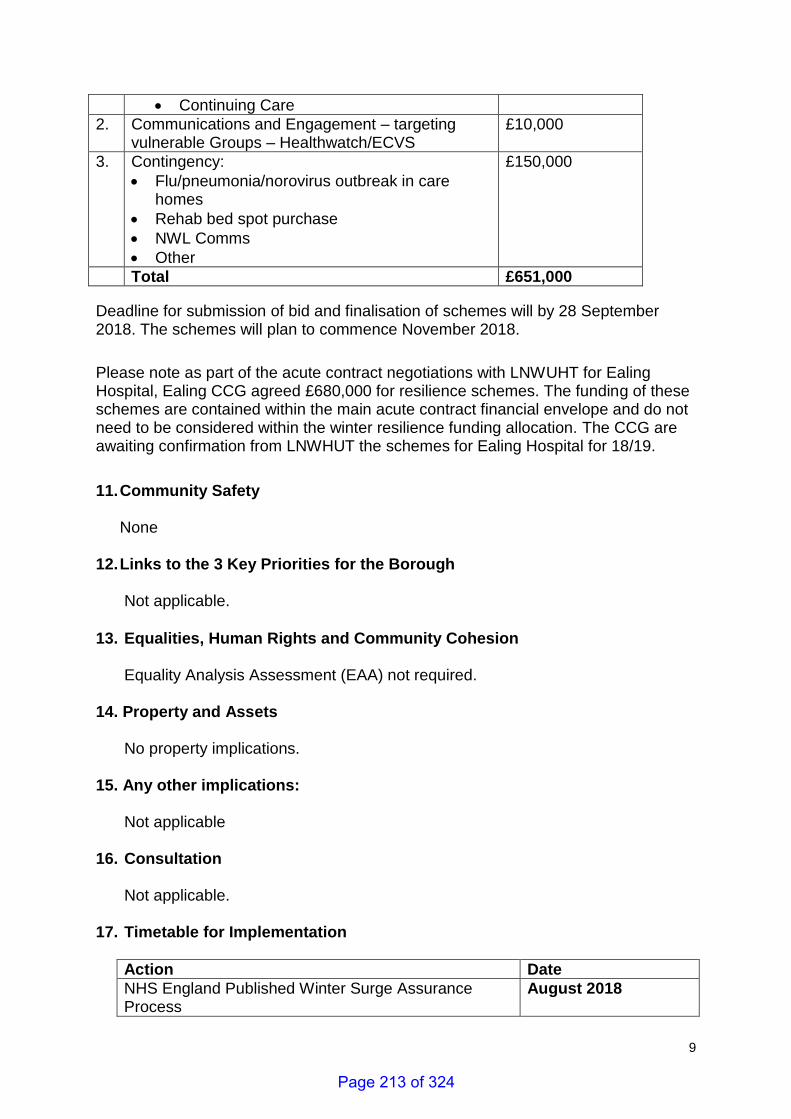
9
Continuing Care
2. Communications and Engagement – targeting vulnerable Groups – Healthwatch/ECVS
£10,000
3. Contingency:
Flu/pneumonia/norovirus outbreak in care homes
Rehab bed spot purchase
NWL Comms
Other
£150,000
Total £651,000
Deadline for submission of bid and finalisation of schemes will by 28 September 2018. The schemes will plan to commence November 2018.
Please note as part of the acute contract negotiations with LNWUHT for Ealing Hospital, Ealing CCG agreed £680,000 for resilience schemes. The funding of these schemes are contained within the main acute contract financial envelope and do not need to be considered within the winter resilience funding allocation. The CCG are awaiting confirmation from LNWHUT the schemes for Ealing Hospital for 18/19.
11. Community Safety
None
12. Links to the 3 Key Priorities for the Borough Not applicable.
13. Equalities, Human Rights and Community Cohesion Equality Analysis Assessment (EAA) not required.
14. Property and Assets
No property implications.
15. Any other implications: Not applicable
16. Consultation
Not applicable.
17. Timetable for Implementation
Action Date
NHS England Published Winter Surge Assurance Process
August 2018
Page 213 of 324
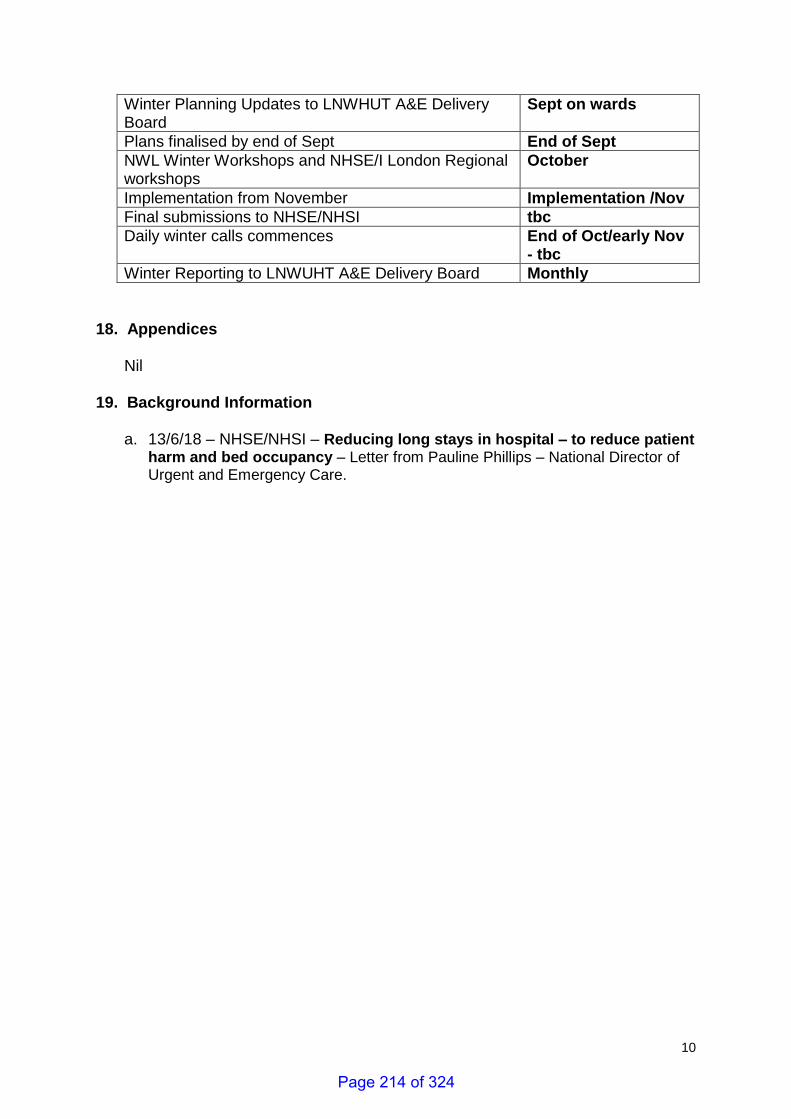
10
Winter Planning Updates to LNWHUT A&E Delivery Board
Sept on wards
Plans finalised by end of Sept End of Sept
NWL Winter Workshops and NHSE/I London Regional workshops
October
Implementation from November Implementation /Nov
Final submissions to NHSE/NHSI tbc
Daily winter calls commences End of Oct/early Nov - tbc
Winter Reporting to LNWUHT A&E Delivery Board Monthly
18. Appendices Nil 19. Background Information
a. 13/6/18 – NHSE/NHSI – Reducing long stays in hospital – to reduce patient harm and bed occupancy – Letter from Pauline Phillips – National Director of Urgent and Emergency Care.
Page 214 of 324
11
Consultation
Name of consultee
Post held Date sent to
consultee
Date response received
Comments appear in
paragraph:
Internal
External
Report History
Decision type: Urgency item?
For information For Information
Report no.: Report author and contact for queries:
First and surname, job title Usha Prema Assistant Director – Unplanned Care Ealing CCG Email:[email protected]
Page 215 of 324

Page 216 of 324
1
Contains Confidential or Exempt Information
NO
Title Response to the LGA Green Paper consultation on Adult Social Care
Responsible Officer(s) Kim Carey, Interim Director of Adult Services
Author(s) Jackie Fisk, Policy Officer
Portfolio(s) Leader of the Council, Cllr Julian Bell, Policy Overview Cllr Binda Rai, Health and Adult Services
For Consideration By Health and Wellbeing Board
Date to be Considered 18 September 2018
Implementation Date if Not Called In
N/A
Affected Wards All
Keywords/Index Social Care, Health, Wellbeing
Purpose of Report: There is wide agreement that Adult Social Care funding is unsustainable and at crisis point. In anticipation of the Government’s Green Paper on Adult Social Care due later this year, the LGA has produced ‘The lives we want to lead – the LGA green paper for adult social care and wellbeing’. The consultation responses will inform the LGA’s proactive influencing of the government on its future policy and funding position. Given the importance of this topic to the health and wellbeing of Ealing’s residents, and the implications across both local government and the wider health economy, this paper seeks the Health and Wellbeing Board’s endorsement of a joint response to the LGA consultation, which closes on 26 September. It also recommends sharing our response with wider partners and with residents to raise awareness of the risks to Ealing if a sustainable future for Adult Social Care is not found, and the urgency of resolving the issues.
1. Recommendations
The Health and Wellbeing Board is asked to:
Confirm its support for the direction of travel in the LGA consultation document, discuss the draft consultation response at Appendix A and agree the final content of a joint Ealing Council/Health and Wellbeing Board submission.
Agree to the council publishing the response on its website and circulating to partners to ensure transparency and to encourage wider debate on the LGA consultation.
Report for: ACTION/INFORMATION Item Number: 12
Page 217 of 324
2
2. Reason for Decision and Options Considered
The pressures on adult social care, and the lack of a sustainable long-term national funding solution, are key risks to the health and wellbeing system nationally and in Ealing and to the wellbeing of residents. With growing demands on adult social care, and reducing budgets for local government, councils are experiencing disproportionate impacts on their wider services. In Ealing, despite the council’s ambitious approach to savings and innovation across the breadth of its services, it is increasingly difficult to manage the pressures on care packages and placements budgets. The issues are complex and cannot be tackled by one partner alone. The national policy direction needs to be reviewed in the light of demand and needs, and this is likely to impact the way in which health partners as well as local government work. Any potential future approaches must ensure that priority is given to the ways in which social care and the NHS are integrated to help make the whole system work effectively. The solutions which are finally chosen must balance both short and long-term pressures, and ensure that the wellbeing focus, including the critical role of public health, is suitably prioritised. Any proposed solutions need to be critiqued to guard against additional burdens such as new regulations or their potential to drain capacity or divert from a focus on the whole system. This high-profile consultation is an important opportunity to contribute a cohesive partnership response from the borough in order to influence Government’s Green Paper. An alternative is to not submit a response, but given the importance of the issues highlighted this would be a key opportunity lost to articulate Ealing’s perspective.
3. Key Implications Councils spend over £15 billion on social care every year, with over £97 million being spent in the borough of Ealing. Demography, inflation and National Wage pressures mean that the gap in adult social care funding will be £3.56 billion nationally by 2025, just to stand still – pressures which Ealing shares. At a national level, by 2019/20, councils could be spending as much as 38 pence in every £1 of council tax on adult social care (up from 28 pence in 2010/11). The way in which social care is paid for is complex, convoluted and little understood by most of the population. Across the country, 45% of people self-pay for their care home costs, 11% pay top-ups, 35% are state-funded and 9% are NHS funded. Additionally, it is estimated that 1.4m people have unmet needs and are not receiving support. The history of social care, and its genesis at a time when people often lived only a few years into retirement and when there were fewer complex cases, has resulted in an opaque system that is unfit for the 21st century. There is general agreement across political parties, the health and wellbeing sectors and the public that change is needed urgently.
Page 218 of 324
3
The LGA consultation sets out comprehensive arguments on ways to set adult social care on a sustainable path and to position it holistically in a wellbeing policy landscape, including arguing for parity of esteem with the NHS. In deliberating on the joint response to the consultation, the council and the Health and Wellbeing Board may wish to argue for an approach which:
Fosters more resident engagement and communication: a sustainable system will need the support of those who will use it and will need them to make lifestyle changes – open engagement is imperative to achieve this.
Has an outcomes and community focus: health and care funding is an investment in the social and economic outcomes of our communities.
Supports subsidiarity and devolution: the assumption should be that improvement should be led as close to the patient/user as possible, with national and regional reform and funding enabling change.
Takes into account that our users are often extremely vulnerable and at very sensitive points in their lives. This is a reality that demands careful and credible plans rather than transformation rhetoric.
Articulates the benefits clearly: Investment and improvement in community services and prevention activity is needed.
Focuses on whole systems: Any solution should bring and be judged on its ability to bring partners closer to making the whole system work, not its effectiveness in successfully competing for resources to make just a part of the system work.
Has sustainable funding: Reform and improvement are crucial, but alone, without a short and long-term funding solution to go with it, will not produce the high-quality outcomes our residents expect and deserve.
4. Financial
This is addressed through the consultation response.
5. Legal 5.1 The Health and Social Care Act 2012 (“the 2012 Act”) makes it a requirement for the Council to establish a Health and Wellbeing Board (“HWB”). S.195 of the 2012 Act requires the HWB to encourage persons who arrange for the provision of any health or social care services in their area to work in an integrated manner. The coordination and support of the response to the LGA Green paper is likely to assist with this requirement on the Council. 6. Value for Money
None
7. Sustainability Impact Appraisal
N/A 8. Risk Management
Page 219 of 324
4
The council’s risk management approach takes into account the issues highlighted in the consultation response.
9. Community Safety None.
10. Links to the 3 Key Priorities for the Borough
The future of funding for adult social care has a cross-cutting impact on the three
key priorities for the council’s administration, in particular the ‘health and great place to live’ priority. The three priorities are:
Good, genuinely affordable homes
Opportunities and living incomes
A healthy and great place
11. Equalities, Human Rights and Community Cohesion This is a response to a national consultation by the LGA, the outcomes from which will be used to influence the discussions on the Government’s future policy direction. There is no direct impact currently on local policy or service delivery. An Equality Analysis Assessment (EAA) is not required at this point.
12. Staffing/Workforce and Accommodation implications:
None. 13. Property and Assets None
14. Any other implications:
None
15. Consultation N/A
16. Timetable for Implementation This is a response to a national consultation, the key dates for which are:
Activity Date
HWBB agrees content of joint consultation response 18 September
Deadline for submissions to LGA Green Paper consultation
26 September
LGA release publications, including consultation findings, ahead of Government’s ASC Green Paper, Budget, NHS Plan and also Spending Review
Autumn, date tbc
Government issues ASC Green Paper Date tbc, expected late 2018
Page 220 of 324
5
17. Appendices Appendix A: Draft consultation joint response from Ealing Council and Ealing Health and Wellbeing Board Appendix B: Local Government Association, ‘The lives we want to lead – the LGA green paper for adult social care and wellbeing’ consultation document
18. Background Information https://futureofadultsocialcare.co.uk/the-green-paper/ Consultation
Name of consultee
Post held Date sent to
consultee
Date response received
Comments appear in
paragraph:
Internal
Paul Najsarek Chief Executive 23 August 24 August & ongoing
Throughout
Judith Finlay Executive Director, Children and Adults
23 August 31 August & ongoing
Throughout
Justin Morley Head of Legal Services (Social Care &Education)
5 September 7 Sept 5. Legal
Nick Penny Finance 14 August 23 August Finance elements
Nish Popat Head of Accountancy 14 August 23 August Finance elements
Pat Main Interim Head of Corporate Finance
22 August 23 August Finance elements
Noel Hatch Head of Strategy and Performance
14 August 23 August Throughout
Kim Carey Interim Director of Adult Services
14 August Ongoing, & approved 7 Sept
Throughout
Rubinder Bains Public Health Consultant 30 August 5 Sept Throughout
Wendy Meredith Interim Director of Public Health
24 August As above Through R. Bains response
Cllr. J. Bell Leader 5 Sept
Cllr. B. Rai Health and Adult Services 5 Sept
Report History
Decision type: Urgency item?
EITHER: Key decision OR Non-key decision OR For information (delete as applicable)
For information
Report no.: Report author and contact for queries: Jackie Fisk, 0208 825 6853
Page 221 of 324
6
Appendix A: LGA Adult Social Care Green Paper consultation & draft responses 1. What role, if any, do you think local government should have in helping to
improve health and wellbeing in local areas? This is a key function of local government and is fundamental to the ambitions of Ealing Council, its community leadership role and its offer to local residents. Our ‘Future Ealing’ outcome-based approach focuses relentlessly on those things that will make the biggest difference to residents, a key aspect of which is health and wellbeing. The council has a key leadership role in bringing partners together to collaborate on shared outcomes.
Through Future Ealing, the council and partners have agreed nine outcomes, which are the things that will have the greatest impact in helping us to improve life in the borough. Focusing on these things will allow us to improve the lives and opportunities of our residents and make the best use of our limited resources, as demand on our services grows. By focusing on these agreed outcomes, we will work as one public service, to focus on prevention, encourage collaboration and reduce duplication – all of which contribute to improving health and wellbeing across the borough.
2. In what ways, if any, is adult social care and support important? Adult social care is fundamental to supporting some of the most vulnerable members of the community – older residents as well as work aged adults with disabilities. But Adult Social Care needs to work with other statutory and voluntary and community services to enable people to live as independently and healthily as possible. Appropriate levels of Adult Social Care have been cited by health partners as fundamental to the health system coping with increasing demand.
3. How important or not do you think it is that decisions about adult social care and
support are made at a local level? Decisions need to be made at a local level to ensure that the specific needs of local populations are met. Allocations of resources need to be made at a local level wherever possible – flexibility at the local level allows the optimum targeting of resources around our locally agreed outcomes. Decisions about adult social care are inextricably linked to the wider wellbeing of individuals and their communities, linked to the many local responsibilities of local authorities in their community leadership role.
Page 222 of 324
7
4. What evidence or examples can you provide, if any, that demonstrate improvement and innovation in adult social care and support in recent years in local areas? In line with our Future Ealing approach, the Council has embarked on a challenging and innovative transformational change programme in Ealing called Better Lives. The programme delivers over a three-year period, aiming to enable people to remain as independent as possible for as long as possible, but that where services and support is needed this is of sufficient quality and quantity to meet demand. This is being delivered to bring demand back in line with available resources as far as possible, thus decreasing the need for other parts of the Council to make additional efficiencies. Key features of our Better Lives programme include: - Promotes primary prevention to maintain wellbeing in the community for
longer - Makes best use of the opportunities available in the wider community and
universal offer - Maximises opportunities to work across the council and with partners to
target existing resources to prevent, reduce or delay demands for formal care and promote wellbeing
- Promotes support to informal carers, social capital, strength and asset based approaches to create more empowering support and care arrangements
- Focuses on delivering clear service user outcomes informed by individual choice, control and promoting as much independence as possible
- Keeps in touch with users to regularly assess how they, their networks, formal and informal arrangements are supporting them to achieve and sustain their goals, outcomes and expectations for their quality of life
- Proves value for money, supports a diverse, sustainable and accessible market for informal and formal care and support
5. What evidence or examples can you provide, if any, that demonstrate the
funding challenges in adult social care and support in recent years in local areas? The care packages and placements budgets have experienced considerable pressures in the last few years. The council has continually striven to handle these pressures through savings and innovation elsewhere, but this is becoming increasingly difficult and unsustainable. The impact of growing demand and funding pressures in adult social care has impacted the council more broadly. As the demand for adult social care services increases as a proportion of the council’s business, it has a disproportionate effect on the remaining areas of the business resulting in severe financial pressures on wider services.
6. What, if anything, has been the impact of funding challenges on local
government’s efforts to improve adult social care?
Page 223 of 324
8
Despite our determination in focusing on innovation and integration locally, the funding challenges have inevitably slowed progress as well as placing additional pressures on other council services. Whilst the Council has proactively sought ways to make service users’ experience of receiving adult social care services better, the funding pressures make this very challenging. The Adult Social Care service has had to reduce staffing and business support costs to ensure front line service is sufficiently supported, however this has created a challenge on the Council’s ability to deliver further improvements to the service. With demand continuing to increase this poses a significant risk to service delivery. Through the council’s Better Lives transformation programme, we are focusing on efficiency, partnership, culture and importantly the way we support residents to receive the right level and type of support, at the right time to maximise people’s independence. This development of our staff and the culture change required are key to delivering our ambition for quality social care – but the degree of funding pressures is putting workforce development and the success of Better Lives under huge pressure.
7. What, if anything, are you most concerned about if adult social care and support
continues to be underfunded? Without a sustainable funding solution, the council will experience overspends and increasing pressures, necessitating further reductions in spend in other budget areas as well as people waiting longer for care, remaining in hospital for longer or care providers failing due to lack of appropriate funding levels. This would affect the whole of the health and wellbeing system in the borough.
8. Do you agree or disagree that the Care Act 2014 remains fit for purpose?
We agree that the Care Act remains fit for purpose but argue strongly that the national funding element must be addressed since this was never implemented.
9. What, if any, do you believe are the main barriers to fully implementing the Care
Act 2014? See answer to 8 above. New responsibilities were introduced through the Care Act, but the funding streams were not, resulting in increased demand and underfunding.
10. Beyond the issue of funding what, if any, are the other key issues which must be
resolved to improve the adult social care and support system? Adult Social Care must have commensurate status with the health system. We consider that the future of Adult Social Care must be integrated with the NHS plan to help make the whole system work. Any solutions must deal with both short and long-term pressures. A focus on wider wellbeing is critical – including addressing the prioritization of public health. It is also important that care is
Page 224 of 324
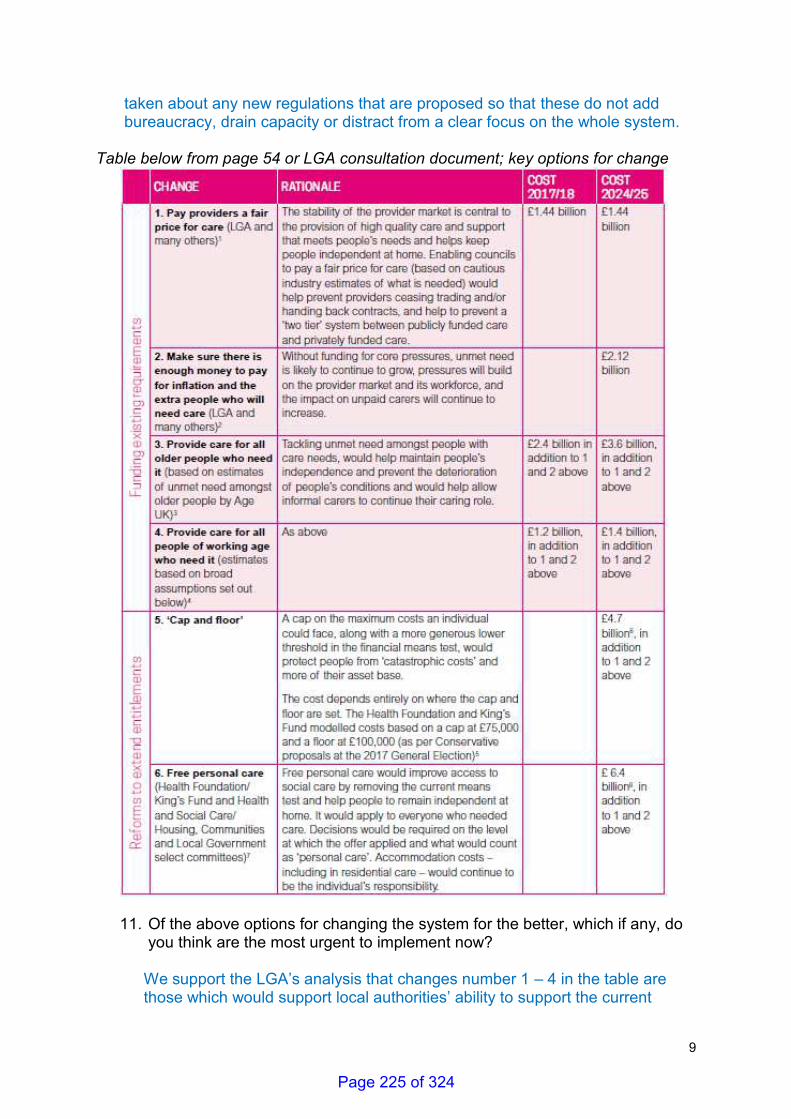
9
taken about any new regulations that are proposed so that these do not add bureaucracy, drain capacity or distract from a clear focus on the whole system.
Table below from page 54 or LGA consultation document; key options for change
11. Of the above options for changing the system for the better, which if any, do you think are the most urgent to implement now?
We support the LGA’s analysis that changes number 1 – 4 in the table are those which would support local authorities’ ability to support the current
Page 225 of 324
10
system and implement their statutory duties fully. Most urgent amongst these are changes 1 and 2 as these would help bring stability to the precarious provider market and fund core pressures. Whilst this would only bring us to a position of stasis, it is a critical first step in stabilising the current crisis situation.
12. Of the above options for changing the system for the better, which if any, do
you think are the most important to implement now?
In terms of bringing adult social care to a stable position, meeting the unmet needs identified in changes 3 and 4 in the table are essential to making a shift to a preventative agenda, by enabling residents to help themselves and each other – including the crucial role of informal carers.
13.Thinking longer-term, and about the type of changes to the system that the above options would help deliver, which options do you think are most important for the future? It is imperative that Government addresses the funding model for adult social care – whether through a cap and floor model or through a shift to free personal care – including negotiating the basis of this with the electorate. This is because it touches on issues of demographics, perceptions of inter-generational fairness and a need for increased personal responsibility whichever model is chosen. There is a danger that doing nothing still remains the default route – which would be a disaster for the future wellbeing of our residents. The difficult decisions which need to be made involve choosing between different perceptions of unfairness. Adult social care needs to be seen on a footing with health services – whether or not all personal care is free. We are agnostic on the final model, so long as the principles of transparency and adequate support for the most vulnerable in our society are met. Through its recent funding announcement on the NHS 5 year plan, the government has shown willingness to invest in public services and that they value the NHS – both very welcome signs. However, the absence of adequate, long-term funding for adult social care and other preventative services has already had significant impact on increasing demand for NHS services. We want to support people to live independent, fulfilled lives where they are most comfortable, and we have shown to be effective in doing this when we have the right funding. Investing in the social care and prevention services is a long-term strategy for ensuring a sustainable model of health and care in England. Funding in the NHS needs to be mirrored by investment in social care and prevention so that we move towards a place based budget rather than separate pots. 14.Aside from the options given for improving the adult social care and support system in local areas, do you have any other suggestions to add? The breadth of issues highlighted in the LGA Green Paper are a reflection of the views of the council and the Health and Wellbeing Board
Page 226 of 324
11
15.What is the role of individuals, families and communities in supporting people’s wellbeing, in your opinion? Where our residents have clear information and are supported to be well-connected in their communities, we know they are motivated to do as much for themselves as possible to remain independent and also there is a wealth of community assets from residents motivated to help each other. Such active citizenship is fundamental to the delivery of the council’s Future Ealing transformation programme. Building on the key contributions of carers and existing voluntary and community sector support, our Better Lives approach seeks a shift whereby demand is met within the community as much as possible, involving a substantial increase in enabling those who can help themselves to do so.
Table below from pages 58/59 or LGA document; key options for funding
Page 227 of 324
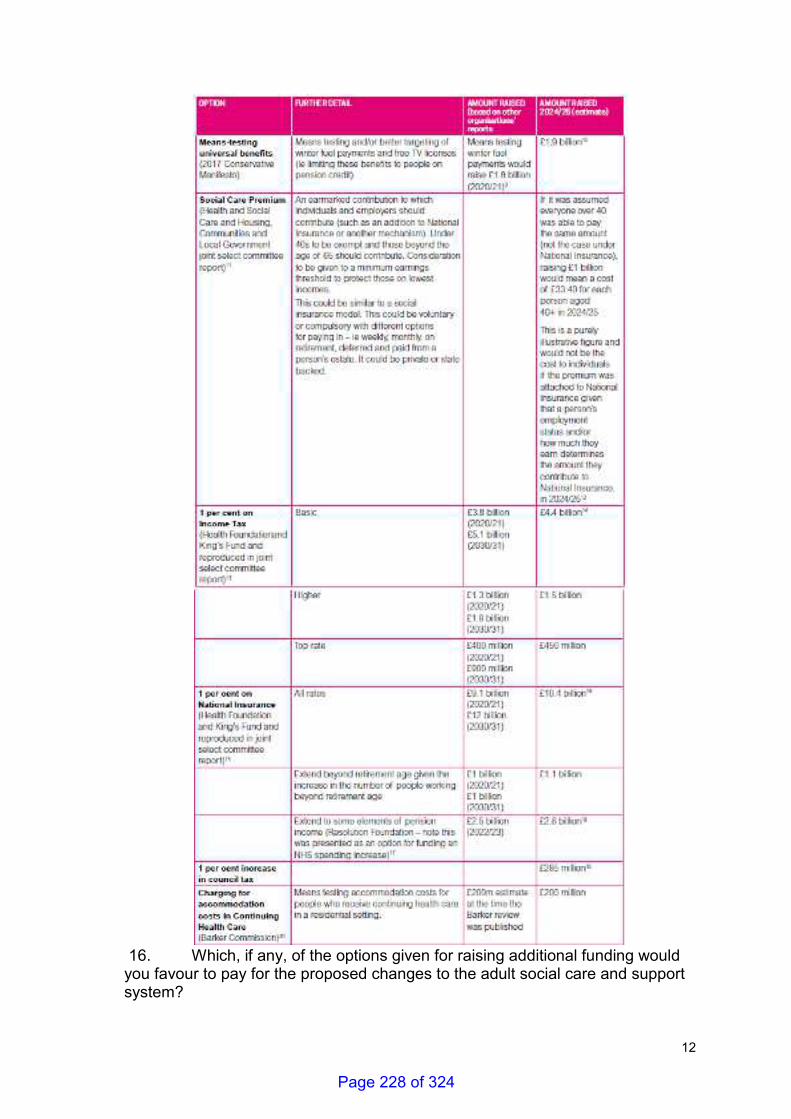
12
16. Which, if any, of the options given for raising additional funding would you favour to pay for the proposed changes to the adult social care and support system?
Page 228 of 324
13
We do not advocate one particular option over another, other than noting any proposed solution must take into account the anticipated demographic and societal changes, and is addressed on a cross-party basis. We agree that it is likely that a mix of solutions will be required, and the deliberation on these is inextricably linked with a need for the Government to be transparent and direct in engaging with citizens on the adult social care funding debate, in particular giving the debate parity of esteem with funding for health. 17. Aside from the options given for raising additional funding for the adult social care and support system in local areas, do you have any other suggestions to add? We suggest that the debate on funding for social care needs to be set in an holistic context of wider government funding. It also needs to factor in the increasing impact of demand on other aspects of social care – specifically children’s social care. The demand of children with disabilities living longer is an issue which, whilst positive, has an adverse impact on both school and council budgets, which link clearly into increasing pressures. Given the imbalance in funding pressures on local government in recent years, consideration should also be given to re-prioritising other governmental departments’ spending. 18. What, if any, are your views on bringing wider welfare benefits (such as Attendance Allowance) together with other funding to help meet lower levels of need for adult social care and support? Depending on the options shortlisted, it is likely to require revisiting other funding streams – such as Attendance Allowance - to consider the cumulative impact on different cohorts of citizens, so that the most vulnerable are protected and ‘fairness’ across the system defined and understood. 19. What are your views on the suggested tests for judging the merits of any solution/s the Government puts forward in its green paper? We support the suggested tests – of wellbeing, fairness, sufficiency, sustainability, clarity and transparency, and subsidiarity – as set out by the LGA. 20. In your opinion, to achieve a long-term funding solution for adult social care and support, to what extent is cross-party co-operation and/or cross-party consensus needed? Learning lessons from the past, and the impact a lack of cross-party support has had on delivering a sustainable solution for adult social care, it is clear that cross-party collaboration is essential. 21. What role, if any, do you think public health services should have in helping to improve health and wellbeing in local areas?
Page 229 of 324
14
Public health services are fundamental to delivery of health and wellbeing since they take into account the wider determinants of health. As illustrated below, the relative contribution of determinants of health are wide-ranging and cut across organizational boundaries:
Public Health is a catalyst for linking the wellbeing elements of a wide range of opportunities for self-help, community and public sector support. The Health in all policies (HiAP) approach is an important contribution in this space since it fosters a collaborative approach to improving the health of all people by incorporating health considerations into decision making across sectors and policy areas. https://local.gov.uk/health-all-policies-manual-local-government 22. What evidence or examples, if any, can you provide that demonstrate the impact of other local services (both council services outside of adult social care and support, and those provided by other organisations) on improving health and wellbeing? We are collaborating on innovative approaches to mitigate funding pressures and to prompt behaviour change amongst residents. For example, we have a partnership neighbourhood-based approach to increasing physical activity in Southall – ‘Let’s Go Southall’ which is predicated on a whole-systems approach to health and wellbeing. We recognise the important link between housing and health and wellbeing, and are seeking to mitigate the immense housing challenges through increased political prioritisation of genuinely affordable housing in Ealing. 23. To what extent, if any, are you seeing a reduction in these other local services?
Page 230 of 324
15
The funding pressures on our and our partners’ finances mean that there are huge pressures on local services, with cuts to many services. This includes the necessity of putting pressure on evidence-based Public Health services such as smoking cessation that improve the health and wellbeing of residents, so that some services are being decommissioned or reduced due to competing resources. The effects impact both the NHS and social care. The impact of funding pressures is felt across both the whole spectrum of statutory and voluntary sector partners, with reduced spending impacting on key areas such as safeguarding, homelessness and mental health provision. 24. What principles, if any, do you believe should underpin the way the adult social care and support service and the NHS work together? Both should work together to get better outcomes for the population. Where service development changes patterns of care, then the money should follow the activity.
25. In your opinion, how important or unimportant is it that decisions made by local health services are understood by local people, and the decision-makers are answerable to them? It is essential - the Health and Wellbeing Board provides the forum for this and local decisions should be transparent. 26. Do you think the role of health and wellbeing boards should be strengthened or not? For HWB discussion. 27. Which, if any, of the options for strengthening the role of health and wellbeing boards do you support? For HWB discussion 28. Do you have any suggestions as to how the accountability of the health service locally could be strengthened? For HWB discussion 29. Which, if any, of the options for spending new NHS funding on the adult social care and support system would you favour? We emphasise the need to focus on integration, with partnership shared endeavours to improve patient/resident outcomes. Our Future Ealing approach is outcome-based and we have reached consensus, expressed through our upcoming Borough Plan, on local shared outcomes around which partners collaborate to deliver. New NHS funding should not be just invested in the
Page 231 of 324
16
existing STPs. With sufficient local flexibility, new NHS funding could have maximum impact on supporting delivery of these shared partnership outcomes.
30. Do you have any other comments or stories from your own experience to add?
N/A
Page 232 of 324
The lives we want to leadThe LGA green paper for adult social care and wellbeing
July 2018
ADULT SOCIAL CARE
FUTURE OF
Page 233 of 324
2 | The lives we want to lead
Your views matter. Our green paper is only a starting point and we want to build momentum for a debate across the country about how to fund the care we want to see in all our communities for adults of all ages and how our wider care and health system can be better geared towards supporting and improving people’s wellbeing.
Throughout this green paper we pose a series of consultation questions and we would welcome your views on all those that are important to you. The consultation will run from 31 July to 26 September. Once the consultation closes we will analyse all responses and publish a response in the autumn.
To complete the consultation you can either visit www.futureofadultsocialcare.co.uk or you can submit your answers to the questions below to: [email protected]
If you are responding as an individual there is also an option to answer the questions in the 'Summary Green Paper' section which are primarily focussed on gathering experience-based evidence and opinions. You will find these at www.futureofadultsocialcare.co.uk/summary-green-paper
Page 234 of 324
The LGA green paper for adult social care and wellbeing | 3
Contents
What our partners have said ..................................................................................................................................4
Foreword .......................................................................................................................................................................8
Executive summary .............................................................................................................................................. 12
Who is this green paper aimed at? ....................................................................................................................16
Adult social care at a glance ...............................................................................................................................18
1. The voice of people who use services ....................................................................................................... 20
2. Delivering and improving wellbeing ..............................................................................................................26
3. Setting the scene – the case for change ..................................................................................................29
4. The options for change ....................................................................................................................................49
5. Adult social care and wider wellbeing .........................................................................................................61
6. Adult social care and the NHS .......................................................................................................................66
7. Summary of key points.....................................................................................................................................74
8. Have your say ......................................................................................................................................................76
Annex A: case studies of innovation, delivery and performance ...........................................................80
References from tables .......................................................................................................................................86
Page 235 of 324
4 | The lives we want to lead
“We support the LGA’s objective to show how local government can be at the forefront of developing pragmatic solutions, this should be the time for an informed debate with the public on the future of social care. The absence of adequate, long-term funding and reform for adult social care has already had a significant impact on increasing demand both in the NHS and across council services. As a sector we want to support people to live independent, fulfilled lives and we have shown to be effective in doing this when we have the right tools and funding. Ensuring that people and place are at heart of any reform is the right approach to take – we now need to pick up the pace of planning to address the urgency of need.”Paul Najsarek, Solace lead spokesperson for wellbeing and Chief Executive of the London Borough of Ealing
“Local government and the voluntary, community and social enterprise [VCSE] sector share a vision for social care which helps us all to live good lives in our own homes with the people we love. Immediate investment is needed to stabilise social care. Then councils and the VCSE sector must work with people who need support and their community organisations to co-design a social care system which intervenes early, sees the whole person and can stay with people and families for the long haul. Human, effective and sustainable approaches already exist: great councils have been pioneering their development. Now they must be scaled up and become the norm.”Alex Fox OBE, Chief Executive of Shared Lives Plus and independent chair of the Joint VCSE Review
What our partners have said
Page 236 of 324
The LGA green paper for adult social care and wellbeing | 5
“The LGA publication of their version of a ‘green paper’ for social care represents an important contribution to the debate about what we want society to look like from one of the key contributors to delivering that future. ADASS will work with the LGA alongside all stakeholders in this critical debate to ensure the voice of adult social care remains prominent throughout. This document maintains a much needed profile in the lead up to the Government's formal green paper due now in the autumn.”Glen Garrod, President of the Association of Directors of Adult Social Services
“It is vital that we keep the focus on the plight of social care, in spite of the succession of government postponements of their own green paper. The LGA is to be congratulated on keeping the debate going and we will respond to the issues it raises.” Niall Dickson, Chief Executive, NHS Confederation
“The issue of how to fund social care cannot continue to be avoided. Decades of indecision has led to one in three people with MS (multiple sclerosis) being denied the care they need and this can’t go on. The LGA’s consultation raises many of the key challenges that must be tackled, including the need for proper government funding and a fair system that works for everyone who needs care. We hope that when it does arrive, the Government’s own green paper will set out a bold and ambitious plan that addresses these challenges. People with MS shouldn’t have to keep paying the price for a system in crisis.”Genevieve Edwards, Director of External Affairs, MS Society
Page 237 of 324
6 | The lives we want to lead
“Fixing social care has been stuck in the too difficult to-do box for far too long. This is not just about the money, it’s also how we do care differently, make it more predictive, proactive and personalised.
“The Care Act provides a 21st Century framing for social care but it needs funding to deliver. By setting out its own green paper the LGA is demonstrating the sort of cross party dialogue and collaboration necessary to deliver the sustainable settlement we desperately need. We are running out of road for the Government to kick the can down.”Professor Paul Burstow FRSA, Chair, Social Care Institute for Excellence
“I am glad the LGA is continuing the debate for a long-term sustainable solution for adult social care. Of course funding and resources are a critical part of the debate but to ensure we focus on quality too, the needs and aspirations of all those using services, their families and carers, must be at the heart of what that future should be.”Andrea Sutcliffe CBE, Chief Inspector of Adult Social Care, Care Quality Commission
“We need to prioritise prevention to ensure a sustainable NHS, to ensure that people can enjoy the best possible quality of life using our hospitals less often and later in life. We can do this through helping people spend more years in good health, and when unwell, to stay in their own homes for longer. And as people retire later, we need to extend their healthy working life.
“40 per cent of all morbidity is preventable and 60 per cent of 60 year olds have at least one longer term condition. In 15 years we will have 1.3 million more people aged over 85, so prevention has to be at the heart of both the new NHS Ten Year Plan and the future work programme of its most critical partner, local government.”Duncan Selbie, Chief Executive, Public Health England
Page 238 of 324
The LGA green paper for adult social care and wellbeing | 7
“We expect to see a fair and well-funded social care sector to enable older and disabled people to live the lives they choose. It is unfair that successive governments have continued to delay decisions about social care reforms.
“The lives we want to lead from the Local Government Association is a very welcome initiative. Where central government stalls, local government is helping to keep adult social care firmly on the agenda. We all need to engage with the questions in this report, raise the debate and fill the void left by central government’s lack of policy progress.”Dr Rhidian Hughes, Chief Executive, Voluntary Organisations Disability Group and Chair, Care Provider Alliance
“It’s great to see health and wellbeing at the very heart of this paper. We support this consultation and it’s essential that the whole system comes together to agree a workable way forward. This must include a strong focus on prevention to deliver sustainable services.”Nicola Close, Chief Executive, Association of Directors of Public Health
“Social care and health are two sides of the same coin. The LGA’s conversation about social care is vital to understand how we provide high quality, timely, cost effective support to everyone who needs it. Gathering views from the frontline about how we change has never been more important.”Saffron Cordery, Deputy Chief Executive, NHS Providers
“This LGA green paper consultation provides a great opportunity for everyone to comment and hopefully help inform the future shape of adult social care.”Lyn Romeo, Chief Social Worker for Adults, Department of Health and Social Care
“Big choices loom for social care policy: how much should the state help individuals with the costs of care? how should funding be raised to pay for that help? And what is the balance in responsibilities between local and national government? With such important and contentious issues, it is vital to consult widely and broadly with stakeholders and citizens to help build consensus on the way forward.” David Phillips, Associate Director, Institute for Fiscal Studies
Page 239 of 324
8 | The lives we want to lead
Adult social care and support matters. High quality social care and support helps people live the life they want to live. It helps bind our communities, it sustains our NHS and it provides essential economic value to our country.
The Local Government Association (LGA), like its many partners in the social care sector, has worked hard to ensure that the question of how to fund social care for the long-term has had the time in the national spotlight that it deserves. But we have still not secured the action we urgently need.
The continued absence of a sustainable, long-term solution has brought care and support to breaking point. It now also means that, across the country, local government is struggling to sustain universal local public services like roads and waste collection as it has to prioritise statutory duties like social care for children and adults, and support for the NHS. The failure to address this creates a deeply uncertain future outlook for people who use social care services now, and the growing number of people who will need the service in the years to come.
This is a collective failure that impacts most on the very people least able to help themselves.
National governments past and present have tended to put political prospects ahead of difficult but necessary decision-making. When they have put forward proposals, national opposition parties have sought to discredit them instead of trying to find common ground. The national media has latched on to this disharmony, further fuelling the politicisation of the question of social care funding. Faced with a frustrating political stalemate, the wider social care sector at times inevitably seeks to rebuild momentum by focusing on the ‘crisis’ in care, despite knowing better than most that a more balanced narrative that emphasises the inherent value of social care is more conducive to winning hearts and minds. The preoccupation of successive governments with the state of our hospitals has impacted on the use of new money for social care.
Foreword
Page 240 of 324
The LGA green paper for adult social care and wellbeing | 9
The result is at least two decades in which the question of how to fund social care for the long-term has never enjoyed more than a few brief periods in the national spotlight. All the while, the concerns and experiences of the people who matter most – those who need care and support and their families – have struggled to get the attention they deserve. More widely, the public has largely remained detached from the debate, finding it difficult to engage with a set of questions and issues that have so many conflicting viewpoints. Most people still do not have a good sense of why social care matters, how it works and how it is funded.
Against this backdrop, the approach of governments past and present in dealing with mounting pressures in social care has been to limp along with piecemeal measures from one year to the next. Local government is widely acknowledged as the most efficient part of the public sector and councils, along with providers and third sector organisations, have responded admirably to help maximise every pound and drive innovation in the interests of people and the public purse. But with demand growing, costs rising, people’s expectations rightly increasing and funding declining, this approach of short-term sticking plasters must be abandoned. The need to resolve the long-term future of care and support is now urgent.
We cannot duck the issue any longer.
It is time to confront the hard choices, be honest about the options and make some clear decisions.
We need to come together as a society and be positive and inspiring, making the case that investment in social care and support for people who need it helps them to reach their full potential and, in turn, our nation's.
Across the country there are many examples that show how our sector has innovated and transformed itself through world-leading initiatives such as direct payments. Positive futures for care and support, which draw on all the assets of councils, communities and civil society, can already be glimpsed and built upon.
Page 241 of 324
10 | The lives we want to lead
The Government’s recent decision to delay its own green paper is disappointing and frustrating. In the context outlined above, it is also hardly surprising. More importantly, it provides an opportunity for local government – so often the pragmatic front-runner on difficult agendas and at the forefront of developing solutions to difficult issues on a cross-party basis – to seize the initiative and take the lead in forging a way ahead. That process begins here with the LGA’s green paper for adult social care and wellbeing, The lives we want to lead. It is supported by all political parties within the LGA, demonstrating the required level of cross-party support amongst local politicians that we need to see matched by our national politicians.
Much of our green paper is about the future of care and support for all adults and how we pay for it. But if our starting point is the individual person and what is important to them, then one service alone can never support them to live the life they want to lead, no matter how good it is. Our green paper therefore looks beyond social care and considers the importance of housing, public health, other council services, including those delivered by district councils, in supporting wellbeing and prevention, and the vital work with councils’ local partners, families and communities. And of course, we consider the NHS. This year we rightly celebrate the 70th birthday of our health service, but if we are to look ahead with confidence to its centenary then it too must change for the benefit of those it serves.
This is therefore a green paper for wellbeing. It seeks to lay the ground to secure both immediate and long-term funding for social care as well as make the case for a shift in approach from acute treatment to community prevention. It is about people, population and place, not structures, systems and silos. It is also just a starting point. Too often policy is developed in isolation. With this green paper we are seeking as wide a selection of viewpoints as possible, recognising that this is complex territory. There are no single or easy solutions and even within the sector there are different views on how we should move forward. Throughout this publication, we therefore pose a series of consultation questions to understand those views and identify where there is consensus or overlap. We encourage you to respond. We have also produced a separate set of tools to help gather the views of the public which you can find on our website www.futureofadultsocialcare.co.uk. Your support in promoting these would be valued as we seek to reach as wide an audience as possible on the questions at the heart of the debate.
Page 242 of 324

The LGA green paper for adult social care and wellbeing | 11
We want to build momentum and help stimulate a truly nationwide debate about how best to fund the care we want to see in all our communities up and down the country for adults of all ages, and how our wider care and health system can be better geared towards supporting and improving people’s wellbeing. We will reflect on our consultation findings in a further publication later in the autumn, in time to influence the Government’s plans; not just their green paper, but also the Budget, the NHS Plan and the Spending Review. This is our chance to put social care and wellbeing right at the very heart of the Government’s thinking.
We have a vision for people’s wellbeing that is rooted in local areas and backed by clear and strong local democratic accountability. It is about helping to build a society where everyone receives the care they need for a good life: well, independent, at home for as long as possible and contributing to family and community life.
It is our time to drive this agenda forward.
Lord Porter of Spalding CBE LGA Chairman
Cllr Nick Forbes Labour Group Leader and LGA Senior Vice Chair
Cllr James Jamieson Conservative Group Leader and LGA Vice Chairman
Cllr Howard Sykes MBE Liberal Democrat Group Leader and LGA Vice Chairman
Cllr Marianne Overton MBE Independent Group Leader and LGA Vice Chairman
Page 243 of 324

12 | The lives we want to lead
Too often adult social care is seen as an adjunct of the NHS, existing simply to relieve pressure on hard pressed acute services. While it is true that social care and the NHS are inextricably linked, it should be seen an essential service in its own right and the people who work hard to deliver the service should be seen as just as valuable as staff in the NHS. It helps people with life-long disabilities, those who acquire disabilities during adulthood, older people with care and support needs and unpaid carers of all ages to live their lives with dignity and in the way they see fit. But it is more than that. It creates services and partnerships – particularly with the voluntary sector – that help strengthen our communities, it allows the NHS to focus on what it does best and it is important for the future of our economy and national productivity; as the Government’s own Industrial Strategy acknowledges, helping people to live independent lives and continue to contribute to society will create “an economy which works for everyone, regardless of age'1.
People working in local government care passionately about adult social care and take pride in the role it plays in supporting people’s lives and improving their outcomes. With the right level of funding, councils can continue to make a positive difference to people’s wellbeing. With the right level of freedoms and flexibilities, they
1 https://www.gov.uk/government/publications/industrial-strategy-the-grand-challenges/industrial-strategy-the-grand-challenges
can work with health and community partners to drive local action across the public, private and voluntary sectors to reshape care and support around the needs of individuals and in the communities they cherish. With the right training and career opportunities, good quality staff can be attracted to the sector and, as importantly, stay in it. Adult social care has a central role to play in this. But it is also embedded in a wider network of local government services and functions which promote health, independence and wellbeing: all council services contribute to health and wellbeing.
Whilst councils and their partners have a strong story to tell on improving people’s wellbeing, progress to date is now unquestionably at risk. Local government has kept the worst consequences of austerity at bay in recent years but its impact is now catching up with councils, threatening services that improve our lives and our communities. This is certainly the case with adult social care and the service now faces a funding gap of £3.56 billion by 2025. This must be closed as a matter of urgency. If it is not, we will see a worsening of the consequences of funding pressures we have seen to date. These include fewer people being able to get the high quality care they need, providers under increasing threat of financial failure,
Executive summary
We all strive for a happy and fulfilling life. We should all have the support we need to live one. Many of us can live the life we want without much, if any, help. Others may need a great deal, receiving it from a range of sources including family, friends, neighbours, community and voluntary groups, and statutory services. What matters most is that everyone can exercise their right to opportunity, independence and control.
Page 244 of 324
The LGA green paper for adult social care and wellbeing | 13
and a disinvestment in prevention driven by the requirement to meet people’s higher level needs. In particular, funding pressures on social care have severe consequences for the NHS, increasing demand on hospitals and more costly acute care. Of course, this is a two-way street and what the NHS does or does not do can impact equally on social care. Reductions in services such as incontinence treatment, stroke rehabilitation and NHS continuing care increase pressures on social care. We know these problems are only going to get worse as demand grows with the needs of our ageing population. The question of how we pay for adult social care for the long-term is therefore getting even more urgent. The fact the question has remained unanswered for at least the last two decades shows the scale of the challenge.
In part, that difficulty stems from a lack of awareness amongst the public of what adult social care is, why it matters and how it is funded. Not so in the NHS, which people intuitively understand, both morally and
2 See, for instance, https://www.lgiu.org.uk/wp-content/uploads/2012/04/Independent-Ageing.pdf
operationally. By paying our taxes we pool the risk and cost of treatment we may need if we become sick. We pay in, the NHS pays out, free at the point of delivery, free at the point of need. It is a simple equation and a powerful contract between citizen and state.
It is a far less clear cut picture in adult social care. Not all care needs count as ‘eligible’ for support under the legislation, and the amount you have to pay depends on the level of your own financial resource, which itself is treated differently depending on whether you receive care at home or in a care or nursing home. If you have more than what many would say is only a modest degree of savings, you pay for everything yourself becoming one of a growing population of ‘self-funders’ who are largely left to navigate the system themselves and make their own arrangements. Without the right information and support, wrong decisions can be made, personal savings can reduce rapidly and people fall back on publicly-funded care, compounding the pressure on local services2.
Page 245 of 324

14 | The lives we want to lead
The situation is often summed up by the simple example of cancer and dementia. Develop the former and the NHS will, in general, take care of you for free. Develop the latter and you risk losing the majority of your savings because you will have to pay for your care. This inevitably raises a host of questions which tend to gravitate towards a broad idea of ‘fairness’. Over the years this has been articulated in different ways, whether it be about people who have paid taxes all their lives, those who have saved and made provision for the future, the importance of protecting people’s housing assets, the opportunities different generations have (or have not) enjoyed, and how we should approach a person’s ability to pay. Fairness means different things to different people, but the level of concern clearly points to a pressing problem that needs to be resolved. The question here is therefore twofold: how can we change the system for the better, and how do we pay for the changes involved?
Even answers to these questions will not bring about the change we need. Securing the long-term financial sustainability of adult social care is of course important. But the benefits of sustainable social care will be even greater if our wider care and health system can be made to work better as a whole. This requires a fundamental rebalancing of priorities – moving away from treating long-term conditions and illness caused by ageing and lifestyle factors and moving towards community-based models of both early intervention and support. There are many potential benefits of health and social care working more closely together and the role councils can play in commissioning, particularly in terms of NHS community-based services integrating with adult social care. It could also help to manage pressures on public spending more effectively. This would help maximise people’s health, wellbeing and independence for as long as possible, and continue to take
a whole-person and whole-family approach to those who develop support needs.
We have many of the key ingredients that are needed to help bring about this shift and focus investment in low cost prevention and support to help bend the demand curve for high cost health care. Under councils’ stewardship we have a better performing and more cost effective system of public health. We have significant new funding for the NHS. In health and wellbeing boards we have a means of joining up clinical, professional and service user voices. We have led the way in re-designing services with – not for – citizens, and we work imaginatively with provider organisations and the third sector. Most importantly, we have democratic accountability through local councils. It is clear we are not starting from scratch. The question here is what level of change is needed to realise the full potential of each of these components?
Through this green paper we want to open up the debate on the core questions outlined above. Our focus in this work is people, and councils across the country want to rise to the challenge and do our bit to make sure people get the care and support they need to live the lives they want. We know that driving continuous improvement amongst councils is just as important as bringing about changes required in other parts of the sector. Whether that is improving our performance, working better with our health and community partners or taking greater responsibility for leading change locally; councils can do more and are committed to doing so. We will need to take risks, scaling up the most successful of the many innovations we have developed and supported. And we know there are no easy answers and that any additional investment must deliver real benefits for local people and communities. This is particularly true for people from black, Asian and
Page 246 of 324
The LGA green paper for adult social care and wellbeing | 15
minority ethnic (BAME) backgrounds and other excluded groups who do not yet enjoy equal access to social care consistently: delivering on equalities will be a key test of any new system. The stakes are high. A failure to be bold today will impact on people, our communities, our hospitals and our economy tomorrow and for decades to come.
Our green paper deliberately steers clear of pushing particular solutions at this stage. Instead, it articulates why this debate is so important, the scale of the challenge and the sorts of questions we need to tackle to drive the conversation forward. We will work with our many partners to engage professionals, politicians, people who need care and support and the public alike in the weeks ahead, before producing a further report in the autumn that reflects on our consultation findings. We hope this will help shape the Government’s own green paper, moving it more towards actual solutions, rather than consulting on territory that has been covered before.
Chapter one of our green paper sets the tone for the remainder, starting with the most important voice in the debate: the people who use services to help them live the life they want to lead. In chapter two we recognise that we are all unique and therefore require different support to fulfil our ambitions. Wellbeing is defined and the role of local government and the wider public, private and independent sectors in supporting this is briefly explored. Chapter three sets out the case for change – why social care matters, how the sector has delivered in challenging times and how it remains committed to doing so, and the scale and consequences of underfunding. In chapter four we explore some of the attitudes and beliefs of the public and other key groups in the debate about the future of long-term funding for social care. We set out a series of options for changing the system for the better before setting out a second set of options for how we might pay for those changes. Chapter five moves the debate along to consider the wider changes we need to see across care and health to help bring out a greater focus on community-based and person-centred prevention. It looks at the role of public health, other council services and those of councils’ partners in supporting and improving wellbeing. Chapter six continues this wider exploration of issues by looking at the nature of the relationship between social care and health, integration, accountability and how the new NHS funding could be used for maximum impact.
Page 247 of 324
16 | The lives we want to lead
“All too often, the funding of adult social care is seen as an economic and a technical issue: what’s the best mechanism for raising the funding we need? While this is important, the more fundamental questions are personal, political and philosophical: what kind of life do we want to have together as a society? How much do we value disabled and older people with care needs? What sort of support would we want available to any of us if we needed care? How much do we really value this and how much might we therefore be prepared to pay for whatever quality of life we decide we want?”Professor Jon Glasby, University of Birmingham LGA think piece series, 2018
Questions about the future of adult social care and support, and the wider changes we need to make to our care and health system to improve wellbeing, should be everyone’s business. They are questions that impact on us all – in our personal and professional capacities, as members of local communities, and as citizens of wider society.
For this reason, our green paper and accompanying consultation aims deliberately high. It seeks the views of people who use care and health services and their carers, people who are experts on various elements of these services, and people who have no knowledge of the system at all. We are ambitious precisely because the views of all these people matter.
Who is this green paper aimed at?
Page 248 of 324
The LGA green paper for adult social care and wellbeing | 17
We want to hear from:
People who use services and their carers: your wellbeing is what matters most and your experiences and expertise should be the single most important force in understanding and shaping the change we need to bring about.
Local and national politicians: as representatives of us all it is in your gift to help bring about the change that is sought –promoting it, putting it on the map and helping to deliver it.
Professionals involved in the commissioning and delivery of care and health: your knowledge of the operational aspects of care and health can help identify all the barriers to progress that need to be overcome and how we might do so.
Public: the chances are that you, or someone you know, will at some point have contact with social care, be that needing services, working in the sector, or being an unpaid carer for someone you love. What you would want for yourself, or someone you care about, must shape the future.
All of us: we cannot move forward without knowing our level of ambition and what we are willing to pay to achieve it.
Page 249 of 324
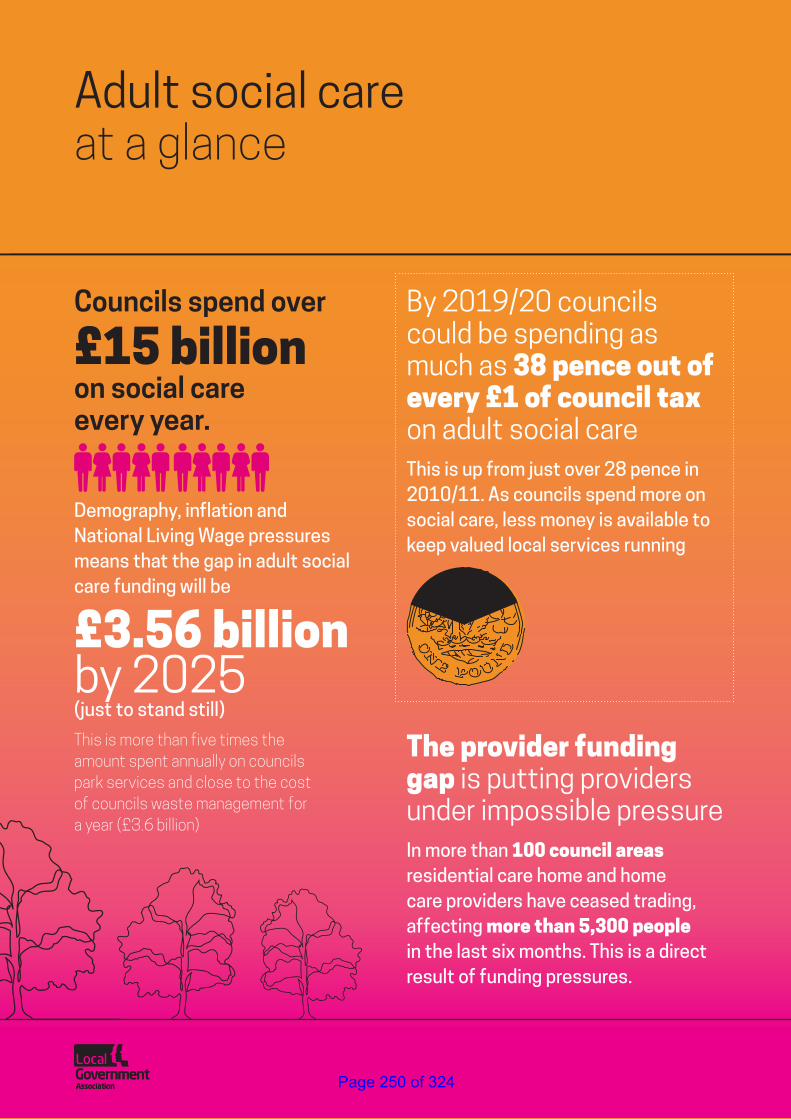
18 | The lives we want to lead
Adult social care at a glance
Councils spend over
£15 billion on social care every year.
Demography, inflation and National Living Wage pressures means that the gap in adult social care funding will be
£3.56 billion by 2025 (just to stand still)
By 2019/20 councils could be spending as much as 38 pence out of every £1 of council tax on adult social careThis is up from just over 28 pence in 2010/11. As councils spend more on social care, less money is available to keep valued local services running
The provider funding gap is putting providers under impossible pressureIn more than 100 council areas residential care home and home care providers have ceased trading, affecting more than 5,300 people in the last six months. This is a direct result of funding pressures.
This is more than five times the amount spent annually on councils park services and close to the cost of councils waste management for a year (£3.6 billion)
Page 250 of 324
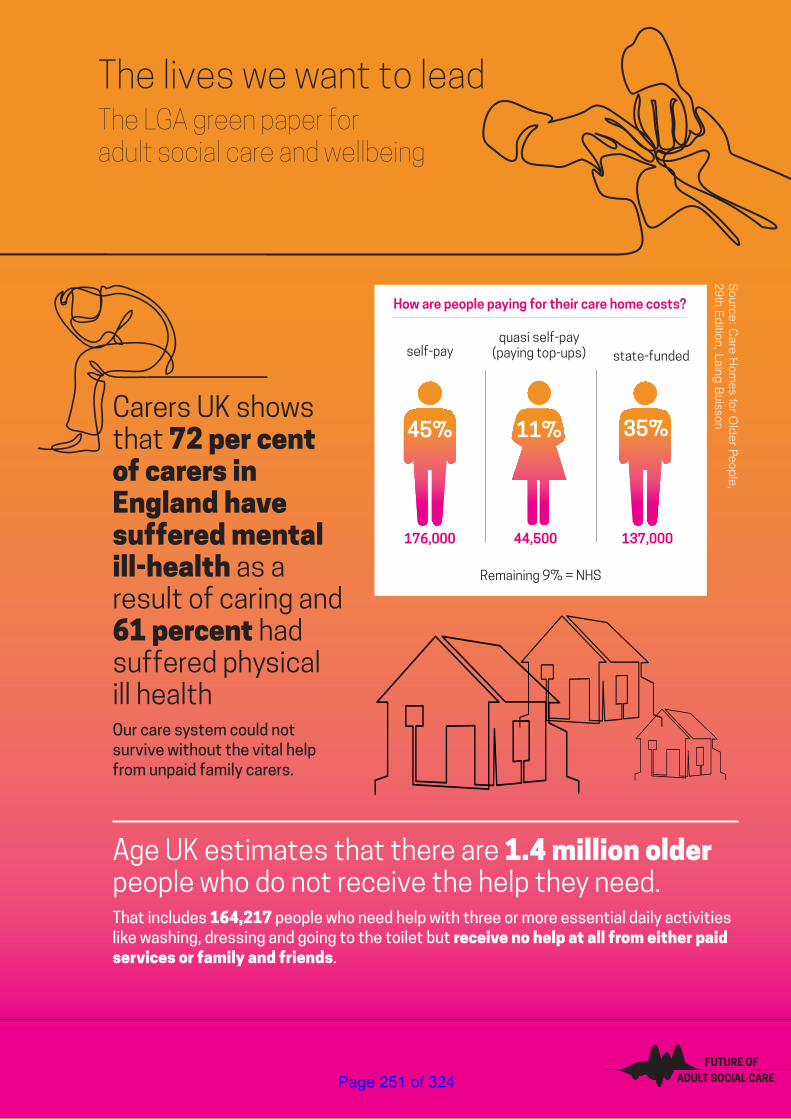
The LGA green paper for adult social care and wellbeing | 19
The lives we want to leadThe LGA green paper for adult social care and wellbeing
ADULT SOCIAL CARE
FUTURE OF
How are people paying for their care home costs?
176,000
self-payquasi self-pay
(paying top-ups) state-funded
44,500 137,000
45% 35%11%
Source: C
are Hom
es for Old
er Peop
le, 29th E
dition, Laing
BuissonCarers UK shows
that 72 per cent of carers in England have suffered mental ill-health as a result of caring and 61 percent had suffered physical ill healthOur care system could not survive without the vital help from unpaid family carers.
Age UK estimates that there are 1.4 million older people who do not receive the help they need.That includes 164,217 people who need help with three or more essential daily activities like washing, dressing and going to the toilet but receive no help at all from either paid services or family and friends.
Remaining 9% = NHS
Page 251 of 324
20 | The lives we want to lead
People must come first. Organisations’ structures, governance, strategy, policy and partnerships all matter. But they must only ever be secondary, serving to help a primary aim of understanding people’s aspirations, needs and the support required to live a life.
There is no such thing as a ‘typical’ person who uses health and social care services. Every individual who needs help and support has their own unique set of circumstances, needs and assets. And there are no neat and clear-cut categories of people who require adult social care and support. Instead, there is a complex interplay between mental and physical conditions that has to be taken into account when deciding the best care and support package. For example, people with learning disabilities have a higher prevalence of mental health problems compared to those without3. More than 15 million people – 30 per cent of the UK population – live with one or more long-term condition(s) and more than four million of these will also have a mental health problem4.
Our first full chapter therefore starts with the voice of people with experience of our care and health system, illustrating the diversity of people supported by the social care and support sector. These are powerful stories, which at times are hard to read. They expose – in the most human terms – the consequences of a system that lacks all the tools required to be the best that it can be for people that need it. They are also a challenge to us all to keep this subject firmly on the public and political radar.
3 Cooper, S.A., Smiley, E., Morrison, J., Williamson, A., & Allan, L. (2007). Mental ill-health in adults with intellectual disabilities: Prevalence and associated factors. The British Journal of Psychiatry, 190, 27–35.
4 Naylor, C., Parsonage, M., McDaid, D., Knapp, M., Fossy, M., & Galea, A. (2012). Long-term conditions and mental health – The cost of co-morbidities. London: The King’s Fund, & Centre for Mental Health.
As you read through our green paper and consider the questions it raises, we encourage you to return to these stories as essential grounding in why this debate is so fundamentally important to the future of people across our country, and our country itself.
1. The voice of people who use services
Page 252 of 324
The LGA green paper for adult social care and wellbeing | 21
Josie’s storyAt the moment, I get three short visits a day from a care worker to cook my meals, help me shower, and keep the house clean.
I get two hours every two weeks 'social' time which at best on a good day gets me over to the park and back. It’s not long enough to join in any activities but I value this time hugely as it’s uninterrupted time with actual real conversation, not just “what do you need to eat?” or similar.
My basic needs are met – I’m clean and I’m fed. But I haven’t got enough support to actually get me out of the house. It means that some days I barely get to speak to anyone, let alone have a social life. If I get an infection and have to ask my carer to pick up a prescription, I don’t get to have a shower that day. There just isn’t enough time. A little more support – for example, a support worker to go with me to new places – would give me so much more opportunity to take part in life, but at the moment that feels like an impossible utopia!
People like me, who were professionals and could make a contribution with the right support, are being cut out of the workforce. Working in an office or a hospital isn’t really possible for me, but I still have skills and experience that I would like to use, if I had the means of doing so. In the end, it is a question of equality. I don’t feel like I’m living, just existing.
Vicki and Keegan’s story I was diagnosed with Muscular Dystrophy when I was young. As a degenerative condition every day is an increasing challenge.
I am now 36 years old and I need assistance to get out of bed, to eat, to use the bathroom and to leave the house. I need someone with me day and night.
My partner Keegan cares for me around the clock. If he didn’t, I would need a full-time carer or I would have to live in a residential home. Yet, Keegan is only paid for four hours a day and we have no funding for respite. I worry every day about what would happen to me if he couldn’t look after me anymore. He is my independence and my dignity.
In the past I have been offered some support to help me at home but as my condition worsens and my needs grow, I am being offered less and less because there is no money available to help me. Something as simple as getting a hoist to help me in and out of bed has become a battle. At times, this has meant that my more preventable symptoms have got so bad I have had to call an ambulance. I am only too aware that every minute I spend with paramedics is taking this costly service away from someone else who needs it, but I am left with no choice. Sadly, I am not the only person I know who has to do this and while I want to feel positive about the future, if I keep being told there is no money for the help me and Keegan need, we feel totally helpless.
It’s hard enough living with this condition without feeling like I have to face a challenge every time I ask for help. The sad thing is none of us know when or if we will need people to care for us one day so it is vital that everyone is aware of the issues before it is too late to do anything about it.
Page 253 of 324
22 | The lives we want to lead
Glyn and Kristin’s storyMy wife Kristin is just 47 years old but has had Multiple Sclerosis for 17 years. Each year, as it inevitably progresses, it becomes a bigger aspect of our life together.
I was caring for Kristin at home but just two years ago this became too much and I collapsed under the strain. We had carers coming in morning and night to get Kristin in and out of bed, but all other hours of the day I was left to care for Kristin on my own.
At the same time, I was trying to run my own business to supplement the modest carer’s allowance I received. I got no respite and was exhausted.
Kristin fell ill with a simple respiratory issue and got stuck in hospital for three months because she wasn’t allowed to leave until a package of full-time care was in place. When she finally left hospital she came home for four months until I collapsed from looking after her with no respite.
She was then placed in an NHS funded nursing home under the continuing healthcare scheme. I think she could have come home full time with the right care in place or if the money being spent on her care home was invested in making the right adaptations to our home. Devastatingly, the council couldn’t pay for all of the changes we needed and I couldn’t fund it on a reduced income so we had no choice.
It’s so hard for people who are not in our situation to understand the enormous impact this has had on our family. Kristin is the most important person in the world to me and I still find it hard that instead of spending our lives together she is left feeling isolated in a home where she is the youngest person by many years. I see her every day, but I miss her terribly and feel so guilty every time I leave her there.
Before Kristin became ill we had never considered that we might one day rely on carers, which terrifyingly made us realise this could happen to anyone – young or old. What is important is that we have a system that makes sure people get looked after in the way they want because that’s the very least we all deserve.
Page 254 of 324
The LGA green paper for adult social care and wellbeing | 23
Sandy’s storyMum was diagnosed with dementia in her early 70s. Dad cared for her at home for many years until the stress became too much and he had a heart attack. We then tried to access home assistance from the local council, but this proved impossible.
The only real option was to move Mum into a care home. Dad sold the family home and bought a small bungalow nearby. We all contributed to the top up fees for over seven years, amounting to hundreds of thousands of pounds. We then tried to access NHS funding for Mum, who was by now in an advanced stage of dementia. [She was] doubly incontinent, no longer able to communicate verbally and unable to feed or dress herself. The funding was refused. We couldn’t understand why.
Eventually we negotiated social care funding for Mum. However, the amount the council pay is significantly less than the fees charged. This subsidisation by private payers is another example of a system riddled with inequalities.
Our Mum is elderly, vulnerable and unable to vote. She no longer has a voice and has become effectively disenfranchised. So we must speak for her and others like her. Society is judged by its treatment of the elderly and this state of affairs is nothing less than shameful. Dementia is an illness. We cannot throw our hands up and say it’s all too difficult.
Governments can no longer turn a blind eye and say we can’t afford it. We have to act now to ensure that people affected by dementia are treated fairly and properly. We must fund a social care programme which will allow the most vulnerable in our society to be cared for in an environment which allows them to live with dignity. Government must step up to the plate and be honest with the electorate.
This situation is not going to go away. Everyone affected by dementia, either those living with the disease or their carers and relatives, deserves so much better.
Page 255 of 324
24 | The lives we want to lead
What adult social care and support desperately needs: sustainable funding for the long-term
Steve’s story I was living with my partner, running a B&B when I had a serious stroke and later two minor heart attacks. After four months in hospital, I was depressed, frail and my memory and cognition had deteriorated.
We knew I needed more support with daily living than my partner could provide. I was unable to return home and it made me frightened about my future, with clinicians uncertain about my further recovery.
I wanted to live locally, so I could continue seeing my partner and I missed my dogs. The Shared Lives scheme matched me, with two trained and approved Shared Lives carers who shared my sarcastic sense of humour, had dogs, and lived close by. They helped me through it all. When I arrived at their home, I never dreamt of being so independent again. I couldn’t walk down the drive. Now I can nip up to town.
My Shared Lives carers helped me gain strength and confidence, walking a little bit further each time, until I could walk independently again. They helped me adapt to my memory loss with strategies for managing money and banking, and supported me to make meals and manage my diet.
Since then I have booked a holiday and travelled on my own. I am very optimistic about life and planning a move into my own flat.
Without the Shared Lives scheme I would have undoubtedly spent longer in hospital, had less choice about where I lived, and had a slower recovery. It is so important that money is available to ensure that schemes like this exist.
Page 256 of 324
The LGA green paper for adult social care and wellbeing | 25
Lucy’s storyMy daughter Lucy has a learning disability and spent 12 years in hospital after being sectioned under the Mental Health Act.
Lucy went through a very stressful time in her life which was when things started to go wrong for her. This caused her to suffer from severe anxiety. She began having more epileptic seizures. When she was hospitalised, we struggled to get her out. As a family, we didn’t know what to do or where to get help. After 12 long years Lucy came out of hospital, supported by the local commissioner and a care and support provider who worked with Lucy and us to plan what she needed and wanted from her life.
They worked with us and Lucy while she was in hospital and supported her transition back into the community. They really helped us to know what was possible. They really listened to us.
Lucy now lives in her own bungalow, close by to us. She is supported by a staff team that she chose and who are trained to support her in a way that works for her.
When she first came home she was very shy and didn’t go out much. Now her confidence has really grown and Lucy has joined the empowerment steering group for the Transforming Care programme, to help improve services and support for people with a learning disability, autism or both. She is learning to travel independently and loves to do the things that we all take for granted – like going out and about,
visiting us but most importantly her niece, and looking after her cat, Smudge.
Good support is about saying that people have a right to a good life in the community with the right support. Lucy is doing really well, but there are always worries in the back of your mind that something will change and the support might stop or get less. We need to recognise that good support now will prevent more expensive hospital stays down the line.
Page 257 of 324
26 | The lives we want to lead
“Local government has many responsibilities but none more core than creating places that are inspiring of good health, leading improvements for local people, encouraging businesses to grow and creating jobs that local people can get. By being ambitious for the health of local people they can create years full of life as well as life full of years.”Duncan Selbie, Chief Executive, Public Health EnglandLGA think piece series, 2018
Key points:• We are best able to live the life we want to
live if we are independent, well and live in communities that support and encourage the many aspects that make us unique
• This is true for everyone but the support we may need is unique to us as individuals and must therefore be personalised
• Local government exists for this very purpose, affecting multiple dimensions of our communities and lives, throughout our lives
• Supporting and improving people’s mental and physical wellbeing is at the heart of local government’s work and that of many other local public, private and voluntary sector organisations. It can only be delivered with communities
2. Delivering and improving wellbeing
“I am very optimistic about life and planning a move into my own flat” Steve’s story
Page 258 of 324
The LGA green paper for adult social care and wellbeing | 27
Our lives are precious and unique and we want to live them as we each see fit.
For the benefit of those who need support to live the life they want to lead, we must start by asking the individual person, ‘What matters to you?’ rather than ‘What is the matter with you?’ However, starting the conversation this way, with the right question and full emphasis on personalisation, means little if we do not have what is required to act on the answer.
Acting most effectively means changing our model of care and support from one which tries to treat the ever-growing burden of long-term conditions and illness caused by demographic and lifestyle factors – doing to the person – to one which helps people maximise their health, wellbeing and independence for as long as possible – doing with the person at all stages of their life. Changing the model in this way requires an equal partnership between local political, clinical, professional and community leaders in which each area develops its own vision and range of services to suit their own unique local circumstances.
Many services support the process of wellbeing. The police service deters, detects and deals with crime. The NHS treats us when we are ill. Our education system helps us learn and be curious. But as essential as these services are, they ultimately only really focus on one element of our lives. And while we alone tend to shape our own aspirations, it is the places in which we live, grow, work and relax that give us opportunities for fulfilling lives and the confidence that the choices we make will result in safe, quality and rewarding experiences.
Local government helps shape the fullness of the places in which we live. From the mix of shops on our high street to the removal and recycling of waste, councils lead and engage with their communities to deliver more than 800 services. This helps keep every aspect of our communities running and improving for the benefit of all people.
Because our lives do not start and stop, neither do councils. Local government services operate both in the background of all our lives and more at the forefront of others’. Councils support people at some of the happiest moments of their lives and some of the hardest.
Page 259 of 324
28 | The lives we want to lead
At the heart of every council’s relationship with its local population is a commitment to improving people’s physical and mental wellbeing. This is a tradition that can be traced back through the decades as local efforts have pieced together to improve our nation’s wellbeing. In more recent times it found expression in the 2014 Care Act, which cemented the idea that a council’s general responsibility in respect of the legislation is to promote an individual’s wellbeing. Helpfully, this was defined in broad terms, recognising that a person’s wellbeing is shaped as much by their participation in work and their personal relationships, to name but two examples, as it is by the practical support they may need with daily tasks such as washing, eating and dressing.
In this way, wellbeing cannot and should not be the preserve of adult social care and support alone. If we are serious about preventing ill health we need a strong public health offer. If we are to help people remain independent at home we need the right kind of housing and neighbourhoods. If we are to encourage physical activity we need vibrant leisure and recreation amenities. If we are to combat loneliness we need reliable transport links, a diverse and resilient community and voluntary sector, and comprehensive employment services. If we are to support people’s mental wellbeing we need to build safe and inclusive communities. The list could easily continue.
Wellbeing goes well beyond local government. The essential input from the local voluntary sector, the care provider market and its workforce and the local NHS all have a clear and fundamental role to play in creating local places where wellbeing can thrive. It is precisely because this is a local endeavour that councils, as democratically accountable local leaders of place, are perfectly positioned to marshal all local aspiration and resources around a common vision for a population’s wellbeing and independence.
CONSULTATION QUESTION:
1. What role, if any, do you think local government should have in helping to improve health and wellbeing in local areas?
Page 260 of 324
The LGA green paper for adult social care and wellbeing | 29
“Adult social care…matters because it’s fundamentally about the business of protecting people’s rights as individuals.”Lyn Romeo, Chief Social Worker for AdultsLGA think piece series, 2018
“What is clear to me is that local government in general and social care in particular have the advantage of being close to communities, being of those communities and able to take decisions where consequences are clear to us because of our perspective and our roots.”Glen Garrod, President, ADASSLGA think piece series, 2018
Key points:• Social care and support matters to individuals,
our communities, our NHS and our economy
• The local dimension of social care matters because it ensures the service is accountable to local people
• Despite a challenging financial environment, social care has delivered – it has improved and innovated
• While diversity of local care and support is the positive result of a health and care system that is responsive to the diversity of the community it serves, unwarranted variation in quality, access and outcome is not acceptable. Local government is committed to addressing this and is best equipped to lead improvement.
• Significant reductions to councils’ funding from national government is now jeopardising the impact local government can have in communities across the country
• In particular, the scale of funding pressures within adult social care threatens progress made to date and now risks people’s wellbeing and outcomes and the stability of the wider system
• There are continuing recruitment and retention challenges in the adult social care workforce
• The Care Act remains the right legal basis for social care but funding pressures are threatening the spirit and letter of the law
3. Setting the scene – the case for change
Page 261 of 324
30 | The lives we want to lead
Why does adult social care matter?
Living the life we want to lead
The first publication in the LGA’s recent think piece series5 on the future of adult social care and support posed the question: why does social care matter? A clear picture emerged from across our expert contributors that the core value of social care lies in supporting people of all ages, with a range of mental and physical health conditions and needs, to live with maximum opportunity, independence, connection to others and control. This is the core value of adult social care and support: it helps people to live the lives they want to lead, building on their own aspirations.
A service that we are all connected to
One in five people have some contact with the social care and support system. That might be as part of its workforce, as a user of services, or as one of the millions of invaluable unpaid carers6. Therefore, while you might not need care now or in the future, you are almost certainly going to be connected to it because of those around you.
5 https://www.local.gov.uk/about/campaigns/towards-sustainable-adult-social-care-and-support-system
6 https://www.adass.org.uk/media/4475/distinctive-valued-personal-adass-march-2015-1.pdf
7 https://voluntarycommunitysocialenterprisereview.files.wordpress.com/2018/05/vcse-review-action-plan-may-2018.pdf
Connecting communities
Social care is also a vital piece of the puzzle that is needed to hold our communities together, making connections to other council services and those provided by local partners. This can help create a network of local support that enables people to be themselves and to fully participate in and contribute to their communities. In the process, this makes those communities more resilient and sustainable; more human.
Links to voluntary, community and social enterprise (VCSE) organisations are particularly important. For instance, the Joint VCSE Review initiated by the Department of Health and Social Care, Public Health England and NHS England notes that:
“There is wide agreement that community organisations, charities and social enterprises are key to establishing a more community-based health, care and public health system which will help people live well, longer and at home, rather than spending long periods within health and care services. They are particularly vital to groups and communities which experience health inequalities and are currently less well reached and supported.7”
“Good support is about saying that people have a right to a good life in the community with the right support” Lucy’s story
Page 262 of 324
The LGA green paper for adult social care and wellbeing | 31
The Review pointed to two key system shifts. First, towards greater personalised care and the building of wellbeing and resilience through co-designing health and care systems with citizens and communities. And second, a bigger and more strategically resourced role for VCSE organisations “which thinks and acts whole-person, whole-family and whole-community”8.
Sustaining our NHS
Social care is also central to the fortunes of our NHS and managing pressures on our hospitals in particular. Care and support, and its links with primary care and public and community health, helps keep numbers at the front door of hospitals down. For those who require time in hospital, that same support in the community helps keep the back door open so people can return home in a safe and timely fashion. Latest statistics for May 2018 show that delays leaving hospital due to social care are down by 39 per cent since July 20179. To put that into perspective, delays due to the NHS are down 13 per cent over the same period.
8 https://voluntarycommunitysocialenterprisereview.files.wordpress.com/2018/05/vcse-review-action-plan-may-2018.pdf
9 https://www.local.gov.uk/about/news/lga-responds-latest-delayed-transfers-care-figures-9
10 https://www.skillsforcare.org.uk/About/News/News-Archive/Adult-social-care-employers-contribute-46-billion-to-the-UK-economy.aspx
11 https://www.carersuk.org/for-professionals/policy/policy-library/valuing-carers-2015
12 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/664563/industrial-strategy-white-paper-web-ready-version.pdf
Supporting our economy and productivity
Finally, the scale of social care is huge. It comprises more than 20,000 organisations and a workforce of more than 1.5 million. Skills for Care estimates that the sector contributes £46 billion annually to the UK economy (£38.5 billion to the English economy)10 and independent care providers are an integral part of many local economies and a driver of employment and local economic growth. Carers UK estimate that the economic value of the contribution made by unpaid family carers in the United Kingdom is a staggering £132 billion a year, more than annual spending by the NHS11.
Supporting people’s wellbeing has wider benefits for our economy. As the Government’s Industrial Strategy notes, “Innovation in age-related products and services can make a significant difference to UK productivity and individuals’ wellbeing”12.
“People like me, who were professionals and could make a contribution with the right support, are being cut out of the workforce” Josie’s story
Page 263 of 324

32 | The lives we want to lead
The Strategy’s ambition to create “an economy that works for everyone, regardless of age” must recognise the link between good health and greater economic participation – both as workers and consumers. The percentage of people aged 65+ who work has risen to 10.4 per cent from 6.6 per cent since 199213 and people aged 65+ contributed or spent £37 billion to the UK hospitality sector in 2015 (27 per cent more than people aged 35-54)14. If everyone worked for a year longer, GDP would rise by 1 per cent15. More broadly, it is estimated that grandparents now provide up to 40 per cent of childcare, enabling their children to pursue their careers without restriction from prohibitive childcare costs16.
The focus must not be confined to older people. Demographic trends do not just forecast a growing elderly population but a growing number of working age adults with learning disabilities, mental health problems or long-term conditions who will need adult social care and support for them to lead independent productive and fulfilling lives. Putting the right support in place
13 https://www.local.gov.uk/sites/default/files/documents/22.11%20Healthy%20Ageing_web_0.pdf
14 https://www.barclayscorporate.com/content/dam/corppublic/corporate/Documents/AgeingPopulation/Ageing-Population-North-West.pdf
15 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/32172/10-1047-default-retirement-age-consultation.pdf
16 https://www.local.gov.uk/sites/default/files/documents/22.11%20Healthy%20Ageing_web_0.pdf
17 https://www.citizensadvice.org.uk/Global/CitizensAdvice/Families%20Publications/Halvingthedisabilityemploymentgap.pdf
18 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/658145/thriving-at-work-stevenson-farmer-review.pdf
to help tackle the disability employment gap – the difference between employment rates of disabled (49 per cent) and non-disabled people (80 per cent)17 – would support working age disabled people into meaningful employment and contribute to local economies. Just as important is supporting people with a mental health condition to remain in, and thrive at, work. The 2016 Stevenson and Farmer review noted that, “300,000 people with a long-term mental health problem lose their jobs each year”. The review found that, “The cost of poor mental to government is between £24 billion and £27 billion” (costs associated with providing benefits, loss of tax revenue and costs to the NHS) and that, “the cost of poor mental health to the economy as whole is…between £74 billion and £99 billion a year”18. Neither should we just consider the national picture. Locally, and particularly in areas with lower employment rates and lower economic output, the care sector is a major and vital employer of local people who, in turn, support the local economy.
Page 264 of 324
The LGA green paper for adult social care and wellbeing | 33
A locally led service
When it comes to the importance of social care being a local service, expert contributors to our think piece series were equally clear that ‘local’ matters. At the heart of this principle lies the greatest strength of local government: its democratic accountability to the people it serves. As all communities are different and require a unique arrangement of services, the importance of local accountability cannot be overstated.
Recent LGA polling on resident satisfaction shows that councils are the most trusted form of government to make local decisions about services in a local area, selected by 72 per cent of respondents. Just 17 per cent of respondents selected national government. Similarly, local councillors were selected by 68 per cent of respondents as the individuals most trusted to make decisions about local services. By comparison, 13 per cent of respondents selected MPs and just 7 per cent selected government ministers19.
CONSULTATION QUESTIONS:
2. In what ways, if any, is adult social care and support important?
3. How important or not do you think it is that decisions about adult social care and support are made at a local level?
19 https://local.gov.uk/sites/default/files/documents/research%20-%20Resident%20Satisfaction%20Polling%20Round%2020%20-%2025%20july%202018.pdf
20 https://www.adass.org.uk/media/6434/adass-budget-survey-report-2018.pdf
Social care innovation and improvementDespite a challenging financial environment, adult social care and linked services have worked hard to continue to deliver, improving people’s lives in a number of ways.
Prioritising care and support: Between 2010 and 2017, adult social care has had to make savings and reductions worth £6 billion as part of wider council efforts to balance the books. But the service continues to be protected relative to other services. The latest ADASS budget survey shows that adult social care accounts for a growing total of councils’ overall budgets, up from 36.9 per cent in 2017/18 to 37.8 per cent in 2018/1920. As a result, by 2019/20, 38p of every £1 of council tax will go towards funding adult social care.
Innovating: Councils are committed to innovation to help reduce costs while maintaining or improving services to the public. This has included changing the way that demand is managed, more effectively using the capacity in communities to help find new care solutions, and working more closely with partners in the NHS to reduce pressures in the care and health system. Innovative approaches can be found in all parts of the country.
Page 265 of 324
34 | The lives we want to lead
Intervening early and preventing needs: Investing in prevention has clear benefits for people and reduces costs to the wider care and health system. There is a great deal of work across the country to help people avoid unnecessary hospital admission and support to increase people’s independence.
Performing: Even in the deeply challenging financial environment in which the wider social care sector has operated over the last few years, there are many instances of performance having been maintained or improved. This includes performance on satisfaction levels, adults with a learning disability living in their own home or with family and the proportion of people using services who say they feel safe and secure.
A range of case studies demonstrating the work of councils and their partners on the above areas can be found at Annex A. These illustrate the significant improvements and innovations which the social care sector has delivered, despite the most challenging circumstances. It is a sector worth investing in.
21 See Industrial Strategy White Paper – Healthy Ageing Grand Challenge
22 Care Quality Commission, Beyond Barriers 2018
The role of digital and technologyWe increasingly live in a connected and digital society. Of course, digital and care-related technology is not on its own the solution to addressing our adult social care or public health related challenges and it is not a replacement for person-centred care and support.
However, better use of data in adult social care offers the potential for more preventative and personalised approaches to care to be established, and emerging technologies offer the potential for new business models to flourish amongst providers of care whether they be large or micro care providers21. Councils have an important role to play in shaping their care market and areas such as Liverpool and Luton are collaborating with care providers to support innovation.
Digital approaches are enabling valuable time of our workforce to be freed up, allowing them to spend more time with those they are supporting whilst at the same time improving the quality of care.
It has the potential not only to enable staff to more effectively communicate with one another (helping to address the quarter of care providers who say the quality of information they receive on discharge is not sufficient22) but also reduce the chances that people have to tell their story multiple times by joining up information from organisations. Progress has been made but still
Page 266 of 324
The LGA green paper for adult social care and wellbeing | 35
only three in 10 councils say that they have the information they need from health partners23.
Technology has the potential to help people live more independently for longer, supporting the focus on prevention. Many of us are increasingly adopting smart technologies around the home and increasingly homes are being designed in a way that can both meet but also adapt to our everyday needs.
Understandably, people’s expectations are increasing. People want to be able to make quicker and more informed decisions about their care choices which means providing the right information at the time they need it.
At the same time people want to be more in control. This might include giving people more opportunities to easily request the support they need and manage their personal budgets (such as in Harrow) or allow some of the worry to be taken out of caring by giving much more useful and timely information to those in a caring role.
Of course, digital is not right in every situation and where it is introduced it needs to remain person-focused, building trust with individuals. This means starting by understanding the aspirations and needs of individuals and co-designing approaches with them. Councils such as Salford are working with local organisations to support the city’s most vulnerable.
23 LGA Digital Self-Assessment with councils 2017
24 www.local.gov.uk/scdip
The 2016 LGA publication ‘Transforming social care through the use of information and technology’ provides evidence from across the country of how both social care and public health are designing approaches that incorporate aspects of digital and data – not only saving money but importantly delivering better outcomes for individuals, carers and the workforce.
But as our green paper demonstrates there is still a significant way to go and only with much needed sustainable investment alongside local leadership can existing good practice be extended. Our LGA innovation programme in social care24, funded by NHS Digital, demonstrates examples of where councils are co-designing approaches that use digital and data. However, these small-scale funding initiatives whilst helpful are not sufficient. The national priority being given to data and technology needs to be re-balanced and show a greater commitment to support local but scalable innovation in adult social care helping to address the systemic challenges that the sector is currently experiencing.
Page 267 of 324
36 | The lives we want to lead
The need for continuous improvementWhilst there is a huge amount of impressive work going on across the country, there is much more we can do to improve, even within existing funding arrangements. Polling suggests that the public remain concerned about achieving a consistent standard of care both in social care and the NHS, and preventing a ‘postcode lottery’. Variation in itself is not a bad thing; diversity of care and support is needed to address the diversity of different communities, and it would be wholly wrong to suggest that every area should have exactly the same set of priorities or range of services for their local population. But nobody wants to see radically different experiences of, or access to, services based solely on where you live rather than on what you need and want. This is one of the reasons that the Care Act introduced a national eligibility framework, to ensure that people across the country are entitled to care on broadly consistent criteria.
There is little evidence that running services nationally makes them more uniform than services planned and delivered locally. The idea that more national systems and approaches would necessarily help eradicate unwanted local variation is flawed: it could exacerbate inequalities which only a highly localised response can address. As is any notion that local government is more variable than other public services. Within the NHS for instance, there is still very significant variation in access, quality and outcomes, including delayed transfers of care attributable to the NHS, Continuing Healthcare eligibility, the rate of patient safety incidents and
25 https://www.parliament.uk/documents/commons-committees/liaison/Prime-Minister-oral-evidence-session-transcript-20-12-2017.pdf
26 https://www.webarchive.org.uk/wayback/archive/20070428120000/http:/www.lyonsinquiry.org.uk/submissions/20060308%20National%20Audit%20Office%20Response%20to%20Interim%20Report.pdf
the availability of IVF treatments. More broadly, variability is not unique to the public sector and is instead an inevitable feature of life. The accessibility and availability of banks, shops, transport connections and restaurants is part and parcel of what makes every area different.
We need a system in which variation reflects positive choices in local areas to reflect local needs and wishes, and to build communities that are inclusive, cohesive and promote the life chances of everyone within them. Councils’ bespoke solutions to local challenges also allow greater space for innovation and improvement to flourish, which is harder to achieve with national-level services. Local investment decisions help change the way things are done on the ground, creating services and partnerships – particularly with the voluntary sector – that benefit our communities. It is no coincidence that many national programmes start from best practice from within local government.
The Prime Minister rightly wants best practice to be shared25. And councils are keen to embrace learning through sector-led improvement, and have welcomed the findings of the CQC reviews of health and care systems. However it would be wrong to presume that a mandatory national inspection programme of council commissioning would necessarily improve matters. Local government has worked with Government to develop its own sector-led improvement approach and it has been shown to be more cost effective than national inspection. The National Audit Office estimates that the cost of the previous top down inspection regime was in excess of £2 billion annually26 whilst the LGA receives just 1 per cent of that to facilitate its wider improvement support in councils. Large
“What is important is that we have a system that makes sure people get looked after in the way they want because that’s the very least we all deserve” Glyn and Kristin’s story
Page 268 of 324
The LGA green paper for adult social care and wellbeing | 37
parts of the previous inspection regime were abolished by Government in 2010 due to the expense. Sector-led support also delivers good results, with 95 per cent of chief executives and 96 per cent of leaders saying that it has had a positive impact on their authority27.
We recognise that the public expect, and have a right to, a consistent level of access, quality and effectiveness of care and support. Councils, working alongside national and local partners, are identifying where unacceptable variation exists and taking steps to tackle it. Local government is committed to working with national government to build on this work, and the sector-led improvement approach that underpins it, to ensure that any new funding for social care is used effectively. Examples of this work are set out below.
Working together for a system-wide focus
• Local government political and professional leadership increasingly recognises that significant improvements to people’s wellbeing cannot be made by just focusing on their part of the health and care system. The recent focus on delayed transfers of care (DTOC) attributable to adult social care is a case in point. Research undertaken for the LGA by Newton Europe28 into DTOCs attributable to
27 http://lga.moderngov.co.uk/documents/s17081/LGA%20Perceptions%20Survey%202017-18.pdf
28 https://www.local.gov.uk/our-support/our-improvement-offer/care-and-health-improvement/systems-resilience/resources/emerging-practice
social care in 17 health economies found that focusing on just one part of the system risks either ignoring underlying causes of the blockage or simply shifting pressure elsewhere. The work found that the best way to help patients through discharge is to ensure the focus on their longer term recovery. DTOC is a symptom of system malfunction, not of itself a root cause. Put the patient first and the rest will follow.
• The CQC local system reviews made a similar finding in relation to managing the flow of older people from community settings into hospital and back again. It found that the key driver to overcoming barriers to effective joined up working was local leaders sharing a clear vision to provide a shared purpose for people and organisations across the local health and social care system. Fragmented and separated systems for local government and social care get in the way of person-centred and place-based working. In particular, separate financial frameworks, performance management regimes, workforce planning and regulatory frameworks for the NHS and local government make it difficult to work together. We would welcome the continuation of these cross-sector reviews alongside a sector-led improvement approach to adult social care.
Page 269 of 324
38 | The lives we want to lead
System leadership
• Some health and wellbeing boards (HWBs) are the driving force for transforming care and support in local communities. They bring together political, health and community leaders to agree a vision and a shared approach to health and wellbeing which addresses the challenges facing their care and health systems. But others are not providing clear leadership and direction. We recognise that if they are to maintain their status as leaders of place, all health and wellbeing boards need to be effective. A key strand of our improvement work focuses on strengthening HWBs in this respect, equipping council leaders with the tools they need to work alongside clinical and community counterparts.
29 https://www.local.gov.uk/icbo
Integrated commissioning
• Councils recognise the importance of strong commissioning and are taking steps to ensure this drives improvement. Building on our framework for commissioning for better outcomes in social care, we are working with councils to focus on Integrated Commissioning for Better Outcomes29. A future model of social care will need to continue to develop and strengthen integrated commissioning.
Shaping the local care market
• Market Position Statements (MPS) are a requirement of the Care Act and encourage commissioners, people who use services, unpaid carers and providers to come together to consider what care and support services are needed in an area, why, and how they might be delivered. Councils recognise the value of MPSs and the need to ensure their robustness and quality.
• The LGA is working with councils and providers to develop the next generation of MPSs that focus much more on: the services needed in a local area; how they can support people to stay out of hospital and live independently at home; support to providers to recruit, retain and develop the care workforce.
CONSULTATION QUESTION:
4. What evidence or examples can you provide, if any, that demonstrate improvement and innovation in adult social care and support in recent years in local areas?
Page 270 of 324
The LGA green paper for adult social care and wellbeing | 39
Improving system-wide performance and effectiveness
• All of our work on systems has the primary objective of supporting councils to work with all relevant local partners to help keep people out of hospital and, if they do need inpatient care, return them to their communities and full independence as far as possible.
• An example is the Transforming Care Partnership, which helps ensure that more people with complex learning disabilities are moving from secure Assessment and Treatment Units to better placements in their own community near family and friends.
Data sharing
• Councils increasingly recognise the need for sound data sharing across health, social care and providers to deliver person-centred care and the role of technology to improve integration, efficiency and commissioning.
Support to challenged areas
• Some areas face a particularly challenging financial environment and require expert support to steer their way through to steadier and more stable times. We have worked with 20 such areas to address real and present financial problems. This is our fastest growing area of support.
• Other areas need support to deliver efficiencies, particularly in learning disability and mental health services, and a range of work is being taken forward to help councils to manage demand.
• As financial circumstances become ever strained, more areas are identifying the need to be better prepared on contingency planning in the event of large scale provider failure. Most councils are experiencing contract hand backs, but the risk of large scale failure is increasing as evidenced by the changing numbers in CQC’s market oversight regime.
Managing risk
• More generally, councils recognise the need to be smarter and more nimble at managing risk. All councils have used our risk tool in some form to aid their understanding of risk in key areas including leadership and governance, performance, quality, resources, workforce and delivering national priorities.
Page 271 of 324
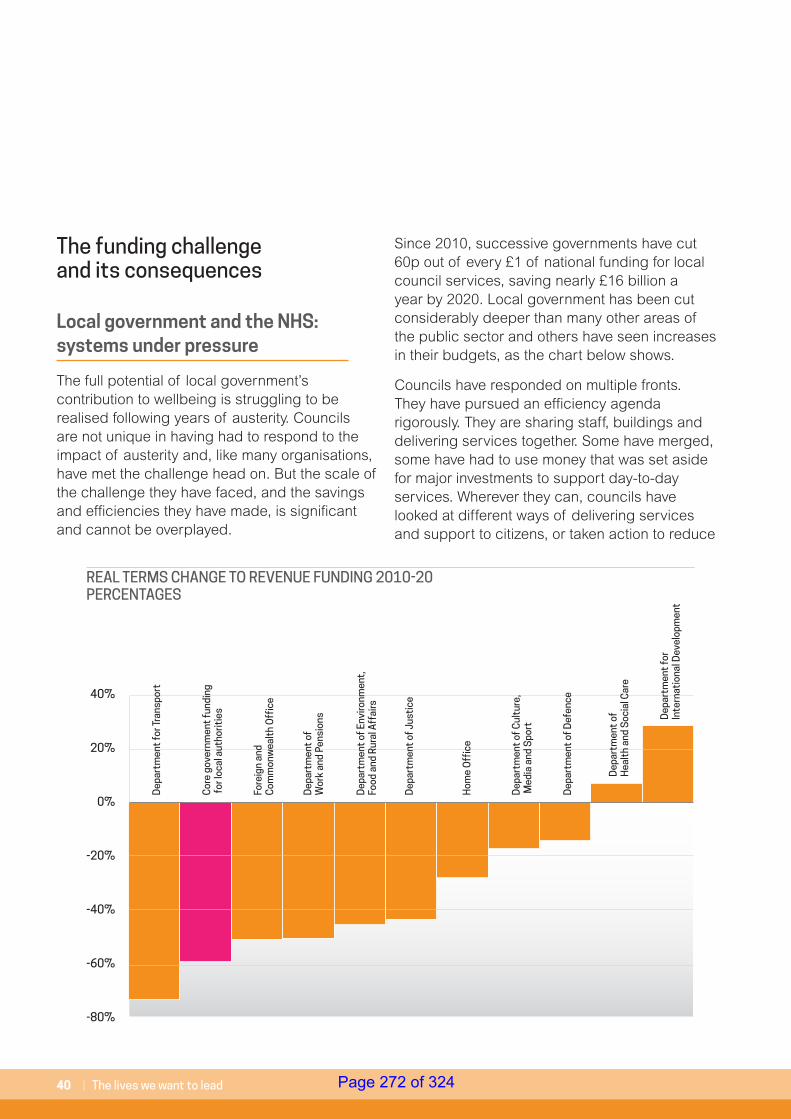
40 | The lives we want to lead
The funding challenge and its consequences
Local government and the NHS: systems under pressure
The full potential of local government’s contribution to wellbeing is struggling to be realised following years of austerity. Councils are not unique in having had to respond to the impact of austerity and, like many organisations, have met the challenge head on. But the scale of the challenge they have faced, and the savings and efficiencies they have made, is significant and cannot be overplayed.
Since 2010, successive governments have cut 60p out of every £1 of national funding for local council services, saving nearly £16 billion a year by 2020. Local government has been cut considerably deeper than many other areas of the public sector and others have seen increases in their budgets, as the chart below shows.
Councils have responded on multiple fronts. They have pursued an efficiency agenda rigorously. They are sharing staff, buildings and delivering services together. Some have merged, some have had to use money that was set aside for major investments to support day-to-day services. Wherever they can, councils have looked at different ways of delivering services and support to citizens, or taken action to reduce
40%
20%
0%
-20%
-40%
-60%
-80%
Dep
artm
ent
for T
rans
port
Cor
e go
vern
men
t fu
ndin
g fo
r loc
al a
utho
ritie
s
Dep
artm
ent
of
Wor
k an
d Pe
nsio
ns
Dep
artm
ent
of J
usti
ce
Dep
artm
ent
of E
nviro
nmen
t,
Food
and
Rur
al A
ffai
rs
Fore
ign
and
Com
mon
wea
lth
Off
ice
Hom
e O
ffic
e
Dep
artm
ent
of C
ultu
re,
Med
ia a
nd S
port
Dep
artm
ent
of D
efen
ce
Dep
artm
ent
of
Hea
lth
and
Soc
ial C
are
Dep
artm
ent
for
Inte
rnat
iona
l Dev
elop
men
t
REAL TERMS CHANGE TO REVENUE FUNDING 2010-20 PERCENTAGES
Page 272 of 324
The LGA green paper for adult social care and wellbeing | 41
demand rather than making cuts. But against the scale of the reduction outlined, these efforts can only go so far. As the Public Accounts Committee has noted, “The harsh reality is that more and more local authorities are now showing signs of financial stress”30. Today, more councils are struggling to balance their books and some are considering whether they have the funding to even deliver their statutory requirements. Put simply, councils no longer have the resources to support people in their communities31.
The local government funding position has serious consequences for wellbeing. It constrains adult social care which, in turn, constrains the voluntary sector and care providers. This is happening now and impacting on people’s quality of life today. The response has been to protect social care relative to other council services. But those other services are crucial to support people’s wellbeing, such as bus services, libraries and road maintenance. In this way, sorting out the long-term funding of adult social care therefore goes hand-in-hand with helping to sort out the long-term funding of local government. And that can only help improve people’s wellbeing.
The NHS is also struggling. A report by NHS Providers shows that community health services are also under pressure. More than half of community trusts surveyed (52 per cent) for the report believed funding had fallen this financial year and 82 per cent were worried that community health services would not receive the investment needed to realise the ambitions of the Five Year Forward View32.
30 https://publications.parliament.uk/pa/cm201719/cmselect/cmpubacc/970/970.pdf
31 For further information visit: https://www.local.gov.uk/sites/default/files/documents/Moving%20the%20conversation%20on.pdf
32 http://nhsproviders.org/state-of-the-provider-sector-05-18
33 https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Understanding-GP-pressures-Kings-Fund-May-2016.pdf
It is a similar picture with GPs with the King’s Fund noting that:
“General practice is in crisis. Workload has increased substantially in recent years and has not been matched by growth in either funding or in workforce…Funding for primary care as share of the NHS overall budget fell every year in our five year study period.33”
As social, community health and primary care face growing pressure, wellbeing deteriorates. As a result, people increasingly seek to have their needs met by turning to the part of our public sector which has arguably been protected from the full force of austerity: hospitals. But targeting investment primarily at the acute sector represents poor investment of public money. And more importantly, it is a poor outcome for most people needing care and support. The argument is bigger than simply saying we spend too much on hospitals. It is about arguing for investment for prevention across the wider system – social care, public health, the third sector and parts of the NHS – as part of a truly system-wide approach to embedding prevention and early intervention within our communities and in everything we do. Good investment and good outcomes for people requires a focus on these communities, ensuring people have the care and support (in the broadest sense) they need to live a good life – to be well, independent, living at home for as long as possible and contributing to family and community life.
“I am only too aware that every minute I spend with paramedics is taking this costly service away from someone else who needs it, but I am left with no choice” Vicki and Keegan’s story
Page 273 of 324
42 | The lives we want to lead
Adult social care funding
As with local government overall, adult social care funding is at its absolute limit, threatening the great progress that has been made in challenging circumstances. Innovation, prevention and performance may be some of the hallmarks of the last few years as social care has sought to insulate itself from the full impact of austerity. But looking ahead, the scope to continue in this way is greatly reduced.
New research by the LGA shows that local government overall faces a funding gap of £7.8 billion by 2025, just to sustain current – and much reduced – levels of service. This includes, within adult social care, an immediate and annually recurring market provider gap of £1.44 billion; the difference between the estimated costs of delivering care and what councils pay. As demography, inflation and National Living Wage pressures build in subsequent years, the adult social care gap rises to £3.56 billion by 202534. And again, this is purely to stand still. To put this in perspective, this is more than five times the amount spent annually on councils’ park services, and close to the total cost of councils’ waste management for a year (£3.6 billion). The short-term funding gap must be closed as an urgent priority and as an initial step in securing the sustainability of care and support.
34 https://www.local.gov.uk/sites/default/files/documents/Technical%20Annex%20%281%29.pdf
35 https://www.adass.org.uk/media/6434/adass-budget-survey-report-2018.pdf
Governments’ response to the challenge of adult social care funding in recent years has been short-term and incremental in nature. One-off grants, the council tax precept for social care and increases in improved Better Care Fund funding have been helpful. But each mechanism has its limitations and they have not been sufficient to deal with all short-term pressures, let alone address the issue of longer-term sustainability. They also cease in 2019/20 with no clarity from 2020 onwards, which makes even short- and medium-term planning extremely difficult.
Furthermore, the major Government narrative and focus of attention has been on services to support older people, largely overlooking the fact that much of the growth in cost pressures comes from the increasing needs of working age adults. As the ADASS budget survey35 shows, services for working age adults now account for 58 per cent of the demographic pressure on social care budgets, including 39 per cent relating to services for people with a learning disability. The demographic pressure relating to older people accounts for 42 per cent of total pressure. This might explain why the proportion of directors most worried about the financial pressures relating to services for working age adults has doubled since last year to 32 per cent and compares to only 12 per cent who are most worried about services for older people.
Page 274 of 324
The LGA green paper for adult social care and wellbeing | 43
The council tax precept is not a sustainable solution. First, it shifts the burden of tackling a clear national crisis on to councils and their residents – and this after years of councils being encouraged to keep council tax as low as possible, or frozen. Second, the value of the precept varies greatly based on the strength of a council’s tax base. Areas facing the greatest demand for services are those that are able to raise the least amount of money through the precept.
Already in 2017/18, the adult social care precept was worth 3.8p of every £1 of council tax raised in England. If all councils with social care responsibility used the precept flexibility and the 2.99 per cent core increase in 2018/19 and 2019/20, this would rise to 6.5p of every £1 of council tax. By the same point, councils could be spending as much as 38p of every £1 of council tax on adult social care, up from just over 28p of every pound in 2010/11.
Improved Better Care Fund resources are also problematic. As explored further below, this funding has become subject to an increasing and concerning degree of oversight and influence from both government and the NHS nationally. The funding also stops at the end of 2019/20.
36 https://www.local.gov.uk/sites/default/files/documents/Securing%20the%20long-term%20sustainability%20of%20adult%20social%20care%20%E2%80%93%20Quality%20-%20Andrea%20Sutcliffe%20CBE.pptx_.pdf
The consequences of underfunding in adult social care
The consequences of this immediate and medium-term funding gap will likely include a deepening of the consequences seen to date in a range of areas.
Quality: Latest information from the Care Quality Commission shows a broadly encouraging picture on quality, with more than four fifths of adult social care services in England rated as ‘good’ (79 per cent) or ‘outstanding’ (2 per cent) following inspection. However, a more worrying trend is emerging amongst services that have been re-inspected. For those services previously rated ‘good’, 76 per cent saw no change to their rating, but 18 per cent dropped to ‘requires improvement’ and 3 per cent dropped to 'inadequate'. Amongst those services previously rated ‘outstanding’, 64 per cent saw no change to their rating, 19 per cent dropped to ‘good’, 14 per cent dropped to ‘requires improvement’ and 3 per cent dropped to 'inadequate'. Improving quality is one thing, sustaining it is clearly another and it is becoming harder to achieve36.
Provider market stability: providers of social care are an absolutely vital part of the social care landscape, delivering practical care services with an essential human touch both to self-funders who pay for their own care and those who are funded by their council. But the provider funding gap outlined above, coupled
Page 275 of 324
44 | The lives we want to lead
with new pressures (such as the potential future uncertainty on liabilities for ‘sleep in’ care) is putting providers under impossible pressure. In the last six months, this has resulted in providers ceasing trading across home and residential care in more than 100 council areas, impacting more than 5,300 people. It has also resulted in providers handing back contracts to more than 60 councils, impacting just under 3,000 people37. Providers make these decisions reluctantly, especially having worked with local communities and individuals over many years. These are difficult decisions that are made when the full costs of care cannot be covered. Some providers are having to reduce the amount of their capacity used by local authorities because it is not profitable. They may seek to increase their income from self funders or others, such as NHS commissioners. The impact is a loss of capacity for local authorities and a knock-on impact on their customers and the NHS.
Unmet and under-met need: under the Care Act, councils are required to follow a national minimum threshold for eligibility. This means that there is a single and consistent framework for determining whether a person’s needs are eligible for public support. The level at which this is currently set, combined with the pressures on social care described above, has arguably been
37 https://www.adass.org.uk/media/6434/adass-budget-survey-report-2018.pdf
38 https://www.ageuk.org.uk/latest-press/articles/july-2018/new-analysis-shows-number-of-older-people-with-unmet-care-needs-soars-to-record-high/
39 https://www.ageuk.org.uk/latest-news/articles/2018/july/1.4-million-older-people-arent-getting-the-care-and-support-they-need--a-staggering-increase-of-almost-20-in-just-two-years/
40 Our estimate of the cost uses Age UK figures as a starting point. We take their figure of 164,217 – the number of older people who receive no support with three or more essential daily activities – and assume support for those people based on the profile of existing support for older people in terms of home care and residential care. We then apply unit costs: for home care we cost 1 hour per day; for residential we cost a year of residential care.
41 We apply the same method used for estimating the cost of meeting unmet need amongst older people. However, as we do not have a starting number (equivalent to the Age UK figure of 164,217) we link to the number of working age adults currently receiving services. The number of working age adults supported is roughly 40 per cent of the number of older people supported so we apply that percentage to the Age UK figure and apply working age adult unit costs for home and residential care.
42 https://www.carersuk.org/images/Downloads/SoC2018/State-of-Caring-report-2018.pdf
partly responsible for an increase in unmet and under-met need.
Age UK estimates38 that there are 1.4 million older people who do not receive the help they need. This includes 164,217 people who need help with three or more essential daily activities (such as washing, dressing and going to the toilet) and who receive no help at all from either paid services or family and friends39. As a purely indicative figure, the LGA estimates that if councils were to support this group of 164,217 older people, £2.4 billion additional funding would be needed40. Looking to working age adults, and again purely as an indicative figure using estimates based on broad assumptions set out below, the LGA estimates that addressing unmet need amongst the 18-64 population would require an additional £1.2 billion41. Unpaid carers also experience unmet need. New research by Carers UK shows that one in seven carers (or those they support) received less care or support in the previous year42.
Unmet (and under-met) need is bad for people and can lead to the worsening of their conditions, and the costs involved in meeting them. But more broadly, it is bad for our economy and can lead to a huge loss of economic input. As we set out above, supporting people’s wellbeing plays an important role in helping
“I don’t feel like I’m living, just existing” Josie’s story
Page 276 of 324
The LGA green paper for adult social care and wellbeing | 45
people to be employed, to be active consumers and to be a support for relatives juggling work and family commitments.
Carers: our care system could not survive without the invaluable input provided by unpaid family carers. But as pressures mount on social care, carers shoulder an increasing strain and this impacts on their own physical and mental wellbeing. New research by Carers UK shows that 72 per cent of carers in England have suffered mental ill health (such as stress and depression) as a result of caring and 61 per cent had suffered physical ill health. A clear majority of carers believe their mental (57 per cent) and physical (58 per cent) health will get worse in the next two years43. When an unpaid caring role breaks down, everyone suffers and costs rise. The research by Carers UK also shows that one fifth of carers had not received a carer’s
43 https://www.carersweek.org/images/Resources/CW18_Research_Report.pdf
44 https://www.carersuk.org/images/Downloads/SoC2018/State-of-Caring-report-2018.pdf
45 https://www.skillsforcare.org.uk/NMDS-SC-intelligence/Workforce-intelligence/documents/State-of-the-adult-social-care-sector/2State-of-the-adult-social-care-sector-and-workforce-2017.pdf
assessment in the last year44. The LGA estimates that it would cost an additional £150 million to provide those assessments.
Workforce: like unpaid carers, the social care workforce is at the core of our care and support system. Its scale is significant.
“Adult social care is a growing sector that, in 2016, had around 20,300 organisations, 40,400 care providing locations and a workforce of around 1.58 million jobs. The number of full-time equivalent jobs was estimated at 1.11 million and the number of people working in adult social care was estimated at 1.45 million45.”
Page 277 of 324

46 | The lives we want to lead
But it too is under significant pressure. Skills for Care estimates that the staff turnover rate of directly employed staff working in social care was 27.8 per cent in 2016/17, approximately 350,000 leavers during the year46. This compares to average labour turnover across the economy of 15 per cent, and 13.4 per cent across local government direct employment.
The National Audit Office has shown that the “growth in the number of jobs has fallen behind growth in demand for care” and that, as we set out above, “The failure of formal care to meet this increased demand may have contributed to the growth in individuals’ care needs not being met”47. This trend looks set to continue. Skills for Care forecasts show that if the social care workforce grows proportionally to the increase in the number of older people aged 75 and over, an increase of 44 per cent (700,000 jobs) will be needed48.
This will be challenging. Directors of adult services believe increasing salaries for care workers is the most important factor in recruitment and retention, which will only increase pressures on budgets. Furthermore, pay rises of 29 per cent over the next three years for the lowest paid NHS staff across England will make the challenge even greater. Directors believe a similar pay rise for social care staff would cost an additional £3 billion a year49. But it is not simply a matter of money. As the National Audit Office has pointed out, care work – particularly lower level roles – suffers from negative perceptions and “is viewed by the public as low skilled and offering limited opportunities for career progression50”
46 https://www.skillsforcare.org.uk/NMDS-SC-intelligence/Workforce-intelligence/documents/State-of-the-adult-social-care-sector/2State-of-the-adult-social-care-sector-and-workforce-2017.pdf
47 https://www.nao.org.uk/wp-content/uploads/2018/02/The-adult-social-care-workforce-in-England.pdf
48 https://www.skillsforcare.org.uk/NMDS-SC-intelligence/Workforce-intelligence/documents/State-of-the-adult-social-care-sector/2State-of-the-adult-social-care-sector-and-workforce-2017.pdf
49 https://www.adass.org.uk/media/6434/adass-budget-survey-report-2018.pdf
50 https://www.nao.org.uk/wp-content/uploads/2018/02/The-adult-social-care-workforce-in-England.pdf
In terms of the workforce directly employed by councils, social workers and occupational therapists are key regulated social care professionals in local authority social care departments responsible for ensuring the protection of people’s human rights and promoting safety, inclusion and citizenship outcomes. Social work has one of the highest vacancy rates at 10.8 per cent and a staff turnover rate of 15.6 per cent, and only a third of social work graduates enter adult social care.
Escalating problems: more generally, the underfunding of social care and support results in people’s wellbeing and outcomes deteriorating as their needs rise and go unmet. This can lead to increased loneliness or the worsening of long-term conditions and results in further demand pressures on the NHS.
CONSULTATION QUESTIONS:
5. What evidence or examples can you provide, if any, that demonstrate the funding challenges in adult social care and support in recent years in local areas?
6. What, if anything, has been the impact of funding challenges on local government’s efforts to improve adult social care?
7. What, if anything, are you most concerned about if adult social care and support continues to be underfunded?
Page 278 of 324
The LGA green paper for adult social care and wellbeing | 47
“Government has already done two of the three jobs we need it to do on social care. It has put in place an excellent piece of legislation – the Care Act – that could provide the right enabling framework for a generation. It has also put in place a trusted inspection system with public confidence. Its third task is to properly fund the system and that should be the primary focus of the green paper”Jon Rouse, Chief Officer, Greater Manchester Health and Social Care PartnershipLGA think piece series, 2018
The Care Act: a legal foundation for care and supportSocial care has already been reformed. Between July 2012 and April 2015, the wider social care sector – people with experience of using services, local government, the NHS, providers, the community, voluntary and social enterprise sector, think tanks, academics and the public – came together with Government to help shape a landmark piece of legislation and prepare for its implementation: the 2014 Care Act. This was a model for how laws should be made; collaboratively, with the voices of those who use services front and centre, and with our national politicians and government in genuine listening mode. It is not perfect, no legislation is. But it is close.
It puts people’s wellbeing – broadly defined – at the heart of the Act and stresses the importance of preventing or delaying the development of care needs. It makes a clear link to integration with health in achieving both wellbeing and prevention. It promotes the development of a local provider market offering diverse and quality services for both self-funders and publicly-funded care. It puts unpaid carers on a par with those they care for and embeds person-centred care and personalised approaches to care through the care planning process. It promotes personal budgets and direct payments in order to give people choice and control over their care.
Page 279 of 324
48 | The lives we want to lead
However, in spite of a deep commitment to the legislation, councils are increasingly struggling to even meet the ‘letter’ of the law. In a 2018 survey of adult services directors, just 34 per cent stated that they were ‘fully confident’ in meeting all of their statutory duties in 2018/19. The figure dropped to one in ten in 2019/20, with no director ‘fully confident’ of meeting all statutory duties in 2020/2151. We can and must do better.
Implementing Part II of the Care Act
Despite widespread support for the legislation, the Care Act has not yet been fully implemented, with the Part II reforms to introduce a cap on the amount people might have to pay and an extension to the financial means test limits still waiting to be enacted, partly due to the lack of funding for the system as a whole. The LGA supported the decision, arguing that the funding earmarked for a cap should be used to support the existing social care system before adding new duties and reforms on top of it. Full implementation of the 'Dilnot Cap' as set out in the Care Act is one of the reform options considered in the next section.
51 https://www.adass.org.uk/media/6434/adass-budget-survey-report-2018.pdf
CONSULTATION QUESTIONS:
8. Do you agree or disagree that the Care Act 2014 remains fit for purpose?
9. What, if any, do you believe are the main barriers to fully implementing the Care Act 2014?
Page 280 of 324
The LGA green paper for adult social care and wellbeing | 49
“There’s a great deal for us to be worried about. The good news is that there’s widespread agreement about an urgent need for action. There’s political consensus that something must be done, but the question is what?”Ben Page, Chief Executive and Anna Quigley, Director of Health Research, Ipsos MORILGA think piece series, 2018
Key points:• Social care is becoming a greater public
priority
• The public and politicians (local and national) support greater funding for social care
• People find the social care system complex and confusing, it is hard to understand, particularly for those facing the immediate pressures of requiring care and having to engage with a system they have never encountered before
• People worry about the costs of social care but are not making preparation for them and the rules are not clear
• Although it is hard to define, people want a greater sense of fairness within social care
• There are a number of options for making social care better
• Making these changes will require more funding. There are different ways of raising this
• Cross-party consensus or cooperation must be sought to secure a workable long-term solution
4. The options for change
Page 281 of 324
50 | The lives we want to lead
“The last 20 years have seen at least five independent reviews of social care funding and 12 white papers, green papers and consultations of one kind or another under five governments. It has been a story of delay, dashed hopes and disappointment.”Richard Humphries, Senior Fellow, The King’s FundLGA think piece series, 2018
Why is it so hard to change?
Public support
Many of the most significant problems facing social care are primarily driven by a lack of funding, as set out in the previous chapter. Whilst the Care Act remains a widely supported broad legislative framework, more funding is needed to implement it fully. So why has it proved so hard for successive governments to deliver sustainable long-term funding for this crucial service?
The answer lies partly in how the public view social care, which is linked to the fact it is complex and hard to understand. Adult social care and support is not free for everyone. An individual who thinks they need support through adult social services is assessed by their council to identify their care needs and determine whether or not those needs are eligible. If they are, a separate assessment is made of the individual’s financial circumstances to determine whether they must contribute to the cost of their care.
Page 282 of 324
The LGA green paper for adult social care and wellbeing | 51
Two recent reports are extremely helpful in understanding the public’s concerns: a recent Ipsos MORI report on attitudes to social care funding reform, prepared for the King’s Fund and Health Foundation52; and a report by public participation charity, Involve, summarising the findings of a ‘Citizens’ Assembly’ they held on behalf of the Health and Social Care Select Committee and the Communities, Housing and Local Government Select Committee53.
• A complex and confusing system: People do not have a detailed understanding of social care services and are unsure about how to access them. Participants with experience of social care said the system was complex, bureaucratic and difficult to navigate. Forty-five per cent of Citizens’ Assembly members selected an ‘easily accessible’ system in their top five principles for a reformed system. Thirty-eight per cent of assembly members put a ‘simple clear’ system in their top five.
• Complex and unclear funding arrangements: Unless they have experience of it, people have limited understanding of how social care funding works. Most people think social care is funded similarly to the NHS, through tax, or that an entitlement based on National Insurance contributions will be available. People with no or limited experience of social care are largely unaware that the system is means tested. Upon learning this, many are “shocked”, as they had assumed there is a more generous offer for more people.
52 https://www.ipsos.com/sites/default/files/ct/publication/documents/2018-06/public-attitudes-social-care-funding-reform-ipsos-mori-2018.pdf
53 https://publications.parliament.uk/pa/cm201719/cmselect/cmcomloc/citizens-assembly-report.pdf
• Transparency and fairness: People want more transparency – both in terms of the costs of social care (individually and nationally), and in terms of being able to see where funding for social care is being raised and where it is being spent. On fairness, there are a range of views reflecting the different interpretations of what fairness is. These include fairness to older people who have paid taxes all their lives, fairness in protecting people’s housing assets, fairness between different generations and fairness based on a person’s ability to pay. In respect of private funding, people want an ‘asset floor’ below which an individual would not have to contribute to their care costs, as well as a ‘cap’ on the costs of care beyond which an individual would not have to pay. In terms of public funding, there is broad support for increases to Income Tax, a social insurance scheme (a stand-alone compulsory payment as a percentage of income paid by everyone aged 40 and over), and an extension of National Insurance to people working beyond state pension age.
“The sad thing is none of us know when or if we will need people to care for us one day so it is vital that everyone is aware of the issues before it is too late to do anything about it” Vicki and Keegan’s story
Page 283 of 324
52 | The lives we want to lead
This detailed work helps to explain the many examples of public polls which show that few people understand social care or how the system is meant to work. For instance, a 2017 Ipsos MORI poll suggested 63 per cent of people believed the NHS provides social care for older people, and 47 per cent believed social care is free at the point of need54.
It is no surprise, given the difficulty of explaining how the existing system works, that governments have struggled to build the political momentum to make proper and long-term improvements to social care funding, when such changes would require tax increases or cuts to other services to pay for it. But that is no excuse. Public and political opinion is changing, and people who need care and support should not be asked to wait any longer.
That is why we are, as part of this consultation, undertaking further work with the public, building on the excellent studies above, to try and get a clearer sense of which changes are most important and acceptable to them.Read more on our website: www.futureofadultsocialcare.co.uk
CONSULTATION QUESTION:
10. Beyond the issue of funding what, if any, are the other key issues which must be resolved to improve the adult social care and support system?
54 https://www.slideshare.net/IpsosMORI/the-state-of-the-state-20172018
55 https://www.health.org.uk/sites/health/files/A-fork-in-the-road-Next-steps-for-social-care-funding-reform-0.pdf
56 https://publications.parliament.uk/pa/cm201719/cmselect/cmcomloc/768/768.pdf
Changing the system for the better‘Standing still’ is not an option and never has been. This was certainly the message from the public in the Ipsos MORI and Citizens’ Assembly work. And doing so would impact on people’s wellbeing and destabilise the care and support system as we have set out above. Building on what we know the public thinks, and thinking about some of the consequences of repeated under-funding of social care that we would like to tackle, the following table summarises a range of key options set out in recent papers for how we might change social care for the better.
This draws on the excellent recent work by Age UK, the Health Foundation and King’s Fund55 and the joint select committee report, ‘Long term funding of adult social care’56. The Health Foundation/Kings Fund and joint select committee reports compare a range of proposals, along with costings and the table below provides only a summary. For further details please see the links provided.
We have not included the option, set out in the Health Foundation and King’s Fund report, of restoring levels of funding to 2009/10 levels. But it is worth noting that they estimate the costs of that at an additional £8 billion in 2021. All of the options below are compared to current funding and, consequently, current levels of access and quality.
“Governments can no longer turn a blind eye and say we can’t afford it… Government must step up to the plate and be honest with the electorate” Sandy’s story
Page 284 of 324
The LGA green paper for adult social care and wellbeing | 53
The options set out in the table do not, in general, overlap, except that free personal care would mean there was no need for a cap on care costs. They would each help different groups, and are not limited to older people; people with life-long disabilities, or working age adults who acquire a disability, require sustainable funding for care and support in their own right.
In thinking about how we can make the system better there are two broad categories of changes to consider. The first, shaded in the table below, are primarily about making the current system work as intended and relate to implementing statutory duties fully. These would help stabilise the ‘here and now’, help address the consequences of underfunding as described above, and create a more solid foundation from which to deliver the second, unshaded, options in the table. These are additional proposals for change, which would help address the separate set of concerns identified above that are more to do with notions of fairness, complexity and transparency. They would signal a change to current requirements (although the ‘cap and floor’ would only require implementation of current legislation, not a new Bill).
The table projects estimated costs in 2024/25 but in considering the long-term future of adult social care we take a longer horizon; the system we build now must be fit for at least the next decade and beyond. In considering the changes we want to make, the question is therefore not simply about preferences for the short- to medium-term, but for the longer-term as well.
Page 285 of 324
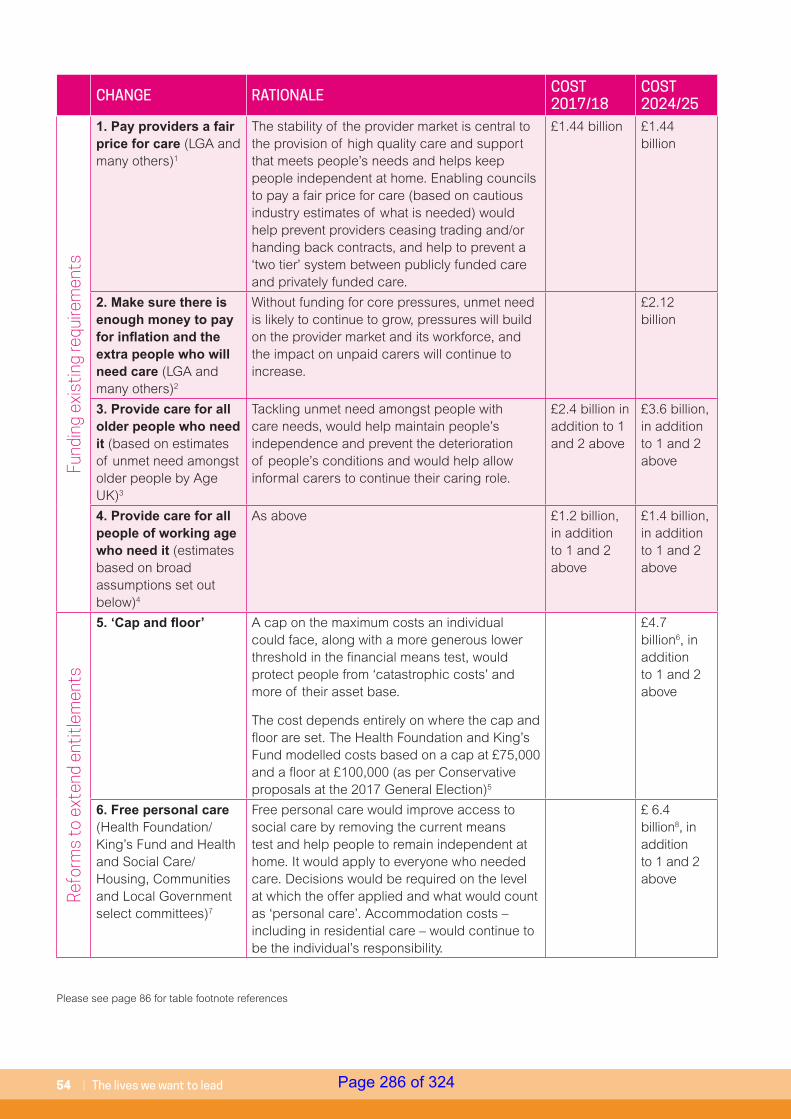
54 | The lives we want to lead
CHANGE RATIONALE COST 2017/18
COST 2024/25
Fund
ing
exis
ting
requ
irem
ents
1. Pay providers a fair price for care (LGA and many others)1
The stability of the provider market is central to the provision of high quality care and support that meets people’s needs and helps keep people independent at home. Enabling councils to pay a fair price for care (based on cautious industry estimates of what is needed) would help prevent providers ceasing trading and/or handing back contracts, and help to prevent a ‘two tier’ system between publicly funded care and privately funded care.
£1.44 billion £1.44 billion
2. Make sure there is enough money to pay for inflation and the extra people who will need care (LGA and many others)2
Without funding for core pressures, unmet need is likely to continue to grow, pressures will build on the provider market and its workforce, and the impact on unpaid carers will continue to increase.
£2.12 billion
3. Provide care for all older people who need it (based on estimates of unmet need amongst older people by Age UK)3
Tackling unmet need amongst people with care needs, would help maintain people’s independence and prevent the deterioration of people’s conditions and would help allow informal carers to continue their caring role.
£2.4 billion in addition to 1 and 2 above
£3.6 billion, in addition to 1 and 2 above
4. Provide care for all people of working age who need it (estimates based on broad assumptions set out below)4
As above £1.2 billion, in addition to 1 and 2 above
£1.4 billion, in addition to 1 and 2 above
Refo
rms
to e
xten
d en
titl
emen
ts
5. ‘Cap and floor’ A cap on the maximum costs an individual could face, along with a more generous lower threshold in the financial means test, would protect people from ‘catastrophic costs’ and more of their asset base.
The cost depends entirely on where the cap and floor are set. The Health Foundation and King’s Fund modelled costs based on a cap at £75,000 and a floor at £100,000 (as per Conservative proposals at the 2017 General Election)5
£4.7 billion6, in addition to 1 and 2 above
6. Free personal care (Health Foundation/King’s Fund and Health and Social Care/Housing, Communities and Local Government select committees)7
Free personal care would improve access to social care by removing the current means test and help people to remain independent at home. It would apply to everyone who needed care. Decisions would be required on the level at which the offer applied and what would count as ‘personal care’. Accommodation costs – including in residential care – would continue to be the individual’s responsibility.
£ 6.4 billion8, in addition to 1 and 2 above
Please see page 86 for table footnote references
Page 286 of 324
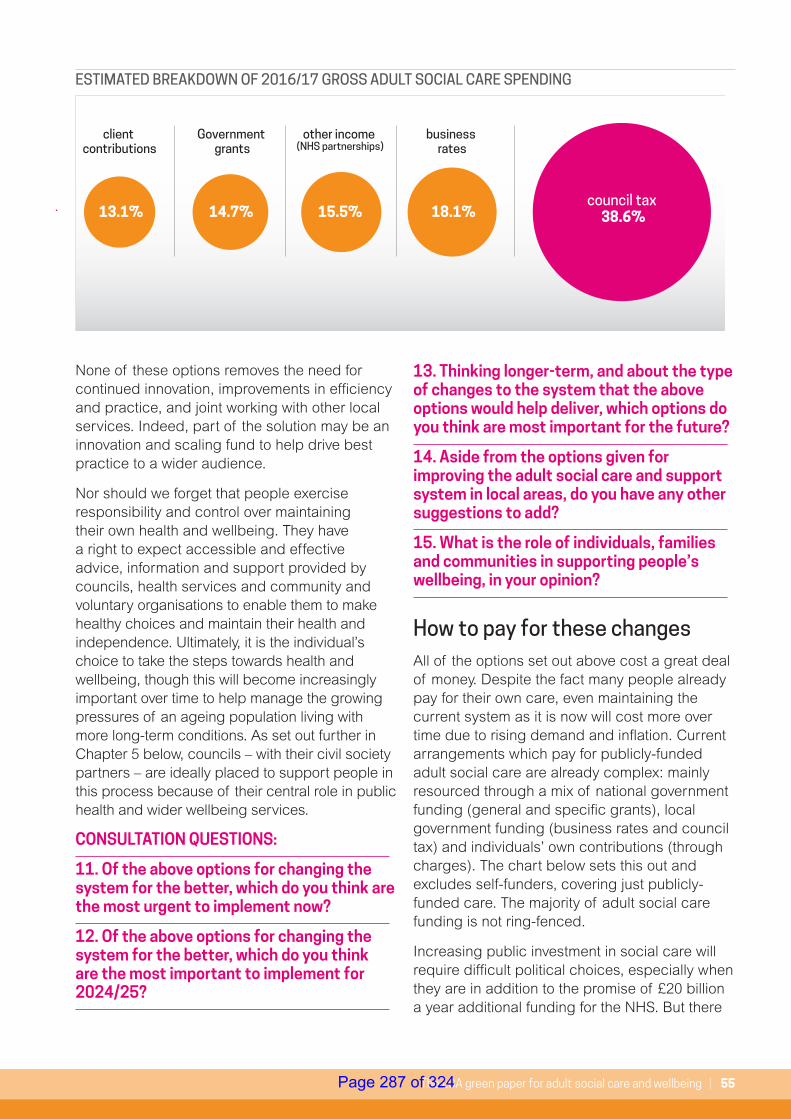
The LGA green paper for adult social care and wellbeing | 55
None of these options removes the need for continued innovation, improvements in efficiency and practice, and joint working with other local services. Indeed, part of the solution may be an innovation and scaling fund to help drive best practice to a wider audience.
Nor should we forget that people exercise responsibility and control over maintaining their own health and wellbeing. They have a right to expect accessible and effective advice, information and support provided by councils, health services and community and voluntary organisations to enable them to make healthy choices and maintain their health and independence. Ultimately, it is the individual’s choice to take the steps towards health and wellbeing, though this will become increasingly important over time to help manage the growing pressures of an ageing population living with more long-term conditions. As set out further in Chapter 5 below, councils – with their civil society partners – are ideally placed to support people in this process because of their central role in public health and wider wellbeing services.
CONSULTATION QUESTIONS:
11. Of the above options for changing the system for the better, which do you think are the most urgent to implement now?
12. Of the above options for changing the system for the better, which do you think are the most important to implement for 2024/25?
13. Thinking longer-term, and about the type of changes to the system that the above options would help deliver, which options do you think are most important for the future?
14. Aside from the options given for improving the adult social care and support system in local areas, do you have any other suggestions to add?
15. What is the role of individuals, families and communities in supporting people’s wellbeing, in your opinion?
How to pay for these changesAll of the options set out above cost a great deal of money. Despite the fact many people already pay for their own care, even maintaining the current system as it is now will cost more over time due to rising demand and inflation. Current arrangements which pay for publicly-funded adult social care are already complex: mainly resourced through a mix of national government funding (general and specific grants), local government funding (business rates and council tax) and individuals’ own contributions (through charges). The chart below sets this out and excludes self-funders, covering just publicly-funded care. The majority of adult social care funding is not ring-fenced.
Increasing public investment in social care will require difficult political choices, especially when they are in addition to the promise of £20 billion a year additional funding for the NHS. But there
ESTIMATED BREAKDOWN OF 2016/17 GROSS ADULT SOCIAL CARE SPENDING
council tax 38.6% 18.1%
business rates
15.5%
other income (NHS partnerships)
14.7%
Government grants
13.1%
client contributions
Page 287 of 324
56 | The lives we want to lead
is public support for this. Recent public polling consistently demonstrates that the British public are proud of the NHS and want to see funding for it increase, even if that means paying more tax. We are starting to see similar consensus on the need for more funding for adult social care. This reflects a shift in public opinion over time about the reality and priority of social care funding.
• In the latest King’s Fund quarterly monitoring report of changes and challenges facing health and social care, ‘social care’ was selected by NHS trust finance directors as the highest priority for investment of the new NHS funding.57
• 82 per cent of respondents to a 2018 NHS Confederation survey said that they support increasing public spending on social care by 3.9 per cent a year – compared to 77 per cent who support increasing healthcare spending by a similar amount (4 per cent).58
• In a 2017 Ipsos MORI poll, 71 per cent of respondents said that they would support an increase in income tax to pay for adult socialcare.59
• In a 2018 Ipsos MORI poll, four out of 10 named community and social care services as one of their top three priorities for any new funding – more support even than for routine surgery and primary care, and outstripped only by support for mental health services and urgent and emergency care.60
57 https://www.kingsfund.org.uk/publications/how-nhs-performing-june-2018
58 http://www.nhsconfed.org/news/2018/06/british-public-backs-increase-in-social-care-spending
59 https://www.ipsos.com/ipsos-mori/en-uk/majority-support-income-tax-rises-increase-funding-available-adult-social-care
60 http://nhsproviders.org/public-attitudes-to-health-and-care-new-nhs-providers-polling
61 ComRes surveyed 155 MPs (56 Conservative, 75 Labour, 12 SNP and 12 Other) and 103 Peers (30 Conservative, 40 Labour, 15 Liberal Democrat and 18 Crossbench/other) using a combination of paper and online surveys between 23 October 2017 and 11 December 2017. The key aims of this research were to track advocacy and efficacy against a comparator set of organisations; and measure attitudes towards local government funding and powers.
62 https://www.local.gov.uk/about/news/nine-ten-councils-say-national-taxation-key-solving-adult-social-care-funding-crisis
• A recent ComRes poll commissioned by the LGA found that 84 per cent of MPs and 81 per cent of Peers agree that additional funding should go to councils’ social care budgets to tackle the funding crisis.
• Recent LGA public polling61 suggests that 87 per cent of the public agree that councils should be given additional central government funding to deal with the funding gap in adult social care.
• A 2018 LGA poll of council leaders and social care cabinet members suggests that 96 per cent believe there is a major national funding problem in this area. 89 per cent said taxation must be part of the solution to securing the long-term sustainability of care and support.62
There has been considerable helpful recent debate about the different ways additional funding could be raised. They have included taxes on income, on property wealth, and cuts to other public spending. The table below summarises the key proposals which have been set out in public, drawing largely on previous reports, and the amount of money they are estimated to raise. We have conducted work to provide a broad estimate of the amount raised by the different options in 2024/25 (where others’ work uses a different timescale) to ensure consistency between the figures used in the tables on page 54 and 58-59.
Page 288 of 324
The LGA green paper for adult social care and wellbeing | 57
There are, of course, other broad options. For instance, during the 2017 General Election, the Conservative Party proposed aligning the means-test for domiciliary care with that for residential care63 so that the value of a person's home would be taken account of along with other assets and income. Linked, they proposed extending deferred payments64 to domiciliary care.
Some organisations have suggested that Attendance Allowance65 and other benefits that support the same group of people could be reformed. For instance, the Barker Commission proposed repurposing Attendance Allowance as part of a new ‘care and support allowance’ to help meet lower levels of need. It could also be means tested. Roughly £5.5 billion a year is spent on Attendance Allowance, although some people spend their allocation on their care needs and others are charged against it so the full amount would not be in scope. More broadly, some people may argue that reprioritising Government expenditure is called for and it is of course in the national interest that we root out tax avoidance to ensure the Exchequer has the full extent of revenue it is owed by individuals and organisations. HMRC estimate that more than £30 billion of tax goes uncollected each year66. The default position, if additional funding is not raised by the above options or others, would be continued cuts to other local council services to protect adult social care, as we have described above.
63 https://s3.eu-west-2.amazonaws.com/conservative-party-manifestos/Forward+Together+-+Our+Plan+for+a+Stronger+Britain+and+a+More+Prosperous....pdf
64 A deferred payment is an arrangement in which a council will (subject to eligibility criteria) pay for an individual’s care home costs and recover those costs at a later point once the person’s home is sold.
65 Attendance Allowance helps with personal support costs if you have a physical or mental disability and are aged 65 and over. It is paid at two rates, depending on the level of care you need (£57.30 or £85.60 a week). Unlike social care, it is not currently means-tested.
66 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/715742/HMRC-measuring-tax-gaps-2018.pdf
CONSULTATION QUESTIONS:
16. Which, if any, of the options given for raising additional funding would you favour to pay for the proposed changes to the adult social care and support system?
17. Aside from the options given for raising additional funding for the adult social care and support system in local areas, do you have any other suggestions to add?
18. What, if any, are your views on bringing wider welfare benefits (such as Attendance Allowance) together with other funding to help meet lower levels of need for adult social care and support?
The LGA is not suggesting a preferred option. However, we are clear that a mix of solutions is likely to be required, both to reflect the scale of the funding challenge we face, which will continue to grow over time, and to reflect different individuals’ and different generations’ particular circumstances.
Page 289 of 324
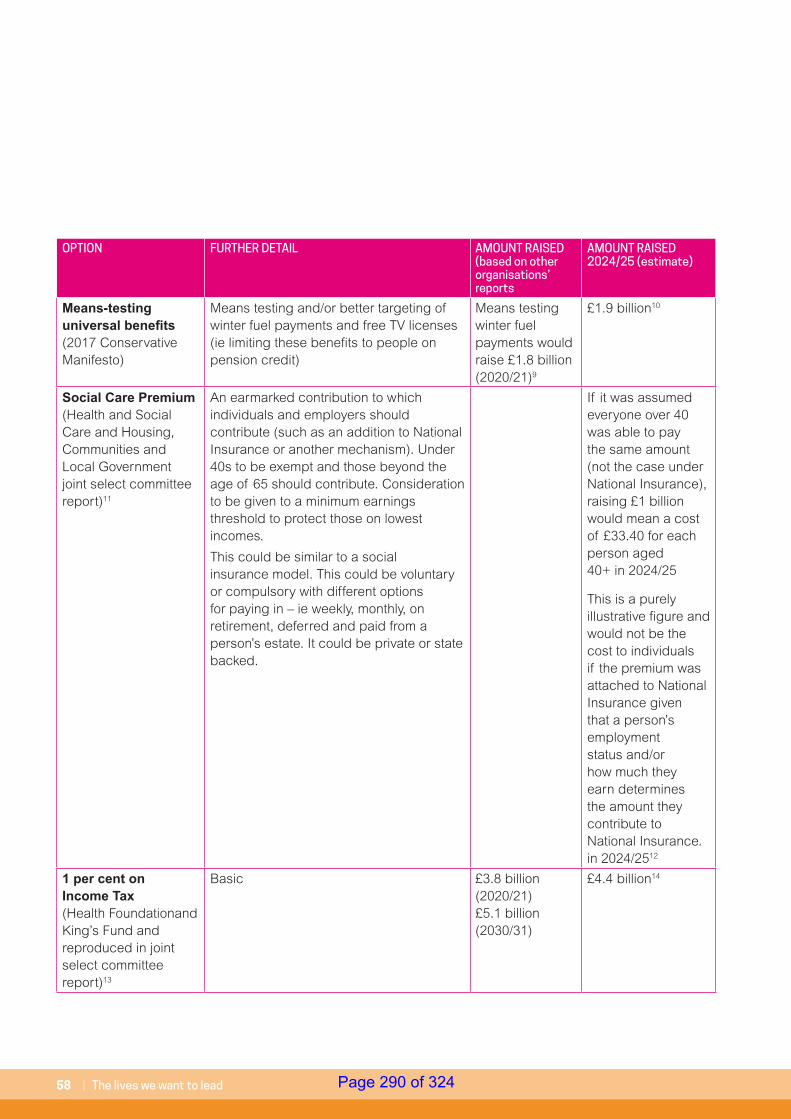
58 | The lives we want to lead
OPTION FURTHER DETAIL AMOUNT RAISED (based on other organisations’ reports
AMOUNT RAISED 2024/25 (estimate)
Means-testing universal benefits (2017 Conservative Manifesto)
Means testing and/or better targeting of winter fuel payments and free TV licenses (ie limiting these benefits to people on pension credit)
Means testing winter fuel payments would raise £1.8 billion (2020/21)9
£1.9 billion10
Social Care Premium (Health and Social Care and Housing, Communities and Local Government joint select committee report)11
An earmarked contribution to which individuals and employers should contribute (such as an addition to National Insurance or another mechanism). Under 40s to be exempt and those beyond the age of 65 should contribute. Consideration to be given to a minimum earnings threshold to protect those on lowest incomes.
This could be similar to a social insurance model. This could be voluntary or compulsory with different options for paying in – ie weekly, monthly, on retirement, deferred and paid from a person’s estate. It could be private or state backed.
If it was assumed everyone over 40 was able to pay the same amount (not the case under National Insurance), raising £1 billion would mean a cost of £33.40 for each person aged 40+ in 2024/25
This is a purely illustrative figure and would not be the cost to individuals if the premium was attached to National Insurance given that a person’s employment status and/or how much they earn determines the amount they contribute to National Insurance.in 2024/2512
1 per cent on Income Tax (Health Foundationand King’s Fund and reproduced in joint select committee report)13
Basic £3.8 billion (2020/21) £5.1 billion (2030/31)
£4.4 billion14
Page 290 of 324
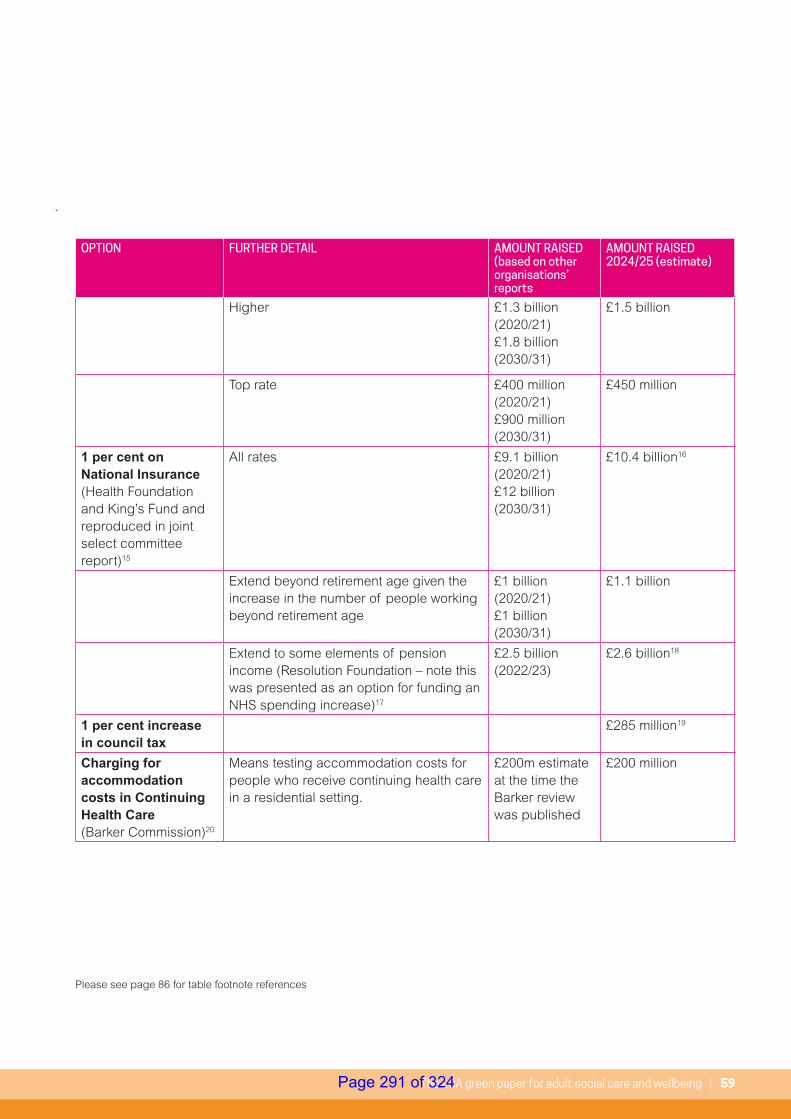
The LGA green paper for adult social care and wellbeing | 59
Higher £1.3 billion (2020/21) £1.8 billion (2030/31)
£1.5 billion
Top rate £400 million (2020/21) £900 million (2030/31)
£450 million
1 per cent on National Insurance (Health Foundation and King’s Fund and reproduced in joint select committee report)15
All rates £9.1 billion (2020/21) £12 billion (2030/31)
£10.4 billion16
Extend beyond retirement age given the increase in the number of people working beyond retirement age
£1 billion (2020/21) £1 billion (2030/31)
£1.1 billion
Extend to some elements of pension income (Resolution Foundation – note this was presented as an option for funding an NHS spending increase)17
£2.5 billion (2022/23)
£2.6 billion18
1 per cent increase in council tax
£285 million19
Charging for accommodation costs in Continuing Health Care (Barker Commission)20
Means testing accommodation costs for people who receive continuing health care in a residential setting.
£200m estimate at the time the Barker review was published
£200 million
Please see page 86 for table footnote references
OPTION FURTHER DETAIL AMOUNT RAISED (based on other organisations’ reports
AMOUNT RAISED 2024/25 (estimate)
Page 291 of 324
60 | The lives we want to lead
Beyond this, there are other tests we may wish to apply to judge the relative merits of any solution/s the Government puts forward in its green paper. These might include, for instance:
• Wellbeing: do the solution/s help advance the core aims of improving and supporting people’s wellbeing, putting the individual at the centre of their care and support, and investing in the social and economic outcomes of our communities?
• Fairness: to what extent, and in what ways, do the solution/s help achieve a greater level of fairness for people? Do we understand the overall impact of the whole package of changes on different groups?
• Sufficiency: how much does the proposed solution/s raise in the short, medium and long-term? How does this compare to the costs of the type of options for change set out above?
• Sustainability: can we be confident that the funding is sufficient over time? If it is sufficient on day 1, will it be sufficient on day 2, day 100, day 1,000, and so on?
• Clarity and transparency: are the solution/s easy enough to understand and will they allow for clear lines of accountability on spending decisions?
• Subsidiarity: can national-level reforms be led as close as possible to the individual they are designed for?
Cross-party political co-operation
“Whatever colour your rosette, I urge all politicians to come together and unite around the common aim that got us into politics in the first place: to improve our communities and the lives of the people who live within them.”Baroness Margaret Eaton DBE DLLGA think piece series, 2018
Potentially difficult reforms to deliver a sustainable and fully funded care system in the future stand a greater chance of success if they are built on a degree of political consensus which can deliver cross-party co-operation, particularly in a parliament with a narrow majority.
Creating a constructive space in which the real issues and the full range of possible solutions can be debated could pave the way for a shared and concerted effort to raise awareness of social care with the public. This might include, for instance, an agreed cross-party narrative on why adult social care matters, how the system works, the challenges it faces, the level of funding required in the sort, medium- and long-term, and the types of options that are most likely and realistic to raise that level of funding.
This is not an impossible task. The recent joint report on long-term funding for adult social care by the Health and Social Care and Housing, Communities and Local Government select committees was a coming together of 22 MPs across four political parties. They reached consensus – not just in terms of articulating the problem but also in identifying, and crucially backing, a set of solutions for a way forward. Through this process, the LGA is seeking to develop a similar position, with similar cross-party support.
CONSULTATION QUESTIONS:
19. What are your views on the suggested tests for judging the merits of any solution/s the Government puts forward in its green paper?
20. In your opinion, to achieve a long-term funding solution for adult social care and support, to what extent is cross-party co-operation and/or cross-party consensus needed?
Page 292 of 324
The LGA green paper for adult social care and wellbeing | 61
“Doctors and nurses can treat illness, but they cannot deliver health. Only healthy local communities can do that – and that is the role of local government.”Rt Hon Stephen Dorrell, Chairman, NHS ConfederationLGA think piece series, 2018
Key points:• Tackling the full extent of future demand
requires a shift in focus and a far greater emphasis on prevention and early intervention
• Public health has a fundamental role to play in this – investing in public health helps to deliver the wider prevention agenda that is critical to our health and care system overall
• Council services – including those provided by district councils – support people’s wellbeing, as do those of councils’ many local partners
As we have set out, adequately funding social care is a key part of the solution for a more secure long-term future for health and wellbeing. But if we are to really tackle the full extent of future demand with quality services we need to refocus our efforts on intervening earlier and preventing needs developing in the first place (or slowing their escalation). This is better for people and better for the public purse. Promoting healthy choices, protecting health, preventing sickness, intervening early to minimise the need for costly hospital treatment, supporting people to manage their own conditions or ‘self-care’, or providing support to unpaid carers requires the input of many council services and many of councils’ local partners.
5. Adult social care and wider wellbeing
Page 293 of 324
62 | The lives we want to lead
The role of public health
The public health challenge in numbers…
Two thirds of adults and a quarter of two to 10 year olds are overweight or obese. Treating the consequences of obesity costs £5.5 billion to the health and social care system and has significant impacts on the quality of lives of people.
The proportion of adults who are overweight or obese is predicted to reach 70 per cent by 2034.
Alcohol-related crime accounts for about 920,000 violent incidents each year – accounting for 47 per cent of violent offences committed. The total annual cost to society of alcohol-related harm is estimated to be £21 billion. The NHS incurs £3.5 billion a year in costs related to alcohol.
Trips and falls cost the NHS more than £2 billion each year, with a 35 per cent increase in acute care costs in the year following a fall.
Loneliness and social isolation are as damaging to our health as smoking 15 cigarettes a day.
Local government is unanimous in its support for taking leadership of public health and working with local partners to achieve shared priorities. Councils are committed to making a difference to the lives of people in local communities by helping them live longer, healthier and more fulfilling lives. But this can only be achieved if we do things differently and resource public health services appropriately as part of wider investment across the system to help embed community-based prevention at all key points, including social care, the NHS and the voluntary sector.
In the 21st century, a huge part of the burden of ill health is avoidable. About a third of all deaths are classed as premature – that is they could have been prevented by lifestyle changes undertaken at an earlier time of life. The World Health Organization (WHO) estimateS that almost one third of the disease burden in industrialised countries can be attributed to four main behaviours: smoking, alcohol intake, poor diet, and lack of physical activity.
Without investment in prevention and early intervention, we will only ever see a continuation of the current vicious circle in which inadequate investment in these areas puts increasing pressure on hospitals, which then attract scarce resources. To put it another way, we need to tackle the cause of the pressures on hospitals and their budgets, not just keep treating the symptoms. Adequately resourcing public health is a sound investment precisely because it helps deliver the wider prevention agenda that is critical to the stability of our care and health services.
But when considering the cost of that illness it is not just the bill for treatment and care that should be taken into account. The economic consequences of premature death and
“We need to recognise that good support now will prevent more expensive hospital stays down the line” Lucy’s story
Page 294 of 324
The LGA green paper for adult social care and wellbeing | 63
preventable illness are considerable, too. These can include loss of productivity in the workplace and the cost of crime and antisocial behaviour.
This is not a new argument. In 2002, the Wanless Report67 put forward a strong case for investing more in public health, estimating that effective public health policy could save the NHS £30 billion a year by 2022/23. The report warned that, without investment in preventing ill health and changing our model of care services, the NHS would be financially unsustainable by 2014. This has come to pass. Spending on NHS care has more than doubled from £61 billion in 1994/95 to over £140 billion in 2016/17 (at 2016/17 prices)68. And even this has not been enough. Latest performance information from NHS Improvement shows that, for the year ending 31 March 2018, providers reported an aggregate deficit of £985 million. This was worse than both the forecast deficit at 2018/18 quarter three (£931 million) and the deficit in the previous financial year (£791 million)69.
67 http://webarchive.nationalarchives.gov.uk/+/http://www.dh.gov.uk/en/Publichealth/Healthinequalities/Healthinequalitiesguidancepublications/DH_066213
68 HM Treasury Public Expenditure Statistical Analyses 2017
69 https://improvement.nhs.uk/documents/2852/Quarter_4_2017-18_performance_report.pdf
Councils are thinking creatively about their public health responsibilities and asking the central question: how do we use all of our resources for council-commissioned or provided services (and not just the modest ring fenced budget) to improve the health of our residents? This discussion is leading councils to think differently about how they affect the wider determinants of health and challenge established ways of working. Where services are not delivering value or significant outcomes they are being decommissioned and replaced by services that can deliver on local government’s huge ambitions for local people.
The LGA has consistently highlighted that the potential contribution of public health is being undermined by funding constraints. Services and interventions that are vital for improving population health are not being implemented, or are being cut back, risking the future sustainability of the NHS. Council leaders have expressed particular concern that recent budget reductions will result in public health services that are inadequate for meeting the needs of the local populations they serve. And they have long warned that planned cuts by Government of £600 million between 2015 and 2020 are counterproductive and will only exacerbate the problems facing the NHS and social care.
CONSULTATION QUESTION:
21. What role, if any, do you think public health services should have in helping to improve health and wellbeing in local areas?
“If the nation fails to get serious about prevention then recent progress in healthy life expectancies will stall, health inequalities will widen, and our ability to fund beneficial new treatments will be crowded-out by the need to spend billions of pounds on wholly avoidable illness”NHS Five Year Forward View, 2014
Page 295 of 324

64 | The lives we want to lead
The role of other council services and those of local partnersAs we have outlined already, council services make an important contribution to supporting people’s wellbeing in the broadest sense. Within councils’ highways and transport services for instance, close on £2.2 billion is spent on road maintenance, street lighting, traffic management and road safety, parking and concessionary fares, which all help create environments that are accessible and safe. Further spending totally nearly £2.1 billion is spent on councils’ culture and related services, such as culture and heritage, recreation and sport, open spaces and library services. Such services help provide opportunities that get people out and about in their local communities. £332 million is spent on regulatory services that ensure high standards in trading, water safety, food safety and noise and nuisance protection. £266 million is spent on community safety measures and nearly £4.3 billion is spent on street cleaning, recycling and waste collection and disposal, creating communities that are safe, clean and accessible.
70 http://www.apse.org.uk/apse/assets/File/Neighbourhood%20Services%20(web).pdf
As the Association for Public Service Excellence has said:
“The provision of high quality local neighbourhood services has a positive impact on the perception of an area, encourages physical activity in a community setting and fosters a sense of wellbeing with citizens. High quality neighbourhood services are complementary to social care, health services, police and fire services, education and housing. All other services thrive better in neighbourhoods that are deemed to be well managed, clean and safe.70”
It is precisely these sort of universal services that have been cut deeper to protect adult social care. To reiterate an earlier point, sorting out the long-term funding of social care therefore goes hand-in-hand with sorting out the long-term funding of services that play an essential role in creating communities we want to live in and which support our wider wellbeing. This includes the many vital frontline services commissioned and delivered by district councils that significantly impact the wider determinants of health and mitigate pressure on primary and social care. Of particular note are housing adaptations which help keep people out of hospital and allow them to return home safely in cases where time in hospital is required.
Page 296 of 324
The LGA green paper for adult social care and wellbeing | 65
As the Association for Public Service Excellence has said:
“The provision of high quality local neighbourhood services has a positive impact on the perception of an area, encourages physical activity in a community setting and fosters a sense of wellbeing with citizens. High quality neighbourhood services are complementary to social care, health services, police and fire services, education and housing. All other services thrive better in neighbourhoods that are deemed to be well managed, clean and safe.70”
It is precisely these sort of universal services that have been cut deeper to protect adult social care. To reiterate an earlier point, sorting out the long-term funding of social care therefore goes hand-in-hand with sorting out the long-term funding of services that play an essential role in creating communities we want to live in and which support our wider wellbeing. This includes the many vital frontline services commissioned and delivered by district councils that significantly impact the wider determinants of health and mitigate pressure on primary and social care. Of particular note are housing adaptations which help keep people out of hospital and allow them to return home safely in cases where time in hospital is required.
District councils are an equally important part of the equation when it comes to designing a system-wide focus on community-based prevention.
Housing more generally is a key component of health and care and the foundation upon which people, including those in vulnerable circumstances, can achieve a positive quality of life. The impact of poor housing on health is similar to that of smoking or alcohol and costs the NHS at least £1.4 billion a year, as well as creating housing worries that can end in homelessness for too many families71.
The lack of available and appropriate general needs, social and private housing is putting pressure on supported housing provision, which provides a vital bridge between housing, support, care and health. Supported housing reduces cost pressures on public services by keeping people out of more costly health and care settings and providing the necessary support to address issues that might otherwise prevent independent living. Around £2.05 billion is spent on support and care services for people living in supported housing72.
This comes from a variety of sources, including council adult social care and housing and homelessness funding.
71 https://www.housinglin.org.uk/_assets/Resources/Housing/Support_materials/87741-Cost-of-Poor-Housing-Briefing-Paper-v3.pdf
72 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/655990/Funding_supported_housing_-_policy_statement_and_consultation.pdf
73 https://www.kingsfund.org.uk/sites/default/files/2018-02/Commissioner_perspectives_on_working_with_the_voluntary_community_and_social_enterprise_sector_1.pdf
74 https://www.thinknpc.org/publications/boldness-in-times-of-change/
75 https://richmondgroupofcharities.org.uk/sites/default/files/final_aw_5902_the_richmond_group_a4_10pp_report.pdf
It is not just councils that help support people’s wellbeing. There are an estimated 36,000 voluntary, community and social enterprise (VCSE) organisations that support and provide health and social care services. The vast majority (nearly 90 per cent) are small, community-based organisations supported by an estimated three million volunteers73. This is an essential sector but one which faces its own pressures as demand for its services rises but state funding is constrained. This pressure is felt all the more by organisations that have relied, in part, on grants and contracts for their local councils, further reducing the impact of the local voluntary sector74. A sustainable voluntary sector is therefore a key component of wellbeing. As the Richmond Group of charities notes:
“Funding for interventions and services that provide vital support for people with long-term conditions or that tackle our serious public health challenges needs to be more sustainable – moving away from the current situation in which as soon as public finances get tight, effective voluntary and community sector approaches get cut75”
CONSULTATION QUESTIONS:
22. What evidence or examples, if any, can you provide that demonstrate the impact of other local services (both council services outside of adult social care and support, and those provided by other organisations) on improving health and wellbeing?
23.To what extent, if any, are you seeing a reduction in these other local services?
Page 297 of 324
66 | The lives we want to lead
Key points:• Our care model must change so that people
experience it as a seamless package of care and support to address their specific needs and aspirations, helping them to live independent and fulfilling lives.
• Integration is not an end in itself but a means of improving health and wellbeing outcomes for individuals and communities, improving the planning and delivery of services and making the best possible use of resources
• The Better Care Fund has been a driver for joined-up planning but it should be locally-led by health and wellbeing boards
• Local government provides vital local leadership and democratic accountability. This must be harnessed, particularly through strengthened health and wellbeing boards, to address the democratic deficit in the NHS
• Council and health leaders are also best placed to drive improvement at the local level. The LGA, working with national partners, is committed to supporting local areas to improve and spread good practice.
• Extracting maximum value from the new NHS funding requires priorities to be set at the local level, with minimum top-down influence from government and the NHS nationally
76 The Better Care Fund was announced by the Government in the June 2013 Spending Round. It creates a local single pooled budget to incentivise the NHS and local government to work more closely together around people, placing their wellbeing as the focus of health and care services, and shifting resources into social care and community services for the benefit of the people. For further information, visit: https://www.local.gov.uk/our-support/our-improvement-offer/care-and-health-improvement/integration-and-better-care-fund/better-care-fund
Adult social care and health working together‘Integration’ is not an end in itself but a means of achieving the triple aims of: improving health and wellbeing outcomes for individuals and communities; improving the planning and delivery of services; and making the best possible use of health and council resources. Neither is integration a panacea for the financial challenges of the health service and local government. Joining up care and support and intervening and offering early support to keep people well is a more efficient use of resources but efficiency alone is not enough to ensure the long-term sustainability of the health and care system.
The primary role of central government and national bodies in integration is to support and enable local leaders by removing the financial, cultural and structural barriers which prevent them acting for the good of their population, rather than the good of their own organisations. However, there has been increasing pressure from central government and the NHS at national level to direct integration and narrow its focus to reducing pressure on acute hospitals. In particular, the Better Care Fund (BCF)76, originally intended as a spur to local leaders to create their own shared plans for joined up community based services, has been used as a tool of performance management.
The introduction of a new requirement in October 2017 for local BCF plans to comply with national targets for delayed transfers of care, or risk national direction or a review of their allocations, was a step too far in central influence. Developments such as these have,
6. Adult social care and the NHS
Page 298 of 324
The LGA green paper for adult social care and wellbeing | 67
in many areas, undermined local partnerships rather than supported them.
The LGA continues to support the original intentions of the BCF77. Local leaders should have freedom to develop their own plans to promote integrated services, with national government playing a supportive and enabling role. But a number of factors, including financial challenges facing health and social care and the increase in national direction of local BCF plans, are identified as major barriers to greater joined up working. A recent LGA survey of council leaders and cabinet members for adult social care asked them to select the single biggest barrier to integration out of a list of ten possible choices. The top four barriers were identified as:
• Financial challenges (33 per cent)
• National direction and pressure to meet national targets (15 per cent)
• Workforce challenges (11 per cent)
• Lack of agreement between health and care leadership (10 per cent)
While local leaders can do their best to use the resources they have to support local joined-up working, there is a clear demand for national government to provide sufficient funding to support integration and give local leaders the space to develop and deliver their own plans.
If this cannot be achieved, the BCF should be reformed with resources going directly to councils and deployed according to locally agreed plans overseen and assured by health and wellbeing boards.
77 The Better Care Fund was announced by the Government in the June 2013 Spending Round. It creates a local single pooled budget to incentivise the NHS and local government to work more closely together around people, placing their wellbeing as the focus of health and care services, and shifting resources into social care and community services for the benefit of the people. For further information, visit: https://www.local.gov.uk/our-support/our-improvement-offer/care-and-health-improvement/integration-and-better-care-fund/better-care-fund
CONSULTATION QUESTION:
24. What principles, if any, do you believe should underpin the way the adult social care and support service and the NHS work together?
Joining up support around the personThe primary purpose of integration is to provide better and more effective care and support to people, enabling them to live more fulfilling and independent lives. Professionals across health and care working together to join up or coordinate services undoubtedly improves people’s experience of services. But on its own it is not sufficient to deliver personalised care. To make real progress on this ambition, we need to put the person at the centre of our planning and for professionals to work with them to identify what they most value in their lives and how we can enable them to achieve it.
Personalisation is not a new concept in social care. For well over a decade, adult social care has worked with people who use services to design and recommission services to ensure that they have more choice and control. Through the Think Local Act Personal (TLAP) partnership initiative, local government and partners have committed to transforming health and social care through personalisation and community-based support.
Page 299 of 324
68 | The lives we want to lead
The ‘Making it Real’ (MiR)78, framework developed by TLAP in partnership with people who use services and carers, describes the outcomes that genuinely personalised care and support should achieve in delivering more choice and control.
The MiR approach uses first person ‘I’ statements or ‘progress markers’ to express what service users and carers would expect to find, if personalisation is working and supporting them to be active, healthy citizens. A review by TLAP of the MiR approach demonstrated that those councils who have signed up and completed their MiR action plans:
• have a greater increase in the numbers of people who use direct payments
• have higher satisfaction levels of people who feel they have control over their life
• have provided more support to carers.
Local government has shown that personalised care at scale is possible. For example, over 500,000 people have a personal budget of whom 154,000 people have a direct payment or part-direct payment79 in order to purchase the support they need.
78 Making it Real website (which includes support materials, case studies, films and examples of Making it Real action plans): www.thinklocalactpersonal.org.uk/Browse/mir
79 NHS Digital (2016), Adult social care activity and finance report, England 2016-17 – table T27 Available online: https://digital.nhs.uk/data-and-information/publications/statistical/adult-social-care-activity-and-finance-report/adult-social-care-activity-and-finance-report-england-2016-17 (accessed 7 June 2018)
80 NHS England (2014), Five Year Forward View. Available online: https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf (accessed 3 June 2018)
81 https://www.gov.uk/government/speeches/we-need-to-do-better-on-social-care
Though it originated in adult social care, personalisation is now a central principle of health care as demonstrated by The Five Year Forward View80 which recognised that many people have the knowledge, skills and confidence to manage their mental and physical health and wellbeing and want to make choices and have control of the care and support they receive. The LGA has worked with NHS England to develop the Integrated Personal Commissioning programme to spread joined-up and personalised care across health and social care, focusing on shared decision making; personalised care and support planning; enabling choice, including legal rights to choice; social prescribing and community-based support; supported self-management and greater access to personal health budgets and integrated personal budgets.
We support the commitment to ensuring that whole-person integrated care is a founding pillar of a future care and support system81. A sustainable approach to health and social care must have personalisation at its heart. Not just because this is what people want, but also because it has the power to transform the way professionals work with people and the way the system works, and this can help to transform lives.
CONSULTATION QUESTION:
25. In your opinion, how important or unimportant is it that decisions made by local health services are understood by local people, and the decision-makers are answerable to them?
Page 300 of 324
The LGA green paper for adult social care and wellbeing | 69
The ‘Making it Real’ (MiR)78, framework developed by TLAP in partnership with people who use services and carers, describes the outcomes that genuinely personalised care and support should achieve in delivering more choice and control.
The MiR approach uses first person ‘I’ statements or ‘progress markers’ to express what service users and carers would expect to find, if personalisation is working and supporting them to be active, healthy citizens. A review by TLAP of the MiR approach demonstrated that those councils who have signed up and completed their MiR action plans:
• have a greater increase in the numbers of people who use direct payments
• have higher satisfaction levels of people who feel they have control over their life
• have provided more support to carers.
Local government has shown that personalised care at scale is possible. For example, over 500,000 people have a personal budget of whom 154,000 people have a direct payment or part-direct payment79 in order to purchase the support they need.
78 Making it Real website (which includes support materials, case studies, films and examples of Making it Real action plans): www.thinklocalactpersonal.org.uk/Browse/mir
79 NHS Digital (2016), Adult social care activity and finance report, England 2016-17 – table T27 Available online: https://digital.nhs.uk/data-and-information/publications/statistical/adult-social-care-activity-and-finance-report/adult-social-care-activity-and-finance-report-england-2016-17 (accessed 7 June 2018)
80 NHS England (2014), Five Year Forward View. Available online: https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf (accessed 3 June 2018)
81 https://www.gov.uk/government/speeches/we-need-to-do-better-on-social-care
CONSULTATION QUESTION:
25. In your opinion, how important or unimportant is it that decisions made by local health services are understood by local people, and the decision-makers are answerable to them?
All of this will necessitate identifying the new roles and skills which will be needed in the system and funding for sustainable skills development. For instance, it may be worth exploring ways in which the new apprenticeship levy can be used more flexibly to help here but other funding will be needed given the anticipated demand for carers.
Local government, local leadershipLocal government leadership is highly effective in driving forward an inclusive, place-based approach to improving health and care services and outcomes. Though only two integrated care systems82 are led by local council senior officers, they have demonstrated how local government can firmly embed plans to transform health and wellbeing into the wider local landscape. Local government is able to use its direct connections with communities through its democratic mandate to have honest and inclusive conversations about the rights and responsibilities of citizens with regard to their health and wellbeing. And it can also link community-based health and wellbeing services to existing community-based services, which are easily accessible to and trusted by people.
A good example of this is the Nottingham and Nottinghamshire Integrated Care System, which is led by David Pearson, Director of Adult Social Care, Health and Public Protection at Nottinghamshire County Council. It has worked closely and inclusively with its communities, workforce and partners to develop a plan that is very much grounded in the promotion of health and wellbeing, prevention, independence and self-care, through supporting community
82 Integrated care systems are a new type of even closer collaboration in which NHS organisations, local councils and others, take collective responsibility for managing resources, delivering NHS standards, and improving the health of the population they serve.
resilience and capacity building. It also recognises the vital need to strengthen primary, community, social care and carer services and the role of housing in supporting wellbeing. The fact that Nottinghamshire was selected as one of the first 10 integrated care systems is evidence that local government leadership is effective in developing a strongly inclusive place-based approach.
Accountability in the NHSPublic polling shows that people trust local councillors more than national politicians to make the right decision for their area. However, the NHS is accountable upwards to the Government, through NHS England, rather than outwards to its communities, through local councillors. The 2012 Health and Social Care Act went some way to addressing the democratic deficit in the NHS by creating health and wellbeing boards (HWBs). The boards are an equal partnership of political, clinical, professional and community leaders, with powers and duties to develop their own place-based strategy for improving the health and wellbeing outcomes of the population. HWBs are variable in their impact and influence. The front runners have undoubtedly driven local plans to develop a new approach to health and wellbeing, which invests in promoting wellbeing, early help and support delivered through joined-up community-based services and advice and information to help people manage their own health. However, not all HWBs have been effective in leading the transformation of health and care services. The LGA continues to support HWBs to ensure that they have an impact on the health and wellbeing of their communities and lead the transformation agenda.
Page 301 of 324
70 | The lives we want to lead
Yet the democratic deficit in the NHS continues, in part due to the disconnect between HWBs and Sustainability and Transformation Partnerships (STPs), set up in 2015 to deliver the NHS Five Year Forward View. Though the LGA supports the intentions of STPs, the way in which they have been implemented in many areas has largely excluded existing democratic processes and has failed to engage councillors or communities in developing plans to transform services. In a recent LGA survey of council leaders and cabinet members for health and social care were asked about the extent to which they were making progress with various partners on integration in their local area. The responses are summarised below:
TO WHAT EXTENT ARE YOU MAKING GOOD OR MODERATE PROGRESS ON INTEGRATION WITH YOUR PARTNERS?
• Council – 87 per cent
• Health and wellbeing board – 84 per cent
• Clinical commissioning group – 81 per cent
• NHS providers – 72 per cent
• Integrated care system – 54 per cent
• Sustainability and transformation partnership – 48 per cent
• NHS England – 26 per cent
It is clear that council leaders and lead members feel strongly that local councillors working with their health commissioning and provider partners are best placed to lead integration, with only 48 per cent reporting good or moderate progress in working with STPs. This is a serious cause for concern as STPs have been given the leadership of place-based integration within the NHS. Unless HWBs are given additional powers they will continue to be bypassed by STPs and people will remain unclear about how decisions are taken within the NHS at the local level. Strengthening the role of HWBs could take various forms:
• STPs could be required to engage with HWBs in the development of STP plans
• HWBs could be given a statutory duty and powers to lead the integration agenda at the local level
• HWBs could assume responsibility for commissioning primary and community care
CONSULTATION QUESTIONS:
25. In your opinion, how important or unimportant is it that decisions made by local health services are understood by local people, and the decision-makers are answerable to them?
26. Do you think the role of health and wellbeing boards should be strengthened or not?
27. Which, if any, of the options for strengthening the role of health and wellbeing boards do you support?
28. Do you have any suggestions as to how the accountability of the health service locally could be strengthened?
Page 302 of 324
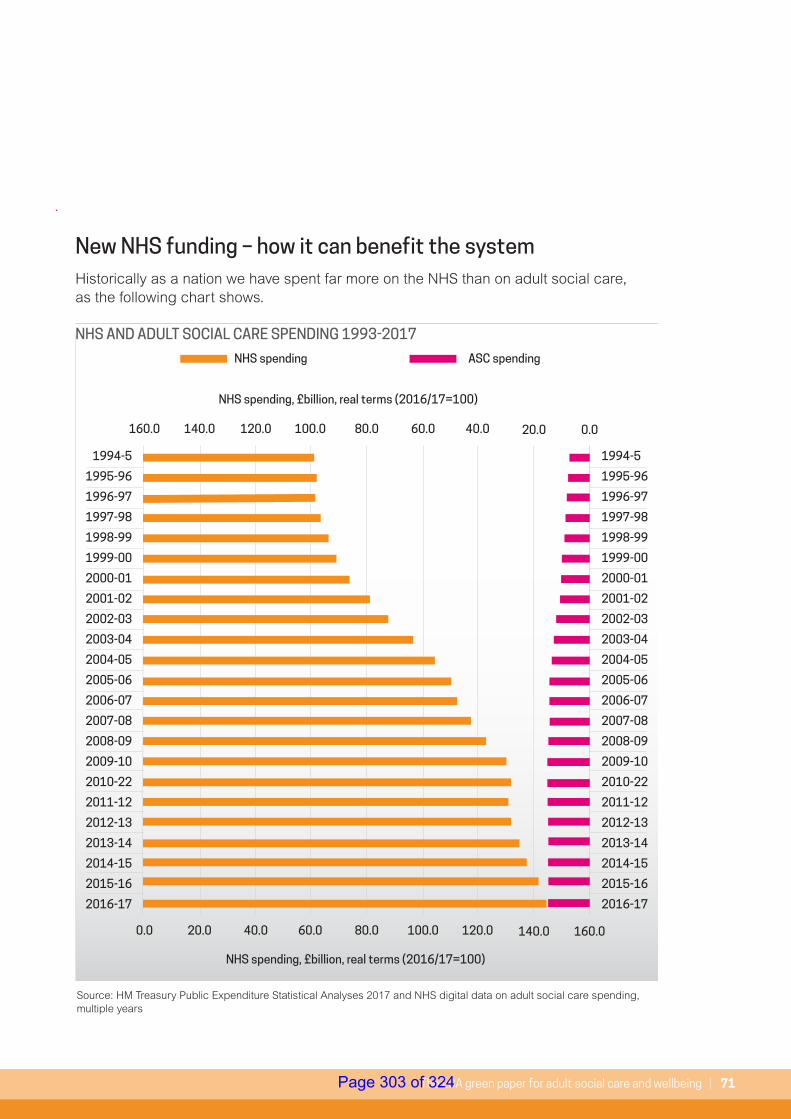
The LGA green paper for adult social care and wellbeing | 71
New NHS funding – how it can benefit the systemHistorically as a nation we have spent far more on the NHS than on adult social care, as the following chart shows.
1994-5
1995-96
1996-97
1997-98
1998-99
1999-00
2000-01
2001-02
2002-03
2003-04
2004-05
2005-06
2006-07
2007-08
2008-09
2009-10
2010-22
2011-12
2012-13
2013-14
2014-15
2015-16
2016-17
1994-5
1995-96
1996-97
1997-98
1998-99
1999-00
2000-01
2001-02
2002-03
2003-04
2004-05
2005-06
2006-07
2007-08
2008-09
2009-10
2010-22
2011-12
2012-13
2013-14
2014-15
2015-16
2016-17
0.0 20.0 40.0
NHS spending, £billion, real terms (2016/17=100)
NHS spending, £billion, real terms (2016/17=100)
NHS spending ASC spending
60.0 80.0 100.0 120.0 140.0 160.0
160.0 140.0 120.0 100.0 80.0 60.0 40.0 20.0 0.0
NHS AND ADULT SOCIAL CARE SPENDING 1993-2017
Source: HM Treasury Public Expenditure Statistical Analyses 2017 and NHS digital data on adult social care spending, multiple years
Page 303 of 324
72 | The lives we want to lead
Bringing about the shift from treating conditions to maximising wellbeing requires rethinking how additional resources are used to best effect. The NHS has been promised significant additional new funding, rising to £20.5 billion by 2023/24, an average of 3.4 per cent growth over the next five years. The linked NHS ten year plan is an opportunity to set out how our health service will develop over the next decade as part of efforts to ensure a world-class NHS. That aspiration can only be achieved if the NHS plan, and the new NHS funding, is used to best effect. But that assumes that the new NHS funding is sufficient and many commentators have already questioned this. For example, the Institute of Fiscal Studies and Health Foundation suggest that “spending on healthcare will have to rise by an average 3.3 per cent a year over the next 15 years just to maintain NHS provision at current levels, and by at least 4 per cent a year if services are to be improved”83.
83 https://www.ifs.org.uk/uploads/R143.pdf#page=6
84 http://nhsproviders.org/news-blogs/news/recovering-nhs-performance-risks-swallowing-up-new-funding
Similarly, NHS Providers have warned that “filling the gaps that have opened up in the health service after almost a decade of austerity will account for much if not most of the new money”84. If such commentators are right, we run the risk of yet again using scarce new resources to manage demand pressures on our hospitals. This would be a missed opportunity to bring about more fundamental change and ensure maximum value is extracted from the £20 billion. Maximum value of the new funding should be defined at the local level, with minimal top-down initiatives from government and NHS England and maximum input from communities, workforce, service users and patients.
Page 304 of 324
The LGA green paper for adult social care and wellbeing | 73
With sufficient local flexibility, the funding could be used to:
• Invest in prevention, primary care and community health services, with multiagency teams working closely alongside the voluntary sector to put in place early help and support
• Reinvigorate investment in intermediate care
• Reverse the cuts to district nursing, particularly so that district nurses can support care homes and extra care facilities
• Fund GP support in nursing homes and care homes to keep people out of hospital
• Fund care navigators in GP surgeries
• Invest in joined-up infrastructure, such as joint commissioning, joint assessment and shared information to track people through the health and care system and joint workforce planning
• Invest in skills development with councils taking more responsibility
• Take personalisation further with a single assessment and care planning process, which is centred on the individual and what matters to them
• Ensure that what digital activity gets delivered through the NHS Plan recognises – and funds – the critical interface with councils and the care sector, with support being given to the sharing of information through local shared records
CONSULTATION QUESTIONS:
29. Which, if any, of the options for spending new NHS funding on the adult social care and support system would you favour?
30. Do you have any other comments or stories from your own experience to add?
Page 305 of 324
74 | The lives we want to lead
7. Summary of key points
Delivering and improving wellbeing
• We are best able to live the life we want to live if we are independent, well and live in communities that support and encourage the many aspects that make us unique.
• This is true for everyone but the support we may need is unique to us as individuals and must therefore be personalised.
• Local government exists for this very purpose, affecting multiple dimensions of our communities and lives, throughout our lives.
• Supporting and improving people’s mental and physical wellbeing is at the heart of local government’s work and that of many other local public, private and voluntary sector organisations, it can only be delivered with communities.
Setting the scene – the case for change
• Social care and support matters to individuals, our communities, our NHS and our economy.
• The local dimension of social care matters because it ensures the service is accountable to local people.
• Despite a challenging financial environment, social care has delivered – it has improved and innovated.
• While diversity of local care and support is the positive result of a health and care system that is responsive to the diversity of the community it serves, unwarranted variation in quality, access and outcome is not acceptable. Local government is committed to addressing this and is best equipped to lead improvement.
• Significant reductions to councils’ funding from national government is now jeopardising the impact local government can have in communities across the country.
• In particular, the scale of funding pressures within adult social care threatens progress made to date and now risks people’s wellbeing and outcomes and the stability of the wider system.
• There are continuing recruitment and retention challenges in the adult social care workforce.
• The Care Act remains the right legal basis for social care but funding pressures are threatening the spirit and letter of the law.
The options for change
• Social care is becoming a greater public priority.
• The public and politicians (local and national) support greater funding for social care.
• People find the social care system complex and confusing, it is hard to understand, particularly for those facing the immediate pressures of requiring care and having to engage with a system they have never encountered before.
• People worry about the costs of social care but are not making preparation for them and the rules are not clear.
• Although it is hard to define, people want a greater sense of fairness within social care.
• There are a number of options for making social care better.
Page 306 of 324
The LGA green paper for adult social care and wellbeing | 75
• Making these changes will require more funding. There are different ways of raising this.
• Cross-party consensus or co-operation must be sought to secure a workable long-term solution.
Adult social care and wider wellbeing
• Tackling the full extent of future demand requires a shift in focus and a far greater emphasis on prevention and early intervention.
• Public health has a fundamental role to play in this – investing in public health helps to deliver the wider prevention agenda that is critical to our health and care system overall.
• Council services – including those provided by district councils – support people’s wellbeing, as do those of councils’ many local partners.
Adult social care and the NHS
• Our care model must change so that people experience it as a seamless package of care and support to address their specific needs and aspirations, helping them to live independent and fulfilling lives.
• Integration is not an end in itself but a means of improving health and wellbeing outcomes for individuals and communities, improving the planning and delivery of services and making the best possible use of resources.
• The Better Care Fund has been a driver for joined-up planning but it should be locally-led by health and wellbeing boards.
• Local government provides vital local leadership and democratic accountability. This must be harnessed, particularly through strengthened health and wellbeing boards, to address the democratic deficit in the NHS.
• Council and health leaders are also best placed to drive improvement at the local level. The LGA, working with national partners, is committed to supporting local areas to improve and spread good practice.
• Extracting maximum value from the new NHS funding requires priorities to be set at the local level, with minimum top-down influence from government and the NHS nationally.
Page 307 of 324
76 | The lives we want to lead
Your views matter. Our green paper is only a starting point and we want to build momentum for a debate across the country about how to fund the care we want to see in all our communities for adults of all ages and how our wider care and health system can be better geared towards supporting and improving people’s wellbeing.
8. Have your say
Throughout our green paper we have posed a series of consultation questions (set out below) and we would welcome your views on all those that are important to you. The consultation will run from 31 July to 26 September. Once the consultation closes we will analyse all responses and publish a response in the autumn.
To complete the consultation you can either visit www.futureofadultsocialcare.co.uk and complete the online survey under the section titled 'The Green Paper', alternatively you can submit your answers to the questions below to: [email protected].
If you are responding as an individual there is also an option to answer the questions in the 'Summary Green Paper' section which are primarily focussed on gathering experience-based evidence and opinions. Again, this can be done online or via the [email protected] inbox.
1. What role, if any, do you think local government should have in helping to improve health and wellbeing in local areas?
2. In what ways, if any, is adult social care and support important?
3. How important or not do you think it is that decisions about adult social care and support are made at a local level?
4. What evidence or examples can you provide, if any, that demonstrate improvement and innovation in adult social care and support in recent years in local areas?
Page 308 of 324
The LGA green paper for adult social care and wellbeing | 77
5. What evidence or examples can you provide, if any, that demonstrate the funding challenges in adult social care and support in recent years in local areas?
6. What, if anything, has been the impact of funding challenges on local government’s efforts to improve adult social care?
7. What, if anything, are you most concerned about if adult social care and support continues to be underfunded?
8. Do you agree or disagree that the Care Act 2014 remains fit for purpose?
9. What, if any, do you believe are the main barriers to fully implementing the Care Act 2014?
10. Beyond the issue of funding what, if any, are the other key issues which must be resolved to improve the adult social care and support system?
11. Of the above options for changing the system for the better, which if any, do you think are the most urgent to implement now?
12. Of the above options for changing the system for the better, which if any, do you think are the most important to implement now?
Page 309 of 324
78 | The lives we want to lead
13. Thinking longer-term, and about the type of changes to the system that the above options would help deliver, which options do you think are most important for the future?
14. Aside from the options given for improving the adult social care and support system in local areas, do you have any other suggestions to add?
15. What is the role of individuals, families and communities in supporting people’s wellbeing, in your opinion?
16. Which, if any, of the options given for raising additional funding would you favour to pay for the proposed changes to the adult social care and support system?
17. Aside from the options given for raising additional funding for the adult social care and support system in local areas, do you have any other suggestions to add?
18. What, if any, are your views on bringing wider welfare benefits (such as Attendance Allowance) together with other funding to help meet lower levels of need for adult social care and support?
19. What are your views on the suggested tests for judging the merits of any solution/s the Government puts forward in its green paper?
20. In your opinion, to achieve a long-term funding solution for adult social care and support, to what extent is cross-party co-operation and/or cross-party consensus needed?
21. What role, if any, do you think public health services should have in helping to improve health and wellbeing in local areas?
Page 310 of 324
The LGA green paper for adult social care and wellbeing | 79
22. What evidence or examples, if any, can you provide that demonstrate the impact of other local services (both council services outside of adult social care and support, and those provided by other organisations) on improving health and wellbeing?
23. To what extent, if any, are you seeing a reduction in these other local services?
24. What principles, if any, do you believe should underpin the way the adult social care and support service and the NHS work together?
25. In your opinion, how important or unimportant is it that decisions made by local health services are understood by local people, and the decision-makers are answerable to them?
26. Do you think the role of health and wellbeing boards should be strengthened or not?
27. Which, if any, of the options for strengthening the role of health and wellbeing boards do you support?
28. Do you have any suggestions as to how the accountability of the health service locally could be strengthened?
29. Which, if any, of the options for spending new NHS funding on the adult social care and support system would you favour?
30. Do you have any other comments or stories from your own experience to add?
Page 311 of 324
80 | The lives we want to lead
Prioritising care and support: Between 2010 and 2017, adult social care has had to make savings and reductions worth £6 billion as part of wider council efforts to balance the books. But the service continues to be protected relative to other services. The latest ADASS budget survey shows that adult social care accounts for a growing total of councils’ overall budgets, up from 36.9 per cent in 2017/18 to 37.8 per cent in 2018/1985. As a result, by 2019/20, 38p of every £1 of council tax will go towards funding adult social care.
Innovating: Councils are committed to innovation to help reduce costs while maintaining or improving services to the public. This has included changing the way that demand is managed, more effectively using the capacity in communities to help find new care solutions, and working more closely with partners in the NHS to reduce pressures in the care and health system. Innovative approaches can be found in all parts of the country.
• Kent County Council is driven, like many councils, by the daily challenge of ensuring people have what they need to enable them to leave hospital safely. Daily multi-disciplinary meetings help to identify and reduce delayed transfers of care and weekly improvement cycle meetings address the reasons for the delays. Staff training and good performance management have helped to embed the ethos, resulting in a 59 per cent reduction of people being discharged into residential care and a 54 per cent reduction in people being discharged into short-term beds. This equates to 350 additional people going to live
85 https://www.adass.org.uk/media/6434/adass-budget-survey-report-2018.pdf
86 https://www.local.gov.uk/sites/default/files/documents/25.43%20Chip%20Efficiency%20Project_03_1.pdf
back at home each year. In 2017 Kent saw 911 fewer residential and nursing care placements compared to 2013.
• Kirklees Metropolitan District Council’s ‘Gateway to care’, co-located with community health, is a multidisciplinary ‘front door’ which provides simple care packages for a rapid response, care navigation, assistive technology provision and safeguarding support. Care navigators, located in four community hubs, help to embed a strengths-based approach by building community capacity and supporting people to find solutions in those communities. The front door deals with the majority of contacts first time, with just 6 per cent going on to a full assessment. In 2017/18 almost half of those with eligible care needs achieved good outcomes through community support, saving the council over £1.9 million.
• Bristol City Council is changing the conversation it has with residents when they first make contact with adult social care, focusing on finding help and support from communities rather than from formal care services. This has resulted in 75 per cent of first contacts being referred to community support, with two thirds of those making contact saying that they felt positive about how they had been treated. In the first year, this approach has saved £6 million86.
• In Swindon Borough Council, a review of patient cases showed that when someone was discharged to a residential care setting, 45 per cent of the time they would have achieved
Annex A: Case studies of innovation, delivery and performance
Page 312 of 324
The LGA green paper for adult social care and wellbeing | 81
a better outcome had they been supported to return home (either with domiciliary reablement, or via intermediate residential reablement). However, neither of these services had the capacity or capability to take the additional volume of patients. Swindon’s health and social care teams designed and led a change programme which has achieved a 163 per cent increase in patients receiving reablement services, daily internal coordination meetings and a reduction in social care delayed transfers of care from 450 days in May 2017 to 30 days in March 2018. It has also resulted in an annual saving of over £1.9 million to the health and social care economy.
• Somerset County Council has worked with the social enterprise Community Catalysts to stimulate micro-providers to develop care and support services in rural areas. This enables people to get support from community enterprises in ways, times and places that suit them and their families, rather than from formal support services. This initiative has led to the development of a flourishing social enterprise sector with 178 providers offering low cost, flexible care and support to older and disabled people and their families. In the first year, care has been offered to over 700 people, collectively delivering 3,600 hours of care a week. The council estimates that this approach has saved over £800,000 a year while offering people a far more flexible and accessible service87.
87 https://www.local.gov.uk/sites/default/files/documents/25.43%20Chip%20Efficiency%20Project_03_1.pdf
88 https://www.local.gov.uk/sites/default/files/documents/5.17%20-%20Housing%20our%20ageing%20population_07_0.pdf
• Bristol City Council, North Somerset Council and Bath and North East Somerset Council jointly commission sector-leading care and repair services across all three council areas from a single organisation, West of England Care & Repair (WEC&R). The councils have pooled their resources to secure economies of scale in the delivery of a range of services to support older and disabled people to live well in their existing homes, for example through providing home improvements, handyperson services, adaptions and support with hospital discharge. The scale of the contract has enabled WEC&R to ‘lever in’ additional funding from grants, and to secure additional private funding to complement the funding from councils. More older and disabled people are receiving a service in addition to what can be delivered from the core funding and for WEC&R it provides a viable and sustainable business.88
• Patients in Mendip seeing a doctor can be referred to Health Connections Mendip, a team employed by the 11 Mendip general practices. Patients can discuss what is important to them and the team can help them access the support they might want. The End Loneliness Campaign in Mendip signposts people to clubs and activities, such as Talking Cafes, line dancing classes, community transport, men’s sheds and befriending services. Health Connections Mendip have a team of more than 600 Community Connectors – such as café owners, drivers, supermarket staff – who on average talk to about 20 people a year which means more than 12,000 signposting conversations a year. Health Connections
Page 313 of 324
82 | The lives we want to lead
Mendip works as part of a team which includes primary care, secondary care, adult social care, voluntary sector, town and district councils and the wider community. This partnership working has led to a 20 per cent reduction in local hospital admissions which is saving £2 million on the public purse. Every £1 spent on the scheme saves the NHS £6.89
• Central Bedfordshire Council has addressed the housing needs of its older population by using a detailed qualitative and quantitative evidence base to produce an ‘investment prospectus’ that sets out its vision and development opportunities. It is a more attractive and engaging approach to stimulating the market than a traditional ‘market shaping’ document. The prospectus specifically identifies the range of opportunities that will, collectively, address the identified demographic, housing and care/support needs, as well as the aspirations and requirements of older people. Delivery outcomes from this innovative way of engaging providers and promoting investment in housing solutions for older people include:
• A council-developed extra care housing scheme of 83 units in Dunstable.
• A private sector ‘rightsizer’ housing scheme of 32 units in Dunstable.
• Two new care homes with 141 beds in Dunstable enabling the council to close some of its in-house outdated care home provision.
89 https://www.local.gov.uk/about/news/loneliness-initiatives-cutting-emergency-hospital-admissions-20-cent
90 https://www.local.gov.uk/sites/default/files/documents/5.17%20-%20Housing%20our%20ageing%20population_07_0.pdf
91 London Borough of Harrow Case Study, Care and Health Improvement Programme, April 2018, https://www.local.gov.uk/sites/default/files/documents/London%20Borough%20of%20Harrow%20LIP%20Case%20Study.pdf
92 https://sharedlivesplus.org.uk/short-breaks/item/484-my-shared-life
• A housing association extra care housing scheme of 81 units in Leighton Buzzard.90
• Councils are at the forefront of promoting choice and control through personal budgets. For example, in Harrow the council is working with the CCG to extend the My Community e-Purse system, which supports purchasing social care services and equipment via personal budgets to people with a personal health budget. This project will benefit people, their carers and their families by giving them more control and choice over their carer and support choices. It will also enable closer working between health and social care and find ways of releasing funding tied up in secondary care that could be more effectively used in social care. The council will manage 259 personal health budgets on behalf of the CCG and it is estimated that the savings – to be realised in 2018/19 – will be £147,000 based on the estimated 7 per cent savings that the council’s e-Purse system has already achieved.91
• Shared Lives is a vital and highly praised approach which matches young people or adults who need support with an approved Shared Lives carer, who provides personal care and either a home or a place to visit regularly. Of the 14,000 people using Shared Lives, half live with their Shared Lives carer and half visit for day support or overnight breaks. My Shared Life92 is an online platform that enables people to give their experience of the service. Responses from over 200 people in Shared Lives shows that:
Page 314 of 324
The LGA green paper for adult social care and wellbeing | 83
• 92 per cent of people felt that their Shared Lives carer’s support improved their social life.
• 81 per cent of people felt that their Shared Lives carer’s support made it easier for them to have friends.
• 73 per cent of people felt involved with their community but 93 per cent felt their Shared Lives carer’s support helped them feel more involved.
• 85 per cent of people felt their Shared Lives carer’s support helped them have more choice in their daily life.
• 84 per cent of people felt their Shared Lives carer’s support improved their physical health.
• 88 per cent of people felt their Shared Lives carer’s support made their emotional health better.
• Councils are supporting people with dementia. Sutton Council funds Admiral Nurses to give support to people living with dementia and their families. This has been supported by the local CCG, which recognises the value of providing extra support to these families. And Cumbria County Council is building three new council care homes to cater for residents with advanced frailty and dementia. This has been identified as an area where not enough private provision is available.
• Digital and technology can play a key role in wider service redesign. It can help make the shift from treatment to prevention and there is a growth in consumer-based technology that can be purchased on the high street to support people remain independent at home. It can also help providers deliver more effective person-centred care and we are
seeing examples of providers (across care settings) using technology to help improve communication with friends, family and those receiving care.
• A number of councils including Hampshire, Barnet, Lancashire and Wolverhampton are using care technology to support people to remain independent at home for longer. In Hampshire, 8,600 people are being supported with 94 per cent of people saying that these approaches increase their feelings of safety and security. Ninety-eight per cent of people would recommend the service to others. It is a similar picture in Lancashire where 8,400 people are being helped to maintain independence and safety.
• Areas such as Leeds, Stockport, Bristol, Dorset and Bracknell Forest are bringing information together from the council and health providers which is reducing the need for service users to have to tell their story multiple times. In Luton and Central Bedfordshire, care homes are being supported to improve sharing of information through access to NHS Mail and shared care records. The project with the ultimate goal of fully shared records is now being expanded to all care homes in the region.
• There are a number of new social care technology-based start-ups emerging, which are using technology to improve the delivery of person-centred care. These providers are using technology to better match care workers to clients and digitising the care records so that carers can log on to information about their clients using their smartphone. Other care providers are using technology to store notes about
Page 315 of 324
84 | The lives we want to lead
clients, read up on those they are visiting and using it as a way to raise the alert if anything is wrong. Families and friends can receive notifications and log in to see how care for their family member is proceeding. These forms of technology are enabling care providers to improve the delivery of person-centred care whilst improving business efficiency of care providers. In Liverpool the council has worked to bring the home care provider sector together with technology suppliers which has resulted in the digitisation of care records and introduction of a network that allows for improved monitoring of people requiring care and support at home.
Intervening early and preventing needs: Investing in prevention has clear benefits for people and reduces costs to the wider care and health system.
• Falls prevention programmes run by councils and their partners reduce the number of falls requiring hospital admission by 29 per cent. This represents a return on investment of more than £3 for every £1 spent.93
• Research on Disabled Facilities Grant (a council grant to help disabled people make changes to their home) shows that every £1 spent on housing adaptations is worth more than £2 in care savings and quality of life gains.94
• Evaluation of the Handyperson Programme has shown that handyperson services support large numbers of older and disabled people to live independently at home for longer and
93 https://www.local.gov.uk/about/news/hospital-admissions-due-falls-older-people-set-reach-nearly-1000-day
94 https://www.local.gov.uk/sites/default/files/documents/building-our-homes-commun-740.pdf
95 https://www.local.gov.uk/sites/default/files/documents/prevention-shared-commitm-4e7.pdf
96 For further information, visit: https://www.local.gov.uk/leicester-journey-improving-discharge-and-avoiding-admissions
97 https://www.local.gov.uk/sites/default/files/documents/lga-learning-disability-s-d9a.pdf
with greater comfort and security. Services include small repairs and minor adaptations that reduce the risk of falls, home security measures to help maintain independent living, and energy efficiency checks to help reduce excess winter deaths95.
• Partners in Leicester are improving hospital discharge and avoiding unnecessary admissions through, for instance, an ‘integrated lifestyle hub’ tackling the wider determinants of health, GP-led care planning for patients identified via a risk stratification system, wrap-around rapid access to services such as assistive technology, falls assessment and equipment, and proactive discharge follow-up for at-risk groups. As a result, attendances in A&E in quarter one of 2017/18 were down by 2.9 per cent from the same point in 2016/17.96
• The Kent Pathway Service supports adults with a learning disability to achieve a more independent life. It supports people for between one and 12 weeks to learn or re-learn skills that help them become more independent and need less support. This has also led to an outcomes-focused practice project for people with a learning disability which aims to adopt a strength-based approach by setting goals and monitoring that providers are delivering and undertaking practice reflection sessions.97
Page 316 of 324
The LGA green paper for adult social care and wellbeing | 85
• Darlington Council adopted the progression model, making enablement a priority. High cost packages of care and in-house services in supported tenancies, day opportunities and short break stays were prioritised as areas of greatest opportunity. Following a strengths-based assessment, James, an individual with a learning disability, moved from residential care to his own tenancy and transferred to tenancy support, making an annual saving of £88,600 to adult social care.98
Performing: The Adult Social Care Outcomes Framework (ASCOF) measures how well care and support services achieve the outcomes that matter most to people. Latest information from October 2017 (for 2016/17)99 shows that, even in the deeply challenging financial environment social care has operated in over the last few years, performance has improved or been maintained in several key areas. The Personal Social Services Adult Social Care Survey (for 2016/17)100 also provides encouraging findings:
• 64.7 per cent of service users are extremely or very satisfied with the care and support services they received.
• 67.6 per cent of service users in the community reported that they have enough choice over the care and support services they receive.
• The proportion of people who use services who have control over their daily life is currently at its highest level (77.7 per cent) in the reporting period (2014/15 to 2016/17).
98 https://www.local.gov.uk/sites/default/files/documents/lga-learning-disability-s-d9a.pdf
99 https://digital.nhs.uk/data-and-information/publications/clinical-indicators/adult-social-care-outcomes-framework-ascof/current
100 https://files.digital.nhs.uk/pdf/d/5/pss-ascs-eng-1617-report.pdf
• The proportion of adults with a learning disability who live in their own home or with their family is currently at its highest level (76.2 per cent) in the reporting period.
• The proportion of people aged 65+ still at home 91 days after discharge from hospital into reablement/rehabilitation services is currently at its second highest level (82.5 per cent) in the reporting period.
The proportion of people who use services who say that those services have made them feel safe and secure is currently at its highest level (86.4 per cent) in the reporting period.
The City of Wolverhampton Council is improving outcomes whilst creating a financially sustainable service through the creation of a ‘Promoting Independence Team’ to undertake overdue reviews. To date, 700 cases have been reviewed, 22 per cent of which resulted in a decrease in the size of the care package, delivering a saving of £900,000 per annum. Use of the ASCOF tool to measure quality of life at start and end of intervention indicated that people felt more in control and were achieving better quality of life outcomes following the review.
Page 317 of 324
86 | The lives we want to lead
Page 54:
1. See here for further explanation: https://www.local.gov.uk/sites/default/files/documents/Technical%20Annex%20%281%29.pdf
2. See here for further explanation: https://www.local.gov.uk/sites/ default/files/documents/Technical%20Annex%20%281%29.pdf
3. Our estimate of the cost uses Age UK figures as a starting point. We take their figure of 164,217 – the number of older people who receive no support with three or more essential daily activities – and assume support for those people based on the profile of existing support for older people in terms of home care and residential care. We then apply unit costs: for home care we cost 1 hour per day; for residential we cost a year of residential care.
4. We apply the same method used for estimating the cost of meeting unmet need amongst older people. However, as we do not have a starting number (equivalent to the Age UK figure of 164,217) we link to the number of working age adults currently receiving services. The number of working age adults supported is roughly 40 per cent of the number of older people supported so we apply that percentage to the Age UK figure and apply working age adult unit costs for home and residential care.
5. https://www.health.org.uk/sites/health/files/A-fork-in-the-road-Next-steps-for-social-care-funding-reform-0.pdf
6. As per under-pinning analysis conducted by the Health Foundation and King’s Fund: https://www.health.org.uk/sites/health/files/A-fork-in-the-road-Next-steps-for-social-care-funding-reform-0.pdf
7. See for instance: https://www.health.org.uk/sites/health/files/A-fork-in-the-road-Next-steps-for-social-care-funding-reform-0.pdf and https://publications.parliament.uk/pa/cm201719/cmselect/cmcomloc/768/768.pdf
8. As per underpinning analysis conducted by the Health Foundation and King’s Fund: https://www.health.org.uk/sites/health/files/A-fork-in-the-road-Next-steps-for-social-care-funding-reform-0.pdf
Page 58-59:
9. https://www.health.org.uk/sites/health/files/Social-care-funding-options-May-2018.pdf
10. We take the estimate as put forward by the Health Foundation and King’s Fund (see 61) and uprate it by OBR forecasts for CPI inflation.
11. https://publications.parliament.uk/pa/cm201719/cmselect/cmcomloc/768/768.pdf
12. For illustrative purposes only, we take a figure of £1 billion and divide this by ONS projections for people aged 40+ in 2024/25. In practice there are many different ways to approach this option, and this cost illustration is intended to give an indication of likely average costs.
13. https://www.health.org.uk/sites/health/files/A-fork-in-the-road-Next-steps-for-social-care-funding-reform-0.pdf / https://publications.parliament.uk/pa/cm201719/cmselect/cmcomloc/768/768.pdf
14. For Income Tax estimates, we take the 2020/21 estimate as put forward by the King’s Fund and Health Foundation, and uprate it on the basis of OBR forecasts of income tax take (themselves extended using the long term average rate of growth to get to 2024/25). In effect this is a 1p increase in the rate, not a 1 per cent increase in income.
15. https://www.kingsfund.org.uk/publications/how-nhs-performing-june-2018
16. For National Insurance, we take the 2020/21 estimate as put forward by the King’s Fund and Health Foundation, and uprate it on the basis of OBR NIC revenue forecasts (themselves extended to get to 2024/25 as above). In effect this is a 1p increase in the rate, not a 1 per cent increase in income.
17. https://www.resolutionfoundation.org/app/uploads/2018/06/Healthy-Finances.pdf
18. We assume pensions rise with inflation.
19. Councils with responsibility for adult social care are only raising around £23 billion in council tax this financial year. 1 per cent of this is £230m. We uprate this in line with expected growth in council tax income so that we apply the 1 per cent to the expected tax base in 2024-25.
20. https://www.kingsfund.org.uk/sites/default/files/field/field_ publication_file/Commission%20Final%20%20interactive.pdf
References from tables:
Page 318 of 324
The LGA green paper for adult social care and wellbeing | 87Page 319 of 324

Local Government Association 18 Smith Square London SW1P 3HZ
Telephone 020 7664 3000 Fax 020 7664 3030 Email [email protected] www.local.gov.uk
For a copy in Braille, larger print or audio, please contact us on 020 7664 3000. We consider requests on an individual basis. REF 29.2
© Local Government Association, July 2018
Page 320 of 324
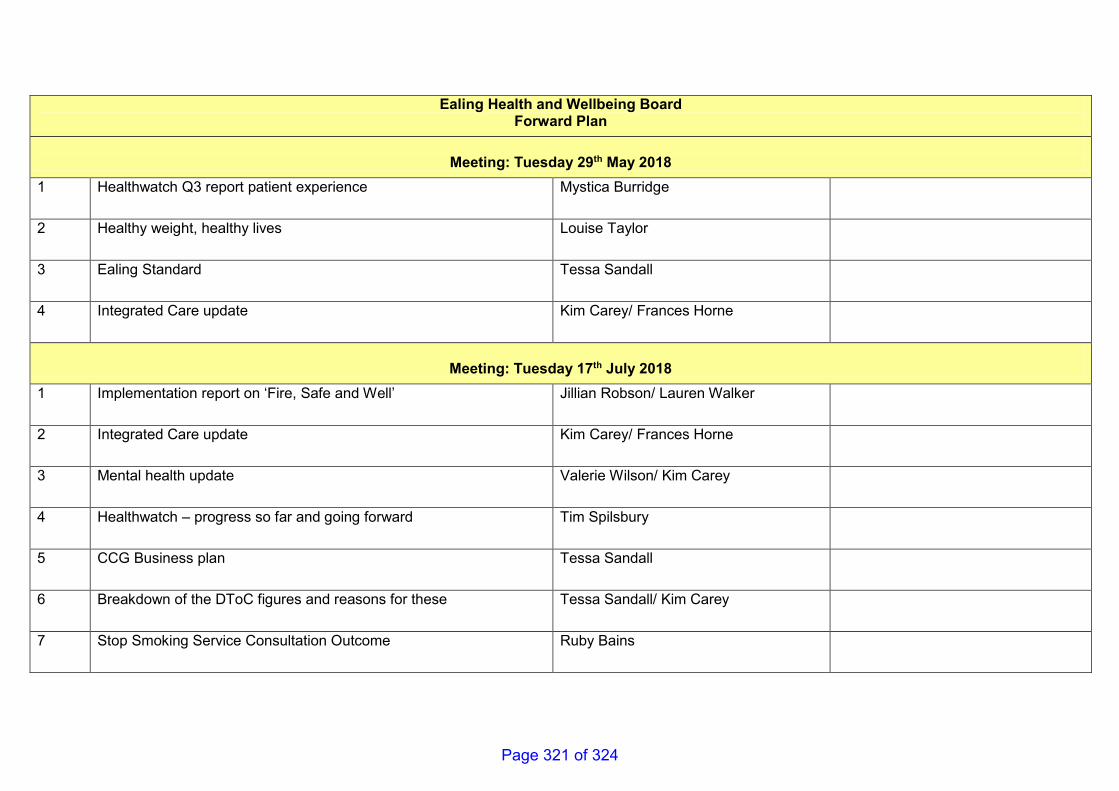
Ealing Health and Wellbeing Board Forward Plan
Meeting: Tuesday 29th May 2018
1 Healthwatch Q3 report patient experience Mystica Burridge
2 Healthy weight, healthy lives Louise Taylor
3 Ealing Standard Tessa Sandall
4 Integrated Care update Kim Carey/ Frances Horne
Meeting: Tuesday 17th July 2018
1 Implementation report on ‘Fire, Safe and Well’ Jillian Robson/ Lauren Walker
2 Integrated Care update Kim Carey/ Frances Horne
3 Mental health update Valerie Wilson/ Kim Carey
4 Healthwatch – progress so far and going forward Tim Spilsbury
5 CCG Business plan Tessa Sandall
6 Breakdown of the DToC figures and reasons for these Tessa Sandall/ Kim Carey
7 Stop Smoking Service Consultation Outcome Ruby Bains
Page 321 of 324
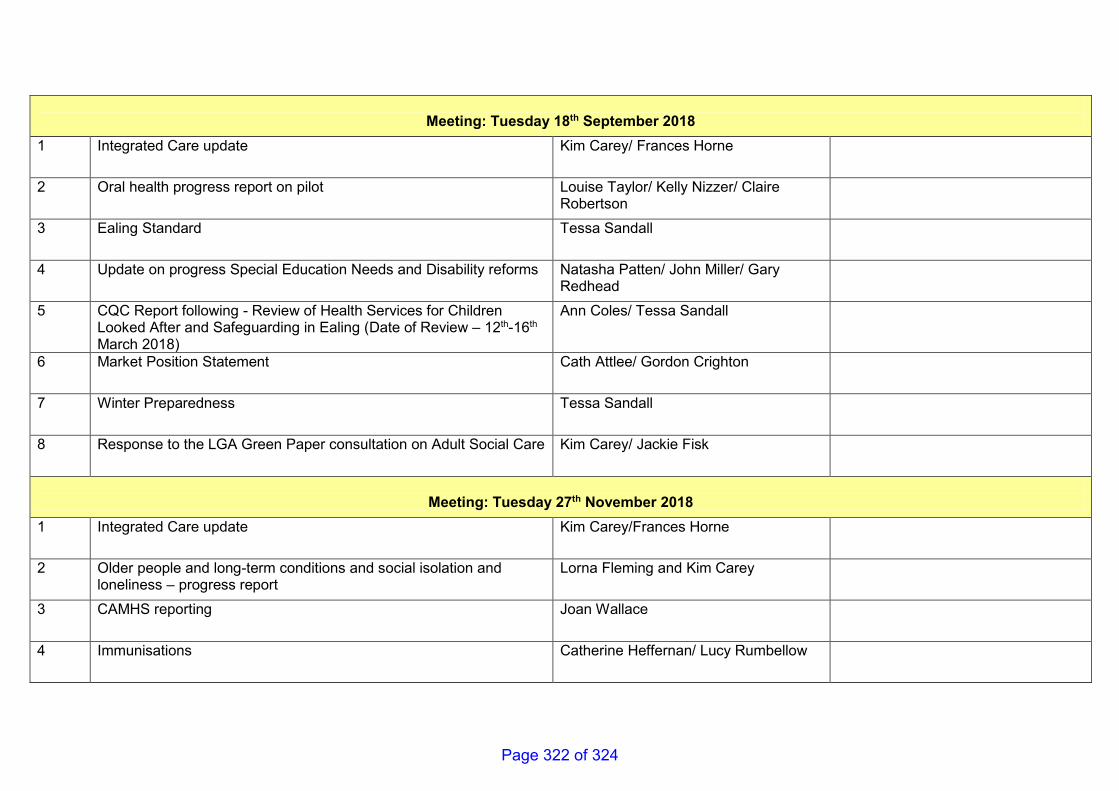
Meeting: Tuesday 18th September 2018
1 Integrated Care update Kim Carey/ Frances Horne
2 Oral health progress report on pilot Louise Taylor/ Kelly Nizzer/ Claire Robertson
3 Ealing Standard Tessa Sandall
4 Update on progress Special Education Needs and Disability reforms Natasha Patten/ John Miller/ Gary Redhead
5 CQC Report following - Review of Health Services for Children Looked After and Safeguarding in Ealing (Date of Review – 12th-16th March 2018)
Ann Coles/ Tessa Sandall
6 Market Position Statement Cath Attlee/ Gordon Crighton
7 Winter Preparedness Tessa Sandall
8 Response to the LGA Green Paper consultation on Adult Social Care Kim Carey/ Jackie Fisk
Meeting: Tuesday 27th November 2018
1 Integrated Care update Kim Carey/Frances Horne
2 Older people and long-term conditions and social isolation and loneliness – progress report
Lorna Fleming and Kim Carey
3 CAMHS reporting Joan Wallace
4 Immunisations Catherine Heffernan/ Lucy Rumbellow
Page 322 of 324
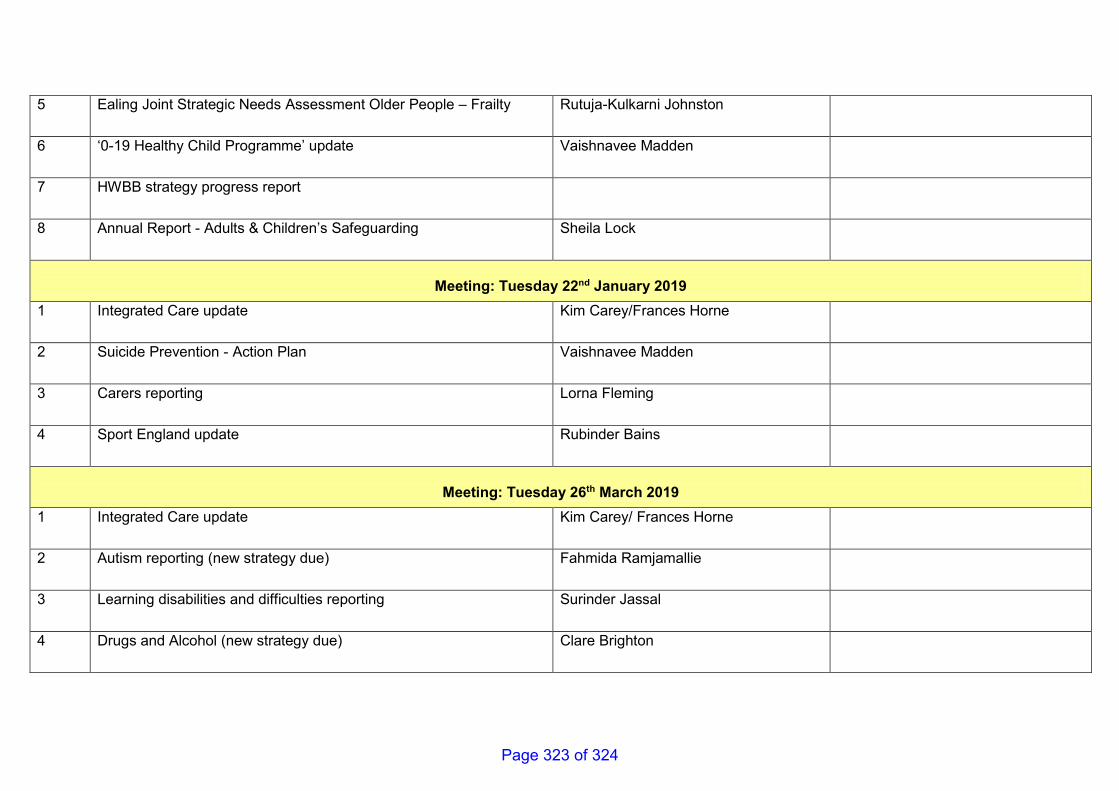
5 Ealing Joint Strategic Needs Assessment Older People – Frailty Rutuja-Kulkarni Johnston
6 ‘0-19 Healthy Child Programme’ update Vaishnavee Madden
7 HWBB strategy progress report
8 Annual Report - Adults & Children’s Safeguarding Sheila Lock
Meeting: Tuesday 22nd January 2019
1 Integrated Care update Kim Carey/Frances Horne
2 Suicide Prevention - Action Plan Vaishnavee Madden
3 Carers reporting Lorna Fleming
4 Sport England update Rubinder Bains
Meeting: Tuesday 26th March 2019
1 Integrated Care update Kim Carey/ Frances Horne
2 Autism reporting (new strategy due) Fahmida Ramjamallie
3 Learning disabilities and difficulties reporting Surinder Jassal
4 Drugs and Alcohol (new strategy due) Clare Brighton
Page 323 of 324

Page 324 of 324





























