Embed Size (px)
Citation preview
PHN Technical Note 86-6
CONTRACEPTIVE SOCIAL MARKETING
by
Lauren A. Chester
February 1986
Population, Health and Nutrition DepartmentWorld Bank
The World Bank does not accept responsibility for the views expressed
herein which are those of the author(s) and should not be attributed to
the World Bank or to its affiliated organizations. The findings,
interpretations, and conclusions are the results of research supported
by the Bank; they do not necessarily represent official policy of the
Bank. The designations employed, the presentation of material, and any
maps. used in this document are solely for the convenience of the reader
and do not imply the expression of any opinion whatsover on the part of
the World Bank or its affiliates concerning the legal status of any
country, territory, city area, or of its authorities, or concerning the
delimitations of its boundaries, or national affiliation.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
PHN Technical Note 36-6
CONTRACEPTIVE SOCIAL MARKETING
ABS T R A CT
This paper presents the results of a survey of the literature oncontraceptive social marketing. Contraceptive social marketing is definedas the sale of contraceptives at subsidized prices through commercialnetworks. The main objective of this approach to contraceptivedistribution is to improve access to family planning products, usingmarketing strategies, at affordable prices to segments of the population
not adequately served by either the commercial sector or government
programs. Contraceptive social marketing projects, unlike free clinicprograms, raise revenue. They utilize the existing commercial distributionnetworks to sell their products. Margins and assorted bonus schemes are
allocated to the members of the distribution chain to encourage
participation and program growth. Contraceptive social marketing strivesto supplement and complement other family planning programs by reaching adifferent target group and providing an alternative source of contraceptive
supplies. There is, however, an inherent tension between the social goalsof sales maximization and program self-sufficiency--these goals need to beprioritized to minimize conflict. Contraceptive social marketing projectscan be only as extensive as the existing commercial network; a weak
infrastructure hampers program growth.
The first national contraceptive social marketing program began
in India in 1967. Today there are 13 ongoing contraceptive socialmarketing projects; the majority are supported by the U.S. Agency forInternational Development. All of these projects sell more than one
method of contraception except India, which sells only condoms (althoughoral contraceptives are being added to its product line). The points-of-purchase for socially marketed contraceptive products include supermarkets,tea stalls, vending machines and pharmacies. In several countriesprescription requirements limit purchase of oral contraceptives topharmacies. Product prices are generally low although a significant rangeexists: one condom costs less than US$.01 in Bangladesh, $.25 in Barbadosand Honduras. The proportion of all contraceptors served by thecontraceptive social marketing project is minimal in Mexico (1.1%) andThailand (3.4%), but significant in Bangladesh (40.5%), Colombia (31.2%)and Egypt (30.0%). The fact that three programs serve at least 30% of allcurrent family planning users and two serve more than 20% suggests thatprograms are acting, to some extent, as an important supply source and areexpanding the availability of contraceptives.
Prepared by: Lauren A. ChesterPopulation, Health & Nutrition Department
February 1986
CONTRACEPTIVE SOCIAL MARKETING
Table of Contents
Page No.
I. Introduction . . . . . . * * n . . . . . . . . . . . . . . 1
II. Pros and Cons of CS Approach . . . . . . . . . . . . . . 2
Advantages. . . . . . . . . . . . . . . . . . . . . . 2Disadvantages . . . . . . . . . . . . . . . . . . . . 2
III. Strategies Used to Achieve CSM Objectives . . . . . . . . 3
Management. * * * * * * . * * . . . . . . . . . . . 3Products. . . . . . . . . . . . . . . . . . . . . . . 4Target Population . . . . * * p * . t . . . . . . 5Brand Name and Packaging. . . . . . . . . . . . . . . 6Distribution Systems. . . . . . . . . . . . . . . . . 6Points of Purchase . . . . . . . . . . . . . . . . . 7Promotion and Advertising . . . . . . . . . . . . . . 7
IV. Evolution of CSM Projects . . . . . . . . . . . . . . . . 9
A. History. . . . . . . . . . . . . . . . . . . . . 9B. Ongoing Projects . . . . . . . . . . . . . . . . . . . 11
India . . . . . . . . . . . . . . . . . . . . . . . 14Sri Lanka . . . . . . . . . . . . . . . . . . . . . 16Bangladesh. . . . . . . . . . . . . . . . . . . . . 17Jamaica . . . . . . . . . . . . . . . . . . . . . . 20Egypt . . . . . . . . . . . . . . . . . . . . . . . 21Caribbean Region. . . . . . . . . . . . . . . . . . 22El Salvador . . . . . . . . . . . . . . . . . . . . 23Nepal . . . . . . . . . . . . . . . . . . . . . . 24Honduras. . . . . . . . . . . . . . . . . . . . . . 24
V. Pricing . . . . . . . . . . . . . . . . . . . . . . . . . 25
A. Pricing Objectives . . . . . . . . . . . . . . . . . . 25B. Determining Appropriate Prices . . . . . . . . . . . . 26C. Current Product Prices and Consumer Outlays for
Protection by CSM Products. . . . . . . . . . . . . 29D. Margins. . . . . . . . . . . . . . . . . . . . . . . 31E. Cost-Effectiveness of CSM Projects . . . . . . . . . . 37F. Mechanisms for Increasing Project Revenue. . . . . . . 41G. Expanded Product Line. . . . . . . . . . . . . . . . . 44H. Substitution . . . . . . . . . . . . . . . . . . . . . 46
VI. CSM Project Evaluation . . . . . . . . . . . . . . . . . . 47
A. Existing Evaluation. . . . . . . . . . . . . . . . . . 47B. Evaluation Findings. . . . . . . . . . . . . . . . . . 48
Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . 51
CONTRACEPTIVE SOCIAL MARKETING
I. Introduction
Marketing can be defined as a managerial process seeking to
achieve a market response via carefully formulated actions with attention
to target markets a distinguishing feature (Greenberg, Novelli and Curtin,
1983). Social marketing involves coordinating the "4P's": product, price,
place (distribution) and promotion to "maximally motivate and facilitate
desired forms of behavior" (Fox and Kotler, 1980). Marketing techniques
are applied to develop and promote a specific goal using commercial
channels of distribution.
The main objective for contraceptive social marketing (CSM) is to
provide family planning products, using marketing strategies, at affordable
(subsidized) prices to segments of the population not adequately served by
either the commercial sector or government programs, in order to improve
access and thus individual welfare. CSM is based on the premises that 1) a
substantial number of people exist in any society that will, if
sufficiently informed, make a rational decision to allot a portion of their
resources to contraceptive purchases; and 2) consumers want alternatives to
government supply sources which are typically family planning or health
clinics.
Selling contraceptives constitutes only part of the marketing
process; marketing tools must also be utilized. Strategies used to achieve
CSM goals are discussed in Sections III and V. The history of CSM projects
and a synopsis of ongoing projects is given in Section IV, and Section VI
looks at project evaluations. A brief description of the advantages and
disadvantages to the CSM approach follows below.
-2-
II. Pros and Cons of CSH Approach
Advantages. CSM projects, as opposed to free clinic programs,
raise revenue. Theoretically, they can be mounted quickly with little
capital expenditure by making use of the established commercial network
(assuming potential problems such as delays in product price approval can
be averted). The number of retail outlets exceeds the actual or potential
number of clinics thereby increasing the potential reach of distribution to
those far from government service points. By utilizing the established
network of distributors and its corresponding administrative bureaucracy,
costs can be kept below those of dispensing the same contraceptives in
clinical programs. Margins alloted to the various members of the
distribution chain and assorted bonus schemes offered to participants can
encourage program growth (see p. 34 for more on bonus schemes). As
commercial entities, CSM projects can detect and respond more quickly to
changing market conditions than government bureaucracies which tend to
operate more slowly and cautiously. CSM serves to supplement and
complement other family planning programs by: 1) reaching a different
target group; 2) providing an alternative to clients who cannot afford
commercially distributed products but are reluctant to use free services
(often seen as inferior--see Price Sensitivity, p. 41; Ylanan and Verzosa,
1979); and 3) increasing product awareness by promotion and advertising.
Disadvantages. There is an inherent tension in CSM between the
social goals of sales maximization and self-sufficiency--these goals need
to be prioritized to minimize conflict. CSM projects can be only as
extensive as the existing commercial network; a weak infrastructure will
hamper program reach. Bureaucratic procedures such as
-3-
registration requirements for pharmaceutical products and the price
approval process can impede project implementation. The CSM product line
can get lost if: there is not sufficient interest in the product and its
promotion along the distribution chain; potential profit is too low because
of small profit margins allowed (coupled with low-priced products); and/or
incentive schemes, meant to supplement profit margins, are insufficient to
motivate distributors. Additionally, it is difficult to assess whether
consumers receive proper instruction on product use from retailers who may
not be highly motivated; for these reasons a number of CSM projects have
opted not to rely solely on the commercial system but to add a back-up
system of promoters (e.g., in-house sales force) to their projects (see
Distribution Systems, p. 6). Retailers tend to respond to rather than
create demand. It also is possible that CSM projects are not reaching new
users but, rather, established users who are substituting CSM project-
supplied products for those obtained from a former supply source.
III. Strategies Used to Achieve CSM Objectives
There are eight key elements to CSM programs (Altman and Piotrow,
1980). These shall each be described briefly in the following except for
pricing which is discussed in Section V.
Management. There are three prevailing management models among
ongoing CSM projects, distinguished by the degree of government
involvement. The first is direct government management, where projects are
implemented directly by the government ministry responsible. The next
involves project management by semi-autonomous agencies which may exercise
management authority or take an advisory role. Projects are subject to an
agreement with the government, specifying project accountability and
-4-
operating conditions. U.S. contractors, local institutions or both are
usually responsible for project operation. The third model is private
organization management. While government is not directly involved, the
projects must comply with general government regulations. Private
organizations operating CSM projects include: independent, non-profit
organizations, including FPAs; and for-profit organizations. One CSM
project (the Caribbean) is now managed by a commercial distributor.
Products. Condoms, oral contraceptives (OCs) and foaming tablets
are the most frequently offered products in CSM projects. All projects
except India market more than one type contraceptive method (see Table 1).
Condoms are supplied in all projects. Their advantages are many and
commonly known; particularly important for CSM is that they are usually
free of legal and medical restrictions, and thus can be sold in a variety
of outlets. OCs are sold by all projects except India (a USAID-supported
CSM project to sell OCs is planned--see p. 16 for details). The main
disadvantage to social marketing of OCs is prescription requirements: 4 of
the 12 projects shown in Table 1 which sell OCs have this requirement,
thereby limiting sales to pharmacies. In two others, prescriptions are not
necessary but sale of OCs is restricted to pharmacies. Pharmacies
constitute a small proportion of commercial outlets and are typically
concentrated in urban areas; accessibility to OCs in rural areas can
therefore be limited. Seven of the projects sell spermicides, but only one
(Mexico) markets injectables. Two projects sell IUDs but only the Egyptian
project sells them at subsidized prices (Mexico sells IUDs at commercial
prices). Egypt has had considerable success at marketing IUDs: IUDs sold
through pharmacies and physicians now account for nearly two-thirds of all
couple years of protection (CYP) provided by the CSM organization, and
-5-
provide coverage to 19 percent of all contraceptors (Social Marketing Forum
(SMF), Spring 1985).1/
Products are donated by USAID and/or IPPF to all but 2 projects.
In Colombia, although some commodities are still received from IPPF,
PROFAMILTA (an FPA) purchases most of the products it sells. In Mexico,
PROFA.M (a private, non-profit organization) purchases packaged commodities
from Mexican manufacturers, as required by law, but hopes to develop its
own production capability for spermicides and condoms. The Indian
government buys condoms directly from Indian manufacturers and gives them
to the CSM project.
Target Population. The target population will be defined by the
objectives of the program. Ideally it will be those not currently using FP
with enough disposable income to buy contraceptives but unable to afford
the full price of commercially marketed products.
Determining the characteristics of the target population through
marketing research can play an important role in designing the CSM project
so that it effectively reaches its target population. It therefore should
be considered an integral part of program design. Investigating willing-
ness to pay and buyer habits and preferences, and testing acceptability of
the product, packaging and promotion techniques contribute to successfully
providing the targeted customers in a non-offensive manner with a product
they can afford. That market research has been used only sporadically and
insufficiently in most ongoing CSM projects is probably due to a lack of
both funds and expertise. An exception to this pattern is Egypt, where
marketing research results are used to guide program operations (see
Egypt, p. 21).
1/ Derived, based on data in Table 2.
-6-
Brand Name and Packaging. Packaging serves the dual purpose of
physically protecting the product and promoting a specific product image;
the latter purpose is usually stressed in CSM projects. Even though
repackaging donated products can be expensive, it has the advantage of
adding distinctive brand names, package design (often needed to
differentiate CSM products from those distributed free in government-run
clinics) and local instruction materials, all of which can be chosen on the
basis of consumer research. Research findings suggest that brand names may
be important to the promotion of a product: condoms tend to be popular
when their names depict manliness and strength (e.g., Panther or Raja
(king)), whereas OCs are favored when their names imply femininity and
affection (Sherris, Ravenholt and Blackburn, 1985).
Distribution Systems. In countries with developed commercial
distribution networks CSM products tend to move from distributors to
wholesalers and stockists to retailers. In countries with less developed
commercial infrastructure the CSM distribution system may be comprised only
of a few salesmen delivering to retailers. Exclusive reliance on
commercial distributors has proven successful in only a few projects (e.g.,
India and Jamaica) because few CSM countries have a developed distribution
network. Problems experienced, such as unwillingness of the distributor to
take on sometimes controversial products with uncertain profit potential,
and little active promoting and selling of CSM products, have prompted the
use of additional distribution systems to supplement, or replace,
commercial distribution. Government and quasi-government distributors
have often been used. In-house sales forces, made up of CSM project staff,
are being used in a number of projects, most notably, Bangladesh. They are
responsible for the distribution tasks of transporting, promoting and
-7-
selling CSM products to retail outlets. Another system occasionally used
consists of village distributors who sell products either to retailers or
directly to consumers. The last two systems tend to have greater
flexibility and mobility to reach more remote areas not well serviced by
the commercial network.
Points of Purchase. The points of purchase constitute the last
link in the distribution chain. Retail outlets (e.g., food stores,
barbershops, street hawkers, etc.) and medical establishments (where
medical personnel promote and sell CSM products, as in Bangladesh; or where
OC prescriptions are required) are primary purchasing locales. Other
purchase points, tried with varying degrees of success, include vending
machines, which are subject to maintenance problems and vandalism; and mail
orders, which have constituted a small part of CSM projects where they were
tried. Using a mail order system usually involves direct consumer
response, and is feasible only in countries with high levels of literacy
and newspaper coverage combined with reliable mail service. Sri Lanka's
experience with this method was relatively successful and cost-effective:
18 months after the project was started, 2 percent of condoms sold were via
mail order (Binnendijk, 1985; Davies and Louis, 1977). Mobile sales units
are being successfully used in Bangladesh: vans travel throughout rural
areas showing family planning films and selling CSM products. House-to-
house sales have had mixed results and are generally expensive compared to
use of an existing commercial system.
Promotion and Advertising. Promotional messages and materials
are used to call attention to CSM products; to inform potential users of
the product's advantages, price, and availability; and ultimately to
persuade consumers to buy CSM products. Promotion to consumers, retailers,
-8-
distributors and other influential groups is considered an essential
component of CSM projects (Sherris, 1985; Altman and Piotrow, 1980). Two
major constraints exist for social marketing promotion: resistance to
advertising and cost. Promotion is often the largest line item in the
operating budget.
CSM projvcts basically utilize four types of promotion:
mass-media; point-of-purchase (posters, displays); public relations
campaigns (rallies at sports events); and the interpersonal approach
(education activities of village promoters). Most programs use print and
broadcast media, and all use some type of point-of-purchase promotions,
e.g., pop-up counter top OC dispensers in Jamaica. Many countries do not
allow public advertising of prescription drugs (see Table 1); in such
countries, or in isolated areas with few or no TVs or radios, other
techniques are used. For example, in Nepal decorated jeeps travel
throughout remote areas broadcasting family planning messages on
loudspeakers and the drivers sell the products.
Advertising messages should be tested to establish that they are
acceptable to their intended audience and accomplish their motivational
goal. The effectivc ness of different family planning themes was pre-tested
in Bangladesh: the most effective messages were those stressing family
economics (food and shelter) and children's (sons') future; least effective
were ads stressing benefits for the wife (Harvey, 1984a). In Ghana, where
the advertisement for the CSM condom was not adequately pretested, the
reaction to mass media promotion of the product was negative and eventually
contributed to the termination of the project.
Even though advertising has been an integral part of CSM
campaigns, ti- effect of advcrzising cn -ales volume has not been
-9-
adequately studied. Available information indicates that it does indeed
lead to increased sales (and conversely to a sales decrease when
advertising is discontinued): evidence from Bangladesh and India in the
mid 1970s showed that advertising restrictions and cuts in the promotional
budget corresponded to decreased sales (Altman and Piotrow, 1980); in
Honduras, sales of OCs doubled in the two months following a five week
advertising campaign, dropped sharply in the months after advertising was
stopped, and rose again when advertising was resumed (Levy, 1984). Such
evidence, while interesting, is much too fragmented, too correlational and
covers periods too short to allow firm conclusions to be drawn.
IV. Evolution of CSM Projects
A. History
The first national CSM program began in India in 1967 and was
designed and supported by the Ford Foundation. Rural Kenya was the site of
the first private CSM project, where Population Services International
(PSI) established a two-year experimental program in 1972 with funds
provided by USAID. In 1973, CSM projects began in Colombia and in Sri
Lanka.
IPPF has been active in initiating and supporting projects in
Colombia, Sri Lanka and Thailand. But by far the greatest amount of
support for CSM projects has come from USAID. Programs funded by USAID
generally begin with full financial support under the management of U.S.
contractors. Technical assistance and assistance for operational expenses
tend to be reduced as programs mature and become more cost-effective.
Commodity support typically continues indefinitely. USAID has supported
the start of 18 full-scale projects since 1974: of these 10 are ongoing
- 10 -
(although Mexico is no longer funded by USAID), 5 are in preparation and 3
have been terminated or suspended. Termination of projects, begun in the
1970s in Tunisia and Ghana, resulted from lack of host government
commitment, government restrictions and from institutional problems. In
Ghana, political sensitivity to mass media advertising of CSM products (see
p. 8), which was not adequately assessed, contributed to the project's
demise. Difficulties with hiring and retaining program managers also
contributed to project failure. More recently, USAID withdrew support from
the Ecuador CSM project, in which no sales transactions had occurred over
the 2-1/2 year project life. Failure to obtain product price approval,
government objections to sale of donated commodities, and changes in
government all contributed to the suspension of this project.
A CSM project launched in Mexico in 1977 with the support of
USAID, proceeded well until 1980, when a change of government led to vastly
diminished support of family planning. New officials rescinded the
project's sales permits for all contraceptives except condoms. They
restricted contraceptive advertising and denied requests for price
increases. Project performance declined markedly, lead,ng to withdrawal of
USAID support. This project has continued without USAID support, although
coverage has fallen markedly, from about 5 percent of the target population
in 1980 to less than 1 percent in 1984. The project has also been selling
a mix of non-contraceptive products (e.g., Bic pens, Q-tips, key-chains,
etc.) in efforts to achieve self-sufficiency and fill the gap created by
lost USAID support (see Section V.H. for more information on product mix).
- 11 -
B. Ongoing Projects
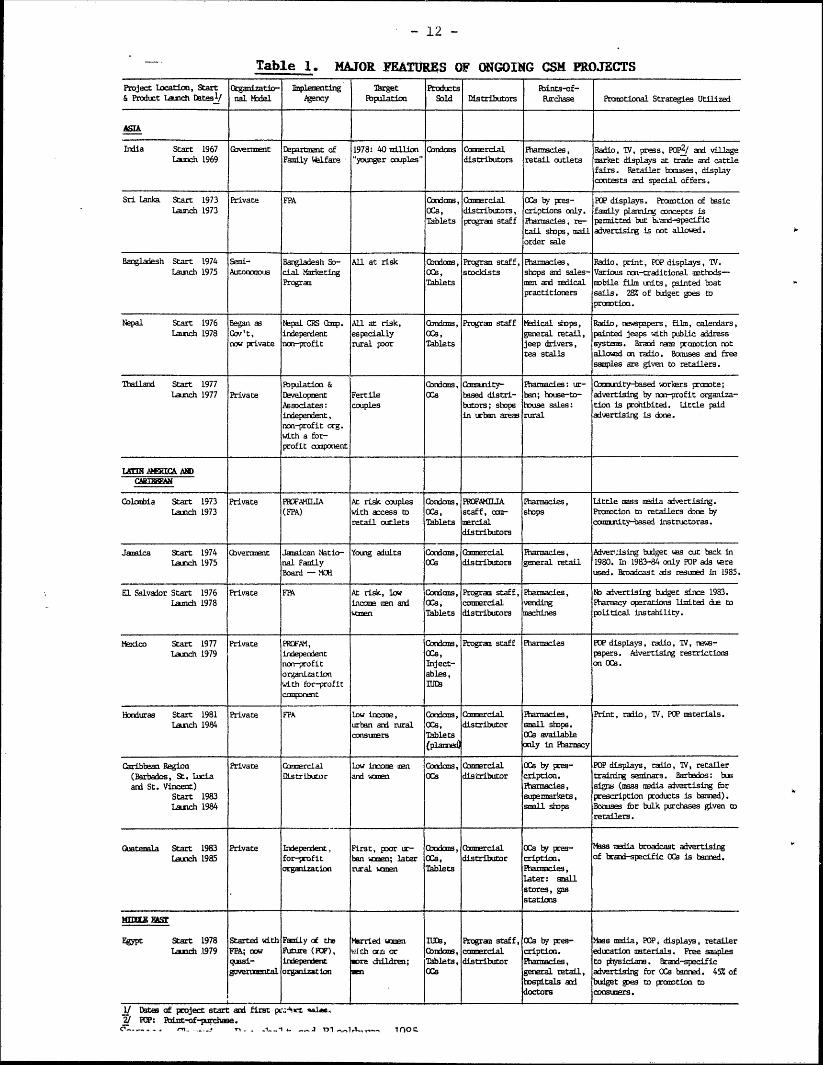
There are currently 13 CSM projects considered to be ongoing,
including one project that has only recently begun sales (Guatemala).
Eight are supported directly by USAID, two by IPPF, those in India and
Thailand by their governments, 2 / and that in Mexico with no outside
funding. The major features of and promotional strategies used by these
projects are given in Table 1.
While the literature does attempt to define CSM, it provides no
clear-cut delineations as to what features constitute a true CSM project.
There is disagreement as to whether the projects in Colombia and Thailand
qualify as true CSM endeavors because their operations are not geared
toward obtaining the typical CSM objective. Instead, they strive to
maximize commercial objectives rather than to provide affordably priced
products to the underserved population; they do not restrict their target
population to low income groups; and they rely heavily on door-to-door
sales in rural areas, not the usual sales method used in CSM projects.
They also employ few of the marketing techniques that are characteristic of
CSM projects (e.g., both do little or no advertising, a major component of
the CSM approach).
Both of these projects use village level workers to promote and
distribute products: these workers operate door-to-door and sell directly
to the consumer. This practice is more typical of a community distribution
program than a CSM program. The goal of Colombia's project is to meet
contraceptive demand as well as subsidize other programs operated by
2/ Thailand also receives some support from USAID and IPPF.
- 12 -
Table 1. MAJOR FEATURES OF ONGOING CSM PROJECTS
Project location, Start organizatio- Implermenting Target Products Fints-of-& Product Lauich Dates/ nal Model Agency opulation Sold Distributors Purchase Ponotional Strategies Utilized
AMIA
Irdia Start 1967 Government Department of 1978: 40 millicn Condsan Camercial Pharmacies, Radio, V, press, POp2/ ad village
Launch 1969 Family Wlfare "younger couples" distributors retail outlets uarket displays at trade and cattlefairs. Retailer bonuses, displaycontests and special offers.
Sri Lanka Start 1973 Private FPA Condoas, Cnercial ('s by pes- POP displays. Prountion of basicLaunch 1973 ocs, distributors, criptions only. family planning concepts is
Tablets progran staff Pharmacies, re- permitted but bLand-specifictail shops, mail advertising is not allowed.order sale
Bangladesh Start 1974 Semi- Bangladesh So- All at risk Condas, Program staff, Pharmacies, Radio, print, POP displays, TV.launch 1975 Autonmous cial Marketing oce, stockists shops and sales- Various ton-tralitional mathods-
Progran Tablets an and uedical nobile film units, painted hatpractitioners sails . 28% of budget goes to
prootion.
Nepal Start 1976 Began as Nepal CRS Gomp. All at risk, ondoas, Progran staff Medical stops, Radio, newspapers, film, calendars,launch 1978 Gov 't, independent especially ocs, general retail, painted jeeps with public address
now private nm-profit rural poor Tablets jeep drivers, systems. Brand name promntion nottea stalls allowd on radio. Bonuses ad free
samples are given to retailers.
Thailand Start 1977 IbpaLation & Cnioms, Cnmnity- Pharmacies: ur- Cammuity-based uorloars promnote;launch 1977 Private Development Fertile CCs tesA distri- ban; house-to- advertising by tn-profit organiza-
Associates: couples butors; shape house sales: tion is prohibitel. Little paidindependent, in trban areas rural aivertising is done.norn-profit org.with a for-profit conponent
LAMM AHERIC& AN)
Colabia Start 1973 Private PROFAMILJA At risk couples Condas, PRIXILIA Pharmacies, Little mass media advertising.Launch 1973 (FPA) with access to ocs, staff, con- shops Prorotion to retailers done by
retail cutlets Tablets Mercial community-based instructoras.distributors
Jamaica Start 1974 (bverment Jamaican Natio- Young adults Ccxas, Gamercial Pharmacies, Adverl;ising badget as cat back inLaunch 1975 nal Family OS distributors general retail 1980. In 1983-84 only POP ads nere
Board - MCt used. Broadcast als resuned in 1985.
El Salvador Start 1976 Private FPA At risk, low Condoms, Progran staff, Pharmacies, No aivertising budget since 1983.Lainch 1978 income can ad OCs, commercial vending Pharmacy operations limited due to
vonen Tablets distributors machines political instability.
Mexico Start 1977 Private PROFM, Cordams, Program staff Pharmacies POP displays, radio, TV, news-launch 1979 indepernent ocs, papers. Advertising restrictions
non-profit Inject- on OCs.
organization ables,with for-profit IUD9canrPnent
Bonduras Start 1981 Private FPA tow income, Coniams, mercial Phrmacies, Print, radio, W, POP materials.Lanch 1984 urban and rural Cs, distributor snall shops.
consumers Tablets CEs available(Planned) only in Pharmacy
Caribbean Region Private C33mercial Low ixome arn Condans, Cnmorcial OCs by pres- POP displays, radio, V, retailer(Barbados, St. Lucia istribucor and woaen (Es distributor cription. training seminars. Barbedos: busand St. Vincent) Pharmacies, signs (mass nadia avertising for
Start 1983 supennarkets, prescription products is banned).Laxinch 1984 smell stops BoUS for bulk purchases given to
retailers.
Guatemala Start 1983 Private adependent, First, poor ur- Oxxkas, Clercial OCs by pres- as media broadcast advertisingLaunch 1985 for-profit ban wonen; later OCs, distributor cription. of brand-pecific Cs is banned.
organization rural woaen Tablets Pharmacies,later: snallstores, gasstations
KWITZ EASZ
Egypt Start 1978 Started with Family at thL Married aomen IUD9, Program staff, OCa by pres- Mass nails, POP, displays, retailarlaunch 1979 FPA; now Future (FUF), with ctr or (brios, commercial cription. education naterials. Free sales
quai- indepenient more ildren; Tablets, distributor Pharmaies, to physician. Brand-specificaveromental organization CES general retail, advertising for (es ernd. 45% of
hospitals ad buget 9yes to pranotion todoctors consumars.
1/ Dates of project start and first pc,Aat sale,2/ Pa: thLat-of-purchase.
- 13 -
PROFAMILIA.3/ In urban areas, PROFAMILIA targets the middle class: it
sells products at high prices to pharmacies, which in turn sell them to
consumers at price levels similar to those for commercially distributed
products. At these price levels the programs cannot adequately serve the
low income population (a typical CSM objective). The urban pharmacy
component, which accounts for two-thirds of total program sales, does cover
nearly 11 percent of all married women of reproductive age (MWRA) and the
total project covers 15 percent of all MWRA and 31 percent of all
contraceptors in Colombia.
The Colombia and Thailand projects do not seek to maximize
distribution but gear marketing efforts toward achieving commercial rather
than demographic objectives. For this reason, as well as those given
above, they will not be discussed extensively in this text.
Not unexpectedly, of the remaining 11 projects, the most
protection measured in terms of couple years of protection (CYP)4 / is
provided in the two countries with the largest populations: the projects
in India and Bangladesh provided 2 million CYP and 1.3 million CYP,
respectively, in 1984 (see Table 2). But, the India program served only
1.4 percent of all married women of reproductive age (MWRA), the Bangladesh
project, 7.7 percent. However, it is estimated that of all contraceptors
in Bangladesh (representing 19 percent of all MWRA), about 40 percent are
served by the CSM program, the highest coverage of users among the
3/ In Colombia's case, some feel that while lack of advertising and high
urban prices remove it from true CSM ranks, the higher urban pricessubsidize the rural program and help it reach the true CSM objective ofserving low income, isolated populations.
4/ For a definition of CYP, see Table 2.
-14
established CSM projects (compared to e.g., 6 percent in India). 5 / This
project accounted for 50 percent of all CYP provided by the total national
program's distribution of condoms, OCs and spermicides in 1983. Egypt
ranks third in CYP provided by projects shown in Table 2, and 30 percent of
all contraceptors are served by its CSM project. In Nepal, the CSM project
reaches 21 percent of contraceptors and accounts for 50 percent of all
condoms distributed in the country, for all spermicides and for 20 percent
of OCs. Coverage in El Salvador, Sri Lanka and Mexico (p. 10) is low and
in the latter two has declined since 1980 (see forthcoming discussion for
explanation). A further description of ongoing CS projects is given
below. 6 /
India 7/. This project is a Government-sponsorea (MOH) effort in
which the Government buys condoms from Indian manufacturers at very low
prices and gives them to the CSM project. Various distributors arrange for
marketing through existing commercial channels, such as tea companies.
Over 400,000 retail outlets distributed Nirodh condoms in 1983/84.
Promotion has been designed and executed within the government; extensive
advertising and point-of-purchase campaigns have accompanied distribution.
The level of sales has increased from less than 25 million in 1968 to
nearly 200 million in 1983. Coverage is estimated to be about 1.4 percent
of MWRA. Nirodh condoms are sold for $0.01 each (see Table 3 on CSM
product prices).
5/ As a comparison, annual sales of the 10 leading OC brands in the U.S.represents about 11.5 percent of all MWRA. Sherris, Ravenholt andBlackburn, 1985.
6/ No further discussion of Mexico, Colombia or Thailand is given.Because Guatemala has just begun sales, no further descriptionadditional to information in Table 1 is given.
7/ Less information is available for this project because it is not USAIDsupported.
- 15 -
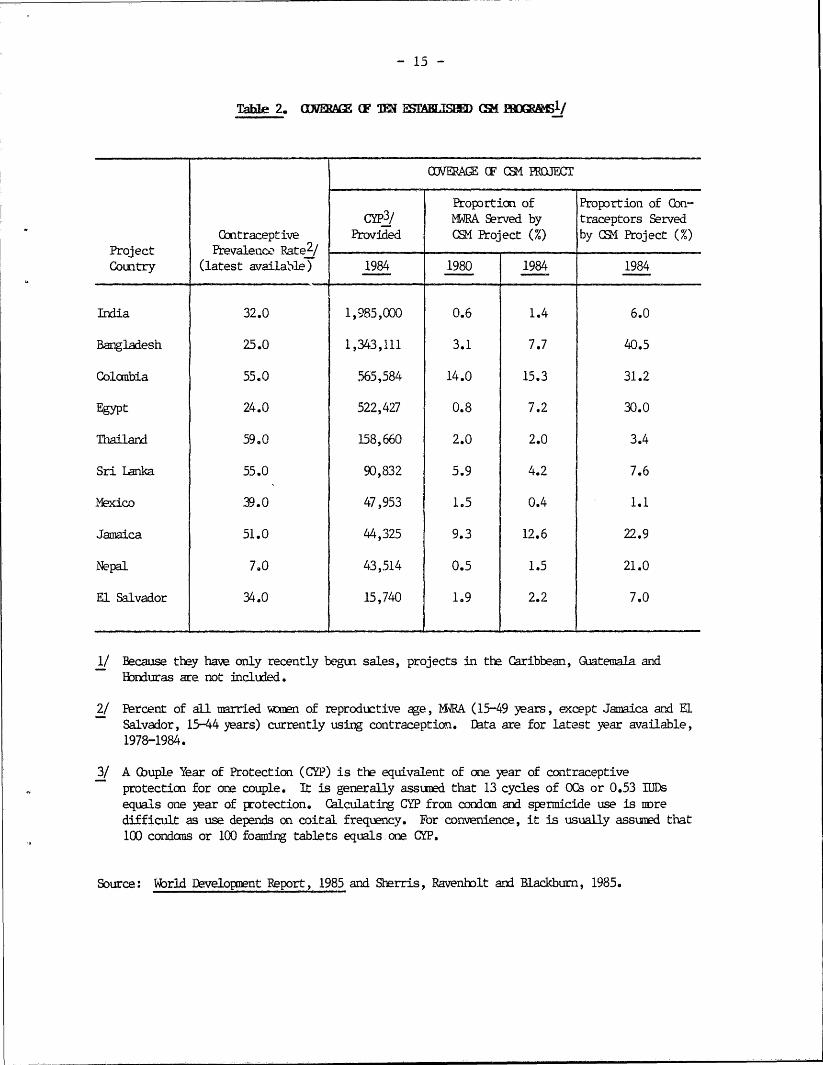
Table 2. (IMWM ( TM ULMSAITSH EM 1RORMSI/
(INERAGE OF (SM PROJECT
Proportion of Proportion of Con-Cyp3/ WRA Served by traceptors Served
Contraceptive Provided CSM Project (%) by C4 Project (%)Project Prevalence Rate2 /Country (latest available) 1984 1980 1984 1984
India 32.0 1,985,000 0.6 1.4 6.0
Bangladesh 25.0 1,343,111 3.1 7.7 40.5
Colombia 55.0 565,584 14.0 15.3 31.2
Egypt 24.0 522,427 0.8 7.2 30.0
Thailand 59.0 158,660 2.0 2.0 3.4
Sri Lanka 55.0 90,832 5.9 4.2 7.6
Mexico 39.0 47,953 1.5 0.4 1.1
Jamaica 51.0 44,325 9.3 12.6 22.9
Nepal 7.0 43,514 0.5 1.5 21.0
El Salvador 34.0 15,740 1.9 2.2 7.0
1/ Because they have only recently begun sales, projects in the Caribbean, Guatemala andHonduras are not included.
2/ Percent of all married wmen of reproductive age, RA (15-49 years, except Jamaica and ElSalvador, 15-44 years) currently using contraception. Data are for latest year available,1978-1984.
3/ A (buple Year of Protection (CYP) is the equivalent of one year of contraceptiveprotection for one couple. It is generally assumed that 13 cycles of OCs or 0.53 IJDsequals one year of protection. Calculating CYP from condom and spermicide use is nredifficult as use depends on coital frequency. For convenience, it is usually assumed that100 condoms or 100 foaming tablets equals one GYP.
Source: World Development Report, 1985 and Sherris, Ravenbolt and Blackburn, 1985.
- 16 -
The Nirodh program has successfully marketed a tremendous number
of condoms during its existence, but sales have lagged in recent years. A
basic problem arose because marketing management had been placed under the
authority of the MOH. Marketing executives have been frustrated by trying
to operate in the commercial world while constrained by government
bureaucracy, budget processes and the involvement of other Ministries,
which have differing and sometimes conflicting priorities and objectives.
When the Marketing Director, placed in the MOH, wanted to hire a
photographer to try out ideas for a new package design, he was unable to,
because all such activity had to be carried out by the Ministry of
Information and Broadcasting, the purveyor of advertising.
There is also some question as to whether the large corporations
(e.g., Union Carbide), which buy condoms from the government and market
them with a margin through their distribution systems, receive adequate
compensation from condom sales. Their activity level has often seemed
dependent on the extent of public relations value they received and/or
government pressure exerted on them to sell condoms (Schellstede, 1985).
In 1984, 15 years after product launch, a second condom was added
to the product line: Nirodh Deluxe, a higher quality, lubricated condom
priced at $0.016. In addition, to help alleviate program stresses and to
spur sales the government plans to set up a semi-autonomous, non-profit
Contraceptive Marketing Organization (CMO) to manage a CSM project that
will sell OCs through pharmacies. This project will target literate, urban
couples with some disposable income, and hopes to have 1.6 to 2.0 million
customers by 1988 (representing 20 percent coverage of the targeted group).
Sri Lanka. Designed to operate on a national scale, this project
was implemented in 1973 by PSI. It is now managed by the national FPA;
- 17 -
both commercial distributors and CSM staff distribute condoms. OCs are
distributed by CSM staff only. For Preethi condoms, the first product
sold, sales reached their highest level in 1980. However, because donor
funding was reduced in the early 1980's, the project was forced to begin
selling many products at commercial prices and to drop the most popular,
low-priced Preethi ($0.03) condom in order to raise needed revenue. The
project now promotes a low priced condom ($0.015), 2 moderately priced
condoms ($0.04-0.05) and two brands sold at higher, commercial prices
(about $0.22 per condom), as well as 1 OC and 1 spermicide. It is also
selling consumer goods such as plastic bags in order to raise additional
income. While this move toward self-sufficiency has been successful in
terms of income generation (by 1984 the program made a profit of about
$0.34 per CYP), the emphasis on higher-priced products has meant lower
total sales and lower coverage (in 1984, 4.2 percent of MWRA were covered,
down from 5.9 percent in 1980).
Bangladesh. This CSM project, managed by the Social Marketing
Program (SMP--a semi-autonomous organization) and assisted by PSI, began
sales with Raja condoms and Maya OCs in 1975. In 1979 foaming tablets were
added, followed by a low dose OC in 1980 and Panther condoms in 1983. It
is one of the more successful projects in terms of both coverage and sales
levels. Initially distribution relied on the existing commercial network,
but it was found that products were not reaching rural areas and
distributors seemed unwilling to expand to these areas. SMP therefore
started its own in-house distribution system using its own sales force: a
300-person staff consists of, among others, a national sales manager, who
supervises 8 regional sales managers, and 70 salesmen (Schellstede and
Ciszewski, 1984). Wholesalers, relieved of having to provide salesmen,
- 18 -
participated more willingly. Emphasis on rural outreach has been such that
up to 60 percent of CSM products may now be sold ultimately to the rural
population. SMP salesmen and medical representatives sell products to
tradesmen. Sales have been made to more than 100,000 various
establishments, including "stockists" who sell products to small retailers
and consumers.
This project distributed enough contraceptive products in 1984 to
cover nearly 8 percent of MWRA (up from 3.1 percent in 1980); of the 11
ongoing CSM projects, only Jamaica reaches a greater share of the
population at risk. In 1983, SMP provided 67 percent of national condom
protection, 21 percent of OC protection and 70 percent of spermicide
protection. In FY 1975-76, SMP provided a total of 80,000 CYP, or 8
percent of nationally provided CYP; in the 12-month period ending June
1983, it provided 931,000 CYP, or 50 percent of the national program output
(Davies, 1983).
"Raja" has virtually become the generic name for condoms.
Extensive and intensive promotion, such as use of riverine junks displaying
Raja logo on the sails, is seen as largely responsible for the 690 percent
sales increase in Raja from 1976 to 1982. Sales increases have paralleled
improvements in the SMP's ability to contact, supply and service
increasingly more distribution outlets. Three brands of condoms are now
offered by the project, although sales are dominated by Raja. "Raja"
condoms sell for less than $0.01 each, about one-tenth the commercial
price. Condoms now account for 86 percent of the total CYP provided
annually by the SMP.
There have been some questions raised concerning actual condom
usage: there is a substantial "gap" between usage implied by national
- 19 -
program records (4-5 percent) and usage measured in the Contraceptive
Prevalence Survey (1.8 percent). Non-cqntaceptive use--the "balloon
factor"--and smuggling (7-8 million condoms to Burma and India annually)
can account for only a small portion of the gap (Davies, 1983). A study by
Family Health International (FHI) concludes that underreporting of condom
use by women appears to be the major cause of the gap.
Davies estimates total condom prevalence to be about 5.4-6.2 percent.
"Maya" has become synonymous with oral contraceptive (OC). Early
use of widespread distribution on a non-prescription basis was not
effective--sales plateaued in 1978 and 1979. Market research found that
people were afraid of the pill, and that rural medical practitioners were
using OCs as a convenient explana'ion for various medical complaints of
clients, Because extensive promotion apparently could not overcome
people's negative perception of the pill, mass marketing does not seem to
have been well suited to dealing with concerns surrounding this product.
The problem of mass marketing may have been accentuated in Bangladesh where
most purchases are made by men--their effectiveness at relaying information
received at point-of-purchase to their wives is problematic.8 /
A new distribution strategy was adopted late in 1980 with the
addition of Ovacon, a low-dose pill. Medical representatives, added to the
sales force, now handle OC distribution to pharmacies and medical
personnel; the idea being to use these "detail men" to counter, through
education, the negative image of OCs that practitioners were portraying,
and to motivate them to actively promote and sell OCs. The plan was that
over-the-counter sales would resume only after OCs were carefully
8/ Low price and an "unscientific" name may also have affected salesperformance.
- 20 -
introduced through medical channels. The new strategy appears to be
working. OC sales over the past two years have grown faster than those of
condoms, doubling from 1982 to 1984, and in 1984 exceeded 2 million cycles
for the first time. Ovacon accounted for 40% of 1984 OC sales (Sherris,
Ravenholt and Blackburn, 1985).
Jamaica. Jamaica's Commercial Distribution of Contraceptives
(JCDC) program is a leader among CSM projects, reaching a large proportion
of MWRA (12.6 percent) and covering nearly one-quarter of all
contraceptors. This success has been accomplished despite a number of
management problems and only a modest growth in sales over recent years.
The ability of the Jamaica project to successfully utilize commercial
distributors is probably due to its commercial infrastructure being
stronger than many other project countries.
Under the management of Westinghouse Health Systems (WHS), sales
of Panther condoms and Perle OCs began in 1975. Sales levels in 1976 were
twice those in 1975. The MOR assumed project responsibility in 1977 when
WHS's contract was not renewed. Starting in 1978, USAID supplied only
commodities and technical assistance, discontinuing funds for advertising.
The MOH had difficulty recruiting a good marketing director because they
were paying only on the civil servant pay scale, and project management
ceased to be consumer-oriented. The country's economic problems
contributed to rising JCDC operating costs, and product prices could not
keep pace with inflation. Condom sales continued to rise but at a slower
rate of 9 percent from 1977 to 1980. During the same period pill sales
increased by 19 percent. Inflation and price controls were eating into
distributor margins during this period and the number of retail outlets
selling CSM products declined. After three years of negotiations, the
government fiaslly approved an increase in product prices in 1981.
- 21 -
However, in real terms, the new prices are actually lower than the 1975
prices due to devaluations in the Jamaican dollar: a Panther condom now
costs $0.03, half the 1975 price; one Perle cycle sells for $0.16 compared
to $0.36 in 1975. After 1980 the rate of increase for product sales slowed
further: to 4 percent for condoms, 9 percent for OCs. Part of this
slowdown was to be expected as the absolute quantity of sales increased,
but it is likely that the change to government management (along with the
problems just mentioned) may have contributed to the reduced rate of sales
growth.
Despite the managerial and financial difficulties, however, the
project remains viable. Targeting the teenage market (because of the high
rate of adolescent pregnancy) is one of the new strategies being tried to
restore the JCDC's earlier momentum. Products are sold, in retail outlets
patronized by young people and pharmacists have been instructed not to
impede teenagers from buying contraceptives.
Egypt. When this project began in 1978 it was part of the FPA;
it became institutionalized as a separate, semi-autonomous organization,
Family of the Future (FOF), in 1979. Sales growth has been significant and
product sales are third highest among the 11 ongoing CSM projects. It now
covers about 7.2 percent of married women of childbearing age (up from 0.8
in 1980), and 30 percent of all contraceptors. The project operates under
a product management system in which each product has its own manager,
responsible for setting objectives and developing marketing strategies.
Condoms, foaming tablets and low-dose OCs are sold by this
project through a combination of in-house and commercial distribution. FOF
contraceptives are promoted at popular beaches and through rallies at
sports events; free samples of condoms and tablets are distributed as are
- 22 -
hats and T-shirts bearing product logos. This project in fact spends 37
percent of its budget on promotion. It has conducted extensive market
research which has enabled it to segment its target market according to
education, attitudes, buying habits, etc. Promotional efforts have been
addressed to the identified segments.
The unique feature of the Egyptian project is that it is the only
one to market IUDs at subsidized prices. The Copper T and Copper 7 IUDs
account for 61 percent of the CYP provided by the project. IUDs are sold
almost exclusively to married women with children who typically buy them at
pharmacies and take them to their doctors for insertion. Early attempts to
gain medical staff participation using printed educational material were
far less successful than was the approach of detailing, personal visits by
medical representatives to physicians and pharmacists to introduce, promote
and sell IUDs, and training programs on IUD insertion. While an aggressive
public relations program helps maintain project visibility and legitimacy
among physicians, it also has its price: in the last quarter of 1984,
promotion to doctors consumed over 20% of the CSM program's budget
(Sherris, Ravenholt and Blackburn, 1985).
Caribbean Region. Barbados, St. Lucia and St. Vincent comprise
the first regional CSM project. The reasoning behind trying this multiple
country approach is that "the bigger market allows savings for countries
too small to run cost-efficient projects of their own." The project is
modeled after Jamaica's CSM project and has adopted its advertising
materials and brand name products; the package for the Perle OC has been
redesigned. The Barbados FPA originally managed the project; it is now
operated by a commercial distributor with technical support from the SOMARC
project of the Futures Group.
- 23 -
Condoms are available in pharmacies, mini-markets, and small
shops. There is a prescription requirement in each country and OC sales
are restricted to pharmacies except in St. Vincent where OCs may also be
made available at non-pharmacy outlets.9 / Because Barbados has banned mass
media advertising of prescription products, bus signs, posters and
detailing to pharmacists and doctors are the chief promotional techniques
used. Retailer incentives in the region include giving the retailer two
free cycles of OCs for every 24 bought and one free condom for every ten
purchased. Physician orientation seminars, to provide project information
and product samples, were held when the project started.
Even though the regional structure probably has financial
benefits, it undoubtedly complicates bureaucratic procedures. Some
difficulties have arisen from cultural and language differences, but the
biggest problem has been overcoming the economic disparity between Barbados
and its two less affluent neighbors. A two-tiered pricing strategy was
devised to address this problem: higher prices are charged in Barbados
($1.75 per OC cycle and $0.75 per condom 3 pack) than in St. Lucia and St.
Vincent ($1.26 and $0.42, respectively). These prices are high relative to
other CSM projects but they are 25 to 50 percent lower than prices for
commercially distributed products in these countries.
It is hoped that this project can be expanded; feasibility
studies are underway on Antigua, Dominica and St. Kitts.
El Salvador. This project is managed by the country's FPA. It
continues to operate despite the political instability in the country, much
turnover in project management personnel, and declining sales levels.
9/ In St. Lucia and St. Vincent, the prescription requirement is very"relaxed." Bayley and Washchuck, 1983.
-24-
Condoms, OCs and tablets are sold mostly through pharmacies. Pharmacies
are only open periodically and have put bars on the windows: clients can
no longer go into pharmacies, they must purchase products through the
barred windows (Blackburn, 1985). The project reaches about 2.2 percent of
MWRA.
Nepal. The early years of this project, which began selling
condoms and OCs in 1978, were plagued by cultural, distributional and
promotional impediments; products were promoted but not available in many
areas, creating a bad image for the project. Multiple languages, difficult
terrain and a weak commercial infrastructure hampered sales growth. In
response to the problems, an in-house sales force was established to
distribute products to wholesalers, stockists and retailers. Two
additional steps were taken in 1981 to help alleviate these problems:
jeeps were acquired to ease mobility and promotional problems, and the
government rescinded its ban on contraceptive brand name advertising on
radio. As a result, sales of Dhaal condoms (which sell for $0.01 each)
increased 95 percent in 1982. Foaming tablets were added to the product
line in 1983. The project covers 21 percent of all contraceptors but only
1.5 percent of MWRA.
After 7 years of quasi-governmental management with technical
assistance from WHS, the CSM project was incorporated as an independent,
non-profit organization in 1983; The Nepal Contraceptive Retail Sales
program has recently become a private company. In 1984 the program hired a
woman sales representative for its products, the first Nepalese woman to
sell contraceptives (SMF, Fall 1984).
Honduras. One of the 4 CSM projects managed by an FPA, this
project officially began in 1981 but organizational and legal problems, and
- 25 -
difficulty in getting the OC registered delayed product launch until March
1984. Sales of condoms and OCs were low in the remainder of 1984 (7,900
CYP) and costs were high (the cost per CYP was $42). In general these
results constitute a poor performance for a 4-year old project. However,
because product sales only began in 1984, it is still too early to evaluate
the eventual success of the project.
V. Pricing
CSM projects are meant to complement government-sponsored and
other commercial distribution programs by reaching a target population that
these programs fail to adequately service. From the consumer point-of-view
there is little difference between CSM products and commercially sold
products except the price: both are usually distributed via retail
outlets, but the CSM products are generally priced to increase sales rather
than to maximize profits (Huber, et. al., 1985). Government and donor
subsidies, which cover product and some start-up costs, allow for
contraceptives to be sold at a low price but one sufficient to generate
some revenue for the distributor, retailer and the project itself.
A. Pricing Objectives
The basic goal of the CSM program has a direct bearing on
determination of pricing objectives. The social objective to increase
accessibility to and availability of family planning products to
populations not presently served means that sales maximization and market
penetration are primary goals in setting prices,, with efforts to attain
self-sufficiency a secondary purpose (Ylanan and Verzosa, 1979). USAID no
longer promotes self-sufficiency as a long-term goal; instead it stresses
cost-effectiveness and maximizing cost recovery without reducing
- 26 -
coverage (Ravenholt, 1985).10/ Project experience to date indicates that
most projects are not ready for financial self-sufficiency "unless the
social objective of expanding contraceptive prevalence is to be sacrificed"
(Harvey, 1984b). As has been mentioned, Mexico's CSM project is considered
self-sufficient and Sri Lanka's is making a profit but in both coverage has
been marketedly reduced; Colombia's project raises considerable revenue but
is not targeted toward low-income market segments.
B. Determining Appropriate Prices
Determining prices for contraceptive products is a critical task
in the planning of a CSM project. Product prices can influence the
behavior of all of the links in the distribution chain--consumers',
retailers, etc. The process of price selection requires considerable study
and analysis if the needs and interest of the CSM project and the target
population are to be served. Arriving at the optimum price is complicated
by the difficulty in identifying the actual costs to the user: consumers
face a number of opportunity costs additional to product costs.
Project designers determine the prices to be charged for CSM
products. They must take into account program goals (coverage and cost
recovery); consumer expectations; government pricing laws; distributor,
wholesaler and retailer margins; and prices relative to target market
income and prices of other consumer products. The process of setting
prices entails a number of steps. First is consideration of what have
become the basic "rules of thumb:" the price of a one month supply of the
product should be less than one percent of the monthly income of lower
10/ "Self-sufficiency" generally means project operation continueswithout subsidies. Subsidies usually cover contraceptive commodities,advertising and some start-up costs. Lewis, 1984.
- 27 -
income groups of the target population; CSM product prices should be in the
same ballpark as prices of frequently purchased items (e.g., loaf of bread,
toothpaste, razors, cigarettes)--this allows the monthly purchase of
contraceptives to fit into the buying habits and cash availability of the
target groups; and CSM products should be about half of the price of other
commercially distributed products. In general these "rules" have been used
as guidelines in price setting by the ongoing projects (Ravenholt, 1982).
The Nirodh program in India chose a price low enough for the "user to
perceive the condom as an everyday necessity, like soap, tea and coffee"
(SMF, Summer 1984). In Bangladesh, the cost of one year's supply of
contraceptives equals about one day's wages at the prevailing rate of farm
labor (Schellstede and Ciszewski, 1984). In Honduras the monthly income of
some groups was $50 in 1980; accordingly the recommended price for a one
month's supply of CSM products was $0.50. But the "rules" are not always
followed: in Egypt CSM products are not as cheap as the lowest priced
contraceptives available through commercial channels and in Honduras OCs
are sold for $0.75 per cycle, more than the recommended price (see
Table 4).
Market research to investigate consumer ability and willingness
to pay, and the price sensitivity of the target market (e.g., consumer
perception of the product quality and price link) should be conducted to
help determine appropriate price levels. It is generally stated that if
prices are set too high the product becomes too expensive for the target
group, and if set too low, the product will be perceived as being of poor
quality. Although the evidence is somewhat mixed, available information
suggests that these assumptions are valid. A review of studies of
developing countries presented by Lewis (1984) shows that while there is
- 28 -
little difference in demand for free and moderately priced products, demand
is reduced for higher priced products. In Jamaica and Thailand, Akin and
Schwartz (1985) found that as product prices increase, product use
decreases, although not markedly (see Price Sensitivity, p. 41 for more
information). On the other hand, survey results from Egypt indicate
existence of the consumer perception that "anything free or cheap can
hardly be good" (Howell and Novelli, 1980). In Thailand, OC users
suffering from side effects often switch to higher priced OCs seen as
higher quality and Ath fewer side effects. "Indirect marketing evidence
from India and post-price rise increases in demand in Jamaica and Sri Lanka
suggest that prices can be too low, depressing demand by reducing consumer
confidence in the contraceptive market" (Lewis, 1984).
Use of pre-launch surveys can help identify consumer attitudes
toward price levels. For example, such a study done in Bangladesh
confirmed that proposed OC and condom prices were acceptable to consumers;
in Nepal OC prices were found to be acceptable but survey respondents in
remote area: felt condom prices were too high.
Distributor, wholesaler and retailer margins to be offered for
sale of CSM products must also be considered in determining product prices
(see Margins, p. 31). These margins, designed to cover expenses and
provide profit, are added to the base price of the product. Margins
provided for CSM items are usually comparable to those for other consumer
products, although some programs (e.g., Nepal, Guatemala and Jamaica) offer
higher margins as an incentive to sell CSM products. Any government
pricing laws must also be accounted for in setting prices.
Based on the program objectives, "rules of thumb," market
research, margins to be offered, etc., project management sets a price for
- 29 -
its products. Many. governments must approve initial prices for new
pharmaceutical products. This process has caused serious problems for some
CSM projects. For example, the project in Ecuador, which had planned to
begin sales in the summer of 1984, was suspended in April 1985 because the
government had failed to approve proposed prices for OCs and spermicides.
Government approval is also necessary in some countries to change (usually
increase) product prices. This process runs more smoothly in some
countries (e.g., when import duties were imposed on tablets in Egypt the
project had little trouble getting approval for a price increase) than in
others (e.g., Jamaica--see p. 20).
C. Current Product Prices and Consumer Outlays for Protection
by CSM Products
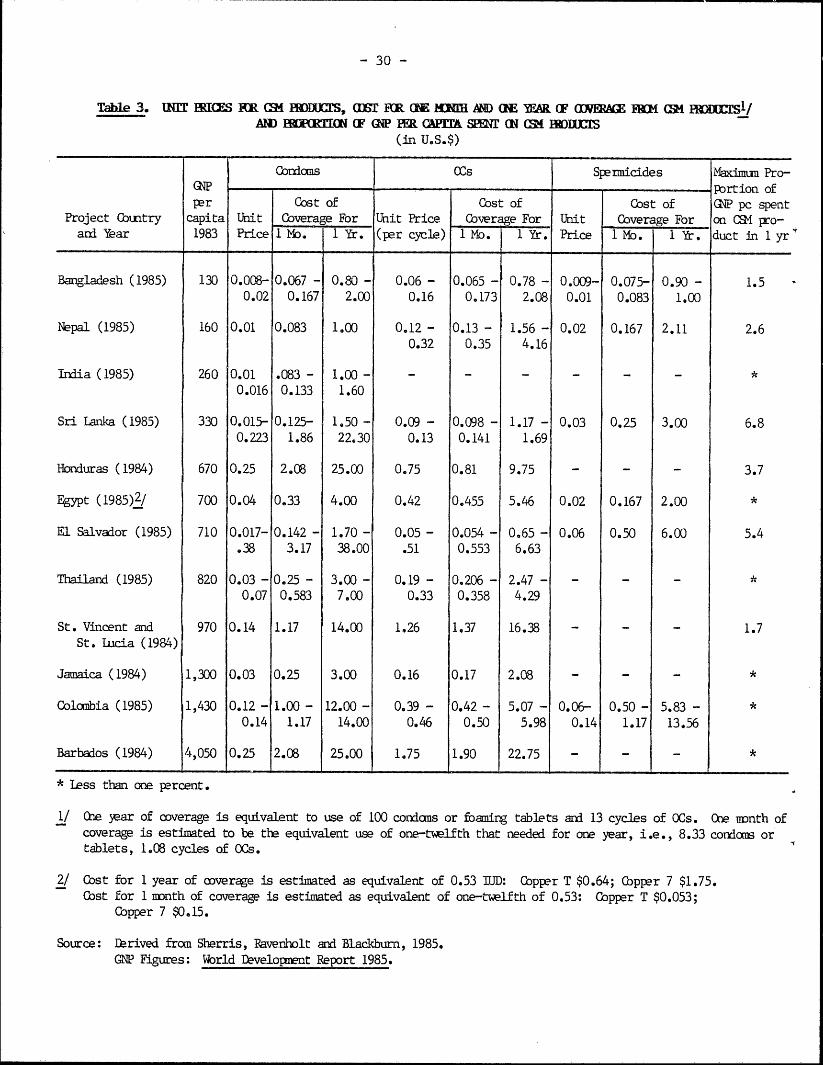
Table 3 shows an estimate of what consumers pay for monthly and
yearly coverage from CSM contraceptive products based on current product
prices, and how that relates to GNP per capita in the CSM countries.11 In
general, there is consistency across projects with consumers in the poorest
countries paying the lowest prices (Bangladesh, Nepal, India, Sri Lanka).
Consumers typically pay more in the Latin American and Caribbean countries
than in Asia, with the exception of Jamaica, where the price of one cycle
of OCs ($0.16) is notably low given its middle income status (see p. 20 for
pricing problems in Jamaica). Overall prices are lowest in Bangladesh and
highest in the Caribbean project (see p. 23 for discussion of Caribbean
project).
Half of the project countries shown in Table 3 offer multiple
products at different prices. The lowest cost of a month's supply of
11/ See Footnote 1/ Table 3 for explanation of calculations.
- 30 -
Table 3. MNIT RICES KR SK PlMlUClS, (If RR (1E IDII AND GCE )EAR (F MME FRM CS1 RMESl/AM HRET(ON F GP ( ER CAPTIA SUE W CS24 HRrS
(in U.S.$)
Condoms OCs Spermicides Maximum Pro-GNP Prtion ofper Cost of Cost of Cost of GNP pc spent
Project Country capita Unit Coverage For Unit Price Coverage For Unit Coverage For on CSM pro-ani Year 1983 Price 1,M. 1 Yr. (per cycle) I Mo. 1 Yr. Price 1 Mo. 1 Yr. duct in l yr
Bangladesh (1985) 130 0.008- 0.067 - 0.80 - 0.06 - 0.065 - 0.78 - 0.009- 0.075- 0.90 - 1.50.02 0.167 2.00 0.16 0.173 2.08 0.01 0.083 1.00
Nepal (1985) 160 0.01 0.083 1.00 0.12 - 0.13 - 1.56 - 0.02 0.167 2.11 2.60.32 0.35 4.16
India (1985) 260 0.01 .083 - 1.00 - - - - - - - *0.016 0.133 1.60
Sri Lanka (1985) 330 0.015- 0.125- 1.50 - 0.09 - 0.098 - 1.17 - 0.03 0.25 3.00 6.80.223 1.86 22.30 0.13 0.141 1.69
Honduras (1984) 670 0.25 2.08 25.00 0.75 0.81 9.75 - - - 3.7
Egypt (1985)2/ 700 0.04 0.33 4.00 0.42 0.455 5.46 0.02 0.167 2.00 *
El Salvador (1985) 710 0.017- 0.142 - 1.70 - 0.05 - 0.054 - 0.65 - 0.06 0.50 6.00 5.4.38 3.17 38.00 .51 0.553 6.63
Thailand (1985) 820 0.03 - 0.25 - 3.00 - 0.19 - 0.206 - 2.47 - - - - *0.07 0.583 7.00 0.33 0.358 4.29
St. Vincent and 970 0.14 1.17 14.00 1.26 1.37 16.38 - - - 1.7St. Lucia (1984)
Jamaica (1984) 1,300 0.03 0.25 3.00 0.16 0.17 2.08 - - - *
Colombia (1985) 1,430 0.12 - 1.00 - 12.00 - 0.39 - 0.42 - 5.07 - 0.06- 0.50 - 5.83 - *0.14 1.17 14.00 0.46 0.50 5.98 0.14 1.17 13.56
Barbados (1984) 4,050 0.25 2.08 25.00 1.75 1.90 22.75 - - - *
* less than one percent.
1/ Cne year of coverage is equivalent to use of 100 condoms or foaming tablets and 13 cycles of OCs. COe month ofcoverage is estimated to be the equivalent use of one-twelfth that needed for one year, i.e., 8.33 condoms ortablets, 1.08 cycles of OCs.
2/ Cost for 1 year of coverage is estimated as equivalent of 0.53 IUD: Copper T $0.64; Cbpper 7 $1.75.Cost for 1 month of coverage is estimated as equivalent of one-twelfth of 0.53: Copper T $0.053;
Copper 7 $0.15.
Source: Darived from Sherris, Ravenlolt and Blackburn, 1985.GNP Figures: Wbrld Development Report 1985.
- 31 -
condoms by country ranges from $0.067 in Bangladesh to $2.08 in Barbados
and Honduras. In seven countries, a month's supply costs $0.25 or less.
Six countries offer more than one brand, thus providing a choice of product
and price. The range for one month of protection from the lowest priced
OCs available by country is $0.05-$1.90 (El Salvador and Barbados are the
outliers); all but two fall below $1.00, and most are $0.50 or less. A
number of projects offer different dose levels of OCs with low-dose pills
often priced higher: they are seen as more desirable and of better
quality. In Nepal the low-dose OC was priced higher ($0.32 per cycle) than
the regular dose ($0.12) to "coincide with its high quality, more effective
image" (SMF, Spring 1984). The cost of coverage from spermicides is
generally close to that for condoms. By country, consumers pay more for
condoms on a monthly basis than for OCs in seven of the countries offering
both, less in three and about the same in one (Bangladesh).
Expenditures for a year's supply of CSM products generally
accounts for a small proportion of GNP per capita in project countries:
2.6 percent or less in 9 countries (less than 1 percent in six of those
nine). This supports Lewis' assertion that spending on family planning
does not represent a large proportion of household expenditures even in low
income countries.
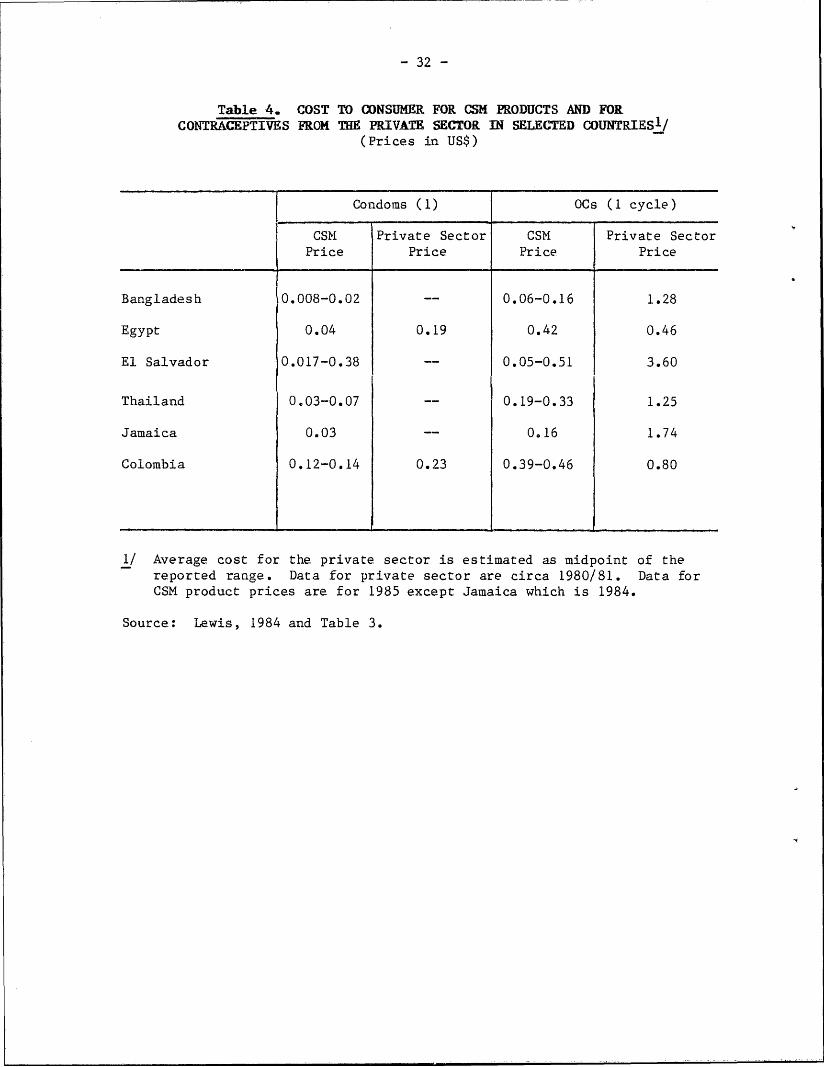
CSM product prices are generally much lower than those found in
the private sector (Table 4). The exception to this is found in Egypt
where OCs from the private sector cost only slightly more per cycle ($0.46)
than those from the CSM project ($0.42).
D. Margins
Most CSM programs rely at least partially on the commercial
distribution system to market their products. Profits to distributors,
- 32 -
Table 4. COST TO CONSUMER FOR CSH PRODUCTS AND FORCONTRACEPTIVES FROM THE PRIVATE SECTOR IN SELECTED COUNTRIESI!
(Prices in US$)
Condoms (1) OCs (1 cycle)
CSM Private Sector CSM Private SectorPrice Price Price Price
Bangladesh 0.008-0.02 -- 0.06-0.16 1.28
Egypt 0.04 0.19 0.42 0.46
El Salvador 0.017-0.38 -- 0.05-0.51 3.60
Thailand 0.03-0.07 -- 0.19-0.33 1.25
Jamaica 0.03 -- 0.16 1.74
Colombia 0.12-0.14 0.23 0.39-0.46 0.80
1/ Average cost for the private sector is estimated as midpoint of thereported range. Data for private sector are circa 1980/81. Data forCSM product prices are for 1985 except Jamaica which is 1984.
Source: Lewis, 1984 and Table 3.
- 33 -
wholesalers and retailers who sell CSM products are determined by the level
of markup they are allowed. Margins for CSM products are usually
comparable to those for other commercial products. While there is a
considerable range in the level of margins allowed, distributor margins
typically range from 15 to 20 percent; wholesaler margins: 4 to 8 perdent;
and retailer margins: 15 to 25 percent. In a few countries margins for
pharmaceuticals are dictated by law (e.g., Mexico). Some programs have
offered higher-than-standard margins to increase profit levels and thereby
encourage the participation of the commercial distribution system. In
India, distributors and wholesalers are allowed a 13 percent margin on CSM
condoms compared to 6 percent offered on most other goods; retailers
receive a 20 percent margin, nearly twice that for other goods (see
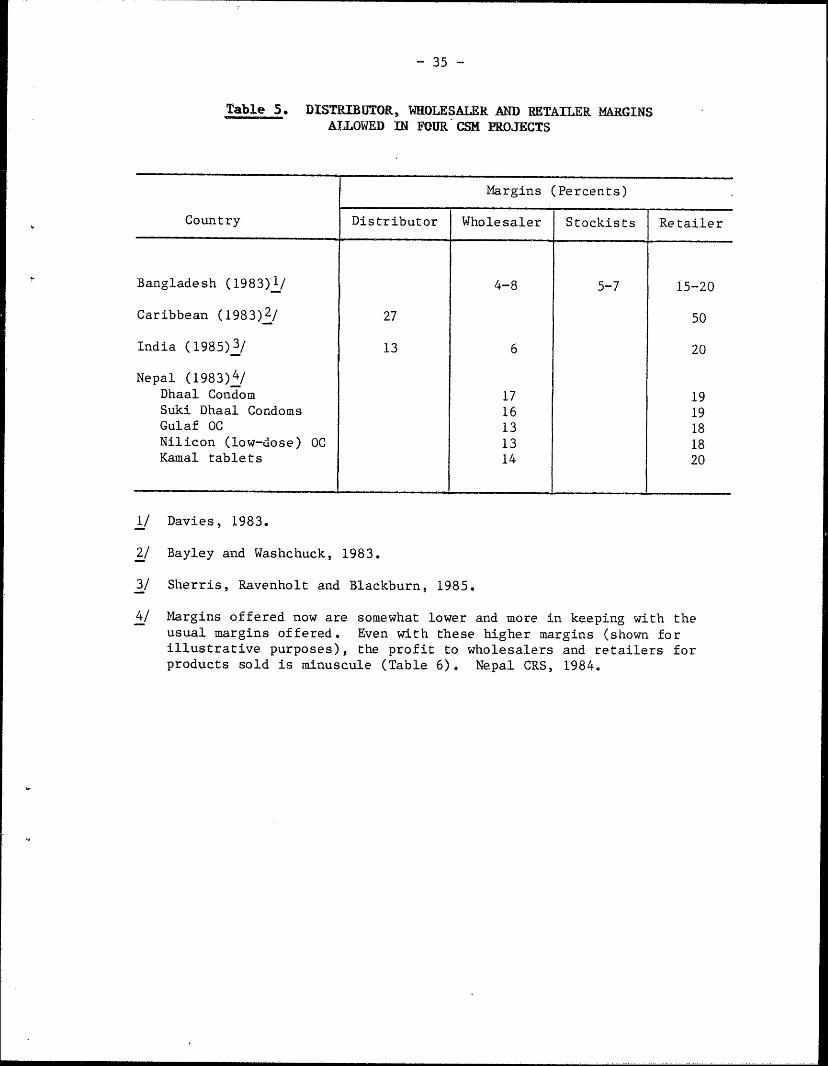
Table 5). In Nepal, the retailer and wholesaler margins were originally
set higher than the usual margin allowed: 18 to 20 percent rather than 15
percent for retailers and 13 to 17 percent, instead of 8 to 10 percent for
wholesalers. These have since been revised downward: wholesalers selling
Gulaf OCs now get a 12 percent margin, while retailers are allowed a
15 percent margin (Sherris, Ravenholt and Blackburn, 1985).
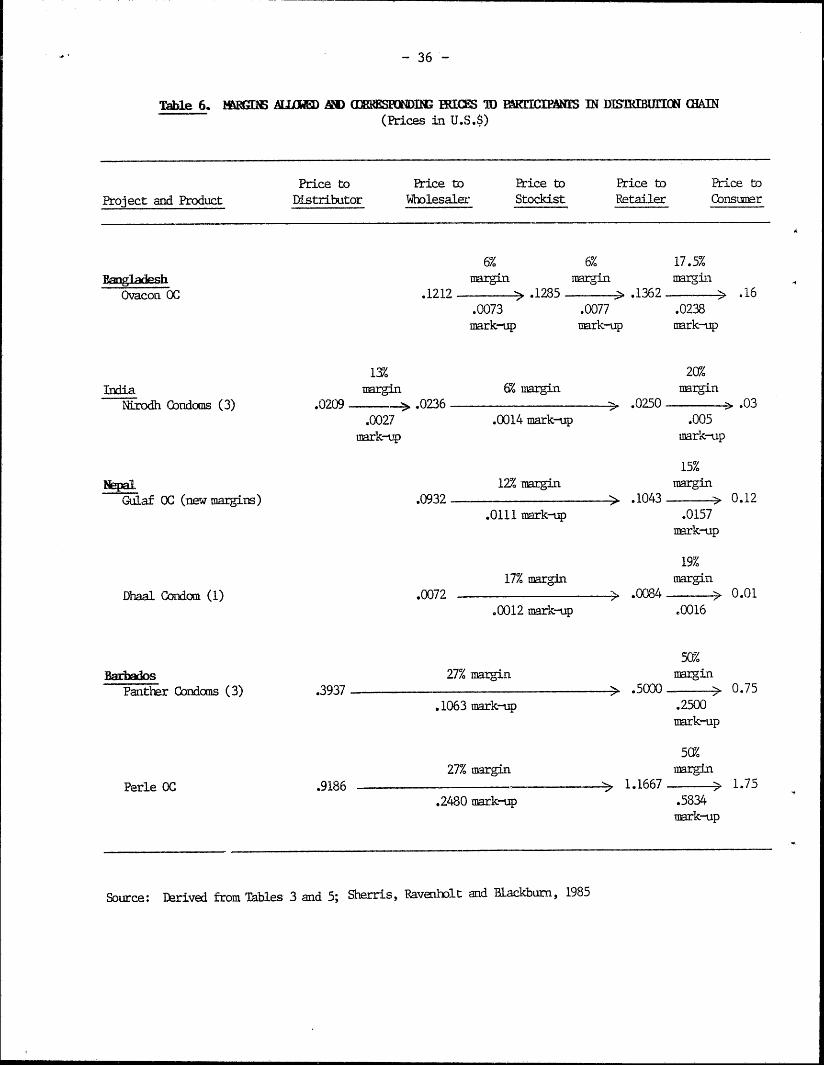
Despite increased margins, profit levels are often very low, not
because the margin itself is low but because the product prices are so
low. For example, in Jamaica, where Panther condoms sell for $0.03 each,
retailers earn very little ($0.0064 per condom sold) even though the
retailer margin is quite high (27 percent); in contrast, the least
expensive, commercially distributed condom in Jamaica provides seven times
more actual profit on each sale because of its higher price (Sherris,
Ravenholt and Blackburn, 1985). Table 6 provides additional examples of
margins and profits received by the different members of the distribution
- 34 -
chain. In Barbados, where the product price and margins are high, profit
levels are considerably greater.12/
Profits earned from margins on product prices which have not been
changed during a project to keep pace with inflation appear to have
declined. In a study by the International Contraceptive Social Marketing
Project (ICSMP), most of the 10 CSM projects examined showed retailer
profit declined to one-third to one-half its initial value since project
launch (ICSMP, 1983a).
CSM projects have developed a number of tactics to help alleviate
these problems. For distributors and wholesalers profit margins are
typically the incentive for involvement, although occasionally they may be
induced to participate as a public relations gimmick or by strong govern-
ment support (i.e., political appeal to sense of patriotism--India). A
number of projects offer bonuses or discounts additional to margins to
encourage retailer participation. In Egypt pharmacies receive a credit
subsidy: they are allowed relaxed payment terms (30 days) on large orders
of CSM products; free displays are also given on bulk purchases of
condoms. Nepal and the Caribbean projects offer free samples with bulk
purchases: in the latter, retailers receive two free cycles of OCs for
every 24 purchased and one free condom for every 10 bought. Nepal offers
one free bonus condom for each one purchased: the scheme reportedly led to
a 60 percent increase in sales to retailers in 1978. Nepal also offers
free calendars and prescription pads to retailers. Nepal has found these
strategies more effective than high margins for increasing retailer
12/ Product prices in Barbados are the highest among all CSM projectcondom and OC prices.
- 35 -
Table 5. DISTRIBUTOR, WHOLESALER AND RETAILER MARGINSALLOWED IN FOUR CSH PROJECTS
Margins (Percents)
Country Distributor Wholesaler Stockists Retailer
Bangladesh (1983)1/ 4-8 5-7 15-20
Caribbean (1983)2/ 27 50
India (1985)3/ 13 6 20
Nepal (1983)4/Dhaal Condom 17 19Suki Dhaal Condoms 16 19Gulaf OC 13 18Nilicon (low-dose) OC 13 18Kamal tablets 14 20
1/ Davies, 1983.
2/ Bayley and Washchuck, 1983.
3/ Sherris, Ravenholt and Blackburn, 1985.
4/ Margins offered now are somewhat lower and more in keeping with theusual margins offered. Even with these higher margins (shown forillustrative purposes), the profit to wholesalers and retailers forproducts sold is minuscule (Table 6). Nepal CRS, 1984.
-36-
Table 6. WlGD AUlMD A O0dOMOM RICS TD BURCIPAIES IN DSMBUICN CHAIN(Prices in U.S.$)
Price to Price to Price to Price to Price to
Project and Product Distributor Wholesaler Stockist Retailer Consumer
6% 6% 17.5%
anglaesh margin margin margin
Ovacon OC .1212 ).1285 .1362 .16
.0073 .0077 .0238mark-up mark-up mark-up
13 20%
India margin 6% margin margin
Nirodh (ondoms (3) .0209 > .0236 > .0250 > .03
.0027 .0014 mark-up .005mark-tp mark-up
15%Nepal 12% margin margin
Gulaf OC (newmargins) .0932 > .1043 0.12.0111 mark-up .0157
mark-up
19%
17% margin margin
Dhaal Condom (1) .0072 .0084 0.01
.0012 mark-up .0016
50%
Barbados 27% margin margin
Pantber Condoms (3) .3937 > .5000 - 0.75.1063 mark-up .2500
mark-up
50%
27% margin margin
Perle OC .9186 > 1.1667 ; 1.75
.2480 mark-up .5834mark-up
Source: Derived from Tables 3 and 5; Sherris, Raveabolt and Blackburn, 1985
- 37 -
participation. In Jamaica, pharmacists may take a retailer training course
offered as part of the CSM project.
Retailers (and others along the distribution chain) are supposed
to charge the official price approved by the government for CSM products.
There appears to be little mechanism for enforcing those prices on the part
of the project and little disincentive to inhibit retailers from increasing
prices (unofficially) and correspondingly, their profits. Studies have
found a wide range of prices charged for CSM products within countries,
indicating that retailers (and others) are manipulating prices.
E. Cost-Effectiveness of CSH Projects
The objectives of individual CSM projects and priorities accorded
them in the different countries will affect costs: those with primarily a
social objective--rural outreach and a low income target nopulation (e.g.,
Bangladesh)--will likely have higher project costs (and charge lower
prices) than a project which emphasizes income generation and
urban-oriented markets (e.g., Sri Lanka, Mexico, Colombia). The cost-
effectiveness of CSM projects is typically measured in terms of annual net
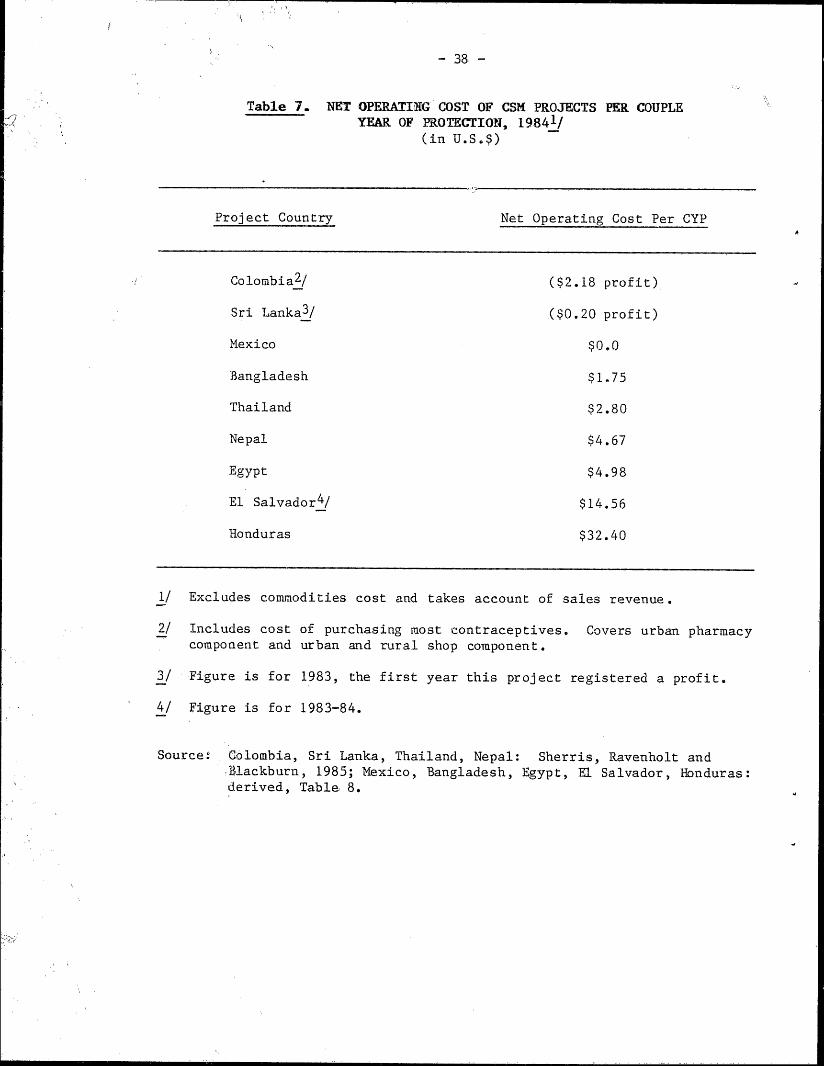
project costs per CYP (see Table 7)13/. Colombia and Sri Lanka are the
only CSM projects making a profit (in Colombia $2.18 per CYP in 1984; in
Sri Lanka $.20 per CYP in 1983, up from a net cost of $0.02 per CYP in
1982). In Sri Lanka, the ability to earn a profit is attributed to the
13/ These figures are based on estimates of CYP and population coverageand should be considered as approximate indicators of program coverageand efficiency.
- 38 -
Table 7. NET OPERATING COST OF CSM PROJECTS PER COUPLEYEAR OF PROTECTION, 19841/
(in U.S.$)
Project Country Net Operating Cost Per CYP
Colombia 2 / ($2.18 profit)
Sri Lanka3 / ($0.20 profit)
Mexico $0.0
Bangladesh $1.75
Thailand $2.80
Nepal $4.67
Egypt $4.98
El Salvador4 / $14.56
Honduras $32.40
1/ Excludes commodities cost and takes account of sales revenue.
2/ Includes cost of purchasing most contraceptives. Covers urban pharmacycomponent and urban and rural shop component.
3/ Figure is for 1983, the first year this project registered a profit.
4/ Figure is for 1983-84.
Source: Colombia, Sri Lanka, Thailand, Nepal: Sherris, Ravenholt andtlackburn, 1985; Mexico, Bangladesh, Egypt, El Salvador, Honduras:derived, Table 8.
- 39 -
addition of products sold at commercial prices in the early 1980's to the
product line. During that period, however, coverage of MWRA dropped by 29
percent (see Table 2). The Mexico project had zero net cost in 1984:
following withdrawal of donor support in 1981, the project began selling
spermicides, IUDs and a number of household items at commercial prices to
raise revenue (see Expanded Product Line, p. 44). Coverage since 1981 has
dropped by 60 percent. The Bangladesh CSM project appears to be
cost-effective given its emphasis on rural outreach and the low price of
its products. Its net cost per CYP ($1.75 in 1984) is less than the cost
for most other agencies providing family planning, including the government
through free programs, which range from $3-18 per CYP. Only the private
voluntary sterilization program approaches the CSM project's low cost per
CYP (SMF, Winter 1984; Davies, 1983).
Cost-effectiveness of these projects is also affected by the
social and economic circumstances existing in the country. For example,
Binnendijk (1985) asserts that "multiple cultures and languages, the
mountainous terrain and weak infrastructural and commercial sector of Nepal
place constraints and costs on the project there not encountered in more
homogenous and developed societies." It is implied that the somewhat
higher costs and low coverage in Nepal are at least partially the result of
these factors, although no specific data are offered to support this view
(the net cost per CYP in Nepal is high but has declined over the
years--discussed below). Sherris, Ravenholt and Blackburn (1985) attribute
at least part of the high net cost per CYP in El Salvador ($14.56) to the
social unrest there which has disrupted sales.
Among the many factors that influence cost-effectiveness, prices
charged, size of project and length of program operation are considered
V -40-
very important, with the latter the most significant. Altman and Piotrow
(1980) state that new programs tend to have high costs (e.g., start--up
costs for market research, packaging, promotion and distribution), while
revenues from sales are low. As programs become established costs level
off while revenue increases from growth in sales. They cite the
significant decreases in net costs per CYP from project inception to 1979
in India ($2.51 to $1.67 in 8 years) and Sri Lanka ($9.83 to $3.79 in 4
years) as evidence. In Bangladesh, the net cost per CYP was $2.86 in 1976,
the first full year of operation when about 10 million condoms and 500,000
cycles of OCs were sold; in 1984 the cost was $1.75 with sales of about 130
million condoms and 2 million OC cycles (and coverage of 40 percent of all
contraceptors). In Nepal, net total cost (including commodities cost) per
CYP went from $49 in 1978 to $19 in 1981 and $8.30 in 1984. During that
period condom sales went from less than 100,000 to 3.4 million and OC sales
from 10,000 cycles to about 110,000 cycles. On the other hand in the young
Honduras project, where sales only began in 1984, the net project cost was
much higher at $32.40.
Large programs tend to be more cost-effective than small ones.
As sales volume increases the program can achieve economies of scale
thereby improving its cost-effectiveness. Fixed costs, e.g., for
contractors, become smaller as a proportion of total expenditures. In
Bangladesh where net operating costs were over $3 million in 1984, the
sales volume was the equivalent of nearly 1.4 million CYPs, yielding a net
cost of $1.75 per CYP. Projects launched in small countries will never be
able to reach a comparable sales volume. For example, in the Caribbean,
where only about 100,000 women of reproductive age live, the budget was
$172,000 in 1983-84 and the cost was over $140 per CYP (without sales
-41-
revenue). At least part of the cause for the high cost per CYP in El
Salvador is attributed to the project size (project sales were the
equivalent of 15,000 CYP from April 1984 to March 1985).
A more in-depth look at project costs and revenue generated
through sales is given in Table 8. Egypt is the most expensive project in
terms of total costs, and generates the most revenue followed by
Bangladesh. Sri Lanka's project is earning a profit of $0.34 per CYP and
Mexico's project has zero net costs. Of the remaining five projects shown,
three generate enough revenue to cover about one-quarter of their costs.
The level of cost recovery is lowest in Nepal at 16%.
F. Mechanisms for Increasing Project Revenue
The intention of CSM projects is to set a low price so that high
sales volume will eventually be generated thereby providing a satisfactory
return to retailers. But retailer profits have generally been low and
where subsidies have been withdrawn (e.g., Mexico, and partially in Jamaica
and Sri Lanka) projects have had to come up with additional ways to raise
revenue. Two such mechanisms have been raising product prices and
expanding the project product line.
Price Sensitivity. How sensitive are consumers to changes in
price? A study by Lewis (1984) on price elasticities found that small
price increases resulted in only temporary decreases in sales followed by a
return to original sales levels. The effect of the price increase in
Jamaica on sales volume was similar to that experienced in other countries
(e.g., Sri Lanka) where prices were raised: demand declined immediately
following the price hike, then gradually moved back to (and in Jamaica's
case, surpassed) original levels. In Egypt, price increases for IUDs (from
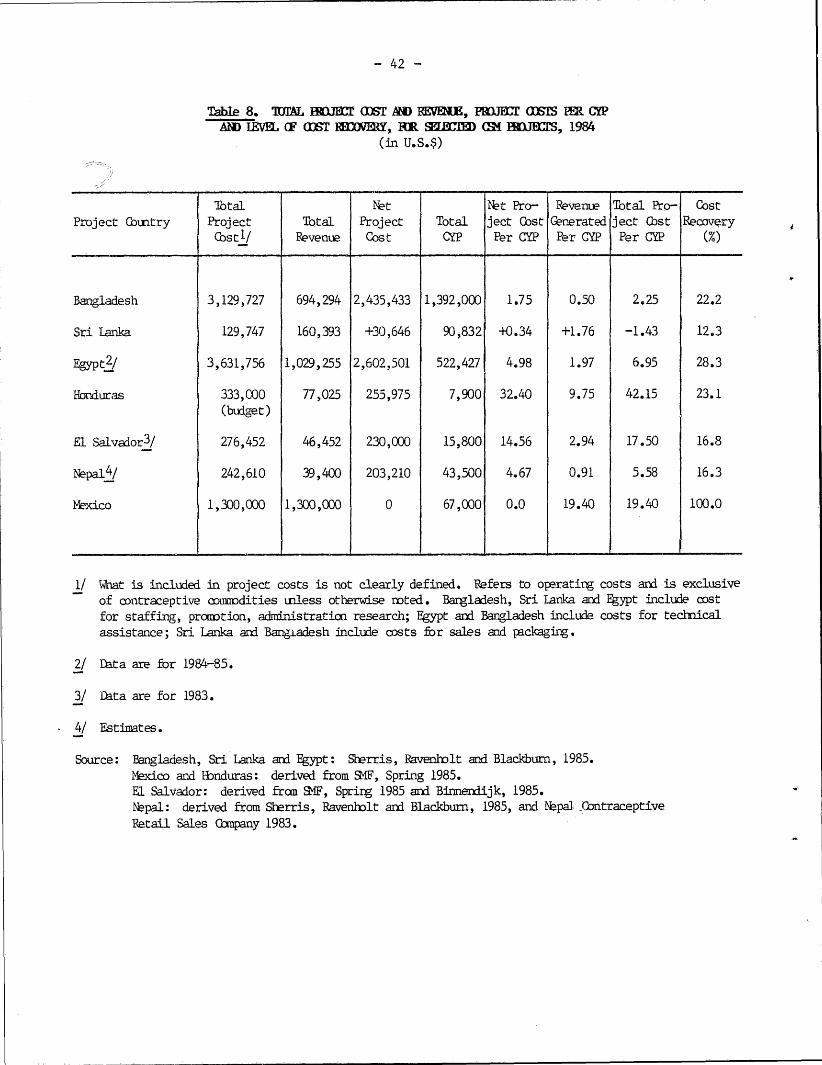
-42-
Table 8. 1TAL W1B= GDST AND REVEM E, PRJECT COTS IM R CYPAlM IEVUZ (F COET RHCOMY, IR SELiWMD GM IBMCJS, 1984
(in U.S.$)
Total Net 1t Pro- Revenue Total Pro- CostProject Country Project Total Project Total ject Cost Generated ject Cost Recovery
Cost'/ Revenue Cost CYP Per CYP Per CYP Per CYP (%)
Bangladesh 3,129,727 694,294 2,435,433 1,392,000 1.75 0.50 2.25 22.2
Sri Lanka 129,747 160,393 +30,646 90,832 +0.34 +1.76 -1.43 12.3
Egypt 2! 3,631,756 1,029,255 2,602,501 522,427 4.98 1.97 6.95 28.3
Honduras 333,000 77,025 255,975 7,900 32.40 9.75 42.15 23.1(budget)
El Salvador3/ 276,452 46,452 230,000 15,800 14.56 2.94 17.50 16.8
Nepal 4/ 242,610 39,400 203,210 43,500 4.67 0.91 5.58 16.3
Mexico 1,300,000 1,300,000 0 67,000 0.0 19.40 19.40 100.0
1/ What is included in project costs is not clearly defined. Refers to operating costs and is exclusiveof contraceptive comodities unless otherwise noted. Bangladesh, Sri Lanka and Egypt include costfor staffing, promotion, administration research; Egypt and Bangladesh include costs for technicalassistance; Sri Lanka and Bangadesh include costs for sales and packaging.
2/ Data are for 1984-85.
3/ Data are for 1983.
4/ Estimates.
Source: Bangladesh, Sri Lanka and Egypt: Sherris, Ravenbolt and Blackburn, 1985.Mexico and Bonduras: derived from SWF, Spring 1985.El Salvador: derived fran SMF, Spring 1985 and Binnendijk, 1985.Npal: derived from Sherris, Ravenholt and Blackburn, 1985, and Nepal ContraceptiveRetail Sales Cbmpany 1983.
- 43
$2.14 to $2.85) and tablets (from $0.022 to $0.036 each) did not affect
sales. In Thailand, doubling the price of injectables (from $0.75 to
$1.50) at public clinics had no effect on current users or new acceptor
levels. However, it appears that a major price increase can reduce demand
significantly in some countries. A doubling of product prices in 1983 in
El Salvador is blamed, in part, for a 50 percent drop in sales.1 4 / In
India, a doubling of the price of Nirodh condoms in 1974 coincided with a
drop in sales (a simultaneous reduction in the promotional budget may also
have contributed).
A study by Akin and Schwartz (1985) on Jamaica and Thailand found
that "as price [for a method] increases consumers become less likely to use
the method, but the magnitude of this price effect is not large".... For
those choosing priced products (instead of free ones), rising prices appear
to have only a small deterent effect on use of each priced method. Data
suggest that if prices were raised 50 percent, usage xould change by less
than 5 percent, and that less than 3 percent would switch to natural
methods, the remainder moving to a less expensive "modern" method.
The results for these two countries suggest that prices do not
significantly affect the decision as to whether to use free contraceptives
or priced products. Oth.. ctudies indicate that where free and modestly
priced contraceptives a l'fered through similar, known outlets (e.g., in
Colombia, Korea and rgp) there is little difference in demand for free
and low priced products. In an experiment in Taiwan, consumers were
presented with a choice of OCs at 3 price levels. The response to the
14/ One must also qonsider how much other factors--political instability--contributed to this drop. SMF, Spring 1984.
-44-
moderately priced OC ($.13) was identical to that for the free product; the
OC which sold for $0.25 per cycle attracted half as many acceptors.
A study of CSK programs in 11 developing countries by Boone, et
al., (1985) found condom sales more sensitive to price (to which they were
negatively related) and less sensitive to income than were OCs.
Apart from the Taiwan study, there have not been any
experimental studies that have actually evaluated how varying prices affect
buying. Data available seem to indicate that there may be some room for
raising prices in CSM projects without affecting demand. This would
increase revenue, provide additional profits and reduce the level of
subsidy needed. But available information also indicates that too high a
price discourages contraceptive usage or leads to shifts to traditional
methods. What is considered too high a price will vary by socioeconomic
conditions of the target group, the value of children, etc. Additional
research on price elasticities of demand and willingness to pay could help
projects set more appropriate prices and provide guidelines as to what the
upper limit of price increases would be in order not to significantly
affect demand.
G. Expanded Product Line
As an alternative to raising CSM product prices in order to
increase revenue, a number of projects provide a product mix: they have
added higher priced brands to their product line to increase product
revenue. Sri Lanka has introduced a new higher priced condom, Preethi
Gold, and sells Rough Rider and Stimula condoms at commercial prices;
Bangladesh added a higher priced, low-dose OC (Ovacon) in 1983.
-45-
Another mechanism for increasing revenue that is being used by
some projects is the addition of non-contraceptive products to the sales
line. In Bangladesh, delivery kits are sold for $1.00; in Nepal ORS
packages are sold for $0.07 a pack. Colombia's PROFAMILIA project added
many products, including disposable diapers, sanitary napkins, Nandol
(analgesic) and distilled water, but only the last continues to be sold;
selling the water is meeting a need not yet duplicated by competitors.
Price competition from the commercial market, the bulk of the items,
storage problems, etc., led to termination of sales of the other items
(Andreasen, 1985). Mexico's PROFAM project also added a number of products
(as many as 8 in 1983) after USAID funding was withdrawn e.g., Bic pens,
sanitary napkins, CONTAC, a health magazine, and key chains (with embedded
condoms for "emergency use"). Economic crisis in 1983 caused severe cash
flow problems forcing PROFA4 to delay payments to non-contraceptive
suppliers. This, coupled with low sales for some items resulted in
discontinuation of sales of many of these products. In 1985, syringes,
disposable diapers and key chains were being sold. Different products are
sold at different times depending on demand and competition. The sale of
non-contraceptive products has generated substantial revenue for PROFAM.
It appears that projects must resist the temptation to
haphazardly add products to their sales line. Careful study should be
conducted to assess which products should be added, if any, and to assure
that they will meet a need of potential consumers. The question of whether
sales of other products is an appropriate activity of CSM projects should
also be addressed. Allowing the revenues raised from other profitable
lines to be used to subsidize CSM projects is effectively a political
-46-
choice of how to use revenues that could be used for other purposes. The
answer as to whether CSM projects should sell non-contraceptive products
and, if so, what types is not immediately obvious.
H. Substitution
The extent to which CSM projects reach those with unmet demand
for contraception and/or actually increase demand, rather than simply
provide products which are substituted for products available from other
sources or for natural methods, has not been systematically studied. Data
presently available are circumstantial and inconclusive. CSM project
evaluation studies done in Bangladesh, Nepal, Mexico and Kenya concluded
"that sales and distribution of contraceptives from existing sources
continued to grow and that if there was substitution it was probably
marginal" (Binnendijk, 1985). In Bangladesh, public and private sector
family planning program managers were found to be supportive of the CSM
project because they saw their increased sales as resulting from the CSM
project's extensive advertising. In fact the Bangladesh program provides
an example of a case where the CSM project may have helped to increase
overall contraceptive prevalence. Available data show that as CYP provided
by the project increased, the CYP provided by all government programs
(except from IUDs and voluntary sterilization) grew proportionally. This
suggests that the CSM project contributed to meeting unmet demand rather
than simply providing an alternative supply source to existing
contraceptive users. This conclusion is speculative, however, as it is not
known how fast demand would have grown without the project. Conversely,
other CSM project data imply that substitution may be considerable in some
countries: data from Sri Lanka, Thailand and Colombia (described as
-47
"inconclusive") suggest that CSM projects contributed to a reduction in
private sector sales. Survey data for Sri Lanka indicate "that as much as
35 percent of CSM condom sales may have been substitution for other family
planning methods." Colombia's PROFAMILIA project, directed at higher
income groups, probably contributed to a decline in commercially
distributed products (Binnendijk, 1985).
This indirect and circumstantial evidence suggests that in
countries where contraceptive use is low and a large market of couples who
are non-users exists (e.g., Bangladesh, Egypt, Nepal and India), CSM
projects probably provide products without having a large impact on other
supply sources. Therefore, substitution may not be a significant factor in
such countries. It may be an issue for countries with higher contraceptive
prevalence and with more government and commercial supply sources (e.g.,
Jamaica, Sri Lanka and Thailand) and in projects that target higher income
groups. More research is needed to determine to what extent CSM programs
reach new users or provide a substitute for conventional commercial sales
or clinic service.
VI. CSM Project Evaluation
A. Existing Evaluations
CSM projects have not been extensively evaluated. Quantitative
evaluations have not been consistently executed: no set approach to
evaluation exists, and appropriate measures of success (sales, CYP,
demographic impact) have not been determined, making assessment of project
performance and effectiveness difficult and cross-country comparisons crude
estimates at best. Data collection has been poor; few baseline studies
have been done. "There have been too few appropriately controlled
-48-
quasi-experimental designs/surveys to conclude with any certainty the
extent to which CSM projects have impacted overall contraceptive prevalence
rates and fertility levels" (Binnendijk, 1985).
None of the ongoing projects cover more than 15.3 percent of the
married women of reproductive age and six cover fewer than 5 percent. At
what level should CSM projects be considered successful? Many health-
oriented efforts strive for very high coverage levels (e.g., EPI--the
Expanded Program for Immunization); should CSM projects similarly try to
reach the masses or should they be content with 5-15 percent coverage?
What coverage level should a marketing manager (as opposed to a health or
family planning manager) consider satisfactory, given budget constraints,
advertising restrictions, etc.?1 5/ These are some of the questions that
evaluations should address.
There appears to be a trend toward doing qualitative evaluations
(e.g., Davies' of Bangladesh, 1983) rather than quantitative evaluations.
This may be necessary where ongoing projects have limited data available.
New projects should be designed so that data which are necessary for more
quantitative assessments will be collected for the project implementation
period.
B. Evaluation Findings
Given the limitations just mentioned, the literature does cite a
number of constraints to project success and factors necessary for good
project performance. These are discussed below.
15/ Pharmaceutical companies selling OCs in the U.S. consider a new
product successful if sales reach $20 million annually: this
represents about 166,500 CYP, or about 0.5 percent of MWRA in the
U.S. Sales of many consumer packaged products are regarded as
successful if they reach as few as 5% of the target population.Sherris, Ravenholt and Blackburn, 1985.
-49-
CSM projects tend to perform best when not implemented directly
by the government. Projects run by FPAs have more management problems and
are less successful than those managed by independent, non-profit
organizations that can operate with more flexibility (Binnendijk, 1985).
Flexibility to adapt to change and reality, and authority to make changes
are keys to success (Altman and Piotrow, 1980). Discontinuity in
management has caused serious problems in some projects (Ravenholt, 1985).
Government support and assistance with overcoming procedural
constraints, however, is critical to program success. Even where
government is not managing a project it can have significant impact on the
operation of a project: absence of political commitment; customs
regulations; restrictions on advertising and price changes; and
prescription requirements have all been mentioned as constraints to project
performance (Osborn and Reinke, 1981; Perkin, 1977; Boone, Farley and
Samuel, 1985). In addition to government "imposed" constraints, multiple
languages and cultures prevalent in a country can complicate advertising
and communication aspects of a project. Lack of resources--financial,
manpower, etc., can restrict execution of the complete marketing process
(Greenberg, Novelli and Curtin, 1983). Marketing (and management)
expertise needs to be available and/or obtainable (ICSMP, 1983b). General
economic problems (Jamaica) and political stability (or lack thereof--El
Salvador) will influence CSM performance. The strength of the commercial
distribution infrastructure will at least partially determine the coverage
of the CSM project: thus far projects have been most successful in
reaching urban and peri-urban areas because it is there that the delivery
systems are strongest; in general, remote rural areas have not benefitted
- 50 -
substantially from CSR projects (except in Bangladesh) (Ravenholt., 1985;
Sherris, 1985). In general, external involvement of other organizations is
considered almost as problematic as management issues, while marketing
becomes more important during the operational stage (ICSMP, 1983b).
Use of donated products has created some problems for CSM project
managers. For example, USAID commodity procurement procedures have
sometimes negatively affected the performance of CSM projects supported by
USAID (most of those discussed in this paper). The lengthy procurement
process can cause supply shortages: lead time for supply orders is long
(18 months for condoms) because contraceptives are purchased in bulk on a
competitive basis to obtain the lowest price. USAID's practice of awarding
contracts to the lowest bidder has, in the past, resulted in changes in the
product supplies and disruption of CSM sales performance. Early problems,
such as the lack of distinction between package designs for CSM products
and those distributed free in government programs, and the limited types of
products available to CSM projects, were alleviated when USAID developed
different packaging for CSM products and made available a variety of
condoms and different dose level OCs so CSM programs could increase their
product line (Sherris, Ravenholt and Blackburn, 1985).
In general, available evidence indicates that CSM programs can
play an important part in meeting the family planning needs in a country if
they are well managed, have government support, are appropriately
publicized and are adapted to the local culture and environment. The fact
that three programs serve at least 30 percent of all current family
planning users and two serve more than 20 percent indicates that programs
are acting, to varying degrees, as important supply services and expanding
the availability of contraceptives.
- 51 -
Bibliography
Akin, John S. and J. Brad Schwartz. "Price Elasticity of Demand forContraceptives: Jamaica and Thailand." Mimeo. 1985.
Altman, Diana L. and Phyllis T. Piotrow. "Social Marketing: Does itWork?" Population Reports 8(1), January 1980.
Andreasen, Alan R. "Growth Opportunities for Contraceptive SocialMarketing Programs." Mimeo. February 1985.
Bayley, Ronald and Gail Washchuck. "Caribbean Contraceptive SpcialMarketing Project--Initial Marketing Plan," Mimeo. Pepared forICSMP, 1983.
Binnendijk, A. "AID's Experience with Contraceptive Social Marketing; ASynthesis of Project Evaluation Findings." Draft. Mimeo. January1985.
Blackburn, Richard. Personal Communication, April 17, 1985.
Boone, M.S., J.U. Farley and S.J. Samuel. "A Cross-Country Study ofCommercial Contraceptive Sales Programs: Factors the Lead toSuccess," Studies in Family Planning 16(1), January/February 1985,30-39.
Davies, J. "Evaluation of the Social Marketing Project." Dacca, U.S.Agency for International Development, Mission to Bangladesh, Office ofPopulation and Health. 1983.
Davies, J., and T.D.J. Louis, "Measuring the Effectiveness of ContraceptiveMarketing Programs: Preethi in Sri Lanka," Studies in FamilyPlanning, 8 (4), April 1977, 82-90.
Fox, Karen F.A. and Philip Kotler. "The Marketing of Social Causes: TheFirst 10 Years," Journal of Marketing 44, Fall 1980, 24-33.
Greenberg, Rachael, William D. Novelli and Leslie Curtin. "A Model forMarket Research in Contraceptive Social Marketing." Prepared forICSMP. February 1983.
Harvey, P.D. (1984a). "Advertising Family Planning in the Press: DirectResponse Results from Bangladesh." Studies in Family Planning, 15(1), January/February 1984, 40-42.
Harvey, P.D. (1984b). "CSM and the Myth of Self-Sufficiency." SocialMarketing Forum, (3), Spring 1984, 2.
Howell, Betty B. and William D. Novelli. "Technical Assistance Report onthe 'Family of the Future' Contraceptive Sales Program, November 23 -December 4, 1980." Mimeo.
Huber, S.C., et.al. "Contraceptive Distribution--Taking Supplies toVillages and Households," Population Reports Series, J(5), July 1985.
-52-
International Contraceptive Social Marketing Project (ICSMP 1983a)."Determining Pricing Policies in Contraceptive Social Marketing."
International Contraceptive Social Marketing Project (ICSMP 1983b)"Contraceptive Social Marketing Strategy Workshop, May 2-5, 1983."
Levy, Tennyson (Don). "Trip Report: Honduras CSM Program, June 11-18,1984." Mimeo. Prepared for ICSMP.
Lewis, Maureen A. "Price Elasticity and Cost Recovery Experience in LDCFamily Planning Programs," Draft, September 1984.
Nepal Contraceptive Retail Sales Company Pvt. Ltd. at a Glance." Mimeo.February 1984.
Osborn, R.W, and W.A. Reinke. "Community-Based Distribution ofContraception -- A Review of Field Experience," January 1981.
Perkin, Gordon W. "Forum: Population Planning--Family Planning ServiceDelivery--Options and Trends." Preventive Medicine 6, 1977, 74-91.
Ravenholt, Betty Butler. "Contraceptive Social Marketing-Guidelines forProject Development," Prepared for ICSMP, September 1982.
Ravenholt, Betty. Personal Communication, February 22, 1985.
Schellstede, W.P. (1985b) "Contraceptive Social Marketing." Washington,D.C. Population Services International, Draft. July 1985.
Schellstede, W.P. and Robert L. Ciszewski. "Social Marketing ofContraceptives in Bangladesh." Studies in Family Planning 15 (1),January/February 1984, 30-39.
Sherris, Jacqueline. "Contraceptive Social Marketing: Lessons Learnedfrom Experience" Review Draft. Mimeo, May 1985.
Sherris, Jacqueline D., Betty B. Ravenholt and Richard Blackburn."Contraceptive Social Marketing: Lessons from Experience."Population Reports 8(3), July-August 1985.
Social Marketing Forum (SMF), 1(2), Winter 1984.
Social Marketing Forum (SMF), 1(3), Spring 1984.
Social Marketing Forum (SMF), 1(4), Summer 1984.
Social Marketing Forum (SMF), 1(5), Fall 1984.
Social Marketing Forum (SMF), 2(2), Spring 1985.
World Development Report 1985. New York: Oxford University Press, 1985.
Ylanan, D., and C.C. Verzosa. "Commercial Retail Sales of Contraceptives,"PIACT Paper No. 6, 1979.





























